User login
Elderly Woman with Shoulder Pain
ANSWER
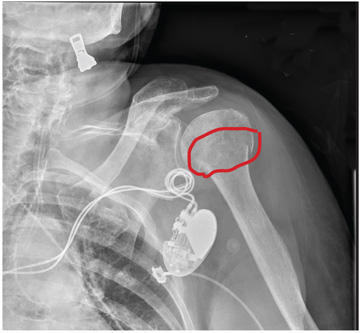
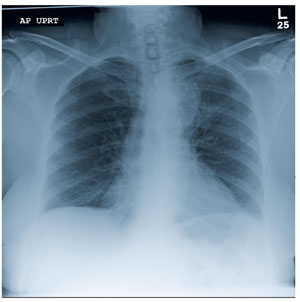
The radiograph demonstrates significant osteopenia. In addition, there is a slightly impacted subcapital fracture of the humeral neck.
Orthopedics was consulted, and the patient was to be treated with nonoperative management. She was given a swathe for immobilization and comfort.
ANSWER
The radiograph demonstrates significant osteopenia. In addition, there is a slightly impacted subcapital fracture of the humeral neck.
Orthopedics was consulted, and the patient was to be treated with nonoperative management. She was given a swathe for immobilization and comfort.
ANSWER
The radiograph demonstrates significant osteopenia. In addition, there is a slightly impacted subcapital fracture of the humeral neck.
Orthopedics was consulted, and the patient was to be treated with nonoperative management. She was given a swathe for immobilization and comfort.

A 90-year-old woman is transferred to your facility from an outside hospital for evaluation of an intracranial hemorrhage secondary to a fall. The patient normally resides in a nursing home and has dementia. She was reportedly ambulating with her walker when she tripped and fell forward. In addition to dementia, her medical history is significant for sick sinus syndrome, for which she has a pacemaker. She also has hypertension and degenerative joint disease. Examination reveals an elderly female who is alert but very confused. Her vital signs are normal. She has moderate swelling and bruising on the left side of her forehead and left orbit. Her pupils react well. As you examine her, you note her unwillingness to use or move her left arm. When you inquire, she states, “It hurts.” Close examination of the left upper extremity shows no obvious deformity or swelling. She does have some tenderness over the left shoulder. You order a radiograph of the left shoulder (shown). What is your impression?

Dyspnea Confines Woman to Wheelchair
ANSWER
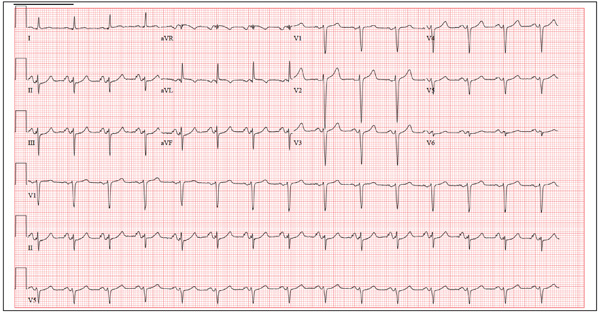
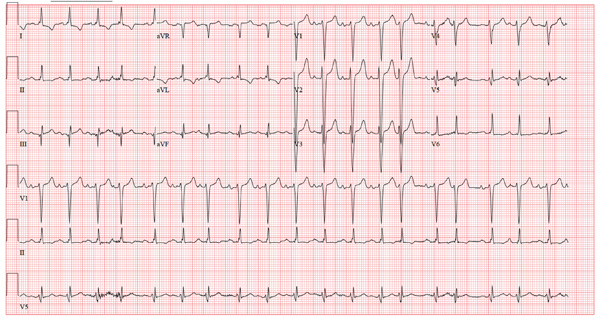
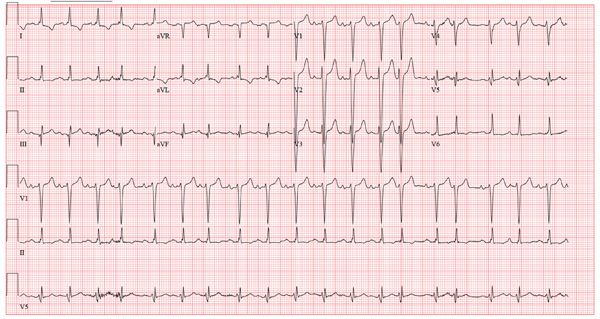
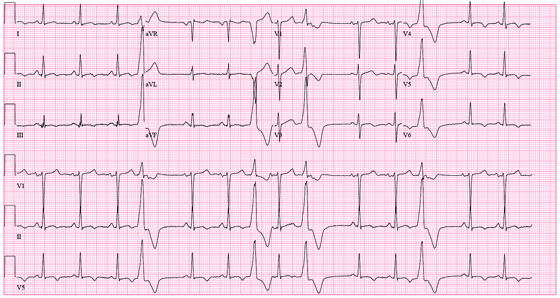
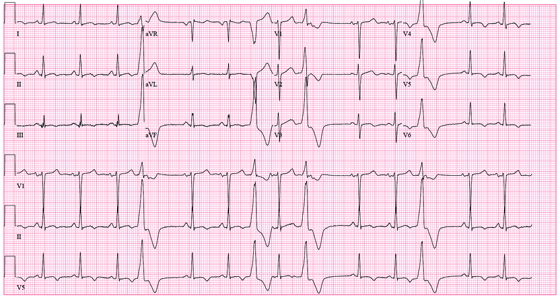
The ECG shows normal sinus rhythm, right atrial enlargement, a left anterior fascicular block, and evidence of an old anterolateral MI. Normal sinus rhythm is evidenced by the presence of a P wave for each QRS complex at a rate of 60 to 100 beats/min. Right atrial enlargement is diagnosed by the presence of tall, peaked P waves ≥ 2.5 mm in leads II, III, and aVF, and is a result of the patient’s pulmonary hypertension (P pulmonale).
A left anterior fascicular block is evidenced by the presence of left-axis deviation (typically between –45° and –90°), small R and large S complexes in leads II, III, and aVF, small Q waves in leads I and aVL, a QRS duration < 120 ms, and poor R-wave progression in leads V1 to V3 and deep S waves in V5 to V6.
The usual criteria for an anterolateral MI include Q, QS, or QRS complexes in leads V4 to V6 with ST-T wave changes. Poor R-wave progression in the absence of Q, QS, or QRS complexes in the anterolateral precordial leads (seen in this ECG) is also consistent with an old anterolateral MI.
ANSWER
The ECG shows normal sinus rhythm, right atrial enlargement, a left anterior fascicular block, and evidence of an old anterolateral MI. Normal sinus rhythm is evidenced by the presence of a P wave for each QRS complex at a rate of 60 to 100 beats/min. Right atrial enlargement is diagnosed by the presence of tall, peaked P waves ≥ 2.5 mm in leads II, III, and aVF, and is a result of the patient’s pulmonary hypertension (P pulmonale).
A left anterior fascicular block is evidenced by the presence of left-axis deviation (typically between –45° and –90°), small R and large S complexes in leads II, III, and aVF, small Q waves in leads I and aVL, a QRS duration < 120 ms, and poor R-wave progression in leads V1 to V3 and deep S waves in V5 to V6.
