User login
The Rising Tide of Atrial Fibrillation: Is Primary Care Ready?
The incidence of atrial fibrillation (AF) is on the rise, and recent joint guidelines from the American College of Cardiology and American Heart Association (ACC/AHA) stress the role of primary care clinicians in prevention and management.
One in three White and one in five Black Americans will develop AF in their lifetime, and the projected number of individuals diagnosed with AF in the United States is expected to double by 2050.
Cardiologists who spoke to Medscape Medical News said primary care clinicians can help control AF by focusing on diabetes and hypertension, along with lifestyle factors such as diet, exercise, and alcohol intake.
“It’s not just a rhythm abnormality, but a complex disease that needs to be addressed in a multidisciplinary, holistic way,” said Jose Joglar, MD, a professor in the Department of Internal Medicine at the UT Southwestern Medical Center in Dallas and lead author of the guidelines.
Joglar said primary care clinicians can play an important role in counseling on lifestyle changes for patients with the most common etiologies such as poorly controlled hypertension, diabetes, and obesity.
The Primary Care Physicians ABCs: Risk Factors and Comorbidities
“As a primary care physician or as a cardiologist, I often think that if I do these things, I’m going to help with a lot of conditions, not just atrial fibrillation,” said Manesh Patel, MD, chief of the Divisions of Cardiology and Clinical Pharmacology at the Duke University School of Medicine in Durham, North Carolina.
Lifestyle choices such as sleeping habits can play a big part in AF outcomes. Although the guidelines specifically address obstructive sleep apnea as a risk factor, he said more data are needed on the effect of sleep hygiene — getting 8 hours of sleep a night — a goal few people attain.
“What we do know is people that can routinely try to go to sleep and sleep with some regularity seem to have less cardiovascular risk,” Patel said.
Although existing data are limited, literature reviews have found evidence that sleep disruptions, sleep duration, circadian rhythm, and insomnia are associated with heart disease, independent of obstructive sleep apnea.
Use of alcohol should also be discussed with patients, as many are unaware of the effects of the drug on cardiovascular disease, said Joglar, who is also the program director of the Clinical Cardiac Electrophysiology Fellowship program at the UT Southwestern Medical Center.
“Doctors can inform the patient that this is not a judgment call but simple medical fact,” he said.
Joglar also said many physicians need to become educated on a common misconception.
“Every time a patient develops palpitations or atrial fibrillation, the first thing every patient tells me is, I quit drinking coffee,” Joglar said.
However, as the guidelines point out, the link between caffeine and AF is uncertain at best.
Preventing AF
A newer class of drugs may help clinicians manage comorbidities that contribute to AF, such as hypertension, sleep apnea, and obesity, said John Mandrola, MD, an electrophysiologist in Louisville, Kentucky, who hosts This Week in Cardiology on Medscape.
Although originally approved for treatment of diabetes, sodium-glucose cotransporter-2 inhibitors are also approved for management of heart failure. Mandrola started prescribing these drugs 2 years ago for patients, given the links of both conditions with AF.
“I think the next frontier for us in cardiology and AF management will be the GLP-1 agonists,” Mandrola said. He hasn’t started prescribing these drugs for his patients yet but said they will likely play a role in the management of patients with AF with the common constellation of comorbidities such as obesity, hypertension, and sleep apnea.
“The GLP-1 agonists have a really good chance of competing with AF ablation for rhythm control over the long term,” he said.
Decisions, Decisions: Stroke Risk Scoring Systems
The risk for stroke varies widely among patients with AF, so primary care clinicians can pick among several scoring systems to estimate the risk for stroke and guide the decision on whether to initiate anticoagulation therapy.
The ACC/AHA guidelines do not state a preference for a particular instrument. The Congestive heart failure, Hypertension, Age, Diabetes mellitus, Stroke, Vascular disease, Sex (CHA2DS2-VASc) score is the most widely used and validated instrument, Joglar said. He usually recommends anticoagulation if the CHA2DS2-VASc score is > 2, dependent on individual patient factors.
“If you have a CHA2DS2-VASc score of 1, and you only had one episode of AF for a few hours a year ago, then your risk of stroke is not as high as somebody who has a score of 1 but has more frequent or persistent AF,” Joglar said.
None of the systems is perfect at predicting risk for stroke, so clinicians should discuss options with patients.
“The real message is, are you talking about the risk of stroke and systemic embolism to your patient, so that the patient understands that risk?” he said.
Patel also said measuring creatine clearance can be analogous to using an instrument like CHA2DS2-VASc.
“I often think about renal disease as a very good risk marker and something that does elevate your risk,” he said.
Which Anticoagulant?
Although the ACC/AHA guidelines still recommend warfarin for patients with AF with mechanical heart valves or moderate to severe rheumatic fever, direct oral anticoagulants (DOACs) are the first-line therapy for all other patients with AF.
In terms of which DOACs to use, the differences are subtle, according to Patel.
“I don’t know that they’re that different from each other,” he said. “All of the new drugs are better than warfarin by far.”
Patel pointed out that dabigatran at 150 mg is the only DOAC shown to reduce the incidence of ischemic stroke. For patients with renal dysfunction, he has a slight preference for a 15-mg dose of rivaroxaban.
Mandrola said he mainly prescribes apixaban and rivaroxaban, the latter of which requires only once a day dosing.
“We stopped using dabigatran because 10% of people get gastrointestinal upset,” he said.
Although studies suggest aspirin is less effective than either warfarin or DOACs for the prevention of stroke, Joglar said he still sees patients who come to him after being prescribed low-dose aspirin from primary care clinicians.
“We made it very clear that it should not be recommended just for mitigating stroke risk in atrial fibrillation,” Joglar said. “You could use it if the patient has another indication, such as a prior heart attack.”
Does My Patient Have to Be in Normal Sinus Rhythm?
The new guidelines present evidence maintaining sinus rhythm should be favored over controlling heart rate for managing AF.
“We’ve focused on rhythm control as a better strategy, especially catheter ablation, which seems to be particularly effective in parallel to lifestyle interventions and management of comorbidities,” Joglar said. Rhythm control is of particular benefit for patients with AF triggered by heart failure. Control of rhythm in these patients has been shown to improve multiple outcomes such as ejection fraction, symptoms, and survival.
Patel said as a patient’s symptoms increase, the more likely a clinician will be able to control sinus rhythm. Some patients do not notice their arrhythmia, but others feel dizzy or have chest pain.
“The less symptomatic the patient is, the more likely they’re going to tolerate it, especially if they’re older, and it’s hard to get them into sinus rhythm,” Patel said.
When to Refer for Catheter Ablation?
The new guidelines upgraded the recommendation for catheter ablation to class I (strong recommendation) for patients with symptomatic AF in whom anti-arrhythmic therapy is unsuccessful, not tolerated, or contraindicated; patients with symptomatic paroxysmal AF (typically younger patients with few comorbidities); and patients with symptomatic or clinically significant atrial flutter. The previous iteration recommended trying drug therapy first.
Multiple randomized clinical trials have demonstrated the effectiveness of catheter ablation.
“In somebody who is younger, with a healthy heart, the 1-year success rate of the procedure might be about 70%,” Joglar said. While 70% of patients receiving a catheter have no AF episodes in the following year, Joglar said 20%-25% of those who do have recurrences will experience fewer or shorter episodes.
Conversations about rate vs rhythm control and whether to pursue catheter ablation often come down to preference, Patel said. He would tend to intervene earlier using ablation in patients with heart failure or those experiencing symptoms of AF who cannot be controlled with a heart rate < 100 beats/min.
But he said he prefers using medication for rate control in many of his patients who are older, have chronic AF, and do not have heart failure.
Mandrola takes a more conservative approach, reserving catheter ablation for patients in whom risk factor management and anti-arrhythmic drugs have not been successful.
“In my hospital, it’s done for patients who have symptomatic AF that’s really impacting their quality of life,” he said. But for those with fewer symptoms, his advice is to provide education, reassurance, and time because AF can resolve on its own.
What About Data From Implantables and Wearables?
The guidelines provide an algorithm for when to treat non-symptomatic atrial high-rate episodes detected by a cardiovascular implantable electronic device such as a pacemaker or defibrillator. Episodes less than 5 minutes can be ignored, while treatment could be considered for those with episodes lasting 5 minutes up to 24 hours with a CHA2DS2-VASc score ≥ 3, or lasting longer than 24 hours with a CHA2DS2-VASc score ≥ 2.
But whether anticoagulation improves outcomes is unclear.
“That is a $64,000 question,” Mandrola said. “I would bet every day I get a notification in the electronic health record that says Mr. Smith had 2 hours of AFib 2 weeks ago.”
He also hears from patients who report their Apple Watch has detected an episode of AF.
Mandrola cited evidence from two recent studies of patients who had an atrial high-rate episode longer than 6 minutes detected by implantable devices. The NOAH-AFNET 6 trial randomized patients over 65 years with one or more risk factors for stroke to receive a DOAC or placebo, while the ARTESIA trial used similar inclusion criteria to assign patients to receive either DOAC or aspirin. Both studies reported modest reductions in stroke that were outweighed by a higher incidence of major bleeding in the group receiving anticoagulation.
Shared decision-making should play a role in deciding how aggressively to treat episodes of AF detected by implantable or wearable devices.
He said some patients fear having a stroke, while others are adamantly opposed to taking an anticoagulant.
For patients who present with a documented episode of AF but who otherwise have no symptoms, Patel said clinicians should consider risk for stroke and frequency and duration of episodes.
“One way clinicians should be thinking about it is, the more risk factors they have, the lower burden of AF I need to treat,” Patel said. Even for patients who are having only short episodes of AF, he has a low threshold for recommending an anticoagulation drug if the patient’s CHA2DS2-VASc score is high.
Patel reported research grants from Bayer, Novartis, Idorsia, NHLBI, and Janssen Pharmaceuticals and served as a consultant on the advisory boards of Bayer, Janssen Pharmaceuticals, and Esperion Therapeutics.
Joglar and Mandrola had no disclosures.
A version of this article appeared on Medscape.com.
The incidence of atrial fibrillation (AF) is on the rise, and recent joint guidelines from the American College of Cardiology and American Heart Association (ACC/AHA) stress the role of primary care clinicians in prevention and management.
One in three White and one in five Black Americans will develop AF in their lifetime, and the projected number of individuals diagnosed with AF in the United States is expected to double by 2050.
Cardiologists who spoke to Medscape Medical News said primary care clinicians can help control AF by focusing on diabetes and hypertension, along with lifestyle factors such as diet, exercise, and alcohol intake.
“It’s not just a rhythm abnormality, but a complex disease that needs to be addressed in a multidisciplinary, holistic way,” said Jose Joglar, MD, a professor in the Department of Internal Medicine at the UT Southwestern Medical Center in Dallas and lead author of the guidelines.
Joglar said primary care clinicians can play an important role in counseling on lifestyle changes for patients with the most common etiologies such as poorly controlled hypertension, diabetes, and obesity.
The Primary Care Physicians ABCs: Risk Factors and Comorbidities
“As a primary care physician or as a cardiologist, I often think that if I do these things, I’m going to help with a lot of conditions, not just atrial fibrillation,” said Manesh Patel, MD, chief of the Divisions of Cardiology and Clinical Pharmacology at the Duke University School of Medicine in Durham, North Carolina.
Lifestyle choices such as sleeping habits can play a big part in AF outcomes. Although the guidelines specifically address obstructive sleep apnea as a risk factor, he said more data are needed on the effect of sleep hygiene — getting 8 hours of sleep a night — a goal few people attain.
“What we do know is people that can routinely try to go to sleep and sleep with some regularity seem to have less cardiovascular risk,” Patel said.
Although existing data are limited, literature reviews have found evidence that sleep disruptions, sleep duration, circadian rhythm, and insomnia are associated with heart disease, independent of obstructive sleep apnea.
Use of alcohol should also be discussed with patients, as many are unaware of the effects of the drug on cardiovascular disease, said Joglar, who is also the program director of the Clinical Cardiac Electrophysiology Fellowship program at the UT Southwestern Medical Center.
“Doctors can inform the patient that this is not a judgment call but simple medical fact,” he said.
Joglar also said many physicians need to become educated on a common misconception.
“Every time a patient develops palpitations or atrial fibrillation, the first thing every patient tells me is, I quit drinking coffee,” Joglar said.
However, as the guidelines point out, the link between caffeine and AF is uncertain at best.
Preventing AF
A newer class of drugs may help clinicians manage comorbidities that contribute to AF, such as hypertension, sleep apnea, and obesity, said John Mandrola, MD, an electrophysiologist in Louisville, Kentucky, who hosts This Week in Cardiology on Medscape.
Although originally approved for treatment of diabetes, sodium-glucose cotransporter-2 inhibitors are also approved for management of heart failure. Mandrola started prescribing these drugs 2 years ago for patients, given the links of both conditions with AF.
“I think the next frontier for us in cardiology and AF management will be the GLP-1 agonists,” Mandrola said. He hasn’t started prescribing these drugs for his patients yet but said they will likely play a role in the management of patients with AF with the common constellation of comorbidities such as obesity, hypertension, and sleep apnea.
“The GLP-1 agonists have a really good chance of competing with AF ablation for rhythm control over the long term,” he said.
Decisions, Decisions: Stroke Risk Scoring Systems
The risk for stroke varies widely among patients with AF, so primary care clinicians can pick among several scoring systems to estimate the risk for stroke and guide the decision on whether to initiate anticoagulation therapy.
The ACC/AHA guidelines do not state a preference for a particular instrument. The Congestive heart failure, Hypertension, Age, Diabetes mellitus, Stroke, Vascular disease, Sex (CHA2DS2-VASc) score is the most widely used and validated instrument, Joglar said. He usually recommends anticoagulation if the CHA2DS2-VASc score is > 2, dependent on individual patient factors.
“If you have a CHA2DS2-VASc score of 1, and you only had one episode of AF for a few hours a year ago, then your risk of stroke is not as high as somebody who has a score of 1 but has more frequent or persistent AF,” Joglar said.
None of the systems is perfect at predicting risk for stroke, so clinicians should discuss options with patients.
“The real message is, are you talking about the risk of stroke and systemic embolism to your patient, so that the patient understands that risk?” he said.
Patel also said measuring creatine clearance can be analogous to using an instrument like CHA2DS2-VASc.
“I often think about renal disease as a very good risk marker and something that does elevate your risk,” he said.
Which Anticoagulant?
Although the ACC/AHA guidelines still recommend warfarin for patients with AF with mechanical heart valves or moderate to severe rheumatic fever, direct oral anticoagulants (DOACs) are the first-line therapy for all other patients with AF.
In terms of which DOACs to use, the differences are subtle, according to Patel.
“I don’t know that they’re that different from each other,” he said. “All of the new drugs are better than warfarin by far.”
Patel pointed out that dabigatran at 150 mg is the only DOAC shown to reduce the incidence of ischemic stroke. For patients with renal dysfunction, he has a slight preference for a 15-mg dose of rivaroxaban.
Mandrola said he mainly prescribes apixaban and rivaroxaban, the latter of which requires only once a day dosing.
“We stopped using dabigatran because 10% of people get gastrointestinal upset,” he said.
Although studies suggest aspirin is less effective than either warfarin or DOACs for the prevention of stroke, Joglar said he still sees patients who come to him after being prescribed low-dose aspirin from primary care clinicians.
“We made it very clear that it should not be recommended just for mitigating stroke risk in atrial fibrillation,” Joglar said. “You could use it if the patient has another indication, such as a prior heart attack.”
Does My Patient Have to Be in Normal Sinus Rhythm?
The new guidelines present evidence maintaining sinus rhythm should be favored over controlling heart rate for managing AF.
“We’ve focused on rhythm control as a better strategy, especially catheter ablation, which seems to be particularly effective in parallel to lifestyle interventions and management of comorbidities,” Joglar said. Rhythm control is of particular benefit for patients with AF triggered by heart failure. Control of rhythm in these patients has been shown to improve multiple outcomes such as ejection fraction, symptoms, and survival.
Patel said as a patient’s symptoms increase, the more likely a clinician will be able to control sinus rhythm. Some patients do not notice their arrhythmia, but others feel dizzy or have chest pain.
“The less symptomatic the patient is, the more likely they’re going to tolerate it, especially if they’re older, and it’s hard to get them into sinus rhythm,” Patel said.
When to Refer for Catheter Ablation?
The new guidelines upgraded the recommendation for catheter ablation to class I (strong recommendation) for patients with symptomatic AF in whom anti-arrhythmic therapy is unsuccessful, not tolerated, or contraindicated; patients with symptomatic paroxysmal AF (typically younger patients with few comorbidities); and patients with symptomatic or clinically significant atrial flutter. The previous iteration recommended trying drug therapy first.
Multiple randomized clinical trials have demonstrated the effectiveness of catheter ablation.
“In somebody who is younger, with a healthy heart, the 1-year success rate of the procedure might be about 70%,” Joglar said. While 70% of patients receiving a catheter have no AF episodes in the following year, Joglar said 20%-25% of those who do have recurrences will experience fewer or shorter episodes.
Conversations about rate vs rhythm control and whether to pursue catheter ablation often come down to preference, Patel said. He would tend to intervene earlier using ablation in patients with heart failure or those experiencing symptoms of AF who cannot be controlled with a heart rate < 100 beats/min.
But he said he prefers using medication for rate control in many of his patients who are older, have chronic AF, and do not have heart failure.
Mandrola takes a more conservative approach, reserving catheter ablation for patients in whom risk factor management and anti-arrhythmic drugs have not been successful.
“In my hospital, it’s done for patients who have symptomatic AF that’s really impacting their quality of life,” he said. But for those with fewer symptoms, his advice is to provide education, reassurance, and time because AF can resolve on its own.
What About Data From Implantables and Wearables?
The guidelines provide an algorithm for when to treat non-symptomatic atrial high-rate episodes detected by a cardiovascular implantable electronic device such as a pacemaker or defibrillator. Episodes less than 5 minutes can be ignored, while treatment could be considered for those with episodes lasting 5 minutes up to 24 hours with a CHA2DS2-VASc score ≥ 3, or lasting longer than 24 hours with a CHA2DS2-VASc score ≥ 2.
But whether anticoagulation improves outcomes is unclear.
“That is a $64,000 question,” Mandrola said. “I would bet every day I get a notification in the electronic health record that says Mr. Smith had 2 hours of AFib 2 weeks ago.”
He also hears from patients who report their Apple Watch has detected an episode of AF.
Mandrola cited evidence from two recent studies of patients who had an atrial high-rate episode longer than 6 minutes detected by implantable devices. The NOAH-AFNET 6 trial randomized patients over 65 years with one or more risk factors for stroke to receive a DOAC or placebo, while the ARTESIA trial used similar inclusion criteria to assign patients to receive either DOAC or aspirin. Both studies reported modest reductions in stroke that were outweighed by a higher incidence of major bleeding in the group receiving anticoagulation.
Shared decision-making should play a role in deciding how aggressively to treat episodes of AF detected by implantable or wearable devices.
He said some patients fear having a stroke, while others are adamantly opposed to taking an anticoagulant.
For patients who present with a documented episode of AF but who otherwise have no symptoms, Patel said clinicians should consider risk for stroke and frequency and duration of episodes.
“One way clinicians should be thinking about it is, the more risk factors they have, the lower burden of AF I need to treat,” Patel said. Even for patients who are having only short episodes of AF, he has a low threshold for recommending an anticoagulation drug if the patient’s CHA2DS2-VASc score is high.
Patel reported research grants from Bayer, Novartis, Idorsia, NHLBI, and Janssen Pharmaceuticals and served as a consultant on the advisory boards of Bayer, Janssen Pharmaceuticals, and Esperion Therapeutics.
Joglar and Mandrola had no disclosures.
A version of this article appeared on Medscape.com.
The incidence of atrial fibrillation (AF) is on the rise, and recent joint guidelines from the American College of Cardiology and American Heart Association (ACC/AHA) stress the role of primary care clinicians in prevention and management.
One in three White and one in five Black Americans will develop AF in their lifetime, and the projected number of individuals diagnosed with AF in the United States is expected to double by 2050.
Cardiologists who spoke to Medscape Medical News said primary care clinicians can help control AF by focusing on diabetes and hypertension, along with lifestyle factors such as diet, exercise, and alcohol intake.
“It’s not just a rhythm abnormality, but a complex disease that needs to be addressed in a multidisciplinary, holistic way,” said Jose Joglar, MD, a professor in the Department of Internal Medicine at the UT Southwestern Medical Center in Dallas and lead author of the guidelines.
Joglar said primary care clinicians can play an important role in counseling on lifestyle changes for patients with the most common etiologies such as poorly controlled hypertension, diabetes, and obesity.
The Primary Care Physicians ABCs: Risk Factors and Comorbidities
“As a primary care physician or as a cardiologist, I often think that if I do these things, I’m going to help with a lot of conditions, not just atrial fibrillation,” said Manesh Patel, MD, chief of the Divisions of Cardiology and Clinical Pharmacology at the Duke University School of Medicine in Durham, North Carolina.
Lifestyle choices such as sleeping habits can play a big part in AF outcomes. Although the guidelines specifically address obstructive sleep apnea as a risk factor, he said more data are needed on the effect of sleep hygiene — getting 8 hours of sleep a night — a goal few people attain.
“What we do know is people that can routinely try to go to sleep and sleep with some regularity seem to have less cardiovascular risk,” Patel said.
Although existing data are limited, literature reviews have found evidence that sleep disruptions, sleep duration, circadian rhythm, and insomnia are associated with heart disease, independent of obstructive sleep apnea.
Use of alcohol should also be discussed with patients, as many are unaware of the effects of the drug on cardiovascular disease, said Joglar, who is also the program director of the Clinical Cardiac Electrophysiology Fellowship program at the UT Southwestern Medical Center.
“Doctors can inform the patient that this is not a judgment call but simple medical fact,” he said.
Joglar also said many physicians need to become educated on a common misconception.
“Every time a patient develops palpitations or atrial fibrillation, the first thing every patient tells me is, I quit drinking coffee,” Joglar said.
However, as the guidelines point out, the link between caffeine and AF is uncertain at best.
Preventing AF
A newer class of drugs may help clinicians manage comorbidities that contribute to AF, such as hypertension, sleep apnea, and obesity, said John Mandrola, MD, an electrophysiologist in Louisville, Kentucky, who hosts This Week in Cardiology on Medscape.
Although originally approved for treatment of diabetes, sodium-glucose cotransporter-2 inhibitors are also approved for management of heart failure. Mandrola started prescribing these drugs 2 years ago for patients, given the links of both conditions with AF.
“I think the next frontier for us in cardiology and AF management will be the GLP-1 agonists,” Mandrola said. He hasn’t started prescribing these drugs for his patients yet but said they will likely play a role in the management of patients with AF with the common constellation of comorbidities such as obesity, hypertension, and sleep apnea.
“The GLP-1 agonists have a really good chance of competing with AF ablation for rhythm control over the long term,” he said.
Decisions, Decisions: Stroke Risk Scoring Systems
The risk for stroke varies widely among patients with AF, so primary care clinicians can pick among several scoring systems to estimate the risk for stroke and guide the decision on whether to initiate anticoagulation therapy.
The ACC/AHA guidelines do not state a preference for a particular instrument. The Congestive heart failure, Hypertension, Age, Diabetes mellitus, Stroke, Vascular disease, Sex (CHA2DS2-VASc) score is the most widely used and validated instrument, Joglar said. He usually recommends anticoagulation if the CHA2DS2-VASc score is > 2, dependent on individual patient factors.
“If you have a CHA2DS2-VASc score of 1, and you only had one episode of AF for a few hours a year ago, then your risk of stroke is not as high as somebody who has a score of 1 but has more frequent or persistent AF,” Joglar said.
