User login
Why Do MDs Have Such a High Rate of Eating Disorders?
Ten years ago, Clare Gerada, FRCGP, an advocate for physician well-being and today president of the UK’s Royal College of General Practitioners, made a prediction to the audience at the International Conference on Physician Health.
“We have seen a massive increase in eating disorders [among doctors],” she said. “I’m not sure anybody is quite aware of the tsunami of eating disorders,” she believed would soon strike predominantly female physicians.
That was 2014. Did the tsunami hit?
Quite possibly. Data are limited on the prevalence of eating disorders (EDs) among healthcare workers, but studies do exist. A 2019 global review and meta-analysis determined “the summary prevalence of eating disorder (ED) risk among medical students was 10.4%.”
A 2022 update of that review boosted the estimate to 17.35%.
Tsunami or not, that’s nearly double the 9% rate within the US general public (from a 2020 report from STRIPED and the Academy of Eating Disorders). And while the following stat isn’t an indicator of EDs per se,
To her credit, Dr. Gerada, awarded a damehood in 2020, was in a position to know what was coming. Her statement was informed by research showing an increasing number of young doctors seeking treatment for mental health issues, including EDs, through the NHS Practitioner Health program, a mental health service she established in 2008.
So ... what puts doctors at such a high risk for EDs?
Be Careful of ‘Overlap Traits’
As with many mental health issues, EDs have no single cause. Researchers believe they stem from a complex interaction of genetic, biological, behavioral, psychological, and social factors. But the medical field should take note: Some personality traits commonly associated with EDs are often shared by successful physicians.
“I think some of the overlap traits would be being highly driven, goal-oriented and self-critical,” said Lesley Williams, MD, a family medicine physician at the Mayo Clinic in Phoenix, Arizona. “A lot of those traits can make you a very successful physician and physician-in-training but could also potentially spill over into body image and rigidity around food.”
Of course, we want physicians to strive for excellence, and the majority of diligent, driven doctors will not develop an ED.
But when pushed too far, those admirable qualities can easily become perfectionism — which has long been recognized as a risk factor for EDs, an association supported by decades of research.
Medical School: Where EDs Begin and Little Education About Them Happens
“I think medicine in general attracts people that often share similar characteristics to those who struggle with EDs — high-achieving, hardworking perfectionists who put a lot of pressure on themselves,” said Elizabeth McNaught, MD, a general practitioner and medical director at Family Mental Wealth.
Diagnosed with an ED at 14, Dr. McNaught has experienced this firsthand and shared her story in a 2020 memoir, Life Hurts: A Doctor’s Personal Journey Through Anorexia.
Competitive, high-stress environments can also be a trigger, Dr. McNaught explained. “The pressure of medical school,” for example, “can perpetuate an eating disorder if that’s something that you’re struggling with,” she said.
Pressure to perform may not be the only problem. Medical students are taught to view weight as a key indicator of health. Multiple studies suggested that not only does weight stigma exist in healthcare but also it has increased over time and negatively affects patients’ psychological well-being and physical health.
There is far less public discourse about how weight stigma can be harmful to medical students and physicians themselves. Dr. Williams believed the weight-centric paradigm was key.
“For so long, we believed that health presents itself within these confines on a BMI chart and anything outside of that is unhealthy and must be fixed,” she said. “I can say from having gone through medical education, having that continual messaging does make someone feel that if I myself am not within those confines, then I need to do something to fix that immediately if I’m going to continue to care for patients.”
In general, Dr. Williams, and Dr. McNaught agreed that medical training around EDs is lacking, producing doctors who are ill-equipped to diagnose, treat, or even discuss them with patients. Dr. Williams recalled only one lecture on the topic in med school.
“And yet, anorexia carries the second highest death rate of all mental illnesses after opioid-use disorders,” she said, “so it’s astonishing that that just wasn’t included.”
MDs Hiding Mental Health Issues
Claire Anderson, MD (a pseudonym), emphatically stated she would never tell anyone at the hospital where she works in the emergency department that she has an ED.
“There is still a lot of misunderstanding about mental health, and I never want people to doubt my ability to care for people,” Dr. Anderson said. “There’s so much stigma around eating disorders, and I also feel like once it’s out there, I can’t take it back, and I don’t want to feel like people are watching me.”
Melissa Klein, PhD, a clinical psychologist specializing in EDs, has more than 25 years of experience working the inpatient ED unit at New York Presbyterian. Having treated medical professionals, Dr. Klein said they have legitimate concerns about revealing their struggles.
“Sometimes, they do get reported to higher ups — the boards,” Dr. Klein said, “and they’re told that they have to get help in order for them to continue to work in their profession. I think people might be scared to ask for help because of that reason.”
Doctors Often Ignore EDs or Teach ‘Bad Habits’
Dr. Anderson firmly believed that if her early treatment from doctors had been better, she might not be struggling so much today.
The first time Dr. Anderson’s mother brought up her daughter’s sudden weight loss at 14, their family doctor conferred with a chart and said there was no reason to worry; Dr. Anderson’s weight was “normal.” “I was eating like 500 calories a day and swimming for 3 hours, and [by saying that], they assured me I was fine,” she recalls.
At 15, when Dr. Anderson went in for an initial assessment for an ED, she thought she’d be connected with a nutritionist and sent home. “I didn’t have a lot of classic thoughts of wanting to be thin or wanting to lose weight,” she said.
Instead, Dr. Anderson was sent to inpatient care, which she credits with escalating her ED. “I picked up on a lot of really bad habits when I went there — I sort of learned how to have an eating disorder,” she said. “When I left, it was very different than when I went in, which is kind of sad.”
Throughout high school, Dr. Anderson went in and out of so many hospitals and treatment programs that she’s lost track of them. Then, in 2008, she left formal treatment altogether. “I had been really angry with the treatment programs for trying to fit me into their box with a rigid schedule of inpatient and outpatient care,” she recalled. “I didn’t want to live in that world anymore.”
After working with a new psychiatrist, Dr. Anderson’s situation improved until a particularly stressful second year of residency. “That’s when I just tanked,” she said. “Residency, and especially being on my own and with COVID, things have not been great for me.”
Dr. Anderson now sees an eating disorder specialist, but she pays for this out-of-pocket. “I have terrible insurance,” she said with a laugh, aware of that irony.
If You Are Struggling, Don’t Be Ashamed
Some physicians who’ve experienced EDs firsthand are working to improve training on diagnosing and treating the conditions. Dr. McNaught has developed and launched a new eLearning program for healthcare workers on how to recognize the early signs and symptoms of an ED and provide support.
“It’s not only so they can recognize it in their patients but also if colleagues and family and friends are struggling,” she said.
In 2021, the American Psychiatric Association (APA) approved the APA Practice Guideline for the Treatment of Patients With Eating Disorders, which aims to improve patient care and treatment outcomes.
But Dr. Klein is concerned that increased stress since the COVID-19 pandemic may be putting healthcare workers at even greater risk.
“When people are under stress or when they feel like there are things in their life that maybe they can’t control, sometimes turning to an eating disorder is a way to cope,” she said, “In that sense, the stress on medical professionals is something that could lead to eating disorder behaviors.”
Dr. Klein’s message to healthcare workers: Don’t be ashamed. She described an ED as “a monster that takes over your brain. Once it starts, it’s very hard to turn it around on your own. So, I hope anyone who is suffering, in whatever field they’re in, that they are able to ask for help.”
A version of this article appeared on Medscape.com.
Ten years ago, Clare Gerada, FRCGP, an advocate for physician well-being and today president of the UK’s Royal College of General Practitioners, made a prediction to the audience at the International Conference on Physician Health.
“We have seen a massive increase in eating disorders [among doctors],” she said. “I’m not sure anybody is quite aware of the tsunami of eating disorders,” she believed would soon strike predominantly female physicians.
That was 2014. Did the tsunami hit?
Quite possibly. Data are limited on the prevalence of eating disorders (EDs) among healthcare workers, but studies do exist. A 2019 global review and meta-analysis determined “the summary prevalence of eating disorder (ED) risk among medical students was 10.4%.”
A 2022 update of that review boosted the estimate to 17.35%.
Tsunami or not, that’s nearly double the 9% rate within the US general public (from a 2020 report from STRIPED and the Academy of Eating Disorders). And while the following stat isn’t an indicator of EDs per se,
To her credit, Dr. Gerada, awarded a damehood in 2020, was in a position to know what was coming. Her statement was informed by research showing an increasing number of young doctors seeking treatment for mental health issues, including EDs, through the NHS Practitioner Health program, a mental health service she established in 2008.
So ... what puts doctors at such a high risk for EDs?
Be Careful of ‘Overlap Traits’
As with many mental health issues, EDs have no single cause. Researchers believe they stem from a complex interaction of genetic, biological, behavioral, psychological, and social factors. But the medical field should take note: Some personality traits commonly associated with EDs are often shared by successful physicians.
“I think some of the overlap traits would be being highly driven, goal-oriented and self-critical,” said Lesley Williams, MD, a family medicine physician at the Mayo Clinic in Phoenix, Arizona. “A lot of those traits can make you a very successful physician and physician-in-training but could also potentially spill over into body image and rigidity around food.”
Of course, we want physicians to strive for excellence, and the majority of diligent, driven doctors will not develop an ED.
But when pushed too far, those admirable qualities can easily become perfectionism — which has long been recognized as a risk factor for EDs, an association supported by decades of research.
Medical School: Where EDs Begin and Little Education About Them Happens
“I think medicine in general attracts people that often share similar characteristics to those who struggle with EDs — high-achieving, hardworking perfectionists who put a lot of pressure on themselves,” said Elizabeth McNaught, MD, a general practitioner and medical director at Family Mental Wealth.
Diagnosed with an ED at 14, Dr. McNaught has experienced this firsthand and shared her story in a 2020 memoir, Life Hurts: A Doctor’s Personal Journey Through Anorexia.
Competitive, high-stress environments can also be a trigger, Dr. McNaught explained. “The pressure of medical school,” for example, “can perpetuate an eating disorder if that’s something that you’re struggling with,” she said.
Pressure to perform may not be the only problem. Medical students are taught to view weight as a key indicator of health. Multiple studies suggested that not only does weight stigma exist in healthcare but also it has increased over time and negatively affects patients’ psychological well-being and physical health.
There is far less public discourse about how weight stigma can be harmful to medical students and physicians themselves. Dr. Williams believed the weight-centric paradigm was key.
“For so long, we believed that health presents itself within these confines on a BMI chart and anything outside of that is unhealthy and must be fixed,” she said. “I can say from having gone through medical education, having that continual messaging does make someone feel that if I myself am not within those confines, then I need to do something to fix that immediately if I’m going to continue to care for patients.”
In general, Dr. Williams, and Dr. McNaught agreed that medical training around EDs is lacking, producing doctors who are ill-equipped to diagnose, treat, or even discuss them with patients. Dr. Williams recalled only one lecture on the topic in med school.
“And yet, anorexia carries the second highest death rate of all mental illnesses after opioid-use disorders,” she said, “so it’s astonishing that that just wasn’t included.”
MDs Hiding Mental Health Issues
Claire Anderson, MD (a pseudonym), emphatically stated she would never tell anyone at the hospital where she works in the emergency department that she has an ED.
“There is still a lot of misunderstanding about mental health, and I never want people to doubt my ability to care for people,” Dr. Anderson said. “There’s so much stigma around eating disorders, and I also feel like once it’s out there, I can’t take it back, and I don’t want to feel like people are watching me.”
Melissa Klein, PhD, a clinical psychologist specializing in EDs, has more than 25 years of experience working the inpatient ED unit at New York Presbyterian. Having treated medical professionals, Dr. Klein said they have legitimate concerns about revealing their struggles.
“Sometimes, they do get reported to higher ups — the boards,” Dr. Klein said, “and they’re told that they have to get help in order for them to continue to work in their profession. I think people might be scared to ask for help because of that reason.”
Doctors Often Ignore EDs or Teach ‘Bad Habits’
Dr. Anderson firmly believed that if her early treatment from doctors had been better, she might not be struggling so much today.
The first time Dr. Anderson’s mother brought up her daughter’s sudden weight loss at 14, their family doctor conferred with a chart and said there was no reason to worry; Dr. Anderson’s weight was “normal.” “I was eating like 500 calories a day and swimming for 3 hours, and [by saying that], they assured me I was fine,” she recalls.
At 15, when Dr. Anderson went in for an initial assessment for an ED, she thought she’d be connected with a nutritionist and sent home. “I didn’t have a lot of classic thoughts of wanting to be thin or wanting to lose weight,” she said.
Instead, Dr. Anderson was sent to inpatient care, which she credits with escalating her ED. “I picked up on a lot of really bad habits when I went there — I sort of learned how to have an eating disorder,” she said. “When I left, it was very different than when I went in, which is kind of sad.”
Throughout high school, Dr. Anderson went in and out of so many hospitals and treatment programs that she’s lost track of them. Then, in 2008, she left formal treatment altogether. “I had been really angry with the treatment programs for trying to fit me into their box with a rigid schedule of inpatient and outpatient care,” she recalled. “I didn’t want to live in that world anymore.”
After working with a new psychiatrist, Dr. Anderson’s situation improved until a particularly stressful second year of residency. “That’s when I just tanked,” she said. “Residency, and especially being on my own and with COVID, things have not been great for me.”
Dr. Anderson now sees an eating disorder specialist, but she pays for this out-of-pocket. “I have terrible insurance,” she said with a laugh, aware of that irony.
If You Are Struggling, Don’t Be Ashamed
Some physicians who’ve experienced EDs firsthand are working to improve training on diagnosing and treating the conditions. Dr. McNaught has developed and launched a new eLearning program for healthcare workers on how to recognize the early signs and symptoms of an ED and provide support.
“It’s not only so they can recognize it in their patients but also if colleagues and family and friends are struggling,” she said.
In 2021, the American Psychiatric Association (APA) approved the APA Practice Guideline for the Treatment of Patients With Eating Disorders, which aims to improve patient care and treatment outcomes.
But Dr. Klein is concerned that increased stress since the COVID-19 pandemic may be putting healthcare workers at even greater risk.
“When people are under stress or when they feel like there are things in their life that maybe they can’t control, sometimes turning to an eating disorder is a way to cope,” she said, “In that sense, the stress on medical professionals is something that could lead to eating disorder behaviors.”
Dr. Klein’s message to healthcare workers: Don’t be ashamed. She described an ED as “a monster that takes over your brain. Once it starts, it’s very hard to turn it around on your own. So, I hope anyone who is suffering, in whatever field they’re in, that they are able to ask for help.”
A version of this article appeared on Medscape.com.
Ten years ago, Clare Gerada, FRCGP, an advocate for physician well-being and today president of the UK’s Royal College of General Practitioners, made a prediction to the audience at the International Conference on Physician Health.
“We have seen a massive increase in eating disorders [among doctors],” she said. “I’m not sure anybody is quite aware of the tsunami of eating disorders,” she believed would soon strike predominantly female physicians.
That was 2014. Did the tsunami hit?
Quite possibly. Data are limited on the prevalence of eating disorders (EDs) among healthcare workers, but studies do exist. A 2019 global review and meta-analysis determined “the summary prevalence of eating disorder (ED) risk among medical students was 10.4%.”
A 2022 update of that review boosted the estimate to 17.35%.
Tsunami or not, that’s nearly double the 9% rate within the US general public (from a 2020 report from STRIPED and the Academy of Eating Disorders). And while the following stat isn’t an indicator of EDs per se,
To her credit, Dr. Gerada, awarded a damehood in 2020, was in a position to know what was coming. Her statement was informed by research showing an increasing number of young doctors seeking treatment for mental health issues, including EDs, through the NHS Practitioner Health program, a mental health service she established in 2008.
So ... what puts doctors at such a high risk for EDs?
Be Careful of ‘Overlap Traits’
As with many mental health issues, EDs have no single cause. Researchers believe they stem from a complex interaction of genetic, biological, behavioral, psychological, and social factors. But the medical field should take note: Some personality traits commonly associated with EDs are often shared by successful physicians.
“I think some of the overlap traits would be being highly driven, goal-oriented and self-critical,” said Lesley Williams, MD, a family medicine physician at the Mayo Clinic in Phoenix, Arizona. “A lot of those traits can make you a very successful physician and physician-in-training but could also potentially spill over into body image and rigidity around food.”
Of course, we want physicians to strive for excellence, and the majority of diligent, driven doctors will not develop an ED.
But when pushed too far, those admirable qualities can easily become perfectionism — which has long been recognized as a risk factor for EDs, an association supported by decades of research.
Medical School: Where EDs Begin and Little Education About Them Happens
“I think medicine in general attracts people that often share similar characteristics to those who struggle with EDs — high-achieving, hardworking perfectionists who put a lot of pressure on themselves,” said Elizabeth McNaught, MD, a general practitioner and medical director at Family Mental Wealth.
Diagnosed with an ED at 14, Dr. McNaught has experienced this firsthand and shared her story in a 2020 memoir, Life Hurts: A Doctor’s Personal Journey Through Anorexia.
Competitive, high-stress environments can also be a trigger, Dr. McNaught explained. “The pressure of medical school,” for example, “can perpetuate an eating disorder if that’s something that you’re struggling with,” she said.
