User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
New Research Dissects Transgenerational Obesity and Diabetes
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1). 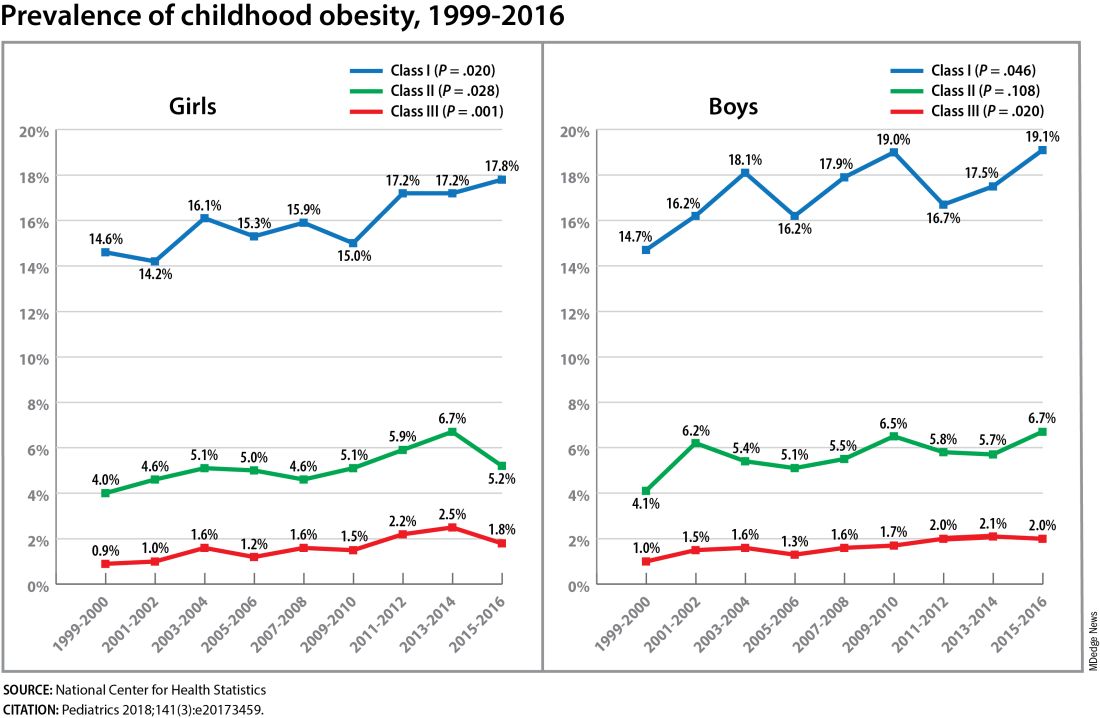
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FROM DPSG-NA 2023
Hormones and Viruses Influence Each Other: Consider These Connections in Your Patients
Stefan Bornstein, MD, PhD, professor, made it clear during a press conference at the 67th Congress of the German Society of Endocrinology (DGE) that there is more than one interaction between them. Nowadays, one can almost speak of an “endocrine virology and even of the virome as an additional, hormonally metabolically active gland,” said Dr. Bornstein, who will receive the Berthold Medal from the DGE in 2024.
Many questions remain unanswered: “We need a better understanding of the interaction of hormone systems with infectious agents — from basics to therapeutic applications,” emphasized the director of the Medical Clinic and Polyclinic III and the Center for Internal Medicine at the Carl Gustav Carus University Hospital, Dresden, Germany.
If infectious diseases could trigger diabetes and other metabolic diseases, this means that “through vaccination programs, we may be able to prevent the occurrence of common metabolic diseases such as diabetes,” said Dr. Bornstein. He highlighted that many people who experienced severe COVID-19 during the pandemic, or died from it, exhibited diabetes or a pre-metabolic syndrome.
“SARS-CoV-2 has utilized an endocrine signaling pathway to invade our cells and cause damage in the organ systems and inflammation,” said Dr. Bornstein. Conversely, it is now known that infections with coronaviruses or other infectious agents like influenza can significantly worsen metabolic status, diabetes, and other endocrine diseases.
SARS-CoV-2 Infects the Beta Cells
Data from the COVID-19 pandemic showed that the likelihood of developing type 1 diabetes significantly increases with a SARS-CoV-2 infection. Researchers led by Dr. Bornstein demonstrated in 2021 that SARS-CoV-2 can infect the insulin-producing cells of the organ. They examined pancreatic tissue from 20 patients who died from COVID-19 using immunofluorescence, immunohistochemistry, RNA in situ hybridization, and electron microscopy.
They found viral SARS-CoV-2 infiltration of the beta cells in all patients. In 11 patients with COVID-19, the expression of ACE2, TMPRSS, and other receptors and factors like DPP4, HMBG1, and NRP1 that can facilitate virus entry was examined. They found that even in the absence of manifest newly onset diabetes, necroptotic cell death, immune cell infiltration, and SARS-CoV-2 infection of the pancreas beta cells can contribute to varying degrees of metabolic disturbance in patients with COVID-19.
In a report published in October 2020, Tim Hollstein, MD, from the Institute for Diabetology and Clinical Metabolic Research at UKSH in Kiel, Germany, and colleagues described the case of a 19-year-old man who developed symptoms of insulin-dependent diabetes after a SARS-CoV-2 infection, without the presence of autoantibodies typical for type 1 diabetes.
The man presented to the emergency department with diabetic ketoacidosis, a C-peptide level of 0.62 µg/L, a blood glucose concentration of 30.6 mmol/L (552 mg/dL), and an A1c level of 16.8%. The patient’s history revealed a probable SARS-CoV-2 infection 5-7 weeks before admission, based on a positive antibody test against SARS-CoV-2.
Some Viruses Produce Insulin-Like Proteins
Recent studies have shown that some viruses can produce insulin-like proteins or hormones that interfere with the metabolism of the affected organism, reported Dr. Bornstein. In addition to metabolic regulation, these “viral hormones” also seem to influence cell turnover and cell death.
Dr. Bornstein pointed out that antiviral medications can delay the onset of type 1 diabetes by preserving the function of insulin-producing beta cells. It has also been shown that conventional medications used to treat hormonal disorders can reduce the susceptibility of the organism to infections — such as antidiabetic preparations like DPP-4 inhibitors or metformin.
In a review published in 2023, Nikolaos Perakakis, MD, professor, research group leader at the Paul Langerhans Institute Dresden, Dresden, Germany, Dr. Bornstein, and colleagues discussed scientific evidence for a close mutual dependence between various virus infections and metabolic diseases. They discussed how viruses can lead to the development or progression of metabolic diseases and vice versa and how metabolic diseases can increase the severity of a virus infection.
Viruses Favor Metabolic Diseases...
Viruses can favor metabolic diseases by, for example, influencing the regulation of cell survival and specific signaling pathways relevant for cell death, proliferation, or dedifferentiation in important endocrine and metabolic organs. Viruses are also capable of controlling cellular glucose metabolism by modulating glucose transporters, altering glucose uptake, regulating signaling pathways, and stimulating glycolysis in infected cells.
Due to the destruction of beta cells, enteroviruses, but also the mumps virus, parainfluenza virus, or human herpes virus 6, are associated with the development of diabetes. The timing of infection often precedes or coincides with the peak of development of islet autoantibodies. The fact that only a small proportion of patients actually develop type 1 diabetes suggests that genetic background, and likely the timing of infection, play an important role.
...And Metabolic Diseases Influence the Course of Infection
Infection with hepatitis C virus (HCV), on the other hand, is associated with an increased risk for type 2 diabetes, with the risk being higher for older individuals with a family history of diabetes. The negative effects of HCV on glucose balance are mainly attributed to increased insulin resistance in the liver. HCV reduces hepatic glucose uptake by downregulating the expression of glucose transporters and additionally impairs insulin signal transduction by inhibiting the PI3K/Akt signaling pathway.
People with obesity, diabetes, or insulin resistance show significant changes in the innate and adaptive functions of the immune system. Regarding the innate immune system, impaired chemotaxis and phagocytosis of neutrophils have been observed in patients with type 2 diabetes.
In the case of obesity, the number of natural killer T cells in adipose tissue decreases, whereas B cells accumulate in adipose tissue and secrete more proinflammatory cytokines. Longitudinal multiomics analyses of various biopsies from individuals with insulin resistance showed a delayed immune response to respiratory virus infections compared with individuals with normal insulin sensitivity.
This story was translated from Medscape Germany using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Stefan Bornstein, MD, PhD, professor, made it clear during a press conference at the 67th Congress of the German Society of Endocrinology (DGE) that there is more than one interaction between them. Nowadays, one can almost speak of an “endocrine virology and even of the virome as an additional, hormonally metabolically active gland,” said Dr. Bornstein, who will receive the Berthold Medal from the DGE in 2024.
Many questions remain unanswered: “We need a better understanding of the interaction of hormone systems with infectious agents — from basics to therapeutic applications,” emphasized the director of the Medical Clinic and Polyclinic III and the Center for Internal Medicine at the Carl Gustav Carus University Hospital, Dresden, Germany.
If infectious diseases could trigger diabetes and other metabolic diseases, this means that “through vaccination programs, we may be able to prevent the occurrence of common metabolic diseases such as diabetes,” said Dr. Bornstein. He highlighted that many people who experienced severe COVID-19 during the pandemic, or died from it, exhibited diabetes or a pre-metabolic syndrome.
“SARS-CoV-2 has utilized an endocrine signaling pathway to invade our cells and cause damage in the organ systems and inflammation,” said Dr. Bornstein. Conversely, it is now known that infections with coronaviruses or other infectious agents like influenza can significantly worsen metabolic status, diabetes, and other endocrine diseases.
SARS-CoV-2 Infects the Beta Cells
Data from the COVID-19 pandemic showed that the likelihood of developing type 1 diabetes significantly increases with a SARS-CoV-2 infection. Researchers led by Dr. Bornstein demonstrated in 2021 that SARS-CoV-2 can infect the insulin-producing cells of the organ. They examined pancreatic tissue from 20 patients who died from COVID-19 using immunofluorescence, immunohistochemistry, RNA in situ hybridization, and electron microscopy.
They found viral SARS-CoV-2 infiltration of the beta cells in all patients. In 11 patients with COVID-19, the expression of ACE2, TMPRSS, and other receptors and factors like DPP4, HMBG1, and NRP1 that can facilitate virus entry was examined. They found that even in the absence of manifest newly onset diabetes, necroptotic cell death, immune cell infiltration, and SARS-CoV-2 infection of the pancreas beta cells can contribute to varying degrees of metabolic disturbance in patients with COVID-19.
In a report published in October 2020, Tim Hollstein, MD, from the Institute for Diabetology and Clinical Metabolic Research at UKSH in Kiel, Germany, and colleagues described the case of a 19-year-old man who developed symptoms of insulin-dependent diabetes after a SARS-CoV-2 infection, without the presence of autoantibodies typical for type 1 diabetes.
The man presented to the emergency department with diabetic ketoacidosis, a C-peptide level of 0.62 µg/L, a blood glucose concentration of 30.6 mmol/L (552 mg/dL), and an A1c level of 16.8%. The patient’s history revealed a probable SARS-CoV-2 infection 5-7 weeks before admission, based on a positive antibody test against SARS-CoV-2.
Some Viruses Produce Insulin-Like Proteins
Recent studies have shown that some viruses can produce insulin-like proteins or hormones that interfere with the metabolism of the affected organism, reported Dr. Bornstein. In addition to metabolic regulation, these “viral hormones” also seem to influence cell turnover and cell death.
Dr. Bornstein pointed out that antiviral medications can delay the onset of type 1 diabetes by preserving the function of insulin-producing beta cells. It has also been shown that conventional medications used to treat hormonal disorders can reduce the susceptibility of the organism to infections — such as antidiabetic preparations like DPP-4 inhibitors or metformin.
In a review published in 2023, Nikolaos Perakakis, MD, professor, research group leader at the Paul Langerhans Institute Dresden, Dresden, Germany, Dr. Bornstein, and colleagues discussed scientific evidence for a close mutual dependence between various virus infections and metabolic diseases. They discussed how viruses can lead to the development or progression of metabolic diseases and vice versa and how metabolic diseases can increase the severity of a virus infection.
Viruses Favor Metabolic Diseases...
Viruses can favor metabolic diseases by, for example, influencing the regulation of cell survival and specific signaling pathways relevant for cell death, proliferation, or dedifferentiation in important endocrine and metabolic organs. Viruses are also capable of controlling cellular glucose metabolism by modulating glucose transporters, altering glucose uptake, regulating signaling pathways, and stimulating glycolysis in infected cells.
Due to the destruction of beta cells, enteroviruses, but also the mumps virus, parainfluenza virus, or human herpes virus 6, are associated with the development of diabetes. The timing of infection often precedes or coincides with the peak of development of islet autoantibodies. The fact that only a small proportion of patients actually develop type 1 diabetes suggests that genetic background, and likely the timing of infection, play an important role.
...And Metabolic Diseases Influence the Course of Infection
Infection with hepatitis C virus (HCV), on the other hand, is associated with an increased risk for type 2 diabetes, with the risk being higher for older individuals with a family history of diabetes. The negative effects of HCV on glucose balance are mainly attributed to increased insulin resistance in the liver. HCV reduces hepatic glucose uptake by downregulating the expression of glucose transporters and additionally impairs insulin signal transduction by inhibiting the PI3K/Akt signaling pathway.
People with obesity, diabetes, or insulin resistance show significant changes in the innate and adaptive functions of the immune system. Regarding the innate immune system, impaired chemotaxis and phagocytosis of neutrophils have been observed in patients with type 2 diabetes.
In the case of obesity, the number of natural killer T cells in adipose tissue decreases, whereas B cells accumulate in adipose tissue and secrete more proinflammatory cytokines. Longitudinal multiomics analyses of various biopsies from individuals with insulin resistance showed a delayed immune response to respiratory virus infections compared with individuals with normal insulin sensitivity.
This story was translated from Medscape Germany using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Stefan Bornstein, MD, PhD, professor, made it clear during a press conference at the 67th Congress of the German Society of Endocrinology (DGE) that there is more than one interaction between them. Nowadays, one can almost speak of an “endocrine virology and even of the virome as an additional, hormonally metabolically active gland,” said Dr. Bornstein, who will receive the Berthold Medal from the DGE in 2024.
Many questions remain unanswered: “We need a better understanding of the interaction of hormone systems with infectious agents — from basics to therapeutic applications,” emphasized the director of the Medical Clinic and Polyclinic III and the Center for Internal Medicine at the Carl Gustav Carus University Hospital, Dresden, Germany.
If infectious diseases could trigger diabetes and other metabolic diseases, this means that “through vaccination programs, we may be able to prevent the occurrence of common metabolic diseases such as diabetes,” said Dr. Bornstein. He highlighted that many people who experienced severe COVID-19 during the pandemic, or died from it, exhibited diabetes or a pre-metabolic syndrome.
“SARS-CoV-2 has utilized an endocrine signaling pathway to invade our cells and cause damage in the organ systems and inflammation,” said Dr. Bornstein. Conversely, it is now known that infections with coronaviruses or other infectious agents like influenza can significantly worsen metabolic status, diabetes, and other endocrine diseases.
SARS-CoV-2 Infects the Beta Cells
Data from the COVID-19 pandemic showed that the likelihood of developing type 1 diabetes significantly increases with a SARS-CoV-2 infection. Researchers led by Dr. Bornstein demonstrated in 2021 that SARS-CoV-2 can infect the insulin-producing cells of the organ. They examined pancreatic tissue from 20 patients who died from COVID-19 using immunofluorescence, immunohistochemistry, RNA in situ hybridization, and electron microscopy.
They found viral SARS-CoV-2 infiltration of the beta cells in all patients. In 11 patients with COVID-19, the expression of ACE2, TMPRSS, and other receptors and factors like DPP4, HMBG1, and NRP1 that can facilitate virus entry was examined. They found that even in the absence of manifest newly onset diabetes, necroptotic cell death, immune cell infiltration, and SARS-CoV-2 infection of the pancreas beta cells can contribute to varying degrees of metabolic disturbance in patients with COVID-19.
In a report published in October 2020, Tim Hollstein, MD, from the Institute for Diabetology and Clinical Metabolic Research at UKSH in Kiel, Germany, and colleagues described the case of a 19-year-old man who developed symptoms of insulin-dependent diabetes after a SARS-CoV-2 infection, without the presence of autoantibodies typical for type 1 diabetes.
The man presented to the emergency department with diabetic ketoacidosis, a C-peptide level of 0.62 µg/L, a blood glucose concentration of 30.6 mmol/L (552 mg/dL), and an A1c level of 16.8%. The patient’s history revealed a probable SARS-CoV-2 infection 5-7 weeks before admission, based on a positive antibody test against SARS-CoV-2.
Some Viruses Produce Insulin-Like Proteins
Recent studies have shown that some viruses can produce insulin-like proteins or hormones that interfere with the metabolism of the affected organism, reported Dr. Bornstein. In addition to metabolic regulation, these “viral hormones” also seem to influence cell turnover and cell death.
Dr. Bornstein pointed out that antiviral medications can delay the onset of type 1 diabetes by preserving the function of insulin-producing beta cells. It has also been shown that conventional medications used to treat hormonal disorders can reduce the susceptibility of the organism to infections — such as antidiabetic preparations like DPP-4 inhibitors or metformin.
In a review published in 2023, Nikolaos Perakakis, MD, professor, research group leader at the Paul Langerhans Institute Dresden, Dresden, Germany, Dr. Bornstein, and colleagues discussed scientific evidence for a close mutual dependence between various virus infections and metabolic diseases. They discussed how viruses can lead to the development or progression of metabolic diseases and vice versa and how metabolic diseases can increase the severity of a virus infection.
Viruses Favor Metabolic Diseases...
Viruses can favor metabolic diseases by, for example, influencing the regulation of cell survival and specific signaling pathways relevant for cell death, proliferation, or dedifferentiation in important endocrine and metabolic organs. Viruses are also capable of controlling cellular glucose metabolism by modulating glucose transporters, altering glucose uptake, regulating signaling pathways, and stimulating glycolysis in infected cells.
Due to the destruction of beta cells, enteroviruses, but also the mumps virus, parainfluenza virus, or human herpes virus 6, are associated with the development of diabetes. The timing of infection often precedes or coincides with the peak of development of islet autoantibodies. The fact that only a small proportion of patients actually develop type 1 diabetes suggests that genetic background, and likely the timing of infection, play an important role.
...And Metabolic Diseases Influence the Course of Infection
Infection with hepatitis C virus (HCV), on the other hand, is associated with an increased risk for type 2 diabetes, with the risk being higher for older individuals with a family history of diabetes. The negative effects of HCV on glucose balance are mainly attributed to increased insulin resistance in the liver. HCV reduces hepatic glucose uptake by downregulating the expression of glucose transporters and additionally impairs insulin signal transduction by inhibiting the PI3K/Akt signaling pathway.
People with obesity, diabetes, or insulin resistance show significant changes in the innate and adaptive functions of the immune system. Regarding the innate immune system, impaired chemotaxis and phagocytosis of neutrophils have been observed in patients with type 2 diabetes.
In the case of obesity, the number of natural killer T cells in adipose tissue decreases, whereas B cells accumulate in adipose tissue and secrete more proinflammatory cytokines. Longitudinal multiomics analyses of various biopsies from individuals with insulin resistance showed a delayed immune response to respiratory virus infections compared with individuals with normal insulin sensitivity.
This story was translated from Medscape Germany using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Sustained Control Reported for Anti–IL-17, Anti–IL-23 Psoriasis Treatments
SAN DIEGO — , but late-breaker data presented at the annual meeting of the American Academy of Dermatology show that these types of responses are sustained for as long as patients have remained on therapy.
Of the two, the longer follow up is with the IL-17 inhibitor bimekizumab (Bimzelx). In a 4-year open-label extension study, the Psoriasis Area and Severity Index (PASI) 90 rate was approximately 85% in treated patients, according to Mark Lebwohl, MD, professor and chairman emeritus of the Department of Dermatology, Icahn School of Medicine at Mount Sinai in New York City
A PASI 90 score signifies that 90% of skin surface area is cleared. The proportion of patients who achieved a PASI 100 score, signifying total clearance, approached 70% at 4 years in the group with the greatest response. PASI 90 and PASI 100 rates at this point were only modestly lower than those reported at the end of the double-blind phase 3 trial when evaluated 3 years earlier.
