User login
Smoking Out Meth Use
With methamphetamine use spreading across the country like a flu epidemic, hospitalists see more meth addicts and deal increasingly with the physical and psychiatric conditions common in these individuals. In overcoming the challenges and frustrations of working with these patients, hospitalists in regions where meth use is rampant have become experts of sorts, and they have messages for their colleagues nationwide: Learn our lessons, because you could be next.
The Meth Evolution
Methamphetamine has become popular for obvious reasons. The drug is cheap, and because it is manufactured using common and easily obtained ingredients, it is accessible anywhere.
The meth epidemic is not a new phenomenon. It started in the 1970s in the American heartland—Iowa and parts of Missouri. Since then, it has spread from West to East—hitting California and Hawaii in the ’80s and moving to Southeastern states such as Georgia and South Carolina in the late ’90s.
According to Richard A. Rawson, PhD, associate director and professor-in-residence for the Integrated Substance Abuse Programs at the Semel Institute for Neuroscience and Human Behavior in the David Geffen School of Medicine at the University of California at Los Angeles, “The spread of meth in the U.S. looks much like that of an infectious disease. It has spread in a very systematic way.”
It is a particular problem in rural communities, where it’s easily accessible and cheap. In fact, Dr. Rawson suggests that the drug doesn’t really present a major problem in urban areas—with the exception of cities that have a concentration of gay men. “Meth use in this population is a unique phenomenon that doesn’t follow the same homogenous spread from west to east,” he says.
Compounding this problem is the fact that HIV and sexually transmitted diseases often accompany meth use. “The drug is uniquely connected to sexual behavior because it increases sex drive, sexual performance, and pleasure,” observes Dr. Rawson. At the same time, hepatitis C is a broad concern in communities in which users inject the drug instead of smoking it. In fact, he says, about 50% of meth injectors are hepatitis-C-positive.
Meth Addicts: Routine for Some Hospitalists
For those hospitalists who see many meth users, working with these patients is fairly routine. As Emory University, Atlanta, assistant professor of medicine and hospitalist J. Allen Garner, MD, says, “As many as 30% of the patients I deal with on any given day are addicted to something—cocaine, alcohol, meth. I can’t say it’s a greater burden than anything else.”
Establishing rapport with these patients can be challenging. “Some say, ‘I’m really strung out and need help.’ Many come in with some physical complaint and don’t tell me that they’re high on meth and haven’t slept for 72 hours,” says Dr. Garner. “Basically, this has to do with the denial that goes along with chemical dependency.
Even patients who readily admit that they have a problem are often in denial about the depth of their addiction. “They’ll say that they have it under control, that they only did it once, or that someone slipped them the drug—all ‘party lines’ that take the heat off of them,” he says.
Gaining the trust of meth addicts is a major challenge, “because the drug produces paranoia, agitation, and nervousness,” says Dr. Rawson, noting that “quick urine tests” can be used to identify meth users, and drug use shows up for hours. These tests are great because they only cost $5-$10 each.
Many meth patients come into the hospital because of a physical ailment. “They present with chest pain, palpitations, and/or shortness of breath, although these conditions clear up pretty quickly,” says Dr. Garner.
Tip-offs that the problem might be drug related include poor hygiene, disheveled appearance, and edgy, antsy behavior. Additionally, says Dr. Rawson, “Weight loss, skin sores and scabs, dental disorders, nervous behavior, and paranoid ideation are blue-ribbon signs of meth use. In places where users inject meth, look for needle marks. In regions where users smoke meth, pulmonary disease and coughing are common.”
In the patients Dr. Garner sees, meth’s lasting effects affect their physical health less than their mental health and quality of life. “Meth deteriorates them to the point that they can’t work, and they detach themselves from family, friends, and society as a whole,” he explains. “They require a lot of deep-seated [psychiatric] therapy to deal with multiple issues.”
While most of the meth users Dr. Garner sees are poorly educated and come from the working class, meth is increasingly popular among college students and professionals. In fact, he says, “I know of several doctors for whom meth was the drug of choice.” It is important for hospitalists to remember that addiction knows no socioeconomic boundaries. Many clinicians view meth addicts in an unsympathetic light and as people who have caused their own problems. This is a barrier that needs to be overcome, stresses Dr. Garner.
What Hospitalists Can Do
Meth users often aren’t even admitted to the hospital. “Treatment is mostly supportive. There is no drug you can give them to bring them down,” says Dr. Garner. “Withdrawal is a terrible thing—a sensation like Satan is crawling up their chest. We give them valium, but they basically have to weather it out.”
Even if the hospitalist addresses the physical effects and discusses treatment options with the meth user, it’s common for these patients to go back to their drug use when they leave the hospital. “Because meth doesn’t have life-threatening withdrawal symptoms—although you feel like you’re going to die—it’s easy for them to keep going back and using. Detox centers generally won’t touch these people,” says Dr. Garner. As a result, many patients end up in a catch-22, repeatedly going back to meth use.
While Dr. Garner does everything he can to help these patients, “they already are slaves to the drug by the time I see them,” he says. “Meth is highly addictive, and many people get hooked after using it just once or twice.”
This lack of available treatment for meth addicts is one of the greatest frustrations Dr. Garner faces as a hospitalist. “We keep putting resources into catching addicts as criminals and not getting them treatment and help before they become burdens on society,” he says.
He is pleased to note that this is changing in some states. “A few of the courts in our locale are starting to incorporate treatment programs through the court systems,” he explains.
Meth and Youth
While meth has become a popular drug among all age groups, “very few teens end up in the hospital because of meth,” says Wendy Wright, MD, a hospitalist at Rady Children’s Hospital in San Diego. “If kids are high on meth, they generally aren’t admitted when they are coming down. And, unlike many adults, they don’t have physical or medical issues that require hospitalization,” she explains. “Kids tolerate meth really well from the physical standpoint. We don’t see the arrhythmias or heart attacks that we see in adult addicts.”
When teen addicts do come in with medical conditions, Dr. Wright suggests, hospitalists often see problems such as skin or urinary tract infections. Teen meth users more frequently come to the hospital with psychiatric problems. “They have paranoid delusions, and some are fairly aggressive,” says Dr. Wright.
While hospitalists dealing with teens face the usual challenge of establishing rapport quickly, Dr. Wright observes that teens tend to be much more open than adults about their drug use. “They are pretty up front; they tell me right off the bat what drugs they use,” she says. “Of course I’m mostly seeing kids [who] aren’t living in an upper-class environment, and they’re not trying to hide things from their parents. The kids I see are streetwise and no nonsense. They have a sense of what their medical needs are and think nothing of asking for HIV or STD testing.”
Because of their youth and general good physical health, teens don’t necessarily create a burden for the hospitals and professionals who care for them. The biggest burden of meth-using teenagers, she suggests, “has to do with social issues. These kids often don’t grow into productive adults. They also have a lot of mental health issues such as bipolar disorder or severe depression, and these are the biggest burdens on the community as a whole. We also see a lot of chlamydia and gonorrhea in our kids.”
Although Dr. Wright strictly sees young patients, she acknowledges intergenerational meth use in families. Her facility sees many children who are brought into protective custody because their parents are meth users and unfit to care for them.
“These kids end up staying in the system, which is a bad place for them to be,” says Dr. Wright. “They grow up with a lot of insecurities and mental health issues, and many go on to be users themselves. While she sees many kids whose grandmothers and mothers are addicts, she believes the problem is situational and not hereditary. Nonetheless, “We’re not sure how to break this cycle,” she says.
Some kids are hospitalized because they are hurt or sick as a result of being in an unsafe environment where parents are meth users. These children are often malnourished or sick because of neglect.
Helping Hospitalists Manage Meth
It helps hospitalists if their facility has clear protocols for handling meth intoxication. “It is especially good to establish a procedure in the emergency department,” advises Dr. Rawson. He stresses that these procedures should address ways to de-escalate aggressive behavior. There are also clinical training techniques and brief interventions used to treat alcoholics that can be useful for dealing with meth addicts. These interventions involve efforts to change behaviors. Specifically, helping patients understand that their substance abuse is putting them at risk and encouraging them to reduce or stop their drug use altogether. The elements of brief interventions for substance abuse have been summarized in the acronym “FRAMES,” which stands for feedback, responsibility, advice, menu of options, empathy, and self-efficacy.
“These tools can help get people to talk about their meth problem[s] and deal with [them],” says Dr. Rawson. “Some of these brief interventions can be amazing in terms of deferring further drug use.”
Burdens of Meth
What hospitalists see in their meth-using patients depends on the maturity of the problem in their community. “In communities where the problem is newer, you are likely to see younger users and fewer physical problems,” says Dr. Rawson.
In areas where the problem has existed for years, hospitalists can expect to see older addicts with physical problems that range from heart conditions to widespread tooth decay (a condition known as “meth mouth”). The longer a community has had a meth problem, the more likely the epidemic is placing a financial burden on the healthcare system.
Dr. Garner urges his colleagues to learn about meth. “A couple of years ago, this was a nonexistent problem,” he says. “Now it has reached crisis proportions in many communities.”
Gina DiRenzo-Coffey, MD, director of inpatient pediatrics and a pediatric hospitalist at Alegent Health/Bergan Mercy Medical Center in Omaha, Neb., agrees: “You can lull yourself into believing that this can’t happen in your community. But no one has been able to stop meth use [among members of their community], and it keeps spreading. It is our job to learn everything we can about this drug and help meth addicts as much as we can.” TH
Joanne Kaldy also writes about a day in the life of a pediatric hospitalist in this issue.
With methamphetamine use spreading across the country like a flu epidemic, hospitalists see more meth addicts and deal increasingly with the physical and psychiatric conditions common in these individuals. In overcoming the challenges and frustrations of working with these patients, hospitalists in regions where meth use is rampant have become experts of sorts, and they have messages for their colleagues nationwide: Learn our lessons, because you could be next.
The Meth Evolution
Methamphetamine has become popular for obvious reasons. The drug is cheap, and because it is manufactured using common and easily obtained ingredients, it is accessible anywhere.
The meth epidemic is not a new phenomenon. It started in the 1970s in the American heartland—Iowa and parts of Missouri. Since then, it has spread from West to East—hitting California and Hawaii in the ’80s and moving to Southeastern states such as Georgia and South Carolina in the late ’90s.
According to Richard A. Rawson, PhD, associate director and professor-in-residence for the Integrated Substance Abuse Programs at the Semel Institute for Neuroscience and Human Behavior in the David Geffen School of Medicine at the University of California at Los Angeles, “The spread of meth in the U.S. looks much like that of an infectious disease. It has spread in a very systematic way.”
It is a particular problem in rural communities, where it’s easily accessible and cheap. In fact, Dr. Rawson suggests that the drug doesn’t really present a major problem in urban areas—with the exception of cities that have a concentration of gay men. “Meth use in this population is a unique phenomenon that doesn’t follow the same homogenous spread from west to east,” he says.
Compounding this problem is the fact that HIV and sexually transmitted diseases often accompany meth use. “The drug is uniquely connected to sexual behavior because it increases sex drive, sexual performance, and pleasure,” observes Dr. Rawson. At the same time, hepatitis C is a broad concern in communities in which users inject the drug instead of smoking it. In fact, he says, about 50% of meth injectors are hepatitis-C-positive.
Meth Addicts: Routine for Some Hospitalists
For those hospitalists who see many meth users, working with these patients is fairly routine. As Emory University, Atlanta, assistant professor of medicine and hospitalist J. Allen Garner, MD, says, “As many as 30% of the patients I deal with on any given day are addicted to something—cocaine, alcohol, meth. I can’t say it’s a greater burden than anything else.”
Establishing rapport with these patients can be challenging. “Some say, ‘I’m really strung out and need help.’ Many come in with some physical complaint and don’t tell me that they’re high on meth and haven’t slept for 72 hours,” says Dr. Garner. “Basically, this has to do with the denial that goes along with chemical dependency.
Even patients who readily admit that they have a problem are often in denial about the depth of their addiction. “They’ll say that they have it under control, that they only did it once, or that someone slipped them the drug—all ‘party lines’ that take the heat off of them,” he says.
Gaining the trust of meth addicts is a major challenge, “because the drug produces paranoia, agitation, and nervousness,” says Dr. Rawson, noting that “quick urine tests” can be used to identify meth users, and drug use shows up for hours. These tests are great because they only cost $5-$10 each.
Many meth patients come into the hospital because of a physical ailment. “They present with chest pain, palpitations, and/or shortness of breath, although these conditions clear up pretty quickly,” says Dr. Garner.
Tip-offs that the problem might be drug related include poor hygiene, disheveled appearance, and edgy, antsy behavior. Additionally, says Dr. Rawson, “Weight loss, skin sores and scabs, dental disorders, nervous behavior, and paranoid ideation are blue-ribbon signs of meth use. In places where users inject meth, look for needle marks. In regions where users smoke meth, pulmonary disease and coughing are common.”
In the patients Dr. Garner sees, meth’s lasting effects affect their physical health less than their mental health and quality of life. “Meth deteriorates them to the point that they can’t work, and they detach themselves from family, friends, and society as a whole,” he explains. “They require a lot of deep-seated [psychiatric] therapy to deal with multiple issues.”
