User login
Mid-Life Hospitalists
Look at hospitalists and you’ll find more gray hair, crow’s feet, and accumulated wisdom than you might expect. While many hospitalists are physicians fresh from residency, the average age of a hospitalist is actually 40—in part because some hospitalist are docs who have left office practices in favor of hospital work.
These docs, who we’ll call “mid-career hospitalists,” take diverse paths to this change. Some miss the adrenaline rush of acute care. Others have become weary of the flat reimbursements and high patient volumes needed to maintain office practices today. Whatever their paths, they’re an interesting lot.
The most common scenario by which mid-career hospitalists make a transition is when hospital administrators recruit their own. That’s how Robert Brannon, MD, an Ob/Gyn in private practice since 1968, became a hospitalist at Presbyterian Hospital of Dallas in July 2005. Shrinking reimbursements, the costs of running an office, having to cover night call, and a national request for proposal (RFP) by the hospital precipitated Dr. Brannon’s career move.
He and nine other Ob/Gyns submitted a proposal in response to the RFP; hospital administrators awarded the group, OB on Call, LLP, a contract to start a hospitalist service for a largely indigent population in a hospital with more than 7,000 births annually.

I had already started to phase out the office practice and was working in a Medicaid clinic and an osteoporosis clinic when the hospital decided it had to do better with its indigent patients, particularly the 80 to 90 each month who came in with no prenatal care,” says Dr. Brannon. “The medical staff knew that resident work rules precluded their work off hours, so patient needs indicated that full-time hospitalists were in order.”
Now Dr. Brannon has the camaraderie of working with other hospitalists and neonatologists, delivering many babies, but still eliminating on-call obligations when he’s off duty.
“I’m doing more significant obstetrics work, re-honing my skills, and doing high-risk deliveries,” he says. “I’m doing what I love without the administrative hassles of a private practice.”
Jeffrey Frank, MD, had an even bigger nut to crack when he switched from an office-based practice to start a hospitalist medicine service at Doctors Medical Center (DMC) in San Pablo, Calif. The 45-year-old internist graduated from medical school in 1987 and worked in a four-person medical group in the area he describes as “very industrial, with oil refineries all around and the home base of the Hells Angels.”
—Scott Oxenhandler, MD
Helping to cover hospitalized patients for five HMOs precipitated his career change. “That was a mini-hospitalist assignment, and I felt I could adapt to full-time,” says Dr. Frank.
On DMC’s medical staff for years, Dr. Frank saw the hospital go from first in market share to a distant second after entrepreneurial doctors built a newer hospital north of town. Dr. Frank’s patients were aging and the prospects for improving the office practice were poor. Then there was Dr. Frank’s 800-pound gorilla: Kaiser-Permanente, a giant with 45% market share, with plans geared to younger patients, and physician salaries that his group couldn’t match. DMC continued slowly downhill, with closure a real risk.
In 2004, with his family’s acceptance of the long hours that launching a hospitalist program would take, Dr. Frank initiated discussions with hospital administrators to become its first chief hospitalist. Rather than leaving the office practice and launching a hospitalist service simultaneously, Dr. Frank approached established vendors for help. He chose IPC for its technology infrastructure and electronic medical records, competitive salaries, and the hope of attracting more physicians, whom Dr. Frank eventually recruited locally.
He built the hospitalist patient base by admitting all patients of the two largest medical groups. His entrepreneurial spirit intrigued both IPC and the hospital’s chief financial officer by reducing the average length of stay from 5.3 to 4.0 days, which improved the bottom line. Dr. Frank’s salary then increased by 30%. He says he loves doing acute care again and sees many of his former patients because the medical group has transferred hospital work to the hospitalists.

—Jeffrey Frank, MD
“I was worried about being at the hospital all the time,” says Dr. Frank. “I’m 45 years old, but energetic because there’s lots of work. I can keep up with three of the hospitalists just out of residency. Seeing my old patients also connects me to my old practice.”
Across the country in Hollywood, Fla., Scott Oxenhandler, MD, a geriatrician, couldn’t be happier with his mid-career change from office-based doctor to hospitalist. He left a thriving practice of eight physicians he helped start in 1987 to be chief hospitalist at Hollywood Memorial Regional Hospital (Fla.). Seeing five to eight hospitalized patients every day as their primary physician, he knew the hospital’s inner workings and how to start a hospitalist program—largely for unassigned patients.
“I wanted a free hand practicing acute care medicine, good compensation and benefits, lack of paperwork hassles, and a great schedule,” says Dr. Oxenhandler.
When he started in July 2004 Dr. Oxenhandler had no problem structuring a hospital medicine service that attracted physicians with competitive salaries and schedules to accommodate individual needs. He now has 21 full- and part-time hospitalists. They mostly work 8 a.m. to 5 p.m. with an average daily census of 12 to 15 and several consults. A nocturnist admits patients from 8 p.m. to 8 a.m., and 10 doctors handle 5 p.m. to 8 p.m. short call four times per month.
Overall, the transition for the 48-year-old veteran was surprisingly easy. “I was in the hospital all the time anyway, and the way internal medicine is evolving there have to be connections between inpatient and outpatient doctors,” says Dr. Oxenhandler. As the hospitalist leader he mentors young doctors, knows how to distribute the workload, and loves to share clinical insights.
Other Paths
For a doctor who finished residency at nearly 40, “mid-career change” takes on new meaning. Ron Jacobs, MD, internist, chief medical officer, and co-founder of PrimeDoc Management Services of Asheville, N.C., was a businessman in his 20s, then studied medicine and started an office practice in 1997. That practice—with four internists, a pulmonologist, and a cardiologist—was thriving. But Dr. Jacobs was bored. He missed the hospital’s intensity, was used to visiting six or eight hospitalized patients daily, and decided that seeing 16 or 18 patients without the office practice would suit him. So he co-founded PrimeDoc, which now has 100 hospitalists practicing in 15 programs throughout the Southeast and Mid-Atlantic.
The 49-year-old doctor eases the transition for other mid-lifers, recognizing that avoiding burnout as a hospitalist requires mental and physical preparation.
“The sheer volume of rounding, whether for an [average daily census] of 18 or 13 consults a day is tough,” says Dr. Jacobs. “They’ve got to be solid internists with strong ICU skills. I like diverse teams of older and younger docs. They work well because a team of hospitalists all just out of residency can easily burn out. They need the experience and mentoring of older docs to augment their up-to-date clinical skills.”
Academia is also fertile ground for mid-career changes. A doctor with an office practice and a faculty appointment may someday close the office and return to the hospital he or she loves. (See the profile of Joseph Snitzer, MD: “Sibling Rivalry,” in The Hospitalist, Sept. 2005.) Scott Wilson, MD, of The University of Iowa Hospitals and Clinic, Rapid City, left to start a hospitalist program in 2000 for the 880-bed University Hospital and its 250-bed Veterans Affairs Hospital after many years of teaching in the medical school. Dr. Wilson was tapped to start the hospitalist program because of improvements he had made in educating physicians.

—Ron Jacobs, MD
“Our program has some unique features, particularly our interaction with residents, improving the med school curriculum, and building research into our practice,” says Dr. Wilson.
In 2004 that included a study showing that patients managed by hospitalists had shorter length of stay (LOS) and lower costs than patients managed by non-hospitalists, but had higher costs per day. (Kaboli PJ, Barnett MJ, Rosenthal GE. Associations with reduced length of stay and costs on an academic hospitalist service. Am J Manag Care. 2004 Aug;10 (8):561-568). The schedule’s tough for a non-20-something: call every fourth night, three-week blocks for six months, then six months of research.
Dr. Wilson enjoys the challenge and the $1 million hospital support the program garnered in 2005. “We meet their needs to reduce LOS and improve quality, and we keep growing our program through new tasks such as surgical co-management of orthopedics,” he says.
Recruiting Them
Hospital administrators who want to recruit mid-career physicians as hospitalists need look no further than their own backyards. The internist or family practice doctor who relishes hospital rounds but has to rush back to the office, such as Dr. Oxenhandler, is a prime candidate for hospitalist recruitment. Areas where medical groups have trouble recruiting new doctors because reimbursements are flat (e.g., San Pablo) are also fertile ground for recruiting. Entrepreneurial physicians like Drs. Brannon and Jacobs, who had already dabbled in other medical careers before becoming hospitalists, are another choice.
Doctors in each of these categories are still brimming with energy and enthusiasm for medicine and are a looking for ways to make things better for patients and themselves. They might be your next hospitalist recruit. TH
Look at hospitalists and you’ll find more gray hair, crow’s feet, and accumulated wisdom than you might expect. While many hospitalists are physicians fresh from residency, the average age of a hospitalist is actually 40—in part because some hospitalist are docs who have left office practices in favor of hospital work.
These docs, who we’ll call “mid-career hospitalists,” take diverse paths to this change. Some miss the adrenaline rush of acute care. Others have become weary of the flat reimbursements and high patient volumes needed to maintain office practices today. Whatever their paths, they’re an interesting lot.
The most common scenario by which mid-career hospitalists make a transition is when hospital administrators recruit their own. That’s how Robert Brannon, MD, an Ob/Gyn in private practice since 1968, became a hospitalist at Presbyterian Hospital of Dallas in July 2005. Shrinking reimbursements, the costs of running an office, having to cover night call, and a national request for proposal (RFP) by the hospital precipitated Dr. Brannon’s career move.
He and nine other Ob/Gyns submitted a proposal in response to the RFP; hospital administrators awarded the group, OB on Call, LLP, a contract to start a hospitalist service for a largely indigent population in a hospital with more than 7,000 births annually.
I had already started to phase out the office practice and was working in a Medicaid clinic and an osteoporosis clinic when the hospital decided it had to do better with its indigent patients, particularly the 80 to 90 each month who came in with no prenatal care,” says Dr. Brannon. “The medical staff knew that resident work rules precluded their work off hours, so patient needs indicated that full-time hospitalists were in order.”
Now Dr. Brannon has the camaraderie of working with other hospitalists and neonatologists, delivering many babies, but still eliminating on-call obligations when he’s off duty.
“I’m doing more significant obstetrics work, re-honing my skills, and doing high-risk deliveries,” he says. “I’m doing what I love without the administrative hassles of a private practice.”
Jeffrey Frank, MD, had an even bigger nut to crack when he switched from an office-based practice to start a hospitalist medicine service at Doctors Medical Center (DMC) in San Pablo, Calif. The 45-year-old internist graduated from medical school in 1987 and worked in a four-person medical group in the area he describes as “very industrial, with oil refineries all around and the home base of the Hells Angels.”
—Scott Oxenhandler, MD
Helping to cover hospitalized patients for five HMOs precipitated his career change. “That was a mini-hospitalist assignment, and I felt I could adapt to full-time,” says Dr. Frank.
On DMC’s medical staff for years, Dr. Frank saw the hospital go from first in market share to a distant second after entrepreneurial doctors built a newer hospital north of town. Dr. Frank’s patients were aging and the prospects for improving the office practice were poor. Then there was Dr. Frank’s 800-pound gorilla: Kaiser-Permanente, a giant with 45% market share, with plans geared to younger patients, and physician salaries that his group couldn’t match. DMC continued slowly downhill, with closure a real risk.
In 2004, with his family’s acceptance of the long hours that launching a hospitalist program would take, Dr. Frank initiated discussions with hospital administrators to become its first chief hospitalist. Rather than leaving the office practice and launching a hospitalist service simultaneously, Dr. Frank approached established vendors for help. He chose IPC for its technology infrastructure and electronic medical records, competitive salaries, and the hope of attracting more physicians, whom Dr. Frank eventually recruited locally.
He built the hospitalist patient base by admitting all patients of the two largest medical groups. His entrepreneurial spirit intrigued both IPC and the hospital’s chief financial officer by reducing the average length of stay from 5.3 to 4.0 days, which improved the bottom line. Dr. Frank’s salary then increased by 30%. He says he loves doing acute care again and sees many of his former patients because the medical group has transferred hospital work to the hospitalists.
—Jeffrey Frank, MD
“I was worried about being at the hospital all the time,” says Dr. Frank. “I’m 45 years old, but energetic because there’s lots of work. I can keep up with three of the hospitalists just out of residency. Seeing my old patients also connects me to my old practice.”
Across the country in Hollywood, Fla., Scott Oxenhandler, MD, a geriatrician, couldn’t be happier with his mid-career change from office-based doctor to hospitalist. He left a thriving practice of eight physicians he helped start in 1987 to be chief hospitalist at Hollywood Memorial Regional Hospital (Fla.). Seeing five to eight hospitalized patients every day as their primary physician, he knew the hospital’s inner workings and how to start a hospitalist program—largely for unassigned patients.
“I wanted a free hand practicing acute care medicine, good compensation and benefits, lack of paperwork hassles, and a great schedule,” says Dr. Oxenhandler.
When he started in July 2004 Dr. Oxenhandler had no problem structuring a hospital medicine service that attracted physicians with competitive salaries and schedules to accommodate individual needs. He now has 21 full- and part-time hospitalists. They mostly work 8 a.m. to 5 p.m. with an average daily census of 12 to 15 and several consults. A nocturnist admits patients from 8 p.m. to 8 a.m., and 10 doctors handle 5 p.m. to 8 p.m. short call four times per month.
Overall, the transition for the 48-year-old veteran was surprisingly easy. “I was in the hospital all the time anyway, and the way internal medicine is evolving there have to be connections between inpatient and outpatient doctors,” says Dr. Oxenhandler. As the hospitalist leader he mentors young doctors, knows how to distribute the workload, and loves to share clinical insights.
Other Paths
For a doctor who finished residency at nearly 40, “mid-career change” takes on new meaning. Ron Jacobs, MD, internist, chief medical officer, and co-founder of PrimeDoc Management Services of Asheville, N.C., was a businessman in his 20s, then studied medicine and started an office practice in 1997. That practice—with four internists, a pulmonologist, and a cardiologist—was thriving. But Dr. Jacobs was bored. He missed the hospital’s intensity, was used to visiting six or eight hospitalized patients daily, and decided that seeing 16 or 18 patients without the office practice would suit him. So he co-founded PrimeDoc, which now has 100 hospitalists practicing in 15 programs throughout the Southeast and Mid-Atlantic.
The 49-year-old doctor eases the transition for other mid-lifers, recognizing that avoiding burnout as a hospitalist requires mental and physical preparation.
“The sheer volume of rounding, whether for an [average daily census] of 18 or 13 consults a day is tough,” says Dr. Jacobs. “They’ve got to be solid internists with strong ICU skills. I like diverse teams of older and younger docs. They work well because a team of hospitalists all just out of residency can easily burn out. They need the experience and mentoring of older docs to augment their up-to-date clinical skills.”
Academia is also fertile ground for mid-career changes. A doctor with an office practice and a faculty appointment may someday close the office and return to the hospital he or she loves. (See the profile of Joseph Snitzer, MD: “Sibling Rivalry,” in The Hospitalist, Sept. 2005.) Scott Wilson, MD, of The University of Iowa Hospitals and Clinic, Rapid City, left to start a hospitalist program in 2000 for the 880-bed University Hospital and its 250-bed Veterans Affairs Hospital after many years of teaching in the medical school. Dr. Wilson was tapped to start the hospitalist program because of improvements he had made in educating physicians.
—Ron Jacobs, MD
“Our program has some unique features, particularly our interaction with residents, improving the med school curriculum, and building research into our practice,” says Dr. Wilson.
In 2004 that included a study showing that patients managed by hospitalists had shorter length of stay (LOS) and lower costs than patients managed by non-hospitalists, but had higher costs per day. (Kaboli PJ, Barnett MJ, Rosenthal GE. Associations with reduced length of stay and costs on an academic hospitalist service. Am J Manag Care. 2004 Aug;10 (8):561-568). The schedule’s tough for a non-20-something: call every fourth night, three-week blocks for six months, then six months of research.
Dr. Wilson enjoys the challenge and the $1 million hospital support the program garnered in 2005. “We meet their needs to reduce LOS and improve quality, and we keep growing our program through new tasks such as surgical co-management of orthopedics,” he says.
Recruiting Them
Hospital administrators who want to recruit mid-career physicians as hospitalists need look no further than their own backyards. The internist or family practice doctor who relishes hospital rounds but has to rush back to the office, such as Dr. Oxenhandler, is a prime candidate for hospitalist recruitment. Areas where medical groups have trouble recruiting new doctors because reimbursements are flat (e.g., San Pablo) are also fertile ground for recruiting. Entrepreneurial physicians like Drs. Brannon and Jacobs, who had already dabbled in other medical careers before becoming hospitalists, are another choice.
Doctors in each of these categories are still brimming with energy and enthusiasm for medicine and are a looking for ways to make things better for patients and themselves. They might be your next hospitalist recruit. TH
Look at hospitalists and you’ll find more gray hair, crow’s feet, and accumulated wisdom than you might expect. While many hospitalists are physicians fresh from residency, the average age of a hospitalist is actually 40—in part because some hospitalist are docs who have left office practices in favor of hospital work.
These docs, who we’ll call “mid-career hospitalists,” take diverse paths to this change. Some miss the adrenaline rush of acute care. Others have become weary of the flat reimbursements and high patient volumes needed to maintain office practices today. Whatever their paths, they’re an interesting lot.
The most common scenario by which mid-career hospitalists make a transition is when hospital administrators recruit their own. That’s how Robert Brannon, MD, an Ob/Gyn in private practice since 1968, became a hospitalist at Presbyterian Hospital of Dallas in July 2005. Shrinking reimbursements, the costs of running an office, having to cover night call, and a national request for proposal (RFP) by the hospital precipitated Dr. Brannon’s career move.
He and nine other Ob/Gyns submitted a proposal in response to the RFP; hospital administrators awarded the group, OB on Call, LLP, a contract to start a hospitalist service for a largely indigent population in a hospital with more than 7,000 births annually.
I had already started to phase out the office practice and was working in a Medicaid clinic and an osteoporosis clinic when the hospital decided it had to do better with its indigent patients, particularly the 80 to 90 each month who came in with no prenatal care,” says Dr. Brannon. “The medical staff knew that resident work rules precluded their work off hours, so patient needs indicated that full-time hospitalists were in order.”
Now Dr. Brannon has the camaraderie of working with other hospitalists and neonatologists, delivering many babies, but still eliminating on-call obligations when he’s off duty.
“I’m doing more significant obstetrics work, re-honing my skills, and doing high-risk deliveries,” he says. “I’m doing what I love without the administrative hassles of a private practice.”
Jeffrey Frank, MD, had an even bigger nut to crack when he switched from an office-based practice to start a hospitalist medicine service at Doctors Medical Center (DMC) in San Pablo, Calif. The 45-year-old internist graduated from medical school in 1987 and worked in a four-person medical group in the area he describes as “very industrial, with oil refineries all around and the home base of the Hells Angels.”
—Scott Oxenhandler, MD
Helping to cover hospitalized patients for five HMOs precipitated his career change. “That was a mini-hospitalist assignment, and I felt I could adapt to full-time,” says Dr. Frank.
On DMC’s medical staff for years, Dr. Frank saw the hospital go from first in market share to a distant second after entrepreneurial doctors built a newer hospital north of town. Dr. Frank’s patients were aging and the prospects for improving the office practice were poor. Then there was Dr. Frank’s 800-pound gorilla: Kaiser-Permanente, a giant with 45% market share, with plans geared to younger patients, and physician salaries that his group couldn’t match. DMC continued slowly downhill, with closure a real risk.
In 2004, with his family’s acceptance of the long hours that launching a hospitalist program would take, Dr. Frank initiated discussions with hospital administrators to become its first chief hospitalist. Rather than leaving the office practice and launching a hospitalist service simultaneously, Dr. Frank approached established vendors for help. He chose IPC for its technology infrastructure and electronic medical records, competitive salaries, and the hope of attracting more physicians, whom Dr. Frank eventually recruited locally.
He built the hospitalist patient base by admitting all patients of the two largest medical groups. His entrepreneurial spirit intrigued both IPC and the hospital’s chief financial officer by reducing the average length of stay from 5.3 to 4.0 days, which improved the bottom line. Dr. Frank’s salary then increased by 30%. He says he loves doing acute care again and sees many of his former patients because the medical group has transferred hospital work to the hospitalists.
—Jeffrey Frank, MD
“I was worried about being at the hospital all the time,” says Dr. Frank. “I’m 45 years old, but energetic because there’s lots of work. I can keep up with three of the hospitalists just out of residency. Seeing my old patients also connects me to my old practice.”
Across the country in Hollywood, Fla., Scott Oxenhandler, MD, a geriatrician, couldn’t be happier with his mid-career change from office-based doctor to hospitalist. He left a thriving practice of eight physicians he helped start in 1987 to be chief hospitalist at Hollywood Memorial Regional Hospital (Fla.). Seeing five to eight hospitalized patients every day as their primary physician, he knew the hospital’s inner workings and how to start a hospitalist program—largely for unassigned patients.
“I wanted a free hand practicing acute care medicine, good compensation and benefits, lack of paperwork hassles, and a great schedule,” says Dr. Oxenhandler.
When he started in July 2004 Dr. Oxenhandler had no problem structuring a hospital medicine service that attracted physicians with competitive salaries and schedules to accommodate individual needs. He now has 21 full- and part-time hospitalists. They mostly work 8 a.m. to 5 p.m. with an average daily census of 12 to 15 and several consults. A nocturnist admits patients from 8 p.m. to 8 a.m., and 10 doctors handle 5 p.m. to 8 p.m. short call four times per month.
Overall, the transition for the 48-year-old veteran was surprisingly easy. “I was in the hospital all the time anyway, and the way internal medicine is evolving there have to be connections between inpatient and outpatient doctors,” says Dr. Oxenhandler. As the hospitalist leader he mentors young doctors, knows how to distribute the workload, and loves to share clinical insights.
Other Paths
For a doctor who finished residency at nearly 40, “mid-career change” takes on new meaning. Ron Jacobs, MD, internist, chief medical officer, and co-founder of PrimeDoc Management Services of Asheville, N.C., was a businessman in his 20s, then studied medicine and started an office practice in 1997. That practice—with four internists, a pulmonologist, and a cardiologist—was thriving. But Dr. Jacobs was bored. He missed the hospital’s intensity, was used to visiting six or eight hospitalized patients daily, and decided that seeing 16 or 18 patients without the office practice would suit him. So he co-founded PrimeDoc, which now has 100 hospitalists practicing in 15 programs throughout the Southeast and Mid-Atlantic.
The 49-year-old doctor eases the transition for other mid-lifers, recognizing that avoiding burnout as a hospitalist requires mental and physical preparation.
“The sheer volume of rounding, whether for an [average daily census] of 18 or 13 consults a day is tough,” says Dr. Jacobs. “They’ve got to be solid internists with strong ICU skills. I like diverse teams of older and younger docs. They work well because a team of hospitalists all just out of residency can easily burn out. They need the experience and mentoring of older docs to augment their up-to-date clinical skills.”
Academia is also fertile ground for mid-career changes. A doctor with an office practice and a faculty appointment may someday close the office and return to the hospital he or she loves. (See the profile of Joseph Snitzer, MD: “Sibling Rivalry,” in The Hospitalist, Sept. 2005.) Scott Wilson, MD, of The University of Iowa Hospitals and Clinic, Rapid City, left to start a hospitalist program in 2000 for the 880-bed University Hospital and its 250-bed Veterans Affairs Hospital after many years of teaching in the medical school. Dr. Wilson was tapped to start the hospitalist program because of improvements he had made in educating physicians.
—Ron Jacobs, MD
“Our program has some unique features, particularly our interaction with residents, improving the med school curriculum, and building research into our practice,” says Dr. Wilson.
In 2004 that included a study showing that patients managed by hospitalists had shorter length of stay (LOS) and lower costs than patients managed by non-hospitalists, but had higher costs per day. (Kaboli PJ, Barnett MJ, Rosenthal GE. Associations with reduced length of stay and costs on an academic hospitalist service. Am J Manag Care. 2004 Aug;10 (8):561-568). The schedule’s tough for a non-20-something: call every fourth night, three-week blocks for six months, then six months of research.
Dr. Wilson enjoys the challenge and the $1 million hospital support the program garnered in 2005. “We meet their needs to reduce LOS and improve quality, and we keep growing our program through new tasks such as surgical co-management of orthopedics,” he says.
Recruiting Them
Hospital administrators who want to recruit mid-career physicians as hospitalists need look no further than their own backyards. The internist or family practice doctor who relishes hospital rounds but has to rush back to the office, such as Dr. Oxenhandler, is a prime candidate for hospitalist recruitment. Areas where medical groups have trouble recruiting new doctors because reimbursements are flat (e.g., San Pablo) are also fertile ground for recruiting. Entrepreneurial physicians like Drs. Brannon and Jacobs, who had already dabbled in other medical careers before becoming hospitalists, are another choice.
Doctors in each of these categories are still brimming with energy and enthusiasm for medicine and are a looking for ways to make things better for patients and themselves. They might be your next hospitalist recruit. TH
HELPS Really Helps
Spend time with hospitalists and their competitive natures readily emerge. Striving for excellence in clinical care, hospital efficiency, and patient satisfaction, they are their hospitals’ beacons for attracting patients from referring physicians. As hospitalists’ capabilities grow, they hone pathways and procedures, improving their hospitals over time. What would happen if those hospitalists systematically shared their collective knowledge?
That’s what’s happening for hospitalists from nine health systems in southeast Michigan. Transcending their individual pursuits of excellence, they have united as Hospitalists as Emerging Leaders in Patient Safety (HELPS), a unique two-year consortium to improve patient safety regionally. Through large and small group meetings, HELPS is defining and tackling paramount patient safety issues, and collecting and sharing data about what works best.
