Frequent and prolonged fasting can lead to patient dissatisfaction and distress.1 It may also cause malnutrition and negatively affect outcomes in high-risk populations such as the elderly.2 Evidence suggests that patients are commonly kept fasting longer than necessary.3,4 However, the extent to which nil per os (NPO) orders are necessary or adhere to evidence-based duration is unknown.
Our study showed half of patients admitted to the general medicine services experienced a period of fasting, and 1 in 4 NPO orders may be avoidable.5 In this study, we aimed to provide action-oriented recommendations by 1) assessing why some interventions did not occur after NPO orders were placed and 2) analyzing NPO orders by indication and comparing them with the best available evidence.
METHOD
This retrospective study was conducted at an academic medical center in the United States. The study protocol was approved by the Mayo Clinic Institutional Review Board.
Detailed data handling and NPO order review processes have been described elsewhere.5 Briefly, we identified 1200 NPO orders of 120 or more minutes’ duration that were written for patients on the general medicine services at our institution in 2013. After blinded duplicate review, we excluded 70 orders written in the intensive care unit or on other services, 24 with unknown indications, 101 primarily indicated for clinical reasons, and 81 that had multiple indications. Consequently, 924 orders indicated for a single intervention (eg, imaging study, procedure, or operation) were included in the main analysis.
We assessed if the indicated intervention was performed. If performed, we recorded the time when the intervention was started. If not performed, we assessed reasons why it was not performed. We also performed exploratory analyses to investigate factors associated with performing the indicated intervention. The variables were 1) NPO starting at midnight, 2) NPO starting within 12 hours of admission, and 3) indication (eg, imaging study, procedure, or operation). We also conducted sensitivity analyses limited to 1 NPO order per patient (N = 673) to assess independence of the orders.
We then further categorized indications for the orders in detail and identified those with a sample size >10. This resulted in 779 orders that were included in the analysis by indication. We reviewed the literature by indication to determine suggested minimally required fasting durations to compare fasting duration in our patients to current evidence-based recommendations.
For descriptive statistics, we used median with interquartile range (IQR) for continuous variables and percentage for discrete variables; chi-square tests were used for comparison of discrete variables. All P values were two-tailed and P < 0.05 was considered significant.
RESULTS
Median length of 924 orders was 12.7 hours (IQR, 10.1-15.7 hours); 190 (20.1%), 577 (62.4%), and 157 (21.0%) orders were indicated for imaging studies, procedures, and operations, respectively. NPO started at midnight in 662 (71.6%) and within 12 hours of admission in 210 (22.7%) orders.
The indicated interventions were not performed in 183 (19.8%) orders, mostly as a result of a change in plan (75/183, 41.0%) or scheduling barriers (43/183, 23.5%). Plan changes occurred when, for example, input from a consulting service was obtained or the supervising physician decided not to pursue the intervention. Scheduling barriers included slots being unavailable and conflicts with other tasks/tests. Notably, only in 1 of 183 (0.5%) orders, the intervention was cancelled because the patient ate (Table 1).
Table 1
NPO orders starting at midnight were associated with higher likelihood of indicated interventions being performed (546/662, 82.5% vs. 195/262, 74.4%; P = 0.006), as were NPO orders starting more than 12 hours after admission (601/714, 84.2% vs. 140/210, 66.7%; P < 0.001). Imaging studies were more likely to be performed than procedures or operations (170/190, 89.5% vs. 452/577, 78.3% vs. 119/157, 75.8%; P = 0.001). These results were unchanged when the analyses were limited to 1 order per patient.
When analyzed by indication, the median durations of NPO orders ranged from 8.3 hours in kidney ultrasound to 13.9 hours in upper endoscopy. These were slightly shortened, most by 1 to 2 hours, when the duration was calculated from start of the order to initiation of the intervention. The literature review identified, for most indications, that the minimally required length of NPO were 2 to 4 hours, generally 6 to 8 hours shorter than the median NPO length in this study sample. Furthermore, for indications such as computed tomography with intravenous contrast and abdominal ultrasound, the literature suggested NPO may be unnecessary (Table 2).6-9,16-30
Table 2
DISCUSSION
We analyzed a comprehensive set of NPO orders written for interventions in medical inpatients at an academic medical center. NPO started at midnight in 71.6% of the analyzed orders. In 1 in 5 NPO orders, the indicated intervention was not performed largely due to a change in plan or scheduling barriers. In most NPO orders in which the indicated interventions were performed, patients were kept fasting either unnecessarily or much longer than needed. This study is the first of its kind in evaluating NPO-ordering practices across multiple indications and comparing them with the best available evidence.
These results suggest current NPO practice in the hospital is suboptimal, and limited literature measures the magnitude of this issue.6,7 An important aspect of our study findings is that, in a substantial number of NPO orders, the indicated interventions were not performed for seemingly avoidable reasons. These issues may be attributable to clinicians’ preemptive decisions or lack of knowledge, or inefficiency in the healthcare system. Minimizing anticipatory NPO may carry drawbacks such as delays in interventions, and limited evidence links excessive NPO with clinical outcomes (eg, length of stay, readmission, or death). However, from the patients’ perspective, it is important to be kept fasting only for clinical benefit. Hence, this calls for substantial improvement of NPO practices.
Furthermore, results indicated that the duration of most NPO orders was longer than the minimal duration currently suggested in the literature. Whereas strong evidence suggests that no longer than 2 hours of fasting is generally required for preoperative purposes,8 limited studies have evaluated the required length of NPO orders in imaging studies and procedures,9-11 which comprised most of the orders in the study cohort. For example, in upper endoscopy, 2 small studies suggested fasting for 1 or 2 hours may provide as good visualization as with the conventional 6 to 8 hours of fasting.9,10 In coronary angiography, a retrospective study demonstrated fasting may be unnecessary.11 Due to lack of robust evidence, guidelines for these interventions either do not specify the required length of fasting or have not changed the conventional recommendations for fasting, leading to large variations in fasting policies by institution.6,12 Therefore, more studies are needed to define required length of fasting for those indications and to measure the exact magnitude of excessive fasting in the hospital.
One of the limitations of this study is generalizability because NPO practice may considerably vary by institution as suggested in the literature.4,6,12 Conversely, studies have suggested that excessive fasting exists in other institutions.3,4,13 Thus, this study adds further evidence of the prevalence of suboptimal NPO practice to the literature and provides a benchmark that other institutions can refer to when evaluating their own NPO practice. Another limitation is the assumption that the evidence for minimally required NPO duration can be applied to our patient samples. Specifically, the American Society of Anesthesiologists guideline states that preoperative or preprocedural fasting may need to be longer than 2 hours for 1) patients with comorbidities that can affect gastric emptying or fluid volume such as obesity, diabetes, emergency care, and enteral tube feeding, and 2) patients in whom airway management might be difficult.8 We did not consider these possibilities, and as these conditions are prevalent in medical inpatients, we may be overstating the excessiveness of fasting orders. On the other hand, especially in patients with diabetes, prolonged fasting may cause harm by inducing hypoglycemia.14 Further, no study rigorously evaluated safety of shortening the fasting period for these subsets of patients. Therefore, it is necessary to establish optimal duration of NPO and to improve NPO ordering practice even in these patient subsets.
While more research is needed to define optimal duration of NPO for various interventions and specific subsets of patients and to establish linkage of excessive NPO with clinical outcomes, our data provide insights into immediate actions that can be taken by clinicians to improve NPO practices using our data as a benchmark. First, institutions can establish more robust practice guidelines or institutional protocols for NPO orders. Successful interventions have been reported,15 and breaking the habit of ordering NPO after midnight is certainly possible. We recommend each institution does so by indication, potentially through interdepartmental work groups involving appropriate departments such as radiology, surgery, and medicine. Second, institutional guidelines or protocols can be incorporated in the ordering system to enable appropriate NPO ordering. For example, at our institution, we are modifying the order screens for ultrasound-guided paracentesis and thoracentesis to indicate that NPO is not necessary for these procedures unless sedation is anticipated. We conclude that, at any institution, efforts in improving the NPO practice are urgently warranted to minimize unnecessary fasting.
Disclosures
This publication was supported by Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. The authors report no financial conflicts of interest.
References
1. Carey SK, Conchin S, Bloomfield-Stone S. A qualitative study into the impact of fasting within a large tertiary hospital in Australia - the patients’ perspective. J Clin Nurs. 2015;24:1946-1954. PubMed
2. Kyriakos G, Calleja-Fernández A, Ávila-Turcios D, Cano-Rodríguez I, Ballesteros Pomar MD, Vidal-Casariego A. Prolonged fasting with fluid therapy is related to poorer outcomes in medical patients. Nutr Hosp. 2013;28:1710-1716. PubMed
3. Rycroft-Malone J, Seers K, Crichton N, et al. A pragmatic cluster randomised trial evaluating three implementation interventions. Implement Sci. 2012;7:80. PubMed
4. Breuer JP, Bosse G, Seifert S, et al. Pre-operative fasting: a nationwide survey of German anaesthesia departments. Acta Anaesthesiol Scand. 2010;54:313-320. PubMed
5. Sorita A, Thongprayoon C, Ahmed A, et al. Frequency and appropriateness of fasting orders in the hospital. Mayo Clin Proc. 2015;90:1225-1232. PubMed
6. Lee BY, Ok JJ, Abdelaziz Elsayed AA, Kim Y, Han DH. Preparative fasting for contrast-enhanced CT: reconsideration. Radiology. 2012;263:444-450. PubMed
7. Manchikanti L, Malla Y, Wargo BW, Fellows B. Preoperative fasting before interventional techniques: is it necessary or evidence-based? Pain Physician. 2011;14:459-467. PubMed
8. American Society of Anesthesiologists Committee. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology. 2011;114:495-511. PubMed
9. Koeppe AT, Lubini M, Bonadeo NM, Moraes I Jr, Fornari F. Comfort, safety and quality of upper gastrointestinal endoscopy after 2 hours fasting: a randomized controlled trial. BMC Gastroenterol. 2013;13:158. PubMed
10. De Silva AP, Amarasiri L, Liyanage MN, Kottachchi D, Dassanayake AS, de Silva HJ. One-hour fast for water and six-hour fast for solids prior to endoscopy provides good endoscopic vision and results in minimum patient discomfort. J Gastroenterol Hepatol. 2009;24:1095-1097. PubMed
11. Hamid T, Aleem Q, Lau Y, et al. Pre-procedural fasting for coronary interventions: is it time to change practice? Heart. 2014;100:658-661. PubMed
12. Ahmed SU, Tonidandel W, Trella J, Martin NM, Chang Y. Peri-procedural protocols for interventional pain management techniques: a survey of US pain centers. Pain Physician. 2005;8:181-185. PubMed
13. Franklin GA, McClave SA, Hurt RT, et al. Physician-delivered malnutrition: why do patients receive nothing by mouth or a clear liquid diet in a university hospital setting? JPEN J Parenter Enteral Nutr. 2011;35:337-342. PubMed
14. Aldasouqi S, Sheikh A, Klosterman P, et al. Hypoglycemia in patients with diabetes who are fasting for laboratory blood tests: the Cape Girardeau Hypoglycemia En Route Prevention Program. Postgrad Med. 2013;125:136-143. PubMed
15. Aguilar-Nascimento JE, Salomão AB, Caporossi C, Diniz BN. Clinical benefits after the implementation of a multimodal perioperative protocol in elderly patients. Arq Gastroenterol. 2010;47:178-183. PubMed
16. Hilberath JN, Oakes DA, Shernan SK, Bulwer BE, D’Ambra MN, Eltzschig HK. Safety of transesophageal echocardiography. J Am Soc Echocardiogr. 2010;23: 1115-1127. PubMed
17. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26:921-964. PubMed
18. Sinan T, Leven H, Sheikh M. Is fasting a necessary preparation for abdominal ultrasound? BMC Med Imaging. 2003;3:1. PubMed
19. Garcia DA, Froes TR. Importance of fasting in preparing dogs for abdominal ultrasound examination of specific organs. J Small Anim Pract. 2014;55:630-634. PubMed
20. Kidney ultrasound. The Johns Hopkins University, The Johns Hopkins Hospital, and Johns Hopkins Health System. Health Library, Johns Hopkins Medicine. Available at: http://www.hopkinsmedicine.org/healthlibrary/test_procedures/urology/kidney_ultrasound_92,P07709/. Accessed August 17, 2015.
