User login
Does Dupilumab Treatment in Atopic Dermatitis Increase Infection Risk in Infants and Children?
Key clinical point: In infants and young children with atopic dermatitis (AD), dupilumab treatment with concomitant low-potency topical corticosteroids (TCS) does not increase infection rates and is associated with a reduced risk for bacterial and non-herpetic skin infections.
Major finding: Patients receiving dupilumab vs placebo had similar total infection rates week 16 (rate ratio [RR] 0.75; P = .223) and a significantly lower frequency of non-herpetic skin infections (RR 0.46; P = .047) and bacterial infections (RR 0.09; P = .019).
Study details: This post hoc analysis of the phase 3 LIBERTY AD PRESCHOOL trial included 162 patients (age 6 months to 5 years) with moderate to severe AD who were randomly assigned to receive 200 or 300 mg dupilumab (n = 83) or placebo (n = 79) every 4 weeks with concomitant low-potency TCS.
Disclosures: This study was funded by Sanofi and Regeneron Pharmaceuticals Inc. Four authors declared being employees or shareholders of Sanofi or Regeneron. The remaining authors declared having ties with Sanofi, Regeneron, or others.
Source: Paller AS, Siegfried EC, Cork MJ, et al. Infections in children aged 6 months to 5 years treated with dupilumab in a placebo-controlled clinical trial of moderate-to-severe atopic dermatitis. Paediatr Drugs. 2024 (Jan 24). doi: 10.1007/s40272-023-00611-9 Source
Key clinical point: In infants and young children with atopic dermatitis (AD), dupilumab treatment with concomitant low-potency topical corticosteroids (TCS) does not increase infection rates and is associated with a reduced risk for bacterial and non-herpetic skin infections.
Major finding: Patients receiving dupilumab vs placebo had similar total infection rates week 16 (rate ratio [RR] 0.75; P = .223) and a significantly lower frequency of non-herpetic skin infections (RR 0.46; P = .047) and bacterial infections (RR 0.09; P = .019).
Study details: This post hoc analysis of the phase 3 LIBERTY AD PRESCHOOL trial included 162 patients (age 6 months to 5 years) with moderate to severe AD who were randomly assigned to receive 200 or 300 mg dupilumab (n = 83) or placebo (n = 79) every 4 weeks with concomitant low-potency TCS.
Disclosures: This study was funded by Sanofi and Regeneron Pharmaceuticals Inc. Four authors declared being employees or shareholders of Sanofi or Regeneron. The remaining authors declared having ties with Sanofi, Regeneron, or others.
Source: Paller AS, Siegfried EC, Cork MJ, et al. Infections in children aged 6 months to 5 years treated with dupilumab in a placebo-controlled clinical trial of moderate-to-severe atopic dermatitis. Paediatr Drugs. 2024 (Jan 24). doi: 10.1007/s40272-023-00611-9 Source
Key clinical point: In infants and young children with atopic dermatitis (AD), dupilumab treatment with concomitant low-potency topical corticosteroids (TCS) does not increase infection rates and is associated with a reduced risk for bacterial and non-herpetic skin infections.
Major finding: Patients receiving dupilumab vs placebo had similar total infection rates week 16 (rate ratio [RR] 0.75; P = .223) and a significantly lower frequency of non-herpetic skin infections (RR 0.46; P = .047) and bacterial infections (RR 0.09; P = .019).
Study details: This post hoc analysis of the phase 3 LIBERTY AD PRESCHOOL trial included 162 patients (age 6 months to 5 years) with moderate to severe AD who were randomly assigned to receive 200 or 300 mg dupilumab (n = 83) or placebo (n = 79) every 4 weeks with concomitant low-potency TCS.
Disclosures: This study was funded by Sanofi and Regeneron Pharmaceuticals Inc. Four authors declared being employees or shareholders of Sanofi or Regeneron. The remaining authors declared having ties with Sanofi, Regeneron, or others.
Source: Paller AS, Siegfried EC, Cork MJ, et al. Infections in children aged 6 months to 5 years treated with dupilumab in a placebo-controlled clinical trial of moderate-to-severe atopic dermatitis. Paediatr Drugs. 2024 (Jan 24). doi: 10.1007/s40272-023-00611-9 Source
Dupilumab Dose Reduction Achievable in Persistently Controlled Atopic Dermatitis
Key clinical point: Dose reduction of 300 mg dupilumab was successfully achieved by dose spacing to >2 weeks without loss of efficacy in most patients with persistently controlled atopic dermatitis (AD), regardless of previous exposure to biologics and Janus kinase inhibitors (JAKi).
Major finding: At a median follow-up of 10 months, dose spacing of 300 mg dupilumab without loss in efficacy was achieved in 35 of 37 patients with controlled AD receiving dupilumab treatment for a median duration of 20.1 months. Similar findings were observed in patients with vs without previous exposure to biologics or JAKi (P > .05).
Study details: Findings are from a retrospective cohort study including 37 patients with controlled AD for more than a year, who were treated with 300 mg dupilumab at intervals > 2 weeks, and of whom 7 patients were classified as non-naive to biologics and JAKi.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Lasheras-Pérez MA, Palacios-Diaz RD, González-Delgado VA, et al. Dose tapering of dupilumab in patients with persistently controlled atopic dermatitis: A Spanish multicenter cohort study. Int J Dermatol. 2024 (Jan 16). doi: 10.1111/ijd.17030 Source
Key clinical point: Dose reduction of 300 mg dupilumab was successfully achieved by dose spacing to >2 weeks without loss of efficacy in most patients with persistently controlled atopic dermatitis (AD), regardless of previous exposure to biologics and Janus kinase inhibitors (JAKi).
