Exposure to more traffic-related air pollution is associated with greater levels of amyloid plaques in the brain, with exposure in the 3 years before death having the greatest risk, a new postmortem study showed.
METHODOLOGY:
Investigators examined the brain tissue of 224 people living in the Atlanta area who agreed to donate their brains after death (average age of death, 76 years) for the presence of amyloid plaques and tau tangles.
They also studied the amount of fine particulate matter < 2.5 microns (PM2.5) from traffic-related air pollution at participants’ home addresses at 1, 3, and 5 years before death.
The presence of the APOE e4 gene was examined for evidence of any effect on the relationship between air pollution and evidence of Alzheimer’s disease (AD).
TAKEAWAY:
The average level of exposure in the year before death was 1.32 µg/m3 and 1.35 µg/m3 in the 3 years before death.
People with 1 µg/m3 higher PM2.5 exposure in the year before death were nearly twice as likely to have higher levels of plaques (odds ratio [OR], 1.92; 95% CI, 1.12-3.30), while those with higher exposure in the 3 years before death were 87% more likely to have higher levels of plaques (OR, 1.87; 95% CI, 1.01-3.17).
A little more than half (56%) of the sample were positive for the APOE e4 genotype, but the strongest association between pollution and neuropathology markers was for noncarriers of the genotype, although this relationship did not reach statistical significance.
IN PRACTICE:
“More research is needed to establish causality for the association between PM2.5 and AD, including epidemiologic and mechanistic studies. Future studies should also investigate the association between PM2.5 and other dementia-related pathologies, including cerebrovascular pathology,” the study authors wrote.
SOURCE:
Anke Hüls, PhD, of Emory University in Atlanta, led the study, which was published online on February 21, 2024, in Neurology.
LIMITATIONS:
The sample was not population-based but a convenience sample composed mostly of highly educated White participants.
DISCLOSURES:
The study was funded by the National Institute of Environmental Health Sciences, the Goizueta Alzheimer’s Disease Research Center, the National Institute on Aging, and the National Institutes of Health. There were no relevant disclosures.
A version of this article appeared on Medscape.com.
Exposure to more traffic-related air pollution is associated with greater levels of amyloid plaques in the brain, with exposure in the 3 years before death having the greatest risk, a new postmortem study showed.
METHODOLOGY:
Investigators examined the brain tissue of 224 people living in the Atlanta area who agreed to donate their brains after death (average age of death, 76 years) for the presence of amyloid plaques and tau tangles.
They also studied the amount of fine particulate matter < 2.5 microns (PM2.5) from traffic-related air pollution at participants’ home addresses at 1, 3, and 5 years before death.
The presence of the APOE e4 gene was examined for evidence of any effect on the relationship between air pollution and evidence of Alzheimer’s disease (AD).
TAKEAWAY:
The average level of exposure in the year before death was 1.32 µg/m3 and 1.35 µg/m3 in the 3 years before death.
People with 1 µg/m3 higher PM2.5 exposure in the year before death were nearly twice as likely to have higher levels of plaques (odds ratio [OR], 1.92; 95% CI, 1.12-3.30), while those with higher exposure in the 3 years before death were 87% more likely to have higher levels of plaques (OR, 1.87; 95% CI, 1.01-3.17).
A little more than half (56%) of the sample were positive for the APOE e4 genotype, but the strongest association between pollution and neuropathology markers was for noncarriers of the genotype, although this relationship did not reach statistical significance.
IN PRACTICE:
“More research is needed to establish causality for the association between PM2.5 and AD, including epidemiologic and mechanistic studies. Future studies should also investigate the association between PM2.5 and other dementia-related pathologies, including cerebrovascular pathology,” the study authors wrote.
SOURCE:
Anke Hüls, PhD, of Emory University in Atlanta, led the study, which was published online on February 21, 2024, in Neurology.
LIMITATIONS:
The sample was not population-based but a convenience sample composed mostly of highly educated White participants.
DISCLOSURES:
The study was funded by the National Institute of Environmental Health Sciences, the Goizueta Alzheimer’s Disease Research Center, the National Institute on Aging, and the National Institutes of Health. There were no relevant disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
Exposure to more traffic-related air pollution is associated with greater levels of amyloid plaques in the brain, with exposure in the 3 years before death having the greatest risk, a new postmortem study showed.
METHODOLOGY:
Investigators examined the brain tissue of 224 people living in the Atlanta area who agreed to donate their brains after death (average age of death, 76 years) for the presence of amyloid plaques and tau tangles.
They also studied the amount of fine particulate matter < 2.5 microns (PM2.5) from traffic-related air pollution at participants’ home addresses at 1, 3, and 5 years before death.
The presence of the APOE e4 gene was examined for evidence of any effect on the relationship between air pollution and evidence of Alzheimer’s disease (AD).
TAKEAWAY:
The average level of exposure in the year before death was 1.32 µg/m3 and 1.35 µg/m3 in the 3 years before death.
People with 1 µg/m3 higher PM2.5 exposure in the year before death were nearly twice as likely to have higher levels of plaques (odds ratio [OR], 1.92; 95% CI, 1.12-3.30), while those with higher exposure in the 3 years before death were 87% more likely to have higher levels of plaques (OR, 1.87; 95% CI, 1.01-3.17).
A little more than half (56%) of the sample were positive for the APOE e4 genotype, but the strongest association between pollution and neuropathology markers was for noncarriers of the genotype, although this relationship did not reach statistical significance.
IN PRACTICE:
“More research is needed to establish causality for the association between PM2.5 and AD, including epidemiologic and mechanistic studies. Future studies should also investigate the association between PM2.5 and other dementia-related pathologies, including cerebrovascular pathology,” the study authors wrote.
SOURCE:
Anke Hüls, PhD, of Emory University in Atlanta, led the study, which was published online on February 21, 2024, in Neurology.
LIMITATIONS:
The sample was not population-based but a convenience sample composed mostly of highly educated White participants.
DISCLOSURES:
The study was funded by the National Institute of Environmental Health Sciences, the Goizueta Alzheimer’s Disease Research Center, the National Institute on Aging, and the National Institutes of Health. There were no relevant disclosures.
A version of this article appeared on Medscape.com.
Thunderstorm asthma can strike with little warning, leaving people with the symptoms of an asthma attack during or after the dark clouds pass.
If you’re unfamiliar, the risk for a thunderstorm asthma attack grows when heavy storms arrive on a day with very high pollen or spores. The storm uplifts these particles, adds water, and causes them to explode into smaller grains. The electrical activity in a storm can do the same. Next, strong winds sweep these particles down and across the ground. People in the path of the storm can experience shortness of breath, coughing, and wheezing.
If thunderstorms are predicted to become more frequent and more severe with climate change, will the same hold true for thunderstorm asthma?
“Yes, if only because the amount of pollen appears to be increasing in many areas due to climate change,” said Frank S. Virant, MD, chief of the Allergy Division at Seattle Children’s Hospital in Washington.
Most cases of thunderstorm asthma occur in the spring and early summer, but that also could change. Pollen seasons “have been getting longer and more intense,” said Shaan M. Waqar, MD, an allergist at ENT and Allergy Associates in Plainview, NY.
“Thunderstorm asthma events are rare, but our changing environment and the increase in the number of people with allergies may make such events more common and more severe into the future,” agreed Paul J. Beggs, PhD, associate professor in the School of Natural Sciences at Macquarie University in Sydney, Australia.
How to Minimize Your Risk
If your patients are sensitive to pollen, advise them to continue to monitor outdoor levels, particularly during tree, grass, and weed pollen season, Dr. Virant recommended. Also patients should pay attention to weather reports. Watch for thunderstorms that could “amplify exposure to the pollen with 40-plus mile per hour winds and often colder air downdrafts.” Cold is an additional asthma trigger, he noted.
People with asthma should try to stay indoors with windows and doors closed during strong thunderstorms and for several hours afterward. Using air filters can also help reduce risk, said Deepti V. Manian, MD, an allergist and immunologist at Stormont Vail Health in Topeka, Kansas.
Patients should continue controller therapies -- such as longer-acting inhalers and allergy medications -- and use a rescue inhaler or nebulizer for prompt treatment of symptoms, recommended Donald J. Dvorin, MD, of The Allergy and Asthma Doctors in Mount Laurel, NJ. Ideally, people seeking shelter indoors during storms should be “accompanied by friends or family who can help them transport quickly to a hospital if needed.”
Asthma Diagnosis Not Required
Even peoples who would not consider themselves to have asthma can be seriously affected. For example, people with hay fever, or allergic rhinitis as it’s also known, are also at risk, said Ajay Kevat, MBBS, MPH, of the respiratory department at Queensland Children’s Hospital in Brisbane, Australia.
People with hay fever can also experience stronger symptoms during and after thunderstorms. Optimally treating allergic rhinitis during the pollen season with non-sedation antihistamines and nasal steroids can help, Dr. Virant said, instead of “chasing symptoms with medication after they are already severe.”
Part of the challenge is connecting severe weather to worse asthma symptoms. “In my experience, there is a lack of awareness surrounding thunderstorm asthma,” Dr. Manian said. For example, people with non-allergic rhinitis, also known as vasomotor rhinitis, can also experience the effects. “It often surprises many of my patients when I introduce the concept of vasomotor rhinitis, which can be triggered by environmental fluctuations.”
Gathering Clouds, Gathering Evidence
Climate change could also change which Americans experience the most storms. Researchers in a June 2022 study predicted fewer storms in the Southern plains and more storms in the Midwest and the Southeastern United States in the future.
Dr. Dvorin practices in Southern New Jersey, and in this area, “we fortunate in this area not to experience thunderstorm-induced asthma exacerbations,” he said.
But climate change means that in the future, thunderstorm asthma could strike in places it has never been seen before, said Dr. Kevat, who wrote a thunderstorm asthma review article published online June 2020 in the Journal of Asthma and Allergy.
And this is not just a concern in the United States. Major thunderstorm asthma events have been reported in Italy, the United Kingdom, the Middle East, Asia, and Australia. In November 2016, for instance, a strong set of storms swept across Melbourne, Australia. Temperatures dropped 10C (about 18F), humidity rose above 70%, and particulate matter like pollen became more concentrated in the air.
This event spurred a “thunderstorm asthma epidemic of unprecedented magnitude, tempo, and geographical range and severity,” Dr. Beggs and colleagues wrote in their June 2018 report in The Lancet Planetary Health.
Large-scale events like this can affect entire communities and quickly overwhelm local health care resources. Within 30 hours of the Melbourne storms, 3,365 people more than usual came to local emergency departments with respiratory issues — and 476 with asthma were admitted to the hospital. Ten people died: five in the hospital and five who could not be resuscitated or died while waiting for emergency services.
More research is needed “so as to best prepare for this unpredictable, significant public health threat,” Dr. Kevat wrote.
People whose asthma is triggered by pollen or mold spores are particularly at risk for thunderstorm asthma, Dr. Waqar said. If you’re unsure, an allergist can help diagnose and treat your allergic risks.
More severe thunderstorms are just one asthma trigger associated with climate change. Last summer, Canadian wildfires sent smoke across the northern U.S. and triggered widespread asthma exacerbations.
Thunderstorm asthma can strike with little warning, leaving people with the symptoms of an asthma attack during or after the dark clouds pass.
If you’re unfamiliar, the risk for a thunderstorm asthma attack grows when heavy storms arrive on a day with very high pollen or spores. The storm uplifts these particles, adds water, and causes them to explode into smaller grains. The electrical activity in a storm can do the same. Next, strong winds sweep these particles down and across the ground. People in the path of the storm can experience shortness of breath, coughing, and wheezing.
If thunderstorms are predicted to become more frequent and more severe with climate change, will the same hold true for thunderstorm asthma?
“Yes, if only because the amount of pollen appears to be increasing in many areas due to climate change,” said Frank S. Virant, MD, chief of the Allergy Division at Seattle Children’s Hospital in Washington.
Most cases of thunderstorm asthma occur in the spring and early summer, but that also could change. Pollen seasons “have been getting longer and more intense,” said Shaan M. Waqar, MD, an allergist at ENT and Allergy Associates in Plainview, NY.
“Thunderstorm asthma events are rare, but our changing environment and the increase in the number of people with allergies may make such events more common and more severe into the future,” agreed Paul J. Beggs, PhD, associate professor in the School of Natural Sciences at Macquarie University in Sydney, Australia.
How to Minimize Your Risk
If your patients are sensitive to pollen, advise them to continue to monitor outdoor levels, particularly during tree, grass, and weed pollen season, Dr. Virant recommended. Also patients should pay attention to weather reports. Watch for thunderstorms that could “amplify exposure to the pollen with 40-plus mile per hour winds and often colder air downdrafts.” Cold is an additional asthma trigger, he noted.
People with asthma should try to stay indoors with windows and doors closed during strong thunderstorms and for several hours afterward. Using air filters can also help reduce risk, said Deepti V. Manian, MD, an allergist and immunologist at Stormont Vail Health in Topeka, Kansas.
Patients should continue controller therapies -- such as longer-acting inhalers and allergy medications -- and use a rescue inhaler or nebulizer for prompt treatment of symptoms, recommended Donald J. Dvorin, MD, of The Allergy and Asthma Doctors in Mount Laurel, NJ. Ideally, people seeking shelter indoors during storms should be “accompanied by friends or family who can help them transport quickly to a hospital if needed.”
Asthma Diagnosis Not Required
Even peoples who would not consider themselves to have asthma can be seriously affected. For example, people with hay fever, or allergic rhinitis as it’s also known, are also at risk, said Ajay Kevat, MBBS, MPH, of the respiratory department at Queensland Children’s Hospital in Brisbane, Australia.
People with hay fever can also experience stronger symptoms during and after thunderstorms. Optimally treating allergic rhinitis during the pollen season with non-sedation antihistamines and nasal steroids can help, Dr. Virant said, instead of “chasing symptoms with medication after they are already severe.”
Part of the challenge is connecting severe weather to worse asthma symptoms. “In my experience, there is a lack of awareness surrounding thunderstorm asthma,” Dr. Manian said. For example, people with non-allergic rhinitis, also known as vasomotor rhinitis, can also experience the effects. “It often surprises many of my patients when I introduce the concept of vasomotor rhinitis, which can be triggered by environmental fluctuations.”
Gathering Clouds, Gathering Evidence
Climate change could also change which Americans experience the most storms. Researchers in a June 2022 study predicted fewer storms in the Southern plains and more storms in the Midwest and the Southeastern United States in the future.
Dr. Dvorin practices in Southern New Jersey, and in this area, “we fortunate in this area not to experience thunderstorm-induced asthma exacerbations,” he said.
But climate change means that in the future, thunderstorm asthma could strike in places it has never been seen before, said Dr. Kevat, who wrote a thunderstorm asthma review article published online June 2020 in the Journal of Asthma and Allergy.
And this is not just a concern in the United States. Major thunderstorm asthma events have been reported in Italy, the United Kingdom, the Middle East, Asia, and Australia. In November 2016, for instance, a strong set of storms swept across Melbourne, Australia. Temperatures dropped 10C (about 18F), humidity rose above 70%, and particulate matter like pollen became more concentrated in the air.
This event spurred a “thunderstorm asthma epidemic of unprecedented magnitude, tempo, and geographical range and severity,” Dr. Beggs and colleagues wrote in their June 2018 report in The Lancet Planetary Health.