While most of the meth users Dr. Garner sees are poorly educated and come from the working class, meth is increasingly popular among college students and professionals. In fact, he says, “I know of several doctors for whom meth was the drug of choice.” It is important for hospitalists to remember that addiction knows no socioeconomic boundaries. Many clinicians view meth addicts in an unsympathetic light and as people who have caused their own problems. This is a barrier that needs to be overcome, stresses Dr. Garner.
What Hospitalists Can Do
Meth users often aren’t even admitted to the hospital. “Treatment is mostly supportive. There is no drug you can give them to bring them down,” says Dr. Garner. “Withdrawal is a terrible thing—a sensation like Satan is crawling up their chest. We give them valium, but they basically have to weather it out.”
Even if the hospitalist addresses the physical effects and discusses treatment options with the meth user, it’s common for these patients to go back to their drug use when they leave the hospital. “Because meth doesn’t have life-threatening withdrawal symptoms—although you feel like you’re going to die—it’s easy for them to keep going back and using. Detox centers generally won’t touch these people,” says Dr. Garner. As a result, many patients end up in a catch-22, repeatedly going back to meth use.
While Dr. Garner does everything he can to help these patients, “they already are slaves to the drug by the time I see them,” he says. “Meth is highly addictive, and many people get hooked after using it just once or twice.”
This lack of available treatment for meth addicts is one of the greatest frustrations Dr. Garner faces as a hospitalist. “We keep putting resources into catching addicts as criminals and not getting them treatment and help before they become burdens on society,” he says.
He is pleased to note that this is changing in some states. “A few of the courts in our locale are starting to incorporate treatment programs through the court systems,” he explains.
Meth and Youth
While meth has become a popular drug among all age groups, “very few teens end up in the hospital because of meth,” says Wendy Wright, MD, a hospitalist at Rady Children’s Hospital in San Diego. “If kids are high on meth, they generally aren’t admitted when they are coming down. And, unlike many adults, they don’t have physical or medical issues that require hospitalization,” she explains. “Kids tolerate meth really well from the physical standpoint. We don’t see the arrhythmias or heart attacks that we see in adult addicts.”
When teen addicts do come in with medical conditions, Dr. Wright suggests, hospitalists often see problems such as skin or urinary tract infections. Teen meth users more frequently come to the hospital with psychiatric problems. “They have paranoid delusions, and some are fairly aggressive,” says Dr. Wright.
While hospitalists dealing with teens face the usual challenge of establishing rapport quickly, Dr. Wright observes that teens tend to be much more open than adults about their drug use. “They are pretty up front; they tell me right off the bat what drugs they use,” she says. “Of course I’m mostly seeing kids [who] aren’t living in an upper-class environment, and they’re not trying to hide things from their parents. The kids I see are streetwise and no nonsense. They have a sense of what their medical needs are and think nothing of asking for HIV or STD testing.”
Because of their youth and general good physical health, teens don’t necessarily create a burden for the hospitals and professionals who care for them. The biggest burden of meth-using teenagers, she suggests, “has to do with social issues. These kids often don’t grow into productive adults. They also have a lot of mental health issues such as bipolar disorder or severe depression, and these are the biggest burdens on the community as a whole. We also see a lot of chlamydia and gonorrhea in our kids.”
Although Dr. Wright strictly sees young patients, she acknowledges intergenerational meth use in families. Her facility sees many children who are brought into protective custody because their parents are meth users and unfit to care for them.
“These kids end up staying in the system, which is a bad place for them to be,” says Dr. Wright. “They grow up with a lot of insecurities and mental health issues, and many go on to be users themselves. While she sees many kids whose grandmothers and mothers are addicts, she believes the problem is situational and not hereditary. Nonetheless, “We’re not sure how to break this cycle,” she says.
Some kids are hospitalized because they are hurt or sick as a result of being in an unsafe environment where parents are meth users. These children are often malnourished or sick because of neglect.
Helping Hospitalists Manage Meth
It helps hospitalists if their facility has clear protocols for handling meth intoxication. “It is especially good to establish a procedure in the emergency department,” advises Dr. Rawson. He stresses that these procedures should address ways to de-escalate aggressive behavior. There are also clinical training techniques and brief interventions used to treat alcoholics that can be useful for dealing with meth addicts. These interventions involve efforts to change behaviors. Specifically, helping patients understand that their substance abuse is putting them at risk and encouraging them to reduce or stop their drug use altogether. The elements of brief interventions for substance abuse have been summarized in the acronym “FRAMES,” which stands for feedback, responsibility, advice, menu of options, empathy, and self-efficacy.
“These tools can help get people to talk about their meth problem[s] and deal with [them],” says Dr. Rawson. “Some of these brief interventions can be amazing in terms of deferring further drug use.”
Burdens of Meth
What hospitalists see in their meth-using patients depends on the maturity of the problem in their community. “In communities where the problem is newer, you are likely to see younger users and fewer physical problems,” says Dr. Rawson.
In areas where the problem has existed for years, hospitalists can expect to see older addicts with physical problems that range from heart conditions to widespread tooth decay (a condition known as “meth mouth”). The longer a community has had a meth problem, the more likely the epidemic is placing a financial burden on the healthcare system.
Dr. Garner urges his colleagues to learn about meth. “A couple of years ago, this was a nonexistent problem,” he says. “Now it has reached crisis proportions in many communities.”
Gina DiRenzo-Coffey, MD, director of inpatient pediatrics and a pediatric hospitalist at Alegent Health/Bergan Mercy Medical Center in Omaha, Neb., agrees: “You can lull yourself into believing that this can’t happen in your community. But no one has been able to stop meth use [among members of their community], and it keeps spreading. It is our job to learn everything we can about this drug and help meth addicts as much as we can.” TH
Joanne Kaldy also writes about a day in the life of a pediatric hospitalist in this issue.
With methamphetamine use spreading across the country like a flu epidemic, hospitalists see more meth addicts and deal increasingly with the physical and psychiatric conditions common in these individuals. In overcoming the challenges and frustrations of working with these patients, hospitalists in regions where meth use is rampant have become experts of sorts, and they have messages for their colleagues nationwide: Learn our lessons, because you could be next.
The Meth Evolution
Methamphetamine has become popular for obvious reasons. The drug is cheap, and because it is manufactured using common and easily obtained ingredients, it is accessible anywhere.
The meth epidemic is not a new phenomenon. It started in the 1970s in the American heartland—Iowa and parts of Missouri. Since then, it has spread from West to East—hitting California and Hawaii in the ’80s and moving to Southeastern states such as Georgia and South Carolina in the late ’90s.
According to Richard A. Rawson, PhD, associate director and professor-in-residence for the Integrated Substance Abuse Programs at the Semel Institute for Neuroscience and Human Behavior in the David Geffen School of Medicine at the University of California at Los Angeles, “The spread of meth in the U.S. looks much like that of an infectious disease. It has spread in a very systematic way.”
It is a particular problem in rural communities, where it’s easily accessible and cheap. In fact, Dr. Rawson suggests that the drug doesn’t really present a major problem in urban areas—with the exception of cities that have a concentration of gay men. “Meth use in this population is a unique phenomenon that doesn’t follow the same homogenous spread from west to east,” he says.
Compounding this problem is the fact that HIV and sexually transmitted diseases often accompany meth use. “The drug is uniquely connected to sexual behavior because it increases sex drive, sexual performance, and pleasure,” observes Dr. Rawson. At the same time, hepatitis C is a broad concern in communities in which users inject the drug instead of smoking it. In fact, he says, about 50% of meth injectors are hepatitis-C-positive.
Meth Addicts: Routine for Some Hospitalists
For those hospitalists who see many meth users, working with these patients is fairly routine. As Emory University, Atlanta, assistant professor of medicine and hospitalist J. Allen Garner, MD, says, “As many as 30% of the patients I deal with on any given day are addicted to something—cocaine, alcohol, meth. I can’t say it’s a greater burden than anything else.”
Establishing rapport with these patients can be challenging. “Some say, ‘I’m really strung out and need help.’ Many come in with some physical complaint and don’t tell me that they’re high on meth and haven’t slept for 72 hours,” says Dr. Garner. “Basically, this has to do with the denial that goes along with chemical dependency.
Even patients who readily admit that they have a problem are often in denial about the depth of their addiction. “They’ll say that they have it under control, that they only did it once, or that someone slipped them the drug—all ‘party lines’ that take the heat off of them,” he says.
Gaining the trust of meth addicts is a major challenge, “because the drug produces paranoia, agitation, and nervousness,” says Dr. Rawson, noting that “quick urine tests” can be used to identify meth users, and drug use shows up for hours. These tests are great because they only cost $5-$10 each.
Many meth patients come into the hospital because of a physical ailment. “They present with chest pain, palpitations, and/or shortness of breath, although these conditions clear up pretty quickly,” says Dr. Garner.
Tip-offs that the problem might be drug related include poor hygiene, disheveled appearance, and edgy, antsy behavior. Additionally, says Dr. Rawson, “Weight loss, skin sores and scabs, dental disorders, nervous behavior, and paranoid ideation are blue-ribbon signs of meth use. In places where users inject meth, look for needle marks. In regions where users smoke meth, pulmonary disease and coughing are common.”
In the patients Dr. Garner sees, meth’s lasting effects affect their physical health less than their mental health and quality of life. “Meth deteriorates them to the point that they can’t work, and they detach themselves from family, friends, and society as a whole,” he explains. “They require a lot of deep-seated [psychiatric] therapy to deal with multiple issues.”
While most of the meth users Dr. Garner sees are poorly educated and come from the working class, meth is increasingly popular among college students and professionals. In fact, he says, “I know of several doctors for whom meth was the drug of choice.” It is important for hospitalists to remember that addiction knows no socioeconomic boundaries. Many clinicians view meth addicts in an unsympathetic light and as people who have caused their own problems. This is a barrier that needs to be overcome, stresses Dr. Garner.
What Hospitalists Can Do
Meth users often aren’t even admitted to the hospital. “Treatment is mostly supportive. There is no drug you can give them to bring them down,” says Dr. Garner. “Withdrawal is a terrible thing—a sensation like Satan is crawling up their chest. We give them valium, but they basically have to weather it out.”
Even if the hospitalist addresses the physical effects and discusses treatment options with the meth user, it’s common for these patients to go back to their drug use when they leave the hospital. “Because meth doesn’t have life-threatening withdrawal symptoms—although you feel like you’re going to die—it’s easy for them to keep going back and using. Detox centers generally won’t touch these people,” says Dr. Garner. As a result, many patients end up in a catch-22, repeatedly going back to meth use.
While Dr. Garner does everything he can to help these patients, “they already are slaves to the drug by the time I see them,” he says. “Meth is highly addictive, and many people get hooked after using it just once or twice.”
This lack of available treatment for meth addicts is one of the greatest frustrations Dr. Garner faces as a hospitalist. “We keep putting resources into catching addicts as criminals and not getting them treatment and help before they become burdens on society,” he says.
He is pleased to note that this is changing in some states. “A few of the courts in our locale are starting to incorporate treatment programs through the court systems,” he explains.
Meth and Youth
While meth has become a popular drug among all age groups, “very few teens end up in the hospital because of meth,” says Wendy Wright, MD, a hospitalist at Rady Children’s Hospital in San Diego. “If kids are high on meth, they generally aren’t admitted when they are coming down. And, unlike many adults, they don’t have physical or medical issues that require hospitalization,” she explains. “Kids tolerate meth really well from the physical standpoint. We don’t see the arrhythmias or heart attacks that we see in adult addicts.”
When teen addicts do come in with medical conditions, Dr. Wright suggests, hospitalists often see problems such as skin or urinary tract infections. Teen meth users more frequently come to the hospital with psychiatric problems. “They have paranoid delusions, and some are fairly aggressive,” says Dr. Wright.
While hospitalists dealing with teens face the usual challenge of establishing rapport quickly, Dr. Wright observes that teens tend to be much more open than adults about their drug use. “They are pretty up front; they tell me right off the bat what drugs they use,” she says. “Of course I’m mostly seeing kids [who] aren’t living in an upper-class environment, and they’re not trying to hide things from their parents. The kids I see are streetwise and no nonsense. They have a sense of what their medical needs are and think nothing of asking for HIV or STD testing.”
Because of their youth and general good physical health, teens don’t necessarily create a burden for the hospitals and professionals who care for them. The biggest burden of meth-using teenagers, she suggests, “has to do with social issues. These kids often don’t grow into productive adults. They also have a lot of mental health issues such as bipolar disorder or severe depression, and these are the biggest burdens on the community as a whole. We also see a lot of chlamydia and gonorrhea in our kids.”
Although Dr. Wright strictly sees young patients, she acknowledges intergenerational meth use in families. Her facility sees many children who are brought into protective custody because their parents are meth users and unfit to care for them.
“These kids end up staying in the system, which is a bad place for them to be,” says Dr. Wright. “They grow up with a lot of insecurities and mental health issues, and many go on to be users themselves. While she sees many kids whose grandmothers and mothers are addicts, she believes the problem is situational and not hereditary. Nonetheless, “We’re not sure how to break this cycle,” she says.
Some kids are hospitalized because they are hurt or sick as a result of being in an unsafe environment where parents are meth users. These children are often malnourished or sick because of neglect.