Major finding: At a median follow-up of 10 months, dose spacing of 300 mg dupilumab without loss in efficacy was achieved in 35 of 37 patients with controlled AD receiving dupilumab treatment for a median duration of 20.1 months. Similar findings were observed in patients with vs without previous exposure to biologics or JAKi (P > .05).
Study details: Findings are from a retrospective cohort study including 37 patients with controlled AD for more than a year, who were treated with 300 mg dupilumab at intervals > 2 weeks, and of whom 7 patients were classified as non-naive to biologics and JAKi.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Lasheras-Pérez MA, Palacios-Diaz RD, González-Delgado VA, et al. Dose tapering of dupilumab in patients with persistently controlled atopic dermatitis: A Spanish multicenter cohort study. Int J Dermatol. 2024 (Jan 16). doi: 10.1111/ijd.17030 Source
Key clinical point: Dose reduction of 300 mg dupilumab was successfully achieved by dose spacing to >2 weeks without loss of efficacy in most patients with persistently controlled atopic dermatitis (AD), regardless of previous exposure to biologics and Janus kinase inhibitors (JAKi).
Major finding: At a median follow-up of 10 months, dose spacing of 300 mg dupilumab without loss in efficacy was achieved in 35 of 37 patients with controlled AD receiving dupilumab treatment for a median duration of 20.1 months. Similar findings were observed in patients with vs without previous exposure to biologics or JAKi (P > .05).
Study details: Findings are from a retrospective cohort study including 37 patients with controlled AD for more than a year, who were treated with 300 mg dupilumab at intervals > 2 weeks, and of whom 7 patients were classified as non-naive to biologics and JAKi.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Lasheras-Pérez MA, Palacios-Diaz RD, González-Delgado VA, et al. Dose tapering of dupilumab in patients with persistently controlled atopic dermatitis: A Spanish multicenter cohort study. Int J Dermatol. 2024 (Jan 16). doi: 10.1111/ijd.17030 Source
Dupilumab Effective in Patients With Atopic Dermatitis and Comorbidities Including Malignancies
Key clinical point: In real-world settings, dupilumab is safe and leads to significant and sustained improvements in the severity of atopic dermatitis (AD) in patients with moderate-to-severe AD, including those with malignancies and other comorbidities.
Major finding: At week 52, 64% of patients showed a decrease in disease severity, achieving a Physician Global Assessment score of 0 or 1 compared with a score of 3 or 4 at baseline. No adverse effect on current malignancy or recurrence of prior malignancy was reported with dupilumab use.
Study details: This real-world retrospective study analyzed the data of 155 adult patients with moderate-to-severe AD, including those with other significant comorbidities like malignancies, who were treated with dupilumab.
Disclosures: This study did not receive any funding. Mohannad Abu-Hilal declared serving as an advisor, consultant, or speaker for or receiving grants or honoraria from various sources.
Source: Metko D, Alkofide M, Abu-Hilal M. A real-world study of dupilumab in patients with atopic dermatitis including patients with malignancy and other medical comorbidities. JAAD Int. 2024;15:5-11 (Jan 15). doi: 10.1016/j.jdin.2024.01.002 Source
Key clinical point: In real-world settings, dupilumab is safe and leads to significant and sustained improvements in the severity of atopic dermatitis (AD) in patients with moderate-to-severe AD, including those with malignancies and other comorbidities.
Major finding: At week 52, 64% of patients showed a decrease in disease severity, achieving a Physician Global Assessment score of 0 or 1 compared with a score of 3 or 4 at baseline. No adverse effect on current malignancy or recurrence of prior malignancy was reported with dupilumab use.
Study details: This real-world retrospective study analyzed the data of 155 adult patients with moderate-to-severe AD, including those with other significant comorbidities like malignancies, who were treated with dupilumab.
Disclosures: This study did not receive any funding. Mohannad Abu-Hilal declared serving as an advisor, consultant, or speaker for or receiving grants or honoraria from various sources.
Source: Metko D, Alkofide M, Abu-Hilal M. A real-world study of dupilumab in patients with atopic dermatitis including patients with malignancy and other medical comorbidities. JAAD Int. 2024;15:5-11 (Jan 15). doi: 10.1016/j.jdin.2024.01.002 Source
Key clinical point: In real-world settings, dupilumab is safe and leads to significant and sustained improvements in the severity of atopic dermatitis (AD) in patients with moderate-to-severe AD, including those with malignancies and other comorbidities.
Major finding: At week 52, 64% of patients showed a decrease in disease severity, achieving a Physician Global Assessment score of 0 or 1 compared with a score of 3 or 4 at baseline. No adverse effect on current malignancy or recurrence of prior malignancy was reported with dupilumab use.
Study details: This real-world retrospective study analyzed the data of 155 adult patients with moderate-to-severe AD, including those with other significant comorbidities like malignancies, who were treated with dupilumab.
Disclosures: This study did not receive any funding. Mohannad Abu-Hilal declared serving as an advisor, consultant, or speaker for or receiving grants or honoraria from various sources.
Source: Metko D, Alkofide M, Abu-Hilal M. A real-world study of dupilumab in patients with atopic dermatitis including patients with malignancy and other medical comorbidities. JAAD Int. 2024;15:5-11 (Jan 15). doi: 10.1016/j.jdin.2024.01.002 Source
Atopic Dermatitis Remission in Children Unaffected by Washing With Water or Cleanser During Summer
Key clinical point: Skin care by washing with water alone is not inferior to washing with a cleanser for the maintenance of remission in children with atopic dermatitis (AD) during the summer.
