User login
Hospital Medicine: Where We’ve Been and Where We’re Going

Robert M. Wachter, MD, professor and chief of the medical service at the University of California, San Francisco (UCSF) Medical Center and director of its hospital medicine group, addressed the audience at the 8th Annual Meeting of the Society of Hospital Medicine (SHM), along with several other noted leaders. Shortly before the meeting, Wachter shared his insight on the initial years of hospital medicine as well as the complexities, challenges, and opportunities the future holds for hospital medicine groups with The Hospitalist.
Well known for having coined the term “hospitalist” in a 1996 New England Journal of Medicine article, Wachter provided a brief outline of the birth of the hospital medicine discipline. He recalled that the initial growth of the field was slow, but it gained momentum as healthcare facilities began to perceive this specialty as an effective way to fulfill a need. During the last 10 years, hospitalists have made clear their value as agents of throughput, systems management, resource utilization, physician practice improvement, round the clock availability, and medical student education, always placing patient safety, satisfaction, and quality at the forefront of the practice. During the next 10 years―and beyond―Wachter envisions an evolution in the critical role hospitalists will play in the continued delivery of quality health care, although he does admit there are some obstacles in the path.
Surgical Co-management
Having established their core role as managers of medical inpatients, hospitalists are setting their sights on other goals. “It’s logical and inevitable that hospitalists will take on roles in surgical co-management,” Wachter says. “Patients who are sick enough to be inpatients for surgery often have multiple medical illnesses. And surgeons are in the OR for much of the day, in some ways like primary care doctors’ being in the office.” Although the data to support this model are limited presently, he believes that good co-management programs will likely lead to an increase in the quality of care, efficiency and patient satisfaction as well as surgeon satisfaction. “This makes … intuitive sense, just as the whole hospitalist idea made sense 10 years ago,” he says.
Wachter admits that the transition will probably be gradual, because of the many clinical, economic, and political complexities. In many cases, surgeons receive a global fee , linked to the expectation that they will administer preoperative and postoperative care. “It will be tricky to try to figure out how to compensate the hospitalist for surgical co-management,” Wachter says. However, he expects the financial aspect of surgical co-management to eventually work itself out. “If there is a more efficient way to manage patients and a way to free up beds, hospitals will be interested in supporting it,” he says. Wachter anticipates a 5- to 10-year evolution before this model becomes widely embraced.
Patient Safety and Quality Improvement
Timing is everything, and for hospitalists the timing could not have been better. “The hospital medicine movement evolved precisely when American medicine began to care about safety and quality,” says Wachter. ”When I first read the Institute of Medicine report on patient safety, ‘To Err is Human,’ in 1999, I knew that we had a tremendous opportunity to make a difference.” Wachter notes that in the past, incentives for high quality performance were lacking. “That is changing rapidly,” he says. With the profusion of Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates, Centers for Medicare and Medicaid Services (CMS) metrics, Leapfrog initiatives, and other quality measures, patient safety and quality have become top priorities. Since hospital medicine encompasses all the vital aspects of quality improvement and patient safety―from understanding transitions and working collaboratively with other medical specialists to improving systems and more effective oversight―hospitalists are becoming the “goto people,” according to Wachter. This is incredibly healthy for our field, he notes, “but more importantly, it will help save.”
As one measure of how the world has changed in just a few years, Wachter reflects on the experience of editing his textbook, Hospital Medicine, in 2000, and again in 2005 for the second edition. He was particularly struck by the chapter he wrote (in the 2005 edition, with his UCSF colleague Niraj Sehgal) on quality measurement and improvement. “It was staggering how much the area had changed,” he says. In the 2000 edition, there were 2 inpatient quality measures: aspirin and beta blockers for patients with myocardial infarction. In the 2005 edition, “we needed a 2-page table to catalogue all of the hospital quality measures produced by an alphabet soup of agencies and organizations.” In fact, he notes, of the 122 chapters in the book, the chapter that had changed the most in 5 years was the one on quality measurement. “This is a complex science that is still evolving,” Wachter says. “I fully expect that the chapter in the 3rd edition will change even more.”
Wachter has spearheaded several other initiatives designed to improve hospital conditions and care of patients. He leads a team of editors for the website, AHRQ Web M&M: Morbidity and Mortality Rounds on the Web (www.webmm.ahrq.gov), which provides expert analyses on medical errors, as well as a forum and online discussions on patient safety issues. He and his colleagues recently launched a second federally sponsored portal for patient safety, “AHRQ Patient Safety Network” (www.psnet.ahrq.gov), which offers regularly updated tools, new literature, surveys, videos, and links to other useful resources and experts and is customizable according to users’ interests.
Burnout
With all the responsibilities assigned to hospitalists, the issue of burnout might become a concern. Defined as mental and/or physical exhaustion caused by excessive and prolonged stress, burnout can afflict medical professionals who spend long hours caring for complicated patients. Wachter worries about burnout, but not unduly so. “There is nothing fundamental about our field that will cause burnout,” he says. He cites 4 factors that contribute to burnout: doing uninteresting, unimportant work; receiving little or no respect from peers; having little or no time to “catch your breath”; and earning an inadequate and unreasonable income. With the diverse responsibilities and personally and professionally satisfying work in which a hospitalist engages, these risks can be mitigated. “I’ve certainly visited hospital medicine groups that were rife with burned out providers,” he says. “But more often, I’ve seen terrific doctors doing work they love, making a difference in the lives of their patients and their institutions. When that’s the case, you don’t see much burnout.” Wachter believes that the way in which hospital medicine groups are designed influences the potential burnout factor. Considerable thought and planning should precede the creation of a hospital medicine group, he asserts. “Some groups are well constructed,” he says. “They’ve created jobs with reasonable amounts of downtime, an opportunity to earn a good income, and the chance to spend time improving the system and deliver high quality patient care.” On the other hand, groups that care for an unsustainable number of patients with lower recompense might well have burnout; some have even collapsed after the physicians led. “You can be sure,” he notes, “that the second iteration of the hospital medicine programs at these institutions will be structured much more carefully so as not to repeat the same mistakes.”
Using his own UCSF Medical Center as an example, Wachter notes virtually no burnout or attrition among his faculty, even though salaries are on an academic scale, below the prevailing community rate. “We feel supported and have time to catch our breath,” he says. “We are respected by our colleagues and the institution, we have a chance to teach, and we genuinely enjoy each other’s company. And we have a chance to work on other things, not just patient care.” And that makes all the difference.
The Future of Hospital Medicine
Wachter was recently elected to the American Board of Internal Medicine, the only new member and the sole hospitalist to earn this honor. In this role, he will have the opportunity to provide input that will influence the development and expansion of the hospital medicine movement. “The Board is interested in the growth of the hospitalist field and what it means for the future,” he says. “They would like to know how to support the field and how best to attract students to it.” Many members of the Board who were skeptical at first about the hospitalist field have now recognized that “hospitalists have brought back the excitement of being an internist.” Wachter believes that students exposed to hospitalists soon realize that these doctors have fulfilling, diverse careers. “Hospitalists interact with patients, act as leaders to make patient care better, increase quality, and write guidelines,” he says. “This is a rich job description.” At the UCSF Medical Center, students involved in various clerkships have the opportunity to work under the tutelage of hospitalists. These collaborative relationships bring greater understanding of the work a hospitalist does and promotes the future of the field, according to Wachter.
Specialized Certification
As each new specialty evolves, different requirements for certification arise. Since hospital medicine is still a fairly young field, educational and training qualifications have yet to be determined. In his role on the American Board of Internal Medicine, Wachter will probably contribute to the discussion on what certification can and should look like. “This is an area of active investigation,” he says. “Will there be a separate certification for hospitalists? Should it be given at initial certification or when a physician recertifies after having been a practicing hospitalist with demonstrated competency? Right now there is no widespread model for hospitalist training at the residency level,” says Wachter. “I would not be surprised if in 10 or 15 years specialized training evolves for hospitalists. If so, then it would be logical that there be some type of separate certification. It’ll be fascinating working with the Board and SHM to determine the best course in the meantime.”
Robert M. Wachter, MD, professor and chief of the medical service at the University of California, San Francisco (UCSF) Medical Center and director of its hospital medicine group, addressed the audience at the 8th Annual Meeting of the Society of Hospital Medicine (SHM), along with several other noted leaders. Shortly before the meeting, Wachter shared his insight on the initial years of hospital medicine as well as the complexities, challenges, and opportunities the future holds for hospital medicine groups with The Hospitalist.
Well known for having coined the term “hospitalist” in a 1996 New England Journal of Medicine article, Wachter provided a brief outline of the birth of the hospital medicine discipline. He recalled that the initial growth of the field was slow, but it gained momentum as healthcare facilities began to perceive this specialty as an effective way to fulfill a need. During the last 10 years, hospitalists have made clear their value as agents of throughput, systems management, resource utilization, physician practice improvement, round the clock availability, and medical student education, always placing patient safety, satisfaction, and quality at the forefront of the practice. During the next 10 years―and beyond―Wachter envisions an evolution in the critical role hospitalists will play in the continued delivery of quality health care, although he does admit there are some obstacles in the path.
Surgical Co-management
Having established their core role as managers of medical inpatients, hospitalists are setting their sights on other goals. “It’s logical and inevitable that hospitalists will take on roles in surgical co-management,” Wachter says. “Patients who are sick enough to be inpatients for surgery often have multiple medical illnesses. And surgeons are in the OR for much of the day, in some ways like primary care doctors’ being in the office.” Although the data to support this model are limited presently, he believes that good co-management programs will likely lead to an increase in the quality of care, efficiency and patient satisfaction as well as surgeon satisfaction. “This makes … intuitive sense, just as the whole hospitalist idea made sense 10 years ago,” he says.
Wachter admits that the transition will probably be gradual, because of the many clinical, economic, and political complexities. In many cases, surgeons receive a global fee , linked to the expectation that they will administer preoperative and postoperative care. “It will be tricky to try to figure out how to compensate the hospitalist for surgical co-management,” Wachter says. However, he expects the financial aspect of surgical co-management to eventually work itself out. “If there is a more efficient way to manage patients and a way to free up beds, hospitals will be interested in supporting it,” he says. Wachter anticipates a 5- to 10-year evolution before this model becomes widely embraced.
Patient Safety and Quality Improvement
Timing is everything, and for hospitalists the timing could not have been better. “The hospital medicine movement evolved precisely when American medicine began to care about safety and quality,” says Wachter. ”When I first read the Institute of Medicine report on patient safety, ‘To Err is Human,’ in 1999, I knew that we had a tremendous opportunity to make a difference.” Wachter notes that in the past, incentives for high quality performance were lacking. “That is changing rapidly,” he says. With the profusion of Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates, Centers for Medicare and Medicaid Services (CMS) metrics, Leapfrog initiatives, and other quality measures, patient safety and quality have become top priorities. Since hospital medicine encompasses all the vital aspects of quality improvement and patient safety―from understanding transitions and working collaboratively with other medical specialists to improving systems and more effective oversight―hospitalists are becoming the “goto people,” according to Wachter. This is incredibly healthy for our field, he notes, “but more importantly, it will help save.”
As one measure of how the world has changed in just a few years, Wachter reflects on the experience of editing his textbook, Hospital Medicine, in 2000, and again in 2005 for the second edition. He was particularly struck by the chapter he wrote (in the 2005 edition, with his UCSF colleague Niraj Sehgal) on quality measurement and improvement. “It was staggering how much the area had changed,” he says. In the 2000 edition, there were 2 inpatient quality measures: aspirin and beta blockers for patients with myocardial infarction. In the 2005 edition, “we needed a 2-page table to catalogue all of the hospital quality measures produced by an alphabet soup of agencies and organizations.” In fact, he notes, of the 122 chapters in the book, the chapter that had changed the most in 5 years was the one on quality measurement. “This is a complex science that is still evolving,” Wachter says. “I fully expect that the chapter in the 3rd edition will change even more.”
Wachter has spearheaded several other initiatives designed to improve hospital conditions and care of patients. He leads a team of editors for the website, AHRQ Web M&M: Morbidity and Mortality Rounds on the Web (www.webmm.ahrq.gov), which provides expert analyses on medical errors, as well as a forum and online discussions on patient safety issues. He and his colleagues recently launched a second federally sponsored portal for patient safety, “AHRQ Patient Safety Network” (www.psnet.ahrq.gov), which offers regularly updated tools, new literature, surveys, videos, and links to other useful resources and experts and is customizable according to users’ interests.
Burnout
With all the responsibilities assigned to hospitalists, the issue of burnout might become a concern. Defined as mental and/or physical exhaustion caused by excessive and prolonged stress, burnout can afflict medical professionals who spend long hours caring for complicated patients. Wachter worries about burnout, but not unduly so. “There is nothing fundamental about our field that will cause burnout,” he says. He cites 4 factors that contribute to burnout: doing uninteresting, unimportant work; receiving little or no respect from peers; having little or no time to “catch your breath”; and earning an inadequate and unreasonable income. With the diverse responsibilities and personally and professionally satisfying work in which a hospitalist engages, these risks can be mitigated. “I’ve certainly visited hospital medicine groups that were rife with burned out providers,” he says. “But more often, I’ve seen terrific doctors doing work they love, making a difference in the lives of their patients and their institutions. When that’s the case, you don’t see much burnout.” Wachter believes that the way in which hospital medicine groups are designed influences the potential burnout factor. Considerable thought and planning should precede the creation of a hospital medicine group, he asserts. “Some groups are well constructed,” he says. “They’ve created jobs with reasonable amounts of downtime, an opportunity to earn a good income, and the chance to spend time improving the system and deliver high quality patient care.” On the other hand, groups that care for an unsustainable number of patients with lower recompense might well have burnout; some have even collapsed after the physicians led. “You can be sure,” he notes, “that the second iteration of the hospital medicine programs at these institutions will be structured much more carefully so as not to repeat the same mistakes.”
Using his own UCSF Medical Center as an example, Wachter notes virtually no burnout or attrition among his faculty, even though salaries are on an academic scale, below the prevailing community rate. “We feel supported and have time to catch our breath,” he says. “We are respected by our colleagues and the institution, we have a chance to teach, and we genuinely enjoy each other’s company. And we have a chance to work on other things, not just patient care.” And that makes all the difference.
The Future of Hospital Medicine
Wachter was recently elected to the American Board of Internal Medicine, the only new member and the sole hospitalist to earn this honor. In this role, he will have the opportunity to provide input that will influence the development and expansion of the hospital medicine movement. “The Board is interested in the growth of the hospitalist field and what it means for the future,” he says. “They would like to know how to support the field and how best to attract students to it.” Many members of the Board who were skeptical at first about the hospitalist field have now recognized that “hospitalists have brought back the excitement of being an internist.” Wachter believes that students exposed to hospitalists soon realize that these doctors have fulfilling, diverse careers. “Hospitalists interact with patients, act as leaders to make patient care better, increase quality, and write guidelines,” he says. “This is a rich job description.” At the UCSF Medical Center, students involved in various clerkships have the opportunity to work under the tutelage of hospitalists. These collaborative relationships bring greater understanding of the work a hospitalist does and promotes the future of the field, according to Wachter.
Specialized Certification
As each new specialty evolves, different requirements for certification arise. Since hospital medicine is still a fairly young field, educational and training qualifications have yet to be determined. In his role on the American Board of Internal Medicine, Wachter will probably contribute to the discussion on what certification can and should look like. “This is an area of active investigation,” he says. “Will there be a separate certification for hospitalists? Should it be given at initial certification or when a physician recertifies after having been a practicing hospitalist with demonstrated competency? Right now there is no widespread model for hospitalist training at the residency level,” says Wachter. “I would not be surprised if in 10 or 15 years specialized training evolves for hospitalists. If so, then it would be logical that there be some type of separate certification. It’ll be fascinating working with the Board and SHM to determine the best course in the meantime.”
Robert M. Wachter, MD, professor and chief of the medical service at the University of California, San Francisco (UCSF) Medical Center and director of its hospital medicine group, addressed the audience at the 8th Annual Meeting of the Society of Hospital Medicine (SHM), along with several other noted leaders. Shortly before the meeting, Wachter shared his insight on the initial years of hospital medicine as well as the complexities, challenges, and opportunities the future holds for hospital medicine groups with The Hospitalist.
Well known for having coined the term “hospitalist” in a 1996 New England Journal of Medicine article, Wachter provided a brief outline of the birth of the hospital medicine discipline. He recalled that the initial growth of the field was slow, but it gained momentum as healthcare facilities began to perceive this specialty as an effective way to fulfill a need. During the last 10 years, hospitalists have made clear their value as agents of throughput, systems management, resource utilization, physician practice improvement, round the clock availability, and medical student education, always placing patient safety, satisfaction, and quality at the forefront of the practice. During the next 10 years―and beyond―Wachter envisions an evolution in the critical role hospitalists will play in the continued delivery of quality health care, although he does admit there are some obstacles in the path.
Surgical Co-management
Having established their core role as managers of medical inpatients, hospitalists are setting their sights on other goals. “It’s logical and inevitable that hospitalists will take on roles in surgical co-management,” Wachter says. “Patients who are sick enough to be inpatients for surgery often have multiple medical illnesses. And surgeons are in the OR for much of the day, in some ways like primary care doctors’ being in the office.” Although the data to support this model are limited presently, he believes that good co-management programs will likely lead to an increase in the quality of care, efficiency and patient satisfaction as well as surgeon satisfaction. “This makes … intuitive sense, just as the whole hospitalist idea made sense 10 years ago,” he says.
Wachter admits that the transition will probably be gradual, because of the many clinical, economic, and political complexities. In many cases, surgeons receive a global fee , linked to the expectation that they will administer preoperative and postoperative care. “It will be tricky to try to figure out how to compensate the hospitalist for surgical co-management,” Wachter says. However, he expects the financial aspect of surgical co-management to eventually work itself out. “If there is a more efficient way to manage patients and a way to free up beds, hospitals will be interested in supporting it,” he says. Wachter anticipates a 5- to 10-year evolution before this model becomes widely embraced.
Patient Safety and Quality Improvement
Timing is everything, and for hospitalists the timing could not have been better. “The hospital medicine movement evolved precisely when American medicine began to care about safety and quality,” says Wachter. ”When I first read the Institute of Medicine report on patient safety, ‘To Err is Human,’ in 1999, I knew that we had a tremendous opportunity to make a difference.” Wachter notes that in the past, incentives for high quality performance were lacking. “That is changing rapidly,” he says. With the profusion of Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates, Centers for Medicare and Medicaid Services (CMS) metrics, Leapfrog initiatives, and other quality measures, patient safety and quality have become top priorities. Since hospital medicine encompasses all the vital aspects of quality improvement and patient safety―from understanding transitions and working collaboratively with other medical specialists to improving systems and more effective oversight―hospitalists are becoming the “goto people,” according to Wachter. This is incredibly healthy for our field, he notes, “but more importantly, it will help save.”
As one measure of how the world has changed in just a few years, Wachter reflects on the experience of editing his textbook, Hospital Medicine, in 2000, and again in 2005 for the second edition. He was particularly struck by the chapter he wrote (in the 2005 edition, with his UCSF colleague Niraj Sehgal) on quality measurement and improvement. “It was staggering how much the area had changed,” he says. In the 2000 edition, there were 2 inpatient quality measures: aspirin and beta blockers for patients with myocardial infarction. In the 2005 edition, “we needed a 2-page table to catalogue all of the hospital quality measures produced by an alphabet soup of agencies and organizations.” In fact, he notes, of the 122 chapters in the book, the chapter that had changed the most in 5 years was the one on quality measurement. “This is a complex science that is still evolving,” Wachter says. “I fully expect that the chapter in the 3rd edition will change even more.”
Wachter has spearheaded several other initiatives designed to improve hospital conditions and care of patients. He leads a team of editors for the website, AHRQ Web M&M: Morbidity and Mortality Rounds on the Web (www.webmm.ahrq.gov), which provides expert analyses on medical errors, as well as a forum and online discussions on patient safety issues. He and his colleagues recently launched a second federally sponsored portal for patient safety, “AHRQ Patient Safety Network” (www.psnet.ahrq.gov), which offers regularly updated tools, new literature, surveys, videos, and links to other useful resources and experts and is customizable according to users’ interests.
Burnout
With all the responsibilities assigned to hospitalists, the issue of burnout might become a concern. Defined as mental and/or physical exhaustion caused by excessive and prolonged stress, burnout can afflict medical professionals who spend long hours caring for complicated patients. Wachter worries about burnout, but not unduly so. “There is nothing fundamental about our field that will cause burnout,” he says. He cites 4 factors that contribute to burnout: doing uninteresting, unimportant work; receiving little or no respect from peers; having little or no time to “catch your breath”; and earning an inadequate and unreasonable income. With the diverse responsibilities and personally and professionally satisfying work in which a hospitalist engages, these risks can be mitigated. “I’ve certainly visited hospital medicine groups that were rife with burned out providers,” he says. “But more often, I’ve seen terrific doctors doing work they love, making a difference in the lives of their patients and their institutions. When that’s the case, you don’t see much burnout.” Wachter believes that the way in which hospital medicine groups are designed influences the potential burnout factor. Considerable thought and planning should precede the creation of a hospital medicine group, he asserts. “Some groups are well constructed,” he says. “They’ve created jobs with reasonable amounts of downtime, an opportunity to earn a good income, and the chance to spend time improving the system and deliver high quality patient care.” On the other hand, groups that care for an unsustainable number of patients with lower recompense might well have burnout; some have even collapsed after the physicians led. “You can be sure,” he notes, “that the second iteration of the hospital medicine programs at these institutions will be structured much more carefully so as not to repeat the same mistakes.”
Using his own UCSF Medical Center as an example, Wachter notes virtually no burnout or attrition among his faculty, even though salaries are on an academic scale, below the prevailing community rate. “We feel supported and have time to catch our breath,” he says. “We are respected by our colleagues and the institution, we have a chance to teach, and we genuinely enjoy each other’s company. And we have a chance to work on other things, not just patient care.” And that makes all the difference.
