User login
40 Year Old "Wart" Suddenly Changes
Answer
Digital mucous cysts (choice “c”), also known as myxoid cysts, are quite common and are found often on fingers and occasionally on toes. But they are almost always located on the distal dorsal portion of the digit, between the cuticle and distal interphalangeal joint—close enough, in many cases, to compress the nail matrix, which leads to a longitudinal trough in the nail plate. Surface erosion of these lesions is unusual but is occasionally seen.
However, given the history, appearance, and especially the location of this patient’s lesion, this is the one diagnosis our patient almost certainly did not have. The others, discussed below, were all real possibilities, and since “common things occur commonly,” squamous cell carcinoma was the most likely.
Discussion
With this clinical picture, cancer is assumed until proven otherwise. In that regard, the presence of a longstanding wart in this location is especially significant, since human papillomavirus (HPV) is known to be potentially oncogenic. The patient’s heavily sun-damaged skin adds another layer of risk for malignant transformation.
The only way to sort through this differential diagnosis was to perform a shave biopsy, which confirmed the diagnosis of squamous cell carcinoma (SCC)—one that showed evidence of arising from a long-standing wart. The patient was referred for Mohs micrographic surgery, for two reasons: (1) this location does not lend itself to simple excision and closure, both because of the paucity of adjacent skin and because of the potential for damage to the underlying tendons, nerves, and blood supply, and (2) SCCs of nonsolar causation (besides HPV, these include ionizing radiation, arsenic, and chronic ulcers) have more potential for metastasis than do the far more common sun-caused SCCs. This is all the more reason to obtain adequate margins. Often in such cases, irradiation of the site is also done, postoperatively.
Had the biopsy not shown clear evidence of cancer, the other items in the differential diagnosis would have come into play. This would have necessitated an additional biopsy, this time to obtain tissue for acid-fast bacilli and bacterial and fungal cultures.
As of this writing, the patient is awaiting Mohs surgery. He will have to be followed closely for at least a year to watch for any signs of metastasis. With an intact immune system, his prognosis is excellent.
Answer
Digital mucous cysts (choice “c”), also known as myxoid cysts, are quite common and are found often on fingers and occasionally on toes. But they are almost always located on the distal dorsal portion of the digit, between the cuticle and distal interphalangeal joint—close enough, in many cases, to compress the nail matrix, which leads to a longitudinal trough in the nail plate. Surface erosion of these lesions is unusual but is occasionally seen.
However, given the history, appearance, and especially the location of this patient’s lesion, this is the one diagnosis our patient almost certainly did not have. The others, discussed below, were all real possibilities, and since “common things occur commonly,” squamous cell carcinoma was the most likely.
Discussion
With this clinical picture, cancer is assumed until proven otherwise. In that regard, the presence of a longstanding wart in this location is especially significant, since human papillomavirus (HPV) is known to be potentially oncogenic. The patient’s heavily sun-damaged skin adds another layer of risk for malignant transformation.
The only way to sort through this differential diagnosis was to perform a shave biopsy, which confirmed the diagnosis of squamous cell carcinoma (SCC)—one that showed evidence of arising from a long-standing wart. The patient was referred for Mohs micrographic surgery, for two reasons: (1) this location does not lend itself to simple excision and closure, both because of the paucity of adjacent skin and because of the potential for damage to the underlying tendons, nerves, and blood supply, and (2) SCCs of nonsolar causation (besides HPV, these include ionizing radiation, arsenic, and chronic ulcers) have more potential for metastasis than do the far more common sun-caused SCCs. This is all the more reason to obtain adequate margins. Often in such cases, irradiation of the site is also done, postoperatively.
Had the biopsy not shown clear evidence of cancer, the other items in the differential diagnosis would have come into play. This would have necessitated an additional biopsy, this time to obtain tissue for acid-fast bacilli and bacterial and fungal cultures.
As of this writing, the patient is awaiting Mohs surgery. He will have to be followed closely for at least a year to watch for any signs of metastasis. With an intact immune system, his prognosis is excellent.
Answer
Digital mucous cysts (choice “c”), also known as myxoid cysts, are quite common and are found often on fingers and occasionally on toes. But they are almost always located on the distal dorsal portion of the digit, between the cuticle and distal interphalangeal joint—close enough, in many cases, to compress the nail matrix, which leads to a longitudinal trough in the nail plate. Surface erosion of these lesions is unusual but is occasionally seen.
However, given the history, appearance, and especially the location of this patient’s lesion, this is the one diagnosis our patient almost certainly did not have. The others, discussed below, were all real possibilities, and since “common things occur commonly,” squamous cell carcinoma was the most likely.
Discussion
With this clinical picture, cancer is assumed until proven otherwise. In that regard, the presence of a longstanding wart in this location is especially significant, since human papillomavirus (HPV) is known to be potentially oncogenic. The patient’s heavily sun-damaged skin adds another layer of risk for malignant transformation.
The only way to sort through this differential diagnosis was to perform a shave biopsy, which confirmed the diagnosis of squamous cell carcinoma (SCC)—one that showed evidence of arising from a long-standing wart. The patient was referred for Mohs micrographic surgery, for two reasons: (1) this location does not lend itself to simple excision and closure, both because of the paucity of adjacent skin and because of the potential for damage to the underlying tendons, nerves, and blood supply, and (2) SCCs of nonsolar causation (besides HPV, these include ionizing radiation, arsenic, and chronic ulcers) have more potential for metastasis than do the far more common sun-caused SCCs. This is all the more reason to obtain adequate margins. Often in such cases, irradiation of the site is also done, postoperatively.