21. Surasi DS, Bhambhvani P, Baldwin JA, Almodovar SE, O’Malley JP. 18F-FDG PET and PET/CT patient preparation: a review of the literature. J Nucl Med Technol. 2014;42:5-13. PubMed
22. Kang SH, Hyun JJ. Preparation and patient evaluation for safe gastrointestinal endoscopy. Clin Endosc. 2013;46:212-218. PubMed
23. Smith I, Kranke P, Murat I, et al. Perioperative fasting in adults and children: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol. 2011;28:556-569. PubMed
24. ASGE Standards of Practice Committee, Saltzman JR, Cash BD, Pasha SF, et al. Bowel preparation before colonoscopy. Gastrointest Endosc. 2015;81:781-794. PubMed
25. Hassan C, Bretthauer M, Kaminski MF, et al; European Society of Gastrointestinal Endoscopy. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2013;45:142-150. PubMed
26. Du Rand IA, Blaikley J, Booton R, et al; British Thoracic Society Bronchoscopy Guideline Group. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: accredited by NICE. Thorax. 2013;68(suppl 1):i1-i44. PubMed
27. Thoracentesis. The Johns Hopkins University, The Johns Hopkins Hospital, and Johns Hopkins Health System. Health Library, Johns Hopkins Medicine. Available at: http://www.hopkinsmedicine.org/healthlibrary/test_procedures/pulmonary/thoracentesis_92,P07761/. Accessed August 18, 2015.
28. Runyon BA. Diagnostic and therapeutic abdominal paracentesis. UpToDate. Available at: http://www.uptodate.com/contents/diagnostic-and-therapeutic-abdominal-paracentesis. Published February 18, 2014. Accessed August 18, 2015.
29. Granata A, Fiorini F, Andrulli S, et al. Doppler ultrasound and renal artery stenosis: An overview. J Ultrasound. 2009;12:133-143. PubMed
30. Gerhard-Herman M, Gardin JM, Jaff M, et al. Guidelines for noninvasive vascular laboratory testing: a report from the American Society of Echocardiography and the Society for Vascular Medicine and Biology. Vasc Med. 2006;11:183-200. PubMed
Frequent and prolonged fasting can lead to patient dissatisfaction and distress.1 It may also cause malnutrition and negatively affect outcomes in high-risk populations such as the elderly.2 Evidence suggests that patients are commonly kept fasting longer than necessary.3,4 However, the extent to which nil per os (NPO) orders are necessary or adhere to evidence-based duration is unknown.
Our study showed half of patients admitted to the general medicine services experienced a period of fasting, and 1 in 4 NPO orders may be avoidable.5 In this study, we aimed to provide action-oriented recommendations by 1) assessing why some interventions did not occur after NPO orders were placed and 2) analyzing NPO orders by indication and comparing them with the best available evidence.
METHOD
This retrospective study was conducted at an academic medical center in the United States. The study protocol was approved by the Mayo Clinic Institutional Review Board.
Detailed data handling and NPO order review processes have been described elsewhere.5 Briefly, we identified 1200 NPO orders of 120 or more minutes’ duration that were written for patients on the general medicine services at our institution in 2013. After blinded duplicate review, we excluded 70 orders written in the intensive care unit or on other services, 24 with unknown indications, 101 primarily indicated for clinical reasons, and 81 that had multiple indications. Consequently, 924 orders indicated for a single intervention (eg, imaging study, procedure, or operation) were included in the main analysis.
We assessed if the indicated intervention was performed. If performed, we recorded the time when the intervention was started. If not performed, we assessed reasons why it was not performed. We also performed exploratory analyses to investigate factors associated with performing the indicated intervention. The variables were 1) NPO starting at midnight, 2) NPO starting within 12 hours of admission, and 3) indication (eg, imaging study, procedure, or operation). We also conducted sensitivity analyses limited to 1 NPO order per patient (N = 673) to assess independence of the orders.
We then further categorized indications for the orders in detail and identified those with a sample size >10. This resulted in 779 orders that were included in the analysis by indication. We reviewed the literature by indication to determine suggested minimally required fasting durations to compare fasting duration in our patients to current evidence-based recommendations.
For descriptive statistics, we used median with interquartile range (IQR) for continuous variables and percentage for discrete variables; chi-square tests were used for comparison of discrete variables. All P values were two-tailed and P < 0.05 was considered significant.
RESULTS
Median length of 924 orders was 12.7 hours (IQR, 10.1-15.7 hours); 190 (20.1%), 577 (62.4%), and 157 (21.0%) orders were indicated for imaging studies, procedures, and operations, respectively. NPO started at midnight in 662 (71.6%) and within 12 hours of admission in 210 (22.7%) orders.
The indicated interventions were not performed in 183 (19.8%) orders, mostly as a result of a change in plan (75/183, 41.0%) or scheduling barriers (43/183, 23.5%). Plan changes occurred when, for example, input from a consulting service was obtained or the supervising physician decided not to pursue the intervention. Scheduling barriers included slots being unavailable and conflicts with other tasks/tests. Notably, only in 1 of 183 (0.5%) orders, the intervention was cancelled because the patient ate (Table 1).
Table 1
NPO orders starting at midnight were associated with higher likelihood of indicated interventions being performed (546/662, 82.5% vs. 195/262, 74.4%; P = 0.006), as were NPO orders starting more than 12 hours after admission (601/714, 84.2% vs. 140/210, 66.7%; P < 0.001). Imaging studies were more likely to be performed than procedures or operations (170/190, 89.5% vs. 452/577, 78.3% vs. 119/157, 75.8%; P = 0.001). These results were unchanged when the analyses were limited to 1 order per patient.
When analyzed by indication, the median durations of NPO orders ranged from 8.3 hours in kidney ultrasound to 13.9 hours in upper endoscopy. These were slightly shortened, most by 1 to 2 hours, when the duration was calculated from start of the order to initiation of the intervention. The literature review identified, for most indications, that the minimally required length of NPO were 2 to 4 hours, generally 6 to 8 hours shorter than the median NPO length in this study sample. Furthermore, for indications such as computed tomography with intravenous contrast and abdominal ultrasound, the literature suggested NPO may be unnecessary (Table 2).6-9,16-30
Table 2
DISCUSSION
We analyzed a comprehensive set of NPO orders written for interventions in medical inpatients at an academic medical center. NPO started at midnight in 71.6% of the analyzed orders. In 1 in 5 NPO orders, the indicated intervention was not performed largely due to a change in plan or scheduling barriers. In most NPO orders in which the indicated interventions were performed, patients were kept fasting either unnecessarily or much longer than needed. This study is the first of its kind in evaluating NPO-ordering practices across multiple indications and comparing them with the best available evidence.
These results suggest current NPO practice in the hospital is suboptimal, and limited literature measures the magnitude of this issue.6,7 An important aspect of our study findings is that, in a substantial number of NPO orders, the indicated interventions were not performed for seemingly avoidable reasons. These issues may be attributable to clinicians’ preemptive decisions or lack of knowledge, or inefficiency in the healthcare system. Minimizing anticipatory NPO may carry drawbacks such as delays in interventions, and limited evidence links excessive NPO with clinical outcomes (eg, length of stay, readmission, or death). However, from the patients’ perspective, it is important to be kept fasting only for clinical benefit. Hence, this calls for substantial improvement of NPO practices.
Furthermore, results indicated that the duration of most NPO orders was longer than the minimal duration currently suggested in the literature. Whereas strong evidence suggests that no longer than 2 hours of fasting is generally required for preoperative purposes,8 limited studies have evaluated the required length of NPO orders in imaging studies and procedures,9-11 which comprised most of the orders in the study cohort. For example, in upper endoscopy, 2 small studies suggested fasting for 1 or 2 hours may provide as good visualization as with the conventional 6 to 8 hours of fasting.9,10 In coronary angiography, a retrospective study demonstrated fasting may be unnecessary.11 Due to lack of robust evidence, guidelines for these interventions either do not specify the required length of fasting or have not changed the conventional recommendations for fasting, leading to large variations in fasting policies by institution.6,12 Therefore, more studies are needed to define required length of fasting for those indications and to measure the exact magnitude of excessive fasting in the hospital.
One of the limitations of this study is generalizability because NPO practice may considerably vary by institution as suggested in the literature.4,6,12 Conversely, studies have suggested that excessive fasting exists in other institutions.3,4,13 Thus, this study adds further evidence of the prevalence of suboptimal NPO practice to the literature and provides a benchmark that other institutions can refer to when evaluating their own NPO practice. Another limitation is the assumption that the evidence for minimally required NPO duration can be applied to our patient samples. Specifically, the American Society of Anesthesiologists guideline states that preoperative or preprocedural fasting may need to be longer than 2 hours for 1) patients with comorbidities that can affect gastric emptying or fluid volume such as obesity, diabetes, emergency care, and enteral tube feeding, and 2) patients in whom airway management might be difficult.8 We did not consider these possibilities, and as these conditions are prevalent in medical inpatients, we may be overstating the excessiveness of fasting orders. On the other hand, especially in patients with diabetes, prolonged fasting may cause harm by inducing hypoglycemia.14 Further, no study rigorously evaluated safety of shortening the fasting period for these subsets of patients. Therefore, it is necessary to establish optimal duration of NPO and to improve NPO ordering practice even in these patient subsets.
While more research is needed to define optimal duration of NPO for various interventions and specific subsets of patients and to establish linkage of excessive NPO with clinical outcomes, our data provide insights into immediate actions that can be taken by clinicians to improve NPO practices using our data as a benchmark. First, institutions can establish more robust practice guidelines or institutional protocols for NPO orders. Successful interventions have been reported,15 and breaking the habit of ordering NPO after midnight is certainly possible. We recommend each institution does so by indication, potentially through interdepartmental work groups involving appropriate departments such as radiology, surgery, and medicine. Second, institutional guidelines or protocols can be incorporated in the ordering system to enable appropriate NPO ordering. For example, at our institution, we are modifying the order screens for ultrasound-guided paracentesis and thoracentesis to indicate that NPO is not necessary for these procedures unless sedation is anticipated. We conclude that, at any institution, efforts in improving the NPO practice are urgently warranted to minimize unnecessary fasting.
Disclosures
This publication was supported by Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. The authors report no financial conflicts of interest.
Frequent and prolonged fasting can lead to patient dissatisfaction and distress.1 It may also cause malnutrition and negatively affect outcomes in high-risk populations such as the elderly.2 Evidence suggests that patients are commonly kept fasting longer than necessary.3,4 However, the extent to which nil per os (NPO) orders are necessary or adhere to evidence-based duration is unknown.
Our study showed half of patients admitted to the general medicine services experienced a period of fasting, and 1 in 4 NPO orders may be avoidable.5 In this study, we aimed to provide action-oriented recommendations by 1) assessing why some interventions did not occur after NPO orders were placed and 2) analyzing NPO orders by indication and comparing them with the best available evidence.
METHOD
This retrospective study was conducted at an academic medical center in the United States. The study protocol was approved by the Mayo Clinic Institutional Review Board.
Detailed data handling and NPO order review processes have been described elsewhere.5 Briefly, we identified 1200 NPO orders of 120 or more minutes’ duration that were written for patients on the general medicine services at our institution in 2013. After blinded duplicate review, we excluded 70 orders written in the intensive care unit or on other services, 24 with unknown indications, 101 primarily indicated for clinical reasons, and 81 that had multiple indications. Consequently, 924 orders indicated for a single intervention (eg, imaging study, procedure, or operation) were included in the main analysis.
We assessed if the indicated intervention was performed. If performed, we recorded the time when the intervention was started. If not performed, we assessed reasons why it was not performed. We also performed exploratory analyses to investigate factors associated with performing the indicated intervention. The variables were 1) NPO starting at midnight, 2) NPO starting within 12 hours of admission, and 3) indication (eg, imaging study, procedure, or operation). We also conducted sensitivity analyses limited to 1 NPO order per patient (N = 673) to assess independence of the orders.
We then further categorized indications for the orders in detail and identified those with a sample size >10. This resulted in 779 orders that were included in the analysis by indication. We reviewed the literature by indication to determine suggested minimally required fasting durations to compare fasting duration in our patients to current evidence-based recommendations.
For descriptive statistics, we used median with interquartile range (IQR) for continuous variables and percentage for discrete variables; chi-square tests were used for comparison of discrete variables. All P values were two-tailed and P < 0.05 was considered significant.
RESULTS
Median length of 924 orders was 12.7 hours (IQR, 10.1-15.7 hours); 190 (20.1%), 577 (62.4%), and 157 (21.0%) orders were indicated for imaging studies, procedures, and operations, respectively. NPO started at midnight in 662 (71.6%) and within 12 hours of admission in 210 (22.7%) orders.
The indicated interventions were not performed in 183 (19.8%) orders, mostly as a result of a change in plan (75/183, 41.0%) or scheduling barriers (43/183, 23.5%). Plan changes occurred when, for example, input from a consulting service was obtained or the supervising physician decided not to pursue the intervention. Scheduling barriers included slots being unavailable and conflicts with other tasks/tests. Notably, only in 1 of 183 (0.5%) orders, the intervention was cancelled because the patient ate (Table 1).
Table 1
NPO orders starting at midnight were associated with higher likelihood of indicated interventions being performed (546/662, 82.5% vs. 195/262, 74.4%; P = 0.006), as were NPO orders starting more than 12 hours after admission (601/714, 84.2% vs. 140/210, 66.7%; P < 0.001). Imaging studies were more likely to be performed than procedures or operations (170/190, 89.5% vs. 452/577, 78.3% vs. 119/157, 75.8%; P = 0.001). These results were unchanged when the analyses were limited to 1 order per patient.