None of the systems is perfect at predicting risk for stroke, so clinicians should discuss options with patients.
“The real message is, are you talking about the risk of stroke and systemic embolism to your patient, so that the patient understands that risk?” he said.
Patel also said measuring creatine clearance can be analogous to using an instrument like CHA2DS2-VASc.
“I often think about renal disease as a very good risk marker and something that does elevate your risk,” he said.
Which Anticoagulant?
Although the ACC/AHA guidelines still recommend warfarin for patients with AF with mechanical heart valves or moderate to severe rheumatic fever, direct oral anticoagulants (DOACs) are the first-line therapy for all other patients with AF.
In terms of which DOACs to use, the differences are subtle, according to Patel.
“I don’t know that they’re that different from each other,” he said. “All of the new drugs are better than warfarin by far.”
Patel pointed out that dabigatran at 150 mg is the only DOAC shown to reduce the incidence of ischemic stroke. For patients with renal dysfunction, he has a slight preference for a 15-mg dose of rivaroxaban.
Mandrola said he mainly prescribes apixaban and rivaroxaban, the latter of which requires only once a day dosing.
“We stopped using dabigatran because 10% of people get gastrointestinal upset,” he said.
Although studies suggest aspirin is less effective than either warfarin or DOACs for the prevention of stroke, Joglar said he still sees patients who come to him after being prescribed low-dose aspirin from primary care clinicians.
“We made it very clear that it should not be recommended just for mitigating stroke risk in atrial fibrillation,” Joglar said. “You could use it if the patient has another indication, such as a prior heart attack.”
Does My Patient Have to Be in Normal Sinus Rhythm?
The new guidelines present evidence maintaining sinus rhythm should be favored over controlling heart rate for managing AF.
“We’ve focused on rhythm control as a better strategy, especially catheter ablation, which seems to be particularly effective in parallel to lifestyle interventions and management of comorbidities,” Joglar said. Rhythm control is of particular benefit for patients with AF triggered by heart failure. Control of rhythm in these patients has been shown to improve multiple outcomes such as ejection fraction, symptoms, and survival.
Patel said as a patient’s symptoms increase, the more likely a clinician will be able to control sinus rhythm. Some patients do not notice their arrhythmia, but others feel dizzy or have chest pain.
“The less symptomatic the patient is, the more likely they’re going to tolerate it, especially if they’re older, and it’s hard to get them into sinus rhythm,” Patel said.
When to Refer for Catheter Ablation?
The new guidelines upgraded the recommendation for catheter ablation to class I (strong recommendation) for patients with symptomatic AF in whom anti-arrhythmic therapy is unsuccessful, not tolerated, or contraindicated; patients with symptomatic paroxysmal AF (typically younger patients with few comorbidities); and patients with symptomatic or clinically significant atrial flutter. The previous iteration recommended trying drug therapy first.
Multiple randomized clinical trials have demonstrated the effectiveness of catheter ablation.
“In somebody who is younger, with a healthy heart, the 1-year success rate of the procedure might be about 70%,” Joglar said. While 70% of patients receiving a catheter have no AF episodes in the following year, Joglar said 20%-25% of those who do have recurrences will experience fewer or shorter episodes.
Conversations about rate vs rhythm control and whether to pursue catheter ablation often come down to preference, Patel said. He would tend to intervene earlier using ablation in patients with heart failure or those experiencing symptoms of AF who cannot be controlled with a heart rate < 100 beats/min.
But he said he prefers using medication for rate control in many of his patients who are older, have chronic AF, and do not have heart failure.
Mandrola takes a more conservative approach, reserving catheter ablation for patients in whom risk factor management and anti-arrhythmic drugs have not been successful.
“In my hospital, it’s done for patients who have symptomatic AF that’s really impacting their quality of life,” he said. But for those with fewer symptoms, his advice is to provide education, reassurance, and time because AF can resolve on its own.
What About Data From Implantables and Wearables?
The guidelines provide an algorithm for when to treat non-symptomatic atrial high-rate episodes detected by a cardiovascular implantable electronic device such as a pacemaker or defibrillator. Episodes less than 5 minutes can be ignored, while treatment could be considered for those with episodes lasting 5 minutes up to 24 hours with a CHA2DS2-VASc score ≥ 3, or lasting longer than 24 hours with a CHA2DS2-VASc score ≥ 2.
But whether anticoagulation improves outcomes is unclear.
“That is a $64,000 question,” Mandrola said. “I would bet every day I get a notification in the electronic health record that says Mr. Smith had 2 hours of AFib 2 weeks ago.”
He also hears from patients who report their Apple Watch has detected an episode of AF.
Mandrola cited evidence from two recent studies of patients who had an atrial high-rate episode longer than 6 minutes detected by implantable devices. The NOAH-AFNET 6 trial randomized patients over 65 years with one or more risk factors for stroke to receive a DOAC or placebo, while the ARTESIA trial used similar inclusion criteria to assign patients to receive either DOAC or aspirin. Both studies reported modest reductions in stroke that were outweighed by a higher incidence of major bleeding in the group receiving anticoagulation.
Shared decision-making should play a role in deciding how aggressively to treat episodes of AF detected by implantable or wearable devices.
He said some patients fear having a stroke, while others are adamantly opposed to taking an anticoagulant.
For patients who present with a documented episode of AF but who otherwise have no symptoms, Patel said clinicians should consider risk for stroke and frequency and duration of episodes.
“One way clinicians should be thinking about it is, the more risk factors they have, the lower burden of AF I need to treat,” Patel said. Even for patients who are having only short episodes of AF, he has a low threshold for recommending an anticoagulation drug if the patient’s CHA2DS2-VASc score is high.
Patel reported research grants from Bayer, Novartis, Idorsia, NHLBI, and Janssen Pharmaceuticals and served as a consultant on the advisory boards of Bayer, Janssen Pharmaceuticals, and Esperion Therapeutics.
Joglar and Mandrola had no disclosures.
A version of this article appeared on Medscape.com.
Does the Road to Treating Endometriosis Start in the Gut?
Researchers may be on track to develop a much-needed tool for studying endometriosis: A noninvasive stool test that could replace the current gold standard of laparoscopy.
Their approach, which focuses on the link between the gut microbiome and endometriosis, also identified a bacterial metabolite they said might be developed as an oral medication for the condition, which affects at least 11% of women.
In previous research, Rama Kommagani, PhD, an associate professor in the Department of Pathology & Immunology at Baylor College of Medicine in Houston, Texas, worked with a mouse model in which endometrial tissue from donor rodents was injected into the peritoneal space of healthy rodents to induce the disorder.
Transfer of fecal microbiota from mice with endometriosis to those without the condition induced the trademark lesions, suggesting the microbiome influences the development of endometriosis. Treating the animals with the antibiotic metronidazole inhibited the progression of endometrial lesions.
Kommagani speculated the microbes release metabolites that stimulate the growth of the endometrial lesions. “Bad bacteria release metabolites, you know, which actually promote the disease,” Kommagani said. “But the good bacteria might release some protective metabolites such as short-chain fatty acids.”
In a new study, Kommagani and his colleagues sought to identify a unique profile of bacteria-derived metabolites that could reliably diagnose endometriosis. Using stool specimens from 18 women with the condition and 31 without the disease, his team conducted whole metabolic profiling of the gut microbiota.
After identifying hundreds of metabolites in the samples, further analysis revealed a subset of 12 metabolites that consistently differentiated women with and without endometriosis.
These findings led to more questions. “If a metabolite is lower in women with endometriosis, does it have any functional relevance?” Kommagani said.
One candidate was 4-hydroxyindole (4HI), which was found in lower levels in the stool of patients. This substance is a little-understood derivative of its parent compound, indole, which occurs naturally in plants and has a wide range of therapeutic uses.
Using a mouse model, Kommagani’s lab demonstrated that feeding mice 4HI before receiving an endometrial transplant prevented the development of lesions typical of endometriosis. Mice given 4HI after they had developed endometriosis showed regression of lesions and decreased response to painful stimuli.
“In a nutshell, we found a specific set of bacterial metabolites in stool, which could be used towards a noninvasive diagnostic test,” Kommagani said. “But we also found this distinct, specific metabolite that could be used as a therapeutic molecule.”
Tatnai Burnett, MD, an assistant professor of obstetrics and gynecology at Mayo Clinic in Rochester, Minnesota, who is not associated with the study, said a noninvasive test would have several advantages over the current methods of diagnosing endometriosis. Clinicians could detect and treat women earlier in the course of their disease. Secondly, a test with sufficient negative predictive value would be helpful in deciding whether to initiate treatment with hormones or other oral medications or go straight to surgery. “I would choose not to do a surgery if I knew with enough certainty that I wasn’t going to find anything,” said Burnett.
Lastly, a test that was quantitative and showed a response to treatment could be used as a disease activity marker to monitor the course of someone’s treatment.
But Burnett said more data on the approach are necessary. “This is a fairly small study, as it goes, for developing a screening test,” he said. “We need to see what its positive predictive value, negative predictive value, sensitivity, and specificity are in a bigger group.”
The road to a cure is even longer than the path to developing a screening test. Kommagani’s lab is now conducting more studies in mice to elucidate the pharmacokinetics and toxicology of 4HI before human trials can be attempted.
And as Burnett pointed out, although mouse models are great for experimentation and generating hypotheses, “We’ve seen way too many times in the past where something’s really exciting in a mouse model or a rat model or a monkey model, and it just doesn’t pan out in humans.”
Kommagani received funding from National Institutes of Health/Eunice Kennedy Shriver National Institute of Child Health and Human Development grants (R01HD102680, R01HD104813) and a Research Scholar Grant from the American Cancer Society. Burnett reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Researchers may be on track to develop a much-needed tool for studying endometriosis: A noninvasive stool test that could replace the current gold standard of laparoscopy.
Their approach, which focuses on the link between the gut microbiome and endometriosis, also identified a bacterial metabolite they said might be developed as an oral medication for the condition, which affects at least 11% of women.
In previous research, Rama Kommagani, PhD, an associate professor in the Department of Pathology & Immunology at Baylor College of Medicine in Houston, Texas, worked with a mouse model in which endometrial tissue from donor rodents was injected into the peritoneal space of healthy rodents to induce the disorder.
Transfer of fecal microbiota from mice with endometriosis to those without the condition induced the trademark lesions, suggesting the microbiome influences the development of endometriosis. Treating the animals with the antibiotic metronidazole inhibited the progression of endometrial lesions.
Kommagani speculated the microbes release metabolites that stimulate the growth of the endometrial lesions. “Bad bacteria release metabolites, you know, which actually promote the disease,” Kommagani said. “But the good bacteria might release some protective metabolites such as short-chain fatty acids.”
In a new study, Kommagani and his colleagues sought to identify a unique profile of bacteria-derived metabolites that could reliably diagnose endometriosis. Using stool specimens from 18 women with the condition and 31 without the disease, his team conducted whole metabolic profiling of the gut microbiota.
After identifying hundreds of metabolites in the samples, further analysis revealed a subset of 12 metabolites that consistently differentiated women with and without endometriosis.
These findings led to more questions. “If a metabolite is lower in women with endometriosis, does it have any functional relevance?” Kommagani said.
One candidate was 4-hydroxyindole (4HI), which was found in lower levels in the stool of patients. This substance is a little-understood derivative of its parent compound, indole, which occurs naturally in plants and has a wide range of therapeutic uses.
Using a mouse model, Kommagani’s lab demonstrated that feeding mice 4HI before receiving an endometrial transplant prevented the development of lesions typical of endometriosis. Mice given 4HI after they had developed endometriosis showed regression of lesions and decreased response to painful stimuli.
“In a nutshell, we found a specific set of bacterial metabolites in stool, which could be used towards a noninvasive diagnostic test,” Kommagani said. “But we also found this distinct, specific metabolite that could be used as a therapeutic molecule.”
Tatnai Burnett, MD, an assistant professor of obstetrics and gynecology at Mayo Clinic in Rochester, Minnesota, who is not associated with the study, said a noninvasive test would have several advantages over the current methods of diagnosing endometriosis. Clinicians could detect and treat women earlier in the course of their disease. Secondly, a test with sufficient negative predictive value would be helpful in deciding whether to initiate treatment with hormones or other oral medications or go straight to surgery. “I would choose not to do a surgery if I knew with enough certainty that I wasn’t going to find anything,” said Burnett.
Lastly, a test that was quantitative and showed a response to treatment could be used as a disease activity marker to monitor the course of someone’s treatment.
But Burnett said more data on the approach are necessary. “This is a fairly small study, as it goes, for developing a screening test,” he said. “We need to see what its positive predictive value, negative predictive value, sensitivity, and specificity are in a bigger group.”
The road to a cure is even longer than the path to developing a screening test. Kommagani’s lab is now conducting more studies in mice to elucidate the pharmacokinetics and toxicology of 4HI before human trials can be attempted.
And as Burnett pointed out, although mouse models are great for experimentation and generating hypotheses, “We’ve seen way too many times in the past where something’s really exciting in a mouse model or a rat model or a monkey model, and it just doesn’t pan out in humans.”
Kommagani received funding from National Institutes of Health/Eunice Kennedy Shriver National Institute of Child Health and Human Development grants (R01HD102680, R01HD104813) and a Research Scholar Grant from the American Cancer Society. Burnett reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Researchers may be on track to develop a much-needed tool for studying endometriosis: A noninvasive stool test that could replace the current gold standard of laparoscopy.
Their approach, which focuses on the link between the gut microbiome and endometriosis, also identified a bacterial metabolite they said might be developed as an oral medication for the condition, which affects at least 11% of women.
In previous research, Rama Kommagani, PhD, an associate professor in the Department of Pathology & Immunology at Baylor College of Medicine in Houston, Texas, worked with a mouse model in which endometrial tissue from donor rodents was injected into the peritoneal space of healthy rodents to induce the disorder.
Transfer of fecal microbiota from mice with endometriosis to those without the condition induced the trademark lesions, suggesting the microbiome influences the development of endometriosis. Treating the animals with the antibiotic metronidazole inhibited the progression of endometrial lesions.
Kommagani speculated the microbes release metabolites that stimulate the growth of the endometrial lesions. “Bad bacteria release metabolites, you know, which actually promote the disease,” Kommagani said. “But the good bacteria might release some protective metabolites such as short-chain fatty acids.”
In a new study, Kommagani and his colleagues sought to identify a unique profile of bacteria-derived metabolites that could reliably diagnose endometriosis. Using stool specimens from 18 women with the condition and 31 without the disease, his team conducted whole metabolic profiling of the gut microbiota.
After identifying hundreds of metabolites in the samples, further analysis revealed a subset of 12 metabolites that consistently differentiated women with and without endometriosis.
These findings led to more questions. “If a metabolite is lower in women with endometriosis, does it have any functional relevance?” Kommagani said.
One candidate was 4-hydroxyindole (4HI), which was found in lower levels in the stool of patients. This substance is a little-understood derivative of its parent compound, indole, which occurs naturally in plants and has a wide range of therapeutic uses.
Using a mouse model, Kommagani’s lab demonstrated that feeding mice 4HI before receiving an endometrial transplant prevented the development of lesions typical of endometriosis. Mice given 4HI after they had developed endometriosis showed regression of lesions and decreased response to painful stimuli.
“In a nutshell, we found a specific set of bacterial metabolites in stool, which could be used towards a noninvasive diagnostic test,” Kommagani said. “But we also found this distinct, specific metabolite that could be used as a therapeutic molecule.”
Tatnai Burnett, MD, an assistant professor of obstetrics and gynecology at Mayo Clinic in Rochester, Minnesota, who is not associated with the study, said a noninvasive test would have several advantages over the current methods of diagnosing endometriosis. Clinicians could detect and treat women earlier in the course of their disease. Secondly, a test with sufficient negative predictive value would be helpful in deciding whether to initiate treatment with hormones or other oral medications or go straight to surgery. “I would choose not to do a surgery if I knew with enough certainty that I wasn’t going to find anything,” said Burnett.
Lastly, a test that was quantitative and showed a response to treatment could be used as a disease activity marker to monitor the course of someone’s treatment.
But Burnett said more data on the approach are necessary. “This is a fairly small study, as it goes, for developing a screening test,” he said. “We need to see what its positive predictive value, negative predictive value, sensitivity, and specificity are in a bigger group.”
The road to a cure is even longer than the path to developing a screening test. Kommagani’s lab is now conducting more studies in mice to elucidate the pharmacokinetics and toxicology of 4HI before human trials can be attempted.
And as Burnett pointed out, although mouse models are great for experimentation and generating hypotheses, “We’ve seen way too many times in the past where something’s really exciting in a mouse model or a rat model or a monkey model, and it just doesn’t pan out in humans.”
Kommagani received funding from National Institutes of Health/Eunice Kennedy Shriver National Institute of Child Health and Human Development grants (R01HD102680, R01HD104813) and a Research Scholar Grant from the American Cancer Society. Burnett reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Abnormal TSH: Forget it or Fret it?
If you’re like most primary care clinicians, your email inbox is flooded with messages from patients with questions about lab results. A common query: Should I be worried about an abnormal value on a test of thyroid-stimulating hormone (TSH)?
For guidance, this news organization spoke with Angela Leung, MD, associate professor of medicine in the Division of Endocrinology, Diabetes & Metabolism at the UCLA David Geffen School of Medicine and an endocrinologist at UCLA and the VA Greater Los Angeles Healthcare System, and Karen Tsai, MD, assistant clinical professor of endocrinology at City of Hope Comprehensive Cancer Center in Duarte, California. The following interview has been edited for length and clarity.
Question: Why do you usually start by measuring TSH levels?
Dr. Leung: We need to measure the thyroid status in a way that integrates more information about the long-term thyroid status and not small changes in thyroid hormone levels. TSH is made by the pituitary gland in the brain, which integrates information about the signals of high and low levels from each of the different thyroid hormones.
Now we can measure the actual thyroid hormones — primarily we’re talking about T3 and T4 — but if we do that, we are relying on a single snapshot in the bloodstream at that moment. The levels might change throughout the day in response to ongoing metabolism and outside stresses. So we usually start by measuring the TSH level, which is a good representation of the compilation of all those things over the past 30 days or so.
Question: How do you describe a low TSH result to patients?
Dr. Leung: Whenever we encounter a low TSH level, we want to repeat the test because it is a dynamic test, and it can change in response to several factors. If it is indeed low, we’re thinking that perhaps there’s a little bit of extra thyroid hormone in the body. It can be either temporary or more chronic, but that higher amount of thyroid hormone is telling the pituitary gland in the brain to start making less. So TSH levels go low when we need less thyroid hormone.
Question: What are some of the reasons for a low TSH level?
Dr. Leung: One of the most common situations for a temporarily low TSH level I see is what we call nonthyroidal illness, like a common cold or just being under the weather. Other things that can artifactually lower the TSH level could be the use of steroids, such as prednisone for asthma or some sort of a rheumatologic condition. Also, the TSH level could be low if a person has been recently exposed to very high amounts of iodine, such as iodinated contrast needed for a CT scan.
If the TSH level remains persistently low, usually in the presence of high thyroid hormone (T3 and/or T4) levels, the most common reason for hyperthyroidism is Graves disease, in which there are autoantibodies — measurable in the blood — that can stimulate the thyroid gland in the neck to make extra thyroid hormone.
Question: And what does an elevated TSH level mean?
Dr. Leung: Again, we want to confirm that it is elevated. We need at least two tests to confirm a high TSH level. A persistently elevated TSH level is a signal there might be low thyroid hormone levels in the body, which could be transient or more longer lasting.
Question: What are some of the most common causes of an elevated TSH level?
Dr. Leung: If the TSH level is confirmed high and the thyroid hormone levels are low, the most common cause of hypothyroidism here in the United States is Hashimoto thyroiditis.
Globally, iodine deficiency is the most common reason for hypothyroidism and may be a problem in parts of the globe where there are endemically low iodine levels in soil, crops, and the food supply like not having enough iodized salt. The thyroid is reliant on having enough iodine as a micronutrient to make thyroid hormone. If it doesn’t, the thyroid really can’t make thyroid hormone. It’s important to also remember, though, that having too much iodine can result in hypo- or hyperthyroidism.
Dr. Tsai: I take a glance at their medication list. Some of the patients are on methimazole or levothyroxine, and those medications should be adjusted first to normalize the TSH level. Other medications like lithium and amiodarone can also cause elevated TSH levels. We are also seeing a lot of patients on cancer therapies, such as tyrosine kinase inhibitors or immunotherapy, that can cause an elevated TSH level.
Question: If the repeat TSH test shows that TSH levels are still elevated, what comes next in your workup?
Dr. Tsai: If there’s not a real clear-cut diagnosis, I’ll order the thyroid peroxidase antibody and the thyroglobulin antibody, although thyroid peroxidase antibody, which is indicative of autoimmune thyroid disease, alone is usually sufficient to make that diagnosis.
Question: Should clinicians follow thyroid antibodies over time?
Dr. Tsai: I usually don’t repeat the antibody tests. In those circumstances where patients who were diagnosed 50-60 years ago and perhaps it is unknown if they had the thyroid antibodies measured at the time and now they’re saying, “Do I actually have Hashimoto’s?” or “Do I really need to continue this for the rest of my life?” I do repeat antibody tests to help gauge if the patient’s levothyroxine can be stopped.
Question: How important is it to follow T4 or T3 levels?
Dr. Tsai: T4 and T3 levels can help differentiate overt thyroid dysfunction — where T3 and/or T4 levels will be abnormal — from subclinical thyroid dysfunction — where T3 and T4 levels would be normal. In general, although we do not fully appreciate the best metric to monitor hypo- or hyperthyroidism, because some patients with a normal TSH level still may have symptoms of thyroid dysfunction, these peripheral thyroid hormone levels are usually the most helpful at the time of initial diagnosis.
Question: What are your criteria for initiating treatment for hypothyroidism?
Dr. Tsai: If the TSH level > 10 mIU/L, I recommend levothyroxine hormone replacement. A lot of published data support clinical benefit in this group.
There is a gray area in those patients who have a TSH level higher than the upper limit of the reference range but less than 10. If the patient doesn’t have overt hypothyroid symptoms, I discuss the findings with the patient but don’t really feel eager to treat. I recommend checking the levels again in 6 months to see where that TSH goes, and if it worsens or becomes greater than 10 mIU/L, I then recommend levothyroxine hormone replacement.
It is also important to note that a TSH level of 5-7 may be an acceptable range for older patients, and they do not require levothyroxine.
The other category is patients whose TSH level is greater than the upper limit of the normal reference range but less than 10 and with overt hypothyroid symptoms such as fatigue, unintentional weight gain, constipation, or cold intolerance. In these patients, it is worthwhile to try a low dose of levothyroxine (25-50 mcg/d) and repeat TSH and free T4 tests in 6-8 weeks and see if the TSH level normalizes.
Dr. Leung: When you look at subclinical hypothyroidism, the situation of an isolated high TSH level in the setting of normal T4 levels, if the TSH level is mildly elevated in the 5-7 mIU/L range, there’s a 60% chance that it will normalize within 6 months.
Going back to Karen’s point, a lot of people are started and maintained on low doses of thyroid hormone forever and ever. A recent study on levothyroxine use found half of the prescriptions were unnecessary.
Question: In an era where many patients obtain much of their health information from TikTok, what’s your approach with patients with a normal TSH level who feel that they should have more testing or start treatment?
Dr. Tsai: Fatigue is one of the common referrals we get into our endocrinology practice, and everyone is convinced that their thyroid is the culprit. It is important to note, however, that fatigue can be due to different diseases such as anemia, depression, sleep disorders, or a recent viral illness.
