User login
Surgery for bowel obstruction in cancer patients didn’t increase 90-day mortality
CORONADO, CALIF. – Among advanced cancer patients with bowel obstruction, surgery was not an independent predictor of the ability to eat at discharge or survival within 90 days of consultation, results from a long-term retrospective study showed.
“I think this represents the complexity in treating these patients,” lead study author Brian D. Badgwell, MD, said at the annual meeting of the Western Surgical Association. “We need future studies to identify the optimal outcome measures.”
For the current study, the researchers retrospectively reviewed the medical records of 490 patients who required surgical consultation for bowel obstruction at MD Anderson Cancer Center between January 2000 and May 2014. They set out to determine the incidence of obstruction due to intra-abdominal tumor and to identify variables associated with the ability to eat at hospital discharge and 90-day survival. They excluded patients without clinical or radiologic features of mechanical bowel obstruction. Clinical variables of interest included obstruction site, tumor vs. non-tumor cause, laboratory parameters, radiologic extent of malignancy, and the type of treatment performed (surgical, medical, or interventional, defined as interventional radiology or endoscopy). Overall survival was calculated from the date of first surgical evaluation for bowel obstruction to any cause mortality or last follow-up. Univariate and multivariate analyses were performed for ability to eat and a Cox proportional hazards model for 90-day survival.
Dr. Badgwell reported that the most common obstruction site in the 490 patients was the small bowel (64%), followed by large bowel (20%) and gastric outlet (16%). Obstruction etiology was identified as tumor-related in 68% of cases, followed by adhesion-related (20%) and unclear (12%). Nearly half of patients (46%) received chemotherapy within 6 weeks of their surgical consultation, but only 4% were neutropenic. More than half of patients (52%) had an albumin level of less than 3.5 g/dL, 52% had a hemoglobin of 10 g/dL or greater, 36% had lymphadenopathy, 35% had ascites, 34% had peritoneal disease, and 31% had a primary or recurrent tumor in place. In addition, 53% had an abdominal visceral malignancy, 9% had bone metastases, and 14% had lung metastases.
About half of patients (49%) received medical management as their treatment, followed by surgical and procedural treatment (32% and 17%, respectively). Fifteen percent were discharged to in-home hospice or to an inpatient hospice facility. More than two-thirds (68%) were able to eat at the time of discharge, and 43% died within 90 days of surgical consultation.
Multivariate analysis revealed that the following factors were negatively associated with eating at discharge: an intact/primary local recurrence (odds ratio, 0.46), carcinomatosis (OR, 0.34), and albumin level of less than 3.5 g/dL (OR, 0.55). At the same time, variables associated with death within 90 days of consultation included having an intact primary/local recurrence (hazard ratio, 1.75), carcinomatosis (HR, 1.98), and abdominal visceral metastasis (HR, 1.75). Finally, compared with procedural treatment, both medical management and surgical management were negatively associated with death within 90 days (HR of 0.51 and 0.44, respectively).
“There is a high rate of non-mechanical bowel dysfunction in patients undergoing surgical consultation for bowel obstruction,” Dr. Badgwell concluded. “It’s very difficult to categorize these cases preoperatively. They do require a selective approach. Variables associated with outcome measures support caution in patients with carcinomatosis, hypoalbuminemia, and multiple sites of disease on imaging.”
Dr. Badgwell reported having no financial disclosures.
CORONADO, CALIF. – Among advanced cancer patients with bowel obstruction, surgery was not an independent predictor of the ability to eat at discharge or survival within 90 days of consultation, results from a long-term retrospective study showed.
“I think this represents the complexity in treating these patients,” lead study author Brian D. Badgwell, MD, said at the annual meeting of the Western Surgical Association. “We need future studies to identify the optimal outcome measures.”
For the current study, the researchers retrospectively reviewed the medical records of 490 patients who required surgical consultation for bowel obstruction at MD Anderson Cancer Center between January 2000 and May 2014. They set out to determine the incidence of obstruction due to intra-abdominal tumor and to identify variables associated with the ability to eat at hospital discharge and 90-day survival. They excluded patients without clinical or radiologic features of mechanical bowel obstruction. Clinical variables of interest included obstruction site, tumor vs. non-tumor cause, laboratory parameters, radiologic extent of malignancy, and the type of treatment performed (surgical, medical, or interventional, defined as interventional radiology or endoscopy). Overall survival was calculated from the date of first surgical evaluation for bowel obstruction to any cause mortality or last follow-up. Univariate and multivariate analyses were performed for ability to eat and a Cox proportional hazards model for 90-day survival.
Dr. Badgwell reported that the most common obstruction site in the 490 patients was the small bowel (64%), followed by large bowel (20%) and gastric outlet (16%). Obstruction etiology was identified as tumor-related in 68% of cases, followed by adhesion-related (20%) and unclear (12%). Nearly half of patients (46%) received chemotherapy within 6 weeks of their surgical consultation, but only 4% were neutropenic. More than half of patients (52%) had an albumin level of less than 3.5 g/dL, 52% had a hemoglobin of 10 g/dL or greater, 36% had lymphadenopathy, 35% had ascites, 34% had peritoneal disease, and 31% had a primary or recurrent tumor in place. In addition, 53% had an abdominal visceral malignancy, 9% had bone metastases, and 14% had lung metastases.
About half of patients (49%) received medical management as their treatment, followed by surgical and procedural treatment (32% and 17%, respectively). Fifteen percent were discharged to in-home hospice or to an inpatient hospice facility. More than two-thirds (68%) were able to eat at the time of discharge, and 43% died within 90 days of surgical consultation.
Multivariate analysis revealed that the following factors were negatively associated with eating at discharge: an intact/primary local recurrence (odds ratio, 0.46), carcinomatosis (OR, 0.34), and albumin level of less than 3.5 g/dL (OR, 0.55). At the same time, variables associated with death within 90 days of consultation included having an intact primary/local recurrence (hazard ratio, 1.75), carcinomatosis (HR, 1.98), and abdominal visceral metastasis (HR, 1.75). Finally, compared with procedural treatment, both medical management and surgical management were negatively associated with death within 90 days (HR of 0.51 and 0.44, respectively).
“There is a high rate of non-mechanical bowel dysfunction in patients undergoing surgical consultation for bowel obstruction,” Dr. Badgwell concluded. “It’s very difficult to categorize these cases preoperatively. They do require a selective approach. Variables associated with outcome measures support caution in patients with carcinomatosis, hypoalbuminemia, and multiple sites of disease on imaging.”
Dr. Badgwell reported having no financial disclosures.
CORONADO, CALIF. – Among advanced cancer patients with bowel obstruction, surgery was not an independent predictor of the ability to eat at discharge or survival within 90 days of consultation, results from a long-term retrospective study showed.
“I think this represents the complexity in treating these patients,” lead study author Brian D. Badgwell, MD, said at the annual meeting of the Western Surgical Association. “We need future studies to identify the optimal outcome measures.”
For the current study, the researchers retrospectively reviewed the medical records of 490 patients who required surgical consultation for bowel obstruction at MD Anderson Cancer Center between January 2000 and May 2014. They set out to determine the incidence of obstruction due to intra-abdominal tumor and to identify variables associated with the ability to eat at hospital discharge and 90-day survival. They excluded patients without clinical or radiologic features of mechanical bowel obstruction. Clinical variables of interest included obstruction site, tumor vs. non-tumor cause, laboratory parameters, radiologic extent of malignancy, and the type of treatment performed (surgical, medical, or interventional, defined as interventional radiology or endoscopy). Overall survival was calculated from the date of first surgical evaluation for bowel obstruction to any cause mortality or last follow-up. Univariate and multivariate analyses were performed for ability to eat and a Cox proportional hazards model for 90-day survival.
Dr. Badgwell reported that the most common obstruction site in the 490 patients was the small bowel (64%), followed by large bowel (20%) and gastric outlet (16%). Obstruction etiology was identified as tumor-related in 68% of cases, followed by adhesion-related (20%) and unclear (12%). Nearly half of patients (46%) received chemotherapy within 6 weeks of their surgical consultation, but only 4% were neutropenic. More than half of patients (52%) had an albumin level of less than 3.5 g/dL, 52% had a hemoglobin of 10 g/dL or greater, 36% had lymphadenopathy, 35% had ascites, 34% had peritoneal disease, and 31% had a primary or recurrent tumor in place. In addition, 53% had an abdominal visceral malignancy, 9% had bone metastases, and 14% had lung metastases.
About half of patients (49%) received medical management as their treatment, followed by surgical and procedural treatment (32% and 17%, respectively). Fifteen percent were discharged to in-home hospice or to an inpatient hospice facility. More than two-thirds (68%) were able to eat at the time of discharge, and 43% died within 90 days of surgical consultation.
Multivariate analysis revealed that the following factors were negatively associated with eating at discharge: an intact/primary local recurrence (odds ratio, 0.46), carcinomatosis (OR, 0.34), and albumin level of less than 3.5 g/dL (OR, 0.55). At the same time, variables associated with death within 90 days of consultation included having an intact primary/local recurrence (hazard ratio, 1.75), carcinomatosis (HR, 1.98), and abdominal visceral metastasis (HR, 1.75). Finally, compared with procedural treatment, both medical management and surgical management were negatively associated with death within 90 days (HR of 0.51 and 0.44, respectively).
“There is a high rate of non-mechanical bowel dysfunction in patients undergoing surgical consultation for bowel obstruction,” Dr. Badgwell concluded. “It’s very difficult to categorize these cases preoperatively. They do require a selective approach. Variables associated with outcome measures support caution in patients with carcinomatosis, hypoalbuminemia, and multiple sites of disease on imaging.”
Dr. Badgwell reported having no financial disclosures.
AT WSA 2016
Key clinical point:
Major finding: Compared with procedural treatment of bowel obstruction, both medical management and surgical management were negatively associated with death within 90 days (HR of 0.51 and 0.44, respectively).
Data source: A retrospective review of 490 patients with advanced cancer who required surgical consultation for bowel obstruction at MD Anderson Cancer Center, Houston, between January 2000 and May 2014.
Disclosures: Dr. Badgwell reported having no financial disclosures.
VIDEO: Biologics: Proposed guideline addresses perioperative management
WASHINGTON – Biologic agents should be stopped prior to elective total knee or hip arthroplasty in patients with rheumatic diseases, according to a draft guideline developed by the American College of Rheumatology and the American Association of Hip and Knee Surgeons.
The guideline, which address the perioperative management of antirheumatic medications in patients with rheumatoid arthritis, spondyloarthritis, psoriatic arthritis, juvenile idiopathic arthritis (JIA), or lupus who are undergoing such surgery, is currently under review, Dr. Susan Goodman, MD, coprincipal investigator, reported at the annual meeting of the American College of Rheumatology.
The draft guideline was created because “guidance was needed for common clinical situations, even where data were sparse. We didn’t want to configure treatment mandates – that’s not what these are,” Dr. Goodman of Cornell University, New York, said.
The recommendations are conditional, she said, meaning that the benefits probably outweigh the harms, that the recommendations apply to most but not all patients, and that future research may lead to changes.
“They’re also preference sensitive,” she said, explaining that patients’ values and preferences should be carefully considered, as they might differ from those of the patient panel consulted during guideline development; the panel expressed greater concern about the risk of infection following surgery than about perioperative flares resulting from medication discontinuation.
Based on agreement by at least 80% of a voting panel which considered available evidence in the context of their clinical experience along with the input from the patient panel, the draft guideline states that:
• Current doses of methotrexate, leflunomide, hydroxychloroquine, and sulfasalazine should be continued in patients with rheumatic diseases undergoing elective hip and knee replacement. This recommendation is based on an extensive literature review that showed the infection rate is decreased in patients who continue these medications, Dr. Goodman said.
• All biologics should be withheld prior to surgery in patients with inflammatory arthritis, and surgery should be planned for the end of the dosing cycle. This matter wasn’t specifically addressed in the literature; however, numerous randomized controlled trials outside of the surgical setting demonstrate an increased risk of infection associated with their use, she noted.
“All of the biologic medications were found to be associated with an increased risk of infection,” she said. “Because of this and the level of importance patients place on minimizing infection risk, we’ve recommended that biologics be withheld prior to surgery.”
• Tofacitinib, which was considered in a separate oral, targeted therapy category, should be withheld for at least 7 days prior to surgery in patients with RA, spondyloarthritis, and JIA. Data from systematic reviews and meta-analyses showed an increased risk of infection with tofacitinib, although more research is needed in order to “firm up” this recommendation, Dr. Goodman said.
• In lupus patients, rituximab and belimumab should be withheld prior to surgery, and surgery should be planned for the end of the dosing period.
“Again, this was not answered in the literature. We depended on observational studies that we reviewed that did show that patients with severe active lupus were at much higher risk for adverse events. But since rituximab isn’t approved by the [Food and Drug Administration] for use in lupus, and belimumab isn’t approved for use in severe lupus – and those seem to be the high-risk patients – we thought withholding them was more prudent,” she said.
• Patients with severe lupus should continue on current doses of methotrexate, mycophenolic acid, azathioprine, mizoribine, cyclosporine, and tacrolimus through surgery. This recommendation is based on indirect data from experience in organ transplant patients.
• All medications should be discontinued in patients whose lupus is not severe.
“Our recommendation is to withhold for 7 days to 2-5 days after surgery in the absence of any wound healing complications or any other complications,” she said, noting that the literature does not directly address this; the recommendation is based on indirect evidence in patients with either active infection or who are at risk for infection.
“We thought that careful monitoring of the patient would permit us to identify flare and intervene quickly. … and that, for mild cases of lupus, the morbidity associated with infection might not be greater than the morbidity associated with the disease flare,” she said.