Large-scale events like this can affect entire communities and quickly overwhelm local health care resources. Within 30 hours of the Melbourne storms, 3,365 people more than usual came to local emergency departments with respiratory issues — and 476 with asthma were admitted to the hospital. Ten people died: five in the hospital and five who could not be resuscitated or died while waiting for emergency services.
More research is needed “so as to best prepare for this unpredictable, significant public health threat,” Dr. Kevat wrote.
People whose asthma is triggered by pollen or mold spores are particularly at risk for thunderstorm asthma, Dr. Waqar said. If you’re unsure, an allergist can help diagnose and treat your allergic risks.
More severe thunderstorms are just one asthma trigger associated with climate change. Last summer, Canadian wildfires sent smoke across the northern U.S. and triggered widespread asthma exacerbations.
Thunderstorm asthma can strike with little warning, leaving people with the symptoms of an asthma attack during or after the dark clouds pass.
If you’re unfamiliar, the risk for a thunderstorm asthma attack grows when heavy storms arrive on a day with very high pollen or spores. The storm uplifts these particles, adds water, and causes them to explode into smaller grains. The electrical activity in a storm can do the same. Next, strong winds sweep these particles down and across the ground. People in the path of the storm can experience shortness of breath, coughing, and wheezing.
If thunderstorms are predicted to become more frequent and more severe with climate change, will the same hold true for thunderstorm asthma?
“Yes, if only because the amount of pollen appears to be increasing in many areas due to climate change,” said Frank S. Virant, MD, chief of the Allergy Division at Seattle Children’s Hospital in Washington.
Most cases of thunderstorm asthma occur in the spring and early summer, but that also could change. Pollen seasons “have been getting longer and more intense,” said Shaan M. Waqar, MD, an allergist at ENT and Allergy Associates in Plainview, NY.
“Thunderstorm asthma events are rare, but our changing environment and the increase in the number of people with allergies may make such events more common and more severe into the future,” agreed Paul J. Beggs, PhD, associate professor in the School of Natural Sciences at Macquarie University in Sydney, Australia.
How to Minimize Your Risk
If your patients are sensitive to pollen, advise them to continue to monitor outdoor levels, particularly during tree, grass, and weed pollen season, Dr. Virant recommended. Also patients should pay attention to weather reports. Watch for thunderstorms that could “amplify exposure to the pollen with 40-plus mile per hour winds and often colder air downdrafts.” Cold is an additional asthma trigger, he noted.
People with asthma should try to stay indoors with windows and doors closed during strong thunderstorms and for several hours afterward. Using air filters can also help reduce risk, said Deepti V. Manian, MD, an allergist and immunologist at Stormont Vail Health in Topeka, Kansas.
Patients should continue controller therapies -- such as longer-acting inhalers and allergy medications -- and use a rescue inhaler or nebulizer for prompt treatment of symptoms, recommended Donald J. Dvorin, MD, of The Allergy and Asthma Doctors in Mount Laurel, NJ. Ideally, people seeking shelter indoors during storms should be “accompanied by friends or family who can help them transport quickly to a hospital if needed.”
Asthma Diagnosis Not Required
Even peoples who would not consider themselves to have asthma can be seriously affected. For example, people with hay fever, or allergic rhinitis as it’s also known, are also at risk, said Ajay Kevat, MBBS, MPH, of the respiratory department at Queensland Children’s Hospital in Brisbane, Australia.
People with hay fever can also experience stronger symptoms during and after thunderstorms. Optimally treating allergic rhinitis during the pollen season with non-sedation antihistamines and nasal steroids can help, Dr. Virant said, instead of “chasing symptoms with medication after they are already severe.”
Part of the challenge is connecting severe weather to worse asthma symptoms. “In my experience, there is a lack of awareness surrounding thunderstorm asthma,” Dr. Manian said. For example, people with non-allergic rhinitis, also known as vasomotor rhinitis, can also experience the effects. “It often surprises many of my patients when I introduce the concept of vasomotor rhinitis, which can be triggered by environmental fluctuations.”
Gathering Clouds, Gathering Evidence
Climate change could also change which Americans experience the most storms. Researchers in a June 2022 study predicted fewer storms in the Southern plains and more storms in the Midwest and the Southeastern United States in the future.
Dr. Dvorin practices in Southern New Jersey, and in this area, “we fortunate in this area not to experience thunderstorm-induced asthma exacerbations,” he said.
But climate change means that in the future, thunderstorm asthma could strike in places it has never been seen before, said Dr. Kevat, who wrote a thunderstorm asthma review article published online June 2020 in the Journal of Asthma and Allergy.
And this is not just a concern in the United States. Major thunderstorm asthma events have been reported in Italy, the United Kingdom, the Middle East, Asia, and Australia. In November 2016, for instance, a strong set of storms swept across Melbourne, Australia. Temperatures dropped 10C (about 18F), humidity rose above 70%, and particulate matter like pollen became more concentrated in the air.
This event spurred a “thunderstorm asthma epidemic of unprecedented magnitude, tempo, and geographical range and severity,” Dr. Beggs and colleagues wrote in their June 2018 report in The Lancet Planetary Health.
Large-scale events like this can affect entire communities and quickly overwhelm local health care resources. Within 30 hours of the Melbourne storms, 3,365 people more than usual came to local emergency departments with respiratory issues — and 476 with asthma were admitted to the hospital. Ten people died: five in the hospital and five who could not be resuscitated or died while waiting for emergency services.
More research is needed “so as to best prepare for this unpredictable, significant public health threat,” Dr. Kevat wrote.
People whose asthma is triggered by pollen or mold spores are particularly at risk for thunderstorm asthma, Dr. Waqar said. If you’re unsure, an allergist can help diagnose and treat your allergic risks.
More severe thunderstorms are just one asthma trigger associated with climate change. Last summer, Canadian wildfires sent smoke across the northern U.S. and triggered widespread asthma exacerbations.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
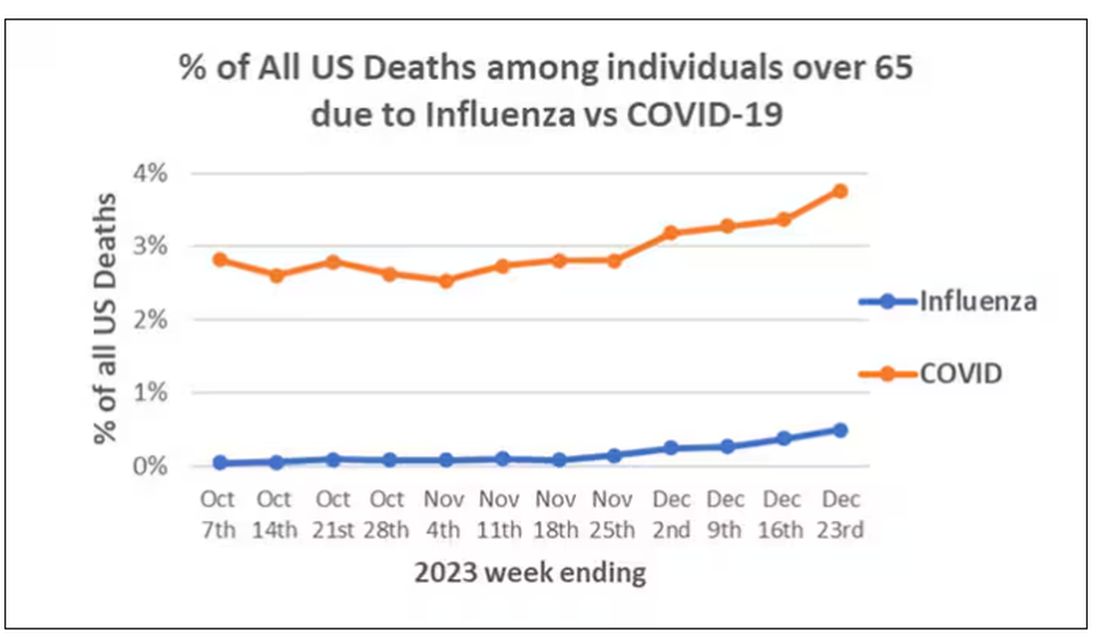
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
Centers for Disease Control and Prevention
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
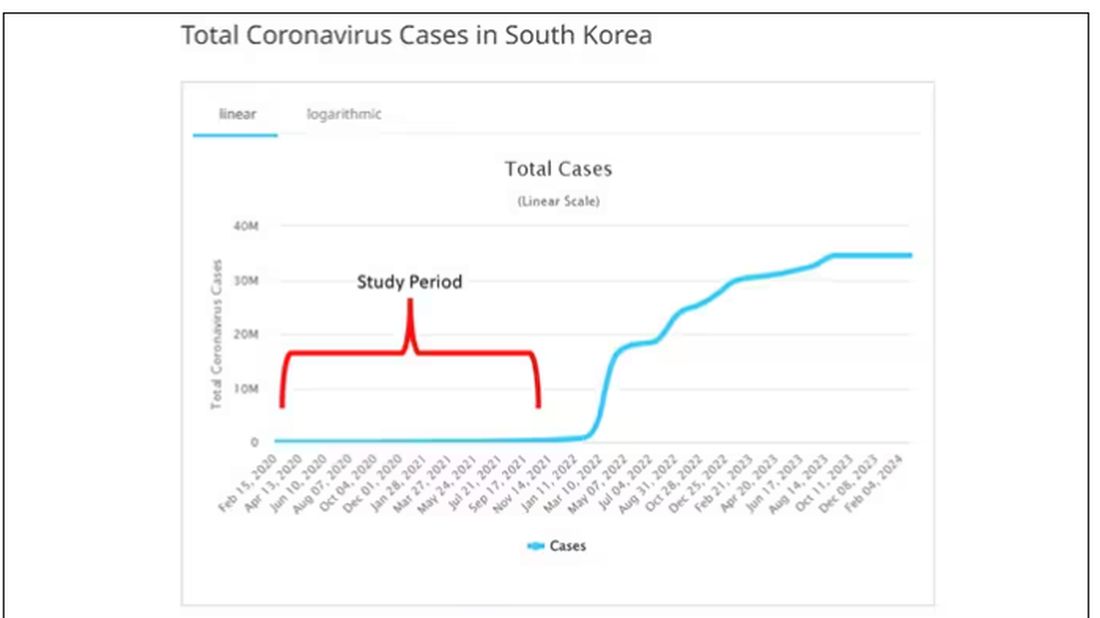
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
Worldometer
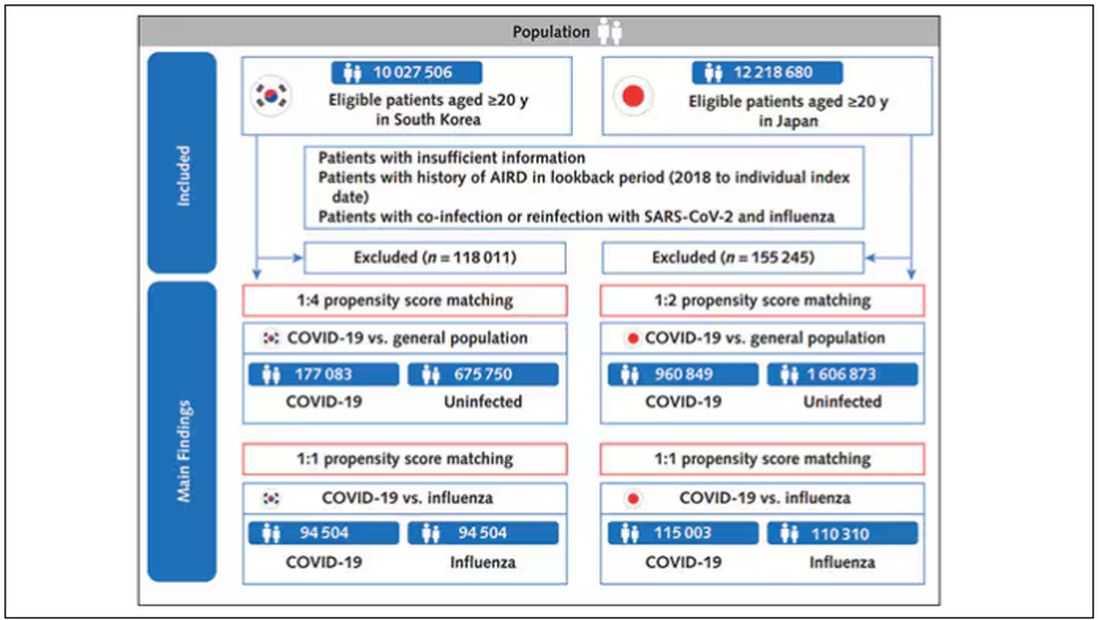
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
Annals of Internal Medicine
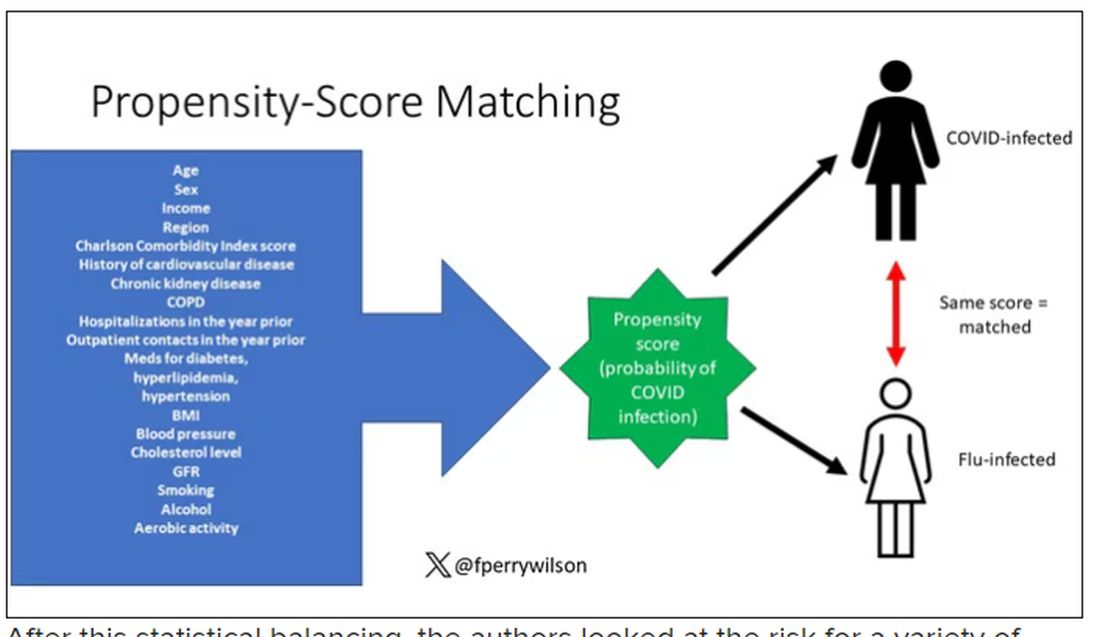
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
Dr. Wilson
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
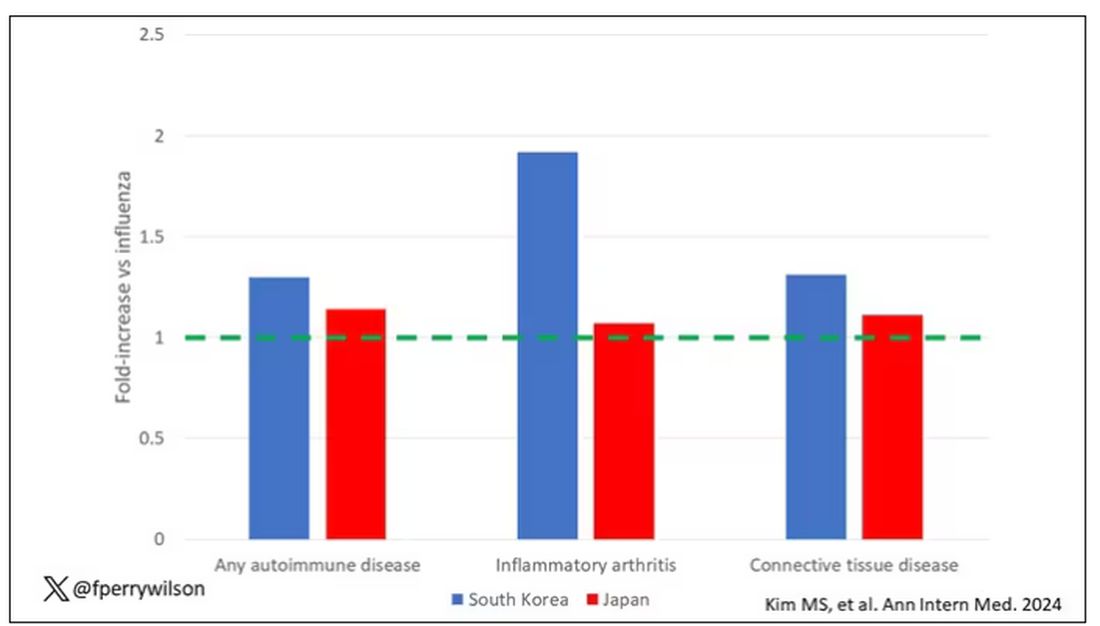
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
Dr. Wilson
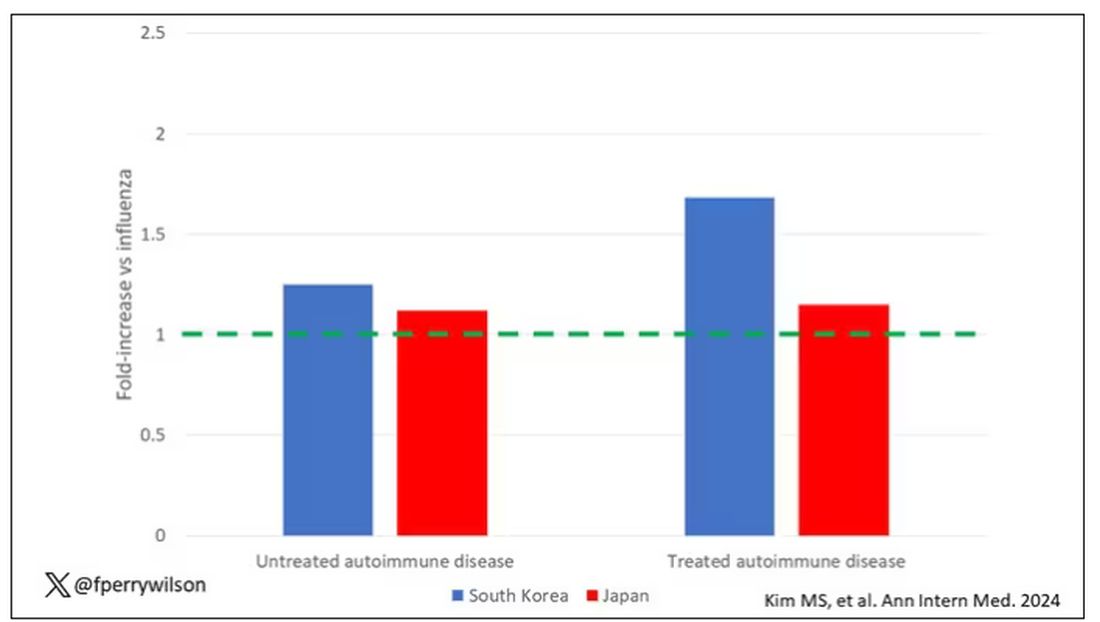
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
Dr. Wilson
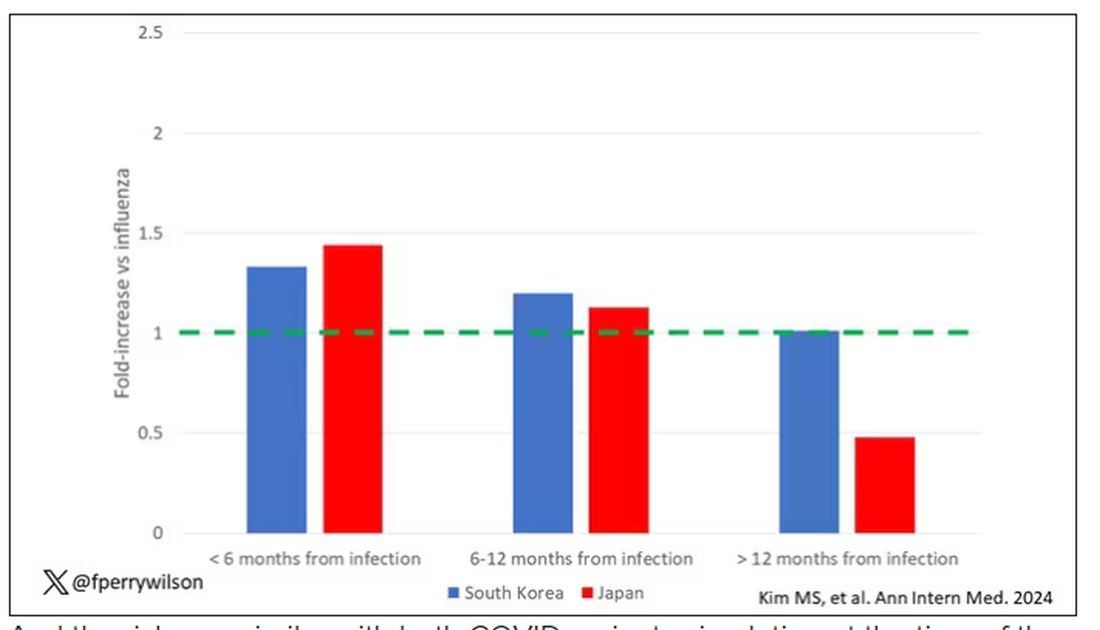
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
Dr. Wilson
And the risk was similar with both COVID variants circulating at the time of the study.
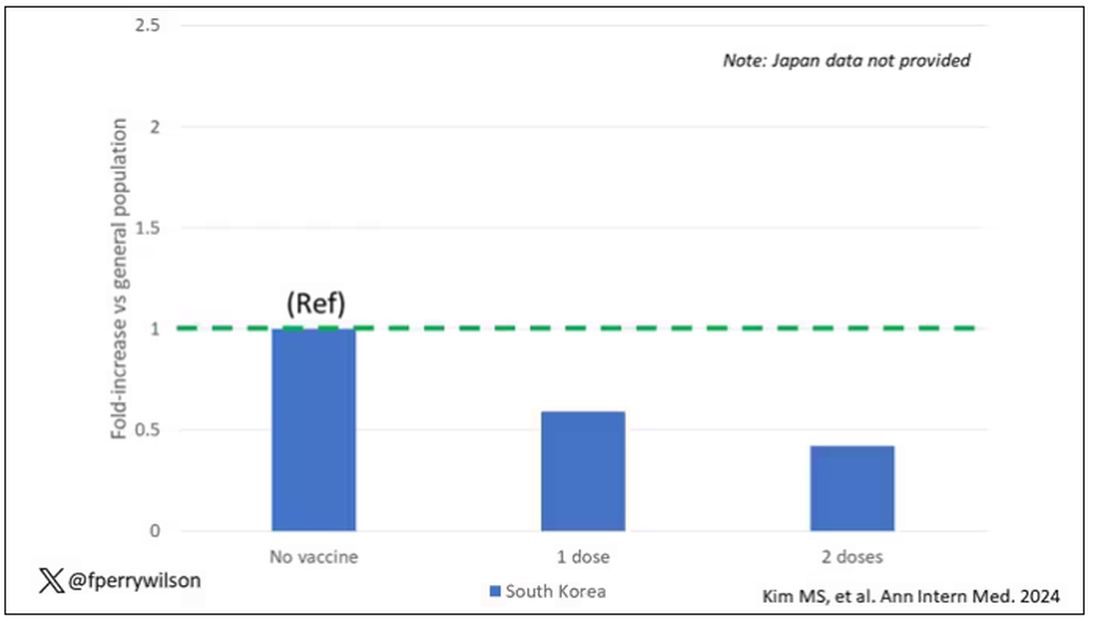
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Dr. WIlson
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
Centers for Disease Control and Prevention
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
Worldometer
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
Annals of Internal Medicine
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
Dr. Wilson
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
Dr. Wilson
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
Dr. Wilson