TSH tests are readily available and cheap. I don’t mind ordering the lab test again if it helps give the patient some reassurance. I also find that patients are relieved once they hear from their endocrinologist that their thyroid is unlikely to be the cause of their fatigue.
Some other endocrine causes we may consider additionally working up include adrenal insufficiency, vitamin D deficiency, and diabetes. A comprehensive metabolic panel and complete blood count is part of my workup to rule out any gross electrolyte abnormalities or any new diagnosis of anemia, liver disease, or chronic kidney disease.
Question: What are your criteria for recommending that someone see an endocrinologist?
Dr. Tsai: Our primary care colleagues can do a workup and interpretation of thyroid function tests in most cases. In the situations where the thyroid function test results are discordant (ie, elevated TSH and elevated free T4 levels or low TSH and low free T4 levels) or difficult to interpret, it would be appropriate to refer the patient to an endocrinologist.
One of the common referrals that we do get from the community is a patient’s thyroid function tests going from hyperthyroid to hypothyroid without a clear explanation or the patient is suboptimally controlled with levothyroxine or methimazole. In those circumstances, it would be worthwhile to send to an endocrinologist try to discern an underlying cause or for optimization of medication.
Dr. Leung and Dr. Tsai had no financial disclosures.
A version of this article appeared on Medscape.com.
If you’re like most primary care clinicians, your email inbox is flooded with messages from patients with questions about lab results. A common query: Should I be worried about an abnormal value on a test of thyroid-stimulating hormone (TSH)?
For guidance, this news organization spoke with Angela Leung, MD, associate professor of medicine in the Division of Endocrinology, Diabetes & Metabolism at the UCLA David Geffen School of Medicine and an endocrinologist at UCLA and the VA Greater Los Angeles Healthcare System, and Karen Tsai, MD, assistant clinical professor of endocrinology at City of Hope Comprehensive Cancer Center in Duarte, California. The following interview has been edited for length and clarity.
Question: Why do you usually start by measuring TSH levels?
Dr. Leung: We need to measure the thyroid status in a way that integrates more information about the long-term thyroid status and not small changes in thyroid hormone levels. TSH is made by the pituitary gland in the brain, which integrates information about the signals of high and low levels from each of the different thyroid hormones.
Now we can measure the actual thyroid hormones — primarily we’re talking about T3 and T4 — but if we do that, we are relying on a single snapshot in the bloodstream at that moment. The levels might change throughout the day in response to ongoing metabolism and outside stresses. So we usually start by measuring the TSH level, which is a good representation of the compilation of all those things over the past 30 days or so.
Question: How do you describe a low TSH result to patients?
Dr. Leung: Whenever we encounter a low TSH level, we want to repeat the test because it is a dynamic test, and it can change in response to several factors. If it is indeed low, we’re thinking that perhaps there’s a little bit of extra thyroid hormone in the body. It can be either temporary or more chronic, but that higher amount of thyroid hormone is telling the pituitary gland in the brain to start making less. So TSH levels go low when we need less thyroid hormone.
Question: What are some of the reasons for a low TSH level?
Dr. Leung: One of the most common situations for a temporarily low TSH level I see is what we call nonthyroidal illness, like a common cold or just being under the weather. Other things that can artifactually lower the TSH level could be the use of steroids, such as prednisone for asthma or some sort of a rheumatologic condition. Also, the TSH level could be low if a person has been recently exposed to very high amounts of iodine, such as iodinated contrast needed for a CT scan.
If the TSH level remains persistently low, usually in the presence of high thyroid hormone (T3 and/or T4) levels, the most common reason for hyperthyroidism is Graves disease, in which there are autoantibodies — measurable in the blood — that can stimulate the thyroid gland in the neck to make extra thyroid hormone.
Question: And what does an elevated TSH level mean?
Dr. Leung: Again, we want to confirm that it is elevated. We need at least two tests to confirm a high TSH level. A persistently elevated TSH level is a signal there might be low thyroid hormone levels in the body, which could be transient or more longer lasting.
Question: What are some of the most common causes of an elevated TSH level?
Dr. Leung: If the TSH level is confirmed high and the thyroid hormone levels are low, the most common cause of hypothyroidism here in the United States is Hashimoto thyroiditis.
Globally, iodine deficiency is the most common reason for hypothyroidism and may be a problem in parts of the globe where there are endemically low iodine levels in soil, crops, and the food supply like not having enough iodized salt. The thyroid is reliant on having enough iodine as a micronutrient to make thyroid hormone. If it doesn’t, the thyroid really can’t make thyroid hormone. It’s important to also remember, though, that having too much iodine can result in hypo- or hyperthyroidism.
Dr. Tsai: I take a glance at their medication list. Some of the patients are on methimazole or levothyroxine, and those medications should be adjusted first to normalize the TSH level. Other medications like lithium and amiodarone can also cause elevated TSH levels. We are also seeing a lot of patients on cancer therapies, such as tyrosine kinase inhibitors or immunotherapy, that can cause an elevated TSH level.
Question: If the repeat TSH test shows that TSH levels are still elevated, what comes next in your workup?
Dr. Tsai: If there’s not a real clear-cut diagnosis, I’ll order the thyroid peroxidase antibody and the thyroglobulin antibody, although thyroid peroxidase antibody, which is indicative of autoimmune thyroid disease, alone is usually sufficient to make that diagnosis.
Question: Should clinicians follow thyroid antibodies over time?
Dr. Tsai: I usually don’t repeat the antibody tests. In those circumstances where patients who were diagnosed 50-60 years ago and perhaps it is unknown if they had the thyroid antibodies measured at the time and now they’re saying, “Do I actually have Hashimoto’s?” or “Do I really need to continue this for the rest of my life?” I do repeat antibody tests to help gauge if the patient’s levothyroxine can be stopped.
Question: How important is it to follow T4 or T3 levels?
Dr. Tsai: T4 and T3 levels can help differentiate overt thyroid dysfunction — where T3 and/or T4 levels will be abnormal — from subclinical thyroid dysfunction — where T3 and T4 levels would be normal. In general, although we do not fully appreciate the best metric to monitor hypo- or hyperthyroidism, because some patients with a normal TSH level still may have symptoms of thyroid dysfunction, these peripheral thyroid hormone levels are usually the most helpful at the time of initial diagnosis.
Question: What are your criteria for initiating treatment for hypothyroidism?
Dr. Tsai: If the TSH level > 10 mIU/L, I recommend levothyroxine hormone replacement. A lot of published data support clinical benefit in this group.
There is a gray area in those patients who have a TSH level higher than the upper limit of the reference range but less than 10. If the patient doesn’t have overt hypothyroid symptoms, I discuss the findings with the patient but don’t really feel eager to treat. I recommend checking the levels again in 6 months to see where that TSH goes, and if it worsens or becomes greater than 10 mIU/L, I then recommend levothyroxine hormone replacement.
It is also important to note that a TSH level of 5-7 may be an acceptable range for older patients, and they do not require levothyroxine.
The other category is patients whose TSH level is greater than the upper limit of the normal reference range but less than 10 and with overt hypothyroid symptoms such as fatigue, unintentional weight gain, constipation, or cold intolerance. In these patients, it is worthwhile to try a low dose of levothyroxine (25-50 mcg/d) and repeat TSH and free T4 tests in 6-8 weeks and see if the TSH level normalizes.
Dr. Leung: When you look at subclinical hypothyroidism, the situation of an isolated high TSH level in the setting of normal T4 levels, if the TSH level is mildly elevated in the 5-7 mIU/L range, there’s a 60% chance that it will normalize within 6 months.
Going back to Karen’s point, a lot of people are started and maintained on low doses of thyroid hormone forever and ever. A recent study on levothyroxine use found half of the prescriptions were unnecessary.
Question: In an era where many patients obtain much of their health information from TikTok, what’s your approach with patients with a normal TSH level who feel that they should have more testing or start treatment?
Dr. Tsai: Fatigue is one of the common referrals we get into our endocrinology practice, and everyone is convinced that their thyroid is the culprit. It is important to note, however, that fatigue can be due to different diseases such as anemia, depression, sleep disorders, or a recent viral illness.
TSH tests are readily available and cheap. I don’t mind ordering the lab test again if it helps give the patient some reassurance. I also find that patients are relieved once they hear from their endocrinologist that their thyroid is unlikely to be the cause of their fatigue.
Some other endocrine causes we may consider additionally working up include adrenal insufficiency, vitamin D deficiency, and diabetes. A comprehensive metabolic panel and complete blood count is part of my workup to rule out any gross electrolyte abnormalities or any new diagnosis of anemia, liver disease, or chronic kidney disease.
Question: What are your criteria for recommending that someone see an endocrinologist?
Dr. Tsai: Our primary care colleagues can do a workup and interpretation of thyroid function tests in most cases. In the situations where the thyroid function test results are discordant (ie, elevated TSH and elevated free T4 levels or low TSH and low free T4 levels) or difficult to interpret, it would be appropriate to refer the patient to an endocrinologist.
One of the common referrals that we do get from the community is a patient’s thyroid function tests going from hyperthyroid to hypothyroid without a clear explanation or the patient is suboptimally controlled with levothyroxine or methimazole. In those circumstances, it would be worthwhile to send to an endocrinologist try to discern an underlying cause or for optimization of medication.
Dr. Leung and Dr. Tsai had no financial disclosures.
A version of this article appeared on Medscape.com.
If you’re like most primary care clinicians, your email inbox is flooded with messages from patients with questions about lab results. A common query: Should I be worried about an abnormal value on a test of thyroid-stimulating hormone (TSH)?
For guidance, this news organization spoke with Angela Leung, MD, associate professor of medicine in the Division of Endocrinology, Diabetes & Metabolism at the UCLA David Geffen School of Medicine and an endocrinologist at UCLA and the VA Greater Los Angeles Healthcare System, and Karen Tsai, MD, assistant clinical professor of endocrinology at City of Hope Comprehensive Cancer Center in Duarte, California. The following interview has been edited for length and clarity.
Question: Why do you usually start by measuring TSH levels?
Dr. Leung: We need to measure the thyroid status in a way that integrates more information about the long-term thyroid status and not small changes in thyroid hormone levels. TSH is made by the pituitary gland in the brain, which integrates information about the signals of high and low levels from each of the different thyroid hormones.
Now we can measure the actual thyroid hormones — primarily we’re talking about T3 and T4 — but if we do that, we are relying on a single snapshot in the bloodstream at that moment. The levels might change throughout the day in response to ongoing metabolism and outside stresses. So we usually start by measuring the TSH level, which is a good representation of the compilation of all those things over the past 30 days or so.
Question: How do you describe a low TSH result to patients?
Dr. Leung: Whenever we encounter a low TSH level, we want to repeat the test because it is a dynamic test, and it can change in response to several factors. If it is indeed low, we’re thinking that perhaps there’s a little bit of extra thyroid hormone in the body. It can be either temporary or more chronic, but that higher amount of thyroid hormone is telling the pituitary gland in the brain to start making less. So TSH levels go low when we need less thyroid hormone.
Question: What are some of the reasons for a low TSH level?
Dr. Leung: One of the most common situations for a temporarily low TSH level I see is what we call nonthyroidal illness, like a common cold or just being under the weather. Other things that can artifactually lower the TSH level could be the use of steroids, such as prednisone for asthma or some sort of a rheumatologic condition. Also, the TSH level could be low if a person has been recently exposed to very high amounts of iodine, such as iodinated contrast needed for a CT scan.
If the TSH level remains persistently low, usually in the presence of high thyroid hormone (T3 and/or T4) levels, the most common reason for hyperthyroidism is Graves disease, in which there are autoantibodies — measurable in the blood — that can stimulate the thyroid gland in the neck to make extra thyroid hormone.
Question: And what does an elevated TSH level mean?
Dr. Leung: Again, we want to confirm that it is elevated. We need at least two tests to confirm a high TSH level. A persistently elevated TSH level is a signal there might be low thyroid hormone levels in the body, which could be transient or more longer lasting.
Question: What are some of the most common causes of an elevated TSH level?
Dr. Leung: If the TSH level is confirmed high and the thyroid hormone levels are low, the most common cause of hypothyroidism here in the United States is Hashimoto thyroiditis.
Globally, iodine deficiency is the most common reason for hypothyroidism and may be a problem in parts of the globe where there are endemically low iodine levels in soil, crops, and the food supply like not having enough iodized salt. The thyroid is reliant on having enough iodine as a micronutrient to make thyroid hormone. If it doesn’t, the thyroid really can’t make thyroid hormone. It’s important to also remember, though, that having too much iodine can result in hypo- or hyperthyroidism.
Dr. Tsai: I take a glance at their medication list. Some of the patients are on methimazole or levothyroxine, and those medications should be adjusted first to normalize the TSH level. Other medications like lithium and amiodarone can also cause elevated TSH levels. We are also seeing a lot of patients on cancer therapies, such as tyrosine kinase inhibitors or immunotherapy, that can cause an elevated TSH level.
Question: If the repeat TSH test shows that TSH levels are still elevated, what comes next in your workup?
Dr. Tsai: If there’s not a real clear-cut diagnosis, I’ll order the thyroid peroxidase antibody and the thyroglobulin antibody, although thyroid peroxidase antibody, which is indicative of autoimmune thyroid disease, alone is usually sufficient to make that diagnosis.
Question: Should clinicians follow thyroid antibodies over time?
Dr. Tsai: I usually don’t repeat the antibody tests. In those circumstances where patients who were diagnosed 50-60 years ago and perhaps it is unknown if they had the thyroid antibodies measured at the time and now they’re saying, “Do I actually have Hashimoto’s?” or “Do I really need to continue this for the rest of my life?” I do repeat antibody tests to help gauge if the patient’s levothyroxine can be stopped.
Question: How important is it to follow T4 or T3 levels?
Dr. Tsai: T4 and T3 levels can help differentiate overt thyroid dysfunction — where T3 and/or T4 levels will be abnormal — from subclinical thyroid dysfunction — where T3 and T4 levels would be normal. In general, although we do not fully appreciate the best metric to monitor hypo- or hyperthyroidism, because some patients with a normal TSH level still may have symptoms of thyroid dysfunction, these peripheral thyroid hormone levels are usually the most helpful at the time of initial diagnosis.
Question: What are your criteria for initiating treatment for hypothyroidism?
Dr. Tsai: If the TSH level > 10 mIU/L, I recommend levothyroxine hormone replacement. A lot of published data support clinical benefit in this group.
There is a gray area in those patients who have a TSH level higher than the upper limit of the reference range but less than 10. If the patient doesn’t have overt hypothyroid symptoms, I discuss the findings with the patient but don’t really feel eager to treat. I recommend checking the levels again in 6 months to see where that TSH goes, and if it worsens or becomes greater than 10 mIU/L, I then recommend levothyroxine hormone replacement.
It is also important to note that a TSH level of 5-7 may be an acceptable range for older patients, and they do not require levothyroxine.
The other category is patients whose TSH level is greater than the upper limit of the normal reference range but less than 10 and with overt hypothyroid symptoms such as fatigue, unintentional weight gain, constipation, or cold intolerance. In these patients, it is worthwhile to try a low dose of levothyroxine (25-50 mcg/d) and repeat TSH and free T4 tests in 6-8 weeks and see if the TSH level normalizes.
Dr. Leung: When you look at subclinical hypothyroidism, the situation of an isolated high TSH level in the setting of normal T4 levels, if the TSH level is mildly elevated in the 5-7 mIU/L range, there’s a 60% chance that it will normalize within 6 months.
Going back to Karen’s point, a lot of people are started and maintained on low doses of thyroid hormone forever and ever. A recent study on levothyroxine use found half of the prescriptions were unnecessary.
Question: In an era where many patients obtain much of their health information from TikTok, what’s your approach with patients with a normal TSH level who feel that they should have more testing or start treatment?
Dr. Tsai: Fatigue is one of the common referrals we get into our endocrinology practice, and everyone is convinced that their thyroid is the culprit. It is important to note, however, that fatigue can be due to different diseases such as anemia, depression, sleep disorders, or a recent viral illness.
TSH tests are readily available and cheap. I don’t mind ordering the lab test again if it helps give the patient some reassurance. I also find that patients are relieved once they hear from their endocrinologist that their thyroid is unlikely to be the cause of their fatigue.
Some other endocrine causes we may consider additionally working up include adrenal insufficiency, vitamin D deficiency, and diabetes. A comprehensive metabolic panel and complete blood count is part of my workup to rule out any gross electrolyte abnormalities or any new diagnosis of anemia, liver disease, or chronic kidney disease.
Question: What are your criteria for recommending that someone see an endocrinologist?
Dr. Tsai: Our primary care colleagues can do a workup and interpretation of thyroid function tests in most cases. In the situations where the thyroid function test results are discordant (ie, elevated TSH and elevated free T4 levels or low TSH and low free T4 levels) or difficult to interpret, it would be appropriate to refer the patient to an endocrinologist.
One of the common referrals that we do get from the community is a patient’s thyroid function tests going from hyperthyroid to hypothyroid without a clear explanation or the patient is suboptimally controlled with levothyroxine or methimazole. In those circumstances, it would be worthwhile to send to an endocrinologist try to discern an underlying cause or for optimization of medication.
Dr. Leung and Dr. Tsai had no financial disclosures.
A version of this article appeared on Medscape.com.
Primary Care: Re Carpe Your Diem
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
Primary Care: Try These Steps to Boost Lung Cancer Screens
A few years ago, Kim Lori Sandler, MD, realized many patients newly diagnosed with lung cancer had never been screened for the disease — they received CT scans only because they were symptomatic.
But Dr. Sandler, a radiologist at Vanderbilt University Medical Center in Nashville, Tennessee, could see in medical charts that most of these patients had been eligible for a screening before becoming symptomatic. And for women, most had received decades worth of mammograms. She saw an opportunity and launched a study to find out if an intervention would work.
Low-dose CT and mammography services often are available in the same imaging facility, so women who qualified for a lung cancer screening were offered the scan during their mammography visit. Over a 3-year period, monthly rates of lung scans in women rose by 50% at one facility and 36% at the other.
“What we found is that women are really receptive, if you talk to them about it,” Dr. Sandler said. “I don’t think that lung cancer is thought of as a disease in women.”
Although lung cancer is the leading cause of cancer deaths in the United States, a recent study in JAMA Internal Medicine found only 18% of eligible patients were screened in 2022, a far cry from the rates of 72% for colon cancer — which itself falls short of goals from US medical groups like the American Cancer Society (ACS). Among those eligible, rates of lung screenings were lowest among younger people without comorbid conditions, who did not have health insurance or a usual source of care, and those living in southern states and states that did not expand Medicaid as part of the Affordable Care Act.
Getting patients screened is lifesaving: 27% of people with lung cancer survive 5 years after diagnosis. But the survival rate rises to 63% when cases are diagnosed at an early stage.
Increasing Uptake
The formal recommendation to use low-dose chest CT to screen for lung cancer is only a decade old. The approach was first endorsed by the United States Preventive Services Task Force (USPSTF) on the basis of an influential trial that found such testing was linked to a 20% reduction in mortality from the disease. Updated 2021 USPSTF guidelines call for annual screening of people aged 50-80 years who have a 20 pack-year history of smoking and currently smoke or have quit within the past 15 years.
But implementing the recommendation is not always simple. Unlike a colorectal or breast cancer screening, which is recommended primarily on patient age, eligibility for a lung cancer screening requires calculating pack-years of smoking, and, for past smokers, knowledge of when they quit.
The structured fields in most electronic medical records (EMRs) inquire about current or past use of cigarettes and the number of daily packs smoked. But few EMRs can calculate when a patient starts smoking two cigarettes a day but then increases to a pack a day and cuts down again. EMRs also do not track when a patient has stopped smoking permanently. Individual clinicians or health systems must identify patients who are eligible for screening, but the lack of automated calculations makes that job more difficult.
Dr. Sandler and colleagues turned to the informatics team at Vanderbilt to develop a natural language processing approach that extracts smoking data directly from clinician notes instead of using standard variables in their EMR.
The number of patients identified as needing a screening using the algorithm nearly doubled from baseline, from 5887 to 10,231 over a 3-year period, according to results from another study that Dr. Sandler published.
Although the algorithm may occasionally flag someone who does not need screening as eligible, “you can always have a conversation with the patient to determine if they actually meet eligibility criteria,” Dr. Sandler said.
Patient Navigators to the Rescue?
About a decade ago, Travis Baggett, MD, MPH, an associate professor of internal medicine at Harvard Medical School, Boston, Massachusetts, received pilot funding from the ACS to study cancer epidemiology among patients at Boston Health Care for the Homeless Program (BHCHP), which serves nearly 10,000 patients at a variety of Boston-area clinics each year.
“We found that both the incidence and mortality rates for lung cancer were more than twofold higher than in the general population,” Dr. Baggett, who is also the director of research at BHCHP, said.
He also discovered that BHCHP patients were diagnosed at significantly later stages than people in the general population for malignancies like breast and colorectal cancer.
Screening for lung cancer was a new recommendation at the time. With additional funding from the ACS, he launched a clinical trial in 2020 that randomized patients who were eligible for lung cancer screening to either work with a patient navigator or receive usual care.
The navigators eased the burden on primary care clinicians: They facilitated shared decision-making visits, helped participants make and attend appointments for low-dose CT, assisted with transportation, and arranged follow-up as needed.
The 3-year study found 43% of patients who received navigation services underwent screening for lung cancer, compared with 9% in the usual-care arm. Participants said the navigators played a critical role in educating them about the importance of screening, coordinating care, and providing emotional support.
“At the root of it all, it was quite clear that one thing that made the navigator successful was their interpersonal qualities and having someone that the patient could trust to help guide them through the process,” Dr. Baggett said.
The navigator program, however, stopped when the funding for the study ended.
But another health system has implemented navigators in a sustainable way through a quality improvement project. Michael Gieske, MD, director of lung cancer screening at St. Elizabeth Healthcare in Edgewood, Kentucky, starts his Friday morning meeting with a multidisciplinary group, including a thoracic surgeon, radiologist, pulmonologist, and several screening nurse navigators. They review the week’s chest CTs, with approximately one-third from patients who underwent lung cancer screening.
Nurse navigators at St. Elizabeth Healthcare follow up with any patient whose scan is suspicious for lung cancer and guide them through the process of seeing specialists and obtaining additional testing.
“They essentially hold the patient’s hand through this scary time in their life and make sure that everything flows smoothly and efficiently,” said Dr. Gieske, a family medicine physician.
St. Elizabeth’s program also draws on several evidence-based strategies used for other cancer screening programs, such as patient and provider education and quarterly feedback to their 194 primary care clinicians on rates of lung cancer screening among their eligible patients.
Several requirements for reimbursement for a lung cancer screening from the US Centers for Medicare & Medicaid Services can also serve as barriers to getting patients screened: Clinicians must identify who is eligible, provide tobacco cessation counseling, and document the shared decision-making process.
To streamline the steps, St. Elizabeth’s clinicians use an EMR smart set that reminds clinicians to verify smoking history and helps them document the required counseling.
Last year, 47% of eligible patients received their recommended screening, and Dr. Gieske said he expects even more improvement.
“We’re on track this year to complete 60% uptake if things continue,” he said, adding that 76% of the new cases of lung cancer are now diagnosed in stage I, with only 5% diagnosed in stage IV.
Dr. Gieske has shared his experience with many clinics in Appalachia, home to some of the highest rates of mortality from lung cancer in the country. A major part of his role with the Appalachian Community Cancer Alliance is helping educate primary care clinicians in the region about the importance of early detection of lung cancer.
“I think one of the most important things is just to convey a message of hope,” he said. “We’re trying to get the good word out there that if you screen individuals, you’re going to catch it early, when you have an extremely high chance of curing the lung cancer.”
