User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
Confronting Healthcare Disinformation on Social Media
More than 90% of internet users are active on social media, which had 4.76 billion users worldwide in January 2023. The digital revolution has reshaped the news landscape and changed how users interact with information. Social media has fostered an active relationship with the media, including the ability to interact directly with the content presented. It also has augmented media’s ability to reach a large audience with tight deadlines.
These developments suggest that social media can be a useful tool in everyday medical practice for professionals and patients. But social media also can spread misinformation, as happened during the COVID-19 pandemic.
This characteristic is the focus of the latest research by Fabiana Zollo, a computer science professor at Ca’ Foscari University of Venice, Italy, and coordinator of the Data Science for Society laboratory. The research was published in The BMJ. Ms. Zollo’s research group aims to assess the effect of social media on misinformation and consequent behaviors related to health. “The study results focus primarily on two topics, the COVID-19 pandemic and vaccinations, but can also be applied to other health-related behaviors such as smoking and diet,” Ms. Zollo told Univadis Italy.
Social media has become an important tool for public health organizations to inform and educate citizens. Institutions can use it to monitor choices and understand which topics are being discussed most at a given time, thus comprehending how the topics evolve and take shape in public discourse. “This could lead to the emergence of people’s perceptions, allowing us to understand, among other things, what the population’s needs might be, including informational needs,” said Ms. Zollo.
Tenuous Causal Link
While social media offers public health organizations the opportunity to inform and engage the public, it also raises concerns about misinformation and the difficulty of measuring its effect on health behavior. Although some studies have observed correlations between exposure to misinformation on social media and levels of adherence to vaccination campaigns, establishing a causal link is complex. As the authors emphasize, “despite the importance of the effect of social media and misinformation on people’s behavior and the broad hypotheses within public and political debates, the current state of the art cannot provide definitive conclusions on a clear causal association between social media and health behaviors.” Establishing a clear causal link between information obtained from social media and offline behavior is challenging due to methodologic limitations and the complexity of connections between online and offline behaviors. Studies often rely on self-reported data, which may not accurately reflect real behaviors, and struggle to isolate the effect of social media from other external influences. Moreover, many studies primarily focus on Western countries, limiting the generalizability of the results to other cultural and geographical conditions.
Another issue highlighted by Ms. Zollo and colleagues is the lack of complete and representative data. Studies often lack detailed information about participants, such as demographic or geolocation data, and rely on limited samples. This lack makes it difficult to assess the effect of misinformation on different segments of the population and in different geographic areas.
“The main methodologic difficulty concerns behavior, which is difficult to measure because it would require tracking a person’s actions over time and having a shared methodology to do so. We need to understand whether online stated intentions do or do not translate into actual behaviors,” said Ms. Zollo. Therefore, despite the recognized importance of the effect of social media and misinformation on people’s general behavior and the broad hypotheses expressed within public and political debates, the current state of the art cannot provide definitive conclusions on a causal association between social media and health behaviors.
Institutions’ Role
Social media is a fertile ground for the formation of echo chambers (where users find themselves dialoguing with like-minded people, forming a distorted impression of the real prevalence of that opinion) and for reinforcing polarized positions around certain topics. “We know that on certain topics, especially those related to health, there is a lot of misinformation circulating precisely because it is easy to leverage factors such as fear and beliefs, even the difficulties in understanding the technical aspects of a message,” said Ms. Zollo. Moreover, institutions have not always provided timely information during the pandemic. “Often, when there is a gap in response to a specific informational need, people turn elsewhere, where those questions find answers. And even if the response is not of high quality, it sometimes confirms the idea that the user had already created in their mind.”
The article published in The BMJ aims primarily to provide information and evaluation insights to institutions rather than professionals or healthcare workers. “We would like to spark the interest of institutions and ministries that can analyze this type of data and integrate it into their monitoring system. Social monitoring (the observation of what happens on social media) is a practice that the World Health Organization is also evaluating and trying to integrate with more traditional tools, such as questionnaires. The aim is to understand as well as possible what a population thinks about a particular health measure, such as a vaccine: Through data obtained from social monitoring, a more realistic and comprehensive view of the problem could be achieved,” said Ms. Zollo.
A Doctor’s Role
And this is where the doctor comes in: All the information thus obtained allows for identifying the needs that the population expresses and that “could push a patient to turn elsewhere, toward sources that provide answers even if of dubious quality or extremely oversimplified.” The doctor can enter this landscape by trying to understand, even with the data provided by institutions, what needs the patients are trying to fill and what drives them to seek elsewhere and to look for a reference community that offers the relevant confirmations.
From the doctor’s perspective, therefore, it can be useful to understand how these dynamics arise and evolve because they could help improve interactions with patients. At the institutional level, social monitoring would be an excellent tool for providing services to doctors who, in turn, offer a service to patients. If it were possible to identify areas where a disinformation narrative is developing from the outset, both the doctor and the institutions would benefit.
Misinformation vs Disinformation
The rapid spread of false or misleading information on social media can undermine trust in healthcare institutions and negatively influence health-related behaviors. Ms. Zollo and colleagues, in fact, speak of misinformation in their discussion, not disinformation. “In English, a distinction is made between misinformation and disinformation, a distinction that we are also adopting in Italian. When we talk about misinformation, we mean information that is generally false, inaccurate, or misleading but has not been created with the intention to harm, an intention that is present in disinformation,” said Ms. Zollo.
The distinction is often not easy to define even at the operational level, but in her studies, Ms. Zollo is mainly interested in understanding how the end user interacts with content, not the purposes for which that content was created. “This allows us to focus on users and the relationships that are created on various social platforms, thus bypassing the author of that information and focusing on how misinformation arises and evolves so that it can be effectively combated before it translates into action (ie, into incorrect health choices),” said Ms. Zollo.
This story was translated from Univadis Italy, which is part of the Medscape Professional Network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
More than 90% of internet users are active on social media, which had 4.76 billion users worldwide in January 2023. The digital revolution has reshaped the news landscape and changed how users interact with information. Social media has fostered an active relationship with the media, including the ability to interact directly with the content presented. It also has augmented media’s ability to reach a large audience with tight deadlines.
These developments suggest that social media can be a useful tool in everyday medical practice for professionals and patients. But social media also can spread misinformation, as happened during the COVID-19 pandemic.
This characteristic is the focus of the latest research by Fabiana Zollo, a computer science professor at Ca’ Foscari University of Venice, Italy, and coordinator of the Data Science for Society laboratory. The research was published in The BMJ. Ms. Zollo’s research group aims to assess the effect of social media on misinformation and consequent behaviors related to health. “The study results focus primarily on two topics, the COVID-19 pandemic and vaccinations, but can also be applied to other health-related behaviors such as smoking and diet,” Ms. Zollo told Univadis Italy.
Social media has become an important tool for public health organizations to inform and educate citizens. Institutions can use it to monitor choices and understand which topics are being discussed most at a given time, thus comprehending how the topics evolve and take shape in public discourse. “This could lead to the emergence of people’s perceptions, allowing us to understand, among other things, what the population’s needs might be, including informational needs,” said Ms. Zollo.
Tenuous Causal Link
While social media offers public health organizations the opportunity to inform and engage the public, it also raises concerns about misinformation and the difficulty of measuring its effect on health behavior. Although some studies have observed correlations between exposure to misinformation on social media and levels of adherence to vaccination campaigns, establishing a causal link is complex. As the authors emphasize, “despite the importance of the effect of social media and misinformation on people’s behavior and the broad hypotheses within public and political debates, the current state of the art cannot provide definitive conclusions on a clear causal association between social media and health behaviors.” Establishing a clear causal link between information obtained from social media and offline behavior is challenging due to methodologic limitations and the complexity of connections between online and offline behaviors. Studies often rely on self-reported data, which may not accurately reflect real behaviors, and struggle to isolate the effect of social media from other external influences. Moreover, many studies primarily focus on Western countries, limiting the generalizability of the results to other cultural and geographical conditions.
Another issue highlighted by Ms. Zollo and colleagues is the lack of complete and representative data. Studies often lack detailed information about participants, such as demographic or geolocation data, and rely on limited samples. This lack makes it difficult to assess the effect of misinformation on different segments of the population and in different geographic areas.
“The main methodologic difficulty concerns behavior, which is difficult to measure because it would require tracking a person’s actions over time and having a shared methodology to do so. We need to understand whether online stated intentions do or do not translate into actual behaviors,” said Ms. Zollo. Therefore, despite the recognized importance of the effect of social media and misinformation on people’s general behavior and the broad hypotheses expressed within public and political debates, the current state of the art cannot provide definitive conclusions on a causal association between social media and health behaviors.
Institutions’ Role
Social media is a fertile ground for the formation of echo chambers (where users find themselves dialoguing with like-minded people, forming a distorted impression of the real prevalence of that opinion) and for reinforcing polarized positions around certain topics. “We know that on certain topics, especially those related to health, there is a lot of misinformation circulating precisely because it is easy to leverage factors such as fear and beliefs, even the difficulties in understanding the technical aspects of a message,” said Ms. Zollo. Moreover, institutions have not always provided timely information during the pandemic. “Often, when there is a gap in response to a specific informational need, people turn elsewhere, where those questions find answers. And even if the response is not of high quality, it sometimes confirms the idea that the user had already created in their mind.”
The article published in The BMJ aims primarily to provide information and evaluation insights to institutions rather than professionals or healthcare workers. “We would like to spark the interest of institutions and ministries that can analyze this type of data and integrate it into their monitoring system. Social monitoring (the observation of what happens on social media) is a practice that the World Health Organization is also evaluating and trying to integrate with more traditional tools, such as questionnaires. The aim is to understand as well as possible what a population thinks about a particular health measure, such as a vaccine: Through data obtained from social monitoring, a more realistic and comprehensive view of the problem could be achieved,” said Ms. Zollo.
A Doctor’s Role
And this is where the doctor comes in: All the information thus obtained allows for identifying the needs that the population expresses and that “could push a patient to turn elsewhere, toward sources that provide answers even if of dubious quality or extremely oversimplified.” The doctor can enter this landscape by trying to understand, even with the data provided by institutions, what needs the patients are trying to fill and what drives them to seek elsewhere and to look for a reference community that offers the relevant confirmations.
From the doctor’s perspective, therefore, it can be useful to understand how these dynamics arise and evolve because they could help improve interactions with patients. At the institutional level, social monitoring would be an excellent tool for providing services to doctors who, in turn, offer a service to patients. If it were possible to identify areas where a disinformation narrative is developing from the outset, both the doctor and the institutions would benefit.
Misinformation vs Disinformation
The rapid spread of false or misleading information on social media can undermine trust in healthcare institutions and negatively influence health-related behaviors. Ms. Zollo and colleagues, in fact, speak of misinformation in their discussion, not disinformation. “In English, a distinction is made between misinformation and disinformation, a distinction that we are also adopting in Italian. When we talk about misinformation, we mean information that is generally false, inaccurate, or misleading but has not been created with the intention to harm, an intention that is present in disinformation,” said Ms. Zollo.
The distinction is often not easy to define even at the operational level, but in her studies, Ms. Zollo is mainly interested in understanding how the end user interacts with content, not the purposes for which that content was created. “This allows us to focus on users and the relationships that are created on various social platforms, thus bypassing the author of that information and focusing on how misinformation arises and evolves so that it can be effectively combated before it translates into action (ie, into incorrect health choices),” said Ms. Zollo.
This story was translated from Univadis Italy, which is part of the Medscape Professional Network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
More than 90% of internet users are active on social media, which had 4.76 billion users worldwide in January 2023. The digital revolution has reshaped the news landscape and changed how users interact with information. Social media has fostered an active relationship with the media, including the ability to interact directly with the content presented. It also has augmented media’s ability to reach a large audience with tight deadlines.
These developments suggest that social media can be a useful tool in everyday medical practice for professionals and patients. But social media also can spread misinformation, as happened during the COVID-19 pandemic.
This characteristic is the focus of the latest research by Fabiana Zollo, a computer science professor at Ca’ Foscari University of Venice, Italy, and coordinator of the Data Science for Society laboratory. The research was published in The BMJ. Ms. Zollo’s research group aims to assess the effect of social media on misinformation and consequent behaviors related to health. “The study results focus primarily on two topics, the COVID-19 pandemic and vaccinations, but can also be applied to other health-related behaviors such as smoking and diet,” Ms. Zollo told Univadis Italy.
Social media has become an important tool for public health organizations to inform and educate citizens. Institutions can use it to monitor choices and understand which topics are being discussed most at a given time, thus comprehending how the topics evolve and take shape in public discourse. “This could lead to the emergence of people’s perceptions, allowing us to understand, among other things, what the population’s needs might be, including informational needs,” said Ms. Zollo.
Tenuous Causal Link
While social media offers public health organizations the opportunity to inform and engage the public, it also raises concerns about misinformation and the difficulty of measuring its effect on health behavior. Although some studies have observed correlations between exposure to misinformation on social media and levels of adherence to vaccination campaigns, establishing a causal link is complex. As the authors emphasize, “despite the importance of the effect of social media and misinformation on people’s behavior and the broad hypotheses within public and political debates, the current state of the art cannot provide definitive conclusions on a clear causal association between social media and health behaviors.” Establishing a clear causal link between information obtained from social media and offline behavior is challenging due to methodologic limitations and the complexity of connections between online and offline behaviors. Studies often rely on self-reported data, which may not accurately reflect real behaviors, and struggle to isolate the effect of social media from other external influences. Moreover, many studies primarily focus on Western countries, limiting the generalizability of the results to other cultural and geographical conditions.
Another issue highlighted by Ms. Zollo and colleagues is the lack of complete and representative data. Studies often lack detailed information about participants, such as demographic or geolocation data, and rely on limited samples. This lack makes it difficult to assess the effect of misinformation on different segments of the population and in different geographic areas.
“The main methodologic difficulty concerns behavior, which is difficult to measure because it would require tracking a person’s actions over time and having a shared methodology to do so. We need to understand whether online stated intentions do or do not translate into actual behaviors,” said Ms. Zollo. Therefore, despite the recognized importance of the effect of social media and misinformation on people’s general behavior and the broad hypotheses expressed within public and political debates, the current state of the art cannot provide definitive conclusions on a causal association between social media and health behaviors.
Institutions’ Role
Social media is a fertile ground for the formation of echo chambers (where users find themselves dialoguing with like-minded people, forming a distorted impression of the real prevalence of that opinion) and for reinforcing polarized positions around certain topics. “We know that on certain topics, especially those related to health, there is a lot of misinformation circulating precisely because it is easy to leverage factors such as fear and beliefs, even the difficulties in understanding the technical aspects of a message,” said Ms. Zollo. Moreover, institutions have not always provided timely information during the pandemic. “Often, when there is a gap in response to a specific informational need, people turn elsewhere, where those questions find answers. And even if the response is not of high quality, it sometimes confirms the idea that the user had already created in their mind.”
The article published in The BMJ aims primarily to provide information and evaluation insights to institutions rather than professionals or healthcare workers. “We would like to spark the interest of institutions and ministries that can analyze this type of data and integrate it into their monitoring system. Social monitoring (the observation of what happens on social media) is a practice that the World Health Organization is also evaluating and trying to integrate with more traditional tools, such as questionnaires. The aim is to understand as well as possible what a population thinks about a particular health measure, such as a vaccine: Through data obtained from social monitoring, a more realistic and comprehensive view of the problem could be achieved,” said Ms. Zollo.
A Doctor’s Role
And this is where the doctor comes in: All the information thus obtained allows for identifying the needs that the population expresses and that “could push a patient to turn elsewhere, toward sources that provide answers even if of dubious quality or extremely oversimplified.” The doctor can enter this landscape by trying to understand, even with the data provided by institutions, what needs the patients are trying to fill and what drives them to seek elsewhere and to look for a reference community that offers the relevant confirmations.
From the doctor’s perspective, therefore, it can be useful to understand how these dynamics arise and evolve because they could help improve interactions with patients. At the institutional level, social monitoring would be an excellent tool for providing services to doctors who, in turn, offer a service to patients. If it were possible to identify areas where a disinformation narrative is developing from the outset, both the doctor and the institutions would benefit.
Misinformation vs Disinformation
The rapid spread of false or misleading information on social media can undermine trust in healthcare institutions and negatively influence health-related behaviors. Ms. Zollo and colleagues, in fact, speak of misinformation in their discussion, not disinformation. “In English, a distinction is made between misinformation and disinformation, a distinction that we are also adopting in Italian. When we talk about misinformation, we mean information that is generally false, inaccurate, or misleading but has not been created with the intention to harm, an intention that is present in disinformation,” said Ms. Zollo.
The distinction is often not easy to define even at the operational level, but in her studies, Ms. Zollo is mainly interested in understanding how the end user interacts with content, not the purposes for which that content was created. “This allows us to focus on users and the relationships that are created on various social platforms, thus bypassing the author of that information and focusing on how misinformation arises and evolves so that it can be effectively combated before it translates into action (ie, into incorrect health choices),” said Ms. Zollo.
This story was translated from Univadis Italy, which is part of the Medscape Professional Network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Severe Salt Restriction May Not Benefit Heart Failure
Strict sodium intake — with or without restrictions on fluid intake — is unlikely to confer clinical benefits on patients with heart failure, reported investigators.
Their review of
In fact, moderate daily intake of sodium (3.0-4.5 g) may improve the quality of life and functional status of these patients, even if it will not improve life expectancy or the hospitalization rate, Paolo Raggi, MD, from the University of Alberta, Edmonton, Alberta, Canada, explained in his narrative review published online in the European Journal of Clinical Investigation.
“It is always a little hard to give up long-held beliefs, and you try to find fault in the new evidence before your eyes,” he said.
Dr. Raggi, who is also coeditor of Atherosclerosis, explained this work was prompted in part by the large, multicenter SODIUM-HF study, which showed that sodium restriction did not reduce the composite outcome of all-cause mortality, cardiovascular hospitalization, and cardiovascular-related emergency department visits, although it did improve quality of life and New York Heart Association class.
And “excessive fluid restriction — typically we were taught to restrict fluid intake to 1 L/d or, at the most, 1.5 L — does not reduce mortality or hospitalization rates and inflicts unnecessary strain and pain on patients,” he said. “Clinicians need to get on board with this novel information.”
Examining the Evidence
For the narrative review, the researchers conducted a literature search for the terms heart failure, salt, sodium, and fluid intake to identify relevant reports.
Most randomized trials were small and examined widely heterogeneous interventions. The identified trials published from 2000 to 2021 had populations that ranged from 12 to 203 participants, had inpatients and outpatients, and included people with reduced and preserved ejection fraction. Sodium interventions varied from extreme reductions (< 800 mg/d) to more moderate approaches (2-3 g/d). No study, regardless of the level of restriction, showed a reduction in mortality or hospitalization rates.