The Future of Hospital Medicine
Wachter was recently elected to the American Board of Internal Medicine, the only new member and the sole hospitalist to earn this honor. In this role, he will have the opportunity to provide input that will influence the development and expansion of the hospital medicine movement. “The Board is interested in the growth of the hospitalist field and what it means for the future,” he says. “They would like to know how to support the field and how best to attract students to it.” Many members of the Board who were skeptical at first about the hospitalist field have now recognized that “hospitalists have brought back the excitement of being an internist.” Wachter believes that students exposed to hospitalists soon realize that these doctors have fulfilling, diverse careers. “Hospitalists interact with patients, act as leaders to make patient care better, increase quality, and write guidelines,” he says. “This is a rich job description.” At the UCSF Medical Center, students involved in various clerkships have the opportunity to work under the tutelage of hospitalists. These collaborative relationships bring greater understanding of the work a hospitalist does and promotes the future of the field, according to Wachter.
Specialized Certification
As each new specialty evolves, different requirements for certification arise. Since hospital medicine is still a fairly young field, educational and training qualifications have yet to be determined. In his role on the American Board of Internal Medicine, Wachter will probably contribute to the discussion on what certification can and should look like. “This is an area of active investigation,” he says. “Will there be a separate certification for hospitalists? Should it be given at initial certification or when a physician recertifies after having been a practicing hospitalist with demonstrated competency? Right now there is no widespread model for hospitalist training at the residency level,” says Wachter. “I would not be surprised if in 10 or 15 years specialized training evolves for hospitalists. If so, then it would be logical that there be some type of separate certification. It’ll be fascinating working with the Board and SHM to determine the best course in the meantime.”
A View of the SHM Annual Meeting in Chicago
Editor’s Note:
Having returned from the 8th SHM Annual Meeting at the time of this writing, it is clear that this was not only the biggest but also the best Annual Meeting to date. As Larry Wellikson and Joe Miller describe more fully in this issue, the lectures, workshops and networking activities available far outstripped the ability of attendees to take part in all of them. In fact, it was common to feel that there were 2, 3, or even more “must attend” sessions taking place simultaneously and if this was sometimes frustrating, it also spoke to the fact that the meeting’s quality was strikingly high. With the realization that a collection of articles is unable to fully convey the vibrancy of the meeting, we have assembled in the following section a “Big Picture” from imbedded reporter Joe Miller, overviews of 2 of the plenary lectures, and recaps of several outstanding breakout sessions. A separate monograph that will include other highlights of the Annual Meeting is under development and will be mailed in August.―JP
I was invited to write a short piece for The Hospitalist summarizing SHM’s 8th Annual Meeting on Thursday, April 28 through Saturday, April 30 in Chicago. As I sat on the airplane on my return flight to Boston, I reflected on what would define a “successful” annual meeting for the professional society representing hospitalists. I concluded that three criteria would define success. Specifically that the conference would:
- Demonstrate the strength and resiliency of the hospital medicine movement
- Provide quality content and learning opportunities to a diverse group of attendees
- Demonstrate that SHM is a competent and effective organization meeting the needs of its members.
I believe the meeting measured up extremely well on all three criteria.
With regard to demonstrating the vibrancy of the hospital medicine movement:
- At the conference, there was recognition by three significant stakeholders in the healthcare industry (hospitals, employers, and regulators) of the critical role of hospitalists. In the opening keynote address, Rick Wade, Senior Vice President of the American Hospital Association, described the growing pressure on hospitals to be “transparent,” sharing information with patients and the public on their performance. Mr. Wade’s address was followed by a presentation by Arnold Milstein, MD, Medical Director of the Pacific Business Group on Health and cofounder of the Leapfrog Group. Dr. Milstein used the metaphor of a shark’s jaws to describe the threat of the continued escalation of healthcare costs, and he indicated that the key to addressing this crisis is to “re-engineer” clinical processes to make them more efficient. On Saturday, Dennis O’Leary, CEO of JCAHO, described the challenge of evaluating the performance of hospitals in the era of patient safety. All three speakers indicated that hospitalists will be critical resources to healthcare leaders faced with these challenges. Another measure of the recognition of hospitalists as a force in the healthcare industry was the fact that over 90 exhibitors wanted the opportunity to get the ear of the conference attendees. The exhibit floor was teeming with hospitalists interested in learning about programs, products, and services.
- The growth of the hospital medicine movement was clearly evident to attendees of the conference. This year’s conference had over 1000 attendees,a growth of 15% over the 2004 annual meeting. When Alpesh Amin, MD, co-director of the course, opened the meeting, the attendees responded to a series of questions through the audience response system. For over 50% of the attendees, this was their first SHM Annual Meeting, indicating that the specialty of hospital medicine has a constant influx of “new blood.” And at the President’s Luncheon, the presentation by Larry Wellikson, MD, CEO of SHM, conveyed a broad array of statistics on the status of the hospital medicine movement, including the fact that the 12,000+ hospitalists in the U.S. makes the specialty bigger than gastroenterology and neurology. Approximately 30% of all U.S. Hospitals have hospital medicine programs; for hospitals with over 200 beds, 55% have hospitalists.
- The excellence of the hospital medicine movement was evident through the quality of the 120+ research, innovation, and clinical vignette posters presented on Friday. Furthermore, the accomplishments of the SHM award winners announced at the President’s Luncheon were quite impressive. Joseph Li, MD, won the award for Outstanding Service in Hospital Medicine, Sunil Kripalani, MD, was named the Outstanding Young Investigator, Shaun Frost, MD, won the Clinical Excellence award, and Jeff Wiese, MD, won the award for Excellence in Teaching. Hospitalists are demonstrating their ability to be innovative, high impact physicians.
With regard to providing learning opportunities for a diverse audience:
- The pre-courses on Thursday allowed attendees to gain in-depth knowledge on practice management, perioperative medicine, and critical care medicine.
- There were 35 separate presentations in 7 tracks over the 2 days of the main meeting. The clinical, adult clinical, and pediatric clinical tracks covered a wide array of topics, from maternal fetal medicine to acquired pediatric heart disease to addiction medicine. Tracks on quality and patient safety were very well attended, and the academic track included an important update on the hospitalist core curriculum being developed by SHM.
- There were 10 special interest forums allowing attendees interested in the following subjects to exchange ideas: community based hospitalists, research, education, medical directors, women hospitalists, pediatric hospitalists, family practice hospitalists, geriatric hospitalists, early career hospitalists, and nurse practitioners and physician assistants.
- The plenary sessions on updates in hospital medicine and pediatric hospital medicine provided excellent reviews of recent research relevant to hospitalists. Bob Wachter’s annual presentation, this year entitled “Hospital Medicine: Still Crazy After All These Years” laid out some important challenges for the hospital medicine movement as it moves into adolescence.
Finally, with regard to demonstrating SHM’s competence and its ability to meet the needs of its members:
- At the President’s Luncheon, the depth of SHM leadership was evident. Jeanne Huddleston, MD, reported on the significant accomplishments of the past year and handed the torch to SHM’s new President, Steve Pantilat, MD. Steve described his two goals for the upcoming year, the development ofan SHM Research Foundation and an emphasis on the role of hospitalists in palliative care. And Larry Wellikson, MD, SHM’s CEO, displayed energy and charisma throughout the meeting.
- The power of SHM volunteerism was unmistakable throughout the meeting. Preetha Basaviah, MD, the overall course director, harnessed group of SHM members participating in a planning committee to decide on the topics and choose the speakers for the meeting. A broad cross-section of SHM members participated in over 15 committee meetings in Chicago, as they donated their time to improving the field of hospital medicine.
- The conference was a vehicle to display the public relations capabilities of SHM. Melanie Bloom, wife of NBC newscaster David Bloom who died in Iraq of DVT complications, described the awareness campaign that SHM led. The attendees then viewed a short video of the television appearances by hospitalists in the last year, as hospital medicine has received increasing attention in the media. Larry Wellikson announced that every SHM member will receive a DVD with these video news segments.
- The strength of SHM staff and organization was on display in Chicago. Larry Wellikson reported that the staff has more than doubled and he cited a litany of accomplishments, including a new improved website, electronic registration for meetings, a broad range of educational offerings, and a healthy financial outlook. Furthermore, SHM has continued to experience significant membership growth, as the number of members now exceeds 4700, an increase of more than 40% in the past 12 months.
- Finally, and perhaps most importantly, Wellikson described a wide variety of initiatives that are being pursued to meet the needs of SHM members. These initiatives include a long range plan for the formal certification of hospitalists, strategic partnerships with key organizations, public policy initiatives, and the continued strengthening of historical efforts regarding education, leadership, and surveys.
In summary, the SHM conference was greater than the sum of the parts. It was successfully executed on multiple fronts. However I have not yet discussed perhaps the most important achievement of this meeting. It served as an opportunity for hospitalists to meet new friends and to reconnect with old colleagues. The Annual Meeting in Chicago created a positive energy that will carry SHM members until we have the opportunity to meet again next year in Washington, DC.
Editor’s Note:
Having returned from the 8th SHM Annual Meeting at the time of this writing, it is clear that this was not only the biggest but also the best Annual Meeting to date. As Larry Wellikson and Joe Miller describe more fully in this issue, the lectures, workshops and networking activities available far outstripped the ability of attendees to take part in all of them. In fact, it was common to feel that there were 2, 3, or even more “must attend” sessions taking place simultaneously and if this was sometimes frustrating, it also spoke to the fact that the meeting’s quality was strikingly high. With the realization that a collection of articles is unable to fully convey the vibrancy of the meeting, we have assembled in the following section a “Big Picture” from imbedded reporter Joe Miller, overviews of 2 of the plenary lectures, and recaps of several outstanding breakout sessions. A separate monograph that will include other highlights of the Annual Meeting is under development and will be mailed in August.―JP
I was invited to write a short piece for The Hospitalist summarizing SHM’s 8th Annual Meeting on Thursday, April 28 through Saturday, April 30 in Chicago. As I sat on the airplane on my return flight to Boston, I reflected on what would define a “successful” annual meeting for the professional society representing hospitalists. I concluded that three criteria would define success. Specifically that the conference would:
- Demonstrate the strength and resiliency of the hospital medicine movement
- Provide quality content and learning opportunities to a diverse group of attendees
- Demonstrate that SHM is a competent and effective organization meeting the needs of its members.
I believe the meeting measured up extremely well on all three criteria.
With regard to demonstrating the vibrancy of the hospital medicine movement:
- At the conference, there was recognition by three significant stakeholders in the healthcare industry (hospitals, employers, and regulators) of the critical role of hospitalists. In the opening keynote address, Rick Wade, Senior Vice President of the American Hospital Association, described the growing pressure on hospitals to be “transparent,” sharing information with patients and the public on their performance. Mr. Wade’s address was followed by a presentation by Arnold Milstein, MD, Medical Director of the Pacific Business Group on Health and cofounder of the Leapfrog Group. Dr. Milstein used the metaphor of a shark’s jaws to describe the threat of the continued escalation of healthcare costs, and he indicated that the key to addressing this crisis is to “re-engineer” clinical processes to make them more efficient. On Saturday, Dennis O’Leary, CEO of JCAHO, described the challenge of evaluating the performance of hospitals in the era of patient safety. All three speakers indicated that hospitalists will be critical resources to healthcare leaders faced with these challenges. Another measure of the recognition of hospitalists as a force in the healthcare industry was the fact that over 90 exhibitors wanted the opportunity to get the ear of the conference attendees. The exhibit floor was teeming with hospitalists interested in learning about programs, products, and services.
- The growth of the hospital medicine movement was clearly evident to attendees of the conference. This year’s conference had over 1000 attendees,a growth of 15% over the 2004 annual meeting. When Alpesh Amin, MD, co-director of the course, opened the meeting, the attendees responded to a series of questions through the audience response system. For over 50% of the attendees, this was their first SHM Annual Meeting, indicating that the specialty of hospital medicine has a constant influx of “new blood.” And at the President’s Luncheon, the presentation by Larry Wellikson, MD, CEO of SHM, conveyed a broad array of statistics on the status of the hospital medicine movement, including the fact that the 12,000+ hospitalists in the U.S. makes the specialty bigger than gastroenterology and neurology. Approximately 30% of all U.S. Hospitals have hospital medicine programs; for hospitals with over 200 beds, 55% have hospitalists.
- The excellence of the hospital medicine movement was evident through the quality of the 120+ research, innovation, and clinical vignette posters presented on Friday. Furthermore, the accomplishments of the SHM award winners announced at the President’s Luncheon were quite impressive. Joseph Li, MD, won the award for Outstanding Service in Hospital Medicine, Sunil Kripalani, MD, was named the Outstanding Young Investigator, Shaun Frost, MD, won the Clinical Excellence award, and Jeff Wiese, MD, won the award for Excellence in Teaching. Hospitalists are demonstrating their ability to be innovative, high impact physicians.
With regard to providing learning opportunities for a diverse audience:
- The pre-courses on Thursday allowed attendees to gain in-depth knowledge on practice management, perioperative medicine, and critical care medicine.
- There were 35 separate presentations in 7 tracks over the 2 days of the main meeting. The clinical, adult clinical, and pediatric clinical tracks covered a wide array of topics, from maternal fetal medicine to acquired pediatric heart disease to addiction medicine. Tracks on quality and patient safety were very well attended, and the academic track included an important update on the hospitalist core curriculum being developed by SHM.
- There were 10 special interest forums allowing attendees interested in the following subjects to exchange ideas: community based hospitalists, research, education, medical directors, women hospitalists, pediatric hospitalists, family practice hospitalists, geriatric hospitalists, early career hospitalists, and nurse practitioners and physician assistants.
- The plenary sessions on updates in hospital medicine and pediatric hospital medicine provided excellent reviews of recent research relevant to hospitalists. Bob Wachter’s annual presentation, this year entitled “Hospital Medicine: Still Crazy After All These Years” laid out some important challenges for the hospital medicine movement as it moves into adolescence.
Finally, with regard to demonstrating SHM’s competence and its ability to meet the needs of its members:
- At the President’s Luncheon, the depth of SHM leadership was evident. Jeanne Huddleston, MD, reported on the significant accomplishments of the past year and handed the torch to SHM’s new President, Steve Pantilat, MD. Steve described his two goals for the upcoming year, the development ofan SHM Research Foundation and an emphasis on the role of hospitalists in palliative care. And Larry Wellikson, MD, SHM’s CEO, displayed energy and charisma throughout the meeting.
- The power of SHM volunteerism was unmistakable throughout the meeting. Preetha Basaviah, MD, the overall course director, harnessed group of SHM members participating in a planning committee to decide on the topics and choose the speakers for the meeting. A broad cross-section of SHM members participated in over 15 committee meetings in Chicago, as they donated their time to improving the field of hospital medicine.
- The conference was a vehicle to display the public relations capabilities of SHM. Melanie Bloom, wife of NBC newscaster David Bloom who died in Iraq of DVT complications, described the awareness campaign that SHM led. The attendees then viewed a short video of the television appearances by hospitalists in the last year, as hospital medicine has received increasing attention in the media. Larry Wellikson announced that every SHM member will receive a DVD with these video news segments.
- The strength of SHM staff and organization was on display in Chicago. Larry Wellikson reported that the staff has more than doubled and he cited a litany of accomplishments, including a new improved website, electronic registration for meetings, a broad range of educational offerings, and a healthy financial outlook. Furthermore, SHM has continued to experience significant membership growth, as the number of members now exceeds 4700, an increase of more than 40% in the past 12 months.
- Finally, and perhaps most importantly, Wellikson described a wide variety of initiatives that are being pursued to meet the needs of SHM members. These initiatives include a long range plan for the formal certification of hospitalists, strategic partnerships with key organizations, public policy initiatives, and the continued strengthening of historical efforts regarding education, leadership, and surveys.
In summary, the SHM conference was greater than the sum of the parts. It was successfully executed on multiple fronts. However I have not yet discussed perhaps the most important achievement of this meeting. It served as an opportunity for hospitalists to meet new friends and to reconnect with old colleagues. The Annual Meeting in Chicago created a positive energy that will carry SHM members until we have the opportunity to meet again next year in Washington, DC.
Editor’s Note:
Having returned from the 8th SHM Annual Meeting at the time of this writing, it is clear that this was not only the biggest but also the best Annual Meeting to date. As Larry Wellikson and Joe Miller describe more fully in this issue, the lectures, workshops and networking activities available far outstripped the ability of attendees to take part in all of them. In fact, it was common to feel that there were 2, 3, or even more “must attend” sessions taking place simultaneously and if this was sometimes frustrating, it also spoke to the fact that the meeting’s quality was strikingly high. With the realization that a collection of articles is unable to fully convey the vibrancy of the meeting, we have assembled in the following section a “Big Picture” from imbedded reporter Joe Miller, overviews of 2 of the plenary lectures, and recaps of several outstanding breakout sessions. A separate monograph that will include other highlights of the Annual Meeting is under development and will be mailed in August.―JP
I was invited to write a short piece for The Hospitalist summarizing SHM’s 8th Annual Meeting on Thursday, April 28 through Saturday, April 30 in Chicago. As I sat on the airplane on my return flight to Boston, I reflected on what would define a “successful” annual meeting for the professional society representing hospitalists. I concluded that three criteria would define success. Specifically that the conference would:
- Demonstrate the strength and resiliency of the hospital medicine movement
- Provide quality content and learning opportunities to a diverse group of attendees
- Demonstrate that SHM is a competent and effective organization meeting the needs of its members.
I believe the meeting measured up extremely well on all three criteria.
With regard to demonstrating the vibrancy of the hospital medicine movement:
- At the conference, there was recognition by three significant stakeholders in the healthcare industry (hospitals, employers, and regulators) of the critical role of hospitalists. In the opening keynote address, Rick Wade, Senior Vice President of the American Hospital Association, described the growing pressure on hospitals to be “transparent,” sharing information with patients and the public on their performance. Mr. Wade’s address was followed by a presentation by Arnold Milstein, MD, Medical Director of the Pacific Business Group on Health and cofounder of the Leapfrog Group. Dr. Milstein used the metaphor of a shark’s jaws to describe the threat of the continued escalation of healthcare costs, and he indicated that the key to addressing this crisis is to “re-engineer” clinical processes to make them more efficient. On Saturday, Dennis O’Leary, CEO of JCAHO, described the challenge of evaluating the performance of hospitals in the era of patient safety. All three speakers indicated that hospitalists will be critical resources to healthcare leaders faced with these challenges. Another measure of the recognition of hospitalists as a force in the healthcare industry was the fact that over 90 exhibitors wanted the opportunity to get the ear of the conference attendees. The exhibit floor was teeming with hospitalists interested in learning about programs, products, and services.
- The growth of the hospital medicine movement was clearly evident to attendees of the conference. This year’s conference had over 1000 attendees,a growth of 15% over the 2004 annual meeting. When Alpesh Amin, MD, co-director of the course, opened the meeting, the attendees responded to a series of questions through the audience response system. For over 50% of the attendees, this was their first SHM Annual Meeting, indicating that the specialty of hospital medicine has a constant influx of “new blood.” And at the President’s Luncheon, the presentation by Larry Wellikson, MD, CEO of SHM, conveyed a broad array of statistics on the status of the hospital medicine movement, including the fact that the 12,000+ hospitalists in the U.S. makes the specialty bigger than gastroenterology and neurology. Approximately 30% of all U.S. Hospitals have hospital medicine programs; for hospitals with over 200 beds, 55% have hospitalists.
- The excellence of the hospital medicine movement was evident through the quality of the 120+ research, innovation, and clinical vignette posters presented on Friday. Furthermore, the accomplishments of the SHM award winners announced at the President’s Luncheon were quite impressive. Joseph Li, MD, won the award for Outstanding Service in Hospital Medicine, Sunil Kripalani, MD, was named the Outstanding Young Investigator, Shaun Frost, MD, won the Clinical Excellence award, and Jeff Wiese, MD, won the award for Excellence in Teaching. Hospitalists are demonstrating their ability to be innovative, high impact physicians.
With regard to providing learning opportunities for a diverse audience:
- The pre-courses on Thursday allowed attendees to gain in-depth knowledge on practice management, perioperative medicine, and critical care medicine.
- There were 35 separate presentations in 7 tracks over the 2 days of the main meeting. The clinical, adult clinical, and pediatric clinical tracks covered a wide array of topics, from maternal fetal medicine to acquired pediatric heart disease to addiction medicine. Tracks on quality and patient safety were very well attended, and the academic track included an important update on the hospitalist core curriculum being developed by SHM.
- There were 10 special interest forums allowing attendees interested in the following subjects to exchange ideas: community based hospitalists, research, education, medical directors, women hospitalists, pediatric hospitalists, family practice hospitalists, geriatric hospitalists, early career hospitalists, and nurse practitioners and physician assistants.
- The plenary sessions on updates in hospital medicine and pediatric hospital medicine provided excellent reviews of recent research relevant to hospitalists. Bob Wachter’s annual presentation, this year entitled “Hospital Medicine: Still Crazy After All These Years” laid out some important challenges for the hospital medicine movement as it moves into adolescence.
Finally, with regard to demonstrating SHM’s competence and its ability to meet the needs of its members:
- At the President’s Luncheon, the depth of SHM leadership was evident. Jeanne Huddleston, MD, reported on the significant accomplishments of the past year and handed the torch to SHM’s new President, Steve Pantilat, MD. Steve described his two goals for the upcoming year, the development ofan SHM Research Foundation and an emphasis on the role of hospitalists in palliative care. And Larry Wellikson, MD, SHM’s CEO, displayed energy and charisma throughout the meeting.
- The power of SHM volunteerism was unmistakable throughout the meeting. Preetha Basaviah, MD, the overall course director, harnessed group of SHM members participating in a planning committee to decide on the topics and choose the speakers for the meeting. A broad cross-section of SHM members participated in over 15 committee meetings in Chicago, as they donated their time to improving the field of hospital medicine.