Helping Hospitalists Manage Meth
It helps hospitalists if their facility has clear protocols for handling meth intoxication. “It is especially good to establish a procedure in the emergency department,” advises Dr. Rawson. He stresses that these procedures should address ways to de-escalate aggressive behavior. There are also clinical training techniques and brief interventions used to treat alcoholics that can be useful for dealing with meth addicts. These interventions involve efforts to change behaviors. Specifically, helping patients understand that their substance abuse is putting them at risk and encouraging them to reduce or stop their drug use altogether. The elements of brief interventions for substance abuse have been summarized in the acronym “FRAMES,” which stands for feedback, responsibility, advice, menu of options, empathy, and self-efficacy.
“These tools can help get people to talk about their meth problem[s] and deal with [them],” says Dr. Rawson. “Some of these brief interventions can be amazing in terms of deferring further drug use.”
Burdens of Meth
What hospitalists see in their meth-using patients depends on the maturity of the problem in their community. “In communities where the problem is newer, you are likely to see younger users and fewer physical problems,” says Dr. Rawson.
In areas where the problem has existed for years, hospitalists can expect to see older addicts with physical problems that range from heart conditions to widespread tooth decay (a condition known as “meth mouth”). The longer a community has had a meth problem, the more likely the epidemic is placing a financial burden on the healthcare system.
Dr. Garner urges his colleagues to learn about meth. “A couple of years ago, this was a nonexistent problem,” he says. “Now it has reached crisis proportions in many communities.”
Gina DiRenzo-Coffey, MD, director of inpatient pediatrics and a pediatric hospitalist at Alegent Health/Bergan Mercy Medical Center in Omaha, Neb., agrees: “You can lull yourself into believing that this can’t happen in your community. But no one has been able to stop meth use [among members of their community], and it keeps spreading. It is our job to learn everything we can about this drug and help meth addicts as much as we can.” TH
Joanne Kaldy also writes about a day in the life of a pediatric hospitalist in this issue.
X-Ray Has Left the Building
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Perilious Prescriptions
Medication-related errors jeopardize patient safety and commonly result in otherwise unnecessary hospitalizations. Approximately 7% of hospital admissions result from drug-related errors, of which 59% are considered preventable.1 It is estimated that adverse drug events affect 2% to 5% of hospitalized patients.2,3 These errors result in increased hospital costs of $4,700 per admission, or about $2 billion annually for U.S. hospitals.2 Calculations indicate that in the nursing home, for each dollar spent on a medication, there is another $1.33 spent on healthcare resources for the treatment of a drug-related morbidity or mortality.
Unfortunately, older folks are particularly susceptible to medication-related problems. Age-associated changes in body composition and physiology, multiple comorbidities, and—last but not least—polypharmacy, are contributing factors. In the United States, patients older than 65 fill an average of 12 prescriptions per year, compared with five fills for patients between ages 25 and 40. In addition, the use of nonprescription medications is more common in the elderly. This opens up the possibility of increased drug-drug or drug-herbal interactions.
Depending on the healthcare setting, as well as the criteria that define inappropriate medication use, studies alert us that between 7% and 21% of ambulatory older folks receive at least one potentially inappropriate medication.4,5 About 60% of nursing home residents, and a staggering 92% of frail elderly hospitalized veterans, receive at least one potentially inappropriate medication.6,7 The consequences of inappropriate drug use in the elderly can be significant. Weakness, resulting in loss of independence and falls that end in bone fractures, is only one possible negative consequence. Between 10% and 20% of the elderly are hospitalized as a result of receiving these inappropriate medications.8,9
Screening Inappropriate Medication
So, what are inappropriate medications for the elderly? Overly simplified, they include any medication that has a greater potential for doing more harm than good. In 1991, Beers and colleagues published criteria for screening inappropriate medication use in elderly patients.10 The authors reviewed the literature and identified 14 nationally recognized authorities in the fields of geriatric pharmacology, epidemiology, geriatrics, and long-term care. Among these experts, consensus was reached on a list of inappropriate medications for elderly nursing home residents. The list was intended to identify medications that should be avoided except under unusual circumstances. The experts also developed criteria for optimal doses, frequencies, and duration of use for these medications.
Since 1991, the criteria have been updated twice (in 1997 and 2002) to include ambulatory elderly. The 2002 Beers list included 48 inappropriate drugs or medication classes, regardless of diagnosis or conditions.11 Because drug-disease interactions in the elderly are increasingly recognized, the 2003 Beers list also included inappropriate medications or medication classes for 20 medical conditions. The consensus panel of experts identified 66 inappropriate drugs with adverse outcomes of potentially high severity. The authors stated specifically that the criteria were not meant to regulate practice to the point at which they would supersede the clinical judgment and assessment of the medical practitioner.
Drug-Drug Interaction
Based on Beers’ criteria for inappropriate prescribing, a literature review of studies conducted between 1992 and 1999 found that between 14% and 23% of the elderly filled a prescription for one or more drugs on the Beers list.12 Long-acting benzodiazepines, dipyridamole, propoxyphene, and amitriptyline were among the most frequently prescribed inappropriate medications.
Cardiovascular and psychotropic drugs are most commonly involved in drug-drug interactions. The most common adverse effects are acute renal failure, hypotension, and neuropsychological presentations such as delirium. Risk factors predisposing to adverse reactions are using multiple medications, receiving care from several prescribing clinicians, and filling prescriptions at more than one pharmacy. Physicians should also be vigilant for drug-herbal interactions.
Drug-Disease Interaction
Another phenomenon responsible for adverse drug events is a drug-disease interaction. For example, renal failure or hepatic insufficiency can interfere with detoxification and excretion; ascites can alter the volume of distribution of hydrophilic drugs, while obesity has an altering effect on lipophilic drugs. Patients with advanced cognitive impairment may have increased sensitivity or paradoxical reactions to drugs with central nervous system or anticholinergic activities.
Optimal Prescribing
As with safety, effective drug therapy for older people is also far from optimal. Optimal drug prescribing should aim for a balance between overprescribing and underprescribing while keeping a safe environment in mind (i.e., monitoring for adverse drug reactions and reducing medication errors). More than 50% of outpatient prescriptions are without indication, while necessary drugs are withheld in the cases of about 55% of elderly outpatients and 25% of hospitalized elderly patients.13
Overprescribing refers not only to the use of multiple medications but also implies a lack of appropriateness in selection, dosing, or use of the medication. For example, the term “prescribing cascade” refers to adding a new medication to treat symptoms of an adverse drug event that is mistakenly assumed to be a separate new diagnosis. Potential consequences of overprescribing include adverse drug events, drug-drug interactions, decreased quality of life, and unnecessary costs. Common factors connected to overprescribing include, but are not limited to, advanced age, multiple comorbidities, multiple prescribers, poor record-keeping, and failure for healthcare providers to thoroughly review a patient’s medication regimen.
Underprescribing of medications to older people is also of concern. Underprescribing results from efforts to avoid complex medication regimens, fear for adverse events, problems with patient adherence to medications, and economic barriers. Underprescribing can result from the notion that older folks will not benefit from medications intended for primary or secondary prevention or for aggressive management of chronic conditions (e.g., angiotensin-converting enzyme inhibitors and beta blockers prescribed for congestive heart failure and after a myocardial infarction).
New Prescribing Initiatives
There have been new initiatives to emphasize optimal prescribing. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates medication reconciliation across inpatient and outpatient practices. In 1999, the Centers for Medicare and Medicaid Services (CMS) expanded the drug use review policy for nursing home certification. Using specific criteria, surveyors and pharmacists must assess resident records for potentially inappropriate medication exposures and associated adverse drug reactions. The “Assessing Care for Vulnerable Elders” (ACOVE) initiative implemented use of quality indicators for prescribing appropriate medications, documentation, education, and medication monitoring. The White House Conference on Aging, held in December 2005, also addressed medication management issues in its resolution entitled “Optimize Medication Management Programs.”
Prescribing Principles
There are a few principles for prescribing that the clinician can keep in mind while caring for the older person. When starting therapy, the basic principle should be to start low and go slow. New complaints or worsening of an existing condition after a drug has been introduced should be scrutinized for the possibility of a drug-induced problem. When choosing treatment for a new medical condition, always consider non-pharmacologic approaches first.
Overprescribing can also be prevented by regularly reviewing a patient’s medication list each time a new medication is started or changed. It is important to know what other providers have prescribed and where prescriptions were filled. It is essential to maintain accurate records. In this regard, the use of electronic medical records can be both an advantage and a disadvantage. Inaccurate drug lists can be self-perpetuating when providers simply copy and paste these sections of the medical records. It is best if the patient can bring all medications, including those purchased over the counter, to the visit. Discontinue any medications that are deemed to be unnecessary after review.
A Few Final Suggestions
For many reasons, patient compliance and adherence can be problematic in older patients.14 Patients often don’t admit not taking their medications as directed. If nonadherence is suspected, the care provider should consider the patient’s financial, cognitive, and functional status, as well as the patient’s beliefs about and understanding of the medications and disease. A simple regimen (such as once daily dosing) and a caregiver who is involved in overseeing medication management are helpful. Medication trays or drug calendars are handy tools. Many older folks may need the reassurance regarding safety that additional education or reinforcement can provide.
Regardless of the steps the physician takes to ensure safe prescribing for the elderly, provider-patient communication is of utmost importance. TH
Dr. Egger works in General Internal Medicine, Section Hospital Medicine, at the Mayo Clinic in Rochester, Minn.
References
- Winterstein AG, Sauer BC, Hepler CD, et al. Preventable drug-related hospital admissions. Ann Pharmacother. 2002;36(7-8):1238-1248.
- Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, D.C.: National Academies Press; 2000.
- Bond CA, Raehl CL, Franke T. Medication errors in United States hospitals. Pharmacotherapy. 2001 Sep;21(9):1023-1036.
- Goulding MR. Inappropriate medication prescribing for elderly ambulatory care patients. Arch Intern Med. 2004 Feb;164(3):305-312.
- Zhan C, Sangl J, Bierman AS, et al. Potentially inappropriate medication use in the community-dwelling elderly: findings from the 1996 Medical Expenditure Panel Survey. JAMA. 2001 Dec 12;286(22):2823-2829.
- Cooper JW. Probable adverse drug reactions in a rural geriatric nursing home population: a four-year study. J Am Geriatr Soc. 1996 Feb;44(2):194-197.
- Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother. 2004 Jan;38(1):9-14.
- Beard K. Adverse reactions as a cause of hospital admission in the aged. Drugs Aging. 1992 Jul-Aug;2(4):356-367.
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998 Apr 15;279(15):1200-1205.
- Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med. 1991 Sep;151(9):1825-1832.
- Fick DM, Cooper JW, Wade WE, et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med. 2003 Dec 8-22;163(22):2716-2724.
- Aparasu RR, Mort JR. Inappropriate prescribing for the elderly: beers criteria-based review. Ann Pharmacother. 2000 Mar;34(3):338-346.
- Hanlon JT, Schmader KE, Ruby CM, et al. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc. 2001 Feb;49(2):200-209.
- Moisan J, Gaudet M, Gregoire JP, et al. Non-compliance with drug treatment and reading difficulties with regard to prescription labelling among seniors. Gerontology. 2002 Jan-Feb;48(1):44-51.
Medication-related errors jeopardize patient safety and commonly result in otherwise unnecessary hospitalizations. Approximately 7% of hospital admissions result from drug-related errors, of which 59% are considered preventable.1 It is estimated that adverse drug events affect 2% to 5% of hospitalized patients.2,3 These errors result in increased hospital costs of $4,700 per admission, or about $2 billion annually for U.S. hospitals.2 Calculations indicate that in the nursing home, for each dollar spent on a medication, there is another $1.33 spent on healthcare resources for the treatment of a drug-related morbidity or mortality.
Unfortunately, older folks are particularly susceptible to medication-related problems. Age-associated changes in body composition and physiology, multiple comorbidities, and—last but not least—polypharmacy, are contributing factors. In the United States, patients older than 65 fill an average of 12 prescriptions per year, compared with five fills for patients between ages 25 and 40. In addition, the use of nonprescription medications is more common in the elderly. This opens up the possibility of increased drug-drug or drug-herbal interactions.
Depending on the healthcare setting, as well as the criteria that define inappropriate medication use, studies alert us that between 7% and 21% of ambulatory older folks receive at least one potentially inappropriate medication.4,5 About 60% of nursing home residents, and a staggering 92% of frail elderly hospitalized veterans, receive at least one potentially inappropriate medication.6,7 The consequences of inappropriate drug use in the elderly can be significant. Weakness, resulting in loss of independence and falls that end in bone fractures, is only one possible negative consequence. Between 10% and 20% of the elderly are hospitalized as a result of receiving these inappropriate medications.8,9
Screening Inappropriate Medication
So, what are inappropriate medications for the elderly? Overly simplified, they include any medication that has a greater potential for doing more harm than good. In 1991, Beers and colleagues published criteria for screening inappropriate medication use in elderly patients.10 The authors reviewed the literature and identified 14 nationally recognized authorities in the fields of geriatric pharmacology, epidemiology, geriatrics, and long-term care. Among these experts, consensus was reached on a list of inappropriate medications for elderly nursing home residents. The list was intended to identify medications that should be avoided except under unusual circumstances. The experts also developed criteria for optimal doses, frequencies, and duration of use for these medications.