Major finding: The mean modified Eczema Area and Severity Index scores at 8 ± 4 weeks were similar in children who washed their upper and lower limbs with water and those who used a cleanser (0.00 and 0.15, respectively; P = .74). No difference was observed in the occurrence of skin infection, Patient-Oriented Eczema Measure, and other secondary outcomes with water vs cleanser use (all P > .05).
Study details: This noninferiority study included 43 children (age < 15 years) with AD having controlled eczema following regular steroid ointment application, who washed the randomly assigned left or right limb with a cleanser and the other limb with water alone.
Disclosures: This study was funded by the Maruho Scholarship Donations Support Program, Japan. Osamu Natsume declared receiving grants from several sources. The other authors declared no conflicts of interest.
Source: Katoh Y, Natsume O, Yasuoka R, et al. Skin care by washing with water is not inferior to washing with a cleanser in children with atopic dermatitis in remission in summer: WASH study. Allergol Int. 2024 (Feb 2). doi: 10.1016/j.alit.2024.01.007 Source
Key clinical point: Skin care by washing with water alone is not inferior to washing with a cleanser for the maintenance of remission in children with atopic dermatitis (AD) during the summer.
Major finding: The mean modified Eczema Area and Severity Index scores at 8 ± 4 weeks were similar in children who washed their upper and lower limbs with water and those who used a cleanser (0.00 and 0.15, respectively; P = .74). No difference was observed in the occurrence of skin infection, Patient-Oriented Eczema Measure, and other secondary outcomes with water vs cleanser use (all P > .05).
Study details: This noninferiority study included 43 children (age < 15 years) with AD having controlled eczema following regular steroid ointment application, who washed the randomly assigned left or right limb with a cleanser and the other limb with water alone.
Disclosures: This study was funded by the Maruho Scholarship Donations Support Program, Japan. Osamu Natsume declared receiving grants from several sources. The other authors declared no conflicts of interest.
Source: Katoh Y, Natsume O, Yasuoka R, et al. Skin care by washing with water is not inferior to washing with a cleanser in children with atopic dermatitis in remission in summer: WASH study. Allergol Int. 2024 (Feb 2). doi: 10.1016/j.alit.2024.01.007 Source
Key clinical point: Skin care by washing with water alone is not inferior to washing with a cleanser for the maintenance of remission in children with atopic dermatitis (AD) during the summer.
Major finding: The mean modified Eczema Area and Severity Index scores at 8 ± 4 weeks were similar in children who washed their upper and lower limbs with water and those who used a cleanser (0.00 and 0.15, respectively; P = .74). No difference was observed in the occurrence of skin infection, Patient-Oriented Eczema Measure, and other secondary outcomes with water vs cleanser use (all P > .05).
Study details: This noninferiority study included 43 children (age < 15 years) with AD having controlled eczema following regular steroid ointment application, who washed the randomly assigned left or right limb with a cleanser and the other limb with water alone.
Disclosures: This study was funded by the Maruho Scholarship Donations Support Program, Japan. Osamu Natsume declared receiving grants from several sources. The other authors declared no conflicts of interest.
Source: Katoh Y, Natsume O, Yasuoka R, et al. Skin care by washing with water is not inferior to washing with a cleanser in children with atopic dermatitis in remission in summer: WASH study. Allergol Int. 2024 (Feb 2). doi: 10.1016/j.alit.2024.01.007 Source
Air Quality Index Tied to the Incidence of Atopic Dermatitis
Key clinical point: A significant positive, dose-dependent association was observed between air quality index (AQI) and the incidence of atopic dermatitis (AD).
Major finding: The participants were classified into four AQI value quantiles (Q), with the mean AQI values from the lowest Q1 to the highest Q4 being 69.0, 78.9, 89.8, and 104.0, respectively. Compared with Q1, the risk for AD increased significantly in Q2 (adjusted hazard ratio [aHR] 1.29; 95% CI 1.04-1.65), Q3 (aHR 4.71; 95% CI 3.78-6.04), and Q4 (aHR 13.20; 95% CI 10.86-16.60). An increase of one unit in the AQI value increased the risk for AD by 7%.
Study details: This cohort study included 21,278,938 individuals without AD, with the long-term average AQI value before AD diagnosis being calculated and linked for each of the individuals.
Disclosures: This study was sponsored by grants from the Ministry of Science and Technology, Taiwan, Republic of China. The authors declared no conflicts of interest.
Source: Wu CY, Wu CY, Li MC, Ho HJ, Ao CK. Association of air quality index (AQI) with incidence of atopic dermatitis in Taiwan: A nationwide population-based cohort study. J Am Acad Dermatol. 2024 (Feb 1). doi: 10.1016/j.jaad.2024.01.058 Source
Key clinical point: A significant positive, dose-dependent association was observed between air quality index (AQI) and the incidence of atopic dermatitis (AD).
Major finding: The participants were classified into four AQI value quantiles (Q), with the mean AQI values from the lowest Q1 to the highest Q4 being 69.0, 78.9, 89.8, and 104.0, respectively. Compared with Q1, the risk for AD increased significantly in Q2 (adjusted hazard ratio [aHR] 1.29; 95% CI 1.04-1.65), Q3 (aHR 4.71; 95% CI 3.78-6.04), and Q4 (aHR 13.20; 95% CI 10.86-16.60). An increase of one unit in the AQI value increased the risk for AD by 7%.
