User login
James J. Stevermer is in the Department of Family and Community Medicine at the University of Missouri–Columbia.
“Go low” or say “No” to aggressive systolic BP goals?
Consider treating non-diabetic patients age ≥50 years to a systolic blood pressure (SBP) target <120 mm Hg as compared to <140 mm Hg when the benefits—lower rates of fatal and nonfatal cardiovascular (CV) events and death from any cause—are likely to outweigh the risks from possible additional medication.1
Strength of recommendation
B: Based on a single, good-quality randomized controlled trial (RCT).
Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
Illustrative Case
A 55-year-old man with hypertension and stage 3 chronic kidney disease (CKD) comes in to your office for routine care. His blood pressure is 135/85 mm Hg, and he is presently taking lisinopril 40 mg daily. Should you increase his antihypertensive regimen?
Hypertension is common and leads to significant morbidity and mortality, but pharmacologic treatment reduces incidence of stroke by 35% to 40%, myocardial infarction (MI) by 15% to 25%, and heart failure by up to 64%.2-4 Specific blood pressure targets for defined populations continue to be studied.
In patients with diabetes, the ACCORD (Action to Control Cardiovascular Risk in Diabetes) trial found that more intensive BP targets did not reduce the rate of major CV events, but the study may have been underpowered.5 The members of The Eighth Joint National Committee recommended treating patients over age 60 years to BP goals <150/90 mm Hg.6 This was based on evidence from 6 randomized controlled trials (RCTs),7-12 but there remains debate—even among the members of the Committee—as to appropriate BP goals in patients of any age without CV disease who have BP measurements of 140-159/90-99 mm Hg.13
Study Summary
Treating to SBP <120 mm Hg lowers mortality
The Systolic Blood Pressure Intervention Trial (SPRINT) was a multicenter RCT designed to determine if treating to lower SBP targets in non-diabetic patients at high risk for CV events improves outcomes as compared to standard care. Patients were at least 50 years of age with SBP of 130 to 180 mm Hg and were at increased CV risk as defined by clinical or subclinical CV disease other than stroke, CKD with glomerular filtration rate (GFR) 20 to 60 mL/min/1.73 m2, 10-year risk of CV disease >15% on Framingham risk score, or age ≥75 years of age. Patients with diabetes; prior stroke; polycystic kidney disease; significant proteinuria within the past 6 months; symptomatic heart failure within the past 6 months; or left ventricular ejection fraction <35% were excluded.1
Patients (N=9361) were randomly assigned to an SBP target <120 mm Hg in the intensive group or <140 mm Hg in the standard treatment group, in an open-label design. Allocation was concealed. The study protocol encouraged, but did not require, the use of thiazide-type diuretics, loop diuretics (for those with advanced renal disease), angiotensin-converting enzyme inhibitors or angiotensin receptor blocker agents, calcium channel blockers, and beta-blockers. Clinicians could add other agents as needed. All major classes of antihypertensives were used.
Medication dosing adjustments were based on the average of 3 BP measurements taken with an automated measurement system (Omron Healthcare, Model 907) with the patient seated after 5 minutes of quiet rest. Target SBP in the standard therapy group was 135 to 139 mm Hg. Medication dosages were lowered if SBP was <130 mm Hg at a single visit or <135 mm Hg at 2 consecutive visits.1
The primary composite outcome included the first occurrence of MI, acute coronary syndrome, stroke, heart failure, or death from CV causes. Secondary outcomes were the individual components of the primary composite outcome, death from any cause, and the composite of the primary outcome or death from any cause.1
Study halted early. The study was stopped early due to significantly lower rates of the primary outcome in the intensive therapy group vs the standard therapy group (1.65% per year vs 2.19% per year, respectively, hazard ratio [HR] with intensive treatment=0.75; 95% confidence interval [CI], 0.64-0.89; P<.001). The resulting median follow-up time was 3.26 years.1 This corresponds to a 25% lower relative risk of the primary outcome, with a decrease in event rates from 6.8% to 5.2% over the trial period. All-cause mortality was also lower in the intensive therapy group: 3.4% vs 4.5% (HR=0.73; 95% CI, 0.60-0.90; P=.003).
The number needed to treat (NNT) over 3.26 years to prevent a primary outcome event, death from any cause, and death from CV causes was 61, 90, and 172, respectively. Serious adverse events occurred more frequently in the intensive therapy group than in the standard therapy group (38.3% vs 37.1%; HR=1.04; P=.25) with a number needed to harm (NNH) of 46 over the study period.1 (When looking at serious adverse events identified as likely associated with the intervention, rates were 4.7% vs 2.5%, respectively [P<.001].) Hypotension, syncope, electrolyte abnormalities, and acute kidney injury/acute renal failure reached statistical significance. The incidence of bradycardia and injurious falls was higher in the intensive treatment group, but did not reach statistical significance. In the subgroup of patients ≥75 years of age, 48% in each study group experienced a serious adverse event.1
Throughout the study, mean SBP was 121.5 mm Hg in the intensive therapy group and 134.6 mm Hg in the standard treatment group. This required an average of one additional BP medication in the intensive therapy group (2.8 vs 1.8, respectively).1
What’s New
Lower SBP produces mortality benefits in those under, and over, age 75
This trial builds on a body of evidence that shows the advantages of lowering SBP to <150 mm Hg7,11,12 by demonstrating benefits, including lower all-cause mortality, for lower SBP targets in non-diabetic patients at high risk of CV disease. The SPRINT trial also showed that the benefits of intensive therapy remained true in a subgroup of patients ≥75 years of age.
The incidence of the primary outcome in the cohort ≥75 years of age receiving intensive therapy was 7.7% vs 10.9% for those receiving standard therapy (HR=0.67; 95% CI, 0.51-0.86; NNT=31). All-cause mortality was also lower in the intensive therapy group than in the standard therapy group among patients ≥75 years of age: 5.5% vs 8.04% (HR=0.68; 95% CI, 0.50-0.92; NNT=38).1
Caveats
Many do not benefit from—or are harmed by—increased medication
The absolute risk reduction for the primary outcome is 1.6%, meaning 98.4% of patients receiving more intensive treatment will not benefit. In a group of 1000 patients, an estimated 16 patients will benefit, 22 patients will be seriously harmed, and 962 patients will experience neither benefit nor harm.14 The difference between how BP was measured in this trial (an average of 3 readings after the patient had rested for 5 minutes) and that which occurs typically in clinical practice could potentially lead to overtreatment in practice.
Also, reducing antihypertensive therapies when the SBP was about 130 to 135 mm Hg in the standard therapy group likely exaggerated the difference in outcomes between the intensive and standard therapy groups, and is neither routine nor recommended in clinical practice.6 Finally, the trial specifically studied non-diabetic patients at high risk of CV disease ≥50 years of age, limiting generalizability to other populations.
Challenges to implementation
Who will benefit/who can achieve intensive SBP goals?
Identifying patients most likely to benefit from more intensive BP targets remains challenging. The SPRINT trial showed a mortality benefit, but at a cost of increased morbidity.1,14 In particular, caution should be exercised in the subgroup of patients ≥75 years. Despite a lower NNT than the rest of the study population, serious adverse events happened more frequently. Also, this particular cohort of volunteers may not be representative of those ≥75 years of age in the general population.
Additionally, achieving intensive SBP goals can be challenging. In the SPRINT trial, only half of the intensive target group achieved an SBP <120 mm Hg.1 And in a 2011-12 National Health and Nutrition Examination Survey, only 52% of patients in the general population achieved a BP target <140/90 mm Hg.15 Lower morbidity and mortality should remain the ultimate goals to the management of hypertension, requiring physicians to carefully assess an individual patient’s likelihood of benefit vs harm.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
2. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
3. Neal B, MacMahon S, Chapman N. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Lancet. 2000;356:1955-1964.
4. Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA. 1997;277:739-745.
5. Margolis KL, O’Connor PJ, Morgan TM, et al. Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: the ACCORD randomized trial. Diabetes Care. 2014;37:1721-1728.
6. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
7. Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887-1898.
8. Verdecchia P, Staessen JA, Angeli F, et al. Usual versus tight control of systolic blood pressure in non-diabetic patients with hypertension (Cardio-Sis): an open-label randomised trial. Lancet. 2009;374:525-533.
9. JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res. 2008;31:2115-2127.
10. Ogihara T, Saruta T, Rakugi H, et al. Target blood pressure for treatment of isolated systolic hypertension in the elderly: valsartan in elderly isolated systolic hypertension study. Hypertension. 2010;56:196-202.
11. Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet. 1997;350:757-764.
12. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). SHEP Cooperative Research Group. JAMA. 1991;265:3255-3264.
13. Cundiff DK, Gueyffier F, Wright JM. Guidelines for managing high blood pressure. JAMA. 2014; 312:294.
14. Ortiz E, James PA. Let’s not SPRINT to judgment about new blood pressure goals. Ann Intern Med. 2016.
15. Nwankwo T, Yoon SS, Burt V, et al. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;1-8.
Consider treating non-diabetic patients age ≥50 years to a systolic blood pressure (SBP) target <120 mm Hg as compared to <140 mm Hg when the benefits—lower rates of fatal and nonfatal cardiovascular (CV) events and death from any cause—are likely to outweigh the risks from possible additional medication.1
Strength of recommendation
B: Based on a single, good-quality randomized controlled trial (RCT).
Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
Illustrative Case
A 55-year-old man with hypertension and stage 3 chronic kidney disease (CKD) comes in to your office for routine care. His blood pressure is 135/85 mm Hg, and he is presently taking lisinopril 40 mg daily. Should you increase his antihypertensive regimen?
Hypertension is common and leads to significant morbidity and mortality, but pharmacologic treatment reduces incidence of stroke by 35% to 40%, myocardial infarction (MI) by 15% to 25%, and heart failure by up to 64%.2-4 Specific blood pressure targets for defined populations continue to be studied.
In patients with diabetes, the ACCORD (Action to Control Cardiovascular Risk in Diabetes) trial found that more intensive BP targets did not reduce the rate of major CV events, but the study may have been underpowered.5 The members of The Eighth Joint National Committee recommended treating patients over age 60 years to BP goals <150/90 mm Hg.6 This was based on evidence from 6 randomized controlled trials (RCTs),7-12 but there remains debate—even among the members of the Committee—as to appropriate BP goals in patients of any age without CV disease who have BP measurements of 140-159/90-99 mm Hg.13
Study Summary
Treating to SBP <120 mm Hg lowers mortality
The Systolic Blood Pressure Intervention Trial (SPRINT) was a multicenter RCT designed to determine if treating to lower SBP targets in non-diabetic patients at high risk for CV events improves outcomes as compared to standard care. Patients were at least 50 years of age with SBP of 130 to 180 mm Hg and were at increased CV risk as defined by clinical or subclinical CV disease other than stroke, CKD with glomerular filtration rate (GFR) 20 to 60 mL/min/1.73 m2, 10-year risk of CV disease >15% on Framingham risk score, or age ≥75 years of age. Patients with diabetes; prior stroke; polycystic kidney disease; significant proteinuria within the past 6 months; symptomatic heart failure within the past 6 months; or left ventricular ejection fraction <35% were excluded.1
Patients (N=9361) were randomly assigned to an SBP target <120 mm Hg in the intensive group or <140 mm Hg in the standard treatment group, in an open-label design. Allocation was concealed. The study protocol encouraged, but did not require, the use of thiazide-type diuretics, loop diuretics (for those with advanced renal disease), angiotensin-converting enzyme inhibitors or angiotensin receptor blocker agents, calcium channel blockers, and beta-blockers. Clinicians could add other agents as needed. All major classes of antihypertensives were used.
Medication dosing adjustments were based on the average of 3 BP measurements taken with an automated measurement system (Omron Healthcare, Model 907) with the patient seated after 5 minutes of quiet rest. Target SBP in the standard therapy group was 135 to 139 mm Hg. Medication dosages were lowered if SBP was <130 mm Hg at a single visit or <135 mm Hg at 2 consecutive visits.1
The primary composite outcome included the first occurrence of MI, acute coronary syndrome, stroke, heart failure, or death from CV causes. Secondary outcomes were the individual components of the primary composite outcome, death from any cause, and the composite of the primary outcome or death from any cause.1
Study halted early. The study was stopped early due to significantly lower rates of the primary outcome in the intensive therapy group vs the standard therapy group (1.65% per year vs 2.19% per year, respectively, hazard ratio [HR] with intensive treatment=0.75; 95% confidence interval [CI], 0.64-0.89; P<.001). The resulting median follow-up time was 3.26 years.1 This corresponds to a 25% lower relative risk of the primary outcome, with a decrease in event rates from 6.8% to 5.2% over the trial period. All-cause mortality was also lower in the intensive therapy group: 3.4% vs 4.5% (HR=0.73; 95% CI, 0.60-0.90; P=.003).
The number needed to treat (NNT) over 3.26 years to prevent a primary outcome event, death from any cause, and death from CV causes was 61, 90, and 172, respectively. Serious adverse events occurred more frequently in the intensive therapy group than in the standard therapy group (38.3% vs 37.1%; HR=1.04; P=.25) with a number needed to harm (NNH) of 46 over the study period.1 (When looking at serious adverse events identified as likely associated with the intervention, rates were 4.7% vs 2.5%, respectively [P<.001].) Hypotension, syncope, electrolyte abnormalities, and acute kidney injury/acute renal failure reached statistical significance. The incidence of bradycardia and injurious falls was higher in the intensive treatment group, but did not reach statistical significance. In the subgroup of patients ≥75 years of age, 48% in each study group experienced a serious adverse event.1
Throughout the study, mean SBP was 121.5 mm Hg in the intensive therapy group and 134.6 mm Hg in the standard treatment group. This required an average of one additional BP medication in the intensive therapy group (2.8 vs 1.8, respectively).1
What’s New
Lower SBP produces mortality benefits in those under, and over, age 75
This trial builds on a body of evidence that shows the advantages of lowering SBP to <150 mm Hg7,11,12 by demonstrating benefits, including lower all-cause mortality, for lower SBP targets in non-diabetic patients at high risk of CV disease. The SPRINT trial also showed that the benefits of intensive therapy remained true in a subgroup of patients ≥75 years of age.
