User login
DUR-928 shows promise for alcoholic hepatitis
BOSTON – Treatment with novel agent DUR-928 may be able to reduce mortality rates among patients with severe alcoholic hepatitis, investigators predicted.
In an open-label, phase IIa trial, 89% of patients with alcoholic hepatitis responded to treatment with the new therapy, reported lead author Tarek Hassanein, MD, of Southern California Research Center in Coronado, Calif., and colleagues.
In an abstract that will be presented at the annual meeting of the American Association for the Study of Liver Diseases, the investigators explained the urgent need for an agent such as DUR-928: “The mortality of severe alcoholic hepatitis remains high in the absence of effective treatment,” they wrote, noting that corticosteroids are only suitable for select patients. According to the investigators, DUR-928 is an endogenous sulfated oxysterol that has been shown to control lipotoxicity and inflammation while increasing hepatic regeneration and cell survival.
The agent was tested among 19 patients with alcoholic hepatitis, many of whom had severe disease; at baseline, 15 had Maddrey’s discriminant function (DF) scores of 32 or less, 12 had Model for End-stage Liver Disease (MELD) scores between 12 and 30, and 11 had serum bilirubin levels higher than 8 mg/dL.
Via intravenous infusion, three dose levels were given: 30 mg, 90 mg, or 150 mg. All patients received at least one dose on day 1, and if still hospitalized, a second dose on day 4, with a total follow-up of 28 days. Treatment response was defined by a Lille score of less than 0.45.
DUR-928 was well tolerated; no serious drug-related adverse events occurred and all patients survived the 28-day follow-up period. Across the population, the response rate was 89%. This figure fell slightly to 87% when considering only patients with severe disease (DF scores of 32 or less), and marginally further still to 83% for those with MELD scores between 21 and 30. Among patients with severe disease, MELD scores decreased by a median of 17.5% (P = .01) over the 28-day period, and in cases with bilirubin starting higher than 8 mg/dL, levels dropped by a median of 25.1% (P = .02) within the first week.
A comparison of these results with historical data revealed that treatment with DUR-928 led to significantly better Lille scores than previously reported (P less than .0001).
“These initial findings are encouraging for further development of DUR-928 in patients with alcoholic hepatitis, including severe alcoholic hepatitis,” the investigators concluded.
The investigators disclosed relationships with DURECT Corporation, Assembly Biosciences, Gilead, and others.
SOURCE: Hassanein T et al. The Liver Meeting 2019, Abstract LO9.
BOSTON – Treatment with novel agent DUR-928 may be able to reduce mortality rates among patients with severe alcoholic hepatitis, investigators predicted.
In an open-label, phase IIa trial, 89% of patients with alcoholic hepatitis responded to treatment with the new therapy, reported lead author Tarek Hassanein, MD, of Southern California Research Center in Coronado, Calif., and colleagues.
In an abstract that will be presented at the annual meeting of the American Association for the Study of Liver Diseases, the investigators explained the urgent need for an agent such as DUR-928: “The mortality of severe alcoholic hepatitis remains high in the absence of effective treatment,” they wrote, noting that corticosteroids are only suitable for select patients. According to the investigators, DUR-928 is an endogenous sulfated oxysterol that has been shown to control lipotoxicity and inflammation while increasing hepatic regeneration and cell survival.
The agent was tested among 19 patients with alcoholic hepatitis, many of whom had severe disease; at baseline, 15 had Maddrey’s discriminant function (DF) scores of 32 or less, 12 had Model for End-stage Liver Disease (MELD) scores between 12 and 30, and 11 had serum bilirubin levels higher than 8 mg/dL.
Via intravenous infusion, three dose levels were given: 30 mg, 90 mg, or 150 mg. All patients received at least one dose on day 1, and if still hospitalized, a second dose on day 4, with a total follow-up of 28 days. Treatment response was defined by a Lille score of less than 0.45.
DUR-928 was well tolerated; no serious drug-related adverse events occurred and all patients survived the 28-day follow-up period. Across the population, the response rate was 89%. This figure fell slightly to 87% when considering only patients with severe disease (DF scores of 32 or less), and marginally further still to 83% for those with MELD scores between 21 and 30. Among patients with severe disease, MELD scores decreased by a median of 17.5% (P = .01) over the 28-day period, and in cases with bilirubin starting higher than 8 mg/dL, levels dropped by a median of 25.1% (P = .02) within the first week.
A comparison of these results with historical data revealed that treatment with DUR-928 led to significantly better Lille scores than previously reported (P less than .0001).
“These initial findings are encouraging for further development of DUR-928 in patients with alcoholic hepatitis, including severe alcoholic hepatitis,” the investigators concluded.
The investigators disclosed relationships with DURECT Corporation, Assembly Biosciences, Gilead, and others.
SOURCE: Hassanein T et al. The Liver Meeting 2019, Abstract LO9.
BOSTON – Treatment with novel agent DUR-928 may be able to reduce mortality rates among patients with severe alcoholic hepatitis, investigators predicted.
In an open-label, phase IIa trial, 89% of patients with alcoholic hepatitis responded to treatment with the new therapy, reported lead author Tarek Hassanein, MD, of Southern California Research Center in Coronado, Calif., and colleagues.
In an abstract that will be presented at the annual meeting of the American Association for the Study of Liver Diseases, the investigators explained the urgent need for an agent such as DUR-928: “The mortality of severe alcoholic hepatitis remains high in the absence of effective treatment,” they wrote, noting that corticosteroids are only suitable for select patients. According to the investigators, DUR-928 is an endogenous sulfated oxysterol that has been shown to control lipotoxicity and inflammation while increasing hepatic regeneration and cell survival.
The agent was tested among 19 patients with alcoholic hepatitis, many of whom had severe disease; at baseline, 15 had Maddrey’s discriminant function (DF) scores of 32 or less, 12 had Model for End-stage Liver Disease (MELD) scores between 12 and 30, and 11 had serum bilirubin levels higher than 8 mg/dL.
Via intravenous infusion, three dose levels were given: 30 mg, 90 mg, or 150 mg. All patients received at least one dose on day 1, and if still hospitalized, a second dose on day 4, with a total follow-up of 28 days. Treatment response was defined by a Lille score of less than 0.45.
DUR-928 was well tolerated; no serious drug-related adverse events occurred and all patients survived the 28-day follow-up period. Across the population, the response rate was 89%. This figure fell slightly to 87% when considering only patients with severe disease (DF scores of 32 or less), and marginally further still to 83% for those with MELD scores between 21 and 30. Among patients with severe disease, MELD scores decreased by a median of 17.5% (P = .01) over the 28-day period, and in cases with bilirubin starting higher than 8 mg/dL, levels dropped by a median of 25.1% (P = .02) within the first week.
A comparison of these results with historical data revealed that treatment with DUR-928 led to significantly better Lille scores than previously reported (P less than .0001).
“These initial findings are encouraging for further development of DUR-928 in patients with alcoholic hepatitis, including severe alcoholic hepatitis,” the investigators concluded.
The investigators disclosed relationships with DURECT Corporation, Assembly Biosciences, Gilead, and others.
SOURCE: Hassanein T et al. The Liver Meeting 2019, Abstract LO9.
REPORTING FROM THE LIVER MEETING 2019
Key clinical point: For patients with alcoholic hepatitis, treatment with novel agent DUR-928 could offer better outcomes than those of existing therapies.
Major finding: Among 15 patients with severe alcoholic hepatitis, 87% responded to treatment (Lille score less than 0.45).
Study details: A phase IIa open-label trial involving 19 patients with alcoholic hepatitis.
Disclosures: The investigators disclosed relationships with DURECT Corporation, Assembly Biosciences, Gilead, and others.
Source: Hassanein T et al. The Liver Meeting 2019, Abstract LO9.
Glecaprevir/pibrentasvir highly effective in HCV genotype 3, among others
BOSTON – Specifically in patients with hepatitis C virus (HCV) genotype 3 infection and compensated cirrhosis, glecaprevir/pibrentasvir (Mavyret) was safe and had high efficacy in a phase 3 clinical trial, echoing an earlier report describing clinical results for the fixed-dose combination in multiple other genotypes.
Treatment with glecaprevir/pibrentasvir was safe and produced high rates of sustained virologic response 12 weeks after treatment (SVR12) for the genotype 3 patients and compensated cirrhosis in the recent results from the EXPEDITION-8 study, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
In a previous report from EXPEDITION-8, investigators said that the treatment was well tolerated and effective in patients with HCV genotypes 1, 2, 4, 5, and 6.
“The availability of an 8-week, pangenotypic regimen for all treatment-naive HCV-infected patients regardless of cirrhosis status may simplify the HCV care pathway, furthering progress towards HCV elimination,” said investigator Robert S. Brown Jr., MD, MPH, and coinvestigators in a late-breaking abstract of the latest study results.
The nonrandomized, multicenter, phase 3b study included 343 adults with HCV genotypes 1-6 who received glecaprevir 300 mg and pibrentasvir 120 mg once daily for 8 weeks. A total of 63% of patients were male, 83% were white; 18% had HCV genotype 3, while the majority (67%) had HCV genotype 1.
For the genotype 3 patients, SVR12 rates were 95.2% in the intention-to-treat population, and 98.4% in the per-protocol population, Dr. Brown and coauthors said in their report on the study. For genotype 1, 2, 4, 5, and 6 patients, the intention-to-treat and per-protocol SVR12 rates were 98.2% and 100%.
Taken together, the SVR12 rates for all genotypes were 97.7% and 99.7%, respectively, for the intention-to-treat and per-protocol populations, according to the investigators.
There were no virologic failures on treatment, and one patients with genotype 3 relapsed in week 4 posttreatment, while one genotype 1 patient discontinued treatment though not because of adverse events, they said.
Most adverse events were grade 1 in severity, and included fatigue, pruritus, headache, and nausea. There were no liver-related toxicities, and no serious adverse events that were related to the study treatment, according to the investigators.
Glecaprevir/pibrentasvir is indicated for patients aged 12 years and older with treatment-naive HCV genotype 1-6 infection without cirrhosis or with compensated cirrhosis, and in patients with HCV genotype 1 infection previously treated with an HCV NS5A inhibitor or an NS3/4A protease inhibitor.
Dr. Brown reported disclosures related to pharmaceutical companies including AbbVie, which markets Mavyret.
SOURCE: Brown RS et al. The Liver Meeting 2019. Abstract LP9.
BOSTON – Specifically in patients with hepatitis C virus (HCV) genotype 3 infection and compensated cirrhosis, glecaprevir/pibrentasvir (Mavyret) was safe and had high efficacy in a phase 3 clinical trial, echoing an earlier report describing clinical results for the fixed-dose combination in multiple other genotypes.
Treatment with glecaprevir/pibrentasvir was safe and produced high rates of sustained virologic response 12 weeks after treatment (SVR12) for the genotype 3 patients and compensated cirrhosis in the recent results from the EXPEDITION-8 study, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
In a previous report from EXPEDITION-8, investigators said that the treatment was well tolerated and effective in patients with HCV genotypes 1, 2, 4, 5, and 6.
“The availability of an 8-week, pangenotypic regimen for all treatment-naive HCV-infected patients regardless of cirrhosis status may simplify the HCV care pathway, furthering progress towards HCV elimination,” said investigator Robert S. Brown Jr., MD, MPH, and coinvestigators in a late-breaking abstract of the latest study results.
The nonrandomized, multicenter, phase 3b study included 343 adults with HCV genotypes 1-6 who received glecaprevir 300 mg and pibrentasvir 120 mg once daily for 8 weeks. A total of 63% of patients were male, 83% were white; 18% had HCV genotype 3, while the majority (67%) had HCV genotype 1.
For the genotype 3 patients, SVR12 rates were 95.2% in the intention-to-treat population, and 98.4% in the per-protocol population, Dr. Brown and coauthors said in their report on the study. For genotype 1, 2, 4, 5, and 6 patients, the intention-to-treat and per-protocol SVR12 rates were 98.2% and 100%.
Taken together, the SVR12 rates for all genotypes were 97.7% and 99.7%, respectively, for the intention-to-treat and per-protocol populations, according to the investigators.
There were no virologic failures on treatment, and one patients with genotype 3 relapsed in week 4 posttreatment, while one genotype 1 patient discontinued treatment though not because of adverse events, they said.
Most adverse events were grade 1 in severity, and included fatigue, pruritus, headache, and nausea. There were no liver-related toxicities, and no serious adverse events that were related to the study treatment, according to the investigators.
Glecaprevir/pibrentasvir is indicated for patients aged 12 years and older with treatment-naive HCV genotype 1-6 infection without cirrhosis or with compensated cirrhosis, and in patients with HCV genotype 1 infection previously treated with an HCV NS5A inhibitor or an NS3/4A protease inhibitor.
Dr. Brown reported disclosures related to pharmaceutical companies including AbbVie, which markets Mavyret.
SOURCE: Brown RS et al. The Liver Meeting 2019. Abstract LP9.
BOSTON – Specifically in patients with hepatitis C virus (HCV) genotype 3 infection and compensated cirrhosis, glecaprevir/pibrentasvir (Mavyret) was safe and had high efficacy in a phase 3 clinical trial, echoing an earlier report describing clinical results for the fixed-dose combination in multiple other genotypes.
Treatment with glecaprevir/pibrentasvir was safe and produced high rates of sustained virologic response 12 weeks after treatment (SVR12) for the genotype 3 patients and compensated cirrhosis in the recent results from the EXPEDITION-8 study, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
In a previous report from EXPEDITION-8, investigators said that the treatment was well tolerated and effective in patients with HCV genotypes 1, 2, 4, 5, and 6.
“The availability of an 8-week, pangenotypic regimen for all treatment-naive HCV-infected patients regardless of cirrhosis status may simplify the HCV care pathway, furthering progress towards HCV elimination,” said investigator Robert S. Brown Jr., MD, MPH, and coinvestigators in a late-breaking abstract of the latest study results.
The nonrandomized, multicenter, phase 3b study included 343 adults with HCV genotypes 1-6 who received glecaprevir 300 mg and pibrentasvir 120 mg once daily for 8 weeks. A total of 63% of patients were male, 83% were white; 18% had HCV genotype 3, while the majority (67%) had HCV genotype 1.
For the genotype 3 patients, SVR12 rates were 95.2% in the intention-to-treat population, and 98.4% in the per-protocol population, Dr. Brown and coauthors said in their report on the study. For genotype 1, 2, 4, 5, and 6 patients, the intention-to-treat and per-protocol SVR12 rates were 98.2% and 100%.
Taken together, the SVR12 rates for all genotypes were 97.7% and 99.7%, respectively, for the intention-to-treat and per-protocol populations, according to the investigators.
There were no virologic failures on treatment, and one patients with genotype 3 relapsed in week 4 posttreatment, while one genotype 1 patient discontinued treatment though not because of adverse events, they said.
Most adverse events were grade 1 in severity, and included fatigue, pruritus, headache, and nausea. There were no liver-related toxicities, and no serious adverse events that were related to the study treatment, according to the investigators.
Glecaprevir/pibrentasvir is indicated for patients aged 12 years and older with treatment-naive HCV genotype 1-6 infection without cirrhosis or with compensated cirrhosis, and in patients with HCV genotype 1 infection previously treated with an HCV NS5A inhibitor or an NS3/4A protease inhibitor.
Dr. Brown reported disclosures related to pharmaceutical companies including AbbVie, which markets Mavyret.
SOURCE: Brown RS et al. The Liver Meeting 2019. Abstract LP9.
REPORTING FROM THE LIVER MEETING 2019
Key clinical point: In patients with hepatitis C virus (HCV) genotype 3 infection and compensated cirrhosis, glecaprevir/pibrentasvir was safe and had high efficacy, echoing an earlier result for the fixed-dose combination in genotypes 1, 2, and 4-6.
Major finding: For the genotype 3 patients, the rate of sustained virologic response 12 weeks after treatment (SVR12) was 95.2% in the intention-to-treat population, and 98.4% in the per-protocol population.
Study details: Further results from EXPEDITION-8, a single-arm phase 3b study including 343 adult patients with HCV genotypes 1-6.
Disclosures: Dr. Brown reported disclosures related to AbbVie, Gilead, Intercept, Dova, Shionogi, Merck, and Bristol-Myers Squibb.
Source: Brown RS et al. The Liver Meeting 2019. Abstract LP9.
Hepatitis C vaccine alters viral trajectory, but fails in chronic infection protection
BOSTON – A prime-boost hepatitis C virus (HCV) vaccine regimen did not protect against chronic infection, but it did evoke immune responses and differences in viral trajectory, according to investigators in what is believed to be the first randomized, placebo-controlled efficacy trial in this setting.
There were no apparent safety concerns with the vaccine according to investigators, led by Kimberly Page, PhD, MPH, of the University of New Mexico, Albuquerque.
“A safe and effective vaccine to prevent chronic hepatitis C virus infection is essential to reduce transmission,” Dr. Page and coauthors said in a late-breaking abstract of the study results, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
The phase 1/2 trial described by Dr. Page and colleagues included 455 adults at risk of HCV infection because of injection drug use. They were randomized to vaccine, which consisted of a recombinant chimpanzee adenovirus-3 vectored vaccine prime plus a recombinant Modified Vaccinia virus Ankara boost, or to two doses of placebo at days 0 and 56 of the study.
There was no difference in chronic HCV infection at 6 months, the primary endpoint of the study. There were 14 chronically infected participants in the vaccine group, as well as 14 in the placebo group, for an overall incidence of infection of 13.0/100 person-years, Dr. Page and coauthors reported in the abstract.
However, there were significant differences in HCV RNA geometric mean peak at 1 month, which was 193,795 IU/L in the vaccine group and 1,078,092 IU/L in the placebo group, according to investigators. Similarly, geometric mean fold rise after infection was 0.2 in the vaccine group and 13.5 in the placebo group.
A total of 78% of vaccinated individuals had T-cell responses to at least one vaccine antigen pool, investigators said, adding that the vaccine was safe, well tolerated, and not associated with any serious adverse events.
Dr. Page had no disclosures related to the abstract.
SOURCE: Page K et al. The Liver Meeting 2019. Abstract LP17.
BOSTON – A prime-boost hepatitis C virus (HCV) vaccine regimen did not protect against chronic infection, but it did evoke immune responses and differences in viral trajectory, according to investigators in what is believed to be the first randomized, placebo-controlled efficacy trial in this setting.
There were no apparent safety concerns with the vaccine according to investigators, led by Kimberly Page, PhD, MPH, of the University of New Mexico, Albuquerque.
“A safe and effective vaccine to prevent chronic hepatitis C virus infection is essential to reduce transmission,” Dr. Page and coauthors said in a late-breaking abstract of the study results, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
The phase 1/2 trial described by Dr. Page and colleagues included 455 adults at risk of HCV infection because of injection drug use. They were randomized to vaccine, which consisted of a recombinant chimpanzee adenovirus-3 vectored vaccine prime plus a recombinant Modified Vaccinia virus Ankara boost, or to two doses of placebo at days 0 and 56 of the study.
There was no difference in chronic HCV infection at 6 months, the primary endpoint of the study. There were 14 chronically infected participants in the vaccine group, as well as 14 in the placebo group, for an overall incidence of infection of 13.0/100 person-years, Dr. Page and coauthors reported in the abstract.
However, there were significant differences in HCV RNA geometric mean peak at 1 month, which was 193,795 IU/L in the vaccine group and 1,078,092 IU/L in the placebo group, according to investigators. Similarly, geometric mean fold rise after infection was 0.2 in the vaccine group and 13.5 in the placebo group.
A total of 78% of vaccinated individuals had T-cell responses to at least one vaccine antigen pool, investigators said, adding that the vaccine was safe, well tolerated, and not associated with any serious adverse events.
Dr. Page had no disclosures related to the abstract.
SOURCE: Page K et al. The Liver Meeting 2019. Abstract LP17.
BOSTON – A prime-boost hepatitis C virus (HCV) vaccine regimen did not protect against chronic infection, but it did evoke immune responses and differences in viral trajectory, according to investigators in what is believed to be the first randomized, placebo-controlled efficacy trial in this setting.
There were no apparent safety concerns with the vaccine according to investigators, led by Kimberly Page, PhD, MPH, of the University of New Mexico, Albuquerque.
“A safe and effective vaccine to prevent chronic hepatitis C virus infection is essential to reduce transmission,” Dr. Page and coauthors said in a late-breaking abstract of the study results, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
The phase 1/2 trial described by Dr. Page and colleagues included 455 adults at risk of HCV infection because of injection drug use. They were randomized to vaccine, which consisted of a recombinant chimpanzee adenovirus-3 vectored vaccine prime plus a recombinant Modified Vaccinia virus Ankara boost, or to two doses of placebo at days 0 and 56 of the study.