Since 1991, the criteria have been updated twice (in 1997 and 2002) to include ambulatory elderly. The 2002 Beers list included 48 inappropriate drugs or medication classes, regardless of diagnosis or conditions.11 Because drug-disease interactions in the elderly are increasingly recognized, the 2003 Beers list also included inappropriate medications or medication classes for 20 medical conditions. The consensus panel of experts identified 66 inappropriate drugs with adverse outcomes of potentially high severity. The authors stated specifically that the criteria were not meant to regulate practice to the point at which they would supersede the clinical judgment and assessment of the medical practitioner.
Drug-Drug Interaction
Based on Beers’ criteria for inappropriate prescribing, a literature review of studies conducted between 1992 and 1999 found that between 14% and 23% of the elderly filled a prescription for one or more drugs on the Beers list.12 Long-acting benzodiazepines, dipyridamole, propoxyphene, and amitriptyline were among the most frequently prescribed inappropriate medications.
Cardiovascular and psychotropic drugs are most commonly involved in drug-drug interactions. The most common adverse effects are acute renal failure, hypotension, and neuropsychological presentations such as delirium. Risk factors predisposing to adverse reactions are using multiple medications, receiving care from several prescribing clinicians, and filling prescriptions at more than one pharmacy. Physicians should also be vigilant for drug-herbal interactions.
Drug-Disease Interaction
Another phenomenon responsible for adverse drug events is a drug-disease interaction. For example, renal failure or hepatic insufficiency can interfere with detoxification and excretion; ascites can alter the volume of distribution of hydrophilic drugs, while obesity has an altering effect on lipophilic drugs. Patients with advanced cognitive impairment may have increased sensitivity or paradoxical reactions to drugs with central nervous system or anticholinergic activities.
Optimal Prescribing
As with safety, effective drug therapy for older people is also far from optimal. Optimal drug prescribing should aim for a balance between overprescribing and underprescribing while keeping a safe environment in mind (i.e., monitoring for adverse drug reactions and reducing medication errors). More than 50% of outpatient prescriptions are without indication, while necessary drugs are withheld in the cases of about 55% of elderly outpatients and 25% of hospitalized elderly patients.13
Overprescribing refers not only to the use of multiple medications but also implies a lack of appropriateness in selection, dosing, or use of the medication. For example, the term “prescribing cascade” refers to adding a new medication to treat symptoms of an adverse drug event that is mistakenly assumed to be a separate new diagnosis. Potential consequences of overprescribing include adverse drug events, drug-drug interactions, decreased quality of life, and unnecessary costs. Common factors connected to overprescribing include, but are not limited to, advanced age, multiple comorbidities, multiple prescribers, poor record-keeping, and failure for healthcare providers to thoroughly review a patient’s medication regimen.
Underprescribing of medications to older people is also of concern. Underprescribing results from efforts to avoid complex medication regimens, fear for adverse events, problems with patient adherence to medications, and economic barriers. Underprescribing can result from the notion that older folks will not benefit from medications intended for primary or secondary prevention or for aggressive management of chronic conditions (e.g., angiotensin-converting enzyme inhibitors and beta blockers prescribed for congestive heart failure and after a myocardial infarction).
New Prescribing Initiatives
There have been new initiatives to emphasize optimal prescribing. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates medication reconciliation across inpatient and outpatient practices. In 1999, the Centers for Medicare and Medicaid Services (CMS) expanded the drug use review policy for nursing home certification. Using specific criteria, surveyors and pharmacists must assess resident records for potentially inappropriate medication exposures and associated adverse drug reactions. The “Assessing Care for Vulnerable Elders” (ACOVE) initiative implemented use of quality indicators for prescribing appropriate medications, documentation, education, and medication monitoring. The White House Conference on Aging, held in December 2005, also addressed medication management issues in its resolution entitled “Optimize Medication Management Programs.”
Prescribing Principles
There are a few principles for prescribing that the clinician can keep in mind while caring for the older person. When starting therapy, the basic principle should be to start low and go slow. New complaints or worsening of an existing condition after a drug has been introduced should be scrutinized for the possibility of a drug-induced problem. When choosing treatment for a new medical condition, always consider non-pharmacologic approaches first.
Overprescribing can also be prevented by regularly reviewing a patient’s medication list each time a new medication is started or changed. It is important to know what other providers have prescribed and where prescriptions were filled. It is essential to maintain accurate records. In this regard, the use of electronic medical records can be both an advantage and a disadvantage. Inaccurate drug lists can be self-perpetuating when providers simply copy and paste these sections of the medical records. It is best if the patient can bring all medications, including those purchased over the counter, to the visit. Discontinue any medications that are deemed to be unnecessary after review.
A Few Final Suggestions
For many reasons, patient compliance and adherence can be problematic in older patients.14 Patients often don’t admit not taking their medications as directed. If nonadherence is suspected, the care provider should consider the patient’s financial, cognitive, and functional status, as well as the patient’s beliefs about and understanding of the medications and disease. A simple regimen (such as once daily dosing) and a caregiver who is involved in overseeing medication management are helpful. Medication trays or drug calendars are handy tools. Many older folks may need the reassurance regarding safety that additional education or reinforcement can provide.
Regardless of the steps the physician takes to ensure safe prescribing for the elderly, provider-patient communication is of utmost importance. TH
Dr. Egger works in General Internal Medicine, Section Hospital Medicine, at the Mayo Clinic in Rochester, Minn.
References
- Winterstein AG, Sauer BC, Hepler CD, et al. Preventable drug-related hospital admissions. Ann Pharmacother. 2002;36(7-8):1238-1248.
- Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, D.C.: National Academies Press; 2000.
- Bond CA, Raehl CL, Franke T. Medication errors in United States hospitals. Pharmacotherapy. 2001 Sep;21(9):1023-1036.
- Goulding MR. Inappropriate medication prescribing for elderly ambulatory care patients. Arch Intern Med. 2004 Feb;164(3):305-312.
- Zhan C, Sangl J, Bierman AS, et al. Potentially inappropriate medication use in the community-dwelling elderly: findings from the 1996 Medical Expenditure Panel Survey. JAMA. 2001 Dec 12;286(22):2823-2829.
- Cooper JW. Probable adverse drug reactions in a rural geriatric nursing home population: a four-year study. J Am Geriatr Soc. 1996 Feb;44(2):194-197.
- Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother. 2004 Jan;38(1):9-14.
- Beard K. Adverse reactions as a cause of hospital admission in the aged. Drugs Aging. 1992 Jul-Aug;2(4):356-367.
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998 Apr 15;279(15):1200-1205.
- Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med. 1991 Sep;151(9):1825-1832.
- Fick DM, Cooper JW, Wade WE, et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med. 2003 Dec 8-22;163(22):2716-2724.
- Aparasu RR, Mort JR. Inappropriate prescribing for the elderly: beers criteria-based review. Ann Pharmacother. 2000 Mar;34(3):338-346.
- Hanlon JT, Schmader KE, Ruby CM, et al. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc. 2001 Feb;49(2):200-209.
- Moisan J, Gaudet M, Gregoire JP, et al. Non-compliance with drug treatment and reading difficulties with regard to prescription labelling among seniors. Gerontology. 2002 Jan-Feb;48(1):44-51.
Medication-related errors jeopardize patient safety and commonly result in otherwise unnecessary hospitalizations. Approximately 7% of hospital admissions result from drug-related errors, of which 59% are considered preventable.1 It is estimated that adverse drug events affect 2% to 5% of hospitalized patients.2,3 These errors result in increased hospital costs of $4,700 per admission, or about $2 billion annually for U.S. hospitals.2 Calculations indicate that in the nursing home, for each dollar spent on a medication, there is another $1.33 spent on healthcare resources for the treatment of a drug-related morbidity or mortality.
Unfortunately, older folks are particularly susceptible to medication-related problems. Age-associated changes in body composition and physiology, multiple comorbidities, and—last but not least—polypharmacy, are contributing factors. In the United States, patients older than 65 fill an average of 12 prescriptions per year, compared with five fills for patients between ages 25 and 40. In addition, the use of nonprescription medications is more common in the elderly. This opens up the possibility of increased drug-drug or drug-herbal interactions.
Depending on the healthcare setting, as well as the criteria that define inappropriate medication use, studies alert us that between 7% and 21% of ambulatory older folks receive at least one potentially inappropriate medication.4,5 About 60% of nursing home residents, and a staggering 92% of frail elderly hospitalized veterans, receive at least one potentially inappropriate medication.6,7 The consequences of inappropriate drug use in the elderly can be significant. Weakness, resulting in loss of independence and falls that end in bone fractures, is only one possible negative consequence. Between 10% and 20% of the elderly are hospitalized as a result of receiving these inappropriate medications.8,9
Screening Inappropriate Medication
So, what are inappropriate medications for the elderly? Overly simplified, they include any medication that has a greater potential for doing more harm than good. In 1991, Beers and colleagues published criteria for screening inappropriate medication use in elderly patients.10 The authors reviewed the literature and identified 14 nationally recognized authorities in the fields of geriatric pharmacology, epidemiology, geriatrics, and long-term care. Among these experts, consensus was reached on a list of inappropriate medications for elderly nursing home residents. The list was intended to identify medications that should be avoided except under unusual circumstances. The experts also developed criteria for optimal doses, frequencies, and duration of use for these medications.
Since 1991, the criteria have been updated twice (in 1997 and 2002) to include ambulatory elderly. The 2002 Beers list included 48 inappropriate drugs or medication classes, regardless of diagnosis or conditions.11 Because drug-disease interactions in the elderly are increasingly recognized, the 2003 Beers list also included inappropriate medications or medication classes for 20 medical conditions. The consensus panel of experts identified 66 inappropriate drugs with adverse outcomes of potentially high severity. The authors stated specifically that the criteria were not meant to regulate practice to the point at which they would supersede the clinical judgment and assessment of the medical practitioner.
Drug-Drug Interaction
Based on Beers’ criteria for inappropriate prescribing, a literature review of studies conducted between 1992 and 1999 found that between 14% and 23% of the elderly filled a prescription for one or more drugs on the Beers list.12 Long-acting benzodiazepines, dipyridamole, propoxyphene, and amitriptyline were among the most frequently prescribed inappropriate medications.
Cardiovascular and psychotropic drugs are most commonly involved in drug-drug interactions. The most common adverse effects are acute renal failure, hypotension, and neuropsychological presentations such as delirium. Risk factors predisposing to adverse reactions are using multiple medications, receiving care from several prescribing clinicians, and filling prescriptions at more than one pharmacy. Physicians should also be vigilant for drug-herbal interactions.
Drug-Disease Interaction
Another phenomenon responsible for adverse drug events is a drug-disease interaction. For example, renal failure or hepatic insufficiency can interfere with detoxification and excretion; ascites can alter the volume of distribution of hydrophilic drugs, while obesity has an altering effect on lipophilic drugs. Patients with advanced cognitive impairment may have increased sensitivity or paradoxical reactions to drugs with central nervous system or anticholinergic activities.
Optimal Prescribing
As with safety, effective drug therapy for older people is also far from optimal. Optimal drug prescribing should aim for a balance between overprescribing and underprescribing while keeping a safe environment in mind (i.e., monitoring for adverse drug reactions and reducing medication errors). More than 50% of outpatient prescriptions are without indication, while necessary drugs are withheld in the cases of about 55% of elderly outpatients and 25% of hospitalized elderly patients.13
Overprescribing refers not only to the use of multiple medications but also implies a lack of appropriateness in selection, dosing, or use of the medication. For example, the term “prescribing cascade” refers to adding a new medication to treat symptoms of an adverse drug event that is mistakenly assumed to be a separate new diagnosis. Potential consequences of overprescribing include adverse drug events, drug-drug interactions, decreased quality of life, and unnecessary costs. Common factors connected to overprescribing include, but are not limited to, advanced age, multiple comorbidities, multiple prescribers, poor record-keeping, and failure for healthcare providers to thoroughly review a patient’s medication regimen.
Underprescribing of medications to older people is also of concern. Underprescribing results from efforts to avoid complex medication regimens, fear for adverse events, problems with patient adherence to medications, and economic barriers. Underprescribing can result from the notion that older folks will not benefit from medications intended for primary or secondary prevention or for aggressive management of chronic conditions (e.g., angiotensin-converting enzyme inhibitors and beta blockers prescribed for congestive heart failure and after a myocardial infarction).
New Prescribing Initiatives
There have been new initiatives to emphasize optimal prescribing. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates medication reconciliation across inpatient and outpatient practices. In 1999, the Centers for Medicare and Medicaid Services (CMS) expanded the drug use review policy for nursing home certification. Using specific criteria, surveyors and pharmacists must assess resident records for potentially inappropriate medication exposures and associated adverse drug reactions. The “Assessing Care for Vulnerable Elders” (ACOVE) initiative implemented use of quality indicators for prescribing appropriate medications, documentation, education, and medication monitoring. The White House Conference on Aging, held in December 2005, also addressed medication management issues in its resolution entitled “Optimize Medication Management Programs.”
Prescribing Principles
There are a few principles for prescribing that the clinician can keep in mind while caring for the older person. When starting therapy, the basic principle should be to start low and go slow. New complaints or worsening of an existing condition after a drug has been introduced should be scrutinized for the possibility of a drug-induced problem. When choosing treatment for a new medical condition, always consider non-pharmacologic approaches first.