Dr. Baggett reported support from grants from the ACS and the Massachusetts General Hospital Research Scholars Program. Dr. Sandler and Dr. Gieske reported no financial conflicts.
A version of this article first appeared on Medscape.com.
A few years ago, Kim Lori Sandler, MD, realized many patients newly diagnosed with lung cancer had never been screened for the disease — they received CT scans only because they were symptomatic.
But Dr. Sandler, a radiologist at Vanderbilt University Medical Center in Nashville, Tennessee, could see in medical charts that most of these patients had been eligible for a screening before becoming symptomatic. And for women, most had received decades worth of mammograms. She saw an opportunity and launched a study to find out if an intervention would work.
Low-dose CT and mammography services often are available in the same imaging facility, so women who qualified for a lung cancer screening were offered the scan during their mammography visit. Over a 3-year period, monthly rates of lung scans in women rose by 50% at one facility and 36% at the other.
“What we found is that women are really receptive, if you talk to them about it,” Dr. Sandler said. “I don’t think that lung cancer is thought of as a disease in women.”
Although lung cancer is the leading cause of cancer deaths in the United States, a recent study in JAMA Internal Medicine found only 18% of eligible patients were screened in 2022, a far cry from the rates of 72% for colon cancer — which itself falls short of goals from US medical groups like the American Cancer Society (ACS). Among those eligible, rates of lung screenings were lowest among younger people without comorbid conditions, who did not have health insurance or a usual source of care, and those living in southern states and states that did not expand Medicaid as part of the Affordable Care Act.
Getting patients screened is lifesaving: 27% of people with lung cancer survive 5 years after diagnosis. But the survival rate rises to 63% when cases are diagnosed at an early stage.
Increasing Uptake
The formal recommendation to use low-dose chest CT to screen for lung cancer is only a decade old. The approach was first endorsed by the United States Preventive Services Task Force (USPSTF) on the basis of an influential trial that found such testing was linked to a 20% reduction in mortality from the disease. Updated 2021 USPSTF guidelines call for annual screening of people aged 50-80 years who have a 20 pack-year history of smoking and currently smoke or have quit within the past 15 years.
But implementing the recommendation is not always simple. Unlike a colorectal or breast cancer screening, which is recommended primarily on patient age, eligibility for a lung cancer screening requires calculating pack-years of smoking, and, for past smokers, knowledge of when they quit.
The structured fields in most electronic medical records (EMRs) inquire about current or past use of cigarettes and the number of daily packs smoked. But few EMRs can calculate when a patient starts smoking two cigarettes a day but then increases to a pack a day and cuts down again. EMRs also do not track when a patient has stopped smoking permanently. Individual clinicians or health systems must identify patients who are eligible for screening, but the lack of automated calculations makes that job more difficult.
Dr. Sandler and colleagues turned to the informatics team at Vanderbilt to develop a natural language processing approach that extracts smoking data directly from clinician notes instead of using standard variables in their EMR.
The number of patients identified as needing a screening using the algorithm nearly doubled from baseline, from 5887 to 10,231 over a 3-year period, according to results from another study that Dr. Sandler published.
Although the algorithm may occasionally flag someone who does not need screening as eligible, “you can always have a conversation with the patient to determine if they actually meet eligibility criteria,” Dr. Sandler said.
Patient Navigators to the Rescue?
About a decade ago, Travis Baggett, MD, MPH, an associate professor of internal medicine at Harvard Medical School, Boston, Massachusetts, received pilot funding from the ACS to study cancer epidemiology among patients at Boston Health Care for the Homeless Program (BHCHP), which serves nearly 10,000 patients at a variety of Boston-area clinics each year.
“We found that both the incidence and mortality rates for lung cancer were more than twofold higher than in the general population,” Dr. Baggett, who is also the director of research at BHCHP, said.
He also discovered that BHCHP patients were diagnosed at significantly later stages than people in the general population for malignancies like breast and colorectal cancer.
Screening for lung cancer was a new recommendation at the time. With additional funding from the ACS, he launched a clinical trial in 2020 that randomized patients who were eligible for lung cancer screening to either work with a patient navigator or receive usual care.
The navigators eased the burden on primary care clinicians: They facilitated shared decision-making visits, helped participants make and attend appointments for low-dose CT, assisted with transportation, and arranged follow-up as needed.
The 3-year study found 43% of patients who received navigation services underwent screening for lung cancer, compared with 9% in the usual-care arm. Participants said the navigators played a critical role in educating them about the importance of screening, coordinating care, and providing emotional support.
“At the root of it all, it was quite clear that one thing that made the navigator successful was their interpersonal qualities and having someone that the patient could trust to help guide them through the process,” Dr. Baggett said.
The navigator program, however, stopped when the funding for the study ended.
But another health system has implemented navigators in a sustainable way through a quality improvement project. Michael Gieske, MD, director of lung cancer screening at St. Elizabeth Healthcare in Edgewood, Kentucky, starts his Friday morning meeting with a multidisciplinary group, including a thoracic surgeon, radiologist, pulmonologist, and several screening nurse navigators. They review the week’s chest CTs, with approximately one-third from patients who underwent lung cancer screening.
Nurse navigators at St. Elizabeth Healthcare follow up with any patient whose scan is suspicious for lung cancer and guide them through the process of seeing specialists and obtaining additional testing.
“They essentially hold the patient’s hand through this scary time in their life and make sure that everything flows smoothly and efficiently,” said Dr. Gieske, a family medicine physician.
St. Elizabeth’s program also draws on several evidence-based strategies used for other cancer screening programs, such as patient and provider education and quarterly feedback to their 194 primary care clinicians on rates of lung cancer screening among their eligible patients.
Several requirements for reimbursement for a lung cancer screening from the US Centers for Medicare & Medicaid Services can also serve as barriers to getting patients screened: Clinicians must identify who is eligible, provide tobacco cessation counseling, and document the shared decision-making process.
To streamline the steps, St. Elizabeth’s clinicians use an EMR smart set that reminds clinicians to verify smoking history and helps them document the required counseling.
Last year, 47% of eligible patients received their recommended screening, and Dr. Gieske said he expects even more improvement.
“We’re on track this year to complete 60% uptake if things continue,” he said, adding that 76% of the new cases of lung cancer are now diagnosed in stage I, with only 5% diagnosed in stage IV.
Dr. Gieske has shared his experience with many clinics in Appalachia, home to some of the highest rates of mortality from lung cancer in the country. A major part of his role with the Appalachian Community Cancer Alliance is helping educate primary care clinicians in the region about the importance of early detection of lung cancer.
“I think one of the most important things is just to convey a message of hope,” he said. “We’re trying to get the good word out there that if you screen individuals, you’re going to catch it early, when you have an extremely high chance of curing the lung cancer.”
Dr. Baggett reported support from grants from the ACS and the Massachusetts General Hospital Research Scholars Program. Dr. Sandler and Dr. Gieske reported no financial conflicts.
A version of this article first appeared on Medscape.com.
A few years ago, Kim Lori Sandler, MD, realized many patients newly diagnosed with lung cancer had never been screened for the disease — they received CT scans only because they were symptomatic.
But Dr. Sandler, a radiologist at Vanderbilt University Medical Center in Nashville, Tennessee, could see in medical charts that most of these patients had been eligible for a screening before becoming symptomatic. And for women, most had received decades worth of mammograms. She saw an opportunity and launched a study to find out if an intervention would work.
Low-dose CT and mammography services often are available in the same imaging facility, so women who qualified for a lung cancer screening were offered the scan during their mammography visit. Over a 3-year period, monthly rates of lung scans in women rose by 50% at one facility and 36% at the other.
“What we found is that women are really receptive, if you talk to them about it,” Dr. Sandler said. “I don’t think that lung cancer is thought of as a disease in women.”
Although lung cancer is the leading cause of cancer deaths in the United States, a recent study in JAMA Internal Medicine found only 18% of eligible patients were screened in 2022, a far cry from the rates of 72% for colon cancer — which itself falls short of goals from US medical groups like the American Cancer Society (ACS). Among those eligible, rates of lung screenings were lowest among younger people without comorbid conditions, who did not have health insurance or a usual source of care, and those living in southern states and states that did not expand Medicaid as part of the Affordable Care Act.
Getting patients screened is lifesaving: 27% of people with lung cancer survive 5 years after diagnosis. But the survival rate rises to 63% when cases are diagnosed at an early stage.
Increasing Uptake
The formal recommendation to use low-dose chest CT to screen for lung cancer is only a decade old. The approach was first endorsed by the United States Preventive Services Task Force (USPSTF) on the basis of an influential trial that found such testing was linked to a 20% reduction in mortality from the disease. Updated 2021 USPSTF guidelines call for annual screening of people aged 50-80 years who have a 20 pack-year history of smoking and currently smoke or have quit within the past 15 years.
But implementing the recommendation is not always simple. Unlike a colorectal or breast cancer screening, which is recommended primarily on patient age, eligibility for a lung cancer screening requires calculating pack-years of smoking, and, for past smokers, knowledge of when they quit.
The structured fields in most electronic medical records (EMRs) inquire about current or past use of cigarettes and the number of daily packs smoked. But few EMRs can calculate when a patient starts smoking two cigarettes a day but then increases to a pack a day and cuts down again. EMRs also do not track when a patient has stopped smoking permanently. Individual clinicians or health systems must identify patients who are eligible for screening, but the lack of automated calculations makes that job more difficult.
Dr. Sandler and colleagues turned to the informatics team at Vanderbilt to develop a natural language processing approach that extracts smoking data directly from clinician notes instead of using standard variables in their EMR.
The number of patients identified as needing a screening using the algorithm nearly doubled from baseline, from 5887 to 10,231 over a 3-year period, according to results from another study that Dr. Sandler published.
Although the algorithm may occasionally flag someone who does not need screening as eligible, “you can always have a conversation with the patient to determine if they actually meet eligibility criteria,” Dr. Sandler said.
Patient Navigators to the Rescue?
About a decade ago, Travis Baggett, MD, MPH, an associate professor of internal medicine at Harvard Medical School, Boston, Massachusetts, received pilot funding from the ACS to study cancer epidemiology among patients at Boston Health Care for the Homeless Program (BHCHP), which serves nearly 10,000 patients at a variety of Boston-area clinics each year.
“We found that both the incidence and mortality rates for lung cancer were more than twofold higher than in the general population,” Dr. Baggett, who is also the director of research at BHCHP, said.
He also discovered that BHCHP patients were diagnosed at significantly later stages than people in the general population for malignancies like breast and colorectal cancer.
Screening for lung cancer was a new recommendation at the time. With additional funding from the ACS, he launched a clinical trial in 2020 that randomized patients who were eligible for lung cancer screening to either work with a patient navigator or receive usual care.
The navigators eased the burden on primary care clinicians: They facilitated shared decision-making visits, helped participants make and attend appointments for low-dose CT, assisted with transportation, and arranged follow-up as needed.
The 3-year study found 43% of patients who received navigation services underwent screening for lung cancer, compared with 9% in the usual-care arm. Participants said the navigators played a critical role in educating them about the importance of screening, coordinating care, and providing emotional support.
“At the root of it all, it was quite clear that one thing that made the navigator successful was their interpersonal qualities and having someone that the patient could trust to help guide them through the process,” Dr. Baggett said.
The navigator program, however, stopped when the funding for the study ended.
But another health system has implemented navigators in a sustainable way through a quality improvement project. Michael Gieske, MD, director of lung cancer screening at St. Elizabeth Healthcare in Edgewood, Kentucky, starts his Friday morning meeting with a multidisciplinary group, including a thoracic surgeon, radiologist, pulmonologist, and several screening nurse navigators. They review the week’s chest CTs, with approximately one-third from patients who underwent lung cancer screening.
Nurse navigators at St. Elizabeth Healthcare follow up with any patient whose scan is suspicious for lung cancer and guide them through the process of seeing specialists and obtaining additional testing.
“They essentially hold the patient’s hand through this scary time in their life and make sure that everything flows smoothly and efficiently,” said Dr. Gieske, a family medicine physician.
St. Elizabeth’s program also draws on several evidence-based strategies used for other cancer screening programs, such as patient and provider education and quarterly feedback to their 194 primary care clinicians on rates of lung cancer screening among their eligible patients.
Several requirements for reimbursement for a lung cancer screening from the US Centers for Medicare & Medicaid Services can also serve as barriers to getting patients screened: Clinicians must identify who is eligible, provide tobacco cessation counseling, and document the shared decision-making process.
To streamline the steps, St. Elizabeth’s clinicians use an EMR smart set that reminds clinicians to verify smoking history and helps them document the required counseling.
Last year, 47% of eligible patients received their recommended screening, and Dr. Gieske said he expects even more improvement.
“We’re on track this year to complete 60% uptake if things continue,” he said, adding that 76% of the new cases of lung cancer are now diagnosed in stage I, with only 5% diagnosed in stage IV.
Dr. Gieske has shared his experience with many clinics in Appalachia, home to some of the highest rates of mortality from lung cancer in the country. A major part of his role with the Appalachian Community Cancer Alliance is helping educate primary care clinicians in the region about the importance of early detection of lung cancer.
“I think one of the most important things is just to convey a message of hope,” he said. “We’re trying to get the good word out there that if you screen individuals, you’re going to catch it early, when you have an extremely high chance of curing the lung cancer.”
Dr. Baggett reported support from grants from the ACS and the Massachusetts General Hospital Research Scholars Program. Dr. Sandler and Dr. Gieske reported no financial conflicts.
A version of this article first appeared on Medscape.com.
The History of Aspirin in Heart Disease Prevention
As the pendulum has swung against recommending aspirin for the primary prevention of heart attacks and strokes, clinicians should focus on other ways to help patients avoid cardiovascular events.
A landmark study published in 1988 in The New England Journal of Medicine reported an astonishing 44% drop in the number of heart attacks among US male physicians aged 40-84 years who took aspirin.
Aspirin subsequently became a daily habit for millions of Americans. In 2017, nearly a quarter of Americans over age 40 who did not have cardiovascular disease (CVD) took the drug, and over 20% of those were doing so without a physician’s recommendation.
But in 2018, three studies (ASCEND, ARRIVE, and ASPREE) showed a stunning reversal in the purported benefit, according to John Wong, MD, vice-chair of the US Preventive Services Task Force (USPSTF).
The calculus for taking aspirin appeared to have changed dramatically: The drug decreased the risk for myocardial infarction by only 11% among study subjects, while its potential harms were much more pronounced.
According to Dr. Wong, who is also a professor of medicine and a primary care physician at Tufts University School of Medicine in Boston, Massachusetts, patients taking low-dose aspirin had a 58% increase in their risk for gastrointestinal bleeding compared with those not on aspirin, as well as a 31% increased risk for intracranial bleeding.
who haven’t had a heart attack or stroke.”
Fewer Americans smoke cigarettes, more realize the benefits of a healthy diet and physical activity, and the medical community better recognizes and treats hypertension. New classes of medications such as statins for high cholesterol are also moving the needle.
But a newer class of drugs may provide a safer replacement for aspirin, according to Muhammad Maqsood, MD, a cardiology fellow at DeBakey Heart and Vascular Center at Methodist Hospital in Houston, Texas. P2Y purinoceptor 12 (P2Y12) inhibitors are effective in lowering the risk for heart attack and stroke in patients with acute coronary syndrome or those undergoing elective percutaneous coronary interventions.
“They have shown a better bleeding profile, especially clopidogrel compared to aspirin,” Dr. Maqsood said.
However, the findings come from trials of patients who already had CVD, so results cannot yet be extrapolated to primary prevention. Dr. Maqsood said the gap highlights the need for clinical trials that evaluate P2Y12 inhibitors for primary prevention, but no such study is registered on clinicaltrials.gov.
Benefits Persist for Some Patients
The new evidence led the USPSTF to publish new guidelines in 2022, downgrading the recommendation for low-dose aspirin use for primary prevention. Previously, the organization stated that clinicians “should” initiate daily low-dose aspirin in adults aged 50-59 years and “consider” its use in adults aged 60-69 years whose 10-year risk for CVD was higher than 10%.
The updated guidelines stated that the decision to initiate low-dose aspirin in adults aged 40-59 years with a greater than 10% risk for CVD “should be an individual one,” based on professional judgment and individual patient preferences. The USPSTF also recommended against the use of aspirin in anyone over the age of 60.
Meanwhile, the American College of Cardiology and American Heart Association also dialed down previously strong recommendations on low-dose aspirin to a more nuanced recommendation stating, “low-dose aspirin might be considered for primary prevention of ASCVD among select adults 40-70 years of age.”
With a varying age limit for recommending aspirin, clinicians may take into consideration several variables.
“Is there a magic age? I don’t think there is,” said Douglas Lloyd-Jones, the former president of the American Heart Association and current chair of the Department of Preventive Medicine and a practicing cardiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
For a patient over age 60 who is at a high risk for adverse cardiovascular outcomes, is unable to quit smoking, and is not likely to experience problematic bleeding, a clinician might recommend aspirin, Dr. Lloyd-Jones said. He said he sometimes also assesses coronary artery calcium to guide his clinical decisions: If elevated (an Agatston score above 100), he might recommend low-dose aspirin.
Dr. Lloyd-Jones also reiterated that patients should continue taking low-dose aspirin if they have already experienced a heart attack, stroke, episode of atrial fibrillation, or required a vascular stent.
Unless a patient with established CVD has intractable bleeding, “the aspirin is really for life,” Dr. Lloyd-Jones said. Patients who have a stent or who are at high risk for recurrence of stroke are more likely to experience thrombosis, and aspirin can decrease the risk.
“In our cardiology community, we don’t just strictly use the age of 70; the decision is always individualized,” Dr. Maqsood said.
Dr. Wong said primary care providers should focus on the USPSTF’s other recommendations that address CVD (Table), such as smoking cessation and screening for hypertension.
“I think our challenge is that we have so many of those A and B recommendations,” Dr. Wong said. “And I think part of the challenge for us is working with the patient to find out what’s most important to them.”
Discussing heart attacks and strokes often will strike a chord with patients because someone they know has been affected.
Dr. Maqsood emphasized the importance of behavioral interventions, such as helping patients decrease their body mass index and control their hyperlipidemia.
“The behavioral interventions are those which are the most cost-effective without any side effects,” he said.
His other piece of advice is to inquire with younger patients about a family history of heart attacks. Familial hypercholesteremia is unlikely to be controlled by diet and exercise and will need medical therapy.
Dr. Lloyd-Jones described the discussions he has with patients about preventing heart attacks as “the most important conversations we can have: Remember that cardiovascular disease is still the leading cause of death and disability in the world and in the United States.”
Dr. Wong, Dr. Lloyd-Jones, and Dr. Maqsood reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As the pendulum has swung against recommending aspirin for the primary prevention of heart attacks and strokes, clinicians should focus on other ways to help patients avoid cardiovascular events.
A landmark study published in 1988 in The New England Journal of Medicine reported an astonishing 44% drop in the number of heart attacks among US male physicians aged 40-84 years who took aspirin.
Aspirin subsequently became a daily habit for millions of Americans. In 2017, nearly a quarter of Americans over age 40 who did not have cardiovascular disease (CVD) took the drug, and over 20% of those were doing so without a physician’s recommendation.
But in 2018, three studies (ASCEND, ARRIVE, and ASPREE) showed a stunning reversal in the purported benefit, according to John Wong, MD, vice-chair of the US Preventive Services Task Force (USPSTF).
The calculus for taking aspirin appeared to have changed dramatically: The drug decreased the risk for myocardial infarction by only 11% among study subjects, while its potential harms were much more pronounced.
According to Dr. Wong, who is also a professor of medicine and a primary care physician at Tufts University School of Medicine in Boston, Massachusetts, patients taking low-dose aspirin had a 58% increase in their risk for gastrointestinal bleeding compared with those not on aspirin, as well as a 31% increased risk for intracranial bleeding.
who haven’t had a heart attack or stroke.”
Fewer Americans smoke cigarettes, more realize the benefits of a healthy diet and physical activity, and the medical community better recognizes and treats hypertension. New classes of medications such as statins for high cholesterol are also moving the needle.
But a newer class of drugs may provide a safer replacement for aspirin, according to Muhammad Maqsood, MD, a cardiology fellow at DeBakey Heart and Vascular Center at Methodist Hospital in Houston, Texas. P2Y purinoceptor 12 (P2Y12) inhibitors are effective in lowering the risk for heart attack and stroke in patients with acute coronary syndrome or those undergoing elective percutaneous coronary interventions.
“They have shown a better bleeding profile, especially clopidogrel compared to aspirin,” Dr. Maqsood said.
However, the findings come from trials of patients who already had CVD, so results cannot yet be extrapolated to primary prevention. Dr. Maqsood said the gap highlights the need for clinical trials that evaluate P2Y12 inhibitors for primary prevention, but no such study is registered on clinicaltrials.gov.
Benefits Persist for Some Patients
The new evidence led the USPSTF to publish new guidelines in 2022, downgrading the recommendation for low-dose aspirin use for primary prevention. Previously, the organization stated that clinicians “should” initiate daily low-dose aspirin in adults aged 50-59 years and “consider” its use in adults aged 60-69 years whose 10-year risk for CVD was higher than 10%.
The updated guidelines stated that the decision to initiate low-dose aspirin in adults aged 40-59 years with a greater than 10% risk for CVD “should be an individual one,” based on professional judgment and individual patient preferences. The USPSTF also recommended against the use of aspirin in anyone over the age of 60.
Meanwhile, the American College of Cardiology and American Heart Association also dialed down previously strong recommendations on low-dose aspirin to a more nuanced recommendation stating, “low-dose aspirin might be considered for primary prevention of ASCVD among select adults 40-70 years of age.”
With a varying age limit for recommending aspirin, clinicians may take into consideration several variables.
“Is there a magic age? I don’t think there is,” said Douglas Lloyd-Jones, the former president of the American Heart Association and current chair of the Department of Preventive Medicine and a practicing cardiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
For a patient over age 60 who is at a high risk for adverse cardiovascular outcomes, is unable to quit smoking, and is not likely to experience problematic bleeding, a clinician might recommend aspirin, Dr. Lloyd-Jones said. He said he sometimes also assesses coronary artery calcium to guide his clinical decisions: If elevated (an Agatston score above 100), he might recommend low-dose aspirin.
Dr. Lloyd-Jones also reiterated that patients should continue taking low-dose aspirin if they have already experienced a heart attack, stroke, episode of atrial fibrillation, or required a vascular stent.
Unless a patient with established CVD has intractable bleeding, “the aspirin is really for life,” Dr. Lloyd-Jones said. Patients who have a stent or who are at high risk for recurrence of stroke are more likely to experience thrombosis, and aspirin can decrease the risk.
“In our cardiology community, we don’t just strictly use the age of 70; the decision is always individualized,” Dr. Maqsood said.
Dr. Wong said primary care providers should focus on the USPSTF’s other recommendations that address CVD (Table), such as smoking cessation and screening for hypertension.
“I think our challenge is that we have so many of those A and B recommendations,” Dr. Wong said. “And I think part of the challenge for us is working with the patient to find out what’s most important to them.”
Discussing heart attacks and strokes often will strike a chord with patients because someone they know has been affected.
Dr. Maqsood emphasized the importance of behavioral interventions, such as helping patients decrease their body mass index and control their hyperlipidemia.
“The behavioral interventions are those which are the most cost-effective without any side effects,” he said.
His other piece of advice is to inquire with younger patients about a family history of heart attacks. Familial hypercholesteremia is unlikely to be controlled by diet and exercise and will need medical therapy.
Dr. Lloyd-Jones described the discussions he has with patients about preventing heart attacks as “the most important conversations we can have: Remember that cardiovascular disease is still the leading cause of death and disability in the world and in the United States.”