The incidence of the primary outcome in the cohort ≥75 years of age receiving intensive therapy was 7.7% vs 10.9% for those receiving standard therapy (HR=0.67; 95% CI, 0.51-0.86; NNT=31). All-cause mortality was also lower in the intensive therapy group than in the standard therapy group among patients ≥75 years of age: 5.5% vs 8.04% (HR=0.68; 95% CI, 0.50-0.92; NNT=38).1
Caveats
Many do not benefit from—or are harmed by—increased medication
The absolute risk reduction for the primary outcome is 1.6%, meaning 98.4% of patients receiving more intensive treatment will not benefit. In a group of 1000 patients, an estimated 16 patients will benefit, 22 patients will be seriously harmed, and 962 patients will experience neither benefit nor harm.14 The difference between how BP was measured in this trial (an average of 3 readings after the patient had rested for 5 minutes) and that which occurs typically in clinical practice could potentially lead to overtreatment in practice.
Also, reducing antihypertensive therapies when the SBP was about 130 to 135 mm Hg in the standard therapy group likely exaggerated the difference in outcomes between the intensive and standard therapy groups, and is neither routine nor recommended in clinical practice.6 Finally, the trial specifically studied non-diabetic patients at high risk of CV disease ≥50 years of age, limiting generalizability to other populations.
Challenges to implementation
Who will benefit/who can achieve intensive SBP goals?
Identifying patients most likely to benefit from more intensive BP targets remains challenging. The SPRINT trial showed a mortality benefit, but at a cost of increased morbidity.1,14 In particular, caution should be exercised in the subgroup of patients ≥75 years. Despite a lower NNT than the rest of the study population, serious adverse events happened more frequently. Also, this particular cohort of volunteers may not be representative of those ≥75 years of age in the general population.
Additionally, achieving intensive SBP goals can be challenging. In the SPRINT trial, only half of the intensive target group achieved an SBP <120 mm Hg.1 And in a 2011-12 National Health and Nutrition Examination Survey, only 52% of patients in the general population achieved a BP target <140/90 mm Hg.15 Lower morbidity and mortality should remain the ultimate goals to the management of hypertension, requiring physicians to carefully assess an individual patient’s likelihood of benefit vs harm.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Consider treating non-diabetic patients age ≥50 years to a systolic blood pressure (SBP) target <120 mm Hg as compared to <140 mm Hg when the benefits—lower rates of fatal and nonfatal cardiovascular (CV) events and death from any cause—are likely to outweigh the risks from possible additional medication.1
Strength of recommendation
B: Based on a single, good-quality randomized controlled trial (RCT).
Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
Illustrative Case
A 55-year-old man with hypertension and stage 3 chronic kidney disease (CKD) comes in to your office for routine care. His blood pressure is 135/85 mm Hg, and he is presently taking lisinopril 40 mg daily. Should you increase his antihypertensive regimen?
Hypertension is common and leads to significant morbidity and mortality, but pharmacologic treatment reduces incidence of stroke by 35% to 40%, myocardial infarction (MI) by 15% to 25%, and heart failure by up to 64%.2-4 Specific blood pressure targets for defined populations continue to be studied.
In patients with diabetes, the ACCORD (Action to Control Cardiovascular Risk in Diabetes) trial found that more intensive BP targets did not reduce the rate of major CV events, but the study may have been underpowered.5 The members of The Eighth Joint National Committee recommended treating patients over age 60 years to BP goals <150/90 mm Hg.6 This was based on evidence from 6 randomized controlled trials (RCTs),7-12 but there remains debate—even among the members of the Committee—as to appropriate BP goals in patients of any age without CV disease who have BP measurements of 140-159/90-99 mm Hg.13
Study Summary
Treating to SBP <120 mm Hg lowers mortality
The Systolic Blood Pressure Intervention Trial (SPRINT) was a multicenter RCT designed to determine if treating to lower SBP targets in non-diabetic patients at high risk for CV events improves outcomes as compared to standard care. Patients were at least 50 years of age with SBP of 130 to 180 mm Hg and were at increased CV risk as defined by clinical or subclinical CV disease other than stroke, CKD with glomerular filtration rate (GFR) 20 to 60 mL/min/1.73 m2, 10-year risk of CV disease >15% on Framingham risk score, or age ≥75 years of age. Patients with diabetes; prior stroke; polycystic kidney disease; significant proteinuria within the past 6 months; symptomatic heart failure within the past 6 months; or left ventricular ejection fraction <35% were excluded.1
Patients (N=9361) were randomly assigned to an SBP target <120 mm Hg in the intensive group or <140 mm Hg in the standard treatment group, in an open-label design. Allocation was concealed. The study protocol encouraged, but did not require, the use of thiazide-type diuretics, loop diuretics (for those with advanced renal disease), angiotensin-converting enzyme inhibitors or angiotensin receptor blocker agents, calcium channel blockers, and beta-blockers. Clinicians could add other agents as needed. All major classes of antihypertensives were used.
Medication dosing adjustments were based on the average of 3 BP measurements taken with an automated measurement system (Omron Healthcare, Model 907) with the patient seated after 5 minutes of quiet rest. Target SBP in the standard therapy group was 135 to 139 mm Hg. Medication dosages were lowered if SBP was <130 mm Hg at a single visit or <135 mm Hg at 2 consecutive visits.1
The primary composite outcome included the first occurrence of MI, acute coronary syndrome, stroke, heart failure, or death from CV causes. Secondary outcomes were the individual components of the primary composite outcome, death from any cause, and the composite of the primary outcome or death from any cause.1
Study halted early. The study was stopped early due to significantly lower rates of the primary outcome in the intensive therapy group vs the standard therapy group (1.65% per year vs 2.19% per year, respectively, hazard ratio [HR] with intensive treatment=0.75; 95% confidence interval [CI], 0.64-0.89; P<.001). The resulting median follow-up time was 3.26 years.1 This corresponds to a 25% lower relative risk of the primary outcome, with a decrease in event rates from 6.8% to 5.2% over the trial period. All-cause mortality was also lower in the intensive therapy group: 3.4% vs 4.5% (HR=0.73; 95% CI, 0.60-0.90; P=.003).
The number needed to treat (NNT) over 3.26 years to prevent a primary outcome event, death from any cause, and death from CV causes was 61, 90, and 172, respectively. Serious adverse events occurred more frequently in the intensive therapy group than in the standard therapy group (38.3% vs 37.1%; HR=1.04; P=.25) with a number needed to harm (NNH) of 46 over the study period.1 (When looking at serious adverse events identified as likely associated with the intervention, rates were 4.7% vs 2.5%, respectively [P<.001].) Hypotension, syncope, electrolyte abnormalities, and acute kidney injury/acute renal failure reached statistical significance. The incidence of bradycardia and injurious falls was higher in the intensive treatment group, but did not reach statistical significance. In the subgroup of patients ≥75 years of age, 48% in each study group experienced a serious adverse event.1
Throughout the study, mean SBP was 121.5 mm Hg in the intensive therapy group and 134.6 mm Hg in the standard treatment group. This required an average of one additional BP medication in the intensive therapy group (2.8 vs 1.8, respectively).1
What’s New
Lower SBP produces mortality benefits in those under, and over, age 75
This trial builds on a body of evidence that shows the advantages of lowering SBP to <150 mm Hg7,11,12 by demonstrating benefits, including lower all-cause mortality, for lower SBP targets in non-diabetic patients at high risk of CV disease. The SPRINT trial also showed that the benefits of intensive therapy remained true in a subgroup of patients ≥75 years of age.
The incidence of the primary outcome in the cohort ≥75 years of age receiving intensive therapy was 7.7% vs 10.9% for those receiving standard therapy (HR=0.67; 95% CI, 0.51-0.86; NNT=31). All-cause mortality was also lower in the intensive therapy group than in the standard therapy group among patients ≥75 years of age: 5.5% vs 8.04% (HR=0.68; 95% CI, 0.50-0.92; NNT=38).1
Caveats
Many do not benefit from—or are harmed by—increased medication
The absolute risk reduction for the primary outcome is 1.6%, meaning 98.4% of patients receiving more intensive treatment will not benefit. In a group of 1000 patients, an estimated 16 patients will benefit, 22 patients will be seriously harmed, and 962 patients will experience neither benefit nor harm.14 The difference between how BP was measured in this trial (an average of 3 readings after the patient had rested for 5 minutes) and that which occurs typically in clinical practice could potentially lead to overtreatment in practice.
Also, reducing antihypertensive therapies when the SBP was about 130 to 135 mm Hg in the standard therapy group likely exaggerated the difference in outcomes between the intensive and standard therapy groups, and is neither routine nor recommended in clinical practice.6 Finally, the trial specifically studied non-diabetic patients at high risk of CV disease ≥50 years of age, limiting generalizability to other populations.
Challenges to implementation
Who will benefit/who can achieve intensive SBP goals?
Identifying patients most likely to benefit from more intensive BP targets remains challenging. The SPRINT trial showed a mortality benefit, but at a cost of increased morbidity.1,14 In particular, caution should be exercised in the subgroup of patients ≥75 years. Despite a lower NNT than the rest of the study population, serious adverse events happened more frequently. Also, this particular cohort of volunteers may not be representative of those ≥75 years of age in the general population.
Additionally, achieving intensive SBP goals can be challenging. In the SPRINT trial, only half of the intensive target group achieved an SBP <120 mm Hg.1 And in a 2011-12 National Health and Nutrition Examination Survey, only 52% of patients in the general population achieved a BP target <140/90 mm Hg.15 Lower morbidity and mortality should remain the ultimate goals to the management of hypertension, requiring physicians to carefully assess an individual patient’s likelihood of benefit vs harm.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
2. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
3. Neal B, MacMahon S, Chapman N. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Lancet. 2000;356:1955-1964.
4. Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA. 1997;277:739-745.
5. Margolis KL, O’Connor PJ, Morgan TM, et al. Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: the ACCORD randomized trial. Diabetes Care. 2014;37:1721-1728.
6. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
7. Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887-1898.
8. Verdecchia P, Staessen JA, Angeli F, et al. Usual versus tight control of systolic blood pressure in non-diabetic patients with hypertension (Cardio-Sis): an open-label randomised trial. Lancet. 2009;374:525-533.
9. JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res. 2008;31:2115-2127.
10. Ogihara T, Saruta T, Rakugi H, et al. Target blood pressure for treatment of isolated systolic hypertension in the elderly: valsartan in elderly isolated systolic hypertension study. Hypertension. 2010;56:196-202.
11. Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet. 1997;350:757-764.
12. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). SHEP Cooperative Research Group. JAMA. 1991;265:3255-3264.
13. Cundiff DK, Gueyffier F, Wright JM. Guidelines for managing high blood pressure. JAMA. 2014; 312:294.
14. Ortiz E, James PA. Let’s not SPRINT to judgment about new blood pressure goals. Ann Intern Med. 2016.
15. Nwankwo T, Yoon SS, Burt V, et al. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;1-8.
1. Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
2. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
3. Neal B, MacMahon S, Chapman N. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Lancet. 2000;356:1955-1964.
4. Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA. 1997;277:739-745.
5. Margolis KL, O’Connor PJ, Morgan TM, et al. Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: the ACCORD randomized trial. Diabetes Care. 2014;37:1721-1728.
6. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
7. Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887-1898.
8. Verdecchia P, Staessen JA, Angeli F, et al. Usual versus tight control of systolic blood pressure in non-diabetic patients with hypertension (Cardio-Sis): an open-label randomised trial. Lancet. 2009;374:525-533.
9. JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res. 2008;31:2115-2127.
10. Ogihara T, Saruta T, Rakugi H, et al. Target blood pressure for treatment of isolated systolic hypertension in the elderly: valsartan in elderly isolated systolic hypertension study. Hypertension. 2010;56:196-202.
11. Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet. 1997;350:757-764.
12. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). SHEP Cooperative Research Group. JAMA. 1991;265:3255-3264.
13. Cundiff DK, Gueyffier F, Wright JM. Guidelines for managing high blood pressure. JAMA. 2014; 312:294.
14. Ortiz E, James PA. Let’s not SPRINT to judgment about new blood pressure goals. Ann Intern Med. 2016.
15. Nwankwo T, Yoon SS, Burt V, et al. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;1-8.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.

New Adjunctive Treatment Option for Venous Stasis Ulcers
PRACTICE CHANGER
Consider adding simvastatin (40 mg/d) to standard wound care and compression for patients with venous stasis ulcers.1
STRENGTH OF RECOMMENDATION
B: Based on a high-quality randomized controlled trial (RCT).1
ILLUSTRATIVE CASE
A 74-year-old woman with chronic lower extremity edema seeks treatment for a nonhealing venous stasis ulcer. For the past nine months, she’s been wearing compression stockings and receiving intermittent home-based wound care, but nothing seems to help. She asks if there’s anything else she can try.
Venous stasis ulcers affect 1% of US adults and lead to substantial morbidity and more than $2 billion in annual health care expenditures.1,2 Edema management—generally limb elevation and compression therapy—has been the mainstay of therapy. Treatment can be lengthy, and ulcer recurrence is common.2,3
Statins have been found to aid wound healing through their diverse physiologic (pleiotropic) effects. Evidence indicates they can be beneficial in treatment of diabetic foot ulcers,4 pressure ulcers,5 and ulcerations associated with systemic sclerosis and Raynaud phenomenon.6 Evangelista et al1 investigated whether adding a statin to standard wound care and compression could improve venous stasis ulcer healing.
