User login
Residents Improving Quality
To Err Is Human revealed the underappreciated tension between the enormous benefits of medical care and the potential for harm.1 Following this report, there has been an explosion of research and commentary detailing quality improvement (QI) opportunities. One area of growing emphasis has been resident physician training.2, 3 If medical care is dangerous, then a substantial contributor to the hazard must be the apprentice‐style process of physician training and the novice skill set of the trainees.4, 5 Many resident training programs have devised efforts to decrease the errors committed by physicians‐in‐training,6 change the culture of residency training,7 engage residents in quality improvement,8, 9 and improve resident training in quality improvement.10
Many of the programs devised to teach QI in the residency setting require substantial funding, a large pool of QI experts, or redesign of resident training programs.410 While effective, these programs are not feasible for many resource‐constrained residency programs. A less intense program, using resident‐led, hospitalist‐facilitated, limited root cause analysis (RCA), has been adopted at the Internal Medicine Residency Program at the Mount Sinai Hospital (MSH). We describe our 2‐year experience using this technique, including cases discussed, improvement strategies suggested, projects implemented, and resident perceptions.
METHODS
Setting
Departmental QI leaders developed this initiative in the Internal Medicine Residency Program at the MSH in New York City, New York. This residency program trains over 140 residents annually in categorical, preliminary, and research track positions, as well as an affiliated medicine/pediatrics program. The program's residents rotate at 3 clinic sites: a tertiary care hospital, a public safety‐net hospital, and a Veterans Affairs hospital. The QI program was only implemented at the MSH. Over 90% of the program's graduates go on to complete a subspecialty fellowship.
Intervention Description
The QI program was designed around a noon‐time quality improvement conference (QIC) occurring once every 4 weeks. In the weeks prior to the session, chief residents and a hospitalist mentor selected a case related to an inpatient care issue. Potential cases were solicited, and/or offered, from a range of sources including attending physicians, nurse managers, residents, and quality officers. Only cases from the teaching services were chosen. To ensure that participants on the case were able to recall relevant details, preference was given to more recent cases. A third‐year resident on an elective or outpatient block was chosen to investigate the case. To maximize the objectivity of the investigation, every effort was made to select a resident who was not involved in the care of the patient.
The resident was instructed to complete a limited RCA (fewer fact‐finding interviews and only 1 group meeting) and was directed to online resources.11 Each resident presenter worked closely with the chief residents and hospitalist mentor to identify appropriate strategies for collecting data and interviewing involved parties. If necessary, either due to volume of work or sensitivity of the case, the chief resident or hospitalist would assist with the data gathering. The resident contacted multiple parties involved in the patient care issue including, nurses, residents, attendings, pharmacists, social workers, and, if appropriate, the patient. The resident constructed a timeline for each case, and identified specific points in the patient care experience, where errors, near misses, or misunderstandings occurred. During the QIC, these findings were presented to Internal Medicine residents, chief residents, representatives from the Chief Medical Officer's office, attending physicians overseeing the residents on inpatient rotations, and representatives from any group (social work nursing, housekeeping, pharmacy, etc) that may have impacted patient care for the particular case being investigated. On average, 50 healthcare providers attended the QIC. Lunch was provided.
After the findings were presented, a chief resident and a lead hospitalist facilitated a group discussion on the circumstances surrounding the case. Discussions were focused on identifying system‐wide failures and proposing systems‐based solutions. Great efforts were made to remind all participants to refrain from individual blame. At the end of each QIC, participants summarized and prioritized suggestions to reduce the discussed error. Interested residents were invited to form improvement committees for cases with viable solutions. Each committee attempted to implement improvements discussed during the QIC. Committees, led by a representative from the Division of Hospital Medicine, included 2 to 4 residents as well as healthcare workers from other disciplines if appropriate. For all improvement efforts, the focus was on the interventions which appeared high yield with low cost.
Intervention Evaluation
The program was exempt from Institutional Review Board review as a part of the Department of Medicine's quality improvement and assurance portfolio.
The results of the QICs were tracked. After each case, a QI team consisting of chief residents and representatives from the Division of Hospital Medicine recorded the cases presented, and interventions suggested for each case, in an online database. After implementation, the success of each intervention was recorded. To evaluate the types of interventions suggested by residents, the 3 physician‐authors, who regularly attend these conferences and have a focused career interest in QI, grouped all suggestions into 4 broad categories: Educational, Reminder Systems, Design Changes (protocol‐based), and Design Changes (Information Technology [IT]‐based). Design change interventions (IT‐based) consisted of an adjustment to electronic systems, such as displaying specific lab results on a medication ordering system. Design changes (protocol‐based) consisted of changes made to standing protocols such as nursing protocols for reporting abnormal lab values. Reminder system interventions were endeavors such as a checklist for discharge planning. Educational interventions focused on providing additional training sessions or conferences.
The 3 physician‐authors independently reviewed each suggested intervention to determine its success. They first evaluated whether the change was attempted or not. For all attempted interventions, the reviewer then assessed if there was either objective permanent system‐wide change, subjective behavior change, or no change. To meet the objective change threshold, the intervention either had to have permanently changed provider workflow or have data demonstrating behavior change or improved outcome. Interventions with anecdotal evidence that behavior was improved or modified, but lacking systematic data, were qualified as subjective behavior change. For each assessment, 2 of the 3 reviewers needed to agree for an intervention to be recorded as a success.
Resident views on the monthly conferences were solicited via an anonymous and voluntary questionnaire. A first survey was designed to assess whether residents felt that the conferences provided them with the ability to recognize and improve systems errors which compromise patient care. This survey was administered at the conclusion of the first year of the program to residents who attended the final 2 QICs. A second survey assessed whether the tone of the conferences was constructive and blame‐free. This survey was administered at the conclusion of the second year of the program to residents who attended the year's final 2 QICs.
RESULTS
Over the first 22 months of the program, 20 conferences were held (Table 1). The topics covered ranged considerably and included: deficits in supervision, medication errors, patient satisfaction, staff safety, and 30‐day readmissions. Forty‐six distinct interventions were suggested during these conferences. Of those, an attempt was made to initiate 25 (54%) of these suggestions (Table 2). Of the 25 interventions that were initiated, 18 (72%) were determined to be successful. Eight resulted in objective permanent system‐wide change and 10 resulted in subjective behavior change among residents.
| QIC Topic | Interventions Suggested by Residents | Suggestion Results (Attempted/Not Attempted, Successful/Unsuccessful) |
|---|---|---|
| ||
| Central venous catheter guide wire lost during code placement | Improved supervision and training for line placement | Attempted, but unsuccessful |
| Avoid unnecessary line placement during codes | Attempted, but unsuccessful | |
| Inappropriate administration of warfarin | Decision support providing real‐time coagulation profile | Attempted and successful |
| Central line bloodstream infection | Clarified and encouraged use of line service | Attempted and successful |
| Daily documentation of catheter placement date | Not attempted | |
| Delayed administration of pain medication | Training nurses to use text paging communication system | Attempted and successful |
| Patient discharged on wrong medication dose | Do not use abbreviations | Not attempted |
| Electronic medication reconciliation | Attempted and successful | |
| Confusion over code status | Clarification of various forms used for DNR | Not attempted |
| Better communication of code status during signout | Not attempted | |
| Patient received hydromorphone IV instead of PO during verbal order at end‐of‐life | Verbal orders should have talk back verification | Attempted, but unsuccessful |
| Encourage informing patients of medical errors | Attempted, but unsuccessful | |
| Premature closure of diagnosis during transfer from MICU | Improve comfort level disagreeing with supervisors | Attempted, but unsuccessful |
| Reassessment of patient prior to late‐day MICU transfers | Not attempted | |
| Patient erroneously received clopidogrel bisulfate (Plavix) for years due to poor medication reconciliation | Improved discharge summary interface | Attempted and successful |
| Encourage physicians to call PCP on discharge | Attempted and successful | |
| Modified barium swallow ordered incorrectly, resulting in patient aspiration | Simplify electronic order entry system to clearly identify tests | Not attempted |
| Change radiology requisition form to facilitate communication | Not attempted | |
| Fingersticks leading to blood exposure | Train PGY1s on the needles used at all 3 hospitals | Not attempted |
| Improve mask with face shields and gown availability | Attempted and successful | |
| Patient discharged with central venous catheter still in place | Check list for lines and Foleys | Not attempted |
| Improved discharge documentation | Not attempted | |
| 30‐Day readmission | Mandatory discharge summary completion prior to discharge | Attempted and successful |
| Discharge summary training during intern year | Attempted and successful | |
| DKA developed in house when insulin not administered | Improve communication between floor and dialysis RNs | Not attempted |
| Better PA supervision by residents regarding order writing | Attempted and successful | |
| Compromised patient satisfaction | Patient handouts with name and role of each care team member | Attempted, but unsuccessful |
| Patient satisfaction coaching | Attempted and successful | |
| Elevated PTT and poor documentation | Improved feedback to residents regarding daily notes | Not attempted |
| Nurses must call physicians with alert values | Not attempted | |
| Hospital‐acquired MRSA | Improve availability of contact precaution gowns | Attempted, but unsuccessful |
| Direct observation of hand washing on morning rounds | Attempted and successful | |
| Staff safety with deranged family member | Education of staff regarding safety protocols | Attempted, but unsuccessful |
| Transfer of unstable patient from outside hospital ICU to general medicine floor | Standardization of OSH transfer guidelines | Not attempted |
| Improved documentation of transferring MD contract data | Attempted and successful | |
| Consult called, patient not seen by attending | Education of faculty on existing institutional consult policy | Attempted, but unsuccessful |
| Clarification of violations reporting process for hospital consults | Attempted, but unsuccessful | |
| Type of Intervention | No. of Interventions Suggested | No. of Interventions Implemented (%) | Of Implemented Interventions, No. Which Were Successful (%) | No. of Attempted Interventions With Objective Change (%) | No. of Attempted Interventions With Subjective Change (%) |
|---|---|---|---|---|---|
| Design changes: information technology‐based | 5 | 2 (40) | 2 (100%) | 2 (100) | 0 (0) |
| Design changes: protocol‐based | 17 | 10 (59) | 8 (80%) | 5 (50) | 3 (30) |
| Educational | 20 | 11 (55) | 7 (64) | 1 (9) | 6 (55) |
| Reminder systems | 4 | 2 (50) | 1 (50) | 0 (0) | 1 (50) |
| Total | 46 | 25 (54) | 18 (72) | 8 (32) | 10 (40) |
Two IT‐based system design changes were implemented; both resulted in objective system‐wide change. Eight protocol‐based design changes were implemented successfully, 5 objectively, and 3 subjectively. Seven educational interventions and 1 reminder system intervention were initiated.
The most successful intervention to come from these conferences was the implementation of an electronic medication reconciliation program. The reconciliation program was suggested following a conference on a patient who was discharged home on the wrong dose of a medication. The institution's paper‐based medication reconciliation process, particularly for heart‐failure patients, had long been known to be deficient. The QIC brought this issue to life by highlighting a cases that may have been ameliorated with a more robust medication reconciliation process. Enthusiastic residents were invited to build a case for medication reconciliation to the Chief Medical Officer, and this helped garner resources for the hospital‐wide project. Another successful IT‐based intervention was initiated after a case of inappropriate administration of warfarin to a patient with an already elevated international normalized ratio (INR). The computerized order entry system was changed so that, at the point of ordering warfarin, the most recent coagulation profile and platelet values appear before an order can be finalized.
An example of a protocol‐based intervention came from a conference that focused on poor communication at the time of discharge, which resulted in a 30‐day readmission. As a result, resident work flow was changed so that discharge summaries are expected to be completed at the time of discharge. Along with this protocol change was an educational initiative to improve the quality of discharge summaries by including essential data for the transition of care.
Overall, residents reviewed the conferences very positively (Table 3). The response rate for the first year survey was 40% (56/140) and the second year survey was 18% (26/143). The vast majority of participants felt that the conferences were of high quality (96%) and that the exercise could lead to improvement in quality (98%). Residents felt that the conference focused more on system issues than individual shortcomings (92%). A majority felt comfortable expressing their opinions during the conferences (77%).
| Overall Conference Quality | ||
|---|---|---|
| Question | Mean Score (n = 53) | Rating Question a 4 or 5 |
| Conference Tone | ||
| Question | Mean Score (n = 26) | Rating Question With a 4 or 5 |
| ||
| Please rate the overall quality of the QIC conferences. | 4.49* | 98% |
| The case highlighted an issue that is highly relevant to the quality of patient care. | 4.81 | 100% |
| Solutions discussed at this conference could lead to improved patient care and/or patient satisfaction. | 4.65 | 96% |
| My knowledge of issues related to hospital quality and patient safety has been enhanced by this conference. | 4.61 | 96% |
| The QIC focused on individuals, individual actions, or omissions, which compromised high quality care. | 3.35 | 50% |
| The QIC focused on system failures that compromised high quality care. | 4.35 | 92% |
| I felt comfortable sharing my honest opinions about the medical events presented during the conferences. | 4.15 | 77% |
| I avoided expressing my opinions about the medical events presented during the conferences because I did not want to criticize my peers. | 2.5 | 19% |
DISCUSSION
The first 20 sessions from this resident‐led, hospitalist‐facilitated QI program provided evidence that residents can contribute to patient safety within a large tertiary care center. The role of residents in actively addressing errors and unsatisfactory outcomes in the hospital has not been a traditional QI focus.12 Involvement has typically been a passive process for physician trainees, while more senior clinical staff members decide on and prioritize QI activities. We have observed that empowering residents to take a more active role in performance improvement yields significant change and does more than simply educate about basic QI methodology.
One reason for the success of these conferences was leveraging insights of residents as key front line providers. Residents spend more time than perhaps any other category of hospital employee working within clinical care systems. They are deeply aware of the quality struggles inherent to large healthcare organizations, and this insight can lead to high impact suggestions for improvement. Often, suggestions were simple proposals that were overlooked or unappreciated by other administrative leaders. An example of this type of contribution was when residents brought the lack of infection control equipment, on certain units, to the attention of the infection control staff and facility engineers. At a separate conference, residents informed the transfer office staff that valuable contact information for physicians accepting outside hospital transfers was not being collected. Both of these observations led to quick change, with better infection control gown availability and improved documentation by transfer office staff.
Our program also demonstrated that including residents in QI provides momentum for either a training program or an institution to pursue solutions that might have otherwise been resisted. The improvement suggestion to complete discharge summaries prior to the patient leaving the hospital had long been a goal for the residency program leadership, but there was hesitation to force this work flow change on the residents. After a QI conference, when a number of the residents themselves made the suggestion, implementing the change was much easier. Similarly, after several cases of clear errors relating to a suboptimal process of medication reconciliation, the institution dedicated scarce IT personnel to work with providers to develop a robust, user‐friendly medication reconciliation application to decrease transition of care errors.
Through this program, residents also demonstrated their ability to deconstruct patient care problems. For each case, resident session leaders interviewed physician providers, physician extenders, nurses, nurse managers, pharmacists, security staff, engineering staff, and administrative staff. They gathered crucial information regarding the patient care event and the gaps or errors that led to a poor outcome. After many of the conferences, the resident presenters commented on how the investigative exercise left them more appreciative of the complexity of the medical system and interested in fixing the problems uncovered.
The feedback from the resident surveys demonstrated that residents valued the QI program. The data collected also shows that such programs can be executed in a manner which highlights system flaws. Our data do, however, suggest that there is room to improve the tone of the conference to further decrease the sense from residents that quality discussions focus on individuals. Residents often struggle to master the myriad new expectations inherent in the transition from student to physician.13 A quality process which discourages already overworked and uncertain trainees, by creating a process which assigns blame for unintentional quality shortcomings, would be counterproductive.
Lessons Learned
While this QI program has had success uncovering clinical care issues, and creating a climate and process for resident participation in improvement, there has been a number of limitations and lessons learned. Most importantly, including busy residents in any process that requires regular participation and follow‐through is difficult. A number of suggested improvements which created substantial interest and early momentum were ultimately left unfinished, as residents and even faculty facilitators became overwhelmed by clinical responsibilities. In fact, the majority of suggestions have not been successfully implemented and even fewer have created lasting change. This must be carefully monitored, as experiencing multiple failures can undermine the empowerment that such QI programs are created to foster.
Regular reflection on the successful and unsuccessful projects yielded several important insights that resulted in changes over the course of the program. Suggestions were more likely to move from idea generation to execution if the QIC was attended by administrators with decision‐making authority. Several of the suggestionsimproved medication reconciliation, better transfer documentation, and improved availability of infection control productswere able to be acted upon because conference attendees were administrators with purview over these issues. Many times, these leaders were more than willing to implement helpful suggestions, but simply needed them to be brought to their attention. As a result, we have been more attentive to inviting as many stakeholders as possible to the QICs.
It was also clear that suggestions would not be realized without a physician leader and were more successful when resident interest was substantial. After each QIC, residents who had made promising suggestions were approached to continue to participate. If the residents agreed, the projects were pursued and a faculty or chief resident leader was assigned. Lastly, we have also made use of one of the department's QI data analysts to assist with project completion. This individual has been made available to provide administrative support (organizing meetings, paperwork, etc) but also to provide data for projects, should the need arise.
Another important finding is that the tone of the QI program must be constantly monitored. Despite reminding residents at each session that the exercise was for the purpose of identifying systems barriers to delivering high quality care, there were times when residents felt targeted or blamed. At one point, a number of residents voiced their concerns that the conferences had spent too much time highlighting quality failures without recognizing the many positive performances on the teaching service. As a result, subsequent conferences often began by highlighting quality improvements made. Additionally, a part of 1 session each year had been dedicated to reading letters and e‐mails sent by patients or families which highlight memorably positive performances by the residents. Finally, care was taken to make sure invited guests to the sessions were reminded of the session's blame‐free ground rules.
Care must be taken when investigating clinical cases. On several occasions, attending physicians expressed discomfort with having residents scrutinize a clinical event. Although this process was protected under the QI umbrella and faculty names were never shared at the conferences, some faculty believed that this process was the purview of departmental or hospital QI staff, not untrained residents. Given the support provided for this program by the department chair and program director, as well as the professional nature with which the residents conducted their inquiries, there was little difficulty rejecting this line of objection. This feedback did lead supervisors to be more involved with the resident presenters, coaching them regarding data gathering and interviewing. If a case appears that it will be particularly sensitive, the hospitalist mentor or chief resident will reach out to involved residents and faculty to notify them that the case will be reviewed.
A final development secured, in part, as a result of this quality program has been more protected faculty time. At the start of this program, all faculty time was donated time on top of other administrative and patient care responsibilities. After the first 18 months of the QIC program, the residency program named an assistant program director for quality. At the time of writing this manuscript, the program further invested in quality by naming both an assistant and associate program director for quality. These positions combined amount to at least 0.4 full‐time equivalents (FTE). Of that, roughly 0.1 FTE is spent working on the QICs and subsequent project implementation.
Limitations
The evaluation of the success of the interventions potentially biased our findings. The qualitative method of using multiple reviewers, all of whom were invested in the program's outcomes, to gauge the success of initiated interventions may have resulted in an overestimate of the project's effectiveness. Furthermore, the category of subjective change lacks measurable criteria, making replication of the findings difficult.
The results presented here are from a single institution, conceived of and executed by a group of dedicated faculty. Moreover, both the chair of the department and the program director were very supportive of this endeavor. Possibly, because of these aspects, the findings presented here would not be readily replicated at another institution.
The percentage of residents who completed the feedback surveys was low. This may result in an overestimate of quality, value, and tone of the conferences, as well as potentially missing an opportunity for improving the program. We will address this issue through more rigorous quantitative and qualitative feedback at the end of the third year of the program.
CONCLUSIONS
Residents are willing and effective participants in a QI program. As front line providers, their experiences are valuable and their willingness to share insights can be an impetus for change. Finally, a process which includes modest investigation by third year residents, has faculty support and oversight, and provides minimal administrative support can overcome the difficulty of involving overworked residents in quality efforts.
Acknowledgements
The authors acknowledge Michael Pourdehnad for his role in developing the quality program.
- ,,.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press;1999.
- ,,,,.Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144:920–926.
- Accreditation Council for Graduate Medical Education. Program directors guide to the common program requirements. Available at: http://www.acgme.org/acWebsite/navPages/commonpr_documents/ CompleteGuide_v2%20.pdf. Accessed May 5,2010.
- ,,,.Medical errors involving trainees: a study of closed malpractice claims from 5 insurers.Arch Intern Med.2007;167:2030–2036.
- ,,,,,.Residents report on adverse events and their causes.Arch Intern Med.2005;165:2607–2613.
- ,.A system of analyzing medical errors to improve GMA curricula and programs.Acad Med.2001;76:125–133.
- ,,, et al.Changing conversations: teaching safety and quality in residency training.Acad Med.2008;83(11):1080–1087.
- ,,.Practice‐based learning and improvement: a curriculum in continuous quality improvement for surgery residents.Arch Surg.2007;142:479–483.
- .Involving residents in quality improvement: contrasting “top‐down” and “bottom‐up” approaches. Accreditation Council for Graduate Medical Education and Institute for Healthcare Improvement‐day project.ACGME Bulletin. August2008.
- ,,,,.Creating a quality improvement elective for medical house officers.Gen Intern Med.2004;19(8):861–867.
- National Center for Patient Safety. United States Department for Veteran Affairs. Root cause analysis tools. Available at: http://www.patientsafety.gov/CogAids/RCA/. Accessed August 17,2010.
- ,,, et al.Residents' engagement in quality improvement: a systematic review of the literature.Acad Med.2009;84:1757–1764.
- ,,.Graduates from a traditional medical curriculum evaluate the effectiveness of their medical curriculum through interviews.BMC Med Educ.2009;9:64.
To Err Is Human revealed the underappreciated tension between the enormous benefits of medical care and the potential for harm.1 Following this report, there has been an explosion of research and commentary detailing quality improvement (QI) opportunities. One area of growing emphasis has been resident physician training.2, 3 If medical care is dangerous, then a substantial contributor to the hazard must be the apprentice‐style process of physician training and the novice skill set of the trainees.4, 5 Many resident training programs have devised efforts to decrease the errors committed by physicians‐in‐training,6 change the culture of residency training,7 engage residents in quality improvement,8, 9 and improve resident training in quality improvement.10
Many of the programs devised to teach QI in the residency setting require substantial funding, a large pool of QI experts, or redesign of resident training programs.410 While effective, these programs are not feasible for many resource‐constrained residency programs. A less intense program, using resident‐led, hospitalist‐facilitated, limited root cause analysis (RCA), has been adopted at the Internal Medicine Residency Program at the Mount Sinai Hospital (MSH). We describe our 2‐year experience using this technique, including cases discussed, improvement strategies suggested, projects implemented, and resident perceptions.
METHODS
Setting
Departmental QI leaders developed this initiative in the Internal Medicine Residency Program at the MSH in New York City, New York. This residency program trains over 140 residents annually in categorical, preliminary, and research track positions, as well as an affiliated medicine/pediatrics program. The program's residents rotate at 3 clinic sites: a tertiary care hospital, a public safety‐net hospital, and a Veterans Affairs hospital. The QI program was only implemented at the MSH. Over 90% of the program's graduates go on to complete a subspecialty fellowship.
Intervention Description
The QI program was designed around a noon‐time quality improvement conference (QIC) occurring once every 4 weeks. In the weeks prior to the session, chief residents and a hospitalist mentor selected a case related to an inpatient care issue. Potential cases were solicited, and/or offered, from a range of sources including attending physicians, nurse managers, residents, and quality officers. Only cases from the teaching services were chosen. To ensure that participants on the case were able to recall relevant details, preference was given to more recent cases. A third‐year resident on an elective or outpatient block was chosen to investigate the case. To maximize the objectivity of the investigation, every effort was made to select a resident who was not involved in the care of the patient.
The resident was instructed to complete a limited RCA (fewer fact‐finding interviews and only 1 group meeting) and was directed to online resources.11 Each resident presenter worked closely with the chief residents and hospitalist mentor to identify appropriate strategies for collecting data and interviewing involved parties. If necessary, either due to volume of work or sensitivity of the case, the chief resident or hospitalist would assist with the data gathering. The resident contacted multiple parties involved in the patient care issue including, nurses, residents, attendings, pharmacists, social workers, and, if appropriate, the patient. The resident constructed a timeline for each case, and identified specific points in the patient care experience, where errors, near misses, or misunderstandings occurred. During the QIC, these findings were presented to Internal Medicine residents, chief residents, representatives from the Chief Medical Officer's office, attending physicians overseeing the residents on inpatient rotations, and representatives from any group (social work nursing, housekeeping, pharmacy, etc) that may have impacted patient care for the particular case being investigated. On average, 50 healthcare providers attended the QIC. Lunch was provided.
After the findings were presented, a chief resident and a lead hospitalist facilitated a group discussion on the circumstances surrounding the case. Discussions were focused on identifying system‐wide failures and proposing systems‐based solutions. Great efforts were made to remind all participants to refrain from individual blame. At the end of each QIC, participants summarized and prioritized suggestions to reduce the discussed error. Interested residents were invited to form improvement committees for cases with viable solutions. Each committee attempted to implement improvements discussed during the QIC. Committees, led by a representative from the Division of Hospital Medicine, included 2 to 4 residents as well as healthcare workers from other disciplines if appropriate. For all improvement efforts, the focus was on the interventions which appeared high yield with low cost.
Intervention Evaluation
The program was exempt from Institutional Review Board review as a part of the Department of Medicine's quality improvement and assurance portfolio.