Study details: This cohort study included 21,278,938 individuals without AD, with the long-term average AQI value before AD diagnosis being calculated and linked for each of the individuals.
Disclosures: This study was sponsored by grants from the Ministry of Science and Technology, Taiwan, Republic of China. The authors declared no conflicts of interest.
Source: Wu CY, Wu CY, Li MC, Ho HJ, Ao CK. Association of air quality index (AQI) with incidence of atopic dermatitis in Taiwan: A nationwide population-based cohort study. J Am Acad Dermatol. 2024 (Feb 1). doi: 10.1016/j.jaad.2024.01.058 Source
Key clinical point: A significant positive, dose-dependent association was observed between air quality index (AQI) and the incidence of atopic dermatitis (AD).
Major finding: The participants were classified into four AQI value quantiles (Q), with the mean AQI values from the lowest Q1 to the highest Q4 being 69.0, 78.9, 89.8, and 104.0, respectively. Compared with Q1, the risk for AD increased significantly in Q2 (adjusted hazard ratio [aHR] 1.29; 95% CI 1.04-1.65), Q3 (aHR 4.71; 95% CI 3.78-6.04), and Q4 (aHR 13.20; 95% CI 10.86-16.60). An increase of one unit in the AQI value increased the risk for AD by 7%.
Study details: This cohort study included 21,278,938 individuals without AD, with the long-term average AQI value before AD diagnosis being calculated and linked for each of the individuals.
Disclosures: This study was sponsored by grants from the Ministry of Science and Technology, Taiwan, Republic of China. The authors declared no conflicts of interest.
Source: Wu CY, Wu CY, Li MC, Ho HJ, Ao CK. Association of air quality index (AQI) with incidence of atopic dermatitis in Taiwan: A nationwide population-based cohort study. J Am Acad Dermatol. 2024 (Feb 1). doi: 10.1016/j.jaad.2024.01.058 Source
Dupilumab Monotherapy Safe and Effective Against Hand and Foot Atopic Dermatitis
Key clinical point: Dupilumab monotherapy is safe and leads to rapid and significant improvements in disease signs and symptoms in patients with hand and foot (HF) atopic dermatitis (AD).
Major finding: At week 16, a significantly higher number of patients receiving dupilumab vs placebo achieved an HF Investigator’s Global Assessment score of 0 or 1 (P = .003) and ≥4-point reduction in HF Peak Pruritus Numeric Rating Scale score (P < .0001), with the difference between groups evident from weeks 4 and 1, respectively. Safety was consistent with the known dupilumab profile.
Study details: Findings are from the phase 3 LIBERTY-AD-HAFT study, which included 106 adults and 27 adolescents (≥ 12 to < 18 years) with moderate to severe HF AD who were randomized (1:1) to receive dupilumab or placebo.
Disclosures: This study was funded by Sanofi and Regeneron Pharmaceuticals Inc. Ten authors declared being employees or shareholders of Sanofi or Regeneron. The remaining authors, except Ewa Sygula, declared serving as investigators, consultants, etc., for or receiving personal fees, grants, honoraria, etc., from Sanofi, Regeneron, or others.
Source: Simpson E, Silverberg JI, Worm M, et al. Dupilumab treatment improves signs, symptoms, quality of life and work productivity in patients with atopic hand and foot dermatitis: Results from a phase 3, randomized, double-blind, placebo-controlled trial. J Am Acad Dermatol. 2024 (Jan 29). doi: 10.1016/j.jaad.2023.12.066 Source
Key clinical point: Dupilumab monotherapy is safe and leads to rapid and significant improvements in disease signs and symptoms in patients with hand and foot (HF) atopic dermatitis (AD).
Major finding: At week 16, a significantly higher number of patients receiving dupilumab vs placebo achieved an HF Investigator’s Global Assessment score of 0 or 1 (P = .003) and ≥4-point reduction in HF Peak Pruritus Numeric Rating Scale score (P < .0001), with the difference between groups evident from weeks 4 and 1, respectively. Safety was consistent with the known dupilumab profile.
Study details: Findings are from the phase 3 LIBERTY-AD-HAFT study, which included 106 adults and 27 adolescents (≥ 12 to < 18 years) with moderate to severe HF AD who were randomized (1:1) to receive dupilumab or placebo.
Disclosures: This study was funded by Sanofi and Regeneron Pharmaceuticals Inc. Ten authors declared being employees or shareholders of Sanofi or Regeneron. The remaining authors, except Ewa Sygula, declared serving as investigators, consultants, etc., for or receiving personal fees, grants, honoraria, etc., from Sanofi, Regeneron, or others.
Source: Simpson E, Silverberg JI, Worm M, et al. Dupilumab treatment improves signs, symptoms, quality of life and work productivity in patients with atopic hand and foot dermatitis: Results from a phase 3, randomized, double-blind, placebo-controlled trial. J Am Acad Dermatol. 2024 (Jan 29). doi: 10.1016/j.jaad.2023.12.066 Source
Key clinical point: Dupilumab monotherapy is safe and leads to rapid and significant improvements in disease signs and symptoms in patients with hand and foot (HF) atopic dermatitis (AD).
Major finding: At week 16, a significantly higher number of patients receiving dupilumab vs placebo achieved an HF Investigator’s Global Assessment score of 0 or 1 (P = .003) and ≥4-point reduction in HF Peak Pruritus Numeric Rating Scale score (P < .0001), with the difference between groups evident from weeks 4 and 1, respectively. Safety was consistent with the known dupilumab profile.