• Biologics should be restarted once surgical wounds show evidence of healing and there is no clinical evidence of infection. The literature does not directly address this; the recommendation is based on the rationale for use of these medications in patients with either active infection or risk for infection.
• Current daily doses of glucocorticoids, rather than supraphysiologic doses, should be continued in adults with RA, lupus, or inflammatory arthritis. A meta-analysis and systematic review of randomized controlled trial data and observational data showed no hemodynamic difference between daily doses and stress doses.
“In addition, there are abundant observational data demonstrating an increase in infection in patients on chronic steroids greater than 15 mg, and we thought that part of the optimization of the patient would be getting them on the lowest possible steroid dose,” she said, stressing that this refers only to adults receiving glucocorticoids for their rheumatic disease, and not to those with a history of JIA who may have received steroids during development, or to those receiving glucocorticoids for primary, adrenal, or hypothalamic disease.
According to Dr. Goodman, the time is right for the introduction of these recommendations, because the increased use of disease-modifying drugs and biologics means that most patients coming in for these surgeries will be taking these medications.
Further, despite the widespread use of the medications, the rate of total knee and hip arthroplasty surgeries among patients with rheumatic diseases is about the same as it was 20 or 30 years ago – and their risk for devastating complications, including infections, remains high, she said, noting that appropriate medication management provides an opportunity to mitigate risk.
Coprincipal investigator, Bryan Springer, MD, further emphasized the importance of the guideline, noting that the 5-year survival among rheumatic disease patients who develop certain perioperative complications is lower than for many common cancers, and that the literature offers little guidance on managing medications in the perioperative period.
“We now have a document that’s based on the available evidence, and also based on expert opinion, to help us manage these patients much more thoroughly in the perioperative period,” Dr. Springer, an orthopedic surgeon in Charlotte, N.C., said during a press briefing on the guideline.
Dr. Springer highlighted the value of the unique collaboration between the ACR and the AAHKS, calling the effort a win both for patients, and for “collaborative efforts, collaborative research, which we just really don’t do enough of,” he said. “I hope this is a huge step towards that direction.”
This guideline development process was funded by the ACR and AAHKS.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Biologic agents should be stopped prior to elective total knee or hip arthroplasty in patients with rheumatic diseases, according to a draft guideline developed by the American College of Rheumatology and the American Association of Hip and Knee Surgeons.
The guideline, which address the perioperative management of antirheumatic medications in patients with rheumatoid arthritis, spondyloarthritis, psoriatic arthritis, juvenile idiopathic arthritis (JIA), or lupus who are undergoing such surgery, is currently under review, Dr. Susan Goodman, MD, coprincipal investigator, reported at the annual meeting of the American College of Rheumatology.
The draft guideline was created because “guidance was needed for common clinical situations, even where data were sparse. We didn’t want to configure treatment mandates – that’s not what these are,” Dr. Goodman of Cornell University, New York, said.
The recommendations are conditional, she said, meaning that the benefits probably outweigh the harms, that the recommendations apply to most but not all patients, and that future research may lead to changes.
“They’re also preference sensitive,” she said, explaining that patients’ values and preferences should be carefully considered, as they might differ from those of the patient panel consulted during guideline development; the panel expressed greater concern about the risk of infection following surgery than about perioperative flares resulting from medication discontinuation.
Based on agreement by at least 80% of a voting panel which considered available evidence in the context of their clinical experience along with the input from the patient panel, the draft guideline states that:
• Current doses of methotrexate, leflunomide, hydroxychloroquine, and sulfasalazine should be continued in patients with rheumatic diseases undergoing elective hip and knee replacement. This recommendation is based on an extensive literature review that showed the infection rate is decreased in patients who continue these medications, Dr. Goodman said.
• All biologics should be withheld prior to surgery in patients with inflammatory arthritis, and surgery should be planned for the end of the dosing cycle. This matter wasn’t specifically addressed in the literature; however, numerous randomized controlled trials outside of the surgical setting demonstrate an increased risk of infection associated with their use, she noted.
“All of the biologic medications were found to be associated with an increased risk of infection,” she said. “Because of this and the level of importance patients place on minimizing infection risk, we’ve recommended that biologics be withheld prior to surgery.”
• Tofacitinib, which was considered in a separate oral, targeted therapy category, should be withheld for at least 7 days prior to surgery in patients with RA, spondyloarthritis, and JIA. Data from systematic reviews and meta-analyses showed an increased risk of infection with tofacitinib, although more research is needed in order to “firm up” this recommendation, Dr. Goodman said.
• In lupus patients, rituximab and belimumab should be withheld prior to surgery, and surgery should be planned for the end of the dosing period.
“Again, this was not answered in the literature. We depended on observational studies that we reviewed that did show that patients with severe active lupus were at much higher risk for adverse events. But since rituximab isn’t approved by the [Food and Drug Administration] for use in lupus, and belimumab isn’t approved for use in severe lupus – and those seem to be the high-risk patients – we thought withholding them was more prudent,” she said.
• Patients with severe lupus should continue on current doses of methotrexate, mycophenolic acid, azathioprine, mizoribine, cyclosporine, and tacrolimus through surgery. This recommendation is based on indirect data from experience in organ transplant patients.
• All medications should be discontinued in patients whose lupus is not severe.
“Our recommendation is to withhold for 7 days to 2-5 days after surgery in the absence of any wound healing complications or any other complications,” she said, noting that the literature does not directly address this; the recommendation is based on indirect evidence in patients with either active infection or who are at risk for infection.
“We thought that careful monitoring of the patient would permit us to identify flare and intervene quickly. … and that, for mild cases of lupus, the morbidity associated with infection might not be greater than the morbidity associated with the disease flare,” she said.
• Biologics should be restarted once surgical wounds show evidence of healing and there is no clinical evidence of infection. The literature does not directly address this; the recommendation is based on the rationale for use of these medications in patients with either active infection or risk for infection.
• Current daily doses of glucocorticoids, rather than supraphysiologic doses, should be continued in adults with RA, lupus, or inflammatory arthritis. A meta-analysis and systematic review of randomized controlled trial data and observational data showed no hemodynamic difference between daily doses and stress doses.
“In addition, there are abundant observational data demonstrating an increase in infection in patients on chronic steroids greater than 15 mg, and we thought that part of the optimization of the patient would be getting them on the lowest possible steroid dose,” she said, stressing that this refers only to adults receiving glucocorticoids for their rheumatic disease, and not to those with a history of JIA who may have received steroids during development, or to those receiving glucocorticoids for primary, adrenal, or hypothalamic disease.
According to Dr. Goodman, the time is right for the introduction of these recommendations, because the increased use of disease-modifying drugs and biologics means that most patients coming in for these surgeries will be taking these medications.
Further, despite the widespread use of the medications, the rate of total knee and hip arthroplasty surgeries among patients with rheumatic diseases is about the same as it was 20 or 30 years ago – and their risk for devastating complications, including infections, remains high, she said, noting that appropriate medication management provides an opportunity to mitigate risk.
Coprincipal investigator, Bryan Springer, MD, further emphasized the importance of the guideline, noting that the 5-year survival among rheumatic disease patients who develop certain perioperative complications is lower than for many common cancers, and that the literature offers little guidance on managing medications in the perioperative period.
“We now have a document that’s based on the available evidence, and also based on expert opinion, to help us manage these patients much more thoroughly in the perioperative period,” Dr. Springer, an orthopedic surgeon in Charlotte, N.C., said during a press briefing on the guideline.
Dr. Springer highlighted the value of the unique collaboration between the ACR and the AAHKS, calling the effort a win both for patients, and for “collaborative efforts, collaborative research, which we just really don’t do enough of,” he said. “I hope this is a huge step towards that direction.”
This guideline development process was funded by the ACR and AAHKS.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Biologic agents should be stopped prior to elective total knee or hip arthroplasty in patients with rheumatic diseases, according to a draft guideline developed by the American College of Rheumatology and the American Association of Hip and Knee Surgeons.
The guideline, which address the perioperative management of antirheumatic medications in patients with rheumatoid arthritis, spondyloarthritis, psoriatic arthritis, juvenile idiopathic arthritis (JIA), or lupus who are undergoing such surgery, is currently under review, Dr. Susan Goodman, MD, coprincipal investigator, reported at the annual meeting of the American College of Rheumatology.
The draft guideline was created because “guidance was needed for common clinical situations, even where data were sparse. We didn’t want to configure treatment mandates – that’s not what these are,” Dr. Goodman of Cornell University, New York, said.
The recommendations are conditional, she said, meaning that the benefits probably outweigh the harms, that the recommendations apply to most but not all patients, and that future research may lead to changes.
“They’re also preference sensitive,” she said, explaining that patients’ values and preferences should be carefully considered, as they might differ from those of the patient panel consulted during guideline development; the panel expressed greater concern about the risk of infection following surgery than about perioperative flares resulting from medication discontinuation.
Based on agreement by at least 80% of a voting panel which considered available evidence in the context of their clinical experience along with the input from the patient panel, the draft guideline states that:
• Current doses of methotrexate, leflunomide, hydroxychloroquine, and sulfasalazine should be continued in patients with rheumatic diseases undergoing elective hip and knee replacement. This recommendation is based on an extensive literature review that showed the infection rate is decreased in patients who continue these medications, Dr. Goodman said.
• All biologics should be withheld prior to surgery in patients with inflammatory arthritis, and surgery should be planned for the end of the dosing cycle. This matter wasn’t specifically addressed in the literature; however, numerous randomized controlled trials outside of the surgical setting demonstrate an increased risk of infection associated with their use, she noted.
“All of the biologic medications were found to be associated with an increased risk of infection,” she said. “Because of this and the level of importance patients place on minimizing infection risk, we’ve recommended that biologics be withheld prior to surgery.”
• Tofacitinib, which was considered in a separate oral, targeted therapy category, should be withheld for at least 7 days prior to surgery in patients with RA, spondyloarthritis, and JIA. Data from systematic reviews and meta-analyses showed an increased risk of infection with tofacitinib, although more research is needed in order to “firm up” this recommendation, Dr. Goodman said.
• In lupus patients, rituximab and belimumab should be withheld prior to surgery, and surgery should be planned for the end of the dosing period.
“Again, this was not answered in the literature. We depended on observational studies that we reviewed that did show that patients with severe active lupus were at much higher risk for adverse events. But since rituximab isn’t approved by the [Food and Drug Administration] for use in lupus, and belimumab isn’t approved for use in severe lupus – and those seem to be the high-risk patients – we thought withholding them was more prudent,” she said.
• Patients with severe lupus should continue on current doses of methotrexate, mycophenolic acid, azathioprine, mizoribine, cyclosporine, and tacrolimus through surgery. This recommendation is based on indirect data from experience in organ transplant patients.
• All medications should be discontinued in patients whose lupus is not severe.
“Our recommendation is to withhold for 7 days to 2-5 days after surgery in the absence of any wound healing complications or any other complications,” she said, noting that the literature does not directly address this; the recommendation is based on indirect evidence in patients with either active infection or who are at risk for infection.
“We thought that careful monitoring of the patient would permit us to identify flare and intervene quickly. … and that, for mild cases of lupus, the morbidity associated with infection might not be greater than the morbidity associated with the disease flare,” she said.
• Biologics should be restarted once surgical wounds show evidence of healing and there is no clinical evidence of infection. The literature does not directly address this; the recommendation is based on the rationale for use of these medications in patients with either active infection or risk for infection.
• Current daily doses of glucocorticoids, rather than supraphysiologic doses, should be continued in adults with RA, lupus, or inflammatory arthritis. A meta-analysis and systematic review of randomized controlled trial data and observational data showed no hemodynamic difference between daily doses and stress doses.
“In addition, there are abundant observational data demonstrating an increase in infection in patients on chronic steroids greater than 15 mg, and we thought that part of the optimization of the patient would be getting them on the lowest possible steroid dose,” she said, stressing that this refers only to adults receiving glucocorticoids for their rheumatic disease, and not to those with a history of JIA who may have received steroids during development, or to those receiving glucocorticoids for primary, adrenal, or hypothalamic disease.
According to Dr. Goodman, the time is right for the introduction of these recommendations, because the increased use of disease-modifying drugs and biologics means that most patients coming in for these surgeries will be taking these medications.
Further, despite the widespread use of the medications, the rate of total knee and hip arthroplasty surgeries among patients with rheumatic diseases is about the same as it was 20 or 30 years ago – and their risk for devastating complications, including infections, remains high, she said, noting that appropriate medication management provides an opportunity to mitigate risk.
Coprincipal investigator, Bryan Springer, MD, further emphasized the importance of the guideline, noting that the 5-year survival among rheumatic disease patients who develop certain perioperative complications is lower than for many common cancers, and that the literature offers little guidance on managing medications in the perioperative period.
“We now have a document that’s based on the available evidence, and also based on expert opinion, to help us manage these patients much more thoroughly in the perioperative period,” Dr. Springer, an orthopedic surgeon in Charlotte, N.C., said during a press briefing on the guideline.
Dr. Springer highlighted the value of the unique collaboration between the ACR and the AAHKS, calling the effort a win both for patients, and for “collaborative efforts, collaborative research, which we just really don’t do enough of,” he said. “I hope this is a huge step towards that direction.”
This guideline development process was funded by the ACR and AAHKS.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ACR ANNUAL MEETING

Continue DMARDs, biologics in RA surgery patients
WASHINGTON – The perioperative use of disease-modifying antirheumatic drug monotherapy or combined therapy with methotrexate and a tumor necrosis factor (TNF) inhibitor is not associated with increased rates of postoperative infectious complications or wound infections in patients with rheumatoid arthritis, according to findings from a retrospective review of more than 9,000 surgeries.