Notably, SODIUM-HF — the randomized clinical trial of sodium restriction to a target of 1.5 g/d — was stopped early after an interim analysis demonstrated the futility of the intervention, and the COVID pandemic made it difficult to continue the trial.
Although a moderate sodium intake of 3-4.5 g/d “seems prudent” for patients with recurrent hospital admissions and fluid overload, an intake of 2-3 g/d may be a more acceptable level. “A more aggressive sodium restriction may be necessary in the presence of chronic kidney disease, where the handling of sodium by the kidneys is hampered,” Dr. Raggi reported.
“The debate on tight sodium restriction in heart failure continues to appear in major medical journals, yet it would seem that after many years of controversy, the time has come to close it,” he said.
‘One Approach Does Not Fit All’
Sodium restriction is difficult to quantify in a large cohort of patients because many studies are based on recall questionnaires and qualitative measurements, said Johanna Contreras, MD, an advanced heart failure and transplant cardiologist at the Mount Sinai Fuster Heart Hospital in New York City.
“Many patients are not aware that processed and precooked foods are very high in sodium and don’t count them as sodium-rich foods,” she said.
Nevertheless, heart failure has many etiologies and stages, so “one approach does not fit all,” she said. For example, patients with stage C heart failure “will clearly get more decompensated when they consume sodium-rich diets, which will increase water absorption.” And patients with heart failure secondary to hypertension are “particularly susceptible” and are likely to become more symptomatic and acutely congestive on diets high in sodium and water, which can increase both morbidity and mortality.
“It is important to understand the kinds of patients we are referring to, how advanced they are, and what comorbidities the patients have,” she said. “We also know that there are race, ethnicity, and gender differences in sensitivity to sodium.”
We should aim for a moderate sodium intake, she said, but patients with high sensitivity, multiple comorbidities, kidney disease, and certain demographic characteristics “need to be more careful.”
Overall, “patients should aim to consume fresh fruits and vegetables and [be aware of] processed foods and adding salt at the table when they are eating,” Dr. Contreras said.
A version of this article first appeared on Medscape.com.
Strict sodium intake — with or without restrictions on fluid intake — is unlikely to confer clinical benefits on patients with heart failure, reported investigators.
Their review of
In fact, moderate daily intake of sodium (3.0-4.5 g) may improve the quality of life and functional status of these patients, even if it will not improve life expectancy or the hospitalization rate, Paolo Raggi, MD, from the University of Alberta, Edmonton, Alberta, Canada, explained in his narrative review published online in the European Journal of Clinical Investigation.
“It is always a little hard to give up long-held beliefs, and you try to find fault in the new evidence before your eyes,” he said.
Dr. Raggi, who is also coeditor of Atherosclerosis, explained this work was prompted in part by the large, multicenter SODIUM-HF study, which showed that sodium restriction did not reduce the composite outcome of all-cause mortality, cardiovascular hospitalization, and cardiovascular-related emergency department visits, although it did improve quality of life and New York Heart Association class.
And “excessive fluid restriction — typically we were taught to restrict fluid intake to 1 L/d or, at the most, 1.5 L — does not reduce mortality or hospitalization rates and inflicts unnecessary strain and pain on patients,” he said. “Clinicians need to get on board with this novel information.”
Examining the Evidence
For the narrative review, the researchers conducted a literature search for the terms heart failure, salt, sodium, and fluid intake to identify relevant reports.
Most randomized trials were small and examined widely heterogeneous interventions. The identified trials published from 2000 to 2021 had populations that ranged from 12 to 203 participants, had inpatients and outpatients, and included people with reduced and preserved ejection fraction. Sodium interventions varied from extreme reductions (< 800 mg/d) to more moderate approaches (2-3 g/d). No study, regardless of the level of restriction, showed a reduction in mortality or hospitalization rates.
Notably, SODIUM-HF — the randomized clinical trial of sodium restriction to a target of 1.5 g/d — was stopped early after an interim analysis demonstrated the futility of the intervention, and the COVID pandemic made it difficult to continue the trial.
Although a moderate sodium intake of 3-4.5 g/d “seems prudent” for patients with recurrent hospital admissions and fluid overload, an intake of 2-3 g/d may be a more acceptable level. “A more aggressive sodium restriction may be necessary in the presence of chronic kidney disease, where the handling of sodium by the kidneys is hampered,” Dr. Raggi reported.
“The debate on tight sodium restriction in heart failure continues to appear in major medical journals, yet it would seem that after many years of controversy, the time has come to close it,” he said.
‘One Approach Does Not Fit All’
Sodium restriction is difficult to quantify in a large cohort of patients because many studies are based on recall questionnaires and qualitative measurements, said Johanna Contreras, MD, an advanced heart failure and transplant cardiologist at the Mount Sinai Fuster Heart Hospital in New York City.
“Many patients are not aware that processed and precooked foods are very high in sodium and don’t count them as sodium-rich foods,” she said.
Nevertheless, heart failure has many etiologies and stages, so “one approach does not fit all,” she said. For example, patients with stage C heart failure “will clearly get more decompensated when they consume sodium-rich diets, which will increase water absorption.” And patients with heart failure secondary to hypertension are “particularly susceptible” and are likely to become more symptomatic and acutely congestive on diets high in sodium and water, which can increase both morbidity and mortality.
“It is important to understand the kinds of patients we are referring to, how advanced they are, and what comorbidities the patients have,” she said. “We also know that there are race, ethnicity, and gender differences in sensitivity to sodium.”
We should aim for a moderate sodium intake, she said, but patients with high sensitivity, multiple comorbidities, kidney disease, and certain demographic characteristics “need to be more careful.”
Overall, “patients should aim to consume fresh fruits and vegetables and [be aware of] processed foods and adding salt at the table when they are eating,” Dr. Contreras said.
A version of this article first appeared on Medscape.com.
Strict sodium intake — with or without restrictions on fluid intake — is unlikely to confer clinical benefits on patients with heart failure, reported investigators.
Their review of
In fact, moderate daily intake of sodium (3.0-4.5 g) may improve the quality of life and functional status of these patients, even if it will not improve life expectancy or the hospitalization rate, Paolo Raggi, MD, from the University of Alberta, Edmonton, Alberta, Canada, explained in his narrative review published online in the European Journal of Clinical Investigation.
“It is always a little hard to give up long-held beliefs, and you try to find fault in the new evidence before your eyes,” he said.
Dr. Raggi, who is also coeditor of Atherosclerosis, explained this work was prompted in part by the large, multicenter SODIUM-HF study, which showed that sodium restriction did not reduce the composite outcome of all-cause mortality, cardiovascular hospitalization, and cardiovascular-related emergency department visits, although it did improve quality of life and New York Heart Association class.
And “excessive fluid restriction — typically we were taught to restrict fluid intake to 1 L/d or, at the most, 1.5 L — does not reduce mortality or hospitalization rates and inflicts unnecessary strain and pain on patients,” he said. “Clinicians need to get on board with this novel information.”
Examining the Evidence
For the narrative review, the researchers conducted a literature search for the terms heart failure, salt, sodium, and fluid intake to identify relevant reports.
Most randomized trials were small and examined widely heterogeneous interventions. The identified trials published from 2000 to 2021 had populations that ranged from 12 to 203 participants, had inpatients and outpatients, and included people with reduced and preserved ejection fraction. Sodium interventions varied from extreme reductions (< 800 mg/d) to more moderate approaches (2-3 g/d). No study, regardless of the level of restriction, showed a reduction in mortality or hospitalization rates.
Notably, SODIUM-HF — the randomized clinical trial of sodium restriction to a target of 1.5 g/d — was stopped early after an interim analysis demonstrated the futility of the intervention, and the COVID pandemic made it difficult to continue the trial.
Although a moderate sodium intake of 3-4.5 g/d “seems prudent” for patients with recurrent hospital admissions and fluid overload, an intake of 2-3 g/d may be a more acceptable level. “A more aggressive sodium restriction may be necessary in the presence of chronic kidney disease, where the handling of sodium by the kidneys is hampered,” Dr. Raggi reported.
“The debate on tight sodium restriction in heart failure continues to appear in major medical journals, yet it would seem that after many years of controversy, the time has come to close it,” he said.
‘One Approach Does Not Fit All’
Sodium restriction is difficult to quantify in a large cohort of patients because many studies are based on recall questionnaires and qualitative measurements, said Johanna Contreras, MD, an advanced heart failure and transplant cardiologist at the Mount Sinai Fuster Heart Hospital in New York City.
“Many patients are not aware that processed and precooked foods are very high in sodium and don’t count them as sodium-rich foods,” she said.
Nevertheless, heart failure has many etiologies and stages, so “one approach does not fit all,” she said. For example, patients with stage C heart failure “will clearly get more decompensated when they consume sodium-rich diets, which will increase water absorption.” And patients with heart failure secondary to hypertension are “particularly susceptible” and are likely to become more symptomatic and acutely congestive on diets high in sodium and water, which can increase both morbidity and mortality.
“It is important to understand the kinds of patients we are referring to, how advanced they are, and what comorbidities the patients have,” she said. “We also know that there are race, ethnicity, and gender differences in sensitivity to sodium.”
We should aim for a moderate sodium intake, she said, but patients with high sensitivity, multiple comorbidities, kidney disease, and certain demographic characteristics “need to be more careful.”
Overall, “patients should aim to consume fresh fruits and vegetables and [be aware of] processed foods and adding salt at the table when they are eating,” Dr. Contreras said.
A version of this article first appeared on Medscape.com.
FROM THE EUROPEAN JOURNAL OF CLINICAL INVESTIGATION
Meat Alternatives May Benefit the Heart
Replacing meat with plant-based meat alternatives (PBMAs) can improve cardiovascular disease risk factors, including low-density lipoprotein cholesterol (LDL-C), a review of randomized controlled trials suggested.
Long-term randomized controlled trials and prospective cohort studies that evaluate cardiovascular disease events such as myocardial infarction and stroke are needed to draw definitive conclusions, according to the authors.
said senior author Ehud Ur, MB, professor of medicine at the University of British Columbia, Vancouver, in Canada, and an endocrinologist at St. Paul’s Hospital in Vancouver.
“However, we also found that there’s a lack of clinical outcome trials that would determine definitively whether plant-based meats are healthy. But certainly, everything points in the direction of cardiovascular benefit,” said Dr. Ur.
The review was published on June 25 in the Canadian Journal of Cardiology.
Ultraprocessed Foods
PBMAs are foods that mimic meats and contain ingredients such as protein derivatives from soy, pea, wheat, and fungi. A growing number of Canadians are limiting meat or excluding it from their diets. Some are opting to eat PBMAs instead.
But most PBMAs are classified as ultraprocessed foods. Such foods are produced primarily from substances extracted from whole food sources, such as sugar, salt, oil, and protein. Alternatively, they may be created in a laboratory using flavor enhancers and food coloring. This classification has caused the public and health professionals to question the potential health implications of PBMAs, said Dr. Ur.
“One of the concerns is that these products are highly processed, and things that are highly processed are considered bad. And so, are you swapping one set of risks for another?” he said.
To shed more light on this question, Dr. Ur’s team, which was led by Matthew Nagra, ND, of the Vancouver Naturopathic Clinic, assessed the literature on PBMAs and their impact on health.
“While the plant-based meat market has experienced significant growth in recent years and more and more Canadians are enjoying plant-based burgers, surprisingly little is known about how these meat alternatives may impact health and, in particular, cardiovascular disease risk,” Dr. Nagra said in a statement. “Thus, we sought to review the available literature on the topic to identify what is currently known and to provide direction for future research.”
Less Saturated Fat, Cholesterol
The researchers assessed the literature that was published from 1970 to 2023 on PBMAs, their contents, nutritional profiles, and impact on cardiovascular disease risk factors, such as cholesterol levels and blood pressure.
They found that, compared with meat, PBMAs had less saturated fat, less cholesterol, more fiber, more carbohydrates, fewer calories, less monounsaturated fat, more polyunsaturated fat, and more sodium.
In addition, several randomized controlled trials showed that PBMAs reduced total cholesterol and LDL-C, as well as apolipoprotein B-100, body weight, and waist circumference. PBMAs were not shown to raise blood pressure, despite some products’ high sodium content.
“No currently available evidence suggests that the concerning aspects of PBMAs (eg, food processing and high sodium content) negate the potential cardiovascular benefits,” wrote the researchers.
Unfortunately, no long-term research has evaluated how these alternatives may affect the risk of developing a myocardial infarction or stroke. Similarly, there is little research on the healthfulness of some common components of PBMAs, such as vital wheat gluten.
To shed light on these important issues would require large clinical trials, involving many patients, and great expense, said Dr. Ur. “Drug companies can afford to do large clinical trials, even if they are expensive to do, because they must do them to get approval for their drug. But these plant-based meats are produced by companies that most likely are not able to do clinical outcome trials. Such trials would have to be done by the National Institutes of Health in the United States, or in Canada, the National Research Council,” he said.
There are many reasons to avoid meat, Dr. Ur added. “There are ethical reasons against killing animals. Then there is the issue of global warming. Meat is a very expensive source of food energy. As an individual, the biggest impact you can make on global warming is to not eat meat. Then there is the argument about personal health, which is where our study comes in. For those people who like the taste of meat and who struggle with giving it up, the PBMAs allow them to have a reasonably diverse diet,” he said.
Are Eggs Healthy?
Meat substitutes are helpful for people who want to reduce their cardiovascular disease risk, J. David Spence, MD, professor emeritus of neurology and clinical pharmacology at the University of Western Ontario in London, Canada, wrote in an accompanying editorial.
“Eating too much meat and egg yolk increases cardiovascular risk, and it’s a challenge for patients to learn to eat less meat and cut out egg yolks. If we can find good substitutes that are tasty and enjoyable, that’s a good thing,” Dr. Spence told this news organization.
“Besides plant-based meat substitutes, there is great potential for reduction of cardiovascular risk with the use of egg substitutes,” he said.
Dr. Spence pointed out that two large egg yolks contain 474 mg of cholesterol, almost twice the amount contained in a Hardee’s Monster Thickburger (265 mg).
Cholesterol elevates plasma levels of toxic metabolites of the intestinal microbiome, such as trimethylamine N-oxide (TMAO). Plasma levels of TMAO increase in a linear fashion with egg consumption, and TMAO is bad for the arteries, said Dr. Spence.
“Eggs are terrible and should not be eaten by people at risk for cardiovascular disease. But people don’t understand that because the egg marketing propaganda has been so effective. The yolk is terrible. The egg marketing board is extremely effective in persuading people that eggs are healthy, and they’re not.”
Dr. Spence recommends using egg substitutes, such as Egg Beaters or Better’n Eggs, instead of whole eggs, and says it’s never too late to switch. “That’s the mistake people make, but the arteries can actually improve,” he said.
No funding source for the study was reported. Dr. Ur and Dr. Spence reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Replacing meat with plant-based meat alternatives (PBMAs) can improve cardiovascular disease risk factors, including low-density lipoprotein cholesterol (LDL-C), a review of randomized controlled trials suggested.
Long-term randomized controlled trials and prospective cohort studies that evaluate cardiovascular disease events such as myocardial infarction and stroke are needed to draw definitive conclusions, according to the authors.
said senior author Ehud Ur, MB, professor of medicine at the University of British Columbia, Vancouver, in Canada, and an endocrinologist at St. Paul’s Hospital in Vancouver.
“However, we also found that there’s a lack of clinical outcome trials that would determine definitively whether plant-based meats are healthy. But certainly, everything points in the direction of cardiovascular benefit,” said Dr. Ur.
The review was published on June 25 in the Canadian Journal of Cardiology.
Ultraprocessed Foods
PBMAs are foods that mimic meats and contain ingredients such as protein derivatives from soy, pea, wheat, and fungi. A growing number of Canadians are limiting meat or excluding it from their diets. Some are opting to eat PBMAs instead.
But most PBMAs are classified as ultraprocessed foods. Such foods are produced primarily from substances extracted from whole food sources, such as sugar, salt, oil, and protein. Alternatively, they may be created in a laboratory using flavor enhancers and food coloring. This classification has caused the public and health professionals to question the potential health implications of PBMAs, said Dr. Ur.
“One of the concerns is that these products are highly processed, and things that are highly processed are considered bad. And so, are you swapping one set of risks for another?” he said.
To shed more light on this question, Dr. Ur’s team, which was led by Matthew Nagra, ND, of the Vancouver Naturopathic Clinic, assessed the literature on PBMAs and their impact on health.
“While the plant-based meat market has experienced significant growth in recent years and more and more Canadians are enjoying plant-based burgers, surprisingly little is known about how these meat alternatives may impact health and, in particular, cardiovascular disease risk,” Dr. Nagra said in a statement. “Thus, we sought to review the available literature on the topic to identify what is currently known and to provide direction for future research.”
Less Saturated Fat, Cholesterol
The researchers assessed the literature that was published from 1970 to 2023 on PBMAs, their contents, nutritional profiles, and impact on cardiovascular disease risk factors, such as cholesterol levels and blood pressure.
They found that, compared with meat, PBMAs had less saturated fat, less cholesterol, more fiber, more carbohydrates, fewer calories, less monounsaturated fat, more polyunsaturated fat, and more sodium.
In addition, several randomized controlled trials showed that PBMAs reduced total cholesterol and LDL-C, as well as apolipoprotein B-100, body weight, and waist circumference. PBMAs were not shown to raise blood pressure, despite some products’ high sodium content.
“No currently available evidence suggests that the concerning aspects of PBMAs (eg, food processing and high sodium content) negate the potential cardiovascular benefits,” wrote the researchers.
Unfortunately, no long-term research has evaluated how these alternatives may affect the risk of developing a myocardial infarction or stroke. Similarly, there is little research on the healthfulness of some common components of PBMAs, such as vital wheat gluten.
To shed light on these important issues would require large clinical trials, involving many patients, and great expense, said Dr. Ur. “Drug companies can afford to do large clinical trials, even if they are expensive to do, because they must do them to get approval for their drug. But these plant-based meats are produced by companies that most likely are not able to do clinical outcome trials. Such trials would have to be done by the National Institutes of Health in the United States, or in Canada, the National Research Council,” he said.
There are many reasons to avoid meat, Dr. Ur added. “There are ethical reasons against killing animals. Then there is the issue of global warming. Meat is a very expensive source of food energy. As an individual, the biggest impact you can make on global warming is to not eat meat. Then there is the argument about personal health, which is where our study comes in. For those people who like the taste of meat and who struggle with giving it up, the PBMAs allow them to have a reasonably diverse diet,” he said.
Are Eggs Healthy?
Meat substitutes are helpful for people who want to reduce their cardiovascular disease risk, J. David Spence, MD, professor emeritus of neurology and clinical pharmacology at the University of Western Ontario in London, Canada, wrote in an accompanying editorial.
“Eating too much meat and egg yolk increases cardiovascular risk, and it’s a challenge for patients to learn to eat less meat and cut out egg yolks. If we can find good substitutes that are tasty and enjoyable, that’s a good thing,” Dr. Spence told this news organization.