Continue for study summary >>
STUDY SUMMARY
Ulcers more likely to close when statin added
This randomized, double-blind, placebo-controlled trial was performed at a large medical center in the Philippines. It was designed to assess the efficacy and safety of simvastatin (40 mg/d) for venous ulcer healing when combined with standard treatment (compression therapy, limb elevation, and standard wound care).1
Study subjects were 66 patients, ages 41 to 71, who’d had one or more venous ulcers for at least three months. They were randomly assigned to receive either simvastatin (40 mg/d; n = 32) or an identical-appearing placebo (n = 34). Patients were excluded if they were pregnant, had an ulcer that was infected or > 10 cm in diameter, or were taking any medication that could interact with a statin. Patients were stratified according to ulcer diameter (≤ 5 cm and > 5 cm). There was no statistically significant difference between the two groups in the duration of venous ulceration (3.80 y in the placebo group vs 3.93 y in the simvastatin group) or incidence of diabetes (5% vs 3%, respectively).
The primary outcome was the proportion of patients whose ulcers completely healed at 10 weeks. Secondary outcomes were measures of the total surface area healed, healing time, and Dermatology Life Quality Index (DLQI) scores. Baseline ulcer diameter and surface area and DLQI scores were obtained prior to therapy initiation. The same dermatologist, who was blinded to the patients’ group assignments, evaluated all patients every two weeks until wound closure or for a maximum of 10 weeks.
Overall, 90% of the patients who received simvastatin had complete ulcer closure at 10 weeks, compared with 34% of patients in the control group (relative risk [RR], 0.16; number needed to treat [NNT], 2).
Among patients with ulcers ≤ 5 cm, 100% of the ulcers healed in the simvastatin group, compared to 50% in the control group (RR, 0.10; NNT, 2). Perhaps more importantly, in patients with ulcers > 5 cm, 67% in the simvastatin group had closure with a mean healing time of nine weeks, whereas none of the ulcers of this size closed in the control group (RR, 0.33; NNT, 1.5), and the mean healed area was significantly larger in patients who received simvastatin (28.9 cm2 vs 19.6 cm2).
In addition, in the simvastatin group, healing times were significantly reduced (7.53 ± 1.34 wk vs 8.55 ± 1.13 wk) and quality of life (as evaluated by DLQI scoring) significantly improved compared to the control group.
Study dropouts were minimal (8%; two in the placebo group and three in the intervention group). Using intention-to-treat analysis and worst-case scenarios for those who dropped out did not affect the primary outcome. There were no withdrawals due to adverse reactions.
WHAT’S NEW
Statins offer significant benefits for treating venous stasis ulcers
This is the first human study to investigate the use of a statin in venous stasis ulcer healing. This intervention demonstrated significant improvements in healing rate and time, a very small NNT for benefit, and improved patient quality of life compared to placebo.
Next page: Caveats >>
CAVEATS
Carefully selected patients
Many wounds will heal with compression therapy alone, as occurred in this study, in which 50% of ulcers ≤ 5 cm treated with standard therapy healed, albeit at a somewhat slower rate. Adding another medication to the regimen when target patients generally have multiple comorbidities should always prompt caution.
The study by Evangelista et al1 was performed in a select population, and the exclusion criteria included the use of some commonly prescribed medications, such as ACE inhibitors. No data were collected on patient BMI, which is a risk factor for delayed healing.
The prevalence of obesity is lower in the Philippines than in the US. It is uncertain what role this difference would have in the statin’s effectiveness.
Further studies, especially those conducted with a less selective population, would better clarify the generalizability of this intervention.
Nontheless, we found the results of this study impressive. The methods reported are rigorous and consistent with standard RCT methodologies.
This is the only study of a statin in human venous stasis disease, but studies in animals—and studies of statins for other types of ulcers in humans—have consistently suggested benefit. It seems hard to argue against adding this low-cost, low-risk intervention.
CHALLENGES TO IMPLEMENTATION
There are no known barriers to implementation of this practice.
REFERENCES
1. Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014; 170:1151-1157.
2. Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010;81: 989-996.
3. The Australian Wound Management Association Inc, New Zealand Wound Care Society Inc. Australian and New Zealand clinical practice guideline for prevention and management of venous leg ulcers (2011). www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ext003_venous_leg_ulcers_aust_nz_0.pdf. Accessed March 21, 2015.
4. Johansen OE, Birkeland KI, Jørgensen AP, et al. Diabetic foot ulcer burden may be modified by high-dose atorvastatin: a 6-month randomized controlled pilot trial. J Diabetes. 2009; 1:182-187.
5. Farsaei S, Khalili H, Farboud ES, et al. Efficacy of topical atorvastatin for the treatment of pressure ulcers: a randomized clinical trial. Pharmacotherapy. 2014;34:19-27.
6. Abou-Raya A, Abou-Raya S, Helmii M. Statins: potentially useful in therapy of systemic sclerosis-related Raynaud’s phenomenon and digital ulcers. J Rheumatol. 2008;35:1801-1808.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2015. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2015;64(3):182-184.
PRACTICE CHANGER
Consider adding simvastatin (40 mg/d) to standard wound care and compression for patients with venous stasis ulcers.1
STRENGTH OF RECOMMENDATION
B: Based on a high-quality randomized controlled trial (RCT).1
ILLUSTRATIVE CASE
A 74-year-old woman with chronic lower extremity edema seeks treatment for a nonhealing venous stasis ulcer. For the past nine months, she’s been wearing compression stockings and receiving intermittent home-based wound care, but nothing seems to help. She asks if there’s anything else she can try.
Venous stasis ulcers affect 1% of US adults and lead to substantial morbidity and more than $2 billion in annual health care expenditures.1,2 Edema management—generally limb elevation and compression therapy—has been the mainstay of therapy. Treatment can be lengthy, and ulcer recurrence is common.2,3
Statins have been found to aid wound healing through their diverse physiologic (pleiotropic) effects. Evidence indicates they can be beneficial in treatment of diabetic foot ulcers,4 pressure ulcers,5 and ulcerations associated with systemic sclerosis and Raynaud phenomenon.6 Evangelista et al1 investigated whether adding a statin to standard wound care and compression could improve venous stasis ulcer healing.
Continue for study summary >>
STUDY SUMMARY
Ulcers more likely to close when statin added
This randomized, double-blind, placebo-controlled trial was performed at a large medical center in the Philippines. It was designed to assess the efficacy and safety of simvastatin (40 mg/d) for venous ulcer healing when combined with standard treatment (compression therapy, limb elevation, and standard wound care).1
Study subjects were 66 patients, ages 41 to 71, who’d had one or more venous ulcers for at least three months. They were randomly assigned to receive either simvastatin (40 mg/d; n = 32) or an identical-appearing placebo (n = 34). Patients were excluded if they were pregnant, had an ulcer that was infected or > 10 cm in diameter, or were taking any medication that could interact with a statin. Patients were stratified according to ulcer diameter (≤ 5 cm and > 5 cm). There was no statistically significant difference between the two groups in the duration of venous ulceration (3.80 y in the placebo group vs 3.93 y in the simvastatin group) or incidence of diabetes (5% vs 3%, respectively).
The primary outcome was the proportion of patients whose ulcers completely healed at 10 weeks. Secondary outcomes were measures of the total surface area healed, healing time, and Dermatology Life Quality Index (DLQI) scores. Baseline ulcer diameter and surface area and DLQI scores were obtained prior to therapy initiation. The same dermatologist, who was blinded to the patients’ group assignments, evaluated all patients every two weeks until wound closure or for a maximum of 10 weeks.
Overall, 90% of the patients who received simvastatin had complete ulcer closure at 10 weeks, compared with 34% of patients in the control group (relative risk [RR], 0.16; number needed to treat [NNT], 2).
Among patients with ulcers ≤ 5 cm, 100% of the ulcers healed in the simvastatin group, compared to 50% in the control group (RR, 0.10; NNT, 2). Perhaps more importantly, in patients with ulcers > 5 cm, 67% in the simvastatin group had closure with a mean healing time of nine weeks, whereas none of the ulcers of this size closed in the control group (RR, 0.33; NNT, 1.5), and the mean healed area was significantly larger in patients who received simvastatin (28.9 cm2 vs 19.6 cm2).
In addition, in the simvastatin group, healing times were significantly reduced (7.53 ± 1.34 wk vs 8.55 ± 1.13 wk) and quality of life (as evaluated by DLQI scoring) significantly improved compared to the control group.
Study dropouts were minimal (8%; two in the placebo group and three in the intervention group). Using intention-to-treat analysis and worst-case scenarios for those who dropped out did not affect the primary outcome. There were no withdrawals due to adverse reactions.
WHAT’S NEW
Statins offer significant benefits for treating venous stasis ulcers
This is the first human study to investigate the use of a statin in venous stasis ulcer healing. This intervention demonstrated significant improvements in healing rate and time, a very small NNT for benefit, and improved patient quality of life compared to placebo.
Next page: Caveats >>
CAVEATS
Carefully selected patients
Many wounds will heal with compression therapy alone, as occurred in this study, in which 50% of ulcers ≤ 5 cm treated with standard therapy healed, albeit at a somewhat slower rate. Adding another medication to the regimen when target patients generally have multiple comorbidities should always prompt caution.
The study by Evangelista et al1 was performed in a select population, and the exclusion criteria included the use of some commonly prescribed medications, such as ACE inhibitors. No data were collected on patient BMI, which is a risk factor for delayed healing.
The prevalence of obesity is lower in the Philippines than in the US. It is uncertain what role this difference would have in the statin’s effectiveness.
Further studies, especially those conducted with a less selective population, would better clarify the generalizability of this intervention.
Nontheless, we found the results of this study impressive. The methods reported are rigorous and consistent with standard RCT methodologies.
This is the only study of a statin in human venous stasis disease, but studies in animals—and studies of statins for other types of ulcers in humans—have consistently suggested benefit. It seems hard to argue against adding this low-cost, low-risk intervention.
CHALLENGES TO IMPLEMENTATION
There are no known barriers to implementation of this practice.
REFERENCES
1. Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014; 170:1151-1157.
2. Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010;81: 989-996.
3. The Australian Wound Management Association Inc, New Zealand Wound Care Society Inc. Australian and New Zealand clinical practice guideline for prevention and management of venous leg ulcers (2011). www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ext003_venous_leg_ulcers_aust_nz_0.pdf. Accessed March 21, 2015.
4. Johansen OE, Birkeland KI, Jørgensen AP, et al. Diabetic foot ulcer burden may be modified by high-dose atorvastatin: a 6-month randomized controlled pilot trial. J Diabetes. 2009; 1:182-187.
5. Farsaei S, Khalili H, Farboud ES, et al. Efficacy of topical atorvastatin for the treatment of pressure ulcers: a randomized clinical trial. Pharmacotherapy. 2014;34:19-27.
6. Abou-Raya A, Abou-Raya S, Helmii M. Statins: potentially useful in therapy of systemic sclerosis-related Raynaud’s phenomenon and digital ulcers. J Rheumatol. 2008;35:1801-1808.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2015. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2015;64(3):182-184.
PRACTICE CHANGER
Consider adding simvastatin (40 mg/d) to standard wound care and compression for patients with venous stasis ulcers.1
STRENGTH OF RECOMMENDATION
B: Based on a high-quality randomized controlled trial (RCT).1
ILLUSTRATIVE CASE
A 74-year-old woman with chronic lower extremity edema seeks treatment for a nonhealing venous stasis ulcer. For the past nine months, she’s been wearing compression stockings and receiving intermittent home-based wound care, but nothing seems to help. She asks if there’s anything else she can try.
Venous stasis ulcers affect 1% of US adults and lead to substantial morbidity and more than $2 billion in annual health care expenditures.1,2 Edema management—generally limb elevation and compression therapy—has been the mainstay of therapy. Treatment can be lengthy, and ulcer recurrence is common.2,3
Statins have been found to aid wound healing through their diverse physiologic (pleiotropic) effects. Evidence indicates they can be beneficial in treatment of diabetic foot ulcers,4 pressure ulcers,5 and ulcerations associated with systemic sclerosis and Raynaud phenomenon.6 Evangelista et al1 investigated whether adding a statin to standard wound care and compression could improve venous stasis ulcer healing.
Continue for study summary >>
STUDY SUMMARY
Ulcers more likely to close when statin added
This randomized, double-blind, placebo-controlled trial was performed at a large medical center in the Philippines. It was designed to assess the efficacy and safety of simvastatin (40 mg/d) for venous ulcer healing when combined with standard treatment (compression therapy, limb elevation, and standard wound care).1
Study subjects were 66 patients, ages 41 to 71, who’d had one or more venous ulcers for at least three months. They were randomly assigned to receive either simvastatin (40 mg/d; n = 32) or an identical-appearing placebo (n = 34). Patients were excluded if they were pregnant, had an ulcer that was infected or > 10 cm in diameter, or were taking any medication that could interact with a statin. Patients were stratified according to ulcer diameter (≤ 5 cm and > 5 cm). There was no statistically significant difference between the two groups in the duration of venous ulceration (3.80 y in the placebo group vs 3.93 y in the simvastatin group) or incidence of diabetes (5% vs 3%, respectively).
The primary outcome was the proportion of patients whose ulcers completely healed at 10 weeks. Secondary outcomes were measures of the total surface area healed, healing time, and Dermatology Life Quality Index (DLQI) scores. Baseline ulcer diameter and surface area and DLQI scores were obtained prior to therapy initiation. The same dermatologist, who was blinded to the patients’ group assignments, evaluated all patients every two weeks until wound closure or for a maximum of 10 weeks.
Overall, 90% of the patients who received simvastatin had complete ulcer closure at 10 weeks, compared with 34% of patients in the control group (relative risk [RR], 0.16; number needed to treat [NNT], 2).