There was no difference in chronic HCV infection at 6 months, the primary endpoint of the study. There were 14 chronically infected participants in the vaccine group, as well as 14 in the placebo group, for an overall incidence of infection of 13.0/100 person-years, Dr. Page and coauthors reported in the abstract.
However, there were significant differences in HCV RNA geometric mean peak at 1 month, which was 193,795 IU/L in the vaccine group and 1,078,092 IU/L in the placebo group, according to investigators. Similarly, geometric mean fold rise after infection was 0.2 in the vaccine group and 13.5 in the placebo group.
A total of 78% of vaccinated individuals had T-cell responses to at least one vaccine antigen pool, investigators said, adding that the vaccine was safe, well tolerated, and not associated with any serious adverse events.
Dr. Page had no disclosures related to the abstract.
SOURCE: Page K et al. The Liver Meeting 2019. Abstract LP17.
REPORTING FROM THE LIVER MEETING 2019
Key clinical point: A prime-boost HCV vaccine altered viral trajectory but did not protect against chronic infection.
Major finding: At 6 months after vaccination, there were 14 chronically infected participants in the vaccine group, and 14 in the placebo group.
Study details: A randomized, placebo controlled phase 1/2 trial including 455 adults at risk of HCV infection.
Disclosures: The first author reported no disclosures.
Source: Page K et al. The Liver Meeting 2019. Abstract LP17.
Fenofibrate fights increased triglycerides in NASH
BOSTON – Fenofibrate is safe and effective for limiting triglyceride increases in patients with nonalcoholic steatohepatitis and advanced fibrosis, based on data from 31 adults.
Treatment of NASH with acetyl-CoA carboxylase inhibitors has been shown to improve liver fat and other liver conditions but may be associated with hyperlipidemia, according to Eric J. Lawitz, MD, of the University of Texas Health, San Antonio, and colleagues. The researchers examined the safety and effectiveness of fenofibrate to mitigate serum triglyceride increases in a study be presented in a late-breaking session at the annual meeting of the American Association for the Study of Liver Diseases.
The researchers randomized 15 patients to treatment with 48 mg of fenofibrate or 145 mg of fenofibrate once daily for 2 weeks, followed by a combination of the fenofibrate doses plus 20 mg of ACC inhibitor firsocostat daily for 24 weeks.
The median fasting triglycerides (TG) in the 48-mg and 145-mg fenofibrate groups were 218 mg/dL and 202 mg/dL, respectively. After 2 weeks, the median change in TG was +2 mg/dL in the 48-mg group and –42 mg/dL in the 145-mg group. After 24 weeks of combination therapy, TG levels were not significantly different from baseline in either group (+19 mg/dL in 48-mg group and +6 mg/dL in the 145-mg group). Significant reductions in serum alanine aminotransferase from baseline to week 24 occurred in the combined groups (median of 39 U/L vs. 27 U/L, respectively). In addition, 43% of patients overall showed at least a 30% reduction in protein density fat fraction.
Both firsocostat and fenofibrate were well tolerated, the researchers said. One treatment-emergent grade 3 TG elevation (defined as greater than 500 mg/dL) occurred in the 48-mg group at week 24. No hepatotoxicity was noted, no patients discontinued therapy because of adverse events, and no other grade 3 or 4 adverse events were reported.
“The combination of firsocostat and fenofibrate led to improvements in hepatic fat, liver biochemistry, and markers of fibrosis,” the researchers concluded in their abstract.
Lead author Dr. Lawitz disclosed financial relationships with Allergan, Akcea Therapeutics, Bristol-Myers Squibb, Boehringer Ingelheim, Gilead Sciences, Madrigal Pharmaceuticals, and Novartis.
The AGA GI Patient Center provides education to help your patients understand NASH at https://www.gastro.org/practice-guidance/gi-patient-center/topic/nonalcoholic-steatohepatitis-nash.
SOURCE: Lawitz E et al. The Liver Meeting 2019. Presentation LP5.
BOSTON – Fenofibrate is safe and effective for limiting triglyceride increases in patients with nonalcoholic steatohepatitis and advanced fibrosis, based on data from 31 adults.
Treatment of NASH with acetyl-CoA carboxylase inhibitors has been shown to improve liver fat and other liver conditions but may be associated with hyperlipidemia, according to Eric J. Lawitz, MD, of the University of Texas Health, San Antonio, and colleagues. The researchers examined the safety and effectiveness of fenofibrate to mitigate serum triglyceride increases in a study be presented in a late-breaking session at the annual meeting of the American Association for the Study of Liver Diseases.
The researchers randomized 15 patients to treatment with 48 mg of fenofibrate or 145 mg of fenofibrate once daily for 2 weeks, followed by a combination of the fenofibrate doses plus 20 mg of ACC inhibitor firsocostat daily for 24 weeks.
The median fasting triglycerides (TG) in the 48-mg and 145-mg fenofibrate groups were 218 mg/dL and 202 mg/dL, respectively. After 2 weeks, the median change in TG was +2 mg/dL in the 48-mg group and –42 mg/dL in the 145-mg group. After 24 weeks of combination therapy, TG levels were not significantly different from baseline in either group (+19 mg/dL in 48-mg group and +6 mg/dL in the 145-mg group). Significant reductions in serum alanine aminotransferase from baseline to week 24 occurred in the combined groups (median of 39 U/L vs. 27 U/L, respectively). In addition, 43% of patients overall showed at least a 30% reduction in protein density fat fraction.
Both firsocostat and fenofibrate were well tolerated, the researchers said. One treatment-emergent grade 3 TG elevation (defined as greater than 500 mg/dL) occurred in the 48-mg group at week 24. No hepatotoxicity was noted, no patients discontinued therapy because of adverse events, and no other grade 3 or 4 adverse events were reported.
“The combination of firsocostat and fenofibrate led to improvements in hepatic fat, liver biochemistry, and markers of fibrosis,” the researchers concluded in their abstract.
Lead author Dr. Lawitz disclosed financial relationships with Allergan, Akcea Therapeutics, Bristol-Myers Squibb, Boehringer Ingelheim, Gilead Sciences, Madrigal Pharmaceuticals, and Novartis.
The AGA GI Patient Center provides education to help your patients understand NASH at https://www.gastro.org/practice-guidance/gi-patient-center/topic/nonalcoholic-steatohepatitis-nash.
SOURCE: Lawitz E et al. The Liver Meeting 2019. Presentation LP5.
BOSTON – Fenofibrate is safe and effective for limiting triglyceride increases in patients with nonalcoholic steatohepatitis and advanced fibrosis, based on data from 31 adults.
Treatment of NASH with acetyl-CoA carboxylase inhibitors has been shown to improve liver fat and other liver conditions but may be associated with hyperlipidemia, according to Eric J. Lawitz, MD, of the University of Texas Health, San Antonio, and colleagues. The researchers examined the safety and effectiveness of fenofibrate to mitigate serum triglyceride increases in a study be presented in a late-breaking session at the annual meeting of the American Association for the Study of Liver Diseases.
The researchers randomized 15 patients to treatment with 48 mg of fenofibrate or 145 mg of fenofibrate once daily for 2 weeks, followed by a combination of the fenofibrate doses plus 20 mg of ACC inhibitor firsocostat daily for 24 weeks.
The median fasting triglycerides (TG) in the 48-mg and 145-mg fenofibrate groups were 218 mg/dL and 202 mg/dL, respectively. After 2 weeks, the median change in TG was +2 mg/dL in the 48-mg group and –42 mg/dL in the 145-mg group. After 24 weeks of combination therapy, TG levels were not significantly different from baseline in either group (+19 mg/dL in 48-mg group and +6 mg/dL in the 145-mg group). Significant reductions in serum alanine aminotransferase from baseline to week 24 occurred in the combined groups (median of 39 U/L vs. 27 U/L, respectively). In addition, 43% of patients overall showed at least a 30% reduction in protein density fat fraction.
Both firsocostat and fenofibrate were well tolerated, the researchers said. One treatment-emergent grade 3 TG elevation (defined as greater than 500 mg/dL) occurred in the 48-mg group at week 24. No hepatotoxicity was noted, no patients discontinued therapy because of adverse events, and no other grade 3 or 4 adverse events were reported.
“The combination of firsocostat and fenofibrate led to improvements in hepatic fat, liver biochemistry, and markers of fibrosis,” the researchers concluded in their abstract.
Lead author Dr. Lawitz disclosed financial relationships with Allergan, Akcea Therapeutics, Bristol-Myers Squibb, Boehringer Ingelheim, Gilead Sciences, Madrigal Pharmaceuticals, and Novartis.
The AGA GI Patient Center provides education to help your patients understand NASH at https://www.gastro.org/practice-guidance/gi-patient-center/topic/nonalcoholic-steatohepatitis-nash.
SOURCE: Lawitz E et al. The Liver Meeting 2019. Presentation LP5.
REPORTING FROM THE LIVER MEETING 2019
Key clinical point: Fenofibrate mitigated serum triglyceride increases in patients with NASH.
Major finding: After 24 weeks of fenofibrate treatment, 43% of patients showed a relative reduction of at least 30% in protein density fat fraction with an average of 40% at a 48 mg-dose and 47% at a 145-mg dose.
Study details: The data come from a 24-week study of 31 adults with advanced fibrosis caused by NASH.
Disclosures: Lead author Dr. Lawitz disclosed financial relationships with Allergan, Akcea Therapeutics, Bristol-Myers Squibb, Boehringer Ingelheim, Gilead Sciences, Madrigal Pharmaceuticals, and Novartis.
Source: Lawitz E et al. The Liver Meeting 2019. Presentation LP5.
High doses of FXR agonist tropifexor reduce hepatic fat, serum ALT in patients with NASH
BOSTON – Alanine aminotransferase, hepatic fat, and body weight all decreased in patients with nonalcoholic steatohepatitis (NASH) treated for 12 weeks with higher doses of tropifexor, an investigational farnesoid X receptor agonist, according to interim results of a randomized trial.
Mild pruritus and minor decreases in LDL cholesterol were seen with tropifexor, similar to what has been seen with other farnesoid X receptor agonists, according to investigators, including senior study author Arun Sanyal, MD, professor in the gastroenterology division of the department of internal medicine at Virgina Commonwealth University in Richmond.
“Changes in liver histology resulting from this trial, along with trials of tropifexor in combination with drugs with other mechanisms of action, will define future therapeutic options in fibrotic NASH,” Dr. Sanyal and coauthors said in a late-breaking abstract for the study, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
That randomized, double-blind, placebo-controlled, phase 2 study, called FLIGHT-FXR, is designed to evaluate tropifexor (LJN452) in patients with NASH at several different doses, according to Dr. Sanyal and coinvestigators.
Previous reports on the trial demonstrated that lower doses of tropifexor (60 and 90 mcg) had favorable safety with anti-inflammatory and antisteatotic efficacy based on biomarker analysis, according to investigators.
This latest report from FLIGHT-FXR includes 152 patients randomly allocated to receive placebo or tropifexor at one of two higher doses (140 or 200 mcg).
At the highest tropifexor dose of 200 mcg, decreases in alanine aminotransferase (ALT), hepatic fat fraction (HFF), gamma-glutamyl transferase (GGT), and body weight were all significant, compared with the decreases in the placebo arm, according to reported data, while in the 140-mcg arm, the findings were significant versus placebo for GGT and body weight.
Relative HFF reduction by at least 30% was seen in 64% of patients in the tropifexor 200-mcg arm, 32% in the tropifexor 140-mcg arm, and 20% in the placebo arm, the investigators reported.
Pruritus was mild among tropifexor-treated patients in more than 60% of cases, investigators said, and pruritus-related discontinuation rates were low, at 2% (1 patient) for the 140-mcg dose and 6% (3 patients) for 200 mcg.
Investigators noted a dose-related increase in LDL cholesterol with tropifexor treatment, but those lipid changes didn’t lead to reduced doses or stopped treatment, they said.
Serious adverse events were infrequent, with a comparable incidence across treatment and placebo groups, investigators added.
Dr. Sanyal provided disclosures related to Sanyal Bio, Exhalenz, Akarna, Fractyl Laboratories, Genfit, Durect, Tiziana, Novartis, Merck, Galectin, and Janssen, among others.
BOSTON – Alanine aminotransferase, hepatic fat, and body weight all decreased in patients with nonalcoholic steatohepatitis (NASH) treated for 12 weeks with higher doses of tropifexor, an investigational farnesoid X receptor agonist, according to interim results of a randomized trial.
Mild pruritus and minor decreases in LDL cholesterol were seen with tropifexor, similar to what has been seen with other farnesoid X receptor agonists, according to investigators, including senior study author Arun Sanyal, MD, professor in the gastroenterology division of the department of internal medicine at Virgina Commonwealth University in Richmond.
“Changes in liver histology resulting from this trial, along with trials of tropifexor in combination with drugs with other mechanisms of action, will define future therapeutic options in fibrotic NASH,” Dr. Sanyal and coauthors said in a late-breaking abstract for the study, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
That randomized, double-blind, placebo-controlled, phase 2 study, called FLIGHT-FXR, is designed to evaluate tropifexor (LJN452) in patients with NASH at several different doses, according to Dr. Sanyal and coinvestigators.
Previous reports on the trial demonstrated that lower doses of tropifexor (60 and 90 mcg) had favorable safety with anti-inflammatory and antisteatotic efficacy based on biomarker analysis, according to investigators.
This latest report from FLIGHT-FXR includes 152 patients randomly allocated to receive placebo or tropifexor at one of two higher doses (140 or 200 mcg).
At the highest tropifexor dose of 200 mcg, decreases in alanine aminotransferase (ALT), hepatic fat fraction (HFF), gamma-glutamyl transferase (GGT), and body weight were all significant, compared with the decreases in the placebo arm, according to reported data, while in the 140-mcg arm, the findings were significant versus placebo for GGT and body weight.
Relative HFF reduction by at least 30% was seen in 64% of patients in the tropifexor 200-mcg arm, 32% in the tropifexor 140-mcg arm, and 20% in the placebo arm, the investigators reported.
Pruritus was mild among tropifexor-treated patients in more than 60% of cases, investigators said, and pruritus-related discontinuation rates were low, at 2% (1 patient) for the 140-mcg dose and 6% (3 patients) for 200 mcg.
Investigators noted a dose-related increase in LDL cholesterol with tropifexor treatment, but those lipid changes didn’t lead to reduced doses or stopped treatment, they said.
Serious adverse events were infrequent, with a comparable incidence across treatment and placebo groups, investigators added.
Dr. Sanyal provided disclosures related to Sanyal Bio, Exhalenz, Akarna, Fractyl Laboratories, Genfit, Durect, Tiziana, Novartis, Merck, Galectin, and Janssen, among others.
BOSTON – Alanine aminotransferase, hepatic fat, and body weight all decreased in patients with nonalcoholic steatohepatitis (NASH) treated for 12 weeks with higher doses of tropifexor, an investigational farnesoid X receptor agonist, according to interim results of a randomized trial.
Mild pruritus and minor decreases in LDL cholesterol were seen with tropifexor, similar to what has been seen with other farnesoid X receptor agonists, according to investigators, including senior study author Arun Sanyal, MD, professor in the gastroenterology division of the department of internal medicine at Virgina Commonwealth University in Richmond.
“Changes in liver histology resulting from this trial, along with trials of tropifexor in combination with drugs with other mechanisms of action, will define future therapeutic options in fibrotic NASH,” Dr. Sanyal and coauthors said in a late-breaking abstract for the study, which will be presented at the annual meeting of the American Association for the Study of Liver Diseases.
That randomized, double-blind, placebo-controlled, phase 2 study, called FLIGHT-FXR, is designed to evaluate tropifexor (LJN452) in patients with NASH at several different doses, according to Dr. Sanyal and coinvestigators.
Previous reports on the trial demonstrated that lower doses of tropifexor (60 and 90 mcg) had favorable safety with anti-inflammatory and antisteatotic efficacy based on biomarker analysis, according to investigators.
This latest report from FLIGHT-FXR includes 152 patients randomly allocated to receive placebo or tropifexor at one of two higher doses (140 or 200 mcg).
At the highest tropifexor dose of 200 mcg, decreases in alanine aminotransferase (ALT), hepatic fat fraction (HFF), gamma-glutamyl transferase (GGT), and body weight were all significant, compared with the decreases in the placebo arm, according to reported data, while in the 140-mcg arm, the findings were significant versus placebo for GGT and body weight.
Relative HFF reduction by at least 30% was seen in 64% of patients in the tropifexor 200-mcg arm, 32% in the tropifexor 140-mcg arm, and 20% in the placebo arm, the investigators reported.
Pruritus was mild among tropifexor-treated patients in more than 60% of cases, investigators said, and pruritus-related discontinuation rates were low, at 2% (1 patient) for the 140-mcg dose and 6% (3 patients) for 200 mcg.
Investigators noted a dose-related increase in LDL cholesterol with tropifexor treatment, but those lipid changes didn’t lead to reduced doses or stopped treatment, they said.
Serious adverse events were infrequent, with a comparable incidence across treatment and placebo groups, investigators added.
Dr. Sanyal provided disclosures related to Sanyal Bio, Exhalenz, Akarna, Fractyl Laboratories, Genfit, Durect, Tiziana, Novartis, Merck, Galectin, and Janssen, among others.
REPORTING FROM THE LIVER MEETING 2019
Key clinical point: Alanine aminotransferase, hepatic fat fraction, gamma-glutamyl transferase, and body weight decreased in patients with nonalcoholic steatohepatitis (NASH) treated for 12 weeks with higher doses of tropifexor, an investigational farnesoid X receptor agonist.
Major finding: ALT, HFF, GGT, and body weight were all significantly decreased versus placebo in patients treated with tropifexor at 200-mcg dose.
Study details: Interim results from the randomized FLIGHT-FXR trial, including 152 patients with NASH.
Disclosures: Dr. Sanyal provided disclosures related to Sanyal Bio, Exhalenz, Akarna, Fractyl Laboratories, Genfit, Durect, Tiziana, Novartis, Merck, Galectin, and Janssen, among others.
Source: Lucas KJ et al. The Liver Meeting 2019, Presentation LO4.
Duodenal mucosal resurfacing has metabolic effects in type 2 diabetes
BOSTON – An ablative procedure intended to promote regrowth of duodenal mucosa was safe and had disease-modifying metabolic effects in a randomized study including patients with type 2 diabetes, according to investigators.
A single duodenal mucosal resurfacing (DMR) procedure improved glycemic, hepatic, and body-weight measures at 24 weeks in the multicenter study, investigators will report at the annual meeting of the American Association for the Study of Liver Diseases.
The novel and minimally invasive endoscopic procedure treats the duodenum, which is increasingly recognized as a key metabolic signaling center, according to the study authors, including senior author Arun Sanyal, MD, professor in the gastroenterology division of the department of internal medicine at Virginia Commonwealth University, Richmond.
“Duodenal mucosal hyperplasia is a potential therapeutic target for insulin-resistance–related metabolic diseases,” Dr. Sanyal and coauthors said in a late-breaking abstract for the study published in the AASLD meeting proceedings.
In a previous international open-label, prospective, multicenter study, published in July in Gut, DMR was feasible and safe, producing durable glycemic improvement in patients with type 2 diabetes with suboptimal control on oral glucose-lowering mediation, according to investigators.
The present study, conducted at nine sites in the European Union and two in Brazil, is the first sham-controlled, double-blind, prospective study of the modality in patients with suboptimally controlled type 2 diabetes, according to Dr. Sanyal and coauthors.
A total of 39 patients in the study underwent DMR, while 36 underwent a sham procedure, according to the published abstract. The mean hemoglobin A1c for those patients was 8.3, the mean body mass index was 31.1 kg/m2, and most (77%) were male.
Median change in hemoglobin A1c from baseline to 24 weeks, one of two primary endpoints in the study, was –0.6% for DMR and –0.3% for the sham procedure (P less than 0.05), according to the study abstract.
Likewise, the primary efficacy endpoint of change in a nonalcoholic steatohepatitis biomarker favored the DMR arm. The median change in liver MRI–proton density fat fraction (MRI-PDFF) from baseline to 12 weeks was –5.4% for DMR and –2.4% for the sham procedure (P less than 0.05), according to the reported data.