The usual criteria for an anterolateral MI include Q, QS, or QRS complexes in leads V4 to V6 with ST-T wave changes. Poor R-wave progression in the absence of Q, QS, or QRS complexes in the anterolateral precordial leads (seen in this ECG) is also consistent with an old anterolateral MI.
ANSWER
The ECG shows normal sinus rhythm, right atrial enlargement, a left anterior fascicular block, and evidence of an old anterolateral MI. Normal sinus rhythm is evidenced by the presence of a P wave for each QRS complex at a rate of 60 to 100 beats/min. Right atrial enlargement is diagnosed by the presence of tall, peaked P waves ≥ 2.5 mm in leads II, III, and aVF, and is a result of the patient’s pulmonary hypertension (P pulmonale).
A left anterior fascicular block is evidenced by the presence of left-axis deviation (typically between –45° and –90°), small R and large S complexes in leads II, III, and aVF, small Q waves in leads I and aVL, a QRS duration < 120 ms, and poor R-wave progression in leads V1 to V3 and deep S waves in V5 to V6.
The usual criteria for an anterolateral MI include Q, QS, or QRS complexes in leads V4 to V6 with ST-T wave changes. Poor R-wave progression in the absence of Q, QS, or QRS complexes in the anterolateral precordial leads (seen in this ECG) is also consistent with an old anterolateral MI.
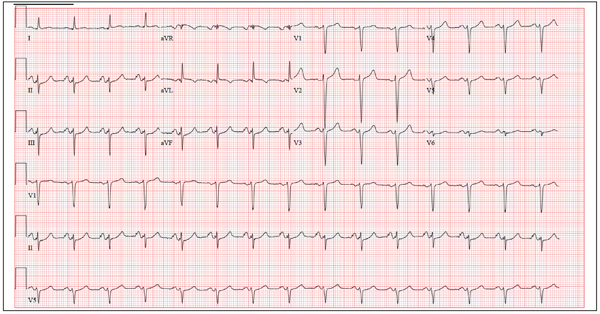
A 46-year-old woman is undergoing evaluation for consideration of heart transplantation versus left ventricular assist device placement as destination therapy. She has had a significant decline in her functional capacity in the past six months (sharpest in the past two months), and now can walk for only half a block be-fore becoming short of breath. For the past month, she has been unable to walk more than 100 feet without dyspnea and now confines herself to a wheelchair. Medical history is remarkable for type 1 diabetes requiring insulin pump therapy; multivessel coronary artery disease (CAD) with angioplasty and stent placement; coronary artery bypass grafting (CABG; left internal thoracic artery graft to left anterior descending artery and reverse saphenous vein graft to the first obtuse marginal branch); an anterior wall myocardial infarction (MI) one year after her CABG; severe ischemic cardiomyopathy with a left ventricular ejection fraction of 18%; implantable defibrillator system for primary prevention of sudden cardiac death; pulmonary hypertension; and hyperlipidemia. Family history is remarkable for diabetes, MI, and sudden death. Social history reveals that despite her ill health, she continues to smoke 1½ packs of cigarettes per day, as she has for the past 30 years. She denies alcohol or illicit drug use. Her medication list is extensive: digoxin, atorvastatin, metoprolol, ramipril, spironolactone, torsemide, aspirin, clopidogrel, omeprazole, ondansetron, insulin pump, sildenafil, and sublingual nitroglycerin. She is allergic to penicillin and cephalosporins. The review of systems is remarkable for early satiety with occasional nausea and vomiting. She states she has difficulty sleeping, and her spouse states she snores very loudly and has witnessed several apneic spells. Physical examination reveals an anxious, obese woman sitting in a wheelchair. Blood pressure is 89/50 mm Hg; pulse, 90 beats/min and regular; respiratory rate, 14 breaths/min; O2 saturation, 94% on room air; and temperature, 36.4°C. Pertinent physical findings include bilateral diabetic retinopathy, jugular venous pressures at 8 to 9 cm, brisk carotid upstrokes without bruits, and late expiratory wheezes in both lung bases. An implantable defibrillator is noted in the infraclavicular area on the left chest. The heart rate is regular, with a 3/6 holosystolic murmur (best heard at the left sternal border) that radiates to the left axilla. The abdomen is large, with the liver span palpable at the right costal margin, and an insulin pump is noted. The extremities reveal 2+ pitting edema to the knees bilaterally, and evidence of recent cellulitis is noted on the left leg below the knee. The neurologic exam is remarkable for diabetic paresthesias in both feet. As part of her work-up, an ECG is obtained and shows the following: a ventricular rate of 90 beats/min; PR interval, 138 ms; QRS duration, 88 ms; QT/QTc inter-val, 370/450 ms; P axis, 81°; R axis, –48°; and T axis, 75°. What is your interpretation of this ECG?
Woman with Discomfort and Discoloration on Back
ANSWER
The correct answer is erythema ab igne (choice “a”) caused, of course, by the effects of the heating pad. The reticular pattern and acute onset are quite characteristic of this unusual condition.
Contact dermatitis (choice “b”) would not have presented in this reticular pattern and would typically have itched intensely.
Cellulitis (choice “c”) represents a superficial infection usually caused by strep and/or staph. It would not have been reticular, would have been painful, and would have required a break in the skin for the offending organism to gain entrance.
Poikiloderma vasculare atrophicans (PVA; choice “d”) describes vascular changes seen focally in patches that evolve slowly over months or even years. It is significant because of its reported potential to evolve into cutaneous T-cell lymphoma; however, PVA does not present with a reticular pattern, nor does it appear acutely.
DISCUSSION
The superficial vascular plexus, configured in a reticular pattern and normally invisible, is sensitive to repeated exposure to the infrared portion of the magnetic spectrum (wavelength 700 to 1,100 nm). This exposure initially produces erythema, which over time turns livid, then permanently hyperpigmented.
Erythema ab igne (EAI) was classically seen in those sitting close to an open fire or stove (producing temperatures of 43°C to 47°C) for extended periods, often for hours each day. With the advent of central heating, other triggers of EAI evolved, including prolonged use of laptop computers, heating fans, and as in this case, heating pads. It can even be due to occupational exposure to intense heat, as with glassblowers, bakers, and steelworkers.
Most of the skin changes seen with EAI resemble those seen with chronic sun damage, including vasodilatation and melanin incontinence with melanophages in the upper dermis.
This particular patient had only one exposure to the heating pad, but had turned it on high and lain on it all night. This produced the changes seen, which will likely become permanently etched in her skin in the exact pattern of the causative heating pad. Months of dexamethasone therapy may also have contributed to the problem, by thinning the patient’s skin enough to render her susceptible to this single exposure to heat.
With EAI patients in general, thought needs to be given to possible underlying issues, such as the source of pain being treated with the heating pad—most commonly, on the low back—or the possible reason for constantly feeling cold, such as anemia or hypothyroidism.
Treatment choices include the application of tretinoin cream or 5-fluorouracil cream, or ablation with laser (YAG, ruby, alexandrite).
ANSWER
The correct answer is erythema ab igne (choice “a”) caused, of course, by the effects of the heating pad. The reticular pattern and acute onset are quite characteristic of this unusual condition.
Contact dermatitis (choice “b”) would not have presented in this reticular pattern and would typically have itched intensely.