Among patients with ulcers ≤ 5 cm, 100% of the ulcers healed in the simvastatin group, compared to 50% in the control group (RR, 0.10; NNT, 2). Perhaps more importantly, in patients with ulcers > 5 cm, 67% in the simvastatin group had closure with a mean healing time of nine weeks, whereas none of the ulcers of this size closed in the control group (RR, 0.33; NNT, 1.5), and the mean healed area was significantly larger in patients who received simvastatin (28.9 cm2 vs 19.6 cm2).
In addition, in the simvastatin group, healing times were significantly reduced (7.53 ± 1.34 wk vs 8.55 ± 1.13 wk) and quality of life (as evaluated by DLQI scoring) significantly improved compared to the control group.
Study dropouts were minimal (8%; two in the placebo group and three in the intervention group). Using intention-to-treat analysis and worst-case scenarios for those who dropped out did not affect the primary outcome. There were no withdrawals due to adverse reactions.
WHAT’S NEW
Statins offer significant benefits for treating venous stasis ulcers
This is the first human study to investigate the use of a statin in venous stasis ulcer healing. This intervention demonstrated significant improvements in healing rate and time, a very small NNT for benefit, and improved patient quality of life compared to placebo.
Next page: Caveats >>
CAVEATS
Carefully selected patients
Many wounds will heal with compression therapy alone, as occurred in this study, in which 50% of ulcers ≤ 5 cm treated with standard therapy healed, albeit at a somewhat slower rate. Adding another medication to the regimen when target patients generally have multiple comorbidities should always prompt caution.
The study by Evangelista et al1 was performed in a select population, and the exclusion criteria included the use of some commonly prescribed medications, such as ACE inhibitors. No data were collected on patient BMI, which is a risk factor for delayed healing.
The prevalence of obesity is lower in the Philippines than in the US. It is uncertain what role this difference would have in the statin’s effectiveness.
Further studies, especially those conducted with a less selective population, would better clarify the generalizability of this intervention.
Nontheless, we found the results of this study impressive. The methods reported are rigorous and consistent with standard RCT methodologies.
This is the only study of a statin in human venous stasis disease, but studies in animals—and studies of statins for other types of ulcers in humans—have consistently suggested benefit. It seems hard to argue against adding this low-cost, low-risk intervention.
CHALLENGES TO IMPLEMENTATION
There are no known barriers to implementation of this practice.
REFERENCES
1. Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014; 170:1151-1157.
2. Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010;81: 989-996.
3. The Australian Wound Management Association Inc, New Zealand Wound Care Society Inc. Australian and New Zealand clinical practice guideline for prevention and management of venous leg ulcers (2011). www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ext003_venous_leg_ulcers_aust_nz_0.pdf. Accessed March 21, 2015.
4. Johansen OE, Birkeland KI, Jørgensen AP, et al. Diabetic foot ulcer burden may be modified by high-dose atorvastatin: a 6-month randomized controlled pilot trial. J Diabetes. 2009; 1:182-187.
5. Farsaei S, Khalili H, Farboud ES, et al. Efficacy of topical atorvastatin for the treatment of pressure ulcers: a randomized clinical trial. Pharmacotherapy. 2014;34:19-27.
6. Abou-Raya A, Abou-Raya S, Helmii M. Statins: potentially useful in therapy of systemic sclerosis-related Raynaud’s phenomenon and digital ulcers. J Rheumatol. 2008;35:1801-1808.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2015. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2015;64(3):182-184.
A new adjunctive Tx option for venous stasis ulcers
Consider adding simvastatin 40 mg/d to standard wound care and compression for patients with venous stasis ulcers.1
Strength of recommendation
B: Based on a high-quality randomized controlled trial (RCT).
Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014;170:1151-1157.
Illustrative case
A 74-year-old woman with chronic lower extremity edema seeks treatment for a nonhealing venous stasis ulcer. For the past 9 months, she’s been wearing compression stockings and receiving intermittent home-based wound care, but nothing seems to help. She asks if there’s anything else she can try.
Venous stasis ulcers affect 1% of US adults and lead to substantial morbidity and more than $2 billion in annual health care expenditures.1,2 Edema management—generally limb elevation and compression therapy—has been the mainstay of therapy. Treatment can be lengthy, and ulcer recurrences are common.2,3
Statins have been found to help wound healing through their diverse physiologic (pleiotropic) effects. Evidence shows they can be beneficial for treating diabetic foot ulcers,4 pressure ulcers,5 and ulcerations associated with systemic sclerosis and Raynaud’s phenomenon.6 Evangelista et al1 investigated whether adding a statin to standard wound care and compression could improve venous stasis ulcer healing.
STUDY SUMMARY: Ulcers are more likely to close when a statin is added to standard care
This randomized, double-blind, placebo-controlled trial was performed at a large medical center in the Philippines. It was designed to assess the efficacy and safety of simvastatin 40 mg/d for venous ulcer healing when combined with standard treatment (compression therapy, limb elevation, and standard wound care).1
Researchers randomized 66 patients ages 41 to 71 who’d had one or more venous ulcers for at least 3 months to receive either simvastatin 40 mg/d (N=32) or an identical appearing placebo (N=34). Patients were excluded if they were pregnant, had an ulcer that was infected or >10 cm in diameter, or were taking any medication that could interact with a statin. Patients were stratified according to ulcer diameter (≤5 cm and >5 cm). There was no statistically significant difference between the 2 groups in the duration of venous ulceration (3.80 years in the placebo group vs 3.93 years in the simvastatin group) or incidence of diabetes (5% in the placebo group vs 3% in the simvastatin group).
The primary outcome was the proportion of patients whose ulcers completely healed at 10 weeks. Secondary outcomes were measures of the total surface area healed and healing time, and Dermatology Life Quality Index (DLQI) scores. Baseline ulcer diameter and surface area and DLQI scores were obtained prior to therapy. The same dermatologist, who was blinded to the patients’ assigned group, evaluated all patients every 2 weeks until wound closure or for a maximum of 10 weeks.
Overall, 90% of the patients who received simvastatin had complete ulcer closure at 10 weeks, compared with 34% of patients in the control group (relative risk [RR]=0.16; 95% confidence interval [CI], 0.05-0.47; number needed to treat [NNT]=2).
Among patients with ulcers ≤5 cm, 100% of the ulcers healed in the simvastatin group, compared to 50% in the control group (RR=0.10; 95% CI, 0.01-0.71; NNT=2). Perhaps more importantly, in patients with ulcers >5 cm, 67% of the ulcers in the simvastatin group had closure with a mean healing time of 9 weeks, whereas none of the ulcers of this size closed in the control group (RR=0.33; 95% CI, 0.12-0.84; NNT=1.5), and the mean healed area was significantly larger in patients who received simvastatin (28.9 cm2 vs 19.6 cm2; P=.03).
In addition, in the simvastatin group, healing times were significantly reduced (7.53±1.34 weeks vs 8.55±1.13 weeks) and quality of life (as evaluated by DLQI scoring) significantly improved compared to the control group.
Study dropouts (8%; 2 in the placebo group and 3 in the intervention group) were minimal. Using intention-to-treat analysis and worst-case scenarios for dropouts did not affect the primary outcome. There were no withdrawals for adverse reactions.
WHAT’S NEW: Statins offer significant benefits for treating venous stasis ulcers
This is the first human study to investigate the use of a statin in venous stasis ulcer healing. This intervention demonstrated significant improvements in healing rate and time, a very small NNT for benefit, and improved patient quality of life compared to placebo.
CAVEATS: Results were found in a carefully selected group of patients
Many wounds will heal with compression therapy alone, as occurred in this study, where 50% of ulcers ≤5 cm treated with standard therapy healed, albeit at a somewhat slower rate. Adding another medication to the regimen when these patients generally have multiple comorbidities should always prompt caution.
The study by Evangelista et al1 was performed in a select population, and the exclusion criteria included the use of some commonly prescribed medications, such as angiotensin-converting enzyme inhibitors. No data were collected on patient body mass index, which is a risk factor for delayed healing. The prevalence of obesity is lower in the Philippines than in the United States, and it is uncertain what role this difference would have in the statin’s effectiveness. Further studies, especially those conducted with a less selective population, would better clarify the generalizability of this intervention.
We found the results of this study impressive. The methods reported are rigorous and consistent with standard RCT methodologies. This is the only study of a statin in human venous stasis disease, but studies in animals—and studies of statins for other types of ulcers in humans—have consistently suggested benefit. It seems hard to argue against adding this low-cost, low-risk intervention.
CHALLENGES TO IMPLEMENTATION
There are no known barriers to implementing this practice.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014;170:1151-1157.
2. Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010;81:989-996.
3. The Australian Wound Management Association Inc, New Zealand Wound Care Society Inc. Australian and New Zealand clinical practice guideline for prevention and management of venous leg ulcers. 2011. Australian Government National Health and Medical Research Council Web site. Available at: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ext003_venous_leg_ulcers_aust_nz_0.pdf. Accessed February 13, 2015.
4. Johansen OE, Birkeland KI, Jørgensen AP, et al. Diabetic foot ulcer burden may be modified by high-dose atorvastatin: A 6-month randomized controlled pilot trial. J Diabetes. 2009;1:182-187.
5. Farsaei S, Khalili H, Farboud ES, et al. Efficacy of topical atorvastatin for the treatment of pressure ulcers: a randomized clinical trial. Pharmacotherapy. 2014;34:19-27.
6. Abou-Raya A, Abou-Raya S, Helmii M. Statins: potentially useful in therapy of systemic sclerosis-related Raynaud’s phenomenon and digital ulcers. J Rheumatol. 2008;35:1801-1808.
Consider adding simvastatin 40 mg/d to standard wound care and compression for patients with venous stasis ulcers.1
Strength of recommendation
B: Based on a high-quality randomized controlled trial (RCT).
Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014;170:1151-1157.
Illustrative case
A 74-year-old woman with chronic lower extremity edema seeks treatment for a nonhealing venous stasis ulcer. For the past 9 months, she’s been wearing compression stockings and receiving intermittent home-based wound care, but nothing seems to help. She asks if there’s anything else she can try.
Venous stasis ulcers affect 1% of US adults and lead to substantial morbidity and more than $2 billion in annual health care expenditures.1,2 Edema management—generally limb elevation and compression therapy—has been the mainstay of therapy. Treatment can be lengthy, and ulcer recurrences are common.2,3
Statins have been found to help wound healing through their diverse physiologic (pleiotropic) effects. Evidence shows they can be beneficial for treating diabetic foot ulcers,4 pressure ulcers,5 and ulcerations associated with systemic sclerosis and Raynaud’s phenomenon.6 Evangelista et al1 investigated whether adding a statin to standard wound care and compression could improve venous stasis ulcer healing.
STUDY SUMMARY: Ulcers are more likely to close when a statin is added to standard care
This randomized, double-blind, placebo-controlled trial was performed at a large medical center in the Philippines. It was designed to assess the efficacy and safety of simvastatin 40 mg/d for venous ulcer healing when combined with standard treatment (compression therapy, limb elevation, and standard wound care).1
Researchers randomized 66 patients ages 41 to 71 who’d had one or more venous ulcers for at least 3 months to receive either simvastatin 40 mg/d (N=32) or an identical appearing placebo (N=34). Patients were excluded if they were pregnant, had an ulcer that was infected or >10 cm in diameter, or were taking any medication that could interact with a statin. Patients were stratified according to ulcer diameter (≤5 cm and >5 cm). There was no statistically significant difference between the 2 groups in the duration of venous ulceration (3.80 years in the placebo group vs 3.93 years in the simvastatin group) or incidence of diabetes (5% in the placebo group vs 3% in the simvastatin group).
The primary outcome was the proportion of patients whose ulcers completely healed at 10 weeks. Secondary outcomes were measures of the total surface area healed and healing time, and Dermatology Life Quality Index (DLQI) scores. Baseline ulcer diameter and surface area and DLQI scores were obtained prior to therapy. The same dermatologist, who was blinded to the patients’ assigned group, evaluated all patients every 2 weeks until wound closure or for a maximum of 10 weeks.
Overall, 90% of the patients who received simvastatin had complete ulcer closure at 10 weeks, compared with 34% of patients in the control group (relative risk [RR]=0.16; 95% confidence interval [CI], 0.05-0.47; number needed to treat [NNT]=2).
Among patients with ulcers ≤5 cm, 100% of the ulcers healed in the simvastatin group, compared to 50% in the control group (RR=0.10; 95% CI, 0.01-0.71; NNT=2). Perhaps more importantly, in patients with ulcers >5 cm, 67% of the ulcers in the simvastatin group had closure with a mean healing time of 9 weeks, whereas none of the ulcers of this size closed in the control group (RR=0.33; 95% CI, 0.12-0.84; NNT=1.5), and the mean healed area was significantly larger in patients who received simvastatin (28.9 cm2 vs 19.6 cm2; P=.03).
In addition, in the simvastatin group, healing times were significantly reduced (7.53±1.34 weeks vs 8.55±1.13 weeks) and quality of life (as evaluated by DLQI scoring) significantly improved compared to the control group.
Study dropouts (8%; 2 in the placebo group and 3 in the intervention group) were minimal. Using intention-to-treat analysis and worst-case scenarios for dropouts did not affect the primary outcome. There were no withdrawals for adverse reactions.
WHAT’S NEW: Statins offer significant benefits for treating venous stasis ulcers
This is the first human study to investigate the use of a statin in venous stasis ulcer healing. This intervention demonstrated significant improvements in healing rate and time, a very small NNT for benefit, and improved patient quality of life compared to placebo.
CAVEATS: Results were found in a carefully selected group of patients
Many wounds will heal with compression therapy alone, as occurred in this study, where 50% of ulcers ≤5 cm treated with standard therapy healed, albeit at a somewhat slower rate. Adding another medication to the regimen when these patients generally have multiple comorbidities should always prompt caution.
The study by Evangelista et al1 was performed in a select population, and the exclusion criteria included the use of some commonly prescribed medications, such as angiotensin-converting enzyme inhibitors. No data were collected on patient body mass index, which is a risk factor for delayed healing. The prevalence of obesity is lower in the Philippines than in the United States, and it is uncertain what role this difference would have in the statin’s effectiveness. Further studies, especially those conducted with a less selective population, would better clarify the generalizability of this intervention.