Pressure to perform may not be the only problem. Medical students are taught to view weight as a key indicator of health. Multiple studies suggested that not only does weight stigma exist in healthcare but also it has increased over time and negatively affects patients’ psychological well-being and physical health.
There is far less public discourse about how weight stigma can be harmful to medical students and physicians themselves. Dr. Williams believed the weight-centric paradigm was key.
“For so long, we believed that health presents itself within these confines on a BMI chart and anything outside of that is unhealthy and must be fixed,” she said. “I can say from having gone through medical education, having that continual messaging does make someone feel that if I myself am not within those confines, then I need to do something to fix that immediately if I’m going to continue to care for patients.”
In general, Dr. Williams, and Dr. McNaught agreed that medical training around EDs is lacking, producing doctors who are ill-equipped to diagnose, treat, or even discuss them with patients. Dr. Williams recalled only one lecture on the topic in med school.
“And yet, anorexia carries the second highest death rate of all mental illnesses after opioid-use disorders,” she said, “so it’s astonishing that that just wasn’t included.”
MDs Hiding Mental Health Issues
Claire Anderson, MD (a pseudonym), emphatically stated she would never tell anyone at the hospital where she works in the emergency department that she has an ED.
“There is still a lot of misunderstanding about mental health, and I never want people to doubt my ability to care for people,” Dr. Anderson said. “There’s so much stigma around eating disorders, and I also feel like once it’s out there, I can’t take it back, and I don’t want to feel like people are watching me.”
Melissa Klein, PhD, a clinical psychologist specializing in EDs, has more than 25 years of experience working the inpatient ED unit at New York Presbyterian. Having treated medical professionals, Dr. Klein said they have legitimate concerns about revealing their struggles.
“Sometimes, they do get reported to higher ups — the boards,” Dr. Klein said, “and they’re told that they have to get help in order for them to continue to work in their profession. I think people might be scared to ask for help because of that reason.”
Doctors Often Ignore EDs or Teach ‘Bad Habits’
Dr. Anderson firmly believed that if her early treatment from doctors had been better, she might not be struggling so much today.
The first time Dr. Anderson’s mother brought up her daughter’s sudden weight loss at 14, their family doctor conferred with a chart and said there was no reason to worry; Dr. Anderson’s weight was “normal.” “I was eating like 500 calories a day and swimming for 3 hours, and [by saying that], they assured me I was fine,” she recalls.
At 15, when Dr. Anderson went in for an initial assessment for an ED, she thought she’d be connected with a nutritionist and sent home. “I didn’t have a lot of classic thoughts of wanting to be thin or wanting to lose weight,” she said.
Instead, Dr. Anderson was sent to inpatient care, which she credits with escalating her ED. “I picked up on a lot of really bad habits when I went there — I sort of learned how to have an eating disorder,” she said. “When I left, it was very different than when I went in, which is kind of sad.”
Throughout high school, Dr. Anderson went in and out of so many hospitals and treatment programs that she’s lost track of them. Then, in 2008, she left formal treatment altogether. “I had been really angry with the treatment programs for trying to fit me into their box with a rigid schedule of inpatient and outpatient care,” she recalled. “I didn’t want to live in that world anymore.”
After working with a new psychiatrist, Dr. Anderson’s situation improved until a particularly stressful second year of residency. “That’s when I just tanked,” she said. “Residency, and especially being on my own and with COVID, things have not been great for me.”
Dr. Anderson now sees an eating disorder specialist, but she pays for this out-of-pocket. “I have terrible insurance,” she said with a laugh, aware of that irony.
If You Are Struggling, Don’t Be Ashamed
Some physicians who’ve experienced EDs firsthand are working to improve training on diagnosing and treating the conditions. Dr. McNaught has developed and launched a new eLearning program for healthcare workers on how to recognize the early signs and symptoms of an ED and provide support.
“It’s not only so they can recognize it in their patients but also if colleagues and family and friends are struggling,” she said.
In 2021, the American Psychiatric Association (APA) approved the APA Practice Guideline for the Treatment of Patients With Eating Disorders, which aims to improve patient care and treatment outcomes.
But Dr. Klein is concerned that increased stress since the COVID-19 pandemic may be putting healthcare workers at even greater risk.
“When people are under stress or when they feel like there are things in their life that maybe they can’t control, sometimes turning to an eating disorder is a way to cope,” she said, “In that sense, the stress on medical professionals is something that could lead to eating disorder behaviors.”
Dr. Klein’s message to healthcare workers: Don’t be ashamed. She described an ED as “a monster that takes over your brain. Once it starts, it’s very hard to turn it around on your own. So, I hope anyone who is suffering, in whatever field they’re in, that they are able to ask for help.”
A version of this article appeared on Medscape.com.
Nodal Radiation May Make BC Axillary Dissection Unnecessary
SAN ANTONIO — Axillary lymph node dissection may be unnecessary if breast cancer patients with one or two positive sentinel lymph nodes plan to have adjuvant nodal radiation, according to a major Scandinavian trial presented at the San Antonio Breast Cancer Symposium.
“It means that you don’t need to dissect the axilla if you” are going to “radiate the axilla.” “For the U.S., that’s the conclusion because there are still centers that do both, and that’s out,” lead investigator Jana de Boniface, MD, PhD, a breast cancer surgeon at the Karolinska Institutet, Stockholm, said in an interview.
Some even wondered if 5 years of endocrine therapy is necessary.
Dr. Boniface shared her thoughts after presenting the Scandinavian trial, SENOMAC, which she led.
SENOMAC randomized 1,204 patients with one or two positive sentinel lymph nodes to axillary dissection; 1,335 with the same finding were randomized to no dissection.
Subjects had clinically T1-3, N0 primary breast cancer. About 89% in both arms went on to adjuvant radiation, including nodal radiation, and almost all also went on to systemic therapy, which included endocrine therapy in over 90%. Only about 2% of subjects had neoadjuvant therapy.
At a median follow-up of nearly 4 years, recurrence-free survival was virtually identical in both groups, with 8% of patients in the dissection arm and 7.1% in the no-dissection group having recurrences. Estimated 5-year recurrence-free survival was just shy of 90% in both groups. Skipping dissection was strongly non-inferior to having one (P < .001).
SENOMAC “clearly shows that you don’t need to dissect the axilla if you have one to two positive sentinel lymph nodes” so long as patients have adjuvant nodal radiation. Recurrence-free survival “curves practically overlap, and we cannot see any difference between the two groups,” Dr. Boniface said.
Meanwhile, the dissection group fared worse on patient reported outcomes. Overall survival outcomes, the primary endpoint of the trial, are expected within 2 years.
The goal of the trial, the largest to date to look into the issue, was to fill gaps in the literature. Similar outcomes were reported around a decade ago in patients with low sentinel lymph node burdens, but the extensive exclusion criteria raised questions about general applicability.
In contrast, SENOMAC was widely inclusive. Over a third of patients had mastectomies, over a third had sentinel lymph node extracapsular extension, almost 6% had T3 disease, almost 20% had lobular carcinoma, 40% were 65 years or older, and tumors were as large as 15.5 cm.
The findings held regardless of those and other factors on subgroup analyses, including estrogen receptor and HER2 status and the number of additional positive nodes retrieved in the dissection group.
Andrea V. Barrio, MD, the study discussant and a breast cancer surgeon at Memorial Sloan Kettering Cancer Center, New York, agreed with the message from SENOMAC.
“Based on this, ALND [axillary lymph node dissection] should not be considered standard in patients with clinical T1-3, N0 breast cancer with one to two positive sentinel nodes, with or without microscopic extracapsular extension, undergoing lumpectomy or mastectomy,” provided nodal adjuvant radiotherapy is indicated, she said.
Although adjuvant nodal radiation for patients with one to three positive sentinel nodes is standard of care in Denmark and Sweden, where most of the patients in SENOMAC were located, practices vary widely in the United States. If adjuvant radiation isn’t used, “then ALND [is still] indicated,” Dr. Barrio said, but in either case, “only one is needed.”
In keeping with the de-escalation theme at the 2023 symposium, both Dr. Boniface and Dr. Barrio noted that trials are now underway to find patients who can avoid any axillary treatment at all if they have just one or two positive sentinel lymph nodes.
Preoperative axillary ultrasound was mandatory in SENOMAC and patients with non-palpable suspicious axillary lymph nodes were enrolled.
Thirty-six were positive on fine needle aspiration and randomized into the study, but when asked, Dr. Boniface didn’t have the data immediately at hand on how they fared.
The work was funded by the Swedish Research Council, Nordic Cancer Union, and others. Dr. Boniface and Dr. Barrio didn’t have any disclosures.
SAN ANTONIO — Axillary lymph node dissection may be unnecessary if breast cancer patients with one or two positive sentinel lymph nodes plan to have adjuvant nodal radiation, according to a major Scandinavian trial presented at the San Antonio Breast Cancer Symposium.
“It means that you don’t need to dissect the axilla if you” are going to “radiate the axilla.” “For the U.S., that’s the conclusion because there are still centers that do both, and that’s out,” lead investigator Jana de Boniface, MD, PhD, a breast cancer surgeon at the Karolinska Institutet, Stockholm, said in an interview.
Some even wondered if 5 years of endocrine therapy is necessary.
Dr. Boniface shared her thoughts after presenting the Scandinavian trial, SENOMAC, which she led.
SENOMAC randomized 1,204 patients with one or two positive sentinel lymph nodes to axillary dissection; 1,335 with the same finding were randomized to no dissection.
Subjects had clinically T1-3, N0 primary breast cancer. About 89% in both arms went on to adjuvant radiation, including nodal radiation, and almost all also went on to systemic therapy, which included endocrine therapy in over 90%. Only about 2% of subjects had neoadjuvant therapy.
At a median follow-up of nearly 4 years, recurrence-free survival was virtually identical in both groups, with 8% of patients in the dissection arm and 7.1% in the no-dissection group having recurrences. Estimated 5-year recurrence-free survival was just shy of 90% in both groups. Skipping dissection was strongly non-inferior to having one (P < .001).
SENOMAC “clearly shows that you don’t need to dissect the axilla if you have one to two positive sentinel lymph nodes” so long as patients have adjuvant nodal radiation. Recurrence-free survival “curves practically overlap, and we cannot see any difference between the two groups,” Dr. Boniface said.
Meanwhile, the dissection group fared worse on patient reported outcomes. Overall survival outcomes, the primary endpoint of the trial, are expected within 2 years.
The goal of the trial, the largest to date to look into the issue, was to fill gaps in the literature. Similar outcomes were reported around a decade ago in patients with low sentinel lymph node burdens, but the extensive exclusion criteria raised questions about general applicability.
In contrast, SENOMAC was widely inclusive. Over a third of patients had mastectomies, over a third had sentinel lymph node extracapsular extension, almost 6% had T3 disease, almost 20% had lobular carcinoma, 40% were 65 years or older, and tumors were as large as 15.5 cm.
The findings held regardless of those and other factors on subgroup analyses, including estrogen receptor and HER2 status and the number of additional positive nodes retrieved in the dissection group.
Andrea V. Barrio, MD, the study discussant and a breast cancer surgeon at Memorial Sloan Kettering Cancer Center, New York, agreed with the message from SENOMAC.
“Based on this, ALND [axillary lymph node dissection] should not be considered standard in patients with clinical T1-3, N0 breast cancer with one to two positive sentinel nodes, with or without microscopic extracapsular extension, undergoing lumpectomy or mastectomy,” provided nodal adjuvant radiotherapy is indicated, she said.
Although adjuvant nodal radiation for patients with one to three positive sentinel nodes is standard of care in Denmark and Sweden, where most of the patients in SENOMAC were located, practices vary widely in the United States. If adjuvant radiation isn’t used, “then ALND [is still] indicated,” Dr. Barrio said, but in either case, “only one is needed.”
In keeping with the de-escalation theme at the 2023 symposium, both Dr. Boniface and Dr. Barrio noted that trials are now underway to find patients who can avoid any axillary treatment at all if they have just one or two positive sentinel lymph nodes.
Preoperative axillary ultrasound was mandatory in SENOMAC and patients with non-palpable suspicious axillary lymph nodes were enrolled.
Thirty-six were positive on fine needle aspiration and randomized into the study, but when asked, Dr. Boniface didn’t have the data immediately at hand on how they fared.
The work was funded by the Swedish Research Council, Nordic Cancer Union, and others. Dr. Boniface and Dr. Barrio didn’t have any disclosures.
SAN ANTONIO — Axillary lymph node dissection may be unnecessary if breast cancer patients with one or two positive sentinel lymph nodes plan to have adjuvant nodal radiation, according to a major Scandinavian trial presented at the San Antonio Breast Cancer Symposium.
“It means that you don’t need to dissect the axilla if you” are going to “radiate the axilla.” “For the U.S., that’s the conclusion because there are still centers that do both, and that’s out,” lead investigator Jana de Boniface, MD, PhD, a breast cancer surgeon at the Karolinska Institutet, Stockholm, said in an interview.
Some even wondered if 5 years of endocrine therapy is necessary.
Dr. Boniface shared her thoughts after presenting the Scandinavian trial, SENOMAC, which she led.
SENOMAC randomized 1,204 patients with one or two positive sentinel lymph nodes to axillary dissection; 1,335 with the same finding were randomized to no dissection.
Subjects had clinically T1-3, N0 primary breast cancer. About 89% in both arms went on to adjuvant radiation, including nodal radiation, and almost all also went on to systemic therapy, which included endocrine therapy in over 90%. Only about 2% of subjects had neoadjuvant therapy.
At a median follow-up of nearly 4 years, recurrence-free survival was virtually identical in both groups, with 8% of patients in the dissection arm and 7.1% in the no-dissection group having recurrences. Estimated 5-year recurrence-free survival was just shy of 90% in both groups. Skipping dissection was strongly non-inferior to having one (P < .001).
SENOMAC “clearly shows that you don’t need to dissect the axilla if you have one to two positive sentinel lymph nodes” so long as patients have adjuvant nodal radiation. Recurrence-free survival “curves practically overlap, and we cannot see any difference between the two groups,” Dr. Boniface said.
Meanwhile, the dissection group fared worse on patient reported outcomes. Overall survival outcomes, the primary endpoint of the trial, are expected within 2 years.
The goal of the trial, the largest to date to look into the issue, was to fill gaps in the literature. Similar outcomes were reported around a decade ago in patients with low sentinel lymph node burdens, but the extensive exclusion criteria raised questions about general applicability.
In contrast, SENOMAC was widely inclusive. Over a third of patients had mastectomies, over a third had sentinel lymph node extracapsular extension, almost 6% had T3 disease, almost 20% had lobular carcinoma, 40% were 65 years or older, and tumors were as large as 15.5 cm.
The findings held regardless of those and other factors on subgroup analyses, including estrogen receptor and HER2 status and the number of additional positive nodes retrieved in the dissection group.
Andrea V. Barrio, MD, the study discussant and a breast cancer surgeon at Memorial Sloan Kettering Cancer Center, New York, agreed with the message from SENOMAC.
“Based on this, ALND [axillary lymph node dissection] should not be considered standard in patients with clinical T1-3, N0 breast cancer with one to two positive sentinel nodes, with or without microscopic extracapsular extension, undergoing lumpectomy or mastectomy,” provided nodal adjuvant radiotherapy is indicated, she said.
Although adjuvant nodal radiation for patients with one to three positive sentinel nodes is standard of care in Denmark and Sweden, where most of the patients in SENOMAC were located, practices vary widely in the United States. If adjuvant radiation isn’t used, “then ALND [is still] indicated,” Dr. Barrio said, but in either case, “only one is needed.”
In keeping with the de-escalation theme at the 2023 symposium, both Dr. Boniface and Dr. Barrio noted that trials are now underway to find patients who can avoid any axillary treatment at all if they have just one or two positive sentinel lymph nodes.
Preoperative axillary ultrasound was mandatory in SENOMAC and patients with non-palpable suspicious axillary lymph nodes were enrolled.
Thirty-six were positive on fine needle aspiration and randomized into the study, but when asked, Dr. Boniface didn’t have the data immediately at hand on how they fared.
The work was funded by the Swedish Research Council, Nordic Cancer Union, and others. Dr. Boniface and Dr. Barrio didn’t have any disclosures.
FROM SABCS 2023
Male Surgeons Linked With Higher Subsequent Healthcare Costs
, data suggested.
A retrospective, population-based cohort study that included more than 1 million adults undergoing any of 25 common surgical procedures found that total healthcare costs assessed at 1 year following surgery were more than $6000 higher when the surgery was performed by a male surgeon. Costs were also higher at 30 and 90 days for patients treated by male surgeons.
“As a male surgeon, I think our results should cause me and my colleagues to pause and consider why this may be,” said lead author Christopher J. D. Wallis, MD, PhD, assistant professor of surgery at the University of Toronto.
“None of us believe that the presence of a Y chromosome in surgeons means there are worse outcomes, it’s just that generally speaking, men and women, as we have known for decades, practice medicine a little differently. Things like communication style, time they spend with their patients, and even things like guideline adherence are different, and understanding how those differences translate into patient outcomes is the goal of this whole body of work,” said Wallis.
The study was published online November 29 in JAMA Surgery.
Explanation Is Elusive
In earlier work, Dr. Wallis and his team reported that patients treated by female surgeons had a small but statistically significant decrease in 30-day mortality, were less likely to be readmitted to the hospital, and had fewer complications than those treated by male surgeons. In another study, they found worse outcomes among female patients treated by male surgeons.
