User login
Subclinical Enthesitis Is More Common in Psoriatic Arthritis
VICTORIA, B.C. – Subclinical enthesitis occurs more commonly in patients with psoriatic arthritis than in those with psoriasis, possibly as a result of age and obesity rather than disease severity, to judge from the findings of a cross-sectional study conducted by investigators at Toronto Western Hospital.
The investigators used ultrasound as well as clinical examination to assess the extent, if any, of enthesitis in study participants, who were 59 patients with psoriatic arthritis and 79 patients with psoriasis. Study participants were recruited from longitudinal cohorts. The control group was made up of 60 healthy volunteers who did not have any personal or family history of spondyloarthropathy. They were evaluated for enthesitis at sites in the calcaneus, knee, and olecranon.

Findings on ultrasound – any enthesophytes, bony erosions, tendon thickness, and bursitis, within tendons – were scored using GUESS (Glasgow Ultrasound Enthesitis Scoring System), which reflects the overall burden bilaterally of enthesitis from abnormalities in five lower limb sites, and the MASEI (Madrid Sonography Enthesitis Index), which additionally includes calcifications and Doppler signals as elemental lesions as well as abnormalities of the olecranon tuberosity enthesis.
The average ages were 52, 53, and 42 years in the psoriasis, psoriatic arthritis, and healthy volunteer groups, respectively, and men accounted for 64%, 57%, and 32% of participants. Corresponding mean body mass indices were 27, 30, and 26 kg/m2, respectively.
In all, 12 anatomical sites were assessed. The mean number showing ultrasonographic enthesitis differed significantly across groups, reported study coauthor Jai P. Jayakar at the annual meeting of the Canadian Rheumatology Association. The number of anatomical sites that showed enthesitis was highest in the psoriatic arthritis group (7.1), intermediate in the psoriasis group (5), and lowest in healthy volunteers (4).
There was also a significant, graded difference across groups in GUESS scores (8.9, 5.6, and 4.4 out of a possible 36, respectively, for psoriatic arthritis, psoriasis, and healthy controls) and in MASEI scores (18.5, 9.9, and 7.7 respectively for psoriatic arthritis, psoriasis, and healthy controls out of a possible 136). However, in multivariate analyses, disease status was not associated with these scores; only increasing age and BMI showed significant associations.
"Our study is one of the first comparative assessments of subclinical enthesitis in psoriasis vs. psoriatic arthritis," noted Mr. Jayakar. "Our results reveal that the prevalence of ultrasonographic entheseal abnormalities and indices of entheseal burden ... are greater in psoriatic arthritis than in psoriasis; however, this relationship may be modulated in a multifactorial manner by factors other than disease status, such as age and body mass index.
"Now, it is possible that enthesitis could be of predictive value in specific patient subgroups – for example, age- or obesity-stratified subgroups," he added. "However, larger studies are needed to confirm the utility of subclinical enthesitis as a predictive factor for the development of psoriatic arthritis in patients with psoriasis."
How could the investigators be certain, a session attendee asked, that they were detecting disease-related enthesitis and not simply mechanical tendonitis?
That is a valid concern, given the lack of consensus among rheumatologists as to which ultrasonographic abnormalities result from degeneration, inflammation, mechanical stress, or other etiologies, acknowledged Mr. Jayakar, a medical student at the University of Western Ontario, London. Large cohorts with well-defined disease status would be required to investigate this further, he said.
"One direction in which we could move forward is if we can find specific elemental lesions – or aggregates of elemental lesions – that are of predictive value, then perhaps those could be used pragmatically to help us in our clinical management," he noted. "But as of now, the pathophysiological underpinnings of these abnormalities are not very well described."
Mr. Jayakar disclosed no relevant conflicts of interest.
VICTORIA, B.C. – Subclinical enthesitis occurs more commonly in patients with psoriatic arthritis than in those with psoriasis, possibly as a result of age and obesity rather than disease severity, to judge from the findings of a cross-sectional study conducted by investigators at Toronto Western Hospital.
The investigators used ultrasound as well as clinical examination to assess the extent, if any, of enthesitis in study participants, who were 59 patients with psoriatic arthritis and 79 patients with psoriasis. Study participants were recruited from longitudinal cohorts. The control group was made up of 60 healthy volunteers who did not have any personal or family history of spondyloarthropathy. They were evaluated for enthesitis at sites in the calcaneus, knee, and olecranon.
Findings on ultrasound – any enthesophytes, bony erosions, tendon thickness, and bursitis, within tendons – were scored using GUESS (Glasgow Ultrasound Enthesitis Scoring System), which reflects the overall burden bilaterally of enthesitis from abnormalities in five lower limb sites, and the MASEI (Madrid Sonography Enthesitis Index), which additionally includes calcifications and Doppler signals as elemental lesions as well as abnormalities of the olecranon tuberosity enthesis.
The average ages were 52, 53, and 42 years in the psoriasis, psoriatic arthritis, and healthy volunteer groups, respectively, and men accounted for 64%, 57%, and 32% of participants. Corresponding mean body mass indices were 27, 30, and 26 kg/m2, respectively.
In all, 12 anatomical sites were assessed. The mean number showing ultrasonographic enthesitis differed significantly across groups, reported study coauthor Jai P. Jayakar at the annual meeting of the Canadian Rheumatology Association. The number of anatomical sites that showed enthesitis was highest in the psoriatic arthritis group (7.1), intermediate in the psoriasis group (5), and lowest in healthy volunteers (4).
There was also a significant, graded difference across groups in GUESS scores (8.9, 5.6, and 4.4 out of a possible 36, respectively, for psoriatic arthritis, psoriasis, and healthy controls) and in MASEI scores (18.5, 9.9, and 7.7 respectively for psoriatic arthritis, psoriasis, and healthy controls out of a possible 136). However, in multivariate analyses, disease status was not associated with these scores; only increasing age and BMI showed significant associations.
"Our study is one of the first comparative assessments of subclinical enthesitis in psoriasis vs. psoriatic arthritis," noted Mr. Jayakar. "Our results reveal that the prevalence of ultrasonographic entheseal abnormalities and indices of entheseal burden ... are greater in psoriatic arthritis than in psoriasis; however, this relationship may be modulated in a multifactorial manner by factors other than disease status, such as age and body mass index.
"Now, it is possible that enthesitis could be of predictive value in specific patient subgroups – for example, age- or obesity-stratified subgroups," he added. "However, larger studies are needed to confirm the utility of subclinical enthesitis as a predictive factor for the development of psoriatic arthritis in patients with psoriasis."
How could the investigators be certain, a session attendee asked, that they were detecting disease-related enthesitis and not simply mechanical tendonitis?
That is a valid concern, given the lack of consensus among rheumatologists as to which ultrasonographic abnormalities result from degeneration, inflammation, mechanical stress, or other etiologies, acknowledged Mr. Jayakar, a medical student at the University of Western Ontario, London. Large cohorts with well-defined disease status would be required to investigate this further, he said.
"One direction in which we could move forward is if we can find specific elemental lesions – or aggregates of elemental lesions – that are of predictive value, then perhaps those could be used pragmatically to help us in our clinical management," he noted. "But as of now, the pathophysiological underpinnings of these abnormalities are not very well described."
Mr. Jayakar disclosed no relevant conflicts of interest.
VICTORIA, B.C. – Subclinical enthesitis occurs more commonly in patients with psoriatic arthritis than in those with psoriasis, possibly as a result of age and obesity rather than disease severity, to judge from the findings of a cross-sectional study conducted by investigators at Toronto Western Hospital.
The investigators used ultrasound as well as clinical examination to assess the extent, if any, of enthesitis in study participants, who were 59 patients with psoriatic arthritis and 79 patients with psoriasis. Study participants were recruited from longitudinal cohorts. The control group was made up of 60 healthy volunteers who did not have any personal or family history of spondyloarthropathy. They were evaluated for enthesitis at sites in the calcaneus, knee, and olecranon.
Findings on ultrasound – any enthesophytes, bony erosions, tendon thickness, and bursitis, within tendons – were scored using GUESS (Glasgow Ultrasound Enthesitis Scoring System), which reflects the overall burden bilaterally of enthesitis from abnormalities in five lower limb sites, and the MASEI (Madrid Sonography Enthesitis Index), which additionally includes calcifications and Doppler signals as elemental lesions as well as abnormalities of the olecranon tuberosity enthesis.
The average ages were 52, 53, and 42 years in the psoriasis, psoriatic arthritis, and healthy volunteer groups, respectively, and men accounted for 64%, 57%, and 32% of participants. Corresponding mean body mass indices were 27, 30, and 26 kg/m2, respectively.
In all, 12 anatomical sites were assessed. The mean number showing ultrasonographic enthesitis differed significantly across groups, reported study coauthor Jai P. Jayakar at the annual meeting of the Canadian Rheumatology Association. The number of anatomical sites that showed enthesitis was highest in the psoriatic arthritis group (7.1), intermediate in the psoriasis group (5), and lowest in healthy volunteers (4).
There was also a significant, graded difference across groups in GUESS scores (8.9, 5.6, and 4.4 out of a possible 36, respectively, for psoriatic arthritis, psoriasis, and healthy controls) and in MASEI scores (18.5, 9.9, and 7.7 respectively for psoriatic arthritis, psoriasis, and healthy controls out of a possible 136). However, in multivariate analyses, disease status was not associated with these scores; only increasing age and BMI showed significant associations.
"Our study is one of the first comparative assessments of subclinical enthesitis in psoriasis vs. psoriatic arthritis," noted Mr. Jayakar. "Our results reveal that the prevalence of ultrasonographic entheseal abnormalities and indices of entheseal burden ... are greater in psoriatic arthritis than in psoriasis; however, this relationship may be modulated in a multifactorial manner by factors other than disease status, such as age and body mass index.
"Now, it is possible that enthesitis could be of predictive value in specific patient subgroups – for example, age- or obesity-stratified subgroups," he added. "However, larger studies are needed to confirm the utility of subclinical enthesitis as a predictive factor for the development of psoriatic arthritis in patients with psoriasis."
How could the investigators be certain, a session attendee asked, that they were detecting disease-related enthesitis and not simply mechanical tendonitis?
That is a valid concern, given the lack of consensus among rheumatologists as to which ultrasonographic abnormalities result from degeneration, inflammation, mechanical stress, or other etiologies, acknowledged Mr. Jayakar, a medical student at the University of Western Ontario, London. Large cohorts with well-defined disease status would be required to investigate this further, he said.
"One direction in which we could move forward is if we can find specific elemental lesions – or aggregates of elemental lesions – that are of predictive value, then perhaps those could be used pragmatically to help us in our clinical management," he noted. "But as of now, the pathophysiological underpinnings of these abnormalities are not very well described."
Mr. Jayakar disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING OF THE CANADIAN RHEUMATOLOGY ASSOCIATION
Major Finding: Patients with psoriatic arthritis had subclinical enthesitis at seven anatomical sites, compared with five for patients with psoriasis and four for healthy controls.
Data Source: Data come from a cross-sectional study of 79 patients with psoriasis, 59 patients with psoriatic arthritis, and 60 healthy volunteers.
Disclosures: Mr. Jayakar disclosed no relevant conflicts of interest.
Medical Food, Supplement Appear Helpful for Dementias
VANCOUVER, B.C. – Medical foods and supplements designed to support neural health and function may soon expand treatment options for common forms of dementia based on the results of two studies.
One study found that a cocktail of compounds designed to support synapse formation and function improved memory in patients with mild Alzheimer’s disease. The other found that oral citicoline, a substrate for acetylcholine synthesis that inhibits neurodegeneration, yielded better memory than no treatment in patients with mild cognitive impairment (MCI) due to vascular causes.

The findings may signal the start of an era in which Alzheimer’s disease and other dementias are managed with a multimodality approach involving a variety of pharmacologic and nonpharmacologic strategies, according to Maria Carrillo, Ph.D., senior director of medical and scientific relations for the Alzheimer’s Association. "We need to continue to be open to different therapeutic avenues and approaches," she commented while moderating a press briefing at the Alzheimer’s Association International Conference 2012, where the data were first presented.
Souvenaid for Mild Alzheimer’s Disease