The results of the QICs were tracked. After each case, a QI team consisting of chief residents and representatives from the Division of Hospital Medicine recorded the cases presented, and interventions suggested for each case, in an online database. After implementation, the success of each intervention was recorded. To evaluate the types of interventions suggested by residents, the 3 physician‐authors, who regularly attend these conferences and have a focused career interest in QI, grouped all suggestions into 4 broad categories: Educational, Reminder Systems, Design Changes (protocol‐based), and Design Changes (Information Technology [IT]‐based). Design change interventions (IT‐based) consisted of an adjustment to electronic systems, such as displaying specific lab results on a medication ordering system. Design changes (protocol‐based) consisted of changes made to standing protocols such as nursing protocols for reporting abnormal lab values. Reminder system interventions were endeavors such as a checklist for discharge planning. Educational interventions focused on providing additional training sessions or conferences.
The 3 physician‐authors independently reviewed each suggested intervention to determine its success. They first evaluated whether the change was attempted or not. For all attempted interventions, the reviewer then assessed if there was either objective permanent system‐wide change, subjective behavior change, or no change. To meet the objective change threshold, the intervention either had to have permanently changed provider workflow or have data demonstrating behavior change or improved outcome. Interventions with anecdotal evidence that behavior was improved or modified, but lacking systematic data, were qualified as subjective behavior change. For each assessment, 2 of the 3 reviewers needed to agree for an intervention to be recorded as a success.
Resident views on the monthly conferences were solicited via an anonymous and voluntary questionnaire. A first survey was designed to assess whether residents felt that the conferences provided them with the ability to recognize and improve systems errors which compromise patient care. This survey was administered at the conclusion of the first year of the program to residents who attended the final 2 QICs. A second survey assessed whether the tone of the conferences was constructive and blame‐free. This survey was administered at the conclusion of the second year of the program to residents who attended the year's final 2 QICs.
RESULTS
Over the first 22 months of the program, 20 conferences were held (Table 1). The topics covered ranged considerably and included: deficits in supervision, medication errors, patient satisfaction, staff safety, and 30‐day readmissions. Forty‐six distinct interventions were suggested during these conferences. Of those, an attempt was made to initiate 25 (54%) of these suggestions (Table 2). Of the 25 interventions that were initiated, 18 (72%) were determined to be successful. Eight resulted in objective permanent system‐wide change and 10 resulted in subjective behavior change among residents.
| QIC Topic | Interventions Suggested by Residents | Suggestion Results (Attempted/Not Attempted, Successful/Unsuccessful) |
|---|---|---|
| ||
| Central venous catheter guide wire lost during code placement | Improved supervision and training for line placement | Attempted, but unsuccessful |
| Avoid unnecessary line placement during codes | Attempted, but unsuccessful | |
| Inappropriate administration of warfarin | Decision support providing real‐time coagulation profile | Attempted and successful |
| Central line bloodstream infection | Clarified and encouraged use of line service | Attempted and successful |
| Daily documentation of catheter placement date | Not attempted | |
| Delayed administration of pain medication | Training nurses to use text paging communication system | Attempted and successful |
| Patient discharged on wrong medication dose | Do not use abbreviations | Not attempted |
| Electronic medication reconciliation | Attempted and successful | |
| Confusion over code status | Clarification of various forms used for DNR | Not attempted |
| Better communication of code status during signout | Not attempted | |
| Patient received hydromorphone IV instead of PO during verbal order at end‐of‐life | Verbal orders should have talk back verification | Attempted, but unsuccessful |
| Encourage informing patients of medical errors | Attempted, but unsuccessful | |
| Premature closure of diagnosis during transfer from MICU | Improve comfort level disagreeing with supervisors | Attempted, but unsuccessful |
| Reassessment of patient prior to late‐day MICU transfers | Not attempted | |
| Patient erroneously received clopidogrel bisulfate (Plavix) for years due to poor medication reconciliation | Improved discharge summary interface | Attempted and successful |
| Encourage physicians to call PCP on discharge | Attempted and successful | |
| Modified barium swallow ordered incorrectly, resulting in patient aspiration | Simplify electronic order entry system to clearly identify tests | Not attempted |
| Change radiology requisition form to facilitate communication | Not attempted | |
| Fingersticks leading to blood exposure | Train PGY1s on the needles used at all 3 hospitals | Not attempted |
| Improve mask with face shields and gown availability | Attempted and successful | |
| Patient discharged with central venous catheter still in place | Check list for lines and Foleys | Not attempted |
| Improved discharge documentation | Not attempted | |
| 30‐Day readmission | Mandatory discharge summary completion prior to discharge | Attempted and successful |
| Discharge summary training during intern year | Attempted and successful | |
| DKA developed in house when insulin not administered | Improve communication between floor and dialysis RNs | Not attempted |
| Better PA supervision by residents regarding order writing | Attempted and successful | |
| Compromised patient satisfaction | Patient handouts with name and role of each care team member | Attempted, but unsuccessful |
| Patient satisfaction coaching | Attempted and successful | |
| Elevated PTT and poor documentation | Improved feedback to residents regarding daily notes | Not attempted |
| Nurses must call physicians with alert values | Not attempted | |
| Hospital‐acquired MRSA | Improve availability of contact precaution gowns | Attempted, but unsuccessful |
| Direct observation of hand washing on morning rounds | Attempted and successful | |
| Staff safety with deranged family member | Education of staff regarding safety protocols | Attempted, but unsuccessful |
| Transfer of unstable patient from outside hospital ICU to general medicine floor | Standardization of OSH transfer guidelines | Not attempted |
| Improved documentation of transferring MD contract data | Attempted and successful | |
| Consult called, patient not seen by attending | Education of faculty on existing institutional consult policy | Attempted, but unsuccessful |
| Clarification of violations reporting process for hospital consults | Attempted, but unsuccessful | |
| Type of Intervention | No. of Interventions Suggested | No. of Interventions Implemented (%) | Of Implemented Interventions, No. Which Were Successful (%) | No. of Attempted Interventions With Objective Change (%) | No. of Attempted Interventions With Subjective Change (%) |
|---|---|---|---|---|---|
| Design changes: information technology‐based | 5 | 2 (40) | 2 (100%) | 2 (100) | 0 (0) |
| Design changes: protocol‐based | 17 | 10 (59) | 8 (80%) | 5 (50) | 3 (30) |
| Educational | 20 | 11 (55) | 7 (64) | 1 (9) | 6 (55) |
| Reminder systems | 4 | 2 (50) | 1 (50) | 0 (0) | 1 (50) |
| Total | 46 | 25 (54) | 18 (72) | 8 (32) | 10 (40) |
Two IT‐based system design changes were implemented; both resulted in objective system‐wide change. Eight protocol‐based design changes were implemented successfully, 5 objectively, and 3 subjectively. Seven educational interventions and 1 reminder system intervention were initiated.
The most successful intervention to come from these conferences was the implementation of an electronic medication reconciliation program. The reconciliation program was suggested following a conference on a patient who was discharged home on the wrong dose of a medication. The institution's paper‐based medication reconciliation process, particularly for heart‐failure patients, had long been known to be deficient. The QIC brought this issue to life by highlighting a cases that may have been ameliorated with a more robust medication reconciliation process. Enthusiastic residents were invited to build a case for medication reconciliation to the Chief Medical Officer, and this helped garner resources for the hospital‐wide project. Another successful IT‐based intervention was initiated after a case of inappropriate administration of warfarin to a patient with an already elevated international normalized ratio (INR). The computerized order entry system was changed so that, at the point of ordering warfarin, the most recent coagulation profile and platelet values appear before an order can be finalized.
An example of a protocol‐based intervention came from a conference that focused on poor communication at the time of discharge, which resulted in a 30‐day readmission. As a result, resident work flow was changed so that discharge summaries are expected to be completed at the time of discharge. Along with this protocol change was an educational initiative to improve the quality of discharge summaries by including essential data for the transition of care.
Overall, residents reviewed the conferences very positively (Table 3). The response rate for the first year survey was 40% (56/140) and the second year survey was 18% (26/143). The vast majority of participants felt that the conferences were of high quality (96%) and that the exercise could lead to improvement in quality (98%). Residents felt that the conference focused more on system issues than individual shortcomings (92%). A majority felt comfortable expressing their opinions during the conferences (77%).
| Overall Conference Quality | ||
|---|---|---|
| Question | Mean Score (n = 53) | Rating Question a 4 or 5 |
| Conference Tone | ||
| Question | Mean Score (n = 26) | Rating Question With a 4 or 5 |
| ||
| Please rate the overall quality of the QIC conferences. | 4.49* | 98% |
| The case highlighted an issue that is highly relevant to the quality of patient care. | 4.81 | 100% |
| Solutions discussed at this conference could lead to improved patient care and/or patient satisfaction. | 4.65 | 96% |
| My knowledge of issues related to hospital quality and patient safety has been enhanced by this conference. | 4.61 | 96% |
| The QIC focused on individuals, individual actions, or omissions, which compromised high quality care. | 3.35 | 50% |
| The QIC focused on system failures that compromised high quality care. | 4.35 | 92% |
| I felt comfortable sharing my honest opinions about the medical events presented during the conferences. | 4.15 | 77% |
| I avoided expressing my opinions about the medical events presented during the conferences because I did not want to criticize my peers. | 2.5 | 19% |
DISCUSSION
The first 20 sessions from this resident‐led, hospitalist‐facilitated QI program provided evidence that residents can contribute to patient safety within a large tertiary care center. The role of residents in actively addressing errors and unsatisfactory outcomes in the hospital has not been a traditional QI focus.12 Involvement has typically been a passive process for physician trainees, while more senior clinical staff members decide on and prioritize QI activities. We have observed that empowering residents to take a more active role in performance improvement yields significant change and does more than simply educate about basic QI methodology.
One reason for the success of these conferences was leveraging insights of residents as key front line providers. Residents spend more time than perhaps any other category of hospital employee working within clinical care systems. They are deeply aware of the quality struggles inherent to large healthcare organizations, and this insight can lead to high impact suggestions for improvement. Often, suggestions were simple proposals that were overlooked or unappreciated by other administrative leaders. An example of this type of contribution was when residents brought the lack of infection control equipment, on certain units, to the attention of the infection control staff and facility engineers. At a separate conference, residents informed the transfer office staff that valuable contact information for physicians accepting outside hospital transfers was not being collected. Both of these observations led to quick change, with better infection control gown availability and improved documentation by transfer office staff.
Our program also demonstrated that including residents in QI provides momentum for either a training program or an institution to pursue solutions that might have otherwise been resisted. The improvement suggestion to complete discharge summaries prior to the patient leaving the hospital had long been a goal for the residency program leadership, but there was hesitation to force this work flow change on the residents. After a QI conference, when a number of the residents themselves made the suggestion, implementing the change was much easier. Similarly, after several cases of clear errors relating to a suboptimal process of medication reconciliation, the institution dedicated scarce IT personnel to work with providers to develop a robust, user‐friendly medication reconciliation application to decrease transition of care errors.
Through this program, residents also demonstrated their ability to deconstruct patient care problems. For each case, resident session leaders interviewed physician providers, physician extenders, nurses, nurse managers, pharmacists, security staff, engineering staff, and administrative staff. They gathered crucial information regarding the patient care event and the gaps or errors that led to a poor outcome. After many of the conferences, the resident presenters commented on how the investigative exercise left them more appreciative of the complexity of the medical system and interested in fixing the problems uncovered.
The feedback from the resident surveys demonstrated that residents valued the QI program. The data collected also shows that such programs can be executed in a manner which highlights system flaws. Our data do, however, suggest that there is room to improve the tone of the conference to further decrease the sense from residents that quality discussions focus on individuals. Residents often struggle to master the myriad new expectations inherent in the transition from student to physician.13 A quality process which discourages already overworked and uncertain trainees, by creating a process which assigns blame for unintentional quality shortcomings, would be counterproductive.
Lessons Learned
While this QI program has had success uncovering clinical care issues, and creating a climate and process for resident participation in improvement, there has been a number of limitations and lessons learned. Most importantly, including busy residents in any process that requires regular participation and follow‐through is difficult. A number of suggested improvements which created substantial interest and early momentum were ultimately left unfinished, as residents and even faculty facilitators became overwhelmed by clinical responsibilities. In fact, the majority of suggestions have not been successfully implemented and even fewer have created lasting change. This must be carefully monitored, as experiencing multiple failures can undermine the empowerment that such QI programs are created to foster.
Regular reflection on the successful and unsuccessful projects yielded several important insights that resulted in changes over the course of the program. Suggestions were more likely to move from idea generation to execution if the QIC was attended by administrators with decision‐making authority. Several of the suggestionsimproved medication reconciliation, better transfer documentation, and improved availability of infection control productswere able to be acted upon because conference attendees were administrators with purview over these issues. Many times, these leaders were more than willing to implement helpful suggestions, but simply needed them to be brought to their attention. As a result, we have been more attentive to inviting as many stakeholders as possible to the QICs.
It was also clear that suggestions would not be realized without a physician leader and were more successful when resident interest was substantial. After each QIC, residents who had made promising suggestions were approached to continue to participate. If the residents agreed, the projects were pursued and a faculty or chief resident leader was assigned. Lastly, we have also made use of one of the department's QI data analysts to assist with project completion. This individual has been made available to provide administrative support (organizing meetings, paperwork, etc) but also to provide data for projects, should the need arise.
Another important finding is that the tone of the QI program must be constantly monitored. Despite reminding residents at each session that the exercise was for the purpose of identifying systems barriers to delivering high quality care, there were times when residents felt targeted or blamed. At one point, a number of residents voiced their concerns that the conferences had spent too much time highlighting quality failures without recognizing the many positive performances on the teaching service. As a result, subsequent conferences often began by highlighting quality improvements made. Additionally, a part of 1 session each year had been dedicated to reading letters and e‐mails sent by patients or families which highlight memorably positive performances by the residents. Finally, care was taken to make sure invited guests to the sessions were reminded of the session's blame‐free ground rules.
Care must be taken when investigating clinical cases. On several occasions, attending physicians expressed discomfort with having residents scrutinize a clinical event. Although this process was protected under the QI umbrella and faculty names were never shared at the conferences, some faculty believed that this process was the purview of departmental or hospital QI staff, not untrained residents. Given the support provided for this program by the department chair and program director, as well as the professional nature with which the residents conducted their inquiries, there was little difficulty rejecting this line of objection. This feedback did lead supervisors to be more involved with the resident presenters, coaching them regarding data gathering and interviewing. If a case appears that it will be particularly sensitive, the hospitalist mentor or chief resident will reach out to involved residents and faculty to notify them that the case will be reviewed.
A final development secured, in part, as a result of this quality program has been more protected faculty time. At the start of this program, all faculty time was donated time on top of other administrative and patient care responsibilities. After the first 18 months of the QIC program, the residency program named an assistant program director for quality. At the time of writing this manuscript, the program further invested in quality by naming both an assistant and associate program director for quality. These positions combined amount to at least 0.4 full‐time equivalents (FTE). Of that, roughly 0.1 FTE is spent working on the QICs and subsequent project implementation.
Limitations
The evaluation of the success of the interventions potentially biased our findings. The qualitative method of using multiple reviewers, all of whom were invested in the program's outcomes, to gauge the success of initiated interventions may have resulted in an overestimate of the project's effectiveness. Furthermore, the category of subjective change lacks measurable criteria, making replication of the findings difficult.
The results presented here are from a single institution, conceived of and executed by a group of dedicated faculty. Moreover, both the chair of the department and the program director were very supportive of this endeavor. Possibly, because of these aspects, the findings presented here would not be readily replicated at another institution.
The percentage of residents who completed the feedback surveys was low. This may result in an overestimate of quality, value, and tone of the conferences, as well as potentially missing an opportunity for improving the program. We will address this issue through more rigorous quantitative and qualitative feedback at the end of the third year of the program.
CONCLUSIONS
Residents are willing and effective participants in a QI program. As front line providers, their experiences are valuable and their willingness to share insights can be an impetus for change. Finally, a process which includes modest investigation by third year residents, has faculty support and oversight, and provides minimal administrative support can overcome the difficulty of involving overworked residents in quality efforts.
Acknowledgements
The authors acknowledge Michael Pourdehnad for his role in developing the quality program.
To Err Is Human revealed the underappreciated tension between the enormous benefits of medical care and the potential for harm.1 Following this report, there has been an explosion of research and commentary detailing quality improvement (QI) opportunities. One area of growing emphasis has been resident physician training.2, 3 If medical care is dangerous, then a substantial contributor to the hazard must be the apprentice‐style process of physician training and the novice skill set of the trainees.4, 5 Many resident training programs have devised efforts to decrease the errors committed by physicians‐in‐training,6 change the culture of residency training,7 engage residents in quality improvement,8, 9 and improve resident training in quality improvement.10
Many of the programs devised to teach QI in the residency setting require substantial funding, a large pool of QI experts, or redesign of resident training programs.410 While effective, these programs are not feasible for many resource‐constrained residency programs. A less intense program, using resident‐led, hospitalist‐facilitated, limited root cause analysis (RCA), has been adopted at the Internal Medicine Residency Program at the Mount Sinai Hospital (MSH). We describe our 2‐year experience using this technique, including cases discussed, improvement strategies suggested, projects implemented, and resident perceptions.
METHODS
Setting
Departmental QI leaders developed this initiative in the Internal Medicine Residency Program at the MSH in New York City, New York. This residency program trains over 140 residents annually in categorical, preliminary, and research track positions, as well as an affiliated medicine/pediatrics program. The program's residents rotate at 3 clinic sites: a tertiary care hospital, a public safety‐net hospital, and a Veterans Affairs hospital. The QI program was only implemented at the MSH. Over 90% of the program's graduates go on to complete a subspecialty fellowship.
Intervention Description
The QI program was designed around a noon‐time quality improvement conference (QIC) occurring once every 4 weeks. In the weeks prior to the session, chief residents and a hospitalist mentor selected a case related to an inpatient care issue. Potential cases were solicited, and/or offered, from a range of sources including attending physicians, nurse managers, residents, and quality officers. Only cases from the teaching services were chosen. To ensure that participants on the case were able to recall relevant details, preference was given to more recent cases. A third‐year resident on an elective or outpatient block was chosen to investigate the case. To maximize the objectivity of the investigation, every effort was made to select a resident who was not involved in the care of the patient.
The resident was instructed to complete a limited RCA (fewer fact‐finding interviews and only 1 group meeting) and was directed to online resources.11 Each resident presenter worked closely with the chief residents and hospitalist mentor to identify appropriate strategies for collecting data and interviewing involved parties. If necessary, either due to volume of work or sensitivity of the case, the chief resident or hospitalist would assist with the data gathering. The resident contacted multiple parties involved in the patient care issue including, nurses, residents, attendings, pharmacists, social workers, and, if appropriate, the patient. The resident constructed a timeline for each case, and identified specific points in the patient care experience, where errors, near misses, or misunderstandings occurred. During the QIC, these findings were presented to Internal Medicine residents, chief residents, representatives from the Chief Medical Officer's office, attending physicians overseeing the residents on inpatient rotations, and representatives from any group (social work nursing, housekeeping, pharmacy, etc) that may have impacted patient care for the particular case being investigated. On average, 50 healthcare providers attended the QIC. Lunch was provided.
After the findings were presented, a chief resident and a lead hospitalist facilitated a group discussion on the circumstances surrounding the case. Discussions were focused on identifying system‐wide failures and proposing systems‐based solutions. Great efforts were made to remind all participants to refrain from individual blame. At the end of each QIC, participants summarized and prioritized suggestions to reduce the discussed error. Interested residents were invited to form improvement committees for cases with viable solutions. Each committee attempted to implement improvements discussed during the QIC. Committees, led by a representative from the Division of Hospital Medicine, included 2 to 4 residents as well as healthcare workers from other disciplines if appropriate. For all improvement efforts, the focus was on the interventions which appeared high yield with low cost.
Intervention Evaluation
The program was exempt from Institutional Review Board review as a part of the Department of Medicine's quality improvement and assurance portfolio.
The results of the QICs were tracked. After each case, a QI team consisting of chief residents and representatives from the Division of Hospital Medicine recorded the cases presented, and interventions suggested for each case, in an online database. After implementation, the success of each intervention was recorded. To evaluate the types of interventions suggested by residents, the 3 physician‐authors, who regularly attend these conferences and have a focused career interest in QI, grouped all suggestions into 4 broad categories: Educational, Reminder Systems, Design Changes (protocol‐based), and Design Changes (Information Technology [IT]‐based). Design change interventions (IT‐based) consisted of an adjustment to electronic systems, such as displaying specific lab results on a medication ordering system. Design changes (protocol‐based) consisted of changes made to standing protocols such as nursing protocols for reporting abnormal lab values. Reminder system interventions were endeavors such as a checklist for discharge planning. Educational interventions focused on providing additional training sessions or conferences.
The 3 physician‐authors independently reviewed each suggested intervention to determine its success. They first evaluated whether the change was attempted or not. For all attempted interventions, the reviewer then assessed if there was either objective permanent system‐wide change, subjective behavior change, or no change. To meet the objective change threshold, the intervention either had to have permanently changed provider workflow or have data demonstrating behavior change or improved outcome. Interventions with anecdotal evidence that behavior was improved or modified, but lacking systematic data, were qualified as subjective behavior change. For each assessment, 2 of the 3 reviewers needed to agree for an intervention to be recorded as a success.
Resident views on the monthly conferences were solicited via an anonymous and voluntary questionnaire. A first survey was designed to assess whether residents felt that the conferences provided them with the ability to recognize and improve systems errors which compromise patient care. This survey was administered at the conclusion of the first year of the program to residents who attended the final 2 QICs. A second survey assessed whether the tone of the conferences was constructive and blame‐free. This survey was administered at the conclusion of the second year of the program to residents who attended the year's final 2 QICs.
RESULTS
Over the first 22 months of the program, 20 conferences were held (Table 1). The topics covered ranged considerably and included: deficits in supervision, medication errors, patient satisfaction, staff safety, and 30‐day readmissions. Forty‐six distinct interventions were suggested during these conferences. Of those, an attempt was made to initiate 25 (54%) of these suggestions (Table 2). Of the 25 interventions that were initiated, 18 (72%) were determined to be successful. Eight resulted in objective permanent system‐wide change and 10 resulted in subjective behavior change among residents.
| QIC Topic | Interventions Suggested by Residents | Suggestion Results (Attempted/Not Attempted, Successful/Unsuccessful) |
|---|---|---|
| ||
| Central venous catheter guide wire lost during code placement | Improved supervision and training for line placement | Attempted, but unsuccessful |
| Avoid unnecessary line placement during codes | Attempted, but unsuccessful | |
| Inappropriate administration of warfarin | Decision support providing real‐time coagulation profile | Attempted and successful |
| Central line bloodstream infection | Clarified and encouraged use of line service | Attempted and successful |
| Daily documentation of catheter placement date | Not attempted | |
| Delayed administration of pain medication | Training nurses to use text paging communication system | Attempted and successful |
| Patient discharged on wrong medication dose | Do not use abbreviations | Not attempted |
| Electronic medication reconciliation | Attempted and successful | |
| Confusion over code status | Clarification of various forms used for DNR | Not attempted |
| Better communication of code status during signout | Not attempted | |
| Patient received hydromorphone IV instead of PO during verbal order at end‐of‐life | Verbal orders should have talk back verification | Attempted, but unsuccessful |
| Encourage informing patients of medical errors | Attempted, but unsuccessful | |
| Premature closure of diagnosis during transfer from MICU | Improve comfort level disagreeing with supervisors | Attempted, but unsuccessful |
| Reassessment of patient prior to late‐day MICU transfers | Not attempted | |
| Patient erroneously received clopidogrel bisulfate (Plavix) for years due to poor medication reconciliation | Improved discharge summary interface | Attempted and successful |
| Encourage physicians to call PCP on discharge | Attempted and successful | |
| Modified barium swallow ordered incorrectly, resulting in patient aspiration | Simplify electronic order entry system to clearly identify tests | Not attempted |
| Change radiology requisition form to facilitate communication | Not attempted | |
| Fingersticks leading to blood exposure | Train PGY1s on the needles used at all 3 hospitals | Not attempted |
| Improve mask with face shields and gown availability | Attempted and successful | |
| Patient discharged with central venous catheter still in place | Check list for lines and Foleys | Not attempted |
| Improved discharge documentation | Not attempted | |
| 30‐Day readmission | Mandatory discharge summary completion prior to discharge | Attempted and successful |
| Discharge summary training during intern year | Attempted and successful | |
| DKA developed in house when insulin not administered | Improve communication between floor and dialysis RNs | Not attempted |
| Better PA supervision by residents regarding order writing | Attempted and successful | |
| Compromised patient satisfaction | Patient handouts with name and role of each care team member | Attempted, but unsuccessful |
| Patient satisfaction coaching | Attempted and successful | |
| Elevated PTT and poor documentation | Improved feedback to residents regarding daily notes | Not attempted |
| Nurses must call physicians with alert values | Not attempted | |
| Hospital‐acquired MRSA | Improve availability of contact precaution gowns | Attempted, but unsuccessful |
| Direct observation of hand washing on morning rounds | Attempted and successful | |
| Staff safety with deranged family member | Education of staff regarding safety protocols | Attempted, but unsuccessful |
| Transfer of unstable patient from outside hospital ICU to general medicine floor | Standardization of OSH transfer guidelines | Not attempted |
| Improved documentation of transferring MD contract data | Attempted and successful | |
| Consult called, patient not seen by attending | Education of faculty on existing institutional consult policy | Attempted, but unsuccessful |
| Clarification of violations reporting process for hospital consults | Attempted, but unsuccessful | |
| Type of Intervention | No. of Interventions Suggested | No. of Interventions Implemented (%) | Of Implemented Interventions, No. Which Were Successful (%) | No. of Attempted Interventions With Objective Change (%) | No. of Attempted Interventions With Subjective Change (%) |
|---|---|---|---|---|---|
| Design changes: information technology‐based | 5 | 2 (40) | 2 (100%) | 2 (100) | 0 (0) |
| Design changes: protocol‐based | 17 | 10 (59) | 8 (80%) | 5 (50) | 3 (30) |
| Educational | 20 | 11 (55) | 7 (64) | 1 (9) | 6 (55) |
| Reminder systems | 4 | 2 (50) | 1 (50) | 0 (0) | 1 (50) |
| Total | 46 | 25 (54) | 18 (72) | 8 (32) | 10 (40) |
Two IT‐based system design changes were implemented; both resulted in objective system‐wide change. Eight protocol‐based design changes were implemented successfully, 5 objectively, and 3 subjectively. Seven educational interventions and 1 reminder system intervention were initiated.