Follow-up with a novel oral anti-IL-23 inhibitor JNJ-2113 (JNJ-77242113) was only 52 weeks, far shorter. But again, the response for the most effective dose at the end of this period was essentially unchanged from that at 16 weeks. Among those on the highest and most effective test dose of once-daily 100 mg, the PASI 90 at 1 year was 64.3%, a rate that was essentially unchanged from week 16.
No Apparent Loss of Benefit Over Time
“We can really look at those dose-response curves and see that there is, overall, a maintenance of response,” reported Laura K. Ferris, MD, PhD, professor and director of clinical trials, Department of Dermatology, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania. In her presentation of the data, she showed similar sustained control for the most effective doses of JNJ-2113 for multiple clinical outcomes, including an investigator’s global assessment (IGA) score of 0 or 1, also signifying clear or near clear skin.
Bimekizumab, a monoclonal antibody that inhibits both IL-17A and IL-17F, is already approved for the treatment of plaque psoriasis. The 52-week BE SURE trial, which provided the 478 patients who entered into the BE BRIGHT open label extension study, was published in The New England Journal of Medicine in July 2021.
In the 4-year data reported by Dr. Lebwohl, three groups were compared: Those initially randomized to an every-4-week dosing schedule of bimekizumab over the course of the 52-week BE SURE trial; those randomized to an every-4-week bimekizumab schedule who were then subsequently switched to an every-8-week schedule; and those initiated on the TNF-inhibitor adalimumab (Humira) and were then switched at week 24 to every-4-week bimekizumab.
The PASI 90 responses at 52 weeks in these three groups, respectively, were 91.2%, 89.3%, and 95.2%. At 4 years, this almost clear response was observed in 82.4%, 83.2%, and 87.6%, respectively. At 52 weeks, the PASI 100 responses in these three groups, respectively, were 75.3%, 74.2%, and 72.9%. At 4 years, 61.9%, 58.5%, and 69.5% still had complete skin clearance.
Bimekizumab was well tolerated during the randomized trial, reported Dr. Lebwohl. The rates of nasopharyngitis and oral candidiasis, which were observed in approximately 12% and 8%, respectively, of treated patients during the randomized phase remained at about the same level in the long-term follow up. There were no new safety signals, he said.
JNJ-2113 Is First Potential Oral IL-23 Inhibitor
JNJ-2113 is a first-in-class oral peptide that binds to the IL-23 receptor, blocking the IL-23 signaling pathway. If approved, it would be the first oral therapy targeting IL-23. The 16-week outcomes of the dose-finding FRONTIER 1 phase 2b trial were published in The New England Journal of Medicine earlier this year. The primary endpoint was PASI 75, achieved by 79% of those on the 100 mg twice daily dose at week 16, vs 9% on placebo, and at 52 weeks, was 76%.
“The proportion of patients achieving the FRONTIER 1 primary endpoint was maintained from week 16 to the end of week 52 in the extension study,” Dr. Ferris said, but further pointed out that rates of near or complete clearance achieved at week 16 were also essentially unchanged at week 52. This was true of PASI scores and IGA.
Clearance of psoriatic lesions on the scalp was particularly impressive. By scalp-specific IGA, rates of clear or near clear (0/1) were not just maintained but improved over the course of follow-up, reaching 75.1% at 52 weeks in the highest dose group, she said.
JNJ-2113 was well tolerated in FRONTIER 1 and remained so during long-term follow-up, in the FRONTIER 2 extension study, according to Dr. Ferris. The most common complaints with JNJ-2113, such as nasopharyngitis (18.1% vs 25.7% in placebo), did not appear to differ significantly from placebo and the treatment remained well tolerated over the course of the extended follow-up.
There are limited direct comparisons of different biologics active in the treatment of plaque psoriasis for efficacy and safety, but these data appear to show a depth and durability of benefit for psoriasis that is exceptional, Dr. Lebwohl told this news organization. “The PASI 100 scores achieved by bimekizumab exceed anything we have seen to date,” he said. “And the durability of those exceedingly high scores is remarkable.”
Dr. Lebwohl reports financial relationships with approximately 40 pharmaceutical companies, including UCB Pharma, which developed bimekizumab. Dr. Ferris reports financial relationships with more than 20 pharmaceutical companies, including Janssen, which is developing JNJ-2113.
A version of this article appeared on Medscape.com.
SAN DIEGO — , but late-breaker data presented at the annual meeting of the American Academy of Dermatology show that these types of responses are sustained for as long as patients have remained on therapy.
Of the two, the longer follow up is with the IL-17 inhibitor bimekizumab (Bimzelx). In a 4-year open-label extension study, the Psoriasis Area and Severity Index (PASI) 90 rate was approximately 85% in treated patients, according to Mark Lebwohl, MD, professor and chairman emeritus of the Department of Dermatology, Icahn School of Medicine at Mount Sinai in New York City
A PASI 90 score signifies that 90% of skin surface area is cleared. The proportion of patients who achieved a PASI 100 score, signifying total clearance, approached 70% at 4 years in the group with the greatest response. PASI 90 and PASI 100 rates at this point were only modestly lower than those reported at the end of the double-blind phase 3 trial when evaluated 3 years earlier.
Follow-up with a novel oral anti-IL-23 inhibitor JNJ-2113 (JNJ-77242113) was only 52 weeks, far shorter. But again, the response for the most effective dose at the end of this period was essentially unchanged from that at 16 weeks. Among those on the highest and most effective test dose of once-daily 100 mg, the PASI 90 at 1 year was 64.3%, a rate that was essentially unchanged from week 16.
No Apparent Loss of Benefit Over Time
“We can really look at those dose-response curves and see that there is, overall, a maintenance of response,” reported Laura K. Ferris, MD, PhD, professor and director of clinical trials, Department of Dermatology, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania. In her presentation of the data, she showed similar sustained control for the most effective doses of JNJ-2113 for multiple clinical outcomes, including an investigator’s global assessment (IGA) score of 0 or 1, also signifying clear or near clear skin.
Bimekizumab, a monoclonal antibody that inhibits both IL-17A and IL-17F, is already approved for the treatment of plaque psoriasis. The 52-week BE SURE trial, which provided the 478 patients who entered into the BE BRIGHT open label extension study, was published in The New England Journal of Medicine in July 2021.
In the 4-year data reported by Dr. Lebwohl, three groups were compared: Those initially randomized to an every-4-week dosing schedule of bimekizumab over the course of the 52-week BE SURE trial; those randomized to an every-4-week bimekizumab schedule who were then subsequently switched to an every-8-week schedule; and those initiated on the TNF-inhibitor adalimumab (Humira) and were then switched at week 24 to every-4-week bimekizumab.
The PASI 90 responses at 52 weeks in these three groups, respectively, were 91.2%, 89.3%, and 95.2%. At 4 years, this almost clear response was observed in 82.4%, 83.2%, and 87.6%, respectively. At 52 weeks, the PASI 100 responses in these three groups, respectively, were 75.3%, 74.2%, and 72.9%. At 4 years, 61.9%, 58.5%, and 69.5% still had complete skin clearance.
Bimekizumab was well tolerated during the randomized trial, reported Dr. Lebwohl. The rates of nasopharyngitis and oral candidiasis, which were observed in approximately 12% and 8%, respectively, of treated patients during the randomized phase remained at about the same level in the long-term follow up. There were no new safety signals, he said.
JNJ-2113 Is First Potential Oral IL-23 Inhibitor
JNJ-2113 is a first-in-class oral peptide that binds to the IL-23 receptor, blocking the IL-23 signaling pathway. If approved, it would be the first oral therapy targeting IL-23. The 16-week outcomes of the dose-finding FRONTIER 1 phase 2b trial were published in The New England Journal of Medicine earlier this year. The primary endpoint was PASI 75, achieved by 79% of those on the 100 mg twice daily dose at week 16, vs 9% on placebo, and at 52 weeks, was 76%.
“The proportion of patients achieving the FRONTIER 1 primary endpoint was maintained from week 16 to the end of week 52 in the extension study,” Dr. Ferris said, but further pointed out that rates of near or complete clearance achieved at week 16 were also essentially unchanged at week 52. This was true of PASI scores and IGA.
Clearance of psoriatic lesions on the scalp was particularly impressive. By scalp-specific IGA, rates of clear or near clear (0/1) were not just maintained but improved over the course of follow-up, reaching 75.1% at 52 weeks in the highest dose group, she said.
JNJ-2113 was well tolerated in FRONTIER 1 and remained so during long-term follow-up, in the FRONTIER 2 extension study, according to Dr. Ferris. The most common complaints with JNJ-2113, such as nasopharyngitis (18.1% vs 25.7% in placebo), did not appear to differ significantly from placebo and the treatment remained well tolerated over the course of the extended follow-up.
There are limited direct comparisons of different biologics active in the treatment of plaque psoriasis for efficacy and safety, but these data appear to show a depth and durability of benefit for psoriasis that is exceptional, Dr. Lebwohl told this news organization. “The PASI 100 scores achieved by bimekizumab exceed anything we have seen to date,” he said. “And the durability of those exceedingly high scores is remarkable.”
Dr. Lebwohl reports financial relationships with approximately 40 pharmaceutical companies, including UCB Pharma, which developed bimekizumab. Dr. Ferris reports financial relationships with more than 20 pharmaceutical companies, including Janssen, which is developing JNJ-2113.
A version of this article appeared on Medscape.com.
SAN DIEGO — , but late-breaker data presented at the annual meeting of the American Academy of Dermatology show that these types of responses are sustained for as long as patients have remained on therapy.
Of the two, the longer follow up is with the IL-17 inhibitor bimekizumab (Bimzelx). In a 4-year open-label extension study, the Psoriasis Area and Severity Index (PASI) 90 rate was approximately 85% in treated patients, according to Mark Lebwohl, MD, professor and chairman emeritus of the Department of Dermatology, Icahn School of Medicine at Mount Sinai in New York City
A PASI 90 score signifies that 90% of skin surface area is cleared. The proportion of patients who achieved a PASI 100 score, signifying total clearance, approached 70% at 4 years in the group with the greatest response. PASI 90 and PASI 100 rates at this point were only modestly lower than those reported at the end of the double-blind phase 3 trial when evaluated 3 years earlier.
Follow-up with a novel oral anti-IL-23 inhibitor JNJ-2113 (JNJ-77242113) was only 52 weeks, far shorter. But again, the response for the most effective dose at the end of this period was essentially unchanged from that at 16 weeks. Among those on the highest and most effective test dose of once-daily 100 mg, the PASI 90 at 1 year was 64.3%, a rate that was essentially unchanged from week 16.
No Apparent Loss of Benefit Over Time
“We can really look at those dose-response curves and see that there is, overall, a maintenance of response,” reported Laura K. Ferris, MD, PhD, professor and director of clinical trials, Department of Dermatology, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania. In her presentation of the data, she showed similar sustained control for the most effective doses of JNJ-2113 for multiple clinical outcomes, including an investigator’s global assessment (IGA) score of 0 or 1, also signifying clear or near clear skin.
Bimekizumab, a monoclonal antibody that inhibits both IL-17A and IL-17F, is already approved for the treatment of plaque psoriasis. The 52-week BE SURE trial, which provided the 478 patients who entered into the BE BRIGHT open label extension study, was published in The New England Journal of Medicine in July 2021.
In the 4-year data reported by Dr. Lebwohl, three groups were compared: Those initially randomized to an every-4-week dosing schedule of bimekizumab over the course of the 52-week BE SURE trial; those randomized to an every-4-week bimekizumab schedule who were then subsequently switched to an every-8-week schedule; and those initiated on the TNF-inhibitor adalimumab (Humira) and were then switched at week 24 to every-4-week bimekizumab.
The PASI 90 responses at 52 weeks in these three groups, respectively, were 91.2%, 89.3%, and 95.2%. At 4 years, this almost clear response was observed in 82.4%, 83.2%, and 87.6%, respectively. At 52 weeks, the PASI 100 responses in these three groups, respectively, were 75.3%, 74.2%, and 72.9%. At 4 years, 61.9%, 58.5%, and 69.5% still had complete skin clearance.
Bimekizumab was well tolerated during the randomized trial, reported Dr. Lebwohl. The rates of nasopharyngitis and oral candidiasis, which were observed in approximately 12% and 8%, respectively, of treated patients during the randomized phase remained at about the same level in the long-term follow up. There were no new safety signals, he said.
JNJ-2113 Is First Potential Oral IL-23 Inhibitor
JNJ-2113 is a first-in-class oral peptide that binds to the IL-23 receptor, blocking the IL-23 signaling pathway. If approved, it would be the first oral therapy targeting IL-23. The 16-week outcomes of the dose-finding FRONTIER 1 phase 2b trial were published in The New England Journal of Medicine earlier this year. The primary endpoint was PASI 75, achieved by 79% of those on the 100 mg twice daily dose at week 16, vs 9% on placebo, and at 52 weeks, was 76%.
“The proportion of patients achieving the FRONTIER 1 primary endpoint was maintained from week 16 to the end of week 52 in the extension study,” Dr. Ferris said, but further pointed out that rates of near or complete clearance achieved at week 16 were also essentially unchanged at week 52. This was true of PASI scores and IGA.
Clearance of psoriatic lesions on the scalp was particularly impressive. By scalp-specific IGA, rates of clear or near clear (0/1) were not just maintained but improved over the course of follow-up, reaching 75.1% at 52 weeks in the highest dose group, she said.
JNJ-2113 was well tolerated in FRONTIER 1 and remained so during long-term follow-up, in the FRONTIER 2 extension study, according to Dr. Ferris. The most common complaints with JNJ-2113, such as nasopharyngitis (18.1% vs 25.7% in placebo), did not appear to differ significantly from placebo and the treatment remained well tolerated over the course of the extended follow-up.
There are limited direct comparisons of different biologics active in the treatment of plaque psoriasis for efficacy and safety, but these data appear to show a depth and durability of benefit for psoriasis that is exceptional, Dr. Lebwohl told this news organization. “The PASI 100 scores achieved by bimekizumab exceed anything we have seen to date,” he said. “And the durability of those exceedingly high scores is remarkable.”
Dr. Lebwohl reports financial relationships with approximately 40 pharmaceutical companies, including UCB Pharma, which developed bimekizumab. Dr. Ferris reports financial relationships with more than 20 pharmaceutical companies, including Janssen, which is developing JNJ-2113.
A version of this article appeared on Medscape.com.
FROM AAD 2024
Phase 2 Results: Zerlasiran siRNA Drug Lowers Lp(a) by 90%
Silence Therapeutics shared positive topline 36-week data from its ongoing phase 2 study of zerlasiran, a long-acting agent directed at lowering Lp(a) levels.
In a statement, the company said the study shows a highly significant reduction from baseline in Lp(a) levels with zerlasiran compared with placebo at 36 weeks, the primary endpoint.
Zerlasiran (formerly known as SLN360), is a short interfering RNA (siRNA) agent, or “ gene silencing” therapy. It binds to and temporarily blocks the action of the LPA gene which encodes for apolipoprotein(a), a dominant and a rate-limiting component in the hepatic synthesis of the Lp(a) particle.
A previous phase 1 study showed that single subcutaneous doses of the drug, ranging from 30 mg to 600 mg, produced a dose-dependent reduction in Lp(a) plasma levels at 45-60 days.
The current double-blind placebo-controlled phase 2 trial — known as ALPACAR-360 — enrolled 178 patients at high risk for atherosclerotic cardiovascular events who had elevated levels of Lp(a), ie, ≥ 125 nmol/L (median baseline Lp(a) was approximately 215 nmol/L). They were randomized to zerlasiran or placebo.
Zerlasiran was administered at 300 mg subcutaneously every 16 or 24 weeks or at 450 mg every 24 weeks.
The 60-week study is ongoing, and secondary endpoints, including change in Lp(a) from baseline to 48 weeks (end of treatment period) and 60 weeks (end of study) and potential effects on other lipids/lipoproteins, will be evaluated.
Silence says it plans to report topline 48-week data from the ALPACAR-360 study in the second quarter of this year.
Elevated levels of Lp(a) represent a genetic risk factor for cardiovascular disease, which is believed to affect approximately 20% of the population. Although there are currently no approved Lp(a)-lowering therapies, several drug candidates are in late-stage clinical testing.
A version of this article appeared on Medscape.com.
Silence Therapeutics shared positive topline 36-week data from its ongoing phase 2 study of zerlasiran, a long-acting agent directed at lowering Lp(a) levels.
In a statement, the company said the study shows a highly significant reduction from baseline in Lp(a) levels with zerlasiran compared with placebo at 36 weeks, the primary endpoint.
Zerlasiran (formerly known as SLN360), is a short interfering RNA (siRNA) agent, or “ gene silencing” therapy. It binds to and temporarily blocks the action of the LPA gene which encodes for apolipoprotein(a), a dominant and a rate-limiting component in the hepatic synthesis of the Lp(a) particle.
A previous phase 1 study showed that single subcutaneous doses of the drug, ranging from 30 mg to 600 mg, produced a dose-dependent reduction in Lp(a) plasma levels at 45-60 days.
The current double-blind placebo-controlled phase 2 trial — known as ALPACAR-360 — enrolled 178 patients at high risk for atherosclerotic cardiovascular events who had elevated levels of Lp(a), ie, ≥ 125 nmol/L (median baseline Lp(a) was approximately 215 nmol/L). They were randomized to zerlasiran or placebo.
Zerlasiran was administered at 300 mg subcutaneously every 16 or 24 weeks or at 450 mg every 24 weeks.
The 60-week study is ongoing, and secondary endpoints, including change in Lp(a) from baseline to 48 weeks (end of treatment period) and 60 weeks (end of study) and potential effects on other lipids/lipoproteins, will be evaluated.
Silence says it plans to report topline 48-week data from the ALPACAR-360 study in the second quarter of this year.
Elevated levels of Lp(a) represent a genetic risk factor for cardiovascular disease, which is believed to affect approximately 20% of the population. Although there are currently no approved Lp(a)-lowering therapies, several drug candidates are in late-stage clinical testing.
A version of this article appeared on Medscape.com.
Silence Therapeutics shared positive topline 36-week data from its ongoing phase 2 study of zerlasiran, a long-acting agent directed at lowering Lp(a) levels.
In a statement, the company said the study shows a highly significant reduction from baseline in Lp(a) levels with zerlasiran compared with placebo at 36 weeks, the primary endpoint.
Zerlasiran (formerly known as SLN360), is a short interfering RNA (siRNA) agent, or “ gene silencing” therapy. It binds to and temporarily blocks the action of the LPA gene which encodes for apolipoprotein(a), a dominant and a rate-limiting component in the hepatic synthesis of the Lp(a) particle.
A previous phase 1 study showed that single subcutaneous doses of the drug, ranging from 30 mg to 600 mg, produced a dose-dependent reduction in Lp(a) plasma levels at 45-60 days.
The current double-blind placebo-controlled phase 2 trial — known as ALPACAR-360 — enrolled 178 patients at high risk for atherosclerotic cardiovascular events who had elevated levels of Lp(a), ie, ≥ 125 nmol/L (median baseline Lp(a) was approximately 215 nmol/L). They were randomized to zerlasiran or placebo.
Zerlasiran was administered at 300 mg subcutaneously every 16 or 24 weeks or at 450 mg every 24 weeks.
The 60-week study is ongoing, and secondary endpoints, including change in Lp(a) from baseline to 48 weeks (end of treatment period) and 60 weeks (end of study) and potential effects on other lipids/lipoproteins, will be evaluated.
Silence says it plans to report topline 48-week data from the ALPACAR-360 study in the second quarter of this year.
Elevated levels of Lp(a) represent a genetic risk factor for cardiovascular disease, which is believed to affect approximately 20% of the population. Although there are currently no approved Lp(a)-lowering therapies, several drug candidates are in late-stage clinical testing.
A version of this article appeared on Medscape.com.
Tirzepatide Weight Loss Consistent Regardless of BMI
Tirzepatide (Zepbound for weight loss; Mounjaro for type 2 diabetes; Eli Lilly) consistently reduced body weight regardless of pretreatment body mass index (BMI) and reduced body weight and waist circumference regardless of duration of overweight or obesity.
The analyses — firstly of the impact of baseline BMI and secondly investigating the impact of the duration of overweight/obesity — are drawn from combined findings from the SURMOUNT 1-4 studies that examined the efficacy and safety of tirzepatide vs placebo. They are scheduled to be presented at May’s European Congress on Obesity (ECO) by Carel Le Roux, MD, University College Dublin, Ireland, and Giovanna Dr. Muscogiuri, MD, endocrinologist from the University of Naples Federico II, Naples, Italy, respectively.
The first analysis of tirzepatide, a dual glucose-dependent insulinotropic polypeptide and glucagon-like peptide 1 receptor agonist, aimed to analyze the impact of baseline BMI category on weight reduction across the series of phase 3 trials.
