User login
Tailored Health IT Improves VTE Rates
Electronic decision support significantly improves VTE prophylaxis and hospital-acquired VTE rates, according to a new study in the Journal of Hospital Medicine.
The report, "Improving Hospital Venous Thromboembolism Prophylaxis With Electronic Decision Report," saw overall medical service prophylaxis rise to 82.1% from 61.9% (P<0.001) and pharmacologic VTE prophylaxis increase to 74.5% from 59% (P<0.001).
"Healthcare leaders talk about information technology (IT) as a means toward effecting improvements in quality and patient safety and, most of the time, they view that and discuss that in terms of the actual IT system being implemented," says lead author Rohit Bhalla, MD, MPH, associate professor of clinical medicine at Albert Einstein College of Medicine in New York City. "What our intervention really got to was once you've implemented an IT system ... how can it be modified, vis-à-vis decision support, so that it provides an even better result than you get with the product that comes out of the box."
Tailoring a health IT system to improve outcomes requires interdisciplinary work that includes quality officers, physicians, IT staff, and programmers. Hospitalist and fellow author Jason Adelman, MD, MS, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., where the study was conducted, says that the research can help generate future buy-in from physicians who don't value electronic decision support tools.
It can "ease the swallowing of the bitter pill to know that it really makes a difference," Dr. Adelman says. "Don't be up in arms when you're forced to do something a little bit extra, because it really works."
Visit our website for more information about health information technology.
Electronic decision support significantly improves VTE prophylaxis and hospital-acquired VTE rates, according to a new study in the Journal of Hospital Medicine.
The report, "Improving Hospital Venous Thromboembolism Prophylaxis With Electronic Decision Report," saw overall medical service prophylaxis rise to 82.1% from 61.9% (P<0.001) and pharmacologic VTE prophylaxis increase to 74.5% from 59% (P<0.001).
"Healthcare leaders talk about information technology (IT) as a means toward effecting improvements in quality and patient safety and, most of the time, they view that and discuss that in terms of the actual IT system being implemented," says lead author Rohit Bhalla, MD, MPH, associate professor of clinical medicine at Albert Einstein College of Medicine in New York City. "What our intervention really got to was once you've implemented an IT system ... how can it be modified, vis-à-vis decision support, so that it provides an even better result than you get with the product that comes out of the box."
Tailoring a health IT system to improve outcomes requires interdisciplinary work that includes quality officers, physicians, IT staff, and programmers. Hospitalist and fellow author Jason Adelman, MD, MS, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., where the study was conducted, says that the research can help generate future buy-in from physicians who don't value electronic decision support tools.
It can "ease the swallowing of the bitter pill to know that it really makes a difference," Dr. Adelman says. "Don't be up in arms when you're forced to do something a little bit extra, because it really works."
Visit our website for more information about health information technology.
Electronic decision support significantly improves VTE prophylaxis and hospital-acquired VTE rates, according to a new study in the Journal of Hospital Medicine.
The report, "Improving Hospital Venous Thromboembolism Prophylaxis With Electronic Decision Report," saw overall medical service prophylaxis rise to 82.1% from 61.9% (P<0.001) and pharmacologic VTE prophylaxis increase to 74.5% from 59% (P<0.001).
"Healthcare leaders talk about information technology (IT) as a means toward effecting improvements in quality and patient safety and, most of the time, they view that and discuss that in terms of the actual IT system being implemented," says lead author Rohit Bhalla, MD, MPH, associate professor of clinical medicine at Albert Einstein College of Medicine in New York City. "What our intervention really got to was once you've implemented an IT system ... how can it be modified, vis-à-vis decision support, so that it provides an even better result than you get with the product that comes out of the box."
Tailoring a health IT system to improve outcomes requires interdisciplinary work that includes quality officers, physicians, IT staff, and programmers. Hospitalist and fellow author Jason Adelman, MD, MS, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., where the study was conducted, says that the research can help generate future buy-in from physicians who don't value electronic decision support tools.
It can "ease the swallowing of the bitter pill to know that it really makes a difference," Dr. Adelman says. "Don't be up in arms when you're forced to do something a little bit extra, because it really works."
Visit our website for more information about health information technology.
TeamSTEPPS Initiative Teaches Teamwork to Healthcare Providers
University of Minnesota hospitalist Karyn Baum, MD, MSEd, directs one of six regional training centers for Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS), an evidence-based, multimedia curriculum, tool set, and system for healthcare organizations to improve their teamwork.