The most successful intervention to come from these conferences was the implementation of an electronic medication reconciliation program. The reconciliation program was suggested following a conference on a patient who was discharged home on the wrong dose of a medication. The institution's paper‐based medication reconciliation process, particularly for heart‐failure patients, had long been known to be deficient. The QIC brought this issue to life by highlighting a cases that may have been ameliorated with a more robust medication reconciliation process. Enthusiastic residents were invited to build a case for medication reconciliation to the Chief Medical Officer, and this helped garner resources for the hospital‐wide project. Another successful IT‐based intervention was initiated after a case of inappropriate administration of warfarin to a patient with an already elevated international normalized ratio (INR). The computerized order entry system was changed so that, at the point of ordering warfarin, the most recent coagulation profile and platelet values appear before an order can be finalized.
An example of a protocol‐based intervention came from a conference that focused on poor communication at the time of discharge, which resulted in a 30‐day readmission. As a result, resident work flow was changed so that discharge summaries are expected to be completed at the time of discharge. Along with this protocol change was an educational initiative to improve the quality of discharge summaries by including essential data for the transition of care.
Overall, residents reviewed the conferences very positively (Table 3). The response rate for the first year survey was 40% (56/140) and the second year survey was 18% (26/143). The vast majority of participants felt that the conferences were of high quality (96%) and that the exercise could lead to improvement in quality (98%). Residents felt that the conference focused more on system issues than individual shortcomings (92%). A majority felt comfortable expressing their opinions during the conferences (77%).
| Overall Conference Quality | ||
|---|---|---|
| Question | Mean Score (n = 53) | Rating Question a 4 or 5 |
| Conference Tone | ||
| Question | Mean Score (n = 26) | Rating Question With a 4 or 5 |
| ||
| Please rate the overall quality of the QIC conferences. | 4.49* | 98% |
| The case highlighted an issue that is highly relevant to the quality of patient care. | 4.81 | 100% |
| Solutions discussed at this conference could lead to improved patient care and/or patient satisfaction. | 4.65 | 96% |
| My knowledge of issues related to hospital quality and patient safety has been enhanced by this conference. | 4.61 | 96% |
| The QIC focused on individuals, individual actions, or omissions, which compromised high quality care. | 3.35 | 50% |
| The QIC focused on system failures that compromised high quality care. | 4.35 | 92% |
| I felt comfortable sharing my honest opinions about the medical events presented during the conferences. | 4.15 | 77% |
| I avoided expressing my opinions about the medical events presented during the conferences because I did not want to criticize my peers. | 2.5 | 19% |
DISCUSSION
The first 20 sessions from this resident‐led, hospitalist‐facilitated QI program provided evidence that residents can contribute to patient safety within a large tertiary care center. The role of residents in actively addressing errors and unsatisfactory outcomes in the hospital has not been a traditional QI focus.12 Involvement has typically been a passive process for physician trainees, while more senior clinical staff members decide on and prioritize QI activities. We have observed that empowering residents to take a more active role in performance improvement yields significant change and does more than simply educate about basic QI methodology.
One reason for the success of these conferences was leveraging insights of residents as key front line providers. Residents spend more time than perhaps any other category of hospital employee working within clinical care systems. They are deeply aware of the quality struggles inherent to large healthcare organizations, and this insight can lead to high impact suggestions for improvement. Often, suggestions were simple proposals that were overlooked or unappreciated by other administrative leaders. An example of this type of contribution was when residents brought the lack of infection control equipment, on certain units, to the attention of the infection control staff and facility engineers. At a separate conference, residents informed the transfer office staff that valuable contact information for physicians accepting outside hospital transfers was not being collected. Both of these observations led to quick change, with better infection control gown availability and improved documentation by transfer office staff.
Our program also demonstrated that including residents in QI provides momentum for either a training program or an institution to pursue solutions that might have otherwise been resisted. The improvement suggestion to complete discharge summaries prior to the patient leaving the hospital had long been a goal for the residency program leadership, but there was hesitation to force this work flow change on the residents. After a QI conference, when a number of the residents themselves made the suggestion, implementing the change was much easier. Similarly, after several cases of clear errors relating to a suboptimal process of medication reconciliation, the institution dedicated scarce IT personnel to work with providers to develop a robust, user‐friendly medication reconciliation application to decrease transition of care errors.
Through this program, residents also demonstrated their ability to deconstruct patient care problems. For each case, resident session leaders interviewed physician providers, physician extenders, nurses, nurse managers, pharmacists, security staff, engineering staff, and administrative staff. They gathered crucial information regarding the patient care event and the gaps or errors that led to a poor outcome. After many of the conferences, the resident presenters commented on how the investigative exercise left them more appreciative of the complexity of the medical system and interested in fixing the problems uncovered.
The feedback from the resident surveys demonstrated that residents valued the QI program. The data collected also shows that such programs can be executed in a manner which highlights system flaws. Our data do, however, suggest that there is room to improve the tone of the conference to further decrease the sense from residents that quality discussions focus on individuals. Residents often struggle to master the myriad new expectations inherent in the transition from student to physician.13 A quality process which discourages already overworked and uncertain trainees, by creating a process which assigns blame for unintentional quality shortcomings, would be counterproductive.
Lessons Learned
While this QI program has had success uncovering clinical care issues, and creating a climate and process for resident participation in improvement, there has been a number of limitations and lessons learned. Most importantly, including busy residents in any process that requires regular participation and follow‐through is difficult. A number of suggested improvements which created substantial interest and early momentum were ultimately left unfinished, as residents and even faculty facilitators became overwhelmed by clinical responsibilities. In fact, the majority of suggestions have not been successfully implemented and even fewer have created lasting change. This must be carefully monitored, as experiencing multiple failures can undermine the empowerment that such QI programs are created to foster.
Regular reflection on the successful and unsuccessful projects yielded several important insights that resulted in changes over the course of the program. Suggestions were more likely to move from idea generation to execution if the QIC was attended by administrators with decision‐making authority. Several of the suggestionsimproved medication reconciliation, better transfer documentation, and improved availability of infection control productswere able to be acted upon because conference attendees were administrators with purview over these issues. Many times, these leaders were more than willing to implement helpful suggestions, but simply needed them to be brought to their attention. As a result, we have been more attentive to inviting as many stakeholders as possible to the QICs.
It was also clear that suggestions would not be realized without a physician leader and were more successful when resident interest was substantial. After each QIC, residents who had made promising suggestions were approached to continue to participate. If the residents agreed, the projects were pursued and a faculty or chief resident leader was assigned. Lastly, we have also made use of one of the department's QI data analysts to assist with project completion. This individual has been made available to provide administrative support (organizing meetings, paperwork, etc) but also to provide data for projects, should the need arise.
Another important finding is that the tone of the QI program must be constantly monitored. Despite reminding residents at each session that the exercise was for the purpose of identifying systems barriers to delivering high quality care, there were times when residents felt targeted or blamed. At one point, a number of residents voiced their concerns that the conferences had spent too much time highlighting quality failures without recognizing the many positive performances on the teaching service. As a result, subsequent conferences often began by highlighting quality improvements made. Additionally, a part of 1 session each year had been dedicated to reading letters and e‐mails sent by patients or families which highlight memorably positive performances by the residents. Finally, care was taken to make sure invited guests to the sessions were reminded of the session's blame‐free ground rules.
Care must be taken when investigating clinical cases. On several occasions, attending physicians expressed discomfort with having residents scrutinize a clinical event. Although this process was protected under the QI umbrella and faculty names were never shared at the conferences, some faculty believed that this process was the purview of departmental or hospital QI staff, not untrained residents. Given the support provided for this program by the department chair and program director, as well as the professional nature with which the residents conducted their inquiries, there was little difficulty rejecting this line of objection. This feedback did lead supervisors to be more involved with the resident presenters, coaching them regarding data gathering and interviewing. If a case appears that it will be particularly sensitive, the hospitalist mentor or chief resident will reach out to involved residents and faculty to notify them that the case will be reviewed.
A final development secured, in part, as a result of this quality program has been more protected faculty time. At the start of this program, all faculty time was donated time on top of other administrative and patient care responsibilities. After the first 18 months of the QIC program, the residency program named an assistant program director for quality. At the time of writing this manuscript, the program further invested in quality by naming both an assistant and associate program director for quality. These positions combined amount to at least 0.4 full‐time equivalents (FTE). Of that, roughly 0.1 FTE is spent working on the QICs and subsequent project implementation.
Limitations
The evaluation of the success of the interventions potentially biased our findings. The qualitative method of using multiple reviewers, all of whom were invested in the program's outcomes, to gauge the success of initiated interventions may have resulted in an overestimate of the project's effectiveness. Furthermore, the category of subjective change lacks measurable criteria, making replication of the findings difficult.
The results presented here are from a single institution, conceived of and executed by a group of dedicated faculty. Moreover, both the chair of the department and the program director were very supportive of this endeavor. Possibly, because of these aspects, the findings presented here would not be readily replicated at another institution.
The percentage of residents who completed the feedback surveys was low. This may result in an overestimate of quality, value, and tone of the conferences, as well as potentially missing an opportunity for improving the program. We will address this issue through more rigorous quantitative and qualitative feedback at the end of the third year of the program.
CONCLUSIONS
Residents are willing and effective participants in a QI program. As front line providers, their experiences are valuable and their willingness to share insights can be an impetus for change. Finally, a process which includes modest investigation by third year residents, has faculty support and oversight, and provides minimal administrative support can overcome the difficulty of involving overworked residents in quality efforts.
Acknowledgements
The authors acknowledge Michael Pourdehnad for his role in developing the quality program.
- ,,.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press;1999.
- ,,,,.Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144:920–926.
- Accreditation Council for Graduate Medical Education. Program directors guide to the common program requirements. Available at: http://www.acgme.org/acWebsite/navPages/commonpr_documents/ CompleteGuide_v2%20.pdf. Accessed May 5,2010.
- ,,,.Medical errors involving trainees: a study of closed malpractice claims from 5 insurers.Arch Intern Med.2007;167:2030–2036.
- ,,,,,.Residents report on adverse events and their causes.Arch Intern Med.2005;165:2607–2613.
- ,.A system of analyzing medical errors to improve GMA curricula and programs.Acad Med.2001;76:125–133.
- ,,, et al.Changing conversations: teaching safety and quality in residency training.Acad Med.2008;83(11):1080–1087.
- ,,.Practice‐based learning and improvement: a curriculum in continuous quality improvement for surgery residents.Arch Surg.2007;142:479–483.
- .Involving residents in quality improvement: contrasting “top‐down” and “bottom‐up” approaches. Accreditation Council for Graduate Medical Education and Institute for Healthcare Improvement‐day project.ACGME Bulletin. August2008.
- ,,,,.Creating a quality improvement elective for medical house officers.Gen Intern Med.2004;19(8):861–867.
- National Center for Patient Safety. United States Department for Veteran Affairs. Root cause analysis tools. Available at: http://www.patientsafety.gov/CogAids/RCA/. Accessed August 17,2010.
- ,,, et al.Residents' engagement in quality improvement: a systematic review of the literature.Acad Med.2009;84:1757–1764.
- ,,.Graduates from a traditional medical curriculum evaluate the effectiveness of their medical curriculum through interviews.BMC Med Educ.2009;9:64.
- ,,.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press;1999.
- ,,,,.Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144:920–926.
- Accreditation Council for Graduate Medical Education. Program directors guide to the common program requirements. Available at: http://www.acgme.org/acWebsite/navPages/commonpr_documents/ CompleteGuide_v2%20.pdf. Accessed May 5,2010.
- ,,,.Medical errors involving trainees: a study of closed malpractice claims from 5 insurers.Arch Intern Med.2007;167:2030–2036.
- ,,,,,.Residents report on adverse events and their causes.Arch Intern Med.2005;165:2607–2613.
- ,.A system of analyzing medical errors to improve GMA curricula and programs.Acad Med.2001;76:125–133.
- ,,, et al.Changing conversations: teaching safety and quality in residency training.Acad Med.2008;83(11):1080–1087.
- ,,.Practice‐based learning and improvement: a curriculum in continuous quality improvement for surgery residents.Arch Surg.2007;142:479–483.
- .Involving residents in quality improvement: contrasting “top‐down” and “bottom‐up” approaches. Accreditation Council for Graduate Medical Education and Institute for Healthcare Improvement‐day project.ACGME Bulletin. August2008.
- ,,,,.Creating a quality improvement elective for medical house officers.Gen Intern Med.2004;19(8):861–867.
- National Center for Patient Safety. United States Department for Veteran Affairs. Root cause analysis tools. Available at: http://www.patientsafety.gov/CogAids/RCA/. Accessed August 17,2010.
- ,,, et al.Residents' engagement in quality improvement: a systematic review of the literature.Acad Med.2009;84:1757–1764.
- ,,.Graduates from a traditional medical curriculum evaluate the effectiveness of their medical curriculum through interviews.BMC Med Educ.2009;9:64.
Care Model for ED Boarders
Emergency Department (ED) overcrowding has become an important problem in North American hospitals.13 A national survey identified the prolonged length of stay of admitted patients in the ED as the most frequent reason for overcrowding.4 This complex problem occurs when hospital inpatient census increases and prevents admitted patients from being assigned and transported to hospital beds in a timely manner.5 The practice of holding admitted patients in the ED, known as boarding, is typically defined as the length of stay (LOS) in ED beginning 2 hours after the time of admission to the time of transfer to the wards.
In a study of daily mean ED LOS, Rathlev et al.6 concluded that a 5% increase in hospital occupancy resulted in 14 hours of holding time for all patients in the ED, and an observational study found that when hospital occupancy exceeds a threshold of 90%, the ED LOS for admitted patients correspondingly increased.7 Thus, efforts to decrease overcrowding will need to address both ED and hospital throughput and LOS. Most importantly, overcrowding has important consequences on physician and patient satisfaction and the quality of patient care.811
Between 1995 and 2005, ED visits rose 20% from 96.5 million to 115.3 million visits annually, while the number of hospital EDs decreased from 4176 to 3795, making an overall 7% increase in ED utilization rate.12 Similarly, there was a 12% increase in the total inpatient admissions for all registered hospitals in the United States from 31 million in 1995 to 35.3 million in 2005.13 However, despite this increase in demand of ED utilization and inpatient admissions, there had been a steady decline in the supply of hospital beds, from 874,000 in 1995, to 805,000 in 2006.13 These factors have exacerbated the problem of ED overcrowding and boarding.
Not only does boarding entail additional consumption of space, resources, equipment, and manpower, it also potentially compromises patient safety. Typically, hospitalists and inpatient medical teams are engaged in providing care to patients in the wards, while ED physicians and nurses are busy taking care of newly‐arrived ED patients. Non‐ED physicians may have the false impression that their boarded patients, while in the ED, are receiving continuous care and so may decide to delay seeing these patients, which can jeopardize the quality and timeliness of care. Studies have shown that ED overcrowding may potentially lead to poor patient care and outcomes and increased risk for medical errors.1416 ED overcrowding potentially causes multiple effects, including prolonging patient pain and suffering, long patient waiting time, patient dissatisfaction, ambulance diversions, decreased physician productivity, and increased frustration among medical staff.15 In a report by the Joint Commission Accreditation of Healthcare Organizations,17 ED overcrowding was cited as a significant contributing factor in sentinel event cases of patient death or permanent injury due to delays in treatment. Boarding critically ill patients who are physiologically vulnerable and unstable can allow them to be subjected to treatment delays at a pivotal point when time‐sensitive interventions are necessary, ie, sepsis or cardiogenic shockthe golden hour in trauma.16 Medical errors are usually not caused by individual errors but by complex hospital systems; and ED overcrowding is a prime example of a system problem that creates a high‐risk environment for medical errors and threatens patient safety.18
Our hospital commonly has 5 to 15 boarders and often has 20 to 30 boarders at any time. Approximately 90% of these patients are admitted to the Medical Service. In response to this challenge, our institution has designated a full‐time hospitalist to manage boarded patients. The primary goal of this new role is to ensure patient safety and the delivery of high‐quality care while admitted patients are in the ED (Table 1).
| |
| 1 | Round on all patients admitted to the Department of Medicine located in the ED, including those on the Teaching and Nonteaching Services. Rounds focus on patient safety, such as ensuring vital home and hospital medications are administered and changes in stability are noted. All patient updates are documented in the ED electronic medical records (IBEX). |
| 2 | Identify admitted patients who may be downgraded from telemetry to nontelemetry status. Telemetry and cardiac beds are in high demand, and decreasing utilization facilitates obtaining the appropriate ward bed for ED patients. |
| 3 | Assess admitted patients for possible discharge. The patient's condition may have improved or results may indicate that admission is no longer required. The ED hospitalist communicates with the ED physician and wards teams, facilitates management, implements the discharge, and ensures adequate follow‐up. |
| 4 | Refer patients to an ED social worker as needed. |
| 5 | Facilitate referrals to other medical or surgical specialties if indicated. |
| 6 | Clarify the plan of care with the ED staff and facilitates ED communication with the ward team. Acts as a liaison and a resource for the ED physicians and nursing staff. |
| 7 | Supervise the triage duties of the medical admitting resident. |
| 8 | Provide medical consultation to ED physicians for patients not being admitted to the hospital or who are being admitted to other services (eg, surgery). |
The objectives of the study were to determine: (1) the impact on quality of care by assessing laboratory results acted upon and medication follow‐up by the ED hospitalist, and (2) the impact on throughput by assessing the number of ED discharges and telemetry downgrades.
Methods
Setting
The Mount Sinai Medical Center is a tertiary‐care 1121‐bed acute care teaching hospital located in New York City. The hospital borders East Harlem and the Upper East Side of Manhattan. The Medical Service is composed of a Teaching Service, composed of house staff and attendings, and a non‐Teaching Service, composed of nurse practitioners, physician assistants, and attendings. Hospitalists and private attendings may have patients on either the Teaching or the non‐Teaching Service. In 2007, there were 56,541 patients admitted for a total of 332,368 days. The mean LOS for medical inpatients was 5.89 days. The total ED visit was 79,500 with a total inpatient and critical care admissions of 24,522. The mean and median LOS for all ED patients were 623 minutes and 493 minutes, respectively. There were 11,488 patients who qualified as boarders, averaging 31.5 boarders per 24 hours; with a mean and median LOS per boarder of 288 minutes and 198 minutes, respectively. The ED LOS for admitted patients ranged from 2 minutes to 4074 minutes (2.83 days).
Admission Process
Once an ED attending physician decides that a patient is to be admitted, the patient is placed on a computerized list in the ED's electronic medical record (IBEX software). The Medical Admitting Resident (MAR) evaluates and triages admitted patients, and assigns and gives a verbal report to the appropriate Medicine Service (ie, Teaching, non‐Teaching, cardiac telemetry unit, intensive care, etc.). The Admitting Office searches for and assigns the appropriate unit and bed for the patient. A hospitalist or resident physician performs the patient's initial assessment and evaluation in the ED, and admission orders are placed in the inpatient computerized order entry system (TDS). When the bed is ready, the ED nurse gives a verbal report to the floor nurse, and the patient is transported to the ward.
Responsibilities
The specific responsibilities of the ED hospitalist are listed in Table 1. The primary role is to round on patients admitted to the Medicine Service who are located in the ED. This encompasses a wide array of patients and services, including patients assigned to a hospitalist service attending or who have a private attending, patients admitted to the Teaching or non‐Teaching Service, patients admitted to the intensive care unit, and patients admitted to a general medicine or specialty service (eg, telemetry, oncology, human immunodeficiency virus [HIV]). Rounding includes review of the ED's electronic medical record as well as direct examination of patients. The hospitalist focuses on patients with longer ED LOS and on aspects of care that may lapse while patients remain in the ED for prolonged periods. At our institution, the follow‐up of subsequent tests, laboratory values, and medications for ED boarders is the responsibility of the primary inpatient team, though the ED physicians act on urgent and critical results and continue to deliver all emergency care. Through rounding, the ED hospitalist is able to identify abnormal results in a timely manner, alert the ED physician and primary inpatient team, and address abnormalities. Specific examples of laboratory results acted upon include hypokalemia, hyperglycemia, and elevated cardiac enzymes. The ED hospitalist is also able to determine whether any outpatient medications have not yet been administered (eg, antihypertensives, immune suppressants) and ensure that subsequent doses of medications initiated in the ED (eg, antibiotics) are administered during the appropriate timeframe.
Communication is emphasized, as contact with ED physicians, ward physicians, and often the outpatient primary care physician is required when any change in management is considered. The ED hospitalist also provides the capability of rapid response to changes in patient status (eg, a new complaint or fever). In addition, the hospitalist is available to consult on medical patients who may not require admission and on nonmedical patients for whom an internal medicine consult may be beneficial (eg, preoperative optimization of a surgical patient). The ED hospitalist documents the evaluation in the IBEX system. Bills were submitted for visits in which patients were discharged as these encounters are comprehensive, but not for other encounters.
Data Collection
The ED hospitalist role began March 10, 2008 and is a 10‐hour shift (8 AM to 6 PM) on weekdays. The study period was from March 10, 2008 through June 30, 2008. The study was approved by the hospital's institutional review board.
Data were collected on aspects of care that could have been impacted by the ED hospitalist, including medication and laboratory orders, ED discharges, ED admissions avoided, and telemetry downgrades. Discharges from ED refers to boarded admitted patients in the ED, who by the judgment of the ED hospitalist were ready for discharge. Admissions avoided refers to patients who the ED physician planned to admit but had not yet been admitted, and whose admission was avoided through the recommendations made by the ED hospitalist. The ED LOS was defined as the duration of time from when the patient was admitted to the Medicine Service to the time the patient was transferred to a medical ward. Telemetry downgrades were defined as patients assigned to the cardiac telemetry unit who the hospitalist determined required only telemetry on a general medical unit or did not require telemetry, or patients assigned to telemetry on a general medicine unit who the hospitalist determined no longer required telemetry.
Results were expressed as percentages of patients admitted to a Medicine Service and percentage of patients evaluated by the ED hospitalist, as indicated. 95% confidence intervals (CI) were calculated.
Results
During the study period, there were 4363 patients admitted to the Medicine Service and 3555 patients who qualified as boarders (mean of 29 boarders per 24 hours). The mean boarding time of admitted patients was 440 minutes. A total of 634 patients (17.8% of all boarded patients) were evaluated by the ED hospitalist. The mean daily number of patients seen by the ED hospitalist was 8.0.
The key elements of the delivery of care by the ED hospitalist are summarized in Table 2.
| Elements | Boarders (n = 3555) [n (%)] | Patients Intervened on (n = 634) [n (%)] |
|---|---|---|
| ||
| Laboratory results acted upon | 472 (13.2) | 472 (74.5) |
| Medication follow‐up | 506 (14.2) | 506 (79.8) |
| Discharges from the ED* | 46 (1.3) | 46 (7.3) |
| Admissions avoided | 6 (0.2) | 6 (0.95) |
| Telemetry downgrades | 61 (1.8) | 61 (9.6) |
The care of boarded patients included follow‐up of laboratory tests for 74.5% (95% CI, 71‐78%) and medication orders for 79.8% (95% CI, 77‐83%) of patients. A total of 46 patients were discharged by the ED hospitalist (0.6 discharges/day) and telemetry was discontinued for 61 patients (0.8 downgrades/day). The discharge rate was 7.3% (95% CI, 5‐10%) and telemetry downgrade rate was 9.6% (95% CI, 8‐12%) of those patients assessed by the ED hospitalist. Expressed as a percentage of the total ED boarders (n = 3555), the combined discharge rate and the admissions avoided rate was 1.5%.
Table 3 shows the discharge diagnoses made from the ED. Chest pain was the most common diagnosis, followed by syncope, pneumonia, and chronic obstructive pulmonary disease (COPD).
| Diagnoses | Patients (n = 46) [n (%)] |
|---|---|
| |
| Chest pain | 12 (26) |
| Syncope/dizziness | 7 (15) |
| Pneumonia | 4 (9) |
| COPD | 4 (9) |
| Congestive heart failure | 3 (7) |
| Gastroenteritis | 3 (7) |
| Dermatitis/rash | 3 (7) |
| Alcohol abuse | 3 (7) |
| Abdominal pain | 3 (7) |
| End stage renal disease | 2 (4) |
| Vaginal bleeding | 1 (2) |
| Fall | 1 (2) |
| Asthma | 1 (2) |
Discussion
Our hospital has successfully implemented an innovative strategy utilizing a hospitalist to help provide seamless care to medical patients located in the ED. Other solutions at our hospital had previously been implemented, but had not adequately addressed the problem, including: (1) protocols to monitor length of stay patterns and deviations, (2) discharge planning activities, (3) organized computerized bed tracking, (4) improvement in the timeliness of ancillary services, (5) daily bed briefing among nurse managers, and (6) 24‐hour presence of a MAR to facilitate triage in the ED.
The current study demonstrates the potential for substantial impact on patient care. The substantial number of the assessed boarder patients for whom laboratory tests (74.5%) and medications (79.8%) were ordered by the ED hospitalists suggests that the quality and timeliness of care was enhanced by this initiative. In addition, the considerable number of patients discharged from the ED and downgraded from telemetry (1.5% and 1.8% of all boarder patients, respectively) suggests that an ED hospitalist may have a meaningful impact on bed utilization and thus decrease ED overcrowding. In 2007, there were 11,488 who qualified as boarders; our data suggest that an ED hospitalist would result in approximately 172 boarders not being admitted annually.