More participants on tirzepatide than on placebo achieved the body weight reduction targets of 5%, 10%, and 15%. “Across the SURMOUNT 1-4 trials, treatment with tirzepatide, along with a reduced-calorie diet and increased physical activity, consistently resulted in clinically significant weight reductions of 5% or more, 10% or more, or 15% or more, as compared to placebo, regardless of baseline BMI subgroup, in adults with obesity or overweight (BMI of 27 and above),” said obesity specialist, Louis J. Aronne, MD, from the Comprehensive Weight Control Center, Weill Cornell Medicine, New York City, and coauthor of the BMI-related analysis.
Dr. Muscogiuri, who is first author of the second analysis that looked at the impact of duration of adiposity, and her coauthors concluded that, “Tirzepatide consistently reduced body weight and waist circumference in people living with obesity or overweight with weight-related comorbidities regardless of the duration of disease. These results are consistent with the overall findings from each study in the SURMOUNT program.”
Weight Loss Consistent Regardless of BMI
The SURMOUNT series of trials involved people with a BMI of 30 kg/m2 and above, or 27 kg/m2 with at least one weight-related comorbidity without type 2 diabetes (SURMOUNT-1, 72 weeks), with type 2 diabetes (SURMOUNT-2, 72 weeks), and without type 2 diabetes after a 12-week intensive lifestyle intervention (SURMOUNT-3, 72 weeks from randomization) or after an 88 week intervention (SURMOUNT-4, 36-week open label tirzepatide lead-in and 52 weeks following randomization).
BMI subgroups were defined by 27-30 (overweight), 30-35 (obesity class I), 35-40 (obesity class II), and 40 kg/m2 and above (obesity class III). Percentage change in body weight from randomization to week 72 (SURMOUNT-1, -2, and -3) or to week 52 (SURMOUNT-4) was determined, as well as the proportions of participants achieving the weight reduction targets of 5%, 10%, and 15%. The per protocol analyses included all participants who received at least one dose of tirzepatide or placebo.
Across these BMI levels, up to 100% of tirzepatide-treated participants achieved weight reduction of 5% or more compared with 30% on placebo in SURMOUNT-1, up to 93% vs 43% in SURMOUNT-2, and up to 97% vs 15%, respectively, in SURMOUNT-3.
At least 10% weight reduction was achieved by up to 93% vs 16%, respectively, in SURMOUNT-1, up to 76% vs 14% in SURMOUNT-2, and up to 92% vs 8% in SURMOUNT-3.
Weight reduction of 15% was achieved by up to 85% compared with 7% of patients on tirzepatide and placebo, respectively, in SURMOUNT-1; up to 60% vs 3%, respectively, in SURMOUNT-2; and up to 78% vs 4% in SURMOUNT-3.
In SURMOUNT-4, during the 36-week open-label tirzepatide treatment, the mean body weight % or more reduction was 21%. Following this lead-in period, further weight reductions of 5% or more, 10%, and 15% or more were achieved by up to 70%, 39%, and 22%, respectively, of participants treated with tirzepatide compared with 2%, 2%, and 0% of patients on placebo.
Body Weight and Waist Circumference Reduced Regardless of Disease Duration
In this second presentation, participants were categorized based on duration with overweight/obesity at baseline (10 years or less, between 10 and 20 years, and above 20 years). Percentage body weight change; the proportions achieving weight loss targets of 5%, 10%, 15%, 20%, and 25%; and the change in waist circumference were analyzed.
Greater weight reductions were found in participants who took tirzepatide than in those who took placebo across the SURMOUNT 1-4 study endpoints, including weight reduction targets of 5%, 10%, 15%, 20%, and 25% compared with placebo-treated participants, regardless of disease duration, reported the authors in an early press release from ECO. The magnitude of weight reductions was generally similar across the disease duration categories.
For example, in the SURMOUNT-1 trial, for patients given 10-mg dose of tirzepatide, those with disease duration under 10 years lost 21% of their weight after 72 weeks compared with 20% body weight loss for those with 10-20 years disease duration and 23% for those with over 20 years disease duration.
In the SURMOUNT-2 trial (where all participants were also living with type 2 diabetes), for patients given the 10-mg dose of tirzepatide, those with disease duration under 10 years lost 12.6% of their body weight, while those with disease duration of 10-20 years lost 12.5%; in people living with overweight or obesity for over 20 years, 14.4% of body weight was lost.
Waist circumference also reduced to a greater extent than placebo for each disease duration category across the four studies, and again, these reductions were consistent across disease duration subgroups.
A difference between patients with and without type 2 diabetes was evident and requires further analysis to explore and understand why patients with type 2 diabetes have less weight loss in these trials than those without type 2 diabetes.
Asked to comment on the findings, Jens Juul Holst, MD, from the Department of Biomedical Sciences and Novo Nordisk Foundation Center for Basic Metabolic Research, University of Copenhagen, Copenhagen, Denmark, said that the results were as expected.
“The first abstract is said to show that there is the same effect regardless of the baseline BMI, but this is the expected outcome — nothing exciting there,” he told this news organization. “The second deals with the effects in people with different duration of adiposity. Again, it was equally effective in all groups and that was also the expected outcome, although important.”
“One question is whether one should treat people with BMI < 30 at all, and that depends on preexisting comorbidities — in particular metabolic syndrome, where treatment could be lifesaving and prevent complications,” added Dr. Holst.
This news organization also asked Jason Halford, ECO president, for his view on the findings. He remarked that with these weight loss drugs overall, “Usually weight loss tends to be proportional and actually greater in the lower BMI categories. This is partly because dosing is not done by body weight, and everyone gets the same doses irrespective of how they weigh. There is an argument that doses should be adjusted. The data suggests these drugs are so potent this does not occur for some reason.”
Dr. Holst added that, “In principle, for a given reduction in food intake, one would expect a similar reduction in body mass, and these agents should be dosed according to the size of the individual — since energy expenditure depends linearly on body weight, this is probably a reasonable measure. But what actually happens is dosing is according to the occurrence of side effects, which is a good pragmatic principle.”
Dr. Holst pointed out that the interesting question here is whether the very obese would somehow be resistant to the GLP-1 RAs (like leptin) — “they are not,” he noted.
He added that to his knowledge, the question around the role played by duration of the adiposity had not been explicitly looked at before. “However, the many individuals with obesity studied after GLP-1 RA treatment have varied widely with respect to duration and weight loss has not previously been known to depend on this, but there is no known physiological mechanism underpinning this.”
Tirzepatide (Mounjaro) was approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for the treatment of type 2 diabetes in 2022. In November 2023, the FDA approved tirzepatide (Zepbound) for chronic weight management in adults with BMI ≥ 30 kg/m2 or BMI ≥ 27 kg/m2 with at least one weight-related comorbidity. Also in November 2023, the EMA Committee for Medicinal Products for Human Use offered a positive opinion on extension of the Mounjaro label to include weight management in adults with BMI ≥ 30 kg/m2 or BMI ≥ 27 kg/m2 and at least one weight-related comorbid condition.
Dr. Holst had no conflicting interest with Eli Lilly but is a member of advisory boards for Novo Nordisk. This work (abstract 014) was funded by Eli Lilly and Company. Dr. Le Roux reported grants from the Irish Research Council, Science Foundation Ireland, Anabio, and the Health Research Board. He served on advisory boards and speaker panels of Novo Nordisk, Herbalife, GI Dynamics, Eli Lilly, Johnson & Johnson, Glia, Irish Life Health, Boehringer Ingelheim, Currax, Zealand Pharma, and Rhythm Pharma. Dr. Le Roux is a member of the Irish Society for Nutrition and Metabolism outside the area of work commented on here. He was the chief medical officer and director of the Medical Device Division of Keyron in 2021. Both of these are unremunerated positions. Dr. Le Roux was a previous investor in Keyron, which develops endoscopically implantable medical devices intended to mimic the surgical procedures of sleeve gastrectomy and gastric bypass. No patients have been included in any of Keyron’s studies, and they are not listed on the stock market. Dr. Le Roux was gifted stock holdings in September 2021 and divested all stock holdings in Keyron in September 2021. He continues to provide scientific advice to Keyron for no remuneration. Dr. Le Roux provides obesity clinical care in the Beyond BMI clinic and is a shareholder in the clinic. Dr. Aronne reported receiving grants or personal fees from Altimmune, AstraZeneca, Boehringer Ingelheim, Eli Lilly, ERX, Gelesis, Intellihealth, Jamieson Wellness, Janssen, Novo Nordisk, Optum, Pfizer, Senda Biosciences, and Versanis and being a shareholder of Allurion, ERX Pharmaceuticals, Gelesis, Intellihealth, and Jamieson Wellness. FJ, TF, MM, LG, and LN are employees and shareholders of Eli Lilly and Company.
A version of this article appeared on Medscape.com.
Tirzepatide (Zepbound for weight loss; Mounjaro for type 2 diabetes; Eli Lilly) consistently reduced body weight regardless of pretreatment body mass index (BMI) and reduced body weight and waist circumference regardless of duration of overweight or obesity.
The analyses — firstly of the impact of baseline BMI and secondly investigating the impact of the duration of overweight/obesity — are drawn from combined findings from the SURMOUNT 1-4 studies that examined the efficacy and safety of tirzepatide vs placebo. They are scheduled to be presented at May’s European Congress on Obesity (ECO) by Carel Le Roux, MD, University College Dublin, Ireland, and Giovanna Dr. Muscogiuri, MD, endocrinologist from the University of Naples Federico II, Naples, Italy, respectively.
The first analysis of tirzepatide, a dual glucose-dependent insulinotropic polypeptide and glucagon-like peptide 1 receptor agonist, aimed to analyze the impact of baseline BMI category on weight reduction across the series of phase 3 trials.
More participants on tirzepatide than on placebo achieved the body weight reduction targets of 5%, 10%, and 15%. “Across the SURMOUNT 1-4 trials, treatment with tirzepatide, along with a reduced-calorie diet and increased physical activity, consistently resulted in clinically significant weight reductions of 5% or more, 10% or more, or 15% or more, as compared to placebo, regardless of baseline BMI subgroup, in adults with obesity or overweight (BMI of 27 and above),” said obesity specialist, Louis J. Aronne, MD, from the Comprehensive Weight Control Center, Weill Cornell Medicine, New York City, and coauthor of the BMI-related analysis.
Dr. Muscogiuri, who is first author of the second analysis that looked at the impact of duration of adiposity, and her coauthors concluded that, “Tirzepatide consistently reduced body weight and waist circumference in people living with obesity or overweight with weight-related comorbidities regardless of the duration of disease. These results are consistent with the overall findings from each study in the SURMOUNT program.”
Weight Loss Consistent Regardless of BMI
The SURMOUNT series of trials involved people with a BMI of 30 kg/m2 and above, or 27 kg/m2 with at least one weight-related comorbidity without type 2 diabetes (SURMOUNT-1, 72 weeks), with type 2 diabetes (SURMOUNT-2, 72 weeks), and without type 2 diabetes after a 12-week intensive lifestyle intervention (SURMOUNT-3, 72 weeks from randomization) or after an 88 week intervention (SURMOUNT-4, 36-week open label tirzepatide lead-in and 52 weeks following randomization).
BMI subgroups were defined by 27-30 (overweight), 30-35 (obesity class I), 35-40 (obesity class II), and 40 kg/m2 and above (obesity class III). Percentage change in body weight from randomization to week 72 (SURMOUNT-1, -2, and -3) or to week 52 (SURMOUNT-4) was determined, as well as the proportions of participants achieving the weight reduction targets of 5%, 10%, and 15%. The per protocol analyses included all participants who received at least one dose of tirzepatide or placebo.
Across these BMI levels, up to 100% of tirzepatide-treated participants achieved weight reduction of 5% or more compared with 30% on placebo in SURMOUNT-1, up to 93% vs 43% in SURMOUNT-2, and up to 97% vs 15%, respectively, in SURMOUNT-3.
At least 10% weight reduction was achieved by up to 93% vs 16%, respectively, in SURMOUNT-1, up to 76% vs 14% in SURMOUNT-2, and up to 92% vs 8% in SURMOUNT-3.
Weight reduction of 15% was achieved by up to 85% compared with 7% of patients on tirzepatide and placebo, respectively, in SURMOUNT-1; up to 60% vs 3%, respectively, in SURMOUNT-2; and up to 78% vs 4% in SURMOUNT-3.
In SURMOUNT-4, during the 36-week open-label tirzepatide treatment, the mean body weight % or more reduction was 21%. Following this lead-in period, further weight reductions of 5% or more, 10%, and 15% or more were achieved by up to 70%, 39%, and 22%, respectively, of participants treated with tirzepatide compared with 2%, 2%, and 0% of patients on placebo.
Body Weight and Waist Circumference Reduced Regardless of Disease Duration
In this second presentation, participants were categorized based on duration with overweight/obesity at baseline (10 years or less, between 10 and 20 years, and above 20 years). Percentage body weight change; the proportions achieving weight loss targets of 5%, 10%, 15%, 20%, and 25%; and the change in waist circumference were analyzed.
Greater weight reductions were found in participants who took tirzepatide than in those who took placebo across the SURMOUNT 1-4 study endpoints, including weight reduction targets of 5%, 10%, 15%, 20%, and 25% compared with placebo-treated participants, regardless of disease duration, reported the authors in an early press release from ECO. The magnitude of weight reductions was generally similar across the disease duration categories.
For example, in the SURMOUNT-1 trial, for patients given 10-mg dose of tirzepatide, those with disease duration under 10 years lost 21% of their weight after 72 weeks compared with 20% body weight loss for those with 10-20 years disease duration and 23% for those with over 20 years disease duration.
In the SURMOUNT-2 trial (where all participants were also living with type 2 diabetes), for patients given the 10-mg dose of tirzepatide, those with disease duration under 10 years lost 12.6% of their body weight, while those with disease duration of 10-20 years lost 12.5%; in people living with overweight or obesity for over 20 years, 14.4% of body weight was lost.
Waist circumference also reduced to a greater extent than placebo for each disease duration category across the four studies, and again, these reductions were consistent across disease duration subgroups.
A difference between patients with and without type 2 diabetes was evident and requires further analysis to explore and understand why patients with type 2 diabetes have less weight loss in these trials than those without type 2 diabetes.
Asked to comment on the findings, Jens Juul Holst, MD, from the Department of Biomedical Sciences and Novo Nordisk Foundation Center for Basic Metabolic Research, University of Copenhagen, Copenhagen, Denmark, said that the results were as expected.
“The first abstract is said to show that there is the same effect regardless of the baseline BMI, but this is the expected outcome — nothing exciting there,” he told this news organization. “The second deals with the effects in people with different duration of adiposity. Again, it was equally effective in all groups and that was also the expected outcome, although important.”
“One question is whether one should treat people with BMI < 30 at all, and that depends on preexisting comorbidities — in particular metabolic syndrome, where treatment could be lifesaving and prevent complications,” added Dr. Holst.
This news organization also asked Jason Halford, ECO president, for his view on the findings. He remarked that with these weight loss drugs overall, “Usually weight loss tends to be proportional and actually greater in the lower BMI categories. This is partly because dosing is not done by body weight, and everyone gets the same doses irrespective of how they weigh. There is an argument that doses should be adjusted. The data suggests these drugs are so potent this does not occur for some reason.”
Dr. Holst added that, “In principle, for a given reduction in food intake, one would expect a similar reduction in body mass, and these agents should be dosed according to the size of the individual — since energy expenditure depends linearly on body weight, this is probably a reasonable measure. But what actually happens is dosing is according to the occurrence of side effects, which is a good pragmatic principle.”
Dr. Holst pointed out that the interesting question here is whether the very obese would somehow be resistant to the GLP-1 RAs (like leptin) — “they are not,” he noted.
He added that to his knowledge, the question around the role played by duration of the adiposity had not been explicitly looked at before. “However, the many individuals with obesity studied after GLP-1 RA treatment have varied widely with respect to duration and weight loss has not previously been known to depend on this, but there is no known physiological mechanism underpinning this.”
Tirzepatide (Mounjaro) was approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for the treatment of type 2 diabetes in 2022. In November 2023, the FDA approved tirzepatide (Zepbound) for chronic weight management in adults with BMI ≥ 30 kg/m2 or BMI ≥ 27 kg/m2 with at least one weight-related comorbidity. Also in November 2023, the EMA Committee for Medicinal Products for Human Use offered a positive opinion on extension of the Mounjaro label to include weight management in adults with BMI ≥ 30 kg/m2 or BMI ≥ 27 kg/m2 and at least one weight-related comorbid condition.
Dr. Holst had no conflicting interest with Eli Lilly but is a member of advisory boards for Novo Nordisk. This work (abstract 014) was funded by Eli Lilly and Company. Dr. Le Roux reported grants from the Irish Research Council, Science Foundation Ireland, Anabio, and the Health Research Board. He served on advisory boards and speaker panels of Novo Nordisk, Herbalife, GI Dynamics, Eli Lilly, Johnson & Johnson, Glia, Irish Life Health, Boehringer Ingelheim, Currax, Zealand Pharma, and Rhythm Pharma. Dr. Le Roux is a member of the Irish Society for Nutrition and Metabolism outside the area of work commented on here. He was the chief medical officer and director of the Medical Device Division of Keyron in 2021. Both of these are unremunerated positions. Dr. Le Roux was a previous investor in Keyron, which develops endoscopically implantable medical devices intended to mimic the surgical procedures of sleeve gastrectomy and gastric bypass. No patients have been included in any of Keyron’s studies, and they are not listed on the stock market. Dr. Le Roux was gifted stock holdings in September 2021 and divested all stock holdings in Keyron in September 2021. He continues to provide scientific advice to Keyron for no remuneration. Dr. Le Roux provides obesity clinical care in the Beyond BMI clinic and is a shareholder in the clinic. Dr. Aronne reported receiving grants or personal fees from Altimmune, AstraZeneca, Boehringer Ingelheim, Eli Lilly, ERX, Gelesis, Intellihealth, Jamieson Wellness, Janssen, Novo Nordisk, Optum, Pfizer, Senda Biosciences, and Versanis and being a shareholder of Allurion, ERX Pharmaceuticals, Gelesis, Intellihealth, and Jamieson Wellness. FJ, TF, MM, LG, and LN are employees and shareholders of Eli Lilly and Company.
A version of this article appeared on Medscape.com.
Tirzepatide (Zepbound for weight loss; Mounjaro for type 2 diabetes; Eli Lilly) consistently reduced body weight regardless of pretreatment body mass index (BMI) and reduced body weight and waist circumference regardless of duration of overweight or obesity.
The analyses — firstly of the impact of baseline BMI and secondly investigating the impact of the duration of overweight/obesity — are drawn from combined findings from the SURMOUNT 1-4 studies that examined the efficacy and safety of tirzepatide vs placebo. They are scheduled to be presented at May’s European Congress on Obesity (ECO) by Carel Le Roux, MD, University College Dublin, Ireland, and Giovanna Dr. Muscogiuri, MD, endocrinologist from the University of Naples Federico II, Naples, Italy, respectively.
The first analysis of tirzepatide, a dual glucose-dependent insulinotropic polypeptide and glucagon-like peptide 1 receptor agonist, aimed to analyze the impact of baseline BMI category on weight reduction across the series of phase 3 trials.
More participants on tirzepatide than on placebo achieved the body weight reduction targets of 5%, 10%, and 15%. “Across the SURMOUNT 1-4 trials, treatment with tirzepatide, along with a reduced-calorie diet and increased physical activity, consistently resulted in clinically significant weight reductions of 5% or more, 10% or more, or 15% or more, as compared to placebo, regardless of baseline BMI subgroup, in adults with obesity or overweight (BMI of 27 and above),” said obesity specialist, Louis J. Aronne, MD, from the Comprehensive Weight Control Center, Weill Cornell Medicine, New York City, and coauthor of the BMI-related analysis.
Dr. Muscogiuri, who is first author of the second analysis that looked at the impact of duration of adiposity, and her coauthors concluded that, “Tirzepatide consistently reduced body weight and waist circumference in people living with obesity or overweight with weight-related comorbidities regardless of the duration of disease. These results are consistent with the overall findings from each study in the SURMOUNT program.”
Weight Loss Consistent Regardless of BMI
The SURMOUNT series of trials involved people with a BMI of 30 kg/m2 and above, or 27 kg/m2 with at least one weight-related comorbidity without type 2 diabetes (SURMOUNT-1, 72 weeks), with type 2 diabetes (SURMOUNT-2, 72 weeks), and without type 2 diabetes after a 12-week intensive lifestyle intervention (SURMOUNT-3, 72 weeks from randomization) or after an 88 week intervention (SURMOUNT-4, 36-week open label tirzepatide lead-in and 52 weeks following randomization).