In the current study, the researchers examined the association between surgeon sex and healthcare costs among patients undergoing various surgical procedures, including coronary artery bypass grafting, appendectomy, hysterectomy, anterior spinal decompression, and knee replacement. They included all adult patients who underwent these procedures at hospitals in Ontario, Canada, between January 2007 and December 2019 in their analysis.
The study sample included 1,165,711 patients. Of this group, 151,054 patients were treated by a female surgeon, and 1,014,657 were treated by a male surgeon.
After adjusting for patient-, surgeon-, anesthesiologist-, and hospital-related factors, they found that 1-year total healthcare costs were $24,882 for patients treated by male surgeons vs $18,517 for patients treated by female surgeons. Healthcare costs were also higher at 30 days (adjusted absolute difference, $3115) and at 90 days (adjusted absolute difference, $4228).
“This translates into a 9%-10% higher risk of costs with male surgeons compared with women surgeons at these time points,” said Dr. Wallis.
“This study cannot provide a specific answer as to why these differences are occurring,” Dr. Wallis said.
“We are currently undertaking more research to better understand the reasons. Our previous studies have shown that patients treated by male physicians have higher rates of death, readmission, and complications. Managing these adverse postoperative events is costly and likely contributes to these differences. Given the size of our study and similar training pathways, we do not think there are technical differences between male and female surgeons. Rather, we are hypothesizing that there may be differences in how physicians practice, make decisions, and consult with patients,” he said.
Ultimately, Dr. Wallis said he would like his research to prompt “a moment of introspection” among his surgical colleagues.
“Hopefully, these data will provide the impetus for further efforts to make surgery, and medicine in general, a field that is welcoming to women,” he said.
Potential Confounding Factors
This study expands the evidence suggesting significant practice differences between male and female surgeons, Ursula Adams, MD, a resident; Caprice C. Greenberg, MD, MPH, chair; and Jared Gallaher, MD, MPH, adjunct assistant professor, all from the Department of Surgery at the University of North Carolina in Chapel Hill, wrote in an accompanying editorial.
They cautioned, however, that “there are many potential confounding factors and possible explanatory mechanisms associated with surgeon sex that make it challenging to untangle influences on costs. Sex may be an easily captured data point, but is understanding the mechanism by which it affects cost the right next step? Surgeons control how and where they practice; they do not have control over their own demographics.”
The editorialists added that while recruiting and retaining women in surgery is important, it is not a solution to controlling costs.
“We must provide surgeons with better data to understand how practice approach and decisions affect cost and support for practice improvement. Only with these insights will we ensure patients of male surgeons receive care that is just as cost-effective as that provided by female surgeons, while also helping to bend the cost curve and improve the quality of surgical care,” they concluded.
‘Admirable’ Data Use
Commenting on the findings, Oluwadamilola “Lola” Fayanju, MD, chief of breast surgery at Penn Medicine in Philadelphia, said, “It is interesting that the study was performed in Canada with its different healthcare system.” Dr. Fayanju did not participate in the study.
“They used administrative data from a national database, and it is admirable that they were able to do that. These data allow us to make large-scale geographical assessments, although they are subject to errors and unmeasured confounders,” said Dr. Fayanju.
Women surgeons may do things that result in better outcomes, she suggested. “In this study, the women were younger and so perhaps were more up to date. They might have optimized management of their patients in the pre-op phase, including better patient selection, which led to better costs. Or in the post-op phase, they might have made themselves readily accessible. For instance, I remove all barriers about getting in touch with me, and I tell my students to make sure the patient can reach you easily,” said Dr. Fayanju.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care, and the Data Sciences Institute at the University of Toronto. Dr. Wallis, Dr. Adams, Dr. Greenberg, Dr. Gallaher, and Dr. Fayanju reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
, data suggested.
A retrospective, population-based cohort study that included more than 1 million adults undergoing any of 25 common surgical procedures found that total healthcare costs assessed at 1 year following surgery were more than $6000 higher when the surgery was performed by a male surgeon. Costs were also higher at 30 and 90 days for patients treated by male surgeons.
“As a male surgeon, I think our results should cause me and my colleagues to pause and consider why this may be,” said lead author Christopher J. D. Wallis, MD, PhD, assistant professor of surgery at the University of Toronto.
“None of us believe that the presence of a Y chromosome in surgeons means there are worse outcomes, it’s just that generally speaking, men and women, as we have known for decades, practice medicine a little differently. Things like communication style, time they spend with their patients, and even things like guideline adherence are different, and understanding how those differences translate into patient outcomes is the goal of this whole body of work,” said Wallis.
The study was published online November 29 in JAMA Surgery.
Explanation Is Elusive
In earlier work, Dr. Wallis and his team reported that patients treated by female surgeons had a small but statistically significant decrease in 30-day mortality, were less likely to be readmitted to the hospital, and had fewer complications than those treated by male surgeons. In another study, they found worse outcomes among female patients treated by male surgeons.
In the current study, the researchers examined the association between surgeon sex and healthcare costs among patients undergoing various surgical procedures, including coronary artery bypass grafting, appendectomy, hysterectomy, anterior spinal decompression, and knee replacement. They included all adult patients who underwent these procedures at hospitals in Ontario, Canada, between January 2007 and December 2019 in their analysis.
The study sample included 1,165,711 patients. Of this group, 151,054 patients were treated by a female surgeon, and 1,014,657 were treated by a male surgeon.
After adjusting for patient-, surgeon-, anesthesiologist-, and hospital-related factors, they found that 1-year total healthcare costs were $24,882 for patients treated by male surgeons vs $18,517 for patients treated by female surgeons. Healthcare costs were also higher at 30 days (adjusted absolute difference, $3115) and at 90 days (adjusted absolute difference, $4228).
“This translates into a 9%-10% higher risk of costs with male surgeons compared with women surgeons at these time points,” said Dr. Wallis.
“This study cannot provide a specific answer as to why these differences are occurring,” Dr. Wallis said.
“We are currently undertaking more research to better understand the reasons. Our previous studies have shown that patients treated by male physicians have higher rates of death, readmission, and complications. Managing these adverse postoperative events is costly and likely contributes to these differences. Given the size of our study and similar training pathways, we do not think there are technical differences between male and female surgeons. Rather, we are hypothesizing that there may be differences in how physicians practice, make decisions, and consult with patients,” he said.
Ultimately, Dr. Wallis said he would like his research to prompt “a moment of introspection” among his surgical colleagues.
“Hopefully, these data will provide the impetus for further efforts to make surgery, and medicine in general, a field that is welcoming to women,” he said.
Potential Confounding Factors
This study expands the evidence suggesting significant practice differences between male and female surgeons, Ursula Adams, MD, a resident; Caprice C. Greenberg, MD, MPH, chair; and Jared Gallaher, MD, MPH, adjunct assistant professor, all from the Department of Surgery at the University of North Carolina in Chapel Hill, wrote in an accompanying editorial.
They cautioned, however, that “there are many potential confounding factors and possible explanatory mechanisms associated with surgeon sex that make it challenging to untangle influences on costs. Sex may be an easily captured data point, but is understanding the mechanism by which it affects cost the right next step? Surgeons control how and where they practice; they do not have control over their own demographics.”
The editorialists added that while recruiting and retaining women in surgery is important, it is not a solution to controlling costs.
“We must provide surgeons with better data to understand how practice approach and decisions affect cost and support for practice improvement. Only with these insights will we ensure patients of male surgeons receive care that is just as cost-effective as that provided by female surgeons, while also helping to bend the cost curve and improve the quality of surgical care,” they concluded.
‘Admirable’ Data Use
Commenting on the findings, Oluwadamilola “Lola” Fayanju, MD, chief of breast surgery at Penn Medicine in Philadelphia, said, “It is interesting that the study was performed in Canada with its different healthcare system.” Dr. Fayanju did not participate in the study.
“They used administrative data from a national database, and it is admirable that they were able to do that. These data allow us to make large-scale geographical assessments, although they are subject to errors and unmeasured confounders,” said Dr. Fayanju.
Women surgeons may do things that result in better outcomes, she suggested. “In this study, the women were younger and so perhaps were more up to date. They might have optimized management of their patients in the pre-op phase, including better patient selection, which led to better costs. Or in the post-op phase, they might have made themselves readily accessible. For instance, I remove all barriers about getting in touch with me, and I tell my students to make sure the patient can reach you easily,” said Dr. Fayanju.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care, and the Data Sciences Institute at the University of Toronto. Dr. Wallis, Dr. Adams, Dr. Greenberg, Dr. Gallaher, and Dr. Fayanju reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
, data suggested.
A retrospective, population-based cohort study that included more than 1 million adults undergoing any of 25 common surgical procedures found that total healthcare costs assessed at 1 year following surgery were more than $6000 higher when the surgery was performed by a male surgeon. Costs were also higher at 30 and 90 days for patients treated by male surgeons.
“As a male surgeon, I think our results should cause me and my colleagues to pause and consider why this may be,” said lead author Christopher J. D. Wallis, MD, PhD, assistant professor of surgery at the University of Toronto.
“None of us believe that the presence of a Y chromosome in surgeons means there are worse outcomes, it’s just that generally speaking, men and women, as we have known for decades, practice medicine a little differently. Things like communication style, time they spend with their patients, and even things like guideline adherence are different, and understanding how those differences translate into patient outcomes is the goal of this whole body of work,” said Wallis.
The study was published online November 29 in JAMA Surgery.
Explanation Is Elusive
In earlier work, Dr. Wallis and his team reported that patients treated by female surgeons had a small but statistically significant decrease in 30-day mortality, were less likely to be readmitted to the hospital, and had fewer complications than those treated by male surgeons. In another study, they found worse outcomes among female patients treated by male surgeons.
In the current study, the researchers examined the association between surgeon sex and healthcare costs among patients undergoing various surgical procedures, including coronary artery bypass grafting, appendectomy, hysterectomy, anterior spinal decompression, and knee replacement. They included all adult patients who underwent these procedures at hospitals in Ontario, Canada, between January 2007 and December 2019 in their analysis.
The study sample included 1,165,711 patients. Of this group, 151,054 patients were treated by a female surgeon, and 1,014,657 were treated by a male surgeon.
After adjusting for patient-, surgeon-, anesthesiologist-, and hospital-related factors, they found that 1-year total healthcare costs were $24,882 for patients treated by male surgeons vs $18,517 for patients treated by female surgeons. Healthcare costs were also higher at 30 days (adjusted absolute difference, $3115) and at 90 days (adjusted absolute difference, $4228).
“This translates into a 9%-10% higher risk of costs with male surgeons compared with women surgeons at these time points,” said Dr. Wallis.
“This study cannot provide a specific answer as to why these differences are occurring,” Dr. Wallis said.
“We are currently undertaking more research to better understand the reasons. Our previous studies have shown that patients treated by male physicians have higher rates of death, readmission, and complications. Managing these adverse postoperative events is costly and likely contributes to these differences. Given the size of our study and similar training pathways, we do not think there are technical differences between male and female surgeons. Rather, we are hypothesizing that there may be differences in how physicians practice, make decisions, and consult with patients,” he said.
Ultimately, Dr. Wallis said he would like his research to prompt “a moment of introspection” among his surgical colleagues.
“Hopefully, these data will provide the impetus for further efforts to make surgery, and medicine in general, a field that is welcoming to women,” he said.
Potential Confounding Factors
This study expands the evidence suggesting significant practice differences between male and female surgeons, Ursula Adams, MD, a resident; Caprice C. Greenberg, MD, MPH, chair; and Jared Gallaher, MD, MPH, adjunct assistant professor, all from the Department of Surgery at the University of North Carolina in Chapel Hill, wrote in an accompanying editorial.
They cautioned, however, that “there are many potential confounding factors and possible explanatory mechanisms associated with surgeon sex that make it challenging to untangle influences on costs. Sex may be an easily captured data point, but is understanding the mechanism by which it affects cost the right next step? Surgeons control how and where they practice; they do not have control over their own demographics.”
The editorialists added that while recruiting and retaining women in surgery is important, it is not a solution to controlling costs.
“We must provide surgeons with better data to understand how practice approach and decisions affect cost and support for practice improvement. Only with these insights will we ensure patients of male surgeons receive care that is just as cost-effective as that provided by female surgeons, while also helping to bend the cost curve and improve the quality of surgical care,” they concluded.
‘Admirable’ Data Use
Commenting on the findings, Oluwadamilola “Lola” Fayanju, MD, chief of breast surgery at Penn Medicine in Philadelphia, said, “It is interesting that the study was performed in Canada with its different healthcare system.” Dr. Fayanju did not participate in the study.
“They used administrative data from a national database, and it is admirable that they were able to do that. These data allow us to make large-scale geographical assessments, although they are subject to errors and unmeasured confounders,” said Dr. Fayanju.
Women surgeons may do things that result in better outcomes, she suggested. “In this study, the women were younger and so perhaps were more up to date. They might have optimized management of their patients in the pre-op phase, including better patient selection, which led to better costs. Or in the post-op phase, they might have made themselves readily accessible. For instance, I remove all barriers about getting in touch with me, and I tell my students to make sure the patient can reach you easily,” said Dr. Fayanju.
The study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care, and the Data Sciences Institute at the University of Toronto. Dr. Wallis, Dr. Adams, Dr. Greenberg, Dr. Gallaher, and Dr. Fayanju reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
AGA Tech Summit: Bridging the Gap Between Innovation, Industry, and Gastroenterologists
Medicine is transforming at a remarkable pace. It is therefore imperative for the future of the field that physicians understand innovation and collaborate with industry partners. Innovation can be defined as invention, adoption, and diffusion.1 During my training in gastroenterology and advanced fellowships, I learned about multiple endoscopic tools and techniques and became familiar with industry names that I frequently encountered in the endoscopy unit or clinic.
I was nominated to attend the AGA Tech Summit Fellows Program by my advanced endoscopy fellowship program director. A total of 22 fellows from around the United States at various stages of their training and interests in the field of gastroenterology and hepatology were selected for the program through an application process. The program included registration, travel, and accommodations to attend the AGA Tech Summit and Fellows Immersion Day at Medtronic.
The first event in the program was a visit to the Medtronic Santa Clara office, where our initial stop was at the research and development lab. We were introduced to design and biomedical engineers who reviewed with us the extensive testing that devices and endoscopy equipment undergo before coming to the market. These labs have a heavy focus on prototyping and experimentation and exist to promote in-house innovation and inventions.
During the day, we met physicians who shared their journeys on how they developed and advanced their careers in partnership with industry. Our visit also included a session with the business development and strategy manager at Medtronic, who discussed strategy and steps involved in product development — from the inception of an idea, institutional policies, and patents, to industry collaboration, and finally to successful commercialization. During medical school and training, we are focused on appropriately learning and applying medical knowledge to clinical care. The Medtronic Fellows Immersion Day experience offered a different perspective and showed other ways by which clinical knowledge and experience can be used to make an impact, in collaboration with industry and stakeholders. It also highlighted alternative career paths for medical professionals. The evening concluded with a meet and greet with the AGA Center for GI Innovation & Technology (CGIT) members and leadership.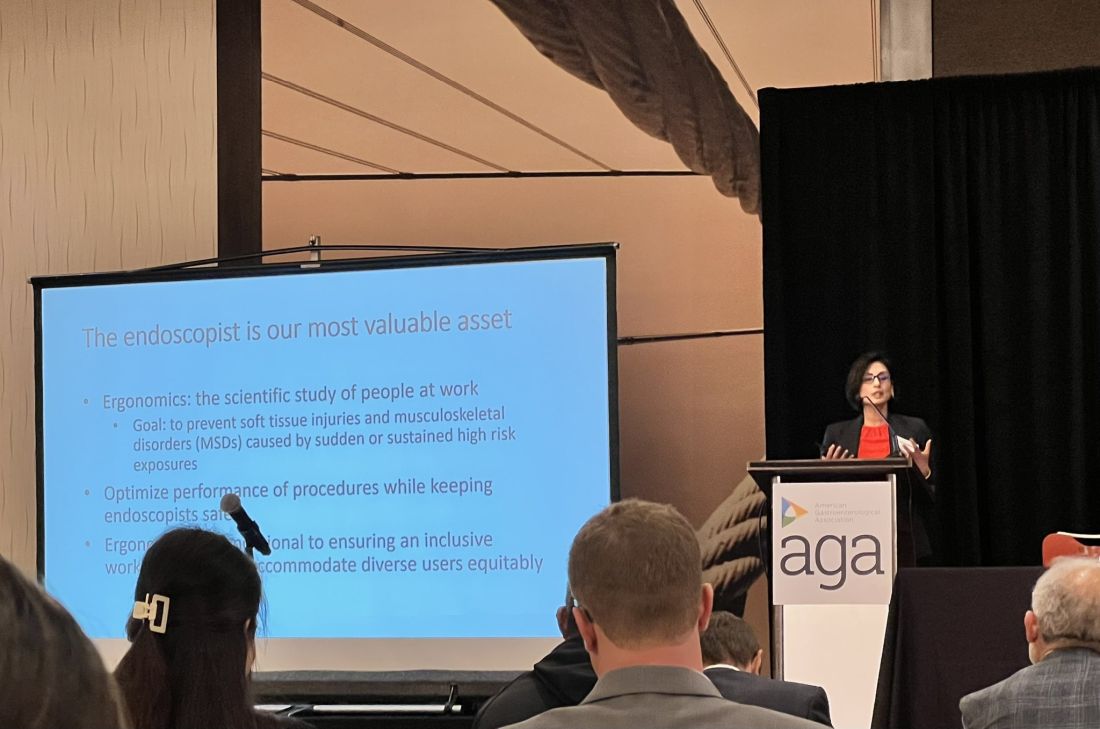
The AGA Tech Summit was unlike any conference I have been to in my 13 years of training in medicine (which included mostly clinically focused scientific meetings). Sessions involved ergonomics, applications of artificial intelligence, advances in imaging, environmental endoscopy, the role of the FDA, and innovations around the world. The audience included but was not limited to industry executives, AGA CGIT leadership, physician innovators, gastroenterologists, venture capitalists, and others. Attendees represented the diversity of our field in terms of organizational structures and backgrounds. This resulted in an opportunity to hear and learn different perspectives about products, emerging technology, and the costs involved for physicians, industry, and patients.