“Besides plant-based meat substitutes, there is great potential for reduction of cardiovascular risk with the use of egg substitutes,” he said.
Dr. Spence pointed out that two large egg yolks contain 474 mg of cholesterol, almost twice the amount contained in a Hardee’s Monster Thickburger (265 mg).
Cholesterol elevates plasma levels of toxic metabolites of the intestinal microbiome, such as trimethylamine N-oxide (TMAO). Plasma levels of TMAO increase in a linear fashion with egg consumption, and TMAO is bad for the arteries, said Dr. Spence.
“Eggs are terrible and should not be eaten by people at risk for cardiovascular disease. But people don’t understand that because the egg marketing propaganda has been so effective. The yolk is terrible. The egg marketing board is extremely effective in persuading people that eggs are healthy, and they’re not.”
Dr. Spence recommends using egg substitutes, such as Egg Beaters or Better’n Eggs, instead of whole eggs, and says it’s never too late to switch. “That’s the mistake people make, but the arteries can actually improve,” he said.
No funding source for the study was reported. Dr. Ur and Dr. Spence reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Replacing meat with plant-based meat alternatives (PBMAs) can improve cardiovascular disease risk factors, including low-density lipoprotein cholesterol (LDL-C), a review of randomized controlled trials suggested.
Long-term randomized controlled trials and prospective cohort studies that evaluate cardiovascular disease events such as myocardial infarction and stroke are needed to draw definitive conclusions, according to the authors.
said senior author Ehud Ur, MB, professor of medicine at the University of British Columbia, Vancouver, in Canada, and an endocrinologist at St. Paul’s Hospital in Vancouver.
“However, we also found that there’s a lack of clinical outcome trials that would determine definitively whether plant-based meats are healthy. But certainly, everything points in the direction of cardiovascular benefit,” said Dr. Ur.
The review was published on June 25 in the Canadian Journal of Cardiology.
Ultraprocessed Foods
PBMAs are foods that mimic meats and contain ingredients such as protein derivatives from soy, pea, wheat, and fungi. A growing number of Canadians are limiting meat or excluding it from their diets. Some are opting to eat PBMAs instead.
But most PBMAs are classified as ultraprocessed foods. Such foods are produced primarily from substances extracted from whole food sources, such as sugar, salt, oil, and protein. Alternatively, they may be created in a laboratory using flavor enhancers and food coloring. This classification has caused the public and health professionals to question the potential health implications of PBMAs, said Dr. Ur.
“One of the concerns is that these products are highly processed, and things that are highly processed are considered bad. And so, are you swapping one set of risks for another?” he said.
To shed more light on this question, Dr. Ur’s team, which was led by Matthew Nagra, ND, of the Vancouver Naturopathic Clinic, assessed the literature on PBMAs and their impact on health.
“While the plant-based meat market has experienced significant growth in recent years and more and more Canadians are enjoying plant-based burgers, surprisingly little is known about how these meat alternatives may impact health and, in particular, cardiovascular disease risk,” Dr. Nagra said in a statement. “Thus, we sought to review the available literature on the topic to identify what is currently known and to provide direction for future research.”
Less Saturated Fat, Cholesterol
The researchers assessed the literature that was published from 1970 to 2023 on PBMAs, their contents, nutritional profiles, and impact on cardiovascular disease risk factors, such as cholesterol levels and blood pressure.
They found that, compared with meat, PBMAs had less saturated fat, less cholesterol, more fiber, more carbohydrates, fewer calories, less monounsaturated fat, more polyunsaturated fat, and more sodium.
In addition, several randomized controlled trials showed that PBMAs reduced total cholesterol and LDL-C, as well as apolipoprotein B-100, body weight, and waist circumference. PBMAs were not shown to raise blood pressure, despite some products’ high sodium content.
“No currently available evidence suggests that the concerning aspects of PBMAs (eg, food processing and high sodium content) negate the potential cardiovascular benefits,” wrote the researchers.
Unfortunately, no long-term research has evaluated how these alternatives may affect the risk of developing a myocardial infarction or stroke. Similarly, there is little research on the healthfulness of some common components of PBMAs, such as vital wheat gluten.
To shed light on these important issues would require large clinical trials, involving many patients, and great expense, said Dr. Ur. “Drug companies can afford to do large clinical trials, even if they are expensive to do, because they must do them to get approval for their drug. But these plant-based meats are produced by companies that most likely are not able to do clinical outcome trials. Such trials would have to be done by the National Institutes of Health in the United States, or in Canada, the National Research Council,” he said.
There are many reasons to avoid meat, Dr. Ur added. “There are ethical reasons against killing animals. Then there is the issue of global warming. Meat is a very expensive source of food energy. As an individual, the biggest impact you can make on global warming is to not eat meat. Then there is the argument about personal health, which is where our study comes in. For those people who like the taste of meat and who struggle with giving it up, the PBMAs allow them to have a reasonably diverse diet,” he said.
Are Eggs Healthy?
Meat substitutes are helpful for people who want to reduce their cardiovascular disease risk, J. David Spence, MD, professor emeritus of neurology and clinical pharmacology at the University of Western Ontario in London, Canada, wrote in an accompanying editorial.
“Eating too much meat and egg yolk increases cardiovascular risk, and it’s a challenge for patients to learn to eat less meat and cut out egg yolks. If we can find good substitutes that are tasty and enjoyable, that’s a good thing,” Dr. Spence told this news organization.
“Besides plant-based meat substitutes, there is great potential for reduction of cardiovascular risk with the use of egg substitutes,” he said.
Dr. Spence pointed out that two large egg yolks contain 474 mg of cholesterol, almost twice the amount contained in a Hardee’s Monster Thickburger (265 mg).
Cholesterol elevates plasma levels of toxic metabolites of the intestinal microbiome, such as trimethylamine N-oxide (TMAO). Plasma levels of TMAO increase in a linear fashion with egg consumption, and TMAO is bad for the arteries, said Dr. Spence.
“Eggs are terrible and should not be eaten by people at risk for cardiovascular disease. But people don’t understand that because the egg marketing propaganda has been so effective. The yolk is terrible. The egg marketing board is extremely effective in persuading people that eggs are healthy, and they’re not.”
Dr. Spence recommends using egg substitutes, such as Egg Beaters or Better’n Eggs, instead of whole eggs, and says it’s never too late to switch. “That’s the mistake people make, but the arteries can actually improve,” he said.
No funding source for the study was reported. Dr. Ur and Dr. Spence reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Feds May End Hospital System’s Noncompete Contract for Part-Time Docs
Mount Sinai Health System in New York City is forcing part-time physicians to sign employment contracts that violate their labor rights, according to a June 2024 complaint by the National Labor Relations Board (NLRB).
The complaint stems from no-poaching and confidentiality clauses in the agreements required as a condition of employment, NLRB officials alleged.
according to a copy of the terms included in NLRB’s June 18 complaint.
By requiring the agreements, NLRB officials claimed, Mount Sinai is “interfering with, restraining, and coercing employees” in violation of the National Labor Relations Act. The health system’s “unfair labor practices” affects commerce as outlined under the law, according to the NLRB. The Act bans employers from burdening or obstructing commerce or the free flow of commerce.
Mount Sinai did not respond to requests for comment.
The NLRB’s complaint follows a landmark decision by the Federal Trade Commission (FTC) to ban noncompete agreements nationwide. In April 2024, the FTC voted to prohibit noncompetes indefinitely in an effort to protect workers.
“Noncompete clauses keep wages low, suppress new ideas, and rob the American economy of dynamism, including from the more than 8500 new startups that would be created a year once noncompetes are banned,” FTC Chair Lina M. Khan said in a statement. “The FTC’s final rule to ban noncompetes will ensure Americans have the freedom to pursue a new job, start a new business, or bring a new idea to market.”
Business groups and agencies have since sued to challenge against the ban, including the Chamber of Commerce. The Chamber and other business groups argue that noncompete agreements are important for companies to protect trade secrets, shield recruiting investments, and hide confidential information. The lawsuits are ongoing.
A Physician Blows the Whistle
An anonymous physician first alerted the NLRB to the contract language in November 2023. The doctor was required the sign the hospital system’s agreement for part-time physicians. The complaint does not say if the employee is still employed by the hospital system.
To remedy the unfair labor practices alleged, the NLRB seeks an order requiring the health system to rescind the contract language, stop any actions against current or former employees to enforce the provisions, and make whole any employees who suffered financial losses related to the contract terms.
The allegation against Mount Sinai is among a rising number of grievances filed with the NLRB that claim unfair labor practices. During the first 6 months of fiscal year 2024, unfair labor practice charges filed across the NLRB’s field offices increased 7% — from 9612 in 2023 to 10,278 in 2024, according to a news release.
NLRB, meanwhile has been cracking down on anticompetitive labor practices and confidentiality provisions that prevent employees from speaking out.
In a February 2023 decision for instance, NLRB ruled that an employer violates the National Labor Relations Act by offering severance agreements to workers that include restrictive confidentiality and nondisparagement terms. In 2022, the NLRB and the Federal Trade Commission forged a partnership to more widely combat unfair, anticompetitive, and deceptive business practices.
“Noncompete provisions reasonably tend to chill employees in the exercise of Section 7 rights when the provisions could reasonably be construed by employees to deny them the ability to quit or change jobs by cutting off their access to other employment opportunities that they are qualified for,” NLRB General Counsel Jennifer Abruzzo said in a 2023 release.
Ms. Abruzzo stressed in a memo that NLR Act is committed to an interagency approach to restrictions on the exercise of employee rights, “including limits to workers’ job mobility, information sharing, and referrals to other agencies.”
Mount Sinai Health System must respond to the NLRB’s complaint by July 16, and an administrative law judge is scheduled to hear the case on September 24.
A version of this article first appeared on Medscape.com.
Mount Sinai Health System in New York City is forcing part-time physicians to sign employment contracts that violate their labor rights, according to a June 2024 complaint by the National Labor Relations Board (NLRB).
The complaint stems from no-poaching and confidentiality clauses in the agreements required as a condition of employment, NLRB officials alleged.
according to a copy of the terms included in NLRB’s June 18 complaint.
By requiring the agreements, NLRB officials claimed, Mount Sinai is “interfering with, restraining, and coercing employees” in violation of the National Labor Relations Act. The health system’s “unfair labor practices” affects commerce as outlined under the law, according to the NLRB. The Act bans employers from burdening or obstructing commerce or the free flow of commerce.
Mount Sinai did not respond to requests for comment.
The NLRB’s complaint follows a landmark decision by the Federal Trade Commission (FTC) to ban noncompete agreements nationwide. In April 2024, the FTC voted to prohibit noncompetes indefinitely in an effort to protect workers.
“Noncompete clauses keep wages low, suppress new ideas, and rob the American economy of dynamism, including from the more than 8500 new startups that would be created a year once noncompetes are banned,” FTC Chair Lina M. Khan said in a statement. “The FTC’s final rule to ban noncompetes will ensure Americans have the freedom to pursue a new job, start a new business, or bring a new idea to market.”
Business groups and agencies have since sued to challenge against the ban, including the Chamber of Commerce. The Chamber and other business groups argue that noncompete agreements are important for companies to protect trade secrets, shield recruiting investments, and hide confidential information. The lawsuits are ongoing.
A Physician Blows the Whistle
An anonymous physician first alerted the NLRB to the contract language in November 2023. The doctor was required the sign the hospital system’s agreement for part-time physicians. The complaint does not say if the employee is still employed by the hospital system.
To remedy the unfair labor practices alleged, the NLRB seeks an order requiring the health system to rescind the contract language, stop any actions against current or former employees to enforce the provisions, and make whole any employees who suffered financial losses related to the contract terms.
The allegation against Mount Sinai is among a rising number of grievances filed with the NLRB that claim unfair labor practices. During the first 6 months of fiscal year 2024, unfair labor practice charges filed across the NLRB’s field offices increased 7% — from 9612 in 2023 to 10,278 in 2024, according to a news release.
NLRB, meanwhile has been cracking down on anticompetitive labor practices and confidentiality provisions that prevent employees from speaking out.
In a February 2023 decision for instance, NLRB ruled that an employer violates the National Labor Relations Act by offering severance agreements to workers that include restrictive confidentiality and nondisparagement terms. In 2022, the NLRB and the Federal Trade Commission forged a partnership to more widely combat unfair, anticompetitive, and deceptive business practices.
“Noncompete provisions reasonably tend to chill employees in the exercise of Section 7 rights when the provisions could reasonably be construed by employees to deny them the ability to quit or change jobs by cutting off their access to other employment opportunities that they are qualified for,” NLRB General Counsel Jennifer Abruzzo said in a 2023 release.
Ms. Abruzzo stressed in a memo that NLR Act is committed to an interagency approach to restrictions on the exercise of employee rights, “including limits to workers’ job mobility, information sharing, and referrals to other agencies.”
Mount Sinai Health System must respond to the NLRB’s complaint by July 16, and an administrative law judge is scheduled to hear the case on September 24.
A version of this article first appeared on Medscape.com.
Mount Sinai Health System in New York City is forcing part-time physicians to sign employment contracts that violate their labor rights, according to a June 2024 complaint by the National Labor Relations Board (NLRB).
The complaint stems from no-poaching and confidentiality clauses in the agreements required as a condition of employment, NLRB officials alleged.
according to a copy of the terms included in NLRB’s June 18 complaint.
By requiring the agreements, NLRB officials claimed, Mount Sinai is “interfering with, restraining, and coercing employees” in violation of the National Labor Relations Act. The health system’s “unfair labor practices” affects commerce as outlined under the law, according to the NLRB. The Act bans employers from burdening or obstructing commerce or the free flow of commerce.
Mount Sinai did not respond to requests for comment.
The NLRB’s complaint follows a landmark decision by the Federal Trade Commission (FTC) to ban noncompete agreements nationwide. In April 2024, the FTC voted to prohibit noncompetes indefinitely in an effort to protect workers.
“Noncompete clauses keep wages low, suppress new ideas, and rob the American economy of dynamism, including from the more than 8500 new startups that would be created a year once noncompetes are banned,” FTC Chair Lina M. Khan said in a statement. “The FTC’s final rule to ban noncompetes will ensure Americans have the freedom to pursue a new job, start a new business, or bring a new idea to market.”
Business groups and agencies have since sued to challenge against the ban, including the Chamber of Commerce. The Chamber and other business groups argue that noncompete agreements are important for companies to protect trade secrets, shield recruiting investments, and hide confidential information. The lawsuits are ongoing.
A Physician Blows the Whistle
An anonymous physician first alerted the NLRB to the contract language in November 2023. The doctor was required the sign the hospital system’s agreement for part-time physicians. The complaint does not say if the employee is still employed by the hospital system.
To remedy the unfair labor practices alleged, the NLRB seeks an order requiring the health system to rescind the contract language, stop any actions against current or former employees to enforce the provisions, and make whole any employees who suffered financial losses related to the contract terms.
The allegation against Mount Sinai is among a rising number of grievances filed with the NLRB that claim unfair labor practices. During the first 6 months of fiscal year 2024, unfair labor practice charges filed across the NLRB’s field offices increased 7% — from 9612 in 2023 to 10,278 in 2024, according to a news release.
NLRB, meanwhile has been cracking down on anticompetitive labor practices and confidentiality provisions that prevent employees from speaking out.
In a February 2023 decision for instance, NLRB ruled that an employer violates the National Labor Relations Act by offering severance agreements to workers that include restrictive confidentiality and nondisparagement terms. In 2022, the NLRB and the Federal Trade Commission forged a partnership to more widely combat unfair, anticompetitive, and deceptive business practices.
“Noncompete provisions reasonably tend to chill employees in the exercise of Section 7 rights when the provisions could reasonably be construed by employees to deny them the ability to quit or change jobs by cutting off their access to other employment opportunities that they are qualified for,” NLRB General Counsel Jennifer Abruzzo said in a 2023 release.
Ms. Abruzzo stressed in a memo that NLR Act is committed to an interagency approach to restrictions on the exercise of employee rights, “including limits to workers’ job mobility, information sharing, and referrals to other agencies.”
Mount Sinai Health System must respond to the NLRB’s complaint by July 16, and an administrative law judge is scheduled to hear the case on September 24.
A version of this article first appeared on Medscape.com.
Stroke Recurrence Risk Doubles in Patients With AF Who Stop Anticoagulation Therapy
, a new Danish nationwide cohort study finds.
Among 8,119 patients aged 50 years and older (54.1% male, mean age 78.4), 4.3% had a recurrent stroke within 1 year following discharge for the initial stroke, reported David Gaist, PhD, of Odense University Hospital, Odense, Denmark, and colleagues in JAMA Neurology.
An adjusted analysis found that those who stopped therapy were more than twice as likely to experience another stroke over a mean 2.9 years (13.4% vs 6.8%, adjusted odds ratio [aOR] = 2.13; 95% confidence interval [CI], 1.57-2.89).
The findings highlight the preventive power of OAC therapy, Dr. Gaist said in an interview, and point to the importance of counseling patients about the benefits of the drugs. “Clinicians can provide balanced information on the pros and cons of discontinuing oral anticoagulants as well as lay out plans on when to restart the medication,” he said.
The researchers launched the study “to provide data on how often recurrent ischemic strokes occur in a large, unselected cohort of patients with atrial fibrillation who had a stroke and started or restarted oral anticoagulants, a situation mirroring what we see in our everyday lives as clinicians,” Dr. Gaist said. “We also wanted to see if patients with breakthrough strokes had particular characteristics compared with patients who did not have a recurrent stroke. Finally, we wanted to quantify a very simple cause of breakthrough stroke by answering the following question: How many of these patients had stopped taking their oral anticoagulant?”
A Large, Unselected Patient Cohort
Dr. Gaist and colleagues tracked 8,119 patients with ischemic stroke and atrial fibrillation who started or restarted OAC therapy within 30 days following their discharge between 2014 and 2021. Patients either had atrial fibrillation before their stroke or developed it afterward.
Eighty-one percent of patients had hypertension, 19.7% had diabetes, and 27.3% had ischemic heart disease; 35.3% had never smoked and smoking information was missing for 15.9%. Race/ethnicity information was not provided.
Patients were followed for an average of 2.9 years until 2022, and all were alive at least 30 days after discharge. During that time, 663 patients had a recurrent ischemic stroke (4.3%), of whom 80.4% were on OAC therapy. The percentage who had stroke at 2 years rose to 6.5%.
While the researchers thought the number of strokes was high, Dr. Gaist said, this isn’t a sign that the drugs aren’t working. “Oral anticoagulant use in secondary prevention in atrial fibrillation is guideline-supported as it has been proven to reduce the risk of stroke by roughly two thirds.”