BMI subgroups were defined by 27-30 (overweight), 30-35 (obesity class I), 35-40 (obesity class II), and 40 kg/m2 and above (obesity class III). Percentage change in body weight from randomization to week 72 (SURMOUNT-1, -2, and -3) or to week 52 (SURMOUNT-4) was determined, as well as the proportions of participants achieving the weight reduction targets of 5%, 10%, and 15%. The per protocol analyses included all participants who received at least one dose of tirzepatide or placebo.
Across these BMI levels, up to 100% of tirzepatide-treated participants achieved weight reduction of 5% or more compared with 30% on placebo in SURMOUNT-1, up to 93% vs 43% in SURMOUNT-2, and up to 97% vs 15%, respectively, in SURMOUNT-3.
At least 10% weight reduction was achieved by up to 93% vs 16%, respectively, in SURMOUNT-1, up to 76% vs 14% in SURMOUNT-2, and up to 92% vs 8% in SURMOUNT-3.
Weight reduction of 15% was achieved by up to 85% compared with 7% of patients on tirzepatide and placebo, respectively, in SURMOUNT-1; up to 60% vs 3%, respectively, in SURMOUNT-2; and up to 78% vs 4% in SURMOUNT-3.
In SURMOUNT-4, during the 36-week open-label tirzepatide treatment, the mean body weight % or more reduction was 21%. Following this lead-in period, further weight reductions of 5% or more, 10%, and 15% or more were achieved by up to 70%, 39%, and 22%, respectively, of participants treated with tirzepatide compared with 2%, 2%, and 0% of patients on placebo.
Body Weight and Waist Circumference Reduced Regardless of Disease Duration
In this second presentation, participants were categorized based on duration with overweight/obesity at baseline (10 years or less, between 10 and 20 years, and above 20 years). Percentage body weight change; the proportions achieving weight loss targets of 5%, 10%, 15%, 20%, and 25%; and the change in waist circumference were analyzed.
Greater weight reductions were found in participants who took tirzepatide than in those who took placebo across the SURMOUNT 1-4 study endpoints, including weight reduction targets of 5%, 10%, 15%, 20%, and 25% compared with placebo-treated participants, regardless of disease duration, reported the authors in an early press release from ECO. The magnitude of weight reductions was generally similar across the disease duration categories.
For example, in the SURMOUNT-1 trial, for patients given 10-mg dose of tirzepatide, those with disease duration under 10 years lost 21% of their weight after 72 weeks compared with 20% body weight loss for those with 10-20 years disease duration and 23% for those with over 20 years disease duration.
In the SURMOUNT-2 trial (where all participants were also living with type 2 diabetes), for patients given the 10-mg dose of tirzepatide, those with disease duration under 10 years lost 12.6% of their body weight, while those with disease duration of 10-20 years lost 12.5%; in people living with overweight or obesity for over 20 years, 14.4% of body weight was lost.
Waist circumference also reduced to a greater extent than placebo for each disease duration category across the four studies, and again, these reductions were consistent across disease duration subgroups.
A difference between patients with and without type 2 diabetes was evident and requires further analysis to explore and understand why patients with type 2 diabetes have less weight loss in these trials than those without type 2 diabetes.
Asked to comment on the findings, Jens Juul Holst, MD, from the Department of Biomedical Sciences and Novo Nordisk Foundation Center for Basic Metabolic Research, University of Copenhagen, Copenhagen, Denmark, said that the results were as expected.
“The first abstract is said to show that there is the same effect regardless of the baseline BMI, but this is the expected outcome — nothing exciting there,” he told this news organization. “The second deals with the effects in people with different duration of adiposity. Again, it was equally effective in all groups and that was also the expected outcome, although important.”
“One question is whether one should treat people with BMI < 30 at all, and that depends on preexisting comorbidities — in particular metabolic syndrome, where treatment could be lifesaving and prevent complications,” added Dr. Holst.
This news organization also asked Jason Halford, ECO president, for his view on the findings. He remarked that with these weight loss drugs overall, “Usually weight loss tends to be proportional and actually greater in the lower BMI categories. This is partly because dosing is not done by body weight, and everyone gets the same doses irrespective of how they weigh. There is an argument that doses should be adjusted. The data suggests these drugs are so potent this does not occur for some reason.”
Dr. Holst added that, “In principle, for a given reduction in food intake, one would expect a similar reduction in body mass, and these agents should be dosed according to the size of the individual — since energy expenditure depends linearly on body weight, this is probably a reasonable measure. But what actually happens is dosing is according to the occurrence of side effects, which is a good pragmatic principle.”
Dr. Holst pointed out that the interesting question here is whether the very obese would somehow be resistant to the GLP-1 RAs (like leptin) — “they are not,” he noted.
He added that to his knowledge, the question around the role played by duration of the adiposity had not been explicitly looked at before. “However, the many individuals with obesity studied after GLP-1 RA treatment have varied widely with respect to duration and weight loss has not previously been known to depend on this, but there is no known physiological mechanism underpinning this.”
Tirzepatide (Mounjaro) was approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for the treatment of type 2 diabetes in 2022. In November 2023, the FDA approved tirzepatide (Zepbound) for chronic weight management in adults with BMI ≥ 30 kg/m2 or BMI ≥ 27 kg/m2 with at least one weight-related comorbidity. Also in November 2023, the EMA Committee for Medicinal Products for Human Use offered a positive opinion on extension of the Mounjaro label to include weight management in adults with BMI ≥ 30 kg/m2 or BMI ≥ 27 kg/m2 and at least one weight-related comorbid condition.
Dr. Holst had no conflicting interest with Eli Lilly but is a member of advisory boards for Novo Nordisk. This work (abstract 014) was funded by Eli Lilly and Company. Dr. Le Roux reported grants from the Irish Research Council, Science Foundation Ireland, Anabio, and the Health Research Board. He served on advisory boards and speaker panels of Novo Nordisk, Herbalife, GI Dynamics, Eli Lilly, Johnson & Johnson, Glia, Irish Life Health, Boehringer Ingelheim, Currax, Zealand Pharma, and Rhythm Pharma. Dr. Le Roux is a member of the Irish Society for Nutrition and Metabolism outside the area of work commented on here. He was the chief medical officer and director of the Medical Device Division of Keyron in 2021. Both of these are unremunerated positions. Dr. Le Roux was a previous investor in Keyron, which develops endoscopically implantable medical devices intended to mimic the surgical procedures of sleeve gastrectomy and gastric bypass. No patients have been included in any of Keyron’s studies, and they are not listed on the stock market. Dr. Le Roux was gifted stock holdings in September 2021 and divested all stock holdings in Keyron in September 2021. He continues to provide scientific advice to Keyron for no remuneration. Dr. Le Roux provides obesity clinical care in the Beyond BMI clinic and is a shareholder in the clinic. Dr. Aronne reported receiving grants or personal fees from Altimmune, AstraZeneca, Boehringer Ingelheim, Eli Lilly, ERX, Gelesis, Intellihealth, Jamieson Wellness, Janssen, Novo Nordisk, Optum, Pfizer, Senda Biosciences, and Versanis and being a shareholder of Allurion, ERX Pharmaceuticals, Gelesis, Intellihealth, and Jamieson Wellness. FJ, TF, MM, LG, and LN are employees and shareholders of Eli Lilly and Company.
A version of this article appeared on Medscape.com.
Epilepsy Linked to Higher COVID Hospitalization, Death Rates
, data from two linked studies showed.
Results showed that individuals with epilepsy had a 60% higher risk for hospitalization and a 33% higher risk of dying from COVID-19 than those without the disorder. However, during the pandemic, the number of hospitalizations and ER visits by people with epilepsy dropped by as much as 30%.
“The neurotropic effects of Sars-CoV-2 might explain some of this increased risk for people with epilepsy, or epilepsy might be associated with alterations in the immune system, predisposing to more severe COVID-19,” wrote the investigators, led by Owen Pickrell, MBBChirm, PhD, Swansea University, United Kingdom.
The findings were published online March 5 in Epilepsia.
Skill Shifting
Epilepsy is one of the most common neurological conditions and affects approximately 50 million people worldwide, with significant comorbidity and an increased risk for early death.
During the pandemic, clinicians treating people with epilepsy and other conditions shifted their skills to treat an ever-increasing number of patients with COVID-19, which may have hindered epilepsy-specific services for a time.
To further explore how the COVID-19 pandemic may have affected the health of this patient population, researchers analyzed health records from a large database with information about hospital admissions, primary care visits, COVID-19 vaccination status, and demographics of 90% of Welsh residents.
Those living with epilepsy before or during the study period (March 1, 2020, to June 31, 2021) were identified and compared with controls without epilepsy.
The analysis included approximately 27,280 people with epilepsy and 136,400 matched controls. Among those with epilepsy, there were 158 deaths (0.58%) and 933 hospitalizations (3.4%). In comparison, there were 370 deaths (0.27%) and 1871 hospitalizations (1.4%) in the control group.
Unadjusted analyses showed the risk of dying from COVID-19 for those with epilepsy vs controls was more than twofold higher (hazard ratio [HR], 2.15; 95% CI; 1.78-2.59) and the increase in the risk for hospitalization was similar (HR, 2.15; 95% CI; 1.94-2.37).
After adjusting for 40 comorbidities, including serious mental illness, asthma, and diabetes, those with epilepsy had a 60% increased risk for hospitalization (adjusted HR [aHR], 1.60) and a 33% increased risk for death (aHR, 1.33) than those without epilepsy (all P < .0001).
The findings “may have implications for prioritizing future COVID-19 treatments and vaccinations for people with epilepsy,” the investigators wrote.
Study limitations included the inability to account for the effect of vaccinations or prior infections with SARS-CoV-2. Moreover, the study did not account for geographical or temporal variations in prevalence and COVID-19 variants.
Consultations Canceled
In the related study, researchers analyzed healthcare utilization by people with epilepsy before and after the pandemic using the same database. Results showed hospital admissions, ER visits, and outpatient visits significantly decreased during the pandemic.
In the year before the pandemic, people with epilepsy had double the rate of ER visits (rate ratio [RR], 2.36), hospital admissions (RR, 2.08), and outpatient appointments (RR, 1.92) compared with matched controls.
However, during the pandemic there was a greater reduction in hospital admissions (RR, 0.70; 95% CI, 0.69-0.72) and ER visits (RR, 0.78; 95% CI, 0.77-0.70) in those with epilepsy versus matched controls (RR, 0.82; 95% CI, 0.81-0.83) as well as hospital visits and ER visits (RR, 0.87; 95% CI, 0.86-0.88; all P < .0001). New epilepsy diagnoses also decreased during the pandemic (RR, 0.73; P < .0001)
The redeployment of epileptologists during the pandemic also meant that epilepsy consultations and investigations were canceled, making it harder for people with epilepsy to access specialty care, the researchers noted.
“Our research also showed that there were fewer new diagnoses of epilepsy and fewer contacts with health services by people with epilepsy, during the period we examined,” Huw Strafford, lead data analyst for the studies, said in a release.
Both studies were funded by Health and Care Research Wales. Dr. Pickrell reported receiving speaker fees from UCB Pharma and Angelini Pharma, travel grants from Angelini Pharma, and an unrestricted grant from UCB Pharma.
A version of this article appeared on Medscape.com .
, data from two linked studies showed.
Results showed that individuals with epilepsy had a 60% higher risk for hospitalization and a 33% higher risk of dying from COVID-19 than those without the disorder. However, during the pandemic, the number of hospitalizations and ER visits by people with epilepsy dropped by as much as 30%.
“The neurotropic effects of Sars-CoV-2 might explain some of this increased risk for people with epilepsy, or epilepsy might be associated with alterations in the immune system, predisposing to more severe COVID-19,” wrote the investigators, led by Owen Pickrell, MBBChirm, PhD, Swansea University, United Kingdom.
The findings were published online March 5 in Epilepsia.
Skill Shifting
Epilepsy is one of the most common neurological conditions and affects approximately 50 million people worldwide, with significant comorbidity and an increased risk for early death.
During the pandemic, clinicians treating people with epilepsy and other conditions shifted their skills to treat an ever-increasing number of patients with COVID-19, which may have hindered epilepsy-specific services for a time.
To further explore how the COVID-19 pandemic may have affected the health of this patient population, researchers analyzed health records from a large database with information about hospital admissions, primary care visits, COVID-19 vaccination status, and demographics of 90% of Welsh residents.
Those living with epilepsy before or during the study period (March 1, 2020, to June 31, 2021) were identified and compared with controls without epilepsy.
The analysis included approximately 27,280 people with epilepsy and 136,400 matched controls. Among those with epilepsy, there were 158 deaths (0.58%) and 933 hospitalizations (3.4%). In comparison, there were 370 deaths (0.27%) and 1871 hospitalizations (1.4%) in the control group.
Unadjusted analyses showed the risk of dying from COVID-19 for those with epilepsy vs controls was more than twofold higher (hazard ratio [HR], 2.15; 95% CI; 1.78-2.59) and the increase in the risk for hospitalization was similar (HR, 2.15; 95% CI; 1.94-2.37).
After adjusting for 40 comorbidities, including serious mental illness, asthma, and diabetes, those with epilepsy had a 60% increased risk for hospitalization (adjusted HR [aHR], 1.60) and a 33% increased risk for death (aHR, 1.33) than those without epilepsy (all P < .0001).
The findings “may have implications for prioritizing future COVID-19 treatments and vaccinations for people with epilepsy,” the investigators wrote.
Study limitations included the inability to account for the effect of vaccinations or prior infections with SARS-CoV-2. Moreover, the study did not account for geographical or temporal variations in prevalence and COVID-19 variants.
Consultations Canceled
In the related study, researchers analyzed healthcare utilization by people with epilepsy before and after the pandemic using the same database. Results showed hospital admissions, ER visits, and outpatient visits significantly decreased during the pandemic.
In the year before the pandemic, people with epilepsy had double the rate of ER visits (rate ratio [RR], 2.36), hospital admissions (RR, 2.08), and outpatient appointments (RR, 1.92) compared with matched controls.
However, during the pandemic there was a greater reduction in hospital admissions (RR, 0.70; 95% CI, 0.69-0.72) and ER visits (RR, 0.78; 95% CI, 0.77-0.70) in those with epilepsy versus matched controls (RR, 0.82; 95% CI, 0.81-0.83) as well as hospital visits and ER visits (RR, 0.87; 95% CI, 0.86-0.88; all P < .0001). New epilepsy diagnoses also decreased during the pandemic (RR, 0.73; P < .0001)
The redeployment of epileptologists during the pandemic also meant that epilepsy consultations and investigations were canceled, making it harder for people with epilepsy to access specialty care, the researchers noted.
“Our research also showed that there were fewer new diagnoses of epilepsy and fewer contacts with health services by people with epilepsy, during the period we examined,” Huw Strafford, lead data analyst for the studies, said in a release.
Both studies were funded by Health and Care Research Wales. Dr. Pickrell reported receiving speaker fees from UCB Pharma and Angelini Pharma, travel grants from Angelini Pharma, and an unrestricted grant from UCB Pharma.
A version of this article appeared on Medscape.com .
, data from two linked studies showed.
Results showed that individuals with epilepsy had a 60% higher risk for hospitalization and a 33% higher risk of dying from COVID-19 than those without the disorder. However, during the pandemic, the number of hospitalizations and ER visits by people with epilepsy dropped by as much as 30%.
“The neurotropic effects of Sars-CoV-2 might explain some of this increased risk for people with epilepsy, or epilepsy might be associated with alterations in the immune system, predisposing to more severe COVID-19,” wrote the investigators, led by Owen Pickrell, MBBChirm, PhD, Swansea University, United Kingdom.
The findings were published online March 5 in Epilepsia.
Skill Shifting
Epilepsy is one of the most common neurological conditions and affects approximately 50 million people worldwide, with significant comorbidity and an increased risk for early death.
During the pandemic, clinicians treating people with epilepsy and other conditions shifted their skills to treat an ever-increasing number of patients with COVID-19, which may have hindered epilepsy-specific services for a time.
To further explore how the COVID-19 pandemic may have affected the health of this patient population, researchers analyzed health records from a large database with information about hospital admissions, primary care visits, COVID-19 vaccination status, and demographics of 90% of Welsh residents.
Those living with epilepsy before or during the study period (March 1, 2020, to June 31, 2021) were identified and compared with controls without epilepsy.
The analysis included approximately 27,280 people with epilepsy and 136,400 matched controls. Among those with epilepsy, there were 158 deaths (0.58%) and 933 hospitalizations (3.4%). In comparison, there were 370 deaths (0.27%) and 1871 hospitalizations (1.4%) in the control group.
Unadjusted analyses showed the risk of dying from COVID-19 for those with epilepsy vs controls was more than twofold higher (hazard ratio [HR], 2.15; 95% CI; 1.78-2.59) and the increase in the risk for hospitalization was similar (HR, 2.15; 95% CI; 1.94-2.37).
After adjusting for 40 comorbidities, including serious mental illness, asthma, and diabetes, those with epilepsy had a 60% increased risk for hospitalization (adjusted HR [aHR], 1.60) and a 33% increased risk for death (aHR, 1.33) than those without epilepsy (all P < .0001).
The findings “may have implications for prioritizing future COVID-19 treatments and vaccinations for people with epilepsy,” the investigators wrote.
Study limitations included the inability to account for the effect of vaccinations or prior infections with SARS-CoV-2. Moreover, the study did not account for geographical or temporal variations in prevalence and COVID-19 variants.
Consultations Canceled
In the related study, researchers analyzed healthcare utilization by people with epilepsy before and after the pandemic using the same database. Results showed hospital admissions, ER visits, and outpatient visits significantly decreased during the pandemic.
In the year before the pandemic, people with epilepsy had double the rate of ER visits (rate ratio [RR], 2.36), hospital admissions (RR, 2.08), and outpatient appointments (RR, 1.92) compared with matched controls.
However, during the pandemic there was a greater reduction in hospital admissions (RR, 0.70; 95% CI, 0.69-0.72) and ER visits (RR, 0.78; 95% CI, 0.77-0.70) in those with epilepsy versus matched controls (RR, 0.82; 95% CI, 0.81-0.83) as well as hospital visits and ER visits (RR, 0.87; 95% CI, 0.86-0.88; all P < .0001). New epilepsy diagnoses also decreased during the pandemic (RR, 0.73; P < .0001)
The redeployment of epileptologists during the pandemic also meant that epilepsy consultations and investigations were canceled, making it harder for people with epilepsy to access specialty care, the researchers noted.
“Our research also showed that there were fewer new diagnoses of epilepsy and fewer contacts with health services by people with epilepsy, during the period we examined,” Huw Strafford, lead data analyst for the studies, said in a release.
Both studies were funded by Health and Care Research Wales. Dr. Pickrell reported receiving speaker fees from UCB Pharma and Angelini Pharma, travel grants from Angelini Pharma, and an unrestricted grant from UCB Pharma.
A version of this article appeared on Medscape.com .
FROM EPILEPSIA
Next Gen Smart Pills Could Transform Personalized Care
On a November morning in 2022, James Messenger opened wide and swallowed a capsule like no other.
Messenger was no stranger to taking pills.
He’d first experimented with prescription opioids as a teenager in Morgantown, West Virginia, battled addiction on-and-off since, and known more than 70 people who had fatally overdosed. So, when asked to test a new “smart pill” that could detect an overdose in progress and call for help, he didn’t hesitate to join the study.
“I’ve lost pretty much every good friend I’ve ever had to this,” said Mr. Messenger. “This pill could save a lot of lives.”
The new Vitals Monitoring capsule he tested is just one example in a growing effort to radically rethink what the humble pill is capable of.
As far back as 1965, scientists introduced the Heidelberg capsule, an electronic pill that measured acidity from within the gut. In 1994, the University of Buffalo coined the term “smart pill” with a device promising to ferry medicine to a precise spot in the intestine, “like the tiny ship in the film Fantastic Voyage.” And in 2001, the US Food and Drug Administration (FDA) approved the first video capsule endoscope, a miniature-camera-toting pill that enabled noninvasive imaging of the small intestine.
But now, nearly 300 iterations are in various stages of development, according to a 2022 analysis. Advances in materials, imaging, and artificial intelligence (AI) are helping address everything from sleep apnea to HIV/AIDS to gut disorders via real-time tracking and real-time help.