Using the TeamSTEPPS approach, Dr. Baum collaborated with hospitalist Albertine Beard, MD, and the charge nurse on a 28-bed medical unit at the Minneapolis VA Medical Center to present a half-day training session for all VA staff, including four hospitalists. The seminar mixed didactics, discussions, and simulations, similar to traditional role-playing techniques but using a high-fidelity manikin that talks and displays vital signs.
"Teamwork is a set of knowledge, skills, and attitudes that lead to the creation of a culture where it’s about us as a team, not about who is highest in the hierarchy," Dr. Baum says. Hospitalists want to be leaders, "but we have a responsibility to be intentional leaders, learning the skills and modeling them," she adds.
Improved teamwork benefits patients through more effective communication and reduction in medical errors, Dr. Baum says, "but it also helps to create a healthy environment in which to work, where we all have each other’s backs."
TeamSTEPPS, developed jointly by the federal Agency for Healthcare Research and Quality (AHRQ) and the Department of Defense, has reached 25% to 30% of U.S. hospitals by annually training about 700 masters. The masters then go back to their institutions and share the techniques.
Read more about why improving teamwork is good for your patients.
University of Minnesota hospitalist Karyn Baum, MD, MSEd, directs one of six regional training centers for Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS), an evidence-based, multimedia curriculum, tool set, and system for healthcare organizations to improve their teamwork.
Using the TeamSTEPPS approach, Dr. Baum collaborated with hospitalist Albertine Beard, MD, and the charge nurse on a 28-bed medical unit at the Minneapolis VA Medical Center to present a half-day training session for all VA staff, including four hospitalists. The seminar mixed didactics, discussions, and simulations, similar to traditional role-playing techniques but using a high-fidelity manikin that talks and displays vital signs.
"Teamwork is a set of knowledge, skills, and attitudes that lead to the creation of a culture where it’s about us as a team, not about who is highest in the hierarchy," Dr. Baum says. Hospitalists want to be leaders, "but we have a responsibility to be intentional leaders, learning the skills and modeling them," she adds.
Improved teamwork benefits patients through more effective communication and reduction in medical errors, Dr. Baum says, "but it also helps to create a healthy environment in which to work, where we all have each other’s backs."
TeamSTEPPS, developed jointly by the federal Agency for Healthcare Research and Quality (AHRQ) and the Department of Defense, has reached 25% to 30% of U.S. hospitals by annually training about 700 masters. The masters then go back to their institutions and share the techniques.
Read more about why improving teamwork is good for your patients.
University of Minnesota hospitalist Karyn Baum, MD, MSEd, directs one of six regional training centers for Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS), an evidence-based, multimedia curriculum, tool set, and system for healthcare organizations to improve their teamwork.
Using the TeamSTEPPS approach, Dr. Baum collaborated with hospitalist Albertine Beard, MD, and the charge nurse on a 28-bed medical unit at the Minneapolis VA Medical Center to present a half-day training session for all VA staff, including four hospitalists. The seminar mixed didactics, discussions, and simulations, similar to traditional role-playing techniques but using a high-fidelity manikin that talks and displays vital signs.
"Teamwork is a set of knowledge, skills, and attitudes that lead to the creation of a culture where it’s about us as a team, not about who is highest in the hierarchy," Dr. Baum says. Hospitalists want to be leaders, "but we have a responsibility to be intentional leaders, learning the skills and modeling them," she adds.
Improved teamwork benefits patients through more effective communication and reduction in medical errors, Dr. Baum says, "but it also helps to create a healthy environment in which to work, where we all have each other’s backs."
TeamSTEPPS, developed jointly by the federal Agency for Healthcare Research and Quality (AHRQ) and the Department of Defense, has reached 25% to 30% of U.S. hospitals by annually training about 700 masters. The masters then go back to their institutions and share the techniques.
Read more about why improving teamwork is good for your patients.
Hospitalist Approach Good Model for Managing Patients
Applying the HM model to specialties that can dedicate themselves to managing inpatients could improve care efficiency, says the coauthor of a new report from the American Hospital Association's (AHA) Physician Leadership Forum.
The 20-page report, "Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice [PDF]," codified a daylong summit of hospitalist leaders and hospital administrators following the annual Health Forum/AHA Leadership Summit last July in San Francisco. SHM helped organize the meeting, which focused on the growing role and importance of "hyphenated hospitalists."