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
Dr. Wilson
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Dr. WIlson
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
In the early days of the pandemic, before we really understood what COVID was, two specialties in the hospital had a foreboding sense that something was very strange about this virus. The first was the pulmonologists, who noticed the striking levels of hypoxemia — low oxygen in the blood — and the rapidity with which patients who had previously been stable would crash in the intensive care unit.
The second, and I mark myself among this group, were the nephrologists. The dialysis machines stopped working right. I remember rounding on patients in the hospital who were on dialysis for kidney failure in the setting of severe COVID infection and seeing clots forming on the dialysis filters. Some patients could barely get in a full treatment because the filters would clog so quickly.
We knew it was worse than flu because of the mortality rates, but these oddities made us realize that it was different too — not just a particularly nasty respiratory virus but one that had effects on the body that we hadn’t really seen before.
Centers for Disease Control and Prevention
That’s why I’ve always been interested in studies that compare what happens to patients after COVID infection vs what happens to patients after other respiratory infections. This week, we’ll look at an intriguing study that suggests that COVID may lead to autoimmune diseases like rheumatoid arthritis, lupus, and vasculitis.
The study appears in the Annals of Internal Medicine and is made possible by the universal electronic health record systems of South Korea and Japan, who collaborated to create a truly staggering cohort of more than 20 million individuals living in those countries from 2020 to 2021.
The exposure of interest? COVID infection, experienced by just under 5% of that cohort over the study period. (Remember, there was a time when COVID infections were relatively controlled, particularly in some countries.)
Worldometer
The researchers wanted to compare the risk for autoimmune disease among COVID-infected individuals against two control groups. The first control group was the general population. This is interesting but a difficult analysis, because people who become infected with COVID might be very different from the general population. The second control group was people infected with influenza. I like this a lot better; the risk factors for COVID and influenza are quite similar, and the fact that this group was diagnosed with flu means at least that they are getting medical care and are sort of “in the system,” so to speak.
Annals of Internal Medicine
But it’s not enough to simply identify these folks and see who ends up with more autoimmune disease. The authors used propensity score matching to pair individuals infected with COVID with individuals from the control groups who were very similar to them. I’ve talked about this strategy before, but the basic idea is that you build a model predicting the likelihood of infection with COVID, based on a slew of factors — and the slew these authors used is pretty big, as shown below — and then stick people with similar risk for COVID together, with one member of the pair having had COVID and the other having eluded it (at least for the study period).
Dr. Wilson
After this statistical balancing, the authors looked at the risk for a variety of autoimmune diseases.
Compared with those infected with flu, those infected with COVID were more likely to be diagnosed with any autoimmune condition, connective tissue disease, and, in Japan at least, inflammatory arthritis.
Dr. Wilson
The authors acknowledge that being diagnosed with a disease might not be the same as actually having the disease, so in another analysis they looked only at people who received treatment for the autoimmune conditions, and the signals were even stronger in that group.
Dr. Wilson
This risk seemed to be highest in the 6 months following the COVID infection, which makes sense biologically if we think that the infection is somehow screwing up the immune system.
Dr. Wilson
And the risk was similar with both COVID variants circulating at the time of the study.
The only factor that reduced the risk? You guessed it: vaccination. This is a particularly interesting finding because the exposure cohort was defined by having been infected with COVID. Therefore, the mechanism of protection is not prevention of infection; it’s something else. Perhaps vaccination helps to get the immune system in a state to respond to COVID infection more… appropriately?
Dr. WIlson
Yes, this study is observational. We can’t draw causal conclusions here. But it does reinforce my long-held belief that COVID is a weird virus, one with effects that are different from the respiratory viruses we are used to. I can’t say for certain whether COVID causes immune system dysfunction that puts someone at risk for autoimmunity — not from this study. But I can say it wouldn’t surprise me.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
I’m Dr. Neil Skolnik, and today I am going to talk about the 2023 update to the Global Strategy for Asthma Management and Prevention. We treat a lot of asthma, and there are some important changes, particularly around the use of albuterol. There are two main guidelines when it comes to asthma, the Global Initiative for Asthma (GINA) guideline and the US National Heart, Lung, and Blood Institute Guidelines. While I had the privilege of serving on the expert working group for the US guidelines, what I like about the GINA guidelines is that they are updated annually, and so they really help us keep up with rapid changes in the field.
Today, I’m going to focus on assessment and treatment.
Four Questions to Assess Asthma Control
Because over half of patients with asthma are not well controlled, it is important to assess control at every asthma visit. Asthma control has two domains: symptom control and the risk for future exacerbations. It is not enough to simply ask, “How is your asthma?” because many patients overrate their control and live with ongoing symptoms. There are many assessment tools; the Asthma Control Test (ACT) focuses on symptoms, and the new Asthma Impairment and Risk Questionnaire (AIRQ) assesses both symptoms and risk for exacerbations. The GINA assessment is probably the easiest to implement, with just four questions relevant to the past 4 weeks:
Have you had daytime symptoms more than twice in one week?
Have you had any night waking due to asthma?
Have you needed short-acting beta-agonist (SABA), such as albuterol, rescue more than twice in one week?
Have you had any activity limitation due to asthma?
Well-controlled asthma is defined as a negative response to all four of these questions, partly controlled asthma is one or two “yes” answers, and uncontrolled asthma is three to four positive responses. You can’t modify a patient’s therapy if you don’t know whether their asthma is well or poorly controlled. You’ll notice that these questions focus on symptom control. It is important also to ask about risk factors for exacerbations, particularly previous exacerbations.
Asthma Treatment Changes
The goals of treatment are control of symptoms and avoidance of exacerbations. The GINA guidelines emphasize that even patients with mild asthma can have severe or fatal exacerbations.
GINA recommends two management tracks. The preferred track uses inhaled corticosteroid (ICS)-formoterol as both maintenance and reliever therapy (MART). Track 2, without the use of ICS-formoterol for MART, is also offered, recognizing that the use of ICS-formoterol for MART is not approved by the US Food and Drug Administration. There is an easy-to-follow stepped-care diagram that is worth looking at; it’s on page 66 of the GINA guideline PDF.
For patients who have symptoms less than twice a month, begin with Step 1 therapy:
Track 1: as-needed low-dose ICS-formoterol.
Track 2: treatment with albuterol; also use ICS whenever albuterol is used.
For patients with symptoms more than twice a month (but not most days of the week) treatment can start with Step 2 therapy:
Track 1: as-needed low-dose ICS-formoterol
Track 2: daily low-dose ICS plus as-needed SABA
An option for rescue therapy for Track 2 across all steps of therapy is to use an ICS whenever a SABA is used for rescue to reduce the likelihood of exacerbation.