- The conference was a vehicle to display the public relations capabilities of SHM. Melanie Bloom, wife of NBC newscaster David Bloom who died in Iraq of DVT complications, described the awareness campaign that SHM led. The attendees then viewed a short video of the television appearances by hospitalists in the last year, as hospital medicine has received increasing attention in the media. Larry Wellikson announced that every SHM member will receive a DVD with these video news segments.
- The strength of SHM staff and organization was on display in Chicago. Larry Wellikson reported that the staff has more than doubled and he cited a litany of accomplishments, including a new improved website, electronic registration for meetings, a broad range of educational offerings, and a healthy financial outlook. Furthermore, SHM has continued to experience significant membership growth, as the number of members now exceeds 4700, an increase of more than 40% in the past 12 months.
- Finally, and perhaps most importantly, Wellikson described a wide variety of initiatives that are being pursued to meet the needs of SHM members. These initiatives include a long range plan for the formal certification of hospitalists, strategic partnerships with key organizations, public policy initiatives, and the continued strengthening of historical efforts regarding education, leadership, and surveys.
In summary, the SHM conference was greater than the sum of the parts. It was successfully executed on multiple fronts. However I have not yet discussed perhaps the most important achievement of this meeting. It served as an opportunity for hospitalists to meet new friends and to reconnect with old colleagues. The Annual Meeting in Chicago created a positive energy that will carry SHM members until we have the opportunity to meet again next year in Washington, DC.
Be There or Be Square

The bomb. The franchise. Sine qua non. Must see. Must be there. How do you say it when something or someone just seems to be in the middle of everything? That is hospital medicine, and that is SHM.
Nowhere was this more evident than at the largest gathering of hospitalists to date, the SHM Annual Meeting held in Chicago at the end of April. If you have a stake in hospital medicine or in building and improving the hospital of the future, all roads led to Chicago and SHM.
Not only was the CME content cutting edge and geared specifically for hospitalists, but also the sessions were greeted with standing room attendance. Clearly we struck a nerve with our 1-day in-depth pre-courses on Perioperative Care and Critical Care. The Practice Management course continues to attract 250 to 300 people as everyone tries to figure out how to get the most out of their hospital medicine group.
SHM virtually took over the entire Sheraton Hotel in downtown Chicago. Everywhere you looked, all you saw were hospitalists or people who needed to talk to hospitalists. The exhibit hall was sold out, and the networking between all the industries that support and depend on hospitalists continued well beyond the boundaries of the exhibit hall.
The Research Abstract, Clinical Vignette, and Innovation Poster session had almost 200 entries. On display here was the new thinking that is so characteristic of hospital medicine. As much as anything, this gathering displayed the youthful energy and innovation that will continue to propel hospital medicine into the future.
Important people came to be heard and to hear from hospitalists. Dennis O’Leary, the CEO of JCAHO, challenged hospitalists to lead their hospitals into a future with improved measurable quality. Rick Wade, a senior leader at the American Hospital Association, saw hospitalists as key partners with other stakeholders to meet the increasing demands on hospitals to do a better job. Arnie Milstein, the CMO and one of the founders of the Leapfrog Group, placed hospitalists squarely in the center of delivering the effective and efficient health care now demanded by America’s businesses and patients. And our own Bob Wachter challenged hospitalists to continue to lead the patient safety revolution.
But hospitalists did not just come to Chicago to sit and listen. Hospitalists are faced with so many new and difficult challenges that they clearly came to ask questions and give answers. Networking was both informal and formal and almost constant. With hospitalists everywhere you turned it was clear that people were out seeking the next new idea, the solution to a real life problem back home, and maybe even their next job.
The SHM Special Interest Forums were lively and well attended. This is where SHM gets its ideas. This is where hospitalists have their voices heard. This is where the diversity of hospital medicine can be seen up close and personal. The world of the hospital and our specialty looks different if you are a pediatrician or a family practitioner or a woman or an NP or a PA or a group leader or a young hospitalist. The demands, and your needs to meet them, can be different if you are in academics or a community hospital. SHM must hear your perspective and, boy, did we hear from you in Chicago.
For me personally, it was an opportunity to see and talk to over 1000 people connected in some way to the growing hospital medicine movement. Many of the people I spoke with were frontline hospitalists, earnest and dedicated to making hospital medicine their life’s work. They want to work with SHM to create a specialty and a career that is satisfying and fulfilling.
Some were representatives from publishers or pharmaceutical companies or hospitalist staffing and recruitment companies trying to bring their unique take on hospital medicine to SHM’s attention. Some were key leaders of other national healthcare organizations looking to partner with hospital medicine, the fastest growing workforce component of the hospital of the future and a force for change and improvement.
There were so many good ideas flying around that there is enough to keep SHM busy for years to come. And you will be hearing and reading about these in the coming months and years. It is clear that the energy around hospital medicine is not waning any time in the near future. There will be much for us to do. And if the talent and the drive to succeed of those who came to Chicago last month are any indication, SHM and our nation’s hospitalists are up to the challenge. Stay tuned.
The bomb. The franchise. Sine qua non. Must see. Must be there. How do you say it when something or someone just seems to be in the middle of everything? That is hospital medicine, and that is SHM.
Nowhere was this more evident than at the largest gathering of hospitalists to date, the SHM Annual Meeting held in Chicago at the end of April. If you have a stake in hospital medicine or in building and improving the hospital of the future, all roads led to Chicago and SHM.
Not only was the CME content cutting edge and geared specifically for hospitalists, but also the sessions were greeted with standing room attendance. Clearly we struck a nerve with our 1-day in-depth pre-courses on Perioperative Care and Critical Care. The Practice Management course continues to attract 250 to 300 people as everyone tries to figure out how to get the most out of their hospital medicine group.
SHM virtually took over the entire Sheraton Hotel in downtown Chicago. Everywhere you looked, all you saw were hospitalists or people who needed to talk to hospitalists. The exhibit hall was sold out, and the networking between all the industries that support and depend on hospitalists continued well beyond the boundaries of the exhibit hall.
The Research Abstract, Clinical Vignette, and Innovation Poster session had almost 200 entries. On display here was the new thinking that is so characteristic of hospital medicine. As much as anything, this gathering displayed the youthful energy and innovation that will continue to propel hospital medicine into the future.
Important people came to be heard and to hear from hospitalists. Dennis O’Leary, the CEO of JCAHO, challenged hospitalists to lead their hospitals into a future with improved measurable quality. Rick Wade, a senior leader at the American Hospital Association, saw hospitalists as key partners with other stakeholders to meet the increasing demands on hospitals to do a better job. Arnie Milstein, the CMO and one of the founders of the Leapfrog Group, placed hospitalists squarely in the center of delivering the effective and efficient health care now demanded by America’s businesses and patients. And our own Bob Wachter challenged hospitalists to continue to lead the patient safety revolution.
But hospitalists did not just come to Chicago to sit and listen. Hospitalists are faced with so many new and difficult challenges that they clearly came to ask questions and give answers. Networking was both informal and formal and almost constant. With hospitalists everywhere you turned it was clear that people were out seeking the next new idea, the solution to a real life problem back home, and maybe even their next job.
The SHM Special Interest Forums were lively and well attended. This is where SHM gets its ideas. This is where hospitalists have their voices heard. This is where the diversity of hospital medicine can be seen up close and personal. The world of the hospital and our specialty looks different if you are a pediatrician or a family practitioner or a woman or an NP or a PA or a group leader or a young hospitalist. The demands, and your needs to meet them, can be different if you are in academics or a community hospital. SHM must hear your perspective and, boy, did we hear from you in Chicago.
For me personally, it was an opportunity to see and talk to over 1000 people connected in some way to the growing hospital medicine movement. Many of the people I spoke with were frontline hospitalists, earnest and dedicated to making hospital medicine their life’s work. They want to work with SHM to create a specialty and a career that is satisfying and fulfilling.
Some were representatives from publishers or pharmaceutical companies or hospitalist staffing and recruitment companies trying to bring their unique take on hospital medicine to SHM’s attention. Some were key leaders of other national healthcare organizations looking to partner with hospital medicine, the fastest growing workforce component of the hospital of the future and a force for change and improvement.
There were so many good ideas flying around that there is enough to keep SHM busy for years to come. And you will be hearing and reading about these in the coming months and years. It is clear that the energy around hospital medicine is not waning any time in the near future. There will be much for us to do. And if the talent and the drive to succeed of those who came to Chicago last month are any indication, SHM and our nation’s hospitalists are up to the challenge. Stay tuned.
The bomb. The franchise. Sine qua non. Must see. Must be there. How do you say it when something or someone just seems to be in the middle of everything? That is hospital medicine, and that is SHM.
Nowhere was this more evident than at the largest gathering of hospitalists to date, the SHM Annual Meeting held in Chicago at the end of April. If you have a stake in hospital medicine or in building and improving the hospital of the future, all roads led to Chicago and SHM.
Not only was the CME content cutting edge and geared specifically for hospitalists, but also the sessions were greeted with standing room attendance. Clearly we struck a nerve with our 1-day in-depth pre-courses on Perioperative Care and Critical Care. The Practice Management course continues to attract 250 to 300 people as everyone tries to figure out how to get the most out of their hospital medicine group.
SHM virtually took over the entire Sheraton Hotel in downtown Chicago. Everywhere you looked, all you saw were hospitalists or people who needed to talk to hospitalists. The exhibit hall was sold out, and the networking between all the industries that support and depend on hospitalists continued well beyond the boundaries of the exhibit hall.
The Research Abstract, Clinical Vignette, and Innovation Poster session had almost 200 entries. On display here was the new thinking that is so characteristic of hospital medicine. As much as anything, this gathering displayed the youthful energy and innovation that will continue to propel hospital medicine into the future.
Important people came to be heard and to hear from hospitalists. Dennis O’Leary, the CEO of JCAHO, challenged hospitalists to lead their hospitals into a future with improved measurable quality. Rick Wade, a senior leader at the American Hospital Association, saw hospitalists as key partners with other stakeholders to meet the increasing demands on hospitals to do a better job. Arnie Milstein, the CMO and one of the founders of the Leapfrog Group, placed hospitalists squarely in the center of delivering the effective and efficient health care now demanded by America’s businesses and patients. And our own Bob Wachter challenged hospitalists to continue to lead the patient safety revolution.
But hospitalists did not just come to Chicago to sit and listen. Hospitalists are faced with so many new and difficult challenges that they clearly came to ask questions and give answers. Networking was both informal and formal and almost constant. With hospitalists everywhere you turned it was clear that people were out seeking the next new idea, the solution to a real life problem back home, and maybe even their next job.
The SHM Special Interest Forums were lively and well attended. This is where SHM gets its ideas. This is where hospitalists have their voices heard. This is where the diversity of hospital medicine can be seen up close and personal. The world of the hospital and our specialty looks different if you are a pediatrician or a family practitioner or a woman or an NP or a PA or a group leader or a young hospitalist. The demands, and your needs to meet them, can be different if you are in academics or a community hospital. SHM must hear your perspective and, boy, did we hear from you in Chicago.
For me personally, it was an opportunity to see and talk to over 1000 people connected in some way to the growing hospital medicine movement. Many of the people I spoke with were frontline hospitalists, earnest and dedicated to making hospital medicine their life’s work. They want to work with SHM to create a specialty and a career that is satisfying and fulfilling.
Some were representatives from publishers or pharmaceutical companies or hospitalist staffing and recruitment companies trying to bring their unique take on hospital medicine to SHM’s attention. Some were key leaders of other national healthcare organizations looking to partner with hospital medicine, the fastest growing workforce component of the hospital of the future and a force for change and improvement.
There were so many good ideas flying around that there is enough to keep SHM busy for years to come. And you will be hearing and reading about these in the coming months and years. It is clear that the energy around hospital medicine is not waning any time in the near future. There will be much for us to do. And if the talent and the drive to succeed of those who came to Chicago last month are any indication, SHM and our nation’s hospitalists are up to the challenge. Stay tuned.
Terri Schiavo and the Pope: My Lessons Learned

As I write first column as President of SHM, palliative care has been much in the news. As a hospitalist who spends much of my time caring for people approaching the end of life and teaching about palliative care, these 2 weeks have kept me busy talking about end of life issues with family, friends, patients, colleagues, and the media. At the same time, these events have reaffirmed for me my choice of a career as a hospitalist and the central role that hospitalists play in providing the highest quality care for the sickest patients, in continually improving that care, and in refining the systems to deliver it.
Terri Schiavo died 2 weeks after her feeding tube was removed. Her life and death sparked protests and political debate. Yet in the end, what seems most profound is the great sadness and loss for her family. Soon after Terri Schiavo died, Pope John Paul II became acutely ill. Several days after a feeding tube was placed, the Pope died in his apartment at the Vatican, triggering a global outpouring of love and grief.
In modern American health care, probably Terri Schiavo and the Pope would have received care from a hospitalist. If she were to arrive in a hospital after a cardiac arrest today, Terri Schiavo would likely be cared for by a hospitalist. It is the hospitalist who would have the first discussions with her family about her condition and prognosis. Similarly, most 84-year-old men with Parkinson’s disease, pneumonia, and a urinary tract infection would be cared for by a hospitalist. Hospitalists are serving as de facto ethicists and palliative care physicians, as we care for increasing numbers of people with serious and terminal illness. This shift in care provides an unprecedented opportunity for us to improve the quality of care for the half of all Americans who die in hospitals. Providing state of the art palliative care reinforces our efforts globally to improve the quality of care for all hospitalized patients. Furthermore, these cases highlight the need for research to define the best ways to deliver that care. As I thought about Terri Schiavo and the Pope, and saw the intense media spotlight on them, I kept thinking, “What does this mean for me?”
I have given this question a great deal of thought over the past week. What, if anything, do the deaths of Terri Schiavo and the Pope teach us? As I see it there are at least 3 important lessons for us as individuals and as hospitalists.
The first lesson is that each of us should consider the kind of care we would want if we were to suffer a devastating injury, as did Terri Schiavo, or be stricken with a progressive, debilitating illness, like the Pope. We should discuss our preferences for care with our loved ones and write them down. As hospitalists we should have these discussions routinely with our patients, document the conversations, notify the patient’s primary care physician, and encourage patients to share their thoughts with their loved ones. As a son, husband, brother, nephew, grandson, and father, I realized that one of the most important obligations I owed to my family was to make my wishes known, and to learn about the wishes of my loved ones. As a hospitalist, I realized that I owed it to my patients to help them express their preferences for care. What I learned echoed what we know about advance directives: You cannot predict what someone will say. Not unexpectedly, my mother, grandmother, and aunt told me that they would never want to live like Terri Schiavo. But in a complete surprise my aunt told me that my favorite uncle, who is blessed with a quick wit and brilliant sense of humor, wants to be kept alive as long as possible.
As a hospitalist, I know that my patients care deeply about these issues and are quite eager to discuss them. Talking with patients about these issues is not just a good thing to do, but ultimately improves quality of care by promoting care that is consistent with patient preferences and emphasizes our commitment to respect patients and advocate on their behalf. I still remember early concerns about hospitalists that we would be cowboys more interested in procedures and yelling “Stat!” than in being caring providers who took time to get to know our patients. Yet an early study of hospitalists that I was involved in found just the opposite. Hospitalists recognized the importance of palliative care and good communication with patients. As I made rounds in the hospital in late March, many patients were watching the vigil outside the hospice in Florida and talking about the Pope. Many patients wanted to know my thoughts. Using the communication skills I have honed over the years, and my cultural background of always answering a question with a question, I turned it around and asked them, “What do you think?” I suspect that patients will be using Terri Schiavo as an example of how they do or do not want to live―and die―for a long time. I will do my best to use this shared touchstone as a starting point for understanding their preferences: “Tell me what it is about Terri Schiavo that worries you?” By helping our patients express their preferences and encouraging them to discuss these with their loved ones, we may ease the burden of families who would otherwise have to make a difficult decision without direct knowledge of the patient’s choice.
The second lesson for us to embrace is that palliative care is a core competency for hospitalists. Palliative care is already identified as a core competency in the Core Curriculum under development by SHM. As part of our goal of improving the quality of care for all of our patients, we have the opportunity to dramatically improve end of life care and to identify people who would benefit from palliative care earlier in the course of illness. This opportunity represents a sacred trust and speaks to the most basic role of the physician to “cure sometimes and comfort always.” Ultimately, the deaths of Terri Schiavo and the Pope, although fundamentally different from each other, and unique in many respects, reaffirmed for me the importance of my role as a hospitalist in providing the highest possible quality of care for people facing serious illness and death. With these skills, we will secure our place as leaders in quality care and reap the rich rewards of using our humanity to help patients and families at one of the most important, profound, and intimate times.
The third lesson for us as hospitalists is that more research is needed to define the optimal ways to care for hospitalized patients. While the case of Terri Schiavo raised particularly thorny family issues that might defy the ability of research to clarify, issues of how best to care for patients like Terri Schiavo and the Pope and the millions of people like them with heart failure, deep vein thromboses, aspiration pneumonia, gastrointestinal bleeding, cancer, and myriad other conditions can be, must be, and will be investigated. The only question will be, by whom? As the providers of an increasingly large percentage of hospital care, we are on the front-lines of recognizing the clinical questions that arise and understanding the systems of care in which solutions must be implemented. Therefore we must play a central role in defining the questions and discovering the answers. Further, because we need research not only in how best to treat patients but also in how to ensure that patients receive these treatments, we need to conduct this research in community hospitals, where the majority of patients are cared for, and not just at academic centers.
In my year as President of SHM, I will continue to develop our organization’s founding mission and to serve hospitalists in their goal of providing the best quality of care to their patients and having satisfying, sustainable, and rewarding jobs. SHM will continue to lead and define the field of hospital medicine in education, leadership, quality, patient safety, and teamwork. In addition, I hope to use my unique skills and insights to focus our members on the central role of research in defining our field and the need for SHM to help direct that research. I will also highlight the importance of hospitalists in providing palliative care and in improving the care of patients with serious and terminal illness. I encourage each hospitalist to embrace these critical issues and invite you to join me in implementing this vision to advance research in hospital medicine and to improve palliative care in hospitals. The research committee has already completed a report on the potential role of SHM in research in hospital medicine that the Board of Directors will discuss at our meeting in May, and I am planning an initiative in palliative care. If you would like to participate in either initiative or simply want to share your thoughts and ideas about these or other important issues in hospital medicine, please contact me by email (stevep@medicine.ucsf.edu). My closing wish is that Terri Schiavo’s family will find comfort and closure, out of the media spotlight, and that the memory of the Pope is honored by the ongoing lessons of tolerance and peace that he taught.
As I write first column as President of SHM, palliative care has been much in the news. As a hospitalist who spends much of my time caring for people approaching the end of life and teaching about palliative care, these 2 weeks have kept me busy talking about end of life issues with family, friends, patients, colleagues, and the media. At the same time, these events have reaffirmed for me my choice of a career as a hospitalist and the central role that hospitalists play in providing the highest quality care for the sickest patients, in continually improving that care, and in refining the systems to deliver it.
Terri Schiavo died 2 weeks after her feeding tube was removed. Her life and death sparked protests and political debate. Yet in the end, what seems most profound is the great sadness and loss for her family. Soon after Terri Schiavo died, Pope John Paul II became acutely ill. Several days after a feeding tube was placed, the Pope died in his apartment at the Vatican, triggering a global outpouring of love and grief.
In modern American health care, probably Terri Schiavo and the Pope would have received care from a hospitalist. If she were to arrive in a hospital after a cardiac arrest today, Terri Schiavo would likely be cared for by a hospitalist. It is the hospitalist who would have the first discussions with her family about her condition and prognosis. Similarly, most 84-year-old men with Parkinson’s disease, pneumonia, and a urinary tract infection would be cared for by a hospitalist. Hospitalists are serving as de facto ethicists and palliative care physicians, as we care for increasing numbers of people with serious and terminal illness. This shift in care provides an unprecedented opportunity for us to improve the quality of care for the half of all Americans who die in hospitals. Providing state of the art palliative care reinforces our efforts globally to improve the quality of care for all hospitalized patients. Furthermore, these cases highlight the need for research to define the best ways to deliver that care. As I thought about Terri Schiavo and the Pope, and saw the intense media spotlight on them, I kept thinking, “What does this mean for me?”
I have given this question a great deal of thought over the past week. What, if anything, do the deaths of Terri Schiavo and the Pope teach us? As I see it there are at least 3 important lessons for us as individuals and as hospitalists.
The first lesson is that each of us should consider the kind of care we would want if we were to suffer a devastating injury, as did Terri Schiavo, or be stricken with a progressive, debilitating illness, like the Pope. We should discuss our preferences for care with our loved ones and write them down. As hospitalists we should have these discussions routinely with our patients, document the conversations, notify the patient’s primary care physician, and encourage patients to share their thoughts with their loved ones. As a son, husband, brother, nephew, grandson, and father, I realized that one of the most important obligations I owed to my family was to make my wishes known, and to learn about the wishes of my loved ones. As a hospitalist, I realized that I owed it to my patients to help them express their preferences for care. What I learned echoed what we know about advance directives: You cannot predict what someone will say. Not unexpectedly, my mother, grandmother, and aunt told me that they would never want to live like Terri Schiavo. But in a complete surprise my aunt told me that my favorite uncle, who is blessed with a quick wit and brilliant sense of humor, wants to be kept alive as long as possible.
As a hospitalist, I know that my patients care deeply about these issues and are quite eager to discuss them. Talking with patients about these issues is not just a good thing to do, but ultimately improves quality of care by promoting care that is consistent with patient preferences and emphasizes our commitment to respect patients and advocate on their behalf. I still remember early concerns about hospitalists that we would be cowboys more interested in procedures and yelling “Stat!” than in being caring providers who took time to get to know our patients. Yet an early study of hospitalists that I was involved in found just the opposite. Hospitalists recognized the importance of palliative care and good communication with patients. As I made rounds in the hospital in late March, many patients were watching the vigil outside the hospice in Florida and talking about the Pope. Many patients wanted to know my thoughts. Using the communication skills I have honed over the years, and my cultural background of always answering a question with a question, I turned it around and asked them, “What do you think?” I suspect that patients will be using Terri Schiavo as an example of how they do or do not want to live―and die―for a long time. I will do my best to use this shared touchstone as a starting point for understanding their preferences: “Tell me what it is about Terri Schiavo that worries you?” By helping our patients express their preferences and encouraging them to discuss these with their loved ones, we may ease the burden of families who would otherwise have to make a difficult decision without direct knowledge of the patient’s choice.