Had the biopsy not shown clear evidence of cancer, the other items in the differential diagnosis would have come into play. This would have necessitated an additional biopsy, this time to obtain tissue for acid-fast bacilli and bacterial and fungal cultures.
As of this writing, the patient is awaiting Mohs surgery. He will have to be followed closely for at least a year to watch for any signs of metastasis. With an intact immune system, his prognosis is excellent.

An 87-year-old man presents for evaluation of a lesion on his left fifth finger that has grown and become ulcerated in the past five months. There is almost no pain in the lesion, which the patient insists was a “wart” for the 40 years prior to these recent changes. Over the years, he has treated his wart with acids, curettement, and liquid nitrogen, to no effect. A recent seven-day course of cephalexin (500 mg tid) also failed to help. Additional history taking reveals that the patient is a farmer who spent his entire life working outdoors every day, year-round. There is no history of immunosuppression. His medications include metoprolol and hydrochlorothiazide. Closer inspection of the lesion reveals a 9-mm, centrally eroded nodule overlying the dorsal proximal interphalangeal joint. The lesion is quite firm on palpation, with a surface that looks and feels smooth and is nontender, with minimal redness. There are no palpable nodes in the epitrochlear or axillary locations. Elsewhere, the patient’s skin is remarkably sun-damaged, with numerous actinic keratoses, solar lentigines, and solar atrophy evident, especially on his hands.

A History of Palpitations and Dizziness
ANSWER
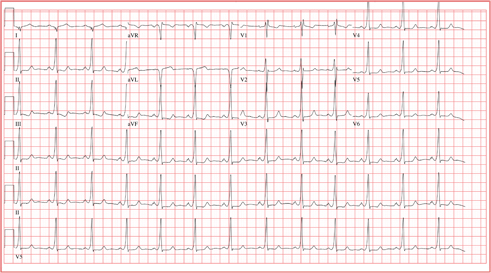
This ECG is diagnostic for Wolff-Parkinson-White (WPW) syndrome. Criteria for WPW syndrome include a normal P wave with a PR interval generally (but not always) of 0.12 sec (120 ms) or greater, initial slurring of the QRS (delta wave), a wide QRS interval > 0.10 sec (100 ms), and secondary ST/T wave changes.
In WPW syndrome, one (or multiple) accessory pathway between the atria and ventricles allows conduction impulses to bypass the atrioventricular node and activate the ventricles prematurely. This premature ventricular activation is responsible for the initial slurring of the QRS complex and produces the characteristic delta wave. The presence of an accessory pathway allows a reentrant tachycardia circuit to occur and is the source of this patient’s palpitations. Subsequent electrophysiology studies identified a single left lateral accessory pathway.
ANSWER
This ECG is diagnostic for Wolff-Parkinson-White (WPW) syndrome. Criteria for WPW syndrome include a normal P wave with a PR interval generally (but not always) of 0.12 sec (120 ms) or greater, initial slurring of the QRS (delta wave), a wide QRS interval > 0.10 sec (100 ms), and secondary ST/T wave changes.
In WPW syndrome, one (or multiple) accessory pathway between the atria and ventricles allows conduction impulses to bypass the atrioventricular node and activate the ventricles prematurely. This premature ventricular activation is responsible for the initial slurring of the QRS complex and produces the characteristic delta wave. The presence of an accessory pathway allows a reentrant tachycardia circuit to occur and is the source of this patient’s palpitations. Subsequent electrophysiology studies identified a single left lateral accessory pathway.
ANSWER
This ECG is diagnostic for Wolff-Parkinson-White (WPW) syndrome. Criteria for WPW syndrome include a normal P wave with a PR interval generally (but not always) of 0.12 sec (120 ms) or greater, initial slurring of the QRS (delta wave), a wide QRS interval > 0.10 sec (100 ms), and secondary ST/T wave changes.
In WPW syndrome, one (or multiple) accessory pathway between the atria and ventricles allows conduction impulses to bypass the atrioventricular node and activate the ventricles prematurely. This premature ventricular activation is responsible for the initial slurring of the QRS complex and produces the characteristic delta wave. The presence of an accessory pathway allows a reentrant tachycardia circuit to occur and is the source of this patient’s palpitations. Subsequent electrophysiology studies identified a single left lateral accessory pathway.

A 20-year-old woman is involved in a motor vehicle accident. Her car was hit from behind while stopped at a light, with the force of impact sufficient to deploy the airbags in both vehicles. When the paramedics arrive, the patient is conscious and responsive but is found to have a rapid pulse (approximately 170 beats/min). During transport to the hospital, her tachycardia abruptly terminates and sinus rhythm returns at rates between 80 and 90 beats/min. In the emergency department, the patient’s physical examination and x-rays reveal no injuries. Review of the rhythm strips from the paramedics in the field shows a narrow complex tachycardia at a rate of 176 beats/min. When interviewed, the patient reveals a history of palpitations, lasting from five minutes up to two hours, over the past several years. When they occur, she says, she gets dizzy and feels a pounding sensation in her chest, but she has never had chest pain or syncope. She cannot identify any specific trigger that initiates her palpitations, but has noticed that if she holds her breath and bears down (Valsalva maneuver), her palpitations will sometimes stop. Her medical history is positive for mild asthma and an allergy to peanuts. She is taking no medications and denies tobacco, alcohol, or recreational drug use. Family history is remarkable for hypertension (father) and type 2 diabetes (mother). She is the oldest of three children, and one of her sisters experiences similar bouts of palpitations. A 14-point review of systems is negative. She denies she could be pregnant; she is currently menstruating. She is 61” tall, weighs 110 lb, and is of small stature and body habitus. She is in no acute distress. Her blood pressure is 110/72 mm Hg; pulse, 80 beats/min and regular; and respiratory rate, 14 breaths/min. The physical exam is unremarkable, with the exception of abrasions on her hands and left forearm. Given the documentation of a tachycardia by the paramedics in the field and a history of recurring palpitations, an ECG is obtained, which reveals the following: a ventricular rate of 77 beats/min; PR interval, 128 ms; QRS duration, 116 ms; QT/QTc interval, 416/470 ms; P axis, 61°; R axis, 98°; and T axis, 5°. What is your interpretation of this ECG?
