User login
Formerly Skin & Allergy News
ass lick
assault rifle
balls
ballsac
black jack
bleach
Boko Haram
bondage
causas
cheap
child abuse
cocaine
compulsive behaviors
cost of miracles
cunt
Daech
display network stats
drug paraphernalia
explosion
fart
fda and death
fda AND warn
fda AND warning
fda AND warns
feom
fuck
gambling
gfc
gun
human trafficking
humira AND expensive
illegal
ISIL
ISIS
Islamic caliphate
Islamic state
madvocate
masturbation
mixed martial arts
MMA
molestation
national rifle association
NRA
nsfw
nuccitelli
pedophile
pedophilia
poker
porn
porn
pornography
psychedelic drug
recreational drug
sex slave rings
shit
slot machine
snort
substance abuse
terrorism
terrorist
texarkana
Texas hold 'em
UFC
section[contains(@class, 'nav-hidden')]
section[contains(@class, 'nav-hidden active')]
The leading independent newspaper covering dermatology news and commentary.
Cosmetic Tattoo Ingredients Associated With Contact Dermatitis
TOPLINE:
, but the ability to identify these allergies in patients is limited.
METHODOLOGY:
- While the allergenic potential of pigments in traditional tattoos has been documented, there is less clarity about pigments used in inks contained in cosmetic tattoos, also known as permanent makeup, and their association with ACD.
- Researchers conducted an Internet search and identified 974 individual permanent makeup ink products sold in the United States and also identified 79 unique pigments in those products.
- They evaluated the safety data sheets of these products and performed a PubMed search to identify documented ACD cases related to these pigments.
TAKEAWAY:
- Of the 79 pigments, 20 contained inorganic metals, which included iron, aluminum, silicone, chromium, copper, titanium, molybdenum, and manganese.
- Organic pigments were more common: 59 of the remaining pigments were organic compounds, mostly azo, quinacridone, or anthraquinone dyes, including 4 black pigments made from carbon only.
- A literature search identified 29 cases where patients had developed ACD thought to be caused by at least one of the 79 pigments identified by the authors of the current study and included 10 of the 79 pigments (12%).
- In 18 of the 29 cases in the literature, patch testing to the suspected pigment had been performed; in 3 cases, ACD was suspected without confirmatory testing.
IN PRACTICE:
Permanent makeup is becoming more popular, and there have been reports of ACD related to pigments contained in the inks, the authors wrote. “Traditional patch testing methods may not be useful in confirming the presence of a pigment allergy, even if one is suspect,” they added. “Consumers and patch testing physicians would benefit from better labeling of tattoo inks and the development of protocols designed to specifically test for tattoo pigment allergies.”
SOURCE:
The study was led by Sarah Rigali, MS, of Rosalind Franklin University, Chicago Medical School, Chicago, and coauthors from the Department of Dermatology, Northwestern University, Chicago, published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The study is limited by incomplete safety data sheets. So, many brands of permanent makeup ink could not be investigated. In addition, some pigments may not be fully disclosed in ingredient lists and precise ink content measurements were not available.
DISCLOSURES:
The study reported receiving no funding. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
, but the ability to identify these allergies in patients is limited.
METHODOLOGY:
- While the allergenic potential of pigments in traditional tattoos has been documented, there is less clarity about pigments used in inks contained in cosmetic tattoos, also known as permanent makeup, and their association with ACD.
- Researchers conducted an Internet search and identified 974 individual permanent makeup ink products sold in the United States and also identified 79 unique pigments in those products.
- They evaluated the safety data sheets of these products and performed a PubMed search to identify documented ACD cases related to these pigments.
TAKEAWAY:
- Of the 79 pigments, 20 contained inorganic metals, which included iron, aluminum, silicone, chromium, copper, titanium, molybdenum, and manganese.
- Organic pigments were more common: 59 of the remaining pigments were organic compounds, mostly azo, quinacridone, or anthraquinone dyes, including 4 black pigments made from carbon only.
- A literature search identified 29 cases where patients had developed ACD thought to be caused by at least one of the 79 pigments identified by the authors of the current study and included 10 of the 79 pigments (12%).
- In 18 of the 29 cases in the literature, patch testing to the suspected pigment had been performed; in 3 cases, ACD was suspected without confirmatory testing.
IN PRACTICE:
Permanent makeup is becoming more popular, and there have been reports of ACD related to pigments contained in the inks, the authors wrote. “Traditional patch testing methods may not be useful in confirming the presence of a pigment allergy, even if one is suspect,” they added. “Consumers and patch testing physicians would benefit from better labeling of tattoo inks and the development of protocols designed to specifically test for tattoo pigment allergies.”
SOURCE:
The study was led by Sarah Rigali, MS, of Rosalind Franklin University, Chicago Medical School, Chicago, and coauthors from the Department of Dermatology, Northwestern University, Chicago, published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The study is limited by incomplete safety data sheets. So, many brands of permanent makeup ink could not be investigated. In addition, some pigments may not be fully disclosed in ingredient lists and precise ink content measurements were not available.
DISCLOSURES:
The study reported receiving no funding. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
, but the ability to identify these allergies in patients is limited.
METHODOLOGY:
- While the allergenic potential of pigments in traditional tattoos has been documented, there is less clarity about pigments used in inks contained in cosmetic tattoos, also known as permanent makeup, and their association with ACD.
- Researchers conducted an Internet search and identified 974 individual permanent makeup ink products sold in the United States and also identified 79 unique pigments in those products.
- They evaluated the safety data sheets of these products and performed a PubMed search to identify documented ACD cases related to these pigments.
TAKEAWAY:
- Of the 79 pigments, 20 contained inorganic metals, which included iron, aluminum, silicone, chromium, copper, titanium, molybdenum, and manganese.
- Organic pigments were more common: 59 of the remaining pigments were organic compounds, mostly azo, quinacridone, or anthraquinone dyes, including 4 black pigments made from carbon only.
- A literature search identified 29 cases where patients had developed ACD thought to be caused by at least one of the 79 pigments identified by the authors of the current study and included 10 of the 79 pigments (12%).
- In 18 of the 29 cases in the literature, patch testing to the suspected pigment had been performed; in 3 cases, ACD was suspected without confirmatory testing.
IN PRACTICE:
Permanent makeup is becoming more popular, and there have been reports of ACD related to pigments contained in the inks, the authors wrote. “Traditional patch testing methods may not be useful in confirming the presence of a pigment allergy, even if one is suspect,” they added. “Consumers and patch testing physicians would benefit from better labeling of tattoo inks and the development of protocols designed to specifically test for tattoo pigment allergies.”
SOURCE:
The study was led by Sarah Rigali, MS, of Rosalind Franklin University, Chicago Medical School, Chicago, and coauthors from the Department of Dermatology, Northwestern University, Chicago, published online in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The study is limited by incomplete safety data sheets. So, many brands of permanent makeup ink could not be investigated. In addition, some pigments may not be fully disclosed in ingredient lists and precise ink content measurements were not available.
DISCLOSURES:
The study reported receiving no funding. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Study Highlights Melanoma Survival Disparities in Rural vs Urban Settings
, results from an analysis of data from the National Cancer Institute showed.
“Melanoma is currently the fifth most common malignancy in the United States, with approximately 106,000 new cases and 7180 reported deaths occurring in 2021,” the study’s first author, Mitchell Taylor, MD, a dermatology research fellow at the University of Nebraska, Omaha, and colleagues wrote in the abstract, which was presented during a poster session at the annual meeting of the Society for Investigative Dermatology. “Rural areas have been shown to bear a higher melanoma disease burden, yet there is a paucity of national-level studies examining these disparities.”
To characterize the rural population diagnosed with cutaneous melanoma and assess associated disparities in the United States, the researchers queried the NCI’s Surveillance, Epidemiology, and End Results database to identify individuals diagnosed with cutaneous melanoma from 2000 to 2020 (International Classification of Diseases, 3rd Edition, 8720/3 — 8780/3; Primary Site codes C44.0-C44.9). They drew from US Office of Management and Budget terminology to define and categorize rural and urban communities.
Among 391,047 patients included during the study period, binary logistic regression analysis revealed that patients in rural areas had a greater odds of being older, from ages 50 to 75 years (odds ratio [OR], 1.10; P < .001); had annual incomes < $70,000 (OR, 16.80; P < .001); had tumors located on the head and neck (OR, 1.24; P < .001); and presented with regional/distant disease (OR, 1.13; P < .001).
As for disease-specific survival, patients living in rural areas had significantly reduced survival compared with those living in urban areas (a mean of 207.3 vs 216.3 months, respectively; P < .001). Multivariate Cox regression revealed that living in a rural setting was significantly associated with reduced disease-specific survival (hazard ratio [HR], 1.10; P < .001), as was having head and neck tumors (HR, 1.41; P < .001).“Overall, this study underscores a significant decrease in disease-specific survival among rural patients diagnosed with cutaneous melanoma and establishes a significant association between rural living and high-risk primary tumor locations, particularly the head and neck,” the authors concluded.
Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, Colorado, who was asked to comment on the results, said the findings echo the results of a recent study which characterized melanoma rates among non-Hispanic American Indian/Alaska Native individuals from 1999 to 2019.
“I suspect this decreased disease-specific survival highlights the issues our rural-residing patients face with access to dermatology care,” Dr. Kohn told this news organization. “Dermatologists are able to detect thinner melanomas than patients [and] are preferentially concentrated in metropolitan areas. Dermatologists are also the most skilled and knowledgeable to screen, diagnose, and manage melanomas. Having fewer dermatologists in rural areas impedes melanoma care for our rural-residing patients.”
Neither the researchers nor Dr. Kohn reported any relevant disclosures.
A version of this article first appeared on Medscape.com.
, results from an analysis of data from the National Cancer Institute showed.
“Melanoma is currently the fifth most common malignancy in the United States, with approximately 106,000 new cases and 7180 reported deaths occurring in 2021,” the study’s first author, Mitchell Taylor, MD, a dermatology research fellow at the University of Nebraska, Omaha, and colleagues wrote in the abstract, which was presented during a poster session at the annual meeting of the Society for Investigative Dermatology. “Rural areas have been shown to bear a higher melanoma disease burden, yet there is a paucity of national-level studies examining these disparities.”
To characterize the rural population diagnosed with cutaneous melanoma and assess associated disparities in the United States, the researchers queried the NCI’s Surveillance, Epidemiology, and End Results database to identify individuals diagnosed with cutaneous melanoma from 2000 to 2020 (International Classification of Diseases, 3rd Edition, 8720/3 — 8780/3; Primary Site codes C44.0-C44.9). They drew from US Office of Management and Budget terminology to define and categorize rural and urban communities.
Among 391,047 patients included during the study period, binary logistic regression analysis revealed that patients in rural areas had a greater odds of being older, from ages 50 to 75 years (odds ratio [OR], 1.10; P < .001); had annual incomes < $70,000 (OR, 16.80; P < .001); had tumors located on the head and neck (OR, 1.24; P < .001); and presented with regional/distant disease (OR, 1.13; P < .001).
As for disease-specific survival, patients living in rural areas had significantly reduced survival compared with those living in urban areas (a mean of 207.3 vs 216.3 months, respectively; P < .001). Multivariate Cox regression revealed that living in a rural setting was significantly associated with reduced disease-specific survival (hazard ratio [HR], 1.10; P < .001), as was having head and neck tumors (HR, 1.41; P < .001).“Overall, this study underscores a significant decrease in disease-specific survival among rural patients diagnosed with cutaneous melanoma and establishes a significant association between rural living and high-risk primary tumor locations, particularly the head and neck,” the authors concluded.
Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, Colorado, who was asked to comment on the results, said the findings echo the results of a recent study which characterized melanoma rates among non-Hispanic American Indian/Alaska Native individuals from 1999 to 2019.
“I suspect this decreased disease-specific survival highlights the issues our rural-residing patients face with access to dermatology care,” Dr. Kohn told this news organization. “Dermatologists are able to detect thinner melanomas than patients [and] are preferentially concentrated in metropolitan areas. Dermatologists are also the most skilled and knowledgeable to screen, diagnose, and manage melanomas. Having fewer dermatologists in rural areas impedes melanoma care for our rural-residing patients.”
Neither the researchers nor Dr. Kohn reported any relevant disclosures.
A version of this article first appeared on Medscape.com.
, results from an analysis of data from the National Cancer Institute showed.
“Melanoma is currently the fifth most common malignancy in the United States, with approximately 106,000 new cases and 7180 reported deaths occurring in 2021,” the study’s first author, Mitchell Taylor, MD, a dermatology research fellow at the University of Nebraska, Omaha, and colleagues wrote in the abstract, which was presented during a poster session at the annual meeting of the Society for Investigative Dermatology. “Rural areas have been shown to bear a higher melanoma disease burden, yet there is a paucity of national-level studies examining these disparities.”