Of study participants at baseline, 37.9% took oral anticoagulants, 23.5% took direct oral anticoagulants (DOACs; dabigatran, rivaroxaban, apixaban, and edoxaban), and 15.1% took vitamin K antagonists. In a nested case-control analysis of 663 cases (58.7% men, mean age 80.1) matched to 2,652 controls, at admission for ischemic stroke, 80.4% were on OAC therapy, and 8%-11% of patients stopped OAC therapy after their strokes, the researchers reported.
Patients who stopped OAC therapy had more severe strokes than those who didn’t at 7 days (median recurrent ischemic stroke Scandinavian Stroke Scale [SSS] score = 40.0 vs 46.0, respectively; aOR = 2.10; 95% CI, 1.31-3.36). Those who stopped OAC therapy also had higher mortality rates at 7 days (11.2% vs 3.9%, respectively) and 30 days (28.1% vs 10.9%, respectively).
It’s not clear why some patients discontinued OAC therapy. “We looked for evidence of serious bleeding or surgical procedures around the time of anticoagulant discontinuation but found this only to be the case in roughly 10% of these patients,” Dr. Gaist said.
He added that the study probably “underestimates the issue of anticoagulant discontinuation, particularly for DOACs, where a shorter half-life compared with warfarin means that even a short drug-break of a few days puts the patient at increased risk of stroke.”
The authors noted study limitations, including the lack of data on actual medication usage, alcohol usage, stroke etiology, lesion location, and socioeconomic status. And, they wrote, the study population is mostly of European origin.
No Surprises
Steven R. Messe, MD, professor of neurology at the Hospital of the University of Pennsylvania, Philadelphia, who didn’t take part in the study but is familiar with its findings, said in an interview that the study is a “well-done analysis.”
The findings are not surprising, he said. “The overall risk of stroke recurrence was 4.3% at 1 year while the mortality rate was higher at 15.4%. Given that the median CHA2DS2-VASc score was 4 and the average age was 79, the stroke recurrence rate and mortality rate are in line with prior studies.”
In regard to the power of OAC therapy to prevent recurrent strokes, Dr. Messe noted that patients may not be adhering to prescribed regimens. Also, “while DOACs are clearly safer that vitamin K–dependent anticoagulants, the medications are generally not dose adjusted. It is possible that adjusting the dose based on measured anti-Xa levels to insure therapeutic anticoagulant effects may reduce the stroke risk further.”
He added that “most of these patients with prior stroke and atrial fibrillation are vasculopathic and at risk of additional strokes due to other mechanisms such as small vessel or large vessel disease.”
In the big picture, the study “confirms again that anticoagulation should be prescribed to all patients with atrial fibrillation and prior stroke, unless there is a strong bleeding risk contraindication,” Dr. Messe said. These patients are clearly at high risk of stroke recurrence and mortality, and all risk factors should be aggressively managed.”
Researchers are exploring other options, he said. “For example, there are studies of factor XI inhibitors that could be added to a DOAC for additional reductions in ischemic stroke. In addition, in patients undergoing cardiac surgery, the randomized trial LAOS III demonstrated that surgical left atrial occlusion in addition to anticoagulation may provide additional stroke prevention.”
Dr. Gaist disclosed personal fees from Pfizer and Bristol Myers Squibb, and grants from Bayer. Several other authors reported various relationships with industry. Dr. Messe has no disclosures.
, a new Danish nationwide cohort study finds.
Among 8,119 patients aged 50 years and older (54.1% male, mean age 78.4), 4.3% had a recurrent stroke within 1 year following discharge for the initial stroke, reported David Gaist, PhD, of Odense University Hospital, Odense, Denmark, and colleagues in JAMA Neurology.
An adjusted analysis found that those who stopped therapy were more than twice as likely to experience another stroke over a mean 2.9 years (13.4% vs 6.8%, adjusted odds ratio [aOR] = 2.13; 95% confidence interval [CI], 1.57-2.89).
The findings highlight the preventive power of OAC therapy, Dr. Gaist said in an interview, and point to the importance of counseling patients about the benefits of the drugs. “Clinicians can provide balanced information on the pros and cons of discontinuing oral anticoagulants as well as lay out plans on when to restart the medication,” he said.
The researchers launched the study “to provide data on how often recurrent ischemic strokes occur in a large, unselected cohort of patients with atrial fibrillation who had a stroke and started or restarted oral anticoagulants, a situation mirroring what we see in our everyday lives as clinicians,” Dr. Gaist said. “We also wanted to see if patients with breakthrough strokes had particular characteristics compared with patients who did not have a recurrent stroke. Finally, we wanted to quantify a very simple cause of breakthrough stroke by answering the following question: How many of these patients had stopped taking their oral anticoagulant?”
A Large, Unselected Patient Cohort
Dr. Gaist and colleagues tracked 8,119 patients with ischemic stroke and atrial fibrillation who started or restarted OAC therapy within 30 days following their discharge between 2014 and 2021. Patients either had atrial fibrillation before their stroke or developed it afterward.
Eighty-one percent of patients had hypertension, 19.7% had diabetes, and 27.3% had ischemic heart disease; 35.3% had never smoked and smoking information was missing for 15.9%. Race/ethnicity information was not provided.
Patients were followed for an average of 2.9 years until 2022, and all were alive at least 30 days after discharge. During that time, 663 patients had a recurrent ischemic stroke (4.3%), of whom 80.4% were on OAC therapy. The percentage who had stroke at 2 years rose to 6.5%.
While the researchers thought the number of strokes was high, Dr. Gaist said, this isn’t a sign that the drugs aren’t working. “Oral anticoagulant use in secondary prevention in atrial fibrillation is guideline-supported as it has been proven to reduce the risk of stroke by roughly two thirds.”
Of study participants at baseline, 37.9% took oral anticoagulants, 23.5% took direct oral anticoagulants (DOACs; dabigatran, rivaroxaban, apixaban, and edoxaban), and 15.1% took vitamin K antagonists. In a nested case-control analysis of 663 cases (58.7% men, mean age 80.1) matched to 2,652 controls, at admission for ischemic stroke, 80.4% were on OAC therapy, and 8%-11% of patients stopped OAC therapy after their strokes, the researchers reported.
Patients who stopped OAC therapy had more severe strokes than those who didn’t at 7 days (median recurrent ischemic stroke Scandinavian Stroke Scale [SSS] score = 40.0 vs 46.0, respectively; aOR = 2.10; 95% CI, 1.31-3.36). Those who stopped OAC therapy also had higher mortality rates at 7 days (11.2% vs 3.9%, respectively) and 30 days (28.1% vs 10.9%, respectively).
It’s not clear why some patients discontinued OAC therapy. “We looked for evidence of serious bleeding or surgical procedures around the time of anticoagulant discontinuation but found this only to be the case in roughly 10% of these patients,” Dr. Gaist said.
He added that the study probably “underestimates the issue of anticoagulant discontinuation, particularly for DOACs, where a shorter half-life compared with warfarin means that even a short drug-break of a few days puts the patient at increased risk of stroke.”
The authors noted study limitations, including the lack of data on actual medication usage, alcohol usage, stroke etiology, lesion location, and socioeconomic status. And, they wrote, the study population is mostly of European origin.
No Surprises
Steven R. Messe, MD, professor of neurology at the Hospital of the University of Pennsylvania, Philadelphia, who didn’t take part in the study but is familiar with its findings, said in an interview that the study is a “well-done analysis.”
The findings are not surprising, he said. “The overall risk of stroke recurrence was 4.3% at 1 year while the mortality rate was higher at 15.4%. Given that the median CHA2DS2-VASc score was 4 and the average age was 79, the stroke recurrence rate and mortality rate are in line with prior studies.”
In regard to the power of OAC therapy to prevent recurrent strokes, Dr. Messe noted that patients may not be adhering to prescribed regimens. Also, “while DOACs are clearly safer that vitamin K–dependent anticoagulants, the medications are generally not dose adjusted. It is possible that adjusting the dose based on measured anti-Xa levels to insure therapeutic anticoagulant effects may reduce the stroke risk further.”
He added that “most of these patients with prior stroke and atrial fibrillation are vasculopathic and at risk of additional strokes due to other mechanisms such as small vessel or large vessel disease.”
In the big picture, the study “confirms again that anticoagulation should be prescribed to all patients with atrial fibrillation and prior stroke, unless there is a strong bleeding risk contraindication,” Dr. Messe said. These patients are clearly at high risk of stroke recurrence and mortality, and all risk factors should be aggressively managed.”
Researchers are exploring other options, he said. “For example, there are studies of factor XI inhibitors that could be added to a DOAC for additional reductions in ischemic stroke. In addition, in patients undergoing cardiac surgery, the randomized trial LAOS III demonstrated that surgical left atrial occlusion in addition to anticoagulation may provide additional stroke prevention.”
Dr. Gaist disclosed personal fees from Pfizer and Bristol Myers Squibb, and grants from Bayer. Several other authors reported various relationships with industry. Dr. Messe has no disclosures.
, a new Danish nationwide cohort study finds.
Among 8,119 patients aged 50 years and older (54.1% male, mean age 78.4), 4.3% had a recurrent stroke within 1 year following discharge for the initial stroke, reported David Gaist, PhD, of Odense University Hospital, Odense, Denmark, and colleagues in JAMA Neurology.
An adjusted analysis found that those who stopped therapy were more than twice as likely to experience another stroke over a mean 2.9 years (13.4% vs 6.8%, adjusted odds ratio [aOR] = 2.13; 95% confidence interval [CI], 1.57-2.89).
The findings highlight the preventive power of OAC therapy, Dr. Gaist said in an interview, and point to the importance of counseling patients about the benefits of the drugs. “Clinicians can provide balanced information on the pros and cons of discontinuing oral anticoagulants as well as lay out plans on when to restart the medication,” he said.
The researchers launched the study “to provide data on how often recurrent ischemic strokes occur in a large, unselected cohort of patients with atrial fibrillation who had a stroke and started or restarted oral anticoagulants, a situation mirroring what we see in our everyday lives as clinicians,” Dr. Gaist said. “We also wanted to see if patients with breakthrough strokes had particular characteristics compared with patients who did not have a recurrent stroke. Finally, we wanted to quantify a very simple cause of breakthrough stroke by answering the following question: How many of these patients had stopped taking their oral anticoagulant?”
A Large, Unselected Patient Cohort
Dr. Gaist and colleagues tracked 8,119 patients with ischemic stroke and atrial fibrillation who started or restarted OAC therapy within 30 days following their discharge between 2014 and 2021. Patients either had atrial fibrillation before their stroke or developed it afterward.
Eighty-one percent of patients had hypertension, 19.7% had diabetes, and 27.3% had ischemic heart disease; 35.3% had never smoked and smoking information was missing for 15.9%. Race/ethnicity information was not provided.
Patients were followed for an average of 2.9 years until 2022, and all were alive at least 30 days after discharge. During that time, 663 patients had a recurrent ischemic stroke (4.3%), of whom 80.4% were on OAC therapy. The percentage who had stroke at 2 years rose to 6.5%.
While the researchers thought the number of strokes was high, Dr. Gaist said, this isn’t a sign that the drugs aren’t working. “Oral anticoagulant use in secondary prevention in atrial fibrillation is guideline-supported as it has been proven to reduce the risk of stroke by roughly two thirds.”
Of study participants at baseline, 37.9% took oral anticoagulants, 23.5% took direct oral anticoagulants (DOACs; dabigatran, rivaroxaban, apixaban, and edoxaban), and 15.1% took vitamin K antagonists. In a nested case-control analysis of 663 cases (58.7% men, mean age 80.1) matched to 2,652 controls, at admission for ischemic stroke, 80.4% were on OAC therapy, and 8%-11% of patients stopped OAC therapy after their strokes, the researchers reported.
Patients who stopped OAC therapy had more severe strokes than those who didn’t at 7 days (median recurrent ischemic stroke Scandinavian Stroke Scale [SSS] score = 40.0 vs 46.0, respectively; aOR = 2.10; 95% CI, 1.31-3.36). Those who stopped OAC therapy also had higher mortality rates at 7 days (11.2% vs 3.9%, respectively) and 30 days (28.1% vs 10.9%, respectively).
It’s not clear why some patients discontinued OAC therapy. “We looked for evidence of serious bleeding or surgical procedures around the time of anticoagulant discontinuation but found this only to be the case in roughly 10% of these patients,” Dr. Gaist said.
He added that the study probably “underestimates the issue of anticoagulant discontinuation, particularly for DOACs, where a shorter half-life compared with warfarin means that even a short drug-break of a few days puts the patient at increased risk of stroke.”
The authors noted study limitations, including the lack of data on actual medication usage, alcohol usage, stroke etiology, lesion location, and socioeconomic status. And, they wrote, the study population is mostly of European origin.
No Surprises
Steven R. Messe, MD, professor of neurology at the Hospital of the University of Pennsylvania, Philadelphia, who didn’t take part in the study but is familiar with its findings, said in an interview that the study is a “well-done analysis.”
The findings are not surprising, he said. “The overall risk of stroke recurrence was 4.3% at 1 year while the mortality rate was higher at 15.4%. Given that the median CHA2DS2-VASc score was 4 and the average age was 79, the stroke recurrence rate and mortality rate are in line with prior studies.”
In regard to the power of OAC therapy to prevent recurrent strokes, Dr. Messe noted that patients may not be adhering to prescribed regimens. Also, “while DOACs are clearly safer that vitamin K–dependent anticoagulants, the medications are generally not dose adjusted. It is possible that adjusting the dose based on measured anti-Xa levels to insure therapeutic anticoagulant effects may reduce the stroke risk further.”
He added that “most of these patients with prior stroke and atrial fibrillation are vasculopathic and at risk of additional strokes due to other mechanisms such as small vessel or large vessel disease.”
In the big picture, the study “confirms again that anticoagulation should be prescribed to all patients with atrial fibrillation and prior stroke, unless there is a strong bleeding risk contraindication,” Dr. Messe said. These patients are clearly at high risk of stroke recurrence and mortality, and all risk factors should be aggressively managed.”
Researchers are exploring other options, he said. “For example, there are studies of factor XI inhibitors that could be added to a DOAC for additional reductions in ischemic stroke. In addition, in patients undergoing cardiac surgery, the randomized trial LAOS III demonstrated that surgical left atrial occlusion in addition to anticoagulation may provide additional stroke prevention.”
Dr. Gaist disclosed personal fees from Pfizer and Bristol Myers Squibb, and grants from Bayer. Several other authors reported various relationships with industry. Dr. Messe has no disclosures.
FROM JAMA NEUROLOGY
Does An Elevated Lp(a) Call for Low-dose Aspirin?
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
Should a patient with high lipoprotein (a), or Lp(a), be started on low-dose aspirin?
This is the conundrum facing many physicians and patients, but even getting to that point will require more availability and coverage of tests and a greater appreciation of the risk associated with Lp(a), said cardiologists.
Lp(a): The Silent Risk
On Lp(a) Awareness Day, C. Michael Gibson, MD, MA, CEO of the Baim Institute for Clinical Research, Boston, Massachusetts, and PERFUSE took the opportunity to talk about his experiences with testing on X.
The professor of medicine at Harvard Medical School, also in Boston, said he was surprised to find that he had a very high calcium score, despite a low-density lipoprotein (LDL) cholesterol level of just 70 mg/dL. Eventually, he found out that he had a “very, very high Lp(a),” which was particularly concerning because his grandfather died of a heart attack at 45 years of age.
But how much risk does that represent?
A 2022 consensus statement from the European Atherosclerosis Society (EAS) highlighted that epidemiologic and genetic studies “strongly support a causal and continuous association between Lp(a) concentration and cardiovascular outcomes,” even at very low LDL cholesterol levels.
This is because Lp(a) has proinflammatory and proatherosclerotic properties, and high levels are associated with both micro- and macrocalcification of the aortic valve. Findings from a US registry study also suggest the threshold related to increased cardiovascular risk may differ for primary and secondary prevention populations (J Am Coll Cardiol. 2024 Mar 5;83[9]:873-886).
Lp(a) is, however, genetically determined, and there are no drugs available that directly lower levels, although some are on the horizon. In the meantime, the experts behind the consensus statement recommend that all adults be tested at least once in their lifetime.
Testing Cost and Availability
This recommendation has been translated into guidelines in “many, many” countries, said lead author Florian Kronenberg, MD, MAE, Institute of Genetic Epidemiology, Medical University of Innsbruck, Innsbruck, Austria, but “we are far away from reaching that goal.”
“We’ve got a real problem,” added Stephen Nicholls, MD, PhD, director of the Victorian Heart Institute and a professor of cardiology at Monash University, Melbourne, Australia, as there is “not a country in the world where there’s good access to Lp(a) testing.”
Dr. Kronenberg said that the consensus statement “created a kind of momentum” toward universal testing.
Ulrich Laufs, MD, PhD, professor and chair, Department of Cardiology, University Hospital Leipzig, Leipzig, Germany, agreed, saying that, overall, Lp(a) testing has “increased dramatically,” albeit from “extremely low levels.”
Dr. Kronenberg believes that “we have to be really patient.” He cited a lack of knowledge among physicians as one of the biggest barriers to greater uptake of testing.
“There is still no appreciation of the role of Lp(a),” agreed Alberico L. Catapano, MD, PhD, director of Cardiovascular Research and of the Lipoproteins and Atherosclerosis Laboratory of IRCCS Multimedica, Milan, Italy, and past president of the EAS.
“That’s why it’s not mentioned” to patients, he said. “What is really needed is to inform physician colleagues that Lp(a) is not only a risk factor but is the cause” of atherosclerotic cardiovascular disease (ASCVD).
Dr. Kronenberg said that the pressure for testing can often come from the patient themselves.
Physicians then question why the patient wants to be tested when there are no medications to treat it, he added. “We really tried very hard when we did the consensus paper to say that we should perform the test and give people advice on what to do.”
Dr. Catapano believes that another major obstacle is the cost of the test, which remains high “because very few people do it,” and there is some debate over which test to use.
Taken together, these issues have meant that “payers are really struggling with the idea of funding Lp(a),” said Dr. Nicholls, adding that “there seems to be this fixation on: ‘Well, if you can’t lower Lp(a), why measure it?’ ”
Rather than blame the payers, he says there is a need to educate about the science behind testing and underline that Lp(a) is an “important risk enhancer” for cardiovascular disease.
“Because if we’re going to make people pay out of pocket, then you’re creating a massive equity issue in that only those who can afford the test have it.”
High Lp(a) Now What?
But once the test has been performed, there then comes the question as to what to do about the result.
“Before we get anywhere near an agent that effectively lowers Lp(a) and get it into the clinic, there are lots of things that we can do today,” said Dr. Nicholls.
If someone has an intermediate or high background cardiovascular risk and they have got a high Lp(a) level, they “should be treated more intensively, as we know that high Lp(a) patients do better if their LDL cholesterol and their blood pressure is lower.”
For Dr. Catapano, this means having the “same mindset as you do with [a patient with] high blood pressure, high LDL cholesterol, and so on, because it’s exactly the same thing: It’s interacting with your other risk factors to increase your overall risk.”
