User login
Five personal finance questions for the young GI
While this article will get you started, these are complex topics, and each could warrant several standalone articles. I strongly encourage you to develop some basic understanding of personal finance through books, websites, and podcasts. If you can manage Barrett’s esophagus, Crohn’s, and cirrhosis, you can understand the basics of personal finance.
1. What should I do about my student loans? Go for public service loan forgiveness or pay them off?
The first step is knowing your debt burden, knowing your options, and developing a plan to pay off student loans. Public service loan forgiveness (PSLF) can be a good option in many situations. For borrowers staying in academic or other 501(c)(3) positions, PSLF is often an obvious move. Importantly, a fall 2022 statement by the U.S. Department of Education clarified that physicians working as contractors for nonprofit hospitals in California and Texas may now qualify for PSLF.1,2
For trainees debating an academic/501(c)(3) position vs. private practice, I would generally not advise making a career choice based purely on PSLF eligibility. However, borrowers with very high federal student loan burdens (e.g., debt to income ratio of > 2:1), or who are very close to the PSLF 10-year requirement may want to consider choosing a qualifying position for a few years to receive PSLF student loan forgiveness. Please see TNG’s 2020 article3 for a deeper discussion. Consultation with a company specializing in student loan advice for physicians may be well worth the upfront cost.
2. Do I need disability insurance? What should I look for?
I would strongly advise getting disability insurance as soon as possible (including while in training). While disability insurance is not cheap, it is one of the first steps you should take and one of the most important ways to protect your financial future. It is essential to look for a specialty-specific own occupation policy. Such a policy will provide disability payments if you are no longer able to work as a gastroenterologist/hepatologist (including an injury which prevents you from doing endoscopies).
There are two major types of disability policies: group policies and individual policies. See table 1 for a detailed comparison.
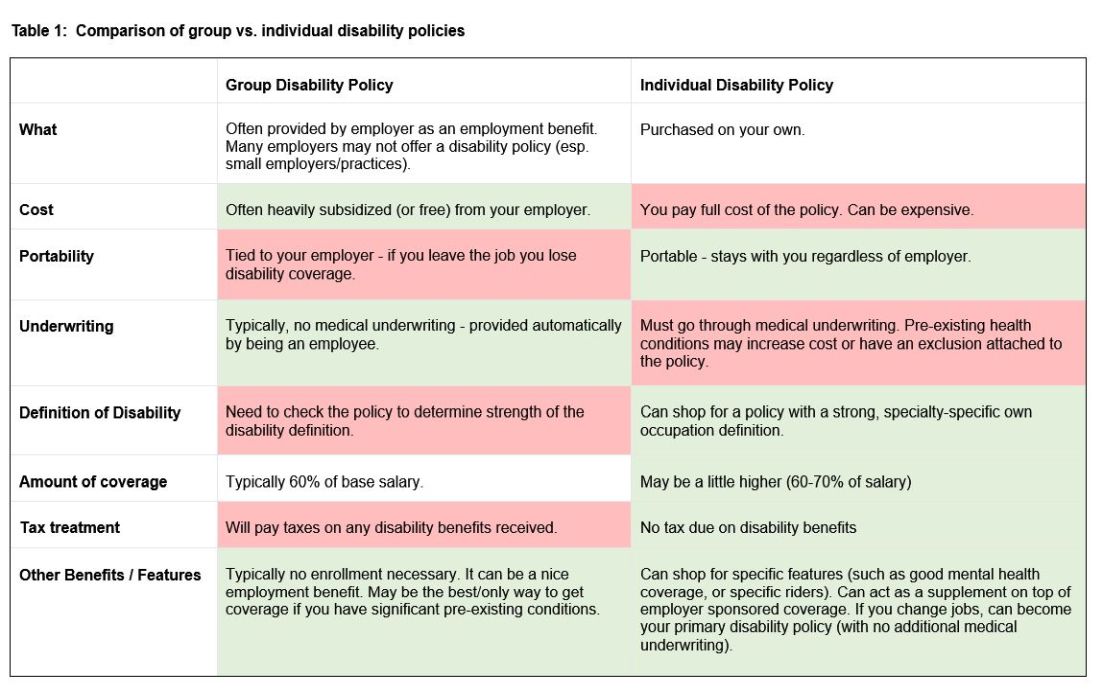
Your hospital/employer may provide a group policy at a heavily subsidized rate. Alternatively, you can purchase an individual disability policy, which is independent of your employer and will stay with you even if you change jobs. Currently, the only companies providing high quality own-occupation policies for physicians are Mass Mutual, Principal, Guardian, The Standard, and Ameritas. Because disability insurance is complicated, it is highly advisable to work with an agent experienced in physician disability policies.
Importantly, even if you have a group disability policy, you can purchase an individual policy as a supplement to provide extra coverage. If you leave employers, the individual policy can then become your primary disability policy without any additional medical underwriting.
3. Do I need life insurance? What type should I get?
If anyone is dependent on your income (partner, child, etc.), you should have life insurance. Moreover, if you expect to have dependents in the near future (e.g., children), you could consider getting life insurance now while you are younger and healthier. For a young GI with multiple financial obligations, term life insurance is generally the right product. Term life insurance is a straightforward, affordable product that can be purchased from multiple high-quality insurance carriers. There are two major considerations: The amount of coverage ($2 million, $3 million, etc.) and the length of coverage (20 years, 30 years, etc.). To estimate the appropriate amount of coverage, start with your expected annual household living expenses, and multiply by 25-30. While this is a rule of thumb, it will get you in the ballpark. For many young physicians, a $2-$5 million policy with 20- to 30-year coverage is reasonable.
Many financial advisers may suggest whole life insurance policies. These are typically not the ideal policy for young GIs who are just starting their careers. While whole life insurance may be the right choice in select cases, term life insurance will be the best product for most of TNG’s audience. As an example, a $3 million, 25-year term policy for a healthy, nonsmoking 35-year-old male would cost approximately $175 per month. A similar $3 million whole life policy could cost $2,000 per month or more.
4. What do I need to know about retirement accounts and investing?
The alphabet soup of retirement accounts can be confusing – IRA, 401k, 457. Retirement accounts provide a tax break to incentivize saving for retirement. Traditional (“non-Roth”) accounts provide a tax break today, but you will pay taxes when withdrawing the money in retirement. Roth accounts provide no tax break now but provide tax-free growth for decades, and no taxes are due when withdrawing money. See table 2 for a detailed comparison of retirement accounts.
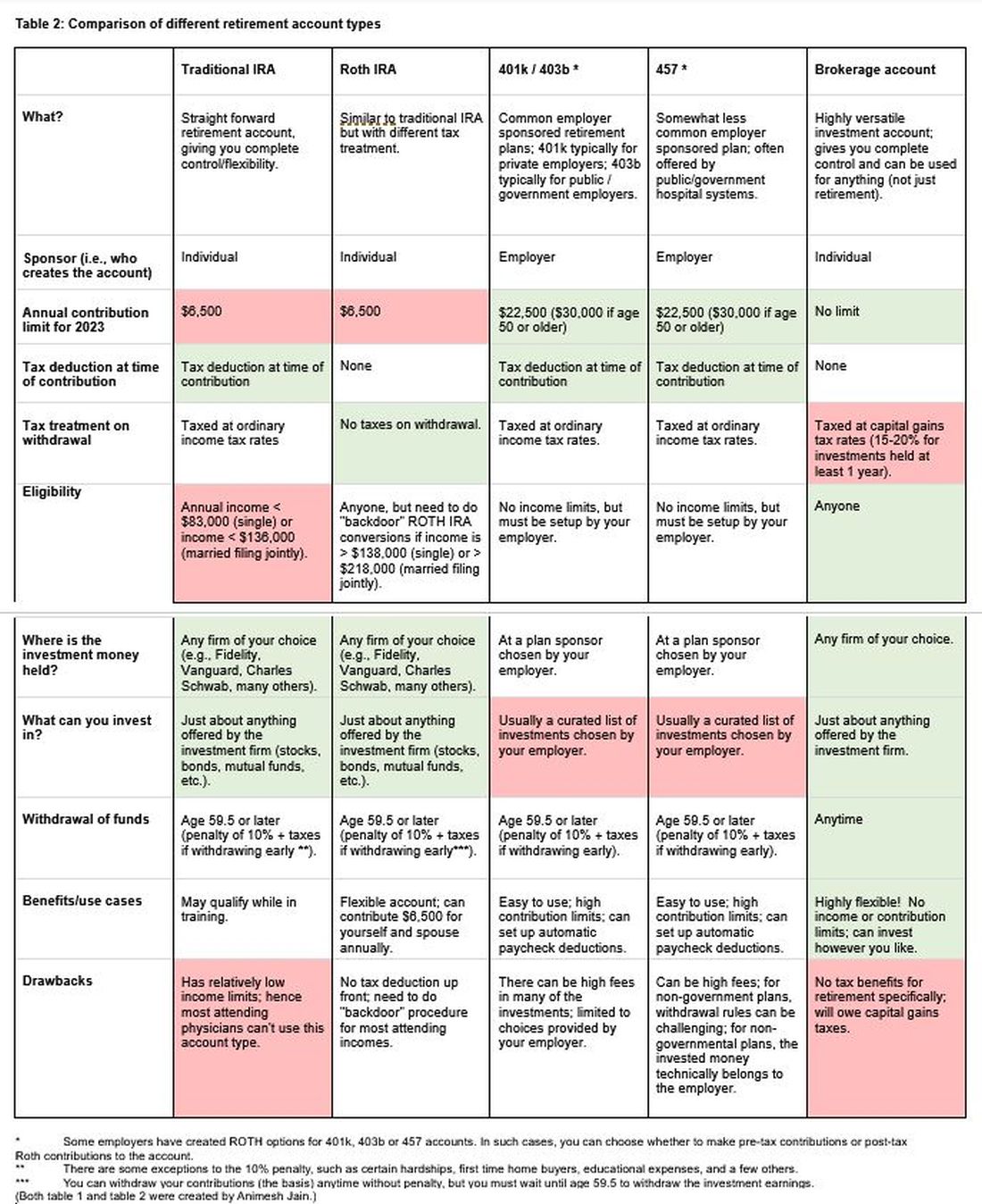
Once you place money into a retirement account, you will need to choose specific investments to grow your money. The two most common asset classes are stocks and bonds, though there are many other reasonable assets, such as real estate, commodities, and alternative currencies. It is generally recommended to have a higher proportion of stock-based investments early on (60%-90%) and then increase the ratio of bonds closer to retirement. Using low cost, passive index funds (or exchange traded funds) is a good way to get stock exposure. Target date retirement funds can be a nice tool for beginning investors since they will automatically adjust the stock/bond ratio for you.
Calculating the amount needed for retirement is beyond the scope of this article. However, saving at least 20% of your gross income specifically for retirement is a good starting point and should set you up for a reasonable retirement in about 30 years. For the average GI physician, this would mean saving $4,000 or more per month for retirement. If you aim to retire earlier, consider investing a higher percentage.
5. What do I need to know about buying a house?
The first question to ask is whether it makes sense to rent or buy a house. This is a personal and lifestyle decision, not just a financial decision. Today’s market is difficult with both high home prices and high rent costs. If there is a reasonable chance that you will be moving within 3-5 years, I would consider not buying until your long-term plans are more stable. Moreover, a high proportion of physicians change jobs.4,5,6 If you are just starting a new job, it is often wise to wait at least 6-12 months before buying a house to ensure the new job is a good fit. If you are in a stable long-term situation, it may be reasonable to buy a house. While it is commonly believed that buying a house is a “good financial move,” there are many hidden costs to home ownership, including big ticket repairs, property taxes, and real estate fees when selling a home.
First-time physician home buyers can often secure a physician mortgage with competitive interest rates and a low down payment of 0%-10% instead of the traditional 20% down payment. Moreover, a good physician mortgage should not have private mortgage insurance (PMI). Given the variation between mortgage companies, my most important piece of advice is to shop around for a good mortgage. An independent mortgage broker can be very valuable.
Dr. Jain is associate professor of medicine in the division of gastroenterology and hepatology, University of North Carolina School of Medicine, Chapel Hill. He has no conflicts of interest. The information in this article is meant for general educational purposes only. For individualized personal finance advice, please seek your own financial advisor, tax accountant, insurance broker, attorney, or other financial professional. Follow Dr. Jain @AJainMD on X.
References
1. Future of PSLF Fact Sheet
2. The Loophole That Can Get Thousands of Doctors into PSLF
3. Student loan management: An introduction for the young gastroenterologist
4. Study Shows First Job after Medical Residency Often Doesn’t Last
5. More physicians want to leave their jobs as pay rates fall, survey finds
6. Physician turnover rates are climbing as they clamor for better work-life balance
While this article will get you started, these are complex topics, and each could warrant several standalone articles. I strongly encourage you to develop some basic understanding of personal finance through books, websites, and podcasts. If you can manage Barrett’s esophagus, Crohn’s, and cirrhosis, you can understand the basics of personal finance.
1. What should I do about my student loans? Go for public service loan forgiveness or pay them off?
The first step is knowing your debt burden, knowing your options, and developing a plan to pay off student loans. Public service loan forgiveness (PSLF) can be a good option in many situations. For borrowers staying in academic or other 501(c)(3) positions, PSLF is often an obvious move. Importantly, a fall 2022 statement by the U.S. Department of Education clarified that physicians working as contractors for nonprofit hospitals in California and Texas may now qualify for PSLF.1,2
For trainees debating an academic/501(c)(3) position vs. private practice, I would generally not advise making a career choice based purely on PSLF eligibility. However, borrowers with very high federal student loan burdens (e.g., debt to income ratio of > 2:1), or who are very close to the PSLF 10-year requirement may want to consider choosing a qualifying position for a few years to receive PSLF student loan forgiveness. Please see TNG’s 2020 article3 for a deeper discussion. Consultation with a company specializing in student loan advice for physicians may be well worth the upfront cost.
2. Do I need disability insurance? What should I look for?
I would strongly advise getting disability insurance as soon as possible (including while in training). While disability insurance is not cheap, it is one of the first steps you should take and one of the most important ways to protect your financial future. It is essential to look for a specialty-specific own occupation policy. Such a policy will provide disability payments if you are no longer able to work as a gastroenterologist/hepatologist (including an injury which prevents you from doing endoscopies).
There are two major types of disability policies: group policies and individual policies. See table 1 for a detailed comparison.
Your hospital/employer may provide a group policy at a heavily subsidized rate. Alternatively, you can purchase an individual disability policy, which is independent of your employer and will stay with you even if you change jobs. Currently, the only companies providing high quality own-occupation policies for physicians are Mass Mutual, Principal, Guardian, The Standard, and Ameritas. Because disability insurance is complicated, it is highly advisable to work with an agent experienced in physician disability policies.
Importantly, even if you have a group disability policy, you can purchase an individual policy as a supplement to provide extra coverage. If you leave employers, the individual policy can then become your primary disability policy without any additional medical underwriting.
3. Do I need life insurance? What type should I get?
If anyone is dependent on your income (partner, child, etc.), you should have life insurance. Moreover, if you expect to have dependents in the near future (e.g., children), you could consider getting life insurance now while you are younger and healthier. For a young GI with multiple financial obligations, term life insurance is generally the right product. Term life insurance is a straightforward, affordable product that can be purchased from multiple high-quality insurance carriers. There are two major considerations: The amount of coverage ($2 million, $3 million, etc.) and the length of coverage (20 years, 30 years, etc.). To estimate the appropriate amount of coverage, start with your expected annual household living expenses, and multiply by 25-30. While this is a rule of thumb, it will get you in the ballpark. For many young physicians, a $2-$5 million policy with 20- to 30-year coverage is reasonable.
Many financial advisers may suggest whole life insurance policies. These are typically not the ideal policy for young GIs who are just starting their careers. While whole life insurance may be the right choice in select cases, term life insurance will be the best product for most of TNG’s audience. As an example, a $3 million, 25-year term policy for a healthy, nonsmoking 35-year-old male would cost approximately $175 per month. A similar $3 million whole life policy could cost $2,000 per month or more.
4. What do I need to know about retirement accounts and investing?
The alphabet soup of retirement accounts can be confusing – IRA, 401k, 457. Retirement accounts provide a tax break to incentivize saving for retirement. Traditional (“non-Roth”) accounts provide a tax break today, but you will pay taxes when withdrawing the money in retirement. Roth accounts provide no tax break now but provide tax-free growth for decades, and no taxes are due when withdrawing money. See table 2 for a detailed comparison of retirement accounts.
Once you place money into a retirement account, you will need to choose specific investments to grow your money. The two most common asset classes are stocks and bonds, though there are many other reasonable assets, such as real estate, commodities, and alternative currencies. It is generally recommended to have a higher proportion of stock-based investments early on (60%-90%) and then increase the ratio of bonds closer to retirement. Using low cost, passive index funds (or exchange traded funds) is a good way to get stock exposure. Target date retirement funds can be a nice tool for beginning investors since they will automatically adjust the stock/bond ratio for you.
Calculating the amount needed for retirement is beyond the scope of this article. However, saving at least 20% of your gross income specifically for retirement is a good starting point and should set you up for a reasonable retirement in about 30 years. For the average GI physician, this would mean saving $4,000 or more per month for retirement. If you aim to retire earlier, consider investing a higher percentage.
5. What do I need to know about buying a house?
The first question to ask is whether it makes sense to rent or buy a house. This is a personal and lifestyle decision, not just a financial decision. Today’s market is difficult with both high home prices and high rent costs. If there is a reasonable chance that you will be moving within 3-5 years, I would consider not buying until your long-term plans are more stable. Moreover, a high proportion of physicians change jobs.4,5,6 If you are just starting a new job, it is often wise to wait at least 6-12 months before buying a house to ensure the new job is a good fit. If you are in a stable long-term situation, it may be reasonable to buy a house. While it is commonly believed that buying a house is a “good financial move,” there are many hidden costs to home ownership, including big ticket repairs, property taxes, and real estate fees when selling a home.
First-time physician home buyers can often secure a physician mortgage with competitive interest rates and a low down payment of 0%-10% instead of the traditional 20% down payment. Moreover, a good physician mortgage should not have private mortgage insurance (PMI). Given the variation between mortgage companies, my most important piece of advice is to shop around for a good mortgage. An independent mortgage broker can be very valuable.
Dr. Jain is associate professor of medicine in the division of gastroenterology and hepatology, University of North Carolina School of Medicine, Chapel Hill. He has no conflicts of interest. The information in this article is meant for general educational purposes only. For individualized personal finance advice, please seek your own financial advisor, tax accountant, insurance broker, attorney, or other financial professional. Follow Dr. Jain @AJainMD on X.
References
1. Future of PSLF Fact Sheet
2. The Loophole That Can Get Thousands of Doctors into PSLF
3. Student loan management: An introduction for the young gastroenterologist
4. Study Shows First Job after Medical Residency Often Doesn’t Last
5. More physicians want to leave their jobs as pay rates fall, survey finds
6. Physician turnover rates are climbing as they clamor for better work-life balance
While this article will get you started, these are complex topics, and each could warrant several standalone articles. I strongly encourage you to develop some basic understanding of personal finance through books, websites, and podcasts. If you can manage Barrett’s esophagus, Crohn’s, and cirrhosis, you can understand the basics of personal finance.
1. What should I do about my student loans? Go for public service loan forgiveness or pay them off?
The first step is knowing your debt burden, knowing your options, and developing a plan to pay off student loans. Public service loan forgiveness (PSLF) can be a good option in many situations. For borrowers staying in academic or other 501(c)(3) positions, PSLF is often an obvious move. Importantly, a fall 2022 statement by the U.S. Department of Education clarified that physicians working as contractors for nonprofit hospitals in California and Texas may now qualify for PSLF.1,2
For trainees debating an academic/501(c)(3) position vs. private practice, I would generally not advise making a career choice based purely on PSLF eligibility. However, borrowers with very high federal student loan burdens (e.g., debt to income ratio of > 2:1), or who are very close to the PSLF 10-year requirement may want to consider choosing a qualifying position for a few years to receive PSLF student loan forgiveness. Please see TNG’s 2020 article3 for a deeper discussion. Consultation with a company specializing in student loan advice for physicians may be well worth the upfront cost.
2. Do I need disability insurance? What should I look for?
I would strongly advise getting disability insurance as soon as possible (including while in training). While disability insurance is not cheap, it is one of the first steps you should take and one of the most important ways to protect your financial future. It is essential to look for a specialty-specific own occupation policy. Such a policy will provide disability payments if you are no longer able to work as a gastroenterologist/hepatologist (including an injury which prevents you from doing endoscopies).
There are two major types of disability policies: group policies and individual policies. See table 1 for a detailed comparison.
Your hospital/employer may provide a group policy at a heavily subsidized rate. Alternatively, you can purchase an individual disability policy, which is independent of your employer and will stay with you even if you change jobs. Currently, the only companies providing high quality own-occupation policies for physicians are Mass Mutual, Principal, Guardian, The Standard, and Ameritas. Because disability insurance is complicated, it is highly advisable to work with an agent experienced in physician disability policies.
Importantly, even if you have a group disability policy, you can purchase an individual policy as a supplement to provide extra coverage. If you leave employers, the individual policy can then become your primary disability policy without any additional medical underwriting.
3. Do I need life insurance? What type should I get?
If anyone is dependent on your income (partner, child, etc.), you should have life insurance. Moreover, if you expect to have dependents in the near future (e.g., children), you could consider getting life insurance now while you are younger and healthier. For a young GI with multiple financial obligations, term life insurance is generally the right product. Term life insurance is a straightforward, affordable product that can be purchased from multiple high-quality insurance carriers. There are two major considerations: The amount of coverage ($2 million, $3 million, etc.) and the length of coverage (20 years, 30 years, etc.). To estimate the appropriate amount of coverage, start with your expected annual household living expenses, and multiply by 25-30. While this is a rule of thumb, it will get you in the ballpark. For many young physicians, a $2-$5 million policy with 20- to 30-year coverage is reasonable.
Many financial advisers may suggest whole life insurance policies. These are typically not the ideal policy for young GIs who are just starting their careers. While whole life insurance may be the right choice in select cases, term life insurance will be the best product for most of TNG’s audience. As an example, a $3 million, 25-year term policy for a healthy, nonsmoking 35-year-old male would cost approximately $175 per month. A similar $3 million whole life policy could cost $2,000 per month or more.
4. What do I need to know about retirement accounts and investing?
The alphabet soup of retirement accounts can be confusing – IRA, 401k, 457. Retirement accounts provide a tax break to incentivize saving for retirement. Traditional (“non-Roth”) accounts provide a tax break today, but you will pay taxes when withdrawing the money in retirement. Roth accounts provide no tax break now but provide tax-free growth for decades, and no taxes are due when withdrawing money. See table 2 for a detailed comparison of retirement accounts.