“These technologies could enable us to shift the paradigm from ‘Let’s wait until the patient comes to us and find out what happened’ to ‘Let’s see how things are changing in real time, intervene now, and personalize that intervention,’ ” said Peter Chai, MD, associate professor of emergency medicine and health technology researcher at Brigham and Women’s Hospital in Boston.
Tracking Vitals From the Inside Out
Already, overdose-reversal agents like naloxone are saving lives. But more than 60% of overdoses occur when no one is around to administer them.
“While we need to focus on treatment, we also need to come up with more acute ways to save individuals when treatment doesn’t work or relapse occurs,” said James J. Mahoney III, PhD, director of addictions research at the Rockefeller Neuroscience Institute at West Virginia University (WVU), Morgantown.
Enter Celero Systems, a Massachusetts-based digital health company that has developed a vitamin-sized capsule packed with tiny sensors, microprocessors, and a radio antenna. It can measure breathing, heart rate, and core temperature — all from deep within the gut.
Respiratory distress is a hallmark early sign of an overdose. But it can be hard to monitor from a distance, especially in populations without access to a charged smartwatch.
Dr. Mahoney imagines a day when patients at risk could be given a weekly pill like Celero’s. If their respiratory rate drops below a dangerous level, it could alert loved ones or, better yet, release an overdose-reversal drug.
“It’s early days,” stressed Dr. Mahoney, whose team has been conducting pilot tests of the pill. “But initial data look promising.”
For one study, published in the journal Device in November 2023, the research team administered an overdose of fentanyl to anesthetized pigs with the pill in their stomachs. The capsule was able to detect respiratory depression within a minute and alert researchers via their laptop in time to step in.
When they gave the pill to 10 volunteers undergoing sleep studies at WVU, they found it could detect respiration rate with an accuracy of 93% compared with external monitoring devices — a feature that could also help diagnose sleep apnea or chronic obstructive pulmonary disease without expensive, intrusive tests.
Accuracy for heart rate was nearly 97%.
In another yet-to-be published trial, Dr. Mahoney tested the device with 10 volunteers in a residential treatment center to determine how well it could be tolerated.
Among the participants was Mr. Messenger, who said the thought of being tracked didn’t bother him.
“It was simple — just like taking a multivitamin,” said Mr. Messenger, now 34, sober, and working as a peer recovery support specialist at a hospital in his hometown. “It could be a great way to keep people alive long enough for them to get their head wrapped around the idea of treatment.”
Boosting Medication Adherence
At Brigham and Women’s Hospital, Dr. Chai is experimenting with a different smart pill — one he believes could help curb the ongoing HIV/AIDS epidemic.
Developed by Florida-based etectRx, the ID-Cap consists of a gelatin capsule embedded with a tiny radiofrequency transmitter, similar to the kind in retail antitheft devices. The capsule can be filled with a variety of medications. When swallowed, stomach acid dissolves the gel and activates the transmitter, which sends a signal to a receiver on a smartwatch, smartphone, or wall-mounted reader to confirm the medication was taken. If it isn’t, the patient’s smartphone or smart speaker might nudge them with a reminder or a family member might be notified.
In recent trials of men at a high risk for HIV, the system improved adherence to the once-daily prevention regimen pre-exposure prophylaxis (PrEP) by double digits.
“PrEP is almost 99% effective in preventing HIV, but you have to take it,” said Dr. Chai, who led the trials. “That seems like such a simple thing, but anyone who is chronically on medication can tell you just how difficult it can be.”
The pill is not the first designed to improve adherence. In 2017, the FDA approved the first digital ingestion tracking system, Abilify MyCite, for the treatment of schizophrenia and bipolar disorder. But its maker, Proteus Digital Health, filed for bankruptcy in 2020 after struggling to recruit patients willing to be tracked. (Some expressed privacy concerns. Others disliked the uncomfortable patch that received and forwarded the signal.)
More recent designs have been streamlined to ditch the patch, said etectRx senior vice president of operations Chris Carnes, PhD. And the cost of making a pill this kind of “smart” has come down to about a dollar.
So far, said Dr. Chai, in the patients he’s worked with, perceived benefits generally outweigh privacy concerns.
Studies are now underway in patients with heart disease and tuberculosis, and the company hopes to move into the aging and memory care space where medication-adherence is a serious problem.
“For us, or any company in this space, to succeed, you have to have a strong business case,” said Dr. Carnes. “If family members can keep their loved ones at home a little longer at an additional cost of $30 a month, that’s a no-brainer.”
Pillcams 2.0
Twenty-three years ago, the first video capsule endoscopy made it possible to image the small intestine via a tiny camera you swallow.
Such “pillcams” offered a more patient-friendly way to diagnose small bowel disorders, such as gastrointestinal bleeding and Crohn’s disease. Rather than undergoing sedation or anesthesia, as required during tube-based endoscopy, patients can go about their day as the pill painlessly passes through their gastrointestinal (GI) tract, capturing and recording data and images.
But the pills have their downsides.
Because they move passively, driven by movement in the intestine, they can miss trouble spots. Their ability to image the esophagus, stomach, and colon has proven limited. And unlike other procedures, like colonoscopy, they can’t intervene with therapy, like removing polyps.
The pillcam “had so much promise, to sort of revolutionize endoscopy, but it never really got the adoption that it seemed like it might,” said Andrew Meltzer, MD, professor of emergency medicine at the GW School of Medicine and Health Sciences in Washington.
That could soon change, he said, thanks to advances in locomotion and AI.
In a recent study of 40 patients, Dr. Meltzer tested a new magnetically controlled capsule endoscopy. Standing at a patient’s side, he could use a joystick to steer the pill around the stomach, capturing images in real time.
The pilot study, published in June 2023, found that the pill clearly identified six key stomach landmarks accurately 95% of the time and didn’t miss any lesions caught with traditional endoscopy. Notably, 80% of the patients preferred the pillcam over the tube.
“They are awake. They can go to work as soon as they leave. And it’s easy for them to tolerate,” Dr. Meltzer said.
More research is necessary, but Dr. Meltzer believes the technology could be particularly useful in the emergency department, allowing doctors to rule out high-risk bleeds in the stomach on the spot without admitting patients unnecessarily or making them return for a traditional scope.
“It has the potential to increase screening and provide more cost-effective care in emergencies,” he said.
It could also be useful in the telemedicine space, allowing a doctor to “drive” the pill from afar to diagnose a distant patient.
Someday, AI could enable the capsule to drive itself, so a doctor could merely press a button and wait. Or it could be adapted to treat what it finds, like administering a drug or cauterizing a bleed.
“If we can come up with a Mars rover which can explore other planets, we should be able to have something that can explore the stomach remotely,” Dr. Meltzer said.
Swallowing the Future
At the California Institute of Technology, researchers have developed a “location-aware” smart pill that uses magnetic fields to help pinpoint its location in the twists and turns of intestines. This could be useful for monitoring food in the GI tract to determine why things aren’t moving.
Other researchers are using AI models to enhance the transmission of video from inside the body and reduce the time it takes to interpret images.
One group at the Massachusetts Institute of Technology has developed a vibrating weight loss capsule designed to stimulate receptors in the gut to signal the brain that the person is full.
Not everyone is a fan of the smart-pill revolution. Some critics have raised concerns about privacy. Others fear that doctors risk yielding too much power to technology. Even those who are excited about the pills’ possibilities temper their optimism with caution.
None of these smart pills have gone mainstream yet in clinical practice, said Vivek Kaul, MD, professor of medicine at the University of Rochester Medical Center, Rochester, New York, and secretary general of the World Gastroenterology Organization.
Clinical validation, accessibility, and insurance coverage “will be critical in shaping their role,” he said. “But overall, it would be fair to state that this technology has come of age and the future is bright.”
A version of this article appeared on Medscape.com.
On a November morning in 2022, James Messenger opened wide and swallowed a capsule like no other.
Messenger was no stranger to taking pills.
He’d first experimented with prescription opioids as a teenager in Morgantown, West Virginia, battled addiction on-and-off since, and known more than 70 people who had fatally overdosed. So, when asked to test a new “smart pill” that could detect an overdose in progress and call for help, he didn’t hesitate to join the study.
“I’ve lost pretty much every good friend I’ve ever had to this,” said Mr. Messenger. “This pill could save a lot of lives.”
The new Vitals Monitoring capsule he tested is just one example in a growing effort to radically rethink what the humble pill is capable of.
As far back as 1965, scientists introduced the Heidelberg capsule, an electronic pill that measured acidity from within the gut. In 1994, the University of Buffalo coined the term “smart pill” with a device promising to ferry medicine to a precise spot in the intestine, “like the tiny ship in the film Fantastic Voyage.” And in 2001, the US Food and Drug Administration (FDA) approved the first video capsule endoscope, a miniature-camera-toting pill that enabled noninvasive imaging of the small intestine.
But now, nearly 300 iterations are in various stages of development, according to a 2022 analysis. Advances in materials, imaging, and artificial intelligence (AI) are helping address everything from sleep apnea to HIV/AIDS to gut disorders via real-time tracking and real-time help.
“These technologies could enable us to shift the paradigm from ‘Let’s wait until the patient comes to us and find out what happened’ to ‘Let’s see how things are changing in real time, intervene now, and personalize that intervention,’ ” said Peter Chai, MD, associate professor of emergency medicine and health technology researcher at Brigham and Women’s Hospital in Boston.
Tracking Vitals From the Inside Out
Already, overdose-reversal agents like naloxone are saving lives. But more than 60% of overdoses occur when no one is around to administer them.
“While we need to focus on treatment, we also need to come up with more acute ways to save individuals when treatment doesn’t work or relapse occurs,” said James J. Mahoney III, PhD, director of addictions research at the Rockefeller Neuroscience Institute at West Virginia University (WVU), Morgantown.
Enter Celero Systems, a Massachusetts-based digital health company that has developed a vitamin-sized capsule packed with tiny sensors, microprocessors, and a radio antenna. It can measure breathing, heart rate, and core temperature — all from deep within the gut.
Respiratory distress is a hallmark early sign of an overdose. But it can be hard to monitor from a distance, especially in populations without access to a charged smartwatch.
Dr. Mahoney imagines a day when patients at risk could be given a weekly pill like Celero’s. If their respiratory rate drops below a dangerous level, it could alert loved ones or, better yet, release an overdose-reversal drug.
“It’s early days,” stressed Dr. Mahoney, whose team has been conducting pilot tests of the pill. “But initial data look promising.”
For one study, published in the journal Device in November 2023, the research team administered an overdose of fentanyl to anesthetized pigs with the pill in their stomachs. The capsule was able to detect respiratory depression within a minute and alert researchers via their laptop in time to step in.
When they gave the pill to 10 volunteers undergoing sleep studies at WVU, they found it could detect respiration rate with an accuracy of 93% compared with external monitoring devices — a feature that could also help diagnose sleep apnea or chronic obstructive pulmonary disease without expensive, intrusive tests.
Accuracy for heart rate was nearly 97%.
In another yet-to-be published trial, Dr. Mahoney tested the device with 10 volunteers in a residential treatment center to determine how well it could be tolerated.
Among the participants was Mr. Messenger, who said the thought of being tracked didn’t bother him.
“It was simple — just like taking a multivitamin,” said Mr. Messenger, now 34, sober, and working as a peer recovery support specialist at a hospital in his hometown. “It could be a great way to keep people alive long enough for them to get their head wrapped around the idea of treatment.”
Boosting Medication Adherence
At Brigham and Women’s Hospital, Dr. Chai is experimenting with a different smart pill — one he believes could help curb the ongoing HIV/AIDS epidemic.
Developed by Florida-based etectRx, the ID-Cap consists of a gelatin capsule embedded with a tiny radiofrequency transmitter, similar to the kind in retail antitheft devices. The capsule can be filled with a variety of medications. When swallowed, stomach acid dissolves the gel and activates the transmitter, which sends a signal to a receiver on a smartwatch, smartphone, or wall-mounted reader to confirm the medication was taken. If it isn’t, the patient’s smartphone or smart speaker might nudge them with a reminder or a family member might be notified.
In recent trials of men at a high risk for HIV, the system improved adherence to the once-daily prevention regimen pre-exposure prophylaxis (PrEP) by double digits.
“PrEP is almost 99% effective in preventing HIV, but you have to take it,” said Dr. Chai, who led the trials. “That seems like such a simple thing, but anyone who is chronically on medication can tell you just how difficult it can be.”
The pill is not the first designed to improve adherence. In 2017, the FDA approved the first digital ingestion tracking system, Abilify MyCite, for the treatment of schizophrenia and bipolar disorder. But its maker, Proteus Digital Health, filed for bankruptcy in 2020 after struggling to recruit patients willing to be tracked. (Some expressed privacy concerns. Others disliked the uncomfortable patch that received and forwarded the signal.)
More recent designs have been streamlined to ditch the patch, said etectRx senior vice president of operations Chris Carnes, PhD. And the cost of making a pill this kind of “smart” has come down to about a dollar.
So far, said Dr. Chai, in the patients he’s worked with, perceived benefits generally outweigh privacy concerns.
Studies are now underway in patients with heart disease and tuberculosis, and the company hopes to move into the aging and memory care space where medication-adherence is a serious problem.
“For us, or any company in this space, to succeed, you have to have a strong business case,” said Dr. Carnes. “If family members can keep their loved ones at home a little longer at an additional cost of $30 a month, that’s a no-brainer.”
Pillcams 2.0
Twenty-three years ago, the first video capsule endoscopy made it possible to image the small intestine via a tiny camera you swallow.
Such “pillcams” offered a more patient-friendly way to diagnose small bowel disorders, such as gastrointestinal bleeding and Crohn’s disease. Rather than undergoing sedation or anesthesia, as required during tube-based endoscopy, patients can go about their day as the pill painlessly passes through their gastrointestinal (GI) tract, capturing and recording data and images.
But the pills have their downsides.
Because they move passively, driven by movement in the intestine, they can miss trouble spots. Their ability to image the esophagus, stomach, and colon has proven limited. And unlike other procedures, like colonoscopy, they can’t intervene with therapy, like removing polyps.
The pillcam “had so much promise, to sort of revolutionize endoscopy, but it never really got the adoption that it seemed like it might,” said Andrew Meltzer, MD, professor of emergency medicine at the GW School of Medicine and Health Sciences in Washington.
That could soon change, he said, thanks to advances in locomotion and AI.
In a recent study of 40 patients, Dr. Meltzer tested a new magnetically controlled capsule endoscopy. Standing at a patient’s side, he could use a joystick to steer the pill around the stomach, capturing images in real time.
The pilot study, published in June 2023, found that the pill clearly identified six key stomach landmarks accurately 95% of the time and didn’t miss any lesions caught with traditional endoscopy. Notably, 80% of the patients preferred the pillcam over the tube.
“They are awake. They can go to work as soon as they leave. And it’s easy for them to tolerate,” Dr. Meltzer said.
More research is necessary, but Dr. Meltzer believes the technology could be particularly useful in the emergency department, allowing doctors to rule out high-risk bleeds in the stomach on the spot without admitting patients unnecessarily or making them return for a traditional scope.
“It has the potential to increase screening and provide more cost-effective care in emergencies,” he said.
It could also be useful in the telemedicine space, allowing a doctor to “drive” the pill from afar to diagnose a distant patient.
Someday, AI could enable the capsule to drive itself, so a doctor could merely press a button and wait. Or it could be adapted to treat what it finds, like administering a drug or cauterizing a bleed.
“If we can come up with a Mars rover which can explore other planets, we should be able to have something that can explore the stomach remotely,” Dr. Meltzer said.
Swallowing the Future
At the California Institute of Technology, researchers have developed a “location-aware” smart pill that uses magnetic fields to help pinpoint its location in the twists and turns of intestines. This could be useful for monitoring food in the GI tract to determine why things aren’t moving.
Other researchers are using AI models to enhance the transmission of video from inside the body and reduce the time it takes to interpret images.
One group at the Massachusetts Institute of Technology has developed a vibrating weight loss capsule designed to stimulate receptors in the gut to signal the brain that the person is full.
Not everyone is a fan of the smart-pill revolution. Some critics have raised concerns about privacy. Others fear that doctors risk yielding too much power to technology. Even those who are excited about the pills’ possibilities temper their optimism with caution.
None of these smart pills have gone mainstream yet in clinical practice, said Vivek Kaul, MD, professor of medicine at the University of Rochester Medical Center, Rochester, New York, and secretary general of the World Gastroenterology Organization.
Clinical validation, accessibility, and insurance coverage “will be critical in shaping their role,” he said. “But overall, it would be fair to state that this technology has come of age and the future is bright.”
A version of this article appeared on Medscape.com.
On a November morning in 2022, James Messenger opened wide and swallowed a capsule like no other.
Messenger was no stranger to taking pills.
He’d first experimented with prescription opioids as a teenager in Morgantown, West Virginia, battled addiction on-and-off since, and known more than 70 people who had fatally overdosed. So, when asked to test a new “smart pill” that could detect an overdose in progress and call for help, he didn’t hesitate to join the study.
“I’ve lost pretty much every good friend I’ve ever had to this,” said Mr. Messenger. “This pill could save a lot of lives.”
The new Vitals Monitoring capsule he tested is just one example in a growing effort to radically rethink what the humble pill is capable of.
As far back as 1965, scientists introduced the Heidelberg capsule, an electronic pill that measured acidity from within the gut. In 1994, the University of Buffalo coined the term “smart pill” with a device promising to ferry medicine to a precise spot in the intestine, “like the tiny ship in the film Fantastic Voyage.” And in 2001, the US Food and Drug Administration (FDA) approved the first video capsule endoscope, a miniature-camera-toting pill that enabled noninvasive imaging of the small intestine.
But now, nearly 300 iterations are in various stages of development, according to a 2022 analysis. Advances in materials, imaging, and artificial intelligence (AI) are helping address everything from sleep apnea to HIV/AIDS to gut disorders via real-time tracking and real-time help.
“These technologies could enable us to shift the paradigm from ‘Let’s wait until the patient comes to us and find out what happened’ to ‘Let’s see how things are changing in real time, intervene now, and personalize that intervention,’ ” said Peter Chai, MD, associate professor of emergency medicine and health technology researcher at Brigham and Women’s Hospital in Boston.
Tracking Vitals From the Inside Out
Already, overdose-reversal agents like naloxone are saving lives. But more than 60% of overdoses occur when no one is around to administer them.
“While we need to focus on treatment, we also need to come up with more acute ways to save individuals when treatment doesn’t work or relapse occurs,” said James J. Mahoney III, PhD, director of addictions research at the Rockefeller Neuroscience Institute at West Virginia University (WVU), Morgantown.
Enter Celero Systems, a Massachusetts-based digital health company that has developed a vitamin-sized capsule packed with tiny sensors, microprocessors, and a radio antenna. It can measure breathing, heart rate, and core temperature — all from deep within the gut.
Respiratory distress is a hallmark early sign of an overdose. But it can be hard to monitor from a distance, especially in populations without access to a charged smartwatch.
Dr. Mahoney imagines a day when patients at risk could be given a weekly pill like Celero’s. If their respiratory rate drops below a dangerous level, it could alert loved ones or, better yet, release an overdose-reversal drug.
“It’s early days,” stressed Dr. Mahoney, whose team has been conducting pilot tests of the pill. “But initial data look promising.”
For one study, published in the journal Device in November 2023, the research team administered an overdose of fentanyl to anesthetized pigs with the pill in their stomachs. The capsule was able to detect respiratory depression within a minute and alert researchers via their laptop in time to step in.
When they gave the pill to 10 volunteers undergoing sleep studies at WVU, they found it could detect respiration rate with an accuracy of 93% compared with external monitoring devices — a feature that could also help diagnose sleep apnea or chronic obstructive pulmonary disease without expensive, intrusive tests.
Accuracy for heart rate was nearly 97%.
In another yet-to-be published trial, Dr. Mahoney tested the device with 10 volunteers in a residential treatment center to determine how well it could be tolerated.
Among the participants was Mr. Messenger, who said the thought of being tracked didn’t bother him.
“It was simple — just like taking a multivitamin,” said Mr. Messenger, now 34, sober, and working as a peer recovery support specialist at a hospital in his hometown. “It could be a great way to keep people alive long enough for them to get their head wrapped around the idea of treatment.”
Boosting Medication Adherence
At Brigham and Women’s Hospital, Dr. Chai is experimenting with a different smart pill — one he believes could help curb the ongoing HIV/AIDS epidemic.
Developed by Florida-based etectRx, the ID-Cap consists of a gelatin capsule embedded with a tiny radiofrequency transmitter, similar to the kind in retail antitheft devices. The capsule can be filled with a variety of medications. When swallowed, stomach acid dissolves the gel and activates the transmitter, which sends a signal to a receiver on a smartwatch, smartphone, or wall-mounted reader to confirm the medication was taken. If it isn’t, the patient’s smartphone or smart speaker might nudge them with a reminder or a family member might be notified.