A $117,000 grant from the Blue Cross/Blue Shield Foundation of Michigan awarded in 2005 to the University of Michigan Health Systems (UMHS) spurred the regional collaboration. Co-principal Investigator Scott Flanders, MD, UMHS’ chief of the hospitalist service and an SHM board member, conceived the project several years ago.
“What galvanized me is when I realized that we are a relatively small number of hospitalists overseeing a large number of patients—between 80,000 to 85,000 admissions annually,” he explains. “Those numbers indicated that we need to share our knowledge, treatment guidelines, and processes if we are to significantly improve patient safety.
—Scott Flanders, MD
“I assumed that many hospitalist groups wanted to improve patient safety,” continues Dr. Flanders. “But we were all working in isolation and were too busy caring for our patients to take the time to collaborate with colleagues in other programs.”
Dr. Flanders and HELPS’ other co-principal investigator, Sanjay Saint, MD, MPH, a hospitalist who heads UMHS’ Patient Safety Enhancement Program, were willing to spearhead a regional patient safety initiative with input from fellow hospitalists and patient safety officers. The Blue Cross/Blue Shield Foundation grant allowed the hospitalists to meet face-to-face periodically, target patient safety concerns, share hospitalist medicine group initiatives, collect data, and disseminate findings and best practices among the participants.
Dr. Saint and his colleagues provided one template for change. By using reminders and automatic order sets to prompt doctors to remove urinary catheters in a timely manner and by using anti-bacterial catheters, the team has shown that it can reduce bloodstream and urinary tract infections among its patients.
Drs. Flanders and Saint outlined a broad range of targets for the consortium hospitalists, including eliminating medication errors, creating a culture of safety, increasing the use of prophylactic medications for surgical patients, improving intensive care practices including pneumonia prevention, and examining end-of-life care practices such as pain management and the use of advance directives. Focusing on the elderly, who often fare poorly during hospitalizations, HELPS is looking for ways to prevent falls and delirium for that patient population. Through regular meetings, the hospitalists are developing techniques and benchmarks for performing quality improvement research and compiling lessons learned.
Nora Maloy, who works for Blue Cross/Blue Shield Foundation and who is Michigan’s senior program officer, positions the hospitalist collaboration as part of her foundation’s broader initiative to improve patient safety in response to the Institute of Medicine’s 1999 “Crossing the Quality Chasm” report that 98,000 unnecessary deaths occur annually in U.S. hospitals.
“We are very excited about the HELPS initiative,” says Maloy. “We hope to see outcomes data and best practices emerge from the nine different systems in the project, and to support a hospitalist consortium that can serve as a national model.”
At early meetings the hospitalists developed this process for their work together:
- Identify a common problem to study;
- Present data on the individual hospitalist or hospitalist group’s experience with the problem and a patient safety initiative to correct it;
- Create a steering committee and a team to research and present data on the initiative;
- Capture and organize data;
- Have an on-site visit from a principal investigator who participates in rounds and discusses data collection capabilities;
- Present to the group key steps in performing the patient safety initiative;
- Implement the initiative in as many of the nine hospitals that want to participate;
- Collect data from the larger group and report to the consortium; and
- Disseminate results through other regional and national meetings, and peer-reviewed journals.
HELPS’ funding frees participating hospitalists to attend quarterly meetings. Reflecting on their busy professional lives, Dr. Flanders says that groups are participating on different levels.
“We know that some hospitalist groups are stable, and they will propose initiatives, collect data, etc.,” he explains. “Other groups that may have recruiting and turnover issues and are just surviving won’t be able to do so, but their attendance at the meetings is very important. There are also small ad hoc meetings for those working on specific patient safety projects.
Took the Challenge
Bobby Lee, MD, director of inpatient medical education at the 600-bed Oakwood Hospital and Medical Center in Dearborn, Mich., eagerly joined the consortium when he realized that a large number of patients were being managed by a small number of hospitalist physicians.
“Scott [Flanders] and Sanjay [Saint] were very inclusive of hospitalists from different programs,” says Dr. Lee. “They articulated what’s important to us as hospitalists—that we bring something special to a hospital, to make it a safer place than when we got there.”
Sharing an Idea
Dr. Lee’s initiative, “Preventing Failure to Resuscitate,” addresses the issue that—on average—between 66% and 70% of patients outside the ICU on whom a code blue is called have alterations in their vital signs six to eight hours before the code. Dr. Lee’s solution was a rapid response team (RRT), developed after process analysis and data collection. And he has shared the initiative with HELPS.
“We did a literature review and then collected historical data on code blues at Oakwood,” explains Dr. Lee. “I took the data to our director of accreditation, an RN, and we felt that we could do better.”
After conducting several small pilot projects on different units to determine optimal staffing, equipment, and medications necessary for a quick response to a code, Dr. Lee presented his findings to Oakwood’s senior management, who committed the necessary resources. That includes a CCU nurse, respiratory therapist, either a hospitalist or intensivist, and a medical service resident—four teams in all for 24/7 coverage.
“There were a surprising number of models and variables we had to look at, such as streamlining lab results, getting test results to the bedside faster, and getting emergency boxes with the right pharmaceuticals on each unit,” adds Dr. Lee.
One interesting twist was Oakwood’s inclusion of hospitalists from private hospital medicine groups on the RRT. “Involving both community-based and academic medicine hospitalists has fostered a culture of inclusiveness, and that works,” says Dr. Lee. His final word: “We can’t leave our patients on the edge of the quality chasm. For not a lot of money, an RRT can help us help someone survive a code blue, and beat the odds that only 17% of code blues live to be discharged from the hospital.”
As the HELPS team continues on its two-year journey to better patient safety, the hospitalists will share what works, what doesn’t work, and what obstacles need to be removed. Overall, though, the HELPS’ vision that a small number of hospitalists joining together can have a huge effect on the care of upward of 80,000 patients has already succeeded. TH
Marlene Piturro is a frequent contributor to The Hospitalist.
Spend time with hospitalists and their competitive natures readily emerge. Striving for excellence in clinical care, hospital efficiency, and patient satisfaction, they are their hospitals’ beacons for attracting patients from referring physicians. As hospitalists’ capabilities grow, they hone pathways and procedures, improving their hospitals over time. What would happen if those hospitalists systematically shared their collective knowledge?
That’s what’s happening for hospitalists from nine health systems in southeast Michigan. Transcending their individual pursuits of excellence, they have united as Hospitalists as Emerging Leaders in Patient Safety (HELPS), a unique two-year consortium to improve patient safety regionally. Through large and small group meetings, HELPS is defining and tackling paramount patient safety issues, and collecting and sharing data about what works best.
A $117,000 grant from the Blue Cross/Blue Shield Foundation of Michigan awarded in 2005 to the University of Michigan Health Systems (UMHS) spurred the regional collaboration. Co-principal Investigator Scott Flanders, MD, UMHS’ chief of the hospitalist service and an SHM board member, conceived the project several years ago.
“What galvanized me is when I realized that we are a relatively small number of hospitalists overseeing a large number of patients—between 80,000 to 85,000 admissions annually,” he explains. “Those numbers indicated that we need to share our knowledge, treatment guidelines, and processes if we are to significantly improve patient safety.
—Scott Flanders, MD
“I assumed that many hospitalist groups wanted to improve patient safety,” continues Dr. Flanders. “But we were all working in isolation and were too busy caring for our patients to take the time to collaborate with colleagues in other programs.”
Dr. Flanders and HELPS’ other co-principal investigator, Sanjay Saint, MD, MPH, a hospitalist who heads UMHS’ Patient Safety Enhancement Program, were willing to spearhead a regional patient safety initiative with input from fellow hospitalists and patient safety officers. The Blue Cross/Blue Shield Foundation grant allowed the hospitalists to meet face-to-face periodically, target patient safety concerns, share hospitalist medicine group initiatives, collect data, and disseminate findings and best practices among the participants.
Dr. Saint and his colleagues provided one template for change. By using reminders and automatic order sets to prompt doctors to remove urinary catheters in a timely manner and by using anti-bacterial catheters, the team has shown that it can reduce bloodstream and urinary tract infections among its patients.
Drs. Flanders and Saint outlined a broad range of targets for the consortium hospitalists, including eliminating medication errors, creating a culture of safety, increasing the use of prophylactic medications for surgical patients, improving intensive care practices including pneumonia prevention, and examining end-of-life care practices such as pain management and the use of advance directives. Focusing on the elderly, who often fare poorly during hospitalizations, HELPS is looking for ways to prevent falls and delirium for that patient population. Through regular meetings, the hospitalists are developing techniques and benchmarks for performing quality improvement research and compiling lessons learned.
Nora Maloy, who works for Blue Cross/Blue Shield Foundation and who is Michigan’s senior program officer, positions the hospitalist collaboration as part of her foundation’s broader initiative to improve patient safety in response to the Institute of Medicine’s 1999 “Crossing the Quality Chasm” report that 98,000 unnecessary deaths occur annually in U.S. hospitals.
“We are very excited about the HELPS initiative,” says Maloy. “We hope to see outcomes data and best practices emerge from the nine different systems in the project, and to support a hospitalist consortium that can serve as a national model.”
At early meetings the hospitalists developed this process for their work together:
- Identify a common problem to study;
- Present data on the individual hospitalist or hospitalist group’s experience with the problem and a patient safety initiative to correct it;
- Create a steering committee and a team to research and present data on the initiative;
- Capture and organize data;
- Have an on-site visit from a principal investigator who participates in rounds and discusses data collection capabilities;
- Present to the group key steps in performing the patient safety initiative;
- Implement the initiative in as many of the nine hospitals that want to participate;
- Collect data from the larger group and report to the consortium; and
- Disseminate results through other regional and national meetings, and peer-reviewed journals.
HELPS’ funding frees participating hospitalists to attend quarterly meetings. Reflecting on their busy professional lives, Dr. Flanders says that groups are participating on different levels.
“We know that some hospitalist groups are stable, and they will propose initiatives, collect data, etc.,” he explains. “Other groups that may have recruiting and turnover issues and are just surviving won’t be able to do so, but their attendance at the meetings is very important. There are also small ad hoc meetings for those working on specific patient safety projects.
Took the Challenge
Bobby Lee, MD, director of inpatient medical education at the 600-bed Oakwood Hospital and Medical Center in Dearborn, Mich., eagerly joined the consortium when he realized that a large number of patients were being managed by a small number of hospitalist physicians.
“Scott [Flanders] and Sanjay [Saint] were very inclusive of hospitalists from different programs,” says Dr. Lee. “They articulated what’s important to us as hospitalists—that we bring something special to a hospital, to make it a safer place than when we got there.”
Sharing an Idea
Dr. Lee’s initiative, “Preventing Failure to Resuscitate,” addresses the issue that—on average—between 66% and 70% of patients outside the ICU on whom a code blue is called have alterations in their vital signs six to eight hours before the code. Dr. Lee’s solution was a rapid response team (RRT), developed after process analysis and data collection. And he has shared the initiative with HELPS.
“We did a literature review and then collected historical data on code blues at Oakwood,” explains Dr. Lee. “I took the data to our director of accreditation, an RN, and we felt that we could do better.”
After conducting several small pilot projects on different units to determine optimal staffing, equipment, and medications necessary for a quick response to a code, Dr. Lee presented his findings to Oakwood’s senior management, who committed the necessary resources. That includes a CCU nurse, respiratory therapist, either a hospitalist or intensivist, and a medical service resident—four teams in all for 24/7 coverage.
“There were a surprising number of models and variables we had to look at, such as streamlining lab results, getting test results to the bedside faster, and getting emergency boxes with the right pharmaceuticals on each unit,” adds Dr. Lee.
One interesting twist was Oakwood’s inclusion of hospitalists from private hospital medicine groups on the RRT. “Involving both community-based and academic medicine hospitalists has fostered a culture of inclusiveness, and that works,” says Dr. Lee. His final word: “We can’t leave our patients on the edge of the quality chasm. For not a lot of money, an RRT can help us help someone survive a code blue, and beat the odds that only 17% of code blues live to be discharged from the hospital.”
As the HELPS team continues on its two-year journey to better patient safety, the hospitalists will share what works, what doesn’t work, and what obstacles need to be removed. Overall, though, the HELPS’ vision that a small number of hospitalists joining together can have a huge effect on the care of upward of 80,000 patients has already succeeded. TH
Marlene Piturro is a frequent contributor to The Hospitalist.
Spend time with hospitalists and their competitive natures readily emerge. Striving for excellence in clinical care, hospital efficiency, and patient satisfaction, they are their hospitals’ beacons for attracting patients from referring physicians. As hospitalists’ capabilities grow, they hone pathways and procedures, improving their hospitals over time. What would happen if those hospitalists systematically shared their collective knowledge?
That’s what’s happening for hospitalists from nine health systems in southeast Michigan. Transcending their individual pursuits of excellence, they have united as Hospitalists as Emerging Leaders in Patient Safety (HELPS), a unique two-year consortium to improve patient safety regionally. Through large and small group meetings, HELPS is defining and tackling paramount patient safety issues, and collecting and sharing data about what works best.
A $117,000 grant from the Blue Cross/Blue Shield Foundation of Michigan awarded in 2005 to the University of Michigan Health Systems (UMHS) spurred the regional collaboration. Co-principal Investigator Scott Flanders, MD, UMHS’ chief of the hospitalist service and an SHM board member, conceived the project several years ago.
“What galvanized me is when I realized that we are a relatively small number of hospitalists overseeing a large number of patients—between 80,000 to 85,000 admissions annually,” he explains. “Those numbers indicated that we need to share our knowledge, treatment guidelines, and processes if we are to significantly improve patient safety.
—Scott Flanders, MD
“I assumed that many hospitalist groups wanted to improve patient safety,” continues Dr. Flanders. “But we were all working in isolation and were too busy caring for our patients to take the time to collaborate with colleagues in other programs.”
Dr. Flanders and HELPS’ other co-principal investigator, Sanjay Saint, MD, MPH, a hospitalist who heads UMHS’ Patient Safety Enhancement Program, were willing to spearhead a regional patient safety initiative with input from fellow hospitalists and patient safety officers. The Blue Cross/Blue Shield Foundation grant allowed the hospitalists to meet face-to-face periodically, target patient safety concerns, share hospitalist medicine group initiatives, collect data, and disseminate findings and best practices among the participants.
Dr. Saint and his colleagues provided one template for change. By using reminders and automatic order sets to prompt doctors to remove urinary catheters in a timely manner and by using anti-bacterial catheters, the team has shown that it can reduce bloodstream and urinary tract infections among its patients.
Drs. Flanders and Saint outlined a broad range of targets for the consortium hospitalists, including eliminating medication errors, creating a culture of safety, increasing the use of prophylactic medications for surgical patients, improving intensive care practices including pneumonia prevention, and examining end-of-life care practices such as pain management and the use of advance directives. Focusing on the elderly, who often fare poorly during hospitalizations, HELPS is looking for ways to prevent falls and delirium for that patient population. Through regular meetings, the hospitalists are developing techniques and benchmarks for performing quality improvement research and compiling lessons learned.
Nora Maloy, who works for Blue Cross/Blue Shield Foundation and who is Michigan’s senior program officer, positions the hospitalist collaboration as part of her foundation’s broader initiative to improve patient safety in response to the Institute of Medicine’s 1999 “Crossing the Quality Chasm” report that 98,000 unnecessary deaths occur annually in U.S. hospitals.
“We are very excited about the HELPS initiative,” says Maloy. “We hope to see outcomes data and best practices emerge from the nine different systems in the project, and to support a hospitalist consortium that can serve as a national model.”
At early meetings the hospitalists developed this process for their work together:
- Identify a common problem to study;
- Present data on the individual hospitalist or hospitalist group’s experience with the problem and a patient safety initiative to correct it;
- Create a steering committee and a team to research and present data on the initiative;
- Capture and organize data;
- Have an on-site visit from a principal investigator who participates in rounds and discusses data collection capabilities;
- Present to the group key steps in performing the patient safety initiative;
- Implement the initiative in as many of the nine hospitals that want to participate;
- Collect data from the larger group and report to the consortium; and
- Disseminate results through other regional and national meetings, and peer-reviewed journals.
HELPS’ funding frees participating hospitalists to attend quarterly meetings. Reflecting on their busy professional lives, Dr. Flanders says that groups are participating on different levels.
“We know that some hospitalist groups are stable, and they will propose initiatives, collect data, etc.,” he explains. “Other groups that may have recruiting and turnover issues and are just surviving won’t be able to do so, but their attendance at the meetings is very important. There are also small ad hoc meetings for those working on specific patient safety projects.
Took the Challenge
Bobby Lee, MD, director of inpatient medical education at the 600-bed Oakwood Hospital and Medical Center in Dearborn, Mich., eagerly joined the consortium when he realized that a large number of patients were being managed by a small number of hospitalist physicians.
“Scott [Flanders] and Sanjay [Saint] were very inclusive of hospitalists from different programs,” says Dr. Lee. “They articulated what’s important to us as hospitalists—that we bring something special to a hospital, to make it a safer place than when we got there.”
Sharing an Idea
Dr. Lee’s initiative, “Preventing Failure to Resuscitate,” addresses the issue that—on average—between 66% and 70% of patients outside the ICU on whom a code blue is called have alterations in their vital signs six to eight hours before the code. Dr. Lee’s solution was a rapid response team (RRT), developed after process analysis and data collection. And he has shared the initiative with HELPS.
“We did a literature review and then collected historical data on code blues at Oakwood,” explains Dr. Lee. “I took the data to our director of accreditation, an RN, and we felt that we could do better.”
After conducting several small pilot projects on different units to determine optimal staffing, equipment, and medications necessary for a quick response to a code, Dr. Lee presented his findings to Oakwood’s senior management, who committed the necessary resources. That includes a CCU nurse, respiratory therapist, either a hospitalist or intensivist, and a medical service resident—four teams in all for 24/7 coverage.
“There were a surprising number of models and variables we had to look at, such as streamlining lab results, getting test results to the bedside faster, and getting emergency boxes with the right pharmaceuticals on each unit,” adds Dr. Lee.
One interesting twist was Oakwood’s inclusion of hospitalists from private hospital medicine groups on the RRT. “Involving both community-based and academic medicine hospitalists has fostered a culture of inclusiveness, and that works,” says Dr. Lee. His final word: “We can’t leave our patients on the edge of the quality chasm. For not a lot of money, an RRT can help us help someone survive a code blue, and beat the odds that only 17% of code blues live to be discharged from the hospital.”
As the HELPS team continues on its two-year journey to better patient safety, the hospitalists will share what works, what doesn’t work, and what obstacles need to be removed. Overall, though, the HELPS’ vision that a small number of hospitalists joining together can have a huge effect on the care of upward of 80,000 patients has already succeeded. TH
Marlene Piturro is a frequent contributor to The Hospitalist.
Start Me Up
Hospital medicine groups, like the people who design and populate them, come in all shapes and sizes. Because the field has matured rapidly with the number of hospitalists growing from 8,700 to 12,000 in the past two years and 50% of hospitals with 200 beds or more having hospitalist programs according to Health and Hospitals Network, there’s naturally been some excessive exuberance, fits and starts, and successes and failures along the way. These stories from the trenches of hospitalist group start-ups reveal just how tricky it is to get it right.
Norma Malgoza, MPA, assistant vice president of Chicago-based Sinai Health Systems, launched that 532-bed academic medical center’s
hospital medicine program in July 2005. The department of internal medicine, which wanted to decrease patients’ length of stay, improve care quality, handle large numbers of unassigned patients, and provide 24/7 coverage, prompted Sinai to hire hospitalists.
After conducting a feasibility study and networking with peers at local hospitals that had hospitalist services, Malgoza struggled to start a program that wouldn’t bust the budget but would attract hospitalists attuned to the department of internal medicine’s goals. Attending an SHM one-day conference, “Best Practices in Managing a Hospital Medicine Program,” (see www.hospitalmedicine.org) helped her with financial modeling, projecting volumes, and devising schedules and compensation packages.
With a grasp of what’s involved in starting a hospitalist service, Malgoza launched the program with 6.5 full-time employees and a physician’s assistant who helped with busy emergency department (ED) night admissions. Now, with a hospitalist average daily census (ADC) of 22 and an attractive compensation system, Malgoza says of the hospitalists, “They are so energetic, always accessible, and will find a pharmacist to get a prescription filled, or push the social workers and nurses to get assessments done. It’s wonderful.”
Recognizing the limited amenities of the aging inner-city hospital, Malgoza hopes to offer hospitalists better facilities. “We want to keep them happy, to give them their own space and a library,” she says. In hindsight she’d add a case manager’s salary to the start-up budget and is working on getting that support.
Developing hospitalist programs using a business plan, such as that developed by Sinai Hospital Systems, is one approach. Anne Borik, MD, created an alternative plan. In the 1990s she grew a program in Phoenix from “ground zero,” as she calls it. Unsatisfied professionally in a large multi-specialty group, she sought a transition to inpatient work only.
“Something ignited the fire within me to be a hospitalist,” she says. “I knew I could reduce bed days and increase patient satisfaction because I wouldn’t be in a rush when I saw patients.”
She sent resumes to hospital administrators, colleagues, and her mentor, who introduced Dr. Borik to North Hollywood, Calif.-based IPC-The Hospitalist Company. Dr. Borik and two other physicians launched IPC-Phoenix at Phoenix Arizona Heart Hospital, generating initial referrals by knocking on primary care physicians’ doors, offering to cover night call and vacations. They agreed to take all unassigned patients at the hospital. “We did things that didn’t threaten other doctors. Only what would make their lives easier,” she adds.
Much has changed since the program’s launch. All IPC physicians now use PDAs with proprietary software, leading to 100% compliance with billing, and discharge reports sent directly to primary care physicians. Call centers contact every patient within 48 hours of discharge to follow-up on recommendations. Recognizing that becoming a hospitalist is a difficult transition for any physician, IPC has a six-month orientation period, especially vital for doctors just out of residency.
“We helped kick off this medical specialty,” says Dr. Borik. “What a great feeling that is.”
—Michael Pistoria, DO
Second Time’s a Charm
Sometimes all the planning for a hospitalist program doesn’t produce expected results, and the launch has to be rethought. Mark Krivopal, MD, director of the Hospitalist Program at Beth Israel Deaconess (BID), Needham (Mass.) faced that challenge. Although BID’s main hospital (an academic medical center) had a thriving hospitalist program, the first attempt three years ago to start one at BID-Needham, a 45-bed community hospital, went awry.
“The community physicians didn’t want to cover night call so they hired third-year residents and moonlighters to do so,” says Dr. Krivopal. “There were problems: no 24/7 coverage, the residents capped the number of admissions and called the medical staff to come in beyond that number, the billing system was sub par, and the community doctors felt they were overcharged.”
The program foundered and BID went back to the drawing board with an internal request for proposals to hospital medicine groups. Dr. Krivopal’s group, Affiliated Physicians Group Hospitalists, proposed a program starting with three hospitalists taking referrals from seven of Needham’s medical groups already familiar with them. They eliminated caps on admissions, implemented 24/7 coverage, fixed the billing system, started covering the seven-bed ICU, and decreased moonlighters’ hours.
Twenty medical groups now use Affiliated Physicians Group Hospitalists. As for relationships among the hospitalists, Dr. Krivopal aims for democratic decision-making held over quarterly dinners, frequent e-mails to share information and derail hidden agendas, and financial incentives that reward a steady increase in ADC. He has integrated hospitalists into BID-Needham’s committees, including the executive committee, P&T, medical review, and patient safety. “It’s not billable hours, but committee work gives us knowledge of what goes on in the hospital, from A to Z,” he concludes.
The hospitalists at Dallas’ Presbyterian Hospital also did better the second time around. In 1992 local physicians grew tired of night admissions; they paid two residents to cover for them and then billed payers. Several years later the referring physicians became unhappy with these arrangements and approached the hospital to start a hospitalist service. In 1997 Scott Fitzgerald, MD, who was then chief resident, contemplated the debt and hassles of opening an office, saw a good fit for Dallas Presbyterian’s need for a hospitalist service and his professional goals. He founded MD on Call, a private hospital medicine group, which still serves Dallas Presbyterian and now employs 16 hospitalists. Having experimented with staffing for a 180 patient load, each physician has an ADC of 12-13. “We keep it lower than most groups’ 16-20 patients,” says Dr. Fitzgerald. “Because I scrutinize quarterly data I know that above 16 our costs and LOS creep up.”
In 1999 the program hit a speed bump when the hospital threatened to reduce the group’s rates. The group, in turn, threatened to leave. “We resolved it by demonstrating that every dollar they paid us earned seven dollars for the hospital, not to mention the growing scope of our activities,” says Dr. Fitzgerald. “In the beginning we were forbidden to do consults, particularly for surgeons. Two years later, we were doing it all.”
He says that the hospital loves the group because it serves the medical staff’s goals and helps grow market share, as hospitalists continue to market to physician practices in outlying suburbs.
Rundsarah Tahboub, MD, medical director of the Hospital Medicine Service at Grant Medical Center in Columbus, Ohio, also succeeded the second time around. With a passion for inpatient medicine, she helped launched a hospitalist program in response to restrictions on residents’ hours at Ohio State University. Having just completed a residency herself, Dr. Tahboub struggled with her lack of experience and, she felt, credibility to lead the program.
“I felt I wasn’t being heard, that I had no autonomy or support,” she says. “When my mentor, the program director of family practice residency at Grant, contacted me to establish a hospitalist program there, I took the challenge.”
Dr. Tahboub evaluated her management style, realizing that she values communication and congeniality with colleagues, getting input and analysis before moving ahead, and flexibility in dealing with obstacles. Citing the example of night call, she explains that hospitalists started with day hours only, leaving residents swamped at night and needing an attending physician.
