User login
COVID-19, hearings on Jan. 6 attack reignite interest in PTSD
After Sept. 11, 2001, and the subsequent long war in Iraq and Afghanistan, both mental health providers and the general public focused on posttraumatic stress disorder (PTSD). However, after almost 20 years of war and the COVID-19 epidemic, attention waned away from military service members and PTSD.

COVID-19–related PTSD and the hearings on the Jan. 6 attack on the Capitol have reignited interest in PTSD diagnosis and treatment. Testimony from police officers at the House select committee hearing about their experiences during the assault and PTSD was harrowing. One of the police officers had also served in Iraq, perhaps leading to “layered PTSD” – symptoms from war abroad and at home.
Thus, I thought a brief review of updates about diagnosis and treatment would be useful. Note: These are my opinions based on my extensive experience and do not represent the official opinion of my employer (MedStar Health).
PTSD was first classified as a disorder in 1980, based mainly on the experiences of military service members in Vietnam, as well as sexual assault victims and disaster survivors. Readers may look elsewhere for a fuller history of the disorder.
However, in brief, we have evolved from strict reliance on a variety of symptoms in the DSM (Diagnostic and Statistical Manual of Mental Disorders) to a more global determination of the experience of trauma and related symptoms of distress. We still rely for diagnosis on trauma-related anxiety and depression symptoms, such as nightmare, flashbacks, numbness, and disassociation.
Treatment has evolved. Patients may benefit from treatment even if they do not meet all the PTSD criteria. As many of my colleagues who treat patients have said, “if it smells like PTSD, treat it like PTSD.”
What is the most effective treatment? The literature declares that evidence-based treatments include two selective serotonin reuptake inhibitors (Zoloft and Paxil) and several psychotherapies. The psychotherapies include cognitive-behavioral therapies, exposure therapy, and EMDR (eye movement desensitization reprocessing).
The problem is that many patients cannot tolerate these therapies. SSRIs do have side effects, the most distressing being sexual dysfunction. Many service members do not enter the psychotherapies, or they drop out of trials, because they cannot tolerate the reimagining of their trauma.
I now counsel patients about the “three buckets” of treatment. The first bucket is medication, which as a psychiatrist is what I focus on. The second bucket is psychotherapy as discussed above. The third bucket is “everything else.”
“Everything else” includes a variety of methods the patients can use to reduce symptoms of anxiety, depression, and PTSD symptoms: exercising; deep breathing through the nose; doing yoga; doing meditation; playing or working with animals; gardening; and engaging in other activities that “self sooth.” I also recommend always doing “small acts of kindness” for others. I myself contribute to food banks and bring cookies or watermelons to the staff at my hospital.
Why is this approach useful? A menu of options gives control back to the patient. It provides activities that can reduce anxiety. Thinking about caring for others helps patients get out of their own “swamp of distress.”
We do live in very difficult times. We’re coping with COVID-19 Delta variant, attacks on the Capitol, and gun violence. I have not yet mentioned climate change, which is extremely frightening to many of us. So all providers need to be aware of all the strategies at our disposal to treat anxiety, depression, and PTSD.
Dr. Ritchie is chair of psychiatry at Medstar Washington (D.C.) Hospital Center. She has no conflicts of interest.
After Sept. 11, 2001, and the subsequent long war in Iraq and Afghanistan, both mental health providers and the general public focused on posttraumatic stress disorder (PTSD). However, after almost 20 years of war and the COVID-19 epidemic, attention waned away from military service members and PTSD.
COVID-19–related PTSD and the hearings on the Jan. 6 attack on the Capitol have reignited interest in PTSD diagnosis and treatment. Testimony from police officers at the House select committee hearing about their experiences during the assault and PTSD was harrowing. One of the police officers had also served in Iraq, perhaps leading to “layered PTSD” – symptoms from war abroad and at home.
Thus, I thought a brief review of updates about diagnosis and treatment would be useful. Note: These are my opinions based on my extensive experience and do not represent the official opinion of my employer (MedStar Health).
PTSD was first classified as a disorder in 1980, based mainly on the experiences of military service members in Vietnam, as well as sexual assault victims and disaster survivors. Readers may look elsewhere for a fuller history of the disorder.
However, in brief, we have evolved from strict reliance on a variety of symptoms in the DSM (Diagnostic and Statistical Manual of Mental Disorders) to a more global determination of the experience of trauma and related symptoms of distress. We still rely for diagnosis on trauma-related anxiety and depression symptoms, such as nightmare, flashbacks, numbness, and disassociation.
Treatment has evolved. Patients may benefit from treatment even if they do not meet all the PTSD criteria. As many of my colleagues who treat patients have said, “if it smells like PTSD, treat it like PTSD.”
What is the most effective treatment? The literature declares that evidence-based treatments include two selective serotonin reuptake inhibitors (Zoloft and Paxil) and several psychotherapies. The psychotherapies include cognitive-behavioral therapies, exposure therapy, and EMDR (eye movement desensitization reprocessing).
The problem is that many patients cannot tolerate these therapies. SSRIs do have side effects, the most distressing being sexual dysfunction. Many service members do not enter the psychotherapies, or they drop out of trials, because they cannot tolerate the reimagining of their trauma.
I now counsel patients about the “three buckets” of treatment. The first bucket is medication, which as a psychiatrist is what I focus on. The second bucket is psychotherapy as discussed above. The third bucket is “everything else.”
“Everything else” includes a variety of methods the patients can use to reduce symptoms of anxiety, depression, and PTSD symptoms: exercising; deep breathing through the nose; doing yoga; doing meditation; playing or working with animals; gardening; and engaging in other activities that “self sooth.” I also recommend always doing “small acts of kindness” for others. I myself contribute to food banks and bring cookies or watermelons to the staff at my hospital.
Why is this approach useful? A menu of options gives control back to the patient. It provides activities that can reduce anxiety. Thinking about caring for others helps patients get out of their own “swamp of distress.”
We do live in very difficult times. We’re coping with COVID-19 Delta variant, attacks on the Capitol, and gun violence. I have not yet mentioned climate change, which is extremely frightening to many of us. So all providers need to be aware of all the strategies at our disposal to treat anxiety, depression, and PTSD.
Dr. Ritchie is chair of psychiatry at Medstar Washington (D.C.) Hospital Center. She has no conflicts of interest.
After Sept. 11, 2001, and the subsequent long war in Iraq and Afghanistan, both mental health providers and the general public focused on posttraumatic stress disorder (PTSD). However, after almost 20 years of war and the COVID-19 epidemic, attention waned away from military service members and PTSD.
COVID-19–related PTSD and the hearings on the Jan. 6 attack on the Capitol have reignited interest in PTSD diagnosis and treatment. Testimony from police officers at the House select committee hearing about their experiences during the assault and PTSD was harrowing. One of the police officers had also served in Iraq, perhaps leading to “layered PTSD” – symptoms from war abroad and at home.
Thus, I thought a brief review of updates about diagnosis and treatment would be useful. Note: These are my opinions based on my extensive experience and do not represent the official opinion of my employer (MedStar Health).
PTSD was first classified as a disorder in 1980, based mainly on the experiences of military service members in Vietnam, as well as sexual assault victims and disaster survivors. Readers may look elsewhere for a fuller history of the disorder.
However, in brief, we have evolved from strict reliance on a variety of symptoms in the DSM (Diagnostic and Statistical Manual of Mental Disorders) to a more global determination of the experience of trauma and related symptoms of distress. We still rely for diagnosis on trauma-related anxiety and depression symptoms, such as nightmare, flashbacks, numbness, and disassociation.
Treatment has evolved. Patients may benefit from treatment even if they do not meet all the PTSD criteria. As many of my colleagues who treat patients have said, “if it smells like PTSD, treat it like PTSD.”
What is the most effective treatment? The literature declares that evidence-based treatments include two selective serotonin reuptake inhibitors (Zoloft and Paxil) and several psychotherapies. The psychotherapies include cognitive-behavioral therapies, exposure therapy, and EMDR (eye movement desensitization reprocessing).
The problem is that many patients cannot tolerate these therapies. SSRIs do have side effects, the most distressing being sexual dysfunction. Many service members do not enter the psychotherapies, or they drop out of trials, because they cannot tolerate the reimagining of their trauma.
I now counsel patients about the “three buckets” of treatment. The first bucket is medication, which as a psychiatrist is what I focus on. The second bucket is psychotherapy as discussed above. The third bucket is “everything else.”
“Everything else” includes a variety of methods the patients can use to reduce symptoms of anxiety, depression, and PTSD symptoms: exercising; deep breathing through the nose; doing yoga; doing meditation; playing or working with animals; gardening; and engaging in other activities that “self sooth.” I also recommend always doing “small acts of kindness” for others. I myself contribute to food banks and bring cookies or watermelons to the staff at my hospital.
Why is this approach useful? A menu of options gives control back to the patient. It provides activities that can reduce anxiety. Thinking about caring for others helps patients get out of their own “swamp of distress.”
We do live in very difficult times. We’re coping with COVID-19 Delta variant, attacks on the Capitol, and gun violence. I have not yet mentioned climate change, which is extremely frightening to many of us. So all providers need to be aware of all the strategies at our disposal to treat anxiety, depression, and PTSD.
Dr. Ritchie is chair of psychiatry at Medstar Washington (D.C.) Hospital Center. She has no conflicts of interest.
Let’s talk about race
“I feel like my aggression is being racialized.” “Of course I wouldn’t call the cops if I felt like hurting myself. I’m Black.”

Those statements represent the heightened trauma our Black and Brown patients with mental health issues have been experiencing. In the wake of increasingly publicized police brutality against Black and Brown communities, the role race plays in mental health decompensation is evident. At this moment in time, we must continue to improve our understanding of the role race plays in psychiatric disorders. We must also ask ourselves: At times, does psychiatry worsen the traumas of the communities we serve?
Some psychiatrists are afraid to speak about race. They may believe it to be too “political.” But avoiding these necessary conversations perpetuates the trauma of those we treat. It suggests that physicians are ignorant of an issue at the forefront of patients’ mental health. Psychiatry, today, is primarily focused on the biological aspects of disease. We must not forget that psychiatry is biopsychosocial. It is imperative that psychiatrists have conversations about race – and its significance to our patients and their care.
Only 10.4% of psychiatrists in the United States comprise those considered underrepresented in medicine (URM). Yet, those very groups make up 32.6% of the U.S. population and are overrepresented in psychiatric hospitals.1 Many studies have shown that concordant racial backgrounds between patient and physician lead to a more positive patient experience2 and arguably, the subsequent potential for better health outcomes. Our efforts in addressing this disparity often fall short. URM applicants may be hesitant to join an institution where diversity is lacking or where they may be the only minority.3 While there is no simple solution, I propose that psychiatrists promote the importance of mental health to Black and Brown students of all ages by collaborating with schools and community leaders.
It is important to acknowledge that the lack of diversity within psychiatry is reflective of that among all physicians. This in part stems from the barriers to medical education that Black and Brown communities face. Those who start off with more resources or have parents who are physicians are at an advantage when trying to get into medical school. In fact, one in five medical students have a parent who is a physician4 and about three-fourths of students come from families whose income falls among the top two quintiles.5 Impoverished communities, which have a disproportionate share of Black and Brown people, cannot afford to take MCAT preparatory classes or to accept unpaid “resume building” opportunities. Many medical schools continue to place more weight on test scores and research/medical experiences, despite a shift to a more holistic review process. Institutions that have tried a different approach and accepted students from more diverse backgrounds may often overlook the challenges that URM students face while in medical school and fail to provide appropriate support resources.
The result is a failure to retain such students. A study conducted at Stony Brook (N.Y.) University showed that those underrepresented in medicine were six times more likely to get dismissed from medical school, and three times more likely to both withdraw or graduate beyond 4 years, compared with their White counterparts.6 This is a serious issue that needs to change on a structural and systemic level.
Any discussion of race and psychiatry must acknowledge psychiatry’s history of racism against Black and Brown communities to engage in racially informed discussions with our patients. Only then can we play a better role advocating against racism within the field in the future. Dating back to the 18th century, psychiatry has promoted ideologies that promote racism. Benjamin Rush, considered the “father of American Psychiatry,” believed that Black skin was a disease derived from leprosy called “negritude.” In the late 19th century, this twisted ideology continued with the invention of the term “drapetomania,” which was used to describe enslaved people who ran away as having a mental disorder.7 Black prisoners were subjected to experimental treatment with substances such as LSD and bulbocapnine to subdue them.8 This idea that minorities were dangerous and needed to be subdued translated into a higher number of schizophrenia diagnoses, particularly among Black men, as it was used as a tool to vilify them in the 1970s. Although schizophrenia is equally prevalent among Whites and non-Whites, Black people are four times more likely to be diagnosed, compared with their White counterparts, while Hispanics are three times more likely. Studies have shown that Black and Brown men are also more likely to receive higher doses of antipsychotics.9
Given this history, it is not surprising that Black and Brown representation within the field is lacking and that patients may be hesitant to share their feelings about race with us. While we can’t change history, we can take a stance condemning the harmful behavior of the past. The American Psychiatric Association issued an apology earlier this year to Black, Indigenous, and People of Color for its support in structural racism.10 This is a step in the right direction, but we need more than statements or performative actions. We need to amplify the voices of Black and Brown psychiatrists and patients, as well as highlight their current and past contributions to the field. While my educational experiences focused on the work of prominent White scholars, medical curricula should showcase the work of people like Solomon Carter Fuller, MD, a Black psychiatrist who was essential to understanding Alzheimer’s, or Joseph White, PhD, sometimes referred to as the “godfather of Black psychology.”11
At times, I have found myself witness to situations where colleagues make statements that not only do not condemn racism, but in fact encourage it. I have unfortunately heard some use the all-too-familiar rhetoric of reverse racism, such as: “They just assume I am racist because I am a White male” or “They’re being racist against me” or statements like “Don’t you think it is far-fetched to believe she was just sitting on a college campus doing nothing when the police were called?” Rhetoric such as this is problematic to the field of psychiatry and medicine as a whole – and only serves to further invalidate the feelings of our Black and Brown patients. We must increase exposure and education regarding racism to address this, especially the meaning of microaggressions, a concept many fail to understand.
Attention to the subject of racism has increased within medical schools and residency training programs in the wake of George Floyd’s death. However, most programs often make these lectures optional or only have one to two limited sessions. Furthermore, many do not make it mandatory for faculty to attend; they are arguably the most in need of this training given that they set the precedent of how to practice psychiatry. Some institutions have incorporated comprehensive antiracist curriculums into medical training. One model that has been successful is the Social Justice and Health Equity program within Yale University’s psychiatry residency. The curriculum has four tracks:
- Structural competency, which focuses on the mental health impact of extraclinical structures, for example a patient’s neighborhood and associated barriers of access.
- Human experience, which explores the interaction of patients and providers and how biases play a role.
- Advocacy, which teaches residents the written and oral skills to lobby for patient interests on a community and legislative level.
- History of psychiatry, which focuses on understanding psychiatry’s prior role in racism.
In each track, there are group discussions, cases led by faculty, and meetings with community leaders. Through this curriculum, residents learn about power, privilege, and how to interact with and advocate for patients in a way that promotes equity, rather than racial disparity.12,13 This is a model that other psychiatric residency programs can promote, emulate, and benefit from.
Educating ourselves will hopefully lead to a deeper introspection of how we interact with patients and if we are promoting antiracism through our attitude and actions. Reflecting on my own personal practice, I have noted that the interplay of race, mental health, and provider decision-making becomes particularly complex when dealing with situations in which a patient exhibits increased aggression or agitation. As a second-year psychiatric resident immersed in the inpatient world, I have become familiar with patients at higher risk and greater need. The first attempt toward de-escalation involves verbal cues without any other more intrusive measures. If that fails, intramuscular (IM) medications are typically considered. If a patient has a history of aggressive behavior, the threshold to use IM medications can decrease dramatically. This is mainly to protect ourselves and our nursing staff and to prioritize safety. While I understand this rationale, I wonder about the patient’s experience. What constitutes “aggressive” behavior? For patients who have had violence used against them because of their race or who have suffered from police brutality, having police present or threatening IM medications will increasingly trigger them and escalate the situation. The aftermath can deepen the distrust of psychiatry by Black and Brown people.
How do we then handle such situations in a way that both protects our staff from physical harm and protects our patients from racial trauma? While I don’t have a great answer, I think we can benefit from standardizing what we consider aggressive behavior and have specific criteria that patients need to exhibit before administering an IM medication. In addition, discussions with the team, including residents, nurses, and attending physicians, about how to address an emergent situation before it actually happens are essential. Specifically discussing the patient’s history and race and how it may affect the situation is not something to be shied away from. Lastly, in the event that an IM medication is administered and police are present, debriefing with the patient afterward is necessary. The patient may not be willing or able to listen to you or trust you, but taking accountability and acknowledging what happened, justified or not, is a part of the process of rebuilding rapport.
Both in the purview of the individual psychiatrist and the field of psychiatry as a whole, we need to examine our behavior and not be afraid to make changes for the betterment of our patients. We must learn to talk about race with our patients and in the process, advocate for more representation of Black and Brown psychiatrists, understanding the barriers faced by these communities when pursuing the medical field. We must educate ourselves on psychiatry’s history, and equip ourselves with knowledge and tools to promote antiracism and shape psychiatry’s future. We can then apply these very tools to challenging situations we may encounter daily with the ultimate goal of improving the mental health of our patients. This is the only way we will progress and ensure that psychiatry is an equitable, antiracist field. As Ibram X. Kendi, PhD, has written, “The heartbeat of antiracism is self-reflection, recognition, admission, and fundamentally self-critique.”
Dr. Malik is a second-year psychiatry resident at the University of California, San Diego. She has a background in policy and grassroots organizing through her time working at the National Coalition for the Homeless and the Women’s Law Project. Dr. Malik has no disclosures.
References
1. Wyse R et al. Acad Psychiatry. 2020 Oct;44(5):523-30.
2. Cooper LA et al. Ann Intern Med. 2003;139:907-15.
3. Pierre JM et al. Acad Psychiatry. 2017;41:226-32.
4. Hartocollis A. “Getting into med school without hard sciences.” New York Times. 2010 Jul 29.
5. AAMC. An updated look at the economic diversity of U.S. medical students. Analysis in Brief. 2018 Oct;18(5).
6. Rainey ML. How do we retain minority health professions students. In: Smedley BD et al. The right thing to do, the smart thing to do: Enhancing diversity in the health professions: Summary of the Symposium on Diversity in Health Professions in Honor of Herbert W. Nickens, M.D. Institute of Medicine. National Academies Press. 2001.
7. Geller J. “Structural racism in American psychiatry and APA: Part 1.” Psychiatric News. 2020 Jun 23.
8. Mohr CL and Gordon JE. Tulane: The emergence of a modern university, 1945-1980. Louisiana State University Press, Baton Rouge. 2001.
9. Metzl JM. The protest psychosis: How schizophrenia became a Black disease. Beacon Press. 2010.
10. APA’s apology to Black, indigenous and people of color for its support of structural racism in psychiatry. American Psychiatric Association. 2021 Jan 18.
11. Black pioneers in mental health. Mental Health America. 2021.
12. Belli B. For Yale’s emerging psychiatrists, confronting racism is in the curriculum. Yale News. 2020 Jul 30.
13. Jordan A and Jackson D. Social justice and health equity curriculum. Yale School of Medicine. 2019 Sep 24.
“I feel like my aggression is being racialized.” “Of course I wouldn’t call the cops if I felt like hurting myself. I’m Black.”
Those statements represent the heightened trauma our Black and Brown patients with mental health issues have been experiencing. In the wake of increasingly publicized police brutality against Black and Brown communities, the role race plays in mental health decompensation is evident. At this moment in time, we must continue to improve our understanding of the role race plays in psychiatric disorders. We must also ask ourselves: At times, does psychiatry worsen the traumas of the communities we serve?
Some psychiatrists are afraid to speak about race. They may believe it to be too “political.” But avoiding these necessary conversations perpetuates the trauma of those we treat. It suggests that physicians are ignorant of an issue at the forefront of patients’ mental health. Psychiatry, today, is primarily focused on the biological aspects of disease. We must not forget that psychiatry is biopsychosocial. It is imperative that psychiatrists have conversations about race – and its significance to our patients and their care.
