User login
Heart Disease in SLE Called 'Startlingly Worrying'
LONDON — The incidence of coronary heart disease among young women with systemic lupus erythematosus is “startlingly worrying,” Ian Bruce, M.D., said at the Sixth European Lupus Meeting.
Studies have shown that the annual incidence of ischemic heart disease in lupus patients is 1.3%-1.5%. In comparison, the incidence among those with newly diagnosed type 2 diabetes and among those who have had a first myocardial infarction is 2%-2.2% per annum. “This latter number may be higher, but you have to remember that these are men in their mid- to late 50s, while the lupus patients in these studies are women whose average age is 35-37,” said Dr. Bruce, of the University of Manchester (England).
The prevalence of myocardial infarction or angina in lupus cohorts ranges from 7% to 10%, depending on patient age and duration of follow-up, he said.
Moreover, as survival improves, the prevalence of the disease increases, as does the proportion of lupus patients who are older and at even greater risk for cardiovascular disease, he said.
Some epidemiologic work has suggested that the peak age of onset also is increasing and now occurs between the fifth to seventh decades. Damage accrues more quickly among patients who are older at onset, he added.
Atherosclerosis also occurs much earlier in women with lupus than in healthy women. “In women younger than 45 in the general population, you virtually do not see plaque, whereas women with lupus are beginning to acquire plaque at that early age,” Dr. Bruce said.
Classic risk factors clearly are implicated in the premature atherosclerosis and coronary heart disease seen in lupus. There is a much higher prevalence of hypertension, diabetes, and renal impairment, and lupus patients typically have other risk factors such as higher levels of LDL cholesterol and triglycerides (Arthritis Rheum. 2003;48:3159-67).
And these risk factors do have an impact. “In a cohort study, we stratified patients according to their total cholesterol levels and found that among those with persistently elevated cholesterol, 24% developed a cardiac event during 12 years of follow-up, compared with 3% whose cholesterol level was normal or varied only slightly with disease flares,” Dr. Bruce said at the meeting, sponsored by the British Society for Rheumatology.
But classic risk factors do not tell the whole story. (See box.) In the general population, risk for a cardiac event increases as risk factors accumulate. “Lupus patients, however, seem to be set at an intrinsically higher baseline, and the accumulation of risk factors has an even more devastating effect,” he said.
A great need exists for properly conducted clinical trials of potential interventions for these patients. “We need to see if what we think will work actually does work and what the magnitude of risk reduction is with a particular intervention,” he said.
Statins are an example. “Everywhere they have been used so far, they have been associated with a reduction in risk of coronary-disease events by about 30%. You could assume that also might be the case in lupus, but that could be a dangerous assumption, because these drugs might not be as well tolerated by lupus patients,” he said.
The larger scope of the disease also must be addressed. Future work must focus on the worldwide burden of atherosclerosis in lupus and consider the ethnic gradient of risk, which might reveal some interesting things about the pathogenesis, he said.
Classic Risk Factors Don't Tell the Whole Story
As the magnitude and severity of atherosclerosis and heart disease in systemic lupus erythematosus (SLE) become clearer, so do some possible mediators and markers. A series of posters presented at the meeting by researchers from the Karolinska Institute, Stockholm, explored various potential contributing factors:
▸ LDL cholesterol. Increased LDL-cholesterol oxidation contributes to lupus-related cardiovascular disease, reported Anna Cederholm, M.D. She compared levels of several risk and protective factors in three groups: 26 women with lupus plus cardiovascular disease, 26 women with lupus but no clinical manifestations of cardiovascular disease, and 26 normal controls. Circulating levels of oxidized LDL cholesterol were increased in both lupus groups, as was platelet-activating factor acetylhydrolase (PAF-AH). Levels of oxidized LDL cholesterol and PAF-AH also were significantly higher in the lupus patients with cardiovascular disease than in those with lupus and no heart disease. Because PAF-AH binds to LDL cholesterol, it also may contribute to atherogenesis, Dr. Cederholm said.
▸ Anti-HDL cholesterol antibodies. SLE-related dyslipidemia showed a surprising pattern in a study of women with a history of cardiovascular disease, reported J. Su, M.D. Large, rather than small, LDL- and HDL-cholesterol particles characterized the dyslipidemia profile. This was not an expected atherogenic lipid profile, Dr. Su explained.
Antibodies against apolipoprotein A1 in HDL cholesterol also were elevated and were associated with the presence of tumor necrosis factor. Whether these anti-apo A1 antibodies play a pathogenic role—for example, by inhibiting the anti-inflammatory properties of HDL—is under investigation, Dr. Su said.
▸ Homocysteine. Hyperhomocysteinemia in patients with lupus correlates with markers of inflammatory activity and is a risk factor for cardiovascular disease, said Elisabet Svenungsson, M.D. In fasting blood samples obtained from a cohort of 208 patients, homocysteine levels were associated with acute phase reactants including C-reactive protein, serum amyloid A protein, fibrinogen, and complement.
Hyperhomocysteinemia also correlated with the presence of arterial disease and nephritis. “It may cause endothelial activation and damage and thus adds to the inflammatory burden that we believe renders SLE patients highly susceptible to cardiovascular disease,” she said.
—Nancy Walsh
LONDON — The incidence of coronary heart disease among young women with systemic lupus erythematosus is “startlingly worrying,” Ian Bruce, M.D., said at the Sixth European Lupus Meeting.
Studies have shown that the annual incidence of ischemic heart disease in lupus patients is 1.3%-1.5%. In comparison, the incidence among those with newly diagnosed type 2 diabetes and among those who have had a first myocardial infarction is 2%-2.2% per annum. “This latter number may be higher, but you have to remember that these are men in their mid- to late 50s, while the lupus patients in these studies are women whose average age is 35-37,” said Dr. Bruce, of the University of Manchester (England).
The prevalence of myocardial infarction or angina in lupus cohorts ranges from 7% to 10%, depending on patient age and duration of follow-up, he said.
Moreover, as survival improves, the prevalence of the disease increases, as does the proportion of lupus patients who are older and at even greater risk for cardiovascular disease, he said.
Some epidemiologic work has suggested that the peak age of onset also is increasing and now occurs between the fifth to seventh decades. Damage accrues more quickly among patients who are older at onset, he added.
Atherosclerosis also occurs much earlier in women with lupus than in healthy women. “In women younger than 45 in the general population, you virtually do not see plaque, whereas women with lupus are beginning to acquire plaque at that early age,” Dr. Bruce said.
Classic risk factors clearly are implicated in the premature atherosclerosis and coronary heart disease seen in lupus. There is a much higher prevalence of hypertension, diabetes, and renal impairment, and lupus patients typically have other risk factors such as higher levels of LDL cholesterol and triglycerides (Arthritis Rheum. 2003;48:3159-67).
And these risk factors do have an impact. “In a cohort study, we stratified patients according to their total cholesterol levels and found that among those with persistently elevated cholesterol, 24% developed a cardiac event during 12 years of follow-up, compared with 3% whose cholesterol level was normal or varied only slightly with disease flares,” Dr. Bruce said at the meeting, sponsored by the British Society for Rheumatology.
But classic risk factors do not tell the whole story. (See box.) In the general population, risk for a cardiac event increases as risk factors accumulate. “Lupus patients, however, seem to be set at an intrinsically higher baseline, and the accumulation of risk factors has an even more devastating effect,” he said.
A great need exists for properly conducted clinical trials of potential interventions for these patients. “We need to see if what we think will work actually does work and what the magnitude of risk reduction is with a particular intervention,” he said.
Statins are an example. “Everywhere they have been used so far, they have been associated with a reduction in risk of coronary-disease events by about 30%. You could assume that also might be the case in lupus, but that could be a dangerous assumption, because these drugs might not be as well tolerated by lupus patients,” he said.
The larger scope of the disease also must be addressed. Future work must focus on the worldwide burden of atherosclerosis in lupus and consider the ethnic gradient of risk, which might reveal some interesting things about the pathogenesis, he said.
Classic Risk Factors Don't Tell the Whole Story
As the magnitude and severity of atherosclerosis and heart disease in systemic lupus erythematosus (SLE) become clearer, so do some possible mediators and markers. A series of posters presented at the meeting by researchers from the Karolinska Institute, Stockholm, explored various potential contributing factors:
▸ LDL cholesterol. Increased LDL-cholesterol oxidation contributes to lupus-related cardiovascular disease, reported Anna Cederholm, M.D. She compared levels of several risk and protective factors in three groups: 26 women with lupus plus cardiovascular disease, 26 women with lupus but no clinical manifestations of cardiovascular disease, and 26 normal controls. Circulating levels of oxidized LDL cholesterol were increased in both lupus groups, as was platelet-activating factor acetylhydrolase (PAF-AH). Levels of oxidized LDL cholesterol and PAF-AH also were significantly higher in the lupus patients with cardiovascular disease than in those with lupus and no heart disease. Because PAF-AH binds to LDL cholesterol, it also may contribute to atherogenesis, Dr. Cederholm said.
▸ Anti-HDL cholesterol antibodies. SLE-related dyslipidemia showed a surprising pattern in a study of women with a history of cardiovascular disease, reported J. Su, M.D. Large, rather than small, LDL- and HDL-cholesterol particles characterized the dyslipidemia profile. This was not an expected atherogenic lipid profile, Dr. Su explained.
Antibodies against apolipoprotein A1 in HDL cholesterol also were elevated and were associated with the presence of tumor necrosis factor. Whether these anti-apo A1 antibodies play a pathogenic role—for example, by inhibiting the anti-inflammatory properties of HDL—is under investigation, Dr. Su said.
▸ Homocysteine. Hyperhomocysteinemia in patients with lupus correlates with markers of inflammatory activity and is a risk factor for cardiovascular disease, said Elisabet Svenungsson, M.D. In fasting blood samples obtained from a cohort of 208 patients, homocysteine levels were associated with acute phase reactants including C-reactive protein, serum amyloid A protein, fibrinogen, and complement.
Hyperhomocysteinemia also correlated with the presence of arterial disease and nephritis. “It may cause endothelial activation and damage and thus adds to the inflammatory burden that we believe renders SLE patients highly susceptible to cardiovascular disease,” she said.
—Nancy Walsh
LONDON — The incidence of coronary heart disease among young women with systemic lupus erythematosus is “startlingly worrying,” Ian Bruce, M.D., said at the Sixth European Lupus Meeting.
Studies have shown that the annual incidence of ischemic heart disease in lupus patients is 1.3%-1.5%. In comparison, the incidence among those with newly diagnosed type 2 diabetes and among those who have had a first myocardial infarction is 2%-2.2% per annum. “This latter number may be higher, but you have to remember that these are men in their mid- to late 50s, while the lupus patients in these studies are women whose average age is 35-37,” said Dr. Bruce, of the University of Manchester (England).
The prevalence of myocardial infarction or angina in lupus cohorts ranges from 7% to 10%, depending on patient age and duration of follow-up, he said.
Moreover, as survival improves, the prevalence of the disease increases, as does the proportion of lupus patients who are older and at even greater risk for cardiovascular disease, he said.
Some epidemiologic work has suggested that the peak age of onset also is increasing and now occurs between the fifth to seventh decades. Damage accrues more quickly among patients who are older at onset, he added.
Atherosclerosis also occurs much earlier in women with lupus than in healthy women. “In women younger than 45 in the general population, you virtually do not see plaque, whereas women with lupus are beginning to acquire plaque at that early age,” Dr. Bruce said.
Classic risk factors clearly are implicated in the premature atherosclerosis and coronary heart disease seen in lupus. There is a much higher prevalence of hypertension, diabetes, and renal impairment, and lupus patients typically have other risk factors such as higher levels of LDL cholesterol and triglycerides (Arthritis Rheum. 2003;48:3159-67).
And these risk factors do have an impact. “In a cohort study, we stratified patients according to their total cholesterol levels and found that among those with persistently elevated cholesterol, 24% developed a cardiac event during 12 years of follow-up, compared with 3% whose cholesterol level was normal or varied only slightly with disease flares,” Dr. Bruce said at the meeting, sponsored by the British Society for Rheumatology.
But classic risk factors do not tell the whole story. (See box.) In the general population, risk for a cardiac event increases as risk factors accumulate. “Lupus patients, however, seem to be set at an intrinsically higher baseline, and the accumulation of risk factors has an even more devastating effect,” he said.
A great need exists for properly conducted clinical trials of potential interventions for these patients. “We need to see if what we think will work actually does work and what the magnitude of risk reduction is with a particular intervention,” he said.
Statins are an example. “Everywhere they have been used so far, they have been associated with a reduction in risk of coronary-disease events by about 30%. You could assume that also might be the case in lupus, but that could be a dangerous assumption, because these drugs might not be as well tolerated by lupus patients,” he said.
The larger scope of the disease also must be addressed. Future work must focus on the worldwide burden of atherosclerosis in lupus and consider the ethnic gradient of risk, which might reveal some interesting things about the pathogenesis, he said.
Classic Risk Factors Don't Tell the Whole Story
As the magnitude and severity of atherosclerosis and heart disease in systemic lupus erythematosus (SLE) become clearer, so do some possible mediators and markers. A series of posters presented at the meeting by researchers from the Karolinska Institute, Stockholm, explored various potential contributing factors:
▸ LDL cholesterol. Increased LDL-cholesterol oxidation contributes to lupus-related cardiovascular disease, reported Anna Cederholm, M.D. She compared levels of several risk and protective factors in three groups: 26 women with lupus plus cardiovascular disease, 26 women with lupus but no clinical manifestations of cardiovascular disease, and 26 normal controls. Circulating levels of oxidized LDL cholesterol were increased in both lupus groups, as was platelet-activating factor acetylhydrolase (PAF-AH). Levels of oxidized LDL cholesterol and PAF-AH also were significantly higher in the lupus patients with cardiovascular disease than in those with lupus and no heart disease. Because PAF-AH binds to LDL cholesterol, it also may contribute to atherogenesis, Dr. Cederholm said.
▸ Anti-HDL cholesterol antibodies. SLE-related dyslipidemia showed a surprising pattern in a study of women with a history of cardiovascular disease, reported J. Su, M.D. Large, rather than small, LDL- and HDL-cholesterol particles characterized the dyslipidemia profile. This was not an expected atherogenic lipid profile, Dr. Su explained.
Antibodies against apolipoprotein A1 in HDL cholesterol also were elevated and were associated with the presence of tumor necrosis factor. Whether these anti-apo A1 antibodies play a pathogenic role—for example, by inhibiting the anti-inflammatory properties of HDL—is under investigation, Dr. Su said.
▸ Homocysteine. Hyperhomocysteinemia in patients with lupus correlates with markers of inflammatory activity and is a risk factor for cardiovascular disease, said Elisabet Svenungsson, M.D. In fasting blood samples obtained from a cohort of 208 patients, homocysteine levels were associated with acute phase reactants including C-reactive protein, serum amyloid A protein, fibrinogen, and complement.
Hyperhomocysteinemia also correlated with the presence of arterial disease and nephritis. “It may cause endothelial activation and damage and thus adds to the inflammatory burden that we believe renders SLE patients highly susceptible to cardiovascular disease,” she said.
—Nancy Walsh
Warfarin Less Effective in Real Life Than in Trials
NEW ORLEANS — Real world experience with warfarin suggests that it is not as good at preventing strokes in patients with atrial fibrillation as clinical trial results have suggested, especially among African Americans.
A review of more than 23,000 Medicare patients with atrial fibrillation showed that overall, warfarin prophylaxis cut the stroke rate by 34%, compared with a 65% cut in strokes that's been consistently seen in clinical trials, Brian F. Gage, M.D., reported at the 30th International Stroke Conference.
This lower efficacy in a real-world setting is “disappointing,” said Dr. Gage, an internist at Washington University in St. Louis.
But warfarin performed even worse in the African Americans in the study. In this group, warfarin use was associated with a trend toward more strokes, although this increase was not statistically significant, compared with African Americans not on warfarin.
In this analysis, the 95% confidence interval showed that, at best, warfarin prophylaxis in African Americans produced an 18% reduction in strokes, compared with untreated patients. This benefit is close to the 22% stroke reduction from aspirin prophylaxis in all patients, a suggestion that aspirin prophylaxis may be just as good as or better than warfarin prophylaxis in African Americans. This hypothesis should be tested by analyzing results already collected in prior randomized, controlled studies, Dr. Gage told this newspaper.
The study used a national sample of 23,657 Medicare patients with atrial fibrillation who were treated during April 1998 through March 1999. Warfarin prophylaxis was used by 43% of African Americans in the study and by 50% of white patients.
Information culled from the medical records of the patients on warfarin therapy showed that this prophylaxis was often used in a less-than-ideal manner. Patients who regularly receive warfarin should have their dosage adjusted based on their international normalized ratio (INR), a measure of clotting time. Ideally, INRs should be measured about every 28 days in patients who regularly take warfarin.
Among all white patients, the average time between INR measurements was 26 days, and among African Americans the average interval was 30 days. But 25% of the white patients on warfarin had an interval of 39 days or longer between INR measurements. Among African Americans on warfarin, 25% had an interval of 57 days or longer between measurements, Dr. Gage said at the conference, sponsored by the American Stroke Association. For these subgroups, the interval between INR measurements was “way too long,” he said.
But substandard INR monitoring was not the only reason patients got less benefit from warfarin prophylaxis, compared with the benchmark of clinical trials. The rate of protection from stroke remained unexpectedly low among African Americans even in an analysis that controlled for the frequency of INR monitoring as well as clinical variables that predispose patients to strokes.
Other factors that were not controlled for in this analysis, and that may help explain warfarin's underachievement, include poor compliance with the warfarin regimen, inadequacies in the health care setting, and inadequate access to anticoagulant services, said Dr. Gage, who is also medical director of the Blood Thinner Clinic at Barnes-Jewish Hospital in St. Louis.
The clinical trials that assessed warfarin's efficacy for preventing strokes in patients with atrial fibrillation were highly selective; more than 90% of patients who were initially assessed for these trials were eventually excluded. The clinical trial results therefore came from patients that were mostly white, less than age 75 years, and followed very closely, and these results may not be generalizable to other health care settings, Dr. Gage said.
NEW ORLEANS — Real world experience with warfarin suggests that it is not as good at preventing strokes in patients with atrial fibrillation as clinical trial results have suggested, especially among African Americans.
A review of more than 23,000 Medicare patients with atrial fibrillation showed that overall, warfarin prophylaxis cut the stroke rate by 34%, compared with a 65% cut in strokes that's been consistently seen in clinical trials, Brian F. Gage, M.D., reported at the 30th International Stroke Conference.
This lower efficacy in a real-world setting is “disappointing,” said Dr. Gage, an internist at Washington University in St. Louis.
But warfarin performed even worse in the African Americans in the study. In this group, warfarin use was associated with a trend toward more strokes, although this increase was not statistically significant, compared with African Americans not on warfarin.
In this analysis, the 95% confidence interval showed that, at best, warfarin prophylaxis in African Americans produced an 18% reduction in strokes, compared with untreated patients. This benefit is close to the 22% stroke reduction from aspirin prophylaxis in all patients, a suggestion that aspirin prophylaxis may be just as good as or better than warfarin prophylaxis in African Americans. This hypothesis should be tested by analyzing results already collected in prior randomized, controlled studies, Dr. Gage told this newspaper.
The study used a national sample of 23,657 Medicare patients with atrial fibrillation who were treated during April 1998 through March 1999. Warfarin prophylaxis was used by 43% of African Americans in the study and by 50% of white patients.
Information culled from the medical records of the patients on warfarin therapy showed that this prophylaxis was often used in a less-than-ideal manner. Patients who regularly receive warfarin should have their dosage adjusted based on their international normalized ratio (INR), a measure of clotting time. Ideally, INRs should be measured about every 28 days in patients who regularly take warfarin.
Among all white patients, the average time between INR measurements was 26 days, and among African Americans the average interval was 30 days. But 25% of the white patients on warfarin had an interval of 39 days or longer between INR measurements. Among African Americans on warfarin, 25% had an interval of 57 days or longer between measurements, Dr. Gage said at the conference, sponsored by the American Stroke Association. For these subgroups, the interval between INR measurements was “way too long,” he said.
But substandard INR monitoring was not the only reason patients got less benefit from warfarin prophylaxis, compared with the benchmark of clinical trials. The rate of protection from stroke remained unexpectedly low among African Americans even in an analysis that controlled for the frequency of INR monitoring as well as clinical variables that predispose patients to strokes.
Other factors that were not controlled for in this analysis, and that may help explain warfarin's underachievement, include poor compliance with the warfarin regimen, inadequacies in the health care setting, and inadequate access to anticoagulant services, said Dr. Gage, who is also medical director of the Blood Thinner Clinic at Barnes-Jewish Hospital in St. Louis.