“We [hospitalists] all talked about it,” says Dr. Tahboub. “While we weren’t thrilled to take night call, we each agreed to cover every fourth night because it was necessary for us to do so.”
Dr. Tahboub also had to figure out how to integrate two previously hired nurse practitioners (NPs) into the hospitalist service. “At first we were unsure how to work with them, but we learned that they enable us to see up to 17 patients on average per day rather than the 12-15 without them. They help us with ED admissions, patient education, and discharges,” says Dr. Tahboub. “The hospitalists love having NPs around and it has become a recruiting point in our favor.”
A recent hire—an office manager—helps the physicians keep paperwork on track.
Hindsight
Looking back, the professionals who have started hospitalist programs have some important lessons to share. Discerning the practice climate, both internal and external, is task number one.
“Make sure you understand the political climate in which you are starting the program, give community doctors time to get used to the idea, expect hospitalist turnover in the early stages, and be ready to hire new hospitalists quickly as demand builds,” advises Michael Pistoria, DO, chief of hospital medicine at Lehigh Valley Hospital and Health Network, Allentown, Pa.
Dr. Tahboub emphasizes the importance of hiring hospitalists in tune with the internal practice climate. “Rigid rules don’t work with us, and some physicians can’t tolerate the amount of flexibility in our program,” she notes.
For executives such as Sinai’s Malgoza, speaking with administrators at other institutions and going to conferences to learn about different hospitalist models helps design a program that fits the hospital’s culture.
Dallas Presbyterian’s Dr. Fitzgerald focuses on hiring great physicians. “Hire the best doctors from the best training programs you can,” he says. “Hiring warm bodies just doesn’t cut it. If you have poor quality docs someone else will take your spot.”
Dr. Fitzgerald also advises that slow program growth allows the chief hospitalist to find physicians who mesh with the group’s personalities and culture. “Find those who want a career as hospitalists rather than those putting in a year or two,” he concludes.
Dr. Borik points out that the hospitalist movement has boomed since she started in the 1990s, with hospitals much more in tune with hospitalist values because they save money and rates for malpractice insurance.
“After you’ve done the groundwork the program can operate like a well-oiled machine to accommodate physicians who want to work in this specialty,” she says, cautioning that ”we can’t ever forget that we don’t own the patients. Their loyalty is to their PCPs. If we drop the ball, either in service or communication, we can lose them.” TH
Marlene Piturro wrote about hospital business drivers in the March 2006 issue.
Hospital medicine groups, like the people who design and populate them, come in all shapes and sizes. Because the field has matured rapidly with the number of hospitalists growing from 8,700 to 12,000 in the past two years and 50% of hospitals with 200 beds or more having hospitalist programs according to Health and Hospitals Network, there’s naturally been some excessive exuberance, fits and starts, and successes and failures along the way. These stories from the trenches of hospitalist group start-ups reveal just how tricky it is to get it right.
Norma Malgoza, MPA, assistant vice president of Chicago-based Sinai Health Systems, launched that 532-bed academic medical center’s
hospital medicine program in July 2005. The department of internal medicine, which wanted to decrease patients’ length of stay, improve care quality, handle large numbers of unassigned patients, and provide 24/7 coverage, prompted Sinai to hire hospitalists.
After conducting a feasibility study and networking with peers at local hospitals that had hospitalist services, Malgoza struggled to start a program that wouldn’t bust the budget but would attract hospitalists attuned to the department of internal medicine’s goals. Attending an SHM one-day conference, “Best Practices in Managing a Hospital Medicine Program,” (see www.hospitalmedicine.org) helped her with financial modeling, projecting volumes, and devising schedules and compensation packages.
With a grasp of what’s involved in starting a hospitalist service, Malgoza launched the program with 6.5 full-time employees and a physician’s assistant who helped with busy emergency department (ED) night admissions. Now, with a hospitalist average daily census (ADC) of 22 and an attractive compensation system, Malgoza says of the hospitalists, “They are so energetic, always accessible, and will find a pharmacist to get a prescription filled, or push the social workers and nurses to get assessments done. It’s wonderful.”
Recognizing the limited amenities of the aging inner-city hospital, Malgoza hopes to offer hospitalists better facilities. “We want to keep them happy, to give them their own space and a library,” she says. In hindsight she’d add a case manager’s salary to the start-up budget and is working on getting that support.
Developing hospitalist programs using a business plan, such as that developed by Sinai Hospital Systems, is one approach. Anne Borik, MD, created an alternative plan. In the 1990s she grew a program in Phoenix from “ground zero,” as she calls it. Unsatisfied professionally in a large multi-specialty group, she sought a transition to inpatient work only.
“Something ignited the fire within me to be a hospitalist,” she says. “I knew I could reduce bed days and increase patient satisfaction because I wouldn’t be in a rush when I saw patients.”
She sent resumes to hospital administrators, colleagues, and her mentor, who introduced Dr. Borik to North Hollywood, Calif.-based IPC-The Hospitalist Company. Dr. Borik and two other physicians launched IPC-Phoenix at Phoenix Arizona Heart Hospital, generating initial referrals by knocking on primary care physicians’ doors, offering to cover night call and vacations. They agreed to take all unassigned patients at the hospital. “We did things that didn’t threaten other doctors. Only what would make their lives easier,” she adds.
Much has changed since the program’s launch. All IPC physicians now use PDAs with proprietary software, leading to 100% compliance with billing, and discharge reports sent directly to primary care physicians. Call centers contact every patient within 48 hours of discharge to follow-up on recommendations. Recognizing that becoming a hospitalist is a difficult transition for any physician, IPC has a six-month orientation period, especially vital for doctors just out of residency.
“We helped kick off this medical specialty,” says Dr. Borik. “What a great feeling that is.”
—Michael Pistoria, DO
Second Time’s a Charm
Sometimes all the planning for a hospitalist program doesn’t produce expected results, and the launch has to be rethought. Mark Krivopal, MD, director of the Hospitalist Program at Beth Israel Deaconess (BID), Needham (Mass.) faced that challenge. Although BID’s main hospital (an academic medical center) had a thriving hospitalist program, the first attempt three years ago to start one at BID-Needham, a 45-bed community hospital, went awry.
“The community physicians didn’t want to cover night call so they hired third-year residents and moonlighters to do so,” says Dr. Krivopal. “There were problems: no 24/7 coverage, the residents capped the number of admissions and called the medical staff to come in beyond that number, the billing system was sub par, and the community doctors felt they were overcharged.”
The program foundered and BID went back to the drawing board with an internal request for proposals to hospital medicine groups. Dr. Krivopal’s group, Affiliated Physicians Group Hospitalists, proposed a program starting with three hospitalists taking referrals from seven of Needham’s medical groups already familiar with them. They eliminated caps on admissions, implemented 24/7 coverage, fixed the billing system, started covering the seven-bed ICU, and decreased moonlighters’ hours.
Twenty medical groups now use Affiliated Physicians Group Hospitalists. As for relationships among the hospitalists, Dr. Krivopal aims for democratic decision-making held over quarterly dinners, frequent e-mails to share information and derail hidden agendas, and financial incentives that reward a steady increase in ADC. He has integrated hospitalists into BID-Needham’s committees, including the executive committee, P&T, medical review, and patient safety. “It’s not billable hours, but committee work gives us knowledge of what goes on in the hospital, from A to Z,” he concludes.
The hospitalists at Dallas’ Presbyterian Hospital also did better the second time around. In 1992 local physicians grew tired of night admissions; they paid two residents to cover for them and then billed payers. Several years later the referring physicians became unhappy with these arrangements and approached the hospital to start a hospitalist service. In 1997 Scott Fitzgerald, MD, who was then chief resident, contemplated the debt and hassles of opening an office, saw a good fit for Dallas Presbyterian’s need for a hospitalist service and his professional goals. He founded MD on Call, a private hospital medicine group, which still serves Dallas Presbyterian and now employs 16 hospitalists. Having experimented with staffing for a 180 patient load, each physician has an ADC of 12-13. “We keep it lower than most groups’ 16-20 patients,” says Dr. Fitzgerald. “Because I scrutinize quarterly data I know that above 16 our costs and LOS creep up.”
In 1999 the program hit a speed bump when the hospital threatened to reduce the group’s rates. The group, in turn, threatened to leave. “We resolved it by demonstrating that every dollar they paid us earned seven dollars for the hospital, not to mention the growing scope of our activities,” says Dr. Fitzgerald. “In the beginning we were forbidden to do consults, particularly for surgeons. Two years later, we were doing it all.”
He says that the hospital loves the group because it serves the medical staff’s goals and helps grow market share, as hospitalists continue to market to physician practices in outlying suburbs.
Rundsarah Tahboub, MD, medical director of the Hospital Medicine Service at Grant Medical Center in Columbus, Ohio, also succeeded the second time around. With a passion for inpatient medicine, she helped launched a hospitalist program in response to restrictions on residents’ hours at Ohio State University. Having just completed a residency herself, Dr. Tahboub struggled with her lack of experience and, she felt, credibility to lead the program.
“I felt I wasn’t being heard, that I had no autonomy or support,” she says. “When my mentor, the program director of family practice residency at Grant, contacted me to establish a hospitalist program there, I took the challenge.”
Dr. Tahboub evaluated her management style, realizing that she values communication and congeniality with colleagues, getting input and analysis before moving ahead, and flexibility in dealing with obstacles. Citing the example of night call, she explains that hospitalists started with day hours only, leaving residents swamped at night and needing an attending physician.
“We [hospitalists] all talked about it,” says Dr. Tahboub. “While we weren’t thrilled to take night call, we each agreed to cover every fourth night because it was necessary for us to do so.”
Dr. Tahboub also had to figure out how to integrate two previously hired nurse practitioners (NPs) into the hospitalist service. “At first we were unsure how to work with them, but we learned that they enable us to see up to 17 patients on average per day rather than the 12-15 without them. They help us with ED admissions, patient education, and discharges,” says Dr. Tahboub. “The hospitalists love having NPs around and it has become a recruiting point in our favor.”
A recent hire—an office manager—helps the physicians keep paperwork on track.
Hindsight
Looking back, the professionals who have started hospitalist programs have some important lessons to share. Discerning the practice climate, both internal and external, is task number one.
“Make sure you understand the political climate in which you are starting the program, give community doctors time to get used to the idea, expect hospitalist turnover in the early stages, and be ready to hire new hospitalists quickly as demand builds,” advises Michael Pistoria, DO, chief of hospital medicine at Lehigh Valley Hospital and Health Network, Allentown, Pa.
Dr. Tahboub emphasizes the importance of hiring hospitalists in tune with the internal practice climate. “Rigid rules don’t work with us, and some physicians can’t tolerate the amount of flexibility in our program,” she notes.
For executives such as Sinai’s Malgoza, speaking with administrators at other institutions and going to conferences to learn about different hospitalist models helps design a program that fits the hospital’s culture.
Dallas Presbyterian’s Dr. Fitzgerald focuses on hiring great physicians. “Hire the best doctors from the best training programs you can,” he says. “Hiring warm bodies just doesn’t cut it. If you have poor quality docs someone else will take your spot.”
Dr. Fitzgerald also advises that slow program growth allows the chief hospitalist to find physicians who mesh with the group’s personalities and culture. “Find those who want a career as hospitalists rather than those putting in a year or two,” he concludes.
Dr. Borik points out that the hospitalist movement has boomed since she started in the 1990s, with hospitals much more in tune with hospitalist values because they save money and rates for malpractice insurance.
“After you’ve done the groundwork the program can operate like a well-oiled machine to accommodate physicians who want to work in this specialty,” she says, cautioning that ”we can’t ever forget that we don’t own the patients. Their loyalty is to their PCPs. If we drop the ball, either in service or communication, we can lose them.” TH
Marlene Piturro wrote about hospital business drivers in the March 2006 issue.
Hospital medicine groups, like the people who design and populate them, come in all shapes and sizes. Because the field has matured rapidly with the number of hospitalists growing from 8,700 to 12,000 in the past two years and 50% of hospitals with 200 beds or more having hospitalist programs according to Health and Hospitals Network, there’s naturally been some excessive exuberance, fits and starts, and successes and failures along the way. These stories from the trenches of hospitalist group start-ups reveal just how tricky it is to get it right.
Norma Malgoza, MPA, assistant vice president of Chicago-based Sinai Health Systems, launched that 532-bed academic medical center’s
hospital medicine program in July 2005. The department of internal medicine, which wanted to decrease patients’ length of stay, improve care quality, handle large numbers of unassigned patients, and provide 24/7 coverage, prompted Sinai to hire hospitalists.
After conducting a feasibility study and networking with peers at local hospitals that had hospitalist services, Malgoza struggled to start a program that wouldn’t bust the budget but would attract hospitalists attuned to the department of internal medicine’s goals. Attending an SHM one-day conference, “Best Practices in Managing a Hospital Medicine Program,” (see www.hospitalmedicine.org) helped her with financial modeling, projecting volumes, and devising schedules and compensation packages.
With a grasp of what’s involved in starting a hospitalist service, Malgoza launched the program with 6.5 full-time employees and a physician’s assistant who helped with busy emergency department (ED) night admissions. Now, with a hospitalist average daily census (ADC) of 22 and an attractive compensation system, Malgoza says of the hospitalists, “They are so energetic, always accessible, and will find a pharmacist to get a prescription filled, or push the social workers and nurses to get assessments done. It’s wonderful.”
Recognizing the limited amenities of the aging inner-city hospital, Malgoza hopes to offer hospitalists better facilities. “We want to keep them happy, to give them their own space and a library,” she says. In hindsight she’d add a case manager’s salary to the start-up budget and is working on getting that support.
Developing hospitalist programs using a business plan, such as that developed by Sinai Hospital Systems, is one approach. Anne Borik, MD, created an alternative plan. In the 1990s she grew a program in Phoenix from “ground zero,” as she calls it. Unsatisfied professionally in a large multi-specialty group, she sought a transition to inpatient work only.
“Something ignited the fire within me to be a hospitalist,” she says. “I knew I could reduce bed days and increase patient satisfaction because I wouldn’t be in a rush when I saw patients.”
She sent resumes to hospital administrators, colleagues, and her mentor, who introduced Dr. Borik to North Hollywood, Calif.-based IPC-The Hospitalist Company. Dr. Borik and two other physicians launched IPC-Phoenix at Phoenix Arizona Heart Hospital, generating initial referrals by knocking on primary care physicians’ doors, offering to cover night call and vacations. They agreed to take all unassigned patients at the hospital. “We did things that didn’t threaten other doctors. Only what would make their lives easier,” she adds.
Much has changed since the program’s launch. All IPC physicians now use PDAs with proprietary software, leading to 100% compliance with billing, and discharge reports sent directly to primary care physicians. Call centers contact every patient within 48 hours of discharge to follow-up on recommendations. Recognizing that becoming a hospitalist is a difficult transition for any physician, IPC has a six-month orientation period, especially vital for doctors just out of residency.
“We helped kick off this medical specialty,” says Dr. Borik. “What a great feeling that is.”
—Michael Pistoria, DO
Second Time’s a Charm
Sometimes all the planning for a hospitalist program doesn’t produce expected results, and the launch has to be rethought. Mark Krivopal, MD, director of the Hospitalist Program at Beth Israel Deaconess (BID), Needham (Mass.) faced that challenge. Although BID’s main hospital (an academic medical center) had a thriving hospitalist program, the first attempt three years ago to start one at BID-Needham, a 45-bed community hospital, went awry.
“The community physicians didn’t want to cover night call so they hired third-year residents and moonlighters to do so,” says Dr. Krivopal. “There were problems: no 24/7 coverage, the residents capped the number of admissions and called the medical staff to come in beyond that number, the billing system was sub par, and the community doctors felt they were overcharged.”
The program foundered and BID went back to the drawing board with an internal request for proposals to hospital medicine groups. Dr. Krivopal’s group, Affiliated Physicians Group Hospitalists, proposed a program starting with three hospitalists taking referrals from seven of Needham’s medical groups already familiar with them. They eliminated caps on admissions, implemented 24/7 coverage, fixed the billing system, started covering the seven-bed ICU, and decreased moonlighters’ hours.
Twenty medical groups now use Affiliated Physicians Group Hospitalists. As for relationships among the hospitalists, Dr. Krivopal aims for democratic decision-making held over quarterly dinners, frequent e-mails to share information and derail hidden agendas, and financial incentives that reward a steady increase in ADC. He has integrated hospitalists into BID-Needham’s committees, including the executive committee, P&T, medical review, and patient safety. “It’s not billable hours, but committee work gives us knowledge of what goes on in the hospital, from A to Z,” he concludes.
The hospitalists at Dallas’ Presbyterian Hospital also did better the second time around. In 1992 local physicians grew tired of night admissions; they paid two residents to cover for them and then billed payers. Several years later the referring physicians became unhappy with these arrangements and approached the hospital to start a hospitalist service. In 1997 Scott Fitzgerald, MD, who was then chief resident, contemplated the debt and hassles of opening an office, saw a good fit for Dallas Presbyterian’s need for a hospitalist service and his professional goals. He founded MD on Call, a private hospital medicine group, which still serves Dallas Presbyterian and now employs 16 hospitalists. Having experimented with staffing for a 180 patient load, each physician has an ADC of 12-13. “We keep it lower than most groups’ 16-20 patients,” says Dr. Fitzgerald. “Because I scrutinize quarterly data I know that above 16 our costs and LOS creep up.”
In 1999 the program hit a speed bump when the hospital threatened to reduce the group’s rates. The group, in turn, threatened to leave. “We resolved it by demonstrating that every dollar they paid us earned seven dollars for the hospital, not to mention the growing scope of our activities,” says Dr. Fitzgerald. “In the beginning we were forbidden to do consults, particularly for surgeons. Two years later, we were doing it all.”
He says that the hospital loves the group because it serves the medical staff’s goals and helps grow market share, as hospitalists continue to market to physician practices in outlying suburbs.
Rundsarah Tahboub, MD, medical director of the Hospital Medicine Service at Grant Medical Center in Columbus, Ohio, also succeeded the second time around. With a passion for inpatient medicine, she helped launched a hospitalist program in response to restrictions on residents’ hours at Ohio State University. Having just completed a residency herself, Dr. Tahboub struggled with her lack of experience and, she felt, credibility to lead the program.
“I felt I wasn’t being heard, that I had no autonomy or support,” she says. “When my mentor, the program director of family practice residency at Grant, contacted me to establish a hospitalist program there, I took the challenge.”
Dr. Tahboub evaluated her management style, realizing that she values communication and congeniality with colleagues, getting input and analysis before moving ahead, and flexibility in dealing with obstacles. Citing the example of night call, she explains that hospitalists started with day hours only, leaving residents swamped at night and needing an attending physician.
“We [hospitalists] all talked about it,” says Dr. Tahboub. “While we weren’t thrilled to take night call, we each agreed to cover every fourth night because it was necessary for us to do so.”
Dr. Tahboub also had to figure out how to integrate two previously hired nurse practitioners (NPs) into the hospitalist service. “At first we were unsure how to work with them, but we learned that they enable us to see up to 17 patients on average per day rather than the 12-15 without them. They help us with ED admissions, patient education, and discharges,” says Dr. Tahboub. “The hospitalists love having NPs around and it has become a recruiting point in our favor.”
A recent hire—an office manager—helps the physicians keep paperwork on track.
Hindsight
Looking back, the professionals who have started hospitalist programs have some important lessons to share. Discerning the practice climate, both internal and external, is task number one.
“Make sure you understand the political climate in which you are starting the program, give community doctors time to get used to the idea, expect hospitalist turnover in the early stages, and be ready to hire new hospitalists quickly as demand builds,” advises Michael Pistoria, DO, chief of hospital medicine at Lehigh Valley Hospital and Health Network, Allentown, Pa.
Dr. Tahboub emphasizes the importance of hiring hospitalists in tune with the internal practice climate. “Rigid rules don’t work with us, and some physicians can’t tolerate the amount of flexibility in our program,” she notes.
For executives such as Sinai’s Malgoza, speaking with administrators at other institutions and going to conferences to learn about different hospitalist models helps design a program that fits the hospital’s culture.
Dallas Presbyterian’s Dr. Fitzgerald focuses on hiring great physicians. “Hire the best doctors from the best training programs you can,” he says. “Hiring warm bodies just doesn’t cut it. If you have poor quality docs someone else will take your spot.”
Dr. Fitzgerald also advises that slow program growth allows the chief hospitalist to find physicians who mesh with the group’s personalities and culture. “Find those who want a career as hospitalists rather than those putting in a year or two,” he concludes.
Dr. Borik points out that the hospitalist movement has boomed since she started in the 1990s, with hospitals much more in tune with hospitalist values because they save money and rates for malpractice insurance.
“After you’ve done the groundwork the program can operate like a well-oiled machine to accommodate physicians who want to work in this specialty,” she says, cautioning that ”we can’t ever forget that we don’t own the patients. Their loyalty is to their PCPs. If we drop the ball, either in service or communication, we can lose them.” TH
Marlene Piturro wrote about hospital business drivers in the March 2006 issue.
Hospitalist Business Drivers
As physicians, including hospitalists, focus on the now—getting the patient in front of them better—they may lose sight of the trends shaping their professional lives. Those trends, called “business drivers” occupy CEOs, CFOs, and other top managers who build strategies by understanding what drivers make organizations successful.
It’s not an easy job. Even the Delphic Oracle might have trouble divining which of the myriad competing drivers will make a hospital better and more profitable than its rivals. Take your pick: Sluggish inpatient volumes, shifts to outpatient procedures, high construction costs, expensive new technologies, an aging population, and consumer-driven care are among the business drivers currently on managers’ minds. (See “Trend Spotters,” p. 48.)
Michael Guthrie, MD, MBA, an executive-in-residence at the University of Colorado, School of Business (Boulder), Health Administration and a presenter at SHM’s September 2005 Leadership Conference in Vail, Colo., sees our aging population as a key business driver shaping hospital and physician livelihoods.
“The aging population and the shift to consumerism in healthcare are definitely on the hospital CEO’s mind,” he says. “Hospitalists need to understand how patient satisfaction drives market share and is highly correlated with the hospital’s business objectives.” By extension, hospitalists’ key metrics, such as compliance with Medicare core measures, reducing length of stay (LOS), and costs per case, mesh well with administration’s.
Keeping the CEO’s need to enhance the organization’s reputation and growth in mind, Dr. Guthrie suggests that hospitalists have their hands full. By focusing on measuring quality, providing the 24/7 coverage that patients want and the hospital needs and finding ways to decrease LOS and costs per case, their interests and those of the hospital’s align.
“Based on their conversations and observations of the hospital’s senior managers, hospitalists can figure out what business drivers are preoccupying them,” adds Dr. Guthrie.
Smart hospitalists can significantly boost their hospital’s bottom line according to Tom Hochhausler, Deloitte & Touche USA LLP’s partner of Life Sciences and Health Care Practice and director of the firm’s biennial survey on trends concerning hospital CEOs. Hochhausler says that with hospitals operating on razor-thin margins, hospitalists can increase their value to hospital CEOs and CFOs by improving communication among clinical staff, better adherence to guidelines, and shortening LOS. “They also have some of the best insights into improving quality in hospitals and are powerful teachers of interns and residents,” he adds. (See “What Worries Hospital CEOs,” at left.)
The difficult part for hospitalists is keeping focused on the hospital’s big picture while doing their jobs. For example, Michael Freed, CFO of Grand Rapids, Mich.-based Spectrum Health, ponders the financial aspects of a huge integrated delivery system with seven hospitals, 12,000 employees, a medical staff of 1,400 and a $2.1 billion budget. Rather than day-to-day concerns he focuses on the future—not one year, but five to 10 years ahead.
“Since the hospitalist team’s job is to cover the hospital 24/7, they don’t always connect the dots of what’s happening throughout the system,” says Ford. That’s why top managers must focus on the future. “If management has the right road map and vision for the future, a lot of good things happen for hospitalists: Patients get better care, which leads to better outcomes, [and] we lower costs and pass the savings along to payers. That, in turn, drives higher market share and increases the hospital’s value proposition.”
Hospital medicine groups rather than individual physicians may be best suited to track the hospital’s business drivers, and align incentives accordingly. Davin Juckett, CPA, MBA, of the Charlotte, N.C., Piedmont Healthcare Management Group, a physician-owned consultancy to more than 100 hospitalists in the southeast, advises hospitalists to use their billing and encounter data to improve their decision-making.
“Hospitalists tend to be very focused on their LOS and quality indicators but there’s a lot more out there,” says Juckett. “Business drivers such as consumer-directed care and P4P [pay for performance] make quantifiable data extremely important. Some MCOs have started star ratings of hospitalist and ER groups, and some doctors are up in arms because they feel it’s subjective. But that’s the future.”
Juckett sees another key business driver for 2006 and 2007: an increasingly competitive business environment for hospitalists. “Hospital medicine groups will have to defend their contracts,” he says. “True, the newness of the specialty makes recruitment an issue, but supply will eventually catch up with demand, and P4P will happen.”
Hospitalists might examine how another major business driver—aggressive competition for payer dollars—can put them at odds with office-based colleagues. By competing with hospitals for lucrative procedures in orthopedics, gynecology, cardiology, and other specialties, community physicians can lure market share away. Hospitalists are well positioned to mediate the conflict, although a report by VHA of Irving, Texas, says hospitalists often don’t keep community doctors informed of issues facing their hospitals. That report adds that hospitalists do a poor job of bringing hospital administrators and physicians together to forge common solutions.