Only 10.4% of psychiatrists in the United States comprise those considered underrepresented in medicine (URM). Yet, those very groups make up 32.6% of the U.S. population and are overrepresented in psychiatric hospitals.1 Many studies have shown that concordant racial backgrounds between patient and physician lead to a more positive patient experience2 and arguably, the subsequent potential for better health outcomes. Our efforts in addressing this disparity often fall short. URM applicants may be hesitant to join an institution where diversity is lacking or where they may be the only minority.3 While there is no simple solution, I propose that psychiatrists promote the importance of mental health to Black and Brown students of all ages by collaborating with schools and community leaders.
It is important to acknowledge that the lack of diversity within psychiatry is reflective of that among all physicians. This in part stems from the barriers to medical education that Black and Brown communities face. Those who start off with more resources or have parents who are physicians are at an advantage when trying to get into medical school. In fact, one in five medical students have a parent who is a physician4 and about three-fourths of students come from families whose income falls among the top two quintiles.5 Impoverished communities, which have a disproportionate share of Black and Brown people, cannot afford to take MCAT preparatory classes or to accept unpaid “resume building” opportunities. Many medical schools continue to place more weight on test scores and research/medical experiences, despite a shift to a more holistic review process. Institutions that have tried a different approach and accepted students from more diverse backgrounds may often overlook the challenges that URM students face while in medical school and fail to provide appropriate support resources.
The result is a failure to retain such students. A study conducted at Stony Brook (N.Y.) University showed that those underrepresented in medicine were six times more likely to get dismissed from medical school, and three times more likely to both withdraw or graduate beyond 4 years, compared with their White counterparts.6 This is a serious issue that needs to change on a structural and systemic level.
Any discussion of race and psychiatry must acknowledge psychiatry’s history of racism against Black and Brown communities to engage in racially informed discussions with our patients. Only then can we play a better role advocating against racism within the field in the future. Dating back to the 18th century, psychiatry has promoted ideologies that promote racism. Benjamin Rush, considered the “father of American Psychiatry,” believed that Black skin was a disease derived from leprosy called “negritude.” In the late 19th century, this twisted ideology continued with the invention of the term “drapetomania,” which was used to describe enslaved people who ran away as having a mental disorder.7 Black prisoners were subjected to experimental treatment with substances such as LSD and bulbocapnine to subdue them.8 This idea that minorities were dangerous and needed to be subdued translated into a higher number of schizophrenia diagnoses, particularly among Black men, as it was used as a tool to vilify them in the 1970s. Although schizophrenia is equally prevalent among Whites and non-Whites, Black people are four times more likely to be diagnosed, compared with their White counterparts, while Hispanics are three times more likely. Studies have shown that Black and Brown men are also more likely to receive higher doses of antipsychotics.9
Given this history, it is not surprising that Black and Brown representation within the field is lacking and that patients may be hesitant to share their feelings about race with us. While we can’t change history, we can take a stance condemning the harmful behavior of the past. The American Psychiatric Association issued an apology earlier this year to Black, Indigenous, and People of Color for its support in structural racism.10 This is a step in the right direction, but we need more than statements or performative actions. We need to amplify the voices of Black and Brown psychiatrists and patients, as well as highlight their current and past contributions to the field. While my educational experiences focused on the work of prominent White scholars, medical curricula should showcase the work of people like Solomon Carter Fuller, MD, a Black psychiatrist who was essential to understanding Alzheimer’s, or Joseph White, PhD, sometimes referred to as the “godfather of Black psychology.”11
At times, I have found myself witness to situations where colleagues make statements that not only do not condemn racism, but in fact encourage it. I have unfortunately heard some use the all-too-familiar rhetoric of reverse racism, such as: “They just assume I am racist because I am a White male” or “They’re being racist against me” or statements like “Don’t you think it is far-fetched to believe she was just sitting on a college campus doing nothing when the police were called?” Rhetoric such as this is problematic to the field of psychiatry and medicine as a whole – and only serves to further invalidate the feelings of our Black and Brown patients. We must increase exposure and education regarding racism to address this, especially the meaning of microaggressions, a concept many fail to understand.
Attention to the subject of racism has increased within medical schools and residency training programs in the wake of George Floyd’s death. However, most programs often make these lectures optional or only have one to two limited sessions. Furthermore, many do not make it mandatory for faculty to attend; they are arguably the most in need of this training given that they set the precedent of how to practice psychiatry. Some institutions have incorporated comprehensive antiracist curriculums into medical training. One model that has been successful is the Social Justice and Health Equity program within Yale University’s psychiatry residency. The curriculum has four tracks:
- Structural competency, which focuses on the mental health impact of extraclinical structures, for example a patient’s neighborhood and associated barriers of access.
- Human experience, which explores the interaction of patients and providers and how biases play a role.
- Advocacy, which teaches residents the written and oral skills to lobby for patient interests on a community and legislative level.
- History of psychiatry, which focuses on understanding psychiatry’s prior role in racism.
In each track, there are group discussions, cases led by faculty, and meetings with community leaders. Through this curriculum, residents learn about power, privilege, and how to interact with and advocate for patients in a way that promotes equity, rather than racial disparity.12,13 This is a model that other psychiatric residency programs can promote, emulate, and benefit from.
Educating ourselves will hopefully lead to a deeper introspection of how we interact with patients and if we are promoting antiracism through our attitude and actions. Reflecting on my own personal practice, I have noted that the interplay of race, mental health, and provider decision-making becomes particularly complex when dealing with situations in which a patient exhibits increased aggression or agitation. As a second-year psychiatric resident immersed in the inpatient world, I have become familiar with patients at higher risk and greater need. The first attempt toward de-escalation involves verbal cues without any other more intrusive measures. If that fails, intramuscular (IM) medications are typically considered. If a patient has a history of aggressive behavior, the threshold to use IM medications can decrease dramatically. This is mainly to protect ourselves and our nursing staff and to prioritize safety. While I understand this rationale, I wonder about the patient’s experience. What constitutes “aggressive” behavior? For patients who have had violence used against them because of their race or who have suffered from police brutality, having police present or threatening IM medications will increasingly trigger them and escalate the situation. The aftermath can deepen the distrust of psychiatry by Black and Brown people.
How do we then handle such situations in a way that both protects our staff from physical harm and protects our patients from racial trauma? While I don’t have a great answer, I think we can benefit from standardizing what we consider aggressive behavior and have specific criteria that patients need to exhibit before administering an IM medication. In addition, discussions with the team, including residents, nurses, and attending physicians, about how to address an emergent situation before it actually happens are essential. Specifically discussing the patient’s history and race and how it may affect the situation is not something to be shied away from. Lastly, in the event that an IM medication is administered and police are present, debriefing with the patient afterward is necessary. The patient may not be willing or able to listen to you or trust you, but taking accountability and acknowledging what happened, justified or not, is a part of the process of rebuilding rapport.
Both in the purview of the individual psychiatrist and the field of psychiatry as a whole, we need to examine our behavior and not be afraid to make changes for the betterment of our patients. We must learn to talk about race with our patients and in the process, advocate for more representation of Black and Brown psychiatrists, understanding the barriers faced by these communities when pursuing the medical field. We must educate ourselves on psychiatry’s history, and equip ourselves with knowledge and tools to promote antiracism and shape psychiatry’s future. We can then apply these very tools to challenging situations we may encounter daily with the ultimate goal of improving the mental health of our patients. This is the only way we will progress and ensure that psychiatry is an equitable, antiracist field. As Ibram X. Kendi, PhD, has written, “The heartbeat of antiracism is self-reflection, recognition, admission, and fundamentally self-critique.”
Dr. Malik is a second-year psychiatry resident at the University of California, San Diego. She has a background in policy and grassroots organizing through her time working at the National Coalition for the Homeless and the Women’s Law Project. Dr. Malik has no disclosures.
References
1. Wyse R et al. Acad Psychiatry. 2020 Oct;44(5):523-30.
2. Cooper LA et al. Ann Intern Med. 2003;139:907-15.
3. Pierre JM et al. Acad Psychiatry. 2017;41:226-32.
4. Hartocollis A. “Getting into med school without hard sciences.” New York Times. 2010 Jul 29.
5. AAMC. An updated look at the economic diversity of U.S. medical students. Analysis in Brief. 2018 Oct;18(5).
6. Rainey ML. How do we retain minority health professions students. In: Smedley BD et al. The right thing to do, the smart thing to do: Enhancing diversity in the health professions: Summary of the Symposium on Diversity in Health Professions in Honor of Herbert W. Nickens, M.D. Institute of Medicine. National Academies Press. 2001.
7. Geller J. “Structural racism in American psychiatry and APA: Part 1.” Psychiatric News. 2020 Jun 23.
8. Mohr CL and Gordon JE. Tulane: The emergence of a modern university, 1945-1980. Louisiana State University Press, Baton Rouge. 2001.
9. Metzl JM. The protest psychosis: How schizophrenia became a Black disease. Beacon Press. 2010.
10. APA’s apology to Black, indigenous and people of color for its support of structural racism in psychiatry. American Psychiatric Association. 2021 Jan 18.
11. Black pioneers in mental health. Mental Health America. 2021.
12. Belli B. For Yale’s emerging psychiatrists, confronting racism is in the curriculum. Yale News. 2020 Jul 30.
13. Jordan A and Jackson D. Social justice and health equity curriculum. Yale School of Medicine. 2019 Sep 24.
“I feel like my aggression is being racialized.” “Of course I wouldn’t call the cops if I felt like hurting myself. I’m Black.”
Those statements represent the heightened trauma our Black and Brown patients with mental health issues have been experiencing. In the wake of increasingly publicized police brutality against Black and Brown communities, the role race plays in mental health decompensation is evident. At this moment in time, we must continue to improve our understanding of the role race plays in psychiatric disorders. We must also ask ourselves: At times, does psychiatry worsen the traumas of the communities we serve?
Some psychiatrists are afraid to speak about race. They may believe it to be too “political.” But avoiding these necessary conversations perpetuates the trauma of those we treat. It suggests that physicians are ignorant of an issue at the forefront of patients’ mental health. Psychiatry, today, is primarily focused on the biological aspects of disease. We must not forget that psychiatry is biopsychosocial. It is imperative that psychiatrists have conversations about race – and its significance to our patients and their care.
Only 10.4% of psychiatrists in the United States comprise those considered underrepresented in medicine (URM). Yet, those very groups make up 32.6% of the U.S. population and are overrepresented in psychiatric hospitals.1 Many studies have shown that concordant racial backgrounds between patient and physician lead to a more positive patient experience2 and arguably, the subsequent potential for better health outcomes. Our efforts in addressing this disparity often fall short. URM applicants may be hesitant to join an institution where diversity is lacking or where they may be the only minority.3 While there is no simple solution, I propose that psychiatrists promote the importance of mental health to Black and Brown students of all ages by collaborating with schools and community leaders.
It is important to acknowledge that the lack of diversity within psychiatry is reflective of that among all physicians. This in part stems from the barriers to medical education that Black and Brown communities face. Those who start off with more resources or have parents who are physicians are at an advantage when trying to get into medical school. In fact, one in five medical students have a parent who is a physician4 and about three-fourths of students come from families whose income falls among the top two quintiles.5 Impoverished communities, which have a disproportionate share of Black and Brown people, cannot afford to take MCAT preparatory classes or to accept unpaid “resume building” opportunities. Many medical schools continue to place more weight on test scores and research/medical experiences, despite a shift to a more holistic review process. Institutions that have tried a different approach and accepted students from more diverse backgrounds may often overlook the challenges that URM students face while in medical school and fail to provide appropriate support resources.
The result is a failure to retain such students. A study conducted at Stony Brook (N.Y.) University showed that those underrepresented in medicine were six times more likely to get dismissed from medical school, and three times more likely to both withdraw or graduate beyond 4 years, compared with their White counterparts.6 This is a serious issue that needs to change on a structural and systemic level.
Any discussion of race and psychiatry must acknowledge psychiatry’s history of racism against Black and Brown communities to engage in racially informed discussions with our patients. Only then can we play a better role advocating against racism within the field in the future. Dating back to the 18th century, psychiatry has promoted ideologies that promote racism. Benjamin Rush, considered the “father of American Psychiatry,” believed that Black skin was a disease derived from leprosy called “negritude.” In the late 19th century, this twisted ideology continued with the invention of the term “drapetomania,” which was used to describe enslaved people who ran away as having a mental disorder.7 Black prisoners were subjected to experimental treatment with substances such as LSD and bulbocapnine to subdue them.8 This idea that minorities were dangerous and needed to be subdued translated into a higher number of schizophrenia diagnoses, particularly among Black men, as it was used as a tool to vilify them in the 1970s. Although schizophrenia is equally prevalent among Whites and non-Whites, Black people are four times more likely to be diagnosed, compared with their White counterparts, while Hispanics are three times more likely. Studies have shown that Black and Brown men are also more likely to receive higher doses of antipsychotics.9
Given this history, it is not surprising that Black and Brown representation within the field is lacking and that patients may be hesitant to share their feelings about race with us. While we can’t change history, we can take a stance condemning the harmful behavior of the past. The American Psychiatric Association issued an apology earlier this year to Black, Indigenous, and People of Color for its support in structural racism.10 This is a step in the right direction, but we need more than statements or performative actions. We need to amplify the voices of Black and Brown psychiatrists and patients, as well as highlight their current and past contributions to the field. While my educational experiences focused on the work of prominent White scholars, medical curricula should showcase the work of people like Solomon Carter Fuller, MD, a Black psychiatrist who was essential to understanding Alzheimer’s, or Joseph White, PhD, sometimes referred to as the “godfather of Black psychology.”11
At times, I have found myself witness to situations where colleagues make statements that not only do not condemn racism, but in fact encourage it. I have unfortunately heard some use the all-too-familiar rhetoric of reverse racism, such as: “They just assume I am racist because I am a White male” or “They’re being racist against me” or statements like “Don’t you think it is far-fetched to believe she was just sitting on a college campus doing nothing when the police were called?” Rhetoric such as this is problematic to the field of psychiatry and medicine as a whole – and only serves to further invalidate the feelings of our Black and Brown patients. We must increase exposure and education regarding racism to address this, especially the meaning of microaggressions, a concept many fail to understand.
Attention to the subject of racism has increased within medical schools and residency training programs in the wake of George Floyd’s death. However, most programs often make these lectures optional or only have one to two limited sessions. Furthermore, many do not make it mandatory for faculty to attend; they are arguably the most in need of this training given that they set the precedent of how to practice psychiatry. Some institutions have incorporated comprehensive antiracist curriculums into medical training. One model that has been successful is the Social Justice and Health Equity program within Yale University’s psychiatry residency. The curriculum has four tracks:
- Structural competency, which focuses on the mental health impact of extraclinical structures, for example a patient’s neighborhood and associated barriers of access.
- Human experience, which explores the interaction of patients and providers and how biases play a role.
- Advocacy, which teaches residents the written and oral skills to lobby for patient interests on a community and legislative level.
- History of psychiatry, which focuses on understanding psychiatry’s prior role in racism.
In each track, there are group discussions, cases led by faculty, and meetings with community leaders. Through this curriculum, residents learn about power, privilege, and how to interact with and advocate for patients in a way that promotes equity, rather than racial disparity.12,13 This is a model that other psychiatric residency programs can promote, emulate, and benefit from.
Educating ourselves will hopefully lead to a deeper introspection of how we interact with patients and if we are promoting antiracism through our attitude and actions. Reflecting on my own personal practice, I have noted that the interplay of race, mental health, and provider decision-making becomes particularly complex when dealing with situations in which a patient exhibits increased aggression or agitation. As a second-year psychiatric resident immersed in the inpatient world, I have become familiar with patients at higher risk and greater need. The first attempt toward de-escalation involves verbal cues without any other more intrusive measures. If that fails, intramuscular (IM) medications are typically considered. If a patient has a history of aggressive behavior, the threshold to use IM medications can decrease dramatically. This is mainly to protect ourselves and our nursing staff and to prioritize safety. While I understand this rationale, I wonder about the patient’s experience. What constitutes “aggressive” behavior? For patients who have had violence used against them because of their race or who have suffered from police brutality, having police present or threatening IM medications will increasingly trigger them and escalate the situation. The aftermath can deepen the distrust of psychiatry by Black and Brown people.
How do we then handle such situations in a way that both protects our staff from physical harm and protects our patients from racial trauma? While I don’t have a great answer, I think we can benefit from standardizing what we consider aggressive behavior and have specific criteria that patients need to exhibit before administering an IM medication. In addition, discussions with the team, including residents, nurses, and attending physicians, about how to address an emergent situation before it actually happens are essential. Specifically discussing the patient’s history and race and how it may affect the situation is not something to be shied away from. Lastly, in the event that an IM medication is administered and police are present, debriefing with the patient afterward is necessary. The patient may not be willing or able to listen to you or trust you, but taking accountability and acknowledging what happened, justified or not, is a part of the process of rebuilding rapport.
Both in the purview of the individual psychiatrist and the field of psychiatry as a whole, we need to examine our behavior and not be afraid to make changes for the betterment of our patients. We must learn to talk about race with our patients and in the process, advocate for more representation of Black and Brown psychiatrists, understanding the barriers faced by these communities when pursuing the medical field. We must educate ourselves on psychiatry’s history, and equip ourselves with knowledge and tools to promote antiracism and shape psychiatry’s future. We can then apply these very tools to challenging situations we may encounter daily with the ultimate goal of improving the mental health of our patients. This is the only way we will progress and ensure that psychiatry is an equitable, antiracist field. As Ibram X. Kendi, PhD, has written, “The heartbeat of antiracism is self-reflection, recognition, admission, and fundamentally self-critique.”
Dr. Malik is a second-year psychiatry resident at the University of California, San Diego. She has a background in policy and grassroots organizing through her time working at the National Coalition for the Homeless and the Women’s Law Project. Dr. Malik has no disclosures.
References
1. Wyse R et al. Acad Psychiatry. 2020 Oct;44(5):523-30.
2. Cooper LA et al. Ann Intern Med. 2003;139:907-15.
3. Pierre JM et al. Acad Psychiatry. 2017;41:226-32.
4. Hartocollis A. “Getting into med school without hard sciences.” New York Times. 2010 Jul 29.
5. AAMC. An updated look at the economic diversity of U.S. medical students. Analysis in Brief. 2018 Oct;18(5).
6. Rainey ML. How do we retain minority health professions students. In: Smedley BD et al. The right thing to do, the smart thing to do: Enhancing diversity in the health professions: Summary of the Symposium on Diversity in Health Professions in Honor of Herbert W. Nickens, M.D. Institute of Medicine. National Academies Press. 2001.
7. Geller J. “Structural racism in American psychiatry and APA: Part 1.” Psychiatric News. 2020 Jun 23.
8. Mohr CL and Gordon JE. Tulane: The emergence of a modern university, 1945-1980. Louisiana State University Press, Baton Rouge. 2001.
9. Metzl JM. The protest psychosis: How schizophrenia became a Black disease. Beacon Press. 2010.
10. APA’s apology to Black, indigenous and people of color for its support of structural racism in psychiatry. American Psychiatric Association. 2021 Jan 18.
11. Black pioneers in mental health. Mental Health America. 2021.
12. Belli B. For Yale’s emerging psychiatrists, confronting racism is in the curriculum. Yale News. 2020 Jul 30.
13. Jordan A and Jackson D. Social justice and health equity curriculum. Yale School of Medicine. 2019 Sep 24.
Church-based services may help close gaps in mental health care
Black individuals who received mental health services through a church-based program reported high levels of satisfaction, data from a small, qualitative study show.
“This model of providing mental health services adjacent to or supported by a trusted institution, with providers who may have a more nuanced and intimate knowledge of the experiences of and perceptions held by community members, may facilitate important therapy-mediating factors, such as trust,” wrote Angela Coombs, MD, of Columbia University, New York, and colleagues.
Black Americans continue to face barriers to mental health services, and fewer than one-third of Black Americans with a mental health condition receive formal mental health care, Dr. Coombs and colleagues reported. Barriers to treatment include stigma and distrust of medical institutions, and strategies are needed to address these barriers to improve access. Consequently, “one approach includes the development of mental health programming and supports with trusted institutions, such as churches,” they said. Data are limited, however, on the perspectives of individuals who have used church-based services.
In the study, published in Psychiatric Services, Dr. Coombs and colleagues recruited 15 adults aged 27-69 years who were receiving or had received mental health services at the HOPE (Healing On Purpose and Evolving) Center, a freestanding mental health clinic affiliated with the First Corinthian Baptist Church in Harlem, New York. At the time of the study in 2019, those attending the center (referred to as “innovators” rather than patients or clients to reduce stigma) received 10 free sessions of evidence-based psychotherapy.