In recent trials of men at a high risk for HIV, the system improved adherence to the once-daily prevention regimen pre-exposure prophylaxis (PrEP) by double digits.
“PrEP is almost 99% effective in preventing HIV, but you have to take it,” said Dr. Chai, who led the trials. “That seems like such a simple thing, but anyone who is chronically on medication can tell you just how difficult it can be.”
The pill is not the first designed to improve adherence. In 2017, the FDA approved the first digital ingestion tracking system, Abilify MyCite, for the treatment of schizophrenia and bipolar disorder. But its maker, Proteus Digital Health, filed for bankruptcy in 2020 after struggling to recruit patients willing to be tracked. (Some expressed privacy concerns. Others disliked the uncomfortable patch that received and forwarded the signal.)
More recent designs have been streamlined to ditch the patch, said etectRx senior vice president of operations Chris Carnes, PhD. And the cost of making a pill this kind of “smart” has come down to about a dollar.
So far, said Dr. Chai, in the patients he’s worked with, perceived benefits generally outweigh privacy concerns.
Studies are now underway in patients with heart disease and tuberculosis, and the company hopes to move into the aging and memory care space where medication-adherence is a serious problem.
“For us, or any company in this space, to succeed, you have to have a strong business case,” said Dr. Carnes. “If family members can keep their loved ones at home a little longer at an additional cost of $30 a month, that’s a no-brainer.”
Pillcams 2.0
Twenty-three years ago, the first video capsule endoscopy made it possible to image the small intestine via a tiny camera you swallow.
Such “pillcams” offered a more patient-friendly way to diagnose small bowel disorders, such as gastrointestinal bleeding and Crohn’s disease. Rather than undergoing sedation or anesthesia, as required during tube-based endoscopy, patients can go about their day as the pill painlessly passes through their gastrointestinal (GI) tract, capturing and recording data and images.
But the pills have their downsides.
Because they move passively, driven by movement in the intestine, they can miss trouble spots. Their ability to image the esophagus, stomach, and colon has proven limited. And unlike other procedures, like colonoscopy, they can’t intervene with therapy, like removing polyps.
The pillcam “had so much promise, to sort of revolutionize endoscopy, but it never really got the adoption that it seemed like it might,” said Andrew Meltzer, MD, professor of emergency medicine at the GW School of Medicine and Health Sciences in Washington.
That could soon change, he said, thanks to advances in locomotion and AI.
In a recent study of 40 patients, Dr. Meltzer tested a new magnetically controlled capsule endoscopy. Standing at a patient’s side, he could use a joystick to steer the pill around the stomach, capturing images in real time.
The pilot study, published in June 2023, found that the pill clearly identified six key stomach landmarks accurately 95% of the time and didn’t miss any lesions caught with traditional endoscopy. Notably, 80% of the patients preferred the pillcam over the tube.
“They are awake. They can go to work as soon as they leave. And it’s easy for them to tolerate,” Dr. Meltzer said.
More research is necessary, but Dr. Meltzer believes the technology could be particularly useful in the emergency department, allowing doctors to rule out high-risk bleeds in the stomach on the spot without admitting patients unnecessarily or making them return for a traditional scope.
“It has the potential to increase screening and provide more cost-effective care in emergencies,” he said.
It could also be useful in the telemedicine space, allowing a doctor to “drive” the pill from afar to diagnose a distant patient.
Someday, AI could enable the capsule to drive itself, so a doctor could merely press a button and wait. Or it could be adapted to treat what it finds, like administering a drug or cauterizing a bleed.
“If we can come up with a Mars rover which can explore other planets, we should be able to have something that can explore the stomach remotely,” Dr. Meltzer said.
Swallowing the Future
At the California Institute of Technology, researchers have developed a “location-aware” smart pill that uses magnetic fields to help pinpoint its location in the twists and turns of intestines. This could be useful for monitoring food in the GI tract to determine why things aren’t moving.
Other researchers are using AI models to enhance the transmission of video from inside the body and reduce the time it takes to interpret images.
One group at the Massachusetts Institute of Technology has developed a vibrating weight loss capsule designed to stimulate receptors in the gut to signal the brain that the person is full.
Not everyone is a fan of the smart-pill revolution. Some critics have raised concerns about privacy. Others fear that doctors risk yielding too much power to technology. Even those who are excited about the pills’ possibilities temper their optimism with caution.
None of these smart pills have gone mainstream yet in clinical practice, said Vivek Kaul, MD, professor of medicine at the University of Rochester Medical Center, Rochester, New York, and secretary general of the World Gastroenterology Organization.
Clinical validation, accessibility, and insurance coverage “will be critical in shaping their role,” he said. “But overall, it would be fair to state that this technology has come of age and the future is bright.”
A version of this article appeared on Medscape.com.
ACC Consensus Guidance on What’s New in HFrEF Treatment
The American College of Cardiology has published a new update to its consensus decision pathway for the treatment of heart failure with reduced ejection fraction (HFrEF).
Chair of the consensus document Writing Committee Thomas M. Maddox, MD, explained to this news organization that this new Decision Pathway provides a practical, streamlined update to frontline clinicians treating patients with heart failure and incorporates evidence from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“While the AHA/ACC/HFSA Guidelines are wonderful in that they collate all the latest scientific evidence, they don’t speak as much to the practicalities of delivering the care. This is what this Decision Pathway document comes in — it is designed to help frontline clinicians with the practical reality of managing these patients,” Dr. Maddox, who is director of the Healthcare Innovation Lab at BJC HealthCare and the Washington University School of Medicine in St Louis, Missouri, commented.
The document, “Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction,” was published online on March 8 in the Journal of the American College of Cardiology.
The authors provided guidance on introducing the numerous evidence-based therapies now available for HFrEF, improving adherence, overcoming treatment barriers, acknowledging contraindications and situations for which few data exist, affording expensive therapies, treating special cohorts, and making the transition to palliative care.
Rather than focusing on extensive text, the document provided practical tips, tables, and figures to make clear the steps, tools, and provisos needed to treat patients with heart failure successfully and expeditiously, they added.
Dr. Maddox reported that there are three main updated areas of advice on the treatment of heart failure in the new document.
Valsartan/Sacubitril First Line
One of the major changes involves an elevation for the status of the angiotensin receptor-neprilysin inhibitor (ARNI), Entresto (valsartan/sacubitril).
“It is now clear that this agent is superior to ACE-inhibitors or angiotensin receptor blockers in terms of reducing heart failure hospitalization and death, whereas previously it was seen as somewhat equivalent,” Dr. Maddox said. “So, barring a contraindication or another problem with getting the medication, this agent should be one of the first line medicines for all patients with heart failure and a reduced ejection fraction.”
Dual Sodium-Glucose Cotransporter 1/2 (SGLT1/2) Inhibitor
A second update involves the addition of sotagliflozin (a dual inhibitor of both SGLT1 and SGLT2) to the SGLT2 inhibitors as another first-line medication for patients with heart failure and reduced ejection fraction.
“We now have evidence that both SGLT2 and SGLT1 inhibitors are beneficial in reducing heart failure hospitalization and death. Previously we only had evidence on SGLT2 inhibitors — dapagliflozin and empagliflozin. Sotagliflozin is a newer agent, which inhibits both SGLT1 and SGLT2, and it turns out that inhibiting both are beneficial in heart failure. So, this gives us a third med in this category,” Dr. Maddox noted.
Rapid Initiation of the Four Pillars of Therapy
The document stated that more data have emerged recently to support early and rapid initiation and titration of the “four pillars” of medical therapy in heart failure to maximize the benefits of patient-reported outcomes and reduction in hospitalizations and mortality.
The four pillars of therapy are ARNI, a beta-blocker, a mineralocorticoid antagonist, and an SGLT inhibitor.
As an example, four-class medication initiation reduced the hazard of cardiovascular death or hospital admission for heart failure significantly (hazard ratio, 0.38) compared with therapy with just an angiotensin-converting enzyme inhibitor/angiotensin receptor blocker plus a beta-blocker, the document reported.
“What we realize now is that the more quickly we can get patients on all four of these drug classes and escalate to target doses or maximally tolerated doses ideally within 3 months, the better the outcome,” Dr. Maddox said.
“Unfortunately, right now there is very incomplete realization and recognition of that in clinical practice. So, we are trying to highlight the importance of this to encourage clinicians to be more aggressive in making this happen.”
“In all patients with heart failure and reduced ejection fraction, getting them on all four of these medicines as quickly as possible will give the best outcome. We’ve seen evidence in support of this from several broad population trials,” he added. “There are times when they can’t take all four but we should do our best to get there.”
Practical Considerations
Dr. Maddox pointed out that the Consensus Document is also trying to account for practical realities and barriers to heart failure treatment.
“When we think about these recommendations — and evidence that getting patients on all these medicines is valuable, we also focus on the fact that there are three major barriers that can get in the way of this and how to think about overcoming those barriers,” he said.
The barriers are comorbidities/side effects of medications, costs of the medicines, and systems of care that are needed to ensure patients can be treated with multiple medications in a timely fashion.
In terms of comorbidities/side effects, Dr. Maddox explained that patients with heart failure are generally older and are likely to have other comorbidities. “The more medicines we give, the more likely we are to run into side effects. So, we have produced some guidance on how to monitor for adverse effects and ways to mitigate these effects so the guideline recommended therapies can be continued without creating new harms.”
He gave the example of mineralocorticoid antagonists, which can sometimes elevate potassium levels, particularly if there is some underlying kidney disease, so clinicians are advised to recommend a low-potassium diet for these patients or the use of potassium binding agents that will also lower the amount of potassium in the blood stream; in this way, patients are able to continue the mineralocorticoid antagonist.
On costs, Dr. Maddox noted that the valsartan/sacubitril combination drug and SGLT inhibitors are new medicines and are expensive.
“They can be prohibitively expensive for patients who have suboptimal pharmacy benefits or who are uninsured.”
The Consensus Document therefore provided some guidance on ways to identify rebate programs, access insurance, and find different pathways to obtaining those drugs at a more reasonable price. It also advocated for policy changes to allow these medicines to be more accessible to more people.
More Use of Digital Tools
On the issue of systems of care, Dr. Maddox noted that the preexisting model of delivering care, which almost always involves the patient coming into the doctor’s office, invokes a high burden on both the system and most especially, the patient.
“Patients do not want to come back and forth to the doctor’s office multiple times in a few weeks. This is often a nonstarter, particularly for patients with busy lives,” he commented.
The Consensus Document advised more use of digital tools to provide remote care and contact with patients including sensors that can measure variables such as heart rate and blood pressure and video appointments.
“We are still working out what are the right models of care and how they can be performed safely and how they can be funded. But I think at the end of the day, this will give us more practical ways of getting people on multiple heart failure medicines and monitoring them safely without causing an undue burden for them logistically,” Dr. Maddox said.
He pointed out that there are a record number of medicines now available to treat heart failure, and while this is welcome, many of these patients are also on multiple other medications for other comorbidities as well.
“If you start giving patients seven, eight, or nine different medicines that they have to take every day, sometimes multiple times a day — that’s complicated medically, logistically, and financially. The potential for interaction and complications increases with every additional medication.”
Dr. Maddox also noted that patients have limits on how many medications they will accept. “It really helps if we have an engaged patient who has a good relationship with the care team to try to develop the right treatment plan that is going to meet their needs and give them the best possible health outcomes.”
It can take many visits to get the patient on all these medications and then up-titrate to target doses.
“We try and do a couple of things in each appointment. Often, we tend to start one or maybe two drugs at a time at a relatively low dose to avoid side effects, so we can be talking about 12-16 different encounters in total,” he said.
He recommended making a plan and the use of new technologies to manage each incremental step.
A Team Approach
Another issue that is discussed in the document is the use of a healthcare team to manage all the necessary appointments.
“It is no longer practical that one person can be the engineer for all this. It should be a team effort,” Dr. Maddox stated.
Responsibilities can be allocated across physicians, nurses, pharmacists, and even case managers, so that the team can take more of a population approach and develop a system to get patients on the multiple medications as quickly as possible.
“While this can still be quite a big burden for the patient, we need to figure out a system to make this as palatable as possible for them. Practices need to tailor this themselves according to what resources they have,” he added.
While most new patients will be routed to cardiologists to start their treatment plans, once on their initial medications and these have been up titrated to target levels, they should be able to be managed by primary care doctors, who will have the most holistic view of the patient and their other comorbidities, Dr. Maddox advised.
“Following this guidance should lead to more patients receiving evidence-based care which leads to better health outcomes, but delivered in a practical way that fits with their life reality and logistical needs,” he concluded.
A version of this article appeared on Medscape.com.
The American College of Cardiology has published a new update to its consensus decision pathway for the treatment of heart failure with reduced ejection fraction (HFrEF).
Chair of the consensus document Writing Committee Thomas M. Maddox, MD, explained to this news organization that this new Decision Pathway provides a practical, streamlined update to frontline clinicians treating patients with heart failure and incorporates evidence from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“While the AHA/ACC/HFSA Guidelines are wonderful in that they collate all the latest scientific evidence, they don’t speak as much to the practicalities of delivering the care. This is what this Decision Pathway document comes in — it is designed to help frontline clinicians with the practical reality of managing these patients,” Dr. Maddox, who is director of the Healthcare Innovation Lab at BJC HealthCare and the Washington University School of Medicine in St Louis, Missouri, commented.
The document, “Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction,” was published online on March 8 in the Journal of the American College of Cardiology.
The authors provided guidance on introducing the numerous evidence-based therapies now available for HFrEF, improving adherence, overcoming treatment barriers, acknowledging contraindications and situations for which few data exist, affording expensive therapies, treating special cohorts, and making the transition to palliative care.
Rather than focusing on extensive text, the document provided practical tips, tables, and figures to make clear the steps, tools, and provisos needed to treat patients with heart failure successfully and expeditiously, they added.
Dr. Maddox reported that there are three main updated areas of advice on the treatment of heart failure in the new document.
Valsartan/Sacubitril First Line
One of the major changes involves an elevation for the status of the angiotensin receptor-neprilysin inhibitor (ARNI), Entresto (valsartan/sacubitril).
“It is now clear that this agent is superior to ACE-inhibitors or angiotensin receptor blockers in terms of reducing heart failure hospitalization and death, whereas previously it was seen as somewhat equivalent,” Dr. Maddox said. “So, barring a contraindication or another problem with getting the medication, this agent should be one of the first line medicines for all patients with heart failure and a reduced ejection fraction.”
Dual Sodium-Glucose Cotransporter 1/2 (SGLT1/2) Inhibitor
A second update involves the addition of sotagliflozin (a dual inhibitor of both SGLT1 and SGLT2) to the SGLT2 inhibitors as another first-line medication for patients with heart failure and reduced ejection fraction.
“We now have evidence that both SGLT2 and SGLT1 inhibitors are beneficial in reducing heart failure hospitalization and death. Previously we only had evidence on SGLT2 inhibitors — dapagliflozin and empagliflozin. Sotagliflozin is a newer agent, which inhibits both SGLT1 and SGLT2, and it turns out that inhibiting both are beneficial in heart failure. So, this gives us a third med in this category,” Dr. Maddox noted.
Rapid Initiation of the Four Pillars of Therapy
The document stated that more data have emerged recently to support early and rapid initiation and titration of the “four pillars” of medical therapy in heart failure to maximize the benefits of patient-reported outcomes and reduction in hospitalizations and mortality.
The four pillars of therapy are ARNI, a beta-blocker, a mineralocorticoid antagonist, and an SGLT inhibitor.
As an example, four-class medication initiation reduced the hazard of cardiovascular death or hospital admission for heart failure significantly (hazard ratio, 0.38) compared with therapy with just an angiotensin-converting enzyme inhibitor/angiotensin receptor blocker plus a beta-blocker, the document reported.
“What we realize now is that the more quickly we can get patients on all four of these drug classes and escalate to target doses or maximally tolerated doses ideally within 3 months, the better the outcome,” Dr. Maddox said.
“Unfortunately, right now there is very incomplete realization and recognition of that in clinical practice. So, we are trying to highlight the importance of this to encourage clinicians to be more aggressive in making this happen.”
“In all patients with heart failure and reduced ejection fraction, getting them on all four of these medicines as quickly as possible will give the best outcome. We’ve seen evidence in support of this from several broad population trials,” he added. “There are times when they can’t take all four but we should do our best to get there.”
Practical Considerations
Dr. Maddox pointed out that the Consensus Document is also trying to account for practical realities and barriers to heart failure treatment.
“When we think about these recommendations — and evidence that getting patients on all these medicines is valuable, we also focus on the fact that there are three major barriers that can get in the way of this and how to think about overcoming those barriers,” he said.
The barriers are comorbidities/side effects of medications, costs of the medicines, and systems of care that are needed to ensure patients can be treated with multiple medications in a timely fashion.
In terms of comorbidities/side effects, Dr. Maddox explained that patients with heart failure are generally older and are likely to have other comorbidities. “The more medicines we give, the more likely we are to run into side effects. So, we have produced some guidance on how to monitor for adverse effects and ways to mitigate these effects so the guideline recommended therapies can be continued without creating new harms.”
He gave the example of mineralocorticoid antagonists, which can sometimes elevate potassium levels, particularly if there is some underlying kidney disease, so clinicians are advised to recommend a low-potassium diet for these patients or the use of potassium binding agents that will also lower the amount of potassium in the blood stream; in this way, patients are able to continue the mineralocorticoid antagonist.
On costs, Dr. Maddox noted that the valsartan/sacubitril combination drug and SGLT inhibitors are new medicines and are expensive.
“They can be prohibitively expensive for patients who have suboptimal pharmacy benefits or who are uninsured.”
The Consensus Document therefore provided some guidance on ways to identify rebate programs, access insurance, and find different pathways to obtaining those drugs at a more reasonable price. It also advocated for policy changes to allow these medicines to be more accessible to more people.
More Use of Digital Tools
On the issue of systems of care, Dr. Maddox noted that the preexisting model of delivering care, which almost always involves the patient coming into the doctor’s office, invokes a high burden on both the system and most especially, the patient.
“Patients do not want to come back and forth to the doctor’s office multiple times in a few weeks. This is often a nonstarter, particularly for patients with busy lives,” he commented.
The Consensus Document advised more use of digital tools to provide remote care and contact with patients including sensors that can measure variables such as heart rate and blood pressure and video appointments.
“We are still working out what are the right models of care and how they can be performed safely and how they can be funded. But I think at the end of the day, this will give us more practical ways of getting people on multiple heart failure medicines and monitoring them safely without causing an undue burden for them logistically,” Dr. Maddox said.
He pointed out that there are a record number of medicines now available to treat heart failure, and while this is welcome, many of these patients are also on multiple other medications for other comorbidities as well.
“If you start giving patients seven, eight, or nine different medicines that they have to take every day, sometimes multiple times a day — that’s complicated medically, logistically, and financially. The potential for interaction and complications increases with every additional medication.”
Dr. Maddox also noted that patients have limits on how many medications they will accept. “It really helps if we have an engaged patient who has a good relationship with the care team to try to develop the right treatment plan that is going to meet their needs and give them the best possible health outcomes.”
It can take many visits to get the patient on all these medications and then up-titrate to target doses.
“We try and do a couple of things in each appointment. Often, we tend to start one or maybe two drugs at a time at a relatively low dose to avoid side effects, so we can be talking about 12-16 different encounters in total,” he said.
He recommended making a plan and the use of new technologies to manage each incremental step.
A Team Approach
Another issue that is discussed in the document is the use of a healthcare team to manage all the necessary appointments.
“It is no longer practical that one person can be the engineer for all this. It should be a team effort,” Dr. Maddox stated.
Responsibilities can be allocated across physicians, nurses, pharmacists, and even case managers, so that the team can take more of a population approach and develop a system to get patients on the multiple medications as quickly as possible.
“While this can still be quite a big burden for the patient, we need to figure out a system to make this as palatable as possible for them. Practices need to tailor this themselves according to what resources they have,” he added.
While most new patients will be routed to cardiologists to start their treatment plans, once on their initial medications and these have been up titrated to target levels, they should be able to be managed by primary care doctors, who will have the most holistic view of the patient and their other comorbidities, Dr. Maddox advised.
“Following this guidance should lead to more patients receiving evidence-based care which leads to better health outcomes, but delivered in a practical way that fits with their life reality and logistical needs,” he concluded.
A version of this article appeared on Medscape.com.