Dr. Wong, Dr. Lloyd-Jones, and Dr. Maqsood reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As the pendulum has swung against recommending aspirin for the primary prevention of heart attacks and strokes, clinicians should focus on other ways to help patients avoid cardiovascular events.
A landmark study published in 1988 in The New England Journal of Medicine reported an astonishing 44% drop in the number of heart attacks among US male physicians aged 40-84 years who took aspirin.
Aspirin subsequently became a daily habit for millions of Americans. In 2017, nearly a quarter of Americans over age 40 who did not have cardiovascular disease (CVD) took the drug, and over 20% of those were doing so without a physician’s recommendation.
But in 2018, three studies (ASCEND, ARRIVE, and ASPREE) showed a stunning reversal in the purported benefit, according to John Wong, MD, vice-chair of the US Preventive Services Task Force (USPSTF).
The calculus for taking aspirin appeared to have changed dramatically: The drug decreased the risk for myocardial infarction by only 11% among study subjects, while its potential harms were much more pronounced.
According to Dr. Wong, who is also a professor of medicine and a primary care physician at Tufts University School of Medicine in Boston, Massachusetts, patients taking low-dose aspirin had a 58% increase in their risk for gastrointestinal bleeding compared with those not on aspirin, as well as a 31% increased risk for intracranial bleeding.
who haven’t had a heart attack or stroke.”
Fewer Americans smoke cigarettes, more realize the benefits of a healthy diet and physical activity, and the medical community better recognizes and treats hypertension. New classes of medications such as statins for high cholesterol are also moving the needle.
But a newer class of drugs may provide a safer replacement for aspirin, according to Muhammad Maqsood, MD, a cardiology fellow at DeBakey Heart and Vascular Center at Methodist Hospital in Houston, Texas. P2Y purinoceptor 12 (P2Y12) inhibitors are effective in lowering the risk for heart attack and stroke in patients with acute coronary syndrome or those undergoing elective percutaneous coronary interventions.
“They have shown a better bleeding profile, especially clopidogrel compared to aspirin,” Dr. Maqsood said.
However, the findings come from trials of patients who already had CVD, so results cannot yet be extrapolated to primary prevention. Dr. Maqsood said the gap highlights the need for clinical trials that evaluate P2Y12 inhibitors for primary prevention, but no such study is registered on clinicaltrials.gov.
Benefits Persist for Some Patients
The new evidence led the USPSTF to publish new guidelines in 2022, downgrading the recommendation for low-dose aspirin use for primary prevention. Previously, the organization stated that clinicians “should” initiate daily low-dose aspirin in adults aged 50-59 years and “consider” its use in adults aged 60-69 years whose 10-year risk for CVD was higher than 10%.
The updated guidelines stated that the decision to initiate low-dose aspirin in adults aged 40-59 years with a greater than 10% risk for CVD “should be an individual one,” based on professional judgment and individual patient preferences. The USPSTF also recommended against the use of aspirin in anyone over the age of 60.
Meanwhile, the American College of Cardiology and American Heart Association also dialed down previously strong recommendations on low-dose aspirin to a more nuanced recommendation stating, “low-dose aspirin might be considered for primary prevention of ASCVD among select adults 40-70 years of age.”
With a varying age limit for recommending aspirin, clinicians may take into consideration several variables.
“Is there a magic age? I don’t think there is,” said Douglas Lloyd-Jones, the former president of the American Heart Association and current chair of the Department of Preventive Medicine and a practicing cardiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
For a patient over age 60 who is at a high risk for adverse cardiovascular outcomes, is unable to quit smoking, and is not likely to experience problematic bleeding, a clinician might recommend aspirin, Dr. Lloyd-Jones said. He said he sometimes also assesses coronary artery calcium to guide his clinical decisions: If elevated (an Agatston score above 100), he might recommend low-dose aspirin.
Dr. Lloyd-Jones also reiterated that patients should continue taking low-dose aspirin if they have already experienced a heart attack, stroke, episode of atrial fibrillation, or required a vascular stent.
Unless a patient with established CVD has intractable bleeding, “the aspirin is really for life,” Dr. Lloyd-Jones said. Patients who have a stent or who are at high risk for recurrence of stroke are more likely to experience thrombosis, and aspirin can decrease the risk.
“In our cardiology community, we don’t just strictly use the age of 70; the decision is always individualized,” Dr. Maqsood said.
Dr. Wong said primary care providers should focus on the USPSTF’s other recommendations that address CVD (Table), such as smoking cessation and screening for hypertension.
“I think our challenge is that we have so many of those A and B recommendations,” Dr. Wong said. “And I think part of the challenge for us is working with the patient to find out what’s most important to them.”
Discussing heart attacks and strokes often will strike a chord with patients because someone they know has been affected.
Dr. Maqsood emphasized the importance of behavioral interventions, such as helping patients decrease their body mass index and control their hyperlipidemia.
“The behavioral interventions are those which are the most cost-effective without any side effects,” he said.
His other piece of advice is to inquire with younger patients about a family history of heart attacks. Familial hypercholesteremia is unlikely to be controlled by diet and exercise and will need medical therapy.
Dr. Lloyd-Jones described the discussions he has with patients about preventing heart attacks as “the most important conversations we can have: Remember that cardiovascular disease is still the leading cause of death and disability in the world and in the United States.”
Dr. Wong, Dr. Lloyd-Jones, and Dr. Maqsood reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Lead Has Not Gone Away — What Should Pediatric Clinicians Do?
following a 2023 outbreak of elevated levels of lead in children associated with consumption of contaminated applesauce.
Federal legislation in the 1970s eliminated lead from gasoline, paints, and other consumer products, and resulted in significantly reduced blood lead levels (BLLs) in children throughout the United States.
But recently published studies highlight persistent issues with lead in drinking water and consumer products, suggesting that the fight is not over.
It’s in the Water
In 2014 the city of Flint, Michigan, changed its water supply and high levels of lead were later found in the municipal water supply.
Effects of that crisis still plague the city today. An initial study found that elevated BLLs had doubled among children between 2013 and 2015.
Lead exposure in young children is associated with several negative outcomes, including decreased cognitive ability, brain volume, and social mobility, and increased anxiety/depression and impulsivity, and higher rates of criminal offenses later in life.
Many other water systems still contain lead pipes, despite a 1986 ban by the US Environmental Protection Agency on using them for installing or repairing public water systems. The mayor of Chicago announced a plan to start replacing lead service lines in 2020; however, 400,000 households are still served by these pipes, the most in the nation.
Benjamin Huynh, a native of Chicago, was curious about the impact of all those lead service lines. Now an assistant professor in the Department of Environmental Health and Engineering at Johns Hopkins University in Baltimore, Maryland, he and his colleagues researched how many children under the age of 6 years were exposed to contaminated water.
The results showed that lead contamination of water is widespread.
“We’re estimating that 68% of kids under the age of 6 in Chicago were exposed to lead-contaminated drinking water,” Mr. Huynh said.
He added that residents in predominantly Black and Latino neighborhoods had the highest risk for lead contamination in their water, but children living on these blocks were less likely to get tested, suggesting a need for more outreach to raise awareness.
Meanwhile, a little over one third of Chicago residents reported drinking bottled water as their main source of drinking water.
But even bottled water could contain lead. The US Food and Drug Administration (FDA) has set a limit for lead in bottled water to five parts per billion. The FDA threshold for taking action in public drinking water systems is 15 parts per billion. But the American Academy of Pediatrics states that no amount of lead in drinking water is considered safe for drinking.
Mr. Huynh also pointed out that not all home water filters remove lead. Only devices that meet National Sanitation Foundation 53 standards are certified for lead removal. Consumers should verify that the filter package specifically lists the device as certified for removing contaminant lead.
Lead-tainted Cinnamon
Last fall, the North Carolina Department of Health and Human Services identified several children with elevated levels of lead who had consumed WanaBana Apple Cinnamon Fruit Puree pouches.
An investigation by the FDA identified additional brands containing lead and issued a recall of applesauce pouches sold by retailers like Dollar Tree and Amazon.
According to the US Centers for Disease Control and Prevention, nearly 500 children were affected by the tainted applesauce. The FDA traced the source of the lead to cinnamon from a supplier in Ecuador.
An FDA spokesperson told this news organization the episode appears to have resulted from “economically motivated adulteration,” which occurs when a manufacturer leaves out or substitutes a valuable ingredient or part of a food. In the case of spices, lead may be added as a coloring agent or to increase the product weight.
“When we look at domestically made products from large, reputable companies, in general, they do a pretty good job of following safe product guidelines and regulations,” said Kevin Osterhoudt, MD, professor of pediatrics at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “But when we use third-party sellers and we import things from other countries that aren’t regulated as closely, we certainly take a lot more risk in the products that we receive.”
While the Food Safety Modernization Act of 2011 aimed to improve agency’s capacity to manage the ever-rising volume of food produced domestically and imported from overseas, the funding has stayed flat while the volume of inspections has increased. In the early 1990s, the number of shipments screened by the agency numbered in the thousands annually. Last year the FDA screened 15 million shipments from more than 200 countries, according to the agency.
Prompted by the finding of lead in applesauce, the FDA began a wider investigation into ground cinnamon by sampling the product from discount retail stores. It recalled an additional six brands of cinnamon sold in the United States containing lead.
Dr. Osterhoudt’s message to families who think their child might have been exposed to a contaminated product is to dispose of it as directed by FDA and CDC guidelines.
In Philadelphia, where Dr. Osterhoudt practices as an emergency room physician, baseline rates of childhood lead poisoning are already high, so he advises families to “do a larger inventory of all the source potential sources of lead in their life and to reduce all the exposures as low as possible.”
He also advises parents that a nutritious diet high in calcium and iron can protect their children from the deleterious effects of lead.
Current Standards for Lead Screening and Testing
Lead is ubiquitous. The common routes of exposure to humans include use of fossil fuels such as leaded gasoline, some types of industrial facilities, and past use of lead-based paint in homes. In addition to spices, lead has been found in a wide variety of products such as toys, jewelry, antiques, cosmetics, and dietary supplements imported from other countries.
Noah Buncher, DO, is a primary care pediatrician in South Philadelphia at Children’s Hospital of Pennsylvania and the former director of a lead clinic in Boston that provides care for children with lead poisoning. He follows guidelines from the American Academy of Pediatrics that define an elevated BLL as ≥ 3.5 µg/dL. The guidelines recommend screening children for lead exposures during well child visits starting at age 6 months up to 6 years and obtaining a BLL if risks for lead exposure are present.
Dr. Buncher starts with a basic environmental history that covers items like the age, condition, zip code of home, parental occupations, or hobbies that might result in exposing family members to lead, and if another child in the home has a history of elevated BLLs.
But a careful history for potential lead exposures can be time-consuming.
“There’s a lot to cover in a routine well child visit,” Dr. Buncher said. “We have maybe 15-20 minutes to cover a lot.”
Clinics also vary on whether lead screening questions are put into workflows in the electronic medical record. Although parents can complete a written questionnaire about possible lead exposures, they may have difficulty answering questions about the age of their home or not know whether their occupation is high risk.
Transportation to a clinic is often a barrier for families, and sometimes patients must travel to a separate lab to be tested for lead.
Dr. Buncher also pointed to the patchwork of local and state requirements that can lead to confusion among providers. Massachusetts, where he formerly practiced, has a universal requirement to test all children at ages 1, 2, and 3 years. But in Pennsylvania, screening laws vary from county to county.
“Pennsylvania should implement universal screening recommendations for all kids under 6 regardless of what county you live in,” Dr. Buncher said.
Protective Measures
Alan Woolf, MD, a professor of pediatrics at Harvard Medical School, Boston, Massachusetts, and director of the Pediatric Environmental Health Center at Boston Children’s Hospital, has a few ideas about how providers can step up their lead game, including partnering with their local health department.
The CDC funds Childhood Lead Poisoning Prevention Programs based in state and local health departments to work with clinicians to improve rates of blood lead testing, monitor the prevalence of lead in their jurisdictions, and ensure that a system of referral is available for treatment and lead remediation services in the home.
Dr. Woolf also suggested that clinicians refer patients under age 3 years with high BLLs to their local Early Intervention Program.
“They’ll assess their child’s development, their speech, their motor skills, their social skills, and if they qualify, it’s free,” Dr. Woolf said.
He cited research showing children with elevated lead levels who received early intervention services performed better in grade school than equally exposed children who did not access similar services.
Another key strategy for pediatric clinicians is to learn local or state regulations for testing children for lead and how to access lead surveillance data in their practice area. Children who reside in high-risk areas are automatic candidates for screening.
Dr. Woolf pointed out that big cities are not the only localities with lead in the drinking water. If families are drawing water from their own well, they should collect that water annually to have it tested for lead and microbes.
At the clinic-wide level, Dr. Woolf recommends the use of blood lead testing as a quality improvement measure. For example, Akron Children’s Hospital developed a quality improvement initiative using a clinical decision support tool to raise screening rates in their network of 30 clinics. One year after beginning the project, lead screenings during 12-month well visits increased from 71% to 96%.
“What we’re interested in as pediatric health professionals is eliminating all background sources of lead in a child’s environment,” Dr. Woolf said. “Whether that’s applesauce pouches, whether that’s lead-containing paint, lead in water, lead in spices, or lead in imported pottery or cookware — there are just a tremendous number of sources of lead that we can do something about.”
None of the subjects reported financial conflicts of interest.
A former pediatrician, Dr. Thomas is a freelance science writer living in Portland, Oregon.
A version of this article appeared on Medscape.com.
following a 2023 outbreak of elevated levels of lead in children associated with consumption of contaminated applesauce.
Federal legislation in the 1970s eliminated lead from gasoline, paints, and other consumer products, and resulted in significantly reduced blood lead levels (BLLs) in children throughout the United States.
But recently published studies highlight persistent issues with lead in drinking water and consumer products, suggesting that the fight is not over.
It’s in the Water
In 2014 the city of Flint, Michigan, changed its water supply and high levels of lead were later found in the municipal water supply.
Effects of that crisis still plague the city today. An initial study found that elevated BLLs had doubled among children between 2013 and 2015.
Lead exposure in young children is associated with several negative outcomes, including decreased cognitive ability, brain volume, and social mobility, and increased anxiety/depression and impulsivity, and higher rates of criminal offenses later in life.
Many other water systems still contain lead pipes, despite a 1986 ban by the US Environmental Protection Agency on using them for installing or repairing public water systems. The mayor of Chicago announced a plan to start replacing lead service lines in 2020; however, 400,000 households are still served by these pipes, the most in the nation.
Benjamin Huynh, a native of Chicago, was curious about the impact of all those lead service lines. Now an assistant professor in the Department of Environmental Health and Engineering at Johns Hopkins University in Baltimore, Maryland, he and his colleagues researched how many children under the age of 6 years were exposed to contaminated water.
The results showed that lead contamination of water is widespread.
“We’re estimating that 68% of kids under the age of 6 in Chicago were exposed to lead-contaminated drinking water,” Mr. Huynh said.
He added that residents in predominantly Black and Latino neighborhoods had the highest risk for lead contamination in their water, but children living on these blocks were less likely to get tested, suggesting a need for more outreach to raise awareness.
Meanwhile, a little over one third of Chicago residents reported drinking bottled water as their main source of drinking water.
But even bottled water could contain lead. The US Food and Drug Administration (FDA) has set a limit for lead in bottled water to five parts per billion. The FDA threshold for taking action in public drinking water systems is 15 parts per billion. But the American Academy of Pediatrics states that no amount of lead in drinking water is considered safe for drinking.
Mr. Huynh also pointed out that not all home water filters remove lead. Only devices that meet National Sanitation Foundation 53 standards are certified for lead removal. Consumers should verify that the filter package specifically lists the device as certified for removing contaminant lead.
Lead-tainted Cinnamon
Last fall, the North Carolina Department of Health and Human Services identified several children with elevated levels of lead who had consumed WanaBana Apple Cinnamon Fruit Puree pouches.
An investigation by the FDA identified additional brands containing lead and issued a recall of applesauce pouches sold by retailers like Dollar Tree and Amazon.
According to the US Centers for Disease Control and Prevention, nearly 500 children were affected by the tainted applesauce. The FDA traced the source of the lead to cinnamon from a supplier in Ecuador.
An FDA spokesperson told this news organization the episode appears to have resulted from “economically motivated adulteration,” which occurs when a manufacturer leaves out or substitutes a valuable ingredient or part of a food. In the case of spices, lead may be added as a coloring agent or to increase the product weight.
“When we look at domestically made products from large, reputable companies, in general, they do a pretty good job of following safe product guidelines and regulations,” said Kevin Osterhoudt, MD, professor of pediatrics at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “But when we use third-party sellers and we import things from other countries that aren’t regulated as closely, we certainly take a lot more risk in the products that we receive.”
While the Food Safety Modernization Act of 2011 aimed to improve agency’s capacity to manage the ever-rising volume of food produced domestically and imported from overseas, the funding has stayed flat while the volume of inspections has increased. In the early 1990s, the number of shipments screened by the agency numbered in the thousands annually. Last year the FDA screened 15 million shipments from more than 200 countries, according to the agency.
Prompted by the finding of lead in applesauce, the FDA began a wider investigation into ground cinnamon by sampling the product from discount retail stores. It recalled an additional six brands of cinnamon sold in the United States containing lead.
Dr. Osterhoudt’s message to families who think their child might have been exposed to a contaminated product is to dispose of it as directed by FDA and CDC guidelines.
In Philadelphia, where Dr. Osterhoudt practices as an emergency room physician, baseline rates of childhood lead poisoning are already high, so he advises families to “do a larger inventory of all the source potential sources of lead in their life and to reduce all the exposures as low as possible.”
He also advises parents that a nutritious diet high in calcium and iron can protect their children from the deleterious effects of lead.
Current Standards for Lead Screening and Testing
Lead is ubiquitous. The common routes of exposure to humans include use of fossil fuels such as leaded gasoline, some types of industrial facilities, and past use of lead-based paint in homes. In addition to spices, lead has been found in a wide variety of products such as toys, jewelry, antiques, cosmetics, and dietary supplements imported from other countries.
Noah Buncher, DO, is a primary care pediatrician in South Philadelphia at Children’s Hospital of Pennsylvania and the former director of a lead clinic in Boston that provides care for children with lead poisoning. He follows guidelines from the American Academy of Pediatrics that define an elevated BLL as ≥ 3.5 µg/dL. The guidelines recommend screening children for lead exposures during well child visits starting at age 6 months up to 6 years and obtaining a BLL if risks for lead exposure are present.
Dr. Buncher starts with a basic environmental history that covers items like the age, condition, zip code of home, parental occupations, or hobbies that might result in exposing family members to lead, and if another child in the home has a history of elevated BLLs.
But a careful history for potential lead exposures can be time-consuming.
“There’s a lot to cover in a routine well child visit,” Dr. Buncher said. “We have maybe 15-20 minutes to cover a lot.”
Clinics also vary on whether lead screening questions are put into workflows in the electronic medical record. Although parents can complete a written questionnaire about possible lead exposures, they may have difficulty answering questions about the age of their home or not know whether their occupation is high risk.
Transportation to a clinic is often a barrier for families, and sometimes patients must travel to a separate lab to be tested for lead.
Dr. Buncher also pointed to the patchwork of local and state requirements that can lead to confusion among providers. Massachusetts, where he formerly practiced, has a universal requirement to test all children at ages 1, 2, and 3 years. But in Pennsylvania, screening laws vary from county to county.
“Pennsylvania should implement universal screening recommendations for all kids under 6 regardless of what county you live in,” Dr. Buncher said.
Protective Measures
Alan Woolf, MD, a professor of pediatrics at Harvard Medical School, Boston, Massachusetts, and director of the Pediatric Environmental Health Center at Boston Children’s Hospital, has a few ideas about how providers can step up their lead game, including partnering with their local health department.
The CDC funds Childhood Lead Poisoning Prevention Programs based in state and local health departments to work with clinicians to improve rates of blood lead testing, monitor the prevalence of lead in their jurisdictions, and ensure that a system of referral is available for treatment and lead remediation services in the home.
Dr. Woolf also suggested that clinicians refer patients under age 3 years with high BLLs to their local Early Intervention Program.
“They’ll assess their child’s development, their speech, their motor skills, their social skills, and if they qualify, it’s free,” Dr. Woolf said.
He cited research showing children with elevated lead levels who received early intervention services performed better in grade school than equally exposed children who did not access similar services.
Another key strategy for pediatric clinicians is to learn local or state regulations for testing children for lead and how to access lead surveillance data in their practice area. Children who reside in high-risk areas are automatic candidates for screening.
Dr. Woolf pointed out that big cities are not the only localities with lead in the drinking water. If families are drawing water from their own well, they should collect that water annually to have it tested for lead and microbes.
At the clinic-wide level, Dr. Woolf recommends the use of blood lead testing as a quality improvement measure. For example, Akron Children’s Hospital developed a quality improvement initiative using a clinical decision support tool to raise screening rates in their network of 30 clinics. One year after beginning the project, lead screenings during 12-month well visits increased from 71% to 96%.
“What we’re interested in as pediatric health professionals is eliminating all background sources of lead in a child’s environment,” Dr. Woolf said. “Whether that’s applesauce pouches, whether that’s lead-containing paint, lead in water, lead in spices, or lead in imported pottery or cookware — there are just a tremendous number of sources of lead that we can do something about.”
None of the subjects reported financial conflicts of interest.
A former pediatrician, Dr. Thomas is a freelance science writer living in Portland, Oregon.
A version of this article appeared on Medscape.com.
following a 2023 outbreak of elevated levels of lead in children associated with consumption of contaminated applesauce.
Federal legislation in the 1970s eliminated lead from gasoline, paints, and other consumer products, and resulted in significantly reduced blood lead levels (BLLs) in children throughout the United States.
But recently published studies highlight persistent issues with lead in drinking water and consumer products, suggesting that the fight is not over.
It’s in the Water
In 2014 the city of Flint, Michigan, changed its water supply and high levels of lead were later found in the municipal water supply.
Effects of that crisis still plague the city today. An initial study found that elevated BLLs had doubled among children between 2013 and 2015.
Lead exposure in young children is associated with several negative outcomes, including decreased cognitive ability, brain volume, and social mobility, and increased anxiety/depression and impulsivity, and higher rates of criminal offenses later in life.
Many other water systems still contain lead pipes, despite a 1986 ban by the US Environmental Protection Agency on using them for installing or repairing public water systems. The mayor of Chicago announced a plan to start replacing lead service lines in 2020; however, 400,000 households are still served by these pipes, the most in the nation.
Benjamin Huynh, a native of Chicago, was curious about the impact of all those lead service lines. Now an assistant professor in the Department of Environmental Health and Engineering at Johns Hopkins University in Baltimore, Maryland, he and his colleagues researched how many children under the age of 6 years were exposed to contaminated water.
The results showed that lead contamination of water is widespread.
“We’re estimating that 68% of kids under the age of 6 in Chicago were exposed to lead-contaminated drinking water,” Mr. Huynh said.
He added that residents in predominantly Black and Latino neighborhoods had the highest risk for lead contamination in their water, but children living on these blocks were less likely to get tested, suggesting a need for more outreach to raise awareness.
Meanwhile, a little over one third of Chicago residents reported drinking bottled water as their main source of drinking water.
But even bottled water could contain lead. The US Food and Drug Administration (FDA) has set a limit for lead in bottled water to five parts per billion. The FDA threshold for taking action in public drinking water systems is 15 parts per billion. But the American Academy of Pediatrics states that no amount of lead in drinking water is considered safe for drinking.
Mr. Huynh also pointed out that not all home water filters remove lead. Only devices that meet National Sanitation Foundation 53 standards are certified for lead removal. Consumers should verify that the filter package specifically lists the device as certified for removing contaminant lead.