Hypoglycemia rates were similar in the DMR and sham arms, and over 24 weeks of study, there were no unanticipated adverse effects attributable to the device and no serious adverse events, Dr. Sanyal and colleagues reported.
Dr. Sanyal reported disclosures related to Fractyl Laboratories, Sanyal Biotechnology, Exalenz Bioscience, Akarna Therapeutics, Genfit, Durect, Indalo, Tiziana, Novartis, Merck, Galectin Therapeutics, Janssen, and others.
BOSTON – An ablative procedure intended to promote regrowth of duodenal mucosa was safe and had disease-modifying metabolic effects in a randomized study including patients with type 2 diabetes, according to investigators.
A single duodenal mucosal resurfacing (DMR) procedure improved glycemic, hepatic, and body-weight measures at 24 weeks in the multicenter study, investigators will report at the annual meeting of the American Association for the Study of Liver Diseases.
The novel and minimally invasive endoscopic procedure treats the duodenum, which is increasingly recognized as a key metabolic signaling center, according to the study authors, including senior author Arun Sanyal, MD, professor in the gastroenterology division of the department of internal medicine at Virginia Commonwealth University, Richmond.
“Duodenal mucosal hyperplasia is a potential therapeutic target for insulin-resistance–related metabolic diseases,” Dr. Sanyal and coauthors said in a late-breaking abstract for the study published in the AASLD meeting proceedings.
In a previous international open-label, prospective, multicenter study, published in July in Gut, DMR was feasible and safe, producing durable glycemic improvement in patients with type 2 diabetes with suboptimal control on oral glucose-lowering mediation, according to investigators.
The present study, conducted at nine sites in the European Union and two in Brazil, is the first sham-controlled, double-blind, prospective study of the modality in patients with suboptimally controlled type 2 diabetes, according to Dr. Sanyal and coauthors.
A total of 39 patients in the study underwent DMR, while 36 underwent a sham procedure, according to the published abstract. The mean hemoglobin A1c for those patients was 8.3, the mean body mass index was 31.1 kg/m2, and most (77%) were male.
Median change in hemoglobin A1c from baseline to 24 weeks, one of two primary endpoints in the study, was –0.6% for DMR and –0.3% for the sham procedure (P less than 0.05), according to the study abstract.
Likewise, the primary efficacy endpoint of change in a nonalcoholic steatohepatitis biomarker favored the DMR arm. The median change in liver MRI–proton density fat fraction (MRI-PDFF) from baseline to 12 weeks was –5.4% for DMR and –2.4% for the sham procedure (P less than 0.05), according to the reported data.
Hypoglycemia rates were similar in the DMR and sham arms, and over 24 weeks of study, there were no unanticipated adverse effects attributable to the device and no serious adverse events, Dr. Sanyal and colleagues reported.
Dr. Sanyal reported disclosures related to Fractyl Laboratories, Sanyal Biotechnology, Exalenz Bioscience, Akarna Therapeutics, Genfit, Durect, Indalo, Tiziana, Novartis, Merck, Galectin Therapeutics, Janssen, and others.
BOSTON – An ablative procedure intended to promote regrowth of duodenal mucosa was safe and had disease-modifying metabolic effects in a randomized study including patients with type 2 diabetes, according to investigators.
A single duodenal mucosal resurfacing (DMR) procedure improved glycemic, hepatic, and body-weight measures at 24 weeks in the multicenter study, investigators will report at the annual meeting of the American Association for the Study of Liver Diseases.
The novel and minimally invasive endoscopic procedure treats the duodenum, which is increasingly recognized as a key metabolic signaling center, according to the study authors, including senior author Arun Sanyal, MD, professor in the gastroenterology division of the department of internal medicine at Virginia Commonwealth University, Richmond.
“Duodenal mucosal hyperplasia is a potential therapeutic target for insulin-resistance–related metabolic diseases,” Dr. Sanyal and coauthors said in a late-breaking abstract for the study published in the AASLD meeting proceedings.
In a previous international open-label, prospective, multicenter study, published in July in Gut, DMR was feasible and safe, producing durable glycemic improvement in patients with type 2 diabetes with suboptimal control on oral glucose-lowering mediation, according to investigators.
The present study, conducted at nine sites in the European Union and two in Brazil, is the first sham-controlled, double-blind, prospective study of the modality in patients with suboptimally controlled type 2 diabetes, according to Dr. Sanyal and coauthors.
A total of 39 patients in the study underwent DMR, while 36 underwent a sham procedure, according to the published abstract. The mean hemoglobin A1c for those patients was 8.3, the mean body mass index was 31.1 kg/m2, and most (77%) were male.
Median change in hemoglobin A1c from baseline to 24 weeks, one of two primary endpoints in the study, was –0.6% for DMR and –0.3% for the sham procedure (P less than 0.05), according to the study abstract.
Likewise, the primary efficacy endpoint of change in a nonalcoholic steatohepatitis biomarker favored the DMR arm. The median change in liver MRI–proton density fat fraction (MRI-PDFF) from baseline to 12 weeks was –5.4% for DMR and –2.4% for the sham procedure (P less than 0.05), according to the reported data.
Hypoglycemia rates were similar in the DMR and sham arms, and over 24 weeks of study, there were no unanticipated adverse effects attributable to the device and no serious adverse events, Dr. Sanyal and colleagues reported.
Dr. Sanyal reported disclosures related to Fractyl Laboratories, Sanyal Biotechnology, Exalenz Bioscience, Akarna Therapeutics, Genfit, Durect, Indalo, Tiziana, Novartis, Merck, Galectin Therapeutics, Janssen, and others.
REPORTING FROM THE LIVER MEETING 2019
Key clinical point: Duodenal mucosal resurfacing was safe and had disease-modifying metabolic effects in patients with type 2 diabetes.
Major finding: Results favored duodenal mucosal resurfacing over sham procedure for changes in median HbA1c (–0.6% vs. –0.3%; P less than .05) and liver MRI–proton density fat fraction (–5.4% vs. –2.4%; P less than 0.05).
Study details: A report on 75 patients treated in a randomized, sham-controlled, double-blind, prospective study.
Disclosures: Dr. Sanyal reported disclosures related to Fractyl Laboratories, Sanyal Biotechnology, Exalenz Bioscience, Akarna Therapeutics, Genfit, Durect, Indalo, Tiziana, Novartis, Merck, Galectin Therapeutics, Janssen, and others.
Source: Sanyal A et al. Liver Meeting 2019, Presentation LO2.
Terlipressin reversed hepatorenal syndrome in large prospective study
BOSTON – Terlipressin, an investigational vasopressin analogue, improved renal function and reversed hepatorenal syndrome type 1 (HRS-1) among patients with progressive advanced liver disease in a randomized trial, according to investigators.
Compared with albumin alone, terlipressin plus albumin significantly reversed worsening of renal function in cirrhotic patients, including those meeting systemic inflammatory response syndrome (SIRS) criteria, said investigators, led by Florence Wong, MD, from the University of Toronto.
“This response was durable and associated with less need for early renal replacement therapy,” said Dr. Wong and coauthors of an abstract describing the study, which will be presented in a late-breaking study session here at the annual meeting of the American Association for the Study of Liver Diseases.
The North American randomized, controlled trial, known as CONFIRM, was designed to confirm the safety and efficacy of terlipressin/albumin as a treatment for HRS-1, a serious but potentially reversible type of acute kidney injury seen in patients with cirrhosis and ascites, investigators said in their communication.
Patients in CONFIRM had “well-defined” HRS-1, based on diagnostic criteria as outlined by the International Club of Ascites, investigators said.
A total of 300 participants were randomized, 199 to terlipressin 1 mg IV every 6 hours and 101 to placebo, with both groups also receiving albumin, for up to 14 days of treatment. According to the report, 132 subjects (44%) met SIRS criteria.
Verified HRS reversal was documented in 29.1% of terlipressin-treated patients versus just 15.8% of the placebo group (P less than .012), investigators reported in their abstract. Among the SIRS patients, verified HRS reversal was seen in 33.3% and 6.3% of the terlipressin- and placebo-treated groups, respectively (P less than .001).
As the primary endpoint of the study, verified HRS reversal is an outcome that combines improvement in renal function, short-term survival following improvement, and avoidance of renal replacement therapy, investigators explained in their report.
Liver transplantation occurred in 23.1% of the terlipressin group and 28.7% of the placebo group, investigators also reported in their abstract.
Ischemia-associated adverse events were seen in 4.5% of the terlipressin arm and 0% for placebo, though in general the rate of adverse events were similar for the treatment and control arms, Dr. Wong and colleagues noted in their report.
The CONFIRM study is supported by Mallinckrodt. Dr. Wong provided disclosures related to Mallinckrodt, Ferring, and Sequana.
BOSTON – Terlipressin, an investigational vasopressin analogue, improved renal function and reversed hepatorenal syndrome type 1 (HRS-1) among patients with progressive advanced liver disease in a randomized trial, according to investigators.
Compared with albumin alone, terlipressin plus albumin significantly reversed worsening of renal function in cirrhotic patients, including those meeting systemic inflammatory response syndrome (SIRS) criteria, said investigators, led by Florence Wong, MD, from the University of Toronto.
“This response was durable and associated with less need for early renal replacement therapy,” said Dr. Wong and coauthors of an abstract describing the study, which will be presented in a late-breaking study session here at the annual meeting of the American Association for the Study of Liver Diseases.
The North American randomized, controlled trial, known as CONFIRM, was designed to confirm the safety and efficacy of terlipressin/albumin as a treatment for HRS-1, a serious but potentially reversible type of acute kidney injury seen in patients with cirrhosis and ascites, investigators said in their communication.
Patients in CONFIRM had “well-defined” HRS-1, based on diagnostic criteria as outlined by the International Club of Ascites, investigators said.
A total of 300 participants were randomized, 199 to terlipressin 1 mg IV every 6 hours and 101 to placebo, with both groups also receiving albumin, for up to 14 days of treatment. According to the report, 132 subjects (44%) met SIRS criteria.
Verified HRS reversal was documented in 29.1% of terlipressin-treated patients versus just 15.8% of the placebo group (P less than .012), investigators reported in their abstract. Among the SIRS patients, verified HRS reversal was seen in 33.3% and 6.3% of the terlipressin- and placebo-treated groups, respectively (P less than .001).
As the primary endpoint of the study, verified HRS reversal is an outcome that combines improvement in renal function, short-term survival following improvement, and avoidance of renal replacement therapy, investigators explained in their report.
Liver transplantation occurred in 23.1% of the terlipressin group and 28.7% of the placebo group, investigators also reported in their abstract.
Ischemia-associated adverse events were seen in 4.5% of the terlipressin arm and 0% for placebo, though in general the rate of adverse events were similar for the treatment and control arms, Dr. Wong and colleagues noted in their report.
The CONFIRM study is supported by Mallinckrodt. Dr. Wong provided disclosures related to Mallinckrodt, Ferring, and Sequana.
BOSTON – Terlipressin, an investigational vasopressin analogue, improved renal function and reversed hepatorenal syndrome type 1 (HRS-1) among patients with progressive advanced liver disease in a randomized trial, according to investigators.
Compared with albumin alone, terlipressin plus albumin significantly reversed worsening of renal function in cirrhotic patients, including those meeting systemic inflammatory response syndrome (SIRS) criteria, said investigators, led by Florence Wong, MD, from the University of Toronto.
“This response was durable and associated with less need for early renal replacement therapy,” said Dr. Wong and coauthors of an abstract describing the study, which will be presented in a late-breaking study session here at the annual meeting of the American Association for the Study of Liver Diseases.
The North American randomized, controlled trial, known as CONFIRM, was designed to confirm the safety and efficacy of terlipressin/albumin as a treatment for HRS-1, a serious but potentially reversible type of acute kidney injury seen in patients with cirrhosis and ascites, investigators said in their communication.
Patients in CONFIRM had “well-defined” HRS-1, based on diagnostic criteria as outlined by the International Club of Ascites, investigators said.
A total of 300 participants were randomized, 199 to terlipressin 1 mg IV every 6 hours and 101 to placebo, with both groups also receiving albumin, for up to 14 days of treatment. According to the report, 132 subjects (44%) met SIRS criteria.
Verified HRS reversal was documented in 29.1% of terlipressin-treated patients versus just 15.8% of the placebo group (P less than .012), investigators reported in their abstract. Among the SIRS patients, verified HRS reversal was seen in 33.3% and 6.3% of the terlipressin- and placebo-treated groups, respectively (P less than .001).
As the primary endpoint of the study, verified HRS reversal is an outcome that combines improvement in renal function, short-term survival following improvement, and avoidance of renal replacement therapy, investigators explained in their report.
Liver transplantation occurred in 23.1% of the terlipressin group and 28.7% of the placebo group, investigators also reported in their abstract.
Ischemia-associated adverse events were seen in 4.5% of the terlipressin arm and 0% for placebo, though in general the rate of adverse events were similar for the treatment and control arms, Dr. Wong and colleagues noted in their report.
The CONFIRM study is supported by Mallinckrodt. Dr. Wong provided disclosures related to Mallinckrodt, Ferring, and Sequana.
REPORTING FROM THE LIVER MEETING 2019
Key clinical point: Terlipressin, an investigational vasopressin analogue, improved renal function and reversed hepatorenal syndrome type 1 (HRS-1) among patients with progressive advanced liver disease.
Major finding: Verified HRS reversal was documented in 29.1% of patients treated with terlipressin/albumin versus 15.8% with placebo/albumin (P less than .012).
Study details: CONFIRM, a randomized, controlled trial including 300 patients with HRS-1.
Disclosures: The CONFIRM study is supported by Mallinckrodt. Dr. Wong provided disclosures related to Mallinckrodt, Ferring, and Sequana.
Source: Wong F et al. The Liver Meeting 2019, Presentation LO5.
Heart Failure in Older Adults: A Geriatrician Call for Action (FULL)
As the population ages, heart failure is becoming a major public health challenge; clinicians need further evidence-based treatments to bridge the existing gap between guidelines and real-world clinical practice.
In 2050, persons aged ≥ 85 years, also known as the oldest old, are projected to reach 18 million, accounting for 4.5% of the US population, up from 2.5% in 2030.1 These patients are the fastest growing segment of the US population.
Advances in treating cardiovascular (CV) disease over the past 2 decades have led to an increased incidence of heart failure (HF) and hospitalizations among older patients.2 Total costs of care for persons with HF have exceeded $30 billion annually and are expected to rise to more than $70 billion by 2030 due to growth of the aging population.3,4 Moreover, the Framingham Study reported mortality increases with advancing age (HR 1.27 and 1.61 per decade in men and women, respectively).5
The prevalence of HF is also high and increasing over time. The National Health and Nutrition Examination Survey reported that about 5.7 million Americans have HF.6 The prevalence of HF is expected to reach 8 million by 2030.6 The higher numbers of HF among patients with advanced age is associated with age-related changes in CV structure and function, including reduced responsiveness to β-adrenergic stimulation, impaired left ventricular diastolic filling, and increased vascular stiffness. In addition, age-related changes in other systems might contribute to a HF diagnosis or worsening of the condition.7
Older adults experience physiologic changes in pharmacokinetics and pharmacodynamics, including decreased volume of distribution and creatinine clearance, which lead to significant changes in drug concentration and effectiveness.8
Geriatric patients aged > 65 years who have comorbidities and those who reside in long-term care settings are underrepresented in clinical trials, leading clinicians to make treatment decisions based on data from younger, community-dwelling individuals. Researchers have questioned whether to include elderly patients and those with comorbidities in clinical trials, given that their diminished response may produce less conclusive results with smaller treatment effects. Exclusion criteria based on comorbid conditions or functional status disqualify many older adults from clinical trials.
This article reviews evidence from major randomized controlled trials over the past 2 decades and explores their applicability to support HF treatment guidelines in patients with advanced age (Table). 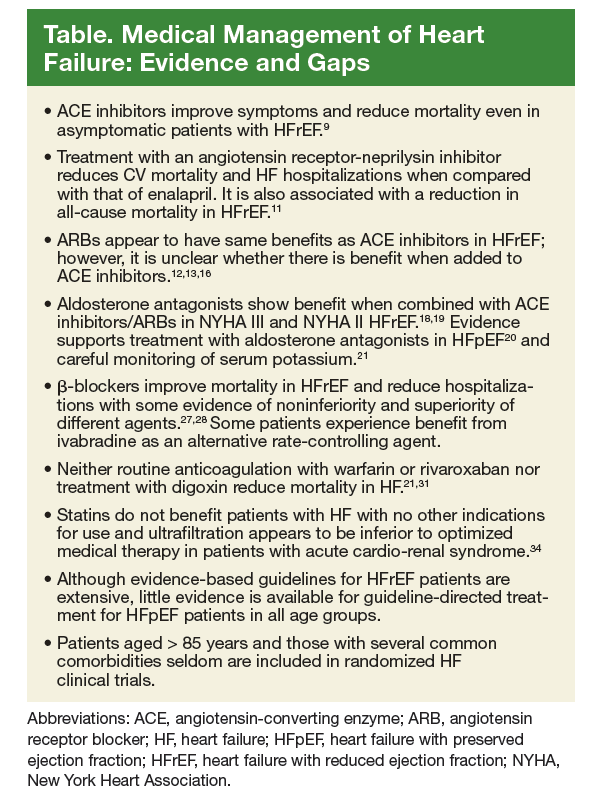
Pharmacotherapy for Heart Failure
Angiotensin-Converting Enzyme Inhibitors
Several randomized clinical trials have found that angiotensin-converting enzyme (ACE) inhibitors improve symptoms in patients with HF. The CooperativeNorth Scandinavian Enalapril Survival Study (CONSENSUS), demonstrated that enalapril improves survival in patients with New York Heart Association (NYHA) class IV HF with reduced ejection fraction (HFrEF) when added to standard therapy.9 However, the duration of beneficial effect of reduced mortality could not be assessed because the benefit of enalapril in NYHA class I to III HF was not evaluated, and follow-up data are limited. The average age of patients in the study was 71 years, and individuals with significant comorbidities were excluded.
ACE inhibitors also were found to reduce mortality even in asymptomatic patients with HFrEF in the Studies of Left Ventricular Dysfunction trial (SOLVD).10 Enalapril was found to reduce 4-year mortality by 16% and decrease HF hospitalizations when added to conventional therapy consisting primarily of digitalis, diuretics, and nitrates in patients with HFrEF. In this trial, patients aged ≥ 80 years were excluded as well as those with serum creatinine > 2 mg/dL or other conditions that could shorten survival or otherwise impede participation in a long-term trial.
PARADIGM-HF trial patients with HFrEF were randomized to enalapril or the angiotensin receptor-neprilysin inhibitor LCZ696. After a median of 27 months of follow-up, treatment with the angiotensin receptor-neprilysin inhibitor demonstrated greater reduction in CV mortality and HF hospitalizations than enalapril did and was associated with reduced all-cause mortality.11 The trial was stopped early because of evidence of overwhelming benefit with LCZ696. This study of mainly white men included no patients aged ≥ 75 years.
Angiotensin Receptor Blockers
Although less studied than ACE inhibitors, angiotensin receptor blockers (ARBs) share similar benefits. Among patients with symptomatic HFrEF taking an ACE inhibitor, the addition of candesartan reduced the risk of CV death and HF hospitalization as demonstrated in the Candesartan in Heart Failure Assessment of Reduction Mortality and Morbidity (CHARM-added and CHARM-alternative trials).12,13 The CHARM-added trial targeted patients with left ventricular ejection fraction (LVEF) ≤ 40% and NYHA class II to IV HF symptoms who were taking an ACE inhibitor. Adding candesartan reduced CV mortality by 37.9% and HF hospitalization by 42.3% compared with that of placebo.
The CHARM-alternative study found that use of candesartan in symptomatic HFrEF patients who do not tolerate ACE inhibitors,resulted in a 20% reduction in CV mortality as well as a 40% reduction in hospitalization for HF. Among patients with HF with preserved ejection fraction (HFpEF) and NYHA class II to IV symptoms, adding candesartan modestly reduced the rate of HF-related hospitalizations and had no effect on CV mortality in the CHARM-preserved study.14 The CHARM trials examined mostly white men, but 26% of patients were aged > 75 years. However, there was no subgroup analysis for patients aged > 75 years. The study excluded patients with serum creatinine > 2 mg/dL.
Other ARB trials included the following:
- The I-PRESERVE trial, which found that irbesartan did not improve outcomes of patients with HF with preserved ejection fraction (HFpEF).15 The study of mostly white patients did not include patients aged ≥ 80 years.