When analyzed by indication, the median durations of NPO orders ranged from 8.3 hours in kidney ultrasound to 13.9 hours in upper endoscopy. These were slightly shortened, most by 1 to 2 hours, when the duration was calculated from start of the order to initiation of the intervention. The literature review identified, for most indications, that the minimally required length of NPO were 2 to 4 hours, generally 6 to 8 hours shorter than the median NPO length in this study sample. Furthermore, for indications such as computed tomography with intravenous contrast and abdominal ultrasound, the literature suggested NPO may be unnecessary (Table 2).6-9,16-30
Table 2
DISCUSSION
We analyzed a comprehensive set of NPO orders written for interventions in medical inpatients at an academic medical center. NPO started at midnight in 71.6% of the analyzed orders. In 1 in 5 NPO orders, the indicated intervention was not performed largely due to a change in plan or scheduling barriers. In most NPO orders in which the indicated interventions were performed, patients were kept fasting either unnecessarily or much longer than needed. This study is the first of its kind in evaluating NPO-ordering practices across multiple indications and comparing them with the best available evidence.
These results suggest current NPO practice in the hospital is suboptimal, and limited literature measures the magnitude of this issue.6,7 An important aspect of our study findings is that, in a substantial number of NPO orders, the indicated interventions were not performed for seemingly avoidable reasons. These issues may be attributable to clinicians’ preemptive decisions or lack of knowledge, or inefficiency in the healthcare system. Minimizing anticipatory NPO may carry drawbacks such as delays in interventions, and limited evidence links excessive NPO with clinical outcomes (eg, length of stay, readmission, or death). However, from the patients’ perspective, it is important to be kept fasting only for clinical benefit. Hence, this calls for substantial improvement of NPO practices.
Furthermore, results indicated that the duration of most NPO orders was longer than the minimal duration currently suggested in the literature. Whereas strong evidence suggests that no longer than 2 hours of fasting is generally required for preoperative purposes,8 limited studies have evaluated the required length of NPO orders in imaging studies and procedures,9-11 which comprised most of the orders in the study cohort. For example, in upper endoscopy, 2 small studies suggested fasting for 1 or 2 hours may provide as good visualization as with the conventional 6 to 8 hours of fasting.9,10 In coronary angiography, a retrospective study demonstrated fasting may be unnecessary.11 Due to lack of robust evidence, guidelines for these interventions either do not specify the required length of fasting or have not changed the conventional recommendations for fasting, leading to large variations in fasting policies by institution.6,12 Therefore, more studies are needed to define required length of fasting for those indications and to measure the exact magnitude of excessive fasting in the hospital.
One of the limitations of this study is generalizability because NPO practice may considerably vary by institution as suggested in the literature.4,6,12 Conversely, studies have suggested that excessive fasting exists in other institutions.3,4,13 Thus, this study adds further evidence of the prevalence of suboptimal NPO practice to the literature and provides a benchmark that other institutions can refer to when evaluating their own NPO practice. Another limitation is the assumption that the evidence for minimally required NPO duration can be applied to our patient samples. Specifically, the American Society of Anesthesiologists guideline states that preoperative or preprocedural fasting may need to be longer than 2 hours for 1) patients with comorbidities that can affect gastric emptying or fluid volume such as obesity, diabetes, emergency care, and enteral tube feeding, and 2) patients in whom airway management might be difficult.8 We did not consider these possibilities, and as these conditions are prevalent in medical inpatients, we may be overstating the excessiveness of fasting orders. On the other hand, especially in patients with diabetes, prolonged fasting may cause harm by inducing hypoglycemia.14 Further, no study rigorously evaluated safety of shortening the fasting period for these subsets of patients. Therefore, it is necessary to establish optimal duration of NPO and to improve NPO ordering practice even in these patient subsets.
While more research is needed to define optimal duration of NPO for various interventions and specific subsets of patients and to establish linkage of excessive NPO with clinical outcomes, our data provide insights into immediate actions that can be taken by clinicians to improve NPO practices using our data as a benchmark. First, institutions can establish more robust practice guidelines or institutional protocols for NPO orders. Successful interventions have been reported,15 and breaking the habit of ordering NPO after midnight is certainly possible. We recommend each institution does so by indication, potentially through interdepartmental work groups involving appropriate departments such as radiology, surgery, and medicine. Second, institutional guidelines or protocols can be incorporated in the ordering system to enable appropriate NPO ordering. For example, at our institution, we are modifying the order screens for ultrasound-guided paracentesis and thoracentesis to indicate that NPO is not necessary for these procedures unless sedation is anticipated. We conclude that, at any institution, efforts in improving the NPO practice are urgently warranted to minimize unnecessary fasting.
Disclosures
This publication was supported by Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. The authors report no financial conflicts of interest.
References
1. Carey SK, Conchin S, Bloomfield-Stone S. A qualitative study into the impact of fasting within a large tertiary hospital in Australia - the patients’ perspective. J Clin Nurs. 2015;24:1946-1954. PubMed
2. Kyriakos G, Calleja-Fernández A, Ávila-Turcios D, Cano-Rodríguez I, Ballesteros Pomar MD, Vidal-Casariego A. Prolonged fasting with fluid therapy is related to poorer outcomes in medical patients. Nutr Hosp. 2013;28:1710-1716. PubMed
3. Rycroft-Malone J, Seers K, Crichton N, et al. A pragmatic cluster randomised trial evaluating three implementation interventions. Implement Sci. 2012;7:80. PubMed
4. Breuer JP, Bosse G, Seifert S, et al. Pre-operative fasting: a nationwide survey of German anaesthesia departments. Acta Anaesthesiol Scand. 2010;54:313-320. PubMed
5. Sorita A, Thongprayoon C, Ahmed A, et al. Frequency and appropriateness of fasting orders in the hospital. Mayo Clin Proc. 2015;90:1225-1232. PubMed
6. Lee BY, Ok JJ, Abdelaziz Elsayed AA, Kim Y, Han DH. Preparative fasting for contrast-enhanced CT: reconsideration. Radiology. 2012;263:444-450. PubMed
7. Manchikanti L, Malla Y, Wargo BW, Fellows B. Preoperative fasting before interventional techniques: is it necessary or evidence-based? Pain Physician. 2011;14:459-467. PubMed
8. American Society of Anesthesiologists Committee. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology. 2011;114:495-511. PubMed
9. Koeppe AT, Lubini M, Bonadeo NM, Moraes I Jr, Fornari F. Comfort, safety and quality of upper gastrointestinal endoscopy after 2 hours fasting: a randomized controlled trial. BMC Gastroenterol. 2013;13:158. PubMed
10. De Silva AP, Amarasiri L, Liyanage MN, Kottachchi D, Dassanayake AS, de Silva HJ. One-hour fast for water and six-hour fast for solids prior to endoscopy provides good endoscopic vision and results in minimum patient discomfort. J Gastroenterol Hepatol. 2009;24:1095-1097. PubMed
11. Hamid T, Aleem Q, Lau Y, et al. Pre-procedural fasting for coronary interventions: is it time to change practice? Heart. 2014;100:658-661. PubMed
12. Ahmed SU, Tonidandel W, Trella J, Martin NM, Chang Y. Peri-procedural protocols for interventional pain management techniques: a survey of US pain centers. Pain Physician. 2005;8:181-185. PubMed
13. Franklin GA, McClave SA, Hurt RT, et al. Physician-delivered malnutrition: why do patients receive nothing by mouth or a clear liquid diet in a university hospital setting? JPEN J Parenter Enteral Nutr. 2011;35:337-342. PubMed
14. Aldasouqi S, Sheikh A, Klosterman P, et al. Hypoglycemia in patients with diabetes who are fasting for laboratory blood tests: the Cape Girardeau Hypoglycemia En Route Prevention Program. Postgrad Med. 2013;125:136-143. PubMed
15. Aguilar-Nascimento JE, Salomão AB, Caporossi C, Diniz BN. Clinical benefits after the implementation of a multimodal perioperative protocol in elderly patients. Arq Gastroenterol. 2010;47:178-183. PubMed
16. Hilberath JN, Oakes DA, Shernan SK, Bulwer BE, D’Ambra MN, Eltzschig HK. Safety of transesophageal echocardiography. J Am Soc Echocardiogr. 2010;23: 1115-1127. PubMed
17. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26:921-964. PubMed
18. Sinan T, Leven H, Sheikh M. Is fasting a necessary preparation for abdominal ultrasound? BMC Med Imaging. 2003;3:1. PubMed
19. Garcia DA, Froes TR. Importance of fasting in preparing dogs for abdominal ultrasound examination of specific organs. J Small Anim Pract. 2014;55:630-634. PubMed
20. Kidney ultrasound. The Johns Hopkins University, The Johns Hopkins Hospital, and Johns Hopkins Health System. Health Library, Johns Hopkins Medicine. Available at: http://www.hopkinsmedicine.org/healthlibrary/test_procedures/urology/kidney_ultrasound_92,P07709/. Accessed August 17, 2015.
21. Surasi DS, Bhambhvani P, Baldwin JA, Almodovar SE, O’Malley JP. 18F-FDG PET and PET/CT patient preparation: a review of the literature. J Nucl Med Technol. 2014;42:5-13. PubMed
22. Kang SH, Hyun JJ. Preparation and patient evaluation for safe gastrointestinal endoscopy. Clin Endosc. 2013;46:212-218. PubMed
23. Smith I, Kranke P, Murat I, et al. Perioperative fasting in adults and children: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol. 2011;28:556-569. PubMed
24. ASGE Standards of Practice Committee, Saltzman JR, Cash BD, Pasha SF, et al. Bowel preparation before colonoscopy. Gastrointest Endosc. 2015;81:781-794. PubMed
25. Hassan C, Bretthauer M, Kaminski MF, et al; European Society of Gastrointestinal Endoscopy. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2013;45:142-150. PubMed
26. Du Rand IA, Blaikley J, Booton R, et al; British Thoracic Society Bronchoscopy Guideline Group. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: accredited by NICE. Thorax. 2013;68(suppl 1):i1-i44. PubMed
27. Thoracentesis. The Johns Hopkins University, The Johns Hopkins Hospital, and Johns Hopkins Health System. Health Library, Johns Hopkins Medicine. Available at: http://www.hopkinsmedicine.org/healthlibrary/test_procedures/pulmonary/thoracentesis_92,P07761/. Accessed August 18, 2015.
28. Runyon BA. Diagnostic and therapeutic abdominal paracentesis. UpToDate. Available at: http://www.uptodate.com/contents/diagnostic-and-therapeutic-abdominal-paracentesis. Published February 18, 2014. Accessed August 18, 2015.