With respect to monotherapy, treatment was continued in 1,951 of 2,601 surgeries among patients receiving methotrexate, in 1,496 of 2,012 surgeries among patients receiving hydroxychloroquine, and in 508 of 652 surgeries among patient receiving leflunomide. The odds ratios for postoperative infection (including urinary tract, pneumonia, or sepsis) and postoperative wound infection, respectively, were 0.79 and 0.77 with methotrexate continuation, 0.93 and 0.86 with hydroxychloroquine continuation, and 0.78 and 0.87 with leflunomide continuation, Hsin-Hsuan Juo, MD, reported at the annual meeting of the American College of Rheumatology.
Data for this study were derived from the U.S. Department of Veterans Affairs administrative database and surgical quality registry. Rheumatoid arthritis patients who underwent a surgical procedure and who were on at least one disease-modifying antirheumatic drug (DMARD) or one biologic agent in the perioperative period during the study period of Oct. 1, 1999, through Sept. 30, 2009, were included. Subjects had a mean age of 67 years, and 91% were men.
The finding that the continuation of DMARD monotherapy or the combination of methotrexate and TNF inhibitor therapy for RA in the perioperative setting was not associated with increased rates of overall postoperative infectious complications and wound infections is important, because many patients are advised to stop taking these drugs prior to surgery because of concerns about increased susceptibility to infection. Discontinuing RA medication can increase the risk of disease flares requiring treatment with prednisone, which can further increase the risk of postsurgical complications, Dr. Juo said.
Clear, consistent guidance on the continuation of treatment among RA patients undergoing surgery has been lacking, she said, noting that guidelines over the years from the ACR, the British Society for Rheumatology, and the Canadian Rheumatology Association have differed in their recommendations.
A new draft guideline reported the morning of Dr. Juo’s presentation at the ACR annual meeting recommended continuing DMARDs but discontinuing biologics prior to surgery, but that guideline is limited to orthopedic surgery among patients with various rheumatic diseases.
“With literature review, the results are conflicting as well; some recommend continuing medication, and others recommend discontinuing medications prior to surgery,” she said.
The current findings, though limited by the study’s observational design and generally older, male population, suggest that continuing antirheumatic medications during the perioperative period is not associated with increased rates of postoperative complications.
“Our study results suggest that discontinuing DMARDs and biologic agents prior to surgery may not be necessary. Therefore, being on DMARDs or biologic agents should not preclude patients from receiving urgent surgeries,” Dr. Juo concluded.
Dr. Juo reported having no disclosures.
WASHINGTON – The perioperative use of disease-modifying antirheumatic drug monotherapy or combined therapy with methotrexate and a tumor necrosis factor (TNF) inhibitor is not associated with increased rates of postoperative infectious complications or wound infections in patients with rheumatoid arthritis, according to findings from a retrospective review of more than 9,000 surgeries.
With respect to monotherapy, treatment was continued in 1,951 of 2,601 surgeries among patients receiving methotrexate, in 1,496 of 2,012 surgeries among patients receiving hydroxychloroquine, and in 508 of 652 surgeries among patient receiving leflunomide. The odds ratios for postoperative infection (including urinary tract, pneumonia, or sepsis) and postoperative wound infection, respectively, were 0.79 and 0.77 with methotrexate continuation, 0.93 and 0.86 with hydroxychloroquine continuation, and 0.78 and 0.87 with leflunomide continuation, Hsin-Hsuan Juo, MD, reported at the annual meeting of the American College of Rheumatology.
Data for this study were derived from the U.S. Department of Veterans Affairs administrative database and surgical quality registry. Rheumatoid arthritis patients who underwent a surgical procedure and who were on at least one disease-modifying antirheumatic drug (DMARD) or one biologic agent in the perioperative period during the study period of Oct. 1, 1999, through Sept. 30, 2009, were included. Subjects had a mean age of 67 years, and 91% were men.
The finding that the continuation of DMARD monotherapy or the combination of methotrexate and TNF inhibitor therapy for RA in the perioperative setting was not associated with increased rates of overall postoperative infectious complications and wound infections is important, because many patients are advised to stop taking these drugs prior to surgery because of concerns about increased susceptibility to infection. Discontinuing RA medication can increase the risk of disease flares requiring treatment with prednisone, which can further increase the risk of postsurgical complications, Dr. Juo said.
Clear, consistent guidance on the continuation of treatment among RA patients undergoing surgery has been lacking, she said, noting that guidelines over the years from the ACR, the British Society for Rheumatology, and the Canadian Rheumatology Association have differed in their recommendations.
A new draft guideline reported the morning of Dr. Juo’s presentation at the ACR annual meeting recommended continuing DMARDs but discontinuing biologics prior to surgery, but that guideline is limited to orthopedic surgery among patients with various rheumatic diseases.
“With literature review, the results are conflicting as well; some recommend continuing medication, and others recommend discontinuing medications prior to surgery,” she said.
The current findings, though limited by the study’s observational design and generally older, male population, suggest that continuing antirheumatic medications during the perioperative period is not associated with increased rates of postoperative complications.
“Our study results suggest that discontinuing DMARDs and biologic agents prior to surgery may not be necessary. Therefore, being on DMARDs or biologic agents should not preclude patients from receiving urgent surgeries,” Dr. Juo concluded.
Dr. Juo reported having no disclosures.
WASHINGTON – The perioperative use of disease-modifying antirheumatic drug monotherapy or combined therapy with methotrexate and a tumor necrosis factor (TNF) inhibitor is not associated with increased rates of postoperative infectious complications or wound infections in patients with rheumatoid arthritis, according to findings from a retrospective review of more than 9,000 surgeries.
With respect to monotherapy, treatment was continued in 1,951 of 2,601 surgeries among patients receiving methotrexate, in 1,496 of 2,012 surgeries among patients receiving hydroxychloroquine, and in 508 of 652 surgeries among patient receiving leflunomide. The odds ratios for postoperative infection (including urinary tract, pneumonia, or sepsis) and postoperative wound infection, respectively, were 0.79 and 0.77 with methotrexate continuation, 0.93 and 0.86 with hydroxychloroquine continuation, and 0.78 and 0.87 with leflunomide continuation, Hsin-Hsuan Juo, MD, reported at the annual meeting of the American College of Rheumatology.
Data for this study were derived from the U.S. Department of Veterans Affairs administrative database and surgical quality registry. Rheumatoid arthritis patients who underwent a surgical procedure and who were on at least one disease-modifying antirheumatic drug (DMARD) or one biologic agent in the perioperative period during the study period of Oct. 1, 1999, through Sept. 30, 2009, were included. Subjects had a mean age of 67 years, and 91% were men.
The finding that the continuation of DMARD monotherapy or the combination of methotrexate and TNF inhibitor therapy for RA in the perioperative setting was not associated with increased rates of overall postoperative infectious complications and wound infections is important, because many patients are advised to stop taking these drugs prior to surgery because of concerns about increased susceptibility to infection. Discontinuing RA medication can increase the risk of disease flares requiring treatment with prednisone, which can further increase the risk of postsurgical complications, Dr. Juo said.
Clear, consistent guidance on the continuation of treatment among RA patients undergoing surgery has been lacking, she said, noting that guidelines over the years from the ACR, the British Society for Rheumatology, and the Canadian Rheumatology Association have differed in their recommendations.
A new draft guideline reported the morning of Dr. Juo’s presentation at the ACR annual meeting recommended continuing DMARDs but discontinuing biologics prior to surgery, but that guideline is limited to orthopedic surgery among patients with various rheumatic diseases.
“With literature review, the results are conflicting as well; some recommend continuing medication, and others recommend discontinuing medications prior to surgery,” she said.
The current findings, though limited by the study’s observational design and generally older, male population, suggest that continuing antirheumatic medications during the perioperative period is not associated with increased rates of postoperative complications.
“Our study results suggest that discontinuing DMARDs and biologic agents prior to surgery may not be necessary. Therefore, being on DMARDs or biologic agents should not preclude patients from receiving urgent surgeries,” Dr. Juo concluded.
Dr. Juo reported having no disclosures.
AT THE ACR ANNUAL MEETING
Key clinical point:
Major finding: Odds ratios for postoperative infection and postoperative wound infection, respectively, were 0.79 and 0.77 with methotrexate continuation, 0.93 and 0.86 with hydroxychloroquine continuation, 0.78 and 0.87 with leflunomide continuation, and 0.35 and 0.38 with combined methotrexate/TNF inhibitor continuation.
Data source: A retrospective review of more than 9,000 surgeries.
Disclosures: Dr. Juo reported having no disclosures.
VIDEO: For CABG, double arterial grafts found no better than single
NEW ORLEANS – Patients undergoing coronary artery bypass graft (CABG) surgery do not see any 5-year survival advantage when their surgeon uses both internal mammary (thoracic) arteries for grafting rather than just one of them along with a vein, finds an interim analysis from the randomized Arterial Revascularization Trial (ART).
Overall, about 8.5% of the 3,102 patients randomized had died 5 years after surgery, with no significant difference between the bilateral graft and single graft groups, according to data reported at the American Heart Association scientific sessions and simultaneously published (N Engl J Med. 2016 Nov 14. doi: 10.1056/NEJMoa1610021). The former had roughly triple the rate of sternal reconstruction, mainly driven by complications in insulin-dependent diabetes patients having high body mass index.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There is strong angiographic evidence that vein grafts have a high rate of failure over time because of atherosclerosis, but internal mammary artery grafts retain excellent patency, he elaborated. “People have speculated that this superior patency of internal mammary arteries will translate into a clinical survival benefit,” and observational data indeed suggest that the bilateral artery strategy reduces mortality by about one-fifth relative to the single artery strategy.
Yet uptake of the bilateral procedure has been low. It is used in fewer than 5% of patients undergoing CABG in the United States and fewer than 10% of those in Europe, reflecting concerns about its greater technical complexity, potentially increased mortality and morbidity, and – until now – lack of evidence from randomized trials.
“What I think we can conclude today is that there are excellent 5-year outcomes of CABG in both groups. This study confirms that it’s at least safe to use bilateral grafts over the medium term,” Dr. Taggart commented. He discussed the results in a video interview conducted at the meeting.
These interim ART data probably won’t sway practice one way or the other, he said. “People who believe in arterial grafts will continue to do them, and those who are not enthusiastic about the prospect of a slightly technically more difficult operation [can now] remain comfortable as to why they are not using both internal mammary arteries.”
Pointed questions

The lack of difference was possibly due to a very high level of guideline-based medical therapy in the trial (which may have especially protected the vein grafts) or to the fact that the annual failure rate of vein grafts is modest and steady up to 5 years but accelerates thereafter, Dr. Taggart proposed. The trial’s primary outcome of 10-year survival, expected in 2018, will likely differ, speculated Dr. Sellke, who is also program chair for the AHA scientific sessions.
“Do you think multiple arterial grafting is superior to single internal mammary artery grafting considering the lack of improvement in survival and other outcomes in the study, with the increase in sternal wound infections?” he asked.
“I personally, if I needed the operation, would insist on having bilateral internal mammary artery grafts done by an experienced operator because it is totally counterintuitive to believe that having more patent grafts in your heart at 10 to 20 years of follow-up is of no benefit,” Dr. Taggart maintained.
When data meet clinical practice
It may require time for the benefit of the bilateral artery graft to emerge, he agreed. “I’m undeterred from my belief that ... in patients who are getting CABG done in their 40s or 50s or early 60s, betting on a graft that’s going to outperform vein grafts is the better strategy.”
Until the trial’s 10-year results become available, physicians may wish to put these interim results in the context when counseling patients, according to Dr. Gardner.
“We have indisputable evidence that arterial grafts have better long-term patency than vein grafts,” he elaborated. “If we had a very sophisticated patient, we might tell them that we were a little surprised that this head-to-head trial of single versus double didn’t show any survival benefit at 5 years, but we still are persuaded by the data that shows the better patency, and we think in the situation that the patient’s in, that we would still recommend a double mammary, assuming that the patient doesn’t have comorbidities that would make that more dangerous.”
Trial details
ART enrolled patients from 28 cardiac surgical centers in seven countries. The patients, all of whom had multivessel coronary disease and were scheduled to undergo CABG, were randomized evenly to single or bilateral internal thoracic artery grafts.
The interim results showed differences in nonadherence to the randomized operation: 2.4% of patients in the single graft group ultimately underwent got bilateral grafts, whereas 14% of patients in the bilateral graft group ultimately got a single graft.
“This raises questions about how experienced some surgeons were with the use of bilateral internal mammary artery grafts,” Dr. Taggart commented.
At 5 years of follow-up, 8.7% of patients in the bilateral graft group and 8.4% of patients in the single graft group had died, a nonsignificant difference. “Those mortalities are similar to what has been observed in other contemporary trials of CABG,” he noted. There was no difference between diabetic and nondiabetic patients with respect to this outcome.
The rate of the composite outcome of death, myocardial infarction, or stroke was 12.2% in the bilateral graft group and 12.7% in the single graft group, also a nonsignificant difference.
On the other hand, patients in the bilateral graft group had higher rates of sternal wound complications (3.5% vs. 1.9%; P = .005) and sternal reconstruction (1.9% vs. 0.6%; P = .002).
The groups were statistically indistinguishable with respect to rates of mortality, major bleeding, or need for repeat revascularization, as well as angina status and quality of life measures, according to Dr. Taggart, who disclosed that he had no relevant conflicts of interest.
NEW ORLEANS – Patients undergoing coronary artery bypass graft (CABG) surgery do not see any 5-year survival advantage when their surgeon uses both internal mammary (thoracic) arteries for grafting rather than just one of them along with a vein, finds an interim analysis from the randomized Arterial Revascularization Trial (ART).