- A randomized trial of valsartan in HF improved symptoms and mortality in NYHA II to IV HF but showed no benefit when added to ACE inhibitors.16 The trial had no patients aged ≥ 75 years and excluded those with several common comorbidities.
- A randomized, double-blind trial studied the effects of high-dose vs low-dose losartan on clinical outcomes in 3,846 patients with HF and demonstrated that high-dose losartan (150 mg/d) reduces all-cause mortality and hospitalization for HF more effectively than does low-dose losartan (50 mg/d).17 The study, however, had several exclusion criteria, and no patients were aged ≥ 75 years.
Mineralocorticoid Receptor Antagonists
Major studies of aldosterone antagonists demonstrated extra benefit when added to ACE inhibitors/ARBs in patients with HFrEF and NYHA class II HF.18,19
In the RALES study, spironolactone was found to reduce all-cause mortality by 30% and symptoms in NYHA III HF without a significant increase in the risk of serious hyperkalemia or renal failure.18 Most patients were white men aged < 80 years. This study demonstrated the importance of closely following serum potassium levels after initiating aldosterone antagonists in patients with subclinical renal disease because extensive structural damage within the kidney occurs before serum creatinine increases. Patients with advanced renal failure or those who cannot have close monitoring of serum potassium levels have an unfavorable risk–benefit ratio with aldosterone antagonists. Patients with cancer and liver failure were excluded from this trial.
In the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure study, (EMPHASIS-HF Study) eplerenone was found to reduce all-cause mortality and hospitalization for HFrEF.19 Similar to RALES, patients were mostly white males aged < 80 years, and patients with clinically significant, coexisting conditions were excluded.
The 2014 Treatment of Preserved Cardiac FunctionHeart Failure with an Aldosterone Antagonist Trial (TOPCAT) randomized 3,445 patients with well-controlled blood pressure to spironolactone or placebo.20 Inclusion criteria were LVEF ≥ 45%, findings of HF, and either a HF hospitalization or elevated B-type natriuretic peptide level. There was no difference in the primary composite outcome of CV mortality, aborted cardiac arrest, or HF hospitalization over the 3.3-year follow-up period. The study found that among patients with HFpEF, spironolactone does not reduce the composite endpoint of CV mortality, aborted cardiac arrest, or HF hospitalizations compared with that of placebo.20 In the trial, 29% of patients were aged > 75 years, and most were white men. There was no subgroup analysis for older patients.20 In all 3 trials, patients with kidney injury (serum creatinine of ≥ 2.5 or estimated glomerular filtration rate of ≤ 30 mL/min) were excluded because of the risk of hyperkalemia.
An observational study after the RALES trial demonstrated a nearly 4-fold increase in admissions for hyperkalemia with a 6-fold increase in associated mortality in patients taking spirolactone.21 Therefore, it is important to closely follow serum potassium levels after initiating aldosterone antagonists in older patients with subclinical renal disease. Patients with advanced renal failure or those without close monitoring of serum potassium levels have an unfavorable risk–benefit ratio with aldosterone antagonists.
Antithrombotic Therapy
The large multicenter, double-blind randomized trial WARCEF found no added benefit with warfarin vs aspirin for patients with HFrEF in sinus rhythm.22 There was no reduced time to first stroke or death, and the reduced ischemic stroke risk was offset by an increase in major hemorrhage. It is not clear whether subgroup analysis for the etiology of patients’ HF was performed in WARCEF.
The Warfarin and Antiplatelet Therapy in Chronic Heart Failure (WATCH) trial (N = 1,587) found that treatment with warfarin resulted in significantly fewer strokes in patients with ischemic cardiomyopathy.23 Randomization was not stratified by age group in both trials, and baseline characteristics included mostly white men, and no patients were older than aged > 75 years.
The risk of bleeding with prophylactic aspirin use for CV disease is dose dependent and increases with higher aspirin doses.24 The use of aspirin, 325 mg/d, in the WARCEF study might have contributed to the increased risk of hemorrhage.
Recently published results of COMMANDER HF found that the addition of rivaroxaban at a dose of 2.5 mg twice daily to standard care, including clinically selected antiplatelet therapies was not associated with a significantly lower rate of the composite primary outcome composite outcome of death, myocardial infarction (MI), or stroke among 5,022 patients with a recent episode of worsening heart failure compared with that of placebo.25
Several medical conditions are known to increase bleeding risk, including hypertension, cerebrovascular disease, ischemic stroke, serious heart disease, diabetes mellitus, renal insufficiency, alcoholism, liver disease, and falls.26 Many of these conditions are common among very old patients and should be considered when estimating risk–benefit ratio of oral anticoagulation therapy.
β-blockers
In several large studies, β-blockers have been shown to be effective in reducing mortality in patients with HFrEF. In the Cardiac Insufficiency Bisoprolol Study II, bisoprolol improved all-cause mortality and all-cause hospitalizations, and reduced sudden death in patients with NYHA III or IV HF.27 In the Carvedilol or Metoprolol European Trial (COMET), carvedilol was superior to metoprolol in reducing all-cause mortality for patients with NYHA II or IV HF.28 Both trials included mostly white men; patients with several comorbidities were excluded, and no patients were aged > 80 years.
COMET compared carvedilol with metoprolol tartrate, the short-acting form of metoprolol that has not shown a survival benefit for patients with HF. However, the Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure trial demonstrated survival benefits with metoprolol CR/XL and included patients aged > 80 years.29
In the SENIORS study, patients treated with nebivolol had a 4.2% absolute risk reduction in a composite of mortality or hospital admission at a mean follow-up of 21 months.30 It is reasonable to use nebivolol for managing HF in older patients. Careful monitoring of heart rate is necessary when prescribing β-blockers for older patients.
Cardiac Glycosides
Digoxin with diuretics was the first-line treatment for HF for many decades and the mainstay of HF therapy until the first large HF trials were performed in the 1980s. One trial initiated by the Digoxin Investigation Group (DIG) studied patients with HFrEF who were already receiving treatment for HF (including 94% taking ACE inhibitors and 82% on diuretics) and randomized them to either digoxin or placebo.31 The study found no significant difference in mortality between the groups at the 3-year follow-up; however, the digoxin group had significantly fewer hospitalizations compared with that of the placebo group.
A post-hoc analysis of patients by age found no difference in mortality between patients aged 70 to 79 years and those ≥ 80 years, with a persistent benefit in fewer hospitalizations. Digoxin continues to be recommended as a reasonable medication for treating symptomatic HFrEF. However, caution is advised in older patients, especially women, who are at higher risk of digoxin toxicity.
No current evidence exists that digoxin adds any benefits for patients with HFpEF of any age and therefore, it should not be used.
Diuretics
Diuretic therapy is important for managing shortness of breath and congestion related to fluid volume overload in patients with HF. Although diuretics have not been shown to reduce mortality in patients with HF, they are the mainstay treatment for patients with HFpEF.32 In a post-hoc analysis of the DIG study, diuretic use was associated with increased risk of mortality and hospitalizations in patients aged > 65 years.33 Hyponatremia is one of the most serious adverse effects (AEs) with these agents and occurs in about one-fifth of elderly patients taking diuretics.
In severe cases hyponatremia can cause a range of problems, including weakness, confusion, postural giddiness, postural hypotension, falls, transient hemiparesis, and seizures. In older patients with diminished renal reserve, diuretics are more likely to precipitate prerenal uremia than it does in younger patients. Prerequisites for diuretic use are an accurate diagnosis, careful monitoring of blood pressure and serum electrolytes, and regular review of their efficacy, AEs, and the need for continued treatment.
Statins
The Controlled Rosuvastatin Multinational Trial in Heart Failure demonstrated that low-dose rosuvastatin (10 mg/d) does not improve survival among patients with moderate-to-severe ischemic cardiomyopathy but could reduce the rate of CV hospitalizations.34 Patients in this study had a mean age of 73 years, and 41% of them were aged ≥ 75 years. However, the study used a low-dose rosuvastatin, and patients with several common comorbidities were excluded. Evidence exists that treatment with other statins may improve outcomes in patients with HF. There is also evidence that among elderly patients with HF, low serum total cholesterol is independently associated with a worse prognosis.35
Comorbidities
Anemia
In patients with iron-deficiency anemia (ferritin 15-100 ng/mL or 100-299 ng/mL with transferrin saturation < 20%) and symptomatic HFrEF (LVEF ≤ 40% with NYHA II to IV HF), oral iron replacement had no effect on exercise capacity as measured using change in peak oxygen uptake.36 However, IV iron replacement might be a reasonable option to improve functional status and quality of life (QOL) for patients with HF.37 In these studies, participants were aged < 75 years, and there is no evidence that treating other types of anemia improves outcomes in patients with HF.
Hypertension
The Systolic Blood Pressure Intervention Trial (SPRINT) demonstrated that controlling blood pressure to a goal systolic pressure of < 120 mm Hg is associated with significant reduction in the mortality among patients with increased CV risk (aged > 75 years, vascular disease, kidney injury, or a Framingham Risk Score >15%).38 The SPRINT study included patients aged > 75 (25%); however, the study excluded older adults living in nursing homes and those with diabetes mellitus, symptomatic HF, dementia, or stroke. The subgroup analysis did not stratify patients based on age nor provided sufficient evidence regarding treatment targets for this vulnerable population. Therefore, clinicians cannot draw any conclusions about managing hypertension among patients with HF from this study.
Sleep Apnea
Sleep apnea is common among patients with HF. A study of adults with chronic HF treated with evidence-based therapies found that 61% of participants had central or obstructive sleep apnea.39 In elderly patients, sleep apnea is further complicated by insomnia and disturbance of sleep cycle that often occur with the aging process.
It is crucial to differentiate central sleep apnea from obstructive sleep apnea, because the treatment approaches differ. Central sleep apnea is associated with poor prognosis in patients with HF.40 Adaptive servo ventilation for central sleep apnea uses a noninvasive ventilator to delivering servo controlled inspiratory pressure support on top of expiratory positive airway pressure. Adaptive servo ventilation for central sleep apnea is associated with higher all-cause mortality and CV mortality.41 Continuous positive airway pressure for obstructive sleep apnea improves sleep quality, reduces the apnea-hypopnea index, and improves nocturnal oxygenation.42
Depression
Clinically significant depression occurs in 21% of patients with HF, and the relationship between depression and poor HF outcomes is consistent and strong across several endpoints. However, in a randomized, 12-week study, the selective serotonin reuptake inhibitor sertraline did not improve depression symptoms or clinical status among patients with HF.43 Depression symptoms might overlap with fatigue and low energy expenditure experienced by oldest old patients with HF who do not have depression.
Furthermore, studies describing depression treatments among patients with HF are too small and heterogeneous to permit definitive conclusions about intervention effectiveness. These results identify areas requiring further development, raise questions regarding the association between depression and clinical outcomes in patients with HF, and provide information on depression prevalence that may help researchers design studies with appropriate depression measures and adequately powered sample sizes.
Frailty
Although frailty is prevalent in the elderly and is independently associated with poor outcomes, there is no standardized definition for frailty. The Fried Frailty Index is a widely used scale that incorporates criteria including weakness, slowness, exhaustion, and low physical activity in the diagnosis of frailty.44 However these symptoms are common among patients with advanced HF with and without depression or frailty.
Frailty should be defined collaboratively by the clinician and the patient and should include multidimensional aspects of health, function, and well-being. The treatment goal for patients with HF with frailty is to establish patient-centered goals based on preferences of care.45
Discussion
Although several novel approaches to improve outcomes of patients with HF have been developed, it continues to be the leading cause of cardiovascular death among older patients and the leading cause of hospital admissions.46 About 50% of newly diagnosed patients with HF die within 5 years.47 Current guidelines for managing HF are based on clinical trials that either include few or completely exclude patients aged > 80 years, minorities, and patients with comorbidities clinicians encounter daily in clinical practice.
Furthermore, most clinical trials are designed with mortality as the primary endpoint, which might be as important to our patients with advanced age as their ability to function with a reasonable QOL and less dependence on caregivers.
Decision making in managing HF in our oldest patients should start with an open discussion of the disease and its prognosis, goals of care, and available treatment options. The discussion should also cover all dimensions of suffering, including physical, spiritual, and psychosocial domains. Interviews of patients dying of HF and their caregivers conducted in the United Kingdom identified several communication and transition of care challenges specific to treating this population.48 The study revealed in most cases, patients did not recall receiving any written information about the severity of their disease and often did not understand the association among symptoms, such as shortness of breath, edema, and HF. Patients and caregivers did not feel involved in the decision-making process regarding their illness.
The concurrent presence of comorbidity, frailty, and cognitive impairment in our aging population with HF might add to the burden of the primary condition. Care often is perceived as fragmented. Polypharmacy negatively impacts HF management by increasing risk of drug nonadherence, drug interactions, and AEs in an already vulnerable population. There is a need for more effective interpersonal and easy to understand communication and resources.
In many situations, support services might be best facilitated by a dedicated palliative medicine team with significant experience in managing patients with HF.Although palliative medicine should always be considered for patients with HF with advanced age,consultations often are not obtained unless the patient decides to forgo medical treatment or until the last month of life.49
Although not all end-of-life symptoms can realistically be palliated, earlier involvement of multidisciplinary palliative medicine specialists may improve symptom control, functional status, and QOL. The team may help patients and caregivers cope with uncertainty, and make informed decisions that are person centered based on value system and beliefs.51
Conclusion
Randomized control trials as well as thoughtful observational studies of HF in patients with advanced age and comorbidities, although challenging, are needed to create the evidence base for treatment interventions and assessing their impact on mortality, morbidity, and QOL in this rapidly growing segment of our population.
Given the lack of evidence for HF treatment in patients with advanced age, the clinician should weigh the knowledge of the effect of aging on the CV system, and the lived experience of patients with HF, with the evidence that exists for making the best decision to relieve bothersome symptoms and improve outcomes of care as determined by patients and their caregivers.
Often the most important intervention we can offer our patients, especially those nearing the end of life, is dedicating our time to truly and actively listen with empathy, understating, and respect for their autonomy and for their decision making. And in doing so we accept our own limitations with humility.
Acknowledgments
Dr. Kheirbek received funds from the Veterans Affairs Capitol Health Care Network to establish the Center for Health and Aging at the Washington DC VA Medical Center.
1. Ortman JM, Velkoff AV, Hogan H. An aging nation: the older population in the United States. https://www.census.gov/prod/2014pubs/p25-1140.pdf. Published May 2014. Accessed September 30, 2018.
2. Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the U.S., 1979 to 2004. J Am Coll Cardiol. 2008;52(6):428-434.
3. Heidenreich PA, Albert NM, Allen LA, et al; American Heart Association Advocacy Coordinating Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Stroke Council. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606-619.
4. National Heart, Lung, and Blood Institute, National Institutes of Health. Incidence and Prevalence: 2006 Chart Book on Cardiovascular and Lung Diseases. Bethesda, MD: National Institutes of Health; 2006.
5. Curtis LH, Whellan DJ, Hammill BG, et al. Incidence and prevalence of heart failure in elderly persons, 1994-2003. Arch Intern Med. 2008;168(4):418-424.
6. Writing Group, Mozaffarian D, Benjamin EJ, et al; American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360.
7. Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a “set up” for vascular disease. Circulation. 2003;107(1):139-146.
8. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14.
9. CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. 1987;316(23):1429-1435.
10. SOLVD Investigators; Yusuf S, Pitt B, Davis CE, Hood WB Jr, Cohn JN. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med. 1992;327(10):685-691.
11. McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004.
12. McMurray JJ, Ostergren J, Swedberg K, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trial. Lancet. 2003;362(9386):767-771.
13. Granger CB, McMurray JJ, Yusuf S, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-Alternative trial. Lancet. 2003;362(9386):772-776.
14. Yusuf S, Pfeffer MA, Swedberg K, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362(9386):777-781.
15. Massie BM, Carson PE, McMurray JJ, et al; I-PRESERVE Investigators. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med. 2008;359(23):2456-2467.
16. Cohn JN, Tognoni G; Valsartan Heart Failure Trial Investigators. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N Engl J Med. 2001;345(23):1667-1675.
17. Konstam MA, Neaton JD, Dickstein K, et al; HEAAL Investigators. Effects of high-dose versus low-dose losartan on clinical outcomes in patients with heart failure (HEAAL study): a randomised, double-blind trial. Lancet. 2009;374(9704):1840-1848.
18. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341(10):709-717.
19. Zannad F, McMurray JJ, Krum H, et al; EMPHASIS-HF Study Group. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364(1):11-21.
20. Pitt B, Pfeffer MA, Assmann SF, et al; TOPCAT Investigators. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370(15):1383-1392.
21. Juurlink DN, Mamdani MM, Lee DS, et al. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004;351(6):543-551.
22. Homma S, Thompson JL, Pullicino PM, et al; WARCEF Investigators. Warfarin and aspirin in patients with heart failure and sinus rhythm. N Engl J Med. 2012;366(20):1859-1869.
23. Massie BM, Collins JF, Ammon SE, et al; WATCH Trial Investigators. Randomized trial of warfarin, aspirin, and clopidogrel in patients with chronic heart failure: the Warfarin and Antiplatelet Therapy in Chronic Heart Failure (WATCH) trial. Circulation. 2009;119(12):1616-1624.
24. Campbell CL, Smyth S, Montalescot G, Steinhubl SR. Aspirin dose for the prevention of cardiovascular disease: a systematic review. JAMA. 2007;297(18):2018-2024.
25. Zannad F, Anker, SD, Byra WM, et al; COMMANDER HF Investigators. Rivaroxaban in patients with heart failure, sinus rhythm, and coronary disease. N Engl J Med. 2018;379(14):1332-1342.
26. Schulman S, Beyth RJ, Kearon C, Levine MN. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):257S-298S.
27. CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999;353(9146):9-13.
28. Poole-Wilson PA, Swedberg K, Cleland JG, et al; Carvedilol Or Metoprolol European Trial Investigators. Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET): randomized controlled trial. Lancet. 2003;362(9377):7-13.
29. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet. 1999;353(9169):2001-2007.
30. Flather MD, Shibata MC, Coats AJ, et al; SENIORS Investigators. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J. 2005;26(3):215-225.
31. Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336(8):525-533.
32. Yancy CW, Jessup M, Bozkurt B, et al; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.
33 Juurlink DN, Mamdani MM, Lee DS, et al. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004;351(6):543-551.
34. Kjekshus J, Apetrei E, Barrios V, et al; CORONA Group. Rosuvastatin in older patients with systolic heart failure. N Engl J Med. 2007;357(22):2248-2261.
35. Rauchhaus M, Clark AL, Doehner W, et al. The relationship between cholesterol and survival in patients with chronic heart failure. J Am Coll Cardiol. 2003;42(11):1933-1940.
36. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e161.
37. Ponikowski P, van Veldhuisen DJ, Comin-Colet J, et al; CONFIRM-HF Investigators. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. Eur Heart J. 2015;36(11):657-668.
38. SPRINT Research Group, Wright JT Jr, Williamson JD, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-2116.
39. MacDonald M, Fang J, Pittman SD, White DP, Malhotra A. The current prevalence of sleep disordered breathing in congestive heart failure patients treated with beta-blockers. J Clin Sleep Med. 2008;4(1):38-42.
40. Bradley TD, Floras JS. Sleep Apnea and heart failure: part II: Central sleep apnea. Circulation. 2003;107(13):1822-1826.
41. Cowie MR, Woehrle H, Wegscheider K, et al. Adaptive servo-ventilation for central sleep apnea in systolic heart failure. N Engl J Med. 2015;373(12):1095-1105.
42. McEvoy RD, Antic NA, Heeley E, et al; SAVE Investigators and Coordinators. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919-931.
43. O’Connor CM, Jiang W, Kuchibhatla M, et al; SADHART-CHF Investigators. Safety and efficacy of sertraline for depression in patients with heart failure: results of the SADHART-CHF (Sertraline Against Depression and Heart Disease in Chronic Heart Failure) trial. J Am Coll Cardiol. 2010;56(9):692-699.
44. Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-156.
45. Pilotto A, Addante F, Franceschi M, et al. Multidimensional Prognostic Index based on a comprehensive geriatric assessment predicts short-term mortality in older patients with heart failure. Circ Heart Fail. 2010;3(1):14-20.
46. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
47. Goldberg, RJ, Ciampa, J, Lessard D,, et al. Long-term survival after heart failure: a contemporary population-based perspective. Arch Intern Med. 2007;167(5):490-496.