Study details: Findings are from the phase 3 LIBERTY-AD-HAFT study, which included 106 adults and 27 adolescents (≥ 12 to < 18 years) with moderate to severe HF AD who were randomized (1:1) to receive dupilumab or placebo.
Disclosures: This study was funded by Sanofi and Regeneron Pharmaceuticals Inc. Ten authors declared being employees or shareholders of Sanofi or Regeneron. The remaining authors, except Ewa Sygula, declared serving as investigators, consultants, etc., for or receiving personal fees, grants, honoraria, etc., from Sanofi, Regeneron, or others.
Source: Simpson E, Silverberg JI, Worm M, et al. Dupilumab treatment improves signs, symptoms, quality of life and work productivity in patients with atopic hand and foot dermatitis: Results from a phase 3, randomized, double-blind, placebo-controlled trial. J Am Acad Dermatol. 2024 (Jan 29). doi: 10.1016/j.jaad.2023.12.066 Source
Atopic Dermatitis Increases the Risk for Subsequent Autoimmune Disease
Key clinical point: A significant causal relationship was observed between atopic dermatitis (AD) and autoimmune diseases in children, and this was supported by the presence of shared genetic factors.
Major finding: At a follow-up of 12 years, children with vs without AD had a significantly increased risk for autoimmune diseases (adjusted hazard ratio [aHR] 1.27; 95% CI 1.23-1.32), particularly psoriasis vulgaris (aHR 2.55; 95% CI 2.25-2.80). Boys were significantly more susceptible to autoimmune diseases than girls (P for interaction = .04). Sixteen shared genes were identified between AD and autoimmune diseases and were associated with comorbidities, such as asthma and bronchiolitis.
Study details: This large-scale cohort study included 39,832 children with AD born between 2002 and 2018, who were matched with 159,328 children without AD.
Disclosures: This study was supported by the Korea Health Technology R&D. The authors declared no conflicts of interest.
Source: Ahn J, Shin S, Lee GC, et al. Unraveling the link between atopic dermatitis and autoimmune diseases in children: Insights from a large-scale cohort study with 15-year follow-up and shared gene ontology analysis. Allergol Int. 2024 (Jan 17). doi: 10.1016/j.alit.2023.12.005 Source
Key clinical point: A significant causal relationship was observed between atopic dermatitis (AD) and autoimmune diseases in children, and this was supported by the presence of shared genetic factors.
Major finding: At a follow-up of 12 years, children with vs without AD had a significantly increased risk for autoimmune diseases (adjusted hazard ratio [aHR] 1.27; 95% CI 1.23-1.32), particularly psoriasis vulgaris (aHR 2.55; 95% CI 2.25-2.80). Boys were significantly more susceptible to autoimmune diseases than girls (P for interaction = .04). Sixteen shared genes were identified between AD and autoimmune diseases and were associated with comorbidities, such as asthma and bronchiolitis.
Study details: This large-scale cohort study included 39,832 children with AD born between 2002 and 2018, who were matched with 159,328 children without AD.
Disclosures: This study was supported by the Korea Health Technology R&D. The authors declared no conflicts of interest.
Source: Ahn J, Shin S, Lee GC, et al. Unraveling the link between atopic dermatitis and autoimmune diseases in children: Insights from a large-scale cohort study with 15-year follow-up and shared gene ontology analysis. Allergol Int. 2024 (Jan 17). doi: 10.1016/j.alit.2023.12.005 Source
Key clinical point: A significant causal relationship was observed between atopic dermatitis (AD) and autoimmune diseases in children, and this was supported by the presence of shared genetic factors.
Major finding: At a follow-up of 12 years, children with vs without AD had a significantly increased risk for autoimmune diseases (adjusted hazard ratio [aHR] 1.27; 95% CI 1.23-1.32), particularly psoriasis vulgaris (aHR 2.55; 95% CI 2.25-2.80). Boys were significantly more susceptible to autoimmune diseases than girls (P for interaction = .04). Sixteen shared genes were identified between AD and autoimmune diseases and were associated with comorbidities, such as asthma and bronchiolitis.
Study details: This large-scale cohort study included 39,832 children with AD born between 2002 and 2018, who were matched with 159,328 children without AD.
Disclosures: This study was supported by the Korea Health Technology R&D. The authors declared no conflicts of interest.