Rash Emerges After 18 Holes of Golf
ANSWER
The correct answer is golfer’s vasculitis (choice “d”), which favors older patients who spend extended periods on their feet in hot weather.
Schamberg’s disease (choice “a”), a type of capillaritis, presents with nonblanchable, true purpura that are classically described and seen as having a peculiar brown color (which has been called cinnamon or cayenne pepper).
Those who experience a true contact dermatitis (choice “b”) almost invariably itch and would most likely present with vesiculation of the skin surface.
Leukocytoclastic vasculitis (LCV; choice “c”) presents as a nonblanchable purpuric condition that, on biopsy, demonstrates classic findings of red blood cell (RBC) extravasation from venules damaged by neutrophils.
DISCUSSION
“Golfer’s vasculitis” has been described in nongolfers who are older and who have spent considerable time on their feet in hot weather. Fair-goers, amusement park patrons, and hikers are just as likely to develop it, but it was first studied in golfers—and at first, it was thought to represent a sensitivity to chemical grass treatment.
However, the lack of symptoms and vesiculation (blistering) suggested otherwise, and biopsies of the affected skin confirmed gravity-related hyperemia with mild extravasation of RBCs. They also failed to show any signs of contact dermatitis. The sharply defined linear inferior border of the rash is clearly caused by the compressive effects of socks, which prevent the leakage of RBCs.
The other items in the differential were rightly considered—particularly LCV, which can be associated with conditions such as hypersensitivity reactions to medications or can be a presenting sign of lupus and rheumatoid arthritis, among several other possibilities. But the key differentiating finding was the highly blanchable nature of this patient’s condition, in marked contrast to the nonblanchable, purpuric nature of classic LCV.
Often enough, blanchability is partial, or at least questionable, and a punch biopsy is necessary to clarify the picture. When histologic signs of LCV are found, blood work is necessary to rule out similar damage to “end organs,” such as kidneys and liver, as well as to attempt to establish the causative trigger.
ANSWER
The correct answer is golfer’s vasculitis (choice “d”), which favors older patients who spend extended periods on their feet in hot weather.
Schamberg’s disease (choice “a”), a type of capillaritis, presents with nonblanchable, true purpura that are classically described and seen as having a peculiar brown color (which has been called cinnamon or cayenne pepper).
Those who experience a true contact dermatitis (choice “b”) almost invariably itch and would most likely present with vesiculation of the skin surface.
Leukocytoclastic vasculitis (LCV; choice “c”) presents as a nonblanchable purpuric condition that, on biopsy, demonstrates classic findings of red blood cell (RBC) extravasation from venules damaged by neutrophils.
DISCUSSION
“Golfer’s vasculitis” has been described in nongolfers who are older and who have spent considerable time on their feet in hot weather. Fair-goers, amusement park patrons, and hikers are just as likely to develop it, but it was first studied in golfers—and at first, it was thought to represent a sensitivity to chemical grass treatment.
However, the lack of symptoms and vesiculation (blistering) suggested otherwise, and biopsies of the affected skin confirmed gravity-related hyperemia with mild extravasation of RBCs. They also failed to show any signs of contact dermatitis. The sharply defined linear inferior border of the rash is clearly caused by the compressive effects of socks, which prevent the leakage of RBCs.
The other items in the differential were rightly considered—particularly LCV, which can be associated with conditions such as hypersensitivity reactions to medications or can be a presenting sign of lupus and rheumatoid arthritis, among several other possibilities. But the key differentiating finding was the highly blanchable nature of this patient’s condition, in marked contrast to the nonblanchable, purpuric nature of classic LCV.
Often enough, blanchability is partial, or at least questionable, and a punch biopsy is necessary to clarify the picture. When histologic signs of LCV are found, blood work is necessary to rule out similar damage to “end organs,” such as kidneys and liver, as well as to attempt to establish the causative trigger.
ANSWER
The correct answer is golfer’s vasculitis (choice “d”), which favors older patients who spend extended periods on their feet in hot weather.
Schamberg’s disease (choice “a”), a type of capillaritis, presents with nonblanchable, true purpura that are classically described and seen as having a peculiar brown color (which has been called cinnamon or cayenne pepper).
Those who experience a true contact dermatitis (choice “b”) almost invariably itch and would most likely present with vesiculation of the skin surface.
Leukocytoclastic vasculitis (LCV; choice “c”) presents as a nonblanchable purpuric condition that, on biopsy, demonstrates classic findings of red blood cell (RBC) extravasation from venules damaged by neutrophils.
DISCUSSION
“Golfer’s vasculitis” has been described in nongolfers who are older and who have spent considerable time on their feet in hot weather. Fair-goers, amusement park patrons, and hikers are just as likely to develop it, but it was first studied in golfers—and at first, it was thought to represent a sensitivity to chemical grass treatment.