Once you place money into a retirement account, you will need to choose specific investments to grow your money. The two most common asset classes are stocks and bonds, though there are many other reasonable assets, such as real estate, commodities, and alternative currencies. It is generally recommended to have a higher proportion of stock-based investments early on (60%-90%) and then increase the ratio of bonds closer to retirement. Using low cost, passive index funds (or exchange traded funds) is a good way to get stock exposure. Target date retirement funds can be a nice tool for beginning investors since they will automatically adjust the stock/bond ratio for you.
Calculating the amount needed for retirement is beyond the scope of this article. However, saving at least 20% of your gross income specifically for retirement is a good starting point and should set you up for a reasonable retirement in about 30 years. For the average GI physician, this would mean saving $4,000 or more per month for retirement. If you aim to retire earlier, consider investing a higher percentage.
5. What do I need to know about buying a house?
The first question to ask is whether it makes sense to rent or buy a house. This is a personal and lifestyle decision, not just a financial decision. Today’s market is difficult with both high home prices and high rent costs. If there is a reasonable chance that you will be moving within 3-5 years, I would consider not buying until your long-term plans are more stable. Moreover, a high proportion of physicians change jobs.4,5,6 If you are just starting a new job, it is often wise to wait at least 6-12 months before buying a house to ensure the new job is a good fit. If you are in a stable long-term situation, it may be reasonable to buy a house. While it is commonly believed that buying a house is a “good financial move,” there are many hidden costs to home ownership, including big ticket repairs, property taxes, and real estate fees when selling a home.
First-time physician home buyers can often secure a physician mortgage with competitive interest rates and a low down payment of 0%-10% instead of the traditional 20% down payment. Moreover, a good physician mortgage should not have private mortgage insurance (PMI). Given the variation between mortgage companies, my most important piece of advice is to shop around for a good mortgage. An independent mortgage broker can be very valuable.
Dr. Jain is associate professor of medicine in the division of gastroenterology and hepatology, University of North Carolina School of Medicine, Chapel Hill. He has no conflicts of interest. The information in this article is meant for general educational purposes only. For individualized personal finance advice, please seek your own financial advisor, tax accountant, insurance broker, attorney, or other financial professional. Follow Dr. Jain @AJainMD on X.
References
1. Future of PSLF Fact Sheet
2. The Loophole That Can Get Thousands of Doctors into PSLF
3. Student loan management: An introduction for the young gastroenterologist
4. Study Shows First Job after Medical Residency Often Doesn’t Last
5. More physicians want to leave their jobs as pay rates fall, survey finds
6. Physician turnover rates are climbing as they clamor for better work-life balance

Stripped privileges: An alarming precedent for community oncologists?
, Alliance Cancer Specialists.
The outcome, some community oncologists say, could set a new precedent in how far large health care organizations will go to take their patients or drive them out of business.
The case
On Sept. 5, Alliance sued Jefferson Health after Jefferson canceled the inpatient oncology/hematology privileges of five Alliance oncologists at three Jefferson Health-Northeast hospitals, primarily alleging that Jefferson was attempting to monopolize cancer care in the area.
Jefferson – one of the largest health care systems in the Philadelphia area that includes the NCI-designated Sidney Kimmel Cancer Center – made the move because it had entered into an exclusive agreement with its own medical group to provide inpatient and outpatient oncology/hematology services at the hospitals.
In its court filings, Jefferson said it entered into the exclusive agreement because doing so was in “the best interest of patients, as it would ensure better integration and availability of care and help ensure that Jefferson consistently provides high-quality medical care in accordance with evidence-based standards.”
Tensions had been building between Alliance and Jefferson for years, ever since, according to Alliance, the community practice declined a buyout offer from Jefferson almost a decade ago.
But the revocation of privileges ultimately tipped the scales for Alliance, sparking the lawsuit.
“For us, that crossed a line,” said Moshe Chasky, MD, one of the five Alliance oncologists and a plaintiff in the suit.
Dr. Chasky and his colleagues had provided care at the hospitals for years, with about 10-15 patients admitted at any one time. The quality of their care is not in dispute. Dr. Chasky, for instance, routinely makes Philadelphia Magazine’s Top Doc List.
Under the new arrangement, the five Alliance oncologists have to hand over care of their admitted patients to Jefferson oncologists or send their patients to another hospital farther away where they do have admitting privileges.
“Without having admitting privileges,” community oncologists “can’t look a patient in the eye and say, ‘No matter what, I’ve got you,’ ” explained Nicolas Ferreyros, managing director of policy, advocacy, and communications at the Community Oncology Alliance, a DC-based lobbying group for independent oncologists.
“A doctor doesn’t want to tell a patient that ‘once you go in the hospital, I have to hand you off.’ ” It undermines their practice, Mr. Ferreyros said.
The situation has caught the attention of other community oncologists who are worried that hospitals canceling admitting privileges might become a new tactic in what they characterize as an ongoing effort to elbow-out independent practitioners and corner the oncology market.
Dr. Chasky said he is getting “calls every day from independent oncologists throughout the country” who “are very concerned. People are watching this for sure.”
Alliance attorney Daniel Frier said that there is nothing unusual about hospitals entering into exclusive contracts with hospital-based practices.
But Mr. Frier said he’s never heard of a hospital entering into an exclusive contract and then terminating the privileges of community oncologists.
“There’s no direct precedent” for the move, he said.
Jefferson Health did not respond to requests for comment.
The ruling
U.S. District Court Judge Kai Scott, who ruled on Alliance’s motion to block the contract and preserve its oncologists’ admitting privileges, ultimately sided with Jefferson and allowed the contract to go forward.
Judge Scott wrote that, “while the court understands the plaintiffs’ concerns and desires to maintain the continuity of care for their own patients,” the court “is not persuaded that either of the two threshold elements for a temporary restraining order or preliminary injunction are met” – first, that Jefferson’s actions violate antitrust laws and second that the plaintiffs “will suffer immediate, irreparable harm” from having their admitting privileges rescinded.
Alliance argued that Jefferson’s contract violated federal antitrust laws and would allow Jefferson to monopolize the local oncology market.
However, Judge Scott called Alliance’s antitrust argument “lifeless” under the strict requirements for antitrust violations, explaining that, among other reasons, a monopoly is unlikely given that Jefferson competes with several high-profile oncology programs in the Philadelphia area, including the Fox Chase Cancer Center.
Judge Scott also expressed doubt that the Jefferson’s actions would cause irreparable harm to Alliance’s business. Alliance employs more than thirty oncologists affiliated with over a dozen hospitals in the greater Philadelphia area, and the inpatient services provided at Jefferson Health-Northeast did not represent a major part of its business.
Despite her ruling, Judge Scott did voice skepticism about some of Jefferson’s arguments.
“The court notes that the Jefferson defendants have briefly argued that Jefferson will be better able to ensure that its own patients receive fully integrated and coordinated care” under the exclusive provider agreement, but “it is unclear how the cooperation of ACS [Alliance Cancer Specialists] and JNE [Jefferson Health-Northeast] hospitalists really caused any problems for the coordinated care of” patients in the many years that they worked together.
It also “does not seem to necessarily serve the community to quickly sever the artery between the services that ACS provides and the services that JNE provides,” Judge Scott wrote.
She added that she would consider another motion from Alliance if the practice makes stronger arguments illustrating antitrust violations and demonstrating irreparable harm.
Currently, Dr. Chasky and Mr. Frier are considering their next steps in the case. The oncologists said they can appeal the judge’s decision or file a new complaint.
Meanwhile, Dr. Chasky and his four colleagues requested and were granted internal medicine privileges at Jefferson Health-Northeast, but given the considerable overlap between oncology and internal medicine, the line between what they can and cannot do remains unclear.
“It’s a mess,” he said.
A familiar story
Large health care entities have increasingly worked to push out or swallow up smaller, independent practices for years.
“What Dr. Chasky and his practice are going through is a little bit more of an aggressive version of what’s going on in the rest of the country,” said Michael Diaz, MD, a community oncologist at Florida Cancer Specialists, the largest independent medical oncology/hematology group in the United States. “The larger institutional hospitals try to make it a closed system so they can keep everything in-house and refer to their own physicians.”
The incentive, Dr. Diaz said, is the financial windfall that Section 340B of the 1992 Public Health Service Act generates for hospital-based oncology services at nonprofit hospitals, such as the Jefferson Health-Northeast facilities.
The 340B program allows nonprofit hospitals to buy primarily outpatient oncology drugs at steep discounts, sometimes 50% or more, and be reimbursed at full price.
When launched in 1992, the program was meant to help a handful of safety-net hospitals cover the cost of charity care, and now approximately more than half of U.S. hospitals participate in the program, particularly after requirements were loosened by the Affordable Care Act. But there’s little transparency on how the money is spent.
Critics say the incentives have created a feeding frenzy among 340B hospitals to either acquire outpatient oncology practices or take their business because of the particularly high margins on oncology drugs. There are similar incentives for hospital-based infusion centers.
In its lawsuit, Alliance alleged that such incentives are what motivated Jefferson’s recent actions.
“It’s all about the money at the end of the day,” said Christian Thomas, MD, a community oncologist with New England Cancer Specialists, Scarborough, Maine, who, like Dr. Diaz, said he’s seen the dynamic play out repeatedly in his career.
The American Hospital Association has been a vigorous defender of 340B in the courts and elsewhere, but the Association’s communications staff had little to say when this news organization reached out about the Jefferson-Alliance situation, except that they do not comment on “specific hospital circumstance.”
Reverberations around the country
Many community oncologists are keeping close tabs on the Jefferson-Alliance situation.
“Our group has been watching Jefferson closely because our [local] hospital is following the same playbook, but they have not yet gone after our privileges,” said Scott Herbert, MD, a community oncologist with the independent Nexus Health system, Sante Fe, N.M.
Dr. Herbert was referring to what has happened since he and his colleagues declined to renew an exclusive provider agreement early this year with St. Vincent Regional Medical Center, a nonprofit hospital in Sante Fe. The agreement allowed the hospital to take advantage of the 340B program because Nexus oncologists acted on its behalf.
St. Vincent’s owner, Christus Health, did not respond to inquiries from this news organization.
Nexus let the contract lapse because its oncologists wanted to provide services at a second, newer hospital in Santa Fe where some of their patients had begun seeking treatment.
The nonprofit hospital in Sante Fe is now building its own oncology practice. Similar to Dr. Chasky’s experience in Philadelphia, Dr. Herbert said his group has seen referrals from the hospital dry up and existing patients rechanneled to the hospital’s oncologists.
“We found over 109 patients in January and February that were referred to one of our docs that got rerouted to one of their docs,” he said.
Dr. Herbert has sent cease-and-desist letters, but “after we saw what Jefferson did, my group said, ‘You better back off of the hospital, or it’s going to take our privileges.’ ”
The Jefferson situation “is sending a message,” he said. “Frankly, we’ve been terrified” at the thought of losing privileges there. “It’s the busiest hospital in our area.”
The future of community oncology
Despite the challenges, Mr. Ferreyros at the Community Oncology Alliance remains optimistic about the future of independent oncology.
Under the competitive pressures, a lot of independent oncology practices have folded in recent years, but the ones that remain are strong. Payers are also increasingly noticing that community oncology practices are less expensive than hospital-based practices for comparable care, he said.
Relationships with hospitals aren’t always adversarial, either. “A lot of practices have collaborative agreements with local hospitals” that work out well, Mr. Ferreyros said, adding that sometimes hospitals even hand over oncology care to local independents after finding that starting and maintaining an oncology service is harder than they imagined.
“The last two decades have been difficult,” but the remaining community oncology practices “are going strong,” he said, and “we’ve never seen more engagement on our issues,” particularly around the issue of cost savings.
A version of this article first appeared on Medscape.com.
, Alliance Cancer Specialists.
The outcome, some community oncologists say, could set a new precedent in how far large health care organizations will go to take their patients or drive them out of business.
The case
On Sept. 5, Alliance sued Jefferson Health after Jefferson canceled the inpatient oncology/hematology privileges of five Alliance oncologists at three Jefferson Health-Northeast hospitals, primarily alleging that Jefferson was attempting to monopolize cancer care in the area.
Jefferson – one of the largest health care systems in the Philadelphia area that includes the NCI-designated Sidney Kimmel Cancer Center – made the move because it had entered into an exclusive agreement with its own medical group to provide inpatient and outpatient oncology/hematology services at the hospitals.
In its court filings, Jefferson said it entered into the exclusive agreement because doing so was in “the best interest of patients, as it would ensure better integration and availability of care and help ensure that Jefferson consistently provides high-quality medical care in accordance with evidence-based standards.”
Tensions had been building between Alliance and Jefferson for years, ever since, according to Alliance, the community practice declined a buyout offer from Jefferson almost a decade ago.
But the revocation of privileges ultimately tipped the scales for Alliance, sparking the lawsuit.
“For us, that crossed a line,” said Moshe Chasky, MD, one of the five Alliance oncologists and a plaintiff in the suit.
Dr. Chasky and his colleagues had provided care at the hospitals for years, with about 10-15 patients admitted at any one time. The quality of their care is not in dispute. Dr. Chasky, for instance, routinely makes Philadelphia Magazine’s Top Doc List.
Under the new arrangement, the five Alliance oncologists have to hand over care of their admitted patients to Jefferson oncologists or send their patients to another hospital farther away where they do have admitting privileges.
“Without having admitting privileges,” community oncologists “can’t look a patient in the eye and say, ‘No matter what, I’ve got you,’ ” explained Nicolas Ferreyros, managing director of policy, advocacy, and communications at the Community Oncology Alliance, a DC-based lobbying group for independent oncologists.
“A doctor doesn’t want to tell a patient that ‘once you go in the hospital, I have to hand you off.’ ” It undermines their practice, Mr. Ferreyros said.
The situation has caught the attention of other community oncologists who are worried that hospitals canceling admitting privileges might become a new tactic in what they characterize as an ongoing effort to elbow-out independent practitioners and corner the oncology market.
Dr. Chasky said he is getting “calls every day from independent oncologists throughout the country” who “are very concerned. People are watching this for sure.”
Alliance attorney Daniel Frier said that there is nothing unusual about hospitals entering into exclusive contracts with hospital-based practices.
But Mr. Frier said he’s never heard of a hospital entering into an exclusive contract and then terminating the privileges of community oncologists.
“There’s no direct precedent” for the move, he said.
Jefferson Health did not respond to requests for comment.
The ruling
U.S. District Court Judge Kai Scott, who ruled on Alliance’s motion to block the contract and preserve its oncologists’ admitting privileges, ultimately sided with Jefferson and allowed the contract to go forward.
Judge Scott wrote that, “while the court understands the plaintiffs’ concerns and desires to maintain the continuity of care for their own patients,” the court “is not persuaded that either of the two threshold elements for a temporary restraining order or preliminary injunction are met” – first, that Jefferson’s actions violate antitrust laws and second that the plaintiffs “will suffer immediate, irreparable harm” from having their admitting privileges rescinded.
Alliance argued that Jefferson’s contract violated federal antitrust laws and would allow Jefferson to monopolize the local oncology market.
However, Judge Scott called Alliance’s antitrust argument “lifeless” under the strict requirements for antitrust violations, explaining that, among other reasons, a monopoly is unlikely given that Jefferson competes with several high-profile oncology programs in the Philadelphia area, including the Fox Chase Cancer Center.
Judge Scott also expressed doubt that the Jefferson’s actions would cause irreparable harm to Alliance’s business. Alliance employs more than thirty oncologists affiliated with over a dozen hospitals in the greater Philadelphia area, and the inpatient services provided at Jefferson Health-Northeast did not represent a major part of its business.
Despite her ruling, Judge Scott did voice skepticism about some of Jefferson’s arguments.
“The court notes that the Jefferson defendants have briefly argued that Jefferson will be better able to ensure that its own patients receive fully integrated and coordinated care” under the exclusive provider agreement, but “it is unclear how the cooperation of ACS [Alliance Cancer Specialists] and JNE [Jefferson Health-Northeast] hospitalists really caused any problems for the coordinated care of” patients in the many years that they worked together.
It also “does not seem to necessarily serve the community to quickly sever the artery between the services that ACS provides and the services that JNE provides,” Judge Scott wrote.
She added that she would consider another motion from Alliance if the practice makes stronger arguments illustrating antitrust violations and demonstrating irreparable harm.
Currently, Dr. Chasky and Mr. Frier are considering their next steps in the case. The oncologists said they can appeal the judge’s decision or file a new complaint.
Meanwhile, Dr. Chasky and his four colleagues requested and were granted internal medicine privileges at Jefferson Health-Northeast, but given the considerable overlap between oncology and internal medicine, the line between what they can and cannot do remains unclear.
“It’s a mess,” he said.
A familiar story
Large health care entities have increasingly worked to push out or swallow up smaller, independent practices for years.
“What Dr. Chasky and his practice are going through is a little bit more of an aggressive version of what’s going on in the rest of the country,” said Michael Diaz, MD, a community oncologist at Florida Cancer Specialists, the largest independent medical oncology/hematology group in the United States. “The larger institutional hospitals try to make it a closed system so they can keep everything in-house and refer to their own physicians.”
The incentive, Dr. Diaz said, is the financial windfall that Section 340B of the 1992 Public Health Service Act generates for hospital-based oncology services at nonprofit hospitals, such as the Jefferson Health-Northeast facilities.
The 340B program allows nonprofit hospitals to buy primarily outpatient oncology drugs at steep discounts, sometimes 50% or more, and be reimbursed at full price.
When launched in 1992, the program was meant to help a handful of safety-net hospitals cover the cost of charity care, and now approximately more than half of U.S. hospitals participate in the program, particularly after requirements were loosened by the Affordable Care Act. But there’s little transparency on how the money is spent.
Critics say the incentives have created a feeding frenzy among 340B hospitals to either acquire outpatient oncology practices or take their business because of the particularly high margins on oncology drugs. There are similar incentives for hospital-based infusion centers.
In its lawsuit, Alliance alleged that such incentives are what motivated Jefferson’s recent actions.
“It’s all about the money at the end of the day,” said Christian Thomas, MD, a community oncologist with New England Cancer Specialists, Scarborough, Maine, who, like Dr. Diaz, said he’s seen the dynamic play out repeatedly in his career.
The American Hospital Association has been a vigorous defender of 340B in the courts and elsewhere, but the Association’s communications staff had little to say when this news organization reached out about the Jefferson-Alliance situation, except that they do not comment on “specific hospital circumstance.”
Reverberations around the country
Many community oncologists are keeping close tabs on the Jefferson-Alliance situation.
“Our group has been watching Jefferson closely because our [local] hospital is following the same playbook, but they have not yet gone after our privileges,” said Scott Herbert, MD, a community oncologist with the independent Nexus Health system, Sante Fe, N.M.
Dr. Herbert was referring to what has happened since he and his colleagues declined to renew an exclusive provider agreement early this year with St. Vincent Regional Medical Center, a nonprofit hospital in Sante Fe. The agreement allowed the hospital to take advantage of the 340B program because Nexus oncologists acted on its behalf.
St. Vincent’s owner, Christus Health, did not respond to inquiries from this news organization.
Nexus let the contract lapse because its oncologists wanted to provide services at a second, newer hospital in Santa Fe where some of their patients had begun seeking treatment.
The nonprofit hospital in Sante Fe is now building its own oncology practice. Similar to Dr. Chasky’s experience in Philadelphia, Dr. Herbert said his group has seen referrals from the hospital dry up and existing patients rechanneled to the hospital’s oncologists.
“We found over 109 patients in January and February that were referred to one of our docs that got rerouted to one of their docs,” he said.
Dr. Herbert has sent cease-and-desist letters, but “after we saw what Jefferson did, my group said, ‘You better back off of the hospital, or it’s going to take our privileges.’ ”
The Jefferson situation “is sending a message,” he said. “Frankly, we’ve been terrified” at the thought of losing privileges there. “It’s the busiest hospital in our area.”
The future of community oncology
Despite the challenges, Mr. Ferreyros at the Community Oncology Alliance remains optimistic about the future of independent oncology.
Under the competitive pressures, a lot of independent oncology practices have folded in recent years, but the ones that remain are strong. Payers are also increasingly noticing that community oncology practices are less expensive than hospital-based practices for comparable care, he said.
Relationships with hospitals aren’t always adversarial, either. “A lot of practices have collaborative agreements with local hospitals” that work out well, Mr. Ferreyros said, adding that sometimes hospitals even hand over oncology care to local independents after finding that starting and maintaining an oncology service is harder than they imagined.
“The last two decades have been difficult,” but the remaining community oncology practices “are going strong,” he said, and “we’ve never seen more engagement on our issues,” particularly around the issue of cost savings.
A version of this article first appeared on Medscape.com.
, Alliance Cancer Specialists.
The outcome, some community oncologists say, could set a new precedent in how far large health care organizations will go to take their patients or drive them out of business.
The case
On Sept. 5, Alliance sued Jefferson Health after Jefferson canceled the inpatient oncology/hematology privileges of five Alliance oncologists at three Jefferson Health-Northeast hospitals, primarily alleging that Jefferson was attempting to monopolize cancer care in the area.
Jefferson – one of the largest health care systems in the Philadelphia area that includes the NCI-designated Sidney Kimmel Cancer Center – made the move because it had entered into an exclusive agreement with its own medical group to provide inpatient and outpatient oncology/hematology services at the hospitals.
In its court filings, Jefferson said it entered into the exclusive agreement because doing so was in “the best interest of patients, as it would ensure better integration and availability of care and help ensure that Jefferson consistently provides high-quality medical care in accordance with evidence-based standards.”
Tensions had been building between Alliance and Jefferson for years, ever since, according to Alliance, the community practice declined a buyout offer from Jefferson almost a decade ago.
But the revocation of privileges ultimately tipped the scales for Alliance, sparking the lawsuit.
“For us, that crossed a line,” said Moshe Chasky, MD, one of the five Alliance oncologists and a plaintiff in the suit.
Dr. Chasky and his colleagues had provided care at the hospitals for years, with about 10-15 patients admitted at any one time. The quality of their care is not in dispute. Dr. Chasky, for instance, routinely makes Philadelphia Magazine’s Top Doc List.
Under the new arrangement, the five Alliance oncologists have to hand over care of their admitted patients to Jefferson oncologists or send their patients to another hospital farther away where they do have admitting privileges.
“Without having admitting privileges,” community oncologists “can’t look a patient in the eye and say, ‘No matter what, I’ve got you,’ ” explained Nicolas Ferreyros, managing director of policy, advocacy, and communications at the Community Oncology Alliance, a DC-based lobbying group for independent oncologists.
“A doctor doesn’t want to tell a patient that ‘once you go in the hospital, I have to hand you off.’ ” It undermines their practice, Mr. Ferreyros said.
The situation has caught the attention of other community oncologists who are worried that hospitals canceling admitting privileges might become a new tactic in what they characterize as an ongoing effort to elbow-out independent practitioners and corner the oncology market.