48. Murray SA, Boyd K, Kendall M, Worth A, Benton TF, Clausen H. Dying of lung cancer or cardiac failure: prospective qualitative interview study of patients and their carers in the community. BMJ. 2002;325(7370):929.
49. Gibbs JS, McCoy AS, Gibbs LM, Rogers AE, Addington-Hall JM. Living with and dying from heart failure: the role of palliative care. Heart. 2002;88(suppl 2):ii36-39.
50. Quill TE, Dresser R, Brock DW. The rule of double effect—a critique of its role in end-of-life decision making. N Engl J Med. 1997;337(24):1768-1771.
51. Nieminen MS, Dickstein K, Fonseca C, et al. The patient perspective: quality of life in advanced heart failure with frequent hospitalizations. Int J Cardiol. 2015;191:256-264.
As the population ages, heart failure is becoming a major public health challenge; clinicians need further evidence-based treatments to bridge the existing gap between guidelines and real-world clinical practice.
As the population ages, heart failure is becoming a major public health challenge; clinicians need further evidence-based treatments to bridge the existing gap between guidelines and real-world clinical practice.
In 2050, persons aged ≥ 85 years, also known as the oldest old, are projected to reach 18 million, accounting for 4.5% of the US population, up from 2.5% in 2030.1 These patients are the fastest growing segment of the US population.
Advances in treating cardiovascular (CV) disease over the past 2 decades have led to an increased incidence of heart failure (HF) and hospitalizations among older patients.2 Total costs of care for persons with HF have exceeded $30 billion annually and are expected to rise to more than $70 billion by 2030 due to growth of the aging population.3,4 Moreover, the Framingham Study reported mortality increases with advancing age (HR 1.27 and 1.61 per decade in men and women, respectively).5
The prevalence of HF is also high and increasing over time. The National Health and Nutrition Examination Survey reported that about 5.7 million Americans have HF.6 The prevalence of HF is expected to reach 8 million by 2030.6 The higher numbers of HF among patients with advanced age is associated with age-related changes in CV structure and function, including reduced responsiveness to β-adrenergic stimulation, impaired left ventricular diastolic filling, and increased vascular stiffness. In addition, age-related changes in other systems might contribute to a HF diagnosis or worsening of the condition.7
Older adults experience physiologic changes in pharmacokinetics and pharmacodynamics, including decreased volume of distribution and creatinine clearance, which lead to significant changes in drug concentration and effectiveness.8
Geriatric patients aged > 65 years who have comorbidities and those who reside in long-term care settings are underrepresented in clinical trials, leading clinicians to make treatment decisions based on data from younger, community-dwelling individuals. Researchers have questioned whether to include elderly patients and those with comorbidities in clinical trials, given that their diminished response may produce less conclusive results with smaller treatment effects. Exclusion criteria based on comorbid conditions or functional status disqualify many older adults from clinical trials.
This article reviews evidence from major randomized controlled trials over the past 2 decades and explores their applicability to support HF treatment guidelines in patients with advanced age (Table).
Pharmacotherapy for Heart Failure
Angiotensin-Converting Enzyme Inhibitors
Several randomized clinical trials have found that angiotensin-converting enzyme (ACE) inhibitors improve symptoms in patients with HF. The CooperativeNorth Scandinavian Enalapril Survival Study (CONSENSUS), demonstrated that enalapril improves survival in patients with New York Heart Association (NYHA) class IV HF with reduced ejection fraction (HFrEF) when added to standard therapy.9 However, the duration of beneficial effect of reduced mortality could not be assessed because the benefit of enalapril in NYHA class I to III HF was not evaluated, and follow-up data are limited. The average age of patients in the study was 71 years, and individuals with significant comorbidities were excluded.
ACE inhibitors also were found to reduce mortality even in asymptomatic patients with HFrEF in the Studies of Left Ventricular Dysfunction trial (SOLVD).10 Enalapril was found to reduce 4-year mortality by 16% and decrease HF hospitalizations when added to conventional therapy consisting primarily of digitalis, diuretics, and nitrates in patients with HFrEF. In this trial, patients aged ≥ 80 years were excluded as well as those with serum creatinine > 2 mg/dL or other conditions that could shorten survival or otherwise impede participation in a long-term trial.
PARADIGM-HF trial patients with HFrEF were randomized to enalapril or the angiotensin receptor-neprilysin inhibitor LCZ696. After a median of 27 months of follow-up, treatment with the angiotensin receptor-neprilysin inhibitor demonstrated greater reduction in CV mortality and HF hospitalizations than enalapril did and was associated with reduced all-cause mortality.11 The trial was stopped early because of evidence of overwhelming benefit with LCZ696. This study of mainly white men included no patients aged ≥ 75 years.
Angiotensin Receptor Blockers
Although less studied than ACE inhibitors, angiotensin receptor blockers (ARBs) share similar benefits. Among patients with symptomatic HFrEF taking an ACE inhibitor, the addition of candesartan reduced the risk of CV death and HF hospitalization as demonstrated in the Candesartan in Heart Failure Assessment of Reduction Mortality and Morbidity (CHARM-added and CHARM-alternative trials).12,13 The CHARM-added trial targeted patients with left ventricular ejection fraction (LVEF) ≤ 40% and NYHA class II to IV HF symptoms who were taking an ACE inhibitor. Adding candesartan reduced CV mortality by 37.9% and HF hospitalization by 42.3% compared with that of placebo.
The CHARM-alternative study found that use of candesartan in symptomatic HFrEF patients who do not tolerate ACE inhibitors,resulted in a 20% reduction in CV mortality as well as a 40% reduction in hospitalization for HF. Among patients with HF with preserved ejection fraction (HFpEF) and NYHA class II to IV symptoms, adding candesartan modestly reduced the rate of HF-related hospitalizations and had no effect on CV mortality in the CHARM-preserved study.14 The CHARM trials examined mostly white men, but 26% of patients were aged > 75 years. However, there was no subgroup analysis for patients aged > 75 years. The study excluded patients with serum creatinine > 2 mg/dL.
Other ARB trials included the following:
- The I-PRESERVE trial, which found that irbesartan did not improve outcomes of patients with HF with preserved ejection fraction (HFpEF).15 The study of mostly white patients did not include patients aged ≥ 80 years.
- A randomized trial of valsartan in HF improved symptoms and mortality in NYHA II to IV HF but showed no benefit when added to ACE inhibitors.16 The trial had no patients aged ≥ 75 years and excluded those with several common comorbidities.
- A randomized, double-blind trial studied the effects of high-dose vs low-dose losartan on clinical outcomes in 3,846 patients with HF and demonstrated that high-dose losartan (150 mg/d) reduces all-cause mortality and hospitalization for HF more effectively than does low-dose losartan (50 mg/d).17 The study, however, had several exclusion criteria, and no patients were aged ≥ 75 years.
Mineralocorticoid Receptor Antagonists
Major studies of aldosterone antagonists demonstrated extra benefit when added to ACE inhibitors/ARBs in patients with HFrEF and NYHA class II HF.18,19
In the RALES study, spironolactone was found to reduce all-cause mortality by 30% and symptoms in NYHA III HF without a significant increase in the risk of serious hyperkalemia or renal failure.18 Most patients were white men aged < 80 years. This study demonstrated the importance of closely following serum potassium levels after initiating aldosterone antagonists in patients with subclinical renal disease because extensive structural damage within the kidney occurs before serum creatinine increases. Patients with advanced renal failure or those who cannot have close monitoring of serum potassium levels have an unfavorable risk–benefit ratio with aldosterone antagonists. Patients with cancer and liver failure were excluded from this trial.
In the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure study, (EMPHASIS-HF Study) eplerenone was found to reduce all-cause mortality and hospitalization for HFrEF.19 Similar to RALES, patients were mostly white males aged < 80 years, and patients with clinically significant, coexisting conditions were excluded.
The 2014 Treatment of Preserved Cardiac FunctionHeart Failure with an Aldosterone Antagonist Trial (TOPCAT) randomized 3,445 patients with well-controlled blood pressure to spironolactone or placebo.20 Inclusion criteria were LVEF ≥ 45%, findings of HF, and either a HF hospitalization or elevated B-type natriuretic peptide level. There was no difference in the primary composite outcome of CV mortality, aborted cardiac arrest, or HF hospitalization over the 3.3-year follow-up period. The study found that among patients with HFpEF, spironolactone does not reduce the composite endpoint of CV mortality, aborted cardiac arrest, or HF hospitalizations compared with that of placebo.20 In the trial, 29% of patients were aged > 75 years, and most were white men. There was no subgroup analysis for older patients.20 In all 3 trials, patients with kidney injury (serum creatinine of ≥ 2.5 or estimated glomerular filtration rate of ≤ 30 mL/min) were excluded because of the risk of hyperkalemia.
An observational study after the RALES trial demonstrated a nearly 4-fold increase in admissions for hyperkalemia with a 6-fold increase in associated mortality in patients taking spirolactone.21 Therefore, it is important to closely follow serum potassium levels after initiating aldosterone antagonists in older patients with subclinical renal disease. Patients with advanced renal failure or those without close monitoring of serum potassium levels have an unfavorable risk–benefit ratio with aldosterone antagonists.
Antithrombotic Therapy
The large multicenter, double-blind randomized trial WARCEF found no added benefit with warfarin vs aspirin for patients with HFrEF in sinus rhythm.22 There was no reduced time to first stroke or death, and the reduced ischemic stroke risk was offset by an increase in major hemorrhage. It is not clear whether subgroup analysis for the etiology of patients’ HF was performed in WARCEF.
The Warfarin and Antiplatelet Therapy in Chronic Heart Failure (WATCH) trial (N = 1,587) found that treatment with warfarin resulted in significantly fewer strokes in patients with ischemic cardiomyopathy.23 Randomization was not stratified by age group in both trials, and baseline characteristics included mostly white men, and no patients were older than aged > 75 years.
The risk of bleeding with prophylactic aspirin use for CV disease is dose dependent and increases with higher aspirin doses.24 The use of aspirin, 325 mg/d, in the WARCEF study might have contributed to the increased risk of hemorrhage.
Recently published results of COMMANDER HF found that the addition of rivaroxaban at a dose of 2.5 mg twice daily to standard care, including clinically selected antiplatelet therapies was not associated with a significantly lower rate of the composite primary outcome composite outcome of death, myocardial infarction (MI), or stroke among 5,022 patients with a recent episode of worsening heart failure compared with that of placebo.25
Several medical conditions are known to increase bleeding risk, including hypertension, cerebrovascular disease, ischemic stroke, serious heart disease, diabetes mellitus, renal insufficiency, alcoholism, liver disease, and falls.26 Many of these conditions are common among very old patients and should be considered when estimating risk–benefit ratio of oral anticoagulation therapy.
β-blockers
In several large studies, β-blockers have been shown to be effective in reducing mortality in patients with HFrEF. In the Cardiac Insufficiency Bisoprolol Study II, bisoprolol improved all-cause mortality and all-cause hospitalizations, and reduced sudden death in patients with NYHA III or IV HF.27 In the Carvedilol or Metoprolol European Trial (COMET), carvedilol was superior to metoprolol in reducing all-cause mortality for patients with NYHA II or IV HF.28 Both trials included mostly white men; patients with several comorbidities were excluded, and no patients were aged > 80 years.
COMET compared carvedilol with metoprolol tartrate, the short-acting form of metoprolol that has not shown a survival benefit for patients with HF. However, the Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure trial demonstrated survival benefits with metoprolol CR/XL and included patients aged > 80 years.29
In the SENIORS study, patients treated with nebivolol had a 4.2% absolute risk reduction in a composite of mortality or hospital admission at a mean follow-up of 21 months.30 It is reasonable to use nebivolol for managing HF in older patients. Careful monitoring of heart rate is necessary when prescribing β-blockers for older patients.
Cardiac Glycosides
Digoxin with diuretics was the first-line treatment for HF for many decades and the mainstay of HF therapy until the first large HF trials were performed in the 1980s. One trial initiated by the Digoxin Investigation Group (DIG) studied patients with HFrEF who were already receiving treatment for HF (including 94% taking ACE inhibitors and 82% on diuretics) and randomized them to either digoxin or placebo.31 The study found no significant difference in mortality between the groups at the 3-year follow-up; however, the digoxin group had significantly fewer hospitalizations compared with that of the placebo group.
A post-hoc analysis of patients by age found no difference in mortality between patients aged 70 to 79 years and those ≥ 80 years, with a persistent benefit in fewer hospitalizations. Digoxin continues to be recommended as a reasonable medication for treating symptomatic HFrEF. However, caution is advised in older patients, especially women, who are at higher risk of digoxin toxicity.
No current evidence exists that digoxin adds any benefits for patients with HFpEF of any age and therefore, it should not be used.
Diuretics
Diuretic therapy is important for managing shortness of breath and congestion related to fluid volume overload in patients with HF. Although diuretics have not been shown to reduce mortality in patients with HF, they are the mainstay treatment for patients with HFpEF.32 In a post-hoc analysis of the DIG study, diuretic use was associated with increased risk of mortality and hospitalizations in patients aged > 65 years.33 Hyponatremia is one of the most serious adverse effects (AEs) with these agents and occurs in about one-fifth of elderly patients taking diuretics.
In severe cases hyponatremia can cause a range of problems, including weakness, confusion, postural giddiness, postural hypotension, falls, transient hemiparesis, and seizures. In older patients with diminished renal reserve, diuretics are more likely to precipitate prerenal uremia than it does in younger patients. Prerequisites for diuretic use are an accurate diagnosis, careful monitoring of blood pressure and serum electrolytes, and regular review of their efficacy, AEs, and the need for continued treatment.
Statins
The Controlled Rosuvastatin Multinational Trial in Heart Failure demonstrated that low-dose rosuvastatin (10 mg/d) does not improve survival among patients with moderate-to-severe ischemic cardiomyopathy but could reduce the rate of CV hospitalizations.34 Patients in this study had a mean age of 73 years, and 41% of them were aged ≥ 75 years. However, the study used a low-dose rosuvastatin, and patients with several common comorbidities were excluded. Evidence exists that treatment with other statins may improve outcomes in patients with HF. There is also evidence that among elderly patients with HF, low serum total cholesterol is independently associated with a worse prognosis.35
Comorbidities
Anemia
In patients with iron-deficiency anemia (ferritin 15-100 ng/mL or 100-299 ng/mL with transferrin saturation < 20%) and symptomatic HFrEF (LVEF ≤ 40% with NYHA II to IV HF), oral iron replacement had no effect on exercise capacity as measured using change in peak oxygen uptake.36 However, IV iron replacement might be a reasonable option to improve functional status and quality of life (QOL) for patients with HF.37 In these studies, participants were aged < 75 years, and there is no evidence that treating other types of anemia improves outcomes in patients with HF.
Hypertension
The Systolic Blood Pressure Intervention Trial (SPRINT) demonstrated that controlling blood pressure to a goal systolic pressure of < 120 mm Hg is associated with significant reduction in the mortality among patients with increased CV risk (aged > 75 years, vascular disease, kidney injury, or a Framingham Risk Score >15%).38 The SPRINT study included patients aged > 75 (25%); however, the study excluded older adults living in nursing homes and those with diabetes mellitus, symptomatic HF, dementia, or stroke. The subgroup analysis did not stratify patients based on age nor provided sufficient evidence regarding treatment targets for this vulnerable population. Therefore, clinicians cannot draw any conclusions about managing hypertension among patients with HF from this study.
Sleep Apnea
Sleep apnea is common among patients with HF. A study of adults with chronic HF treated with evidence-based therapies found that 61% of participants had central or obstructive sleep apnea.39 In elderly patients, sleep apnea is further complicated by insomnia and disturbance of sleep cycle that often occur with the aging process.
It is crucial to differentiate central sleep apnea from obstructive sleep apnea, because the treatment approaches differ. Central sleep apnea is associated with poor prognosis in patients with HF.40 Adaptive servo ventilation for central sleep apnea uses a noninvasive ventilator to delivering servo controlled inspiratory pressure support on top of expiratory positive airway pressure. Adaptive servo ventilation for central sleep apnea is associated with higher all-cause mortality and CV mortality.41 Continuous positive airway pressure for obstructive sleep apnea improves sleep quality, reduces the apnea-hypopnea index, and improves nocturnal oxygenation.42
Depression
Clinically significant depression occurs in 21% of patients with HF, and the relationship between depression and poor HF outcomes is consistent and strong across several endpoints. However, in a randomized, 12-week study, the selective serotonin reuptake inhibitor sertraline did not improve depression symptoms or clinical status among patients with HF.43 Depression symptoms might overlap with fatigue and low energy expenditure experienced by oldest old patients with HF who do not have depression.
Furthermore, studies describing depression treatments among patients with HF are too small and heterogeneous to permit definitive conclusions about intervention effectiveness. These results identify areas requiring further development, raise questions regarding the association between depression and clinical outcomes in patients with HF, and provide information on depression prevalence that may help researchers design studies with appropriate depression measures and adequately powered sample sizes.
Frailty
Although frailty is prevalent in the elderly and is independently associated with poor outcomes, there is no standardized definition for frailty. The Fried Frailty Index is a widely used scale that incorporates criteria including weakness, slowness, exhaustion, and low physical activity in the diagnosis of frailty.44 However these symptoms are common among patients with advanced HF with and without depression or frailty.
Frailty should be defined collaboratively by the clinician and the patient and should include multidimensional aspects of health, function, and well-being. The treatment goal for patients with HF with frailty is to establish patient-centered goals based on preferences of care.45
Discussion
Although several novel approaches to improve outcomes of patients with HF have been developed, it continues to be the leading cause of cardiovascular death among older patients and the leading cause of hospital admissions.46 About 50% of newly diagnosed patients with HF die within 5 years.47 Current guidelines for managing HF are based on clinical trials that either include few or completely exclude patients aged > 80 years, minorities, and patients with comorbidities clinicians encounter daily in clinical practice.
Furthermore, most clinical trials are designed with mortality as the primary endpoint, which might be as important to our patients with advanced age as their ability to function with a reasonable QOL and less dependence on caregivers.
Decision making in managing HF in our oldest patients should start with an open discussion of the disease and its prognosis, goals of care, and available treatment options. The discussion should also cover all dimensions of suffering, including physical, spiritual, and psychosocial domains. Interviews of patients dying of HF and their caregivers conducted in the United Kingdom identified several communication and transition of care challenges specific to treating this population.48 The study revealed in most cases, patients did not recall receiving any written information about the severity of their disease and often did not understand the association among symptoms, such as shortness of breath, edema, and HF. Patients and caregivers did not feel involved in the decision-making process regarding their illness.
The concurrent presence of comorbidity, frailty, and cognitive impairment in our aging population with HF might add to the burden of the primary condition. Care often is perceived as fragmented. Polypharmacy negatively impacts HF management by increasing risk of drug nonadherence, drug interactions, and AEs in an already vulnerable population. There is a need for more effective interpersonal and easy to understand communication and resources.
In many situations, support services might be best facilitated by a dedicated palliative medicine team with significant experience in managing patients with HF.Although palliative medicine should always be considered for patients with HF with advanced age,consultations often are not obtained unless the patient decides to forgo medical treatment or until the last month of life.49
Although not all end-of-life symptoms can realistically be palliated, earlier involvement of multidisciplinary palliative medicine specialists may improve symptom control, functional status, and QOL. The team may help patients and caregivers cope with uncertainty, and make informed decisions that are person centered based on value system and beliefs.51
Conclusion
Randomized control trials as well as thoughtful observational studies of HF in patients with advanced age and comorbidities, although challenging, are needed to create the evidence base for treatment interventions and assessing their impact on mortality, morbidity, and QOL in this rapidly growing segment of our population.
Given the lack of evidence for HF treatment in patients with advanced age, the clinician should weigh the knowledge of the effect of aging on the CV system, and the lived experience of patients with HF, with the evidence that exists for making the best decision to relieve bothersome symptoms and improve outcomes of care as determined by patients and their caregivers.
Often the most important intervention we can offer our patients, especially those nearing the end of life, is dedicating our time to truly and actively listen with empathy, understating, and respect for their autonomy and for their decision making. And in doing so we accept our own limitations with humility.
Acknowledgments
Dr. Kheirbek received funds from the Veterans Affairs Capitol Health Care Network to establish the Center for Health and Aging at the Washington DC VA Medical Center.
In 2050, persons aged ≥ 85 years, also known as the oldest old, are projected to reach 18 million, accounting for 4.5% of the US population, up from 2.5% in 2030.1 These patients are the fastest growing segment of the US population.