We found the results of this study impressive. The methods reported are rigorous and consistent with standard RCT methodologies. This is the only study of a statin in human venous stasis disease, but studies in animals—and studies of statins for other types of ulcers in humans—have consistently suggested benefit. It seems hard to argue against adding this low-cost, low-risk intervention.
CHALLENGES TO IMPLEMENTATION
There are no known barriers to implementing this practice.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Consider adding simvastatin 40 mg/d to standard wound care and compression for patients with venous stasis ulcers.1
Strength of recommendation
B: Based on a high-quality randomized controlled trial (RCT).
Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014;170:1151-1157.
Illustrative case
A 74-year-old woman with chronic lower extremity edema seeks treatment for a nonhealing venous stasis ulcer. For the past 9 months, she’s been wearing compression stockings and receiving intermittent home-based wound care, but nothing seems to help. She asks if there’s anything else she can try.
Venous stasis ulcers affect 1% of US adults and lead to substantial morbidity and more than $2 billion in annual health care expenditures.1,2 Edema management—generally limb elevation and compression therapy—has been the mainstay of therapy. Treatment can be lengthy, and ulcer recurrences are common.2,3
Statins have been found to help wound healing through their diverse physiologic (pleiotropic) effects. Evidence shows they can be beneficial for treating diabetic foot ulcers,4 pressure ulcers,5 and ulcerations associated with systemic sclerosis and Raynaud’s phenomenon.6 Evangelista et al1 investigated whether adding a statin to standard wound care and compression could improve venous stasis ulcer healing.
STUDY SUMMARY: Ulcers are more likely to close when a statin is added to standard care
This randomized, double-blind, placebo-controlled trial was performed at a large medical center in the Philippines. It was designed to assess the efficacy and safety of simvastatin 40 mg/d for venous ulcer healing when combined with standard treatment (compression therapy, limb elevation, and standard wound care).1
Researchers randomized 66 patients ages 41 to 71 who’d had one or more venous ulcers for at least 3 months to receive either simvastatin 40 mg/d (N=32) or an identical appearing placebo (N=34). Patients were excluded if they were pregnant, had an ulcer that was infected or >10 cm in diameter, or were taking any medication that could interact with a statin. Patients were stratified according to ulcer diameter (≤5 cm and >5 cm). There was no statistically significant difference between the 2 groups in the duration of venous ulceration (3.80 years in the placebo group vs 3.93 years in the simvastatin group) or incidence of diabetes (5% in the placebo group vs 3% in the simvastatin group).
The primary outcome was the proportion of patients whose ulcers completely healed at 10 weeks. Secondary outcomes were measures of the total surface area healed and healing time, and Dermatology Life Quality Index (DLQI) scores. Baseline ulcer diameter and surface area and DLQI scores were obtained prior to therapy. The same dermatologist, who was blinded to the patients’ assigned group, evaluated all patients every 2 weeks until wound closure or for a maximum of 10 weeks.
Overall, 90% of the patients who received simvastatin had complete ulcer closure at 10 weeks, compared with 34% of patients in the control group (relative risk [RR]=0.16; 95% confidence interval [CI], 0.05-0.47; number needed to treat [NNT]=2).
Among patients with ulcers ≤5 cm, 100% of the ulcers healed in the simvastatin group, compared to 50% in the control group (RR=0.10; 95% CI, 0.01-0.71; NNT=2). Perhaps more importantly, in patients with ulcers >5 cm, 67% of the ulcers in the simvastatin group had closure with a mean healing time of 9 weeks, whereas none of the ulcers of this size closed in the control group (RR=0.33; 95% CI, 0.12-0.84; NNT=1.5), and the mean healed area was significantly larger in patients who received simvastatin (28.9 cm2 vs 19.6 cm2; P=.03).
In addition, in the simvastatin group, healing times were significantly reduced (7.53±1.34 weeks vs 8.55±1.13 weeks) and quality of life (as evaluated by DLQI scoring) significantly improved compared to the control group.
Study dropouts (8%; 2 in the placebo group and 3 in the intervention group) were minimal. Using intention-to-treat analysis and worst-case scenarios for dropouts did not affect the primary outcome. There were no withdrawals for adverse reactions.
WHAT’S NEW: Statins offer significant benefits for treating venous stasis ulcers
This is the first human study to investigate the use of a statin in venous stasis ulcer healing. This intervention demonstrated significant improvements in healing rate and time, a very small NNT for benefit, and improved patient quality of life compared to placebo.
CAVEATS: Results were found in a carefully selected group of patients
Many wounds will heal with compression therapy alone, as occurred in this study, where 50% of ulcers ≤5 cm treated with standard therapy healed, albeit at a somewhat slower rate. Adding another medication to the regimen when these patients generally have multiple comorbidities should always prompt caution.
The study by Evangelista et al1 was performed in a select population, and the exclusion criteria included the use of some commonly prescribed medications, such as angiotensin-converting enzyme inhibitors. No data were collected on patient body mass index, which is a risk factor for delayed healing. The prevalence of obesity is lower in the Philippines than in the United States, and it is uncertain what role this difference would have in the statin’s effectiveness. Further studies, especially those conducted with a less selective population, would better clarify the generalizability of this intervention.
We found the results of this study impressive. The methods reported are rigorous and consistent with standard RCT methodologies. This is the only study of a statin in human venous stasis disease, but studies in animals—and studies of statins for other types of ulcers in humans—have consistently suggested benefit. It seems hard to argue against adding this low-cost, low-risk intervention.
CHALLENGES TO IMPLEMENTATION
There are no known barriers to implementing this practice.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014;170:1151-1157.
2. Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010;81:989-996.
3. The Australian Wound Management Association Inc, New Zealand Wound Care Society Inc. Australian and New Zealand clinical practice guideline for prevention and management of venous leg ulcers. 2011. Australian Government National Health and Medical Research Council Web site. Available at: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ext003_venous_leg_ulcers_aust_nz_0.pdf. Accessed February 13, 2015.
4. Johansen OE, Birkeland KI, Jørgensen AP, et al. Diabetic foot ulcer burden may be modified by high-dose atorvastatin: A 6-month randomized controlled pilot trial. J Diabetes. 2009;1:182-187.
5. Farsaei S, Khalili H, Farboud ES, et al. Efficacy of topical atorvastatin for the treatment of pressure ulcers: a randomized clinical trial. Pharmacotherapy. 2014;34:19-27.
6. Abou-Raya A, Abou-Raya S, Helmii M. Statins: potentially useful in therapy of systemic sclerosis-related Raynaud’s phenomenon and digital ulcers. J Rheumatol. 2008;35:1801-1808.
1. Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: a randomized, double-blind, placebo-controlled trial. Br J Dermatol. 2014;170:1151-1157.
2. Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010;81:989-996.
3. The Australian Wound Management Association Inc, New Zealand Wound Care Society Inc. Australian and New Zealand clinical practice guideline for prevention and management of venous leg ulcers. 2011. Australian Government National Health and Medical Research Council Web site. Available at: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ext003_venous_leg_ulcers_aust_nz_0.pdf. Accessed February 13, 2015.
4. Johansen OE, Birkeland KI, Jørgensen AP, et al. Diabetic foot ulcer burden may be modified by high-dose atorvastatin: A 6-month randomized controlled pilot trial. J Diabetes. 2009;1:182-187.
5. Farsaei S, Khalili H, Farboud ES, et al. Efficacy of topical atorvastatin for the treatment of pressure ulcers: a randomized clinical trial. Pharmacotherapy. 2014;34:19-27.
6. Abou-Raya A, Abou-Raya S, Helmii M. Statins: potentially useful in therapy of systemic sclerosis-related Raynaud’s phenomenon and digital ulcers. J Rheumatol. 2008;35:1801-1808.
Copyright © 2015 Family Physicians Inquiries Network. All rights reserved.
Prescribing Statins for Patients With ACS? No Need to Wait
PRACTICE CHANGER
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis1
ILLUSTRATIVE CASE
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well known for their cholesterol-lowering effect, they also offer benefits independent of lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, those with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk for coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time to start statins in patients with ACS.
Continue for study summary >>
STUDY SUMMARY
Meta-analysis shows statins before PCI cut risk for MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) with those who received low-dose or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8,750 patients. Four studies enrolled only patients with ST elevation MI (STEMI), eight were restricted to NSTEMI, and the remaining eight studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 days before. For those started after PCI, the average time to administration was 3.18 days after.
Administering statins before PCI resulted in a greater reduction in the odds of MI than did starting them afterward. Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3,621) in the statins group and 5% (179 of 3,577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat = 62.5) and a 33% reduction of the odds of MI (odds ratio [OR] = 0.67). There was also a trend toward reduced mortality in the statin group (OR = 0.66).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR = 0.38) than starting them post-PCI (OR = 0.85) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant; these findings persisted past 30 days.
WHAT’S NEW
Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk for subsequent MI.
Next page: Caveats and challenges >>
CAVEATS
Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION
No barriers to earlier start
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the associated risks are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
REFERENCES
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005; 37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57: e215-e367.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(12):735, 738.
PRACTICE CHANGER
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis1
ILLUSTRATIVE CASE
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well known for their cholesterol-lowering effect, they also offer benefits independent of lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, those with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk for coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time to start statins in patients with ACS.
Continue for study summary >>
STUDY SUMMARY
Meta-analysis shows statins before PCI cut risk for MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) with those who received low-dose or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8,750 patients. Four studies enrolled only patients with ST elevation MI (STEMI), eight were restricted to NSTEMI, and the remaining eight studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 days before. For those started after PCI, the average time to administration was 3.18 days after.
Administering statins before PCI resulted in a greater reduction in the odds of MI than did starting them afterward. Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3,621) in the statins group and 5% (179 of 3,577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat = 62.5) and a 33% reduction of the odds of MI (odds ratio [OR] = 0.67). There was also a trend toward reduced mortality in the statin group (OR = 0.66).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR = 0.38) than starting them post-PCI (OR = 0.85) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant; these findings persisted past 30 days.
WHAT’S NEW
Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk for subsequent MI.
Next page: Caveats and challenges >>
CAVEATS
Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION
No barriers to earlier start
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the associated risks are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
REFERENCES
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005; 37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57: e215-e367.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(12):735, 738.
PRACTICE CHANGER
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis1
ILLUSTRATIVE CASE
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well known for their cholesterol-lowering effect, they also offer benefits independent of lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, those with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk for coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time to start statins in patients with ACS.
Continue for study summary >>
STUDY SUMMARY
Meta-analysis shows statins before PCI cut risk for MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) with those who received low-dose or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8,750 patients. Four studies enrolled only patients with ST elevation MI (STEMI), eight were restricted to NSTEMI, and the remaining eight studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 days before. For those started after PCI, the average time to administration was 3.18 days after.
Administering statins before PCI resulted in a greater reduction in the odds of MI than did starting them afterward. Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3,621) in the statins group and 5% (179 of 3,577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat = 62.5) and a 33% reduction of the odds of MI (odds ratio [OR] = 0.67). There was also a trend toward reduced mortality in the statin group (OR = 0.66).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR = 0.38) than starting them post-PCI (OR = 0.85) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant; these findings persisted past 30 days.
WHAT’S NEW
Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk for subsequent MI.
Next page: Caveats and challenges >>
CAVEATS
Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION
No barriers to earlier start
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the associated risks are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
REFERENCES
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005; 37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57: e215-e367.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(12):735, 738.
Prescribing statins for patients with ACS? No need to wait
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
A Simple Way to Reduce Catheter-associated UTIs
PRACTICE CHANGER
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk for urinary tract infections (UTIs).1
STRENGTH OF RECOMMENDATION
B: Based on a meta-analysis.1
ILLUSTRATIVE CASE
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and soon his urinary catheter will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2
Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species comprise the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. CDC guidelines published in 2009 outline which patients are appropriate candidates for catheterization but do not recommend routine use of antibiotics to prevent CAUTIs.2 A 2014 Infectious Diseases Society of America practice recommendation, which was published after the study reported on here, states the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY
Analysis shows prophylactic antibiotics reduce UTIs
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed seven studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of two surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including two that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to three days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics and 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17, with a risk ratio (RR) of .45. The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the two studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT’S NEW
We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
Continue for caveats and challenges >>
CAVEATS
Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk for attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION
Which antibiotics to use—and for how long—remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for three days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administration of antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
REFERENCES
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed November 12, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(5):E10-E12.
PRACTICE CHANGER
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk for urinary tract infections (UTIs).1
STRENGTH OF RECOMMENDATION
B: Based on a meta-analysis.1
ILLUSTRATIVE CASE
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and soon his urinary catheter will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2
Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species comprise the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. CDC guidelines published in 2009 outline which patients are appropriate candidates for catheterization but do not recommend routine use of antibiotics to prevent CAUTIs.2 A 2014 Infectious Diseases Society of America practice recommendation, which was published after the study reported on here, states the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY
Analysis shows prophylactic antibiotics reduce UTIs
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed seven studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of two surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including two that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to three days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics and 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17, with a risk ratio (RR) of .45. The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the two studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT’S NEW
We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
Continue for caveats and challenges >>
CAVEATS
Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk for attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION
Which antibiotics to use—and for how long—remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for three days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administration of antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
REFERENCES
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed November 12, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(5):E10-E12.