The final session of the summit, the AGA Shark Tank, was perhaps the most intriguing one of all. The session showcased landscape-changing technology to AGA investors and venture capitalists. The participants presented their own pitches and faced the sharks (judges). The winner received additional funding, tailored guidance from the AGA CGIT committee, partnering opportunities with interested parties, and the opportunity to represent AGA Shark Tank at the Digestive Disease Week (DDW).
The AGA Tech Summit Fellows Program is a learning platform that not only helps you find your niche in the world of GI innovation but also equips you with resources and connections to make an impact. It is also a great way to infuse new ideas into your practice or research. As healthcare professionals, we must create a culture where innovation can flourish, and where staff and patients feel empowered to contribute to the innovation process and help make change happen — to me, the AGA Tech Summit is one such avenue.
Reference
1. Kelly CJ and Young AJ. Promoting innovation in healthcare. Future Healthc J. 2017 Jun. doi: 10.7861/futurehosp.4-2-121.
Dr. Umar is Assistant Professor of Medicine, Section of Gastroenterology and Hepatology, Baylor College of Medicine, Houston, Texas, and a staff physician at Michael E. DeBakey VA Medical Center, Houston. Dr. Umar has no relevant financial conflicts and is on X, formerly Twitter, @shifaumarMD.
Medicine is transforming at a remarkable pace. It is therefore imperative for the future of the field that physicians understand innovation and collaborate with industry partners. Innovation can be defined as invention, adoption, and diffusion.1 During my training in gastroenterology and advanced fellowships, I learned about multiple endoscopic tools and techniques and became familiar with industry names that I frequently encountered in the endoscopy unit or clinic.
I was nominated to attend the AGA Tech Summit Fellows Program by my advanced endoscopy fellowship program director. A total of 22 fellows from around the United States at various stages of their training and interests in the field of gastroenterology and hepatology were selected for the program through an application process. The program included registration, travel, and accommodations to attend the AGA Tech Summit and Fellows Immersion Day at Medtronic.
The first event in the program was a visit to the Medtronic Santa Clara office, where our initial stop was at the research and development lab. We were introduced to design and biomedical engineers who reviewed with us the extensive testing that devices and endoscopy equipment undergo before coming to the market. These labs have a heavy focus on prototyping and experimentation and exist to promote in-house innovation and inventions.
During the day, we met physicians who shared their journeys on how they developed and advanced their careers in partnership with industry. Our visit also included a session with the business development and strategy manager at Medtronic, who discussed strategy and steps involved in product development — from the inception of an idea, institutional policies, and patents, to industry collaboration, and finally to successful commercialization. During medical school and training, we are focused on appropriately learning and applying medical knowledge to clinical care. The Medtronic Fellows Immersion Day experience offered a different perspective and showed other ways by which clinical knowledge and experience can be used to make an impact, in collaboration with industry and stakeholders. It also highlighted alternative career paths for medical professionals. The evening concluded with a meet and greet with the AGA Center for GI Innovation & Technology (CGIT) members and leadership.
The AGA Tech Summit was unlike any conference I have been to in my 13 years of training in medicine (which included mostly clinically focused scientific meetings). Sessions involved ergonomics, applications of artificial intelligence, advances in imaging, environmental endoscopy, the role of the FDA, and innovations around the world. The audience included but was not limited to industry executives, AGA CGIT leadership, physician innovators, gastroenterologists, venture capitalists, and others. Attendees represented the diversity of our field in terms of organizational structures and backgrounds. This resulted in an opportunity to hear and learn different perspectives about products, emerging technology, and the costs involved for physicians, industry, and patients.
The final session of the summit, the AGA Shark Tank, was perhaps the most intriguing one of all. The session showcased landscape-changing technology to AGA investors and venture capitalists. The participants presented their own pitches and faced the sharks (judges). The winner received additional funding, tailored guidance from the AGA CGIT committee, partnering opportunities with interested parties, and the opportunity to represent AGA Shark Tank at the Digestive Disease Week (DDW).
The AGA Tech Summit Fellows Program is a learning platform that not only helps you find your niche in the world of GI innovation but also equips you with resources and connections to make an impact. It is also a great way to infuse new ideas into your practice or research. As healthcare professionals, we must create a culture where innovation can flourish, and where staff and patients feel empowered to contribute to the innovation process and help make change happen — to me, the AGA Tech Summit is one such avenue.
Reference
1. Kelly CJ and Young AJ. Promoting innovation in healthcare. Future Healthc J. 2017 Jun. doi: 10.7861/futurehosp.4-2-121.
Dr. Umar is Assistant Professor of Medicine, Section of Gastroenterology and Hepatology, Baylor College of Medicine, Houston, Texas, and a staff physician at Michael E. DeBakey VA Medical Center, Houston. Dr. Umar has no relevant financial conflicts and is on X, formerly Twitter, @shifaumarMD.
Medicine is transforming at a remarkable pace. It is therefore imperative for the future of the field that physicians understand innovation and collaborate with industry partners. Innovation can be defined as invention, adoption, and diffusion.1 During my training in gastroenterology and advanced fellowships, I learned about multiple endoscopic tools and techniques and became familiar with industry names that I frequently encountered in the endoscopy unit or clinic.
I was nominated to attend the AGA Tech Summit Fellows Program by my advanced endoscopy fellowship program director. A total of 22 fellows from around the United States at various stages of their training and interests in the field of gastroenterology and hepatology were selected for the program through an application process. The program included registration, travel, and accommodations to attend the AGA Tech Summit and Fellows Immersion Day at Medtronic.
The first event in the program was a visit to the Medtronic Santa Clara office, where our initial stop was at the research and development lab. We were introduced to design and biomedical engineers who reviewed with us the extensive testing that devices and endoscopy equipment undergo before coming to the market. These labs have a heavy focus on prototyping and experimentation and exist to promote in-house innovation and inventions.
During the day, we met physicians who shared their journeys on how they developed and advanced their careers in partnership with industry. Our visit also included a session with the business development and strategy manager at Medtronic, who discussed strategy and steps involved in product development — from the inception of an idea, institutional policies, and patents, to industry collaboration, and finally to successful commercialization. During medical school and training, we are focused on appropriately learning and applying medical knowledge to clinical care. The Medtronic Fellows Immersion Day experience offered a different perspective and showed other ways by which clinical knowledge and experience can be used to make an impact, in collaboration with industry and stakeholders. It also highlighted alternative career paths for medical professionals. The evening concluded with a meet and greet with the AGA Center for GI Innovation & Technology (CGIT) members and leadership.
The AGA Tech Summit was unlike any conference I have been to in my 13 years of training in medicine (which included mostly clinically focused scientific meetings). Sessions involved ergonomics, applications of artificial intelligence, advances in imaging, environmental endoscopy, the role of the FDA, and innovations around the world. The audience included but was not limited to industry executives, AGA CGIT leadership, physician innovators, gastroenterologists, venture capitalists, and others. Attendees represented the diversity of our field in terms of organizational structures and backgrounds. This resulted in an opportunity to hear and learn different perspectives about products, emerging technology, and the costs involved for physicians, industry, and patients.
The final session of the summit, the AGA Shark Tank, was perhaps the most intriguing one of all. The session showcased landscape-changing technology to AGA investors and venture capitalists. The participants presented their own pitches and faced the sharks (judges). The winner received additional funding, tailored guidance from the AGA CGIT committee, partnering opportunities with interested parties, and the opportunity to represent AGA Shark Tank at the Digestive Disease Week (DDW).
The AGA Tech Summit Fellows Program is a learning platform that not only helps you find your niche in the world of GI innovation but also equips you with resources and connections to make an impact. It is also a great way to infuse new ideas into your practice or research. As healthcare professionals, we must create a culture where innovation can flourish, and where staff and patients feel empowered to contribute to the innovation process and help make change happen — to me, the AGA Tech Summit is one such avenue.
Reference
1. Kelly CJ and Young AJ. Promoting innovation in healthcare. Future Healthc J. 2017 Jun. doi: 10.7861/futurehosp.4-2-121.
Dr. Umar is Assistant Professor of Medicine, Section of Gastroenterology and Hepatology, Baylor College of Medicine, Houston, Texas, and a staff physician at Michael E. DeBakey VA Medical Center, Houston. Dr. Umar has no relevant financial conflicts and is on X, formerly Twitter, @shifaumarMD.
Physician-Owned Hospitals: The Answer for Better Care?
This discussion was recorded on November 16, 2023. This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical advisor for Medscape Emergency Medicine. Joining me today is Dr. Brian J. Miller, a hospitalist with Johns Hopkins University School of Medicine and a health policy expert, to discuss the current and renewed interest in physician-owned hospitals.
Welcome, Dr. Miller. It’s a pleasure to have you join me today.
Brian J. Miller, MD, MBA, MPH: Thank you for having me.
History and Controversies Surrounding Physician-Owned Hospitals
Dr. Glatter: I want to start off by having you describe the history associated with the moratorium on new physician-owned hospitals in 2010 that’s related ultimately to the Affordable Care Act, but also, the current and renewed media interest in physician-owned hospitals that’s linked to recent congressional hearings last month.
Dr. Miller: Thank you. I should note that my views are my own and don’t represent those of Hopkins or the American Enterprise Institute, where I’m a nonresident fellow nor the Medicare Payment Advisory Commission, of which I’m a Commissioner.
The story about physician-owned hospitals is an interesting one. Hospitals turned into health systems in the 1980s and 1990s, and physicians started to shift purely from an independent model into a more organized group practice or employed model. Physicians realized that they wanted an alternative operating arrangement. You want a choice of how you practice and what your employment is. And as community hospitals started to buy physicians and also establish their own physician groups de novo, physicians opened physician-owned hospitals.
Physician-owned hospitals fell into a couple of buckets. One is what we call community hospitals, or what the antitrust lawyers would call general acute care hospitals: those offering emergency room (ER) services, labor and delivery, primary care, general surgery — the whole regular gamut, except that some of the owners were physicians.
The other half of the marketplace ended up being specialty hospitals: those built around a specific medical specialty and series of procedures and chronic care. For example, cardiac hospitals often do CABG, TAVR, maybe abdominal aortic aneurysm (triple A) repairs, and they have cardiology clinics, cath labs, a cardiac intensive care unit (ICU), ER, etc. There were also orthopedic surgical specialty hospitals, which were sort of like an ambulatory surgery center (ASC) plus several beds. Then there were general surgical specialty hospitals. At one point, there were some women’s health–focused specialty hospitals.
The hospital industry, of course, as you can understand, didn’t exactly like this. They had a series of concerns about what we would historically call cherry-picking or lemon-dropping of patients. They were worried that physician-owned facilities didn’t want to serve public payer patients, and there was a whole series of reports and investigations.
Around the time the Affordable Care Act passed, the hospital industry had many concerns about physician-owned specialty hospitals, and there was a moratorium as part of the 2003 Medicare Modernization Act. As part of the bargaining over the hospital industry support for the Affordable Care Act, they traded their support for, among other things, their number one priority, which is a statutory prohibition on new or expanded physician-owned hospitals from participating in Medicare. That included both physician-owned community hospitals and physician-owned specialty hospitals.
Dr. Glatter: That was part of the impetus to prevent physicians from referring patients where they had an ownership stake. Certainly, hospitals can be owned by attorneys and nonprofit organizations, and certainly, ASCs can be owned by physicians. There is an ongoing issue in terms of physicians not being able to have an ownership stake. In terms of equity ownership, we know that certain other models allow this, but basically, it sounds like this is an issue with Medicare. That seems to be the crux of it, correct?
Dr. Miller: Yes. I would also add that it’s interesting when we look at other professions. When we look at lawyers, nonlawyers are actually not allowed to own an equity stake in a law practice. In many other professions, you either have corporate ownership or professional ownership, or the alternative is you have only professional ownership. I would say the hospital industry is one of the few areas where professional ownership not only is not allowed, but also is statutorily prohibited functionally through the Medicare program.
Unveiling the Dynamics of Hospital Ownership
Dr. Glatter: A recent study done by two PhDs looked at 2019 data on 20 of the most expensive diagnosis-related groups (DRGs). It examined the cost savings, and we’re talking over $1 billion in expenditures when you look at the data from general acute care hospitals vs physician-owned hospitals. This is what appears to me to be a key driver of the push to loosen restrictions on physician-owned hospitals. Isn’t that correct?
Dr. Miller: I would say that’s one of many components. There’s more history to this issue. I remember sitting at a think tank talking to someone several years ago about hospital consolidation as an issue. We went through the usual levers that us policy wonks go through. We talked about antitrust enforcement, certificate of need, rising hospital costs from consolidation, lower quality (or at least no quality gains, as shown by a New England Journal of Medicine study), and decrements in patient experience that result from the diseconomies of scale. They sort of pooh-poohed many of the policy ideas. They basically said that there was no hope for hospital consolidation as an issue.
Well, what about physician ownership? I started with my research team to comb through the literature and found a variety of studies — some of which were sort of entertaining, because they’d do things like study physician-owned specialty hospitals, nonprofit-owned specialty hospitals, and for-profit specialty hospitals and compare them with nonprofit or for-profit community hospitals, and then say physician-owned hospitals that were specialty were bad.
They mixed ownership and service markets right there in so many ways, I’m not sure where to start. My team did a systematic review of around 30 years of research, looking at the evidence base in this space. We found a couple of things.
We found that physician-owned community hospitals did not have a cost or quality difference, meaning that there was no definitive evidence that the physician-owned community hospitals were cheaper based on historical evidence, which was very old. That means there’s not specific harm from them. When you permit market entry for community hospitals, that promotes competition, which results in lower prices and higher quality.
Then we also looked at the specialty hospital markets — surgical specialty hospitals, orthopedic surgical specialty hospitals, and cardiac hospitals. We noted for cardiac hospitals, there wasn’t clear evidence about cost savings, but there was definitive evidence of higher quality, from things like 30-day mortality for significant procedures like treatment of acute MI, triple A repair, stuff like that.
For orthopedic surgical specialty hospitals, we noted lower costs and higher quality, which again fits with operationally what we would know. If you have a facility that’s doing 20 total hips a day, you’re creating a focused factory. Just like if you think about it for interventional cardiology, your boards have a minimum number of procedures that you have to do to stay certified because we know about the volume-quality relationship.
Then we looked at general surgical specialty hospitals. There wasn’t enough evidence to make a conclusive thought about costs, and there was a clear trend toward higher quality. I would say this recent study is important, but there is a whole bunch of other literature out there, too.
Exploring the Scope of Emergency Care in Physician-Owned Hospitals
Dr. Glatter: Certainly, your colleague Wang from Johns Hopkins has done important research in this sector. The paper, “Reconsidering the Ban on Physician-Owned Hospitals to Combat Consolidation,” by you and several colleagues, mentions and highlights the issues that you just described. I understand that it’s going to be published in the NYU Journal of Legislation and Public Policy.
One thing I want to bring up — and this is an important issue — is that the risk for patients has been talked about by the American Hospital Association and the Federation of American Hospitals, in terms of limited or no emergency services at such physician-owned hospitals and having to call 911 when patients need emergent care or stabilization. That’s been the rebuttal, along with an Office of Inspector General (OIG) report from 2008. Almost, I guess, three quarters of the patients that needed emergent care got this at publicly funded hospitals.
Dr. Miller: I’m familiar with the argument about emergency care. If you actually go and look at it, it differs by specialty market. Physician-owned community hospitals have ERs because that’s how they get their business. If you are running a hospital medicine floor, a general surgical specialty floor, you have a labor delivery unit, a primary care clinic, and a cardiology clinic. You have all the things that all the other hospitals have. The physician-owned community hospitals almost uniformly have an ER.
When you look at the physician-owned specialty hospitals, it’s a little more granular. If you look at the cardiac hospitals, they have ERs. They also have cardiac ICUs, operating rooms, etc. The area where the hospital industry had concerns — which I think is valid to point out — is that physician-owned orthopedic surgical specialty hospitals don’t have ERs. But this makes sense because of what that hospital functionally is: a factory for whatever the scope of procedures is, be it joint replacements or shoulder arthroscopy. The orthopedic surgical specialty hospital is like an ASC plus several hospital beds. Many of those did not have ERs because clinically it didn’t make sense.