Though the ED LOS was higher during the study period compared to 2007, it was lower than the 2 months immediately preceding implementation of the ED hospitalist role. The ED LOS was 732 and 658 minutes for January and February 2008, respectively, which was markedly increased from 2007 (288 minutes), and prompted development of the ED hospitalist role. The ED LOS during the study period subsequently decreased to 440 minutes. Though the wide fluctuations in ED LOS and the short time period with high ED LOS prior to implementation preclude concluding that the ED hospitalist role decreased ED LOS, the data suggest that an ED hospitalist may be able to improve ED throughput.
The majority of the discharges made by the ED hospitalist are patients who had been admitted for chest pain, had improved, and had negative cardiac enzymes and stress tests. Patients with syncope who were discharged were likely patients without any comorbidities. The COPD and pneumonia admissions were likely patients who improved after aggressive treatment in the ED.
The impact of ED overcrowding on the quality of patient care and outcomes may be substantial. Hwang et al.19 found a direct correlation between ED census and time to pain assessment and administration of analgesic medication. A study at an academic medical center found that higher ED volume was associated with less likelihood of antibiotics being administered within 4 hours for patients with community‐acquired pneumonia.20 A comprehensive review of the literature identified 41 studies examining the effects of ED overcrowding on clinical outcomes and the investigators noted that ED overcrowding was associated with increased in‐hospital mortality.8
Causes of poor outcomes during periods of overcrowding may be the high volume of acute patients preventing adequate time and attention for each ED patient, as well as confusion during the transition from ED to ward physicians. For example, a patient may receive their initial dose of antibiotics from the ED physician, but subsequent doses may be overlooked in the transition of care from the ED physician to the inpatient team. In addition, having admitted patients located in the ED for extended periods of time may lead to these patients not being seen as frequently as patients admitted to the inpatient wards. Another potential consequence of prolonged ED stay for admitted patients is delay in inpatient management. Tests done in the ED may prompt further studies that may not be ordered promptly while patients remain in the ED, which subsequently increases LOS. Other potential issues may be an increase in confusion among geriatric patients in a noisy and crowded ED; decreased access to specialized nursing care that may be available on a hospital ward; decreased access to physical therapy and occupational therapy services; and decreased comfort and satisfaction as patients wait in overcrowded EDs for prolonged periods.
Several other potential innovative solutions to ED overcrowding have been proposed, studied, and tested. These measures generally are focused on improving the three interdependent components of ED workflow: INPUT THROUGHPUT OUTPUT.21, 22 However, process redesign and intervention on these 3 interdependent ED workflow components may be difficult to achieve, especially when hospital resources are limited and when inpatient hospital capacity is already maximized. In some institutions, efforts have been reported to successfully streamline the transfer of admitted ED patients to inpatient beds, through transfer‐to‐ward policy interventions (eg, physician coordinators for patient flow and bed management or transfers made within a defined period of time).2326 However, in a study by Quinn et al.,27 implementation of a rapid admission policy resulted in a decrease of only 10.1 minutes in the ED LOS. Several studies have demonstrated the benefits of an acute medical admissions unit in alleviating ED overcrowding.28, 29 Other unconventional solutions by some hospitals include sending admitted patients to the unit's hallways or placing discharged patients in the hallway while waiting for transportation so that the ED bed will be readily available.30
The ED hospitalist is well‐situated to have an impact on several key hospital outcomes. As the ED hospitalist role was shown to affect processes that relate to ED throughput, it is possible that the role will improve ED overcrowding and decrease ED LOS. Specifically, identifying patients who can be discharged and for whom telemetry is no longer indicated decreases unnecessary bed utilization and allows these beds to be available for other ED patients. This initiative also may promote patient satisfaction by assuring patients that their medical and concerns are being fully addressed while they are in the ED. Increased emphasis on hospital reporting will make patient satisfaction a priority for many hospitals, and the ED hospitalist will be in a unique position to meet and greet patients admitted to the Medicine Service and to reassure them that the medical team is present and addressing their concerns. The hospitalist's ability to facilitate diagnostic testing and treatment while patients remain in the ED may also help decrease the total LOS in the hospital. In addition, the ED hospitalist is also in position to recognize social factors at the earliest stage of admission so that they can be immediately addressed. Future studies will need to be done to determine if this model of transitional care impacts these important factors.
Our study has several important limitations. Most notably, the lack of a comparison interval for which a hospitalist was not assigned to this role prevents us from drawing any definitive conclusions on the benefits of the ED hospitalist model. Also, we collected only summary data and do not have demographic data on the patients managed by the ED hospitalist or information on the ED course of patients who were discharged or had telemetry downgraded. This prevents determination of whether discharged patients did not require admission initially or whose condition evolved over a prolonged ED stay. In addition, other key outcomes, such as patient satisfaction and satisfaction of the ED physicians and nursing staff have not yet been formally measured. Future studies will be needed to determine if an ED hospital model can improve important process and clinical outcomes.
The greatest challenge of this initiative was introducing and familiarizing this role to the key stakeholders, including the ED physicians and nursing staff, house staff, and private practice physicians. Though we did not perform structured surveys on satisfaction, through informal discussions we noted that the role was welcomed with enthusiasm by the ED physicians. Notably, several ED physicians expressed appreciation that they were able to focus their care on new ED patients rather than on the boarded ED patients. Through feedback, we noted soon after implementation that ED faculty and nurses needed further clarification about the potential overlapping roles of the ED hospitalist and ED physicians and ward physicians. These concerns were addressed by educational sessions and announcements, including presentations at ED faculty and staff meetings. The hospitalist assigned to the role each month received individualized orientation prior to assuming the role, and an ED Hospitalist Manual was distributed. Possibly due to these focused sessions, the hospitalists assigned to the role became quickly acclimated.
Conclusions
We have found that designating a hospitalist to directly address the care of ED boarders can enhance the quality and timeliness of care and decrease bed and telemetry utilization with the potential to impact ED and hospital LOS. Given the success of the pilot model, the role was expanded at our institution to 10 hours per day, 7 days per week. Hospitals struggling to address the needs of their admitted patients in the ED should consider incorporating an ED hospitalist to enhance clinical care and address issues relating to throughput. A follow‐up study is needed to more precisely describe the impact of the ED hospitalist model.
- , , , et al.Estimating the degree of emergency department overcrowding in academic medical centers: results of the National ED Overcrowding Study (NEDOCS).Acad Emerg Med.2004;11:38–50.
- , , , et al.Frequency, determinants, and impact of overcrowding in emergency departments in Canada: a national survey.Healthc Q.2007;10:32–40.
- , .EMDOC (emergency department overcrowding) internet‐based safety net research.Admin Emerg Med.2008;35:101–107.
- United States General Accounting Office.Hospital Emergency Departments: Crowded Conditions Vary Among Hospitals and Communities. March 2003.Washington, DC:General Accounting Office;2003.
- .Overcrowding in emergency department: increased demand and decreased capacity.Ann Emerg Med.2002;39:430–432.
- , , , et al.Time series analysis of variables associated with daily mean emergency department length of stay.Ann Emerg Med.2007;49:265–271.
- , , , et al.Effect of hospital occupancy on emergency department length of stay and patient disposition.Ann Emerg Med.2003;10:127–133.
- , , , et al.The effect of emergency department crowding on clinically oriented outcomes.Acad Emerg Med.2009;16:1–10.
- , .Emergency department overcrowding: the impact of resource scarcity on physician job satisfaction.J Health Manag.2005;50:327–340.
- , , , , , .The effect of emergency department crowding on patient satisfaction for admitted patients.Acad Emerg Med.2008;15:825–831.
- , .The effect of crowding on access and quality in an academic ED.Am J Emerg Med.2006;24:787–794.
- , , .National Hospital Ambulatory Medical Care Survey: 2005 Emergency Department Summary. Advance Data from Vital and Health Statistics. No. 386.Hyattsville, MD:National Center for Health Statistics;2007.
- American Hospital Association (AHA).Table 1: Historical trends in utilization, personnel, and finances: year 1946–2006.AHA Hospital Statistics.2008 ed.Chicago:Health Forum LLC;2008:3.
- , .Emergency department overcrowding in the US: an emerging threat to patient safety and public health.Emerg Med J.2003;20:402–405.
- , .Overcrowding in the nation's emergency departments: complex causes and disturbing effects.Ann Emerg Med.2000;35:63–68.
- , .Clinical review: emergency department overcrowding and the potential impact on the critically ill.Crit Care.2005;9:291–295.
- Joint Commission on Accreditation of Healthcare Organizations (JCAHO): Sentinel event alert 2002, Issue 26. Available at: http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_26.htm. Accessed October2009.
- , , , et al.Safety net research in emergency medicine: proceedings of the Academic Emergency Consensus Conference on “The Unraveling Safety Net.”Acad Emerg Med.2001;8:1024–1029.
- , , , , , .Emergency department crowding and decreased quality of pain care.Acad Emerg Med.2008;15:1248–1256.
- , , , .Effect of emergency department crowding on time to antibiotics in patients admitted with community‐acquired pneumonia.Ann Emerg Med.2007;50:501–509.
- , , , et al.A conceptual model of emergency department crowding.Ann Emerg Med.2003;42:173–180.
- , , , et al.Emergency department crowding: consensus development of potential measures.Ann Emerg Med.2003;42:824–834.
- , , , et al.Intervention to decrease emergency department crowding: does it have an effect on return visits and hospital readmission?Ann Emerg Med.2003;41:173–185.
- , , , et al.Rapid process design in a university‐based emergency department: decreasing waiting time intervals and improving patient satisfaction.Ann Emerg Med.2002;39:168–177.
- .Emergency department crowding: an action plan.Acad Emerg Med.2001;18:185–187.
- , , .Hospitalists and an innovative emergency department admission process.J Gen Intern Med.2004;19:266–268.
- , , et al.Effects of implementing a rapid admission policy in the ED.Am J Emerg Med.2007;25:559–563.
- , , .Effect of an emergency department managed acute care unit on ED overcrowding and emergency medical services diversion.Acad Emerg Med.2001;8:1085–1100.
- , , , .Emergency department census of patients awaiting admission following reorganization of an admissions process.Emerg Med J.2006;23:363–367.
- .Emergency department flow and the boarded patient: how to get admitted patients upstairs.Ann Emerg Med.2007;49:68–70.
Emergency Department (ED) overcrowding has become an important problem in North American hospitals.13 A national survey identified the prolonged length of stay of admitted patients in the ED as the most frequent reason for overcrowding.4 This complex problem occurs when hospital inpatient census increases and prevents admitted patients from being assigned and transported to hospital beds in a timely manner.5 The practice of holding admitted patients in the ED, known as boarding, is typically defined as the length of stay (LOS) in ED beginning 2 hours after the time of admission to the time of transfer to the wards.
In a study of daily mean ED LOS, Rathlev et al.6 concluded that a 5% increase in hospital occupancy resulted in 14 hours of holding time for all patients in the ED, and an observational study found that when hospital occupancy exceeds a threshold of 90%, the ED LOS for admitted patients correspondingly increased.7 Thus, efforts to decrease overcrowding will need to address both ED and hospital throughput and LOS. Most importantly, overcrowding has important consequences on physician and patient satisfaction and the quality of patient care.811
Between 1995 and 2005, ED visits rose 20% from 96.5 million to 115.3 million visits annually, while the number of hospital EDs decreased from 4176 to 3795, making an overall 7% increase in ED utilization rate.12 Similarly, there was a 12% increase in the total inpatient admissions for all registered hospitals in the United States from 31 million in 1995 to 35.3 million in 2005.13 However, despite this increase in demand of ED utilization and inpatient admissions, there had been a steady decline in the supply of hospital beds, from 874,000 in 1995, to 805,000 in 2006.13 These factors have exacerbated the problem of ED overcrowding and boarding.
Not only does boarding entail additional consumption of space, resources, equipment, and manpower, it also potentially compromises patient safety. Typically, hospitalists and inpatient medical teams are engaged in providing care to patients in the wards, while ED physicians and nurses are busy taking care of newly‐arrived ED patients. Non‐ED physicians may have the false impression that their boarded patients, while in the ED, are receiving continuous care and so may decide to delay seeing these patients, which can jeopardize the quality and timeliness of care. Studies have shown that ED overcrowding may potentially lead to poor patient care and outcomes and increased risk for medical errors.1416 ED overcrowding potentially causes multiple effects, including prolonging patient pain and suffering, long patient waiting time, patient dissatisfaction, ambulance diversions, decreased physician productivity, and increased frustration among medical staff.15 In a report by the Joint Commission Accreditation of Healthcare Organizations,17 ED overcrowding was cited as a significant contributing factor in sentinel event cases of patient death or permanent injury due to delays in treatment. Boarding critically ill patients who are physiologically vulnerable and unstable can allow them to be subjected to treatment delays at a pivotal point when time‐sensitive interventions are necessary, ie, sepsis or cardiogenic shockthe golden hour in trauma.16 Medical errors are usually not caused by individual errors but by complex hospital systems; and ED overcrowding is a prime example of a system problem that creates a high‐risk environment for medical errors and threatens patient safety.18
Our hospital commonly has 5 to 15 boarders and often has 20 to 30 boarders at any time. Approximately 90% of these patients are admitted to the Medical Service. In response to this challenge, our institution has designated a full‐time hospitalist to manage boarded patients. The primary goal of this new role is to ensure patient safety and the delivery of high‐quality care while admitted patients are in the ED (Table 1).
| |
| 1 | Round on all patients admitted to the Department of Medicine located in the ED, including those on the Teaching and Nonteaching Services. Rounds focus on patient safety, such as ensuring vital home and hospital medications are administered and changes in stability are noted. All patient updates are documented in the ED electronic medical records (IBEX). |
| 2 | Identify admitted patients who may be downgraded from telemetry to nontelemetry status. Telemetry and cardiac beds are in high demand, and decreasing utilization facilitates obtaining the appropriate ward bed for ED patients. |
| 3 | Assess admitted patients for possible discharge. The patient's condition may have improved or results may indicate that admission is no longer required. The ED hospitalist communicates with the ED physician and wards teams, facilitates management, implements the discharge, and ensures adequate follow‐up. |
| 4 | Refer patients to an ED social worker as needed. |
| 5 | Facilitate referrals to other medical or surgical specialties if indicated. |
| 6 | Clarify the plan of care with the ED staff and facilitates ED communication with the ward team. Acts as a liaison and a resource for the ED physicians and nursing staff. |
| 7 | Supervise the triage duties of the medical admitting resident. |
| 8 | Provide medical consultation to ED physicians for patients not being admitted to the hospital or who are being admitted to other services (eg, surgery). |
The objectives of the study were to determine: (1) the impact on quality of care by assessing laboratory results acted upon and medication follow‐up by the ED hospitalist, and (2) the impact on throughput by assessing the number of ED discharges and telemetry downgrades.
Methods
Setting
The Mount Sinai Medical Center is a tertiary‐care 1121‐bed acute care teaching hospital located in New York City. The hospital borders East Harlem and the Upper East Side of Manhattan. The Medical Service is composed of a Teaching Service, composed of house staff and attendings, and a non‐Teaching Service, composed of nurse practitioners, physician assistants, and attendings. Hospitalists and private attendings may have patients on either the Teaching or the non‐Teaching Service. In 2007, there were 56,541 patients admitted for a total of 332,368 days. The mean LOS for medical inpatients was 5.89 days. The total ED visit was 79,500 with a total inpatient and critical care admissions of 24,522. The mean and median LOS for all ED patients were 623 minutes and 493 minutes, respectively. There were 11,488 patients who qualified as boarders, averaging 31.5 boarders per 24 hours; with a mean and median LOS per boarder of 288 minutes and 198 minutes, respectively. The ED LOS for admitted patients ranged from 2 minutes to 4074 minutes (2.83 days).
Admission Process
Once an ED attending physician decides that a patient is to be admitted, the patient is placed on a computerized list in the ED's electronic medical record (IBEX software). The Medical Admitting Resident (MAR) evaluates and triages admitted patients, and assigns and gives a verbal report to the appropriate Medicine Service (ie, Teaching, non‐Teaching, cardiac telemetry unit, intensive care, etc.). The Admitting Office searches for and assigns the appropriate unit and bed for the patient. A hospitalist or resident physician performs the patient's initial assessment and evaluation in the ED, and admission orders are placed in the inpatient computerized order entry system (TDS). When the bed is ready, the ED nurse gives a verbal report to the floor nurse, and the patient is transported to the ward.
Responsibilities
The specific responsibilities of the ED hospitalist are listed in Table 1. The primary role is to round on patients admitted to the Medicine Service who are located in the ED. This encompasses a wide array of patients and services, including patients assigned to a hospitalist service attending or who have a private attending, patients admitted to the Teaching or non‐Teaching Service, patients admitted to the intensive care unit, and patients admitted to a general medicine or specialty service (eg, telemetry, oncology, human immunodeficiency virus [HIV]). Rounding includes review of the ED's electronic medical record as well as direct examination of patients. The hospitalist focuses on patients with longer ED LOS and on aspects of care that may lapse while patients remain in the ED for prolonged periods. At our institution, the follow‐up of subsequent tests, laboratory values, and medications for ED boarders is the responsibility of the primary inpatient team, though the ED physicians act on urgent and critical results and continue to deliver all emergency care. Through rounding, the ED hospitalist is able to identify abnormal results in a timely manner, alert the ED physician and primary inpatient team, and address abnormalities. Specific examples of laboratory results acted upon include hypokalemia, hyperglycemia, and elevated cardiac enzymes. The ED hospitalist is also able to determine whether any outpatient medications have not yet been administered (eg, antihypertensives, immune suppressants) and ensure that subsequent doses of medications initiated in the ED (eg, antibiotics) are administered during the appropriate timeframe.
Communication is emphasized, as contact with ED physicians, ward physicians, and often the outpatient primary care physician is required when any change in management is considered. The ED hospitalist also provides the capability of rapid response to changes in patient status (eg, a new complaint or fever). In addition, the hospitalist is available to consult on medical patients who may not require admission and on nonmedical patients for whom an internal medicine consult may be beneficial (eg, preoperative optimization of a surgical patient). The ED hospitalist documents the evaluation in the IBEX system. Bills were submitted for visits in which patients were discharged as these encounters are comprehensive, but not for other encounters.
Data Collection
The ED hospitalist role began March 10, 2008 and is a 10‐hour shift (8 AM to 6 PM) on weekdays. The study period was from March 10, 2008 through June 30, 2008. The study was approved by the hospital's institutional review board.
Data were collected on aspects of care that could have been impacted by the ED hospitalist, including medication and laboratory orders, ED discharges, ED admissions avoided, and telemetry downgrades. Discharges from ED refers to boarded admitted patients in the ED, who by the judgment of the ED hospitalist were ready for discharge. Admissions avoided refers to patients who the ED physician planned to admit but had not yet been admitted, and whose admission was avoided through the recommendations made by the ED hospitalist. The ED LOS was defined as the duration of time from when the patient was admitted to the Medicine Service to the time the patient was transferred to a medical ward. Telemetry downgrades were defined as patients assigned to the cardiac telemetry unit who the hospitalist determined required only telemetry on a general medical unit or did not require telemetry, or patients assigned to telemetry on a general medicine unit who the hospitalist determined no longer required telemetry.
Results were expressed as percentages of patients admitted to a Medicine Service and percentage of patients evaluated by the ED hospitalist, as indicated. 95% confidence intervals (CI) were calculated.
Results
During the study period, there were 4363 patients admitted to the Medicine Service and 3555 patients who qualified as boarders (mean of 29 boarders per 24 hours). The mean boarding time of admitted patients was 440 minutes. A total of 634 patients (17.8% of all boarded patients) were evaluated by the ED hospitalist. The mean daily number of patients seen by the ED hospitalist was 8.0.
The key elements of the delivery of care by the ED hospitalist are summarized in Table 2.
| Elements | Boarders (n = 3555) [n (%)] | Patients Intervened on (n = 634) [n (%)] |
|---|---|---|
| ||
| Laboratory results acted upon | 472 (13.2) | 472 (74.5) |
| Medication follow‐up | 506 (14.2) | 506 (79.8) |
| Discharges from the ED* | 46 (1.3) | 46 (7.3) |
| Admissions avoided | 6 (0.2) | 6 (0.95) |
| Telemetry downgrades | 61 (1.8) | 61 (9.6) |
The care of boarded patients included follow‐up of laboratory tests for 74.5% (95% CI, 71‐78%) and medication orders for 79.8% (95% CI, 77‐83%) of patients. A total of 46 patients were discharged by the ED hospitalist (0.6 discharges/day) and telemetry was discontinued for 61 patients (0.8 downgrades/day). The discharge rate was 7.3% (95% CI, 5‐10%) and telemetry downgrade rate was 9.6% (95% CI, 8‐12%) of those patients assessed by the ED hospitalist. Expressed as a percentage of the total ED boarders (n = 3555), the combined discharge rate and the admissions avoided rate was 1.5%.
Table 3 shows the discharge diagnoses made from the ED. Chest pain was the most common diagnosis, followed by syncope, pneumonia, and chronic obstructive pulmonary disease (COPD).
| Diagnoses | Patients (n = 46) [n (%)] |
|---|---|
| |
| Chest pain | 12 (26) |
| Syncope/dizziness | 7 (15) |
| Pneumonia | 4 (9) |
| COPD | 4 (9) |
| Congestive heart failure | 3 (7) |
| Gastroenteritis | 3 (7) |
| Dermatitis/rash | 3 (7) |
| Alcohol abuse | 3 (7) |
| Abdominal pain | 3 (7) |
| End stage renal disease | 2 (4) |
| Vaginal bleeding | 1 (2) |
| Fall | 1 (2) |
| Asthma | 1 (2) |
Discussion
Our hospital has successfully implemented an innovative strategy utilizing a hospitalist to help provide seamless care to medical patients located in the ED. Other solutions at our hospital had previously been implemented, but had not adequately addressed the problem, including: (1) protocols to monitor length of stay patterns and deviations, (2) discharge planning activities, (3) organized computerized bed tracking, (4) improvement in the timeliness of ancillary services, (5) daily bed briefing among nurse managers, and (6) 24‐hour presence of a MAR to facilitate triage in the ED.
The current study demonstrates the potential for substantial impact on patient care. The substantial number of the assessed boarder patients for whom laboratory tests (74.5%) and medications (79.8%) were ordered by the ED hospitalists suggests that the quality and timeliness of care was enhanced by this initiative. In addition, the considerable number of patients discharged from the ED and downgraded from telemetry (1.5% and 1.8% of all boarder patients, respectively) suggests that an ED hospitalist may have a meaningful impact on bed utilization and thus decrease ED overcrowding. In 2007, there were 11,488 who qualified as boarders; our data suggest that an ED hospitalist would result in approximately 172 boarders not being admitted annually.
Though the ED LOS was higher during the study period compared to 2007, it was lower than the 2 months immediately preceding implementation of the ED hospitalist role. The ED LOS was 732 and 658 minutes for January and February 2008, respectively, which was markedly increased from 2007 (288 minutes), and prompted development of the ED hospitalist role. The ED LOS during the study period subsequently decreased to 440 minutes. Though the wide fluctuations in ED LOS and the short time period with high ED LOS prior to implementation preclude concluding that the ED hospitalist role decreased ED LOS, the data suggest that an ED hospitalist may be able to improve ED throughput.
The majority of the discharges made by the ED hospitalist are patients who had been admitted for chest pain, had improved, and had negative cardiac enzymes and stress tests. Patients with syncope who were discharged were likely patients without any comorbidities. The COPD and pneumonia admissions were likely patients who improved after aggressive treatment in the ED.
The impact of ED overcrowding on the quality of patient care and outcomes may be substantial. Hwang et al.19 found a direct correlation between ED census and time to pain assessment and administration of analgesic medication. A study at an academic medical center found that higher ED volume was associated with less likelihood of antibiotics being administered within 4 hours for patients with community‐acquired pneumonia.20 A comprehensive review of the literature identified 41 studies examining the effects of ED overcrowding on clinical outcomes and the investigators noted that ED overcrowding was associated with increased in‐hospital mortality.8
Causes of poor outcomes during periods of overcrowding may be the high volume of acute patients preventing adequate time and attention for each ED patient, as well as confusion during the transition from ED to ward physicians. For example, a patient may receive their initial dose of antibiotics from the ED physician, but subsequent doses may be overlooked in the transition of care from the ED physician to the inpatient team. In addition, having admitted patients located in the ED for extended periods of time may lead to these patients not being seen as frequently as patients admitted to the inpatient wards. Another potential consequence of prolonged ED stay for admitted patients is delay in inpatient management. Tests done in the ED may prompt further studies that may not be ordered promptly while patients remain in the ED, which subsequently increases LOS. Other potential issues may be an increase in confusion among geriatric patients in a noisy and crowded ED; decreased access to specialized nursing care that may be available on a hospital ward; decreased access to physical therapy and occupational therapy services; and decreased comfort and satisfaction as patients wait in overcrowded EDs for prolonged periods.