Advances in treating cardiovascular (CV) disease over the past 2 decades have led to an increased incidence of heart failure (HF) and hospitalizations among older patients.2 Total costs of care for persons with HF have exceeded $30 billion annually and are expected to rise to more than $70 billion by 2030 due to growth of the aging population.3,4 Moreover, the Framingham Study reported mortality increases with advancing age (HR 1.27 and 1.61 per decade in men and women, respectively).5
The prevalence of HF is also high and increasing over time. The National Health and Nutrition Examination Survey reported that about 5.7 million Americans have HF.6 The prevalence of HF is expected to reach 8 million by 2030.6 The higher numbers of HF among patients with advanced age is associated with age-related changes in CV structure and function, including reduced responsiveness to β-adrenergic stimulation, impaired left ventricular diastolic filling, and increased vascular stiffness. In addition, age-related changes in other systems might contribute to a HF diagnosis or worsening of the condition.7
Older adults experience physiologic changes in pharmacokinetics and pharmacodynamics, including decreased volume of distribution and creatinine clearance, which lead to significant changes in drug concentration and effectiveness.8
Geriatric patients aged > 65 years who have comorbidities and those who reside in long-term care settings are underrepresented in clinical trials, leading clinicians to make treatment decisions based on data from younger, community-dwelling individuals. Researchers have questioned whether to include elderly patients and those with comorbidities in clinical trials, given that their diminished response may produce less conclusive results with smaller treatment effects. Exclusion criteria based on comorbid conditions or functional status disqualify many older adults from clinical trials.
This article reviews evidence from major randomized controlled trials over the past 2 decades and explores their applicability to support HF treatment guidelines in patients with advanced age (Table).
Pharmacotherapy for Heart Failure
Angiotensin-Converting Enzyme Inhibitors
Several randomized clinical trials have found that angiotensin-converting enzyme (ACE) inhibitors improve symptoms in patients with HF. The CooperativeNorth Scandinavian Enalapril Survival Study (CONSENSUS), demonstrated that enalapril improves survival in patients with New York Heart Association (NYHA) class IV HF with reduced ejection fraction (HFrEF) when added to standard therapy.9 However, the duration of beneficial effect of reduced mortality could not be assessed because the benefit of enalapril in NYHA class I to III HF was not evaluated, and follow-up data are limited. The average age of patients in the study was 71 years, and individuals with significant comorbidities were excluded.
ACE inhibitors also were found to reduce mortality even in asymptomatic patients with HFrEF in the Studies of Left Ventricular Dysfunction trial (SOLVD).10 Enalapril was found to reduce 4-year mortality by 16% and decrease HF hospitalizations when added to conventional therapy consisting primarily of digitalis, diuretics, and nitrates in patients with HFrEF. In this trial, patients aged ≥ 80 years were excluded as well as those with serum creatinine > 2 mg/dL or other conditions that could shorten survival or otherwise impede participation in a long-term trial.
PARADIGM-HF trial patients with HFrEF were randomized to enalapril or the angiotensin receptor-neprilysin inhibitor LCZ696. After a median of 27 months of follow-up, treatment with the angiotensin receptor-neprilysin inhibitor demonstrated greater reduction in CV mortality and HF hospitalizations than enalapril did and was associated with reduced all-cause mortality.11 The trial was stopped early because of evidence of overwhelming benefit with LCZ696. This study of mainly white men included no patients aged ≥ 75 years.
Angiotensin Receptor Blockers
Although less studied than ACE inhibitors, angiotensin receptor blockers (ARBs) share similar benefits. Among patients with symptomatic HFrEF taking an ACE inhibitor, the addition of candesartan reduced the risk of CV death and HF hospitalization as demonstrated in the Candesartan in Heart Failure Assessment of Reduction Mortality and Morbidity (CHARM-added and CHARM-alternative trials).12,13 The CHARM-added trial targeted patients with left ventricular ejection fraction (LVEF) ≤ 40% and NYHA class II to IV HF symptoms who were taking an ACE inhibitor. Adding candesartan reduced CV mortality by 37.9% and HF hospitalization by 42.3% compared with that of placebo.
The CHARM-alternative study found that use of candesartan in symptomatic HFrEF patients who do not tolerate ACE inhibitors,resulted in a 20% reduction in CV mortality as well as a 40% reduction in hospitalization for HF. Among patients with HF with preserved ejection fraction (HFpEF) and NYHA class II to IV symptoms, adding candesartan modestly reduced the rate of HF-related hospitalizations and had no effect on CV mortality in the CHARM-preserved study.14 The CHARM trials examined mostly white men, but 26% of patients were aged > 75 years. However, there was no subgroup analysis for patients aged > 75 years. The study excluded patients with serum creatinine > 2 mg/dL.
Other ARB trials included the following:
- The I-PRESERVE trial, which found that irbesartan did not improve outcomes of patients with HF with preserved ejection fraction (HFpEF).15 The study of mostly white patients did not include patients aged ≥ 80 years.
- A randomized trial of valsartan in HF improved symptoms and mortality in NYHA II to IV HF but showed no benefit when added to ACE inhibitors.16 The trial had no patients aged ≥ 75 years and excluded those with several common comorbidities.
- A randomized, double-blind trial studied the effects of high-dose vs low-dose losartan on clinical outcomes in 3,846 patients with HF and demonstrated that high-dose losartan (150 mg/d) reduces all-cause mortality and hospitalization for HF more effectively than does low-dose losartan (50 mg/d).17 The study, however, had several exclusion criteria, and no patients were aged ≥ 75 years.
Mineralocorticoid Receptor Antagonists
Major studies of aldosterone antagonists demonstrated extra benefit when added to ACE inhibitors/ARBs in patients with HFrEF and NYHA class II HF.18,19
In the RALES study, spironolactone was found to reduce all-cause mortality by 30% and symptoms in NYHA III HF without a significant increase in the risk of serious hyperkalemia or renal failure.18 Most patients were white men aged < 80 years. This study demonstrated the importance of closely following serum potassium levels after initiating aldosterone antagonists in patients with subclinical renal disease because extensive structural damage within the kidney occurs before serum creatinine increases. Patients with advanced renal failure or those who cannot have close monitoring of serum potassium levels have an unfavorable risk–benefit ratio with aldosterone antagonists. Patients with cancer and liver failure were excluded from this trial.
In the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure study, (EMPHASIS-HF Study) eplerenone was found to reduce all-cause mortality and hospitalization for HFrEF.19 Similar to RALES, patients were mostly white males aged < 80 years, and patients with clinically significant, coexisting conditions were excluded.
The 2014 Treatment of Preserved Cardiac FunctionHeart Failure with an Aldosterone Antagonist Trial (TOPCAT) randomized 3,445 patients with well-controlled blood pressure to spironolactone or placebo.20 Inclusion criteria were LVEF ≥ 45%, findings of HF, and either a HF hospitalization or elevated B-type natriuretic peptide level. There was no difference in the primary composite outcome of CV mortality, aborted cardiac arrest, or HF hospitalization over the 3.3-year follow-up period. The study found that among patients with HFpEF, spironolactone does not reduce the composite endpoint of CV mortality, aborted cardiac arrest, or HF hospitalizations compared with that of placebo.20 In the trial, 29% of patients were aged > 75 years, and most were white men. There was no subgroup analysis for older patients.20 In all 3 trials, patients with kidney injury (serum creatinine of ≥ 2.5 or estimated glomerular filtration rate of ≤ 30 mL/min) were excluded because of the risk of hyperkalemia.
An observational study after the RALES trial demonstrated a nearly 4-fold increase in admissions for hyperkalemia with a 6-fold increase in associated mortality in patients taking spirolactone.21 Therefore, it is important to closely follow serum potassium levels after initiating aldosterone antagonists in older patients with subclinical renal disease. Patients with advanced renal failure or those without close monitoring of serum potassium levels have an unfavorable risk–benefit ratio with aldosterone antagonists.
Antithrombotic Therapy
The large multicenter, double-blind randomized trial WARCEF found no added benefit with warfarin vs aspirin for patients with HFrEF in sinus rhythm.22 There was no reduced time to first stroke or death, and the reduced ischemic stroke risk was offset by an increase in major hemorrhage. It is not clear whether subgroup analysis for the etiology of patients’ HF was performed in WARCEF.
The Warfarin and Antiplatelet Therapy in Chronic Heart Failure (WATCH) trial (N = 1,587) found that treatment with warfarin resulted in significantly fewer strokes in patients with ischemic cardiomyopathy.23 Randomization was not stratified by age group in both trials, and baseline characteristics included mostly white men, and no patients were older than aged > 75 years.
The risk of bleeding with prophylactic aspirin use for CV disease is dose dependent and increases with higher aspirin doses.24 The use of aspirin, 325 mg/d, in the WARCEF study might have contributed to the increased risk of hemorrhage.
Recently published results of COMMANDER HF found that the addition of rivaroxaban at a dose of 2.5 mg twice daily to standard care, including clinically selected antiplatelet therapies was not associated with a significantly lower rate of the composite primary outcome composite outcome of death, myocardial infarction (MI), or stroke among 5,022 patients with a recent episode of worsening heart failure compared with that of placebo.25
Several medical conditions are known to increase bleeding risk, including hypertension, cerebrovascular disease, ischemic stroke, serious heart disease, diabetes mellitus, renal insufficiency, alcoholism, liver disease, and falls.26 Many of these conditions are common among very old patients and should be considered when estimating risk–benefit ratio of oral anticoagulation therapy.
β-blockers
In several large studies, β-blockers have been shown to be effective in reducing mortality in patients with HFrEF. In the Cardiac Insufficiency Bisoprolol Study II, bisoprolol improved all-cause mortality and all-cause hospitalizations, and reduced sudden death in patients with NYHA III or IV HF.27 In the Carvedilol or Metoprolol European Trial (COMET), carvedilol was superior to metoprolol in reducing all-cause mortality for patients with NYHA II or IV HF.28 Both trials included mostly white men; patients with several comorbidities were excluded, and no patients were aged > 80 years.
COMET compared carvedilol with metoprolol tartrate, the short-acting form of metoprolol that has not shown a survival benefit for patients with HF. However, the Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure trial demonstrated survival benefits with metoprolol CR/XL and included patients aged > 80 years.29
In the SENIORS study, patients treated with nebivolol had a 4.2% absolute risk reduction in a composite of mortality or hospital admission at a mean follow-up of 21 months.30 It is reasonable to use nebivolol for managing HF in older patients. Careful monitoring of heart rate is necessary when prescribing β-blockers for older patients.
Cardiac Glycosides
Digoxin with diuretics was the first-line treatment for HF for many decades and the mainstay of HF therapy until the first large HF trials were performed in the 1980s. One trial initiated by the Digoxin Investigation Group (DIG) studied patients with HFrEF who were already receiving treatment for HF (including 94% taking ACE inhibitors and 82% on diuretics) and randomized them to either digoxin or placebo.31 The study found no significant difference in mortality between the groups at the 3-year follow-up; however, the digoxin group had significantly fewer hospitalizations compared with that of the placebo group.
A post-hoc analysis of patients by age found no difference in mortality between patients aged 70 to 79 years and those ≥ 80 years, with a persistent benefit in fewer hospitalizations. Digoxin continues to be recommended as a reasonable medication for treating symptomatic HFrEF. However, caution is advised in older patients, especially women, who are at higher risk of digoxin toxicity.
No current evidence exists that digoxin adds any benefits for patients with HFpEF of any age and therefore, it should not be used.
Diuretics
Diuretic therapy is important for managing shortness of breath and congestion related to fluid volume overload in patients with HF. Although diuretics have not been shown to reduce mortality in patients with HF, they are the mainstay treatment for patients with HFpEF.32 In a post-hoc analysis of the DIG study, diuretic use was associated with increased risk of mortality and hospitalizations in patients aged > 65 years.33 Hyponatremia is one of the most serious adverse effects (AEs) with these agents and occurs in about one-fifth of elderly patients taking diuretics.
In severe cases hyponatremia can cause a range of problems, including weakness, confusion, postural giddiness, postural hypotension, falls, transient hemiparesis, and seizures. In older patients with diminished renal reserve, diuretics are more likely to precipitate prerenal uremia than it does in younger patients. Prerequisites for diuretic use are an accurate diagnosis, careful monitoring of blood pressure and serum electrolytes, and regular review of their efficacy, AEs, and the need for continued treatment.
Statins
The Controlled Rosuvastatin Multinational Trial in Heart Failure demonstrated that low-dose rosuvastatin (10 mg/d) does not improve survival among patients with moderate-to-severe ischemic cardiomyopathy but could reduce the rate of CV hospitalizations.34 Patients in this study had a mean age of 73 years, and 41% of them were aged ≥ 75 years. However, the study used a low-dose rosuvastatin, and patients with several common comorbidities were excluded. Evidence exists that treatment with other statins may improve outcomes in patients with HF. There is also evidence that among elderly patients with HF, low serum total cholesterol is independently associated with a worse prognosis.35
Comorbidities
Anemia
In patients with iron-deficiency anemia (ferritin 15-100 ng/mL or 100-299 ng/mL with transferrin saturation < 20%) and symptomatic HFrEF (LVEF ≤ 40% with NYHA II to IV HF), oral iron replacement had no effect on exercise capacity as measured using change in peak oxygen uptake.36 However, IV iron replacement might be a reasonable option to improve functional status and quality of life (QOL) for patients with HF.37 In these studies, participants were aged < 75 years, and there is no evidence that treating other types of anemia improves outcomes in patients with HF.
Hypertension
The Systolic Blood Pressure Intervention Trial (SPRINT) demonstrated that controlling blood pressure to a goal systolic pressure of < 120 mm Hg is associated with significant reduction in the mortality among patients with increased CV risk (aged > 75 years, vascular disease, kidney injury, or a Framingham Risk Score >15%).38 The SPRINT study included patients aged > 75 (25%); however, the study excluded older adults living in nursing homes and those with diabetes mellitus, symptomatic HF, dementia, or stroke. The subgroup analysis did not stratify patients based on age nor provided sufficient evidence regarding treatment targets for this vulnerable population. Therefore, clinicians cannot draw any conclusions about managing hypertension among patients with HF from this study.
Sleep Apnea
Sleep apnea is common among patients with HF. A study of adults with chronic HF treated with evidence-based therapies found that 61% of participants had central or obstructive sleep apnea.39 In elderly patients, sleep apnea is further complicated by insomnia and disturbance of sleep cycle that often occur with the aging process.
It is crucial to differentiate central sleep apnea from obstructive sleep apnea, because the treatment approaches differ. Central sleep apnea is associated with poor prognosis in patients with HF.40 Adaptive servo ventilation for central sleep apnea uses a noninvasive ventilator to delivering servo controlled inspiratory pressure support on top of expiratory positive airway pressure. Adaptive servo ventilation for central sleep apnea is associated with higher all-cause mortality and CV mortality.41 Continuous positive airway pressure for obstructive sleep apnea improves sleep quality, reduces the apnea-hypopnea index, and improves nocturnal oxygenation.42
Depression
Clinically significant depression occurs in 21% of patients with HF, and the relationship between depression and poor HF outcomes is consistent and strong across several endpoints. However, in a randomized, 12-week study, the selective serotonin reuptake inhibitor sertraline did not improve depression symptoms or clinical status among patients with HF.43 Depression symptoms might overlap with fatigue and low energy expenditure experienced by oldest old patients with HF who do not have depression.
Furthermore, studies describing depression treatments among patients with HF are too small and heterogeneous to permit definitive conclusions about intervention effectiveness. These results identify areas requiring further development, raise questions regarding the association between depression and clinical outcomes in patients with HF, and provide information on depression prevalence that may help researchers design studies with appropriate depression measures and adequately powered sample sizes.
Frailty
Although frailty is prevalent in the elderly and is independently associated with poor outcomes, there is no standardized definition for frailty. The Fried Frailty Index is a widely used scale that incorporates criteria including weakness, slowness, exhaustion, and low physical activity in the diagnosis of frailty.44 However these symptoms are common among patients with advanced HF with and without depression or frailty.
Frailty should be defined collaboratively by the clinician and the patient and should include multidimensional aspects of health, function, and well-being. The treatment goal for patients with HF with frailty is to establish patient-centered goals based on preferences of care.45
Discussion
Although several novel approaches to improve outcomes of patients with HF have been developed, it continues to be the leading cause of cardiovascular death among older patients and the leading cause of hospital admissions.46 About 50% of newly diagnosed patients with HF die within 5 years.47 Current guidelines for managing HF are based on clinical trials that either include few or completely exclude patients aged > 80 years, minorities, and patients with comorbidities clinicians encounter daily in clinical practice.
Furthermore, most clinical trials are designed with mortality as the primary endpoint, which might be as important to our patients with advanced age as their ability to function with a reasonable QOL and less dependence on caregivers.
Decision making in managing HF in our oldest patients should start with an open discussion of the disease and its prognosis, goals of care, and available treatment options. The discussion should also cover all dimensions of suffering, including physical, spiritual, and psychosocial domains. Interviews of patients dying of HF and their caregivers conducted in the United Kingdom identified several communication and transition of care challenges specific to treating this population.48 The study revealed in most cases, patients did not recall receiving any written information about the severity of their disease and often did not understand the association among symptoms, such as shortness of breath, edema, and HF. Patients and caregivers did not feel involved in the decision-making process regarding their illness.
The concurrent presence of comorbidity, frailty, and cognitive impairment in our aging population with HF might add to the burden of the primary condition. Care often is perceived as fragmented. Polypharmacy negatively impacts HF management by increasing risk of drug nonadherence, drug interactions, and AEs in an already vulnerable population. There is a need for more effective interpersonal and easy to understand communication and resources.
In many situations, support services might be best facilitated by a dedicated palliative medicine team with significant experience in managing patients with HF.Although palliative medicine should always be considered for patients with HF with advanced age,consultations often are not obtained unless the patient decides to forgo medical treatment or until the last month of life.49
Although not all end-of-life symptoms can realistically be palliated, earlier involvement of multidisciplinary palliative medicine specialists may improve symptom control, functional status, and QOL. The team may help patients and caregivers cope with uncertainty, and make informed decisions that are person centered based on value system and beliefs.51
Conclusion
Randomized control trials as well as thoughtful observational studies of HF in patients with advanced age and comorbidities, although challenging, are needed to create the evidence base for treatment interventions and assessing their impact on mortality, morbidity, and QOL in this rapidly growing segment of our population.
Given the lack of evidence for HF treatment in patients with advanced age, the clinician should weigh the knowledge of the effect of aging on the CV system, and the lived experience of patients with HF, with the evidence that exists for making the best decision to relieve bothersome symptoms and improve outcomes of care as determined by patients and their caregivers.
Often the most important intervention we can offer our patients, especially those nearing the end of life, is dedicating our time to truly and actively listen with empathy, understating, and respect for their autonomy and for their decision making. And in doing so we accept our own limitations with humility.
Acknowledgments
Dr. Kheirbek received funds from the Veterans Affairs Capitol Health Care Network to establish the Center for Health and Aging at the Washington DC VA Medical Center.
1. Ortman JM, Velkoff AV, Hogan H. An aging nation: the older population in the United States. https://www.census.gov/prod/2014pubs/p25-1140.pdf. Published May 2014. Accessed September 30, 2018.
2. Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the U.S., 1979 to 2004. J Am Coll Cardiol. 2008;52(6):428-434.
3. Heidenreich PA, Albert NM, Allen LA, et al; American Heart Association Advocacy Coordinating Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Stroke Council. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606-619.
4. National Heart, Lung, and Blood Institute, National Institutes of Health. Incidence and Prevalence: 2006 Chart Book on Cardiovascular and Lung Diseases. Bethesda, MD: National Institutes of Health; 2006.
5. Curtis LH, Whellan DJ, Hammill BG, et al. Incidence and prevalence of heart failure in elderly persons, 1994-2003. Arch Intern Med. 2008;168(4):418-424.
6. Writing Group, Mozaffarian D, Benjamin EJ, et al; American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360.
7. Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a “set up” for vascular disease. Circulation. 2003;107(1):139-146.
8. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14.
9. CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. 1987;316(23):1429-1435.
10. SOLVD Investigators; Yusuf S, Pitt B, Davis CE, Hood WB Jr, Cohn JN. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med. 1992;327(10):685-691.
11. McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004.
12. McMurray JJ, Ostergren J, Swedberg K, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trial. Lancet. 2003;362(9386):767-771.
13. Granger CB, McMurray JJ, Yusuf S, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-Alternative trial. Lancet. 2003;362(9386):772-776.