What’s interesting, though, is that the hospital industry also operates specialty hospitals. If you go into many of the large systems, they have cardiac specialty hospitals and cancer specialty hospitals. I would say that some of them have ERs, as they appropriately should, and some of those specialty hospitals do not. They might have a community hospital down the street that’s part of that health system that has an ER, but some of the specialty hospitals don’t necessarily have a dedicated ER.
I agree, that’s a valid concern. I would say, though, the question is, what are the scope of services in that hospital? Is an ER required? Community hospitals should have ERs. It makes sense also for a cardiac hospital to have one. If you’re running a total joint replacement factory, it might not make clinical sense.
Dr. Glatter: The patients who are treated at that hospital, if they do have emergent conditions, need to have board-certified emergency physicians treating them, in my view because I’m an ER physician. Having surgeons that are not emergency physicians staff a department at a specialty orthopedic hospital or, say, a cancer hospital is not acceptable from my standpoint. That›s my opinion and recommendation, coming from emergency medicine.
Dr. Miller: I would say that anesthesiologists are actually highly qualified in critical care. The question is about clinical decompensation; if you’re doing a procedure, you have an anesthesiologist right there who is capable of critical care. The function of the ER is to either serve as a window into the hospital for patient volume or to serve as a referral for emergent complaints.
Dr. Glatter: An anesthesiologist — I’ll take issue with that — does not have the training of an emergency physician in terms of scope of practice.
Dr. Miller: My anesthesiology colleagues would probably disagree for managing an emergency during an operating room case.
Dr. Glatter: Fair enough, but I think in the general sense. The other issue is that, in terms of emergent responses to patients that decompensate, when you have to transfer a patient, that violates Medicare requirements. How is that even a valid issue or argument if you’re going to have to transfer a patient from your specialty hospital? That happens. Again, I know that you’re saying these hospitals are completely independent and can function, stabilize patients, and treat emergencies, but that’s not the reality across the country, in my opinion.
Dr. Miller: I don’t think that’s the case for the physician-owned specialty cardiac hospitals, for starters. Many of those have ICUs in addition to operating rooms as a matter of routine in addition to ERs. I don’t think that’s the case for physician-owned community hospitals, which have ERs, ICUs, medicine floors, and surgical floors. Physician-owned community hospitals are around half the market. Of that remaining market, a significant percentage are cardiac hospitals. If you’re taking an issue with orthopedic surgical specialty hospitals, that’s a clinical operational question that can and should be answered.
I’d also posit that the nonprofit and for-profit hospital industries also operate specialty hospitals. Any of these questions, we shouldn’t just be asking about physician-owned facilities; we should be asking about them across ownership types, because we’re talking about scope of service and quality and safety. The ownership in that case doesn’t matter. The broader question is, are orthopedic surgical specialty hospitals owned by physicians, tax-exempt hospitals, or tax-paying hospitals? Is that a valid clinical business model? Is it safe? Does it meet Medicare conditions of participation? I would say that’s what that question is, because other ownership models do operate those facilities.
Dr. Glatter: You make some valid points, and I do agree on some of them. I think that, ultimately, these models of care, and certainly cost and quality, are issues. Again, it goes back to being able, in my opinion, to provide emergent care, which seems to me a very important issue.
Dr. Miller: I agree that providing emergent care is an issue. It›s an issue in any site of care. The hospital industry posits that all hospital outpatient departments (HOPDs) have emergent care. I can tell you, having worked in HOPDs (I›ve trained in them during residency), the response if something emergent happens is to either call 911 or wheel the patient down to the ER in a wheelchair or stretcher. I think that these hospital claims about emergency care coverage — these are important questions, but we should be asking them across all clinical settings and say what is the appropriate scope of care provided? What is the appropriate level of acuity and ability to provide emergent or critical care? That›s an important question regardless of ownership model across the entire industry.
Deeper Dive Into Data on Physician-Owned Hospitals
Dr. Glatter: We need to really focus on that. I’ll agree with you on that.
There was a March 2023 report from Dobson | DaVanzo. It showed that physician-owned hospitals had lower Medicaid, dual-eligible, and uncompensated care and charity care discharges than full-service acute care hospitals. Physician-owned hospitals had less than half the proportion of Medicaid discharges compared with non–physician-owned hospitals. They were also less likely to care for dual-eligible patients overall compared with non–physician-owned hospitals.
In addition, when COVID hit, the physician-owned hospitals overall — and again, there may be exceptions — were not equipped to handle these patient surges in the acute setting of a public health emergency. There was a hospital in Texas that did pivot that I’m aware of — Renaissance Hospital, which ramped up a long-term care facility to become a COVID hospital — but I think that’s the exception. I think this report raises some valid concerns; I’ll let you rebut that.
Dr. Miller: A couple of things. One, I am not aware that there’s any clear market evidence or a systematic study that shows that physician-owned hospitals had trouble responding to COVID. I don’t think that assertion has been proven. The study was funded by the hospital industry. First of all, it was not a peer-reviewed study; it was funded by an industry that paid a consulting firm. It doesn’t mean that we still shouldn’t read it, but that brings bias into question. The joke in Washington is, pick your favorite statistician or economist, and they can say what you want and have a battle of economists and statisticians.
For example, in that study, they didn’t include the entire ownership universe of physician-owned hospitals. If we go to the peer-reviewed literature, there’s a great 2015 BMJ paper showing that the Medicaid payer mix is actually the same between physician-owned hospitals vs not. The mix of patients by ethnicity — for example, think about African American patients — was the same. I would be more inclined to believe the peer-reviewed literature in BMJ as opposed to an industry-funded study that was not peer-reviewed and not independent and has methodological questions.
Dr. Glatter: Those data are 8 years old, so I’d like to see more recent data. It would be interesting, just as a follow-up to that, to see where the needle has moved — if it has, for that matter — in terms of Medicaid patients that you’re referring to.
Dr. Miller: I tend to be skeptical of all industry research, regardless of who published it, because they have an economic incentive. If they’re selecting certain age groups or excluding certain hospitals, that makes you wonder about the validity of the study. Your job as an industry-funded researcher is that, essentially, you’re being paid to look for an answer. It’s not necessarily an honest evaluation of the data.
Dr. Glatter: I want to bring up another point about the Hospital Readmissions Reduction Program (HRRP) and the data on how physician-owned hospitals compared with acute care hospitals that are non–physician-owned and have you comment on that. The Dobson | DaVanzo study called into question that physician-owned hospitals treat fewer patients who are dual-eligible, which we know.
Dr. Miller: I don’t think we do know that.
Dr. Glatter: There are data that point to that, again, looking at the studies.
Dr. Miller: I’m saying that’s a single study funded by industry as opposed to an independent, academic, peer-reviewed literature paper. That would be like saying, during the debate of the Inflation Reduction Act (IRA), that you should read the pharmaceutical industries research but take any of it at pure face value as factual. Yes, we should read it. Yes, we should evaluate it on its own merits. I think, again, appropriately, you need to be concerned when people have an economic incentive.
The question about the HRRP I’m going to take a little broader, because I think that program is unfair to the industry overall. There are many factors that drive hospital readmission. Whether Mrs Smith went home and ate potato chips and then took her Lasix, that’s very much outside of the hospital industry’s control, and there’s some evidence that the HRRP increases mortality in some patient populations.
In terms of a quality metric, it’s unfair to the industry. I think we took an operating process, internal metric for the hospital industry, turned it into a quality metric, and attached it to a financial bonus, which is an inappropriate policy decision.
Rethinking Ownership Models and Empowering Clinicians
Dr. Glatter: I agree with you on that. One thing I do want to bring up is that whether the physician-owned hospitals are subject to many of the quality measures that full-service, acute care hospitals are. That really is, I think, a broader context.
Dr. Miller: Fifty-five percent of physician-owned hospitals are full-service community hospitals, so I would say at least half the market is 100% subject to that.
Dr. Glatter: If only 50% are, that’s already an issue.
Dr. Miller: Cardiac specialty hospitals — which, as I said, nonprofit and for-profit hospital chains also operate — are also subject to the appropriate quality measures, readmissions, etc. Just because we don’t necessarily have the best quality measurement in the system in the country, it doesn’t mean that we shouldn’t allow care specialization. As I’d point out, if we’re concerned about specialty hospitals, the concern shouldn’t just be about physician-owned specialty hospitals; it should be about specialty hospitals by and large. Many health systems run cardiac specialty hospitals, cancer specialty hospitals, and orthopedic specialty hospitals. If we’re going to have a discussion about concerns there, it should be about the entire industry of specialty hospitals.
I think specialty hospitals serve an important role in society, allowing for specialization and exploiting in a positive way the volume-quality relationship. Whether those are owned by a for-profit publicly traded company, a tax-exempt facility, or physicians, I think that is an important way to have innovation and care delivery because frankly, we haven’t had much innovation in care delivery. Much of what we do in terms of how we practice clinically hasn’t really changed in the 50 years since my late father graduated from medical school. We still have rounds, we’re still taking notes, we’re still operating in the same way. Many processes are manual. We don’t have the mass production and mass customization of care that we need.
When you have a focused factory, it allows you to design care in a way that drives up quality, not just for the average patient but also the patients at the tail ends, because you have time to focus on that specific service line and that specific patient population.
Physician-owned community hospitals offer an important opportunity for a different employment model. I remember going to the dermatologist and the dermatologist was depressed, shuffling around the room, sad, and I asked him why. He said he didn’t really like his employer, and I said, “Why don’t you pick another one?” He’s like, “There are only two large health systems I can work for. They all have the same clinical practice environment and functionally the same value.”
Physicians are increasingly burned out. They face monopsony power in who purchases their labor. They have little control. They don’t want to go through five committees, seven administrators, and attend 25 meetings just to change a single small process in clinical operations. If you’re an owner operator, you have a much better ability to do it.
Frankly, when many facilities do well now, when they do well clinically and do well financially, who benefits? The hospital administration and the hospital executives. The doctors aren’t benefiting. The nurses aren’t benefiting. The CNA is not benefiting. The secretary is not benefiting. The custodian is not benefiting. Shouldn’t the workers have a right to own and operate the business and do well when the business does well serving the community? That puts me in the weird space of agreeing with both conservatives and progressives.
Dr. Glatter: I agree with you. I think an ownership stake is always attractive. It helps with retention of employed persons. There›s no question that, when they have a stake, when they have skin in the game, they feel more empowered. I will not argue with you about that.
Dr. Miller: We don’t have business models where workers have that option in healthcare. Like the National Academy of Medicine said, one of the key drivers of burnout is the externalization of the locus of control over clinical practice, and the current business operating models guarantee an externalization of the locus of control over clinical practice.
If you actually look at the recent American Medical Association (AMA) meeting, there was a resolution to ban the corporate practice of medicine. They wanted to go more toward the legal professions model where only physicians can own and operate care delivery.
Dr. Glatter: Well, I think the shift is certainly something that the AMA would like and physicians collectively would agree with. Having a better lifestyle and being able to have control are factors in burnout.
Dr. Miller: It’s not just doctors. I think nurses want a better lifestyle. The nurses are treated as interchangeable lines on a spreadsheet. The nurses are an integral part of our clinical team. Why don’t we work together as a clinical unit to build a better delivery system? What better way to do that than to have clinicians in charge of it, right?
My favorite bakery that’s about 30 minutes away is owned by a baker. It is not owned by a large tax-exempt corporation. It’s owned by an owner operator who takes pride in their work. I think that is something that the profession would do well to return to. When I was a resident, one of my colleagues was already planning their retirement. That’s how depressed they were.
I went into medicine to actually care for patients. I think that we can make the world a better place for our patients. What that means is not only treating them with drugs and devices, but also creating a delivery system where they don’t have to wander from lobby to lobby in a 200,000 square-foot facility, wait in line for hours on end, get bills 6 months later, and fill out endless paper forms over and over again.
All of these basic processes in healthcare delivery that are broken could have and should have been fixed — and have been fixed in almost every other industry. I had to replace one of my car tires because I had a flat tire. The local tire shop has an app, and it sends me SMS text messages telling me when my appointment is and when my car is ready. We have solved all of these problems in many other businesses.
We have not solved them in healthcare delivery because, one, we have massive monopolies that are raising prices, have lower quality, and deliver a crappy patient experience, and we have also subjugated the clinical worker into a corporate automaton. We are functionally drones. We don’t have the agency and the authority to improve clinical operations anymore. It’s really depressing, and we should have that option again.
I trust my doctor. I trust the nurses that I work with, and I would like them to help make clinical decisions in a financially responsible and a sensible operational manner. We need to empower our workforce in order to do that so we can recapture the value of what it means to be a clinician again.
The current model of corporate employment: massive scale, more administrators, more processes, more emails, more meetings, more PowerPoint decks, more federal subsidies. The hospital industry has choices. It can improve clinical operations. It can show up in Washington and lobby for increased subsidies. It can invest in the market and not pay taxes for the tax-exempt facilities. Obviously, it makes the logical choices as an economic actor to show up, lobby for increased subsidies, and then also invest in the stock market.
Improving clinical operations is hard. It hasn’t happened. The Bureau of Labor Statistics shows that the private community hospital industry has had flat labor productivity growth, on average, for the past 25 years, and for some years it even declined. This is totally atypical across the economy.
We have failed our clinicians, and most importantly, we have failed our patients. I’ve been sick. My relatives have been sick, waiting hours, not able to get appointments, and redoing forms. It’s a total disaster. It’s time and reasonable to try an alternative ownership and operating model. There are obviously problems. The problems can and should be addressed, but it doesn’t mean that we should have a statutory prohibition on professionals owning and operating their own business.
Dr. Glatter: There was a report that $500 million was saved by limiting or banning or putting a moratorium on physician-owned hospitals by the Congressional Budget Office.
Dr. Miller: Yes, I’m very aware of those data. I’d say that the CBO also is off by 50% on the estimation of the implementation of the Part D program. They overestimated the Affordable Care Act market enrollment by over 10 million people — again, around 50%. They also estimated that the CMS Innovation Center initially would be a savings. Now they’ve re-estimated it as a 10-year expenditure and it has actually cost the taxpayers money.
The CBO is not transparent about what its assumptions are or its analysis and methods. As a researcher, we have to publish our information. It has to go through peer review. I want to know what goes into that $500 million figure — what the assumptions are and what the model is. It’s hard to comment without knowing how they came up with it.
Dr. Glatter: The points you make are very valid. Physicians and nurses want a better lifestyle.
Dr. Miller: It’s not even a better lifestyle. It’s about having a say in how clinical operations work and helping make them better. We want the delivery system to work better. This is an opportunity for us to do so.
Dr. Glatter: That translates into technology: obviously, generative artificial intelligence (AI) coming into the forefront, as we know, and changing care delivery models as you’re referring to, which is going to happen. It’s going to be a slow process. I think that the evolution is happening and will happen, as you accurately described.
Dr. Miller: The other thing that’s different now vs 20 years ago is that managed care is here, there, and everywhere, as Dr Seuss would say. You have utilization review and prior authorization, which I’ve experienced as a patient and a physician, and boy, is it not a fun process. There’s a large amount of friction that needs to be improved. If we’re worried about induced demand or inappropriate utilization, we have managed care right there to help police bad behavior.
Reforming Healthcare Systems and Restoring Patient-Centric Focus
Dr. Glatter: If you were to come up with, say, three bullet points of how we can work our way out of this current morass of where our healthcare systems exist, where do you see the solutions or how can we make and effect change?
Dr. Miller: I’d say there are a couple of things. One is, let business models compete fairly on an equal playing field. Let the physician-owned hospital compete with the tax-exempt hospital and the nonprofit hospital. Put them on an equal playing field. We have things like 340B, which favors tax-exempt hospitals. For-profit or tax-paying hospitals are not able to participate in that. That doesn’t make any sense just from a public policy perspective. Tax-paying hospitals and physician-owned hospitals pay taxes on investments, but tax-exempt hospitals don’t. I think, in public policy, we need to equalize the playing field between business models. Let the best business model win.
The other thing we need to do is to encourage the adoption of technology. The physician will eventually be an arbiter of tech-driven or AI-driven tools. In fact, at some point, the standard of care might be to use those tools. Not using those tools would be seen as negligence. If you think about placing a jugular or central venous catheter, to not use ultrasound would be considered insane. Thirty years ago, to use ultrasound would be considered novel. I think technology and AI will get us to that point of helping make care more efficient and more customized.
Those are the two biggest interventions, I would say. Third, every time we have a conversation in public policy, we need to remember what it is to be a patient. The decision should be driven not around any one industry’s profitability, but what it is to be a patient and how we can make that experience less burdensome, less expensive, or in plain English, suck less.
Dr. Glatter: Safety net hospitals and critical access hospitals are part of this discussion that, yes, we want everything to, in an ideal world, function more efficiently and effectively, with less cost and less red tape. The safety net of our nation is struggling.
Dr. Miller: I 100% agree. The Cook County hospitals of the world are deserving of our support and, frankly, our gratitude. Facilities like that have huge burdens of patients with Medicaid. We also still have millions of uninsured patients. The neighborhoods that they serve are also poorer. I think facilities like that are deserving of public support.
I also think we need to clearly define what those hospitals are. One of the challenges I’ve realized as I waded into this space is that market definitions of what a service market is for a hospital, its specialty type or what a safety net hospital is need to be more clearly defined because those facilities 100% are deserving of our support. We just need to be clear about what they are.