Overprescribing can also be prevented by regularly reviewing a patient’s medication list each time a new medication is started or changed. It is important to know what other providers have prescribed and where prescriptions were filled. It is essential to maintain accurate records. In this regard, the use of electronic medical records can be both an advantage and a disadvantage. Inaccurate drug lists can be self-perpetuating when providers simply copy and paste these sections of the medical records. It is best if the patient can bring all medications, including those purchased over the counter, to the visit. Discontinue any medications that are deemed to be unnecessary after review.
A Few Final Suggestions
For many reasons, patient compliance and adherence can be problematic in older patients.14 Patients often don’t admit not taking their medications as directed. If nonadherence is suspected, the care provider should consider the patient’s financial, cognitive, and functional status, as well as the patient’s beliefs about and understanding of the medications and disease. A simple regimen (such as once daily dosing) and a caregiver who is involved in overseeing medication management are helpful. Medication trays or drug calendars are handy tools. Many older folks may need the reassurance regarding safety that additional education or reinforcement can provide.
Regardless of the steps the physician takes to ensure safe prescribing for the elderly, provider-patient communication is of utmost importance. TH
Dr. Egger works in General Internal Medicine, Section Hospital Medicine, at the Mayo Clinic in Rochester, Minn.
References
- Winterstein AG, Sauer BC, Hepler CD, et al. Preventable drug-related hospital admissions. Ann Pharmacother. 2002;36(7-8):1238-1248.
- Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, D.C.: National Academies Press; 2000.
- Bond CA, Raehl CL, Franke T. Medication errors in United States hospitals. Pharmacotherapy. 2001 Sep;21(9):1023-1036.
- Goulding MR. Inappropriate medication prescribing for elderly ambulatory care patients. Arch Intern Med. 2004 Feb;164(3):305-312.
- Zhan C, Sangl J, Bierman AS, et al. Potentially inappropriate medication use in the community-dwelling elderly: findings from the 1996 Medical Expenditure Panel Survey. JAMA. 2001 Dec 12;286(22):2823-2829.
- Cooper JW. Probable adverse drug reactions in a rural geriatric nursing home population: a four-year study. J Am Geriatr Soc. 1996 Feb;44(2):194-197.
- Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother. 2004 Jan;38(1):9-14.
- Beard K. Adverse reactions as a cause of hospital admission in the aged. Drugs Aging. 1992 Jul-Aug;2(4):356-367.
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998 Apr 15;279(15):1200-1205.
- Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med. 1991 Sep;151(9):1825-1832.
- Fick DM, Cooper JW, Wade WE, et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med. 2003 Dec 8-22;163(22):2716-2724.
- Aparasu RR, Mort JR. Inappropriate prescribing for the elderly: beers criteria-based review. Ann Pharmacother. 2000 Mar;34(3):338-346.
- Hanlon JT, Schmader KE, Ruby CM, et al. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc. 2001 Feb;49(2):200-209.
- Moisan J, Gaudet M, Gregoire JP, et al. Non-compliance with drug treatment and reading difficulties with regard to prescription labelling among seniors. Gerontology. 2002 Jan-Feb;48(1):44-51.
An Intense Rash

A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.
A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.
A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.
PSTF Monitors Quality

In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
Pay Dirt

It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
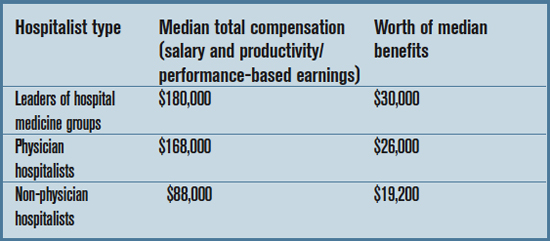
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
Medicare, Money, and Quality Measures

The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
An Historic Moment for Hospital Medicine

In an historic decision at its October 2006 board meeting, the American Board of Internal Medicine (ABIM) agreed to move forward to develop a process for Focused Recognition of Hospital Medicine through ABIM’s Maintenance of Certification (MOC). This is the first time ABIM has offered focused recognition for any subset of internal medicine. In addition, this brings recognition to the uniqueness of hospitalists, who dedicate their professional careers to managing the care of acutely ill patients and creating a better healthcare delivery process at their local hospitals.
This whole concept started when the SHM Board approved a resolution in February 2004, outlining the need to recognize hospitalists as unique providers of healthcare. At the time, the SHM Board asked SHM staff and leadership to work with existing certifying organizations, such as ABIM, to develop a mechanism for hospitalists to have a formal credential recognizing hospital medicine.
Because more than 80% of hospitalists are initially trained in internal medicine, SHM leadership decided that it made sense to first approach ABIM. At the same time SHM had plans to develop similar solutions for hospitalists who are trained initially as pediatricians, family practitioners, and osteopaths (all of which are certified by boards other than ABIM).
Soon after the 2004 SHM Board meeting, SHM executive staff approached key leaders at ABIM. ABIM held a retreat in 2004 to discuss new models of certification. Later the ABIM Board encouraged meetings with SHM to keep hospital medicine within internal medicine.
In April 2005 ABIM and SHM leadership agreed that recognition of hospitalists initially trained in internal medicine might be achieved by modifying the existing MOC process. At that time the ABIM Board was concerned that any changes to the certification system might fragment the internal medicine community. To its credit the ABIM Board did not let these concerns block the process. ABIM soon convened a range of stakeholders in internal medicine to address these issues.
This group of stakeholders was broadly drawn from the leadership at SHM, the American College of Physicians, the Society of General Internal Medicine, all medical subspecialties, the Alliance for Academic Internal Medicine, the Association of American Medical Colleges, the AMA, the Residency Review Committee, and ABIM itself. These stakeholders met in December 2005, May 2006, and again in September 2006.
In preparation for these meetings SHM had developed its comprehensive Core Competencies in Hospital Medicine that was published as a supplement to the first issue of the Journal of Hospital Medicine (JHM) in February 2006. This was a powerful, tangible set of circumstances for hospital medicine.
When people began questioning what made hospital medicine unique among internal medicine disciplines or what was the substance of hospital medicine, being able to hand them the Core Competencies and to walk them through this thoughtful document was very important. In the same way, establishing our own repository for medical advances in hospital medicine via JHM also supported the development of a new field in internal medicine.
It’s been helpful that other key trends have taken shape in the last few years. The Alliance for Academic Internal Medicine (AAIM), representing the Association of Professors of Medicine (APM) and the Association of Directors of Programs in Internal Medicine (APDIM) and others, worked closely with ACP and the rest of the specialties in internal medicine to redesign the internal medicine residency so that it reflects the current and future practice environment.
Further, throughout healthcare there has been an increasing call for performance standards and quality improvement—all in the context of using resources more efficiently. There has been a movement to reshape healthcare centered on the patient and delivered by teams of health professionals, as well as increasing calls to coordinate care across locales and providers so as to improve patient safety and provide the best care.
In addition, the growth of hospital medicine has accelerated in the last few years. The fact that data not only from SHM but also from the American Hospital Association (AHA) and others show that more than 15,000 hospitalists now practice at more than 2,000 hospitals illustrates that that the size and influence of hospitalists comprise an indisputable trend.
And for many hospitals the driver for developing hospital medicine groups is the need to have on-site health professionals who are committed to changes in quality, systems improvement, patient safety, and efficiency.
Whether you call this a tipping point à la Malcolm Gladwell (The Tipping Point, New York City: Little, Brown and Company; 2000) or a perfect storm, to its credit ABIM—with the support of ACP, AAIM, and others—saw an opportunity to develop meaningful changes to MOC as a means of identifying hospitalists and of motivating the self study and improvement in skills and knowledge so important to meet the demands of healthcare delivery in the 21st century.
Now the hard work begins. In October 2006 the ABIM Board of Directors approved appointment of an ABIM Committee on Hospital Medicine Focused Recognition (HMFR). This work group will make recommendations to the ABIM Board in 2007 regarding the requirements for evidence of proficiency in HMFR in the MOC process as well as recommending policy of how HMFR would relate to the rest of ABIM certification and MOC in internal medicine.
SHM and hospital medicine leaders intend to play a key role in helping ABIM shape the details of the HMFR process so that it’s meaningful to the hospitalists who choose to get HMFR during their MOC—as well as to those who employ hospitalists, the physicians and other health professionals that hospitalists work with, the hospitals we work in, and the patients we care for.
At the same time ABIM must approach the American Board of Medical Specialties (ABMS) because the ABMS will ultimately need to accept the HMFR process before ABIM can put this new process in place. This is a significant hurdle to clear, but the ABIM Board is committed to using its resources and powers of persuasion to make this happen.
Even with the hard work and political battles ahead, it is difficult not to sit back and marvel at how far we have come. Our specialty is just 10 years old, but we now have more than 15,000 practitioners and are on our way to 30,000 or even 40,000. We have our own journal, our own specialty society, our own set of competencies, our own growing national annual meeting, our own textbooks, and a growing number of publications aimed at hospitalists.
Now with the help of ABIM and the blessing of ABMS, there is a serious prospect that the first recognition of hospital medicine in the certification process will become a reality.
Will the first hospitalist claim Hospital Medicine Focused Recognition in 2008 or 2009? The exact date is too difficult to predict. That it will happen and that it will be meaningful is more certain now than it has ever been. To all those who have had the foresight and leadership to make this a reality, we thank you. Now let’s get down to the difficult work of creating a process that will help hospitalists provide the best care to their patients and help them to be leaders of change and improvement at their institutions. TH
Dr. Wellikson has been CEO of SHM since 2000.
In an historic decision at its October 2006 board meeting, the American Board of Internal Medicine (ABIM) agreed to move forward to develop a process for Focused Recognition of Hospital Medicine through ABIM’s Maintenance of Certification (MOC). This is the first time ABIM has offered focused recognition for any subset of internal medicine. In addition, this brings recognition to the uniqueness of hospitalists, who dedicate their professional careers to managing the care of acutely ill patients and creating a better healthcare delivery process at their local hospitals.
This whole concept started when the SHM Board approved a resolution in February 2004, outlining the need to recognize hospitalists as unique providers of healthcare. At the time, the SHM Board asked SHM staff and leadership to work with existing certifying organizations, such as ABIM, to develop a mechanism for hospitalists to have a formal credential recognizing hospital medicine.
Because more than 80% of hospitalists are initially trained in internal medicine, SHM leadership decided that it made sense to first approach ABIM. At the same time SHM had plans to develop similar solutions for hospitalists who are trained initially as pediatricians, family practitioners, and osteopaths (all of which are certified by boards other than ABIM).
Soon after the 2004 SHM Board meeting, SHM executive staff approached key leaders at ABIM. ABIM held a retreat in 2004 to discuss new models of certification. Later the ABIM Board encouraged meetings with SHM to keep hospital medicine within internal medicine.
In April 2005 ABIM and SHM leadership agreed that recognition of hospitalists initially trained in internal medicine might be achieved by modifying the existing MOC process. At that time the ABIM Board was concerned that any changes to the certification system might fragment the internal medicine community. To its credit the ABIM Board did not let these concerns block the process. ABIM soon convened a range of stakeholders in internal medicine to address these issues.
This group of stakeholders was broadly drawn from the leadership at SHM, the American College of Physicians, the Society of General Internal Medicine, all medical subspecialties, the Alliance for Academic Internal Medicine, the Association of American Medical Colleges, the AMA, the Residency Review Committee, and ABIM itself. These stakeholders met in December 2005, May 2006, and again in September 2006.
In preparation for these meetings SHM had developed its comprehensive Core Competencies in Hospital Medicine that was published as a supplement to the first issue of the Journal of Hospital Medicine (JHM) in February 2006. This was a powerful, tangible set of circumstances for hospital medicine.
When people began questioning what made hospital medicine unique among internal medicine disciplines or what was the substance of hospital medicine, being able to hand them the Core Competencies and to walk them through this thoughtful document was very important. In the same way, establishing our own repository for medical advances in hospital medicine via JHM also supported the development of a new field in internal medicine.
It’s been helpful that other key trends have taken shape in the last few years. The Alliance for Academic Internal Medicine (AAIM), representing the Association of Professors of Medicine (APM) and the Association of Directors of Programs in Internal Medicine (APDIM) and others, worked closely with ACP and the rest of the specialties in internal medicine to redesign the internal medicine residency so that it reflects the current and future practice environment.
Further, throughout healthcare there has been an increasing call for performance standards and quality improvement—all in the context of using resources more efficiently. There has been a movement to reshape healthcare centered on the patient and delivered by teams of health professionals, as well as increasing calls to coordinate care across locales and providers so as to improve patient safety and provide the best care.
In addition, the growth of hospital medicine has accelerated in the last few years. The fact that data not only from SHM but also from the American Hospital Association (AHA) and others show that more than 15,000 hospitalists now practice at more than 2,000 hospitals illustrates that that the size and influence of hospitalists comprise an indisputable trend.
And for many hospitals the driver for developing hospital medicine groups is the need to have on-site health professionals who are committed to changes in quality, systems improvement, patient safety, and efficiency.
Whether you call this a tipping point à la Malcolm Gladwell (The Tipping Point, New York City: Little, Brown and Company; 2000) or a perfect storm, to its credit ABIM—with the support of ACP, AAIM, and others—saw an opportunity to develop meaningful changes to MOC as a means of identifying hospitalists and of motivating the self study and improvement in skills and knowledge so important to meet the demands of healthcare delivery in the 21st century.