PRACTICE CHANGER
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk for urinary tract infections (UTIs).1
STRENGTH OF RECOMMENDATION
B: Based on a meta-analysis.1
ILLUSTRATIVE CASE
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and soon his urinary catheter will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2
Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species comprise the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. CDC guidelines published in 2009 outline which patients are appropriate candidates for catheterization but do not recommend routine use of antibiotics to prevent CAUTIs.2 A 2014 Infectious Diseases Society of America practice recommendation, which was published after the study reported on here, states the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY
Analysis shows prophylactic antibiotics reduce UTIs
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed seven studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of two surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including two that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to three days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics and 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17, with a risk ratio (RR) of .45. The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the two studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT’S NEW
We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
Continue for caveats and challenges >>
CAVEATS
Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk for attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION
Which antibiotics to use—and for how long—remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for three days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administration of antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
REFERENCES
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed November 12, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(5):E10-E12.
A simple way to reduce catheter-associated UTIs
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk of urinary tract infections (UTIs).1
Strength of recommendation
B: Based on a meta-analysis.
Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
Illustrative case
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and his urinary catheter soon will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2 Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species make up the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. Centers for Disease Control and Prevention (CDC) guidelines published in 2009 outline which patients are appropriate for catheterization, but do not recommend routine use of antibiotics to prevent CAUTIs.2 The 2014 Infectious Diseases Society of America guidelines, which came out before the study reported on here was published, state the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY: Meta-analysis shows prophylactic antibiotics reduce UTI ris
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed 7 studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of 2 surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including 2 that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to 3 days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics vs 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17 (95% confidence interval [CI], 12-30), with a risk ratio (RR) of .45 (95% CI, .28-.72). The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial, and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the 2 studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT'S NEW: We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
CAVEATS: Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk of attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION: Which antibiotics to use, and for how long, remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for 3 days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administering antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. Available at: http://www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed April 15, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk of urinary tract infections (UTIs).1
Strength of recommendation
B: Based on a meta-analysis.
Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
Illustrative case
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and his urinary catheter soon will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2 Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species make up the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. Centers for Disease Control and Prevention (CDC) guidelines published in 2009 outline which patients are appropriate for catheterization, but do not recommend routine use of antibiotics to prevent CAUTIs.2 The 2014 Infectious Diseases Society of America guidelines, which came out before the study reported on here was published, state the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY: Meta-analysis shows prophylactic antibiotics reduce UTI ris
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed 7 studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of 2 surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including 2 that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to 3 days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics vs 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17 (95% confidence interval [CI], 12-30), with a risk ratio (RR) of .45 (95% CI, .28-.72). The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial, and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the 2 studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT'S NEW: We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
CAVEATS: Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk of attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION: Which antibiotics to use, and for how long, remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for 3 days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administering antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk of urinary tract infections (UTIs).1
Strength of recommendation
B: Based on a meta-analysis.
Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
Illustrative case
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and his urinary catheter soon will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2 Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species make up the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. Centers for Disease Control and Prevention (CDC) guidelines published in 2009 outline which patients are appropriate for catheterization, but do not recommend routine use of antibiotics to prevent CAUTIs.2 The 2014 Infectious Diseases Society of America guidelines, which came out before the study reported on here was published, state the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY: Meta-analysis shows prophylactic antibiotics reduce UTI ris
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed 7 studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of 2 surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including 2 that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to 3 days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics vs 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17 (95% confidence interval [CI], 12-30), with a risk ratio (RR) of .45 (95% CI, .28-.72). The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial, and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the 2 studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT'S NEW: We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
CAVEATS: Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk of attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION: Which antibiotics to use, and for how long, remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for 3 days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administering antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. Available at: http://www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed April 15, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. Available at: http://www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed April 15, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
It’s Time to Use an Age-based Approach to D-dimer
PRACTICE CHANGER
Use an age-adjusted d-dimer cutoff (patient age in years × 10 μg/L) for patients older than 50 when evaluating for venous thromboembolism (VTE); it reduces false-positives without substantially increasing false-negatives.1
STRENGTH OF RECOMMENDATION
A: Based on consistent and good-quality patient-centered evidence from a meta-analysis of cohort studies.1
ILLUSTRATIVE CASE
A 78-year-old woman with no significant medical history or recent immobility comes to your clinic complaining of left lower extremity pain and swelling. Her d-dimer is 650 μg/L. What is your next step?
Although d-dimer is recognized as a reasonable screening tool for VTE, the specificity of d-dimer testing using a conventional cutoff value of 500 μg/L is particularly poor in patients older than 50. In low-risk patients older than 80, the specificity is 14.7%.2-5 As a result, conventional d-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1,000 in younger patients to 8:1,000 in older patients,4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and CT pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
Continued on next page >>
STUDY SUMMARY
Using age-adjusted d-dimer cutoffs significantly reduced false-positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had d-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.
Five high-quality studies of 13 cohorts were included in this analysis (N = 12,497; 6,969 patients older than 50). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and d-dimer sensitivity and specificity for patients ages ≤ 50, 51 to 60, 61 to 70, 71 to 80, and > 80.
The specificity of the conventional d-dimer cutoff value for VTE decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 μg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (see table). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1,000 patients older than 80, compared with 124/1,000 when using the conventional cutoff.
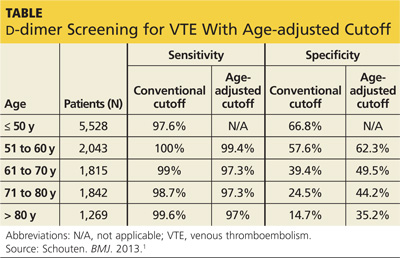
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1,000 patients) is comparable to the false-negative rate in those ages 50 and younger (3 per 1,000). The advantages are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
Continued on next page >>
WHAT’S NEW?
We can now use d-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive d-dimer test was less useful for older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients older than 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted d-dimer cutoff improves the diagnostic accuracy of d-dimer screening in older adults.
CAVEATS
Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of d-dimer results. Not all patients included in this meta-analysis whose d-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of the age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION
You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is its identification of a simple calculation that can directly improve patient care. Clinicians can easily apply an age-adjusted d-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 μg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted d-dimer calculation was provided with the lab results.
REFERENCES
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013;346: f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:
765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. http://bit.ly/1gPkLoE. Accessed March 3, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711-1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Accessed March 3, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(3):155-156, 158.
PRACTICE CHANGER
Use an age-adjusted d-dimer cutoff (patient age in years × 10 μg/L) for patients older than 50 when evaluating for venous thromboembolism (VTE); it reduces false-positives without substantially increasing false-negatives.1
STRENGTH OF RECOMMENDATION
A: Based on consistent and good-quality patient-centered evidence from a meta-analysis of cohort studies.1
ILLUSTRATIVE CASE
A 78-year-old woman with no significant medical history or recent immobility comes to your clinic complaining of left lower extremity pain and swelling. Her d-dimer is 650 μg/L. What is your next step?
Although d-dimer is recognized as a reasonable screening tool for VTE, the specificity of d-dimer testing using a conventional cutoff value of 500 μg/L is particularly poor in patients older than 50. In low-risk patients older than 80, the specificity is 14.7%.2-5 As a result, conventional d-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1,000 in younger patients to 8:1,000 in older patients,4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and CT pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
Continued on next page >>
STUDY SUMMARY
Using age-adjusted d-dimer cutoffs significantly reduced false-positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had d-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.
Five high-quality studies of 13 cohorts were included in this analysis (N = 12,497; 6,969 patients older than 50). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and d-dimer sensitivity and specificity for patients ages ≤ 50, 51 to 60, 61 to 70, 71 to 80, and > 80.
The specificity of the conventional d-dimer cutoff value for VTE decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 μg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (see table). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1,000 patients older than 80, compared with 124/1,000 when using the conventional cutoff.
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1,000 patients) is comparable to the false-negative rate in those ages 50 and younger (3 per 1,000). The advantages are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
Continued on next page >>
WHAT’S NEW?
We can now use d-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive d-dimer test was less useful for older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients older than 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted d-dimer cutoff improves the diagnostic accuracy of d-dimer screening in older adults.
CAVEATS
Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of d-dimer results. Not all patients included in this meta-analysis whose d-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of the age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION
You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is its identification of a simple calculation that can directly improve patient care. Clinicians can easily apply an age-adjusted d-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 μg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted d-dimer calculation was provided with the lab results.
REFERENCES
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013;346: f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:
765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. http://bit.ly/1gPkLoE. Accessed March 3, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711-1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Accessed March 3, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(3):155-156, 158.
PRACTICE CHANGER
Use an age-adjusted d-dimer cutoff (patient age in years × 10 μg/L) for patients older than 50 when evaluating for venous thromboembolism (VTE); it reduces false-positives without substantially increasing false-negatives.1
STRENGTH OF RECOMMENDATION
A: Based on consistent and good-quality patient-centered evidence from a meta-analysis of cohort studies.1
ILLUSTRATIVE CASE
A 78-year-old woman with no significant medical history or recent immobility comes to your clinic complaining of left lower extremity pain and swelling. Her d-dimer is 650 μg/L. What is your next step?
Although d-dimer is recognized as a reasonable screening tool for VTE, the specificity of d-dimer testing using a conventional cutoff value of 500 μg/L is particularly poor in patients older than 50. In low-risk patients older than 80, the specificity is 14.7%.2-5 As a result, conventional d-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1,000 in younger patients to 8:1,000 in older patients,4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and CT pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
Continued on next page >>
STUDY SUMMARY
Using age-adjusted d-dimer cutoffs significantly reduced false-positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had d-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.
Five high-quality studies of 13 cohorts were included in this analysis (N = 12,497; 6,969 patients older than 50). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and d-dimer sensitivity and specificity for patients ages ≤ 50, 51 to 60, 61 to 70, 71 to 80, and > 80.
The specificity of the conventional d-dimer cutoff value for VTE decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 μg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (see table). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1,000 patients older than 80, compared with 124/1,000 when using the conventional cutoff.
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1,000 patients) is comparable to the false-negative rate in those ages 50 and younger (3 per 1,000). The advantages are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
Continued on next page >>
WHAT’S NEW?
We can now use d-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive d-dimer test was less useful for older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients older than 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted d-dimer cutoff improves the diagnostic accuracy of d-dimer screening in older adults.
CAVEATS
Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of d-dimer results. Not all patients included in this meta-analysis whose d-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of the age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION
You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is its identification of a simple calculation that can directly improve patient care. Clinicians can easily apply an age-adjusted d-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 μg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted d-dimer calculation was provided with the lab results.
REFERENCES
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013;346: f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:
765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. http://bit.ly/1gPkLoE. Accessed March 3, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711-1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Accessed March 3, 2014.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Copyright © 2014. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2014;63(3):155-156, 158.
It’s time to use an age-based approach to D-dimer
Use an age-adjusted D-dimer cutoff (patient’s age in years × 10 mcg/L) for patients over age 50 years when evaluating for venous thromboembolism (VTE); it reduces false positives without substantially increasing false negatives.1
Strength of recommendation
A: Based on consistent and good quality patient-centered evidence from a meta-analysis of cohort studies.
Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and metaanalysis. BMJ. 2013;346:f2492.
Illustrative case
A 78-year-old woman with no significant past medical history or recent immobility comes into your clinic complaining of left lower extremity pain and swelling. Her D-dimer is 650 mcg/L. What is your next step?
Although D-dimer is recognized as a reasonable screening tool for VTE, the specificity of D-dimer testing using a conventional cutoff value of 500 mcg/L is particularly poor in patients over 50 years. In low-risk patients over 80 years old, the specificity is 14.7% (95% confidence interval, 11.3%-18.6%).2-5 As a result, conventional D-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1000 in younger patients to 8:1000 in older patients4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and computed tomography pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
STUDY SUMMARY: Using age-adjusted D-dimer cutoffs significantly reduced false positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had D-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies published before June 21, 2012 that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.

Five high-quality studies of 13 cohorts were included in this analysis (N=12,497; 6969 patients >50 years). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and D-dimer sensitivity and specificity for patients ages ≤50, 51 to 60, 61 to 70, 71 to 80, and >80 years.
The specificity of using the conventional D-dimer cutoff value for VTE (500 mcg/L) decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 mcg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (TABLE). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1000 patients >80 years, compared with 124/1000 when using the conventional cutoff.
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than age 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1000 patients) is comparable to the false negative rate in those age, ≤50 (3 per 1000). The advantages of an age-adjusted cutoff are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
WHAT'S NEW?: We can now make use of the D-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive D-dimer test was less useful for our older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients over age 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted D-dimer cutoff improves the diagnostic accuracy of D-dimer screening in older adults.
CAVEATS: Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of D-dimer results. Not all patients included in this meta-analysis whose D-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of using an age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION: You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is it identifies a simple calculation that can directly improve patient care. Physicians can easily apply an age-adjusted D-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 mcg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted D-dimer calculation was provided with the lab results.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013; 346:f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. Available at: http://bit.ly/1vStJtm. Updated January 30, 2014. Accessed February 13, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711–1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Updated January 2013. Accessed October 23, 2013.
Use an age-adjusted D-dimer cutoff (patient’s age in years × 10 mcg/L) for patients over age 50 years when evaluating for venous thromboembolism (VTE); it reduces false positives without substantially increasing false negatives.1
Strength of recommendation
A: Based on consistent and good quality patient-centered evidence from a meta-analysis of cohort studies.
Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and metaanalysis. BMJ. 2013;346:f2492.
Illustrative case
A 78-year-old woman with no significant past medical history or recent immobility comes into your clinic complaining of left lower extremity pain and swelling. Her D-dimer is 650 mcg/L. What is your next step?
Although D-dimer is recognized as a reasonable screening tool for VTE, the specificity of D-dimer testing using a conventional cutoff value of 500 mcg/L is particularly poor in patients over 50 years. In low-risk patients over 80 years old, the specificity is 14.7% (95% confidence interval, 11.3%-18.6%).2-5 As a result, conventional D-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1000 in younger patients to 8:1000 in older patients4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and computed tomography pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
STUDY SUMMARY: Using age-adjusted D-dimer cutoffs significantly reduced false positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had D-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies published before June 21, 2012 that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.