Regarding critical access hospitals, when you practice in a rural area, you have to think differently about care delivery. I’d say many of the rural systems are highly creative in how they structure clinical operations. Before the public health emergency, during the COVID pandemic, when we had a massive change in telehealth, rural hospitals were using — within the very narrow confines — as much telehealth as they could and should.
Rural hospitals also make greater use of nurse practitioners (NPs) and physician assistants (PAs). For many of the specialty services, I remember, your first call was an NP or a PA because the physician was downstairs doing procedures. They’d come up and assess the patient before the procedure, but most of your consult questions were answered by the NP or PA. I’m not saying that’s the model we should use nationwide, but that rural systems are highly innovative and creative; they’re deserving of our time, attention, and support, and frankly, we can learn from them.
Dr. Glatter: I want to thank you for your time and your expertise in this area. We’ll see how the congressional hearings affect the industry as a whole, how the needle moves, and whether the ban or moratorium on physician-owned hospitals continues to exist going forward.
Dr. Miller: I appreciate you having me. The hospital industry is one of the most important industries for health care. This is a time of inflection, right? We need to go back to the value of what it means to be a clinician and serve patients. Hospitals need to reorient themselves around that core concern. How do we help support clinicians — doctors, nurses, pharmacists, whomever it is — in serving patients? Hospitals have become too corporate, so I think that this is an expected pushback.
Dr. Glatter: Again, I want to thank you for your time. This was a very important discussion. Thank you for your expertise.
Robert D. Glatter, MD, is an assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. He is a medical advisor for Medscape and hosts the Hot Topics in EM series. He disclosed no relevant financial relationships.Brian J. Miller, MD, MBA, MPH, is a hospitalist and an assistant professor of medicine at the Johns Hopkins University School of Medicine. He is also a nonresident fellow at the American Enterprise Institute. From 2014 to 2017, Dr. Miller worked at four federal regulatory agencies: Federal Trade Commission (FTC), Federal Communications Commission (FCC), Centers for Medicare & Medicaid Services (CMS), and the Food & Drug Administration (FDA). Dr. Miller disclosed ties with the Medicare Payment Advisory Commission.
A version of this article appeared on Medscape.com.
This discussion was recorded on November 16, 2023. This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical advisor for Medscape Emergency Medicine. Joining me today is Dr. Brian J. Miller, a hospitalist with Johns Hopkins University School of Medicine and a health policy expert, to discuss the current and renewed interest in physician-owned hospitals.
Welcome, Dr. Miller. It’s a pleasure to have you join me today.
Brian J. Miller, MD, MBA, MPH: Thank you for having me.
History and Controversies Surrounding Physician-Owned Hospitals
Dr. Glatter: I want to start off by having you describe the history associated with the moratorium on new physician-owned hospitals in 2010 that’s related ultimately to the Affordable Care Act, but also, the current and renewed media interest in physician-owned hospitals that’s linked to recent congressional hearings last month.
Dr. Miller: Thank you. I should note that my views are my own and don’t represent those of Hopkins or the American Enterprise Institute, where I’m a nonresident fellow nor the Medicare Payment Advisory Commission, of which I’m a Commissioner.
The story about physician-owned hospitals is an interesting one. Hospitals turned into health systems in the 1980s and 1990s, and physicians started to shift purely from an independent model into a more organized group practice or employed model. Physicians realized that they wanted an alternative operating arrangement. You want a choice of how you practice and what your employment is. And as community hospitals started to buy physicians and also establish their own physician groups de novo, physicians opened physician-owned hospitals.
Physician-owned hospitals fell into a couple of buckets. One is what we call community hospitals, or what the antitrust lawyers would call general acute care hospitals: those offering emergency room (ER) services, labor and delivery, primary care, general surgery — the whole regular gamut, except that some of the owners were physicians.
The other half of the marketplace ended up being specialty hospitals: those built around a specific medical specialty and series of procedures and chronic care. For example, cardiac hospitals often do CABG, TAVR, maybe abdominal aortic aneurysm (triple A) repairs, and they have cardiology clinics, cath labs, a cardiac intensive care unit (ICU), ER, etc. There were also orthopedic surgical specialty hospitals, which were sort of like an ambulatory surgery center (ASC) plus several beds. Then there were general surgical specialty hospitals. At one point, there were some women’s health–focused specialty hospitals.
The hospital industry, of course, as you can understand, didn’t exactly like this. They had a series of concerns about what we would historically call cherry-picking or lemon-dropping of patients. They were worried that physician-owned facilities didn’t want to serve public payer patients, and there was a whole series of reports and investigations.
Around the time the Affordable Care Act passed, the hospital industry had many concerns about physician-owned specialty hospitals, and there was a moratorium as part of the 2003 Medicare Modernization Act. As part of the bargaining over the hospital industry support for the Affordable Care Act, they traded their support for, among other things, their number one priority, which is a statutory prohibition on new or expanded physician-owned hospitals from participating in Medicare. That included both physician-owned community hospitals and physician-owned specialty hospitals.
Dr. Glatter: That was part of the impetus to prevent physicians from referring patients where they had an ownership stake. Certainly, hospitals can be owned by attorneys and nonprofit organizations, and certainly, ASCs can be owned by physicians. There is an ongoing issue in terms of physicians not being able to have an ownership stake. In terms of equity ownership, we know that certain other models allow this, but basically, it sounds like this is an issue with Medicare. That seems to be the crux of it, correct?
Dr. Miller: Yes. I would also add that it’s interesting when we look at other professions. When we look at lawyers, nonlawyers are actually not allowed to own an equity stake in a law practice. In many other professions, you either have corporate ownership or professional ownership, or the alternative is you have only professional ownership. I would say the hospital industry is one of the few areas where professional ownership not only is not allowed, but also is statutorily prohibited functionally through the Medicare program.
Unveiling the Dynamics of Hospital Ownership
Dr. Glatter: A recent study done by two PhDs looked at 2019 data on 20 of the most expensive diagnosis-related groups (DRGs). It examined the cost savings, and we’re talking over $1 billion in expenditures when you look at the data from general acute care hospitals vs physician-owned hospitals. This is what appears to me to be a key driver of the push to loosen restrictions on physician-owned hospitals. Isn’t that correct?
Dr. Miller: I would say that’s one of many components. There’s more history to this issue. I remember sitting at a think tank talking to someone several years ago about hospital consolidation as an issue. We went through the usual levers that us policy wonks go through. We talked about antitrust enforcement, certificate of need, rising hospital costs from consolidation, lower quality (or at least no quality gains, as shown by a New England Journal of Medicine study), and decrements in patient experience that result from the diseconomies of scale. They sort of pooh-poohed many of the policy ideas. They basically said that there was no hope for hospital consolidation as an issue.
Well, what about physician ownership? I started with my research team to comb through the literature and found a variety of studies — some of which were sort of entertaining, because they’d do things like study physician-owned specialty hospitals, nonprofit-owned specialty hospitals, and for-profit specialty hospitals and compare them with nonprofit or for-profit community hospitals, and then say physician-owned hospitals that were specialty were bad.
They mixed ownership and service markets right there in so many ways, I’m not sure where to start. My team did a systematic review of around 30 years of research, looking at the evidence base in this space. We found a couple of things.
We found that physician-owned community hospitals did not have a cost or quality difference, meaning that there was no definitive evidence that the physician-owned community hospitals were cheaper based on historical evidence, which was very old. That means there’s not specific harm from them. When you permit market entry for community hospitals, that promotes competition, which results in lower prices and higher quality.
Then we also looked at the specialty hospital markets — surgical specialty hospitals, orthopedic surgical specialty hospitals, and cardiac hospitals. We noted for cardiac hospitals, there wasn’t clear evidence about cost savings, but there was definitive evidence of higher quality, from things like 30-day mortality for significant procedures like treatment of acute MI, triple A repair, stuff like that.
For orthopedic surgical specialty hospitals, we noted lower costs and higher quality, which again fits with operationally what we would know. If you have a facility that’s doing 20 total hips a day, you’re creating a focused factory. Just like if you think about it for interventional cardiology, your boards have a minimum number of procedures that you have to do to stay certified because we know about the volume-quality relationship.
Then we looked at general surgical specialty hospitals. There wasn’t enough evidence to make a conclusive thought about costs, and there was a clear trend toward higher quality. I would say this recent study is important, but there is a whole bunch of other literature out there, too.
Exploring the Scope of Emergency Care in Physician-Owned Hospitals
Dr. Glatter: Certainly, your colleague Wang from Johns Hopkins has done important research in this sector. The paper, “Reconsidering the Ban on Physician-Owned Hospitals to Combat Consolidation,” by you and several colleagues, mentions and highlights the issues that you just described. I understand that it’s going to be published in the NYU Journal of Legislation and Public Policy.
One thing I want to bring up — and this is an important issue — is that the risk for patients has been talked about by the American Hospital Association and the Federation of American Hospitals, in terms of limited or no emergency services at such physician-owned hospitals and having to call 911 when patients need emergent care or stabilization. That’s been the rebuttal, along with an Office of Inspector General (OIG) report from 2008. Almost, I guess, three quarters of the patients that needed emergent care got this at publicly funded hospitals.
Dr. Miller: I’m familiar with the argument about emergency care. If you actually go and look at it, it differs by specialty market. Physician-owned community hospitals have ERs because that’s how they get their business. If you are running a hospital medicine floor, a general surgical specialty floor, you have a labor delivery unit, a primary care clinic, and a cardiology clinic. You have all the things that all the other hospitals have. The physician-owned community hospitals almost uniformly have an ER.
When you look at the physician-owned specialty hospitals, it’s a little more granular. If you look at the cardiac hospitals, they have ERs. They also have cardiac ICUs, operating rooms, etc. The area where the hospital industry had concerns — which I think is valid to point out — is that physician-owned orthopedic surgical specialty hospitals don’t have ERs. But this makes sense because of what that hospital functionally is: a factory for whatever the scope of procedures is, be it joint replacements or shoulder arthroscopy. The orthopedic surgical specialty hospital is like an ASC plus several hospital beds. Many of those did not have ERs because clinically it didn’t make sense.
What’s interesting, though, is that the hospital industry also operates specialty hospitals. If you go into many of the large systems, they have cardiac specialty hospitals and cancer specialty hospitals. I would say that some of them have ERs, as they appropriately should, and some of those specialty hospitals do not. They might have a community hospital down the street that’s part of that health system that has an ER, but some of the specialty hospitals don’t necessarily have a dedicated ER.
I agree, that’s a valid concern. I would say, though, the question is, what are the scope of services in that hospital? Is an ER required? Community hospitals should have ERs. It makes sense also for a cardiac hospital to have one. If you’re running a total joint replacement factory, it might not make clinical sense.
Dr. Glatter: The patients who are treated at that hospital, if they do have emergent conditions, need to have board-certified emergency physicians treating them, in my view because I’m an ER physician. Having surgeons that are not emergency physicians staff a department at a specialty orthopedic hospital or, say, a cancer hospital is not acceptable from my standpoint. That›s my opinion and recommendation, coming from emergency medicine.
Dr. Miller: I would say that anesthesiologists are actually highly qualified in critical care. The question is about clinical decompensation; if you’re doing a procedure, you have an anesthesiologist right there who is capable of critical care. The function of the ER is to either serve as a window into the hospital for patient volume or to serve as a referral for emergent complaints.
Dr. Glatter: An anesthesiologist — I’ll take issue with that — does not have the training of an emergency physician in terms of scope of practice.
Dr. Miller: My anesthesiology colleagues would probably disagree for managing an emergency during an operating room case.
Dr. Glatter: Fair enough, but I think in the general sense. The other issue is that, in terms of emergent responses to patients that decompensate, when you have to transfer a patient, that violates Medicare requirements. How is that even a valid issue or argument if you’re going to have to transfer a patient from your specialty hospital? That happens. Again, I know that you’re saying these hospitals are completely independent and can function, stabilize patients, and treat emergencies, but that’s not the reality across the country, in my opinion.
Dr. Miller: I don’t think that’s the case for the physician-owned specialty cardiac hospitals, for starters. Many of those have ICUs in addition to operating rooms as a matter of routine in addition to ERs. I don’t think that’s the case for physician-owned community hospitals, which have ERs, ICUs, medicine floors, and surgical floors. Physician-owned community hospitals are around half the market. Of that remaining market, a significant percentage are cardiac hospitals. If you’re taking an issue with orthopedic surgical specialty hospitals, that’s a clinical operational question that can and should be answered.
I’d also posit that the nonprofit and for-profit hospital industries also operate specialty hospitals. Any of these questions, we shouldn’t just be asking about physician-owned facilities; we should be asking about them across ownership types, because we’re talking about scope of service and quality and safety. The ownership in that case doesn’t matter. The broader question is, are orthopedic surgical specialty hospitals owned by physicians, tax-exempt hospitals, or tax-paying hospitals? Is that a valid clinical business model? Is it safe? Does it meet Medicare conditions of participation? I would say that’s what that question is, because other ownership models do operate those facilities.
Dr. Glatter: You make some valid points, and I do agree on some of them. I think that, ultimately, these models of care, and certainly cost and quality, are issues. Again, it goes back to being able, in my opinion, to provide emergent care, which seems to me a very important issue.
Dr. Miller: I agree that providing emergent care is an issue. It›s an issue in any site of care. The hospital industry posits that all hospital outpatient departments (HOPDs) have emergent care. I can tell you, having worked in HOPDs (I›ve trained in them during residency), the response if something emergent happens is to either call 911 or wheel the patient down to the ER in a wheelchair or stretcher. I think that these hospital claims about emergency care coverage — these are important questions, but we should be asking them across all clinical settings and say what is the appropriate scope of care provided? What is the appropriate level of acuity and ability to provide emergent or critical care? That›s an important question regardless of ownership model across the entire industry.
Deeper Dive Into Data on Physician-Owned Hospitals
Dr. Glatter: We need to really focus on that. I’ll agree with you on that.
There was a March 2023 report from Dobson | DaVanzo. It showed that physician-owned hospitals had lower Medicaid, dual-eligible, and uncompensated care and charity care discharges than full-service acute care hospitals. Physician-owned hospitals had less than half the proportion of Medicaid discharges compared with non–physician-owned hospitals. They were also less likely to care for dual-eligible patients overall compared with non–physician-owned hospitals.
In addition, when COVID hit, the physician-owned hospitals overall — and again, there may be exceptions — were not equipped to handle these patient surges in the acute setting of a public health emergency. There was a hospital in Texas that did pivot that I’m aware of — Renaissance Hospital, which ramped up a long-term care facility to become a COVID hospital — but I think that’s the exception. I think this report raises some valid concerns; I’ll let you rebut that.
Dr. Miller: A couple of things. One, I am not aware that there’s any clear market evidence or a systematic study that shows that physician-owned hospitals had trouble responding to COVID. I don’t think that assertion has been proven. The study was funded by the hospital industry. First of all, it was not a peer-reviewed study; it was funded by an industry that paid a consulting firm. It doesn’t mean that we still shouldn’t read it, but that brings bias into question. The joke in Washington is, pick your favorite statistician or economist, and they can say what you want and have a battle of economists and statisticians.
For example, in that study, they didn’t include the entire ownership universe of physician-owned hospitals. If we go to the peer-reviewed literature, there’s a great 2015 BMJ paper showing that the Medicaid payer mix is actually the same between physician-owned hospitals vs not. The mix of patients by ethnicity — for example, think about African American patients — was the same. I would be more inclined to believe the peer-reviewed literature in BMJ as opposed to an industry-funded study that was not peer-reviewed and not independent and has methodological questions.
Dr. Glatter: Those data are 8 years old, so I’d like to see more recent data. It would be interesting, just as a follow-up to that, to see where the needle has moved — if it has, for that matter — in terms of Medicaid patients that you’re referring to.
Dr. Miller: I tend to be skeptical of all industry research, regardless of who published it, because they have an economic incentive. If they’re selecting certain age groups or excluding certain hospitals, that makes you wonder about the validity of the study. Your job as an industry-funded researcher is that, essentially, you’re being paid to look for an answer. It’s not necessarily an honest evaluation of the data.
Dr. Glatter: I want to bring up another point about the Hospital Readmissions Reduction Program (HRRP) and the data on how physician-owned hospitals compared with acute care hospitals that are non–physician-owned and have you comment on that. The Dobson | DaVanzo study called into question that physician-owned hospitals treat fewer patients who are dual-eligible, which we know.
Dr. Miller: I don’t think we do know that.
Dr. Glatter: There are data that point to that, again, looking at the studies.
Dr. Miller: I’m saying that’s a single study funded by industry as opposed to an independent, academic, peer-reviewed literature paper. That would be like saying, during the debate of the Inflation Reduction Act (IRA), that you should read the pharmaceutical industries research but take any of it at pure face value as factual. Yes, we should read it. Yes, we should evaluate it on its own merits. I think, again, appropriately, you need to be concerned when people have an economic incentive.
The question about the HRRP I’m going to take a little broader, because I think that program is unfair to the industry overall. There are many factors that drive hospital readmission. Whether Mrs Smith went home and ate potato chips and then took her Lasix, that’s very much outside of the hospital industry’s control, and there’s some evidence that the HRRP increases mortality in some patient populations.