Dr. Chasky said he is getting “calls every day from independent oncologists throughout the country” who “are very concerned. People are watching this for sure.”
Alliance attorney Daniel Frier said that there is nothing unusual about hospitals entering into exclusive contracts with hospital-based practices.
But Mr. Frier said he’s never heard of a hospital entering into an exclusive contract and then terminating the privileges of community oncologists.
“There’s no direct precedent” for the move, he said.
Jefferson Health did not respond to requests for comment.
The ruling
U.S. District Court Judge Kai Scott, who ruled on Alliance’s motion to block the contract and preserve its oncologists’ admitting privileges, ultimately sided with Jefferson and allowed the contract to go forward.
Judge Scott wrote that, “while the court understands the plaintiffs’ concerns and desires to maintain the continuity of care for their own patients,” the court “is not persuaded that either of the two threshold elements for a temporary restraining order or preliminary injunction are met” – first, that Jefferson’s actions violate antitrust laws and second that the plaintiffs “will suffer immediate, irreparable harm” from having their admitting privileges rescinded.
Alliance argued that Jefferson’s contract violated federal antitrust laws and would allow Jefferson to monopolize the local oncology market.
However, Judge Scott called Alliance’s antitrust argument “lifeless” under the strict requirements for antitrust violations, explaining that, among other reasons, a monopoly is unlikely given that Jefferson competes with several high-profile oncology programs in the Philadelphia area, including the Fox Chase Cancer Center.
Judge Scott also expressed doubt that the Jefferson’s actions would cause irreparable harm to Alliance’s business. Alliance employs more than thirty oncologists affiliated with over a dozen hospitals in the greater Philadelphia area, and the inpatient services provided at Jefferson Health-Northeast did not represent a major part of its business.
Despite her ruling, Judge Scott did voice skepticism about some of Jefferson’s arguments.
“The court notes that the Jefferson defendants have briefly argued that Jefferson will be better able to ensure that its own patients receive fully integrated and coordinated care” under the exclusive provider agreement, but “it is unclear how the cooperation of ACS [Alliance Cancer Specialists] and JNE [Jefferson Health-Northeast] hospitalists really caused any problems for the coordinated care of” patients in the many years that they worked together.
It also “does not seem to necessarily serve the community to quickly sever the artery between the services that ACS provides and the services that JNE provides,” Judge Scott wrote.
She added that she would consider another motion from Alliance if the practice makes stronger arguments illustrating antitrust violations and demonstrating irreparable harm.
Currently, Dr. Chasky and Mr. Frier are considering their next steps in the case. The oncologists said they can appeal the judge’s decision or file a new complaint.
Meanwhile, Dr. Chasky and his four colleagues requested and were granted internal medicine privileges at Jefferson Health-Northeast, but given the considerable overlap between oncology and internal medicine, the line between what they can and cannot do remains unclear.
“It’s a mess,” he said.
A familiar story
Large health care entities have increasingly worked to push out or swallow up smaller, independent practices for years.
“What Dr. Chasky and his practice are going through is a little bit more of an aggressive version of what’s going on in the rest of the country,” said Michael Diaz, MD, a community oncologist at Florida Cancer Specialists, the largest independent medical oncology/hematology group in the United States. “The larger institutional hospitals try to make it a closed system so they can keep everything in-house and refer to their own physicians.”
The incentive, Dr. Diaz said, is the financial windfall that Section 340B of the 1992 Public Health Service Act generates for hospital-based oncology services at nonprofit hospitals, such as the Jefferson Health-Northeast facilities.
The 340B program allows nonprofit hospitals to buy primarily outpatient oncology drugs at steep discounts, sometimes 50% or more, and be reimbursed at full price.
When launched in 1992, the program was meant to help a handful of safety-net hospitals cover the cost of charity care, and now approximately more than half of U.S. hospitals participate in the program, particularly after requirements were loosened by the Affordable Care Act. But there’s little transparency on how the money is spent.
Critics say the incentives have created a feeding frenzy among 340B hospitals to either acquire outpatient oncology practices or take their business because of the particularly high margins on oncology drugs. There are similar incentives for hospital-based infusion centers.
In its lawsuit, Alliance alleged that such incentives are what motivated Jefferson’s recent actions.
“It’s all about the money at the end of the day,” said Christian Thomas, MD, a community oncologist with New England Cancer Specialists, Scarborough, Maine, who, like Dr. Diaz, said he’s seen the dynamic play out repeatedly in his career.
The American Hospital Association has been a vigorous defender of 340B in the courts and elsewhere, but the Association’s communications staff had little to say when this news organization reached out about the Jefferson-Alliance situation, except that they do not comment on “specific hospital circumstance.”
Reverberations around the country
Many community oncologists are keeping close tabs on the Jefferson-Alliance situation.
“Our group has been watching Jefferson closely because our [local] hospital is following the same playbook, but they have not yet gone after our privileges,” said Scott Herbert, MD, a community oncologist with the independent Nexus Health system, Sante Fe, N.M.
Dr. Herbert was referring to what has happened since he and his colleagues declined to renew an exclusive provider agreement early this year with St. Vincent Regional Medical Center, a nonprofit hospital in Sante Fe. The agreement allowed the hospital to take advantage of the 340B program because Nexus oncologists acted on its behalf.
St. Vincent’s owner, Christus Health, did not respond to inquiries from this news organization.
Nexus let the contract lapse because its oncologists wanted to provide services at a second, newer hospital in Santa Fe where some of their patients had begun seeking treatment.
The nonprofit hospital in Sante Fe is now building its own oncology practice. Similar to Dr. Chasky’s experience in Philadelphia, Dr. Herbert said his group has seen referrals from the hospital dry up and existing patients rechanneled to the hospital’s oncologists.
“We found over 109 patients in January and February that were referred to one of our docs that got rerouted to one of their docs,” he said.
Dr. Herbert has sent cease-and-desist letters, but “after we saw what Jefferson did, my group said, ‘You better back off of the hospital, or it’s going to take our privileges.’ ”
The Jefferson situation “is sending a message,” he said. “Frankly, we’ve been terrified” at the thought of losing privileges there. “It’s the busiest hospital in our area.”
The future of community oncology
Despite the challenges, Mr. Ferreyros at the Community Oncology Alliance remains optimistic about the future of independent oncology.
Under the competitive pressures, a lot of independent oncology practices have folded in recent years, but the ones that remain are strong. Payers are also increasingly noticing that community oncology practices are less expensive than hospital-based practices for comparable care, he said.
Relationships with hospitals aren’t always adversarial, either. “A lot of practices have collaborative agreements with local hospitals” that work out well, Mr. Ferreyros said, adding that sometimes hospitals even hand over oncology care to local independents after finding that starting and maintaining an oncology service is harder than they imagined.
“The last two decades have been difficult,” but the remaining community oncology practices “are going strong,” he said, and “we’ve never seen more engagement on our issues,” particularly around the issue of cost savings.
A version of this article first appeared on Medscape.com.
Early career considerations for gastroenterologists interested in diversity, equity, and inclusion roles

Highlighting the importance of DEI across all aspects of medicine is long overdue, and the field of gastroenterology is no exception. Diversity in the gastroenterology workforce still has significant room for improvement with only 12% of all gastroenterology fellows in 2018 identifying as Black, Latino/a/x, American Indian or Alaskan Native, or Native Hawaiian or Pacific Islander.1 Moreover, only 4.4% of practicing gastroenterologists identify as Black, 6.7% identify as Latino/a/x, 0.1% as American Indian or Alaskan Native, and 0.003% as Native Hawaiian or Pacific Islander.2
The intensified focus on diversity in GI is welcomed, but increasing physician workforce diversity is only one of the necessary steps. If our ultimate goal is to improve health outcomes and achieve health equity for historically marginalized racial, ethnic, and socioeconomically disadvantaged communities, we must critically evaluate the path beyond just enhancing workforce diversity.
Black and Latino/a/x physicians are more likely to care for historically marginalized communities,3 which has been shown to improve all-cause mortality and reduce racial disparities.4 Additionally, diverse work teams are more innovative and productive.5 Therefore, expanding diversity must include 1) providing equitable policies and access to opportunities and promotions; 2) building inclusive environments in our institutions and practices; and 3) providing space for all people to feel like they can belong, feel respected at work, and genuinely have their opinions and ideas valued. What diversity, equity, inclusion, and belonging provide for us and our patients are avenues to thrive, solve complex problems, and tackle prominent issues within our institutions, workplaces, and communities.
To this end, many academic centers, hospitals, and private practice entities have produced a flurry of new DEI initiatives coupled with titles and roles. Some of these roles have thankfully brought recognition and economic compensation to the people doing this work. Still, as an early career gastroenterologist, you may be offered or are considering taking on a DEI role during your early career. As two underrepresented minority women in medicine who took on DEI roles with their first jobs, we wanted to highlight a few aspects to think about during your early career:
Does the DEI role come with resources?
Historically, DEI efforts were treated as “extra work,” or an activity that was done using one’s own personal time. In addition, this work called upon the small number of physicians underrepresented in medicine, largely uncompensated and with an exorbitant minority tax during a critical moment in establishing their early careers. DEI should no longer be seen as an extracurricular activity but as a vital component of an institution’s success.
If you are considering a DEI role, the first question to ask is, “Does this role come with extra compensation or protected time?” We highly recommend not taking on the role if the answer is no. If your institution or employer is only offering increased minority tax, you are being set up to either fail, burn out, or both. Your employer or institution does not appear to value your time or effort in DEI, and you should interpret their lack of compensation or protected time as such.
If the answer is yes, then here are a few other things to consider: Is there institutional support for you to be successful in your new role? As DEI work challenges you to come up with solutions to combat years of historic marginalization for racial and ethnic minorities, this work can sometimes feel overwhelming and isolating. The importance of the DEI community and mentorship within and outside your institution is critical. You should consider joining DEI working groups or committees through GI national societies, the Association of American Medical Colleges, or the Accreditation Council for Graduate Medical Education. You can also connect with a fantastic network of people engaged in this work via social media and lean on friends and colleagues leading similar initiatives across the country.
Other critical logistical questions are if your role will come with administrative support, whether there is a budget for programs or events, and whether your institution/employer will support you in seeking continued professional development for your DEI role.6
Make sure to understand the “ask” from your division, department, or company.
Before confirming you are willing to take on this role, get a clear vision of what you are being asked to accomplish. There are so many opportunities to improve the DEI landscape. Therefore, knowing what you are specifically being asked to do will be critical to your success.
Are you being asked to work on diversity?
Does your institution want you to focus on and improve the recruitment and retention of trainees, physicians, or staff underrepresented in medicine? If so, you will need to have access to all the prior work and statistics. Capture the landscape before your interventions (% underrepresented in medicine [URiM] trainees, % URiM faculty at each level, % of URiM trainees retained as faculty, % of URiM faculty being promoted each year, etc.) This will allow you to determine the outcomes of your proposed improvements or programs.
Is your employer focused on equity?
Are you being asked to think about ways to operationalize improved patient health equity, or are you being asked to build equitable opportunities/programs for career advancement for URiMs at your institution? For either equity issue, you first need to understand the scope of the problem to ask for the necessary resources for a potential solution. Discuss timeline expectations, as equity work is a marathon and may take years to move the needle on any particular issue. This timeline is also critical for your employer to be aware of and support, as unrealistic timelines and expectations will also set you up for failure.
Or, are you being asked to concentrate on inclusion?
Does your institution need an assessment of how inclusive the climate is for trainees, staff, or physicians? Does this assessment align with your division or department’s impression, and how do you plan to work toward potential solutions for improvement?
Although diversity, equity, and inclusion are interconnected entities, they all have distinct objectives and solutions. It is essential to understand your vision and your employer’s vision for this role. If they are not aligned, having early and in-depth conversations about aligning your visions will set you on a path to success in your early career.
Know your why or more importantly, your who?
Early career physicians who are considering taking on DEI work do so for a reason. Being passionate about this type of work is usually born from a personal experience or your deep-rooted values. For us, experiencing and witnessing health disparities for our family members and people who look like us are what initially fueled our passion for this work. Additional experiences with trainees and patients keep us invigorated to continue highlighting the importance of DEI and encourage others to be passionate about DEI’s huge value added. As DEI work can come with challenges, remembering and re-centering on why you are passionate about this work or who you are engaging in this work for can keep you going.
There are several aspects to consider before taking on a DEI role, but overall, the work is rewarding and can be a great addition to the building blocks of your early career. In the short term, you build a DEI community network of peers, mentors, colleagues, and friends beyond your immediate institution and specialty. You also can demonstrate your leadership skills and potential early on in your career. In the long-term, engaging in these types of roles helps build a climate and culture that is conducive to enacting change for our patients and communities, including advancing healthcare equity and working toward recruitment, retention, and expansion efforts for our trainees and faculty. Overall, we think this type of work in your early career can be an integral part of your personal and professional development, while also having an impact that ripples beyond the walls of the endoscopy suite.
Dr. Fritz is an assistant professor of medicine in the division of gastroenterology at Washington University School of Medicine, St. Louis. Dr. Rodriguez is a gastroenterologist with Brigham and Women’s Hospital in Boston. Neither Dr. Rodriguez nor Dr. Fritz disclosed no conflicts of interest.
References
1. Santhosh L,Babik JM. Trends in racial and ethnic diversity in internal medicine subspecialty fellowships from 2006 to 2018. JAMA Network Open 2020;3:e1920482-e1920482.
2. Colleges AoAM. Physician Specialty Data Report/Active physicians who identified as Black or African-American, 2021. 2022.
3. Komaromy M et al. The role of black and Hispanic physicians in providing health care for underserved populations. New England Journal of Medicine 1996;334:1305-10.
4. Snyder JE et al. Black representation in the primary care physician workforce and its association with population life expectancy and mortality rates in the US. JAMA Network Open 2023;6:e236687-e236687.
5. Page S. Diversity bonuses and the business case. The Diversity Bonus: Princeton University Press, 2017:184-208.
6. Vela MB et al. Diversity, equity, and inclusion officer position available: Proceed with caution. Journal of Graduate Medical Education 2021;13:771-3.
Helpful resources
Diversity and Inclusion Toolkit Resources, AAMC
Blackinggastro.org, The Association of Black Gastroenterologists and Hepatologists (ABGH)
Podcast: Clinical Problem Solvers: Anti-Racism in Medicine
Highlighting the importance of DEI across all aspects of medicine is long overdue, and the field of gastroenterology is no exception. Diversity in the gastroenterology workforce still has significant room for improvement with only 12% of all gastroenterology fellows in 2018 identifying as Black, Latino/a/x, American Indian or Alaskan Native, or Native Hawaiian or Pacific Islander.1 Moreover, only 4.4% of practicing gastroenterologists identify as Black, 6.7% identify as Latino/a/x, 0.1% as American Indian or Alaskan Native, and 0.003% as Native Hawaiian or Pacific Islander.2
The intensified focus on diversity in GI is welcomed, but increasing physician workforce diversity is only one of the necessary steps. If our ultimate goal is to improve health outcomes and achieve health equity for historically marginalized racial, ethnic, and socioeconomically disadvantaged communities, we must critically evaluate the path beyond just enhancing workforce diversity.
Black and Latino/a/x physicians are more likely to care for historically marginalized communities,3 which has been shown to improve all-cause mortality and reduce racial disparities.4 Additionally, diverse work teams are more innovative and productive.5 Therefore, expanding diversity must include 1) providing equitable policies and access to opportunities and promotions; 2) building inclusive environments in our institutions and practices; and 3) providing space for all people to feel like they can belong, feel respected at work, and genuinely have their opinions and ideas valued. What diversity, equity, inclusion, and belonging provide for us and our patients are avenues to thrive, solve complex problems, and tackle prominent issues within our institutions, workplaces, and communities.
To this end, many academic centers, hospitals, and private practice entities have produced a flurry of new DEI initiatives coupled with titles and roles. Some of these roles have thankfully brought recognition and economic compensation to the people doing this work. Still, as an early career gastroenterologist, you may be offered or are considering taking on a DEI role during your early career. As two underrepresented minority women in medicine who took on DEI roles with their first jobs, we wanted to highlight a few aspects to think about during your early career:
Does the DEI role come with resources?
Historically, DEI efforts were treated as “extra work,” or an activity that was done using one’s own personal time. In addition, this work called upon the small number of physicians underrepresented in medicine, largely uncompensated and with an exorbitant minority tax during a critical moment in establishing their early careers. DEI should no longer be seen as an extracurricular activity but as a vital component of an institution’s success.
If you are considering a DEI role, the first question to ask is, “Does this role come with extra compensation or protected time?” We highly recommend not taking on the role if the answer is no. If your institution or employer is only offering increased minority tax, you are being set up to either fail, burn out, or both. Your employer or institution does not appear to value your time or effort in DEI, and you should interpret their lack of compensation or protected time as such.
If the answer is yes, then here are a few other things to consider: Is there institutional support for you to be successful in your new role? As DEI work challenges you to come up with solutions to combat years of historic marginalization for racial and ethnic minorities, this work can sometimes feel overwhelming and isolating. The importance of the DEI community and mentorship within and outside your institution is critical. You should consider joining DEI working groups or committees through GI national societies, the Association of American Medical Colleges, or the Accreditation Council for Graduate Medical Education. You can also connect with a fantastic network of people engaged in this work via social media and lean on friends and colleagues leading similar initiatives across the country.
Other critical logistical questions are if your role will come with administrative support, whether there is a budget for programs or events, and whether your institution/employer will support you in seeking continued professional development for your DEI role.6
Make sure to understand the “ask” from your division, department, or company.
Before confirming you are willing to take on this role, get a clear vision of what you are being asked to accomplish. There are so many opportunities to improve the DEI landscape. Therefore, knowing what you are specifically being asked to do will be critical to your success.
Are you being asked to work on diversity?
Does your institution want you to focus on and improve the recruitment and retention of trainees, physicians, or staff underrepresented in medicine? If so, you will need to have access to all the prior work and statistics. Capture the landscape before your interventions (% underrepresented in medicine [URiM] trainees, % URiM faculty at each level, % of URiM trainees retained as faculty, % of URiM faculty being promoted each year, etc.) This will allow you to determine the outcomes of your proposed improvements or programs.
Is your employer focused on equity?
Are you being asked to think about ways to operationalize improved patient health equity, or are you being asked to build equitable opportunities/programs for career advancement for URiMs at your institution? For either equity issue, you first need to understand the scope of the problem to ask for the necessary resources for a potential solution. Discuss timeline expectations, as equity work is a marathon and may take years to move the needle on any particular issue. This timeline is also critical for your employer to be aware of and support, as unrealistic timelines and expectations will also set you up for failure.
Or, are you being asked to concentrate on inclusion?
Does your institution need an assessment of how inclusive the climate is for trainees, staff, or physicians? Does this assessment align with your division or department’s impression, and how do you plan to work toward potential solutions for improvement?
Although diversity, equity, and inclusion are interconnected entities, they all have distinct objectives and solutions. It is essential to understand your vision and your employer’s vision for this role. If they are not aligned, having early and in-depth conversations about aligning your visions will set you on a path to success in your early career.
Know your why or more importantly, your who?
Early career physicians who are considering taking on DEI work do so for a reason. Being passionate about this type of work is usually born from a personal experience or your deep-rooted values. For us, experiencing and witnessing health disparities for our family members and people who look like us are what initially fueled our passion for this work. Additional experiences with trainees and patients keep us invigorated to continue highlighting the importance of DEI and encourage others to be passionate about DEI’s huge value added. As DEI work can come with challenges, remembering and re-centering on why you are passionate about this work or who you are engaging in this work for can keep you going.
There are several aspects to consider before taking on a DEI role, but overall, the work is rewarding and can be a great addition to the building blocks of your early career. In the short term, you build a DEI community network of peers, mentors, colleagues, and friends beyond your immediate institution and specialty. You also can demonstrate your leadership skills and potential early on in your career. In the long-term, engaging in these types of roles helps build a climate and culture that is conducive to enacting change for our patients and communities, including advancing healthcare equity and working toward recruitment, retention, and expansion efforts for our trainees and faculty. Overall, we think this type of work in your early career can be an integral part of your personal and professional development, while also having an impact that ripples beyond the walls of the endoscopy suite.
Dr. Fritz is an assistant professor of medicine in the division of gastroenterology at Washington University School of Medicine, St. Louis. Dr. Rodriguez is a gastroenterologist with Brigham and Women’s Hospital in Boston. Neither Dr. Rodriguez nor Dr. Fritz disclosed no conflicts of interest.
References
1. Santhosh L,Babik JM. Trends in racial and ethnic diversity in internal medicine subspecialty fellowships from 2006 to 2018. JAMA Network Open 2020;3:e1920482-e1920482.
2. Colleges AoAM. Physician Specialty Data Report/Active physicians who identified as Black or African-American, 2021. 2022.
3. Komaromy M et al. The role of black and Hispanic physicians in providing health care for underserved populations. New England Journal of Medicine 1996;334:1305-10.
4. Snyder JE et al. Black representation in the primary care physician workforce and its association with population life expectancy and mortality rates in the US. JAMA Network Open 2023;6:e236687-e236687.
5. Page S. Diversity bonuses and the business case. The Diversity Bonus: Princeton University Press, 2017:184-208.
6. Vela MB et al. Diversity, equity, and inclusion officer position available: Proceed with caution. Journal of Graduate Medical Education 2021;13:771-3.
Helpful resources
Diversity and Inclusion Toolkit Resources, AAMC
Blackinggastro.org, The Association of Black Gastroenterologists and Hepatologists (ABGH)
Podcast: Clinical Problem Solvers: Anti-Racism in Medicine
Highlighting the importance of DEI across all aspects of medicine is long overdue, and the field of gastroenterology is no exception. Diversity in the gastroenterology workforce still has significant room for improvement with only 12% of all gastroenterology fellows in 2018 identifying as Black, Latino/a/x, American Indian or Alaskan Native, or Native Hawaiian or Pacific Islander.1 Moreover, only 4.4% of practicing gastroenterologists identify as Black, 6.7% identify as Latino/a/x, 0.1% as American Indian or Alaskan Native, and 0.003% as Native Hawaiian or Pacific Islander.2
The intensified focus on diversity in GI is welcomed, but increasing physician workforce diversity is only one of the necessary steps. If our ultimate goal is to improve health outcomes and achieve health equity for historically marginalized racial, ethnic, and socioeconomically disadvantaged communities, we must critically evaluate the path beyond just enhancing workforce diversity.
Black and Latino/a/x physicians are more likely to care for historically marginalized communities,3 which has been shown to improve all-cause mortality and reduce racial disparities.4 Additionally, diverse work teams are more innovative and productive.5 Therefore, expanding diversity must include 1) providing equitable policies and access to opportunities and promotions; 2) building inclusive environments in our institutions and practices; and 3) providing space for all people to feel like they can belong, feel respected at work, and genuinely have their opinions and ideas valued. What diversity, equity, inclusion, and belonging provide for us and our patients are avenues to thrive, solve complex problems, and tackle prominent issues within our institutions, workplaces, and communities.