29. Granata A, Fiorini F, Andrulli S, et al. Doppler ultrasound and renal artery stenosis: An overview. J Ultrasound. 2009;12:133-143. PubMed
30. Gerhard-Herman M, Gardin JM, Jaff M, et al. Guidelines for noninvasive vascular laboratory testing: a report from the American Society of Echocardiography and the Society for Vascular Medicine and Biology. Vasc Med. 2006;11:183-200. PubMed
References
1. Carey SK, Conchin S, Bloomfield-Stone S. A qualitative study into the impact of fasting within a large tertiary hospital in Australia - the patients’ perspective. J Clin Nurs. 2015;24:1946-1954. PubMed
2. Kyriakos G, Calleja-Fernández A, Ávila-Turcios D, Cano-Rodríguez I, Ballesteros Pomar MD, Vidal-Casariego A. Prolonged fasting with fluid therapy is related to poorer outcomes in medical patients. Nutr Hosp. 2013;28:1710-1716. PubMed
3. Rycroft-Malone J, Seers K, Crichton N, et al. A pragmatic cluster randomised trial evaluating three implementation interventions. Implement Sci. 2012;7:80. PubMed
4. Breuer JP, Bosse G, Seifert S, et al. Pre-operative fasting: a nationwide survey of German anaesthesia departments. Acta Anaesthesiol Scand. 2010;54:313-320. PubMed
5. Sorita A, Thongprayoon C, Ahmed A, et al. Frequency and appropriateness of fasting orders in the hospital. Mayo Clin Proc. 2015;90:1225-1232. PubMed
6. Lee BY, Ok JJ, Abdelaziz Elsayed AA, Kim Y, Han DH. Preparative fasting for contrast-enhanced CT: reconsideration. Radiology. 2012;263:444-450. PubMed
7. Manchikanti L, Malla Y, Wargo BW, Fellows B. Preoperative fasting before interventional techniques: is it necessary or evidence-based? Pain Physician. 2011;14:459-467. PubMed
8. American Society of Anesthesiologists Committee. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology. 2011;114:495-511. PubMed
9. Koeppe AT, Lubini M, Bonadeo NM, Moraes I Jr, Fornari F. Comfort, safety and quality of upper gastrointestinal endoscopy after 2 hours fasting: a randomized controlled trial. BMC Gastroenterol. 2013;13:158. PubMed
10. De Silva AP, Amarasiri L, Liyanage MN, Kottachchi D, Dassanayake AS, de Silva HJ. One-hour fast for water and six-hour fast for solids prior to endoscopy provides good endoscopic vision and results in minimum patient discomfort. J Gastroenterol Hepatol. 2009;24:1095-1097. PubMed
11. Hamid T, Aleem Q, Lau Y, et al. Pre-procedural fasting for coronary interventions: is it time to change practice? Heart. 2014;100:658-661. PubMed
12. Ahmed SU, Tonidandel W, Trella J, Martin NM, Chang Y. Peri-procedural protocols for interventional pain management techniques: a survey of US pain centers. Pain Physician. 2005;8:181-185. PubMed
13. Franklin GA, McClave SA, Hurt RT, et al. Physician-delivered malnutrition: why do patients receive nothing by mouth or a clear liquid diet in a university hospital setting? JPEN J Parenter Enteral Nutr. 2011;35:337-342. PubMed
14. Aldasouqi S, Sheikh A, Klosterman P, et al. Hypoglycemia in patients with diabetes who are fasting for laboratory blood tests: the Cape Girardeau Hypoglycemia En Route Prevention Program. Postgrad Med. 2013;125:136-143. PubMed
15. Aguilar-Nascimento JE, Salomão AB, Caporossi C, Diniz BN. Clinical benefits after the implementation of a multimodal perioperative protocol in elderly patients. Arq Gastroenterol. 2010;47:178-183. PubMed
16. Hilberath JN, Oakes DA, Shernan SK, Bulwer BE, D’Ambra MN, Eltzschig HK. Safety of transesophageal echocardiography. J Am Soc Echocardiogr. 2010;23: 1115-1127. PubMed
17. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26:921-964. PubMed
18. Sinan T, Leven H, Sheikh M. Is fasting a necessary preparation for abdominal ultrasound? BMC Med Imaging. 2003;3:1. PubMed
19. Garcia DA, Froes TR. Importance of fasting in preparing dogs for abdominal ultrasound examination of specific organs. J Small Anim Pract. 2014;55:630-634. PubMed
20. Kidney ultrasound. The Johns Hopkins University, The Johns Hopkins Hospital, and Johns Hopkins Health System. Health Library, Johns Hopkins Medicine. Available at: http://www.hopkinsmedicine.org/healthlibrary/test_procedures/urology/kidney_ultrasound_92,P07709/. Accessed August 17, 2015.
21. Surasi DS, Bhambhvani P, Baldwin JA, Almodovar SE, O’Malley JP. 18F-FDG PET and PET/CT patient preparation: a review of the literature. J Nucl Med Technol. 2014;42:5-13. PubMed
22. Kang SH, Hyun JJ. Preparation and patient evaluation for safe gastrointestinal endoscopy. Clin Endosc. 2013;46:212-218. PubMed
23. Smith I, Kranke P, Murat I, et al. Perioperative fasting in adults and children: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol. 2011;28:556-569. PubMed
24. ASGE Standards of Practice Committee, Saltzman JR, Cash BD, Pasha SF, et al. Bowel preparation before colonoscopy. Gastrointest Endosc. 2015;81:781-794. PubMed
25. Hassan C, Bretthauer M, Kaminski MF, et al; European Society of Gastrointestinal Endoscopy. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2013;45:142-150. PubMed
26. Du Rand IA, Blaikley J, Booton R, et al; British Thoracic Society Bronchoscopy Guideline Group. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: accredited by NICE. Thorax. 2013;68(suppl 1):i1-i44. PubMed
27. Thoracentesis. The Johns Hopkins University, The Johns Hopkins Hospital, and Johns Hopkins Health System. Health Library, Johns Hopkins Medicine. Available at: http://www.hopkinsmedicine.org/healthlibrary/test_procedures/pulmonary/thoracentesis_92,P07761/. Accessed August 18, 2015.
28. Runyon BA. Diagnostic and therapeutic abdominal paracentesis. UpToDate. Available at: http://www.uptodate.com/contents/diagnostic-and-therapeutic-abdominal-paracentesis. Published February 18, 2014. Accessed August 18, 2015.
29. Granata A, Fiorini F, Andrulli S, et al. Doppler ultrasound and renal artery stenosis: An overview. J Ultrasound. 2009;12:133-143. PubMed
30. Gerhard-Herman M, Gardin JM, Jaff M, et al. Guidelines for noninvasive vascular laboratory testing: a report from the American Society of Echocardiography and the Society for Vascular Medicine and Biology. Vasc Med. 2006;11:183-200. PubMed
Address for Correspondence and Reprint Requests: Deanne T. Kashiwagi, MD, Mayo Clinic, Division of Hospital Internal Medicine, 200 First Street SW, Rochester, MN 55905; Telephone: 507-255-8715; Fax: 507-255-9189; Email: kashiwagi.deanne@mayo.edu
Content Gating
Open Access (article Unlocked/Open Access)
Alternative CME
Consolidated Pubs: Do Not Show Source Publication Logo
Hospital medicine (HM), which is the fastest growing medical specialty in the United States, includes more than 40,000 healthcare providers.[1] Hospitalists include practitioners from a variety of medical specialties, including internal medicine and pediatrics, and professional backgrounds such as physicians, nurse practitioners. and physician assistants.[2, 3] Originally defined as specialists of inpatient medicine, hospitalists must diagnose and manage a wide variety of clinical conditions, coordinate transitions of care, provide perioperative management to surgical patients, and contribute to quality improvement and hospital administration.[4, 5]
With the evolution of the HM, the need for effective continuing medical education (CME) has become increasingly important. Courses make up the largest percentage of CME activity types,[6] which also include regularly scheduled lecture series, internet materials, and journal‐related CME. Successful CME courses require educational content that matches the learning needs of its participants.[7] In 2006, the Society for Hospital Medicine (SHM) developed core competencies in HM to guide educators in identifying professional practice gaps for useful CME.[8] However, knowing a population's characteristics and learning needs is a key first step to recognizing a practice gap.[9] Understanding these components is important to ensuring that competencies in the field of HM remain relevant to address existing practice gaps.[10] Currently, little is known about the demographic characteristics of participants in HM CME.
Research on the characteristics of effective clinical teachers in medicine has revealed the importance of establishing a positive learning climate, asking questions, diagnosing learners needs, giving feedback, utilizing established teaching frameworks, and developing a personalized philosophy of teaching.[11] Within CME, research has generally demonstrated that courses lead to improvements in lower level outcomes,[12] such as satisfaction and learning, yet higher level outcomes such as behavior change and impacts on patients are inconsistent.[13, 14, 15] Additionally, we have shown that participant reflection on CME is enhanced by presenters who have prior teaching experience and higher teaching effectiveness scores, by the use of audience participation and by incorporating relevant content.[16, 17] Despite the existence of research on CME in general, we are not aware of prior studies regarding characteristics of effective CME in the field of HM.
To better understand and improve the quality of HM CME, we sought to describe the characteristics of participants at a large, national HM CME course, and to identify associations between characteristics of presentations and CME teaching effectiveness (CMETE) scores using a previously validated instrument.
METHODS
Study Design and Participants
This cross‐sectional study included all participants (n=368) and presenters (n=29) at the Mayo Clinic Hospital Medicine Managing Complex Patients (MCP) course in October 2014. MCP is a CME course designed for hospitalists (defined as those who spend most of their professional practice caring for hospitalized patients) and provides up to 24.5 American Medical Association Physician's Recognition Award category 1 credits. The course took place over 4 days and consisted of 32 didactic presentations, which comprised the context for data collection for this study. The structure of the course day consisted of early and late morning sessions, each made up of 3 to 5 presentations, followed by a question and answer session with presenters and a 15‐minute break. The study was deemed exempt by the Mayo Clinic Institutional Review Board.
Independent Variables: Characteristics of Participants and Presentations
Demographic characteristics of participants were obtained through anonymous surveys attached to CME teaching effectiveness forms. Variables included participant sex, professional degree, self‐identified hospitalist, medical specialty, geographic practice location, age, years in practice/level of training, practice setting, American Board of Internal Medicine (ABIM) certification of Focused Practice in Hospital Medicine, number of CME credits earned, and number of CME programs attended in the past year. These variables were selected in an effort to describe potentially relevant demographics of a national cohort of HM CME participants.
Presentation variables included use of clinical cases, audience response system (ARS), number of slides, defined goals/objectives, summary slide and presentation length in minutes, and are supported by previous CME effectiveness research.[16, 17, 18, 19]
The CMETE scores for this study were obtained from an instrument described in our previous research.[16] The instrument contains 7 items on 5‐point scales (range: strongly disagree to strongly agree) that address speaker clarity and organization, relevant content, use of case examples, effective slides, interactive learning methods (eg, audience response), use of supporting evidence, appropriate amount of content, and summary of key points. Additionally, the instrument includes 2 open‐ended questions: (1) What did the speaker do well? (Please describe specific behaviors and examples) and (2) What could the speaker improve on? (Please describe specific behaviors and examples). Validity evidence for CMETE scores included factor analysis demonstrating a unidimensional model for measuring presenter feedback, along with excellent internal consistency and inter‐rater reliability.[16]
Data Analysis
A CMETE score per presentation from each attendee was calculated as the average over the 7 instrument items. A composite presentation‐level CMETE score was then computed as the average overall score within each presentation. CMETE scores were summarized using means and standard deviations (SDs). The overall CMETE scores were compared by presentation characteristics using Kruskal‐Wallis tests. To illustrate the size of observed differences, Cohen effect sizes are presented as the average difference between groups divided by the common SD. All analyses were performed using SAS version 9 (SAS Institute Inc., Cary, NC).
RESULTS
There were 32 presentations during the MCP conference in 2014. A total of 277 (75.2%) out of 368 participants completed the survey. This yielded 7947 CMETE evaluations for analysis, with an average of 28.7 per person (median: 31, interquartile range: 2732, range: 632).
Demographic characteristics of course participants are listed in Table 1. Participants (number, %), described themselves as hospitalists (181, 70.4%), ABIM certified with HM focus (48, 18.8%), physicians with MD or MBBS degrees (181, 70.4%), nurse practitioners or physician assistants (52; 20.2%), and in practice 20 years (73, 28%). The majority of participants (148, 58.3%) worked in private practice, whereas only 63 (24.8%) worked in academic settings.
Participant Characteristics
Variable
No. of Attendees (%), N=277
NOTE: Abbreviations: ABIM, American Board of Internal Medicine; CME, continuing medical education; DO, doctor of osteopathic medicine; HM, hospital medicine; IM, internal medicine; MBBS, bachelor of medicine, bachelor of surgery; MD, medical doctor; NP, nurse practitioner; PA, physician assistant.