The clinical trials that assessed warfarin's efficacy for preventing strokes in patients with atrial fibrillation were highly selective; more than 90% of patients who were initially assessed for these trials were eventually excluded. The clinical trial results therefore came from patients that were mostly white, less than age 75 years, and followed very closely, and these results may not be generalizable to other health care settings, Dr. Gage said.
NEW ORLEANS — Real world experience with warfarin suggests that it is not as good at preventing strokes in patients with atrial fibrillation as clinical trial results have suggested, especially among African Americans.
A review of more than 23,000 Medicare patients with atrial fibrillation showed that overall, warfarin prophylaxis cut the stroke rate by 34%, compared with a 65% cut in strokes that's been consistently seen in clinical trials, Brian F. Gage, M.D., reported at the 30th International Stroke Conference.
This lower efficacy in a real-world setting is “disappointing,” said Dr. Gage, an internist at Washington University in St. Louis.
But warfarin performed even worse in the African Americans in the study. In this group, warfarin use was associated with a trend toward more strokes, although this increase was not statistically significant, compared with African Americans not on warfarin.
In this analysis, the 95% confidence interval showed that, at best, warfarin prophylaxis in African Americans produced an 18% reduction in strokes, compared with untreated patients. This benefit is close to the 22% stroke reduction from aspirin prophylaxis in all patients, a suggestion that aspirin prophylaxis may be just as good as or better than warfarin prophylaxis in African Americans. This hypothesis should be tested by analyzing results already collected in prior randomized, controlled studies, Dr. Gage told this newspaper.
The study used a national sample of 23,657 Medicare patients with atrial fibrillation who were treated during April 1998 through March 1999. Warfarin prophylaxis was used by 43% of African Americans in the study and by 50% of white patients.
Information culled from the medical records of the patients on warfarin therapy showed that this prophylaxis was often used in a less-than-ideal manner. Patients who regularly receive warfarin should have their dosage adjusted based on their international normalized ratio (INR), a measure of clotting time. Ideally, INRs should be measured about every 28 days in patients who regularly take warfarin.
Among all white patients, the average time between INR measurements was 26 days, and among African Americans the average interval was 30 days. But 25% of the white patients on warfarin had an interval of 39 days or longer between INR measurements. Among African Americans on warfarin, 25% had an interval of 57 days or longer between measurements, Dr. Gage said at the conference, sponsored by the American Stroke Association. For these subgroups, the interval between INR measurements was “way too long,” he said.
But substandard INR monitoring was not the only reason patients got less benefit from warfarin prophylaxis, compared with the benchmark of clinical trials. The rate of protection from stroke remained unexpectedly low among African Americans even in an analysis that controlled for the frequency of INR monitoring as well as clinical variables that predispose patients to strokes.
Other factors that were not controlled for in this analysis, and that may help explain warfarin's underachievement, include poor compliance with the warfarin regimen, inadequacies in the health care setting, and inadequate access to anticoagulant services, said Dr. Gage, who is also medical director of the Blood Thinner Clinic at Barnes-Jewish Hospital in St. Louis.
The clinical trials that assessed warfarin's efficacy for preventing strokes in patients with atrial fibrillation were highly selective; more than 90% of patients who were initially assessed for these trials were eventually excluded. The clinical trial results therefore came from patients that were mostly white, less than age 75 years, and followed very closely, and these results may not be generalizable to other health care settings, Dr. Gage said.
Sirolimus-Eluting Stents Edge Past Paclitaxel Stents
ORLANDO, FLA. — Three more salvos were fired in the battle of competing drug-eluting coronary stents. When the smoke cleared and findings from the new head-to-head trials were reported at the annual meeting of the American College of Cardiology, the sirolimus-eluting stent, Cypher, had edged the paclitaxel stent, Taxus, in two studies, with the third and largest trial ending in a draw.
With the results from at least four head-to-head studies now reported (results from the fourth were reported in January), the sirolimus-eluting stent has shown some consistent advantages.
The biggest difference between the two types of stents was seen in a study with 1,012 patients who were randomized to treatment with either sirolimus- or paclitaxel-eluting stents at two Swiss university hospitals. The study, named SIRTAX, was completely funded by the hospitals and received no industry sponsorship, said Stephan Windecker, M.D., a cardiologist at the University Hospital in Bern.
The study randomized all comers who required coronary stenting. Slightly more than half of the patients had acute coronary syndrome, almost a quarter had triple-vessel disease, and about 20% had diabetes. About 8% had ostial lesions, another 8% had lesions at bifurcations, 35% had calcified lesions, 37% had lesions of moderate or excessive tortuosity, and 2% of lesions were in saphenous vein grafts.
All patients were treated with 75 mg clopidogrel daily for a year following stenting, and all received 100 mg aspirin daily indefinitely.
The study's primary end point was the combined incidence of cardiac death, myocardial infarction, or ischemia-driven target lesion revascularization (TLR) within 9 months of treatment. The rate of this end point was 6.2% in the 503 patients who received sirolimus-eluting stents and 10.8% in the 509 who received paclitaxel-eluting stents, a statistically significant difference.
This outcome was driven largely by the difference in the need for TLR: 4.8% in patients who received sirolimus-eluting stents and 8.3% in those who got paclitaxel-eluting stents, also a statistically significant difference. All of the secondary end points also favored the sirolimus-eluting stent, although some of these were not statistically significant.
The advantage in the primary, combined end point for the sirolimus-eluting stents was especially dramatic in patients with diabetes. In this subgroup, sirolimus-eluting stents were associated with a better than threefold reduction in events, compared with the paclitaxel-eluting stents. The advantage was half as large in patients without diabetes. The two groups had identical rates of stent thrombosis.
An even larger, higher-profile trial failed to show a clear advantage for either type of stent. The highly anticipated prospective randomized multicenter head-to-head comparison of the two stents, named REALITY, was done at 90 centers in Europe, Asia, South America, and Mexico (but not in the United States), enrolled 1,353 patients, and was sponsored by Cordis, the company that makes and markets the sirolimus-eluting coronary stent.
This study involved a more highly selected group of patients, excluding those with ostial lesions, recent MIs, total occlusions, and certain other high-risk conditions. But 28% of patients had diabetes. After stenting, all patients received 100 mg of aspirin indefinitely. Daily treatment with a thienopyridine (clopidogrel or ticlopidine) was used for at least 2 months in all patients who received sirolimus-eluting stents and for at least 6 months in all patients who got paclitaxel-eluting stents.
The study's primary end point was the rate of in-lesion binary restenosis at 8 months after stenting, as measured by angiography. This rate was 9.6% in the sirolimus-eluting stents and 11.1% in the paclitaxel-eluting stents, a difference that was not statistically significant, reported Marie-Claude Morice, M.D., a cardiologist at the Cardiovascular Institute in Paris.
Other important clinical end points also failed to show a statistically significant difference between the two stent types. The combined rate of major coronary end points—cardiac death, MI, and TLR, was 9.2% in the patients who received sirolimus-eluting stents and 10.6% in those who received paclitaxel-eluting stents. The difference in the revascularization rate only was even tighter: 5.0% in the sirolimus-eluting stent group and 5.4% in those who got paclitaxel-eluting stents.
The only major differences between stent types in this study were in late in-stent lumen loss after 8 months, and in the rate of stent thrombosis during the first 30 days of treatment. Late loss averaged 0.1 mm with the sirolimus stents and 0.3 mm with the paclitaxel stents. Stent thrombosis occurred in 0.4% of patients who received sirolimus stents and in 1.8% of those who received paclitaxel stents. But the rate of stent thrombosis was not a prespecified end point for this study and a difference between the two stent types for this measure was unexpected. As a result, the clinical significance of this finding was unclear, Dr. Morice said.
The third set of study results presented at the meeting came from a single-center study with a total of 250 patients, all of whom had diabetes. Like the larger Swiss trial, this study, called ISAR-DIABETES, had no commercial funding and was sponsored solely by the German Heart Center in Munich.
This study had fewer exclusion criteria than the REALITY study. Exclusions were limited to patients with acute MI, left-main disease, in-stent restenosis, or an allergy to one of the study drugs.
The study's primary end point was the rate of in-segment, late lumen loss at 6-8 months after stenting, as measured by angiography. The average amount of late loss was 0.43 mm in patients who received sirolimus stents and 0.67 mm in those who got paclitaxel stents, a difference that was statistically significant, reported Adnan Kastrati, M.D., professor of cardiology at the German Heart Center.
Patients who received sirolimus stents also had significantly less angiographic restenosis than did those who got paclitaxel stents, 6.9% vs. 16.5%, respectively. But there were no statistically significant differences in clinical end points, including clinical restenosis and the rates of death and MI at 9 months after stenting.
Although the results from this third study showed differences only for angiographic end points, Dr. Kastrati said that he was convinced by the outcome. “The results will push us to select sirolimus-eluting stents for patients with diabetes,” he said.
In January, results were reported from a fourth study by Dr. Kastrati and associates that compared the two stent types, in 200 patients with in-stent restenosis. In that study, patients who received sirolimus-eluting stents had significantly less clinical restenosis compared with the patients who received paclitaxel-eluting stents (JAMA 2005;293:165-71).
ORLANDO, FLA. — Three more salvos were fired in the battle of competing drug-eluting coronary stents. When the smoke cleared and findings from the new head-to-head trials were reported at the annual meeting of the American College of Cardiology, the sirolimus-eluting stent, Cypher, had edged the paclitaxel stent, Taxus, in two studies, with the third and largest trial ending in a draw.
With the results from at least four head-to-head studies now reported (results from the fourth were reported in January), the sirolimus-eluting stent has shown some consistent advantages.
The biggest difference between the two types of stents was seen in a study with 1,012 patients who were randomized to treatment with either sirolimus- or paclitaxel-eluting stents at two Swiss university hospitals. The study, named SIRTAX, was completely funded by the hospitals and received no industry sponsorship, said Stephan Windecker, M.D., a cardiologist at the University Hospital in Bern.
The study randomized all comers who required coronary stenting. Slightly more than half of the patients had acute coronary syndrome, almost a quarter had triple-vessel disease, and about 20% had diabetes. About 8% had ostial lesions, another 8% had lesions at bifurcations, 35% had calcified lesions, 37% had lesions of moderate or excessive tortuosity, and 2% of lesions were in saphenous vein grafts.
All patients were treated with 75 mg clopidogrel daily for a year following stenting, and all received 100 mg aspirin daily indefinitely.
The study's primary end point was the combined incidence of cardiac death, myocardial infarction, or ischemia-driven target lesion revascularization (TLR) within 9 months of treatment. The rate of this end point was 6.2% in the 503 patients who received sirolimus-eluting stents and 10.8% in the 509 who received paclitaxel-eluting stents, a statistically significant difference.
This outcome was driven largely by the difference in the need for TLR: 4.8% in patients who received sirolimus-eluting stents and 8.3% in those who got paclitaxel-eluting stents, also a statistically significant difference. All of the secondary end points also favored the sirolimus-eluting stent, although some of these were not statistically significant.
The advantage in the primary, combined end point for the sirolimus-eluting stents was especially dramatic in patients with diabetes. In this subgroup, sirolimus-eluting stents were associated with a better than threefold reduction in events, compared with the paclitaxel-eluting stents. The advantage was half as large in patients without diabetes. The two groups had identical rates of stent thrombosis.
An even larger, higher-profile trial failed to show a clear advantage for either type of stent. The highly anticipated prospective randomized multicenter head-to-head comparison of the two stents, named REALITY, was done at 90 centers in Europe, Asia, South America, and Mexico (but not in the United States), enrolled 1,353 patients, and was sponsored by Cordis, the company that makes and markets the sirolimus-eluting coronary stent.
This study involved a more highly selected group of patients, excluding those with ostial lesions, recent MIs, total occlusions, and certain other high-risk conditions. But 28% of patients had diabetes. After stenting, all patients received 100 mg of aspirin indefinitely. Daily treatment with a thienopyridine (clopidogrel or ticlopidine) was used for at least 2 months in all patients who received sirolimus-eluting stents and for at least 6 months in all patients who got paclitaxel-eluting stents.
The study's primary end point was the rate of in-lesion binary restenosis at 8 months after stenting, as measured by angiography. This rate was 9.6% in the sirolimus-eluting stents and 11.1% in the paclitaxel-eluting stents, a difference that was not statistically significant, reported Marie-Claude Morice, M.D., a cardiologist at the Cardiovascular Institute in Paris.
Other important clinical end points also failed to show a statistically significant difference between the two stent types. The combined rate of major coronary end points—cardiac death, MI, and TLR, was 9.2% in the patients who received sirolimus-eluting stents and 10.6% in those who received paclitaxel-eluting stents. The difference in the revascularization rate only was even tighter: 5.0% in the sirolimus-eluting stent group and 5.4% in those who got paclitaxel-eluting stents.
The only major differences between stent types in this study were in late in-stent lumen loss after 8 months, and in the rate of stent thrombosis during the first 30 days of treatment. Late loss averaged 0.1 mm with the sirolimus stents and 0.3 mm with the paclitaxel stents. Stent thrombosis occurred in 0.4% of patients who received sirolimus stents and in 1.8% of those who received paclitaxel stents. But the rate of stent thrombosis was not a prespecified end point for this study and a difference between the two stent types for this measure was unexpected. As a result, the clinical significance of this finding was unclear, Dr. Morice said.
The third set of study results presented at the meeting came from a single-center study with a total of 250 patients, all of whom had diabetes. Like the larger Swiss trial, this study, called ISAR-DIABETES, had no commercial funding and was sponsored solely by the German Heart Center in Munich.
This study had fewer exclusion criteria than the REALITY study. Exclusions were limited to patients with acute MI, left-main disease, in-stent restenosis, or an allergy to one of the study drugs.
The study's primary end point was the rate of in-segment, late lumen loss at 6-8 months after stenting, as measured by angiography. The average amount of late loss was 0.43 mm in patients who received sirolimus stents and 0.67 mm in those who got paclitaxel stents, a difference that was statistically significant, reported Adnan Kastrati, M.D., professor of cardiology at the German Heart Center.
Patients who received sirolimus stents also had significantly less angiographic restenosis than did those who got paclitaxel stents, 6.9% vs. 16.5%, respectively. But there were no statistically significant differences in clinical end points, including clinical restenosis and the rates of death and MI at 9 months after stenting.
Although the results from this third study showed differences only for angiographic end points, Dr. Kastrati said that he was convinced by the outcome. “The results will push us to select sirolimus-eluting stents for patients with diabetes,” he said.
In January, results were reported from a fourth study by Dr. Kastrati and associates that compared the two stent types, in 200 patients with in-stent restenosis. In that study, patients who received sirolimus-eluting stents had significantly less clinical restenosis compared with the patients who received paclitaxel-eluting stents (JAMA 2005;293:165-71).
ORLANDO, FLA. — Three more salvos were fired in the battle of competing drug-eluting coronary stents. When the smoke cleared and findings from the new head-to-head trials were reported at the annual meeting of the American College of Cardiology, the sirolimus-eluting stent, Cypher, had edged the paclitaxel stent, Taxus, in two studies, with the third and largest trial ending in a draw.
With the results from at least four head-to-head studies now reported (results from the fourth were reported in January), the sirolimus-eluting stent has shown some consistent advantages.
The biggest difference between the two types of stents was seen in a study with 1,012 patients who were randomized to treatment with either sirolimus- or paclitaxel-eluting stents at two Swiss university hospitals. The study, named SIRTAX, was completely funded by the hospitals and received no industry sponsorship, said Stephan Windecker, M.D., a cardiologist at the University Hospital in Bern.
The study randomized all comers who required coronary stenting. Slightly more than half of the patients had acute coronary syndrome, almost a quarter had triple-vessel disease, and about 20% had diabetes. About 8% had ostial lesions, another 8% had lesions at bifurcations, 35% had calcified lesions, 37% had lesions of moderate or excessive tortuosity, and 2% of lesions were in saphenous vein grafts.
All patients were treated with 75 mg clopidogrel daily for a year following stenting, and all received 100 mg aspirin daily indefinitely.
The study's primary end point was the combined incidence of cardiac death, myocardial infarction, or ischemia-driven target lesion revascularization (TLR) within 9 months of treatment. The rate of this end point was 6.2% in the 503 patients who received sirolimus-eluting stents and 10.8% in the 509 who received paclitaxel-eluting stents, a statistically significant difference.
This outcome was driven largely by the difference in the need for TLR: 4.8% in patients who received sirolimus-eluting stents and 8.3% in those who got paclitaxel-eluting stents, also a statistically significant difference. All of the secondary end points also favored the sirolimus-eluting stent, although some of these were not statistically significant.
The advantage in the primary, combined end point for the sirolimus-eluting stents was especially dramatic in patients with diabetes. In this subgroup, sirolimus-eluting stents were associated with a better than threefold reduction in events, compared with the paclitaxel-eluting stents. The advantage was half as large in patients without diabetes. The two groups had identical rates of stent thrombosis.
An even larger, higher-profile trial failed to show a clear advantage for either type of stent. The highly anticipated prospective randomized multicenter head-to-head comparison of the two stents, named REALITY, was done at 90 centers in Europe, Asia, South America, and Mexico (but not in the United States), enrolled 1,353 patients, and was sponsored by Cordis, the company that makes and markets the sirolimus-eluting coronary stent.
This study involved a more highly selected group of patients, excluding those with ostial lesions, recent MIs, total occlusions, and certain other high-risk conditions. But 28% of patients had diabetes. After stenting, all patients received 100 mg of aspirin indefinitely. Daily treatment with a thienopyridine (clopidogrel or ticlopidine) was used for at least 2 months in all patients who received sirolimus-eluting stents and for at least 6 months in all patients who got paclitaxel-eluting stents.
The study's primary end point was the rate of in-lesion binary restenosis at 8 months after stenting, as measured by angiography. This rate was 9.6% in the sirolimus-eluting stents and 11.1% in the paclitaxel-eluting stents, a difference that was not statistically significant, reported Marie-Claude Morice, M.D., a cardiologist at the Cardiovascular Institute in Paris.
Other important clinical end points also failed to show a statistically significant difference between the two stent types. The combined rate of major coronary end points—cardiac death, MI, and TLR, was 9.2% in the patients who received sirolimus-eluting stents and 10.6% in those who received paclitaxel-eluting stents. The difference in the revascularization rate only was even tighter: 5.0% in the sirolimus-eluting stent group and 5.4% in those who got paclitaxel-eluting stents.
The only major differences between stent types in this study were in late in-stent lumen loss after 8 months, and in the rate of stent thrombosis during the first 30 days of treatment. Late loss averaged 0.1 mm with the sirolimus stents and 0.3 mm with the paclitaxel stents. Stent thrombosis occurred in 0.4% of patients who received sirolimus stents and in 1.8% of those who received paclitaxel stents. But the rate of stent thrombosis was not a prespecified end point for this study and a difference between the two stent types for this measure was unexpected. As a result, the clinical significance of this finding was unclear, Dr. Morice said.
The third set of study results presented at the meeting came from a single-center study with a total of 250 patients, all of whom had diabetes. Like the larger Swiss trial, this study, called ISAR-DIABETES, had no commercial funding and was sponsored solely by the German Heart Center in Munich.
This study had fewer exclusion criteria than the REALITY study. Exclusions were limited to patients with acute MI, left-main disease, in-stent restenosis, or an allergy to one of the study drugs.
The study's primary end point was the rate of in-segment, late lumen loss at 6-8 months after stenting, as measured by angiography. The average amount of late loss was 0.43 mm in patients who received sirolimus stents and 0.67 mm in those who got paclitaxel stents, a difference that was statistically significant, reported Adnan Kastrati, M.D., professor of cardiology at the German Heart Center.
Patients who received sirolimus stents also had significantly less angiographic restenosis than did those who got paclitaxel stents, 6.9% vs. 16.5%, respectively. But there were no statistically significant differences in clinical end points, including clinical restenosis and the rates of death and MI at 9 months after stenting.
Although the results from this third study showed differences only for angiographic end points, Dr. Kastrati said that he was convinced by the outcome. “The results will push us to select sirolimus-eluting stents for patients with diabetes,” he said.
In January, results were reported from a fourth study by Dr. Kastrati and associates that compared the two stent types, in 200 patients with in-stent restenosis. In that study, patients who received sirolimus-eluting stents had significantly less clinical restenosis compared with the patients who received paclitaxel-eluting stents (JAMA 2005;293:165-71).
Uses for Drug-Eluting Stents Are Rising Rapidly
Despite their higher cost, and despite recent concerns about late thrombosis, drug-eluting stents now dominate.
In the final 3 months of 2004, drug-eluting stents were estimated to have been used for 87% of all interventional coronary procedures in the United States, Martin B. Leon, M.D., said last November at the American Heart Association's scientific sessions in New Orleans. Less than 2 years earlier, not a single drug-eluting stent had been used in the United States outside of a clinical trial. The Food and Drug Administration first approved a drug-eluting stent in April 2003.