Bricks and Mortar
Balancing soaring construction costs with the need to give picky consumers and physicians the latest technology in gleaming new buildings is another trend. Big-ticket items keep Joann Marqusee, MPP, senior vice-president of operations and facilities at Boston-based Beth Israel Deaconess Medical Center occupied. Her job—prioritizing capital projects, keeping facilities up to date, and tailoring spending to reduce future maintenance needs—got even more challenging with Hurricane Katrina. “Things are always difficult, but now the price of oil and steel are rising,” says Marqusee. “And we can’t find dehumidifiers to help with our little floods; they’re all in New Orleans.”
She has capital-spending decisions down to a disciplined process: Match projects with the strategic plan (e.g., neurosurgery ahead of ob/gyn), assess impact on patient volume and return on investment, and improve patient safety and quality. Explaining those decisions to physicians who get feisty when a favored project is delayed or cancelled is the tough part.
To gain doctors’ support for management’s spending priorities, Marqusee has a PowerPoint presentation for them: “Space: The Final Frontier.” She raves about hospitalists’ response: ”The hospitalists’ input has been fantastic because of their analytic training. For example, they understand ED throughput, and we use their expertise to improve design. And when we tell them that the new ICU can’t open as soon as they’d like because it’s being built above the bone marrow transplant center, and we need a new HVAC system installed first, they get it. They care about patients and when we introduce bottom line issues as well, we strengthen our working relationship.”
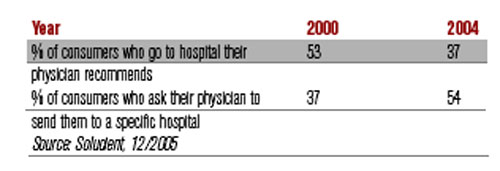
Where the (Aging) Consumer Is King
Consumerism is another business driver that hospitals can’t ignore. Individuals are increasingly willing to push their physicians to send them to the hospitals the consumers prefer, according to Solucient, a healthcare market intelligence firm in Evanston, Ill. In a survey of nearly 20,000 households Solucient identified a group of “responsive consumers,” (i.e., those proactive about managing their healthcare). Slightly older than the average consumer surveyed, the respondents have between 20% and 80% higher incidence of chronic diseases, and increasingly choose where they’re hospitalized rather than accept their physician’s recommendation:
Solucient’s data also show that responsive consumers heavily research and utilize hospital and physician ratings.
Homegrown Effort
While consultants are oracles of healthcare trends, some physician administrators rely on themselves instead. Akram Boutrous, MD, executive vice-president and CMO of South Nassau Community Hospital (Oceanside, N.Y.), turned the hospital around with an eight-year business improvement program based on understanding business trends. Some achievements: a 73% increase in patient revenues, 57% jump in outpatient services, and 27% increase in inpatient discharges.
Dr. Boutros considered using consultants, but disliked their high fees and lack of ongoing involvement. Instead he read stacks of books and articles on business drivers and strategies before selecting General Electric’s Accelerated Action Approach to Success. The method uses teams to solve problems that make organizations non-competitive.
“Hospitals face incredibly complex problems and competing demands from different departments,” says Dr. Boutros. “As a physician administrator I felt I could translate for all sides.”
He cites consumer-directed care as a key trend blindsiding most doctors. “They are completely unprepared for the changing market dynamics of consumer choice,” he says.
Consultants, administrators, and physicians agree: Hospitalists need to avoid the tunnel vision when it comes to their own metrics and pay attention to the business drivers changing healthcare. If they learn to spot key trends, they’re perfectly situated to work with hospital administrators and their office-based colleagues on using that knowledge to increase market share, and to have better and more profitable hospitals. TH
Writer Marlene Piturro covered SHM’s Leadership Conference in Vail for The Hospitalist.
As physicians, including hospitalists, focus on the now—getting the patient in front of them better—they may lose sight of the trends shaping their professional lives. Those trends, called “business drivers” occupy CEOs, CFOs, and other top managers who build strategies by understanding what drivers make organizations successful.
It’s not an easy job. Even the Delphic Oracle might have trouble divining which of the myriad competing drivers will make a hospital better and more profitable than its rivals. Take your pick: Sluggish inpatient volumes, shifts to outpatient procedures, high construction costs, expensive new technologies, an aging population, and consumer-driven care are among the business drivers currently on managers’ minds. (See “Trend Spotters,” p. 48.)
Michael Guthrie, MD, MBA, an executive-in-residence at the University of Colorado, School of Business (Boulder), Health Administration and a presenter at SHM’s September 2005 Leadership Conference in Vail, Colo., sees our aging population as a key business driver shaping hospital and physician livelihoods.
“The aging population and the shift to consumerism in healthcare are definitely on the hospital CEO’s mind,” he says. “Hospitalists need to understand how patient satisfaction drives market share and is highly correlated with the hospital’s business objectives.” By extension, hospitalists’ key metrics, such as compliance with Medicare core measures, reducing length of stay (LOS), and costs per case, mesh well with administration’s.
Keeping the CEO’s need to enhance the organization’s reputation and growth in mind, Dr. Guthrie suggests that hospitalists have their hands full. By focusing on measuring quality, providing the 24/7 coverage that patients want and the hospital needs and finding ways to decrease LOS and costs per case, their interests and those of the hospital’s align.
“Based on their conversations and observations of the hospital’s senior managers, hospitalists can figure out what business drivers are preoccupying them,” adds Dr. Guthrie.
Smart hospitalists can significantly boost their hospital’s bottom line according to Tom Hochhausler, Deloitte & Touche USA LLP’s partner of Life Sciences and Health Care Practice and director of the firm’s biennial survey on trends concerning hospital CEOs. Hochhausler says that with hospitals operating on razor-thin margins, hospitalists can increase their value to hospital CEOs and CFOs by improving communication among clinical staff, better adherence to guidelines, and shortening LOS. “They also have some of the best insights into improving quality in hospitals and are powerful teachers of interns and residents,” he adds. (See “What Worries Hospital CEOs,” at left.)
The difficult part for hospitalists is keeping focused on the hospital’s big picture while doing their jobs. For example, Michael Freed, CFO of Grand Rapids, Mich.-based Spectrum Health, ponders the financial aspects of a huge integrated delivery system with seven hospitals, 12,000 employees, a medical staff of 1,400 and a $2.1 billion budget. Rather than day-to-day concerns he focuses on the future—not one year, but five to 10 years ahead.
“Since the hospitalist team’s job is to cover the hospital 24/7, they don’t always connect the dots of what’s happening throughout the system,” says Ford. That’s why top managers must focus on the future. “If management has the right road map and vision for the future, a lot of good things happen for hospitalists: Patients get better care, which leads to better outcomes, [and] we lower costs and pass the savings along to payers. That, in turn, drives higher market share and increases the hospital’s value proposition.”
Hospital medicine groups rather than individual physicians may be best suited to track the hospital’s business drivers, and align incentives accordingly. Davin Juckett, CPA, MBA, of the Charlotte, N.C., Piedmont Healthcare Management Group, a physician-owned consultancy to more than 100 hospitalists in the southeast, advises hospitalists to use their billing and encounter data to improve their decision-making.
“Hospitalists tend to be very focused on their LOS and quality indicators but there’s a lot more out there,” says Juckett. “Business drivers such as consumer-directed care and P4P [pay for performance] make quantifiable data extremely important. Some MCOs have started star ratings of hospitalist and ER groups, and some doctors are up in arms because they feel it’s subjective. But that’s the future.”
Juckett sees another key business driver for 2006 and 2007: an increasingly competitive business environment for hospitalists. “Hospital medicine groups will have to defend their contracts,” he says. “True, the newness of the specialty makes recruitment an issue, but supply will eventually catch up with demand, and P4P will happen.”
Hospitalists might examine how another major business driver—aggressive competition for payer dollars—can put them at odds with office-based colleagues. By competing with hospitals for lucrative procedures in orthopedics, gynecology, cardiology, and other specialties, community physicians can lure market share away. Hospitalists are well positioned to mediate the conflict, although a report by VHA of Irving, Texas, says hospitalists often don’t keep community doctors informed of issues facing their hospitals. That report adds that hospitalists do a poor job of bringing hospital administrators and physicians together to forge common solutions.
Bricks and Mortar
Balancing soaring construction costs with the need to give picky consumers and physicians the latest technology in gleaming new buildings is another trend. Big-ticket items keep Joann Marqusee, MPP, senior vice-president of operations and facilities at Boston-based Beth Israel Deaconess Medical Center occupied. Her job—prioritizing capital projects, keeping facilities up to date, and tailoring spending to reduce future maintenance needs—got even more challenging with Hurricane Katrina. “Things are always difficult, but now the price of oil and steel are rising,” says Marqusee. “And we can’t find dehumidifiers to help with our little floods; they’re all in New Orleans.”
She has capital-spending decisions down to a disciplined process: Match projects with the strategic plan (e.g., neurosurgery ahead of ob/gyn), assess impact on patient volume and return on investment, and improve patient safety and quality. Explaining those decisions to physicians who get feisty when a favored project is delayed or cancelled is the tough part.
To gain doctors’ support for management’s spending priorities, Marqusee has a PowerPoint presentation for them: “Space: The Final Frontier.” She raves about hospitalists’ response: ”The hospitalists’ input has been fantastic because of their analytic training. For example, they understand ED throughput, and we use their expertise to improve design. And when we tell them that the new ICU can’t open as soon as they’d like because it’s being built above the bone marrow transplant center, and we need a new HVAC system installed first, they get it. They care about patients and when we introduce bottom line issues as well, we strengthen our working relationship.”
Where the (Aging) Consumer Is King
Consumerism is another business driver that hospitals can’t ignore. Individuals are increasingly willing to push their physicians to send them to the hospitals the consumers prefer, according to Solucient, a healthcare market intelligence firm in Evanston, Ill. In a survey of nearly 20,000 households Solucient identified a group of “responsive consumers,” (i.e., those proactive about managing their healthcare). Slightly older than the average consumer surveyed, the respondents have between 20% and 80% higher incidence of chronic diseases, and increasingly choose where they’re hospitalized rather than accept their physician’s recommendation:
Solucient’s data also show that responsive consumers heavily research and utilize hospital and physician ratings.
Homegrown Effort
While consultants are oracles of healthcare trends, some physician administrators rely on themselves instead. Akram Boutrous, MD, executive vice-president and CMO of South Nassau Community Hospital (Oceanside, N.Y.), turned the hospital around with an eight-year business improvement program based on understanding business trends. Some achievements: a 73% increase in patient revenues, 57% jump in outpatient services, and 27% increase in inpatient discharges.
Dr. Boutros considered using consultants, but disliked their high fees and lack of ongoing involvement. Instead he read stacks of books and articles on business drivers and strategies before selecting General Electric’s Accelerated Action Approach to Success. The method uses teams to solve problems that make organizations non-competitive.
“Hospitals face incredibly complex problems and competing demands from different departments,” says Dr. Boutros. “As a physician administrator I felt I could translate for all sides.”
He cites consumer-directed care as a key trend blindsiding most doctors. “They are completely unprepared for the changing market dynamics of consumer choice,” he says.
Consultants, administrators, and physicians agree: Hospitalists need to avoid the tunnel vision when it comes to their own metrics and pay attention to the business drivers changing healthcare. If they learn to spot key trends, they’re perfectly situated to work with hospital administrators and their office-based colleagues on using that knowledge to increase market share, and to have better and more profitable hospitals. TH
Writer Marlene Piturro covered SHM’s Leadership Conference in Vail for The Hospitalist.
As physicians, including hospitalists, focus on the now—getting the patient in front of them better—they may lose sight of the trends shaping their professional lives. Those trends, called “business drivers” occupy CEOs, CFOs, and other top managers who build strategies by understanding what drivers make organizations successful.
It’s not an easy job. Even the Delphic Oracle might have trouble divining which of the myriad competing drivers will make a hospital better and more profitable than its rivals. Take your pick: Sluggish inpatient volumes, shifts to outpatient procedures, high construction costs, expensive new technologies, an aging population, and consumer-driven care are among the business drivers currently on managers’ minds. (See “Trend Spotters,” p. 48.)
Michael Guthrie, MD, MBA, an executive-in-residence at the University of Colorado, School of Business (Boulder), Health Administration and a presenter at SHM’s September 2005 Leadership Conference in Vail, Colo., sees our aging population as a key business driver shaping hospital and physician livelihoods.
“The aging population and the shift to consumerism in healthcare are definitely on the hospital CEO’s mind,” he says. “Hospitalists need to understand how patient satisfaction drives market share and is highly correlated with the hospital’s business objectives.” By extension, hospitalists’ key metrics, such as compliance with Medicare core measures, reducing length of stay (LOS), and costs per case, mesh well with administration’s.
Keeping the CEO’s need to enhance the organization’s reputation and growth in mind, Dr. Guthrie suggests that hospitalists have their hands full. By focusing on measuring quality, providing the 24/7 coverage that patients want and the hospital needs and finding ways to decrease LOS and costs per case, their interests and those of the hospital’s align.
“Based on their conversations and observations of the hospital’s senior managers, hospitalists can figure out what business drivers are preoccupying them,” adds Dr. Guthrie.
Smart hospitalists can significantly boost their hospital’s bottom line according to Tom Hochhausler, Deloitte & Touche USA LLP’s partner of Life Sciences and Health Care Practice and director of the firm’s biennial survey on trends concerning hospital CEOs. Hochhausler says that with hospitals operating on razor-thin margins, hospitalists can increase their value to hospital CEOs and CFOs by improving communication among clinical staff, better adherence to guidelines, and shortening LOS. “They also have some of the best insights into improving quality in hospitals and are powerful teachers of interns and residents,” he adds. (See “What Worries Hospital CEOs,” at left.)
The difficult part for hospitalists is keeping focused on the hospital’s big picture while doing their jobs. For example, Michael Freed, CFO of Grand Rapids, Mich.-based Spectrum Health, ponders the financial aspects of a huge integrated delivery system with seven hospitals, 12,000 employees, a medical staff of 1,400 and a $2.1 billion budget. Rather than day-to-day concerns he focuses on the future—not one year, but five to 10 years ahead.
“Since the hospitalist team’s job is to cover the hospital 24/7, they don’t always connect the dots of what’s happening throughout the system,” says Ford. That’s why top managers must focus on the future. “If management has the right road map and vision for the future, a lot of good things happen for hospitalists: Patients get better care, which leads to better outcomes, [and] we lower costs and pass the savings along to payers. That, in turn, drives higher market share and increases the hospital’s value proposition.”
Hospital medicine groups rather than individual physicians may be best suited to track the hospital’s business drivers, and align incentives accordingly. Davin Juckett, CPA, MBA, of the Charlotte, N.C., Piedmont Healthcare Management Group, a physician-owned consultancy to more than 100 hospitalists in the southeast, advises hospitalists to use their billing and encounter data to improve their decision-making.
“Hospitalists tend to be very focused on their LOS and quality indicators but there’s a lot more out there,” says Juckett. “Business drivers such as consumer-directed care and P4P [pay for performance] make quantifiable data extremely important. Some MCOs have started star ratings of hospitalist and ER groups, and some doctors are up in arms because they feel it’s subjective. But that’s the future.”
Juckett sees another key business driver for 2006 and 2007: an increasingly competitive business environment for hospitalists. “Hospital medicine groups will have to defend their contracts,” he says. “True, the newness of the specialty makes recruitment an issue, but supply will eventually catch up with demand, and P4P will happen.”
Hospitalists might examine how another major business driver—aggressive competition for payer dollars—can put them at odds with office-based colleagues. By competing with hospitals for lucrative procedures in orthopedics, gynecology, cardiology, and other specialties, community physicians can lure market share away. Hospitalists are well positioned to mediate the conflict, although a report by VHA of Irving, Texas, says hospitalists often don’t keep community doctors informed of issues facing their hospitals. That report adds that hospitalists do a poor job of bringing hospital administrators and physicians together to forge common solutions.
Bricks and Mortar
Balancing soaring construction costs with the need to give picky consumers and physicians the latest technology in gleaming new buildings is another trend. Big-ticket items keep Joann Marqusee, MPP, senior vice-president of operations and facilities at Boston-based Beth Israel Deaconess Medical Center occupied. Her job—prioritizing capital projects, keeping facilities up to date, and tailoring spending to reduce future maintenance needs—got even more challenging with Hurricane Katrina. “Things are always difficult, but now the price of oil and steel are rising,” says Marqusee. “And we can’t find dehumidifiers to help with our little floods; they’re all in New Orleans.”
She has capital-spending decisions down to a disciplined process: Match projects with the strategic plan (e.g., neurosurgery ahead of ob/gyn), assess impact on patient volume and return on investment, and improve patient safety and quality. Explaining those decisions to physicians who get feisty when a favored project is delayed or cancelled is the tough part.
To gain doctors’ support for management’s spending priorities, Marqusee has a PowerPoint presentation for them: “Space: The Final Frontier.” She raves about hospitalists’ response: ”The hospitalists’ input has been fantastic because of their analytic training. For example, they understand ED throughput, and we use their expertise to improve design. And when we tell them that the new ICU can’t open as soon as they’d like because it’s being built above the bone marrow transplant center, and we need a new HVAC system installed first, they get it. They care about patients and when we introduce bottom line issues as well, we strengthen our working relationship.”
Where the (Aging) Consumer Is King
Consumerism is another business driver that hospitals can’t ignore. Individuals are increasingly willing to push their physicians to send them to the hospitals the consumers prefer, according to Solucient, a healthcare market intelligence firm in Evanston, Ill. In a survey of nearly 20,000 households Solucient identified a group of “responsive consumers,” (i.e., those proactive about managing their healthcare). Slightly older than the average consumer surveyed, the respondents have between 20% and 80% higher incidence of chronic diseases, and increasingly choose where they’re hospitalized rather than accept their physician’s recommendation:
Solucient’s data also show that responsive consumers heavily research and utilize hospital and physician ratings.
Homegrown Effort
While consultants are oracles of healthcare trends, some physician administrators rely on themselves instead. Akram Boutrous, MD, executive vice-president and CMO of South Nassau Community Hospital (Oceanside, N.Y.), turned the hospital around with an eight-year business improvement program based on understanding business trends. Some achievements: a 73% increase in patient revenues, 57% jump in outpatient services, and 27% increase in inpatient discharges.
Dr. Boutros considered using consultants, but disliked their high fees and lack of ongoing involvement. Instead he read stacks of books and articles on business drivers and strategies before selecting General Electric’s Accelerated Action Approach to Success. The method uses teams to solve problems that make organizations non-competitive.
“Hospitals face incredibly complex problems and competing demands from different departments,” says Dr. Boutros. “As a physician administrator I felt I could translate for all sides.”
He cites consumer-directed care as a key trend blindsiding most doctors. “They are completely unprepared for the changing market dynamics of consumer choice,” he says.
Consultants, administrators, and physicians agree: Hospitalists need to avoid the tunnel vision when it comes to their own metrics and pay attention to the business drivers changing healthcare. If they learn to spot key trends, they’re perfectly situated to work with hospital administrators and their office-based colleagues on using that knowledge to increase market share, and to have better and more profitable hospitals. TH
Writer Marlene Piturro covered SHM’s Leadership Conference in Vail for The Hospitalist.
A Midwest Partnership
Quite likely things are different in Minnesota than they are on either coast. People are polite, know how to work together, and are respectful about consuming resources. Or as Tom Anderson, MD, a HealthPartners Medical Group (HPMG) hospitalist says: “In Minnesota affable usually beats good.” Fortunately, the 25 physician members of the hospitalist team who belong to the 580-member HPMG, are beyond affable and good. By many measures they are excellent, and they are shaping the field of hospital medicine.
At the heart of the HPMG hospitalist program’s quality are its people. Burke Kealey, MD, HPMG’s assistant medical director, helped start the program in 1997, recruiting young, energetic, and personable physicians who liked practicing big city hospital medicine, Midwestern style. “Our hospitalist program was one of the early ones operating before the term ‘hospitalist’ was well-known,” says Dr. Kealey.
The hospitalists are employed neither by an academic medical nor a community hospital. Instead, they are members of a 580-multispecialty physician group that anchors HealthPartners Network, an organization that consistently ranks among The National Committee for Quality Assurance’s (NCQA) top five health plans regionally and top 10 nationally. Yet excellence has its price, as the perverse incentives of the U.S. healthcare system reveal. Mary Brainerd, HealthPartner’s CEO, comments that although the company consistently ranks high, it gets paid thousands of dollars less per patient by Medicare than poor performing plans.
“The way Medicare is set up, it actually punishes you for being good,” says Brainerd, referring to Medicare’s rules that qualify hospitals to receive additional payments each time a patient returns for more treatment—even if their return was caused by sub-par diagnosis and treatment. Under Medicare’s incentives, hospitals and doctors who order unnecessary tests, provide poor care, or even make patients worse often receive higher payments than those who provide efficient, high-quality care. That doesn’t stop HPMG from doing things correctly.
With the physician group employing both clinic and inpatient physicians, it’s more straightforward getting metrics and incentives aligned than in a healthcare environment where the outpatient physician’s loss may be the hospitalist’s gain—or vice versa. “Working closely with clinic and ER doctors decreases length of stay, improves clinical outcomes, and decreases costs,” says Dr. Kealey. “That helps the whole medical group.”
Another major contributor to clinical excellence goes beyond HPMG. Using the Minnesota mindset, HPMG’s physicians work with the area’s other medical heavyweights, the Mayo Clinic (Rochester, Minn.) and the Allina Medical Group (Minneapolis), forging a consensus on best practices and evidence-based guidelines (www.icsi.org). An example of HPMG’s outpatient and inpatient physician collaboration is their approach to CHF. After both groups tackled the job of operationalizing “perfect” CHF care in a one-day Rapid Design Workshop, “perfect treatment” outcomes rose from 22% in January 2005 to 50% in March 2005.
Nuts and Bolts
Scheduling logistics is among the challenges a hospitalist program’s manager faces, and Dr. Kealey and his colleagues have—through experience—done well. Each hospitalist selects a block schedule (either one week on, one week off or 14 days straight for 24 weeks). They also serve two night shift weeks (6 p.m.—8 a.m.), although residents run things at night. Hospitalists reconfigure their schedules every six months, helping to avoid burnout. Geographic deployment is another energy saver. Each hospitalist works in one or two units, allowing them to know patients, family, and the nursing staff well. It also cuts the nine-story hospital down to a size.
To communicate effectively, physicians use electronic technology. Voice pagers connect all HPMG physicians. Other devices sound alerts, allow for co-management of patients with chronic diseases, quick referrals to specialists within the group, in-box messaging, and a discharge summary to the primary physician in six to eight hours.
As for compensation, physicians receive a base salary, set at 80% of SHM’s annual average for the Midwest, accounting for 65% of pay. Of the balance, productivity as measured by relative value units (RVUs) accounts for 40%, with 20% each for high marks on patient and provider satisfaction surveys, and the medical director’s discretion.
Myriad Opportunities
The HPMG hospitalist program offers opportunities to pursue many professional paths, as its SHM award roster shows. SHM’s Award for Outstanding Service in Clinical Medicine to HPMG Hospitalists have included:
- 2002 Rusty Holman, Outstanding Service in Hospital Medicine;
- 2003 Burke Kealey, Clinical Excellence; and
- 2005 Shaun Frost, Clinical Excellence.
Adding depth to the program involves embracing physicians on unusual career paths, such as Tom Anderson, MD, one of HPMG’s family practice hospitalists. After finishing training at Ramsey County Hospital of St. Paul, Minn., which became Regions Hospital in 1997 (and where Dr. Kealey also trained), Dr. Anderson joined a seven-doctor rural practice in Iron Range, Wis.
“It was in a hard-working blue collar town, and we were throwbacks,” says Dr. Anderson, “doing all our own obstetrics, covering the ER, helping surgeons. I was a real person in that community. Everyone knew each other from the church or hardware store.” If the doctors wanted to change anything, they talked over doughnuts and coffee, deciding how it would affect them and their patients. Dr. Anderson loved the work, but wanted more family time than the all-consuming rural practice allowed.
A recruiting call from Dr. Kealey changed everything. Dr. Kealey calls Dr. Anderson “a bright and shining star, someone who sits in the front row and asks all the questions.”
Dr. Anderson joined HPMG’s hospitalist team in 2004, enjoying the one-week-on/one-week-off schedule and the continuity of care afforded by a large team. “This is a big busy hospital,” he says. “The patients are really sick, and we plan our 12-hour shift around them.” He starts with a 7 a.m. huddle of nurses and physicians to plan the day by prioritizing patient needs, reviewing orders, arranging time to talk to specialists, and visiting all patients. “By 9 a.m. we’ve planned the day, including 3 p.m. patient discharges. I like prioritizing what has to be done, and defining what has to be fixed.”
Rick Hilger, MD, board certified in internal medicine and pediatrics, is on another mission. After residency at the University of Minnesota Medical School (Duluth), he became Regions Hospital’s chief resident and then stayed on. He wanted a pediatrics hospitalist practice, which proved impractical because 95% of Regions’ pediatric cases now go to another hospital. “Down the line I’d like a 50/50 adult/peds mix, but that’s hard to accomplish in a hospitalist program,” he says.
Still looking for a challenge, Dr. Hilger chose the Institute for Healthcare Improvement’s “100K Lives” initiative, becoming the lead physician for Region’s rapid response team to prevent unnecessary code-blue calls. With the hospitalists’ geographic deployment to specific units that meant planning who would respond to codes and how that would be communicated. Dr. Hilger encouraged administration to hire full-time employees to field a rapid response team and created a pre-code team.
“At least 30%-40% of patients code outside the ICU,” he says. “We’ve observed that they often have unstable vital signs six to eight hours before coding. We’ve cut through administrative minutiae and red tape so that patients don’t sit there with unstable vitals for long.”
The pre-code team—an ICU trained nurse and respiratory therapist—are alerted to those signs and respond in five minutes or less, 24/7. The rest of the team is alerted via pagers, with hospitalists fielding an average of three calls per day.