Several other potential innovative solutions to ED overcrowding have been proposed, studied, and tested. These measures generally are focused on improving the three interdependent components of ED workflow: INPUT THROUGHPUT OUTPUT.21, 22 However, process redesign and intervention on these 3 interdependent ED workflow components may be difficult to achieve, especially when hospital resources are limited and when inpatient hospital capacity is already maximized. In some institutions, efforts have been reported to successfully streamline the transfer of admitted ED patients to inpatient beds, through transfer‐to‐ward policy interventions (eg, physician coordinators for patient flow and bed management or transfers made within a defined period of time).2326 However, in a study by Quinn et al.,27 implementation of a rapid admission policy resulted in a decrease of only 10.1 minutes in the ED LOS. Several studies have demonstrated the benefits of an acute medical admissions unit in alleviating ED overcrowding.28, 29 Other unconventional solutions by some hospitals include sending admitted patients to the unit's hallways or placing discharged patients in the hallway while waiting for transportation so that the ED bed will be readily available.30
The ED hospitalist is well‐situated to have an impact on several key hospital outcomes. As the ED hospitalist role was shown to affect processes that relate to ED throughput, it is possible that the role will improve ED overcrowding and decrease ED LOS. Specifically, identifying patients who can be discharged and for whom telemetry is no longer indicated decreases unnecessary bed utilization and allows these beds to be available for other ED patients. This initiative also may promote patient satisfaction by assuring patients that their medical and concerns are being fully addressed while they are in the ED. Increased emphasis on hospital reporting will make patient satisfaction a priority for many hospitals, and the ED hospitalist will be in a unique position to meet and greet patients admitted to the Medicine Service and to reassure them that the medical team is present and addressing their concerns. The hospitalist's ability to facilitate diagnostic testing and treatment while patients remain in the ED may also help decrease the total LOS in the hospital. In addition, the ED hospitalist is also in position to recognize social factors at the earliest stage of admission so that they can be immediately addressed. Future studies will need to be done to determine if this model of transitional care impacts these important factors.
Our study has several important limitations. Most notably, the lack of a comparison interval for which a hospitalist was not assigned to this role prevents us from drawing any definitive conclusions on the benefits of the ED hospitalist model. Also, we collected only summary data and do not have demographic data on the patients managed by the ED hospitalist or information on the ED course of patients who were discharged or had telemetry downgraded. This prevents determination of whether discharged patients did not require admission initially or whose condition evolved over a prolonged ED stay. In addition, other key outcomes, such as patient satisfaction and satisfaction of the ED physicians and nursing staff have not yet been formally measured. Future studies will be needed to determine if an ED hospital model can improve important process and clinical outcomes.
The greatest challenge of this initiative was introducing and familiarizing this role to the key stakeholders, including the ED physicians and nursing staff, house staff, and private practice physicians. Though we did not perform structured surveys on satisfaction, through informal discussions we noted that the role was welcomed with enthusiasm by the ED physicians. Notably, several ED physicians expressed appreciation that they were able to focus their care on new ED patients rather than on the boarded ED patients. Through feedback, we noted soon after implementation that ED faculty and nurses needed further clarification about the potential overlapping roles of the ED hospitalist and ED physicians and ward physicians. These concerns were addressed by educational sessions and announcements, including presentations at ED faculty and staff meetings. The hospitalist assigned to the role each month received individualized orientation prior to assuming the role, and an ED Hospitalist Manual was distributed. Possibly due to these focused sessions, the hospitalists assigned to the role became quickly acclimated.
Conclusions
We have found that designating a hospitalist to directly address the care of ED boarders can enhance the quality and timeliness of care and decrease bed and telemetry utilization with the potential to impact ED and hospital LOS. Given the success of the pilot model, the role was expanded at our institution to 10 hours per day, 7 days per week. Hospitals struggling to address the needs of their admitted patients in the ED should consider incorporating an ED hospitalist to enhance clinical care and address issues relating to throughput. A follow‐up study is needed to more precisely describe the impact of the ED hospitalist model.
Emergency Department (ED) overcrowding has become an important problem in North American hospitals.13 A national survey identified the prolonged length of stay of admitted patients in the ED as the most frequent reason for overcrowding.4 This complex problem occurs when hospital inpatient census increases and prevents admitted patients from being assigned and transported to hospital beds in a timely manner.5 The practice of holding admitted patients in the ED, known as boarding, is typically defined as the length of stay (LOS) in ED beginning 2 hours after the time of admission to the time of transfer to the wards.
In a study of daily mean ED LOS, Rathlev et al.6 concluded that a 5% increase in hospital occupancy resulted in 14 hours of holding time for all patients in the ED, and an observational study found that when hospital occupancy exceeds a threshold of 90%, the ED LOS for admitted patients correspondingly increased.7 Thus, efforts to decrease overcrowding will need to address both ED and hospital throughput and LOS. Most importantly, overcrowding has important consequences on physician and patient satisfaction and the quality of patient care.811
Between 1995 and 2005, ED visits rose 20% from 96.5 million to 115.3 million visits annually, while the number of hospital EDs decreased from 4176 to 3795, making an overall 7% increase in ED utilization rate.12 Similarly, there was a 12% increase in the total inpatient admissions for all registered hospitals in the United States from 31 million in 1995 to 35.3 million in 2005.13 However, despite this increase in demand of ED utilization and inpatient admissions, there had been a steady decline in the supply of hospital beds, from 874,000 in 1995, to 805,000 in 2006.13 These factors have exacerbated the problem of ED overcrowding and boarding.
Not only does boarding entail additional consumption of space, resources, equipment, and manpower, it also potentially compromises patient safety. Typically, hospitalists and inpatient medical teams are engaged in providing care to patients in the wards, while ED physicians and nurses are busy taking care of newly‐arrived ED patients. Non‐ED physicians may have the false impression that their boarded patients, while in the ED, are receiving continuous care and so may decide to delay seeing these patients, which can jeopardize the quality and timeliness of care. Studies have shown that ED overcrowding may potentially lead to poor patient care and outcomes and increased risk for medical errors.1416 ED overcrowding potentially causes multiple effects, including prolonging patient pain and suffering, long patient waiting time, patient dissatisfaction, ambulance diversions, decreased physician productivity, and increased frustration among medical staff.15 In a report by the Joint Commission Accreditation of Healthcare Organizations,17 ED overcrowding was cited as a significant contributing factor in sentinel event cases of patient death or permanent injury due to delays in treatment. Boarding critically ill patients who are physiologically vulnerable and unstable can allow them to be subjected to treatment delays at a pivotal point when time‐sensitive interventions are necessary, ie, sepsis or cardiogenic shockthe golden hour in trauma.16 Medical errors are usually not caused by individual errors but by complex hospital systems; and ED overcrowding is a prime example of a system problem that creates a high‐risk environment for medical errors and threatens patient safety.18
Our hospital commonly has 5 to 15 boarders and often has 20 to 30 boarders at any time. Approximately 90% of these patients are admitted to the Medical Service. In response to this challenge, our institution has designated a full‐time hospitalist to manage boarded patients. The primary goal of this new role is to ensure patient safety and the delivery of high‐quality care while admitted patients are in the ED (Table 1).
| |
| 1 | Round on all patients admitted to the Department of Medicine located in the ED, including those on the Teaching and Nonteaching Services. Rounds focus on patient safety, such as ensuring vital home and hospital medications are administered and changes in stability are noted. All patient updates are documented in the ED electronic medical records (IBEX). |
| 2 | Identify admitted patients who may be downgraded from telemetry to nontelemetry status. Telemetry and cardiac beds are in high demand, and decreasing utilization facilitates obtaining the appropriate ward bed for ED patients. |
| 3 | Assess admitted patients for possible discharge. The patient's condition may have improved or results may indicate that admission is no longer required. The ED hospitalist communicates with the ED physician and wards teams, facilitates management, implements the discharge, and ensures adequate follow‐up. |
| 4 | Refer patients to an ED social worker as needed. |
| 5 | Facilitate referrals to other medical or surgical specialties if indicated. |
| 6 | Clarify the plan of care with the ED staff and facilitates ED communication with the ward team. Acts as a liaison and a resource for the ED physicians and nursing staff. |
| 7 | Supervise the triage duties of the medical admitting resident. |
| 8 | Provide medical consultation to ED physicians for patients not being admitted to the hospital or who are being admitted to other services (eg, surgery). |
The objectives of the study were to determine: (1) the impact on quality of care by assessing laboratory results acted upon and medication follow‐up by the ED hospitalist, and (2) the impact on throughput by assessing the number of ED discharges and telemetry downgrades.
Methods
Setting
The Mount Sinai Medical Center is a tertiary‐care 1121‐bed acute care teaching hospital located in New York City. The hospital borders East Harlem and the Upper East Side of Manhattan. The Medical Service is composed of a Teaching Service, composed of house staff and attendings, and a non‐Teaching Service, composed of nurse practitioners, physician assistants, and attendings. Hospitalists and private attendings may have patients on either the Teaching or the non‐Teaching Service. In 2007, there were 56,541 patients admitted for a total of 332,368 days. The mean LOS for medical inpatients was 5.89 days. The total ED visit was 79,500 with a total inpatient and critical care admissions of 24,522. The mean and median LOS for all ED patients were 623 minutes and 493 minutes, respectively. There were 11,488 patients who qualified as boarders, averaging 31.5 boarders per 24 hours; with a mean and median LOS per boarder of 288 minutes and 198 minutes, respectively. The ED LOS for admitted patients ranged from 2 minutes to 4074 minutes (2.83 days).
Admission Process
Once an ED attending physician decides that a patient is to be admitted, the patient is placed on a computerized list in the ED's electronic medical record (IBEX software). The Medical Admitting Resident (MAR) evaluates and triages admitted patients, and assigns and gives a verbal report to the appropriate Medicine Service (ie, Teaching, non‐Teaching, cardiac telemetry unit, intensive care, etc.). The Admitting Office searches for and assigns the appropriate unit and bed for the patient. A hospitalist or resident physician performs the patient's initial assessment and evaluation in the ED, and admission orders are placed in the inpatient computerized order entry system (TDS). When the bed is ready, the ED nurse gives a verbal report to the floor nurse, and the patient is transported to the ward.
Responsibilities
The specific responsibilities of the ED hospitalist are listed in Table 1. The primary role is to round on patients admitted to the Medicine Service who are located in the ED. This encompasses a wide array of patients and services, including patients assigned to a hospitalist service attending or who have a private attending, patients admitted to the Teaching or non‐Teaching Service, patients admitted to the intensive care unit, and patients admitted to a general medicine or specialty service (eg, telemetry, oncology, human immunodeficiency virus [HIV]). Rounding includes review of the ED's electronic medical record as well as direct examination of patients. The hospitalist focuses on patients with longer ED LOS and on aspects of care that may lapse while patients remain in the ED for prolonged periods. At our institution, the follow‐up of subsequent tests, laboratory values, and medications for ED boarders is the responsibility of the primary inpatient team, though the ED physicians act on urgent and critical results and continue to deliver all emergency care. Through rounding, the ED hospitalist is able to identify abnormal results in a timely manner, alert the ED physician and primary inpatient team, and address abnormalities. Specific examples of laboratory results acted upon include hypokalemia, hyperglycemia, and elevated cardiac enzymes. The ED hospitalist is also able to determine whether any outpatient medications have not yet been administered (eg, antihypertensives, immune suppressants) and ensure that subsequent doses of medications initiated in the ED (eg, antibiotics) are administered during the appropriate timeframe.
Communication is emphasized, as contact with ED physicians, ward physicians, and often the outpatient primary care physician is required when any change in management is considered. The ED hospitalist also provides the capability of rapid response to changes in patient status (eg, a new complaint or fever). In addition, the hospitalist is available to consult on medical patients who may not require admission and on nonmedical patients for whom an internal medicine consult may be beneficial (eg, preoperative optimization of a surgical patient). The ED hospitalist documents the evaluation in the IBEX system. Bills were submitted for visits in which patients were discharged as these encounters are comprehensive, but not for other encounters.
Data Collection
The ED hospitalist role began March 10, 2008 and is a 10‐hour shift (8 AM to 6 PM) on weekdays. The study period was from March 10, 2008 through June 30, 2008. The study was approved by the hospital's institutional review board.
Data were collected on aspects of care that could have been impacted by the ED hospitalist, including medication and laboratory orders, ED discharges, ED admissions avoided, and telemetry downgrades. Discharges from ED refers to boarded admitted patients in the ED, who by the judgment of the ED hospitalist were ready for discharge. Admissions avoided refers to patients who the ED physician planned to admit but had not yet been admitted, and whose admission was avoided through the recommendations made by the ED hospitalist. The ED LOS was defined as the duration of time from when the patient was admitted to the Medicine Service to the time the patient was transferred to a medical ward. Telemetry downgrades were defined as patients assigned to the cardiac telemetry unit who the hospitalist determined required only telemetry on a general medical unit or did not require telemetry, or patients assigned to telemetry on a general medicine unit who the hospitalist determined no longer required telemetry.
Results were expressed as percentages of patients admitted to a Medicine Service and percentage of patients evaluated by the ED hospitalist, as indicated. 95% confidence intervals (CI) were calculated.
Results
During the study period, there were 4363 patients admitted to the Medicine Service and 3555 patients who qualified as boarders (mean of 29 boarders per 24 hours). The mean boarding time of admitted patients was 440 minutes. A total of 634 patients (17.8% of all boarded patients) were evaluated by the ED hospitalist. The mean daily number of patients seen by the ED hospitalist was 8.0.
The key elements of the delivery of care by the ED hospitalist are summarized in Table 2.
| Elements | Boarders (n = 3555) [n (%)] | Patients Intervened on (n = 634) [n (%)] |
|---|---|---|
| ||
| Laboratory results acted upon | 472 (13.2) | 472 (74.5) |
| Medication follow‐up | 506 (14.2) | 506 (79.8) |
| Discharges from the ED* | 46 (1.3) | 46 (7.3) |
| Admissions avoided | 6 (0.2) | 6 (0.95) |
| Telemetry downgrades | 61 (1.8) | 61 (9.6) |
The care of boarded patients included follow‐up of laboratory tests for 74.5% (95% CI, 71‐78%) and medication orders for 79.8% (95% CI, 77‐83%) of patients. A total of 46 patients were discharged by the ED hospitalist (0.6 discharges/day) and telemetry was discontinued for 61 patients (0.8 downgrades/day). The discharge rate was 7.3% (95% CI, 5‐10%) and telemetry downgrade rate was 9.6% (95% CI, 8‐12%) of those patients assessed by the ED hospitalist. Expressed as a percentage of the total ED boarders (n = 3555), the combined discharge rate and the admissions avoided rate was 1.5%.
Table 3 shows the discharge diagnoses made from the ED. Chest pain was the most common diagnosis, followed by syncope, pneumonia, and chronic obstructive pulmonary disease (COPD).
| Diagnoses | Patients (n = 46) [n (%)] |
|---|---|
| |
| Chest pain | 12 (26) |
| Syncope/dizziness | 7 (15) |
| Pneumonia | 4 (9) |
| COPD | 4 (9) |
| Congestive heart failure | 3 (7) |
| Gastroenteritis | 3 (7) |
| Dermatitis/rash | 3 (7) |
| Alcohol abuse | 3 (7) |
| Abdominal pain | 3 (7) |
| End stage renal disease | 2 (4) |
| Vaginal bleeding | 1 (2) |
| Fall | 1 (2) |
| Asthma | 1 (2) |
Discussion
Our hospital has successfully implemented an innovative strategy utilizing a hospitalist to help provide seamless care to medical patients located in the ED. Other solutions at our hospital had previously been implemented, but had not adequately addressed the problem, including: (1) protocols to monitor length of stay patterns and deviations, (2) discharge planning activities, (3) organized computerized bed tracking, (4) improvement in the timeliness of ancillary services, (5) daily bed briefing among nurse managers, and (6) 24‐hour presence of a MAR to facilitate triage in the ED.
The current study demonstrates the potential for substantial impact on patient care. The substantial number of the assessed boarder patients for whom laboratory tests (74.5%) and medications (79.8%) were ordered by the ED hospitalists suggests that the quality and timeliness of care was enhanced by this initiative. In addition, the considerable number of patients discharged from the ED and downgraded from telemetry (1.5% and 1.8% of all boarder patients, respectively) suggests that an ED hospitalist may have a meaningful impact on bed utilization and thus decrease ED overcrowding. In 2007, there were 11,488 who qualified as boarders; our data suggest that an ED hospitalist would result in approximately 172 boarders not being admitted annually.
Though the ED LOS was higher during the study period compared to 2007, it was lower than the 2 months immediately preceding implementation of the ED hospitalist role. The ED LOS was 732 and 658 minutes for January and February 2008, respectively, which was markedly increased from 2007 (288 minutes), and prompted development of the ED hospitalist role. The ED LOS during the study period subsequently decreased to 440 minutes. Though the wide fluctuations in ED LOS and the short time period with high ED LOS prior to implementation preclude concluding that the ED hospitalist role decreased ED LOS, the data suggest that an ED hospitalist may be able to improve ED throughput.
The majority of the discharges made by the ED hospitalist are patients who had been admitted for chest pain, had improved, and had negative cardiac enzymes and stress tests. Patients with syncope who were discharged were likely patients without any comorbidities. The COPD and pneumonia admissions were likely patients who improved after aggressive treatment in the ED.
The impact of ED overcrowding on the quality of patient care and outcomes may be substantial. Hwang et al.19 found a direct correlation between ED census and time to pain assessment and administration of analgesic medication. A study at an academic medical center found that higher ED volume was associated with less likelihood of antibiotics being administered within 4 hours for patients with community‐acquired pneumonia.20 A comprehensive review of the literature identified 41 studies examining the effects of ED overcrowding on clinical outcomes and the investigators noted that ED overcrowding was associated with increased in‐hospital mortality.8
Causes of poor outcomes during periods of overcrowding may be the high volume of acute patients preventing adequate time and attention for each ED patient, as well as confusion during the transition from ED to ward physicians. For example, a patient may receive their initial dose of antibiotics from the ED physician, but subsequent doses may be overlooked in the transition of care from the ED physician to the inpatient team. In addition, having admitted patients located in the ED for extended periods of time may lead to these patients not being seen as frequently as patients admitted to the inpatient wards. Another potential consequence of prolonged ED stay for admitted patients is delay in inpatient management. Tests done in the ED may prompt further studies that may not be ordered promptly while patients remain in the ED, which subsequently increases LOS. Other potential issues may be an increase in confusion among geriatric patients in a noisy and crowded ED; decreased access to specialized nursing care that may be available on a hospital ward; decreased access to physical therapy and occupational therapy services; and decreased comfort and satisfaction as patients wait in overcrowded EDs for prolonged periods.
Several other potential innovative solutions to ED overcrowding have been proposed, studied, and tested. These measures generally are focused on improving the three interdependent components of ED workflow: INPUT THROUGHPUT OUTPUT.21, 22 However, process redesign and intervention on these 3 interdependent ED workflow components may be difficult to achieve, especially when hospital resources are limited and when inpatient hospital capacity is already maximized. In some institutions, efforts have been reported to successfully streamline the transfer of admitted ED patients to inpatient beds, through transfer‐to‐ward policy interventions (eg, physician coordinators for patient flow and bed management or transfers made within a defined period of time).2326 However, in a study by Quinn et al.,27 implementation of a rapid admission policy resulted in a decrease of only 10.1 minutes in the ED LOS. Several studies have demonstrated the benefits of an acute medical admissions unit in alleviating ED overcrowding.28, 29 Other unconventional solutions by some hospitals include sending admitted patients to the unit's hallways or placing discharged patients in the hallway while waiting for transportation so that the ED bed will be readily available.30
The ED hospitalist is well‐situated to have an impact on several key hospital outcomes. As the ED hospitalist role was shown to affect processes that relate to ED throughput, it is possible that the role will improve ED overcrowding and decrease ED LOS. Specifically, identifying patients who can be discharged and for whom telemetry is no longer indicated decreases unnecessary bed utilization and allows these beds to be available for other ED patients. This initiative also may promote patient satisfaction by assuring patients that their medical and concerns are being fully addressed while they are in the ED. Increased emphasis on hospital reporting will make patient satisfaction a priority for many hospitals, and the ED hospitalist will be in a unique position to meet and greet patients admitted to the Medicine Service and to reassure them that the medical team is present and addressing their concerns. The hospitalist's ability to facilitate diagnostic testing and treatment while patients remain in the ED may also help decrease the total LOS in the hospital. In addition, the ED hospitalist is also in position to recognize social factors at the earliest stage of admission so that they can be immediately addressed. Future studies will need to be done to determine if this model of transitional care impacts these important factors.
Our study has several important limitations. Most notably, the lack of a comparison interval for which a hospitalist was not assigned to this role prevents us from drawing any definitive conclusions on the benefits of the ED hospitalist model. Also, we collected only summary data and do not have demographic data on the patients managed by the ED hospitalist or information on the ED course of patients who were discharged or had telemetry downgraded. This prevents determination of whether discharged patients did not require admission initially or whose condition evolved over a prolonged ED stay. In addition, other key outcomes, such as patient satisfaction and satisfaction of the ED physicians and nursing staff have not yet been formally measured. Future studies will be needed to determine if an ED hospital model can improve important process and clinical outcomes.
The greatest challenge of this initiative was introducing and familiarizing this role to the key stakeholders, including the ED physicians and nursing staff, house staff, and private practice physicians. Though we did not perform structured surveys on satisfaction, through informal discussions we noted that the role was welcomed with enthusiasm by the ED physicians. Notably, several ED physicians expressed appreciation that they were able to focus their care on new ED patients rather than on the boarded ED patients. Through feedback, we noted soon after implementation that ED faculty and nurses needed further clarification about the potential overlapping roles of the ED hospitalist and ED physicians and ward physicians. These concerns were addressed by educational sessions and announcements, including presentations at ED faculty and staff meetings. The hospitalist assigned to the role each month received individualized orientation prior to assuming the role, and an ED Hospitalist Manual was distributed. Possibly due to these focused sessions, the hospitalists assigned to the role became quickly acclimated.
Conclusions
We have found that designating a hospitalist to directly address the care of ED boarders can enhance the quality and timeliness of care and decrease bed and telemetry utilization with the potential to impact ED and hospital LOS. Given the success of the pilot model, the role was expanded at our institution to 10 hours per day, 7 days per week. Hospitals struggling to address the needs of their admitted patients in the ED should consider incorporating an ED hospitalist to enhance clinical care and address issues relating to throughput. A follow‐up study is needed to more precisely describe the impact of the ED hospitalist model.
- , , , et al.Estimating the degree of emergency department overcrowding in academic medical centers: results of the National ED Overcrowding Study (NEDOCS).Acad Emerg Med.2004;11:38–50.
- , , , et al.Frequency, determinants, and impact of overcrowding in emergency departments in Canada: a national survey.Healthc Q.2007;10:32–40.
- , .EMDOC (emergency department overcrowding) internet‐based safety net research.Admin Emerg Med.2008;35:101–107.
- United States General Accounting Office.Hospital Emergency Departments: Crowded Conditions Vary Among Hospitals and Communities. March 2003.Washington, DC:General Accounting Office;2003.
- .Overcrowding in emergency department: increased demand and decreased capacity.Ann Emerg Med.2002;39:430–432.
- , , , et al.Time series analysis of variables associated with daily mean emergency department length of stay.Ann Emerg Med.2007;49:265–271.
- , , , et al.Effect of hospital occupancy on emergency department length of stay and patient disposition.Ann Emerg Med.2003;10:127–133.
- , , , et al.The effect of emergency department crowding on clinically oriented outcomes.Acad Emerg Med.2009;16:1–10.
- , .Emergency department overcrowding: the impact of resource scarcity on physician job satisfaction.J Health Manag.2005;50:327–340.
- , , , , , .The effect of emergency department crowding on patient satisfaction for admitted patients.Acad Emerg Med.2008;15:825–831.
- , .The effect of crowding on access and quality in an academic ED.Am J Emerg Med.2006;24:787–794.
- , , .National Hospital Ambulatory Medical Care Survey: 2005 Emergency Department Summary. Advance Data from Vital and Health Statistics. No. 386.Hyattsville, MD:National Center for Health Statistics;2007.
- American Hospital Association (AHA).Table 1: Historical trends in utilization, personnel, and finances: year 1946–2006.AHA Hospital Statistics.2008 ed.Chicago:Health Forum LLC;2008:3.
- , .Emergency department overcrowding in the US: an emerging threat to patient safety and public health.Emerg Med J.2003;20:402–405.
- , .Overcrowding in the nation's emergency departments: complex causes and disturbing effects.Ann Emerg Med.2000;35:63–68.
- , .Clinical review: emergency department overcrowding and the potential impact on the critically ill.Crit Care.2005;9:291–295.
- Joint Commission on Accreditation of Healthcare Organizations (JCAHO): Sentinel event alert 2002, Issue 26. Available at: http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_26.htm. Accessed October2009.
- , , , et al.Safety net research in emergency medicine: proceedings of the Academic Emergency Consensus Conference on “The Unraveling Safety Net.”Acad Emerg Med.2001;8:1024–1029.
- , , , , , .Emergency department crowding and decreased quality of pain care.Acad Emerg Med.2008;15:1248–1256.
- , , , .Effect of emergency department crowding on time to antibiotics in patients admitted with community‐acquired pneumonia.Ann Emerg Med.2007;50:501–509.
- , , , et al.A conceptual model of emergency department crowding.Ann Emerg Med.2003;42:173–180.
- , , , et al.Emergency department crowding: consensus development of potential measures.Ann Emerg Med.2003;42:824–834.
- , , , et al.Intervention to decrease emergency department crowding: does it have an effect on return visits and hospital readmission?Ann Emerg Med.2003;41:173–185.
- , , , et al.Rapid process design in a university‐based emergency department: decreasing waiting time intervals and improving patient satisfaction.Ann Emerg Med.2002;39:168–177.
- .Emergency department crowding: an action plan.Acad Emerg Med.2001;18:185–187.
- , , .Hospitalists and an innovative emergency department admission process.J Gen Intern Med.2004;19:266–268.
- , , et al.Effects of implementing a rapid admission policy in the ED.Am J Emerg Med.2007;25:559–563.
- , , .Effect of an emergency department managed acute care unit on ED overcrowding and emergency medical services diversion.Acad Emerg Med.2001;8:1085–1100.