Sex
Unknown
22
Male
124 (48.6%)
Female
131 (51.4%)
Age
Unknown
17
2029 years
11 (4.2%)
3039 years
83 (31.9%)
4049 years
61 (23.5%)
5059 years
56 (21.5%)
6069 years
38 (14.6%)
70+ years
11 (4.2%)
Professional degree
Unknown
20
MD/MBBS
181 (70.4%)
DO
23 (8.9%)
NP
28 (10.9%)
PA
24 (9.3%)
Other
1 (0.4%)
Medical specialty
Unknown
26
Internal medicine
149 (59.4%)
Family medicine
47 (18.7%)
IM subspecialty
14 (5.6%)
Other
41 (16.3%)
Geographic location
Unknown
16
Western US
48 (18.4%)
Northeastern US
33 (12.6%)
Midwestern US
98 (37.5%)
Southern US
40 (15.3%)
Canada
13 (5.0%)
Other
29 (11.1%)
Years of practice/training
Unknown
16
Currently in training
1 (0.4%)
Practice 04 years
68 (26.1%)
Practice 59 years
55 (21.1%)
Practice 1019 years
64 (24.5%)
Practice 20+ years
73 (28.0%)
Practice setting
Unknown
23
Academic
63 (24.8%)
Privateurban
99 (39.0%)
Privaterural
49 (19.3%)
Other
43 (16.9%)
ABIM certification HM
Unknown
22
Yes
48 (18.8%)
No
207 (81.2%)
Hospitalist
Unknown
20
Yes
181 (70.4%)
No
76 (29.6%)
CME credits claimed
Unknown
20
024
54 (21.0%)
2549
105 (40.9%)
5074
61 (23.7%)
7599
15 (5.8%)
100+
22 (8.6%)
CME programs attended
Unknown
18
0
38 (14.7%)
12
166 (64.1%)
35
52 (20.1%)
6+
3 (1.2%)
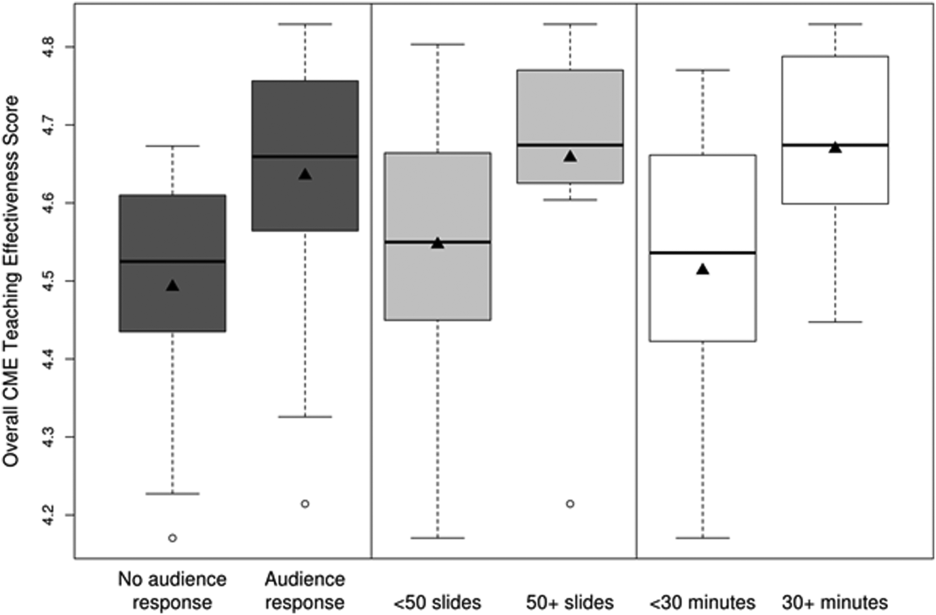
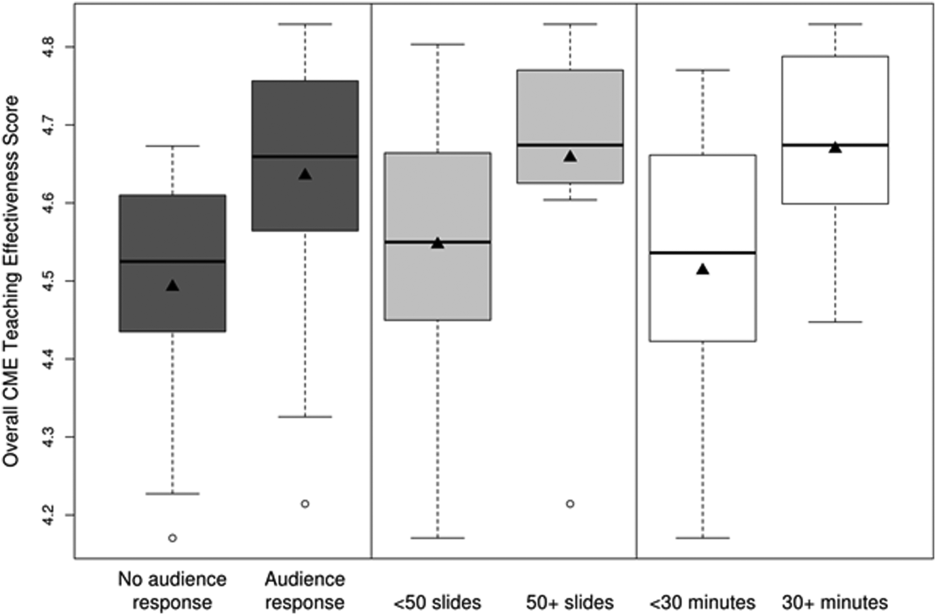
CMETE scores (mean [SD]) were significantly associated with the use of ARS (4.64 [0.16]) vs no ARS (4.49 [0.16]; P=0.01, Table 2, Figure 1), longer presentations (30 minutes: 4.67 [0.13] vs <30 minutes: 4.51 [0.18]; P=0.02), and larger number of slides (50: 4.66 [0.17] vs <50: 4.55 [0.17]; P=0.04). There were no significant associations between CMETE scores and use of clinical cases, defined goals, or summary slides.
Associations Between Presentation Characteristics and Validated Continuing Medical Education Teaching Effectiveness Scores
Presentation Variable
No. (%)
Mean Score
Standard Deviation
P Value
Use of clinical cases
Yes
28 (87.5%)
4.60
0.18
0.14
No
4 (12.5%)
4.49
0.14
Audience response system
Yes
20 (62.5%)
4.64
0.16
0.01
No
12 (37.5%)
4.49
0.16
No. of slides
50
10 (31.3%)
4.66
0.17
0.04
<50
22 (68.8%)
4.55
0.17
Defined goals/objectives
Yes
29 (90.6%)
4.58
0.18
0.87
No
3 (9.4%)
4.61
0.17
Summary slide
Yes
22 (68.8%)
4.56
0.18
0.44
No
10 (31.3%)
4.62
0.15
Presentation length
30 minutes
14 (43.8%)
4.67
0.13
0.02
<30 minutes
18 (56.3%)
4.51
0.18
Figure 1
Overall teaching effectiveness score distribution by audience response, number of slides, and presentation length. The boxes represent the interquartile range (IQR) (25th to 75th percentiles) with the median (middle horizontal line) and mean (triangle). The dashed lines extend to the last observation within a distance equal to 1.5*IQR from the top and bottom of the box. Any observations beyond that distance are plotted separately. Abbreviations: CME, continuing medical education.
The magnitude of score differences observed in this study are substantial when considered in terms of Cohen's effect sizes. For number of slides, the effect size is 0.65, for audience response the effect size is 0.94, and for presentation length the effect size is approximately 1. According to Cohen, effect sizes of 0.5 to 0.8 are moderate, and effect sizes >0.8 are large. Consequently, the effect sizes of our observed differences are moderate to large.[20, 21]
DISCUSSION
To our knowledge, this is the first study to measure associations between validated teaching effectiveness scores and characteristics of presentations in HM CME. We found that the use of ARS and longer presentations were associated with significantly higher CMETE scores. Our findings have implications for HM CME course directors and presenters as they attempt to develop methods to improve the quality of CME.
CME participants in our study crossed a wide range of ages and experience, which is consistent with national surveys of hospitalists.[22, 23] Interestingly, however, nearly 1 in 3 participants trained in a specialty other than internal medicine. Additionally, the professional degrees of participants were diverse, with 20% of participants having trained as nurse practitioners or physician assistants. These findings are at odds with an early national survey of inpatient practitioners,[22] but consistent with recent literature that the diversity of training backgrounds among hospitalists is increasing as the field of HM evolves.[24] Hospital medicine CME providers will need to be cognizant of these demographic changes as they work to identify practice gaps and apply appropriate educational methods.
The use of an ARS allows for increased participation and engagement among lecture attendees, which in turn promotes active learning.[25, 26, 27] The association of higher teaching scores with the use of ARS is consistent with previous research in other CME settings such as clinical round tables and medical grand rounds.[17, 28] As it pertains to HM specifically, our findings also build upon a recent study by Sehgal et al., which reported on the novel use of bedside CME to enhance interactive learning and discussion among hospitalists, and which was viewed favorably by course participants.[29]
The reasons why longer presentations in our study were linked to higher CMETE scores are not entirely clear, as previous CME research has failed to demonstrate this relationship.[18] One possibility is that course participants prefer learning from presentations that provide granular, content‐rich information. Another possibility may be that characteristics of effective presenters who gave longer presentations and that were not measured in this study, such as presenter experience and expertise, were responsible for the observed increase in CMETE scores. Yet another possibility is that effective presentations were longer due to the use of ARS, which was also associated with better CMETE scores. This explanation may be plausible because the ARS requires additional slides and provides opportunities for audience interaction, which may lengthen the duration of any given presentation.
This study has several limitations. This was a single CME conference sponsored by a large academic medical center, which may limit generalizability, especially to smaller conferences in community settings. However, the audience was large and diverse in terms of participants experiences, practice settings, professional backgrounds, and geographic locations. Furthermore, the demographic characteristics of hospitalists at our course appear very similar to a recently reported national cross‐section of hospitalist groups.[30] Second, this is a cross‐sectional study without a comparison group. Nonetheless, a systematic review showed that most published education research studies involved single‐group designs without comparison groups.[31] Last, the outcomes of the study include attitudes and objectively measured presenter behaviors such as the use of ARS, but not patient‐related outcomes. Nonetheless, evidence indicates that the majority of medical education research does not present outcomes beyond knowledge,[31] and it has been noted that behavior‐related outcomes strike the ideal balance between feasibility and rigor.[32, 33] Finally, the instrument used in this study to measure teaching effectiveness is supported by prior validity evidence.[16]
In summary, we found that hospital medicine CME presentations, which are longer and use audience responses, are associated with greater teaching effectiveness ratings by CME course participants. These findings build upon previous CME research and suggest that CME course directors and presenters should strive to incorporate opportunities that promote audience engagement and participation. Additionally, this study adds to the existing validity of evidence for the CMETE assessment tool. We believe that future research should explore potential associations between teacher effectiveness and patient‐related outcomes, and determine whether course content that reflects the SHM core competencies improves CME teaching effectiveness scores.
Society of Hospital Medicine. 2013/2014 press kit. Available at: http://www.hospitalmedicine.org/Web/Media_Center/Web/Media_Center/Media_Center.aspx?hkey=e26ceba7-ba93-4e50-8eb1-1ccc75d6f0fd. Accessed May 18, 2015.
Kleinpell RM, Hanson NA, Buchner BR, Winters R, Wilson MJ, Keck AC. Hospitalist services: an evolving opportunity. Nurse Pract.2008;33:9–10.
Wall S, Scudamore D, Chin J, et al. The evolving role of the pediatric nurse practitioner in hospital medicine. J Hosp Med.2014;9:261–265.
Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med.1996;335:514–517.
Society of Hospital Medicine. Definition of a hospitalist and hospital medicine. Available at: http://www.hospitalmedicine.org/Web/About_SHM/Hospitalist_Definition/Web/About_SHM/Industry/Hospital_Medicine_Hospital_Definition.aspx. Accessed February 16, 2015.
Accreditation Council for Continuing Medical Education. 2013 annual report data executive summary. Available at: http://www.accme.org/sites/default/files/630_2013_Annual_Report_20140715_0.pdf. Accessed February 16, 2015.
Muroff LR. The anatomy of an outstanding CME meeting. J Am Coll Radiol.2005;2:534–540.
McKean SC, Budnitz TL, Dressler DD, Amin AN, Pistoria MJ. How to use The Core Competencies in Hospital Medicine: a framework for curriculum development. J Hosp Med.2006;1:57–67.
Wittich CM, Chutka DS, Mauck KF, Berger RA, Litin SC, Beckman TJ. Perspective: a practical approach to defining professional practice gaps for continuing medical education. Acad Med.2012;87:582–585.
Dressler DD, Pistoria MJ, Budnitz TL, McKean SC, Amin AN. Core competencies in hospital medicine: development and methodology. J Hosp Med. 2006;1(suppl 1):148–156.
Beckman TJ, Lee MC. Proposal for a collaborative approach to clinical teaching. Mayo Clin Proc.2009;84:339–344.
Beckman TJ, Cook DA. Developing scholarly projects in education: a primer for medical teachers. Med Teach.2007;29:210–218.
Mansouri M, Lockyer J. A meta‐analysis of continuing medical education effectiveness. J Contin Educ Health Prof.2007;27:6–15.
Moore DE, Green JS, Gallis HA. Achieving desired results and improved outcomes: integrating planning and assessment throughout learning activities. J Contin Educ Health Prof.2009;29:1–15.
Cervero RM, Gaines JK. Effectiveness of continuing medical education: updated synthesis of systematic reviews. Available at: http://www.accme.org/sites/default/files/652_20141104_Effectiveness_of_Continuing_Medical_Education_Cervero_and_Gaines.pdf. Accessed March 25, 2015.
Wittich CM, Mauck KF, Mandrekar JN, et al. Improving participant feedback to continuing medical education presenters in internal medicine: a mixed‐methods study. J Gen Intern Med.2012;27:425–431.
Wittich CM, Szostek JH, Reed DA, et al. Measuring faculty reflection on medical grand rounds at Mayo Clinic: associations with teaching experience, clinical exposure, and presenter effectiveness. Mayo Clin Proc.2013;88:277–284.
Copeland HL, Longworth DL, Hewson MG, Stoller JK. Successful lecturing: a prospective study to validate attributes of the effective medical lecture. J Gen Intern Med.2000;15:366–371.
Shewchuk RM, Schmidt HJ, Benarous A, Bennett NL, Abdolrasulnia M, Casebeer LL. A standardized approach to assessing physician expectations and perceptions of continuing medical education. J Contin Educ Health Prof.2007;27:173–182.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York, NY: Academic Press; 1977.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed.Hillsdale, NJ: Erlbaum; 1988.
Lindenauer PK, Pantilat SZ, Katz PP, Wachter RM. Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians. Ann Intern Med.1999;130:343–349.
Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med.2012;27:28–36.
Kartha A, Restuccia JD, Burgess JF, et al. Nurse practitioner and physician assistant scope of practice in 118 acute care hospitals. J Hosp Med.2014;9:615–620.