Other hospitalists find their special niches. Shaun Frost, MD, is breaking ground in peri-surgical care in orthopedics, urology and neurology, and is active in process improvement teams. Howard Epstein, MD, leads the palliative care team, while John Degelau, MD, chief of hospital medical at North Memorial, pursues his interest in geriatrics. Rich Mahr, MD, is the physician champion for electronic health records.
So being an HPMG hospitalist allows physicians to pursue many avenues of clinical and process improvement, including national initiatives and teaching. Dr. Anderson sums up what HPMG is about: “I joined this group because of its passion for medicine. When we get older we’ll look back and say that we had our moment, our time to give it 100%.”
Dr. Kealey calls them “an energized creative group. Everyone wants to go to national meetings and to keep ahead of the pack, to ask what’s next to learn?” TH
Writer Marlene Piturro regularly writes practice profiles for The Hospitalist.
Quite likely things are different in Minnesota than they are on either coast. People are polite, know how to work together, and are respectful about consuming resources. Or as Tom Anderson, MD, a HealthPartners Medical Group (HPMG) hospitalist says: “In Minnesota affable usually beats good.” Fortunately, the 25 physician members of the hospitalist team who belong to the 580-member HPMG, are beyond affable and good. By many measures they are excellent, and they are shaping the field of hospital medicine.
At the heart of the HPMG hospitalist program’s quality are its people. Burke Kealey, MD, HPMG’s assistant medical director, helped start the program in 1997, recruiting young, energetic, and personable physicians who liked practicing big city hospital medicine, Midwestern style. “Our hospitalist program was one of the early ones operating before the term ‘hospitalist’ was well-known,” says Dr. Kealey.
The hospitalists are employed neither by an academic medical nor a community hospital. Instead, they are members of a 580-multispecialty physician group that anchors HealthPartners Network, an organization that consistently ranks among The National Committee for Quality Assurance’s (NCQA) top five health plans regionally and top 10 nationally. Yet excellence has its price, as the perverse incentives of the U.S. healthcare system reveal. Mary Brainerd, HealthPartner’s CEO, comments that although the company consistently ranks high, it gets paid thousands of dollars less per patient by Medicare than poor performing plans.
“The way Medicare is set up, it actually punishes you for being good,” says Brainerd, referring to Medicare’s rules that qualify hospitals to receive additional payments each time a patient returns for more treatment—even if their return was caused by sub-par diagnosis and treatment. Under Medicare’s incentives, hospitals and doctors who order unnecessary tests, provide poor care, or even make patients worse often receive higher payments than those who provide efficient, high-quality care. That doesn’t stop HPMG from doing things correctly.
With the physician group employing both clinic and inpatient physicians, it’s more straightforward getting metrics and incentives aligned than in a healthcare environment where the outpatient physician’s loss may be the hospitalist’s gain—or vice versa. “Working closely with clinic and ER doctors decreases length of stay, improves clinical outcomes, and decreases costs,” says Dr. Kealey. “That helps the whole medical group.”
Another major contributor to clinical excellence goes beyond HPMG. Using the Minnesota mindset, HPMG’s physicians work with the area’s other medical heavyweights, the Mayo Clinic (Rochester, Minn.) and the Allina Medical Group (Minneapolis), forging a consensus on best practices and evidence-based guidelines (www.icsi.org). An example of HPMG’s outpatient and inpatient physician collaboration is their approach to CHF. After both groups tackled the job of operationalizing “perfect” CHF care in a one-day Rapid Design Workshop, “perfect treatment” outcomes rose from 22% in January 2005 to 50% in March 2005.
Nuts and Bolts
Scheduling logistics is among the challenges a hospitalist program’s manager faces, and Dr. Kealey and his colleagues have—through experience—done well. Each hospitalist selects a block schedule (either one week on, one week off or 14 days straight for 24 weeks). They also serve two night shift weeks (6 p.m.—8 a.m.), although residents run things at night. Hospitalists reconfigure their schedules every six months, helping to avoid burnout. Geographic deployment is another energy saver. Each hospitalist works in one or two units, allowing them to know patients, family, and the nursing staff well. It also cuts the nine-story hospital down to a size.
To communicate effectively, physicians use electronic technology. Voice pagers connect all HPMG physicians. Other devices sound alerts, allow for co-management of patients with chronic diseases, quick referrals to specialists within the group, in-box messaging, and a discharge summary to the primary physician in six to eight hours.
As for compensation, physicians receive a base salary, set at 80% of SHM’s annual average for the Midwest, accounting for 65% of pay. Of the balance, productivity as measured by relative value units (RVUs) accounts for 40%, with 20% each for high marks on patient and provider satisfaction surveys, and the medical director’s discretion.
Myriad Opportunities
The HPMG hospitalist program offers opportunities to pursue many professional paths, as its SHM award roster shows. SHM’s Award for Outstanding Service in Clinical Medicine to HPMG Hospitalists have included:
- 2002 Rusty Holman, Outstanding Service in Hospital Medicine;
- 2003 Burke Kealey, Clinical Excellence; and
- 2005 Shaun Frost, Clinical Excellence.
Adding depth to the program involves embracing physicians on unusual career paths, such as Tom Anderson, MD, one of HPMG’s family practice hospitalists. After finishing training at Ramsey County Hospital of St. Paul, Minn., which became Regions Hospital in 1997 (and where Dr. Kealey also trained), Dr. Anderson joined a seven-doctor rural practice in Iron Range, Wis.
“It was in a hard-working blue collar town, and we were throwbacks,” says Dr. Anderson, “doing all our own obstetrics, covering the ER, helping surgeons. I was a real person in that community. Everyone knew each other from the church or hardware store.” If the doctors wanted to change anything, they talked over doughnuts and coffee, deciding how it would affect them and their patients. Dr. Anderson loved the work, but wanted more family time than the all-consuming rural practice allowed.
A recruiting call from Dr. Kealey changed everything. Dr. Kealey calls Dr. Anderson “a bright and shining star, someone who sits in the front row and asks all the questions.”
Dr. Anderson joined HPMG’s hospitalist team in 2004, enjoying the one-week-on/one-week-off schedule and the continuity of care afforded by a large team. “This is a big busy hospital,” he says. “The patients are really sick, and we plan our 12-hour shift around them.” He starts with a 7 a.m. huddle of nurses and physicians to plan the day by prioritizing patient needs, reviewing orders, arranging time to talk to specialists, and visiting all patients. “By 9 a.m. we’ve planned the day, including 3 p.m. patient discharges. I like prioritizing what has to be done, and defining what has to be fixed.”
Rick Hilger, MD, board certified in internal medicine and pediatrics, is on another mission. After residency at the University of Minnesota Medical School (Duluth), he became Regions Hospital’s chief resident and then stayed on. He wanted a pediatrics hospitalist practice, which proved impractical because 95% of Regions’ pediatric cases now go to another hospital. “Down the line I’d like a 50/50 adult/peds mix, but that’s hard to accomplish in a hospitalist program,” he says.
Still looking for a challenge, Dr. Hilger chose the Institute for Healthcare Improvement’s “100K Lives” initiative, becoming the lead physician for Region’s rapid response team to prevent unnecessary code-blue calls. With the hospitalists’ geographic deployment to specific units that meant planning who would respond to codes and how that would be communicated. Dr. Hilger encouraged administration to hire full-time employees to field a rapid response team and created a pre-code team.
“At least 30%-40% of patients code outside the ICU,” he says. “We’ve observed that they often have unstable vital signs six to eight hours before coding. We’ve cut through administrative minutiae and red tape so that patients don’t sit there with unstable vitals for long.”
The pre-code team—an ICU trained nurse and respiratory therapist—are alerted to those signs and respond in five minutes or less, 24/7. The rest of the team is alerted via pagers, with hospitalists fielding an average of three calls per day.
Other hospitalists find their special niches. Shaun Frost, MD, is breaking ground in peri-surgical care in orthopedics, urology and neurology, and is active in process improvement teams. Howard Epstein, MD, leads the palliative care team, while John Degelau, MD, chief of hospital medical at North Memorial, pursues his interest in geriatrics. Rich Mahr, MD, is the physician champion for electronic health records.
So being an HPMG hospitalist allows physicians to pursue many avenues of clinical and process improvement, including national initiatives and teaching. Dr. Anderson sums up what HPMG is about: “I joined this group because of its passion for medicine. When we get older we’ll look back and say that we had our moment, our time to give it 100%.”
Dr. Kealey calls them “an energized creative group. Everyone wants to go to national meetings and to keep ahead of the pack, to ask what’s next to learn?” TH
Writer Marlene Piturro regularly writes practice profiles for The Hospitalist.
Quite likely things are different in Minnesota than they are on either coast. People are polite, know how to work together, and are respectful about consuming resources. Or as Tom Anderson, MD, a HealthPartners Medical Group (HPMG) hospitalist says: “In Minnesota affable usually beats good.” Fortunately, the 25 physician members of the hospitalist team who belong to the 580-member HPMG, are beyond affable and good. By many measures they are excellent, and they are shaping the field of hospital medicine.
At the heart of the HPMG hospitalist program’s quality are its people. Burke Kealey, MD, HPMG’s assistant medical director, helped start the program in 1997, recruiting young, energetic, and personable physicians who liked practicing big city hospital medicine, Midwestern style. “Our hospitalist program was one of the early ones operating before the term ‘hospitalist’ was well-known,” says Dr. Kealey.
The hospitalists are employed neither by an academic medical nor a community hospital. Instead, they are members of a 580-multispecialty physician group that anchors HealthPartners Network, an organization that consistently ranks among The National Committee for Quality Assurance’s (NCQA) top five health plans regionally and top 10 nationally. Yet excellence has its price, as the perverse incentives of the U.S. healthcare system reveal. Mary Brainerd, HealthPartner’s CEO, comments that although the company consistently ranks high, it gets paid thousands of dollars less per patient by Medicare than poor performing plans.
“The way Medicare is set up, it actually punishes you for being good,” says Brainerd, referring to Medicare’s rules that qualify hospitals to receive additional payments each time a patient returns for more treatment—even if their return was caused by sub-par diagnosis and treatment. Under Medicare’s incentives, hospitals and doctors who order unnecessary tests, provide poor care, or even make patients worse often receive higher payments than those who provide efficient, high-quality care. That doesn’t stop HPMG from doing things correctly.
With the physician group employing both clinic and inpatient physicians, it’s more straightforward getting metrics and incentives aligned than in a healthcare environment where the outpatient physician’s loss may be the hospitalist’s gain—or vice versa. “Working closely with clinic and ER doctors decreases length of stay, improves clinical outcomes, and decreases costs,” says Dr. Kealey. “That helps the whole medical group.”
Another major contributor to clinical excellence goes beyond HPMG. Using the Minnesota mindset, HPMG’s physicians work with the area’s other medical heavyweights, the Mayo Clinic (Rochester, Minn.) and the Allina Medical Group (Minneapolis), forging a consensus on best practices and evidence-based guidelines (www.icsi.org). An example of HPMG’s outpatient and inpatient physician collaboration is their approach to CHF. After both groups tackled the job of operationalizing “perfect” CHF care in a one-day Rapid Design Workshop, “perfect treatment” outcomes rose from 22% in January 2005 to 50% in March 2005.
Nuts and Bolts
Scheduling logistics is among the challenges a hospitalist program’s manager faces, and Dr. Kealey and his colleagues have—through experience—done well. Each hospitalist selects a block schedule (either one week on, one week off or 14 days straight for 24 weeks). They also serve two night shift weeks (6 p.m.—8 a.m.), although residents run things at night. Hospitalists reconfigure their schedules every six months, helping to avoid burnout. Geographic deployment is another energy saver. Each hospitalist works in one or two units, allowing them to know patients, family, and the nursing staff well. It also cuts the nine-story hospital down to a size.
To communicate effectively, physicians use electronic technology. Voice pagers connect all HPMG physicians. Other devices sound alerts, allow for co-management of patients with chronic diseases, quick referrals to specialists within the group, in-box messaging, and a discharge summary to the primary physician in six to eight hours.
As for compensation, physicians receive a base salary, set at 80% of SHM’s annual average for the Midwest, accounting for 65% of pay. Of the balance, productivity as measured by relative value units (RVUs) accounts for 40%, with 20% each for high marks on patient and provider satisfaction surveys, and the medical director’s discretion.
Myriad Opportunities
The HPMG hospitalist program offers opportunities to pursue many professional paths, as its SHM award roster shows. SHM’s Award for Outstanding Service in Clinical Medicine to HPMG Hospitalists have included:
- 2002 Rusty Holman, Outstanding Service in Hospital Medicine;
- 2003 Burke Kealey, Clinical Excellence; and
- 2005 Shaun Frost, Clinical Excellence.
Adding depth to the program involves embracing physicians on unusual career paths, such as Tom Anderson, MD, one of HPMG’s family practice hospitalists. After finishing training at Ramsey County Hospital of St. Paul, Minn., which became Regions Hospital in 1997 (and where Dr. Kealey also trained), Dr. Anderson joined a seven-doctor rural practice in Iron Range, Wis.
“It was in a hard-working blue collar town, and we were throwbacks,” says Dr. Anderson, “doing all our own obstetrics, covering the ER, helping surgeons. I was a real person in that community. Everyone knew each other from the church or hardware store.” If the doctors wanted to change anything, they talked over doughnuts and coffee, deciding how it would affect them and their patients. Dr. Anderson loved the work, but wanted more family time than the all-consuming rural practice allowed.
A recruiting call from Dr. Kealey changed everything. Dr. Kealey calls Dr. Anderson “a bright and shining star, someone who sits in the front row and asks all the questions.”
Dr. Anderson joined HPMG’s hospitalist team in 2004, enjoying the one-week-on/one-week-off schedule and the continuity of care afforded by a large team. “This is a big busy hospital,” he says. “The patients are really sick, and we plan our 12-hour shift around them.” He starts with a 7 a.m. huddle of nurses and physicians to plan the day by prioritizing patient needs, reviewing orders, arranging time to talk to specialists, and visiting all patients. “By 9 a.m. we’ve planned the day, including 3 p.m. patient discharges. I like prioritizing what has to be done, and defining what has to be fixed.”
Rick Hilger, MD, board certified in internal medicine and pediatrics, is on another mission. After residency at the University of Minnesota Medical School (Duluth), he became Regions Hospital’s chief resident and then stayed on. He wanted a pediatrics hospitalist practice, which proved impractical because 95% of Regions’ pediatric cases now go to another hospital. “Down the line I’d like a 50/50 adult/peds mix, but that’s hard to accomplish in a hospitalist program,” he says.
Still looking for a challenge, Dr. Hilger chose the Institute for Healthcare Improvement’s “100K Lives” initiative, becoming the lead physician for Region’s rapid response team to prevent unnecessary code-blue calls. With the hospitalists’ geographic deployment to specific units that meant planning who would respond to codes and how that would be communicated. Dr. Hilger encouraged administration to hire full-time employees to field a rapid response team and created a pre-code team.
“At least 30%-40% of patients code outside the ICU,” he says. “We’ve observed that they often have unstable vital signs six to eight hours before coding. We’ve cut through administrative minutiae and red tape so that patients don’t sit there with unstable vitals for long.”
The pre-code team—an ICU trained nurse and respiratory therapist—are alerted to those signs and respond in five minutes or less, 24/7. The rest of the team is alerted via pagers, with hospitalists fielding an average of three calls per day.
Other hospitalists find their special niches. Shaun Frost, MD, is breaking ground in peri-surgical care in orthopedics, urology and neurology, and is active in process improvement teams. Howard Epstein, MD, leads the palliative care team, while John Degelau, MD, chief of hospital medical at North Memorial, pursues his interest in geriatrics. Rich Mahr, MD, is the physician champion for electronic health records.
So being an HPMG hospitalist allows physicians to pursue many avenues of clinical and process improvement, including national initiatives and teaching. Dr. Anderson sums up what HPMG is about: “I joined this group because of its passion for medicine. When we get older we’ll look back and say that we had our moment, our time to give it 100%.”
Dr. Kealey calls them “an energized creative group. Everyone wants to go to national meetings and to keep ahead of the pack, to ask what’s next to learn?” TH
Writer Marlene Piturro regularly writes practice profiles for The Hospitalist.
Leading Roles
The 100 hospitalists who gathered in September at the Vail Cascade Hotel and Spa among Vail, Colorado’s high peaks for SHM’s second Hospitalist Medicine Leadership Academy showed their character early during a simulation led by David Javitch, PhD, a Harvard University instructor. The exercise usually goes like this: The leader auctions $1 bills, with bidders paying their highest bid whether they win or lose. Participants’ aggressive juices flow and someone usually pays $5 or $10 for the lone dollar. Then they realize that their irrational bidding behavior is fueled by their need to compete rather than to cooperate, and the leader discusses the value of cooperation over greed.
But the SHM Leadership Academy hospitalists played the game differently. Dr. Javitch earmarked the proceeds of the auction for a pediatric AIDS foundation. After early bids to $5, one Mississippi doctor who had worked in a hospital without water and electricity during Hurricane Katrina bid $100. The bidding ceased abruptly. Spontaneously, several groups took up collections to boost the donation’s size. This stopped the facilitator in his tracks.
Instead of giving the participants a lesson on the destructive power of greed and competition, the facilitator got a lesson about hospitalist altruism—a dedication to serving people that is transforming how patients are treated in America’s medical centers. This exercise revealed both the pros and the cons of hospitalists’ leadership tendencies.
The Academy Format
Working at round tables of 10, the hospitalists spent all four days in the same small group. Each group was led by a facilitator who guided its exercises, kept the discussion on track, and encouraged participation in feedback and Q&A sessions. The hospitalists were put through their paces by experts in various disciplines relating to hospital medicine, learning about the field’s leadership challenges, its business metrics, strategic planning, understanding various personality traits and communication styles, and managing change and transformation efforts.
The SHM Leadership Academy, which limits attendance to 100, balances lectures with exercises, simulations, personality and communication inventories, and time for questions and sharing about professional issues. There was also time set aside for networking, including at a cocktail party hosted by IPC: The Hospitalist Company, North Hollywood, Calif., as well as sightseeing, biking, and visits to Vail Village to explore local shops and restaurants
Who Attended
The hospitalist attendees came to the Leadership Academy from diverse paths and at various stages of their careers. Some physicians started hospitalist programs fresh from residency, some worked in large teams, some had been in solo and group practice before becoming hospitalists, some were employed by hospitalist groups and health plans, and one started as a community-based solo practice hospitalist. They work in a wide range of settings, from rural and suburban community hospitals to academic medical centers, and in cities large and small.
Russell (“Rusty”) Holman, MD, and Cogent Healthcare’s, Irvine, Calif., national medical director, spelled out the Leadership Academy’s goals: for hospitalists to run their programs more efficiently, improve morale within their groups, maximize team efficiency, and identify critical drivers of success.
“Our goal at this conference is for you to learn new things, to improve your skills as leaders, and to learn how to continually demonstrate value to your CEOs and CFOs,” says Dr. Holman, who also led participants through the analytic steps of a strategic plan in their small groups.
Leadership Challenges
Laurence Wellikson, MD, SHM CEO, spelled out the challenges confronting hospital medicine.
“In a nation that spent $1.7 trillion on healthcare in 2003, or 15.3% of the nation’s GDP, with rising insurance premiums and out-of-pocket costs to consumers, hospitalists will be part of a systemic solution to controlling costs and providing high quality care,” says Dr. Wellikson.
He points out that hospitals are changing rapidly, requiring hospitalists to adapt to work environments in flux. The 20% annual turnover in nursing staffs, PCPs giving up inpatient care, subspecialists narrowing their hospital work, and overcrowded emergency departments all create both opportunities and challenges for hospitalists.
“Hospital medicine is growing rapidly and so are the demands on hospitalists,” adds Dr. Wellikson, who articulated SHM’s goal of helping hospitalists develop their leadership skills in a rapidly changing and complex field. He urges participants to transcend medicine’s “cult of uniqueness among individual doctors” and to lead teams that will reform hospitals internally and provide measurable improvements in patient care quality and reduce waste.
These trends are playing out in a healthcare system that’s forced to do more with less. Michael Guthrie, MD, MBA, executive in residence at the University of Colorado at Denver, points out that hospitalists must assume their CEOs and CFOs mindsets to understand the myriad challenges that arise from the swelling number of uninsured patients, the demands of aging baby boomers, malpractice liability, competition, rapid changes in technology, the need for new buildings, and the emphasis on patient satisfaction and safety. The rise of consumer-directed care resulting from employers shifting healthcare costs to employees has raised concerns about how “shopping around” among hospitals might affect clinical performance.
Dr. Guthrie stresses that value is in the eyes of the beholder and that the hospitalist’s work greatly affects other care team members’ satisfaction, relationships with other physicians, patient satisfaction and safety, and the hospital’s business interests.
“Hospitalists use their knowledge, ideas, skills, and expertise with process improvement to get things done with and through other people,” he explains. “When we understand what problems need to be solved and what our measures of success are we can have the rapture of accomplishment.”
Turmoil throughout the healthcare system and rapid growth of the hospitalist movement provided an apt backdrop for remarks Jack Silversin, DMD, DrPh, made in a session titled, “Leading and Managing Change.” Dr. Silversin is the president of Amicus Inc., a consultant firm based in Cambridge, Mass. He urges physicians to transcend their traditional roles as protectors of the status quo to become sponsors of change instead. Physicians as change agents publicly demonstrate their commitment to being leaders in several important ways.
“Change is definitely more work than maintaining the status quo,” says Dr. Silversin, “but organizations need doctors who sponsor change rather than resist it.”
Working through a simulation of a headstrong hospitalist trying to strong-arm her way to a 24/7 schedule for hospitalists rather than having the medical staff or moonlighters taking night call, participants developed their own insights into handling change.
“You’ve got to start small and gain credibility with little victories rather than doing something major right away,” said one attendee.
Trying to get non-hospitalists to support change was another idea: “Leadership doesn’t always have an MD credential attached to it,” added Dr. Silversin.
Being a change agent means looking inward as well as outward, and to that end attendees at the Leadership Academy spent time exploring their personal strengths and communication styles. Having completed a “Strength Deployment Inventory,” a self-scored test published by Personal Strength Publishing of Carlsbad, Calif., that measures an individual’s motives and values, prior to the conference, the hospitalists—led by Dr. Javitch—determined their strengths and weaknesses on altruism, assertiveness, and analysis. Small groups and dyads role-played situations where a colleague, an administrator, or a subordinate had a vastly different approach to problem-solving and decision-making.
“There are no right or wrong answers here, just a growing awareness of what our strengths are and things we need to guard against,” says Javitch.
Timothy Keogh, PhD, clinical associate professor of Managerial Communication at Tulane University, New Orleans, discussed that effective communication—both spoken and nonverbal—is a key tool skill mastered by good leaders. Explaining that everyone’s façade masks things that are hidden consciously or unconsciously, self-awareness can help us “enlarge our arena and tap into talents that can flower.” He also points out that 80% of our communication style is due to our personality and 20% to environment, and that it “costs us energy to flex.”
Dr. Keogh encouraged attendees to adapt to other communication styles so the listener can hear what is being said. For example, someone with a dominant communication style might be perceived as pushy by a one with a conscientious perfecting style. Completing the DiSC, a self-scored communication and personality style inventory from Inscape Publishing of Minneapolis, 22% of the hospitalists were predominantly creative, while 18% were perfectionists, and 12% inspirational communicators. Dr. Keogh says that this pattern is consistent with norms for physicians, and urged attendees to study how personality types can improve their handling of emotions, goals, values, fears, and judgments.
Throughout the sessions hospitalists raised issues, some of which mesh with others in the hospital, such as top administrators, and some of which don’t mesh. Many spoke candidly about their difficulties growing a hospitalist program beyond an admitting service into a full-blown inpatient medicine service—particularly with office-based colleagues waiting in the wings to be relieved of hospital work. Physician recruitment and retention were very much on their minds, as were rocky relationships with subspecialists, turnover in top administration that results in having to “resell” the hospitalist program to new leaders, and constant pressures to seek new ways to reduce average length of stay and emergency department throughput. Achieving a balance of patient care, committee responsibilities, and teaching and research for physicians interested in those areas were also mentioned.
Looking to the future, Mary Jo Gorman, MD, MD, SHM president-elect and chief medical officer of IPC: The Hospitalist Company, indicates her organizational vision: “It isn’t easy to build something brand new in only one year, so I plan to build on SHM’s momentum. My goal is to keep defining and building hospital medicine as a career rather than as an extension of the house officer path.”
Conclusion
With 100 hospitalists now armed with a new tool kit, Dr. Wellikson outlined SHM’s plans for upcoming Leadership Academies: “Our next Academy is Jan 9-12, 2006 in Tucson [Ariz.], and we’ve added a medical directors’ forum for managing burnout.” An advanced Leadership Academy is also planned for 2006. TH
The 100 hospitalists who gathered in September at the Vail Cascade Hotel and Spa among Vail, Colorado’s high peaks for SHM’s second Hospitalist Medicine Leadership Academy showed their character early during a simulation led by David Javitch, PhD, a Harvard University instructor. The exercise usually goes like this: The leader auctions $1 bills, with bidders paying their highest bid whether they win or lose. Participants’ aggressive juices flow and someone usually pays $5 or $10 for the lone dollar. Then they realize that their irrational bidding behavior is fueled by their need to compete rather than to cooperate, and the leader discusses the value of cooperation over greed.
But the SHM Leadership Academy hospitalists played the game differently. Dr. Javitch earmarked the proceeds of the auction for a pediatric AIDS foundation. After early bids to $5, one Mississippi doctor who had worked in a hospital without water and electricity during Hurricane Katrina bid $100. The bidding ceased abruptly. Spontaneously, several groups took up collections to boost the donation’s size. This stopped the facilitator in his tracks.