"With the hospitalist movement, it's critical that there is coordination between the inpatient and the outpatient world … but also inpatient-wise, there should be some coordination of services between the various specialties that are dedicated to the hospital," says John Combes, MD, AHA senior vice president. "We have an opportunity here, as more and more subspecialties develop hospital-based and hospital-focused practices, to construct it right."
Dr. Combes says the model is not applicable to all specialties, but early adoption by fields including OBGYN, orthopedics, neurology, and surgery is a good sign. Hospitalist could look at forming large, multispecialty groups to bring all hospital-focused programs under one proverbial roof. "So there's not only coordination at the hospital level, but also at the group level," he adds.
The continued growth of specialty hospitalists might hinge on whether research shows that the approach improves patient outcomes.
"The jury is out on that right now," Dr. Combes says. "As hospitalists get better at defining what their role is within the inpatient setting—particularly around care coordination, care improvement, efficiency, reduction of unnecessary procedures and testing—we'll be able to document more value."
Visit our website for more information about hospital-based medical practices.
Applying the HM model to specialties that can dedicate themselves to managing inpatients could improve care efficiency, says the coauthor of a new report from the American Hospital Association's (AHA) Physician Leadership Forum.
The 20-page report, "Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice [PDF]," codified a daylong summit of hospitalist leaders and hospital administrators following the annual Health Forum/AHA Leadership Summit last July in San Francisco. SHM helped organize the meeting, which focused on the growing role and importance of "hyphenated hospitalists."
"With the hospitalist movement, it's critical that there is coordination between the inpatient and the outpatient world … but also inpatient-wise, there should be some coordination of services between the various specialties that are dedicated to the hospital," says John Combes, MD, AHA senior vice president. "We have an opportunity here, as more and more subspecialties develop hospital-based and hospital-focused practices, to construct it right."
Dr. Combes says the model is not applicable to all specialties, but early adoption by fields including OBGYN, orthopedics, neurology, and surgery is a good sign. Hospitalist could look at forming large, multispecialty groups to bring all hospital-focused programs under one proverbial roof. "So there's not only coordination at the hospital level, but also at the group level," he adds.
The continued growth of specialty hospitalists might hinge on whether research shows that the approach improves patient outcomes.
"The jury is out on that right now," Dr. Combes says. "As hospitalists get better at defining what their role is within the inpatient setting—particularly around care coordination, care improvement, efficiency, reduction of unnecessary procedures and testing—we'll be able to document more value."
Visit our website for more information about hospital-based medical practices.
Applying the HM model to specialties that can dedicate themselves to managing inpatients could improve care efficiency, says the coauthor of a new report from the American Hospital Association's (AHA) Physician Leadership Forum.
The 20-page report, "Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice [PDF]," codified a daylong summit of hospitalist leaders and hospital administrators following the annual Health Forum/AHA Leadership Summit last July in San Francisco. SHM helped organize the meeting, which focused on the growing role and importance of "hyphenated hospitalists."
"With the hospitalist movement, it's critical that there is coordination between the inpatient and the outpatient world … but also inpatient-wise, there should be some coordination of services between the various specialties that are dedicated to the hospital," says John Combes, MD, AHA senior vice president. "We have an opportunity here, as more and more subspecialties develop hospital-based and hospital-focused practices, to construct it right."
Dr. Combes says the model is not applicable to all specialties, but early adoption by fields including OBGYN, orthopedics, neurology, and surgery is a good sign. Hospitalist could look at forming large, multispecialty groups to bring all hospital-focused programs under one proverbial roof. "So there's not only coordination at the hospital level, but also at the group level," he adds.
The continued growth of specialty hospitalists might hinge on whether research shows that the approach improves patient outcomes.
"The jury is out on that right now," Dr. Combes says. "As hospitalists get better at defining what their role is within the inpatient setting—particularly around care coordination, care improvement, efficiency, reduction of unnecessary procedures and testing—we'll be able to document more value."
Visit our website for more information about hospital-based medical practices.
iPad Rollout at UC-Irvine Medical Center Prompts Security Measures
The University of California’s Irvine Medical Center has been issuing iPads to its incoming class of 100 medical students and to all 18 resident physicians in its department of emergency medicine.1 The entire medical curriculum is on the iPad and employs document sharing via the SharePoint collaborative software platform, says Adam Gold, the medical center’s director of emerging technologies.