However, the lack of symptoms and vesiculation (blistering) suggested otherwise, and biopsies of the affected skin confirmed gravity-related hyperemia with mild extravasation of RBCs. They also failed to show any signs of contact dermatitis. The sharply defined linear inferior border of the rash is clearly caused by the compressive effects of socks, which prevent the leakage of RBCs.
The other items in the differential were rightly considered—particularly LCV, which can be associated with conditions such as hypersensitivity reactions to medications or can be a presenting sign of lupus and rheumatoid arthritis, among several other possibilities. But the key differentiating finding was the highly blanchable nature of this patient’s condition, in marked contrast to the nonblanchable, purpuric nature of classic LCV.
Often enough, blanchability is partial, or at least questionable, and a punch biopsy is necessary to clarify the picture. When histologic signs of LCV are found, blood work is necessary to rule out similar damage to “end organs,” such as kidneys and liver, as well as to attempt to establish the causative trigger.

When an asymptomatic rash appeared rather suddenly on both of her legs, a 54-year-old woman sought medical evaluation by her primary care provider. He diagnosed contact dermatitis and prescribed triamcinolone cream 0.1%. Forty-eight hours later, with no signs of improvement evident, the patient seeks and is granted a same-day appointment with dermatology. The patient denies any previous occurrences of such a rash and further denies having joint pain, fever, or malaise. She had not taken any new medications prior to the rash’s onset; furthermore, she only occasionally uses OTC medicines. A thorough history reveals that two days before the rash appeared, on one of the first hot days of the summer (with a temperature above 95°F), the woman played 18 holes of golf. The rash itself is strikingly red and affects both lower legs symmetrically, from mid-calf to just above the ankles. There, it ends abruptly with a linear, transverse border. There is no tenderness or increased warmth appreciated on palpation, nor is there any nodularity, vesiculation, or other disruption of the skin’s surface. Distinct, complete blanching is noted on firm digital palpation.

Severe Injury After Being Struck by a Car
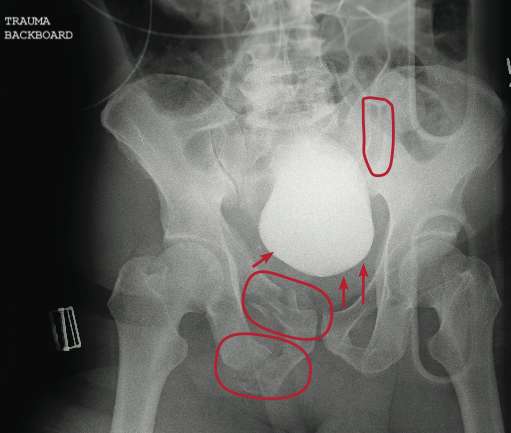
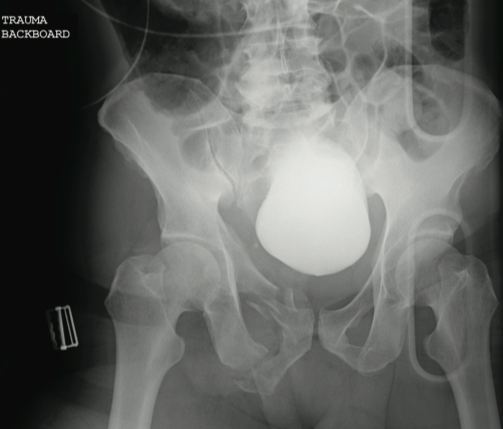
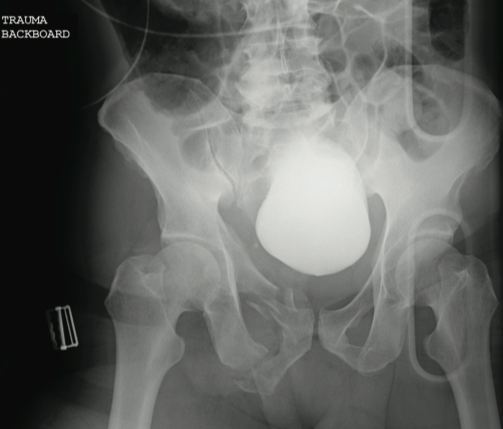
The radiograph reveals several findings. First, there are obvious displaced fractures of the right superior and inferior rami bones. There is also a diastatic fracture of the left sacroiliac joint.
Also, as the bladder is full of contrast (probably from a recent cystogram), note how it appears to be displaced to a more superior position than usual. This is second- ary to formation of a pelvic hematoma.
The radiograph reveals several findings. First, there are obvious displaced fractures of the right superior and inferior rami bones. There is also a diastatic fracture of the left sacroiliac joint.
Also, as the bladder is full of contrast (probably from a recent cystogram), note how it appears to be displaced to a more superior position than usual. This is second- ary to formation of a pelvic hematoma.
The radiograph reveals several findings. First, there are obvious displaced fractures of the right superior and inferior rami bones. There is also a diastatic fracture of the left sacroiliac joint.
Also, as the bladder is full of contrast (probably from a recent cystogram), note how it appears to be displaced to a more superior position than usual. This is second- ary to formation of a pelvic hematoma.
A 59-year-old man was struck by a car while walking. He was initially evaluated at another facility, intubated, resuscitated, and stabilized, then transferred to your facility. He is believed to have a severe head injury and possibly other internal injuries. The man is unresponsive on arrival at your facility. No medical history is available. His vital signs are stable, with a blood pressure of 113/74 mm Hg; heart rate, 101 beats/min; and respiratory rate, 14 breaths/min. Initial Glasgow Coma Scale score is reported as a 3T. It is unclear whether the patient has recently received any sedation. As you are reviewing the results of testing conducted at both your facility and the facility to which the patient was originally taken, you see a portable pelvic radiograph (shown). What is your impression?
