User login
Controversies in Respiratory Protective Equipment Selection and Use During COVID-19
One contentious issue during the COVID-19 crisis has been the appropriate selection and use of respiratory protective equipment (RPE) for healthcare workers (HCWs) in hospitals and long-term care settings. As of April 2020, discrepancies exist in the recommendations from health authorities such as the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and Canadian Standards Association (CSA). The first of these recommends a surgical mask for routine care and a respirator for high-risk care such as aerosol-generating procedures, while the CDC recommends respirators for all aspects of patient care for these SARS-CoV-2–infected patients, and the CSA risk assessment tool would also result in selection of a respirator.1-3
Given the contradictory guidance, we will discuss several important considerations for hospital leaders in the implementation of a healthcare respiratory protection program during the current pandemic, including a focused review of the empirical data on surgical mask vs face-fitted respirator (most commonly available in healthcare as N95 in North America), continuous use of the RPE throughout an entire shift vs targeted use when caring for patients, and key areas of uncertainty.
SURGICAL MASK OR RESPIRATOR
Surgical masks are traditionally used for protection against droplet transmission of respiratory infections, in which large droplets often fall to the ground within short distances; on the other hand, N95 respirators are used for much smaller airborne pathogens, which can remain suspended in the air for long periods of time. Although empiric studies have supported the superiority of respirators over surgical masks in simulated settings (frequently defined as a calculated concentration ratio outside vs inside the RPE), most clinical studies fail to demonstrate a difference in clinical outcomes such as the prevention of respiratory infection. For instance, an exposure study using saline aerosol to simulate viral particles showed that N95 respirators conferred up to 8 to 12 times greater protection against particulate penetration, compared with surgical masks.4 However, these advantages of respirators over surgical masks in carefully controlled laboratory studies do not seem to translate to decreased infection risk in real-world settings.
The effectiveness of N95 respirators vs surgical masks in preventing respiratory infections has been evaluated in a small number of clinical randomized, controlled trials (RCTs). We identified five systematic reviews and/or metanalyses published after 2010 and three RCTs published after 1990.5-12 The RCTs used laboratory-confirmed respiratory virus or clinical infection in HCWs as a clinical outcome, but studies differed in the implementation of RPE use (ie, continuous or targeted use). In a systematic review and metanalysis, Long et al identified six RCTs (9,171 participants) and concluded that, with the exception of laboratory-confirmed bacterial colonization, N95 respirators did not reduce the rate of laboratory-confirmed influenza, viral respiratory infections, or influenza-like illness among HCWs, compared with surgical masks.5 The authors noted risks of bias in these studies owing to the inability to blind and conceal allocation. In addition, the studies focused on infections that are known to transmit via droplet, such as influenza, so the results might not be applicable in the face of a new pandemic in which the important modes of transmission are not yet clear.
WHOLE-SHIFT OR INTERMITTENT USE
The evidence base evaluating continuous vs targeted use of RPE in healthcare settings is quite small. Continuous use refers to using the RPE during an entire shift, whereas targeted use involves using RPE only when caring for confirmed or suspected respiratory patients. In our literature review we identified only one RCT that included separate study arms for continuous and targeted N95 respirator use.13 The authors found a significantly lower rate of clinical respiratory illness among HCWs in the continuous-use group, compared with that in the targeted-use group. Limitations of the study included a relatively short follow-up of 4 weeks and uneven distribution of baseline characteristics, although the authors adjusted for these differences in their analysis. The study, however, did not compare continuous vs targeted use of surgical masks with regard to clinical outcomes. Based on the study results, we can only infer that continuous use of RPE, either surgical mask or N95 respirator, may provide additional benefit to HCWs vs targeted use only.
Given the lack of robust evidence informing continuous or targeted RPE use, we suggest some additional factors to guide decision making. In settings with high HCW compliance with universal RPE (above 50%), even noncompliant HCW are protected against clinical respiratory illness, which suggests a herd protective effect when universal RPE use is implemented, likely owing to the prevention of symptomatic or asymptomatic infectious spread among HCWs.14 It is important to note that the compliance rate may be limited by discomfort of prolonged wear of certain RPEs. One study reported that compliance rate is lower for continuous use (66%) than it is for targeted use (82%).13 Accumulated respiratory pathogen deposition on RPEs from an extended period of use that could result in self-contamination to the wearer is a potential concern, although these risks must be balanced against the repeated donning and doffing required by targeted use. Pilot studies examining viral particles left on surgical masks after being worn for entire shifts (or as long as tolerated) found that there were significantly more viral particles detected after 6 hours of continuous wear, which may increase the risk of self-contamination.15
UNCERTAINTIES
The current literature is applicable to infections that are known to spread via droplet contact, and this is a major limitation in generalizing the available evidence to the SARS-CoV-2 pandemic, in which debate persists regarding the exact mode of transmission. It is postulated that, even in infections traditionally considered to be spread by droplets, such as influenza, aerosol transmission may occur when HCWs are working in close proximity to the exposure source or when the droplet evaporates and becomes droplet nuclei. The United States National Academies of Science, Engineering, and Medicine expert consultation report, published in April 2020, concluded that current studies support the possibility of aerosolization of SARS-CoV-2 virus from normal breathing.16 As of April 2020, the WHO recommendation for SARS-CoV-2 is to use droplet contact precautions with a surgical mask for regular patient care and N95 respirator for aerosol-generating procedures.1 Although we have not come across any studies specifically comparing the efficacy between surgical mask to N95 respirator protection while performing aerosol-generating procedures, a systematic review found that certain aerosol-generating procedures, such as endotracheal intubation and noninvasive ventilation, conferred a significantly higher risk of transmission of SARS-CoV-1 to HCWs in 2003.17 For the current crisis, the CDC is taking a cautious approach in which N95 respirators are recommended for HCWs caring for patients with confirmed or suspected SARS-CoV-2 infection if the supply chain is secure, with advice in place in times of RPE shortage, such as use of expired respirators, other types of equivalent respirators, or respirators not approved by the National Institute for Occupational Safety and Health, as well as optimization of administrative and engineering controls (eg, telemedicine, limiting patient and visitor numbers, physical barriers, optimizing ventilation systems).2,18 This advice is unusual in terms of deviating from advising the most appropriate RPE, and we presume it reflects the present global supply problems.
RPEs are only one component of a necessary personal protective equipment ensemble. Although eye protection (goggles or face shields) is recommended by the WHO and CDC when caring for patients with SARS-CoV-2, there is considerable uncertainty regarding the incremental effectiveness of eye protection because such protection is usually worn in conjunction with RPE. A 2019 Cochrane review did not identify any good-quality studies that could inform judgments regarding the effectiveness of eye protective equipment,19 and a recent rapid review reporting on the efficacy of eye protection in primary care settings reached a similar conclusion.20 A risk-based approach would be to include eye protection in a well-designed personal protective equipment program.
In the absence of aerosol-generating procedures, N95 respirators confer no additional benefit in preventing HCW respiratory infections when droplet transmission is suspected. However, the applicability of the available evidence is limited given the uncertainties surrounding SARS-CoV-2 transmission. When RPE may become scarce during a pandemic, the risk of potential self-contamination must be weighed against RPE conservation strategies. RPE compliance, herd-protection effects of routine RPE use, and RPE contamination from prolonged use are therefore important elements to consider when implementing hospital policies regarding universal masking because they all impact the potential effectiveness of RPE.
CONCLUSIONS
At the present time we lack definitive evidence on the effectiveness of surgical masks vs respirators and continuous vs targeted RPE use in the hospital setting for SARS-CoV-2. If our goal is to minimize risk of HCW infection, continuous use of N95 respirator could be considered. However, a more pragmatic solution in the setting of a limited supply of N95 respirators would be continuous use of surgical masks while engaged in clinical care of patients under investigation or with confirmed COVID-19.
1. World Health Organization. Rational use of personal protective equipment for coronavirus disease (COVID-19): Interim guidance. February 27, 2020. https://apps.who.int/iris/bitstream/handle/10665/331215/WHO-2019-nCov-IPCPPE_use-2020.1-eng.pdf. Accessed April 1, 2020.
2. Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed April 1, 2020.
3. Canadian Standard Association. Selection, Use, and Care of Respirators (CAN/CSA-Z94.4-18). Toronto, Canada: CSA Group; 2018.
4. Lee SA, Grinshpun SA, Reponen T. Respiratory performance offered by N95 respirators and surgical masks: human subject evaluation with NaCl aerosol representing bacterial and viral particle size range. Ann Occup Hyg. 2008;52(3):177-185. https://doi.org/10.1093/annhyg/men005.
5. Long Y, Hu T, Liu L, et al. Effectiveness of N95 respirators versus surgical masks against influenza: a systematic review and meta‐analysis. J Evid Based Med. 2020. https://doi.org/10.1111/jebm.12381.
6. Offeddu V, Yung CF, Low MSF, Tam CC. Effectiveness of masks and respirators against respiratory infections in healthcare workers: a systematic review and meta-analysis. Clin Infect Dis. 2017;65(11):1934-1942. https://doi.org/10.1093/cid/cix681.
7. Smith JD, MacDougall CC, Johnstone J, Copes RA, Schwartz B, Garber GE. Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis. CMAJ. 2016;188(8):567-574. https://doi.org/10.1503/cmaj.150835.
8. Bin-Reza F, Lopez Chavarrias V, Nicoll A, Chamberland ME. The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence. Influenza Other Respir Viruses. 2012;6(4):257-267. https://doi.org/10.1111/j.1750-2659.2011.00307.x.
9. Jefferson T, Del Mar CB, Dooley L, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev. 2011;2011(7):CD006207. https://doi.org/10.1002/14651858.CD006207.pub4.
10. Radonovich LJ Jr, Simberkoff MS, Bessesen MT, et al. N95 respirators vs medical masks for preventing influenza among health care personnel: a randomized clinical trial. JAMA. 2019;322(9):824-833. https://doi.org/10.1001/jama.2019.11645.
11. MacIntyre CR, Chughtai AA, Rahman B, et al. The efficacy of medical masks and respirators against respiratory infection in healthcare workers. Influenza Other Respir Viruses. 2017;11(6):511-517. https://doi.org/10.1111/irv.12474.
12. Loeb M, Dafoe N, Mahony J, et al. Surgical mask vs N95 respirator for preventing influenza among health care workers. JAMA. 2009;302(17):1865-1871. https://doi.org/10.1001/jama.2009.1466.
13. Macintyre CR, Wang Q, Seale H, et al. A randomized clinical trial of three options for N95 respirators and medical masks in health workers. Am J Respir Crit Care Med. 2013;187(9):960-966. https://doi.org/10.1164/rccm.201207-1164OC.
14. Chen X, Chughtai AA, Macintyre CR. Herd protection effect of N95 respirators in healthcare workers. J Int Med Res. 2017;45(6):1760-1767. https://doi.org/10.1177/0300060516665491.
15. Chughtai AA, Stelzer-Braid S, Rawlinson W, et al. Contamination by respiratory viruses on outer surface of medical masks used by hospital healthcare workers. BMC Infect Dis. 2019;19(1):491. https://doi.org/10.1186/s12879-019-4109-x.
16. National Research Council. Rapid Expert Consultation on the Possibility of Bioaerosol Spread of SARS-CoV-2 for the COVID-19 Pandemic (April 1, 2020). Washington, DC: National Academies Press; 2020. https://doi.org/10.17226/25769.
17. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. https://doi.org/10.1371/journal.pone.0035797.
18. Centers for Disease Control and Prevention. Strategies for Optimizing the Supply of N95 Respirators: COVID-19. 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/respirators-strategy/crisis-alternate-strategies.html. Accessed March 31, 2020.
19. Verbeek JH, Rajamaki B, Ijaz S, et al. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst Rev. 2019;7(7):CD011621. https://doi.org/10.1002/14651858.CD011621.pub3.
20. Khunti K, Greenhalgh T, Chan XH, et al. What is the efficacy of eye protection equipment compared to no eye protection equipment in preventing transmission of COVID-19-type respiratory illnesses in primary and community care?. CEBM. April 3, 2020. https://www.cebm.net/covid-19/what-is-the-efficacy-of-eye-protection-equipment-compared-to-no-eye-protection-equipment-in-preventing-transmission-of-covid-19-type-respiratory-illnesses-in-primary-and-community-care/. Accessed April 6, 2020.
One contentious issue during the COVID-19 crisis has been the appropriate selection and use of respiratory protective equipment (RPE) for healthcare workers (HCWs) in hospitals and long-term care settings. As of April 2020, discrepancies exist in the recommendations from health authorities such as the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and Canadian Standards Association (CSA). The first of these recommends a surgical mask for routine care and a respirator for high-risk care such as aerosol-generating procedures, while the CDC recommends respirators for all aspects of patient care for these SARS-CoV-2–infected patients, and the CSA risk assessment tool would also result in selection of a respirator.1-3
Given the contradictory guidance, we will discuss several important considerations for hospital leaders in the implementation of a healthcare respiratory protection program during the current pandemic, including a focused review of the empirical data on surgical mask vs face-fitted respirator (most commonly available in healthcare as N95 in North America), continuous use of the RPE throughout an entire shift vs targeted use when caring for patients, and key areas of uncertainty.
SURGICAL MASK OR RESPIRATOR
Surgical masks are traditionally used for protection against droplet transmission of respiratory infections, in which large droplets often fall to the ground within short distances; on the other hand, N95 respirators are used for much smaller airborne pathogens, which can remain suspended in the air for long periods of time. Although empiric studies have supported the superiority of respirators over surgical masks in simulated settings (frequently defined as a calculated concentration ratio outside vs inside the RPE), most clinical studies fail to demonstrate a difference in clinical outcomes such as the prevention of respiratory infection. For instance, an exposure study using saline aerosol to simulate viral particles showed that N95 respirators conferred up to 8 to 12 times greater protection against particulate penetration, compared with surgical masks.4 However, these advantages of respirators over surgical masks in carefully controlled laboratory studies do not seem to translate to decreased infection risk in real-world settings.
The effectiveness of N95 respirators vs surgical masks in preventing respiratory infections has been evaluated in a small number of clinical randomized, controlled trials (RCTs). We identified five systematic reviews and/or metanalyses published after 2010 and three RCTs published after 1990.5-12 The RCTs used laboratory-confirmed respiratory virus or clinical infection in HCWs as a clinical outcome, but studies differed in the implementation of RPE use (ie, continuous or targeted use). In a systematic review and metanalysis, Long et al identified six RCTs (9,171 participants) and concluded that, with the exception of laboratory-confirmed bacterial colonization, N95 respirators did not reduce the rate of laboratory-confirmed influenza, viral respiratory infections, or influenza-like illness among HCWs, compared with surgical masks.5 The authors noted risks of bias in these studies owing to the inability to blind and conceal allocation. In addition, the studies focused on infections that are known to transmit via droplet, such as influenza, so the results might not be applicable in the face of a new pandemic in which the important modes of transmission are not yet clear.
WHOLE-SHIFT OR INTERMITTENT USE
The evidence base evaluating continuous vs targeted use of RPE in healthcare settings is quite small. Continuous use refers to using the RPE during an entire shift, whereas targeted use involves using RPE only when caring for confirmed or suspected respiratory patients. In our literature review we identified only one RCT that included separate study arms for continuous and targeted N95 respirator use.13 The authors found a significantly lower rate of clinical respiratory illness among HCWs in the continuous-use group, compared with that in the targeted-use group. Limitations of the study included a relatively short follow-up of 4 weeks and uneven distribution of baseline characteristics, although the authors adjusted for these differences in their analysis. The study, however, did not compare continuous vs targeted use of surgical masks with regard to clinical outcomes. Based on the study results, we can only infer that continuous use of RPE, either surgical mask or N95 respirator, may provide additional benefit to HCWs vs targeted use only.
Given the lack of robust evidence informing continuous or targeted RPE use, we suggest some additional factors to guide decision making. In settings with high HCW compliance with universal RPE (above 50%), even noncompliant HCW are protected against clinical respiratory illness, which suggests a herd protective effect when universal RPE use is implemented, likely owing to the prevention of symptomatic or asymptomatic infectious spread among HCWs.14 It is important to note that the compliance rate may be limited by discomfort of prolonged wear of certain RPEs. One study reported that compliance rate is lower for continuous use (66%) than it is for targeted use (82%).13 Accumulated respiratory pathogen deposition on RPEs from an extended period of use that could result in self-contamination to the wearer is a potential concern, although these risks must be balanced against the repeated donning and doffing required by targeted use. Pilot studies examining viral particles left on surgical masks after being worn for entire shifts (or as long as tolerated) found that there were significantly more viral particles detected after 6 hours of continuous wear, which may increase the risk of self-contamination.15
UNCERTAINTIES
The current literature is applicable to infections that are known to spread via droplet contact, and this is a major limitation in generalizing the available evidence to the SARS-CoV-2 pandemic, in which debate persists regarding the exact mode of transmission. It is postulated that, even in infections traditionally considered to be spread by droplets, such as influenza, aerosol transmission may occur when HCWs are working in close proximity to the exposure source or when the droplet evaporates and becomes droplet nuclei. The United States National Academies of Science, Engineering, and Medicine expert consultation report, published in April 2020, concluded that current studies support the possibility of aerosolization of SARS-CoV-2 virus from normal breathing.16 As of April 2020, the WHO recommendation for SARS-CoV-2 is to use droplet contact precautions with a surgical mask for regular patient care and N95 respirator for aerosol-generating procedures.1 Although we have not come across any studies specifically comparing the efficacy between surgical mask to N95 respirator protection while performing aerosol-generating procedures, a systematic review found that certain aerosol-generating procedures, such as endotracheal intubation and noninvasive ventilation, conferred a significantly higher risk of transmission of SARS-CoV-1 to HCWs in 2003.17 For the current crisis, the CDC is taking a cautious approach in which N95 respirators are recommended for HCWs caring for patients with confirmed or suspected SARS-CoV-2 infection if the supply chain is secure, with advice in place in times of RPE shortage, such as use of expired respirators, other types of equivalent respirators, or respirators not approved by the National Institute for Occupational Safety and Health, as well as optimization of administrative and engineering controls (eg, telemedicine, limiting patient and visitor numbers, physical barriers, optimizing ventilation systems).2,18 This advice is unusual in terms of deviating from advising the most appropriate RPE, and we presume it reflects the present global supply problems.
RPEs are only one component of a necessary personal protective equipment ensemble. Although eye protection (goggles or face shields) is recommended by the WHO and CDC when caring for patients with SARS-CoV-2, there is considerable uncertainty regarding the incremental effectiveness of eye protection because such protection is usually worn in conjunction with RPE. A 2019 Cochrane review did not identify any good-quality studies that could inform judgments regarding the effectiveness of eye protective equipment,19 and a recent rapid review reporting on the efficacy of eye protection in primary care settings reached a similar conclusion.20 A risk-based approach would be to include eye protection in a well-designed personal protective equipment program.
In the absence of aerosol-generating procedures, N95 respirators confer no additional benefit in preventing HCW respiratory infections when droplet transmission is suspected. However, the applicability of the available evidence is limited given the uncertainties surrounding SARS-CoV-2 transmission. When RPE may become scarce during a pandemic, the risk of potential self-contamination must be weighed against RPE conservation strategies. RPE compliance, herd-protection effects of routine RPE use, and RPE contamination from prolonged use are therefore important elements to consider when implementing hospital policies regarding universal masking because they all impact the potential effectiveness of RPE.
CONCLUSIONS
At the present time we lack definitive evidence on the effectiveness of surgical masks vs respirators and continuous vs targeted RPE use in the hospital setting for SARS-CoV-2. If our goal is to minimize risk of HCW infection, continuous use of N95 respirator could be considered. However, a more pragmatic solution in the setting of a limited supply of N95 respirators would be continuous use of surgical masks while engaged in clinical care of patients under investigation or with confirmed COVID-19.
One contentious issue during the COVID-19 crisis has been the appropriate selection and use of respiratory protective equipment (RPE) for healthcare workers (HCWs) in hospitals and long-term care settings. As of April 2020, discrepancies exist in the recommendations from health authorities such as the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and Canadian Standards Association (CSA). The first of these recommends a surgical mask for routine care and a respirator for high-risk care such as aerosol-generating procedures, while the CDC recommends respirators for all aspects of patient care for these SARS-CoV-2–infected patients, and the CSA risk assessment tool would also result in selection of a respirator.1-3
Given the contradictory guidance, we will discuss several important considerations for hospital leaders in the implementation of a healthcare respiratory protection program during the current pandemic, including a focused review of the empirical data on surgical mask vs face-fitted respirator (most commonly available in healthcare as N95 in North America), continuous use of the RPE throughout an entire shift vs targeted use when caring for patients, and key areas of uncertainty.
SURGICAL MASK OR RESPIRATOR
Surgical masks are traditionally used for protection against droplet transmission of respiratory infections, in which large droplets often fall to the ground within short distances; on the other hand, N95 respirators are used for much smaller airborne pathogens, which can remain suspended in the air for long periods of time. Although empiric studies have supported the superiority of respirators over surgical masks in simulated settings (frequently defined as a calculated concentration ratio outside vs inside the RPE), most clinical studies fail to demonstrate a difference in clinical outcomes such as the prevention of respiratory infection. For instance, an exposure study using saline aerosol to simulate viral particles showed that N95 respirators conferred up to 8 to 12 times greater protection against particulate penetration, compared with surgical masks.4 However, these advantages of respirators over surgical masks in carefully controlled laboratory studies do not seem to translate to decreased infection risk in real-world settings.
The effectiveness of N95 respirators vs surgical masks in preventing respiratory infections has been evaluated in a small number of clinical randomized, controlled trials (RCTs). We identified five systematic reviews and/or metanalyses published after 2010 and three RCTs published after 1990.5-12 The RCTs used laboratory-confirmed respiratory virus or clinical infection in HCWs as a clinical outcome, but studies differed in the implementation of RPE use (ie, continuous or targeted use). In a systematic review and metanalysis, Long et al identified six RCTs (9,171 participants) and concluded that, with the exception of laboratory-confirmed bacterial colonization, N95 respirators did not reduce the rate of laboratory-confirmed influenza, viral respiratory infections, or influenza-like illness among HCWs, compared with surgical masks.5 The authors noted risks of bias in these studies owing to the inability to blind and conceal allocation. In addition, the studies focused on infections that are known to transmit via droplet, such as influenza, so the results might not be applicable in the face of a new pandemic in which the important modes of transmission are not yet clear.
WHOLE-SHIFT OR INTERMITTENT USE
The evidence base evaluating continuous vs targeted use of RPE in healthcare settings is quite small. Continuous use refers to using the RPE during an entire shift, whereas targeted use involves using RPE only when caring for confirmed or suspected respiratory patients. In our literature review we identified only one RCT that included separate study arms for continuous and targeted N95 respirator use.13 The authors found a significantly lower rate of clinical respiratory illness among HCWs in the continuous-use group, compared with that in the targeted-use group. Limitations of the study included a relatively short follow-up of 4 weeks and uneven distribution of baseline characteristics, although the authors adjusted for these differences in their analysis. The study, however, did not compare continuous vs targeted use of surgical masks with regard to clinical outcomes. Based on the study results, we can only infer that continuous use of RPE, either surgical mask or N95 respirator, may provide additional benefit to HCWs vs targeted use only.
Given the lack of robust evidence informing continuous or targeted RPE use, we suggest some additional factors to guide decision making. In settings with high HCW compliance with universal RPE (above 50%), even noncompliant HCW are protected against clinical respiratory illness, which suggests a herd protective effect when universal RPE use is implemented, likely owing to the prevention of symptomatic or asymptomatic infectious spread among HCWs.14 It is important to note that the compliance rate may be limited by discomfort of prolonged wear of certain RPEs. One study reported that compliance rate is lower for continuous use (66%) than it is for targeted use (82%).13 Accumulated respiratory pathogen deposition on RPEs from an extended period of use that could result in self-contamination to the wearer is a potential concern, although these risks must be balanced against the repeated donning and doffing required by targeted use. Pilot studies examining viral particles left on surgical masks after being worn for entire shifts (or as long as tolerated) found that there were significantly more viral particles detected after 6 hours of continuous wear, which may increase the risk of self-contamination.15
UNCERTAINTIES
The current literature is applicable to infections that are known to spread via droplet contact, and this is a major limitation in generalizing the available evidence to the SARS-CoV-2 pandemic, in which debate persists regarding the exact mode of transmission. It is postulated that, even in infections traditionally considered to be spread by droplets, such as influenza, aerosol transmission may occur when HCWs are working in close proximity to the exposure source or when the droplet evaporates and becomes droplet nuclei. The United States National Academies of Science, Engineering, and Medicine expert consultation report, published in April 2020, concluded that current studies support the possibility of aerosolization of SARS-CoV-2 virus from normal breathing.16 As of April 2020, the WHO recommendation for SARS-CoV-2 is to use droplet contact precautions with a surgical mask for regular patient care and N95 respirator for aerosol-generating procedures.1 Although we have not come across any studies specifically comparing the efficacy between surgical mask to N95 respirator protection while performing aerosol-generating procedures, a systematic review found that certain aerosol-generating procedures, such as endotracheal intubation and noninvasive ventilation, conferred a significantly higher risk of transmission of SARS-CoV-1 to HCWs in 2003.17 For the current crisis, the CDC is taking a cautious approach in which N95 respirators are recommended for HCWs caring for patients with confirmed or suspected SARS-CoV-2 infection if the supply chain is secure, with advice in place in times of RPE shortage, such as use of expired respirators, other types of equivalent respirators, or respirators not approved by the National Institute for Occupational Safety and Health, as well as optimization of administrative and engineering controls (eg, telemedicine, limiting patient and visitor numbers, physical barriers, optimizing ventilation systems).2,18 This advice is unusual in terms of deviating from advising the most appropriate RPE, and we presume it reflects the present global supply problems.
RPEs are only one component of a necessary personal protective equipment ensemble. Although eye protection (goggles or face shields) is recommended by the WHO and CDC when caring for patients with SARS-CoV-2, there is considerable uncertainty regarding the incremental effectiveness of eye protection because such protection is usually worn in conjunction with RPE. A 2019 Cochrane review did not identify any good-quality studies that could inform judgments regarding the effectiveness of eye protective equipment,19 and a recent rapid review reporting on the efficacy of eye protection in primary care settings reached a similar conclusion.20 A risk-based approach would be to include eye protection in a well-designed personal protective equipment program.
In the absence of aerosol-generating procedures, N95 respirators confer no additional benefit in preventing HCW respiratory infections when droplet transmission is suspected. However, the applicability of the available evidence is limited given the uncertainties surrounding SARS-CoV-2 transmission. When RPE may become scarce during a pandemic, the risk of potential self-contamination must be weighed against RPE conservation strategies. RPE compliance, herd-protection effects of routine RPE use, and RPE contamination from prolonged use are therefore important elements to consider when implementing hospital policies regarding universal masking because they all impact the potential effectiveness of RPE.
CONCLUSIONS
At the present time we lack definitive evidence on the effectiveness of surgical masks vs respirators and continuous vs targeted RPE use in the hospital setting for SARS-CoV-2. If our goal is to minimize risk of HCW infection, continuous use of N95 respirator could be considered. However, a more pragmatic solution in the setting of a limited supply of N95 respirators would be continuous use of surgical masks while engaged in clinical care of patients under investigation or with confirmed COVID-19.
1. World Health Organization. Rational use of personal protective equipment for coronavirus disease (COVID-19): Interim guidance. February 27, 2020. https://apps.who.int/iris/bitstream/handle/10665/331215/WHO-2019-nCov-IPCPPE_use-2020.1-eng.pdf. Accessed April 1, 2020.
2. Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed April 1, 2020.
3. Canadian Standard Association. Selection, Use, and Care of Respirators (CAN/CSA-Z94.4-18). Toronto, Canada: CSA Group; 2018.
4. Lee SA, Grinshpun SA, Reponen T. Respiratory performance offered by N95 respirators and surgical masks: human subject evaluation with NaCl aerosol representing bacterial and viral particle size range. Ann Occup Hyg. 2008;52(3):177-185. https://doi.org/10.1093/annhyg/men005.
5. Long Y, Hu T, Liu L, et al. Effectiveness of N95 respirators versus surgical masks against influenza: a systematic review and meta‐analysis. J Evid Based Med. 2020. https://doi.org/10.1111/jebm.12381.
6. Offeddu V, Yung CF, Low MSF, Tam CC. Effectiveness of masks and respirators against respiratory infections in healthcare workers: a systematic review and meta-analysis. Clin Infect Dis. 2017;65(11):1934-1942. https://doi.org/10.1093/cid/cix681.
7. Smith JD, MacDougall CC, Johnstone J, Copes RA, Schwartz B, Garber GE. Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis. CMAJ. 2016;188(8):567-574. https://doi.org/10.1503/cmaj.150835.
8. Bin-Reza F, Lopez Chavarrias V, Nicoll A, Chamberland ME. The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence. Influenza Other Respir Viruses. 2012;6(4):257-267. https://doi.org/10.1111/j.1750-2659.2011.00307.x.
9. Jefferson T, Del Mar CB, Dooley L, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev. 2011;2011(7):CD006207. https://doi.org/10.1002/14651858.CD006207.pub4.
10. Radonovich LJ Jr, Simberkoff MS, Bessesen MT, et al. N95 respirators vs medical masks for preventing influenza among health care personnel: a randomized clinical trial. JAMA. 2019;322(9):824-833. https://doi.org/10.1001/jama.2019.11645.
11. MacIntyre CR, Chughtai AA, Rahman B, et al. The efficacy of medical masks and respirators against respiratory infection in healthcare workers. Influenza Other Respir Viruses. 2017;11(6):511-517. https://doi.org/10.1111/irv.12474.
12. Loeb M, Dafoe N, Mahony J, et al. Surgical mask vs N95 respirator for preventing influenza among health care workers. JAMA. 2009;302(17):1865-1871. https://doi.org/10.1001/jama.2009.1466.
13. Macintyre CR, Wang Q, Seale H, et al. A randomized clinical trial of three options for N95 respirators and medical masks in health workers. Am J Respir Crit Care Med. 2013;187(9):960-966. https://doi.org/10.1164/rccm.201207-1164OC.
14. Chen X, Chughtai AA, Macintyre CR. Herd protection effect of N95 respirators in healthcare workers. J Int Med Res. 2017;45(6):1760-1767. https://doi.org/10.1177/0300060516665491.
15. Chughtai AA, Stelzer-Braid S, Rawlinson W, et al. Contamination by respiratory viruses on outer surface of medical masks used by hospital healthcare workers. BMC Infect Dis. 2019;19(1):491. https://doi.org/10.1186/s12879-019-4109-x.
16. National Research Council. Rapid Expert Consultation on the Possibility of Bioaerosol Spread of SARS-CoV-2 for the COVID-19 Pandemic (April 1, 2020). Washington, DC: National Academies Press; 2020. https://doi.org/10.17226/25769.
17. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. https://doi.org/10.1371/journal.pone.0035797.
18. Centers for Disease Control and Prevention. Strategies for Optimizing the Supply of N95 Respirators: COVID-19. 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/respirators-strategy/crisis-alternate-strategies.html. Accessed March 31, 2020.
19. Verbeek JH, Rajamaki B, Ijaz S, et al. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst Rev. 2019;7(7):CD011621. https://doi.org/10.1002/14651858.CD011621.pub3.
20. Khunti K, Greenhalgh T, Chan XH, et al. What is the efficacy of eye protection equipment compared to no eye protection equipment in preventing transmission of COVID-19-type respiratory illnesses in primary and community care?. CEBM. April 3, 2020. https://www.cebm.net/covid-19/what-is-the-efficacy-of-eye-protection-equipment-compared-to-no-eye-protection-equipment-in-preventing-transmission-of-covid-19-type-respiratory-illnesses-in-primary-and-community-care/. Accessed April 6, 2020.
1. World Health Organization. Rational use of personal protective equipment for coronavirus disease (COVID-19): Interim guidance. February 27, 2020. https://apps.who.int/iris/bitstream/handle/10665/331215/WHO-2019-nCov-IPCPPE_use-2020.1-eng.pdf. Accessed April 1, 2020.
2. Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed April 1, 2020.
3. Canadian Standard Association. Selection, Use, and Care of Respirators (CAN/CSA-Z94.4-18). Toronto, Canada: CSA Group; 2018.
4. Lee SA, Grinshpun SA, Reponen T. Respiratory performance offered by N95 respirators and surgical masks: human subject evaluation with NaCl aerosol representing bacterial and viral particle size range. Ann Occup Hyg. 2008;52(3):177-185. https://doi.org/10.1093/annhyg/men005.
5. Long Y, Hu T, Liu L, et al. Effectiveness of N95 respirators versus surgical masks against influenza: a systematic review and meta‐analysis. J Evid Based Med. 2020. https://doi.org/10.1111/jebm.12381.
6. Offeddu V, Yung CF, Low MSF, Tam CC. Effectiveness of masks and respirators against respiratory infections in healthcare workers: a systematic review and meta-analysis. Clin Infect Dis. 2017;65(11):1934-1942. https://doi.org/10.1093/cid/cix681.
7. Smith JD, MacDougall CC, Johnstone J, Copes RA, Schwartz B, Garber GE. Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis. CMAJ. 2016;188(8):567-574. https://doi.org/10.1503/cmaj.150835.
8. Bin-Reza F, Lopez Chavarrias V, Nicoll A, Chamberland ME. The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence. Influenza Other Respir Viruses. 2012;6(4):257-267. https://doi.org/10.1111/j.1750-2659.2011.00307.x.
9. Jefferson T, Del Mar CB, Dooley L, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev. 2011;2011(7):CD006207. https://doi.org/10.1002/14651858.CD006207.pub4.
10. Radonovich LJ Jr, Simberkoff MS, Bessesen MT, et al. N95 respirators vs medical masks for preventing influenza among health care personnel: a randomized clinical trial. JAMA. 2019;322(9):824-833. https://doi.org/10.1001/jama.2019.11645.
11. MacIntyre CR, Chughtai AA, Rahman B, et al. The efficacy of medical masks and respirators against respiratory infection in healthcare workers. Influenza Other Respir Viruses. 2017;11(6):511-517. https://doi.org/10.1111/irv.12474.
12. Loeb M, Dafoe N, Mahony J, et al. Surgical mask vs N95 respirator for preventing influenza among health care workers. JAMA. 2009;302(17):1865-1871. https://doi.org/10.1001/jama.2009.1466.
13. Macintyre CR, Wang Q, Seale H, et al. A randomized clinical trial of three options for N95 respirators and medical masks in health workers. Am J Respir Crit Care Med. 2013;187(9):960-966. https://doi.org/10.1164/rccm.201207-1164OC.
14. Chen X, Chughtai AA, Macintyre CR. Herd protection effect of N95 respirators in healthcare workers. J Int Med Res. 2017;45(6):1760-1767. https://doi.org/10.1177/0300060516665491.
15. Chughtai AA, Stelzer-Braid S, Rawlinson W, et al. Contamination by respiratory viruses on outer surface of medical masks used by hospital healthcare workers. BMC Infect Dis. 2019;19(1):491. https://doi.org/10.1186/s12879-019-4109-x.
16. National Research Council. Rapid Expert Consultation on the Possibility of Bioaerosol Spread of SARS-CoV-2 for the COVID-19 Pandemic (April 1, 2020). Washington, DC: National Academies Press; 2020. https://doi.org/10.17226/25769.
17. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. https://doi.org/10.1371/journal.pone.0035797.
18. Centers for Disease Control and Prevention. Strategies for Optimizing the Supply of N95 Respirators: COVID-19. 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/respirators-strategy/crisis-alternate-strategies.html. Accessed March 31, 2020.
19. Verbeek JH, Rajamaki B, Ijaz S, et al. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst Rev. 2019;7(7):CD011621. https://doi.org/10.1002/14651858.CD011621.pub3.
20. Khunti K, Greenhalgh T, Chan XH, et al. What is the efficacy of eye protection equipment compared to no eye protection equipment in preventing transmission of COVID-19-type respiratory illnesses in primary and community care?. CEBM. April 3, 2020. https://www.cebm.net/covid-19/what-is-the-efficacy-of-eye-protection-equipment-compared-to-no-eye-protection-equipment-in-preventing-transmission-of-covid-19-type-respiratory-illnesses-in-primary-and-community-care/. Accessed April 6, 2020.
© 2020 Society of Hospital Medicine
Innovation and Knowledge Sharing Can Transform COVID-19 Infection Prevention Response
Emerging studies on coronavirus disease 2019 (COVID-19) confirm high rates of infection among healthcare workers (HCWs).1 As widespread community transmission increases, frontline HCWs, such as hospitalists, are at particularly high risk of exposure to people with undiagnosed COVID-19. Although there is no known effective treatment for COVID-19, early detection is vital to decreasing ongoing transmission through contact tracing and quarantine. However, lack of adequate testing capacity prevented basic public health interventions from curbing the pandemic at an earlier stage. As a result, given high rates of presumed community transmission of COVID-19 and evidence for asymptomatic transmission, there have been moves toward the use of universal personal protective equipment (PPE). This strategy is challenging to implement because of the acute PPE shortage, which has resulted in an urgent need to embrace innovation in infection prevention.
The current pandemic has resulted in an unprecedented volume of data being generated and disseminated, with the potential to impact real-time responses in geographically disparate regions. Here, we focus on the potential for innovation and knowledge sharing from an infection prevention perspective, which could enhance frontline HCW safety in the current COVID-19 pandemic.
DIAGNOSIS MATTERS
Every outbreak begins and ends with a diagnostic test. Widespread population testing coupled with intensive contact tracing had the potential to curb national epidemics if it had been implemented in time. In the United States, which now has the highest number of COVID-19 cases worldwide, there were technical difficulties with the first diagnostic test developed by the Centers for Disease Control and Prevention (CDC) and subsequent delays in scaling up access to COVID-19 diagnostic testing.2 The strategy of initially reserving testing only for those who were critically ill meant that by the time patients with COVID-19 were being diagnosed, widespread community spread had occurred because of the lack of detection of individuals with less severe or asymptomatic infections.
In contrast, scaled-up testing in South Korea has helped limit the spread and consequences of COVID-19. The use of drive-through testing centers enabled safe and efficient testing, while minimizing the risk to HCWs and eliminating the possibility of cross infection among people being tested.3 Although outdoor testing is not feasible in all settings, this approach avoids resources and time typically needed for ventilation (typically a negative pressure room with 12 air changes per hour would be used) and cleaning of specimen collection rooms.
The other major diagnostic gap is the ability to identify individuals who have recovered from COVID-19 and are immune. There is an urgent need to develop and scale up a rapid serological test that avoids cross-reactivity with other coronaviruses. Ideally, this test would permit testing of HCWs to determine who is likely immune and can therefore return safely to work.
RETHINKING PPE
There has been a massive and rapid increase in the need for PPE globally because of overwhelmed health systems having to care for large numbers of patients with suspected or confirmed COVID-19. This has been exacerbated by public fear, which has led to panic buying of medical face masks (primarily used to protect others from infections with a droplet mode of transmission) and filtering facepiece half-mask respirators, which include N95 respirators (used to protect the wearer from infections with an airborne mode of transmission).
COVID-19 is thought to be predominantly spread by transmission of respiratory droplets (>5 and <10 μm in diameter), which occurs when people are in close contact (within 1 meter) with others who typically (but not always) have respiratory symptoms such as cough or sneeze or with fomites that have come into contact with an infected person. This is in contrast to infectious diseases such as tuberculosis (TB) or measles, which are spread by airborne transmission of virus suspended in droplet nuclei (<5 μm in diameter), which can remain in the air for prolonged periods of time and can be transmitted over distances greater than 1 meter.4
While World Health Organization (WHO) and CDC infection prevention guidance have cited droplet transmission as the primary mode of transmission for COVID-19, current CDC guidelines state that respirators are preferred for the care of patients with known or suspected COVID-19, given the potential for opportunistic airborne transmission.5 However, in the setting of respirator shortages, it is recommended that these should be prioritized for HCWs caring for patients with COVID-19 in the context of aerosol-generating procedures or other patients with infections spread by airborne transmission such as TB or varicella until the supply chain is restored. Of note, optimal use of respirators requires fit testing, which is often lacking in nursing homes and outpatient facilities, as well as more widely in resource-limited countries.
Universal masking (use of surgical mask) for HCWs caring for any patient irrespective of symptoms or presenting complaint has also been implemented by many large hospital systems in recent days. Although universal masking adds to the burden of the PPE shortage, in settings with widespread community transmission and given increasing evidence6 demonstrating transmission from people with asymptomatic and presymptomatic infection, universal masking may be useful to decrease transmission. However, particularly in the setting of PPE shortages, it is important to understand that surgical masks are designed to be single use and that dampness and frequent adjustment of the mask affects their effectiveness.
As urgent attempts to coordinate and increase PPE manufacture are being made by health systems, in conjunction with private partnerships, there has also been a burst of public campaigns to sew cloth masks to mitigate the real-time shortages. Although it is likely that cloth masks provide inadequate protection in comparison with surgical masks,7 evidence does suggest that cloth masks provide some degree of protection from the spread of respiratory viruses,8 particularly if these are replaced promptly when damp or damaged and if combined with other interventions such as hand hygiene. This has led to recommendations for the general public in various countries to wear cloth face coverings in public settings, particularly where social distancing may be harder to maintain, but these are not recommended for use by HCWs in healthcare settings.
INNOVATION IN INFECTION PREVENTION
Strategies to navigate the PPE shortage in the era of COVID-19 include importing, reclaiming, reusing, and repurposing PPE; generating and extending supply; eliminating nonessential services; reducing patient contact; and using nonhuman services such as drones to deliver equipment and undertake tasks such as decontamination.9,10 Multidisciplinary teams are working on creative ways to use existing resources to make effective PPE, including alternatives to N95 respirators. An outbreak simulation study at Emory University in Atlanta, Georgia, and the University of Texas Health Science Center at Houston in Texas demonstrated that HCWs could be rapidly trained and fit tested to use elastomeric half-mask respirators, which are reusable.11 A multidisciplinary team at Boston Children’s Hospital in Massachusetts has developed and completed a small pilot study of a reusable elastomeric respirator made using an anesthesia facemask, antimicrobial filter, and elastic straps.12
Given evidence that suggests that COVID-19 involves a component of airborne transmission,13 in addition to droplet spread and surface (fomite) contamination,14 using known infection prevention techniques that work to decrease airborne transmission of other respiratory infectious diseases should also be considered. Germicidal ultraviolet (GUV) air disinfection rapidly disinfects upper room air, which is then continually exchanged with contaminated lower-room air. GUV air disinfection has been demonstrated to be a safe and cost-effective intervention, with an efficacy of approximately 80% for decreasing TB transmission.15 GUV air disinfection is also effective against airborne influenza and measles and may play a role in surface decontamination by accelerating viral inactivation. Enabling GUV in high-risk areas such as the emergency department or intensive care unit could be a high-yield intervention to decrease transmission of COVID-19.
HCWs exposed to other respiratory infections such as influenza or TB may receive preventive therapy to reduce the risk of developing disease. High rates of COVID-19 in HCWs have prompted several initiatives to evaluate innovative approaches to decreasing this risk. Multiple studies are underway to determine whether hydroxychloroquine could be used for pre- or postexposure prophylaxis to prevent COVID-19. Another multisite trial will evaluate whether the BCG vaccine, primarily used to reduce the risk of TB, provides protection against COVID-19 in HCWs, driven by data suggesting a correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19.16
DATA GENERATION AND KNOWLEDGE SHARING
Infection prevention efforts can benefit from the unprecedented amount of data on COVID-19 that is being generated and shared. Successful examples of the rapid intensification of infection prevention measures to decrease transmission in healthcare facilities should be emulated. The hospital authority of Hong Kong implemented a bundle of measures focused on early recognition, isolation, notification, and molecular diagnostics for people being evaluated for COVID-19.17 They subsequently broadened the clinical and epidemiological criteria of surveillance as the outbreak evolved and intensified PPE recommendations to all HCWs (face masks for all and N95 respirators for those performing aerosol-generating procedures), which appears to have resulted in no cases of HCW infection or nosocomial transmission.
Data characterizing the extent of occupational infections in HCWs during acute and chronic epidemics is often lacking and subject to wide variability in reporting, which limits its impact. For example, HCWs in high TB incidence countries have at least twice the risk of developing TB, compared with the general population. Although there are still major gaps in national data collection regarding the incidence of occupational TB, recent attempts by WHO to systematically record this data have resulted in increasing prioritization of this group as an at-risk population who may benefit from TB preventive therapy. We strongly advocate that health systems systematically record and share longitudinal data on numbers of HCWs infected with COVID-19. This transparency will facilitate urgent action to replenish and sustain resources such as PPE and enable institutions to share and adapt successful infection prevention strategies. Examples such as the prevention of central line- associated bloodstream infections demonstrate the potential impact of national collaborative efforts to strengthen infection prevention, although further effort is needed to optimize knowledge sharing in the context of outbreaks.
CONCLUSIONS
The cost of not investing in public health pandemic preparedness including measures to protect HCWs is now widely apparent. HCWs have a right to safety in their workplaces as they fulfil their duty of care to patients.18 Rapid scale-up of diagnostic testing capacity, and bundles of infection prevention interventions including universal masking and drive-through testing, can safeguard HCWs and the patients they serve in the current COVID-19 pandemic. Re-establishing immediate access to quality-assured PPE is imperative to reduce the individual and workforce consequences of HCWs developing COVID-19 or other infectious diseases like TB that are continuously a threat to the workforce. Meanwhile, innovative approaches such as repurposing resources to develop PPE and use of GUV air disinfection may help to mitigate PPE shortages, and use of preventive therapies may also decrease COVID-19 risk in HCWs. Reliable surveillance data on HCW infection rates can help identify and track gaps in infection prevention, as well as identify strategies that impact this outcome. Ultimately greater top-down political commitment is urgently needed to ensure that frontline HCWs have the necessary resources to address the current pandemic and to sustain these interventions to protect HCWs in the future.
1. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11)1061-1069. https://doi.org/10.1001/jama.2020.1585.
2. Sharfstein JM, Becker SJ, Mello MM. Diagnostic testing for the novel coronavirus. JAMA. 2020. https://doi.org/10.1001/jama.2020.3864.
3. Kwon KT, Ko JH, Shin H, Sung M, Kim JY. Drive-through screening center for COVID-19: a safe and efficient screening system against massive community outbreak. J Korean Med Sci. 2020;35(11):e123. https://doi.org/10.3346/jkms.2020.35.e123.
4. World Health Organization. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations. Scientific Brief, March 29, 2020. https://www.who.int/publications-detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations. Accessed April 5, 2020.
5. Centers for Disease Control and Prevention. CDC Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed April 5, 2020.
6. Kimball A, Hatfield KM, Arons M, et al. Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility—King County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69(13):377-381. https://doi.org/10.15585/mmwr.mm6913e1.
7. MacIntyre CR, Seale H, Dung TC, et al. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open. 2015;5(4):e006577. https://doi.org/10.1136/bmjopen-2014-006577.
8. van der Sande M, Teunis P, Sabel R. Professional and home-made face masks reduce exposure to respiratory infections among the general population. PLoS One. 2008;3(7):e2618. https://doi.org/10.1371/journal.pone.0002618.
9. Livingston E, Desai A, Berkwits M. Sourcing Personal Protective Equipment During the COVID-19 Pandemic. JAMA. 2020. https://doi.org/10.1001/jama.2020.5317.
10. Steuart R, Huang FS, Schaffzin JK, Thomson J. Finding the value in personal protective equipment for hospitalized patients during a pandemic and beyond. J Hosp Med. 2020;15(5):xxx-xxx. https://doi.org/10.12788/jhm.3429.
11. Pompeii LA, Kraft CS, Brownsword EA, et al. Training and fit testing of health care personnel for reusable elastomeric half-mask respirators compared with disposable N95 respirators. JAMA. 2020;e204806. https://doi.org/10.1001/jama.2020.4806.
12. Boston Children’s Hospital. Surgical Innovation Fellowship. https://www.childrenshospital.org/research/departments-divisions-programs/departments/surgery/surgical-innovation-fellowship. Accessed April 5, 2020.
13. van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020. https://doi.org/10.1056/NEJMc2004973.
14. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;e203227. https://doi.org/10.1001/jama.2020.3227.
15. Mphaphlele M, Dharmadhikari AS, Jensen PA, et al. Institutional tuberculosis transmission. Controlled trial of upper room ultraviolet air disinfection: a basis for new dosing guidelines. Am J Respir Crit Care Med. 2015;192(4):477-484. https://doi.org/10.1164/rccm.201501-0060OC.
16. Miller A, Reandelar MJ, Fasciglione K, Roumenova V, Li Y, Otazu GH. Correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19: an epidemiological study. medRxiv. 2020. https://doi.org/10.1101/2020.03.24.20042937 .
17. Cheng VCC, Wong SC, Chen JHK, et al. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. 2020. https://doi.org/10.1017/ice.2020.58.
18. Antommaria AHM. Conflicting duties and reciprocal obligations during a pandemic. J Hosp Med. 2020;15(5):xxx-xxx. https://doi.org/10.12788/jhm.3425.
Emerging studies on coronavirus disease 2019 (COVID-19) confirm high rates of infection among healthcare workers (HCWs).1 As widespread community transmission increases, frontline HCWs, such as hospitalists, are at particularly high risk of exposure to people with undiagnosed COVID-19. Although there is no known effective treatment for COVID-19, early detection is vital to decreasing ongoing transmission through contact tracing and quarantine. However, lack of adequate testing capacity prevented basic public health interventions from curbing the pandemic at an earlier stage. As a result, given high rates of presumed community transmission of COVID-19 and evidence for asymptomatic transmission, there have been moves toward the use of universal personal protective equipment (PPE). This strategy is challenging to implement because of the acute PPE shortage, which has resulted in an urgent need to embrace innovation in infection prevention.
The current pandemic has resulted in an unprecedented volume of data being generated and disseminated, with the potential to impact real-time responses in geographically disparate regions. Here, we focus on the potential for innovation and knowledge sharing from an infection prevention perspective, which could enhance frontline HCW safety in the current COVID-19 pandemic.
DIAGNOSIS MATTERS
Every outbreak begins and ends with a diagnostic test. Widespread population testing coupled with intensive contact tracing had the potential to curb national epidemics if it had been implemented in time. In the United States, which now has the highest number of COVID-19 cases worldwide, there were technical difficulties with the first diagnostic test developed by the Centers for Disease Control and Prevention (CDC) and subsequent delays in scaling up access to COVID-19 diagnostic testing.2 The strategy of initially reserving testing only for those who were critically ill meant that by the time patients with COVID-19 were being diagnosed, widespread community spread had occurred because of the lack of detection of individuals with less severe or asymptomatic infections.
In contrast, scaled-up testing in South Korea has helped limit the spread and consequences of COVID-19. The use of drive-through testing centers enabled safe and efficient testing, while minimizing the risk to HCWs and eliminating the possibility of cross infection among people being tested.3 Although outdoor testing is not feasible in all settings, this approach avoids resources and time typically needed for ventilation (typically a negative pressure room with 12 air changes per hour would be used) and cleaning of specimen collection rooms.
The other major diagnostic gap is the ability to identify individuals who have recovered from COVID-19 and are immune. There is an urgent need to develop and scale up a rapid serological test that avoids cross-reactivity with other coronaviruses. Ideally, this test would permit testing of HCWs to determine who is likely immune and can therefore return safely to work.
RETHINKING PPE
There has been a massive and rapid increase in the need for PPE globally because of overwhelmed health systems having to care for large numbers of patients with suspected or confirmed COVID-19. This has been exacerbated by public fear, which has led to panic buying of medical face masks (primarily used to protect others from infections with a droplet mode of transmission) and filtering facepiece half-mask respirators, which include N95 respirators (used to protect the wearer from infections with an airborne mode of transmission).
COVID-19 is thought to be predominantly spread by transmission of respiratory droplets (>5 and <10 μm in diameter), which occurs when people are in close contact (within 1 meter) with others who typically (but not always) have respiratory symptoms such as cough or sneeze or with fomites that have come into contact with an infected person. This is in contrast to infectious diseases such as tuberculosis (TB) or measles, which are spread by airborne transmission of virus suspended in droplet nuclei (<5 μm in diameter), which can remain in the air for prolonged periods of time and can be transmitted over distances greater than 1 meter.4
While World Health Organization (WHO) and CDC infection prevention guidance have cited droplet transmission as the primary mode of transmission for COVID-19, current CDC guidelines state that respirators are preferred for the care of patients with known or suspected COVID-19, given the potential for opportunistic airborne transmission.5 However, in the setting of respirator shortages, it is recommended that these should be prioritized for HCWs caring for patients with COVID-19 in the context of aerosol-generating procedures or other patients with infections spread by airborne transmission such as TB or varicella until the supply chain is restored. Of note, optimal use of respirators requires fit testing, which is often lacking in nursing homes and outpatient facilities, as well as more widely in resource-limited countries.
Universal masking (use of surgical mask) for HCWs caring for any patient irrespective of symptoms or presenting complaint has also been implemented by many large hospital systems in recent days. Although universal masking adds to the burden of the PPE shortage, in settings with widespread community transmission and given increasing evidence6 demonstrating transmission from people with asymptomatic and presymptomatic infection, universal masking may be useful to decrease transmission. However, particularly in the setting of PPE shortages, it is important to understand that surgical masks are designed to be single use and that dampness and frequent adjustment of the mask affects their effectiveness.
As urgent attempts to coordinate and increase PPE manufacture are being made by health systems, in conjunction with private partnerships, there has also been a burst of public campaigns to sew cloth masks to mitigate the real-time shortages. Although it is likely that cloth masks provide inadequate protection in comparison with surgical masks,7 evidence does suggest that cloth masks provide some degree of protection from the spread of respiratory viruses,8 particularly if these are replaced promptly when damp or damaged and if combined with other interventions such as hand hygiene. This has led to recommendations for the general public in various countries to wear cloth face coverings in public settings, particularly where social distancing may be harder to maintain, but these are not recommended for use by HCWs in healthcare settings.
INNOVATION IN INFECTION PREVENTION
Strategies to navigate the PPE shortage in the era of COVID-19 include importing, reclaiming, reusing, and repurposing PPE; generating and extending supply; eliminating nonessential services; reducing patient contact; and using nonhuman services such as drones to deliver equipment and undertake tasks such as decontamination.9,10 Multidisciplinary teams are working on creative ways to use existing resources to make effective PPE, including alternatives to N95 respirators. An outbreak simulation study at Emory University in Atlanta, Georgia, and the University of Texas Health Science Center at Houston in Texas demonstrated that HCWs could be rapidly trained and fit tested to use elastomeric half-mask respirators, which are reusable.11 A multidisciplinary team at Boston Children’s Hospital in Massachusetts has developed and completed a small pilot study of a reusable elastomeric respirator made using an anesthesia facemask, antimicrobial filter, and elastic straps.12
Given evidence that suggests that COVID-19 involves a component of airborne transmission,13 in addition to droplet spread and surface (fomite) contamination,14 using known infection prevention techniques that work to decrease airborne transmission of other respiratory infectious diseases should also be considered. Germicidal ultraviolet (GUV) air disinfection rapidly disinfects upper room air, which is then continually exchanged with contaminated lower-room air. GUV air disinfection has been demonstrated to be a safe and cost-effective intervention, with an efficacy of approximately 80% for decreasing TB transmission.15 GUV air disinfection is also effective against airborne influenza and measles and may play a role in surface decontamination by accelerating viral inactivation. Enabling GUV in high-risk areas such as the emergency department or intensive care unit could be a high-yield intervention to decrease transmission of COVID-19.
HCWs exposed to other respiratory infections such as influenza or TB may receive preventive therapy to reduce the risk of developing disease. High rates of COVID-19 in HCWs have prompted several initiatives to evaluate innovative approaches to decreasing this risk. Multiple studies are underway to determine whether hydroxychloroquine could be used for pre- or postexposure prophylaxis to prevent COVID-19. Another multisite trial will evaluate whether the BCG vaccine, primarily used to reduce the risk of TB, provides protection against COVID-19 in HCWs, driven by data suggesting a correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19.16
DATA GENERATION AND KNOWLEDGE SHARING
Infection prevention efforts can benefit from the unprecedented amount of data on COVID-19 that is being generated and shared. Successful examples of the rapid intensification of infection prevention measures to decrease transmission in healthcare facilities should be emulated. The hospital authority of Hong Kong implemented a bundle of measures focused on early recognition, isolation, notification, and molecular diagnostics for people being evaluated for COVID-19.17 They subsequently broadened the clinical and epidemiological criteria of surveillance as the outbreak evolved and intensified PPE recommendations to all HCWs (face masks for all and N95 respirators for those performing aerosol-generating procedures), which appears to have resulted in no cases of HCW infection or nosocomial transmission.
Data characterizing the extent of occupational infections in HCWs during acute and chronic epidemics is often lacking and subject to wide variability in reporting, which limits its impact. For example, HCWs in high TB incidence countries have at least twice the risk of developing TB, compared with the general population. Although there are still major gaps in national data collection regarding the incidence of occupational TB, recent attempts by WHO to systematically record this data have resulted in increasing prioritization of this group as an at-risk population who may benefit from TB preventive therapy. We strongly advocate that health systems systematically record and share longitudinal data on numbers of HCWs infected with COVID-19. This transparency will facilitate urgent action to replenish and sustain resources such as PPE and enable institutions to share and adapt successful infection prevention strategies. Examples such as the prevention of central line- associated bloodstream infections demonstrate the potential impact of national collaborative efforts to strengthen infection prevention, although further effort is needed to optimize knowledge sharing in the context of outbreaks.
CONCLUSIONS
The cost of not investing in public health pandemic preparedness including measures to protect HCWs is now widely apparent. HCWs have a right to safety in their workplaces as they fulfil their duty of care to patients.18 Rapid scale-up of diagnostic testing capacity, and bundles of infection prevention interventions including universal masking and drive-through testing, can safeguard HCWs and the patients they serve in the current COVID-19 pandemic. Re-establishing immediate access to quality-assured PPE is imperative to reduce the individual and workforce consequences of HCWs developing COVID-19 or other infectious diseases like TB that are continuously a threat to the workforce. Meanwhile, innovative approaches such as repurposing resources to develop PPE and use of GUV air disinfection may help to mitigate PPE shortages, and use of preventive therapies may also decrease COVID-19 risk in HCWs. Reliable surveillance data on HCW infection rates can help identify and track gaps in infection prevention, as well as identify strategies that impact this outcome. Ultimately greater top-down political commitment is urgently needed to ensure that frontline HCWs have the necessary resources to address the current pandemic and to sustain these interventions to protect HCWs in the future.
Emerging studies on coronavirus disease 2019 (COVID-19) confirm high rates of infection among healthcare workers (HCWs).1 As widespread community transmission increases, frontline HCWs, such as hospitalists, are at particularly high risk of exposure to people with undiagnosed COVID-19. Although there is no known effective treatment for COVID-19, early detection is vital to decreasing ongoing transmission through contact tracing and quarantine. However, lack of adequate testing capacity prevented basic public health interventions from curbing the pandemic at an earlier stage. As a result, given high rates of presumed community transmission of COVID-19 and evidence for asymptomatic transmission, there have been moves toward the use of universal personal protective equipment (PPE). This strategy is challenging to implement because of the acute PPE shortage, which has resulted in an urgent need to embrace innovation in infection prevention.
The current pandemic has resulted in an unprecedented volume of data being generated and disseminated, with the potential to impact real-time responses in geographically disparate regions. Here, we focus on the potential for innovation and knowledge sharing from an infection prevention perspective, which could enhance frontline HCW safety in the current COVID-19 pandemic.
DIAGNOSIS MATTERS
Every outbreak begins and ends with a diagnostic test. Widespread population testing coupled with intensive contact tracing had the potential to curb national epidemics if it had been implemented in time. In the United States, which now has the highest number of COVID-19 cases worldwide, there were technical difficulties with the first diagnostic test developed by the Centers for Disease Control and Prevention (CDC) and subsequent delays in scaling up access to COVID-19 diagnostic testing.2 The strategy of initially reserving testing only for those who were critically ill meant that by the time patients with COVID-19 were being diagnosed, widespread community spread had occurred because of the lack of detection of individuals with less severe or asymptomatic infections.
In contrast, scaled-up testing in South Korea has helped limit the spread and consequences of COVID-19. The use of drive-through testing centers enabled safe and efficient testing, while minimizing the risk to HCWs and eliminating the possibility of cross infection among people being tested.3 Although outdoor testing is not feasible in all settings, this approach avoids resources and time typically needed for ventilation (typically a negative pressure room with 12 air changes per hour would be used) and cleaning of specimen collection rooms.
The other major diagnostic gap is the ability to identify individuals who have recovered from COVID-19 and are immune. There is an urgent need to develop and scale up a rapid serological test that avoids cross-reactivity with other coronaviruses. Ideally, this test would permit testing of HCWs to determine who is likely immune and can therefore return safely to work.
RETHINKING PPE
There has been a massive and rapid increase in the need for PPE globally because of overwhelmed health systems having to care for large numbers of patients with suspected or confirmed COVID-19. This has been exacerbated by public fear, which has led to panic buying of medical face masks (primarily used to protect others from infections with a droplet mode of transmission) and filtering facepiece half-mask respirators, which include N95 respirators (used to protect the wearer from infections with an airborne mode of transmission).
COVID-19 is thought to be predominantly spread by transmission of respiratory droplets (>5 and <10 μm in diameter), which occurs when people are in close contact (within 1 meter) with others who typically (but not always) have respiratory symptoms such as cough or sneeze or with fomites that have come into contact with an infected person. This is in contrast to infectious diseases such as tuberculosis (TB) or measles, which are spread by airborne transmission of virus suspended in droplet nuclei (<5 μm in diameter), which can remain in the air for prolonged periods of time and can be transmitted over distances greater than 1 meter.4
While World Health Organization (WHO) and CDC infection prevention guidance have cited droplet transmission as the primary mode of transmission for COVID-19, current CDC guidelines state that respirators are preferred for the care of patients with known or suspected COVID-19, given the potential for opportunistic airborne transmission.5 However, in the setting of respirator shortages, it is recommended that these should be prioritized for HCWs caring for patients with COVID-19 in the context of aerosol-generating procedures or other patients with infections spread by airborne transmission such as TB or varicella until the supply chain is restored. Of note, optimal use of respirators requires fit testing, which is often lacking in nursing homes and outpatient facilities, as well as more widely in resource-limited countries.
Universal masking (use of surgical mask) for HCWs caring for any patient irrespective of symptoms or presenting complaint has also been implemented by many large hospital systems in recent days. Although universal masking adds to the burden of the PPE shortage, in settings with widespread community transmission and given increasing evidence6 demonstrating transmission from people with asymptomatic and presymptomatic infection, universal masking may be useful to decrease transmission. However, particularly in the setting of PPE shortages, it is important to understand that surgical masks are designed to be single use and that dampness and frequent adjustment of the mask affects their effectiveness.
As urgent attempts to coordinate and increase PPE manufacture are being made by health systems, in conjunction with private partnerships, there has also been a burst of public campaigns to sew cloth masks to mitigate the real-time shortages. Although it is likely that cloth masks provide inadequate protection in comparison with surgical masks,7 evidence does suggest that cloth masks provide some degree of protection from the spread of respiratory viruses,8 particularly if these are replaced promptly when damp or damaged and if combined with other interventions such as hand hygiene. This has led to recommendations for the general public in various countries to wear cloth face coverings in public settings, particularly where social distancing may be harder to maintain, but these are not recommended for use by HCWs in healthcare settings.
INNOVATION IN INFECTION PREVENTION
Strategies to navigate the PPE shortage in the era of COVID-19 include importing, reclaiming, reusing, and repurposing PPE; generating and extending supply; eliminating nonessential services; reducing patient contact; and using nonhuman services such as drones to deliver equipment and undertake tasks such as decontamination.9,10 Multidisciplinary teams are working on creative ways to use existing resources to make effective PPE, including alternatives to N95 respirators. An outbreak simulation study at Emory University in Atlanta, Georgia, and the University of Texas Health Science Center at Houston in Texas demonstrated that HCWs could be rapidly trained and fit tested to use elastomeric half-mask respirators, which are reusable.11 A multidisciplinary team at Boston Children’s Hospital in Massachusetts has developed and completed a small pilot study of a reusable elastomeric respirator made using an anesthesia facemask, antimicrobial filter, and elastic straps.12
Given evidence that suggests that COVID-19 involves a component of airborne transmission,13 in addition to droplet spread and surface (fomite) contamination,14 using known infection prevention techniques that work to decrease airborne transmission of other respiratory infectious diseases should also be considered. Germicidal ultraviolet (GUV) air disinfection rapidly disinfects upper room air, which is then continually exchanged with contaminated lower-room air. GUV air disinfection has been demonstrated to be a safe and cost-effective intervention, with an efficacy of approximately 80% for decreasing TB transmission.15 GUV air disinfection is also effective against airborne influenza and measles and may play a role in surface decontamination by accelerating viral inactivation. Enabling GUV in high-risk areas such as the emergency department or intensive care unit could be a high-yield intervention to decrease transmission of COVID-19.
HCWs exposed to other respiratory infections such as influenza or TB may receive preventive therapy to reduce the risk of developing disease. High rates of COVID-19 in HCWs have prompted several initiatives to evaluate innovative approaches to decreasing this risk. Multiple studies are underway to determine whether hydroxychloroquine could be used for pre- or postexposure prophylaxis to prevent COVID-19. Another multisite trial will evaluate whether the BCG vaccine, primarily used to reduce the risk of TB, provides protection against COVID-19 in HCWs, driven by data suggesting a correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19.16
DATA GENERATION AND KNOWLEDGE SHARING
Infection prevention efforts can benefit from the unprecedented amount of data on COVID-19 that is being generated and shared. Successful examples of the rapid intensification of infection prevention measures to decrease transmission in healthcare facilities should be emulated. The hospital authority of Hong Kong implemented a bundle of measures focused on early recognition, isolation, notification, and molecular diagnostics for people being evaluated for COVID-19.17 They subsequently broadened the clinical and epidemiological criteria of surveillance as the outbreak evolved and intensified PPE recommendations to all HCWs (face masks for all and N95 respirators for those performing aerosol-generating procedures), which appears to have resulted in no cases of HCW infection or nosocomial transmission.
Data characterizing the extent of occupational infections in HCWs during acute and chronic epidemics is often lacking and subject to wide variability in reporting, which limits its impact. For example, HCWs in high TB incidence countries have at least twice the risk of developing TB, compared with the general population. Although there are still major gaps in national data collection regarding the incidence of occupational TB, recent attempts by WHO to systematically record this data have resulted in increasing prioritization of this group as an at-risk population who may benefit from TB preventive therapy. We strongly advocate that health systems systematically record and share longitudinal data on numbers of HCWs infected with COVID-19. This transparency will facilitate urgent action to replenish and sustain resources such as PPE and enable institutions to share and adapt successful infection prevention strategies. Examples such as the prevention of central line- associated bloodstream infections demonstrate the potential impact of national collaborative efforts to strengthen infection prevention, although further effort is needed to optimize knowledge sharing in the context of outbreaks.
CONCLUSIONS
The cost of not investing in public health pandemic preparedness including measures to protect HCWs is now widely apparent. HCWs have a right to safety in their workplaces as they fulfil their duty of care to patients.18 Rapid scale-up of diagnostic testing capacity, and bundles of infection prevention interventions including universal masking and drive-through testing, can safeguard HCWs and the patients they serve in the current COVID-19 pandemic. Re-establishing immediate access to quality-assured PPE is imperative to reduce the individual and workforce consequences of HCWs developing COVID-19 or other infectious diseases like TB that are continuously a threat to the workforce. Meanwhile, innovative approaches such as repurposing resources to develop PPE and use of GUV air disinfection may help to mitigate PPE shortages, and use of preventive therapies may also decrease COVID-19 risk in HCWs. Reliable surveillance data on HCW infection rates can help identify and track gaps in infection prevention, as well as identify strategies that impact this outcome. Ultimately greater top-down political commitment is urgently needed to ensure that frontline HCWs have the necessary resources to address the current pandemic and to sustain these interventions to protect HCWs in the future.
1. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11)1061-1069. https://doi.org/10.1001/jama.2020.1585.
2. Sharfstein JM, Becker SJ, Mello MM. Diagnostic testing for the novel coronavirus. JAMA. 2020. https://doi.org/10.1001/jama.2020.3864.
3. Kwon KT, Ko JH, Shin H, Sung M, Kim JY. Drive-through screening center for COVID-19: a safe and efficient screening system against massive community outbreak. J Korean Med Sci. 2020;35(11):e123. https://doi.org/10.3346/jkms.2020.35.e123.
4. World Health Organization. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations. Scientific Brief, March 29, 2020. https://www.who.int/publications-detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations. Accessed April 5, 2020.
5. Centers for Disease Control and Prevention. CDC Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed April 5, 2020.
6. Kimball A, Hatfield KM, Arons M, et al. Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility—King County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69(13):377-381. https://doi.org/10.15585/mmwr.mm6913e1.
7. MacIntyre CR, Seale H, Dung TC, et al. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open. 2015;5(4):e006577. https://doi.org/10.1136/bmjopen-2014-006577.
8. van der Sande M, Teunis P, Sabel R. Professional and home-made face masks reduce exposure to respiratory infections among the general population. PLoS One. 2008;3(7):e2618. https://doi.org/10.1371/journal.pone.0002618.
9. Livingston E, Desai A, Berkwits M. Sourcing Personal Protective Equipment During the COVID-19 Pandemic. JAMA. 2020. https://doi.org/10.1001/jama.2020.5317.
10. Steuart R, Huang FS, Schaffzin JK, Thomson J. Finding the value in personal protective equipment for hospitalized patients during a pandemic and beyond. J Hosp Med. 2020;15(5):xxx-xxx. https://doi.org/10.12788/jhm.3429.
11. Pompeii LA, Kraft CS, Brownsword EA, et al. Training and fit testing of health care personnel for reusable elastomeric half-mask respirators compared with disposable N95 respirators. JAMA. 2020;e204806. https://doi.org/10.1001/jama.2020.4806.
12. Boston Children’s Hospital. Surgical Innovation Fellowship. https://www.childrenshospital.org/research/departments-divisions-programs/departments/surgery/surgical-innovation-fellowship. Accessed April 5, 2020.