Overall, about 8.5% of the 3,102 patients randomized had died 5 years after surgery, with no significant difference between the bilateral graft and single graft groups, according to data reported at the American Heart Association scientific sessions and simultaneously published (N Engl J Med. 2016 Nov 14. doi: 10.1056/NEJMoa1610021). The former had roughly triple the rate of sternal reconstruction, mainly driven by complications in insulin-dependent diabetes patients having high body mass index.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There is strong angiographic evidence that vein grafts have a high rate of failure over time because of atherosclerosis, but internal mammary artery grafts retain excellent patency, he elaborated. “People have speculated that this superior patency of internal mammary arteries will translate into a clinical survival benefit,” and observational data indeed suggest that the bilateral artery strategy reduces mortality by about one-fifth relative to the single artery strategy.
Yet uptake of the bilateral procedure has been low. It is used in fewer than 5% of patients undergoing CABG in the United States and fewer than 10% of those in Europe, reflecting concerns about its greater technical complexity, potentially increased mortality and morbidity, and – until now – lack of evidence from randomized trials.
“What I think we can conclude today is that there are excellent 5-year outcomes of CABG in both groups. This study confirms that it’s at least safe to use bilateral grafts over the medium term,” Dr. Taggart commented. He discussed the results in a video interview conducted at the meeting.
These interim ART data probably won’t sway practice one way or the other, he said. “People who believe in arterial grafts will continue to do them, and those who are not enthusiastic about the prospect of a slightly technically more difficult operation [can now] remain comfortable as to why they are not using both internal mammary arteries.”
Pointed questions
The lack of difference was possibly due to a very high level of guideline-based medical therapy in the trial (which may have especially protected the vein grafts) or to the fact that the annual failure rate of vein grafts is modest and steady up to 5 years but accelerates thereafter, Dr. Taggart proposed. The trial’s primary outcome of 10-year survival, expected in 2018, will likely differ, speculated Dr. Sellke, who is also program chair for the AHA scientific sessions.
“Do you think multiple arterial grafting is superior to single internal mammary artery grafting considering the lack of improvement in survival and other outcomes in the study, with the increase in sternal wound infections?” he asked.
“I personally, if I needed the operation, would insist on having bilateral internal mammary artery grafts done by an experienced operator because it is totally counterintuitive to believe that having more patent grafts in your heart at 10 to 20 years of follow-up is of no benefit,” Dr. Taggart maintained.
When data meet clinical practice
It may require time for the benefit of the bilateral artery graft to emerge, he agreed. “I’m undeterred from my belief that ... in patients who are getting CABG done in their 40s or 50s or early 60s, betting on a graft that’s going to outperform vein grafts is the better strategy.”
Until the trial’s 10-year results become available, physicians may wish to put these interim results in the context when counseling patients, according to Dr. Gardner.
“We have indisputable evidence that arterial grafts have better long-term patency than vein grafts,” he elaborated. “If we had a very sophisticated patient, we might tell them that we were a little surprised that this head-to-head trial of single versus double didn’t show any survival benefit at 5 years, but we still are persuaded by the data that shows the better patency, and we think in the situation that the patient’s in, that we would still recommend a double mammary, assuming that the patient doesn’t have comorbidities that would make that more dangerous.”
Trial details
ART enrolled patients from 28 cardiac surgical centers in seven countries. The patients, all of whom had multivessel coronary disease and were scheduled to undergo CABG, were randomized evenly to single or bilateral internal thoracic artery grafts.
The interim results showed differences in nonadherence to the randomized operation: 2.4% of patients in the single graft group ultimately underwent got bilateral grafts, whereas 14% of patients in the bilateral graft group ultimately got a single graft.
“This raises questions about how experienced some surgeons were with the use of bilateral internal mammary artery grafts,” Dr. Taggart commented.
At 5 years of follow-up, 8.7% of patients in the bilateral graft group and 8.4% of patients in the single graft group had died, a nonsignificant difference. “Those mortalities are similar to what has been observed in other contemporary trials of CABG,” he noted. There was no difference between diabetic and nondiabetic patients with respect to this outcome.
The rate of the composite outcome of death, myocardial infarction, or stroke was 12.2% in the bilateral graft group and 12.7% in the single graft group, also a nonsignificant difference.
On the other hand, patients in the bilateral graft group had higher rates of sternal wound complications (3.5% vs. 1.9%; P = .005) and sternal reconstruction (1.9% vs. 0.6%; P = .002).
The groups were statistically indistinguishable with respect to rates of mortality, major bleeding, or need for repeat revascularization, as well as angina status and quality of life measures, according to Dr. Taggart, who disclosed that he had no relevant conflicts of interest.
NEW ORLEANS – Patients undergoing coronary artery bypass graft (CABG) surgery do not see any 5-year survival advantage when their surgeon uses both internal mammary (thoracic) arteries for grafting rather than just one of them along with a vein, finds an interim analysis from the randomized Arterial Revascularization Trial (ART).
Overall, about 8.5% of the 3,102 patients randomized had died 5 years after surgery, with no significant difference between the bilateral graft and single graft groups, according to data reported at the American Heart Association scientific sessions and simultaneously published (N Engl J Med. 2016 Nov 14. doi: 10.1056/NEJMoa1610021). The former had roughly triple the rate of sternal reconstruction, mainly driven by complications in insulin-dependent diabetes patients having high body mass index.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There is strong angiographic evidence that vein grafts have a high rate of failure over time because of atherosclerosis, but internal mammary artery grafts retain excellent patency, he elaborated. “People have speculated that this superior patency of internal mammary arteries will translate into a clinical survival benefit,” and observational data indeed suggest that the bilateral artery strategy reduces mortality by about one-fifth relative to the single artery strategy.
Yet uptake of the bilateral procedure has been low. It is used in fewer than 5% of patients undergoing CABG in the United States and fewer than 10% of those in Europe, reflecting concerns about its greater technical complexity, potentially increased mortality and morbidity, and – until now – lack of evidence from randomized trials.
“What I think we can conclude today is that there are excellent 5-year outcomes of CABG in both groups. This study confirms that it’s at least safe to use bilateral grafts over the medium term,” Dr. Taggart commented. He discussed the results in a video interview conducted at the meeting.
These interim ART data probably won’t sway practice one way or the other, he said. “People who believe in arterial grafts will continue to do them, and those who are not enthusiastic about the prospect of a slightly technically more difficult operation [can now] remain comfortable as to why they are not using both internal mammary arteries.”
Pointed questions
The lack of difference was possibly due to a very high level of guideline-based medical therapy in the trial (which may have especially protected the vein grafts) or to the fact that the annual failure rate of vein grafts is modest and steady up to 5 years but accelerates thereafter, Dr. Taggart proposed. The trial’s primary outcome of 10-year survival, expected in 2018, will likely differ, speculated Dr. Sellke, who is also program chair for the AHA scientific sessions.
“Do you think multiple arterial grafting is superior to single internal mammary artery grafting considering the lack of improvement in survival and other outcomes in the study, with the increase in sternal wound infections?” he asked.
“I personally, if I needed the operation, would insist on having bilateral internal mammary artery grafts done by an experienced operator because it is totally counterintuitive to believe that having more patent grafts in your heart at 10 to 20 years of follow-up is of no benefit,” Dr. Taggart maintained.
When data meet clinical practice
It may require time for the benefit of the bilateral artery graft to emerge, he agreed. “I’m undeterred from my belief that ... in patients who are getting CABG done in their 40s or 50s or early 60s, betting on a graft that’s going to outperform vein grafts is the better strategy.”
Until the trial’s 10-year results become available, physicians may wish to put these interim results in the context when counseling patients, according to Dr. Gardner.
“We have indisputable evidence that arterial grafts have better long-term patency than vein grafts,” he elaborated. “If we had a very sophisticated patient, we might tell them that we were a little surprised that this head-to-head trial of single versus double didn’t show any survival benefit at 5 years, but we still are persuaded by the data that shows the better patency, and we think in the situation that the patient’s in, that we would still recommend a double mammary, assuming that the patient doesn’t have comorbidities that would make that more dangerous.”
Trial details
ART enrolled patients from 28 cardiac surgical centers in seven countries. The patients, all of whom had multivessel coronary disease and were scheduled to undergo CABG, were randomized evenly to single or bilateral internal thoracic artery grafts.
The interim results showed differences in nonadherence to the randomized operation: 2.4% of patients in the single graft group ultimately underwent got bilateral grafts, whereas 14% of patients in the bilateral graft group ultimately got a single graft.
“This raises questions about how experienced some surgeons were with the use of bilateral internal mammary artery grafts,” Dr. Taggart commented.
At 5 years of follow-up, 8.7% of patients in the bilateral graft group and 8.4% of patients in the single graft group had died, a nonsignificant difference. “Those mortalities are similar to what has been observed in other contemporary trials of CABG,” he noted. There was no difference between diabetic and nondiabetic patients with respect to this outcome.
The rate of the composite outcome of death, myocardial infarction, or stroke was 12.2% in the bilateral graft group and 12.7% in the single graft group, also a nonsignificant difference.
On the other hand, patients in the bilateral graft group had higher rates of sternal wound complications (3.5% vs. 1.9%; P = .005) and sternal reconstruction (1.9% vs. 0.6%; P = .002).
The groups were statistically indistinguishable with respect to rates of mortality, major bleeding, or need for repeat revascularization, as well as angina status and quality of life measures, according to Dr. Taggart, who disclosed that he had no relevant conflicts of interest.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: At 5 years, the rate of all-cause mortality was 8.7% in the bilateral graft group and 8.4% in the single graft group, a nonsignificant difference.
Data source: ART, a randomized trial among 3,102 patients with multivessel coronary disease undergoing CABG.
Disclosures: Dr. Taggart had no relevant conflicts of interest. The trial was funded by the U.K. Medical Research Council, the British Heart Foundation, and the U.K. National Institute of Health Research Efficacy and Mechanistic Evaluation.
Robotic surgery instruments ‘virtually impossible’ to clean completely
Instruments used for robotic surgery are “virtually impossible” to clean completely, according to a report published in Infection Control & Hospital Epidemiology.
“A new standard for the cleaning of complex surgical instruments needs to be established, especially for those used in robotic surgery,” wrote Yuhei Saito of the surgical center at the University of Tokyo Hospital and associates.
They assessed the residual contamination of both robotic and regular surgical instruments at their medical center because “hospital staff in central sterile supply departments are troubled by the reprocessing of robotic instruments because they cannot be disassembled for cleaning like other endoscopic instruments. Their complex structure impairs brushing the inner surface of narrow lumens, resulting in failure to [completely] remove contaminants,” the researchers wrote.
In the first phase of the study, the researchers examined 41 instruments immediately after they were used in robotic surgery (7 radical prostatectomies and 2 anterior resections of the rectum) and 27 regular instruments immediately after they were used for open surgery (gastrectomy and colectomy). The robotic instruments were contaminated with 72.3 × 103 mcg of protein each, compared with 5.5 × 103 mcg of protein on the regular instruments, the investigators reported (Infect Control Hosp Epidemiol. 2016 Oct 31. doi: 10.1017/ice.2016.249).
In the second phase of the study, the researchers examined another 24 robotic instruments and 40 regular instruments after they were used in surgery and then cleaned according to the manufacturers’ instructions three successive times. For the robotic instruments, this involved manually brushing the outer surface while moving the instrument “wrists” through their full range of motion, followed by 15 minutes of ultrasonication with enzymatic detergent, flushing the lumen with a water gun through flush ports, and rinsing the entire instrument. For regular instruments, cleaning involved washer-disinfectors and included 5 minutes of ultrasonication, 10 minutes of spraying with an alkaline detergent, and 10 minutes of disinfection via heating.
The level of contamination declined with each successive cleaning but still remained comparatively high for the robotic instruments. The amount of protein contaminants released in the three cleanings was 650, 550, and 530 mcg per robotic instrument, compared with 16, 17, and 17 mcg per ordinary instrument.
The efficacy of cleaning was 97.6% for robotic instruments and 99.1% for regular instruments, the researchers reported.
This study was not designed to assess whether residual contamination is associated with adverse events such as infection in subsequent patients, and there are few data available on this topic.
“We have to recognize that there might be a considerable volume of insufficient cleaning or occult surgical site infections,” the investigators wrote.
New instrument washers equipped with a specific cleaning function for narrow lumens are becoming available, they noted, and “further study should be conducted using these washers with improved cleaning efficacy.”
The study was supported by the Japan Society for the Promotion of Science. The investigators reported having no relevant financial disclosures.
Instruments used for robotic surgery are “virtually impossible” to clean completely, according to a report published in Infection Control & Hospital Epidemiology.
“A new standard for the cleaning of complex surgical instruments needs to be established, especially for those used in robotic surgery,” wrote Yuhei Saito of the surgical center at the University of Tokyo Hospital and associates.
They assessed the residual contamination of both robotic and regular surgical instruments at their medical center because “hospital staff in central sterile supply departments are troubled by the reprocessing of robotic instruments because they cannot be disassembled for cleaning like other endoscopic instruments. Their complex structure impairs brushing the inner surface of narrow lumens, resulting in failure to [completely] remove contaminants,” the researchers wrote.
In the first phase of the study, the researchers examined 41 instruments immediately after they were used in robotic surgery (7 radical prostatectomies and 2 anterior resections of the rectum) and 27 regular instruments immediately after they were used for open surgery (gastrectomy and colectomy). The robotic instruments were contaminated with 72.3 × 103 mcg of protein each, compared with 5.5 × 103 mcg of protein on the regular instruments, the investigators reported (Infect Control Hosp Epidemiol. 2016 Oct 31. doi: 10.1017/ice.2016.249).