Source: Ahn J, Shin S, Lee GC, et al. Unraveling the link between atopic dermatitis and autoimmune diseases in children: Insights from a large-scale cohort study with 15-year follow-up and shared gene ontology analysis. Allergol Int. 2024 (Jan 17). doi: 10.1016/j.alit.2023.12.005 Source
Alagille Syndrome
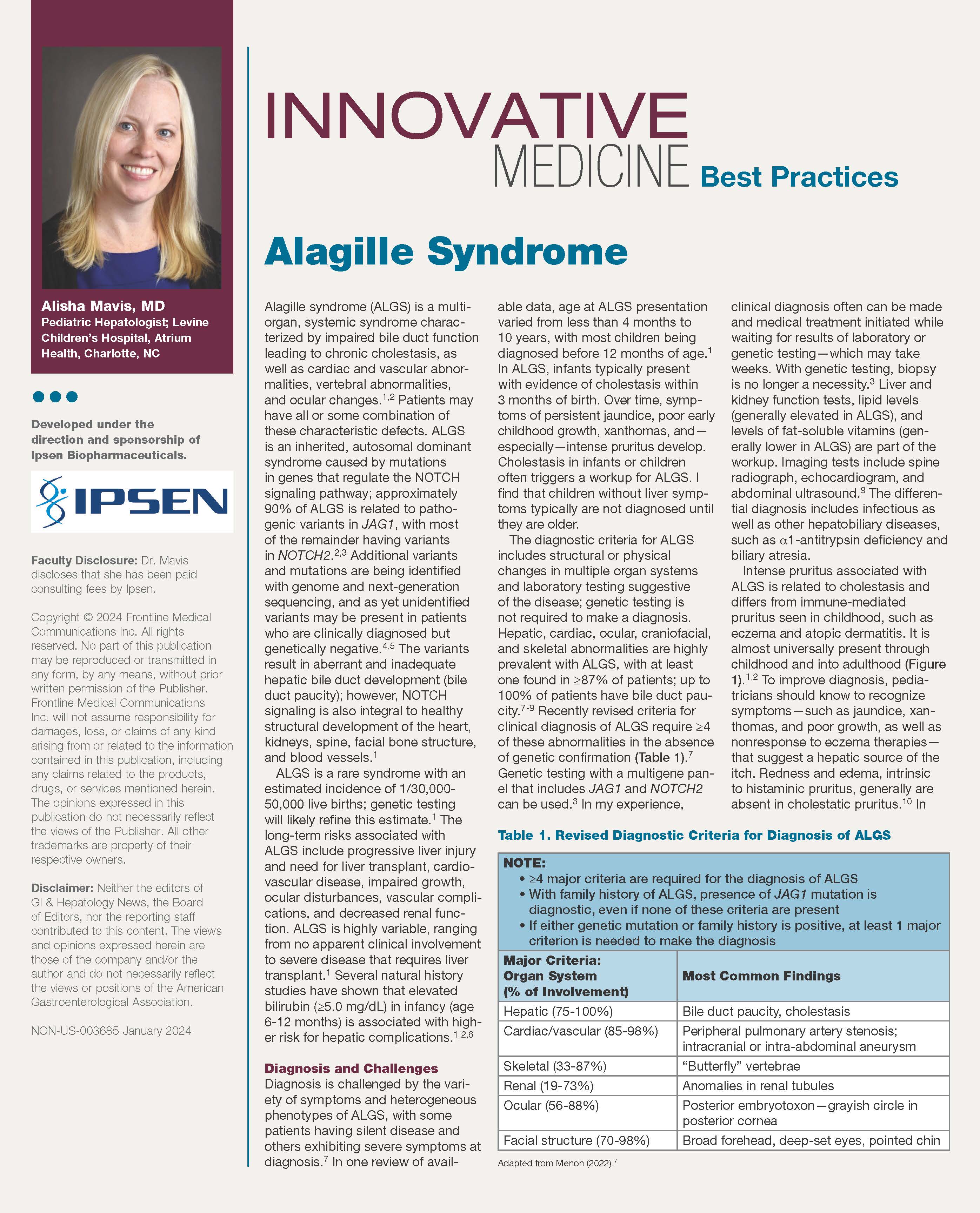
In this article Alisha Mavis, MD, discusses the prevalence, diagnosis, challenges, and management of patients with this Alagille Syndrome, as well as the need for a multidisciplinary approach to care.
In this article Alisha Mavis, MD, discusses the prevalence, diagnosis, challenges, and management of patients with this Alagille Syndrome, as well as the need for a multidisciplinary approach to care.
In this article Alisha Mavis, MD, discusses the prevalence, diagnosis, challenges, and management of patients with this Alagille Syndrome, as well as the need for a multidisciplinary approach to care.
An Ethical Analysis of Treatment of an Active-Duty Service Member With Limited Follow-up
For active-duty service members, dermatologic conditions are among the most common presenting concerns, comprising 15% to 75% of wartime outpatient visits.1 In general, there are unique considerations when caring for active-duty service members, including meeting designated active-duty retention and hierarchical standards.2 We present a hypothetical case: An active-duty military patient presents to a new dermatologist for cosmetic enhancement of facial skin dyspigmentation. The patient will be leaving soon for deployment and will not be able to follow up for 9 months. How should the dermatologist treat a patient who cannot follow up for so long?
The therapeutic modalities offered can be impacted by forthcoming deployments3 that may result in delayed time to administer repeat treatments or follow-up. The patient may have high expectations for a single appointment for a condition that requires prolonged treatment courses. Because there often is no reliable mechanism for patients to obtain refills during deployment, any medications prescribed would need to be provided in advance for the entire deployment duration, which often is 6 to 9 months. Additionally, treatment monitoring or modifications are severely limited, especially in the context of treatment nonresponse or adverse reactions. Considering the unique limitations of this patient population, both military and civilian physicians are faced with a need to maximize beneficence and autonomy while balancing nonmaleficence and justice.
One possible option is to decline to treat until the patient can follow up after returning from deployment. However, denying a request for an active treatable indication for which the patient desires treatment compromises patient autonomy and beneficence. Further, treatment should be provided to patients equitably to maintain justice. Although there may be a role for discussing active monitoring with nonintervention with the patient, denying treatment can negatively impact their physical and mental health and may be harmful. However, the patient should know and fully understand the risks and benefits of nonintervention with limited follow-up, including suboptimal outcomes or adverse events.