- , , , .Emergency department census of patients awaiting admission following reorganization of an admissions process.Emerg Med J.2006;23:363–367.
- .Emergency department flow and the boarded patient: how to get admitted patients upstairs.Ann Emerg Med.2007;49:68–70.
- , , , et al.Estimating the degree of emergency department overcrowding in academic medical centers: results of the National ED Overcrowding Study (NEDOCS).Acad Emerg Med.2004;11:38–50.
- , , , et al.Frequency, determinants, and impact of overcrowding in emergency departments in Canada: a national survey.Healthc Q.2007;10:32–40.
- , .EMDOC (emergency department overcrowding) internet‐based safety net research.Admin Emerg Med.2008;35:101–107.
- United States General Accounting Office.Hospital Emergency Departments: Crowded Conditions Vary Among Hospitals and Communities. March 2003.Washington, DC:General Accounting Office;2003.
- .Overcrowding in emergency department: increased demand and decreased capacity.Ann Emerg Med.2002;39:430–432.
- , , , et al.Time series analysis of variables associated with daily mean emergency department length of stay.Ann Emerg Med.2007;49:265–271.
- , , , et al.Effect of hospital occupancy on emergency department length of stay and patient disposition.Ann Emerg Med.2003;10:127–133.
- , , , et al.The effect of emergency department crowding on clinically oriented outcomes.Acad Emerg Med.2009;16:1–10.
- , .Emergency department overcrowding: the impact of resource scarcity on physician job satisfaction.J Health Manag.2005;50:327–340.
- , , , , , .The effect of emergency department crowding on patient satisfaction for admitted patients.Acad Emerg Med.2008;15:825–831.
- , .The effect of crowding on access and quality in an academic ED.Am J Emerg Med.2006;24:787–794.
- , , .National Hospital Ambulatory Medical Care Survey: 2005 Emergency Department Summary. Advance Data from Vital and Health Statistics. No. 386.Hyattsville, MD:National Center for Health Statistics;2007.
- American Hospital Association (AHA).Table 1: Historical trends in utilization, personnel, and finances: year 1946–2006.AHA Hospital Statistics.2008 ed.Chicago:Health Forum LLC;2008:3.
- , .Emergency department overcrowding in the US: an emerging threat to patient safety and public health.Emerg Med J.2003;20:402–405.
- , .Overcrowding in the nation's emergency departments: complex causes and disturbing effects.Ann Emerg Med.2000;35:63–68.
- , .Clinical review: emergency department overcrowding and the potential impact on the critically ill.Crit Care.2005;9:291–295.
- Joint Commission on Accreditation of Healthcare Organizations (JCAHO): Sentinel event alert 2002, Issue 26. Available at: http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_26.htm. Accessed October2009.
- , , , et al.Safety net research in emergency medicine: proceedings of the Academic Emergency Consensus Conference on “The Unraveling Safety Net.”Acad Emerg Med.2001;8:1024–1029.
- , , , , , .Emergency department crowding and decreased quality of pain care.Acad Emerg Med.2008;15:1248–1256.
- , , , .Effect of emergency department crowding on time to antibiotics in patients admitted with community‐acquired pneumonia.Ann Emerg Med.2007;50:501–509.
- , , , et al.A conceptual model of emergency department crowding.Ann Emerg Med.2003;42:173–180.
- , , , et al.Emergency department crowding: consensus development of potential measures.Ann Emerg Med.2003;42:824–834.
- , , , et al.Intervention to decrease emergency department crowding: does it have an effect on return visits and hospital readmission?Ann Emerg Med.2003;41:173–185.
- , , , et al.Rapid process design in a university‐based emergency department: decreasing waiting time intervals and improving patient satisfaction.Ann Emerg Med.2002;39:168–177.
- .Emergency department crowding: an action plan.Acad Emerg Med.2001;18:185–187.
- , , .Hospitalists and an innovative emergency department admission process.J Gen Intern Med.2004;19:266–268.
- , , et al.Effects of implementing a rapid admission policy in the ED.Am J Emerg Med.2007;25:559–563.
- , , .Effect of an emergency department managed acute care unit on ED overcrowding and emergency medical services diversion.Acad Emerg Med.2001;8:1085–1100.
- , , , .Emergency department census of patients awaiting admission following reorganization of an admissions process.Emerg Med J.2006;23:363–367.
- .Emergency department flow and the boarded patient: how to get admitted patients upstairs.Ann Emerg Med.2007;49:68–70.
Copyright © 2009 Society of Hospital Medicine
Evidence-Based Medicine and the Hospitalist
The terms “hospital medicine” and “evidence-based medicine” (EBM) are both recent arrivals in the history of medicine. Both have spread through medicine at a rapid pace, highlighting the attraction and fundamental soundness of their core ideas. Much has been written about the benefits of the hospitalist movement regarding quality, patient throughput and financial indicators. The next phase in the revolution of patient care is the confluence of technology, EBM, and hospital medicine. One of the pillars for the continued success of the hospital medicine movement will be EBM. EBM must become an integral part of the skill set for all hospitalists.
EBM is an analytical approach with a fundamental knowledge base and a set of tools. The exponential growth of clinical information requires that physicians use an analytical approach for answering clinical questions and keeping up-to-date. This may be easier if you work at an academic center rather than a non-teaching hospital, although this is not guaranteed. Regardless of the working environment, an analytical approach will be needed if we are to build on initial success and unrealized potential to improve quality and patient safety.
The term “EBM” was introduced by a group of clinician researchers and educators at McMaster University during the early 1990s. It was initially defined as “a systemic approach to analyzed published research as the basis of clinical decision making.” Subsequently, as the EBM movement matured as a discipline, the early proponents and developers provided a more complete definition: “Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research (1).”
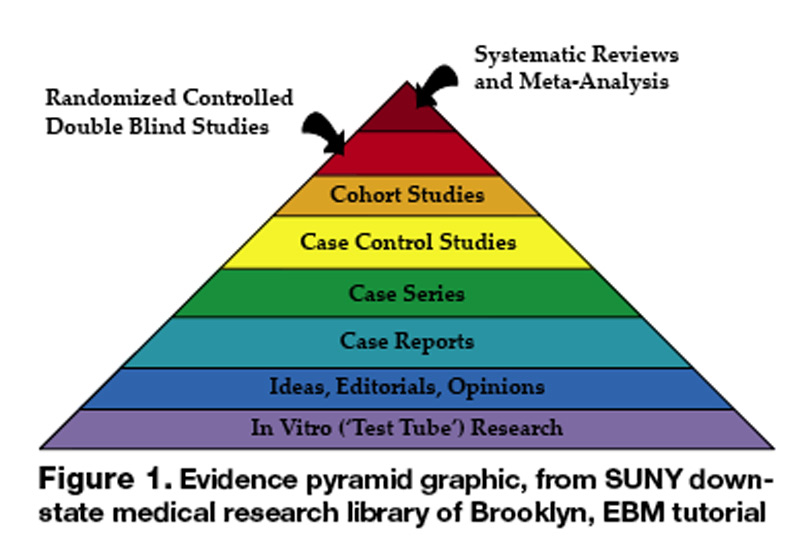
Of course, the concept of practicing medicine based on the scientific method has been around for years. The days of bloodletting with leeches are behind us, but rigorous scientific evaluation of medicine reached critical mass only in the last century. The first double-blind randomized controlled trial (RCT) was conducted in 1931; the study tested the use of sanocrysin for treatment of tuberculosis (2). Since then, there has been an exponential growth in clinical trials. This information explosion requires new approaches to integrating the ever-increasing knowledge with patient care; the concurrent revolution in information technology provides opportunities limited only by our own imaginations.
EBM is not without its critics: “It is cookbook medicine,” “It focuses on cost efficiency,” “I can’t find an RCT that fits my patient,” and “It doesn’t take into account the clinician’s experience” are often argued points. If EBM is not used effectively, all the criticisms are appropriate. Sacket, one of the earliest proponents and likely EBM’s most eloquent champion, refuted the claim that EBM is “cookbook medicine.” He argued that EBM requires a bottom-up approach that integrates the best external evidence with individual clinical expertise and patients’ choice. External clinical evidence informs, but does not replace, individual clinical expertise. The physician must decide whether the external evidence applies to the individual patient at all and, if so, how it should be integrated into a clinical decision (1).
Neither is EBM strictly about RCTs and meta-analysis. It’s about tracking down the best available evidence for your question and, thus, your patient. Sometimes a cohort study is best when you want to find the prognosis of a certain illness. Similarly, a cross-sectional study may be most appropriate when you’re trying to determine the sensitivity and specificity of a test. If a disease once thought universally fatal is proven otherwise in a case report, then a randomized control trial is hardly necessary. Finally, an RCT or meta-analysis is not always going to be available for the disease process you are dealing with, but EBM gives us the skill set to look down the evidence pyramid and find the next best thing (Figure 1).
It is also clear that EBM is not about cost cutting, although many hospital medicine programs were started with this as the primary goal, given the current healthcare environment. Certainly fears exist that EBM is being used by healthcare managers, organizations, and administrators as a cost-efficiency tool. It may be that good evidence is cost-efficient in certain situations, while in others it may require the healthcare system to invest more in itself if available evidence supports doing so. Thus it is imperative that hospitalists accept the challenge of incorporating EBM into their daily practice and become leaders in its application, with patient safety and quality of care as primary goals. If we don’t, others will define the role of EBM for us, with a potential for poor outcomes for the patient and the profession.
The EBM skill set and its tools are being continuously refined, with the evidence pyramid as one of the most basic principles (3). This evidence pyramid is a model for grading the evidence. It puts in perspective the different grades of evidence or study designs. For example, a systematic review of randomized controlled trials that show consistent results provides the highest quality evidence and is ranked accordingly in the pyramid. In contrast, a case report or case series of a treatment would be ranked much lower.
The first step in incorporating EBM into one’s daily practice requires an understanding of its analytical approach and access to the necessary tools. The process begins with asking a question that is answerable. A well-built clinical question is one that benefits the patient and clinician. Such questions are directly relevant to patient problems and phrased in ways that direct your search to relevant and precise answers.
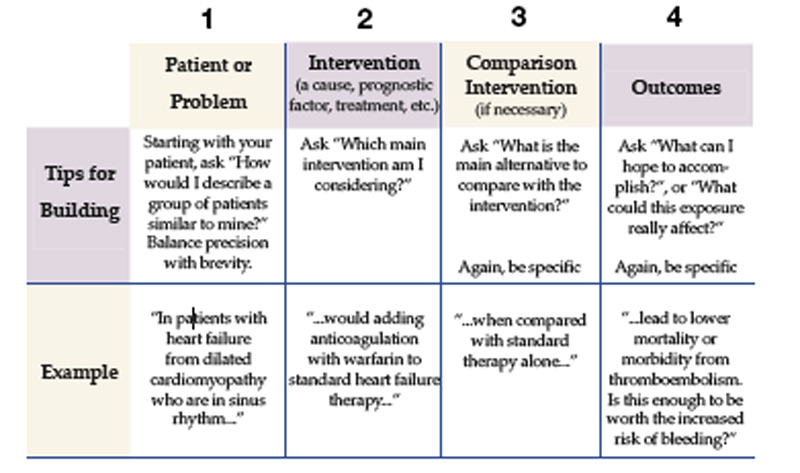
In forming the question the following process, referred to as the PICO method, is helpful (4).
With the question formed, consider what type of question you have. This is often referred to as the typology of the question.
- Clinical Findings: Gathering and interpreting findings from the history, clinical examination, and test results.
- Etiology: Identifying causes for disease.
- Differential Diagnosis: Ranking by likelihood, seriousness, and treatability of the patients problem.
- Prognosis: Figuring out how to estimate the likely clinical course and complications over time of the disease
- Therapy: Selecting treatments to offer that do more good than harm and that are worth the effort and cost of using them.
- Prevention: Reducing the chance of disease by identifying and modifying risk factors and how to diagnose disease early by screening.
- Self-improvement: Keeping up-to-date, improve your clinical skills, and run a better, more efficient clinical practice.
The types of questions can next be matched to the type of research that may provide the answer:
- Diagnosis: prospective cohort study with good quality validation against “gold standard.”
- Prognosis: prospective cohort study.
- Therapy or prevention: prospective, randomized controlled clinical trial (RCT).
- Harm/Etiology: RCT, cohort or case-control study (probably retrospective).
- Economic: analysis of sensible costs against evidence-based outcome.
Once the question has been formed, the following steps lie ahead: finding the evidence, critically appraising the evidence, acting on the evidence, and, finally, evaluating one’s performance. Very much like the formation of the question, each of the subsequent steps involves an analytical approach that can be mastered. Technology—particularly personal computers, the Internet and PDAs—has made the task of mastering EBM easier in many ways. The additional steps in using EBM effectively will be addressed in future articles. A list of useful links is provided below.
http://library.downstate.edu/EBM2/contents.htm
http://healthsystem.virginia.edu/internet/library/collections/ebm/index.cfm
Dr. Kathuria may be reached at Navneet.kathuria@mssm.edu.
Endnotes
- Guyatt GH, Haynes RB, Jaeschke RZ, et al. Users’ guides to the medical literature: XXV. Evidence-based medicine: principles for applying the users’ guides to patient care. Evidence-Based Medicine Working Group. JAMA. 2000;284:1290-6.
- Claridge, J, Fabian, T. History and Development of Evidence Based Medicine. World Journal of Surgery 2005
- Guyatt GH, Haynes RB, et. al. Users’ guides to the medical literature: XXV. Evidence-Based Medicine: Principles for Applying the Users’ Guides to Patient Care. 2000;284:1290-1296
- Sackett DL, Richardson WS, Rosenberg W, Haynes RB (1997). Evidence-based medicine: How to practice and teach EBM. New York: Churchill Livingston
The terms “hospital medicine” and “evidence-based medicine” (EBM) are both recent arrivals in the history of medicine. Both have spread through medicine at a rapid pace, highlighting the attraction and fundamental soundness of their core ideas. Much has been written about the benefits of the hospitalist movement regarding quality, patient throughput and financial indicators. The next phase in the revolution of patient care is the confluence of technology, EBM, and hospital medicine. One of the pillars for the continued success of the hospital medicine movement will be EBM. EBM must become an integral part of the skill set for all hospitalists.
EBM is an analytical approach with a fundamental knowledge base and a set of tools. The exponential growth of clinical information requires that physicians use an analytical approach for answering clinical questions and keeping up-to-date. This may be easier if you work at an academic center rather than a non-teaching hospital, although this is not guaranteed. Regardless of the working environment, an analytical approach will be needed if we are to build on initial success and unrealized potential to improve quality and patient safety.
The term “EBM” was introduced by a group of clinician researchers and educators at McMaster University during the early 1990s. It was initially defined as “a systemic approach to analyzed published research as the basis of clinical decision making.” Subsequently, as the EBM movement matured as a discipline, the early proponents and developers provided a more complete definition: “Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research (1).”
Of course, the concept of practicing medicine based on the scientific method has been around for years. The days of bloodletting with leeches are behind us, but rigorous scientific evaluation of medicine reached critical mass only in the last century. The first double-blind randomized controlled trial (RCT) was conducted in 1931; the study tested the use of sanocrysin for treatment of tuberculosis (2). Since then, there has been an exponential growth in clinical trials. This information explosion requires new approaches to integrating the ever-increasing knowledge with patient care; the concurrent revolution in information technology provides opportunities limited only by our own imaginations.
EBM is not without its critics: “It is cookbook medicine,” “It focuses on cost efficiency,” “I can’t find an RCT that fits my patient,” and “It doesn’t take into account the clinician’s experience” are often argued points. If EBM is not used effectively, all the criticisms are appropriate. Sacket, one of the earliest proponents and likely EBM’s most eloquent champion, refuted the claim that EBM is “cookbook medicine.” He argued that EBM requires a bottom-up approach that integrates the best external evidence with individual clinical expertise and patients’ choice. External clinical evidence informs, but does not replace, individual clinical expertise. The physician must decide whether the external evidence applies to the individual patient at all and, if so, how it should be integrated into a clinical decision (1).
Neither is EBM strictly about RCTs and meta-analysis. It’s about tracking down the best available evidence for your question and, thus, your patient. Sometimes a cohort study is best when you want to find the prognosis of a certain illness. Similarly, a cross-sectional study may be most appropriate when you’re trying to determine the sensitivity and specificity of a test. If a disease once thought universally fatal is proven otherwise in a case report, then a randomized control trial is hardly necessary. Finally, an RCT or meta-analysis is not always going to be available for the disease process you are dealing with, but EBM gives us the skill set to look down the evidence pyramid and find the next best thing (Figure 1).
It is also clear that EBM is not about cost cutting, although many hospital medicine programs were started with this as the primary goal, given the current healthcare environment. Certainly fears exist that EBM is being used by healthcare managers, organizations, and administrators as a cost-efficiency tool. It may be that good evidence is cost-efficient in certain situations, while in others it may require the healthcare system to invest more in itself if available evidence supports doing so. Thus it is imperative that hospitalists accept the challenge of incorporating EBM into their daily practice and become leaders in its application, with patient safety and quality of care as primary goals. If we don’t, others will define the role of EBM for us, with a potential for poor outcomes for the patient and the profession.
The EBM skill set and its tools are being continuously refined, with the evidence pyramid as one of the most basic principles (3). This evidence pyramid is a model for grading the evidence. It puts in perspective the different grades of evidence or study designs. For example, a systematic review of randomized controlled trials that show consistent results provides the highest quality evidence and is ranked accordingly in the pyramid. In contrast, a case report or case series of a treatment would be ranked much lower.
The first step in incorporating EBM into one’s daily practice requires an understanding of its analytical approach and access to the necessary tools. The process begins with asking a question that is answerable. A well-built clinical question is one that benefits the patient and clinician. Such questions are directly relevant to patient problems and phrased in ways that direct your search to relevant and precise answers.
In forming the question the following process, referred to as the PICO method, is helpful (4).
With the question formed, consider what type of question you have. This is often referred to as the typology of the question.
- Clinical Findings: Gathering and interpreting findings from the history, clinical examination, and test results.
- Etiology: Identifying causes for disease.
- Differential Diagnosis: Ranking by likelihood, seriousness, and treatability of the patients problem.
- Prognosis: Figuring out how to estimate the likely clinical course and complications over time of the disease
- Therapy: Selecting treatments to offer that do more good than harm and that are worth the effort and cost of using them.
- Prevention: Reducing the chance of disease by identifying and modifying risk factors and how to diagnose disease early by screening.
- Self-improvement: Keeping up-to-date, improve your clinical skills, and run a better, more efficient clinical practice.
The types of questions can next be matched to the type of research that may provide the answer:
- Diagnosis: prospective cohort study with good quality validation against “gold standard.”
- Prognosis: prospective cohort study.
- Therapy or prevention: prospective, randomized controlled clinical trial (RCT).
- Harm/Etiology: RCT, cohort or case-control study (probably retrospective).
- Economic: analysis of sensible costs against evidence-based outcome.
Once the question has been formed, the following steps lie ahead: finding the evidence, critically appraising the evidence, acting on the evidence, and, finally, evaluating one’s performance. Very much like the formation of the question, each of the subsequent steps involves an analytical approach that can be mastered. Technology—particularly personal computers, the Internet and PDAs—has made the task of mastering EBM easier in many ways. The additional steps in using EBM effectively will be addressed in future articles. A list of useful links is provided below.
http://library.downstate.edu/EBM2/contents.htm
http://healthsystem.virginia.edu/internet/library/collections/ebm/index.cfm
Dr. Kathuria may be reached at Navneet.kathuria@mssm.edu.
Endnotes
- Guyatt GH, Haynes RB, Jaeschke RZ, et al. Users’ guides to the medical literature: XXV. Evidence-based medicine: principles for applying the users’ guides to patient care. Evidence-Based Medicine Working Group. JAMA. 2000;284:1290-6.
- Claridge, J, Fabian, T. History and Development of Evidence Based Medicine. World Journal of Surgery 2005
- Guyatt GH, Haynes RB, et. al. Users’ guides to the medical literature: XXV. Evidence-Based Medicine: Principles for Applying the Users’ Guides to Patient Care. 2000;284:1290-1296
- Sackett DL, Richardson WS, Rosenberg W, Haynes RB (1997). Evidence-based medicine: How to practice and teach EBM. New York: Churchill Livingston
The terms “hospital medicine” and “evidence-based medicine” (EBM) are both recent arrivals in the history of medicine. Both have spread through medicine at a rapid pace, highlighting the attraction and fundamental soundness of their core ideas. Much has been written about the benefits of the hospitalist movement regarding quality, patient throughput and financial indicators. The next phase in the revolution of patient care is the confluence of technology, EBM, and hospital medicine. One of the pillars for the continued success of the hospital medicine movement will be EBM. EBM must become an integral part of the skill set for all hospitalists.
EBM is an analytical approach with a fundamental knowledge base and a set of tools. The exponential growth of clinical information requires that physicians use an analytical approach for answering clinical questions and keeping up-to-date. This may be easier if you work at an academic center rather than a non-teaching hospital, although this is not guaranteed. Regardless of the working environment, an analytical approach will be needed if we are to build on initial success and unrealized potential to improve quality and patient safety.
The term “EBM” was introduced by a group of clinician researchers and educators at McMaster University during the early 1990s. It was initially defined as “a systemic approach to analyzed published research as the basis of clinical decision making.” Subsequently, as the EBM movement matured as a discipline, the early proponents and developers provided a more complete definition: “Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research (1).”
Of course, the concept of practicing medicine based on the scientific method has been around for years. The days of bloodletting with leeches are behind us, but rigorous scientific evaluation of medicine reached critical mass only in the last century. The first double-blind randomized controlled trial (RCT) was conducted in 1931; the study tested the use of sanocrysin for treatment of tuberculosis (2). Since then, there has been an exponential growth in clinical trials. This information explosion requires new approaches to integrating the ever-increasing knowledge with patient care; the concurrent revolution in information technology provides opportunities limited only by our own imaginations.
EBM is not without its critics: “It is cookbook medicine,” “It focuses on cost efficiency,” “I can’t find an RCT that fits my patient,” and “It doesn’t take into account the clinician’s experience” are often argued points. If EBM is not used effectively, all the criticisms are appropriate. Sacket, one of the earliest proponents and likely EBM’s most eloquent champion, refuted the claim that EBM is “cookbook medicine.” He argued that EBM requires a bottom-up approach that integrates the best external evidence with individual clinical expertise and patients’ choice. External clinical evidence informs, but does not replace, individual clinical expertise. The physician must decide whether the external evidence applies to the individual patient at all and, if so, how it should be integrated into a clinical decision (1).
Neither is EBM strictly about RCTs and meta-analysis. It’s about tracking down the best available evidence for your question and, thus, your patient. Sometimes a cohort study is best when you want to find the prognosis of a certain illness. Similarly, a cross-sectional study may be most appropriate when you’re trying to determine the sensitivity and specificity of a test. If a disease once thought universally fatal is proven otherwise in a case report, then a randomized control trial is hardly necessary. Finally, an RCT or meta-analysis is not always going to be available for the disease process you are dealing with, but EBM gives us the skill set to look down the evidence pyramid and find the next best thing (Figure 1).
It is also clear that EBM is not about cost cutting, although many hospital medicine programs were started with this as the primary goal, given the current healthcare environment. Certainly fears exist that EBM is being used by healthcare managers, organizations, and administrators as a cost-efficiency tool. It may be that good evidence is cost-efficient in certain situations, while in others it may require the healthcare system to invest more in itself if available evidence supports doing so. Thus it is imperative that hospitalists accept the challenge of incorporating EBM into their daily practice and become leaders in its application, with patient safety and quality of care as primary goals. If we don’t, others will define the role of EBM for us, with a potential for poor outcomes for the patient and the profession.
The EBM skill set and its tools are being continuously refined, with the evidence pyramid as one of the most basic principles (3). This evidence pyramid is a model for grading the evidence. It puts in perspective the different grades of evidence or study designs. For example, a systematic review of randomized controlled trials that show consistent results provides the highest quality evidence and is ranked accordingly in the pyramid. In contrast, a case report or case series of a treatment would be ranked much lower.
The first step in incorporating EBM into one’s daily practice requires an understanding of its analytical approach and access to the necessary tools. The process begins with asking a question that is answerable. A well-built clinical question is one that benefits the patient and clinician. Such questions are directly relevant to patient problems and phrased in ways that direct your search to relevant and precise answers.
In forming the question the following process, referred to as the PICO method, is helpful (4).
With the question formed, consider what type of question you have. This is often referred to as the typology of the question.
- Clinical Findings: Gathering and interpreting findings from the history, clinical examination, and test results.
- Etiology: Identifying causes for disease.
- Differential Diagnosis: Ranking by likelihood, seriousness, and treatability of the patients problem.
- Prognosis: Figuring out how to estimate the likely clinical course and complications over time of the disease
- Therapy: Selecting treatments to offer that do more good than harm and that are worth the effort and cost of using them.
- Prevention: Reducing the chance of disease by identifying and modifying risk factors and how to diagnose disease early by screening.
- Self-improvement: Keeping up-to-date, improve your clinical skills, and run a better, more efficient clinical practice.
The types of questions can next be matched to the type of research that may provide the answer:
- Diagnosis: prospective cohort study with good quality validation against “gold standard.”
- Prognosis: prospective cohort study.
- Therapy or prevention: prospective, randomized controlled clinical trial (RCT).
- Harm/Etiology: RCT, cohort or case-control study (probably retrospective).
- Economic: analysis of sensible costs against evidence-based outcome.