In the second phase of the study, the researchers examined another 24 robotic instruments and 40 regular instruments after they were used in surgery and then cleaned according to the manufacturers’ instructions three successive times. For the robotic instruments, this involved manually brushing the outer surface while moving the instrument “wrists” through their full range of motion, followed by 15 minutes of ultrasonication with enzymatic detergent, flushing the lumen with a water gun through flush ports, and rinsing the entire instrument. For regular instruments, cleaning involved washer-disinfectors and included 5 minutes of ultrasonication, 10 minutes of spraying with an alkaline detergent, and 10 minutes of disinfection via heating.
The level of contamination declined with each successive cleaning but still remained comparatively high for the robotic instruments. The amount of protein contaminants released in the three cleanings was 650, 550, and 530 mcg per robotic instrument, compared with 16, 17, and 17 mcg per ordinary instrument.
The efficacy of cleaning was 97.6% for robotic instruments and 99.1% for regular instruments, the researchers reported.
This study was not designed to assess whether residual contamination is associated with adverse events such as infection in subsequent patients, and there are few data available on this topic.
“We have to recognize that there might be a considerable volume of insufficient cleaning or occult surgical site infections,” the investigators wrote.
New instrument washers equipped with a specific cleaning function for narrow lumens are becoming available, they noted, and “further study should be conducted using these washers with improved cleaning efficacy.”
The study was supported by the Japan Society for the Promotion of Science. The investigators reported having no relevant financial disclosures.
Instruments used for robotic surgery are “virtually impossible” to clean completely, according to a report published in Infection Control & Hospital Epidemiology.
“A new standard for the cleaning of complex surgical instruments needs to be established, especially for those used in robotic surgery,” wrote Yuhei Saito of the surgical center at the University of Tokyo Hospital and associates.
They assessed the residual contamination of both robotic and regular surgical instruments at their medical center because “hospital staff in central sterile supply departments are troubled by the reprocessing of robotic instruments because they cannot be disassembled for cleaning like other endoscopic instruments. Their complex structure impairs brushing the inner surface of narrow lumens, resulting in failure to [completely] remove contaminants,” the researchers wrote.
In the first phase of the study, the researchers examined 41 instruments immediately after they were used in robotic surgery (7 radical prostatectomies and 2 anterior resections of the rectum) and 27 regular instruments immediately after they were used for open surgery (gastrectomy and colectomy). The robotic instruments were contaminated with 72.3 × 103 mcg of protein each, compared with 5.5 × 103 mcg of protein on the regular instruments, the investigators reported (Infect Control Hosp Epidemiol. 2016 Oct 31. doi: 10.1017/ice.2016.249).
In the second phase of the study, the researchers examined another 24 robotic instruments and 40 regular instruments after they were used in surgery and then cleaned according to the manufacturers’ instructions three successive times. For the robotic instruments, this involved manually brushing the outer surface while moving the instrument “wrists” through their full range of motion, followed by 15 minutes of ultrasonication with enzymatic detergent, flushing the lumen with a water gun through flush ports, and rinsing the entire instrument. For regular instruments, cleaning involved washer-disinfectors and included 5 minutes of ultrasonication, 10 minutes of spraying with an alkaline detergent, and 10 minutes of disinfection via heating.
The level of contamination declined with each successive cleaning but still remained comparatively high for the robotic instruments. The amount of protein contaminants released in the three cleanings was 650, 550, and 530 mcg per robotic instrument, compared with 16, 17, and 17 mcg per ordinary instrument.
The efficacy of cleaning was 97.6% for robotic instruments and 99.1% for regular instruments, the researchers reported.
This study was not designed to assess whether residual contamination is associated with adverse events such as infection in subsequent patients, and there are few data available on this topic.
“We have to recognize that there might be a considerable volume of insufficient cleaning or occult surgical site infections,” the investigators wrote.
New instrument washers equipped with a specific cleaning function for narrow lumens are becoming available, they noted, and “further study should be conducted using these washers with improved cleaning efficacy.”
The study was supported by the Japan Society for the Promotion of Science. The investigators reported having no relevant financial disclosures.
FROM INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY
Key clinical point:
Major finding: Immediately after surgery, robotic instruments were contaminated with 72.3 × 103 mcg of protein each, compared with 5.5 × 103 mcg of protein on regular instruments.
Data source: A single-center analysis of protein contamination before and after three successive cleanings on 65 instruments used for robotic surgery and 67 regular instruments used for open surgery.
Disclosures: This study was supported by the Japan Society for the Promotion of Science. The investigators reported having no relevant financial disclosures.
Long-term opioid use uncommon among trauma patients
WASHINGTON – Patients with traumatic injuries don’t appear to be at undue risk of sustained opioid use, a large database review has demonstrated.
More than half of the 13,000 patients in the study were discharged on opioids, but they were able to discontinue them fairly rapidly, Muhammad Chaudhary, MD, said at the annual clinical congress of the American College of Surgeons. Within 3 months, less than one-third were still using the drugs, and 1 year later, only 1% were still taking an opioid pain medication.
Dr. Chaudhary examined opioid use among 13,624 patients included in the Tricare military insurance database. The patients were treated for traumatic injuries they received during 2007-2013. Most of the patients were men (82%), and the largest age group was 18- to 24-year-olds (39%). Military rank was used as a proxy for socioeconomic status in this study: 15% of the cohort had an officer rank, while the rest were junior or senior enlisted personnel.
The group was very healthy, with a median Charlson Comorbidity Index score of 0. They were somewhat seriously injured, however. The median Injury Severity Score was 13, and the range was 9-17. Anxiety and depression were uncommon (9% and 7%, respectively).
More than half the patients (54%) were discharged on an opioid medication. That percentage dropped very rapidly. By 90 days after discharge, just 9% of patients were still taking the drugs. By 1 year, only 1% were using opioids.
Dr. Chaudhary conducted a multivariate analysis that controlled for a number of factors, including age, gender, marital status, rank, mental health status, injury severity, comorbidities, and treatment environment. Two factors – black race and younger age (18-24 years) – significantly increased the likelihood of early opioid discontinuation (8% and 11%, respectively). There were no significant interactions with anxiety or depression.
Junior enlisted personnel – the proxy group for lower socioeconomic status – and those with a prolonged length of stay were significantly less likely to get off the medications, Dr. Chaudhary said.
“While we strongly believe that these factors should not be used to determine who can get opioids, it might make sense to enhance perioperative surveillance and engage pain management services early on in patients with risk factors, to reduce the risk of sustained opioid use,” he concluded.
Dr. Chaudhary had no financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
WASHINGTON – Patients with traumatic injuries don’t appear to be at undue risk of sustained opioid use, a large database review has demonstrated.
More than half of the 13,000 patients in the study were discharged on opioids, but they were able to discontinue them fairly rapidly, Muhammad Chaudhary, MD, said at the annual clinical congress of the American College of Surgeons. Within 3 months, less than one-third were still using the drugs, and 1 year later, only 1% were still taking an opioid pain medication.
Dr. Chaudhary examined opioid use among 13,624 patients included in the Tricare military insurance database. The patients were treated for traumatic injuries they received during 2007-2013. Most of the patients were men (82%), and the largest age group was 18- to 24-year-olds (39%). Military rank was used as a proxy for socioeconomic status in this study: 15% of the cohort had an officer rank, while the rest were junior or senior enlisted personnel.
The group was very healthy, with a median Charlson Comorbidity Index score of 0. They were somewhat seriously injured, however. The median Injury Severity Score was 13, and the range was 9-17. Anxiety and depression were uncommon (9% and 7%, respectively).
More than half the patients (54%) were discharged on an opioid medication. That percentage dropped very rapidly. By 90 days after discharge, just 9% of patients were still taking the drugs. By 1 year, only 1% were using opioids.
Dr. Chaudhary conducted a multivariate analysis that controlled for a number of factors, including age, gender, marital status, rank, mental health status, injury severity, comorbidities, and treatment environment. Two factors – black race and younger age (18-24 years) – significantly increased the likelihood of early opioid discontinuation (8% and 11%, respectively). There were no significant interactions with anxiety or depression.
Junior enlisted personnel – the proxy group for lower socioeconomic status – and those with a prolonged length of stay were significantly less likely to get off the medications, Dr. Chaudhary said.
“While we strongly believe that these factors should not be used to determine who can get opioids, it might make sense to enhance perioperative surveillance and engage pain management services early on in patients with risk factors, to reduce the risk of sustained opioid use,” he concluded.
Dr. Chaudhary had no financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
WASHINGTON – Patients with traumatic injuries don’t appear to be at undue risk of sustained opioid use, a large database review has demonstrated.
More than half of the 13,000 patients in the study were discharged on opioids, but they were able to discontinue them fairly rapidly, Muhammad Chaudhary, MD, said at the annual clinical congress of the American College of Surgeons. Within 3 months, less than one-third were still using the drugs, and 1 year later, only 1% were still taking an opioid pain medication.
Dr. Chaudhary examined opioid use among 13,624 patients included in the Tricare military insurance database. The patients were treated for traumatic injuries they received during 2007-2013. Most of the patients were men (82%), and the largest age group was 18- to 24-year-olds (39%). Military rank was used as a proxy for socioeconomic status in this study: 15% of the cohort had an officer rank, while the rest were junior or senior enlisted personnel.
The group was very healthy, with a median Charlson Comorbidity Index score of 0. They were somewhat seriously injured, however. The median Injury Severity Score was 13, and the range was 9-17. Anxiety and depression were uncommon (9% and 7%, respectively).
More than half the patients (54%) were discharged on an opioid medication. That percentage dropped very rapidly. By 90 days after discharge, just 9% of patients were still taking the drugs. By 1 year, only 1% were using opioids.
Dr. Chaudhary conducted a multivariate analysis that controlled for a number of factors, including age, gender, marital status, rank, mental health status, injury severity, comorbidities, and treatment environment. Two factors – black race and younger age (18-24 years) – significantly increased the likelihood of early opioid discontinuation (8% and 11%, respectively). There were no significant interactions with anxiety or depression.
Junior enlisted personnel – the proxy group for lower socioeconomic status – and those with a prolonged length of stay were significantly less likely to get off the medications, Dr. Chaudhary said.
“While we strongly believe that these factors should not be used to determine who can get opioids, it might make sense to enhance perioperative surveillance and engage pain management services early on in patients with risk factors, to reduce the risk of sustained opioid use,” he concluded.
Dr. Chaudhary had no financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
AT THE ACS CLINICAL CONGRESS
Key clinical point:
Major finding: A year after discharge, only 1% of the patients were still using a prescription opioid pain medication.
Data source: A database review including 13,642 patients.
Disclosures: Dr. Chaudhary had no financial disclosures.
Fragmented readmission after liver transplant linked to adverse outcomes
CORONADO, CALIF. – Postdischarge surgical care fragmentation significantly increases the risk of both 30-day mortality and subsequent readmission in the first year following orthotopic liver transplantation, results from a study of national data showed.
“In an era of regionalization and centers of excellence, the likelihood for postdischarge fragmentation, defined as readmission to any hospital other than the hospital at which the surgery was performed, is an increasing reality,” Anai N. Kothari, MD, said at the annual meeting of the Western Surgical Association. “In many different surgical subspecialties – major vascular operations, bariatric surgery, oncologic resections – it’s known to be a risk factor for adverse events and poor quality. Postdischarge fragmentation is common, [and related to] as often as one in four readmissions. It increases the risk for short- and long-term morbidity and mortality, decreases survival, and increases cost.”
Dr. Kothari reported results from 2,996 patients with 7,485 readmission encounters at 299 hospitals. Of the 7,485 readmissions, 6,249 (83.5%) were nonfragmented, and 1,236 (16.5%) were fragmented. The mean age of patients was 55 years. There were no significant differences in baseline characteristics between patients with nonfragmented and fragmented admissions in terms of patient age, sex, preoperative and postoperative length of stay, Charlson comorbidity index, and comorbidities, with the exception of renal failure, which was more common among patients in the fragmented admission group.
Compared with the patients in the nonfragmented admission group, those in the fragmented admission group had a greater number of average readmissions per patient (3.3 vs. 2.5, respectively; P less than .0001) and a greater number of average days to readmission (168 vs. 105; P less than .0001). Reasons for readmission differed among the two groups. Patients readmitted to the index transplant center were more likely to have a biliary, hematologic, or neurologic complication, while those in the fragmented admissions group were more likely to be readmitted for things like electrolyte disturbances, respiratory issues, gastrointestinal issues, or hematologic-related issues. There was no difference in overall cost of care between the two groups (an average of $11,621.68 vs. $11.585.39, respectively).
After the investigators adjusted for age, sex, reason for readmission, cost of the index liver transplant, readmission length of stay, number of previous readmissions, and time from transplant, postdischarge fragmentation increased the odds of both 30-day mortality (OR, 1.75) and 30-day readmission (OR, 2.14). “It looks like just having a fragmented readmission is an independent predictor for an adverse event,” Dr. Kothari said.
Significant predictors of adverse events following a fragmented readmission included an increased number of previous readmissions (OR, 1.07) and readmission within 90 days of orthotopic liver transplant (OR, 2.19). “These two factors may be important for guiding providers to say, ‘If you have these things, this patient should likely come back to their index transplant center,’” Dr. Kothari said.
He reported having no relevant financial disclosures.
CORONADO, CALIF. – Postdischarge surgical care fragmentation significantly increases the risk of both 30-day mortality and subsequent readmission in the first year following orthotopic liver transplantation, results from a study of national data showed.