Now the hard work begins. In October 2006 the ABIM Board of Directors approved appointment of an ABIM Committee on Hospital Medicine Focused Recognition (HMFR). This work group will make recommendations to the ABIM Board in 2007 regarding the requirements for evidence of proficiency in HMFR in the MOC process as well as recommending policy of how HMFR would relate to the rest of ABIM certification and MOC in internal medicine.
SHM and hospital medicine leaders intend to play a key role in helping ABIM shape the details of the HMFR process so that it’s meaningful to the hospitalists who choose to get HMFR during their MOC—as well as to those who employ hospitalists, the physicians and other health professionals that hospitalists work with, the hospitals we work in, and the patients we care for.
At the same time ABIM must approach the American Board of Medical Specialties (ABMS) because the ABMS will ultimately need to accept the HMFR process before ABIM can put this new process in place. This is a significant hurdle to clear, but the ABIM Board is committed to using its resources and powers of persuasion to make this happen.
Even with the hard work and political battles ahead, it is difficult not to sit back and marvel at how far we have come. Our specialty is just 10 years old, but we now have more than 15,000 practitioners and are on our way to 30,000 or even 40,000. We have our own journal, our own specialty society, our own set of competencies, our own growing national annual meeting, our own textbooks, and a growing number of publications aimed at hospitalists.
Now with the help of ABIM and the blessing of ABMS, there is a serious prospect that the first recognition of hospital medicine in the certification process will become a reality.
Will the first hospitalist claim Hospital Medicine Focused Recognition in 2008 or 2009? The exact date is too difficult to predict. That it will happen and that it will be meaningful is more certain now than it has ever been. To all those who have had the foresight and leadership to make this a reality, we thank you. Now let’s get down to the difficult work of creating a process that will help hospitalists provide the best care to their patients and help them to be leaders of change and improvement at their institutions. TH
Dr. Wellikson has been CEO of SHM since 2000.
In an historic decision at its October 2006 board meeting, the American Board of Internal Medicine (ABIM) agreed to move forward to develop a process for Focused Recognition of Hospital Medicine through ABIM’s Maintenance of Certification (MOC). This is the first time ABIM has offered focused recognition for any subset of internal medicine. In addition, this brings recognition to the uniqueness of hospitalists, who dedicate their professional careers to managing the care of acutely ill patients and creating a better healthcare delivery process at their local hospitals.
This whole concept started when the SHM Board approved a resolution in February 2004, outlining the need to recognize hospitalists as unique providers of healthcare. At the time, the SHM Board asked SHM staff and leadership to work with existing certifying organizations, such as ABIM, to develop a mechanism for hospitalists to have a formal credential recognizing hospital medicine.
Because more than 80% of hospitalists are initially trained in internal medicine, SHM leadership decided that it made sense to first approach ABIM. At the same time SHM had plans to develop similar solutions for hospitalists who are trained initially as pediatricians, family practitioners, and osteopaths (all of which are certified by boards other than ABIM).
Soon after the 2004 SHM Board meeting, SHM executive staff approached key leaders at ABIM. ABIM held a retreat in 2004 to discuss new models of certification. Later the ABIM Board encouraged meetings with SHM to keep hospital medicine within internal medicine.
In April 2005 ABIM and SHM leadership agreed that recognition of hospitalists initially trained in internal medicine might be achieved by modifying the existing MOC process. At that time the ABIM Board was concerned that any changes to the certification system might fragment the internal medicine community. To its credit the ABIM Board did not let these concerns block the process. ABIM soon convened a range of stakeholders in internal medicine to address these issues.
This group of stakeholders was broadly drawn from the leadership at SHM, the American College of Physicians, the Society of General Internal Medicine, all medical subspecialties, the Alliance for Academic Internal Medicine, the Association of American Medical Colleges, the AMA, the Residency Review Committee, and ABIM itself. These stakeholders met in December 2005, May 2006, and again in September 2006.
In preparation for these meetings SHM had developed its comprehensive Core Competencies in Hospital Medicine that was published as a supplement to the first issue of the Journal of Hospital Medicine (JHM) in February 2006. This was a powerful, tangible set of circumstances for hospital medicine.
When people began questioning what made hospital medicine unique among internal medicine disciplines or what was the substance of hospital medicine, being able to hand them the Core Competencies and to walk them through this thoughtful document was very important. In the same way, establishing our own repository for medical advances in hospital medicine via JHM also supported the development of a new field in internal medicine.
It’s been helpful that other key trends have taken shape in the last few years. The Alliance for Academic Internal Medicine (AAIM), representing the Association of Professors of Medicine (APM) and the Association of Directors of Programs in Internal Medicine (APDIM) and others, worked closely with ACP and the rest of the specialties in internal medicine to redesign the internal medicine residency so that it reflects the current and future practice environment.
Further, throughout healthcare there has been an increasing call for performance standards and quality improvement—all in the context of using resources more efficiently. There has been a movement to reshape healthcare centered on the patient and delivered by teams of health professionals, as well as increasing calls to coordinate care across locales and providers so as to improve patient safety and provide the best care.
In addition, the growth of hospital medicine has accelerated in the last few years. The fact that data not only from SHM but also from the American Hospital Association (AHA) and others show that more than 15,000 hospitalists now practice at more than 2,000 hospitals illustrates that that the size and influence of hospitalists comprise an indisputable trend.
And for many hospitals the driver for developing hospital medicine groups is the need to have on-site health professionals who are committed to changes in quality, systems improvement, patient safety, and efficiency.
Whether you call this a tipping point à la Malcolm Gladwell (The Tipping Point, New York City: Little, Brown and Company; 2000) or a perfect storm, to its credit ABIM—with the support of ACP, AAIM, and others—saw an opportunity to develop meaningful changes to MOC as a means of identifying hospitalists and of motivating the self study and improvement in skills and knowledge so important to meet the demands of healthcare delivery in the 21st century.
Now the hard work begins. In October 2006 the ABIM Board of Directors approved appointment of an ABIM Committee on Hospital Medicine Focused Recognition (HMFR). This work group will make recommendations to the ABIM Board in 2007 regarding the requirements for evidence of proficiency in HMFR in the MOC process as well as recommending policy of how HMFR would relate to the rest of ABIM certification and MOC in internal medicine.
SHM and hospital medicine leaders intend to play a key role in helping ABIM shape the details of the HMFR process so that it’s meaningful to the hospitalists who choose to get HMFR during their MOC—as well as to those who employ hospitalists, the physicians and other health professionals that hospitalists work with, the hospitals we work in, and the patients we care for.
At the same time ABIM must approach the American Board of Medical Specialties (ABMS) because the ABMS will ultimately need to accept the HMFR process before ABIM can put this new process in place. This is a significant hurdle to clear, but the ABIM Board is committed to using its resources and powers of persuasion to make this happen.
Even with the hard work and political battles ahead, it is difficult not to sit back and marvel at how far we have come. Our specialty is just 10 years old, but we now have more than 15,000 practitioners and are on our way to 30,000 or even 40,000. We have our own journal, our own specialty society, our own set of competencies, our own growing national annual meeting, our own textbooks, and a growing number of publications aimed at hospitalists.
Now with the help of ABIM and the blessing of ABMS, there is a serious prospect that the first recognition of hospital medicine in the certification process will become a reality.
Will the first hospitalist claim Hospital Medicine Focused Recognition in 2008 or 2009? The exact date is too difficult to predict. That it will happen and that it will be meaningful is more certain now than it has ever been. To all those who have had the foresight and leadership to make this a reality, we thank you. Now let’s get down to the difficult work of creating a process that will help hospitalists provide the best care to their patients and help them to be leaders of change and improvement at their institutions. TH
Dr. Wellikson has been CEO of SHM since 2000.
Are You Satisfied?

“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
Here, There, Everywhere
Many primary care physicians welcome the introduction of hospital medicine for its potential to help normalize their schedules, reduce interruptions to their clinic work from hospitalized patients, and moderate after-hours on-call demands. Some have found hospital medicine itself such an attractive option for balancing their schedules between work and personal commitments that they have pursued it as a career.
Internist Doyle Detweiler, MD, started closing down his medical office practice in Newton, Kan., a small town 15 miles north of Wichita, in June of this year so he could become the first full-time hospitalist at 81-bed Newton Medical Center. Pulled between his office practice and the demands of visiting his patients at the hospital, Dr. Detweiler had seen his family life suffer, with limited quality time to spend with his daughters Lilly, 4, and Hannah, 18 months.
“The worst thing was that when I’d go to work, I’d kiss my little girls goodbye and they’d still be bed. When I’d come home and kiss them good night, they’d already be in bed,” he says. “My wife would never know even approximately when I’d be heading home. So it would be difficult for us to plan anything in the evenings.” He also spent a lot of time working on the weekends.
Dr. Detweiler still faces significant time demands in his new job—at least until a second hospitalist can be brought on board later this year. But the move has already produced dividends in terms of shorter and more predictable hours. Generally, he wraps up work shortly after 6 p.m., when the last post-operative case has been admitted, and he has been called back to the hospital only three times in two months for after-hours patient crises.
“One big advantage I can see—once we ultimately get the program rolling—is that I’ll know when I’ll be working and when I’m off and checked out,” he explains. “As a hospitalist, there still will be times when I’m really busy, but it will be easier to plan something like going out for dinner at 7 p.m.”
The Needs of Children—and Parents
The classic juggle of work and home life involves the care of young children, although that is only one of the competing personal demands on doctors’ time. As the proportion of women in medicine has grown, employers have been challenged to find ways to accommodate their staffs’ maternity leaves and child-care responsibilities, while working parents seek to accommodate their children’s swimming lessons, ball games, and ballet classes.
The generation that now dominates hospitalist ranks (average age 37, according to SHM’s “Biannual Survey of the Hospital Medicine Movement”) has little taste for the traditional image of the old-fashioned, male family doctor, essentially available to his patients 24/7. Lifestyle issues are important factors in their career choices.
Other working hospitalists want time to travel or to pursue outside interests. Their hours of work may be shorter and more predictable than for other physicians, but the pace can be intense, with life-and-death situations involving critically ill patients occurring every day. Many of today’s hospitalists also belong to the “sandwich generation,” juggling simultaneous caregiving responsibilities for children and aging parents.
Stacy Walton Goldsholl, MD, of Wilmington, N.C., president of the hospital medicine division of TeamHealth, and member of the SHM Board of Directors, faced an extreme version of these competing demands when starting her new managerial position on January 1, 2006. Pregnant with her second child, Richard, who was born in April, she was also caring for her 65-year-old father, who died of cancer in February.
“It was tough watching my dad, formerly a very robust person, truly the motivating force for my professional success, my moral compass, confidant, and advisor, as he got sicker,” says Dr. Goldsholl. “Some days I’d leave my two-year-old, Aiden, with my husband and go care for my dad, giving him his injection of Lovenox [enoxaparin] or replacing his PCA pump. My mom and I were his primary caregivers at home until we physically couldn’t handle it.”
At that point her father was admitted to a hospice inpatient facility, where she would sit by his bedside with a computer in her lap.
Dr. Goldsholl probably would have needed to take a leave of absence if she had been working as a hospitalist, but her new employers at TeamHealth gave her a lot of flexibility, limiting the number of strategic meetings she had to attend. In general, however, she believes hospitalist shift work is more accommodating to family demands than an administrative position. She returned from maternity leave full time on June 1 and now travels every week for her job; her mother, who lives nearby, fills in as her grandchildren’s nanny. But Dr. Goldsholl’s experience has sparked her interest in exploring sustainability issues for other hospitalists.
“TeamHealth’s leaders told me their turnover rate is about 5 percent for hospitalists, versus an industry average of 19 percent,” says Dr. Goldsholl. “I found that hard to believe, but when I interviewed some of our local medical directors, it turned out to be true. They were all extremely positive about their relationship with our operational infrastructure.
“There’s so much to do and so many opportunities out there, but it must be sustainable,” she continues. “In order to sustain a career, you must be fulfilled personally, which is directly related to your work/life balance.”
When she drilled down into the company’s data, trying to find out why TeamHealth is able to retain its doctors, she found that the hours they work average 7.3% less than the industry as a whole, while their compensation is comparable to others.1
For Daniel Dressler, MD, medical director of the Hospital Medicine Group at Emory Healthcare in Atlanta, Ga., hospital medicine can be a juggling act—as can his committee work for SHM—although he is able to conduct some business from home. “When we do the conference calls for SHM, half of the time I’m home taking care of our kids”—one-year-old twins—often with one of them in his lap.
Dr. Dressler and his wife had been building a new home and working closely with contractors and subcontractors when she discovered she was pregnant last year. The construction project experienced multiple delays. When interviewed in September, the Dresslers were living temporarily with his in-laws and hoping the house would be completed within another month. His wife, a physical therapist, was not working but was looking forward to returning to work.
Dr. Dressler estimates that he puts in a 60-hour workweek, including 30 hours of hospitalist shifts and the rest administrative, teaching, and education. “I don’t recommend building a new house and having kids at the same time,” he says. “Taking care of one-year-old twins is more difficult than anything I do at work. But we have a good time.”
He also tries to squeeze in a basketball game with the medical residents every weekend.