To characterize the rural population diagnosed with cutaneous melanoma and assess associated disparities in the United States, the researchers queried the NCI’s Surveillance, Epidemiology, and End Results database to identify individuals diagnosed with cutaneous melanoma from 2000 to 2020 (International Classification of Diseases, 3rd Edition, 8720/3 — 8780/3; Primary Site codes C44.0-C44.9). They drew from US Office of Management and Budget terminology to define and categorize rural and urban communities.
Among 391,047 patients included during the study period, binary logistic regression analysis revealed that patients in rural areas had a greater odds of being older, from ages 50 to 75 years (odds ratio [OR], 1.10; P < .001); had annual incomes < $70,000 (OR, 16.80; P < .001); had tumors located on the head and neck (OR, 1.24; P < .001); and presented with regional/distant disease (OR, 1.13; P < .001).
As for disease-specific survival, patients living in rural areas had significantly reduced survival compared with those living in urban areas (a mean of 207.3 vs 216.3 months, respectively; P < .001). Multivariate Cox regression revealed that living in a rural setting was significantly associated with reduced disease-specific survival (hazard ratio [HR], 1.10; P < .001), as was having head and neck tumors (HR, 1.41; P < .001).“Overall, this study underscores a significant decrease in disease-specific survival among rural patients diagnosed with cutaneous melanoma and establishes a significant association between rural living and high-risk primary tumor locations, particularly the head and neck,” the authors concluded.
Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, Colorado, who was asked to comment on the results, said the findings echo the results of a recent study which characterized melanoma rates among non-Hispanic American Indian/Alaska Native individuals from 1999 to 2019.
“I suspect this decreased disease-specific survival highlights the issues our rural-residing patients face with access to dermatology care,” Dr. Kohn told this news organization. “Dermatologists are able to detect thinner melanomas than patients [and] are preferentially concentrated in metropolitan areas. Dermatologists are also the most skilled and knowledgeable to screen, diagnose, and manage melanomas. Having fewer dermatologists in rural areas impedes melanoma care for our rural-residing patients.”
Neither the researchers nor Dr. Kohn reported any relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SID 2024
Features of Merkel Cell in Hispanic Patients Explored
. In addition, the most affected site was the upper limb/shoulder, which differs from what has been reported in previous studies.
Those are key findings from a retrospective study of national cancer data that was presented during a poster session at the annual meeting of the Society for Investigative Dermatology.
“Merkel cell carcinoma is an infrequent and aggressive form of neuroendocrine skin cancer that mainly impacts individuals of White ethnicity, with a general occurrence rate of 0.7 instances per 100,000 person-years,” one of the study authors, Luis J. Borda, MD, chief dermatology resident at Eastern Virginia Medical School, Norfolk, Virginia, told this news organization. The incidence of MCC is increasing among all racial groups, especially in the Hispanic population, he added.
To determine how age, sex, and primary site of MCC differ in White vs non-White Hispanic patients, the researchers evaluated the 22 population-based cancer registries of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program from 2000 through 2020. They reported categorical variables as counts and percentages and used chi-square test with Yates’s correction to assess the association between categorical variables.
Of the 17,920 MCCs identified by the researchers, 40 (0.22%) were in non-White Hispanic patients. Compared with the White patients with MCC, significantly fewer non-White Hispanic patients were age 70 years or older (50% vs 72.1%, respectively; P < .001), and MCC was more common in female non-White Hispanic patients (23, or 57.5%), while White patients with MCC were predominantly male (11,309, or 63.2%; P < .05). “This suggests that MCC in non-White Hispanic patients may involve different risk factors related to age beyond just cumulative UV exposure and aging-related immunosenescence, which may additionally account for the higher prevalence of females in this cohort, as historically male outdoor occupation has resulted in increased lifetime cumulative UV exposure,” Dr. Borda said.
The head and neck were the most common sites of disease involvement in White patients (41.9% vs 27.5% in non-White Hispanic patients; P = .09), while the upper limb and shoulder were the most common sites of disease involvement in non-White Hispanic patients (37.5% vs 23.8% in White patients; P = .06). This finding “differs from previous studies showing head/neck being the most common site in Hispanics,” Dr. Borda said, adding that this could be a result of White patients not being included in the Hispanic cohort in this study. “Because non-White Hispanic patients have darker skin, they may have proportionally more cases on sun-protected skin, as is described by the present data, suggesting that they are less likely to have UV-driven MCC.”
The study “highlights distinct demographic and clinical characteristics of MCC among non-White Hispanic patients compared to their White counterparts, emphasizing the importance of considering race/ethnicity in understanding the epidemiology of this rare but increasingly prevalent cancer,” Dr. Borda said. He and his co-authors are planning to do further research on the increasing incidence of MCC in non-White Hispanic patients and on staging at diagnosis compared to White patients.
Dr. Borda acknowledged certain limitations of the analysis, including the small sample size in the non-White Hispanic group, the retrospective nature of SEER data, selection bias, and the potential for underreporting. He and his co-authors reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
. In addition, the most affected site was the upper limb/shoulder, which differs from what has been reported in previous studies.
Those are key findings from a retrospective study of national cancer data that was presented during a poster session at the annual meeting of the Society for Investigative Dermatology.
“Merkel cell carcinoma is an infrequent and aggressive form of neuroendocrine skin cancer that mainly impacts individuals of White ethnicity, with a general occurrence rate of 0.7 instances per 100,000 person-years,” one of the study authors, Luis J. Borda, MD, chief dermatology resident at Eastern Virginia Medical School, Norfolk, Virginia, told this news organization. The incidence of MCC is increasing among all racial groups, especially in the Hispanic population, he added.
To determine how age, sex, and primary site of MCC differ in White vs non-White Hispanic patients, the researchers evaluated the 22 population-based cancer registries of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program from 2000 through 2020. They reported categorical variables as counts and percentages and used chi-square test with Yates’s correction to assess the association between categorical variables.
Of the 17,920 MCCs identified by the researchers, 40 (0.22%) were in non-White Hispanic patients. Compared with the White patients with MCC, significantly fewer non-White Hispanic patients were age 70 years or older (50% vs 72.1%, respectively; P < .001), and MCC was more common in female non-White Hispanic patients (23, or 57.5%), while White patients with MCC were predominantly male (11,309, or 63.2%; P < .05). “This suggests that MCC in non-White Hispanic patients may involve different risk factors related to age beyond just cumulative UV exposure and aging-related immunosenescence, which may additionally account for the higher prevalence of females in this cohort, as historically male outdoor occupation has resulted in increased lifetime cumulative UV exposure,” Dr. Borda said.
The head and neck were the most common sites of disease involvement in White patients (41.9% vs 27.5% in non-White Hispanic patients; P = .09), while the upper limb and shoulder were the most common sites of disease involvement in non-White Hispanic patients (37.5% vs 23.8% in White patients; P = .06). This finding “differs from previous studies showing head/neck being the most common site in Hispanics,” Dr. Borda said, adding that this could be a result of White patients not being included in the Hispanic cohort in this study. “Because non-White Hispanic patients have darker skin, they may have proportionally more cases on sun-protected skin, as is described by the present data, suggesting that they are less likely to have UV-driven MCC.”
The study “highlights distinct demographic and clinical characteristics of MCC among non-White Hispanic patients compared to their White counterparts, emphasizing the importance of considering race/ethnicity in understanding the epidemiology of this rare but increasingly prevalent cancer,” Dr. Borda said. He and his co-authors are planning to do further research on the increasing incidence of MCC in non-White Hispanic patients and on staging at diagnosis compared to White patients.
Dr. Borda acknowledged certain limitations of the analysis, including the small sample size in the non-White Hispanic group, the retrospective nature of SEER data, selection bias, and the potential for underreporting. He and his co-authors reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
. In addition, the most affected site was the upper limb/shoulder, which differs from what has been reported in previous studies.
Those are key findings from a retrospective study of national cancer data that was presented during a poster session at the annual meeting of the Society for Investigative Dermatology.
“Merkel cell carcinoma is an infrequent and aggressive form of neuroendocrine skin cancer that mainly impacts individuals of White ethnicity, with a general occurrence rate of 0.7 instances per 100,000 person-years,” one of the study authors, Luis J. Borda, MD, chief dermatology resident at Eastern Virginia Medical School, Norfolk, Virginia, told this news organization. The incidence of MCC is increasing among all racial groups, especially in the Hispanic population, he added.
To determine how age, sex, and primary site of MCC differ in White vs non-White Hispanic patients, the researchers evaluated the 22 population-based cancer registries of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program from 2000 through 2020. They reported categorical variables as counts and percentages and used chi-square test with Yates’s correction to assess the association between categorical variables.
Of the 17,920 MCCs identified by the researchers, 40 (0.22%) were in non-White Hispanic patients. Compared with the White patients with MCC, significantly fewer non-White Hispanic patients were age 70 years or older (50% vs 72.1%, respectively; P < .001), and MCC was more common in female non-White Hispanic patients (23, or 57.5%), while White patients with MCC were predominantly male (11,309, or 63.2%; P < .05). “This suggests that MCC in non-White Hispanic patients may involve different risk factors related to age beyond just cumulative UV exposure and aging-related immunosenescence, which may additionally account for the higher prevalence of females in this cohort, as historically male outdoor occupation has resulted in increased lifetime cumulative UV exposure,” Dr. Borda said.
The head and neck were the most common sites of disease involvement in White patients (41.9% vs 27.5% in non-White Hispanic patients; P = .09), while the upper limb and shoulder were the most common sites of disease involvement in non-White Hispanic patients (37.5% vs 23.8% in White patients; P = .06). This finding “differs from previous studies showing head/neck being the most common site in Hispanics,” Dr. Borda said, adding that this could be a result of White patients not being included in the Hispanic cohort in this study. “Because non-White Hispanic patients have darker skin, they may have proportionally more cases on sun-protected skin, as is described by the present data, suggesting that they are less likely to have UV-driven MCC.”
The study “highlights distinct demographic and clinical characteristics of MCC among non-White Hispanic patients compared to their White counterparts, emphasizing the importance of considering race/ethnicity in understanding the epidemiology of this rare but increasingly prevalent cancer,” Dr. Borda said. He and his co-authors are planning to do further research on the increasing incidence of MCC in non-White Hispanic patients and on staging at diagnosis compared to White patients.
Dr. Borda acknowledged certain limitations of the analysis, including the small sample size in the non-White Hispanic group, the retrospective nature of SEER data, selection bias, and the potential for underreporting. He and his co-authors reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
FROM SID 2024
Study Finds Isotretinoin Effective for Acne in Transgender Patients on Hormone Rx
TOPLINE:
, but more information is needed on dosing and barriers to treatment.
METHODOLOGY:
- Acne can be a side effect of masculinizing hormone therapy for transmasculine individuals. While isotretinoin is an effective treatment option for acne, its effectiveness and safety in transgender and gender-diverse individuals are not well understood.
- This retrospective case series included 55 patients (mean age, 25.4 years) undergoing masculinizing hormone therapy at four medical centers, who were prescribed isotretinoin for acne associated with treatment.
- Isotretinoin treatment was started a median of 22.1 months after hormone therapy was initiated and continued for a median of 6 months with a median cumulative dose of 132.7 mg/kg.
- Researchers assessed acne improvement, clearance, recurrence, adverse effects, and reasons for treatment discontinuation.
TAKEAWAY:
- Overall, 48 patients (87.3%) experienced improvement, and 26 (47.3%) achieved clearance during treatment. A higher proportion of patients experienced improvement (97% vs 72.7%) and achieved clearance (63.6% vs 22.7%) with cumulative doses of ≥ 120 mg/kg than those who received cumulative doses < 120 mg/kg.
- The risk for recurrence was 20% (in four patients) among 20 patients who achieved clearance and had any subsequent health care encounters, with a mean follow-up time of 734.3 days.
- Common adverse effects included dryness (80%), joint pain (14.5%), and headaches (10.9%). Other adverse effects included nose bleeds (9.1%) and depression (5.5%).
- Of the 22 patients with a cumulative dose < 120 mg/kg, 14 (63.6%) were lost to follow-up; among those not lost to follow-up, 2 patients discontinued treatment because of transfer of care, 1 because of adverse effects, and 1 because of gender-affirming surgery, with concerns about wound healing.
IN PRACTICE:
“Although isotretinoin appears to be an effective treatment option for acne among individuals undergoing masculinizing hormone therapy, further efforts are needed to understand optimal dosing and treatment barriers to improve outcomes in transgender and gender-diverse individuals receiving testosterone,” the authors concluded.
SOURCE:
The study, led by James Choe, BS, Department of Dermatology, Brigham and Women’s Hospital, Harvard Medical School, Boston, was published online in JAMA Dermatology.