Instead of giving the participants a lesson on the destructive power of greed and competition, the facilitator got a lesson about hospitalist altruism—a dedication to serving people that is transforming how patients are treated in America’s medical centers. This exercise revealed both the pros and the cons of hospitalists’ leadership tendencies.
The Academy Format
Working at round tables of 10, the hospitalists spent all four days in the same small group. Each group was led by a facilitator who guided its exercises, kept the discussion on track, and encouraged participation in feedback and Q&A sessions. The hospitalists were put through their paces by experts in various disciplines relating to hospital medicine, learning about the field’s leadership challenges, its business metrics, strategic planning, understanding various personality traits and communication styles, and managing change and transformation efforts.
The SHM Leadership Academy, which limits attendance to 100, balances lectures with exercises, simulations, personality and communication inventories, and time for questions and sharing about professional issues. There was also time set aside for networking, including at a cocktail party hosted by IPC: The Hospitalist Company, North Hollywood, Calif., as well as sightseeing, biking, and visits to Vail Village to explore local shops and restaurants
Who Attended
The hospitalist attendees came to the Leadership Academy from diverse paths and at various stages of their careers. Some physicians started hospitalist programs fresh from residency, some worked in large teams, some had been in solo and group practice before becoming hospitalists, some were employed by hospitalist groups and health plans, and one started as a community-based solo practice hospitalist. They work in a wide range of settings, from rural and suburban community hospitals to academic medical centers, and in cities large and small.
Russell (“Rusty”) Holman, MD, and Cogent Healthcare’s, Irvine, Calif., national medical director, spelled out the Leadership Academy’s goals: for hospitalists to run their programs more efficiently, improve morale within their groups, maximize team efficiency, and identify critical drivers of success.
“Our goal at this conference is for you to learn new things, to improve your skills as leaders, and to learn how to continually demonstrate value to your CEOs and CFOs,” says Dr. Holman, who also led participants through the analytic steps of a strategic plan in their small groups.
Leadership Challenges
Laurence Wellikson, MD, SHM CEO, spelled out the challenges confronting hospital medicine.
“In a nation that spent $1.7 trillion on healthcare in 2003, or 15.3% of the nation’s GDP, with rising insurance premiums and out-of-pocket costs to consumers, hospitalists will be part of a systemic solution to controlling costs and providing high quality care,” says Dr. Wellikson.
He points out that hospitals are changing rapidly, requiring hospitalists to adapt to work environments in flux. The 20% annual turnover in nursing staffs, PCPs giving up inpatient care, subspecialists narrowing their hospital work, and overcrowded emergency departments all create both opportunities and challenges for hospitalists.
“Hospital medicine is growing rapidly and so are the demands on hospitalists,” adds Dr. Wellikson, who articulated SHM’s goal of helping hospitalists develop their leadership skills in a rapidly changing and complex field. He urges participants to transcend medicine’s “cult of uniqueness among individual doctors” and to lead teams that will reform hospitals internally and provide measurable improvements in patient care quality and reduce waste.
These trends are playing out in a healthcare system that’s forced to do more with less. Michael Guthrie, MD, MBA, executive in residence at the University of Colorado at Denver, points out that hospitalists must assume their CEOs and CFOs mindsets to understand the myriad challenges that arise from the swelling number of uninsured patients, the demands of aging baby boomers, malpractice liability, competition, rapid changes in technology, the need for new buildings, and the emphasis on patient satisfaction and safety. The rise of consumer-directed care resulting from employers shifting healthcare costs to employees has raised concerns about how “shopping around” among hospitals might affect clinical performance.
Dr. Guthrie stresses that value is in the eyes of the beholder and that the hospitalist’s work greatly affects other care team members’ satisfaction, relationships with other physicians, patient satisfaction and safety, and the hospital’s business interests.
“Hospitalists use their knowledge, ideas, skills, and expertise with process improvement to get things done with and through other people,” he explains. “When we understand what problems need to be solved and what our measures of success are we can have the rapture of accomplishment.”
Turmoil throughout the healthcare system and rapid growth of the hospitalist movement provided an apt backdrop for remarks Jack Silversin, DMD, DrPh, made in a session titled, “Leading and Managing Change.” Dr. Silversin is the president of Amicus Inc., a consultant firm based in Cambridge, Mass. He urges physicians to transcend their traditional roles as protectors of the status quo to become sponsors of change instead. Physicians as change agents publicly demonstrate their commitment to being leaders in several important ways.
“Change is definitely more work than maintaining the status quo,” says Dr. Silversin, “but organizations need doctors who sponsor change rather than resist it.”
Working through a simulation of a headstrong hospitalist trying to strong-arm her way to a 24/7 schedule for hospitalists rather than having the medical staff or moonlighters taking night call, participants developed their own insights into handling change.
“You’ve got to start small and gain credibility with little victories rather than doing something major right away,” said one attendee.
Trying to get non-hospitalists to support change was another idea: “Leadership doesn’t always have an MD credential attached to it,” added Dr. Silversin.
Being a change agent means looking inward as well as outward, and to that end attendees at the Leadership Academy spent time exploring their personal strengths and communication styles. Having completed a “Strength Deployment Inventory,” a self-scored test published by Personal Strength Publishing of Carlsbad, Calif., that measures an individual’s motives and values, prior to the conference, the hospitalists—led by Dr. Javitch—determined their strengths and weaknesses on altruism, assertiveness, and analysis. Small groups and dyads role-played situations where a colleague, an administrator, or a subordinate had a vastly different approach to problem-solving and decision-making.
“There are no right or wrong answers here, just a growing awareness of what our strengths are and things we need to guard against,” says Javitch.
Timothy Keogh, PhD, clinical associate professor of Managerial Communication at Tulane University, New Orleans, discussed that effective communication—both spoken and nonverbal—is a key tool skill mastered by good leaders. Explaining that everyone’s façade masks things that are hidden consciously or unconsciously, self-awareness can help us “enlarge our arena and tap into talents that can flower.” He also points out that 80% of our communication style is due to our personality and 20% to environment, and that it “costs us energy to flex.”
Dr. Keogh encouraged attendees to adapt to other communication styles so the listener can hear what is being said. For example, someone with a dominant communication style might be perceived as pushy by a one with a conscientious perfecting style. Completing the DiSC, a self-scored communication and personality style inventory from Inscape Publishing of Minneapolis, 22% of the hospitalists were predominantly creative, while 18% were perfectionists, and 12% inspirational communicators. Dr. Keogh says that this pattern is consistent with norms for physicians, and urged attendees to study how personality types can improve their handling of emotions, goals, values, fears, and judgments.
Throughout the sessions hospitalists raised issues, some of which mesh with others in the hospital, such as top administrators, and some of which don’t mesh. Many spoke candidly about their difficulties growing a hospitalist program beyond an admitting service into a full-blown inpatient medicine service—particularly with office-based colleagues waiting in the wings to be relieved of hospital work. Physician recruitment and retention were very much on their minds, as were rocky relationships with subspecialists, turnover in top administration that results in having to “resell” the hospitalist program to new leaders, and constant pressures to seek new ways to reduce average length of stay and emergency department throughput. Achieving a balance of patient care, committee responsibilities, and teaching and research for physicians interested in those areas were also mentioned.
Looking to the future, Mary Jo Gorman, MD, MD, SHM president-elect and chief medical officer of IPC: The Hospitalist Company, indicates her organizational vision: “It isn’t easy to build something brand new in only one year, so I plan to build on SHM’s momentum. My goal is to keep defining and building hospital medicine as a career rather than as an extension of the house officer path.”
Conclusion
With 100 hospitalists now armed with a new tool kit, Dr. Wellikson outlined SHM’s plans for upcoming Leadership Academies: “Our next Academy is Jan 9-12, 2006 in Tucson [Ariz.], and we’ve added a medical directors’ forum for managing burnout.” An advanced Leadership Academy is also planned for 2006. TH
The 100 hospitalists who gathered in September at the Vail Cascade Hotel and Spa among Vail, Colorado’s high peaks for SHM’s second Hospitalist Medicine Leadership Academy showed their character early during a simulation led by David Javitch, PhD, a Harvard University instructor. The exercise usually goes like this: The leader auctions $1 bills, with bidders paying their highest bid whether they win or lose. Participants’ aggressive juices flow and someone usually pays $5 or $10 for the lone dollar. Then they realize that their irrational bidding behavior is fueled by their need to compete rather than to cooperate, and the leader discusses the value of cooperation over greed.
But the SHM Leadership Academy hospitalists played the game differently. Dr. Javitch earmarked the proceeds of the auction for a pediatric AIDS foundation. After early bids to $5, one Mississippi doctor who had worked in a hospital without water and electricity during Hurricane Katrina bid $100. The bidding ceased abruptly. Spontaneously, several groups took up collections to boost the donation’s size. This stopped the facilitator in his tracks.
Instead of giving the participants a lesson on the destructive power of greed and competition, the facilitator got a lesson about hospitalist altruism—a dedication to serving people that is transforming how patients are treated in America’s medical centers. This exercise revealed both the pros and the cons of hospitalists’ leadership tendencies.
The Academy Format
Working at round tables of 10, the hospitalists spent all four days in the same small group. Each group was led by a facilitator who guided its exercises, kept the discussion on track, and encouraged participation in feedback and Q&A sessions. The hospitalists were put through their paces by experts in various disciplines relating to hospital medicine, learning about the field’s leadership challenges, its business metrics, strategic planning, understanding various personality traits and communication styles, and managing change and transformation efforts.
The SHM Leadership Academy, which limits attendance to 100, balances lectures with exercises, simulations, personality and communication inventories, and time for questions and sharing about professional issues. There was also time set aside for networking, including at a cocktail party hosted by IPC: The Hospitalist Company, North Hollywood, Calif., as well as sightseeing, biking, and visits to Vail Village to explore local shops and restaurants
Who Attended
The hospitalist attendees came to the Leadership Academy from diverse paths and at various stages of their careers. Some physicians started hospitalist programs fresh from residency, some worked in large teams, some had been in solo and group practice before becoming hospitalists, some were employed by hospitalist groups and health plans, and one started as a community-based solo practice hospitalist. They work in a wide range of settings, from rural and suburban community hospitals to academic medical centers, and in cities large and small.
Russell (“Rusty”) Holman, MD, and Cogent Healthcare’s, Irvine, Calif., national medical director, spelled out the Leadership Academy’s goals: for hospitalists to run their programs more efficiently, improve morale within their groups, maximize team efficiency, and identify critical drivers of success.
“Our goal at this conference is for you to learn new things, to improve your skills as leaders, and to learn how to continually demonstrate value to your CEOs and CFOs,” says Dr. Holman, who also led participants through the analytic steps of a strategic plan in their small groups.
Leadership Challenges
Laurence Wellikson, MD, SHM CEO, spelled out the challenges confronting hospital medicine.
“In a nation that spent $1.7 trillion on healthcare in 2003, or 15.3% of the nation’s GDP, with rising insurance premiums and out-of-pocket costs to consumers, hospitalists will be part of a systemic solution to controlling costs and providing high quality care,” says Dr. Wellikson.
He points out that hospitals are changing rapidly, requiring hospitalists to adapt to work environments in flux. The 20% annual turnover in nursing staffs, PCPs giving up inpatient care, subspecialists narrowing their hospital work, and overcrowded emergency departments all create both opportunities and challenges for hospitalists.
“Hospital medicine is growing rapidly and so are the demands on hospitalists,” adds Dr. Wellikson, who articulated SHM’s goal of helping hospitalists develop their leadership skills in a rapidly changing and complex field. He urges participants to transcend medicine’s “cult of uniqueness among individual doctors” and to lead teams that will reform hospitals internally and provide measurable improvements in patient care quality and reduce waste.
These trends are playing out in a healthcare system that’s forced to do more with less. Michael Guthrie, MD, MBA, executive in residence at the University of Colorado at Denver, points out that hospitalists must assume their CEOs and CFOs mindsets to understand the myriad challenges that arise from the swelling number of uninsured patients, the demands of aging baby boomers, malpractice liability, competition, rapid changes in technology, the need for new buildings, and the emphasis on patient satisfaction and safety. The rise of consumer-directed care resulting from employers shifting healthcare costs to employees has raised concerns about how “shopping around” among hospitals might affect clinical performance.
Dr. Guthrie stresses that value is in the eyes of the beholder and that the hospitalist’s work greatly affects other care team members’ satisfaction, relationships with other physicians, patient satisfaction and safety, and the hospital’s business interests.
“Hospitalists use their knowledge, ideas, skills, and expertise with process improvement to get things done with and through other people,” he explains. “When we understand what problems need to be solved and what our measures of success are we can have the rapture of accomplishment.”
Turmoil throughout the healthcare system and rapid growth of the hospitalist movement provided an apt backdrop for remarks Jack Silversin, DMD, DrPh, made in a session titled, “Leading and Managing Change.” Dr. Silversin is the president of Amicus Inc., a consultant firm based in Cambridge, Mass. He urges physicians to transcend their traditional roles as protectors of the status quo to become sponsors of change instead. Physicians as change agents publicly demonstrate their commitment to being leaders in several important ways.
“Change is definitely more work than maintaining the status quo,” says Dr. Silversin, “but organizations need doctors who sponsor change rather than resist it.”
Working through a simulation of a headstrong hospitalist trying to strong-arm her way to a 24/7 schedule for hospitalists rather than having the medical staff or moonlighters taking night call, participants developed their own insights into handling change.
“You’ve got to start small and gain credibility with little victories rather than doing something major right away,” said one attendee.
Trying to get non-hospitalists to support change was another idea: “Leadership doesn’t always have an MD credential attached to it,” added Dr. Silversin.
Being a change agent means looking inward as well as outward, and to that end attendees at the Leadership Academy spent time exploring their personal strengths and communication styles. Having completed a “Strength Deployment Inventory,” a self-scored test published by Personal Strength Publishing of Carlsbad, Calif., that measures an individual’s motives and values, prior to the conference, the hospitalists—led by Dr. Javitch—determined their strengths and weaknesses on altruism, assertiveness, and analysis. Small groups and dyads role-played situations where a colleague, an administrator, or a subordinate had a vastly different approach to problem-solving and decision-making.
“There are no right or wrong answers here, just a growing awareness of what our strengths are and things we need to guard against,” says Javitch.
Timothy Keogh, PhD, clinical associate professor of Managerial Communication at Tulane University, New Orleans, discussed that effective communication—both spoken and nonverbal—is a key tool skill mastered by good leaders. Explaining that everyone’s façade masks things that are hidden consciously or unconsciously, self-awareness can help us “enlarge our arena and tap into talents that can flower.” He also points out that 80% of our communication style is due to our personality and 20% to environment, and that it “costs us energy to flex.”
Dr. Keogh encouraged attendees to adapt to other communication styles so the listener can hear what is being said. For example, someone with a dominant communication style might be perceived as pushy by a one with a conscientious perfecting style. Completing the DiSC, a self-scored communication and personality style inventory from Inscape Publishing of Minneapolis, 22% of the hospitalists were predominantly creative, while 18% were perfectionists, and 12% inspirational communicators. Dr. Keogh says that this pattern is consistent with norms for physicians, and urged attendees to study how personality types can improve their handling of emotions, goals, values, fears, and judgments.
Throughout the sessions hospitalists raised issues, some of which mesh with others in the hospital, such as top administrators, and some of which don’t mesh. Many spoke candidly about their difficulties growing a hospitalist program beyond an admitting service into a full-blown inpatient medicine service—particularly with office-based colleagues waiting in the wings to be relieved of hospital work. Physician recruitment and retention were very much on their minds, as were rocky relationships with subspecialists, turnover in top administration that results in having to “resell” the hospitalist program to new leaders, and constant pressures to seek new ways to reduce average length of stay and emergency department throughput. Achieving a balance of patient care, committee responsibilities, and teaching and research for physicians interested in those areas were also mentioned.
Looking to the future, Mary Jo Gorman, MD, MD, SHM president-elect and chief medical officer of IPC: The Hospitalist Company, indicates her organizational vision: “It isn’t easy to build something brand new in only one year, so I plan to build on SHM’s momentum. My goal is to keep defining and building hospital medicine as a career rather than as an extension of the house officer path.”
Conclusion
With 100 hospitalists now armed with a new tool kit, Dr. Wellikson outlined SHM’s plans for upcoming Leadership Academies: “Our next Academy is Jan 9-12, 2006 in Tucson [Ariz.], and we’ve added a medical directors’ forum for managing burnout.” An advanced Leadership Academy is also planned for 2006. TH
Top PICS
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.


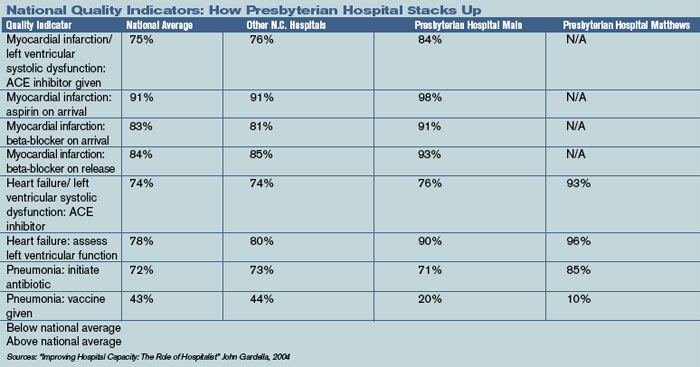
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
PEDIATRIC SPECIAL SECTION: Sibling Rivalry
In the flourishing metropolitan area of Atlanta, hospitalists and community-based physicians at Children’s Healthcare of Atlanta thrive within their niches, riding waves of opportunity fueled by the region’s burgeoning population. Jay Berkelhamer, MD, senior vice president of medical affairs at Children’s Healthcare of Atlanta calls his city “one of the most dynamic growth centers in the United States. Within 10 years we are estimated to have at least 150,000 more kids in Atlanta, leading to even greater opportunities for hospitalists and private practice primary care and specialty pediatricians.”
Two Hospitals, One system
Children’s Hospital of Atlanta’s hospitalist program is, in fact, two separate programs: one at Egleston, the other at Scottish Rite. The parent organization links the two and manages each hospital’s mission, structure, hiring, compensation, and outcomes.

—David Hall, MD
The six Egleston full-time equivalent hospitalists, or “cat herders,” as Corinne Taylor, MD, Egleston’s chief of medical affairs, describes them, are employees of Emory University Medical School. Most Egleston hospitalists are parents of young children and work four days a week, allowing them a balance of career and family life. Employed by the medical school and working at an academic medical center, they receive a salary, benefits, and other support services. Side by side with interns and residents, Egleston’s hospitalists see Atlanta’s sickest, frailest, and most at-risk children: the uninsured, underinsured immigrant and local population.
At Egleston the pediatric hospitalists are like their counterparts who treat adult patients in other settings. They deal with many patients with chronic conditions that lead to repeat hospitalizations.
“We see lots of ex-preemies with multiple problems such as asthma, seizures, cerebral palsy, and gastric problems,” says Dr. Taylor. “Some are ventilator-dependent and need lots of care.”
She relishes the clinical discipline that being a hospitalist at an academic medical center presents. “I do my homework every day and enjoy the stimulation of teaching our house officers,” explains Dr. Taylor. “Working with adult learners on the chronic conditions we manage and the cases with puzzling symptoms is exciting.”
Dr. Taylor’s boss is this hospitalist program’s founder, Joseph Snitzer, MD (see “Joseph Snitzer, MD: A hospital medicine pioneer”). Being hospital-based frees Dr. Snitzer to observe an endless parade of clinical challenges, including complex rheumatology cases, lupus, tumors, infected shunts, seizures, exotic infections, oncology diagnoses, and more.
“People call us from rural hospitals and private practices for help with diagnoses,” explains Dr. Snitzer. “We’re not smarter than anyone else. We just see a lot more than most other physicians.”
Scottish Rite
Across town at Scottish Rite, a nonprofit hospital, the hospitalists cope with the demands of a steady influx of new Atlantans. David Hall, MD, is Scottish Rite’s medical director. He was a former Egleston hospitalist and a private practitioner for 10 years in Baltimore before he relocated to Atlanta.
“We don’t have house officers, and there is a resident on call only one night a week,” says Dr. Hall. “Pediatricians in the community need to have their patients admitted 24/7, and we also have to admit from the emergency department at night. With our hospitalists taking calls at night and working all the next day, sometimes they would be on for 36 hours straight. As our service has grown, we’ve realized that this model was not sustainable.”
To reduce the burnout from their growing patient loads, the hospitalists changed their model. As of August 1, 2005, hospitalists at Scottish Rite began working either eight- or 12-hour shifts.
“Until we gain some experience with the shift system, we know we will struggle with continuity and handoffs,” adds Dr. Hall. Scottish Rite is also increasing its complement of moonlighting private practice pediatricians who want to keep their hospital skills current by covering the heavy workload.
Dr. Hall says recruiting new hospitalists isn’t a problem. Many local physicians want to do this work—especially right after residency. Comparing being a hospitalist with his 10 years in private practice, he says, “In my office practice I’d be sitting 20 feet away from a colleague, and there wasn’t much interaction. Now I’m learning something new every day and discussing interesting patients with other doctors. Building these ongoing relationships is great.”
Benefits, Culture, and More
The compensation and benefits packages at Egleston and Scottish Rite reflect that they are two separate hospitals in one system. Egleston’s hospitalists are employed by the medical school and receive a straight salary, with no incentive or at risk components. Scottish Rite’s hospitalists are hospital employees and have 20% of their salary at risk with productivity, quality improvement, and patient satisfaction incentives.
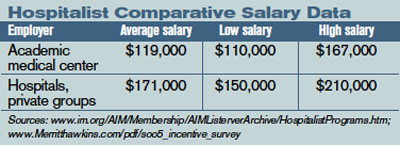
Although the different compensation systems may lead to discrepancies in pay, Dr. Berkelhamer explains that the policy of Children’s Hospital of Atlanta is to offer market-based salaries to all hospitalists. “Part of my job is to ensure that Dr. Snitzer and Dr. Hall are empowered to hire the physicians they want,” he says.
The hospitals have different corporate cultures as well. “The Scottish Rite group is very comfortable with lots of hands-on work while those at Egleston like to spend more time teaching,” says Dr. Berkelhamer.
Dr. Taylor, who trained with Dr. Snitzer and had a private practice in Atlanta for five years before becoming a full-time Egleston hospitalist in 1993, also acknowledges the different cultures at Egleston and Scottish Rite.
“We are two hospitals that come to the table and work together,” she observes. “Although we are in separate locations and may approach things differently, we practice the same type of medicine.”
Dr. Berkelhamer, who works with both sets of hospitalists, reinforces the observation that their clinical practices are consistent: “Surveys on patient and community physician satisfaction are the same, as are outcomes and productivity data.”
Special Issues for Both Hospitals
As part of a growing medical specialty in a dynamic region of the country, hospitalists at Children’s Hospital of Atlanta must confront a number of issues—some unique to them, others that reflect national trends. With different compensation and productivity systems, the two sets of hospitalists must collaborate to practice one brand of medicine.
An important formal step in their collaboration is the computerized medical and order entry system scheduled for spring 2006 implementation. The hospitalists are working together to develop clinical pathways and standardized orders based on their culling through best practices and evidence-based medicine guidelines. A newly appointed chief quality officer will keep the project on track.
Atlanta’s growth presents other issues for the hospitalists. With a constant influx of new community-based pediatricians Dr. Taylor finds that the hospitalists sometimes have trouble communicating with them to coordinate care.
“There are now at least 1,000 primary care and subspecialty pediatricians in Atlanta,” she says. “Trying to build trust and to track personal preferences with so many doctors is difficult. Fortunately we have electronic medical records so we can share important data with them.”
The hospitals’ social workers and case managers represent added glue to hold the communication together. Another of Atlanta’s challenges: It has only two medical schools from which to draw local hospitalists and other pediatricians, Emory University and the smaller Morehouse University. While not insurmountable, it means that most pediatricians practicing in the area must relocate to Atlanta.
What the Future Holds
And then there are issues that transcend Atlanta. Dr. Snitzer feels the national movement for hospitalists to become a specialty will happen sooner rather than later. In line with that movement, Children’s Hospital of Atlanta will have its first hospitalist fellowship in 2007. (For more information on pediatric hospital medicine fellowships, see “Pediatric Fellowship Offered,” below.)
For Dr. Hall, hospitalist compensation in a boomtown rankles. “People can’t really make money being hospitalists,” he explains. “Most need some subsidy to keep the programs going.”
The pay issues are being addressed, albeit slowly. Dr. Hall is encouraged by the campaign of pediatric intensivists to have coding and payment upgrades; he sees it as a template for higher hospitalist reimbursement schedules. “We only get paid for one visit a day, but we often see a patient several times a day,” he says. “Reimbursement should reflect what we really do.”
Both hospitals will have new buildings, each with 250 beds, more surgical suites, and expanded emergency departments by early 2007. That should lead to more hospitalist hiring—not surprising for a hospital that pioneered having inpatient physicians more than 20 years ago. TH
Writer Marlene Piturro is based in New York.
Joseph Snitzer, MD: A hospital medicine pioneer

In 1983—13 years before Robert Wachter, MD, FACP, coined the term “hospitalist”—Egleston Children’s Hospital Department of Pediatrics Chairman Joseph Patterson, MD, asked a former trainee to establish an in-house general pediatric service. That young doctor, Joseph Snitzer III, had been splitting his time equally between a private practice and teaching at Egleston through his affiliation with the Emory University School of Medicine. He said yes to the new assignment.