Dr. Dressler’s schedule demands reflect an additional wrinkle in terms of juggling work and family—especially in a relatively new field with huge growth opportunities and an emphasis on changing the healthcare system. Doctors must balance what is truly required to perform the job and satisfy their employers with what they do to satisfy their own standards and expectations, as well as take advantage of opportunities to advance their careers.
“There’s the balance of what’s reasonable for you at this point in your career. It’s a personal decision for everyone—[deciding] what is an adequate amount of time for each of the priorities in your life … what drives you, and what makes you happy in your life,” says Dr. Dressler. “The things that drive me include teaching and advancing the field, which means seizing opportunities to grow with this new and growing field, but hopefully not to the detriment of the rest of my life.”
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
A Family-Friendly Practice
Arpana Vidyarthi, MD, an academic hospitalist at the University of California-San Francisco (UCSF), has responsibilities for teaching residents and medical students and additional roles in hospital quality and safety. “It’s a somewhat different role than a shift hospitalist, with different stressors,” she says. “But there are many options out there, and one of the things that makes being a hospitalist attractive to me is the flexibility it offers.”
Dr. Vidyarthi’s husband also has a demanding job. She is able to do some of her own work at home with her two-year-old daughter, Anaiya, but estimates that her nanny puts in a 50-hour week. “I came to UCSF to do a hospitalist fellowship, and this is exactly what I want to do, with tremendous job satisfaction and a varied schedule. Yet I feel stretched all the time,” she says.
Dr. Vidyarthi credits her group practice at UCSF and its head, Robert Wachter, MD, for a supportive and family-friendly working environment. Colleague Adrienne Green, MD, agrees, adding that three of the group’s 24 physician members are pregnant at this time.
Dr. Green’s children are very interested in her work and have visited her at the hospital, which makes the work more real to them. “I’ll tell them about some of my patients who are really sick, and I’ll explain that the reason I’m going to work on the weekend is that I’m helping people get better and get out of the hospital,” says Dr. Green. “When I’m working on a Saturday and my son has a baseball game, I’ll tell him I’ll try to get to the game, but I can’t promise. But when we do have family time, we make it quality time.”
Dr. Wachter explains how he promotes a family-friendly work environment for hospitalists at UCSF: “My overarching management philosophy is that the quality of our program is equal to the quality of the people we’re able to recruit and retain. Thus, an environment that is professionally satisfying, collegiate, fun, and supportive of everyone’s personal and family goals is fundamental.”
Balancing life and work requires some give and take among the members of the group, who cover for each other when needed. It also takes a commitment to staffing in anticipation of predictable future needs for maternity leaves, sabbaticals and the like, rather than waiting for the actual need to arrive.
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
Making Good Career Choices
Lisa Kettering, MD, a member of SHM’s Board of Directors, has been a working hospitalist since 1998. Before that she worked in a traditional internal medicine practice. She also believes that hospital medicine offers more flexibility and opportunities for balance, with a full-time hospitalist position roughly comparable to the “part-time” private practice position she once held.
“In private practice, you’re always coming back to phone calls and piles of charts,” says Dr. Kettering. “As a hospitalist, you take care of your business in real time, instead of always playing catch up.”
A year ago, Dr. Kettering assumed medical direction of a practice of nine hospitalists and three intensivists at Exempla-St. Joseph Hospital in Denver, Colo., a position that includes significant clinical duties and requires about 80 hours of her time per week.
“If my children [three sons age 21, 19, and 16] were not almost grown, I could not have accepted this position,” she says. “But this job is my passion. For me, the key to family balance has been a supportive spouse and lots of child care and other supports.”
Dr. Kettering’s sons were born just before or during her medical school and residency, so her long hours have always been part of the equation. “What I gave up [for this career] were aspects of a social life, such as dinners out with our friends and an opportunity to work on my tennis game” and similar hobbies, she says. She has continued to run, a time-efficient form of exercise and stress management. Now that her children are leaving home, there is more time to indulge a love of yoga and Pilates and to resume a more normal social life—although she doesn’t do much cooking.
Don’t be shy about getting help, Dr. Kettering advises. She engages a personal assistant eight hours a week to help with errands such as making travel arrangements, picking up groceries, taking the car in for servicing, or wrapping the birthday presents she buys. “Not that I couldn’t squeeze in a few errands on the way home from work, but it would just be more demands on my time,” she explains.
“I believe I am an optimist, but my advice to young doctors is this: Don’t believe you can do it all,” says Dr. Kettering. “You need to make careful, considered decisions along the way, understanding you do have control over your choices. But there’s no question that you’ll have to give up many things if you choose medicine as a career.”
The biggest recommendation Dr. Kettering offers for future hospitalists is to make career choices based on a passion for the work—not on the flexible hours. Then consider how to make the job work in terms of schedules and the other nuts and bolts of practice, being aware of the varied opportunities that exist.
Although hospital medicine is sometimes described as a young person’s game, Dr. Kettering believes that if it is practiced correctly, with a sustainable work schedule, it doesn’t have to lead to burnout or exhaustion. “My practice is [composed] exclusively of doctors who have chosen hospital medicine as a life’s work—not a stopgap between residency and fellowship,” she says. “We also have a wonderful group of physicians, and there has not been a time when somebody had a family emergency that somebody else didn’t step up to cover.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Reference
- Compensation by Employment Model, Society of Hospital Medicine Benchmark Survey, 2003.
Many primary care physicians welcome the introduction of hospital medicine for its potential to help normalize their schedules, reduce interruptions to their clinic work from hospitalized patients, and moderate after-hours on-call demands. Some have found hospital medicine itself such an attractive option for balancing their schedules between work and personal commitments that they have pursued it as a career.
Internist Doyle Detweiler, MD, started closing down his medical office practice in Newton, Kan., a small town 15 miles north of Wichita, in June of this year so he could become the first full-time hospitalist at 81-bed Newton Medical Center. Pulled between his office practice and the demands of visiting his patients at the hospital, Dr. Detweiler had seen his family life suffer, with limited quality time to spend with his daughters Lilly, 4, and Hannah, 18 months.
“The worst thing was that when I’d go to work, I’d kiss my little girls goodbye and they’d still be bed. When I’d come home and kiss them good night, they’d already be in bed,” he says. “My wife would never know even approximately when I’d be heading home. So it would be difficult for us to plan anything in the evenings.” He also spent a lot of time working on the weekends.
Dr. Detweiler still faces significant time demands in his new job—at least until a second hospitalist can be brought on board later this year. But the move has already produced dividends in terms of shorter and more predictable hours. Generally, he wraps up work shortly after 6 p.m., when the last post-operative case has been admitted, and he has been called back to the hospital only three times in two months for after-hours patient crises.
“One big advantage I can see—once we ultimately get the program rolling—is that I’ll know when I’ll be working and when I’m off and checked out,” he explains. “As a hospitalist, there still will be times when I’m really busy, but it will be easier to plan something like going out for dinner at 7 p.m.”
The Needs of Children—and Parents
The classic juggle of work and home life involves the care of young children, although that is only one of the competing personal demands on doctors’ time. As the proportion of women in medicine has grown, employers have been challenged to find ways to accommodate their staffs’ maternity leaves and child-care responsibilities, while working parents seek to accommodate their children’s swimming lessons, ball games, and ballet classes.
The generation that now dominates hospitalist ranks (average age 37, according to SHM’s “Biannual Survey of the Hospital Medicine Movement”) has little taste for the traditional image of the old-fashioned, male family doctor, essentially available to his patients 24/7. Lifestyle issues are important factors in their career choices.
Other working hospitalists want time to travel or to pursue outside interests. Their hours of work may be shorter and more predictable than for other physicians, but the pace can be intense, with life-and-death situations involving critically ill patients occurring every day. Many of today’s hospitalists also belong to the “sandwich generation,” juggling simultaneous caregiving responsibilities for children and aging parents.
Stacy Walton Goldsholl, MD, of Wilmington, N.C., president of the hospital medicine division of TeamHealth, and member of the SHM Board of Directors, faced an extreme version of these competing demands when starting her new managerial position on January 1, 2006. Pregnant with her second child, Richard, who was born in April, she was also caring for her 65-year-old father, who died of cancer in February.
“It was tough watching my dad, formerly a very robust person, truly the motivating force for my professional success, my moral compass, confidant, and advisor, as he got sicker,” says Dr. Goldsholl. “Some days I’d leave my two-year-old, Aiden, with my husband and go care for my dad, giving him his injection of Lovenox [enoxaparin] or replacing his PCA pump. My mom and I were his primary caregivers at home until we physically couldn’t handle it.”
At that point her father was admitted to a hospice inpatient facility, where she would sit by his bedside with a computer in her lap.
Dr. Goldsholl probably would have needed to take a leave of absence if she had been working as a hospitalist, but her new employers at TeamHealth gave her a lot of flexibility, limiting the number of strategic meetings she had to attend. In general, however, she believes hospitalist shift work is more accommodating to family demands than an administrative position. She returned from maternity leave full time on June 1 and now travels every week for her job; her mother, who lives nearby, fills in as her grandchildren’s nanny. But Dr. Goldsholl’s experience has sparked her interest in exploring sustainability issues for other hospitalists.
“TeamHealth’s leaders told me their turnover rate is about 5 percent for hospitalists, versus an industry average of 19 percent,” says Dr. Goldsholl. “I found that hard to believe, but when I interviewed some of our local medical directors, it turned out to be true. They were all extremely positive about their relationship with our operational infrastructure.
“There’s so much to do and so many opportunities out there, but it must be sustainable,” she continues. “In order to sustain a career, you must be fulfilled personally, which is directly related to your work/life balance.”
When she drilled down into the company’s data, trying to find out why TeamHealth is able to retain its doctors, she found that the hours they work average 7.3% less than the industry as a whole, while their compensation is comparable to others.1
For Daniel Dressler, MD, medical director of the Hospital Medicine Group at Emory Healthcare in Atlanta, Ga., hospital medicine can be a juggling act—as can his committee work for SHM—although he is able to conduct some business from home. “When we do the conference calls for SHM, half of the time I’m home taking care of our kids”—one-year-old twins—often with one of them in his lap.
Dr. Dressler and his wife had been building a new home and working closely with contractors and subcontractors when she discovered she was pregnant last year. The construction project experienced multiple delays. When interviewed in September, the Dresslers were living temporarily with his in-laws and hoping the house would be completed within another month. His wife, a physical therapist, was not working but was looking forward to returning to work.
Dr. Dressler estimates that he puts in a 60-hour workweek, including 30 hours of hospitalist shifts and the rest administrative, teaching, and education. “I don’t recommend building a new house and having kids at the same time,” he says. “Taking care of one-year-old twins is more difficult than anything I do at work. But we have a good time.”
He also tries to squeeze in a basketball game with the medical residents every weekend.
Dr. Dressler’s schedule demands reflect an additional wrinkle in terms of juggling work and family—especially in a relatively new field with huge growth opportunities and an emphasis on changing the healthcare system. Doctors must balance what is truly required to perform the job and satisfy their employers with what they do to satisfy their own standards and expectations, as well as take advantage of opportunities to advance their careers.
“There’s the balance of what’s reasonable for you at this point in your career. It’s a personal decision for everyone—[deciding] what is an adequate amount of time for each of the priorities in your life … what drives you, and what makes you happy in your life,” says Dr. Dressler. “The things that drive me include teaching and advancing the field, which means seizing opportunities to grow with this new and growing field, but hopefully not to the detriment of the rest of my life.”
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
A Family-Friendly Practice
Arpana Vidyarthi, MD, an academic hospitalist at the University of California-San Francisco (UCSF), has responsibilities for teaching residents and medical students and additional roles in hospital quality and safety. “It’s a somewhat different role than a shift hospitalist, with different stressors,” she says. “But there are many options out there, and one of the things that makes being a hospitalist attractive to me is the flexibility it offers.”
Dr. Vidyarthi’s husband also has a demanding job. She is able to do some of her own work at home with her two-year-old daughter, Anaiya, but estimates that her nanny puts in a 50-hour week. “I came to UCSF to do a hospitalist fellowship, and this is exactly what I want to do, with tremendous job satisfaction and a varied schedule. Yet I feel stretched all the time,” she says.
Dr. Vidyarthi credits her group practice at UCSF and its head, Robert Wachter, MD, for a supportive and family-friendly working environment. Colleague Adrienne Green, MD, agrees, adding that three of the group’s 24 physician members are pregnant at this time.
Dr. Green’s children are very interested in her work and have visited her at the hospital, which makes the work more real to them. “I’ll tell them about some of my patients who are really sick, and I’ll explain that the reason I’m going to work on the weekend is that I’m helping people get better and get out of the hospital,” says Dr. Green. “When I’m working on a Saturday and my son has a baseball game, I’ll tell him I’ll try to get to the game, but I can’t promise. But when we do have family time, we make it quality time.”
Dr. Wachter explains how he promotes a family-friendly work environment for hospitalists at UCSF: “My overarching management philosophy is that the quality of our program is equal to the quality of the people we’re able to recruit and retain. Thus, an environment that is professionally satisfying, collegiate, fun, and supportive of everyone’s personal and family goals is fundamental.”
Balancing life and work requires some give and take among the members of the group, who cover for each other when needed. It also takes a commitment to staffing in anticipation of predictable future needs for maternity leaves, sabbaticals and the like, rather than waiting for the actual need to arrive.