In terms of a quality metric, it’s unfair to the industry. I think we took an operating process, internal metric for the hospital industry, turned it into a quality metric, and attached it to a financial bonus, which is an inappropriate policy decision.
Rethinking Ownership Models and Empowering Clinicians
Dr. Glatter: I agree with you on that. One thing I do want to bring up is that whether the physician-owned hospitals are subject to many of the quality measures that full-service, acute care hospitals are. That really is, I think, a broader context.
Dr. Miller: Fifty-five percent of physician-owned hospitals are full-service community hospitals, so I would say at least half the market is 100% subject to that.
Dr. Glatter: If only 50% are, that’s already an issue.
Dr. Miller: Cardiac specialty hospitals — which, as I said, nonprofit and for-profit hospital chains also operate — are also subject to the appropriate quality measures, readmissions, etc. Just because we don’t necessarily have the best quality measurement in the system in the country, it doesn’t mean that we shouldn’t allow care specialization. As I’d point out, if we’re concerned about specialty hospitals, the concern shouldn’t just be about physician-owned specialty hospitals; it should be about specialty hospitals by and large. Many health systems run cardiac specialty hospitals, cancer specialty hospitals, and orthopedic specialty hospitals. If we’re going to have a discussion about concerns there, it should be about the entire industry of specialty hospitals.
I think specialty hospitals serve an important role in society, allowing for specialization and exploiting in a positive way the volume-quality relationship. Whether those are owned by a for-profit publicly traded company, a tax-exempt facility, or physicians, I think that is an important way to have innovation and care delivery because frankly, we haven’t had much innovation in care delivery. Much of what we do in terms of how we practice clinically hasn’t really changed in the 50 years since my late father graduated from medical school. We still have rounds, we’re still taking notes, we’re still operating in the same way. Many processes are manual. We don’t have the mass production and mass customization of care that we need.
When you have a focused factory, it allows you to design care in a way that drives up quality, not just for the average patient but also the patients at the tail ends, because you have time to focus on that specific service line and that specific patient population.
Physician-owned community hospitals offer an important opportunity for a different employment model. I remember going to the dermatologist and the dermatologist was depressed, shuffling around the room, sad, and I asked him why. He said he didn’t really like his employer, and I said, “Why don’t you pick another one?” He’s like, “There are only two large health systems I can work for. They all have the same clinical practice environment and functionally the same value.”
Physicians are increasingly burned out. They face monopsony power in who purchases their labor. They have little control. They don’t want to go through five committees, seven administrators, and attend 25 meetings just to change a single small process in clinical operations. If you’re an owner operator, you have a much better ability to do it.
Frankly, when many facilities do well now, when they do well clinically and do well financially, who benefits? The hospital administration and the hospital executives. The doctors aren’t benefiting. The nurses aren’t benefiting. The CNA is not benefiting. The secretary is not benefiting. The custodian is not benefiting. Shouldn’t the workers have a right to own and operate the business and do well when the business does well serving the community? That puts me in the weird space of agreeing with both conservatives and progressives.
Dr. Glatter: I agree with you. I think an ownership stake is always attractive. It helps with retention of employed persons. There›s no question that, when they have a stake, when they have skin in the game, they feel more empowered. I will not argue with you about that.
Dr. Miller: We don’t have business models where workers have that option in healthcare. Like the National Academy of Medicine said, one of the key drivers of burnout is the externalization of the locus of control over clinical practice, and the current business operating models guarantee an externalization of the locus of control over clinical practice.
If you actually look at the recent American Medical Association (AMA) meeting, there was a resolution to ban the corporate practice of medicine. They wanted to go more toward the legal professions model where only physicians can own and operate care delivery.
Dr. Glatter: Well, I think the shift is certainly something that the AMA would like and physicians collectively would agree with. Having a better lifestyle and being able to have control are factors in burnout.
Dr. Miller: It’s not just doctors. I think nurses want a better lifestyle. The nurses are treated as interchangeable lines on a spreadsheet. The nurses are an integral part of our clinical team. Why don’t we work together as a clinical unit to build a better delivery system? What better way to do that than to have clinicians in charge of it, right?
My favorite bakery that’s about 30 minutes away is owned by a baker. It is not owned by a large tax-exempt corporation. It’s owned by an owner operator who takes pride in their work. I think that is something that the profession would do well to return to. When I was a resident, one of my colleagues was already planning their retirement. That’s how depressed they were.
I went into medicine to actually care for patients. I think that we can make the world a better place for our patients. What that means is not only treating them with drugs and devices, but also creating a delivery system where they don’t have to wander from lobby to lobby in a 200,000 square-foot facility, wait in line for hours on end, get bills 6 months later, and fill out endless paper forms over and over again.
All of these basic processes in healthcare delivery that are broken could have and should have been fixed — and have been fixed in almost every other industry. I had to replace one of my car tires because I had a flat tire. The local tire shop has an app, and it sends me SMS text messages telling me when my appointment is and when my car is ready. We have solved all of these problems in many other businesses.
We have not solved them in healthcare delivery because, one, we have massive monopolies that are raising prices, have lower quality, and deliver a crappy patient experience, and we have also subjugated the clinical worker into a corporate automaton. We are functionally drones. We don’t have the agency and the authority to improve clinical operations anymore. It’s really depressing, and we should have that option again.
I trust my doctor. I trust the nurses that I work with, and I would like them to help make clinical decisions in a financially responsible and a sensible operational manner. We need to empower our workforce in order to do that so we can recapture the value of what it means to be a clinician again.
The current model of corporate employment: massive scale, more administrators, more processes, more emails, more meetings, more PowerPoint decks, more federal subsidies. The hospital industry has choices. It can improve clinical operations. It can show up in Washington and lobby for increased subsidies. It can invest in the market and not pay taxes for the tax-exempt facilities. Obviously, it makes the logical choices as an economic actor to show up, lobby for increased subsidies, and then also invest in the stock market.
Improving clinical operations is hard. It hasn’t happened. The Bureau of Labor Statistics shows that the private community hospital industry has had flat labor productivity growth, on average, for the past 25 years, and for some years it even declined. This is totally atypical across the economy.
We have failed our clinicians, and most importantly, we have failed our patients. I’ve been sick. My relatives have been sick, waiting hours, not able to get appointments, and redoing forms. It’s a total disaster. It’s time and reasonable to try an alternative ownership and operating model. There are obviously problems. The problems can and should be addressed, but it doesn’t mean that we should have a statutory prohibition on professionals owning and operating their own business.
Dr. Glatter: There was a report that $500 million was saved by limiting or banning or putting a moratorium on physician-owned hospitals by the Congressional Budget Office.
Dr. Miller: Yes, I’m very aware of those data. I’d say that the CBO also is off by 50% on the estimation of the implementation of the Part D program. They overestimated the Affordable Care Act market enrollment by over 10 million people — again, around 50%. They also estimated that the CMS Innovation Center initially would be a savings. Now they’ve re-estimated it as a 10-year expenditure and it has actually cost the taxpayers money.
The CBO is not transparent about what its assumptions are or its analysis and methods. As a researcher, we have to publish our information. It has to go through peer review. I want to know what goes into that $500 million figure — what the assumptions are and what the model is. It’s hard to comment without knowing how they came up with it.
Dr. Glatter: The points you make are very valid. Physicians and nurses want a better lifestyle.
Dr. Miller: It’s not even a better lifestyle. It’s about having a say in how clinical operations work and helping make them better. We want the delivery system to work better. This is an opportunity for us to do so.
Dr. Glatter: That translates into technology: obviously, generative artificial intelligence (AI) coming into the forefront, as we know, and changing care delivery models as you’re referring to, which is going to happen. It’s going to be a slow process. I think that the evolution is happening and will happen, as you accurately described.
Dr. Miller: The other thing that’s different now vs 20 years ago is that managed care is here, there, and everywhere, as Dr Seuss would say. You have utilization review and prior authorization, which I’ve experienced as a patient and a physician, and boy, is it not a fun process. There’s a large amount of friction that needs to be improved. If we’re worried about induced demand or inappropriate utilization, we have managed care right there to help police bad behavior.
Reforming Healthcare Systems and Restoring Patient-Centric Focus
Dr. Glatter: If you were to come up with, say, three bullet points of how we can work our way out of this current morass of where our healthcare systems exist, where do you see the solutions or how can we make and effect change?
Dr. Miller: I’d say there are a couple of things. One is, let business models compete fairly on an equal playing field. Let the physician-owned hospital compete with the tax-exempt hospital and the nonprofit hospital. Put them on an equal playing field. We have things like 340B, which favors tax-exempt hospitals. For-profit or tax-paying hospitals are not able to participate in that. That doesn’t make any sense just from a public policy perspective. Tax-paying hospitals and physician-owned hospitals pay taxes on investments, but tax-exempt hospitals don’t. I think, in public policy, we need to equalize the playing field between business models. Let the best business model win.
The other thing we need to do is to encourage the adoption of technology. The physician will eventually be an arbiter of tech-driven or AI-driven tools. In fact, at some point, the standard of care might be to use those tools. Not using those tools would be seen as negligence. If you think about placing a jugular or central venous catheter, to not use ultrasound would be considered insane. Thirty years ago, to use ultrasound would be considered novel. I think technology and AI will get us to that point of helping make care more efficient and more customized.
Those are the two biggest interventions, I would say. Third, every time we have a conversation in public policy, we need to remember what it is to be a patient. The decision should be driven not around any one industry’s profitability, but what it is to be a patient and how we can make that experience less burdensome, less expensive, or in plain English, suck less.
Dr. Glatter: Safety net hospitals and critical access hospitals are part of this discussion that, yes, we want everything to, in an ideal world, function more efficiently and effectively, with less cost and less red tape. The safety net of our nation is struggling.
Dr. Miller: I 100% agree. The Cook County hospitals of the world are deserving of our support and, frankly, our gratitude. Facilities like that have huge burdens of patients with Medicaid. We also still have millions of uninsured patients. The neighborhoods that they serve are also poorer. I think facilities like that are deserving of public support.
I also think we need to clearly define what those hospitals are. One of the challenges I’ve realized as I waded into this space is that market definitions of what a service market is for a hospital, its specialty type or what a safety net hospital is need to be more clearly defined because those facilities 100% are deserving of our support. We just need to be clear about what they are.
Regarding critical access hospitals, when you practice in a rural area, you have to think differently about care delivery. I’d say many of the rural systems are highly creative in how they structure clinical operations. Before the public health emergency, during the COVID pandemic, when we had a massive change in telehealth, rural hospitals were using — within the very narrow confines — as much telehealth as they could and should.
Rural hospitals also make greater use of nurse practitioners (NPs) and physician assistants (PAs). For many of the specialty services, I remember, your first call was an NP or a PA because the physician was downstairs doing procedures. They’d come up and assess the patient before the procedure, but most of your consult questions were answered by the NP or PA. I’m not saying that’s the model we should use nationwide, but that rural systems are highly innovative and creative; they’re deserving of our time, attention, and support, and frankly, we can learn from them.
Dr. Glatter: I want to thank you for your time and your expertise in this area. We’ll see how the congressional hearings affect the industry as a whole, how the needle moves, and whether the ban or moratorium on physician-owned hospitals continues to exist going forward.
Dr. Miller: I appreciate you having me. The hospital industry is one of the most important industries for health care. This is a time of inflection, right? We need to go back to the value of what it means to be a clinician and serve patients. Hospitals need to reorient themselves around that core concern. How do we help support clinicians — doctors, nurses, pharmacists, whomever it is — in serving patients? Hospitals have become too corporate, so I think that this is an expected pushback.
Dr. Glatter: Again, I want to thank you for your time. This was a very important discussion. Thank you for your expertise.
Robert D. Glatter, MD, is an assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. He is a medical advisor for Medscape and hosts the Hot Topics in EM series. He disclosed no relevant financial relationships.Brian J. Miller, MD, MBA, MPH, is a hospitalist and an assistant professor of medicine at the Johns Hopkins University School of Medicine. He is also a nonresident fellow at the American Enterprise Institute. From 2014 to 2017, Dr. Miller worked at four federal regulatory agencies: Federal Trade Commission (FTC), Federal Communications Commission (FCC), Centers for Medicare & Medicaid Services (CMS), and the Food & Drug Administration (FDA). Dr. Miller disclosed ties with the Medicare Payment Advisory Commission.
A version of this article appeared on Medscape.com.
This discussion was recorded on November 16, 2023. This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical advisor for Medscape Emergency Medicine. Joining me today is Dr. Brian J. Miller, a hospitalist with Johns Hopkins University School of Medicine and a health policy expert, to discuss the current and renewed interest in physician-owned hospitals.
Welcome, Dr. Miller. It’s a pleasure to have you join me today.
Brian J. Miller, MD, MBA, MPH: Thank you for having me.
History and Controversies Surrounding Physician-Owned Hospitals
Dr. Glatter: I want to start off by having you describe the history associated with the moratorium on new physician-owned hospitals in 2010 that’s related ultimately to the Affordable Care Act, but also, the current and renewed media interest in physician-owned hospitals that’s linked to recent congressional hearings last month.
Dr. Miller: Thank you. I should note that my views are my own and don’t represent those of Hopkins or the American Enterprise Institute, where I’m a nonresident fellow nor the Medicare Payment Advisory Commission, of which I’m a Commissioner.
The story about physician-owned hospitals is an interesting one. Hospitals turned into health systems in the 1980s and 1990s, and physicians started to shift purely from an independent model into a more organized group practice or employed model. Physicians realized that they wanted an alternative operating arrangement. You want a choice of how you practice and what your employment is. And as community hospitals started to buy physicians and also establish their own physician groups de novo, physicians opened physician-owned hospitals.
Physician-owned hospitals fell into a couple of buckets. One is what we call community hospitals, or what the antitrust lawyers would call general acute care hospitals: those offering emergency room (ER) services, labor and delivery, primary care, general surgery — the whole regular gamut, except that some of the owners were physicians.
The other half of the marketplace ended up being specialty hospitals: those built around a specific medical specialty and series of procedures and chronic care. For example, cardiac hospitals often do CABG, TAVR, maybe abdominal aortic aneurysm (triple A) repairs, and they have cardiology clinics, cath labs, a cardiac intensive care unit (ICU), ER, etc. There were also orthopedic surgical specialty hospitals, which were sort of like an ambulatory surgery center (ASC) plus several beds. Then there were general surgical specialty hospitals. At one point, there were some women’s health–focused specialty hospitals.
The hospital industry, of course, as you can understand, didn’t exactly like this. They had a series of concerns about what we would historically call cherry-picking or lemon-dropping of patients. They were worried that physician-owned facilities didn’t want to serve public payer patients, and there was a whole series of reports and investigations.
Around the time the Affordable Care Act passed, the hospital industry had many concerns about physician-owned specialty hospitals, and there was a moratorium as part of the 2003 Medicare Modernization Act. As part of the bargaining over the hospital industry support for the Affordable Care Act, they traded their support for, among other things, their number one priority, which is a statutory prohibition on new or expanded physician-owned hospitals from participating in Medicare. That included both physician-owned community hospitals and physician-owned specialty hospitals.
Dr. Glatter: That was part of the impetus to prevent physicians from referring patients where they had an ownership stake. Certainly, hospitals can be owned by attorneys and nonprofit organizations, and certainly, ASCs can be owned by physicians. There is an ongoing issue in terms of physicians not being able to have an ownership stake. In terms of equity ownership, we know that certain other models allow this, but basically, it sounds like this is an issue with Medicare. That seems to be the crux of it, correct?
Dr. Miller: Yes. I would also add that it’s interesting when we look at other professions. When we look at lawyers, nonlawyers are actually not allowed to own an equity stake in a law practice. In many other professions, you either have corporate ownership or professional ownership, or the alternative is you have only professional ownership. I would say the hospital industry is one of the few areas where professional ownership not only is not allowed, but also is statutorily prohibited functionally through the Medicare program.
Unveiling the Dynamics of Hospital Ownership
Dr. Glatter: A recent study done by two PhDs looked at 2019 data on 20 of the most expensive diagnosis-related groups (DRGs). It examined the cost savings, and we’re talking over $1 billion in expenditures when you look at the data from general acute care hospitals vs physician-owned hospitals. This is what appears to me to be a key driver of the push to loosen restrictions on physician-owned hospitals. Isn’t that correct?
Dr. Miller: I would say that’s one of many components. There’s more history to this issue. I remember sitting at a think tank talking to someone several years ago about hospital consolidation as an issue. We went through the usual levers that us policy wonks go through. We talked about antitrust enforcement, certificate of need, rising hospital costs from consolidation, lower quality (or at least no quality gains, as shown by a New England Journal of Medicine study), and decrements in patient experience that result from the diseconomies of scale. They sort of pooh-poohed many of the policy ideas. They basically said that there was no hope for hospital consolidation as an issue.
Well, what about physician ownership? I started with my research team to comb through the literature and found a variety of studies — some of which were sort of entertaining, because they’d do things like study physician-owned specialty hospitals, nonprofit-owned specialty hospitals, and for-profit specialty hospitals and compare them with nonprofit or for-profit community hospitals, and then say physician-owned hospitals that were specialty were bad.
They mixed ownership and service markets right there in so many ways, I’m not sure where to start. My team did a systematic review of around 30 years of research, looking at the evidence base in this space. We found a couple of things.