Lead-tainted Cinnamon
Last fall, the North Carolina Department of Health and Human Services identified several children with elevated levels of lead who had consumed WanaBana Apple Cinnamon Fruit Puree pouches.
An investigation by the FDA identified additional brands containing lead and issued a recall of applesauce pouches sold by retailers like Dollar Tree and Amazon.
According to the US Centers for Disease Control and Prevention, nearly 500 children were affected by the tainted applesauce. The FDA traced the source of the lead to cinnamon from a supplier in Ecuador.
An FDA spokesperson told this news organization the episode appears to have resulted from “economically motivated adulteration,” which occurs when a manufacturer leaves out or substitutes a valuable ingredient or part of a food. In the case of spices, lead may be added as a coloring agent or to increase the product weight.
“When we look at domestically made products from large, reputable companies, in general, they do a pretty good job of following safe product guidelines and regulations,” said Kevin Osterhoudt, MD, professor of pediatrics at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “But when we use third-party sellers and we import things from other countries that aren’t regulated as closely, we certainly take a lot more risk in the products that we receive.”
While the Food Safety Modernization Act of 2011 aimed to improve agency’s capacity to manage the ever-rising volume of food produced domestically and imported from overseas, the funding has stayed flat while the volume of inspections has increased. In the early 1990s, the number of shipments screened by the agency numbered in the thousands annually. Last year the FDA screened 15 million shipments from more than 200 countries, according to the agency.
Prompted by the finding of lead in applesauce, the FDA began a wider investigation into ground cinnamon by sampling the product from discount retail stores. It recalled an additional six brands of cinnamon sold in the United States containing lead.
Dr. Osterhoudt’s message to families who think their child might have been exposed to a contaminated product is to dispose of it as directed by FDA and CDC guidelines.
In Philadelphia, where Dr. Osterhoudt practices as an emergency room physician, baseline rates of childhood lead poisoning are already high, so he advises families to “do a larger inventory of all the source potential sources of lead in their life and to reduce all the exposures as low as possible.”
He also advises parents that a nutritious diet high in calcium and iron can protect their children from the deleterious effects of lead.
Current Standards for Lead Screening and Testing
Lead is ubiquitous. The common routes of exposure to humans include use of fossil fuels such as leaded gasoline, some types of industrial facilities, and past use of lead-based paint in homes. In addition to spices, lead has been found in a wide variety of products such as toys, jewelry, antiques, cosmetics, and dietary supplements imported from other countries.
Noah Buncher, DO, is a primary care pediatrician in South Philadelphia at Children’s Hospital of Pennsylvania and the former director of a lead clinic in Boston that provides care for children with lead poisoning. He follows guidelines from the American Academy of Pediatrics that define an elevated BLL as ≥ 3.5 µg/dL. The guidelines recommend screening children for lead exposures during well child visits starting at age 6 months up to 6 years and obtaining a BLL if risks for lead exposure are present.
Dr. Buncher starts with a basic environmental history that covers items like the age, condition, zip code of home, parental occupations, or hobbies that might result in exposing family members to lead, and if another child in the home has a history of elevated BLLs.
But a careful history for potential lead exposures can be time-consuming.
“There’s a lot to cover in a routine well child visit,” Dr. Buncher said. “We have maybe 15-20 minutes to cover a lot.”
Clinics also vary on whether lead screening questions are put into workflows in the electronic medical record. Although parents can complete a written questionnaire about possible lead exposures, they may have difficulty answering questions about the age of their home or not know whether their occupation is high risk.
Transportation to a clinic is often a barrier for families, and sometimes patients must travel to a separate lab to be tested for lead.
Dr. Buncher also pointed to the patchwork of local and state requirements that can lead to confusion among providers. Massachusetts, where he formerly practiced, has a universal requirement to test all children at ages 1, 2, and 3 years. But in Pennsylvania, screening laws vary from county to county.
“Pennsylvania should implement universal screening recommendations for all kids under 6 regardless of what county you live in,” Dr. Buncher said.
Protective Measures
Alan Woolf, MD, a professor of pediatrics at Harvard Medical School, Boston, Massachusetts, and director of the Pediatric Environmental Health Center at Boston Children’s Hospital, has a few ideas about how providers can step up their lead game, including partnering with their local health department.
The CDC funds Childhood Lead Poisoning Prevention Programs based in state and local health departments to work with clinicians to improve rates of blood lead testing, monitor the prevalence of lead in their jurisdictions, and ensure that a system of referral is available for treatment and lead remediation services in the home.
Dr. Woolf also suggested that clinicians refer patients under age 3 years with high BLLs to their local Early Intervention Program.
“They’ll assess their child’s development, their speech, their motor skills, their social skills, and if they qualify, it’s free,” Dr. Woolf said.
He cited research showing children with elevated lead levels who received early intervention services performed better in grade school than equally exposed children who did not access similar services.
Another key strategy for pediatric clinicians is to learn local or state regulations for testing children for lead and how to access lead surveillance data in their practice area. Children who reside in high-risk areas are automatic candidates for screening.
Dr. Woolf pointed out that big cities are not the only localities with lead in the drinking water. If families are drawing water from their own well, they should collect that water annually to have it tested for lead and microbes.
At the clinic-wide level, Dr. Woolf recommends the use of blood lead testing as a quality improvement measure. For example, Akron Children’s Hospital developed a quality improvement initiative using a clinical decision support tool to raise screening rates in their network of 30 clinics. One year after beginning the project, lead screenings during 12-month well visits increased from 71% to 96%.
“What we’re interested in as pediatric health professionals is eliminating all background sources of lead in a child’s environment,” Dr. Woolf said. “Whether that’s applesauce pouches, whether that’s lead-containing paint, lead in water, lead in spices, or lead in imported pottery or cookware — there are just a tremendous number of sources of lead that we can do something about.”
None of the subjects reported financial conflicts of interest.
A former pediatrician, Dr. Thomas is a freelance science writer living in Portland, Oregon.
A version of this article appeared on Medscape.com.
How PCPs Can Contribute to Epilepsy Care
The Centers for Disease Control and Prevention (CDC) estimates that 1.1% of US adults have epilepsy. Although 89% report seeing a physician in the past year about their condition, only 62% of adults saw a neurologist or seizure specialist.
These findings prompted Rosemary Kobau, MPH, the acting team lead for the CDC’s epilepsy program, to take a closer look at referral patterns by primary care providers in the United States.
She also noticed what she calls a “big red flag”: “We found that 40% of primary care providers did not indicate that they would refer their patient with epilepsy to a neurologist when their patient fails to respond to treatment, or if they have a change in seizure activity,” Dr. Kobau told this news organization. Individuals with uncontrolled seizures are at risk for multiple adverse health outcomes, along with emotional problems, social stigma, and decreased life expectancy.
Factors that influenced primary care clinicians to refer to a neurologist included prompt availability of appointments, ability to talk to the neurologist, and whether a patient’s insurance covered specialty visits. Proximity of a specialist also was cited as a barrier, because neurologists can be hard to find outside of urban centers.
Wait lists for neurologist are not like to get shorter any time soon, according to a 2019 report from the American Academy of Neurology (AAN). A 2013 workforce report from the AAN found 35 US states, representing 62% of the US population, had fewer neurologists than needed to meet demand. By 2025, demand is projected to exceed supply in 41 states.
Much of the increasing demand for adult neurologists is driven by aging of the population, resulting in higher rates of stroke, Parkinson’s disease, and dementia. But pediatric neurologists are also overwhelmed: Pediatric neurology is one of the top three pediatric subspecialties with the longest wait times. The shortage is exacerbated by difficulties in transitioning adolescents with epilepsy — many diagnosed early in life with neurodevelopmental and epileptic encephalopathy and problem lists that include learning disorders, behavioral issues, and other chronic medical problems — to adult epilepsy specialists.
Although one of the solutions offered by the AAN is more training in epilepsy management for non-neurologists (such as CME programs developed by the American Epilepsy Society), many primary care providers are overwhelmed already. Still, primary care providers are well-positioned to help answer some of the most important questions about the management of patients with seizure disorders.
How to Help
“There’s a lot the pediatrician can do when a child presents with seizures,” said Sucheta Joshi, MD, who serves as the medical director of the Neurological Institute Comprehensive Epilepsy Center at Children’s Hospital Los Angeles.
Step one is helping to allay the fears of family members who witness a seizure. “They can talk about seizure safety, they can talk about first aid when a seizure happens, they can talk about what to do, what not to do,” she advised. Clinicians who see children can find resources for families on the American Academy of Pediatrics (AAP) National Coordinating Center for Epilepsy website, including a 24/7 helpline, information about local chapters of the Epilepsy Foundation, and first aid training for seizures.
Fred Lado, MD, PhD, a professor of neurology at the Zucker School of Medicine at Hofstra-Norwell in Hempstead, New York, said that primary care clinicians have several decision points when it comes to their patients with epilepsy.
The first is whether to initiate medication after the first episode of seizure. Studies show that the risk for a second seizure decreases in patients started on anticonvulsant therapy after a first event, but many clinicians don›t want to commit patients to long-term therapy without more evidence that the patient has epilepsy. Studies have shown that delaying therapy until a second seizure occurs doesn›t negatively affect quality of life and long-term prognosis.
The International League Against Epilepsy (ILAE) advised treatment for patients with two or more unprovoked seizures but revised its recommendation in 2014 to begin treatment after a first seizure for individuals at high risk for a second seizure. History of a brain insult related to a stroke, mass lesion in the brain, or trauma are risk factors for a second seizure, whereas seizures provoked by a concussion, alcohol withdrawal, or exposure to toxins carry low risk for additional episodes.
Dr. Lado also raised the importance of taking a good history from a patient presenting for medical care for a new-onset seizure to determine whether the recent episode is really the first such incident.
Up to half of patients presenting to emergency departments for convulsive seizures have a history of a preceding nonmotor seizure that the patient or their family members have failed to identify. As many as 60% of people with epilepsy have focal seizures, but the majority of these are nonmotor seizures. As a result, these patients often go without a diagnosis until they develop bilateral tonic-clonic seizures — by which time they may already been injured during a seizure or had an accident while driving.
In terms of imaging and other workup that should be performed prior to the first appointment with a pediatric neurologist or epilepsy specialist, Dr. Joshi generally recommends EEG. She also prefers MRI over CT, which is better for finding lesions that tend to cause seizures in kids such as developmental abnormalities like a cortical malformation or a perinatal process. Obtaining an MRI prior to seeing the neurologist is elective, depending on whether the history and clinical presentation suggest a focal lesion.
For adults, Dr. Lado also recommends an EEG and MRI to start but rarely advises other laboratory studies. When patients present to the emergency department with a new-onset seizure, the workup commonly includes a chemistry panel to rule out hypoglycemia or electrolyte abnormalities. But in the outpatient setting, where a patient describes symptoms of a seizure that occurred a week ago or longer, Dr. Lado said the yield of such assessments is low.
“I think the labs are often more useful as you’re thinking about an anticonvulsant,” Dr. Lado said. Particularly for a patient who is facing a long wait to see specialist, obtaining baseline liver enzymes and a complete blood cell count is worthwhile, because many antiseizure medications can cause anemia or liver damage.
Dr. Lado agreed that referral to a specialist is critical for patients with drug-resistant seizures, defined by the ILAE as seizures that persist despite the use of two or more anticonvulsants.
“One of the great problems in epilepsy care is a sort of sense of complacency,” he said. Some of his own patients have become comfortable with their epilepsy diagnosis and profess to be untroubled by having a few seizures per year. In 2018, Dr. Kobau was a co-author on a study reporting that less than half of US adults taking seizure medications were seizure-free in the past year.
This scenario is an opportunity for primary care providers to help determine whether their patients are taking their antiseizure medication correctly. A referral to a specialist might not be necessary if the seizures are occurring because the patient’s prescription ran out. Similarly, if a patient doesn’t take the medication because of unpleasant side effects, raising the dose won’t help.
Dr. Lado’s advice is to explore why the patient’s management plan is not working and make adjustments tailored to their needs. The solution might be as simple as changing the patient to an extended-release formulation to lower the number of daily doses needed, he said.
But for patients who do have recurrent seizures despite good adherence, Dr. Lado strongly urges a referral to an epilepsy specialist. He serves as president of the National Association of Epilepsy Centers (NAEC), a network of more than 260 epilepsy centers in the United States that offer the services of epileptologists, neurosurgeons, neuropsychologists, nurse specialists, EEG technologists, social workers, and others with training and experience in epilepsy care. In addition to adjusting and monitoring medications, patients seen at an NAEC can be evaluated for surgery, neurostimulators, and ketogenic diets.
Improving Self-Management
Another role that primary care can play is promoting self-efficacy among patients with epilepsy.
“Providers have historically tended to focus on medication adherence alone, ignoring other health enhancing behaviors, even just sleep hygiene,” Dr. Kobau said. But adequate sleep, regular exercise, a healthy diet, avoidance of tobacco and excessive alcohol, and stress management are all important for seizure management.
In 2007, CDC launched the Managing Epilepsy Well (MEW) Network, which has the mission of advancing self-management research in collaboration with patients with epilepsy as well as a broad range of healthcare providers. “It’s a patient-driven kind of approach consistent with community-based, participatory practice research,” said Dr. Kobau, who oversees the initiative.
The MEW network, which consists of six prevention research centers funded by CDC, has piloted and evaluated several evidence-based programs that can help patients better control their epilepsy.
One such intervention is Project Uplift, which delivers mindfulness-based cognitive-behavioral therapy in a virtual group setting. Behavioral therapy is important for people with seizure disorders, whose risk for depression is more than twice that of the general population. The initial trial found the intervention was effective in reducing depressive symptoms in participants, and research since has focused on adapting the program to provide culturally appropriate care to underserved populations. The eight sessions, held weekly, are available in both English and Spanish.
Another program, HOBSCOTCH, allows patients to meet one-on-one virtually with a trained coach to work on skills for improving attention and memory, common problems among people with epilepsy.
MINDSET involves a tablet-based clinical decision tool that patients can use to track their self-management behaviors, such as taking their medications, seizure triggers, symptoms of depression, and keeping their clinic appointments. It also helps them monitor whether they are getting adequate sleep, reducing their stress, and maintaining social networks. The tool generates a printable action plan for patients to prompt discussion and shared decision-making between patient and clinician to prioritize behavioral issues, set goals, and monitor changes over time.
Clinicians can refer patients to any of the MEW interventions, or patients can enroll themselves online.
Emerging Approaches
The AAN’s 2019 report promoted use of technological solutions to bridge the gap between primary care providers and scarce — as well as distant — neurologists. Many health systems support e-consults between clinicians, allowing simple discussions about medications and advice about testing recommended prior to a neurology visit. Initially developed for treatment for infection with hepatitis C virus, Project Extension for Community Healthcare Outcomes (ECHO) uses a central hub of specialists to support primary care providers via teleconference to conduct case reviews and didactic sessions.
Much of Dr. Joshi’s work has focused on ways to coordinate care to children who live far from a pediatric epilepsy center. In a previous position at the University of Michigan, her team was one of four sites funded by the AAP’s National Coordinating Center for Epilepsy to pilot an intervention using telehealth. Implemented in 2017-2019, the initiative used quality improvement methodology to explore a model where patients went to the office of their primary care provider so that both could participate in the call with a neurologist.
The strategy was successful, resulting in reduced out-of-pocket costs, missed school hours, and missed work hours. Patient satisfaction was high (97%), and more parents in the intervention group than the control group agreed that it was easier to obtain appointments with specialists (95% vs 65%, respectively).
And since the pandemic, in-home telehealth visits have become commonplace, adding to the potential convenience and cost savings of telemedicine.
CDC has invested in Project ECHO as a training program for nonspecialist providers to manage epilepsy. Based at the University of Cincinnati, the initial pilot from 2017 to 2019 trained primary care providers in Ohio and neighboring states using monthly 1-hour sessions via Zoom. According to Dr. Kobau, “Of those 164 primary care providers, 97% reported higher interest in improving their care of patients with epilepsy, and at least 98% reported that they were more confident in treating their patients with epilepsy.” Since that time, over 900 providers have received the training, which now attracts participants from all over the country.
Although the current burden of managing epilepsy now seems to be falling heavily on primary care providers, Dr. Lado said he believes they can provide useful insight into their patients’ history and needs: “I think they are in a unique and impactful position, mostly to refer those patients who are still having seizures.”
Additional Resources for Patients and Providers
- American Academy of Pediatrics National Coordinating Center for Epilepsy
- American Epilepsy Society (CME courses designed to designed to increase knowledge about epilepsy diagnosis, treatment, and management; seizure first-aid; epilepsy stigma; and social determinants of health for people with epilepsy)
- Centers for Disease Control and Prevention .
Dr. Joshi, Dr. Kobau, and Dr. Lado report no relevant financial relationships.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com .
The Centers for Disease Control and Prevention (CDC) estimates that 1.1% of US adults have epilepsy. Although 89% report seeing a physician in the past year about their condition, only 62% of adults saw a neurologist or seizure specialist.
These findings prompted Rosemary Kobau, MPH, the acting team lead for the CDC’s epilepsy program, to take a closer look at referral patterns by primary care providers in the United States.
She also noticed what she calls a “big red flag”: “We found that 40% of primary care providers did not indicate that they would refer their patient with epilepsy to a neurologist when their patient fails to respond to treatment, or if they have a change in seizure activity,” Dr. Kobau told this news organization. Individuals with uncontrolled seizures are at risk for multiple adverse health outcomes, along with emotional problems, social stigma, and decreased life expectancy.
Factors that influenced primary care clinicians to refer to a neurologist included prompt availability of appointments, ability to talk to the neurologist, and whether a patient’s insurance covered specialty visits. Proximity of a specialist also was cited as a barrier, because neurologists can be hard to find outside of urban centers.
Wait lists for neurologist are not like to get shorter any time soon, according to a 2019 report from the American Academy of Neurology (AAN). A 2013 workforce report from the AAN found 35 US states, representing 62% of the US population, had fewer neurologists than needed to meet demand. By 2025, demand is projected to exceed supply in 41 states.
Much of the increasing demand for adult neurologists is driven by aging of the population, resulting in higher rates of stroke, Parkinson’s disease, and dementia. But pediatric neurologists are also overwhelmed: Pediatric neurology is one of the top three pediatric subspecialties with the longest wait times. The shortage is exacerbated by difficulties in transitioning adolescents with epilepsy — many diagnosed early in life with neurodevelopmental and epileptic encephalopathy and problem lists that include learning disorders, behavioral issues, and other chronic medical problems — to adult epilepsy specialists.
Although one of the solutions offered by the AAN is more training in epilepsy management for non-neurologists (such as CME programs developed by the American Epilepsy Society), many primary care providers are overwhelmed already. Still, primary care providers are well-positioned to help answer some of the most important questions about the management of patients with seizure disorders.
How to Help
“There’s a lot the pediatrician can do when a child presents with seizures,” said Sucheta Joshi, MD, who serves as the medical director of the Neurological Institute Comprehensive Epilepsy Center at Children’s Hospital Los Angeles.
Step one is helping to allay the fears of family members who witness a seizure. “They can talk about seizure safety, they can talk about first aid when a seizure happens, they can talk about what to do, what not to do,” she advised. Clinicians who see children can find resources for families on the American Academy of Pediatrics (AAP) National Coordinating Center for Epilepsy website, including a 24/7 helpline, information about local chapters of the Epilepsy Foundation, and first aid training for seizures.
Fred Lado, MD, PhD, a professor of neurology at the Zucker School of Medicine at Hofstra-Norwell in Hempstead, New York, said that primary care clinicians have several decision points when it comes to their patients with epilepsy.
The first is whether to initiate medication after the first episode of seizure. Studies show that the risk for a second seizure decreases in patients started on anticonvulsant therapy after a first event, but many clinicians don›t want to commit patients to long-term therapy without more evidence that the patient has epilepsy. Studies have shown that delaying therapy until a second seizure occurs doesn›t negatively affect quality of life and long-term prognosis.
The International League Against Epilepsy (ILAE) advised treatment for patients with two or more unprovoked seizures but revised its recommendation in 2014 to begin treatment after a first seizure for individuals at high risk for a second seizure. History of a brain insult related to a stroke, mass lesion in the brain, or trauma are risk factors for a second seizure, whereas seizures provoked by a concussion, alcohol withdrawal, or exposure to toxins carry low risk for additional episodes.
Dr. Lado also raised the importance of taking a good history from a patient presenting for medical care for a new-onset seizure to determine whether the recent episode is really the first such incident.
Up to half of patients presenting to emergency departments for convulsive seizures have a history of a preceding nonmotor seizure that the patient or their family members have failed to identify. As many as 60% of people with epilepsy have focal seizures, but the majority of these are nonmotor seizures. As a result, these patients often go without a diagnosis until they develop bilateral tonic-clonic seizures — by which time they may already been injured during a seizure or had an accident while driving.
In terms of imaging and other workup that should be performed prior to the first appointment with a pediatric neurologist or epilepsy specialist, Dr. Joshi generally recommends EEG. She also prefers MRI over CT, which is better for finding lesions that tend to cause seizures in kids such as developmental abnormalities like a cortical malformation or a perinatal process. Obtaining an MRI prior to seeing the neurologist is elective, depending on whether the history and clinical presentation suggest a focal lesion.
For adults, Dr. Lado also recommends an EEG and MRI to start but rarely advises other laboratory studies. When patients present to the emergency department with a new-onset seizure, the workup commonly includes a chemistry panel to rule out hypoglycemia or electrolyte abnormalities. But in the outpatient setting, where a patient describes symptoms of a seizure that occurred a week ago or longer, Dr. Lado said the yield of such assessments is low.
“I think the labs are often more useful as you’re thinking about an anticonvulsant,” Dr. Lado said. Particularly for a patient who is facing a long wait to see specialist, obtaining baseline liver enzymes and a complete blood cell count is worthwhile, because many antiseizure medications can cause anemia or liver damage.
Dr. Lado agreed that referral to a specialist is critical for patients with drug-resistant seizures, defined by the ILAE as seizures that persist despite the use of two or more anticonvulsants.
“One of the great problems in epilepsy care is a sort of sense of complacency,” he said. Some of his own patients have become comfortable with their epilepsy diagnosis and profess to be untroubled by having a few seizures per year. In 2018, Dr. Kobau was a co-author on a study reporting that less than half of US adults taking seizure medications were seizure-free in the past year.
This scenario is an opportunity for primary care providers to help determine whether their patients are taking their antiseizure medication correctly. A referral to a specialist might not be necessary if the seizures are occurring because the patient’s prescription ran out. Similarly, if a patient doesn’t take the medication because of unpleasant side effects, raising the dose won’t help.
Dr. Lado’s advice is to explore why the patient’s management plan is not working and make adjustments tailored to their needs. The solution might be as simple as changing the patient to an extended-release formulation to lower the number of daily doses needed, he said.
But for patients who do have recurrent seizures despite good adherence, Dr. Lado strongly urges a referral to an epilepsy specialist. He serves as president of the National Association of Epilepsy Centers (NAEC), a network of more than 260 epilepsy centers in the United States that offer the services of epileptologists, neurosurgeons, neuropsychologists, nurse specialists, EEG technologists, social workers, and others with training and experience in epilepsy care. In addition to adjusting and monitoring medications, patients seen at an NAEC can be evaluated for surgery, neurostimulators, and ketogenic diets.
Improving Self-Management
Another role that primary care can play is promoting self-efficacy among patients with epilepsy.
“Providers have historically tended to focus on medication adherence alone, ignoring other health enhancing behaviors, even just sleep hygiene,” Dr. Kobau said. But adequate sleep, regular exercise, a healthy diet, avoidance of tobacco and excessive alcohol, and stress management are all important for seizure management.