13. van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020. https://doi.org/10.1056/NEJMc2004973.
14. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;e203227. https://doi.org/10.1001/jama.2020.3227.
15. Mphaphlele M, Dharmadhikari AS, Jensen PA, et al. Institutional tuberculosis transmission. Controlled trial of upper room ultraviolet air disinfection: a basis for new dosing guidelines. Am J Respir Crit Care Med. 2015;192(4):477-484. https://doi.org/10.1164/rccm.201501-0060OC.
16. Miller A, Reandelar MJ, Fasciglione K, Roumenova V, Li Y, Otazu GH. Correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19: an epidemiological study. medRxiv. 2020. https://doi.org/10.1101/2020.03.24.20042937 .
17. Cheng VCC, Wong SC, Chen JHK, et al. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. 2020. https://doi.org/10.1017/ice.2020.58.
18. Antommaria AHM. Conflicting duties and reciprocal obligations during a pandemic. J Hosp Med. 2020;15(5):xxx-xxx. https://doi.org/10.12788/jhm.3425.
1. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11)1061-1069. https://doi.org/10.1001/jama.2020.1585.
2. Sharfstein JM, Becker SJ, Mello MM. Diagnostic testing for the novel coronavirus. JAMA. 2020. https://doi.org/10.1001/jama.2020.3864.
3. Kwon KT, Ko JH, Shin H, Sung M, Kim JY. Drive-through screening center for COVID-19: a safe and efficient screening system against massive community outbreak. J Korean Med Sci. 2020;35(11):e123. https://doi.org/10.3346/jkms.2020.35.e123.
4. World Health Organization. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations. Scientific Brief, March 29, 2020. https://www.who.int/publications-detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations. Accessed April 5, 2020.
5. Centers for Disease Control and Prevention. CDC Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed April 5, 2020.
6. Kimball A, Hatfield KM, Arons M, et al. Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility—King County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69(13):377-381. https://doi.org/10.15585/mmwr.mm6913e1.
7. MacIntyre CR, Seale H, Dung TC, et al. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open. 2015;5(4):e006577. https://doi.org/10.1136/bmjopen-2014-006577.
8. van der Sande M, Teunis P, Sabel R. Professional and home-made face masks reduce exposure to respiratory infections among the general population. PLoS One. 2008;3(7):e2618. https://doi.org/10.1371/journal.pone.0002618.
9. Livingston E, Desai A, Berkwits M. Sourcing Personal Protective Equipment During the COVID-19 Pandemic. JAMA. 2020. https://doi.org/10.1001/jama.2020.5317.
10. Steuart R, Huang FS, Schaffzin JK, Thomson J. Finding the value in personal protective equipment for hospitalized patients during a pandemic and beyond. J Hosp Med. 2020;15(5):xxx-xxx. https://doi.org/10.12788/jhm.3429.
11. Pompeii LA, Kraft CS, Brownsword EA, et al. Training and fit testing of health care personnel for reusable elastomeric half-mask respirators compared with disposable N95 respirators. JAMA. 2020;e204806. https://doi.org/10.1001/jama.2020.4806.
12. Boston Children’s Hospital. Surgical Innovation Fellowship. https://www.childrenshospital.org/research/departments-divisions-programs/departments/surgery/surgical-innovation-fellowship. Accessed April 5, 2020.
13. van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020. https://doi.org/10.1056/NEJMc2004973.
14. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;e203227. https://doi.org/10.1001/jama.2020.3227.
15. Mphaphlele M, Dharmadhikari AS, Jensen PA, et al. Institutional tuberculosis transmission. Controlled trial of upper room ultraviolet air disinfection: a basis for new dosing guidelines. Am J Respir Crit Care Med. 2015;192(4):477-484. https://doi.org/10.1164/rccm.201501-0060OC.
16. Miller A, Reandelar MJ, Fasciglione K, Roumenova V, Li Y, Otazu GH. Correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19: an epidemiological study. medRxiv. 2020. https://doi.org/10.1101/2020.03.24.20042937 .
17. Cheng VCC, Wong SC, Chen JHK, et al. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. 2020. https://doi.org/10.1017/ice.2020.58.
18. Antommaria AHM. Conflicting duties and reciprocal obligations during a pandemic. J Hosp Med. 2020;15(5):xxx-xxx. https://doi.org/10.12788/jhm.3425.
© 2020 Society of Hospital Medicine
Implementing Physical Distancing in the Hospital: A Key Strategy to Prevent Nosocomial Transmission of COVID-19
Hospitalists serve as frontline healthcare professionals caring for the increasing number of COVID-19 patients in the United States. The safety of hospitalists and other frontline healthcare workers is paramount to preventing high nosocomial transmission as has been reported in several other countries. Much effort to date has rightly focused on ensuring healthcare workers have appropriate personal protective equipment (PPE) given the known increased risk of nosocomial infection to healthcare workers. However, another important strategy to prevent nosocomial transmission is to implement “social distancing,” or avoiding close contact with others. While this approach has received considerable press with regards to implementation in communities, social, or physical, distancing in the hospital is also a critical way to prevent nosocomial transmission and ensure the health and welfare of our workforce to meet the challenge. The Centers for Disease Control and Prevention (CDC) defines close contact as less than 6 feet away for over 10 minutes.1 Given the myriad clinical interactions that occur within teams in the hospital, such distancing can prove challenging.
At the University of Chicago Medicine in Illinois, our hospitalist group was an early adopter of implementing several strategies to facilitate physical distancing in the context of clinical care to minimize community transmission of COVID-19 among healthcare professionals. We describe how to implement physical distancing effectively in specific hospital settings, including some challenges and strategies to surmount them.
EDUCATIONAL CONFERENCES AND ADMINISTRATIVE MEETINGS
Educational conferences and administrative meetings need to be transitioned to virtual meetings. While it may be easy to broadcast a conference in lieu of meeting in a conference room, it is critical that hospital clinicians do not “huddle close together” in front of a computer, which would defeat the purpose of physical distancing. While “flipping the classroom” in preclinical and higher education is common, this method can be effective to deliver standard education followed by a virtual question and answer session or chat room.2
Educational discussions can also occur asynchronously through learning management systems, such as Canvas, or even closed social media channels, such as Slack, that enable discussions. These tools require training to work, so it is important to invest in education on the chosen platform to ensure that it functions smoothly. It is equally important that administrators become familiar with these tools while working remotely and can facilitate administrative meetings without difficulty. We created a one-page tip sheet to help ease the transition for department administrators. The tip sheet highlighted how to start a virtual meeting and meeting etiquette (eg, mute upon entry into the meeting, mute when not talking, announce yourself when talking) as well as ensuring that dial-ins could easily access the meeting by including one-touch options, when available, on calendar invites in addition to the weblink. A daily email update can be an important adjunct to administrative meetings to ensure critical updates are reaching all clinicians in a group and also preserves meeting time for clarifying questions.
CLINICAL WORKROOMS
Perhaps the biggest challenge is how many clinical workrooms in hospitals today are crowded with computers next to each other. Ventilation can also be poor, making conditions riskier. This makes implemention of social distancing extremely challenging, but also critical, given how much time hospital-based clinicians spend on computers and in their workrooms. The first step to achieving social distancing in the workroom is to take an inventory of how many people work there and get a log of the number of computers. Consider whether existing computers can be rearranged with a goal of keeping people 6 feet apart. For particularly cramped workrooms, this may require assigning computer spaces to physicians across a floor or several floors, using computers out on a unit, or using mobile computers to limit the number of people in the workroom at one time. We suggest working with physical plant leaders and Information Technology to reallocate mobile workstations, laptops, or desktops to conference rooms, patient visiting areas, and offices that are not being used. Because coronavirus can survive on surfaces for several hours, it is also important to stock work rooms with disinfectants to clean surfaces such as keyboards and desktops frequently. One other important thing to consider is whether computers can be assigned to specific teams or people to limit the use of a computer by multiple people.
ROUNDING, SIGN-OUT, AND MULTIDISCIPLINARY ROUNDS
Rounding
Perhaps one of the most fundamental hardships with physical distancing is how to conduct routine clinical care such as rounds, sign-out, or multidisciplinary rounds. Rounds on teaching services are particularly challenging given the number of people. At many teaching institutions, medical students are no longer on clinical rotations, which immediately reduces the number of people on teaching teams. The other thing to consider is how rounds are conducted. As opposed to a large team walking together, assign one person from the team as the liaison for the patient, which also has the added benefit of conserving precious PPE. Virtual rounding enables clinicians, including residents and attendings, to work together and decide the plan for the day without first crowding into a patient room. This is perhaps the most important cultural hurdle that one may face.
Another administrative hurdle and common concern is how to bill for such interactions. While federal guidance evolves, our institution created smartphrases for this type of virtual rounding whereby attendings attest to resident notes even if they did not physically see the patient. Additional information may be obtained from patients by calling them on their patient-room phones or by using telemedicine as some hospitals are implementing.3 For large “mega” teams, split the team into smaller groups to facilitate continuity and easier conversations.
Sign-out
When feasible, it is important to transition to phone sign-out supplemented with viewing an updated shared sign-out, ideally electronically, for shift change. When using phone sign-out, it is ideal to implement a verbal read-back to ensure understanding and to keep your sign-out updated. Because using the telephone is not the most effective communication channel for sign-out, it is key to be vigilant with other sign-out best practices, such as using a standard template like IPASS4 or another framework, prioritizing sick patients, and ensuring a focus on to-do and if/then items that are critical for the receiver to ensure understanding.5
Multidisciplinary Rounds
As multidisciplinary rounds typically occur either at the bedside or in a conference room, it is key to ensure that these occur virtually whenever possible. One option is to use conference calls or video chat (eg, Zoom) for multidisciplinary rounds whenever possible. Calendar invites or paging reminders can be used to prompt teams when to call in to discuss patients. Because multiple people are entering a virtual room at once, it is important to establish an order or have a leader orchestrate who is next. In addition, given the importance of multiple people contributing to the discussion, it is also equally important for those speaking always to announce who they are and their role (eg, social worker, case manager, physical therapist) since it may not be possible to recognize people’s voices alone. This is where visual recognition can be helpful through use of institutional video conferencing that enables hearing and seeing someone. Further, it is important to ensure that the platform being used is HIPAA compliant.
CALL ROOMS
Call rooms in hospitals can be particularly challenging if they are shared. Finding additional call rooms may require use of cots or reallocation of patient rooms. It is also possible for hospitalists to consider air mattresses in their offices or other private spaces to avoid sharing call rooms. Consider assigning the same call room to the same few people over the course of a rotation or period to avoid many people sharing one room. If a hospital is converting units to group patients under investigation or those who are COVID-19 positive, reallocating call rooms may be necessary to accommodate new teams. Lastly, it is important to communicate proactively with environmental services staff to make sure all call rooms are equipped with cleaning supplies and hand sanitizer and are cleaned daily to avoid nosocomial transmission.
CONCLUSION
/section>Containing nosocomial spread of coronavirus is particularly challenging for hospitals because of how contagious the virus is, the extreme shortage of PPE, and lack of mass testing to identify those who are sick. Therefore, physical distancing in the hospital is critical to ensure the health and well-being of the health professional workforce during the pandemic.
1. Centers for Disease Control and Prevention. Interim U.S. Guidance for Risk Assessment and Public Health Management of Healthcare Personnel with Potential Exposure in a Healthcare Setting to Patients with Coronavirus Disease (COVID-19). https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-risk-assesment-hcp.html. Accessed April 2, 2020.
2. Stephenson CR, Wang AT, Szostek JH, et al. Flipping the continuing medical education classroom: validating a measure of attendees’ perceptions. J Contin Educ Health Prof. 2016;36(4):256-262. https://doi.org/10.1097/CEH.0000000000000113.
3. Doshi A, Platt Y, Dressen JR, K Mathews BK, Siy JC. Keep calm and log on: telemedicine for COVID-19 pandemic response. J Hosp Med. 2020;15(4):xxx-xxxx. https://doi.org/10.12788/jhm.3419.
4. Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803-1812. https://doi.org/10.1056/NEJMsa1405556.
5. Gaffney S, Farnan JM, Hirsch K, McGinty M, Arora VM. The modified, multi-patient observed simulated handoff experience (M-OSHE): assessment and feedback for entering residents on handoff performance. J Gen Intern Med. 2016;31(4):438-441. https://doi.org/10.1007/s11606-016-3591-8.
Hospitalists serve as frontline healthcare professionals caring for the increasing number of COVID-19 patients in the United States. The safety of hospitalists and other frontline healthcare workers is paramount to preventing high nosocomial transmission as has been reported in several other countries. Much effort to date has rightly focused on ensuring healthcare workers have appropriate personal protective equipment (PPE) given the known increased risk of nosocomial infection to healthcare workers. However, another important strategy to prevent nosocomial transmission is to implement “social distancing,” or avoiding close contact with others. While this approach has received considerable press with regards to implementation in communities, social, or physical, distancing in the hospital is also a critical way to prevent nosocomial transmission and ensure the health and welfare of our workforce to meet the challenge. The Centers for Disease Control and Prevention (CDC) defines close contact as less than 6 feet away for over 10 minutes.1 Given the myriad clinical interactions that occur within teams in the hospital, such distancing can prove challenging.
At the University of Chicago Medicine in Illinois, our hospitalist group was an early adopter of implementing several strategies to facilitate physical distancing in the context of clinical care to minimize community transmission of COVID-19 among healthcare professionals. We describe how to implement physical distancing effectively in specific hospital settings, including some challenges and strategies to surmount them.
EDUCATIONAL CONFERENCES AND ADMINISTRATIVE MEETINGS
Educational conferences and administrative meetings need to be transitioned to virtual meetings. While it may be easy to broadcast a conference in lieu of meeting in a conference room, it is critical that hospital clinicians do not “huddle close together” in front of a computer, which would defeat the purpose of physical distancing. While “flipping the classroom” in preclinical and higher education is common, this method can be effective to deliver standard education followed by a virtual question and answer session or chat room.2
Educational discussions can also occur asynchronously through learning management systems, such as Canvas, or even closed social media channels, such as Slack, that enable discussions. These tools require training to work, so it is important to invest in education on the chosen platform to ensure that it functions smoothly. It is equally important that administrators become familiar with these tools while working remotely and can facilitate administrative meetings without difficulty. We created a one-page tip sheet to help ease the transition for department administrators. The tip sheet highlighted how to start a virtual meeting and meeting etiquette (eg, mute upon entry into the meeting, mute when not talking, announce yourself when talking) as well as ensuring that dial-ins could easily access the meeting by including one-touch options, when available, on calendar invites in addition to the weblink. A daily email update can be an important adjunct to administrative meetings to ensure critical updates are reaching all clinicians in a group and also preserves meeting time for clarifying questions.
CLINICAL WORKROOMS
Perhaps the biggest challenge is how many clinical workrooms in hospitals today are crowded with computers next to each other. Ventilation can also be poor, making conditions riskier. This makes implemention of social distancing extremely challenging, but also critical, given how much time hospital-based clinicians spend on computers and in their workrooms. The first step to achieving social distancing in the workroom is to take an inventory of how many people work there and get a log of the number of computers. Consider whether existing computers can be rearranged with a goal of keeping people 6 feet apart. For particularly cramped workrooms, this may require assigning computer spaces to physicians across a floor or several floors, using computers out on a unit, or using mobile computers to limit the number of people in the workroom at one time. We suggest working with physical plant leaders and Information Technology to reallocate mobile workstations, laptops, or desktops to conference rooms, patient visiting areas, and offices that are not being used. Because coronavirus can survive on surfaces for several hours, it is also important to stock work rooms with disinfectants to clean surfaces such as keyboards and desktops frequently. One other important thing to consider is whether computers can be assigned to specific teams or people to limit the use of a computer by multiple people.
ROUNDING, SIGN-OUT, AND MULTIDISCIPLINARY ROUNDS
Rounding
Perhaps one of the most fundamental hardships with physical distancing is how to conduct routine clinical care such as rounds, sign-out, or multidisciplinary rounds. Rounds on teaching services are particularly challenging given the number of people. At many teaching institutions, medical students are no longer on clinical rotations, which immediately reduces the number of people on teaching teams. The other thing to consider is how rounds are conducted. As opposed to a large team walking together, assign one person from the team as the liaison for the patient, which also has the added benefit of conserving precious PPE. Virtual rounding enables clinicians, including residents and attendings, to work together and decide the plan for the day without first crowding into a patient room. This is perhaps the most important cultural hurdle that one may face.
Another administrative hurdle and common concern is how to bill for such interactions. While federal guidance evolves, our institution created smartphrases for this type of virtual rounding whereby attendings attest to resident notes even if they did not physically see the patient. Additional information may be obtained from patients by calling them on their patient-room phones or by using telemedicine as some hospitals are implementing.3 For large “mega” teams, split the team into smaller groups to facilitate continuity and easier conversations.
Sign-out
When feasible, it is important to transition to phone sign-out supplemented with viewing an updated shared sign-out, ideally electronically, for shift change. When using phone sign-out, it is ideal to implement a verbal read-back to ensure understanding and to keep your sign-out updated. Because using the telephone is not the most effective communication channel for sign-out, it is key to be vigilant with other sign-out best practices, such as using a standard template like IPASS4 or another framework, prioritizing sick patients, and ensuring a focus on to-do and if/then items that are critical for the receiver to ensure understanding.5
Multidisciplinary Rounds
As multidisciplinary rounds typically occur either at the bedside or in a conference room, it is key to ensure that these occur virtually whenever possible. One option is to use conference calls or video chat (eg, Zoom) for multidisciplinary rounds whenever possible. Calendar invites or paging reminders can be used to prompt teams when to call in to discuss patients. Because multiple people are entering a virtual room at once, it is important to establish an order or have a leader orchestrate who is next. In addition, given the importance of multiple people contributing to the discussion, it is also equally important for those speaking always to announce who they are and their role (eg, social worker, case manager, physical therapist) since it may not be possible to recognize people’s voices alone. This is where visual recognition can be helpful through use of institutional video conferencing that enables hearing and seeing someone. Further, it is important to ensure that the platform being used is HIPAA compliant.
CALL ROOMS
Call rooms in hospitals can be particularly challenging if they are shared. Finding additional call rooms may require use of cots or reallocation of patient rooms. It is also possible for hospitalists to consider air mattresses in their offices or other private spaces to avoid sharing call rooms. Consider assigning the same call room to the same few people over the course of a rotation or period to avoid many people sharing one room. If a hospital is converting units to group patients under investigation or those who are COVID-19 positive, reallocating call rooms may be necessary to accommodate new teams. Lastly, it is important to communicate proactively with environmental services staff to make sure all call rooms are equipped with cleaning supplies and hand sanitizer and are cleaned daily to avoid nosocomial transmission.
CONCLUSION
/section>Containing nosocomial spread of coronavirus is particularly challenging for hospitals because of how contagious the virus is, the extreme shortage of PPE, and lack of mass testing to identify those who are sick. Therefore, physical distancing in the hospital is critical to ensure the health and well-being of the health professional workforce during the pandemic.
Hospitalists serve as frontline healthcare professionals caring for the increasing number of COVID-19 patients in the United States. The safety of hospitalists and other frontline healthcare workers is paramount to preventing high nosocomial transmission as has been reported in several other countries. Much effort to date has rightly focused on ensuring healthcare workers have appropriate personal protective equipment (PPE) given the known increased risk of nosocomial infection to healthcare workers. However, another important strategy to prevent nosocomial transmission is to implement “social distancing,” or avoiding close contact with others. While this approach has received considerable press with regards to implementation in communities, social, or physical, distancing in the hospital is also a critical way to prevent nosocomial transmission and ensure the health and welfare of our workforce to meet the challenge. The Centers for Disease Control and Prevention (CDC) defines close contact as less than 6 feet away for over 10 minutes.1 Given the myriad clinical interactions that occur within teams in the hospital, such distancing can prove challenging.
At the University of Chicago Medicine in Illinois, our hospitalist group was an early adopter of implementing several strategies to facilitate physical distancing in the context of clinical care to minimize community transmission of COVID-19 among healthcare professionals. We describe how to implement physical distancing effectively in specific hospital settings, including some challenges and strategies to surmount them.
EDUCATIONAL CONFERENCES AND ADMINISTRATIVE MEETINGS
Educational conferences and administrative meetings need to be transitioned to virtual meetings. While it may be easy to broadcast a conference in lieu of meeting in a conference room, it is critical that hospital clinicians do not “huddle close together” in front of a computer, which would defeat the purpose of physical distancing. While “flipping the classroom” in preclinical and higher education is common, this method can be effective to deliver standard education followed by a virtual question and answer session or chat room.2
Educational discussions can also occur asynchronously through learning management systems, such as Canvas, or even closed social media channels, such as Slack, that enable discussions. These tools require training to work, so it is important to invest in education on the chosen platform to ensure that it functions smoothly. It is equally important that administrators become familiar with these tools while working remotely and can facilitate administrative meetings without difficulty. We created a one-page tip sheet to help ease the transition for department administrators. The tip sheet highlighted how to start a virtual meeting and meeting etiquette (eg, mute upon entry into the meeting, mute when not talking, announce yourself when talking) as well as ensuring that dial-ins could easily access the meeting by including one-touch options, when available, on calendar invites in addition to the weblink. A daily email update can be an important adjunct to administrative meetings to ensure critical updates are reaching all clinicians in a group and also preserves meeting time for clarifying questions.
CLINICAL WORKROOMS
Perhaps the biggest challenge is how many clinical workrooms in hospitals today are crowded with computers next to each other. Ventilation can also be poor, making conditions riskier. This makes implemention of social distancing extremely challenging, but also critical, given how much time hospital-based clinicians spend on computers and in their workrooms. The first step to achieving social distancing in the workroom is to take an inventory of how many people work there and get a log of the number of computers. Consider whether existing computers can be rearranged with a goal of keeping people 6 feet apart. For particularly cramped workrooms, this may require assigning computer spaces to physicians across a floor or several floors, using computers out on a unit, or using mobile computers to limit the number of people in the workroom at one time. We suggest working with physical plant leaders and Information Technology to reallocate mobile workstations, laptops, or desktops to conference rooms, patient visiting areas, and offices that are not being used. Because coronavirus can survive on surfaces for several hours, it is also important to stock work rooms with disinfectants to clean surfaces such as keyboards and desktops frequently. One other important thing to consider is whether computers can be assigned to specific teams or people to limit the use of a computer by multiple people.
ROUNDING, SIGN-OUT, AND MULTIDISCIPLINARY ROUNDS
Rounding
Perhaps one of the most fundamental hardships with physical distancing is how to conduct routine clinical care such as rounds, sign-out, or multidisciplinary rounds. Rounds on teaching services are particularly challenging given the number of people. At many teaching institutions, medical students are no longer on clinical rotations, which immediately reduces the number of people on teaching teams. The other thing to consider is how rounds are conducted. As opposed to a large team walking together, assign one person from the team as the liaison for the patient, which also has the added benefit of conserving precious PPE. Virtual rounding enables clinicians, including residents and attendings, to work together and decide the plan for the day without first crowding into a patient room. This is perhaps the most important cultural hurdle that one may face.
Another administrative hurdle and common concern is how to bill for such interactions. While federal guidance evolves, our institution created smartphrases for this type of virtual rounding whereby attendings attest to resident notes even if they did not physically see the patient. Additional information may be obtained from patients by calling them on their patient-room phones or by using telemedicine as some hospitals are implementing.3 For large “mega” teams, split the team into smaller groups to facilitate continuity and easier conversations.
Sign-out
When feasible, it is important to transition to phone sign-out supplemented with viewing an updated shared sign-out, ideally electronically, for shift change. When using phone sign-out, it is ideal to implement a verbal read-back to ensure understanding and to keep your sign-out updated. Because using the telephone is not the most effective communication channel for sign-out, it is key to be vigilant with other sign-out best practices, such as using a standard template like IPASS4 or another framework, prioritizing sick patients, and ensuring a focus on to-do and if/then items that are critical for the receiver to ensure understanding.5
Multidisciplinary Rounds
As multidisciplinary rounds typically occur either at the bedside or in a conference room, it is key to ensure that these occur virtually whenever possible. One option is to use conference calls or video chat (eg, Zoom) for multidisciplinary rounds whenever possible. Calendar invites or paging reminders can be used to prompt teams when to call in to discuss patients. Because multiple people are entering a virtual room at once, it is important to establish an order or have a leader orchestrate who is next. In addition, given the importance of multiple people contributing to the discussion, it is also equally important for those speaking always to announce who they are and their role (eg, social worker, case manager, physical therapist) since it may not be possible to recognize people’s voices alone. This is where visual recognition can be helpful through use of institutional video conferencing that enables hearing and seeing someone. Further, it is important to ensure that the platform being used is HIPAA compliant.
CALL ROOMS
Call rooms in hospitals can be particularly challenging if they are shared. Finding additional call rooms may require use of cots or reallocation of patient rooms. It is also possible for hospitalists to consider air mattresses in their offices or other private spaces to avoid sharing call rooms. Consider assigning the same call room to the same few people over the course of a rotation or period to avoid many people sharing one room. If a hospital is converting units to group patients under investigation or those who are COVID-19 positive, reallocating call rooms may be necessary to accommodate new teams. Lastly, it is important to communicate proactively with environmental services staff to make sure all call rooms are equipped with cleaning supplies and hand sanitizer and are cleaned daily to avoid nosocomial transmission.
CONCLUSION
/section>Containing nosocomial spread of coronavirus is particularly challenging for hospitals because of how contagious the virus is, the extreme shortage of PPE, and lack of mass testing to identify those who are sick. Therefore, physical distancing in the hospital is critical to ensure the health and well-being of the health professional workforce during the pandemic.
1. Centers for Disease Control and Prevention. Interim U.S. Guidance for Risk Assessment and Public Health Management of Healthcare Personnel with Potential Exposure in a Healthcare Setting to Patients with Coronavirus Disease (COVID-19). https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-risk-assesment-hcp.html. Accessed April 2, 2020.
2. Stephenson CR, Wang AT, Szostek JH, et al. Flipping the continuing medical education classroom: validating a measure of attendees’ perceptions. J Contin Educ Health Prof. 2016;36(4):256-262. https://doi.org/10.1097/CEH.0000000000000113.
3. Doshi A, Platt Y, Dressen JR, K Mathews BK, Siy JC. Keep calm and log on: telemedicine for COVID-19 pandemic response. J Hosp Med. 2020;15(4):xxx-xxxx. https://doi.org/10.12788/jhm.3419.
4. Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803-1812. https://doi.org/10.1056/NEJMsa1405556.
5. Gaffney S, Farnan JM, Hirsch K, McGinty M, Arora VM. The modified, multi-patient observed simulated handoff experience (M-OSHE): assessment and feedback for entering residents on handoff performance. J Gen Intern Med. 2016;31(4):438-441. https://doi.org/10.1007/s11606-016-3591-8.
1. Centers for Disease Control and Prevention. Interim U.S. Guidance for Risk Assessment and Public Health Management of Healthcare Personnel with Potential Exposure in a Healthcare Setting to Patients with Coronavirus Disease (COVID-19). https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-risk-assesment-hcp.html. Accessed April 2, 2020.
2. Stephenson CR, Wang AT, Szostek JH, et al. Flipping the continuing medical education classroom: validating a measure of attendees’ perceptions. J Contin Educ Health Prof. 2016;36(4):256-262. https://doi.org/10.1097/CEH.0000000000000113.
3. Doshi A, Platt Y, Dressen JR, K Mathews BK, Siy JC. Keep calm and log on: telemedicine for COVID-19 pandemic response. J Hosp Med. 2020;15(4):xxx-xxxx. https://doi.org/10.12788/jhm.3419.
4. Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803-1812. https://doi.org/10.1056/NEJMsa1405556.
5. Gaffney S, Farnan JM, Hirsch K, McGinty M, Arora VM. The modified, multi-patient observed simulated handoff experience (M-OSHE): assessment and feedback for entering residents on handoff performance. J Gen Intern Med. 2016;31(4):438-441. https://doi.org/10.1007/s11606-016-3591-8.
© 2020 Society of Hospital Medicine
Do I Have Coronavirus?
“To journey for the sake of saving our own lives is little by little to cease to live in any sense that really matters, even to ourselves, because it is only by journeying for the world’s sake—even when the world bores and sickens and scares you half to death—that little by little we start to come alive.”
—Frederick Buechner
On February 29, 2020, I find out by text from my intern when the first patient at our hospital in Seattle tests positive for COVID-19. He learns of it from his fellow intern who is caring for the patient. The news quickly spreads through the hospital like the virus itself, going from person to person while official communication channels remain initially silent. The news comes on the heels of a friend’s text that her daughter’s high school is closing for disinfection after a classmate also tested positive for COVID-19. I know the cataclysmic significance of these two events: Public health efforts to contain the SARS-CoV-2 coronavirus have failed, and there is ongoing community spread of the infection in Washington state. I text my intern back with the emoji of The Scream by Edvard Munch.
Could I be asymptomatically infected with the coronavirus? I work in close quarters with my colleagues who cared for the COVID-19–positive patient before he was placed in infection precautions. Social distancing has yet to enter our lexicon and our lives. In our crowded office, shared surfaces abound. Suddenly, every hard surface seems suspect—chairs, phones, dictaphone handsets, code pagers, printers, keypads, and door handles. All can be vectors of viral transmission. Normally insouciant about cleanliness, my coworkers and I start swabbing down every surface with disinfectant wipes. I ponder my likelihood of infection and decide it is possible but not probable.
In the next few days, I have a trip to Sedona, Arizona, planned with my extended family. Originally conceived as a celebration for my mom’s 80th birthday, we repurposed it as a time to grieve together after she unexpectedly passed away. I debate back and forth whether to go on the trip. If there is a chance I am infected with the coronavirus, it feels irresponsible to board an airplane with hundreds of other people. Yet the trip carries such high value for me. My family holds out hope I can get tested for the coronavirus, but I know just how limited testing capability is. It cuts me to the heart, but I cancel my flight. The deciding factor is that my sister has an autoimmune disease and is immunosuppressed. I don’t want to jeopardize her health. The world has truly gone topsy-turvy when the greatest thoughtfulness you can show to someone you love is to stay the hell away from her.
AM I A HYPOCHONDRIAC?
After my work stretch, I hunker down at home to monitor myself. I have a mild sore throat but convince myself it is psychosomatic. My plausible deniability of illness dies when I develop a cough and fatigue. Based on my symptoms, it is impossible to tell if I have the coronavirus or a common cold. I place myself on home quarantine. I don’t pursue coronavirus testing because there are hospitalized patients who need it much more than I do. I diligently monitor my temperature twice daily and it remains normal. My sore throat and fatigue go away, but my cough and some mild shortness of breath persists. I attribute it to my asthma, but the possibility of COVID-19 always lurks in the back of my mind. COVID-19 patients often don’t worsen until their second week of infection. Ordinarily, I would start using my steroid inhaler, but I hold off since steroids are thought to prolong viral replication.
When I tire of staying in the house, I go outside to work in the yard. I get on a low ladder to pull down the English ivy climbing up and smothering a tree. The ivy strand I’m tugging on suddenly breaks and I fall hard onto my back. Like a slap in the face, the accident shocks me into a new state of mental clarity. As a hospitalist, I’m a precious resource to my community right now. I can’t knock myself out of commission for dumb reasons. I ban myself from climbing any more ladders.
WHY CAN’T I GET TESTED?
As my time in quarantine draws to a close, I put my legal and financial affairs in order and pack a just-in-case backpack. The emergency room doctor hospitalized at a nearby hospital with severe COVID-19 is about my age. I am still coughing so I check in with the head of Infection Control to see if I need to be tested before returning to work. He tells me no. As I start working, I realize that coughing is the new leprosy. Even though I wear a mask, I get tense looks from others who carefully keep their distance from me. I tell everyone I have cough variant asthma, but what they all want to know is if I have been tested for the coronavirus. I haven’t been.
When my hospital sets up a new dedicated Employee Health screening phone line, I call right away. The nurse tells me I don’t meet criteria for coronavirus testing even though I am working on the COVID-19 rule-out unit with patients who have tested positive. While I agree with her from a medical standpoint, I don’t from a social or psychological perspective. This is a particularly unpropitious time in history to be a Chinese American doctor who can’t stop coughing. A negative test will reassure my patients and coworkers I am not a risk to them. A positive test, which is a possibility because of known prolonged viral shedding of the coronavirus, will reassure me I’m likely on my way to developing serologic immunity. I don’t get a test. When I tell my colleague, he suggests I resort to lying, but I won’t do it. As I’ve watched how power, wealth, and privilege play out in access to testing, I refuse to manipulate the system. But my experience is pointed commentary on the abysmal failure of testing in the United States when a frontline symptomatic doctor taking care of COVID-19 patients in one of the epicenters of the pandemic can’t get a coronavirus test. During a meeting, the head of Infection Control bluntly states he hopes we know that all of us are going to get the coronavirus at some point, but hopefully it won’t take us out of commission all at once. I feel better hearing him acknowledge that because it confirms my own sense of reality.
ARE WE RUNNING OUT OF PERSONAL PROTECTIVE EQUIPMENT?
While the ongoing pandemic definitely increases stress and anxiety levels in the hospital, there also continues to be caring and kindness. As I don my personal protective equipment (PPE), a nurse notices an exposed gap in the back of my gown and fixes it for me. He has my back, literally and figuratively. Our unit clerk, hearing my persistent cough, braves the 6-foot danger zone to hand me cough drops. Another nurse asks when the last time was I drank anything, and I give her a blank look because I can’t remember. I’m trying to minimize my use of masks, so I have kept my current one on all day. The front of the mask may be contaminated, but as long as I don’t touch that surface, it is still protecting me. She hands me a cup of water and I consider the benefit of staying hydrated versus using up another mask. Having previously landed in the emergency room with a kidney stone from not properly hydrating, I take off the mask, throw it away, wash my hands, and drink the water. But in my mind, I’m acutely aware of our shrinking supply of PPE.
On our time off work, my coworkers and I reach out to everyone we know to ask for mask donations. One friend tells me her husband is fashioning a mask for her from their furnace filter. She considers it the most romantic thing he’s ever done for her. The two of us agree that if we run out of PPE, we will go on caring for our patients anyway. We are doctors and caring for others is not only what we do, but an intrinsic part of who we are. Our journey amid the coronavirus pandemic may at times scare us half to death, but in caring for others “little by little we start to come alive.”
“To journey for the sake of saving our own lives is little by little to cease to live in any sense that really matters, even to ourselves, because it is only by journeying for the world’s sake—even when the world bores and sickens and scares you half to death—that little by little we start to come alive.”
—Frederick Buechner
On February 29, 2020, I find out by text from my intern when the first patient at our hospital in Seattle tests positive for COVID-19. He learns of it from his fellow intern who is caring for the patient. The news quickly spreads through the hospital like the virus itself, going from person to person while official communication channels remain initially silent. The news comes on the heels of a friend’s text that her daughter’s high school is closing for disinfection after a classmate also tested positive for COVID-19. I know the cataclysmic significance of these two events: Public health efforts to contain the SARS-CoV-2 coronavirus have failed, and there is ongoing community spread of the infection in Washington state. I text my intern back with the emoji of The Scream by Edvard Munch.