In the first trial, known as Souvenir II, researchers led by Dr. Philip Scheltens of the VU University Medical Center in Amsterdam studied 259 patients from multiple centers in Europe who had mild Alzheimer’s disease, with a Mini-Mental State Examination (MMSE) score of 25 or greater.
Patients were randomized evenly to receive Souvenaid (125 mL orally once a day) or a control drink for the first 24 weeks. Souvenaid contains a special formulation of omega-3 and -6 fatty acids, choline, phospholipids, B vitamins, and antioxidants designed to promote the formation and function of synapses, he explained.
"Synapse dysfunction is ... critical to causing symptoms in Alzheimer’s disease. It’s not the amyloid load that causes memory problems – it’s the loss of synapses and the loss of neurons that do so," he noted. In a subsequent 24-week extension period, all patients received Souvenaid.
Rates of serious adverse events did not differ between groups, and there were no new safety signals during the extension period, Dr. Scheltens reported.
Compliance was uniformly high in both groups during both periods, ranging from 93% to 97%. "People really liked [Souvenaid] and stayed on the product the whole time," he said. "There are two flavors: strawberry and vanilla. It’s like a drinkable yogurt. ... It tastes very, very good, and that’s why the compliance was so high. Although the amount of fish oil in it is equivalent to three or four herrings, you would be surprised that it doesn’t smell at all like fish or taste like fish."
At 24 weeks, patients in the Souvenaid group had a significantly greater improvement from baseline in z scores for the Neuropsychological Test Battery memory domain (P = .023) and marginally better total composite scores (P = .053), as recently published (J. Alzheimers Dis. 2012;31:225-36).
In additional results, there was a significant improvement between 24 and 48 weeks in the z score for the memory domain of the Neuropsychological Test Battery among both patients who started and continued on Souvenaid (P = .025) and patients who started on the control drink and switched to Souvenaid (P = .009).
"The memory actually even improved further; there was no ceiling effect on memory," Dr. Scheltens commented. "So the mild patients could even improve further."
The effect size in the study was 0.21, "exactly on the order of the cholinesterase inhibitors," he pointed out. "But the risk-benefit ratio is much better, because there are no side effects and people can take it as long as they want."
"We think this may offer a new approach, a dietary management approach, if you like, in people with very early Alzheimer’s disease," Dr. Scheltens concluded. "We are continuing the [research] program because we think it is worthwhile to pursue this in a rigorous, scientifically oriented way. The targeted patient population will be the mild to very mild Alzheimer’s disease patients."
He said it’s unlikely that combining individual dietary supplements could achieve the benefit seen with Souvenaid. Studies of various individual components have shown "they basically don’t work. Only the particular combination of all these nutrients is needed and is necessary to build up the membrane of the synapse. So it’s just not something you can do at home – throw a little bit of this, a little bit of that in a tube. It is the specific combination and the ratio between the [components of the] combination that actually works."
Assuming Souvenaid makes it to the market, it will be classified as a medical food. "That means it has to be prescribed by a doctor and it needs to be delivered by a pharmacist. It is not over the counter," Dr. Scheltens noted. He expects that the product will first be launched in Europe, as the manufacturer is located there.
Citicoline for Vascular MCI
In the second trial, known as IDEALE, Dr. Pietro Gareri, a geriatrician with the Ambulatory Center for Dementia in Catanzaro, Italy, and his colleagues enrolled 349 patients in Italy at least 65 years of age who had evidence of vascular lesions on neuroradiologic imaging, and either an MMSE score of at least 21 or subjective memory complaints. (Those with probable Alzheimer’s disease were excluded.)
The patients were assigned in a 3:1 ratio to open-label treatment with citicoline (500 mg twice a day) or a control condition (no treatment).
"Citicoline has a number of different properties," Dr. Gareri explained. "For example, it inhibits apoptosis associated with cerebral ischemia. And it’s able to inhibit several models of neurodegeneration. It’s able to potentiate neuroplasticity. And it is a natural precursor of phospholipid synthesis."
Trial results showed a nonsignificant increase in MMSE scores over 6 months in the citicoline group (from 22.4 to 22.9), compared with a decrease in scores in the control group (from 21.5 to 19.6). Scores differed significantly between groups at 3 months and at 6 months.
Both groups had improvements in functional dependence, as assessed from activities of daily living and instrumental activities of daily living, with no significant between-group difference.
There was a trend toward better Geriatric Depression Scale scores with citicoline (P = .06). "This was not a surprise, because citicoline increases noradrenaline and dopamine levels in the central nervous system," Dr. Gareri commented. None of the patients experienced adverse events.
"Definitively, this study shows that citicoline is effective and safe. Therefore it can be recommended in vascular mild cognitive impairment," he concluded.
Neither Dr. Scheltens nor Dr. Gareri disclosed any relevant conflicts of interest.
VANCOUVER, B.C. – Medical foods and supplements designed to support neural health and function may soon expand treatment options for common forms of dementia based on the results of two studies.
One study found that a cocktail of compounds designed to support synapse formation and function improved memory in patients with mild Alzheimer’s disease. The other found that oral citicoline, a substrate for acetylcholine synthesis that inhibits neurodegeneration, yielded better memory than no treatment in patients with mild cognitive impairment (MCI) due to vascular causes.
The findings may signal the start of an era in which Alzheimer’s disease and other dementias are managed with a multimodality approach involving a variety of pharmacologic and nonpharmacologic strategies, according to Maria Carrillo, Ph.D., senior director of medical and scientific relations for the Alzheimer’s Association. "We need to continue to be open to different therapeutic avenues and approaches," she commented while moderating a press briefing at the Alzheimer’s Association International Conference 2012, where the data were first presented.
Souvenaid for Mild Alzheimer’s Disease
In the first trial, known as Souvenir II, researchers led by Dr. Philip Scheltens of the VU University Medical Center in Amsterdam studied 259 patients from multiple centers in Europe who had mild Alzheimer’s disease, with a Mini-Mental State Examination (MMSE) score of 25 or greater.
Patients were randomized evenly to receive Souvenaid (125 mL orally once a day) or a control drink for the first 24 weeks. Souvenaid contains a special formulation of omega-3 and -6 fatty acids, choline, phospholipids, B vitamins, and antioxidants designed to promote the formation and function of synapses, he explained.
"Synapse dysfunction is ... critical to causing symptoms in Alzheimer’s disease. It’s not the amyloid load that causes memory problems – it’s the loss of synapses and the loss of neurons that do so," he noted. In a subsequent 24-week extension period, all patients received Souvenaid.
Rates of serious adverse events did not differ between groups, and there were no new safety signals during the extension period, Dr. Scheltens reported.
Compliance was uniformly high in both groups during both periods, ranging from 93% to 97%. "People really liked [Souvenaid] and stayed on the product the whole time," he said. "There are two flavors: strawberry and vanilla. It’s like a drinkable yogurt. ... It tastes very, very good, and that’s why the compliance was so high. Although the amount of fish oil in it is equivalent to three or four herrings, you would be surprised that it doesn’t smell at all like fish or taste like fish."
At 24 weeks, patients in the Souvenaid group had a significantly greater improvement from baseline in z scores for the Neuropsychological Test Battery memory domain (P = .023) and marginally better total composite scores (P = .053), as recently published (J. Alzheimers Dis. 2012;31:225-36).
In additional results, there was a significant improvement between 24 and 48 weeks in the z score for the memory domain of the Neuropsychological Test Battery among both patients who started and continued on Souvenaid (P = .025) and patients who started on the control drink and switched to Souvenaid (P = .009).
"The memory actually even improved further; there was no ceiling effect on memory," Dr. Scheltens commented. "So the mild patients could even improve further."
The effect size in the study was 0.21, "exactly on the order of the cholinesterase inhibitors," he pointed out. "But the risk-benefit ratio is much better, because there are no side effects and people can take it as long as they want."
"We think this may offer a new approach, a dietary management approach, if you like, in people with very early Alzheimer’s disease," Dr. Scheltens concluded. "We are continuing the [research] program because we think it is worthwhile to pursue this in a rigorous, scientifically oriented way. The targeted patient population will be the mild to very mild Alzheimer’s disease patients."
He said it’s unlikely that combining individual dietary supplements could achieve the benefit seen with Souvenaid. Studies of various individual components have shown "they basically don’t work. Only the particular combination of all these nutrients is needed and is necessary to build up the membrane of the synapse. So it’s just not something you can do at home – throw a little bit of this, a little bit of that in a tube. It is the specific combination and the ratio between the [components of the] combination that actually works."
Assuming Souvenaid makes it to the market, it will be classified as a medical food. "That means it has to be prescribed by a doctor and it needs to be delivered by a pharmacist. It is not over the counter," Dr. Scheltens noted. He expects that the product will first be launched in Europe, as the manufacturer is located there.
Citicoline for Vascular MCI
In the second trial, known as IDEALE, Dr. Pietro Gareri, a geriatrician with the Ambulatory Center for Dementia in Catanzaro, Italy, and his colleagues enrolled 349 patients in Italy at least 65 years of age who had evidence of vascular lesions on neuroradiologic imaging, and either an MMSE score of at least 21 or subjective memory complaints. (Those with probable Alzheimer’s disease were excluded.)
The patients were assigned in a 3:1 ratio to open-label treatment with citicoline (500 mg twice a day) or a control condition (no treatment).
"Citicoline has a number of different properties," Dr. Gareri explained. "For example, it inhibits apoptosis associated with cerebral ischemia. And it’s able to inhibit several models of neurodegeneration. It’s able to potentiate neuroplasticity. And it is a natural precursor of phospholipid synthesis."
Trial results showed a nonsignificant increase in MMSE scores over 6 months in the citicoline group (from 22.4 to 22.9), compared with a decrease in scores in the control group (from 21.5 to 19.6). Scores differed significantly between groups at 3 months and at 6 months.
Both groups had improvements in functional dependence, as assessed from activities of daily living and instrumental activities of daily living, with no significant between-group difference.
There was a trend toward better Geriatric Depression Scale scores with citicoline (P = .06). "This was not a surprise, because citicoline increases noradrenaline and dopamine levels in the central nervous system," Dr. Gareri commented. None of the patients experienced adverse events.
"Definitively, this study shows that citicoline is effective and safe. Therefore it can be recommended in vascular mild cognitive impairment," he concluded.
Neither Dr. Scheltens nor Dr. Gareri disclosed any relevant conflicts of interest.
VANCOUVER, B.C. – Medical foods and supplements designed to support neural health and function may soon expand treatment options for common forms of dementia based on the results of two studies.
One study found that a cocktail of compounds designed to support synapse formation and function improved memory in patients with mild Alzheimer’s disease. The other found that oral citicoline, a substrate for acetylcholine synthesis that inhibits neurodegeneration, yielded better memory than no treatment in patients with mild cognitive impairment (MCI) due to vascular causes.
The findings may signal the start of an era in which Alzheimer’s disease and other dementias are managed with a multimodality approach involving a variety of pharmacologic and nonpharmacologic strategies, according to Maria Carrillo, Ph.D., senior director of medical and scientific relations for the Alzheimer’s Association. "We need to continue to be open to different therapeutic avenues and approaches," she commented while moderating a press briefing at the Alzheimer’s Association International Conference 2012, where the data were first presented.
Souvenaid for Mild Alzheimer’s Disease
In the first trial, known as Souvenir II, researchers led by Dr. Philip Scheltens of the VU University Medical Center in Amsterdam studied 259 patients from multiple centers in Europe who had mild Alzheimer’s disease, with a Mini-Mental State Examination (MMSE) score of 25 or greater.
Patients were randomized evenly to receive Souvenaid (125 mL orally once a day) or a control drink for the first 24 weeks. Souvenaid contains a special formulation of omega-3 and -6 fatty acids, choline, phospholipids, B vitamins, and antioxidants designed to promote the formation and function of synapses, he explained.
"Synapse dysfunction is ... critical to causing symptoms in Alzheimer’s disease. It’s not the amyloid load that causes memory problems – it’s the loss of synapses and the loss of neurons that do so," he noted. In a subsequent 24-week extension period, all patients received Souvenaid.
Rates of serious adverse events did not differ between groups, and there were no new safety signals during the extension period, Dr. Scheltens reported.
Compliance was uniformly high in both groups during both periods, ranging from 93% to 97%. "People really liked [Souvenaid] and stayed on the product the whole time," he said. "There are two flavors: strawberry and vanilla. It’s like a drinkable yogurt. ... It tastes very, very good, and that’s why the compliance was so high. Although the amount of fish oil in it is equivalent to three or four herrings, you would be surprised that it doesn’t smell at all like fish or taste like fish."
At 24 weeks, patients in the Souvenaid group had a significantly greater improvement from baseline in z scores for the Neuropsychological Test Battery memory domain (P = .023) and marginally better total composite scores (P = .053), as recently published (J. Alzheimers Dis. 2012;31:225-36).
In additional results, there was a significant improvement between 24 and 48 weeks in the z score for the memory domain of the Neuropsychological Test Battery among both patients who started and continued on Souvenaid (P = .025) and patients who started on the control drink and switched to Souvenaid (P = .009).
"The memory actually even improved further; there was no ceiling effect on memory," Dr. Scheltens commented. "So the mild patients could even improve further."
The effect size in the study was 0.21, "exactly on the order of the cholinesterase inhibitors," he pointed out. "But the risk-benefit ratio is much better, because there are no side effects and people can take it as long as they want."
"We think this may offer a new approach, a dietary management approach, if you like, in people with very early Alzheimer’s disease," Dr. Scheltens concluded. "We are continuing the [research] program because we think it is worthwhile to pursue this in a rigorous, scientifically oriented way. The targeted patient population will be the mild to very mild Alzheimer’s disease patients."
He said it’s unlikely that combining individual dietary supplements could achieve the benefit seen with Souvenaid. Studies of various individual components have shown "they basically don’t work. Only the particular combination of all these nutrients is needed and is necessary to build up the membrane of the synapse. So it’s just not something you can do at home – throw a little bit of this, a little bit of that in a tube. It is the specific combination and the ratio between the [components of the] combination that actually works."
Assuming Souvenaid makes it to the market, it will be classified as a medical food. "That means it has to be prescribed by a doctor and it needs to be delivered by a pharmacist. It is not over the counter," Dr. Scheltens noted. He expects that the product will first be launched in Europe, as the manufacturer is located there.
Citicoline for Vascular MCI
In the second trial, known as IDEALE, Dr. Pietro Gareri, a geriatrician with the Ambulatory Center for Dementia in Catanzaro, Italy, and his colleagues enrolled 349 patients in Italy at least 65 years of age who had evidence of vascular lesions on neuroradiologic imaging, and either an MMSE score of at least 21 or subjective memory complaints. (Those with probable Alzheimer’s disease were excluded.)
The patients were assigned in a 3:1 ratio to open-label treatment with citicoline (500 mg twice a day) or a control condition (no treatment).
"Citicoline has a number of different properties," Dr. Gareri explained. "For example, it inhibits apoptosis associated with cerebral ischemia. And it’s able to inhibit several models of neurodegeneration. It’s able to potentiate neuroplasticity. And it is a natural precursor of phospholipid synthesis."
Trial results showed a nonsignificant increase in MMSE scores over 6 months in the citicoline group (from 22.4 to 22.9), compared with a decrease in scores in the control group (from 21.5 to 19.6). Scores differed significantly between groups at 3 months and at 6 months.
Both groups had improvements in functional dependence, as assessed from activities of daily living and instrumental activities of daily living, with no significant between-group difference.
There was a trend toward better Geriatric Depression Scale scores with citicoline (P = .06). "This was not a surprise, because citicoline increases noradrenaline and dopamine levels in the central nervous system," Dr. Gareri commented. None of the patients experienced adverse events.
"Definitively, this study shows that citicoline is effective and safe. Therefore it can be recommended in vascular mild cognitive impairment," he concluded.
Neither Dr. Scheltens nor Dr. Gareri disclosed any relevant conflicts of interest.
AT THE ALZHEIMER'S ASSOCIATION INTERNATIONAL CONFERENCE 2012

Erlotinib Fails as Maintenance Therapy for Ovarian Cancer
CHICAGO – Maintenance erlotinib was no more efficacious than observation when given to women with ovarian or related cancers who had no evidence of progression after receiving first-line platinum-based chemotherapy.
The 835 women studied in a randomized, phase III trial had a median progression-free survival of about 1 year and an overall survival median of about 4.5 years regardless of whether they were assigned to erlotinib – an oral inhibitor of the EGFR (epidermal growth factor receptor) tyrosine kinase – or simple observation.
The findings were similar in patient subgroups who were stratified according to a wide range of factors, such as stage and (in preliminary analyses) tumor EGFR positivity, investigators reported at the annual meeting of the American Society of Clinical Oncology.
"Maintenance erlotinib after first-line chemotherapy in patients with ovarian, peritoneal, or fallopian tube cancer did not increase progression-free survival nor overall survival," said lead investigator Dr. Ignace B. Vergote. Moreover, a quarter of patients stopped the drug early because of adverse effects.
"At this moment, we cannot identify a subgroup that might benefit from erlotinib maintenance therapy after first-line chemotherapy for ovarian cancer, but we are continuing to look at immunohistochemistry and FISH [fluorescence in situ hybridization] analysis," added Dr. Vergote, chairman of the Leuven (Belgium) Cancer Institute and head of the department of obstetrics and gynecology and gynecologic oncology at the Catholic University of Leuven.
Discussant Dr. Michael V. Seiden of the Fox Chase Cancer Center in Philadelphia noted that there was "a compelling body of basic and preclinical evidence that made the advent or launch of this study very logical." For example, research had shown a correlation between high tumor EGFR levels and poor prognosis in ovarian cancer, as well as an association– in various cancers – of EGFR mutations or expression with response to therapies targeting this receptor.
"Unfortunately, the addition of erlotinib as part of a maintenance schedule did not budge progression-free survival or overall survival," he said. "Perhaps now, in 2012, with the value of ... hindsight, one might have made this prediction, in that there have been now numerous negative single-arm studies or nearly negative single-arm studies with both small-molecule inhibitors and monoclonal antibodies" against EGFR.
Women enrolled in the EORTC (European Organisation for Research and Treatment of Cancer) 55041 trial – a joint effort of six cooperative groups – had high-risk stage I, or stages II to IV epithelial ovarian, primary peritoneal, or fallopian tube cancer and at least stable disease as of the end of first-line platinum-based chemotherapy.
They were assigned to either erlotinib (Tarceva) 150 mg daily for 2 years or observation. Erlotinib is currently approved by the Food and Drug Administration for the treatment of non–small cell lung cancer and pancreatic cancer.
Demographic and clinical data showed that about 62% of patients had serous tumor histology. Nearly all (96%) had received carboplatin and paclitaxel as their first-line therapy. Roughly 70% had had primary debulking surgery, whereas 30% had received neoadjuvant therapy and interval debulking surgery; there was no evidence of disease at surgery in 48% of the former and 62% of the latter.
Overall, 25% of patients in the erlotinib group stopped therapy early because of unacceptable adverse events (mainly rash), Dr. Vergote reported.
Main results showed that with a median follow-up of 4.3 years, erlotinib and observation were statistically indistinguishable in terms of median progression-free survival (12.7 vs. 12.4 months), with progression defined according to RECIST criteria or CA (cancer antigen) 125 levels, and overall survival (51 vs. 59 months). The findings were similar in subgroups stratified by stage, age, performance status, and response at the end of first-line chemotherapy.
Patients in the erlotinib group were more likely to experience grade 3/4 diarrhea (5% vs. 1%) and rash (13% vs. 0%).
Preliminary tumor mutational analysis in 318 patients showed that the most common was PI3KCA mutation (present in about 4% of cases), followed by KRAS mutation (present in about 3%). Only about 1% had an EGFR mutation, and mutations of NRAS and BRAF were similarly uncommon.
Progression-free survival was better for patients having any of these mutations than for those having none (P = .04). But among the former, there was no significant benefit of erlotinib over observation.
Progression-free survival was also similar across subgroups of patients whose tumors were EGFR positive and negative according to either immunohistochemistry or FISH.
Analyses failed to identify any significant relationship between the development of rash during erlotinib therapy and progression-free survival. The investigators plan to analyze quality of life data.
Dr. Vergote disclosed no relevant conflicts of interest. Dr. Seiden disclosed no relevant conflicts of interest.
CHICAGO – Maintenance erlotinib was no more efficacious than observation when given to women with ovarian or related cancers who had no evidence of progression after receiving first-line platinum-based chemotherapy.
The 835 women studied in a randomized, phase III trial had a median progression-free survival of about 1 year and an overall survival median of about 4.5 years regardless of whether they were assigned to erlotinib – an oral inhibitor of the EGFR (epidermal growth factor receptor) tyrosine kinase – or simple observation.
The findings were similar in patient subgroups who were stratified according to a wide range of factors, such as stage and (in preliminary analyses) tumor EGFR positivity, investigators reported at the annual meeting of the American Society of Clinical Oncology.
"Maintenance erlotinib after first-line chemotherapy in patients with ovarian, peritoneal, or fallopian tube cancer did not increase progression-free survival nor overall survival," said lead investigator Dr. Ignace B. Vergote. Moreover, a quarter of patients stopped the drug early because of adverse effects.
"At this moment, we cannot identify a subgroup that might benefit from erlotinib maintenance therapy after first-line chemotherapy for ovarian cancer, but we are continuing to look at immunohistochemistry and FISH [fluorescence in situ hybridization] analysis," added Dr. Vergote, chairman of the Leuven (Belgium) Cancer Institute and head of the department of obstetrics and gynecology and gynecologic oncology at the Catholic University of Leuven.
Discussant Dr. Michael V. Seiden of the Fox Chase Cancer Center in Philadelphia noted that there was "a compelling body of basic and preclinical evidence that made the advent or launch of this study very logical." For example, research had shown a correlation between high tumor EGFR levels and poor prognosis in ovarian cancer, as well as an association– in various cancers – of EGFR mutations or expression with response to therapies targeting this receptor.
"Unfortunately, the addition of erlotinib as part of a maintenance schedule did not budge progression-free survival or overall survival," he said. "Perhaps now, in 2012, with the value of ... hindsight, one might have made this prediction, in that there have been now numerous negative single-arm studies or nearly negative single-arm studies with both small-molecule inhibitors and monoclonal antibodies" against EGFR.
Women enrolled in the EORTC (European Organisation for Research and Treatment of Cancer) 55041 trial – a joint effort of six cooperative groups – had high-risk stage I, or stages II to IV epithelial ovarian, primary peritoneal, or fallopian tube cancer and at least stable disease as of the end of first-line platinum-based chemotherapy.
They were assigned to either erlotinib (Tarceva) 150 mg daily for 2 years or observation. Erlotinib is currently approved by the Food and Drug Administration for the treatment of non–small cell lung cancer and pancreatic cancer.
Demographic and clinical data showed that about 62% of patients had serous tumor histology. Nearly all (96%) had received carboplatin and paclitaxel as their first-line therapy. Roughly 70% had had primary debulking surgery, whereas 30% had received neoadjuvant therapy and interval debulking surgery; there was no evidence of disease at surgery in 48% of the former and 62% of the latter.
Overall, 25% of patients in the erlotinib group stopped therapy early because of unacceptable adverse events (mainly rash), Dr. Vergote reported.
Main results showed that with a median follow-up of 4.3 years, erlotinib and observation were statistically indistinguishable in terms of median progression-free survival (12.7 vs. 12.4 months), with progression defined according to RECIST criteria or CA (cancer antigen) 125 levels, and overall survival (51 vs. 59 months). The findings were similar in subgroups stratified by stage, age, performance status, and response at the end of first-line chemotherapy.
Patients in the erlotinib group were more likely to experience grade 3/4 diarrhea (5% vs. 1%) and rash (13% vs. 0%).
Preliminary tumor mutational analysis in 318 patients showed that the most common was PI3KCA mutation (present in about 4% of cases), followed by KRAS mutation (present in about 3%). Only about 1% had an EGFR mutation, and mutations of NRAS and BRAF were similarly uncommon.
Progression-free survival was better for patients having any of these mutations than for those having none (P = .04). But among the former, there was no significant benefit of erlotinib over observation.
Progression-free survival was also similar across subgroups of patients whose tumors were EGFR positive and negative according to either immunohistochemistry or FISH.
Analyses failed to identify any significant relationship between the development of rash during erlotinib therapy and progression-free survival. The investigators plan to analyze quality of life data.
Dr. Vergote disclosed no relevant conflicts of interest. Dr. Seiden disclosed no relevant conflicts of interest.
CHICAGO – Maintenance erlotinib was no more efficacious than observation when given to women with ovarian or related cancers who had no evidence of progression after receiving first-line platinum-based chemotherapy.
The 835 women studied in a randomized, phase III trial had a median progression-free survival of about 1 year and an overall survival median of about 4.5 years regardless of whether they were assigned to erlotinib – an oral inhibitor of the EGFR (epidermal growth factor receptor) tyrosine kinase – or simple observation.
The findings were similar in patient subgroups who were stratified according to a wide range of factors, such as stage and (in preliminary analyses) tumor EGFR positivity, investigators reported at the annual meeting of the American Society of Clinical Oncology.
"Maintenance erlotinib after first-line chemotherapy in patients with ovarian, peritoneal, or fallopian tube cancer did not increase progression-free survival nor overall survival," said lead investigator Dr. Ignace B. Vergote. Moreover, a quarter of patients stopped the drug early because of adverse effects.
"At this moment, we cannot identify a subgroup that might benefit from erlotinib maintenance therapy after first-line chemotherapy for ovarian cancer, but we are continuing to look at immunohistochemistry and FISH [fluorescence in situ hybridization] analysis," added Dr. Vergote, chairman of the Leuven (Belgium) Cancer Institute and head of the department of obstetrics and gynecology and gynecologic oncology at the Catholic University of Leuven.
Discussant Dr. Michael V. Seiden of the Fox Chase Cancer Center in Philadelphia noted that there was "a compelling body of basic and preclinical evidence that made the advent or launch of this study very logical." For example, research had shown a correlation between high tumor EGFR levels and poor prognosis in ovarian cancer, as well as an association– in various cancers – of EGFR mutations or expression with response to therapies targeting this receptor.
"Unfortunately, the addition of erlotinib as part of a maintenance schedule did not budge progression-free survival or overall survival," he said. "Perhaps now, in 2012, with the value of ... hindsight, one might have made this prediction, in that there have been now numerous negative single-arm studies or nearly negative single-arm studies with both small-molecule inhibitors and monoclonal antibodies" against EGFR.
Women enrolled in the EORTC (European Organisation for Research and Treatment of Cancer) 55041 trial – a joint effort of six cooperative groups – had high-risk stage I, or stages II to IV epithelial ovarian, primary peritoneal, or fallopian tube cancer and at least stable disease as of the end of first-line platinum-based chemotherapy.
They were assigned to either erlotinib (Tarceva) 150 mg daily for 2 years or observation. Erlotinib is currently approved by the Food and Drug Administration for the treatment of non–small cell lung cancer and pancreatic cancer.
Demographic and clinical data showed that about 62% of patients had serous tumor histology. Nearly all (96%) had received carboplatin and paclitaxel as their first-line therapy. Roughly 70% had had primary debulking surgery, whereas 30% had received neoadjuvant therapy and interval debulking surgery; there was no evidence of disease at surgery in 48% of the former and 62% of the latter.
Overall, 25% of patients in the erlotinib group stopped therapy early because of unacceptable adverse events (mainly rash), Dr. Vergote reported.
Main results showed that with a median follow-up of 4.3 years, erlotinib and observation were statistically indistinguishable in terms of median progression-free survival (12.7 vs. 12.4 months), with progression defined according to RECIST criteria or CA (cancer antigen) 125 levels, and overall survival (51 vs. 59 months). The findings were similar in subgroups stratified by stage, age, performance status, and response at the end of first-line chemotherapy.
Patients in the erlotinib group were more likely to experience grade 3/4 diarrhea (5% vs. 1%) and rash (13% vs. 0%).
Preliminary tumor mutational analysis in 318 patients showed that the most common was PI3KCA mutation (present in about 4% of cases), followed by KRAS mutation (present in about 3%). Only about 1% had an EGFR mutation, and mutations of NRAS and BRAF were similarly uncommon.
Progression-free survival was better for patients having any of these mutations than for those having none (P = .04). But among the former, there was no significant benefit of erlotinib over observation.
Progression-free survival was also similar across subgroups of patients whose tumors were EGFR positive and negative according to either immunohistochemistry or FISH.
Analyses failed to identify any significant relationship between the development of rash during erlotinib therapy and progression-free survival. The investigators plan to analyze quality of life data.
Dr. Vergote disclosed no relevant conflicts of interest. Dr. Seiden disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: Compared with observation, erlotinib did not significantly improve either progression-free survival (12.7 vs. 12.4 months) or overall survival (51 vs. 59 months).
Data Source: The phase III EORTC 55041A trial involved 835 women with high-risk stage I or stage II-IV ovarian, peritoneal, or tubal cancer who had no evidence of progression after first-line, platinum-based chemotherapy.
Disclosures: Dr. Vergote and Dr. Seiden disclosed no relevant conflicts of interest.
Benefit of IVIG in Alzheimer's Disease Appears Durable
VANCOUVER, B.C. – Intravenous immunoglobulin continues to slow the decline in cognitive and other functions seen in Alzheimer’s disease for at least 3 years, suggest data from an extended phase II randomized trial among 21 patients with mild to moderate disease.
Compared with their counterparts who started on a placebo and crossed over to intravenous immunoglobulin (IVIG) in the trial, patients who received the pooled antibody preparation continuously had significantly better scores on measures of cognitive, global, and daily function, and behavior, Dr. Norman Relkin reported at the Alzheimer’s Association International Conference 2012.