In 2007, CDC launched the Managing Epilepsy Well (MEW) Network, which has the mission of advancing self-management research in collaboration with patients with epilepsy as well as a broad range of healthcare providers. “It’s a patient-driven kind of approach consistent with community-based, participatory practice research,” said Dr. Kobau, who oversees the initiative.
The MEW network, which consists of six prevention research centers funded by CDC, has piloted and evaluated several evidence-based programs that can help patients better control their epilepsy.
One such intervention is Project Uplift, which delivers mindfulness-based cognitive-behavioral therapy in a virtual group setting. Behavioral therapy is important for people with seizure disorders, whose risk for depression is more than twice that of the general population. The initial trial found the intervention was effective in reducing depressive symptoms in participants, and research since has focused on adapting the program to provide culturally appropriate care to underserved populations. The eight sessions, held weekly, are available in both English and Spanish.
Another program, HOBSCOTCH, allows patients to meet one-on-one virtually with a trained coach to work on skills for improving attention and memory, common problems among people with epilepsy.
MINDSET involves a tablet-based clinical decision tool that patients can use to track their self-management behaviors, such as taking their medications, seizure triggers, symptoms of depression, and keeping their clinic appointments. It also helps them monitor whether they are getting adequate sleep, reducing their stress, and maintaining social networks. The tool generates a printable action plan for patients to prompt discussion and shared decision-making between patient and clinician to prioritize behavioral issues, set goals, and monitor changes over time.
Clinicians can refer patients to any of the MEW interventions, or patients can enroll themselves online.
Emerging Approaches
The AAN’s 2019 report promoted use of technological solutions to bridge the gap between primary care providers and scarce — as well as distant — neurologists. Many health systems support e-consults between clinicians, allowing simple discussions about medications and advice about testing recommended prior to a neurology visit. Initially developed for treatment for infection with hepatitis C virus, Project Extension for Community Healthcare Outcomes (ECHO) uses a central hub of specialists to support primary care providers via teleconference to conduct case reviews and didactic sessions.
Much of Dr. Joshi’s work has focused on ways to coordinate care to children who live far from a pediatric epilepsy center. In a previous position at the University of Michigan, her team was one of four sites funded by the AAP’s National Coordinating Center for Epilepsy to pilot an intervention using telehealth. Implemented in 2017-2019, the initiative used quality improvement methodology to explore a model where patients went to the office of their primary care provider so that both could participate in the call with a neurologist.
The strategy was successful, resulting in reduced out-of-pocket costs, missed school hours, and missed work hours. Patient satisfaction was high (97%), and more parents in the intervention group than the control group agreed that it was easier to obtain appointments with specialists (95% vs 65%, respectively).
And since the pandemic, in-home telehealth visits have become commonplace, adding to the potential convenience and cost savings of telemedicine.
CDC has invested in Project ECHO as a training program for nonspecialist providers to manage epilepsy. Based at the University of Cincinnati, the initial pilot from 2017 to 2019 trained primary care providers in Ohio and neighboring states using monthly 1-hour sessions via Zoom. According to Dr. Kobau, “Of those 164 primary care providers, 97% reported higher interest in improving their care of patients with epilepsy, and at least 98% reported that they were more confident in treating their patients with epilepsy.” Since that time, over 900 providers have received the training, which now attracts participants from all over the country.
Although the current burden of managing epilepsy now seems to be falling heavily on primary care providers, Dr. Lado said he believes they can provide useful insight into their patients’ history and needs: “I think they are in a unique and impactful position, mostly to refer those patients who are still having seizures.”
Additional Resources for Patients and Providers
- American Academy of Pediatrics National Coordinating Center for Epilepsy
- American Epilepsy Society (CME courses designed to designed to increase knowledge about epilepsy diagnosis, treatment, and management; seizure first-aid; epilepsy stigma; and social determinants of health for people with epilepsy)
- Centers for Disease Control and Prevention .
Dr. Joshi, Dr. Kobau, and Dr. Lado report no relevant financial relationships.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com .
The Centers for Disease Control and Prevention (CDC) estimates that 1.1% of US adults have epilepsy. Although 89% report seeing a physician in the past year about their condition, only 62% of adults saw a neurologist or seizure specialist.
These findings prompted Rosemary Kobau, MPH, the acting team lead for the CDC’s epilepsy program, to take a closer look at referral patterns by primary care providers in the United States.
She also noticed what she calls a “big red flag”: “We found that 40% of primary care providers did not indicate that they would refer their patient with epilepsy to a neurologist when their patient fails to respond to treatment, or if they have a change in seizure activity,” Dr. Kobau told this news organization. Individuals with uncontrolled seizures are at risk for multiple adverse health outcomes, along with emotional problems, social stigma, and decreased life expectancy.
Factors that influenced primary care clinicians to refer to a neurologist included prompt availability of appointments, ability to talk to the neurologist, and whether a patient’s insurance covered specialty visits. Proximity of a specialist also was cited as a barrier, because neurologists can be hard to find outside of urban centers.
Wait lists for neurologist are not like to get shorter any time soon, according to a 2019 report from the American Academy of Neurology (AAN). A 2013 workforce report from the AAN found 35 US states, representing 62% of the US population, had fewer neurologists than needed to meet demand. By 2025, demand is projected to exceed supply in 41 states.
Much of the increasing demand for adult neurologists is driven by aging of the population, resulting in higher rates of stroke, Parkinson’s disease, and dementia. But pediatric neurologists are also overwhelmed: Pediatric neurology is one of the top three pediatric subspecialties with the longest wait times. The shortage is exacerbated by difficulties in transitioning adolescents with epilepsy — many diagnosed early in life with neurodevelopmental and epileptic encephalopathy and problem lists that include learning disorders, behavioral issues, and other chronic medical problems — to adult epilepsy specialists.
Although one of the solutions offered by the AAN is more training in epilepsy management for non-neurologists (such as CME programs developed by the American Epilepsy Society), many primary care providers are overwhelmed already. Still, primary care providers are well-positioned to help answer some of the most important questions about the management of patients with seizure disorders.
How to Help
“There’s a lot the pediatrician can do when a child presents with seizures,” said Sucheta Joshi, MD, who serves as the medical director of the Neurological Institute Comprehensive Epilepsy Center at Children’s Hospital Los Angeles.
Step one is helping to allay the fears of family members who witness a seizure. “They can talk about seizure safety, they can talk about first aid when a seizure happens, they can talk about what to do, what not to do,” she advised. Clinicians who see children can find resources for families on the American Academy of Pediatrics (AAP) National Coordinating Center for Epilepsy website, including a 24/7 helpline, information about local chapters of the Epilepsy Foundation, and first aid training for seizures.
Fred Lado, MD, PhD, a professor of neurology at the Zucker School of Medicine at Hofstra-Norwell in Hempstead, New York, said that primary care clinicians have several decision points when it comes to their patients with epilepsy.
The first is whether to initiate medication after the first episode of seizure. Studies show that the risk for a second seizure decreases in patients started on anticonvulsant therapy after a first event, but many clinicians don›t want to commit patients to long-term therapy without more evidence that the patient has epilepsy. Studies have shown that delaying therapy until a second seizure occurs doesn›t negatively affect quality of life and long-term prognosis.
The International League Against Epilepsy (ILAE) advised treatment for patients with two or more unprovoked seizures but revised its recommendation in 2014 to begin treatment after a first seizure for individuals at high risk for a second seizure. History of a brain insult related to a stroke, mass lesion in the brain, or trauma are risk factors for a second seizure, whereas seizures provoked by a concussion, alcohol withdrawal, or exposure to toxins carry low risk for additional episodes.
Dr. Lado also raised the importance of taking a good history from a patient presenting for medical care for a new-onset seizure to determine whether the recent episode is really the first such incident.
Up to half of patients presenting to emergency departments for convulsive seizures have a history of a preceding nonmotor seizure that the patient or their family members have failed to identify. As many as 60% of people with epilepsy have focal seizures, but the majority of these are nonmotor seizures. As a result, these patients often go without a diagnosis until they develop bilateral tonic-clonic seizures — by which time they may already been injured during a seizure or had an accident while driving.
In terms of imaging and other workup that should be performed prior to the first appointment with a pediatric neurologist or epilepsy specialist, Dr. Joshi generally recommends EEG. She also prefers MRI over CT, which is better for finding lesions that tend to cause seizures in kids such as developmental abnormalities like a cortical malformation or a perinatal process. Obtaining an MRI prior to seeing the neurologist is elective, depending on whether the history and clinical presentation suggest a focal lesion.
For adults, Dr. Lado also recommends an EEG and MRI to start but rarely advises other laboratory studies. When patients present to the emergency department with a new-onset seizure, the workup commonly includes a chemistry panel to rule out hypoglycemia or electrolyte abnormalities. But in the outpatient setting, where a patient describes symptoms of a seizure that occurred a week ago or longer, Dr. Lado said the yield of such assessments is low.
“I think the labs are often more useful as you’re thinking about an anticonvulsant,” Dr. Lado said. Particularly for a patient who is facing a long wait to see specialist, obtaining baseline liver enzymes and a complete blood cell count is worthwhile, because many antiseizure medications can cause anemia or liver damage.
Dr. Lado agreed that referral to a specialist is critical for patients with drug-resistant seizures, defined by the ILAE as seizures that persist despite the use of two or more anticonvulsants.
“One of the great problems in epilepsy care is a sort of sense of complacency,” he said. Some of his own patients have become comfortable with their epilepsy diagnosis and profess to be untroubled by having a few seizures per year. In 2018, Dr. Kobau was a co-author on a study reporting that less than half of US adults taking seizure medications were seizure-free in the past year.
This scenario is an opportunity for primary care providers to help determine whether their patients are taking their antiseizure medication correctly. A referral to a specialist might not be necessary if the seizures are occurring because the patient’s prescription ran out. Similarly, if a patient doesn’t take the medication because of unpleasant side effects, raising the dose won’t help.
Dr. Lado’s advice is to explore why the patient’s management plan is not working and make adjustments tailored to their needs. The solution might be as simple as changing the patient to an extended-release formulation to lower the number of daily doses needed, he said.
But for patients who do have recurrent seizures despite good adherence, Dr. Lado strongly urges a referral to an epilepsy specialist. He serves as president of the National Association of Epilepsy Centers (NAEC), a network of more than 260 epilepsy centers in the United States that offer the services of epileptologists, neurosurgeons, neuropsychologists, nurse specialists, EEG technologists, social workers, and others with training and experience in epilepsy care. In addition to adjusting and monitoring medications, patients seen at an NAEC can be evaluated for surgery, neurostimulators, and ketogenic diets.
Improving Self-Management
Another role that primary care can play is promoting self-efficacy among patients with epilepsy.
“Providers have historically tended to focus on medication adherence alone, ignoring other health enhancing behaviors, even just sleep hygiene,” Dr. Kobau said. But adequate sleep, regular exercise, a healthy diet, avoidance of tobacco and excessive alcohol, and stress management are all important for seizure management.
In 2007, CDC launched the Managing Epilepsy Well (MEW) Network, which has the mission of advancing self-management research in collaboration with patients with epilepsy as well as a broad range of healthcare providers. “It’s a patient-driven kind of approach consistent with community-based, participatory practice research,” said Dr. Kobau, who oversees the initiative.
The MEW network, which consists of six prevention research centers funded by CDC, has piloted and evaluated several evidence-based programs that can help patients better control their epilepsy.
One such intervention is Project Uplift, which delivers mindfulness-based cognitive-behavioral therapy in a virtual group setting. Behavioral therapy is important for people with seizure disorders, whose risk for depression is more than twice that of the general population. The initial trial found the intervention was effective in reducing depressive symptoms in participants, and research since has focused on adapting the program to provide culturally appropriate care to underserved populations. The eight sessions, held weekly, are available in both English and Spanish.
Another program, HOBSCOTCH, allows patients to meet one-on-one virtually with a trained coach to work on skills for improving attention and memory, common problems among people with epilepsy.
MINDSET involves a tablet-based clinical decision tool that patients can use to track their self-management behaviors, such as taking their medications, seizure triggers, symptoms of depression, and keeping their clinic appointments. It also helps them monitor whether they are getting adequate sleep, reducing their stress, and maintaining social networks. The tool generates a printable action plan for patients to prompt discussion and shared decision-making between patient and clinician to prioritize behavioral issues, set goals, and monitor changes over time.
Clinicians can refer patients to any of the MEW interventions, or patients can enroll themselves online.
Emerging Approaches
The AAN’s 2019 report promoted use of technological solutions to bridge the gap between primary care providers and scarce — as well as distant — neurologists. Many health systems support e-consults between clinicians, allowing simple discussions about medications and advice about testing recommended prior to a neurology visit. Initially developed for treatment for infection with hepatitis C virus, Project Extension for Community Healthcare Outcomes (ECHO) uses a central hub of specialists to support primary care providers via teleconference to conduct case reviews and didactic sessions.
Much of Dr. Joshi’s work has focused on ways to coordinate care to children who live far from a pediatric epilepsy center. In a previous position at the University of Michigan, her team was one of four sites funded by the AAP’s National Coordinating Center for Epilepsy to pilot an intervention using telehealth. Implemented in 2017-2019, the initiative used quality improvement methodology to explore a model where patients went to the office of their primary care provider so that both could participate in the call with a neurologist.
The strategy was successful, resulting in reduced out-of-pocket costs, missed school hours, and missed work hours. Patient satisfaction was high (97%), and more parents in the intervention group than the control group agreed that it was easier to obtain appointments with specialists (95% vs 65%, respectively).
And since the pandemic, in-home telehealth visits have become commonplace, adding to the potential convenience and cost savings of telemedicine.
CDC has invested in Project ECHO as a training program for nonspecialist providers to manage epilepsy. Based at the University of Cincinnati, the initial pilot from 2017 to 2019 trained primary care providers in Ohio and neighboring states using monthly 1-hour sessions via Zoom. According to Dr. Kobau, “Of those 164 primary care providers, 97% reported higher interest in improving their care of patients with epilepsy, and at least 98% reported that they were more confident in treating their patients with epilepsy.” Since that time, over 900 providers have received the training, which now attracts participants from all over the country.
Although the current burden of managing epilepsy now seems to be falling heavily on primary care providers, Dr. Lado said he believes they can provide useful insight into their patients’ history and needs: “I think they are in a unique and impactful position, mostly to refer those patients who are still having seizures.”
Additional Resources for Patients and Providers
- American Academy of Pediatrics National Coordinating Center for Epilepsy
- American Epilepsy Society (CME courses designed to designed to increase knowledge about epilepsy diagnosis, treatment, and management; seizure first-aid; epilepsy stigma; and social determinants of health for people with epilepsy)
- Centers for Disease Control and Prevention .
Dr. Joshi, Dr. Kobau, and Dr. Lado report no relevant financial relationships.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com .
Breaking the Diagnostic Bottleneck in RA
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).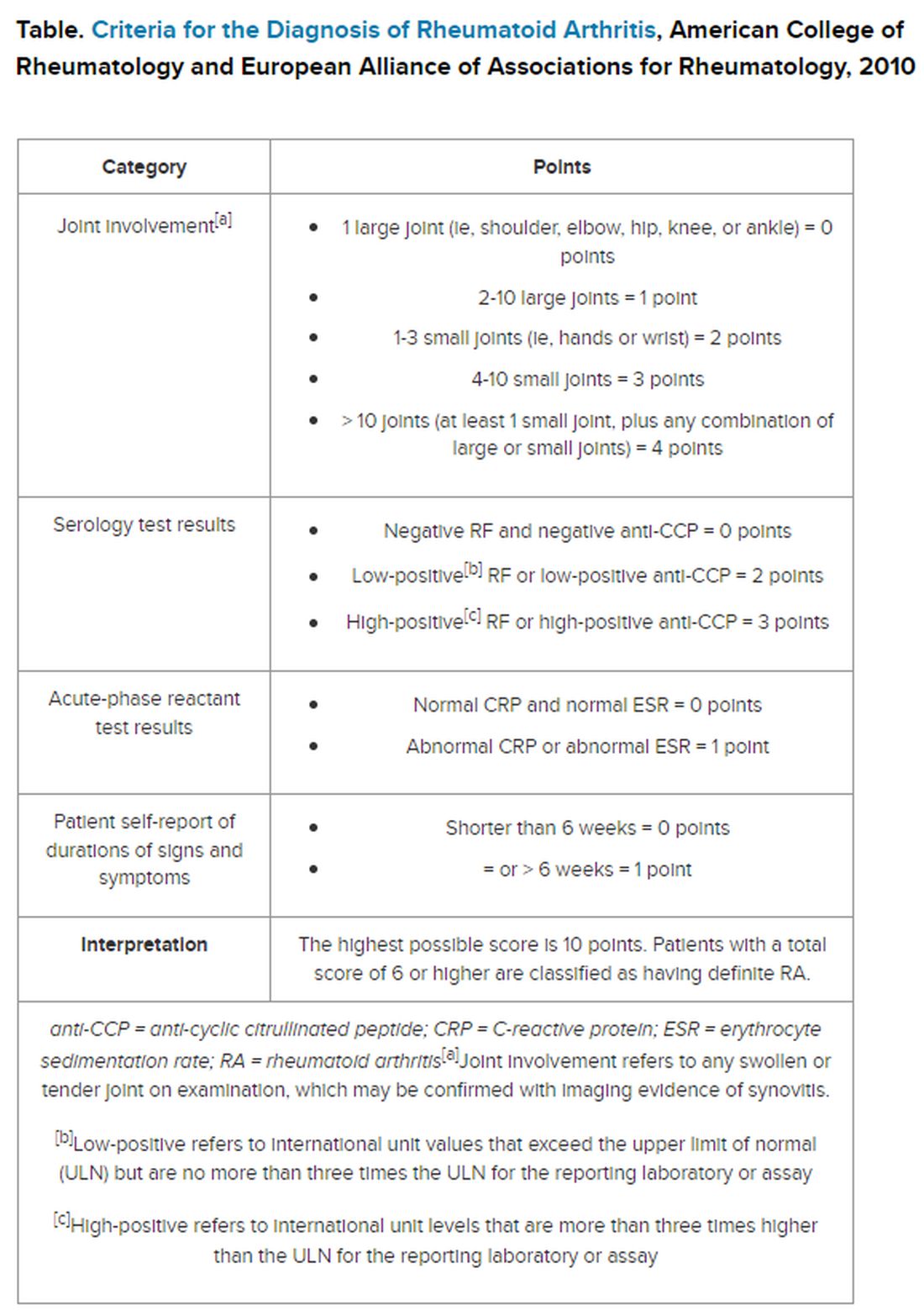
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Why Is Kidney Disease So Often Missed?
Nearly 37 million Americans, or 15%, have chronic kidney disease (CKD), but 9 in 10 adults with the condition are not aware of their diagnosis. A recent study from Stanford University found that
What should primary care providers be doing differently?
The current standard of care is to screen people with underlying conditions that put them at higher risk of developing CKD, most commonly diabetes and hypertension. That’s why the American Diabetes Association recommends annual screening for CKD in patients with type 1 diabetes as well as those with type 2 diabetes.
And the American Heart Association (AHA) released an advisory last year that defined cardiovascular-kidney-metabolic (CKM) syndrome, a constellation of conditions that often occur together: obesity, diabetes, CKD, and cardiovascular disease. They propose a staged approach to identifying and monitoring CKM throughout the lifespan, which includes regular monitoring of the urine albumin-creatinine ratio in patients who have developed diabetes, hypertension, metabolic syndrome, or any signs of kidney disease.
But despite recognition from the subspecialty professional societies of the importance of screening persons with risk factors — additional conditions are obesity and family history of CKD — real-world implementation lags.
Sylvia Rosas, MD, is a nephrologist and associate professor of medicine at Harvard University in Cambridge, Massachusetts, who also serves as president of the National Kidney Foundation. In an interview with this news organization, she cited several alarming facts about the state of CKD screening in the United States.
“Of people with diabetes who have insurance, only 40% get both the glomerular filtration rate (GFR) and the albumin performed, and for those who have hypertension, only 10%,” Dr. Rosas said. She is referring to a urine spot test that measures the amount of albumin in the urine, which is then paired with a serum measurement of creatinine to estimate the glomerular filtration rate. Both tests are needed to detect the asymptomatic stages of CKD, because the presence of albumin in the urine usually precedes drops in the GFR, which indicates more serious disease.
Dr. Rosas said she is frustrated by the low rate of testing compared with other commonly recommended preventive screenings, given the low cost and simplicity of assessment. Serum creatinine often is obtained as part of a routine chemistry panel, and the albumin test requires a single spot urine test. Yet, in 2018, 61% of US adults aged 50-75 years had received a colonoscopy in the past 10 years. Compared with the high price and inconvenience of undergoing colonoscopy, Dr. Rosas has trouble believing that “we cannot get more than 40% of people [with diabetes] to pee in a cup.”
But the biggest issue is that if people with risk factors don’t get screened before they develop symptoms of CKD, it is often too late to avoid dialysis or the need for transplantation.
The early warning symptoms are few, according to Nisha Bansal, MD, a professor in the department of nephrology at the University of Washington in Seattle. “New hypertension is a really important early sign,” Dr. Bansal said. “We know kidney disease almost certainly causes hypertension, so I would definitely think about screening for kidney disease.” Other findings on exam are the appearance of new edema or signs of fluid retention in the hands or around the eyes, along with findings in the urine of albumin, protein, or blood.
But most patients don’t have any symptoms in the early stages, and they can be nonspecific. “It is fatigue and some nausea,” Dr. Rosas said. “It’s only way at the end that you start vomiting, get itchy, or have hiccups.” Data from the Centers for Disease Control and Prevention have shown that over one third of patients at high risk for kidney failure are unaware of their disease. According to Dr. Rosas, these are patients who often receive the diagnosis of CKD and start dialysis the same day.
Why Not Screen Everyone?
For many conditions, like HIV or different types of cancer, the US Preventive Services Task Force (USPSTF) recommends broad screening of asymptomatic individuals so that early treatment can improve outcomes.
But when the USPSTF considered the question in 2012 of whether adults should be screened for CKD regardless of symptoms, it found little evidence that early detection could change the course of their illness. At that time, the standard of care for treating early stages of CKD generally focused on treating the comorbid conditions, such as diabetes, hypertension, and cardiovascular disease.
But the equation has changed with the availability of new drugs to treat CKD, such as sodium-glucose cotransporter 2 (SGLT2) inhibitors and mineralocorticoid receptor antagonists (MRAs).
“I consider these blockbuster drugs,” Dr. Bansal said. “For the first time in decades, we’re showing that this class of medications, the SGLT2 inhibitors, substantially reduce risk of loss of kidney function.”
Expressed in the lumen of the proximal renal tubules, SGLT2 reabsorbs filtered glucose from the tubular lumen. Inhibition of SGLT2 promotes urinary glucose excretion and reduces sodium reabsorption, increasing delivery of sodium to the distal tubule. The first SGLT2 inhibitor, canagliflozin, was approved in 2013 for use as an antihyperglycemic agent but subsequently was shown to have serendipitous benefits for the heart and kidneys.
Clinical trials have documented reductions in the risk for cardiovascular events in patients with type 2 diabetes, as well as decreases in the risk for progression to end-stage renal disease, cardiovascular mortality, and hospitalization for heart failure. Updated international guidelines from 2022 recommend treating all patients with type 2 diabetes and CKD with an estimated GFR ≥ 20 mL/min/1.73 m2 with an SGLT2 inhibitor.
But several trials of SGLT2 inhibitors also demonstrated benefits in reducing the risk for cardiovascular-related death or hospitalization for heart failure, even in patients without diabetes. Although initial approval from the US Food and Drug Administration was limited to patients with diabetes and heart failure, the agency has recently expanded its indications to include adults with CKD who do not have diabetes.