To this end, many academic centers, hospitals, and private practice entities have produced a flurry of new DEI initiatives coupled with titles and roles. Some of these roles have thankfully brought recognition and economic compensation to the people doing this work. Still, as an early career gastroenterologist, you may be offered or are considering taking on a DEI role during your early career. As two underrepresented minority women in medicine who took on DEI roles with their first jobs, we wanted to highlight a few aspects to think about during your early career:
Does the DEI role come with resources?
Historically, DEI efforts were treated as “extra work,” or an activity that was done using one’s own personal time. In addition, this work called upon the small number of physicians underrepresented in medicine, largely uncompensated and with an exorbitant minority tax during a critical moment in establishing their early careers. DEI should no longer be seen as an extracurricular activity but as a vital component of an institution’s success.
If you are considering a DEI role, the first question to ask is, “Does this role come with extra compensation or protected time?” We highly recommend not taking on the role if the answer is no. If your institution or employer is only offering increased minority tax, you are being set up to either fail, burn out, or both. Your employer or institution does not appear to value your time or effort in DEI, and you should interpret their lack of compensation or protected time as such.
If the answer is yes, then here are a few other things to consider: Is there institutional support for you to be successful in your new role? As DEI work challenges you to come up with solutions to combat years of historic marginalization for racial and ethnic minorities, this work can sometimes feel overwhelming and isolating. The importance of the DEI community and mentorship within and outside your institution is critical. You should consider joining DEI working groups or committees through GI national societies, the Association of American Medical Colleges, or the Accreditation Council for Graduate Medical Education. You can also connect with a fantastic network of people engaged in this work via social media and lean on friends and colleagues leading similar initiatives across the country.
Other critical logistical questions are if your role will come with administrative support, whether there is a budget for programs or events, and whether your institution/employer will support you in seeking continued professional development for your DEI role.6
Make sure to understand the “ask” from your division, department, or company.
Before confirming you are willing to take on this role, get a clear vision of what you are being asked to accomplish. There are so many opportunities to improve the DEI landscape. Therefore, knowing what you are specifically being asked to do will be critical to your success.
Are you being asked to work on diversity?
Does your institution want you to focus on and improve the recruitment and retention of trainees, physicians, or staff underrepresented in medicine? If so, you will need to have access to all the prior work and statistics. Capture the landscape before your interventions (% underrepresented in medicine [URiM] trainees, % URiM faculty at each level, % of URiM trainees retained as faculty, % of URiM faculty being promoted each year, etc.) This will allow you to determine the outcomes of your proposed improvements or programs.
Is your employer focused on equity?
Are you being asked to think about ways to operationalize improved patient health equity, or are you being asked to build equitable opportunities/programs for career advancement for URiMs at your institution? For either equity issue, you first need to understand the scope of the problem to ask for the necessary resources for a potential solution. Discuss timeline expectations, as equity work is a marathon and may take years to move the needle on any particular issue. This timeline is also critical for your employer to be aware of and support, as unrealistic timelines and expectations will also set you up for failure.
Or, are you being asked to concentrate on inclusion?
Does your institution need an assessment of how inclusive the climate is for trainees, staff, or physicians? Does this assessment align with your division or department’s impression, and how do you plan to work toward potential solutions for improvement?
Although diversity, equity, and inclusion are interconnected entities, they all have distinct objectives and solutions. It is essential to understand your vision and your employer’s vision for this role. If they are not aligned, having early and in-depth conversations about aligning your visions will set you on a path to success in your early career.
Know your why or more importantly, your who?
Early career physicians who are considering taking on DEI work do so for a reason. Being passionate about this type of work is usually born from a personal experience or your deep-rooted values. For us, experiencing and witnessing health disparities for our family members and people who look like us are what initially fueled our passion for this work. Additional experiences with trainees and patients keep us invigorated to continue highlighting the importance of DEI and encourage others to be passionate about DEI’s huge value added. As DEI work can come with challenges, remembering and re-centering on why you are passionate about this work or who you are engaging in this work for can keep you going.
There are several aspects to consider before taking on a DEI role, but overall, the work is rewarding and can be a great addition to the building blocks of your early career. In the short term, you build a DEI community network of peers, mentors, colleagues, and friends beyond your immediate institution and specialty. You also can demonstrate your leadership skills and potential early on in your career. In the long-term, engaging in these types of roles helps build a climate and culture that is conducive to enacting change for our patients and communities, including advancing healthcare equity and working toward recruitment, retention, and expansion efforts for our trainees and faculty. Overall, we think this type of work in your early career can be an integral part of your personal and professional development, while also having an impact that ripples beyond the walls of the endoscopy suite.
Dr. Fritz is an assistant professor of medicine in the division of gastroenterology at Washington University School of Medicine, St. Louis. Dr. Rodriguez is a gastroenterologist with Brigham and Women’s Hospital in Boston. Neither Dr. Rodriguez nor Dr. Fritz disclosed no conflicts of interest.
References
1. Santhosh L,Babik JM. Trends in racial and ethnic diversity in internal medicine subspecialty fellowships from 2006 to 2018. JAMA Network Open 2020;3:e1920482-e1920482.
2. Colleges AoAM. Physician Specialty Data Report/Active physicians who identified as Black or African-American, 2021. 2022.
3. Komaromy M et al. The role of black and Hispanic physicians in providing health care for underserved populations. New England Journal of Medicine 1996;334:1305-10.
4. Snyder JE et al. Black representation in the primary care physician workforce and its association with population life expectancy and mortality rates in the US. JAMA Network Open 2023;6:e236687-e236687.
5. Page S. Diversity bonuses and the business case. The Diversity Bonus: Princeton University Press, 2017:184-208.
6. Vela MB et al. Diversity, equity, and inclusion officer position available: Proceed with caution. Journal of Graduate Medical Education 2021;13:771-3.
Helpful resources
Diversity and Inclusion Toolkit Resources, AAMC
Blackinggastro.org, The Association of Black Gastroenterologists and Hepatologists (ABGH)
Podcast: Clinical Problem Solvers: Anti-Racism in Medicine
84-year-old MD contests employer’s mandatory cognitive tests for older docs
Lylas G. Mogk, MD, recently sued Henry Ford Health and Henry Ford Medical Group in federal court, alleging that the mandatory cognitive test violates the Americans with Disabilities Act, the Age Discrimination in Employment Act, and two Michigan laws.
Dr. Mogk’s lawsuit follows a widely watched 2020 case in which the U.S. Equal Employment Opportunity Commission sued Yale New Haven Hospital, the teaching hospital of Yale University, for age discrimination. According to the lawsuit, the hospital illegally required neuropsychological and eye examinations of physicians aged 70 or older who sought to gain or renew staff privileges.
According to the lawsuit, Dr. Mogk is a member of Henry Ford Medical Group, which in 2017 required all members aged 70 and older to undergo cognitive screening tests. The tests would be repeated every 5 years thereafter, the lawsuit said, and anyone who refused would have to resign or be fired.
Dr. Mogk completed the screening, although no information about the results or outcome was mentioned in the lawsuit. It’s not clear whether Henry Ford’s cognitive test mandate remains in place; a spokesperson for Henry Ford Health and attorneys for Dr. Mogk declined to comment.
The number of practicing physicians in their 70s and beyond is rising. A 2021 report found that 12% of U.S. licensed physicians in 2020 were least 70 years old, up from 9% in 2010 and an increase from 75,627 to 120,510. The percentage of doctors aged 60-69 grew to 19% from 16% in 2010.
The number of health systems requiring testing of older physicians isn’t known, although various reports suggest at least a dozen have had mandates.
The University of California, San Diego, offers a physical and mental screening program that health organizations can use to evaluate “late-career physicians,” and a 2021 report noted that “Nebraska’s Children’s Hospital requires physicians aged 70 years and older to undergo an assessment by several peers, a complete physical, and unspecified cognitive screening.” Another system, Hartford HealthCare, mandated an annual reappointment process for clinicians aged 70 or older, requiring them to undergo various exams.
There’s evidence that physician performance declines with age. However, age-based cognitive testing can run afoul of federal and state laws against age discrimination, said Sharona Hoffman, JD, professor of law and bioethics at Case Western Reserve University, Cleveland, in an interview.
Federal law prohibits age-related restrictions on employment but allows exceptions in areas like public safety, said Ms. Hoffman, who’s written about age discrimination and testing requirements. Pilots, law enforcement officers, firefighters, and air controllers, for example, can be forced to retire at specific ages.
It’s not clear how many physicians took the cognitive tests required by Henry Ford Medical Group.
However, details are available about the policy at Yale New Haven Hospital: According to the EEOC lawsuit, from 2016 to 2019, 145 physicians aged 70 or older took the mandatory test. Of those, seven individuals failed either or both of the exams, 14 were listed as “borderline deficient,” and one was listed as “deficient.” Another five refused testing and either resigned or changed their status. The EEOC case against the hospital is still pending.
“You can make an argument that health care is like a public safety job because people put their lives in the hands of doctors,” Ms. Hoffman said.
In defending mandatory cognitive tests, she said, health care systems could say, “it’s not really discrimination; we’re not forcing them to retire, we’re not limiting their work in any way. We’re just doing testing to make sure they perform competently, and the ADA allows us to conduct testing that is job-related.”
Indeed, a Yale New Haven Hospital spokesman made an argument along these lines in a statement regarding the 2020 lawsuit: The “policy is designed to protect our patients from potential harm while including safeguards to ensure that our physicians are treated fairly. The policy is modeled on similar standards in other industries, and we are confident that no discrimination has occurred and will vigorously defend ourselves in this matter.”
However, Ms. Hoffman herself doesn’t buy these arguments. Requiring tests only for older physicians does appear to be discrimination based on age, she said. As an alternative, “employers can do close supervision of people. As soon as there are performance problems or patient complaints, you need to see a doctor or get testing done.”
Another option is to mandate tests at specific ages via licensing boards. “I don’t think that would be legally problematic,” Ms. Hoffman said.
What else can be done to protect patients from clinicians whose skills have significantly declined as they’ve aged? The 2021 report in Neurology Clinical Practice notes that there are disadvantages to several strategies.
One common approach, waiting to evaluate a clinician until an error occurs, can lead to patient harm, the report’s authors wrote. Relying on reporting by peers is problematic because “physicians have been very resistant to reporting colleagues who are impaired” and the “medical apprenticeship model discourages physicians from reporting on senior colleagues.”
Physician self-assessment is yet another option, but “loss of insight may be a component of an individual’s impairment,” the authors wrote.
So what’s the best solution? The authors recommended “a relatively brief cognitive screening followed by more extensive testing for the most impaired individuals.” This approach “appears most reliable in confidentially identifying truly impaired physicians while minimizing the chance of a falsely flagging unimpaired individuals. This strategy allows aging physicians to continue working while safeguarding both their reputations and their patients’ health.”
Ms. Hoffman has no disclosures.
A version of this article first appeared on Medscape.com.
Lylas G. Mogk, MD, recently sued Henry Ford Health and Henry Ford Medical Group in federal court, alleging that the mandatory cognitive test violates the Americans with Disabilities Act, the Age Discrimination in Employment Act, and two Michigan laws.
Dr. Mogk’s lawsuit follows a widely watched 2020 case in which the U.S. Equal Employment Opportunity Commission sued Yale New Haven Hospital, the teaching hospital of Yale University, for age discrimination. According to the lawsuit, the hospital illegally required neuropsychological and eye examinations of physicians aged 70 or older who sought to gain or renew staff privileges.
According to the lawsuit, Dr. Mogk is a member of Henry Ford Medical Group, which in 2017 required all members aged 70 and older to undergo cognitive screening tests. The tests would be repeated every 5 years thereafter, the lawsuit said, and anyone who refused would have to resign or be fired.
Dr. Mogk completed the screening, although no information about the results or outcome was mentioned in the lawsuit. It’s not clear whether Henry Ford’s cognitive test mandate remains in place; a spokesperson for Henry Ford Health and attorneys for Dr. Mogk declined to comment.
The number of practicing physicians in their 70s and beyond is rising. A 2021 report found that 12% of U.S. licensed physicians in 2020 were least 70 years old, up from 9% in 2010 and an increase from 75,627 to 120,510. The percentage of doctors aged 60-69 grew to 19% from 16% in 2010.
The number of health systems requiring testing of older physicians isn’t known, although various reports suggest at least a dozen have had mandates.
The University of California, San Diego, offers a physical and mental screening program that health organizations can use to evaluate “late-career physicians,” and a 2021 report noted that “Nebraska’s Children’s Hospital requires physicians aged 70 years and older to undergo an assessment by several peers, a complete physical, and unspecified cognitive screening.” Another system, Hartford HealthCare, mandated an annual reappointment process for clinicians aged 70 or older, requiring them to undergo various exams.
There’s evidence that physician performance declines with age. However, age-based cognitive testing can run afoul of federal and state laws against age discrimination, said Sharona Hoffman, JD, professor of law and bioethics at Case Western Reserve University, Cleveland, in an interview.
Federal law prohibits age-related restrictions on employment but allows exceptions in areas like public safety, said Ms. Hoffman, who’s written about age discrimination and testing requirements. Pilots, law enforcement officers, firefighters, and air controllers, for example, can be forced to retire at specific ages.
It’s not clear how many physicians took the cognitive tests required by Henry Ford Medical Group.
However, details are available about the policy at Yale New Haven Hospital: According to the EEOC lawsuit, from 2016 to 2019, 145 physicians aged 70 or older took the mandatory test. Of those, seven individuals failed either or both of the exams, 14 were listed as “borderline deficient,” and one was listed as “deficient.” Another five refused testing and either resigned or changed their status. The EEOC case against the hospital is still pending.
“You can make an argument that health care is like a public safety job because people put their lives in the hands of doctors,” Ms. Hoffman said.
In defending mandatory cognitive tests, she said, health care systems could say, “it’s not really discrimination; we’re not forcing them to retire, we’re not limiting their work in any way. We’re just doing testing to make sure they perform competently, and the ADA allows us to conduct testing that is job-related.”
Indeed, a Yale New Haven Hospital spokesman made an argument along these lines in a statement regarding the 2020 lawsuit: The “policy is designed to protect our patients from potential harm while including safeguards to ensure that our physicians are treated fairly. The policy is modeled on similar standards in other industries, and we are confident that no discrimination has occurred and will vigorously defend ourselves in this matter.”
However, Ms. Hoffman herself doesn’t buy these arguments. Requiring tests only for older physicians does appear to be discrimination based on age, she said. As an alternative, “employers can do close supervision of people. As soon as there are performance problems or patient complaints, you need to see a doctor or get testing done.”
Another option is to mandate tests at specific ages via licensing boards. “I don’t think that would be legally problematic,” Ms. Hoffman said.
What else can be done to protect patients from clinicians whose skills have significantly declined as they’ve aged? The 2021 report in Neurology Clinical Practice notes that there are disadvantages to several strategies.
One common approach, waiting to evaluate a clinician until an error occurs, can lead to patient harm, the report’s authors wrote. Relying on reporting by peers is problematic because “physicians have been very resistant to reporting colleagues who are impaired” and the “medical apprenticeship model discourages physicians from reporting on senior colleagues.”
Physician self-assessment is yet another option, but “loss of insight may be a component of an individual’s impairment,” the authors wrote.
So what’s the best solution? The authors recommended “a relatively brief cognitive screening followed by more extensive testing for the most impaired individuals.” This approach “appears most reliable in confidentially identifying truly impaired physicians while minimizing the chance of a falsely flagging unimpaired individuals. This strategy allows aging physicians to continue working while safeguarding both their reputations and their patients’ health.”
Ms. Hoffman has no disclosures.
A version of this article first appeared on Medscape.com.
Lylas G. Mogk, MD, recently sued Henry Ford Health and Henry Ford Medical Group in federal court, alleging that the mandatory cognitive test violates the Americans with Disabilities Act, the Age Discrimination in Employment Act, and two Michigan laws.
Dr. Mogk’s lawsuit follows a widely watched 2020 case in which the U.S. Equal Employment Opportunity Commission sued Yale New Haven Hospital, the teaching hospital of Yale University, for age discrimination. According to the lawsuit, the hospital illegally required neuropsychological and eye examinations of physicians aged 70 or older who sought to gain or renew staff privileges.
According to the lawsuit, Dr. Mogk is a member of Henry Ford Medical Group, which in 2017 required all members aged 70 and older to undergo cognitive screening tests. The tests would be repeated every 5 years thereafter, the lawsuit said, and anyone who refused would have to resign or be fired.
Dr. Mogk completed the screening, although no information about the results or outcome was mentioned in the lawsuit. It’s not clear whether Henry Ford’s cognitive test mandate remains in place; a spokesperson for Henry Ford Health and attorneys for Dr. Mogk declined to comment.
The number of practicing physicians in their 70s and beyond is rising. A 2021 report found that 12% of U.S. licensed physicians in 2020 were least 70 years old, up from 9% in 2010 and an increase from 75,627 to 120,510. The percentage of doctors aged 60-69 grew to 19% from 16% in 2010.
The number of health systems requiring testing of older physicians isn’t known, although various reports suggest at least a dozen have had mandates.
The University of California, San Diego, offers a physical and mental screening program that health organizations can use to evaluate “late-career physicians,” and a 2021 report noted that “Nebraska’s Children’s Hospital requires physicians aged 70 years and older to undergo an assessment by several peers, a complete physical, and unspecified cognitive screening.” Another system, Hartford HealthCare, mandated an annual reappointment process for clinicians aged 70 or older, requiring them to undergo various exams.
There’s evidence that physician performance declines with age. However, age-based cognitive testing can run afoul of federal and state laws against age discrimination, said Sharona Hoffman, JD, professor of law and bioethics at Case Western Reserve University, Cleveland, in an interview.
Federal law prohibits age-related restrictions on employment but allows exceptions in areas like public safety, said Ms. Hoffman, who’s written about age discrimination and testing requirements. Pilots, law enforcement officers, firefighters, and air controllers, for example, can be forced to retire at specific ages.
It’s not clear how many physicians took the cognitive tests required by Henry Ford Medical Group.
However, details are available about the policy at Yale New Haven Hospital: According to the EEOC lawsuit, from 2016 to 2019, 145 physicians aged 70 or older took the mandatory test. Of those, seven individuals failed either or both of the exams, 14 were listed as “borderline deficient,” and one was listed as “deficient.” Another five refused testing and either resigned or changed their status. The EEOC case against the hospital is still pending.
“You can make an argument that health care is like a public safety job because people put their lives in the hands of doctors,” Ms. Hoffman said.
In defending mandatory cognitive tests, she said, health care systems could say, “it’s not really discrimination; we’re not forcing them to retire, we’re not limiting their work in any way. We’re just doing testing to make sure they perform competently, and the ADA allows us to conduct testing that is job-related.”
Indeed, a Yale New Haven Hospital spokesman made an argument along these lines in a statement regarding the 2020 lawsuit: The “policy is designed to protect our patients from potential harm while including safeguards to ensure that our physicians are treated fairly. The policy is modeled on similar standards in other industries, and we are confident that no discrimination has occurred and will vigorously defend ourselves in this matter.”
However, Ms. Hoffman herself doesn’t buy these arguments. Requiring tests only for older physicians does appear to be discrimination based on age, she said. As an alternative, “employers can do close supervision of people. As soon as there are performance problems or patient complaints, you need to see a doctor or get testing done.”
Another option is to mandate tests at specific ages via licensing boards. “I don’t think that would be legally problematic,” Ms. Hoffman said.
What else can be done to protect patients from clinicians whose skills have significantly declined as they’ve aged? The 2021 report in Neurology Clinical Practice notes that there are disadvantages to several strategies.
One common approach, waiting to evaluate a clinician until an error occurs, can lead to patient harm, the report’s authors wrote. Relying on reporting by peers is problematic because “physicians have been very resistant to reporting colleagues who are impaired” and the “medical apprenticeship model discourages physicians from reporting on senior colleagues.”
Physician self-assessment is yet another option, but “loss of insight may be a component of an individual’s impairment,” the authors wrote.
So what’s the best solution? The authors recommended “a relatively brief cognitive screening followed by more extensive testing for the most impaired individuals.” This approach “appears most reliable in confidentially identifying truly impaired physicians while minimizing the chance of a falsely flagging unimpaired individuals. This strategy allows aging physicians to continue working while safeguarding both their reputations and their patients’ health.”
Ms. Hoffman has no disclosures.
A version of this article first appeared on Medscape.com.
Addressing supply-demand mismatch in GI
Impacts of this supply-demand mismatch are felt daily in our GI practices as we strive to expand access in our clinics and endoscopy suites, particularly in rural and urban underserved communities. In gastroenterology, increased demand for care has been driven by a perfect storm of population growth, increased patient awareness of GI health, and rising incidence of digestive diseases.
Between 2019 and 2034, the U.S. population is expected to grow by 10.6%, while the population aged 65 and older expands by over 42%. Recent increases in the CRC screening–eligible population also have contributed to unprecedented demand for GI care. Furthermore, care delivery has become more complex and time-consuming with the evolution of personalized medicine and high prevalence of comorbid conditions. At the same time, we are faced with a dwindling supply of gastroenterology providers. In 2021, there were 15,678 practicing gastroenterologists in the U.S., over half of whom were 55 years or older. This translates to 1 gastroenterologist per 20,830 people captured in the U.S. Census.
Addressing this striking supply-demand mismatch in GI requires a multi-pronged approach that addresses its complex drivers. First and foremost, we must expand the number of GI fellowship training slots to boost our pipeline. There are approximately 1,840 GI fellows currently in training, a third of whom enter the workforce each year. While the number of GI fellowship slots in the GI fellowship match has slowly increased over time (from 525 available slots across 199 programs in 2019 to 657 slots across 230 programs in 2023), this incremental growth is dwarfed by overall need. Continued advocacy for increased funding to support expansion of training slots is necessary to further move the needle – such lobbying recently led to the addition of 1,000 new Medicare-supported graduate medical education positions across specialties over a 5-year period starting in 2020, illustrating that change is possible. At the same time, we must address the factors that are causing gastroenterologists to leave the workforce prematurely through early retirement or part-time work by investing in innovative solutions to address burnout, reduce administrative burdens, enhance the efficiency of care delivery, and maintain financial viability. By investing in our physician workforce and its sustainability, we can ensure that our profession is better prepared to meet the needs of our growing and increasingly complex patient population now and in the future.
We hope you enjoy the November issue of GI & Hepatology News and have a wonderful Thanksgiving.
Megan A. Adams, MD, JD, MSc
Editor-in-Chief
Impacts of this supply-demand mismatch are felt daily in our GI practices as we strive to expand access in our clinics and endoscopy suites, particularly in rural and urban underserved communities. In gastroenterology, increased demand for care has been driven by a perfect storm of population growth, increased patient awareness of GI health, and rising incidence of digestive diseases.