Could I be asymptomatically infected with the coronavirus? I work in close quarters with my colleagues who cared for the COVID-19–positive patient before he was placed in infection precautions. Social distancing has yet to enter our lexicon and our lives. In our crowded office, shared surfaces abound. Suddenly, every hard surface seems suspect—chairs, phones, dictaphone handsets, code pagers, printers, keypads, and door handles. All can be vectors of viral transmission. Normally insouciant about cleanliness, my coworkers and I start swabbing down every surface with disinfectant wipes. I ponder my likelihood of infection and decide it is possible but not probable.
In the next few days, I have a trip to Sedona, Arizona, planned with my extended family. Originally conceived as a celebration for my mom’s 80th birthday, we repurposed it as a time to grieve together after she unexpectedly passed away. I debate back and forth whether to go on the trip. If there is a chance I am infected with the coronavirus, it feels irresponsible to board an airplane with hundreds of other people. Yet the trip carries such high value for me. My family holds out hope I can get tested for the coronavirus, but I know just how limited testing capability is. It cuts me to the heart, but I cancel my flight. The deciding factor is that my sister has an autoimmune disease and is immunosuppressed. I don’t want to jeopardize her health. The world has truly gone topsy-turvy when the greatest thoughtfulness you can show to someone you love is to stay the hell away from her.
AM I A HYPOCHONDRIAC?
After my work stretch, I hunker down at home to monitor myself. I have a mild sore throat but convince myself it is psychosomatic. My plausible deniability of illness dies when I develop a cough and fatigue. Based on my symptoms, it is impossible to tell if I have the coronavirus or a common cold. I place myself on home quarantine. I don’t pursue coronavirus testing because there are hospitalized patients who need it much more than I do. I diligently monitor my temperature twice daily and it remains normal. My sore throat and fatigue go away, but my cough and some mild shortness of breath persists. I attribute it to my asthma, but the possibility of COVID-19 always lurks in the back of my mind. COVID-19 patients often don’t worsen until their second week of infection. Ordinarily, I would start using my steroid inhaler, but I hold off since steroids are thought to prolong viral replication.
When I tire of staying in the house, I go outside to work in the yard. I get on a low ladder to pull down the English ivy climbing up and smothering a tree. The ivy strand I’m tugging on suddenly breaks and I fall hard onto my back. Like a slap in the face, the accident shocks me into a new state of mental clarity. As a hospitalist, I’m a precious resource to my community right now. I can’t knock myself out of commission for dumb reasons. I ban myself from climbing any more ladders.
WHY CAN’T I GET TESTED?
As my time in quarantine draws to a close, I put my legal and financial affairs in order and pack a just-in-case backpack. The emergency room doctor hospitalized at a nearby hospital with severe COVID-19 is about my age. I am still coughing so I check in with the head of Infection Control to see if I need to be tested before returning to work. He tells me no. As I start working, I realize that coughing is the new leprosy. Even though I wear a mask, I get tense looks from others who carefully keep their distance from me. I tell everyone I have cough variant asthma, but what they all want to know is if I have been tested for the coronavirus. I haven’t been.
When my hospital sets up a new dedicated Employee Health screening phone line, I call right away. The nurse tells me I don’t meet criteria for coronavirus testing even though I am working on the COVID-19 rule-out unit with patients who have tested positive. While I agree with her from a medical standpoint, I don’t from a social or psychological perspective. This is a particularly unpropitious time in history to be a Chinese American doctor who can’t stop coughing. A negative test will reassure my patients and coworkers I am not a risk to them. A positive test, which is a possibility because of known prolonged viral shedding of the coronavirus, will reassure me I’m likely on my way to developing serologic immunity. I don’t get a test. When I tell my colleague, he suggests I resort to lying, but I won’t do it. As I’ve watched how power, wealth, and privilege play out in access to testing, I refuse to manipulate the system. But my experience is pointed commentary on the abysmal failure of testing in the United States when a frontline symptomatic doctor taking care of COVID-19 patients in one of the epicenters of the pandemic can’t get a coronavirus test. During a meeting, the head of Infection Control bluntly states he hopes we know that all of us are going to get the coronavirus at some point, but hopefully it won’t take us out of commission all at once. I feel better hearing him acknowledge that because it confirms my own sense of reality.
ARE WE RUNNING OUT OF PERSONAL PROTECTIVE EQUIPMENT?
While the ongoing pandemic definitely increases stress and anxiety levels in the hospital, there also continues to be caring and kindness. As I don my personal protective equipment (PPE), a nurse notices an exposed gap in the back of my gown and fixes it for me. He has my back, literally and figuratively. Our unit clerk, hearing my persistent cough, braves the 6-foot danger zone to hand me cough drops. Another nurse asks when the last time was I drank anything, and I give her a blank look because I can’t remember. I’m trying to minimize my use of masks, so I have kept my current one on all day. The front of the mask may be contaminated, but as long as I don’t touch that surface, it is still protecting me. She hands me a cup of water and I consider the benefit of staying hydrated versus using up another mask. Having previously landed in the emergency room with a kidney stone from not properly hydrating, I take off the mask, throw it away, wash my hands, and drink the water. But in my mind, I’m acutely aware of our shrinking supply of PPE.
On our time off work, my coworkers and I reach out to everyone we know to ask for mask donations. One friend tells me her husband is fashioning a mask for her from their furnace filter. She considers it the most romantic thing he’s ever done for her. The two of us agree that if we run out of PPE, we will go on caring for our patients anyway. We are doctors and caring for others is not only what we do, but an intrinsic part of who we are. Our journey amid the coronavirus pandemic may at times scare us half to death, but in caring for others “little by little we start to come alive.”
“To journey for the sake of saving our own lives is little by little to cease to live in any sense that really matters, even to ourselves, because it is only by journeying for the world’s sake—even when the world bores and sickens and scares you half to death—that little by little we start to come alive.”
—Frederick Buechner
On February 29, 2020, I find out by text from my intern when the first patient at our hospital in Seattle tests positive for COVID-19. He learns of it from his fellow intern who is caring for the patient. The news quickly spreads through the hospital like the virus itself, going from person to person while official communication channels remain initially silent. The news comes on the heels of a friend’s text that her daughter’s high school is closing for disinfection after a classmate also tested positive for COVID-19. I know the cataclysmic significance of these two events: Public health efforts to contain the SARS-CoV-2 coronavirus have failed, and there is ongoing community spread of the infection in Washington state. I text my intern back with the emoji of The Scream by Edvard Munch.
Could I be asymptomatically infected with the coronavirus? I work in close quarters with my colleagues who cared for the COVID-19–positive patient before he was placed in infection precautions. Social distancing has yet to enter our lexicon and our lives. In our crowded office, shared surfaces abound. Suddenly, every hard surface seems suspect—chairs, phones, dictaphone handsets, code pagers, printers, keypads, and door handles. All can be vectors of viral transmission. Normally insouciant about cleanliness, my coworkers and I start swabbing down every surface with disinfectant wipes. I ponder my likelihood of infection and decide it is possible but not probable.
In the next few days, I have a trip to Sedona, Arizona, planned with my extended family. Originally conceived as a celebration for my mom’s 80th birthday, we repurposed it as a time to grieve together after she unexpectedly passed away. I debate back and forth whether to go on the trip. If there is a chance I am infected with the coronavirus, it feels irresponsible to board an airplane with hundreds of other people. Yet the trip carries such high value for me. My family holds out hope I can get tested for the coronavirus, but I know just how limited testing capability is. It cuts me to the heart, but I cancel my flight. The deciding factor is that my sister has an autoimmune disease and is immunosuppressed. I don’t want to jeopardize her health. The world has truly gone topsy-turvy when the greatest thoughtfulness you can show to someone you love is to stay the hell away from her.
AM I A HYPOCHONDRIAC?
After my work stretch, I hunker down at home to monitor myself. I have a mild sore throat but convince myself it is psychosomatic. My plausible deniability of illness dies when I develop a cough and fatigue. Based on my symptoms, it is impossible to tell if I have the coronavirus or a common cold. I place myself on home quarantine. I don’t pursue coronavirus testing because there are hospitalized patients who need it much more than I do. I diligently monitor my temperature twice daily and it remains normal. My sore throat and fatigue go away, but my cough and some mild shortness of breath persists. I attribute it to my asthma, but the possibility of COVID-19 always lurks in the back of my mind. COVID-19 patients often don’t worsen until their second week of infection. Ordinarily, I would start using my steroid inhaler, but I hold off since steroids are thought to prolong viral replication.
When I tire of staying in the house, I go outside to work in the yard. I get on a low ladder to pull down the English ivy climbing up and smothering a tree. The ivy strand I’m tugging on suddenly breaks and I fall hard onto my back. Like a slap in the face, the accident shocks me into a new state of mental clarity. As a hospitalist, I’m a precious resource to my community right now. I can’t knock myself out of commission for dumb reasons. I ban myself from climbing any more ladders.
WHY CAN’T I GET TESTED?
As my time in quarantine draws to a close, I put my legal and financial affairs in order and pack a just-in-case backpack. The emergency room doctor hospitalized at a nearby hospital with severe COVID-19 is about my age. I am still coughing so I check in with the head of Infection Control to see if I need to be tested before returning to work. He tells me no. As I start working, I realize that coughing is the new leprosy. Even though I wear a mask, I get tense looks from others who carefully keep their distance from me. I tell everyone I have cough variant asthma, but what they all want to know is if I have been tested for the coronavirus. I haven’t been.
When my hospital sets up a new dedicated Employee Health screening phone line, I call right away. The nurse tells me I don’t meet criteria for coronavirus testing even though I am working on the COVID-19 rule-out unit with patients who have tested positive. While I agree with her from a medical standpoint, I don’t from a social or psychological perspective. This is a particularly unpropitious time in history to be a Chinese American doctor who can’t stop coughing. A negative test will reassure my patients and coworkers I am not a risk to them. A positive test, which is a possibility because of known prolonged viral shedding of the coronavirus, will reassure me I’m likely on my way to developing serologic immunity. I don’t get a test. When I tell my colleague, he suggests I resort to lying, but I won’t do it. As I’ve watched how power, wealth, and privilege play out in access to testing, I refuse to manipulate the system. But my experience is pointed commentary on the abysmal failure of testing in the United States when a frontline symptomatic doctor taking care of COVID-19 patients in one of the epicenters of the pandemic can’t get a coronavirus test. During a meeting, the head of Infection Control bluntly states he hopes we know that all of us are going to get the coronavirus at some point, but hopefully it won’t take us out of commission all at once. I feel better hearing him acknowledge that because it confirms my own sense of reality.
ARE WE RUNNING OUT OF PERSONAL PROTECTIVE EQUIPMENT?
While the ongoing pandemic definitely increases stress and anxiety levels in the hospital, there also continues to be caring and kindness. As I don my personal protective equipment (PPE), a nurse notices an exposed gap in the back of my gown and fixes it for me. He has my back, literally and figuratively. Our unit clerk, hearing my persistent cough, braves the 6-foot danger zone to hand me cough drops. Another nurse asks when the last time was I drank anything, and I give her a blank look because I can’t remember. I’m trying to minimize my use of masks, so I have kept my current one on all day. The front of the mask may be contaminated, but as long as I don’t touch that surface, it is still protecting me. She hands me a cup of water and I consider the benefit of staying hydrated versus using up another mask. Having previously landed in the emergency room with a kidney stone from not properly hydrating, I take off the mask, throw it away, wash my hands, and drink the water. But in my mind, I’m acutely aware of our shrinking supply of PPE.
On our time off work, my coworkers and I reach out to everyone we know to ask for mask donations. One friend tells me her husband is fashioning a mask for her from their furnace filter. She considers it the most romantic thing he’s ever done for her. The two of us agree that if we run out of PPE, we will go on caring for our patients anyway. We are doctors and caring for others is not only what we do, but an intrinsic part of who we are. Our journey amid the coronavirus pandemic may at times scare us half to death, but in caring for others “little by little we start to come alive.”
© 2020 Society of Hospital Medicine
The Importance of Compassion as the Default in Times of Crisis: The Curious Case of “Vertical Interdiction”
Each night, while my 2-year-old is having her dinner of macaroni and cheese or chicken nuggets, we video chat with my elderly parents. It used to be that this time was mainly my daughter showing off her newfound fork skills, but lately it has become “elderly parent education hour.”
“Well, we’re trying to decide if we should go to the bridge club,” announced my mother early in the week of March 13th.
“No, mom! Under no circumstances should you go to the bridge club! Social distance! Stay home! If I’ve given up restaurants and babysitters and am sitting here every night holding a phone covered in mac and cheese grease, you can give up the bridge club!”
I am all for keeping my elderly parents as isolated as possible during these pandemic times. I wasn’t alone in my fear that they weren’t taking my advice seriously: My social media feed was subsequently filled with posts from other physicians who had also been educating their parents about the need for social distancing.
ECONOMIC FEARS AND POLICY PROPOSALS
Then, just as we were all settling into “social distancing,” on March 20, a debate emerged on the opinion pages of The New York Times that took the argument to the next level: A former professor of mine suggested a move from a policy of “horizontal interdiction” (one that restricts the movement of the entire population, without taking risk into consideration) to a “vertical interdiction” strategy that focuses on sequestering those among us most likely to experience poor outcomes from coronavirus infection (eg, the elderly, people with chronic diseases, and the immunologically compromised).1
This first piece was followed 2 days later on March 22 by an article from a regular New York Times contributor who called social distancing “groupthink” and then seconded the vertical interdiction proposal.2 Both pieces referred to the downturn in the economy as the reason the policy would be an improvement on social distancing; they argued that lost jobs and services would cause less suffering and loss than a policy that required extended isolation of the elderly.
NOT A FEASIBLE OPTION
On closer inspection, however, vertical interdiction is different and much scarier than “social distancing.” The words used by the author of the original article gave a clue: “If we were to focus on the especially vulnerable, there would be resources to keep them at home, provide them with needed services and coronavirus testing, and direct our medical system to their early care. I would favor proactive rather than reactive testing.” This was not just a plan to keep my parents from the bridge club. This was a plan for forced quarantine, mandatory testing, and months of isolation. Almost immediately, physicians and policy makers identified feasibility problems with the idea.3 To name a few, it is not clear that the death rate in young people is all that low; even with removing elders from the equation, the demand for hospital and critical care services is rapidly overwhelming supply; testing the “herd immunity” hypothesis in real time with a virus that has a death rate of 1%-3% still runs the risk of causing millions of deaths.
I will add a few more reasons why this idea of vertical interdiction was never feasible: There is no existing structure to facilitate mandatory isolation and quarantine of elders. We have no mechanism for caring for elders who are isolated at home. We cannot rapidly design the digital health monitoring needed. We cannot provide the mobile testing proposed. In the case of seniors who require nursing care, the problems would be even greater. Our recent efforts to protect patients in nursing facilities have proven to be extremely difficult. The greatest problem is finding a way to keep the staff from bringing the virus into the facility (and there are many staff: nutrition services, nursing, patient care technicians, physical therapy, social work). The only possible answer to this issue might mean wearing extensive protective equipment, similar to physicians in Wuhan4 (full-head hood plus goggles). Imagine being a patient in this scenario: months of being bathed, dressed, fed, and helped to the bathroom by a person in an isolation suit.
A CRITICAL NEED TO MAINTAIN A DEFAULT OF COMPASSION
Now, just a few weeks later, with the virus spreading and many nonelders on ventilators, the idea of “elderly sequestration” as it was presented in mid-March feels dated and irrelevant. However, the episode can and should teach us a more important lesson: The idea was fatally flawed not only because it was not feasible but primarily because it was so lacking in compassion.
The lack of compassion was not just related to the fact that patients with end-stage dementia will undoubtedly be confused and frightened when confronted with months of care administered by people in hazmat suits. It is also that the proposed policy, by creating pockets of isolation, felt like a setup for missteps and subsequent rampant infection. My first thought was that these policies would not protect vulnerable elders but hide them from view, causing another situation like the one at Lifecare in Kirkland, Washington, which resulted in more than 35 deaths.5 This time, our policies (and not just our carelessness) would be responsible for creating it.
While writing this article, sadly, such a thing has happened, just miles from my home. The Soldiers Home in Holyoke, Massachusetts, is a skilled nursing facility that has generally been very highly regarded by veterans and their families. Unfortunately, a lack of responsiveness to the current pandemic, including failure to provide protective equipment, failure to remove symptomatic staff from frontline care, and a lack of transparency about symptomatic staff and patients has resulted in a scandal and a tragedy.6 Over 5 days at the end of March, eight veterans died of coronavirus without patients being sent to hospitals and without the cases being reported to either Massachusetts or local officials. Many other patients in the facility also tested positive for coronavirus, as did staff members. While this incident was not driven by a vertical interdiction policy, it was the result of actions taken to isolate and sequester elders from the community. The worst (and most symbolic) injustice was the fact that, because of rules about disposing of bodies with coronavirus (and possibly to cover up the incompetence that led to the deaths), the bodies of deceased veterans were piled into a refrigeration truck sitting in the parking lot of the facility as the tragedy unfolded.
This is a defining moment for physicians, for the healthcare system, and for our society. I am so proud of my colleagues who have stepped up, shown up, worn their (sometimes improvised) personal protective equipment and kept seeing patients because it is our job and it is part of the contract we entered into when we became physicians. Our policy choices in this moment are just as important, and it is not our ability to “get the economy started again” but our sacrifices now (or lack thereof) that will be remembered for a hundred years. Choosing patients over profit, compassion over callousness, are important not just for controlling hospital volumes and reserving intensive care unit beds, but also for preserving our professional integrity and saving our humanity.
1. Katz DL. Is our fight against coronavirus worse than the disease? New York Times. March 20, 2020. https://www.nytimes.com/2020/03/20/opinion/coronavirus-pandemic-social-distancing.html. Accessed April 3, 2020.
2. Friedman TL. A plan to get America back to work. New York Times. March 22, 2020. https://www.nytimes.com/2020/03/22/opinion/coronavirus-economy.html. Accessed April 3, 2020.
3. Apkon M, Forman HP, Sonnenfeld J. Why isolating older Americans would be a huge mistake in fighting the coronavirus. Fortune. March 24, 2020. https://fortune.com/2020/03/24/coronavirus-curve-herd-immunity-deaths/?fbclid=IwAR0K3_40MDmwrP4djtqkcAZBXFaJViIv1_2GGgZBQ269oLcTkJmptuR5G0Q. Accessed April 3, 2020
4. Gawande A. Keeping the coronavirus from infecting health-care workers. New Yorker. March 21, 2020. https://www.newyorker.com/news/news-desk/keeping-the-coronavirus-from-infecting-health-care-workers. Accessed April 3, 2020.5. Read R. Nursing home staff spread coronavirus to other facilities, CDC investigation finds. Los Angeles Times. March 18, 2020. https://www.latimes.com/world-nation/story/2020-03-18/coronavirus-spread-nursing-homes. Accessed April 3, 2020.
6. Christensen D. ‘Just complete chaos’: Soldiers’ Home staff cite dangerous conditions fueling COVID-19 outbreak. Daily Hampshire Gazette. March 31, 2020. https://www.gazettenet.com/Employees-allege-lax-COVID-19-safety-protocols-at-Holyoke-Soldiers-Home-33631412. Accessed April 3, 2020.
Each night, while my 2-year-old is having her dinner of macaroni and cheese or chicken nuggets, we video chat with my elderly parents. It used to be that this time was mainly my daughter showing off her newfound fork skills, but lately it has become “elderly parent education hour.”
“Well, we’re trying to decide if we should go to the bridge club,” announced my mother early in the week of March 13th.
“No, mom! Under no circumstances should you go to the bridge club! Social distance! Stay home! If I’ve given up restaurants and babysitters and am sitting here every night holding a phone covered in mac and cheese grease, you can give up the bridge club!”
I am all for keeping my elderly parents as isolated as possible during these pandemic times. I wasn’t alone in my fear that they weren’t taking my advice seriously: My social media feed was subsequently filled with posts from other physicians who had also been educating their parents about the need for social distancing.
ECONOMIC FEARS AND POLICY PROPOSALS
Then, just as we were all settling into “social distancing,” on March 20, a debate emerged on the opinion pages of The New York Times that took the argument to the next level: A former professor of mine suggested a move from a policy of “horizontal interdiction” (one that restricts the movement of the entire population, without taking risk into consideration) to a “vertical interdiction” strategy that focuses on sequestering those among us most likely to experience poor outcomes from coronavirus infection (eg, the elderly, people with chronic diseases, and the immunologically compromised).1
This first piece was followed 2 days later on March 22 by an article from a regular New York Times contributor who called social distancing “groupthink” and then seconded the vertical interdiction proposal.2 Both pieces referred to the downturn in the economy as the reason the policy would be an improvement on social distancing; they argued that lost jobs and services would cause less suffering and loss than a policy that required extended isolation of the elderly.
NOT A FEASIBLE OPTION
On closer inspection, however, vertical interdiction is different and much scarier than “social distancing.” The words used by the author of the original article gave a clue: “If we were to focus on the especially vulnerable, there would be resources to keep them at home, provide them with needed services and coronavirus testing, and direct our medical system to their early care. I would favor proactive rather than reactive testing.” This was not just a plan to keep my parents from the bridge club. This was a plan for forced quarantine, mandatory testing, and months of isolation. Almost immediately, physicians and policy makers identified feasibility problems with the idea.3 To name a few, it is not clear that the death rate in young people is all that low; even with removing elders from the equation, the demand for hospital and critical care services is rapidly overwhelming supply; testing the “herd immunity” hypothesis in real time with a virus that has a death rate of 1%-3% still runs the risk of causing millions of deaths.
I will add a few more reasons why this idea of vertical interdiction was never feasible: There is no existing structure to facilitate mandatory isolation and quarantine of elders. We have no mechanism for caring for elders who are isolated at home. We cannot rapidly design the digital health monitoring needed. We cannot provide the mobile testing proposed. In the case of seniors who require nursing care, the problems would be even greater. Our recent efforts to protect patients in nursing facilities have proven to be extremely difficult. The greatest problem is finding a way to keep the staff from bringing the virus into the facility (and there are many staff: nutrition services, nursing, patient care technicians, physical therapy, social work). The only possible answer to this issue might mean wearing extensive protective equipment, similar to physicians in Wuhan4 (full-head hood plus goggles). Imagine being a patient in this scenario: months of being bathed, dressed, fed, and helped to the bathroom by a person in an isolation suit.
A CRITICAL NEED TO MAINTAIN A DEFAULT OF COMPASSION
Now, just a few weeks later, with the virus spreading and many nonelders on ventilators, the idea of “elderly sequestration” as it was presented in mid-March feels dated and irrelevant. However, the episode can and should teach us a more important lesson: The idea was fatally flawed not only because it was not feasible but primarily because it was so lacking in compassion.
The lack of compassion was not just related to the fact that patients with end-stage dementia will undoubtedly be confused and frightened when confronted with months of care administered by people in hazmat suits. It is also that the proposed policy, by creating pockets of isolation, felt like a setup for missteps and subsequent rampant infection. My first thought was that these policies would not protect vulnerable elders but hide them from view, causing another situation like the one at Lifecare in Kirkland, Washington, which resulted in more than 35 deaths.5 This time, our policies (and not just our carelessness) would be responsible for creating it.
While writing this article, sadly, such a thing has happened, just miles from my home. The Soldiers Home in Holyoke, Massachusetts, is a skilled nursing facility that has generally been very highly regarded by veterans and their families. Unfortunately, a lack of responsiveness to the current pandemic, including failure to provide protective equipment, failure to remove symptomatic staff from frontline care, and a lack of transparency about symptomatic staff and patients has resulted in a scandal and a tragedy.6 Over 5 days at the end of March, eight veterans died of coronavirus without patients being sent to hospitals and without the cases being reported to either Massachusetts or local officials. Many other patients in the facility also tested positive for coronavirus, as did staff members. While this incident was not driven by a vertical interdiction policy, it was the result of actions taken to isolate and sequester elders from the community. The worst (and most symbolic) injustice was the fact that, because of rules about disposing of bodies with coronavirus (and possibly to cover up the incompetence that led to the deaths), the bodies of deceased veterans were piled into a refrigeration truck sitting in the parking lot of the facility as the tragedy unfolded.
This is a defining moment for physicians, for the healthcare system, and for our society. I am so proud of my colleagues who have stepped up, shown up, worn their (sometimes improvised) personal protective equipment and kept seeing patients because it is our job and it is part of the contract we entered into when we became physicians. Our policy choices in this moment are just as important, and it is not our ability to “get the economy started again” but our sacrifices now (or lack thereof) that will be remembered for a hundred years. Choosing patients over profit, compassion over callousness, are important not just for controlling hospital volumes and reserving intensive care unit beds, but also for preserving our professional integrity and saving our humanity.
Each night, while my 2-year-old is having her dinner of macaroni and cheese or chicken nuggets, we video chat with my elderly parents. It used to be that this time was mainly my daughter showing off her newfound fork skills, but lately it has become “elderly parent education hour.”
“Well, we’re trying to decide if we should go to the bridge club,” announced my mother early in the week of March 13th.
“No, mom! Under no circumstances should you go to the bridge club! Social distance! Stay home! If I’ve given up restaurants and babysitters and am sitting here every night holding a phone covered in mac and cheese grease, you can give up the bridge club!”
I am all for keeping my elderly parents as isolated as possible during these pandemic times. I wasn’t alone in my fear that they weren’t taking my advice seriously: My social media feed was subsequently filled with posts from other physicians who had also been educating their parents about the need for social distancing.
ECONOMIC FEARS AND POLICY PROPOSALS
Then, just as we were all settling into “social distancing,” on March 20, a debate emerged on the opinion pages of The New York Times that took the argument to the next level: A former professor of mine suggested a move from a policy of “horizontal interdiction” (one that restricts the movement of the entire population, without taking risk into consideration) to a “vertical interdiction” strategy that focuses on sequestering those among us most likely to experience poor outcomes from coronavirus infection (eg, the elderly, people with chronic diseases, and the immunologically compromised).1
This first piece was followed 2 days later on March 22 by an article from a regular New York Times contributor who called social distancing “groupthink” and then seconded the vertical interdiction proposal.2 Both pieces referred to the downturn in the economy as the reason the policy would be an improvement on social distancing; they argued that lost jobs and services would cause less suffering and loss than a policy that required extended isolation of the elderly.
NOT A FEASIBLE OPTION
On closer inspection, however, vertical interdiction is different and much scarier than “social distancing.” The words used by the author of the original article gave a clue: “If we were to focus on the especially vulnerable, there would be resources to keep them at home, provide them with needed services and coronavirus testing, and direct our medical system to their early care. I would favor proactive rather than reactive testing.” This was not just a plan to keep my parents from the bridge club. This was a plan for forced quarantine, mandatory testing, and months of isolation. Almost immediately, physicians and policy makers identified feasibility problems with the idea.3 To name a few, it is not clear that the death rate in young people is all that low; even with removing elders from the equation, the demand for hospital and critical care services is rapidly overwhelming supply; testing the “herd immunity” hypothesis in real time with a virus that has a death rate of 1%-3% still runs the risk of causing millions of deaths.
I will add a few more reasons why this idea of vertical interdiction was never feasible: There is no existing structure to facilitate mandatory isolation and quarantine of elders. We have no mechanism for caring for elders who are isolated at home. We cannot rapidly design the digital health monitoring needed. We cannot provide the mobile testing proposed. In the case of seniors who require nursing care, the problems would be even greater. Our recent efforts to protect patients in nursing facilities have proven to be extremely difficult. The greatest problem is finding a way to keep the staff from bringing the virus into the facility (and there are many staff: nutrition services, nursing, patient care technicians, physical therapy, social work). The only possible answer to this issue might mean wearing extensive protective equipment, similar to physicians in Wuhan4 (full-head hood plus goggles). Imagine being a patient in this scenario: months of being bathed, dressed, fed, and helped to the bathroom by a person in an isolation suit.
A CRITICAL NEED TO MAINTAIN A DEFAULT OF COMPASSION
Now, just a few weeks later, with the virus spreading and many nonelders on ventilators, the idea of “elderly sequestration” as it was presented in mid-March feels dated and irrelevant. However, the episode can and should teach us a more important lesson: The idea was fatally flawed not only because it was not feasible but primarily because it was so lacking in compassion.
The lack of compassion was not just related to the fact that patients with end-stage dementia will undoubtedly be confused and frightened when confronted with months of care administered by people in hazmat suits. It is also that the proposed policy, by creating pockets of isolation, felt like a setup for missteps and subsequent rampant infection. My first thought was that these policies would not protect vulnerable elders but hide them from view, causing another situation like the one at Lifecare in Kirkland, Washington, which resulted in more than 35 deaths.5 This time, our policies (and not just our carelessness) would be responsible for creating it.
While writing this article, sadly, such a thing has happened, just miles from my home. The Soldiers Home in Holyoke, Massachusetts, is a skilled nursing facility that has generally been very highly regarded by veterans and their families. Unfortunately, a lack of responsiveness to the current pandemic, including failure to provide protective equipment, failure to remove symptomatic staff from frontline care, and a lack of transparency about symptomatic staff and patients has resulted in a scandal and a tragedy.6 Over 5 days at the end of March, eight veterans died of coronavirus without patients being sent to hospitals and without the cases being reported to either Massachusetts or local officials. Many other patients in the facility also tested positive for coronavirus, as did staff members. While this incident was not driven by a vertical interdiction policy, it was the result of actions taken to isolate and sequester elders from the community. The worst (and most symbolic) injustice was the fact that, because of rules about disposing of bodies with coronavirus (and possibly to cover up the incompetence that led to the deaths), the bodies of deceased veterans were piled into a refrigeration truck sitting in the parking lot of the facility as the tragedy unfolded.
This is a defining moment for physicians, for the healthcare system, and for our society. I am so proud of my colleagues who have stepped up, shown up, worn their (sometimes improvised) personal protective equipment and kept seeing patients because it is our job and it is part of the contract we entered into when we became physicians. Our policy choices in this moment are just as important, and it is not our ability to “get the economy started again” but our sacrifices now (or lack thereof) that will be remembered for a hundred years. Choosing patients over profit, compassion over callousness, are important not just for controlling hospital volumes and reserving intensive care unit beds, but also for preserving our professional integrity and saving our humanity.
1. Katz DL. Is our fight against coronavirus worse than the disease? New York Times. March 20, 2020. https://www.nytimes.com/2020/03/20/opinion/coronavirus-pandemic-social-distancing.html. Accessed April 3, 2020.
2. Friedman TL. A plan to get America back to work. New York Times. March 22, 2020. https://www.nytimes.com/2020/03/22/opinion/coronavirus-economy.html. Accessed April 3, 2020.
3. Apkon M, Forman HP, Sonnenfeld J. Why isolating older Americans would be a huge mistake in fighting the coronavirus. Fortune. March 24, 2020. https://fortune.com/2020/03/24/coronavirus-curve-herd-immunity-deaths/?fbclid=IwAR0K3_40MDmwrP4djtqkcAZBXFaJViIv1_2GGgZBQ269oLcTkJmptuR5G0Q. Accessed April 3, 2020
4. Gawande A. Keeping the coronavirus from infecting health-care workers. New Yorker. March 21, 2020. https://www.newyorker.com/news/news-desk/keeping-the-coronavirus-from-infecting-health-care-workers. Accessed April 3, 2020.5. Read R. Nursing home staff spread coronavirus to other facilities, CDC investigation finds. Los Angeles Times. March 18, 2020. https://www.latimes.com/world-nation/story/2020-03-18/coronavirus-spread-nursing-homes. Accessed April 3, 2020.
6. Christensen D. ‘Just complete chaos’: Soldiers’ Home staff cite dangerous conditions fueling COVID-19 outbreak. Daily Hampshire Gazette. March 31, 2020. https://www.gazettenet.com/Employees-allege-lax-COVID-19-safety-protocols-at-Holyoke-Soldiers-Home-33631412. Accessed April 3, 2020.
1. Katz DL. Is our fight against coronavirus worse than the disease? New York Times. March 20, 2020. https://www.nytimes.com/2020/03/20/opinion/coronavirus-pandemic-social-distancing.html. Accessed April 3, 2020.
2. Friedman TL. A plan to get America back to work. New York Times. March 22, 2020. https://www.nytimes.com/2020/03/22/opinion/coronavirus-economy.html. Accessed April 3, 2020.
3. Apkon M, Forman HP, Sonnenfeld J. Why isolating older Americans would be a huge mistake in fighting the coronavirus. Fortune. March 24, 2020. https://fortune.com/2020/03/24/coronavirus-curve-herd-immunity-deaths/?fbclid=IwAR0K3_40MDmwrP4djtqkcAZBXFaJViIv1_2GGgZBQ269oLcTkJmptuR5G0Q. Accessed April 3, 2020
4. Gawande A. Keeping the coronavirus from infecting health-care workers. New Yorker. March 21, 2020. https://www.newyorker.com/news/news-desk/keeping-the-coronavirus-from-infecting-health-care-workers. Accessed April 3, 2020.5. Read R. Nursing home staff spread coronavirus to other facilities, CDC investigation finds. Los Angeles Times. March 18, 2020. https://www.latimes.com/world-nation/story/2020-03-18/coronavirus-spread-nursing-homes. Accessed April 3, 2020.
6. Christensen D. ‘Just complete chaos’: Soldiers’ Home staff cite dangerous conditions fueling COVID-19 outbreak. Daily Hampshire Gazette. March 31, 2020. https://www.gazettenet.com/Employees-allege-lax-COVID-19-safety-protocols-at-Holyoke-Soldiers-Home-33631412. Accessed April 3, 2020.
© 2020 Society of Hospital Medicine
Understanding the Singapore COVID-19 Experience: Implications for Hospital Medicine
One of the worst public health threats of our generation, coronavirus disease 2019 (COVID-19), first emerged in Wuhan, China, in December 2019 and quickly spread to Singapore, Hong Kong, and Taiwan. These three countries have been praised for their control of the pandemic,1,2 while the number of cases worldwide, including those in the United States, has soared. Political alignment, centralized and integrated healthcare systems, small size, effective technology deployment, widespread testing combined with contact tracing and isolation, and personal protective equipment (PPE) availability underscore their successes.1,3-5 Although these factors differ starkly from those currently employed in the United States, a better understanding their experience may positively influence the myriad US responses. We describe some salient features of Singapore’s infection preparedness, provide examples of how these features guided the National University Hospital (NUH) Singapore COVID-19 response, and illustrate how one facet of the NUH response was translated to develop a new care model at the University of California, San Francisco (UCSF).
THE SINGAPORE EXPERIENCE OVER TIME
Singapore, a small island country (278 square miles) city-state in Southeast Asia has a population of 5.8 million people. Most Singaporeans receive their inpatient care in the public hospitals that are organized and resourced through the Singapore Ministry of Health (MOH). In 2003, severe acute respiratory syndrome (SARS) infected 238 people and killed 33 over 3 months in Singapore, which led to a significant economic downturn. Singapore’s initial SARS experience unveiled limitations in infrastructure, staff preparedness, virus control methodology, and centralized crisis systems. Lessons gleaned from the SARS experience laid the foundation for Singapore’s subsequent disaster preparedness.6
Post-SARS, the MOH created structures and systems to prepare Singapore for future epidemics. All public hospitals expanded isolation capacity by constructing new units or repurposing existing ones and creating colocated Emergency Department (ED) isolation facilities. Additionally, the MOH commissioned the National Centre for Infectious Diseases, a 330-bed high-level isolation hospital.7 They also mandated hospital systems to regularly practice mass casualty and infectious (including respiratory) crisis responses through externally evaluated simulation.8 These are orchestrated down to the smallest detail and involve staff at all levels. For example, healthcare workers (HCW) being “deployed” outside of their specialty, housekeepers practicing novel hazardous waste disposal, and security guards managing crowds interact throughout the exercise.