The second lesson for us to embrace is that palliative care is a core competency for hospitalists. Palliative care is already identified as a core competency in the Core Curriculum under development by SHM. As part of our goal of improving the quality of care for all of our patients, we have the opportunity to dramatically improve end of life care and to identify people who would benefit from palliative care earlier in the course of illness. This opportunity represents a sacred trust and speaks to the most basic role of the physician to “cure sometimes and comfort always.” Ultimately, the deaths of Terri Schiavo and the Pope, although fundamentally different from each other, and unique in many respects, reaffirmed for me the importance of my role as a hospitalist in providing the highest possible quality of care for people facing serious illness and death. With these skills, we will secure our place as leaders in quality care and reap the rich rewards of using our humanity to help patients and families at one of the most important, profound, and intimate times.
The third lesson for us as hospitalists is that more research is needed to define the optimal ways to care for hospitalized patients. While the case of Terri Schiavo raised particularly thorny family issues that might defy the ability of research to clarify, issues of how best to care for patients like Terri Schiavo and the Pope and the millions of people like them with heart failure, deep vein thromboses, aspiration pneumonia, gastrointestinal bleeding, cancer, and myriad other conditions can be, must be, and will be investigated. The only question will be, by whom? As the providers of an increasingly large percentage of hospital care, we are on the front-lines of recognizing the clinical questions that arise and understanding the systems of care in which solutions must be implemented. Therefore we must play a central role in defining the questions and discovering the answers. Further, because we need research not only in how best to treat patients but also in how to ensure that patients receive these treatments, we need to conduct this research in community hospitals, where the majority of patients are cared for, and not just at academic centers.
In my year as President of SHM, I will continue to develop our organization’s founding mission and to serve hospitalists in their goal of providing the best quality of care to their patients and having satisfying, sustainable, and rewarding jobs. SHM will continue to lead and define the field of hospital medicine in education, leadership, quality, patient safety, and teamwork. In addition, I hope to use my unique skills and insights to focus our members on the central role of research in defining our field and the need for SHM to help direct that research. I will also highlight the importance of hospitalists in providing palliative care and in improving the care of patients with serious and terminal illness. I encourage each hospitalist to embrace these critical issues and invite you to join me in implementing this vision to advance research in hospital medicine and to improve palliative care in hospitals. The research committee has already completed a report on the potential role of SHM in research in hospital medicine that the Board of Directors will discuss at our meeting in May, and I am planning an initiative in palliative care. If you would like to participate in either initiative or simply want to share your thoughts and ideas about these or other important issues in hospital medicine, please contact me by email (stevep@medicine.ucsf.edu). My closing wish is that Terri Schiavo’s family will find comfort and closure, out of the media spotlight, and that the memory of the Pope is honored by the ongoing lessons of tolerance and peace that he taught.
As I write first column as President of SHM, palliative care has been much in the news. As a hospitalist who spends much of my time caring for people approaching the end of life and teaching about palliative care, these 2 weeks have kept me busy talking about end of life issues with family, friends, patients, colleagues, and the media. At the same time, these events have reaffirmed for me my choice of a career as a hospitalist and the central role that hospitalists play in providing the highest quality care for the sickest patients, in continually improving that care, and in refining the systems to deliver it.
Terri Schiavo died 2 weeks after her feeding tube was removed. Her life and death sparked protests and political debate. Yet in the end, what seems most profound is the great sadness and loss for her family. Soon after Terri Schiavo died, Pope John Paul II became acutely ill. Several days after a feeding tube was placed, the Pope died in his apartment at the Vatican, triggering a global outpouring of love and grief.
In modern American health care, probably Terri Schiavo and the Pope would have received care from a hospitalist. If she were to arrive in a hospital after a cardiac arrest today, Terri Schiavo would likely be cared for by a hospitalist. It is the hospitalist who would have the first discussions with her family about her condition and prognosis. Similarly, most 84-year-old men with Parkinson’s disease, pneumonia, and a urinary tract infection would be cared for by a hospitalist. Hospitalists are serving as de facto ethicists and palliative care physicians, as we care for increasing numbers of people with serious and terminal illness. This shift in care provides an unprecedented opportunity for us to improve the quality of care for the half of all Americans who die in hospitals. Providing state of the art palliative care reinforces our efforts globally to improve the quality of care for all hospitalized patients. Furthermore, these cases highlight the need for research to define the best ways to deliver that care. As I thought about Terri Schiavo and the Pope, and saw the intense media spotlight on them, I kept thinking, “What does this mean for me?”
I have given this question a great deal of thought over the past week. What, if anything, do the deaths of Terri Schiavo and the Pope teach us? As I see it there are at least 3 important lessons for us as individuals and as hospitalists.
The first lesson is that each of us should consider the kind of care we would want if we were to suffer a devastating injury, as did Terri Schiavo, or be stricken with a progressive, debilitating illness, like the Pope. We should discuss our preferences for care with our loved ones and write them down. As hospitalists we should have these discussions routinely with our patients, document the conversations, notify the patient’s primary care physician, and encourage patients to share their thoughts with their loved ones. As a son, husband, brother, nephew, grandson, and father, I realized that one of the most important obligations I owed to my family was to make my wishes known, and to learn about the wishes of my loved ones. As a hospitalist, I realized that I owed it to my patients to help them express their preferences for care. What I learned echoed what we know about advance directives: You cannot predict what someone will say. Not unexpectedly, my mother, grandmother, and aunt told me that they would never want to live like Terri Schiavo. But in a complete surprise my aunt told me that my favorite uncle, who is blessed with a quick wit and brilliant sense of humor, wants to be kept alive as long as possible.
As a hospitalist, I know that my patients care deeply about these issues and are quite eager to discuss them. Talking with patients about these issues is not just a good thing to do, but ultimately improves quality of care by promoting care that is consistent with patient preferences and emphasizes our commitment to respect patients and advocate on their behalf. I still remember early concerns about hospitalists that we would be cowboys more interested in procedures and yelling “Stat!” than in being caring providers who took time to get to know our patients. Yet an early study of hospitalists that I was involved in found just the opposite. Hospitalists recognized the importance of palliative care and good communication with patients. As I made rounds in the hospital in late March, many patients were watching the vigil outside the hospice in Florida and talking about the Pope. Many patients wanted to know my thoughts. Using the communication skills I have honed over the years, and my cultural background of always answering a question with a question, I turned it around and asked them, “What do you think?” I suspect that patients will be using Terri Schiavo as an example of how they do or do not want to live―and die―for a long time. I will do my best to use this shared touchstone as a starting point for understanding their preferences: “Tell me what it is about Terri Schiavo that worries you?” By helping our patients express their preferences and encouraging them to discuss these with their loved ones, we may ease the burden of families who would otherwise have to make a difficult decision without direct knowledge of the patient’s choice.
The second lesson for us to embrace is that palliative care is a core competency for hospitalists. Palliative care is already identified as a core competency in the Core Curriculum under development by SHM. As part of our goal of improving the quality of care for all of our patients, we have the opportunity to dramatically improve end of life care and to identify people who would benefit from palliative care earlier in the course of illness. This opportunity represents a sacred trust and speaks to the most basic role of the physician to “cure sometimes and comfort always.” Ultimately, the deaths of Terri Schiavo and the Pope, although fundamentally different from each other, and unique in many respects, reaffirmed for me the importance of my role as a hospitalist in providing the highest possible quality of care for people facing serious illness and death. With these skills, we will secure our place as leaders in quality care and reap the rich rewards of using our humanity to help patients and families at one of the most important, profound, and intimate times.
The third lesson for us as hospitalists is that more research is needed to define the optimal ways to care for hospitalized patients. While the case of Terri Schiavo raised particularly thorny family issues that might defy the ability of research to clarify, issues of how best to care for patients like Terri Schiavo and the Pope and the millions of people like them with heart failure, deep vein thromboses, aspiration pneumonia, gastrointestinal bleeding, cancer, and myriad other conditions can be, must be, and will be investigated. The only question will be, by whom? As the providers of an increasingly large percentage of hospital care, we are on the front-lines of recognizing the clinical questions that arise and understanding the systems of care in which solutions must be implemented. Therefore we must play a central role in defining the questions and discovering the answers. Further, because we need research not only in how best to treat patients but also in how to ensure that patients receive these treatments, we need to conduct this research in community hospitals, where the majority of patients are cared for, and not just at academic centers.
In my year as President of SHM, I will continue to develop our organization’s founding mission and to serve hospitalists in their goal of providing the best quality of care to their patients and having satisfying, sustainable, and rewarding jobs. SHM will continue to lead and define the field of hospital medicine in education, leadership, quality, patient safety, and teamwork. In addition, I hope to use my unique skills and insights to focus our members on the central role of research in defining our field and the need for SHM to help direct that research. I will also highlight the importance of hospitalists in providing palliative care and in improving the care of patients with serious and terminal illness. I encourage each hospitalist to embrace these critical issues and invite you to join me in implementing this vision to advance research in hospital medicine and to improve palliative care in hospitals. The research committee has already completed a report on the potential role of SHM in research in hospital medicine that the Board of Directors will discuss at our meeting in May, and I am planning an initiative in palliative care. If you would like to participate in either initiative or simply want to share your thoughts and ideas about these or other important issues in hospital medicine, please contact me by email (stevep@medicine.ucsf.edu). My closing wish is that Terri Schiavo’s family will find comfort and closure, out of the media spotlight, and that the memory of the Pope is honored by the ongoing lessons of tolerance and peace that he taught.
Testing for Helicobacter Pylori
Supplement Editor:
Gary Falk, MD
Contents
Helicobacter pylori: Why it still matters in 2005
M. Brian Fennerty, MD
How to test for Helicobacter pylori in 2005
Nimish Vakil, MD, and A. Mark Fendrick, MD
Pitfalls, pearls, and practicalities in the diagnosis of Helicobacter pylori infection
Gary Falk, MD; Leonard Ehrlich, MD; A. Mark Fendrick, MD; M. Brian Fennerty, MD; Ben Gold, MD; Nimish Vakil, MD; Derek van Amerongen, MD, MS; and David Wyatt, MD
Supplement Editor:
Gary Falk, MD
Contents
Helicobacter pylori: Why it still matters in 2005
M. Brian Fennerty, MD
How to test for Helicobacter pylori in 2005
Nimish Vakil, MD, and A. Mark Fendrick, MD
Pitfalls, pearls, and practicalities in the diagnosis of Helicobacter pylori infection
Gary Falk, MD; Leonard Ehrlich, MD; A. Mark Fendrick, MD; M. Brian Fennerty, MD; Ben Gold, MD; Nimish Vakil, MD; Derek van Amerongen, MD, MS; and David Wyatt, MD
Supplement Editor:
Gary Falk, MD
Contents
Helicobacter pylori: Why it still matters in 2005
M. Brian Fennerty, MD
How to test for Helicobacter pylori in 2005
Nimish Vakil, MD, and A. Mark Fendrick, MD
Pitfalls, pearls, and practicalities in the diagnosis of Helicobacter pylori infection
Gary Falk, MD; Leonard Ehrlich, MD; A. Mark Fendrick, MD; M. Brian Fennerty, MD; Ben Gold, MD; Nimish Vakil, MD; Derek van Amerongen, MD, MS; and David Wyatt, MD
Pitfalls, pearls, and practicalities in the diagnosis of Helicobacter pylori infection
Other Literature of Interest
1. Carratala J, FernandezSabe N, Ortega L, et al. Outpatient care compared with hospitalization for community-acquired pneumonia: a randomized trial in low-risk patients. Ann Intern Med. 2005;142: 165-72.
The appropriate triage and management of patients with community-acquired pneumonia (CAP) has important implications for patient outcomes and the allocation of health care resources. Despite the availability of validated risk stratification tools significant variability in clinical practice which results in hospitalization rates that are often inconsistent with the severity of illness. In this unblinded, randomized controlled trial, 224 patients with CAP and a low-risk pneumonia severity index (PSI) score between 51 and 90 (class II and III) were randomized to outpatient oral levofloxacin therapy versus inpatient sequential intravenous and oral levofloxacin therapy. Exclusion criteria included quinolone allergy or use within the previous 3 months, PaO2 < 60 mm Hg, complicated pleural effusion, lung abscess, metastatic infection, inability to maintain oral intake, and severe psychosocial problems precluding outpatient therapy. In an intention-to-treat analysis, the primary endpoints, of cure of pneumonia (resolution of signs, symptoms, and radiographic changes at 30 days), absence of adverse drug reactions, medical complications, or need for hospitalization at 30 days were achieved in 83.6% of outpatients and in 80.7% of hospitalized patients. For the secondary endpoint of patient satisfaction, 91.2% of outpatients versus 79.1% of hospitalized patients (p=.03) were satisfied, but there were no differences between groups with respect to the secondary endpoint of health-related quality of life. Mortality was similar between the 2 groups, and although the study was not sufficiently powered to address this outcome, and interestingly there was trend toward increased medical complications in the hospitalized patients.
Limitations of this study include lack of blinding by investigators and questions about whether the results can be generalized given the geographic variation in microbial susceptibility to quinolone antibiotics. As the authors suggest, this study also highlights limitations in the PSI scoring system, given that patients with clinical findings and comorbidities who would never be treated in the outpatient setting may in fact fall into low-risk PSI categories. These concerns notwithstanding, this study adds to our ability to identify an additional subset of patients with CAP who can be safely managed as outpatients.
2. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med. 2005;142:260-73.
Early in the hospital medicine movement, when it was clear that hospitalists provided more efficient care than their colleagues, experience was cited as a reason for this difference. If, for example, a hospitalist cares for patients with community-acquired pneumonia daily, he or she is more likely to make the transition to oral antibiotics sooner, resulting in a shorter length of stay. Everyone recognized the hospitalists were younger, but is it plausible their “inexperience” explained the difference in care?
Choudhry and colleagues explored the available data surrounding clinical experience and quality of care delivered by physicians. They found few studies that specifically evaluated the effects of experience on quality of care. They did find articles that looked at quality of care and included experience or age as part of the physician characteristics
that possibly explained the differences. They reviewed 59 articles, available on MEDLINE, published since 1966. Forty-five studies found an inverse relationship between increasing experience and performance. For example, physicians more recently out of training programs were more familiar with evidence-based therapies for myocardial infarction and more familiar with NIH recommendations for treatment of breast cancer. Experienced physicians were less likely to screen for hypertension and more likely to prescribe inappropriate medications for elderly patients. This led them to the unexpected conclusion that experienced physicians may be at risk for providing lower-quality care and may need improvement interventions. An accompanying editorial by Drs. Weinberger, Duffy, and Cassel of the American Board of Internal Medicine stated, “The profession cannot ignore this striking finding and its implications: Practice does not make perfect, but it must be accompanied by ongoing active effort to maintain competence and quality of care.” They urged all physicians to “embrace the concepts behind maintenance of (board) certification.”
The image of Marcus Welby, MD, would lead one to believe that experience promotes higher quality care. But don’t ask a hospitalist: Many aren’t old enough to remember seeing him on television.
3. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352:969-77.
March was DVT (deep vein thrombosis) Awareness Month. Despite the availability of numerous guidelines, providers fail to consistently prescribe prophylactic measures against venous thromboembolism (VTE) for their hospitalized patients who meet criteria for prophylaxis.
Kucher and colleagues tested an innovative approach to remind providers to undertake such measures for their patients. They designed a computer program to identify hospitalized patients at increased risk for VTE who were not presently receiving VTE prophylaxis. The program reviewed the records of inpatients on the medical and surgical services and assigned a VTE risk score for each patient based on their history (i.e., history of cancer, hypercoagulability, etc.) and their present medical treatment (i.e., hormone therapy, prescribed bed rest, etc.). For patients considered “high risk” for VTE, the computer reviewed orders to identify ongoing use of VTE prophylactic measures. High-risk patients not receiving prophylactic therapies were randomized into 2 groups. The responsible physician in the intervention group received an electronic alert about the risk of VTE in their patient. No alerts were sent to the physicians in the control group. Physicians who received the alerts were forced to acknowledge the alert by either actively withholding prophylaxis or ordering prophylaxis (mechanical or pharmacologic measures). Patients were followed for 90 days with a primary endpoint of clinically diagnosed, objectively confirmed deep vein thrombosis (DVT) or pulmonary embolism (PE). The primary endpoint occurred in 8.2% of the control group versus 4.9% in the invention group (p<.001). The alert reduced the risk of DVT or PE at 90 days by 41% (p=.001).
The results of the study are interesting. The authors acknowledged that many physicians had patients in both groups. So receiving 1 alert may have affected their use of prophylaxis in both groups. They also could not eliminate the possibility of diagnostic bias. Prophylaxis was not blinded and VTE testing was not routinely performed. Would physicians be more likely to order an imaging study for symptomatic patients on no prophylaxis than patients on prophylaxis? Nevertheless, for hospitals that have sufficient computer resources, implementation of such alerts can elevate physician awareness about VTE and other clinical conditions.
4. Lau DT, Kasper JD, Pofer DE, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med. 2005;165: 68-74.
Lau and colleagues studied the impact of potentially inappropriate medications among residents of longtermcare facilities. They used information from a 1996 national survey of home residents. The sample included 3372 residents, 65 years and older, who lived in a nursing home for 3 months or longer. Over half of the residents were older than 85 years old and 75% were female. Only 10% were black. Nearly two thirds had dementia or other mental disorders. The study used the Beers Criteria to define potentially inappropriate medications. The potential errors in medications were categorized as 1 of 3 types:
- inappropriate choice of medication
- excessive medication dosage
- drug–disease interactions
Residents were considered to have a potentially inappropriate medication if their medication administration records revealed any of the above findings.
A univariate analysis showed that the risk of hospitalization was almost 30% higher among residents who received potentially inappropriate medications in the preceding month and 33% higher among residents who received potentially inappropriate medications for 2 consecutive months, compared with residents with no inappropriate medication exposure. The odds of death in any month were 21% higher among residents who had inappropriate medication exposure during the month of death or the preceeding month, compared with those with no inappropriate medication exposure.
These findings can be generalized to the inpatient setting, where hospitalists have the opportunity to influence and modify prescribing practices in the elderly population.
5. Lessnau KD. Is chest radiography necessary after uncomplicated insertion of a triplelumen catheter in the right internal jugular vein, using the anterior approach? Chest. 2005;127:220-3.
The routine use of chest radiography to confirm proper triplelumen catheter (TLC) placement may be an unnecessary and costly intervention. Lessnau conducted a prospective observational study of 100 consecutive patients over a 4-month period who required non-urgent TLC placement. The primary operators of the procedure included 18 medical residents, 3 pulmonary fellows, and a pulmonary attending with supervision provided for more junior clinicians. Operators followed a standardized approach to TLC placement utilizing the anterior approach to the right internal jugular vein. Complicated procedures were predefined as any procedure that required more than 3 needle passes, resulted in hemorrhage or hematoma formation (where there was concern for pneumothorax), or an absence of blood return in any of the TLC’s lumens. All subjects underwent routine post-procedure chest radiography to determine proper placement of the catheter and to exclude pneumothorax. A blinded radiologist reviewed these images.
Ninety-eight of the 100 catheters were in proper position. One malpositioned catheter was 7 cm above the right atrium in a patient who was 215 cm (>7 feet) tall. The second was noted to be in an S-shaped position on chest radiography. This procedure had required 20 needle passes and 5 slides of the catheter; additionally, blood return was inadequate in 2 lumens of the catheter. An operator reported a possible complication in 10 other procedures, but the only clinical finding in these cases was the development of a local hematoma in 1 patient. Eighty-eight patients had uncomplicated insertions and had normal chest radiographs. There were no pneumothoraces.
This study demonstrates that in carefully controlled and supervised situations, as described in the study, routine chest radiography may be omitted if the insertion goes smoothly. It is important to note that these results are specific to the technique described in the study (using the anterior approach to the right internal jugular, using a short finder needle to initially locate the vein) and cannot be extrapolated to other methods of TLC insertion. Important limitations of the study include the sample size of only 100 patients and the use of only a single anatomic approach to TLC insertion. These findings, although an important first step, will need to be reproduced on a larger scale before we can recommend the cessation of routine chest radiography after TLC placement on a more widespread basis.
6. Safdar N, Fine JP, Maki DG. Metaanalysis: methods for diagnosing intravascular devicerelated bloodstream infection. Ann Intern Med. 2005;142:451-66.
Intravascular device (IVD)–related blood stream infections are a frequent cause of morbidity and mortality, and yet there is lack of a clear consensus on the most accurate method to make this diagnosis.
In this metaanalysis, Safdar et al. reviewed 185 studies, including 8 different diagnostic tests, for the detection of IVD-related bloodstream infections, of which 51 studies met the inclusion criteria. Tests were divided into IVD-sparing and those requiring IVD removal. Pooled sensitivity and specificity, summary measures of accuracy, and the mean log odds ratio were determined. The most accurate IVD-sparing test was paired quantitative blood cultures (simultaneous blood cultures from the IVD and a peripheral site, with a positive result defined as an IVD-site microorganism concentration 3–5 times greater than peripheral site) with a sensitivity of 0.87 (95% CI: 0.83–0.91) and specificity of 0.98 (95% CI: 0.97–0.99). This was followed by quantitative IVD-drawn blood cultures alone (positive result defined as growth of ≥100 CFU), with a sensitivity of 0.77 (95% CI: 0.69–0.85) and a specificity of 0.90 (95% CI: 0.88–0.92). IVD-drawn qualitative blood cultures had a sensitivity of 0.87 (95% CI: 0.80–0.94) and a specificity of 0.83 (95% CI: 0.78–0.88), and IVD- and peripheral-drawn qualitative blood cultures with differential time to positivity had a sensitivity of 0.85 (95% CI: 0.78–0.92) and specificity of 0.81 (95% CI: 0.81–0.97).