Landscaper Can't Outrun Tree
ANSWER
The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
ANSWER
The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
ANSWER
The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.

A 24-year-old man who works as a landscaper/tree-cutter presents for evaluation of right shoulder pain after a tree fell on him. He states that he attempted to run away as the tree fell, but it struck him nonetheless. He did not lose consciousness. The tree struck the right side of his body. The patient’s medical history is unremarkable. He is complaining of right-side back and shoulder pain. Initial vital signs and primary survey appear to be normal. Secondary survey shows decreased range of motion in the right shoulder, with point tenderness in the scapula. There are no obvious deformities. Distal pulses are strong, and the patient is otherwise neurovascularly intact. Radiograph of the right shoulder is shown. What is your impression?

Landscaper Can't Outrun Tree
ANSWER
The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
ANSWER
The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
ANSWER
The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
A 24-year-old man who works as a landscaper/tree-cutter presents for evaluation of right shoulder pain after a tree fell on him. He states that he attempted to run away as the tree fell, but it struck him nonetheless. He did not lose consciousness. The tree struck the right side of his body. The patient’s medical history is unremarkable. He is complaining of right-side back and shoulder pain. Initial vital signs and primary survey appear to be normal. Secondary survey shows decreased range of motion in the right shoulder, with point tenderness in the scapula. There are no obvious deformities. Distal pulses are strong, and the patient is otherwise neurovascularly intact. Radiograph of the right shoulder is shown. What is your impression?

Spreading Lesions on Sun-damaged Skin
ANSWER
The correct answer is idiopathic guttate hypomelanosis (choice “d”), a common condition primarily seen on sun-damaged patients, but often mistaken for tinea versicolor (choice “b”).
Vitiligo (choice “a”) can present with “confetti” lesions, but would more likely lead to complete loss of pigment in most of the lesions, not the partial loss seen in this patient. Biopsy is indicated in questionable cases.
Tinea versicolor, equally common, is caused by a commensal yeast called Malassezia furfur that feeds on sebum, which is why it favors the oily parts of the body (back and chest, primarily). It is almost never seen on the legs, which have the fewest oil glands on the body. In addition, tinea versicolor is, by its nature, an epidermal process, leading to the formation of a fine KOH-positive scale.
Since lupus (choice “c”) is a form of vasculitis, the associated inflammation can lead to pigment loss, especially in darker-skinned patients. Without a more likely explanation for these lesions, a biopsy might well have been indicated.
DISCUSSION
Biopsy might have suggested any number of other diseases that can also present with hypomelanosis, such as cutaneous T-cell lymphoma or sarcoid. But idiopathic guttate hypomelanosis is far more common, and the patient’s age, gender, and history of chronic UV damage all lend themselves perfectly to this diagnosis.
Idiopathic guttate hypomelanosis, for unknown reasons, tends to appear in women at earlier ages than in men (usually about a decade younger). For either gender, treatment is problematic once the lesions have fully developed. Early in the process, the obvious remedy is better sun protection. Lasers, retinoids, liquid nitrogen, and anti-inflammatory creams have all been tried with little success.
ANSWER
The correct answer is idiopathic guttate hypomelanosis (choice “d”), a common condition primarily seen on sun-damaged patients, but often mistaken for tinea versicolor (choice “b”).
Vitiligo (choice “a”) can present with “confetti” lesions, but would more likely lead to complete loss of pigment in most of the lesions, not the partial loss seen in this patient. Biopsy is indicated in questionable cases.
Tinea versicolor, equally common, is caused by a commensal yeast called Malassezia furfur that feeds on sebum, which is why it favors the oily parts of the body (back and chest, primarily). It is almost never seen on the legs, which have the fewest oil glands on the body. In addition, tinea versicolor is, by its nature, an epidermal process, leading to the formation of a fine KOH-positive scale.
Since lupus (choice “c”) is a form of vasculitis, the associated inflammation can lead to pigment loss, especially in darker-skinned patients. Without a more likely explanation for these lesions, a biopsy might well have been indicated.
DISCUSSION
Biopsy might have suggested any number of other diseases that can also present with hypomelanosis, such as cutaneous T-cell lymphoma or sarcoid. But idiopathic guttate hypomelanosis is far more common, and the patient’s age, gender, and history of chronic UV damage all lend themselves perfectly to this diagnosis.
Idiopathic guttate hypomelanosis, for unknown reasons, tends to appear in women at earlier ages than in men (usually about a decade younger). For either gender, treatment is problematic once the lesions have fully developed. Early in the process, the obvious remedy is better sun protection. Lasers, retinoids, liquid nitrogen, and anti-inflammatory creams have all been tried with little success.
ANSWER
The correct answer is idiopathic guttate hypomelanosis (choice “d”), a common condition primarily seen on sun-damaged patients, but often mistaken for tinea versicolor (choice “b”).
Vitiligo (choice “a”) can present with “confetti” lesions, but would more likely lead to complete loss of pigment in most of the lesions, not the partial loss seen in this patient. Biopsy is indicated in questionable cases.
Tinea versicolor, equally common, is caused by a commensal yeast called Malassezia furfur that feeds on sebum, which is why it favors the oily parts of the body (back and chest, primarily). It is almost never seen on the legs, which have the fewest oil glands on the body. In addition, tinea versicolor is, by its nature, an epidermal process, leading to the formation of a fine KOH-positive scale.