Cain J, Robinson E. A primer on audience response systems: current applications and future considerations. Am J Pharm Educ.2008;72:77.
Davis N, Davis D, Bloch R. Continuing medical education: AMEE education guide no 35. Med Teach.2008;30:652–666.
Caldwell JE. Clickers in the large classroom: current research and best‐practice tips. CBE Life Sci Educ.2007;6:9–20.
Miller RG, Ashar BH, Getz KJ. Evaluation of an audience response system for the continuing education of health professionals. J Contin Educ Health Prof.2003;23:109–115.
Sehgal NL, Wachter RM, Vidyarthi AR. Bringing continuing medical education to the bedside: the University of California, San Francisco Hospitalist Mini‐College. J Hosp Med.2014;9:129–134.
Society of Hospital Medicine. 2014 State of Hospital Medicine Report. Philadelphia, PA: Society of Hospital Medicine; 2014.
Reed DA, Cook DA, Beckman TJ, Levine RB, Kern DE, Wright SM. Association between funding and quality of published medical education research. JAMA.2007;298:1002–1009.
Shea JA. Mind the gap: some reasons why medical education research is different from health services research. Med Educ.2001;35:319–320.
Cook DA, Beckman TJ. Reflections on experimental research in medical education. Adv Health Sci Educ Theory Pract.2010;15:455–464.
Hospital medicine (HM), which is the fastest growing medical specialty in the United States, includes more than 40,000 healthcare providers.[1] Hospitalists include practitioners from a variety of medical specialties, including internal medicine and pediatrics, and professional backgrounds such as physicians, nurse practitioners. and physician assistants.[2, 3] Originally defined as specialists of inpatient medicine, hospitalists must diagnose and manage a wide variety of clinical conditions, coordinate transitions of care, provide perioperative management to surgical patients, and contribute to quality improvement and hospital administration.[4, 5]
With the evolution of the HM, the need for effective continuing medical education (CME) has become increasingly important. Courses make up the largest percentage of CME activity types,[6] which also include regularly scheduled lecture series, internet materials, and journal‐related CME. Successful CME courses require educational content that matches the learning needs of its participants.[7] In 2006, the Society for Hospital Medicine (SHM) developed core competencies in HM to guide educators in identifying professional practice gaps for useful CME.[8] However, knowing a population's characteristics and learning needs is a key first step to recognizing a practice gap.[9] Understanding these components is important to ensuring that competencies in the field of HM remain relevant to address existing practice gaps.[10] Currently, little is known about the demographic characteristics of participants in HM CME.
Research on the characteristics of effective clinical teachers in medicine has revealed the importance of establishing a positive learning climate, asking questions, diagnosing learners needs, giving feedback, utilizing established teaching frameworks, and developing a personalized philosophy of teaching.[11] Within CME, research has generally demonstrated that courses lead to improvements in lower level outcomes,[12] such as satisfaction and learning, yet higher level outcomes such as behavior change and impacts on patients are inconsistent.[13, 14, 15] Additionally, we have shown that participant reflection on CME is enhanced by presenters who have prior teaching experience and higher teaching effectiveness scores, by the use of audience participation and by incorporating relevant content.[16, 17] Despite the existence of research on CME in general, we are not aware of prior studies regarding characteristics of effective CME in the field of HM.
To better understand and improve the quality of HM CME, we sought to describe the characteristics of participants at a large, national HM CME course, and to identify associations between characteristics of presentations and CME teaching effectiveness (CMETE) scores using a previously validated instrument.
METHODS
Study Design and Participants
This cross‐sectional study included all participants (n=368) and presenters (n=29) at the Mayo Clinic Hospital Medicine Managing Complex Patients (MCP) course in October 2014. MCP is a CME course designed for hospitalists (defined as those who spend most of their professional practice caring for hospitalized patients) and provides up to 24.5 American Medical Association Physician's Recognition Award category 1 credits. The course took place over 4 days and consisted of 32 didactic presentations, which comprised the context for data collection for this study. The structure of the course day consisted of early and late morning sessions, each made up of 3 to 5 presentations, followed by a question and answer session with presenters and a 15‐minute break. The study was deemed exempt by the Mayo Clinic Institutional Review Board.
Independent Variables: Characteristics of Participants and Presentations
Demographic characteristics of participants were obtained through anonymous surveys attached to CME teaching effectiveness forms. Variables included participant sex, professional degree, self‐identified hospitalist, medical specialty, geographic practice location, age, years in practice/level of training, practice setting, American Board of Internal Medicine (ABIM) certification of Focused Practice in Hospital Medicine, number of CME credits earned, and number of CME programs attended in the past year. These variables were selected in an effort to describe potentially relevant demographics of a national cohort of HM CME participants.
Presentation variables included use of clinical cases, audience response system (ARS), number of slides, defined goals/objectives, summary slide and presentation length in minutes, and are supported by previous CME effectiveness research.[16, 17, 18, 19]
The CMETE scores for this study were obtained from an instrument described in our previous research.[16] The instrument contains 7 items on 5‐point scales (range: strongly disagree to strongly agree) that address speaker clarity and organization, relevant content, use of case examples, effective slides, interactive learning methods (eg, audience response), use of supporting evidence, appropriate amount of content, and summary of key points. Additionally, the instrument includes 2 open‐ended questions: (1) What did the speaker do well? (Please describe specific behaviors and examples) and (2) What could the speaker improve on? (Please describe specific behaviors and examples). Validity evidence for CMETE scores included factor analysis demonstrating a unidimensional model for measuring presenter feedback, along with excellent internal consistency and inter‐rater reliability.[16]
Data Analysis
A CMETE score per presentation from each attendee was calculated as the average over the 7 instrument items. A composite presentation‐level CMETE score was then computed as the average overall score within each presentation. CMETE scores were summarized using means and standard deviations (SDs). The overall CMETE scores were compared by presentation characteristics using Kruskal‐Wallis tests. To illustrate the size of observed differences, Cohen effect sizes are presented as the average difference between groups divided by the common SD. All analyses were performed using SAS version 9 (SAS Institute Inc., Cary, NC).
RESULTS
There were 32 presentations during the MCP conference in 2014. A total of 277 (75.2%) out of 368 participants completed the survey. This yielded 7947 CMETE evaluations for analysis, with an average of 28.7 per person (median: 31, interquartile range: 2732, range: 632).
Demographic characteristics of course participants are listed in Table 1. Participants (number, %), described themselves as hospitalists (181, 70.4%), ABIM certified with HM focus (48, 18.8%), physicians with MD or MBBS degrees (181, 70.4%), nurse practitioners or physician assistants (52; 20.2%), and in practice 20 years (73, 28%). The majority of participants (148, 58.3%) worked in private practice, whereas only 63 (24.8%) worked in academic settings.
Participant Characteristics
Variable
No. of Attendees (%), N=277
NOTE: Abbreviations: ABIM, American Board of Internal Medicine; CME, continuing medical education; DO, doctor of osteopathic medicine; HM, hospital medicine; IM, internal medicine; MBBS, bachelor of medicine, bachelor of surgery; MD, medical doctor; NP, nurse practitioner; PA, physician assistant.
Sex
Unknown
22
Male
124 (48.6%)
Female
131 (51.4%)
Age
Unknown
17
2029 years
11 (4.2%)
3039 years
83 (31.9%)
4049 years
61 (23.5%)
5059 years
56 (21.5%)
6069 years
38 (14.6%)
70+ years
11 (4.2%)
Professional degree
Unknown
20
MD/MBBS
181 (70.4%)
DO
23 (8.9%)
NP
28 (10.9%)
PA
24 (9.3%)
Other
1 (0.4%)
Medical specialty
Unknown
26
Internal medicine
149 (59.4%)
Family medicine
47 (18.7%)
IM subspecialty
14 (5.6%)
Other
41 (16.3%)
Geographic location
Unknown
16
Western US
48 (18.4%)
Northeastern US
33 (12.6%)
Midwestern US
98 (37.5%)
Southern US
40 (15.3%)
Canada
13 (5.0%)
Other
29 (11.1%)
Years of practice/training
Unknown
16
Currently in training
1 (0.4%)
Practice 04 years
68 (26.1%)
Practice 59 years
55 (21.1%)
Practice 1019 years
64 (24.5%)
Practice 20+ years
73 (28.0%)
Practice setting
Unknown
23
Academic
63 (24.8%)
Privateurban
99 (39.0%)
Privaterural
49 (19.3%)
Other
43 (16.9%)
ABIM certification HM
Unknown
22
Yes
48 (18.8%)
No
207 (81.2%)
Hospitalist
Unknown
20
Yes
181 (70.4%)
No
76 (29.6%)
CME credits claimed
Unknown
20
024
54 (21.0%)
2549
105 (40.9%)
5074
61 (23.7%)
7599
15 (5.8%)
100+
22 (8.6%)
CME programs attended
Unknown
18
0
38 (14.7%)
12
166 (64.1%)
35
52 (20.1%)
6+
3 (1.2%)
CMETE scores (mean [SD]) were significantly associated with the use of ARS (4.64 [0.16]) vs no ARS (4.49 [0.16]; P=0.01, Table 2, Figure 1), longer presentations (30 minutes: 4.67 [0.13] vs <30 minutes: 4.51 [0.18]; P=0.02), and larger number of slides (50: 4.66 [0.17] vs <50: 4.55 [0.17]; P=0.04). There were no significant associations between CMETE scores and use of clinical cases, defined goals, or summary slides.
Associations Between Presentation Characteristics and Validated Continuing Medical Education Teaching Effectiveness Scores
Presentation Variable
No. (%)
Mean Score
Standard Deviation
P Value
Use of clinical cases
Yes
28 (87.5%)
4.60
0.18
0.14
No
4 (12.5%)
4.49
0.14
Audience response system
Yes
20 (62.5%)
4.64
0.16
0.01
No
12 (37.5%)
4.49
0.16
No. of slides
50
10 (31.3%)
4.66
0.17
0.04
<50
22 (68.8%)
4.55
0.17
Defined goals/objectives
Yes
29 (90.6%)
4.58
0.18
0.87
No
3 (9.4%)
4.61
0.17
Summary slide
Yes
22 (68.8%)
4.56
0.18
0.44
No
10 (31.3%)
4.62
0.15
Presentation length
30 minutes
14 (43.8%)
4.67
0.13
0.02
<30 minutes
18 (56.3%)
4.51
0.18
Figure 1
Overall teaching effectiveness score distribution by audience response, number of slides, and presentation length. The boxes represent the interquartile range (IQR) (25th to 75th percentiles) with the median (middle horizontal line) and mean (triangle). The dashed lines extend to the last observation within a distance equal to 1.5*IQR from the top and bottom of the box. Any observations beyond that distance are plotted separately. Abbreviations: CME, continuing medical education.
The magnitude of score differences observed in this study are substantial when considered in terms of Cohen's effect sizes. For number of slides, the effect size is 0.65, for audience response the effect size is 0.94, and for presentation length the effect size is approximately 1. According to Cohen, effect sizes of 0.5 to 0.8 are moderate, and effect sizes >0.8 are large. Consequently, the effect sizes of our observed differences are moderate to large.[20, 21]
DISCUSSION
To our knowledge, this is the first study to measure associations between validated teaching effectiveness scores and characteristics of presentations in HM CME. We found that the use of ARS and longer presentations were associated with significantly higher CMETE scores. Our findings have implications for HM CME course directors and presenters as they attempt to develop methods to improve the quality of CME.
CME participants in our study crossed a wide range of ages and experience, which is consistent with national surveys of hospitalists.[22, 23] Interestingly, however, nearly 1 in 3 participants trained in a specialty other than internal medicine. Additionally, the professional degrees of participants were diverse, with 20% of participants having trained as nurse practitioners or physician assistants. These findings are at odds with an early national survey of inpatient practitioners,[22] but consistent with recent literature that the diversity of training backgrounds among hospitalists is increasing as the field of HM evolves.[24] Hospital medicine CME providers will need to be cognizant of these demographic changes as they work to identify practice gaps and apply appropriate educational methods.
The use of an ARS allows for increased participation and engagement among lecture attendees, which in turn promotes active learning.[25, 26, 27] The association of higher teaching scores with the use of ARS is consistent with previous research in other CME settings such as clinical round tables and medical grand rounds.[17, 28] As it pertains to HM specifically, our findings also build upon a recent study by Sehgal et al., which reported on the novel use of bedside CME to enhance interactive learning and discussion among hospitalists, and which was viewed favorably by course participants.[29]
The reasons why longer presentations in our study were linked to higher CMETE scores are not entirely clear, as previous CME research has failed to demonstrate this relationship.[18] One possibility is that course participants prefer learning from presentations that provide granular, content‐rich information. Another possibility may be that characteristics of effective presenters who gave longer presentations and that were not measured in this study, such as presenter experience and expertise, were responsible for the observed increase in CMETE scores. Yet another possibility is that effective presentations were longer due to the use of ARS, which was also associated with better CMETE scores. This explanation may be plausible because the ARS requires additional slides and provides opportunities for audience interaction, which may lengthen the duration of any given presentation.