But the use of these new technologies and subsequent clamoring by students, professors, physicians, and other staff to connect their own mobile devices to the network have led to the establishment of security and management guidelines for monitoring technology use, now spelled out in the new “Bring Your Own Device” policy, Gold explains.
Reference
The University of California’s Irvine Medical Center has been issuing iPads to its incoming class of 100 medical students and to all 18 resident physicians in its department of emergency medicine.1 The entire medical curriculum is on the iPad and employs document sharing via the SharePoint collaborative software platform, says Adam Gold, the medical center’s director of emerging technologies.
But the use of these new technologies and subsequent clamoring by students, professors, physicians, and other staff to connect their own mobile devices to the network have led to the establishment of security and management guidelines for monitoring technology use, now spelled out in the new “Bring Your Own Device” policy, Gold explains.
Reference
The University of California’s Irvine Medical Center has been issuing iPads to its incoming class of 100 medical students and to all 18 resident physicians in its department of emergency medicine.1 The entire medical curriculum is on the iPad and employs document sharing via the SharePoint collaborative software platform, says Adam Gold, the medical center’s director of emerging technologies.
But the use of these new technologies and subsequent clamoring by students, professors, physicians, and other staff to connect their own mobile devices to the network have led to the establishment of security and management guidelines for monitoring technology use, now spelled out in the new “Bring Your Own Device” policy, Gold explains.
Reference
Innovator of Care Transitions Model for Hospital Patients Honored
University of Colorado at Denver geriatrician Eric Coleman, MD, MPH—who pioneered the celebrated Care Transitions Model (www.caretransitions.org), which sends “coaches” on home visits and has them make phone calls to patients in an effort to smooth post-hospital discharge transitions and enhance self-care—has been honored with a MacArthur Foundation “genius” award.
Dr. Coleman also co-chairs the advisory board for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) national quality initiative.
The MacArthur Fellowship is known for honoring individuals who have shown exceptional originality and creativity, bestowing them with a $500,000 award—no strings attached. Dr. Coleman says the award “promotes the opportunity for approaching complex problems in new light—taking risks with new approaches and serving in the role of a ‘change agent.’”
“I look forward to working collaboratively with hospitalists and hospitals on finding new strategies and solutions for improving the discharge experience,” he says.
University of Colorado at Denver geriatrician Eric Coleman, MD, MPH—who pioneered the celebrated Care Transitions Model (www.caretransitions.org), which sends “coaches” on home visits and has them make phone calls to patients in an effort to smooth post-hospital discharge transitions and enhance self-care—has been honored with a MacArthur Foundation “genius” award.
Dr. Coleman also co-chairs the advisory board for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) national quality initiative.
The MacArthur Fellowship is known for honoring individuals who have shown exceptional originality and creativity, bestowing them with a $500,000 award—no strings attached. Dr. Coleman says the award “promotes the opportunity for approaching complex problems in new light—taking risks with new approaches and serving in the role of a ‘change agent.’”
“I look forward to working collaboratively with hospitalists and hospitals on finding new strategies and solutions for improving the discharge experience,” he says.
University of Colorado at Denver geriatrician Eric Coleman, MD, MPH—who pioneered the celebrated Care Transitions Model (www.caretransitions.org), which sends “coaches” on home visits and has them make phone calls to patients in an effort to smooth post-hospital discharge transitions and enhance self-care—has been honored with a MacArthur Foundation “genius” award.
Dr. Coleman also co-chairs the advisory board for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) national quality initiative.
The MacArthur Fellowship is known for honoring individuals who have shown exceptional originality and creativity, bestowing them with a $500,000 award—no strings attached. Dr. Coleman says the award “promotes the opportunity for approaching complex problems in new light—taking risks with new approaches and serving in the role of a ‘change agent.’”
“I look forward to working collaboratively with hospitalists and hospitals on finding new strategies and solutions for improving the discharge experience,” he says.