“We have not yet identified any subsets of patients who don't benefit from receiving drug-eluting stents [by having less restenosis] compared with bare metal stents,” said David J. Cohen, M.D., associate director of interventional cardiology at Beth Israel Deaconess Medical Center in Boston. “De facto practice in the United States today is to use drug-eluting stents whenever the available stent lengths and diameters fit. At Beth Israel Deaconess, most of the time when patients [who are undergoing coronary stenting] don't receive drug-eluting stents it's because the vessel is too small or too large to accommodate available stent sizes,” he told this newspaper.
They are so widespread that medicolegal concerns may now drive their use even more than purely clinical factors. “When the risk of restenosis is low, operators must balance the need for drug-eluting stents with the medicolegal risk of avoiding what has become the de facto standard of care for all patients,” said Herbert D. Aronow, M.D., director of the cardiac catheterization laboratories at the Veterans Affairs Medical Center in Philadelphia.
According to one study, in 2003, about a third of all sirolimus-eluting (Cypher) stents used in the United States were for off-label coronary artery indications (CARDIOLOGY NEWS, February 2005, p. 15).
As of early this year, no cardiology society had issued formal recommendations on the appropriate uses of drug-eluting stents, although these are expected soon. In the meantime, some experts have given their personal opinions.
One set of standards was laid out by Gregg W. Stone, M.D., in a talk at the AHA scientific session. “In workhorse lesions, in patients undergoing elective coronary interventions with de novo lesions up to 46 mm in length and in vessels with reference diameters of 2.5-3.75 mm without acute coronary syndrome or acute MI, in general the safety and efficacy of two drug-eluting stents, Cypher and Taxus [paclitaxel-eluting], has been proved,” said Dr. Stone, an interventional cardiologist at Columbia University in New York. “Using drug-eluting stents over bare metal stents in these lesions is the appropriate thing to do.”
But, he added, “we desperately need more data regarding the safety and efficacy of drug-eluting stents in unapproved and high-risk indications before their use should be considered routine. … You need to be aware of the evidence so you know what you are doing.”
A step was taken this past March to better define the safety and efficacy of drug-eluting stents in more complex vessels and lesions, with reports from two studies at the annual meeting of the American College of Cardiology. A Danish study with 322 patients compared sirolimus-eluting with bare-metal stents in patients with total occlusions, lesions at bifurcations, ostial lesions, and lesions in angulated arteries. Patients who received drug-eluting stents had better angiographic and clinical outcomes. A second report involved more than 1,100 patients who were treated with either paclitaxel-eluting or bare metal stents. The results showed that the drug-eluting stents were superior in coronaries narrower than 2.25 mm and in wide arteries.
According to Dr. Stone last November, there are also grounds for using a single drug-eluting stent to treat in-stent restenosis within a bare metal stent. But he cautioned physicians to “think twice” about using drug-eluting stents outside of a study for unprotected left main disease, in-stent restenosis following failed brachytherapy, and in patients with acute myocardial infarction. There is even less evidence on using drug-eluting stents for V-stenting of a bifurcation, and it is completely unclear how cardiologists should manage restenosis within a drug-eluting stent.
Despite their higher cost, and despite recent concerns about late thrombosis, drug-eluting stents now dominate.
In the final 3 months of 2004, drug-eluting stents were estimated to have been used for 87% of all interventional coronary procedures in the United States, Martin B. Leon, M.D., said last November at the American Heart Association's scientific sessions in New Orleans. Less than 2 years earlier, not a single drug-eluting stent had been used in the United States outside of a clinical trial. The Food and Drug Administration first approved a drug-eluting stent in April 2003.
“We have not yet identified any subsets of patients who don't benefit from receiving drug-eluting stents [by having less restenosis] compared with bare metal stents,” said David J. Cohen, M.D., associate director of interventional cardiology at Beth Israel Deaconess Medical Center in Boston. “De facto practice in the United States today is to use drug-eluting stents whenever the available stent lengths and diameters fit. At Beth Israel Deaconess, most of the time when patients [who are undergoing coronary stenting] don't receive drug-eluting stents it's because the vessel is too small or too large to accommodate available stent sizes,” he told this newspaper.
They are so widespread that medicolegal concerns may now drive their use even more than purely clinical factors. “When the risk of restenosis is low, operators must balance the need for drug-eluting stents with the medicolegal risk of avoiding what has become the de facto standard of care for all patients,” said Herbert D. Aronow, M.D., director of the cardiac catheterization laboratories at the Veterans Affairs Medical Center in Philadelphia.
According to one study, in 2003, about a third of all sirolimus-eluting (Cypher) stents used in the United States were for off-label coronary artery indications (CARDIOLOGY NEWS, February 2005, p. 15).
As of early this year, no cardiology society had issued formal recommendations on the appropriate uses of drug-eluting stents, although these are expected soon. In the meantime, some experts have given their personal opinions.
One set of standards was laid out by Gregg W. Stone, M.D., in a talk at the AHA scientific session. “In workhorse lesions, in patients undergoing elective coronary interventions with de novo lesions up to 46 mm in length and in vessels with reference diameters of 2.5-3.75 mm without acute coronary syndrome or acute MI, in general the safety and efficacy of two drug-eluting stents, Cypher and Taxus [paclitaxel-eluting], has been proved,” said Dr. Stone, an interventional cardiologist at Columbia University in New York. “Using drug-eluting stents over bare metal stents in these lesions is the appropriate thing to do.”
But, he added, “we desperately need more data regarding the safety and efficacy of drug-eluting stents in unapproved and high-risk indications before their use should be considered routine. … You need to be aware of the evidence so you know what you are doing.”
A step was taken this past March to better define the safety and efficacy of drug-eluting stents in more complex vessels and lesions, with reports from two studies at the annual meeting of the American College of Cardiology. A Danish study with 322 patients compared sirolimus-eluting with bare-metal stents in patients with total occlusions, lesions at bifurcations, ostial lesions, and lesions in angulated arteries. Patients who received drug-eluting stents had better angiographic and clinical outcomes. A second report involved more than 1,100 patients who were treated with either paclitaxel-eluting or bare metal stents. The results showed that the drug-eluting stents were superior in coronaries narrower than 2.25 mm and in wide arteries.
According to Dr. Stone last November, there are also grounds for using a single drug-eluting stent to treat in-stent restenosis within a bare metal stent. But he cautioned physicians to “think twice” about using drug-eluting stents outside of a study for unprotected left main disease, in-stent restenosis following failed brachytherapy, and in patients with acute myocardial infarction. There is even less evidence on using drug-eluting stents for V-stenting of a bifurcation, and it is completely unclear how cardiologists should manage restenosis within a drug-eluting stent.
Despite their higher cost, and despite recent concerns about late thrombosis, drug-eluting stents now dominate.
In the final 3 months of 2004, drug-eluting stents were estimated to have been used for 87% of all interventional coronary procedures in the United States, Martin B. Leon, M.D., said last November at the American Heart Association's scientific sessions in New Orleans. Less than 2 years earlier, not a single drug-eluting stent had been used in the United States outside of a clinical trial. The Food and Drug Administration first approved a drug-eluting stent in April 2003.
“We have not yet identified any subsets of patients who don't benefit from receiving drug-eluting stents [by having less restenosis] compared with bare metal stents,” said David J. Cohen, M.D., associate director of interventional cardiology at Beth Israel Deaconess Medical Center in Boston. “De facto practice in the United States today is to use drug-eluting stents whenever the available stent lengths and diameters fit. At Beth Israel Deaconess, most of the time when patients [who are undergoing coronary stenting] don't receive drug-eluting stents it's because the vessel is too small or too large to accommodate available stent sizes,” he told this newspaper.
They are so widespread that medicolegal concerns may now drive their use even more than purely clinical factors. “When the risk of restenosis is low, operators must balance the need for drug-eluting stents with the medicolegal risk of avoiding what has become the de facto standard of care for all patients,” said Herbert D. Aronow, M.D., director of the cardiac catheterization laboratories at the Veterans Affairs Medical Center in Philadelphia.
According to one study, in 2003, about a third of all sirolimus-eluting (Cypher) stents used in the United States were for off-label coronary artery indications (CARDIOLOGY NEWS, February 2005, p. 15).
As of early this year, no cardiology society had issued formal recommendations on the appropriate uses of drug-eluting stents, although these are expected soon. In the meantime, some experts have given their personal opinions.
One set of standards was laid out by Gregg W. Stone, M.D., in a talk at the AHA scientific session. “In workhorse lesions, in patients undergoing elective coronary interventions with de novo lesions up to 46 mm in length and in vessels with reference diameters of 2.5-3.75 mm without acute coronary syndrome or acute MI, in general the safety and efficacy of two drug-eluting stents, Cypher and Taxus [paclitaxel-eluting], has been proved,” said Dr. Stone, an interventional cardiologist at Columbia University in New York. “Using drug-eluting stents over bare metal stents in these lesions is the appropriate thing to do.”
But, he added, “we desperately need more data regarding the safety and efficacy of drug-eluting stents in unapproved and high-risk indications before their use should be considered routine. … You need to be aware of the evidence so you know what you are doing.”
A step was taken this past March to better define the safety and efficacy of drug-eluting stents in more complex vessels and lesions, with reports from two studies at the annual meeting of the American College of Cardiology. A Danish study with 322 patients compared sirolimus-eluting with bare-metal stents in patients with total occlusions, lesions at bifurcations, ostial lesions, and lesions in angulated arteries. Patients who received drug-eluting stents had better angiographic and clinical outcomes. A second report involved more than 1,100 patients who were treated with either paclitaxel-eluting or bare metal stents. The results showed that the drug-eluting stents were superior in coronaries narrower than 2.25 mm and in wide arteries.
According to Dr. Stone last November, there are also grounds for using a single drug-eluting stent to treat in-stent restenosis within a bare metal stent. But he cautioned physicians to “think twice” about using drug-eluting stents outside of a study for unprotected left main disease, in-stent restenosis following failed brachytherapy, and in patients with acute myocardial infarction. There is even less evidence on using drug-eluting stents for V-stenting of a bifurcation, and it is completely unclear how cardiologists should manage restenosis within a drug-eluting stent.
Health Care Will Be Better and You Will Make It Happen

The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data driven with clear quality measurements, where better performance is rewarded by better compensation is coming to a hospital near you during your professional career. And SHM and hospitalists are at the center of this revolution in the care of the acutely ill patient.
Hospitals are complex organizations with many moving parts and many unique constituencies often with different and, at times, competing definitions of success. What is clear is that even though many people have been talking about rewarding quality or making the hospital work for the patient, the current system is primarily physician centered and driven by increasing units of activity rather than how well a job is done. If we had the ideal system the patient would be able to demand that the physician appear when he wanted him to and we would be paying more for the best quality of care.
In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change from the noisy centralized nurses’ station where the health professionals congregate to a place designed to have data and nurses and doctors at the bedside. This would be the first concrete step to get the important members of the team (physicians, nurses, pharmacists, therapists) closer to the patient and closer to each other. The next step is to figure out how best to use everyone’s knowledge and perspective of the patient to provide more efficient and more effective care. SHM is working with Robert Wood Johnson Foundation and others on this initiative.
We will need to shift the data we collect from being mostly about getting paid to more about measuring how good a job we are doing. And while we are at it, it would be good if we could agree on what should be measured and if we could create a constant format so we can compare performance between institutions and groups. It would also be nice if physicians would agree to even be measured, and even better if physicians would be active participants in validating and responding to the data.
Then we would need to get the payers, the businesses and the insurers, and the government to care enough about quality to put their money where their measurements are and start paying for better performance rather than for more units of service (e.g., more visits, procedures, or surgeries, no matter the indications or the outcomes).
Before you start thinking this is the raving of someone who wants manna from heaven, let me point out what is happening right now in 2005.
SHM has partnered with the Critical Care Institute of the American College of Chest Physicians (ACCP), the American Association of Critical Care Nurses (AACCN), the American Society of Health System Pharmacists (ASHP), and others to form a Critical Care Collaborative. Together these organizations represent over 100,000 healthcare professionals and through their leadership will work towards designing a more patient-focused approach that relies on communication and cooperation from the entire team responsible for delivering patient care. The goal will be to design and test models of care, as well as to increase recognition and awareness of existing models by tapping into the resources of the participating organizations. Efforts will be directed at all elements of the system including the point of care, support systems (IT), administration, payers, and regulatory bodies.
SHM is also actively participating in quality and team-based initiatives with the endocrine societies and the cardiology communities. This will lead to a new way of managing care in diabetes, heart failure, coronary artery disease, and deep vein thrombosis and pulmonary embolism.
On a national level President Bush has appointed David Brailler as the “health IT czar” with the charge to expand and integrate the information capabilities in health care. This coupled with the work being done at the National Quality Forum by Ken Kizer and others will lead to practical front line applications of standards of care and the ability to measure our performance in the reality of today’s hospital.
And even the payers are getting into the mix. The new buzz words are “pay for performance” and it is all the rage. CMS and others are well into beta test programs to see just how this would play out. Peer pressure and restriction of privileges have been the only concrete drivers to improve quality in the past. The prospect that demonstrable, measurable better care will translate into more compensation or greater market share is being tested in today’s hospital.
This is not a pipe dream or a Ralph Waldo Emerson essay. These initiatives are being driven by capable action oriented leaders who have a history of making change happen. And hospitalists, who for the most part are in the beginning of a 20 to 30-year professional career, are primed to play significant roles in this changing dynamic.
In the most basic way, today’s 12,000 hospitalists and the next 20,000 who will join us in the coming years must be much more than just willing participants to make this fly. Sure hospitalists will be the effector arm of health system change in their hospitals, but hospitalists must have
the skills and the vision to help shape this better day in health care. Hospitalists need to embrace the patient-centered, performance-driven acute care system. Hospitalists need to demand care delivered by teams and have the leadership skills to help these teams manage and lead change.
This wasn’t taught in medical school or residency, but that doesn’t matter. Hospital medicine as a new specialty has arrived coincident to (or by design at) a special moment in health care. Our patients have expectations of excellent care. There are plenty of resources available to do the best job. We just aren’t organized to be the best that we can be. But this will all be sorted out in the coming years. It is an exciting time to be a health professional, and hospitalists are at the center. And SHM has the vision and will have the programs to help our hospitalists be an important part in creating this new era of health care.
The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data driven with clear quality measurements, where better performance is rewarded by better compensation is coming to a hospital near you during your professional career. And SHM and hospitalists are at the center of this revolution in the care of the acutely ill patient.
Hospitals are complex organizations with many moving parts and many unique constituencies often with different and, at times, competing definitions of success. What is clear is that even though many people have been talking about rewarding quality or making the hospital work for the patient, the current system is primarily physician centered and driven by increasing units of activity rather than how well a job is done. If we had the ideal system the patient would be able to demand that the physician appear when he wanted him to and we would be paying more for the best quality of care.
In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change from the noisy centralized nurses’ station where the health professionals congregate to a place designed to have data and nurses and doctors at the bedside. This would be the first concrete step to get the important members of the team (physicians, nurses, pharmacists, therapists) closer to the patient and closer to each other. The next step is to figure out how best to use everyone’s knowledge and perspective of the patient to provide more efficient and more effective care. SHM is working with Robert Wood Johnson Foundation and others on this initiative.
We will need to shift the data we collect from being mostly about getting paid to more about measuring how good a job we are doing. And while we are at it, it would be good if we could agree on what should be measured and if we could create a constant format so we can compare performance between institutions and groups. It would also be nice if physicians would agree to even be measured, and even better if physicians would be active participants in validating and responding to the data.
Then we would need to get the payers, the businesses and the insurers, and the government to care enough about quality to put their money where their measurements are and start paying for better performance rather than for more units of service (e.g., more visits, procedures, or surgeries, no matter the indications or the outcomes).
Before you start thinking this is the raving of someone who wants manna from heaven, let me point out what is happening right now in 2005.
SHM has partnered with the Critical Care Institute of the American College of Chest Physicians (ACCP), the American Association of Critical Care Nurses (AACCN), the American Society of Health System Pharmacists (ASHP), and others to form a Critical Care Collaborative. Together these organizations represent over 100,000 healthcare professionals and through their leadership will work towards designing a more patient-focused approach that relies on communication and cooperation from the entire team responsible for delivering patient care. The goal will be to design and test models of care, as well as to increase recognition and awareness of existing models by tapping into the resources of the participating organizations. Efforts will be directed at all elements of the system including the point of care, support systems (IT), administration, payers, and regulatory bodies.
SHM is also actively participating in quality and team-based initiatives with the endocrine societies and the cardiology communities. This will lead to a new way of managing care in diabetes, heart failure, coronary artery disease, and deep vein thrombosis and pulmonary embolism.
On a national level President Bush has appointed David Brailler as the “health IT czar” with the charge to expand and integrate the information capabilities in health care. This coupled with the work being done at the National Quality Forum by Ken Kizer and others will lead to practical front line applications of standards of care and the ability to measure our performance in the reality of today’s hospital.
And even the payers are getting into the mix. The new buzz words are “pay for performance” and it is all the rage. CMS and others are well into beta test programs to see just how this would play out. Peer pressure and restriction of privileges have been the only concrete drivers to improve quality in the past. The prospect that demonstrable, measurable better care will translate into more compensation or greater market share is being tested in today’s hospital.
This is not a pipe dream or a Ralph Waldo Emerson essay. These initiatives are being driven by capable action oriented leaders who have a history of making change happen. And hospitalists, who for the most part are in the beginning of a 20 to 30-year professional career, are primed to play significant roles in this changing dynamic.
In the most basic way, today’s 12,000 hospitalists and the next 20,000 who will join us in the coming years must be much more than just willing participants to make this fly. Sure hospitalists will be the effector arm of health system change in their hospitals, but hospitalists must have
the skills and the vision to help shape this better day in health care. Hospitalists need to embrace the patient-centered, performance-driven acute care system. Hospitalists need to demand care delivered by teams and have the leadership skills to help these teams manage and lead change.
This wasn’t taught in medical school or residency, but that doesn’t matter. Hospital medicine as a new specialty has arrived coincident to (or by design at) a special moment in health care. Our patients have expectations of excellent care. There are plenty of resources available to do the best job. We just aren’t organized to be the best that we can be. But this will all be sorted out in the coming years. It is an exciting time to be a health professional, and hospitalists are at the center. And SHM has the vision and will have the programs to help our hospitalists be an important part in creating this new era of health care.
The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data driven with clear quality measurements, where better performance is rewarded by better compensation is coming to a hospital near you during your professional career. And SHM and hospitalists are at the center of this revolution in the care of the acutely ill patient.
Hospitals are complex organizations with many moving parts and many unique constituencies often with different and, at times, competing definitions of success. What is clear is that even though many people have been talking about rewarding quality or making the hospital work for the patient, the current system is primarily physician centered and driven by increasing units of activity rather than how well a job is done. If we had the ideal system the patient would be able to demand that the physician appear when he wanted him to and we would be paying more for the best quality of care.
In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change from the noisy centralized nurses’ station where the health professionals congregate to a place designed to have data and nurses and doctors at the bedside. This would be the first concrete step to get the important members of the team (physicians, nurses, pharmacists, therapists) closer to the patient and closer to each other. The next step is to figure out how best to use everyone’s knowledge and perspective of the patient to provide more efficient and more effective care. SHM is working with Robert Wood Johnson Foundation and others on this initiative.
We will need to shift the data we collect from being mostly about getting paid to more about measuring how good a job we are doing. And while we are at it, it would be good if we could agree on what should be measured and if we could create a constant format so we can compare performance between institutions and groups. It would also be nice if physicians would agree to even be measured, and even better if physicians would be active participants in validating and responding to the data.
Then we would need to get the payers, the businesses and the insurers, and the government to care enough about quality to put their money where their measurements are and start paying for better performance rather than for more units of service (e.g., more visits, procedures, or surgeries, no matter the indications or the outcomes).
Before you start thinking this is the raving of someone who wants manna from heaven, let me point out what is happening right now in 2005.
SHM has partnered with the Critical Care Institute of the American College of Chest Physicians (ACCP), the American Association of Critical Care Nurses (AACCN), the American Society of Health System Pharmacists (ASHP), and others to form a Critical Care Collaborative. Together these organizations represent over 100,000 healthcare professionals and through their leadership will work towards designing a more patient-focused approach that relies on communication and cooperation from the entire team responsible for delivering patient care. The goal will be to design and test models of care, as well as to increase recognition and awareness of existing models by tapping into the resources of the participating organizations. Efforts will be directed at all elements of the system including the point of care, support systems (IT), administration, payers, and regulatory bodies.
SHM is also actively participating in quality and team-based initiatives with the endocrine societies and the cardiology communities. This will lead to a new way of managing care in diabetes, heart failure, coronary artery disease, and deep vein thrombosis and pulmonary embolism.