This study has several limitations. This was a single CME conference sponsored by a large academic medical center, which may limit generalizability, especially to smaller conferences in community settings. However, the audience was large and diverse in terms of participants experiences, practice settings, professional backgrounds, and geographic locations. Furthermore, the demographic characteristics of hospitalists at our course appear very similar to a recently reported national cross‐section of hospitalist groups.[30] Second, this is a cross‐sectional study without a comparison group. Nonetheless, a systematic review showed that most published education research studies involved single‐group designs without comparison groups.[31] Last, the outcomes of the study include attitudes and objectively measured presenter behaviors such as the use of ARS, but not patient‐related outcomes. Nonetheless, evidence indicates that the majority of medical education research does not present outcomes beyond knowledge,[31] and it has been noted that behavior‐related outcomes strike the ideal balance between feasibility and rigor.[32, 33] Finally, the instrument used in this study to measure teaching effectiveness is supported by prior validity evidence.[16]
In summary, we found that hospital medicine CME presentations, which are longer and use audience responses, are associated with greater teaching effectiveness ratings by CME course participants. These findings build upon previous CME research and suggest that CME course directors and presenters should strive to incorporate opportunities that promote audience engagement and participation. Additionally, this study adds to the existing validity of evidence for the CMETE assessment tool. We believe that future research should explore potential associations between teacher effectiveness and patient‐related outcomes, and determine whether course content that reflects the SHM core competencies improves CME teaching effectiveness scores.
Disclosure
Nothing to report.
Hospital medicine (HM), which is the fastest growing medical specialty in the United States, includes more than 40,000 healthcare providers.[1] Hospitalists include practitioners from a variety of medical specialties, including internal medicine and pediatrics, and professional backgrounds such as physicians, nurse practitioners. and physician assistants.[2, 3] Originally defined as specialists of inpatient medicine, hospitalists must diagnose and manage a wide variety of clinical conditions, coordinate transitions of care, provide perioperative management to surgical patients, and contribute to quality improvement and hospital administration.[4, 5]
With the evolution of the HM, the need for effective continuing medical education (CME) has become increasingly important. Courses make up the largest percentage of CME activity types,[6] which also include regularly scheduled lecture series, internet materials, and journal‐related CME. Successful CME courses require educational content that matches the learning needs of its participants.[7] In 2006, the Society for Hospital Medicine (SHM) developed core competencies in HM to guide educators in identifying professional practice gaps for useful CME.[8] However, knowing a population's characteristics and learning needs is a key first step to recognizing a practice gap.[9] Understanding these components is important to ensuring that competencies in the field of HM remain relevant to address existing practice gaps.[10] Currently, little is known about the demographic characteristics of participants in HM CME.
Research on the characteristics of effective clinical teachers in medicine has revealed the importance of establishing a positive learning climate, asking questions, diagnosing learners needs, giving feedback, utilizing established teaching frameworks, and developing a personalized philosophy of teaching.[11] Within CME, research has generally demonstrated that courses lead to improvements in lower level outcomes,[12] such as satisfaction and learning, yet higher level outcomes such as behavior change and impacts on patients are inconsistent.[13, 14, 15] Additionally, we have shown that participant reflection on CME is enhanced by presenters who have prior teaching experience and higher teaching effectiveness scores, by the use of audience participation and by incorporating relevant content.[16, 17] Despite the existence of research on CME in general, we are not aware of prior studies regarding characteristics of effective CME in the field of HM.
To better understand and improve the quality of HM CME, we sought to describe the characteristics of participants at a large, national HM CME course, and to identify associations between characteristics of presentations and CME teaching effectiveness (CMETE) scores using a previously validated instrument.
METHODS
Study Design and Participants
This cross‐sectional study included all participants (n=368) and presenters (n=29) at the Mayo Clinic Hospital Medicine Managing Complex Patients (MCP) course in October 2014. MCP is a CME course designed for hospitalists (defined as those who spend most of their professional practice caring for hospitalized patients) and provides up to 24.5 American Medical Association Physician's Recognition Award category 1 credits. The course took place over 4 days and consisted of 32 didactic presentations, which comprised the context for data collection for this study. The structure of the course day consisted of early and late morning sessions, each made up of 3 to 5 presentations, followed by a question and answer session with presenters and a 15‐minute break. The study was deemed exempt by the Mayo Clinic Institutional Review Board.
Independent Variables: Characteristics of Participants and Presentations
Demographic characteristics of participants were obtained through anonymous surveys attached to CME teaching effectiveness forms. Variables included participant sex, professional degree, self‐identified hospitalist, medical specialty, geographic practice location, age, years in practice/level of training, practice setting, American Board of Internal Medicine (ABIM) certification of Focused Practice in Hospital Medicine, number of CME credits earned, and number of CME programs attended in the past year. These variables were selected in an effort to describe potentially relevant demographics of a national cohort of HM CME participants.
Presentation variables included use of clinical cases, audience response system (ARS), number of slides, defined goals/objectives, summary slide and presentation length in minutes, and are supported by previous CME effectiveness research.[16, 17, 18, 19]
The CMETE scores for this study were obtained from an instrument described in our previous research.[16] The instrument contains 7 items on 5‐point scales (range: strongly disagree to strongly agree) that address speaker clarity and organization, relevant content, use of case examples, effective slides, interactive learning methods (eg, audience response), use of supporting evidence, appropriate amount of content, and summary of key points. Additionally, the instrument includes 2 open‐ended questions: (1) What did the speaker do well? (Please describe specific behaviors and examples) and (2) What could the speaker improve on? (Please describe specific behaviors and examples). Validity evidence for CMETE scores included factor analysis demonstrating a unidimensional model for measuring presenter feedback, along with excellent internal consistency and inter‐rater reliability.[16]
Data Analysis
A CMETE score per presentation from each attendee was calculated as the average over the 7 instrument items. A composite presentation‐level CMETE score was then computed as the average overall score within each presentation. CMETE scores were summarized using means and standard deviations (SDs). The overall CMETE scores were compared by presentation characteristics using Kruskal‐Wallis tests. To illustrate the size of observed differences, Cohen effect sizes are presented as the average difference between groups divided by the common SD. All analyses were performed using SAS version 9 (SAS Institute Inc., Cary, NC).
RESULTS
There were 32 presentations during the MCP conference in 2014. A total of 277 (75.2%) out of 368 participants completed the survey. This yielded 7947 CMETE evaluations for analysis, with an average of 28.7 per person (median: 31, interquartile range: 2732, range: 632).
Demographic characteristics of course participants are listed in Table 1. Participants (number, %), described themselves as hospitalists (181, 70.4%), ABIM certified with HM focus (48, 18.8%), physicians with MD or MBBS degrees (181, 70.4%), nurse practitioners or physician assistants (52; 20.2%), and in practice 20 years (73, 28%). The majority of participants (148, 58.3%) worked in private practice, whereas only 63 (24.8%) worked in academic settings.
Participant Characteristics
Variable
No. of Attendees (%), N=277
NOTE: Abbreviations: ABIM, American Board of Internal Medicine; CME, continuing medical education; DO, doctor of osteopathic medicine; HM, hospital medicine; IM, internal medicine; MBBS, bachelor of medicine, bachelor of surgery; MD, medical doctor; NP, nurse practitioner; PA, physician assistant.
Sex
Unknown
22
Male
124 (48.6%)
Female
131 (51.4%)
Age
Unknown
17
2029 years
11 (4.2%)
3039 years
83 (31.9%)
4049 years
61 (23.5%)
5059 years
56 (21.5%)
6069 years
38 (14.6%)
70+ years
11 (4.2%)
Professional degree
Unknown
20
MD/MBBS
181 (70.4%)
DO
23 (8.9%)
NP
28 (10.9%)
PA
24 (9.3%)
Other
1 (0.4%)
Medical specialty
Unknown
26
Internal medicine
149 (59.4%)
Family medicine
47 (18.7%)
IM subspecialty
14 (5.6%)
Other
41 (16.3%)
Geographic location
Unknown
16
Western US
48 (18.4%)
Northeastern US
33 (12.6%)
Midwestern US
98 (37.5%)
Southern US
40 (15.3%)
Canada
13 (5.0%)
Other
29 (11.1%)
Years of practice/training
Unknown
16
Currently in training
1 (0.4%)
Practice 04 years
68 (26.1%)
Practice 59 years
55 (21.1%)
Practice 1019 years
64 (24.5%)
Practice 20+ years
73 (28.0%)
Practice setting
Unknown
23
Academic
63 (24.8%)
Privateurban
99 (39.0%)
Privaterural
49 (19.3%)
Other
43 (16.9%)
ABIM certification HM
Unknown
22
Yes
48 (18.8%)
No
207 (81.2%)
Hospitalist
Unknown
20
Yes
181 (70.4%)
No
76 (29.6%)
CME credits claimed
Unknown
20
024
54 (21.0%)
2549
105 (40.9%)
5074
61 (23.7%)
7599
15 (5.8%)
100+
22 (8.6%)
CME programs attended
Unknown
18
0
38 (14.7%)
12
166 (64.1%)
35
52 (20.1%)
6+
3 (1.2%)
CMETE scores (mean [SD]) were significantly associated with the use of ARS (4.64 [0.16]) vs no ARS (4.49 [0.16]; P=0.01, Table 2, Figure 1), longer presentations (30 minutes: 4.67 [0.13] vs <30 minutes: 4.51 [0.18]; P=0.02), and larger number of slides (50: 4.66 [0.17] vs <50: 4.55 [0.17]; P=0.04). There were no significant associations between CMETE scores and use of clinical cases, defined goals, or summary slides.
Associations Between Presentation Characteristics and Validated Continuing Medical Education Teaching Effectiveness Scores
Presentation Variable
No. (%)
Mean Score
Standard Deviation
P Value
Use of clinical cases
Yes
28 (87.5%)
4.60
0.18
0.14
No
4 (12.5%)
4.49
0.14
Audience response system
Yes
20 (62.5%)
4.64
0.16
0.01
No
12 (37.5%)
4.49
0.16
No. of slides
50
10 (31.3%)
4.66
0.17
0.04
<50
22 (68.8%)
4.55
0.17
Defined goals/objectives
Yes
29 (90.6%)
4.58
0.18
0.87
No
3 (9.4%)
4.61
0.17
Summary slide
Yes
22 (68.8%)
4.56
0.18
0.44
No
10 (31.3%)
4.62
0.15
Presentation length
30 minutes
14 (43.8%)
4.67
0.13
0.02
<30 minutes
18 (56.3%)
4.51
0.18
Figure 1
Overall teaching effectiveness score distribution by audience response, number of slides, and presentation length. The boxes represent the interquartile range (IQR) (25th to 75th percentiles) with the median (middle horizontal line) and mean (triangle). The dashed lines extend to the last observation within a distance equal to 1.5*IQR from the top and bottom of the box. Any observations beyond that distance are plotted separately. Abbreviations: CME, continuing medical education.
The magnitude of score differences observed in this study are substantial when considered in terms of Cohen's effect sizes. For number of slides, the effect size is 0.65, for audience response the effect size is 0.94, and for presentation length the effect size is approximately 1. According to Cohen, effect sizes of 0.5 to 0.8 are moderate, and effect sizes >0.8 are large. Consequently, the effect sizes of our observed differences are moderate to large.[20, 21]
DISCUSSION
To our knowledge, this is the first study to measure associations between validated teaching effectiveness scores and characteristics of presentations in HM CME. We found that the use of ARS and longer presentations were associated with significantly higher CMETE scores. Our findings have implications for HM CME course directors and presenters as they attempt to develop methods to improve the quality of CME.
CME participants in our study crossed a wide range of ages and experience, which is consistent with national surveys of hospitalists.[22, 23] Interestingly, however, nearly 1 in 3 participants trained in a specialty other than internal medicine. Additionally, the professional degrees of participants were diverse, with 20% of participants having trained as nurse practitioners or physician assistants. These findings are at odds with an early national survey of inpatient practitioners,[22] but consistent with recent literature that the diversity of training backgrounds among hospitalists is increasing as the field of HM evolves.[24] Hospital medicine CME providers will need to be cognizant of these demographic changes as they work to identify practice gaps and apply appropriate educational methods.
The use of an ARS allows for increased participation and engagement among lecture attendees, which in turn promotes active learning.[25, 26, 27] The association of higher teaching scores with the use of ARS is consistent with previous research in other CME settings such as clinical round tables and medical grand rounds.[17, 28] As it pertains to HM specifically, our findings also build upon a recent study by Sehgal et al., which reported on the novel use of bedside CME to enhance interactive learning and discussion among hospitalists, and which was viewed favorably by course participants.[29]
The reasons why longer presentations in our study were linked to higher CMETE scores are not entirely clear, as previous CME research has failed to demonstrate this relationship.[18] One possibility is that course participants prefer learning from presentations that provide granular, content‐rich information. Another possibility may be that characteristics of effective presenters who gave longer presentations and that were not measured in this study, such as presenter experience and expertise, were responsible for the observed increase in CMETE scores. Yet another possibility is that effective presentations were longer due to the use of ARS, which was also associated with better CMETE scores. This explanation may be plausible because the ARS requires additional slides and provides opportunities for audience interaction, which may lengthen the duration of any given presentation.