LIMITATIONS:
The study population was limited to four centers, and variability in clinician- and patient-reported acne outcomes and missing information could affect the reliability of data. Because of the small sample size, the association of masculinizing hormone therapy regimens with outcomes could not be evaluated.
DISCLOSURES:
One author is supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Three authors reported receiving grants or personal fees from various sources. The other authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, but more information is needed on dosing and barriers to treatment.
METHODOLOGY:
- Acne can be a side effect of masculinizing hormone therapy for transmasculine individuals. While isotretinoin is an effective treatment option for acne, its effectiveness and safety in transgender and gender-diverse individuals are not well understood.
- This retrospective case series included 55 patients (mean age, 25.4 years) undergoing masculinizing hormone therapy at four medical centers, who were prescribed isotretinoin for acne associated with treatment.
- Isotretinoin treatment was started a median of 22.1 months after hormone therapy was initiated and continued for a median of 6 months with a median cumulative dose of 132.7 mg/kg.
- Researchers assessed acne improvement, clearance, recurrence, adverse effects, and reasons for treatment discontinuation.
TAKEAWAY:
- Overall, 48 patients (87.3%) experienced improvement, and 26 (47.3%) achieved clearance during treatment. A higher proportion of patients experienced improvement (97% vs 72.7%) and achieved clearance (63.6% vs 22.7%) with cumulative doses of ≥ 120 mg/kg than those who received cumulative doses < 120 mg/kg.
- The risk for recurrence was 20% (in four patients) among 20 patients who achieved clearance and had any subsequent health care encounters, with a mean follow-up time of 734.3 days.
- Common adverse effects included dryness (80%), joint pain (14.5%), and headaches (10.9%). Other adverse effects included nose bleeds (9.1%) and depression (5.5%).
- Of the 22 patients with a cumulative dose < 120 mg/kg, 14 (63.6%) were lost to follow-up; among those not lost to follow-up, 2 patients discontinued treatment because of transfer of care, 1 because of adverse effects, and 1 because of gender-affirming surgery, with concerns about wound healing.
IN PRACTICE:
“Although isotretinoin appears to be an effective treatment option for acne among individuals undergoing masculinizing hormone therapy, further efforts are needed to understand optimal dosing and treatment barriers to improve outcomes in transgender and gender-diverse individuals receiving testosterone,” the authors concluded.
SOURCE:
The study, led by James Choe, BS, Department of Dermatology, Brigham and Women’s Hospital, Harvard Medical School, Boston, was published online in JAMA Dermatology.
LIMITATIONS:
The study population was limited to four centers, and variability in clinician- and patient-reported acne outcomes and missing information could affect the reliability of data. Because of the small sample size, the association of masculinizing hormone therapy regimens with outcomes could not be evaluated.
DISCLOSURES:
One author is supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Three authors reported receiving grants or personal fees from various sources. The other authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, but more information is needed on dosing and barriers to treatment.
METHODOLOGY:
- Acne can be a side effect of masculinizing hormone therapy for transmasculine individuals. While isotretinoin is an effective treatment option for acne, its effectiveness and safety in transgender and gender-diverse individuals are not well understood.
- This retrospective case series included 55 patients (mean age, 25.4 years) undergoing masculinizing hormone therapy at four medical centers, who were prescribed isotretinoin for acne associated with treatment.
- Isotretinoin treatment was started a median of 22.1 months after hormone therapy was initiated and continued for a median of 6 months with a median cumulative dose of 132.7 mg/kg.
- Researchers assessed acne improvement, clearance, recurrence, adverse effects, and reasons for treatment discontinuation.
TAKEAWAY:
- Overall, 48 patients (87.3%) experienced improvement, and 26 (47.3%) achieved clearance during treatment. A higher proportion of patients experienced improvement (97% vs 72.7%) and achieved clearance (63.6% vs 22.7%) with cumulative doses of ≥ 120 mg/kg than those who received cumulative doses < 120 mg/kg.
- The risk for recurrence was 20% (in four patients) among 20 patients who achieved clearance and had any subsequent health care encounters, with a mean follow-up time of 734.3 days.
- Common adverse effects included dryness (80%), joint pain (14.5%), and headaches (10.9%). Other adverse effects included nose bleeds (9.1%) and depression (5.5%).
- Of the 22 patients with a cumulative dose < 120 mg/kg, 14 (63.6%) were lost to follow-up; among those not lost to follow-up, 2 patients discontinued treatment because of transfer of care, 1 because of adverse effects, and 1 because of gender-affirming surgery, with concerns about wound healing.
IN PRACTICE:
“Although isotretinoin appears to be an effective treatment option for acne among individuals undergoing masculinizing hormone therapy, further efforts are needed to understand optimal dosing and treatment barriers to improve outcomes in transgender and gender-diverse individuals receiving testosterone,” the authors concluded.
SOURCE:
The study, led by James Choe, BS, Department of Dermatology, Brigham and Women’s Hospital, Harvard Medical School, Boston, was published online in JAMA Dermatology.
LIMITATIONS:
The study population was limited to four centers, and variability in clinician- and patient-reported acne outcomes and missing information could affect the reliability of data. Because of the small sample size, the association of masculinizing hormone therapy regimens with outcomes could not be evaluated.
DISCLOSURES:
One author is supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Three authors reported receiving grants or personal fees from various sources. The other authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
Hidradenitis Suppurativa: Clinical Outcomes for Bimekizumab Positive in Phase 3 Studies
TOPLINE:
, in two phase 3 studies.
METHODOLOGY:
- To assess the efficacy and safety of bimekizumab, an interleukin (IL)-17A and IL-17F antagonist, 320 mg for HS, researchers conducted two 48-week phase 3 trials BE HEARD I (n = 505) and II (n = 509), which enrolled patients with moderate to severe HS and a history of inadequate response to systemic antibiotics.
- Patients were randomly assigned to one of four groups: Bimekizumab every 2 weeks, bimekizumab every 2 weeks for 16 weeks followed by every 4 weeks of dosing, bimekizumab every 4 weeks, or placebo for 16 weeks followed by bimekizumab every 2 weeks.
- The primary outcome was an HS clinical response of at least 50% (HiSCR50) at week 16, defined as at least a 50% reduction in total abscess and inflammatory nodule count.
TAKEAWAY:
- A higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved an HiSCR50 response at week 16 in BE HEARD I (48% vs 29%; odds ratio [OR], 2.23; P = .006) and II (52% vs 32%; OR, 2.29; P = .0032) trials.
- Patients receiving bimekizumab every 4 weeks also achieved a higher HiSCR50 response at week 16 vs placebo in the BE HEARD II trial (54% vs 32%; OR, 2.42; P = .0038).
- At week 16, a higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved at least a 75% HiSCR (HiSCR75) in both trials, and a higher proportion of those receiving bimekizumab every 4 weeks achieved HiSCR75 in the BE HEARD II trial.
- At week 48, 45%-68% of patients achieved HiSCR50 in both trials.
- Patients who received bimekizumab vs placebo for the initial 16 weeks had greater improvements in patient-reported outcomes, and bimekizumab was well tolerated with a low number of serious or severe treatment-emergent adverse events.
IN PRACTICE:
“Bimekizumab was well tolerated by patients with hidradenitis suppurativa and produced rapid and deep clinically meaningful responses that were maintained up to 48 weeks,” the authors wrote. “These data support the use of bimekizumab as a promising new therapeutic option for patients with moderate to severe hidradenitis suppurativa.”
SOURCE:
Alexa B. Kimball, MD, MPH, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, led this study, which was published online in The Lancet.
LIMITATIONS:
The placebo-controlled part of this trial was relatively short at 16 weeks and may affect the interpretation of later efficacy data, there was a lack of an active comparator group, and the efficacy of treatment was evaluated in the presence of rescue treatment with systemic antibiotics.
DISCLOSURES:
The studies were funded by bimekizumab manufacturer UCB Pharma. Seven authors disclosed being current or former employees of UCB Pharma. Other authors reported several ties with many companies, including UCB Pharma.
A version of this article first appeared on Medscape.com.
TOPLINE:
, in two phase 3 studies.
METHODOLOGY:
- To assess the efficacy and safety of bimekizumab, an interleukin (IL)-17A and IL-17F antagonist, 320 mg for HS, researchers conducted two 48-week phase 3 trials BE HEARD I (n = 505) and II (n = 509), which enrolled patients with moderate to severe HS and a history of inadequate response to systemic antibiotics.
- Patients were randomly assigned to one of four groups: Bimekizumab every 2 weeks, bimekizumab every 2 weeks for 16 weeks followed by every 4 weeks of dosing, bimekizumab every 4 weeks, or placebo for 16 weeks followed by bimekizumab every 2 weeks.
- The primary outcome was an HS clinical response of at least 50% (HiSCR50) at week 16, defined as at least a 50% reduction in total abscess and inflammatory nodule count.
TAKEAWAY:
- A higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved an HiSCR50 response at week 16 in BE HEARD I (48% vs 29%; odds ratio [OR], 2.23; P = .006) and II (52% vs 32%; OR, 2.29; P = .0032) trials.
- Patients receiving bimekizumab every 4 weeks also achieved a higher HiSCR50 response at week 16 vs placebo in the BE HEARD II trial (54% vs 32%; OR, 2.42; P = .0038).
- At week 16, a higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved at least a 75% HiSCR (HiSCR75) in both trials, and a higher proportion of those receiving bimekizumab every 4 weeks achieved HiSCR75 in the BE HEARD II trial.
- At week 48, 45%-68% of patients achieved HiSCR50 in both trials.
- Patients who received bimekizumab vs placebo for the initial 16 weeks had greater improvements in patient-reported outcomes, and bimekizumab was well tolerated with a low number of serious or severe treatment-emergent adverse events.
IN PRACTICE:
“Bimekizumab was well tolerated by patients with hidradenitis suppurativa and produced rapid and deep clinically meaningful responses that were maintained up to 48 weeks,” the authors wrote. “These data support the use of bimekizumab as a promising new therapeutic option for patients with moderate to severe hidradenitis suppurativa.”
SOURCE:
Alexa B. Kimball, MD, MPH, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, led this study, which was published online in The Lancet.
LIMITATIONS:
The placebo-controlled part of this trial was relatively short at 16 weeks and may affect the interpretation of later efficacy data, there was a lack of an active comparator group, and the efficacy of treatment was evaluated in the presence of rescue treatment with systemic antibiotics.
DISCLOSURES:
The studies were funded by bimekizumab manufacturer UCB Pharma. Seven authors disclosed being current or former employees of UCB Pharma. Other authors reported several ties with many companies, including UCB Pharma.
A version of this article first appeared on Medscape.com.
TOPLINE:
, in two phase 3 studies.
METHODOLOGY:
- To assess the efficacy and safety of bimekizumab, an interleukin (IL)-17A and IL-17F antagonist, 320 mg for HS, researchers conducted two 48-week phase 3 trials BE HEARD I (n = 505) and II (n = 509), which enrolled patients with moderate to severe HS and a history of inadequate response to systemic antibiotics.
- Patients were randomly assigned to one of four groups: Bimekizumab every 2 weeks, bimekizumab every 2 weeks for 16 weeks followed by every 4 weeks of dosing, bimekizumab every 4 weeks, or placebo for 16 weeks followed by bimekizumab every 2 weeks.
- The primary outcome was an HS clinical response of at least 50% (HiSCR50) at week 16, defined as at least a 50% reduction in total abscess and inflammatory nodule count.
TAKEAWAY:
- A higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved an HiSCR50 response at week 16 in BE HEARD I (48% vs 29%; odds ratio [OR], 2.23; P = .006) and II (52% vs 32%; OR, 2.29; P = .0032) trials.
- Patients receiving bimekizumab every 4 weeks also achieved a higher HiSCR50 response at week 16 vs placebo in the BE HEARD II trial (54% vs 32%; OR, 2.42; P = .0038).
- At week 16, a higher proportion of patients receiving bimekizumab every 2 weeks vs placebo achieved at least a 75% HiSCR (HiSCR75) in both trials, and a higher proportion of those receiving bimekizumab every 4 weeks achieved HiSCR75 in the BE HEARD II trial.
- At week 48, 45%-68% of patients achieved HiSCR50 in both trials.
- Patients who received bimekizumab vs placebo for the initial 16 weeks had greater improvements in patient-reported outcomes, and bimekizumab was well tolerated with a low number of serious or severe treatment-emergent adverse events.
IN PRACTICE:
“Bimekizumab was well tolerated by patients with hidradenitis suppurativa and produced rapid and deep clinically meaningful responses that were maintained up to 48 weeks,” the authors wrote. “These data support the use of bimekizumab as a promising new therapeutic option for patients with moderate to severe hidradenitis suppurativa.”
SOURCE:
Alexa B. Kimball, MD, MPH, from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, led this study, which was published online in The Lancet.