Another possibility for the management of this case may be conducting a one-time laser or light-based therapy or a one-time superficial- to medium-depth chemical peel before the patient leaves on deployment. Often, a series of laser- or light-based treatments is required to maximize outcomes for dyspigmentation. Without follow-up and with possible deployment to an environment with high UV exposure, the patient may experience disease exacerbation or other adverse effects. Treatment of those adverse effects may be delayed, as further intervention is not possible during deployment. Lower initial laser settings may be safer but may not be highly effective initially. More rigorous treatment upon return from deployment may be considered. Similar to laser therapies, chemical peels usually require several treatments for optimal outcomes. Without follow-up and with potential deployment to remote environments, there is a risk for adverse events that outweighs the minimal benefit of a single treatment. Therefore, either intervention may violate the principle of nonmaleficence.
A more reasonable approach may be initiating topical therapy and following up via telemedicine evaluation. Topical therapy often is the least-invasive approach and carries a reduced risk for adverse effects. Triple-combination therapy with topical retinoids, hydroquinone, and topical steroids is a common first-line approach.4 Because this approach is patient dependent, therapy can be more easily modulated or halted in the context of undesired results. Additionally, if internet connectivity is available, an asynchronous telemedicine approach could be utilized during deployment to monitor and advise changes as necessary, provided the regulatory framework allows for it.5
Although there is no uniformly correct approach in a scenario of limited patient follow-up, the last solution may be most ethically favorable: to begin therapy with milder and safer therapies (topical) and defer higher-intensity regimens until the patient returns from deployment. This allows some treatment initiation to preserve justice, beneficence, and patient autonomy. Associated virtual follow-up via telemedicine also allows avoidance of nonmaleficence in this context.
- Hwang J, Kakimoto C. Teledermatology in the US military: a historic foundation for current and future applications. Cutis. 2018;101:335;337;345.
- Dodd JG, Grant-Kels JM. Ethical concerns in caring for active duty service members who may be seeking dermatologic care outside the military soon. Int J Womens Dermatol. 2020;6:445-447. doi:10.1016/j.ijwd.2020.07.001
- Burke KR, Larrymore DC, Cho S. Treatment consideration for US military members with skin disease. Cutis. 2019;103:329-332.
- Desai SR. Hyperpigmentation therapy: a review. J Clin Aesthet Dermatol. 2014;7:13-17.
- Hwang JS, Lappan CM, Sperling LC, et al. Utilization of telemedicine in the U.S. military in a deployed setting. Mil Med. 2014;179:1347-1353. doi:10.7205/MILMED-D-14-00115
For active-duty service members, dermatologic conditions are among the most common presenting concerns, comprising 15% to 75% of wartime outpatient visits.1 In general, there are unique considerations when caring for active-duty service members, including meeting designated active-duty retention and hierarchical standards.2 We present a hypothetical case: An active-duty military patient presents to a new dermatologist for cosmetic enhancement of facial skin dyspigmentation. The patient will be leaving soon for deployment and will not be able to follow up for 9 months. How should the dermatologist treat a patient who cannot follow up for so long?
The therapeutic modalities offered can be impacted by forthcoming deployments3 that may result in delayed time to administer repeat treatments or follow-up. The patient may have high expectations for a single appointment for a condition that requires prolonged treatment courses. Because there often is no reliable mechanism for patients to obtain refills during deployment, any medications prescribed would need to be provided in advance for the entire deployment duration, which often is 6 to 9 months. Additionally, treatment monitoring or modifications are severely limited, especially in the context of treatment nonresponse or adverse reactions. Considering the unique limitations of this patient population, both military and civilian physicians are faced with a need to maximize beneficence and autonomy while balancing nonmaleficence and justice.
One possible option is to decline to treat until the patient can follow up after returning from deployment. However, denying a request for an active treatable indication for which the patient desires treatment compromises patient autonomy and beneficence. Further, treatment should be provided to patients equitably to maintain justice. Although there may be a role for discussing active monitoring with nonintervention with the patient, denying treatment can negatively impact their physical and mental health and may be harmful. However, the patient should know and fully understand the risks and benefits of nonintervention with limited follow-up, including suboptimal outcomes or adverse events.
Another possibility for the management of this case may be conducting a one-time laser or light-based therapy or a one-time superficial- to medium-depth chemical peel before the patient leaves on deployment. Often, a series of laser- or light-based treatments is required to maximize outcomes for dyspigmentation. Without follow-up and with possible deployment to an environment with high UV exposure, the patient may experience disease exacerbation or other adverse effects. Treatment of those adverse effects may be delayed, as further intervention is not possible during deployment. Lower initial laser settings may be safer but may not be highly effective initially. More rigorous treatment upon return from deployment may be considered. Similar to laser therapies, chemical peels usually require several treatments for optimal outcomes. Without follow-up and with potential deployment to remote environments, there is a risk for adverse events that outweighs the minimal benefit of a single treatment. Therefore, either intervention may violate the principle of nonmaleficence.
A more reasonable approach may be initiating topical therapy and following up via telemedicine evaluation. Topical therapy often is the least-invasive approach and carries a reduced risk for adverse effects. Triple-combination therapy with topical retinoids, hydroquinone, and topical steroids is a common first-line approach.4 Because this approach is patient dependent, therapy can be more easily modulated or halted in the context of undesired results. Additionally, if internet connectivity is available, an asynchronous telemedicine approach could be utilized during deployment to monitor and advise changes as necessary, provided the regulatory framework allows for it.5
Although there is no uniformly correct approach in a scenario of limited patient follow-up, the last solution may be most ethically favorable: to begin therapy with milder and safer therapies (topical) and defer higher-intensity regimens until the patient returns from deployment. This allows some treatment initiation to preserve justice, beneficence, and patient autonomy. Associated virtual follow-up via telemedicine also allows avoidance of nonmaleficence in this context.