Once the question has been formed, the following steps lie ahead: finding the evidence, critically appraising the evidence, acting on the evidence, and, finally, evaluating one’s performance. Very much like the formation of the question, each of the subsequent steps involves an analytical approach that can be mastered. Technology—particularly personal computers, the Internet and PDAs—has made the task of mastering EBM easier in many ways. The additional steps in using EBM effectively will be addressed in future articles. A list of useful links is provided below.
http://library.downstate.edu/EBM2/contents.htm
http://healthsystem.virginia.edu/internet/library/collections/ebm/index.cfm
Dr. Kathuria may be reached at Navneet.kathuria@mssm.edu.
Endnotes
- Guyatt GH, Haynes RB, Jaeschke RZ, et al. Users’ guides to the medical literature: XXV. Evidence-based medicine: principles for applying the users’ guides to patient care. Evidence-Based Medicine Working Group. JAMA. 2000;284:1290-6.
- Claridge, J, Fabian, T. History and Development of Evidence Based Medicine. World Journal of Surgery 2005
- Guyatt GH, Haynes RB, et. al. Users’ guides to the medical literature: XXV. Evidence-Based Medicine: Principles for Applying the Users’ Guides to Patient Care. 2000;284:1290-1296
- Sackett DL, Richardson WS, Rosenberg W, Haynes RB (1997). Evidence-based medicine: How to practice and teach EBM. New York: Churchill Livingston
In the Literature
Literature at a Glance
- Drug-eluting stents decrease the need for revascularization.
- Case volume is related to hospital performance assessment.
- Prolonged QRS duration in patients with CHF is associated with increased morbidity and mortality.
- For out-of-hospital ACLS, vasopressin plus epinephrine is not better than vasopressin alone.
- Oral rivaroxaban is more efficacious than enoxaparin for VTE prophylaxis after total hip replacement.
- LMWH and UFH offer similar perioperative VTE prophylaxis benefit in patients with cancer.
- Salmeterol added to inhaled corticosteroids decreases severe asthma exacerbations.
- Early invasive strategy has unclear benefit in low-risk women with unstable angina or NSTEMI.
- Strategies to prevent contrast-induced acute kidney injury are not uniform.
- Hyperglycemia in hospitalized children is common and associated with ICU admission.
Do drug-eluting stents improve outcomes after ST-elevation myocardial infarction (STEMI)?
Background: Drug-eluting stents reduce restenosis rates compared to bare-metal stents. However, there is concern drug-eluting stents increase the risk of stent thrombosis leading to MI and death. Prior studies compared patients who received bare-metal versus those who received drug-eluting stents. Outcomes on a population level might provide new insight.
Study design: Observational study.
Setting: 100% national sample of patients 65 and older who received a coronary stent from 2002-05 enrolled in the traditional fee-for-service Medicare program.
Synopsis: 38,917 patients in the pre-drug-eluting-stent era from October 2002 to March 2003 received bare-metal stents. Nearly 62% of 28,086 patients studied from September to December 2003 received drug-eluting stents. The remaining 38.5% received bare-metal stents. Outcomes of percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), STEMI, and death were observed through December 31, 2005.
Patients in the drug-eluting-stent era had a lower two-year risk for repeat revascularization compared to patients in the bare-metal-stent era. In the drug-eluting versus bare-metal eras, repeat PCI was 17.1% versus 20.0% (p<0.001) and need for CABG was 2.7% versus 4.2% (p<0.01). Comparing adjusted outcomes for death, or STEMI, at two years, the two groups appeared similar.
The study did have limitations: the data only reflect sirolimus stents, the authors could not assess dual-antiplatelet therapy or obtain information on coronary anatomy or procedure details to account for selection bias in stent utilization, and the patients were all Medicare beneficiaries.
Bottom line: Drug-eluting stents are associated with fewer repeat revascularization procedures than bare-metal stents, but have not shown a significant improvement in the subsequent risk of STEMI or death.
Citation: Malenka DJ, Kaplan AV, Lucas FL, Sharp SM, Skinner JA. Outcomes following coronary stenting in the era of bare-metal vs. the era of drug-eluting stents. JAMA 2008;299(24):2868-2877.
Does case volume affect hospital performance for publicly reported process measures?
Background: Hospitals are increasingly graded and compared to one another. “Top medical centers” are defined as those within the top 10% of hospitals in specified performance measures. Hospitals with large and small case volumes might not be compared evenly and fairly.
Study design: Eight publicly reported process measures for acute myocardial infarction (AMI) were compared to hospital case volume, process performance, and label as “top hospital.”
Setting: Data were analyzed from the Hospital Quality Alliance for 3,761 hospitals from January to December 2005.
Synopsis: Hospitals with large case volume overall had better process performance. For example, looking at use of beta-blockers in patients with AMI on arrival to a hospital, small-volume hospitals (<10 AMI cases) averaged 72% while large volume (>100 AMI cases) averaged 80% (p<0.001). However, hospitals with small case volumes were more likely to receive “top hospital” rating even when hospitals with very low case volumes were excluded.
Hospital quality reporting that does not account for case volume is misleading to hospitals and consumers. In this study, larger-volume hospitals appeared to perform better in process measures, but were less likely to receive “top hospital” rating.
Bottom line: Hospitals with large and small case volumes can easily be compared to one another for process measures in AMI.
Citation: O’Brien SM, DeLong ER, Peterson ED. Impact of case volume on hospital performance assessment. Arch Intern Med. 2008;168(12):1277-1284.
What is the predictive value of QRS duration in patients hospitalized with worsening CHF?
Background: In outpatients, a prolonged QRS duration (greater than 120 ms) is associated with increased mortality. Its value in the inpatient setting is unclear. For patients hospitalized with CHF exacerbations, establishing the value of QRS duration may allow for tailored management.
Study design: Retrospective post hoc analysis from the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST).
Setting: 4,133 patients were enrolled from North American, South American, and European sites.
Synopsis: Of 2,962 patients included in the final post hoc analysis, 1,321 (44.6%) had a prolonged QRS duration. During a median follow up of 9.9 months, the all-cause mortality rate was 18.7% for patients with a normal baseline QRS duration and 28.1% for patients with a prolonged baseline QRS.
After adjusting for confounding variables, patients with a prolonged baseline QRS had a 24% increased risk of all-cause mortality and a 28% increased risk for a composite endpoint of cardiac mortality or hospitalization for heart failure exacerbation.
The retrospective nature of the analysis represents the major limitation of this study. In addition, most of the enrolled patients were white, which limits the studies generalizability to other ethnic groups.
Bottom Line: A prolonged QRS duration for patients admitted with decompensated left ventricular heart failure is common and may be associated with increased morbidity and mortality.
Citation: Wang NC, Maggioni AP, Konstam MA, Zannad F, Drasa HB, Burnett JC, et al. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA. 2008;299(22):2656-2666.
For patients with out-of-hospital cardiac arrest, does the addition of vasopressin to epinephrine in a protocol for ACLS improve outcomes?
Background: The outcome for patients experiencing cardiac arrest who require vasopressors remains extremely poor. Despite disappointing data on vasopressin as an alternative treatment during cardiac arrest, a recent subgroup analysis suggested patients who received epinephrine and vasopressin together had superior clinical outcomes.
Study Design: Prospective multicenter randomized double-blind controlled trial.
Setting: 31 emergency medical service organizations in France.
Synopsis: Of the 2,894 patients, 20.7% of those receiving combination treatment (vasopressin plus epinephrine) survived to hospital admission versus 21.3% of those in the epinephrine-only group. For those same groups, 1.7% of combination and 2.3% of epinephrine-only patients survived to hospital discharge. No significant outcome differences were found in any group or subgroup analysis.
The study had lower-than-expected overall survival to hospital discharge, which may have handicapped its effort to find a true difference in treatment arms.
Bottom line: The addition of vasopressin to epinephrine in the treatment of out-of-hospital cardiac arrest does not improve outcomes.
Citation: Gueugniaud PY, David JS, Chanzy E, Hubert H, Dubien P, Mauriaucourt P, et al. Vasopressin and epinephrine vs. epinephrine alone in cardiopulmonary resuscitation. N Engl J Med. 2008;359(1):21-30.
Is oral rivaroxaban more efficacious than subcutaneous enoxaparin in preventing VTE after hip-replacement surgery?
Background: Venous thromboembolism (VTE) prophylaxis after total hip replacement (THR) is important but can be cumbersome because the most commonly used anticoagulants are either subcutaneous or require frequent monitoring. Rivaroxaban, an oral direct inhibitor of factor Xa may provide more convenient anticoagulation postoperatively. However, its efficacy and safety are unknown.
Study design: Randomized double-blind trial.
Setting: Multicenter study performed in 27 countries.
Synopsis: Patients undergoing THR surgery were randomized to oral rivaroxaban (10mg once daily without monitoring, started six to eight hours after surgery) or subcutaneous enoxaparin (40mg once daily, started 12 hours prior to surgery). After surgery, prophylaxis was administered for 35 days. The primary outcome was a composite of asymptomatic deep venous thrombosis (DVT), symptomatic DVT or pulmonary embolism (PE), or death from any cause at 36 days after surgery.
In the enoxaparin group, 3.7% of patients experienced the primary outcome. This decreased to 1.1% in the rivaroxaban group. Approximately one-third of events were symptomatic. Major bleeding occurred in 0.1% and 0.3% (p=NS) of patients in the enoxaparin and rivaroxaban groups, respectively.
The study is limited by the exclusion of 1,388 of the 4,541 patients (30.6%) randomized, primarily due to having inadequate venography. Also, because the majority of thromboembolic events were asymptomatic, the primary outcome overemphasizes the clinical difference.
Bottom line: Oral rivaroxaban without monitoring is more efficacious than, and as safe as, subcutaneous enoxaparin when used for VTE prophylaxis for THR.
Citation: Eriksson B, Borris LC, Friedman RJ, Hass S, Huisman MV, Kakkar AK, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med. 2008;358:2765-75.
Is LMWH more efficacious than UFH in preventing postoperative VTE in cancer patients?
Background: Patients with cancer are at increased risk for VTE and require prophylaxis to prevent this complication postoperatively. Low molecular weight heparin (LMWH) has proven more efficacious than subcutaneous unfractionated heparin (UFH) in other settings (e.g., DVT treatment). However, it is still unknown whether LMWH offers better prophylaxis compared to UFH for cancer patients undergoing surgery.
Study design: Systematic review and meta-analysis.
Setting: 14 randomized controlled trials.
Synopsis: Eleven trials exclusively examined patients with cancer (n=4006) and three trials reported data for cancer patients as subgroups (n=1816). There were in differences in mortality, pulmonary embolism, and symptomatic DVT rates between the two groups.
LMWH was associated with a decrease in total (asymptomatic or symptomatic) DVT (RR, 0.72; 95% CI, 0.55-0.94). Rates of major bleeding, minor bleeding, and intraoperative blood loss were similar between the two treatments.
This meta-analysis is limited because 12 remaining trials (n=3185) also enrolled cancer patients but did not provide specific data for the cancer patient subgroup. The study also is limited by the heterogeneity of the original trials, including utilizing varying LMWHs and dosing regimens, numerous types of surgeries, and a wide range of neoplasms.
Bottom line: LMWH does not decrease mortality, pulmonary embolism, or symptomatic DVT compared to UFH in cancer patients undergoing surgery.
Citation: Akl EA, Terrenato I, Barba M, Sperati F, Sempos EV, Muti P, et al. Low-molecular-weight heparin vs. unfractionated heparin for perioperative thromboprophylaxis in patients with cancer. Arch Intern Med. 2008;168:1261-9.
Does salmeterol added to inhaled corticosteroids improve severe asthma-related events?
Background: Asthma is a chronic disease causing major morbidity and mortality worldwide. Disease guidelines recommend all patients with persistent asthma be treated with inhaled corticosteroids. These same guidelines recommend adding a long-acting beta-agonist for patients whose symptoms persist. However, the safety of this practice has come under scrutiny.
Study design: Meta-analysis.
Setting: Sixty-six randomized, controlled trials conducted worldwide.
Synopsis: Analysis included 66 GlaxoSmithKline trials with a total of 20,966 patients with persistent asthma. Patients used either salmeterol (50mcg twice daily) plus inhaled corticosteroid (10,400 patients) or inhaled corticosteroid alone (10,566 patients).
Results showed no differences in asthma-related hospitalizations, asthma-related intubations, or deaths between the two groups. However, due to the low number of events, definitive conclusions are difficult to make. Severe asthma exacerbations requiring systemic corticosteroids significantly decreased in the inhaled corticosteroid plus salmeterol group.
The study is limited by it inclusion of only those trials sponsored by GlaxoSmithKline and by the short duration of most of the studies. Additionally, the studies included in the analysis used clinical outcomes as secondary endpoints.
Bottom line: Adding salmeterol to inhaled corticosteroid decreases severe asthma exacerbations and is likely safe, but does not have an effect on asthma-related hospitalization or death.
Citation: Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et.al. Meta-analysis: Effects of adding salmeterol to inhaled corticosteroids on serious asthma-related events. Annals Intern Med. 2008;149:33-42.
Is an early invasive strategy effective in women with unstable angina or NSTEMI?
Background: Despite many trials showing the value of an early invasive strategy for patients with non-ST-segment elevation acute coronary syndrome (NSTE ACS), data from several trials question this benefit in women. Some trials show higher risk of death and myocardial infarction (MI) in subgroup analysis of women.
Study Design: Meta-analysis.
Setting: Eight randomized, controlled trials conducted worldwide.
Synopsis: Analysis included eight trials with 10,412 patients (3,075 women) with NSTE ACS. The invasive group (5,083 patients) was defined as those referred for coronary angiography with subsequent intervention as needed. The composite endpoint of death, MI, or rehospitalization within 12 months with ACS occurred in 21.1% of the invasive group and 25.9% of the medically managed group (OR, 0.78; CI, 0.61-0.98).
The subgroup, including only women, had a non-statistically significant OR of 0.81 (CI, 0.65-1.01), including no effect on all-cause mortality, nonfatal MI, or the composite of death and MI. However, women with high-risk features (elevated biomarkers) undergoing the invasive strategy had a significant reduction in the composite endpoint (OR, 0.67; CI, 0.50-0.88).
The study is limited by the use of subgroup analysis, secondary endpoints, heterogeneity between trials, and possible publication bias.
Bottom line: Early invasive strategy is effective in men and high-risk women with NSTE ACS, but not in low-risk women.
Citation: O’Donoghue M, Boden W, Braunwald E, Cannon CP, Clayton TC, Winter RJ, et.al. Early invasive vs. conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction. JAMA. 2008;300:71-80.
What strategies are used to prevent contrast-induced acute kidney injury?
Background: Contrast-induced acute kidney injury (CIAKI) is a condition potentially amenable to preventive care. Several trials have identified intravenous hydration, N-acetylcysteine, and withdrawal of NSAIDS as interventions that reduce the possibility of CIAKI in high-risk patients. Little is known about whether healthcare providers routinely use these strategies.
Study design: Prospective observational cohort study.
Setting: Veterans Affairs (VA) Pittsburgh Healthcare System.
Synopsis: 11,410 patients scheduled for radiographic procedures were screened. After exclusion criteria and eligibility, 660 patients with an estimated glomerular filtration rate less than 60ml/min/1.73m2 were identified. Usage of intravenous fluids, N-acetylcysteine, and discontinuation of NSAIDS were recorded. Serum creatinine (SCr) was measured 48 to 96 hours post-procedure. CIAKI was defined as relative increase in SCr from baseline (≥25%, ≥50% and ≥100%) and absolute increase in SCr levels from baseline (≥0.25, ≥0.5, and ≥1.0). CIAKI association with adverse outcomes was evaluated by tracking 30-day mortality, need for dialysis, and hospitalization.
The incidence of CIAKI was less common in patients undergoing CT scans versus those having angiograms. Adverse 30-day outcomes were uncommon. Pre- and post-procedure intravenous hydration was administered to 40% of study patients, more commonly with coronary angiogram than with computed tomography (91.2% vs. 16%, p<0.0001). N-acetylcysteine was administered to 39.2%. Only 6.8% of those taking NSAIDS reported being told to discontinue the medication.
Study limitations include the small sample size and the single site location, both limiting generalizability.
Bottom line: Clinically significant CIAKI is uncommon, and preventive care is not uniformly implemented in patients undergoing contrast-enhanced radiographic procedures.
Citation: Weisbord SD, Mor MK, Resnick AL, Hartwig KC, Sonel AF, Fine MJ, et al. Prevention, incidence, and outcomes of contrast-induced acute kidney injury. Arch Intern Med. 2008;168(12):1325-1332.
How does hyperglycemia affect morbidity and mortality in children admitted to a community pediatric hospital?
Background: Inpatient hyperglycemia in adult patients is a predictor of poor clinical outcomes. The association of hyperglycemia and clinical outcomes in children admitted to a general community hospital has not been studied.
Study design: Retrospective observational cohort study.
Setting: A community pediatric hospital in Atlanta, Ga.
Synopsis: Review of medical records of 903 consecutive pediatric patients admitted to critical and non-critical areas took place. Of these, 542 patients constituted the study population. The study excluded 342 patients who didn’t have a blood glucose measurement. Hyperglycemia was defined as an admission or in-hospital blood glucose greater than 120mg/dl.
One-fourth of the children admitted to the hospital had hyperglycemia, most without a prior history of diabetes. The presence of hyperglycemia on admission was not associated with increased length of stay (LOS) or increased mortality. Children with hyperglycemia were more likely to be admitted to the ICU and had longer ICU LOS.
This was a retrospective study conducted at a single site whose demographics and disease spectrum may differ from those of other institutions. There were an insufficient number of deaths to make any conclusions regarding the impact of hyperglycemia on mortality. Prospective, randomized, multicenter trials are needed to better elucidate the effects of in-patient hyperglycemia.
Bottom line: Hyperglycemia is common in children with or without diabetes admitted to the hospital, and is associated with increased ICU admissions and ICU length of stay. Its connection to mortality is inconclusive.
Citation: Palaio A, Smiley D, Ceron M, Klein R, Cho IS, Mejia R, et al. Prevalence and clinical outcome of inpatient hyperglycemia in a community pediatric hospital. J Hosp Med.2008;3(3):212-217.
Literature at a Glance
- Drug-eluting stents decrease the need for revascularization.
- Case volume is related to hospital performance assessment.
- Prolonged QRS duration in patients with CHF is associated with increased morbidity and mortality.
- For out-of-hospital ACLS, vasopressin plus epinephrine is not better than vasopressin alone.
- Oral rivaroxaban is more efficacious than enoxaparin for VTE prophylaxis after total hip replacement.
- LMWH and UFH offer similar perioperative VTE prophylaxis benefit in patients with cancer.
- Salmeterol added to inhaled corticosteroids decreases severe asthma exacerbations.
- Early invasive strategy has unclear benefit in low-risk women with unstable angina or NSTEMI.
- Strategies to prevent contrast-induced acute kidney injury are not uniform.
- Hyperglycemia in hospitalized children is common and associated with ICU admission.
Do drug-eluting stents improve outcomes after ST-elevation myocardial infarction (STEMI)?
Background: Drug-eluting stents reduce restenosis rates compared to bare-metal stents. However, there is concern drug-eluting stents increase the risk of stent thrombosis leading to MI and death. Prior studies compared patients who received bare-metal versus those who received drug-eluting stents. Outcomes on a population level might provide new insight.
Study design: Observational study.
Setting: 100% national sample of patients 65 and older who received a coronary stent from 2002-05 enrolled in the traditional fee-for-service Medicare program.
Synopsis: 38,917 patients in the pre-drug-eluting-stent era from October 2002 to March 2003 received bare-metal stents. Nearly 62% of 28,086 patients studied from September to December 2003 received drug-eluting stents. The remaining 38.5% received bare-metal stents. Outcomes of percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), STEMI, and death were observed through December 31, 2005.
Patients in the drug-eluting-stent era had a lower two-year risk for repeat revascularization compared to patients in the bare-metal-stent era. In the drug-eluting versus bare-metal eras, repeat PCI was 17.1% versus 20.0% (p<0.001) and need for CABG was 2.7% versus 4.2% (p<0.01). Comparing adjusted outcomes for death, or STEMI, at two years, the two groups appeared similar.
The study did have limitations: the data only reflect sirolimus stents, the authors could not assess dual-antiplatelet therapy or obtain information on coronary anatomy or procedure details to account for selection bias in stent utilization, and the patients were all Medicare beneficiaries.
Bottom line: Drug-eluting stents are associated with fewer repeat revascularization procedures than bare-metal stents, but have not shown a significant improvement in the subsequent risk of STEMI or death.
Citation: Malenka DJ, Kaplan AV, Lucas FL, Sharp SM, Skinner JA. Outcomes following coronary stenting in the era of bare-metal vs. the era of drug-eluting stents. JAMA 2008;299(24):2868-2877.
Does case volume affect hospital performance for publicly reported process measures?
Background: Hospitals are increasingly graded and compared to one another. “Top medical centers” are defined as those within the top 10% of hospitals in specified performance measures. Hospitals with large and small case volumes might not be compared evenly and fairly.
Study design: Eight publicly reported process measures for acute myocardial infarction (AMI) were compared to hospital case volume, process performance, and label as “top hospital.”
Setting: Data were analyzed from the Hospital Quality Alliance for 3,761 hospitals from January to December 2005.
Synopsis: Hospitals with large case volume overall had better process performance. For example, looking at use of beta-blockers in patients with AMI on arrival to a hospital, small-volume hospitals (<10 AMI cases) averaged 72% while large volume (>100 AMI cases) averaged 80% (p<0.001). However, hospitals with small case volumes were more likely to receive “top hospital” rating even when hospitals with very low case volumes were excluded.
Hospital quality reporting that does not account for case volume is misleading to hospitals and consumers. In this study, larger-volume hospitals appeared to perform better in process measures, but were less likely to receive “top hospital” rating.
Bottom line: Hospitals with large and small case volumes can easily be compared to one another for process measures in AMI.
Citation: O’Brien SM, DeLong ER, Peterson ED. Impact of case volume on hospital performance assessment. Arch Intern Med. 2008;168(12):1277-1284.
What is the predictive value of QRS duration in patients hospitalized with worsening CHF?
Background: In outpatients, a prolonged QRS duration (greater than 120 ms) is associated with increased mortality. Its value in the inpatient setting is unclear. For patients hospitalized with CHF exacerbations, establishing the value of QRS duration may allow for tailored management.
Study design: Retrospective post hoc analysis from the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST).
Setting: 4,133 patients were enrolled from North American, South American, and European sites.
Synopsis: Of 2,962 patients included in the final post hoc analysis, 1,321 (44.6%) had a prolonged QRS duration. During a median follow up of 9.9 months, the all-cause mortality rate was 18.7% for patients with a normal baseline QRS duration and 28.1% for patients with a prolonged baseline QRS.
After adjusting for confounding variables, patients with a prolonged baseline QRS had a 24% increased risk of all-cause mortality and a 28% increased risk for a composite endpoint of cardiac mortality or hospitalization for heart failure exacerbation.
The retrospective nature of the analysis represents the major limitation of this study. In addition, most of the enrolled patients were white, which limits the studies generalizability to other ethnic groups.
Bottom Line: A prolonged QRS duration for patients admitted with decompensated left ventricular heart failure is common and may be associated with increased morbidity and mortality.
Citation: Wang NC, Maggioni AP, Konstam MA, Zannad F, Drasa HB, Burnett JC, et al. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA. 2008;299(22):2656-2666.
For patients with out-of-hospital cardiac arrest, does the addition of vasopressin to epinephrine in a protocol for ACLS improve outcomes?
Background: The outcome for patients experiencing cardiac arrest who require vasopressors remains extremely poor. Despite disappointing data on vasopressin as an alternative treatment during cardiac arrest, a recent subgroup analysis suggested patients who received epinephrine and vasopressin together had superior clinical outcomes.
Study Design: Prospective multicenter randomized double-blind controlled trial.
Setting: 31 emergency medical service organizations in France.
Synopsis: Of the 2,894 patients, 20.7% of those receiving combination treatment (vasopressin plus epinephrine) survived to hospital admission versus 21.3% of those in the epinephrine-only group. For those same groups, 1.7% of combination and 2.3% of epinephrine-only patients survived to hospital discharge. No significant outcome differences were found in any group or subgroup analysis.
The study had lower-than-expected overall survival to hospital discharge, which may have handicapped its effort to find a true difference in treatment arms.
Bottom line: The addition of vasopressin to epinephrine in the treatment of out-of-hospital cardiac arrest does not improve outcomes.
Citation: Gueugniaud PY, David JS, Chanzy E, Hubert H, Dubien P, Mauriaucourt P, et al. Vasopressin and epinephrine vs. epinephrine alone in cardiopulmonary resuscitation. N Engl J Med. 2008;359(1):21-30.
Is oral rivaroxaban more efficacious than subcutaneous enoxaparin in preventing VTE after hip-replacement surgery?
Background: Venous thromboembolism (VTE) prophylaxis after total hip replacement (THR) is important but can be cumbersome because the most commonly used anticoagulants are either subcutaneous or require frequent monitoring. Rivaroxaban, an oral direct inhibitor of factor Xa may provide more convenient anticoagulation postoperatively. However, its efficacy and safety are unknown.
Study design: Randomized double-blind trial.
Setting: Multicenter study performed in 27 countries.
Synopsis: Patients undergoing THR surgery were randomized to oral rivaroxaban (10mg once daily without monitoring, started six to eight hours after surgery) or subcutaneous enoxaparin (40mg once daily, started 12 hours prior to surgery). After surgery, prophylaxis was administered for 35 days. The primary outcome was a composite of asymptomatic deep venous thrombosis (DVT), symptomatic DVT or pulmonary embolism (PE), or death from any cause at 36 days after surgery.
In the enoxaparin group, 3.7% of patients experienced the primary outcome. This decreased to 1.1% in the rivaroxaban group. Approximately one-third of events were symptomatic. Major bleeding occurred in 0.1% and 0.3% (p=NS) of patients in the enoxaparin and rivaroxaban groups, respectively.