Treatment included cognitive-behavioral therapy (CBT), religiously integrated CBT, and interpersonal psychotherapy (IPT) to individuals, couples, and families. Group psychotherapy also was an option. Clinicians at the HOPE Center included licensed social workers with doctoral and master’s-level degrees, as well as supervised social work student interns.
Study participants took part in a 30-minute interview, in person or by phone, with a female psychiatrist who was not employed by the HOPE Center or involved in treating the patients. There were 15 participants: 13 women and 2 men, with mean ages of 48 and 51 years, respectively; 14 identified as Black, non-Hispanic. Most (13 individuals) identified as heterosexual, 11 had never married, and 14 had some college or technical school education.
Notably, 11 participants reported attending church once a week, and 13 said they considered religion or spirituality highly important. Participants “reported that services that could integrate their spiritual beliefs with their current mental health challenges enhanced the therapeutic experience,” the researchers said.
Positive messaging about mental health care from the church and senior pastor also encouraged the participants to take advantage of the HOPE Center services.
As one participant said, “I’ve always believed that I can handle my own issues ... but listening to the pastor always talking about the [HOPE] Center and not to be ashamed if you have weaknesses, that’s when I said, ‘You know what, let me just start seeking mental health services because I really need [them].’ ”
, including recognizing cycles of unproductive behavior, processing traumatic experiences and learning self-love, and embracing meditation at home.
“A common theme among participants was that the HOPE Center provided them with tools to destress, process trauma, and manage anxiety,” the researchers wrote. In particular, several participants cited group sessions on teaching and practicing mindfulness as their favorite services. They described the HOPE Center as a positive, peaceful, and welcoming environment where they felt safe.
Cost issues were important as well. Participants noted that the HOPE Center’s ability to provide services that were free made it easier for them to attend. “Although participants said that it was helpful that the HOPE Center provided referrals to external providers and agencies for additional services, some said they wished that the HOPE Center would provide long-term therapy,” the researchers noted.
Overall, “most participants said that establishing more mental health resources within faith-based spaces could accelerate normalization of seeking and receiving mental health care within religious Black communities,” they said.
The study findings were limited by the absence of clinical data – and data on participants’ frequency and location of church attendance, the researchers noted. In addition, the positive results could be tied to selection bias, Dr. Coombs and colleagues said. Another possible limitation is the overrepresentation of cisgender women among the participants. Still, “the perspectives shared by participants suggest that this model of care may address several important barriers to care faced by some Black American populations,” the researchers wrote.
Bridging gap between spirituality and mental health
In an interview, Atasha Jordan, MD, said Black Americans with mental illnesses have long lacked equal access to mental health services. “However, in light of the COVID-19 pandemic, published studies have shown that rates of mental illness increased concurrently with a rise in spirituality and faith. That said, we currently live in a time where mental health and spirituality are more likely to intersect,” noted Dr. Jordan, of the University of Pennsylvania, Philadelphia.
She said it is not surprising that the study participants felt more comfortable receiving mental health services at a clinic that was church affiliated.
“We have known for years that people of faith are more likely to seek comfort for psychological distress from clergy, rather than mental health professionals. Providing a more familiar entry point to mental health services through a church-affiliated mental health clinic helps to bridge the existing gap between spirituality and mental health,” Dr. Jordan said. “For many Black Americans, spirituality is a central component of culturally-informed mental health care.
“Mental health providers may find improved service utilization and outcomes for their patients by collaborating with faith-based organizations or investing time to learn spiritually-based psychotherapies.”
Recently published data, notably a study published May 1, 2021, in Psychiatric Services, continue to support the existing knowledge “that many patients with psychiatric illnesses want increased attention paid to spirituality during their mental health care,” Dr. Jordan noted. “Moreover, they showed that nonreligious clinicians may be more apt than religious clinicians to provide objective, spiritually-oriented mental health care. In this vein, further research aimed at understanding the most effective methods to address spiritual health in times of mental distress can help all mental health providers better meet their patients’ psychiatric and psychological needs.”
Overcoming stigma, mistrust
During the pandemic, clinicians have seen an increase in mental health distress in the form of anxiety, depression, and trauma symptoms, Lorenzo Norris, MD, of George Washington University, Washington, said in an interview.

“Historically, African Americans have faced numerous barriers to mental health care, including stigma and mistrust of medical institutions,” Dr. Norris said. “At this time, perhaps more than in recent decades, novel ways of eliminating and navigating these barriers must be explored in an evidence-based fashion that will inform future interventions.”
Dr. Norris also found that the study findings make sense.
“Historically, the Black church has been a central institution in the community,” he said. “In my personal experience, the church served in a variety of roles, including but not limited to advocacy, employment, social services, peer support, and notably a trusted source of advice pertaining to health. In addition, Black churches may be in an ideal position to serve as culturally sensitive facilitators to build trust,” he said.
The study’s message for clinicians, according to Dr. Norris, is to “carefully consider partnering with faith-based organizations and community leaders if you want to supplement your efforts at decreasing mental health care disparities in the African American community.”
He pointed out, however, that in addition to the small number of participants, the study did not examine clinical outcomes. “So we must be careful how much we take from the initial conclusions,” Dr. Norris said.
Additional research is needed on a much larger scale to add support to the study findings, he said. “This study focused on one church and its particular program,” Dr. Norris noted. “There is likely a great deal of heterogeneity with Black churches and definitely among church members they serve,” he said. “Although it may be tempting to go with an ‘of course it will work’ approach, it is best to have additional qualitative and quantitative research of a much larger scale, with clinical controls that examine the ability of Black churches to address barriers African Americans face in receiving and utilizing mental health services,” he concluded.
Dr. Jordan disclosed receiving a 2021-2022 American Psychiatric Association/Substance Abuse and Mental Health Services Administration Minority Fellowship Program grant to study mental health literacy in the Black church. Dr. Norris disclosed serving as CEO of the Cleveland Clergy Alliance, a nonprofit organization providing outreach assistance as a mechanism to help seniors and the disabled population through community programming. The study authors reported no disclosures.
Black individuals who received mental health services through a church-based program reported high levels of satisfaction, data from a small, qualitative study show.
“This model of providing mental health services adjacent to or supported by a trusted institution, with providers who may have a more nuanced and intimate knowledge of the experiences of and perceptions held by community members, may facilitate important therapy-mediating factors, such as trust,” wrote Angela Coombs, MD, of Columbia University, New York, and colleagues.
Black Americans continue to face barriers to mental health services, and fewer than one-third of Black Americans with a mental health condition receive formal mental health care, Dr. Coombs and colleagues reported. Barriers to treatment include stigma and distrust of medical institutions, and strategies are needed to address these barriers to improve access. Consequently, “one approach includes the development of mental health programming and supports with trusted institutions, such as churches,” they said. Data are limited, however, on the perspectives of individuals who have used church-based services.
In the study, published in Psychiatric Services, Dr. Coombs and colleagues recruited 15 adults aged 27-69 years who were receiving or had received mental health services at the HOPE (Healing On Purpose and Evolving) Center, a freestanding mental health clinic affiliated with the First Corinthian Baptist Church in Harlem, New York. At the time of the study in 2019, those attending the center (referred to as “innovators” rather than patients or clients to reduce stigma) received 10 free sessions of evidence-based psychotherapy.
Treatment included cognitive-behavioral therapy (CBT), religiously integrated CBT, and interpersonal psychotherapy (IPT) to individuals, couples, and families. Group psychotherapy also was an option. Clinicians at the HOPE Center included licensed social workers with doctoral and master’s-level degrees, as well as supervised social work student interns.
Study participants took part in a 30-minute interview, in person or by phone, with a female psychiatrist who was not employed by the HOPE Center or involved in treating the patients. There were 15 participants: 13 women and 2 men, with mean ages of 48 and 51 years, respectively; 14 identified as Black, non-Hispanic. Most (13 individuals) identified as heterosexual, 11 had never married, and 14 had some college or technical school education.
Notably, 11 participants reported attending church once a week, and 13 said they considered religion or spirituality highly important. Participants “reported that services that could integrate their spiritual beliefs with their current mental health challenges enhanced the therapeutic experience,” the researchers said.
Positive messaging about mental health care from the church and senior pastor also encouraged the participants to take advantage of the HOPE Center services.
As one participant said, “I’ve always believed that I can handle my own issues ... but listening to the pastor always talking about the [HOPE] Center and not to be ashamed if you have weaknesses, that’s when I said, ‘You know what, let me just start seeking mental health services because I really need [them].’ ”
, including recognizing cycles of unproductive behavior, processing traumatic experiences and learning self-love, and embracing meditation at home.
“A common theme among participants was that the HOPE Center provided them with tools to destress, process trauma, and manage anxiety,” the researchers wrote. In particular, several participants cited group sessions on teaching and practicing mindfulness as their favorite services. They described the HOPE Center as a positive, peaceful, and welcoming environment where they felt safe.
Cost issues were important as well. Participants noted that the HOPE Center’s ability to provide services that were free made it easier for them to attend. “Although participants said that it was helpful that the HOPE Center provided referrals to external providers and agencies for additional services, some said they wished that the HOPE Center would provide long-term therapy,” the researchers noted.
Overall, “most participants said that establishing more mental health resources within faith-based spaces could accelerate normalization of seeking and receiving mental health care within religious Black communities,” they said.
The study findings were limited by the absence of clinical data – and data on participants’ frequency and location of church attendance, the researchers noted. In addition, the positive results could be tied to selection bias, Dr. Coombs and colleagues said. Another possible limitation is the overrepresentation of cisgender women among the participants. Still, “the perspectives shared by participants suggest that this model of care may address several important barriers to care faced by some Black American populations,” the researchers wrote.
Bridging gap between spirituality and mental health
In an interview, Atasha Jordan, MD, said Black Americans with mental illnesses have long lacked equal access to mental health services. “However, in light of the COVID-19 pandemic, published studies have shown that rates of mental illness increased concurrently with a rise in spirituality and faith. That said, we currently live in a time where mental health and spirituality are more likely to intersect,” noted Dr. Jordan, of the University of Pennsylvania, Philadelphia.
She said it is not surprising that the study participants felt more comfortable receiving mental health services at a clinic that was church affiliated.
“We have known for years that people of faith are more likely to seek comfort for psychological distress from clergy, rather than mental health professionals. Providing a more familiar entry point to mental health services through a church-affiliated mental health clinic helps to bridge the existing gap between spirituality and mental health,” Dr. Jordan said. “For many Black Americans, spirituality is a central component of culturally-informed mental health care.
“Mental health providers may find improved service utilization and outcomes for their patients by collaborating with faith-based organizations or investing time to learn spiritually-based psychotherapies.”
Recently published data, notably a study published May 1, 2021, in Psychiatric Services, continue to support the existing knowledge “that many patients with psychiatric illnesses want increased attention paid to spirituality during their mental health care,” Dr. Jordan noted. “Moreover, they showed that nonreligious clinicians may be more apt than religious clinicians to provide objective, spiritually-oriented mental health care. In this vein, further research aimed at understanding the most effective methods to address spiritual health in times of mental distress can help all mental health providers better meet their patients’ psychiatric and psychological needs.”
Overcoming stigma, mistrust
During the pandemic, clinicians have seen an increase in mental health distress in the form of anxiety, depression, and trauma symptoms, Lorenzo Norris, MD, of George Washington University, Washington, said in an interview.
“Historically, African Americans have faced numerous barriers to mental health care, including stigma and mistrust of medical institutions,” Dr. Norris said. “At this time, perhaps more than in recent decades, novel ways of eliminating and navigating these barriers must be explored in an evidence-based fashion that will inform future interventions.”
Dr. Norris also found that the study findings make sense.
“Historically, the Black church has been a central institution in the community,” he said. “In my personal experience, the church served in a variety of roles, including but not limited to advocacy, employment, social services, peer support, and notably a trusted source of advice pertaining to health. In addition, Black churches may be in an ideal position to serve as culturally sensitive facilitators to build trust,” he said.
The study’s message for clinicians, according to Dr. Norris, is to “carefully consider partnering with faith-based organizations and community leaders if you want to supplement your efforts at decreasing mental health care disparities in the African American community.”
He pointed out, however, that in addition to the small number of participants, the study did not examine clinical outcomes. “So we must be careful how much we take from the initial conclusions,” Dr. Norris said.
Additional research is needed on a much larger scale to add support to the study findings, he said. “This study focused on one church and its particular program,” Dr. Norris noted. “There is likely a great deal of heterogeneity with Black churches and definitely among church members they serve,” he said. “Although it may be tempting to go with an ‘of course it will work’ approach, it is best to have additional qualitative and quantitative research of a much larger scale, with clinical controls that examine the ability of Black churches to address barriers African Americans face in receiving and utilizing mental health services,” he concluded.
Dr. Jordan disclosed receiving a 2021-2022 American Psychiatric Association/Substance Abuse and Mental Health Services Administration Minority Fellowship Program grant to study mental health literacy in the Black church. Dr. Norris disclosed serving as CEO of the Cleveland Clergy Alliance, a nonprofit organization providing outreach assistance as a mechanism to help seniors and the disabled population through community programming. The study authors reported no disclosures.
Black individuals who received mental health services through a church-based program reported high levels of satisfaction, data from a small, qualitative study show.
“This model of providing mental health services adjacent to or supported by a trusted institution, with providers who may have a more nuanced and intimate knowledge of the experiences of and perceptions held by community members, may facilitate important therapy-mediating factors, such as trust,” wrote Angela Coombs, MD, of Columbia University, New York, and colleagues.
Black Americans continue to face barriers to mental health services, and fewer than one-third of Black Americans with a mental health condition receive formal mental health care, Dr. Coombs and colleagues reported. Barriers to treatment include stigma and distrust of medical institutions, and strategies are needed to address these barriers to improve access. Consequently, “one approach includes the development of mental health programming and supports with trusted institutions, such as churches,” they said. Data are limited, however, on the perspectives of individuals who have used church-based services.
In the study, published in Psychiatric Services, Dr. Coombs and colleagues recruited 15 adults aged 27-69 years who were receiving or had received mental health services at the HOPE (Healing On Purpose and Evolving) Center, a freestanding mental health clinic affiliated with the First Corinthian Baptist Church in Harlem, New York. At the time of the study in 2019, those attending the center (referred to as “innovators” rather than patients or clients to reduce stigma) received 10 free sessions of evidence-based psychotherapy.
Treatment included cognitive-behavioral therapy (CBT), religiously integrated CBT, and interpersonal psychotherapy (IPT) to individuals, couples, and families. Group psychotherapy also was an option. Clinicians at the HOPE Center included licensed social workers with doctoral and master’s-level degrees, as well as supervised social work student interns.
Study participants took part in a 30-minute interview, in person or by phone, with a female psychiatrist who was not employed by the HOPE Center or involved in treating the patients. There were 15 participants: 13 women and 2 men, with mean ages of 48 and 51 years, respectively; 14 identified as Black, non-Hispanic. Most (13 individuals) identified as heterosexual, 11 had never married, and 14 had some college or technical school education.
Notably, 11 participants reported attending church once a week, and 13 said they considered religion or spirituality highly important. Participants “reported that services that could integrate their spiritual beliefs with their current mental health challenges enhanced the therapeutic experience,” the researchers said.
Positive messaging about mental health care from the church and senior pastor also encouraged the participants to take advantage of the HOPE Center services.
As one participant said, “I’ve always believed that I can handle my own issues ... but listening to the pastor always talking about the [HOPE] Center and not to be ashamed if you have weaknesses, that’s when I said, ‘You know what, let me just start seeking mental health services because I really need [them].’ ”
, including recognizing cycles of unproductive behavior, processing traumatic experiences and learning self-love, and embracing meditation at home.
“A common theme among participants was that the HOPE Center provided them with tools to destress, process trauma, and manage anxiety,” the researchers wrote. In particular, several participants cited group sessions on teaching and practicing mindfulness as their favorite services. They described the HOPE Center as a positive, peaceful, and welcoming environment where they felt safe.
Cost issues were important as well. Participants noted that the HOPE Center’s ability to provide services that were free made it easier for them to attend. “Although participants said that it was helpful that the HOPE Center provided referrals to external providers and agencies for additional services, some said they wished that the HOPE Center would provide long-term therapy,” the researchers noted.
Overall, “most participants said that establishing more mental health resources within faith-based spaces could accelerate normalization of seeking and receiving mental health care within religious Black communities,” they said.
The study findings were limited by the absence of clinical data – and data on participants’ frequency and location of church attendance, the researchers noted. In addition, the positive results could be tied to selection bias, Dr. Coombs and colleagues said. Another possible limitation is the overrepresentation of cisgender women among the participants. Still, “the perspectives shared by participants suggest that this model of care may address several important barriers to care faced by some Black American populations,” the researchers wrote.
Bridging gap between spirituality and mental health
In an interview, Atasha Jordan, MD, said Black Americans with mental illnesses have long lacked equal access to mental health services. “However, in light of the COVID-19 pandemic, published studies have shown that rates of mental illness increased concurrently with a rise in spirituality and faith. That said, we currently live in a time where mental health and spirituality are more likely to intersect,” noted Dr. Jordan, of the University of Pennsylvania, Philadelphia.
She said it is not surprising that the study participants felt more comfortable receiving mental health services at a clinic that was church affiliated.
“We have known for years that people of faith are more likely to seek comfort for psychological distress from clergy, rather than mental health professionals. Providing a more familiar entry point to mental health services through a church-affiliated mental health clinic helps to bridge the existing gap between spirituality and mental health,” Dr. Jordan said. “For many Black Americans, spirituality is a central component of culturally-informed mental health care.
“Mental health providers may find improved service utilization and outcomes for their patients by collaborating with faith-based organizations or investing time to learn spiritually-based psychotherapies.”
Recently published data, notably a study published May 1, 2021, in Psychiatric Services, continue to support the existing knowledge “that many patients with psychiatric illnesses want increased attention paid to spirituality during their mental health care,” Dr. Jordan noted. “Moreover, they showed that nonreligious clinicians may be more apt than religious clinicians to provide objective, spiritually-oriented mental health care. In this vein, further research aimed at understanding the most effective methods to address spiritual health in times of mental distress can help all mental health providers better meet their patients’ psychiatric and psychological needs.”
Overcoming stigma, mistrust
During the pandemic, clinicians have seen an increase in mental health distress in the form of anxiety, depression, and trauma symptoms, Lorenzo Norris, MD, of George Washington University, Washington, said in an interview.
“Historically, African Americans have faced numerous barriers to mental health care, including stigma and mistrust of medical institutions,” Dr. Norris said. “At this time, perhaps more than in recent decades, novel ways of eliminating and navigating these barriers must be explored in an evidence-based fashion that will inform future interventions.”
Dr. Norris also found that the study findings make sense.
“Historically, the Black church has been a central institution in the community,” he said. “In my personal experience, the church served in a variety of roles, including but not limited to advocacy, employment, social services, peer support, and notably a trusted source of advice pertaining to health. In addition, Black churches may be in an ideal position to serve as culturally sensitive facilitators to build trust,” he said.
The study’s message for clinicians, according to Dr. Norris, is to “carefully consider partnering with faith-based organizations and community leaders if you want to supplement your efforts at decreasing mental health care disparities in the African American community.”
He pointed out, however, that in addition to the small number of participants, the study did not examine clinical outcomes. “So we must be careful how much we take from the initial conclusions,” Dr. Norris said.
Additional research is needed on a much larger scale to add support to the study findings, he said. “This study focused on one church and its particular program,” Dr. Norris noted. “There is likely a great deal of heterogeneity with Black churches and definitely among church members they serve,” he said. “Although it may be tempting to go with an ‘of course it will work’ approach, it is best to have additional qualitative and quantitative research of a much larger scale, with clinical controls that examine the ability of Black churches to address barriers African Americans face in receiving and utilizing mental health services,” he concluded.
Dr. Jordan disclosed receiving a 2021-2022 American Psychiatric Association/Substance Abuse and Mental Health Services Administration Minority Fellowship Program grant to study mental health literacy in the Black church. Dr. Norris disclosed serving as CEO of the Cleveland Clergy Alliance, a nonprofit organization providing outreach assistance as a mechanism to help seniors and the disabled population through community programming. The study authors reported no disclosures.