Five high-quality studies of 13 cohorts were included in this analysis (N=12,497; 6969 patients >50 years). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and D-dimer sensitivity and specificity for patients ages ≤50, 51 to 60, 61 to 70, 71 to 80, and >80 years.
The specificity of using the conventional D-dimer cutoff value for VTE (500 mcg/L) decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 mcg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (TABLE). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1000 patients >80 years, compared with 124/1000 when using the conventional cutoff.
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than age 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1000 patients) is comparable to the false negative rate in those age, ≤50 (3 per 1000). The advantages of an age-adjusted cutoff are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
WHAT'S NEW?: We can now make use of the D-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive D-dimer test was less useful for our older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients over age 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted D-dimer cutoff improves the diagnostic accuracy of D-dimer screening in older adults.
CAVEATS: Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of D-dimer results. Not all patients included in this meta-analysis whose D-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of using an age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION: You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is it identifies a simple calculation that can directly improve patient care. Physicians can easily apply an age-adjusted D-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 mcg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted D-dimer calculation was provided with the lab results.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Use an age-adjusted D-dimer cutoff (patient’s age in years × 10 mcg/L) for patients over age 50 years when evaluating for venous thromboembolism (VTE); it reduces false positives without substantially increasing false negatives.1
Strength of recommendation
A: Based on consistent and good quality patient-centered evidence from a meta-analysis of cohort studies.
Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and metaanalysis. BMJ. 2013;346:f2492.
Illustrative case
A 78-year-old woman with no significant past medical history or recent immobility comes into your clinic complaining of left lower extremity pain and swelling. Her D-dimer is 650 mcg/L. What is your next step?
Although D-dimer is recognized as a reasonable screening tool for VTE, the specificity of D-dimer testing using a conventional cutoff value of 500 mcg/L is particularly poor in patients over 50 years. In low-risk patients over 80 years old, the specificity is 14.7% (95% confidence interval, 11.3%-18.6%).2-5 As a result, conventional D-dimer testing is not very helpful for ruling out VTE in older patients.2-5
Improved testing is needed for a population at heightened risk
In the United States, there are more than 600,000 cases of deep vein thrombosis (DVT) and pulmonary embolism (PE) each year.2 The incidence of PE increases from 1:1000 in younger patients to 8:1000 in older patients4 and the mortality rate can reach 30%.6 The gold standards of venography and pulmonary angiography have been replaced by less burdensome tests, primarily lower extremity duplex ultrasound and computed tomography pulmonary angiogram. However, even these tests are expensive and often present logistical challenges in elderly patients. For these reasons, it is helpful to have a simple, less-expensive tool to rule out VTE in older patients who have signs or symptoms.
STUDY SUMMARY: Using age-adjusted D-dimer cutoffs significantly reduced false positives
Schouten et al1 performed a systematic review and meta-analysis of studies of older patients with suspected VTE who had D-dimer testing using both conventional and age-adjusted cutoff values. The authors searched Medline and Embase for studies published before June 21, 2012 that were performed in outpatient, inpatient, or emergency department settings. They excluded studies of high-risk patients, specifically perioperative patients and those who’d had VTE, cancer, or a coagulation disorder.
Five high-quality studies of 13 cohorts were included in this analysis (N=12,497; 6969 patients >50 years). Each of these studies was a retrospective analysis of patients with a low clinical probability of VTE, as determined by Geneva or Wells scoring. The authors calculated the VTE prevalence and D-dimer sensitivity and specificity for patients ages ≤50, 51 to 60, 61 to 70, 71 to 80, and >80 years.
The specificity of using the conventional D-dimer cutoff value for VTE (500 mcg/L) decreased with age from 57.6% in those ages 51 to 60 to 14.7% in those older than 80. When age-adjusted cutoffs were used (age in years × 10 mcg/L), specificities improved in all age categories, particularly for older patients. For example, using age-adjusted cutoff values improved specificity to 62.3% in patients ages 51 to 60 and to 35.2% in those older than 80 (TABLE). Using a hypothetical model, Schouten et al1 calculated that applying age-adjusted cutoff values would exclude VTE in 303/1000 patients >80 years, compared with 124/1000 when using the conventional cutoff.
The benefit of using an age-adjusted cutoff is the ability to exclude VTE in more patients (1 out of 3 in those older than age 80) while not significantly increasing the number of missed VTE. In fact, the number of missed cases in the older population using the age-adjusted cutoff (approximately 1 to 4 per 1000 patients) is comparable to the false negative rate in those age, ≤50 (3 per 1000). The advantages of an age-adjusted cutoff are most notable with the use of enzyme linked fluorescent assays because these assays have a higher sensitivity and a trend toward lower specificity compared with other assays.
WHAT'S NEW?: We can now make use of the D-dimer in older patients
Up until now, it was acknowledged that the simple and less expensive D-dimer test was less useful for our older patients. In fact, in their 2007 clinical practice guideline on the diagnosis of VTE in primary care, the American Academy of Family Physicians and the American College of Physicians commented on the poor performance of the test in older patients.2 A more recent guideline—released by the Institute for Clinical Systems Improvement in January 2013—provided no specific guidance for patients over age 50.7 The meta-analysis reported on here, however, provides that guidance: Using an age-adjusted D-dimer cutoff improves the diagnostic accuracy of D-dimer screening in older adults.
CAVEATS: Results are not generalizable to patients at higher risk
These findings are not generalizable to all patients, particularly those at higher clinical risk who would undergo imaging regardless of D-dimer results. Not all patients included in this meta-analysis whose D-dimer was negative received imaging to confirm that they did not have VTE. As a result, the diagnostic accuracy of using an age-adjusted cutoff could have been overestimated, although this is likely not clinically important because these cases would have remained symptomatic within the 45-day to 3-month follow-up period.
CHALLENGES TO IMPLEMENTATION: You, not the lab, will need to do the calculation
One of the more valuable aspects of this study is it identifies a simple calculation that can directly improve patient care. Physicians can easily apply an age-adjusted D-dimer cutoff as they interpret lab results by multiplying the patient’s age in years × 10 mcg/L. While this does not require institutional changes by the lab, hospital, or clinic, it would be helpful if the age-adjusted D-dimer calculation was provided with the lab results.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013; 346:f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. Available at: http://bit.ly/1vStJtm. Updated January 30, 2014. Accessed February 13, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711–1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Updated January 2013. Accessed October 23, 2013.
1. Schouten HJ, Geersing GJ, Koek HL, et al. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013; 346:f2492.
2. Qaseem A, Snow V, Barry P, et al; Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
3. Vossen JA, Albrektson J, Sensarma A, et al. Clinical usefulness of adjusted D-dimer cutoff values to exclude pulmonary embolism in a community hospital emergency department patient population. Acta Radiol. 2012;53:765-768.
4. van Es J, Mos I, Douma R, et al. The combination of four different clinical decision rules and an age-adjusted D-dimer cut-off increases the number of patients in whom acute pulmonary embolism can safely be excluded. Thromb Haemost. 2012;107:167-171.
5. Deep vein thrombosis (DVT). DynaMed Web site. Available at: http://bit.ly/1vStJtm. Updated January 30, 2014. Accessed February 13, 2014.
6. Horlander KT, Mannino DM, Leeper KV. Pulmonary embolism mortality in the United States, 1979–1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163:1711–1717.
7. Dupras D, Bluhm J, Felty C, et al. Venous thromboembolism diagnosis and treatment. Institute for Clinical Systems Improvement Web site. Available at: https://www.icsi.org/_asset/sw0pgp/VTE.pdf. Updated January 2013. Accessed October 23, 2013.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
Ramipril for claudication?
Consider prescribing ramipril for patients who have intermittent claudication.1
Strength of recommendation
A: Based on a high-quality placebo-controlled randomized controlled trial (RCT) consistent with prior RCTs.
Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA. 2013;309:453-460.
Illustrative case
A 63-year-old man presents with pain in both legs, which starts with activity and resolves with rest. He has a resting blood pressure of 135/77 mm Hg consistent with past measurements, and an ankle-brachial index (ABI) <0.90, which is consistent with peripheral artery disease (PAD). His daily medications are 81 mg aspirin, 25 mg hydrochlorothiazide, and 40 mg simvastatin. What additional agent could be added for his symptoms?
PAD, defined as an ABI <0.9, affects approximately 5% of Americans older than 40 years. About two-thirds of those with PAD are asymptomatic; the remaining third suffer from intermittent claudication (IC).2
Exercise and smoking cessation are effective at reducing IC symptoms, as well as the long-term cardiovascular event risk associated with PAD.3 But even with these lifestyle changes, patients with PAD are often troubled by persistent symptoms.
Few evidence-based treatments for IC
Compared with placebo, the antiplatelet agents indobufen and picotamide have been shown to improve pain-free walking distance (PFWD).4 So have cilostazol5 and naftidrofuryl,6 as well as lipid-lowering agents.7
In a pilot study of 40 patients, 10 mg ramipril was shown to improve pain-free walking time (PFWT) at 24 weeks by 227 seconds (95% confidence interval [CI]=175-278; P<.001). That represents a 164% increase from baseline, vs no change in PFWT at 24 weeks for the placebo group.8 A recent small (N=33), double-blinded RCT found similar improvements in maximum treadmill walking distance, PFWD, and patient-reported walking distance at 24 weeks with ramipril compared with placebo.9
In the HOPE study, a subsection of patients who were older than 55 years and had PAD were treated with a daily target dose of 10 mg ramipril for a mean of 4.5 years. Compared with placebo, ramipril reduced the primary outcome—cardiovascular mortality, myocardial infarction (MI), or stroke—by 25% (risk ratio=0.75; 95% CI, 0.61-0.92).10
In the study reported on here, Ahimastos et al took a closer look at ramipril.
STUDY SUMMARY: Patients on ramipril can walk longer pain free
The authors conducted a double-blind, randomized placebo-controlled trial evaluating the effectiveness of 10 mg/d ramipril for the improvement of maximum walk time (MWT) and PFWT in patients with PAD.1 Eligible patients had an ABI <0.9 in at least one leg and a history of IC in at least one leg, with stable claudication symptoms and a stable medical regimen for 6 months or more. Exclusion criteria included a resting blood pressure >160/100 mm Hg; use of ACE inhibitors, angiotensin II receptor blockers, potassium sparing diuretics, or potassium supplements in the past 6 months; serum creatinine >2.3 mg/dL; renal artery stenosis; previous coronary or lower extremity revascularization procedure; MI in the past 3 months; major surgery planned for the following year; critical limb ischemia; or any condition other than PAD limiting walking ability.
In total, 212 patients underwent randomization, and either took 10 mg/d ramipril or placebo for 24 weeks. The participants had similar baseline characteristics. Most were male (83.5%), with a mean age of 65.5 years; 33.5% were current smokers; 50% had hypertension; and 24.1% had type 2 diabetes.
Primary outcomes—PFWT and MWT—improved in the ramipril group. Compared with the placebo group, those in the ramipril group had a mean PFWT increase of 75 seconds (95% CI, 60-89; P<.001) and a 255-second increase in MWT (95% CI, 215-295; P<.001), a 52% and 107% increase from baseline, respectively. Most secondary measures (including the Walking Impairment Questionnaire median distance score, the speed score, and the stair-climbing score) also improved significantly, relative to the placebo group. However, ABI did not change significantly in either group.
WHAT'S NEW: Evidence that ramipril improves patient-oriented outcomes
Ramipril not only reduces cardiovascular mortality, MI, and stroke in patients with PAD,10 but is effective in improving patient-oriented outcomes such as duration of walking without developing IC.
CAVEATS: Would ramipril help less stable patients?
Inclusion criteria used by Ahimastos et al limit the generalizability of this study to patients with stable symptoms for 6 months or more. Similarly, because the study lasted for 24 weeks, it is not known whether ramipril’s benefits for patients with claudication would continue indefinitely. Also of note: The ABI did not improve in the treatment cohort at the end of this 24-week period, and the authors did not report objective outcomes such as revascularization or mortality.
CHALLENGES TO IMPLEMENTATION: Monitoring, adverse effects may present problems
Use of ACE inhibitors requires monitoring of renal function and serum potassium. In addition, ACE inhibitors can induce a chronic cough that often limits their use in those affected; 6.6% of the treatment group withdrew from this study due to persistent cough.1
ACKNOWLEDGEMENT
The PURLs surveillance system was supported in part by Grant Number UL1RR024999 from the National center for Research Resources, a clinical Translational science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National center for Research Resources or the National Institutes of Health.
1. Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA. 2013;309:453-460.
2. Centers for Disease Control and Prevention. Lower extremity disease among persons aged ≥40 years with and without diabe- tes—United States, 1999-2002. MMWR Morb Mortal Wkly Rep. 2005;54:1158-1160.
3. Watson L, Ellis B, Leng GC. Exercise for intermittent claudication. Cochrane Database Syst Rev. 2008;(4):CD000990.
4. Wong PF, Chong LY, Mikhailidis DP, et al. Antiplatelet agents for intermittent claudication. Cochrane Database Syst Rev. 2011;(11):CD001272.
5. Robless P, Mikhailidis DP, Stansby GP. Cilostazol for peripheral arterial disease. Cochrane Database Syst Rev. 2008;(1):CD003748.
6. de Backer TL, Vander Stichele R, Lehert P, et al. Naftidrofuryl for intermittent claudication. Cochrane Database Syst Rev. 2012;(12):CD001368.
7. Aung PP, Maxwell HG, Jepson RG, et al. Lipid-lowering for pe- ripheral arterial disease of the lower limb. Cochrane Database Syst Rev. 2007;(4):CD000123.
8. Ahimastos AA, Lawler A, Reid CM, et al. Brief communication: ramipril markedly improves walking ability in patients with pe- ripheral arterial disease: a randomized trial. Ann Intern Med. 2006;144:660-664.