The testing and viral spread control challenges during SARS spawned hospital-system epidemiology capacity building. Infectious diseases reporting guidelines were refined, and communication channels enhanced to include cross-hospital information sharing and direct lines of communication for epidemiology groups to and from the MOH. Enhanced contact tracing methodologies were adopted and practiced regularly. In addition, material stockpiles, supplies, and supply chains were recalibrated.
The Singapore government also adopted the Disease Outbreak Response System Condition (DORSCON) system,9 a color-coded framework for pandemic response that guides activation of crisis interventions broadly (such as temperature screening at airports and restrictions to travel and internal movements), as well as within the healthcare setting.
In addition to prompting these notable preparedness efforts, SARS had a palpable impact on Singaporeans’ collective psychology both within and outside of the hospital system. The very close-knit medical community lost colleagues during the crisis, and the larger community deeply felt the health and economic costs of this crisis.10 The resulting “respect” or “healthy fear” for infectious crises continues to the present day.
THE SINGAPORE COVID-19 RESPONSE: NATIONAL UNIVERSITY HOSPITAL EXPERIENCE
The NUH is a 1,200-bed public tertiary care academic health center in Singapore. Before the first COVID-19 case was diagnosed in Singapore, NUH joined forces with its broader health system, university resources (schools of medicine and public health), and international partners to refine the existing structures and systems in response to this new infectious threat.
One of these structures included the existing NUH ED negative-pressure “fever facility.” In the ED triage, patients are routinely screened for infectious diseases such as H1N1, MERS-CoV, and measles. In early January, these screening criteria were evolved to adapt to COVID-19. High-risk patients bypass common waiting areas and are sent directly to the fever facility for management. From there, patients requiring admission are sent to one of the inpatient isolation wards, each with over 21 negative-pressure isolation rooms. To expand isolation capacity, lower-priority patients were relocated, and the existing negative- and neutral-pressure rooms were converted into COVID-19 pandemic wards.
The pandemic wards are staffed by nurses with previous isolation experience and Internal Medicine and Subspecialty Medicine physicians and trainees working closely with Infectious Diseases experts. Pandemic Ward teams are sequestered from other clinical and administrative teams, wear hospital-laundered scrubs, and use PPE-conserving practices. These strategies, implemented at the outset, are based on international guidelines contextualized to local needs and include extended use (up to 6 hours) of N95 respirators for the pandemic wards, and surgical masks in all other clinical areas. Notably, there have been no documented transmissions to HCW or patients at NUH. The workforce was maximized by limiting nonurgent clinical, administrative, research, and teaching activities.
In February, COVID-19 testing was initiated internally and deployed widely. NUH, at the time of this writing, has performed more than 6,000 swabs with up to 200 tests run per day (with 80 confirmed cases). Testing at this scale has allowed NUH to ensure: (a) prompt isolation of patients, even those with mild symptoms, (b) deisolation of those testing negative thus conserving PPE and isolation facilities, (c) a better understanding of the epidemiology and the wide range of clinical manifestations of COVID-19, and (d) early comprehensive contact tracing including mildly symptomatic patients.
The MOH plays a central role in coordinating COVID-19 activities and supports individual hospital systems such as NUH. Some of their crisis leadership strategies include daily text messages distributed countrywide, two-way communication channels that ensure feedback loops with hospital executives, epidemiology specialists, and operational workgroups, and engendering interhospital collaboration.11
A US HOSPITAL MEDICINE RESPONSE: UC SAN FRANCISCO
In the United States, the Joint Commission provides structures, tools, and processes for hospital systems to prepare for disasters.12 Many hospital systems have experience with natural disasters which, similar to Singapore’s planning, ensures structures and systems are in place during a crisis. Although these are transferable to multiple types of disasters, the US healthcare system’s direct experience with infectious crises is limited. A fairly distinctive facet—and an asset of US healthcare—is the role of hospitalists.
Hospitalists care for the majority of medical inpatients across the United States,13 and as such, they currently, and will increasingly, play a major role in the US COVID-19 response. This is the case at the UCSF Helen Diller Medical Center at Parnassus Heights (UCSFMC), a 600-bed academic medical center. To learn from other’s early experiences with COVID-19, UCSF Health System leadership connected with many outside health systems including NUH. As one of its multiple pandemic responses, they engaged the UCSFMC Division of Hospital Medicine (DHM), a division that includes 117 hospitalists, to work with hospital and health system leadership and launch a respiratory isolation unit (RIU) modeled after the NUH pandemic ward. The aim of the RIU is to group inpatients with either confirmed or suspected COVID-19 patients who do not require critical care.
An interdisciplinary work group comprising hospitalists, infectious disease specialists, emergency department clinicians, nursing, rehabilitation experts, hospital epidemiology and infection-prevention leaders, safety specialists, and systems engineers was assembled to repurpose an existing medical unit and establish new care models for the RIU. This workgroup created clinical guidelines and workflows, and RIU leaders actively solicit feedback from the staff to advance these standards.
Hospitalists and nurses who volunteered to work on the UCSF attending-staffed RIU received extensive training, including online and widely available in-person PPE training delivered by infection-prevention experts. The RIU hospitalists engage with hospitalists nationwide through ongoing conference calls to share best practices and clinical cases. Patients are admitted by hospitalists to the RIU via the emergency department or directly from ambulatory sites. All RIU providers and staff are screened daily for symptoms prior to starting their shifts, wear hospital-laundered scrubs on the unit, and remain on the unit for the duration of their shift. Hospitalists and nurses communicate regularly to cluster their patient visits and interventions while specialists provide virtual consults (as deemed safe and appropriate) to optimize PPE conservation and decrease overall exposure. The Health System establishes and revises PPE protocols based on CDC guidelines, best available evidence, and supply chain realities. These guidelines are evolving and currently include surgical mask, gown, gloves, and eye protection for all patient interactions with suspected or confirmed COVID-19 and respirator use during aerosol-generating procedures. Research studies (eg, clinical trials and evaluations), informatics efforts (eg, patient flow dashboards), and healthcare technology innovations (eg, tablets for telehealth and video visits) are continually integrated into the RIU infrastructure. Robust attention to the well-being of everyone working on the unit includes chaplain visits, daily debriefs, meal delivery, and palliative care service support, which enrich the unit experience and instill a culture of unity.
MOVING FORWARD
The structures and systems born out of the 2003 SARS experience and the “test, trace, and isolate” strategy were arguably key drivers to flatten Singapore’s epidemic curve early in the pandemic.3 Even with these in place, Singapore is now experiencing a second wave with a significantly higher caseload.14 In response, the government instituted strict social distancing measures on April 3, closing schools and most workplaces. This suggests that the COVID-19 pandemic may fluctuate over time and that varying types and levels of interventions will be required to maintain long-term control. The NUH team describes experiencing cognitive overload given the ever-changing nature and volume of information and fatigue due to the effort required and duration of this crisis. New programs addressing these challenges are being developed and rapidly deployed.
Despite early testing limitations and newly minted systems, San Francisco is cautiously optimistic about its epidemic curve. Since the March 17, 2020, “shelter in place” order, COVID-19 hospitalizations have remained manageable and constant.15 This has afforded healthcare systems including UCSF critical time to evolve its clinical operations (eg, the RIU) and to leverage its academic culture coordinating its bench research, global health, epidemiology, clinical research, informatics, and clinical enterprise scholars and experts to advance COVID-19 science and inform pandemic solutions. Although the UCSF frontline teams are challenged by the stresses of being in the throes of the pandemic amidst a rapidly changing landscape (including changes in PPE and testing recommendations specifically), they are working together to build team resilience for what may come.
CONCLUSION
The world is facing a pandemic of tremendous proportions, and the United States is in the midst of a wave the height of which is yet to be seen. As Fisher and colleagues wrote in 2011, “Our response to infectious disease outbreaks is born out of past experience.”4 Singapore and NUH’s structures and systems that were put into place demonstrate this—they are timely, have been effective thus far, and will be tested in this next wave. “However, no two outbreaks are the same,” the authors wrote, “so an understanding of the infectious agent as well as the environment confronting it is fundamental to the response.”4 In the United States, hospitalists are a key asset in our environment to confront this virus. The UCSF experience exemplifies that, by combining new ideas from another system with on-the-ground expertise while working hand-in-hand with the hospital and health system, hospitalists can be a critical facet of the pandemic response. Hospitalists’ intrinsic abilities to collaborate, learn, and innovate will enable them to not only meet this challenge now but also to transform practices and capacities to respond to crises into the future.
Acknowledgment
Bradley Sharpe, MD, Division Chief, Division of Hospital Medicine, University of California, San Francisco, California, for his input on conception and critical review of this manuscript.
1. Wang CJ, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analytics, new technology, and proactive testing. JAMA. 2020. https://doi.org/10.1001/jama.2020.3151.
2. Legido-Quigley H, Asgari N, Teo YY, et al. Are high-performing health systems resilient against the COVID-19 epidemic? Lancet. 2020;395(10227):848-850. https://doi.org/10.1016/S0140-6736(20)30551-1.
3. Wong JEL, Leo YS, Tan CC. COVID-19 in Singapore—current experience: critical global issues that require attention and action. JAMA. 2020;323(13):1243-1244. https://doi.org/10.1001/jama.2020.2467.
4. Fisher D, Hui DS, Gao Z, et al. Pandemic response lessons from influenza H1N1 2009 in Asia. Respirology. 2011;16(6):876-882. https://doi.org/ 10.1111/j.1440-1843.2011.02003.x.
5. Wong ATY, Chen H, Liu SH, et al. From SARS to avian influenza preparedness in Hong Kong. Clin Infect Dis. 2017;64(suppl_2):S98-S104. https://doi.org/ 10.1093/cid/cix123.
6. Tan CC. SARS in Singapore--key lessons from an epidemic. Ann Acad Med Singapore. 2006;35(5):345-349.
7. National Centre for Infectious Diseases. About NCID. https://www.ncid.sg/About-NCID/Pages/default.aspx. Accessed April 5, 2020.
8. Cutter J. Preparing for an influenza pandemic in Singapore. Ann Acad Med Singapore. 2008;37(6):497-503.
9. Singapore Ministry of Health. What do the different DORSCON levels mean. http://www.gov.sg/article/what-do-the-different-dorscon-levels-mean. Accessed April 5, 2020.
10. Lee J-W, McKibbin WJ. Estimating the global economic costs of SARS. In: Knobler S, Mahmoud A, Lemon S, et al, eds. Institute of Medicine (US) Forum on Microbial Threats. Washington, DC: National Academies Press (US); 2004.
11. James EH, Wooten L. Leadership as (un)usual: how to display competence in times of crisis. Organ Dyn. 2005;34(2):141-152. https://doi.org/10.1016/j.orgdyn.2005.03.005
12. The Joint Commission. Emergency Management: Coronavirus Resources. 2020. https://www.jointcommission.org/covid-19/. Accessed April 4, 2020.
13. Wachter RM, Goldman L. Zero to 50,000 – the 20th anniversary of the hospitalist. N Engl J Med. 2016;375(11):1009-1011. https://doi.org/10.1056/NEJMp1607958.
14. Singapore Ministry of Health. Official Update of COVID-19 Situation in Singapore. 2020. https://experience.arcgis.com/experience/7e30edc490a5441a874f9efe67bd8b89. Accessed April 5, 2020.
15. Chronicle Digital Team. Coronavirus tracker. San Francisco Chronicle. https://projects.sfchronicle.com/2020/coronavirus-map/. Accessed April 5, 2020.
One of the worst public health threats of our generation, coronavirus disease 2019 (COVID-19), first emerged in Wuhan, China, in December 2019 and quickly spread to Singapore, Hong Kong, and Taiwan. These three countries have been praised for their control of the pandemic,1,2 while the number of cases worldwide, including those in the United States, has soared. Political alignment, centralized and integrated healthcare systems, small size, effective technology deployment, widespread testing combined with contact tracing and isolation, and personal protective equipment (PPE) availability underscore their successes.1,3-5 Although these factors differ starkly from those currently employed in the United States, a better understanding their experience may positively influence the myriad US responses. We describe some salient features of Singapore’s infection preparedness, provide examples of how these features guided the National University Hospital (NUH) Singapore COVID-19 response, and illustrate how one facet of the NUH response was translated to develop a new care model at the University of California, San Francisco (UCSF).
THE SINGAPORE EXPERIENCE OVER TIME
Singapore, a small island country (278 square miles) city-state in Southeast Asia has a population of 5.8 million people. Most Singaporeans receive their inpatient care in the public hospitals that are organized and resourced through the Singapore Ministry of Health (MOH). In 2003, severe acute respiratory syndrome (SARS) infected 238 people and killed 33 over 3 months in Singapore, which led to a significant economic downturn. Singapore’s initial SARS experience unveiled limitations in infrastructure, staff preparedness, virus control methodology, and centralized crisis systems. Lessons gleaned from the SARS experience laid the foundation for Singapore’s subsequent disaster preparedness.6
Post-SARS, the MOH created structures and systems to prepare Singapore for future epidemics. All public hospitals expanded isolation capacity by constructing new units or repurposing existing ones and creating colocated Emergency Department (ED) isolation facilities. Additionally, the MOH commissioned the National Centre for Infectious Diseases, a 330-bed high-level isolation hospital.7 They also mandated hospital systems to regularly practice mass casualty and infectious (including respiratory) crisis responses through externally evaluated simulation.8 These are orchestrated down to the smallest detail and involve staff at all levels. For example, healthcare workers (HCW) being “deployed” outside of their specialty, housekeepers practicing novel hazardous waste disposal, and security guards managing crowds interact throughout the exercise.
The testing and viral spread control challenges during SARS spawned hospital-system epidemiology capacity building. Infectious diseases reporting guidelines were refined, and communication channels enhanced to include cross-hospital information sharing and direct lines of communication for epidemiology groups to and from the MOH. Enhanced contact tracing methodologies were adopted and practiced regularly. In addition, material stockpiles, supplies, and supply chains were recalibrated.
The Singapore government also adopted the Disease Outbreak Response System Condition (DORSCON) system,9 a color-coded framework for pandemic response that guides activation of crisis interventions broadly (such as temperature screening at airports and restrictions to travel and internal movements), as well as within the healthcare setting.
In addition to prompting these notable preparedness efforts, SARS had a palpable impact on Singaporeans’ collective psychology both within and outside of the hospital system. The very close-knit medical community lost colleagues during the crisis, and the larger community deeply felt the health and economic costs of this crisis.10 The resulting “respect” or “healthy fear” for infectious crises continues to the present day.
THE SINGAPORE COVID-19 RESPONSE: NATIONAL UNIVERSITY HOSPITAL EXPERIENCE
The NUH is a 1,200-bed public tertiary care academic health center in Singapore. Before the first COVID-19 case was diagnosed in Singapore, NUH joined forces with its broader health system, university resources (schools of medicine and public health), and international partners to refine the existing structures and systems in response to this new infectious threat.
One of these structures included the existing NUH ED negative-pressure “fever facility.” In the ED triage, patients are routinely screened for infectious diseases such as H1N1, MERS-CoV, and measles. In early January, these screening criteria were evolved to adapt to COVID-19. High-risk patients bypass common waiting areas and are sent directly to the fever facility for management. From there, patients requiring admission are sent to one of the inpatient isolation wards, each with over 21 negative-pressure isolation rooms. To expand isolation capacity, lower-priority patients were relocated, and the existing negative- and neutral-pressure rooms were converted into COVID-19 pandemic wards.
The pandemic wards are staffed by nurses with previous isolation experience and Internal Medicine and Subspecialty Medicine physicians and trainees working closely with Infectious Diseases experts. Pandemic Ward teams are sequestered from other clinical and administrative teams, wear hospital-laundered scrubs, and use PPE-conserving practices. These strategies, implemented at the outset, are based on international guidelines contextualized to local needs and include extended use (up to 6 hours) of N95 respirators for the pandemic wards, and surgical masks in all other clinical areas. Notably, there have been no documented transmissions to HCW or patients at NUH. The workforce was maximized by limiting nonurgent clinical, administrative, research, and teaching activities.
In February, COVID-19 testing was initiated internally and deployed widely. NUH, at the time of this writing, has performed more than 6,000 swabs with up to 200 tests run per day (with 80 confirmed cases). Testing at this scale has allowed NUH to ensure: (a) prompt isolation of patients, even those with mild symptoms, (b) deisolation of those testing negative thus conserving PPE and isolation facilities, (c) a better understanding of the epidemiology and the wide range of clinical manifestations of COVID-19, and (d) early comprehensive contact tracing including mildly symptomatic patients.
The MOH plays a central role in coordinating COVID-19 activities and supports individual hospital systems such as NUH. Some of their crisis leadership strategies include daily text messages distributed countrywide, two-way communication channels that ensure feedback loops with hospital executives, epidemiology specialists, and operational workgroups, and engendering interhospital collaboration.11
A US HOSPITAL MEDICINE RESPONSE: UC SAN FRANCISCO
In the United States, the Joint Commission provides structures, tools, and processes for hospital systems to prepare for disasters.12 Many hospital systems have experience with natural disasters which, similar to Singapore’s planning, ensures structures and systems are in place during a crisis. Although these are transferable to multiple types of disasters, the US healthcare system’s direct experience with infectious crises is limited. A fairly distinctive facet—and an asset of US healthcare—is the role of hospitalists.
Hospitalists care for the majority of medical inpatients across the United States,13 and as such, they currently, and will increasingly, play a major role in the US COVID-19 response. This is the case at the UCSF Helen Diller Medical Center at Parnassus Heights (UCSFMC), a 600-bed academic medical center. To learn from other’s early experiences with COVID-19, UCSF Health System leadership connected with many outside health systems including NUH. As one of its multiple pandemic responses, they engaged the UCSFMC Division of Hospital Medicine (DHM), a division that includes 117 hospitalists, to work with hospital and health system leadership and launch a respiratory isolation unit (RIU) modeled after the NUH pandemic ward. The aim of the RIU is to group inpatients with either confirmed or suspected COVID-19 patients who do not require critical care.
An interdisciplinary work group comprising hospitalists, infectious disease specialists, emergency department clinicians, nursing, rehabilitation experts, hospital epidemiology and infection-prevention leaders, safety specialists, and systems engineers was assembled to repurpose an existing medical unit and establish new care models for the RIU. This workgroup created clinical guidelines and workflows, and RIU leaders actively solicit feedback from the staff to advance these standards.
Hospitalists and nurses who volunteered to work on the UCSF attending-staffed RIU received extensive training, including online and widely available in-person PPE training delivered by infection-prevention experts. The RIU hospitalists engage with hospitalists nationwide through ongoing conference calls to share best practices and clinical cases. Patients are admitted by hospitalists to the RIU via the emergency department or directly from ambulatory sites. All RIU providers and staff are screened daily for symptoms prior to starting their shifts, wear hospital-laundered scrubs on the unit, and remain on the unit for the duration of their shift. Hospitalists and nurses communicate regularly to cluster their patient visits and interventions while specialists provide virtual consults (as deemed safe and appropriate) to optimize PPE conservation and decrease overall exposure. The Health System establishes and revises PPE protocols based on CDC guidelines, best available evidence, and supply chain realities. These guidelines are evolving and currently include surgical mask, gown, gloves, and eye protection for all patient interactions with suspected or confirmed COVID-19 and respirator use during aerosol-generating procedures. Research studies (eg, clinical trials and evaluations), informatics efforts (eg, patient flow dashboards), and healthcare technology innovations (eg, tablets for telehealth and video visits) are continually integrated into the RIU infrastructure. Robust attention to the well-being of everyone working on the unit includes chaplain visits, daily debriefs, meal delivery, and palliative care service support, which enrich the unit experience and instill a culture of unity.
MOVING FORWARD
The structures and systems born out of the 2003 SARS experience and the “test, trace, and isolate” strategy were arguably key drivers to flatten Singapore’s epidemic curve early in the pandemic.3 Even with these in place, Singapore is now experiencing a second wave with a significantly higher caseload.14 In response, the government instituted strict social distancing measures on April 3, closing schools and most workplaces. This suggests that the COVID-19 pandemic may fluctuate over time and that varying types and levels of interventions will be required to maintain long-term control. The NUH team describes experiencing cognitive overload given the ever-changing nature and volume of information and fatigue due to the effort required and duration of this crisis. New programs addressing these challenges are being developed and rapidly deployed.
Despite early testing limitations and newly minted systems, San Francisco is cautiously optimistic about its epidemic curve. Since the March 17, 2020, “shelter in place” order, COVID-19 hospitalizations have remained manageable and constant.15 This has afforded healthcare systems including UCSF critical time to evolve its clinical operations (eg, the RIU) and to leverage its academic culture coordinating its bench research, global health, epidemiology, clinical research, informatics, and clinical enterprise scholars and experts to advance COVID-19 science and inform pandemic solutions. Although the UCSF frontline teams are challenged by the stresses of being in the throes of the pandemic amidst a rapidly changing landscape (including changes in PPE and testing recommendations specifically), they are working together to build team resilience for what may come.
CONCLUSION
The world is facing a pandemic of tremendous proportions, and the United States is in the midst of a wave the height of which is yet to be seen. As Fisher and colleagues wrote in 2011, “Our response to infectious disease outbreaks is born out of past experience.”4 Singapore and NUH’s structures and systems that were put into place demonstrate this—they are timely, have been effective thus far, and will be tested in this next wave. “However, no two outbreaks are the same,” the authors wrote, “so an understanding of the infectious agent as well as the environment confronting it is fundamental to the response.”4 In the United States, hospitalists are a key asset in our environment to confront this virus. The UCSF experience exemplifies that, by combining new ideas from another system with on-the-ground expertise while working hand-in-hand with the hospital and health system, hospitalists can be a critical facet of the pandemic response. Hospitalists’ intrinsic abilities to collaborate, learn, and innovate will enable them to not only meet this challenge now but also to transform practices and capacities to respond to crises into the future.
Acknowledgment
Bradley Sharpe, MD, Division Chief, Division of Hospital Medicine, University of California, San Francisco, California, for his input on conception and critical review of this manuscript.
One of the worst public health threats of our generation, coronavirus disease 2019 (COVID-19), first emerged in Wuhan, China, in December 2019 and quickly spread to Singapore, Hong Kong, and Taiwan. These three countries have been praised for their control of the pandemic,1,2 while the number of cases worldwide, including those in the United States, has soared. Political alignment, centralized and integrated healthcare systems, small size, effective technology deployment, widespread testing combined with contact tracing and isolation, and personal protective equipment (PPE) availability underscore their successes.1,3-5 Although these factors differ starkly from those currently employed in the United States, a better understanding their experience may positively influence the myriad US responses. We describe some salient features of Singapore’s infection preparedness, provide examples of how these features guided the National University Hospital (NUH) Singapore COVID-19 response, and illustrate how one facet of the NUH response was translated to develop a new care model at the University of California, San Francisco (UCSF).
THE SINGAPORE EXPERIENCE OVER TIME
Singapore, a small island country (278 square miles) city-state in Southeast Asia has a population of 5.8 million people. Most Singaporeans receive their inpatient care in the public hospitals that are organized and resourced through the Singapore Ministry of Health (MOH). In 2003, severe acute respiratory syndrome (SARS) infected 238 people and killed 33 over 3 months in Singapore, which led to a significant economic downturn. Singapore’s initial SARS experience unveiled limitations in infrastructure, staff preparedness, virus control methodology, and centralized crisis systems. Lessons gleaned from the SARS experience laid the foundation for Singapore’s subsequent disaster preparedness.6
Post-SARS, the MOH created structures and systems to prepare Singapore for future epidemics. All public hospitals expanded isolation capacity by constructing new units or repurposing existing ones and creating colocated Emergency Department (ED) isolation facilities. Additionally, the MOH commissioned the National Centre for Infectious Diseases, a 330-bed high-level isolation hospital.7 They also mandated hospital systems to regularly practice mass casualty and infectious (including respiratory) crisis responses through externally evaluated simulation.8 These are orchestrated down to the smallest detail and involve staff at all levels. For example, healthcare workers (HCW) being “deployed” outside of their specialty, housekeepers practicing novel hazardous waste disposal, and security guards managing crowds interact throughout the exercise.
The testing and viral spread control challenges during SARS spawned hospital-system epidemiology capacity building. Infectious diseases reporting guidelines were refined, and communication channels enhanced to include cross-hospital information sharing and direct lines of communication for epidemiology groups to and from the MOH. Enhanced contact tracing methodologies were adopted and practiced regularly. In addition, material stockpiles, supplies, and supply chains were recalibrated.
The Singapore government also adopted the Disease Outbreak Response System Condition (DORSCON) system,9 a color-coded framework for pandemic response that guides activation of crisis interventions broadly (such as temperature screening at airports and restrictions to travel and internal movements), as well as within the healthcare setting.
In addition to prompting these notable preparedness efforts, SARS had a palpable impact on Singaporeans’ collective psychology both within and outside of the hospital system. The very close-knit medical community lost colleagues during the crisis, and the larger community deeply felt the health and economic costs of this crisis.10 The resulting “respect” or “healthy fear” for infectious crises continues to the present day.
THE SINGAPORE COVID-19 RESPONSE: NATIONAL UNIVERSITY HOSPITAL EXPERIENCE
The NUH is a 1,200-bed public tertiary care academic health center in Singapore. Before the first COVID-19 case was diagnosed in Singapore, NUH joined forces with its broader health system, university resources (schools of medicine and public health), and international partners to refine the existing structures and systems in response to this new infectious threat.
One of these structures included the existing NUH ED negative-pressure “fever facility.” In the ED triage, patients are routinely screened for infectious diseases such as H1N1, MERS-CoV, and measles. In early January, these screening criteria were evolved to adapt to COVID-19. High-risk patients bypass common waiting areas and are sent directly to the fever facility for management. From there, patients requiring admission are sent to one of the inpatient isolation wards, each with over 21 negative-pressure isolation rooms. To expand isolation capacity, lower-priority patients were relocated, and the existing negative- and neutral-pressure rooms were converted into COVID-19 pandemic wards.
The pandemic wards are staffed by nurses with previous isolation experience and Internal Medicine and Subspecialty Medicine physicians and trainees working closely with Infectious Diseases experts. Pandemic Ward teams are sequestered from other clinical and administrative teams, wear hospital-laundered scrubs, and use PPE-conserving practices. These strategies, implemented at the outset, are based on international guidelines contextualized to local needs and include extended use (up to 6 hours) of N95 respirators for the pandemic wards, and surgical masks in all other clinical areas. Notably, there have been no documented transmissions to HCW or patients at NUH. The workforce was maximized by limiting nonurgent clinical, administrative, research, and teaching activities.
In February, COVID-19 testing was initiated internally and deployed widely. NUH, at the time of this writing, has performed more than 6,000 swabs with up to 200 tests run per day (with 80 confirmed cases). Testing at this scale has allowed NUH to ensure: (a) prompt isolation of patients, even those with mild symptoms, (b) deisolation of those testing negative thus conserving PPE and isolation facilities, (c) a better understanding of the epidemiology and the wide range of clinical manifestations of COVID-19, and (d) early comprehensive contact tracing including mildly symptomatic patients.
The MOH plays a central role in coordinating COVID-19 activities and supports individual hospital systems such as NUH. Some of their crisis leadership strategies include daily text messages distributed countrywide, two-way communication channels that ensure feedback loops with hospital executives, epidemiology specialists, and operational workgroups, and engendering interhospital collaboration.11
A US HOSPITAL MEDICINE RESPONSE: UC SAN FRANCISCO
In the United States, the Joint Commission provides structures, tools, and processes for hospital systems to prepare for disasters.12 Many hospital systems have experience with natural disasters which, similar to Singapore’s planning, ensures structures and systems are in place during a crisis. Although these are transferable to multiple types of disasters, the US healthcare system’s direct experience with infectious crises is limited. A fairly distinctive facet—and an asset of US healthcare—is the role of hospitalists.
Hospitalists care for the majority of medical inpatients across the United States,13 and as such, they currently, and will increasingly, play a major role in the US COVID-19 response. This is the case at the UCSF Helen Diller Medical Center at Parnassus Heights (UCSFMC), a 600-bed academic medical center. To learn from other’s early experiences with COVID-19, UCSF Health System leadership connected with many outside health systems including NUH. As one of its multiple pandemic responses, they engaged the UCSFMC Division of Hospital Medicine (DHM), a division that includes 117 hospitalists, to work with hospital and health system leadership and launch a respiratory isolation unit (RIU) modeled after the NUH pandemic ward. The aim of the RIU is to group inpatients with either confirmed or suspected COVID-19 patients who do not require critical care.
An interdisciplinary work group comprising hospitalists, infectious disease specialists, emergency department clinicians, nursing, rehabilitation experts, hospital epidemiology and infection-prevention leaders, safety specialists, and systems engineers was assembled to repurpose an existing medical unit and establish new care models for the RIU. This workgroup created clinical guidelines and workflows, and RIU leaders actively solicit feedback from the staff to advance these standards.
Hospitalists and nurses who volunteered to work on the UCSF attending-staffed RIU received extensive training, including online and widely available in-person PPE training delivered by infection-prevention experts. The RIU hospitalists engage with hospitalists nationwide through ongoing conference calls to share best practices and clinical cases. Patients are admitted by hospitalists to the RIU via the emergency department or directly from ambulatory sites. All RIU providers and staff are screened daily for symptoms prior to starting their shifts, wear hospital-laundered scrubs on the unit, and remain on the unit for the duration of their shift. Hospitalists and nurses communicate regularly to cluster their patient visits and interventions while specialists provide virtual consults (as deemed safe and appropriate) to optimize PPE conservation and decrease overall exposure. The Health System establishes and revises PPE protocols based on CDC guidelines, best available evidence, and supply chain realities. These guidelines are evolving and currently include surgical mask, gown, gloves, and eye protection for all patient interactions with suspected or confirmed COVID-19 and respirator use during aerosol-generating procedures. Research studies (eg, clinical trials and evaluations), informatics efforts (eg, patient flow dashboards), and healthcare technology innovations (eg, tablets for telehealth and video visits) are continually integrated into the RIU infrastructure. Robust attention to the well-being of everyone working on the unit includes chaplain visits, daily debriefs, meal delivery, and palliative care service support, which enrich the unit experience and instill a culture of unity.
MOVING FORWARD
The structures and systems born out of the 2003 SARS experience and the “test, trace, and isolate” strategy were arguably key drivers to flatten Singapore’s epidemic curve early in the pandemic.3 Even with these in place, Singapore is now experiencing a second wave with a significantly higher caseload.14 In response, the government instituted strict social distancing measures on April 3, closing schools and most workplaces. This suggests that the COVID-19 pandemic may fluctuate over time and that varying types and levels of interventions will be required to maintain long-term control. The NUH team describes experiencing cognitive overload given the ever-changing nature and volume of information and fatigue due to the effort required and duration of this crisis. New programs addressing these challenges are being developed and rapidly deployed.
Despite early testing limitations and newly minted systems, San Francisco is cautiously optimistic about its epidemic curve. Since the March 17, 2020, “shelter in place” order, COVID-19 hospitalizations have remained manageable and constant.15 This has afforded healthcare systems including UCSF critical time to evolve its clinical operations (eg, the RIU) and to leverage its academic culture coordinating its bench research, global health, epidemiology, clinical research, informatics, and clinical enterprise scholars and experts to advance COVID-19 science and inform pandemic solutions. Although the UCSF frontline teams are challenged by the stresses of being in the throes of the pandemic amidst a rapidly changing landscape (including changes in PPE and testing recommendations specifically), they are working together to build team resilience for what may come.
CONCLUSION
The world is facing a pandemic of tremendous proportions, and the United States is in the midst of a wave the height of which is yet to be seen. As Fisher and colleagues wrote in 2011, “Our response to infectious disease outbreaks is born out of past experience.”4 Singapore and NUH’s structures and systems that were put into place demonstrate this—they are timely, have been effective thus far, and will be tested in this next wave. “However, no two outbreaks are the same,” the authors wrote, “so an understanding of the infectious agent as well as the environment confronting it is fundamental to the response.”4 In the United States, hospitalists are a key asset in our environment to confront this virus. The UCSF experience exemplifies that, by combining new ideas from another system with on-the-ground expertise while working hand-in-hand with the hospital and health system, hospitalists can be a critical facet of the pandemic response. Hospitalists’ intrinsic abilities to collaborate, learn, and innovate will enable them to not only meet this challenge now but also to transform practices and capacities to respond to crises into the future.
Acknowledgment
Bradley Sharpe, MD, Division Chief, Division of Hospital Medicine, University of California, San Francisco, California, for his input on conception and critical review of this manuscript.
1. Wang CJ, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analytics, new technology, and proactive testing. JAMA. 2020. https://doi.org/10.1001/jama.2020.3151.
2. Legido-Quigley H, Asgari N, Teo YY, et al. Are high-performing health systems resilient against the COVID-19 epidemic? Lancet. 2020;395(10227):848-850. https://doi.org/10.1016/S0140-6736(20)30551-1.
3. Wong JEL, Leo YS, Tan CC. COVID-19 in Singapore—current experience: critical global issues that require attention and action. JAMA. 2020;323(13):1243-1244. https://doi.org/10.1001/jama.2020.2467.
4. Fisher D, Hui DS, Gao Z, et al. Pandemic response lessons from influenza H1N1 2009 in Asia. Respirology. 2011;16(6):876-882. https://doi.org/ 10.1111/j.1440-1843.2011.02003.x.
5. Wong ATY, Chen H, Liu SH, et al. From SARS to avian influenza preparedness in Hong Kong. Clin Infect Dis. 2017;64(suppl_2):S98-S104. https://doi.org/ 10.1093/cid/cix123.
6. Tan CC. SARS in Singapore--key lessons from an epidemic. Ann Acad Med Singapore. 2006;35(5):345-349.
7. National Centre for Infectious Diseases. About NCID. https://www.ncid.sg/About-NCID/Pages/default.aspx. Accessed April 5, 2020.
8. Cutter J. Preparing for an influenza pandemic in Singapore. Ann Acad Med Singapore. 2008;37(6):497-503.
9. Singapore Ministry of Health. What do the different DORSCON levels mean. http://www.gov.sg/article/what-do-the-different-dorscon-levels-mean. Accessed April 5, 2020.
10. Lee J-W, McKibbin WJ. Estimating the global economic costs of SARS. In: Knobler S, Mahmoud A, Lemon S, et al, eds. Institute of Medicine (US) Forum on Microbial Threats. Washington, DC: National Academies Press (US); 2004.
11. James EH, Wooten L. Leadership as (un)usual: how to display competence in times of crisis. Organ Dyn. 2005;34(2):141-152. https://doi.org/10.1016/j.orgdyn.2005.03.005
12. The Joint Commission. Emergency Management: Coronavirus Resources. 2020. https://www.jointcommission.org/covid-19/. Accessed April 4, 2020.
13. Wachter RM, Goldman L. Zero to 50,000 – the 20th anniversary of the hospitalist. N Engl J Med. 2016;375(11):1009-1011. https://doi.org/10.1056/NEJMp1607958.