Since becoming a full-time hospitalist more than two decades ago, Dr. Snitzer relishes both his time working with interns and residents and an ever-changing mix of treatment and diagnostic mysteries. He is now the chief, Division of General Pediatrics, Children’s Healthcare of Atlanta at Egleston, and professor of pediatrics, Emory School of Medicine.
“We see everything here, from Kawasaki syndrome to neonatal apnea, seizure disorders, tumors, dehydration, jaundice, and all kinds of infections,” he explains. “About 50% of the children admitted have chronic conditions and the rest have various acute illnesses. There are unique challenges every day.”
Dr. Snitzer trained both Dr. Hall and Dr. Taylor, transmitting knowledge from one generation of physicians to the next. His hospitalist team maintains excellent relationships with the community’s doctors, both general pediatricians and specialists.
What is the main strength of Dr. Snitzer and the other hospitalists? Coordination with Atlanta’s pediatricians on getting things done in the hospital. Phone consultations with Atlanta’s physicians and those in rural areas seeking Children’s Hospital of Atlanta’s expertise on complex diagnoses and cases also keep him busy.
“Our experience with complexity is overwhelming,” he says. “Perhaps we can’t offer a great deal with simple diagnoses, such as diarrhea or simple skin infections, but we can with tough cases.” —MP
PEDIATRIC SPECIAL SECTION:
NEWS
Pediatric Fellowship Offered
Children’s Hospitalists of San Diego offers program

The Pediatric Hospitalist program at Children’s Hospital and Health Center of San Diego (CHHC) began in 1978. The current hospitalists are employed by Children’s Specialists of San Diego (CSSD), a 180-member pediatric-only specialty medical group. Inpatient care is provided for 75% of all general pediatric patients at the 233-bed tertiary care CHHC. Program consultation is offered at nearby Palomar Medical Center, a 23-bed unit within a larger 319-bed community hospital with a trauma center.
The hospitalists are the primary teaching faculty for the house staff and medical students who come from the University of California San Diego (UCSD), Balboa Naval Hospital, Pendleton Naval Medical Center, and Scripps Family Medicine. All hospitalists are board-certified pediatricians and have additional degrees or postresidency training, such as chief residency or fellowship experience.
Hospitalists fulfill many leadership roles in the hospital and community when not on service. A detailed list is available in a previous issue of The Hospitalist (Nov/Dec 2004;8(6):59-60). Current research includes an Agency for Healthcare Research and Quality (AHRQ) safety grant on medication errors, a bronchiolitis clinical trial, juvenile justice research on hepatitis B, a Hispanic cultural competency grant from the California Endowment, spiratory syncytial virus immunoprophylaxis outcomes in a managed population, and primary care perceptions of pediatric dentistry. Thus the hospitalist program has a long history of strong commitment to children and the core aspects of pediatric hospital medicine.
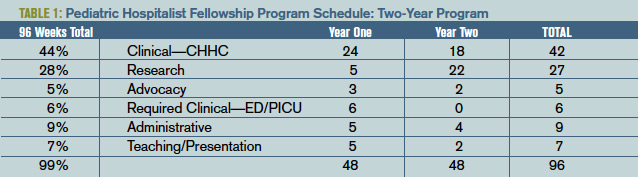
The Fellowship
The CSSD Pediatric Hospitalist Fellowship Program goal is to train highly motivated pediatricians for careers in academic and clinical hospital medicine. Over a two-year period instruction is provided in clinical, advocacy, administrative, teaching, and research aspects of pediatric hospital medicine. Clinical education emphasizes inpatient acute care, including intensive care and emergency transport at the busy main campus at CHHC. Outpatient clinical care offers experiences in adolescent juvenile hall medicine, hospice, and child protection. The diverse clinical exposure, teaching from local and national leaders, and volume of patients ensure graduates of this program are well prepared for any clinical hospitalist position.
The staff gains administrative experience via both hospital and medical group quality improvement activities. This work is directed by the medical director for CSSD and the physician advisor for quality management for CHHC, both of whom are CSSD pediatric hospitalists. Skills in process improvement, continuous quality improvement, risk management, organizational management and leadership are honed during the fellowship. Opportunity exists to take courses through the American College of Physician Executives if the trainee desires a future in administrative hospitalist medicine.
Academics and teaching are a core value of the pediatric hospitalist service. The fellow participates in the monthly division journal club and internal case review. Daily teaching while on the clinical service includes bedside rounds, management rounds, and attending rounds. Pediatric hospitalists are the primary inpatient teaching staff and as such have a significant responsibility for daily house staff education. The fellow participates in noon conferences and other educational venues under the guidance of the director of inpatient teaching (also a pediatric hospitalist).
Advocacy skills are learned through experiences in the juvenile hall system, Center for Child Protection, the American Academy of Pediatrics (AAP), and at the local and state level for children’s services funding. Under the leadership of the medical directors for the Center for Child Protection and the A.B. and Jessie Polinsky Center for Abused Children, the fellow participates in case review and observes expert child abuse testimony in court. Discussions with legislators in Sacramento focus upon protection of the California Children’s Services system, which supports critically ill state-funded children. The fellow learns AAP local and national structure, participating in conferences and chapter events.
Research is expected during this two-year fellowship program. Formal clinical research training is part of the first year curriculum of UCSD’s Clinical Research Enhancement through Supplemental Training (CREST) program. The first year of this two-year CREST program includes weekly classes covering epidemiology, patient-oriented research, health services research, and informatics. Those dedicated to completion of a master’s degree during the two-year program may integrate this training with a more intense curriculum schedule. A research project and mentor is chosen after the first quarter of the first year. Research may be in any area of pediatric hospitalist medicine. Research is presented at either Pediatric Academic Societies, Society of Hospital Medicine, or other similar forum upon completion.
The schedule is flexible, but follows the template. (See Table 1, p. 30: “Pediatric Hospitalist Fellowship Program Schedule.”)
One fellowship position is offered every year, with application submissions accepted through Dec. 1, interviews granted Dec. 15-Feb. 1 and final selection by Feb. 15. You can obtain an application from the CSSD Web site “Fellowships” page (http://childrensspecialists. com/body.cfm?id=580) or by e-mailing Fellowship Coordinator Susan Stafford at sstafford@chsd.org.
PEDIATRIC SPECIAL SECTION:
IN THE LITERATURE
Retrospective Study Attempts Criteria for Diagnosing MAS
Reviews by Julia Simmons, MD
Ravelli A, Magni-Manzoni S, Pistorio A, et al. Preliminary diagnostic guidelines for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. J Pediatr. 2005;146(5):598-604.
Macrophage activating syndrome (MAS) is a complication of connective tissue disorders, most often associated with active systemic juvenile idiopathic arthritis (S-JIA). It is a rare disorder and the exact incidence is unknown. It is characterized by uncontrolled activation and proliferation of T-lymphocytes and macrophages. If not recognized and treated aggressively, MAS can be life threatening.
In this article, the authors’ purpose was to review the available clinical, laboratory, and histopathologic data in patients with active S-JIA and in those with active S-JIA complicated by MAS. The goal was to develop criteria to diagnose MAS.
The retrospective study was designed using the classification, criteria approach. The index cases included patients with MAS complicating S-JIA. The “confusable” condition was active S-JIA. There were 74 patients in the index cases. Seventeen of the cases were observed at the authors’ institution. These patients were diagnosed with S-JIA using the International League of Association for Rheumatology criteria. They were identified using a database search. Fifty-seven of the cases were obtained from a Medline search. Of these 74 patients, eight were disqualified because they did not meet the definition of S-JIA, and 11 were excluded because of insufficient data. The control group contained 37 patients observed at the authors’ sites. The sensitivity rate, specificity rate, area under receiver operating characteristic curve, and diagnostic odds ratio were applied to the data to differentiate MAS complicating S-JIA from S-JIA.
The study results found hemorrhages and central nervous dysfunction were the strongest clinical discriminating factors. The strongest laboratory discriminators included thrombocytopenia, leukopenia, elevated aspartate aminotransferase, and hypofibrinogenemia. Histopathological criterion included evidence of macrophage hemophagocytosis in the bone marrow aspirate. Other useful discriminators included hypertriglyceridemia, elevated ferritin, hepatomegaly, hand hyponatremia. Final guidelines were developed after analyzing the statistics and determining the clinical importance: “The diagnosis of MAS requires the presence of any two or more laboratory criteria or of any two or three or more clinical and/or laboratory criteria. A bone marrow aspirate for the demonstration of hemophagocytosis may be required only in doubtful cases.”
In summary, MAS complicating S-JIA is a disorder without concrete diagnostic criteria. The authors have performed preliminary studies to diagnose MAS. They appropriately recognized the need for prospective larger clinical studies.
HNL Helps Distinguish Infections
Fjaertoft G, Foucard T, Xu S, et al. Human neutrophil lipocalin (HNL) as a diagnostic tool in children with acute infections: a study of the kinetics. Acta Pediatrica costarricense. 2005;94:661-666.
In pediatrics, the clinician is often faced with the diagnostic challenge of differentiating a bacterial infectious process from a viral infection. History, physical exam, and laboratory data make the distinction. In this article, the authors’ purpose was to assess the kinetics of HNL with viral and bacterial infections. Further, they assess the response of HNL when the infection is treated with antibiotics. The response of HNL is compared with that of C-reactive protein.
In the study, 92 patients with a median age of 26 months were hospitalized because they required systemic antibiotics or because of the severity of their medical condition. Upon admission and on hospital days one, two, and three, the C-reactive protein, white blood cell count with differential, and HNL were measured. The patients were retrospectively classified into five groups: true bacterial infection (n=28), true viral infection (n=4), suspected bacterial infection (n=18), suspected viral (n=34), and other.
A true bacterial infection required bacterial isolation from blood, urine, or cerebrospinal fluid culture, or radiographic demonstration of pneumonia. Patients were classified as having a suspected bacterial infection if they had a nonspecific diagnosis, but an elevated C-reactive protein and erythrocyte sedimentation rate. A true viral infection required isolation of a virus. If a patient did not meet any of the above criteria, the person was classified as having a suspected viral infection. Those patients in the “other” group were diagnosed with Kawasaki disease, Borrelia meningitis, and one undiagnosed patient. The patients were classified using history, exam, and laboratory values including white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and cultures. HNL values were not used in the classification.
The results demonstrated that both C-reactive protein and HNL are elevated with true bacterial infections compared with viral illnesses. Neither C-reactive protein nor HNL were significantly different in true bacterial infections versus suspected bacterial infections. The optimal cut-off for C-reactive protein was 59 mg/L with 93% sensitivity and 68% specificity. The optimal cutoff for HNL was 217 micrograms/L with 90% sensitivity and 74% specificity. In patients with true bacterial infections, HNL was highest at admission and decreased one day after admission. In contrast, the C-reactive protein values were similar on the day of admission and on hospital day one. C-reactive protein decreased significantly on days two and three of hospitalization. After hospital day one, HNL was elevated in only 11% of patients with true bacterial infection in contrast to 83% patients with elevated C-reactive protein.
In summary, HNL may be a useful marker to distinguish bacterial and viral illnesses. In comparison with C-reactive protein, it normalizes more rapidly after appropriate antibiotic therapy is initiated. In the future, HNL may be a useful marker in monitoring the response to antibiotic therapy.
CEDKA in Peds
Lawrence SE, Cummings EA, Gaboury I, et al. Population-based study of incidence and risk factors for cerebral edema in pediatric diabetic ketoacidosis. . 2005;146:688-692.
New onset insulin dependent diabetes mellitus is complicated by diabetic ketoacidosis (DKA) in 15% to 67% of patients. The incidence of cerebral edema in diabetic ketoacidosis (CEDKA) has been reported as 0.4-3.1. In the article, the authors seek to determine the incidence, outcome, and risk factors for cerebral edema in DKA in patients younger than 16.
The study was case-controlled with an active Canadian surveillance study. The authors surveyed pediatricians for a two-year period. During this time in Canada, all physicians were requested to submit reports monthly on patients with CEDKA younger than 16.
Thirteen cases were identified and the incidence of CEDKA was 0.51%. Overall mortality from cerebral edema was 0.15%. Increased blood urea nitrogen, degree of dehydration, hyperglycemia, and lower initial bicarbonate were associated with CEDKA. TH
In the flourishing metropolitan area of Atlanta, hospitalists and community-based physicians at Children’s Healthcare of Atlanta thrive within their niches, riding waves of opportunity fueled by the region’s burgeoning population. Jay Berkelhamer, MD, senior vice president of medical affairs at Children’s Healthcare of Atlanta calls his city “one of the most dynamic growth centers in the United States. Within 10 years we are estimated to have at least 150,000 more kids in Atlanta, leading to even greater opportunities for hospitalists and private practice primary care and specialty pediatricians.”
Two Hospitals, One system
Children’s Hospital of Atlanta’s hospitalist program is, in fact, two separate programs: one at Egleston, the other at Scottish Rite. The parent organization links the two and manages each hospital’s mission, structure, hiring, compensation, and outcomes.
—David Hall, MD
The six Egleston full-time equivalent hospitalists, or “cat herders,” as Corinne Taylor, MD, Egleston’s chief of medical affairs, describes them, are employees of Emory University Medical School. Most Egleston hospitalists are parents of young children and work four days a week, allowing them a balance of career and family life. Employed by the medical school and working at an academic medical center, they receive a salary, benefits, and other support services. Side by side with interns and residents, Egleston’s hospitalists see Atlanta’s sickest, frailest, and most at-risk children: the uninsured, underinsured immigrant and local population.
At Egleston the pediatric hospitalists are like their counterparts who treat adult patients in other settings. They deal with many patients with chronic conditions that lead to repeat hospitalizations.
“We see lots of ex-preemies with multiple problems such as asthma, seizures, cerebral palsy, and gastric problems,” says Dr. Taylor. “Some are ventilator-dependent and need lots of care.”
She relishes the clinical discipline that being a hospitalist at an academic medical center presents. “I do my homework every day and enjoy the stimulation of teaching our house officers,” explains Dr. Taylor. “Working with adult learners on the chronic conditions we manage and the cases with puzzling symptoms is exciting.”
Dr. Taylor’s boss is this hospitalist program’s founder, Joseph Snitzer, MD (see “Joseph Snitzer, MD: A hospital medicine pioneer”). Being hospital-based frees Dr. Snitzer to observe an endless parade of clinical challenges, including complex rheumatology cases, lupus, tumors, infected shunts, seizures, exotic infections, oncology diagnoses, and more.
“People call us from rural hospitals and private practices for help with diagnoses,” explains Dr. Snitzer. “We’re not smarter than anyone else. We just see a lot more than most other physicians.”
Scottish Rite
Across town at Scottish Rite, a nonprofit hospital, the hospitalists cope with the demands of a steady influx of new Atlantans. David Hall, MD, is Scottish Rite’s medical director. He was a former Egleston hospitalist and a private practitioner for 10 years in Baltimore before he relocated to Atlanta.
“We don’t have house officers, and there is a resident on call only one night a week,” says Dr. Hall. “Pediatricians in the community need to have their patients admitted 24/7, and we also have to admit from the emergency department at night. With our hospitalists taking calls at night and working all the next day, sometimes they would be on for 36 hours straight. As our service has grown, we’ve realized that this model was not sustainable.”
To reduce the burnout from their growing patient loads, the hospitalists changed their model. As of August 1, 2005, hospitalists at Scottish Rite began working either eight- or 12-hour shifts.
“Until we gain some experience with the shift system, we know we will struggle with continuity and handoffs,” adds Dr. Hall. Scottish Rite is also increasing its complement of moonlighting private practice pediatricians who want to keep their hospital skills current by covering the heavy workload.
Dr. Hall says recruiting new hospitalists isn’t a problem. Many local physicians want to do this work—especially right after residency. Comparing being a hospitalist with his 10 years in private practice, he says, “In my office practice I’d be sitting 20 feet away from a colleague, and there wasn’t much interaction. Now I’m learning something new every day and discussing interesting patients with other doctors. Building these ongoing relationships is great.”
Benefits, Culture, and More
The compensation and benefits packages at Egleston and Scottish Rite reflect that they are two separate hospitals in one system. Egleston’s hospitalists are employed by the medical school and receive a straight salary, with no incentive or at risk components. Scottish Rite’s hospitalists are hospital employees and have 20% of their salary at risk with productivity, quality improvement, and patient satisfaction incentives.
Although the different compensation systems may lead to discrepancies in pay, Dr. Berkelhamer explains that the policy of Children’s Hospital of Atlanta is to offer market-based salaries to all hospitalists. “Part of my job is to ensure that Dr. Snitzer and Dr. Hall are empowered to hire the physicians they want,” he says.
The hospitals have different corporate cultures as well. “The Scottish Rite group is very comfortable with lots of hands-on work while those at Egleston like to spend more time teaching,” says Dr. Berkelhamer.
Dr. Taylor, who trained with Dr. Snitzer and had a private practice in Atlanta for five years before becoming a full-time Egleston hospitalist in 1993, also acknowledges the different cultures at Egleston and Scottish Rite.
“We are two hospitals that come to the table and work together,” she observes. “Although we are in separate locations and may approach things differently, we practice the same type of medicine.”
Dr. Berkelhamer, who works with both sets of hospitalists, reinforces the observation that their clinical practices are consistent: “Surveys on patient and community physician satisfaction are the same, as are outcomes and productivity data.”
Special Issues for Both Hospitals
As part of a growing medical specialty in a dynamic region of the country, hospitalists at Children’s Hospital of Atlanta must confront a number of issues—some unique to them, others that reflect national trends. With different compensation and productivity systems, the two sets of hospitalists must collaborate to practice one brand of medicine.
An important formal step in their collaboration is the computerized medical and order entry system scheduled for spring 2006 implementation. The hospitalists are working together to develop clinical pathways and standardized orders based on their culling through best practices and evidence-based medicine guidelines. A newly appointed chief quality officer will keep the project on track.
Atlanta’s growth presents other issues for the hospitalists. With a constant influx of new community-based pediatricians Dr. Taylor finds that the hospitalists sometimes have trouble communicating with them to coordinate care.
“There are now at least 1,000 primary care and subspecialty pediatricians in Atlanta,” she says. “Trying to build trust and to track personal preferences with so many doctors is difficult. Fortunately we have electronic medical records so we can share important data with them.”
The hospitals’ social workers and case managers represent added glue to hold the communication together. Another of Atlanta’s challenges: It has only two medical schools from which to draw local hospitalists and other pediatricians, Emory University and the smaller Morehouse University. While not insurmountable, it means that most pediatricians practicing in the area must relocate to Atlanta.
What the Future Holds
And then there are issues that transcend Atlanta. Dr. Snitzer feels the national movement for hospitalists to become a specialty will happen sooner rather than later. In line with that movement, Children’s Hospital of Atlanta will have its first hospitalist fellowship in 2007. (For more information on pediatric hospital medicine fellowships, see “Pediatric Fellowship Offered,” below.)
For Dr. Hall, hospitalist compensation in a boomtown rankles. “People can’t really make money being hospitalists,” he explains. “Most need some subsidy to keep the programs going.”
The pay issues are being addressed, albeit slowly. Dr. Hall is encouraged by the campaign of pediatric intensivists to have coding and payment upgrades; he sees it as a template for higher hospitalist reimbursement schedules. “We only get paid for one visit a day, but we often see a patient several times a day,” he says. “Reimbursement should reflect what we really do.”
Both hospitals will have new buildings, each with 250 beds, more surgical suites, and expanded emergency departments by early 2007. That should lead to more hospitalist hiring—not surprising for a hospital that pioneered having inpatient physicians more than 20 years ago. TH
Writer Marlene Piturro is based in New York.
Joseph Snitzer, MD: A hospital medicine pioneer
In 1983—13 years before Robert Wachter, MD, FACP, coined the term “hospitalist”—Egleston Children’s Hospital Department of Pediatrics Chairman Joseph Patterson, MD, asked a former trainee to establish an in-house general pediatric service. That young doctor, Joseph Snitzer III, had been splitting his time equally between a private practice and teaching at Egleston through his affiliation with the Emory University School of Medicine. He said yes to the new assignment.
Since becoming a full-time hospitalist more than two decades ago, Dr. Snitzer relishes both his time working with interns and residents and an ever-changing mix of treatment and diagnostic mysteries. He is now the chief, Division of General Pediatrics, Children’s Healthcare of Atlanta at Egleston, and professor of pediatrics, Emory School of Medicine.
“We see everything here, from Kawasaki syndrome to neonatal apnea, seizure disorders, tumors, dehydration, jaundice, and all kinds of infections,” he explains. “About 50% of the children admitted have chronic conditions and the rest have various acute illnesses. There are unique challenges every day.”
Dr. Snitzer trained both Dr. Hall and Dr. Taylor, transmitting knowledge from one generation of physicians to the next. His hospitalist team maintains excellent relationships with the community’s doctors, both general pediatricians and specialists.
What is the main strength of Dr. Snitzer and the other hospitalists? Coordination with Atlanta’s pediatricians on getting things done in the hospital. Phone consultations with Atlanta’s physicians and those in rural areas seeking Children’s Hospital of Atlanta’s expertise on complex diagnoses and cases also keep him busy.
“Our experience with complexity is overwhelming,” he says. “Perhaps we can’t offer a great deal with simple diagnoses, such as diarrhea or simple skin infections, but we can with tough cases.” —MP
PEDIATRIC SPECIAL SECTION:
NEWS
Pediatric Fellowship Offered
Children’s Hospitalists of San Diego offers program
The Pediatric Hospitalist program at Children’s Hospital and Health Center of San Diego (CHHC) began in 1978. The current hospitalists are employed by Children’s Specialists of San Diego (CSSD), a 180-member pediatric-only specialty medical group. Inpatient care is provided for 75% of all general pediatric patients at the 233-bed tertiary care CHHC. Program consultation is offered at nearby Palomar Medical Center, a 23-bed unit within a larger 319-bed community hospital with a trauma center.
The hospitalists are the primary teaching faculty for the house staff and medical students who come from the University of California San Diego (UCSD), Balboa Naval Hospital, Pendleton Naval Medical Center, and Scripps Family Medicine. All hospitalists are board-certified pediatricians and have additional degrees or postresidency training, such as chief residency or fellowship experience.
Hospitalists fulfill many leadership roles in the hospital and community when not on service. A detailed list is available in a previous issue of The Hospitalist (Nov/Dec 2004;8(6):59-60). Current research includes an Agency for Healthcare Research and Quality (AHRQ) safety grant on medication errors, a bronchiolitis clinical trial, juvenile justice research on hepatitis B, a Hispanic cultural competency grant from the California Endowment, spiratory syncytial virus immunoprophylaxis outcomes in a managed population, and primary care perceptions of pediatric dentistry. Thus the hospitalist program has a long history of strong commitment to children and the core aspects of pediatric hospital medicine.
The Fellowship
The CSSD Pediatric Hospitalist Fellowship Program goal is to train highly motivated pediatricians for careers in academic and clinical hospital medicine. Over a two-year period instruction is provided in clinical, advocacy, administrative, teaching, and research aspects of pediatric hospital medicine. Clinical education emphasizes inpatient acute care, including intensive care and emergency transport at the busy main campus at CHHC. Outpatient clinical care offers experiences in adolescent juvenile hall medicine, hospice, and child protection. The diverse clinical exposure, teaching from local and national leaders, and volume of patients ensure graduates of this program are well prepared for any clinical hospitalist position.
The staff gains administrative experience via both hospital and medical group quality improvement activities. This work is directed by the medical director for CSSD and the physician advisor for quality management for CHHC, both of whom are CSSD pediatric hospitalists. Skills in process improvement, continuous quality improvement, risk management, organizational management and leadership are honed during the fellowship. Opportunity exists to take courses through the American College of Physician Executives if the trainee desires a future in administrative hospitalist medicine.
Academics and teaching are a core value of the pediatric hospitalist service. The fellow participates in the monthly division journal club and internal case review. Daily teaching while on the clinical service includes bedside rounds, management rounds, and attending rounds. Pediatric hospitalists are the primary inpatient teaching staff and as such have a significant responsibility for daily house staff education. The fellow participates in noon conferences and other educational venues under the guidance of the director of inpatient teaching (also a pediatric hospitalist).
Advocacy skills are learned through experiences in the juvenile hall system, Center for Child Protection, the American Academy of Pediatrics (AAP), and at the local and state level for children’s services funding. Under the leadership of the medical directors for the Center for Child Protection and the A.B. and Jessie Polinsky Center for Abused Children, the fellow participates in case review and observes expert child abuse testimony in court. Discussions with legislators in Sacramento focus upon protection of the California Children’s Services system, which supports critically ill state-funded children. The fellow learns AAP local and national structure, participating in conferences and chapter events.
Research is expected during this two-year fellowship program. Formal clinical research training is part of the first year curriculum of UCSD’s Clinical Research Enhancement through Supplemental Training (CREST) program. The first year of this two-year CREST program includes weekly classes covering epidemiology, patient-oriented research, health services research, and informatics. Those dedicated to completion of a master’s degree during the two-year program may integrate this training with a more intense curriculum schedule. A research project and mentor is chosen after the first quarter of the first year. Research may be in any area of pediatric hospitalist medicine. Research is presented at either Pediatric Academic Societies, Society of Hospital Medicine, or other similar forum upon completion.
The schedule is flexible, but follows the template. (See Table 1, p. 30: “Pediatric Hospitalist Fellowship Program Schedule.”)
One fellowship position is offered every year, with application submissions accepted through Dec. 1, interviews granted Dec. 15-Feb. 1 and final selection by Feb. 15. You can obtain an application from the CSSD Web site “Fellowships” page (http://childrensspecialists. com/body.cfm?id=580) or by e-mailing Fellowship Coordinator Susan Stafford at sstafford@chsd.org.