FROM PSYCHIATRIC SERVICES
Trauma, psychiatric comorbidities tied to functional motor disorders
Most adults with functional motor disorders (FMDs) report a history of psychological or physical trauma 6 months before the onset of symptoms, a retrospective study of 482 individuals suggests. Those challenges prevent more than half of those patients – most of whom are women – from working, the researchers found.
“This finding points to the huge socioeconomical burden of FMD and emphasizes the need for better diagnostic procedure and active management,” wrote Béatrice Garcin, MD, of Sorbonne Université, Paris, and associates.
FMDs are a common presentation of functional neurologic disorders, but clinical characteristics of FMDs are not well understood because large series of consecutive patients are limited, Dr. Garcin and associates said.
In the study, published in the Journal of Psychosomatic Research, the investigators reviewed data from consecutive patients with FMD who were seen at a single hospital in France between 2008 and 2016. Half of the patients had functional motor weakness (241) and half had functional movement disorders (241). All of the patients had been referred for transcranial magnetic stimulation (TMS) as treatment for FMD.
The median age of the patients was 40 years, the median age at the onset of symptoms was 35.5 years, and 74% were women. The most common clinical presentations were tremor and dystonia (83.4%), and no demographic differences were observed between patients with functional motor weakness and functional movement disorders. Symptoms were bilateral in about half of the patients (51.7%), with left- and right-sided symptoms in 28.2% and 20.1%, respectively.
More than 80% of the patients reported a history of trauma within 6 months of the onset of their symptoms, mainly psychological trauma (50.6%). Another 20.1% reported a physical trauma, and 8.7% reported trauma from surgical procedures.
In addition, about two-thirds (66.4%) had psychiatric comorbidities; 52.7% of these were mood disorders: 49.3% depression and 3.3% bipolar disorder. “However, these results about psychiatric comorbidities should be taken with caution,” the researchers emphasized. “ and psychiatric diagnosis may lack precision because of the absence of systematic psychiatric interviews and psychiatric questionnaires in the present study.”
No significant differences appeared between the motor weakness and movement disorders groups in terms of occupation, level of education, medical somatic history, symptom onset, psychiatric comorbidities, or self-reported history of trauma. Patients in the motor weakness group were significantly younger at the time of TMS treatment and had a shorter disease duration prior to that treatment. No differences were noted between the groups with regard to clinical FMD phenotypes.
The study findings were limited by several factors, including the potential selection bias because of enrollment at a neurology referral center, lack of a control group, and underrepresentation of children and older adults, the researchers noted. Also, symptom severity was not assessed and could not be compared among phenotypes or demographic groups.
However, the results contribute to the characterization of FMD patients. “Future studies are needed to clarify the characteristics of FMD patients and the consequences of their symptoms on disability and work status,” they said.
The study received no outside funding. Lead author Dr. Garcin had no disclosures.
Most adults with functional motor disorders (FMDs) report a history of psychological or physical trauma 6 months before the onset of symptoms, a retrospective study of 482 individuals suggests. Those challenges prevent more than half of those patients – most of whom are women – from working, the researchers found.
“This finding points to the huge socioeconomical burden of FMD and emphasizes the need for better diagnostic procedure and active management,” wrote Béatrice Garcin, MD, of Sorbonne Université, Paris, and associates.
FMDs are a common presentation of functional neurologic disorders, but clinical characteristics of FMDs are not well understood because large series of consecutive patients are limited, Dr. Garcin and associates said.
In the study, published in the Journal of Psychosomatic Research, the investigators reviewed data from consecutive patients with FMD who were seen at a single hospital in France between 2008 and 2016. Half of the patients had functional motor weakness (241) and half had functional movement disorders (241). All of the patients had been referred for transcranial magnetic stimulation (TMS) as treatment for FMD.
The median age of the patients was 40 years, the median age at the onset of symptoms was 35.5 years, and 74% were women. The most common clinical presentations were tremor and dystonia (83.4%), and no demographic differences were observed between patients with functional motor weakness and functional movement disorders. Symptoms were bilateral in about half of the patients (51.7%), with left- and right-sided symptoms in 28.2% and 20.1%, respectively.
More than 80% of the patients reported a history of trauma within 6 months of the onset of their symptoms, mainly psychological trauma (50.6%). Another 20.1% reported a physical trauma, and 8.7% reported trauma from surgical procedures.
In addition, about two-thirds (66.4%) had psychiatric comorbidities; 52.7% of these were mood disorders: 49.3% depression and 3.3% bipolar disorder. “However, these results about psychiatric comorbidities should be taken with caution,” the researchers emphasized. “ and psychiatric diagnosis may lack precision because of the absence of systematic psychiatric interviews and psychiatric questionnaires in the present study.”
No significant differences appeared between the motor weakness and movement disorders groups in terms of occupation, level of education, medical somatic history, symptom onset, psychiatric comorbidities, or self-reported history of trauma. Patients in the motor weakness group were significantly younger at the time of TMS treatment and had a shorter disease duration prior to that treatment. No differences were noted between the groups with regard to clinical FMD phenotypes.
The study findings were limited by several factors, including the potential selection bias because of enrollment at a neurology referral center, lack of a control group, and underrepresentation of children and older adults, the researchers noted. Also, symptom severity was not assessed and could not be compared among phenotypes or demographic groups.
However, the results contribute to the characterization of FMD patients. “Future studies are needed to clarify the characteristics of FMD patients and the consequences of their symptoms on disability and work status,” they said.
The study received no outside funding. Lead author Dr. Garcin had no disclosures.
Most adults with functional motor disorders (FMDs) report a history of psychological or physical trauma 6 months before the onset of symptoms, a retrospective study of 482 individuals suggests. Those challenges prevent more than half of those patients – most of whom are women – from working, the researchers found.
“This finding points to the huge socioeconomical burden of FMD and emphasizes the need for better diagnostic procedure and active management,” wrote Béatrice Garcin, MD, of Sorbonne Université, Paris, and associates.
FMDs are a common presentation of functional neurologic disorders, but clinical characteristics of FMDs are not well understood because large series of consecutive patients are limited, Dr. Garcin and associates said.
In the study, published in the Journal of Psychosomatic Research, the investigators reviewed data from consecutive patients with FMD who were seen at a single hospital in France between 2008 and 2016. Half of the patients had functional motor weakness (241) and half had functional movement disorders (241). All of the patients had been referred for transcranial magnetic stimulation (TMS) as treatment for FMD.
The median age of the patients was 40 years, the median age at the onset of symptoms was 35.5 years, and 74% were women. The most common clinical presentations were tremor and dystonia (83.4%), and no demographic differences were observed between patients with functional motor weakness and functional movement disorders. Symptoms were bilateral in about half of the patients (51.7%), with left- and right-sided symptoms in 28.2% and 20.1%, respectively.
More than 80% of the patients reported a history of trauma within 6 months of the onset of their symptoms, mainly psychological trauma (50.6%). Another 20.1% reported a physical trauma, and 8.7% reported trauma from surgical procedures.
In addition, about two-thirds (66.4%) had psychiatric comorbidities; 52.7% of these were mood disorders: 49.3% depression and 3.3% bipolar disorder. “However, these results about psychiatric comorbidities should be taken with caution,” the researchers emphasized. “ and psychiatric diagnosis may lack precision because of the absence of systematic psychiatric interviews and psychiatric questionnaires in the present study.”
No significant differences appeared between the motor weakness and movement disorders groups in terms of occupation, level of education, medical somatic history, symptom onset, psychiatric comorbidities, or self-reported history of trauma. Patients in the motor weakness group were significantly younger at the time of TMS treatment and had a shorter disease duration prior to that treatment. No differences were noted between the groups with regard to clinical FMD phenotypes.
The study findings were limited by several factors, including the potential selection bias because of enrollment at a neurology referral center, lack of a control group, and underrepresentation of children and older adults, the researchers noted. Also, symptom severity was not assessed and could not be compared among phenotypes or demographic groups.
However, the results contribute to the characterization of FMD patients. “Future studies are needed to clarify the characteristics of FMD patients and the consequences of their symptoms on disability and work status,” they said.
The study received no outside funding. Lead author Dr. Garcin had no disclosures.
FROM THE JOURNAL OF PSYCHOSOMATIC RESEARCH
Psychiatric genomics has a diversity problem
In combing the genome, scientists can use genetic clues to determine a person’s risk for psychiatric disease and even identify new drug targets. But the benefits of these discoveries will be limited to people of European descent.
Nearly 90% of participants in genome-wide association studies (GWASs), which search for gene variants linked to disease, are of European ancestry. This Eurocentric focus threatens to widen existing disparities in racial and ethnic mental health.

“If you develop certain interventions based on only a single population profile, then you’ll be leaving out the rest of the populations in the world,” says Solomon Teferra, MD, PhD, associate professor of psychiatry at Addis Ababa University, Ethiopia. In a growing trend, psychiatric researchers are diverging from the field’s European bias and are working to correct the imbalance in DNA databases.
The significant downsides of genomics’ one-track mind
One obstacle hindering therapeutic advances in psychiatry is a shallow understanding of the mechanisms of disorders. “The biggest problem in terms of advancing research for mental health conditions is that we don’t understand the underlying biology,” says Laramie Duncan, PhD, assistant professor of psychiatry and behavioral sciences at Stanford (Calif.) University. “Genetics is one of the best ways to systematically look for new clues about the underlying biology.”
At the advent of genomic research, scientists thought it best to study DNA from people of a single ancestry from one continent. “Researchers for a long time held the idea that it was going to be too complicated to include multiple ancestries in the first rounds of genetic analyses,” says Dr. Duncan.
Studying DNA from someone with ancestors from multiple parts of the world wasn’t compatible with methods used in the early days of GWASs. “Individual parts of a person’s DNA can be linked back to one region of the world or another, and most of our methods essentially assume that all of a person’s DNA came from one region of the world,” says Dr. Duncan.
Because many genes are usually involved in psychiatric disorders, scientists need large numbers of participants to detect uncommon, influential variants. Early research was concentrated in North America and Europe so that scientists could readily collect samples from people of European ancestry.
“It then went out of hand because it became routine practice to use only this one group, essentially White, European ancestry people,” says Karoline Kuchenbaecker, PhD, associate professor of psychiatry at University College London.
Yet findings from one population won’t necessarily translate to others. “And that’s exactly what has been shown,” says Dr. Teferra. Polygenic risk scores developed for schizophrenia from European samples, for example, perform poorly among people of African ancestry, although among Europeans, they are strongly effective at differentiating European individuals with and those without schizophrenia. Moreover, drugs that target a gene identified from studies in European populations may be harmful to other groups.
Studies drawn from a diverse pool of participants would benefit a wider swath of humanity. They would also allow scientists to discover small areas of overlap in genomes of different populations, which would help them close in on the true biology of diseases and ensure that “we’re all benefiting from more diverse data in genetics and psychiatric genetics,” says Dr. Kuchenbaecker.
New efforts aim at filling the gaps
, not African, Latin American, or Indigenous ancestry.
Efforts to increase representation of persons of African ancestry have largely focused on African Americans; fewer efforts have extended to the African continent, home to the most genetically diverse populations. Even fewer have focused on mental health. “The little that was being done was on a very small scale,” says Karestan Koenen, PhD, a professor at Harvard School of Public Health, Boston.
With this in mind, researchers from institutions in Kenya, Uganda, South Africa, and Ethiopia partnered with researchers at the Broad Institute of the Massachusetts Institute of Technology and Harvard to conduct the largest GWAS of psychiatric disorders in Africa. Dr. Koenen leads the project, Neuropsychiatric Genetics of African Populations–Psychosis (NeuroGAP-Psychosis), which will analyze DNA from over 35,000 people of African ancestry in each of these four countries. Investigators will compare the half of participants who have no history of psychosis with the half with schizophrenia or bipolar disorder in the hopes of identifying the genetic determinants of psychosis.
“Then any potential intervention or therapeutics that will be developed will also be useful for Africans,” says Dr. Teferra, a NeuroGAP principal investigator. Because of the tremendous degree of genetic diversity among people on the continent, however, findings still might not translate to all African populations.
But correcting equity problems in genomics isn’t as simple as recruiting people with non-European backgrounds, especially if those people are unfamiliar with research or have been subject to scientific exploitation. “Special care needs to be taken to, first of all, provide information that’s appropriate [to participants], but also motivate people to take part and then find ways to keep these communities involved and understand what they’re interested in,” says Dr. Kuchenbaecker, who is not involved with NeuroGAP.
For NeuroGAP, the team needed to work with ethical committees at all of the institutions involved, ensure research materials were appropriate for each community’s cultural context, and gain the trust of local communities.
“One of the biggest criticisms within the scientific world is that people from more endowed countries just fly in, bully everyone, collect the data, and leave, with no credit to the local scientists or communities,” says NeuroGAP principal investigator Lukoye Atwoli, MMed, PhD, professor of psychiatry and dean of the Medical College, East Africa, at the Aga Khan University, Nairobi, Kenya. “That is one of the biggest pitfalls we had to grapple with.”
To address that concern, NeuroGAP is training local researchers and is providing them with requested resources so they can carry out similar studies in the future. “We will be looking to address a real need in the academic community and in clinical service delivery,” says Dr. Atwoli.
Dr. Kuchenbaecker says that NeuroGAP demonstrates features necessary for projects seeking to improve equity in psychiatric genomics. “What they’re doing right is recruiting really large numbers, recruiting from different African countries, and involving African investigators,” she says.
In the Americas, Janitza Montalvo-Ortiz, PhD, assistant professor in the Division of Genetics, department of psychiatry, Yale University, New Haven, Conn., and her colleagues are expanding psychiatric genomics projects in Latin America. She co-founded the Latin American Genomics Consortium in 2019, a network of scientists supporting psychiatric genomic research in the region. The consortium also involves the Neuropsychiatric Genetics in Mexican Populations project, which is similar to NeuroGAP and is also led by Dr. Koenan.
The study of Latin American populations is complicated, because genes in these populations reflect Indigenous American, European, and African ancestries. Even when investigators sampled DNA from Latin American individuals, that data often went unused. “Now with new methods emerging to allow us to properly analyze admixed populations in GWAS studies, we’re making efforts to compile different datasets scattered across different large-scale cohorts,” says Dr. Montalvo-Ortiz. “Our ultimate goal is to conduct the first large-scale LatinX GWAS of psychiatry,” she says.
With these projects, researchers hope that new psychiatric research will produce clinical advances for people historically left on the sidelines of genomic studies. By involving their communities in genomic research, “whatever is going to be developed will also benefit our community,” says Dr. Teferra. “We will not be left out.”
A version of this article first appeared on Medscape.com.
In combing the genome, scientists can use genetic clues to determine a person’s risk for psychiatric disease and even identify new drug targets. But the benefits of these discoveries will be limited to people of European descent.
Nearly 90% of participants in genome-wide association studies (GWASs), which search for gene variants linked to disease, are of European ancestry. This Eurocentric focus threatens to widen existing disparities in racial and ethnic mental health.
“If you develop certain interventions based on only a single population profile, then you’ll be leaving out the rest of the populations in the world,” says Solomon Teferra, MD, PhD, associate professor of psychiatry at Addis Ababa University, Ethiopia. In a growing trend, psychiatric researchers are diverging from the field’s European bias and are working to correct the imbalance in DNA databases.
The significant downsides of genomics’ one-track mind
One obstacle hindering therapeutic advances in psychiatry is a shallow understanding of the mechanisms of disorders. “The biggest problem in terms of advancing research for mental health conditions is that we don’t understand the underlying biology,” says Laramie Duncan, PhD, assistant professor of psychiatry and behavioral sciences at Stanford (Calif.) University. “Genetics is one of the best ways to systematically look for new clues about the underlying biology.”
At the advent of genomic research, scientists thought it best to study DNA from people of a single ancestry from one continent. “Researchers for a long time held the idea that it was going to be too complicated to include multiple ancestries in the first rounds of genetic analyses,” says Dr. Duncan.
Studying DNA from someone with ancestors from multiple parts of the world wasn’t compatible with methods used in the early days of GWASs. “Individual parts of a person’s DNA can be linked back to one region of the world or another, and most of our methods essentially assume that all of a person’s DNA came from one region of the world,” says Dr. Duncan.
Because many genes are usually involved in psychiatric disorders, scientists need large numbers of participants to detect uncommon, influential variants. Early research was concentrated in North America and Europe so that scientists could readily collect samples from people of European ancestry.
“It then went out of hand because it became routine practice to use only this one group, essentially White, European ancestry people,” says Karoline Kuchenbaecker, PhD, associate professor of psychiatry at University College London.
Yet findings from one population won’t necessarily translate to others. “And that’s exactly what has been shown,” says Dr. Teferra. Polygenic risk scores developed for schizophrenia from European samples, for example, perform poorly among people of African ancestry, although among Europeans, they are strongly effective at differentiating European individuals with and those without schizophrenia. Moreover, drugs that target a gene identified from studies in European populations may be harmful to other groups.
Studies drawn from a diverse pool of participants would benefit a wider swath of humanity. They would also allow scientists to discover small areas of overlap in genomes of different populations, which would help them close in on the true biology of diseases and ensure that “we’re all benefiting from more diverse data in genetics and psychiatric genetics,” says Dr. Kuchenbaecker.
New efforts aim at filling the gaps
, not African, Latin American, or Indigenous ancestry.
Efforts to increase representation of persons of African ancestry have largely focused on African Americans; fewer efforts have extended to the African continent, home to the most genetically diverse populations. Even fewer have focused on mental health. “The little that was being done was on a very small scale,” says Karestan Koenen, PhD, a professor at Harvard School of Public Health, Boston.
With this in mind, researchers from institutions in Kenya, Uganda, South Africa, and Ethiopia partnered with researchers at the Broad Institute of the Massachusetts Institute of Technology and Harvard to conduct the largest GWAS of psychiatric disorders in Africa. Dr. Koenen leads the project, Neuropsychiatric Genetics of African Populations–Psychosis (NeuroGAP-Psychosis), which will analyze DNA from over 35,000 people of African ancestry in each of these four countries. Investigators will compare the half of participants who have no history of psychosis with the half with schizophrenia or bipolar disorder in the hopes of identifying the genetic determinants of psychosis.
“Then any potential intervention or therapeutics that will be developed will also be useful for Africans,” says Dr. Teferra, a NeuroGAP principal investigator. Because of the tremendous degree of genetic diversity among people on the continent, however, findings still might not translate to all African populations.
But correcting equity problems in genomics isn’t as simple as recruiting people with non-European backgrounds, especially if those people are unfamiliar with research or have been subject to scientific exploitation. “Special care needs to be taken to, first of all, provide information that’s appropriate [to participants], but also motivate people to take part and then find ways to keep these communities involved and understand what they’re interested in,” says Dr. Kuchenbaecker, who is not involved with NeuroGAP.
For NeuroGAP, the team needed to work with ethical committees at all of the institutions involved, ensure research materials were appropriate for each community’s cultural context, and gain the trust of local communities.
“One of the biggest criticisms within the scientific world is that people from more endowed countries just fly in, bully everyone, collect the data, and leave, with no credit to the local scientists or communities,” says NeuroGAP principal investigator Lukoye Atwoli, MMed, PhD, professor of psychiatry and dean of the Medical College, East Africa, at the Aga Khan University, Nairobi, Kenya. “That is one of the biggest pitfalls we had to grapple with.”
To address that concern, NeuroGAP is training local researchers and is providing them with requested resources so they can carry out similar studies in the future. “We will be looking to address a real need in the academic community and in clinical service delivery,” says Dr. Atwoli.
Dr. Kuchenbaecker says that NeuroGAP demonstrates features necessary for projects seeking to improve equity in psychiatric genomics. “What they’re doing right is recruiting really large numbers, recruiting from different African countries, and involving African investigators,” she says.
In the Americas, Janitza Montalvo-Ortiz, PhD, assistant professor in the Division of Genetics, department of psychiatry, Yale University, New Haven, Conn., and her colleagues are expanding psychiatric genomics projects in Latin America. She co-founded the Latin American Genomics Consortium in 2019, a network of scientists supporting psychiatric genomic research in the region. The consortium also involves the Neuropsychiatric Genetics in Mexican Populations project, which is similar to NeuroGAP and is also led by Dr. Koenan.
The study of Latin American populations is complicated, because genes in these populations reflect Indigenous American, European, and African ancestries. Even when investigators sampled DNA from Latin American individuals, that data often went unused. “Now with new methods emerging to allow us to properly analyze admixed populations in GWAS studies, we’re making efforts to compile different datasets scattered across different large-scale cohorts,” says Dr. Montalvo-Ortiz. “Our ultimate goal is to conduct the first large-scale LatinX GWAS of psychiatry,” she says.