On a national level President Bush has appointed David Brailler as the “health IT czar” with the charge to expand and integrate the information capabilities in health care. This coupled with the work being done at the National Quality Forum by Ken Kizer and others will lead to practical front line applications of standards of care and the ability to measure our performance in the reality of today’s hospital.
And even the payers are getting into the mix. The new buzz words are “pay for performance” and it is all the rage. CMS and others are well into beta test programs to see just how this would play out. Peer pressure and restriction of privileges have been the only concrete drivers to improve quality in the past. The prospect that demonstrable, measurable better care will translate into more compensation or greater market share is being tested in today’s hospital.
This is not a pipe dream or a Ralph Waldo Emerson essay. These initiatives are being driven by capable action oriented leaders who have a history of making change happen. And hospitalists, who for the most part are in the beginning of a 20 to 30-year professional career, are primed to play significant roles in this changing dynamic.
In the most basic way, today’s 12,000 hospitalists and the next 20,000 who will join us in the coming years must be much more than just willing participants to make this fly. Sure hospitalists will be the effector arm of health system change in their hospitals, but hospitalists must have
the skills and the vision to help shape this better day in health care. Hospitalists need to embrace the patient-centered, performance-driven acute care system. Hospitalists need to demand care delivered by teams and have the leadership skills to help these teams manage and lead change.
This wasn’t taught in medical school or residency, but that doesn’t matter. Hospital medicine as a new specialty has arrived coincident to (or by design at) a special moment in health care. Our patients have expectations of excellent care. There are plenty of resources available to do the best job. We just aren’t organized to be the best that we can be. But this will all be sorted out in the coming years. It is an exciting time to be a health professional, and hospitalists are at the center. And SHM has the vision and will have the programs to help our hospitalists be an important part in creating this new era of health care.
Five-Year Review of Codes Begins
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
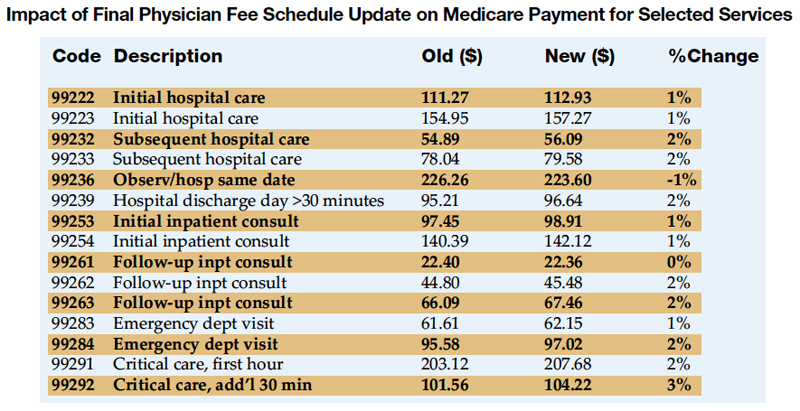
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at mjgorman@ipcm.com.
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at mjgorman@ipcm.com.
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at mjgorman@ipcm.com.
Other Pediatric Literature of Interest
1. Uehara R, Yashiro M, Nakamura Y, Yanagawa H. Clinical features of patients with Kawasaki disease whose parents had the same disease. Arch Pediatr Adolesc Med. 2004;158:1166-9.
Authors from the Department of Public Heath, Jichi Medical School and Saitama Prefectural University in Japan note that in the 35 years that have passed since the initial descriptions of Kawasaki disease some patients who had the disease have reached reproductive age and, thus, familial cases of two generations occur. Based on responses to nationwide surveys of hospitals and pediatric departments 65 cases of Kawasaki disease were identified in children whose parents had the same diagnosis. The odds for having sibling cases of Kawasaki disease were significantly increased for patients whose parents had the disease (OR, 6.94; 95% CI, 2.77–17.38). Patients with parental Kawasaki disease were also more likely to have recurrent disease, receive additional intravenous immunoglobulin administrations, and to have coronary artery abnormalities. The authors aptly discuss significant limitations to the study design; however, they conclude that these results highlight the need for exploration of a possible genetic contribution to pathogenesis of Kawasaki disease.
2. Jacobs RF, Maples HD, Aranda JV, et al. Pharmacokinetics of intravenously administered azithromycin in pediatric patients. Pediatr Infect Dis J. 2005;24:34-9.
Azithromyin is an azalide antibiotic with in vitro activity against a spectrum of bacterial pathogens commonly treated in pediatric infections. Currently intravenous (IV) azithromycin is only approved for use in adults. These researchers from three sites of the Pediatric Pharmacology Research Unit Network report results of an open-label single-dose pharmacokinetic and tolerance study of intravenous azithromycin in a pediatric population. This information will be required to facilitate approval for use in the pediatric population, as well as guide dosing for therapeutic trials. The authors studied pharmacokinetics in 29 patients ages 0.5 to <e;16 years of age and conclude that the disposition of IV administered azithromycin is comparable in patients in this age range; however, there was a tendency for increased clearance in younger children. The most common adverse effect was nausea that did not require intervention reported in 25% of the subjects.
3. Berger WE, Qaqundah PY, Blake, K, et al. Safety of budesonide inhalation suspension in infants aged six to twelve months with mild to moderate persistent asthma or recurrent wheeze. J Pediatr. 2005;146:91-5.
Current guidelines recommend inhaled corticosteroids (ICS) for long-term management of persistent asthma in children regardless of age. Currently the only nebulized ICS approved for use by the US Food and Drug Administration is budesonide. Controlled studies analyzing the safety and efficacy of budesonide exclusively in infants is lacking. Therefore, these researchers present a multicenter, randomized, double-blinded, parallel group, placebo-controlled study of 141 patients assessing the safety of once-daily administered nebulized budesonide in infants with persistent asthma. The primary outcome variable was adrenal function measured as mean changes from baseline to study end in postcosyntropin-stimulated plasma cortisol levels. The study was not powered to measure efficacy. The study concludes that the safety profile for nebulized budesonide was similar to that of placebo, with no suppression of adrenal function.
1. Uehara R, Yashiro M, Nakamura Y, Yanagawa H. Clinical features of patients with Kawasaki disease whose parents had the same disease. Arch Pediatr Adolesc Med. 2004;158:1166-9.
Authors from the Department of Public Heath, Jichi Medical School and Saitama Prefectural University in Japan note that in the 35 years that have passed since the initial descriptions of Kawasaki disease some patients who had the disease have reached reproductive age and, thus, familial cases of two generations occur. Based on responses to nationwide surveys of hospitals and pediatric departments 65 cases of Kawasaki disease were identified in children whose parents had the same diagnosis. The odds for having sibling cases of Kawasaki disease were significantly increased for patients whose parents had the disease (OR, 6.94; 95% CI, 2.77–17.38). Patients with parental Kawasaki disease were also more likely to have recurrent disease, receive additional intravenous immunoglobulin administrations, and to have coronary artery abnormalities. The authors aptly discuss significant limitations to the study design; however, they conclude that these results highlight the need for exploration of a possible genetic contribution to pathogenesis of Kawasaki disease.
2. Jacobs RF, Maples HD, Aranda JV, et al. Pharmacokinetics of intravenously administered azithromycin in pediatric patients. Pediatr Infect Dis J. 2005;24:34-9.
Azithromyin is an azalide antibiotic with in vitro activity against a spectrum of bacterial pathogens commonly treated in pediatric infections. Currently intravenous (IV) azithromycin is only approved for use in adults. These researchers from three sites of the Pediatric Pharmacology Research Unit Network report results of an open-label single-dose pharmacokinetic and tolerance study of intravenous azithromycin in a pediatric population. This information will be required to facilitate approval for use in the pediatric population, as well as guide dosing for therapeutic trials. The authors studied pharmacokinetics in 29 patients ages 0.5 to <e;16 years of age and conclude that the disposition of IV administered azithromycin is comparable in patients in this age range; however, there was a tendency for increased clearance in younger children. The most common adverse effect was nausea that did not require intervention reported in 25% of the subjects.
3. Berger WE, Qaqundah PY, Blake, K, et al. Safety of budesonide inhalation suspension in infants aged six to twelve months with mild to moderate persistent asthma or recurrent wheeze. J Pediatr. 2005;146:91-5.
Current guidelines recommend inhaled corticosteroids (ICS) for long-term management of persistent asthma in children regardless of age. Currently the only nebulized ICS approved for use by the US Food and Drug Administration is budesonide. Controlled studies analyzing the safety and efficacy of budesonide exclusively in infants is lacking. Therefore, these researchers present a multicenter, randomized, double-blinded, parallel group, placebo-controlled study of 141 patients assessing the safety of once-daily administered nebulized budesonide in infants with persistent asthma. The primary outcome variable was adrenal function measured as mean changes from baseline to study end in postcosyntropin-stimulated plasma cortisol levels. The study was not powered to measure efficacy. The study concludes that the safety profile for nebulized budesonide was similar to that of placebo, with no suppression of adrenal function.
1. Uehara R, Yashiro M, Nakamura Y, Yanagawa H. Clinical features of patients with Kawasaki disease whose parents had the same disease. Arch Pediatr Adolesc Med. 2004;158:1166-9.
Authors from the Department of Public Heath, Jichi Medical School and Saitama Prefectural University in Japan note that in the 35 years that have passed since the initial descriptions of Kawasaki disease some patients who had the disease have reached reproductive age and, thus, familial cases of two generations occur. Based on responses to nationwide surveys of hospitals and pediatric departments 65 cases of Kawasaki disease were identified in children whose parents had the same diagnosis. The odds for having sibling cases of Kawasaki disease were significantly increased for patients whose parents had the disease (OR, 6.94; 95% CI, 2.77–17.38). Patients with parental Kawasaki disease were also more likely to have recurrent disease, receive additional intravenous immunoglobulin administrations, and to have coronary artery abnormalities. The authors aptly discuss significant limitations to the study design; however, they conclude that these results highlight the need for exploration of a possible genetic contribution to pathogenesis of Kawasaki disease.
2. Jacobs RF, Maples HD, Aranda JV, et al. Pharmacokinetics of intravenously administered azithromycin in pediatric patients. Pediatr Infect Dis J. 2005;24:34-9.
Azithromyin is an azalide antibiotic with in vitro activity against a spectrum of bacterial pathogens commonly treated in pediatric infections. Currently intravenous (IV) azithromycin is only approved for use in adults. These researchers from three sites of the Pediatric Pharmacology Research Unit Network report results of an open-label single-dose pharmacokinetic and tolerance study of intravenous azithromycin in a pediatric population. This information will be required to facilitate approval for use in the pediatric population, as well as guide dosing for therapeutic trials. The authors studied pharmacokinetics in 29 patients ages 0.5 to <e;16 years of age and conclude that the disposition of IV administered azithromycin is comparable in patients in this age range; however, there was a tendency for increased clearance in younger children. The most common adverse effect was nausea that did not require intervention reported in 25% of the subjects.
3. Berger WE, Qaqundah PY, Blake, K, et al. Safety of budesonide inhalation suspension in infants aged six to twelve months with mild to moderate persistent asthma or recurrent wheeze. J Pediatr. 2005;146:91-5.
Current guidelines recommend inhaled corticosteroids (ICS) for long-term management of persistent asthma in children regardless of age. Currently the only nebulized ICS approved for use by the US Food and Drug Administration is budesonide. Controlled studies analyzing the safety and efficacy of budesonide exclusively in infants is lacking. Therefore, these researchers present a multicenter, randomized, double-blinded, parallel group, placebo-controlled study of 141 patients assessing the safety of once-daily administered nebulized budesonide in infants with persistent asthma. The primary outcome variable was adrenal function measured as mean changes from baseline to study end in postcosyntropin-stimulated plasma cortisol levels. The study was not powered to measure efficacy. The study concludes that the safety profile for nebulized budesonide was similar to that of placebo, with no suppression of adrenal function.
Pediatric in the Literature
Parents' Priorities and Satisfaction with Acute Pediatric Care
Ammentorp J, Mainz J, Sabroe S. Parents’ priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med. 2005;159:127-31.
Researchers from Kolding Hospital in Denmark designed this study to identify parents’ priorities of and satisfaction with care provided to pediatric patients by nurses and physicians. The cross-sectional study took place on the pediatric ward by enrolling consecutively admitted patients between 0800 and 2200 who spoke and understood Danish. The researchers designed and validated a 36 item questionnaire with input from 13 previous studies about patient satisfaction. The items were assessed using a 5-point Likert scale and were grouped into six dimensions of service: 1) Access to care and treatment, 2) Information and communication related to care and treatment, 3) Information related to practical conditions (i.e., orientation to the ward), 4) Physicians’ behavior, 5) Nurses’ behavior, and 6) Access to service. The survey consisted of two parts. Section 1 addressed priorities and was to be filled out by the parent(s) at admission. Section 2 addressed satisfaction and was to be filled out at discharge. The response rates for Section 1 and Section 2 were 84% and 67%, respectively. Statistical analysis demonstrated that parents could differentiate between priority and satisfaction.
Parents generally rated most aspects of care as important, and aspects related directly to treatment were rated highest. The three most important priorities with the assigned scores with 5 being the highest possible score were: 1) Find(ing) out what is wrong with the child (4.6), 2) Taking care of the child’s pain if it is relevant (4.6), and 3) Explanation of the diagnosis/problem (4.5). The least important items for parents in general were related to orientation of the ward. Interestingly, the least important item for parents in the study was having the child discharged the same day as admission (2.7).
Parents were most satisfied with the kindness of the nurses (4.4) and understanding the nurses information (4.3). The lowest satisfaction level was found with waiting time on the ward for medication evaluation, and this was also the greatest gap between priority and satisfaction for the parents in the study (priority 4.5, satisfaction 3.0)
The researchers present satisfaction and priority data together in a scatter plot with priority mean score on the vertical axis and satisfaction mean score on the horizontal access and in so doing create four quadrants that aid in focusing attention on improving quality on their ward. The researchers conclude that items that plot in the upper left quadrant deserve special attention as items that parents believe are important but are not satisfied with. Items differentiating between physician and nursing involvement in the same service areas were plotted as well, and results indicated that, in general, parents gave physician service higher priority but were more satisfied with nursing service.
The researchers conclude that the tool they describe is a validated questionnaire that can be used to evaluate parent priorities for and satisfaction with care provided on pediatric inpatient wards. This information can be used to guide further investigations and quality development. For the study ward this tool demonstrated that waiting time and communication with parents represented the most important areas for improvement.
Satisfaction is an important aspect of quality of care, as well an important attribute of the potential value added by physicians dedicated to inpatient medicine. Several important factors limit generalizing the specific conclusions of this study, including not including the non-Danish speaking minority and not identifying parents whose children have had multiple inpatient admissions. Regardless, the survey and scatter plot analysis with a “special attention” quadrant have obvious utility in the effort to produce quality improvement with regard to parents’ perception of the quality of care their children receive. Other interesting applications not specifically addressed in the study include measuring the priorities and satisfaction level of patients old enough to respond, including questions regarding service provided by nurse practitioners or physician’s assistants and testing to see if parents’ and/or patients’ priorities change from admission, through hospitalization, and at discharge.
Evaluation of a Staff-Only Hospitalist System in a Tertiary Care, Academic Children's Hospital
Dwight P, MacArthur C, Friedman JN, et al. Evaluation of a staff-only hospitalist system in a tertiary care, academic children’s hospital. Pediatrics. 2004;114:1545-9.
The division of pediatrics at The Hospital for Sick Children in Toronto, a tertiary care, academic center, operates a pediatric inpatient unit with approximately 4000 admissions each year. In 1995, limited resident duty hours led to a reorganization of inpatient pediatric teams to include two distinct hospitalist models: A hospitalist/housestaff model (CTU) and hospitalist staff -only model (CPU). The authors review recent research that has demonstrated the efficiency of hospitalist/housestaff systems in both adult and pediatric medicine and accurately point out that published data is lacking assessing the staff -only pediatric hospitalist model. Therefore, the authors designed a cohort study of 3807 admissions to the general inpatient pediatric unit between July 1, 1996 and June 30, 1997.
The primary outcome measure was length of stay, and secondary outcome measures included frequency of subspecialty consultation, readmission to the hospital, and death. Consultations were measured as none or >1 and readmissions were defined as admission within 7 days of discharge for the same or a related diagnosis. Clinically relevant information collected for each patient included age, gender, referral source, stay in a special care unit, most responsible diagnosis, and comorbidity. Comorbidity was defined as either an uncomplicated stay or a stay complicated by a chronic illness, series or important conditions, and/or a potentially life-threatening condition. The CTU team had a daily census of 24 to 30 patients and consisted of 1 attending pediatrician, 3 or 4 pediatric residents, and 2 medical students. CTU pediatricians attended this service 4–8 weeks each year. The CPU was staffed with 3 pediatricians who were responsible for all aspects of care Monday through Friday from 0800 to 1700 and on weekends. Medical students were included on this team. Overnight and weekends clinical fellows not part of the CPU team provided coverage. Each CPU physicians maintained a daily census of 8–10 patients. These physicians spent approximately 11 months of the year providing inpatient care.
During the study there were 3807 admissions, of which 33% were to the CPU and 67% were to the CTU. Patients admitted to the CPU were older (median age: 95 weeks vs. 69 weeks, p < .01) and less likely to have comorbidity (24% vs. 30%; p < .01). The diagnoses admitted to the two teams were not significantly different. The median length of hospital stay for the CPU team was 2.5 days (interquartile range [IQR]: 1.6–4.4 days) versus 2.9 days (IQR: 1.8–4.9) for the CTU team (p < .01). Multivariate linear regression showed a significant difference in length of stay after adjustment for age, gender and comorbidity (p < .04). The authors performed a stratified analysis of the 10 most frequent diagnoses admitted during the study period, and the median length of stay for these groups combined was shorter on the CPU team compared with the CTU team (2.1 days vs. 2.6 days, p < .01). There was no significant difference between the two teams with readmissions, frequency of consultation, or death.
The authors discuss some important limitations to the study. First, the unique characteristics of the individual unit studied inhibit the ability to generalize the results. Second, there were some differences in the baseline characteristics between the two groups, although multivariate analysis of theses differences did not change the statistical significance of the results. Finally, satisfaction of patients, families, and care providers was not measured.
These researchers conclude that within this system the hospitalist staff -only team reduced the length of stay by 14% compared with an attending staff/housestaff team. Although statistically significant, the clinical significance of this reduction in length of stay is unclear and the authors did not include financial data in the study design. Despite these facts, the authors make an important assertion that the difference in stay of 8 hours may be enough to promote throughput by decreasing wait times for admissions from the emergency departments and/or special care units. Additional studies are required to test this assertion.
Parents' Priorities and Satisfaction with Acute Pediatric Care
Ammentorp J, Mainz J, Sabroe S. Parents’ priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med. 2005;159:127-31.
Researchers from Kolding Hospital in Denmark designed this study to identify parents’ priorities of and satisfaction with care provided to pediatric patients by nurses and physicians. The cross-sectional study took place on the pediatric ward by enrolling consecutively admitted patients between 0800 and 2200 who spoke and understood Danish. The researchers designed and validated a 36 item questionnaire with input from 13 previous studies about patient satisfaction. The items were assessed using a 5-point Likert scale and were grouped into six dimensions of service: 1) Access to care and treatment, 2) Information and communication related to care and treatment, 3) Information related to practical conditions (i.e., orientation to the ward), 4) Physicians’ behavior, 5) Nurses’ behavior, and 6) Access to service. The survey consisted of two parts. Section 1 addressed priorities and was to be filled out by the parent(s) at admission. Section 2 addressed satisfaction and was to be filled out at discharge. The response rates for Section 1 and Section 2 were 84% and 67%, respectively. Statistical analysis demonstrated that parents could differentiate between priority and satisfaction.
Parents generally rated most aspects of care as important, and aspects related directly to treatment were rated highest. The three most important priorities with the assigned scores with 5 being the highest possible score were: 1) Find(ing) out what is wrong with the child (4.6), 2) Taking care of the child’s pain if it is relevant (4.6), and 3) Explanation of the diagnosis/problem (4.5). The least important items for parents in general were related to orientation of the ward. Interestingly, the least important item for parents in the study was having the child discharged the same day as admission (2.7).
Parents were most satisfied with the kindness of the nurses (4.4) and understanding the nurses information (4.3). The lowest satisfaction level was found with waiting time on the ward for medication evaluation, and this was also the greatest gap between priority and satisfaction for the parents in the study (priority 4.5, satisfaction 3.0)
The researchers present satisfaction and priority data together in a scatter plot with priority mean score on the vertical axis and satisfaction mean score on the horizontal access and in so doing create four quadrants that aid in focusing attention on improving quality on their ward. The researchers conclude that items that plot in the upper left quadrant deserve special attention as items that parents believe are important but are not satisfied with. Items differentiating between physician and nursing involvement in the same service areas were plotted as well, and results indicated that, in general, parents gave physician service higher priority but were more satisfied with nursing service.