Moreover, the subset of patients who received the optimal dose of IVIG for the entire 3-year period had little to no decline in these measures from baseline, suggesting that clinical progression of the disease had been effectively halted.
Adverse effects seen with IVIG were consistent with what was expected, given 30 years of experience with this agent in other diseases – mainly short-lived infusion-related reactions such as rash and fever, although a single patient did experience a stroke. The majority of patients received all planned infusions.
"By the results that we have shown here, we have established that IVIG is potentially a viable therapy for as long as 36 months and perhaps longer," Dr. Relkin commented in a press briefing. However, he cautioned, the number of patients studied was small, and IVIG is not currently approved to treat Alzheimer’s disease.
"My coinvestigators and I want to really emphasize that this work is investigational, and it’s not intended to promote the off-label use of this particular product to treat Alzheimer’s disease. This is a very important point because this agent is in limited supply, and the indications for which it is approved, some of them represent disorders in which patients can only survive by getting this particular product," he explained. "So we don’t want to bankrupt the available supplies by creating false hope or premature use of this product."
The promising results seen in the extended trial prompted initiation of the phase III Gammaglobulin Alzheimer Partnership (GAP) study, which has been further testing the optimal dose of IVIG against placebo. "The last patient should be through that study by December of this year, and we expect readout [of the results] by the middle of 2013," he said.
The patients enrolled in the phase II trial had mild to moderate Alzheimer’s disease, with a Mini-Mental State Examination score of 14-26. Those who had experienced myocardial infarction or stroke were generally excluded to reduce the risk of thromboembolic complications.
During the initial 6 months, patients received randomized double-blind treatment with placebo or various doses of IVIG (Gammagard). In a first extension out to 18 months, placebo patients were switched to IVIG and treatment became open-label. In a second extension out to 36 months, all patients were given the dose that had emerged as the optimal one (0.4 g/kg every 2 weeks).
Cognitive function was assessed with the Alzheimer’s Disease Assessment Scale cognitive subscale (ADAS-Cog), global functioning with the Clinical Global Impression of Change (CGIC) scale, daily functioning from Activities of Daily Living (ADL), and behavior from the Neuropsychiatric Inventory (NPI).
Results at 6 months and at 18 months favored IVIG over placebo, according to Dr. Relkin, director of the memory disorders program at Weill Cornell Medical College, New York.
Results for the full 36 months, reported for the first time in a poster session at the meeting, showed that in a comparison of all patients given IVIG continuously in the trial (regardless of dose) with patients who had a delay because they started with placebo, the decline in the four main measures was slower in the former group, with significant differences at nearly all time points.
"Particularly if you look at the global measure and daily function measure, there is a bend in the curve of the group that got placebo, and that bend occurs when they were switched to the optimum dose," Dr. Relkin noted. "We think that’s important because it shows that even patients who are a little bit further along in the disease state can benefit."
In what he characterized as "the most striking finding," analyses restricted to the four patients who received the optimal dose of IVIG continuously showed virtually no decline in the four main measures over 36 months.
"To put this in perspective, when we see patients with Alzheimer’s disease in our clinic untreated, there is usually a measurable decline below baseline within 3-6 months. If we treat them with the currently available agents, they typically drop below their baseline between 6 and 12 months," he commented. "If we have a patient who goes out to 18 or 24 months without changing, we usually begin to doubt if they have Alzheimer’s disease. If we have two patients like that in our practice, we begin to doubt our own diagnostic prowess. To have four patients, all of whom received the same dose [and] are effectively unchanged after 3 years, is a remarkable result."
It is still too premature to conclude that IVIG had a disease-modifying effect, according to Dr. Relkin. "However, the shapes of those graphs are exactly what people model when they are predicting what a disease-modifying therapy would look like, which is that there is a divergence of slopes, which means that the curves widen as time goes on. I think we have to wait for the results of the phase III study before we can answer that question," he concluded.
Dr. Relkin disclosed that he receives research support from Baxter Healthcare, which supported the trial.
VANCOUVER, B.C. – Intravenous immunoglobulin continues to slow the decline in cognitive and other functions seen in Alzheimer’s disease for at least 3 years, suggest data from an extended phase II randomized trial among 21 patients with mild to moderate disease.
Compared with their counterparts who started on a placebo and crossed over to intravenous immunoglobulin (IVIG) in the trial, patients who received the pooled antibody preparation continuously had significantly better scores on measures of cognitive, global, and daily function, and behavior, Dr. Norman Relkin reported at the Alzheimer’s Association International Conference 2012.
Moreover, the subset of patients who received the optimal dose of IVIG for the entire 3-year period had little to no decline in these measures from baseline, suggesting that clinical progression of the disease had been effectively halted.
Adverse effects seen with IVIG were consistent with what was expected, given 30 years of experience with this agent in other diseases – mainly short-lived infusion-related reactions such as rash and fever, although a single patient did experience a stroke. The majority of patients received all planned infusions.
"By the results that we have shown here, we have established that IVIG is potentially a viable therapy for as long as 36 months and perhaps longer," Dr. Relkin commented in a press briefing. However, he cautioned, the number of patients studied was small, and IVIG is not currently approved to treat Alzheimer’s disease.
"My coinvestigators and I want to really emphasize that this work is investigational, and it’s not intended to promote the off-label use of this particular product to treat Alzheimer’s disease. This is a very important point because this agent is in limited supply, and the indications for which it is approved, some of them represent disorders in which patients can only survive by getting this particular product," he explained. "So we don’t want to bankrupt the available supplies by creating false hope or premature use of this product."
The promising results seen in the extended trial prompted initiation of the phase III Gammaglobulin Alzheimer Partnership (GAP) study, which has been further testing the optimal dose of IVIG against placebo. "The last patient should be through that study by December of this year, and we expect readout [of the results] by the middle of 2013," he said.
The patients enrolled in the phase II trial had mild to moderate Alzheimer’s disease, with a Mini-Mental State Examination score of 14-26. Those who had experienced myocardial infarction or stroke were generally excluded to reduce the risk of thromboembolic complications.
During the initial 6 months, patients received randomized double-blind treatment with placebo or various doses of IVIG (Gammagard). In a first extension out to 18 months, placebo patients were switched to IVIG and treatment became open-label. In a second extension out to 36 months, all patients were given the dose that had emerged as the optimal one (0.4 g/kg every 2 weeks).
Cognitive function was assessed with the Alzheimer’s Disease Assessment Scale cognitive subscale (ADAS-Cog), global functioning with the Clinical Global Impression of Change (CGIC) scale, daily functioning from Activities of Daily Living (ADL), and behavior from the Neuropsychiatric Inventory (NPI).
Results at 6 months and at 18 months favored IVIG over placebo, according to Dr. Relkin, director of the memory disorders program at Weill Cornell Medical College, New York.
Results for the full 36 months, reported for the first time in a poster session at the meeting, showed that in a comparison of all patients given IVIG continuously in the trial (regardless of dose) with patients who had a delay because they started with placebo, the decline in the four main measures was slower in the former group, with significant differences at nearly all time points.
"Particularly if you look at the global measure and daily function measure, there is a bend in the curve of the group that got placebo, and that bend occurs when they were switched to the optimum dose," Dr. Relkin noted. "We think that’s important because it shows that even patients who are a little bit further along in the disease state can benefit."
In what he characterized as "the most striking finding," analyses restricted to the four patients who received the optimal dose of IVIG continuously showed virtually no decline in the four main measures over 36 months.
"To put this in perspective, when we see patients with Alzheimer’s disease in our clinic untreated, there is usually a measurable decline below baseline within 3-6 months. If we treat them with the currently available agents, they typically drop below their baseline between 6 and 12 months," he commented. "If we have a patient who goes out to 18 or 24 months without changing, we usually begin to doubt if they have Alzheimer’s disease. If we have two patients like that in our practice, we begin to doubt our own diagnostic prowess. To have four patients, all of whom received the same dose [and] are effectively unchanged after 3 years, is a remarkable result."
It is still too premature to conclude that IVIG had a disease-modifying effect, according to Dr. Relkin. "However, the shapes of those graphs are exactly what people model when they are predicting what a disease-modifying therapy would look like, which is that there is a divergence of slopes, which means that the curves widen as time goes on. I think we have to wait for the results of the phase III study before we can answer that question," he concluded.
Dr. Relkin disclosed that he receives research support from Baxter Healthcare, which supported the trial.
VANCOUVER, B.C. – Intravenous immunoglobulin continues to slow the decline in cognitive and other functions seen in Alzheimer’s disease for at least 3 years, suggest data from an extended phase II randomized trial among 21 patients with mild to moderate disease.
Compared with their counterparts who started on a placebo and crossed over to intravenous immunoglobulin (IVIG) in the trial, patients who received the pooled antibody preparation continuously had significantly better scores on measures of cognitive, global, and daily function, and behavior, Dr. Norman Relkin reported at the Alzheimer’s Association International Conference 2012.
Moreover, the subset of patients who received the optimal dose of IVIG for the entire 3-year period had little to no decline in these measures from baseline, suggesting that clinical progression of the disease had been effectively halted.
Adverse effects seen with IVIG were consistent with what was expected, given 30 years of experience with this agent in other diseases – mainly short-lived infusion-related reactions such as rash and fever, although a single patient did experience a stroke. The majority of patients received all planned infusions.
"By the results that we have shown here, we have established that IVIG is potentially a viable therapy for as long as 36 months and perhaps longer," Dr. Relkin commented in a press briefing. However, he cautioned, the number of patients studied was small, and IVIG is not currently approved to treat Alzheimer’s disease.
"My coinvestigators and I want to really emphasize that this work is investigational, and it’s not intended to promote the off-label use of this particular product to treat Alzheimer’s disease. This is a very important point because this agent is in limited supply, and the indications for which it is approved, some of them represent disorders in which patients can only survive by getting this particular product," he explained. "So we don’t want to bankrupt the available supplies by creating false hope or premature use of this product."
The promising results seen in the extended trial prompted initiation of the phase III Gammaglobulin Alzheimer Partnership (GAP) study, which has been further testing the optimal dose of IVIG against placebo. "The last patient should be through that study by December of this year, and we expect readout [of the results] by the middle of 2013," he said.
The patients enrolled in the phase II trial had mild to moderate Alzheimer’s disease, with a Mini-Mental State Examination score of 14-26. Those who had experienced myocardial infarction or stroke were generally excluded to reduce the risk of thromboembolic complications.
During the initial 6 months, patients received randomized double-blind treatment with placebo or various doses of IVIG (Gammagard). In a first extension out to 18 months, placebo patients were switched to IVIG and treatment became open-label. In a second extension out to 36 months, all patients were given the dose that had emerged as the optimal one (0.4 g/kg every 2 weeks).
Cognitive function was assessed with the Alzheimer’s Disease Assessment Scale cognitive subscale (ADAS-Cog), global functioning with the Clinical Global Impression of Change (CGIC) scale, daily functioning from Activities of Daily Living (ADL), and behavior from the Neuropsychiatric Inventory (NPI).
Results at 6 months and at 18 months favored IVIG over placebo, according to Dr. Relkin, director of the memory disorders program at Weill Cornell Medical College, New York.
Results for the full 36 months, reported for the first time in a poster session at the meeting, showed that in a comparison of all patients given IVIG continuously in the trial (regardless of dose) with patients who had a delay because they started with placebo, the decline in the four main measures was slower in the former group, with significant differences at nearly all time points.
"Particularly if you look at the global measure and daily function measure, there is a bend in the curve of the group that got placebo, and that bend occurs when they were switched to the optimum dose," Dr. Relkin noted. "We think that’s important because it shows that even patients who are a little bit further along in the disease state can benefit."
In what he characterized as "the most striking finding," analyses restricted to the four patients who received the optimal dose of IVIG continuously showed virtually no decline in the four main measures over 36 months.
"To put this in perspective, when we see patients with Alzheimer’s disease in our clinic untreated, there is usually a measurable decline below baseline within 3-6 months. If we treat them with the currently available agents, they typically drop below their baseline between 6 and 12 months," he commented. "If we have a patient who goes out to 18 or 24 months without changing, we usually begin to doubt if they have Alzheimer’s disease. If we have two patients like that in our practice, we begin to doubt our own diagnostic prowess. To have four patients, all of whom received the same dose [and] are effectively unchanged after 3 years, is a remarkable result."
It is still too premature to conclude that IVIG had a disease-modifying effect, according to Dr. Relkin. "However, the shapes of those graphs are exactly what people model when they are predicting what a disease-modifying therapy would look like, which is that there is a divergence of slopes, which means that the curves widen as time goes on. I think we have to wait for the results of the phase III study before we can answer that question," he concluded.
Dr. Relkin disclosed that he receives research support from Baxter Healthcare, which supported the trial.
AT THE ALZHEIMER'S ASSOCIATION INTERNATIONAL CONFERENCE 2012
Major Finding: Patients who continuously received IVIG for 3 years had significantly better scores on measures of cognitive, global, and daily function, as well as behavior, than did patients who started on placebo and switched to IVIG after 18 months.
Data Source: This was an open-label extension out to 36 months of a randomized, placebo-controlled phase II trial among 21 patients with mild to moderate Alzheimer’s disease.
Disclosures: Dr. Relkin disclosed that he receives research support from Baxter Healthcare, which supported the trial.