Cellulitis (choice “c”) represents a superficial infection usually caused by strep and/or staph. It would not have been reticular, would have been painful, and would have required a break in the skin for the offending organism to gain entrance.
Poikiloderma vasculare atrophicans (PVA; choice “d”) describes vascular changes seen focally in patches that evolve slowly over months or even years. It is significant because of its reported potential to evolve into cutaneous T-cell lymphoma; however, PVA does not present with a reticular pattern, nor does it appear acutely.
DISCUSSION
The superficial vascular plexus, configured in a reticular pattern and normally invisible, is sensitive to repeated exposure to the infrared portion of the magnetic spectrum (wavelength 700 to 1,100 nm). This exposure initially produces erythema, which over time turns livid, then permanently hyperpigmented.
Erythema ab igne (EAI) was classically seen in those sitting close to an open fire or stove (producing temperatures of 43°C to 47°C) for extended periods, often for hours each day. With the advent of central heating, other triggers of EAI evolved, including prolonged use of laptop computers, heating fans, and as in this case, heating pads. It can even be due to occupational exposure to intense heat, as with glassblowers, bakers, and steelworkers.
Most of the skin changes seen with EAI resemble those seen with chronic sun damage, including vasodilatation and melanin incontinence with melanophages in the upper dermis.
This particular patient had only one exposure to the heating pad, but had turned it on high and lain on it all night. This produced the changes seen, which will likely become permanently etched in her skin in the exact pattern of the causative heating pad. Months of dexamethasone therapy may also have contributed to the problem, by thinning the patient’s skin enough to render her susceptible to this single exposure to heat.
With EAI patients in general, thought needs to be given to possible underlying issues, such as the source of pain being treated with the heating pad—most commonly, on the low back—or the possible reason for constantly feeling cold, such as anemia or hypothyroidism.
Treatment choices include the application of tretinoin cream or 5-fluorouracil cream, or ablation with laser (YAG, ruby, alexandrite).
ANSWER
The correct answer is erythema ab igne (choice “a”) caused, of course, by the effects of the heating pad. The reticular pattern and acute onset are quite characteristic of this unusual condition.
Contact dermatitis (choice “b”) would not have presented in this reticular pattern and would typically have itched intensely.
Cellulitis (choice “c”) represents a superficial infection usually caused by strep and/or staph. It would not have been reticular, would have been painful, and would have required a break in the skin for the offending organism to gain entrance.
Poikiloderma vasculare atrophicans (PVA; choice “d”) describes vascular changes seen focally in patches that evolve slowly over months or even years. It is significant because of its reported potential to evolve into cutaneous T-cell lymphoma; however, PVA does not present with a reticular pattern, nor does it appear acutely.
DISCUSSION
The superficial vascular plexus, configured in a reticular pattern and normally invisible, is sensitive to repeated exposure to the infrared portion of the magnetic spectrum (wavelength 700 to 1,100 nm). This exposure initially produces erythema, which over time turns livid, then permanently hyperpigmented.
Erythema ab igne (EAI) was classically seen in those sitting close to an open fire or stove (producing temperatures of 43°C to 47°C) for extended periods, often for hours each day. With the advent of central heating, other triggers of EAI evolved, including prolonged use of laptop computers, heating fans, and as in this case, heating pads. It can even be due to occupational exposure to intense heat, as with glassblowers, bakers, and steelworkers.
Most of the skin changes seen with EAI resemble those seen with chronic sun damage, including vasodilatation and melanin incontinence with melanophages in the upper dermis.
This particular patient had only one exposure to the heating pad, but had turned it on high and lain on it all night. This produced the changes seen, which will likely become permanently etched in her skin in the exact pattern of the causative heating pad. Months of dexamethasone therapy may also have contributed to the problem, by thinning the patient’s skin enough to render her susceptible to this single exposure to heat.
With EAI patients in general, thought needs to be given to possible underlying issues, such as the source of pain being treated with the heating pad—most commonly, on the low back—or the possible reason for constantly feeling cold, such as anemia or hypothyroidism.
Treatment choices include the application of tretinoin cream or 5-fluorouracil cream, or ablation with laser (YAG, ruby, alexandrite).

A 42-year-old woman presents with discoloration and discomfort involving her back. The discomfort, which started less than 24 hours ago, is not severe, but she is worried about the changes in color she can see in the mirror. Her history is significant for metastatic melanoma. She has been undergoing treatment with chemotherapy and localized radiation and for several months has been taking systemic steroids for intracerebral edema. Additional history taking reveals that the night before the appearance of the skin changes, she fell asleep lying on a heating pad because she was cold. She denies doing this habitually. Examination reveals a large patch of reticular erythema covering the entire central back, sharply sparing the area under the bra strap. The erythema is bounded laterally by sharply demarcated linear margins that mimic the exact shape and size of the heating pad in question. Focal blisters can be seen within the erythema, but the overall effect is macular (flat). Neither tenderness nor increased warmth is noted on palpation.

Elderly Man Failed To Mention Hip Pain After Fall
ANSWER
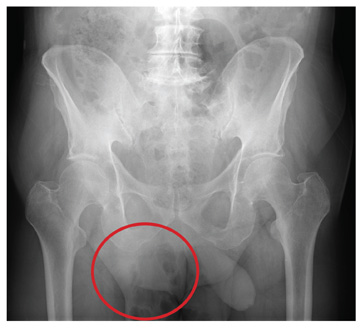
The radiograph demonstrates diffuse bony demineralization, as well as generalized degenerative changes. No obvious fracture or dislocation of the hip joint is seen.
Of note, though, are air lucencies within the area of the scrotum. This most likely represents a bowel finding and is strongly suggestive of an inguinal hernia. No acute intervention is warranted for this incidental finding; outpatient follow-up with general surgery was arranged.
ANSWER
The radiograph demonstrates diffuse bony demineralization, as well as generalized degenerative changes. No obvious fracture or dislocation of the hip joint is seen.
Of note, though, are air lucencies within the area of the scrotum. This most likely represents a bowel finding and is strongly suggestive of an inguinal hernia. No acute intervention is warranted for this incidental finding; outpatient follow-up with general surgery was arranged.
ANSWER
The radiograph demonstrates diffuse bony demineralization, as well as generalized degenerative changes. No obvious fracture or dislocation of the hip joint is seen.
Of note, though, are air lucencies within the area of the scrotum. This most likely represents a bowel finding and is strongly suggestive of an inguinal hernia. No acute intervention is warranted for this incidental finding; outpatient follow-up with general surgery was arranged.

An 87-year-old man is admitted to the hospital with a traumatic subarachnoid hemorrhage secondary to a fall down some steps. He is taking warfarin for atrial fibrillation; because his INR is elevated, he is placed in the ICU for close observation and warfarin reversal. His medical history is otherwise unremarkable, except for mild hypertension. During rounds, he complains of severe hip pain, possibly related to the fall. He admits that he “probably didn’t mention this” while he was in the emergency department. Physical examination demonstrates moderate tenderness and bruising in the left hip. No obvious leg shortening is noted. There is pain in the left hip with abduction and adduction, as well as with internal and external rotation. Good distal pulses are noted, as well as good color and sensation. His vital signs are normal. You order a portable pelvis radiograph (shown). What is your impression?

Should This Fitness Instructor Worry About Her Heart?