Between 2019 and 2034, the U.S. population is expected to grow by 10.6%, while the population aged 65 and older expands by over 42%. Recent increases in the CRC screening–eligible population also have contributed to unprecedented demand for GI care. Furthermore, care delivery has become more complex and time-consuming with the evolution of personalized medicine and high prevalence of comorbid conditions. At the same time, we are faced with a dwindling supply of gastroenterology providers. In 2021, there were 15,678 practicing gastroenterologists in the U.S., over half of whom were 55 years or older. This translates to 1 gastroenterologist per 20,830 people captured in the U.S. Census.
Addressing this striking supply-demand mismatch in GI requires a multi-pronged approach that addresses its complex drivers. First and foremost, we must expand the number of GI fellowship training slots to boost our pipeline. There are approximately 1,840 GI fellows currently in training, a third of whom enter the workforce each year. While the number of GI fellowship slots in the GI fellowship match has slowly increased over time (from 525 available slots across 199 programs in 2019 to 657 slots across 230 programs in 2023), this incremental growth is dwarfed by overall need. Continued advocacy for increased funding to support expansion of training slots is necessary to further move the needle – such lobbying recently led to the addition of 1,000 new Medicare-supported graduate medical education positions across specialties over a 5-year period starting in 2020, illustrating that change is possible. At the same time, we must address the factors that are causing gastroenterologists to leave the workforce prematurely through early retirement or part-time work by investing in innovative solutions to address burnout, reduce administrative burdens, enhance the efficiency of care delivery, and maintain financial viability. By investing in our physician workforce and its sustainability, we can ensure that our profession is better prepared to meet the needs of our growing and increasingly complex patient population now and in the future.
We hope you enjoy the November issue of GI & Hepatology News and have a wonderful Thanksgiving.
Megan A. Adams, MD, JD, MSc
Editor-in-Chief
Impacts of this supply-demand mismatch are felt daily in our GI practices as we strive to expand access in our clinics and endoscopy suites, particularly in rural and urban underserved communities. In gastroenterology, increased demand for care has been driven by a perfect storm of population growth, increased patient awareness of GI health, and rising incidence of digestive diseases.
Between 2019 and 2034, the U.S. population is expected to grow by 10.6%, while the population aged 65 and older expands by over 42%. Recent increases in the CRC screening–eligible population also have contributed to unprecedented demand for GI care. Furthermore, care delivery has become more complex and time-consuming with the evolution of personalized medicine and high prevalence of comorbid conditions. At the same time, we are faced with a dwindling supply of gastroenterology providers. In 2021, there were 15,678 practicing gastroenterologists in the U.S., over half of whom were 55 years or older. This translates to 1 gastroenterologist per 20,830 people captured in the U.S. Census.
Addressing this striking supply-demand mismatch in GI requires a multi-pronged approach that addresses its complex drivers. First and foremost, we must expand the number of GI fellowship training slots to boost our pipeline. There are approximately 1,840 GI fellows currently in training, a third of whom enter the workforce each year. While the number of GI fellowship slots in the GI fellowship match has slowly increased over time (from 525 available slots across 199 programs in 2019 to 657 slots across 230 programs in 2023), this incremental growth is dwarfed by overall need. Continued advocacy for increased funding to support expansion of training slots is necessary to further move the needle – such lobbying recently led to the addition of 1,000 new Medicare-supported graduate medical education positions across specialties over a 5-year period starting in 2020, illustrating that change is possible. At the same time, we must address the factors that are causing gastroenterologists to leave the workforce prematurely through early retirement or part-time work by investing in innovative solutions to address burnout, reduce administrative burdens, enhance the efficiency of care delivery, and maintain financial viability. By investing in our physician workforce and its sustainability, we can ensure that our profession is better prepared to meet the needs of our growing and increasingly complex patient population now and in the future.
We hope you enjoy the November issue of GI & Hepatology News and have a wonderful Thanksgiving.
Megan A. Adams, MD, JD, MSc
Editor-in-Chief

Seven metrics oncology practices can track to be successful
and see how they measure up against their peers.
“Once practices figure out what they want to measure, and obviously they want to measure things that they’re not doing so well, they can look for opportunities for improvement,” said Diana Berich Brieva, DHA, MBA, CPC-A, the CEO of Ambulatory Care Consultants, which partners with medical practices to optimize operations and increase revenue.
Benchmarking your practice against others shows you how your numbers stack up to other practices’ metrics by percentile – for instance, whether your revenue is in the 25th, 50th, or 75th percentile against similar practices.
The 2024 MIPS Value Pathways (MVP) for Advancing Cancer Care is a new CMS program with specific metric criteria. The voluntary program has a Nov. 30, 2023, deadline for practices to sign up. The purpose of the program is to help practices identify areas where they can improve. Also, oncology societies such as the American Society of Clinical Oncology (ASCO) have developed metrics for this specialty.
Still, for many practices, it’s essential to develop your own metrics according to your patient population and available resources, explained Dr. Brieva.
Here are seven popular oncology metrics that many practices track to measure success.
1. Productivity
Every practice may think about productivity differently depending on whether it focuses on new patients, revenue, business development, or a combination. You can measure physician productivity in many ways: by the number of new patients per full-time employee (FTE), work relative value units (wRVU) per FTE, which measures physician work, and established patient visits.
Some clinics measure for wRVU for chemotherapy administration and per-hospital visits as a percentage of total patients as well. “We’re a community-based oncology practice, so we don’t use RVUs, but we do use other production numbers,” said Emily Touloukian, DO, an oncologist-hematologist and president of Coastal Cancer Center with four locations around South Carolina. She is assistant professor of internal medicine at the University of South Carolina, Columbia.
“There are lots of quality programs out there that measure how well oncology practices are meeting guidelines. The one we’ve participated with since its inception is [the] Quality Oncology Practice Initiative (QOPI) through [the] American Society of Clinical Oncology (ASCO),” said Dr. Touloukian. “Basically, it’s a chart review and extraction of various indicators in accordance with quality measures.”
Pontchartrain Cancer Center, with four locations around Louisiana, tracks the number of new patients in hematology and oncology by location and provider. They also track follow-up patients. New and follow-up patient metrics are broken down by visit code.
“The E&M code tells me the level of acuity that the physician coded for,” said Kathy Oubre, MS, the CEO of Pontchartrain. Patients with complicated cases get a higher-paying code since clinics get paid differently for each code. Ms. Oubre tracks the codes by provider and says if they bill every patient with the same code, it can put your practice at risk for an audit, even when it’s the lowest billable code.
In the 2019 ASCO survey, the number of new patient visits reported by participants averaged 301 visits per FTE. Established patient visits averaged 3,334.
“When we talk about metrics and how we measure things and how successful our practice is, productivity also has to do with how satisfied the people working for you and with you are,” said Dr. Touloukian.
“If you’re not providing a supportive workplace for your physicians and employees, you’re not going to be successful,” she said. “You’ll end up with doctors coming and going every 2 years, employees quitting all the time, and a need for retraining.” Instead, if you can create a welcoming, sustainable environment where people are happy to come to work, physicians aren’t burnt out, and get to spend time away from the clinic to recharge, productivity will be more successful.
2. Revenue
When participating in their voluntary survey, practices can get a copy of revenue metric data annually from the Medical Group Management Association (MGMA). It collects the number of FTEs, gross revenue, net revenue, and collection rate and is broken down by specialties so your practice can benchmark against others. Total revenue, including oncologists’ salaries per FTE from the ASCO survey, was $7,323,900, but comparisons are difficult since practices differ in services.
Revenue metrics can consist of total revenue (cash collections), net medical excluding radiation services, drug revenue for infusion services, cash expenses including salaries, net accounts receivable, and gross accounts receivable minus contractual allowances and bad debt. Practices can differ on bad debt collection because of the emotional nature of cancer treatment. However, some use revenue cycle management companies with debt collection services; others find charity foundation funds for patients who can’t pay.
Pontchartrain also tracks when its clinic gets paid. Ms. Oubre said the best practice is that your claims receive payment within 21 days. They send claims out every 24 hours. “For example, most of that money is in drugs we’ve administered to patients we’ve likely already paid for.” Since there is a gap between paying their wholesaler for drugs and receiving reimbursement, they closely track claims and payment metrics.
Any claims that get sent back are refiled and sent out again within 24 hours. When claims hit 31 days without a response, the practice reaches out to learn the problem. “We’re proactive rather than waiting for the denial to come,” Ms. Oubre told this news organization. Dr. Brieva said for every revenue metric a practice tracks in which they’re not performing well, the practice has to find a solution. Are too many claims being denied? Do claim forms contain errors? Are most claims being paid in the 21-day window? Is the problem a user error, an issue with the clearinghouse, or an intake error on the other end? The key to successful metric use is to drill down for answers to these questions.
3. Patient satisfaction
Patient satisfaction may be one of the more straightforward metrics practices can track, though not specific to oncology. Dr. Brieva said most metric programs include patient satisfaction surveys against which you can benchmark your practice. You can also create your own emailed patient surveys. The metric can show how satisfied your patients are and how you compare against other practices.
Ms. Oubre said Pontchartrain also tracks metrics around participating in advanced care planning, survivorship care, and transitional care management. Even though most insurers require copays for these services, they’ve found patients who participate in them have an overall better experience.
“The Biden administration also has a Cancer Moon Shot initiative, which intends to reduce cancer deaths by 50% by 2047,” said Dr. Brieva. “They want to reduce deaths and improve the experience of patients. So, tracking survival rates will also be key for this program.”
4. Referrals
Oncology is typically a referral business. So, keeping track of the top referring physicians every quarter is the best way to ensure your referring clinicians are happy with your practice’s service. A best practice is that all new oncology referrals are seen within 48 hours. If your referral metric drops off, especially for top referrers, a physician from your practice should check in with the referrer.
Ms. Oubre runs reports out of the EMR and scrubs for referring providers, so she’s alerted to any issues. “It can be as simple as a front office staff who was rude on the phone,” she said. “We had an issue years ago with one of our schedulers who didn’t want to risk staying after 5:00 p.m., so she wouldn’t put anyone on the schedule after 3:00. But if I hadn’t called and identified that from the referring practitioner, I wouldn’t have known that they couldn’t get late-afternoon appointments at our clinic.”
5. No-show appointments
Practices track no-shows per week to determine which patients did not show up for their visits vs. those who rescheduled. If a patient on active treatment starts no-showing, practices must find out why. Is it a social or a transportation issue, or do they want to discontinue treatment? Often, you can help with the problem if you know what it is.
“Sometimes we can help from a social determinants of health perspective, helping to provide services like transportation, financial assistance, or other things, and patients appreciate that we would care enough to reach out to see if we can help,” said Ms. Oubre.
For recurring no-shows, practices should notify the referring provider. Letting the referring clinician know that the patient stopped coming is a professional courtesy that helps strengthen your referral relationships. You wouldn’t want the referring physician to think the patient is being treated for cancer only to find out later that they discontinued treatment.
6. Injections and infusions
By tracking the number of injections and infusions per location per week, clinics can assess how busy their chemo chairs are and how many injections they give. Benchmarks include the number of initial intravenous infusions/injections and the total number of drug administration services per patient per chair. Similar metrics in radiation oncology are helpful.
7. Pharmacy prescriptions
For practices with an in-house pharmacy, tracking how many prescriptions are written per week by each provider and whether they could fill them in-house or had to send them out to a specialty pharmacy because of an insurance issue tells you the volume of drugs your pharmacy is fulfilling. Point-of-care dispensing pharmacy revenue averaged $1,843,342 in the ASCO survey.
Dr. Brieva mentioned many other trackable metrics, such as the time to start treatment, adherence to treatment guidelines, rates of side effects and complications, patient retention rates, treatment completion rates, and coordination of care with other providers, which may be additional metrics your practice wants to track.
Dr. Touloukian said that practices must be careful how they measure some metrics because if you’re extracting data from the EMR and someone hasn’t entered it correctly, you won’t get accurate information. “I like programs like QOPI because while it’s a little labor intensive, my staff actually goes in and extracts the data from the charts and shows the proof.
“Comparing yourself to other [oncology] practices across the nation helps to ensure you’re achieving a certain level of success on some of these traditional metrics,” said Dr. Touloukian.
A version of this article first appeared on Medscape.com.
and see how they measure up against their peers.
“Once practices figure out what they want to measure, and obviously they want to measure things that they’re not doing so well, they can look for opportunities for improvement,” said Diana Berich Brieva, DHA, MBA, CPC-A, the CEO of Ambulatory Care Consultants, which partners with medical practices to optimize operations and increase revenue.
Benchmarking your practice against others shows you how your numbers stack up to other practices’ metrics by percentile – for instance, whether your revenue is in the 25th, 50th, or 75th percentile against similar practices.
The 2024 MIPS Value Pathways (MVP) for Advancing Cancer Care is a new CMS program with specific metric criteria. The voluntary program has a Nov. 30, 2023, deadline for practices to sign up. The purpose of the program is to help practices identify areas where they can improve. Also, oncology societies such as the American Society of Clinical Oncology (ASCO) have developed metrics for this specialty.
Still, for many practices, it’s essential to develop your own metrics according to your patient population and available resources, explained Dr. Brieva.
Here are seven popular oncology metrics that many practices track to measure success.
1. Productivity
Every practice may think about productivity differently depending on whether it focuses on new patients, revenue, business development, or a combination. You can measure physician productivity in many ways: by the number of new patients per full-time employee (FTE), work relative value units (wRVU) per FTE, which measures physician work, and established patient visits.
Some clinics measure for wRVU for chemotherapy administration and per-hospital visits as a percentage of total patients as well. “We’re a community-based oncology practice, so we don’t use RVUs, but we do use other production numbers,” said Emily Touloukian, DO, an oncologist-hematologist and president of Coastal Cancer Center with four locations around South Carolina. She is assistant professor of internal medicine at the University of South Carolina, Columbia.
“There are lots of quality programs out there that measure how well oncology practices are meeting guidelines. The one we’ve participated with since its inception is [the] Quality Oncology Practice Initiative (QOPI) through [the] American Society of Clinical Oncology (ASCO),” said Dr. Touloukian. “Basically, it’s a chart review and extraction of various indicators in accordance with quality measures.”
Pontchartrain Cancer Center, with four locations around Louisiana, tracks the number of new patients in hematology and oncology by location and provider. They also track follow-up patients. New and follow-up patient metrics are broken down by visit code.
“The E&M code tells me the level of acuity that the physician coded for,” said Kathy Oubre, MS, the CEO of Pontchartrain. Patients with complicated cases get a higher-paying code since clinics get paid differently for each code. Ms. Oubre tracks the codes by provider and says if they bill every patient with the same code, it can put your practice at risk for an audit, even when it’s the lowest billable code.
In the 2019 ASCO survey, the number of new patient visits reported by participants averaged 301 visits per FTE. Established patient visits averaged 3,334.
“When we talk about metrics and how we measure things and how successful our practice is, productivity also has to do with how satisfied the people working for you and with you are,” said Dr. Touloukian.
“If you’re not providing a supportive workplace for your physicians and employees, you’re not going to be successful,” she said. “You’ll end up with doctors coming and going every 2 years, employees quitting all the time, and a need for retraining.” Instead, if you can create a welcoming, sustainable environment where people are happy to come to work, physicians aren’t burnt out, and get to spend time away from the clinic to recharge, productivity will be more successful.
2. Revenue
When participating in their voluntary survey, practices can get a copy of revenue metric data annually from the Medical Group Management Association (MGMA). It collects the number of FTEs, gross revenue, net revenue, and collection rate and is broken down by specialties so your practice can benchmark against others. Total revenue, including oncologists’ salaries per FTE from the ASCO survey, was $7,323,900, but comparisons are difficult since practices differ in services.
Revenue metrics can consist of total revenue (cash collections), net medical excluding radiation services, drug revenue for infusion services, cash expenses including salaries, net accounts receivable, and gross accounts receivable minus contractual allowances and bad debt. Practices can differ on bad debt collection because of the emotional nature of cancer treatment. However, some use revenue cycle management companies with debt collection services; others find charity foundation funds for patients who can’t pay.
Pontchartrain also tracks when its clinic gets paid. Ms. Oubre said the best practice is that your claims receive payment within 21 days. They send claims out every 24 hours. “For example, most of that money is in drugs we’ve administered to patients we’ve likely already paid for.” Since there is a gap between paying their wholesaler for drugs and receiving reimbursement, they closely track claims and payment metrics.
Any claims that get sent back are refiled and sent out again within 24 hours. When claims hit 31 days without a response, the practice reaches out to learn the problem. “We’re proactive rather than waiting for the denial to come,” Ms. Oubre told this news organization. Dr. Brieva said for every revenue metric a practice tracks in which they’re not performing well, the practice has to find a solution. Are too many claims being denied? Do claim forms contain errors? Are most claims being paid in the 21-day window? Is the problem a user error, an issue with the clearinghouse, or an intake error on the other end? The key to successful metric use is to drill down for answers to these questions.
3. Patient satisfaction
Patient satisfaction may be one of the more straightforward metrics practices can track, though not specific to oncology. Dr. Brieva said most metric programs include patient satisfaction surveys against which you can benchmark your practice. You can also create your own emailed patient surveys. The metric can show how satisfied your patients are and how you compare against other practices.
Ms. Oubre said Pontchartrain also tracks metrics around participating in advanced care planning, survivorship care, and transitional care management. Even though most insurers require copays for these services, they’ve found patients who participate in them have an overall better experience.
“The Biden administration also has a Cancer Moon Shot initiative, which intends to reduce cancer deaths by 50% by 2047,” said Dr. Brieva. “They want to reduce deaths and improve the experience of patients. So, tracking survival rates will also be key for this program.”
4. Referrals
Oncology is typically a referral business. So, keeping track of the top referring physicians every quarter is the best way to ensure your referring clinicians are happy with your practice’s service. A best practice is that all new oncology referrals are seen within 48 hours. If your referral metric drops off, especially for top referrers, a physician from your practice should check in with the referrer.
Ms. Oubre runs reports out of the EMR and scrubs for referring providers, so she’s alerted to any issues. “It can be as simple as a front office staff who was rude on the phone,” she said. “We had an issue years ago with one of our schedulers who didn’t want to risk staying after 5:00 p.m., so she wouldn’t put anyone on the schedule after 3:00. But if I hadn’t called and identified that from the referring practitioner, I wouldn’t have known that they couldn’t get late-afternoon appointments at our clinic.”
5. No-show appointments
Practices track no-shows per week to determine which patients did not show up for their visits vs. those who rescheduled. If a patient on active treatment starts no-showing, practices must find out why. Is it a social or a transportation issue, or do they want to discontinue treatment? Often, you can help with the problem if you know what it is.
“Sometimes we can help from a social determinants of health perspective, helping to provide services like transportation, financial assistance, or other things, and patients appreciate that we would care enough to reach out to see if we can help,” said Ms. Oubre.
For recurring no-shows, practices should notify the referring provider. Letting the referring clinician know that the patient stopped coming is a professional courtesy that helps strengthen your referral relationships. You wouldn’t want the referring physician to think the patient is being treated for cancer only to find out later that they discontinued treatment.
6. Injections and infusions
By tracking the number of injections and infusions per location per week, clinics can assess how busy their chemo chairs are and how many injections they give. Benchmarks include the number of initial intravenous infusions/injections and the total number of drug administration services per patient per chair. Similar metrics in radiation oncology are helpful.
7. Pharmacy prescriptions
For practices with an in-house pharmacy, tracking how many prescriptions are written per week by each provider and whether they could fill them in-house or had to send them out to a specialty pharmacy because of an insurance issue tells you the volume of drugs your pharmacy is fulfilling. Point-of-care dispensing pharmacy revenue averaged $1,843,342 in the ASCO survey.
Dr. Brieva mentioned many other trackable metrics, such as the time to start treatment, adherence to treatment guidelines, rates of side effects and complications, patient retention rates, treatment completion rates, and coordination of care with other providers, which may be additional metrics your practice wants to track.
Dr. Touloukian said that practices must be careful how they measure some metrics because if you’re extracting data from the EMR and someone hasn’t entered it correctly, you won’t get accurate information. “I like programs like QOPI because while it’s a little labor intensive, my staff actually goes in and extracts the data from the charts and shows the proof.
“Comparing yourself to other [oncology] practices across the nation helps to ensure you’re achieving a certain level of success on some of these traditional metrics,” said Dr. Touloukian.
A version of this article first appeared on Medscape.com.
and see how they measure up against their peers.
“Once practices figure out what they want to measure, and obviously they want to measure things that they’re not doing so well, they can look for opportunities for improvement,” said Diana Berich Brieva, DHA, MBA, CPC-A, the CEO of Ambulatory Care Consultants, which partners with medical practices to optimize operations and increase revenue.
Benchmarking your practice against others shows you how your numbers stack up to other practices’ metrics by percentile – for instance, whether your revenue is in the 25th, 50th, or 75th percentile against similar practices.
The 2024 MIPS Value Pathways (MVP) for Advancing Cancer Care is a new CMS program with specific metric criteria. The voluntary program has a Nov. 30, 2023, deadline for practices to sign up. The purpose of the program is to help practices identify areas where they can improve. Also, oncology societies such as the American Society of Clinical Oncology (ASCO) have developed metrics for this specialty.
Still, for many practices, it’s essential to develop your own metrics according to your patient population and available resources, explained Dr. Brieva.
Here are seven popular oncology metrics that many practices track to measure success.
1. Productivity
Every practice may think about productivity differently depending on whether it focuses on new patients, revenue, business development, or a combination. You can measure physician productivity in many ways: by the number of new patients per full-time employee (FTE), work relative value units (wRVU) per FTE, which measures physician work, and established patient visits.
Some clinics measure for wRVU for chemotherapy administration and per-hospital visits as a percentage of total patients as well. “We’re a community-based oncology practice, so we don’t use RVUs, but we do use other production numbers,” said Emily Touloukian, DO, an oncologist-hematologist and president of Coastal Cancer Center with four locations around South Carolina. She is assistant professor of internal medicine at the University of South Carolina, Columbia.
“There are lots of quality programs out there that measure how well oncology practices are meeting guidelines. The one we’ve participated with since its inception is [the] Quality Oncology Practice Initiative (QOPI) through [the] American Society of Clinical Oncology (ASCO),” said Dr. Touloukian. “Basically, it’s a chart review and extraction of various indicators in accordance with quality measures.”
Pontchartrain Cancer Center, with four locations around Louisiana, tracks the number of new patients in hematology and oncology by location and provider. They also track follow-up patients. New and follow-up patient metrics are broken down by visit code.