Mild Cognitive Impairment Carries Adverse Prognosis
VANCOUVER, B.C. – Mild cognitive impairment warrants clinical attention as it confers a sharply elevated risk of death and also portends increasing social isolation, according to a pair of longitudinal studies.
Amnestic MCI Is Independent Risk Factor for Death
In the first study, investigators led by Mindy J. Katz, a senior associate in the neurology department of the Albert Einstein College of Medicine, New York, followed 733 community-dwelling participants aged 70 years or older from the Einstein Aging Study.

Results showed that after confounders were taken into account, individuals with the amnestic type of mild cognitive impairment (MCI), which affects memory, were more than twice as likely to die in the next 5 years as were their cognitively intact counterparts. But those with nonamnestic MCI, which affects executive function, judgment, visuospatial ability, and/or language, were not at increased risk.
The heightened mortality with the former may be related both to its frequent progression to Alzheimer’s disease and to its impact on adherence to medical therapy for comorbidities such as hypertension and diabetes, according to Ms. Katz. "If they can’t remember to take their medications, if they don’t keep their appointments with their doctors, their medical care might not be as good as that of someone who is ... capable of keeping these appointments and taking their medications," she said in an interview at the Alzheimer’s Association International Conference 2012.
The findings apply only to people who meet diagnostic criteria for amnestic MCI, she stressed. "Just because you forget where you put your keys or you can’t remember why you walked into a room, that’s not a reason to panic." However, "after you’ve been clinically evaluated and the clinician feels that you really do have a true memory impairment, then it’s a warning sign for both the individual to prepare for the future and for caretakers to be aware that maybe this person might need more care or a plan for care in the future, and to make provisions both financially and in terms of caretaking that might be involved going forward for that individual."

Senior author Dr. Richard B. Lipton, also of the Albert Einstein College of Medicine, noted that there has been some question as to whether MCI is an important entity. "Well, if it’s associated with an increased risk of death, then presumably it’s important, because death is the ultimate hard end point that is face-valid to all parties," he said.
Identifying MCI is now key for two reasons, according to Dr. Lipton. "Ultimately ... that will be a group that’s treated to keep them from progressing and developing full-blown Alzheimer’s disease. But even today, it’s important because adherence to medical therapy for people with memory impairment requires planning and family support."
In the study, 10% of participants had amnestic MCI and 9% had nonamnestic MCI at baseline. Additionally, 3% developed dementia at some time after their first evaluation.
During follow-up, nearly a third of study participants died. In a multivariate analysis, those with amnestic MCI had a significantly elevated risk of death relative to their cognitively intact peers (hazard ratio, 2.17). The other significant independent risk factors were dementia (3.26), advancing age (1.10), Geriatric Depression Scale score (1.09), and comorbidity index (1.34).
In contrast, nonamnestic MCI did not significantly affect risk, nor did educational attainment. APOE e4 allele status showed a trend toward increased mortality.
Withdrawal From Community Life
In the second study, a team led by Dr. Jeffrey Kaye of Oregon Health and Science University in Portland followed 140 community-dwelling, nondepressed older adults from the Intelligent Systems for Assessing Aging Change (ISAAC) cohort who had a mean age of 84 years at baseline.

The investigators used new technology called pervasive computing or embedded ambient sensing, outfitting the participants’ homes with motion sensors and with contact sensors on doors to detect 24/7 activity patterns, including travel outside the home.
At baseline, the 20% of participants who had MCI were statistically indistinguishable from their cognitively intact counterparts in terms of the amount of time spent outside the home each day, with both averaging about 4.2 hours daily.
However, during a follow-up period of more than 3 years, there was a steady decline in this measure in the adults with MCI, compared with little change in the cognitively intact participants. In the last month of monitoring, the participants with MCI left their home for 2.9 hours daily on average, which was significantly shorter than the 3.8 hours recorded for cognitively intact participants.
"With progression of MCI, there is increasingly less time spent outside the home, and it’s independent of mood or health status, so it’s not simply because they are depressed or they are sicker," Dr. Kaye noted in an interview at the conference. "It seems to be more intrinsically a part of having MCI. This to us suggests that there is a progressive narrowing of opportunity to interact with the outside world."
The community withdrawal seen in the MCI group might occur for several reasons. "One of the highest suspicions is that as you develop increasing difficulty with your memory and thinking, you become less confident and more apprehensive about interacting with other people," he proposed. "There may also be just the practical forgetting of appointments and just not attending to things that they would usually be doing. So they are just not remembering to remember."
The participants with MCI were unaware of the change in their activity, according to Dr. Kaye. "We asked them on an annual basis about their activities, and this is very subtle. They don’t actually see this, at least using a sort of subjectively reported series of questions that were asked about their participation in clubs, classes, and social events, and going out to eat, things like that."
By enabling more accurate assessment of time spent outside the home, the technology used could have implications for both clinical care and research.
"For those of us interested in trying to get more real-time measurement of activity and behavior, we think that this kind of measure can be used to unobtrusively assess very early activity changes that may be indicative of evolving MCI," he explained. "It would be much more meaningful, rather than saying, ‘I remembered one more animal on that memory test’ [to instead say,] ‘I actually had two more outings a day or spent 20 minutes outside more often than I did previously, on this treatment.’ "
None of the investigators had relevant conflicts of interest.
VANCOUVER, B.C. – Mild cognitive impairment warrants clinical attention as it confers a sharply elevated risk of death and also portends increasing social isolation, according to a pair of longitudinal studies.
Amnestic MCI Is Independent Risk Factor for Death
In the first study, investigators led by Mindy J. Katz, a senior associate in the neurology department of the Albert Einstein College of Medicine, New York, followed 733 community-dwelling participants aged 70 years or older from the Einstein Aging Study.
Results showed that after confounders were taken into account, individuals with the amnestic type of mild cognitive impairment (MCI), which affects memory, were more than twice as likely to die in the next 5 years as were their cognitively intact counterparts. But those with nonamnestic MCI, which affects executive function, judgment, visuospatial ability, and/or language, were not at increased risk.
The heightened mortality with the former may be related both to its frequent progression to Alzheimer’s disease and to its impact on adherence to medical therapy for comorbidities such as hypertension and diabetes, according to Ms. Katz. "If they can’t remember to take their medications, if they don’t keep their appointments with their doctors, their medical care might not be as good as that of someone who is ... capable of keeping these appointments and taking their medications," she said in an interview at the Alzheimer’s Association International Conference 2012.
The findings apply only to people who meet diagnostic criteria for amnestic MCI, she stressed. "Just because you forget where you put your keys or you can’t remember why you walked into a room, that’s not a reason to panic." However, "after you’ve been clinically evaluated and the clinician feels that you really do have a true memory impairment, then it’s a warning sign for both the individual to prepare for the future and for caretakers to be aware that maybe this person might need more care or a plan for care in the future, and to make provisions both financially and in terms of caretaking that might be involved going forward for that individual."
Senior author Dr. Richard B. Lipton, also of the Albert Einstein College of Medicine, noted that there has been some question as to whether MCI is an important entity. "Well, if it’s associated with an increased risk of death, then presumably it’s important, because death is the ultimate hard end point that is face-valid to all parties," he said.
Identifying MCI is now key for two reasons, according to Dr. Lipton. "Ultimately ... that will be a group that’s treated to keep them from progressing and developing full-blown Alzheimer’s disease. But even today, it’s important because adherence to medical therapy for people with memory impairment requires planning and family support."
In the study, 10% of participants had amnestic MCI and 9% had nonamnestic MCI at baseline. Additionally, 3% developed dementia at some time after their first evaluation.
During follow-up, nearly a third of study participants died. In a multivariate analysis, those with amnestic MCI had a significantly elevated risk of death relative to their cognitively intact peers (hazard ratio, 2.17). The other significant independent risk factors were dementia (3.26), advancing age (1.10), Geriatric Depression Scale score (1.09), and comorbidity index (1.34).
In contrast, nonamnestic MCI did not significantly affect risk, nor did educational attainment. APOE e4 allele status showed a trend toward increased mortality.
Withdrawal From Community Life
In the second study, a team led by Dr. Jeffrey Kaye of Oregon Health and Science University in Portland followed 140 community-dwelling, nondepressed older adults from the Intelligent Systems for Assessing Aging Change (ISAAC) cohort who had a mean age of 84 years at baseline.
The investigators used new technology called pervasive computing or embedded ambient sensing, outfitting the participants’ homes with motion sensors and with contact sensors on doors to detect 24/7 activity patterns, including travel outside the home.
At baseline, the 20% of participants who had MCI were statistically indistinguishable from their cognitively intact counterparts in terms of the amount of time spent outside the home each day, with both averaging about 4.2 hours daily.
However, during a follow-up period of more than 3 years, there was a steady decline in this measure in the adults with MCI, compared with little change in the cognitively intact participants. In the last month of monitoring, the participants with MCI left their home for 2.9 hours daily on average, which was significantly shorter than the 3.8 hours recorded for cognitively intact participants.
"With progression of MCI, there is increasingly less time spent outside the home, and it’s independent of mood or health status, so it’s not simply because they are depressed or they are sicker," Dr. Kaye noted in an interview at the conference. "It seems to be more intrinsically a part of having MCI. This to us suggests that there is a progressive narrowing of opportunity to interact with the outside world."
The community withdrawal seen in the MCI group might occur for several reasons. "One of the highest suspicions is that as you develop increasing difficulty with your memory and thinking, you become less confident and more apprehensive about interacting with other people," he proposed. "There may also be just the practical forgetting of appointments and just not attending to things that they would usually be doing. So they are just not remembering to remember."
The participants with MCI were unaware of the change in their activity, according to Dr. Kaye. "We asked them on an annual basis about their activities, and this is very subtle. They don’t actually see this, at least using a sort of subjectively reported series of questions that were asked about their participation in clubs, classes, and social events, and going out to eat, things like that."
By enabling more accurate assessment of time spent outside the home, the technology used could have implications for both clinical care and research.
"For those of us interested in trying to get more real-time measurement of activity and behavior, we think that this kind of measure can be used to unobtrusively assess very early activity changes that may be indicative of evolving MCI," he explained. "It would be much more meaningful, rather than saying, ‘I remembered one more animal on that memory test’ [to instead say,] ‘I actually had two more outings a day or spent 20 minutes outside more often than I did previously, on this treatment.’ "
None of the investigators had relevant conflicts of interest.
VANCOUVER, B.C. – Mild cognitive impairment warrants clinical attention as it confers a sharply elevated risk of death and also portends increasing social isolation, according to a pair of longitudinal studies.
Amnestic MCI Is Independent Risk Factor for Death
In the first study, investigators led by Mindy J. Katz, a senior associate in the neurology department of the Albert Einstein College of Medicine, New York, followed 733 community-dwelling participants aged 70 years or older from the Einstein Aging Study.
Results showed that after confounders were taken into account, individuals with the amnestic type of mild cognitive impairment (MCI), which affects memory, were more than twice as likely to die in the next 5 years as were their cognitively intact counterparts. But those with nonamnestic MCI, which affects executive function, judgment, visuospatial ability, and/or language, were not at increased risk.
The heightened mortality with the former may be related both to its frequent progression to Alzheimer’s disease and to its impact on adherence to medical therapy for comorbidities such as hypertension and diabetes, according to Ms. Katz. "If they can’t remember to take their medications, if they don’t keep their appointments with their doctors, their medical care might not be as good as that of someone who is ... capable of keeping these appointments and taking their medications," she said in an interview at the Alzheimer’s Association International Conference 2012.
The findings apply only to people who meet diagnostic criteria for amnestic MCI, she stressed. "Just because you forget where you put your keys or you can’t remember why you walked into a room, that’s not a reason to panic." However, "after you’ve been clinically evaluated and the clinician feels that you really do have a true memory impairment, then it’s a warning sign for both the individual to prepare for the future and for caretakers to be aware that maybe this person might need more care or a plan for care in the future, and to make provisions both financially and in terms of caretaking that might be involved going forward for that individual."
Senior author Dr. Richard B. Lipton, also of the Albert Einstein College of Medicine, noted that there has been some question as to whether MCI is an important entity. "Well, if it’s associated with an increased risk of death, then presumably it’s important, because death is the ultimate hard end point that is face-valid to all parties," he said.
Identifying MCI is now key for two reasons, according to Dr. Lipton. "Ultimately ... that will be a group that’s treated to keep them from progressing and developing full-blown Alzheimer’s disease. But even today, it’s important because adherence to medical therapy for people with memory impairment requires planning and family support."
In the study, 10% of participants had amnestic MCI and 9% had nonamnestic MCI at baseline. Additionally, 3% developed dementia at some time after their first evaluation.
During follow-up, nearly a third of study participants died. In a multivariate analysis, those with amnestic MCI had a significantly elevated risk of death relative to their cognitively intact peers (hazard ratio, 2.17). The other significant independent risk factors were dementia (3.26), advancing age (1.10), Geriatric Depression Scale score (1.09), and comorbidity index (1.34).
In contrast, nonamnestic MCI did not significantly affect risk, nor did educational attainment. APOE e4 allele status showed a trend toward increased mortality.
Withdrawal From Community Life
In the second study, a team led by Dr. Jeffrey Kaye of Oregon Health and Science University in Portland followed 140 community-dwelling, nondepressed older adults from the Intelligent Systems for Assessing Aging Change (ISAAC) cohort who had a mean age of 84 years at baseline.
The investigators used new technology called pervasive computing or embedded ambient sensing, outfitting the participants’ homes with motion sensors and with contact sensors on doors to detect 24/7 activity patterns, including travel outside the home.
At baseline, the 20% of participants who had MCI were statistically indistinguishable from their cognitively intact counterparts in terms of the amount of time spent outside the home each day, with both averaging about 4.2 hours daily.
However, during a follow-up period of more than 3 years, there was a steady decline in this measure in the adults with MCI, compared with little change in the cognitively intact participants. In the last month of monitoring, the participants with MCI left their home for 2.9 hours daily on average, which was significantly shorter than the 3.8 hours recorded for cognitively intact participants.
"With progression of MCI, there is increasingly less time spent outside the home, and it’s independent of mood or health status, so it’s not simply because they are depressed or they are sicker," Dr. Kaye noted in an interview at the conference. "It seems to be more intrinsically a part of having MCI. This to us suggests that there is a progressive narrowing of opportunity to interact with the outside world."
The community withdrawal seen in the MCI group might occur for several reasons. "One of the highest suspicions is that as you develop increasing difficulty with your memory and thinking, you become less confident and more apprehensive about interacting with other people," he proposed. "There may also be just the practical forgetting of appointments and just not attending to things that they would usually be doing. So they are just not remembering to remember."
The participants with MCI were unaware of the change in their activity, according to Dr. Kaye. "We asked them on an annual basis about their activities, and this is very subtle. They don’t actually see this, at least using a sort of subjectively reported series of questions that were asked about their participation in clubs, classes, and social events, and going out to eat, things like that."
By enabling more accurate assessment of time spent outside the home, the technology used could have implications for both clinical care and research.
"For those of us interested in trying to get more real-time measurement of activity and behavior, we think that this kind of measure can be used to unobtrusively assess very early activity changes that may be indicative of evolving MCI," he explained. "It would be much more meaningful, rather than saying, ‘I remembered one more animal on that memory test’ [to instead say,] ‘I actually had two more outings a day or spent 20 minutes outside more often than I did previously, on this treatment.’ "
None of the investigators had relevant conflicts of interest.
AT THE ALZHEIMER'S ASSOCIATION INTERNATIONAL CONFERENCE 2012

Oral Taxane Shows Spunk in Metastatic Breast Cancer
CHICAGO – Tesetaxel, an investigational oral taxane, is highly active when used to treat chemotherapy-naive metastatic breast cancer, a phase II trial suggests. And in contrast to the main intravenously administered taxanes, it does not require steroidal premedication and can cause little-to-no peripheral neuropathy.
A total of 46 women were treated with tesetaxel just once every 3 weeks during an office visit in the trial. The overall response rate was 45% – at least a bit higher than the roughly 20%-35% previously seen with the intravenously administered taxanes paclitaxel (Taxol) and docetaxel (Taxotere), according to presenting author Dr. Loretta M. Itri.