ANSWER
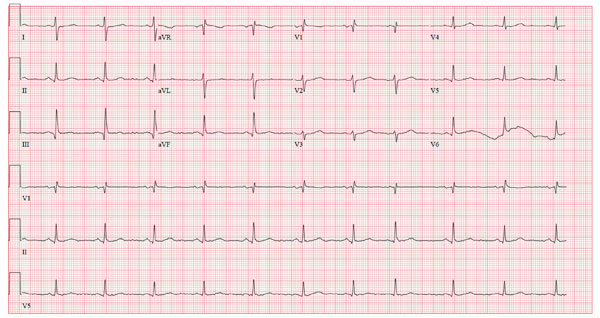
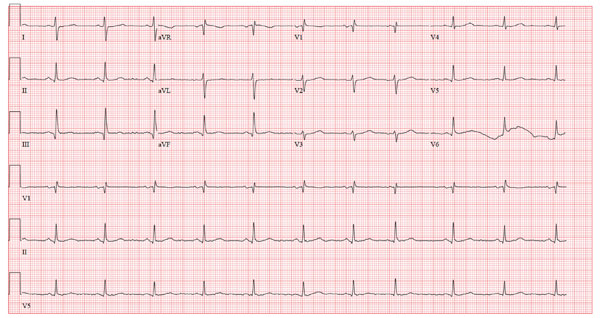
The ECG shows sinus tachycardia with premature atrial contractions. The premature atrial contractions occur at the 14th and 16th beats on the rhythm strip. They are evident by the shortened R-R interval preceding the beat, with the QRS complex appearing similar to the normal QRS complexes, signifying they propagate through the normal conduction system.
The P waves are hidden from view in the previous T wave. The nonspecific S- and T-wave abnormalities are physiologic in nature and of no consequence. Finally, the large S waves seen in the precordial leads are due to the patient’s thin body habitus and not to ventricular hypertrophy.
The patient was reassured that there were no structural abnormalities of her heart, and that there was no need to treat the premature contractions at this time. She was also asked to monitor her caffeine and energy drink intake to determine whether there was a correlation with her palpitations.
She was relieved to hear that there are no restrictions in her physical activity
ANSWER
The ECG shows sinus tachycardia with premature atrial contractions. The premature atrial contractions occur at the 14th and 16th beats on the rhythm strip. They are evident by the shortened R-R interval preceding the beat, with the QRS complex appearing similar to the normal QRS complexes, signifying they propagate through the normal conduction system.
The P waves are hidden from view in the previous T wave. The nonspecific S- and T-wave abnormalities are physiologic in nature and of no consequence. Finally, the large S waves seen in the precordial leads are due to the patient’s thin body habitus and not to ventricular hypertrophy.
The patient was reassured that there were no structural abnormalities of her heart, and that there was no need to treat the premature contractions at this time. She was also asked to monitor her caffeine and energy drink intake to determine whether there was a correlation with her palpitations.
She was relieved to hear that there are no restrictions in her physical activity
ANSWER
The ECG shows sinus tachycardia with premature atrial contractions. The premature atrial contractions occur at the 14th and 16th beats on the rhythm strip. They are evident by the shortened R-R interval preceding the beat, with the QRS complex appearing similar to the normal QRS complexes, signifying they propagate through the normal conduction system.
The P waves are hidden from view in the previous T wave. The nonspecific S- and T-wave abnormalities are physiologic in nature and of no consequence. Finally, the large S waves seen in the precordial leads are due to the patient’s thin body habitus and not to ventricular hypertrophy.
The patient was reassured that there were no structural abnormalities of her heart, and that there was no need to treat the premature contractions at this time. She was also asked to monitor her caffeine and energy drink intake to determine whether there was a correlation with her palpitations.
She was relieved to hear that there are no restrictions in her physical activity
A 38-year-old woman presents to your clinic with a two-year history of palpitations that have not increased in severity or frequency. Although they are bother-some, she has had no chest pain, shortness of breath, dyspnea on exertion, or peripheral edema. She denies any symptoms of tachycardia, bradycardia, syn-cope, or near syncope. She works at a local health club as a Zumba instructor and teaches four spinning classes per week. She recently learned that the health club will be closing. As a result, until she finds another position, she will be without benefits. She states she wants to “get this checked out” before she loses her medical insurance. Medical history is unremarkable, with the exception of a right clavicle fracture sustained at age 15. She began menses at age 12, has never been pregnant, and has never had surgery. Family history is remarkable for hypertension and diabetes. Her parents and three siblings are alive and well. The patient has no known drug allergies. Her medications include ibuprofen as needed for musculoskeletal pain and an oral contraceptive. She denies recreational drug use. The review of systems is unremarkable, and her last menstrual period was 11 days ago. On physical exam, she is a thin, well-developed, athletic-appearing woman in no distress. Her height is 69”, and her weight is 144 lb. Blood pressure is 108/56 mm Hg; pulse, 58 beats/min and regular; respiratory rate, 14 beats/min; and temperature, 98.4°F. There are no murmurs, gallops, or rubs on her cardiac exam. Her lungs are clear. Her abdomen is flat and nontender, with good bowel tones in all quadrants. There is no peripheral edema. Peripheral pulses are full and bounding bilaterally in all four extremities. The neurologic exam is normal. A chemistry panel, complete blood count, lipid panel, and thyroid function studies are ordered; the results are all within normal limits. A transthoracic echocardiogram shows normal valves, normal wall motion, and a left ventricular ejection fraction of 75%. A baseline ECG shows no ectopic beats. She is placed on a continuous rhythm monitor for 10 minutes, and no ectopic, premature, or dropped beats are seen. At that point, the patient remembers that the palpitations often occur just as she starts exercising, then go away once her heart rate is elevated. You have her do jumping jacks in the examination room for 30 seconds, and she states she can feel the palpitations. You quickly obtain an ECG, which reveals the following: a ventricular rate of 117 beats/min; PR interval, 158 ms; QRS duration, 110 ms; QT/QTc interval, 336/468 ms; P axis, 57°; R axis, 15°; and T axis, 153°. What is your interpretation of this ECG?
Skin Change and Fatigue Forces Woman to Take Leave of Absence
ANSWER
The correct answer is dermatomyositis (choice “c”), thought to be a vasculopathy mediated by the deposition of complement and lysis of capillaries in skin and muscle.
Carcinoid (choice “a”) is a rare tumor that can release vasoactive peptides, which cause episodic flushing, and if prolonged, can cause permanent changes in the skin. But carcinoid involves neither muscle weakness nor the particular skin changes seen with dermatomyositis.
Lupus erythematosus (choice “b”) can present with similar symptoms. However, when it affects the fingers, it specifically affects the interphalangeal skin, sharply sparing the knuckles. Both lupus erythematosus and mixed connective tissue disease (MCTD; choice “d”) can present with similar changes in the cuticles, but neither present with such profound muscle weakness.
DISCUSSION
Dermatomyositis is one of three main conditions that present with characteristic changes in the cuticular vasculature (the other two being scleroderma and MCTD). The definitive diagnosis is usually made by a rheumatologist, who is able to distinguish dermatomyositis from the rest of the differential—a process that can be rather complex.
The first diagnostic step is to identify the changes to the cuticular vasculature. These must be specifically sought; they are not always as obvious as in this case. Fortunately, magnification can easily be carried out with either an ophthalmoscope or dermatoscope, an examination enhanced by the application of oil first.