PEDIATRIC SPECIAL SECTION:
IN THE LITERATURE
Retrospective Study Attempts Criteria for Diagnosing MAS
Reviews by Julia Simmons, MD
Ravelli A, Magni-Manzoni S, Pistorio A, et al. Preliminary diagnostic guidelines for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. J Pediatr. 2005;146(5):598-604.
Macrophage activating syndrome (MAS) is a complication of connective tissue disorders, most often associated with active systemic juvenile idiopathic arthritis (S-JIA). It is a rare disorder and the exact incidence is unknown. It is characterized by uncontrolled activation and proliferation of T-lymphocytes and macrophages. If not recognized and treated aggressively, MAS can be life threatening.
In this article, the authors’ purpose was to review the available clinical, laboratory, and histopathologic data in patients with active S-JIA and in those with active S-JIA complicated by MAS. The goal was to develop criteria to diagnose MAS.
The retrospective study was designed using the classification, criteria approach. The index cases included patients with MAS complicating S-JIA. The “confusable” condition was active S-JIA. There were 74 patients in the index cases. Seventeen of the cases were observed at the authors’ institution. These patients were diagnosed with S-JIA using the International League of Association for Rheumatology criteria. They were identified using a database search. Fifty-seven of the cases were obtained from a Medline search. Of these 74 patients, eight were disqualified because they did not meet the definition of S-JIA, and 11 were excluded because of insufficient data. The control group contained 37 patients observed at the authors’ sites. The sensitivity rate, specificity rate, area under receiver operating characteristic curve, and diagnostic odds ratio were applied to the data to differentiate MAS complicating S-JIA from S-JIA.
The study results found hemorrhages and central nervous dysfunction were the strongest clinical discriminating factors. The strongest laboratory discriminators included thrombocytopenia, leukopenia, elevated aspartate aminotransferase, and hypofibrinogenemia. Histopathological criterion included evidence of macrophage hemophagocytosis in the bone marrow aspirate. Other useful discriminators included hypertriglyceridemia, elevated ferritin, hepatomegaly, hand hyponatremia. Final guidelines were developed after analyzing the statistics and determining the clinical importance: “The diagnosis of MAS requires the presence of any two or more laboratory criteria or of any two or three or more clinical and/or laboratory criteria. A bone marrow aspirate for the demonstration of hemophagocytosis may be required only in doubtful cases.”
In summary, MAS complicating S-JIA is a disorder without concrete diagnostic criteria. The authors have performed preliminary studies to diagnose MAS. They appropriately recognized the need for prospective larger clinical studies.
HNL Helps Distinguish Infections
Fjaertoft G, Foucard T, Xu S, et al. Human neutrophil lipocalin (HNL) as a diagnostic tool in children with acute infections: a study of the kinetics. Acta Pediatrica costarricense. 2005;94:661-666.
In pediatrics, the clinician is often faced with the diagnostic challenge of differentiating a bacterial infectious process from a viral infection. History, physical exam, and laboratory data make the distinction. In this article, the authors’ purpose was to assess the kinetics of HNL with viral and bacterial infections. Further, they assess the response of HNL when the infection is treated with antibiotics. The response of HNL is compared with that of C-reactive protein.
In the study, 92 patients with a median age of 26 months were hospitalized because they required systemic antibiotics or because of the severity of their medical condition. Upon admission and on hospital days one, two, and three, the C-reactive protein, white blood cell count with differential, and HNL were measured. The patients were retrospectively classified into five groups: true bacterial infection (n=28), true viral infection (n=4), suspected bacterial infection (n=18), suspected viral (n=34), and other.
A true bacterial infection required bacterial isolation from blood, urine, or cerebrospinal fluid culture, or radiographic demonstration of pneumonia. Patients were classified as having a suspected bacterial infection if they had a nonspecific diagnosis, but an elevated C-reactive protein and erythrocyte sedimentation rate. A true viral infection required isolation of a virus. If a patient did not meet any of the above criteria, the person was classified as having a suspected viral infection. Those patients in the “other” group were diagnosed with Kawasaki disease, Borrelia meningitis, and one undiagnosed patient. The patients were classified using history, exam, and laboratory values including white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and cultures. HNL values were not used in the classification.
The results demonstrated that both C-reactive protein and HNL are elevated with true bacterial infections compared with viral illnesses. Neither C-reactive protein nor HNL were significantly different in true bacterial infections versus suspected bacterial infections. The optimal cut-off for C-reactive protein was 59 mg/L with 93% sensitivity and 68% specificity. The optimal cutoff for HNL was 217 micrograms/L with 90% sensitivity and 74% specificity. In patients with true bacterial infections, HNL was highest at admission and decreased one day after admission. In contrast, the C-reactive protein values were similar on the day of admission and on hospital day one. C-reactive protein decreased significantly on days two and three of hospitalization. After hospital day one, HNL was elevated in only 11% of patients with true bacterial infection in contrast to 83% patients with elevated C-reactive protein.
In summary, HNL may be a useful marker to distinguish bacterial and viral illnesses. In comparison with C-reactive protein, it normalizes more rapidly after appropriate antibiotic therapy is initiated. In the future, HNL may be a useful marker in monitoring the response to antibiotic therapy.
CEDKA in Peds
Lawrence SE, Cummings EA, Gaboury I, et al. Population-based study of incidence and risk factors for cerebral edema in pediatric diabetic ketoacidosis. . 2005;146:688-692.
New onset insulin dependent diabetes mellitus is complicated by diabetic ketoacidosis (DKA) in 15% to 67% of patients. The incidence of cerebral edema in diabetic ketoacidosis (CEDKA) has been reported as 0.4-3.1. In the article, the authors seek to determine the incidence, outcome, and risk factors for cerebral edema in DKA in patients younger than 16.
The study was case-controlled with an active Canadian surveillance study. The authors surveyed pediatricians for a two-year period. During this time in Canada, all physicians were requested to submit reports monthly on patients with CEDKA younger than 16.
Thirteen cases were identified and the incidence of CEDKA was 0.51%. Overall mortality from cerebral edema was 0.15%. Increased blood urea nitrogen, degree of dehydration, hyperglycemia, and lower initial bicarbonate were associated with CEDKA. TH
In the flourishing metropolitan area of Atlanta, hospitalists and community-based physicians at Children’s Healthcare of Atlanta thrive within their niches, riding waves of opportunity fueled by the region’s burgeoning population. Jay Berkelhamer, MD, senior vice president of medical affairs at Children’s Healthcare of Atlanta calls his city “one of the most dynamic growth centers in the United States. Within 10 years we are estimated to have at least 150,000 more kids in Atlanta, leading to even greater opportunities for hospitalists and private practice primary care and specialty pediatricians.”
Two Hospitals, One system
Children’s Hospital of Atlanta’s hospitalist program is, in fact, two separate programs: one at Egleston, the other at Scottish Rite. The parent organization links the two and manages each hospital’s mission, structure, hiring, compensation, and outcomes.
—David Hall, MD
The six Egleston full-time equivalent hospitalists, or “cat herders,” as Corinne Taylor, MD, Egleston’s chief of medical affairs, describes them, are employees of Emory University Medical School. Most Egleston hospitalists are parents of young children and work four days a week, allowing them a balance of career and family life. Employed by the medical school and working at an academic medical center, they receive a salary, benefits, and other support services. Side by side with interns and residents, Egleston’s hospitalists see Atlanta’s sickest, frailest, and most at-risk children: the uninsured, underinsured immigrant and local population.
At Egleston the pediatric hospitalists are like their counterparts who treat adult patients in other settings. They deal with many patients with chronic conditions that lead to repeat hospitalizations.
“We see lots of ex-preemies with multiple problems such as asthma, seizures, cerebral palsy, and gastric problems,” says Dr. Taylor. “Some are ventilator-dependent and need lots of care.”
She relishes the clinical discipline that being a hospitalist at an academic medical center presents. “I do my homework every day and enjoy the stimulation of teaching our house officers,” explains Dr. Taylor. “Working with adult learners on the chronic conditions we manage and the cases with puzzling symptoms is exciting.”
Dr. Taylor’s boss is this hospitalist program’s founder, Joseph Snitzer, MD (see “Joseph Snitzer, MD: A hospital medicine pioneer”). Being hospital-based frees Dr. Snitzer to observe an endless parade of clinical challenges, including complex rheumatology cases, lupus, tumors, infected shunts, seizures, exotic infections, oncology diagnoses, and more.
“People call us from rural hospitals and private practices for help with diagnoses,” explains Dr. Snitzer. “We’re not smarter than anyone else. We just see a lot more than most other physicians.”
Scottish Rite
Across town at Scottish Rite, a nonprofit hospital, the hospitalists cope with the demands of a steady influx of new Atlantans. David Hall, MD, is Scottish Rite’s medical director. He was a former Egleston hospitalist and a private practitioner for 10 years in Baltimore before he relocated to Atlanta.
“We don’t have house officers, and there is a resident on call only one night a week,” says Dr. Hall. “Pediatricians in the community need to have their patients admitted 24/7, and we also have to admit from the emergency department at night. With our hospitalists taking calls at night and working all the next day, sometimes they would be on for 36 hours straight. As our service has grown, we’ve realized that this model was not sustainable.”
To reduce the burnout from their growing patient loads, the hospitalists changed their model. As of August 1, 2005, hospitalists at Scottish Rite began working either eight- or 12-hour shifts.
“Until we gain some experience with the shift system, we know we will struggle with continuity and handoffs,” adds Dr. Hall. Scottish Rite is also increasing its complement of moonlighting private practice pediatricians who want to keep their hospital skills current by covering the heavy workload.
Dr. Hall says recruiting new hospitalists isn’t a problem. Many local physicians want to do this work—especially right after residency. Comparing being a hospitalist with his 10 years in private practice, he says, “In my office practice I’d be sitting 20 feet away from a colleague, and there wasn’t much interaction. Now I’m learning something new every day and discussing interesting patients with other doctors. Building these ongoing relationships is great.”
Benefits, Culture, and More
The compensation and benefits packages at Egleston and Scottish Rite reflect that they are two separate hospitals in one system. Egleston’s hospitalists are employed by the medical school and receive a straight salary, with no incentive or at risk components. Scottish Rite’s hospitalists are hospital employees and have 20% of their salary at risk with productivity, quality improvement, and patient satisfaction incentives.
Although the different compensation systems may lead to discrepancies in pay, Dr. Berkelhamer explains that the policy of Children’s Hospital of Atlanta is to offer market-based salaries to all hospitalists. “Part of my job is to ensure that Dr. Snitzer and Dr. Hall are empowered to hire the physicians they want,” he says.
The hospitals have different corporate cultures as well. “The Scottish Rite group is very comfortable with lots of hands-on work while those at Egleston like to spend more time teaching,” says Dr. Berkelhamer.
Dr. Taylor, who trained with Dr. Snitzer and had a private practice in Atlanta for five years before becoming a full-time Egleston hospitalist in 1993, also acknowledges the different cultures at Egleston and Scottish Rite.
“We are two hospitals that come to the table and work together,” she observes. “Although we are in separate locations and may approach things differently, we practice the same type of medicine.”
Dr. Berkelhamer, who works with both sets of hospitalists, reinforces the observation that their clinical practices are consistent: “Surveys on patient and community physician satisfaction are the same, as are outcomes and productivity data.”
Special Issues for Both Hospitals
As part of a growing medical specialty in a dynamic region of the country, hospitalists at Children’s Hospital of Atlanta must confront a number of issues—some unique to them, others that reflect national trends. With different compensation and productivity systems, the two sets of hospitalists must collaborate to practice one brand of medicine.
An important formal step in their collaboration is the computerized medical and order entry system scheduled for spring 2006 implementation. The hospitalists are working together to develop clinical pathways and standardized orders based on their culling through best practices and evidence-based medicine guidelines. A newly appointed chief quality officer will keep the project on track.
Atlanta’s growth presents other issues for the hospitalists. With a constant influx of new community-based pediatricians Dr. Taylor finds that the hospitalists sometimes have trouble communicating with them to coordinate care.
“There are now at least 1,000 primary care and subspecialty pediatricians in Atlanta,” she says. “Trying to build trust and to track personal preferences with so many doctors is difficult. Fortunately we have electronic medical records so we can share important data with them.”
The hospitals’ social workers and case managers represent added glue to hold the communication together. Another of Atlanta’s challenges: It has only two medical schools from which to draw local hospitalists and other pediatricians, Emory University and the smaller Morehouse University. While not insurmountable, it means that most pediatricians practicing in the area must relocate to Atlanta.
What the Future Holds
And then there are issues that transcend Atlanta. Dr. Snitzer feels the national movement for hospitalists to become a specialty will happen sooner rather than later. In line with that movement, Children’s Hospital of Atlanta will have its first hospitalist fellowship in 2007. (For more information on pediatric hospital medicine fellowships, see “Pediatric Fellowship Offered,” below.)
For Dr. Hall, hospitalist compensation in a boomtown rankles. “People can’t really make money being hospitalists,” he explains. “Most need some subsidy to keep the programs going.”
The pay issues are being addressed, albeit slowly. Dr. Hall is encouraged by the campaign of pediatric intensivists to have coding and payment upgrades; he sees it as a template for higher hospitalist reimbursement schedules. “We only get paid for one visit a day, but we often see a patient several times a day,” he says. “Reimbursement should reflect what we really do.”
Both hospitals will have new buildings, each with 250 beds, more surgical suites, and expanded emergency departments by early 2007. That should lead to more hospitalist hiring—not surprising for a hospital that pioneered having inpatient physicians more than 20 years ago. TH
Writer Marlene Piturro is based in New York.
Joseph Snitzer, MD: A hospital medicine pioneer
In 1983—13 years before Robert Wachter, MD, FACP, coined the term “hospitalist”—Egleston Children’s Hospital Department of Pediatrics Chairman Joseph Patterson, MD, asked a former trainee to establish an in-house general pediatric service. That young doctor, Joseph Snitzer III, had been splitting his time equally between a private practice and teaching at Egleston through his affiliation with the Emory University School of Medicine. He said yes to the new assignment.
Since becoming a full-time hospitalist more than two decades ago, Dr. Snitzer relishes both his time working with interns and residents and an ever-changing mix of treatment and diagnostic mysteries. He is now the chief, Division of General Pediatrics, Children’s Healthcare of Atlanta at Egleston, and professor of pediatrics, Emory School of Medicine.
“We see everything here, from Kawasaki syndrome to neonatal apnea, seizure disorders, tumors, dehydration, jaundice, and all kinds of infections,” he explains. “About 50% of the children admitted have chronic conditions and the rest have various acute illnesses. There are unique challenges every day.”
Dr. Snitzer trained both Dr. Hall and Dr. Taylor, transmitting knowledge from one generation of physicians to the next. His hospitalist team maintains excellent relationships with the community’s doctors, both general pediatricians and specialists.
What is the main strength of Dr. Snitzer and the other hospitalists? Coordination with Atlanta’s pediatricians on getting things done in the hospital. Phone consultations with Atlanta’s physicians and those in rural areas seeking Children’s Hospital of Atlanta’s expertise on complex diagnoses and cases also keep him busy.
“Our experience with complexity is overwhelming,” he says. “Perhaps we can’t offer a great deal with simple diagnoses, such as diarrhea or simple skin infections, but we can with tough cases.” —MP
PEDIATRIC SPECIAL SECTION:
NEWS
Pediatric Fellowship Offered
Children’s Hospitalists of San Diego offers program
The Pediatric Hospitalist program at Children’s Hospital and Health Center of San Diego (CHHC) began in 1978. The current hospitalists are employed by Children’s Specialists of San Diego (CSSD), a 180-member pediatric-only specialty medical group. Inpatient care is provided for 75% of all general pediatric patients at the 233-bed tertiary care CHHC. Program consultation is offered at nearby Palomar Medical Center, a 23-bed unit within a larger 319-bed community hospital with a trauma center.
The hospitalists are the primary teaching faculty for the house staff and medical students who come from the University of California San Diego (UCSD), Balboa Naval Hospital, Pendleton Naval Medical Center, and Scripps Family Medicine. All hospitalists are board-certified pediatricians and have additional degrees or postresidency training, such as chief residency or fellowship experience.
Hospitalists fulfill many leadership roles in the hospital and community when not on service. A detailed list is available in a previous issue of The Hospitalist (Nov/Dec 2004;8(6):59-60). Current research includes an Agency for Healthcare Research and Quality (AHRQ) safety grant on medication errors, a bronchiolitis clinical trial, juvenile justice research on hepatitis B, a Hispanic cultural competency grant from the California Endowment, spiratory syncytial virus immunoprophylaxis outcomes in a managed population, and primary care perceptions of pediatric dentistry. Thus the hospitalist program has a long history of strong commitment to children and the core aspects of pediatric hospital medicine.
The Fellowship
The CSSD Pediatric Hospitalist Fellowship Program goal is to train highly motivated pediatricians for careers in academic and clinical hospital medicine. Over a two-year period instruction is provided in clinical, advocacy, administrative, teaching, and research aspects of pediatric hospital medicine. Clinical education emphasizes inpatient acute care, including intensive care and emergency transport at the busy main campus at CHHC. Outpatient clinical care offers experiences in adolescent juvenile hall medicine, hospice, and child protection. The diverse clinical exposure, teaching from local and national leaders, and volume of patients ensure graduates of this program are well prepared for any clinical hospitalist position.
The staff gains administrative experience via both hospital and medical group quality improvement activities. This work is directed by the medical director for CSSD and the physician advisor for quality management for CHHC, both of whom are CSSD pediatric hospitalists. Skills in process improvement, continuous quality improvement, risk management, organizational management and leadership are honed during the fellowship. Opportunity exists to take courses through the American College of Physician Executives if the trainee desires a future in administrative hospitalist medicine.
Academics and teaching are a core value of the pediatric hospitalist service. The fellow participates in the monthly division journal club and internal case review. Daily teaching while on the clinical service includes bedside rounds, management rounds, and attending rounds. Pediatric hospitalists are the primary inpatient teaching staff and as such have a significant responsibility for daily house staff education. The fellow participates in noon conferences and other educational venues under the guidance of the director of inpatient teaching (also a pediatric hospitalist).
Advocacy skills are learned through experiences in the juvenile hall system, Center for Child Protection, the American Academy of Pediatrics (AAP), and at the local and state level for children’s services funding. Under the leadership of the medical directors for the Center for Child Protection and the A.B. and Jessie Polinsky Center for Abused Children, the fellow participates in case review and observes expert child abuse testimony in court. Discussions with legislators in Sacramento focus upon protection of the California Children’s Services system, which supports critically ill state-funded children. The fellow learns AAP local and national structure, participating in conferences and chapter events.
Research is expected during this two-year fellowship program. Formal clinical research training is part of the first year curriculum of UCSD’s Clinical Research Enhancement through Supplemental Training (CREST) program. The first year of this two-year CREST program includes weekly classes covering epidemiology, patient-oriented research, health services research, and informatics. Those dedicated to completion of a master’s degree during the two-year program may integrate this training with a more intense curriculum schedule. A research project and mentor is chosen after the first quarter of the first year. Research may be in any area of pediatric hospitalist medicine. Research is presented at either Pediatric Academic Societies, Society of Hospital Medicine, or other similar forum upon completion.
The schedule is flexible, but follows the template. (See Table 1, p. 30: “Pediatric Hospitalist Fellowship Program Schedule.”)
One fellowship position is offered every year, with application submissions accepted through Dec. 1, interviews granted Dec. 15-Feb. 1 and final selection by Feb. 15. You can obtain an application from the CSSD Web site “Fellowships” page (http://childrensspecialists. com/body.cfm?id=580) or by e-mailing Fellowship Coordinator Susan Stafford at sstafford@chsd.org.
PEDIATRIC SPECIAL SECTION:
IN THE LITERATURE
Retrospective Study Attempts Criteria for Diagnosing MAS
Reviews by Julia Simmons, MD
Ravelli A, Magni-Manzoni S, Pistorio A, et al. Preliminary diagnostic guidelines for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. J Pediatr. 2005;146(5):598-604.
Macrophage activating syndrome (MAS) is a complication of connective tissue disorders, most often associated with active systemic juvenile idiopathic arthritis (S-JIA). It is a rare disorder and the exact incidence is unknown. It is characterized by uncontrolled activation and proliferation of T-lymphocytes and macrophages. If not recognized and treated aggressively, MAS can be life threatening.
In this article, the authors’ purpose was to review the available clinical, laboratory, and histopathologic data in patients with active S-JIA and in those with active S-JIA complicated by MAS. The goal was to develop criteria to diagnose MAS.
The retrospective study was designed using the classification, criteria approach. The index cases included patients with MAS complicating S-JIA. The “confusable” condition was active S-JIA. There were 74 patients in the index cases. Seventeen of the cases were observed at the authors’ institution. These patients were diagnosed with S-JIA using the International League of Association for Rheumatology criteria. They were identified using a database search. Fifty-seven of the cases were obtained from a Medline search. Of these 74 patients, eight were disqualified because they did not meet the definition of S-JIA, and 11 were excluded because of insufficient data. The control group contained 37 patients observed at the authors’ sites. The sensitivity rate, specificity rate, area under receiver operating characteristic curve, and diagnostic odds ratio were applied to the data to differentiate MAS complicating S-JIA from S-JIA.
The study results found hemorrhages and central nervous dysfunction were the strongest clinical discriminating factors. The strongest laboratory discriminators included thrombocytopenia, leukopenia, elevated aspartate aminotransferase, and hypofibrinogenemia. Histopathological criterion included evidence of macrophage hemophagocytosis in the bone marrow aspirate. Other useful discriminators included hypertriglyceridemia, elevated ferritin, hepatomegaly, hand hyponatremia. Final guidelines were developed after analyzing the statistics and determining the clinical importance: “The diagnosis of MAS requires the presence of any two or more laboratory criteria or of any two or three or more clinical and/or laboratory criteria. A bone marrow aspirate for the demonstration of hemophagocytosis may be required only in doubtful cases.”
In summary, MAS complicating S-JIA is a disorder without concrete diagnostic criteria. The authors have performed preliminary studies to diagnose MAS. They appropriately recognized the need for prospective larger clinical studies.
HNL Helps Distinguish Infections
Fjaertoft G, Foucard T, Xu S, et al. Human neutrophil lipocalin (HNL) as a diagnostic tool in children with acute infections: a study of the kinetics. Acta Pediatrica costarricense. 2005;94:661-666.
In pediatrics, the clinician is often faced with the diagnostic challenge of differentiating a bacterial infectious process from a viral infection. History, physical exam, and laboratory data make the distinction. In this article, the authors’ purpose was to assess the kinetics of HNL with viral and bacterial infections. Further, they assess the response of HNL when the infection is treated with antibiotics. The response of HNL is compared with that of C-reactive protein.
In the study, 92 patients with a median age of 26 months were hospitalized because they required systemic antibiotics or because of the severity of their medical condition. Upon admission and on hospital days one, two, and three, the C-reactive protein, white blood cell count with differential, and HNL were measured. The patients were retrospectively classified into five groups: true bacterial infection (n=28), true viral infection (n=4), suspected bacterial infection (n=18), suspected viral (n=34), and other.
A true bacterial infection required bacterial isolation from blood, urine, or cerebrospinal fluid culture, or radiographic demonstration of pneumonia. Patients were classified as having a suspected bacterial infection if they had a nonspecific diagnosis, but an elevated C-reactive protein and erythrocyte sedimentation rate. A true viral infection required isolation of a virus. If a patient did not meet any of the above criteria, the person was classified as having a suspected viral infection. Those patients in the “other” group were diagnosed with Kawasaki disease, Borrelia meningitis, and one undiagnosed patient. The patients were classified using history, exam, and laboratory values including white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and cultures. HNL values were not used in the classification.
The results demonstrated that both C-reactive protein and HNL are elevated with true bacterial infections compared with viral illnesses. Neither C-reactive protein nor HNL were significantly different in true bacterial infections versus suspected bacterial infections. The optimal cut-off for C-reactive protein was 59 mg/L with 93% sensitivity and 68% specificity. The optimal cutoff for HNL was 217 micrograms/L with 90% sensitivity and 74% specificity. In patients with true bacterial infections, HNL was highest at admission and decreased one day after admission. In contrast, the C-reactive protein values were similar on the day of admission and on hospital day one. C-reactive protein decreased significantly on days two and three of hospitalization. After hospital day one, HNL was elevated in only 11% of patients with true bacterial infection in contrast to 83% patients with elevated C-reactive protein.
In summary, HNL may be a useful marker to distinguish bacterial and viral illnesses. In comparison with C-reactive protein, it normalizes more rapidly after appropriate antibiotic therapy is initiated. In the future, HNL may be a useful marker in monitoring the response to antibiotic therapy.
CEDKA in Peds
Lawrence SE, Cummings EA, Gaboury I, et al. Population-based study of incidence and risk factors for cerebral edema in pediatric diabetic ketoacidosis. . 2005;146:688-692.
New onset insulin dependent diabetes mellitus is complicated by diabetic ketoacidosis (DKA) in 15% to 67% of patients. The incidence of cerebral edema in diabetic ketoacidosis (CEDKA) has been reported as 0.4-3.1. In the article, the authors seek to determine the incidence, outcome, and risk factors for cerebral edema in DKA in patients younger than 16.
The study was case-controlled with an active Canadian surveillance study. The authors surveyed pediatricians for a two-year period. During this time in Canada, all physicians were requested to submit reports monthly on patients with CEDKA younger than 16.
Thirteen cases were identified and the incidence of CEDKA was 0.51%. Overall mortality from cerebral edema was 0.15%. Increased blood urea nitrogen, degree of dehydration, hyperglycemia, and lower initial bicarbonate were associated with CEDKA. TH