The most accurate test requiring IVD removal was quantitative catheter segment culture (segment of catheter is flushed or sonicated and plated, positive if ≥1000 CFU), with sensitivity of 0.83 (95% CI: 0.78–0.88) and specificity of 0.87 (95% CI: 0.85–0.89), followed by semi-quantitative catheter segment culture (5cm segment plated, positive if ≥ 15 CFU) with sensitivity of 0.82 (95% CI: 0.81–0.89) and specificity of 0.82 (95% CI: 0.80–0.84). The least accurate was qualitative catheter segment culture (positive if any growth) with a sensitivity of 0.90 (95% CI: 0.83–0.97) and specificity of 0.72 (95% CI: 0.66–0.78).
The limitations of this study include heterogeneity of study design, including limited data on the use of antibiotics before culture data was obtained and the baseline prevalence of bacteremia in the study populations. In addition, all data was obtained prior to the widespread use of antibiotic-coated catheters. While these results support the catheter-tip quantitative culture techniques that are already widely in use, they are less applicable to blood culture testing techniques, because quantitative assays are rarely used. Fortunately, all of these assays have a high negative predictive value, and false-positive results can be minimized by reserving testing for patients in whom there is moderate-to-high pretest probability of IVD related bloodstream infection.
7. Sopena N, Sabria M, Neunos 2000 Study Group. Multicenter study of hospital-acquired pneumonia in non-ICU patients. Chest. 2005;127:213-9.
A growing body of literature exists on hospital-acquired pneumonia (HAP) in the ICU setting. Sopena and colleagues extend the HAP literature to the non-ICU setting in a multicenter cross-sectional study. Cases of HAP were identified if clinical or radiographic evidence of pneumonia developed 72 hours after admission or within 10 days of a previous discharge. Patients who developed pneumonia in the ICU were excluded from analysis.
During an 18-month study period, 165 cases were identified with complete clinical and microbiologic data. The incidence of HAP was 3.1 ± 1.4 per 1000 hospital admissions. Ninety-eight (59.4%) patients diagnosed with HAP had severe underlying diseases that were classified as fatal (<1 year) or ultimately fatal (in 5 years). Extrinsic risk factors observed in patients with HAP included concurrent steroid use (29%), antibiotic therapy (53.3%), use of H2 blockers (37%), and hospitalization greater than 5 days (76%). Microbiologic data were positive in 60 (36.4%) cases. Streptococcus pneumoniae was diagnosed in 16 cases (9.7%), enterobacteriaceae in 8 (4.8%), Legionella pneumophila in 7 (4.2%), Aspergillus sp in 7 (4.2%), Pseudomonas aeruginosa in 7 (4.2%). Four cases of Staphylococcus aureus were diagnosed (3%), only one of which was methicillin resistant.
Complications of HAP occurred in 52.1% of cases and included respiratory failure (34.5%), pleural effusion (20.6%), septic shock (9.6%), renal failure (4.8%), and empyema (2.4%). Forty-three (26%) patients died during the hospitalization; 23 of these cases were directly attributed to HAP.
A limitation of the study is that the incidence of HAP was somewhat lower than reported in the literature and thus might represent an unintended sampling bias. Moreover, the study demonstrated underlying factors seen in patients with HAP, but these are not necessarily causative. Results useful to hospitalists include a higher than expected rate of Legionella and Aspergillus sp causing HAP in this population. A Legionella outbreak was not the explanation, as these cases were diagnosed in 5 different hospitals. The high frequency of adverse outcomes associated with HAP should alert hospitalists to the risk of nosocomial pneumonia in the non-ICU setting.
1. Carratala J, FernandezSabe N, Ortega L, et al. Outpatient care compared with hospitalization for community-acquired pneumonia: a randomized trial in low-risk patients. Ann Intern Med. 2005;142: 165-72.
The appropriate triage and management of patients with community-acquired pneumonia (CAP) has important implications for patient outcomes and the allocation of health care resources. Despite the availability of validated risk stratification tools significant variability in clinical practice which results in hospitalization rates that are often inconsistent with the severity of illness. In this unblinded, randomized controlled trial, 224 patients with CAP and a low-risk pneumonia severity index (PSI) score between 51 and 90 (class II and III) were randomized to outpatient oral levofloxacin therapy versus inpatient sequential intravenous and oral levofloxacin therapy. Exclusion criteria included quinolone allergy or use within the previous 3 months, PaO2 < 60 mm Hg, complicated pleural effusion, lung abscess, metastatic infection, inability to maintain oral intake, and severe psychosocial problems precluding outpatient therapy. In an intention-to-treat analysis, the primary endpoints, of cure of pneumonia (resolution of signs, symptoms, and radiographic changes at 30 days), absence of adverse drug reactions, medical complications, or need for hospitalization at 30 days were achieved in 83.6% of outpatients and in 80.7% of hospitalized patients. For the secondary endpoint of patient satisfaction, 91.2% of outpatients versus 79.1% of hospitalized patients (p=.03) were satisfied, but there were no differences between groups with respect to the secondary endpoint of health-related quality of life. Mortality was similar between the 2 groups, and although the study was not sufficiently powered to address this outcome, and interestingly there was trend toward increased medical complications in the hospitalized patients.
Limitations of this study include lack of blinding by investigators and questions about whether the results can be generalized given the geographic variation in microbial susceptibility to quinolone antibiotics. As the authors suggest, this study also highlights limitations in the PSI scoring system, given that patients with clinical findings and comorbidities who would never be treated in the outpatient setting may in fact fall into low-risk PSI categories. These concerns notwithstanding, this study adds to our ability to identify an additional subset of patients with CAP who can be safely managed as outpatients.
2. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med. 2005;142:260-73.
Early in the hospital medicine movement, when it was clear that hospitalists provided more efficient care than their colleagues, experience was cited as a reason for this difference. If, for example, a hospitalist cares for patients with community-acquired pneumonia daily, he or she is more likely to make the transition to oral antibiotics sooner, resulting in a shorter length of stay. Everyone recognized the hospitalists were younger, but is it plausible their “inexperience” explained the difference in care?
Choudhry and colleagues explored the available data surrounding clinical experience and quality of care delivered by physicians. They found few studies that specifically evaluated the effects of experience on quality of care. They did find articles that looked at quality of care and included experience or age as part of the physician characteristics
that possibly explained the differences. They reviewed 59 articles, available on MEDLINE, published since 1966. Forty-five studies found an inverse relationship between increasing experience and performance. For example, physicians more recently out of training programs were more familiar with evidence-based therapies for myocardial infarction and more familiar with NIH recommendations for treatment of breast cancer. Experienced physicians were less likely to screen for hypertension and more likely to prescribe inappropriate medications for elderly patients. This led them to the unexpected conclusion that experienced physicians may be at risk for providing lower-quality care and may need improvement interventions. An accompanying editorial by Drs. Weinberger, Duffy, and Cassel of the American Board of Internal Medicine stated, “The profession cannot ignore this striking finding and its implications: Practice does not make perfect, but it must be accompanied by ongoing active effort to maintain competence and quality of care.” They urged all physicians to “embrace the concepts behind maintenance of (board) certification.”
The image of Marcus Welby, MD, would lead one to believe that experience promotes higher quality care. But don’t ask a hospitalist: Many aren’t old enough to remember seeing him on television.
3. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352:969-77.
March was DVT (deep vein thrombosis) Awareness Month. Despite the availability of numerous guidelines, providers fail to consistently prescribe prophylactic measures against venous thromboembolism (VTE) for their hospitalized patients who meet criteria for prophylaxis.
Kucher and colleagues tested an innovative approach to remind providers to undertake such measures for their patients. They designed a computer program to identify hospitalized patients at increased risk for VTE who were not presently receiving VTE prophylaxis. The program reviewed the records of inpatients on the medical and surgical services and assigned a VTE risk score for each patient based on their history (i.e., history of cancer, hypercoagulability, etc.) and their present medical treatment (i.e., hormone therapy, prescribed bed rest, etc.). For patients considered “high risk” for VTE, the computer reviewed orders to identify ongoing use of VTE prophylactic measures. High-risk patients not receiving prophylactic therapies were randomized into 2 groups. The responsible physician in the intervention group received an electronic alert about the risk of VTE in their patient. No alerts were sent to the physicians in the control group. Physicians who received the alerts were forced to acknowledge the alert by either actively withholding prophylaxis or ordering prophylaxis (mechanical or pharmacologic measures). Patients were followed for 90 days with a primary endpoint of clinically diagnosed, objectively confirmed deep vein thrombosis (DVT) or pulmonary embolism (PE). The primary endpoint occurred in 8.2% of the control group versus 4.9% in the invention group (p<.001). The alert reduced the risk of DVT or PE at 90 days by 41% (p=.001).
The results of the study are interesting. The authors acknowledged that many physicians had patients in both groups. So receiving 1 alert may have affected their use of prophylaxis in both groups. They also could not eliminate the possibility of diagnostic bias. Prophylaxis was not blinded and VTE testing was not routinely performed. Would physicians be more likely to order an imaging study for symptomatic patients on no prophylaxis than patients on prophylaxis? Nevertheless, for hospitals that have sufficient computer resources, implementation of such alerts can elevate physician awareness about VTE and other clinical conditions.
4. Lau DT, Kasper JD, Pofer DE, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med. 2005;165: 68-74.
Lau and colleagues studied the impact of potentially inappropriate medications among residents of longtermcare facilities. They used information from a 1996 national survey of home residents. The sample included 3372 residents, 65 years and older, who lived in a nursing home for 3 months or longer. Over half of the residents were older than 85 years old and 75% were female. Only 10% were black. Nearly two thirds had dementia or other mental disorders. The study used the Beers Criteria to define potentially inappropriate medications. The potential errors in medications were categorized as 1 of 3 types:
- inappropriate choice of medication
- excessive medication dosage
- drug–disease interactions
Residents were considered to have a potentially inappropriate medication if their medication administration records revealed any of the above findings.
A univariate analysis showed that the risk of hospitalization was almost 30% higher among residents who received potentially inappropriate medications in the preceding month and 33% higher among residents who received potentially inappropriate medications for 2 consecutive months, compared with residents with no inappropriate medication exposure. The odds of death in any month were 21% higher among residents who had inappropriate medication exposure during the month of death or the preceeding month, compared with those with no inappropriate medication exposure.
These findings can be generalized to the inpatient setting, where hospitalists have the opportunity to influence and modify prescribing practices in the elderly population.
5. Lessnau KD. Is chest radiography necessary after uncomplicated insertion of a triplelumen catheter in the right internal jugular vein, using the anterior approach? Chest. 2005;127:220-3.
The routine use of chest radiography to confirm proper triplelumen catheter (TLC) placement may be an unnecessary and costly intervention. Lessnau conducted a prospective observational study of 100 consecutive patients over a 4-month period who required non-urgent TLC placement. The primary operators of the procedure included 18 medical residents, 3 pulmonary fellows, and a pulmonary attending with supervision provided for more junior clinicians. Operators followed a standardized approach to TLC placement utilizing the anterior approach to the right internal jugular vein. Complicated procedures were predefined as any procedure that required more than 3 needle passes, resulted in hemorrhage or hematoma formation (where there was concern for pneumothorax), or an absence of blood return in any of the TLC’s lumens. All subjects underwent routine post-procedure chest radiography to determine proper placement of the catheter and to exclude pneumothorax. A blinded radiologist reviewed these images.
Ninety-eight of the 100 catheters were in proper position. One malpositioned catheter was 7 cm above the right atrium in a patient who was 215 cm (>7 feet) tall. The second was noted to be in an S-shaped position on chest radiography. This procedure had required 20 needle passes and 5 slides of the catheter; additionally, blood return was inadequate in 2 lumens of the catheter. An operator reported a possible complication in 10 other procedures, but the only clinical finding in these cases was the development of a local hematoma in 1 patient. Eighty-eight patients had uncomplicated insertions and had normal chest radiographs. There were no pneumothoraces.
This study demonstrates that in carefully controlled and supervised situations, as described in the study, routine chest radiography may be omitted if the insertion goes smoothly. It is important to note that these results are specific to the technique described in the study (using the anterior approach to the right internal jugular, using a short finder needle to initially locate the vein) and cannot be extrapolated to other methods of TLC insertion. Important limitations of the study include the sample size of only 100 patients and the use of only a single anatomic approach to TLC insertion. These findings, although an important first step, will need to be reproduced on a larger scale before we can recommend the cessation of routine chest radiography after TLC placement on a more widespread basis.
6. Safdar N, Fine JP, Maki DG. Metaanalysis: methods for diagnosing intravascular devicerelated bloodstream infection. Ann Intern Med. 2005;142:451-66.
Intravascular device (IVD)–related blood stream infections are a frequent cause of morbidity and mortality, and yet there is lack of a clear consensus on the most accurate method to make this diagnosis.
In this metaanalysis, Safdar et al. reviewed 185 studies, including 8 different diagnostic tests, for the detection of IVD-related bloodstream infections, of which 51 studies met the inclusion criteria. Tests were divided into IVD-sparing and those requiring IVD removal. Pooled sensitivity and specificity, summary measures of accuracy, and the mean log odds ratio were determined. The most accurate IVD-sparing test was paired quantitative blood cultures (simultaneous blood cultures from the IVD and a peripheral site, with a positive result defined as an IVD-site microorganism concentration 3–5 times greater than peripheral site) with a sensitivity of 0.87 (95% CI: 0.83–0.91) and specificity of 0.98 (95% CI: 0.97–0.99). This was followed by quantitative IVD-drawn blood cultures alone (positive result defined as growth of ≥100 CFU), with a sensitivity of 0.77 (95% CI: 0.69–0.85) and a specificity of 0.90 (95% CI: 0.88–0.92). IVD-drawn qualitative blood cultures had a sensitivity of 0.87 (95% CI: 0.80–0.94) and a specificity of 0.83 (95% CI: 0.78–0.88), and IVD- and peripheral-drawn qualitative blood cultures with differential time to positivity had a sensitivity of 0.85 (95% CI: 0.78–0.92) and specificity of 0.81 (95% CI: 0.81–0.97).
The most accurate test requiring IVD removal was quantitative catheter segment culture (segment of catheter is flushed or sonicated and plated, positive if ≥1000 CFU), with sensitivity of 0.83 (95% CI: 0.78–0.88) and specificity of 0.87 (95% CI: 0.85–0.89), followed by semi-quantitative catheter segment culture (5cm segment plated, positive if ≥ 15 CFU) with sensitivity of 0.82 (95% CI: 0.81–0.89) and specificity of 0.82 (95% CI: 0.80–0.84). The least accurate was qualitative catheter segment culture (positive if any growth) with a sensitivity of 0.90 (95% CI: 0.83–0.97) and specificity of 0.72 (95% CI: 0.66–0.78).
The limitations of this study include heterogeneity of study design, including limited data on the use of antibiotics before culture data was obtained and the baseline prevalence of bacteremia in the study populations. In addition, all data was obtained prior to the widespread use of antibiotic-coated catheters. While these results support the catheter-tip quantitative culture techniques that are already widely in use, they are less applicable to blood culture testing techniques, because quantitative assays are rarely used. Fortunately, all of these assays have a high negative predictive value, and false-positive results can be minimized by reserving testing for patients in whom there is moderate-to-high pretest probability of IVD related bloodstream infection.
7. Sopena N, Sabria M, Neunos 2000 Study Group. Multicenter study of hospital-acquired pneumonia in non-ICU patients. Chest. 2005;127:213-9.
A growing body of literature exists on hospital-acquired pneumonia (HAP) in the ICU setting. Sopena and colleagues extend the HAP literature to the non-ICU setting in a multicenter cross-sectional study. Cases of HAP were identified if clinical or radiographic evidence of pneumonia developed 72 hours after admission or within 10 days of a previous discharge. Patients who developed pneumonia in the ICU were excluded from analysis.
During an 18-month study period, 165 cases were identified with complete clinical and microbiologic data. The incidence of HAP was 3.1 ± 1.4 per 1000 hospital admissions. Ninety-eight (59.4%) patients diagnosed with HAP had severe underlying diseases that were classified as fatal (<1 year) or ultimately fatal (in 5 years). Extrinsic risk factors observed in patients with HAP included concurrent steroid use (29%), antibiotic therapy (53.3%), use of H2 blockers (37%), and hospitalization greater than 5 days (76%). Microbiologic data were positive in 60 (36.4%) cases. Streptococcus pneumoniae was diagnosed in 16 cases (9.7%), enterobacteriaceae in 8 (4.8%), Legionella pneumophila in 7 (4.2%), Aspergillus sp in 7 (4.2%), Pseudomonas aeruginosa in 7 (4.2%). Four cases of Staphylococcus aureus were diagnosed (3%), only one of which was methicillin resistant.
Complications of HAP occurred in 52.1% of cases and included respiratory failure (34.5%), pleural effusion (20.6%), septic shock (9.6%), renal failure (4.8%), and empyema (2.4%). Forty-three (26%) patients died during the hospitalization; 23 of these cases were directly attributed to HAP.
A limitation of the study is that the incidence of HAP was somewhat lower than reported in the literature and thus might represent an unintended sampling bias. Moreover, the study demonstrated underlying factors seen in patients with HAP, but these are not necessarily causative. Results useful to hospitalists include a higher than expected rate of Legionella and Aspergillus sp causing HAP in this population. A Legionella outbreak was not the explanation, as these cases were diagnosed in 5 different hospitals. The high frequency of adverse outcomes associated with HAP should alert hospitalists to the risk of nosocomial pneumonia in the non-ICU setting.
1. Carratala J, FernandezSabe N, Ortega L, et al. Outpatient care compared with hospitalization for community-acquired pneumonia: a randomized trial in low-risk patients. Ann Intern Med. 2005;142: 165-72.
The appropriate triage and management of patients with community-acquired pneumonia (CAP) has important implications for patient outcomes and the allocation of health care resources. Despite the availability of validated risk stratification tools significant variability in clinical practice which results in hospitalization rates that are often inconsistent with the severity of illness. In this unblinded, randomized controlled trial, 224 patients with CAP and a low-risk pneumonia severity index (PSI) score between 51 and 90 (class II and III) were randomized to outpatient oral levofloxacin therapy versus inpatient sequential intravenous and oral levofloxacin therapy. Exclusion criteria included quinolone allergy or use within the previous 3 months, PaO2 < 60 mm Hg, complicated pleural effusion, lung abscess, metastatic infection, inability to maintain oral intake, and severe psychosocial problems precluding outpatient therapy. In an intention-to-treat analysis, the primary endpoints, of cure of pneumonia (resolution of signs, symptoms, and radiographic changes at 30 days), absence of adverse drug reactions, medical complications, or need for hospitalization at 30 days were achieved in 83.6% of outpatients and in 80.7% of hospitalized patients. For the secondary endpoint of patient satisfaction, 91.2% of outpatients versus 79.1% of hospitalized patients (p=.03) were satisfied, but there were no differences between groups with respect to the secondary endpoint of health-related quality of life. Mortality was similar between the 2 groups, and although the study was not sufficiently powered to address this outcome, and interestingly there was trend toward increased medical complications in the hospitalized patients.
Limitations of this study include lack of blinding by investigators and questions about whether the results can be generalized given the geographic variation in microbial susceptibility to quinolone antibiotics. As the authors suggest, this study also highlights limitations in the PSI scoring system, given that patients with clinical findings and comorbidities who would never be treated in the outpatient setting may in fact fall into low-risk PSI categories. These concerns notwithstanding, this study adds to our ability to identify an additional subset of patients with CAP who can be safely managed as outpatients.
2. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med. 2005;142:260-73.
Early in the hospital medicine movement, when it was clear that hospitalists provided more efficient care than their colleagues, experience was cited as a reason for this difference. If, for example, a hospitalist cares for patients with community-acquired pneumonia daily, he or she is more likely to make the transition to oral antibiotics sooner, resulting in a shorter length of stay. Everyone recognized the hospitalists were younger, but is it plausible their “inexperience” explained the difference in care?
Choudhry and colleagues explored the available data surrounding clinical experience and quality of care delivered by physicians. They found few studies that specifically evaluated the effects of experience on quality of care. They did find articles that looked at quality of care and included experience or age as part of the physician characteristics
that possibly explained the differences. They reviewed 59 articles, available on MEDLINE, published since 1966. Forty-five studies found an inverse relationship between increasing experience and performance. For example, physicians more recently out of training programs were more familiar with evidence-based therapies for myocardial infarction and more familiar with NIH recommendations for treatment of breast cancer. Experienced physicians were less likely to screen for hypertension and more likely to prescribe inappropriate medications for elderly patients. This led them to the unexpected conclusion that experienced physicians may be at risk for providing lower-quality care and may need improvement interventions. An accompanying editorial by Drs. Weinberger, Duffy, and Cassel of the American Board of Internal Medicine stated, “The profession cannot ignore this striking finding and its implications: Practice does not make perfect, but it must be accompanied by ongoing active effort to maintain competence and quality of care.” They urged all physicians to “embrace the concepts behind maintenance of (board) certification.”
The image of Marcus Welby, MD, would lead one to believe that experience promotes higher quality care. But don’t ask a hospitalist: Many aren’t old enough to remember seeing him on television.
3. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352:969-77.
March was DVT (deep vein thrombosis) Awareness Month. Despite the availability of numerous guidelines, providers fail to consistently prescribe prophylactic measures against venous thromboembolism (VTE) for their hospitalized patients who meet criteria for prophylaxis.