The American College of Cardiology has published a new update to its consensus decision pathway for the treatment of heart failure with reduced ejection fraction (HFrEF).
Chair of the consensus document Writing Committee Thomas M. Maddox, MD, explained to this news organization that this new Decision Pathway provides a practical, streamlined update to frontline clinicians treating patients with heart failure and incorporates evidence from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“While the AHA/ACC/HFSA Guidelines are wonderful in that they collate all the latest scientific evidence, they don’t speak as much to the practicalities of delivering the care. This is what this Decision Pathway document comes in — it is designed to help frontline clinicians with the practical reality of managing these patients,” Dr. Maddox, who is director of the Healthcare Innovation Lab at BJC HealthCare and the Washington University School of Medicine in St Louis, Missouri, commented.
The document, “Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction,” was published online on March 8 in the Journal of the American College of Cardiology.
The authors provided guidance on introducing the numerous evidence-based therapies now available for HFrEF, improving adherence, overcoming treatment barriers, acknowledging contraindications and situations for which few data exist, affording expensive therapies, treating special cohorts, and making the transition to palliative care.
Rather than focusing on extensive text, the document provided practical tips, tables, and figures to make clear the steps, tools, and provisos needed to treat patients with heart failure successfully and expeditiously, they added.
Dr. Maddox reported that there are three main updated areas of advice on the treatment of heart failure in the new document.
Valsartan/Sacubitril First Line
One of the major changes involves an elevation for the status of the angiotensin receptor-neprilysin inhibitor (ARNI), Entresto (valsartan/sacubitril).
“It is now clear that this agent is superior to ACE-inhibitors or angiotensin receptor blockers in terms of reducing heart failure hospitalization and death, whereas previously it was seen as somewhat equivalent,” Dr. Maddox said. “So, barring a contraindication or another problem with getting the medication, this agent should be one of the first line medicines for all patients with heart failure and a reduced ejection fraction.”
Dual Sodium-Glucose Cotransporter 1/2 (SGLT1/2) Inhibitor
A second update involves the addition of sotagliflozin (a dual inhibitor of both SGLT1 and SGLT2) to the SGLT2 inhibitors as another first-line medication for patients with heart failure and reduced ejection fraction.
“We now have evidence that both SGLT2 and SGLT1 inhibitors are beneficial in reducing heart failure hospitalization and death. Previously we only had evidence on SGLT2 inhibitors — dapagliflozin and empagliflozin. Sotagliflozin is a newer agent, which inhibits both SGLT1 and SGLT2, and it turns out that inhibiting both are beneficial in heart failure. So, this gives us a third med in this category,” Dr. Maddox noted.
Rapid Initiation of the Four Pillars of Therapy
The document stated that more data have emerged recently to support early and rapid initiation and titration of the “four pillars” of medical therapy in heart failure to maximize the benefits of patient-reported outcomes and reduction in hospitalizations and mortality.
The four pillars of therapy are ARNI, a beta-blocker, a mineralocorticoid antagonist, and an SGLT inhibitor.
As an example, four-class medication initiation reduced the hazard of cardiovascular death or hospital admission for heart failure significantly (hazard ratio, 0.38) compared with therapy with just an angiotensin-converting enzyme inhibitor/angiotensin receptor blocker plus a beta-blocker, the document reported.
“What we realize now is that the more quickly we can get patients on all four of these drug classes and escalate to target doses or maximally tolerated doses ideally within 3 months, the better the outcome,” Dr. Maddox said.
“Unfortunately, right now there is very incomplete realization and recognition of that in clinical practice. So, we are trying to highlight the importance of this to encourage clinicians to be more aggressive in making this happen.”
“In all patients with heart failure and reduced ejection fraction, getting them on all four of these medicines as quickly as possible will give the best outcome. We’ve seen evidence in support of this from several broad population trials,” he added. “There are times when they can’t take all four but we should do our best to get there.”
Practical Considerations
Dr. Maddox pointed out that the Consensus Document is also trying to account for practical realities and barriers to heart failure treatment.
“When we think about these recommendations — and evidence that getting patients on all these medicines is valuable, we also focus on the fact that there are three major barriers that can get in the way of this and how to think about overcoming those barriers,” he said.
The barriers are comorbidities/side effects of medications, costs of the medicines, and systems of care that are needed to ensure patients can be treated with multiple medications in a timely fashion.
In terms of comorbidities/side effects, Dr. Maddox explained that patients with heart failure are generally older and are likely to have other comorbidities. “The more medicines we give, the more likely we are to run into side effects. So, we have produced some guidance on how to monitor for adverse effects and ways to mitigate these effects so the guideline recommended therapies can be continued without creating new harms.”
He gave the example of mineralocorticoid antagonists, which can sometimes elevate potassium levels, particularly if there is some underlying kidney disease, so clinicians are advised to recommend a low-potassium diet for these patients or the use of potassium binding agents that will also lower the amount of potassium in the blood stream; in this way, patients are able to continue the mineralocorticoid antagonist.
On costs, Dr. Maddox noted that the valsartan/sacubitril combination drug and SGLT inhibitors are new medicines and are expensive.
“They can be prohibitively expensive for patients who have suboptimal pharmacy benefits or who are uninsured.”
The Consensus Document therefore provided some guidance on ways to identify rebate programs, access insurance, and find different pathways to obtaining those drugs at a more reasonable price. It also advocated for policy changes to allow these medicines to be more accessible to more people.
More Use of Digital Tools
On the issue of systems of care, Dr. Maddox noted that the preexisting model of delivering care, which almost always involves the patient coming into the doctor’s office, invokes a high burden on both the system and most especially, the patient.
“Patients do not want to come back and forth to the doctor’s office multiple times in a few weeks. This is often a nonstarter, particularly for patients with busy lives,” he commented.
The Consensus Document advised more use of digital tools to provide remote care and contact with patients including sensors that can measure variables such as heart rate and blood pressure and video appointments.
“We are still working out what are the right models of care and how they can be performed safely and how they can be funded. But I think at the end of the day, this will give us more practical ways of getting people on multiple heart failure medicines and monitoring them safely without causing an undue burden for them logistically,” Dr. Maddox said.
He pointed out that there are a record number of medicines now available to treat heart failure, and while this is welcome, many of these patients are also on multiple other medications for other comorbidities as well.
“If you start giving patients seven, eight, or nine different medicines that they have to take every day, sometimes multiple times a day — that’s complicated medically, logistically, and financially. The potential for interaction and complications increases with every additional medication.”
Dr. Maddox also noted that patients have limits on how many medications they will accept. “It really helps if we have an engaged patient who has a good relationship with the care team to try to develop the right treatment plan that is going to meet their needs and give them the best possible health outcomes.”
It can take many visits to get the patient on all these medications and then up-titrate to target doses.
“We try and do a couple of things in each appointment. Often, we tend to start one or maybe two drugs at a time at a relatively low dose to avoid side effects, so we can be talking about 12-16 different encounters in total,” he said.
He recommended making a plan and the use of new technologies to manage each incremental step.
A Team Approach
Another issue that is discussed in the document is the use of a healthcare team to manage all the necessary appointments.
“It is no longer practical that one person can be the engineer for all this. It should be a team effort,” Dr. Maddox stated.
Responsibilities can be allocated across physicians, nurses, pharmacists, and even case managers, so that the team can take more of a population approach and develop a system to get patients on the multiple medications as quickly as possible.
“While this can still be quite a big burden for the patient, we need to figure out a system to make this as palatable as possible for them. Practices need to tailor this themselves according to what resources they have,” he added.
While most new patients will be routed to cardiologists to start their treatment plans, once on their initial medications and these have been up titrated to target levels, they should be able to be managed by primary care doctors, who will have the most holistic view of the patient and their other comorbidities, Dr. Maddox advised.
“Following this guidance should lead to more patients receiving evidence-based care which leads to better health outcomes, but delivered in a practical way that fits with their life reality and logistical needs,” he concluded.
A version of this article appeared on Medscape.com.
Allergens Present in Most ‘Hypoallergenic’ Baby Cleansers, Study Finds
TOPLINE:
METHODOLOGY:
- Many baby cleansers are marketed as “hypoallergenic,” but these claims are not validated.
- This study assessed the potential allergens and marketing claims in best-selling baby cleansers.
- The researchers collected ingredients and marketing claims of the top 50 best-selling baby body wash products sold on Amazon on April 4, 2023.
- Ingredient lists were checked for potential allergens using the 2020 American Contact Dermatitis Society (ACDS) core allergen series, which lists 90 common allergens for adults and children.
TAKEAWAY:
- In the 50 cleansers tested, 10 allergens were identified. Overall, 94% of the cleansers contained at least one allergen, averaging 2.9 allergens per product; cocamidopropyl betaine (72%), fragrance (64%), and sodium benzoate (54%) were the most common allergens.
- All cleansers had at least five marketing claims, with an average of 10.9 claims per product; the most common claims were “paraben-free” (88%), “phthalate-free” (84%), “tear-free” (74%), and “hypoallergenic” or “allergy-tested” (74%).
- There was no significant difference in the number of allergens in the cleansers marketed as “hypoallergenic” or “allergy tested” compared with cleansers that did not have these claims (P = .843).
- Fewer allergens were found in cleansers endorsed by the National Eczema Association (P = .004) or labeled “synthetic fragrance-free” (P = .003).
- There was a positive correlation between a greater number of allergens and an increased number of marketing claims (r = 0.547, P < .001) and a negative correlation between cost and number of allergens (r = −0.450, P = .001).
IN PRACTICE:
Because marketing claims like “hypoallergenic” may be misleading, “clinicians should counsel parents to carefully examine cleanser ingredients or consider selecting cleansers” endorsed by the National Eczema Association or another international eczema organization, especially for infants and children with a history of atopic dermatitis, the authors wrote.
SOURCE:
The study, led by Sasan D. Noveir, BA, from the University of California, Los Angeles, and coauthors from the division of dermatology at UCLA, was published online in Pediatric Dermatology.
LIMITATIONS:
The study only evaluated top-selling products from a single online source at a specific time, which may limit generalizability. Potential allergens not included in the ACDS core series may be present.
DISCLOSURES:
The study did not disclose any funding source. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Many baby cleansers are marketed as “hypoallergenic,” but these claims are not validated.
- This study assessed the potential allergens and marketing claims in best-selling baby cleansers.
- The researchers collected ingredients and marketing claims of the top 50 best-selling baby body wash products sold on Amazon on April 4, 2023.
- Ingredient lists were checked for potential allergens using the 2020 American Contact Dermatitis Society (ACDS) core allergen series, which lists 90 common allergens for adults and children.
TAKEAWAY:
- In the 50 cleansers tested, 10 allergens were identified. Overall, 94% of the cleansers contained at least one allergen, averaging 2.9 allergens per product; cocamidopropyl betaine (72%), fragrance (64%), and sodium benzoate (54%) were the most common allergens.
- All cleansers had at least five marketing claims, with an average of 10.9 claims per product; the most common claims were “paraben-free” (88%), “phthalate-free” (84%), “tear-free” (74%), and “hypoallergenic” or “allergy-tested” (74%).
- There was no significant difference in the number of allergens in the cleansers marketed as “hypoallergenic” or “allergy tested” compared with cleansers that did not have these claims (P = .843).
- Fewer allergens were found in cleansers endorsed by the National Eczema Association (P = .004) or labeled “synthetic fragrance-free” (P = .003).
- There was a positive correlation between a greater number of allergens and an increased number of marketing claims (r = 0.547, P < .001) and a negative correlation between cost and number of allergens (r = −0.450, P = .001).
IN PRACTICE:
Because marketing claims like “hypoallergenic” may be misleading, “clinicians should counsel parents to carefully examine cleanser ingredients or consider selecting cleansers” endorsed by the National Eczema Association or another international eczema organization, especially for infants and children with a history of atopic dermatitis, the authors wrote.
SOURCE:
The study, led by Sasan D. Noveir, BA, from the University of California, Los Angeles, and coauthors from the division of dermatology at UCLA, was published online in Pediatric Dermatology.
LIMITATIONS:
The study only evaluated top-selling products from a single online source at a specific time, which may limit generalizability. Potential allergens not included in the ACDS core series may be present.
DISCLOSURES:
The study did not disclose any funding source. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Many baby cleansers are marketed as “hypoallergenic,” but these claims are not validated.
- This study assessed the potential allergens and marketing claims in best-selling baby cleansers.
- The researchers collected ingredients and marketing claims of the top 50 best-selling baby body wash products sold on Amazon on April 4, 2023.
- Ingredient lists were checked for potential allergens using the 2020 American Contact Dermatitis Society (ACDS) core allergen series, which lists 90 common allergens for adults and children.
TAKEAWAY:
- In the 50 cleansers tested, 10 allergens were identified. Overall, 94% of the cleansers contained at least one allergen, averaging 2.9 allergens per product; cocamidopropyl betaine (72%), fragrance (64%), and sodium benzoate (54%) were the most common allergens.
- All cleansers had at least five marketing claims, with an average of 10.9 claims per product; the most common claims were “paraben-free” (88%), “phthalate-free” (84%), “tear-free” (74%), and “hypoallergenic” or “allergy-tested” (74%).
- There was no significant difference in the number of allergens in the cleansers marketed as “hypoallergenic” or “allergy tested” compared with cleansers that did not have these claims (P = .843).
- Fewer allergens were found in cleansers endorsed by the National Eczema Association (P = .004) or labeled “synthetic fragrance-free” (P = .003).
- There was a positive correlation between a greater number of allergens and an increased number of marketing claims (r = 0.547, P < .001) and a negative correlation between cost and number of allergens (r = −0.450, P = .001).
IN PRACTICE:
Because marketing claims like “hypoallergenic” may be misleading, “clinicians should counsel parents to carefully examine cleanser ingredients or consider selecting cleansers” endorsed by the National Eczema Association or another international eczema organization, especially for infants and children with a history of atopic dermatitis, the authors wrote.
SOURCE:
The study, led by Sasan D. Noveir, BA, from the University of California, Los Angeles, and coauthors from the division of dermatology at UCLA, was published online in Pediatric Dermatology.
LIMITATIONS:
The study only evaluated top-selling products from a single online source at a specific time, which may limit generalizability. Potential allergens not included in the ACDS core series may be present.
DISCLOSURES:
The study did not disclose any funding source. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Diet and Exercise in a Pill Are Real: How Mimetics Work
If couch-potato lab mice had beach-body dreams and if they could speak, they might tell you they’re thrilled by advances in the science of exercise and calorie-restriction (CR) mimetics.
In recent studies conducted at research centers across the United States, mice have chowed down, fattened up, exercised only if they felt like it, and still managed to lose body fat, improve their blood lipids, increase muscle power, avoid blood sugar problems, and boost heart function.
How did these mice get so lucky? They were given mimetics, experimental drugs that “mimic” the effects of exercise and calorie reduction in the body without the need to break a sweat or eat less.
“The mice looked like they’d done endurance training,” said Thomas Burris, PhD, chair of the Department of Pharmacodynamics at the University of Florida, Gainesville, Florida, and coauthor of a September 2023 study of the exercise mimetic SLU-PP-332, published in The Journal of Pharmacology and Experimental Therapeutics.
Meanwhile, the CR mimetic mannoheptulose (MH) “was incredibly effective at stopping the negative effects of a high-fat diet in mice,” said Donald K. Ingram, PhD, an adjunct professor at Louisiana State University’s Pennington Biomedical Research Center, Baton Rouge, Louisiana, who began studying CR mimetics at the National Institute on Aging in the 1980s. In a 2022 study published in Nutrients, MH also increased insulin sensitivity.
These “have your cake and eat it, too” drugs aren’t on the market for human use — but they’re edging closer. Several have moved into human trials with encouraging results. The National Institutes of Health and the pharmaceutical industry are taking notice, anteing up big research dollars. At the earliest, one could win US Food and Drug Administration (FDA) approval in 4-5 years, Dr. Burris said.
The medical appeal is clear: Mimetics could one day prevent and treat serious conditions such as age- and disease-related muscle loss, diabetes, heart failure, and even neurodegenerative disorders like Parkinson’s disease and Alzheimer’s disease, said the scientists studying them.
The commercial appeal is unavoidable: Mimetics have the potential to help nondieters avoid weight gain and allow dieters to build and/or preserve more calorie-burning muscle — a boon because losing weight can reduce muscle, especially with rapid loss.
How do these drugs work? What’s their downside? Like the “miracle” glucagon-like peptide 1 (GLP-1) weight-loss drugs that are now ubiquitous, are mimetics an effective pharmaceutical way to replicate two of society’s biggest lifestyle sticking points — diet and exercise?
It’s possible…
CR Mimetics: The Healthspan Drug?
From nematodes and fruit flies to yeast, Labrador Retrievers, and people, plenty of research shows that reducing calorie intake may improve health and prolong life. By how much? Cutting calories by 25% for 2 years slowed the pace of aging 2%-3% in the landmark CALERIE study of 197 adults, according to a 2023 study in Nature Aging. Sounds small, but the researchers said that equals a 10%-15% lower risk for an early death — on par with the longevity bonus you’d get from quitting smoking.
Trouble is low-cal living isn’t easy. “Diets work,” said George Roth, PhD, of GeroScience, Inc., in Pylesville, MD, who began studying CR at the National Institute on Aging in the 1980s with Ingram. “But it’s hard to sustain.”
That’s where CR mimetics come in. They activate the same health-promoting genes switched on by dieting, fasting, and extended periods of hunger, Dr. Roth said. The end result isn’t big weight loss. Instead, CR mimetics may keep us healthier and younger as we age. “Calorie restriction shifts metabolic processes in the body to protect against damage and stress,” he said.
Dr. Roth and Dr. Ingram are currently focused on the CR mimetic mannoheptulose (MH), a sugar found in unripe avocados. “It works at the first step in carbohydrate metabolism in cells throughout the body, so less energy goes through that pathway,” he said. “Glucose metabolism is reduced by 10%-15%. It’s the closest thing to actually eating less food.”
Their 2022 study found that while mice on an all-you-can-eat high-fat diet gained weight and body fat and saw blood lipids increase while insulin sensitivity decreased, mice that also got MH avoided these problems. A 2023 human study in Nutrients coauthored by Dr. Roth and Dr. Ingram found that a group consuming freeze-dried avocado had lower insulin levels than a placebo group.
Other researchers are looking at ways to stimulate the CR target nicotinamide adenine dinucleotide (NAD+). NAD+ assists sirtuins — a group of seven enzymes central to the beneficial effects of CR on aging — but levels drop with age. University of Colorado researchers are studying the effects of nicotinamide riboside (NR), an NAD+ precursor, in older adults with a $2.5 million National Institute on Aging grant. Small, preliminary human studies have found the compound reduced indicators of insulin resistance in the brain, in a January 2023 study in Aging Cell, and reduced blood pressure and arterial stiffness in a 2018 study published in Nature Communications.
Another NAD+ precursor, nicotinamide mononucleotide, reduced low-density lipoprotein cholesterol, diastolic blood pressure, and body weight in a Harvard Medical School study of 30 midlife and older adults with overweight and obesity, published in August 2023 in The Journal of Clinical Endocrinology & Metabolism. And in an April 2022 study published in Hepatology of people with nonalcoholic fatty liver disease, a proprietary supplement that included NR didn’t reduce liver fat but had a significant (vs placebo) reduction in ceramide and the liver enzyme alanine aminotransferase, a marker of inflammation.
“I think it was a pretty interesting result,” said lead researcher Leonard Guarente, PhD, professor of biology at Massachusetts Institute of Technology and founder of the supplement company Elysium. “Fatty liver progressively damages the liver. This has the potential to slow that down.”
Exercise Mimetics: Fitness in a Pill?
Physical activity builds muscle and fitness, helps keeps bones strong, sharpens thinking and memory, guards against depression, and helps discourage a slew of health concerns from weight gain and high blood pressure to diabetes and heart disease. Muscle becomes more dense, more powerful and may even burn more calories, said Dr. Burris. The problem: That pesky part about actually moving. Fewer than half of American adults get recommended amounts of aerobic exercise and fewer than a quarter fit in strength training, according to the Centers for Disease Control and Prevention.
Enter the exercise mimetics. Unlike CR mimetics, exercise mimetics affect mitochondria — the tiny power plants in muscle and every other cell in the body. They switch on genes that encourage the growth of more mitochondria and encourage them to burn fatty acids, not just glucose, for fuel.
In mice, this can keep them from gaining weight, increase insulin sensitivity, and boost exercise endurance. “We can use a drug to activate the same networks that are activated by physical activity,” said Ronald Evans, PhD, professor and director of the Gene Expression Laboratory at the Salk Institute for Biological Studies in La Jolla, California.