Win Whitcomb: Introducing Neuroquality and Neurosafety

The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
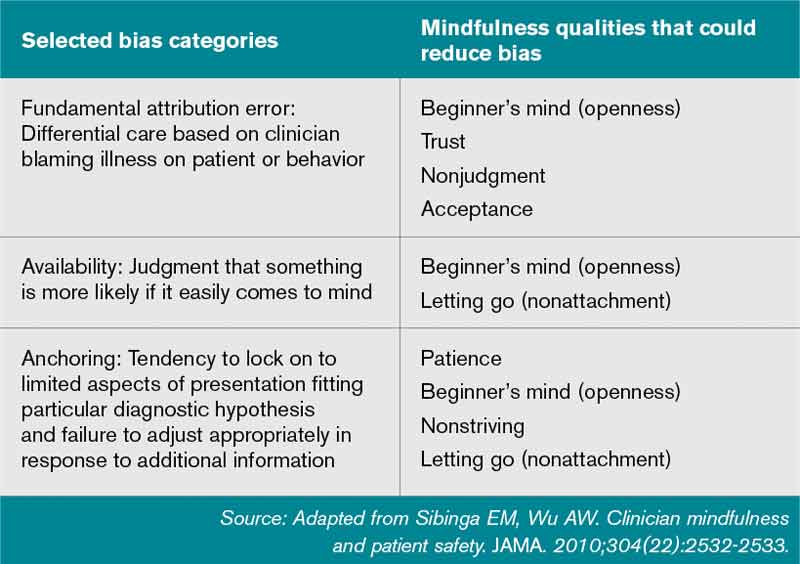
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Federal Grant Supports "eHospitalist" Pilot Program in Wisconsin
John Almquist, MD, FHM, director of hospitalist services for Ministry Health Care, a 15-hospital system serving rural Wisconsin, believes that an "e-hospitalist" pilot project now being tested at Ministry St. Mary's Hospital in Rhinelander, Wis., could be a boon for rural communities that have difficulty recruiting primary-care physicians (PCPs).
When the hospitals in those communities are unable to offer hospitalist coverage, it makes the setting less attractive to PCPs because they might have to follow their patients in the hospital day and night, he explains.
Ministry recruited and trained two nurse practitioners who will soon be deployed at a critical-access hospital in Eagle River, population 1,443, supported remotely by the eight-member HM group in Rhinelander for consultations, supervision, and multidisciplinary rounds. The training is bolstered by written order sets focused on 30 common medical conditions that lead to admissions to rural hospitals.
"The hospitalist in Rhinelander is also able to talk directly to the patient at the remote site," Dr. Almquist says.
The e-hospitalist program uses a telehealth network developed by Marshfield Clinic, a multispecialty physician group practice based in Marshfield, Wis. The clinic recently received a $1 million grant from the federal government to expand its 15-year-old telemedicine program. Part of the grant money is being used to expand the ehospitalist approach to new sites.
Visit our website for more information about hospitalists and telemedicine.
John Almquist, MD, FHM, director of hospitalist services for Ministry Health Care, a 15-hospital system serving rural Wisconsin, believes that an "e-hospitalist" pilot project now being tested at Ministry St. Mary's Hospital in Rhinelander, Wis., could be a boon for rural communities that have difficulty recruiting primary-care physicians (PCPs).
When the hospitals in those communities are unable to offer hospitalist coverage, it makes the setting less attractive to PCPs because they might have to follow their patients in the hospital day and night, he explains.
Ministry recruited and trained two nurse practitioners who will soon be deployed at a critical-access hospital in Eagle River, population 1,443, supported remotely by the eight-member HM group in Rhinelander for consultations, supervision, and multidisciplinary rounds. The training is bolstered by written order sets focused on 30 common medical conditions that lead to admissions to rural hospitals.
"The hospitalist in Rhinelander is also able to talk directly to the patient at the remote site," Dr. Almquist says.
The e-hospitalist program uses a telehealth network developed by Marshfield Clinic, a multispecialty physician group practice based in Marshfield, Wis. The clinic recently received a $1 million grant from the federal government to expand its 15-year-old telemedicine program. Part of the grant money is being used to expand the ehospitalist approach to new sites.
Visit our website for more information about hospitalists and telemedicine.
John Almquist, MD, FHM, director of hospitalist services for Ministry Health Care, a 15-hospital system serving rural Wisconsin, believes that an "e-hospitalist" pilot project now being tested at Ministry St. Mary's Hospital in Rhinelander, Wis., could be a boon for rural communities that have difficulty recruiting primary-care physicians (PCPs).
When the hospitals in those communities are unable to offer hospitalist coverage, it makes the setting less attractive to PCPs because they might have to follow their patients in the hospital day and night, he explains.
Ministry recruited and trained two nurse practitioners who will soon be deployed at a critical-access hospital in Eagle River, population 1,443, supported remotely by the eight-member HM group in Rhinelander for consultations, supervision, and multidisciplinary rounds. The training is bolstered by written order sets focused on 30 common medical conditions that lead to admissions to rural hospitals.