For patients with more severe asthma symptoms most days of the week, or whose asthma is waking them from sleep one or more times weekly, then you can start with Step 3 therapy as follows:
Track 1: low dose ICS-formoterol as MART
Track 2: low-dose ICS with long-acting beta-agonist (LABA) for maintenance, plus as needed SABA or as needed ICS-SABA
That’s going to cover most of our patients. As we see people back, if escalation of therapy is needed, then Step 4 therapy is:
Track 1: medium-dose ICS-formoterol as MART
Track 2: medium-dose ICS-LABA plus as needed SABA or as-needed ICS-SABA
For patients who remain uncontrolled, it’s important to realize that Step 5 gives you the option to add a long-acting muscarinic antagonist (LAMA). In my experience this can be very helpful. We can also consider going to high-dose ICS-LABS for maintenance. At this step, the patient usually has pretty severe, uncontrolled asthma and we can think about checking eosinophil counts, ordering pulmonary function tests, and referring to our specialist colleagues for consideration of biologic therapy.
It is important to see patients back regularly, and to assess asthma control. If a patient is not well controlled or has had exacerbations, consider stepping up therapy, or changing from albuterol alone as rescue to albuterol plus ICS for rescue. If they have been well controlled for a long time, consider de-escalation of therapy among patients on one of the higher therapy steps.
Dr. Skolnik has disclosed the following relevant financial relationships: Serve(d) on the advisory board for AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck; and Bayer; serve(d) as a speaker or a member of a speakers bureau for AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, GlaxoSmithKline. Received research grant from Sanofi, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Bayer; and received income in an amount equal to or greater than $250 from AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article appeared on Medscape.com.
I’m Dr. Neil Skolnik, and today I am going to talk about the 2023 update to the Global Strategy for Asthma Management and Prevention. We treat a lot of asthma, and there are some important changes, particularly around the use of albuterol. There are two main guidelines when it comes to asthma, the Global Initiative for Asthma (GINA) guideline and the US National Heart, Lung, and Blood Institute Guidelines. While I had the privilege of serving on the expert working group for the US guidelines, what I like about the GINA guidelines is that they are updated annually, and so they really help us keep up with rapid changes in the field.
Today, I’m going to focus on assessment and treatment.
Four Questions to Assess Asthma Control
Because over half of patients with asthma are not well controlled, it is important to assess control at every asthma visit. Asthma control has two domains: symptom control and the risk for future exacerbations. It is not enough to simply ask, “How is your asthma?” because many patients overrate their control and live with ongoing symptoms. There are many assessment tools; the Asthma Control Test (ACT) focuses on symptoms, and the new Asthma Impairment and Risk Questionnaire (AIRQ) assesses both symptoms and risk for exacerbations. The GINA assessment is probably the easiest to implement, with just four questions relevant to the past 4 weeks:
Have you had daytime symptoms more than twice in one week?
Have you had any night waking due to asthma?
Have you needed short-acting beta-agonist (SABA), such as albuterol, rescue more than twice in one week?
Have you had any activity limitation due to asthma?
Well-controlled asthma is defined as a negative response to all four of these questions, partly controlled asthma is one or two “yes” answers, and uncontrolled asthma is three to four positive responses. You can’t modify a patient’s therapy if you don’t know whether their asthma is well or poorly controlled. You’ll notice that these questions focus on symptom control. It is important also to ask about risk factors for exacerbations, particularly previous exacerbations.
Asthma Treatment Changes
The goals of treatment are control of symptoms and avoidance of exacerbations. The GINA guidelines emphasize that even patients with mild asthma can have severe or fatal exacerbations.
GINA recommends two management tracks. The preferred track uses inhaled corticosteroid (ICS)-formoterol as both maintenance and reliever therapy (MART). Track 2, without the use of ICS-formoterol for MART, is also offered, recognizing that the use of ICS-formoterol for MART is not approved by the US Food and Drug Administration. There is an easy-to-follow stepped-care diagram that is worth looking at; it’s on page 66 of the GINA guideline PDF.
For patients who have symptoms less than twice a month, begin with Step 1 therapy:
Track 1: as-needed low-dose ICS-formoterol.
Track 2: treatment with albuterol; also use ICS whenever albuterol is used.
For patients with symptoms more than twice a month (but not most days of the week) treatment can start with Step 2 therapy:
Track 1: as-needed low-dose ICS-formoterol
Track 2: daily low-dose ICS plus as-needed SABA
An option for rescue therapy for Track 2 across all steps of therapy is to use an ICS whenever a SABA is used for rescue to reduce the likelihood of exacerbation.
For patients with more severe asthma symptoms most days of the week, or whose asthma is waking them from sleep one or more times weekly, then you can start with Step 3 therapy as follows:
Track 1: low dose ICS-formoterol as MART
Track 2: low-dose ICS with long-acting beta-agonist (LABA) for maintenance, plus as needed SABA or as needed ICS-SABA
That’s going to cover most of our patients. As we see people back, if escalation of therapy is needed, then Step 4 therapy is:
Track 1: medium-dose ICS-formoterol as MART
Track 2: medium-dose ICS-LABA plus as needed SABA or as-needed ICS-SABA
For patients who remain uncontrolled, it’s important to realize that Step 5 gives you the option to add a long-acting muscarinic antagonist (LAMA). In my experience this can be very helpful. We can also consider going to high-dose ICS-LABS for maintenance. At this step, the patient usually has pretty severe, uncontrolled asthma and we can think about checking eosinophil counts, ordering pulmonary function tests, and referring to our specialist colleagues for consideration of biologic therapy.
It is important to see patients back regularly, and to assess asthma control. If a patient is not well controlled or has had exacerbations, consider stepping up therapy, or changing from albuterol alone as rescue to albuterol plus ICS for rescue. If they have been well controlled for a long time, consider de-escalation of therapy among patients on one of the higher therapy steps.
Dr. Skolnik has disclosed the following relevant financial relationships: Serve(d) on the advisory board for AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck; and Bayer; serve(d) as a speaker or a member of a speakers bureau for AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, GlaxoSmithKline. Received research grant from Sanofi, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Bayer; and received income in an amount equal to or greater than $250 from AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Dr. Neil Skolnik, and today I am going to talk about the 2023 update to the Global Strategy for Asthma Management and Prevention. We treat a lot of asthma, and there are some important changes, particularly around the use of albuterol. There are two main guidelines when it comes to asthma, the Global Initiative for Asthma (GINA) guideline and the US National Heart, Lung, and Blood Institute Guidelines. While I had the privilege of serving on the expert working group for the US guidelines, what I like about the GINA guidelines is that they are updated annually, and so they really help us keep up with rapid changes in the field.
Today, I’m going to focus on assessment and treatment.
Four Questions to Assess Asthma Control
Because over half of patients with asthma are not well controlled, it is important to assess control at every asthma visit. Asthma control has two domains: symptom control and the risk for future exacerbations. It is not enough to simply ask, “How is your asthma?” because many patients overrate their control and live with ongoing symptoms. There are many assessment tools; the Asthma Control Test (ACT) focuses on symptoms, and the new Asthma Impairment and Risk Questionnaire (AIRQ) assesses both symptoms and risk for exacerbations. The GINA assessment is probably the easiest to implement, with just four questions relevant to the past 4 weeks:
Have you had daytime symptoms more than twice in one week?
Have you had any night waking due to asthma?
Have you needed short-acting beta-agonist (SABA), such as albuterol, rescue more than twice in one week?
Have you had any activity limitation due to asthma?
Well-controlled asthma is defined as a negative response to all four of these questions, partly controlled asthma is one or two “yes” answers, and uncontrolled asthma is three to four positive responses. You can’t modify a patient’s therapy if you don’t know whether their asthma is well or poorly controlled. You’ll notice that these questions focus on symptom control. It is important also to ask about risk factors for exacerbations, particularly previous exacerbations.
Asthma Treatment Changes
The goals of treatment are control of symptoms and avoidance of exacerbations. The GINA guidelines emphasize that even patients with mild asthma can have severe or fatal exacerbations.
GINA recommends two management tracks. The preferred track uses inhaled corticosteroid (ICS)-formoterol as both maintenance and reliever therapy (MART). Track 2, without the use of ICS-formoterol for MART, is also offered, recognizing that the use of ICS-formoterol for MART is not approved by the US Food and Drug Administration. There is an easy-to-follow stepped-care diagram that is worth looking at; it’s on page 66 of the GINA guideline PDF.
For patients who have symptoms less than twice a month, begin with Step 1 therapy:
Track 1: as-needed low-dose ICS-formoterol.
Track 2: treatment with albuterol; also use ICS whenever albuterol is used.
For patients with symptoms more than twice a month (but not most days of the week) treatment can start with Step 2 therapy:
Track 1: as-needed low-dose ICS-formoterol
Track 2: daily low-dose ICS plus as-needed SABA
An option for rescue therapy for Track 2 across all steps of therapy is to use an ICS whenever a SABA is used for rescue to reduce the likelihood of exacerbation.
For patients with more severe asthma symptoms most days of the week, or whose asthma is waking them from sleep one or more times weekly, then you can start with Step 3 therapy as follows:
Track 1: low dose ICS-formoterol as MART
Track 2: low-dose ICS with long-acting beta-agonist (LABA) for maintenance, plus as needed SABA or as needed ICS-SABA
That’s going to cover most of our patients. As we see people back, if escalation of therapy is needed, then Step 4 therapy is:
Track 1: medium-dose ICS-formoterol as MART
Track 2: medium-dose ICS-LABA plus as needed SABA or as-needed ICS-SABA
For patients who remain uncontrolled, it’s important to realize that Step 5 gives you the option to add a long-acting muscarinic antagonist (LAMA). In my experience this can be very helpful. We can also consider going to high-dose ICS-LABS for maintenance. At this step, the patient usually has pretty severe, uncontrolled asthma and we can think about checking eosinophil counts, ordering pulmonary function tests, and referring to our specialist colleagues for consideration of biologic therapy.
It is important to see patients back regularly, and to assess asthma control. If a patient is not well controlled or has had exacerbations, consider stepping up therapy, or changing from albuterol alone as rescue to albuterol plus ICS for rescue. If they have been well controlled for a long time, consider de-escalation of therapy among patients on one of the higher therapy steps.
Dr. Skolnik has disclosed the following relevant financial relationships: Serve(d) on the advisory board for AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck; and Bayer; serve(d) as a speaker or a member of a speakers bureau for AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, GlaxoSmithKline. Received research grant from Sanofi, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Bayer; and received income in an amount equal to or greater than $250 from AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article appeared on Medscape.com.
Viral infections frequently cause acute respiratory failure requiring ICU admission. In the United States, influenza causes over 50,000 deaths annually and SARS-CoV2 resulted in 170,000 hospitalizations in December 2023 alone.1 2 RSV lacks precise incidence data due to inconsistent testing but is increasingly implicated in respiratory failure.
Patients with underlying pulmonary comorbidities are at increased risk of severe infection. RSV induces bronchospasm and increases the risk for severe infection in patients with obstructive lung disease.3 Additionally, COPD patients with viral respiratory infections have higher rates of ICU admission, mechanical ventilation, and death compared with similar patients admitted for other etiologies.4
Diagnosis typically is achieved with nasopharyngeal PCR swabs. Positive viral swabs correlate with higher ICU admission and ventilation rates in patients with COPD.4 Coinfection with multiple respiratory viruses leads to higher mortality rates and bacterial and fungal coinfection further increases morbidity and mortality.5
Treatment includes respiratory support with noninvasive ventilation and high-flow nasal cannula, reducing the need for mechanical ventilation.6 Inhaled bronchodilators are particularly beneficial in patients with RSV infection.5 Oseltamivir reduces mortality in severe influenza cases, while remdesivir shows efficacy in SARS-CoV2 infection not requiring invasive ventilation.7 Severe SARS-CoV2 infection can be treated with immunomodulators. However, their availability is limited. Corticosteroids reduce mortality and mechanical ventilation in patients with SARS-CoV2; however, their use is associated with worse outcomes in influenza and RSV.7 8
Vaccination remains crucial for prevention of severe disease. RSV vaccination, in addition to influenza and SARS-CoV2 immunization, presents an opportunity to reduce morbidity and mortality.
References
1. Troeger C, et al. Lancet Infect Dis. 2018;18[11]:1191-1210.
2. WHO COVID-19 Epidemiological Update, 2024.
3. Coussement J, et al. Chest. 2022;161[6]:1475-1484.
4. Mulpuru S, et al. Influenza Other Respir Viruses. 2022;16[6]:1172-1182.
5. Saura O, et al. Expert Rev Anti Infect Ther. 2022;20[12]:1537-1550.
6. Inglis R, Ayebale E, Schultz MJ. Curr Opin Crit Care. 2019;25[1]:45-53.
7. O’Driscoll LS, Martin-Loeches I. Semin Respir Crit Care Med. 2021;42[6]:771-787.
Viral infections frequently cause acute respiratory failure requiring ICU admission. In the United States, influenza causes over 50,000 deaths annually and SARS-CoV2 resulted in 170,000 hospitalizations in December 2023 alone.1 2 RSV lacks precise incidence data due to inconsistent testing but is increasingly implicated in respiratory failure.
Patients with underlying pulmonary comorbidities are at increased risk of severe infection. RSV induces bronchospasm and increases the risk for severe infection in patients with obstructive lung disease.3 Additionally, COPD patients with viral respiratory infections have higher rates of ICU admission, mechanical ventilation, and death compared with similar patients admitted for other etiologies.4
Diagnosis typically is achieved with nasopharyngeal PCR swabs. Positive viral swabs correlate with higher ICU admission and ventilation rates in patients with COPD.4 Coinfection with multiple respiratory viruses leads to higher mortality rates and bacterial and fungal coinfection further increases morbidity and mortality.5
Treatment includes respiratory support with noninvasive ventilation and high-flow nasal cannula, reducing the need for mechanical ventilation.6 Inhaled bronchodilators are particularly beneficial in patients with RSV infection.5 Oseltamivir reduces mortality in severe influenza cases, while remdesivir shows efficacy in SARS-CoV2 infection not requiring invasive ventilation.7 Severe SARS-CoV2 infection can be treated with immunomodulators. However, their availability is limited. Corticosteroids reduce mortality and mechanical ventilation in patients with SARS-CoV2; however, their use is associated with worse outcomes in influenza and RSV.7 8
Vaccination remains crucial for prevention of severe disease. RSV vaccination, in addition to influenza and SARS-CoV2 immunization, presents an opportunity to reduce morbidity and mortality.
References
1. Troeger C, et al. Lancet Infect Dis. 2018;18[11]:1191-1210.
2. WHO COVID-19 Epidemiological Update, 2024.
3. Coussement J, et al. Chest. 2022;161[6]:1475-1484.
4. Mulpuru S, et al. Influenza Other Respir Viruses. 2022;16[6]:1172-1182.
5. Saura O, et al. Expert Rev Anti Infect Ther. 2022;20[12]:1537-1550.
6. Inglis R, Ayebale E, Schultz MJ. Curr Opin Crit Care. 2019;25[1]:45-53.
7. O’Driscoll LS, Martin-Loeches I. Semin Respir Crit Care Med. 2021;42[6]:771-787.
8. Bhimraj, A et al. Clin Inf Dis. 2022.
Chest Infections and Disaster Response Network
Disaster Response and Global Health Section
Zein Kattih, MD
Kathryn Hughes, MD
Brian Tran, MD
Viral infections frequently cause acute respiratory failure requiring ICU admission. In the United States, influenza causes over 50,000 deaths annually and SARS-CoV2 resulted in 170,000 hospitalizations in December 2023 alone.1 2 RSV lacks precise incidence data due to inconsistent testing but is increasingly implicated in respiratory failure.