The researchers conclude that the tool they describe is a validated questionnaire that can be used to evaluate parent priorities for and satisfaction with care provided on pediatric inpatient wards. This information can be used to guide further investigations and quality development. For the study ward this tool demonstrated that waiting time and communication with parents represented the most important areas for improvement.
Satisfaction is an important aspect of quality of care, as well an important attribute of the potential value added by physicians dedicated to inpatient medicine. Several important factors limit generalizing the specific conclusions of this study, including not including the non-Danish speaking minority and not identifying parents whose children have had multiple inpatient admissions. Regardless, the survey and scatter plot analysis with a “special attention” quadrant have obvious utility in the effort to produce quality improvement with regard to parents’ perception of the quality of care their children receive. Other interesting applications not specifically addressed in the study include measuring the priorities and satisfaction level of patients old enough to respond, including questions regarding service provided by nurse practitioners or physician’s assistants and testing to see if parents’ and/or patients’ priorities change from admission, through hospitalization, and at discharge.
Evaluation of a Staff-Only Hospitalist System in a Tertiary Care, Academic Children's Hospital
Dwight P, MacArthur C, Friedman JN, et al. Evaluation of a staff-only hospitalist system in a tertiary care, academic children’s hospital. Pediatrics. 2004;114:1545-9.
The division of pediatrics at The Hospital for Sick Children in Toronto, a tertiary care, academic center, operates a pediatric inpatient unit with approximately 4000 admissions each year. In 1995, limited resident duty hours led to a reorganization of inpatient pediatric teams to include two distinct hospitalist models: A hospitalist/housestaff model (CTU) and hospitalist staff -only model (CPU). The authors review recent research that has demonstrated the efficiency of hospitalist/housestaff systems in both adult and pediatric medicine and accurately point out that published data is lacking assessing the staff -only pediatric hospitalist model. Therefore, the authors designed a cohort study of 3807 admissions to the general inpatient pediatric unit between July 1, 1996 and June 30, 1997.
The primary outcome measure was length of stay, and secondary outcome measures included frequency of subspecialty consultation, readmission to the hospital, and death. Consultations were measured as none or >1 and readmissions were defined as admission within 7 days of discharge for the same or a related diagnosis. Clinically relevant information collected for each patient included age, gender, referral source, stay in a special care unit, most responsible diagnosis, and comorbidity. Comorbidity was defined as either an uncomplicated stay or a stay complicated by a chronic illness, series or important conditions, and/or a potentially life-threatening condition. The CTU team had a daily census of 24 to 30 patients and consisted of 1 attending pediatrician, 3 or 4 pediatric residents, and 2 medical students. CTU pediatricians attended this service 4–8 weeks each year. The CPU was staffed with 3 pediatricians who were responsible for all aspects of care Monday through Friday from 0800 to 1700 and on weekends. Medical students were included on this team. Overnight and weekends clinical fellows not part of the CPU team provided coverage. Each CPU physicians maintained a daily census of 8–10 patients. These physicians spent approximately 11 months of the year providing inpatient care.
During the study there were 3807 admissions, of which 33% were to the CPU and 67% were to the CTU. Patients admitted to the CPU were older (median age: 95 weeks vs. 69 weeks, p < .01) and less likely to have comorbidity (24% vs. 30%; p < .01). The diagnoses admitted to the two teams were not significantly different. The median length of hospital stay for the CPU team was 2.5 days (interquartile range [IQR]: 1.6–4.4 days) versus 2.9 days (IQR: 1.8–4.9) for the CTU team (p < .01). Multivariate linear regression showed a significant difference in length of stay after adjustment for age, gender and comorbidity (p < .04). The authors performed a stratified analysis of the 10 most frequent diagnoses admitted during the study period, and the median length of stay for these groups combined was shorter on the CPU team compared with the CTU team (2.1 days vs. 2.6 days, p < .01). There was no significant difference between the two teams with readmissions, frequency of consultation, or death.
The authors discuss some important limitations to the study. First, the unique characteristics of the individual unit studied inhibit the ability to generalize the results. Second, there were some differences in the baseline characteristics between the two groups, although multivariate analysis of theses differences did not change the statistical significance of the results. Finally, satisfaction of patients, families, and care providers was not measured.
These researchers conclude that within this system the hospitalist staff -only team reduced the length of stay by 14% compared with an attending staff/housestaff team. Although statistically significant, the clinical significance of this reduction in length of stay is unclear and the authors did not include financial data in the study design. Despite these facts, the authors make an important assertion that the difference in stay of 8 hours may be enough to promote throughput by decreasing wait times for admissions from the emergency departments and/or special care units. Additional studies are required to test this assertion.
Parents' Priorities and Satisfaction with Acute Pediatric Care
Ammentorp J, Mainz J, Sabroe S. Parents’ priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med. 2005;159:127-31.
Researchers from Kolding Hospital in Denmark designed this study to identify parents’ priorities of and satisfaction with care provided to pediatric patients by nurses and physicians. The cross-sectional study took place on the pediatric ward by enrolling consecutively admitted patients between 0800 and 2200 who spoke and understood Danish. The researchers designed and validated a 36 item questionnaire with input from 13 previous studies about patient satisfaction. The items were assessed using a 5-point Likert scale and were grouped into six dimensions of service: 1) Access to care and treatment, 2) Information and communication related to care and treatment, 3) Information related to practical conditions (i.e., orientation to the ward), 4) Physicians’ behavior, 5) Nurses’ behavior, and 6) Access to service. The survey consisted of two parts. Section 1 addressed priorities and was to be filled out by the parent(s) at admission. Section 2 addressed satisfaction and was to be filled out at discharge. The response rates for Section 1 and Section 2 were 84% and 67%, respectively. Statistical analysis demonstrated that parents could differentiate between priority and satisfaction.
Parents generally rated most aspects of care as important, and aspects related directly to treatment were rated highest. The three most important priorities with the assigned scores with 5 being the highest possible score were: 1) Find(ing) out what is wrong with the child (4.6), 2) Taking care of the child’s pain if it is relevant (4.6), and 3) Explanation of the diagnosis/problem (4.5). The least important items for parents in general were related to orientation of the ward. Interestingly, the least important item for parents in the study was having the child discharged the same day as admission (2.7).
Parents were most satisfied with the kindness of the nurses (4.4) and understanding the nurses information (4.3). The lowest satisfaction level was found with waiting time on the ward for medication evaluation, and this was also the greatest gap between priority and satisfaction for the parents in the study (priority 4.5, satisfaction 3.0)
The researchers present satisfaction and priority data together in a scatter plot with priority mean score on the vertical axis and satisfaction mean score on the horizontal access and in so doing create four quadrants that aid in focusing attention on improving quality on their ward. The researchers conclude that items that plot in the upper left quadrant deserve special attention as items that parents believe are important but are not satisfied with. Items differentiating between physician and nursing involvement in the same service areas were plotted as well, and results indicated that, in general, parents gave physician service higher priority but were more satisfied with nursing service.
The researchers conclude that the tool they describe is a validated questionnaire that can be used to evaluate parent priorities for and satisfaction with care provided on pediatric inpatient wards. This information can be used to guide further investigations and quality development. For the study ward this tool demonstrated that waiting time and communication with parents represented the most important areas for improvement.
Satisfaction is an important aspect of quality of care, as well an important attribute of the potential value added by physicians dedicated to inpatient medicine. Several important factors limit generalizing the specific conclusions of this study, including not including the non-Danish speaking minority and not identifying parents whose children have had multiple inpatient admissions. Regardless, the survey and scatter plot analysis with a “special attention” quadrant have obvious utility in the effort to produce quality improvement with regard to parents’ perception of the quality of care their children receive. Other interesting applications not specifically addressed in the study include measuring the priorities and satisfaction level of patients old enough to respond, including questions regarding service provided by nurse practitioners or physician’s assistants and testing to see if parents’ and/or patients’ priorities change from admission, through hospitalization, and at discharge.
Evaluation of a Staff-Only Hospitalist System in a Tertiary Care, Academic Children's Hospital
Dwight P, MacArthur C, Friedman JN, et al. Evaluation of a staff-only hospitalist system in a tertiary care, academic children’s hospital. Pediatrics. 2004;114:1545-9.
The division of pediatrics at The Hospital for Sick Children in Toronto, a tertiary care, academic center, operates a pediatric inpatient unit with approximately 4000 admissions each year. In 1995, limited resident duty hours led to a reorganization of inpatient pediatric teams to include two distinct hospitalist models: A hospitalist/housestaff model (CTU) and hospitalist staff -only model (CPU). The authors review recent research that has demonstrated the efficiency of hospitalist/housestaff systems in both adult and pediatric medicine and accurately point out that published data is lacking assessing the staff -only pediatric hospitalist model. Therefore, the authors designed a cohort study of 3807 admissions to the general inpatient pediatric unit between July 1, 1996 and June 30, 1997.
The primary outcome measure was length of stay, and secondary outcome measures included frequency of subspecialty consultation, readmission to the hospital, and death. Consultations were measured as none or >1 and readmissions were defined as admission within 7 days of discharge for the same or a related diagnosis. Clinically relevant information collected for each patient included age, gender, referral source, stay in a special care unit, most responsible diagnosis, and comorbidity. Comorbidity was defined as either an uncomplicated stay or a stay complicated by a chronic illness, series or important conditions, and/or a potentially life-threatening condition. The CTU team had a daily census of 24 to 30 patients and consisted of 1 attending pediatrician, 3 or 4 pediatric residents, and 2 medical students. CTU pediatricians attended this service 4–8 weeks each year. The CPU was staffed with 3 pediatricians who were responsible for all aspects of care Monday through Friday from 0800 to 1700 and on weekends. Medical students were included on this team. Overnight and weekends clinical fellows not part of the CPU team provided coverage. Each CPU physicians maintained a daily census of 8–10 patients. These physicians spent approximately 11 months of the year providing inpatient care.
During the study there were 3807 admissions, of which 33% were to the CPU and 67% were to the CTU. Patients admitted to the CPU were older (median age: 95 weeks vs. 69 weeks, p < .01) and less likely to have comorbidity (24% vs. 30%; p < .01). The diagnoses admitted to the two teams were not significantly different. The median length of hospital stay for the CPU team was 2.5 days (interquartile range [IQR]: 1.6–4.4 days) versus 2.9 days (IQR: 1.8–4.9) for the CTU team (p < .01). Multivariate linear regression showed a significant difference in length of stay after adjustment for age, gender and comorbidity (p < .04). The authors performed a stratified analysis of the 10 most frequent diagnoses admitted during the study period, and the median length of stay for these groups combined was shorter on the CPU team compared with the CTU team (2.1 days vs. 2.6 days, p < .01). There was no significant difference between the two teams with readmissions, frequency of consultation, or death.
The authors discuss some important limitations to the study. First, the unique characteristics of the individual unit studied inhibit the ability to generalize the results. Second, there were some differences in the baseline characteristics between the two groups, although multivariate analysis of theses differences did not change the statistical significance of the results. Finally, satisfaction of patients, families, and care providers was not measured.
These researchers conclude that within this system the hospitalist staff -only team reduced the length of stay by 14% compared with an attending staff/housestaff team. Although statistically significant, the clinical significance of this reduction in length of stay is unclear and the authors did not include financial data in the study design. Despite these facts, the authors make an important assertion that the difference in stay of 8 hours may be enough to promote throughput by decreasing wait times for admissions from the emergency departments and/or special care units. Additional studies are required to test this assertion.
TIPs Case Report
A 10-month-old Hispanic female presents to the emergency department with a chief complaint of being limp. The mother states that the first day of the child’s illness began with tactile fever. The patient did not have any diarrhea or vomiting. After presenting to the emergency department she was diagnosed with a left otitis media. At that time, intramuscular ceftriaxone was given and amoxicillin was prescribed. The second day the patient was doing well and there were no new problems. On the third day the patient woke up and was not moving her arms and legs as much as usual, did not want to sit up on her own, and was lying limp. Additionally, she had some decreased oral intake that day and one loose stool.
Upon follow up at the pediatrician’s office there was concern about how limp the child seemed and she was sent back to the emergency department for transfer to the children’s hospital. However, the emergency department did blood work, gave intravenous fluids, and after observing slight improvement in limb movement, discharged the child to home.
At home, the child spiked a temperature. She was brought to the pediatrician’s office the next day where slight improvement in movement and more alert affect were noted; however, concern remained regarding her overall decreased activity. The child was again sent to the emergency department for transport to the pediatric hospital.
Review of systems revealed one vomiting episode and one loose stool, slight runny nose, and decrease in oral intake 1 day prior to admission. They had recently returned form California from a weekend trip. There was no significant past medical history aside from an otitis media 4 months ago. The child was born full-term without any complications. The child does not take any chronic medications, but did take two doses of amoxicillin for one and a half days in addition to acetaminophen for fever. The child does not have any known allergies. Her diet includes breastmilk and table foods. Six month vaccinations are not completed, but prior vaccines had been given on schedule. The child lives with her mother only and family history was not significant. Developmentally the child rolled over at 4 months, sits without support, pulls to stand, and stands with help.
Physical exam showed a temperature of 100.5F, heart rate of 148, respiratory rate of 30, blood pressure 103/70, and a weight of 10.5 kg (90%). Patient is well developed and well nourished without any acute distress. Physical exam was pertinent for supple neck with head lag, generalized weakness with decreased muscular strength in the upper and lower extremities. Upper extremities strength was 4/5 and lower extremities were 3/5. Neck laxity was present, sitting required support, and she refused to stand. Neurologically the patient was alert with reflexes mildly decreased in the lower extremities.
Laboratory evaluation included a complete blood count with a white blood cell (WBC) count of 11.7 and of hemoglobin of 11.4. A comprehensive metabolic panel was within normal limits. Lumbar puncture showed glucose of 50, protein of 38, 2 WBCs, 2 red blood cells, and a negative gram stain. Urinalysis was negative. Erythrocyte sedimentation rate was 17, CPK was 57, and chest radiograph was negative.

At this time stool was sent for botulism toxin; however, there was no history of eating canned food or honey. While waiting for results the patient showed slight improvement in movement and activity and demonstrated good oral intake. Physical therapy and speech therapy were working with the patient and lower extremity movement was improving, but she still had diffi culty standing. At this time an MRI of the brain and cervical spine was ordered and showed an intramedullary lesion involving the cervical and upper thoracic cord with localized cord enlargement. Enhancement was seen along C5 and C6 to the T1 level without canal stenosis and normal anatomic alignment was noted (Figure 1). In the meantime, stool for botulism toxin returned negative. Treatment was started for the diagnosis of transverse myelitis and included dexamethasone 2 mg/kg once daily with a taper over 5 weeks. She had minimal improvement prior to discharge, but showed slow and steady resolution of symptoms. Follow up with neurology was to be done on an outpatient basis, as well as continuation of physical therapy and occupational therapy.
Discussion
Transverse myelitis or transverse myelopathy (TM) is a syndrome of acute or subacute inflammation involving the spinal cord with partial or complete loss of neurologic function. It is usually limited to a number of spinal segments. The incidence is 1.3 new cases per one million residents annually. It affects all ages and both sexes; however, is uncommon in children less than 10 years of age. There are three theories for the etiology: cell-mediated autoimmune inflammation and/or demyelination of the spinal cord, a direct viral infection of the cord, and a paraneoplastic remote effect of cancer.
Clinical features include abrupt onset of symptoms varying from hours to a few days. One third of patients have a preceding viral illness. An early sign is muscle weakness, especially of the lower limbs. There may be numbness at the midthoracic region, strength loss as extreme as paraplegia, loss of bowel or bladder control, or sensory loss, most commonly involves pain and temperature. Fifty percent may experience a sharp, gnawing back pain at the level of the myelitis. Progression of the disease can lead to spasticity and hyperreflexia.
There is not a confirmation of any pathophysiologic mechanism. Demyelination, neuronal injury, and incomplete or complete necrosis of neural tissue may be associated with inflammatory changes on biopsy.
Differential diagnosis includes idiopathic autoimmune transverse myelitis, acute disseminated encephalomyelitis, multiple sclerosis (MS), Guillain-Barre, viral myelitis, vasculitis, spinal cord infarction, paraneoplastic myelopathy, vascular malformations, and nutritional myelopathy. Additionally, infectious etiologies include HIV myelopathy, spirochetal infection, and poliomyelitis.
Diagnosis is by exclusion. First, a mechanical, compressive lesion must be excluded from the differential. MRI of the spine visualizes the myelin and excludes compression and is used primarily to exclude these possible etiologies. MRI of the brain is useful to diagnose multiple sclerosis. Lumbar puncture results are variable ranging from normal to nonspecifi c inflammatory changes including a mild increase in protein or leukocytosis with an increase in polymorponuclear cells. Glucose is usually normal.
It is important, especially in adolescents, to differentiate TM from MS and Guillain-Barre. In MS symptoms are more likely separated by time, with “attacks” and a relapsing and remitting presentation. MS patients typically present with numbness and weakness in more than one extremity. In Guillain-Barre syndrome the presentation may be similar to TM in that there is weakness in the lower extremity, areflexia, and a possible viral illness precedent. However, a dermatome localization of sensory loss on neurologic exam can differentiate between a spinal cord lesion and a peripheral nerve etiology.
Treatment for TM symptoms is nonspecifi c. If a specific etiology is found then specific treatment should be rendered, otherwise one must rule out infectious or systemic inflammatory disorders. Pharmacologic treatment commonly includes high dose steroids, for example methylprednisone 1 g IV daily for 3–5 days followed with an
oral steroid taper. The evidence in the literature supporting this therapeutic approach includes mostly small studies with inconsistent results. In addition, small, uncontrolled or pilot studies have demonstrated that cyclophosphamide, azathioprine and plasmapheresis alone or in addition to corticosteroids may improve outcomes. Larger scale randomized, blinded, and controlled studies are required to more clearly define the most safe and efficacious treatment for this uncommon pediatric diagnosis.
References
- Knebusch M, Strassburg HM, Reiners K. Acute myelitis in childhood: nine cases and review of the literature. Dev Med Child Neurol. 1998;40:631-9.
- Rolad L. Pathophysiology and clinical feature of Multiple sclerosis. Immune and Infectious Disease.408-11.
- Transverse Myelitis consortium working group. Proposed diagnostic and nosology of acute transverse myelitis. Neurology. 2002;59(4).
- Andronikou S, Albuquerque-Jonathan G, Wilmshurst J, Hewlett R. MRI fi nding in acute idiopathic transverse myelopathy in children. Pediatr Radiol. 2003;33:624-9.
- Corboy J, Price R. Myelitis and toxic, infl ammatory, and infectious disorders. Curr Opin Neurol Neurosurg. 1993;6:564-70.
- Rust R. Multiple sclerosis, acute disseminated encephalomyelitis, and related conditions. Semin Pediatr Neurol. 2000;7:66-90.
- Mewashingh L, Christiaens F, et al. Cervical myelitis from herpes simplex virus type 1. Pediatr Neurol. 2004;30:54-6.
- Dhiwakar M, Buxton N. Acute transverse myelitis mimicking and intramedullary neoplasm. Br J Neurosurg. 2004;18:72-3.
- Fegan, Cheng, Demmeller, Kaplan. Textbook of Pediatric Infectious Disease. 5th Ed. 2004:518-31.
- Samuels, Feske. Offi ce Practice of Neurology. 2nd Ed. 2003
A 10-month-old Hispanic female presents to the emergency department with a chief complaint of being limp. The mother states that the first day of the child’s illness began with tactile fever. The patient did not have any diarrhea or vomiting. After presenting to the emergency department she was diagnosed with a left otitis media. At that time, intramuscular ceftriaxone was given and amoxicillin was prescribed. The second day the patient was doing well and there were no new problems. On the third day the patient woke up and was not moving her arms and legs as much as usual, did not want to sit up on her own, and was lying limp. Additionally, she had some decreased oral intake that day and one loose stool.
Upon follow up at the pediatrician’s office there was concern about how limp the child seemed and she was sent back to the emergency department for transfer to the children’s hospital. However, the emergency department did blood work, gave intravenous fluids, and after observing slight improvement in limb movement, discharged the child to home.
At home, the child spiked a temperature. She was brought to the pediatrician’s office the next day where slight improvement in movement and more alert affect were noted; however, concern remained regarding her overall decreased activity. The child was again sent to the emergency department for transport to the pediatric hospital.