LIMITATIONS:
The placebo-controlled part of this trial was relatively short at 16 weeks and may affect the interpretation of later efficacy data, there was a lack of an active comparator group, and the efficacy of treatment was evaluated in the presence of rescue treatment with systemic antibiotics.
DISCLOSURES:
The studies were funded by bimekizumab manufacturer UCB Pharma. Seven authors disclosed being current or former employees of UCB Pharma. Other authors reported several ties with many companies, including UCB Pharma.
A version of this article first appeared on Medscape.com.
Are Children Born Through ART at Higher Risk for Cancer?
The results of a large French study comparing the cancer risk in children conceived through assisted reproductive technology (ART) with that of naturally conceived children were published recently in JAMA Network Open. This study is one of the largest to date on this subject: It included 8,526,306 children born in France between 2010 and 2021, of whom 260,236 (3%) were conceived through ART, and followed them up to a median age of 6.7 years.
Motivations for the Study
ART (including artificial insemination, in vitro fertilization [IVF], or intracytoplasmic sperm injection [ICSI] with fresh or frozen embryo transfer) accounts for about 1 in 30 births in France. However, limited and heterogeneous data have suggested an increased risk for certain health disorders, including cancer, among children conceived through ART. Therefore, a large-scale evaluation of cancer risk in these children is important.
No Overall Increase
In all, 9256 children developed cancer, including 292 who were conceived through ART. Thus, Nevertheless, a slight increase in the risk for leukemia was observed in children conceived through IVF or ICSI. The investigators observed approximately one additional case for every 5000 newborns conceived through IVF or ICSI who reached age 10 years.
Epidemiological monitoring should be continued to better evaluate long-term risks and see whether the risk for leukemia is confirmed. If it is, then it will be useful to investigate the mechanisms related to ART techniques or the fertility disorders of parents that could lead to an increased risk for leukemia.
This story was translated from Univadis France, which is part of the Medscape Professional Network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
The results of a large French study comparing the cancer risk in children conceived through assisted reproductive technology (ART) with that of naturally conceived children were published recently in JAMA Network Open. This study is one of the largest to date on this subject: It included 8,526,306 children born in France between 2010 and 2021, of whom 260,236 (3%) were conceived through ART, and followed them up to a median age of 6.7 years.
Motivations for the Study
ART (including artificial insemination, in vitro fertilization [IVF], or intracytoplasmic sperm injection [ICSI] with fresh or frozen embryo transfer) accounts for about 1 in 30 births in France. However, limited and heterogeneous data have suggested an increased risk for certain health disorders, including cancer, among children conceived through ART. Therefore, a large-scale evaluation of cancer risk in these children is important.
No Overall Increase
In all, 9256 children developed cancer, including 292 who were conceived through ART. Thus, Nevertheless, a slight increase in the risk for leukemia was observed in children conceived through IVF or ICSI. The investigators observed approximately one additional case for every 5000 newborns conceived through IVF or ICSI who reached age 10 years.
Epidemiological monitoring should be continued to better evaluate long-term risks and see whether the risk for leukemia is confirmed. If it is, then it will be useful to investigate the mechanisms related to ART techniques or the fertility disorders of parents that could lead to an increased risk for leukemia.
This story was translated from Univadis France, which is part of the Medscape Professional Network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
The results of a large French study comparing the cancer risk in children conceived through assisted reproductive technology (ART) with that of naturally conceived children were published recently in JAMA Network Open. This study is one of the largest to date on this subject: It included 8,526,306 children born in France between 2010 and 2021, of whom 260,236 (3%) were conceived through ART, and followed them up to a median age of 6.7 years.
Motivations for the Study
ART (including artificial insemination, in vitro fertilization [IVF], or intracytoplasmic sperm injection [ICSI] with fresh or frozen embryo transfer) accounts for about 1 in 30 births in France. However, limited and heterogeneous data have suggested an increased risk for certain health disorders, including cancer, among children conceived through ART. Therefore, a large-scale evaluation of cancer risk in these children is important.
No Overall Increase
In all, 9256 children developed cancer, including 292 who were conceived through ART. Thus, Nevertheless, a slight increase in the risk for leukemia was observed in children conceived through IVF or ICSI. The investigators observed approximately one additional case for every 5000 newborns conceived through IVF or ICSI who reached age 10 years.
Epidemiological monitoring should be continued to better evaluate long-term risks and see whether the risk for leukemia is confirmed. If it is, then it will be useful to investigate the mechanisms related to ART techniques or the fertility disorders of parents that could lead to an increased risk for leukemia.
This story was translated from Univadis France, which is part of the Medscape Professional Network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Celiac Disease: Five Things to Know
Celiac disease is a chronic, immune-mediated, systemic disorder caused by intolerance to gluten — a protein present in rye, barley, and wheat grains — that affects genetically predisposed individuals.
Due to its wide spectrum of clinical manifestations, celiac disease resembles a multisystemic disorder. Its most common gastrointestinal (GI) symptoms include chronic diarrhea, weight loss, and abdominal distention. However, celiac disease can also manifest in myriad extraintestinal symptoms, ranging from headache and fatigue to delayed puberty and psychiatric disorders, with differing presentations in children and adults.
To date, the only treatment is adopting a gluten-free diet (GFD). Although key to preventing persistent villous atrophy, the main cause of complications in celiac disease, lifelong adherence to GFD is challenging and may not resolve all clinical issues. These shortcomings have driven recent efforts to develop novel therapeutic options for patients with this disease.
Here are five things to know about celiac disease.
1. Rising Prevalence of Celiac Disease and Other Autoimmune Disorders Suggests Environmental Factors May Be at Play
Gluten was first identified as the cause of celiac disease in the 1950s. At that time, the condition was thought to be a relatively rare GI disease of childhood that primarily affected people of European descent, but it is now known to be a common disease affecting those of various ages, races, and ethnicities.
A 2018 meta-analysis found the pooled global prevalence of celiac disease was 1.4%. Incidence has increased by as much as 7.5% annually over the past several decades.
Increased awareness among clinicians and improved detection likely play a role in the trend. However, the growth in celiac disease is consistent with that seen for other autoimmune disorders, according to a 2024 update of evidence surrounding celiac disease. Shared environmental factors have been proposed as triggers for celiac disease and other autoimmune diseases and appear to be influencing their rise, the authors noted. These factors include migration and population growth, changing dietary patterns and food processing practices, and altered wheat consumption.
2. No-Biopsy Diagnosis Is Accepted for Children and Shows Promise for Adults
It is estimated that almost 60 million people worldwide have celiac disease, but most remain undiagnosed or misdiagnosed, or they experience significant diagnostic delays.
Prospective data indicate that children with first-degree relatives with celiac disease are at a significantly higher risk of developing the condition, which should prompt screening efforts in this population.
The 2023 updated guidelines from the American College of Gastroenterology (ACG) state that serology testing plays a central role in screening. This commonly involves serological testing for positive serological markers of the disease, including immunoglobulin A (IgA), anti-tissue transglutaminase IgA (tTG-IgA), anti-deamidated gliadin peptide, or endomysial antibodies.
To confirm diagnosis, clinicians have relied on intestinal biopsy since the late 1950s. The ACG still recommends esophagogastroduodenoscopy with multiple duodenal biopsies for confirmation of diagnosis in both children and adults with suspicion of celiac disease. However, recent years have seen a shift toward a no-biopsy approach.
For more than a decade in Europe, a no-biopsy approach has been established practice in pediatric patients, for whom the burden of obtaining a histological confirmation is understandably greater. Most guidelines now permit children to be diagnosed with celiac disease in the absence of a biopsy under specific circumstances (eg, characteristic symptoms of celiac disease and tTG-IgA levels > 10 times the upper limit of normal). The ACG guidelines state that “this approach is a reasonable alternative to the standard approach to a [celiac disease] diagnosis in selected children.”
The ACG does not recommend a no-biopsy approach in adults, noting that, in comparison with children, there is a relative lack of data indicating that serology is predictive in this population. However, it does recognize that physicians may encounter patients for whom a biopsy diagnosis may not be safe or practical. In such cases, an “after-the-fact” diagnosis of likely celiac disease can be given to symptomatic adult patients with a ≥ 10-fold elevation of tTG-IgA and a positive endomysial antibody in a second blood sample.
A 2024 meta-analysis of 18 studies involving over 12,103 adult patients from 15 countries concluded that a no-biopsy approach using tTG-IgA antibody levels ≥ 10 times the upper limit of normal was highly specific and predictive of celiac disease.
3. Celiac Disease Is Associated With Several Life-Threatening Conditions
Emerging data indicate that gastroenterologists should be vigilant in screening patients with celiac disease for several other GI conditions.
Inflammatory bowel disease and celiac disease have a strong bidirectional association, suggesting a possible genetic link between the conditions and indicating that physicians should consider the alternate diagnosis when symptoms persist after treatment.
Given the hypervigilance around food and diet inherent to celiac disease, patients are at an increased risk of developing avoidant/restrictive food intake disorder, according to a 2022 retrospective study.
In 2023, Italian investigators showed that children with celiac disease have an elevated prevalence of functional GI disorders even after adopting a GFD for a year, regardless of whether they consumed processed or natural foods. It was unclear whether this was due to a chronic inflammatory process or to nutritional factors.
Complications resulting from celiac disease are not limited to GI disorders. For a variety of underlying pathophysiological reasons, including intestinal permeability, hyposplenism, and malabsorption of nutrients, patients with celiac disease may be at a higher risk for non-GI conditions, such as osteopenia, women’s health disorders (eg, ovarian failure, endometriosis, or pregnancy loss), juvenile idiopathic arthritis in children and rheumatoid arthritis in adults, certain forms of cancer, infectious diseases, and cardiomyopathy.
4. GFD Is the Only Treatment, but It’s Imperfect and Frustrating for Patients
GFD is the only treatment for celiac disease and must be adhered to without deviation throughout a patient’s life.
Maintaining unwavering adherence reaps considerable benefits: Improved clinical symptoms, robust mucosal healing, and normalization of serological markers. Yet it also takes a considerable toll on patients. Patients with celiac disease struggle with a host of negative physical, psychological, and social impacts. They also report a higher treatment burden than those with gastroesophageal reflux disease or hypertension, and comparable with end-stage renal disease.
GFD also poses financial challenges. Although the price of gluten-free products has decreased in recent years, they still cost significantly more than items with gluten.
Adherence to GFD does not always equate to complete mucosal recovery. While mucosal recovery is achieved in 95% of children within 2 years of the diet’s adoption, only 34% and 66% of adults obtain it within 2 and 5 years, respectively.
GFD may lead to nutrient imbalances because gluten-free foods are typically low in alimentary fiber, micronutrients (eg, vitamin D, vitamin B12, or folate), and minerals (eg, iron, zinc, magnesium, or calcium). With higher sugar and fat content, GFD may leave patients susceptible to unwanted weight gain.
The pervasiveness of gluten in the food production system makes the risk for cross-contamination high. Gluten is often found in both naturally gluten-free foods and products labeled as such. Gluten-sensing technologies, some of which can be used via smartphone apps, have been developed to help patients identify possible cross-contamination. However, the ACG guidelines recommend against the use of these technologies until there is sufficient evidence supporting their ability to improve adherence and clinical outcomes.
5. Novel Therapies for Celiac Disease Are in the Pipeline
The limitations of GFD as the standard treatment for celiac disease have led to an increased focus on developing novel therapeutic interventions. They can be sorted into five key categories: Modulation of the immunostimulatory effects of toxic gluten peptides, elimination of toxic gluten peptides before they reach the intestine, induction of gluten tolerance, modulation of intestinal permeability, and restoration of gut microbiota balance.
Three therapies designed to block antigen presentation by HLA-DQ2/8, the gene alleles that predispose people to celiac disease, show promise: TPM502, an agent that contains three gluten-specific antigenic peptides with overlapping T-cell epitopes for the HLA-DQ2.5 gene; KAN-101, designed to induce gluten tolerance by targeting receptors on the liver; and DONQ52, a multi-specific antibody that targets HLA-DQ2. The KAN-101 therapy received Fast Track designation by the US Food and Drug Administration in 2022.
These and several other agents in clinical and preclinical development are discussed in detail in a 2024 review article. Although no therapies have reached phase 3 testing, when they do, it will undoubtedly be welcomed by those with celiac disease.
A version of this article first appeared on Medscape.com.
Celiac disease is a chronic, immune-mediated, systemic disorder caused by intolerance to gluten — a protein present in rye, barley, and wheat grains — that affects genetically predisposed individuals.
Due to its wide spectrum of clinical manifestations, celiac disease resembles a multisystemic disorder. Its most common gastrointestinal (GI) symptoms include chronic diarrhea, weight loss, and abdominal distention. However, celiac disease can also manifest in myriad extraintestinal symptoms, ranging from headache and fatigue to delayed puberty and psychiatric disorders, with differing presentations in children and adults.