The study is limited by the exclusion of 1,388 of the 4,541 patients (30.6%) randomized, primarily due to having inadequate venography. Also, because the majority of thromboembolic events were asymptomatic, the primary outcome overemphasizes the clinical difference.
Bottom line: Oral rivaroxaban without monitoring is more efficacious than, and as safe as, subcutaneous enoxaparin when used for VTE prophylaxis for THR.
Citation: Eriksson B, Borris LC, Friedman RJ, Hass S, Huisman MV, Kakkar AK, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med. 2008;358:2765-75.
Is LMWH more efficacious than UFH in preventing postoperative VTE in cancer patients?
Background: Patients with cancer are at increased risk for VTE and require prophylaxis to prevent this complication postoperatively. Low molecular weight heparin (LMWH) has proven more efficacious than subcutaneous unfractionated heparin (UFH) in other settings (e.g., DVT treatment). However, it is still unknown whether LMWH offers better prophylaxis compared to UFH for cancer patients undergoing surgery.
Study design: Systematic review and meta-analysis.
Setting: 14 randomized controlled trials.
Synopsis: Eleven trials exclusively examined patients with cancer (n=4006) and three trials reported data for cancer patients as subgroups (n=1816). There were in differences in mortality, pulmonary embolism, and symptomatic DVT rates between the two groups.
LMWH was associated with a decrease in total (asymptomatic or symptomatic) DVT (RR, 0.72; 95% CI, 0.55-0.94). Rates of major bleeding, minor bleeding, and intraoperative blood loss were similar between the two treatments.
This meta-analysis is limited because 12 remaining trials (n=3185) also enrolled cancer patients but did not provide specific data for the cancer patient subgroup. The study also is limited by the heterogeneity of the original trials, including utilizing varying LMWHs and dosing regimens, numerous types of surgeries, and a wide range of neoplasms.
Bottom line: LMWH does not decrease mortality, pulmonary embolism, or symptomatic DVT compared to UFH in cancer patients undergoing surgery.
Citation: Akl EA, Terrenato I, Barba M, Sperati F, Sempos EV, Muti P, et al. Low-molecular-weight heparin vs. unfractionated heparin for perioperative thromboprophylaxis in patients with cancer. Arch Intern Med. 2008;168:1261-9.
Does salmeterol added to inhaled corticosteroids improve severe asthma-related events?
Background: Asthma is a chronic disease causing major morbidity and mortality worldwide. Disease guidelines recommend all patients with persistent asthma be treated with inhaled corticosteroids. These same guidelines recommend adding a long-acting beta-agonist for patients whose symptoms persist. However, the safety of this practice has come under scrutiny.
Study design: Meta-analysis.
Setting: Sixty-six randomized, controlled trials conducted worldwide.
Synopsis: Analysis included 66 GlaxoSmithKline trials with a total of 20,966 patients with persistent asthma. Patients used either salmeterol (50mcg twice daily) plus inhaled corticosteroid (10,400 patients) or inhaled corticosteroid alone (10,566 patients).
Results showed no differences in asthma-related hospitalizations, asthma-related intubations, or deaths between the two groups. However, due to the low number of events, definitive conclusions are difficult to make. Severe asthma exacerbations requiring systemic corticosteroids significantly decreased in the inhaled corticosteroid plus salmeterol group.
The study is limited by it inclusion of only those trials sponsored by GlaxoSmithKline and by the short duration of most of the studies. Additionally, the studies included in the analysis used clinical outcomes as secondary endpoints.
Bottom line: Adding salmeterol to inhaled corticosteroid decreases severe asthma exacerbations and is likely safe, but does not have an effect on asthma-related hospitalization or death.
Citation: Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et.al. Meta-analysis: Effects of adding salmeterol to inhaled corticosteroids on serious asthma-related events. Annals Intern Med. 2008;149:33-42.
Is an early invasive strategy effective in women with unstable angina or NSTEMI?
Background: Despite many trials showing the value of an early invasive strategy for patients with non-ST-segment elevation acute coronary syndrome (NSTE ACS), data from several trials question this benefit in women. Some trials show higher risk of death and myocardial infarction (MI) in subgroup analysis of women.
Study Design: Meta-analysis.
Setting: Eight randomized, controlled trials conducted worldwide.
Synopsis: Analysis included eight trials with 10,412 patients (3,075 women) with NSTE ACS. The invasive group (5,083 patients) was defined as those referred for coronary angiography with subsequent intervention as needed. The composite endpoint of death, MI, or rehospitalization within 12 months with ACS occurred in 21.1% of the invasive group and 25.9% of the medically managed group (OR, 0.78; CI, 0.61-0.98).
The subgroup, including only women, had a non-statistically significant OR of 0.81 (CI, 0.65-1.01), including no effect on all-cause mortality, nonfatal MI, or the composite of death and MI. However, women with high-risk features (elevated biomarkers) undergoing the invasive strategy had a significant reduction in the composite endpoint (OR, 0.67; CI, 0.50-0.88).
The study is limited by the use of subgroup analysis, secondary endpoints, heterogeneity between trials, and possible publication bias.
Bottom line: Early invasive strategy is effective in men and high-risk women with NSTE ACS, but not in low-risk women.
Citation: O’Donoghue M, Boden W, Braunwald E, Cannon CP, Clayton TC, Winter RJ, et.al. Early invasive vs. conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction. JAMA. 2008;300:71-80.
What strategies are used to prevent contrast-induced acute kidney injury?
Background: Contrast-induced acute kidney injury (CIAKI) is a condition potentially amenable to preventive care. Several trials have identified intravenous hydration, N-acetylcysteine, and withdrawal of NSAIDS as interventions that reduce the possibility of CIAKI in high-risk patients. Little is known about whether healthcare providers routinely use these strategies.
Study design: Prospective observational cohort study.
Setting: Veterans Affairs (VA) Pittsburgh Healthcare System.
Synopsis: 11,410 patients scheduled for radiographic procedures were screened. After exclusion criteria and eligibility, 660 patients with an estimated glomerular filtration rate less than 60ml/min/1.73m2 were identified. Usage of intravenous fluids, N-acetylcysteine, and discontinuation of NSAIDS were recorded. Serum creatinine (SCr) was measured 48 to 96 hours post-procedure. CIAKI was defined as relative increase in SCr from baseline (≥25%, ≥50% and ≥100%) and absolute increase in SCr levels from baseline (≥0.25, ≥0.5, and ≥1.0). CIAKI association with adverse outcomes was evaluated by tracking 30-day mortality, need for dialysis, and hospitalization.
The incidence of CIAKI was less common in patients undergoing CT scans versus those having angiograms. Adverse 30-day outcomes were uncommon. Pre- and post-procedure intravenous hydration was administered to 40% of study patients, more commonly with coronary angiogram than with computed tomography (91.2% vs. 16%, p<0.0001). N-acetylcysteine was administered to 39.2%. Only 6.8% of those taking NSAIDS reported being told to discontinue the medication.
Study limitations include the small sample size and the single site location, both limiting generalizability.
Bottom line: Clinically significant CIAKI is uncommon, and preventive care is not uniformly implemented in patients undergoing contrast-enhanced radiographic procedures.
Citation: Weisbord SD, Mor MK, Resnick AL, Hartwig KC, Sonel AF, Fine MJ, et al. Prevention, incidence, and outcomes of contrast-induced acute kidney injury. Arch Intern Med. 2008;168(12):1325-1332.
How does hyperglycemia affect morbidity and mortality in children admitted to a community pediatric hospital?
Background: Inpatient hyperglycemia in adult patients is a predictor of poor clinical outcomes. The association of hyperglycemia and clinical outcomes in children admitted to a general community hospital has not been studied.
Study design: Retrospective observational cohort study.
Setting: A community pediatric hospital in Atlanta, Ga.
Synopsis: Review of medical records of 903 consecutive pediatric patients admitted to critical and non-critical areas took place. Of these, 542 patients constituted the study population. The study excluded 342 patients who didn’t have a blood glucose measurement. Hyperglycemia was defined as an admission or in-hospital blood glucose greater than 120mg/dl.
One-fourth of the children admitted to the hospital had hyperglycemia, most without a prior history of diabetes. The presence of hyperglycemia on admission was not associated with increased length of stay (LOS) or increased mortality. Children with hyperglycemia were more likely to be admitted to the ICU and had longer ICU LOS.
This was a retrospective study conducted at a single site whose demographics and disease spectrum may differ from those of other institutions. There were an insufficient number of deaths to make any conclusions regarding the impact of hyperglycemia on mortality. Prospective, randomized, multicenter trials are needed to better elucidate the effects of in-patient hyperglycemia.
Bottom line: Hyperglycemia is common in children with or without diabetes admitted to the hospital, and is associated with increased ICU admissions and ICU length of stay. Its connection to mortality is inconclusive.
Citation: Palaio A, Smiley D, Ceron M, Klein R, Cho IS, Mejia R, et al. Prevalence and clinical outcome of inpatient hyperglycemia in a community pediatric hospital. J Hosp Med.2008;3(3):212-217.
Literature at a Glance
- Drug-eluting stents decrease the need for revascularization.
- Case volume is related to hospital performance assessment.
- Prolonged QRS duration in patients with CHF is associated with increased morbidity and mortality.
- For out-of-hospital ACLS, vasopressin plus epinephrine is not better than vasopressin alone.
- Oral rivaroxaban is more efficacious than enoxaparin for VTE prophylaxis after total hip replacement.
- LMWH and UFH offer similar perioperative VTE prophylaxis benefit in patients with cancer.
- Salmeterol added to inhaled corticosteroids decreases severe asthma exacerbations.
- Early invasive strategy has unclear benefit in low-risk women with unstable angina or NSTEMI.
- Strategies to prevent contrast-induced acute kidney injury are not uniform.
- Hyperglycemia in hospitalized children is common and associated with ICU admission.
Do drug-eluting stents improve outcomes after ST-elevation myocardial infarction (STEMI)?
Background: Drug-eluting stents reduce restenosis rates compared to bare-metal stents. However, there is concern drug-eluting stents increase the risk of stent thrombosis leading to MI and death. Prior studies compared patients who received bare-metal versus those who received drug-eluting stents. Outcomes on a population level might provide new insight.
Study design: Observational study.
Setting: 100% national sample of patients 65 and older who received a coronary stent from 2002-05 enrolled in the traditional fee-for-service Medicare program.
Synopsis: 38,917 patients in the pre-drug-eluting-stent era from October 2002 to March 2003 received bare-metal stents. Nearly 62% of 28,086 patients studied from September to December 2003 received drug-eluting stents. The remaining 38.5% received bare-metal stents. Outcomes of percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), STEMI, and death were observed through December 31, 2005.
Patients in the drug-eluting-stent era had a lower two-year risk for repeat revascularization compared to patients in the bare-metal-stent era. In the drug-eluting versus bare-metal eras, repeat PCI was 17.1% versus 20.0% (p<0.001) and need for CABG was 2.7% versus 4.2% (p<0.01). Comparing adjusted outcomes for death, or STEMI, at two years, the two groups appeared similar.
The study did have limitations: the data only reflect sirolimus stents, the authors could not assess dual-antiplatelet therapy or obtain information on coronary anatomy or procedure details to account for selection bias in stent utilization, and the patients were all Medicare beneficiaries.
Bottom line: Drug-eluting stents are associated with fewer repeat revascularization procedures than bare-metal stents, but have not shown a significant improvement in the subsequent risk of STEMI or death.
Citation: Malenka DJ, Kaplan AV, Lucas FL, Sharp SM, Skinner JA. Outcomes following coronary stenting in the era of bare-metal vs. the era of drug-eluting stents. JAMA 2008;299(24):2868-2877.
Does case volume affect hospital performance for publicly reported process measures?
Background: Hospitals are increasingly graded and compared to one another. “Top medical centers” are defined as those within the top 10% of hospitals in specified performance measures. Hospitals with large and small case volumes might not be compared evenly and fairly.
Study design: Eight publicly reported process measures for acute myocardial infarction (AMI) were compared to hospital case volume, process performance, and label as “top hospital.”
Setting: Data were analyzed from the Hospital Quality Alliance for 3,761 hospitals from January to December 2005.
Synopsis: Hospitals with large case volume overall had better process performance. For example, looking at use of beta-blockers in patients with AMI on arrival to a hospital, small-volume hospitals (<10 AMI cases) averaged 72% while large volume (>100 AMI cases) averaged 80% (p<0.001). However, hospitals with small case volumes were more likely to receive “top hospital” rating even when hospitals with very low case volumes were excluded.
Hospital quality reporting that does not account for case volume is misleading to hospitals and consumers. In this study, larger-volume hospitals appeared to perform better in process measures, but were less likely to receive “top hospital” rating.
Bottom line: Hospitals with large and small case volumes can easily be compared to one another for process measures in AMI.
Citation: O’Brien SM, DeLong ER, Peterson ED. Impact of case volume on hospital performance assessment. Arch Intern Med. 2008;168(12):1277-1284.
What is the predictive value of QRS duration in patients hospitalized with worsening CHF?
Background: In outpatients, a prolonged QRS duration (greater than 120 ms) is associated with increased mortality. Its value in the inpatient setting is unclear. For patients hospitalized with CHF exacerbations, establishing the value of QRS duration may allow for tailored management.
Study design: Retrospective post hoc analysis from the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST).
Setting: 4,133 patients were enrolled from North American, South American, and European sites.
Synopsis: Of 2,962 patients included in the final post hoc analysis, 1,321 (44.6%) had a prolonged QRS duration. During a median follow up of 9.9 months, the all-cause mortality rate was 18.7% for patients with a normal baseline QRS duration and 28.1% for patients with a prolonged baseline QRS.
After adjusting for confounding variables, patients with a prolonged baseline QRS had a 24% increased risk of all-cause mortality and a 28% increased risk for a composite endpoint of cardiac mortality or hospitalization for heart failure exacerbation.
The retrospective nature of the analysis represents the major limitation of this study. In addition, most of the enrolled patients were white, which limits the studies generalizability to other ethnic groups.
Bottom Line: A prolonged QRS duration for patients admitted with decompensated left ventricular heart failure is common and may be associated with increased morbidity and mortality.
Citation: Wang NC, Maggioni AP, Konstam MA, Zannad F, Drasa HB, Burnett JC, et al. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA. 2008;299(22):2656-2666.
For patients with out-of-hospital cardiac arrest, does the addition of vasopressin to epinephrine in a protocol for ACLS improve outcomes?
Background: The outcome for patients experiencing cardiac arrest who require vasopressors remains extremely poor. Despite disappointing data on vasopressin as an alternative treatment during cardiac arrest, a recent subgroup analysis suggested patients who received epinephrine and vasopressin together had superior clinical outcomes.
Study Design: Prospective multicenter randomized double-blind controlled trial.
Setting: 31 emergency medical service organizations in France.
Synopsis: Of the 2,894 patients, 20.7% of those receiving combination treatment (vasopressin plus epinephrine) survived to hospital admission versus 21.3% of those in the epinephrine-only group. For those same groups, 1.7% of combination and 2.3% of epinephrine-only patients survived to hospital discharge. No significant outcome differences were found in any group or subgroup analysis.
The study had lower-than-expected overall survival to hospital discharge, which may have handicapped its effort to find a true difference in treatment arms.
Bottom line: The addition of vasopressin to epinephrine in the treatment of out-of-hospital cardiac arrest does not improve outcomes.
Citation: Gueugniaud PY, David JS, Chanzy E, Hubert H, Dubien P, Mauriaucourt P, et al. Vasopressin and epinephrine vs. epinephrine alone in cardiopulmonary resuscitation. N Engl J Med. 2008;359(1):21-30.
Is oral rivaroxaban more efficacious than subcutaneous enoxaparin in preventing VTE after hip-replacement surgery?
Background: Venous thromboembolism (VTE) prophylaxis after total hip replacement (THR) is important but can be cumbersome because the most commonly used anticoagulants are either subcutaneous or require frequent monitoring. Rivaroxaban, an oral direct inhibitor of factor Xa may provide more convenient anticoagulation postoperatively. However, its efficacy and safety are unknown.
Study design: Randomized double-blind trial.
Setting: Multicenter study performed in 27 countries.
Synopsis: Patients undergoing THR surgery were randomized to oral rivaroxaban (10mg once daily without monitoring, started six to eight hours after surgery) or subcutaneous enoxaparin (40mg once daily, started 12 hours prior to surgery). After surgery, prophylaxis was administered for 35 days. The primary outcome was a composite of asymptomatic deep venous thrombosis (DVT), symptomatic DVT or pulmonary embolism (PE), or death from any cause at 36 days after surgery.
In the enoxaparin group, 3.7% of patients experienced the primary outcome. This decreased to 1.1% in the rivaroxaban group. Approximately one-third of events were symptomatic. Major bleeding occurred in 0.1% and 0.3% (p=NS) of patients in the enoxaparin and rivaroxaban groups, respectively.
The study is limited by the exclusion of 1,388 of the 4,541 patients (30.6%) randomized, primarily due to having inadequate venography. Also, because the majority of thromboembolic events were asymptomatic, the primary outcome overemphasizes the clinical difference.
Bottom line: Oral rivaroxaban without monitoring is more efficacious than, and as safe as, subcutaneous enoxaparin when used for VTE prophylaxis for THR.
Citation: Eriksson B, Borris LC, Friedman RJ, Hass S, Huisman MV, Kakkar AK, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med. 2008;358:2765-75.
Is LMWH more efficacious than UFH in preventing postoperative VTE in cancer patients?
Background: Patients with cancer are at increased risk for VTE and require prophylaxis to prevent this complication postoperatively. Low molecular weight heparin (LMWH) has proven more efficacious than subcutaneous unfractionated heparin (UFH) in other settings (e.g., DVT treatment). However, it is still unknown whether LMWH offers better prophylaxis compared to UFH for cancer patients undergoing surgery.
Study design: Systematic review and meta-analysis.
Setting: 14 randomized controlled trials.
Synopsis: Eleven trials exclusively examined patients with cancer (n=4006) and three trials reported data for cancer patients as subgroups (n=1816). There were in differences in mortality, pulmonary embolism, and symptomatic DVT rates between the two groups.
LMWH was associated with a decrease in total (asymptomatic or symptomatic) DVT (RR, 0.72; 95% CI, 0.55-0.94). Rates of major bleeding, minor bleeding, and intraoperative blood loss were similar between the two treatments.
This meta-analysis is limited because 12 remaining trials (n=3185) also enrolled cancer patients but did not provide specific data for the cancer patient subgroup. The study also is limited by the heterogeneity of the original trials, including utilizing varying LMWHs and dosing regimens, numerous types of surgeries, and a wide range of neoplasms.
Bottom line: LMWH does not decrease mortality, pulmonary embolism, or symptomatic DVT compared to UFH in cancer patients undergoing surgery.
Citation: Akl EA, Terrenato I, Barba M, Sperati F, Sempos EV, Muti P, et al. Low-molecular-weight heparin vs. unfractionated heparin for perioperative thromboprophylaxis in patients with cancer. Arch Intern Med. 2008;168:1261-9.
Does salmeterol added to inhaled corticosteroids improve severe asthma-related events?
Background: Asthma is a chronic disease causing major morbidity and mortality worldwide. Disease guidelines recommend all patients with persistent asthma be treated with inhaled corticosteroids. These same guidelines recommend adding a long-acting beta-agonist for patients whose symptoms persist. However, the safety of this practice has come under scrutiny.
Study design: Meta-analysis.
Setting: Sixty-six randomized, controlled trials conducted worldwide.
Synopsis: Analysis included 66 GlaxoSmithKline trials with a total of 20,966 patients with persistent asthma. Patients used either salmeterol (50mcg twice daily) plus inhaled corticosteroid (10,400 patients) or inhaled corticosteroid alone (10,566 patients).
Results showed no differences in asthma-related hospitalizations, asthma-related intubations, or deaths between the two groups. However, due to the low number of events, definitive conclusions are difficult to make. Severe asthma exacerbations requiring systemic corticosteroids significantly decreased in the inhaled corticosteroid plus salmeterol group.
The study is limited by it inclusion of only those trials sponsored by GlaxoSmithKline and by the short duration of most of the studies. Additionally, the studies included in the analysis used clinical outcomes as secondary endpoints.
Bottom line: Adding salmeterol to inhaled corticosteroid decreases severe asthma exacerbations and is likely safe, but does not have an effect on asthma-related hospitalization or death.
Citation: Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et.al. Meta-analysis: Effects of adding salmeterol to inhaled corticosteroids on serious asthma-related events. Annals Intern Med. 2008;149:33-42.
Is an early invasive strategy effective in women with unstable angina or NSTEMI?
Background: Despite many trials showing the value of an early invasive strategy for patients with non-ST-segment elevation acute coronary syndrome (NSTE ACS), data from several trials question this benefit in women. Some trials show higher risk of death and myocardial infarction (MI) in subgroup analysis of women.
Study Design: Meta-analysis.
Setting: Eight randomized, controlled trials conducted worldwide.
Synopsis: Analysis included eight trials with 10,412 patients (3,075 women) with NSTE ACS. The invasive group (5,083 patients) was defined as those referred for coronary angiography with subsequent intervention as needed. The composite endpoint of death, MI, or rehospitalization within 12 months with ACS occurred in 21.1% of the invasive group and 25.9% of the medically managed group (OR, 0.78; CI, 0.61-0.98).
The subgroup, including only women, had a non-statistically significant OR of 0.81 (CI, 0.65-1.01), including no effect on all-cause mortality, nonfatal MI, or the composite of death and MI. However, women with high-risk features (elevated biomarkers) undergoing the invasive strategy had a significant reduction in the composite endpoint (OR, 0.67; CI, 0.50-0.88).
The study is limited by the use of subgroup analysis, secondary endpoints, heterogeneity between trials, and possible publication bias.
Bottom line: Early invasive strategy is effective in men and high-risk women with NSTE ACS, but not in low-risk women.
Citation: O’Donoghue M, Boden W, Braunwald E, Cannon CP, Clayton TC, Winter RJ, et.al. Early invasive vs. conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction. JAMA. 2008;300:71-80.
What strategies are used to prevent contrast-induced acute kidney injury?
Background: Contrast-induced acute kidney injury (CIAKI) is a condition potentially amenable to preventive care. Several trials have identified intravenous hydration, N-acetylcysteine, and withdrawal of NSAIDS as interventions that reduce the possibility of CIAKI in high-risk patients. Little is known about whether healthcare providers routinely use these strategies.
Study design: Prospective observational cohort study.
Setting: Veterans Affairs (VA) Pittsburgh Healthcare System.
Synopsis: 11,410 patients scheduled for radiographic procedures were screened. After exclusion criteria and eligibility, 660 patients with an estimated glomerular filtration rate less than 60ml/min/1.73m2 were identified. Usage of intravenous fluids, N-acetylcysteine, and discontinuation of NSAIDS were recorded. Serum creatinine (SCr) was measured 48 to 96 hours post-procedure. CIAKI was defined as relative increase in SCr from baseline (≥25%, ≥50% and ≥100%) and absolute increase in SCr levels from baseline (≥0.25, ≥0.5, and ≥1.0). CIAKI association with adverse outcomes was evaluated by tracking 30-day mortality, need for dialysis, and hospitalization.
The incidence of CIAKI was less common in patients undergoing CT scans versus those having angiograms. Adverse 30-day outcomes were uncommon. Pre- and post-procedure intravenous hydration was administered to 40% of study patients, more commonly with coronary angiogram than with computed tomography (91.2% vs. 16%, p<0.0001). N-acetylcysteine was administered to 39.2%. Only 6.8% of those taking NSAIDS reported being told to discontinue the medication.
Study limitations include the small sample size and the single site location, both limiting generalizability.
Bottom line: Clinically significant CIAKI is uncommon, and preventive care is not uniformly implemented in patients undergoing contrast-enhanced radiographic procedures.
Citation: Weisbord SD, Mor MK, Resnick AL, Hartwig KC, Sonel AF, Fine MJ, et al. Prevention, incidence, and outcomes of contrast-induced acute kidney injury. Arch Intern Med. 2008;168(12):1325-1332.
How does hyperglycemia affect morbidity and mortality in children admitted to a community pediatric hospital?
Background: Inpatient hyperglycemia in adult patients is a predictor of poor clinical outcomes. The association of hyperglycemia and clinical outcomes in children admitted to a general community hospital has not been studied.
Study design: Retrospective observational cohort study.
Setting: A community pediatric hospital in Atlanta, Ga.
Synopsis: Review of medical records of 903 consecutive pediatric patients admitted to critical and non-critical areas took place. Of these, 542 patients constituted the study population. The study excluded 342 patients who didn’t have a blood glucose measurement. Hyperglycemia was defined as an admission or in-hospital blood glucose greater than 120mg/dl.
One-fourth of the children admitted to the hospital had hyperglycemia, most without a prior history of diabetes. The presence of hyperglycemia on admission was not associated with increased length of stay (LOS) or increased mortality. Children with hyperglycemia were more likely to be admitted to the ICU and had longer ICU LOS.
This was a retrospective study conducted at a single site whose demographics and disease spectrum may differ from those of other institutions. There were an insufficient number of deaths to make any conclusions regarding the impact of hyperglycemia on mortality. Prospective, randomized, multicenter trials are needed to better elucidate the effects of in-patient hyperglycemia.
Bottom line: Hyperglycemia is common in children with or without diabetes admitted to the hospital, and is associated with increased ICU admissions and ICU length of stay. Its connection to mortality is inconclusive.
Citation: Palaio A, Smiley D, Ceron M, Klein R, Cho IS, Mejia R, et al. Prevalence and clinical outcome of inpatient hyperglycemia in a community pediatric hospital. J Hosp Med.2008;3(3):212-217.