Since lupus (choice “c”) is a form of vasculitis, the associated inflammation can lead to pigment loss, especially in darker-skinned patients. Without a more likely explanation for these lesions, a biopsy might well have been indicated.
DISCUSSION
Biopsy might have suggested any number of other diseases that can also present with hypomelanosis, such as cutaneous T-cell lymphoma or sarcoid. But idiopathic guttate hypomelanosis is far more common, and the patient’s age, gender, and history of chronic UV damage all lend themselves perfectly to this diagnosis.
Idiopathic guttate hypomelanosis, for unknown reasons, tends to appear in women at earlier ages than in men (usually about a decade younger). For either gender, treatment is problematic once the lesions have fully developed. Early in the process, the obvious remedy is better sun protection. Lasers, retinoids, liquid nitrogen, and anti-inflammatory creams have all been tried with little success.

A few years ago, a woman first noticed lesions developing on her legs. The patient sought care from her primary care provider; however, despite a number of treatment regimens, including topical clotrimazole and terbinafine creams, the lesions have not only failed to resolve but have also grown in number and spread to other areas of her body. The woman, now 48, is referred to dermatology for evaluation of her persistent but asymptomatic condition. The patient claims that her health is otherwise excellent, although she has seasonal allergies, was a long-time smoker until two months ago, and has just begun estrogen replacement therapy. She is especially concerned that the lesions have started to appear on the skin of her abdomen. She specifically denies shortness of breath, joint pain, fever, unexplained weight loss, or cough. An examination of her skin reveals a multitude of 2- to 6-mm partially depigmented, roughly round macules uniformly distributed on her legs, arms, and trunk. The lesions, which average about 3 mm, have no palpable component and no observable scale or underlying induration. There is a concentration of them on the anterior tibial areas, as well as on the dorsal forearms; however, none are seen on her face, and the volar surfaces of her forearms are almost completely spared. Significantly, the patient’s exposed skin is tremendously sun-damaged, evidenced by a deep brown color and a weathered, wrinkled look, with many telangiectasias and brown to tan–orange macules on her face.

Infant "Fell Out of Car Seat"
ANSWER
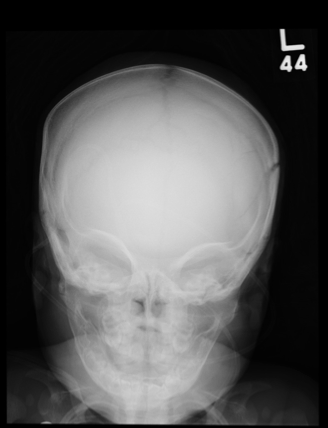
The plain film demonstrates bilateral parietal skull fractures, more evident on the left than right side. Subsequent noncontrast CT of the skull confirmed these fractures, and also showed bilateral subdural hematomas.
Such findings, both clinically and radiographically, are highly worrisome and suggestive of nonaccidental injury (ie, abuse). This unfortunate infant was placed immediately under the care of the Department of Family and Children Services and moved to the pediatric ICU for close monitoring.
ANSWER
The plain film demonstrates bilateral parietal skull fractures, more evident on the left than right side. Subsequent noncontrast CT of the skull confirmed these fractures, and also showed bilateral subdural hematomas.
Such findings, both clinically and radiographically, are highly worrisome and suggestive of nonaccidental injury (ie, abuse). This unfortunate infant was placed immediately under the care of the Department of Family and Children Services and moved to the pediatric ICU for close monitoring.
ANSWER
The plain film demonstrates bilateral parietal skull fractures, more evident on the left than right side. Subsequent noncontrast CT of the skull confirmed these fractures, and also showed bilateral subdural hematomas.
Such findings, both clinically and radiographically, are highly worrisome and suggestive of nonaccidental injury (ie, abuse). This unfortunate infant was placed immediately under the care of the Department of Family and Children Services and moved to the pediatric ICU for close monitoring.
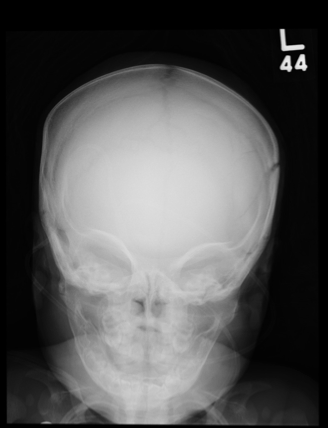
A 5-month-old girl is brought to your facility for decreased level of consciousness. According to the parents, the infant reportedly fell out of her car seat earlier this morning. Prenatal history is unremarkable; immunizations are up to date. Initial examination shows a lethargic female infant with vital signs as follows: temperature, 99.7°F; blood pressure, 91/65 mm Hg; heart rate; 180 beats/min; and initial O2 saturation, 86% on room air. Supplemental oxygen and an IV fluid bolus are given, which correct the hypoxia and tachycardia. Physical exam shows a depressed anterior fontanelle and bilateral periorbital ecchymosis, as well as multiple bruises of varying ages on the face and body. An old scar on the left side of the forehead is noted as well. While still somewhat lethargic, the infant does move all extremities to painful stimuli. A weak cry is present. Initial radiographs of the chest and skull are obtained; the one of the skull is shown. What is your impression?
It "Must" Be a Fungal Infection—Right?
ANSWER
The correct answer is ED&C (choice “a”); see below for discussion. Imiquimod cream (choice “b”) is indicated in such cases, although it is not without shortcomings as a treatment choice (more information below).