“In an era of regionalization and centers of excellence, the likelihood for postdischarge fragmentation, defined as readmission to any hospital other than the hospital at which the surgery was performed, is an increasing reality,” Anai N. Kothari, MD, said at the annual meeting of the Western Surgical Association. “In many different surgical subspecialties – major vascular operations, bariatric surgery, oncologic resections – it’s known to be a risk factor for adverse events and poor quality. Postdischarge fragmentation is common, [and related to] as often as one in four readmissions. It increases the risk for short- and long-term morbidity and mortality, decreases survival, and increases cost.”
Dr. Kothari reported results from 2,996 patients with 7,485 readmission encounters at 299 hospitals. Of the 7,485 readmissions, 6,249 (83.5%) were nonfragmented, and 1,236 (16.5%) were fragmented. The mean age of patients was 55 years. There were no significant differences in baseline characteristics between patients with nonfragmented and fragmented admissions in terms of patient age, sex, preoperative and postoperative length of stay, Charlson comorbidity index, and comorbidities, with the exception of renal failure, which was more common among patients in the fragmented admission group.
Compared with the patients in the nonfragmented admission group, those in the fragmented admission group had a greater number of average readmissions per patient (3.3 vs. 2.5, respectively; P less than .0001) and a greater number of average days to readmission (168 vs. 105; P less than .0001). Reasons for readmission differed among the two groups. Patients readmitted to the index transplant center were more likely to have a biliary, hematologic, or neurologic complication, while those in the fragmented admissions group were more likely to be readmitted for things like electrolyte disturbances, respiratory issues, gastrointestinal issues, or hematologic-related issues. There was no difference in overall cost of care between the two groups (an average of $11,621.68 vs. $11.585.39, respectively).
After the investigators adjusted for age, sex, reason for readmission, cost of the index liver transplant, readmission length of stay, number of previous readmissions, and time from transplant, postdischarge fragmentation increased the odds of both 30-day mortality (OR, 1.75) and 30-day readmission (OR, 2.14). “It looks like just having a fragmented readmission is an independent predictor for an adverse event,” Dr. Kothari said.
Significant predictors of adverse events following a fragmented readmission included an increased number of previous readmissions (OR, 1.07) and readmission within 90 days of orthotopic liver transplant (OR, 2.19). “These two factors may be important for guiding providers to say, ‘If you have these things, this patient should likely come back to their index transplant center,’” Dr. Kothari said.
He reported having no relevant financial disclosures.
CORONADO, CALIF. – Postdischarge surgical care fragmentation significantly increases the risk of both 30-day mortality and subsequent readmission in the first year following orthotopic liver transplantation, results from a study of national data showed.
“In an era of regionalization and centers of excellence, the likelihood for postdischarge fragmentation, defined as readmission to any hospital other than the hospital at which the surgery was performed, is an increasing reality,” Anai N. Kothari, MD, said at the annual meeting of the Western Surgical Association. “In many different surgical subspecialties – major vascular operations, bariatric surgery, oncologic resections – it’s known to be a risk factor for adverse events and poor quality. Postdischarge fragmentation is common, [and related to] as often as one in four readmissions. It increases the risk for short- and long-term morbidity and mortality, decreases survival, and increases cost.”
Dr. Kothari reported results from 2,996 patients with 7,485 readmission encounters at 299 hospitals. Of the 7,485 readmissions, 6,249 (83.5%) were nonfragmented, and 1,236 (16.5%) were fragmented. The mean age of patients was 55 years. There were no significant differences in baseline characteristics between patients with nonfragmented and fragmented admissions in terms of patient age, sex, preoperative and postoperative length of stay, Charlson comorbidity index, and comorbidities, with the exception of renal failure, which was more common among patients in the fragmented admission group.
Compared with the patients in the nonfragmented admission group, those in the fragmented admission group had a greater number of average readmissions per patient (3.3 vs. 2.5, respectively; P less than .0001) and a greater number of average days to readmission (168 vs. 105; P less than .0001). Reasons for readmission differed among the two groups. Patients readmitted to the index transplant center were more likely to have a biliary, hematologic, or neurologic complication, while those in the fragmented admissions group were more likely to be readmitted for things like electrolyte disturbances, respiratory issues, gastrointestinal issues, or hematologic-related issues. There was no difference in overall cost of care between the two groups (an average of $11,621.68 vs. $11.585.39, respectively).
After the investigators adjusted for age, sex, reason for readmission, cost of the index liver transplant, readmission length of stay, number of previous readmissions, and time from transplant, postdischarge fragmentation increased the odds of both 30-day mortality (OR, 1.75) and 30-day readmission (OR, 2.14). “It looks like just having a fragmented readmission is an independent predictor for an adverse event,” Dr. Kothari said.
Significant predictors of adverse events following a fragmented readmission included an increased number of previous readmissions (OR, 1.07) and readmission within 90 days of orthotopic liver transplant (OR, 2.19). “These two factors may be important for guiding providers to say, ‘If you have these things, this patient should likely come back to their index transplant center,’” Dr. Kothari said.
He reported having no relevant financial disclosures.
AT WSA 2016
Key clinical point:
Major finding: After investigators adjusted for numerous variables, postdischarge fragmentation following orthotopic liver transplantation increased the odds of both 30-day mortality (OR, 1.75) and 30-day readmission (OR, 2.14).
Data source: An analysis of data from the Healthcare Cost and Utilization Project State Inpatient Databases for Florida and California between 2006 and 2011 to identify 2,996 patients who underwent orthotopic liver transplantation.
Disclosures: Dr. Kothari reported having no relevant financial disclosures.
In era of infliximab, ulcerative colitis surgical outcomes worsen
WASHINGTON – The era of powerful biologics has led to unforeseen surgical outcomes in patients with ulcerative colitis.
Patients undergoing surgery for ulcerative colitis now are 38% more likely to die in the hospital than they were 15 years ago, before infliximab and other biologics were adopted as medical therapy for the disease. A database review covering 18 years found that other surgical outcomes are worse, too, Jonathan Abelson, MD, said at the annual clinical congress of the American College of Surgeons.
“These very powerful agents could be completely eliminating the need for surgery in patients with mild disease, leaving surgery for those who have very advanced disease and didn’t respond well to medical therapy,” said Dr. Abelson, a clinical research fellow at New York–Presbyterian Hospital, N.Y. “We are operating now only on patients with very severe disease, not the wider range of patients we had 15 years ago, when there weren’t as effective medical options.”
He and his colleagues used the New York Statewide Planning and Research Cooperative System (SPARCS) database to identify 7,070 patients who had undergone bowel resection for ulcerative colitis during two epochs: prebiologics (1995-2005) and postbiologics (2006-2013). The cohorts were about evenly split in numbers.
There were some statistically significant differences in baseline characteristics. Patients in epoch 2 were about a year older (51 vs. 50 years). Significantly more of them had at least two major comorbidities (28% vs. 18%). Minimally invasive surgery was significantly more common in epoch 2 (28% vs. 3%).
Significantly more surgeries in epoch 2 were staged into three or more procedures (14% vs. 9%). This finding probably reflects the level of disease severity in those presenting for surgery or the fact that they underwent surgery after recently receiving biologics, Dr. Abelson said.
“One of the limits of this study is that we don’t know exactly the reasons for these one-, two-, or three-stage surgeries. The theory is that patients who were more ill at presentation are more likely to have a multistaged surgery. Another reason could be that if they are on these powerful immunosuppressive regimens, the surgeon might be concerned about not healing well from a definitive one- or two-stage surgery.”
He then conducted a multivariate analysis that controlled for baseline factors, including a variety of individual comorbid conditions. In this analysis, patients in epoch 2 were 38% more likely to die in the hospital and 51% more likely to experience a major postoperative event, like shock, pulmonary embolism, stroke, or heart attack. The chance of a surgical complication was increased by 39%, and these patients were 25% more likely to need a transfusion during surgery than those from epoch 1.
The poorer outcomes held for an at least an entire year after surgery, Dr. Abelson said. At 1 year, patients in epoch 2 were 36% more likely to have a readmission than those in epoch 1. Major events and procedural complications were both 46% more likely. Patients were also 36% more likely to require an additional procedure.
“These are not the outcomes we want to see, especially in this era when our surgical techniques have improved so much,” Dr. Abelson said. “If what this represents, though, is that we are now operating on a higher-risk population, we can’t just say, ‘Well, that’s how it’s going to be.’ We need to figure out how to minimize morbidity and mortality in this high-risk patient population.”
One goal, he suggested, would be to assess response to a biologic regimen earlier in the hopes of determining who will respond well, and moving ahead with surgery in those who don’t.
This is a tough sell for patients, he said.
“There is a big fear of this surgery. It usually requires a temporary ileostomy and a stoma bag, and patients are terrified of that. There have been a few studies demonstrating that earlier referral to surgery improves quality of life; living with advanced ulcerative colitis can be extremely difficult and patients often feel a lot better after we remove their diseased colon. But getting there is a challenge.”
Dr. Abelson had no financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_Gal
WASHINGTON – The era of powerful biologics has led to unforeseen surgical outcomes in patients with ulcerative colitis.
Patients undergoing surgery for ulcerative colitis now are 38% more likely to die in the hospital than they were 15 years ago, before infliximab and other biologics were adopted as medical therapy for the disease. A database review covering 18 years found that other surgical outcomes are worse, too, Jonathan Abelson, MD, said at the annual clinical congress of the American College of Surgeons.
“These very powerful agents could be completely eliminating the need for surgery in patients with mild disease, leaving surgery for those who have very advanced disease and didn’t respond well to medical therapy,” said Dr. Abelson, a clinical research fellow at New York–Presbyterian Hospital, N.Y. “We are operating now only on patients with very severe disease, not the wider range of patients we had 15 years ago, when there weren’t as effective medical options.”
He and his colleagues used the New York Statewide Planning and Research Cooperative System (SPARCS) database to identify 7,070 patients who had undergone bowel resection for ulcerative colitis during two epochs: prebiologics (1995-2005) and postbiologics (2006-2013). The cohorts were about evenly split in numbers.
There were some statistically significant differences in baseline characteristics. Patients in epoch 2 were about a year older (51 vs. 50 years). Significantly more of them had at least two major comorbidities (28% vs. 18%). Minimally invasive surgery was significantly more common in epoch 2 (28% vs. 3%).
Significantly more surgeries in epoch 2 were staged into three or more procedures (14% vs. 9%). This finding probably reflects the level of disease severity in those presenting for surgery or the fact that they underwent surgery after recently receiving biologics, Dr. Abelson said.
“One of the limits of this study is that we don’t know exactly the reasons for these one-, two-, or three-stage surgeries. The theory is that patients who were more ill at presentation are more likely to have a multistaged surgery. Another reason could be that if they are on these powerful immunosuppressive regimens, the surgeon might be concerned about not healing well from a definitive one- or two-stage surgery.”
He then conducted a multivariate analysis that controlled for baseline factors, including a variety of individual comorbid conditions. In this analysis, patients in epoch 2 were 38% more likely to die in the hospital and 51% more likely to experience a major postoperative event, like shock, pulmonary embolism, stroke, or heart attack. The chance of a surgical complication was increased by 39%, and these patients were 25% more likely to need a transfusion during surgery than those from epoch 1.
The poorer outcomes held for an at least an entire year after surgery, Dr. Abelson said. At 1 year, patients in epoch 2 were 36% more likely to have a readmission than those in epoch 1. Major events and procedural complications were both 46% more likely. Patients were also 36% more likely to require an additional procedure.
“These are not the outcomes we want to see, especially in this era when our surgical techniques have improved so much,” Dr. Abelson said. “If what this represents, though, is that we are now operating on a higher-risk population, we can’t just say, ‘Well, that’s how it’s going to be.’ We need to figure out how to minimize morbidity and mortality in this high-risk patient population.”
One goal, he suggested, would be to assess response to a biologic regimen earlier in the hopes of determining who will respond well, and moving ahead with surgery in those who don’t.
This is a tough sell for patients, he said.
“There is a big fear of this surgery. It usually requires a temporary ileostomy and a stoma bag, and patients are terrified of that. There have been a few studies demonstrating that earlier referral to surgery improves quality of life; living with advanced ulcerative colitis can be extremely difficult and patients often feel a lot better after we remove their diseased colon. But getting there is a challenge.”
Dr. Abelson had no financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_Gal
WASHINGTON – The era of powerful biologics has led to unforeseen surgical outcomes in patients with ulcerative colitis.
Patients undergoing surgery for ulcerative colitis now are 38% more likely to die in the hospital than they were 15 years ago, before infliximab and other biologics were adopted as medical therapy for the disease. A database review covering 18 years found that other surgical outcomes are worse, too, Jonathan Abelson, MD, said at the annual clinical congress of the American College of Surgeons.
“These very powerful agents could be completely eliminating the need for surgery in patients with mild disease, leaving surgery for those who have very advanced disease and didn’t respond well to medical therapy,” said Dr. Abelson, a clinical research fellow at New York–Presbyterian Hospital, N.Y. “We are operating now only on patients with very severe disease, not the wider range of patients we had 15 years ago, when there weren’t as effective medical options.”
He and his colleagues used the New York Statewide Planning and Research Cooperative System (SPARCS) database to identify 7,070 patients who had undergone bowel resection for ulcerative colitis during two epochs: prebiologics (1995-2005) and postbiologics (2006-2013). The cohorts were about evenly split in numbers.
There were some statistically significant differences in baseline characteristics. Patients in epoch 2 were about a year older (51 vs. 50 years). Significantly more of them had at least two major comorbidities (28% vs. 18%). Minimally invasive surgery was significantly more common in epoch 2 (28% vs. 3%).
Significantly more surgeries in epoch 2 were staged into three or more procedures (14% vs. 9%). This finding probably reflects the level of disease severity in those presenting for surgery or the fact that they underwent surgery after recently receiving biologics, Dr. Abelson said.