14. Yusuf S, Pfeffer MA, Swedberg K, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362(9386):777-781.
15. Massie BM, Carson PE, McMurray JJ, et al; I-PRESERVE Investigators. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med. 2008;359(23):2456-2467.
16. Cohn JN, Tognoni G; Valsartan Heart Failure Trial Investigators. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N Engl J Med. 2001;345(23):1667-1675.
17. Konstam MA, Neaton JD, Dickstein K, et al; HEAAL Investigators. Effects of high-dose versus low-dose losartan on clinical outcomes in patients with heart failure (HEAAL study): a randomised, double-blind trial. Lancet. 2009;374(9704):1840-1848.
18. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341(10):709-717.
19. Zannad F, McMurray JJ, Krum H, et al; EMPHASIS-HF Study Group. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364(1):11-21.
20. Pitt B, Pfeffer MA, Assmann SF, et al; TOPCAT Investigators. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370(15):1383-1392.
21. Juurlink DN, Mamdani MM, Lee DS, et al. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004;351(6):543-551.
22. Homma S, Thompson JL, Pullicino PM, et al; WARCEF Investigators. Warfarin and aspirin in patients with heart failure and sinus rhythm. N Engl J Med. 2012;366(20):1859-1869.
23. Massie BM, Collins JF, Ammon SE, et al; WATCH Trial Investigators. Randomized trial of warfarin, aspirin, and clopidogrel in patients with chronic heart failure: the Warfarin and Antiplatelet Therapy in Chronic Heart Failure (WATCH) trial. Circulation. 2009;119(12):1616-1624.
24. Campbell CL, Smyth S, Montalescot G, Steinhubl SR. Aspirin dose for the prevention of cardiovascular disease: a systematic review. JAMA. 2007;297(18):2018-2024.
25. Zannad F, Anker, SD, Byra WM, et al; COMMANDER HF Investigators. Rivaroxaban in patients with heart failure, sinus rhythm, and coronary disease. N Engl J Med. 2018;379(14):1332-1342.
26. Schulman S, Beyth RJ, Kearon C, Levine MN. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):257S-298S.
27. CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999;353(9146):9-13.
28. Poole-Wilson PA, Swedberg K, Cleland JG, et al; Carvedilol Or Metoprolol European Trial Investigators. Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET): randomized controlled trial. Lancet. 2003;362(9377):7-13.
29. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet. 1999;353(9169):2001-2007.
30. Flather MD, Shibata MC, Coats AJ, et al; SENIORS Investigators. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J. 2005;26(3):215-225.
31. Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336(8):525-533.
32. Yancy CW, Jessup M, Bozkurt B, et al; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.
33 Juurlink DN, Mamdani MM, Lee DS, et al. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004;351(6):543-551.
34. Kjekshus J, Apetrei E, Barrios V, et al; CORONA Group. Rosuvastatin in older patients with systolic heart failure. N Engl J Med. 2007;357(22):2248-2261.
35. Rauchhaus M, Clark AL, Doehner W, et al. The relationship between cholesterol and survival in patients with chronic heart failure. J Am Coll Cardiol. 2003;42(11):1933-1940.
36. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e161.
37. Ponikowski P, van Veldhuisen DJ, Comin-Colet J, et al; CONFIRM-HF Investigators. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. Eur Heart J. 2015;36(11):657-668.
38. SPRINT Research Group, Wright JT Jr, Williamson JD, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-2116.
39. MacDonald M, Fang J, Pittman SD, White DP, Malhotra A. The current prevalence of sleep disordered breathing in congestive heart failure patients treated with beta-blockers. J Clin Sleep Med. 2008;4(1):38-42.
40. Bradley TD, Floras JS. Sleep Apnea and heart failure: part II: Central sleep apnea. Circulation. 2003;107(13):1822-1826.
41. Cowie MR, Woehrle H, Wegscheider K, et al. Adaptive servo-ventilation for central sleep apnea in systolic heart failure. N Engl J Med. 2015;373(12):1095-1105.
42. McEvoy RD, Antic NA, Heeley E, et al; SAVE Investigators and Coordinators. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919-931.
43. O’Connor CM, Jiang W, Kuchibhatla M, et al; SADHART-CHF Investigators. Safety and efficacy of sertraline for depression in patients with heart failure: results of the SADHART-CHF (Sertraline Against Depression and Heart Disease in Chronic Heart Failure) trial. J Am Coll Cardiol. 2010;56(9):692-699.
44. Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-156.
45. Pilotto A, Addante F, Franceschi M, et al. Multidimensional Prognostic Index based on a comprehensive geriatric assessment predicts short-term mortality in older patients with heart failure. Circ Heart Fail. 2010;3(1):14-20.
46. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
47. Goldberg, RJ, Ciampa, J, Lessard D,, et al. Long-term survival after heart failure: a contemporary population-based perspective. Arch Intern Med. 2007;167(5):490-496.
48. Murray SA, Boyd K, Kendall M, Worth A, Benton TF, Clausen H. Dying of lung cancer or cardiac failure: prospective qualitative interview study of patients and their carers in the community. BMJ. 2002;325(7370):929.
49. Gibbs JS, McCoy AS, Gibbs LM, Rogers AE, Addington-Hall JM. Living with and dying from heart failure: the role of palliative care. Heart. 2002;88(suppl 2):ii36-39.
50. Quill TE, Dresser R, Brock DW. The rule of double effect—a critique of its role in end-of-life decision making. N Engl J Med. 1997;337(24):1768-1771.
51. Nieminen MS, Dickstein K, Fonseca C, et al. The patient perspective: quality of life in advanced heart failure with frequent hospitalizations. Int J Cardiol. 2015;191:256-264.
1. Ortman JM, Velkoff AV, Hogan H. An aging nation: the older population in the United States. https://www.census.gov/prod/2014pubs/p25-1140.pdf. Published May 2014. Accessed September 30, 2018.
2. Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the U.S., 1979 to 2004. J Am Coll Cardiol. 2008;52(6):428-434.
3. Heidenreich PA, Albert NM, Allen LA, et al; American Heart Association Advocacy Coordinating Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Stroke Council. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606-619.
4. National Heart, Lung, and Blood Institute, National Institutes of Health. Incidence and Prevalence: 2006 Chart Book on Cardiovascular and Lung Diseases. Bethesda, MD: National Institutes of Health; 2006.
5. Curtis LH, Whellan DJ, Hammill BG, et al. Incidence and prevalence of heart failure in elderly persons, 1994-2003. Arch Intern Med. 2008;168(4):418-424.
6. Writing Group, Mozaffarian D, Benjamin EJ, et al; American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360.
7. Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a “set up” for vascular disease. Circulation. 2003;107(1):139-146.
8. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14.
9. CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. 1987;316(23):1429-1435.
10. SOLVD Investigators; Yusuf S, Pitt B, Davis CE, Hood WB Jr, Cohn JN. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med. 1992;327(10):685-691.
11. McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004.
12. McMurray JJ, Ostergren J, Swedberg K, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trial. Lancet. 2003;362(9386):767-771.
13. Granger CB, McMurray JJ, Yusuf S, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-Alternative trial. Lancet. 2003;362(9386):772-776.
14. Yusuf S, Pfeffer MA, Swedberg K, et al; CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362(9386):777-781.
15. Massie BM, Carson PE, McMurray JJ, et al; I-PRESERVE Investigators. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med. 2008;359(23):2456-2467.
16. Cohn JN, Tognoni G; Valsartan Heart Failure Trial Investigators. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N Engl J Med. 2001;345(23):1667-1675.
17. Konstam MA, Neaton JD, Dickstein K, et al; HEAAL Investigators. Effects of high-dose versus low-dose losartan on clinical outcomes in patients with heart failure (HEAAL study): a randomised, double-blind trial. Lancet. 2009;374(9704):1840-1848.
18. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341(10):709-717.
19. Zannad F, McMurray JJ, Krum H, et al; EMPHASIS-HF Study Group. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364(1):11-21.
20. Pitt B, Pfeffer MA, Assmann SF, et al; TOPCAT Investigators. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370(15):1383-1392.
21. Juurlink DN, Mamdani MM, Lee DS, et al. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004;351(6):543-551.
22. Homma S, Thompson JL, Pullicino PM, et al; WARCEF Investigators. Warfarin and aspirin in patients with heart failure and sinus rhythm. N Engl J Med. 2012;366(20):1859-1869.
23. Massie BM, Collins JF, Ammon SE, et al; WATCH Trial Investigators. Randomized trial of warfarin, aspirin, and clopidogrel in patients with chronic heart failure: the Warfarin and Antiplatelet Therapy in Chronic Heart Failure (WATCH) trial. Circulation. 2009;119(12):1616-1624.
24. Campbell CL, Smyth S, Montalescot G, Steinhubl SR. Aspirin dose for the prevention of cardiovascular disease: a systematic review. JAMA. 2007;297(18):2018-2024.
25. Zannad F, Anker, SD, Byra WM, et al; COMMANDER HF Investigators. Rivaroxaban in patients with heart failure, sinus rhythm, and coronary disease. N Engl J Med. 2018;379(14):1332-1342.
26. Schulman S, Beyth RJ, Kearon C, Levine MN. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):257S-298S.
27. CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999;353(9146):9-13.
28. Poole-Wilson PA, Swedberg K, Cleland JG, et al; Carvedilol Or Metoprolol European Trial Investigators. Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET): randomized controlled trial. Lancet. 2003;362(9377):7-13.
29. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet. 1999;353(9169):2001-2007.
30. Flather MD, Shibata MC, Coats AJ, et al; SENIORS Investigators. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J. 2005;26(3):215-225.
31. Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336(8):525-533.
32. Yancy CW, Jessup M, Bozkurt B, et al; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147-e239.
33 Juurlink DN, Mamdani MM, Lee DS, et al. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004;351(6):543-551.
34. Kjekshus J, Apetrei E, Barrios V, et al; CORONA Group. Rosuvastatin in older patients with systolic heart failure. N Engl J Med. 2007;357(22):2248-2261.
35. Rauchhaus M, Clark AL, Doehner W, et al. The relationship between cholesterol and survival in patients with chronic heart failure. J Am Coll Cardiol. 2003;42(11):1933-1940.
36. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e161.
37. Ponikowski P, van Veldhuisen DJ, Comin-Colet J, et al; CONFIRM-HF Investigators. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. Eur Heart J. 2015;36(11):657-668.
38. SPRINT Research Group, Wright JT Jr, Williamson JD, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-2116.
39. MacDonald M, Fang J, Pittman SD, White DP, Malhotra A. The current prevalence of sleep disordered breathing in congestive heart failure patients treated with beta-blockers. J Clin Sleep Med. 2008;4(1):38-42.
40. Bradley TD, Floras JS. Sleep Apnea and heart failure: part II: Central sleep apnea. Circulation. 2003;107(13):1822-1826.
41. Cowie MR, Woehrle H, Wegscheider K, et al. Adaptive servo-ventilation for central sleep apnea in systolic heart failure. N Engl J Med. 2015;373(12):1095-1105.
42. McEvoy RD, Antic NA, Heeley E, et al; SAVE Investigators and Coordinators. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919-931.
43. O’Connor CM, Jiang W, Kuchibhatla M, et al; SADHART-CHF Investigators. Safety and efficacy of sertraline for depression in patients with heart failure: results of the SADHART-CHF (Sertraline Against Depression and Heart Disease in Chronic Heart Failure) trial. J Am Coll Cardiol. 2010;56(9):692-699.
44. Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-156.
45. Pilotto A, Addante F, Franceschi M, et al. Multidimensional Prognostic Index based on a comprehensive geriatric assessment predicts short-term mortality in older patients with heart failure. Circ Heart Fail. 2010;3(1):14-20.
46. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
47. Goldberg, RJ, Ciampa, J, Lessard D,, et al. Long-term survival after heart failure: a contemporary population-based perspective. Arch Intern Med. 2007;167(5):490-496.
48. Murray SA, Boyd K, Kendall M, Worth A, Benton TF, Clausen H. Dying of lung cancer or cardiac failure: prospective qualitative interview study of patients and their carers in the community. BMJ. 2002;325(7370):929.
49. Gibbs JS, McCoy AS, Gibbs LM, Rogers AE, Addington-Hall JM. Living with and dying from heart failure: the role of palliative care. Heart. 2002;88(suppl 2):ii36-39.
50. Quill TE, Dresser R, Brock DW. The rule of double effect—a critique of its role in end-of-life decision making. N Engl J Med. 1997;337(24):1768-1771.
51. Nieminen MS, Dickstein K, Fonseca C, et al. The patient perspective: quality of life in advanced heart failure with frequent hospitalizations. Int J Cardiol. 2015;191:256-264.
Bariatric surgery shows metabolic benefits in lower-BMI patients
LAS VEGAS – It’s time to take bariatric out of bariatric surgery.
“The way forward is to not call it bariatric surgery or weight-loss surgery but surgery to treat diabetes, hypertension, hyperlipidemia, and other metabolic diseases,” said Oliver A. Varban, MD, at a meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery. “We need to reframe the conversation with patients about what success [with bariatric surgery] looks like. Weight loss can be a side effect of the operation if patients have surgery to resolve their diabetes. It’s not about BMI; it’s about treating metabolic disease.”
Dr. Varban, a bariatric surgeon at the University of Michigan in Ann Arbor, reported data showing that bariatric surgery with sleeve gastrectomy in patients with baseline body mass index (BMI) levels below 35 kg/m2 was as effective at normalizing a range of metabolically associated disorders as it was in more obese patients in an observational study of more than 45,000 patients who underwent surgery in Michigan.
The findings add to an already extensive pool of evidence for loosening current guidelines that restrict bariatric surgery to patients with a BMI of 35 kg/m2 or greater, Dr. Varban said. But an influential bariatric surgery consensus statement from the National Institutes of Health that dates from 1991 and remains in place, recommends this surgery only for people with a BMI of at least 35 kg/m2, and this guidance often limits access to the surgery for patients at lower BMI, he noted.
A more inclusive assessment of patients as potential candidates for bariatric surgery should include a range of considerations in addition to weight and height, he explained in an interview. “Even if people have a BMI of less than 30 kg/m2 but have, or are at high risk for developing, metabolic disease, they should also be offered the operation.”
The guidance from the NIH results in a U.S. bariatric surgery population that effectively centers mainly on women with a BMI of 40 kg/m2 or greater and makes procedures like sleeve gastrectomy unavailable to many other types of patients who could benefit from it, Dr. Varban said. In 2018, the American Society for Metabolic and Bariatric Surgery released a position statement that summarized the evidence for the safety and efficacy of bariatric surgery in people with a BMI of 30-34 kg/m2, and cited the lingering and restrictive impact of the 1991 NIH consensus statement.
The study run by Dr. Varban and his associates used data collected by 43 programs in the Michigan Bariatric Surgery Collaborative during 2006-2018 that included 1,073 patients who had a BMI of less than 35 kg/m2 on the day they underwent sleeve gastrectomy, and 44,511 patients who had the same procedure and had a BMI of at least 35 kg/m2. The operations were performed by any one of 81 surgeons who worked at the centers during this time.
The patients with lower BMIs were older, with an average age of 51 years, compared with 45 years in the higher-BMI group, and they had higher prevalences of certain metabolic disorders. Diabetes affected 37% of those in the lower-BMI group and 31% of those with higher BMIs; hyperlipidemia affected 57% and 45%, respectively; and gastroesophageal reflux disease affected 56% and 49%, respectively. Obstructive sleep apnea was more common in the group with higher BMIs, at 47%, compared with 41% of those with lower BMIs.
The average BMI in the lower group was 33.7 kg/m2; in the higher group it was 46.7 kg/m2. Dr. Varban did not have data on whether any patients in the lower-BMI group had a BMI below 30 kg/m2. Roughly a third of the patients in the lower-BMI group had a BMI of less than 35 kg/m2 at the time of their initial examination, whereas the other two-thirds had a BMI that low only on the day of their surgery.At follow-up 1 year after their surgery, patients who started with lower BMIs had, in general, a very similar pattern of responses as those who started with higher BMIs, with rates of discontinuation of treatments for diabetes, hypertension, hyperlipidemia, obstructive sleep apnea, and gastroesophageal reflux of about 50%-80% and similar in both treatment arms. For example, discontinuation of oral diabetes drugs occurred in 79% and 78% of those with low and high BMIs, respectively, and discontinuation of hypertension medications occurred in 60% and 54%, respectively. Although the average absolute weight loss in the patients with lower BMIs was nearly half that of patients with higher starting BMIs, a much greater percentage of patients in the lower-BMI group achieved a BMI of less than 25 kg/m2, compared with the higher-BMI group (36% vs. 6%, respectively).
Patients from the lower-BMI group also showed high levels of satisfaction with their surgery and its results after 1 year. Questionnaire results from roughly half the patients in each treatment group showed that 90% were very satisfied in the lower-BMI group, compared with 84% of those who began with higher BMIs, with a dissatisfaction rate of 1% and 2%, respectively. The average body-image score at 1 year follow-up was significantly higher in those who started with lower BMIs. The rate of complications was low and similar in the two groups, with a 6% rate in the lower-BMI group and 5% in those with higher BMIs.
The study received no commercial funding. Dr. Varban receives salary support from Blue Cross Blue Shield of Michigan.
SOURCE: Varban et al. Obesity Week 2019, Abstract A105.
This article was updated 11/8/2020.
This is a very important topic and study, and its findings are very positive and reinforcing for more liberal use of bariatric surgery. Results from several prior studies had documented the safety and efficacy of bariatric surgery in patients with lower body mass index, and its fantastic to now have additional data that show the same outcomes. A major challenge is making patients and more physicians aware of the range of comorbidities that can be effectively managed with bariatric surgery, even in patients with lower body mass index.
Mona Misra, MD, is associate director of the Bariatric Program at Cedars-Sinai Marina Del Rey Hospital in Los Angeles. She had no relevant disclosures. She made these comments as designated discussant for the study.
This is a very important topic and study, and its findings are very positive and reinforcing for more liberal use of bariatric surgery. Results from several prior studies had documented the safety and efficacy of bariatric surgery in patients with lower body mass index, and its fantastic to now have additional data that show the same outcomes. A major challenge is making patients and more physicians aware of the range of comorbidities that can be effectively managed with bariatric surgery, even in patients with lower body mass index.
Mona Misra, MD, is associate director of the Bariatric Program at Cedars-Sinai Marina Del Rey Hospital in Los Angeles. She had no relevant disclosures. She made these comments as designated discussant for the study.
This is a very important topic and study, and its findings are very positive and reinforcing for more liberal use of bariatric surgery. Results from several prior studies had documented the safety and efficacy of bariatric surgery in patients with lower body mass index, and its fantastic to now have additional data that show the same outcomes. A major challenge is making patients and more physicians aware of the range of comorbidities that can be effectively managed with bariatric surgery, even in patients with lower body mass index.
Mona Misra, MD, is associate director of the Bariatric Program at Cedars-Sinai Marina Del Rey Hospital in Los Angeles. She had no relevant disclosures. She made these comments as designated discussant for the study.
LAS VEGAS – It’s time to take bariatric out of bariatric surgery.
“The way forward is to not call it bariatric surgery or weight-loss surgery but surgery to treat diabetes, hypertension, hyperlipidemia, and other metabolic diseases,” said Oliver A. Varban, MD, at a meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery. “We need to reframe the conversation with patients about what success [with bariatric surgery] looks like. Weight loss can be a side effect of the operation if patients have surgery to resolve their diabetes. It’s not about BMI; it’s about treating metabolic disease.”
Dr. Varban, a bariatric surgeon at the University of Michigan in Ann Arbor, reported data showing that bariatric surgery with sleeve gastrectomy in patients with baseline body mass index (BMI) levels below 35 kg/m2 was as effective at normalizing a range of metabolically associated disorders as it was in more obese patients in an observational study of more than 45,000 patients who underwent surgery in Michigan.
The findings add to an already extensive pool of evidence for loosening current guidelines that restrict bariatric surgery to patients with a BMI of 35 kg/m2 or greater, Dr. Varban said. But an influential bariatric surgery consensus statement from the National Institutes of Health that dates from 1991 and remains in place, recommends this surgery only for people with a BMI of at least 35 kg/m2, and this guidance often limits access to the surgery for patients at lower BMI, he noted.
A more inclusive assessment of patients as potential candidates for bariatric surgery should include a range of considerations in addition to weight and height, he explained in an interview. “Even if people have a BMI of less than 30 kg/m2 but have, or are at high risk for developing, metabolic disease, they should also be offered the operation.”