Given the size of the lesion, one could argue that two-stage excision (choice “c”), in which two-thirds of the lesion is removed initially, the wound allowed to heal, then the rest of the lesion removed later, would be a good option. Again, however, it is not perfect.
Mohs surgery (choice “d”) is the only option offered that takes care of the entire lesion in one step, with microscopically controlled margins to ensure complete removal and primary closure all in one session.
DISCUSSION
There are at least five types of BCC; of these, the superficial BCC is the one that looks the least like a skin cancer. The back is one of the more common areas for a BCC to appear, where it is often mistaken for fungal infection. The latter condition is actually quite uncommon on the back; furthermore, this patient had no particular reason to be exposed to such an organism or to be susceptible to it. Lack of response to treatment for fungal infection was further evidence against such a diagnosis.
Knowing that BCCs can look like this is a priceless piece of information. Corroboration for the diagnosis of this sun-caused skin cancer comes readily from the presence of sun damage elsewhere on the skin. Superficial BCCs are so common that biopsy is often unnecessary, although insurance providers frequently require it before excision can be done.
ED&C, a perfectly acceptable mode of treatment for many minor BCCs, is not a good choice in this area and with a lesion of this size, as it is likely to produce a large, nonhealing, raw wound covered by inappropriate granulation (so-called pyogenic granuloma).
Treatment with imiquimod cream, two to four times a week for at least a month, has the potential to be curative, but involves the creation of a large oozing site while it’s working. Even after several months’ treatment on a lesion of this size, biopsies may still be necessary to check for residual cancer. In selected patients and lesions, cases in which surgery is problematic, imiquimod can be an excellent treatment choice.
Two-stage excision does ensure the complete removal of the lesion but has the obvious disadvantage of taking several weeks and requiring two surgery sessions.
Even if the patient is sent for Mohs surgery, closure will be problematic with a lesion this size and in this keloid-prone area.
But job #1 in such cases is to make a correct diagnosis, then select from among the various treatment choices. Without a biopsy, that diagnosis is uncertain. But without the suspicion of BCC, biopsy may not appear to be indicated.
ANSWER
The correct answer is ED&C (choice “a”); see below for discussion. Imiquimod cream (choice “b”) is indicated in such cases, although it is not without shortcomings as a treatment choice (more information below).
Given the size of the lesion, one could argue that two-stage excision (choice “c”), in which two-thirds of the lesion is removed initially, the wound allowed to heal, then the rest of the lesion removed later, would be a good option. Again, however, it is not perfect.
Mohs surgery (choice “d”) is the only option offered that takes care of the entire lesion in one step, with microscopically controlled margins to ensure complete removal and primary closure all in one session.
DISCUSSION
There are at least five types of BCC; of these, the superficial BCC is the one that looks the least like a skin cancer. The back is one of the more common areas for a BCC to appear, where it is often mistaken for fungal infection. The latter condition is actually quite uncommon on the back; furthermore, this patient had no particular reason to be exposed to such an organism or to be susceptible to it. Lack of response to treatment for fungal infection was further evidence against such a diagnosis.
Knowing that BCCs can look like this is a priceless piece of information. Corroboration for the diagnosis of this sun-caused skin cancer comes readily from the presence of sun damage elsewhere on the skin. Superficial BCCs are so common that biopsy is often unnecessary, although insurance providers frequently require it before excision can be done.
ED&C, a perfectly acceptable mode of treatment for many minor BCCs, is not a good choice in this area and with a lesion of this size, as it is likely to produce a large, nonhealing, raw wound covered by inappropriate granulation (so-called pyogenic granuloma).
Treatment with imiquimod cream, two to four times a week for at least a month, has the potential to be curative, but involves the creation of a large oozing site while it’s working. Even after several months’ treatment on a lesion of this size, biopsies may still be necessary to check for residual cancer. In selected patients and lesions, cases in which surgery is problematic, imiquimod can be an excellent treatment choice.
Two-stage excision does ensure the complete removal of the lesion but has the obvious disadvantage of taking several weeks and requiring two surgery sessions.
Even if the patient is sent for Mohs surgery, closure will be problematic with a lesion this size and in this keloid-prone area.
But job #1 in such cases is to make a correct diagnosis, then select from among the various treatment choices. Without a biopsy, that diagnosis is uncertain. But without the suspicion of BCC, biopsy may not appear to be indicated.
ANSWER
The correct answer is ED&C (choice “a”); see below for discussion. Imiquimod cream (choice “b”) is indicated in such cases, although it is not without shortcomings as a treatment choice (more information below).
Given the size of the lesion, one could argue that two-stage excision (choice “c”), in which two-thirds of the lesion is removed initially, the wound allowed to heal, then the rest of the lesion removed later, would be a good option. Again, however, it is not perfect.
Mohs surgery (choice “d”) is the only option offered that takes care of the entire lesion in one step, with microscopically controlled margins to ensure complete removal and primary closure all in one session.
DISCUSSION
There are at least five types of BCC; of these, the superficial BCC is the one that looks the least like a skin cancer. The back is one of the more common areas for a BCC to appear, where it is often mistaken for fungal infection. The latter condition is actually quite uncommon on the back; furthermore, this patient had no particular reason to be exposed to such an organism or to be susceptible to it. Lack of response to treatment for fungal infection was further evidence against such a diagnosis.
Knowing that BCCs can look like this is a priceless piece of information. Corroboration for the diagnosis of this sun-caused skin cancer comes readily from the presence of sun damage elsewhere on the skin. Superficial BCCs are so common that biopsy is often unnecessary, although insurance providers frequently require it before excision can be done.