“One of the limits of this study is that we don’t know exactly the reasons for these one-, two-, or three-stage surgeries. The theory is that patients who were more ill at presentation are more likely to have a multistaged surgery. Another reason could be that if they are on these powerful immunosuppressive regimens, the surgeon might be concerned about not healing well from a definitive one- or two-stage surgery.”
He then conducted a multivariate analysis that controlled for baseline factors, including a variety of individual comorbid conditions. In this analysis, patients in epoch 2 were 38% more likely to die in the hospital and 51% more likely to experience a major postoperative event, like shock, pulmonary embolism, stroke, or heart attack. The chance of a surgical complication was increased by 39%, and these patients were 25% more likely to need a transfusion during surgery than those from epoch 1.
The poorer outcomes held for an at least an entire year after surgery, Dr. Abelson said. At 1 year, patients in epoch 2 were 36% more likely to have a readmission than those in epoch 1. Major events and procedural complications were both 46% more likely. Patients were also 36% more likely to require an additional procedure.
“These are not the outcomes we want to see, especially in this era when our surgical techniques have improved so much,” Dr. Abelson said. “If what this represents, though, is that we are now operating on a higher-risk population, we can’t just say, ‘Well, that’s how it’s going to be.’ We need to figure out how to minimize morbidity and mortality in this high-risk patient population.”
One goal, he suggested, would be to assess response to a biologic regimen earlier in the hopes of determining who will respond well, and moving ahead with surgery in those who don’t.
This is a tough sell for patients, he said.
“There is a big fear of this surgery. It usually requires a temporary ileostomy and a stoma bag, and patients are terrified of that. There have been a few studies demonstrating that earlier referral to surgery improves quality of life; living with advanced ulcerative colitis can be extremely difficult and patients often feel a lot better after we remove their diseased colon. But getting there is a challenge.”
Dr. Abelson had no financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_Gal
AT THE ACS CLINICAL CONGRESS
Key clinical point:
Major finding: Patients are 38% more likely to die in the hospital than they were 15 years ago.
Data source: The 18-year database review comprised more than 7,000 surgeries.
Disclosures: Dr. Abelson had no financial disclosures.
Infection, readmission linked after open lower-extremity procedures
COLUMBUS, OHIO – Infections account for more than one-third of readmissions after endovascular lower-extremity procedures, but an analysis of these procedures over a 6-year period has identified a handful of factors, including an extended hospital stay, that may help vascular surgeons identify patients at greatest risk and reduce infection-related readmissions.
“Of a little over 7,000 patients that we evaluated with peripheral artery disease who underwent an elective lower-extremity procedure, we found an overall readmission rate of 10.9%; about 9.5% for those who underwent an open procedure and just over 12% for those who underwent an endovascular procedure,” Joseph C. Melvin, MD, of the University of Missouri Hospitals & Clinics in Columbia said at the annual meeting of the Midwestern Vascular Surgery Society.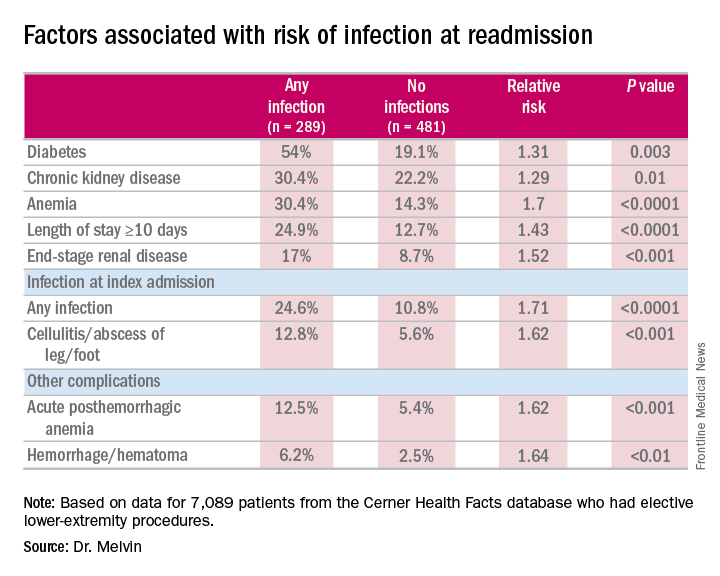
While the readmission rate for open operations was lower, the infection rate at readmission was higher for open procedures: 45.5% (157 of 345 readmissions) vs. 31.1% (132 of 425 readmissions), Dr. Melvin said.
“The risk factors for diagnosis of infection at readmission we found to be significant were anemia, chronic kidney disease, and end-stage renal disease, any infection at the time of the index admission, specifically cellulitis or abscess of the lower extremity given the patient’s peripheral artery disease status, diabetes, and then complications including posthemorrhagic anemia,” Dr. Melvin said. Laboratory testing values at the time of index admissions confirmed the risk factors.
The investigators also used multivariable logistic regression models in the analysis and found that factors most predictive of an infection-related readmission were length of stay, having the procedure at a teaching facility, anemia, and infection at the index admission, Dr. Melvin said.
The surgical site was the most common source of the infection, and Staphylococcus “not surprisingly” accounted for 25% of pathogens, Dr. Melvin said. “But what we did find to be interesting was that just over 40% of patients were found to have a gram-negative bacteria isolated, which would come into play with our decision with regards to antibiotic treatment,” he said.
The data suggest that further evaluation of ways to decrease postoperative infections and use of broad-spectrum antibiotics during readmissions may improve outcomes after open lower-extremity procedures, Dr. Melvin said.
Dr. Melvin had no financial relationships to disclose.
COLUMBUS, OHIO – Infections account for more than one-third of readmissions after endovascular lower-extremity procedures, but an analysis of these procedures over a 6-year period has identified a handful of factors, including an extended hospital stay, that may help vascular surgeons identify patients at greatest risk and reduce infection-related readmissions.
“Of a little over 7,000 patients that we evaluated with peripheral artery disease who underwent an elective lower-extremity procedure, we found an overall readmission rate of 10.9%; about 9.5% for those who underwent an open procedure and just over 12% for those who underwent an endovascular procedure,” Joseph C. Melvin, MD, of the University of Missouri Hospitals & Clinics in Columbia said at the annual meeting of the Midwestern Vascular Surgery Society.
While the readmission rate for open operations was lower, the infection rate at readmission was higher for open procedures: 45.5% (157 of 345 readmissions) vs. 31.1% (132 of 425 readmissions), Dr. Melvin said.
“The risk factors for diagnosis of infection at readmission we found to be significant were anemia, chronic kidney disease, and end-stage renal disease, any infection at the time of the index admission, specifically cellulitis or abscess of the lower extremity given the patient’s peripheral artery disease status, diabetes, and then complications including posthemorrhagic anemia,” Dr. Melvin said. Laboratory testing values at the time of index admissions confirmed the risk factors.
The investigators also used multivariable logistic regression models in the analysis and found that factors most predictive of an infection-related readmission were length of stay, having the procedure at a teaching facility, anemia, and infection at the index admission, Dr. Melvin said.
The surgical site was the most common source of the infection, and Staphylococcus “not surprisingly” accounted for 25% of pathogens, Dr. Melvin said. “But what we did find to be interesting was that just over 40% of patients were found to have a gram-negative bacteria isolated, which would come into play with our decision with regards to antibiotic treatment,” he said.
The data suggest that further evaluation of ways to decrease postoperative infections and use of broad-spectrum antibiotics during readmissions may improve outcomes after open lower-extremity procedures, Dr. Melvin said.
Dr. Melvin had no financial relationships to disclose.
COLUMBUS, OHIO – Infections account for more than one-third of readmissions after endovascular lower-extremity procedures, but an analysis of these procedures over a 6-year period has identified a handful of factors, including an extended hospital stay, that may help vascular surgeons identify patients at greatest risk and reduce infection-related readmissions.
“Of a little over 7,000 patients that we evaluated with peripheral artery disease who underwent an elective lower-extremity procedure, we found an overall readmission rate of 10.9%; about 9.5% for those who underwent an open procedure and just over 12% for those who underwent an endovascular procedure,” Joseph C. Melvin, MD, of the University of Missouri Hospitals & Clinics in Columbia said at the annual meeting of the Midwestern Vascular Surgery Society.
While the readmission rate for open operations was lower, the infection rate at readmission was higher for open procedures: 45.5% (157 of 345 readmissions) vs. 31.1% (132 of 425 readmissions), Dr. Melvin said.
“The risk factors for diagnosis of infection at readmission we found to be significant were anemia, chronic kidney disease, and end-stage renal disease, any infection at the time of the index admission, specifically cellulitis or abscess of the lower extremity given the patient’s peripheral artery disease status, diabetes, and then complications including posthemorrhagic anemia,” Dr. Melvin said. Laboratory testing values at the time of index admissions confirmed the risk factors.
The investigators also used multivariable logistic regression models in the analysis and found that factors most predictive of an infection-related readmission were length of stay, having the procedure at a teaching facility, anemia, and infection at the index admission, Dr. Melvin said.
The surgical site was the most common source of the infection, and Staphylococcus “not surprisingly” accounted for 25% of pathogens, Dr. Melvin said. “But what we did find to be interesting was that just over 40% of patients were found to have a gram-negative bacteria isolated, which would come into play with our decision with regards to antibiotic treatment,” he said.
The data suggest that further evaluation of ways to decrease postoperative infections and use of broad-spectrum antibiotics during readmissions may improve outcomes after open lower-extremity procedures, Dr. Melvin said.
Dr. Melvin had no financial relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: Extended hospital stay and other factors can help identify patients at greatest risk for readmission due to infection.
Major finding: More than one-third of readmissions from lower-extremity procedures are the result of infections.
Data source: 7,089 elective lower extremity procedures selected from the Cerner Health Facts database.
Disclosures: Dr. Melvin reported having no financial disclosures.
Staple line reinforcement linked to increased leak risk in bariatric surgery
Laparoscopic sleeve gastrectomy is safe and effective overall, but staple line reinforcement appears to increase the rate of postsurgical leaks – which were associated with readmissions and, in some cases, reoperations.
A large review of quality improvement data found that staple line reinforcement – an extremely common technique – was associated with a 60% increased risk of leak, compared with closures without staple line reinforcement, Elizabeth R. Berger, MD, and her colleagues reported in the October issue of the Annals of Surgery (2016;264:464-73).
“This study also demonstrates that leaks were significantly more morbid than bleeding with higher readmission and reoperation rates in patients with a leak vs. a bleed,” wrote Dr. Berger of Loyola University, Chicago, and her coauthors. “Therefore, a surgeon should consider the benefits, risks, and costs of each surgical technique in performing a laparoscopic sleeve gastrectomy and selectively utilize those that, in their hands, minimize morbidity while maximizing clinical effectiveness.”
The team examined outcomes in 189,477 laparoscopic sleeve gastrectomies performed by 1,634 surgeons at 720 centers from 2012 to 2014. All of the data were extracted from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, created in 2012 by the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery.
They examined the impact of staple line reinforcement, oversewing the staple line, bougie size, and distance of the staple line from the pylorus on 30-day outcomes, and their effect on weight loss and weight-related comorbidities at 1 year. Outcomes included morbidity, leak rates, and bleeding, which were examined at both the patient and surgeon levels.
Most patients (126,904; 67%) patients had some type of staple line reinforcement (SLR); the rest had only oversewn staple lines (OSL) or no reinforcement. Leaks occurred in 1,703 patients and bleeds in 1,436 patients. Leaks were more serious than bleeds: Patients with a leak were almost 28% more likely to readmitted and 11% more likely to need a reoperation than were patients who had only a bleed.
At the patient level, those with SLR with or without OSL were 20%-46% more likely to experience a leak than were those who had neither. Bleeding rates were about 70% lower in the SLR groups.
Most surgeons in the analysis (80%) used some type of SLR; almost 20% routinely used only OSL, and 30% routinely used only SLR. At the surgeon level, SLR was associated with a 60% increased risk of a postoperative leak, compared with no reinforcement. There was no association between SLR and bleeding risk, however.
Oversewing had an effect on 1-year weight loss. Patients with oversewn staple lines lost an additional 1.3 points on the body mass index (BMI) scale, compared with patients with no type of reinforcement.
“The reason for increased leaks from SLR is relatively unclear,” the authors wrote. “The two layers of material that are placed within the staple line could increase ischemia or decrease the relative staple heights. At the notches, where one staple firing ends and the next one begins, there is sandwiching of the two layers of staples and a combined four layers of SLR. This bulk may predispose to leaks.”
Larger bougie sizes (BS) seemed more beneficial than did smaller ones, in both the surgeon- and patient-level analyses. A BS of at least 38 French was associated with a 28% decreased risk of a leak (odds ratio 0.72) at the patient level and a 10% decreased risk at the surgeon level (OR 0.90). There were no associations with bleeding.
“Our findings support literature that describes narrower BSs leads to increased ischemia secondary to increased intraluminal pressure, causing more leaks,” the authors wrote.
A BS of at least 40 French had a significant impact on weight loss. At 1 year, patients with the larger BS had lost 2.45 points more on the BMI scale than did those with smaller sizes.
This finding is in accord with other studies, including one that found the best weight-loss outcomes associated with a BS of more than 60 French. “Perhaps the sleeve works because of more rapid emptying, which is favored by a relatively larger BS, rather than because of restriction,” they said.
The distance to the pylorus (DP) from the staple line initiation point was divided into four sections: less than 4 cm; 4-5 cm; 5-6 cm; and 6 cm or more.
On a patient level, there was no association between DP and leak rates. There was, however, an association with bleeding. A DP of 4-4.99 cm had the highest rate, 90%, while a DP of 5-5.99 cm had the lowest (71%). DP was also associated with weight loss on this level, with a distance of more than 6 cm being associated with the biggest BMI decrease (3.7 points).