Review of systems revealed one vomiting episode and one loose stool, slight runny nose, and decrease in oral intake 1 day prior to admission. They had recently returned form California from a weekend trip. There was no significant past medical history aside from an otitis media 4 months ago. The child was born full-term without any complications. The child does not take any chronic medications, but did take two doses of amoxicillin for one and a half days in addition to acetaminophen for fever. The child does not have any known allergies. Her diet includes breastmilk and table foods. Six month vaccinations are not completed, but prior vaccines had been given on schedule. The child lives with her mother only and family history was not significant. Developmentally the child rolled over at 4 months, sits without support, pulls to stand, and stands with help.
Physical exam showed a temperature of 100.5F, heart rate of 148, respiratory rate of 30, blood pressure 103/70, and a weight of 10.5 kg (90%). Patient is well developed and well nourished without any acute distress. Physical exam was pertinent for supple neck with head lag, generalized weakness with decreased muscular strength in the upper and lower extremities. Upper extremities strength was 4/5 and lower extremities were 3/5. Neck laxity was present, sitting required support, and she refused to stand. Neurologically the patient was alert with reflexes mildly decreased in the lower extremities.
Laboratory evaluation included a complete blood count with a white blood cell (WBC) count of 11.7 and of hemoglobin of 11.4. A comprehensive metabolic panel was within normal limits. Lumbar puncture showed glucose of 50, protein of 38, 2 WBCs, 2 red blood cells, and a negative gram stain. Urinalysis was negative. Erythrocyte sedimentation rate was 17, CPK was 57, and chest radiograph was negative.
At this time stool was sent for botulism toxin; however, there was no history of eating canned food or honey. While waiting for results the patient showed slight improvement in movement and activity and demonstrated good oral intake. Physical therapy and speech therapy were working with the patient and lower extremity movement was improving, but she still had diffi culty standing. At this time an MRI of the brain and cervical spine was ordered and showed an intramedullary lesion involving the cervical and upper thoracic cord with localized cord enlargement. Enhancement was seen along C5 and C6 to the T1 level without canal stenosis and normal anatomic alignment was noted (Figure 1). In the meantime, stool for botulism toxin returned negative. Treatment was started for the diagnosis of transverse myelitis and included dexamethasone 2 mg/kg once daily with a taper over 5 weeks. She had minimal improvement prior to discharge, but showed slow and steady resolution of symptoms. Follow up with neurology was to be done on an outpatient basis, as well as continuation of physical therapy and occupational therapy.
Discussion
Transverse myelitis or transverse myelopathy (TM) is a syndrome of acute or subacute inflammation involving the spinal cord with partial or complete loss of neurologic function. It is usually limited to a number of spinal segments. The incidence is 1.3 new cases per one million residents annually. It affects all ages and both sexes; however, is uncommon in children less than 10 years of age. There are three theories for the etiology: cell-mediated autoimmune inflammation and/or demyelination of the spinal cord, a direct viral infection of the cord, and a paraneoplastic remote effect of cancer.
Clinical features include abrupt onset of symptoms varying from hours to a few days. One third of patients have a preceding viral illness. An early sign is muscle weakness, especially of the lower limbs. There may be numbness at the midthoracic region, strength loss as extreme as paraplegia, loss of bowel or bladder control, or sensory loss, most commonly involves pain and temperature. Fifty percent may experience a sharp, gnawing back pain at the level of the myelitis. Progression of the disease can lead to spasticity and hyperreflexia.
There is not a confirmation of any pathophysiologic mechanism. Demyelination, neuronal injury, and incomplete or complete necrosis of neural tissue may be associated with inflammatory changes on biopsy.
Differential diagnosis includes idiopathic autoimmune transverse myelitis, acute disseminated encephalomyelitis, multiple sclerosis (MS), Guillain-Barre, viral myelitis, vasculitis, spinal cord infarction, paraneoplastic myelopathy, vascular malformations, and nutritional myelopathy. Additionally, infectious etiologies include HIV myelopathy, spirochetal infection, and poliomyelitis.
Diagnosis is by exclusion. First, a mechanical, compressive lesion must be excluded from the differential. MRI of the spine visualizes the myelin and excludes compression and is used primarily to exclude these possible etiologies. MRI of the brain is useful to diagnose multiple sclerosis. Lumbar puncture results are variable ranging from normal to nonspecifi c inflammatory changes including a mild increase in protein or leukocytosis with an increase in polymorponuclear cells. Glucose is usually normal.
It is important, especially in adolescents, to differentiate TM from MS and Guillain-Barre. In MS symptoms are more likely separated by time, with “attacks” and a relapsing and remitting presentation. MS patients typically present with numbness and weakness in more than one extremity. In Guillain-Barre syndrome the presentation may be similar to TM in that there is weakness in the lower extremity, areflexia, and a possible viral illness precedent. However, a dermatome localization of sensory loss on neurologic exam can differentiate between a spinal cord lesion and a peripheral nerve etiology.
Treatment for TM symptoms is nonspecifi c. If a specific etiology is found then specific treatment should be rendered, otherwise one must rule out infectious or systemic inflammatory disorders. Pharmacologic treatment commonly includes high dose steroids, for example methylprednisone 1 g IV daily for 3–5 days followed with an
oral steroid taper. The evidence in the literature supporting this therapeutic approach includes mostly small studies with inconsistent results. In addition, small, uncontrolled or pilot studies have demonstrated that cyclophosphamide, azathioprine and plasmapheresis alone or in addition to corticosteroids may improve outcomes. Larger scale randomized, blinded, and controlled studies are required to more clearly define the most safe and efficacious treatment for this uncommon pediatric diagnosis.
References
- Knebusch M, Strassburg HM, Reiners K. Acute myelitis in childhood: nine cases and review of the literature. Dev Med Child Neurol. 1998;40:631-9.
- Rolad L. Pathophysiology and clinical feature of Multiple sclerosis. Immune and Infectious Disease.408-11.
- Transverse Myelitis consortium working group. Proposed diagnostic and nosology of acute transverse myelitis. Neurology. 2002;59(4).
- Andronikou S, Albuquerque-Jonathan G, Wilmshurst J, Hewlett R. MRI fi nding in acute idiopathic transverse myelopathy in children. Pediatr Radiol. 2003;33:624-9.
- Corboy J, Price R. Myelitis and toxic, infl ammatory, and infectious disorders. Curr Opin Neurol Neurosurg. 1993;6:564-70.
- Rust R. Multiple sclerosis, acute disseminated encephalomyelitis, and related conditions. Semin Pediatr Neurol. 2000;7:66-90.
- Mewashingh L, Christiaens F, et al. Cervical myelitis from herpes simplex virus type 1. Pediatr Neurol. 2004;30:54-6.
- Dhiwakar M, Buxton N. Acute transverse myelitis mimicking and intramedullary neoplasm. Br J Neurosurg. 2004;18:72-3.
- Fegan, Cheng, Demmeller, Kaplan. Textbook of Pediatric Infectious Disease. 5th Ed. 2004:518-31.
- Samuels, Feske. Offi ce Practice of Neurology. 2nd Ed. 2003
A 10-month-old Hispanic female presents to the emergency department with a chief complaint of being limp. The mother states that the first day of the child’s illness began with tactile fever. The patient did not have any diarrhea or vomiting. After presenting to the emergency department she was diagnosed with a left otitis media. At that time, intramuscular ceftriaxone was given and amoxicillin was prescribed. The second day the patient was doing well and there were no new problems. On the third day the patient woke up and was not moving her arms and legs as much as usual, did not want to sit up on her own, and was lying limp. Additionally, she had some decreased oral intake that day and one loose stool.
Upon follow up at the pediatrician’s office there was concern about how limp the child seemed and she was sent back to the emergency department for transfer to the children’s hospital. However, the emergency department did blood work, gave intravenous fluids, and after observing slight improvement in limb movement, discharged the child to home.
At home, the child spiked a temperature. She was brought to the pediatrician’s office the next day where slight improvement in movement and more alert affect were noted; however, concern remained regarding her overall decreased activity. The child was again sent to the emergency department for transport to the pediatric hospital.
Review of systems revealed one vomiting episode and one loose stool, slight runny nose, and decrease in oral intake 1 day prior to admission. They had recently returned form California from a weekend trip. There was no significant past medical history aside from an otitis media 4 months ago. The child was born full-term without any complications. The child does not take any chronic medications, but did take two doses of amoxicillin for one and a half days in addition to acetaminophen for fever. The child does not have any known allergies. Her diet includes breastmilk and table foods. Six month vaccinations are not completed, but prior vaccines had been given on schedule. The child lives with her mother only and family history was not significant. Developmentally the child rolled over at 4 months, sits without support, pulls to stand, and stands with help.
Physical exam showed a temperature of 100.5F, heart rate of 148, respiratory rate of 30, blood pressure 103/70, and a weight of 10.5 kg (90%). Patient is well developed and well nourished without any acute distress. Physical exam was pertinent for supple neck with head lag, generalized weakness with decreased muscular strength in the upper and lower extremities. Upper extremities strength was 4/5 and lower extremities were 3/5. Neck laxity was present, sitting required support, and she refused to stand. Neurologically the patient was alert with reflexes mildly decreased in the lower extremities.
Laboratory evaluation included a complete blood count with a white blood cell (WBC) count of 11.7 and of hemoglobin of 11.4. A comprehensive metabolic panel was within normal limits. Lumbar puncture showed glucose of 50, protein of 38, 2 WBCs, 2 red blood cells, and a negative gram stain. Urinalysis was negative. Erythrocyte sedimentation rate was 17, CPK was 57, and chest radiograph was negative.
At this time stool was sent for botulism toxin; however, there was no history of eating canned food or honey. While waiting for results the patient showed slight improvement in movement and activity and demonstrated good oral intake. Physical therapy and speech therapy were working with the patient and lower extremity movement was improving, but she still had diffi culty standing. At this time an MRI of the brain and cervical spine was ordered and showed an intramedullary lesion involving the cervical and upper thoracic cord with localized cord enlargement. Enhancement was seen along C5 and C6 to the T1 level without canal stenosis and normal anatomic alignment was noted (Figure 1). In the meantime, stool for botulism toxin returned negative. Treatment was started for the diagnosis of transverse myelitis and included dexamethasone 2 mg/kg once daily with a taper over 5 weeks. She had minimal improvement prior to discharge, but showed slow and steady resolution of symptoms. Follow up with neurology was to be done on an outpatient basis, as well as continuation of physical therapy and occupational therapy.
Discussion
Transverse myelitis or transverse myelopathy (TM) is a syndrome of acute or subacute inflammation involving the spinal cord with partial or complete loss of neurologic function. It is usually limited to a number of spinal segments. The incidence is 1.3 new cases per one million residents annually. It affects all ages and both sexes; however, is uncommon in children less than 10 years of age. There are three theories for the etiology: cell-mediated autoimmune inflammation and/or demyelination of the spinal cord, a direct viral infection of the cord, and a paraneoplastic remote effect of cancer.
Clinical features include abrupt onset of symptoms varying from hours to a few days. One third of patients have a preceding viral illness. An early sign is muscle weakness, especially of the lower limbs. There may be numbness at the midthoracic region, strength loss as extreme as paraplegia, loss of bowel or bladder control, or sensory loss, most commonly involves pain and temperature. Fifty percent may experience a sharp, gnawing back pain at the level of the myelitis. Progression of the disease can lead to spasticity and hyperreflexia.
There is not a confirmation of any pathophysiologic mechanism. Demyelination, neuronal injury, and incomplete or complete necrosis of neural tissue may be associated with inflammatory changes on biopsy.
Differential diagnosis includes idiopathic autoimmune transverse myelitis, acute disseminated encephalomyelitis, multiple sclerosis (MS), Guillain-Barre, viral myelitis, vasculitis, spinal cord infarction, paraneoplastic myelopathy, vascular malformations, and nutritional myelopathy. Additionally, infectious etiologies include HIV myelopathy, spirochetal infection, and poliomyelitis.
Diagnosis is by exclusion. First, a mechanical, compressive lesion must be excluded from the differential. MRI of the spine visualizes the myelin and excludes compression and is used primarily to exclude these possible etiologies. MRI of the brain is useful to diagnose multiple sclerosis. Lumbar puncture results are variable ranging from normal to nonspecifi c inflammatory changes including a mild increase in protein or leukocytosis with an increase in polymorponuclear cells. Glucose is usually normal.
It is important, especially in adolescents, to differentiate TM from MS and Guillain-Barre. In MS symptoms are more likely separated by time, with “attacks” and a relapsing and remitting presentation. MS patients typically present with numbness and weakness in more than one extremity. In Guillain-Barre syndrome the presentation may be similar to TM in that there is weakness in the lower extremity, areflexia, and a possible viral illness precedent. However, a dermatome localization of sensory loss on neurologic exam can differentiate between a spinal cord lesion and a peripheral nerve etiology.
Treatment for TM symptoms is nonspecifi c. If a specific etiology is found then specific treatment should be rendered, otherwise one must rule out infectious or systemic inflammatory disorders. Pharmacologic treatment commonly includes high dose steroids, for example methylprednisone 1 g IV daily for 3–5 days followed with an
oral steroid taper. The evidence in the literature supporting this therapeutic approach includes mostly small studies with inconsistent results. In addition, small, uncontrolled or pilot studies have demonstrated that cyclophosphamide, azathioprine and plasmapheresis alone or in addition to corticosteroids may improve outcomes. Larger scale randomized, blinded, and controlled studies are required to more clearly define the most safe and efficacious treatment for this uncommon pediatric diagnosis.
References
- Knebusch M, Strassburg HM, Reiners K. Acute myelitis in childhood: nine cases and review of the literature. Dev Med Child Neurol. 1998;40:631-9.
- Rolad L. Pathophysiology and clinical feature of Multiple sclerosis. Immune and Infectious Disease.408-11.
- Transverse Myelitis consortium working group. Proposed diagnostic and nosology of acute transverse myelitis. Neurology. 2002;59(4).
- Andronikou S, Albuquerque-Jonathan G, Wilmshurst J, Hewlett R. MRI fi nding in acute idiopathic transverse myelopathy in children. Pediatr Radiol. 2003;33:624-9.
- Corboy J, Price R. Myelitis and toxic, infl ammatory, and infectious disorders. Curr Opin Neurol Neurosurg. 1993;6:564-70.
- Rust R. Multiple sclerosis, acute disseminated encephalomyelitis, and related conditions. Semin Pediatr Neurol. 2000;7:66-90.
- Mewashingh L, Christiaens F, et al. Cervical myelitis from herpes simplex virus type 1. Pediatr Neurol. 2004;30:54-6.
- Dhiwakar M, Buxton N. Acute transverse myelitis mimicking and intramedullary neoplasm. Br J Neurosurg. 2004;18:72-3.
- Fegan, Cheng, Demmeller, Kaplan. Textbook of Pediatric Infectious Disease. 5th Ed. 2004:518-31.
- Samuels, Feske. Offi ce Practice of Neurology. 2nd Ed. 2003
Other Literature of Interest
1. Dexter PR, Perkins SM, Mahany KS, Jones K, McDonald CJ. Inpatient computer-based standing orders vs. physician reminders to increase influenza and pneumococcal vaccination rates: a randomized trial. JAMA. 2004; 292: 2366-71.
Past studies have suggested that most patients admitted with severe pneumococcal infections have been hospitalized in the preceding 5 years, and simply being hospitalized is a potential risk factor for later pneumococcal infection. Likewise, hospitalization provides an opportunity to vaccinate high-risk patients against influenza, and raising pneumococcal and influenza immunization rates is a CMS quality improvement priority. Prior investigations have supported the use of labor-intensive manual standing orders as well as computerized reminders, but this prospective trial was conducted in 1998 and 1999 to assess the effectiveness of a computer-based system to screen for eligible patients and then generate orders to perform pneumonia and influenza vaccinations on inpatients at the time of discharge.
Over 13 months, a total of 3777 inpatients were entered into the study. The hospital computer identified patients eligible for vaccination based on common criteria and randomized them to one of two groups of physician teams. For one group of teams, the computer order-entry system would automatically generate vaccination orders at the time of discharge for vaccine-eligible patients; for the other group of teams, only computer reminders were provided to physicians. The outcome measure was administration of vaccine; long-term outcomes such as incidence of subsequent disease or mortality were not measured.
During the study period, 50% of all hospitalized patients were identified as eligible for influenza vaccination; 22% were eligible for pneumococcal vaccination. In each case, the “standing order” group received vaccine more often (influenza: 42% vs. 30%, p<.001; pneumococcal vaccine: 51% vs. 31%). The numbers were subsequently adjusted to allow for patients who had previously received vaccine, but the impressive differences persisted. Nurses reported reasons for non-administration in 98% of the eligible patients who were not vaccinated; the most common reason was patient refusal. It is not clear if the physicians knew that a study was being conducted. No adverse reactions were reported.
CMS has pushed for the development of institutional standing order sets as a tool to improve compliance with vaccination rate targets. Where the technology is available, computer systems that can screen eligible patients and generate automatic orders are an effective tool in implementing many quality-improvement initiatives, and hospitalists are in a crucial position to take an active role in their development and implementation.
2. Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for a trial fibrillation. Ann Intern Med. 2004; 141: 745-52.
Warfarin has been shown to reduce risk of stroke in patients with chronic and paroxysmal atrial fibrillation. Intracranial hemorrhage remains one of the most feared complications of warfarin, especially among older patients, prompting suggestions to consider lower intensity anticoagulation among patients older than 75 years who have atrial fibrillation.
This study evaluated the relationship between the intensity of anticoagulation, risk of intracranial hemorrhage, and age of patients with atrial fibrillation.
This was a retrospective case control study conducted at a tertiary care medical center. One-hundred and seventy patients on warfarin and admitted with intracranial hemorrhage from 1993 to 2002 were matched with 1020 patients who were on warfarin but without intracranial bleed. After controlling for comorbid conditions and aspirin use, authors conducted multivariable logistic regression analysis to determine the odds of intracranial hemorrhage with regard to age and INR. The risk of intracranial hemorrhage increased at 85 years of age and at INR values of 3.5 or greater. The risk of intracranial hemorrhage at INR less than 2.0 did not differ statistically from the risk at INR of 2.0–3.0.
This study shows the risk of intracranial hemorrhage is not decreased by choosing lower intensity anticoagulation, and target INR should still be kept at 2.5 among elderly patients. However, patients older than 85 years should be counseled about their higher risk of intracranial hemorrhage.
3. Heeschen C, Hamm CW, Mitrovic V, et al. N-terminal pro-B-type natriuretic peptide levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation. 2004;110: 3206-12.
Recent data demonstrate the prognostic value of assessment of neurohormonal activation in patients with acute coronary syndromes (ACS). B-type natriuretic peptide levels (BNP) and levels of the N-terminal fragment of the BNP prohormone (NT-proBNP) predict adverse long-term outcomes in patients with ACS. Investigators reviewed plasma samples of Troponin T (TnT) and NT-proBNP obtained from patients with ACS enrolled in the Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) trial, which randomized patients to tirofiban or heparin for 48 hours and assessed mortality and myocardial infarction at 30 day follow-up. TnT and NT-proBNP determinations were available at baseline for 1791 patients, and at 48 and 72 hours from 1401 patients. Baseline NT-proBNP levels >250 ng/L were associated with significantly higher rates of death and myocardial infarction at 7 and 30 day follow-up. After adjustment for TnT and C-reactive protein levels, elevated NTproBNP levels maintained its predictive value (OR 2.7; p<.001). In patients with normal TnT levels, NT-proBNP levels identified a subgroup of patients at increased risk (OR 3.0; p=.004). However, in patients with high TnT levels (>0.1 mcg/L), NT-proBNP lost its predictive value (p=.58). More importantly, patients with normal levels of both TnT and NT-proBNP were at very low risk (0.6% event rate at 30 day follow-up).
Serial determinations of NT-proBNP levels at 48 and 72 hours were reviewed in patients without major adverse cardiac events (death or myocardial infarction); these patients were subdivided into groups with and without refractory ischemia. Patients without refractory ischemia showed a significant decline in NT-proBNP levels, whereas patients with refractory ischemia had no significant change. Persistently elevated NT-proBNP levels at 72 hours were associated with a 17.2% risk of death or MI at 30 days, compared with 0.6% risk if NT-proBNP returned to normal at 72 hours (p<.001). Neither TnT nor C-reactive protein demonstrated similar predictive value.
The study is limited by its retrospective nature, by potential selection bias by including only patients with direct evidence of coronary artery disease, and by limitations of the generalizability of its findings (e.g., to emergency department patients with chest pain).
As BNP and NT-proBNP are counter-regulatory hormones that play an active role in the response to ischemic injury, the authors suggest that NT-proBNP is a promising tool for dynamic risk assessment in patients with ACS. The authors also do not differentiate between BNP and NT-proBNP with regard to use in risk stratification, which might lead one to believe that these tests share similar predictive value. (Of note, the study was entirely funded by a company that produces an assay for NT-proBNP). Prospective trials to validate this tool are warranted
4. Heuschmann PU, Kolominsky-Rabas PL, Roether J, et al. Predictors of in-hospital mortality in patients with acute ischemic stroke treated with thrombolytic therapy. JAMA. 2004;292:1831-38.