With these projects, researchers hope that new psychiatric research will produce clinical advances for people historically left on the sidelines of genomic studies. By involving their communities in genomic research, “whatever is going to be developed will also benefit our community,” says Dr. Teferra. “We will not be left out.”
A version of this article first appeared on Medscape.com.
In combing the genome, scientists can use genetic clues to determine a person’s risk for psychiatric disease and even identify new drug targets. But the benefits of these discoveries will be limited to people of European descent.
Nearly 90% of participants in genome-wide association studies (GWASs), which search for gene variants linked to disease, are of European ancestry. This Eurocentric focus threatens to widen existing disparities in racial and ethnic mental health.
“If you develop certain interventions based on only a single population profile, then you’ll be leaving out the rest of the populations in the world,” says Solomon Teferra, MD, PhD, associate professor of psychiatry at Addis Ababa University, Ethiopia. In a growing trend, psychiatric researchers are diverging from the field’s European bias and are working to correct the imbalance in DNA databases.
The significant downsides of genomics’ one-track mind
One obstacle hindering therapeutic advances in psychiatry is a shallow understanding of the mechanisms of disorders. “The biggest problem in terms of advancing research for mental health conditions is that we don’t understand the underlying biology,” says Laramie Duncan, PhD, assistant professor of psychiatry and behavioral sciences at Stanford (Calif.) University. “Genetics is one of the best ways to systematically look for new clues about the underlying biology.”
At the advent of genomic research, scientists thought it best to study DNA from people of a single ancestry from one continent. “Researchers for a long time held the idea that it was going to be too complicated to include multiple ancestries in the first rounds of genetic analyses,” says Dr. Duncan.
Studying DNA from someone with ancestors from multiple parts of the world wasn’t compatible with methods used in the early days of GWASs. “Individual parts of a person’s DNA can be linked back to one region of the world or another, and most of our methods essentially assume that all of a person’s DNA came from one region of the world,” says Dr. Duncan.
Because many genes are usually involved in psychiatric disorders, scientists need large numbers of participants to detect uncommon, influential variants. Early research was concentrated in North America and Europe so that scientists could readily collect samples from people of European ancestry.
“It then went out of hand because it became routine practice to use only this one group, essentially White, European ancestry people,” says Karoline Kuchenbaecker, PhD, associate professor of psychiatry at University College London.
Yet findings from one population won’t necessarily translate to others. “And that’s exactly what has been shown,” says Dr. Teferra. Polygenic risk scores developed for schizophrenia from European samples, for example, perform poorly among people of African ancestry, although among Europeans, they are strongly effective at differentiating European individuals with and those without schizophrenia. Moreover, drugs that target a gene identified from studies in European populations may be harmful to other groups.
Studies drawn from a diverse pool of participants would benefit a wider swath of humanity. They would also allow scientists to discover small areas of overlap in genomes of different populations, which would help them close in on the true biology of diseases and ensure that “we’re all benefiting from more diverse data in genetics and psychiatric genetics,” says Dr. Kuchenbaecker.
New efforts aim at filling the gaps
, not African, Latin American, or Indigenous ancestry.
Efforts to increase representation of persons of African ancestry have largely focused on African Americans; fewer efforts have extended to the African continent, home to the most genetically diverse populations. Even fewer have focused on mental health. “The little that was being done was on a very small scale,” says Karestan Koenen, PhD, a professor at Harvard School of Public Health, Boston.
With this in mind, researchers from institutions in Kenya, Uganda, South Africa, and Ethiopia partnered with researchers at the Broad Institute of the Massachusetts Institute of Technology and Harvard to conduct the largest GWAS of psychiatric disorders in Africa. Dr. Koenen leads the project, Neuropsychiatric Genetics of African Populations–Psychosis (NeuroGAP-Psychosis), which will analyze DNA from over 35,000 people of African ancestry in each of these four countries. Investigators will compare the half of participants who have no history of psychosis with the half with schizophrenia or bipolar disorder in the hopes of identifying the genetic determinants of psychosis.
“Then any potential intervention or therapeutics that will be developed will also be useful for Africans,” says Dr. Teferra, a NeuroGAP principal investigator. Because of the tremendous degree of genetic diversity among people on the continent, however, findings still might not translate to all African populations.
But correcting equity problems in genomics isn’t as simple as recruiting people with non-European backgrounds, especially if those people are unfamiliar with research or have been subject to scientific exploitation. “Special care needs to be taken to, first of all, provide information that’s appropriate [to participants], but also motivate people to take part and then find ways to keep these communities involved and understand what they’re interested in,” says Dr. Kuchenbaecker, who is not involved with NeuroGAP.
For NeuroGAP, the team needed to work with ethical committees at all of the institutions involved, ensure research materials were appropriate for each community’s cultural context, and gain the trust of local communities.
“One of the biggest criticisms within the scientific world is that people from more endowed countries just fly in, bully everyone, collect the data, and leave, with no credit to the local scientists or communities,” says NeuroGAP principal investigator Lukoye Atwoli, MMed, PhD, professor of psychiatry and dean of the Medical College, East Africa, at the Aga Khan University, Nairobi, Kenya. “That is one of the biggest pitfalls we had to grapple with.”
To address that concern, NeuroGAP is training local researchers and is providing them with requested resources so they can carry out similar studies in the future. “We will be looking to address a real need in the academic community and in clinical service delivery,” says Dr. Atwoli.
Dr. Kuchenbaecker says that NeuroGAP demonstrates features necessary for projects seeking to improve equity in psychiatric genomics. “What they’re doing right is recruiting really large numbers, recruiting from different African countries, and involving African investigators,” she says.
In the Americas, Janitza Montalvo-Ortiz, PhD, assistant professor in the Division of Genetics, department of psychiatry, Yale University, New Haven, Conn., and her colleagues are expanding psychiatric genomics projects in Latin America. She co-founded the Latin American Genomics Consortium in 2019, a network of scientists supporting psychiatric genomic research in the region. The consortium also involves the Neuropsychiatric Genetics in Mexican Populations project, which is similar to NeuroGAP and is also led by Dr. Koenan.
The study of Latin American populations is complicated, because genes in these populations reflect Indigenous American, European, and African ancestries. Even when investigators sampled DNA from Latin American individuals, that data often went unused. “Now with new methods emerging to allow us to properly analyze admixed populations in GWAS studies, we’re making efforts to compile different datasets scattered across different large-scale cohorts,” says Dr. Montalvo-Ortiz. “Our ultimate goal is to conduct the first large-scale LatinX GWAS of psychiatry,” she says.
With these projects, researchers hope that new psychiatric research will produce clinical advances for people historically left on the sidelines of genomic studies. By involving their communities in genomic research, “whatever is going to be developed will also benefit our community,” says Dr. Teferra. “We will not be left out.”
A version of this article first appeared on Medscape.com.
Health anxiety common as COVID restrictions loosen
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
State-of-the-art psych unit designed with recovery in mind
Calming wall colors, nature-themed murals, and soft nighttime lighting are all part of a unique new state-of-the-art inpatient psychiatric unit that focuses especially on children and adolescents who have experienced significant trauma.
The 16-bed unit, which has been in the works for 3½ years and opened June 30 at the University of Maryland Medical Center (UMMC), in Baltimore, Maryland, treats youth aged 5 to 17 years. It has separate wings for younger children and for adolescents.

“We offer a really warm and welcoming environment that we think is going to promote health and healing,” the unit’s head, Sarah Edwards, DO, director of child and adolescent psychiatry at UMMC and assistant professor of psychiatry, University of Maryland School of Medicine (UMSOM), Baltimore, said in an interview.
Previous research shows that 1 in 4 children experience some kind of maltreatment, whether physical, sexual, or emotional, and that 1 in 5 develop a diagnosable mental health disorder.
, Dr. Edwards noted. Recent data show that the rate of suicidal ideation among youth has increased significantly during the COVID-19 crisis.
“Urban children have unfortunately suffered a lot of what we call traumatic stress, so they might be victims of physical or sexual abuse but also face layers of stressful situations – for example, living in unsafe neighborhoods and attending schools that might not be so welcoming and safe,” said Dr. Edwards.
Safety first
Typical conditions treated at the new unit will include depression, anxiety, attention-deficit/hyperactivity disorder, psychotic spectrum, as well as trauma disorders.
Some of these young patients have been through the foster care system and show signs of trauma and poor attachment, Dr. Edwards noted. As a result, they may have difficulty regulating their thoughts and emotions and at times exhibit dangerous behavior.
The new unit is designed both architecturally and clinically to deliver “trauma-informed” care. This type of approach “recognizes the pervasive nature of trauma” and promotes settings that facilitate recovery, Dr. Edwards added.
The idea is to treat individuals “in a way that doesn’t re-traumatize them or make their condition worse,” she added.

Safety is of the utmost importance in the unit, Jill RachBeisel, MD, chief of psychiatry at UMMC and professor and chair in the department of psychiatry at UMSOM, said in an interview.
“Health care workers must recognize and respond to the effects of trauma – and one very important way is to provide care in settings that emphasize physical and emotional safety, which helps instill a sense of control and empowerment,” Dr. RachBeisel said.
Providing youth with options is an important way to provide that sense of control, Dr. Edwards added. For example, residents can choose their own music in their bedroom, such as sounds of nature, running water, or birds chirping. They can also draw or write personal notes on a large whiteboard in their unit.
Circadian-rhythm lighting
Other unique elements of the new unit include walls painted soothing shades and murals of natural scenery, created by a local artist.

These murals perfectly capture “the kind of overall spirit of what we were trying to induce,” said Dr. Edwards.
A part of the unit dubbed the “front porch” has a large mural depicting “a landscape of beautiful trees and water and animals,” she noted. Kids can gather here to relax or just hang out.
The lighting at the unit mirrors circadian rhythms. It’s brighter during the day to promote wakefulness and participation in activities and gradually dims toward the evening hours to help induce restful nighttime sleep.
Safe and empowering and adopt productive behaviors and coping skills, Dr. Edwards noted.
The staff for the interprofessional unit includes psychiatrists, psychologists, psychiatric nurses, occupational therapists, and others trained in pediatric care.
Advice for other centers
“Our new unit is designed to provide the highest standard in mental health care and incorporates a high-tech approach to create a calming, soothing, and engaging setting,” said Dr. RachBeisel.
School-transition specialists help connect discharged patients and their families to vital services and peer support. These services represent “an essential component of the continuum of care” for youth experiencing mental distress, she added.
Other organizations considering establishing a similar type of psychiatric unit should consult all stakeholders.
“We had staff, no matter what their role, be part of every step of this process, including helping with the design, picking out furniture they thought would make the most sense, and helping choose the artwork,” she said.
It is also important to incorporate feedback from youth themselves, Dr. Edwards added.
A version of this article first appeared on Medscape.com.
Calming wall colors, nature-themed murals, and soft nighttime lighting are all part of a unique new state-of-the-art inpatient psychiatric unit that focuses especially on children and adolescents who have experienced significant trauma.
The 16-bed unit, which has been in the works for 3½ years and opened June 30 at the University of Maryland Medical Center (UMMC), in Baltimore, Maryland, treats youth aged 5 to 17 years. It has separate wings for younger children and for adolescents.
“We offer a really warm and welcoming environment that we think is going to promote health and healing,” the unit’s head, Sarah Edwards, DO, director of child and adolescent psychiatry at UMMC and assistant professor of psychiatry, University of Maryland School of Medicine (UMSOM), Baltimore, said in an interview.
Previous research shows that 1 in 4 children experience some kind of maltreatment, whether physical, sexual, or emotional, and that 1 in 5 develop a diagnosable mental health disorder.
, Dr. Edwards noted. Recent data show that the rate of suicidal ideation among youth has increased significantly during the COVID-19 crisis.
“Urban children have unfortunately suffered a lot of what we call traumatic stress, so they might be victims of physical or sexual abuse but also face layers of stressful situations – for example, living in unsafe neighborhoods and attending schools that might not be so welcoming and safe,” said Dr. Edwards.
Safety first
Typical conditions treated at the new unit will include depression, anxiety, attention-deficit/hyperactivity disorder, psychotic spectrum, as well as trauma disorders.
Some of these young patients have been through the foster care system and show signs of trauma and poor attachment, Dr. Edwards noted. As a result, they may have difficulty regulating their thoughts and emotions and at times exhibit dangerous behavior.
The new unit is designed both architecturally and clinically to deliver “trauma-informed” care. This type of approach “recognizes the pervasive nature of trauma” and promotes settings that facilitate recovery, Dr. Edwards added.
The idea is to treat individuals “in a way that doesn’t re-traumatize them or make their condition worse,” she added.
Safety is of the utmost importance in the unit, Jill RachBeisel, MD, chief of psychiatry at UMMC and professor and chair in the department of psychiatry at UMSOM, said in an interview.
“Health care workers must recognize and respond to the effects of trauma – and one very important way is to provide care in settings that emphasize physical and emotional safety, which helps instill a sense of control and empowerment,” Dr. RachBeisel said.
Providing youth with options is an important way to provide that sense of control, Dr. Edwards added. For example, residents can choose their own music in their bedroom, such as sounds of nature, running water, or birds chirping. They can also draw or write personal notes on a large whiteboard in their unit.
Circadian-rhythm lighting
Other unique elements of the new unit include walls painted soothing shades and murals of natural scenery, created by a local artist.
These murals perfectly capture “the kind of overall spirit of what we were trying to induce,” said Dr. Edwards.
A part of the unit dubbed the “front porch” has a large mural depicting “a landscape of beautiful trees and water and animals,” she noted. Kids can gather here to relax or just hang out.
The lighting at the unit mirrors circadian rhythms. It’s brighter during the day to promote wakefulness and participation in activities and gradually dims toward the evening hours to help induce restful nighttime sleep.
Safe and empowering and adopt productive behaviors and coping skills, Dr. Edwards noted.
The staff for the interprofessional unit includes psychiatrists, psychologists, psychiatric nurses, occupational therapists, and others trained in pediatric care.
Advice for other centers
“Our new unit is designed to provide the highest standard in mental health care and incorporates a high-tech approach to create a calming, soothing, and engaging setting,” said Dr. RachBeisel.
School-transition specialists help connect discharged patients and their families to vital services and peer support. These services represent “an essential component of the continuum of care” for youth experiencing mental distress, she added.
Other organizations considering establishing a similar type of psychiatric unit should consult all stakeholders.
“We had staff, no matter what their role, be part of every step of this process, including helping with the design, picking out furniture they thought would make the most sense, and helping choose the artwork,” she said.
It is also important to incorporate feedback from youth themselves, Dr. Edwards added.
A version of this article first appeared on Medscape.com.
Calming wall colors, nature-themed murals, and soft nighttime lighting are all part of a unique new state-of-the-art inpatient psychiatric unit that focuses especially on children and adolescents who have experienced significant trauma.
The 16-bed unit, which has been in the works for 3½ years and opened June 30 at the University of Maryland Medical Center (UMMC), in Baltimore, Maryland, treats youth aged 5 to 17 years. It has separate wings for younger children and for adolescents.
“We offer a really warm and welcoming environment that we think is going to promote health and healing,” the unit’s head, Sarah Edwards, DO, director of child and adolescent psychiatry at UMMC and assistant professor of psychiatry, University of Maryland School of Medicine (UMSOM), Baltimore, said in an interview.
Previous research shows that 1 in 4 children experience some kind of maltreatment, whether physical, sexual, or emotional, and that 1 in 5 develop a diagnosable mental health disorder.
, Dr. Edwards noted. Recent data show that the rate of suicidal ideation among youth has increased significantly during the COVID-19 crisis.
“Urban children have unfortunately suffered a lot of what we call traumatic stress, so they might be victims of physical or sexual abuse but also face layers of stressful situations – for example, living in unsafe neighborhoods and attending schools that might not be so welcoming and safe,” said Dr. Edwards.
Safety first
Typical conditions treated at the new unit will include depression, anxiety, attention-deficit/hyperactivity disorder, psychotic spectrum, as well as trauma disorders.
Some of these young patients have been through the foster care system and show signs of trauma and poor attachment, Dr. Edwards noted. As a result, they may have difficulty regulating their thoughts and emotions and at times exhibit dangerous behavior.
The new unit is designed both architecturally and clinically to deliver “trauma-informed” care. This type of approach “recognizes the pervasive nature of trauma” and promotes settings that facilitate recovery, Dr. Edwards added.
The idea is to treat individuals “in a way that doesn’t re-traumatize them or make their condition worse,” she added.
Safety is of the utmost importance in the unit, Jill RachBeisel, MD, chief of psychiatry at UMMC and professor and chair in the department of psychiatry at UMSOM, said in an interview.
“Health care workers must recognize and respond to the effects of trauma – and one very important way is to provide care in settings that emphasize physical and emotional safety, which helps instill a sense of control and empowerment,” Dr. RachBeisel said.
Providing youth with options is an important way to provide that sense of control, Dr. Edwards added. For example, residents can choose their own music in their bedroom, such as sounds of nature, running water, or birds chirping. They can also draw or write personal notes on a large whiteboard in their unit.
Circadian-rhythm lighting
Other unique elements of the new unit include walls painted soothing shades and murals of natural scenery, created by a local artist.
These murals perfectly capture “the kind of overall spirit of what we were trying to induce,” said Dr. Edwards.
A part of the unit dubbed the “front porch” has a large mural depicting “a landscape of beautiful trees and water and animals,” she noted. Kids can gather here to relax or just hang out.
The lighting at the unit mirrors circadian rhythms. It’s brighter during the day to promote wakefulness and participation in activities and gradually dims toward the evening hours to help induce restful nighttime sleep.
Safe and empowering and adopt productive behaviors and coping skills, Dr. Edwards noted.
The staff for the interprofessional unit includes psychiatrists, psychologists, psychiatric nurses, occupational therapists, and others trained in pediatric care.
Advice for other centers
“Our new unit is designed to provide the highest standard in mental health care and incorporates a high-tech approach to create a calming, soothing, and engaging setting,” said Dr. RachBeisel.
School-transition specialists help connect discharged patients and their families to vital services and peer support. These services represent “an essential component of the continuum of care” for youth experiencing mental distress, she added.
Other organizations considering establishing a similar type of psychiatric unit should consult all stakeholders.
“We had staff, no matter what their role, be part of every step of this process, including helping with the design, picking out furniture they thought would make the most sense, and helping choose the artwork,” she said.
It is also important to incorporate feedback from youth themselves, Dr. Edwards added.
A version of this article first appeared on Medscape.com.
High rates of work-related trauma, PTSD in intern physicians
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.

Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”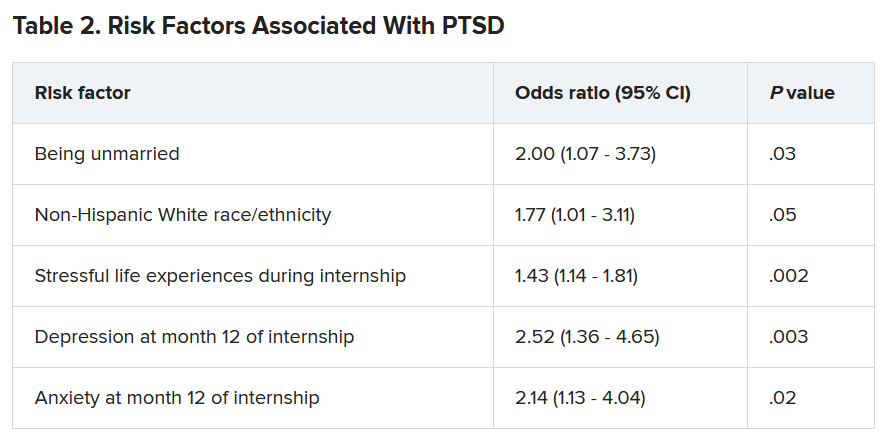
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.
Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.
Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A Veteran Presenting With Shortness of Breath, Cough, and Leukocytosis
Case Presentation: A 62-year-old male presented with shortness of breath and a cough productive of green sputum. He had a history of hyperlipidemia, posttraumatic stress disorder, bipolar disorder, obstructive sleep apnea, and a 50 pack-year history of smoking. His medications included prazosin, melatonin, lithium, and gabapentin. He also had a significant exposure history including asbestos and chemical paints following his leave from the military. At the initial evaluation, laboratory work revealed a leukocytosis with white blood cell (WBC) count 20 k/cm3and otherwise normal transaminases, albumin, and electrolytes. A chest X-ray revealed a new left hilar mass.