To date, the only treatment is adopting a gluten-free diet (GFD). Although key to preventing persistent villous atrophy, the main cause of complications in celiac disease, lifelong adherence to GFD is challenging and may not resolve all clinical issues. These shortcomings have driven recent efforts to develop novel therapeutic options for patients with this disease.
Here are five things to know about celiac disease.
1. Rising Prevalence of Celiac Disease and Other Autoimmune Disorders Suggests Environmental Factors May Be at Play
Gluten was first identified as the cause of celiac disease in the 1950s. At that time, the condition was thought to be a relatively rare GI disease of childhood that primarily affected people of European descent, but it is now known to be a common disease affecting those of various ages, races, and ethnicities.
A 2018 meta-analysis found the pooled global prevalence of celiac disease was 1.4%. Incidence has increased by as much as 7.5% annually over the past several decades.
Increased awareness among clinicians and improved detection likely play a role in the trend. However, the growth in celiac disease is consistent with that seen for other autoimmune disorders, according to a 2024 update of evidence surrounding celiac disease. Shared environmental factors have been proposed as triggers for celiac disease and other autoimmune diseases and appear to be influencing their rise, the authors noted. These factors include migration and population growth, changing dietary patterns and food processing practices, and altered wheat consumption.
2. No-Biopsy Diagnosis Is Accepted for Children and Shows Promise for Adults
It is estimated that almost 60 million people worldwide have celiac disease, but most remain undiagnosed or misdiagnosed, or they experience significant diagnostic delays.
Prospective data indicate that children with first-degree relatives with celiac disease are at a significantly higher risk of developing the condition, which should prompt screening efforts in this population.
The 2023 updated guidelines from the American College of Gastroenterology (ACG) state that serology testing plays a central role in screening. This commonly involves serological testing for positive serological markers of the disease, including immunoglobulin A (IgA), anti-tissue transglutaminase IgA (tTG-IgA), anti-deamidated gliadin peptide, or endomysial antibodies.
To confirm diagnosis, clinicians have relied on intestinal biopsy since the late 1950s. The ACG still recommends esophagogastroduodenoscopy with multiple duodenal biopsies for confirmation of diagnosis in both children and adults with suspicion of celiac disease. However, recent years have seen a shift toward a no-biopsy approach.
For more than a decade in Europe, a no-biopsy approach has been established practice in pediatric patients, for whom the burden of obtaining a histological confirmation is understandably greater. Most guidelines now permit children to be diagnosed with celiac disease in the absence of a biopsy under specific circumstances (eg, characteristic symptoms of celiac disease and tTG-IgA levels > 10 times the upper limit of normal). The ACG guidelines state that “this approach is a reasonable alternative to the standard approach to a [celiac disease] diagnosis in selected children.”
The ACG does not recommend a no-biopsy approach in adults, noting that, in comparison with children, there is a relative lack of data indicating that serology is predictive in this population. However, it does recognize that physicians may encounter patients for whom a biopsy diagnosis may not be safe or practical. In such cases, an “after-the-fact” diagnosis of likely celiac disease can be given to symptomatic adult patients with a ≥ 10-fold elevation of tTG-IgA and a positive endomysial antibody in a second blood sample.
A 2024 meta-analysis of 18 studies involving over 12,103 adult patients from 15 countries concluded that a no-biopsy approach using tTG-IgA antibody levels ≥ 10 times the upper limit of normal was highly specific and predictive of celiac disease.
3. Celiac Disease Is Associated With Several Life-Threatening Conditions
Emerging data indicate that gastroenterologists should be vigilant in screening patients with celiac disease for several other GI conditions.
Inflammatory bowel disease and celiac disease have a strong bidirectional association, suggesting a possible genetic link between the conditions and indicating that physicians should consider the alternate diagnosis when symptoms persist after treatment.
Given the hypervigilance around food and diet inherent to celiac disease, patients are at an increased risk of developing avoidant/restrictive food intake disorder, according to a 2022 retrospective study.
In 2023, Italian investigators showed that children with celiac disease have an elevated prevalence of functional GI disorders even after adopting a GFD for a year, regardless of whether they consumed processed or natural foods. It was unclear whether this was due to a chronic inflammatory process or to nutritional factors.
Complications resulting from celiac disease are not limited to GI disorders. For a variety of underlying pathophysiological reasons, including intestinal permeability, hyposplenism, and malabsorption of nutrients, patients with celiac disease may be at a higher risk for non-GI conditions, such as osteopenia, women’s health disorders (eg, ovarian failure, endometriosis, or pregnancy loss), juvenile idiopathic arthritis in children and rheumatoid arthritis in adults, certain forms of cancer, infectious diseases, and cardiomyopathy.
4. GFD Is the Only Treatment, but It’s Imperfect and Frustrating for Patients
GFD is the only treatment for celiac disease and must be adhered to without deviation throughout a patient’s life.
Maintaining unwavering adherence reaps considerable benefits: Improved clinical symptoms, robust mucosal healing, and normalization of serological markers. Yet it also takes a considerable toll on patients. Patients with celiac disease struggle with a host of negative physical, psychological, and social impacts. They also report a higher treatment burden than those with gastroesophageal reflux disease or hypertension, and comparable with end-stage renal disease.
GFD also poses financial challenges. Although the price of gluten-free products has decreased in recent years, they still cost significantly more than items with gluten.
Adherence to GFD does not always equate to complete mucosal recovery. While mucosal recovery is achieved in 95% of children within 2 years of the diet’s adoption, only 34% and 66% of adults obtain it within 2 and 5 years, respectively.
GFD may lead to nutrient imbalances because gluten-free foods are typically low in alimentary fiber, micronutrients (eg, vitamin D, vitamin B12, or folate), and minerals (eg, iron, zinc, magnesium, or calcium). With higher sugar and fat content, GFD may leave patients susceptible to unwanted weight gain.
The pervasiveness of gluten in the food production system makes the risk for cross-contamination high. Gluten is often found in both naturally gluten-free foods and products labeled as such. Gluten-sensing technologies, some of which can be used via smartphone apps, have been developed to help patients identify possible cross-contamination. However, the ACG guidelines recommend against the use of these technologies until there is sufficient evidence supporting their ability to improve adherence and clinical outcomes.
5. Novel Therapies for Celiac Disease Are in the Pipeline
The limitations of GFD as the standard treatment for celiac disease have led to an increased focus on developing novel therapeutic interventions. They can be sorted into five key categories: Modulation of the immunostimulatory effects of toxic gluten peptides, elimination of toxic gluten peptides before they reach the intestine, induction of gluten tolerance, modulation of intestinal permeability, and restoration of gut microbiota balance.
Three therapies designed to block antigen presentation by HLA-DQ2/8, the gene alleles that predispose people to celiac disease, show promise: TPM502, an agent that contains three gluten-specific antigenic peptides with overlapping T-cell epitopes for the HLA-DQ2.5 gene; KAN-101, designed to induce gluten tolerance by targeting receptors on the liver; and DONQ52, a multi-specific antibody that targets HLA-DQ2. The KAN-101 therapy received Fast Track designation by the US Food and Drug Administration in 2022.
These and several other agents in clinical and preclinical development are discussed in detail in a 2024 review article. Although no therapies have reached phase 3 testing, when they do, it will undoubtedly be welcomed by those with celiac disease.
A version of this article first appeared on Medscape.com.
Celiac disease is a chronic, immune-mediated, systemic disorder caused by intolerance to gluten — a protein present in rye, barley, and wheat grains — that affects genetically predisposed individuals.
Due to its wide spectrum of clinical manifestations, celiac disease resembles a multisystemic disorder. Its most common gastrointestinal (GI) symptoms include chronic diarrhea, weight loss, and abdominal distention. However, celiac disease can also manifest in myriad extraintestinal symptoms, ranging from headache and fatigue to delayed puberty and psychiatric disorders, with differing presentations in children and adults.
To date, the only treatment is adopting a gluten-free diet (GFD). Although key to preventing persistent villous atrophy, the main cause of complications in celiac disease, lifelong adherence to GFD is challenging and may not resolve all clinical issues. These shortcomings have driven recent efforts to develop novel therapeutic options for patients with this disease.
Here are five things to know about celiac disease.
1. Rising Prevalence of Celiac Disease and Other Autoimmune Disorders Suggests Environmental Factors May Be at Play
Gluten was first identified as the cause of celiac disease in the 1950s. At that time, the condition was thought to be a relatively rare GI disease of childhood that primarily affected people of European descent, but it is now known to be a common disease affecting those of various ages, races, and ethnicities.
A 2018 meta-analysis found the pooled global prevalence of celiac disease was 1.4%. Incidence has increased by as much as 7.5% annually over the past several decades.
Increased awareness among clinicians and improved detection likely play a role in the trend. However, the growth in celiac disease is consistent with that seen for other autoimmune disorders, according to a 2024 update of evidence surrounding celiac disease. Shared environmental factors have been proposed as triggers for celiac disease and other autoimmune diseases and appear to be influencing their rise, the authors noted. These factors include migration and population growth, changing dietary patterns and food processing practices, and altered wheat consumption.
2. No-Biopsy Diagnosis Is Accepted for Children and Shows Promise for Adults
It is estimated that almost 60 million people worldwide have celiac disease, but most remain undiagnosed or misdiagnosed, or they experience significant diagnostic delays.
Prospective data indicate that children with first-degree relatives with celiac disease are at a significantly higher risk of developing the condition, which should prompt screening efforts in this population.
The 2023 updated guidelines from the American College of Gastroenterology (ACG) state that serology testing plays a central role in screening. This commonly involves serological testing for positive serological markers of the disease, including immunoglobulin A (IgA), anti-tissue transglutaminase IgA (tTG-IgA), anti-deamidated gliadin peptide, or endomysial antibodies.
To confirm diagnosis, clinicians have relied on intestinal biopsy since the late 1950s. The ACG still recommends esophagogastroduodenoscopy with multiple duodenal biopsies for confirmation of diagnosis in both children and adults with suspicion of celiac disease. However, recent years have seen a shift toward a no-biopsy approach.
For more than a decade in Europe, a no-biopsy approach has been established practice in pediatric patients, for whom the burden of obtaining a histological confirmation is understandably greater. Most guidelines now permit children to be diagnosed with celiac disease in the absence of a biopsy under specific circumstances (eg, characteristic symptoms of celiac disease and tTG-IgA levels > 10 times the upper limit of normal). The ACG guidelines state that “this approach is a reasonable alternative to the standard approach to a [celiac disease] diagnosis in selected children.”
The ACG does not recommend a no-biopsy approach in adults, noting that, in comparison with children, there is a relative lack of data indicating that serology is predictive in this population. However, it does recognize that physicians may encounter patients for whom a biopsy diagnosis may not be safe or practical. In such cases, an “after-the-fact” diagnosis of likely celiac disease can be given to symptomatic adult patients with a ≥ 10-fold elevation of tTG-IgA and a positive endomysial antibody in a second blood sample.
A 2024 meta-analysis of 18 studies involving over 12,103 adult patients from 15 countries concluded that a no-biopsy approach using tTG-IgA antibody levels ≥ 10 times the upper limit of normal was highly specific and predictive of celiac disease.
3. Celiac Disease Is Associated With Several Life-Threatening Conditions
Emerging data indicate that gastroenterologists should be vigilant in screening patients with celiac disease for several other GI conditions.
Inflammatory bowel disease and celiac disease have a strong bidirectional association, suggesting a possible genetic link between the conditions and indicating that physicians should consider the alternate diagnosis when symptoms persist after treatment.
Given the hypervigilance around food and diet inherent to celiac disease, patients are at an increased risk of developing avoidant/restrictive food intake disorder, according to a 2022 retrospective study.
In 2023, Italian investigators showed that children with celiac disease have an elevated prevalence of functional GI disorders even after adopting a GFD for a year, regardless of whether they consumed processed or natural foods. It was unclear whether this was due to a chronic inflammatory process or to nutritional factors.
Complications resulting from celiac disease are not limited to GI disorders. For a variety of underlying pathophysiological reasons, including intestinal permeability, hyposplenism, and malabsorption of nutrients, patients with celiac disease may be at a higher risk for non-GI conditions, such as osteopenia, women’s health disorders (eg, ovarian failure, endometriosis, or pregnancy loss), juvenile idiopathic arthritis in children and rheumatoid arthritis in adults, certain forms of cancer, infectious diseases, and cardiomyopathy.
4. GFD Is the Only Treatment, but It’s Imperfect and Frustrating for Patients
GFD is the only treatment for celiac disease and must be adhered to without deviation throughout a patient’s life.
Maintaining unwavering adherence reaps considerable benefits: Improved clinical symptoms, robust mucosal healing, and normalization of serological markers. Yet it also takes a considerable toll on patients. Patients with celiac disease struggle with a host of negative physical, psychological, and social impacts. They also report a higher treatment burden than those with gastroesophageal reflux disease or hypertension, and comparable with end-stage renal disease.