Kucher and colleagues tested an innovative approach to remind providers to undertake such measures for their patients. They designed a computer program to identify hospitalized patients at increased risk for VTE who were not presently receiving VTE prophylaxis. The program reviewed the records of inpatients on the medical and surgical services and assigned a VTE risk score for each patient based on their history (i.e., history of cancer, hypercoagulability, etc.) and their present medical treatment (i.e., hormone therapy, prescribed bed rest, etc.). For patients considered “high risk” for VTE, the computer reviewed orders to identify ongoing use of VTE prophylactic measures. High-risk patients not receiving prophylactic therapies were randomized into 2 groups. The responsible physician in the intervention group received an electronic alert about the risk of VTE in their patient. No alerts were sent to the physicians in the control group. Physicians who received the alerts were forced to acknowledge the alert by either actively withholding prophylaxis or ordering prophylaxis (mechanical or pharmacologic measures). Patients were followed for 90 days with a primary endpoint of clinically diagnosed, objectively confirmed deep vein thrombosis (DVT) or pulmonary embolism (PE). The primary endpoint occurred in 8.2% of the control group versus 4.9% in the invention group (p<.001). The alert reduced the risk of DVT or PE at 90 days by 41% (p=.001).
The results of the study are interesting. The authors acknowledged that many physicians had patients in both groups. So receiving 1 alert may have affected their use of prophylaxis in both groups. They also could not eliminate the possibility of diagnostic bias. Prophylaxis was not blinded and VTE testing was not routinely performed. Would physicians be more likely to order an imaging study for symptomatic patients on no prophylaxis than patients on prophylaxis? Nevertheless, for hospitals that have sufficient computer resources, implementation of such alerts can elevate physician awareness about VTE and other clinical conditions.
4. Lau DT, Kasper JD, Pofer DE, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med. 2005;165: 68-74.
Lau and colleagues studied the impact of potentially inappropriate medications among residents of longtermcare facilities. They used information from a 1996 national survey of home residents. The sample included 3372 residents, 65 years and older, who lived in a nursing home for 3 months or longer. Over half of the residents were older than 85 years old and 75% were female. Only 10% were black. Nearly two thirds had dementia or other mental disorders. The study used the Beers Criteria to define potentially inappropriate medications. The potential errors in medications were categorized as 1 of 3 types:
- inappropriate choice of medication
- excessive medication dosage
- drug–disease interactions
Residents were considered to have a potentially inappropriate medication if their medication administration records revealed any of the above findings.
A univariate analysis showed that the risk of hospitalization was almost 30% higher among residents who received potentially inappropriate medications in the preceding month and 33% higher among residents who received potentially inappropriate medications for 2 consecutive months, compared with residents with no inappropriate medication exposure. The odds of death in any month were 21% higher among residents who had inappropriate medication exposure during the month of death or the preceeding month, compared with those with no inappropriate medication exposure.
These findings can be generalized to the inpatient setting, where hospitalists have the opportunity to influence and modify prescribing practices in the elderly population.
5. Lessnau KD. Is chest radiography necessary after uncomplicated insertion of a triplelumen catheter in the right internal jugular vein, using the anterior approach? Chest. 2005;127:220-3.
The routine use of chest radiography to confirm proper triplelumen catheter (TLC) placement may be an unnecessary and costly intervention. Lessnau conducted a prospective observational study of 100 consecutive patients over a 4-month period who required non-urgent TLC placement. The primary operators of the procedure included 18 medical residents, 3 pulmonary fellows, and a pulmonary attending with supervision provided for more junior clinicians. Operators followed a standardized approach to TLC placement utilizing the anterior approach to the right internal jugular vein. Complicated procedures were predefined as any procedure that required more than 3 needle passes, resulted in hemorrhage or hematoma formation (where there was concern for pneumothorax), or an absence of blood return in any of the TLC’s lumens. All subjects underwent routine post-procedure chest radiography to determine proper placement of the catheter and to exclude pneumothorax. A blinded radiologist reviewed these images.
Ninety-eight of the 100 catheters were in proper position. One malpositioned catheter was 7 cm above the right atrium in a patient who was 215 cm (>7 feet) tall. The second was noted to be in an S-shaped position on chest radiography. This procedure had required 20 needle passes and 5 slides of the catheter; additionally, blood return was inadequate in 2 lumens of the catheter. An operator reported a possible complication in 10 other procedures, but the only clinical finding in these cases was the development of a local hematoma in 1 patient. Eighty-eight patients had uncomplicated insertions and had normal chest radiographs. There were no pneumothoraces.
This study demonstrates that in carefully controlled and supervised situations, as described in the study, routine chest radiography may be omitted if the insertion goes smoothly. It is important to note that these results are specific to the technique described in the study (using the anterior approach to the right internal jugular, using a short finder needle to initially locate the vein) and cannot be extrapolated to other methods of TLC insertion. Important limitations of the study include the sample size of only 100 patients and the use of only a single anatomic approach to TLC insertion. These findings, although an important first step, will need to be reproduced on a larger scale before we can recommend the cessation of routine chest radiography after TLC placement on a more widespread basis.
6. Safdar N, Fine JP, Maki DG. Metaanalysis: methods for diagnosing intravascular devicerelated bloodstream infection. Ann Intern Med. 2005;142:451-66.
Intravascular device (IVD)–related blood stream infections are a frequent cause of morbidity and mortality, and yet there is lack of a clear consensus on the most accurate method to make this diagnosis.
In this metaanalysis, Safdar et al. reviewed 185 studies, including 8 different diagnostic tests, for the detection of IVD-related bloodstream infections, of which 51 studies met the inclusion criteria. Tests were divided into IVD-sparing and those requiring IVD removal. Pooled sensitivity and specificity, summary measures of accuracy, and the mean log odds ratio were determined. The most accurate IVD-sparing test was paired quantitative blood cultures (simultaneous blood cultures from the IVD and a peripheral site, with a positive result defined as an IVD-site microorganism concentration 3–5 times greater than peripheral site) with a sensitivity of 0.87 (95% CI: 0.83–0.91) and specificity of 0.98 (95% CI: 0.97–0.99). This was followed by quantitative IVD-drawn blood cultures alone (positive result defined as growth of ≥100 CFU), with a sensitivity of 0.77 (95% CI: 0.69–0.85) and a specificity of 0.90 (95% CI: 0.88–0.92). IVD-drawn qualitative blood cultures had a sensitivity of 0.87 (95% CI: 0.80–0.94) and a specificity of 0.83 (95% CI: 0.78–0.88), and IVD- and peripheral-drawn qualitative blood cultures with differential time to positivity had a sensitivity of 0.85 (95% CI: 0.78–0.92) and specificity of 0.81 (95% CI: 0.81–0.97).
The most accurate test requiring IVD removal was quantitative catheter segment culture (segment of catheter is flushed or sonicated and plated, positive if ≥1000 CFU), with sensitivity of 0.83 (95% CI: 0.78–0.88) and specificity of 0.87 (95% CI: 0.85–0.89), followed by semi-quantitative catheter segment culture (5cm segment plated, positive if ≥ 15 CFU) with sensitivity of 0.82 (95% CI: 0.81–0.89) and specificity of 0.82 (95% CI: 0.80–0.84). The least accurate was qualitative catheter segment culture (positive if any growth) with a sensitivity of 0.90 (95% CI: 0.83–0.97) and specificity of 0.72 (95% CI: 0.66–0.78).
The limitations of this study include heterogeneity of study design, including limited data on the use of antibiotics before culture data was obtained and the baseline prevalence of bacteremia in the study populations. In addition, all data was obtained prior to the widespread use of antibiotic-coated catheters. While these results support the catheter-tip quantitative culture techniques that are already widely in use, they are less applicable to blood culture testing techniques, because quantitative assays are rarely used. Fortunately, all of these assays have a high negative predictive value, and false-positive results can be minimized by reserving testing for patients in whom there is moderate-to-high pretest probability of IVD related bloodstream infection.
7. Sopena N, Sabria M, Neunos 2000 Study Group. Multicenter study of hospital-acquired pneumonia in non-ICU patients. Chest. 2005;127:213-9.
A growing body of literature exists on hospital-acquired pneumonia (HAP) in the ICU setting. Sopena and colleagues extend the HAP literature to the non-ICU setting in a multicenter cross-sectional study. Cases of HAP were identified if clinical or radiographic evidence of pneumonia developed 72 hours after admission or within 10 days of a previous discharge. Patients who developed pneumonia in the ICU were excluded from analysis.
During an 18-month study period, 165 cases were identified with complete clinical and microbiologic data. The incidence of HAP was 3.1 ± 1.4 per 1000 hospital admissions. Ninety-eight (59.4%) patients diagnosed with HAP had severe underlying diseases that were classified as fatal (<1 year) or ultimately fatal (in 5 years). Extrinsic risk factors observed in patients with HAP included concurrent steroid use (29%), antibiotic therapy (53.3%), use of H2 blockers (37%), and hospitalization greater than 5 days (76%). Microbiologic data were positive in 60 (36.4%) cases. Streptococcus pneumoniae was diagnosed in 16 cases (9.7%), enterobacteriaceae in 8 (4.8%), Legionella pneumophila in 7 (4.2%), Aspergillus sp in 7 (4.2%), Pseudomonas aeruginosa in 7 (4.2%). Four cases of Staphylococcus aureus were diagnosed (3%), only one of which was methicillin resistant.
Complications of HAP occurred in 52.1% of cases and included respiratory failure (34.5%), pleural effusion (20.6%), septic shock (9.6%), renal failure (4.8%), and empyema (2.4%). Forty-three (26%) patients died during the hospitalization; 23 of these cases were directly attributed to HAP.
A limitation of the study is that the incidence of HAP was somewhat lower than reported in the literature and thus might represent an unintended sampling bias. Moreover, the study demonstrated underlying factors seen in patients with HAP, but these are not necessarily causative. Results useful to hospitalists include a higher than expected rate of Legionella and Aspergillus sp causing HAP in this population. A Legionella outbreak was not the explanation, as these cases were diagnosed in 5 different hospitals. The high frequency of adverse outcomes associated with HAP should alert hospitalists to the risk of nosocomial pneumonia in the non-ICU setting.
Opportunity to Partner in Improving Care: The Medicare Chronic Care improvement Programs
The Medicare Modernization Act of 2003 (MMA) authorized development and testing of voluntary programs focused on improving the quality of care and quality of life for beneficiaries with multiple chronic illnesses. These Chronic Care Improvement Programs (CCIPs) represent the first large-scale chronic care improvement initiative under the Medicare fee-for-service (FFS) program. The programs also may represent an opportunity for SHM members to partner with the selected organizations.
CMS selected organizations that will offer self-care guidance and support to chronically ill beneficiaries. These organizations will help beneficiaries manage their health, adhere to their physicians’ plans of care, and assure that they seek or obtain medical care as needed to reduce their health risks. Chronic conditions are currently a leading cause of illness, disability, and death among beneficiaries and account for a disproportionate share of health care expenditures.
Each selected organization may design its own program, with the potential for a variety of unique models. Some vendors are partnering with physician groups and others may reach out to physicians in their regions. The selected regions and respective vendors are:
- Brooklyn and Queens in New York City (Visiting Nurse Service of New York in partnership with United-Healthcare Services, Inc.–Evercare)
- Chicago (Aetna Health Management)
- District of Columbia and Maryland (American Healthways, Inc.)
- Central Florida (Humana, Inc.)
- Georgia (CIGNA HealthCare)
- Mississippi (McKesson Health Solutions)
- Oklahoma (LifeMasters Supported SelfCare, Inc.)
- Pennsylvania (Health Dialog Services Corporation)
- Tennessee (XLHealth)
Performance-based contracting is one of the most important features of the CCIP design. The CCIPs will be paid based on achieving measurable improvements in clinical and financial outcomes, as well as satisfaction levels across their assigned populations. Payment is not based on services provided. CCIP organizations will be paid monthly fees, but those fees will be fully at risk. The organizations will be required to refund some or all of their fees to the federal government if they do not meet agreed-upon standards for quality improvement, savings to Medicare, and increased beneficiary satisfaction levels.
Phase I programs will collectively serve 150,000 to 300,000 chronically ill beneficiaries who are enrolled in traditional fee-for-service Medicare. This is the phase currentlyunder development, with the first programs expected to begin implementation in spring 2005. The programs are intended to help increase adherence to evidence-based care, reduce unnecessary hospital stays and emergency room visits, and help beneficiaries avoid costly and debilitating complications and comorbidities. With attention to reducing hospital costs, hospitalists may play an important role in CCIPs.
CCIPs include collaboration with participants’ providers to improve communication regarding relevant clinical information. The programs are being designed to assist beneficiaries in managing all of their health problems (not just a single disease). The programs to be tested vary in types of interventions to be used to improve outcomes. Across all programs, payments will be based on performance results.
Patient participation will be entirely voluntary. Eligible beneficiaries do not have to change plans or providers to participate, and there is no charge to the beneficiaries to participate. Once the program begins, beneficiaries may stop participating at any time. These programs may not restrict access to care. CMS will use historical claims data to identify beneficiaries by geographic area and screen them for eligibility. The selected beneficiaries will be assigned randomly to either an intervention group or a control group. Those in the intervention group will be notified of the opportunity to participate via a letter from the Medicare program. The letter will describe the CCIP and give the beneficiary the opportunity to decline to participate.
Phase II, which is the expansion of successful CCIPs, may begin within 2 to 31/2 years after Phase I. Entire CCIPs, or components of programs, may be expanded either regionally or nationally. SHM will continue to track the progress of the CCIPs and to encourage members to participate in the development and implementation of this exciting new chapter of Medicare services.
Please check the list above. If you are interested in partnering with any of the organizations, please email Lillian Higgins at lhiggins@hospitalistmedicine.org. She will provide you with contact information for the CCIP vendor.
The Medicare Modernization Act of 2003 (MMA) authorized development and testing of voluntary programs focused on improving the quality of care and quality of life for beneficiaries with multiple chronic illnesses. These Chronic Care Improvement Programs (CCIPs) represent the first large-scale chronic care improvement initiative under the Medicare fee-for-service (FFS) program. The programs also may represent an opportunity for SHM members to partner with the selected organizations.
CMS selected organizations that will offer self-care guidance and support to chronically ill beneficiaries. These organizations will help beneficiaries manage their health, adhere to their physicians’ plans of care, and assure that they seek or obtain medical care as needed to reduce their health risks. Chronic conditions are currently a leading cause of illness, disability, and death among beneficiaries and account for a disproportionate share of health care expenditures.
Each selected organization may design its own program, with the potential for a variety of unique models. Some vendors are partnering with physician groups and others may reach out to physicians in their regions. The selected regions and respective vendors are:
- Brooklyn and Queens in New York City (Visiting Nurse Service of New York in partnership with United-Healthcare Services, Inc.–Evercare)
- Chicago (Aetna Health Management)
- District of Columbia and Maryland (American Healthways, Inc.)
- Central Florida (Humana, Inc.)
- Georgia (CIGNA HealthCare)
- Mississippi (McKesson Health Solutions)
- Oklahoma (LifeMasters Supported SelfCare, Inc.)
- Pennsylvania (Health Dialog Services Corporation)
- Tennessee (XLHealth)
Performance-based contracting is one of the most important features of the CCIP design. The CCIPs will be paid based on achieving measurable improvements in clinical and financial outcomes, as well as satisfaction levels across their assigned populations. Payment is not based on services provided. CCIP organizations will be paid monthly fees, but those fees will be fully at risk. The organizations will be required to refund some or all of their fees to the federal government if they do not meet agreed-upon standards for quality improvement, savings to Medicare, and increased beneficiary satisfaction levels.
Phase I programs will collectively serve 150,000 to 300,000 chronically ill beneficiaries who are enrolled in traditional fee-for-service Medicare. This is the phase currentlyunder development, with the first programs expected to begin implementation in spring 2005. The programs are intended to help increase adherence to evidence-based care, reduce unnecessary hospital stays and emergency room visits, and help beneficiaries avoid costly and debilitating complications and comorbidities. With attention to reducing hospital costs, hospitalists may play an important role in CCIPs.
CCIPs include collaboration with participants’ providers to improve communication regarding relevant clinical information. The programs are being designed to assist beneficiaries in managing all of their health problems (not just a single disease). The programs to be tested vary in types of interventions to be used to improve outcomes. Across all programs, payments will be based on performance results.
Patient participation will be entirely voluntary. Eligible beneficiaries do not have to change plans or providers to participate, and there is no charge to the beneficiaries to participate. Once the program begins, beneficiaries may stop participating at any time. These programs may not restrict access to care. CMS will use historical claims data to identify beneficiaries by geographic area and screen them for eligibility. The selected beneficiaries will be assigned randomly to either an intervention group or a control group. Those in the intervention group will be notified of the opportunity to participate via a letter from the Medicare program. The letter will describe the CCIP and give the beneficiary the opportunity to decline to participate.
Phase II, which is the expansion of successful CCIPs, may begin within 2 to 31/2 years after Phase I. Entire CCIPs, or components of programs, may be expanded either regionally or nationally. SHM will continue to track the progress of the CCIPs and to encourage members to participate in the development and implementation of this exciting new chapter of Medicare services.
Please check the list above. If you are interested in partnering with any of the organizations, please email Lillian Higgins at lhiggins@hospitalistmedicine.org. She will provide you with contact information for the CCIP vendor.
The Medicare Modernization Act of 2003 (MMA) authorized development and testing of voluntary programs focused on improving the quality of care and quality of life for beneficiaries with multiple chronic illnesses. These Chronic Care Improvement Programs (CCIPs) represent the first large-scale chronic care improvement initiative under the Medicare fee-for-service (FFS) program. The programs also may represent an opportunity for SHM members to partner with the selected organizations.
CMS selected organizations that will offer self-care guidance and support to chronically ill beneficiaries. These organizations will help beneficiaries manage their health, adhere to their physicians’ plans of care, and assure that they seek or obtain medical care as needed to reduce their health risks. Chronic conditions are currently a leading cause of illness, disability, and death among beneficiaries and account for a disproportionate share of health care expenditures.
Each selected organization may design its own program, with the potential for a variety of unique models. Some vendors are partnering with physician groups and others may reach out to physicians in their regions. The selected regions and respective vendors are:
- Brooklyn and Queens in New York City (Visiting Nurse Service of New York in partnership with United-Healthcare Services, Inc.–Evercare)
- Chicago (Aetna Health Management)
- District of Columbia and Maryland (American Healthways, Inc.)
- Central Florida (Humana, Inc.)
- Georgia (CIGNA HealthCare)
- Mississippi (McKesson Health Solutions)
- Oklahoma (LifeMasters Supported SelfCare, Inc.)
- Pennsylvania (Health Dialog Services Corporation)
- Tennessee (XLHealth)
Performance-based contracting is one of the most important features of the CCIP design. The CCIPs will be paid based on achieving measurable improvements in clinical and financial outcomes, as well as satisfaction levels across their assigned populations. Payment is not based on services provided. CCIP organizations will be paid monthly fees, but those fees will be fully at risk. The organizations will be required to refund some or all of their fees to the federal government if they do not meet agreed-upon standards for quality improvement, savings to Medicare, and increased beneficiary satisfaction levels.
Phase I programs will collectively serve 150,000 to 300,000 chronically ill beneficiaries who are enrolled in traditional fee-for-service Medicare. This is the phase currentlyunder development, with the first programs expected to begin implementation in spring 2005. The programs are intended to help increase adherence to evidence-based care, reduce unnecessary hospital stays and emergency room visits, and help beneficiaries avoid costly and debilitating complications and comorbidities. With attention to reducing hospital costs, hospitalists may play an important role in CCIPs.
CCIPs include collaboration with participants’ providers to improve communication regarding relevant clinical information. The programs are being designed to assist beneficiaries in managing all of their health problems (not just a single disease). The programs to be tested vary in types of interventions to be used to improve outcomes. Across all programs, payments will be based on performance results.
Patient participation will be entirely voluntary. Eligible beneficiaries do not have to change plans or providers to participate, and there is no charge to the beneficiaries to participate. Once the program begins, beneficiaries may stop participating at any time. These programs may not restrict access to care. CMS will use historical claims data to identify beneficiaries by geographic area and screen them for eligibility. The selected beneficiaries will be assigned randomly to either an intervention group or a control group. Those in the intervention group will be notified of the opportunity to participate via a letter from the Medicare program. The letter will describe the CCIP and give the beneficiary the opportunity to decline to participate.
Phase II, which is the expansion of successful CCIPs, may begin within 2 to 31/2 years after Phase I. Entire CCIPs, or components of programs, may be expanded either regionally or nationally. SHM will continue to track the progress of the CCIPs and to encourage members to participate in the development and implementation of this exciting new chapter of Medicare services.
Please check the list above. If you are interested in partnering with any of the organizations, please email Lillian Higgins at lhiggins@hospitalistmedicine.org. She will provide you with contact information for the CCIP vendor.
SHM Elects Jack Percelay, MD, FAAP, to newly Created Pediatrics Seat on Board of Directors

SHM has created a new seat on the Board of Directors that must be filled by a pediatric hospitalist and has elected Jack Percelay, MD, FAAP as its new pediatric board member. Dr. Percelay began serving a 1-year term on the SHM board beginning April 29, 2005. In the Fall of 2005, during the next board elections, the new position will become a 3-year pediatric board seat.
“The addition of a pediatrics seat to the board is important because pediatric hospitalists have a unique and important perspective on our growing specialty of hospital medicine,” said new SHM President, Steven Pantilat, MD, FACP. “Jack Percelay has long been a leader in field of pediatric hospital medicine, has nurtured the development of pediatric hospitalists, and has been a key link in our work with the American Academy of Pediatrics for many years now. We welcome his insights and vision as we continue to expand the role of education and leadership for pediatric hospitalists.”
“For many years SHM has had a pediatrician represented on the board―first with Mike Ruhlen from Toledo and more recently with David Zipes from Indianapolis,“ added SHM immediate past President Jeanne Huddleston. “At this stage in the growth of hospital medicine, the SHM board felt it was important to ensure that we continue to have a pediatric voice represented on the board.”
Dr. Percelay currently is director, Virtua Inpatient Pediatrics and CARES at Children’s Health Associates in Vorhees, NJ. Virtua Inpatient Pediatrics is a 13-person pediatric hospitalist group providing coverage at West Jersey Vorhees and Burlington Memorial Hospitals in southern New Jersey. The group covers the pediatric ward, pediatric ICU and emergency room.