“Our data show significantly increased excess weight loss in a stepwise fashion as the DP increases,” the authors said. “Our data suggest that as DP increased, there was an increased excess weight loss, possibly explained by preserving the ‘antral mill.’ Stapling further from the pylorus perhaps keeps the antrum’s functional component intact and allows food to enter the distal gut more quickly, leading to earlier satiety and increased weight loss.”
Only 114 surgeons (8%) used a DP of less than 4 cm. There were no significant associations with any 30-day outcomes and DP after adjustment.
The authors had no financial disclosures.
Before drawing overarching conclusions and implementing recommendations based on this study, there are several limitations that must be borne in mind when considering data-mining exercises such as this one:
• It should be taken into account that there was significant intraoperative variation in technique and experience among the surgeons that was not captured through the data acquisition.
• Similarly, the true distance between the stapler and the selected bougie is also variable, adding an inherent lack of accuracy of the true real diameter of the completed gastric tube.
• There is a lack of granular information, including the type of SLR or staplers used, thereby also limiting any reliable conclusions that could be drawn.
• There are additional techniques, such as omental buttressing, and the use of clips, sutures, or hemostatic agents that are not reported, yet may have an impact on leak and bleeding rates.
• The reported follow-up rate of 39.4% at 1 year is typically considered to be suboptimal.
• SLR techniques may also include oversewing, and these are also subject to wide variation, including the type of suture material used, and the actual suturing technique that was implemented.
• Only those patients whose bleeding was severe enough to warrant transfusions were included, such that lower level bleeding would have not been represented in this report.
• There were also deficiencies in correlating leaks or bleeding rates with staple height selection, or the experience and learning curve of the surgeon.

Samer Mattar, MD, is a bariatric surgeon and professor of surgery at Oregon Health and Science University, Portland. Dr. Mattar has no disclosures.
Before drawing overarching conclusions and implementing recommendations based on this study, there are several limitations that must be borne in mind when considering data-mining exercises such as this one:
• It should be taken into account that there was significant intraoperative variation in technique and experience among the surgeons that was not captured through the data acquisition.
• Similarly, the true distance between the stapler and the selected bougie is also variable, adding an inherent lack of accuracy of the true real diameter of the completed gastric tube.
• There is a lack of granular information, including the type of SLR or staplers used, thereby also limiting any reliable conclusions that could be drawn.
• There are additional techniques, such as omental buttressing, and the use of clips, sutures, or hemostatic agents that are not reported, yet may have an impact on leak and bleeding rates.
• The reported follow-up rate of 39.4% at 1 year is typically considered to be suboptimal.
• SLR techniques may also include oversewing, and these are also subject to wide variation, including the type of suture material used, and the actual suturing technique that was implemented.
• Only those patients whose bleeding was severe enough to warrant transfusions were included, such that lower level bleeding would have not been represented in this report.
• There were also deficiencies in correlating leaks or bleeding rates with staple height selection, or the experience and learning curve of the surgeon.
Samer Mattar, MD, is a bariatric surgeon and professor of surgery at Oregon Health and Science University, Portland. Dr. Mattar has no disclosures.
Before drawing overarching conclusions and implementing recommendations based on this study, there are several limitations that must be borne in mind when considering data-mining exercises such as this one:
• It should be taken into account that there was significant intraoperative variation in technique and experience among the surgeons that was not captured through the data acquisition.
• Similarly, the true distance between the stapler and the selected bougie is also variable, adding an inherent lack of accuracy of the true real diameter of the completed gastric tube.
• There is a lack of granular information, including the type of SLR or staplers used, thereby also limiting any reliable conclusions that could be drawn.
• There are additional techniques, such as omental buttressing, and the use of clips, sutures, or hemostatic agents that are not reported, yet may have an impact on leak and bleeding rates.
• The reported follow-up rate of 39.4% at 1 year is typically considered to be suboptimal.
• SLR techniques may also include oversewing, and these are also subject to wide variation, including the type of suture material used, and the actual suturing technique that was implemented.
• Only those patients whose bleeding was severe enough to warrant transfusions were included, such that lower level bleeding would have not been represented in this report.
• There were also deficiencies in correlating leaks or bleeding rates with staple height selection, or the experience and learning curve of the surgeon.
Samer Mattar, MD, is a bariatric surgeon and professor of surgery at Oregon Health and Science University, Portland. Dr. Mattar has no disclosures.
Laparoscopic sleeve gastrectomy is safe and effective overall, but staple line reinforcement appears to increase the rate of postsurgical leaks – which were associated with readmissions and, in some cases, reoperations.
A large review of quality improvement data found that staple line reinforcement – an extremely common technique – was associated with a 60% increased risk of leak, compared with closures without staple line reinforcement, Elizabeth R. Berger, MD, and her colleagues reported in the October issue of the Annals of Surgery (2016;264:464-73).
“This study also demonstrates that leaks were significantly more morbid than bleeding with higher readmission and reoperation rates in patients with a leak vs. a bleed,” wrote Dr. Berger of Loyola University, Chicago, and her coauthors. “Therefore, a surgeon should consider the benefits, risks, and costs of each surgical technique in performing a laparoscopic sleeve gastrectomy and selectively utilize those that, in their hands, minimize morbidity while maximizing clinical effectiveness.”
The team examined outcomes in 189,477 laparoscopic sleeve gastrectomies performed by 1,634 surgeons at 720 centers from 2012 to 2014. All of the data were extracted from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, created in 2012 by the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery.
They examined the impact of staple line reinforcement, oversewing the staple line, bougie size, and distance of the staple line from the pylorus on 30-day outcomes, and their effect on weight loss and weight-related comorbidities at 1 year. Outcomes included morbidity, leak rates, and bleeding, which were examined at both the patient and surgeon levels.
Most patients (126,904; 67%) patients had some type of staple line reinforcement (SLR); the rest had only oversewn staple lines (OSL) or no reinforcement. Leaks occurred in 1,703 patients and bleeds in 1,436 patients. Leaks were more serious than bleeds: Patients with a leak were almost 28% more likely to readmitted and 11% more likely to need a reoperation than were patients who had only a bleed.
At the patient level, those with SLR with or without OSL were 20%-46% more likely to experience a leak than were those who had neither. Bleeding rates were about 70% lower in the SLR groups.
Most surgeons in the analysis (80%) used some type of SLR; almost 20% routinely used only OSL, and 30% routinely used only SLR. At the surgeon level, SLR was associated with a 60% increased risk of a postoperative leak, compared with no reinforcement. There was no association between SLR and bleeding risk, however.
Oversewing had an effect on 1-year weight loss. Patients with oversewn staple lines lost an additional 1.3 points on the body mass index (BMI) scale, compared with patients with no type of reinforcement.
“The reason for increased leaks from SLR is relatively unclear,” the authors wrote. “The two layers of material that are placed within the staple line could increase ischemia or decrease the relative staple heights. At the notches, where one staple firing ends and the next one begins, there is sandwiching of the two layers of staples and a combined four layers of SLR. This bulk may predispose to leaks.”
Larger bougie sizes (BS) seemed more beneficial than did smaller ones, in both the surgeon- and patient-level analyses. A BS of at least 38 French was associated with a 28% decreased risk of a leak (odds ratio 0.72) at the patient level and a 10% decreased risk at the surgeon level (OR 0.90). There were no associations with bleeding.
“Our findings support literature that describes narrower BSs leads to increased ischemia secondary to increased intraluminal pressure, causing more leaks,” the authors wrote.
A BS of at least 40 French had a significant impact on weight loss. At 1 year, patients with the larger BS had lost 2.45 points more on the BMI scale than did those with smaller sizes.
This finding is in accord with other studies, including one that found the best weight-loss outcomes associated with a BS of more than 60 French. “Perhaps the sleeve works because of more rapid emptying, which is favored by a relatively larger BS, rather than because of restriction,” they said.
The distance to the pylorus (DP) from the staple line initiation point was divided into four sections: less than 4 cm; 4-5 cm; 5-6 cm; and 6 cm or more.
On a patient level, there was no association between DP and leak rates. There was, however, an association with bleeding. A DP of 4-4.99 cm had the highest rate, 90%, while a DP of 5-5.99 cm had the lowest (71%). DP was also associated with weight loss on this level, with a distance of more than 6 cm being associated with the biggest BMI decrease (3.7 points).
“Our data show significantly increased excess weight loss in a stepwise fashion as the DP increases,” the authors said. “Our data suggest that as DP increased, there was an increased excess weight loss, possibly explained by preserving the ‘antral mill.’ Stapling further from the pylorus perhaps keeps the antrum’s functional component intact and allows food to enter the distal gut more quickly, leading to earlier satiety and increased weight loss.”
Only 114 surgeons (8%) used a DP of less than 4 cm. There were no significant associations with any 30-day outcomes and DP after adjustment.
The authors had no financial disclosures.
Laparoscopic sleeve gastrectomy is safe and effective overall, but staple line reinforcement appears to increase the rate of postsurgical leaks – which were associated with readmissions and, in some cases, reoperations.
A large review of quality improvement data found that staple line reinforcement – an extremely common technique – was associated with a 60% increased risk of leak, compared with closures without staple line reinforcement, Elizabeth R. Berger, MD, and her colleagues reported in the October issue of the Annals of Surgery (2016;264:464-73).
“This study also demonstrates that leaks were significantly more morbid than bleeding with higher readmission and reoperation rates in patients with a leak vs. a bleed,” wrote Dr. Berger of Loyola University, Chicago, and her coauthors. “Therefore, a surgeon should consider the benefits, risks, and costs of each surgical technique in performing a laparoscopic sleeve gastrectomy and selectively utilize those that, in their hands, minimize morbidity while maximizing clinical effectiveness.”
The team examined outcomes in 189,477 laparoscopic sleeve gastrectomies performed by 1,634 surgeons at 720 centers from 2012 to 2014. All of the data were extracted from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, created in 2012 by the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery.
They examined the impact of staple line reinforcement, oversewing the staple line, bougie size, and distance of the staple line from the pylorus on 30-day outcomes, and their effect on weight loss and weight-related comorbidities at 1 year. Outcomes included morbidity, leak rates, and bleeding, which were examined at both the patient and surgeon levels.
Most patients (126,904; 67%) patients had some type of staple line reinforcement (SLR); the rest had only oversewn staple lines (OSL) or no reinforcement. Leaks occurred in 1,703 patients and bleeds in 1,436 patients. Leaks were more serious than bleeds: Patients with a leak were almost 28% more likely to readmitted and 11% more likely to need a reoperation than were patients who had only a bleed.
At the patient level, those with SLR with or without OSL were 20%-46% more likely to experience a leak than were those who had neither. Bleeding rates were about 70% lower in the SLR groups.
Most surgeons in the analysis (80%) used some type of SLR; almost 20% routinely used only OSL, and 30% routinely used only SLR. At the surgeon level, SLR was associated with a 60% increased risk of a postoperative leak, compared with no reinforcement. There was no association between SLR and bleeding risk, however.
Oversewing had an effect on 1-year weight loss. Patients with oversewn staple lines lost an additional 1.3 points on the body mass index (BMI) scale, compared with patients with no type of reinforcement.
“The reason for increased leaks from SLR is relatively unclear,” the authors wrote. “The two layers of material that are placed within the staple line could increase ischemia or decrease the relative staple heights. At the notches, where one staple firing ends and the next one begins, there is sandwiching of the two layers of staples and a combined four layers of SLR. This bulk may predispose to leaks.”
Larger bougie sizes (BS) seemed more beneficial than did smaller ones, in both the surgeon- and patient-level analyses. A BS of at least 38 French was associated with a 28% decreased risk of a leak (odds ratio 0.72) at the patient level and a 10% decreased risk at the surgeon level (OR 0.90). There were no associations with bleeding.
“Our findings support literature that describes narrower BSs leads to increased ischemia secondary to increased intraluminal pressure, causing more leaks,” the authors wrote.
A BS of at least 40 French had a significant impact on weight loss. At 1 year, patients with the larger BS had lost 2.45 points more on the BMI scale than did those with smaller sizes.
This finding is in accord with other studies, including one that found the best weight-loss outcomes associated with a BS of more than 60 French. “Perhaps the sleeve works because of more rapid emptying, which is favored by a relatively larger BS, rather than because of restriction,” they said.
The distance to the pylorus (DP) from the staple line initiation point was divided into four sections: less than 4 cm; 4-5 cm; 5-6 cm; and 6 cm or more.
On a patient level, there was no association between DP and leak rates. There was, however, an association with bleeding. A DP of 4-4.99 cm had the highest rate, 90%, while a DP of 5-5.99 cm had the lowest (71%). DP was also associated with weight loss on this level, with a distance of more than 6 cm being associated with the biggest BMI decrease (3.7 points).
“Our data show significantly increased excess weight loss in a stepwise fashion as the DP increases,” the authors said. “Our data suggest that as DP increased, there was an increased excess weight loss, possibly explained by preserving the ‘antral mill.’ Stapling further from the pylorus perhaps keeps the antrum’s functional component intact and allows food to enter the distal gut more quickly, leading to earlier satiety and increased weight loss.”
Only 114 surgeons (8%) used a DP of less than 4 cm. There were no significant associations with any 30-day outcomes and DP after adjustment.
The authors had no financial disclosures.
FROM THE ANNALS OF SURGERY
Key clinical point:
Major finding: Compared to not reinforcing the staple line, doing sow as associated with up to a 60% increase in the risk of a postsurgical leak.
Data source: The database review contained outcomes on 189,477 laparoscopic sleeve gastrectomies.
Disclosures: None of the study authors had any financial disclosures.