“The E&M code tells me the level of acuity that the physician coded for,” said Kathy Oubre, MS, the CEO of Pontchartrain. Patients with complicated cases get a higher-paying code since clinics get paid differently for each code. Ms. Oubre tracks the codes by provider and says if they bill every patient with the same code, it can put your practice at risk for an audit, even when it’s the lowest billable code.
In the 2019 ASCO survey, the number of new patient visits reported by participants averaged 301 visits per FTE. Established patient visits averaged 3,334.
“When we talk about metrics and how we measure things and how successful our practice is, productivity also has to do with how satisfied the people working for you and with you are,” said Dr. Touloukian.
“If you’re not providing a supportive workplace for your physicians and employees, you’re not going to be successful,” she said. “You’ll end up with doctors coming and going every 2 years, employees quitting all the time, and a need for retraining.” Instead, if you can create a welcoming, sustainable environment where people are happy to come to work, physicians aren’t burnt out, and get to spend time away from the clinic to recharge, productivity will be more successful.
2. Revenue
When participating in their voluntary survey, practices can get a copy of revenue metric data annually from the Medical Group Management Association (MGMA). It collects the number of FTEs, gross revenue, net revenue, and collection rate and is broken down by specialties so your practice can benchmark against others. Total revenue, including oncologists’ salaries per FTE from the ASCO survey, was $7,323,900, but comparisons are difficult since practices differ in services.
Revenue metrics can consist of total revenue (cash collections), net medical excluding radiation services, drug revenue for infusion services, cash expenses including salaries, net accounts receivable, and gross accounts receivable minus contractual allowances and bad debt. Practices can differ on bad debt collection because of the emotional nature of cancer treatment. However, some use revenue cycle management companies with debt collection services; others find charity foundation funds for patients who can’t pay.
Pontchartrain also tracks when its clinic gets paid. Ms. Oubre said the best practice is that your claims receive payment within 21 days. They send claims out every 24 hours. “For example, most of that money is in drugs we’ve administered to patients we’ve likely already paid for.” Since there is a gap between paying their wholesaler for drugs and receiving reimbursement, they closely track claims and payment metrics.
Any claims that get sent back are refiled and sent out again within 24 hours. When claims hit 31 days without a response, the practice reaches out to learn the problem. “We’re proactive rather than waiting for the denial to come,” Ms. Oubre told this news organization. Dr. Brieva said for every revenue metric a practice tracks in which they’re not performing well, the practice has to find a solution. Are too many claims being denied? Do claim forms contain errors? Are most claims being paid in the 21-day window? Is the problem a user error, an issue with the clearinghouse, or an intake error on the other end? The key to successful metric use is to drill down for answers to these questions.
3. Patient satisfaction
Patient satisfaction may be one of the more straightforward metrics practices can track, though not specific to oncology. Dr. Brieva said most metric programs include patient satisfaction surveys against which you can benchmark your practice. You can also create your own emailed patient surveys. The metric can show how satisfied your patients are and how you compare against other practices.
Ms. Oubre said Pontchartrain also tracks metrics around participating in advanced care planning, survivorship care, and transitional care management. Even though most insurers require copays for these services, they’ve found patients who participate in them have an overall better experience.
“The Biden administration also has a Cancer Moon Shot initiative, which intends to reduce cancer deaths by 50% by 2047,” said Dr. Brieva. “They want to reduce deaths and improve the experience of patients. So, tracking survival rates will also be key for this program.”
4. Referrals
Oncology is typically a referral business. So, keeping track of the top referring physicians every quarter is the best way to ensure your referring clinicians are happy with your practice’s service. A best practice is that all new oncology referrals are seen within 48 hours. If your referral metric drops off, especially for top referrers, a physician from your practice should check in with the referrer.
Ms. Oubre runs reports out of the EMR and scrubs for referring providers, so she’s alerted to any issues. “It can be as simple as a front office staff who was rude on the phone,” she said. “We had an issue years ago with one of our schedulers who didn’t want to risk staying after 5:00 p.m., so she wouldn’t put anyone on the schedule after 3:00. But if I hadn’t called and identified that from the referring practitioner, I wouldn’t have known that they couldn’t get late-afternoon appointments at our clinic.”
5. No-show appointments
Practices track no-shows per week to determine which patients did not show up for their visits vs. those who rescheduled. If a patient on active treatment starts no-showing, practices must find out why. Is it a social or a transportation issue, or do they want to discontinue treatment? Often, you can help with the problem if you know what it is.
“Sometimes we can help from a social determinants of health perspective, helping to provide services like transportation, financial assistance, or other things, and patients appreciate that we would care enough to reach out to see if we can help,” said Ms. Oubre.
For recurring no-shows, practices should notify the referring provider. Letting the referring clinician know that the patient stopped coming is a professional courtesy that helps strengthen your referral relationships. You wouldn’t want the referring physician to think the patient is being treated for cancer only to find out later that they discontinued treatment.
6. Injections and infusions
By tracking the number of injections and infusions per location per week, clinics can assess how busy their chemo chairs are and how many injections they give. Benchmarks include the number of initial intravenous infusions/injections and the total number of drug administration services per patient per chair. Similar metrics in radiation oncology are helpful.
7. Pharmacy prescriptions
For practices with an in-house pharmacy, tracking how many prescriptions are written per week by each provider and whether they could fill them in-house or had to send them out to a specialty pharmacy because of an insurance issue tells you the volume of drugs your pharmacy is fulfilling. Point-of-care dispensing pharmacy revenue averaged $1,843,342 in the ASCO survey.
Dr. Brieva mentioned many other trackable metrics, such as the time to start treatment, adherence to treatment guidelines, rates of side effects and complications, patient retention rates, treatment completion rates, and coordination of care with other providers, which may be additional metrics your practice wants to track.
Dr. Touloukian said that practices must be careful how they measure some metrics because if you’re extracting data from the EMR and someone hasn’t entered it correctly, you won’t get accurate information. “I like programs like QOPI because while it’s a little labor intensive, my staff actually goes in and extracts the data from the charts and shows the proof.
“Comparing yourself to other [oncology] practices across the nation helps to ensure you’re achieving a certain level of success on some of these traditional metrics,” said Dr. Touloukian.
A version of this article first appeared on Medscape.com.
Teledermatology: A Postpandemic Update
The rapid expansion of teledermatology in the United States due to the COVID-19 pandemic has been well documented, 1 but where do we stand now that health care and society as a whole are back to a new version of normal? It is important to consider why telemedicine was able to grow so quickly during that period—the Centers for Medicare & Medicaid Services (CMS) unilaterally changed policies related to provision of services and reimbursement thereof due to the public health emergency (PHE), which was declared by the Department of Health and Human Services in January 2020 to provide increased access to care for patients. Under the PHE, reimbursement rates for virtual visits improved, providers could care for patients from their homes and across state lines, and the use of video platforms that were not Health Insurance Portability and Accountability Act compliant was allowed. 2,3
The trajectory of teledermatology after the pandemic, however, remains unclear. In a survey assessing dermatologists’ perceptions of telemedicine (N=4356), 97% used telemedicine during the pandemic but only 58% reported that they intended to continue using teledermatology postpandemic,1 which is driven, at least in part, by the potential concern that dermatologists will again experience the same regulatory and logistical barriers that limited teledermatology utilization prepandemic.
What has changed in reimbursement for teledermatology since the PHE ended?
The PHE ended on May 11, 2023, and already video platforms that were used during the pandemic to provide telemedicine visits but are not Health Insurance Portability and Accountability Act compliant are now forbidden,2 Medicare virtual check-in appointments can only be conducted with established patients,4 and medical licensing requirements have been reinstated in most states such that patients must be located in the state where the provider is licensed to practice medicine at the time of a virtual visit.3 Although the CMS was granted wide freedoms to waive and suspend certain rules, this was only in the context of the PHE, and any lasting changes must be established by Congress.
Reassuringly, recent legislation via the Consolidated Appropriations Act, 2023, authorized an extension of many of the CMS telehealth flexibilities that were in place during the PHE through December 31, 2024 (Table),2 such as allowing access to telehealth services in any geographic area in the United States rather than only rural areas, allowing patients to stay in their homes for telehealth visits rather than traveling to an approved health care facility, and allowing the delivery of telemedicine via audio-only technology if a patient is unable to use both audio and video. As of now, the place of service (POS) designation for telehealth visits will not revert back to the former code (POS 02) but will remain at POS 11 with the telehealth modifier -95 so physicians will be reimbursed at the full level of a non-facility physician’s office rate.4 The CMS has indicated that there will be no change in the reimbursement policy until after December 31, 20234; however, the sense of uncertainty around what happens after this date has made it hard for organizations and practices to fully commit to teledermatology services without knowing what the long-term financial impact may be. Some organizations have already noted that they plan to continue supporting telemedicine after the CMS flexibilities expire. Accountable Care Organizations have the ability to offer services that allow participating practitioners to continue the use of telemedicine visits to expand access to care. Medicaid and Children’s Health Insurance Program policies vary by state and private health insurance policies vary by individual plans, but it should be noted that commercial coverage for telemedicine visits was already strong prior to the pandemic.2

What medical licensing requirements are in place now for telehealth?
During the PHE, medical licensing requirements also were relaxed, enabling providers to deliver telemedicine service in states where they were not licensed.3 As the PHE orders ended, some states including New York discontinued cross-state licensing waivers altogether,6 whereas others have enacted legislation to make them permanent or extend them for brief periods of time.3,6 One potential solution is the Interstate Medical Licensure Compact (https://www.imlcc.org/), which includes 39 states as of October 2023. This program expedites the process for physicians already licensed in participating states to obtain their medical license in another participating state, though licensing fees are required for each state in which a physician wants to practice. Furthermore, some states such as North Dakota, Hawaii, and Virginia have licensure by endorsement policies, which enable licensed physicians with specific qualifications to provide telehealth services in the endorsing state. Other states such as Florida, New Jersey, Louisiana, Minnesota, Nevada, and New Mexico have special telehealth registries that allow physicians in good standing who are licensed in other states to deliver telehealth services to in-state residents barring they do not provide in-person, in-state services.6 Lastly, some states have temporary practice laws to allow existing patients who need medical attention while traveling out of state to see their home providers virtually or in person under certain circumstances for a limited period of time.3,5 In Hawaii and New Hampshire, physicians with out-of-state licenses can provide consultative services in some circumstances.5
What changes have been made to make it easier for patients to use telehealth?
As the legislation around telemedicine is shifting postpandemic, it is important to address additional logistical barriers to teledermatology on a larger scale if the discipline is to stay in practice. On November 15, 2021, the Infrastructure Investment and Jobs Act provided $65 billion in funding for broadband to expand access to high-speed internet. Some of this money was allocated to the Affordable Connectivity Program, which provides eligible households with a discount on broadband service and internet-connected devices. Eligible patrons can qualify for a discount of up to $75 per month for internet service and a one-time discount up to $100 on a laptop, desktop computer, or tablet purchased through a participating provider.6 Although a step in the right direction, the effects of this program on telemedicine encounters remains to be proven. Additionally, these programs do not address educational barriers to understanding how to utilize telemedicine platforms or provide incentives for practitioners to offer telemedicine services.
Final Thoughts
The pandemic taught our specialty a great deal about how to utilize telemedicine. For many dermatologists a return to in-person business as usual could not come fast enough; however, many practices have continued to offer at least some teledermatology services. Although the PHE waivers have ended, the extension of numerous CMS flexibilities through the end of 2024 allows us more time to develop sustainable policies to support the long-term health of telemedicine as a whole, both to sustain practices and to expand access to care in dermatology. The favorable attitudes of both patients and physicians about teledermatology have been clearly documented,1,7 and we should continue to safely expand the use of this technology.
- Kennedy J, Arey S, Hopkins Z, et al. Dermatologist perceptions of teledermatology implementation and future use after COVID-19: demographics, barriers, and insights. JAMA Dermatol. 2021;157:595-597.
- US Department of Health and Human Services. HHS fact sheet: telehealth flexibilities and resources and the COVID-19 public health emergency. Published May 10, 2023. Accessed October 18, 2023. https://www.hhs.gov/aboutnews/2023/05/10/hhs-fact-sheet-telehealth-flexibilities-resources-covid-19-public-health-emergency.html
- US Department of Health and Human Services. Licensing across state lines. Updated May 11, 2023. Accessed October 25, 2023. https://telehealth.hhs.gov/licensure/licensing-across-state-lines
- American Academy of Dermatology. Teledermatology and the COVID-19 pandemic. Accessed October 12, 2023. https://www.aad.org/member/practice/telederm/covid-19
- American Medical Association. Licensure & Telehealth. Accessed October 12, 2023. https://www.ama-assn.org/system/files/issue-brief-licensure-telehealth.pdf
- Federal Communications Commission. Affordable Connectivity Program. Updated June 29, 2023. Accessed October 12, 2023. https://www.fcc.gov/affordable-connectivity-program
- Tensen E, van der Heijden JP, Jaspers MWM, et al. Two decades of teledermatology: current status and integration in national healthcare systems. Curr Dermatol Rep. 2016;5:96-104.
The rapid expansion of teledermatology in the United States due to the COVID-19 pandemic has been well documented, 1 but where do we stand now that health care and society as a whole are back to a new version of normal? It is important to consider why telemedicine was able to grow so quickly during that period—the Centers for Medicare & Medicaid Services (CMS) unilaterally changed policies related to provision of services and reimbursement thereof due to the public health emergency (PHE), which was declared by the Department of Health and Human Services in January 2020 to provide increased access to care for patients. Under the PHE, reimbursement rates for virtual visits improved, providers could care for patients from their homes and across state lines, and the use of video platforms that were not Health Insurance Portability and Accountability Act compliant was allowed. 2,3
The trajectory of teledermatology after the pandemic, however, remains unclear. In a survey assessing dermatologists’ perceptions of telemedicine (N=4356), 97% used telemedicine during the pandemic but only 58% reported that they intended to continue using teledermatology postpandemic,1 which is driven, at least in part, by the potential concern that dermatologists will again experience the same regulatory and logistical barriers that limited teledermatology utilization prepandemic.
What has changed in reimbursement for teledermatology since the PHE ended?
The PHE ended on May 11, 2023, and already video platforms that were used during the pandemic to provide telemedicine visits but are not Health Insurance Portability and Accountability Act compliant are now forbidden,2 Medicare virtual check-in appointments can only be conducted with established patients,4 and medical licensing requirements have been reinstated in most states such that patients must be located in the state where the provider is licensed to practice medicine at the time of a virtual visit.3 Although the CMS was granted wide freedoms to waive and suspend certain rules, this was only in the context of the PHE, and any lasting changes must be established by Congress.
Reassuringly, recent legislation via the Consolidated Appropriations Act, 2023, authorized an extension of many of the CMS telehealth flexibilities that were in place during the PHE through December 31, 2024 (Table),2 such as allowing access to telehealth services in any geographic area in the United States rather than only rural areas, allowing patients to stay in their homes for telehealth visits rather than traveling to an approved health care facility, and allowing the delivery of telemedicine via audio-only technology if a patient is unable to use both audio and video. As of now, the place of service (POS) designation for telehealth visits will not revert back to the former code (POS 02) but will remain at POS 11 with the telehealth modifier -95 so physicians will be reimbursed at the full level of a non-facility physician’s office rate.4 The CMS has indicated that there will be no change in the reimbursement policy until after December 31, 20234; however, the sense of uncertainty around what happens after this date has made it hard for organizations and practices to fully commit to teledermatology services without knowing what the long-term financial impact may be. Some organizations have already noted that they plan to continue supporting telemedicine after the CMS flexibilities expire. Accountable Care Organizations have the ability to offer services that allow participating practitioners to continue the use of telemedicine visits to expand access to care. Medicaid and Children’s Health Insurance Program policies vary by state and private health insurance policies vary by individual plans, but it should be noted that commercial coverage for telemedicine visits was already strong prior to the pandemic.2
What medical licensing requirements are in place now for telehealth?
During the PHE, medical licensing requirements also were relaxed, enabling providers to deliver telemedicine service in states where they were not licensed.3 As the PHE orders ended, some states including New York discontinued cross-state licensing waivers altogether,6 whereas others have enacted legislation to make them permanent or extend them for brief periods of time.3,6 One potential solution is the Interstate Medical Licensure Compact (https://www.imlcc.org/), which includes 39 states as of October 2023. This program expedites the process for physicians already licensed in participating states to obtain their medical license in another participating state, though licensing fees are required for each state in which a physician wants to practice. Furthermore, some states such as North Dakota, Hawaii, and Virginia have licensure by endorsement policies, which enable licensed physicians with specific qualifications to provide telehealth services in the endorsing state. Other states such as Florida, New Jersey, Louisiana, Minnesota, Nevada, and New Mexico have special telehealth registries that allow physicians in good standing who are licensed in other states to deliver telehealth services to in-state residents barring they do not provide in-person, in-state services.6 Lastly, some states have temporary practice laws to allow existing patients who need medical attention while traveling out of state to see their home providers virtually or in person under certain circumstances for a limited period of time.3,5 In Hawaii and New Hampshire, physicians with out-of-state licenses can provide consultative services in some circumstances.5
What changes have been made to make it easier for patients to use telehealth?
As the legislation around telemedicine is shifting postpandemic, it is important to address additional logistical barriers to teledermatology on a larger scale if the discipline is to stay in practice. On November 15, 2021, the Infrastructure Investment and Jobs Act provided $65 billion in funding for broadband to expand access to high-speed internet. Some of this money was allocated to the Affordable Connectivity Program, which provides eligible households with a discount on broadband service and internet-connected devices. Eligible patrons can qualify for a discount of up to $75 per month for internet service and a one-time discount up to $100 on a laptop, desktop computer, or tablet purchased through a participating provider.6 Although a step in the right direction, the effects of this program on telemedicine encounters remains to be proven. Additionally, these programs do not address educational barriers to understanding how to utilize telemedicine platforms or provide incentives for practitioners to offer telemedicine services.
Final Thoughts
The pandemic taught our specialty a great deal about how to utilize telemedicine. For many dermatologists a return to in-person business as usual could not come fast enough; however, many practices have continued to offer at least some teledermatology services. Although the PHE waivers have ended, the extension of numerous CMS flexibilities through the end of 2024 allows us more time to develop sustainable policies to support the long-term health of telemedicine as a whole, both to sustain practices and to expand access to care in dermatology. The favorable attitudes of both patients and physicians about teledermatology have been clearly documented,1,7 and we should continue to safely expand the use of this technology.
The rapid expansion of teledermatology in the United States due to the COVID-19 pandemic has been well documented, 1 but where do we stand now that health care and society as a whole are back to a new version of normal? It is important to consider why telemedicine was able to grow so quickly during that period—the Centers for Medicare & Medicaid Services (CMS) unilaterally changed policies related to provision of services and reimbursement thereof due to the public health emergency (PHE), which was declared by the Department of Health and Human Services in January 2020 to provide increased access to care for patients. Under the PHE, reimbursement rates for virtual visits improved, providers could care for patients from their homes and across state lines, and the use of video platforms that were not Health Insurance Portability and Accountability Act compliant was allowed. 2,3
The trajectory of teledermatology after the pandemic, however, remains unclear. In a survey assessing dermatologists’ perceptions of telemedicine (N=4356), 97% used telemedicine during the pandemic but only 58% reported that they intended to continue using teledermatology postpandemic,1 which is driven, at least in part, by the potential concern that dermatologists will again experience the same regulatory and logistical barriers that limited teledermatology utilization prepandemic.
What has changed in reimbursement for teledermatology since the PHE ended?
The PHE ended on May 11, 2023, and already video platforms that were used during the pandemic to provide telemedicine visits but are not Health Insurance Portability and Accountability Act compliant are now forbidden,2 Medicare virtual check-in appointments can only be conducted with established patients,4 and medical licensing requirements have been reinstated in most states such that patients must be located in the state where the provider is licensed to practice medicine at the time of a virtual visit.3 Although the CMS was granted wide freedoms to waive and suspend certain rules, this was only in the context of the PHE, and any lasting changes must be established by Congress.
Reassuringly, recent legislation via the Consolidated Appropriations Act, 2023, authorized an extension of many of the CMS telehealth flexibilities that were in place during the PHE through December 31, 2024 (Table),2 such as allowing access to telehealth services in any geographic area in the United States rather than only rural areas, allowing patients to stay in their homes for telehealth visits rather than traveling to an approved health care facility, and allowing the delivery of telemedicine via audio-only technology if a patient is unable to use both audio and video. As of now, the place of service (POS) designation for telehealth visits will not revert back to the former code (POS 02) but will remain at POS 11 with the telehealth modifier -95 so physicians will be reimbursed at the full level of a non-facility physician’s office rate.4 The CMS has indicated that there will be no change in the reimbursement policy until after December 31, 20234; however, the sense of uncertainty around what happens after this date has made it hard for organizations and practices to fully commit to teledermatology services without knowing what the long-term financial impact may be. Some organizations have already noted that they plan to continue supporting telemedicine after the CMS flexibilities expire. Accountable Care Organizations have the ability to offer services that allow participating practitioners to continue the use of telemedicine visits to expand access to care. Medicaid and Children’s Health Insurance Program policies vary by state and private health insurance policies vary by individual plans, but it should be noted that commercial coverage for telemedicine visits was already strong prior to the pandemic.2
What medical licensing requirements are in place now for telehealth?
During the PHE, medical licensing requirements also were relaxed, enabling providers to deliver telemedicine service in states where they were not licensed.3 As the PHE orders ended, some states including New York discontinued cross-state licensing waivers altogether,6 whereas others have enacted legislation to make them permanent or extend them for brief periods of time.3,6 One potential solution is the Interstate Medical Licensure Compact (https://www.imlcc.org/), which includes 39 states as of October 2023. This program expedites the process for physicians already licensed in participating states to obtain their medical license in another participating state, though licensing fees are required for each state in which a physician wants to practice. Furthermore, some states such as North Dakota, Hawaii, and Virginia have licensure by endorsement policies, which enable licensed physicians with specific qualifications to provide telehealth services in the endorsing state. Other states such as Florida, New Jersey, Louisiana, Minnesota, Nevada, and New Mexico have special telehealth registries that allow physicians in good standing who are licensed in other states to deliver telehealth services to in-state residents barring they do not provide in-person, in-state services.6 Lastly, some states have temporary practice laws to allow existing patients who need medical attention while traveling out of state to see their home providers virtually or in person under certain circumstances for a limited period of time.3,5 In Hawaii and New Hampshire, physicians with out-of-state licenses can provide consultative services in some circumstances.5
What changes have been made to make it easier for patients to use telehealth?