In 2003, Dr. Percelay coauthored a survey initiated by the American Association of Pediatrics entitled “Attitudes Toward and Experiences with Pediatric Hospitalists: A National Survey.” The goal of the survey was to explore the extent to which the pediatric hospitalist practice has developed and to examine pediatricians’ attitudes and experiences with pediatric hospitalists. It was the first survey the AAP has conducted on hospitalists.
Dr. Percelay also was a lead author for the recent AAP Policy statement “Guiding Principles for Pediatric Hospitalist Programs” (Pediatrics 2005;115: 11012).
A charter member of SHM, Dr. Percelay has served on numerous committees, including chair of the Pediatric Committee and a member of the Public Policy committee.
SHM has created a new seat on the Board of Directors that must be filled by a pediatric hospitalist and has elected Jack Percelay, MD, FAAP as its new pediatric board member. Dr. Percelay began serving a 1-year term on the SHM board beginning April 29, 2005. In the Fall of 2005, during the next board elections, the new position will become a 3-year pediatric board seat.
“The addition of a pediatrics seat to the board is important because pediatric hospitalists have a unique and important perspective on our growing specialty of hospital medicine,” said new SHM President, Steven Pantilat, MD, FACP. “Jack Percelay has long been a leader in field of pediatric hospital medicine, has nurtured the development of pediatric hospitalists, and has been a key link in our work with the American Academy of Pediatrics for many years now. We welcome his insights and vision as we continue to expand the role of education and leadership for pediatric hospitalists.”
“For many years SHM has had a pediatrician represented on the board―first with Mike Ruhlen from Toledo and more recently with David Zipes from Indianapolis,“ added SHM immediate past President Jeanne Huddleston. “At this stage in the growth of hospital medicine, the SHM board felt it was important to ensure that we continue to have a pediatric voice represented on the board.”
Dr. Percelay currently is director, Virtua Inpatient Pediatrics and CARES at Children’s Health Associates in Vorhees, NJ. Virtua Inpatient Pediatrics is a 13-person pediatric hospitalist group providing coverage at West Jersey Vorhees and Burlington Memorial Hospitals in southern New Jersey. The group covers the pediatric ward, pediatric ICU and emergency room.
In 2003, Dr. Percelay coauthored a survey initiated by the American Association of Pediatrics entitled “Attitudes Toward and Experiences with Pediatric Hospitalists: A National Survey.” The goal of the survey was to explore the extent to which the pediatric hospitalist practice has developed and to examine pediatricians’ attitudes and experiences with pediatric hospitalists. It was the first survey the AAP has conducted on hospitalists.
Dr. Percelay also was a lead author for the recent AAP Policy statement “Guiding Principles for Pediatric Hospitalist Programs” (Pediatrics 2005;115: 11012).
A charter member of SHM, Dr. Percelay has served on numerous committees, including chair of the Pediatric Committee and a member of the Public Policy committee.
SHM has created a new seat on the Board of Directors that must be filled by a pediatric hospitalist and has elected Jack Percelay, MD, FAAP as its new pediatric board member. Dr. Percelay began serving a 1-year term on the SHM board beginning April 29, 2005. In the Fall of 2005, during the next board elections, the new position will become a 3-year pediatric board seat.
“The addition of a pediatrics seat to the board is important because pediatric hospitalists have a unique and important perspective on our growing specialty of hospital medicine,” said new SHM President, Steven Pantilat, MD, FACP. “Jack Percelay has long been a leader in field of pediatric hospital medicine, has nurtured the development of pediatric hospitalists, and has been a key link in our work with the American Academy of Pediatrics for many years now. We welcome his insights and vision as we continue to expand the role of education and leadership for pediatric hospitalists.”
“For many years SHM has had a pediatrician represented on the board―first with Mike Ruhlen from Toledo and more recently with David Zipes from Indianapolis,“ added SHM immediate past President Jeanne Huddleston. “At this stage in the growth of hospital medicine, the SHM board felt it was important to ensure that we continue to have a pediatric voice represented on the board.”
Dr. Percelay currently is director, Virtua Inpatient Pediatrics and CARES at Children’s Health Associates in Vorhees, NJ. Virtua Inpatient Pediatrics is a 13-person pediatric hospitalist group providing coverage at West Jersey Vorhees and Burlington Memorial Hospitals in southern New Jersey. The group covers the pediatric ward, pediatric ICU and emergency room.
In 2003, Dr. Percelay coauthored a survey initiated by the American Association of Pediatrics entitled “Attitudes Toward and Experiences with Pediatric Hospitalists: A National Survey.” The goal of the survey was to explore the extent to which the pediatric hospitalist practice has developed and to examine pediatricians’ attitudes and experiences with pediatric hospitalists. It was the first survey the AAP has conducted on hospitalists.
Dr. Percelay also was a lead author for the recent AAP Policy statement “Guiding Principles for Pediatric Hospitalist Programs” (Pediatrics 2005;115: 11012).
A charter member of SHM, Dr. Percelay has served on numerous committees, including chair of the Pediatric Committee and a member of the Public Policy committee.
Managing Physician Performance in Hospital Medicine
Joel Barker describes leadership as “…the ability to take people where they otherwise would not go.” In other words, leadership is about creating change in something that exists today. Management, on the other hand, may be considered a series of steps to ensure that things happen the desired and consistent way. Although this article is not of scope sufficient to explore the differences between management and leadership, it will address a domain in which the 2 intimately intersect. Managing others relies upon many foundations of leadership, such as establishing the group’s vision and setting key strategic goals. In like manner, successful leadership in stimulating change is dependent on the effective management of personnel to ensure that the culture, work habits, outcomes, and behaviors are consistent with the change efforts. This article will focus on the management of physicians in hospital medicine groups. The 8 steps outlined are applicable regardless of employer type, group size, or mission. Almost all of the skills necessary to effectively implement a performance management system can be learned and are best practiced on a regular basis. Furthermore, there are many existing resources for further education and development in these areas based on one’s current level of competency.
The author wishes to acknowledge the faculty of the American College of Physician Executives for their work in assembling many of the concepts found in this article. The course “Managing Physician Performance in Organizations” serves to underscore an integrated model of performance management and explores some of the theoretical bases of human behavior not included here.
Defining Your Group
Before you can manage performance, you must know the parameters by which the group is defined. The prerequisites for performance management include salient statements of mission, vision, and values. The mission defines the purpose for the group being in place and usually reflects the interests of the hospital(s) or medical group affiliated with or actually employing the hospital medicine group. The mission statement should be able to answer the questions “Why does our hospital medicine group exist? What purpose does it serve? In very broad terms, what scope of services do we provide?” The vision is a concise summary of what the group would like to be or achieve in the future, and it may relate to growth, range of services, outcomes, or other dimensions. Most often the vision is the leader’s platform for change in order to articulate the rationale for creating a better future. Values are those characteristics that guide decision making and provide guidance for everyone’s expected behavior and conduct in the group. Values can be thought of as the “lens” through which the vision is carried out and the mission upheld.
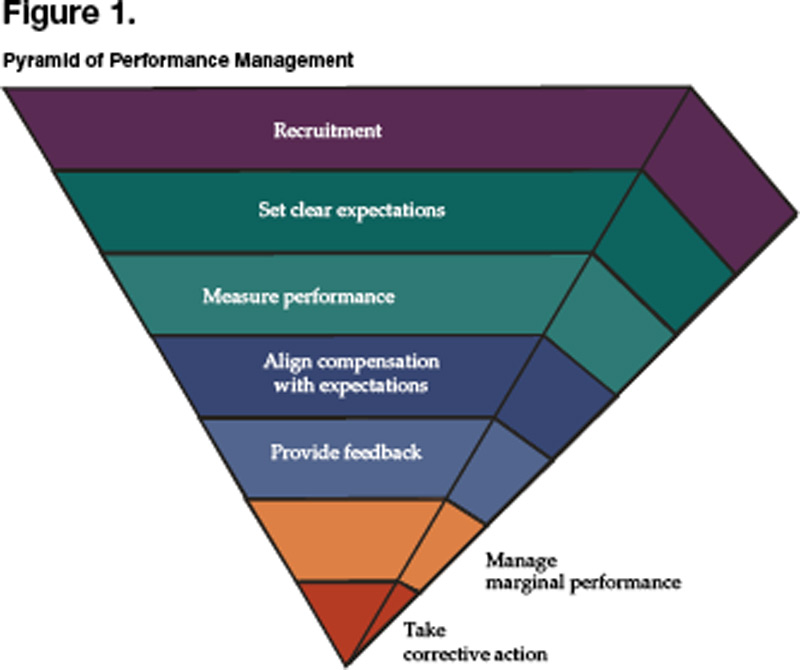
From the mission, vision, and values come strategies for achieving successful change and the more specific goals that the group is to attain. In some cases the group may have undertaken a formal strategic planning process that rendered a series of goals, objectives, and/or programs to be carried out in the immediate to intermediate term. We now reach the vital area in which a well structured and supported performance management system can play a pivotal role in ensuring the successful implementation of strategic thinking. Until now, the thought and planning process had focused on the right thing to do. From here, the focus becomes doing things right. Once you have completely answered the questions above and have a confident sense of where your group is heading and why, then the steps that follow will enable you to stack the deck in favor of achieving the level of performance you desire. Note that each step is embedded in action. Figure 1 represents the pyramid of performance management, a prioritized approach to managing others.
Recruiting the Right People
Not everyone has the luxury of personally hiring each physician in their group, much less having a surplus of candidates that are outstanding in every dimension. The reality in 2005 is that there continues to be demand for hospitalists far exceeding the available supply. This “seller’s market” (i.e., a hospitalist “sells” his or her services to an employer) represents a challenging dynamic for new or growing hospital medicine groups attempting to recruit the top candidates. It gets even worse when you consider hospital medicine as a new specialty, often finding itself in hospitals where the medical staff are skeptical or apprehensive in accepting the new group, and one bad hire can undermine the group’s chances of success. Furthermore, there may not be adequate experience or expertise in recruiting new physicians or correctly identifying those who would be a proper fit for the group. So how does one go about recruiting the right people?
Planning begins with having defined the group in terms of the mission and values. Knowing the vision and specific strategies to be employed lends insight into what type of individual would best fit with the needs and culture of the group. It is important to list the desired qualities on paper and plan for assessing each one, knowing that there is no perfect candidate and these characteristics must therefore be prioritized. Remember, what makes a good hospitalist in your group does not mean they will be good somewhere else; be sure you define very clearly what exactly “good” means. At the same time, it is also critical to outline the selling points of potentially joining your group in terms of 3 areas: the practice itself, compensation, and location.
The next step consists of preparing a slate of candidates for interviews. There are many methods of finding (i.e., sourcing) strong candidates, one of the best of which is to ask members of your current group or other trusted colleagues for referrals. If you are interested in filling a position with a more specific skill set such as information technology, palliative care, or clinical teaching, then a “make or buy” decision needs to be made to either recruit for the individual already in possession of such credentials or to hire more generically and then train accordingly. Once candidates are identified, a deliberate process of reviewing their written materials and interviewing them by telephone will determine the appropriateness of an in person interview. Speaking with references can occur at any time, and some advocate for this to occur prior to bringing a candidate for formal interview, as another mechanism of screening and to focus interview questions on site. The formal interview itself should be well structured and enable your key stakeholders to meet with the candidate and submit an immediate assessment. The shorter the turnaround time to extend an offer, the more decisive and committed to the candidate you will appear. Likewise, if you have a diverse composition of interviewers who weigh in with their perspectives, then there should be little to delay a hiring decision.
There are 3 additional points to remember when looking to hire an additional hospitalist into your group. First, it is estimated that 70% of physicians who leave a job do so because of spousal discontent. To mitigate this possibility, invite the spouse to accompany the candidate to the interview location, and assemble a parallel agenda for him or her.. Do not consider yourself on a “best behavior” basis during courtship alone; you need to continue nurturing the candidate and family well into the first year of employment to ensure a good transition. Second, be realistic about your expectations. There is no perfect candidate, so you must prioritize those qualities you want most from them. If you wait for perfection, the delay will cause you to overlook many very good physicians. Finally, take another look at the performance management pyramid. The reason the area for recruitment is so large is because of the disproportionate amount of time that one should invest in recruitment processes. Hiring the right people up front will make the rest of the steps far easier and minimize the likelihood of your being drawn into the nadir of the pyramid.
Setting Clear Expectations
Do you have a job description? When you read it, does it adequately describe what is expected of your hospitalists? Do you have an orientation for new members to your group? How long does it last? Is additional training offered? Are there outcomes that you expect from this training? And once you have oriented, trained, and offered a job description, does the actual work environment support or negate your efforts―i.e., does culture trump your formal process?
The cycle of setting clear expectations about work performance begins during the recruitment phase. Being absolutely forthcoming about what it is like to work in your group and what you expect from each and every member is paramount to allow both you and the candidate to determine a good fit. Once the physician has joined your group, orientation and training should hardly be a 1-, 2- or 3-day exercise. These are continuous and ongoing processes, given our rapidly changing practice environment. In fact, change is one of the only reliable characteristics of what we do, and extending the welcome “The job you take today is unlikely to be the job you will have next year” is hardly inappropriate. Be mindful that setting clear expectations with all of your hospitalists is the bedrock of a functional performance management system. Defining expectations alone will often improve performance, vis-à-vis the Hawthorne effect.
Expectations should always be depersonalized and focus on behavior. Behavior itself may be regarded in 2 distinct domains: those behaviors that are observed, and those outcomes that are measurable. Examples of observable behaviors include interpersonal interactions with nurses and consultants, pager response times, and attendance at monthly team meetings. Measurable outcomes include work RVU productivity, patient satisfaction, readmission rates, and compliance with coding and documentation guidelines. There are many ways to organize dimensions of performance that you may expect from your physicians―the 6 aims of quality (safe, timely, effective, efficient, equitable, and patient centered, as outlined in the IOM report Crossing the Quality Chasm), maintenance of a healthy workplace, citizenship, relationships with others, etc.―yet the key is to define and communicate them, then check often for understanding.
Measuring Actual Performance
Be the first to admit “the numbers are wrong,” and you will save hearing it from many others. There are many inherent problems in measuring actual performance, and the data may never be perfect. As an exercise, try assigning individual readmission rates within your group, and you will find that because of handoffs within the group and lack of precision in identifying who actually discharged the patient, there will be many arguments over whether the data is valid. However, in most circumstances, if the data is flawed, it still may serve a strong purpose to highlight the relative variation within the group. Searching for quantifiable systemic data and being transparent about the limitations of the data will be an exercise worth undertaking. In like manner, behavioral observation data are potentially fraught with conflict if the data are focused on judgment of character traits (I believe this hospitalist has a good bedside manner) rather than on observable behaviors (This hospitalist always/sometimes/never comes to meetings on time). Measures are best when they are objective, relevant to the position, and interpretable. Remember: All measures are flawed; some are useful.
Aligning Compensation With Expectations
Conventional wisdom states that people will do more of what they are incentivized to do. The corollary to this is to be sure what you incentivize is actually what you want. For the group that is trying to improve individual productivity and reduce length of stay, providing financial rewards for work RVU’s alone may result in less assertiveness in managing timely discharges and bickering over who picks up the 11 p.m. vs. 2 a.m. overnight admission the following morning. Ultimately, compensation must be intimately linked with the mission of the group, and tremendous care must be taken in determining the construct of any system. Although it is well beyond the scope of this article to detail the many considerations of designing a compensation system, one must understand that it is only one component―and not the most important component―of a performance management program.
Here are a few points to consider as you integrate your compensation system into the rest of the steps in the pyramid:
- A straight salary with or without a “guaranteed” bonus is unlikely to reward or motivate any new behaviors.
- For a performance-based compensation plan to have sufficient impact, at least 20%–30% of compensation must be tied to performance.
- Consider having both group and individual measures as part of your plan to engender a sense of teamwork and collective effort in performing well.
- Limit the number of variables in the plan to 3–5; otherwise, measures are too diluted to carry meaningful weight.
- Perform a local market comparison for benchmarking your goal median compensation; often administrative staff are more willing to share this information with other administrative staff if the understanding is that all market results will be shared.
- The process of constructing or evolving your plan, being inclusive of members of your group as well as any group sponsors, ends up being far more valuable than the final plan itself.
Providing Regular Feedback
Have you ever had a complaint that sounded like “I get way too much feedback around here?” Probably not. More likely is the case that your hospitalists wonder how they stand in terms of being compared to others and to themselves over time. The creed “no news must be good news” is hardly supportive of promoting top performance. Feedback itself can be highly influential and reflects the expectations explained by the group leader. Expectations not measured or fed back to the individual hospitalists will be expectations soon forgotten or ignored, because they may be felt not to matter.
Effective feedback is both formal and informal. The annual performance review is a common example of the former, but it is in no way meant to be the only feedback a hospitalist should receive, nor is it the most powerful. The annual review should be well structured, can outline longer term goals and ideas for self-improvement, and may serve in some key administrative functions like compensation and promotion. Informal, regular feedback, however, may serve you much better in driving performance, because it is timelier, more relevant to daily work, and more specific to the individual. Individuals also respond much more constructively to positive feedback, and some experts believe the ratio of positive to negative feedback should be on the order of 9 to 1. Be sure that feedback is done in a coaching manner and focuses on the behavior (You may try sitting down when you talk with patients as a way of making them feel more at ease) rather than on the person themselves (You’re really not a good communicator).
Managing Marginal Performance
Marginal performance can be defined as a physician whose observed behaviors or measured outcomes are at significant variance from what is expected. This pattern takes place over time and happens in spite of having in place all the other elements of a performance management system. Consider the “clock puncher” who rarely helps out the rest of the team on busy days and never shows up to group meetings or committees. Or the “tortoise” that has wonderful staff relations but chronically arrives at work late and repeatedly forgets to submit inpatient charges. Then there’s the “hothead” who is clinically adept and has high patient satisfaction but loses his or her temper with nursing and is pervasively confrontational with consultants. The steps to be taken in these and other cases like them include ensuring adequate documentation, reaching an agreement with the individual in recognizing that there is a problem, generating options for causality, negotiating a contract for improvement, and then letting future behavior determine the consequences.
Taking Corrective Action
Sometimes you simply cannot fix everything, and you need to be easy on yourself for having reached the point where the situation is no longer remediable in spite of your best efforts. In the end, everyone will be better off. When physician conduct becomes detrimental to patient safety, staff safety or quality patient care; is disruptive to the organization; or is otherwise chronically aberrant, then it is time to take adverse action. Since there are many pitfalls that have HR and legal implications, it is advisable to consult with relevant personnel to avoid problems with inadequate documentation and the potential need to report actions to state agencies and the National Practitioner Data Bank (per the Healthcare Quality Improvement Act of 1986).
Resources
- Ury W, Fisher R. Getting to Yes: Negotiating Agreement Without Giving In. 2nd ed. New York: Penguin Books; 1991.
- Reinertsen J. Physicians as leaders in the improvement of health care systems. Ann Intern Med. 1998;128:833-8.
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
- American College of Physician Executives. Managing Physician Performance in Organizations. Ongoing courses available at www.acpe.org.
Joel Barker describes leadership as “…the ability to take people where they otherwise would not go.” In other words, leadership is about creating change in something that exists today. Management, on the other hand, may be considered a series of steps to ensure that things happen the desired and consistent way. Although this article is not of scope sufficient to explore the differences between management and leadership, it will address a domain in which the 2 intimately intersect. Managing others relies upon many foundations of leadership, such as establishing the group’s vision and setting key strategic goals. In like manner, successful leadership in stimulating change is dependent on the effective management of personnel to ensure that the culture, work habits, outcomes, and behaviors are consistent with the change efforts. This article will focus on the management of physicians in hospital medicine groups. The 8 steps outlined are applicable regardless of employer type, group size, or mission. Almost all of the skills necessary to effectively implement a performance management system can be learned and are best practiced on a regular basis. Furthermore, there are many existing resources for further education and development in these areas based on one’s current level of competency.
The author wishes to acknowledge the faculty of the American College of Physician Executives for their work in assembling many of the concepts found in this article. The course “Managing Physician Performance in Organizations” serves to underscore an integrated model of performance management and explores some of the theoretical bases of human behavior not included here.
Defining Your Group
Before you can manage performance, you must know the parameters by which the group is defined. The prerequisites for performance management include salient statements of mission, vision, and values. The mission defines the purpose for the group being in place and usually reflects the interests of the hospital(s) or medical group affiliated with or actually employing the hospital medicine group. The mission statement should be able to answer the questions “Why does our hospital medicine group exist? What purpose does it serve? In very broad terms, what scope of services do we provide?” The vision is a concise summary of what the group would like to be or achieve in the future, and it may relate to growth, range of services, outcomes, or other dimensions. Most often the vision is the leader’s platform for change in order to articulate the rationale for creating a better future. Values are those characteristics that guide decision making and provide guidance for everyone’s expected behavior and conduct in the group. Values can be thought of as the “lens” through which the vision is carried out and the mission upheld.
From the mission, vision, and values come strategies for achieving successful change and the more specific goals that the group is to attain. In some cases the group may have undertaken a formal strategic planning process that rendered a series of goals, objectives, and/or programs to be carried out in the immediate to intermediate term. We now reach the vital area in which a well structured and supported performance management system can play a pivotal role in ensuring the successful implementation of strategic thinking. Until now, the thought and planning process had focused on the right thing to do. From here, the focus becomes doing things right. Once you have completely answered the questions above and have a confident sense of where your group is heading and why, then the steps that follow will enable you to stack the deck in favor of achieving the level of performance you desire. Note that each step is embedded in action. Figure 1 represents the pyramid of performance management, a prioritized approach to managing others.