For active-duty service members, dermatologic conditions are among the most common presenting concerns, comprising 15% to 75% of wartime outpatient visits.1 In general, there are unique considerations when caring for active-duty service members, including meeting designated active-duty retention and hierarchical standards.2 We present a hypothetical case: An active-duty military patient presents to a new dermatologist for cosmetic enhancement of facial skin dyspigmentation. The patient will be leaving soon for deployment and will not be able to follow up for 9 months. How should the dermatologist treat a patient who cannot follow up for so long?
The therapeutic modalities offered can be impacted by forthcoming deployments3 that may result in delayed time to administer repeat treatments or follow-up. The patient may have high expectations for a single appointment for a condition that requires prolonged treatment courses. Because there often is no reliable mechanism for patients to obtain refills during deployment, any medications prescribed would need to be provided in advance for the entire deployment duration, which often is 6 to 9 months. Additionally, treatment monitoring or modifications are severely limited, especially in the context of treatment nonresponse or adverse reactions. Considering the unique limitations of this patient population, both military and civilian physicians are faced with a need to maximize beneficence and autonomy while balancing nonmaleficence and justice.
One possible option is to decline to treat until the patient can follow up after returning from deployment. However, denying a request for an active treatable indication for which the patient desires treatment compromises patient autonomy and beneficence. Further, treatment should be provided to patients equitably to maintain justice. Although there may be a role for discussing active monitoring with nonintervention with the patient, denying treatment can negatively impact their physical and mental health and may be harmful. However, the patient should know and fully understand the risks and benefits of nonintervention with limited follow-up, including suboptimal outcomes or adverse events.
Another possibility for the management of this case may be conducting a one-time laser or light-based therapy or a one-time superficial- to medium-depth chemical peel before the patient leaves on deployment. Often, a series of laser- or light-based treatments is required to maximize outcomes for dyspigmentation. Without follow-up and with possible deployment to an environment with high UV exposure, the patient may experience disease exacerbation or other adverse effects. Treatment of those adverse effects may be delayed, as further intervention is not possible during deployment. Lower initial laser settings may be safer but may not be highly effective initially. More rigorous treatment upon return from deployment may be considered. Similar to laser therapies, chemical peels usually require several treatments for optimal outcomes. Without follow-up and with potential deployment to remote environments, there is a risk for adverse events that outweighs the minimal benefit of a single treatment. Therefore, either intervention may violate the principle of nonmaleficence.
A more reasonable approach may be initiating topical therapy and following up via telemedicine evaluation. Topical therapy often is the least-invasive approach and carries a reduced risk for adverse effects. Triple-combination therapy with topical retinoids, hydroquinone, and topical steroids is a common first-line approach.4 Because this approach is patient dependent, therapy can be more easily modulated or halted in the context of undesired results. Additionally, if internet connectivity is available, an asynchronous telemedicine approach could be utilized during deployment to monitor and advise changes as necessary, provided the regulatory framework allows for it.5
Although there is no uniformly correct approach in a scenario of limited patient follow-up, the last solution may be most ethically favorable: to begin therapy with milder and safer therapies (topical) and defer higher-intensity regimens until the patient returns from deployment. This allows some treatment initiation to preserve justice, beneficence, and patient autonomy. Associated virtual follow-up via telemedicine also allows avoidance of nonmaleficence in this context.
- Hwang J, Kakimoto C. Teledermatology in the US military: a historic foundation for current and future applications. Cutis. 2018;101:335;337;345.
- Dodd JG, Grant-Kels JM. Ethical concerns in caring for active duty service members who may be seeking dermatologic care outside the military soon. Int J Womens Dermatol. 2020;6:445-447. doi:10.1016/j.ijwd.2020.07.001
- Burke KR, Larrymore DC, Cho S. Treatment consideration for US military members with skin disease. Cutis. 2019;103:329-332.
- Desai SR. Hyperpigmentation therapy: a review. J Clin Aesthet Dermatol. 2014;7:13-17.
- Hwang JS, Lappan CM, Sperling LC, et al. Utilization of telemedicine in the U.S. military in a deployed setting. Mil Med. 2014;179:1347-1353. doi:10.7205/MILMED-D-14-00115
- Hwang J, Kakimoto C. Teledermatology in the US military: a historic foundation for current and future applications. Cutis. 2018;101:335;337;345.
- Dodd JG, Grant-Kels JM. Ethical concerns in caring for active duty service members who may be seeking dermatologic care outside the military soon. Int J Womens Dermatol. 2020;6:445-447. doi:10.1016/j.ijwd.2020.07.001
- Burke KR, Larrymore DC, Cho S. Treatment consideration for US military members with skin disease. Cutis. 2019;103:329-332.
- Desai SR. Hyperpigmentation therapy: a review. J Clin Aesthet Dermatol. 2014;7:13-17.
- Hwang JS, Lappan CM, Sperling LC, et al. Utilization of telemedicine in the U.S. military in a deployed setting. Mil Med. 2014;179:1347-1353. doi:10.7205/MILMED-D-14-00115
PRACTICE POINTS
- Dermatologic conditions are among the most common concerns reported by active-duty service members.
- The unique considerations of deployments are important for dermatologists to consider in the treatment of skin disease.