GFD also poses financial challenges. Although the price of gluten-free products has decreased in recent years, they still cost significantly more than items with gluten.
Adherence to GFD does not always equate to complete mucosal recovery. While mucosal recovery is achieved in 95% of children within 2 years of the diet’s adoption, only 34% and 66% of adults obtain it within 2 and 5 years, respectively.
GFD may lead to nutrient imbalances because gluten-free foods are typically low in alimentary fiber, micronutrients (eg, vitamin D, vitamin B12, or folate), and minerals (eg, iron, zinc, magnesium, or calcium). With higher sugar and fat content, GFD may leave patients susceptible to unwanted weight gain.
The pervasiveness of gluten in the food production system makes the risk for cross-contamination high. Gluten is often found in both naturally gluten-free foods and products labeled as such. Gluten-sensing technologies, some of which can be used via smartphone apps, have been developed to help patients identify possible cross-contamination. However, the ACG guidelines recommend against the use of these technologies until there is sufficient evidence supporting their ability to improve adherence and clinical outcomes.
5. Novel Therapies for Celiac Disease Are in the Pipeline
The limitations of GFD as the standard treatment for celiac disease have led to an increased focus on developing novel therapeutic interventions. They can be sorted into five key categories: Modulation of the immunostimulatory effects of toxic gluten peptides, elimination of toxic gluten peptides before they reach the intestine, induction of gluten tolerance, modulation of intestinal permeability, and restoration of gut microbiota balance.
Three therapies designed to block antigen presentation by HLA-DQ2/8, the gene alleles that predispose people to celiac disease, show promise: TPM502, an agent that contains three gluten-specific antigenic peptides with overlapping T-cell epitopes for the HLA-DQ2.5 gene; KAN-101, designed to induce gluten tolerance by targeting receptors on the liver; and DONQ52, a multi-specific antibody that targets HLA-DQ2. The KAN-101 therapy received Fast Track designation by the US Food and Drug Administration in 2022.
These and several other agents in clinical and preclinical development are discussed in detail in a 2024 review article. Although no therapies have reached phase 3 testing, when they do, it will undoubtedly be welcomed by those with celiac disease.
A version of this article first appeared on Medscape.com.
Clear Coverage Preference for Humira Over Biosimilars Seen in Most Medicare Part D Plans
Despite the influx of adalimumab biosimilars entering the market in 2023, Humira remains on top.
As of January 2024, both high and low concentrations of Humira, the originator adalimumab product, are nearly universally covered by Medicare Part D plans, while only half of these plans covered adalimumab biosimilars, according to a new research letter published online on June 6, 2024, in JAMA.
Of the plans that covered both, only 1.5% had lower-tier placement for biosimilars.
“This study of formulary coverage helps explain limited uptake of adalimumab biosimilars,” wrote the authors, led by Matthew J. Klebanoff, MD, of the University of Pennsylvania, Philadelphia. “Subpar biosimilar adoption will not only undermine their potential to reduce spending but also may deter investments in biosimilar development.”
The analysis included the formulary and enrollment files for 5609 Medicare Part D plans, representing 44.4 million beneficiaries. Drug list prices and whole acquisition costs (WAC) were pulled from the Red Book database, which provides prices for prescription and over-the-counter drugs as well as medical devices and supplies.
Nearly all (98.9%) of Part D plans covered the high-concentration (100 mg/mL) version of adalimumab with a WAC of $6923. This higher concentration is the most popular formulation of the drug, making up an estimated 85% of prescriptions. By comparison, 26.8% of plans covered the high-concentration version of adalimumab-adaz (Hyrimoz), with a WAC 5% less than the reference product.
The unbranded version of adalimumab-adaz, sold at an 81% discount from the reference product, was covered by 13% of plans. Only 4.6% of plans covered high-concentration adalimumab-bwwd (Hadlima), manufactured by Samsung Bioepis.
In January 2024, no high-concentration adalimumab biosimilar had been granted interchangeability status by the US Food and Drug Administration (FDA). Adalimumab-ryvk (Simlandi) was the first biosimilar to receive this designation and was launched in late May 2024.
Coverage for the lower concentration of adalimumab was nearly universal (98.7% of plans). About half of the plans (50.7%) covered adalimumab-adbm (Cyltezo) at a 5% discount. Adalimumab-adbm (Boehringer Ingelheim) was the first interchangeable Humira biosimilar approved by the FDA, but it is only interchangeable with the less popular, lower concentration formulation of adalimumab.
All other biosimilars were covered by less than 5% of Medicare Part D plans, even with some having a WAC 86% below Humira.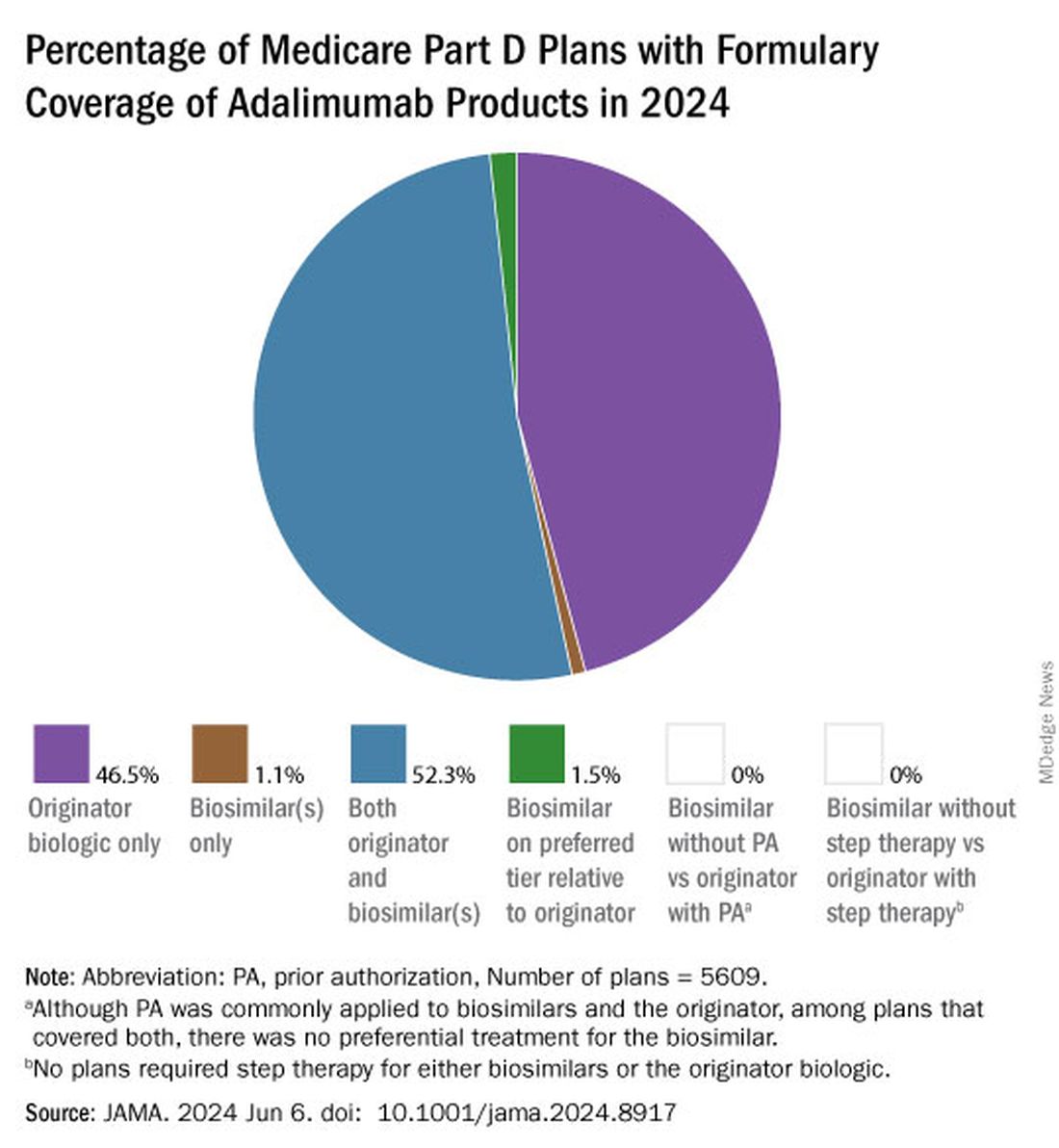
Few plans (1.5%) had biosimilars on preferred tiers compared with the reference product, and no plans used prior authorization to incentivize use of biosimilars. Most plans preferred the higher-priced version of adalimumab biosimilars, which appeals to pharmacy benefit managers who can therefore receive higher rebates, the authors noted.
“Ultimately, biosimilars’ true effect on spending will depend not on their list price but rather on their net price (after rebates) and their influence on originator biologics’ net price,” they wrote. They pointed to the 38% drop in Humira’s annual net price at the end of 2023 compared with the prior year.
“Despite this price decrease, biosimilars offer far greater potential savings: Several adalimumab biosimilars have list prices that are less than half of Humira’s net price,” the authors continued, and encouraged policy makers to mandate coverage for these lower-priced options.
Dr. Klebanoff was supported by a grant from the Health Resources and Services Administration. Two coauthors were supported by a grant from the National Institute on Aging. One author reported receiving consulting fees from AbbVie, which manufactures Humira.
A version of this article appeared on Medscape.com .
Despite the influx of adalimumab biosimilars entering the market in 2023, Humira remains on top.
As of January 2024, both high and low concentrations of Humira, the originator adalimumab product, are nearly universally covered by Medicare Part D plans, while only half of these plans covered adalimumab biosimilars, according to a new research letter published online on June 6, 2024, in JAMA.
Of the plans that covered both, only 1.5% had lower-tier placement for biosimilars.
“This study of formulary coverage helps explain limited uptake of adalimumab biosimilars,” wrote the authors, led by Matthew J. Klebanoff, MD, of the University of Pennsylvania, Philadelphia. “Subpar biosimilar adoption will not only undermine their potential to reduce spending but also may deter investments in biosimilar development.”
The analysis included the formulary and enrollment files for 5609 Medicare Part D plans, representing 44.4 million beneficiaries. Drug list prices and whole acquisition costs (WAC) were pulled from the Red Book database, which provides prices for prescription and over-the-counter drugs as well as medical devices and supplies.
Nearly all (98.9%) of Part D plans covered the high-concentration (100 mg/mL) version of adalimumab with a WAC of $6923. This higher concentration is the most popular formulation of the drug, making up an estimated 85% of prescriptions. By comparison, 26.8% of plans covered the high-concentration version of adalimumab-adaz (Hyrimoz), with a WAC 5% less than the reference product.
The unbranded version of adalimumab-adaz, sold at an 81% discount from the reference product, was covered by 13% of plans. Only 4.6% of plans covered high-concentration adalimumab-bwwd (Hadlima), manufactured by Samsung Bioepis.
In January 2024, no high-concentration adalimumab biosimilar had been granted interchangeability status by the US Food and Drug Administration (FDA). Adalimumab-ryvk (Simlandi) was the first biosimilar to receive this designation and was launched in late May 2024.
Coverage for the lower concentration of adalimumab was nearly universal (98.7% of plans). About half of the plans (50.7%) covered adalimumab-adbm (Cyltezo) at a 5% discount. Adalimumab-adbm (Boehringer Ingelheim) was the first interchangeable Humira biosimilar approved by the FDA, but it is only interchangeable with the less popular, lower concentration formulation of adalimumab.
All other biosimilars were covered by less than 5% of Medicare Part D plans, even with some having a WAC 86% below Humira.
Few plans (1.5%) had biosimilars on preferred tiers compared with the reference product, and no plans used prior authorization to incentivize use of biosimilars. Most plans preferred the higher-priced version of adalimumab biosimilars, which appeals to pharmacy benefit managers who can therefore receive higher rebates, the authors noted.
“Ultimately, biosimilars’ true effect on spending will depend not on their list price but rather on their net price (after rebates) and their influence on originator biologics’ net price,” they wrote. They pointed to the 38% drop in Humira’s annual net price at the end of 2023 compared with the prior year.
“Despite this price decrease, biosimilars offer far greater potential savings: Several adalimumab biosimilars have list prices that are less than half of Humira’s net price,” the authors continued, and encouraged policy makers to mandate coverage for these lower-priced options.
Dr. Klebanoff was supported by a grant from the Health Resources and Services Administration. Two coauthors were supported by a grant from the National Institute on Aging. One author reported receiving consulting fees from AbbVie, which manufactures Humira.
A version of this article appeared on Medscape.com .
Despite the influx of adalimumab biosimilars entering the market in 2023, Humira remains on top.