These findings, along with sunburn-like eruptions on the neck and face, should prompt laboratory testing. Significant results would include a positive antinuclear antibody test and elevations of the muscle enzymes creatine kinase and aldolase. Skin biopsy is helpful, though not diagnostic by itself. Additional studies might include a barium swallow, which would show weak pharyngeal muscles, and either an electromyography or MRI, which would demonstrate characteristic muscle changes secondary to inflammation.
Perhaps the most important aspect of dermatomyositis is its connection to cancer. A significant percentage of adults diagnosed with dermatomyositis will also have an associated and often occult malignancy, which may be found before, during, or after the diagnosis of dermatomyositis. (Juvenile dermatomyositis is not associated with malignancy.)
Patient age, constitutional symptoms, rapidity of onset, high level of serum muscle enzymes, grossly elevated erythrocyte sedimentation rate, and severity of dermatomyositis are all factors that would prompt an aggressive search for malignancies, the types of which mirror those seen in the general population. In such cases, surgical and/or medical cures of causative cancer usually stop the dermatomyositis as well.
The workup on this particular patient is still underway, but she is already responding to therapy with prednisone (1 mg/kg/d), to be taken until muscle enzymes are normal. This can take months, with dosage reduced as symptoms respond. Steroid-sparing agents, such as methotrexate or azathioprine, are often begun as prednisone levels are reduced.
SUGGESTED READING
James WD, Berger T, Elston D. Andrews’ Diseases of the Skin: Clinical Dermatology. 10th ed. Saunders; 2005:166-170.
Bergman R, Sharony L, Schapira D, et al. The handheld dermatoscope as a nail-fold capillaroscopic instrument. Arch Dermatol. 2003;139(8): 1027-1030.
ANSWER
The correct answer is dermatomyositis (choice “c”), thought to be a vasculopathy mediated by the deposition of complement and lysis of capillaries in skin and muscle.
Carcinoid (choice “a”) is a rare tumor that can release vasoactive peptides, which cause episodic flushing, and if prolonged, can cause permanent changes in the skin. But carcinoid involves neither muscle weakness nor the particular skin changes seen with dermatomyositis.
Lupus erythematosus (choice “b”) can present with similar symptoms. However, when it affects the fingers, it specifically affects the interphalangeal skin, sharply sparing the knuckles. Both lupus erythematosus and mixed connective tissue disease (MCTD; choice “d”) can present with similar changes in the cuticles, but neither present with such profound muscle weakness.
DISCUSSION
Dermatomyositis is one of three main conditions that present with characteristic changes in the cuticular vasculature (the other two being scleroderma and MCTD). The definitive diagnosis is usually made by a rheumatologist, who is able to distinguish dermatomyositis from the rest of the differential—a process that can be rather complex.
The first diagnostic step is to identify the changes to the cuticular vasculature. These must be specifically sought; they are not always as obvious as in this case. Fortunately, magnification can easily be carried out with either an ophthalmoscope or dermatoscope, an examination enhanced by the application of oil first.
These findings, along with sunburn-like eruptions on the neck and face, should prompt laboratory testing. Significant results would include a positive antinuclear antibody test and elevations of the muscle enzymes creatine kinase and aldolase. Skin biopsy is helpful, though not diagnostic by itself. Additional studies might include a barium swallow, which would show weak pharyngeal muscles, and either an electromyography or MRI, which would demonstrate characteristic muscle changes secondary to inflammation.
Perhaps the most important aspect of dermatomyositis is its connection to cancer. A significant percentage of adults diagnosed with dermatomyositis will also have an associated and often occult malignancy, which may be found before, during, or after the diagnosis of dermatomyositis. (Juvenile dermatomyositis is not associated with malignancy.)
Patient age, constitutional symptoms, rapidity of onset, high level of serum muscle enzymes, grossly elevated erythrocyte sedimentation rate, and severity of dermatomyositis are all factors that would prompt an aggressive search for malignancies, the types of which mirror those seen in the general population. In such cases, surgical and/or medical cures of causative cancer usually stop the dermatomyositis as well.
The workup on this particular patient is still underway, but she is already responding to therapy with prednisone (1 mg/kg/d), to be taken until muscle enzymes are normal. This can take months, with dosage reduced as symptoms respond. Steroid-sparing agents, such as methotrexate or azathioprine, are often begun as prednisone levels are reduced.
SUGGESTED READING
James WD, Berger T, Elston D. Andrews’ Diseases of the Skin: Clinical Dermatology. 10th ed. Saunders; 2005:166-170.
Bergman R, Sharony L, Schapira D, et al. The handheld dermatoscope as a nail-fold capillaroscopic instrument. Arch Dermatol. 2003;139(8): 1027-1030.
ANSWER
The correct answer is dermatomyositis (choice “c”), thought to be a vasculopathy mediated by the deposition of complement and lysis of capillaries in skin and muscle.
Carcinoid (choice “a”) is a rare tumor that can release vasoactive peptides, which cause episodic flushing, and if prolonged, can cause permanent changes in the skin. But carcinoid involves neither muscle weakness nor the particular skin changes seen with dermatomyositis.
Lupus erythematosus (choice “b”) can present with similar symptoms. However, when it affects the fingers, it specifically affects the interphalangeal skin, sharply sparing the knuckles. Both lupus erythematosus and mixed connective tissue disease (MCTD; choice “d”) can present with similar changes in the cuticles, but neither present with such profound muscle weakness.
DISCUSSION
Dermatomyositis is one of three main conditions that present with characteristic changes in the cuticular vasculature (the other two being scleroderma and MCTD). The definitive diagnosis is usually made by a rheumatologist, who is able to distinguish dermatomyositis from the rest of the differential—a process that can be rather complex.
The first diagnostic step is to identify the changes to the cuticular vasculature. These must be specifically sought; they are not always as obvious as in this case. Fortunately, magnification can easily be carried out with either an ophthalmoscope or dermatoscope, an examination enhanced by the application of oil first.
These findings, along with sunburn-like eruptions on the neck and face, should prompt laboratory testing. Significant results would include a positive antinuclear antibody test and elevations of the muscle enzymes creatine kinase and aldolase. Skin biopsy is helpful, though not diagnostic by itself. Additional studies might include a barium swallow, which would show weak pharyngeal muscles, and either an electromyography or MRI, which would demonstrate characteristic muscle changes secondary to inflammation.
Perhaps the most important aspect of dermatomyositis is its connection to cancer. A significant percentage of adults diagnosed with dermatomyositis will also have an associated and often occult malignancy, which may be found before, during, or after the diagnosis of dermatomyositis. (Juvenile dermatomyositis is not associated with malignancy.)
Patient age, constitutional symptoms, rapidity of onset, high level of serum muscle enzymes, grossly elevated erythrocyte sedimentation rate, and severity of dermatomyositis are all factors that would prompt an aggressive search for malignancies, the types of which mirror those seen in the general population. In such cases, surgical and/or medical cures of causative cancer usually stop the dermatomyositis as well.
The workup on this particular patient is still underway, but she is already responding to therapy with prednisone (1 mg/kg/d), to be taken until muscle enzymes are normal. This can take months, with dosage reduced as symptoms respond. Steroid-sparing agents, such as methotrexate or azathioprine, are often begun as prednisone levels are reduced.