Patients with underlying pulmonary comorbidities are at increased risk of severe infection. RSV induces bronchospasm and increases the risk for severe infection in patients with obstructive lung disease.3 Additionally, COPD patients with viral respiratory infections have higher rates of ICU admission, mechanical ventilation, and death compared with similar patients admitted for other etiologies.4
Diagnosis typically is achieved with nasopharyngeal PCR swabs. Positive viral swabs correlate with higher ICU admission and ventilation rates in patients with COPD.4 Coinfection with multiple respiratory viruses leads to higher mortality rates and bacterial and fungal coinfection further increases morbidity and mortality.5
Treatment includes respiratory support with noninvasive ventilation and high-flow nasal cannula, reducing the need for mechanical ventilation.6 Inhaled bronchodilators are particularly beneficial in patients with RSV infection.5 Oseltamivir reduces mortality in severe influenza cases, while remdesivir shows efficacy in SARS-CoV2 infection not requiring invasive ventilation.7 Severe SARS-CoV2 infection can be treated with immunomodulators. However, their availability is limited. Corticosteroids reduce mortality and mechanical ventilation in patients with SARS-CoV2; however, their use is associated with worse outcomes in influenza and RSV.7 8
Vaccination remains crucial for prevention of severe disease. RSV vaccination, in addition to influenza and SARS-CoV2 immunization, presents an opportunity to reduce morbidity and mortality.
References
1. Troeger C, et al. Lancet Infect Dis. 2018;18[11]:1191-1210.
2. WHO COVID-19 Epidemiological Update, 2024.
3. Coussement J, et al. Chest. 2022;161[6]:1475-1484.
4. Mulpuru S, et al. Influenza Other Respir Viruses. 2022;16[6]:1172-1182.
5. Saura O, et al. Expert Rev Anti Infect Ther. 2022;20[12]:1537-1550.
6. Inglis R, Ayebale E, Schultz MJ. Curr Opin Crit Care. 2019;25[1]:45-53.
7. O’Driscoll LS, Martin-Loeches I. Semin Respir Crit Care Med. 2021;42[6]:771-787.
Chronic obstructive pulmonary disease (COPD) is a respiratory disorder associated with slowly progressive systemic inflammation. It includes emphysema, chronic bronchitis, and small airway disease. Patients with COPD have an incomplete reversibility of airway obstruction, the key differentiating factor between it and asthma.1
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend a combination inhaler consisting of a long-acting β-2 agonist (LABA) and inhaled corticosteroid (ICS) for patients with a history of COPD exacerbations.2 Blood eosinophil count is another marker for the initiation of an ICS in patients with COPD. According to the 2023 GOLD Report, ICS therapy is appropriate for patients who experience frequent exacerbations and have a blood eosinophil count > 100 cells/μL, while on maximum tolerated inhaler therapy.3 A 2019 meta-analysis found an overall reduction in the risk of exacerbations in patients with blood eosinophil counts ≥ 100 cells/µL after initiating an ICS.4
Common ICS-LABA inhalers include the combination of budesonide/formoterol as well as fluticasone/salmeterol. Though these combinations are within the same therapeutic class, they have different delivery systems: budesonide/formoterol is a metered dose inhaler, while fluticasone/salmeterol is a dry powder inhaler. The PATHOS study compared the exacerbation rates for the 2 inhalers in primary care patients with COPD. Patients treated long-term with the budesonide/formoterol inhaler were significantly less likely to experience a COPD exacerbation than those treated with the fluticasone/salmeterol inhaler.5
In 2021, The Veteran Health Administration transitioned patients from budesonide/formoterol inhalers to fluticasone/salmeterol inhalers through a formulary conversion. The purpose of this study was to examine the outcomes for patients undergoing the transition.
Methods
A retrospective chart review was conducted on patients at the Hershel “Woody” Williams Veterans Affairs Medical Center in Huntington, West Virginia, with COPD and prescriptions for both budesonide/formoterol and fluticasone/salmeterol inhalers between February 1, 2021, and May 30, 2022. In 2018, the prevalence of COPD in West Virginia was 13.9%, highest in the US.6 Data was obtained through the US Department of Veteran Affairs (VA) Corporate Data Warehouse and stored on a VA Informatics and Computing Infrastructure server. Patients were randomly selected from this cohort and included if they were aged 18 to 89 years, prescribed both inhalers, and had a confirmed COPD diagnosis. Patients were excluded if they also had an asthma diagnosis, if they had an interstitial lung disease, or any tracheostomy tubes. The date of transition from a budesonide/formoterol inhaler to a fluticasone/salmeterol inhaler was collected to establish a timeline of 6 months before and 6 months after the transition.
The primary endpoint was to assess clinical outcomes such as the number of COPD exacerbations and hospitalizations within 6 months of the transition for patients affected by the formulary conversion. Secondary outcomes included the incidence of adverse effects (AEs), treatment failure, tobacco use, and systemic corticosteroid/antimicrobial utilization.
Statistical analyses were performed using STATA v.15. Numerical data was analyzed using a Wilcoxon signed rank test. Categorical data was analyzed by a logistic regression analysis.
Results
Of 1497 included patients who transitioned from budesonide/formoterol to fluticasone/salmeterol inhalers, 165 were randomly selected and 100 patients were included in this analysis. Of the 100 patients, 99 were male with a mean (SEM) age of 71 (0.69) years (range, 54-87) (Table).
The transition from budesonide/formoterol to fluticasone/salmeterol inhalers did not have a statistically significant impact on exacerbations (P = .56). Thirty patients had ≥ 1 exacerbation: 12 had an exacerbation before the transition, 10 had an exacerbation after the transition, and 8 had exacerbations before and after the transition. In the 6 months prior to the transition while on a budesonide/formoterol inhaler, there were 24 exacerbations among 20 patients. Five patients had > 1 exacerbation, accounting for 11 of the 24 exacerbations. There were 29 exacerbations among 19 patients while on a fluticasone/salmeterol inhaler in the 6 months after the transition. Four of these patients had > 1 exacerbation, accounting for 14 of 29 exacerbations (Figure).
Secondary endpoints showed 3 patients experienced an AE related to fluticasone/salmeterol, including thrush, coughing and throat irritation, and dyspnea. Eighteen fluticasone/salmeterol therapeutic failures were indicated by related prior authorization medication requests in the electronic health record. Twelve of 18 patients experienced no difference in exacerbations before vs after the transition to budesonide/formoterol. Twenty-three patients transitioned from fluticasone/salmeterol to a different ICS-LABA therapy; 20 of those 23 patients transitioned back to a budesonide/formoterol inhaler.
There were 48 documented active tobacco users in the study. There was no statistically significant correlation (P = .52) when comparing tobacco use at time of conversion and exacerbation frequency, although the coefficient showed a negative correlation of -0.387. In the 6 months prior to the transition, there were 17 prescriptions for systemic corticosteroids and 24 for antibiotics to treat COPD exacerbations. Following the transition, there were only 12 prescriptions for systemic corticosteroids and 23 for antibiotics. Fifty-two patients had an active prescription for a fluticasone/salmeterol inhaler at the time of the data review (November to December 2022); of the 48 patients who did not, 10 were no longer active due to patient death between the study period and data retrieval.
Discussion
Patients who transitioned from budesonide/formoterol to fluticasone/salmeterol inhalers did not show a significant difference in clinical COPD outcomes. While the total number of exacerbations increased after switching to the fluticasone/salmeterol inhaler, fewer patients had exacerbations during fluticasone/salmeterol therapy when compared with budesonide/fluticasone therapy. The number of patients receiving systemic corticosteroids and antibiotics to treat exacerbations before and after the transition were similar.
The frequency of treatment failures and AEs to the fluticasone/salmeterol inhaler could be due to the change of the inhaler delivery systems. Budesonide/formoterol is a metered dose inhaler (MDI). It is equipped with a pressurized canister that allows a spacer to be used to maximize benefit. Spacers can assist in preventing oral candidiasis by reducing the amount of medication that touches the back of the throat. Spacers are an option for patients, but not all use them for their MDIs, which can result in a less effective administered dose. Fluticasone/salmeterol is a dry powder inhaler, which requires a deep, fast breath to maximize the benefit, and spacers cannot be used with them. MDIs have been shown to be responsible for a negative impact on climate change, which can be reduced by switching to a dry powder inhaler.7
Tobacco cessation is very important in limiting the progression of COPD. As shown with the negative coefficient correlation, not being an active tobacco user at the time of transition correlated (although not significantly) with less frequent exacerbations. When comparing this study to similar research, such as the PATHOS study, several differences are observed.5 The PATHOS study compared long term treatment (> 1 year) of budesonide/formoterol or fluticasone/salmeterol, a longer period than this study. It regarded similar outcomes for the definition of an exacerbation, such as antibiotic/steroid use or hospital admission. While the current study showed no significant difference between the 2 inhalers and their effect on exacerbations, the PATHOS study found that those treated with a budesonide/formoterol inhaler were less likely to experience COPD-related exacerbations than those treated with the fluticasone/salmeterol inhaler. The PATHOS study had a larger mainly Scandinavian sample (N = 5500). This population could exhibit baseline differences from a study of US veterans.5 A similar Canadian matched cohort study of 2262 patients compared the 2 inhalers to assess their relative effectiveness. It found that COPD exacerbations did not differ between the 2 groups, but the budesonide/formoterol group was significantly less likely to have an emergency department visit compared to the fluticasone salmeterol group.8 Like the PATHOS study, the Canadian study had a larger sample size and longer timeframe than did our study.
Limitations
There are various limitations to this study. It was a retrospective, single-center study and the patient population was relatively homogenous, with only 1 female and a mean age of 71 years. As a study conducted in a veteran population in West Virginia, the findings may not be representative of the general population with COPD, which includes more women and more racial diversity.9 The American Lung Association discusses how environmental exposures to hazardous conditions increase the risks of pulmonary diseases for veterans.10 It has been reported that the prevalence of COPD is higher among veterans compared to the general population, but it is not different in terms of disease manifestation.10
Another limitation is the short time frame. Clinical guidelines, including the GOLD Report, typically track the number of exacerbations for 1 year to escalate therapy.3 Six months was a relatively short time frame, and it is possible that more exacerbations may have occurred beyond the study time frame. Ten patients in the sample died between the end of the study period and data retrieval, which might have been caught by a longer study period. An additional limitation was the inability to measure adherence. As this was a formulary conversion, many patients had been mailed a 30- or 90-day prescription of the budesonide/formoterol inhaler when transitioned to the fluticasone/salmeterol inhaler. There was no way to accurately determine when the patient made the switch to the fluticasone/salmeterol inhaler. This study also had a small sample group (a pre-post analysis of the same group), a limitation when evaluating the impact of this formulary change on a small percentage of the population transitioned.
This formulary conversion occurred during the COVID-19 pandemic, and some exacerbations could have been the result of a misdiagnosed COVID-19 infection. Respiratory infections, including COVID-19, are common causes of exacerbations. It is also possible that some patients elected not to receive medical care for symptoms of an exacerbation during the pandemic.11
Conclusions
Switching from the budesonide/formoterol inhaler to the fluticasone/salmeterol inhaler through formulary conversion did not have a significant impact on the clinical outcomes in patients with COPD. This study found that although the inhalers contain different active ingredients, products within the same therapeutic class yielded nonsignificant changes. When conducting formulary conversions, intolerances and treatment failures should be expected when switching from different inhaler delivery systems. This study further justifies the ability to be cost effective by making formulary conversions within the same therapeutic class within a veterans population.
Acknowledgments
The authors would like to acknowledge James Brown, PharmD, PhD.
References
1. US Department of Veterans Affairs. VA/DOD Clinical Practice Guideline. Management of Outpatient Chronic Obstructive Pulmonary Disease. 2021. Accessed January 22, 2024. https://www.healthquality.va.gov/guidelines/cd/copd/
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD Report. 2022. Accessed January 22, 2024. https://goldcopd.org/2022-gold-reports/
3. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis management, and prevention of chronic obstructive pulmonary disease 2023 report. Accessed January 26, 2024. https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf
4. Oshagbemi OA, Odiba JO, Daniel A, Yunusa I. Absolute blood eosinophil counts to guide inhaled corticosteroids therapy among patients with COPD: systematic review and meta-analysis. Curr Drug Targets. 2019;20(16):1670-1679. doi:10.2174/1389450120666190808141625
5. Larsson K, Janson C, Lisspers K, et al. Combination of budesonide/formoterol more effective than fluticasone/salmeterol in preventing exacerbations in chronic obstructive pulmonary disease: the PATHOS study. J Intern Med. 2013;273(6):584-594. doi:10.1111/joim.12067
6. West Virginia Department of Health and Human Resources, Division of Health Promotion and Chronic Disease. Statistics about the population of West Virginia. 2018. Accessed January 22, 2024. https://dhhr.wv.gov/hpcd/data_reports/ Pages/Fast-Facts.aspx
7. Fidler L, Green S, Wintemute K. Pressurized metered-dose inhalers and their impact on climate change. CMAJ. 2022;194(12):E460. doi:10.1503/cmaj.211747
8. Blais L, Forget A, Ramachandran S. Relative effectiveness of budesonide/formoterol and fluticasone propionate/salmeterol in a 1-year, population-based, matched cohort study of patients with chronic obstructive pulmonary disease (COPD): Effect on COPD-related exacerbations, emergency department visits and hospitalizations, medication utilization, and treatment adherence. Clin Ther. 2010;32(7):1320-1328. doi:10.1016/j.clinthera.2010.06.022
9. Wheaton AG, Cunningham TJ, Ford ES, Croft JB; Centers for Disease Control and Prevention (CDC). Employment and activity limitations among adults with chronic obstructive pulmonary disease — United States, 2013. MMWR Morb Mortal Wkly Rep. 2015:64(11):289-295.