"The hospitalist in Rhinelander is also able to talk directly to the patient at the remote site," Dr. Almquist says.
The e-hospitalist program uses a telehealth network developed by Marshfield Clinic, a multispecialty physician group practice based in Marshfield, Wis. The clinic recently received a $1 million grant from the federal government to expand its 15-year-old telemedicine program. Part of the grant money is being used to expand the ehospitalist approach to new sites.
Visit our website for more information about hospitalists and telemedicine.
ONLINE EXCLUSIVE: Listen to Derek C. Angus discuss incorporating hospitalists into a tiered system of ICU care
Click here to listen to Dr. Angus
Click here to listen to Dr. Angus
Click here to listen to Dr. Angus
Study: Neurohospitalists Benefit Academic Medical Centers
Bringing a neurohospitalist service into an academic medical center can reduce neurological patients' length of stay (LOS) at the facility, according to a study in Neurology.
The retrospective cohort study, "Effect of a Neurohospitalist Service on Outcomes at an Academic Medical Center," found that the mean LOS dropped to 4.6 days while the neurohospitalist service was in place, compared with 6.3 days during the pre-neurohospitalist period. However, adding the service didn't significantly reduce the median cost of care delivery ($6,758 vs. $7,241; P=0.25) or in-hospital mortality rate (1.6% vs. 1.2%; P=0.61), the study noted.
Lead author Vanja Douglas, MD, health sciences assistant clinical professor in the department of neurology at the University of California at San Francisco (UCSF) School of Medicine, says the study's impact is limited by its single-center universe of data. The study was conducted at a UCSF Medical Center in October 2006, but Dr. Douglas hopes similar studies at other academic or community centers will replicate the findings.
"If the current model people have in place is not necessarily focused on outcomes like LOS and cost, then making a change to a neurohospitalist model is likely to positively affect those outcomes," says Dr. Douglas, editor in chief of The Neurohospitalist.
Investigators tracked administrative data starting 21 months before UCSF added a neurohospitalist service and 27 months after. The service was comprised of one neurohospitalist focused solely on inpatients, which allowed other staff neurologists to focus on consultative cases throughout the hospital. Dr. Douglas says as HM groups look to improve their scope of practice and bottom line, studies such as his can lay the groundwork to make the investment.
"A lot of the groups that contract with hospitals are interested in partnering with subspecialty hospitalists," Dr. Douglas adds. "A neurohospitalist model has the potential to work, and the potential to improve outcomes."
Bringing a neurohospitalist service into an academic medical center can reduce neurological patients' length of stay (LOS) at the facility, according to a study in Neurology.
The retrospective cohort study, "Effect of a Neurohospitalist Service on Outcomes at an Academic Medical Center," found that the mean LOS dropped to 4.6 days while the neurohospitalist service was in place, compared with 6.3 days during the pre-neurohospitalist period. However, adding the service didn't significantly reduce the median cost of care delivery ($6,758 vs. $7,241; P=0.25) or in-hospital mortality rate (1.6% vs. 1.2%; P=0.61), the study noted.
Lead author Vanja Douglas, MD, health sciences assistant clinical professor in the department of neurology at the University of California at San Francisco (UCSF) School of Medicine, says the study's impact is limited by its single-center universe of data. The study was conducted at a UCSF Medical Center in October 2006, but Dr. Douglas hopes similar studies at other academic or community centers will replicate the findings.
"If the current model people have in place is not necessarily focused on outcomes like LOS and cost, then making a change to a neurohospitalist model is likely to positively affect those outcomes," says Dr. Douglas, editor in chief of The Neurohospitalist.
Investigators tracked administrative data starting 21 months before UCSF added a neurohospitalist service and 27 months after. The service was comprised of one neurohospitalist focused solely on inpatients, which allowed other staff neurologists to focus on consultative cases throughout the hospital. Dr. Douglas says as HM groups look to improve their scope of practice and bottom line, studies such as his can lay the groundwork to make the investment.
"A lot of the groups that contract with hospitals are interested in partnering with subspecialty hospitalists," Dr. Douglas adds. "A neurohospitalist model has the potential to work, and the potential to improve outcomes."
Bringing a neurohospitalist service into an academic medical center can reduce neurological patients' length of stay (LOS) at the facility, according to a study in Neurology.