ED&C, a perfectly acceptable mode of treatment for many minor BCCs, is not a good choice in this area and with a lesion of this size, as it is likely to produce a large, nonhealing, raw wound covered by inappropriate granulation (so-called pyogenic granuloma).
Treatment with imiquimod cream, two to four times a week for at least a month, has the potential to be curative, but involves the creation of a large oozing site while it’s working. Even after several months’ treatment on a lesion of this size, biopsies may still be necessary to check for residual cancer. In selected patients and lesions, cases in which surgery is problematic, imiquimod can be an excellent treatment choice.
Two-stage excision does ensure the complete removal of the lesion but has the obvious disadvantage of taking several weeks and requiring two surgery sessions.
Even if the patient is sent for Mohs surgery, closure will be problematic with a lesion this size and in this keloid-prone area.
But job #1 in such cases is to make a correct diagnosis, then select from among the various treatment choices. Without a biopsy, that diagnosis is uncertain. But without the suspicion of BCC, biopsy may not appear to be indicated.

A 50-year-old man has had a nonhealing but otherwise asymptomatic lesion on his back for more than three years. The lesion has slowly grown, despite the use of a number of treatments, including OTC and prescription antifungal creams and OTC steroid creams. The consensus from his primary care providers is that this must represent some form of fungal infection, although they are at a loss to explain why it has not responded to treatment for that condition. The patient presents to dermatology because his wife insisted on referral to a specialist when the lesion finally became focally eroded around its margins. Further history taking reveals that there are no pets or children at home, there is no personal history of atopy, and the patient has never worked with livestock. For 30 years, he worked outdoors for the power company, but he is now assigned to a desk job. He is not immunosuppressed, and his only medication is for hypertension. During the physical examination, you observe an arciform, faintly and focally eroded border surrounding a 5-cm pink patch on the patient’s left upper back. Closer inspection reveals prominent pilosebaceous units confined by well-defined borders, with a background of uniformly atrophic, glassy-looking telangiectatic skin. No scale is seen on or around the lesion. Elsewhere, you see a moderate number of solar lentigines across the patient’s shoulders and note that his posterior neck has a deeply lined appearance. The rest of his trunk and face have similar lesions, although none is especially worrisome. To confirm your clinical suspicions, you perform a shave biopsy on the central portion of the lesion, which shows superficial basal cell carcinoma (BCC). Treatment options are then discussed at length with the patient.

Postoperative Patient Experiencing Respiratory Distress
ANSWER
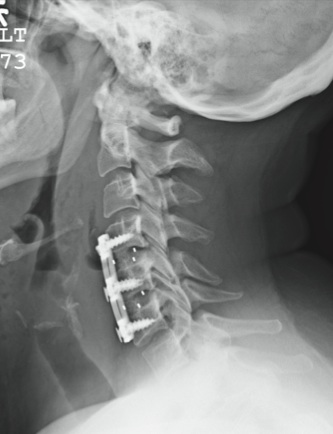
The patient is status post two-level anterior cervical diskectomy and fusion, with interbody grafts and hardware appearing intact. The radiograph demonstrates significant prevertebral soft-tissue swelling greater than 2 cm over several levels. This results in significant posterior compression of the oropharynx. Such findings are typically seen in patients who develop retropharyngeal hematomas.
This patient was urgently returned to the operating room, where she underwent successful evacuation of a hematoma that was under a moderate amount of pressure. No specific source was identified, which is not uncommon.
The patient made a full recovery.
ANSWER
The patient is status post two-level anterior cervical diskectomy and fusion, with interbody grafts and hardware appearing intact. The radiograph demonstrates significant prevertebral soft-tissue swelling greater than 2 cm over several levels. This results in significant posterior compression of the oropharynx. Such findings are typically seen in patients who develop retropharyngeal hematomas.
This patient was urgently returned to the operating room, where she underwent successful evacuation of a hematoma that was under a moderate amount of pressure. No specific source was identified, which is not uncommon.
The patient made a full recovery.
ANSWER
The patient is status post two-level anterior cervical diskectomy and fusion, with interbody grafts and hardware appearing intact. The radiograph demonstrates significant prevertebral soft-tissue swelling greater than 2 cm over several levels. This results in significant posterior compression of the oropharynx. Such findings are typically seen in patients who develop retropharyngeal hematomas.
This patient was urgently returned to the operating room, where she underwent successful evacuation of a hematoma that was under a moderate amount of pressure. No specific source was identified, which is not uncommon.
The patient made a full recovery.
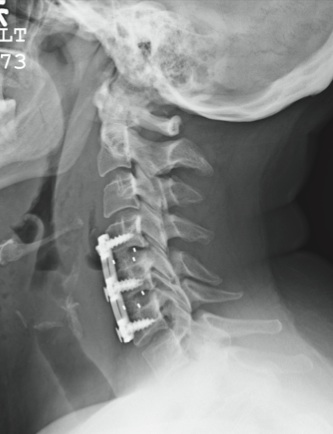
You receive a call from the nursing staff stating that a postoperative patient is experiencing respiratory distress. The patient is a 41-year-old woman who underwent a two-level anterior cervical diskectomy and fusion yesterday. There were no problems during the surgery. Earlier this morning, when the patient was examined during rounds, she was experiencing mild dysphagia, and steroids were ordered. Now, the patient says she cannot breathe well unless she is sitting upright. Her vital signs are stable, with an O2 saturation of 93%. Her incision is swollen and appears full. Stat radiograph of the cervical spine is obtained (shown). What is your impression?