The objective of this study was to identify factors associated with in-hospital mortality in ischemic stroke patients treated with recombinant tissue plasminogen activator (tPA). It was a prospective observational cohort study of 1658 patients conducted at 225 community and academic hospitals throughout Germany with main outcome of in-hospital mortality.
In this study 10% of patients who were treated with tPA died during their hospital stay, with 2/3 of deaths occurring in the first 7 days. Relative probability of in-hospital mortality increased with increasing patient age, with an odds ratio (OR) of 1.6 for each 10-year increment in age. Age was an independent predictor of in hospital mortality irrespective of tPA administration, with patients older than 75 years age having 4 fold higher mortality than the youngest cohort of less than 55 years age.
Other factors predicting in hospital mortality were altered level of consciousness and relative lack of experience with tPA treatment in the center. Altered level of consciousness was a predictor of stroke severity and an independent predictor of in-hospital mortality (OR 3.4). The increase in mortality in centers with limited experience with tPA administration (OR 0.97) reflected learning curve issues with these patients. The study was not designed to separate out the confounders of operator experience curve from institutional experience curves, or to derive the exact relationship between experience and outcomes.
5. McAlister FA, Bertsch K, Man J, et al. Incidence of and risk factors for pulmonary complications after non-thoracic surgery. Am J Respir Crit Care Med. 2004; published ahead of print on November 24, 2004 as doi:10.1164/rccm.200408-1069OC. Accessed January 27, 2005.
Postoperative pulmonary complications after nonthoracic surgery are a cause of significant morbidity and increased length of hospital stay. Previous studies of preoperative pulmonary assessment were limited by non-representative patient samples, conflicting results, and lack of explicit definitions of these complications. The authors conducted a prospective cohort study of 1055 patients seen in a Pre-Admission Clinic of a tertiary care university hospital. Mean age was 55 years, 50% male, and the cohort consisted of patients scheduled for intermediate risk elective surgery (upper abdominal, lower abdominal, orthopedic). They evaluated physical exam maneuvers (cough test, wheeze test, maximal laryngeal height, and forced expiratory time, all of which are described in an online data supplement) and preoperative spirometry values, and collected information on clinically significant postoperative pulmonary complications, including pneumonia, respiratory failure requiring mechanical ventilation, atelectasis requiring bronchoscopy, or pneumothorax or pleural effusion requiring percutaneous intervention. Twenty-eight patients (2.7%) suffered a pulmonary complication within 7 days of surgery, one of whom died. Length of stay was significantly prolonged in this group (mean 27.9 days vs 4.5 days, p=.006). Multivariate regression analysis revealed four variables that were independently associated with increased risk for postoperative pulmonary complications: age > 65 years, positive cough test (repeated coughing after asking the patient to inhale deeply and cough once), perioperative nasogastric tube, and anesthesia duration 2.5 hours or greater. Number of pack years smoked, FEV1, FEV1/FVC ratio, and upper abdominal surgery were associated with postoperative pulmonary complications but were not found to be independently associated by multivariate analysis.
While it is not surprising that the above risk factors are predictive of postoperative complications, this is the first study to incorporate specific exam maneuvers and spirometry into a risk prediction analysis. Limitations of this model are lack of independent validation and lack of generalizability to other populations, e.g., inpatients awaiting urgent surgery. Of note, the study further provides further support for not routinely obtaining pulmonary function testing for risk stratification prior to noncardiac surgery.
6. Mortenson, EM, Restrepo M, Anzeuto A, Pugh J. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J Med. 2004;117:726-31.
The American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) have published guidelines for the management of community acquired pneumonia that include recommendations for antibiotic selection. This retrospective cohort study attempted to measure the association between adherence to such guidelines and 30-day mortality in patients admitted with pneumonia to two Texas hospitals.
The characteristics of the patients studied reflect a reasonable cross-section of typical pneumonia patients, with the exception that the patients were mostly (85%) men. Of the study population, 78% were admitted through the ER, 20% admitted to the ICU, and 9% were nursing home residents. Antibiotics were considered “concordant” if they were consistent with either the most recent IDSA or ATS recommendations. The “nonconcordant” group was slightly older (66 vs. 61), generally sicker (higher rate of comorbid COPD and CVD), had more cerebrovascular disease, was more likely to present with altered mental status, and less frequently received antibiotics within 8 hours of presentation. The study did not comment on patients’ vaccination status. Thirty-day mortality was 6.2% in the guideline-concordant group, versus 21.7% in the other group (p < .001). The most common “non-concordant” regimen described was use of a beta-lactam alone, although specific antibiotic regimens were not evaluated.
While the results of this study are not surprising, they provide us with both the validation to continue practice according to existing recommendations, particularly the avoidance of monotherapy with beta-lactam antibiotics. The study also provides us with the imperative to take the lead in developing evidence-based pneumonia pathways at our own hospitals.
7. Pham MX, Whooley MA, Evans GT Jr, et al. Prognostic value of low-level cardiac troponin-I elevations in patients without definite acute coronary syndromes. Am Heart J. 2004;148: 776-82.
With the availability of rapid and highly sensitive and specific troponin testing, many patients admitted to the hospital with non-cardiac diagnoses have been recognized as having abnormal serum troponin-I or troponin-T levels, often just slightly above the reference cutoff for “normal.” While the clinical assumption is often that the elevated enzyme level does not reflect an acute coronary syndrome per se, its significance regarding the patient’s underlying cardiac health is often unclear.
Pham et al. retrospectively reviewed the 1-year mortality of 366 patients who were admitted to the San Francisco VA without evidence of acute MI or ACS either clinically or by EKG, but who had low-level troponin-I elevations (up to 3.0 ng/mL—a level that the authors state was reached by institutional consensus, and which was measured by a “first-generation” assay). These patients were admitted for a broad spectrum of diagnoses ranging from CHF to COPD to sepsis. Ninety-six percent of the patients were men; their average age was 69.
Follow-up was accomplished after a mean of 288 days and included 97% of patients. The primary endpoint was MI or death due to cardiac disease at one year; secondary endpoints were revascularization or admission for unstable angina. The primary endpoint was reached by 11% of patients with cTn-I between 1.0 and 3.0 ng/mL, and 4% of the patients with cTn-I up to 1.0 ng/mL (adjusted HR 3.4, 95% CI, 1.3 to 9.4), and the higher the cTn-I, the higher the risk. However, the authors did not test for the level of risk by specific diagnosis, so they caution against overgeneralizing their findings.
The findings of this study add to the evidence that any evidence of myocardial injury implies an increased risk of underlying heart disease and accompanying long—term cardiac complications– even if such injury occurs in the absence of ACS or known heart disease. Hospitalists often see such injury in the setting of acute infection and pulmonary disease and may be the first to recognize the possibility of CHD in a given patient. To date, guidelines addressing optimal prospective risk stratification have not been developed. Until they are, hospitalists should be aware of the ramifications of “troponin leak” and be prepared to initiate necessary inpatient monitoring and treatments, and to coordinate appropriate follow-up for these patients.
8. Saposnik G, Young B, Silver B, et al. Lack of improvement in patients with acute stroke after treatment with thrombolytic therapy: predictors and association with outcome. JAMA. 2004; 292: 1839-44.
Recombinant tissue plasminogen activator (tPA) has been shown to be one of the most efficacious therapies for acute stroke treatment. This was a systematic evaluation of predictors for outcomes at 24 hours after tPA therapy and of the prognostic significance of lack of improvement at 24 hours for long-term outcomes at 3 months.
The trial was a prospective cohort study of 216 consecutive patients admitted with acute ischemic stroke to a university hospital. The decision to treat with tPA was based on the NINDS protocol with one difference: patients with involvement of more than one third of the middle cerebral artery on the baseline CT scan were excluded. A control CT scan was performed at 24 hours to determine the presence of new infarction, cortical involvement, and extension of the ischemic lesion.
Lack of improvement was defined as a difference between the NIHSS score at baseline and at 24 hours of 3 points or less. Poor outcome at 3 months was defined by a modified Rankin Scale score of 3 to 5 or death.
After adjusting for age, gender, and stroke severity, hyperglycemia at admission (glucose > 144 mg/dL), cortical involvement, and time to treatment were independent predictors of lack of improvement at 24 hours. After adjusting for age, gender, and stroke severity, lack of improvement at 24 hours was an independent predictor of poor outcome and death at 3 months. Patients with lack of improvement at 24 hours also had longer lengths of hospitalization.
9. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004;351:2049-57.
Neurohormonal changes, endothelial dysfunction, impaired nitric oxide availability, and oxidant stress all contribute to the structural remodeling of the left ventricle in congestive heart failure. The combination of isosorbide dinitrate, an organic nitrate that stimulates nitric oxide signaling, and the antioxidant and vasodilator hydralazine improves survival in heart failure. Based on more recent data that black patients have a clinically significant response to this combination therapy, the authors of the African-American Heart Failure Trial (A-HeFT) evaluated 1050 black patients with congestive heart failure in a randomized, double-blind, placebo controlled trial. Patients were randomized to fixed doses of isosorbide dinitrate and hydralazine plus background therapy (i.e., digoxin, ACE inhibitors, beta-blockers, diuretics, angiotensin receptor blockers) or to placebo plus background therapy. After 18 months, the trial was stopped due to a significantly higher mortality rate in the placebo group (10.2% in the placebo group vs. 6.2% with combination
therapy, p=.02); survival differences emerged at 180 days and increased progressively thereafter. The combination therapy group reported more headache and dizziness but suffered fewer exacerbations of congestive heart failure and reported improvement in subjective assessments of quality of life as measured by questionnaires. Accompanying editorials discuss the role of nitric oxide and prevention of oxidative stress in the treatment of heart failure, as well as the controversial issues surrounding race-based therapeutics.
1. Dexter PR, Perkins SM, Mahany KS, Jones K, McDonald CJ. Inpatient computer-based standing orders vs. physician reminders to increase influenza and pneumococcal vaccination rates: a randomized trial. JAMA. 2004; 292: 2366-71.
Past studies have suggested that most patients admitted with severe pneumococcal infections have been hospitalized in the preceding 5 years, and simply being hospitalized is a potential risk factor for later pneumococcal infection. Likewise, hospitalization provides an opportunity to vaccinate high-risk patients against influenza, and raising pneumococcal and influenza immunization rates is a CMS quality improvement priority. Prior investigations have supported the use of labor-intensive manual standing orders as well as computerized reminders, but this prospective trial was conducted in 1998 and 1999 to assess the effectiveness of a computer-based system to screen for eligible patients and then generate orders to perform pneumonia and influenza vaccinations on inpatients at the time of discharge.
Over 13 months, a total of 3777 inpatients were entered into the study. The hospital computer identified patients eligible for vaccination based on common criteria and randomized them to one of two groups of physician teams. For one group of teams, the computer order-entry system would automatically generate vaccination orders at the time of discharge for vaccine-eligible patients; for the other group of teams, only computer reminders were provided to physicians. The outcome measure was administration of vaccine; long-term outcomes such as incidence of subsequent disease or mortality were not measured.
During the study period, 50% of all hospitalized patients were identified as eligible for influenza vaccination; 22% were eligible for pneumococcal vaccination. In each case, the “standing order” group received vaccine more often (influenza: 42% vs. 30%, p<.001; pneumococcal vaccine: 51% vs. 31%). The numbers were subsequently adjusted to allow for patients who had previously received vaccine, but the impressive differences persisted. Nurses reported reasons for non-administration in 98% of the eligible patients who were not vaccinated; the most common reason was patient refusal. It is not clear if the physicians knew that a study was being conducted. No adverse reactions were reported.
CMS has pushed for the development of institutional standing order sets as a tool to improve compliance with vaccination rate targets. Where the technology is available, computer systems that can screen eligible patients and generate automatic orders are an effective tool in implementing many quality-improvement initiatives, and hospitalists are in a crucial position to take an active role in their development and implementation.
2. Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for a trial fibrillation. Ann Intern Med. 2004; 141: 745-52.
Warfarin has been shown to reduce risk of stroke in patients with chronic and paroxysmal atrial fibrillation. Intracranial hemorrhage remains one of the most feared complications of warfarin, especially among older patients, prompting suggestions to consider lower intensity anticoagulation among patients older than 75 years who have atrial fibrillation.
This study evaluated the relationship between the intensity of anticoagulation, risk of intracranial hemorrhage, and age of patients with atrial fibrillation.
This was a retrospective case control study conducted at a tertiary care medical center. One-hundred and seventy patients on warfarin and admitted with intracranial hemorrhage from 1993 to 2002 were matched with 1020 patients who were on warfarin but without intracranial bleed. After controlling for comorbid conditions and aspirin use, authors conducted multivariable logistic regression analysis to determine the odds of intracranial hemorrhage with regard to age and INR. The risk of intracranial hemorrhage increased at 85 years of age and at INR values of 3.5 or greater. The risk of intracranial hemorrhage at INR less than 2.0 did not differ statistically from the risk at INR of 2.0–3.0.
This study shows the risk of intracranial hemorrhage is not decreased by choosing lower intensity anticoagulation, and target INR should still be kept at 2.5 among elderly patients. However, patients older than 85 years should be counseled about their higher risk of intracranial hemorrhage.
3. Heeschen C, Hamm CW, Mitrovic V, et al. N-terminal pro-B-type natriuretic peptide levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation. 2004;110: 3206-12.
Recent data demonstrate the prognostic value of assessment of neurohormonal activation in patients with acute coronary syndromes (ACS). B-type natriuretic peptide levels (BNP) and levels of the N-terminal fragment of the BNP prohormone (NT-proBNP) predict adverse long-term outcomes in patients with ACS. Investigators reviewed plasma samples of Troponin T (TnT) and NT-proBNP obtained from patients with ACS enrolled in the Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) trial, which randomized patients to tirofiban or heparin for 48 hours and assessed mortality and myocardial infarction at 30 day follow-up. TnT and NT-proBNP determinations were available at baseline for 1791 patients, and at 48 and 72 hours from 1401 patients. Baseline NT-proBNP levels >250 ng/L were associated with significantly higher rates of death and myocardial infarction at 7 and 30 day follow-up. After adjustment for TnT and C-reactive protein levels, elevated NTproBNP levels maintained its predictive value (OR 2.7; p<.001). In patients with normal TnT levels, NT-proBNP levels identified a subgroup of patients at increased risk (OR 3.0; p=.004). However, in patients with high TnT levels (>0.1 mcg/L), NT-proBNP lost its predictive value (p=.58). More importantly, patients with normal levels of both TnT and NT-proBNP were at very low risk (0.6% event rate at 30 day follow-up).
Serial determinations of NT-proBNP levels at 48 and 72 hours were reviewed in patients without major adverse cardiac events (death or myocardial infarction); these patients were subdivided into groups with and without refractory ischemia. Patients without refractory ischemia showed a significant decline in NT-proBNP levels, whereas patients with refractory ischemia had no significant change. Persistently elevated NT-proBNP levels at 72 hours were associated with a 17.2% risk of death or MI at 30 days, compared with 0.6% risk if NT-proBNP returned to normal at 72 hours (p<.001). Neither TnT nor C-reactive protein demonstrated similar predictive value.
The study is limited by its retrospective nature, by potential selection bias by including only patients with direct evidence of coronary artery disease, and by limitations of the generalizability of its findings (e.g., to emergency department patients with chest pain).
As BNP and NT-proBNP are counter-regulatory hormones that play an active role in the response to ischemic injury, the authors suggest that NT-proBNP is a promising tool for dynamic risk assessment in patients with ACS. The authors also do not differentiate between BNP and NT-proBNP with regard to use in risk stratification, which might lead one to believe that these tests share similar predictive value. (Of note, the study was entirely funded by a company that produces an assay for NT-proBNP). Prospective trials to validate this tool are warranted
4. Heuschmann PU, Kolominsky-Rabas PL, Roether J, et al. Predictors of in-hospital mortality in patients with acute ischemic stroke treated with thrombolytic therapy. JAMA. 2004;292:1831-38.
The objective of this study was to identify factors associated with in-hospital mortality in ischemic stroke patients treated with recombinant tissue plasminogen activator (tPA). It was a prospective observational cohort study of 1658 patients conducted at 225 community and academic hospitals throughout Germany with main outcome of in-hospital mortality.
In this study 10% of patients who were treated with tPA died during their hospital stay, with 2/3 of deaths occurring in the first 7 days. Relative probability of in-hospital mortality increased with increasing patient age, with an odds ratio (OR) of 1.6 for each 10-year increment in age. Age was an independent predictor of in hospital mortality irrespective of tPA administration, with patients older than 75 years age having 4 fold higher mortality than the youngest cohort of less than 55 years age.
Other factors predicting in hospital mortality were altered level of consciousness and relative lack of experience with tPA treatment in the center. Altered level of consciousness was a predictor of stroke severity and an independent predictor of in-hospital mortality (OR 3.4). The increase in mortality in centers with limited experience with tPA administration (OR 0.97) reflected learning curve issues with these patients. The study was not designed to separate out the confounders of operator experience curve from institutional experience curves, or to derive the exact relationship between experience and outcomes.
5. McAlister FA, Bertsch K, Man J, et al. Incidence of and risk factors for pulmonary complications after non-thoracic surgery. Am J Respir Crit Care Med. 2004; published ahead of print on November 24, 2004 as doi:10.1164/rccm.200408-1069OC. Accessed January 27, 2005.
Postoperative pulmonary complications after nonthoracic surgery are a cause of significant morbidity and increased length of hospital stay. Previous studies of preoperative pulmonary assessment were limited by non-representative patient samples, conflicting results, and lack of explicit definitions of these complications. The authors conducted a prospective cohort study of 1055 patients seen in a Pre-Admission Clinic of a tertiary care university hospital. Mean age was 55 years, 50% male, and the cohort consisted of patients scheduled for intermediate risk elective surgery (upper abdominal, lower abdominal, orthopedic). They evaluated physical exam maneuvers (cough test, wheeze test, maximal laryngeal height, and forced expiratory time, all of which are described in an online data supplement) and preoperative spirometry values, and collected information on clinically significant postoperative pulmonary complications, including pneumonia, respiratory failure requiring mechanical ventilation, atelectasis requiring bronchoscopy, or pneumothorax or pleural effusion requiring percutaneous intervention. Twenty-eight patients (2.7%) suffered a pulmonary complication within 7 days of surgery, one of whom died. Length of stay was significantly prolonged in this group (mean 27.9 days vs 4.5 days, p=.006). Multivariate regression analysis revealed four variables that were independently associated with increased risk for postoperative pulmonary complications: age > 65 years, positive cough test (repeated coughing after asking the patient to inhale deeply and cough once), perioperative nasogastric tube, and anesthesia duration 2.5 hours or greater. Number of pack years smoked, FEV1, FEV1/FVC ratio, and upper abdominal surgery were associated with postoperative pulmonary complications but were not found to be independently associated by multivariate analysis.
While it is not surprising that the above risk factors are predictive of postoperative complications, this is the first study to incorporate specific exam maneuvers and spirometry into a risk prediction analysis. Limitations of this model are lack of independent validation and lack of generalizability to other populations, e.g., inpatients awaiting urgent surgery. Of note, the study further provides further support for not routinely obtaining pulmonary function testing for risk stratification prior to noncardiac surgery.
6. Mortenson, EM, Restrepo M, Anzeuto A, Pugh J. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J Med. 2004;117:726-31.
The American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) have published guidelines for the management of community acquired pneumonia that include recommendations for antibiotic selection. This retrospective cohort study attempted to measure the association between adherence to such guidelines and 30-day mortality in patients admitted with pneumonia to two Texas hospitals.
The characteristics of the patients studied reflect a reasonable cross-section of typical pneumonia patients, with the exception that the patients were mostly (85%) men. Of the study population, 78% were admitted through the ER, 20% admitted to the ICU, and 9% were nursing home residents. Antibiotics were considered “concordant” if they were consistent with either the most recent IDSA or ATS recommendations. The “nonconcordant” group was slightly older (66 vs. 61), generally sicker (higher rate of comorbid COPD and CVD), had more cerebrovascular disease, was more likely to present with altered mental status, and less frequently received antibiotics within 8 hours of presentation. The study did not comment on patients’ vaccination status. Thirty-day mortality was 6.2% in the guideline-concordant group, versus 21.7% in the other group (p < .001). The most common “non-concordant” regimen described was use of a beta-lactam alone, although specific antibiotic regimens were not evaluated.
While the results of this study are not surprising, they provide us with both the validation to continue practice according to existing recommendations, particularly the avoidance of monotherapy with beta-lactam antibiotics. The study also provides us with the imperative to take the lead in developing evidence-based pneumonia pathways at our own hospitals.