The retrospective cohort study, "Effect of a Neurohospitalist Service on Outcomes at an Academic Medical Center," found that the mean LOS dropped to 4.6 days while the neurohospitalist service was in place, compared with 6.3 days during the pre-neurohospitalist period. However, adding the service didn't significantly reduce the median cost of care delivery ($6,758 vs. $7,241; P=0.25) or in-hospital mortality rate (1.6% vs. 1.2%; P=0.61), the study noted.
Lead author Vanja Douglas, MD, health sciences assistant clinical professor in the department of neurology at the University of California at San Francisco (UCSF) School of Medicine, says the study's impact is limited by its single-center universe of data. The study was conducted at a UCSF Medical Center in October 2006, but Dr. Douglas hopes similar studies at other academic or community centers will replicate the findings.
"If the current model people have in place is not necessarily focused on outcomes like LOS and cost, then making a change to a neurohospitalist model is likely to positively affect those outcomes," says Dr. Douglas, editor in chief of The Neurohospitalist.
Investigators tracked administrative data starting 21 months before UCSF added a neurohospitalist service and 27 months after. The service was comprised of one neurohospitalist focused solely on inpatients, which allowed other staff neurologists to focus on consultative cases throughout the hospital. Dr. Douglas says as HM groups look to improve their scope of practice and bottom line, studies such as his can lay the groundwork to make the investment.
"A lot of the groups that contract with hospitals are interested in partnering with subspecialty hospitalists," Dr. Douglas adds. "A neurohospitalist model has the potential to work, and the potential to improve outcomes."
ICU Hospitalist Model Improves Quality of Care for Critically Ill Patients
Despite calls for board-certified intensivists to manage all critically ill patients, only a third of hospitalized ICU patients currently are seen by such a specialist—mostly because there are not enough of them to go around.1,2 More and more hospitalists, especially those in community hospitals, are working in ICUs (see “The Critical-Care Debate,”). With the proper training, that can be a good thing for patients and hospitalists, according to a Research, Innovations, and Clinical Vignettes (RIV) abstract presented at HM12 in San Diego.3
Lead author and hospitalist Mark Krivopal, MD, SFHM, formerly with TeamHealth in California and now vice president and medical director of clinical integration and hospital medicine at Steward Health Care in Boston, outlined a program at California’s Lodi Memorial Hospital that identified a group of hospitalists who had experience in caring for critically ill patients and credentials to perform such procedures as central-line placements, intubations, and ventilator management. The select group of TeamHealth hospitalists completed a two-day “Fundamentals of Critical Care Support” course offered by the Society of Critical Care Medicine (www.sccm.org), then began covering the ICU in shifts from 7 a.m. to 7 p.m. The program was so successful early on that hospital administration requested that it expand to a 24-hour service.
An ICU hospitalist program needs to be a partnership, Dr. Krivopal says. Essential oversight at Lodi Memorial is provided by the hospital’s sole pulmonologist.
Preliminary data showed a 35% reduction in ventilator days and 22% reduction in ICU stays, Dr. Krivopal says. The hospital also reports high satisfaction from nurses and other staff. Additional metrics, such as cost savings and patient satisfaction, are under review.
“So long as the level of training is sufficient, this is an approach that definitely should be explored,” he says, adding that young internists have many of the skills needed for ICU work. “But if you don’t keep those skills up [with practice] after residency, you lose them.”
References
- The Leapfrog Group. ICU physician staffing fact sheet. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/media/file/Leapfrog-ICU_Physician_Staffing_Fact_Sheet.pdf. Accessed Aug. 29, 2012.
- Health Resources & Services Administration. Report to Congress: The critical care workforce: a study of the supply and demand for critical care physicians. U.S. Department of Health & Human Services website. Available at: http://bhpr.hrsa.gov/healthworkforce/reports/studycriticalcarephys.pdf. Accessed Aug. 29, 2012.
- Krivopal M, Hlaing M, Felber R, Himebaugh R. ICU hospitalist: a novel method of care for the critically ill patients in economically lean times. J Hosp Med. 2012;7(Suppl 2):192.