SUGGESTED READING
James WD, Berger T, Elston D. Andrews’ Diseases of the Skin: Clinical Dermatology. 10th ed. Saunders; 2005:166-170.
Bergman R, Sharony L, Schapira D, et al. The handheld dermatoscope as a nail-fold capillaroscopic instrument. Arch Dermatol. 2003;139(8): 1027-1030.
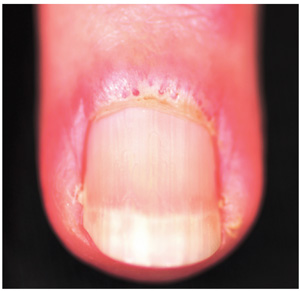
A three-month history of muscle weakness, fatigue, and skin changes prompts a 59-year-old woman to self-refer to dermatology. Otherwise healthy prior to the onset of these symptoms, she has had to take a leave of absence from work due to her inability to carry out her duties, which include light lifting and prolonged periods of time on her feet as a clerk in a pharmacy. She first consulted her primary care provider (PCP), who informed her that she was not anemic and did not have thyroid disease; the PCP felt that stress was probably a factor. She then purchased a number of products from her health food store, which she started taking until the skin on her hands began to change. On examination, atrophic pinkish red planar plaques are noted on 10/10 fingers, confined to the dorsal aspects of her joints and sharply sparing the interphalangeal spaces. The cuticles demonstrate the presence of dilated and irregularly shaped capillary loops. Several of her cuticles are also overgrown and frayed. Examination of the rest of the patient’s skin reveals a blanchable, faintly sunburned appearance to her anterior neck.

Woman with Metabolic Syndrome
ANSWER
The correct interpretation of this ECG includes sinus rhythm with frequent premature ventricular complexes (PVCs), a T-wave abnormality suggesting lateral ischemia, and a prolonged QT interval.
PVCs occur when conduction of the ventricular myocardium occurs without involving the normal His-Purkinje system. They are responsible for the patient’s irregular pulse.
A prolonged QT interval is evidenced by a QTc interval > 440 ms. The QTc is calculated from Bazett’s formula, which states the QTc = QT interval divided by the square root of the previous R-R interval. The normal range for a QTc is generally considered to be 350 to 440 ms.
Inverted T waves in leads V3 to V6 are suggestive of lateral ischemia. However, they are also seen in subacute or old pericarditis and myocarditis, so clinical correlation is required. The patient has had no recent or remote episodes of chest pain or chest discomfort in the past year.
ANSWER
The correct interpretation of this ECG includes sinus rhythm with frequent premature ventricular complexes (PVCs), a T-wave abnormality suggesting lateral ischemia, and a prolonged QT interval.
PVCs occur when conduction of the ventricular myocardium occurs without involving the normal His-Purkinje system. They are responsible for the patient’s irregular pulse.
A prolonged QT interval is evidenced by a QTc interval > 440 ms. The QTc is calculated from Bazett’s formula, which states the QTc = QT interval divided by the square root of the previous R-R interval. The normal range for a QTc is generally considered to be 350 to 440 ms.
Inverted T waves in leads V3 to V6 are suggestive of lateral ischemia. However, they are also seen in subacute or old pericarditis and myocarditis, so clinical correlation is required. The patient has had no recent or remote episodes of chest pain or chest discomfort in the past year.
ANSWER
The correct interpretation of this ECG includes sinus rhythm with frequent premature ventricular complexes (PVCs), a T-wave abnormality suggesting lateral ischemia, and a prolonged QT interval.
PVCs occur when conduction of the ventricular myocardium occurs without involving the normal His-Purkinje system. They are responsible for the patient’s irregular pulse.
A prolonged QT interval is evidenced by a QTc interval > 440 ms. The QTc is calculated from Bazett’s formula, which states the QTc = QT interval divided by the square root of the previous R-R interval. The normal range for a QTc is generally considered to be 350 to 440 ms.
Inverted T waves in leads V3 to V6 are suggestive of lateral ischemia. However, they are also seen in subacute or old pericarditis and myocarditis, so clinical correlation is required. The patient has had no recent or remote episodes of chest pain or chest discomfort in the past year.
A 50-year-old woman with metabolic syndrome presents for a routine clinic appointment. You quickly review the five criteria of metabolic syndrome: • Fasting blood glucose ≥ 110 mg/dL • Waist circumference ≥ 40” in men or ≥ 35” in women • Triglycerides ≥ 150 mg/dL • HDL cholesterol < 40 ¬mg/dL in men or < 50 mg/dL in women • Blood pressure ≥ 130/85 mm Hg. The patient’s last clinic visit was four months ago; since then, she has done well and has no specific complaints or concerns. She denies angina, palpitations, dizziness, syncope, or dyspnea. Medical history is significant for New York Heart Association class III heart failure and cardiomyopathy secondary to myopericarditis with small-vessel coronary artery disease, as well as depression with anxiety. She also has a history of obstructive sleep apnea, but refuses to use a constant positive airway pressure (CPAP) machine at night due to claustrophobia. She attempts to control her diabetes with diet and exercise but admits she isn’t very compliant. Her medication list includes amlodipine, furosemide, carvedilol, lisinopril, isosorbide dinitrate, hydralazine, spironolactone, simvastatin, citalopram, omeprazole, and oxybutynin. She is allergic to ampicillin, methocarbamol, and codeine. The patient’s family history is unknown, as she was adopted. She works as a comptroller for a municipality in the suburbs, is recently divorced, and does not smoke or drink. Her review of systems is remarkable for headaches, anxiety, and loneliness following her divorce. She denies thoughts of injuring herself or suicide. Physical examination reveals a blood pressure of 118/64 mm Hg; pulse, 88 beats/min and irregular; respiratory rate, 16 breaths/min-1; and temperature, 99.2°F. Her weight is unchanged from her last visit. Her lungs are clear bilaterally, the jugular venous pressure is approximately 4 cm, and her cardiac exam reveals no murmurs, rubs, or extra heart sounds. Her abdomen is benign, and she has strong pulses bilaterally with 1+ pitting edema in both lower extremities, limited to the ankles. Laboratory data demonstrate chemical and lipid profiles and complete blood count within normal limits. An echocardiogram performed at her previous visit showed a left ventricular ejection fraction of 45%, with a mildly enlarged left ventricle, normal right ventricular size and function, and no valvular anomalies. It has been a year since her last ECG, so you decide to order one. It reveals the following: a ventricular rate of 87 beats/min; PR interval, 138 ms; QRS duration, 86 ms; QT/QTc interval, 388/466 ms; P axis, 61°; R axis, 43°; and T axis, 9°. What is your interpretation of this ECG?
Immunosuppressed Woman with Lesion on Her Thumb
ANSWER
The correct answer is basal cell carcinoma (choice “d”), which only rarely affects the hands; it is far more common on more directly sun-exposed skin (eg, face, neck, and back).
Immunosuppressed individuals are at increased risk for squamous cell carcinoma (SCC; choice “a”), particularly those cancers associated with the human papillomavirus. These can present as odd plaques on the hands, so SCC belongs in the differential.
Mycobacterial infection (choice “b”) will demonstrate caseating (necrotic) granulomas and positive stains for acid-fast bacilli such as M marinum or M fortuitum; however, it can manifest with plaques.