►Manisha Apte, MD, Chief Medical Resident, VA Boston Healthcare System (VABHS) and Boston Medical Center (BMC): To work up his new left hilar mass, a computed tomography (CT) of the chest was ordered (Figure 1), which revealed an apical left lower lobe mass extending into the left hilum encasing part of the ascending aorta. Enlarged mediastinal subcentimeter paratracheal and superior mediastinal lymph nodes also were identified and the pattern raised the concern for lymphangitic carcinomatosis. Dr. Fine, what do you make of the CT findings?
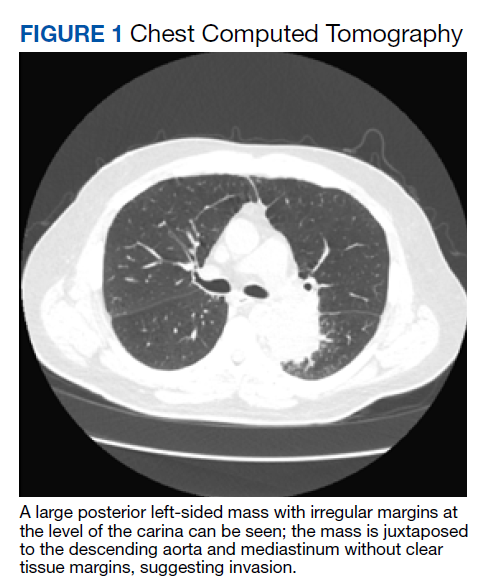
► Alan Fine, MD, Section of Pulmonary and Critical Care, VABHS and Professor of Medicine, Boston University School of Medicine: This mass had irregular edges with septal thickening, which may be why there was a concern for lymphangitic spread. There were no clear tissue planes to see if this process was invading the mediastinum. The mass was irregular, a single lesion, and proximal, making it consistent with a lung cancer. In fact, with his history of smoking, asbestos exposure, the numbers 1 to 10 diagnoses were lung cancer. The lack of demarcation of tissue planes supports this. There are some infections, classically actinomycosis, that do cross and invade anatomical barriers.1 But this looked like a primary lung cancer.
► Dr. Apte: The patient was referred to a pulmonologist where an additional history of night sweats and weight loss were noted. Dr. Fine, we have a patient with a newly identified lung mass, and while we have reason to suspect malignancy as you have already noted, there are many other etiologies to consider, including infections (histoplasmosis, cryptococcosis, bacterial abscess), inflammatory processes (sarcoidosis, rheumatoid nodule) and vasculitis (granulomatosis with polyangiitis). What should be the next step taken to make a diagnosis?
►Dr. Fine: For cancer specifically, we would like to both stage and make a diagnosis with one procedure. That’s part of the utility of a positron emission tomography (PET) scan: We can see lymph node involvement and stage the cancer. We must consider the patient’s comorbidities and the location of the lesion (ie, is it amenable to needle biopsy?). In this case, there are enlarged mediastinal lymph nodes, so one could perform a bronchoscopy with endobronchial ultrasound, which is a relatively noninvasive way to sample the lymph nodes to ideally stage and make a diagnosis as safely as possible. If we are considering infection, needle aspiration is not as sensitive.2
► Dr. Apte: The patient underwent a PET CT, which redemonstrated the lung mass with a loss of aortic fat plane suspicious for aortic involvement as well as lymph nodes in levels 7 and 8 that were concerning for malignancy. Subsequent bronchoscopy with biopsy and endobronchial ultrasound did not show evidence of malignancy; washing and brushing from the mass and lymph node specimens did not identify malignant cells. Benign respiratory mucosa with mild chronic inflammation was noted. Dr. Fine, given the nonspecific findings on the PET scan, negative findings on our bronchoscopy, and a negative biopsy, should we be satisfied that we have ruled out cancer?
► Dr. Fine: No, bronchoscopy has its limitations. It’s highly sensitive to the diagnosis of malignancy if you can see an endobronchial lesion, but we did not see one here. You can only go so far with the scope, and it’s not uncommon for us not to be able to make the diagnosis with bronchoscopy. Malignancy is still the most likely diagnosis, and we need to work this up further. I would perform another biopsy.
►Dr. Apte: Four weeks later, the patient presented with continued shortness of breath, fatigue, and fever. A repeat chest CT showed an opacity suggestive of pneumonia. Given the continued concern for cancer a CT-guided needle biopsy was performed and was once again negative for malignancy. The decision was made to pursue a video-assisted thorascopic surgery (VATS). Following the VATS, the patient developed rigors, fever, and tachycardia with new atrial fibrillation. While being evaluated hypercalcemia was identified, with further workup revealing a low parathyroid hormone (PTH) and low PTH-related peptide. Dr. Fine, the presence of hypercalcemia and a new arrythmia raised the possibility of sarcoidosis. Could this be sarcoidosis?
►Dr. Fine: Sarcoidosis is one of the great masqueraders in medicine. There is a type of sarcoidosis called nodular sarcoidosis where you see masslike distribution in the lung, but generally there are multiple masses and so this presentation would be atypical.3 There is also a phenomenon called sarcoidal reactions usually in the presence of cancer. Again, one tends to see multiple tiny lesions in the lung. It is certainly on the differential, but I would consider it to be less likely than cancer. It is also relatively common to develop atrial fibrillation after manipulation from a lung surgery.4 The other possibility I am concerned about is whether the mass is invading the mediastinum and involving the pericardium.
►Dr. Apte: Results from the VATS biopsy once again returned negative for malignancy and instead showed signs of focal micro-abscesses, atypical pneumocytes, and prominent neutrophils. A diagnosis of acute fibrinous organizing pneumonia (AFOP) was offered. Dr. Fine, what is AFOP?
►Dr. Fine: This is the first case of AFOP I had seen and probably the first case many in our department have seen. This is a relatively new entity with limited reported cases in the literature and is a pathological diagnosis originally recorded in autopsies from patients at the National Institutes of Health.5,6 Given the complexity of the lesion, the diagnosis is difficult to make. Most commonly, AFOP is associated with other systemic entities, most commonly hematologic malignancies like lymphomas and leukemias. It has also been associated with vasculitis and certain drugs. The mechanism is poorly understood, and although pneumonia is a part of the term, this just implies there is inflammation of the lung (ie, pneumonitis).
► Dr. Apte: Given the association of AFOP with underlying hematologic malignancies, an emphasis was placed on another finding: the patient’s increasing WBC count. The total WBC count had been 20 k/cm3 at the time of his lung mass discovery but had increased to > 40 k/cm3 with a differential of neutrophils > 80%. Flow cytometry was negative, and his peripheral smear was read as normal. Dr. Gilbert, what might explain this patient’s leukocytosis?
►Gary Gilbert, MD, Section of Hematology and Oncology, VABHS and Associate Professor of Medicine, Harvard Medical School (HMS): This patient had an elevated WBC for 4 months. Initially, the cause was likely lithium as this is known to cause a leukocytosis.7 More recently, the total WBC had increased and there were a couple of other abnormalities: A consistently elevated absolute monocyte count and a markedly elevated mature neutrophil count. These findings are consistent with a leukemoid reaction (ie, a WBC count > 50,000/µL from causes other than leukemia). The question becomes what is this a leukemoid reaction in response to? Once we have excluded a lung malignancy (a well-known common cause of a leukemoid reaction) we must consider a clonal myeloproliferative disorder. This is particularly true because many things that cause a leukemoid reaction (eg, lobar pneumonia) do not cause a persistently elevated neutrophil count. That this patient does have a persistently elevated neutrophil count suggests something abnormal about the neutrophils themselves.
► Dr. Apte: A bone marrow biopsy was performed. Dr. Gilbert, can you comment on this patient’s bone marrow biopsy and whether a myeloproliferative disorder may have played a role in the marked leukocytosis?
► Dr. Gilbert: The bone marrow biopsy was hyperplastic with myeloid predominance and normal maturation in all lineages. A deep sequencing analysis demonstrated the absence of chromosomal abnormalities or genetic mutations that are associated with myeloproliferative disorders. This excludes the possibility of a myeloproliferative disorder.
► Dr. Apte: The patient was started on 60 mg of prednisone daily, which led to marked improvement in his symptoms. He was discharged in stable condition but presented again with abdominal pain. A complete blood count once again showed increased WBC and new thrombocytosis. A CT angiogram (CTA) showed the prior lung mass with new signs of central necrosis. In the abdomen, new splenic and renal infarct were identified, along with signs of multiple arterial thrombi in the abdomen and internal and external iliac vessel wall thickening. These findings were read as concerning for a medium vessel vasculitis. Dr. Kaur, what are some of the imaging findings you would expect to see in vasculitis, and what about this patient’s CT is consistent with a medium vessel vasculitis?
► Maneet Kaur, MD, Section of Rheumatology, VABHS: Vasculitis is inflammation of the vessel wall that can lead to vascular injury and activation of the coagulation cascade. Sometimes these findings can be seen on imaging with evidence of stenosis, microaneurysms, and thrombosis distal to the stenosis. The nomenclature of vasculitis is not simple and has been revised many times. Medium-vessel vasculitis does not just affect the medium vessels (eg, visceral arteries) but can overlap with distal large vessels and smaller cutaneous vessels.
The first thing that comes to mind in this case is polyarteritis nodosa (PAN), an immune complex-mediated medium vessel disease that can involve large and small vessels in muscle, nerve, and skin. It can also present with masses.
►Dr. Apte: To address the arterial thrombi seen on CTA, arterial-brachial indices were obtained and showed bilateral occlusive disease in his distal extremities; findings that could be explained by vasculitis. His VATS biopsy pathology was reviewed for signs of vasculitis. Dr. Huang, can you review these slides for us please?
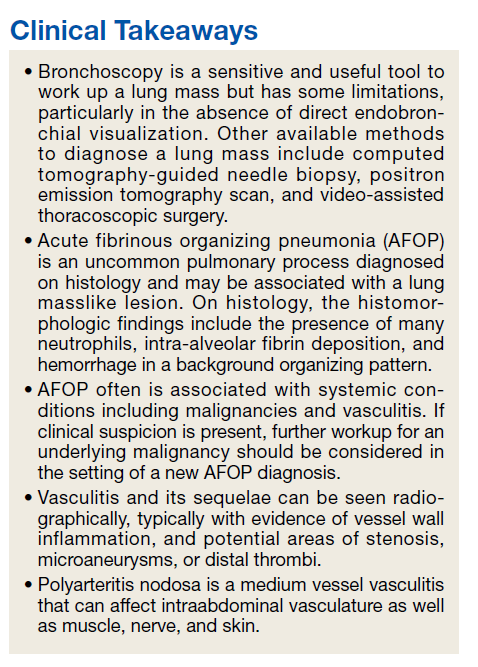
►Qin Huang, MD, Department of Pathology and Laboratory Medicine, VABHS and Assistant Professor of Pathology, HMS: This patient had a history of smoking, and there are many black pigment-laden macrophages present in the lung tissue. There were areas of hemorrhage and fibrin deposition and an overall picture of organizing pneumonia. At a lower power, you can see neutrophils everywhere, some in the form of micro-abscesses. The arterial walls did not show signs of vasculitis (Figure 2). Based on the clinical information and radiology findings, we suspected an acute infection-related pneumonia or a primary lung malignancy causing obstruction pneumonia. We suggested a rebiopsy of the lung mass to rule out a primary lung malignancy.
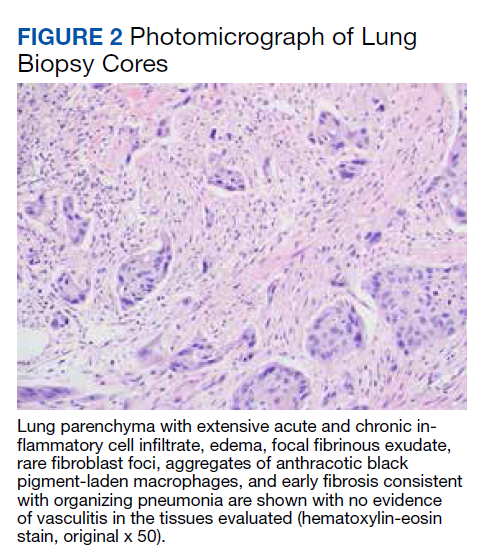
► Dr. Apte: Given his CT findings, a serologic rheumatologic workup including antineutrophil cytoplasmic antibody, antinuclear antibody, and rheumatoid factors were sent and returned negative. The location of arterial wall inflammation on imaging made it unamenable for biopsy. The patient began to experience bilateral temporal pain, which raised the concern for a large vessel vasculitis, specifically giant cell arteritis. Bilateral temporal artery biopsies were obtained and were not suggestive of vasculitis. Dr. Kaur, we still do not have any serologic or biopsy confirmation to support a diagnosis of vasculitis. Can we still call this a vasculitis?
►Dr. Kaur: Few things can cause the picture that was seen radiographically. A few noninflammatory causes like fibromuscular dysplasia can cause both large and small vessel stenosis, but the elevations in erythrocyte sedimentation rate and C-reactive protein along with response to steroids makes these diagnoses unlikely. Sometimes we must make a clinical diagnosis for vasculitis based on the clinical picture, and I would feel comfortable treating this patient for vasculitis.
With that said, I remain concerned that this patient also has a malignancy. His WBC increased to > 70 k/cm3 and his calcium to > 13 mg/dL. These findings are hard to explain by vasculitis alone. There are cancer-associated vasculitis, and I suspect this is the explanation here.8 His temporal pain was pointing to large vessel involvement, so he could have an undifferentiated vasculitis.
► Dr. Apte: A decision was made to empirically treat with tocilizumab, an IL-6 receptor antagonist, for an undifferentiated autoimmune disease, in addition to tapering steroids. The patient underwent a second VATS, which again revealed AFOP but no signs of malignancy. Unfortunately, he developed multiple complications over the subsequent weeks and passed away. An autopsy was requested by family members and pathology from his lung mass was reviewed. (Figure 3). Dr. Huang, can you review these slides for us?
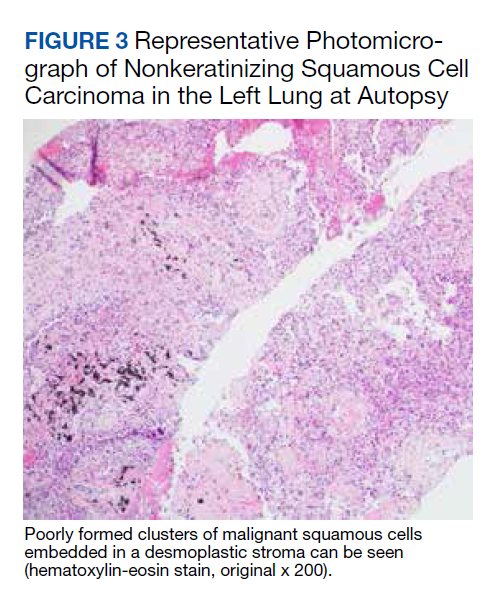
► Dr. Huang: The left lung mass at autopsy shows nests, poorly formed clusters, and individuals of malignant neoplastic nonkeratinizing squamous cells embedded in a desmoplastic stroma in the mass center, consistent with poorly differentiated squamous cell carcinoma, and a circumscribed area of residual subacute organizing pneumonia with abscess, granulomatous changes, and early fibrosis at the periphery of this mass.
►Dr. Apte: Based on autopsy findings, the final diagnosis was poorly differentiated squamous cell carcinoma associated with subacute organizing pneumonia and medium vessel vasculitis, which presented with a severe leukocytosis ultimately thought to be a leukemoid reaction from his lung cancer.
1. Valour F, Sénéchal A, Dupieux C, et al. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014;7:183-197. Published 2014 Jul 5. doi:10.2147/IDR.S39601
2. de Bazelaire C, Coffin A, Cohen-Zarade S, et al. CT-guided biopsies in lung infections in patients with haematological malignancies. Diagn Interv Imaging. 2013;94(2):202-215. doi:10.1016/j.diii.2012.12.008
3. Sweidan AJ, Singh NK, Stein A, Tanios M. Nodular sarcoidosis masquerading as cancer. Clin Med Insights Circ Respir Pulm Med. 2017;11:1179548417703123. Published 2017 Apr 12. doi:10.1177/1179548417703123
4. Bagheri R, Yousefi Y, Rezai R, Azemonfar V, Keshtan FG. Atrial fibrillation after lung surgery: incidence, underlying factors, and predictors. Kardiochir Torakochirurgia Pol. 2019;16(2):53-56. doi:10.5114/kitp.2019.86355
5. Lu J, Yin Q, Zha Y, et al. Acute fibrinous and organizing pneumonia: two case reports and literature review. BMC Pulm Med. 2019;19(1):141. Published 2019 Aug 5. doi:10.1186/s12890-019-0861-3
6. Beasley MB, Franks TJ, Galvin JR, Gochuico B, Travis WD. Acute fibrinous and organizing pneumonia: a histological pattern of lung injury and possible variant of diffuse alveolar damage. Arch Pathol Lab Med. 2002;126(9):1064-1070. doi:10.5858/2002-126-1064-AFAOP
7. Murphy DL, Goodwin FK, Bunney WE Jr. Leukocytosis during lithium treatment. Am J Psychiatry. 1971;127(11):1559-1561. doi:10.1176/ajp.127.11.1559
8. Fain O, Hamidou M, Cacoub P, et al. Vasculitides associated with malignancies: analysis of sixty patients. Arthritis Rheum. 2007;57(8):1473-1480. doi:10.1002/art.23085
Case Presentation: A 62-year-old male presented with shortness of breath and a cough productive of green sputum. He had a history of hyperlipidemia, posttraumatic stress disorder, bipolar disorder, obstructive sleep apnea, and a 50 pack-year history of smoking. His medications included prazosin, melatonin, lithium, and gabapentin. He also had a significant exposure history including asbestos and chemical paints following his leave from the military. At the initial evaluation, laboratory work revealed a leukocytosis with white blood cell (WBC) count 20 k/cm3and otherwise normal transaminases, albumin, and electrolytes. A chest X-ray revealed a new left hilar mass.
►Manisha Apte, MD, Chief Medical Resident, VA Boston Healthcare System (VABHS) and Boston Medical Center (BMC): To work up his new left hilar mass, a computed tomography (CT) of the chest was ordered (Figure 1), which revealed an apical left lower lobe mass extending into the left hilum encasing part of the ascending aorta. Enlarged mediastinal subcentimeter paratracheal and superior mediastinal lymph nodes also were identified and the pattern raised the concern for lymphangitic carcinomatosis. Dr. Fine, what do you make of the CT findings?
► Alan Fine, MD, Section of Pulmonary and Critical Care, VABHS and Professor of Medicine, Boston University School of Medicine: This mass had irregular edges with septal thickening, which may be why there was a concern for lymphangitic spread. There were no clear tissue planes to see if this process was invading the mediastinum. The mass was irregular, a single lesion, and proximal, making it consistent with a lung cancer. In fact, with his history of smoking, asbestos exposure, the numbers 1 to 10 diagnoses were lung cancer. The lack of demarcation of tissue planes supports this. There are some infections, classically actinomycosis, that do cross and invade anatomical barriers.1 But this looked like a primary lung cancer.
► Dr. Apte: The patient was referred to a pulmonologist where an additional history of night sweats and weight loss were noted. Dr. Fine, we have a patient with a newly identified lung mass, and while we have reason to suspect malignancy as you have already noted, there are many other etiologies to consider, including infections (histoplasmosis, cryptococcosis, bacterial abscess), inflammatory processes (sarcoidosis, rheumatoid nodule) and vasculitis (granulomatosis with polyangiitis). What should be the next step taken to make a diagnosis?
►Dr. Fine: For cancer specifically, we would like to both stage and make a diagnosis with one procedure. That’s part of the utility of a positron emission tomography (PET) scan: We can see lymph node involvement and stage the cancer. We must consider the patient’s comorbidities and the location of the lesion (ie, is it amenable to needle biopsy?). In this case, there are enlarged mediastinal lymph nodes, so one could perform a bronchoscopy with endobronchial ultrasound, which is a relatively noninvasive way to sample the lymph nodes to ideally stage and make a diagnosis as safely as possible. If we are considering infection, needle aspiration is not as sensitive.2
► Dr. Apte: The patient underwent a PET CT, which redemonstrated the lung mass with a loss of aortic fat plane suspicious for aortic involvement as well as lymph nodes in levels 7 and 8 that were concerning for malignancy. Subsequent bronchoscopy with biopsy and endobronchial ultrasound did not show evidence of malignancy; washing and brushing from the mass and lymph node specimens did not identify malignant cells. Benign respiratory mucosa with mild chronic inflammation was noted. Dr. Fine, given the nonspecific findings on the PET scan, negative findings on our bronchoscopy, and a negative biopsy, should we be satisfied that we have ruled out cancer?