"This compares favorably. This is a phase II open-label study. I’m sure the response rate is going to fall a little bit over time, but ... I think we are going to be nothing less than equivalent to the other taxanes," she said in an interview at the annual meeting of the American Society of Clinical Oncology.
A provision for dose escalation from 27 mg/m2 to 35 mg/m2 was halted halfway through the trial because there was minimal gain in efficacy but substantially more toxicity. "So this [27 mg/m2] is the dose that we will be taking forward in our clinical trials, and we are abandoning escalation," she said. There were no cases of hypersensitivity reaction regardless of dose used; the rate of grade 3 peripheral neuropathy was 16% with dose escalation but 0% without it.
The majority of the patients having progression on treatment had triple-negative disease, Dr. Itri noted. "Now that we know that it’s the triple-negatives who have recently received a taxane who are the ones who don’t respond, we will probably begin excluding that population ... so that we can further enrich [the study population]. We want to give the drug to people whom we can do something good for," she said.
The next step in breast cancer is an ongoing three-arm phase IIb trial comparing tesetaxel given every 3 weeks vs. weekly, and also comparing it with capecitabine (Xeloda), in about 200 patients.
"What’s interesting about the weekly dose is that we have seen in the phase I study no significant neutropenia. So we feel obligated to evaluate the weekly dose, because if we truly had a taxane regimen with no neutropenia, that could be important," said Dr. Itri, an oncologist and chief medical officer of Genta, the company that is developing tesetaxel.
"I will tell you that I have a real bias here ... The weekly dosing is going to really have to be something special for us to abandon the every-3-week dosing, because the convenience and the compliance are so easy," she continued. "These women have a life to live, and the drug was designed to be as user friendly as possible, and I personally don’t like the idea of sending patients home with cytotoxic chemotherapy."
Discussant Dr. Stacy L. Moulder of the University of Texas M.D. Anderson Cancer Center, Houston, noted the advantages of tesetaxel over intravenous taxanes with respect to factors such as oral administration, no need for premedication, and, possibly, reduced toxicity. "But the question that remains is, is this the best microtubule inhibitor?"
She pointed out that a trial of nab-paclitaxel (Abraxane) found approximately double the median duration of progression-free survival seen with tesetaxel in this trial and a fairly similar rate of higher-grade peripheral neuropathy (J. Clin. Oncol. 2009;27:3611-9). "So I think it remains unanswered whether this drug is as good as some of the currently existing novel taxanes," she maintained.
Unlike the intravenous taxanes, tesetaxel is not a substrate for P-glycoprotein (PGP), a transmembrane pump that is likely the main mechanism of taxane resistance, according to Dr. Itri. Thus, it is highly concentrated in cells that overexpress PGP. In preclinical studies, tesetaxel’s cytotoxic activity has been 3-10 times greater than that of the intravenous taxanes in cells not expressing PGP and 10-100 times greater in multidrug-resistant tumor cells overexpressing PGP.
Women were eligible for the trial if they had HER2-negative, chemotherapy-naive metastatic breast cancer. (Those with hormone receptor–positive disease could have received hormonal therapy for their metastases.) Prior adjuvant taxane therapy given more than a year before enrollment was permitted.
The women received single-agent tesetaxel orally once every 3 weeks and without any antiallergy premedication but with an oral antiemetic as a precaution. "We have completed an effect-of-food study; the drug can be administered with or without food, so there is no need for fasting," Dr. Itri said.
"The patient takes their pill in front of the doctor, so the doctor knows that the patient has gotten a full dose. There is no compliance question," she further noted. "Then they go home and they come back 3 weeks later."
The starting dose was 27 mg/m2 every 3 weeks. For the first half of the trial, the dose was escalated up to 35 mg/m2 every 3 weeks if tolerated.
Overall, 20% of women had triple-negative disease, according to results reported in a poster session. More than half each had liver metastases (52%) and lung metastases (57%). Fifty-seven percent had received a taxane as part of their adjuvant therapy.
The median number of cycles of tesetaxel received was 4 (range, 1-17). The overall response rate was 45% (49% in women with estrogen receptor–positive disease and 33% in women with triple-negative disease).
The overall response rate was nearly the same among women who received only the nonescalated dose (44%) and among women who received the escalated dose (47%).
An additional 36% of patients achieved stable disease. Median progression-free survival was 5.8 months for all treated patients and 7.3 months for those with estrogen receptor–positive disease.
"Pretty much, the tolerability profile looks really good," Dr. Itri commented. In particular, none of the patients had hypersensitivity reactions.
By far, the most common grade 3/4 adverse event was neutropenia, seen in 33% of patients overall (26% without dose escalation and 43% with it). However, "none of these patients required a colony-stimulating factor or were febrile. So this now becomes a true outpatient regimen," she said.
The rate of grade 3 peripheral neuropathy was 7% overall (0% without dose escalation and 16% with it), and there was no grade 4 peripheral neuropathy. The rate of grade 2 alopecia was 15% regardless of dose.
Genta sponsored the trial. Dr. Itri disclosed employment and stock ownership in Genta. Dr. Moulder disclosed no relevant conflicts of interest.
CHICAGO – Tesetaxel, an investigational oral taxane, is highly active when used to treat chemotherapy-naive metastatic breast cancer, a phase II trial suggests. And in contrast to the main intravenously administered taxanes, it does not require steroidal premedication and can cause little-to-no peripheral neuropathy.
A total of 46 women were treated with tesetaxel just once every 3 weeks during an office visit in the trial. The overall response rate was 45% – at least a bit higher than the roughly 20%-35% previously seen with the intravenously administered taxanes paclitaxel (Taxol) and docetaxel (Taxotere), according to presenting author Dr. Loretta M. Itri.
"This compares favorably. This is a phase II open-label study. I’m sure the response rate is going to fall a little bit over time, but ... I think we are going to be nothing less than equivalent to the other taxanes," she said in an interview at the annual meeting of the American Society of Clinical Oncology.
A provision for dose escalation from 27 mg/m2 to 35 mg/m2 was halted halfway through the trial because there was minimal gain in efficacy but substantially more toxicity. "So this [27 mg/m2] is the dose that we will be taking forward in our clinical trials, and we are abandoning escalation," she said. There were no cases of hypersensitivity reaction regardless of dose used; the rate of grade 3 peripheral neuropathy was 16% with dose escalation but 0% without it.
The majority of the patients having progression on treatment had triple-negative disease, Dr. Itri noted. "Now that we know that it’s the triple-negatives who have recently received a taxane who are the ones who don’t respond, we will probably begin excluding that population ... so that we can further enrich [the study population]. We want to give the drug to people whom we can do something good for," she said.
The next step in breast cancer is an ongoing three-arm phase IIb trial comparing tesetaxel given every 3 weeks vs. weekly, and also comparing it with capecitabine (Xeloda), in about 200 patients.
"What’s interesting about the weekly dose is that we have seen in the phase I study no significant neutropenia. So we feel obligated to evaluate the weekly dose, because if we truly had a taxane regimen with no neutropenia, that could be important," said Dr. Itri, an oncologist and chief medical officer of Genta, the company that is developing tesetaxel.
"I will tell you that I have a real bias here ... The weekly dosing is going to really have to be something special for us to abandon the every-3-week dosing, because the convenience and the compliance are so easy," she continued. "These women have a life to live, and the drug was designed to be as user friendly as possible, and I personally don’t like the idea of sending patients home with cytotoxic chemotherapy."
Discussant Dr. Stacy L. Moulder of the University of Texas M.D. Anderson Cancer Center, Houston, noted the advantages of tesetaxel over intravenous taxanes with respect to factors such as oral administration, no need for premedication, and, possibly, reduced toxicity. "But the question that remains is, is this the best microtubule inhibitor?"
She pointed out that a trial of nab-paclitaxel (Abraxane) found approximately double the median duration of progression-free survival seen with tesetaxel in this trial and a fairly similar rate of higher-grade peripheral neuropathy (J. Clin. Oncol. 2009;27:3611-9). "So I think it remains unanswered whether this drug is as good as some of the currently existing novel taxanes," she maintained.
Unlike the intravenous taxanes, tesetaxel is not a substrate for P-glycoprotein (PGP), a transmembrane pump that is likely the main mechanism of taxane resistance, according to Dr. Itri. Thus, it is highly concentrated in cells that overexpress PGP. In preclinical studies, tesetaxel’s cytotoxic activity has been 3-10 times greater than that of the intravenous taxanes in cells not expressing PGP and 10-100 times greater in multidrug-resistant tumor cells overexpressing PGP.
Women were eligible for the trial if they had HER2-negative, chemotherapy-naive metastatic breast cancer. (Those with hormone receptor–positive disease could have received hormonal therapy for their metastases.) Prior adjuvant taxane therapy given more than a year before enrollment was permitted.
The women received single-agent tesetaxel orally once every 3 weeks and without any antiallergy premedication but with an oral antiemetic as a precaution. "We have completed an effect-of-food study; the drug can be administered with or without food, so there is no need for fasting," Dr. Itri said.
"The patient takes their pill in front of the doctor, so the doctor knows that the patient has gotten a full dose. There is no compliance question," she further noted. "Then they go home and they come back 3 weeks later."
The starting dose was 27 mg/m2 every 3 weeks. For the first half of the trial, the dose was escalated up to 35 mg/m2 every 3 weeks if tolerated.
Overall, 20% of women had triple-negative disease, according to results reported in a poster session. More than half each had liver metastases (52%) and lung metastases (57%). Fifty-seven percent had received a taxane as part of their adjuvant therapy.
The median number of cycles of tesetaxel received was 4 (range, 1-17). The overall response rate was 45% (49% in women with estrogen receptor–positive disease and 33% in women with triple-negative disease).
The overall response rate was nearly the same among women who received only the nonescalated dose (44%) and among women who received the escalated dose (47%).
An additional 36% of patients achieved stable disease. Median progression-free survival was 5.8 months for all treated patients and 7.3 months for those with estrogen receptor–positive disease.
"Pretty much, the tolerability profile looks really good," Dr. Itri commented. In particular, none of the patients had hypersensitivity reactions.
By far, the most common grade 3/4 adverse event was neutropenia, seen in 33% of patients overall (26% without dose escalation and 43% with it). However, "none of these patients required a colony-stimulating factor or were febrile. So this now becomes a true outpatient regimen," she said.
The rate of grade 3 peripheral neuropathy was 7% overall (0% without dose escalation and 16% with it), and there was no grade 4 peripheral neuropathy. The rate of grade 2 alopecia was 15% regardless of dose.
Genta sponsored the trial. Dr. Itri disclosed employment and stock ownership in Genta. Dr. Moulder disclosed no relevant conflicts of interest.
CHICAGO – Tesetaxel, an investigational oral taxane, is highly active when used to treat chemotherapy-naive metastatic breast cancer, a phase II trial suggests. And in contrast to the main intravenously administered taxanes, it does not require steroidal premedication and can cause little-to-no peripheral neuropathy.
A total of 46 women were treated with tesetaxel just once every 3 weeks during an office visit in the trial. The overall response rate was 45% – at least a bit higher than the roughly 20%-35% previously seen with the intravenously administered taxanes paclitaxel (Taxol) and docetaxel (Taxotere), according to presenting author Dr. Loretta M. Itri.
"This compares favorably. This is a phase II open-label study. I’m sure the response rate is going to fall a little bit over time, but ... I think we are going to be nothing less than equivalent to the other taxanes," she said in an interview at the annual meeting of the American Society of Clinical Oncology.
A provision for dose escalation from 27 mg/m2 to 35 mg/m2 was halted halfway through the trial because there was minimal gain in efficacy but substantially more toxicity. "So this [27 mg/m2] is the dose that we will be taking forward in our clinical trials, and we are abandoning escalation," she said. There were no cases of hypersensitivity reaction regardless of dose used; the rate of grade 3 peripheral neuropathy was 16% with dose escalation but 0% without it.
The majority of the patients having progression on treatment had triple-negative disease, Dr. Itri noted. "Now that we know that it’s the triple-negatives who have recently received a taxane who are the ones who don’t respond, we will probably begin excluding that population ... so that we can further enrich [the study population]. We want to give the drug to people whom we can do something good for," she said.
The next step in breast cancer is an ongoing three-arm phase IIb trial comparing tesetaxel given every 3 weeks vs. weekly, and also comparing it with capecitabine (Xeloda), in about 200 patients.
"What’s interesting about the weekly dose is that we have seen in the phase I study no significant neutropenia. So we feel obligated to evaluate the weekly dose, because if we truly had a taxane regimen with no neutropenia, that could be important," said Dr. Itri, an oncologist and chief medical officer of Genta, the company that is developing tesetaxel.
"I will tell you that I have a real bias here ... The weekly dosing is going to really have to be something special for us to abandon the every-3-week dosing, because the convenience and the compliance are so easy," she continued. "These women have a life to live, and the drug was designed to be as user friendly as possible, and I personally don’t like the idea of sending patients home with cytotoxic chemotherapy."
Discussant Dr. Stacy L. Moulder of the University of Texas M.D. Anderson Cancer Center, Houston, noted the advantages of tesetaxel over intravenous taxanes with respect to factors such as oral administration, no need for premedication, and, possibly, reduced toxicity. "But the question that remains is, is this the best microtubule inhibitor?"
She pointed out that a trial of nab-paclitaxel (Abraxane) found approximately double the median duration of progression-free survival seen with tesetaxel in this trial and a fairly similar rate of higher-grade peripheral neuropathy (J. Clin. Oncol. 2009;27:3611-9). "So I think it remains unanswered whether this drug is as good as some of the currently existing novel taxanes," she maintained.
Unlike the intravenous taxanes, tesetaxel is not a substrate for P-glycoprotein (PGP), a transmembrane pump that is likely the main mechanism of taxane resistance, according to Dr. Itri. Thus, it is highly concentrated in cells that overexpress PGP. In preclinical studies, tesetaxel’s cytotoxic activity has been 3-10 times greater than that of the intravenous taxanes in cells not expressing PGP and 10-100 times greater in multidrug-resistant tumor cells overexpressing PGP.
Women were eligible for the trial if they had HER2-negative, chemotherapy-naive metastatic breast cancer. (Those with hormone receptor–positive disease could have received hormonal therapy for their metastases.) Prior adjuvant taxane therapy given more than a year before enrollment was permitted.
The women received single-agent tesetaxel orally once every 3 weeks and without any antiallergy premedication but with an oral antiemetic as a precaution. "We have completed an effect-of-food study; the drug can be administered with or without food, so there is no need for fasting," Dr. Itri said.
"The patient takes their pill in front of the doctor, so the doctor knows that the patient has gotten a full dose. There is no compliance question," she further noted. "Then they go home and they come back 3 weeks later."
The starting dose was 27 mg/m2 every 3 weeks. For the first half of the trial, the dose was escalated up to 35 mg/m2 every 3 weeks if tolerated.
Overall, 20% of women had triple-negative disease, according to results reported in a poster session. More than half each had liver metastases (52%) and lung metastases (57%). Fifty-seven percent had received a taxane as part of their adjuvant therapy.
The median number of cycles of tesetaxel received was 4 (range, 1-17). The overall response rate was 45% (49% in women with estrogen receptor–positive disease and 33% in women with triple-negative disease).
The overall response rate was nearly the same among women who received only the nonescalated dose (44%) and among women who received the escalated dose (47%).
An additional 36% of patients achieved stable disease. Median progression-free survival was 5.8 months for all treated patients and 7.3 months for those with estrogen receptor–positive disease.
"Pretty much, the tolerability profile looks really good," Dr. Itri commented. In particular, none of the patients had hypersensitivity reactions.
By far, the most common grade 3/4 adverse event was neutropenia, seen in 33% of patients overall (26% without dose escalation and 43% with it). However, "none of these patients required a colony-stimulating factor or were febrile. So this now becomes a true outpatient regimen," she said.
The rate of grade 3 peripheral neuropathy was 7% overall (0% without dose escalation and 16% with it), and there was no grade 4 peripheral neuropathy. The rate of grade 2 alopecia was 15% regardless of dose.
Genta sponsored the trial. Dr. Itri disclosed employment and stock ownership in Genta. Dr. Moulder disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY

Biochemotherapy Gets Mixed Results in High-Risk Melanoma
CHICAGO – Biochemotherapy is efficacious when used as adjuvant treatment for high-risk melanoma, but not enough to displace the current standard of care, suggests a randomized phase III trial of the Southwest Oncology Group.
The trial, known as S0008, pitted biochemotherapy (chemotherapy plus interleukin-2 and interferon) against high-dose interferon in 402 patients who had undergone wide local excision and lymphadenectomy for stage III melanoma that had features conferring a high risk of recurrence.
Biochemotherapy was associated with a 24% lower risk of relapse, compared with interferon, but there was no significant difference in overall survival, according to trial results reported at the annual meeting of the American Society of Clinical Oncology. Adverse event profiles differed somewhat.
"Biochemotherapy is the first and only therapy to demonstrate a significant improvement in relapse-free survival compared to high-dose interferon in stage III melanoma patients. Biochemotherapy, however, was not associated with an improvement in overall survival," said lead investigator Dr. Lawrence E. Flaherty of the Karmanos Cancer Institute in Detroit.
"Further follow-up will be done on the trial to provide additional insights on longer-term outcomes, but they are not expected to be statistically significant."
"Without an overall survival benefit, biochemotherapy does not replace interferon as the standard of care. However, this may be an attractive alternative to interferon for high-risk melanoma patients," he added, noting biochemotherapy’s advantages of a much shorter treatment duration (2 vs. 12 months) and higher rate of treatment completion.
"Probably more important for our research community is the ability to modify all of the elements that we see here – all of the chemotherapy and biotherapy – as newer elements enter into our field," Dr. Flaherty commented. "This is a template that we can move forward with much more easily and effectively, and efforts of that nature are already ongoing in the stage IV setting."
A session attendee asked, "Would you care to speculate why there was no impact on survival? The disease-free survival impact is very reasonable ... [but] the [overall survival] curves never separated. Any thoughts?"
Dr. Flaherty proposed that it may be related to salvage therapies received after progression, which have improved since the trial. "Certainly, [with] these patients’ having progressed on biochemotherapy, the question would be, what other agents are available then to treat them at progression? I think that that would be less of an issue today with newer agents out, [such as] vemurafenib [and] ipilimumab. It might look differently today than it did with data in the 2000s," he said.
Another attendee questioned whether the short duration of biochemotherapy in the study compromised its efficacy. "Maybe one of the issues here is, by doing 2 months of treatment, you are not really fully exploiting the value of biochemotherapy," he said. "But I know that in community settings, it’s very hard to go beyond this, so it’s a tricky situation."
"We agree," Dr. Flaherty replied. "We had to look for a regimen that could be done throughout the United States with the potential of safety as well as efficacy. And that may be different than what can be done in specialty comprehensive cancer centers."
Discussant Dr. Lynn Schuchter of the Abramson Cancer Center at the University of Pennsylvania, Philadelphia, said, "It’s reasonable to consider biochemotherapy in the adjuvant setting in highly selected patients with melanoma. When I’ve used it, it’s been in young patients with multiple positive lymph nodes."
"I would say that the study results that we heard today do not change the standard of care for our patients with stage III melanoma," she agreed. "And importantly, I would say that further tweaking of the interferon dose, schedule, or route, or type of interferon is not going to move the field forward. ... It’s time that we really look at the new phase III adjuvant trials," such as those involving ipilimumab, vemurafenib, and dabrafenib, and vaccines.
Patients in the S0008 trial were randomized in balanced fashion to biochemotherapy (a 2-month course involving cisplatin, vinblastine, dacarbazine, IL-2, and interferon) or high-dose interferon (4-week induction followed by 48-week maintenance).
Results showed that patients in the biochemotherapy arm were significantly more likely to complete treatment (80% vs. 43%; P less than .001).
With a median 6.25-year follow-up, "the relapse-free survival is strikingly in favor of the biochemotherapy arm" over the high-dose interferon arm, Dr. Flaherty reported (median, 4.3 vs. 1.9 years; hazard ratio, 0.76; P = .03). The 5-year rate of relapse-free survival was 47% and 39%, respectively.
Findings were generally similar across subgroups, although "the more favorable groups appear to be younger individuals, females, those with one to three positive nodes, macroscopic nodes, and those without ulceration," he noted.
There was no significant difference between groups in overall survival. The median duration was 8.4 years with high-dose interferon and was not reached with biochemotherapy. The 5-year rate was 56% in both groups. And findings again were generally similar across patient subgroups.
The two treatments had differing grade 3/4 adverse event profiles: Biochemotherapy was associated with higher rates of gastrointestinal, hematologic, and metabolic toxicities, but lower rates of hepatic and neuropsychiatric toxicities.
Dr. Flaherty disclosed that he is a consultant to and receives honoraria and research funding from Merck and Novartis. Dr. Schuchter disclosed that she receives research funding from Genentech, GlaxoSmithKline, Merck, and Roche.
CHICAGO – Biochemotherapy is efficacious when used as adjuvant treatment for high-risk melanoma, but not enough to displace the current standard of care, suggests a randomized phase III trial of the Southwest Oncology Group.
The trial, known as S0008, pitted biochemotherapy (chemotherapy plus interleukin-2 and interferon) against high-dose interferon in 402 patients who had undergone wide local excision and lymphadenectomy for stage III melanoma that had features conferring a high risk of recurrence.
Biochemotherapy was associated with a 24% lower risk of relapse, compared with interferon, but there was no significant difference in overall survival, according to trial results reported at the annual meeting of the American Society of Clinical Oncology. Adverse event profiles differed somewhat.
"Biochemotherapy is the first and only therapy to demonstrate a significant improvement in relapse-free survival compared to high-dose interferon in stage III melanoma patients. Biochemotherapy, however, was not associated with an improvement in overall survival," said lead investigator Dr. Lawrence E. Flaherty of the Karmanos Cancer Institute in Detroit.
"Further follow-up will be done on the trial to provide additional insights on longer-term outcomes, but they are not expected to be statistically significant."
"Without an overall survival benefit, biochemotherapy does not replace interferon as the standard of care. However, this may be an attractive alternative to interferon for high-risk melanoma patients," he added, noting biochemotherapy’s advantages of a much shorter treatment duration (2 vs. 12 months) and higher rate of treatment completion.
"Probably more important for our research community is the ability to modify all of the elements that we see here – all of the chemotherapy and biotherapy – as newer elements enter into our field," Dr. Flaherty commented. "This is a template that we can move forward with much more easily and effectively, and efforts of that nature are already ongoing in the stage IV setting."
A session attendee asked, "Would you care to speculate why there was no impact on survival? The disease-free survival impact is very reasonable ... [but] the [overall survival] curves never separated. Any thoughts?"
Dr. Flaherty proposed that it may be related to salvage therapies received after progression, which have improved since the trial. "Certainly, [with] these patients’ having progressed on biochemotherapy, the question would be, what other agents are available then to treat them at progression? I think that that would be less of an issue today with newer agents out, [such as] vemurafenib [and] ipilimumab. It might look differently today than it did with data in the 2000s," he said.
Another attendee questioned whether the short duration of biochemotherapy in the study compromised its efficacy. "Maybe one of the issues here is, by doing 2 months of treatment, you are not really fully exploiting the value of biochemotherapy," he said. "But I know that in community settings, it’s very hard to go beyond this, so it’s a tricky situation."
"We agree," Dr. Flaherty replied. "We had to look for a regimen that could be done throughout the United States with the potential of safety as well as efficacy. And that may be different than what can be done in specialty comprehensive cancer centers."
Discussant Dr. Lynn Schuchter of the Abramson Cancer Center at the University of Pennsylvania, Philadelphia, said, "It’s reasonable to consider biochemotherapy in the adjuvant setting in highly selected patients with melanoma. When I’ve used it, it’s been in young patients with multiple positive lymph nodes."
"I would say that the study results that we heard today do not change the standard of care for our patients with stage III melanoma," she agreed. "And importantly, I would say that further tweaking of the interferon dose, schedule, or route, or type of interferon is not going to move the field forward. ... It’s time that we really look at the new phase III adjuvant trials," such as those involving ipilimumab, vemurafenib, and dabrafenib, and vaccines.
Patients in the S0008 trial were randomized in balanced fashion to biochemotherapy (a 2-month course involving cisplatin, vinblastine, dacarbazine, IL-2, and interferon) or high-dose interferon (4-week induction followed by 48-week maintenance).
Results showed that patients in the biochemotherapy arm were significantly more likely to complete treatment (80% vs. 43%; P less than .001).
With a median 6.25-year follow-up, "the relapse-free survival is strikingly in favor of the biochemotherapy arm" over the high-dose interferon arm, Dr. Flaherty reported (median, 4.3 vs. 1.9 years; hazard ratio, 0.76; P = .03). The 5-year rate of relapse-free survival was 47% and 39%, respectively.
Findings were generally similar across subgroups, although "the more favorable groups appear to be younger individuals, females, those with one to three positive nodes, macroscopic nodes, and those without ulceration," he noted.
There was no significant difference between groups in overall survival. The median duration was 8.4 years with high-dose interferon and was not reached with biochemotherapy. The 5-year rate was 56% in both groups. And findings again were generally similar across patient subgroups.
The two treatments had differing grade 3/4 adverse event profiles: Biochemotherapy was associated with higher rates of gastrointestinal, hematologic, and metabolic toxicities, but lower rates of hepatic and neuropsychiatric toxicities.
Dr. Flaherty disclosed that he is a consultant to and receives honoraria and research funding from Merck and Novartis. Dr. Schuchter disclosed that she receives research funding from Genentech, GlaxoSmithKline, Merck, and Roche.
CHICAGO – Biochemotherapy is efficacious when used as adjuvant treatment for high-risk melanoma, but not enough to displace the current standard of care, suggests a randomized phase III trial of the Southwest Oncology Group.
The trial, known as S0008, pitted biochemotherapy (chemotherapy plus interleukin-2 and interferon) against high-dose interferon in 402 patients who had undergone wide local excision and lymphadenectomy for stage III melanoma that had features conferring a high risk of recurrence.
Biochemotherapy was associated with a 24% lower risk of relapse, compared with interferon, but there was no significant difference in overall survival, according to trial results reported at the annual meeting of the American Society of Clinical Oncology. Adverse event profiles differed somewhat.
"Biochemotherapy is the first and only therapy to demonstrate a significant improvement in relapse-free survival compared to high-dose interferon in stage III melanoma patients. Biochemotherapy, however, was not associated with an improvement in overall survival," said lead investigator Dr. Lawrence E. Flaherty of the Karmanos Cancer Institute in Detroit.
"Further follow-up will be done on the trial to provide additional insights on longer-term outcomes, but they are not expected to be statistically significant."
"Without an overall survival benefit, biochemotherapy does not replace interferon as the standard of care. However, this may be an attractive alternative to interferon for high-risk melanoma patients," he added, noting biochemotherapy’s advantages of a much shorter treatment duration (2 vs. 12 months) and higher rate of treatment completion.
"Probably more important for our research community is the ability to modify all of the elements that we see here – all of the chemotherapy and biotherapy – as newer elements enter into our field," Dr. Flaherty commented. "This is a template that we can move forward with much more easily and effectively, and efforts of that nature are already ongoing in the stage IV setting."
A session attendee asked, "Would you care to speculate why there was no impact on survival? The disease-free survival impact is very reasonable ... [but] the [overall survival] curves never separated. Any thoughts?"
Dr. Flaherty proposed that it may be related to salvage therapies received after progression, which have improved since the trial. "Certainly, [with] these patients’ having progressed on biochemotherapy, the question would be, what other agents are available then to treat them at progression? I think that that would be less of an issue today with newer agents out, [such as] vemurafenib [and] ipilimumab. It might look differently today than it did with data in the 2000s," he said.
Another attendee questioned whether the short duration of biochemotherapy in the study compromised its efficacy. "Maybe one of the issues here is, by doing 2 months of treatment, you are not really fully exploiting the value of biochemotherapy," he said. "But I know that in community settings, it’s very hard to go beyond this, so it’s a tricky situation."
"We agree," Dr. Flaherty replied. "We had to look for a regimen that could be done throughout the United States with the potential of safety as well as efficacy. And that may be different than what can be done in specialty comprehensive cancer centers."
Discussant Dr. Lynn Schuchter of the Abramson Cancer Center at the University of Pennsylvania, Philadelphia, said, "It’s reasonable to consider biochemotherapy in the adjuvant setting in highly selected patients with melanoma. When I’ve used it, it’s been in young patients with multiple positive lymph nodes."
"I would say that the study results that we heard today do not change the standard of care for our patients with stage III melanoma," she agreed. "And importantly, I would say that further tweaking of the interferon dose, schedule, or route, or type of interferon is not going to move the field forward. ... It’s time that we really look at the new phase III adjuvant trials," such as those involving ipilimumab, vemurafenib, and dabrafenib, and vaccines.
Patients in the S0008 trial were randomized in balanced fashion to biochemotherapy (a 2-month course involving cisplatin, vinblastine, dacarbazine, IL-2, and interferon) or high-dose interferon (4-week induction followed by 48-week maintenance).
Results showed that patients in the biochemotherapy arm were significantly more likely to complete treatment (80% vs. 43%; P less than .001).
With a median 6.25-year follow-up, "the relapse-free survival is strikingly in favor of the biochemotherapy arm" over the high-dose interferon arm, Dr. Flaherty reported (median, 4.3 vs. 1.9 years; hazard ratio, 0.76; P = .03). The 5-year rate of relapse-free survival was 47% and 39%, respectively.
Findings were generally similar across subgroups, although "the more favorable groups appear to be younger individuals, females, those with one to three positive nodes, macroscopic nodes, and those without ulceration," he noted.
There was no significant difference between groups in overall survival. The median duration was 8.4 years with high-dose interferon and was not reached with biochemotherapy. The 5-year rate was 56% in both groups. And findings again were generally similar across patient subgroups.
The two treatments had differing grade 3/4 adverse event profiles: Biochemotherapy was associated with higher rates of gastrointestinal, hematologic, and metabolic toxicities, but lower rates of hepatic and neuropsychiatric toxicities.
Dr. Flaherty disclosed that he is a consultant to and receives honoraria and research funding from Merck and Novartis. Dr. Schuchter disclosed that she receives research funding from Genentech, GlaxoSmithKline, Merck, and Roche.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: Compared with high-dose interferon, biochemotherapy significantly improved relapse-free survival (HR, 0.76), but not overall survival.
Data Source: The randomized, phase III SWOG S0008 trial involved 402 patients with high-risk, stage III melanoma.
Disclosures: Dr. Flaherty disclosed that he is a consultant to and receives honoraria and research funding from Merck and Novartis. Dr. Schuchter disclosed that she receives research funding from Genentech, GlaxoSmithKline, Merck, and Roche.
Cortical Thickening Observed in Patients With Frequent Migraines
LOS ANGELES – The thickness and functional activation of primary somatosensory cortex mapping to the face differed according to the frequency of migraine in a small study presented at the annual meeting of the American Headache Society.
In the cross-sectional study of 20 patients, investigators conducted anatomic and functional magnetic resonance imaging in 10 patients with a low frequency of migraine attacks (mean age 40 years) and 10 with a high frequency of attacks (mean age 44 years).