Dr. Bansal said she was happy to see this widening of the indications, which makes more patients eligible to receive SGLT2 inhibitors. “I really think this early CKD group is a great group to consider for those medications,” she said.
Dr. Bansal also pointed out that MRAs are another class of drugs with an interesting history. Earlier steroidal MRAs were found to have anti-inflammatory and antifibrotic properties, and in 1960 spironolactone was approved for use as a diuretic for the management of edema, primary aldosteronism, and hypertension. But even as their use in cardiology rose, MRAs had less utility for CKD, given adverse events such as hyperkalemia and hormonal effects like gynecomastia.
But the latest generation of nonsteroidal MRAs (nsMRAs) has higher selectivity for the mineralocorticoid receptor than sex-steroid hormone receptors, reducing androgenic side effects and preventing elevated potassium. Finerenone, the only nsMRA approved in the United States, has been shown in clinical trials to reduce the incidence of cardiovascular events (death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and CKD outcomes, including kidney failure, decrease in estimated GFR, or death from renal causes.
EPIC Changes Coming?
In light of treatment advances that offer hope of preventing progression of CKD in patients identified early, both the National Kidney Foundation and the American Kidney Fund lobbied the USPSTF in 2022 to conduct a fresh review of recent data to evaluate the need for updated screening recommendations.
The task force completed development of a research plan and collection of public comments in early 2023 and is now reviewing evidence before developing a draft recommendation.
A team of health policy researchers from Stanford is hoping that some of their recently published work will attract the panel’s attention. The first study, published in 2022, evaluated the cost-effectiveness of dapagliflozin, an SGLT2 inhibitor that has been shown to reduce mortality by 48% in CKD patients without diabetes.
The Stanford team found that adding dapagliflozin to standard care for these patients improved life expectancy by 2 years and reduced the percentage of those who needed dialysis or kidney transplant from 17% to 11%.
More recently, Marika Cusick, a doctoral candidate in health policy at the Stanford School of Medicine in Stanford, California, served as first author of an evaluation of the cost-effectiveness of screening asymptomatic adults. “We assessed screening for albuminuria in conjunction with conventional CKD therapy in addition to this new SGLT2 inhibitor class of drugs,” she said. They projected how this might change CKD progression in US adults who are aged 35 or older compared with standard therapy alone.
The findings were favorable. “A one-time screening would result in a reduction of 398,000 cases of kidney replacement therapy [defined as needing either dialysis or renal transplant] among 158 million US adults who are currently aged 35-75 years,” Ms. Cusick told this news organization.
In terms of quality-adjusted life years (QALYs), a one-time screening at age 55 years yielded an incremental cost-effectiveness ratio of $86,300 per QALY. Screening every 10 years between the ages of 35 and 75 years cost less than $100,000 per QALY gained.
According to Doug Owens, MD, professor and chair of the department of health policy at Stanford School of Medicine, “There’s a societal decision about how much are we willing to pay for additional length and quality of life. And this fits within what is generally considered reasonable for the US.”
For example, in the United States, screening for breast cancer among women aged 40-64 years costs $51,000 per QALY, whereas screening for lung cancer using USPSTF guidelines ranges from $72,639 to $156,774 per QALY.
A former member of the USPSTF, Owens predicted that the current review process would take at least another year. Meanwhile, he and Ms. Cusick are hoping that their work influences the USPSTF to recommend screening asymptomatic adults. “Increasing the awareness of these drugs and their effectiveness is a crucial first step,” he said.
Although adherence to current recommendations for screening of people at risk is poor, Dr. Rosas suggested that the USPSTF guidelines would be more influential in changing practice among primary care physicians than subspecialty guidelines would.
“When you have a recommendation like that, they’re putting it in the electronic health record,” she said. By adding best practice alerts to their electronic health record systems, health systems can make it easier for primary care doctors to check all the boxes.
In line with the AHA’s holistic approach towards managing cardiovascular illnesses, CKD, and metabolic disease, Dr. Bansal suggested an additional strategy: “I think we’re moving toward more interdisciplinary care models, where primary care doctors, nephrologist, cardiologists, and endocrinologists — all of us — should be working together in a collaborative care model, to help break down some of these barriers in terms of screening as well as implementation of these therapies.”
Dr. Bansal, Ms. Cusick, and Dr. Owens reported no financial conflicts of interest. Dr. Rosas receives funding from AstraZeneca and Bayer for serving on advisory boards and clinical research funding, as well as funding from the National Institute of Diabetes and Digestive and Kidney Diseases for clinical trials.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com.
Nearly 37 million Americans, or 15%, have chronic kidney disease (CKD), but 9 in 10 adults with the condition are not aware of their diagnosis. A recent study from Stanford University found that
What should primary care providers be doing differently?
The current standard of care is to screen people with underlying conditions that put them at higher risk of developing CKD, most commonly diabetes and hypertension. That’s why the American Diabetes Association recommends annual screening for CKD in patients with type 1 diabetes as well as those with type 2 diabetes.
And the American Heart Association (AHA) released an advisory last year that defined cardiovascular-kidney-metabolic (CKM) syndrome, a constellation of conditions that often occur together: obesity, diabetes, CKD, and cardiovascular disease. They propose a staged approach to identifying and monitoring CKM throughout the lifespan, which includes regular monitoring of the urine albumin-creatinine ratio in patients who have developed diabetes, hypertension, metabolic syndrome, or any signs of kidney disease.
But despite recognition from the subspecialty professional societies of the importance of screening persons with risk factors — additional conditions are obesity and family history of CKD — real-world implementation lags.
Sylvia Rosas, MD, is a nephrologist and associate professor of medicine at Harvard University in Cambridge, Massachusetts, who also serves as president of the National Kidney Foundation. In an interview with this news organization, she cited several alarming facts about the state of CKD screening in the United States.
“Of people with diabetes who have insurance, only 40% get both the glomerular filtration rate (GFR) and the albumin performed, and for those who have hypertension, only 10%,” Dr. Rosas said. She is referring to a urine spot test that measures the amount of albumin in the urine, which is then paired with a serum measurement of creatinine to estimate the glomerular filtration rate. Both tests are needed to detect the asymptomatic stages of CKD, because the presence of albumin in the urine usually precedes drops in the GFR, which indicates more serious disease.
Dr. Rosas said she is frustrated by the low rate of testing compared with other commonly recommended preventive screenings, given the low cost and simplicity of assessment. Serum creatinine often is obtained as part of a routine chemistry panel, and the albumin test requires a single spot urine test. Yet, in 2018, 61% of US adults aged 50-75 years had received a colonoscopy in the past 10 years. Compared with the high price and inconvenience of undergoing colonoscopy, Dr. Rosas has trouble believing that “we cannot get more than 40% of people [with diabetes] to pee in a cup.”
But the biggest issue is that if people with risk factors don’t get screened before they develop symptoms of CKD, it is often too late to avoid dialysis or the need for transplantation.
The early warning symptoms are few, according to Nisha Bansal, MD, a professor in the department of nephrology at the University of Washington in Seattle. “New hypertension is a really important early sign,” Dr. Bansal said. “We know kidney disease almost certainly causes hypertension, so I would definitely think about screening for kidney disease.” Other findings on exam are the appearance of new edema or signs of fluid retention in the hands or around the eyes, along with findings in the urine of albumin, protein, or blood.
But most patients don’t have any symptoms in the early stages, and they can be nonspecific. “It is fatigue and some nausea,” Dr. Rosas said. “It’s only way at the end that you start vomiting, get itchy, or have hiccups.” Data from the Centers for Disease Control and Prevention have shown that over one third of patients at high risk for kidney failure are unaware of their disease. According to Dr. Rosas, these are patients who often receive the diagnosis of CKD and start dialysis the same day.
Why Not Screen Everyone?
For many conditions, like HIV or different types of cancer, the US Preventive Services Task Force (USPSTF) recommends broad screening of asymptomatic individuals so that early treatment can improve outcomes.
But when the USPSTF considered the question in 2012 of whether adults should be screened for CKD regardless of symptoms, it found little evidence that early detection could change the course of their illness. At that time, the standard of care for treating early stages of CKD generally focused on treating the comorbid conditions, such as diabetes, hypertension, and cardiovascular disease.
But the equation has changed with the availability of new drugs to treat CKD, such as sodium-glucose cotransporter 2 (SGLT2) inhibitors and mineralocorticoid receptor antagonists (MRAs).
“I consider these blockbuster drugs,” Dr. Bansal said. “For the first time in decades, we’re showing that this class of medications, the SGLT2 inhibitors, substantially reduce risk of loss of kidney function.”
Expressed in the lumen of the proximal renal tubules, SGLT2 reabsorbs filtered glucose from the tubular lumen. Inhibition of SGLT2 promotes urinary glucose excretion and reduces sodium reabsorption, increasing delivery of sodium to the distal tubule. The first SGLT2 inhibitor, canagliflozin, was approved in 2013 for use as an antihyperglycemic agent but subsequently was shown to have serendipitous benefits for the heart and kidneys.
Clinical trials have documented reductions in the risk for cardiovascular events in patients with type 2 diabetes, as well as decreases in the risk for progression to end-stage renal disease, cardiovascular mortality, and hospitalization for heart failure. Updated international guidelines from 2022 recommend treating all patients with type 2 diabetes and CKD with an estimated GFR ≥ 20 mL/min/1.73 m2 with an SGLT2 inhibitor.
But several trials of SGLT2 inhibitors also demonstrated benefits in reducing the risk for cardiovascular-related death or hospitalization for heart failure, even in patients without diabetes. Although initial approval from the US Food and Drug Administration was limited to patients with diabetes and heart failure, the agency has recently expanded its indications to include adults with CKD who do not have diabetes.
Dr. Bansal said she was happy to see this widening of the indications, which makes more patients eligible to receive SGLT2 inhibitors. “I really think this early CKD group is a great group to consider for those medications,” she said.
Dr. Bansal also pointed out that MRAs are another class of drugs with an interesting history. Earlier steroidal MRAs were found to have anti-inflammatory and antifibrotic properties, and in 1960 spironolactone was approved for use as a diuretic for the management of edema, primary aldosteronism, and hypertension. But even as their use in cardiology rose, MRAs had less utility for CKD, given adverse events such as hyperkalemia and hormonal effects like gynecomastia.
But the latest generation of nonsteroidal MRAs (nsMRAs) has higher selectivity for the mineralocorticoid receptor than sex-steroid hormone receptors, reducing androgenic side effects and preventing elevated potassium. Finerenone, the only nsMRA approved in the United States, has been shown in clinical trials to reduce the incidence of cardiovascular events (death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and CKD outcomes, including kidney failure, decrease in estimated GFR, or death from renal causes.
EPIC Changes Coming?
In light of treatment advances that offer hope of preventing progression of CKD in patients identified early, both the National Kidney Foundation and the American Kidney Fund lobbied the USPSTF in 2022 to conduct a fresh review of recent data to evaluate the need for updated screening recommendations.
The task force completed development of a research plan and collection of public comments in early 2023 and is now reviewing evidence before developing a draft recommendation.
A team of health policy researchers from Stanford is hoping that some of their recently published work will attract the panel’s attention. The first study, published in 2022, evaluated the cost-effectiveness of dapagliflozin, an SGLT2 inhibitor that has been shown to reduce mortality by 48% in CKD patients without diabetes.
The Stanford team found that adding dapagliflozin to standard care for these patients improved life expectancy by 2 years and reduced the percentage of those who needed dialysis or kidney transplant from 17% to 11%.
More recently, Marika Cusick, a doctoral candidate in health policy at the Stanford School of Medicine in Stanford, California, served as first author of an evaluation of the cost-effectiveness of screening asymptomatic adults. “We assessed screening for albuminuria in conjunction with conventional CKD therapy in addition to this new SGLT2 inhibitor class of drugs,” she said. They projected how this might change CKD progression in US adults who are aged 35 or older compared with standard therapy alone.
The findings were favorable. “A one-time screening would result in a reduction of 398,000 cases of kidney replacement therapy [defined as needing either dialysis or renal transplant] among 158 million US adults who are currently aged 35-75 years,” Ms. Cusick told this news organization.
In terms of quality-adjusted life years (QALYs), a one-time screening at age 55 years yielded an incremental cost-effectiveness ratio of $86,300 per QALY. Screening every 10 years between the ages of 35 and 75 years cost less than $100,000 per QALY gained.
According to Doug Owens, MD, professor and chair of the department of health policy at Stanford School of Medicine, “There’s a societal decision about how much are we willing to pay for additional length and quality of life. And this fits within what is generally considered reasonable for the US.”
For example, in the United States, screening for breast cancer among women aged 40-64 years costs $51,000 per QALY, whereas screening for lung cancer using USPSTF guidelines ranges from $72,639 to $156,774 per QALY.
A former member of the USPSTF, Owens predicted that the current review process would take at least another year. Meanwhile, he and Ms. Cusick are hoping that their work influences the USPSTF to recommend screening asymptomatic adults. “Increasing the awareness of these drugs and their effectiveness is a crucial first step,” he said.
Although adherence to current recommendations for screening of people at risk is poor, Dr. Rosas suggested that the USPSTF guidelines would be more influential in changing practice among primary care physicians than subspecialty guidelines would.
“When you have a recommendation like that, they’re putting it in the electronic health record,” she said. By adding best practice alerts to their electronic health record systems, health systems can make it easier for primary care doctors to check all the boxes.
In line with the AHA’s holistic approach towards managing cardiovascular illnesses, CKD, and metabolic disease, Dr. Bansal suggested an additional strategy: “I think we’re moving toward more interdisciplinary care models, where primary care doctors, nephrologist, cardiologists, and endocrinologists — all of us — should be working together in a collaborative care model, to help break down some of these barriers in terms of screening as well as implementation of these therapies.”
Dr. Bansal, Ms. Cusick, and Dr. Owens reported no financial conflicts of interest. Dr. Rosas receives funding from AstraZeneca and Bayer for serving on advisory boards and clinical research funding, as well as funding from the National Institute of Diabetes and Digestive and Kidney Diseases for clinical trials.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com.
Nearly 37 million Americans, or 15%, have chronic kidney disease (CKD), but 9 in 10 adults with the condition are not aware of their diagnosis. A recent study from Stanford University found that
What should primary care providers be doing differently?
The current standard of care is to screen people with underlying conditions that put them at higher risk of developing CKD, most commonly diabetes and hypertension. That’s why the American Diabetes Association recommends annual screening for CKD in patients with type 1 diabetes as well as those with type 2 diabetes.
And the American Heart Association (AHA) released an advisory last year that defined cardiovascular-kidney-metabolic (CKM) syndrome, a constellation of conditions that often occur together: obesity, diabetes, CKD, and cardiovascular disease. They propose a staged approach to identifying and monitoring CKM throughout the lifespan, which includes regular monitoring of the urine albumin-creatinine ratio in patients who have developed diabetes, hypertension, metabolic syndrome, or any signs of kidney disease.
But despite recognition from the subspecialty professional societies of the importance of screening persons with risk factors — additional conditions are obesity and family history of CKD — real-world implementation lags.
Sylvia Rosas, MD, is a nephrologist and associate professor of medicine at Harvard University in Cambridge, Massachusetts, who also serves as president of the National Kidney Foundation. In an interview with this news organization, she cited several alarming facts about the state of CKD screening in the United States.
“Of people with diabetes who have insurance, only 40% get both the glomerular filtration rate (GFR) and the albumin performed, and for those who have hypertension, only 10%,” Dr. Rosas said. She is referring to a urine spot test that measures the amount of albumin in the urine, which is then paired with a serum measurement of creatinine to estimate the glomerular filtration rate. Both tests are needed to detect the asymptomatic stages of CKD, because the presence of albumin in the urine usually precedes drops in the GFR, which indicates more serious disease.
Dr. Rosas said she is frustrated by the low rate of testing compared with other commonly recommended preventive screenings, given the low cost and simplicity of assessment. Serum creatinine often is obtained as part of a routine chemistry panel, and the albumin test requires a single spot urine test. Yet, in 2018, 61% of US adults aged 50-75 years had received a colonoscopy in the past 10 years. Compared with the high price and inconvenience of undergoing colonoscopy, Dr. Rosas has trouble believing that “we cannot get more than 40% of people [with diabetes] to pee in a cup.”
But the biggest issue is that if people with risk factors don’t get screened before they develop symptoms of CKD, it is often too late to avoid dialysis or the need for transplantation.
The early warning symptoms are few, according to Nisha Bansal, MD, a professor in the department of nephrology at the University of Washington in Seattle. “New hypertension is a really important early sign,” Dr. Bansal said. “We know kidney disease almost certainly causes hypertension, so I would definitely think about screening for kidney disease.” Other findings on exam are the appearance of new edema or signs of fluid retention in the hands or around the eyes, along with findings in the urine of albumin, protein, or blood.
But most patients don’t have any symptoms in the early stages, and they can be nonspecific. “It is fatigue and some nausea,” Dr. Rosas said. “It’s only way at the end that you start vomiting, get itchy, or have hiccups.” Data from the Centers for Disease Control and Prevention have shown that over one third of patients at high risk for kidney failure are unaware of their disease. According to Dr. Rosas, these are patients who often receive the diagnosis of CKD and start dialysis the same day.
Why Not Screen Everyone?
For many conditions, like HIV or different types of cancer, the US Preventive Services Task Force (USPSTF) recommends broad screening of asymptomatic individuals so that early treatment can improve outcomes.
But when the USPSTF considered the question in 2012 of whether adults should be screened for CKD regardless of symptoms, it found little evidence that early detection could change the course of their illness. At that time, the standard of care for treating early stages of CKD generally focused on treating the comorbid conditions, such as diabetes, hypertension, and cardiovascular disease.
But the equation has changed with the availability of new drugs to treat CKD, such as sodium-glucose cotransporter 2 (SGLT2) inhibitors and mineralocorticoid receptor antagonists (MRAs).
“I consider these blockbuster drugs,” Dr. Bansal said. “For the first time in decades, we’re showing that this class of medications, the SGLT2 inhibitors, substantially reduce risk of loss of kidney function.”
Expressed in the lumen of the proximal renal tubules, SGLT2 reabsorbs filtered glucose from the tubular lumen. Inhibition of SGLT2 promotes urinary glucose excretion and reduces sodium reabsorption, increasing delivery of sodium to the distal tubule. The first SGLT2 inhibitor, canagliflozin, was approved in 2013 for use as an antihyperglycemic agent but subsequently was shown to have serendipitous benefits for the heart and kidneys.
Clinical trials have documented reductions in the risk for cardiovascular events in patients with type 2 diabetes, as well as decreases in the risk for progression to end-stage renal disease, cardiovascular mortality, and hospitalization for heart failure. Updated international guidelines from 2022 recommend treating all patients with type 2 diabetes and CKD with an estimated GFR ≥ 20 mL/min/1.73 m2 with an SGLT2 inhibitor.
But several trials of SGLT2 inhibitors also demonstrated benefits in reducing the risk for cardiovascular-related death or hospitalization for heart failure, even in patients without diabetes. Although initial approval from the US Food and Drug Administration was limited to patients with diabetes and heart failure, the agency has recently expanded its indications to include adults with CKD who do not have diabetes.
Dr. Bansal said she was happy to see this widening of the indications, which makes more patients eligible to receive SGLT2 inhibitors. “I really think this early CKD group is a great group to consider for those medications,” she said.
Dr. Bansal also pointed out that MRAs are another class of drugs with an interesting history. Earlier steroidal MRAs were found to have anti-inflammatory and antifibrotic properties, and in 1960 spironolactone was approved for use as a diuretic for the management of edema, primary aldosteronism, and hypertension. But even as their use in cardiology rose, MRAs had less utility for CKD, given adverse events such as hyperkalemia and hormonal effects like gynecomastia.
But the latest generation of nonsteroidal MRAs (nsMRAs) has higher selectivity for the mineralocorticoid receptor than sex-steroid hormone receptors, reducing androgenic side effects and preventing elevated potassium. Finerenone, the only nsMRA approved in the United States, has been shown in clinical trials to reduce the incidence of cardiovascular events (death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and CKD outcomes, including kidney failure, decrease in estimated GFR, or death from renal causes.
EPIC Changes Coming?
In light of treatment advances that offer hope of preventing progression of CKD in patients identified early, both the National Kidney Foundation and the American Kidney Fund lobbied the USPSTF in 2022 to conduct a fresh review of recent data to evaluate the need for updated screening recommendations.
The task force completed development of a research plan and collection of public comments in early 2023 and is now reviewing evidence before developing a draft recommendation.
A team of health policy researchers from Stanford is hoping that some of their recently published work will attract the panel’s attention. The first study, published in 2022, evaluated the cost-effectiveness of dapagliflozin, an SGLT2 inhibitor that has been shown to reduce mortality by 48% in CKD patients without diabetes.
The Stanford team found that adding dapagliflozin to standard care for these patients improved life expectancy by 2 years and reduced the percentage of those who needed dialysis or kidney transplant from 17% to 11%.
More recently, Marika Cusick, a doctoral candidate in health policy at the Stanford School of Medicine in Stanford, California, served as first author of an evaluation of the cost-effectiveness of screening asymptomatic adults. “We assessed screening for albuminuria in conjunction with conventional CKD therapy in addition to this new SGLT2 inhibitor class of drugs,” she said. They projected how this might change CKD progression in US adults who are aged 35 or older compared with standard therapy alone.
The findings were favorable. “A one-time screening would result in a reduction of 398,000 cases of kidney replacement therapy [defined as needing either dialysis or renal transplant] among 158 million US adults who are currently aged 35-75 years,” Ms. Cusick told this news organization.
In terms of quality-adjusted life years (QALYs), a one-time screening at age 55 years yielded an incremental cost-effectiveness ratio of $86,300 per QALY. Screening every 10 years between the ages of 35 and 75 years cost less than $100,000 per QALY gained.
According to Doug Owens, MD, professor and chair of the department of health policy at Stanford School of Medicine, “There’s a societal decision about how much are we willing to pay for additional length and quality of life. And this fits within what is generally considered reasonable for the US.”
For example, in the United States, screening for breast cancer among women aged 40-64 years costs $51,000 per QALY, whereas screening for lung cancer using USPSTF guidelines ranges from $72,639 to $156,774 per QALY.
A former member of the USPSTF, Owens predicted that the current review process would take at least another year. Meanwhile, he and Ms. Cusick are hoping that their work influences the USPSTF to recommend screening asymptomatic adults. “Increasing the awareness of these drugs and their effectiveness is a crucial first step,” he said.
Although adherence to current recommendations for screening of people at risk is poor, Dr. Rosas suggested that the USPSTF guidelines would be more influential in changing practice among primary care physicians than subspecialty guidelines would.
“When you have a recommendation like that, they’re putting it in the electronic health record,” she said. By adding best practice alerts to their electronic health record systems, health systems can make it easier for primary care doctors to check all the boxes.
In line with the AHA’s holistic approach towards managing cardiovascular illnesses, CKD, and metabolic disease, Dr. Bansal suggested an additional strategy: “I think we’re moving toward more interdisciplinary care models, where primary care doctors, nephrologist, cardiologists, and endocrinologists — all of us — should be working together in a collaborative care model, to help break down some of these barriers in terms of screening as well as implementation of these therapies.”
Dr. Bansal, Ms. Cusick, and Dr. Owens reported no financial conflicts of interest. Dr. Rosas receives funding from AstraZeneca and Bayer for serving on advisory boards and clinical research funding, as well as funding from the National Institute of Diabetes and Digestive and Kidney Diseases for clinical trials.
Dr. Thomas is a pediatrician and epidemiologist living in Portland, Oregon.
A version of this article appeared on Medscape.com.