Dr. Gibson agreed. Through a range of measures, including weight loss and statin therapy, he was able to reduce his overall cardiovascular risk, and his LDL cholesterol level dropped to just 20 mg/dL.
A Role for Aspirin?
It gained added momentum when Pablo Corral, MD, a lipidologist and a professor in the School of Medicine, Pharmacology Department, FASTA University, Mar del Plata, Buenos Aires, Argentina, highlighted the issue on X.
He pointed to a recent study, which showed that regular aspirin use was associated with a significantly lower rate of ASCVD mortality in adults without clinical ASCVD but who had elevated Lp(a).
Dr. Nicholls said that, when you “peel away the layers” of the current evidence, there is some suggestion that Lp(a)may be prothrombotic. “So in theory, perhaps aspirin might be maybe more intuitively useful there.”
He noted that the ASPREE primary prevention study found that low-dose aspirin in older adults resulted in a significantly higher risk for major hemorrhage over placebo and did not significantly reduce the risk for cardiovascular disease.
But an analysis he and his colleagues did suggest that aspirin may indeed benefit older individuals if they have elevated Lp(a) genotypes.
An Individual Decision
For Dr. Kronenberg and Dr. Laufs, there is currently a lack of appropriate data to make a recommendation either way, particularly for primary prevention.
They warned that the risk for thrombosis in patients with mildly elevated Lp(a) cannot be discounted, and in most cases either “the existing risk of bleeding exceeds the beneficial effects [of aspirin], or it’s not indicated,” said Dr. Laufs.
“When we make a recommendation, we should have evidence-based data,” Dr. Kronenberg said, but, at the moment, people “somehow put their finger in the air and see” which way the wind is blowing.
Dr. Catapano urged patients to talk to their physician, as even low-dose aspirin is “very potent” at inhibiting platelets.
Dr. Gibson agreed, saying that he is in two minds, as the potential benefit has to be weighed against the bleeding risk.
He personally takes low-dose aspirin because “I know I have a low bleeding risk,” but it is a decision “that has to be taken individually between a patient and their physician.”
Dr. Gibson, Dr. Kronenberg, Dr. Nicholls, and Dr. Catapano all reported conflicts of interest with numerous pharmaceutical companies and organizations.
A version of this article first appeared on Medscape.com.
Facial Temperature Can Reveal Age and Disease
This transcript has been edited for clarity.
My oldest daughter is at sleepaway camp for a couple of weeks, and the camp has a photographer who goes around all day taking pictures of the kids, which get uploaded to a private Facebook group. In the past, I would go online every day (or, okay, several times a day) and scroll through all those pictures looking for one that features my kid.
I don’t have to do that anymore. This year, I simply uploaded a picture of my daughter to an app and artificial intelligence (AI) takes care of the rest, recognizing her face amidst the sea of smiling children, and flagging just those photos for me to peruse. It’s amazing, really. And a bit scary.
The fact that facial recognition has penetrated the summer camp market should tell you that the tech is truly ubiquitous. But today we’re going to think a bit more about what AI can do with a picture of your face, because the power of facial recognition is not just skin deep.
What’s got me hot and bothered about facial images is this paper, appearing in Cell Metabolism, which adds a new layer to the standard facial-analysis playbook: facial temperature.
To understand this paper, you need to understand a whole field of research that is developing various different “clocks” for age.
It turns out that age really is just a number. Our cells, our proteins, our biochemistry can be analyzed to give different numbers. These “clocks,” as distinct from the calendar we usually use to measure our age, might have more predictive power than the number itself.
There are numerous molecular clocks, such as telomere length, that not only correlate with calendar age but are superior to calendar age in predicting age-related complications. Testing telomere length typically requires a blood sample — and remains costly. But we can use other sources to estimate age; how about a photo?
I mean, we do this all the time when we meet someone new or, as a physician, when we meet a new patient. I have often written that a patient “appears younger than their stated age,” and we’ve all had the experience of hearing how old someone is and being shocked. I mean, have you seen Sharon Stone recently? She’s 66 years old. Okay — to be fair, there might be some outside help there. But you get the point.
Back to the Cell Metabolism paper. Researchers report on multiple algorithms to obtain an “age” from a picture of an individual’s face.
The first algorithm is pretty straightforward. Researchers collected 2811 images, all of Han Chinese individuals ranging in age from 20 to 90 years, and reconstructed a 3D facial map from those. 
They then trained a convolutional neural network to predict the individuals’ ages from the pictures. It was quite accurate, as you can see here.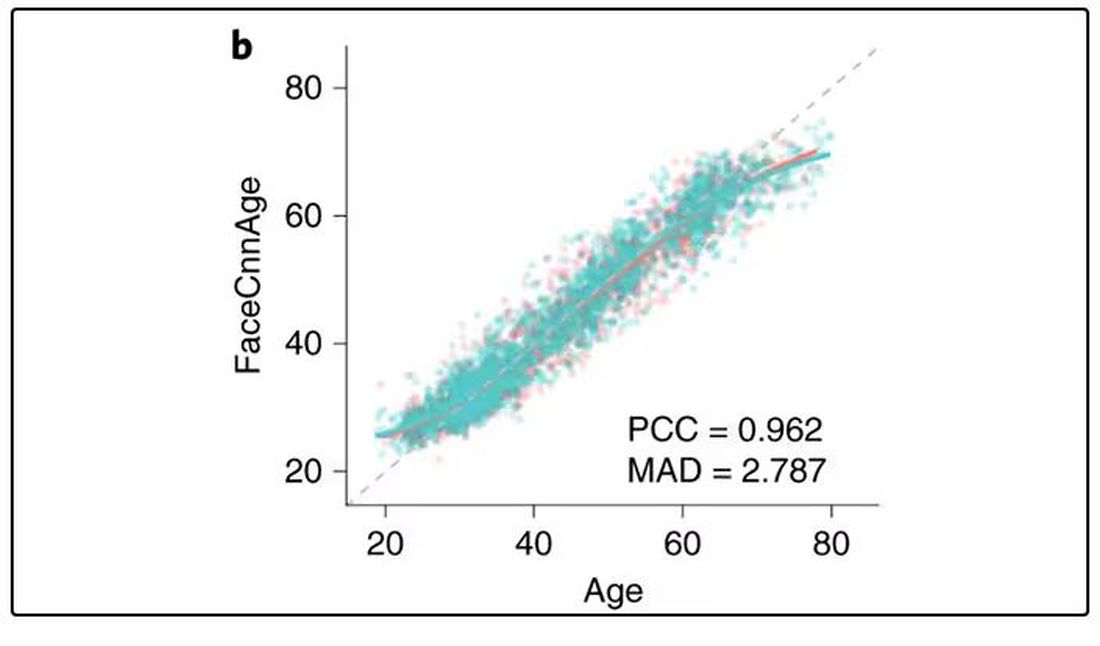
In the AI age, this may not seem that impressive. A brief search online turned up dozens of apps that promised to guess my age from a photo.
I sent this rather unflattering picture of myself to ChatGPT which, after initially demurring and saying it was not designed to guess ages, pegged me at somewhere between 35 and 45, which I am taking as a major victory.
But the Cell Metabolism paper goes deeper. Literally. 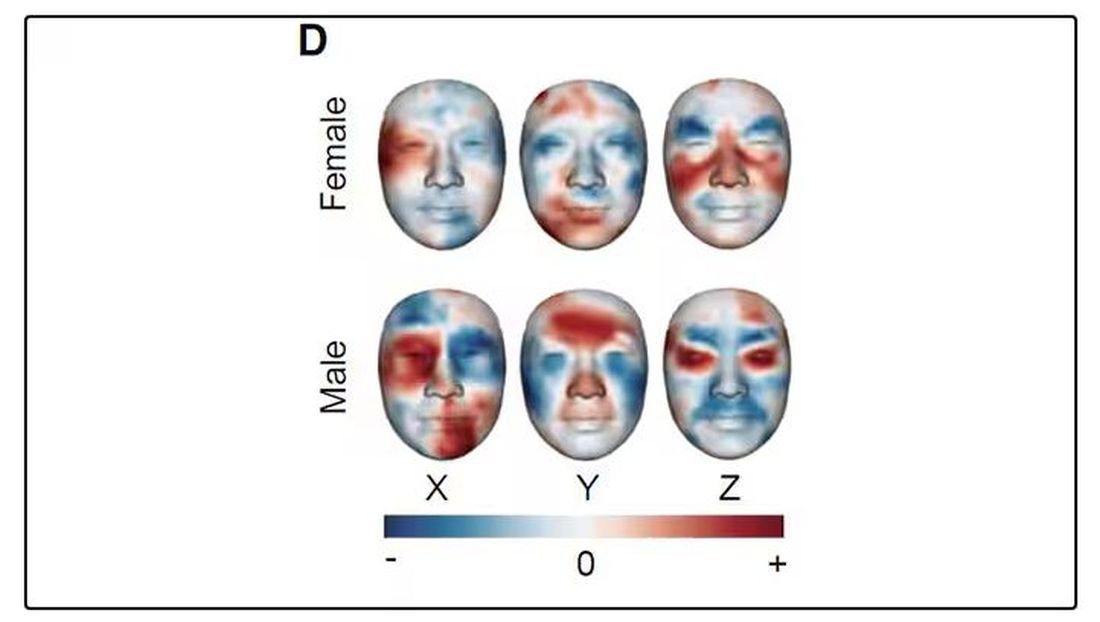
And this is where things start to get interesting. Because sure, the visible part of your face can change depending on makeup, expression, plastic surgery, and the like. But the temperature? That’s harder to fake.
It turns out that the temperature distribution in your face changes as you get older. There is a cooling of the nose and the cheeks, for example.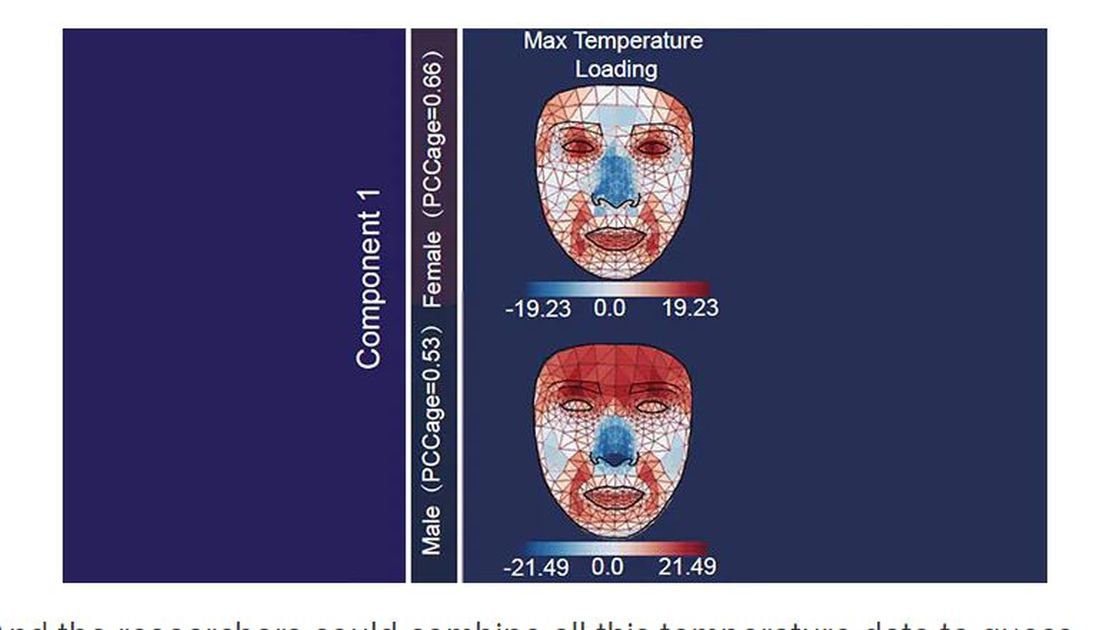
And the researchers could combine all this temperature data to guess someone’s calendar age fairly accurately, though notably not as accurately as the model that just looks at the pictures.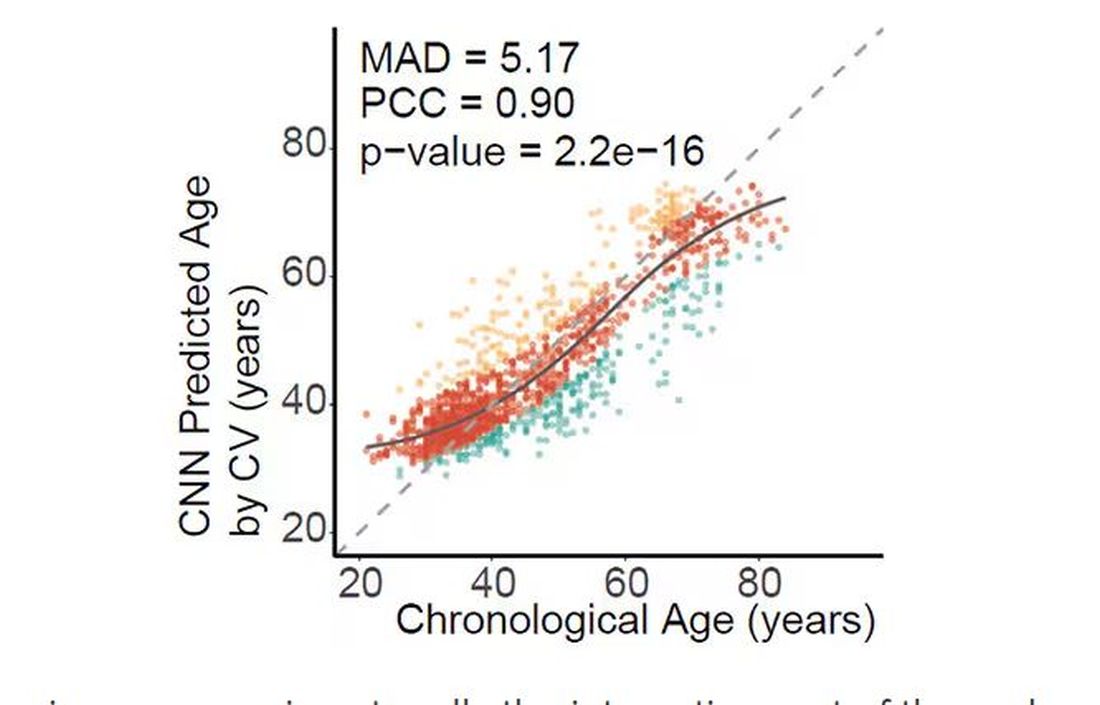
But guessing your age is not really the interesting part of thermal imaging of the face. It’s guessing — or, rather, predicting — the state of your metabolism. All these study participants had extensive metabolic testing performed, as well as detailed analysis of their lifestyle behaviors. And facial images could be used to predict those factors.
For example, the 3D reconstruction of the faces could predict who ate seafood (they tend to look younger than their actual age) compared with who ate poultry and meat (they tend to look older). The thermal imaging could predict who got more sleep (they look younger from a temperature perspective) and who ate more yogurt (also younger-appearing, temperature-wise). Facial temperature patterns could identify those with higher BMI, higher blood pressure, higher fasting glucose.
The researchers used the difference between actual and predicted age as a metric to measure illness as well. You can see here how, on average, individuals with hypertension, diabetes, and even liver cysts are “older,” at least by face temperature.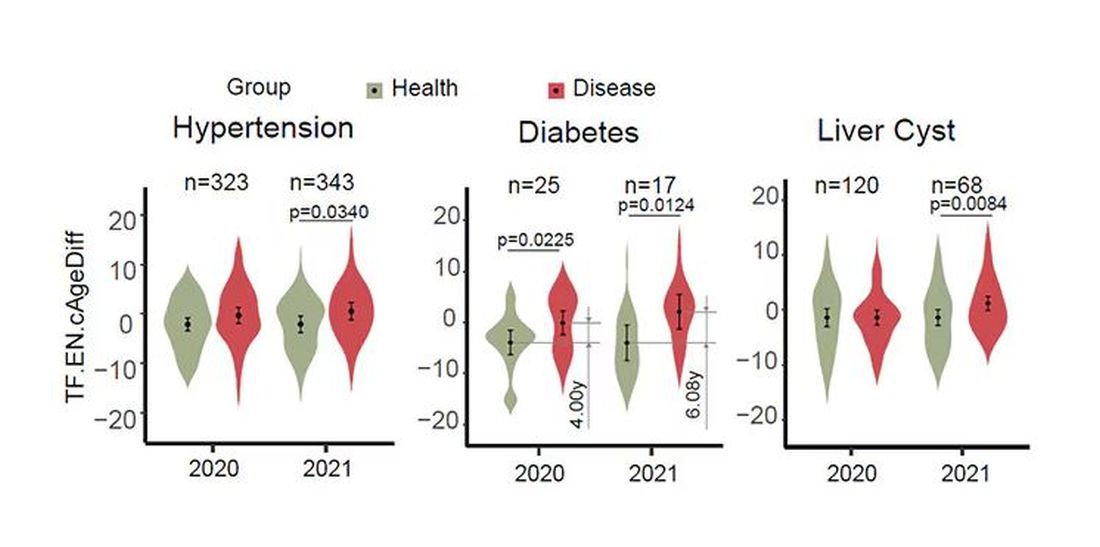
It may even be possible to use facial temperature as biofeedback. In a small study, the researchers measured the difference between facial temperature age and real age before and after 2 weeks of jump-roping. It turns out that 2 weeks of jump-roping can make you look about 5 years younger, at least as judged by a thermal camera. Or like the Predator.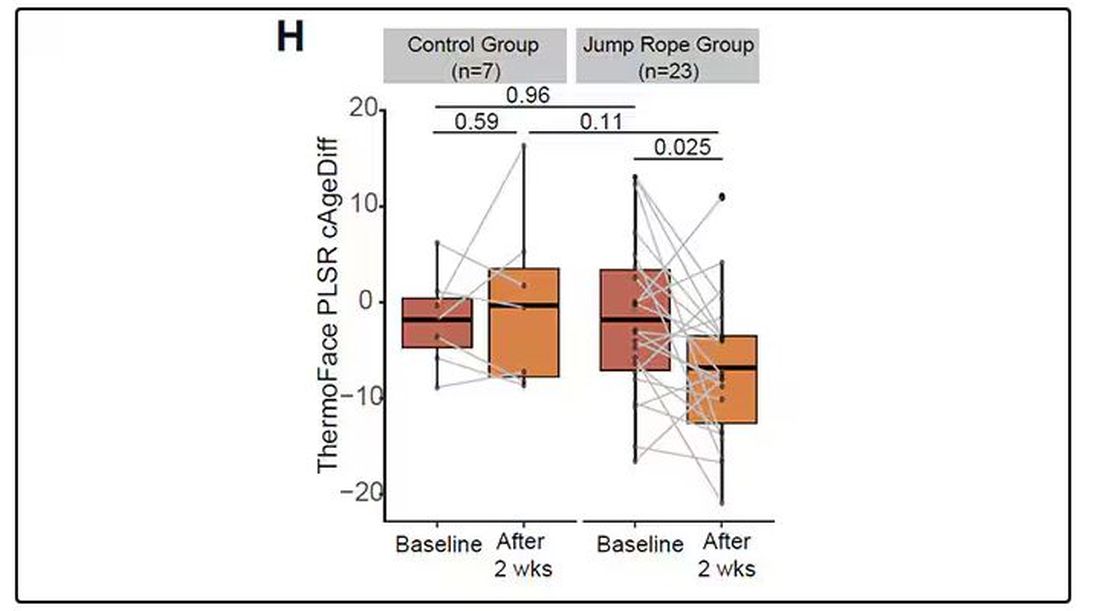
Okay, this is all very cool, but I’m not saying we’ll all be doing facial temperature tests in the near future. No; what this study highlights for me is how much information about ourselves is available to those who know how to decode it. Maybe those data come from the wrinkles in our faces, or the angles of our smiles, or the speed with which we type, or the temperature of our elbows. The data have always been there, actually, but we’ve never had the tools powerful enough to analyze them until now.