As the legislation around telemedicine is shifting postpandemic, it is important to address additional logistical barriers to teledermatology on a larger scale if the discipline is to stay in practice. On November 15, 2021, the Infrastructure Investment and Jobs Act provided $65 billion in funding for broadband to expand access to high-speed internet. Some of this money was allocated to the Affordable Connectivity Program, which provides eligible households with a discount on broadband service and internet-connected devices. Eligible patrons can qualify for a discount of up to $75 per month for internet service and a one-time discount up to $100 on a laptop, desktop computer, or tablet purchased through a participating provider.6 Although a step in the right direction, the effects of this program on telemedicine encounters remains to be proven. Additionally, these programs do not address educational barriers to understanding how to utilize telemedicine platforms or provide incentives for practitioners to offer telemedicine services.
Final Thoughts
The pandemic taught our specialty a great deal about how to utilize telemedicine. For many dermatologists a return to in-person business as usual could not come fast enough; however, many practices have continued to offer at least some teledermatology services. Although the PHE waivers have ended, the extension of numerous CMS flexibilities through the end of 2024 allows us more time to develop sustainable policies to support the long-term health of telemedicine as a whole, both to sustain practices and to expand access to care in dermatology. The favorable attitudes of both patients and physicians about teledermatology have been clearly documented,1,7 and we should continue to safely expand the use of this technology.
- Kennedy J, Arey S, Hopkins Z, et al. Dermatologist perceptions of teledermatology implementation and future use after COVID-19: demographics, barriers, and insights. JAMA Dermatol. 2021;157:595-597.
- US Department of Health and Human Services. HHS fact sheet: telehealth flexibilities and resources and the COVID-19 public health emergency. Published May 10, 2023. Accessed October 18, 2023. https://www.hhs.gov/aboutnews/2023/05/10/hhs-fact-sheet-telehealth-flexibilities-resources-covid-19-public-health-emergency.html
- US Department of Health and Human Services. Licensing across state lines. Updated May 11, 2023. Accessed October 25, 2023. https://telehealth.hhs.gov/licensure/licensing-across-state-lines
- American Academy of Dermatology. Teledermatology and the COVID-19 pandemic. Accessed October 12, 2023. https://www.aad.org/member/practice/telederm/covid-19
- American Medical Association. Licensure & Telehealth. Accessed October 12, 2023. https://www.ama-assn.org/system/files/issue-brief-licensure-telehealth.pdf
- Federal Communications Commission. Affordable Connectivity Program. Updated June 29, 2023. Accessed October 12, 2023. https://www.fcc.gov/affordable-connectivity-program
- Tensen E, van der Heijden JP, Jaspers MWM, et al. Two decades of teledermatology: current status and integration in national healthcare systems. Curr Dermatol Rep. 2016;5:96-104.
- Kennedy J, Arey S, Hopkins Z, et al. Dermatologist perceptions of teledermatology implementation and future use after COVID-19: demographics, barriers, and insights. JAMA Dermatol. 2021;157:595-597.
- US Department of Health and Human Services. HHS fact sheet: telehealth flexibilities and resources and the COVID-19 public health emergency. Published May 10, 2023. Accessed October 18, 2023. https://www.hhs.gov/aboutnews/2023/05/10/hhs-fact-sheet-telehealth-flexibilities-resources-covid-19-public-health-emergency.html
- US Department of Health and Human Services. Licensing across state lines. Updated May 11, 2023. Accessed October 25, 2023. https://telehealth.hhs.gov/licensure/licensing-across-state-lines
- American Academy of Dermatology. Teledermatology and the COVID-19 pandemic. Accessed October 12, 2023. https://www.aad.org/member/practice/telederm/covid-19
- American Medical Association. Licensure & Telehealth. Accessed October 12, 2023. https://www.ama-assn.org/system/files/issue-brief-licensure-telehealth.pdf
- Federal Communications Commission. Affordable Connectivity Program. Updated June 29, 2023. Accessed October 12, 2023. https://www.fcc.gov/affordable-connectivity-program
- Tensen E, van der Heijden JP, Jaspers MWM, et al. Two decades of teledermatology: current status and integration in national healthcare systems. Curr Dermatol Rep. 2016;5:96-104.

‘Why did I choose this?’ Tackling burnout in oncology
MADRID – “Why did I choose this?”
That is the core question a Portuguese oncologist posed from the audience during a session at the annual meeting of the European Society for Medical Oncology (ESMO) that was dedicated to building a sustainable oncology workforce.
“Ten, twenty years ago, being a doctor was a dream,” she said, but right now doctors are underpaid, under strain, and have very few resources.
This oncologist is hardly alone.
A survey from ESMO conducted almost a decade ago found that more than 50% of oncologists across Europe, many of whom were early in their careers, reported being burned out.
This, Dr. Lim said, “was the starting point,” well before the COVID pandemic struck.
More recently, the pandemic has taken its own toll on the well-being of oncologists. A survey presented at ESMO 2020 revealed that 38% of participants, spanning 101 countries, reported experiencing burnout, and 66% said they were not able to perform their job.
Medscape’s 2023 Physician Burnout and Depression Report highlighted similar burnout rates, with 53% of U.S. physicians and 52% of oncologists saying they felt burned out, compared with about 42% in 2018, before the pandemic.
The oncology workforce is in crisis in every country, said Dr. Lim, from the Cancer Dynamics Lab, the Francis Crick Institute, London.
Burnout, characterized by emotional exhaustion, depersonalization or feelings of cynicism, and a low sense of personal accomplishment, can result in a poor work-life balance as well as poor mental and physical health. Factors linked to burnout include social isolation, increased workload, reduced quality of work, lack of control over work, and stressful professional experiences.
Together, these factors can affect patient care and further exacerbate staffing issues, Dr. Lim said.
Staffing shortages are common. Oncologists often work long hours or on weekends to cover gaps caused by staffing shortages. Recent data revealed that in high-income countries, there are on average 0.65 medical oncologists and 0.25 radiation oncologists per 100 patients — a situation made worse by professionals taking early retirement or leaving medicine during the pandemic.
“We have seen that the shortage of human resources in many countries as well as the increasing workload related to the increasing number of cancers,” as well as patients surviving longer, have increased pressures on the healthcare system, Andrés Cervantes, MD, PhD, president of ESMO, explained in a press conference.
While tackling these oncology workforce problems requires smaller, local changes to a physician’s daily routine, “the real change,” Dr. Lim said, lies at an infrastructure level.
In response to this chronic and growing problem, ESMO launched its Resilience Task Force in 2020 to evaluate burnout and well-being. The task force plans to publish a position paper in which it will propose a set of recommendations regarding the psychosocial risks of burnout as well as flexible work patterns, well-being resources, and targeted support.
A panel of experts at the meeting touched on some of these solutions.
Dealing with staff shortages is a must, said Jean-Yves Blay, MD, PhD, during the session. “It’s a simple mathematical equation,” Dr. Blay said. “We must increase the number of doctors in medical schools and the number of nurses and healthcare professionals in all schools.” Improving staffing would also help reduce chronic workload issues.
Resilience training should also be incorporated into physician training starting in medical school. Teaching oncologists how to deal with bad news and to cope when patients dies is particularly important.
“I was not taught that,” said the oncologist from Portugal. “I had to learn that at my own cost.”
The good news is that it’s possible to develop resiliency skills over time, said Claire Hardy, PhD, from Lancaster University, United Kingdom, who agreed that training programs could be one approach to improve oncologists’ work life.
However, a person’s needs are determined by their institution and personal responsibilities. “No one knows your job better than you,” Dr. Hardy said. “No one knows better than you where the inefficiencies are, where the bureaucracy is that could be taken away, or it could be done by somebody whose role it is to sort all that out.”
But having this understanding is not enough. Physician also need to feel “psychological safety to be able to speak out and say that something isn’t working right now or is too much,” or, “I’m spending too much time doing this.”
In other words, oncologists need to be able to set boundaries and say no.
Dr. Hardy said this concept “has been around a while, but it’s really gaining momentum,” and being able to discuss these issues in a forum such as the ESMO Congress is a promising start.
Dr. Lim has relationships with Janseen and SEOM. No other relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
MADRID – “Why did I choose this?”
That is the core question a Portuguese oncologist posed from the audience during a session at the annual meeting of the European Society for Medical Oncology (ESMO) that was dedicated to building a sustainable oncology workforce.
“Ten, twenty years ago, being a doctor was a dream,” she said, but right now doctors are underpaid, under strain, and have very few resources.
This oncologist is hardly alone.
A survey from ESMO conducted almost a decade ago found that more than 50% of oncologists across Europe, many of whom were early in their careers, reported being burned out.
This, Dr. Lim said, “was the starting point,” well before the COVID pandemic struck.
More recently, the pandemic has taken its own toll on the well-being of oncologists. A survey presented at ESMO 2020 revealed that 38% of participants, spanning 101 countries, reported experiencing burnout, and 66% said they were not able to perform their job.
Medscape’s 2023 Physician Burnout and Depression Report highlighted similar burnout rates, with 53% of U.S. physicians and 52% of oncologists saying they felt burned out, compared with about 42% in 2018, before the pandemic.
The oncology workforce is in crisis in every country, said Dr. Lim, from the Cancer Dynamics Lab, the Francis Crick Institute, London.
Burnout, characterized by emotional exhaustion, depersonalization or feelings of cynicism, and a low sense of personal accomplishment, can result in a poor work-life balance as well as poor mental and physical health. Factors linked to burnout include social isolation, increased workload, reduced quality of work, lack of control over work, and stressful professional experiences.
Together, these factors can affect patient care and further exacerbate staffing issues, Dr. Lim said.
Staffing shortages are common. Oncologists often work long hours or on weekends to cover gaps caused by staffing shortages. Recent data revealed that in high-income countries, there are on average 0.65 medical oncologists and 0.25 radiation oncologists per 100 patients — a situation made worse by professionals taking early retirement or leaving medicine during the pandemic.
“We have seen that the shortage of human resources in many countries as well as the increasing workload related to the increasing number of cancers,” as well as patients surviving longer, have increased pressures on the healthcare system, Andrés Cervantes, MD, PhD, president of ESMO, explained in a press conference.
While tackling these oncology workforce problems requires smaller, local changes to a physician’s daily routine, “the real change,” Dr. Lim said, lies at an infrastructure level.
In response to this chronic and growing problem, ESMO launched its Resilience Task Force in 2020 to evaluate burnout and well-being. The task force plans to publish a position paper in which it will propose a set of recommendations regarding the psychosocial risks of burnout as well as flexible work patterns, well-being resources, and targeted support.
A panel of experts at the meeting touched on some of these solutions.
Dealing with staff shortages is a must, said Jean-Yves Blay, MD, PhD, during the session. “It’s a simple mathematical equation,” Dr. Blay said. “We must increase the number of doctors in medical schools and the number of nurses and healthcare professionals in all schools.” Improving staffing would also help reduce chronic workload issues.
Resilience training should also be incorporated into physician training starting in medical school. Teaching oncologists how to deal with bad news and to cope when patients dies is particularly important.
“I was not taught that,” said the oncologist from Portugal. “I had to learn that at my own cost.”
The good news is that it’s possible to develop resiliency skills over time, said Claire Hardy, PhD, from Lancaster University, United Kingdom, who agreed that training programs could be one approach to improve oncologists’ work life.
However, a person’s needs are determined by their institution and personal responsibilities. “No one knows your job better than you,” Dr. Hardy said. “No one knows better than you where the inefficiencies are, where the bureaucracy is that could be taken away, or it could be done by somebody whose role it is to sort all that out.”
But having this understanding is not enough. Physician also need to feel “psychological safety to be able to speak out and say that something isn’t working right now or is too much,” or, “I’m spending too much time doing this.”
In other words, oncologists need to be able to set boundaries and say no.
Dr. Hardy said this concept “has been around a while, but it’s really gaining momentum,” and being able to discuss these issues in a forum such as the ESMO Congress is a promising start.
Dr. Lim has relationships with Janseen and SEOM. No other relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
MADRID – “Why did I choose this?”
That is the core question a Portuguese oncologist posed from the audience during a session at the annual meeting of the European Society for Medical Oncology (ESMO) that was dedicated to building a sustainable oncology workforce.
“Ten, twenty years ago, being a doctor was a dream,” she said, but right now doctors are underpaid, under strain, and have very few resources.
This oncologist is hardly alone.
A survey from ESMO conducted almost a decade ago found that more than 50% of oncologists across Europe, many of whom were early in their careers, reported being burned out.
This, Dr. Lim said, “was the starting point,” well before the COVID pandemic struck.
More recently, the pandemic has taken its own toll on the well-being of oncologists. A survey presented at ESMO 2020 revealed that 38% of participants, spanning 101 countries, reported experiencing burnout, and 66% said they were not able to perform their job.
Medscape’s 2023 Physician Burnout and Depression Report highlighted similar burnout rates, with 53% of U.S. physicians and 52% of oncologists saying they felt burned out, compared with about 42% in 2018, before the pandemic.
The oncology workforce is in crisis in every country, said Dr. Lim, from the Cancer Dynamics Lab, the Francis Crick Institute, London.
Burnout, characterized by emotional exhaustion, depersonalization or feelings of cynicism, and a low sense of personal accomplishment, can result in a poor work-life balance as well as poor mental and physical health. Factors linked to burnout include social isolation, increased workload, reduced quality of work, lack of control over work, and stressful professional experiences.
Together, these factors can affect patient care and further exacerbate staffing issues, Dr. Lim said.
Staffing shortages are common. Oncologists often work long hours or on weekends to cover gaps caused by staffing shortages. Recent data revealed that in high-income countries, there are on average 0.65 medical oncologists and 0.25 radiation oncologists per 100 patients — a situation made worse by professionals taking early retirement or leaving medicine during the pandemic.
“We have seen that the shortage of human resources in many countries as well as the increasing workload related to the increasing number of cancers,” as well as patients surviving longer, have increased pressures on the healthcare system, Andrés Cervantes, MD, PhD, president of ESMO, explained in a press conference.
While tackling these oncology workforce problems requires smaller, local changes to a physician’s daily routine, “the real change,” Dr. Lim said, lies at an infrastructure level.
In response to this chronic and growing problem, ESMO launched its Resilience Task Force in 2020 to evaluate burnout and well-being. The task force plans to publish a position paper in which it will propose a set of recommendations regarding the psychosocial risks of burnout as well as flexible work patterns, well-being resources, and targeted support.
A panel of experts at the meeting touched on some of these solutions.
Dealing with staff shortages is a must, said Jean-Yves Blay, MD, PhD, during the session. “It’s a simple mathematical equation,” Dr. Blay said. “We must increase the number of doctors in medical schools and the number of nurses and healthcare professionals in all schools.” Improving staffing would also help reduce chronic workload issues.
Resilience training should also be incorporated into physician training starting in medical school. Teaching oncologists how to deal with bad news and to cope when patients dies is particularly important.
“I was not taught that,” said the oncologist from Portugal. “I had to learn that at my own cost.”
The good news is that it’s possible to develop resiliency skills over time, said Claire Hardy, PhD, from Lancaster University, United Kingdom, who agreed that training programs could be one approach to improve oncologists’ work life.
However, a person’s needs are determined by their institution and personal responsibilities. “No one knows your job better than you,” Dr. Hardy said. “No one knows better than you where the inefficiencies are, where the bureaucracy is that could be taken away, or it could be done by somebody whose role it is to sort all that out.”
But having this understanding is not enough. Physician also need to feel “psychological safety to be able to speak out and say that something isn’t working right now or is too much,” or, “I’m spending too much time doing this.”
In other words, oncologists need to be able to set boundaries and say no.
Dr. Hardy said this concept “has been around a while, but it’s really gaining momentum,” and being able to discuss these issues in a forum such as the ESMO Congress is a promising start.
Dr. Lim has relationships with Janseen and SEOM. No other relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
FROM ESMO 2023
Employment vs. private practice: Who’s happier?
Alexandra Kharazi, MD, a California-based cardiothoracic surgeon, previously worked as an employed physician and is now in private practice. Though she appreciates that there are some trade-offs to working with her small group of three surgeons, Dr. Kharazi has no qualms about her choice.
“For me, it’s an issue of autonomy,” she said. “While I have to work a lot of hours, I don’t have to adhere to a strict schedule. I also don’t have to follow specific policies and rules.”
In contrast, Cassandra Boduch, MD, an employed psychiatrist with PsychPlus in Houston, is very satisfied with working as an employee. “I looked into private practice, but no one really prepares you for the complications that come with it,” she said. “There’s a lot more that goes into it than people realize.”
By hanging up her own shingle, Dr. Kharazi may be living a rapidly shrinking dream. According to the American Medical Association, between 2012 and 2022, the share of physicians working in private practice fell from 60% to 47%. The share of physicians working in hospitals as direct employees or contractors increased from about 6% to about 10% during the same time period.
, according to the AMA.
Though the traditional dream of owning your own practice may be slipping away, are employed physicians less happy than are their self-employed peers? By many measures, the answer is no.
In Medscape’s Employed Physicians Report 2023, doctors weighed in on the pros and cons of their jobs.
When asked what they like most about their jobs, employed physician respondents reported “not having to run a business” as their number-one benefit, followed closely by a stable income. The fact that employers pay for malpractice insurance ranked third, followed by work-life balance.
“We get no business classes in medical school or residency,” said one employed physician. “Having a good salary feels good,” said another. Yet another respondent chimed in: “Running a practice as a small business has become undoable over the past 10-12 years.”
And 50% of employed physicians said that they were “very satisfied/satisfied” with their degree of autonomy.
Still, employed physicians also had plenty to say about the downsides of their jobs.
Many pointed to “feeling like a cog in the machine,” and one doctor pointed to the hassle of dealing with bureaucracy. Others complained about the fact that nonphysicians ran the business and lacked an understanding of what physicians really need from their jobs. When asked whether administrative rules made sense, 63% of physician respondents said that yes, the rules make sense for the business; but, only 52% said that the rules make sense for the doctors themselves.
Other complaints included the requirement to reach high productivity targets and too low an income potential. In the 9 years since Medscape’s 2104 Employed Physicians Report, the share of employed doctors paid on a straight salary has declined from 46% to 31%. Those compensated on a base salary plus productivity targets and other performance metrics rose from 13% in 2014 to 32% now.
“Many doctors go into private practice because of the freedom it brings and the potential financial incentives,” added Dr. Boduch. “I know that many doctors have a dream of working for themselves, and in many cases, that works out great for them.”
Dr. Boduch noted that in her job as chief medical officer at PsychPlus, she still has flexibility plus the perks of working with a bigger practice. In this scenario, Dr. Boduch said, the company can negotiate with insurance companies, allowing her the financial rewards of private practice.
What’s right for you?
“I think it might be somewhat generational,” said Cody Futch, senior recruiting executive at AMN Healthcare. “It used to be that fewer hospitals offered employment, so private practice was the way to go. Now, there are fewer privates because hospitals and corporations are buying them up.”
This reality has potentially shaped the way younger generations approach their workplace. Also, Gen Z tends to have less intention to stay with a current employer for the long term than did their parents. “Older physicians were trained to expect they’d run their own business and build it over the years,” said Mr. Futch. “The younger generations look at it as a job, something they may want to switch in a few years. It’s a combination of candidates wanting more options, and also the fact that there are more options to be employed.”
Along those lines, younger generations in general tend to place work-life balance as a higher priority than do older generations, and employed physicians place this equation high on the list as well. In the Employed Physicians Report 2023, 54% said that they are satisfied or better with their work-life balance, up from 51% in the 2022 report.
With that in mind, Dr. Kharazi noted that flexibility is one of the chief reasons why she likes private practice. “If my kid has an event I want to attend, I don’t have to adhere to a strict schedule,” she said.
Satisfaction as an employee vs. employed doctor sometimes changes based on the type of medicine you practice too. With specialties that tend to be primarily outpatient, such as dermatology and allergy, private practice may be the best option regardless. “Hospitals don’t seek out those specialists as much and the specialists can operate successfully without a hospital,” said Mr. Futch.
Hospitals try to incentivize doctors with perks like hefty sign-on bonuses, student loan forgiveness, plenty of vacation time, and more. They also put money into marketing their doctors, a time-consuming and expensive aspect that is tough to shoulder in private practice, especially in the early years. Mr. Futch adds that many doctors view employment as a more stable option. “As the government changes reimbursement policies, the income from private practice fluctuates,” he said. “So many doctors worry that if they buy into a private practice, it is a risky endeavor.”
Hospitals aren’t always a sure bet in that regard, either: They go through tough financial times, lay off staff, or make salary cuts. Historically, however, employment tends to be the safer route, which can make it an attractive option.
Ultimately, the pros and cons of each scenario are individual. It’s up to physicians to do their own math and balance sheet before making a decision.
A version of this article first appeared on Medscape.com.
Alexandra Kharazi, MD, a California-based cardiothoracic surgeon, previously worked as an employed physician and is now in private practice. Though she appreciates that there are some trade-offs to working with her small group of three surgeons, Dr. Kharazi has no qualms about her choice.
“For me, it’s an issue of autonomy,” she said. “While I have to work a lot of hours, I don’t have to adhere to a strict schedule. I also don’t have to follow specific policies and rules.”
In contrast, Cassandra Boduch, MD, an employed psychiatrist with PsychPlus in Houston, is very satisfied with working as an employee. “I looked into private practice, but no one really prepares you for the complications that come with it,” she said. “There’s a lot more that goes into it than people realize.”
By hanging up her own shingle, Dr. Kharazi may be living a rapidly shrinking dream. According to the American Medical Association, between 2012 and 2022, the share of physicians working in private practice fell from 60% to 47%. The share of physicians working in hospitals as direct employees or contractors increased from about 6% to about 10% during the same time period.
, according to the AMA.
Though the traditional dream of owning your own practice may be slipping away, are employed physicians less happy than are their self-employed peers? By many measures, the answer is no.
In Medscape’s Employed Physicians Report 2023, doctors weighed in on the pros and cons of their jobs.
When asked what they like most about their jobs, employed physician respondents reported “not having to run a business” as their number-one benefit, followed closely by a stable income. The fact that employers pay for malpractice insurance ranked third, followed by work-life balance.
“We get no business classes in medical school or residency,” said one employed physician. “Having a good salary feels good,” said another. Yet another respondent chimed in: “Running a practice as a small business has become undoable over the past 10-12 years.”
And 50% of employed physicians said that they were “very satisfied/satisfied” with their degree of autonomy.
Still, employed physicians also had plenty to say about the downsides of their jobs.
Many pointed to “feeling like a cog in the machine,” and one doctor pointed to the hassle of dealing with bureaucracy. Others complained about the fact that nonphysicians ran the business and lacked an understanding of what physicians really need from their jobs. When asked whether administrative rules made sense, 63% of physician respondents said that yes, the rules make sense for the business; but, only 52% said that the rules make sense for the doctors themselves.
Other complaints included the requirement to reach high productivity targets and too low an income potential. In the 9 years since Medscape’s 2104 Employed Physicians Report, the share of employed doctors paid on a straight salary has declined from 46% to 31%. Those compensated on a base salary plus productivity targets and other performance metrics rose from 13% in 2014 to 32% now.