Results showed that the area of the postcentral gyrus cortex representing the face was about a quarter thicker in the high-frequency group, compared with the low-frequency group. And activation of this area in response to a painful stimulus was also greater in the former.
"We think that this change that we see in high-frequency migraineurs is probably an adaptive response of the brain in order to accommodate this increased input of painful attacks, to be able to process it more and be able to handle it," commented lead investigator Nasim Maleki, Ph.D., of the Center for Pain and the Brain at Children’s Hospital Boston. Thus, the cortical thickening and increased activation might be a marker of chronification or transformation of migraine due to greater frequency of pain, triptan use, or both, she proposed.
A longitudinal study would be needed to definitively sort out cause versus effect, Dr. Maleki acknowledged. "But it could be a good hypothesis at least if somebody could do a longitudinal study, for example, looking at patients who regress from chronic to episodic migraine and then seeing if that area undergoes changes, both morphometric and functional changes."
Dr. Peter Goadsby of the University of California, San Francisco, asked, "Did you say that the BOLD [blood oxygen level–dependent] effect was being elicited from the dorsum of the hand, and the flow changes were in the face area [of the cortex]?"
"I was surprised by the same thing, too," Dr. Maleki replied. She noted that in results not shown, there was also activation of cortical areas corresponding to the hand. "But I think that maybe because that [face] area is already sensitized and responds to pain in general, the fact that we were seeing it even when we were stimulating the hand ... that’s relevant."
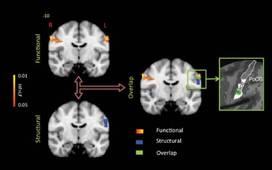
Session attendee Dr. Ronald Andiman of Cedars-Sinai Medical Center in Los Angeles asked, "What is the substance of the increased thickness of the cortex when you see it? Is it cellular? Is it neural fibers?"
It was not possible to tell given that the study used only MRI, Dr. Maleki said. "But ... we are thinking of doing the same thing in rats and seeing if there is the same pattern, and then we will be able to determine if it is density, or if it is just the number of neurons, or what exactly is going on," she said.
In a discussion of research highlights from the meeting and elsewhere, Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia noted that a previous study of new London cab drivers found that their cortical thickness increased when they learned to navigate the city.
In the migraine study, "the question is, is this [thickening] cause or result?" he said. "I suspect this is like the cab drivers: If you have a lot of headaches, you learn what they are, and it affects your cortex. And I agree that this is probably a marker for migraine, not a cause of it."
Dr. Maleki and her colleagues recruited patients who had had episodic migraine for at least 3 years. On the basis of age, sex, and other migraine characteristics, they matched patients with low-frequency attacks (1-2 per month) to patients with high-frequency attacks (8-12 per month). However, she acknowledged, use of analgesic medications was unavoidably greater in the high-frequency group. The investigators also included a group of age- and sex-matched healthy individuals as controls.
Results from anatomical MRI showed that the thickness of the area of the postcentral gyrus representing the face averaged approximately 2.25 mm in patients with high-frequency migraines, compared with 1.75 mm in patients with low-frequency migraines (P less than .05) and 2.0 mm in the control participants (P less than .05).
During functional MRI performed while a noxious heat stimulus was applied to the dorsum of the hand on the migraine-dominant side, there were greater increases in BOLD signals bilaterally in the same area in the high- versus low-frequency group. "Comparing what we saw in the morphometric differences between groups and these functional contrasting results, we saw an overlap between the area that shows this structural thickening and the area that shows this functional difference," Dr. Maleki noted.
Additional functional MRI comparing somatosensory cortex connectivity between migraine groups showed that certain other areas of the brain were also more active in the high-frequency group.
"Interestingly, all of these areas ... are known areas involved in pain processing," she noted. "So again, this confirms that this thicker cortical area in high-frequency migraineurs also has stronger communication with these other areas of the brain that are also involved in pain processing."
Dr. Maleki disclosed no relevant conflicts of interest. Data analysis was supported in part by a grant from Merck.
LOS ANGELES – The thickness and functional activation of primary somatosensory cortex mapping to the face differed according to the frequency of migraine in a small study presented at the annual meeting of the American Headache Society.
In the cross-sectional study of 20 patients, investigators conducted anatomic and functional magnetic resonance imaging in 10 patients with a low frequency of migraine attacks (mean age 40 years) and 10 with a high frequency of attacks (mean age 44 years).
Results showed that the area of the postcentral gyrus cortex representing the face was about a quarter thicker in the high-frequency group, compared with the low-frequency group. And activation of this area in response to a painful stimulus was also greater in the former.
"We think that this change that we see in high-frequency migraineurs is probably an adaptive response of the brain in order to accommodate this increased input of painful attacks, to be able to process it more and be able to handle it," commented lead investigator Nasim Maleki, Ph.D., of the Center for Pain and the Brain at Children’s Hospital Boston. Thus, the cortical thickening and increased activation might be a marker of chronification or transformation of migraine due to greater frequency of pain, triptan use, or both, she proposed.
A longitudinal study would be needed to definitively sort out cause versus effect, Dr. Maleki acknowledged. "But it could be a good hypothesis at least if somebody could do a longitudinal study, for example, looking at patients who regress from chronic to episodic migraine and then seeing if that area undergoes changes, both morphometric and functional changes."
Dr. Peter Goadsby of the University of California, San Francisco, asked, "Did you say that the BOLD [blood oxygen level–dependent] effect was being elicited from the dorsum of the hand, and the flow changes were in the face area [of the cortex]?"
"I was surprised by the same thing, too," Dr. Maleki replied. She noted that in results not shown, there was also activation of cortical areas corresponding to the hand. "But I think that maybe because that [face] area is already sensitized and responds to pain in general, the fact that we were seeing it even when we were stimulating the hand ... that’s relevant."
Session attendee Dr. Ronald Andiman of Cedars-Sinai Medical Center in Los Angeles asked, "What is the substance of the increased thickness of the cortex when you see it? Is it cellular? Is it neural fibers?"
It was not possible to tell given that the study used only MRI, Dr. Maleki said. "But ... we are thinking of doing the same thing in rats and seeing if there is the same pattern, and then we will be able to determine if it is density, or if it is just the number of neurons, or what exactly is going on," she said.
In a discussion of research highlights from the meeting and elsewhere, Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia noted that a previous study of new London cab drivers found that their cortical thickness increased when they learned to navigate the city.
In the migraine study, "the question is, is this [thickening] cause or result?" he said. "I suspect this is like the cab drivers: If you have a lot of headaches, you learn what they are, and it affects your cortex. And I agree that this is probably a marker for migraine, not a cause of it."
Dr. Maleki and her colleagues recruited patients who had had episodic migraine for at least 3 years. On the basis of age, sex, and other migraine characteristics, they matched patients with low-frequency attacks (1-2 per month) to patients with high-frequency attacks (8-12 per month). However, she acknowledged, use of analgesic medications was unavoidably greater in the high-frequency group. The investigators also included a group of age- and sex-matched healthy individuals as controls.
Results from anatomical MRI showed that the thickness of the area of the postcentral gyrus representing the face averaged approximately 2.25 mm in patients with high-frequency migraines, compared with 1.75 mm in patients with low-frequency migraines (P less than .05) and 2.0 mm in the control participants (P less than .05).
During functional MRI performed while a noxious heat stimulus was applied to the dorsum of the hand on the migraine-dominant side, there were greater increases in BOLD signals bilaterally in the same area in the high- versus low-frequency group. "Comparing what we saw in the morphometric differences between groups and these functional contrasting results, we saw an overlap between the area that shows this structural thickening and the area that shows this functional difference," Dr. Maleki noted.
Additional functional MRI comparing somatosensory cortex connectivity between migraine groups showed that certain other areas of the brain were also more active in the high-frequency group.
"Interestingly, all of these areas ... are known areas involved in pain processing," she noted. "So again, this confirms that this thicker cortical area in high-frequency migraineurs also has stronger communication with these other areas of the brain that are also involved in pain processing."
Dr. Maleki disclosed no relevant conflicts of interest. Data analysis was supported in part by a grant from Merck.
LOS ANGELES – The thickness and functional activation of primary somatosensory cortex mapping to the face differed according to the frequency of migraine in a small study presented at the annual meeting of the American Headache Society.
In the cross-sectional study of 20 patients, investigators conducted anatomic and functional magnetic resonance imaging in 10 patients with a low frequency of migraine attacks (mean age 40 years) and 10 with a high frequency of attacks (mean age 44 years).
Results showed that the area of the postcentral gyrus cortex representing the face was about a quarter thicker in the high-frequency group, compared with the low-frequency group. And activation of this area in response to a painful stimulus was also greater in the former.
"We think that this change that we see in high-frequency migraineurs is probably an adaptive response of the brain in order to accommodate this increased input of painful attacks, to be able to process it more and be able to handle it," commented lead investigator Nasim Maleki, Ph.D., of the Center for Pain and the Brain at Children’s Hospital Boston. Thus, the cortical thickening and increased activation might be a marker of chronification or transformation of migraine due to greater frequency of pain, triptan use, or both, she proposed.
A longitudinal study would be needed to definitively sort out cause versus effect, Dr. Maleki acknowledged. "But it could be a good hypothesis at least if somebody could do a longitudinal study, for example, looking at patients who regress from chronic to episodic migraine and then seeing if that area undergoes changes, both morphometric and functional changes."
Dr. Peter Goadsby of the University of California, San Francisco, asked, "Did you say that the BOLD [blood oxygen level–dependent] effect was being elicited from the dorsum of the hand, and the flow changes were in the face area [of the cortex]?"
"I was surprised by the same thing, too," Dr. Maleki replied. She noted that in results not shown, there was also activation of cortical areas corresponding to the hand. "But I think that maybe because that [face] area is already sensitized and responds to pain in general, the fact that we were seeing it even when we were stimulating the hand ... that’s relevant."
Session attendee Dr. Ronald Andiman of Cedars-Sinai Medical Center in Los Angeles asked, "What is the substance of the increased thickness of the cortex when you see it? Is it cellular? Is it neural fibers?"
It was not possible to tell given that the study used only MRI, Dr. Maleki said. "But ... we are thinking of doing the same thing in rats and seeing if there is the same pattern, and then we will be able to determine if it is density, or if it is just the number of neurons, or what exactly is going on," she said.
In a discussion of research highlights from the meeting and elsewhere, Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia noted that a previous study of new London cab drivers found that their cortical thickness increased when they learned to navigate the city.
In the migraine study, "the question is, is this [thickening] cause or result?" he said. "I suspect this is like the cab drivers: If you have a lot of headaches, you learn what they are, and it affects your cortex. And I agree that this is probably a marker for migraine, not a cause of it."
Dr. Maleki and her colleagues recruited patients who had had episodic migraine for at least 3 years. On the basis of age, sex, and other migraine characteristics, they matched patients with low-frequency attacks (1-2 per month) to patients with high-frequency attacks (8-12 per month). However, she acknowledged, use of analgesic medications was unavoidably greater in the high-frequency group. The investigators also included a group of age- and sex-matched healthy individuals as controls.
Results from anatomical MRI showed that the thickness of the area of the postcentral gyrus representing the face averaged approximately 2.25 mm in patients with high-frequency migraines, compared with 1.75 mm in patients with low-frequency migraines (P less than .05) and 2.0 mm in the control participants (P less than .05).
During functional MRI performed while a noxious heat stimulus was applied to the dorsum of the hand on the migraine-dominant side, there were greater increases in BOLD signals bilaterally in the same area in the high- versus low-frequency group. "Comparing what we saw in the morphometric differences between groups and these functional contrasting results, we saw an overlap between the area that shows this structural thickening and the area that shows this functional difference," Dr. Maleki noted.
Additional functional MRI comparing somatosensory cortex connectivity between migraine groups showed that certain other areas of the brain were also more active in the high-frequency group.
"Interestingly, all of these areas ... are known areas involved in pain processing," she noted. "So again, this confirms that this thicker cortical area in high-frequency migraineurs also has stronger communication with these other areas of the brain that are also involved in pain processing."
Dr. Maleki disclosed no relevant conflicts of interest. Data analysis was supported in part by a grant from Merck.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
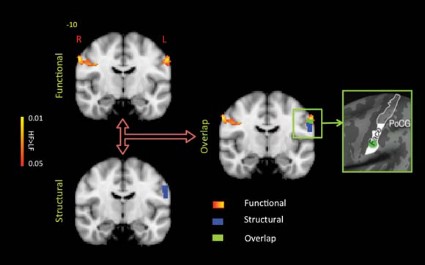
Chronic Migraine Linked to More Stressful Life Events
LOS ANGELES – Chronic migraineurs reported a greater number of stressful major life events than did those with episodic migraines in a large, cross-sectional analysis of the American Migraine Prevalence and Prevention Study.
In the study, 551 chronic migraineurs were 25% more likely report to a higher number of stressful major life events in the past year than were 7,644 episodic migraineurs, after other factors were taken into account.
"We don’t know whether the events occurred before the onset of chronic migraine or because a person was a chronic migraineur," acknowledged Aubrey N. Manack, Ph.D., an epidemiologist with Allergan Inc.

"What I think is most relevant for clinical practice is that events are perceived as stressful based on an individual’s appraisal," she continued; "so cognitive behavioral interventions may be beneficial in helping individuals reframe their perception of events and in teaching more coping skills."
She recommended future study to assess whether this association is influenced by cultural factors, as well as longitudinal research to determine if stressful life events are a risk factor for or a consequence of chronic migraine.
Session attendee Dr. Gretchen Tietjen of the University of Toledo (Ohio) Medical Center noted that she and her colleagues have analyzed data from the AMPPS as well, and found that early stressful life events – in this case, childhood maltreatment – predicted more frequent headache-days. "So I think an interesting thing would be, besides controlling for all of the things you have controlled for, to look at that, since we already have the data, just to see how many of those chronic migraineurs who had perceived stressful life events had very stressful early life events," she said at the annual meeting of the American Headache Society.
Dr. Manack agreed. And Dawn Buse, Ph.D., a psychologist at the Albert Einstein College of Medicine, New York, and a coinvestigator on both studies, noted that "early stressful life events and traumatic events such as abuse and maltreatment actually in kind of an epigenetic sort of way change our responses forever – immune system responses, coping stress mechanisms. It’s very likely that individuals who had early trauma perceive an event as stressful or overwhelming compared to an individual who had a healthier childhood and who may be more hearty."

"And what’s so interesting to remember is that an event in itself inherently is not stressful," rather it is how a person perceives the event, Dr. Buse added. Therefore, "we need to help our patients perceive life events as manageable and enhance coping skills."
In the longitudinal, population-based AMPPS, questionnaires were mailed to 24,000 individuals reporting severe headache who were first identified in 2004 and then followed up annually between 2005 and 2009.
Dr. Manack’s team studied participants in 2007 who met the diagnostic criteria for migraine, and split them into an episodic migraine group (defined as having fewer than 15 headache-days monthly) and a chronic migraine group (15 or more headache-days monthly).
The participants were surveyed about major life events in the past year, including moves; changes in the status of significant relationships; work and school stressors; events related to children; deaths; and other extremely stressful situations. Those who reported experiencing at least one such event were asked to rate its stressfulness on a 1-5 scale, and events were classified as stressful if they were rated as at least 4.
Overall, 82% of patients with chronic migraine and 79% of patients with episodic migraine reported experiencing at least one major life event in the previous year.
"The difference doesn’t seem that significant, but when you look at ... the number of events that happened, you start to see greater separation," Dr. Manack noted.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of major life events in unadjusted analysis (odds ratio, 1.19; P = .03) and even more so after adjustment for age, sex, race, and body mass index (OR, 1.22; P = .01).