7. Pham MX, Whooley MA, Evans GT Jr, et al. Prognostic value of low-level cardiac troponin-I elevations in patients without definite acute coronary syndromes. Am Heart J. 2004;148: 776-82.
With the availability of rapid and highly sensitive and specific troponin testing, many patients admitted to the hospital with non-cardiac diagnoses have been recognized as having abnormal serum troponin-I or troponin-T levels, often just slightly above the reference cutoff for “normal.” While the clinical assumption is often that the elevated enzyme level does not reflect an acute coronary syndrome per se, its significance regarding the patient’s underlying cardiac health is often unclear.
Pham et al. retrospectively reviewed the 1-year mortality of 366 patients who were admitted to the San Francisco VA without evidence of acute MI or ACS either clinically or by EKG, but who had low-level troponin-I elevations (up to 3.0 ng/mL—a level that the authors state was reached by institutional consensus, and which was measured by a “first-generation” assay). These patients were admitted for a broad spectrum of diagnoses ranging from CHF to COPD to sepsis. Ninety-six percent of the patients were men; their average age was 69.
Follow-up was accomplished after a mean of 288 days and included 97% of patients. The primary endpoint was MI or death due to cardiac disease at one year; secondary endpoints were revascularization or admission for unstable angina. The primary endpoint was reached by 11% of patients with cTn-I between 1.0 and 3.0 ng/mL, and 4% of the patients with cTn-I up to 1.0 ng/mL (adjusted HR 3.4, 95% CI, 1.3 to 9.4), and the higher the cTn-I, the higher the risk. However, the authors did not test for the level of risk by specific diagnosis, so they caution against overgeneralizing their findings.
The findings of this study add to the evidence that any evidence of myocardial injury implies an increased risk of underlying heart disease and accompanying long—term cardiac complications– even if such injury occurs in the absence of ACS or known heart disease. Hospitalists often see such injury in the setting of acute infection and pulmonary disease and may be the first to recognize the possibility of CHD in a given patient. To date, guidelines addressing optimal prospective risk stratification have not been developed. Until they are, hospitalists should be aware of the ramifications of “troponin leak” and be prepared to initiate necessary inpatient monitoring and treatments, and to coordinate appropriate follow-up for these patients.
8. Saposnik G, Young B, Silver B, et al. Lack of improvement in patients with acute stroke after treatment with thrombolytic therapy: predictors and association with outcome. JAMA. 2004; 292: 1839-44.
Recombinant tissue plasminogen activator (tPA) has been shown to be one of the most efficacious therapies for acute stroke treatment. This was a systematic evaluation of predictors for outcomes at 24 hours after tPA therapy and of the prognostic significance of lack of improvement at 24 hours for long-term outcomes at 3 months.
The trial was a prospective cohort study of 216 consecutive patients admitted with acute ischemic stroke to a university hospital. The decision to treat with tPA was based on the NINDS protocol with one difference: patients with involvement of more than one third of the middle cerebral artery on the baseline CT scan were excluded. A control CT scan was performed at 24 hours to determine the presence of new infarction, cortical involvement, and extension of the ischemic lesion.
Lack of improvement was defined as a difference between the NIHSS score at baseline and at 24 hours of 3 points or less. Poor outcome at 3 months was defined by a modified Rankin Scale score of 3 to 5 or death.
After adjusting for age, gender, and stroke severity, hyperglycemia at admission (glucose > 144 mg/dL), cortical involvement, and time to treatment were independent predictors of lack of improvement at 24 hours. After adjusting for age, gender, and stroke severity, lack of improvement at 24 hours was an independent predictor of poor outcome and death at 3 months. Patients with lack of improvement at 24 hours also had longer lengths of hospitalization.
9. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004;351:2049-57.
Neurohormonal changes, endothelial dysfunction, impaired nitric oxide availability, and oxidant stress all contribute to the structural remodeling of the left ventricle in congestive heart failure. The combination of isosorbide dinitrate, an organic nitrate that stimulates nitric oxide signaling, and the antioxidant and vasodilator hydralazine improves survival in heart failure. Based on more recent data that black patients have a clinically significant response to this combination therapy, the authors of the African-American Heart Failure Trial (A-HeFT) evaluated 1050 black patients with congestive heart failure in a randomized, double-blind, placebo controlled trial. Patients were randomized to fixed doses of isosorbide dinitrate and hydralazine plus background therapy (i.e., digoxin, ACE inhibitors, beta-blockers, diuretics, angiotensin receptor blockers) or to placebo plus background therapy. After 18 months, the trial was stopped due to a significantly higher mortality rate in the placebo group (10.2% in the placebo group vs. 6.2% with combination
therapy, p=.02); survival differences emerged at 180 days and increased progressively thereafter. The combination therapy group reported more headache and dizziness but suffered fewer exacerbations of congestive heart failure and reported improvement in subjective assessments of quality of life as measured by questionnaires. Accompanying editorials discuss the role of nitric oxide and prevention of oxidative stress in the treatment of heart failure, as well as the controversial issues surrounding race-based therapeutics.
1. Dexter PR, Perkins SM, Mahany KS, Jones K, McDonald CJ. Inpatient computer-based standing orders vs. physician reminders to increase influenza and pneumococcal vaccination rates: a randomized trial. JAMA. 2004; 292: 2366-71.
Past studies have suggested that most patients admitted with severe pneumococcal infections have been hospitalized in the preceding 5 years, and simply being hospitalized is a potential risk factor for later pneumococcal infection. Likewise, hospitalization provides an opportunity to vaccinate high-risk patients against influenza, and raising pneumococcal and influenza immunization rates is a CMS quality improvement priority. Prior investigations have supported the use of labor-intensive manual standing orders as well as computerized reminders, but this prospective trial was conducted in 1998 and 1999 to assess the effectiveness of a computer-based system to screen for eligible patients and then generate orders to perform pneumonia and influenza vaccinations on inpatients at the time of discharge.
Over 13 months, a total of 3777 inpatients were entered into the study. The hospital computer identified patients eligible for vaccination based on common criteria and randomized them to one of two groups of physician teams. For one group of teams, the computer order-entry system would automatically generate vaccination orders at the time of discharge for vaccine-eligible patients; for the other group of teams, only computer reminders were provided to physicians. The outcome measure was administration of vaccine; long-term outcomes such as incidence of subsequent disease or mortality were not measured.
During the study period, 50% of all hospitalized patients were identified as eligible for influenza vaccination; 22% were eligible for pneumococcal vaccination. In each case, the “standing order” group received vaccine more often (influenza: 42% vs. 30%, p<.001; pneumococcal vaccine: 51% vs. 31%). The numbers were subsequently adjusted to allow for patients who had previously received vaccine, but the impressive differences persisted. Nurses reported reasons for non-administration in 98% of the eligible patients who were not vaccinated; the most common reason was patient refusal. It is not clear if the physicians knew that a study was being conducted. No adverse reactions were reported.
CMS has pushed for the development of institutional standing order sets as a tool to improve compliance with vaccination rate targets. Where the technology is available, computer systems that can screen eligible patients and generate automatic orders are an effective tool in implementing many quality-improvement initiatives, and hospitalists are in a crucial position to take an active role in their development and implementation.
2. Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for a trial fibrillation. Ann Intern Med. 2004; 141: 745-52.
Warfarin has been shown to reduce risk of stroke in patients with chronic and paroxysmal atrial fibrillation. Intracranial hemorrhage remains one of the most feared complications of warfarin, especially among older patients, prompting suggestions to consider lower intensity anticoagulation among patients older than 75 years who have atrial fibrillation.
This study evaluated the relationship between the intensity of anticoagulation, risk of intracranial hemorrhage, and age of patients with atrial fibrillation.
This was a retrospective case control study conducted at a tertiary care medical center. One-hundred and seventy patients on warfarin and admitted with intracranial hemorrhage from 1993 to 2002 were matched with 1020 patients who were on warfarin but without intracranial bleed. After controlling for comorbid conditions and aspirin use, authors conducted multivariable logistic regression analysis to determine the odds of intracranial hemorrhage with regard to age and INR. The risk of intracranial hemorrhage increased at 85 years of age and at INR values of 3.5 or greater. The risk of intracranial hemorrhage at INR less than 2.0 did not differ statistically from the risk at INR of 2.0–3.0.
This study shows the risk of intracranial hemorrhage is not decreased by choosing lower intensity anticoagulation, and target INR should still be kept at 2.5 among elderly patients. However, patients older than 85 years should be counseled about their higher risk of intracranial hemorrhage.
3. Heeschen C, Hamm CW, Mitrovic V, et al. N-terminal pro-B-type natriuretic peptide levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation. 2004;110: 3206-12.
Recent data demonstrate the prognostic value of assessment of neurohormonal activation in patients with acute coronary syndromes (ACS). B-type natriuretic peptide levels (BNP) and levels of the N-terminal fragment of the BNP prohormone (NT-proBNP) predict adverse long-term outcomes in patients with ACS. Investigators reviewed plasma samples of Troponin T (TnT) and NT-proBNP obtained from patients with ACS enrolled in the Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) trial, which randomized patients to tirofiban or heparin for 48 hours and assessed mortality and myocardial infarction at 30 day follow-up. TnT and NT-proBNP determinations were available at baseline for 1791 patients, and at 48 and 72 hours from 1401 patients. Baseline NT-proBNP levels >250 ng/L were associated with significantly higher rates of death and myocardial infarction at 7 and 30 day follow-up. After adjustment for TnT and C-reactive protein levels, elevated NTproBNP levels maintained its predictive value (OR 2.7; p<.001). In patients with normal TnT levels, NT-proBNP levels identified a subgroup of patients at increased risk (OR 3.0; p=.004). However, in patients with high TnT levels (>0.1 mcg/L), NT-proBNP lost its predictive value (p=.58). More importantly, patients with normal levels of both TnT and NT-proBNP were at very low risk (0.6% event rate at 30 day follow-up).
Serial determinations of NT-proBNP levels at 48 and 72 hours were reviewed in patients without major adverse cardiac events (death or myocardial infarction); these patients were subdivided into groups with and without refractory ischemia. Patients without refractory ischemia showed a significant decline in NT-proBNP levels, whereas patients with refractory ischemia had no significant change. Persistently elevated NT-proBNP levels at 72 hours were associated with a 17.2% risk of death or MI at 30 days, compared with 0.6% risk if NT-proBNP returned to normal at 72 hours (p<.001). Neither TnT nor C-reactive protein demonstrated similar predictive value.
The study is limited by its retrospective nature, by potential selection bias by including only patients with direct evidence of coronary artery disease, and by limitations of the generalizability of its findings (e.g., to emergency department patients with chest pain).
As BNP and NT-proBNP are counter-regulatory hormones that play an active role in the response to ischemic injury, the authors suggest that NT-proBNP is a promising tool for dynamic risk assessment in patients with ACS. The authors also do not differentiate between BNP and NT-proBNP with regard to use in risk stratification, which might lead one to believe that these tests share similar predictive value. (Of note, the study was entirely funded by a company that produces an assay for NT-proBNP). Prospective trials to validate this tool are warranted
4. Heuschmann PU, Kolominsky-Rabas PL, Roether J, et al. Predictors of in-hospital mortality in patients with acute ischemic stroke treated with thrombolytic therapy. JAMA. 2004;292:1831-38.
The objective of this study was to identify factors associated with in-hospital mortality in ischemic stroke patients treated with recombinant tissue plasminogen activator (tPA). It was a prospective observational cohort study of 1658 patients conducted at 225 community and academic hospitals throughout Germany with main outcome of in-hospital mortality.
In this study 10% of patients who were treated with tPA died during their hospital stay, with 2/3 of deaths occurring in the first 7 days. Relative probability of in-hospital mortality increased with increasing patient age, with an odds ratio (OR) of 1.6 for each 10-year increment in age. Age was an independent predictor of in hospital mortality irrespective of tPA administration, with patients older than 75 years age having 4 fold higher mortality than the youngest cohort of less than 55 years age.
Other factors predicting in hospital mortality were altered level of consciousness and relative lack of experience with tPA treatment in the center. Altered level of consciousness was a predictor of stroke severity and an independent predictor of in-hospital mortality (OR 3.4). The increase in mortality in centers with limited experience with tPA administration (OR 0.97) reflected learning curve issues with these patients. The study was not designed to separate out the confounders of operator experience curve from institutional experience curves, or to derive the exact relationship between experience and outcomes.
5. McAlister FA, Bertsch K, Man J, et al. Incidence of and risk factors for pulmonary complications after non-thoracic surgery. Am J Respir Crit Care Med. 2004; published ahead of print on November 24, 2004 as doi:10.1164/rccm.200408-1069OC. Accessed January 27, 2005.
Postoperative pulmonary complications after nonthoracic surgery are a cause of significant morbidity and increased length of hospital stay. Previous studies of preoperative pulmonary assessment were limited by non-representative patient samples, conflicting results, and lack of explicit definitions of these complications. The authors conducted a prospective cohort study of 1055 patients seen in a Pre-Admission Clinic of a tertiary care university hospital. Mean age was 55 years, 50% male, and the cohort consisted of patients scheduled for intermediate risk elective surgery (upper abdominal, lower abdominal, orthopedic). They evaluated physical exam maneuvers (cough test, wheeze test, maximal laryngeal height, and forced expiratory time, all of which are described in an online data supplement) and preoperative spirometry values, and collected information on clinically significant postoperative pulmonary complications, including pneumonia, respiratory failure requiring mechanical ventilation, atelectasis requiring bronchoscopy, or pneumothorax or pleural effusion requiring percutaneous intervention. Twenty-eight patients (2.7%) suffered a pulmonary complication within 7 days of surgery, one of whom died. Length of stay was significantly prolonged in this group (mean 27.9 days vs 4.5 days, p=.006). Multivariate regression analysis revealed four variables that were independently associated with increased risk for postoperative pulmonary complications: age > 65 years, positive cough test (repeated coughing after asking the patient to inhale deeply and cough once), perioperative nasogastric tube, and anesthesia duration 2.5 hours or greater. Number of pack years smoked, FEV1, FEV1/FVC ratio, and upper abdominal surgery were associated with postoperative pulmonary complications but were not found to be independently associated by multivariate analysis.
While it is not surprising that the above risk factors are predictive of postoperative complications, this is the first study to incorporate specific exam maneuvers and spirometry into a risk prediction analysis. Limitations of this model are lack of independent validation and lack of generalizability to other populations, e.g., inpatients awaiting urgent surgery. Of note, the study further provides further support for not routinely obtaining pulmonary function testing for risk stratification prior to noncardiac surgery.
6. Mortenson, EM, Restrepo M, Anzeuto A, Pugh J. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J Med. 2004;117:726-31.
The American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) have published guidelines for the management of community acquired pneumonia that include recommendations for antibiotic selection. This retrospective cohort study attempted to measure the association between adherence to such guidelines and 30-day mortality in patients admitted with pneumonia to two Texas hospitals.
The characteristics of the patients studied reflect a reasonable cross-section of typical pneumonia patients, with the exception that the patients were mostly (85%) men. Of the study population, 78% were admitted through the ER, 20% admitted to the ICU, and 9% were nursing home residents. Antibiotics were considered “concordant” if they were consistent with either the most recent IDSA or ATS recommendations. The “nonconcordant” group was slightly older (66 vs. 61), generally sicker (higher rate of comorbid COPD and CVD), had more cerebrovascular disease, was more likely to present with altered mental status, and less frequently received antibiotics within 8 hours of presentation. The study did not comment on patients’ vaccination status. Thirty-day mortality was 6.2% in the guideline-concordant group, versus 21.7% in the other group (p < .001). The most common “non-concordant” regimen described was use of a beta-lactam alone, although specific antibiotic regimens were not evaluated.
While the results of this study are not surprising, they provide us with both the validation to continue practice according to existing recommendations, particularly the avoidance of monotherapy with beta-lactam antibiotics. The study also provides us with the imperative to take the lead in developing evidence-based pneumonia pathways at our own hospitals.
7. Pham MX, Whooley MA, Evans GT Jr, et al. Prognostic value of low-level cardiac troponin-I elevations in patients without definite acute coronary syndromes. Am Heart J. 2004;148: 776-82.
With the availability of rapid and highly sensitive and specific troponin testing, many patients admitted to the hospital with non-cardiac diagnoses have been recognized as having abnormal serum troponin-I or troponin-T levels, often just slightly above the reference cutoff for “normal.” While the clinical assumption is often that the elevated enzyme level does not reflect an acute coronary syndrome per se, its significance regarding the patient’s underlying cardiac health is often unclear.
Pham et al. retrospectively reviewed the 1-year mortality of 366 patients who were admitted to the San Francisco VA without evidence of acute MI or ACS either clinically or by EKG, but who had low-level troponin-I elevations (up to 3.0 ng/mL—a level that the authors state was reached by institutional consensus, and which was measured by a “first-generation” assay). These patients were admitted for a broad spectrum of diagnoses ranging from CHF to COPD to sepsis. Ninety-six percent of the patients were men; their average age was 69.
Follow-up was accomplished after a mean of 288 days and included 97% of patients. The primary endpoint was MI or death due to cardiac disease at one year; secondary endpoints were revascularization or admission for unstable angina. The primary endpoint was reached by 11% of patients with cTn-I between 1.0 and 3.0 ng/mL, and 4% of the patients with cTn-I up to 1.0 ng/mL (adjusted HR 3.4, 95% CI, 1.3 to 9.4), and the higher the cTn-I, the higher the risk. However, the authors did not test for the level of risk by specific diagnosis, so they caution against overgeneralizing their findings.
The findings of this study add to the evidence that any evidence of myocardial injury implies an increased risk of underlying heart disease and accompanying long—term cardiac complications– even if such injury occurs in the absence of ACS or known heart disease. Hospitalists often see such injury in the setting of acute infection and pulmonary disease and may be the first to recognize the possibility of CHD in a given patient. To date, guidelines addressing optimal prospective risk stratification have not been developed. Until they are, hospitalists should be aware of the ramifications of “troponin leak” and be prepared to initiate necessary inpatient monitoring and treatments, and to coordinate appropriate follow-up for these patients.
8. Saposnik G, Young B, Silver B, et al. Lack of improvement in patients with acute stroke after treatment with thrombolytic therapy: predictors and association with outcome. JAMA. 2004; 292: 1839-44.
Recombinant tissue plasminogen activator (tPA) has been shown to be one of the most efficacious therapies for acute stroke treatment. This was a systematic evaluation of predictors for outcomes at 24 hours after tPA therapy and of the prognostic significance of lack of improvement at 24 hours for long-term outcomes at 3 months.
The trial was a prospective cohort study of 216 consecutive patients admitted with acute ischemic stroke to a university hospital. The decision to treat with tPA was based on the NINDS protocol with one difference: patients with involvement of more than one third of the middle cerebral artery on the baseline CT scan were excluded. A control CT scan was performed at 24 hours to determine the presence of new infarction, cortical involvement, and extension of the ischemic lesion.
Lack of improvement was defined as a difference between the NIHSS score at baseline and at 24 hours of 3 points or less. Poor outcome at 3 months was defined by a modified Rankin Scale score of 3 to 5 or death.
After adjusting for age, gender, and stroke severity, hyperglycemia at admission (glucose > 144 mg/dL), cortical involvement, and time to treatment were independent predictors of lack of improvement at 24 hours. After adjusting for age, gender, and stroke severity, lack of improvement at 24 hours was an independent predictor of poor outcome and death at 3 months. Patients with lack of improvement at 24 hours also had longer lengths of hospitalization.
9. Taylor AL, Ziesche S, Yancy C, et al. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004;351:2049-57.
Neurohormonal changes, endothelial dysfunction, impaired nitric oxide availability, and oxidant stress all contribute to the structural remodeling of the left ventricle in congestive heart failure. The combination of isosorbide dinitrate, an organic nitrate that stimulates nitric oxide signaling, and the antioxidant and vasodilator hydralazine improves survival in heart failure. Based on more recent data that black patients have a clinically significant response to this combination therapy, the authors of the African-American Heart Failure Trial (A-HeFT) evaluated 1050 black patients with congestive heart failure in a randomized, double-blind, placebo controlled trial. Patients were randomized to fixed doses of isosorbide dinitrate and hydralazine plus background therapy (i.e., digoxin, ACE inhibitors, beta-blockers, diuretics, angiotensin receptor blockers) or to placebo plus background therapy. After 18 months, the trial was stopped due to a significantly higher mortality rate in the placebo group (10.2% in the placebo group vs. 6.2% with combination
therapy, p=.02); survival differences emerged at 180 days and increased progressively thereafter. The combination therapy group reported more headache and dizziness but suffered fewer exacerbations of congestive heart failure and reported improvement in subjective assessments of quality of life as measured by questionnaires. Accompanying editorials discuss the role of nitric oxide and prevention of oxidative stress in the treatment of heart failure, as well as the controversial issues surrounding race-based therapeutics.