As of January 2024, both high and low concentrations of Humira, the originator adalimumab product, are nearly universally covered by Medicare Part D plans, while only half of these plans covered adalimumab biosimilars, according to a new research letter published online on June 6, 2024, in JAMA.
Of the plans that covered both, only 1.5% had lower-tier placement for biosimilars.
“This study of formulary coverage helps explain limited uptake of adalimumab biosimilars,” wrote the authors, led by Matthew J. Klebanoff, MD, of the University of Pennsylvania, Philadelphia. “Subpar biosimilar adoption will not only undermine their potential to reduce spending but also may deter investments in biosimilar development.”
The analysis included the formulary and enrollment files for 5609 Medicare Part D plans, representing 44.4 million beneficiaries. Drug list prices and whole acquisition costs (WAC) were pulled from the Red Book database, which provides prices for prescription and over-the-counter drugs as well as medical devices and supplies.
Nearly all (98.9%) of Part D plans covered the high-concentration (100 mg/mL) version of adalimumab with a WAC of $6923. This higher concentration is the most popular formulation of the drug, making up an estimated 85% of prescriptions. By comparison, 26.8% of plans covered the high-concentration version of adalimumab-adaz (Hyrimoz), with a WAC 5% less than the reference product.
The unbranded version of adalimumab-adaz, sold at an 81% discount from the reference product, was covered by 13% of plans. Only 4.6% of plans covered high-concentration adalimumab-bwwd (Hadlima), manufactured by Samsung Bioepis.
In January 2024, no high-concentration adalimumab biosimilar had been granted interchangeability status by the US Food and Drug Administration (FDA). Adalimumab-ryvk (Simlandi) was the first biosimilar to receive this designation and was launched in late May 2024.
Coverage for the lower concentration of adalimumab was nearly universal (98.7% of plans). About half of the plans (50.7%) covered adalimumab-adbm (Cyltezo) at a 5% discount. Adalimumab-adbm (Boehringer Ingelheim) was the first interchangeable Humira biosimilar approved by the FDA, but it is only interchangeable with the less popular, lower concentration formulation of adalimumab.
All other biosimilars were covered by less than 5% of Medicare Part D plans, even with some having a WAC 86% below Humira.
Few plans (1.5%) had biosimilars on preferred tiers compared with the reference product, and no plans used prior authorization to incentivize use of biosimilars. Most plans preferred the higher-priced version of adalimumab biosimilars, which appeals to pharmacy benefit managers who can therefore receive higher rebates, the authors noted.
“Ultimately, biosimilars’ true effect on spending will depend not on their list price but rather on their net price (after rebates) and their influence on originator biologics’ net price,” they wrote. They pointed to the 38% drop in Humira’s annual net price at the end of 2023 compared with the prior year.
“Despite this price decrease, biosimilars offer far greater potential savings: Several adalimumab biosimilars have list prices that are less than half of Humira’s net price,” the authors continued, and encouraged policy makers to mandate coverage for these lower-priced options.
Dr. Klebanoff was supported by a grant from the Health Resources and Services Administration. Two coauthors were supported by a grant from the National Institute on Aging. One author reported receiving consulting fees from AbbVie, which manufactures Humira.
A version of this article appeared on Medscape.com .
FROM JAMA
FDA Grants New Pediatric Arthritis Indications for Upadacitinib
Upadacitinib (Rinvoq) is now indicated for patients aged 2 years or older with active polyarticular juvenile idiopathic arthritis (pJIA) and psoriatic arthritis (PsA) who cannot tolerate or achieve adequate disease response with one or more tumor necrosis factor (TNF) blockers, according to a press release from manufacturer AbbVie.
For the youngest patients, upadacitinib is also available as a weight-based oral solution (Rinvoq LQ) in addition to the previously available tablets, according to the company. JIA, which includes pJIA and juvenile PsA, affects nearly 300,000 children and adolescents in the United States, and alternatives to TNF inhibitor (TNFi) therapy are limited, according to the company. 
“Pediatric patients with pJIA and PsA can be severely limited in their ability to complete daily physical tasks and participate in everyday activities. Understanding their needs today and knowing the likelihood of disease in adulthood underscores the need for additional treatment options,” Aarat Patel, MD, a pediatric rheumatologist at Bon Secours Rheumatology Center, Richmond, Virginia, said in the press release. “Having a treatment option available for patients who do not respond well to a TNFi addresses a need for the healthcare community, patients, and their families,” he said.
Upadacitinib, a Janus kinase (JAK) inhibitor, is being studied for multiple immune-mediated inflammatory diseases. The new indication was supported by data from adults with rheumatoid arthritis (RA) and PsA, 51 pediatric patients with pJIA and active polyarthritis, and safety data from 83 pediatric patients aged 2 years to younger than 18 years with pJIA and active polyarthritis.
In the studies, the drug’s safety in pediatric patients was similar to the known safety profile in adults, which includes increased risk for serious infections such as tuberculosis, cancer, immune system problems, blood clots, and serious allergic reactions to components of the drug, according to the press release. However, the safety and effectiveness of upadacitinib for pJIA and PsA in patients younger than 2 years are unknown.
“Upadacitinib plasma exposures in pediatric patients with pJIA and PsA at the recommended dosage are predicted to be comparable to those observed in adults with RA and PsA based on population pharmacokinetic modeling and simulation,” according to the press release.
Currently, upadacitinib’s only other pediatric indication is for moderate to severe atopic dermatitis in children aged 12 years or older. Upadacitinib also is indicated for treatment of adults with moderate to severe RA, active PsA, active ankylosing spondylitis, active nonradiographic axial spondyloarthritis, and moderate to severe ulcerative colitis and Crohn’s disease, but safety and efficacy for its use in treatment of these conditions in children and adolescents is unknown.
Upadacitinib also is being studied in phase 3 trials for treatment of conditions including alopecia areata, ankylosing spondylitis, atopic dermatitis, axial spondyloarthritis, Crohn’s disease, giant cell arteritis, hidradenitis suppurativa, psoriatic arthritis, RA, systemic lupus erythematosus, Takayasu arteritis, ulcerative colitis, and vitiligo, according to the press release.
Full prescribing information and safety data for upadacitinib are available here.
A version of this article appeared on Medscape.com.
Upadacitinib (Rinvoq) is now indicated for patients aged 2 years or older with active polyarticular juvenile idiopathic arthritis (pJIA) and psoriatic arthritis (PsA) who cannot tolerate or achieve adequate disease response with one or more tumor necrosis factor (TNF) blockers, according to a press release from manufacturer AbbVie.
For the youngest patients, upadacitinib is also available as a weight-based oral solution (Rinvoq LQ) in addition to the previously available tablets, according to the company. JIA, which includes pJIA and juvenile PsA, affects nearly 300,000 children and adolescents in the United States, and alternatives to TNF inhibitor (TNFi) therapy are limited, according to the company.
“Pediatric patients with pJIA and PsA can be severely limited in their ability to complete daily physical tasks and participate in everyday activities. Understanding their needs today and knowing the likelihood of disease in adulthood underscores the need for additional treatment options,” Aarat Patel, MD, a pediatric rheumatologist at Bon Secours Rheumatology Center, Richmond, Virginia, said in the press release. “Having a treatment option available for patients who do not respond well to a TNFi addresses a need for the healthcare community, patients, and their families,” he said.
Upadacitinib, a Janus kinase (JAK) inhibitor, is being studied for multiple immune-mediated inflammatory diseases. The new indication was supported by data from adults with rheumatoid arthritis (RA) and PsA, 51 pediatric patients with pJIA and active polyarthritis, and safety data from 83 pediatric patients aged 2 years to younger than 18 years with pJIA and active polyarthritis.
In the studies, the drug’s safety in pediatric patients was similar to the known safety profile in adults, which includes increased risk for serious infections such as tuberculosis, cancer, immune system problems, blood clots, and serious allergic reactions to components of the drug, according to the press release. However, the safety and effectiveness of upadacitinib for pJIA and PsA in patients younger than 2 years are unknown.
“Upadacitinib plasma exposures in pediatric patients with pJIA and PsA at the recommended dosage are predicted to be comparable to those observed in adults with RA and PsA based on population pharmacokinetic modeling and simulation,” according to the press release.
Currently, upadacitinib’s only other pediatric indication is for moderate to severe atopic dermatitis in children aged 12 years or older. Upadacitinib also is indicated for treatment of adults with moderate to severe RA, active PsA, active ankylosing spondylitis, active nonradiographic axial spondyloarthritis, and moderate to severe ulcerative colitis and Crohn’s disease, but safety and efficacy for its use in treatment of these conditions in children and adolescents is unknown.
Upadacitinib also is being studied in phase 3 trials for treatment of conditions including alopecia areata, ankylosing spondylitis, atopic dermatitis, axial spondyloarthritis, Crohn’s disease, giant cell arteritis, hidradenitis suppurativa, psoriatic arthritis, RA, systemic lupus erythematosus, Takayasu arteritis, ulcerative colitis, and vitiligo, according to the press release.
Full prescribing information and safety data for upadacitinib are available here.
A version of this article appeared on Medscape.com.
Upadacitinib (Rinvoq) is now indicated for patients aged 2 years or older with active polyarticular juvenile idiopathic arthritis (pJIA) and psoriatic arthritis (PsA) who cannot tolerate or achieve adequate disease response with one or more tumor necrosis factor (TNF) blockers, according to a press release from manufacturer AbbVie.
For the youngest patients, upadacitinib is also available as a weight-based oral solution (Rinvoq LQ) in addition to the previously available tablets, according to the company. JIA, which includes pJIA and juvenile PsA, affects nearly 300,000 children and adolescents in the United States, and alternatives to TNF inhibitor (TNFi) therapy are limited, according to the company.
“Pediatric patients with pJIA and PsA can be severely limited in their ability to complete daily physical tasks and participate in everyday activities. Understanding their needs today and knowing the likelihood of disease in adulthood underscores the need for additional treatment options,” Aarat Patel, MD, a pediatric rheumatologist at Bon Secours Rheumatology Center, Richmond, Virginia, said in the press release. “Having a treatment option available for patients who do not respond well to a TNFi addresses a need for the healthcare community, patients, and their families,” he said.
Upadacitinib, a Janus kinase (JAK) inhibitor, is being studied for multiple immune-mediated inflammatory diseases. The new indication was supported by data from adults with rheumatoid arthritis (RA) and PsA, 51 pediatric patients with pJIA and active polyarthritis, and safety data from 83 pediatric patients aged 2 years to younger than 18 years with pJIA and active polyarthritis.
In the studies, the drug’s safety in pediatric patients was similar to the known safety profile in adults, which includes increased risk for serious infections such as tuberculosis, cancer, immune system problems, blood clots, and serious allergic reactions to components of the drug, according to the press release. However, the safety and effectiveness of upadacitinib for pJIA and PsA in patients younger than 2 years are unknown.
“Upadacitinib plasma exposures in pediatric patients with pJIA and PsA at the recommended dosage are predicted to be comparable to those observed in adults with RA and PsA based on population pharmacokinetic modeling and simulation,” according to the press release.
Currently, upadacitinib’s only other pediatric indication is for moderate to severe atopic dermatitis in children aged 12 years or older. Upadacitinib also is indicated for treatment of adults with moderate to severe RA, active PsA, active ankylosing spondylitis, active nonradiographic axial spondyloarthritis, and moderate to severe ulcerative colitis and Crohn’s disease, but safety and efficacy for its use in treatment of these conditions in children and adolescents is unknown.
Upadacitinib also is being studied in phase 3 trials for treatment of conditions including alopecia areata, ankylosing spondylitis, atopic dermatitis, axial spondyloarthritis, Crohn’s disease, giant cell arteritis, hidradenitis suppurativa, psoriatic arthritis, RA, systemic lupus erythematosus, Takayasu arteritis, ulcerative colitis, and vitiligo, according to the press release.
Full prescribing information and safety data for upadacitinib are available here.
A version of this article appeared on Medscape.com.
High Sodium Intake Linked to Greater Risk for Eczema
In a study of adults, an increase of 1 g in estimated 24-hour urinary sodium excretion was associated with 11% higher odds of an atopic dermatitis (AD) diagnosis, 16% higher odds of having active AD, and 11% higher odds of increased severity of AD.
Those are key findings from a cross-sectional analysis of data from the United Kingdom.
“Excessive dietary sodium, common in fast food, may be associated with AD,” corresponding author Katrina Abuabara, MD, MA, MSCE, and colleagues wrote in the study, which was published online in JAMA Dermatology. They referred to recent research using sodium MRI, which showed that “the majority of the body’s exchangeable sodium is stored in the skin and that skin sodium is associated with autoimmune and chronic inflammatory conditions, including AD.” And in another study published in 2019, lesional skin sodium was 30-fold greater in patients with AD than in healthy controls.