Despite calls for board-certified intensivists to manage all critically ill patients, only a third of hospitalized ICU patients currently are seen by such a specialist—mostly because there are not enough of them to go around.1,2 More and more hospitalists, especially those in community hospitals, are working in ICUs (see “The Critical-Care Debate,”). With the proper training, that can be a good thing for patients and hospitalists, according to a Research, Innovations, and Clinical Vignettes (RIV) abstract presented at HM12 in San Diego.3
Lead author and hospitalist Mark Krivopal, MD, SFHM, formerly with TeamHealth in California and now vice president and medical director of clinical integration and hospital medicine at Steward Health Care in Boston, outlined a program at California’s Lodi Memorial Hospital that identified a group of hospitalists who had experience in caring for critically ill patients and credentials to perform such procedures as central-line placements, intubations, and ventilator management. The select group of TeamHealth hospitalists completed a two-day “Fundamentals of Critical Care Support” course offered by the Society of Critical Care Medicine (www.sccm.org), then began covering the ICU in shifts from 7 a.m. to 7 p.m. The program was so successful early on that hospital administration requested that it expand to a 24-hour service.
An ICU hospitalist program needs to be a partnership, Dr. Krivopal says. Essential oversight at Lodi Memorial is provided by the hospital’s sole pulmonologist.
Preliminary data showed a 35% reduction in ventilator days and 22% reduction in ICU stays, Dr. Krivopal says. The hospital also reports high satisfaction from nurses and other staff. Additional metrics, such as cost savings and patient satisfaction, are under review.
“So long as the level of training is sufficient, this is an approach that definitely should be explored,” he says, adding that young internists have many of the skills needed for ICU work. “But if you don’t keep those skills up [with practice] after residency, you lose them.”
References
- The Leapfrog Group. ICU physician staffing fact sheet. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/media/file/Leapfrog-ICU_Physician_Staffing_Fact_Sheet.pdf. Accessed Aug. 29, 2012.
- Health Resources & Services Administration. Report to Congress: The critical care workforce: a study of the supply and demand for critical care physicians. U.S. Department of Health & Human Services website. Available at: http://bhpr.hrsa.gov/healthworkforce/reports/studycriticalcarephys.pdf. Accessed Aug. 29, 2012.
- Krivopal M, Hlaing M, Felber R, Himebaugh R. ICU hospitalist: a novel method of care for the critically ill patients in economically lean times. J Hosp Med. 2012;7(Suppl 2):192.
Despite calls for board-certified intensivists to manage all critically ill patients, only a third of hospitalized ICU patients currently are seen by such a specialist—mostly because there are not enough of them to go around.1,2 More and more hospitalists, especially those in community hospitals, are working in ICUs (see “The Critical-Care Debate,”). With the proper training, that can be a good thing for patients and hospitalists, according to a Research, Innovations, and Clinical Vignettes (RIV) abstract presented at HM12 in San Diego.3
Lead author and hospitalist Mark Krivopal, MD, SFHM, formerly with TeamHealth in California and now vice president and medical director of clinical integration and hospital medicine at Steward Health Care in Boston, outlined a program at California’s Lodi Memorial Hospital that identified a group of hospitalists who had experience in caring for critically ill patients and credentials to perform such procedures as central-line placements, intubations, and ventilator management. The select group of TeamHealth hospitalists completed a two-day “Fundamentals of Critical Care Support” course offered by the Society of Critical Care Medicine (www.sccm.org), then began covering the ICU in shifts from 7 a.m. to 7 p.m. The program was so successful early on that hospital administration requested that it expand to a 24-hour service.
An ICU hospitalist program needs to be a partnership, Dr. Krivopal says. Essential oversight at Lodi Memorial is provided by the hospital’s sole pulmonologist.
Preliminary data showed a 35% reduction in ventilator days and 22% reduction in ICU stays, Dr. Krivopal says. The hospital also reports high satisfaction from nurses and other staff. Additional metrics, such as cost savings and patient satisfaction, are under review.
“So long as the level of training is sufficient, this is an approach that definitely should be explored,” he says, adding that young internists have many of the skills needed for ICU work. “But if you don’t keep those skills up [with practice] after residency, you lose them.”
References
- The Leapfrog Group. ICU physician staffing fact sheet. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/media/file/Leapfrog-ICU_Physician_Staffing_Fact_Sheet.pdf. Accessed Aug. 29, 2012.
- Health Resources & Services Administration. Report to Congress: The critical care workforce: a study of the supply and demand for critical care physicians. U.S. Department of Health & Human Services website. Available at: http://bhpr.hrsa.gov/healthworkforce/reports/studycriticalcarephys.pdf. Accessed Aug. 29, 2012.
- Krivopal M, Hlaing M, Felber R, Himebaugh R. ICU hospitalist: a novel method of care for the critically ill patients in economically lean times. J Hosp Med. 2012;7(Suppl 2):192.