14. Singapore Ministry of Health. Official Update of COVID-19 Situation in Singapore. 2020. https://experience.arcgis.com/experience/7e30edc490a5441a874f9efe67bd8b89. Accessed April 5, 2020.
15. Chronicle Digital Team. Coronavirus tracker. San Francisco Chronicle. https://projects.sfchronicle.com/2020/coronavirus-map/. Accessed April 5, 2020.
1. Wang CJ, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analytics, new technology, and proactive testing. JAMA. 2020. https://doi.org/10.1001/jama.2020.3151.
2. Legido-Quigley H, Asgari N, Teo YY, et al. Are high-performing health systems resilient against the COVID-19 epidemic? Lancet. 2020;395(10227):848-850. https://doi.org/10.1016/S0140-6736(20)30551-1.
3. Wong JEL, Leo YS, Tan CC. COVID-19 in Singapore—current experience: critical global issues that require attention and action. JAMA. 2020;323(13):1243-1244. https://doi.org/10.1001/jama.2020.2467.
4. Fisher D, Hui DS, Gao Z, et al. Pandemic response lessons from influenza H1N1 2009 in Asia. Respirology. 2011;16(6):876-882. https://doi.org/ 10.1111/j.1440-1843.2011.02003.x.
5. Wong ATY, Chen H, Liu SH, et al. From SARS to avian influenza preparedness in Hong Kong. Clin Infect Dis. 2017;64(suppl_2):S98-S104. https://doi.org/ 10.1093/cid/cix123.
6. Tan CC. SARS in Singapore--key lessons from an epidemic. Ann Acad Med Singapore. 2006;35(5):345-349.
7. National Centre for Infectious Diseases. About NCID. https://www.ncid.sg/About-NCID/Pages/default.aspx. Accessed April 5, 2020.
8. Cutter J. Preparing for an influenza pandemic in Singapore. Ann Acad Med Singapore. 2008;37(6):497-503.
9. Singapore Ministry of Health. What do the different DORSCON levels mean. http://www.gov.sg/article/what-do-the-different-dorscon-levels-mean. Accessed April 5, 2020.
10. Lee J-W, McKibbin WJ. Estimating the global economic costs of SARS. In: Knobler S, Mahmoud A, Lemon S, et al, eds. Institute of Medicine (US) Forum on Microbial Threats. Washington, DC: National Academies Press (US); 2004.
11. James EH, Wooten L. Leadership as (un)usual: how to display competence in times of crisis. Organ Dyn. 2005;34(2):141-152. https://doi.org/10.1016/j.orgdyn.2005.03.005
12. The Joint Commission. Emergency Management: Coronavirus Resources. 2020. https://www.jointcommission.org/covid-19/. Accessed April 4, 2020.
13. Wachter RM, Goldman L. Zero to 50,000 – the 20th anniversary of the hospitalist. N Engl J Med. 2016;375(11):1009-1011. https://doi.org/10.1056/NEJMp1607958.
14. Singapore Ministry of Health. Official Update of COVID-19 Situation in Singapore. 2020. https://experience.arcgis.com/experience/7e30edc490a5441a874f9efe67bd8b89. Accessed April 5, 2020.
15. Chronicle Digital Team. Coronavirus tracker. San Francisco Chronicle. https://projects.sfchronicle.com/2020/coronavirus-map/. Accessed April 5, 2020.
© 2020 Society of Hospital Medicine
Pediatric Hospital Medicine Management, Staffing, and Well-being in the Face of COVID-19
MANAGEMENT AND COMMUNICATION
Establish a Command Team
We benefit from having an existing divisional leadership structure comprising the director, medical directors of our clinical service lines, directors of education and community integration, and associate directors of clinical operations, research, and quality. This established team provides us broad representation of team member expertise and ideas. We maintain our weekly leadership team meeting through video chat and have added daily 30-minute virtual huddles to provide updates from our respective areas and discuss logistical challenges and planning. We use ad hoc phone meetings with relevant team members to address issues of immediate concern.
In the absence of a formal leadership team structure, establish a command team comprising representative leaders of your varied groups (eg, clinical operations, quality improvement, education, research, and business).
Collaborate With Institutional Response
Align divisional command team actions with the institutional response. Our clinical operations leader serves as our primary representative on the institutional emergency preparedness team. This participation allows bidirectional communication, both for institutional updates to be shared with division members and division-specific initiatives to be shared with institutional leadership to facilitate learning across the system.
In conjunction with hospital leadership, our division created a special isolation unit (SIU) to isolate patients positive for COVID-19 and persons under investigation. The institutional emergency preparedness team highlighted the need for such a unit, and our divisional leadership team developed the physician staffing model and medical care delivery system. We collaborated with key stakeholders, including nurses, respiratory therapists, other patient care services members, and subspecialists. The SIU leadership, which includes representatives from hospital medicine, nursing, respiratory therapy, and hospital operations, holds regular phone huddles to provide support and enlist resources based on identified gaps, which allows the frontline SIU physicians to focus on patient care. The calls initially occurred twice daily, but we transitioned to a once-daily schedule after routines were established and resources were procured.
Communicate With Everyone
Frequent communication with the clinical staff is paramount given the rapidly evolving operational changes and medical management recommendations. The divisional leadership team provides frequent email updates to the attending physicians on clinical shifts to communicate clinical updates, send reminders to conserve personal protective equipment (PPE), and share links to COVID-19 resources.
We use our weekly divisional meetings, now held virtually, to provide updates and to allow staff to ask questions and provide input. These meetings routinely include our nonclinical staff, such as administrative assistants and research coordinators, to ensure all team members’ voices are heard and skill sets are utilized. Our divisional infrastructure promotes dialogue and transparency, which is key to our division’s culture. Applying a learning health network approach has allowed us to generate new ideas, accelerate improvement, and encourage everyone to be a part of our community focused on improving outcomes.6 We continue to leverage this approach in our pandemic response.
One idea generated from this approach prompted us to create a centralized communication forum, using Microsoft Teams, to serve as a repository for the most up-to-date information related to COVID-19, the SIU, and general information, including links to divisional and institutional resources.
Maintain Nonclinical Operations
Nonclinical staff are working remotely. The business director and research director hold daily calls with the administrative staff and research coordinators, respectively, to discuss workload and to reallocate responsibilities as needed. This approach allows the business, administrative, and research support teams to function efficiently and redistribute work as the nonclinical priorities shift to meet divisional needs.
STAFFING
Establish a Backup Pool
We anticipate needing a larger pool of backup providers in the event of ill or quarantined staff or in case of increased patient volumes. The latter may be less likely for pediatric patients based on early studies3-5 but could occur if our free-standing children’s hospital expands to include the care of adult patients. We asked physicians to volunteer for backup shifts to augment our existing “jeopardy” backup system with a greater request to those with a lower clinical full-time equivalence. Each day, two backup shift positions are filled by volunteers, with additional positions added on days when medicine-pediatrics providers are scheduled for shifts in case they are needed at the university (adult) hospital.
Minimize Staffing to Reserve Pool
We monitor census closely on all service lines, including our consult service lines and secondary inpatient site, with plans to dissolve unnecessary consult services and combine medical teams, when feasible, to reduce the risk of staff exposure and maintain reserves. For example, after elective procedures were canceled, we reduced physician staffing of our surgical comanagement service to the minimal necessary coverage. We assign nonpatient-facing clinical duties to physicians who are called off their shift, in quarantine, or mildly ill to help off-load the clinical burden. Such duties include accepting direct admission phone calls, triaging patient care calls, entering orders remotely, and assisting with care coordination needs.
Anticipate Adult Care Needs
Our pediatric institution admits select groups of adult patients with congenital or complex healthcare needs who require specialized care. Hospitalists board certified in both pediatrics and internal medicine provide consultative services to many of these patients. Anticipating that these physicians may be needed in adult facilities, we plan to dissolve this consult service and utilize our reserve pool of providers to cover their pediatric shifts if needed. Additionally, if our hospital expands coverage for adult patients, these medicine-pediatrics providers will be instrumental in coordinating that expanded effort and will serve as leaders for teams of physicians and advanced practice providers with limited or no adult medicine training.
Special Isolation Unit
Logistic planning for our SIU evolved over the first few patients with rapid-cycle feedback and learning with each admission. This feedback was facilitated with our twice-daily huddle calls, which involved all key stakeholders, including nursing and respiratory therapy representatives. For division physician staffing, higher-risk team members are excluded from working on this unit. Because the SIU was developed to care for all patients positive for COVID-19 and persons under investigation, subspecialty patients not typically cared for by Hospital Medicine at our institution are being admitted to this unit. Therefore, subspecialty divisions assign attending physicians to provide consultative services to the SIU. These consultants use the unit’s telemedicine capabilities, when feasible, to limit staff exposure and conserve PPE. Our hospital medicine leaders in the SIU proactively worked with subspecialty divisions that are anticipated to have more admissions given their at-risk patient populations, such as pulmonary medicine, cardiology, and oncology. They specifically developed staffing plans for these patients if the SIU census becomes unsustainable under Hospital Medicine alone.
STAFF WELL-BEING
Healthcare workers are experiencing numerous stressors at work and home during this tumultuous time. Our workforce is at risk of developing emotional distress and mental health concerns. A cross-sectional survey of more than 1,200 healthcare workers in China who cared for COVID-19 patients found that many experienced symptoms of psychological distress (71%), as well as depression (51%), anxiety (44%), and insomnia (34%).7 Hospital medicine groups should consider methods to support their staff to mitigate stressors and promote self-care.
Anticipate Childcare Issues
When we were faced with impending school and daycare closures, we surveyed our division to assess childcare needs (Table) and share resources. We created a system of emergency childcare coverage options by connecting parents with similarly aged children and who lived in geographic proximity. This approach to childcare contingency planning was shared with and adopted by other divisions within the institution.
Build Support Measures
To support each other during this particularly stressful time, we divided division members into groups or “support pods,” each facilitated by a leadership team member. Group text messages and weekly phone or video chats have promoted connectivity and peer support.
Promote Self-care
The divisional leadership team provides food and drink for staff on clinical shifts. We also collated self-care resources to share via a central repository. These resources include ideas for meditation, home education for children, parenting, exercise, faith communities, entertainment, methods to support our local community through volunteerism and donations, and mental health resources, as well as online links to these resources.
Adult health systems will be disproportionately affected as this pandemic evolves. Pediatric hospitalists have the unique opportunity to support the response efforts by maintaining teams that are flexible and adaptable to evolving community needs. To do this, team leaders need to promote transparency, share learnings, and leverage the diverse skills of team members to ensure we are ready to meet the challenges of the moment.
1. World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report - 51. [Situation Report]. 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19. Accessed March 26, 2020.
2. Centers for Disease Control and Prevention. Interim Guidance for Healthcare Facilities: Preparing for Community Transmission of COVID-19 in the United States. 2020. https://www.cdc.gov/coronavirus/2019-ncov/healthcare-facilities/guidance-hcf.html. Accessed March 27, 2020.
3. Dong Y, Mo X, Hu Y, et al. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. 2020. https://doi.org/10.1542/peds.2020-0702.
4. Cruz A, Zeichner S. COVID-19 in children: initial characterization of pediatric disease. Pediatrics. 2020;e20200834. https://doi.org/10.1542/peds.2020-0834.
5. Wu Z, McGoogan J. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648.
6. James M Anderson Center of Health Systems Excellence. The Power of Learning Networks. https://www.cincinnatichildrens.org/research/divisions/j/anderson-center/learning-networks. Accessed April 2, 2020.
7. Lai J, Ma S, Wang Y, et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw Open. 2020;3(3):e203976. https://doi.org/10.1001/jamanetworkopen.2020.3976.
MANAGEMENT AND COMMUNICATION
Establish a Command Team
We benefit from having an existing divisional leadership structure comprising the director, medical directors of our clinical service lines, directors of education and community integration, and associate directors of clinical operations, research, and quality. This established team provides us broad representation of team member expertise and ideas. We maintain our weekly leadership team meeting through video chat and have added daily 30-minute virtual huddles to provide updates from our respective areas and discuss logistical challenges and planning. We use ad hoc phone meetings with relevant team members to address issues of immediate concern.
In the absence of a formal leadership team structure, establish a command team comprising representative leaders of your varied groups (eg, clinical operations, quality improvement, education, research, and business).
Collaborate With Institutional Response
Align divisional command team actions with the institutional response. Our clinical operations leader serves as our primary representative on the institutional emergency preparedness team. This participation allows bidirectional communication, both for institutional updates to be shared with division members and division-specific initiatives to be shared with institutional leadership to facilitate learning across the system.
In conjunction with hospital leadership, our division created a special isolation unit (SIU) to isolate patients positive for COVID-19 and persons under investigation. The institutional emergency preparedness team highlighted the need for such a unit, and our divisional leadership team developed the physician staffing model and medical care delivery system. We collaborated with key stakeholders, including nurses, respiratory therapists, other patient care services members, and subspecialists. The SIU leadership, which includes representatives from hospital medicine, nursing, respiratory therapy, and hospital operations, holds regular phone huddles to provide support and enlist resources based on identified gaps, which allows the frontline SIU physicians to focus on patient care. The calls initially occurred twice daily, but we transitioned to a once-daily schedule after routines were established and resources were procured.
Communicate With Everyone
Frequent communication with the clinical staff is paramount given the rapidly evolving operational changes and medical management recommendations. The divisional leadership team provides frequent email updates to the attending physicians on clinical shifts to communicate clinical updates, send reminders to conserve personal protective equipment (PPE), and share links to COVID-19 resources.
We use our weekly divisional meetings, now held virtually, to provide updates and to allow staff to ask questions and provide input. These meetings routinely include our nonclinical staff, such as administrative assistants and research coordinators, to ensure all team members’ voices are heard and skill sets are utilized. Our divisional infrastructure promotes dialogue and transparency, which is key to our division’s culture. Applying a learning health network approach has allowed us to generate new ideas, accelerate improvement, and encourage everyone to be a part of our community focused on improving outcomes.6 We continue to leverage this approach in our pandemic response.
One idea generated from this approach prompted us to create a centralized communication forum, using Microsoft Teams, to serve as a repository for the most up-to-date information related to COVID-19, the SIU, and general information, including links to divisional and institutional resources.
Maintain Nonclinical Operations
Nonclinical staff are working remotely. The business director and research director hold daily calls with the administrative staff and research coordinators, respectively, to discuss workload and to reallocate responsibilities as needed. This approach allows the business, administrative, and research support teams to function efficiently and redistribute work as the nonclinical priorities shift to meet divisional needs.
STAFFING
Establish a Backup Pool
We anticipate needing a larger pool of backup providers in the event of ill or quarantined staff or in case of increased patient volumes. The latter may be less likely for pediatric patients based on early studies3-5 but could occur if our free-standing children’s hospital expands to include the care of adult patients. We asked physicians to volunteer for backup shifts to augment our existing “jeopardy” backup system with a greater request to those with a lower clinical full-time equivalence. Each day, two backup shift positions are filled by volunteers, with additional positions added on days when medicine-pediatrics providers are scheduled for shifts in case they are needed at the university (adult) hospital.
Minimize Staffing to Reserve Pool
We monitor census closely on all service lines, including our consult service lines and secondary inpatient site, with plans to dissolve unnecessary consult services and combine medical teams, when feasible, to reduce the risk of staff exposure and maintain reserves. For example, after elective procedures were canceled, we reduced physician staffing of our surgical comanagement service to the minimal necessary coverage. We assign nonpatient-facing clinical duties to physicians who are called off their shift, in quarantine, or mildly ill to help off-load the clinical burden. Such duties include accepting direct admission phone calls, triaging patient care calls, entering orders remotely, and assisting with care coordination needs.
Anticipate Adult Care Needs
Our pediatric institution admits select groups of adult patients with congenital or complex healthcare needs who require specialized care. Hospitalists board certified in both pediatrics and internal medicine provide consultative services to many of these patients. Anticipating that these physicians may be needed in adult facilities, we plan to dissolve this consult service and utilize our reserve pool of providers to cover their pediatric shifts if needed. Additionally, if our hospital expands coverage for adult patients, these medicine-pediatrics providers will be instrumental in coordinating that expanded effort and will serve as leaders for teams of physicians and advanced practice providers with limited or no adult medicine training.
Special Isolation Unit
Logistic planning for our SIU evolved over the first few patients with rapid-cycle feedback and learning with each admission. This feedback was facilitated with our twice-daily huddle calls, which involved all key stakeholders, including nursing and respiratory therapy representatives. For division physician staffing, higher-risk team members are excluded from working on this unit. Because the SIU was developed to care for all patients positive for COVID-19 and persons under investigation, subspecialty patients not typically cared for by Hospital Medicine at our institution are being admitted to this unit. Therefore, subspecialty divisions assign attending physicians to provide consultative services to the SIU. These consultants use the unit’s telemedicine capabilities, when feasible, to limit staff exposure and conserve PPE. Our hospital medicine leaders in the SIU proactively worked with subspecialty divisions that are anticipated to have more admissions given their at-risk patient populations, such as pulmonary medicine, cardiology, and oncology. They specifically developed staffing plans for these patients if the SIU census becomes unsustainable under Hospital Medicine alone.
STAFF WELL-BEING
Healthcare workers are experiencing numerous stressors at work and home during this tumultuous time. Our workforce is at risk of developing emotional distress and mental health concerns. A cross-sectional survey of more than 1,200 healthcare workers in China who cared for COVID-19 patients found that many experienced symptoms of psychological distress (71%), as well as depression (51%), anxiety (44%), and insomnia (34%).7 Hospital medicine groups should consider methods to support their staff to mitigate stressors and promote self-care.
Anticipate Childcare Issues
When we were faced with impending school and daycare closures, we surveyed our division to assess childcare needs (Table) and share resources. We created a system of emergency childcare coverage options by connecting parents with similarly aged children and who lived in geographic proximity. This approach to childcare contingency planning was shared with and adopted by other divisions within the institution.
Build Support Measures
To support each other during this particularly stressful time, we divided division members into groups or “support pods,” each facilitated by a leadership team member. Group text messages and weekly phone or video chats have promoted connectivity and peer support.
Promote Self-care
The divisional leadership team provides food and drink for staff on clinical shifts. We also collated self-care resources to share via a central repository. These resources include ideas for meditation, home education for children, parenting, exercise, faith communities, entertainment, methods to support our local community through volunteerism and donations, and mental health resources, as well as online links to these resources.
Adult health systems will be disproportionately affected as this pandemic evolves. Pediatric hospitalists have the unique opportunity to support the response efforts by maintaining teams that are flexible and adaptable to evolving community needs. To do this, team leaders need to promote transparency, share learnings, and leverage the diverse skills of team members to ensure we are ready to meet the challenges of the moment.
MANAGEMENT AND COMMUNICATION
Establish a Command Team
We benefit from having an existing divisional leadership structure comprising the director, medical directors of our clinical service lines, directors of education and community integration, and associate directors of clinical operations, research, and quality. This established team provides us broad representation of team member expertise and ideas. We maintain our weekly leadership team meeting through video chat and have added daily 30-minute virtual huddles to provide updates from our respective areas and discuss logistical challenges and planning. We use ad hoc phone meetings with relevant team members to address issues of immediate concern.
In the absence of a formal leadership team structure, establish a command team comprising representative leaders of your varied groups (eg, clinical operations, quality improvement, education, research, and business).
Collaborate With Institutional Response
Align divisional command team actions with the institutional response. Our clinical operations leader serves as our primary representative on the institutional emergency preparedness team. This participation allows bidirectional communication, both for institutional updates to be shared with division members and division-specific initiatives to be shared with institutional leadership to facilitate learning across the system.
In conjunction with hospital leadership, our division created a special isolation unit (SIU) to isolate patients positive for COVID-19 and persons under investigation. The institutional emergency preparedness team highlighted the need for such a unit, and our divisional leadership team developed the physician staffing model and medical care delivery system. We collaborated with key stakeholders, including nurses, respiratory therapists, other patient care services members, and subspecialists. The SIU leadership, which includes representatives from hospital medicine, nursing, respiratory therapy, and hospital operations, holds regular phone huddles to provide support and enlist resources based on identified gaps, which allows the frontline SIU physicians to focus on patient care. The calls initially occurred twice daily, but we transitioned to a once-daily schedule after routines were established and resources were procured.
Communicate With Everyone
Frequent communication with the clinical staff is paramount given the rapidly evolving operational changes and medical management recommendations. The divisional leadership team provides frequent email updates to the attending physicians on clinical shifts to communicate clinical updates, send reminders to conserve personal protective equipment (PPE), and share links to COVID-19 resources.
We use our weekly divisional meetings, now held virtually, to provide updates and to allow staff to ask questions and provide input. These meetings routinely include our nonclinical staff, such as administrative assistants and research coordinators, to ensure all team members’ voices are heard and skill sets are utilized. Our divisional infrastructure promotes dialogue and transparency, which is key to our division’s culture. Applying a learning health network approach has allowed us to generate new ideas, accelerate improvement, and encourage everyone to be a part of our community focused on improving outcomes.6 We continue to leverage this approach in our pandemic response.
One idea generated from this approach prompted us to create a centralized communication forum, using Microsoft Teams, to serve as a repository for the most up-to-date information related to COVID-19, the SIU, and general information, including links to divisional and institutional resources.
Maintain Nonclinical Operations
Nonclinical staff are working remotely. The business director and research director hold daily calls with the administrative staff and research coordinators, respectively, to discuss workload and to reallocate responsibilities as needed. This approach allows the business, administrative, and research support teams to function efficiently and redistribute work as the nonclinical priorities shift to meet divisional needs.
STAFFING
Establish a Backup Pool
We anticipate needing a larger pool of backup providers in the event of ill or quarantined staff or in case of increased patient volumes. The latter may be less likely for pediatric patients based on early studies3-5 but could occur if our free-standing children’s hospital expands to include the care of adult patients. We asked physicians to volunteer for backup shifts to augment our existing “jeopardy” backup system with a greater request to those with a lower clinical full-time equivalence. Each day, two backup shift positions are filled by volunteers, with additional positions added on days when medicine-pediatrics providers are scheduled for shifts in case they are needed at the university (adult) hospital.
Minimize Staffing to Reserve Pool
We monitor census closely on all service lines, including our consult service lines and secondary inpatient site, with plans to dissolve unnecessary consult services and combine medical teams, when feasible, to reduce the risk of staff exposure and maintain reserves. For example, after elective procedures were canceled, we reduced physician staffing of our surgical comanagement service to the minimal necessary coverage. We assign nonpatient-facing clinical duties to physicians who are called off their shift, in quarantine, or mildly ill to help off-load the clinical burden. Such duties include accepting direct admission phone calls, triaging patient care calls, entering orders remotely, and assisting with care coordination needs.
Anticipate Adult Care Needs
Our pediatric institution admits select groups of adult patients with congenital or complex healthcare needs who require specialized care. Hospitalists board certified in both pediatrics and internal medicine provide consultative services to many of these patients. Anticipating that these physicians may be needed in adult facilities, we plan to dissolve this consult service and utilize our reserve pool of providers to cover their pediatric shifts if needed. Additionally, if our hospital expands coverage for adult patients, these medicine-pediatrics providers will be instrumental in coordinating that expanded effort and will serve as leaders for teams of physicians and advanced practice providers with limited or no adult medicine training.
Special Isolation Unit
Logistic planning for our SIU evolved over the first few patients with rapid-cycle feedback and learning with each admission. This feedback was facilitated with our twice-daily huddle calls, which involved all key stakeholders, including nursing and respiratory therapy representatives. For division physician staffing, higher-risk team members are excluded from working on this unit. Because the SIU was developed to care for all patients positive for COVID-19 and persons under investigation, subspecialty patients not typically cared for by Hospital Medicine at our institution are being admitted to this unit. Therefore, subspecialty divisions assign attending physicians to provide consultative services to the SIU. These consultants use the unit’s telemedicine capabilities, when feasible, to limit staff exposure and conserve PPE. Our hospital medicine leaders in the SIU proactively worked with subspecialty divisions that are anticipated to have more admissions given their at-risk patient populations, such as pulmonary medicine, cardiology, and oncology. They specifically developed staffing plans for these patients if the SIU census becomes unsustainable under Hospital Medicine alone.
STAFF WELL-BEING
Healthcare workers are experiencing numerous stressors at work and home during this tumultuous time. Our workforce is at risk of developing emotional distress and mental health concerns. A cross-sectional survey of more than 1,200 healthcare workers in China who cared for COVID-19 patients found that many experienced symptoms of psychological distress (71%), as well as depression (51%), anxiety (44%), and insomnia (34%).7 Hospital medicine groups should consider methods to support their staff to mitigate stressors and promote self-care.
Anticipate Childcare Issues
When we were faced with impending school and daycare closures, we surveyed our division to assess childcare needs (Table) and share resources. We created a system of emergency childcare coverage options by connecting parents with similarly aged children and who lived in geographic proximity. This approach to childcare contingency planning was shared with and adopted by other divisions within the institution.
Build Support Measures
To support each other during this particularly stressful time, we divided division members into groups or “support pods,” each facilitated by a leadership team member. Group text messages and weekly phone or video chats have promoted connectivity and peer support.
Promote Self-care
The divisional leadership team provides food and drink for staff on clinical shifts. We also collated self-care resources to share via a central repository. These resources include ideas for meditation, home education for children, parenting, exercise, faith communities, entertainment, methods to support our local community through volunteerism and donations, and mental health resources, as well as online links to these resources.
Adult health systems will be disproportionately affected as this pandemic evolves. Pediatric hospitalists have the unique opportunity to support the response efforts by maintaining teams that are flexible and adaptable to evolving community needs. To do this, team leaders need to promote transparency, share learnings, and leverage the diverse skills of team members to ensure we are ready to meet the challenges of the moment.
1. World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report - 51. [Situation Report]. 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19. Accessed March 26, 2020.
2. Centers for Disease Control and Prevention. Interim Guidance for Healthcare Facilities: Preparing for Community Transmission of COVID-19 in the United States. 2020. https://www.cdc.gov/coronavirus/2019-ncov/healthcare-facilities/guidance-hcf.html. Accessed March 27, 2020.
3. Dong Y, Mo X, Hu Y, et al. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. 2020. https://doi.org/10.1542/peds.2020-0702.
4. Cruz A, Zeichner S. COVID-19 in children: initial characterization of pediatric disease. Pediatrics. 2020;e20200834. https://doi.org/10.1542/peds.2020-0834.
5. Wu Z, McGoogan J. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648.
6. James M Anderson Center of Health Systems Excellence. The Power of Learning Networks. https://www.cincinnatichildrens.org/research/divisions/j/anderson-center/learning-networks. Accessed April 2, 2020.
7. Lai J, Ma S, Wang Y, et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw Open. 2020;3(3):e203976. https://doi.org/10.1001/jamanetworkopen.2020.3976.
1. World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report - 51. [Situation Report]. 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19. Accessed March 26, 2020.
2. Centers for Disease Control and Prevention. Interim Guidance for Healthcare Facilities: Preparing for Community Transmission of COVID-19 in the United States. 2020. https://www.cdc.gov/coronavirus/2019-ncov/healthcare-facilities/guidance-hcf.html. Accessed March 27, 2020.
3. Dong Y, Mo X, Hu Y, et al. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. 2020. https://doi.org/10.1542/peds.2020-0702.
4. Cruz A, Zeichner S. COVID-19 in children: initial characterization of pediatric disease. Pediatrics. 2020;e20200834. https://doi.org/10.1542/peds.2020-0834.
5. Wu Z, McGoogan J. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648.
6. James M Anderson Center of Health Systems Excellence. The Power of Learning Networks. https://www.cincinnatichildrens.org/research/divisions/j/anderson-center/learning-networks. Accessed April 2, 2020.
7. Lai J, Ma S, Wang Y, et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw Open. 2020;3(3):e203976. https://doi.org/10.1001/jamanetworkopen.2020.3976.
© 2020 Society of Hospital Medicine
Children’s Hospitals Caring for Adults During a Pandemic: Pragmatic Considerations and Approaches
Health systems around the world have been called upon to expand acute care capacity to manage the current and projected surge of adults with COVID-19, the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 There has been mixed guidance on how pediatric facilities should consolidate and coordinate pediatric care in a way that optimizes the capacity of hospital beds, staff, and supplies, such as ventilators and medications, for both adults and children in a community.2 Furthermore, if and how these pediatric facilities should expand capacity to care for adult patients safely is uncertain.
For the last 5 years, both Boston Children’s Hospital and Cincinnati Children’s Hospital Medical Center have been caring for specific adult populations in free-standing pediatric hospitals because of the increasing prevalence of young adults with rare, complex, and historically fatal conditions (eg, chromosomal abnormalities). In the past, low life expectancies for children with such conditions contributed to the evolution of specialized care in pediatric health systems that often does not exist in adult health systems. Our teams in Boston and Cincinnati have gained insight into the multifaceted infrastructure and teams necessary to provide safe care for adults hospitalized in a pediatric setting.
In this perspective piece, we will highlight important principles that pediatric facilities and providers should prioritize if they anticipate caring for hospitalized adults during this pandemic. Designing and implementing an adult care model requires iteratively addressing the following key areas: development of a multistakeholder team, system readiness for intensive care unit (ICU) care of adults, institutional situation awareness, scope of practice, staffing considerations, patient safety, and patient populations and special considerations (eg, adults with chronic conditions of childhood onset). With these areas in mind, pediatric facilities should then consider whether they have the capacity to manage hospitalized adults.
DEVELOPMENT OF A MULTISTAKEHOLDER TEAM
Providing care for any hospitalized patient requires engagement with many health system stakeholders. By involving key stakeholders early in the planning process for our adult care model, we were able to anticipate potential obstacles when caring for a unique subset of patients and gain support of multidisciplinary partners. For instance, inclusion of bedside and support staff highlighted specific needs, such as nurses with adult training and a revised formulary to include common adult medications (eg, clopidogrel for adults with a drug-eluting stent).
Responding to the surge of hospitalized adult patients will require increasing hospital capacity.3 In pediatric settings, this will require consideration of innovative care models. These care models may include pediatric systems flexing to care for adult patients. We recommend hospital leaders from both pediatric and adult facilities have formal discussions on the best ways for pediatric facilities to respond to serve their local population. Inclusion of other key stakeholders will ensure factors imperative to the safe care of adults will not be missed.
SYSTEM READINESS FOR ICU CARE OF ADULTS
There were three levels of consideration for the use of our local pediatric ICU for these patients. First, our institutional policies allow care for adults throughout the system, which we describe in more detail later, in the “Scope of Practice” section. Second, our free-standing pediatric hospital ICUs have accreditation for the care of adults. Third, we developed clear guidelines for subspecialists regarding when adults can safely be admitted or transferred to the pediatric ICU.
Responding to a crisis still necessitates establishing a clear care-escalation plan. An initial barrier may be that some systems do not have a pediatric ICU accredited for care of patients above a certain age. During a crisis, however, as hospital volumes and mortalities rise, states may pursue executive orders, as New York State did, that ease these age restrictions.4 Otherwise, we recommend a clear transfer plan to an adult ICU or emergency credentialing and privileging of adult intensivists. Both of these options may pose challenges during a pandemic because adult ICUs will likely be full.
INSTITUTIONAL SITUATION AWARENESS
Institutional situation awareness for the identification and mitigation of risks inherent in adult care in a pediatric setting is essential for patient safety. Tracking of admitted adult patients via our electronic health record (EHR) occurs daily by an adult care–team member. Our adult care teams partner with physician safety officers and attend daily institutional multidisciplinary safety huddles to create a shared mental model for the care of adult patients. Daily huddle reports include discussion regarding the number of admitted adults, review of illness acuity, consultative advice on management, and contingency planning for potential decompensation.5,6 This integration into institutional huddles has been instrumental in proactively identifying hospitalized adults who are at risk for clinical decompensation and mitigating those risks.
Should a pediatric system admit adults to new sites or units, we recommend leveraging preexisting patient safety infrastructure similarly to identify and mitigate risks. If possible, any institutional communication about adult patients should involve adult-trained staff. Mechanisms for tracking patients will depend on local EHRs but are important to guide regular check-ins with providers caring for those patients.
SCOPE OF PRACTICE
Multiple levels of regulation affect a provider’s scope of practice. The most general of these regulations are state guidelines, followed by local institutional policy. Our institutions require consults for older adults—age varies at our specific institutions—by our adult-care team for assessment of risk and comanagement of adult-specific comorbidities. Additionally, we have agreements with our affiliated adult health facilities that allow in-person adult subspecialty consultation.
While state and institutional policies lay the foundation for pediatric systems considering new adult-care models, provider-level considerations are also needed. Often the patient’s age is a primary consideration, but comorbid conditions also affect the provider’s comfort and ability to care for these patients. We urge practitioners to exercise the full range of their capacities, but also to think critically about the ethical scope of one’s practice. As healthcare providers, it is our duty to hold each other accountable, voice concerns, and advocate to increase health system capacity equitably.7 It’s paramount that channels of communication, in-person or virtual, be arranged for supportive adult subspecialist consultation.
STAFFING CONSIDERATIONS
Med-Peds physicians and advanced practice providers are the foundation of the clinical care provided to adults at our institutions. Our Med-Peds providers practice in both the free-standing pediatric hospital and an affiliated adult health system. They offer expertise in adult clinical care and navigate between pediatric and adult systems when the need arises (eg, adult requiring urgent intervention for an acute myocardial infarction). Adult competencies of other staff must be addressed. For example, our cardiac ICUs include nurses with adult clinical care experience because critically ill adults with congenital heart disease are admitted. Advanced Care Life Support (ACLS) training is also required for staff caring for adults throughout the hospital.
There are many ways, even during a crisis, to develop an adult care model in a pediatric setting. Depending on workforce availability, internal medicine, Med-Peds, family medicine, critical care, and emergency medicine physicians could serve on either a primary service or as a consultant to support pediatrics-trained providers in caring for adults should the patient volume and acuity require staffing restructuring. Adult subspecialty access must be addressed. Telehealth may play a significant role in extending clinicians in all of these clinical roles both during the current crisis but also in underresourced settings.8 A clear process and indication for emergency or temporary credentialing and privileging necessitates understanding and addressing such challenges early. Training in adult care, or lack thereof, for other staff, such as nurses and respiratory therapists, is also crucial to consider.
PATIENT SAFETY
Adults are more likely than children to have comorbidities and clinical deterioration while hospitalized. At our institutions, when a rapid response team is called for an adult patient, an adult care–team provider responds to aid in clinical management and determines the appropriate care setting. Additionally, given that the incidence of coronary artery disease increases starting at age 35 years,9 our systems have developed procedures for managing time-sensitive conditions seen more commonly in adults, such as acute myocardial infarction, stroke, and pulmonary embolism. Despite simulation training for pediatric providers and staff, it is clear that implementing these procedures is highly dependent on involvement of the adult care team.
With the urgency of implementation, pediatric systems should consider increasing the number of providers and staff with ACLS training, especially for rapid response and code teams. Many pediatric systems may need to evaluate how their code carts are stocked and ensure they are equipped with appropriate medication dosages and sizes of supplies. Emergent and accessible adult care will be needed, especially for issues with time-to-intervention criteria like acute myocardial infarction and stroke. Hospitalized adults with COVID-19 may also have a higher incidence of arrhythmia, cardiac ischemia, and stroke.10 Consider proactively simulating common COVID-19–related scenarios to build interdisciplinary teamwork in emergency scenarios. Interhospital agreements and pathways exist for sharing medications. Outreach to pharmacies may be indicated to ensure accessibility for medications not commonly found in pediatric systems.