► Dr. Fine: No, bronchoscopy has its limitations. It’s highly sensitive to the diagnosis of malignancy if you can see an endobronchial lesion, but we did not see one here. You can only go so far with the scope, and it’s not uncommon for us not to be able to make the diagnosis with bronchoscopy. Malignancy is still the most likely diagnosis, and we need to work this up further. I would perform another biopsy.
►Dr. Apte: Four weeks later, the patient presented with continued shortness of breath, fatigue, and fever. A repeat chest CT showed an opacity suggestive of pneumonia. Given the continued concern for cancer a CT-guided needle biopsy was performed and was once again negative for malignancy. The decision was made to pursue a video-assisted thorascopic surgery (VATS). Following the VATS, the patient developed rigors, fever, and tachycardia with new atrial fibrillation. While being evaluated hypercalcemia was identified, with further workup revealing a low parathyroid hormone (PTH) and low PTH-related peptide. Dr. Fine, the presence of hypercalcemia and a new arrythmia raised the possibility of sarcoidosis. Could this be sarcoidosis?
►Dr. Fine: Sarcoidosis is one of the great masqueraders in medicine. There is a type of sarcoidosis called nodular sarcoidosis where you see masslike distribution in the lung, but generally there are multiple masses and so this presentation would be atypical.3 There is also a phenomenon called sarcoidal reactions usually in the presence of cancer. Again, one tends to see multiple tiny lesions in the lung. It is certainly on the differential, but I would consider it to be less likely than cancer. It is also relatively common to develop atrial fibrillation after manipulation from a lung surgery.4 The other possibility I am concerned about is whether the mass is invading the mediastinum and involving the pericardium.
►Dr. Apte: Results from the VATS biopsy once again returned negative for malignancy and instead showed signs of focal micro-abscesses, atypical pneumocytes, and prominent neutrophils. A diagnosis of acute fibrinous organizing pneumonia (AFOP) was offered. Dr. Fine, what is AFOP?
►Dr. Fine: This is the first case of AFOP I had seen and probably the first case many in our department have seen. This is a relatively new entity with limited reported cases in the literature and is a pathological diagnosis originally recorded in autopsies from patients at the National Institutes of Health.5,6 Given the complexity of the lesion, the diagnosis is difficult to make. Most commonly, AFOP is associated with other systemic entities, most commonly hematologic malignancies like lymphomas and leukemias. It has also been associated with vasculitis and certain drugs. The mechanism is poorly understood, and although pneumonia is a part of the term, this just implies there is inflammation of the lung (ie, pneumonitis).
► Dr. Apte: Given the association of AFOP with underlying hematologic malignancies, an emphasis was placed on another finding: the patient’s increasing WBC count. The total WBC count had been 20 k/cm3 at the time of his lung mass discovery but had increased to > 40 k/cm3 with a differential of neutrophils > 80%. Flow cytometry was negative, and his peripheral smear was read as normal. Dr. Gilbert, what might explain this patient’s leukocytosis?
►Gary Gilbert, MD, Section of Hematology and Oncology, VABHS and Associate Professor of Medicine, Harvard Medical School (HMS): This patient had an elevated WBC for 4 months. Initially, the cause was likely lithium as this is known to cause a leukocytosis.7 More recently, the total WBC had increased and there were a couple of other abnormalities: A consistently elevated absolute monocyte count and a markedly elevated mature neutrophil count. These findings are consistent with a leukemoid reaction (ie, a WBC count > 50,000/µL from causes other than leukemia). The question becomes what is this a leukemoid reaction in response to? Once we have excluded a lung malignancy (a well-known common cause of a leukemoid reaction) we must consider a clonal myeloproliferative disorder. This is particularly true because many things that cause a leukemoid reaction (eg, lobar pneumonia) do not cause a persistently elevated neutrophil count. That this patient does have a persistently elevated neutrophil count suggests something abnormal about the neutrophils themselves.
► Dr. Apte: A bone marrow biopsy was performed. Dr. Gilbert, can you comment on this patient’s bone marrow biopsy and whether a myeloproliferative disorder may have played a role in the marked leukocytosis?
► Dr. Gilbert: The bone marrow biopsy was hyperplastic with myeloid predominance and normal maturation in all lineages. A deep sequencing analysis demonstrated the absence of chromosomal abnormalities or genetic mutations that are associated with myeloproliferative disorders. This excludes the possibility of a myeloproliferative disorder.
► Dr. Apte: The patient was started on 60 mg of prednisone daily, which led to marked improvement in his symptoms. He was discharged in stable condition but presented again with abdominal pain. A complete blood count once again showed increased WBC and new thrombocytosis. A CT angiogram (CTA) showed the prior lung mass with new signs of central necrosis. In the abdomen, new splenic and renal infarct were identified, along with signs of multiple arterial thrombi in the abdomen and internal and external iliac vessel wall thickening. These findings were read as concerning for a medium vessel vasculitis. Dr. Kaur, what are some of the imaging findings you would expect to see in vasculitis, and what about this patient’s CT is consistent with a medium vessel vasculitis?
► Maneet Kaur, MD, Section of Rheumatology, VABHS: Vasculitis is inflammation of the vessel wall that can lead to vascular injury and activation of the coagulation cascade. Sometimes these findings can be seen on imaging with evidence of stenosis, microaneurysms, and thrombosis distal to the stenosis. The nomenclature of vasculitis is not simple and has been revised many times. Medium-vessel vasculitis does not just affect the medium vessels (eg, visceral arteries) but can overlap with distal large vessels and smaller cutaneous vessels.
The first thing that comes to mind in this case is polyarteritis nodosa (PAN), an immune complex-mediated medium vessel disease that can involve large and small vessels in muscle, nerve, and skin. It can also present with masses.
►Dr. Apte: To address the arterial thrombi seen on CTA, arterial-brachial indices were obtained and showed bilateral occlusive disease in his distal extremities; findings that could be explained by vasculitis. His VATS biopsy pathology was reviewed for signs of vasculitis. Dr. Huang, can you review these slides for us please?
►Qin Huang, MD, Department of Pathology and Laboratory Medicine, VABHS and Assistant Professor of Pathology, HMS: This patient had a history of smoking, and there are many black pigment-laden macrophages present in the lung tissue. There were areas of hemorrhage and fibrin deposition and an overall picture of organizing pneumonia. At a lower power, you can see neutrophils everywhere, some in the form of micro-abscesses. The arterial walls did not show signs of vasculitis (Figure 2). Based on the clinical information and radiology findings, we suspected an acute infection-related pneumonia or a primary lung malignancy causing obstruction pneumonia. We suggested a rebiopsy of the lung mass to rule out a primary lung malignancy.
► Dr. Apte: Given his CT findings, a serologic rheumatologic workup including antineutrophil cytoplasmic antibody, antinuclear antibody, and rheumatoid factors were sent and returned negative. The location of arterial wall inflammation on imaging made it unamenable for biopsy. The patient began to experience bilateral temporal pain, which raised the concern for a large vessel vasculitis, specifically giant cell arteritis. Bilateral temporal artery biopsies were obtained and were not suggestive of vasculitis. Dr. Kaur, we still do not have any serologic or biopsy confirmation to support a diagnosis of vasculitis. Can we still call this a vasculitis?
►Dr. Kaur: Few things can cause the picture that was seen radiographically. A few noninflammatory causes like fibromuscular dysplasia can cause both large and small vessel stenosis, but the elevations in erythrocyte sedimentation rate and C-reactive protein along with response to steroids makes these diagnoses unlikely. Sometimes we must make a clinical diagnosis for vasculitis based on the clinical picture, and I would feel comfortable treating this patient for vasculitis.
With that said, I remain concerned that this patient also has a malignancy. His WBC increased to > 70 k/cm3 and his calcium to > 13 mg/dL. These findings are hard to explain by vasculitis alone. There are cancer-associated vasculitis, and I suspect this is the explanation here.8 His temporal pain was pointing to large vessel involvement, so he could have an undifferentiated vasculitis.
► Dr. Apte: A decision was made to empirically treat with tocilizumab, an IL-6 receptor antagonist, for an undifferentiated autoimmune disease, in addition to tapering steroids. The patient underwent a second VATS, which again revealed AFOP but no signs of malignancy. Unfortunately, he developed multiple complications over the subsequent weeks and passed away. An autopsy was requested by family members and pathology from his lung mass was reviewed. (Figure 3). Dr. Huang, can you review these slides for us?
► Dr. Huang: The left lung mass at autopsy shows nests, poorly formed clusters, and individuals of malignant neoplastic nonkeratinizing squamous cells embedded in a desmoplastic stroma in the mass center, consistent with poorly differentiated squamous cell carcinoma, and a circumscribed area of residual subacute organizing pneumonia with abscess, granulomatous changes, and early fibrosis at the periphery of this mass.
►Dr. Apte: Based on autopsy findings, the final diagnosis was poorly differentiated squamous cell carcinoma associated with subacute organizing pneumonia and medium vessel vasculitis, which presented with a severe leukocytosis ultimately thought to be a leukemoid reaction from his lung cancer.
Case Presentation: A 62-year-old male presented with shortness of breath and a cough productive of green sputum. He had a history of hyperlipidemia, posttraumatic stress disorder, bipolar disorder, obstructive sleep apnea, and a 50 pack-year history of smoking. His medications included prazosin, melatonin, lithium, and gabapentin. He also had a significant exposure history including asbestos and chemical paints following his leave from the military. At the initial evaluation, laboratory work revealed a leukocytosis with white blood cell (WBC) count 20 k/cm3and otherwise normal transaminases, albumin, and electrolytes. A chest X-ray revealed a new left hilar mass.
►Manisha Apte, MD, Chief Medical Resident, VA Boston Healthcare System (VABHS) and Boston Medical Center (BMC): To work up his new left hilar mass, a computed tomography (CT) of the chest was ordered (Figure 1), which revealed an apical left lower lobe mass extending into the left hilum encasing part of the ascending aorta. Enlarged mediastinal subcentimeter paratracheal and superior mediastinal lymph nodes also were identified and the pattern raised the concern for lymphangitic carcinomatosis. Dr. Fine, what do you make of the CT findings?
► Alan Fine, MD, Section of Pulmonary and Critical Care, VABHS and Professor of Medicine, Boston University School of Medicine: This mass had irregular edges with septal thickening, which may be why there was a concern for lymphangitic spread. There were no clear tissue planes to see if this process was invading the mediastinum. The mass was irregular, a single lesion, and proximal, making it consistent with a lung cancer. In fact, with his history of smoking, asbestos exposure, the numbers 1 to 10 diagnoses were lung cancer. The lack of demarcation of tissue planes supports this. There are some infections, classically actinomycosis, that do cross and invade anatomical barriers.1 But this looked like a primary lung cancer.
► Dr. Apte: The patient was referred to a pulmonologist where an additional history of night sweats and weight loss were noted. Dr. Fine, we have a patient with a newly identified lung mass, and while we have reason to suspect malignancy as you have already noted, there are many other etiologies to consider, including infections (histoplasmosis, cryptococcosis, bacterial abscess), inflammatory processes (sarcoidosis, rheumatoid nodule) and vasculitis (granulomatosis with polyangiitis). What should be the next step taken to make a diagnosis?
►Dr. Fine: For cancer specifically, we would like to both stage and make a diagnosis with one procedure. That’s part of the utility of a positron emission tomography (PET) scan: We can see lymph node involvement and stage the cancer. We must consider the patient’s comorbidities and the location of the lesion (ie, is it amenable to needle biopsy?). In this case, there are enlarged mediastinal lymph nodes, so one could perform a bronchoscopy with endobronchial ultrasound, which is a relatively noninvasive way to sample the lymph nodes to ideally stage and make a diagnosis as safely as possible. If we are considering infection, needle aspiration is not as sensitive.2
► Dr. Apte: The patient underwent a PET CT, which redemonstrated the lung mass with a loss of aortic fat plane suspicious for aortic involvement as well as lymph nodes in levels 7 and 8 that were concerning for malignancy. Subsequent bronchoscopy with biopsy and endobronchial ultrasound did not show evidence of malignancy; washing and brushing from the mass and lymph node specimens did not identify malignant cells. Benign respiratory mucosa with mild chronic inflammation was noted. Dr. Fine, given the nonspecific findings on the PET scan, negative findings on our bronchoscopy, and a negative biopsy, should we be satisfied that we have ruled out cancer?
► Dr. Fine: No, bronchoscopy has its limitations. It’s highly sensitive to the diagnosis of malignancy if you can see an endobronchial lesion, but we did not see one here. You can only go so far with the scope, and it’s not uncommon for us not to be able to make the diagnosis with bronchoscopy. Malignancy is still the most likely diagnosis, and we need to work this up further. I would perform another biopsy.
►Dr. Apte: Four weeks later, the patient presented with continued shortness of breath, fatigue, and fever. A repeat chest CT showed an opacity suggestive of pneumonia. Given the continued concern for cancer a CT-guided needle biopsy was performed and was once again negative for malignancy. The decision was made to pursue a video-assisted thorascopic surgery (VATS). Following the VATS, the patient developed rigors, fever, and tachycardia with new atrial fibrillation. While being evaluated hypercalcemia was identified, with further workup revealing a low parathyroid hormone (PTH) and low PTH-related peptide. Dr. Fine, the presence of hypercalcemia and a new arrythmia raised the possibility of sarcoidosis. Could this be sarcoidosis?
►Dr. Fine: Sarcoidosis is one of the great masqueraders in medicine. There is a type of sarcoidosis called nodular sarcoidosis where you see masslike distribution in the lung, but generally there are multiple masses and so this presentation would be atypical.3 There is also a phenomenon called sarcoidal reactions usually in the presence of cancer. Again, one tends to see multiple tiny lesions in the lung. It is certainly on the differential, but I would consider it to be less likely than cancer. It is also relatively common to develop atrial fibrillation after manipulation from a lung surgery.4 The other possibility I am concerned about is whether the mass is invading the mediastinum and involving the pericardium.
►Dr. Apte: Results from the VATS biopsy once again returned negative for malignancy and instead showed signs of focal micro-abscesses, atypical pneumocytes, and prominent neutrophils. A diagnosis of acute fibrinous organizing pneumonia (AFOP) was offered. Dr. Fine, what is AFOP?
►Dr. Fine: This is the first case of AFOP I had seen and probably the first case many in our department have seen. This is a relatively new entity with limited reported cases in the literature and is a pathological diagnosis originally recorded in autopsies from patients at the National Institutes of Health.5,6 Given the complexity of the lesion, the diagnosis is difficult to make. Most commonly, AFOP is associated with other systemic entities, most commonly hematologic malignancies like lymphomas and leukemias. It has also been associated with vasculitis and certain drugs. The mechanism is poorly understood, and although pneumonia is a part of the term, this just implies there is inflammation of the lung (ie, pneumonitis).
► Dr. Apte: Given the association of AFOP with underlying hematologic malignancies, an emphasis was placed on another finding: the patient’s increasing WBC count. The total WBC count had been 20 k/cm3 at the time of his lung mass discovery but had increased to > 40 k/cm3 with a differential of neutrophils > 80%. Flow cytometry was negative, and his peripheral smear was read as normal. Dr. Gilbert, what might explain this patient’s leukocytosis?
►Gary Gilbert, MD, Section of Hematology and Oncology, VABHS and Associate Professor of Medicine, Harvard Medical School (HMS): This patient had an elevated WBC for 4 months. Initially, the cause was likely lithium as this is known to cause a leukocytosis.7 More recently, the total WBC had increased and there were a couple of other abnormalities: A consistently elevated absolute monocyte count and a markedly elevated mature neutrophil count. These findings are consistent with a leukemoid reaction (ie, a WBC count > 50,000/µL from causes other than leukemia). The question becomes what is this a leukemoid reaction in response to? Once we have excluded a lung malignancy (a well-known common cause of a leukemoid reaction) we must consider a clonal myeloproliferative disorder. This is particularly true because many things that cause a leukemoid reaction (eg, lobar pneumonia) do not cause a persistently elevated neutrophil count. That this patient does have a persistently elevated neutrophil count suggests something abnormal about the neutrophils themselves.
► Dr. Apte: A bone marrow biopsy was performed. Dr. Gilbert, can you comment on this patient’s bone marrow biopsy and whether a myeloproliferative disorder may have played a role in the marked leukocytosis?
► Dr. Gilbert: The bone marrow biopsy was hyperplastic with myeloid predominance and normal maturation in all lineages. A deep sequencing analysis demonstrated the absence of chromosomal abnormalities or genetic mutations that are associated with myeloproliferative disorders. This excludes the possibility of a myeloproliferative disorder.
► Dr. Apte: The patient was started on 60 mg of prednisone daily, which led to marked improvement in his symptoms. He was discharged in stable condition but presented again with abdominal pain. A complete blood count once again showed increased WBC and new thrombocytosis. A CT angiogram (CTA) showed the prior lung mass with new signs of central necrosis. In the abdomen, new splenic and renal infarct were identified, along with signs of multiple arterial thrombi in the abdomen and internal and external iliac vessel wall thickening. These findings were read as concerning for a medium vessel vasculitis. Dr. Kaur, what are some of the imaging findings you would expect to see in vasculitis, and what about this patient’s CT is consistent with a medium vessel vasculitis?
► Maneet Kaur, MD, Section of Rheumatology, VABHS: Vasculitis is inflammation of the vessel wall that can lead to vascular injury and activation of the coagulation cascade. Sometimes these findings can be seen on imaging with evidence of stenosis, microaneurysms, and thrombosis distal to the stenosis. The nomenclature of vasculitis is not simple and has been revised many times. Medium-vessel vasculitis does not just affect the medium vessels (eg, visceral arteries) but can overlap with distal large vessels and smaller cutaneous vessels.
The first thing that comes to mind in this case is polyarteritis nodosa (PAN), an immune complex-mediated medium vessel disease that can involve large and small vessels in muscle, nerve, and skin. It can also present with masses.
►Dr. Apte: To address the arterial thrombi seen on CTA, arterial-brachial indices were obtained and showed bilateral occlusive disease in his distal extremities; findings that could be explained by vasculitis. His VATS biopsy pathology was reviewed for signs of vasculitis. Dr. Huang, can you review these slides for us please?
►Qin Huang, MD, Department of Pathology and Laboratory Medicine, VABHS and Assistant Professor of Pathology, HMS: This patient had a history of smoking, and there are many black pigment-laden macrophages present in the lung tissue. There were areas of hemorrhage and fibrin deposition and an overall picture of organizing pneumonia. At a lower power, you can see neutrophils everywhere, some in the form of micro-abscesses. The arterial walls did not show signs of vasculitis (Figure 2). Based on the clinical information and radiology findings, we suspected an acute infection-related pneumonia or a primary lung malignancy causing obstruction pneumonia. We suggested a rebiopsy of the lung mass to rule out a primary lung malignancy.
► Dr. Apte: Given his CT findings, a serologic rheumatologic workup including antineutrophil cytoplasmic antibody, antinuclear antibody, and rheumatoid factors were sent and returned negative. The location of arterial wall inflammation on imaging made it unamenable for biopsy. The patient began to experience bilateral temporal pain, which raised the concern for a large vessel vasculitis, specifically giant cell arteritis. Bilateral temporal artery biopsies were obtained and were not suggestive of vasculitis. Dr. Kaur, we still do not have any serologic or biopsy confirmation to support a diagnosis of vasculitis. Can we still call this a vasculitis?
►Dr. Kaur: Few things can cause the picture that was seen radiographically. A few noninflammatory causes like fibromuscular dysplasia can cause both large and small vessel stenosis, but the elevations in erythrocyte sedimentation rate and C-reactive protein along with response to steroids makes these diagnoses unlikely. Sometimes we must make a clinical diagnosis for vasculitis based on the clinical picture, and I would feel comfortable treating this patient for vasculitis.