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
Making Good Career Choices
Lisa Kettering, MD, a member of SHM’s Board of Directors, has been a working hospitalist since 1998. Before that she worked in a traditional internal medicine practice. She also believes that hospital medicine offers more flexibility and opportunities for balance, with a full-time hospitalist position roughly comparable to the “part-time” private practice position she once held.
“In private practice, you’re always coming back to phone calls and piles of charts,” says Dr. Kettering. “As a hospitalist, you take care of your business in real time, instead of always playing catch up.”
A year ago, Dr. Kettering assumed medical direction of a practice of nine hospitalists and three intensivists at Exempla-St. Joseph Hospital in Denver, Colo., a position that includes significant clinical duties and requires about 80 hours of her time per week.
“If my children [three sons age 21, 19, and 16] were not almost grown, I could not have accepted this position,” she says. “But this job is my passion. For me, the key to family balance has been a supportive spouse and lots of child care and other supports.”
Dr. Kettering’s sons were born just before or during her medical school and residency, so her long hours have always been part of the equation. “What I gave up [for this career] were aspects of a social life, such as dinners out with our friends and an opportunity to work on my tennis game” and similar hobbies, she says. She has continued to run, a time-efficient form of exercise and stress management. Now that her children are leaving home, there is more time to indulge a love of yoga and Pilates and to resume a more normal social life—although she doesn’t do much cooking.
Don’t be shy about getting help, Dr. Kettering advises. She engages a personal assistant eight hours a week to help with errands such as making travel arrangements, picking up groceries, taking the car in for servicing, or wrapping the birthday presents she buys. “Not that I couldn’t squeeze in a few errands on the way home from work, but it would just be more demands on my time,” she explains.
“I believe I am an optimist, but my advice to young doctors is this: Don’t believe you can do it all,” says Dr. Kettering. “You need to make careful, considered decisions along the way, understanding you do have control over your choices. But there’s no question that you’ll have to give up many things if you choose medicine as a career.”
The biggest recommendation Dr. Kettering offers for future hospitalists is to make career choices based on a passion for the work—not on the flexible hours. Then consider how to make the job work in terms of schedules and the other nuts and bolts of practice, being aware of the varied opportunities that exist.
Although hospital medicine is sometimes described as a young person’s game, Dr. Kettering believes that if it is practiced correctly, with a sustainable work schedule, it doesn’t have to lead to burnout or exhaustion. “My practice is [composed] exclusively of doctors who have chosen hospital medicine as a life’s work—not a stopgap between residency and fellowship,” she says. “We also have a wonderful group of physicians, and there has not been a time when somebody had a family emergency that somebody else didn’t step up to cover.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Reference
- Compensation by Employment Model, Society of Hospital Medicine Benchmark Survey, 2003.
Many primary care physicians welcome the introduction of hospital medicine for its potential to help normalize their schedules, reduce interruptions to their clinic work from hospitalized patients, and moderate after-hours on-call demands. Some have found hospital medicine itself such an attractive option for balancing their schedules between work and personal commitments that they have pursued it as a career.
Internist Doyle Detweiler, MD, started closing down his medical office practice in Newton, Kan., a small town 15 miles north of Wichita, in June of this year so he could become the first full-time hospitalist at 81-bed Newton Medical Center. Pulled between his office practice and the demands of visiting his patients at the hospital, Dr. Detweiler had seen his family life suffer, with limited quality time to spend with his daughters Lilly, 4, and Hannah, 18 months.
“The worst thing was that when I’d go to work, I’d kiss my little girls goodbye and they’d still be bed. When I’d come home and kiss them good night, they’d already be in bed,” he says. “My wife would never know even approximately when I’d be heading home. So it would be difficult for us to plan anything in the evenings.” He also spent a lot of time working on the weekends.
Dr. Detweiler still faces significant time demands in his new job—at least until a second hospitalist can be brought on board later this year. But the move has already produced dividends in terms of shorter and more predictable hours. Generally, he wraps up work shortly after 6 p.m., when the last post-operative case has been admitted, and he has been called back to the hospital only three times in two months for after-hours patient crises.
“One big advantage I can see—once we ultimately get the program rolling—is that I’ll know when I’ll be working and when I’m off and checked out,” he explains. “As a hospitalist, there still will be times when I’m really busy, but it will be easier to plan something like going out for dinner at 7 p.m.”
The Needs of Children—and Parents
The classic juggle of work and home life involves the care of young children, although that is only one of the competing personal demands on doctors’ time. As the proportion of women in medicine has grown, employers have been challenged to find ways to accommodate their staffs’ maternity leaves and child-care responsibilities, while working parents seek to accommodate their children’s swimming lessons, ball games, and ballet classes.
The generation that now dominates hospitalist ranks (average age 37, according to SHM’s “Biannual Survey of the Hospital Medicine Movement”) has little taste for the traditional image of the old-fashioned, male family doctor, essentially available to his patients 24/7. Lifestyle issues are important factors in their career choices.
Other working hospitalists want time to travel or to pursue outside interests. Their hours of work may be shorter and more predictable than for other physicians, but the pace can be intense, with life-and-death situations involving critically ill patients occurring every day. Many of today’s hospitalists also belong to the “sandwich generation,” juggling simultaneous caregiving responsibilities for children and aging parents.
Stacy Walton Goldsholl, MD, of Wilmington, N.C., president of the hospital medicine division of TeamHealth, and member of the SHM Board of Directors, faced an extreme version of these competing demands when starting her new managerial position on January 1, 2006. Pregnant with her second child, Richard, who was born in April, she was also caring for her 65-year-old father, who died of cancer in February.
“It was tough watching my dad, formerly a very robust person, truly the motivating force for my professional success, my moral compass, confidant, and advisor, as he got sicker,” says Dr. Goldsholl. “Some days I’d leave my two-year-old, Aiden, with my husband and go care for my dad, giving him his injection of Lovenox [enoxaparin] or replacing his PCA pump. My mom and I were his primary caregivers at home until we physically couldn’t handle it.”
At that point her father was admitted to a hospice inpatient facility, where she would sit by his bedside with a computer in her lap.
Dr. Goldsholl probably would have needed to take a leave of absence if she had been working as a hospitalist, but her new employers at TeamHealth gave her a lot of flexibility, limiting the number of strategic meetings she had to attend. In general, however, she believes hospitalist shift work is more accommodating to family demands than an administrative position. She returned from maternity leave full time on June 1 and now travels every week for her job; her mother, who lives nearby, fills in as her grandchildren’s nanny. But Dr. Goldsholl’s experience has sparked her interest in exploring sustainability issues for other hospitalists.
“TeamHealth’s leaders told me their turnover rate is about 5 percent for hospitalists, versus an industry average of 19 percent,” says Dr. Goldsholl. “I found that hard to believe, but when I interviewed some of our local medical directors, it turned out to be true. They were all extremely positive about their relationship with our operational infrastructure.
“There’s so much to do and so many opportunities out there, but it must be sustainable,” she continues. “In order to sustain a career, you must be fulfilled personally, which is directly related to your work/life balance.”
When she drilled down into the company’s data, trying to find out why TeamHealth is able to retain its doctors, she found that the hours they work average 7.3% less than the industry as a whole, while their compensation is comparable to others.1
For Daniel Dressler, MD, medical director of the Hospital Medicine Group at Emory Healthcare in Atlanta, Ga., hospital medicine can be a juggling act—as can his committee work for SHM—although he is able to conduct some business from home. “When we do the conference calls for SHM, half of the time I’m home taking care of our kids”—one-year-old twins—often with one of them in his lap.
Dr. Dressler and his wife had been building a new home and working closely with contractors and subcontractors when she discovered she was pregnant last year. The construction project experienced multiple delays. When interviewed in September, the Dresslers were living temporarily with his in-laws and hoping the house would be completed within another month. His wife, a physical therapist, was not working but was looking forward to returning to work.
Dr. Dressler estimates that he puts in a 60-hour workweek, including 30 hours of hospitalist shifts and the rest administrative, teaching, and education. “I don’t recommend building a new house and having kids at the same time,” he says. “Taking care of one-year-old twins is more difficult than anything I do at work. But we have a good time.”
He also tries to squeeze in a basketball game with the medical residents every weekend.
Dr. Dressler’s schedule demands reflect an additional wrinkle in terms of juggling work and family—especially in a relatively new field with huge growth opportunities and an emphasis on changing the healthcare system. Doctors must balance what is truly required to perform the job and satisfy their employers with what they do to satisfy their own standards and expectations, as well as take advantage of opportunities to advance their careers.
“There’s the balance of what’s reasonable for you at this point in your career. It’s a personal decision for everyone—[deciding] what is an adequate amount of time for each of the priorities in your life … what drives you, and what makes you happy in your life,” says Dr. Dressler. “The things that drive me include teaching and advancing the field, which means seizing opportunities to grow with this new and growing field, but hopefully not to the detriment of the rest of my life.”
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
A Family-Friendly Practice
Arpana Vidyarthi, MD, an academic hospitalist at the University of California-San Francisco (UCSF), has responsibilities for teaching residents and medical students and additional roles in hospital quality and safety. “It’s a somewhat different role than a shift hospitalist, with different stressors,” she says. “But there are many options out there, and one of the things that makes being a hospitalist attractive to me is the flexibility it offers.”
Dr. Vidyarthi’s husband also has a demanding job. She is able to do some of her own work at home with her two-year-old daughter, Anaiya, but estimates that her nanny puts in a 50-hour week. “I came to UCSF to do a hospitalist fellowship, and this is exactly what I want to do, with tremendous job satisfaction and a varied schedule. Yet I feel stretched all the time,” she says.
Dr. Vidyarthi credits her group practice at UCSF and its head, Robert Wachter, MD, for a supportive and family-friendly working environment. Colleague Adrienne Green, MD, agrees, adding that three of the group’s 24 physician members are pregnant at this time.
Dr. Green’s children are very interested in her work and have visited her at the hospital, which makes the work more real to them. “I’ll tell them about some of my patients who are really sick, and I’ll explain that the reason I’m going to work on the weekend is that I’m helping people get better and get out of the hospital,” says Dr. Green. “When I’m working on a Saturday and my son has a baseball game, I’ll tell him I’ll try to get to the game, but I can’t promise. But when we do have family time, we make it quality time.”
Dr. Wachter explains how he promotes a family-friendly work environment for hospitalists at UCSF: “My overarching management philosophy is that the quality of our program is equal to the quality of the people we’re able to recruit and retain. Thus, an environment that is professionally satisfying, collegiate, fun, and supportive of everyone’s personal and family goals is fundamental.”
Balancing life and work requires some give and take among the members of the group, who cover for each other when needed. It also takes a commitment to staffing in anticipation of predictable future needs for maternity leaves, sabbaticals and the like, rather than waiting for the actual need to arrive.
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
Making Good Career Choices
Lisa Kettering, MD, a member of SHM’s Board of Directors, has been a working hospitalist since 1998. Before that she worked in a traditional internal medicine practice. She also believes that hospital medicine offers more flexibility and opportunities for balance, with a full-time hospitalist position roughly comparable to the “part-time” private practice position she once held.
“In private practice, you’re always coming back to phone calls and piles of charts,” says Dr. Kettering. “As a hospitalist, you take care of your business in real time, instead of always playing catch up.”
A year ago, Dr. Kettering assumed medical direction of a practice of nine hospitalists and three intensivists at Exempla-St. Joseph Hospital in Denver, Colo., a position that includes significant clinical duties and requires about 80 hours of her time per week.
“If my children [three sons age 21, 19, and 16] were not almost grown, I could not have accepted this position,” she says. “But this job is my passion. For me, the key to family balance has been a supportive spouse and lots of child care and other supports.”
Dr. Kettering’s sons were born just before or during her medical school and residency, so her long hours have always been part of the equation. “What I gave up [for this career] were aspects of a social life, such as dinners out with our friends and an opportunity to work on my tennis game” and similar hobbies, she says. She has continued to run, a time-efficient form of exercise and stress management. Now that her children are leaving home, there is more time to indulge a love of yoga and Pilates and to resume a more normal social life—although she doesn’t do much cooking.
Don’t be shy about getting help, Dr. Kettering advises. She engages a personal assistant eight hours a week to help with errands such as making travel arrangements, picking up groceries, taking the car in for servicing, or wrapping the birthday presents she buys. “Not that I couldn’t squeeze in a few errands on the way home from work, but it would just be more demands on my time,” she explains.
“I believe I am an optimist, but my advice to young doctors is this: Don’t believe you can do it all,” says Dr. Kettering. “You need to make careful, considered decisions along the way, understanding you do have control over your choices. But there’s no question that you’ll have to give up many things if you choose medicine as a career.”
The biggest recommendation Dr. Kettering offers for future hospitalists is to make career choices based on a passion for the work—not on the flexible hours. Then consider how to make the job work in terms of schedules and the other nuts and bolts of practice, being aware of the varied opportunities that exist.
Although hospital medicine is sometimes described as a young person’s game, Dr. Kettering believes that if it is practiced correctly, with a sustainable work schedule, it doesn’t have to lead to burnout or exhaustion. “My practice is [composed] exclusively of doctors who have chosen hospital medicine as a life’s work—not a stopgap between residency and fellowship,” she says. “We also have a wonderful group of physicians, and there has not been a time when somebody had a family emergency that somebody else didn’t step up to cover.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Reference
- Compensation by Employment Model, Society of Hospital Medicine Benchmark Survey, 2003.