When I was a kid, I was obsessed with Star Trek — I know, you’re shocked — and, of course, the famous tricorder, a scanner that could tell everything about someone’s state of health in 5 seconds from 3 feet away. That’s how I thought medicine really would be in the future. Once I got to medical school, I was disabused of that notion. But the age of data, the age of AI, may mean the tricorder age is not actually that far away.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
My oldest daughter is at sleepaway camp for a couple of weeks, and the camp has a photographer who goes around all day taking pictures of the kids, which get uploaded to a private Facebook group. In the past, I would go online every day (or, okay, several times a day) and scroll through all those pictures looking for one that features my kid.
I don’t have to do that anymore. This year, I simply uploaded a picture of my daughter to an app and artificial intelligence (AI) takes care of the rest, recognizing her face amidst the sea of smiling children, and flagging just those photos for me to peruse. It’s amazing, really. And a bit scary.
The fact that facial recognition has penetrated the summer camp market should tell you that the tech is truly ubiquitous. But today we’re going to think a bit more about what AI can do with a picture of your face, because the power of facial recognition is not just skin deep.
What’s got me hot and bothered about facial images is this paper, appearing in Cell Metabolism, which adds a new layer to the standard facial-analysis playbook: facial temperature.
To understand this paper, you need to understand a whole field of research that is developing various different “clocks” for age.
It turns out that age really is just a number. Our cells, our proteins, our biochemistry can be analyzed to give different numbers. These “clocks,” as distinct from the calendar we usually use to measure our age, might have more predictive power than the number itself.
There are numerous molecular clocks, such as telomere length, that not only correlate with calendar age but are superior to calendar age in predicting age-related complications. Testing telomere length typically requires a blood sample — and remains costly. But we can use other sources to estimate age; how about a photo?
I mean, we do this all the time when we meet someone new or, as a physician, when we meet a new patient. I have often written that a patient “appears younger than their stated age,” and we’ve all had the experience of hearing how old someone is and being shocked. I mean, have you seen Sharon Stone recently? She’s 66 years old. Okay — to be fair, there might be some outside help there. But you get the point.
Back to the Cell Metabolism paper. Researchers report on multiple algorithms to obtain an “age” from a picture of an individual’s face.
The first algorithm is pretty straightforward. Researchers collected 2811 images, all of Han Chinese individuals ranging in age from 20 to 90 years, and reconstructed a 3D facial map from those.
They then trained a convolutional neural network to predict the individuals’ ages from the pictures. It was quite accurate, as you can see here.
In the AI age, this may not seem that impressive. A brief search online turned up dozens of apps that promised to guess my age from a photo.
I sent this rather unflattering picture of myself to ChatGPT which, after initially demurring and saying it was not designed to guess ages, pegged me at somewhere between 35 and 45, which I am taking as a major victory.
But the Cell Metabolism paper goes deeper. Literally.
And this is where things start to get interesting. Because sure, the visible part of your face can change depending on makeup, expression, plastic surgery, and the like. But the temperature? That’s harder to fake.
It turns out that the temperature distribution in your face changes as you get older. There is a cooling of the nose and the cheeks, for example.
And the researchers could combine all this temperature data to guess someone’s calendar age fairly accurately, though notably not as accurately as the model that just looks at the pictures.
But guessing your age is not really the interesting part of thermal imaging of the face. It’s guessing — or, rather, predicting — the state of your metabolism. All these study participants had extensive metabolic testing performed, as well as detailed analysis of their lifestyle behaviors. And facial images could be used to predict those factors.
For example, the 3D reconstruction of the faces could predict who ate seafood (they tend to look younger than their actual age) compared with who ate poultry and meat (they tend to look older). The thermal imaging could predict who got more sleep (they look younger from a temperature perspective) and who ate more yogurt (also younger-appearing, temperature-wise). Facial temperature patterns could identify those with higher BMI, higher blood pressure, higher fasting glucose.
The researchers used the difference between actual and predicted age as a metric to measure illness as well. You can see here how, on average, individuals with hypertension, diabetes, and even liver cysts are “older,” at least by face temperature.
It may even be possible to use facial temperature as biofeedback. In a small study, the researchers measured the difference between facial temperature age and real age before and after 2 weeks of jump-roping. It turns out that 2 weeks of jump-roping can make you look about 5 years younger, at least as judged by a thermal camera. Or like the Predator.
Okay, this is all very cool, but I’m not saying we’ll all be doing facial temperature tests in the near future. No; what this study highlights for me is how much information about ourselves is available to those who know how to decode it. Maybe those data come from the wrinkles in our faces, or the angles of our smiles, or the speed with which we type, or the temperature of our elbows. The data have always been there, actually, but we’ve never had the tools powerful enough to analyze them until now.
When I was a kid, I was obsessed with Star Trek — I know, you’re shocked — and, of course, the famous tricorder, a scanner that could tell everything about someone’s state of health in 5 seconds from 3 feet away. That’s how I thought medicine really would be in the future. Once I got to medical school, I was disabused of that notion. But the age of data, the age of AI, may mean the tricorder age is not actually that far away.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
My oldest daughter is at sleepaway camp for a couple of weeks, and the camp has a photographer who goes around all day taking pictures of the kids, which get uploaded to a private Facebook group. In the past, I would go online every day (or, okay, several times a day) and scroll through all those pictures looking for one that features my kid.
I don’t have to do that anymore. This year, I simply uploaded a picture of my daughter to an app and artificial intelligence (AI) takes care of the rest, recognizing her face amidst the sea of smiling children, and flagging just those photos for me to peruse. It’s amazing, really. And a bit scary.
The fact that facial recognition has penetrated the summer camp market should tell you that the tech is truly ubiquitous. But today we’re going to think a bit more about what AI can do with a picture of your face, because the power of facial recognition is not just skin deep.
What’s got me hot and bothered about facial images is this paper, appearing in Cell Metabolism, which adds a new layer to the standard facial-analysis playbook: facial temperature.
To understand this paper, you need to understand a whole field of research that is developing various different “clocks” for age.
It turns out that age really is just a number. Our cells, our proteins, our biochemistry can be analyzed to give different numbers. These “clocks,” as distinct from the calendar we usually use to measure our age, might have more predictive power than the number itself.
There are numerous molecular clocks, such as telomere length, that not only correlate with calendar age but are superior to calendar age in predicting age-related complications. Testing telomere length typically requires a blood sample — and remains costly. But we can use other sources to estimate age; how about a photo?
I mean, we do this all the time when we meet someone new or, as a physician, when we meet a new patient. I have often written that a patient “appears younger than their stated age,” and we’ve all had the experience of hearing how old someone is and being shocked. I mean, have you seen Sharon Stone recently? She’s 66 years old. Okay — to be fair, there might be some outside help there. But you get the point.
Back to the Cell Metabolism paper. Researchers report on multiple algorithms to obtain an “age” from a picture of an individual’s face.
The first algorithm is pretty straightforward. Researchers collected 2811 images, all of Han Chinese individuals ranging in age from 20 to 90 years, and reconstructed a 3D facial map from those.
They then trained a convolutional neural network to predict the individuals’ ages from the pictures. It was quite accurate, as you can see here.
In the AI age, this may not seem that impressive. A brief search online turned up dozens of apps that promised to guess my age from a photo.
I sent this rather unflattering picture of myself to ChatGPT which, after initially demurring and saying it was not designed to guess ages, pegged me at somewhere between 35 and 45, which I am taking as a major victory.
But the Cell Metabolism paper goes deeper. Literally.
And this is where things start to get interesting. Because sure, the visible part of your face can change depending on makeup, expression, plastic surgery, and the like. But the temperature? That’s harder to fake.
It turns out that the temperature distribution in your face changes as you get older. There is a cooling of the nose and the cheeks, for example.
And the researchers could combine all this temperature data to guess someone’s calendar age fairly accurately, though notably not as accurately as the model that just looks at the pictures.
But guessing your age is not really the interesting part of thermal imaging of the face. It’s guessing — or, rather, predicting — the state of your metabolism. All these study participants had extensive metabolic testing performed, as well as detailed analysis of their lifestyle behaviors. And facial images could be used to predict those factors.
For example, the 3D reconstruction of the faces could predict who ate seafood (they tend to look younger than their actual age) compared with who ate poultry and meat (they tend to look older). The thermal imaging could predict who got more sleep (they look younger from a temperature perspective) and who ate more yogurt (also younger-appearing, temperature-wise). Facial temperature patterns could identify those with higher BMI, higher blood pressure, higher fasting glucose.
The researchers used the difference between actual and predicted age as a metric to measure illness as well. You can see here how, on average, individuals with hypertension, diabetes, and even liver cysts are “older,” at least by face temperature.
It may even be possible to use facial temperature as biofeedback. In a small study, the researchers measured the difference between facial temperature age and real age before and after 2 weeks of jump-roping. It turns out that 2 weeks of jump-roping can make you look about 5 years younger, at least as judged by a thermal camera. Or like the Predator.
Okay, this is all very cool, but I’m not saying we’ll all be doing facial temperature tests in the near future. No; what this study highlights for me is how much information about ourselves is available to those who know how to decode it. Maybe those data come from the wrinkles in our faces, or the angles of our smiles, or the speed with which we type, or the temperature of our elbows. The data have always been there, actually, but we’ve never had the tools powerful enough to analyze them until now.
When I was a kid, I was obsessed with Star Trek — I know, you’re shocked — and, of course, the famous tricorder, a scanner that could tell everything about someone’s state of health in 5 seconds from 3 feet away. That’s how I thought medicine really would be in the future. Once I got to medical school, I was disabused of that notion. But the age of data, the age of AI, may mean the tricorder age is not actually that far away.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Time Warp: Fax Machines Still Common in Oncology Practice. Why?
One minute, he’s working on sequencing a tumor genome. The next, he’s sifting through pages of disorganized data from a device that has been around for decades: the fax machine.
“If two doctors’ offices aren’t on the same electronic medical record, one of the main ways to transfer records is still by fax,” said Dr. Lewis, director of gastrointestinal oncology at Intermountain Healthcare in Murray, Utah. “I can go from cutting-edge innovation to relying on, at best, 1980s information technology. It just boggles my mind.”
Dr. Lewis, who has posted about his frustration with fax machines, is far from alone. Oncologists are among the many specialists across the country at the mercy of telecopiers.
According to a 2021 report by the Office of the National Coordinator for Health Information Technology, fax and mail continue to be the most common methods for hospitals and health systems to exchange care record summaries. In 2019, nearly 8 in 10 hospitals used mail or fax to send and receive health information, the report found.
Fax machines are still commonplace across the healthcare spectrum, said Robert Havasy, MS, senior director for informatics strategy at the Healthcare Information and Management Systems Society (HIMSS). Inertia, cost, and more pressing priorities for hospitals and medical institutions contribute to the technology sticking around, he explained.
“Post-COVID, my guess is we’re still at over 50% of healthcare practices using fax for some reason, on a daily basis,” Mr. Havasy said in an interview. “A lot of hospitals just don’t have the time, the money, or the staff to fix that problem because there’s always something a little higher up the priority chain they need to focus on.”
If, for instance, “you’re going to do a process redesign to reduce hospital total acquired infections, your fax machine replacement might be 10th or 12th on the list. It just never gets up to 1 or 2 because it’s ‘not that much of a problem,’ ” he added.
Or is it?
Administrators may not view fax machines as a top concern, but clinicians who deal with the machines daily see it differently.
“What worries me is we’re taking records out of an electronic storehouse [and] converting them to a paper medium,” Dr. Lewis said. “And then we are scanning into another electronic storehouse. The more steps, the more can be lost.”
And when information is lost, patient care can be compromised.
Slower Workflows, Care Concerns
Although there are no published data on fax machine use in oncology specifically, this outdated technology does come into play in a variety of ways along the cancer care continuum.
Radiation oncologist David R. Penberthy, MD, said patients often seek his cancer center’s expertise for second opinions, and that requires collecting patient records from many different practices.
“Ideally, it would come electronically, but sometimes it does come by fax,” said Dr. Penberthy, program director of radiation oncology at the University of Virginia School of Medicine in Charlottesville. “The quality of the fax is not always the best. Sometimes it’s literally a fax of a fax. You’re reading something that’s very difficult to read.”
Orders for new tests are also typically sent and received via fax temporarily while IT teams work to integrate them into the electronic health record (EHR), Dr. Penberthy said.
Insurers and third-party laboratories often send test results back by fax as well.
“Even if I haven’t actually sent my patient out of our institution, this crucial result may only be entered back into the record as a scanned document from a fax, which is not great because it can get lost in the other results that are reported electronically,” Dr. Lewis said. The risk here is that an ordering physician won’t see these results, which can lead to delayed or overlooked care for patients, he explained.
“To me, it’s like a blind spot,” Dr. Lewis said. “Every time we use a fax, I see it actually as an opportunity for oversight and missed opportunity to collect data.”
Dr. Penberthy said faxing can slow things down at his practice, particularly if he faxes a document to another office but receives no confirmation and has to track down what happened.
As for cybersecurity, data that are in transit during faxing are generally considered secure and compliant with the Health Insurance Portability and Accountability Act (HIPAA), said Mr. Havasy of HIMSS. However, the Privacy Rule also requires that data remain secure while at rest, which isn’t always possible, he added.
“That’s where faxes fall down, because generally fax machines are in public, if you will, or open areas in a hospital,” he said. “They just sit on a desk. I don’t know that the next nurse who comes up and looks through that stack was the nurse who was treating the patient.”
Important decisions or results can also be missed when sent by fax, creating headaches for physicians and care problems for patients.
Dr. Lewis recently experienced an insurance-related fax mishap over Memorial Day weekend. He believed his patient had access to the antinausea medication he had prescribed. When Dr. Lewis happened to check the fax machine over the weekend, he found a coverage denial for the medication from the insurer but, at that point, had no recourse to appeal because it was a long holiday weekend.
“Had the denial been sent by an electronic means that was quicker and more readily available, it would have been possible to appeal before the holiday weekend,” he said.
Hematologist Aaron Goodman, MD, encountered a similar problem after an insurer denied coverage of an expensive cancer drug for a patient and faxed over its reason for the denial. Dr. Goodman was not directly notified that the information arrived and didn’t learn about the denial for a week, he said.
“There’s no ‘ding’ in my inbox if something is faxed over and scanned,” said Dr. Goodman, associate professor of medicine at UC San Diego Health. “Once I realized it was denied, I was able to rectify it, but it wasted a week of a patient not getting a drug that I felt would be beneficial for them.”
Broader Health Policy Impacts
The use of outdated technology, such as fax machines, also creates ripple effects that burden the health system, health policy experts say.
Duplicate testing and unnecessary care are top impacts, said Julia Adler-Milstein, PhD, professor of medicine and chief of the division of clinical informatics and digital transformation at the University of California, San Francisco.
Studies show that 20%-30% of the $65 billion spent annually on lab tests is used on unnecessary duplicate tests, and another estimated $30 billion is spent each year on unnecessary duplicate medical imaging. These duplicate tests may be mitigated if hospitals adopt certified EHR technology, research shows.
Still, without EHR interoperability between institutions, new providers may be unaware that tests or past labs for patients exist, leading to repeat tests, said Dr. Adler-Milstein, who researches health IT policy with a focus on EHRs. Patients can sometimes fill in the gaps, but not always.
“Fax machines only help close information gaps if the clinician is aware of where to seek out the information and there is someone at the other organization to locate and transmit the information in a timely manner,” Dr. Adler-Milstein said.
Old technology and poor interoperability also greatly affect data collection for disease surveillance and monitoring, said Janet Hamilton, MPH, executive director for the Council of State and Territorial Epidemiologists. This issue was keenly demonstrated during the pandemic, Ms. Hamilton said.
“It was tragic, quite honestly,” she said. “There was such an immense amount of data that needed to be moved quickly, and that’s when computers are at their best.”
But, she said, “we didn’t have the level of systems in place to do it well.”
Specifically, the lack of electronic case reporting in place during the pandemic — where diagnoses are documented in the record and then immediately sent to the public health system — led to reports that were delayed, not made, or had missing or incomplete information, such as patients’ race and ethnicity or other health conditions, Ms. Hamilton said.
Incomplete or missing data hampered the ability of public health officials and researchers to understand how the virus might affect different patients.
“If you had a chronic condition like cancer, you were less likely to have a positive outcome with COVID,” Ms. Hamilton said. “But because electronic case reporting was not in place, we didn’t get some of those additional pieces of information. We didn’t have people’s underlying oncology status to then say, ‘Here are individuals with these types of characteristics, and these are the things that happen if they also have a cancer.’”
Slow, but Steady, Improvements
Efforts at the state and federal levels have targeted improved health information exchange, but progress takes time, Dr. Adler-Milstein said.
Most states have some form of health information exchange, such as statewide exchanges, regional health information organizations, or clinical data registries. Maryland is often held up as a notable example for its health information exchange, Dr. Adler-Milstein noted.
According to Maryland law, all hospitals under the jurisdiction of the Maryland Health Care Commission are required to electronically connect to the state-designated health information exchange. In 2012, Maryland became the first state to connect all its 46 acute care hospitals in the sharing of real-time data.
The Health Information Technology for Economic and Clinical Health (HITECH) Act provided federal-enhanced Medicaid matching funds to states through 2021 to support efforts to advance electronic exchange. Nearly all states used these funds, and most have identified other sources to sustain the efforts, according to a recent US Government Accountability Office (GAO) report. However, GAO found that small and rural providers are less likely to have the financial and technological resources to participate in or maintain electronic exchange capabilities.