Overall, 77% of patients with chronic migraine and 71% of patients with episodic migraine reported experiencing at least one stressful major life event in the previous year. Again, differences between groups appeared somewhat greater at higher numbers of events.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of stressful major life events in both unadjusted analysis (OR, 1.25; P = .02) and adjusted analysis (OR, 1.26; P = .01).
Dr. Manack disclosed that she is a full-time employee of Allergan Inc. The AMPPS is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics Inc.; additional analyses and manuscript preparation were supported through a grant from Allergan Inc. to the National Headache Foundation.
LOS ANGELES – Chronic migraineurs reported a greater number of stressful major life events than did those with episodic migraines in a large, cross-sectional analysis of the American Migraine Prevalence and Prevention Study.
In the study, 551 chronic migraineurs were 25% more likely report to a higher number of stressful major life events in the past year than were 7,644 episodic migraineurs, after other factors were taken into account.
"We don’t know whether the events occurred before the onset of chronic migraine or because a person was a chronic migraineur," acknowledged Aubrey N. Manack, Ph.D., an epidemiologist with Allergan Inc.
"What I think is most relevant for clinical practice is that events are perceived as stressful based on an individual’s appraisal," she continued; "so cognitive behavioral interventions may be beneficial in helping individuals reframe their perception of events and in teaching more coping skills."
She recommended future study to assess whether this association is influenced by cultural factors, as well as longitudinal research to determine if stressful life events are a risk factor for or a consequence of chronic migraine.
Session attendee Dr. Gretchen Tietjen of the University of Toledo (Ohio) Medical Center noted that she and her colleagues have analyzed data from the AMPPS as well, and found that early stressful life events – in this case, childhood maltreatment – predicted more frequent headache-days. "So I think an interesting thing would be, besides controlling for all of the things you have controlled for, to look at that, since we already have the data, just to see how many of those chronic migraineurs who had perceived stressful life events had very stressful early life events," she said at the annual meeting of the American Headache Society.
Dr. Manack agreed. And Dawn Buse, Ph.D., a psychologist at the Albert Einstein College of Medicine, New York, and a coinvestigator on both studies, noted that "early stressful life events and traumatic events such as abuse and maltreatment actually in kind of an epigenetic sort of way change our responses forever – immune system responses, coping stress mechanisms. It’s very likely that individuals who had early trauma perceive an event as stressful or overwhelming compared to an individual who had a healthier childhood and who may be more hearty."
"And what’s so interesting to remember is that an event in itself inherently is not stressful," rather it is how a person perceives the event, Dr. Buse added. Therefore, "we need to help our patients perceive life events as manageable and enhance coping skills."
In the longitudinal, population-based AMPPS, questionnaires were mailed to 24,000 individuals reporting severe headache who were first identified in 2004 and then followed up annually between 2005 and 2009.
Dr. Manack’s team studied participants in 2007 who met the diagnostic criteria for migraine, and split them into an episodic migraine group (defined as having fewer than 15 headache-days monthly) and a chronic migraine group (15 or more headache-days monthly).
The participants were surveyed about major life events in the past year, including moves; changes in the status of significant relationships; work and school stressors; events related to children; deaths; and other extremely stressful situations. Those who reported experiencing at least one such event were asked to rate its stressfulness on a 1-5 scale, and events were classified as stressful if they were rated as at least 4.
Overall, 82% of patients with chronic migraine and 79% of patients with episodic migraine reported experiencing at least one major life event in the previous year.
"The difference doesn’t seem that significant, but when you look at ... the number of events that happened, you start to see greater separation," Dr. Manack noted.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of major life events in unadjusted analysis (odds ratio, 1.19; P = .03) and even more so after adjustment for age, sex, race, and body mass index (OR, 1.22; P = .01).
Overall, 77% of patients with chronic migraine and 71% of patients with episodic migraine reported experiencing at least one stressful major life event in the previous year. Again, differences between groups appeared somewhat greater at higher numbers of events.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of stressful major life events in both unadjusted analysis (OR, 1.25; P = .02) and adjusted analysis (OR, 1.26; P = .01).
Dr. Manack disclosed that she is a full-time employee of Allergan Inc. The AMPPS is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics Inc.; additional analyses and manuscript preparation were supported through a grant from Allergan Inc. to the National Headache Foundation.
LOS ANGELES – Chronic migraineurs reported a greater number of stressful major life events than did those with episodic migraines in a large, cross-sectional analysis of the American Migraine Prevalence and Prevention Study.
In the study, 551 chronic migraineurs were 25% more likely report to a higher number of stressful major life events in the past year than were 7,644 episodic migraineurs, after other factors were taken into account.
"We don’t know whether the events occurred before the onset of chronic migraine or because a person was a chronic migraineur," acknowledged Aubrey N. Manack, Ph.D., an epidemiologist with Allergan Inc.
"What I think is most relevant for clinical practice is that events are perceived as stressful based on an individual’s appraisal," she continued; "so cognitive behavioral interventions may be beneficial in helping individuals reframe their perception of events and in teaching more coping skills."
She recommended future study to assess whether this association is influenced by cultural factors, as well as longitudinal research to determine if stressful life events are a risk factor for or a consequence of chronic migraine.
Session attendee Dr. Gretchen Tietjen of the University of Toledo (Ohio) Medical Center noted that she and her colleagues have analyzed data from the AMPPS as well, and found that early stressful life events – in this case, childhood maltreatment – predicted more frequent headache-days. "So I think an interesting thing would be, besides controlling for all of the things you have controlled for, to look at that, since we already have the data, just to see how many of those chronic migraineurs who had perceived stressful life events had very stressful early life events," she said at the annual meeting of the American Headache Society.
Dr. Manack agreed. And Dawn Buse, Ph.D., a psychologist at the Albert Einstein College of Medicine, New York, and a coinvestigator on both studies, noted that "early stressful life events and traumatic events such as abuse and maltreatment actually in kind of an epigenetic sort of way change our responses forever – immune system responses, coping stress mechanisms. It’s very likely that individuals who had early trauma perceive an event as stressful or overwhelming compared to an individual who had a healthier childhood and who may be more hearty."
"And what’s so interesting to remember is that an event in itself inherently is not stressful," rather it is how a person perceives the event, Dr. Buse added. Therefore, "we need to help our patients perceive life events as manageable and enhance coping skills."
In the longitudinal, population-based AMPPS, questionnaires were mailed to 24,000 individuals reporting severe headache who were first identified in 2004 and then followed up annually between 2005 and 2009.
Dr. Manack’s team studied participants in 2007 who met the diagnostic criteria for migraine, and split them into an episodic migraine group (defined as having fewer than 15 headache-days monthly) and a chronic migraine group (15 or more headache-days monthly).
The participants were surveyed about major life events in the past year, including moves; changes in the status of significant relationships; work and school stressors; events related to children; deaths; and other extremely stressful situations. Those who reported experiencing at least one such event were asked to rate its stressfulness on a 1-5 scale, and events were classified as stressful if they were rated as at least 4.
Overall, 82% of patients with chronic migraine and 79% of patients with episodic migraine reported experiencing at least one major life event in the previous year.
"The difference doesn’t seem that significant, but when you look at ... the number of events that happened, you start to see greater separation," Dr. Manack noted.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of major life events in unadjusted analysis (odds ratio, 1.19; P = .03) and even more so after adjustment for age, sex, race, and body mass index (OR, 1.22; P = .01).
Overall, 77% of patients with chronic migraine and 71% of patients with episodic migraine reported experiencing at least one stressful major life event in the previous year. Again, differences between groups appeared somewhat greater at higher numbers of events.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of stressful major life events in both unadjusted analysis (OR, 1.25; P = .02) and adjusted analysis (OR, 1.26; P = .01).
Dr. Manack disclosed that she is a full-time employee of Allergan Inc. The AMPPS is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics Inc.; additional analyses and manuscript preparation were supported through a grant from Allergan Inc. to the National Headache Foundation.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: Relative to their counterparts with episodic migraine, patients with chronic migraine were more likely to report a greater number of stressful major life events in the past year (OR, 1.26).
Data Source: This was a cross-sectional study of 551 individuals with chronic migraine and 7,644 individuals with episodic migraine from the AMPPS.
Disclosures: Dr. Manack disclosed that she is a full-time employee of Allergan. The AMPP study is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics; additional analyses and manuscript preparation were supported through a grant from Allergan to the National Headache Foundation.
Platinum Levels Linked to Toxicity in Testicular Cancer Survivors
CHICAGO – Long-term platinum exposure may explain higher rates of certain late adverse effects in men who have undergone treatment for testicular cancer, investigators reported based on a longitudinal study.
Among 96 consecutive men treated with cisplatin for testicular cancer, serum platinum levels 5 years later were 14% higher in those with elevated versus normal blood pressure and 16% higher in those with paresthesia versus those without it.
Dr. Hink Boer and his colleagues collected two or three serum samples and a 24-hour urine sample from the men at various time points after chemotherapy out to 13 years (median, 5 years) for platinum measurement.
The men had a median age of 29 years at the start of treatment, according to results reported in a poster presentation at the annual meeting of the American Society of Clinical Oncology. The median absolute cumulative cisplatin dose was 809 mg.
The findings are especially important as these survivors are young men who "have their whole life ahead of them, actually. Survivor care is very much focused on relapse detection, of course. In the last decade, I think there is more attention on the delayed effects," Dr. Boer, a research fellow in medical oncology at the University of Groningen in the Netherlands, said in an interview.
A population pharmacokinetic model using measured serum platinum concentration and urinary excretion rate, as well as administered cisplatin dosage, age, body surface area, height, and weight, suggested that the mean terminal half-life of platinum in serum was 3.7 years, Dr. Boer reported.
Platinum levels fell steadily and in exponential fashion with time after chemotherapy but were still detectable 13 years later. Serum platinum levels at 3 years and at 5 years after chemotherapy were significantly higher in men administered a higher total dose of cisplatin and in men having lower renal clearance, he said.
Analyses of long-term toxicity showed that, compared with their counterparts with lower blood pressure, men with a blood pressure of at least 130/85 mm Hg or on antihypertensive medication had higher mean serum platinum levels at 3 years (420 vs. 366 pg/g, P = .045) and at 5 years (210 vs. 185 pg/g, P = .04), as well as a higher platinum area under the curve (AUC) for years 1-5 (1,071 vs. 945 pg/g × 103 × day, P = .04).
Similarly, compared with their counterparts who did not have paresthesia, men having this adverse effect had higher mean serum platinum levels at 3 years (456 vs. 387 pg/g, P = .02) and at 5 years (227 vs. 195 pg/g, P = .02), as well as a higher platinum AUC for years 1-5 (1,144 vs. 996 pg/g × 103 × day, P = .02).
In contrast, men with secondary Raynaud disease and men with endothelial damage as assessed from von Willebrand factor levels did not have significantly higher serum platinum levels than their respective counterparts, Dr. Boer said.
"It is a well-known problem now that the chemotherapy has its late effects, and we wanted to look to see if these very small concentrations ... have any relationship with these late toxicities," he said. "If you look at these data, you could assume that there is a relationship, a very small concentration but still, it might have an effect."
"The chemotherapy is very successful, of course; you don’t want to change it. The cure rates are very high in testicular cancer patients," he added. "At the moment it is not possible to get the platinum out of the body. It is not technically possible to chelate it or something.
"But you have to think about it – it could be a mechanism, so it is worthwhile to do more studies on this. Perhaps in the future, it will be possible to chelate it and get it out, if we can confirm that this is really an etiological mechanism," he said.
Current practice at his institution for these patients is regular examinations with special focus on cardiovascular risk factors such as blood pressure and cholesterol. "We are trying to bring more structure in this care and to pay more attention to the late effects. I think [the patients] deserve it because they are so young," Dr. Boer said.
Discussant Dr. Kim Allyson Margolin of the University of Washington, Seattle, noted that accumulating research is casting doubt on the view that this chemotherapy has minimal late effects. However, despite the finding of an association between persistent free platinum and late toxicity, "we don’t know whether the relationship of prior platinum exposure, just by doses given or something different about how the body handles the platinum related to renal function or metabolic polymorphisms, is responsible"
The study is "very interesting and provocative," Dr. Margolin concluded, "but we need more data. Pharmacologic investigations are still needed to enhance the quality of life for this growing number of germ cell tumor survivors."
Although the study focused on serum, Dr. Boer noted that platinum can be found in other tissues as well. "In the ganglia, for example, and also in bone, fat, and the liver ... it’s ... not really known if the platinum in these body compartments is reactive or not. It is really a topic that deserves more research," he said.
Dr. Boer disclosed that he had no relevant conflicts of interest. Dr. Margolin disclosed that she is a consultant to Bristol-Myers Squibb, Genentech, and Johnson & Johnson.
CHICAGO – Long-term platinum exposure may explain higher rates of certain late adverse effects in men who have undergone treatment for testicular cancer, investigators reported based on a longitudinal study.
Among 96 consecutive men treated with cisplatin for testicular cancer, serum platinum levels 5 years later were 14% higher in those with elevated versus normal blood pressure and 16% higher in those with paresthesia versus those without it.
Dr. Hink Boer and his colleagues collected two or three serum samples and a 24-hour urine sample from the men at various time points after chemotherapy out to 13 years (median, 5 years) for platinum measurement.
The men had a median age of 29 years at the start of treatment, according to results reported in a poster presentation at the annual meeting of the American Society of Clinical Oncology. The median absolute cumulative cisplatin dose was 809 mg.
The findings are especially important as these survivors are young men who "have their whole life ahead of them, actually. Survivor care is very much focused on relapse detection, of course. In the last decade, I think there is more attention on the delayed effects," Dr. Boer, a research fellow in medical oncology at the University of Groningen in the Netherlands, said in an interview.
A population pharmacokinetic model using measured serum platinum concentration and urinary excretion rate, as well as administered cisplatin dosage, age, body surface area, height, and weight, suggested that the mean terminal half-life of platinum in serum was 3.7 years, Dr. Boer reported.
Platinum levels fell steadily and in exponential fashion with time after chemotherapy but were still detectable 13 years later. Serum platinum levels at 3 years and at 5 years after chemotherapy were significantly higher in men administered a higher total dose of cisplatin and in men having lower renal clearance, he said.
Analyses of long-term toxicity showed that, compared with their counterparts with lower blood pressure, men with a blood pressure of at least 130/85 mm Hg or on antihypertensive medication had higher mean serum platinum levels at 3 years (420 vs. 366 pg/g, P = .045) and at 5 years (210 vs. 185 pg/g, P = .04), as well as a higher platinum area under the curve (AUC) for years 1-5 (1,071 vs. 945 pg/g × 103 × day, P = .04).
Similarly, compared with their counterparts who did not have paresthesia, men having this adverse effect had higher mean serum platinum levels at 3 years (456 vs. 387 pg/g, P = .02) and at 5 years (227 vs. 195 pg/g, P = .02), as well as a higher platinum AUC for years 1-5 (1,144 vs. 996 pg/g × 103 × day, P = .02).
In contrast, men with secondary Raynaud disease and men with endothelial damage as assessed from von Willebrand factor levels did not have significantly higher serum platinum levels than their respective counterparts, Dr. Boer said.
"It is a well-known problem now that the chemotherapy has its late effects, and we wanted to look to see if these very small concentrations ... have any relationship with these late toxicities," he said. "If you look at these data, you could assume that there is a relationship, a very small concentration but still, it might have an effect."
"The chemotherapy is very successful, of course; you don’t want to change it. The cure rates are very high in testicular cancer patients," he added. "At the moment it is not possible to get the platinum out of the body. It is not technically possible to chelate it or something.
"But you have to think about it – it could be a mechanism, so it is worthwhile to do more studies on this. Perhaps in the future, it will be possible to chelate it and get it out, if we can confirm that this is really an etiological mechanism," he said.
Current practice at his institution for these patients is regular examinations with special focus on cardiovascular risk factors such as blood pressure and cholesterol. "We are trying to bring more structure in this care and to pay more attention to the late effects. I think [the patients] deserve it because they are so young," Dr. Boer said.
Discussant Dr. Kim Allyson Margolin of the University of Washington, Seattle, noted that accumulating research is casting doubt on the view that this chemotherapy has minimal late effects. However, despite the finding of an association between persistent free platinum and late toxicity, "we don’t know whether the relationship of prior platinum exposure, just by doses given or something different about how the body handles the platinum related to renal function or metabolic polymorphisms, is responsible"
The study is "very interesting and provocative," Dr. Margolin concluded, "but we need more data. Pharmacologic investigations are still needed to enhance the quality of life for this growing number of germ cell tumor survivors."
Although the study focused on serum, Dr. Boer noted that platinum can be found in other tissues as well. "In the ganglia, for example, and also in bone, fat, and the liver ... it’s ... not really known if the platinum in these body compartments is reactive or not. It is really a topic that deserves more research," he said.
Dr. Boer disclosed that he had no relevant conflicts of interest. Dr. Margolin disclosed that she is a consultant to Bristol-Myers Squibb, Genentech, and Johnson & Johnson.
CHICAGO – Long-term platinum exposure may explain higher rates of certain late adverse effects in men who have undergone treatment for testicular cancer, investigators reported based on a longitudinal study.
Among 96 consecutive men treated with cisplatin for testicular cancer, serum platinum levels 5 years later were 14% higher in those with elevated versus normal blood pressure and 16% higher in those with paresthesia versus those without it.
Dr. Hink Boer and his colleagues collected two or three serum samples and a 24-hour urine sample from the men at various time points after chemotherapy out to 13 years (median, 5 years) for platinum measurement.
The men had a median age of 29 years at the start of treatment, according to results reported in a poster presentation at the annual meeting of the American Society of Clinical Oncology. The median absolute cumulative cisplatin dose was 809 mg.
The findings are especially important as these survivors are young men who "have their whole life ahead of them, actually. Survivor care is very much focused on relapse detection, of course. In the last decade, I think there is more attention on the delayed effects," Dr. Boer, a research fellow in medical oncology at the University of Groningen in the Netherlands, said in an interview.
A population pharmacokinetic model using measured serum platinum concentration and urinary excretion rate, as well as administered cisplatin dosage, age, body surface area, height, and weight, suggested that the mean terminal half-life of platinum in serum was 3.7 years, Dr. Boer reported.
Platinum levels fell steadily and in exponential fashion with time after chemotherapy but were still detectable 13 years later. Serum platinum levels at 3 years and at 5 years after chemotherapy were significantly higher in men administered a higher total dose of cisplatin and in men having lower renal clearance, he said.
Analyses of long-term toxicity showed that, compared with their counterparts with lower blood pressure, men with a blood pressure of at least 130/85 mm Hg or on antihypertensive medication had higher mean serum platinum levels at 3 years (420 vs. 366 pg/g, P = .045) and at 5 years (210 vs. 185 pg/g, P = .04), as well as a higher platinum area under the curve (AUC) for years 1-5 (1,071 vs. 945 pg/g × 103 × day, P = .04).
Similarly, compared with their counterparts who did not have paresthesia, men having this adverse effect had higher mean serum platinum levels at 3 years (456 vs. 387 pg/g, P = .02) and at 5 years (227 vs. 195 pg/g, P = .02), as well as a higher platinum AUC for years 1-5 (1,144 vs. 996 pg/g × 103 × day, P = .02).
In contrast, men with secondary Raynaud disease and men with endothelial damage as assessed from von Willebrand factor levels did not have significantly higher serum platinum levels than their respective counterparts, Dr. Boer said.
"It is a well-known problem now that the chemotherapy has its late effects, and we wanted to look to see if these very small concentrations ... have any relationship with these late toxicities," he said. "If you look at these data, you could assume that there is a relationship, a very small concentration but still, it might have an effect."
"The chemotherapy is very successful, of course; you don’t want to change it. The cure rates are very high in testicular cancer patients," he added. "At the moment it is not possible to get the platinum out of the body. It is not technically possible to chelate it or something.
"But you have to think about it – it could be a mechanism, so it is worthwhile to do more studies on this. Perhaps in the future, it will be possible to chelate it and get it out, if we can confirm that this is really an etiological mechanism," he said.
Current practice at his institution for these patients is regular examinations with special focus on cardiovascular risk factors such as blood pressure and cholesterol. "We are trying to bring more structure in this care and to pay more attention to the late effects. I think [the patients] deserve it because they are so young," Dr. Boer said.
Discussant Dr. Kim Allyson Margolin of the University of Washington, Seattle, noted that accumulating research is casting doubt on the view that this chemotherapy has minimal late effects. However, despite the finding of an association between persistent free platinum and late toxicity, "we don’t know whether the relationship of prior platinum exposure, just by doses given or something different about how the body handles the platinum related to renal function or metabolic polymorphisms, is responsible"
The study is "very interesting and provocative," Dr. Margolin concluded, "but we need more data. Pharmacologic investigations are still needed to enhance the quality of life for this growing number of germ cell tumor survivors."
Although the study focused on serum, Dr. Boer noted that platinum can be found in other tissues as well. "In the ganglia, for example, and also in bone, fat, and the liver ... it’s ... not really known if the platinum in these body compartments is reactive or not. It is really a topic that deserves more research," he said.
Dr. Boer disclosed that he had no relevant conflicts of interest. Dr. Margolin disclosed that she is a consultant to Bristol-Myers Squibb, Genentech, and Johnson & Johnson.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Major Finding: Circulating levels of platinum at 5 years were significantly higher in patients with elevated blood pressure (210 vs. 185 pg/g) and paresthesias (227 vs. 195 pg/g).
Data Source: Investigators did a longitudinal study of 96 consecutive patients treated with cisplatin for testicular cancer.
Disclosures: Dr. Boer disclosed that he had no relevant conflicts of interest. Dr. Margolin disclosed that she is a consultant to Bristol-Myers Squibb, Genentech, and Johnson & Johnson.