10. Bamonti PM, Robinson SA, Wan ES, Moy ML. Improving physiological, physical, and psychological health outcomes: a narrative review in US veterans with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1269-1283. doi:10.2147/COPD.S339323
11. Czeisler MÉ, Marynak K, Clarke KEN, et al. Delay or avoidance of medical care because of COVID-19–related concerns - United States, June 2020. MMWR Morb Mortal Wkly Rep. 2020;69(36):1250-1257. doi:10.15585/mmwr.mm6936a4
aNorth Florida/South Georgia Veterans Affairs Health System, Gainesville
bHershel “Woody” Williams Veterans Affairs Medical Center, Huntington, West Virginia
Author disclosures
The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Ethics and consent
This study was reviewed and approved by the Marshall University and Hershel “Woody” Williams Veterans Affairs Medical Center institutional review boards
aNorth Florida/South Georgia Veterans Affairs Health System, Gainesville
bHershel “Woody” Williams Veterans Affairs Medical Center, Huntington, West Virginia
Author disclosures
The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Ethics and consent
This study was reviewed and approved by the Marshall University and Hershel “Woody” Williams Veterans Affairs Medical Center institutional review boards
aNorth Florida/South Georgia Veterans Affairs Health System, Gainesville
bHershel “Woody” Williams Veterans Affairs Medical Center, Huntington, West Virginia
Author disclosures
The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Ethics and consent
This study was reviewed and approved by the Marshall University and Hershel “Woody” Williams Veterans Affairs Medical Center institutional review boards
Chronic obstructive pulmonary disease (COPD) is a respiratory disorder associated with slowly progressive systemic inflammation. It includes emphysema, chronic bronchitis, and small airway disease. Patients with COPD have an incomplete reversibility of airway obstruction, the key differentiating factor between it and asthma.1
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend a combination inhaler consisting of a long-acting β-2 agonist (LABA) and inhaled corticosteroid (ICS) for patients with a history of COPD exacerbations.2 Blood eosinophil count is another marker for the initiation of an ICS in patients with COPD. According to the 2023 GOLD Report, ICS therapy is appropriate for patients who experience frequent exacerbations and have a blood eosinophil count > 100 cells/μL, while on maximum tolerated inhaler therapy.3 A 2019 meta-analysis found an overall reduction in the risk of exacerbations in patients with blood eosinophil counts ≥ 100 cells/µL after initiating an ICS.4
Common ICS-LABA inhalers include the combination of budesonide/formoterol as well as fluticasone/salmeterol. Though these combinations are within the same therapeutic class, they have different delivery systems: budesonide/formoterol is a metered dose inhaler, while fluticasone/salmeterol is a dry powder inhaler. The PATHOS study compared the exacerbation rates for the 2 inhalers in primary care patients with COPD. Patients treated long-term with the budesonide/formoterol inhaler were significantly less likely to experience a COPD exacerbation than those treated with the fluticasone/salmeterol inhaler.5
In 2021, The Veteran Health Administration transitioned patients from budesonide/formoterol inhalers to fluticasone/salmeterol inhalers through a formulary conversion. The purpose of this study was to examine the outcomes for patients undergoing the transition.
Methods
A retrospective chart review was conducted on patients at the Hershel “Woody” Williams Veterans Affairs Medical Center in Huntington, West Virginia, with COPD and prescriptions for both budesonide/formoterol and fluticasone/salmeterol inhalers between February 1, 2021, and May 30, 2022. In 2018, the prevalence of COPD in West Virginia was 13.9%, highest in the US.6 Data was obtained through the US Department of Veteran Affairs (VA) Corporate Data Warehouse and stored on a VA Informatics and Computing Infrastructure server. Patients were randomly selected from this cohort and included if they were aged 18 to 89 years, prescribed both inhalers, and had a confirmed COPD diagnosis. Patients were excluded if they also had an asthma diagnosis, if they had an interstitial lung disease, or any tracheostomy tubes. The date of transition from a budesonide/formoterol inhaler to a fluticasone/salmeterol inhaler was collected to establish a timeline of 6 months before and 6 months after the transition.
The primary endpoint was to assess clinical outcomes such as the number of COPD exacerbations and hospitalizations within 6 months of the transition for patients affected by the formulary conversion. Secondary outcomes included the incidence of adverse effects (AEs), treatment failure, tobacco use, and systemic corticosteroid/antimicrobial utilization.
Statistical analyses were performed using STATA v.15. Numerical data was analyzed using a Wilcoxon signed rank test. Categorical data was analyzed by a logistic regression analysis.
Results
Of 1497 included patients who transitioned from budesonide/formoterol to fluticasone/salmeterol inhalers, 165 were randomly selected and 100 patients were included in this analysis. Of the 100 patients, 99 were male with a mean (SEM) age of 71 (0.69) years (range, 54-87) (Table).
The transition from budesonide/formoterol to fluticasone/salmeterol inhalers did not have a statistically significant impact on exacerbations (P = .56). Thirty patients had ≥ 1 exacerbation: 12 had an exacerbation before the transition, 10 had an exacerbation after the transition, and 8 had exacerbations before and after the transition. In the 6 months prior to the transition while on a budesonide/formoterol inhaler, there were 24 exacerbations among 20 patients. Five patients had > 1 exacerbation, accounting for 11 of the 24 exacerbations. There were 29 exacerbations among 19 patients while on a fluticasone/salmeterol inhaler in the 6 months after the transition. Four of these patients had > 1 exacerbation, accounting for 14 of 29 exacerbations (Figure).
Secondary endpoints showed 3 patients experienced an AE related to fluticasone/salmeterol, including thrush, coughing and throat irritation, and dyspnea. Eighteen fluticasone/salmeterol therapeutic failures were indicated by related prior authorization medication requests in the electronic health record. Twelve of 18 patients experienced no difference in exacerbations before vs after the transition to budesonide/formoterol. Twenty-three patients transitioned from fluticasone/salmeterol to a different ICS-LABA therapy; 20 of those 23 patients transitioned back to a budesonide/formoterol inhaler.
There were 48 documented active tobacco users in the study. There was no statistically significant correlation (P = .52) when comparing tobacco use at time of conversion and exacerbation frequency, although the coefficient showed a negative correlation of -0.387. In the 6 months prior to the transition, there were 17 prescriptions for systemic corticosteroids and 24 for antibiotics to treat COPD exacerbations. Following the transition, there were only 12 prescriptions for systemic corticosteroids and 23 for antibiotics. Fifty-two patients had an active prescription for a fluticasone/salmeterol inhaler at the time of the data review (November to December 2022); of the 48 patients who did not, 10 were no longer active due to patient death between the study period and data retrieval.
Discussion
Patients who transitioned from budesonide/formoterol to fluticasone/salmeterol inhalers did not show a significant difference in clinical COPD outcomes. While the total number of exacerbations increased after switching to the fluticasone/salmeterol inhaler, fewer patients had exacerbations during fluticasone/salmeterol therapy when compared with budesonide/fluticasone therapy. The number of patients receiving systemic corticosteroids and antibiotics to treat exacerbations before and after the transition were similar.
The frequency of treatment failures and AEs to the fluticasone/salmeterol inhaler could be due to the change of the inhaler delivery systems. Budesonide/formoterol is a metered dose inhaler (MDI). It is equipped with a pressurized canister that allows a spacer to be used to maximize benefit. Spacers can assist in preventing oral candidiasis by reducing the amount of medication that touches the back of the throat. Spacers are an option for patients, but not all use them for their MDIs, which can result in a less effective administered dose. Fluticasone/salmeterol is a dry powder inhaler, which requires a deep, fast breath to maximize the benefit, and spacers cannot be used with them. MDIs have been shown to be responsible for a negative impact on climate change, which can be reduced by switching to a dry powder inhaler.7
Tobacco cessation is very important in limiting the progression of COPD. As shown with the negative coefficient correlation, not being an active tobacco user at the time of transition correlated (although not significantly) with less frequent exacerbations. When comparing this study to similar research, such as the PATHOS study, several differences are observed.5 The PATHOS study compared long term treatment (> 1 year) of budesonide/formoterol or fluticasone/salmeterol, a longer period than this study. It regarded similar outcomes for the definition of an exacerbation, such as antibiotic/steroid use or hospital admission. While the current study showed no significant difference between the 2 inhalers and their effect on exacerbations, the PATHOS study found that those treated with a budesonide/formoterol inhaler were less likely to experience COPD-related exacerbations than those treated with the fluticasone/salmeterol inhaler. The PATHOS study had a larger mainly Scandinavian sample (N = 5500). This population could exhibit baseline differences from a study of US veterans.5 A similar Canadian matched cohort study of 2262 patients compared the 2 inhalers to assess their relative effectiveness. It found that COPD exacerbations did not differ between the 2 groups, but the budesonide/formoterol group was significantly less likely to have an emergency department visit compared to the fluticasone salmeterol group.8 Like the PATHOS study, the Canadian study had a larger sample size and longer timeframe than did our study.
Limitations
There are various limitations to this study. It was a retrospective, single-center study and the patient population was relatively homogenous, with only 1 female and a mean age of 71 years. As a study conducted in a veteran population in West Virginia, the findings may not be representative of the general population with COPD, which includes more women and more racial diversity.9 The American Lung Association discusses how environmental exposures to hazardous conditions increase the risks of pulmonary diseases for veterans.10 It has been reported that the prevalence of COPD is higher among veterans compared to the general population, but it is not different in terms of disease manifestation.10
Another limitation is the short time frame. Clinical guidelines, including the GOLD Report, typically track the number of exacerbations for 1 year to escalate therapy.3 Six months was a relatively short time frame, and it is possible that more exacerbations may have occurred beyond the study time frame. Ten patients in the sample died between the end of the study period and data retrieval, which might have been caught by a longer study period. An additional limitation was the inability to measure adherence. As this was a formulary conversion, many patients had been mailed a 30- or 90-day prescription of the budesonide/formoterol inhaler when transitioned to the fluticasone/salmeterol inhaler. There was no way to accurately determine when the patient made the switch to the fluticasone/salmeterol inhaler. This study also had a small sample group (a pre-post analysis of the same group), a limitation when evaluating the impact of this formulary change on a small percentage of the population transitioned.
This formulary conversion occurred during the COVID-19 pandemic, and some exacerbations could have been the result of a misdiagnosed COVID-19 infection. Respiratory infections, including COVID-19, are common causes of exacerbations. It is also possible that some patients elected not to receive medical care for symptoms of an exacerbation during the pandemic.11
Conclusions
Switching from the budesonide/formoterol inhaler to the fluticasone/salmeterol inhaler through formulary conversion did not have a significant impact on the clinical outcomes in patients with COPD. This study found that although the inhalers contain different active ingredients, products within the same therapeutic class yielded nonsignificant changes. When conducting formulary conversions, intolerances and treatment failures should be expected when switching from different inhaler delivery systems. This study further justifies the ability to be cost effective by making formulary conversions within the same therapeutic class within a veterans population.
Acknowledgments
The authors would like to acknowledge James Brown, PharmD, PhD.
Chronic obstructive pulmonary disease (COPD) is a respiratory disorder associated with slowly progressive systemic inflammation. It includes emphysema, chronic bronchitis, and small airway disease. Patients with COPD have an incomplete reversibility of airway obstruction, the key differentiating factor between it and asthma.1
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend a combination inhaler consisting of a long-acting β-2 agonist (LABA) and inhaled corticosteroid (ICS) for patients with a history of COPD exacerbations.2 Blood eosinophil count is another marker for the initiation of an ICS in patients with COPD. According to the 2023 GOLD Report, ICS therapy is appropriate for patients who experience frequent exacerbations and have a blood eosinophil count > 100 cells/μL, while on maximum tolerated inhaler therapy.3 A 2019 meta-analysis found an overall reduction in the risk of exacerbations in patients with blood eosinophil counts ≥ 100 cells/µL after initiating an ICS.4
Common ICS-LABA inhalers include the combination of budesonide/formoterol as well as fluticasone/salmeterol. Though these combinations are within the same therapeutic class, they have different delivery systems: budesonide/formoterol is a metered dose inhaler, while fluticasone/salmeterol is a dry powder inhaler. The PATHOS study compared the exacerbation rates for the 2 inhalers in primary care patients with COPD. Patients treated long-term with the budesonide/formoterol inhaler were significantly less likely to experience a COPD exacerbation than those treated with the fluticasone/salmeterol inhaler.5
In 2021, The Veteran Health Administration transitioned patients from budesonide/formoterol inhalers to fluticasone/salmeterol inhalers through a formulary conversion. The purpose of this study was to examine the outcomes for patients undergoing the transition.
Methods
A retrospective chart review was conducted on patients at the Hershel “Woody” Williams Veterans Affairs Medical Center in Huntington, West Virginia, with COPD and prescriptions for both budesonide/formoterol and fluticasone/salmeterol inhalers between February 1, 2021, and May 30, 2022. In 2018, the prevalence of COPD in West Virginia was 13.9%, highest in the US.6 Data was obtained through the US Department of Veteran Affairs (VA) Corporate Data Warehouse and stored on a VA Informatics and Computing Infrastructure server. Patients were randomly selected from this cohort and included if they were aged 18 to 89 years, prescribed both inhalers, and had a confirmed COPD diagnosis. Patients were excluded if they also had an asthma diagnosis, if they had an interstitial lung disease, or any tracheostomy tubes. The date of transition from a budesonide/formoterol inhaler to a fluticasone/salmeterol inhaler was collected to establish a timeline of 6 months before and 6 months after the transition.
The primary endpoint was to assess clinical outcomes such as the number of COPD exacerbations and hospitalizations within 6 months of the transition for patients affected by the formulary conversion. Secondary outcomes included the incidence of adverse effects (AEs), treatment failure, tobacco use, and systemic corticosteroid/antimicrobial utilization.
Statistical analyses were performed using STATA v.15. Numerical data was analyzed using a Wilcoxon signed rank test. Categorical data was analyzed by a logistic regression analysis.
Results
Of 1497 included patients who transitioned from budesonide/formoterol to fluticasone/salmeterol inhalers, 165 were randomly selected and 100 patients were included in this analysis. Of the 100 patients, 99 were male with a mean (SEM) age of 71 (0.69) years (range, 54-87) (Table).
The transition from budesonide/formoterol to fluticasone/salmeterol inhalers did not have a statistically significant impact on exacerbations (P = .56). Thirty patients had ≥ 1 exacerbation: 12 had an exacerbation before the transition, 10 had an exacerbation after the transition, and 8 had exacerbations before and after the transition. In the 6 months prior to the transition while on a budesonide/formoterol inhaler, there were 24 exacerbations among 20 patients. Five patients had > 1 exacerbation, accounting for 11 of the 24 exacerbations. There were 29 exacerbations among 19 patients while on a fluticasone/salmeterol inhaler in the 6 months after the transition. Four of these patients had > 1 exacerbation, accounting for 14 of 29 exacerbations (Figure).
Secondary endpoints showed 3 patients experienced an AE related to fluticasone/salmeterol, including thrush, coughing and throat irritation, and dyspnea. Eighteen fluticasone/salmeterol therapeutic failures were indicated by related prior authorization medication requests in the electronic health record. Twelve of 18 patients experienced no difference in exacerbations before vs after the transition to budesonide/formoterol. Twenty-three patients transitioned from fluticasone/salmeterol to a different ICS-LABA therapy; 20 of those 23 patients transitioned back to a budesonide/formoterol inhaler.
There were 48 documented active tobacco users in the study. There was no statistically significant correlation (P = .52) when comparing tobacco use at time of conversion and exacerbation frequency, although the coefficient showed a negative correlation of -0.387. In the 6 months prior to the transition, there were 17 prescriptions for systemic corticosteroids and 24 for antibiotics to treat COPD exacerbations. Following the transition, there were only 12 prescriptions for systemic corticosteroids and 23 for antibiotics. Fifty-two patients had an active prescription for a fluticasone/salmeterol inhaler at the time of the data review (November to December 2022); of the 48 patients who did not, 10 were no longer active due to patient death between the study period and data retrieval.
Discussion
Patients who transitioned from budesonide/formoterol to fluticasone/salmeterol inhalers did not show a significant difference in clinical COPD outcomes. While the total number of exacerbations increased after switching to the fluticasone/salmeterol inhaler, fewer patients had exacerbations during fluticasone/salmeterol therapy when compared with budesonide/fluticasone therapy. The number of patients receiving systemic corticosteroids and antibiotics to treat exacerbations before and after the transition were similar.