Nationally, several recent initiatives have targeted health data interoperability, including for cancer care. The Centers for Disease Control and Prevention’s Data Modernization Initiative is a multiyear, multi–billion-dollar effort to improve data sharing across the federal and state public health landscape.
Meanwhile, in March 2024, the Biden-Harris administration launched United States Core Data for Interoperability Plus Cancer. The program will define a recommended minimum set of cancer-related data to be included in a patient’s EHR to enhance data exchange for research and clinical care.
EHR vendors are also key to improving the landscape, said Dr. Adler-Milstein. Vendors such as Epic have developed strong sharing capabilities for transmitting health information from site to site, but of course, that only helps if providers have Epic, she said.
“That’s where these national frameworks should help, because we don’t want it to break down by what EHR vendor you have,” she said. “It’s a patchwork. You can go to some places and hear success stories because they have Epic or a state health information exchange, but it’s very heterogeneous. In some places, they have nothing and are using a fax machine.”
Mr. Havasy believes fax machines will ultimately go extinct, particularly as a younger, more digitally savvy generation enters the healthcare workforce. He also foresees that the growing use of artificial intelligence will help eradicate the outdated technology.
But, Ms. Hamilton noted, “unless we have consistent, ongoing, sustained funding, it is very hard to move off [an older] technology that can work. That’s one of the biggest barriers.”
“Public health is about protecting the lives of every single person everywhere,” Ms. Hamilton said, “but when we don’t have the data that comes into the system, we can’t achieve our mission.”
A version of this article appeared on Medscape.com.
One minute, he’s working on sequencing a tumor genome. The next, he’s sifting through pages of disorganized data from a device that has been around for decades: the fax machine.
“If two doctors’ offices aren’t on the same electronic medical record, one of the main ways to transfer records is still by fax,” said Dr. Lewis, director of gastrointestinal oncology at Intermountain Healthcare in Murray, Utah. “I can go from cutting-edge innovation to relying on, at best, 1980s information technology. It just boggles my mind.”
Dr. Lewis, who has posted about his frustration with fax machines, is far from alone. Oncologists are among the many specialists across the country at the mercy of telecopiers.
According to a 2021 report by the Office of the National Coordinator for Health Information Technology, fax and mail continue to be the most common methods for hospitals and health systems to exchange care record summaries. In 2019, nearly 8 in 10 hospitals used mail or fax to send and receive health information, the report found.
Fax machines are still commonplace across the healthcare spectrum, said Robert Havasy, MS, senior director for informatics strategy at the Healthcare Information and Management Systems Society (HIMSS). Inertia, cost, and more pressing priorities for hospitals and medical institutions contribute to the technology sticking around, he explained.
“Post-COVID, my guess is we’re still at over 50% of healthcare practices using fax for some reason, on a daily basis,” Mr. Havasy said in an interview. “A lot of hospitals just don’t have the time, the money, or the staff to fix that problem because there’s always something a little higher up the priority chain they need to focus on.”
If, for instance, “you’re going to do a process redesign to reduce hospital total acquired infections, your fax machine replacement might be 10th or 12th on the list. It just never gets up to 1 or 2 because it’s ‘not that much of a problem,’ ” he added.
Or is it?
Administrators may not view fax machines as a top concern, but clinicians who deal with the machines daily see it differently.
“What worries me is we’re taking records out of an electronic storehouse [and] converting them to a paper medium,” Dr. Lewis said. “And then we are scanning into another electronic storehouse. The more steps, the more can be lost.”
And when information is lost, patient care can be compromised.
Slower Workflows, Care Concerns
Although there are no published data on fax machine use in oncology specifically, this outdated technology does come into play in a variety of ways along the cancer care continuum.
Radiation oncologist David R. Penberthy, MD, said patients often seek his cancer center’s expertise for second opinions, and that requires collecting patient records from many different practices.
“Ideally, it would come electronically, but sometimes it does come by fax,” said Dr. Penberthy, program director of radiation oncology at the University of Virginia School of Medicine in Charlottesville. “The quality of the fax is not always the best. Sometimes it’s literally a fax of a fax. You’re reading something that’s very difficult to read.”
Orders for new tests are also typically sent and received via fax temporarily while IT teams work to integrate them into the electronic health record (EHR), Dr. Penberthy said.
Insurers and third-party laboratories often send test results back by fax as well.
“Even if I haven’t actually sent my patient out of our institution, this crucial result may only be entered back into the record as a scanned document from a fax, which is not great because it can get lost in the other results that are reported electronically,” Dr. Lewis said. The risk here is that an ordering physician won’t see these results, which can lead to delayed or overlooked care for patients, he explained.
“To me, it’s like a blind spot,” Dr. Lewis said. “Every time we use a fax, I see it actually as an opportunity for oversight and missed opportunity to collect data.”
Dr. Penberthy said faxing can slow things down at his practice, particularly if he faxes a document to another office but receives no confirmation and has to track down what happened.
As for cybersecurity, data that are in transit during faxing are generally considered secure and compliant with the Health Insurance Portability and Accountability Act (HIPAA), said Mr. Havasy of HIMSS. However, the Privacy Rule also requires that data remain secure while at rest, which isn’t always possible, he added.
“That’s where faxes fall down, because generally fax machines are in public, if you will, or open areas in a hospital,” he said. “They just sit on a desk. I don’t know that the next nurse who comes up and looks through that stack was the nurse who was treating the patient.”
Important decisions or results can also be missed when sent by fax, creating headaches for physicians and care problems for patients.
Dr. Lewis recently experienced an insurance-related fax mishap over Memorial Day weekend. He believed his patient had access to the antinausea medication he had prescribed. When Dr. Lewis happened to check the fax machine over the weekend, he found a coverage denial for the medication from the insurer but, at that point, had no recourse to appeal because it was a long holiday weekend.
“Had the denial been sent by an electronic means that was quicker and more readily available, it would have been possible to appeal before the holiday weekend,” he said.
Hematologist Aaron Goodman, MD, encountered a similar problem after an insurer denied coverage of an expensive cancer drug for a patient and faxed over its reason for the denial. Dr. Goodman was not directly notified that the information arrived and didn’t learn about the denial for a week, he said.
“There’s no ‘ding’ in my inbox if something is faxed over and scanned,” said Dr. Goodman, associate professor of medicine at UC San Diego Health. “Once I realized it was denied, I was able to rectify it, but it wasted a week of a patient not getting a drug that I felt would be beneficial for them.”
Broader Health Policy Impacts
The use of outdated technology, such as fax machines, also creates ripple effects that burden the health system, health policy experts say.
Duplicate testing and unnecessary care are top impacts, said Julia Adler-Milstein, PhD, professor of medicine and chief of the division of clinical informatics and digital transformation at the University of California, San Francisco.
Studies show that 20%-30% of the $65 billion spent annually on lab tests is used on unnecessary duplicate tests, and another estimated $30 billion is spent each year on unnecessary duplicate medical imaging. These duplicate tests may be mitigated if hospitals adopt certified EHR technology, research shows.
Still, without EHR interoperability between institutions, new providers may be unaware that tests or past labs for patients exist, leading to repeat tests, said Dr. Adler-Milstein, who researches health IT policy with a focus on EHRs. Patients can sometimes fill in the gaps, but not always.
“Fax machines only help close information gaps if the clinician is aware of where to seek out the information and there is someone at the other organization to locate and transmit the information in a timely manner,” Dr. Adler-Milstein said.
Old technology and poor interoperability also greatly affect data collection for disease surveillance and monitoring, said Janet Hamilton, MPH, executive director for the Council of State and Territorial Epidemiologists. This issue was keenly demonstrated during the pandemic, Ms. Hamilton said.
“It was tragic, quite honestly,” she said. “There was such an immense amount of data that needed to be moved quickly, and that’s when computers are at their best.”
But, she said, “we didn’t have the level of systems in place to do it well.”
Specifically, the lack of electronic case reporting in place during the pandemic — where diagnoses are documented in the record and then immediately sent to the public health system — led to reports that were delayed, not made, or had missing or incomplete information, such as patients’ race and ethnicity or other health conditions, Ms. Hamilton said.
Incomplete or missing data hampered the ability of public health officials and researchers to understand how the virus might affect different patients.
“If you had a chronic condition like cancer, you were less likely to have a positive outcome with COVID,” Ms. Hamilton said. “But because electronic case reporting was not in place, we didn’t get some of those additional pieces of information. We didn’t have people’s underlying oncology status to then say, ‘Here are individuals with these types of characteristics, and these are the things that happen if they also have a cancer.’”
Slow, but Steady, Improvements
Efforts at the state and federal levels have targeted improved health information exchange, but progress takes time, Dr. Adler-Milstein said.
Most states have some form of health information exchange, such as statewide exchanges, regional health information organizations, or clinical data registries. Maryland is often held up as a notable example for its health information exchange, Dr. Adler-Milstein noted.
According to Maryland law, all hospitals under the jurisdiction of the Maryland Health Care Commission are required to electronically connect to the state-designated health information exchange. In 2012, Maryland became the first state to connect all its 46 acute care hospitals in the sharing of real-time data.
The Health Information Technology for Economic and Clinical Health (HITECH) Act provided federal-enhanced Medicaid matching funds to states through 2021 to support efforts to advance electronic exchange. Nearly all states used these funds, and most have identified other sources to sustain the efforts, according to a recent US Government Accountability Office (GAO) report. However, GAO found that small and rural providers are less likely to have the financial and technological resources to participate in or maintain electronic exchange capabilities.
Nationally, several recent initiatives have targeted health data interoperability, including for cancer care. The Centers for Disease Control and Prevention’s Data Modernization Initiative is a multiyear, multi–billion-dollar effort to improve data sharing across the federal and state public health landscape.
Meanwhile, in March 2024, the Biden-Harris administration launched United States Core Data for Interoperability Plus Cancer. The program will define a recommended minimum set of cancer-related data to be included in a patient’s EHR to enhance data exchange for research and clinical care.
EHR vendors are also key to improving the landscape, said Dr. Adler-Milstein. Vendors such as Epic have developed strong sharing capabilities for transmitting health information from site to site, but of course, that only helps if providers have Epic, she said.
“That’s where these national frameworks should help, because we don’t want it to break down by what EHR vendor you have,” she said. “It’s a patchwork. You can go to some places and hear success stories because they have Epic or a state health information exchange, but it’s very heterogeneous. In some places, they have nothing and are using a fax machine.”
Mr. Havasy believes fax machines will ultimately go extinct, particularly as a younger, more digitally savvy generation enters the healthcare workforce. He also foresees that the growing use of artificial intelligence will help eradicate the outdated technology.
But, Ms. Hamilton noted, “unless we have consistent, ongoing, sustained funding, it is very hard to move off [an older] technology that can work. That’s one of the biggest barriers.”
“Public health is about protecting the lives of every single person everywhere,” Ms. Hamilton said, “but when we don’t have the data that comes into the system, we can’t achieve our mission.”
A version of this article appeared on Medscape.com.
One minute, he’s working on sequencing a tumor genome. The next, he’s sifting through pages of disorganized data from a device that has been around for decades: the fax machine.
“If two doctors’ offices aren’t on the same electronic medical record, one of the main ways to transfer records is still by fax,” said Dr. Lewis, director of gastrointestinal oncology at Intermountain Healthcare in Murray, Utah. “I can go from cutting-edge innovation to relying on, at best, 1980s information technology. It just boggles my mind.”
Dr. Lewis, who has posted about his frustration with fax machines, is far from alone. Oncologists are among the many specialists across the country at the mercy of telecopiers.
According to a 2021 report by the Office of the National Coordinator for Health Information Technology, fax and mail continue to be the most common methods for hospitals and health systems to exchange care record summaries. In 2019, nearly 8 in 10 hospitals used mail or fax to send and receive health information, the report found.
Fax machines are still commonplace across the healthcare spectrum, said Robert Havasy, MS, senior director for informatics strategy at the Healthcare Information and Management Systems Society (HIMSS). Inertia, cost, and more pressing priorities for hospitals and medical institutions contribute to the technology sticking around, he explained.
“Post-COVID, my guess is we’re still at over 50% of healthcare practices using fax for some reason, on a daily basis,” Mr. Havasy said in an interview. “A lot of hospitals just don’t have the time, the money, or the staff to fix that problem because there’s always something a little higher up the priority chain they need to focus on.”
If, for instance, “you’re going to do a process redesign to reduce hospital total acquired infections, your fax machine replacement might be 10th or 12th on the list. It just never gets up to 1 or 2 because it’s ‘not that much of a problem,’ ” he added.
Or is it?
Administrators may not view fax machines as a top concern, but clinicians who deal with the machines daily see it differently.
“What worries me is we’re taking records out of an electronic storehouse [and] converting them to a paper medium,” Dr. Lewis said. “And then we are scanning into another electronic storehouse. The more steps, the more can be lost.”
And when information is lost, patient care can be compromised.
Slower Workflows, Care Concerns
Although there are no published data on fax machine use in oncology specifically, this outdated technology does come into play in a variety of ways along the cancer care continuum.
Radiation oncologist David R. Penberthy, MD, said patients often seek his cancer center’s expertise for second opinions, and that requires collecting patient records from many different practices.
“Ideally, it would come electronically, but sometimes it does come by fax,” said Dr. Penberthy, program director of radiation oncology at the University of Virginia School of Medicine in Charlottesville. “The quality of the fax is not always the best. Sometimes it’s literally a fax of a fax. You’re reading something that’s very difficult to read.”
Orders for new tests are also typically sent and received via fax temporarily while IT teams work to integrate them into the electronic health record (EHR), Dr. Penberthy said.
Insurers and third-party laboratories often send test results back by fax as well.
“Even if I haven’t actually sent my patient out of our institution, this crucial result may only be entered back into the record as a scanned document from a fax, which is not great because it can get lost in the other results that are reported electronically,” Dr. Lewis said. The risk here is that an ordering physician won’t see these results, which can lead to delayed or overlooked care for patients, he explained.
“To me, it’s like a blind spot,” Dr. Lewis said. “Every time we use a fax, I see it actually as an opportunity for oversight and missed opportunity to collect data.”
Dr. Penberthy said faxing can slow things down at his practice, particularly if he faxes a document to another office but receives no confirmation and has to track down what happened.
As for cybersecurity, data that are in transit during faxing are generally considered secure and compliant with the Health Insurance Portability and Accountability Act (HIPAA), said Mr. Havasy of HIMSS. However, the Privacy Rule also requires that data remain secure while at rest, which isn’t always possible, he added.
“That’s where faxes fall down, because generally fax machines are in public, if you will, or open areas in a hospital,” he said. “They just sit on a desk. I don’t know that the next nurse who comes up and looks through that stack was the nurse who was treating the patient.”
Important decisions or results can also be missed when sent by fax, creating headaches for physicians and care problems for patients.
Dr. Lewis recently experienced an insurance-related fax mishap over Memorial Day weekend. He believed his patient had access to the antinausea medication he had prescribed. When Dr. Lewis happened to check the fax machine over the weekend, he found a coverage denial for the medication from the insurer but, at that point, had no recourse to appeal because it was a long holiday weekend.
“Had the denial been sent by an electronic means that was quicker and more readily available, it would have been possible to appeal before the holiday weekend,” he said.
Hematologist Aaron Goodman, MD, encountered a similar problem after an insurer denied coverage of an expensive cancer drug for a patient and faxed over its reason for the denial. Dr. Goodman was not directly notified that the information arrived and didn’t learn about the denial for a week, he said.
“There’s no ‘ding’ in my inbox if something is faxed over and scanned,” said Dr. Goodman, associate professor of medicine at UC San Diego Health. “Once I realized it was denied, I was able to rectify it, but it wasted a week of a patient not getting a drug that I felt would be beneficial for them.”
Broader Health Policy Impacts
The use of outdated technology, such as fax machines, also creates ripple effects that burden the health system, health policy experts say.
Duplicate testing and unnecessary care are top impacts, said Julia Adler-Milstein, PhD, professor of medicine and chief of the division of clinical informatics and digital transformation at the University of California, San Francisco.
Studies show that 20%-30% of the $65 billion spent annually on lab tests is used on unnecessary duplicate tests, and another estimated $30 billion is spent each year on unnecessary duplicate medical imaging. These duplicate tests may be mitigated if hospitals adopt certified EHR technology, research shows.
Still, without EHR interoperability between institutions, new providers may be unaware that tests or past labs for patients exist, leading to repeat tests, said Dr. Adler-Milstein, who researches health IT policy with a focus on EHRs. Patients can sometimes fill in the gaps, but not always.
“Fax machines only help close information gaps if the clinician is aware of where to seek out the information and there is someone at the other organization to locate and transmit the information in a timely manner,” Dr. Adler-Milstein said.
Old technology and poor interoperability also greatly affect data collection for disease surveillance and monitoring, said Janet Hamilton, MPH, executive director for the Council of State and Territorial Epidemiologists. This issue was keenly demonstrated during the pandemic, Ms. Hamilton said.
“It was tragic, quite honestly,” she said. “There was such an immense amount of data that needed to be moved quickly, and that’s when computers are at their best.”
But, she said, “we didn’t have the level of systems in place to do it well.”
Specifically, the lack of electronic case reporting in place during the pandemic — where diagnoses are documented in the record and then immediately sent to the public health system — led to reports that were delayed, not made, or had missing or incomplete information, such as patients’ race and ethnicity or other health conditions, Ms. Hamilton said.
Incomplete or missing data hampered the ability of public health officials and researchers to understand how the virus might affect different patients.
“If you had a chronic condition like cancer, you were less likely to have a positive outcome with COVID,” Ms. Hamilton said. “But because electronic case reporting was not in place, we didn’t get some of those additional pieces of information. We didn’t have people’s underlying oncology status to then say, ‘Here are individuals with these types of characteristics, and these are the things that happen if they also have a cancer.’”
Slow, but Steady, Improvements
Efforts at the state and federal levels have targeted improved health information exchange, but progress takes time, Dr. Adler-Milstein said.
Most states have some form of health information exchange, such as statewide exchanges, regional health information organizations, or clinical data registries. Maryland is often held up as a notable example for its health information exchange, Dr. Adler-Milstein noted.
According to Maryland law, all hospitals under the jurisdiction of the Maryland Health Care Commission are required to electronically connect to the state-designated health information exchange. In 2012, Maryland became the first state to connect all its 46 acute care hospitals in the sharing of real-time data.
The Health Information Technology for Economic and Clinical Health (HITECH) Act provided federal-enhanced Medicaid matching funds to states through 2021 to support efforts to advance electronic exchange. Nearly all states used these funds, and most have identified other sources to sustain the efforts, according to a recent US Government Accountability Office (GAO) report. However, GAO found that small and rural providers are less likely to have the financial and technological resources to participate in or maintain electronic exchange capabilities.
Nationally, several recent initiatives have targeted health data interoperability, including for cancer care. The Centers for Disease Control and Prevention’s Data Modernization Initiative is a multiyear, multi–billion-dollar effort to improve data sharing across the federal and state public health landscape.