PATIENT POPULATIONS AND SPECIAL CONSIDERATIONS
Our children’s hospitals care for certain adult populations with chronic conditions of childhood origin because of the availability of subspecialty clinical expertise. Our adult care team aids in contingency planning to help determine place of admission (adult vs pediatric hospital) depending on patient clinical needs and system expertise. For instance, an adult with congenital heart disease may have two cardiologists—one for congenital heart disease and one for coronary artery disease. Patients with an acute issue such as new-onset arrhythmia may be admitted to our pediatric hospital; however, for a stroke they would be admitted to the adult hospital.
While important and tempting to address this issue first, creating criteria to determine which patient population to admit should be a last consideration during a pandemic. Consider if the decision to admit should be determined based on COVID-19 infection status. From there, types of conditions thought to be within the purview of pediatric practice can be considered. These include basic infectious diseases pathology (eg, skin/soft-tissue infections and pyelonephritis) and chronic conditions of childhood origin (eg, cystic fibrosis, diabetes, and inflammatory bowel disease), which have specialty providers who could work across an extended age range. Conditions potentially more challenging to safely care for in pediatric facilities include acute cardiac conditions (eg, angina, acute coronary syndrome, and arrhythmias), alcohol withdrawal, end-stage liver or kidney disease, and gastrointestinal bleeds. Considerations need to be made for research protocols and novel therapies only available at adult institutions. Through this whole process, it is especially crucial to note care equity and ensure that all patients have access to the highest attainable care possible.
CONCLUSION
Policymakers at pediatric facilities should think critically about their institution’s capacity to manage adults. In some circumstances, the decision might be to not admit adult patients based on the factors discussed in this paper or other contextual factors of the local healthcare systems. Our role in providing care for adults in pediatric hospitals involves not only ensuring age-appropriate care, but also in supporting patients and other healthcare providers to navigate a fragmented health system. Our adult-care models required building relationships between pediatric and adult health systems. Building these relationships in the setting of crisis can strengthen health systems and healthcare communities beyond the era of COVID-19. Because it’s promoted enhanced collaboration between pediatric and adult facilities, COVID-19 can be a platform to build a better system to support our already vulnerable young adults with chronic conditions of childhood origin for years to come.
1. Cavallo JJ, Donoho DA, Forman HP. Hospital capacity and operations in the coronavirus disease 2019 (COVID-19) Pandemic—planning for the Nth patient. JAMA Health Forum. 2020;1(3):e200345. https://jamanetwork.com/channels/health-forum/fullarticle/2763353. Accessed March 30, 2020.
2. Children’s Hospital Association. Consolidating Pediatric Hospital Care to Increase Capacity for Adults with COVID-19. https://www.childrenshospitals.org/Quality-and-Performance/COVID19/Resources/Consolidating-Pediatric-Hospital-Care-Increase-Capacity-Adults-COVID19. Accessed March 28, 2020.
3. Campbell J. Andrew Cuomo’s order to hospitals: expand capacity or face state takeover. Democrat & Chronicle. April 1, 2020. https://www.democratandchronicle.com/story/news/politics/albany/2020/04/01/coronavirus-cuomo-order-state-hospital-takeover/5100134002/. Accessed April 2, 2020.
4. New York State Education Department, Office of the Professions. COVID-19 Executive Orders. http://www.op.nysed.gov/COVID-19_EO.html. Accessed April 2, 2020.
5. Brady PW, Muething S, Kotagal U, et al. Improving situation awareness to reduce unrecognized clinical deterioration and serious safety events. Pediatrics. 2013;131(1):e298-e308. https://doi.org/10.1542/peds.2012-1364.
6. Conway-Habes EE, Herbst BF, Herbst LA, et al. Using quality improvement to introduce and standardize the National Early Warning Score (NEWS) for adult inpatients at a children’s hospital. Hosp Pediatr. 2017;7(3):156-163. https://doi.org/10.1542/hpeds.2016-0117.
7. Berry JG, Bloom S, Foley S, Palfrey JS. Health inequity in children and youth with chronic health conditions. Pediatrics. 2010;126(Suppl 3):S111-S119. https://doi.org/10.1542/peds.2010-1466D.
8. Smith AC, Thomas E, Snoswell CL, et al. Telehealth for global emergencies: implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020:1357633X20916567. https://doi.org/10.1177/1357633X20916567.
9. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139-e596. https://doi.org/10.1161/CIR.0000000000000757.
10. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648.
Health systems around the world have been called upon to expand acute care capacity to manage the current and projected surge of adults with COVID-19, the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 There has been mixed guidance on how pediatric facilities should consolidate and coordinate pediatric care in a way that optimizes the capacity of hospital beds, staff, and supplies, such as ventilators and medications, for both adults and children in a community.2 Furthermore, if and how these pediatric facilities should expand capacity to care for adult patients safely is uncertain.
For the last 5 years, both Boston Children’s Hospital and Cincinnati Children’s Hospital Medical Center have been caring for specific adult populations in free-standing pediatric hospitals because of the increasing prevalence of young adults with rare, complex, and historically fatal conditions (eg, chromosomal abnormalities). In the past, low life expectancies for children with such conditions contributed to the evolution of specialized care in pediatric health systems that often does not exist in adult health systems. Our teams in Boston and Cincinnati have gained insight into the multifaceted infrastructure and teams necessary to provide safe care for adults hospitalized in a pediatric setting.
In this perspective piece, we will highlight important principles that pediatric facilities and providers should prioritize if they anticipate caring for hospitalized adults during this pandemic. Designing and implementing an adult care model requires iteratively addressing the following key areas: development of a multistakeholder team, system readiness for intensive care unit (ICU) care of adults, institutional situation awareness, scope of practice, staffing considerations, patient safety, and patient populations and special considerations (eg, adults with chronic conditions of childhood onset). With these areas in mind, pediatric facilities should then consider whether they have the capacity to manage hospitalized adults.
DEVELOPMENT OF A MULTISTAKEHOLDER TEAM
Providing care for any hospitalized patient requires engagement with many health system stakeholders. By involving key stakeholders early in the planning process for our adult care model, we were able to anticipate potential obstacles when caring for a unique subset of patients and gain support of multidisciplinary partners. For instance, inclusion of bedside and support staff highlighted specific needs, such as nurses with adult training and a revised formulary to include common adult medications (eg, clopidogrel for adults with a drug-eluting stent).
Responding to the surge of hospitalized adult patients will require increasing hospital capacity.3 In pediatric settings, this will require consideration of innovative care models. These care models may include pediatric systems flexing to care for adult patients. We recommend hospital leaders from both pediatric and adult facilities have formal discussions on the best ways for pediatric facilities to respond to serve their local population. Inclusion of other key stakeholders will ensure factors imperative to the safe care of adults will not be missed.
SYSTEM READINESS FOR ICU CARE OF ADULTS
There were three levels of consideration for the use of our local pediatric ICU for these patients. First, our institutional policies allow care for adults throughout the system, which we describe in more detail later, in the “Scope of Practice” section. Second, our free-standing pediatric hospital ICUs have accreditation for the care of adults. Third, we developed clear guidelines for subspecialists regarding when adults can safely be admitted or transferred to the pediatric ICU.
Responding to a crisis still necessitates establishing a clear care-escalation plan. An initial barrier may be that some systems do not have a pediatric ICU accredited for care of patients above a certain age. During a crisis, however, as hospital volumes and mortalities rise, states may pursue executive orders, as New York State did, that ease these age restrictions.4 Otherwise, we recommend a clear transfer plan to an adult ICU or emergency credentialing and privileging of adult intensivists. Both of these options may pose challenges during a pandemic because adult ICUs will likely be full.
INSTITUTIONAL SITUATION AWARENESS
Institutional situation awareness for the identification and mitigation of risks inherent in adult care in a pediatric setting is essential for patient safety. Tracking of admitted adult patients via our electronic health record (EHR) occurs daily by an adult care–team member. Our adult care teams partner with physician safety officers and attend daily institutional multidisciplinary safety huddles to create a shared mental model for the care of adult patients. Daily huddle reports include discussion regarding the number of admitted adults, review of illness acuity, consultative advice on management, and contingency planning for potential decompensation.5,6 This integration into institutional huddles has been instrumental in proactively identifying hospitalized adults who are at risk for clinical decompensation and mitigating those risks.
Should a pediatric system admit adults to new sites or units, we recommend leveraging preexisting patient safety infrastructure similarly to identify and mitigate risks. If possible, any institutional communication about adult patients should involve adult-trained staff. Mechanisms for tracking patients will depend on local EHRs but are important to guide regular check-ins with providers caring for those patients.
SCOPE OF PRACTICE
Multiple levels of regulation affect a provider’s scope of practice. The most general of these regulations are state guidelines, followed by local institutional policy. Our institutions require consults for older adults—age varies at our specific institutions—by our adult-care team for assessment of risk and comanagement of adult-specific comorbidities. Additionally, we have agreements with our affiliated adult health facilities that allow in-person adult subspecialty consultation.
While state and institutional policies lay the foundation for pediatric systems considering new adult-care models, provider-level considerations are also needed. Often the patient’s age is a primary consideration, but comorbid conditions also affect the provider’s comfort and ability to care for these patients. We urge practitioners to exercise the full range of their capacities, but also to think critically about the ethical scope of one’s practice. As healthcare providers, it is our duty to hold each other accountable, voice concerns, and advocate to increase health system capacity equitably.7 It’s paramount that channels of communication, in-person or virtual, be arranged for supportive adult subspecialist consultation.
STAFFING CONSIDERATIONS
Med-Peds physicians and advanced practice providers are the foundation of the clinical care provided to adults at our institutions. Our Med-Peds providers practice in both the free-standing pediatric hospital and an affiliated adult health system. They offer expertise in adult clinical care and navigate between pediatric and adult systems when the need arises (eg, adult requiring urgent intervention for an acute myocardial infarction). Adult competencies of other staff must be addressed. For example, our cardiac ICUs include nurses with adult clinical care experience because critically ill adults with congenital heart disease are admitted. Advanced Care Life Support (ACLS) training is also required for staff caring for adults throughout the hospital.
There are many ways, even during a crisis, to develop an adult care model in a pediatric setting. Depending on workforce availability, internal medicine, Med-Peds, family medicine, critical care, and emergency medicine physicians could serve on either a primary service or as a consultant to support pediatrics-trained providers in caring for adults should the patient volume and acuity require staffing restructuring. Adult subspecialty access must be addressed. Telehealth may play a significant role in extending clinicians in all of these clinical roles both during the current crisis but also in underresourced settings.8 A clear process and indication for emergency or temporary credentialing and privileging necessitates understanding and addressing such challenges early. Training in adult care, or lack thereof, for other staff, such as nurses and respiratory therapists, is also crucial to consider.
PATIENT SAFETY
Adults are more likely than children to have comorbidities and clinical deterioration while hospitalized. At our institutions, when a rapid response team is called for an adult patient, an adult care–team provider responds to aid in clinical management and determines the appropriate care setting. Additionally, given that the incidence of coronary artery disease increases starting at age 35 years,9 our systems have developed procedures for managing time-sensitive conditions seen more commonly in adults, such as acute myocardial infarction, stroke, and pulmonary embolism. Despite simulation training for pediatric providers and staff, it is clear that implementing these procedures is highly dependent on involvement of the adult care team.
With the urgency of implementation, pediatric systems should consider increasing the number of providers and staff with ACLS training, especially for rapid response and code teams. Many pediatric systems may need to evaluate how their code carts are stocked and ensure they are equipped with appropriate medication dosages and sizes of supplies. Emergent and accessible adult care will be needed, especially for issues with time-to-intervention criteria like acute myocardial infarction and stroke. Hospitalized adults with COVID-19 may also have a higher incidence of arrhythmia, cardiac ischemia, and stroke.10 Consider proactively simulating common COVID-19–related scenarios to build interdisciplinary teamwork in emergency scenarios. Interhospital agreements and pathways exist for sharing medications. Outreach to pharmacies may be indicated to ensure accessibility for medications not commonly found in pediatric systems.
PATIENT POPULATIONS AND SPECIAL CONSIDERATIONS
Our children’s hospitals care for certain adult populations with chronic conditions of childhood origin because of the availability of subspecialty clinical expertise. Our adult care team aids in contingency planning to help determine place of admission (adult vs pediatric hospital) depending on patient clinical needs and system expertise. For instance, an adult with congenital heart disease may have two cardiologists—one for congenital heart disease and one for coronary artery disease. Patients with an acute issue such as new-onset arrhythmia may be admitted to our pediatric hospital; however, for a stroke they would be admitted to the adult hospital.
While important and tempting to address this issue first, creating criteria to determine which patient population to admit should be a last consideration during a pandemic. Consider if the decision to admit should be determined based on COVID-19 infection status. From there, types of conditions thought to be within the purview of pediatric practice can be considered. These include basic infectious diseases pathology (eg, skin/soft-tissue infections and pyelonephritis) and chronic conditions of childhood origin (eg, cystic fibrosis, diabetes, and inflammatory bowel disease), which have specialty providers who could work across an extended age range. Conditions potentially more challenging to safely care for in pediatric facilities include acute cardiac conditions (eg, angina, acute coronary syndrome, and arrhythmias), alcohol withdrawal, end-stage liver or kidney disease, and gastrointestinal bleeds. Considerations need to be made for research protocols and novel therapies only available at adult institutions. Through this whole process, it is especially crucial to note care equity and ensure that all patients have access to the highest attainable care possible.
CONCLUSION
Policymakers at pediatric facilities should think critically about their institution’s capacity to manage adults. In some circumstances, the decision might be to not admit adult patients based on the factors discussed in this paper or other contextual factors of the local healthcare systems. Our role in providing care for adults in pediatric hospitals involves not only ensuring age-appropriate care, but also in supporting patients and other healthcare providers to navigate a fragmented health system. Our adult-care models required building relationships between pediatric and adult health systems. Building these relationships in the setting of crisis can strengthen health systems and healthcare communities beyond the era of COVID-19. Because it’s promoted enhanced collaboration between pediatric and adult facilities, COVID-19 can be a platform to build a better system to support our already vulnerable young adults with chronic conditions of childhood origin for years to come.
Health systems around the world have been called upon to expand acute care capacity to manage the current and projected surge of adults with COVID-19, the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 There has been mixed guidance on how pediatric facilities should consolidate and coordinate pediatric care in a way that optimizes the capacity of hospital beds, staff, and supplies, such as ventilators and medications, for both adults and children in a community.2 Furthermore, if and how these pediatric facilities should expand capacity to care for adult patients safely is uncertain.
For the last 5 years, both Boston Children’s Hospital and Cincinnati Children’s Hospital Medical Center have been caring for specific adult populations in free-standing pediatric hospitals because of the increasing prevalence of young adults with rare, complex, and historically fatal conditions (eg, chromosomal abnormalities). In the past, low life expectancies for children with such conditions contributed to the evolution of specialized care in pediatric health systems that often does not exist in adult health systems. Our teams in Boston and Cincinnati have gained insight into the multifaceted infrastructure and teams necessary to provide safe care for adults hospitalized in a pediatric setting.
In this perspective piece, we will highlight important principles that pediatric facilities and providers should prioritize if they anticipate caring for hospitalized adults during this pandemic. Designing and implementing an adult care model requires iteratively addressing the following key areas: development of a multistakeholder team, system readiness for intensive care unit (ICU) care of adults, institutional situation awareness, scope of practice, staffing considerations, patient safety, and patient populations and special considerations (eg, adults with chronic conditions of childhood onset). With these areas in mind, pediatric facilities should then consider whether they have the capacity to manage hospitalized adults.
DEVELOPMENT OF A MULTISTAKEHOLDER TEAM
Providing care for any hospitalized patient requires engagement with many health system stakeholders. By involving key stakeholders early in the planning process for our adult care model, we were able to anticipate potential obstacles when caring for a unique subset of patients and gain support of multidisciplinary partners. For instance, inclusion of bedside and support staff highlighted specific needs, such as nurses with adult training and a revised formulary to include common adult medications (eg, clopidogrel for adults with a drug-eluting stent).
Responding to the surge of hospitalized adult patients will require increasing hospital capacity.3 In pediatric settings, this will require consideration of innovative care models. These care models may include pediatric systems flexing to care for adult patients. We recommend hospital leaders from both pediatric and adult facilities have formal discussions on the best ways for pediatric facilities to respond to serve their local population. Inclusion of other key stakeholders will ensure factors imperative to the safe care of adults will not be missed.
SYSTEM READINESS FOR ICU CARE OF ADULTS
There were three levels of consideration for the use of our local pediatric ICU for these patients. First, our institutional policies allow care for adults throughout the system, which we describe in more detail later, in the “Scope of Practice” section. Second, our free-standing pediatric hospital ICUs have accreditation for the care of adults. Third, we developed clear guidelines for subspecialists regarding when adults can safely be admitted or transferred to the pediatric ICU.
Responding to a crisis still necessitates establishing a clear care-escalation plan. An initial barrier may be that some systems do not have a pediatric ICU accredited for care of patients above a certain age. During a crisis, however, as hospital volumes and mortalities rise, states may pursue executive orders, as New York State did, that ease these age restrictions.4 Otherwise, we recommend a clear transfer plan to an adult ICU or emergency credentialing and privileging of adult intensivists. Both of these options may pose challenges during a pandemic because adult ICUs will likely be full.
INSTITUTIONAL SITUATION AWARENESS
Institutional situation awareness for the identification and mitigation of risks inherent in adult care in a pediatric setting is essential for patient safety. Tracking of admitted adult patients via our electronic health record (EHR) occurs daily by an adult care–team member. Our adult care teams partner with physician safety officers and attend daily institutional multidisciplinary safety huddles to create a shared mental model for the care of adult patients. Daily huddle reports include discussion regarding the number of admitted adults, review of illness acuity, consultative advice on management, and contingency planning for potential decompensation.5,6 This integration into institutional huddles has been instrumental in proactively identifying hospitalized adults who are at risk for clinical decompensation and mitigating those risks.
Should a pediatric system admit adults to new sites or units, we recommend leveraging preexisting patient safety infrastructure similarly to identify and mitigate risks. If possible, any institutional communication about adult patients should involve adult-trained staff. Mechanisms for tracking patients will depend on local EHRs but are important to guide regular check-ins with providers caring for those patients.
SCOPE OF PRACTICE
Multiple levels of regulation affect a provider’s scope of practice. The most general of these regulations are state guidelines, followed by local institutional policy. Our institutions require consults for older adults—age varies at our specific institutions—by our adult-care team for assessment of risk and comanagement of adult-specific comorbidities. Additionally, we have agreements with our affiliated adult health facilities that allow in-person adult subspecialty consultation.
While state and institutional policies lay the foundation for pediatric systems considering new adult-care models, provider-level considerations are also needed. Often the patient’s age is a primary consideration, but comorbid conditions also affect the provider’s comfort and ability to care for these patients. We urge practitioners to exercise the full range of their capacities, but also to think critically about the ethical scope of one’s practice. As healthcare providers, it is our duty to hold each other accountable, voice concerns, and advocate to increase health system capacity equitably.7 It’s paramount that channels of communication, in-person or virtual, be arranged for supportive adult subspecialist consultation.
STAFFING CONSIDERATIONS
Med-Peds physicians and advanced practice providers are the foundation of the clinical care provided to adults at our institutions. Our Med-Peds providers practice in both the free-standing pediatric hospital and an affiliated adult health system. They offer expertise in adult clinical care and navigate between pediatric and adult systems when the need arises (eg, adult requiring urgent intervention for an acute myocardial infarction). Adult competencies of other staff must be addressed. For example, our cardiac ICUs include nurses with adult clinical care experience because critically ill adults with congenital heart disease are admitted. Advanced Care Life Support (ACLS) training is also required for staff caring for adults throughout the hospital.
There are many ways, even during a crisis, to develop an adult care model in a pediatric setting. Depending on workforce availability, internal medicine, Med-Peds, family medicine, critical care, and emergency medicine physicians could serve on either a primary service or as a consultant to support pediatrics-trained providers in caring for adults should the patient volume and acuity require staffing restructuring. Adult subspecialty access must be addressed. Telehealth may play a significant role in extending clinicians in all of these clinical roles both during the current crisis but also in underresourced settings.8 A clear process and indication for emergency or temporary credentialing and privileging necessitates understanding and addressing such challenges early. Training in adult care, or lack thereof, for other staff, such as nurses and respiratory therapists, is also crucial to consider.
PATIENT SAFETY
Adults are more likely than children to have comorbidities and clinical deterioration while hospitalized. At our institutions, when a rapid response team is called for an adult patient, an adult care–team provider responds to aid in clinical management and determines the appropriate care setting. Additionally, given that the incidence of coronary artery disease increases starting at age 35 years,9 our systems have developed procedures for managing time-sensitive conditions seen more commonly in adults, such as acute myocardial infarction, stroke, and pulmonary embolism. Despite simulation training for pediatric providers and staff, it is clear that implementing these procedures is highly dependent on involvement of the adult care team.
With the urgency of implementation, pediatric systems should consider increasing the number of providers and staff with ACLS training, especially for rapid response and code teams. Many pediatric systems may need to evaluate how their code carts are stocked and ensure they are equipped with appropriate medication dosages and sizes of supplies. Emergent and accessible adult care will be needed, especially for issues with time-to-intervention criteria like acute myocardial infarction and stroke. Hospitalized adults with COVID-19 may also have a higher incidence of arrhythmia, cardiac ischemia, and stroke.10 Consider proactively simulating common COVID-19–related scenarios to build interdisciplinary teamwork in emergency scenarios. Interhospital agreements and pathways exist for sharing medications. Outreach to pharmacies may be indicated to ensure accessibility for medications not commonly found in pediatric systems.
PATIENT POPULATIONS AND SPECIAL CONSIDERATIONS
Our children’s hospitals care for certain adult populations with chronic conditions of childhood origin because of the availability of subspecialty clinical expertise. Our adult care team aids in contingency planning to help determine place of admission (adult vs pediatric hospital) depending on patient clinical needs and system expertise. For instance, an adult with congenital heart disease may have two cardiologists—one for congenital heart disease and one for coronary artery disease. Patients with an acute issue such as new-onset arrhythmia may be admitted to our pediatric hospital; however, for a stroke they would be admitted to the adult hospital.
While important and tempting to address this issue first, creating criteria to determine which patient population to admit should be a last consideration during a pandemic. Consider if the decision to admit should be determined based on COVID-19 infection status. From there, types of conditions thought to be within the purview of pediatric practice can be considered. These include basic infectious diseases pathology (eg, skin/soft-tissue infections and pyelonephritis) and chronic conditions of childhood origin (eg, cystic fibrosis, diabetes, and inflammatory bowel disease), which have specialty providers who could work across an extended age range. Conditions potentially more challenging to safely care for in pediatric facilities include acute cardiac conditions (eg, angina, acute coronary syndrome, and arrhythmias), alcohol withdrawal, end-stage liver or kidney disease, and gastrointestinal bleeds. Considerations need to be made for research protocols and novel therapies only available at adult institutions. Through this whole process, it is especially crucial to note care equity and ensure that all patients have access to the highest attainable care possible.
CONCLUSION
Policymakers at pediatric facilities should think critically about their institution’s capacity to manage adults. In some circumstances, the decision might be to not admit adult patients based on the factors discussed in this paper or other contextual factors of the local healthcare systems. Our role in providing care for adults in pediatric hospitals involves not only ensuring age-appropriate care, but also in supporting patients and other healthcare providers to navigate a fragmented health system. Our adult-care models required building relationships between pediatric and adult health systems. Building these relationships in the setting of crisis can strengthen health systems and healthcare communities beyond the era of COVID-19. Because it’s promoted enhanced collaboration between pediatric and adult facilities, COVID-19 can be a platform to build a better system to support our already vulnerable young adults with chronic conditions of childhood origin for years to come.
1. Cavallo JJ, Donoho DA, Forman HP. Hospital capacity and operations in the coronavirus disease 2019 (COVID-19) Pandemic—planning for the Nth patient. JAMA Health Forum. 2020;1(3):e200345. https://jamanetwork.com/channels/health-forum/fullarticle/2763353. Accessed March 30, 2020.
2. Children’s Hospital Association. Consolidating Pediatric Hospital Care to Increase Capacity for Adults with COVID-19. https://www.childrenshospitals.org/Quality-and-Performance/COVID19/Resources/Consolidating-Pediatric-Hospital-Care-Increase-Capacity-Adults-COVID19. Accessed March 28, 2020.
3. Campbell J. Andrew Cuomo’s order to hospitals: expand capacity or face state takeover. Democrat & Chronicle. April 1, 2020. https://www.democratandchronicle.com/story/news/politics/albany/2020/04/01/coronavirus-cuomo-order-state-hospital-takeover/5100134002/. Accessed April 2, 2020.
4. New York State Education Department, Office of the Professions. COVID-19 Executive Orders. http://www.op.nysed.gov/COVID-19_EO.html. Accessed April 2, 2020.
5. Brady PW, Muething S, Kotagal U, et al. Improving situation awareness to reduce unrecognized clinical deterioration and serious safety events. Pediatrics. 2013;131(1):e298-e308. https://doi.org/10.1542/peds.2012-1364.
6. Conway-Habes EE, Herbst BF, Herbst LA, et al. Using quality improvement to introduce and standardize the National Early Warning Score (NEWS) for adult inpatients at a children’s hospital. Hosp Pediatr. 2017;7(3):156-163. https://doi.org/10.1542/hpeds.2016-0117.
7. Berry JG, Bloom S, Foley S, Palfrey JS. Health inequity in children and youth with chronic health conditions. Pediatrics. 2010;126(Suppl 3):S111-S119. https://doi.org/10.1542/peds.2010-1466D.
8. Smith AC, Thomas E, Snoswell CL, et al. Telehealth for global emergencies: implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020:1357633X20916567. https://doi.org/10.1177/1357633X20916567.
9. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139-e596. https://doi.org/10.1161/CIR.0000000000000757.
10. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648.
1. Cavallo JJ, Donoho DA, Forman HP. Hospital capacity and operations in the coronavirus disease 2019 (COVID-19) Pandemic—planning for the Nth patient. JAMA Health Forum. 2020;1(3):e200345. https://jamanetwork.com/channels/health-forum/fullarticle/2763353. Accessed March 30, 2020.
2. Children’s Hospital Association. Consolidating Pediatric Hospital Care to Increase Capacity for Adults with COVID-19. https://www.childrenshospitals.org/Quality-and-Performance/COVID19/Resources/Consolidating-Pediatric-Hospital-Care-Increase-Capacity-Adults-COVID19. Accessed March 28, 2020.
3. Campbell J. Andrew Cuomo’s order to hospitals: expand capacity or face state takeover. Democrat & Chronicle. April 1, 2020. https://www.democratandchronicle.com/story/news/politics/albany/2020/04/01/coronavirus-cuomo-order-state-hospital-takeover/5100134002/. Accessed April 2, 2020.
4. New York State Education Department, Office of the Professions. COVID-19 Executive Orders. http://www.op.nysed.gov/COVID-19_EO.html. Accessed April 2, 2020.
5. Brady PW, Muething S, Kotagal U, et al. Improving situation awareness to reduce unrecognized clinical deterioration and serious safety events. Pediatrics. 2013;131(1):e298-e308. https://doi.org/10.1542/peds.2012-1364.
6. Conway-Habes EE, Herbst BF, Herbst LA, et al. Using quality improvement to introduce and standardize the National Early Warning Score (NEWS) for adult inpatients at a children’s hospital. Hosp Pediatr. 2017;7(3):156-163. https://doi.org/10.1542/hpeds.2016-0117.
7. Berry JG, Bloom S, Foley S, Palfrey JS. Health inequity in children and youth with chronic health conditions. Pediatrics. 2010;126(Suppl 3):S111-S119. https://doi.org/10.1542/peds.2010-1466D.
8. Smith AC, Thomas E, Snoswell CL, et al. Telehealth for global emergencies: implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020:1357633X20916567. https://doi.org/10.1177/1357633X20916567.
9. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139-e596. https://doi.org/10.1161/CIR.0000000000000757.
10. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648.
© 2020 Society of Hospital Medicine
Finding the Value in Personal Protective Equipment for Hospitalized Patients During a Pandemic and Beyond
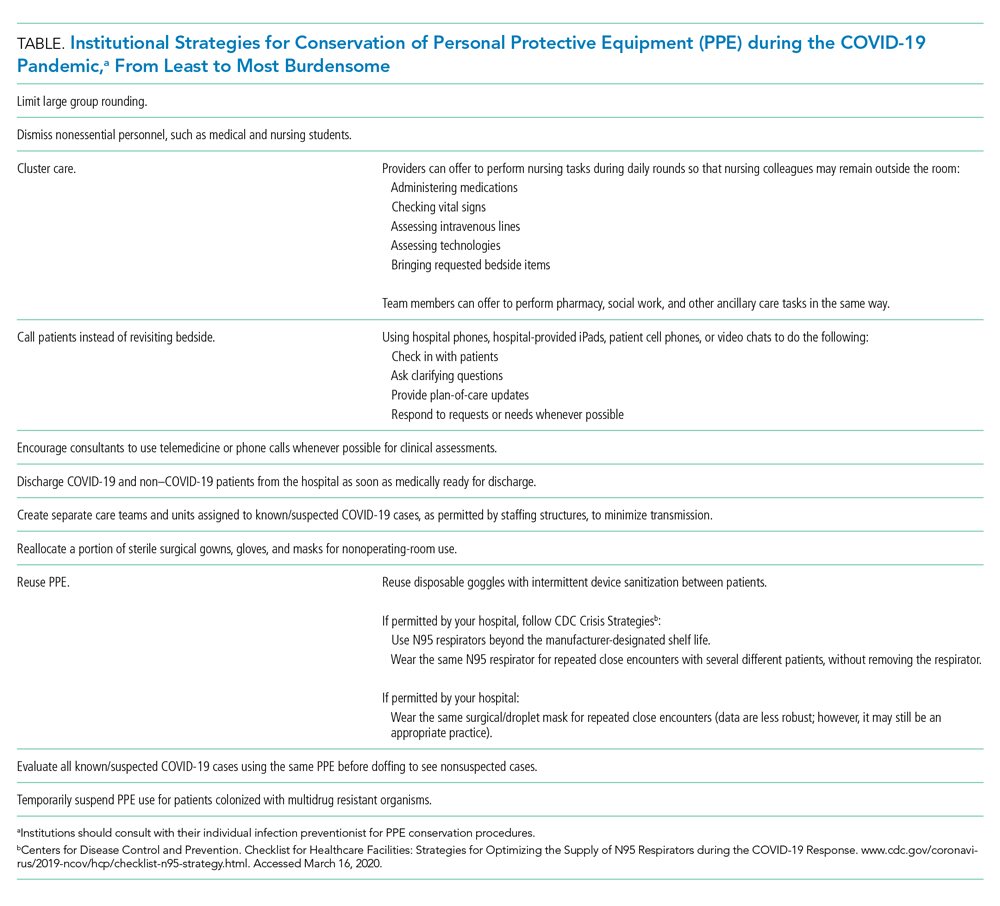
Due to the pandemic spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the cause of COVID-19 infection, there is significant disruption to the global supply of PPE.2 Order volumes of PPE have increased, prices have surged, and distributors are experiencing challenges meeting order demands.3 With decreased overseas exports, suppliers have placed hospitals on PPE allocations, and many hospitals’ orders for PPE have been only partially filled.3,4 Unless hospitals have established stockpiles, most only have supplies for 3-7 days of routine use, leaving them vulnerable to exhausting PPE supplies. At the onset of the pandemic, 86% of United States hospitals reported concerns about their PPE supply.4
The potential for PPE shortages has led both the Centers for Disease Control and Prevention (CDC) and the World Health Organization to call for the rational and appropriate use of PPE in order to conserve supplies.2,3 By the time COVID-19 was declared a pandemic, 54% of hospitals had imposed PPE conservation protocols,4 with more expected to follow in the weeks and months to come. Innovative protocols have been conceptualized and used to conserve PPE in hospitals (Table).
Yet these conservation protocols often fail to identify missed opportunities to improve the value of PPE that already exist in hospital care. By defining the value of inpatient PPE, hospitals can identify opportunities for value improvement. Changes implemented now will maximize PPE value and preserve supply during this pandemic and beyond.
THE VALUE OF PPE
In order to conserve PPE supply, hospitals might consider limiting PPE to cases in which clear evidence exists to support its use. However, evidence for PPE use can be challenging to interpret because the impact of preventing nosocomial infections (an outcome that did not occur) is inherently problematic to measure. This makes assessing the value of PPE in preventing nosocomial transmission in specific situations difficult.
The basis of using PPE is its effectiveness in controlling outbreaks.1 A meta-analysis of 6 case-control studies from the SARS outbreak of 2003, which disproportionately infected healthcare workers, suggested that handwashing and PPE were effective in preventing disease transmission. Handwashing alone reduced transmission by 55%, wearing gloves by 57%, and wearing facemasks by 68%; the cumulative effect of handwashing, masks, gloves, and gowns reduced transmission by 91%.5 A cohort study of healthcare workers exposed to H1N1 influenza A in 2009 found that use of a facemask or an N95 respirator was associated with negative viral serology suggesting noninfected status.6 With respiratory syncytial virus (RSV) outbreaks, a narrative synthesis of 4 studies examining transmission also suggested gowns, facemasks, and eye protection are effective, with eye protection perhaps more effective than gowns and masks.7 Yet these studies’ conclusions are limited by study design differences and small sample sizes.
The evidence supporting PPE use for routine hospital conditions is more challenging to interpret. One pediatric study of seasonal respiratory viruses showed that adding droplet precautions to an existing policy of contact precautions alone decreased nosocomial infections for most viruses evaluated.8 Yet this study, like many of PPE use, is limited by sample size and possible misclassification of exposure and outcome biases. Because PPE is always utilized in conjunction with other preventive measures, isolating the impact of PPE is challenging, let alone isolating the individual effects of PPE components. In the absence of strong empirical evidence, hospitals must rely on the inherent rationale of PPE use for patient and healthcare worker safety in assessing its value.
In order to protect patients from disease transmission during a pandemic, hospitals might also reconsider whether to use PPE in cases in which evidence is absent, such as routine prevention for colonized but noninfected patients. However, evidence of the possible patient harms of PPE are emerging. Healthcare providers spend less time with isolated patients9,10 and document fewer vital signs.11 Patients in PPE may experience delays in admission12 and discharge,13 and have higher rates of falls, pressure ulcers, and medication errors.14,15 They may also experience higher rates of anxiety and depression.16 Yet no evidence suggests PPE use for noninfected patients prevents transmission to patients or to healthcare workers. Using PPE when it is not indicated deemphasizes the value of other preventative precautions (eg, handwashing), unnecessarily depletes PPE supply, and may create patient harm without added benefit. High-value PPE, both during a pandemic and beyond, is defined by a system designed so that healthcare workers use PPE when they need it, and do not use PPE when not indicated.