9. Shahin Y, Cockcroft JR, Chetter IC. Randomized clinical trial of angiotensin-converting enzyme inhibitor, ramipril, in patients with intermittent claudication. Br J Surg. 2013;100:1154-1163.
10. Ostergren J, Sleight P, Dagenais G, et al. Impact of ramipril in pa- tients with evidence of clinical or subclinical peripheral arterial disease. Eur Heart J. 2004;25:17-24.
Consider prescribing ramipril for patients who have intermittent claudication.1
Strength of recommendation
A: Based on a high-quality placebo-controlled randomized controlled trial (RCT) consistent with prior RCTs.
Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA. 2013;309:453-460.
Illustrative case
A 63-year-old man presents with pain in both legs, which starts with activity and resolves with rest. He has a resting blood pressure of 135/77 mm Hg consistent with past measurements, and an ankle-brachial index (ABI) <0.90, which is consistent with peripheral artery disease (PAD). His daily medications are 81 mg aspirin, 25 mg hydrochlorothiazide, and 40 mg simvastatin. What additional agent could be added for his symptoms?
PAD, defined as an ABI <0.9, affects approximately 5% of Americans older than 40 years. About two-thirds of those with PAD are asymptomatic; the remaining third suffer from intermittent claudication (IC).2
Exercise and smoking cessation are effective at reducing IC symptoms, as well as the long-term cardiovascular event risk associated with PAD.3 But even with these lifestyle changes, patients with PAD are often troubled by persistent symptoms.
Few evidence-based treatments for IC
Compared with placebo, the antiplatelet agents indobufen and picotamide have been shown to improve pain-free walking distance (PFWD).4 So have cilostazol5 and naftidrofuryl,6 as well as lipid-lowering agents.7
In a pilot study of 40 patients, 10 mg ramipril was shown to improve pain-free walking time (PFWT) at 24 weeks by 227 seconds (95% confidence interval [CI]=175-278; P<.001). That represents a 164% increase from baseline, vs no change in PFWT at 24 weeks for the placebo group.8 A recent small (N=33), double-blinded RCT found similar improvements in maximum treadmill walking distance, PFWD, and patient-reported walking distance at 24 weeks with ramipril compared with placebo.9
In the HOPE study, a subsection of patients who were older than 55 years and had PAD were treated with a daily target dose of 10 mg ramipril for a mean of 4.5 years. Compared with placebo, ramipril reduced the primary outcome—cardiovascular mortality, myocardial infarction (MI), or stroke—by 25% (risk ratio=0.75; 95% CI, 0.61-0.92).10
In the study reported on here, Ahimastos et al took a closer look at ramipril.
STUDY SUMMARY: Patients on ramipril can walk longer pain free
The authors conducted a double-blind, randomized placebo-controlled trial evaluating the effectiveness of 10 mg/d ramipril for the improvement of maximum walk time (MWT) and PFWT in patients with PAD.1 Eligible patients had an ABI <0.9 in at least one leg and a history of IC in at least one leg, with stable claudication symptoms and a stable medical regimen for 6 months or more. Exclusion criteria included a resting blood pressure >160/100 mm Hg; use of ACE inhibitors, angiotensin II receptor blockers, potassium sparing diuretics, or potassium supplements in the past 6 months; serum creatinine >2.3 mg/dL; renal artery stenosis; previous coronary or lower extremity revascularization procedure; MI in the past 3 months; major surgery planned for the following year; critical limb ischemia; or any condition other than PAD limiting walking ability.
In total, 212 patients underwent randomization, and either took 10 mg/d ramipril or placebo for 24 weeks. The participants had similar baseline characteristics. Most were male (83.5%), with a mean age of 65.5 years; 33.5% were current smokers; 50% had hypertension; and 24.1% had type 2 diabetes.
Primary outcomes—PFWT and MWT—improved in the ramipril group. Compared with the placebo group, those in the ramipril group had a mean PFWT increase of 75 seconds (95% CI, 60-89; P<.001) and a 255-second increase in MWT (95% CI, 215-295; P<.001), a 52% and 107% increase from baseline, respectively. Most secondary measures (including the Walking Impairment Questionnaire median distance score, the speed score, and the stair-climbing score) also improved significantly, relative to the placebo group. However, ABI did not change significantly in either group.
WHAT'S NEW: Evidence that ramipril improves patient-oriented outcomes
Ramipril not only reduces cardiovascular mortality, MI, and stroke in patients with PAD,10 but is effective in improving patient-oriented outcomes such as duration of walking without developing IC.
CAVEATS: Would ramipril help less stable patients?
Inclusion criteria used by Ahimastos et al limit the generalizability of this study to patients with stable symptoms for 6 months or more. Similarly, because the study lasted for 24 weeks, it is not known whether ramipril’s benefits for patients with claudication would continue indefinitely. Also of note: The ABI did not improve in the treatment cohort at the end of this 24-week period, and the authors did not report objective outcomes such as revascularization or mortality.
CHALLENGES TO IMPLEMENTATION: Monitoring, adverse effects may present problems
Use of ACE inhibitors requires monitoring of renal function and serum potassium. In addition, ACE inhibitors can induce a chronic cough that often limits their use in those affected; 6.6% of the treatment group withdrew from this study due to persistent cough.1
ACKNOWLEDGEMENT
The PURLs surveillance system was supported in part by Grant Number UL1RR024999 from the National center for Research Resources, a clinical Translational science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National center for Research Resources or the National Institutes of Health.
Consider prescribing ramipril for patients who have intermittent claudication.1
Strength of recommendation
A: Based on a high-quality placebo-controlled randomized controlled trial (RCT) consistent with prior RCTs.
Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA. 2013;309:453-460.
Illustrative case
A 63-year-old man presents with pain in both legs, which starts with activity and resolves with rest. He has a resting blood pressure of 135/77 mm Hg consistent with past measurements, and an ankle-brachial index (ABI) <0.90, which is consistent with peripheral artery disease (PAD). His daily medications are 81 mg aspirin, 25 mg hydrochlorothiazide, and 40 mg simvastatin. What additional agent could be added for his symptoms?
PAD, defined as an ABI <0.9, affects approximately 5% of Americans older than 40 years. About two-thirds of those with PAD are asymptomatic; the remaining third suffer from intermittent claudication (IC).2
Exercise and smoking cessation are effective at reducing IC symptoms, as well as the long-term cardiovascular event risk associated with PAD.3 But even with these lifestyle changes, patients with PAD are often troubled by persistent symptoms.
Few evidence-based treatments for IC
Compared with placebo, the antiplatelet agents indobufen and picotamide have been shown to improve pain-free walking distance (PFWD).4 So have cilostazol5 and naftidrofuryl,6 as well as lipid-lowering agents.7
In a pilot study of 40 patients, 10 mg ramipril was shown to improve pain-free walking time (PFWT) at 24 weeks by 227 seconds (95% confidence interval [CI]=175-278; P<.001). That represents a 164% increase from baseline, vs no change in PFWT at 24 weeks for the placebo group.8 A recent small (N=33), double-blinded RCT found similar improvements in maximum treadmill walking distance, PFWD, and patient-reported walking distance at 24 weeks with ramipril compared with placebo.9
In the HOPE study, a subsection of patients who were older than 55 years and had PAD were treated with a daily target dose of 10 mg ramipril for a mean of 4.5 years. Compared with placebo, ramipril reduced the primary outcome—cardiovascular mortality, myocardial infarction (MI), or stroke—by 25% (risk ratio=0.75; 95% CI, 0.61-0.92).10
In the study reported on here, Ahimastos et al took a closer look at ramipril.
STUDY SUMMARY: Patients on ramipril can walk longer pain free
The authors conducted a double-blind, randomized placebo-controlled trial evaluating the effectiveness of 10 mg/d ramipril for the improvement of maximum walk time (MWT) and PFWT in patients with PAD.1 Eligible patients had an ABI <0.9 in at least one leg and a history of IC in at least one leg, with stable claudication symptoms and a stable medical regimen for 6 months or more. Exclusion criteria included a resting blood pressure >160/100 mm Hg; use of ACE inhibitors, angiotensin II receptor blockers, potassium sparing diuretics, or potassium supplements in the past 6 months; serum creatinine >2.3 mg/dL; renal artery stenosis; previous coronary or lower extremity revascularization procedure; MI in the past 3 months; major surgery planned for the following year; critical limb ischemia; or any condition other than PAD limiting walking ability.
In total, 212 patients underwent randomization, and either took 10 mg/d ramipril or placebo for 24 weeks. The participants had similar baseline characteristics. Most were male (83.5%), with a mean age of 65.5 years; 33.5% were current smokers; 50% had hypertension; and 24.1% had type 2 diabetes.
Primary outcomes—PFWT and MWT—improved in the ramipril group. Compared with the placebo group, those in the ramipril group had a mean PFWT increase of 75 seconds (95% CI, 60-89; P<.001) and a 255-second increase in MWT (95% CI, 215-295; P<.001), a 52% and 107% increase from baseline, respectively. Most secondary measures (including the Walking Impairment Questionnaire median distance score, the speed score, and the stair-climbing score) also improved significantly, relative to the placebo group. However, ABI did not change significantly in either group.
WHAT'S NEW: Evidence that ramipril improves patient-oriented outcomes
Ramipril not only reduces cardiovascular mortality, MI, and stroke in patients with PAD,10 but is effective in improving patient-oriented outcomes such as duration of walking without developing IC.
CAVEATS: Would ramipril help less stable patients?
Inclusion criteria used by Ahimastos et al limit the generalizability of this study to patients with stable symptoms for 6 months or more. Similarly, because the study lasted for 24 weeks, it is not known whether ramipril’s benefits for patients with claudication would continue indefinitely. Also of note: The ABI did not improve in the treatment cohort at the end of this 24-week period, and the authors did not report objective outcomes such as revascularization or mortality.
CHALLENGES TO IMPLEMENTATION: Monitoring, adverse effects may present problems
Use of ACE inhibitors requires monitoring of renal function and serum potassium. In addition, ACE inhibitors can induce a chronic cough that often limits their use in those affected; 6.6% of the treatment group withdrew from this study due to persistent cough.1
ACKNOWLEDGEMENT
The PURLs surveillance system was supported in part by Grant Number UL1RR024999 from the National center for Research Resources, a clinical Translational science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National center for Research Resources or the National Institutes of Health.
1. Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA. 2013;309:453-460.
2. Centers for Disease Control and Prevention. Lower extremity disease among persons aged ≥40 years with and without diabe- tes—United States, 1999-2002. MMWR Morb Mortal Wkly Rep. 2005;54:1158-1160.
3. Watson L, Ellis B, Leng GC. Exercise for intermittent claudication. Cochrane Database Syst Rev. 2008;(4):CD000990.
4. Wong PF, Chong LY, Mikhailidis DP, et al. Antiplatelet agents for intermittent claudication. Cochrane Database Syst Rev. 2011;(11):CD001272.
5. Robless P, Mikhailidis DP, Stansby GP. Cilostazol for peripheral arterial disease. Cochrane Database Syst Rev. 2008;(1):CD003748.
6. de Backer TL, Vander Stichele R, Lehert P, et al. Naftidrofuryl for intermittent claudication. Cochrane Database Syst Rev. 2012;(12):CD001368.
7. Aung PP, Maxwell HG, Jepson RG, et al. Lipid-lowering for pe- ripheral arterial disease of the lower limb. Cochrane Database Syst Rev. 2007;(4):CD000123.
8. Ahimastos AA, Lawler A, Reid CM, et al. Brief communication: ramipril markedly improves walking ability in patients with pe- ripheral arterial disease: a randomized trial. Ann Intern Med. 2006;144:660-664.
9. Shahin Y, Cockcroft JR, Chetter IC. Randomized clinical trial of angiotensin-converting enzyme inhibitor, ramipril, in patients with intermittent claudication. Br J Surg. 2013;100:1154-1163.
10. Ostergren J, Sleight P, Dagenais G, et al. Impact of ramipril in pa- tients with evidence of clinical or subclinical peripheral arterial disease. Eur Heart J. 2004;25:17-24.
1. Ahimastos AA, Walker PJ, Askew C, et al. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA. 2013;309:453-460.
2. Centers for Disease Control and Prevention. Lower extremity disease among persons aged ≥40 years with and without diabe- tes—United States, 1999-2002. MMWR Morb Mortal Wkly Rep. 2005;54:1158-1160.
3. Watson L, Ellis B, Leng GC. Exercise for intermittent claudication. Cochrane Database Syst Rev. 2008;(4):CD000990.
4. Wong PF, Chong LY, Mikhailidis DP, et al. Antiplatelet agents for intermittent claudication. Cochrane Database Syst Rev. 2011;(11):CD001272.
5. Robless P, Mikhailidis DP, Stansby GP. Cilostazol for peripheral arterial disease. Cochrane Database Syst Rev. 2008;(1):CD003748.
6. de Backer TL, Vander Stichele R, Lehert P, et al. Naftidrofuryl for intermittent claudication. Cochrane Database Syst Rev. 2012;(12):CD001368.
7. Aung PP, Maxwell HG, Jepson RG, et al. Lipid-lowering for pe- ripheral arterial disease of the lower limb. Cochrane Database Syst Rev. 2007;(4):CD000123.
8. Ahimastos AA, Lawler A, Reid CM, et al. Brief communication: ramipril markedly improves walking ability in patients with pe- ripheral arterial disease: a randomized trial. Ann Intern Med. 2006;144:660-664.
9. Shahin Y, Cockcroft JR, Chetter IC. Randomized clinical trial of angiotensin-converting enzyme inhibitor, ramipril, in patients with intermittent claudication. Br J Surg. 2013;100:1154-1163.
10. Ostergren J, Sleight P, Dagenais G, et al. Impact of ramipril in pa- tients with evidence of clinical or subclinical peripheral arterial disease. Eur Heart J. 2004;25:17-24.
Copyright © 2013 Family Physicians Inquiries Network. All rights reserved.