The guidance from the NIH results in a U.S. bariatric surgery population that effectively centers mainly on women with a BMI of 40 kg/m2 or greater and makes procedures like sleeve gastrectomy unavailable to many other types of patients who could benefit from it, Dr. Varban said. In 2018, the American Society for Metabolic and Bariatric Surgery released a position statement that summarized the evidence for the safety and efficacy of bariatric surgery in people with a BMI of 30-34 kg/m2, and cited the lingering and restrictive impact of the 1991 NIH consensus statement.
The study run by Dr. Varban and his associates used data collected by 43 programs in the Michigan Bariatric Surgery Collaborative during 2006-2018 that included 1,073 patients who had a BMI of less than 35 kg/m2 on the day they underwent sleeve gastrectomy, and 44,511 patients who had the same procedure and had a BMI of at least 35 kg/m2. The operations were performed by any one of 81 surgeons who worked at the centers during this time.
The patients with lower BMIs were older, with an average age of 51 years, compared with 45 years in the higher-BMI group, and they had higher prevalences of certain metabolic disorders. Diabetes affected 37% of those in the lower-BMI group and 31% of those with higher BMIs; hyperlipidemia affected 57% and 45%, respectively; and gastroesophageal reflux disease affected 56% and 49%, respectively. Obstructive sleep apnea was more common in the group with higher BMIs, at 47%, compared with 41% of those with lower BMIs.
The average BMI in the lower group was 33.7 kg/m2; in the higher group it was 46.7 kg/m2. Dr. Varban did not have data on whether any patients in the lower-BMI group had a BMI below 30 kg/m2. Roughly a third of the patients in the lower-BMI group had a BMI of less than 35 kg/m2 at the time of their initial examination, whereas the other two-thirds had a BMI that low only on the day of their surgery.At follow-up 1 year after their surgery, patients who started with lower BMIs had, in general, a very similar pattern of responses as those who started with higher BMIs, with rates of discontinuation of treatments for diabetes, hypertension, hyperlipidemia, obstructive sleep apnea, and gastroesophageal reflux of about 50%-80% and similar in both treatment arms. For example, discontinuation of oral diabetes drugs occurred in 79% and 78% of those with low and high BMIs, respectively, and discontinuation of hypertension medications occurred in 60% and 54%, respectively. Although the average absolute weight loss in the patients with lower BMIs was nearly half that of patients with higher starting BMIs, a much greater percentage of patients in the lower-BMI group achieved a BMI of less than 25 kg/m2, compared with the higher-BMI group (36% vs. 6%, respectively).
Patients from the lower-BMI group also showed high levels of satisfaction with their surgery and its results after 1 year. Questionnaire results from roughly half the patients in each treatment group showed that 90% were very satisfied in the lower-BMI group, compared with 84% of those who began with higher BMIs, with a dissatisfaction rate of 1% and 2%, respectively. The average body-image score at 1 year follow-up was significantly higher in those who started with lower BMIs. The rate of complications was low and similar in the two groups, with a 6% rate in the lower-BMI group and 5% in those with higher BMIs.
The study received no commercial funding. Dr. Varban receives salary support from Blue Cross Blue Shield of Michigan.
SOURCE: Varban et al. Obesity Week 2019, Abstract A105.
This article was updated 11/8/2020.
LAS VEGAS – It’s time to take bariatric out of bariatric surgery.
“The way forward is to not call it bariatric surgery or weight-loss surgery but surgery to treat diabetes, hypertension, hyperlipidemia, and other metabolic diseases,” said Oliver A. Varban, MD, at a meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery. “We need to reframe the conversation with patients about what success [with bariatric surgery] looks like. Weight loss can be a side effect of the operation if patients have surgery to resolve their diabetes. It’s not about BMI; it’s about treating metabolic disease.”
Dr. Varban, a bariatric surgeon at the University of Michigan in Ann Arbor, reported data showing that bariatric surgery with sleeve gastrectomy in patients with baseline body mass index (BMI) levels below 35 kg/m2 was as effective at normalizing a range of metabolically associated disorders as it was in more obese patients in an observational study of more than 45,000 patients who underwent surgery in Michigan.
The findings add to an already extensive pool of evidence for loosening current guidelines that restrict bariatric surgery to patients with a BMI of 35 kg/m2 or greater, Dr. Varban said. But an influential bariatric surgery consensus statement from the National Institutes of Health that dates from 1991 and remains in place, recommends this surgery only for people with a BMI of at least 35 kg/m2, and this guidance often limits access to the surgery for patients at lower BMI, he noted.
A more inclusive assessment of patients as potential candidates for bariatric surgery should include a range of considerations in addition to weight and height, he explained in an interview. “Even if people have a BMI of less than 30 kg/m2 but have, or are at high risk for developing, metabolic disease, they should also be offered the operation.”
The guidance from the NIH results in a U.S. bariatric surgery population that effectively centers mainly on women with a BMI of 40 kg/m2 or greater and makes procedures like sleeve gastrectomy unavailable to many other types of patients who could benefit from it, Dr. Varban said. In 2018, the American Society for Metabolic and Bariatric Surgery released a position statement that summarized the evidence for the safety and efficacy of bariatric surgery in people with a BMI of 30-34 kg/m2, and cited the lingering and restrictive impact of the 1991 NIH consensus statement.
The study run by Dr. Varban and his associates used data collected by 43 programs in the Michigan Bariatric Surgery Collaborative during 2006-2018 that included 1,073 patients who had a BMI of less than 35 kg/m2 on the day they underwent sleeve gastrectomy, and 44,511 patients who had the same procedure and had a BMI of at least 35 kg/m2. The operations were performed by any one of 81 surgeons who worked at the centers during this time.
The patients with lower BMIs were older, with an average age of 51 years, compared with 45 years in the higher-BMI group, and they had higher prevalences of certain metabolic disorders. Diabetes affected 37% of those in the lower-BMI group and 31% of those with higher BMIs; hyperlipidemia affected 57% and 45%, respectively; and gastroesophageal reflux disease affected 56% and 49%, respectively. Obstructive sleep apnea was more common in the group with higher BMIs, at 47%, compared with 41% of those with lower BMIs.
The average BMI in the lower group was 33.7 kg/m2; in the higher group it was 46.7 kg/m2. Dr. Varban did not have data on whether any patients in the lower-BMI group had a BMI below 30 kg/m2. Roughly a third of the patients in the lower-BMI group had a BMI of less than 35 kg/m2 at the time of their initial examination, whereas the other two-thirds had a BMI that low only on the day of their surgery.At follow-up 1 year after their surgery, patients who started with lower BMIs had, in general, a very similar pattern of responses as those who started with higher BMIs, with rates of discontinuation of treatments for diabetes, hypertension, hyperlipidemia, obstructive sleep apnea, and gastroesophageal reflux of about 50%-80% and similar in both treatment arms. For example, discontinuation of oral diabetes drugs occurred in 79% and 78% of those with low and high BMIs, respectively, and discontinuation of hypertension medications occurred in 60% and 54%, respectively. Although the average absolute weight loss in the patients with lower BMIs was nearly half that of patients with higher starting BMIs, a much greater percentage of patients in the lower-BMI group achieved a BMI of less than 25 kg/m2, compared with the higher-BMI group (36% vs. 6%, respectively).
Patients from the lower-BMI group also showed high levels of satisfaction with their surgery and its results after 1 year. Questionnaire results from roughly half the patients in each treatment group showed that 90% were very satisfied in the lower-BMI group, compared with 84% of those who began with higher BMIs, with a dissatisfaction rate of 1% and 2%, respectively. The average body-image score at 1 year follow-up was significantly higher in those who started with lower BMIs. The rate of complications was low and similar in the two groups, with a 6% rate in the lower-BMI group and 5% in those with higher BMIs.
The study received no commercial funding. Dr. Varban receives salary support from Blue Cross Blue Shield of Michigan.
SOURCE: Varban et al. Obesity Week 2019, Abstract A105.
This article was updated 11/8/2020.
REPORTING FROM OBESITY WEEK 2019
Key clinical point:
Major finding: Discontinuation of hypertension drugs occurred in 60% of patients with lower BMIs at baseline and 54% of those with higher BMIs.
Study details: Review of prospectively collected data from 45,584 patients who underwent sleeve gastrectomy in Michigan during 2006-2018.
Disclosures: The study received no commercial funding. Dr. Varban receives salary support from Blue Cross Blue Shield of Michigan. Dr. Misra had no relevant disclosures.
Source: Varban OA et al. Obesity Week 2019, Abstract A105.
Ataluren shows real-world benefit for nonsense mutation Duchenne muscular dystrophy
AUSTIN, TEX. – , according to new data.
“Participants in the STRIDE Registry [real-world patients] showed a reduction in functional decline over 48 weeks, compared with patients receiving placebo” in the trial, reported Abdallah Delage of PTC Therapeutics in Zug, Switzerland, and his associates.
Duchenne muscular dystrophy affects an estimated 1 in 3,600-6,000 male births globally, about 10%-15% of whom have nonsense mutation DMD. This mutation causes a truncated, nonfunctional dystrophin protein due to a premature stop codon, the authors explained. Ataluren “promotes ribosomal read-through of the premature stop codon to produce a full-length dystrophin protein,” they explained.
Ataluren is currently approved for ambulatory patients age 2 and older with nonsense mutation DMD in the European Union and several other European countries. Israel, Korea, Chile, and Ukraine have approved it for patients aged 5 and older.
The Strategic Targeting of Registries and International Database of Excellence (STRIDE) Registry contains real-world data from patients using ataluren as part of an ongoing multicenter observational postapproval safety study. The investigators are tracking patients for at least 5 years after enrollment in 14 countries where ataluren is approved or commercially available through early-access programs. Patients take 40 mg/kg daily: 10 mg/kg in the morning, 10 mg/kg midday, and 20 mg/kg in the evening.
The researchers compared outcomes in 216 patients in the STRIDE Registry with participants in a randomized controlled phase 3 study of ataluren involving 228 boys, aged 7-16, who received ataluren (n = 114) or placebo (n = 114) for 48 weeks. Patients were an average 9 years old in STRIDE and in both arms of the randomized controlled trial.
The STRIDE Registry participants, comprising 184 ambulatory and 26 nonambulatory patients at enrollment, had at least 48 weeks between their first and last assessment. All of the patients in the phase 3 study and 88.6% of the STRIDE Registry patients were receiving corticosteroids along with ataluren. The researchers compared the 184 ambulatory STRIDE participants with the participants of the randomized controlled trial for one primary and four secondary endpoints from baseline to 48 weeks.
For the primary endpoint, 6-minute walk distance, average distance was 35 meters shorter than baseline in STRIDE Registry participants (n = 66), 42.2 meters shorter in the patients receiving ataluren in the phase 3 study (n = 109), and 57.6 meters shorter in RCT patients receiving placebo in the phase 3 trial (n = 109).
A secondary endpoint, the time it took patients to walk or run 10 meters, increased 1.6 seconds from baseline to 48 weeks in STRIDE Registry participants (n = 61), 2.3 seconds in participants receiving ataluren in the phase 3 trial (n = 109), and 3.5 seconds in study participants receiving placebo (n = 110).
Another secondary endpoint, the change in time it took for patients to stand from supine position from baseline to 48 weeks, was 2.9 additional seconds for STRIDE participants (n = 55), 3.8 additional seconds in study participants receiving ataluren (n = 101), and 3.9 additional seconds in study participants receiving placebo (n = 96).
Two final secondary endpoints were the changes in time to climb four stairs and to descend four stairs from baseline to 48 weeks. STRIDE participants (n = 47) climbed four stairs 1.2 seconds more slowly at 48 weeks, compared with 2.7 seconds more slowly in the participants who received ataluren in the phase 3 trial (n = 105) and 4.5 seconds more slowly in those who received placebo. Descending four stairs took 0.5 more seconds at 48 weeks in STRIDE participants (n = 40), 2.2 more seconds in participants who received ataluren in the phase 3 trial (n = 106), and 4.0 more seconds in those who received placebo (n = 100).
At least one adverse event occurred in 20.7% of registry participants; seven of these were considered treatment related. Treatment-related side effects included abdominal pain, vomiting, headache, stomach ache, diarrhea, and increased serum lipids.
The study and STRIDE Registry is funded by PTC Therapeutics with TREAT-NMD and the Cooperative International Neuromuscular Research Group. Mr. Delage and five other authors are employees of PTC Therapeutics, and six authors had received speaker or consultancy fees or served on the advisory board of a variety of companies.
SOURCE: Delage A et al. AANEM 2019, Abstract 115.
AUSTIN, TEX. – , according to new data.
“Participants in the STRIDE Registry [real-world patients] showed a reduction in functional decline over 48 weeks, compared with patients receiving placebo” in the trial, reported Abdallah Delage of PTC Therapeutics in Zug, Switzerland, and his associates.
Duchenne muscular dystrophy affects an estimated 1 in 3,600-6,000 male births globally, about 10%-15% of whom have nonsense mutation DMD. This mutation causes a truncated, nonfunctional dystrophin protein due to a premature stop codon, the authors explained. Ataluren “promotes ribosomal read-through of the premature stop codon to produce a full-length dystrophin protein,” they explained.
Ataluren is currently approved for ambulatory patients age 2 and older with nonsense mutation DMD in the European Union and several other European countries. Israel, Korea, Chile, and Ukraine have approved it for patients aged 5 and older.
The Strategic Targeting of Registries and International Database of Excellence (STRIDE) Registry contains real-world data from patients using ataluren as part of an ongoing multicenter observational postapproval safety study. The investigators are tracking patients for at least 5 years after enrollment in 14 countries where ataluren is approved or commercially available through early-access programs. Patients take 40 mg/kg daily: 10 mg/kg in the morning, 10 mg/kg midday, and 20 mg/kg in the evening.
The researchers compared outcomes in 216 patients in the STRIDE Registry with participants in a randomized controlled phase 3 study of ataluren involving 228 boys, aged 7-16, who received ataluren (n = 114) or placebo (n = 114) for 48 weeks. Patients were an average 9 years old in STRIDE and in both arms of the randomized controlled trial.
The STRIDE Registry participants, comprising 184 ambulatory and 26 nonambulatory patients at enrollment, had at least 48 weeks between their first and last assessment. All of the patients in the phase 3 study and 88.6% of the STRIDE Registry patients were receiving corticosteroids along with ataluren. The researchers compared the 184 ambulatory STRIDE participants with the participants of the randomized controlled trial for one primary and four secondary endpoints from baseline to 48 weeks.
For the primary endpoint, 6-minute walk distance, average distance was 35 meters shorter than baseline in STRIDE Registry participants (n = 66), 42.2 meters shorter in the patients receiving ataluren in the phase 3 study (n = 109), and 57.6 meters shorter in RCT patients receiving placebo in the phase 3 trial (n = 109).
A secondary endpoint, the time it took patients to walk or run 10 meters, increased 1.6 seconds from baseline to 48 weeks in STRIDE Registry participants (n = 61), 2.3 seconds in participants receiving ataluren in the phase 3 trial (n = 109), and 3.5 seconds in study participants receiving placebo (n = 110).
Another secondary endpoint, the change in time it took for patients to stand from supine position from baseline to 48 weeks, was 2.9 additional seconds for STRIDE participants (n = 55), 3.8 additional seconds in study participants receiving ataluren (n = 101), and 3.9 additional seconds in study participants receiving placebo (n = 96).
Two final secondary endpoints were the changes in time to climb four stairs and to descend four stairs from baseline to 48 weeks. STRIDE participants (n = 47) climbed four stairs 1.2 seconds more slowly at 48 weeks, compared with 2.7 seconds more slowly in the participants who received ataluren in the phase 3 trial (n = 105) and 4.5 seconds more slowly in those who received placebo. Descending four stairs took 0.5 more seconds at 48 weeks in STRIDE participants (n = 40), 2.2 more seconds in participants who received ataluren in the phase 3 trial (n = 106), and 4.0 more seconds in those who received placebo (n = 100).
At least one adverse event occurred in 20.7% of registry participants; seven of these were considered treatment related. Treatment-related side effects included abdominal pain, vomiting, headache, stomach ache, diarrhea, and increased serum lipids.
The study and STRIDE Registry is funded by PTC Therapeutics with TREAT-NMD and the Cooperative International Neuromuscular Research Group. Mr. Delage and five other authors are employees of PTC Therapeutics, and six authors had received speaker or consultancy fees or served on the advisory board of a variety of companies.
SOURCE: Delage A et al. AANEM 2019, Abstract 115.
AUSTIN, TEX. – , according to new data.
“Participants in the STRIDE Registry [real-world patients] showed a reduction in functional decline over 48 weeks, compared with patients receiving placebo” in the trial, reported Abdallah Delage of PTC Therapeutics in Zug, Switzerland, and his associates.
Duchenne muscular dystrophy affects an estimated 1 in 3,600-6,000 male births globally, about 10%-15% of whom have nonsense mutation DMD. This mutation causes a truncated, nonfunctional dystrophin protein due to a premature stop codon, the authors explained. Ataluren “promotes ribosomal read-through of the premature stop codon to produce a full-length dystrophin protein,” they explained.
Ataluren is currently approved for ambulatory patients age 2 and older with nonsense mutation DMD in the European Union and several other European countries. Israel, Korea, Chile, and Ukraine have approved it for patients aged 5 and older.
The Strategic Targeting of Registries and International Database of Excellence (STRIDE) Registry contains real-world data from patients using ataluren as part of an ongoing multicenter observational postapproval safety study. The investigators are tracking patients for at least 5 years after enrollment in 14 countries where ataluren is approved or commercially available through early-access programs. Patients take 40 mg/kg daily: 10 mg/kg in the morning, 10 mg/kg midday, and 20 mg/kg in the evening.
The researchers compared outcomes in 216 patients in the STRIDE Registry with participants in a randomized controlled phase 3 study of ataluren involving 228 boys, aged 7-16, who received ataluren (n = 114) or placebo (n = 114) for 48 weeks. Patients were an average 9 years old in STRIDE and in both arms of the randomized controlled trial.
The STRIDE Registry participants, comprising 184 ambulatory and 26 nonambulatory patients at enrollment, had at least 48 weeks between their first and last assessment. All of the patients in the phase 3 study and 88.6% of the STRIDE Registry patients were receiving corticosteroids along with ataluren. The researchers compared the 184 ambulatory STRIDE participants with the participants of the randomized controlled trial for one primary and four secondary endpoints from baseline to 48 weeks.
For the primary endpoint, 6-minute walk distance, average distance was 35 meters shorter than baseline in STRIDE Registry participants (n = 66), 42.2 meters shorter in the patients receiving ataluren in the phase 3 study (n = 109), and 57.6 meters shorter in RCT patients receiving placebo in the phase 3 trial (n = 109).
A secondary endpoint, the time it took patients to walk or run 10 meters, increased 1.6 seconds from baseline to 48 weeks in STRIDE Registry participants (n = 61), 2.3 seconds in participants receiving ataluren in the phase 3 trial (n = 109), and 3.5 seconds in study participants receiving placebo (n = 110).
Another secondary endpoint, the change in time it took for patients to stand from supine position from baseline to 48 weeks, was 2.9 additional seconds for STRIDE participants (n = 55), 3.8 additional seconds in study participants receiving ataluren (n = 101), and 3.9 additional seconds in study participants receiving placebo (n = 96).
Two final secondary endpoints were the changes in time to climb four stairs and to descend four stairs from baseline to 48 weeks. STRIDE participants (n = 47) climbed four stairs 1.2 seconds more slowly at 48 weeks, compared with 2.7 seconds more slowly in the participants who received ataluren in the phase 3 trial (n = 105) and 4.5 seconds more slowly in those who received placebo. Descending four stairs took 0.5 more seconds at 48 weeks in STRIDE participants (n = 40), 2.2 more seconds in participants who received ataluren in the phase 3 trial (n = 106), and 4.0 more seconds in those who received placebo (n = 100).
At least one adverse event occurred in 20.7% of registry participants; seven of these were considered treatment related. Treatment-related side effects included abdominal pain, vomiting, headache, stomach ache, diarrhea, and increased serum lipids.
The study and STRIDE Registry is funded by PTC Therapeutics with TREAT-NMD and the Cooperative International Neuromuscular Research Group. Mr. Delage and five other authors are employees of PTC Therapeutics, and six authors had received speaker or consultancy fees or served on the advisory board of a variety of companies.
SOURCE: Delage A et al. AANEM 2019, Abstract 115.
REPORTING FROM AANEM 2019