With that said, I remain concerned that this patient also has a malignancy. His WBC increased to > 70 k/cm3 and his calcium to > 13 mg/dL. These findings are hard to explain by vasculitis alone. There are cancer-associated vasculitis, and I suspect this is the explanation here.8 His temporal pain was pointing to large vessel involvement, so he could have an undifferentiated vasculitis.
► Dr. Apte: A decision was made to empirically treat with tocilizumab, an IL-6 receptor antagonist, for an undifferentiated autoimmune disease, in addition to tapering steroids. The patient underwent a second VATS, which again revealed AFOP but no signs of malignancy. Unfortunately, he developed multiple complications over the subsequent weeks and passed away. An autopsy was requested by family members and pathology from his lung mass was reviewed. (Figure 3). Dr. Huang, can you review these slides for us?
► Dr. Huang: The left lung mass at autopsy shows nests, poorly formed clusters, and individuals of malignant neoplastic nonkeratinizing squamous cells embedded in a desmoplastic stroma in the mass center, consistent with poorly differentiated squamous cell carcinoma, and a circumscribed area of residual subacute organizing pneumonia with abscess, granulomatous changes, and early fibrosis at the periphery of this mass.
►Dr. Apte: Based on autopsy findings, the final diagnosis was poorly differentiated squamous cell carcinoma associated with subacute organizing pneumonia and medium vessel vasculitis, which presented with a severe leukocytosis ultimately thought to be a leukemoid reaction from his lung cancer.
1. Valour F, Sénéchal A, Dupieux C, et al. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014;7:183-197. Published 2014 Jul 5. doi:10.2147/IDR.S39601
2. de Bazelaire C, Coffin A, Cohen-Zarade S, et al. CT-guided biopsies in lung infections in patients with haematological malignancies. Diagn Interv Imaging. 2013;94(2):202-215. doi:10.1016/j.diii.2012.12.008
3. Sweidan AJ, Singh NK, Stein A, Tanios M. Nodular sarcoidosis masquerading as cancer. Clin Med Insights Circ Respir Pulm Med. 2017;11:1179548417703123. Published 2017 Apr 12. doi:10.1177/1179548417703123
4. Bagheri R, Yousefi Y, Rezai R, Azemonfar V, Keshtan FG. Atrial fibrillation after lung surgery: incidence, underlying factors, and predictors. Kardiochir Torakochirurgia Pol. 2019;16(2):53-56. doi:10.5114/kitp.2019.86355
5. Lu J, Yin Q, Zha Y, et al. Acute fibrinous and organizing pneumonia: two case reports and literature review. BMC Pulm Med. 2019;19(1):141. Published 2019 Aug 5. doi:10.1186/s12890-019-0861-3
6. Beasley MB, Franks TJ, Galvin JR, Gochuico B, Travis WD. Acute fibrinous and organizing pneumonia: a histological pattern of lung injury and possible variant of diffuse alveolar damage. Arch Pathol Lab Med. 2002;126(9):1064-1070. doi:10.5858/2002-126-1064-AFAOP
7. Murphy DL, Goodwin FK, Bunney WE Jr. Leukocytosis during lithium treatment. Am J Psychiatry. 1971;127(11):1559-1561. doi:10.1176/ajp.127.11.1559
8. Fain O, Hamidou M, Cacoub P, et al. Vasculitides associated with malignancies: analysis of sixty patients. Arthritis Rheum. 2007;57(8):1473-1480. doi:10.1002/art.23085
1. Valour F, Sénéchal A, Dupieux C, et al. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014;7:183-197. Published 2014 Jul 5. doi:10.2147/IDR.S39601
2. de Bazelaire C, Coffin A, Cohen-Zarade S, et al. CT-guided biopsies in lung infections in patients with haematological malignancies. Diagn Interv Imaging. 2013;94(2):202-215. doi:10.1016/j.diii.2012.12.008
3. Sweidan AJ, Singh NK, Stein A, Tanios M. Nodular sarcoidosis masquerading as cancer. Clin Med Insights Circ Respir Pulm Med. 2017;11:1179548417703123. Published 2017 Apr 12. doi:10.1177/1179548417703123
4. Bagheri R, Yousefi Y, Rezai R, Azemonfar V, Keshtan FG. Atrial fibrillation after lung surgery: incidence, underlying factors, and predictors. Kardiochir Torakochirurgia Pol. 2019;16(2):53-56. doi:10.5114/kitp.2019.86355
5. Lu J, Yin Q, Zha Y, et al. Acute fibrinous and organizing pneumonia: two case reports and literature review. BMC Pulm Med. 2019;19(1):141. Published 2019 Aug 5. doi:10.1186/s12890-019-0861-3
6. Beasley MB, Franks TJ, Galvin JR, Gochuico B, Travis WD. Acute fibrinous and organizing pneumonia: a histological pattern of lung injury and possible variant of diffuse alveolar damage. Arch Pathol Lab Med. 2002;126(9):1064-1070. doi:10.5858/2002-126-1064-AFAOP
7. Murphy DL, Goodwin FK, Bunney WE Jr. Leukocytosis during lithium treatment. Am J Psychiatry. 1971;127(11):1559-1561. doi:10.1176/ajp.127.11.1559
8. Fain O, Hamidou M, Cacoub P, et al. Vasculitides associated with malignancies: analysis of sixty patients. Arthritis Rheum. 2007;57(8):1473-1480. doi:10.1002/art.23085
Psychiatric fallout from long-COVID: How to prepare
As mounting evidence points to a significant psychiatric component of COVID-19, experts are concerned about an influx of survivors presenting with persistent mental health problems and how best to prepare.

Clinicians should be aware that patients who have had COVID frequently develop psychiatric symptoms, Silvia S. Martins, MD, PhD, associate professor of epidemiology, Columbia University, New York, said in an interview.
“There should be more screening of all patients recovering from a COVID infection for anxiety, posttraumatic stress disorder, and depression, as well as referral to services, including psychotherapy, and medication as needed,” said Dr. Martins, who, along with colleagues, uncovered a high rate of these symptoms in patients who had the disease.
The COVID-19 pandemic has taken an enormous social, emotional, and public health toll. It has disrupted lives and caused stress, fear, and uncertainty about loss of health and income, not to mention forced isolation.
In addition, a significant number of patients who contract COVID-19 continue to have symptoms after the acute phase of the illness. This post-COVID, or “long-haul,” syndrome isn’t well defined; experts cite a range of symptoms that persist for weeks or months.
These ongoing symptoms can include cough, fatigue, and chronic pain, as well as psychiatric complaints. As reported by this news organization, an observational study of more than 230,000 U.S. patient health records revealed that one in three COVID-19 survivors received a psychiatric or neurologic diagnosis within 6 months of contracting the virus.
The most common psychiatric diagnoses were anxiety disorders, mood disorders, substance misuse disorders, and insomnia.
Significant symptoms even in mild cases
Another study showed that even those with mild COVID-19 may experience psychiatric symptoms independently of previous psychiatric diagnoses. Results revealed that 26% of the sample of almost 900 patients reported depression, 22% reported anxiety, and 17% reported symptoms of posttraumatic stress 2 months after testing positive for the virus. This finding is important because the majority of individuals who contract COVID-19 have a mild case.

“We saw very high levels of clinically significant depression, anxiety, and posttraumatic stress symptoms in people who had mild disease,” study investigator João Mauricio Castaldelli-Maia, MD, PhD, postdoctoral fellow, department of epidemiology, Columbia University, said in an interview.
He attributed these symptoms in part to long periods of isolation, even from relatives in the same household, in cramped spaces typical of large cities such as São Paulo.
Social isolation can have a huge impact on persons who depend on social connections and relationships, Vivian Pender, MD, president of the American Psychiatric Association and clinical professor of psychiatry, Weill Cornell Medical Center, New York, said in an interview.
“The fact that we have not been able to see our colleagues, our friends, our family, and in the case of psychiatrists, even our patients has taken a toll on everyone, and that leads to more stress, more anxiety,” she said.
National surveys show that psychiatric symptoms occur after acute COVID. One survey revealed that over 50% of 3,900 respondents who had COVID reported having at least moderate symptoms of major depression.
Unique depression subtype?
Another survey, slated for publication later this year, shows that lead investigator Roy Perlis, MD, professor of psychiatry, Harvard Medical School, Boston, said in an interview.
This might suggest a neurobiological element. Researchers are speculating as to whether lingering psychiatric problems that occur after having COVID are linked to the psychosocial impact of the disease or to pathological processes, such as inflammation, that affect the brain.
Although rates of post-COVID psychiatric symptoms vary from study to study, “they seem to be pretty enduring,” noted Faith Gunning, PhD, vice chair of research, department of psychology, Weill Cornell Medicine, who specializes in clinical neuropsychology.
“So they’re not just a brief response” to getting sick, a fact that points to the possible need for treatment, she told this news organization. “In some of the work that’s starting to emerge, it does appear that the symptoms persist, at least for a relatively large subset of individuals.”
Although depression typically affects twice as many women as men, these new surveys show that, after COVID, “that difference is not so distinct,” said Dr. Gunning.
It’s unclear why this is, but it could be cause by financial stresses that may affect men to a greater extent, she added. “There is so much we’re still learning.”
Increased suicide risk?
Other researchers, including Leo Sher, MD, professor of psychiatry, Icahn School of Medicine at Mount Sinai, and director of inpatient psychiatry, James J. Peters Veterans Affairs Medical Center, both in New York, are concerned that higher rates of psychiatric symptoms among patients with long-haul COVID raise the risk for suicidal ideation and behavior.
Studies of suicidality in COVID-19 survivors “are urgently needed,” said Dr. Sher in an article published in the Monthly Journal of the Association of Physicians.
“We need to study what factors may increase suicide risk among the COVID-19 survivors during and after the recovery. We also need to investigate whether there is a long-term increased suicide risk among COVID-19 survivors,” Dr. Sher said.
COVID-19 is not unique among viral respiratory diseases in being associated with long-term mental health problems. Research shows that survivors of the 2003 outbreak of severe acute respiratory syndrome experienced increased psychological distress that persisted for at least a year, as did patients who in 2015 had Middle East respiratory syndrome coronavirus (MERS-CoV).
Some experts believe clinicians should screen patients for mental health symptoms after the acute phase of COVID and offer early and prolonged care.
“Early mental health intervention such as psychotherapy and supportive groups could play an important role in preventing incident mental health problems for post-COVID sufferers,” said Dr. Castaldelli-Maia.
A version of this article first appeared on Medscape.com.
As mounting evidence points to a significant psychiatric component of COVID-19, experts are concerned about an influx of survivors presenting with persistent mental health problems and how best to prepare.
Clinicians should be aware that patients who have had COVID frequently develop psychiatric symptoms, Silvia S. Martins, MD, PhD, associate professor of epidemiology, Columbia University, New York, said in an interview.
“There should be more screening of all patients recovering from a COVID infection for anxiety, posttraumatic stress disorder, and depression, as well as referral to services, including psychotherapy, and medication as needed,” said Dr. Martins, who, along with colleagues, uncovered a high rate of these symptoms in patients who had the disease.
The COVID-19 pandemic has taken an enormous social, emotional, and public health toll. It has disrupted lives and caused stress, fear, and uncertainty about loss of health and income, not to mention forced isolation.
In addition, a significant number of patients who contract COVID-19 continue to have symptoms after the acute phase of the illness. This post-COVID, or “long-haul,” syndrome isn’t well defined; experts cite a range of symptoms that persist for weeks or months.
These ongoing symptoms can include cough, fatigue, and chronic pain, as well as psychiatric complaints. As reported by this news organization, an observational study of more than 230,000 U.S. patient health records revealed that one in three COVID-19 survivors received a psychiatric or neurologic diagnosis within 6 months of contracting the virus.
The most common psychiatric diagnoses were anxiety disorders, mood disorders, substance misuse disorders, and insomnia.
Significant symptoms even in mild cases
Another study showed that even those with mild COVID-19 may experience psychiatric symptoms independently of previous psychiatric diagnoses. Results revealed that 26% of the sample of almost 900 patients reported depression, 22% reported anxiety, and 17% reported symptoms of posttraumatic stress 2 months after testing positive for the virus. This finding is important because the majority of individuals who contract COVID-19 have a mild case.
“We saw very high levels of clinically significant depression, anxiety, and posttraumatic stress symptoms in people who had mild disease,” study investigator João Mauricio Castaldelli-Maia, MD, PhD, postdoctoral fellow, department of epidemiology, Columbia University, said in an interview.
He attributed these symptoms in part to long periods of isolation, even from relatives in the same household, in cramped spaces typical of large cities such as São Paulo.
Social isolation can have a huge impact on persons who depend on social connections and relationships, Vivian Pender, MD, president of the American Psychiatric Association and clinical professor of psychiatry, Weill Cornell Medical Center, New York, said in an interview.
“The fact that we have not been able to see our colleagues, our friends, our family, and in the case of psychiatrists, even our patients has taken a toll on everyone, and that leads to more stress, more anxiety,” she said.
National surveys show that psychiatric symptoms occur after acute COVID. One survey revealed that over 50% of 3,900 respondents who had COVID reported having at least moderate symptoms of major depression.
Unique depression subtype?
Another survey, slated for publication later this year, shows that lead investigator Roy Perlis, MD, professor of psychiatry, Harvard Medical School, Boston, said in an interview.
This might suggest a neurobiological element. Researchers are speculating as to whether lingering psychiatric problems that occur after having COVID are linked to the psychosocial impact of the disease or to pathological processes, such as inflammation, that affect the brain.
Although rates of post-COVID psychiatric symptoms vary from study to study, “they seem to be pretty enduring,” noted Faith Gunning, PhD, vice chair of research, department of psychology, Weill Cornell Medicine, who specializes in clinical neuropsychology.
“So they’re not just a brief response” to getting sick, a fact that points to the possible need for treatment, she told this news organization. “In some of the work that’s starting to emerge, it does appear that the symptoms persist, at least for a relatively large subset of individuals.”
Although depression typically affects twice as many women as men, these new surveys show that, after COVID, “that difference is not so distinct,” said Dr. Gunning.
It’s unclear why this is, but it could be cause by financial stresses that may affect men to a greater extent, she added. “There is so much we’re still learning.”
Increased suicide risk?
Other researchers, including Leo Sher, MD, professor of psychiatry, Icahn School of Medicine at Mount Sinai, and director of inpatient psychiatry, James J. Peters Veterans Affairs Medical Center, both in New York, are concerned that higher rates of psychiatric symptoms among patients with long-haul COVID raise the risk for suicidal ideation and behavior.
Studies of suicidality in COVID-19 survivors “are urgently needed,” said Dr. Sher in an article published in the Monthly Journal of the Association of Physicians.
“We need to study what factors may increase suicide risk among the COVID-19 survivors during and after the recovery. We also need to investigate whether there is a long-term increased suicide risk among COVID-19 survivors,” Dr. Sher said.
COVID-19 is not unique among viral respiratory diseases in being associated with long-term mental health problems. Research shows that survivors of the 2003 outbreak of severe acute respiratory syndrome experienced increased psychological distress that persisted for at least a year, as did patients who in 2015 had Middle East respiratory syndrome coronavirus (MERS-CoV).
Some experts believe clinicians should screen patients for mental health symptoms after the acute phase of COVID and offer early and prolonged care.
“Early mental health intervention such as psychotherapy and supportive groups could play an important role in preventing incident mental health problems for post-COVID sufferers,” said Dr. Castaldelli-Maia.
A version of this article first appeared on Medscape.com.
As mounting evidence points to a significant psychiatric component of COVID-19, experts are concerned about an influx of survivors presenting with persistent mental health problems and how best to prepare.
Clinicians should be aware that patients who have had COVID frequently develop psychiatric symptoms, Silvia S. Martins, MD, PhD, associate professor of epidemiology, Columbia University, New York, said in an interview.
“There should be more screening of all patients recovering from a COVID infection for anxiety, posttraumatic stress disorder, and depression, as well as referral to services, including psychotherapy, and medication as needed,” said Dr. Martins, who, along with colleagues, uncovered a high rate of these symptoms in patients who had the disease.
The COVID-19 pandemic has taken an enormous social, emotional, and public health toll. It has disrupted lives and caused stress, fear, and uncertainty about loss of health and income, not to mention forced isolation.
In addition, a significant number of patients who contract COVID-19 continue to have symptoms after the acute phase of the illness. This post-COVID, or “long-haul,” syndrome isn’t well defined; experts cite a range of symptoms that persist for weeks or months.
These ongoing symptoms can include cough, fatigue, and chronic pain, as well as psychiatric complaints. As reported by this news organization, an observational study of more than 230,000 U.S. patient health records revealed that one in three COVID-19 survivors received a psychiatric or neurologic diagnosis within 6 months of contracting the virus.
The most common psychiatric diagnoses were anxiety disorders, mood disorders, substance misuse disorders, and insomnia.
Significant symptoms even in mild cases
Another study showed that even those with mild COVID-19 may experience psychiatric symptoms independently of previous psychiatric diagnoses. Results revealed that 26% of the sample of almost 900 patients reported depression, 22% reported anxiety, and 17% reported symptoms of posttraumatic stress 2 months after testing positive for the virus. This finding is important because the majority of individuals who contract COVID-19 have a mild case.
“We saw very high levels of clinically significant depression, anxiety, and posttraumatic stress symptoms in people who had mild disease,” study investigator João Mauricio Castaldelli-Maia, MD, PhD, postdoctoral fellow, department of epidemiology, Columbia University, said in an interview.
He attributed these symptoms in part to long periods of isolation, even from relatives in the same household, in cramped spaces typical of large cities such as São Paulo.
Social isolation can have a huge impact on persons who depend on social connections and relationships, Vivian Pender, MD, president of the American Psychiatric Association and clinical professor of psychiatry, Weill Cornell Medical Center, New York, said in an interview.
“The fact that we have not been able to see our colleagues, our friends, our family, and in the case of psychiatrists, even our patients has taken a toll on everyone, and that leads to more stress, more anxiety,” she said.
National surveys show that psychiatric symptoms occur after acute COVID. One survey revealed that over 50% of 3,900 respondents who had COVID reported having at least moderate symptoms of major depression.
Unique depression subtype?
Another survey, slated for publication later this year, shows that lead investigator Roy Perlis, MD, professor of psychiatry, Harvard Medical School, Boston, said in an interview.
This might suggest a neurobiological element. Researchers are speculating as to whether lingering psychiatric problems that occur after having COVID are linked to the psychosocial impact of the disease or to pathological processes, such as inflammation, that affect the brain.
Although rates of post-COVID psychiatric symptoms vary from study to study, “they seem to be pretty enduring,” noted Faith Gunning, PhD, vice chair of research, department of psychology, Weill Cornell Medicine, who specializes in clinical neuropsychology.
“So they’re not just a brief response” to getting sick, a fact that points to the possible need for treatment, she told this news organization. “In some of the work that’s starting to emerge, it does appear that the symptoms persist, at least for a relatively large subset of individuals.”
Although depression typically affects twice as many women as men, these new surveys show that, after COVID, “that difference is not so distinct,” said Dr. Gunning.
It’s unclear why this is, but it could be cause by financial stresses that may affect men to a greater extent, she added. “There is so much we’re still learning.”
Increased suicide risk?
Other researchers, including Leo Sher, MD, professor of psychiatry, Icahn School of Medicine at Mount Sinai, and director of inpatient psychiatry, James J. Peters Veterans Affairs Medical Center, both in New York, are concerned that higher rates of psychiatric symptoms among patients with long-haul COVID raise the risk for suicidal ideation and behavior.
Studies of suicidality in COVID-19 survivors “are urgently needed,” said Dr. Sher in an article published in the Monthly Journal of the Association of Physicians.
“We need to study what factors may increase suicide risk among the COVID-19 survivors during and after the recovery. We also need to investigate whether there is a long-term increased suicide risk among COVID-19 survivors,” Dr. Sher said.
COVID-19 is not unique among viral respiratory diseases in being associated with long-term mental health problems. Research shows that survivors of the 2003 outbreak of severe acute respiratory syndrome experienced increased psychological distress that persisted for at least a year, as did patients who in 2015 had Middle East respiratory syndrome coronavirus (MERS-CoV).
Some experts believe clinicians should screen patients for mental health symptoms after the acute phase of COVID and offer early and prolonged care.
“Early mental health intervention such as psychotherapy and supportive groups could play an important role in preventing incident mental health problems for post-COVID sufferers,” said Dr. Castaldelli-Maia.
A version of this article first appeared on Medscape.com.