ORDERING PPE IN A COMPLEX HEALTHCARE ENVIRONMENT
While all hospitalized patients are admitted using standard precautions, decisions surrounding PPE can be nuanced for even experienced clinicians. Although the CDC does provide guidance for PPE use based on symptoms that correlate with potential for transmission (eg, patients with cough should be placed in at least droplet precautions),1 guidelines must rely on provider evaluation and interpretation. For instance, three etiologies of cough—pneumococcal pneumonia, RSV bronchiolitis, and pulmonary tuberculosis—would all require different PPE. The clinician must weigh the probabilities of each pathogen and assess the harm of not protecting against certain pathogens in his or her decision.
Amidst the stress and cognitive burdens placed on clinicians, accuracy in PPE decisions is easily deprioritized. Clinicians may not completely consider patient-specific indications for PPE, implications for patients and staff, and supply shortages. Although the CDC and many hospitals have PPE initiation and discontinuation criteria, clinicians may favor educated guesswork and reliance on past experience when guidelines are poorly accessible or poorly searchable. Such individual, nonstandardized decisions likely lead to variability in practice patterns, inaccuracies in PPE decisions, and ultimately waste of PPE resources.
WHERE OUR HOSPITAL USES PPE IN A LOW-VALUE WAY
At our institution, the inconveniences, cognitive burden, and perceived benefit of routine PPE interventions have created a system in which PPE is regularly overused. On our hospital medicine wards, we found that PPE was both over-ordered upon admission (eg, contact/droplet precautions ordered for influenza when droplet precautions only would have sufficed) and unnecessarily continued even after children met discontinuation criteria.
On discharge review from our general pediatric ward in 2019, 18% of children discharged with PPE orders no longer met criteria for PPE. Two conditions—community-acquired bacterial pneumonia and skin and soft-tissue infections—accounted for 47% of discharges with unnecessary PPE orders. At an estimated cost of $0.13-$0.53 for droplet precautions per use, $0.69 for contact precautions, and $0.82-$1.22 for both, the absolute cost of continuing PPE without indication could be as high as $61/day per patient when estimating 50 uses per day. This direct cost represents healthcare spending without added value when PPE are not necessary. Furthermore, the additional emotional cost to the patient and family in their hospitalization experience, the cost of clinician time donning and doffing, the environmental cost of PPE waste, and the cost to the limited PPE supply are not considered in these calculations.
During a pandemic characterized by PPE shortages nationwide, allowing missed opportunities for PPE discontinuation to persist is not only wasteful, but inattentive to public health.
OPPORTUNITIES FOR HOSPITALS TO MAXIMIZE THE VALUE OF PPE
For individual clinicians, opportunities exist to improve PPE usage in daily patient care. Clinicians should not overlook PPE decisions; instead they should make it a practice to review PPE orders daily during rounds as they would lab orders. Clinicians and nursing staff should work together to identify PPE discontinuation opportunities, leveraging the electronic medical record when possible. For the benefit of patients and families, clinicians and bedside staff should recognize and assist in managing patient expectations of PPE.
Hospitals should work to make PPE references easily accessible and interpretable by frontline clinicians. To minimize variability of use, PPE ordering for routine conditions should be standardized and streamlined, including discontinuation criteria. Hospitals should invest in behavioral health programs to support patients with conditions necessitating PPE and develop policies to ensure ancillary services are equally available to all patients. To alleviate concerns about limited clinician time spent with isolated patients, hospitals should assign clinician workloads while accounting for the known increased time needed to care for patients with PPE.
For hospitals with extreme supply shortages, conservation might include decreased use of PPE for conditions in which its use is controversial (eg, patients colonized with methicillin-resistant Staphylococcus aureus or multidrug resistant organisms) as has been trialed in institutions prior to this pandemic.17,18 Such PPE policy changes might occur in addition to, or in conjunction with, the conservation strategies suggested by other institutions (Table).
Healthcare systems should continually reassess the value of PPE for their hospitals and make changes accordingly. In the midst of difficulties directly demonstrating PPE’s value, hospitals must rely on the inherent rationale of PPE use in assessing value decisions weighed against harms while balancing healthcare worker protection regulations. Decisions should always occur while continuing other sensible infection-control procedures, such as handwashing and environmental hygiene measures.
To effect maximal change, healthcare systems should invest in redesigning PPE ordering systems at the highest level. This should include harnessing existing technologies to streamline PPE ordering decisions to meet clinicians’ cognitive needs. Decision support and auditing technologies could automate and monitor PPE orders efficiently. Likely to be most effective, an investment in creating and maintaining centralized PPE expert management teams to assess, order, and discontinue PPE would minimize individual ordering variation, minimize cost, and maximize value to patients, staff, and hospitals.
CONCLUSION
In this pandemic, we have the opportunity to rethink how we understand and use PPE in hospitalized patients. It is vitally important now more than ever to consciously conserve the limited supply of PPE resources. As we seek to increase healthcare value while limiting overuse and waste, PPE is a prime target for value improvement efforts as the effective but also burdensome tool that it is. Hospitalists are well-positioned to lead the redesign of how, when, and why PPE is used and to create a more optimized, lasting system that provides maximal value to patients, families, and healthcare workers during this current crisis and beyond.
1. Siegel JD, Rhinehart E, Jackson M, Chiarello L. 2007 Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control. 2007;35(10 Suppl 2):S65-164. https://doi.org/10.1016/j.ajic.2007.10.007.
2. World Health Organization. Shortage of personal protective equipment endangering health workers worldwide. https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide. Accessed March 12, 2020.
3. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19): healthcare supply of personal protective equipment. https://www.cdc.gov/coronavirus/2019-ncov/hcp/healthcare-supply-ppe.html. Accessed March 12, 2020.
4. Premier Inc. Premier Inc survey finds 86 percent of health systems are concerned about personal protective equipment shortages due to coronavirus. https://www.premierinc.com/newsroom/press-releases/premier-inc-survey-finds-86-percent-of-health-systems-are-concerned-about-personal-protective-equipment-shortages-due-to-coronavirus. Accessed March 22, 2020.
5. Jefferson T, Foxlee R, Del Mar C, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ. 2008;336(7635):77-80. https://doi.org/10.1136/bmj.39393.510347.BE.
6. Jaeger JL, Patel M, Dharan N, et al. Transmission of 2009 pandemic influenza A (H1N1) virus among healthcare personnel-Southern California, 2009. Infect Control Hosp Epidemiol. 2011;32(12):1149-1157. https://doi.org/10.1086/662709.
7. French CE, McKenzie BC, Coope C, et al. Risk of nosocomial respiratory syncytial virus infection and effectiveness of control measures to prevent transmission events: a systematic review. Influenza Other Respir Viruses. 2016;10(4):268-290. https://doi.org/10.1111/irv.12379.
8. Rubin LG, Kohn N, Nullet S, Hill M. Reduction in rate of nosocomial respiratory virus infections in a children’s hospital associated with enhanced isolation precautions. Infect Control Hosp Epidemiol. 2018;39(2):152-156. https://doi.org/10.1017/ice.2017.282.
9. Dashiell-Earp CN, Bell DS, Ang AO, Uslan DZ. Do physicians spend less time with patients in contact isolation?: A time-motion study of internal medicine interns. JAMA Intern Med. 2014;174(5):814-815. https://doi.org/10.1001/jamainternmed.2014.537.
10. Saint S, Higgins LA, Nallamothu BK, Chenoweth C. Do physicians examine patients in contact isolation less frequently? A brief report. Am J Infect Control. 2003;31(6):354-356. https://doi.org/10.1016/S0196-6553(02)48250-8.
11. Kirkland KB, Weinstein JM. Adverse effects of contact isolation. Lancet. 1999(354):1177-1178. https://doi.org/10.1016/S0140-6736(99)04196-3.
12. McLemore A, Bearman G, Edmond MB. Effect of contact precautions on wait time from emergency room disposition to inpatient admission. Infect Control Hosp Epidemiol. 2011;32(3):298-299. https://doi.org/10.1086/658913.
13. Tran K, Bell C, Stall N, et al. The effect of hospital isolation precautions on patient outcomes and cost of care: a multi-site, retrospective, propensity score-matched cohort study. J Gen Intern Med. 2017;32(3):262-268. https://doi.org/10.1007/s11606-016-3862-4.
14. Karki S, Leder K, Cheng AC. Patients under contact precautions have an increased risk of injuries and medication errors: a retrospective cohort study. Infect Control Hosp Epidemiol. 2013;34(10):1118-1120. https://doi.org/10.1086/673153.
15. Stelfox HT, Bates DW, Redelmeier DA. Safety of patients isolated for infection control. JAMA. 2003;290(14):1899-1905. https://doi.org/10.1001/jama.290.14.1899.
16. Catalano G, Houston SH, Catalano MC, et al. Anxiety and depression in hospitalized patients in resistant organism isolation. South Med J. 2003;96(2):141-145. https://doi.org/10.1097/01.SMJ.0000050683.36014.2E.
17. Young K, Doernberg SB, Snedecor RF, Mallin E. Things we do for no reason: contact precautions for MRSA and VRE. J Hosp Med. 2019;14(3):178-180. https://doi.org/10.12788/jhm.3126.
18. Bearman G, Abbas S, Masroor N, et al. Impact of discontinuing contact precautions for methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus: an interrupted time series analysis. Infect Control Hosp Epidemiol. 2018;39(6):676-682. https://doi.org/10.1017/ice.2018.57.
Due to the pandemic spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the cause of COVID-19 infection, there is significant disruption to the global supply of PPE.2 Order volumes of PPE have increased, prices have surged, and distributors are experiencing challenges meeting order demands.3 With decreased overseas exports, suppliers have placed hospitals on PPE allocations, and many hospitals’ orders for PPE have been only partially filled.3,4 Unless hospitals have established stockpiles, most only have supplies for 3-7 days of routine use, leaving them vulnerable to exhausting PPE supplies. At the onset of the pandemic, 86% of United States hospitals reported concerns about their PPE supply.4
The potential for PPE shortages has led both the Centers for Disease Control and Prevention (CDC) and the World Health Organization to call for the rational and appropriate use of PPE in order to conserve supplies.2,3 By the time COVID-19 was declared a pandemic, 54% of hospitals had imposed PPE conservation protocols,4 with more expected to follow in the weeks and months to come. Innovative protocols have been conceptualized and used to conserve PPE in hospitals (Table).
Yet these conservation protocols often fail to identify missed opportunities to improve the value of PPE that already exist in hospital care. By defining the value of inpatient PPE, hospitals can identify opportunities for value improvement. Changes implemented now will maximize PPE value and preserve supply during this pandemic and beyond.
THE VALUE OF PPE
In order to conserve PPE supply, hospitals might consider limiting PPE to cases in which clear evidence exists to support its use. However, evidence for PPE use can be challenging to interpret because the impact of preventing nosocomial infections (an outcome that did not occur) is inherently problematic to measure. This makes assessing the value of PPE in preventing nosocomial transmission in specific situations difficult.
The basis of using PPE is its effectiveness in controlling outbreaks.1 A meta-analysis of 6 case-control studies from the SARS outbreak of 2003, which disproportionately infected healthcare workers, suggested that handwashing and PPE were effective in preventing disease transmission. Handwashing alone reduced transmission by 55%, wearing gloves by 57%, and wearing facemasks by 68%; the cumulative effect of handwashing, masks, gloves, and gowns reduced transmission by 91%.5 A cohort study of healthcare workers exposed to H1N1 influenza A in 2009 found that use of a facemask or an N95 respirator was associated with negative viral serology suggesting noninfected status.6 With respiratory syncytial virus (RSV) outbreaks, a narrative synthesis of 4 studies examining transmission also suggested gowns, facemasks, and eye protection are effective, with eye protection perhaps more effective than gowns and masks.7 Yet these studies’ conclusions are limited by study design differences and small sample sizes.
The evidence supporting PPE use for routine hospital conditions is more challenging to interpret. One pediatric study of seasonal respiratory viruses showed that adding droplet precautions to an existing policy of contact precautions alone decreased nosocomial infections for most viruses evaluated.8 Yet this study, like many of PPE use, is limited by sample size and possible misclassification of exposure and outcome biases. Because PPE is always utilized in conjunction with other preventive measures, isolating the impact of PPE is challenging, let alone isolating the individual effects of PPE components. In the absence of strong empirical evidence, hospitals must rely on the inherent rationale of PPE use for patient and healthcare worker safety in assessing its value.
In order to protect patients from disease transmission during a pandemic, hospitals might also reconsider whether to use PPE in cases in which evidence is absent, such as routine prevention for colonized but noninfected patients. However, evidence of the possible patient harms of PPE are emerging. Healthcare providers spend less time with isolated patients9,10 and document fewer vital signs.11 Patients in PPE may experience delays in admission12 and discharge,13 and have higher rates of falls, pressure ulcers, and medication errors.14,15 They may also experience higher rates of anxiety and depression.16 Yet no evidence suggests PPE use for noninfected patients prevents transmission to patients or to healthcare workers. Using PPE when it is not indicated deemphasizes the value of other preventative precautions (eg, handwashing), unnecessarily depletes PPE supply, and may create patient harm without added benefit. High-value PPE, both during a pandemic and beyond, is defined by a system designed so that healthcare workers use PPE when they need it, and do not use PPE when not indicated.
ORDERING PPE IN A COMPLEX HEALTHCARE ENVIRONMENT
While all hospitalized patients are admitted using standard precautions, decisions surrounding PPE can be nuanced for even experienced clinicians. Although the CDC does provide guidance for PPE use based on symptoms that correlate with potential for transmission (eg, patients with cough should be placed in at least droplet precautions),1 guidelines must rely on provider evaluation and interpretation. For instance, three etiologies of cough—pneumococcal pneumonia, RSV bronchiolitis, and pulmonary tuberculosis—would all require different PPE. The clinician must weigh the probabilities of each pathogen and assess the harm of not protecting against certain pathogens in his or her decision.
Amidst the stress and cognitive burdens placed on clinicians, accuracy in PPE decisions is easily deprioritized. Clinicians may not completely consider patient-specific indications for PPE, implications for patients and staff, and supply shortages. Although the CDC and many hospitals have PPE initiation and discontinuation criteria, clinicians may favor educated guesswork and reliance on past experience when guidelines are poorly accessible or poorly searchable. Such individual, nonstandardized decisions likely lead to variability in practice patterns, inaccuracies in PPE decisions, and ultimately waste of PPE resources.
WHERE OUR HOSPITAL USES PPE IN A LOW-VALUE WAY
At our institution, the inconveniences, cognitive burden, and perceived benefit of routine PPE interventions have created a system in which PPE is regularly overused. On our hospital medicine wards, we found that PPE was both over-ordered upon admission (eg, contact/droplet precautions ordered for influenza when droplet precautions only would have sufficed) and unnecessarily continued even after children met discontinuation criteria.
On discharge review from our general pediatric ward in 2019, 18% of children discharged with PPE orders no longer met criteria for PPE. Two conditions—community-acquired bacterial pneumonia and skin and soft-tissue infections—accounted for 47% of discharges with unnecessary PPE orders. At an estimated cost of $0.13-$0.53 for droplet precautions per use, $0.69 for contact precautions, and $0.82-$1.22 for both, the absolute cost of continuing PPE without indication could be as high as $61/day per patient when estimating 50 uses per day. This direct cost represents healthcare spending without added value when PPE are not necessary. Furthermore, the additional emotional cost to the patient and family in their hospitalization experience, the cost of clinician time donning and doffing, the environmental cost of PPE waste, and the cost to the limited PPE supply are not considered in these calculations.
During a pandemic characterized by PPE shortages nationwide, allowing missed opportunities for PPE discontinuation to persist is not only wasteful, but inattentive to public health.
OPPORTUNITIES FOR HOSPITALS TO MAXIMIZE THE VALUE OF PPE
For individual clinicians, opportunities exist to improve PPE usage in daily patient care. Clinicians should not overlook PPE decisions; instead they should make it a practice to review PPE orders daily during rounds as they would lab orders. Clinicians and nursing staff should work together to identify PPE discontinuation opportunities, leveraging the electronic medical record when possible. For the benefit of patients and families, clinicians and bedside staff should recognize and assist in managing patient expectations of PPE.
Hospitals should work to make PPE references easily accessible and interpretable by frontline clinicians. To minimize variability of use, PPE ordering for routine conditions should be standardized and streamlined, including discontinuation criteria. Hospitals should invest in behavioral health programs to support patients with conditions necessitating PPE and develop policies to ensure ancillary services are equally available to all patients. To alleviate concerns about limited clinician time spent with isolated patients, hospitals should assign clinician workloads while accounting for the known increased time needed to care for patients with PPE.
For hospitals with extreme supply shortages, conservation might include decreased use of PPE for conditions in which its use is controversial (eg, patients colonized with methicillin-resistant Staphylococcus aureus or multidrug resistant organisms) as has been trialed in institutions prior to this pandemic.17,18 Such PPE policy changes might occur in addition to, or in conjunction with, the conservation strategies suggested by other institutions (Table).
Healthcare systems should continually reassess the value of PPE for their hospitals and make changes accordingly. In the midst of difficulties directly demonstrating PPE’s value, hospitals must rely on the inherent rationale of PPE use in assessing value decisions weighed against harms while balancing healthcare worker protection regulations. Decisions should always occur while continuing other sensible infection-control procedures, such as handwashing and environmental hygiene measures.
To effect maximal change, healthcare systems should invest in redesigning PPE ordering systems at the highest level. This should include harnessing existing technologies to streamline PPE ordering decisions to meet clinicians’ cognitive needs. Decision support and auditing technologies could automate and monitor PPE orders efficiently. Likely to be most effective, an investment in creating and maintaining centralized PPE expert management teams to assess, order, and discontinue PPE would minimize individual ordering variation, minimize cost, and maximize value to patients, staff, and hospitals.
CONCLUSION
In this pandemic, we have the opportunity to rethink how we understand and use PPE in hospitalized patients. It is vitally important now more than ever to consciously conserve the limited supply of PPE resources. As we seek to increase healthcare value while limiting overuse and waste, PPE is a prime target for value improvement efforts as the effective but also burdensome tool that it is. Hospitalists are well-positioned to lead the redesign of how, when, and why PPE is used and to create a more optimized, lasting system that provides maximal value to patients, families, and healthcare workers during this current crisis and beyond.
Due to the pandemic spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the cause of COVID-19 infection, there is significant disruption to the global supply of PPE.2 Order volumes of PPE have increased, prices have surged, and distributors are experiencing challenges meeting order demands.3 With decreased overseas exports, suppliers have placed hospitals on PPE allocations, and many hospitals’ orders for PPE have been only partially filled.3,4 Unless hospitals have established stockpiles, most only have supplies for 3-7 days of routine use, leaving them vulnerable to exhausting PPE supplies. At the onset of the pandemic, 86% of United States hospitals reported concerns about their PPE supply.4
The potential for PPE shortages has led both the Centers for Disease Control and Prevention (CDC) and the World Health Organization to call for the rational and appropriate use of PPE in order to conserve supplies.2,3 By the time COVID-19 was declared a pandemic, 54% of hospitals had imposed PPE conservation protocols,4 with more expected to follow in the weeks and months to come. Innovative protocols have been conceptualized and used to conserve PPE in hospitals (Table).
Yet these conservation protocols often fail to identify missed opportunities to improve the value of PPE that already exist in hospital care. By defining the value of inpatient PPE, hospitals can identify opportunities for value improvement. Changes implemented now will maximize PPE value and preserve supply during this pandemic and beyond.
THE VALUE OF PPE
In order to conserve PPE supply, hospitals might consider limiting PPE to cases in which clear evidence exists to support its use. However, evidence for PPE use can be challenging to interpret because the impact of preventing nosocomial infections (an outcome that did not occur) is inherently problematic to measure. This makes assessing the value of PPE in preventing nosocomial transmission in specific situations difficult.
The basis of using PPE is its effectiveness in controlling outbreaks.1 A meta-analysis of 6 case-control studies from the SARS outbreak of 2003, which disproportionately infected healthcare workers, suggested that handwashing and PPE were effective in preventing disease transmission. Handwashing alone reduced transmission by 55%, wearing gloves by 57%, and wearing facemasks by 68%; the cumulative effect of handwashing, masks, gloves, and gowns reduced transmission by 91%.5 A cohort study of healthcare workers exposed to H1N1 influenza A in 2009 found that use of a facemask or an N95 respirator was associated with negative viral serology suggesting noninfected status.6 With respiratory syncytial virus (RSV) outbreaks, a narrative synthesis of 4 studies examining transmission also suggested gowns, facemasks, and eye protection are effective, with eye protection perhaps more effective than gowns and masks.7 Yet these studies’ conclusions are limited by study design differences and small sample sizes.
The evidence supporting PPE use for routine hospital conditions is more challenging to interpret. One pediatric study of seasonal respiratory viruses showed that adding droplet precautions to an existing policy of contact precautions alone decreased nosocomial infections for most viruses evaluated.8 Yet this study, like many of PPE use, is limited by sample size and possible misclassification of exposure and outcome biases. Because PPE is always utilized in conjunction with other preventive measures, isolating the impact of PPE is challenging, let alone isolating the individual effects of PPE components. In the absence of strong empirical evidence, hospitals must rely on the inherent rationale of PPE use for patient and healthcare worker safety in assessing its value.
In order to protect patients from disease transmission during a pandemic, hospitals might also reconsider whether to use PPE in cases in which evidence is absent, such as routine prevention for colonized but noninfected patients. However, evidence of the possible patient harms of PPE are emerging. Healthcare providers spend less time with isolated patients9,10 and document fewer vital signs.11 Patients in PPE may experience delays in admission12 and discharge,13 and have higher rates of falls, pressure ulcers, and medication errors.14,15 They may also experience higher rates of anxiety and depression.16 Yet no evidence suggests PPE use for noninfected patients prevents transmission to patients or to healthcare workers. Using PPE when it is not indicated deemphasizes the value of other preventative precautions (eg, handwashing), unnecessarily depletes PPE supply, and may create patient harm without added benefit. High-value PPE, both during a pandemic and beyond, is defined by a system designed so that healthcare workers use PPE when they need it, and do not use PPE when not indicated.
ORDERING PPE IN A COMPLEX HEALTHCARE ENVIRONMENT
While all hospitalized patients are admitted using standard precautions, decisions surrounding PPE can be nuanced for even experienced clinicians. Although the CDC does provide guidance for PPE use based on symptoms that correlate with potential for transmission (eg, patients with cough should be placed in at least droplet precautions),1 guidelines must rely on provider evaluation and interpretation. For instance, three etiologies of cough—pneumococcal pneumonia, RSV bronchiolitis, and pulmonary tuberculosis—would all require different PPE. The clinician must weigh the probabilities of each pathogen and assess the harm of not protecting against certain pathogens in his or her decision.
Amidst the stress and cognitive burdens placed on clinicians, accuracy in PPE decisions is easily deprioritized. Clinicians may not completely consider patient-specific indications for PPE, implications for patients and staff, and supply shortages. Although the CDC and many hospitals have PPE initiation and discontinuation criteria, clinicians may favor educated guesswork and reliance on past experience when guidelines are poorly accessible or poorly searchable. Such individual, nonstandardized decisions likely lead to variability in practice patterns, inaccuracies in PPE decisions, and ultimately waste of PPE resources.
WHERE OUR HOSPITAL USES PPE IN A LOW-VALUE WAY
At our institution, the inconveniences, cognitive burden, and perceived benefit of routine PPE interventions have created a system in which PPE is regularly overused. On our hospital medicine wards, we found that PPE was both over-ordered upon admission (eg, contact/droplet precautions ordered for influenza when droplet precautions only would have sufficed) and unnecessarily continued even after children met discontinuation criteria.
On discharge review from our general pediatric ward in 2019, 18% of children discharged with PPE orders no longer met criteria for PPE. Two conditions—community-acquired bacterial pneumonia and skin and soft-tissue infections—accounted for 47% of discharges with unnecessary PPE orders. At an estimated cost of $0.13-$0.53 for droplet precautions per use, $0.69 for contact precautions, and $0.82-$1.22 for both, the absolute cost of continuing PPE without indication could be as high as $61/day per patient when estimating 50 uses per day. This direct cost represents healthcare spending without added value when PPE are not necessary. Furthermore, the additional emotional cost to the patient and family in their hospitalization experience, the cost of clinician time donning and doffing, the environmental cost of PPE waste, and the cost to the limited PPE supply are not considered in these calculations.
During a pandemic characterized by PPE shortages nationwide, allowing missed opportunities for PPE discontinuation to persist is not only wasteful, but inattentive to public health.
OPPORTUNITIES FOR HOSPITALS TO MAXIMIZE THE VALUE OF PPE
For individual clinicians, opportunities exist to improve PPE usage in daily patient care. Clinicians should not overlook PPE decisions; instead they should make it a practice to review PPE orders daily during rounds as they would lab orders. Clinicians and nursing staff should work together to identify PPE discontinuation opportunities, leveraging the electronic medical record when possible. For the benefit of patients and families, clinicians and bedside staff should recognize and assist in managing patient expectations of PPE.
Hospitals should work to make PPE references easily accessible and interpretable by frontline clinicians. To minimize variability of use, PPE ordering for routine conditions should be standardized and streamlined, including discontinuation criteria. Hospitals should invest in behavioral health programs to support patients with conditions necessitating PPE and develop policies to ensure ancillary services are equally available to all patients. To alleviate concerns about limited clinician time spent with isolated patients, hospitals should assign clinician workloads while accounting for the known increased time needed to care for patients with PPE.
For hospitals with extreme supply shortages, conservation might include decreased use of PPE for conditions in which its use is controversial (eg, patients colonized with methicillin-resistant Staphylococcus aureus or multidrug resistant organisms) as has been trialed in institutions prior to this pandemic.17,18 Such PPE policy changes might occur in addition to, or in conjunction with, the conservation strategies suggested by other institutions (Table).
Healthcare systems should continually reassess the value of PPE for their hospitals and make changes accordingly. In the midst of difficulties directly demonstrating PPE’s value, hospitals must rely on the inherent rationale of PPE use in assessing value decisions weighed against harms while balancing healthcare worker protection regulations. Decisions should always occur while continuing other sensible infection-control procedures, such as handwashing and environmental hygiene measures.
To effect maximal change, healthcare systems should invest in redesigning PPE ordering systems at the highest level. This should include harnessing existing technologies to streamline PPE ordering decisions to meet clinicians’ cognitive needs. Decision support and auditing technologies could automate and monitor PPE orders efficiently. Likely to be most effective, an investment in creating and maintaining centralized PPE expert management teams to assess, order, and discontinue PPE would minimize individual ordering variation, minimize cost, and maximize value to patients, staff, and hospitals.
CONCLUSION
In this pandemic, we have the opportunity to rethink how we understand and use PPE in hospitalized patients. It is vitally important now more than ever to consciously conserve the limited supply of PPE resources. As we seek to increase healthcare value while limiting overuse and waste, PPE is a prime target for value improvement efforts as the effective but also burdensome tool that it is. Hospitalists are well-positioned to lead the redesign of how, when, and why PPE is used and to create a more optimized, lasting system that provides maximal value to patients, families, and healthcare workers during this current crisis and beyond.
1. Siegel JD, Rhinehart E, Jackson M, Chiarello L. 2007 Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control. 2007;35(10 Suppl 2):S65-164. https://doi.org/10.1016/j.ajic.2007.10.007.
2. World Health Organization. Shortage of personal protective equipment endangering health workers worldwide. https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide. Accessed March 12, 2020.
3. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19): healthcare supply of personal protective equipment. https://www.cdc.gov/coronavirus/2019-ncov/hcp/healthcare-supply-ppe.html. Accessed March 12, 2020.
4. Premier Inc. Premier Inc survey finds 86 percent of health systems are concerned about personal protective equipment shortages due to coronavirus. https://www.premierinc.com/newsroom/press-releases/premier-inc-survey-finds-86-percent-of-health-systems-are-concerned-about-personal-protective-equipment-shortages-due-to-coronavirus. Accessed March 22, 2020.
5. Jefferson T, Foxlee R, Del Mar C, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ. 2008;336(7635):77-80. https://doi.org/10.1136/bmj.39393.510347.BE.
6. Jaeger JL, Patel M, Dharan N, et al. Transmission of 2009 pandemic influenza A (H1N1) virus among healthcare personnel-Southern California, 2009. Infect Control Hosp Epidemiol. 2011;32(12):1149-1157. https://doi.org/10.1086/662709.
7. French CE, McKenzie BC, Coope C, et al. Risk of nosocomial respiratory syncytial virus infection and effectiveness of control measures to prevent transmission events: a systematic review. Influenza Other Respir Viruses. 2016;10(4):268-290. https://doi.org/10.1111/irv.12379.
8. Rubin LG, Kohn N, Nullet S, Hill M. Reduction in rate of nosocomial respiratory virus infections in a children’s hospital associated with enhanced isolation precautions. Infect Control Hosp Epidemiol. 2018;39(2):152-156. https://doi.org/10.1017/ice.2017.282.
9. Dashiell-Earp CN, Bell DS, Ang AO, Uslan DZ. Do physicians spend less time with patients in contact isolation?: A time-motion study of internal medicine interns. JAMA Intern Med. 2014;174(5):814-815. https://doi.org/10.1001/jamainternmed.2014.537.
10. Saint S, Higgins LA, Nallamothu BK, Chenoweth C. Do physicians examine patients in contact isolation less frequently? A brief report. Am J Infect Control. 2003;31(6):354-356. https://doi.org/10.1016/S0196-6553(02)48250-8.
11. Kirkland KB, Weinstein JM. Adverse effects of contact isolation. Lancet. 1999(354):1177-1178. https://doi.org/10.1016/S0140-6736(99)04196-3.
12. McLemore A, Bearman G, Edmond MB. Effect of contact precautions on wait time from emergency room disposition to inpatient admission. Infect Control Hosp Epidemiol. 2011;32(3):298-299. https://doi.org/10.1086/658913.
13. Tran K, Bell C, Stall N, et al. The effect of hospital isolation precautions on patient outcomes and cost of care: a multi-site, retrospective, propensity score-matched cohort study. J Gen Intern Med. 2017;32(3):262-268. https://doi.org/10.1007/s11606-016-3862-4.
14. Karki S, Leder K, Cheng AC. Patients under contact precautions have an increased risk of injuries and medication errors: a retrospective cohort study. Infect Control Hosp Epidemiol. 2013;34(10):1118-1120. https://doi.org/10.1086/673153.
15. Stelfox HT, Bates DW, Redelmeier DA. Safety of patients isolated for infection control. JAMA. 2003;290(14):1899-1905. https://doi.org/10.1001/jama.290.14.1899.
16. Catalano G, Houston SH, Catalano MC, et al. Anxiety and depression in hospitalized patients in resistant organism isolation. South Med J. 2003;96(2):141-145. https://doi.org/10.1097/01.SMJ.0000050683.36014.2E.
17. Young K, Doernberg SB, Snedecor RF, Mallin E. Things we do for no reason: contact precautions for MRSA and VRE. J Hosp Med. 2019;14(3):178-180. https://doi.org/10.12788/jhm.3126.
18. Bearman G, Abbas S, Masroor N, et al. Impact of discontinuing contact precautions for methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus: an interrupted time series analysis. Infect Control Hosp Epidemiol. 2018;39(6):676-682. https://doi.org/10.1017/ice.2018.57.
1. Siegel JD, Rhinehart E, Jackson M, Chiarello L. 2007 Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control. 2007;35(10 Suppl 2):S65-164. https://doi.org/10.1016/j.ajic.2007.10.007.
2. World Health Organization. Shortage of personal protective equipment endangering health workers worldwide. https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide. Accessed March 12, 2020.
3. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19): healthcare supply of personal protective equipment. https://www.cdc.gov/coronavirus/2019-ncov/hcp/healthcare-supply-ppe.html. Accessed March 12, 2020.
4. Premier Inc. Premier Inc survey finds 86 percent of health systems are concerned about personal protective equipment shortages due to coronavirus. https://www.premierinc.com/newsroom/press-releases/premier-inc-survey-finds-86-percent-of-health-systems-are-concerned-about-personal-protective-equipment-shortages-due-to-coronavirus. Accessed March 22, 2020.
5. Jefferson T, Foxlee R, Del Mar C, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ. 2008;336(7635):77-80. https://doi.org/10.1136/bmj.39393.510347.BE.
6. Jaeger JL, Patel M, Dharan N, et al. Transmission of 2009 pandemic influenza A (H1N1) virus among healthcare personnel-Southern California, 2009. Infect Control Hosp Epidemiol. 2011;32(12):1149-1157. https://doi.org/10.1086/662709.
7. French CE, McKenzie BC, Coope C, et al. Risk of nosocomial respiratory syncytial virus infection and effectiveness of control measures to prevent transmission events: a systematic review. Influenza Other Respir Viruses. 2016;10(4):268-290. https://doi.org/10.1111/irv.12379.
8. Rubin LG, Kohn N, Nullet S, Hill M. Reduction in rate of nosocomial respiratory virus infections in a children’s hospital associated with enhanced isolation precautions. Infect Control Hosp Epidemiol. 2018;39(2):152-156. https://doi.org/10.1017/ice.2017.282.
9. Dashiell-Earp CN, Bell DS, Ang AO, Uslan DZ. Do physicians spend less time with patients in contact isolation?: A time-motion study of internal medicine interns. JAMA Intern Med. 2014;174(5):814-815. https://doi.org/10.1001/jamainternmed.2014.537.
10. Saint S, Higgins LA, Nallamothu BK, Chenoweth C. Do physicians examine patients in contact isolation less frequently? A brief report. Am J Infect Control. 2003;31(6):354-356. https://doi.org/10.1016/S0196-6553(02)48250-8.
11. Kirkland KB, Weinstein JM. Adverse effects of contact isolation. Lancet. 1999(354):1177-1178. https://doi.org/10.1016/S0140-6736(99)04196-3.
12. McLemore A, Bearman G, Edmond MB. Effect of contact precautions on wait time from emergency room disposition to inpatient admission. Infect Control Hosp Epidemiol. 2011;32(3):298-299. https://doi.org/10.1086/658913.
13. Tran K, Bell C, Stall N, et al. The effect of hospital isolation precautions on patient outcomes and cost of care: a multi-site, retrospective, propensity score-matched cohort study. J Gen Intern Med. 2017;32(3):262-268. https://doi.org/10.1007/s11606-016-3862-4.
14. Karki S, Leder K, Cheng AC. Patients under contact precautions have an increased risk of injuries and medication errors: a retrospective cohort study. Infect Control Hosp Epidemiol. 2013;34(10):1118-1120. https://doi.org/10.1086/673153.
15. Stelfox HT, Bates DW, Redelmeier DA. Safety of patients isolated for infection control. JAMA. 2003;290(14):1899-1905. https://doi.org/10.1001/jama.290.14.1899.
16. Catalano G, Houston SH, Catalano MC, et al. Anxiety and depression in hospitalized patients in resistant organism isolation. South Med J. 2003;96(2):141-145. https://doi.org/10.1097/01.SMJ.0000050683.36014.2E.
17. Young K, Doernberg SB, Snedecor RF, Mallin E. Things we do for no reason: contact precautions for MRSA and VRE. J Hosp Med. 2019;14(3):178-180. https://doi.org/10.12788/jhm.3126.
18. Bearman G, Abbas S, Masroor N, et al. Impact of discontinuing contact precautions for methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus: an interrupted time series analysis. Infect Control Hosp Epidemiol. 2018;39(6):676-682. https://doi.org/10.1017/ice.2018.57.
© 2020 Society of Hospital Medicine