To investigate whether there is an association between higher levels of sodium consumption and AD prevalence, activity, and severity at the population level, Dr. Abuabara, of the program for clinical research in the Department of Dermatology at the University of California, San Francisco, and coauthors drew from the UK Biobank, a population-based cohort of more than 500,000 individuals aged 37-73 years at the time of recruitment by the National Health Service. The primary exposure was 24-hour urinary sodium excretion, which was calculated by using the INTERSALT equation, a sex-specific estimation that incorporates body mass index; age; and urine concentrations of potassium, sodium, and creatinine. The primary study outcome was AD or active AD based on diagnostic and prescription codes from linked electronic medical records. The researchers used multivariable logistic regression models adjusted for age, sex, race and ethnicity, Townsend deprivation index, and education to measure the association.
Of the 215,832 Biobank participants included in the analysis, 54% were female, their mean age was 57 years, 95% were White, their mean estimated 24-hour urine sodium excretion was 3.01 g/day, and 10,839 (5%) had a diagnosis of AD. The researchers observed that on multivariable logistic regression, a 1-g increase in estimated 24-hour urine sodium excretion was associated with increased odds of AD (adjusted odds ratio [AOR], 1.11; 95% CI, 1.07-1.14), increased odds of active AD (AOR, 1.16; 95% CI, 1.05-1.28), and increased odds of increasing severity of AD (AOR, 1.11; 95% CI, 1.07-1.15).
Validating Results With US Data
To validate the findings, the researchers evaluated a cohort of 13,014 participants from the US-based National Health and Nutrition Examination Survey (NHANES), using pooled data from the 1999-2000, 2001-2002, and 2003-2004 samples. Of the 13,014 participants, 796 reported current AD, and 1493 reported AD in the past year. The mean dietary sodium intake of overall NHANES participants estimated with 24-hour dietary recall questionnaires was 3.45 g, with a mean of 3.47 g for those with current AD and a mean of 3.44 g for those without AD.
The researchers observed that a 1-g/day higher dietary sodium intake was associated with a higher risk for current AD (AOR, 1.22; 95%CI, 1.01-1.47) and a somewhat higher risk for AD in the past year (AOR, 1.14; 95% CI, 0.97-1.35).
“Future work should examine whether variation of sodium intake over time might trigger AD flares and whether it helps to explain heterogeneity in response to new immunomodulatory treatments for AD,” the authors wrote. “Reduced sodium intake was recommended as a treatment for AD more than a century ago, but there have yet to be studies examining the association of dietary sodium reduction with skin sodium concentration or AD severity,” they added. Noting that sodium reduction “has been shown to be a cost-effective intervention for hypertension and other cardiovascular disease outcomes,” they said that their data “support experimental studies of this approach in AD.”
They acknowledged certain limitations of the study, including the fact that a single spot urine sample was used in the UK Biobank cohort, “which only captures dietary intake of the last 24 hours and is not the best measure of usual or long-term intake of sodium.” They also noted that the findings may not be generalizable to other populations and that AD was based on self-report in the NHANES validation cohort.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was asked to comment on the results, said the study by Dr. Abuabara and colleagues “gives us another reason to avoid salt, showing that 1 g/day of higher salt intake increases the risk of AD in an adult population and more severe AD.”
He added that, “Now, can you say that reducing salt intake will have a therapeutic effect or clinically relevant impact? No. [That is] certainly worth exploring but at a minimum, gives some more credibility to keeping it bland.”
The study was supported by a grant from the Medical Student in Aging Research Program, the National Institute on Aging, and the National Eczema Association. Dr. Abuabara reported receiving research funding for her institution from Pfizer and Cosmetique Internacional/La Roche-Posay and consulting fees from Target RWE, Sanofi, Nektar, and Amgen. No other disclosures were reported. Dr. Friedman had no relevant disclosures.
A version of this article appeared on Medscape.com.
In a study of adults, an increase of 1 g in estimated 24-hour urinary sodium excretion was associated with 11% higher odds of an atopic dermatitis (AD) diagnosis, 16% higher odds of having active AD, and 11% higher odds of increased severity of AD.
Those are key findings from a cross-sectional analysis of data from the United Kingdom.
“Excessive dietary sodium, common in fast food, may be associated with AD,” corresponding author Katrina Abuabara, MD, MA, MSCE, and colleagues wrote in the study, which was published online in JAMA Dermatology. They referred to recent research using sodium MRI, which showed that “the majority of the body’s exchangeable sodium is stored in the skin and that skin sodium is associated with autoimmune and chronic inflammatory conditions, including AD.” And in another study published in 2019, lesional skin sodium was 30-fold greater in patients with AD than in healthy controls.
To investigate whether there is an association between higher levels of sodium consumption and AD prevalence, activity, and severity at the population level, Dr. Abuabara, of the program for clinical research in the Department of Dermatology at the University of California, San Francisco, and coauthors drew from the UK Biobank, a population-based cohort of more than 500,000 individuals aged 37-73 years at the time of recruitment by the National Health Service. The primary exposure was 24-hour urinary sodium excretion, which was calculated by using the INTERSALT equation, a sex-specific estimation that incorporates body mass index; age; and urine concentrations of potassium, sodium, and creatinine. The primary study outcome was AD or active AD based on diagnostic and prescription codes from linked electronic medical records. The researchers used multivariable logistic regression models adjusted for age, sex, race and ethnicity, Townsend deprivation index, and education to measure the association.
Of the 215,832 Biobank participants included in the analysis, 54% were female, their mean age was 57 years, 95% were White, their mean estimated 24-hour urine sodium excretion was 3.01 g/day, and 10,839 (5%) had a diagnosis of AD. The researchers observed that on multivariable logistic regression, a 1-g increase in estimated 24-hour urine sodium excretion was associated with increased odds of AD (adjusted odds ratio [AOR], 1.11; 95% CI, 1.07-1.14), increased odds of active AD (AOR, 1.16; 95% CI, 1.05-1.28), and increased odds of increasing severity of AD (AOR, 1.11; 95% CI, 1.07-1.15).
Validating Results With US Data
To validate the findings, the researchers evaluated a cohort of 13,014 participants from the US-based National Health and Nutrition Examination Survey (NHANES), using pooled data from the 1999-2000, 2001-2002, and 2003-2004 samples. Of the 13,014 participants, 796 reported current AD, and 1493 reported AD in the past year. The mean dietary sodium intake of overall NHANES participants estimated with 24-hour dietary recall questionnaires was 3.45 g, with a mean of 3.47 g for those with current AD and a mean of 3.44 g for those without AD.
The researchers observed that a 1-g/day higher dietary sodium intake was associated with a higher risk for current AD (AOR, 1.22; 95%CI, 1.01-1.47) and a somewhat higher risk for AD in the past year (AOR, 1.14; 95% CI, 0.97-1.35).
“Future work should examine whether variation of sodium intake over time might trigger AD flares and whether it helps to explain heterogeneity in response to new immunomodulatory treatments for AD,” the authors wrote. “Reduced sodium intake was recommended as a treatment for AD more than a century ago, but there have yet to be studies examining the association of dietary sodium reduction with skin sodium concentration or AD severity,” they added. Noting that sodium reduction “has been shown to be a cost-effective intervention for hypertension and other cardiovascular disease outcomes,” they said that their data “support experimental studies of this approach in AD.”
They acknowledged certain limitations of the study, including the fact that a single spot urine sample was used in the UK Biobank cohort, “which only captures dietary intake of the last 24 hours and is not the best measure of usual or long-term intake of sodium.” They also noted that the findings may not be generalizable to other populations and that AD was based on self-report in the NHANES validation cohort.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was asked to comment on the results, said the study by Dr. Abuabara and colleagues “gives us another reason to avoid salt, showing that 1 g/day of higher salt intake increases the risk of AD in an adult population and more severe AD.”
He added that, “Now, can you say that reducing salt intake will have a therapeutic effect or clinically relevant impact? No. [That is] certainly worth exploring but at a minimum, gives some more credibility to keeping it bland.”
The study was supported by a grant from the Medical Student in Aging Research Program, the National Institute on Aging, and the National Eczema Association. Dr. Abuabara reported receiving research funding for her institution from Pfizer and Cosmetique Internacional/La Roche-Posay and consulting fees from Target RWE, Sanofi, Nektar, and Amgen. No other disclosures were reported. Dr. Friedman had no relevant disclosures.
A version of this article appeared on Medscape.com.
In a study of adults, an increase of 1 g in estimated 24-hour urinary sodium excretion was associated with 11% higher odds of an atopic dermatitis (AD) diagnosis, 16% higher odds of having active AD, and 11% higher odds of increased severity of AD.
Those are key findings from a cross-sectional analysis of data from the United Kingdom.
“Excessive dietary sodium, common in fast food, may be associated with AD,” corresponding author Katrina Abuabara, MD, MA, MSCE, and colleagues wrote in the study, which was published online in JAMA Dermatology. They referred to recent research using sodium MRI, which showed that “the majority of the body’s exchangeable sodium is stored in the skin and that skin sodium is associated with autoimmune and chronic inflammatory conditions, including AD.” And in another study published in 2019, lesional skin sodium was 30-fold greater in patients with AD than in healthy controls.
To investigate whether there is an association between higher levels of sodium consumption and AD prevalence, activity, and severity at the population level, Dr. Abuabara, of the program for clinical research in the Department of Dermatology at the University of California, San Francisco, and coauthors drew from the UK Biobank, a population-based cohort of more than 500,000 individuals aged 37-73 years at the time of recruitment by the National Health Service. The primary exposure was 24-hour urinary sodium excretion, which was calculated by using the INTERSALT equation, a sex-specific estimation that incorporates body mass index; age; and urine concentrations of potassium, sodium, and creatinine. The primary study outcome was AD or active AD based on diagnostic and prescription codes from linked electronic medical records. The researchers used multivariable logistic regression models adjusted for age, sex, race and ethnicity, Townsend deprivation index, and education to measure the association.
Of the 215,832 Biobank participants included in the analysis, 54% were female, their mean age was 57 years, 95% were White, their mean estimated 24-hour urine sodium excretion was 3.01 g/day, and 10,839 (5%) had a diagnosis of AD. The researchers observed that on multivariable logistic regression, a 1-g increase in estimated 24-hour urine sodium excretion was associated with increased odds of AD (adjusted odds ratio [AOR], 1.11; 95% CI, 1.07-1.14), increased odds of active AD (AOR, 1.16; 95% CI, 1.05-1.28), and increased odds of increasing severity of AD (AOR, 1.11; 95% CI, 1.07-1.15).
Validating Results With US Data
To validate the findings, the researchers evaluated a cohort of 13,014 participants from the US-based National Health and Nutrition Examination Survey (NHANES), using pooled data from the 1999-2000, 2001-2002, and 2003-2004 samples. Of the 13,014 participants, 796 reported current AD, and 1493 reported AD in the past year. The mean dietary sodium intake of overall NHANES participants estimated with 24-hour dietary recall questionnaires was 3.45 g, with a mean of 3.47 g for those with current AD and a mean of 3.44 g for those without AD.
The researchers observed that a 1-g/day higher dietary sodium intake was associated with a higher risk for current AD (AOR, 1.22; 95%CI, 1.01-1.47) and a somewhat higher risk for AD in the past year (AOR, 1.14; 95% CI, 0.97-1.35).
“Future work should examine whether variation of sodium intake over time might trigger AD flares and whether it helps to explain heterogeneity in response to new immunomodulatory treatments for AD,” the authors wrote. “Reduced sodium intake was recommended as a treatment for AD more than a century ago, but there have yet to be studies examining the association of dietary sodium reduction with skin sodium concentration or AD severity,” they added. Noting that sodium reduction “has been shown to be a cost-effective intervention for hypertension and other cardiovascular disease outcomes,” they said that their data “support experimental studies of this approach in AD.”
They acknowledged certain limitations of the study, including the fact that a single spot urine sample was used in the UK Biobank cohort, “which only captures dietary intake of the last 24 hours and is not the best measure of usual or long-term intake of sodium.” They also noted that the findings may not be generalizable to other populations and that AD was based on self-report in the NHANES validation cohort.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was asked to comment on the results, said the study by Dr. Abuabara and colleagues “gives us another reason to avoid salt, showing that 1 g/day of higher salt intake increases the risk of AD in an adult population and more severe AD.”
He added that, “Now, can you say that reducing salt intake will have a therapeutic effect or clinically relevant impact? No. [That is] certainly worth exploring but at a minimum, gives some more credibility to keeping it bland.”
The study was supported by a grant from the Medical Student in Aging Research Program, the National Institute on Aging, and the National Eczema Association. Dr. Abuabara reported receiving research funding for her institution from Pfizer and Cosmetique Internacional/La Roche-Posay and consulting fees from Target RWE, Sanofi, Nektar, and Amgen. No other disclosures were reported. Dr. Friedman had no relevant disclosures.
A version of this article appeared on Medscape.com.