The frequency of treatment failures and AEs to the fluticasone/salmeterol inhaler could be due to the change of the inhaler delivery systems. Budesonide/formoterol is a metered dose inhaler (MDI). It is equipped with a pressurized canister that allows a spacer to be used to maximize benefit. Spacers can assist in preventing oral candidiasis by reducing the amount of medication that touches the back of the throat. Spacers are an option for patients, but not all use them for their MDIs, which can result in a less effective administered dose. Fluticasone/salmeterol is a dry powder inhaler, which requires a deep, fast breath to maximize the benefit, and spacers cannot be used with them. MDIs have been shown to be responsible for a negative impact on climate change, which can be reduced by switching to a dry powder inhaler.7
Tobacco cessation is very important in limiting the progression of COPD. As shown with the negative coefficient correlation, not being an active tobacco user at the time of transition correlated (although not significantly) with less frequent exacerbations. When comparing this study to similar research, such as the PATHOS study, several differences are observed.5 The PATHOS study compared long term treatment (> 1 year) of budesonide/formoterol or fluticasone/salmeterol, a longer period than this study. It regarded similar outcomes for the definition of an exacerbation, such as antibiotic/steroid use or hospital admission. While the current study showed no significant difference between the 2 inhalers and their effect on exacerbations, the PATHOS study found that those treated with a budesonide/formoterol inhaler were less likely to experience COPD-related exacerbations than those treated with the fluticasone/salmeterol inhaler. The PATHOS study had a larger mainly Scandinavian sample (N = 5500). This population could exhibit baseline differences from a study of US veterans.5 A similar Canadian matched cohort study of 2262 patients compared the 2 inhalers to assess their relative effectiveness. It found that COPD exacerbations did not differ between the 2 groups, but the budesonide/formoterol group was significantly less likely to have an emergency department visit compared to the fluticasone salmeterol group.8 Like the PATHOS study, the Canadian study had a larger sample size and longer timeframe than did our study.
Limitations
There are various limitations to this study. It was a retrospective, single-center study and the patient population was relatively homogenous, with only 1 female and a mean age of 71 years. As a study conducted in a veteran population in West Virginia, the findings may not be representative of the general population with COPD, which includes more women and more racial diversity.9 The American Lung Association discusses how environmental exposures to hazardous conditions increase the risks of pulmonary diseases for veterans.10 It has been reported that the prevalence of COPD is higher among veterans compared to the general population, but it is not different in terms of disease manifestation.10
Another limitation is the short time frame. Clinical guidelines, including the GOLD Report, typically track the number of exacerbations for 1 year to escalate therapy.3 Six months was a relatively short time frame, and it is possible that more exacerbations may have occurred beyond the study time frame. Ten patients in the sample died between the end of the study period and data retrieval, which might have been caught by a longer study period. An additional limitation was the inability to measure adherence. As this was a formulary conversion, many patients had been mailed a 30- or 90-day prescription of the budesonide/formoterol inhaler when transitioned to the fluticasone/salmeterol inhaler. There was no way to accurately determine when the patient made the switch to the fluticasone/salmeterol inhaler. This study also had a small sample group (a pre-post analysis of the same group), a limitation when evaluating the impact of this formulary change on a small percentage of the population transitioned.
This formulary conversion occurred during the COVID-19 pandemic, and some exacerbations could have been the result of a misdiagnosed COVID-19 infection. Respiratory infections, including COVID-19, are common causes of exacerbations. It is also possible that some patients elected not to receive medical care for symptoms of an exacerbation during the pandemic.11
Conclusions
Switching from the budesonide/formoterol inhaler to the fluticasone/salmeterol inhaler through formulary conversion did not have a significant impact on the clinical outcomes in patients with COPD. This study found that although the inhalers contain different active ingredients, products within the same therapeutic class yielded nonsignificant changes. When conducting formulary conversions, intolerances and treatment failures should be expected when switching from different inhaler delivery systems. This study further justifies the ability to be cost effective by making formulary conversions within the same therapeutic class within a veterans population.
Acknowledgments
The authors would like to acknowledge James Brown, PharmD, PhD.
References
1. US Department of Veterans Affairs. VA/DOD Clinical Practice Guideline. Management of Outpatient Chronic Obstructive Pulmonary Disease. 2021. Accessed January 22, 2024. https://www.healthquality.va.gov/guidelines/cd/copd/
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD Report. 2022. Accessed January 22, 2024. https://goldcopd.org/2022-gold-reports/
3. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis management, and prevention of chronic obstructive pulmonary disease 2023 report. Accessed January 26, 2024. https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf
4. Oshagbemi OA, Odiba JO, Daniel A, Yunusa I. Absolute blood eosinophil counts to guide inhaled corticosteroids therapy among patients with COPD: systematic review and meta-analysis. Curr Drug Targets. 2019;20(16):1670-1679. doi:10.2174/1389450120666190808141625
5. Larsson K, Janson C, Lisspers K, et al. Combination of budesonide/formoterol more effective than fluticasone/salmeterol in preventing exacerbations in chronic obstructive pulmonary disease: the PATHOS study. J Intern Med. 2013;273(6):584-594. doi:10.1111/joim.12067
6. West Virginia Department of Health and Human Resources, Division of Health Promotion and Chronic Disease. Statistics about the population of West Virginia. 2018. Accessed January 22, 2024. https://dhhr.wv.gov/hpcd/data_reports/ Pages/Fast-Facts.aspx
7. Fidler L, Green S, Wintemute K. Pressurized metered-dose inhalers and their impact on climate change. CMAJ. 2022;194(12):E460. doi:10.1503/cmaj.211747
8. Blais L, Forget A, Ramachandran S. Relative effectiveness of budesonide/formoterol and fluticasone propionate/salmeterol in a 1-year, population-based, matched cohort study of patients with chronic obstructive pulmonary disease (COPD): Effect on COPD-related exacerbations, emergency department visits and hospitalizations, medication utilization, and treatment adherence. Clin Ther. 2010;32(7):1320-1328. doi:10.1016/j.clinthera.2010.06.022
9. Wheaton AG, Cunningham TJ, Ford ES, Croft JB; Centers for Disease Control and Prevention (CDC). Employment and activity limitations among adults with chronic obstructive pulmonary disease — United States, 2013. MMWR Morb Mortal Wkly Rep. 2015:64(11):289-295.
10. Bamonti PM, Robinson SA, Wan ES, Moy ML. Improving physiological, physical, and psychological health outcomes: a narrative review in US veterans with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1269-1283. doi:10.2147/COPD.S339323
11. Czeisler MÉ, Marynak K, Clarke KEN, et al. Delay or avoidance of medical care because of COVID-19–related concerns - United States, June 2020. MMWR Morb Mortal Wkly Rep. 2020;69(36):1250-1257. doi:10.15585/mmwr.mm6936a4
References
1. US Department of Veterans Affairs. VA/DOD Clinical Practice Guideline. Management of Outpatient Chronic Obstructive Pulmonary Disease. 2021. Accessed January 22, 2024. https://www.healthquality.va.gov/guidelines/cd/copd/
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD Report. 2022. Accessed January 22, 2024. https://goldcopd.org/2022-gold-reports/
3. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis management, and prevention of chronic obstructive pulmonary disease 2023 report. Accessed January 26, 2024. https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf
4. Oshagbemi OA, Odiba JO, Daniel A, Yunusa I. Absolute blood eosinophil counts to guide inhaled corticosteroids therapy among patients with COPD: systematic review and meta-analysis. Curr Drug Targets. 2019;20(16):1670-1679. doi:10.2174/1389450120666190808141625
5. Larsson K, Janson C, Lisspers K, et al. Combination of budesonide/formoterol more effective than fluticasone/salmeterol in preventing exacerbations in chronic obstructive pulmonary disease: the PATHOS study. J Intern Med. 2013;273(6):584-594. doi:10.1111/joim.12067
6. West Virginia Department of Health and Human Resources, Division of Health Promotion and Chronic Disease. Statistics about the population of West Virginia. 2018. Accessed January 22, 2024. https://dhhr.wv.gov/hpcd/data_reports/ Pages/Fast-Facts.aspx
7. Fidler L, Green S, Wintemute K. Pressurized metered-dose inhalers and their impact on climate change. CMAJ. 2022;194(12):E460. doi:10.1503/cmaj.211747
8. Blais L, Forget A, Ramachandran S. Relative effectiveness of budesonide/formoterol and fluticasone propionate/salmeterol in a 1-year, population-based, matched cohort study of patients with chronic obstructive pulmonary disease (COPD): Effect on COPD-related exacerbations, emergency department visits and hospitalizations, medication utilization, and treatment adherence. Clin Ther. 2010;32(7):1320-1328. doi:10.1016/j.clinthera.2010.06.022
9. Wheaton AG, Cunningham TJ, Ford ES, Croft JB; Centers for Disease Control and Prevention (CDC). Employment and activity limitations among adults with chronic obstructive pulmonary disease — United States, 2013. MMWR Morb Mortal Wkly Rep. 2015:64(11):289-295.
10. Bamonti PM, Robinson SA, Wan ES, Moy ML. Improving physiological, physical, and psychological health outcomes: a narrative review in US veterans with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1269-1283. doi:10.2147/COPD.S339323
11. Czeisler MÉ, Marynak K, Clarke KEN, et al. Delay or avoidance of medical care because of COVID-19–related concerns - United States, June 2020. MMWR Morb Mortal Wkly Rep. 2020;69(36):1250-1257. doi:10.15585/mmwr.mm6936a4
The Food and Drug Administration (FDA) has accepted an application for Priority Review for dupilumab as an add-on therapy for adults with uncontrolled chronic obstructive pulmonary disease (COPD), according to a press release from manufacturer Regeneron.
If approved, dupilumab would be the only biologic option for COPD and the first new treatment option in approximately 10 years, according to the company.
Dupilumab works by blocking signaling by the interleukin (IL) 4 and IL-13 pathways, and Regeneron’s development program focuses on a population of COPD patients who also have type 2 inflammation.
The supplemental Biologics License Application was based on data from a pair of clinical trials in the company’s phase 3 COPD clinical research program.
In the studies, known as BOREAS and NOTUS, adults with uncontrolled COPD and type 2 inflammation who were current or former smokers were randomized to 300 mg of subcutaneous dupilumab or placebo once every 2 weeks. Type 2 inflammation was defined as blood eosinophil counts of at least 300 cells per microliter.
All patients received standard-of-care therapy. The primary endpoint of reduced annualized moderate or severe acute COPD exacerbations was 30% and 34% greater in the dupilumab groups in the two studies, respectively, compared with the placebo groups, and the significant differences in improvement persisted at 52 weeks.
Safety data were similar to previous studies of dupilumab for its approved indications. The most common adverse events seen in 5% or more of dupilumab patients compared with placebo patients across the two studies included back pain, COVID-19, diarrhea, headache, and nasopharyngitis.
Priority Review status is granted to applications for approval for therapies that may offer significant improvements, although the therapies are still in clinical development. The target action date for the FDA decision is June 27, 2024, and regulatory submissions for dupilumab for COPD are under consideration in China and Europe in addition to the United States, according to the company.
A version of this article appeared on Medscape.com.
The Food and Drug Administration (FDA) has accepted an application for Priority Review for dupilumab as an add-on therapy for adults with uncontrolled chronic obstructive pulmonary disease (COPD), according to a press release from manufacturer Regeneron.
If approved, dupilumab would be the only biologic option for COPD and the first new treatment option in approximately 10 years, according to the company.
Dupilumab works by blocking signaling by the interleukin (IL) 4 and IL-13 pathways, and Regeneron’s development program focuses on a population of COPD patients who also have type 2 inflammation.
The supplemental Biologics License Application was based on data from a pair of clinical trials in the company’s phase 3 COPD clinical research program.
In the studies, known as BOREAS and NOTUS, adults with uncontrolled COPD and type 2 inflammation who were current or former smokers were randomized to 300 mg of subcutaneous dupilumab or placebo once every 2 weeks. Type 2 inflammation was defined as blood eosinophil counts of at least 300 cells per microliter.
All patients received standard-of-care therapy. The primary endpoint of reduced annualized moderate or severe acute COPD exacerbations was 30% and 34% greater in the dupilumab groups in the two studies, respectively, compared with the placebo groups, and the significant differences in improvement persisted at 52 weeks.
Safety data were similar to previous studies of dupilumab for its approved indications. The most common adverse events seen in 5% or more of dupilumab patients compared with placebo patients across the two studies included back pain, COVID-19, diarrhea, headache, and nasopharyngitis.
Priority Review status is granted to applications for approval for therapies that may offer significant improvements, although the therapies are still in clinical development. The target action date for the FDA decision is June 27, 2024, and regulatory submissions for dupilumab for COPD are under consideration in China and Europe in addition to the United States, according to the company.
A version of this article appeared on Medscape.com.
The Food and Drug Administration (FDA) has accepted an application for Priority Review for dupilumab as an add-on therapy for adults with uncontrolled chronic obstructive pulmonary disease (COPD), according to a press release from manufacturer Regeneron.
If approved, dupilumab would be the only biologic option for COPD and the first new treatment option in approximately 10 years, according to the company.
Dupilumab works by blocking signaling by the interleukin (IL) 4 and IL-13 pathways, and Regeneron’s development program focuses on a population of COPD patients who also have type 2 inflammation.
The supplemental Biologics License Application was based on data from a pair of clinical trials in the company’s phase 3 COPD clinical research program.
In the studies, known as BOREAS and NOTUS, adults with uncontrolled COPD and type 2 inflammation who were current or former smokers were randomized to 300 mg of subcutaneous dupilumab or placebo once every 2 weeks. Type 2 inflammation was defined as blood eosinophil counts of at least 300 cells per microliter.
All patients received standard-of-care therapy. The primary endpoint of reduced annualized moderate or severe acute COPD exacerbations was 30% and 34% greater in the dupilumab groups in the two studies, respectively, compared with the placebo groups, and the significant differences in improvement persisted at 52 weeks.
Safety data were similar to previous studies of dupilumab for its approved indications. The most common adverse events seen in 5% or more of dupilumab patients compared with placebo patients across the two studies included back pain, COVID-19, diarrhea, headache, and nasopharyngitis.
Priority Review status is granted to applications for approval for therapies that may offer significant improvements, although the therapies are still in clinical development. The target action date for the FDA decision is June 27, 2024, and regulatory submissions for dupilumab for COPD are under consideration in China and Europe in addition to the United States, according to the company.
A version of this article appeared on Medscape.com.
The MightySat Medical, an over-the-counter medical fingertip pulse oximeter, has received clearance from the US Food and Drug Administration (FDA) for use without a prescription, according to a press releasefrom manufacturer Masimo.
The device is the first medical fingertip pulse oximeter available directly to consumers without a prescription that includes the same technology used by many hospitals, according to the company.
According to the FDA, home pulse oximeters are currently generally of two classes: hospital-grade prescription devices which have been vetted for accuracy through clinical trials, and over-the-counter devices which are sold direct to consumers but often estimate oxygen saturation. FDA communication on pulse oximeter accuracy states "OTC oximeters that are sold as either general wellness or sporting/aviation products are not intended for medical purposes, so they do not undergo FDA review."
Pulse oximeter use is important for patients diagnosed with breathing problems or lung diseases such as asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, lung cancer, flu, pneumonia, or COVID-19 to collect accurate data on arterial blood oxygen saturation that they can share with their healthcare providers, according to the company. Patients with cardiac conditions, including pulmonary hypertension and heart failure may also benefit from pulse oximeter monitoring.