Meanwhile, in March 2024, the Biden-Harris administration launched United States Core Data for Interoperability Plus Cancer. The program will define a recommended minimum set of cancer-related data to be included in a patient’s EHR to enhance data exchange for research and clinical care.
EHR vendors are also key to improving the landscape, said Dr. Adler-Milstein. Vendors such as Epic have developed strong sharing capabilities for transmitting health information from site to site, but of course, that only helps if providers have Epic, she said.
“That’s where these national frameworks should help, because we don’t want it to break down by what EHR vendor you have,” she said. “It’s a patchwork. You can go to some places and hear success stories because they have Epic or a state health information exchange, but it’s very heterogeneous. In some places, they have nothing and are using a fax machine.”
Mr. Havasy believes fax machines will ultimately go extinct, particularly as a younger, more digitally savvy generation enters the healthcare workforce. He also foresees that the growing use of artificial intelligence will help eradicate the outdated technology.
But, Ms. Hamilton noted, “unless we have consistent, ongoing, sustained funding, it is very hard to move off [an older] technology that can work. That’s one of the biggest barriers.”
“Public health is about protecting the lives of every single person everywhere,” Ms. Hamilton said, “but when we don’t have the data that comes into the system, we can’t achieve our mission.”
A version of this article appeared on Medscape.com.
Trading TV Time for Physical Activity Boosts Healthy Aging
TOPLINE:
, but substituting it with any physical activity — or even sleeping, in case of women with inadequate sleep — may lead to better overall health.
METHODOLOGY:
- Previous studies have shown that replacing sedentary behavior with physical activity may improve mortality outcomes, but whether this increased lifespan is accompanied by better overall health remains an unanswered question.
- To understand the impact of sedentary behavior and physical activity on healthy aging, researchers analyzed data from the prospective cohort Nurses’ Health Study.
- They included 45,176 women aged > 50 years in 1992 (mean age, 59.2 years) who were free of major chronic diseases and were followed up for 20 years.
- In 1992, validated questionnaires were used to record exposure to sedentary behavior, different levels of physical activity, and sleep. The time spent watching television was the primary exposure in the sedentary behavior category.
- The main outcome was healthy aging, defined as survival to ≥ 70 years of age and maintenance of four domains of health — being free of 11 main chronic diseases and having no impairment of subjective memory, physical function, or mental health.
TAKEAWAY:
- At 20 years of follow-up, 8.6% of the women achieved healthy aging, while 41.4% had none of the 11 chronic diseases, 16.1% had no physical function impairment, 44.1% had no mental health limitation, and 51.9% reported no memory impairment.
- For each increase of 2 hours per day spent sitting and watching television, the odds of healthy aging dropped by 12% (95% confidence interval [CI], 7%-17%).
- Conversely, every additional 2 hours per day of low-level physical activity at work upped the odds of healthy aging by 6% (95% CI, 3%-9%); furthermore, each extra hour per day of standardized moderate to vigorous physical activity (normal pace walking or the equivalent) was associated with 14% higher odds (95% CI, 11%-16%) of healthy aging.
- In a theoretical modeling analysis, individuals could increase their odds of healthy aging by replacing 1 hour of television time per day with low levels of physical activity at home and work or with moderate to vigorous levels of physical activity — or even sleeping, for those who slept for ≤ 7 hours.
IN PRACTICE:
“These findings expand on the literature reporting that replacing sedentary behavior with light or moderate to vigorous physical activity is associated with decreased mortality by suggesting that this increased lifespan might be accompanied by better overall health,” the authors wrote.
SOURCE:
Hongying Shi, PhD, Department of Epidemiology and Health Statistics, School of Public Health, Wenzhou Medical University, Wenzhou, China, led this study, which was published online in JAMA Network Open.
LIMITATIONS:
The measures of different behaviors were self-reported and may, therefore, be less accurate than objective measurement methods. Measurement error may have attenuated the effect of low levels of physical activity. The single exposure assessment at baseline may not reflect the long-term pattern of these activities.
DISCLOSURES:
The lead author was supported by the National Social Science Foundation Project of China and the Zhejiang Provincial Philosophy and Social Sciences Planning Project. A co-author and the Nurses’ Health Study were supported by the US National Institutes of Health. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, but substituting it with any physical activity — or even sleeping, in case of women with inadequate sleep — may lead to better overall health.
METHODOLOGY:
- Previous studies have shown that replacing sedentary behavior with physical activity may improve mortality outcomes, but whether this increased lifespan is accompanied by better overall health remains an unanswered question.
- To understand the impact of sedentary behavior and physical activity on healthy aging, researchers analyzed data from the prospective cohort Nurses’ Health Study.
- They included 45,176 women aged > 50 years in 1992 (mean age, 59.2 years) who were free of major chronic diseases and were followed up for 20 years.
- In 1992, validated questionnaires were used to record exposure to sedentary behavior, different levels of physical activity, and sleep. The time spent watching television was the primary exposure in the sedentary behavior category.
- The main outcome was healthy aging, defined as survival to ≥ 70 years of age and maintenance of four domains of health — being free of 11 main chronic diseases and having no impairment of subjective memory, physical function, or mental health.
TAKEAWAY:
- At 20 years of follow-up, 8.6% of the women achieved healthy aging, while 41.4% had none of the 11 chronic diseases, 16.1% had no physical function impairment, 44.1% had no mental health limitation, and 51.9% reported no memory impairment.
- For each increase of 2 hours per day spent sitting and watching television, the odds of healthy aging dropped by 12% (95% confidence interval [CI], 7%-17%).
- Conversely, every additional 2 hours per day of low-level physical activity at work upped the odds of healthy aging by 6% (95% CI, 3%-9%); furthermore, each extra hour per day of standardized moderate to vigorous physical activity (normal pace walking or the equivalent) was associated with 14% higher odds (95% CI, 11%-16%) of healthy aging.
- In a theoretical modeling analysis, individuals could increase their odds of healthy aging by replacing 1 hour of television time per day with low levels of physical activity at home and work or with moderate to vigorous levels of physical activity — or even sleeping, for those who slept for ≤ 7 hours.
IN PRACTICE:
“These findings expand on the literature reporting that replacing sedentary behavior with light or moderate to vigorous physical activity is associated with decreased mortality by suggesting that this increased lifespan might be accompanied by better overall health,” the authors wrote.
SOURCE:
Hongying Shi, PhD, Department of Epidemiology and Health Statistics, School of Public Health, Wenzhou Medical University, Wenzhou, China, led this study, which was published online in JAMA Network Open.
LIMITATIONS:
The measures of different behaviors were self-reported and may, therefore, be less accurate than objective measurement methods. Measurement error may have attenuated the effect of low levels of physical activity. The single exposure assessment at baseline may not reflect the long-term pattern of these activities.
DISCLOSURES:
The lead author was supported by the National Social Science Foundation Project of China and the Zhejiang Provincial Philosophy and Social Sciences Planning Project. A co-author and the Nurses’ Health Study were supported by the US National Institutes of Health. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, but substituting it with any physical activity — or even sleeping, in case of women with inadequate sleep — may lead to better overall health.
METHODOLOGY:
- Previous studies have shown that replacing sedentary behavior with physical activity may improve mortality outcomes, but whether this increased lifespan is accompanied by better overall health remains an unanswered question.
- To understand the impact of sedentary behavior and physical activity on healthy aging, researchers analyzed data from the prospective cohort Nurses’ Health Study.
- They included 45,176 women aged > 50 years in 1992 (mean age, 59.2 years) who were free of major chronic diseases and were followed up for 20 years.
- In 1992, validated questionnaires were used to record exposure to sedentary behavior, different levels of physical activity, and sleep. The time spent watching television was the primary exposure in the sedentary behavior category.
- The main outcome was healthy aging, defined as survival to ≥ 70 years of age and maintenance of four domains of health — being free of 11 main chronic diseases and having no impairment of subjective memory, physical function, or mental health.
TAKEAWAY:
- At 20 years of follow-up, 8.6% of the women achieved healthy aging, while 41.4% had none of the 11 chronic diseases, 16.1% had no physical function impairment, 44.1% had no mental health limitation, and 51.9% reported no memory impairment.
- For each increase of 2 hours per day spent sitting and watching television, the odds of healthy aging dropped by 12% (95% confidence interval [CI], 7%-17%).
- Conversely, every additional 2 hours per day of low-level physical activity at work upped the odds of healthy aging by 6% (95% CI, 3%-9%); furthermore, each extra hour per day of standardized moderate to vigorous physical activity (normal pace walking or the equivalent) was associated with 14% higher odds (95% CI, 11%-16%) of healthy aging.
- In a theoretical modeling analysis, individuals could increase their odds of healthy aging by replacing 1 hour of television time per day with low levels of physical activity at home and work or with moderate to vigorous levels of physical activity — or even sleeping, for those who slept for ≤ 7 hours.
IN PRACTICE:
“These findings expand on the literature reporting that replacing sedentary behavior with light or moderate to vigorous physical activity is associated with decreased mortality by suggesting that this increased lifespan might be accompanied by better overall health,” the authors wrote.
SOURCE:
Hongying Shi, PhD, Department of Epidemiology and Health Statistics, School of Public Health, Wenzhou Medical University, Wenzhou, China, led this study, which was published online in JAMA Network Open.
LIMITATIONS:
The measures of different behaviors were self-reported and may, therefore, be less accurate than objective measurement methods. Measurement error may have attenuated the effect of low levels of physical activity. The single exposure assessment at baseline may not reflect the long-term pattern of these activities.
DISCLOSURES:
The lead author was supported by the National Social Science Foundation Project of China and the Zhejiang Provincial Philosophy and Social Sciences Planning Project. A co-author and the Nurses’ Health Study were supported by the US National Institutes of Health. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
Does Semaglutide Reduce Inflammation?
LYON, FRANCE — The anti-obesity drug semaglutide is associated with significant reductions in the inflammatory marker high-sensitivity C-reactive protein (CRP), even in patients who do not lose substantial amounts of weight with the drug, according to data from the SELECT clinical trial.
The research, presented at the European Atherosclerosis Society 2024, involved over 17,600 patients with overweight or obesity and had established cardiovascular disease but not diabetes.
“Weight loss was associated with greater high-sensitivity CRP reduction in both treatment groups,” said study presenter Jorge Plutzky, MD, director of Preventive Cardiology at Brigham and Women’s Hospital, Boston, but “with increased high-sensitivity CRP reductions in those receiving semaglutide.”
The drug also “significantly reduced high-sensitivity CRP early,” he said, “prior to major weight loss and in those who did not lose significant amounts of weight.” The reductions reached approximately 12% at 4 weeks and around 20% at 8 weeks, when the weight loss “was still quite modest,” at 2% and 3% of body weight, respectively. Even among patients who achieved weight loss of less than 2% body weight, semaglutide was associated with a reduction in high-sensitivity CRP levels.
In the SELECT trial, semaglutide also resulted in a consistent reduction of around 20% vs placebo in major adverse cardiovascular events such as cardiovascular mortality, nonfatal myocardial infarction, or nonfatal stroke.
But Naveed Sattar, MD, PhD, professor of cardiometabolic medicine at the University of Glasgow, Scotland, said in an interview that body weight “is probably the major driver” of CRP levels in the population, accounting for between 20% and 30% of the variation.
Dr. Sattar, who was not involved in the study, said that because drugs like semaglutide lower weight but also have anti-inflammatory effects, the question becomes: “Could the anti-inflammatory effects be part of the mechanisms by which these drugs affect the risk of major adverse cardiovascular events?”
Reducing Cardiovascular Events
The current analysis, however, cannot answer the question, he said. “All it tells us is about associations.”
“What we do know is semaglutide, predominantly by lowering weight, is lowering CRP levels and equally, we know that when you lose weight, you improve blood pressure, you improve lipids, and you reduce the risk of diabetes,” he said.
Dr. Sattar also took issue with the researchers’ conclusion that the high-sensitivity CRP reductions seen in SELECT occurred prior to major weight loss because the “pattern of CRP reduction and weight reduction is almost identical.”
Dr. Sattar also pointed out in a recent editorial that the drug appears to have a direct effect on blood vessels and the heart, which may lead to improvements in systemic inflammation. Consequently, he said, any assertion that semaglutide is genuinely anti-inflammatory is, at this stage, “speculation.”
Dr. Plutzky said that “systemic, chronic inflammation is implicated as a potential mechanism and therapeutic target in atherosclerosis and major adverse cardiovascular events, as well as obesity,” and high-sensitivity CRP levels are an “established biomarker of inflammation and have been shown to predict cardiovascular risk.”
However, the relationship between high-sensitivity CRP, responses to glucagon-like peptide 1 receptor agonists like semaglutide, and cardiovascular outcomes in obesity “remains incompletely understood,” said Dr. Plutzky.
A version of this article appeared on Medscape.com.
LYON, FRANCE — The anti-obesity drug semaglutide is associated with significant reductions in the inflammatory marker high-sensitivity C-reactive protein (CRP), even in patients who do not lose substantial amounts of weight with the drug, according to data from the SELECT clinical trial.
The research, presented at the European Atherosclerosis Society 2024, involved over 17,600 patients with overweight or obesity and had established cardiovascular disease but not diabetes.
“Weight loss was associated with greater high-sensitivity CRP reduction in both treatment groups,” said study presenter Jorge Plutzky, MD, director of Preventive Cardiology at Brigham and Women’s Hospital, Boston, but “with increased high-sensitivity CRP reductions in those receiving semaglutide.”
The drug also “significantly reduced high-sensitivity CRP early,” he said, “prior to major weight loss and in those who did not lose significant amounts of weight.” The reductions reached approximately 12% at 4 weeks and around 20% at 8 weeks, when the weight loss “was still quite modest,” at 2% and 3% of body weight, respectively. Even among patients who achieved weight loss of less than 2% body weight, semaglutide was associated with a reduction in high-sensitivity CRP levels.
In the SELECT trial, semaglutide also resulted in a consistent reduction of around 20% vs placebo in major adverse cardiovascular events such as cardiovascular mortality, nonfatal myocardial infarction, or nonfatal stroke.
But Naveed Sattar, MD, PhD, professor of cardiometabolic medicine at the University of Glasgow, Scotland, said in an interview that body weight “is probably the major driver” of CRP levels in the population, accounting for between 20% and 30% of the variation.
Dr. Sattar, who was not involved in the study, said that because drugs like semaglutide lower weight but also have anti-inflammatory effects, the question becomes: “Could the anti-inflammatory effects be part of the mechanisms by which these drugs affect the risk of major adverse cardiovascular events?”
Reducing Cardiovascular Events
The current analysis, however, cannot answer the question, he said. “All it tells us is about associations.”
“What we do know is semaglutide, predominantly by lowering weight, is lowering CRP levels and equally, we know that when you lose weight, you improve blood pressure, you improve lipids, and you reduce the risk of diabetes,” he said.
Dr. Sattar also took issue with the researchers’ conclusion that the high-sensitivity CRP reductions seen in SELECT occurred prior to major weight loss because the “pattern of CRP reduction and weight reduction is almost identical.”
Dr. Sattar also pointed out in a recent editorial that the drug appears to have a direct effect on blood vessels and the heart, which may lead to improvements in systemic inflammation. Consequently, he said, any assertion that semaglutide is genuinely anti-inflammatory is, at this stage, “speculation.”
Dr. Plutzky said that “systemic, chronic inflammation is implicated as a potential mechanism and therapeutic target in atherosclerosis and major adverse cardiovascular events, as well as obesity,” and high-sensitivity CRP levels are an “established biomarker of inflammation and have been shown to predict cardiovascular risk.”
However, the relationship between high-sensitivity CRP, responses to glucagon-like peptide 1 receptor agonists like semaglutide, and cardiovascular outcomes in obesity “remains incompletely understood,” said Dr. Plutzky.
A version of this article appeared on Medscape.com.
LYON, FRANCE — The anti-obesity drug semaglutide is associated with significant reductions in the inflammatory marker high-sensitivity C-reactive protein (CRP), even in patients who do not lose substantial amounts of weight with the drug, according to data from the SELECT clinical trial.
The research, presented at the European Atherosclerosis Society 2024, involved over 17,600 patients with overweight or obesity and had established cardiovascular disease but not diabetes.
“Weight loss was associated with greater high-sensitivity CRP reduction in both treatment groups,” said study presenter Jorge Plutzky, MD, director of Preventive Cardiology at Brigham and Women’s Hospital, Boston, but “with increased high-sensitivity CRP reductions in those receiving semaglutide.”
The drug also “significantly reduced high-sensitivity CRP early,” he said, “prior to major weight loss and in those who did not lose significant amounts of weight.” The reductions reached approximately 12% at 4 weeks and around 20% at 8 weeks, when the weight loss “was still quite modest,” at 2% and 3% of body weight, respectively. Even among patients who achieved weight loss of less than 2% body weight, semaglutide was associated with a reduction in high-sensitivity CRP levels.
In the SELECT trial, semaglutide also resulted in a consistent reduction of around 20% vs placebo in major adverse cardiovascular events such as cardiovascular mortality, nonfatal myocardial infarction, or nonfatal stroke.
But Naveed Sattar, MD, PhD, professor of cardiometabolic medicine at the University of Glasgow, Scotland, said in an interview that body weight “is probably the major driver” of CRP levels in the population, accounting for between 20% and 30% of the variation.
Dr. Sattar, who was not involved in the study, said that because drugs like semaglutide lower weight but also have anti-inflammatory effects, the question becomes: “Could the anti-inflammatory effects be part of the mechanisms by which these drugs affect the risk of major adverse cardiovascular events?”
Reducing Cardiovascular Events
The current analysis, however, cannot answer the question, he said. “All it tells us is about associations.”
“What we do know is semaglutide, predominantly by lowering weight, is lowering CRP levels and equally, we know that when you lose weight, you improve blood pressure, you improve lipids, and you reduce the risk of diabetes,” he said.
Dr. Sattar also took issue with the researchers’ conclusion that the high-sensitivity CRP reductions seen in SELECT occurred prior to major weight loss because the “pattern of CRP reduction and weight reduction is almost identical.”
Dr. Sattar also pointed out in a recent editorial that the drug appears to have a direct effect on blood vessels and the heart, which may lead to improvements in systemic inflammation. Consequently, he said, any assertion that semaglutide is genuinely anti-inflammatory is, at this stage, “speculation.”
Dr. Plutzky said that “systemic, chronic inflammation is implicated as a potential mechanism and therapeutic target in atherosclerosis and major adverse cardiovascular events, as well as obesity,” and high-sensitivity CRP levels are an “established biomarker of inflammation and have been shown to predict cardiovascular risk.”
However, the relationship between high-sensitivity CRP, responses to glucagon-like peptide 1 receptor agonists like semaglutide, and cardiovascular outcomes in obesity “remains incompletely understood,” said Dr. Plutzky.
A version of this article appeared on Medscape.com.