“Many doctors go into private practice because of the freedom it brings and the potential financial incentives,” added Dr. Boduch. “I know that many doctors have a dream of working for themselves, and in many cases, that works out great for them.”
Dr. Boduch noted that in her job as chief medical officer at PsychPlus, she still has flexibility plus the perks of working with a bigger practice. In this scenario, Dr. Boduch said, the company can negotiate with insurance companies, allowing her the financial rewards of private practice.
What’s right for you?
“I think it might be somewhat generational,” said Cody Futch, senior recruiting executive at AMN Healthcare. “It used to be that fewer hospitals offered employment, so private practice was the way to go. Now, there are fewer privates because hospitals and corporations are buying them up.”
This reality has potentially shaped the way younger generations approach their workplace. Also, Gen Z tends to have less intention to stay with a current employer for the long term than did their parents. “Older physicians were trained to expect they’d run their own business and build it over the years,” said Mr. Futch. “The younger generations look at it as a job, something they may want to switch in a few years. It’s a combination of candidates wanting more options, and also the fact that there are more options to be employed.”
Along those lines, younger generations in general tend to place work-life balance as a higher priority than do older generations, and employed physicians place this equation high on the list as well. In the Employed Physicians Report 2023, 54% said that they are satisfied or better with their work-life balance, up from 51% in the 2022 report.
With that in mind, Dr. Kharazi noted that flexibility is one of the chief reasons why she likes private practice. “If my kid has an event I want to attend, I don’t have to adhere to a strict schedule,” she said.
Satisfaction as an employee vs. employed doctor sometimes changes based on the type of medicine you practice too. With specialties that tend to be primarily outpatient, such as dermatology and allergy, private practice may be the best option regardless. “Hospitals don’t seek out those specialists as much and the specialists can operate successfully without a hospital,” said Mr. Futch.
Hospitals try to incentivize doctors with perks like hefty sign-on bonuses, student loan forgiveness, plenty of vacation time, and more. They also put money into marketing their doctors, a time-consuming and expensive aspect that is tough to shoulder in private practice, especially in the early years. Mr. Futch adds that many doctors view employment as a more stable option. “As the government changes reimbursement policies, the income from private practice fluctuates,” he said. “So many doctors worry that if they buy into a private practice, it is a risky endeavor.”
Hospitals aren’t always a sure bet in that regard, either: They go through tough financial times, lay off staff, or make salary cuts. Historically, however, employment tends to be the safer route, which can make it an attractive option.
Ultimately, the pros and cons of each scenario are individual. It’s up to physicians to do their own math and balance sheet before making a decision.
A version of this article first appeared on Medscape.com.
Alexandra Kharazi, MD, a California-based cardiothoracic surgeon, previously worked as an employed physician and is now in private practice. Though she appreciates that there are some trade-offs to working with her small group of three surgeons, Dr. Kharazi has no qualms about her choice.
“For me, it’s an issue of autonomy,” she said. “While I have to work a lot of hours, I don’t have to adhere to a strict schedule. I also don’t have to follow specific policies and rules.”
In contrast, Cassandra Boduch, MD, an employed psychiatrist with PsychPlus in Houston, is very satisfied with working as an employee. “I looked into private practice, but no one really prepares you for the complications that come with it,” she said. “There’s a lot more that goes into it than people realize.”
By hanging up her own shingle, Dr. Kharazi may be living a rapidly shrinking dream. According to the American Medical Association, between 2012 and 2022, the share of physicians working in private practice fell from 60% to 47%. The share of physicians working in hospitals as direct employees or contractors increased from about 6% to about 10% during the same time period.
, according to the AMA.
Though the traditional dream of owning your own practice may be slipping away, are employed physicians less happy than are their self-employed peers? By many measures, the answer is no.
In Medscape’s Employed Physicians Report 2023, doctors weighed in on the pros and cons of their jobs.
When asked what they like most about their jobs, employed physician respondents reported “not having to run a business” as their number-one benefit, followed closely by a stable income. The fact that employers pay for malpractice insurance ranked third, followed by work-life balance.
“We get no business classes in medical school or residency,” said one employed physician. “Having a good salary feels good,” said another. Yet another respondent chimed in: “Running a practice as a small business has become undoable over the past 10-12 years.”
And 50% of employed physicians said that they were “very satisfied/satisfied” with their degree of autonomy.
Still, employed physicians also had plenty to say about the downsides of their jobs.
Many pointed to “feeling like a cog in the machine,” and one doctor pointed to the hassle of dealing with bureaucracy. Others complained about the fact that nonphysicians ran the business and lacked an understanding of what physicians really need from their jobs. When asked whether administrative rules made sense, 63% of physician respondents said that yes, the rules make sense for the business; but, only 52% said that the rules make sense for the doctors themselves.
Other complaints included the requirement to reach high productivity targets and too low an income potential. In the 9 years since Medscape’s 2104 Employed Physicians Report, the share of employed doctors paid on a straight salary has declined from 46% to 31%. Those compensated on a base salary plus productivity targets and other performance metrics rose from 13% in 2014 to 32% now.
“Many doctors go into private practice because of the freedom it brings and the potential financial incentives,” added Dr. Boduch. “I know that many doctors have a dream of working for themselves, and in many cases, that works out great for them.”
Dr. Boduch noted that in her job as chief medical officer at PsychPlus, she still has flexibility plus the perks of working with a bigger practice. In this scenario, Dr. Boduch said, the company can negotiate with insurance companies, allowing her the financial rewards of private practice.
What’s right for you?
“I think it might be somewhat generational,” said Cody Futch, senior recruiting executive at AMN Healthcare. “It used to be that fewer hospitals offered employment, so private practice was the way to go. Now, there are fewer privates because hospitals and corporations are buying them up.”
This reality has potentially shaped the way younger generations approach their workplace. Also, Gen Z tends to have less intention to stay with a current employer for the long term than did their parents. “Older physicians were trained to expect they’d run their own business and build it over the years,” said Mr. Futch. “The younger generations look at it as a job, something they may want to switch in a few years. It’s a combination of candidates wanting more options, and also the fact that there are more options to be employed.”
Along those lines, younger generations in general tend to place work-life balance as a higher priority than do older generations, and employed physicians place this equation high on the list as well. In the Employed Physicians Report 2023, 54% said that they are satisfied or better with their work-life balance, up from 51% in the 2022 report.
With that in mind, Dr. Kharazi noted that flexibility is one of the chief reasons why she likes private practice. “If my kid has an event I want to attend, I don’t have to adhere to a strict schedule,” she said.
Satisfaction as an employee vs. employed doctor sometimes changes based on the type of medicine you practice too. With specialties that tend to be primarily outpatient, such as dermatology and allergy, private practice may be the best option regardless. “Hospitals don’t seek out those specialists as much and the specialists can operate successfully without a hospital,” said Mr. Futch.
Hospitals try to incentivize doctors with perks like hefty sign-on bonuses, student loan forgiveness, plenty of vacation time, and more. They also put money into marketing their doctors, a time-consuming and expensive aspect that is tough to shoulder in private practice, especially in the early years. Mr. Futch adds that many doctors view employment as a more stable option. “As the government changes reimbursement policies, the income from private practice fluctuates,” he said. “So many doctors worry that if they buy into a private practice, it is a risky endeavor.”
Hospitals aren’t always a sure bet in that regard, either: They go through tough financial times, lay off staff, or make salary cuts. Historically, however, employment tends to be the safer route, which can make it an attractive option.
Ultimately, the pros and cons of each scenario are individual. It’s up to physicians to do their own math and balance sheet before making a decision.
A version of this article first appeared on Medscape.com.
Employed physicians: A survival guide
The strike by health care workers at Kaiser Permanente may not involve physicians (yet). But as more doctors in the United States are finding themselves working as salaried employees, physicians can – and probably will – become a powerful force for change in a health care system that has shown itself to be increasingly hostile to employee concerns over issues involving patient care, wages and benefits, safety, and well-being.
Salaried employment has its challenges. Physician-employees may have less autonomy and voice in decision-making that affects patients. They may splinter into fragmented work groups; feel isolated; and have different imperatives based on who they are, what they want, and where they work. They may feel more removed from their patients and struggle to build strong relationships, with their employers in the way.
Yet important opportunities exist for doctors when embracing their employee side. Examples of these interests include adequate compensation, wellness, job security, patient and worker safety, health care quality, reasonable workloads and schedules, and fair treatment by employers, including the need to exhibit a strong collective voice in organizational decision-making.
Some believe that physician-employees must be unionized to maximize their rights and power as employees. Many expect physician unionization to take hold more fully over time. Medical residents, the doctors of tomorrow, are already considering unionization in greater numbers. Some are also doing it in the same employment setting alongside other health professionals, such as nurses.
Having studied doctors and their employment situations for years, I am convinced that whether through unionization or another approach, physicians must also change how they think about control; train and learn alongside other health care workers who share similar interests; and elevate at an early career stage their knowledge of the business side of health care.
Adopt a more pragmatic definition of autonomy
Doctors must embrace an updated definition of autonomy – one that matches their status as highly paid labor.
When I have spoken to physicians in my research about what autonomy means to them, many seem unable to reconceptualize it from a vague and absolute form of their profession’s strategic control over their economic fates and technical skills toward an individualized control that is situation-specific, one centered on winning the daily fights about workplace bread-and-butter issues such as those mentioned above.
But a more pragmatic definition of autonomy could get doctors focused on influencing important issues of the patient-care day and enhance their negotiating power with employers. It would allow physicians to break out of what often seems a paralysis of inaction – waiting for employers, insurers, or the government to reinstate the profession’s idealized version of control by handing it back the keys to the health care system through major regulatory, structural, and reimbursement-related changes. This fantasy is unlikely to become reality.
Physician-employees I’ve talked to over the years understand their everyday challenges. But when it comes to engaging in localized and sustained action to overcome them, they often perform less well, leading to feelings of helplessness and burnout. Valuing tactical control over their jobs and work setting will yield smaller but more impactful wins as employees intent on making their everyday work lives better.
Train alongside other health care professionals
Physicians must accept that how they are trained no longer prepares them for the employee world into which most are dropped. For instance, unless doctors are trained collaboratively alongside other health care professionals – such as nurses – they are less likely to identify closely with these colleagues once in practice. There is strength in numbers, so this mutual identification empowers both groups of employees. Yet, medical education remains largely the same: training young medical students in isolation for the first couple of years, then placing them into clerkships and residencies where true interprofessional care opportunities remain stunted and secondary to the “physician as captain of the team” mantra.
Unfortunately, the “hidden curriculum” of medicine helps convince medical students and residents early in their careers that they are the unquestioned leaders in patient care settings. This hierarchy encourages some doctors to keep their psychological distance from other members of the health care team and to resist sharing power, concerns, or insights with less skilled health care workers. This socialization harms the ability of physicians to act in a unified fashion alongside these other workers. Having physicians learn and train alongside other health professionals yields positive benefits for collective advocacy, including a shared sense of purpose, positive views on collaboration with others in the health setting, and greater development of bonds with nonphysician coworkers.
Integrate business with medical training in real time
Medical students and residents generally lack exposure to the everyday business realities of the U.S. health care system. This gap hinders their ability to understand the employee world and push for the types of changes and work conditions that benefit all health care workers. Formal business and management training should be a required part of every U.S. medical school and residency curriculum from day one. If you see it at all in medical schools now, it is mostly by accident, or given separate treatment in the form of standalone MBA or MPH degrees that rarely integrate organically and in real time with actual medical training. Not every doctor needs an MBA or MPH degree. However, all of them require a stronger contextual understanding of how the medicine they wish to practice is shaped by the economic and fiscal circumstances surrounding it – circumstances they do not control.
This is another reason why young doctors are unhappy and burned out. They cannot push for specific changes or properly critique the pros and cons of how their work is structured because they have not been made aware, in real time as they learn clinical practice, how their jobs are shaped by realities such as insurance coverage and reimbursement, the fragmentation of the care delivery system, their employer’s financial health , and the socioeconomic circumstances of their patients. They aren’t given the methods and tools related to process and quality improvement, budgeting, negotiation, risk management, leadership, and talent management that might help them navigate these undermining forces. They also get little advance exposure in their training to important workplace “soft” skills in such areas as how to work in teams, networking, communication and listening, empathy, and problem-solving – all necessary foci for bringing them closer to other health care workers and advocating alongside them effectively with health care employers.
Now is the time for physicians to embrace their identity as employees. Doing so is in their own best interest as professionals. It will help others in the health care workforce as well as patients. Moreover, it provides a needed counterbalance to the powerful corporate ethos now ascendant in U.S. health care.
Timothy Hoff, PhD, is a professor of management and healthcare systems at Northeastern University, Boston, and an associate fellow at the University of Oxford, England. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The strike by health care workers at Kaiser Permanente may not involve physicians (yet). But as more doctors in the United States are finding themselves working as salaried employees, physicians can – and probably will – become a powerful force for change in a health care system that has shown itself to be increasingly hostile to employee concerns over issues involving patient care, wages and benefits, safety, and well-being.
Salaried employment has its challenges. Physician-employees may have less autonomy and voice in decision-making that affects patients. They may splinter into fragmented work groups; feel isolated; and have different imperatives based on who they are, what they want, and where they work. They may feel more removed from their patients and struggle to build strong relationships, with their employers in the way.
Yet important opportunities exist for doctors when embracing their employee side. Examples of these interests include adequate compensation, wellness, job security, patient and worker safety, health care quality, reasonable workloads and schedules, and fair treatment by employers, including the need to exhibit a strong collective voice in organizational decision-making.
Some believe that physician-employees must be unionized to maximize their rights and power as employees. Many expect physician unionization to take hold more fully over time. Medical residents, the doctors of tomorrow, are already considering unionization in greater numbers. Some are also doing it in the same employment setting alongside other health professionals, such as nurses.
Having studied doctors and their employment situations for years, I am convinced that whether through unionization or another approach, physicians must also change how they think about control; train and learn alongside other health care workers who share similar interests; and elevate at an early career stage their knowledge of the business side of health care.
Adopt a more pragmatic definition of autonomy
Doctors must embrace an updated definition of autonomy – one that matches their status as highly paid labor.
When I have spoken to physicians in my research about what autonomy means to them, many seem unable to reconceptualize it from a vague and absolute form of their profession’s strategic control over their economic fates and technical skills toward an individualized control that is situation-specific, one centered on winning the daily fights about workplace bread-and-butter issues such as those mentioned above.
But a more pragmatic definition of autonomy could get doctors focused on influencing important issues of the patient-care day and enhance their negotiating power with employers. It would allow physicians to break out of what often seems a paralysis of inaction – waiting for employers, insurers, or the government to reinstate the profession’s idealized version of control by handing it back the keys to the health care system through major regulatory, structural, and reimbursement-related changes. This fantasy is unlikely to become reality.
Physician-employees I’ve talked to over the years understand their everyday challenges. But when it comes to engaging in localized and sustained action to overcome them, they often perform less well, leading to feelings of helplessness and burnout. Valuing tactical control over their jobs and work setting will yield smaller but more impactful wins as employees intent on making their everyday work lives better.
Train alongside other health care professionals
Physicians must accept that how they are trained no longer prepares them for the employee world into which most are dropped. For instance, unless doctors are trained collaboratively alongside other health care professionals – such as nurses – they are less likely to identify closely with these colleagues once in practice. There is strength in numbers, so this mutual identification empowers both groups of employees. Yet, medical education remains largely the same: training young medical students in isolation for the first couple of years, then placing them into clerkships and residencies where true interprofessional care opportunities remain stunted and secondary to the “physician as captain of the team” mantra.
Unfortunately, the “hidden curriculum” of medicine helps convince medical students and residents early in their careers that they are the unquestioned leaders in patient care settings. This hierarchy encourages some doctors to keep their psychological distance from other members of the health care team and to resist sharing power, concerns, or insights with less skilled health care workers. This socialization harms the ability of physicians to act in a unified fashion alongside these other workers. Having physicians learn and train alongside other health professionals yields positive benefits for collective advocacy, including a shared sense of purpose, positive views on collaboration with others in the health setting, and greater development of bonds with nonphysician coworkers.
Integrate business with medical training in real time
Medical students and residents generally lack exposure to the everyday business realities of the U.S. health care system. This gap hinders their ability to understand the employee world and push for the types of changes and work conditions that benefit all health care workers. Formal business and management training should be a required part of every U.S. medical school and residency curriculum from day one. If you see it at all in medical schools now, it is mostly by accident, or given separate treatment in the form of standalone MBA or MPH degrees that rarely integrate organically and in real time with actual medical training. Not every doctor needs an MBA or MPH degree. However, all of them require a stronger contextual understanding of how the medicine they wish to practice is shaped by the economic and fiscal circumstances surrounding it – circumstances they do not control.
This is another reason why young doctors are unhappy and burned out. They cannot push for specific changes or properly critique the pros and cons of how their work is structured because they have not been made aware, in real time as they learn clinical practice, how their jobs are shaped by realities such as insurance coverage and reimbursement, the fragmentation of the care delivery system, their employer’s financial health , and the socioeconomic circumstances of their patients. They aren’t given the methods and tools related to process and quality improvement, budgeting, negotiation, risk management, leadership, and talent management that might help them navigate these undermining forces. They also get little advance exposure in their training to important workplace “soft” skills in such areas as how to work in teams, networking, communication and listening, empathy, and problem-solving – all necessary foci for bringing them closer to other health care workers and advocating alongside them effectively with health care employers.
Now is the time for physicians to embrace their identity as employees. Doing so is in their own best interest as professionals. It will help others in the health care workforce as well as patients. Moreover, it provides a needed counterbalance to the powerful corporate ethos now ascendant in U.S. health care.
Timothy Hoff, PhD, is a professor of management and healthcare systems at Northeastern University, Boston, and an associate fellow at the University of Oxford, England. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The strike by health care workers at Kaiser Permanente may not involve physicians (yet). But as more doctors in the United States are finding themselves working as salaried employees, physicians can – and probably will – become a powerful force for change in a health care system that has shown itself to be increasingly hostile to employee concerns over issues involving patient care, wages and benefits, safety, and well-being.
Salaried employment has its challenges. Physician-employees may have less autonomy and voice in decision-making that affects patients. They may splinter into fragmented work groups; feel isolated; and have different imperatives based on who they are, what they want, and where they work. They may feel more removed from their patients and struggle to build strong relationships, with their employers in the way.
Yet important opportunities exist for doctors when embracing their employee side. Examples of these interests include adequate compensation, wellness, job security, patient and worker safety, health care quality, reasonable workloads and schedules, and fair treatment by employers, including the need to exhibit a strong collective voice in organizational decision-making.
Some believe that physician-employees must be unionized to maximize their rights and power as employees. Many expect physician unionization to take hold more fully over time. Medical residents, the doctors of tomorrow, are already considering unionization in greater numbers. Some are also doing it in the same employment setting alongside other health professionals, such as nurses.
Having studied doctors and their employment situations for years, I am convinced that whether through unionization or another approach, physicians must also change how they think about control; train and learn alongside other health care workers who share similar interests; and elevate at an early career stage their knowledge of the business side of health care.
Adopt a more pragmatic definition of autonomy
Doctors must embrace an updated definition of autonomy – one that matches their status as highly paid labor.
When I have spoken to physicians in my research about what autonomy means to them, many seem unable to reconceptualize it from a vague and absolute form of their profession’s strategic control over their economic fates and technical skills toward an individualized control that is situation-specific, one centered on winning the daily fights about workplace bread-and-butter issues such as those mentioned above.
But a more pragmatic definition of autonomy could get doctors focused on influencing important issues of the patient-care day and enhance their negotiating power with employers. It would allow physicians to break out of what often seems a paralysis of inaction – waiting for employers, insurers, or the government to reinstate the profession’s idealized version of control by handing it back the keys to the health care system through major regulatory, structural, and reimbursement-related changes. This fantasy is unlikely to become reality.
Physician-employees I’ve talked to over the years understand their everyday challenges. But when it comes to engaging in localized and sustained action to overcome them, they often perform less well, leading to feelings of helplessness and burnout. Valuing tactical control over their jobs and work setting will yield smaller but more impactful wins as employees intent on making their everyday work lives better.
Train alongside other health care professionals
Physicians must accept that how they are trained no longer prepares them for the employee world into which most are dropped. For instance, unless doctors are trained collaboratively alongside other health care professionals – such as nurses – they are less likely to identify closely with these colleagues once in practice. There is strength in numbers, so this mutual identification empowers both groups of employees. Yet, medical education remains largely the same: training young medical students in isolation for the first couple of years, then placing them into clerkships and residencies where true interprofessional care opportunities remain stunted and secondary to the “physician as captain of the team” mantra.
Unfortunately, the “hidden curriculum” of medicine helps convince medical students and residents early in their careers that they are the unquestioned leaders in patient care settings. This hierarchy encourages some doctors to keep their psychological distance from other members of the health care team and to resist sharing power, concerns, or insights with less skilled health care workers. This socialization harms the ability of physicians to act in a unified fashion alongside these other workers. Having physicians learn and train alongside other health professionals yields positive benefits for collective advocacy, including a shared sense of purpose, positive views on collaboration with others in the health setting, and greater development of bonds with nonphysician coworkers.
Integrate business with medical training in real time
Medical students and residents generally lack exposure to the everyday business realities of the U.S. health care system. This gap hinders their ability to understand the employee world and push for the types of changes and work conditions that benefit all health care workers. Formal business and management training should be a required part of every U.S. medical school and residency curriculum from day one. If you see it at all in medical schools now, it is mostly by accident, or given separate treatment in the form of standalone MBA or MPH degrees that rarely integrate organically and in real time with actual medical training. Not every doctor needs an MBA or MPH degree. However, all of them require a stronger contextual understanding of how the medicine they wish to practice is shaped by the economic and fiscal circumstances surrounding it – circumstances they do not control.
This is another reason why young doctors are unhappy and burned out. They cannot push for specific changes or properly critique the pros and cons of how their work is structured because they have not been made aware, in real time as they learn clinical practice, how their jobs are shaped by realities such as insurance coverage and reimbursement, the fragmentation of the care delivery system, their employer’s financial health , and the socioeconomic circumstances of their patients. They aren’t given the methods and tools related to process and quality improvement, budgeting, negotiation, risk management, leadership, and talent management that might help them navigate these undermining forces. They also get little advance exposure in their training to important workplace “soft” skills in such areas as how to work in teams, networking, communication and listening, empathy, and problem-solving – all necessary foci for bringing them closer to other health care workers and advocating alongside them effectively with health care employers.
Now is the time for physicians to embrace their identity as employees. Doing so is in their own best interest as professionals. It will help others in the health care workforce as well as patients. Moreover, it provides a needed counterbalance to the powerful corporate ethos now ascendant in U.S. health care.
Timothy Hoff, PhD, is a professor of management and healthcare systems at Northeastern University, Boston, and an associate fellow at the University of Oxford, England. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.