However, challenges of pulse oximeter use include measuring accuracy when patients are moving, measuring patients with poor circulation, and measuring patients with cool, thick, or darker skin. The MightySat Medical is designed to provide reliable measures of oxygen saturation and pulse rate across all patient groups, the manufacturers wrote in the press release.
Asked for additional comment, Diego J. Maselli, MD, FCCP, Professor and Chief in the division of Pulmonary Diseases and Critical Care at UT Health at San Antonio, noted, "Over the past decades, there has been an increased interest in home monitoring of medical conditions, particulrly with the development of more portable and accessible technology."
"This was heightended by the COVID-19 pandemic where telemedicine was frequently required as a means of delivering care," Dr. Maselli continued. "One of the important characteristics to monitor was the oxgen saturation in patients that had an active COVID-19 infection as it would dictate management and was part of the protocol for monitoring the clinical course of infection. Because of this need, many companies developed portable pulse oximeters for home use. This resulted in widespread use of pulse oximeters at home and other places outside clinic or hospital."
Other over-the-counter pulse oximeters that are not cleared by the FDA may create confusion among patients about the accuracy of their measurements, according to the company.
Dr. Maselli also commented that pulse oximeters' value can vary. "Unfortunately, these devices vary in quality and reliability and patients may not be fully aware of this. Most recently, the FDA approved a hospital-grade pulse oximeter that requires no prescription. This device may provide a more accurate reading in a wide range of clinical situations outside the healthcare setting. Patients should be aware that there are different grades of pulse oximeter before selecting one for home use. In addition, patients should work closely with their providers to better select the monitoring modaility that best fits their clinical situation," he said.
MightySat Medical is indicated for individuals aged 18 years and older who are well or poorly perfused under no motion conditions and is not intended as a diagnostic or screening tool for lung disease, according to the release. Treatment decisions based on data from the device should be made only in consultation with a healthcare provider, the company said. Dr. Maselli serves as a member of the CHEST Physician editorial board.
The FDA’s websiteoffers further guidance related to at-home pulse oximeter use, with recommendations and limitations, as well as information on initiatives to ensure accurate and equitable pulse oximetry for all patients.
A version of this article appeared on Medscape.com.
The MightySat Medical, an over-the-counter medical fingertip pulse oximeter, has received clearance from the US Food and Drug Administration (FDA) for use without a prescription, according to a press releasefrom manufacturer Masimo.
The device is the first medical fingertip pulse oximeter available directly to consumers without a prescription that includes the same technology used by many hospitals, according to the company.
According to the FDA, home pulse oximeters are currently generally of two classes: hospital-grade prescription devices which have been vetted for accuracy through clinical trials, and over-the-counter devices which are sold direct to consumers but often estimate oxygen saturation. FDA communication on pulse oximeter accuracy states "OTC oximeters that are sold as either general wellness or sporting/aviation products are not intended for medical purposes, so they do not undergo FDA review."
Pulse oximeter use is important for patients diagnosed with breathing problems or lung diseases such as asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, lung cancer, flu, pneumonia, or COVID-19 to collect accurate data on arterial blood oxygen saturation that they can share with their healthcare providers, according to the company. Patients with cardiac conditions, including pulmonary hypertension and heart failure may also benefit from pulse oximeter monitoring.
However, challenges of pulse oximeter use include measuring accuracy when patients are moving, measuring patients with poor circulation, and measuring patients with cool, thick, or darker skin. The MightySat Medical is designed to provide reliable measures of oxygen saturation and pulse rate across all patient groups, the manufacturers wrote in the press release.
Asked for additional comment, Diego J. Maselli, MD, FCCP, Professor and Chief in the division of Pulmonary Diseases and Critical Care at UT Health at San Antonio, noted, "Over the past decades, there has been an increased interest in home monitoring of medical conditions, particulrly with the development of more portable and accessible technology."
"This was heightended by the COVID-19 pandemic where telemedicine was frequently required as a means of delivering care," Dr. Maselli continued. "One of the important characteristics to monitor was the oxgen saturation in patients that had an active COVID-19 infection as it would dictate management and was part of the protocol for monitoring the clinical course of infection. Because of this need, many companies developed portable pulse oximeters for home use. This resulted in widespread use of pulse oximeters at home and other places outside clinic or hospital."
Other over-the-counter pulse oximeters that are not cleared by the FDA may create confusion among patients about the accuracy of their measurements, according to the company.
Dr. Maselli also commented that pulse oximeters' value can vary. "Unfortunately, these devices vary in quality and reliability and patients may not be fully aware of this. Most recently, the FDA approved a hospital-grade pulse oximeter that requires no prescription. This device may provide a more accurate reading in a wide range of clinical situations outside the healthcare setting. Patients should be aware that there are different grades of pulse oximeter before selecting one for home use. In addition, patients should work closely with their providers to better select the monitoring modaility that best fits their clinical situation," he said.
MightySat Medical is indicated for individuals aged 18 years and older who are well or poorly perfused under no motion conditions and is not intended as a diagnostic or screening tool for lung disease, according to the release. Treatment decisions based on data from the device should be made only in consultation with a healthcare provider, the company said. Dr. Maselli serves as a member of the CHEST Physician editorial board.
The FDA’s websiteoffers further guidance related to at-home pulse oximeter use, with recommendations and limitations, as well as information on initiatives to ensure accurate and equitable pulse oximetry for all patients.
A version of this article appeared on Medscape.com.
The MightySat Medical, an over-the-counter medical fingertip pulse oximeter, has received clearance from the US Food and Drug Administration (FDA) for use without a prescription, according to a press releasefrom manufacturer Masimo.
The device is the first medical fingertip pulse oximeter available directly to consumers without a prescription that includes the same technology used by many hospitals, according to the company.
According to the FDA, home pulse oximeters are currently generally of two classes: hospital-grade prescription devices which have been vetted for accuracy through clinical trials, and over-the-counter devices which are sold direct to consumers but often estimate oxygen saturation. FDA communication on pulse oximeter accuracy states "OTC oximeters that are sold as either general wellness or sporting/aviation products are not intended for medical purposes, so they do not undergo FDA review."
Pulse oximeter use is important for patients diagnosed with breathing problems or lung diseases such as asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, lung cancer, flu, pneumonia, or COVID-19 to collect accurate data on arterial blood oxygen saturation that they can share with their healthcare providers, according to the company. Patients with cardiac conditions, including pulmonary hypertension and heart failure may also benefit from pulse oximeter monitoring.
However, challenges of pulse oximeter use include measuring accuracy when patients are moving, measuring patients with poor circulation, and measuring patients with cool, thick, or darker skin. The MightySat Medical is designed to provide reliable measures of oxygen saturation and pulse rate across all patient groups, the manufacturers wrote in the press release.
Asked for additional comment, Diego J. Maselli, MD, FCCP, Professor and Chief in the division of Pulmonary Diseases and Critical Care at UT Health at San Antonio, noted, "Over the past decades, there has been an increased interest in home monitoring of medical conditions, particulrly with the development of more portable and accessible technology."
"This was heightended by the COVID-19 pandemic where telemedicine was frequently required as a means of delivering care," Dr. Maselli continued. "One of the important characteristics to monitor was the oxgen saturation in patients that had an active COVID-19 infection as it would dictate management and was part of the protocol for monitoring the clinical course of infection. Because of this need, many companies developed portable pulse oximeters for home use. This resulted in widespread use of pulse oximeters at home and other places outside clinic or hospital."
Other over-the-counter pulse oximeters that are not cleared by the FDA may create confusion among patients about the accuracy of their measurements, according to the company.
Dr. Maselli also commented that pulse oximeters' value can vary. "Unfortunately, these devices vary in quality and reliability and patients may not be fully aware of this. Most recently, the FDA approved a hospital-grade pulse oximeter that requires no prescription. This device may provide a more accurate reading in a wide range of clinical situations outside the healthcare setting. Patients should be aware that there are different grades of pulse oximeter before selecting one for home use. In addition, patients should work closely with their providers to better select the monitoring modaility that best fits their clinical situation," he said.
MightySat Medical is indicated for individuals aged 18 years and older who are well or poorly perfused under no motion conditions and is not intended as a diagnostic or screening tool for lung disease, according to the release. Treatment decisions based on data from the device should be made only in consultation with a healthcare provider, the company said. Dr. Maselli serves as a member of the CHEST Physician editorial board.
The FDA’s websiteoffers further guidance related to at-home pulse oximeter use, with recommendations and limitations, as well as information on initiatives to ensure accurate and equitable pulse oximetry for all patients.
A version of this article appeared on Medscape.com.
Several female reproductive factors across the life cycle were significantly associated with increased COPD risk, including age at menarche, number of children, infertility, pregnancy outcomes, and age at menopause.
METHODOLOGY:
The researchers reviewed data from women in the International Collaboration for a Life Course Approach to Reproductive Health and Chronic Disease Events (InterLACE) consortium, which includes 27 observational studies involving more than 850,000 women in 12 countries.
The current study included 283,070 women, 3.8% of whom developed COPD over a median of 11 years.
The researchers examined the association between COPD and age at menarche, number of children, infertility, miscarriage, stillbirth, and age at natural menopause.
TAKEAWAY:
Higher risk of COPD was significantly associated with menarche at age 11 years or younger (hazard ratio [HR], 1.17), and at 16 years and older (HR, 1.24), as well as having three or more children.
Higher risk of COPD was significantly associated with a history of infertility, and with miscarriage, or stillbirth compared with no miscarriages or stillbirths; the risk increased with the number of miscarriages or stillbirths (HR, 1.36 for ≥ 3 miscarriages and 1.67 for ≥ 2 stillbirths).
COPD risk was significantly increased with earlier age at the time of natural menopause (HR, 1.69 for those aged < 40 years and 1.42 for those aged 40-44 years compared with those aged 50-51 years).
IN PRACTICE:
“Further research is needed to understand the mechanisms linking multiple female reproductive histories and COPD,” which could include autoimmune components and social/environmental factors, the researchers wrote.
SOURCE:
The lead author on the study was Chen Liang, MD, of the University of Queensland, Australia. The study was published online in BMJ Thorax).
LIMITATIONS:
Study limitations included volunteer bias, underreporting of COPD, potential confounders such as childhood respiratory infections and smoking history, and the inability to assess the effects of medications including contraceptives and hormone replacement therapy on COPD.
DISCLOSURES:
The InterLACE project is supported by the Australian National Health and Medical Research Council and Centres of Research Excellence. Corresponding author Gita D. Mishra disclosed support from the Australian National Health and Medical Research Council Leadership Fellowship.
A version of this article appeared on Medscape.com.
Several female reproductive factors across the life cycle were significantly associated with increased COPD risk, including age at menarche, number of children, infertility, pregnancy outcomes, and age at menopause.
METHODOLOGY:
The researchers reviewed data from women in the International Collaboration for a Life Course Approach to Reproductive Health and Chronic Disease Events (InterLACE) consortium, which includes 27 observational studies involving more than 850,000 women in 12 countries.
The current study included 283,070 women, 3.8% of whom developed COPD over a median of 11 years.
The researchers examined the association between COPD and age at menarche, number of children, infertility, miscarriage, stillbirth, and age at natural menopause.
TAKEAWAY:
Higher risk of COPD was significantly associated with menarche at age 11 years or younger (hazard ratio [HR], 1.17), and at 16 years and older (HR, 1.24), as well as having three or more children.
Higher risk of COPD was significantly associated with a history of infertility, and with miscarriage, or stillbirth compared with no miscarriages or stillbirths; the risk increased with the number of miscarriages or stillbirths (HR, 1.36 for ≥ 3 miscarriages and 1.67 for ≥ 2 stillbirths).
COPD risk was significantly increased with earlier age at the time of natural menopause (HR, 1.69 for those aged < 40 years and 1.42 for those aged 40-44 years compared with those aged 50-51 years).
IN PRACTICE:
“Further research is needed to understand the mechanisms linking multiple female reproductive histories and COPD,” which could include autoimmune components and social/environmental factors, the researchers wrote.
SOURCE:
The lead author on the study was Chen Liang, MD, of the University of Queensland, Australia. The study was published online in BMJ Thorax).
LIMITATIONS:
Study limitations included volunteer bias, underreporting of COPD, potential confounders such as childhood respiratory infections and smoking history, and the inability to assess the effects of medications including contraceptives and hormone replacement therapy on COPD.
DISCLOSURES:
The InterLACE project is supported by the Australian National Health and Medical Research Council and Centres of Research Excellence. Corresponding author Gita D. Mishra disclosed support from the Australian National Health and Medical Research Council Leadership Fellowship.
A version of this article appeared on Medscape.com.
TOPLINE:
Several female reproductive factors across the life cycle were significantly associated with increased COPD risk, including age at menarche, number of children, infertility, pregnancy outcomes, and age at menopause.
METHODOLOGY:
The researchers reviewed data from women in the International Collaboration for a Life Course Approach to Reproductive Health and Chronic Disease Events (InterLACE) consortium, which includes 27 observational studies involving more than 850,000 women in 12 countries.
The current study included 283,070 women, 3.8% of whom developed COPD over a median of 11 years.
The researchers examined the association between COPD and age at menarche, number of children, infertility, miscarriage, stillbirth, and age at natural menopause.
TAKEAWAY:
Higher risk of COPD was significantly associated with menarche at age 11 years or younger (hazard ratio [HR], 1.17), and at 16 years and older (HR, 1.24), as well as having three or more children.
Higher risk of COPD was significantly associated with a history of infertility, and with miscarriage, or stillbirth compared with no miscarriages or stillbirths; the risk increased with the number of miscarriages or stillbirths (HR, 1.36 for ≥ 3 miscarriages and 1.67 for ≥ 2 stillbirths).
COPD risk was significantly increased with earlier age at the time of natural menopause (HR, 1.69 for those aged < 40 years and 1.42 for those aged 40-44 years compared with those aged 50-51 years).
IN PRACTICE:
“Further research is needed to understand the mechanisms linking multiple female reproductive histories and COPD,” which could include autoimmune components and social/environmental factors, the researchers wrote.
SOURCE:
The lead author on the study was Chen Liang, MD, of the University of Queensland, Australia. The study was published online in BMJ Thorax).
LIMITATIONS:
Study limitations included volunteer bias, underreporting of COPD, potential confounders such as childhood respiratory infections and smoking history, and the inability to assess the effects of medications including contraceptives and hormone replacement therapy on COPD.
DISCLOSURES:
The InterLACE project is supported by the Australian National Health and Medical Research Council and Centres of Research Excellence. Corresponding author Gita D. Mishra disclosed support from the Australian National Health and Medical Research Council Leadership Fellowship.
A version of this article appeared on Medscape.com.
Lingering postinfectious cough has been a concern across Canada this winter. Patients with this symptom (defined as a subacute cough, with symptoms lasting between 3 and 8 weeks after the infection) have many questions when they come to the clinic. But there is no evidence supporting pharmacologic treatment for postinfectious cough, according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.
Lingering postinfectious cough has been a concern across Canada this winter. Patients with this symptom (defined as a subacute cough, with symptoms lasting between 3 and 8 weeks after the infection) have many questions when they come to the clinic. But there is no evidence supporting pharmacologic treatment for postinfectious cough, according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.
Lingering postinfectious cough has been a concern across Canada this winter. Patients with this symptom (defined as a subacute cough, with symptoms lasting between 3 and 8 weeks after the infection) have many questions when they come to the clinic. But there is no evidence supporting pharmacologic treatment for postinfectious cough, according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.