Sarcoid (choice “c”) can be lesional and is thought to represent a reaction to an unknown antigen. Often reddish brown in color with plaquish morphology, sarcoid also demonstrates granulomatous changes microscopically; however, these are noncaseating epithelioid granulomas with no palisading.
DISCUSSION
Since granuloma annulare (GA) is notorious for appearing as papules and plaques on the extremities of females, this diagnosis was not a surprise. Often, GA is so obvious that a biopsy is unnecessary. However, given the patient’s immunosuppressed state and the many serious diagnostic possibilities to be ruled out (cancer was a possibility, and had the lesion represented sarcoidosis, it could have been the tip of a serious iceberg involving the liver, lung, or even heart), biopsy was the only option. As is often the case, thought was given to the site selected, in order to avoid damage to local structures or the creation of nonhealing wounds.
GA can occur in several forms, this patient’s case representing the most common one. It can also present as a generalized eruption, in a subcutaneous form, or even with blistering. At one time, it was thought that having GA meant that the patient had or was about to develop diabetes, but that assertion has long since been disproven.
Once diagnosed, GA does not really require treatment since it is self-limiting. However, treatment choices for this form include class 2 steroid creams or liquid nitrogen. This patient opted to do nothing, but she was very relieved to have ruled out more serious disease.
ANSWER
The correct answer is basal cell carcinoma (choice “d”), which only rarely affects the hands; it is far more common on more directly sun-exposed skin (eg, face, neck, and back).
Immunosuppressed individuals are at increased risk for squamous cell carcinoma (SCC; choice “a”), particularly those cancers associated with the human papillomavirus. These can present as odd plaques on the hands, so SCC belongs in the differential.
Mycobacterial infection (choice “b”) will demonstrate caseating (necrotic) granulomas and positive stains for acid-fast bacilli such as M marinum or M fortuitum; however, it can manifest with plaques.
Sarcoid (choice “c”) can be lesional and is thought to represent a reaction to an unknown antigen. Often reddish brown in color with plaquish morphology, sarcoid also demonstrates granulomatous changes microscopically; however, these are noncaseating epithelioid granulomas with no palisading.
DISCUSSION
Since granuloma annulare (GA) is notorious for appearing as papules and plaques on the extremities of females, this diagnosis was not a surprise. Often, GA is so obvious that a biopsy is unnecessary. However, given the patient’s immunosuppressed state and the many serious diagnostic possibilities to be ruled out (cancer was a possibility, and had the lesion represented sarcoidosis, it could have been the tip of a serious iceberg involving the liver, lung, or even heart), biopsy was the only option. As is often the case, thought was given to the site selected, in order to avoid damage to local structures or the creation of nonhealing wounds.
GA can occur in several forms, this patient’s case representing the most common one. It can also present as a generalized eruption, in a subcutaneous form, or even with blistering. At one time, it was thought that having GA meant that the patient had or was about to develop diabetes, but that assertion has long since been disproven.
Once diagnosed, GA does not really require treatment since it is self-limiting. However, treatment choices for this form include class 2 steroid creams or liquid nitrogen. This patient opted to do nothing, but she was very relieved to have ruled out more serious disease.
ANSWER
The correct answer is basal cell carcinoma (choice “d”), which only rarely affects the hands; it is far more common on more directly sun-exposed skin (eg, face, neck, and back).
Immunosuppressed individuals are at increased risk for squamous cell carcinoma (SCC; choice “a”), particularly those cancers associated with the human papillomavirus. These can present as odd plaques on the hands, so SCC belongs in the differential.
Mycobacterial infection (choice “b”) will demonstrate caseating (necrotic) granulomas and positive stains for acid-fast bacilli such as M marinum or M fortuitum; however, it can manifest with plaques.
Sarcoid (choice “c”) can be lesional and is thought to represent a reaction to an unknown antigen. Often reddish brown in color with plaquish morphology, sarcoid also demonstrates granulomatous changes microscopically; however, these are noncaseating epithelioid granulomas with no palisading.
DISCUSSION
Since granuloma annulare (GA) is notorious for appearing as papules and plaques on the extremities of females, this diagnosis was not a surprise. Often, GA is so obvious that a biopsy is unnecessary. However, given the patient’s immunosuppressed state and the many serious diagnostic possibilities to be ruled out (cancer was a possibility, and had the lesion represented sarcoidosis, it could have been the tip of a serious iceberg involving the liver, lung, or even heart), biopsy was the only option. As is often the case, thought was given to the site selected, in order to avoid damage to local structures or the creation of nonhealing wounds.
GA can occur in several forms, this patient’s case representing the most common one. It can also present as a generalized eruption, in a subcutaneous form, or even with blistering. At one time, it was thought that having GA meant that the patient had or was about to develop diabetes, but that assertion has long since been disproven.
Once diagnosed, GA does not really require treatment since it is self-limiting. However, treatment choices for this form include class 2 steroid creams or liquid nitrogen. This patient opted to do nothing, but she was very relieved to have ruled out more serious disease.

Referred by her primary care provider, a 63-year-old woman presents to dermatology for evaluation of an asymptomatic lesion on her thumb. The lesion has slowly grown over a period of years and has persisted despite attempted treatment with topical steroid creams, antifungal cream, and cryotherapy. She denies any other similar occurrences or indeed any skin problems in general. She has a dense medical history, mostly revolving around a heart transplant several years ago that necessitated ongoing immune suppression. This apparently played a role in the development of two squamous cell carcinomas (one on the face, the other on an arm), both successfully dealt with surgically. She admits that as a teenager she tanned and sunburned repeatedly. She specifically denies having diabetes. On examination, the lesion proves to be a reddish brown, roughly ovoid plaque measuring about 3 x 2 cm, located on the medial right thumb. Its surface is smooth and nontender to touch, with no focal papularity and no scaling. Given the failure of previous treatments and the patient’s immunosuppressed state, the decision is made to perform punch biopsy on the site. Care is taken to avoid the neurovascular bundle on the mid-lateral aspect of the digit, and the 3-mm defect is closed with a single nylon suture. The pathology report shows foci of degenerative collagen associated with palisaded granulomatous inflammation.

Alaskan Man is Concerned About Going Home
ANSWER
The correct interpretation includes normal sinus rhythm with a premature supraventricular complex, a rightward axis, and a QR pattern in V1 suggestive of right ventricular conduction delay.
The eighth beat in the rhythm strip is the premature supraventricular complex. It occurs earlier than the rate of the normal sinus rhythm, and there is a compensatory pause prior to resumption of the next sinus beat.
A right axis is evidenced by an R-wave axis > 100° and is common in chronic obstructive pulmonary disease. Right ventricular conduction delay, or incomplete right bundle branch block, occurs when conduction is slowed through the right bundle. ECG criteria include an RSR’ or QR pattern with a QRS duration of 100 to 120 ms, with similar terminal features of a normal QRS. In this case, the QRS pattern is < 100 ms; however, the QR pattern in lead V1 is suspicious.
ANSWER
The correct interpretation includes normal sinus rhythm with a premature supraventricular complex, a rightward axis, and a QR pattern in V1 suggestive of right ventricular conduction delay.
The eighth beat in the rhythm strip is the premature supraventricular complex. It occurs earlier than the rate of the normal sinus rhythm, and there is a compensatory pause prior to resumption of the next sinus beat.