Among notable mimetics moving into human studies is ASP0367, a drug in a class called PPAR delta modulators first developed in Evans’ lab. ASP0367 was licensed to the pharmaceutical company Mitobridge, later acquired by Astellas. Astellas is currently running a phase 2/3 human trial of the investigational drug in people with the rare genetic disorder primary mitochondrial myopathy.
At the University of Florida, Dr. Burris and team hope to soon move the exercise mimetic SLU-PP-332 into human studies. “It targets a receptor called ERR that I’ve been working on since the 1980s,” Dr. Burris said. “We knew from genetic studies that ERR has a role in exercise’s effects on mitochondrial function in muscle.” The calorie mimetics he’s studying also activate genes for making more mitochondria and driving them to burn fatty acids. “This generates a lot of energy,” he said. In a January 2024 study in Circulation, Dr. Burris found the drug restores heart function in mice experiencing heart failure. “Very little heart function was lost,” he said. It’s had no serious side effects.
The Future of Exercise and CR Pills
The field has hit some bumps. Some feel inevitable — such as otherwise healthy people misusing the drugs. GW1516, an early experimental exercise mimetic studied by Dr. Evans and abandoned because it triggered tumor growth in lab studies, is used illegally by elite athletes as a performance-enhancing drug despite warnings from the US Anti-Doping Agency. Dr. Burris worries that future CR mimetics could be misused the same way.
But he and others see plenty of benefits in future, FDA-approved drugs. Exercise mimetics like SLU-PP-332 might one day be given to people alongside weight-loss drugs, such as Mounjaro (tirzepatide) or Ozempic (semaglutide) to prevent muscle loss. “SLU-PP-332 doesn’t affect hunger or food intake the way those drugs do,” he said. “It changes muscle.”
Mimetics may one day help older adults and people with muscle disorders rebuild muscle even when they cannot exercise and to delay a range of age-related diseases without onerous dieting. “The chance to intervene and provide a longer healthspan and lifespan — that’s been the moon shot,” Dr. Roth said.
Dr. Guarente noted that CR mimetics may work best for people who aren’t carrying extra pounds but want the health benefits of slashing calories without sacrificing meals and snacks. “Fat is still going to be a problem for joints, cholesterol, inflammation,” he said. “Calorie mimetics are not a panacea for obesity but could help preserve overall health and vitality.”
And what about the billion-dollar question: What happens when these drugs become available to a general public that has issues with actual exercise and healthy diet?
Evans sees only positives. “Our environment is designed to keep people sitting down and consuming high-calorie foods,” he said. “In the absence of people getting motivated to exercise — and there’s no evidence the country is moving in that direction on its own — a pill is an important option to have.”
A version of this article appeared on Medscape.com.
If couch-potato lab mice had beach-body dreams and if they could speak, they might tell you they’re thrilled by advances in the science of exercise and calorie-restriction (CR) mimetics.
In recent studies conducted at research centers across the United States, mice have chowed down, fattened up, exercised only if they felt like it, and still managed to lose body fat, improve their blood lipids, increase muscle power, avoid blood sugar problems, and boost heart function.
How did these mice get so lucky? They were given mimetics, experimental drugs that “mimic” the effects of exercise and calorie reduction in the body without the need to break a sweat or eat less.
“The mice looked like they’d done endurance training,” said Thomas Burris, PhD, chair of the Department of Pharmacodynamics at the University of Florida, Gainesville, Florida, and coauthor of a September 2023 study of the exercise mimetic SLU-PP-332, published in The Journal of Pharmacology and Experimental Therapeutics.
Meanwhile, the CR mimetic mannoheptulose (MH) “was incredibly effective at stopping the negative effects of a high-fat diet in mice,” said Donald K. Ingram, PhD, an adjunct professor at Louisiana State University’s Pennington Biomedical Research Center, Baton Rouge, Louisiana, who began studying CR mimetics at the National Institute on Aging in the 1980s. In a 2022 study published in Nutrients, MH also increased insulin sensitivity.
These “have your cake and eat it, too” drugs aren’t on the market for human use — but they’re edging closer. Several have moved into human trials with encouraging results. The National Institutes of Health and the pharmaceutical industry are taking notice, anteing up big research dollars. At the earliest, one could win US Food and Drug Administration (FDA) approval in 4-5 years, Dr. Burris said.
The medical appeal is clear: Mimetics could one day prevent and treat serious conditions such as age- and disease-related muscle loss, diabetes, heart failure, and even neurodegenerative disorders like Parkinson’s disease and Alzheimer’s disease, said the scientists studying them.
The commercial appeal is unavoidable: Mimetics have the potential to help nondieters avoid weight gain and allow dieters to build and/or preserve more calorie-burning muscle — a boon because losing weight can reduce muscle, especially with rapid loss.
How do these drugs work? What’s their downside? Like the “miracle” glucagon-like peptide 1 (GLP-1) weight-loss drugs that are now ubiquitous, are mimetics an effective pharmaceutical way to replicate two of society’s biggest lifestyle sticking points — diet and exercise?
It’s possible…
CR Mimetics: The Healthspan Drug?
From nematodes and fruit flies to yeast, Labrador Retrievers, and people, plenty of research shows that reducing calorie intake may improve health and prolong life. By how much? Cutting calories by 25% for 2 years slowed the pace of aging 2%-3% in the landmark CALERIE study of 197 adults, according to a 2023 study in Nature Aging. Sounds small, but the researchers said that equals a 10%-15% lower risk for an early death — on par with the longevity bonus you’d get from quitting smoking.
Trouble is low-cal living isn’t easy. “Diets work,” said George Roth, PhD, of GeroScience, Inc., in Pylesville, MD, who began studying CR at the National Institute on Aging in the 1980s with Ingram. “But it’s hard to sustain.”
That’s where CR mimetics come in. They activate the same health-promoting genes switched on by dieting, fasting, and extended periods of hunger, Dr. Roth said. The end result isn’t big weight loss. Instead, CR mimetics may keep us healthier and younger as we age. “Calorie restriction shifts metabolic processes in the body to protect against damage and stress,” he said.
Dr. Roth and Dr. Ingram are currently focused on the CR mimetic mannoheptulose (MH), a sugar found in unripe avocados. “It works at the first step in carbohydrate metabolism in cells throughout the body, so less energy goes through that pathway,” he said. “Glucose metabolism is reduced by 10%-15%. It’s the closest thing to actually eating less food.”
Their 2022 study found that while mice on an all-you-can-eat high-fat diet gained weight and body fat and saw blood lipids increase while insulin sensitivity decreased, mice that also got MH avoided these problems. A 2023 human study in Nutrients coauthored by Dr. Roth and Dr. Ingram found that a group consuming freeze-dried avocado had lower insulin levels than a placebo group.
Other researchers are looking at ways to stimulate the CR target nicotinamide adenine dinucleotide (NAD+). NAD+ assists sirtuins — a group of seven enzymes central to the beneficial effects of CR on aging — but levels drop with age. University of Colorado researchers are studying the effects of nicotinamide riboside (NR), an NAD+ precursor, in older adults with a $2.5 million National Institute on Aging grant. Small, preliminary human studies have found the compound reduced indicators of insulin resistance in the brain, in a January 2023 study in Aging Cell, and reduced blood pressure and arterial stiffness in a 2018 study published in Nature Communications.
Another NAD+ precursor, nicotinamide mononucleotide, reduced low-density lipoprotein cholesterol, diastolic blood pressure, and body weight in a Harvard Medical School study of 30 midlife and older adults with overweight and obesity, published in August 2023 in The Journal of Clinical Endocrinology & Metabolism. And in an April 2022 study published in Hepatology of people with nonalcoholic fatty liver disease, a proprietary supplement that included NR didn’t reduce liver fat but had a significant (vs placebo) reduction in ceramide and the liver enzyme alanine aminotransferase, a marker of inflammation.
“I think it was a pretty interesting result,” said lead researcher Leonard Guarente, PhD, professor of biology at Massachusetts Institute of Technology and founder of the supplement company Elysium. “Fatty liver progressively damages the liver. This has the potential to slow that down.”
Exercise Mimetics: Fitness in a Pill?
Physical activity builds muscle and fitness, helps keeps bones strong, sharpens thinking and memory, guards against depression, and helps discourage a slew of health concerns from weight gain and high blood pressure to diabetes and heart disease. Muscle becomes more dense, more powerful and may even burn more calories, said Dr. Burris. The problem: That pesky part about actually moving. Fewer than half of American adults get recommended amounts of aerobic exercise and fewer than a quarter fit in strength training, according to the Centers for Disease Control and Prevention.
Enter the exercise mimetics. Unlike CR mimetics, exercise mimetics affect mitochondria — the tiny power plants in muscle and every other cell in the body. They switch on genes that encourage the growth of more mitochondria and encourage them to burn fatty acids, not just glucose, for fuel.
In mice, this can keep them from gaining weight, increase insulin sensitivity, and boost exercise endurance. “We can use a drug to activate the same networks that are activated by physical activity,” said Ronald Evans, PhD, professor and director of the Gene Expression Laboratory at the Salk Institute for Biological Studies in La Jolla, California.
Among notable mimetics moving into human studies is ASP0367, a drug in a class called PPAR delta modulators first developed in Evans’ lab. ASP0367 was licensed to the pharmaceutical company Mitobridge, later acquired by Astellas. Astellas is currently running a phase 2/3 human trial of the investigational drug in people with the rare genetic disorder primary mitochondrial myopathy.
At the University of Florida, Dr. Burris and team hope to soon move the exercise mimetic SLU-PP-332 into human studies. “It targets a receptor called ERR that I’ve been working on since the 1980s,” Dr. Burris said. “We knew from genetic studies that ERR has a role in exercise’s effects on mitochondrial function in muscle.” The calorie mimetics he’s studying also activate genes for making more mitochondria and driving them to burn fatty acids. “This generates a lot of energy,” he said. In a January 2024 study in Circulation, Dr. Burris found the drug restores heart function in mice experiencing heart failure. “Very little heart function was lost,” he said. It’s had no serious side effects.
The Future of Exercise and CR Pills
The field has hit some bumps. Some feel inevitable — such as otherwise healthy people misusing the drugs. GW1516, an early experimental exercise mimetic studied by Dr. Evans and abandoned because it triggered tumor growth in lab studies, is used illegally by elite athletes as a performance-enhancing drug despite warnings from the US Anti-Doping Agency. Dr. Burris worries that future CR mimetics could be misused the same way.
But he and others see plenty of benefits in future, FDA-approved drugs. Exercise mimetics like SLU-PP-332 might one day be given to people alongside weight-loss drugs, such as Mounjaro (tirzepatide) or Ozempic (semaglutide) to prevent muscle loss. “SLU-PP-332 doesn’t affect hunger or food intake the way those drugs do,” he said. “It changes muscle.”
Mimetics may one day help older adults and people with muscle disorders rebuild muscle even when they cannot exercise and to delay a range of age-related diseases without onerous dieting. “The chance to intervene and provide a longer healthspan and lifespan — that’s been the moon shot,” Dr. Roth said.
Dr. Guarente noted that CR mimetics may work best for people who aren’t carrying extra pounds but want the health benefits of slashing calories without sacrificing meals and snacks. “Fat is still going to be a problem for joints, cholesterol, inflammation,” he said. “Calorie mimetics are not a panacea for obesity but could help preserve overall health and vitality.”
And what about the billion-dollar question: What happens when these drugs become available to a general public that has issues with actual exercise and healthy diet?
Evans sees only positives. “Our environment is designed to keep people sitting down and consuming high-calorie foods,” he said. “In the absence of people getting motivated to exercise — and there’s no evidence the country is moving in that direction on its own — a pill is an important option to have.”
A version of this article appeared on Medscape.com.
If couch-potato lab mice had beach-body dreams and if they could speak, they might tell you they’re thrilled by advances in the science of exercise and calorie-restriction (CR) mimetics.
In recent studies conducted at research centers across the United States, mice have chowed down, fattened up, exercised only if they felt like it, and still managed to lose body fat, improve their blood lipids, increase muscle power, avoid blood sugar problems, and boost heart function.
How did these mice get so lucky? They were given mimetics, experimental drugs that “mimic” the effects of exercise and calorie reduction in the body without the need to break a sweat or eat less.
“The mice looked like they’d done endurance training,” said Thomas Burris, PhD, chair of the Department of Pharmacodynamics at the University of Florida, Gainesville, Florida, and coauthor of a September 2023 study of the exercise mimetic SLU-PP-332, published in The Journal of Pharmacology and Experimental Therapeutics.
Meanwhile, the CR mimetic mannoheptulose (MH) “was incredibly effective at stopping the negative effects of a high-fat diet in mice,” said Donald K. Ingram, PhD, an adjunct professor at Louisiana State University’s Pennington Biomedical Research Center, Baton Rouge, Louisiana, who began studying CR mimetics at the National Institute on Aging in the 1980s. In a 2022 study published in Nutrients, MH also increased insulin sensitivity.
These “have your cake and eat it, too” drugs aren’t on the market for human use — but they’re edging closer. Several have moved into human trials with encouraging results. The National Institutes of Health and the pharmaceutical industry are taking notice, anteing up big research dollars. At the earliest, one could win US Food and Drug Administration (FDA) approval in 4-5 years, Dr. Burris said.
The medical appeal is clear: Mimetics could one day prevent and treat serious conditions such as age- and disease-related muscle loss, diabetes, heart failure, and even neurodegenerative disorders like Parkinson’s disease and Alzheimer’s disease, said the scientists studying them.
The commercial appeal is unavoidable: Mimetics have the potential to help nondieters avoid weight gain and allow dieters to build and/or preserve more calorie-burning muscle — a boon because losing weight can reduce muscle, especially with rapid loss.
How do these drugs work? What’s their downside? Like the “miracle” glucagon-like peptide 1 (GLP-1) weight-loss drugs that are now ubiquitous, are mimetics an effective pharmaceutical way to replicate two of society’s biggest lifestyle sticking points — diet and exercise?
It’s possible…
CR Mimetics: The Healthspan Drug?
From nematodes and fruit flies to yeast, Labrador Retrievers, and people, plenty of research shows that reducing calorie intake may improve health and prolong life. By how much? Cutting calories by 25% for 2 years slowed the pace of aging 2%-3% in the landmark CALERIE study of 197 adults, according to a 2023 study in Nature Aging. Sounds small, but the researchers said that equals a 10%-15% lower risk for an early death — on par with the longevity bonus you’d get from quitting smoking.
Trouble is low-cal living isn’t easy. “Diets work,” said George Roth, PhD, of GeroScience, Inc., in Pylesville, MD, who began studying CR at the National Institute on Aging in the 1980s with Ingram. “But it’s hard to sustain.”
That’s where CR mimetics come in. They activate the same health-promoting genes switched on by dieting, fasting, and extended periods of hunger, Dr. Roth said. The end result isn’t big weight loss. Instead, CR mimetics may keep us healthier and younger as we age. “Calorie restriction shifts metabolic processes in the body to protect against damage and stress,” he said.
Dr. Roth and Dr. Ingram are currently focused on the CR mimetic mannoheptulose (MH), a sugar found in unripe avocados. “It works at the first step in carbohydrate metabolism in cells throughout the body, so less energy goes through that pathway,” he said. “Glucose metabolism is reduced by 10%-15%. It’s the closest thing to actually eating less food.”
Their 2022 study found that while mice on an all-you-can-eat high-fat diet gained weight and body fat and saw blood lipids increase while insulin sensitivity decreased, mice that also got MH avoided these problems. A 2023 human study in Nutrients coauthored by Dr. Roth and Dr. Ingram found that a group consuming freeze-dried avocado had lower insulin levels than a placebo group.
Other researchers are looking at ways to stimulate the CR target nicotinamide adenine dinucleotide (NAD+). NAD+ assists sirtuins — a group of seven enzymes central to the beneficial effects of CR on aging — but levels drop with age. University of Colorado researchers are studying the effects of nicotinamide riboside (NR), an NAD+ precursor, in older adults with a $2.5 million National Institute on Aging grant. Small, preliminary human studies have found the compound reduced indicators of insulin resistance in the brain, in a January 2023 study in Aging Cell, and reduced blood pressure and arterial stiffness in a 2018 study published in Nature Communications.
Another NAD+ precursor, nicotinamide mononucleotide, reduced low-density lipoprotein cholesterol, diastolic blood pressure, and body weight in a Harvard Medical School study of 30 midlife and older adults with overweight and obesity, published in August 2023 in The Journal of Clinical Endocrinology & Metabolism. And in an April 2022 study published in Hepatology of people with nonalcoholic fatty liver disease, a proprietary supplement that included NR didn’t reduce liver fat but had a significant (vs placebo) reduction in ceramide and the liver enzyme alanine aminotransferase, a marker of inflammation.
“I think it was a pretty interesting result,” said lead researcher Leonard Guarente, PhD, professor of biology at Massachusetts Institute of Technology and founder of the supplement company Elysium. “Fatty liver progressively damages the liver. This has the potential to slow that down.”
Exercise Mimetics: Fitness in a Pill?
Physical activity builds muscle and fitness, helps keeps bones strong, sharpens thinking and memory, guards against depression, and helps discourage a slew of health concerns from weight gain and high blood pressure to diabetes and heart disease. Muscle becomes more dense, more powerful and may even burn more calories, said Dr. Burris. The problem: That pesky part about actually moving. Fewer than half of American adults get recommended amounts of aerobic exercise and fewer than a quarter fit in strength training, according to the Centers for Disease Control and Prevention.
Enter the exercise mimetics. Unlike CR mimetics, exercise mimetics affect mitochondria — the tiny power plants in muscle and every other cell in the body. They switch on genes that encourage the growth of more mitochondria and encourage them to burn fatty acids, not just glucose, for fuel.
In mice, this can keep them from gaining weight, increase insulin sensitivity, and boost exercise endurance. “We can use a drug to activate the same networks that are activated by physical activity,” said Ronald Evans, PhD, professor and director of the Gene Expression Laboratory at the Salk Institute for Biological Studies in La Jolla, California.
Among notable mimetics moving into human studies is ASP0367, a drug in a class called PPAR delta modulators first developed in Evans’ lab. ASP0367 was licensed to the pharmaceutical company Mitobridge, later acquired by Astellas. Astellas is currently running a phase 2/3 human trial of the investigational drug in people with the rare genetic disorder primary mitochondrial myopathy.
At the University of Florida, Dr. Burris and team hope to soon move the exercise mimetic SLU-PP-332 into human studies. “It targets a receptor called ERR that I’ve been working on since the 1980s,” Dr. Burris said. “We knew from genetic studies that ERR has a role in exercise’s effects on mitochondrial function in muscle.” The calorie mimetics he’s studying also activate genes for making more mitochondria and driving them to burn fatty acids. “This generates a lot of energy,” he said. In a January 2024 study in Circulation, Dr. Burris found the drug restores heart function in mice experiencing heart failure. “Very little heart function was lost,” he said. It’s had no serious side effects.
The Future of Exercise and CR Pills
The field has hit some bumps. Some feel inevitable — such as otherwise healthy people misusing the drugs. GW1516, an early experimental exercise mimetic studied by Dr. Evans and abandoned because it triggered tumor growth in lab studies, is used illegally by elite athletes as a performance-enhancing drug despite warnings from the US Anti-Doping Agency. Dr. Burris worries that future CR mimetics could be misused the same way.
But he and others see plenty of benefits in future, FDA-approved drugs. Exercise mimetics like SLU-PP-332 might one day be given to people alongside weight-loss drugs, such as Mounjaro (tirzepatide) or Ozempic (semaglutide) to prevent muscle loss. “SLU-PP-332 doesn’t affect hunger or food intake the way those drugs do,” he said. “It changes muscle.”
Mimetics may one day help older adults and people with muscle disorders rebuild muscle even when they cannot exercise and to delay a range of age-related diseases without onerous dieting. “The chance to intervene and provide a longer healthspan and lifespan — that’s been the moon shot,” Dr. Roth said.
Dr. Guarente noted that CR mimetics may work best for people who aren’t carrying extra pounds but want the health benefits of slashing calories without sacrificing meals and snacks. “Fat is still going to be a problem for joints, cholesterol, inflammation,” he said. “Calorie mimetics are not a panacea for obesity but could help preserve overall health and vitality.”
And what about the billion-dollar question: What happens when these drugs become available to a general public that has issues with actual exercise and healthy diet?
Evans sees only positives. “Our environment is designed to keep people sitting down and consuming high-calorie foods,” he said. “In the absence of people getting motivated to exercise — and there’s no evidence the country is moving in that direction on its own — a pill is an important option to have.”
A version of this article appeared on Medscape.com.