This study has several limitations. This was a single CME conference sponsored by a large academic medical center, which may limit generalizability, especially to smaller conferences in community settings. However, the audience was large and diverse in terms of participants experiences, practice settings, professional backgrounds, and geographic locations. Furthermore, the demographic characteristics of hospitalists at our course appear very similar to a recently reported national cross‐section of hospitalist groups.[30] Second, this is a cross‐sectional study without a comparison group. Nonetheless, a systematic review showed that most published education research studies involved single‐group designs without comparison groups.[31] Last, the outcomes of the study include attitudes and objectively measured presenter behaviors such as the use of ARS, but not patient‐related outcomes. Nonetheless, evidence indicates that the majority of medical education research does not present outcomes beyond knowledge,[31] and it has been noted that behavior‐related outcomes strike the ideal balance between feasibility and rigor.[32, 33] Finally, the instrument used in this study to measure teaching effectiveness is supported by prior validity evidence.[16]
In summary, we found that hospital medicine CME presentations, which are longer and use audience responses, are associated with greater teaching effectiveness ratings by CME course participants. These findings build upon previous CME research and suggest that CME course directors and presenters should strive to incorporate opportunities that promote audience engagement and participation. Additionally, this study adds to the existing validity of evidence for the CMETE assessment tool. We believe that future research should explore potential associations between teacher effectiveness and patient‐related outcomes, and determine whether course content that reflects the SHM core competencies improves CME teaching effectiveness scores.
Disclosure
Nothing to report.
References
Society of Hospital Medicine. 2013/2014 press kit. Available at: http://www.hospitalmedicine.org/Web/Media_Center/Web/Media_Center/Media_Center.aspx?hkey=e26ceba7-ba93-4e50-8eb1-1ccc75d6f0fd. Accessed May 18, 2015.
Kleinpell RM, Hanson NA, Buchner BR, Winters R, Wilson MJ, Keck AC. Hospitalist services: an evolving opportunity. Nurse Pract.2008;33:9–10.
Wall S, Scudamore D, Chin J, et al. The evolving role of the pediatric nurse practitioner in hospital medicine. J Hosp Med.2014;9:261–265.
Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med.1996;335:514–517.
Society of Hospital Medicine. Definition of a hospitalist and hospital medicine. Available at: http://www.hospitalmedicine.org/Web/About_SHM/Hospitalist_Definition/Web/About_SHM/Industry/Hospital_Medicine_Hospital_Definition.aspx. Accessed February 16, 2015.
Accreditation Council for Continuing Medical Education. 2013 annual report data executive summary. Available at: http://www.accme.org/sites/default/files/630_2013_Annual_Report_20140715_0.pdf. Accessed February 16, 2015.
Muroff LR. The anatomy of an outstanding CME meeting. J Am Coll Radiol.2005;2:534–540.
McKean SC, Budnitz TL, Dressler DD, Amin AN, Pistoria MJ. How to use The Core Competencies in Hospital Medicine: a framework for curriculum development. J Hosp Med.2006;1:57–67.
Wittich CM, Chutka DS, Mauck KF, Berger RA, Litin SC, Beckman TJ. Perspective: a practical approach to defining professional practice gaps for continuing medical education. Acad Med.2012;87:582–585.
Dressler DD, Pistoria MJ, Budnitz TL, McKean SC, Amin AN. Core competencies in hospital medicine: development and methodology. J Hosp Med. 2006;1(suppl 1):148–156.
Beckman TJ, Lee MC. Proposal for a collaborative approach to clinical teaching. Mayo Clin Proc.2009;84:339–344.
Beckman TJ, Cook DA. Developing scholarly projects in education: a primer for medical teachers. Med Teach.2007;29:210–218.
Mansouri M, Lockyer J. A meta‐analysis of continuing medical education effectiveness. J Contin Educ Health Prof.2007;27:6–15.
Moore DE, Green JS, Gallis HA. Achieving desired results and improved outcomes: integrating planning and assessment throughout learning activities. J Contin Educ Health Prof.2009;29:1–15.
Cervero RM, Gaines JK. Effectiveness of continuing medical education: updated synthesis of systematic reviews. Available at: http://www.accme.org/sites/default/files/652_20141104_Effectiveness_of_Continuing_Medical_Education_Cervero_and_Gaines.pdf. Accessed March 25, 2015.
Wittich CM, Mauck KF, Mandrekar JN, et al. Improving participant feedback to continuing medical education presenters in internal medicine: a mixed‐methods study. J Gen Intern Med.2012;27:425–431.
Wittich CM, Szostek JH, Reed DA, et al. Measuring faculty reflection on medical grand rounds at Mayo Clinic: associations with teaching experience, clinical exposure, and presenter effectiveness. Mayo Clin Proc.2013;88:277–284.
Copeland HL, Longworth DL, Hewson MG, Stoller JK. Successful lecturing: a prospective study to validate attributes of the effective medical lecture. J Gen Intern Med.2000;15:366–371.
Shewchuk RM, Schmidt HJ, Benarous A, Bennett NL, Abdolrasulnia M, Casebeer LL. A standardized approach to assessing physician expectations and perceptions of continuing medical education. J Contin Educ Health Prof.2007;27:173–182.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York, NY: Academic Press; 1977.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed.Hillsdale, NJ: Erlbaum; 1988.
Lindenauer PK, Pantilat SZ, Katz PP, Wachter RM. Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians. Ann Intern Med.1999;130:343–349.
Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med.2012;27:28–36.
Kartha A, Restuccia JD, Burgess JF, et al. Nurse practitioner and physician assistant scope of practice in 118 acute care hospitals. J Hosp Med.2014;9:615–620.
Cain J, Robinson E. A primer on audience response systems: current applications and future considerations. Am J Pharm Educ.2008;72:77.
Davis N, Davis D, Bloch R. Continuing medical education: AMEE education guide no 35. Med Teach.2008;30:652–666.
Caldwell JE. Clickers in the large classroom: current research and best‐practice tips. CBE Life Sci Educ.2007;6:9–20.
Miller RG, Ashar BH, Getz KJ. Evaluation of an audience response system for the continuing education of health professionals. J Contin Educ Health Prof.2003;23:109–115.
Sehgal NL, Wachter RM, Vidyarthi AR. Bringing continuing medical education to the bedside: the University of California, San Francisco Hospitalist Mini‐College. J Hosp Med.2014;9:129–134.
Society of Hospital Medicine. 2014 State of Hospital Medicine Report. Philadelphia, PA: Society of Hospital Medicine; 2014.
Reed DA, Cook DA, Beckman TJ, Levine RB, Kern DE, Wright SM. Association between funding and quality of published medical education research. JAMA.2007;298:1002–1009.
Shea JA. Mind the gap: some reasons why medical education research is different from health services research. Med Educ.2001;35:319–320.
Cook DA, Beckman TJ. Reflections on experimental research in medical education. Adv Health Sci Educ Theory Pract.2010;15:455–464.
References
Society of Hospital Medicine. 2013/2014 press kit. Available at: http://www.hospitalmedicine.org/Web/Media_Center/Web/Media_Center/Media_Center.aspx?hkey=e26ceba7-ba93-4e50-8eb1-1ccc75d6f0fd. Accessed May 18, 2015.
Kleinpell RM, Hanson NA, Buchner BR, Winters R, Wilson MJ, Keck AC. Hospitalist services: an evolving opportunity. Nurse Pract.2008;33:9–10.
Wall S, Scudamore D, Chin J, et al. The evolving role of the pediatric nurse practitioner in hospital medicine. J Hosp Med.2014;9:261–265.
Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med.1996;335:514–517.
Society of Hospital Medicine. Definition of a hospitalist and hospital medicine. Available at: http://www.hospitalmedicine.org/Web/About_SHM/Hospitalist_Definition/Web/About_SHM/Industry/Hospital_Medicine_Hospital_Definition.aspx. Accessed February 16, 2015.
Accreditation Council for Continuing Medical Education. 2013 annual report data executive summary. Available at: http://www.accme.org/sites/default/files/630_2013_Annual_Report_20140715_0.pdf. Accessed February 16, 2015.
Muroff LR. The anatomy of an outstanding CME meeting. J Am Coll Radiol.2005;2:534–540.
McKean SC, Budnitz TL, Dressler DD, Amin AN, Pistoria MJ. How to use The Core Competencies in Hospital Medicine: a framework for curriculum development. J Hosp Med.2006;1:57–67.
Wittich CM, Chutka DS, Mauck KF, Berger RA, Litin SC, Beckman TJ. Perspective: a practical approach to defining professional practice gaps for continuing medical education. Acad Med.2012;87:582–585.
Dressler DD, Pistoria MJ, Budnitz TL, McKean SC, Amin AN. Core competencies in hospital medicine: development and methodology. J Hosp Med. 2006;1(suppl 1):148–156.
Beckman TJ, Lee MC. Proposal for a collaborative approach to clinical teaching. Mayo Clin Proc.2009;84:339–344.
Beckman TJ, Cook DA. Developing scholarly projects in education: a primer for medical teachers. Med Teach.2007;29:210–218.
Mansouri M, Lockyer J. A meta‐analysis of continuing medical education effectiveness. J Contin Educ Health Prof.2007;27:6–15.
Moore DE, Green JS, Gallis HA. Achieving desired results and improved outcomes: integrating planning and assessment throughout learning activities. J Contin Educ Health Prof.2009;29:1–15.
Cervero RM, Gaines JK. Effectiveness of continuing medical education: updated synthesis of systematic reviews. Available at: http://www.accme.org/sites/default/files/652_20141104_Effectiveness_of_Continuing_Medical_Education_Cervero_and_Gaines.pdf. Accessed March 25, 2015.
Wittich CM, Mauck KF, Mandrekar JN, et al. Improving participant feedback to continuing medical education presenters in internal medicine: a mixed‐methods study. J Gen Intern Med.2012;27:425–431.
Wittich CM, Szostek JH, Reed DA, et al. Measuring faculty reflection on medical grand rounds at Mayo Clinic: associations with teaching experience, clinical exposure, and presenter effectiveness. Mayo Clin Proc.2013;88:277–284.
Copeland HL, Longworth DL, Hewson MG, Stoller JK. Successful lecturing: a prospective study to validate attributes of the effective medical lecture. J Gen Intern Med.2000;15:366–371.
Shewchuk RM, Schmidt HJ, Benarous A, Bennett NL, Abdolrasulnia M, Casebeer LL. A standardized approach to assessing physician expectations and perceptions of continuing medical education. J Contin Educ Health Prof.2007;27:173–182.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York, NY: Academic Press; 1977.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed.Hillsdale, NJ: Erlbaum; 1988.
Lindenauer PK, Pantilat SZ, Katz PP, Wachter RM. Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians. Ann Intern Med.1999;130:343–349.
Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med.2012;27:28–36.
Kartha A, Restuccia JD, Burgess JF, et al. Nurse practitioner and physician assistant scope of practice in 118 acute care hospitals. J Hosp Med.2014;9:615–620.
Cain J, Robinson E. A primer on audience response systems: current applications and future considerations. Am J Pharm Educ.2008;72:77.
Davis N, Davis D, Bloch R. Continuing medical education: AMEE education guide no 35. Med Teach.2008;30:652–666.
Caldwell JE. Clickers in the large classroom: current research and best‐practice tips. CBE Life Sci Educ.2007;6:9–20.
Miller RG, Ashar BH, Getz KJ. Evaluation of an audience response system for the continuing education of health professionals. J Contin Educ Health Prof.2003;23:109–115.
Sehgal NL, Wachter RM, Vidyarthi AR. Bringing continuing medical education to the bedside: the University of California, San Francisco Hospitalist Mini‐College. J Hosp Med.2014;9:129–134.
Society of Hospital Medicine. 2014 State of Hospital Medicine Report. Philadelphia, PA: Society of Hospital Medicine; 2014.
Reed DA, Cook DA, Beckman TJ, Levine RB, Kern DE, Wright SM. Association between funding and quality of published medical education research. JAMA.2007;298:1002–1009.
Shea JA. Mind the gap: some reasons why medical education research is different from health services research. Med Educ.2001;35:319–320.
Cook DA, Beckman TJ. Reflections on experimental research in medical education. Adv Health Sci Educ Theory Pract.2010;15:455–464.
Address for correspondence and reprint requests: John T. Ratelle, MD, Mayo Clinic Rochester, 200 First Street SW, Rochester, MN 55905; Telephone: 507‐284‐3589; Fax: 507‐255‐9189; E‐mail: ratelle.john@mayo.edu