A right axis is evidenced by an R-wave axis > 100° and is common in chronic obstructive pulmonary disease. Right ventricular conduction delay, or incomplete right bundle branch block, occurs when conduction is slowed through the right bundle. ECG criteria include an RSR’ or QR pattern with a QRS duration of 100 to 120 ms, with similar terminal features of a normal QRS. In this case, the QRS pattern is < 100 ms; however, the QR pattern in lead V1 is suspicious.
ANSWER
The correct interpretation includes normal sinus rhythm with a premature supraventricular complex, a rightward axis, and a QR pattern in V1 suggestive of right ventricular conduction delay.
The eighth beat in the rhythm strip is the premature supraventricular complex. It occurs earlier than the rate of the normal sinus rhythm, and there is a compensatory pause prior to resumption of the next sinus beat.
A right axis is evidenced by an R-wave axis > 100° and is common in chronic obstructive pulmonary disease. Right ventricular conduction delay, or incomplete right bundle branch block, occurs when conduction is slowed through the right bundle. ECG criteria include an RSR’ or QR pattern with a QRS duration of 100 to 120 ms, with similar terminal features of a normal QRS. In this case, the QRS pattern is < 100 ms; however, the QR pattern in lead V1 is suspicious.
A 65-year-old man who lives in a remote village in Alaska is in your area on vacation. He presents to your office stating he has had a cold for the past three weeks that “just won’t go away.” He has tried several OTC medications without success, and he now has a productive cough. You notice as you walk into the examining room that it reeks of cigarette smoke. On questioning the patient, you learn that he has smoked two to three packs of cigarettes a day for most of his life. He is proud to announce that now he is down to 1.5 packs per day. He denies chest pain, fevers, chills, or night sweats, but admits that he is more short of breath than usual and has discomfort in his right chest. He can only walk 25 or 30 feet before he must rest, and he cannot climb one flight of stairs without stopping. He plans to return home in four days and is concerned that he won’t be able to function independently, stating, “You can die up there pretty easily if you’re not up to speed.” His medical history is remarkable for coronary artery disease with three-vessel coronary artery revascularization in 2004, paroxysmal atrial fibrillation, dyslipidemia, chronic obstructive pulmonary disease, and arthritis. Current medications include allopurinol, aspirin, atenolol, fluticasone-salmeterol and albuterol inhalers, folic acid, furosemide, isosorbide mononitrate, lisinopril, potassium chloride, rosuvastatin, and warfarin. He acknowledges that he does not take his warfarin routinely. He is allergic to codeine. Family history is remarkable for a father who died of a myocardial infarction at age 63, and two younger brothers who have had coronary revascularization procedures. He is a retired commercial fisherman who lives alone. He admits to drinking one six-pack of beer per day and occasionally smoking marijuana. A review of systems is remarkable for recurring headaches and a 10-lb weight loss over the past three months. The physical exam reveals a disheveled man in no distress. His blood pressure is 160/94 mm Hg; pulse, 70 beats/min; respirations, 18 breaths/min-1; and temperature, 100.4°F. His teeth are in poor repair, with multiple caries. The lungs reveal diminished vesicular breath sounds throughout with late inspiratory crackles in the right upper lung fields and few breath sounds with late expiratory wheezes in the right lower quadrant. The neck veins are flat, and there are no murmurs, rubs, or extra heart sounds. The abdomen is obese but benign, and there are no neurologic findings. Pertinent laboratory findings include a white blood count of 14,300/mm3 with 75% neutrophils, 20% bands, and 15% lymphocytes. A chest x-ray reveals normal cardiac size, sternotomy wires and surgical clips, and right lower-lobe consolidation consistent with right lower lobe pneumonia. An ECG shows the following: a ventricular rate of 65 beats/min; PR interval, 162 ms; QRS duration, 90 ms; QT/QTc interval, 448/465 ms; P axis, 60°; R axis, 101°; and T axis, 55°. What is your interpretation of this ECG?
Woman With Back Pain Unable To Walk
ANSWER
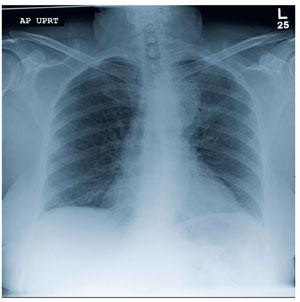
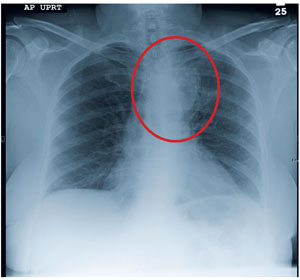
The radiograph demonstrates a fairly large mass on the medial aspect of the left upper lobe. Such findings are usually associated with bronchogenic carcinomas.
Among the documentation from the transferring facility was a copy of a CT scan of the patient’s chest. On that study, the mass is seen; it appears to extend to the posterior chest wall, with extensive involvement and destruction of the ribs and posterior elements of T4 and T5. There is also evidence of some spinal cord compression, which would explain the patient’s presenting complaint.
Subsequent CT-guided biopsy demonstrated the lesion to be a non–small cell carcinoma. Due to the already extensive involvement, surgery was not an option, and the patient was referred for palliative radiation therapy.
ANSWER
The radiograph demonstrates a fairly large mass on the medial aspect of the left upper lobe. Such findings are usually associated with bronchogenic carcinomas.
Among the documentation from the transferring facility was a copy of a CT scan of the patient’s chest. On that study, the mass is seen; it appears to extend to the posterior chest wall, with extensive involvement and destruction of the ribs and posterior elements of T4 and T5. There is also evidence of some spinal cord compression, which would explain the patient’s presenting complaint.
Subsequent CT-guided biopsy demonstrated the lesion to be a non–small cell carcinoma. Due to the already extensive involvement, surgery was not an option, and the patient was referred for palliative radiation therapy.
ANSWER
The radiograph demonstrates a fairly large mass on the medial aspect of the left upper lobe. Such findings are usually associated with bronchogenic carcinomas.
Among the documentation from the transferring facility was a copy of a CT scan of the patient’s chest. On that study, the mass is seen; it appears to extend to the posterior chest wall, with extensive involvement and destruction of the ribs and posterior elements of T4 and T5. There is also evidence of some spinal cord compression, which would explain the patient’s presenting complaint.
Subsequent CT-guided biopsy demonstrated the lesion to be a non–small cell carcinoma. Due to the already extensive involvement, surgery was not an option, and the patient was referred for palliative radiation therapy.
A 63-year-old woman is transferred to your facility for evaluation of acute lower extremity paralysis. She has had ongoing back pain for the past several months. Yesterday, she noticed her legs were dragging; last night, she was unable to walk, which prompted her trip to the local emergency department. She says she had “some sort of scan” there and was told that she had a tumor on her spine. She denies any injury or trauma. Her medical history is significant for reflux, hypertension, and extensive tobacco use. She is in no obvious distress, and her vital signs are normal. Physical exam demonstrates extreme weakness in both lower extremities, from the hips down and worse on the left side. She has decreased sensation and reflexes as well. As you review the rest of her transfer paperwork and try to find any imaging studies or reports, the radiology technician collects the patient for a chest radiograph (the result of which is shown). What is your impression?