Recruiting the Right People
Not everyone has the luxury of personally hiring each physician in their group, much less having a surplus of candidates that are outstanding in every dimension. The reality in 2005 is that there continues to be demand for hospitalists far exceeding the available supply. This “seller’s market” (i.e., a hospitalist “sells” his or her services to an employer) represents a challenging dynamic for new or growing hospital medicine groups attempting to recruit the top candidates. It gets even worse when you consider hospital medicine as a new specialty, often finding itself in hospitals where the medical staff are skeptical or apprehensive in accepting the new group, and one bad hire can undermine the group’s chances of success. Furthermore, there may not be adequate experience or expertise in recruiting new physicians or correctly identifying those who would be a proper fit for the group. So how does one go about recruiting the right people?
Planning begins with having defined the group in terms of the mission and values. Knowing the vision and specific strategies to be employed lends insight into what type of individual would best fit with the needs and culture of the group. It is important to list the desired qualities on paper and plan for assessing each one, knowing that there is no perfect candidate and these characteristics must therefore be prioritized. Remember, what makes a good hospitalist in your group does not mean they will be good somewhere else; be sure you define very clearly what exactly “good” means. At the same time, it is also critical to outline the selling points of potentially joining your group in terms of 3 areas: the practice itself, compensation, and location.
The next step consists of preparing a slate of candidates for interviews. There are many methods of finding (i.e., sourcing) strong candidates, one of the best of which is to ask members of your current group or other trusted colleagues for referrals. If you are interested in filling a position with a more specific skill set such as information technology, palliative care, or clinical teaching, then a “make or buy” decision needs to be made to either recruit for the individual already in possession of such credentials or to hire more generically and then train accordingly. Once candidates are identified, a deliberate process of reviewing their written materials and interviewing them by telephone will determine the appropriateness of an in person interview. Speaking with references can occur at any time, and some advocate for this to occur prior to bringing a candidate for formal interview, as another mechanism of screening and to focus interview questions on site. The formal interview itself should be well structured and enable your key stakeholders to meet with the candidate and submit an immediate assessment. The shorter the turnaround time to extend an offer, the more decisive and committed to the candidate you will appear. Likewise, if you have a diverse composition of interviewers who weigh in with their perspectives, then there should be little to delay a hiring decision.
There are 3 additional points to remember when looking to hire an additional hospitalist into your group. First, it is estimated that 70% of physicians who leave a job do so because of spousal discontent. To mitigate this possibility, invite the spouse to accompany the candidate to the interview location, and assemble a parallel agenda for him or her.. Do not consider yourself on a “best behavior” basis during courtship alone; you need to continue nurturing the candidate and family well into the first year of employment to ensure a good transition. Second, be realistic about your expectations. There is no perfect candidate, so you must prioritize those qualities you want most from them. If you wait for perfection, the delay will cause you to overlook many very good physicians. Finally, take another look at the performance management pyramid. The reason the area for recruitment is so large is because of the disproportionate amount of time that one should invest in recruitment processes. Hiring the right people up front will make the rest of the steps far easier and minimize the likelihood of your being drawn into the nadir of the pyramid.
Setting Clear Expectations
Do you have a job description? When you read it, does it adequately describe what is expected of your hospitalists? Do you have an orientation for new members to your group? How long does it last? Is additional training offered? Are there outcomes that you expect from this training? And once you have oriented, trained, and offered a job description, does the actual work environment support or negate your efforts―i.e., does culture trump your formal process?
The cycle of setting clear expectations about work performance begins during the recruitment phase. Being absolutely forthcoming about what it is like to work in your group and what you expect from each and every member is paramount to allow both you and the candidate to determine a good fit. Once the physician has joined your group, orientation and training should hardly be a 1-, 2- or 3-day exercise. These are continuous and ongoing processes, given our rapidly changing practice environment. In fact, change is one of the only reliable characteristics of what we do, and extending the welcome “The job you take today is unlikely to be the job you will have next year” is hardly inappropriate. Be mindful that setting clear expectations with all of your hospitalists is the bedrock of a functional performance management system. Defining expectations alone will often improve performance, vis-à-vis the Hawthorne effect.
Expectations should always be depersonalized and focus on behavior. Behavior itself may be regarded in 2 distinct domains: those behaviors that are observed, and those outcomes that are measurable. Examples of observable behaviors include interpersonal interactions with nurses and consultants, pager response times, and attendance at monthly team meetings. Measurable outcomes include work RVU productivity, patient satisfaction, readmission rates, and compliance with coding and documentation guidelines. There are many ways to organize dimensions of performance that you may expect from your physicians―the 6 aims of quality (safe, timely, effective, efficient, equitable, and patient centered, as outlined in the IOM report Crossing the Quality Chasm), maintenance of a healthy workplace, citizenship, relationships with others, etc.―yet the key is to define and communicate them, then check often for understanding.
Measuring Actual Performance
Be the first to admit “the numbers are wrong,” and you will save hearing it from many others. There are many inherent problems in measuring actual performance, and the data may never be perfect. As an exercise, try assigning individual readmission rates within your group, and you will find that because of handoffs within the group and lack of precision in identifying who actually discharged the patient, there will be many arguments over whether the data is valid. However, in most circumstances, if the data is flawed, it still may serve a strong purpose to highlight the relative variation within the group. Searching for quantifiable systemic data and being transparent about the limitations of the data will be an exercise worth undertaking. In like manner, behavioral observation data are potentially fraught with conflict if the data are focused on judgment of character traits (I believe this hospitalist has a good bedside manner) rather than on observable behaviors (This hospitalist always/sometimes/never comes to meetings on time). Measures are best when they are objective, relevant to the position, and interpretable. Remember: All measures are flawed; some are useful.
Aligning Compensation With Expectations
Conventional wisdom states that people will do more of what they are incentivized to do. The corollary to this is to be sure what you incentivize is actually what you want. For the group that is trying to improve individual productivity and reduce length of stay, providing financial rewards for work RVU’s alone may result in less assertiveness in managing timely discharges and bickering over who picks up the 11 p.m. vs. 2 a.m. overnight admission the following morning. Ultimately, compensation must be intimately linked with the mission of the group, and tremendous care must be taken in determining the construct of any system. Although it is well beyond the scope of this article to detail the many considerations of designing a compensation system, one must understand that it is only one component―and not the most important component―of a performance management program.
Here are a few points to consider as you integrate your compensation system into the rest of the steps in the pyramid:
- A straight salary with or without a “guaranteed” bonus is unlikely to reward or motivate any new behaviors.
- For a performance-based compensation plan to have sufficient impact, at least 20%–30% of compensation must be tied to performance.
- Consider having both group and individual measures as part of your plan to engender a sense of teamwork and collective effort in performing well.
- Limit the number of variables in the plan to 3–5; otherwise, measures are too diluted to carry meaningful weight.
- Perform a local market comparison for benchmarking your goal median compensation; often administrative staff are more willing to share this information with other administrative staff if the understanding is that all market results will be shared.
- The process of constructing or evolving your plan, being inclusive of members of your group as well as any group sponsors, ends up being far more valuable than the final plan itself.
Providing Regular Feedback
Have you ever had a complaint that sounded like “I get way too much feedback around here?” Probably not. More likely is the case that your hospitalists wonder how they stand in terms of being compared to others and to themselves over time. The creed “no news must be good news” is hardly supportive of promoting top performance. Feedback itself can be highly influential and reflects the expectations explained by the group leader. Expectations not measured or fed back to the individual hospitalists will be expectations soon forgotten or ignored, because they may be felt not to matter.
Effective feedback is both formal and informal. The annual performance review is a common example of the former, but it is in no way meant to be the only feedback a hospitalist should receive, nor is it the most powerful. The annual review should be well structured, can outline longer term goals and ideas for self-improvement, and may serve in some key administrative functions like compensation and promotion. Informal, regular feedback, however, may serve you much better in driving performance, because it is timelier, more relevant to daily work, and more specific to the individual. Individuals also respond much more constructively to positive feedback, and some experts believe the ratio of positive to negative feedback should be on the order of 9 to 1. Be sure that feedback is done in a coaching manner and focuses on the behavior (You may try sitting down when you talk with patients as a way of making them feel more at ease) rather than on the person themselves (You’re really not a good communicator).
Managing Marginal Performance
Marginal performance can be defined as a physician whose observed behaviors or measured outcomes are at significant variance from what is expected. This pattern takes place over time and happens in spite of having in place all the other elements of a performance management system. Consider the “clock puncher” who rarely helps out the rest of the team on busy days and never shows up to group meetings or committees. Or the “tortoise” that has wonderful staff relations but chronically arrives at work late and repeatedly forgets to submit inpatient charges. Then there’s the “hothead” who is clinically adept and has high patient satisfaction but loses his or her temper with nursing and is pervasively confrontational with consultants. The steps to be taken in these and other cases like them include ensuring adequate documentation, reaching an agreement with the individual in recognizing that there is a problem, generating options for causality, negotiating a contract for improvement, and then letting future behavior determine the consequences.
Taking Corrective Action
Sometimes you simply cannot fix everything, and you need to be easy on yourself for having reached the point where the situation is no longer remediable in spite of your best efforts. In the end, everyone will be better off. When physician conduct becomes detrimental to patient safety, staff safety or quality patient care; is disruptive to the organization; or is otherwise chronically aberrant, then it is time to take adverse action. Since there are many pitfalls that have HR and legal implications, it is advisable to consult with relevant personnel to avoid problems with inadequate documentation and the potential need to report actions to state agencies and the National Practitioner Data Bank (per the Healthcare Quality Improvement Act of 1986).
Resources
- Ury W, Fisher R. Getting to Yes: Negotiating Agreement Without Giving In. 2nd ed. New York: Penguin Books; 1991.
- Reinertsen J. Physicians as leaders in the improvement of health care systems. Ann Intern Med. 1998;128:833-8.
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
- American College of Physician Executives. Managing Physician Performance in Organizations. Ongoing courses available at www.acpe.org.
Joel Barker describes leadership as “…the ability to take people where they otherwise would not go.” In other words, leadership is about creating change in something that exists today. Management, on the other hand, may be considered a series of steps to ensure that things happen the desired and consistent way. Although this article is not of scope sufficient to explore the differences between management and leadership, it will address a domain in which the 2 intimately intersect. Managing others relies upon many foundations of leadership, such as establishing the group’s vision and setting key strategic goals. In like manner, successful leadership in stimulating change is dependent on the effective management of personnel to ensure that the culture, work habits, outcomes, and behaviors are consistent with the change efforts. This article will focus on the management of physicians in hospital medicine groups. The 8 steps outlined are applicable regardless of employer type, group size, or mission. Almost all of the skills necessary to effectively implement a performance management system can be learned and are best practiced on a regular basis. Furthermore, there are many existing resources for further education and development in these areas based on one’s current level of competency.
The author wishes to acknowledge the faculty of the American College of Physician Executives for their work in assembling many of the concepts found in this article. The course “Managing Physician Performance in Organizations” serves to underscore an integrated model of performance management and explores some of the theoretical bases of human behavior not included here.
Defining Your Group
Before you can manage performance, you must know the parameters by which the group is defined. The prerequisites for performance management include salient statements of mission, vision, and values. The mission defines the purpose for the group being in place and usually reflects the interests of the hospital(s) or medical group affiliated with or actually employing the hospital medicine group. The mission statement should be able to answer the questions “Why does our hospital medicine group exist? What purpose does it serve? In very broad terms, what scope of services do we provide?” The vision is a concise summary of what the group would like to be or achieve in the future, and it may relate to growth, range of services, outcomes, or other dimensions. Most often the vision is the leader’s platform for change in order to articulate the rationale for creating a better future. Values are those characteristics that guide decision making and provide guidance for everyone’s expected behavior and conduct in the group. Values can be thought of as the “lens” through which the vision is carried out and the mission upheld.
From the mission, vision, and values come strategies for achieving successful change and the more specific goals that the group is to attain. In some cases the group may have undertaken a formal strategic planning process that rendered a series of goals, objectives, and/or programs to be carried out in the immediate to intermediate term. We now reach the vital area in which a well structured and supported performance management system can play a pivotal role in ensuring the successful implementation of strategic thinking. Until now, the thought and planning process had focused on the right thing to do. From here, the focus becomes doing things right. Once you have completely answered the questions above and have a confident sense of where your group is heading and why, then the steps that follow will enable you to stack the deck in favor of achieving the level of performance you desire. Note that each step is embedded in action. Figure 1 represents the pyramid of performance management, a prioritized approach to managing others.
Recruiting the Right People
Not everyone has the luxury of personally hiring each physician in their group, much less having a surplus of candidates that are outstanding in every dimension. The reality in 2005 is that there continues to be demand for hospitalists far exceeding the available supply. This “seller’s market” (i.e., a hospitalist “sells” his or her services to an employer) represents a challenging dynamic for new or growing hospital medicine groups attempting to recruit the top candidates. It gets even worse when you consider hospital medicine as a new specialty, often finding itself in hospitals where the medical staff are skeptical or apprehensive in accepting the new group, and one bad hire can undermine the group’s chances of success. Furthermore, there may not be adequate experience or expertise in recruiting new physicians or correctly identifying those who would be a proper fit for the group. So how does one go about recruiting the right people?
Planning begins with having defined the group in terms of the mission and values. Knowing the vision and specific strategies to be employed lends insight into what type of individual would best fit with the needs and culture of the group. It is important to list the desired qualities on paper and plan for assessing each one, knowing that there is no perfect candidate and these characteristics must therefore be prioritized. Remember, what makes a good hospitalist in your group does not mean they will be good somewhere else; be sure you define very clearly what exactly “good” means. At the same time, it is also critical to outline the selling points of potentially joining your group in terms of 3 areas: the practice itself, compensation, and location.
The next step consists of preparing a slate of candidates for interviews. There are many methods of finding (i.e., sourcing) strong candidates, one of the best of which is to ask members of your current group or other trusted colleagues for referrals. If you are interested in filling a position with a more specific skill set such as information technology, palliative care, or clinical teaching, then a “make or buy” decision needs to be made to either recruit for the individual already in possession of such credentials or to hire more generically and then train accordingly. Once candidates are identified, a deliberate process of reviewing their written materials and interviewing them by telephone will determine the appropriateness of an in person interview. Speaking with references can occur at any time, and some advocate for this to occur prior to bringing a candidate for formal interview, as another mechanism of screening and to focus interview questions on site. The formal interview itself should be well structured and enable your key stakeholders to meet with the candidate and submit an immediate assessment. The shorter the turnaround time to extend an offer, the more decisive and committed to the candidate you will appear. Likewise, if you have a diverse composition of interviewers who weigh in with their perspectives, then there should be little to delay a hiring decision.
There are 3 additional points to remember when looking to hire an additional hospitalist into your group. First, it is estimated that 70% of physicians who leave a job do so because of spousal discontent. To mitigate this possibility, invite the spouse to accompany the candidate to the interview location, and assemble a parallel agenda for him or her.. Do not consider yourself on a “best behavior” basis during courtship alone; you need to continue nurturing the candidate and family well into the first year of employment to ensure a good transition. Second, be realistic about your expectations. There is no perfect candidate, so you must prioritize those qualities you want most from them. If you wait for perfection, the delay will cause you to overlook many very good physicians. Finally, take another look at the performance management pyramid. The reason the area for recruitment is so large is because of the disproportionate amount of time that one should invest in recruitment processes. Hiring the right people up front will make the rest of the steps far easier and minimize the likelihood of your being drawn into the nadir of the pyramid.
Setting Clear Expectations
Do you have a job description? When you read it, does it adequately describe what is expected of your hospitalists? Do you have an orientation for new members to your group? How long does it last? Is additional training offered? Are there outcomes that you expect from this training? And once you have oriented, trained, and offered a job description, does the actual work environment support or negate your efforts―i.e., does culture trump your formal process?
The cycle of setting clear expectations about work performance begins during the recruitment phase. Being absolutely forthcoming about what it is like to work in your group and what you expect from each and every member is paramount to allow both you and the candidate to determine a good fit. Once the physician has joined your group, orientation and training should hardly be a 1-, 2- or 3-day exercise. These are continuous and ongoing processes, given our rapidly changing practice environment. In fact, change is one of the only reliable characteristics of what we do, and extending the welcome “The job you take today is unlikely to be the job you will have next year” is hardly inappropriate. Be mindful that setting clear expectations with all of your hospitalists is the bedrock of a functional performance management system. Defining expectations alone will often improve performance, vis-à-vis the Hawthorne effect.
Expectations should always be depersonalized and focus on behavior. Behavior itself may be regarded in 2 distinct domains: those behaviors that are observed, and those outcomes that are measurable. Examples of observable behaviors include interpersonal interactions with nurses and consultants, pager response times, and attendance at monthly team meetings. Measurable outcomes include work RVU productivity, patient satisfaction, readmission rates, and compliance with coding and documentation guidelines. There are many ways to organize dimensions of performance that you may expect from your physicians―the 6 aims of quality (safe, timely, effective, efficient, equitable, and patient centered, as outlined in the IOM report Crossing the Quality Chasm), maintenance of a healthy workplace, citizenship, relationships with others, etc.―yet the key is to define and communicate them, then check often for understanding.
Measuring Actual Performance
Be the first to admit “the numbers are wrong,” and you will save hearing it from many others. There are many inherent problems in measuring actual performance, and the data may never be perfect. As an exercise, try assigning individual readmission rates within your group, and you will find that because of handoffs within the group and lack of precision in identifying who actually discharged the patient, there will be many arguments over whether the data is valid. However, in most circumstances, if the data is flawed, it still may serve a strong purpose to highlight the relative variation within the group. Searching for quantifiable systemic data and being transparent about the limitations of the data will be an exercise worth undertaking. In like manner, behavioral observation data are potentially fraught with conflict if the data are focused on judgment of character traits (I believe this hospitalist has a good bedside manner) rather than on observable behaviors (This hospitalist always/sometimes/never comes to meetings on time). Measures are best when they are objective, relevant to the position, and interpretable. Remember: All measures are flawed; some are useful.
Aligning Compensation With Expectations
Conventional wisdom states that people will do more of what they are incentivized to do. The corollary to this is to be sure what you incentivize is actually what you want. For the group that is trying to improve individual productivity and reduce length of stay, providing financial rewards for work RVU’s alone may result in less assertiveness in managing timely discharges and bickering over who picks up the 11 p.m. vs. 2 a.m. overnight admission the following morning. Ultimately, compensation must be intimately linked with the mission of the group, and tremendous care must be taken in determining the construct of any system. Although it is well beyond the scope of this article to detail the many considerations of designing a compensation system, one must understand that it is only one component―and not the most important component―of a performance management program.
Here are a few points to consider as you integrate your compensation system into the rest of the steps in the pyramid:
- A straight salary with or without a “guaranteed” bonus is unlikely to reward or motivate any new behaviors.
- For a performance-based compensation plan to have sufficient impact, at least 20%–30% of compensation must be tied to performance.
- Consider having both group and individual measures as part of your plan to engender a sense of teamwork and collective effort in performing well.
- Limit the number of variables in the plan to 3–5; otherwise, measures are too diluted to carry meaningful weight.
- Perform a local market comparison for benchmarking your goal median compensation; often administrative staff are more willing to share this information with other administrative staff if the understanding is that all market results will be shared.
- The process of constructing or evolving your plan, being inclusive of members of your group as well as any group sponsors, ends up being far more valuable than the final plan itself.
Providing Regular Feedback
Have you ever had a complaint that sounded like “I get way too much feedback around here?” Probably not. More likely is the case that your hospitalists wonder how they stand in terms of being compared to others and to themselves over time. The creed “no news must be good news” is hardly supportive of promoting top performance. Feedback itself can be highly influential and reflects the expectations explained by the group leader. Expectations not measured or fed back to the individual hospitalists will be expectations soon forgotten or ignored, because they may be felt not to matter.
Effective feedback is both formal and informal. The annual performance review is a common example of the former, but it is in no way meant to be the only feedback a hospitalist should receive, nor is it the most powerful. The annual review should be well structured, can outline longer term goals and ideas for self-improvement, and may serve in some key administrative functions like compensation and promotion. Informal, regular feedback, however, may serve you much better in driving performance, because it is timelier, more relevant to daily work, and more specific to the individual. Individuals also respond much more constructively to positive feedback, and some experts believe the ratio of positive to negative feedback should be on the order of 9 to 1. Be sure that feedback is done in a coaching manner and focuses on the behavior (You may try sitting down when you talk with patients as a way of making them feel more at ease) rather than on the person themselves (You’re really not a good communicator).
Managing Marginal Performance
Marginal performance can be defined as a physician whose observed behaviors or measured outcomes are at significant variance from what is expected. This pattern takes place over time and happens in spite of having in place all the other elements of a performance management system. Consider the “clock puncher” who rarely helps out the rest of the team on busy days and never shows up to group meetings or committees. Or the “tortoise” that has wonderful staff relations but chronically arrives at work late and repeatedly forgets to submit inpatient charges. Then there’s the “hothead” who is clinically adept and has high patient satisfaction but loses his or her temper with nursing and is pervasively confrontational with consultants. The steps to be taken in these and other cases like them include ensuring adequate documentation, reaching an agreement with the individual in recognizing that there is a problem, generating options for causality, negotiating a contract for improvement, and then letting future behavior determine the consequences.
Taking Corrective Action
Sometimes you simply cannot fix everything, and you need to be easy on yourself for having reached the point where the situation is no longer remediable in spite of your best efforts. In the end, everyone will be better off. When physician conduct becomes detrimental to patient safety, staff safety or quality patient care; is disruptive to the organization; or is otherwise chronically aberrant, then it is time to take adverse action. Since there are many pitfalls that have HR and legal implications, it is advisable to consult with relevant personnel to avoid problems with inadequate documentation and the potential need to report actions to state agencies and the National Practitioner Data Bank (per the Healthcare Quality Improvement Act of 1986).
Resources
- Ury W, Fisher R. Getting to Yes: Negotiating Agreement Without Giving In. 2nd ed. New York: Penguin Books; 1991.
- Reinertsen J. Physicians as leaders in the improvement of health care systems. Ann Intern Med. 1998;128:833-8.
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
- American College of Physician Executives. Managing Physician Performance in Organizations. Ongoing courses available at www.acpe.org.