We found that physician-owned community hospitals did not have a cost or quality difference, meaning that there was no definitive evidence that the physician-owned community hospitals were cheaper based on historical evidence, which was very old. That means there’s not specific harm from them. When you permit market entry for community hospitals, that promotes competition, which results in lower prices and higher quality.
Then we also looked at the specialty hospital markets — surgical specialty hospitals, orthopedic surgical specialty hospitals, and cardiac hospitals. We noted for cardiac hospitals, there wasn’t clear evidence about cost savings, but there was definitive evidence of higher quality, from things like 30-day mortality for significant procedures like treatment of acute MI, triple A repair, stuff like that.
For orthopedic surgical specialty hospitals, we noted lower costs and higher quality, which again fits with operationally what we would know. If you have a facility that’s doing 20 total hips a day, you’re creating a focused factory. Just like if you think about it for interventional cardiology, your boards have a minimum number of procedures that you have to do to stay certified because we know about the volume-quality relationship.
Then we looked at general surgical specialty hospitals. There wasn’t enough evidence to make a conclusive thought about costs, and there was a clear trend toward higher quality. I would say this recent study is important, but there is a whole bunch of other literature out there, too.
Exploring the Scope of Emergency Care in Physician-Owned Hospitals
Dr. Glatter: Certainly, your colleague Wang from Johns Hopkins has done important research in this sector. The paper, “Reconsidering the Ban on Physician-Owned Hospitals to Combat Consolidation,” by you and several colleagues, mentions and highlights the issues that you just described. I understand that it’s going to be published in the NYU Journal of Legislation and Public Policy.
One thing I want to bring up — and this is an important issue — is that the risk for patients has been talked about by the American Hospital Association and the Federation of American Hospitals, in terms of limited or no emergency services at such physician-owned hospitals and having to call 911 when patients need emergent care or stabilization. That’s been the rebuttal, along with an Office of Inspector General (OIG) report from 2008. Almost, I guess, three quarters of the patients that needed emergent care got this at publicly funded hospitals.
Dr. Miller: I’m familiar with the argument about emergency care. If you actually go and look at it, it differs by specialty market. Physician-owned community hospitals have ERs because that’s how they get their business. If you are running a hospital medicine floor, a general surgical specialty floor, you have a labor delivery unit, a primary care clinic, and a cardiology clinic. You have all the things that all the other hospitals have. The physician-owned community hospitals almost uniformly have an ER.
When you look at the physician-owned specialty hospitals, it’s a little more granular. If you look at the cardiac hospitals, they have ERs. They also have cardiac ICUs, operating rooms, etc. The area where the hospital industry had concerns — which I think is valid to point out — is that physician-owned orthopedic surgical specialty hospitals don’t have ERs. But this makes sense because of what that hospital functionally is: a factory for whatever the scope of procedures is, be it joint replacements or shoulder arthroscopy. The orthopedic surgical specialty hospital is like an ASC plus several hospital beds. Many of those did not have ERs because clinically it didn’t make sense.
What’s interesting, though, is that the hospital industry also operates specialty hospitals. If you go into many of the large systems, they have cardiac specialty hospitals and cancer specialty hospitals. I would say that some of them have ERs, as they appropriately should, and some of those specialty hospitals do not. They might have a community hospital down the street that’s part of that health system that has an ER, but some of the specialty hospitals don’t necessarily have a dedicated ER.
I agree, that’s a valid concern. I would say, though, the question is, what are the scope of services in that hospital? Is an ER required? Community hospitals should have ERs. It makes sense also for a cardiac hospital to have one. If you’re running a total joint replacement factory, it might not make clinical sense.
Dr. Glatter: The patients who are treated at that hospital, if they do have emergent conditions, need to have board-certified emergency physicians treating them, in my view because I’m an ER physician. Having surgeons that are not emergency physicians staff a department at a specialty orthopedic hospital or, say, a cancer hospital is not acceptable from my standpoint. That›s my opinion and recommendation, coming from emergency medicine.
Dr. Miller: I would say that anesthesiologists are actually highly qualified in critical care. The question is about clinical decompensation; if you’re doing a procedure, you have an anesthesiologist right there who is capable of critical care. The function of the ER is to either serve as a window into the hospital for patient volume or to serve as a referral for emergent complaints.
Dr. Glatter: An anesthesiologist — I’ll take issue with that — does not have the training of an emergency physician in terms of scope of practice.
Dr. Miller: My anesthesiology colleagues would probably disagree for managing an emergency during an operating room case.
Dr. Glatter: Fair enough, but I think in the general sense. The other issue is that, in terms of emergent responses to patients that decompensate, when you have to transfer a patient, that violates Medicare requirements. How is that even a valid issue or argument if you’re going to have to transfer a patient from your specialty hospital? That happens. Again, I know that you’re saying these hospitals are completely independent and can function, stabilize patients, and treat emergencies, but that’s not the reality across the country, in my opinion.
Dr. Miller: I don’t think that’s the case for the physician-owned specialty cardiac hospitals, for starters. Many of those have ICUs in addition to operating rooms as a matter of routine in addition to ERs. I don’t think that’s the case for physician-owned community hospitals, which have ERs, ICUs, medicine floors, and surgical floors. Physician-owned community hospitals are around half the market. Of that remaining market, a significant percentage are cardiac hospitals. If you’re taking an issue with orthopedic surgical specialty hospitals, that’s a clinical operational question that can and should be answered.
I’d also posit that the nonprofit and for-profit hospital industries also operate specialty hospitals. Any of these questions, we shouldn’t just be asking about physician-owned facilities; we should be asking about them across ownership types, because we’re talking about scope of service and quality and safety. The ownership in that case doesn’t matter. The broader question is, are orthopedic surgical specialty hospitals owned by physicians, tax-exempt hospitals, or tax-paying hospitals? Is that a valid clinical business model? Is it safe? Does it meet Medicare conditions of participation? I would say that’s what that question is, because other ownership models do operate those facilities.
Dr. Glatter: You make some valid points, and I do agree on some of them. I think that, ultimately, these models of care, and certainly cost and quality, are issues. Again, it goes back to being able, in my opinion, to provide emergent care, which seems to me a very important issue.
Dr. Miller: I agree that providing emergent care is an issue. It›s an issue in any site of care. The hospital industry posits that all hospital outpatient departments (HOPDs) have emergent care. I can tell you, having worked in HOPDs (I›ve trained in them during residency), the response if something emergent happens is to either call 911 or wheel the patient down to the ER in a wheelchair or stretcher. I think that these hospital claims about emergency care coverage — these are important questions, but we should be asking them across all clinical settings and say what is the appropriate scope of care provided? What is the appropriate level of acuity and ability to provide emergent or critical care? That›s an important question regardless of ownership model across the entire industry.
Deeper Dive Into Data on Physician-Owned Hospitals
Dr. Glatter: We need to really focus on that. I’ll agree with you on that.
There was a March 2023 report from Dobson | DaVanzo. It showed that physician-owned hospitals had lower Medicaid, dual-eligible, and uncompensated care and charity care discharges than full-service acute care hospitals. Physician-owned hospitals had less than half the proportion of Medicaid discharges compared with non–physician-owned hospitals. They were also less likely to care for dual-eligible patients overall compared with non–physician-owned hospitals.
In addition, when COVID hit, the physician-owned hospitals overall — and again, there may be exceptions — were not equipped to handle these patient surges in the acute setting of a public health emergency. There was a hospital in Texas that did pivot that I’m aware of — Renaissance Hospital, which ramped up a long-term care facility to become a COVID hospital — but I think that’s the exception. I think this report raises some valid concerns; I’ll let you rebut that.
Dr. Miller: A couple of things. One, I am not aware that there’s any clear market evidence or a systematic study that shows that physician-owned hospitals had trouble responding to COVID. I don’t think that assertion has been proven. The study was funded by the hospital industry. First of all, it was not a peer-reviewed study; it was funded by an industry that paid a consulting firm. It doesn’t mean that we still shouldn’t read it, but that brings bias into question. The joke in Washington is, pick your favorite statistician or economist, and they can say what you want and have a battle of economists and statisticians.
For example, in that study, they didn’t include the entire ownership universe of physician-owned hospitals. If we go to the peer-reviewed literature, there’s a great 2015 BMJ paper showing that the Medicaid payer mix is actually the same between physician-owned hospitals vs not. The mix of patients by ethnicity — for example, think about African American patients — was the same. I would be more inclined to believe the peer-reviewed literature in BMJ as opposed to an industry-funded study that was not peer-reviewed and not independent and has methodological questions.
Dr. Glatter: Those data are 8 years old, so I’d like to see more recent data. It would be interesting, just as a follow-up to that, to see where the needle has moved — if it has, for that matter — in terms of Medicaid patients that you’re referring to.
Dr. Miller: I tend to be skeptical of all industry research, regardless of who published it, because they have an economic incentive. If they’re selecting certain age groups or excluding certain hospitals, that makes you wonder about the validity of the study. Your job as an industry-funded researcher is that, essentially, you’re being paid to look for an answer. It’s not necessarily an honest evaluation of the data.
Dr. Glatter: I want to bring up another point about the Hospital Readmissions Reduction Program (HRRP) and the data on how physician-owned hospitals compared with acute care hospitals that are non–physician-owned and have you comment on that. The Dobson | DaVanzo study called into question that physician-owned hospitals treat fewer patients who are dual-eligible, which we know.
Dr. Miller: I don’t think we do know that.
Dr. Glatter: There are data that point to that, again, looking at the studies.
Dr. Miller: I’m saying that’s a single study funded by industry as opposed to an independent, academic, peer-reviewed literature paper. That would be like saying, during the debate of the Inflation Reduction Act (IRA), that you should read the pharmaceutical industries research but take any of it at pure face value as factual. Yes, we should read it. Yes, we should evaluate it on its own merits. I think, again, appropriately, you need to be concerned when people have an economic incentive.
The question about the HRRP I’m going to take a little broader, because I think that program is unfair to the industry overall. There are many factors that drive hospital readmission. Whether Mrs Smith went home and ate potato chips and then took her Lasix, that’s very much outside of the hospital industry’s control, and there’s some evidence that the HRRP increases mortality in some patient populations.
In terms of a quality metric, it’s unfair to the industry. I think we took an operating process, internal metric for the hospital industry, turned it into a quality metric, and attached it to a financial bonus, which is an inappropriate policy decision.
Rethinking Ownership Models and Empowering Clinicians
Dr. Glatter: I agree with you on that. One thing I do want to bring up is that whether the physician-owned hospitals are subject to many of the quality measures that full-service, acute care hospitals are. That really is, I think, a broader context.
Dr. Miller: Fifty-five percent of physician-owned hospitals are full-service community hospitals, so I would say at least half the market is 100% subject to that.
Dr. Glatter: If only 50% are, that’s already an issue.
Dr. Miller: Cardiac specialty hospitals — which, as I said, nonprofit and for-profit hospital chains also operate — are also subject to the appropriate quality measures, readmissions, etc. Just because we don’t necessarily have the best quality measurement in the system in the country, it doesn’t mean that we shouldn’t allow care specialization. As I’d point out, if we’re concerned about specialty hospitals, the concern shouldn’t just be about physician-owned specialty hospitals; it should be about specialty hospitals by and large. Many health systems run cardiac specialty hospitals, cancer specialty hospitals, and orthopedic specialty hospitals. If we’re going to have a discussion about concerns there, it should be about the entire industry of specialty hospitals.
I think specialty hospitals serve an important role in society, allowing for specialization and exploiting in a positive way the volume-quality relationship. Whether those are owned by a for-profit publicly traded company, a tax-exempt facility, or physicians, I think that is an important way to have innovation and care delivery because frankly, we haven’t had much innovation in care delivery. Much of what we do in terms of how we practice clinically hasn’t really changed in the 50 years since my late father graduated from medical school. We still have rounds, we’re still taking notes, we’re still operating in the same way. Many processes are manual. We don’t have the mass production and mass customization of care that we need.
When you have a focused factory, it allows you to design care in a way that drives up quality, not just for the average patient but also the patients at the tail ends, because you have time to focus on that specific service line and that specific patient population.
Physician-owned community hospitals offer an important opportunity for a different employment model. I remember going to the dermatologist and the dermatologist was depressed, shuffling around the room, sad, and I asked him why. He said he didn’t really like his employer, and I said, “Why don’t you pick another one?” He’s like, “There are only two large health systems I can work for. They all have the same clinical practice environment and functionally the same value.”
Physicians are increasingly burned out. They face monopsony power in who purchases their labor. They have little control. They don’t want to go through five committees, seven administrators, and attend 25 meetings just to change a single small process in clinical operations. If you’re an owner operator, you have a much better ability to do it.
Frankly, when many facilities do well now, when they do well clinically and do well financially, who benefits? The hospital administration and the hospital executives. The doctors aren’t benefiting. The nurses aren’t benefiting. The CNA is not benefiting. The secretary is not benefiting. The custodian is not benefiting. Shouldn’t the workers have a right to own and operate the business and do well when the business does well serving the community? That puts me in the weird space of agreeing with both conservatives and progressives.
Dr. Glatter: I agree with you. I think an ownership stake is always attractive. It helps with retention of employed persons. There›s no question that, when they have a stake, when they have skin in the game, they feel more empowered. I will not argue with you about that.
Dr. Miller: We don’t have business models where workers have that option in healthcare. Like the National Academy of Medicine said, one of the key drivers of burnout is the externalization of the locus of control over clinical practice, and the current business operating models guarantee an externalization of the locus of control over clinical practice.
If you actually look at the recent American Medical Association (AMA) meeting, there was a resolution to ban the corporate practice of medicine. They wanted to go more toward the legal professions model where only physicians can own and operate care delivery.
Dr. Glatter: Well, I think the shift is certainly something that the AMA would like and physicians collectively would agree with. Having a better lifestyle and being able to have control are factors in burnout.
Dr. Miller: It’s not just doctors. I think nurses want a better lifestyle. The nurses are treated as interchangeable lines on a spreadsheet. The nurses are an integral part of our clinical team. Why don’t we work together as a clinical unit to build a better delivery system? What better way to do that than to have clinicians in charge of it, right?
My favorite bakery that’s about 30 minutes away is owned by a baker. It is not owned by a large tax-exempt corporation. It’s owned by an owner operator who takes pride in their work. I think that is something that the profession would do well to return to. When I was a resident, one of my colleagues was already planning their retirement. That’s how depressed they were.
I went into medicine to actually care for patients. I think that we can make the world a better place for our patients. What that means is not only treating them with drugs and devices, but also creating a delivery system where they don’t have to wander from lobby to lobby in a 200,000 square-foot facility, wait in line for hours on end, get bills 6 months later, and fill out endless paper forms over and over again.
All of these basic processes in healthcare delivery that are broken could have and should have been fixed — and have been fixed in almost every other industry. I had to replace one of my car tires because I had a flat tire. The local tire shop has an app, and it sends me SMS text messages telling me when my appointment is and when my car is ready. We have solved all of these problems in many other businesses.
We have not solved them in healthcare delivery because, one, we have massive monopolies that are raising prices, have lower quality, and deliver a crappy patient experience, and we have also subjugated the clinical worker into a corporate automaton. We are functionally drones. We don’t have the agency and the authority to improve clinical operations anymore. It’s really depressing, and we should have that option again.
I trust my doctor. I trust the nurses that I work with, and I would like them to help make clinical decisions in a financially responsible and a sensible operational manner. We need to empower our workforce in order to do that so we can recapture the value of what it means to be a clinician again.
The current model of corporate employment: massive scale, more administrators, more processes, more emails, more meetings, more PowerPoint decks, more federal subsidies. The hospital industry has choices. It can improve clinical operations. It can show up in Washington and lobby for increased subsidies. It can invest in the market and not pay taxes for the tax-exempt facilities. Obviously, it makes the logical choices as an economic actor to show up, lobby for increased subsidies, and then also invest in the stock market.
Improving clinical operations is hard. It hasn’t happened. The Bureau of Labor Statistics shows that the private community hospital industry has had flat labor productivity growth, on average, for the past 25 years, and for some years it even declined. This is totally atypical across the economy.
We have failed our clinicians, and most importantly, we have failed our patients. I’ve been sick. My relatives have been sick, waiting hours, not able to get appointments, and redoing forms. It’s a total disaster. It’s time and reasonable to try an alternative ownership and operating model. There are obviously problems. The problems can and should be addressed, but it doesn’t mean that we should have a statutory prohibition on professionals owning and operating their own business.
Dr. Glatter: There was a report that $500 million was saved by limiting or banning or putting a moratorium on physician-owned hospitals by the Congressional Budget Office.
Dr. Miller: Yes, I’m very aware of those data. I’d say that the CBO also is off by 50% on the estimation of the implementation of the Part D program. They overestimated the Affordable Care Act market enrollment by over 10 million people — again, around 50%. They also estimated that the CMS Innovation Center initially would be a savings. Now they’ve re-estimated it as a 10-year expenditure and it has actually cost the taxpayers money.
The CBO is not transparent about what its assumptions are or its analysis and methods. As a researcher, we have to publish our information. It has to go through peer review. I want to know what goes into that $500 million figure — what the assumptions are and what the model is. It’s hard to comment without knowing how they came up with it.
Dr. Glatter: The points you make are very valid. Physicians and nurses want a better lifestyle.
Dr. Miller: It’s not even a better lifestyle. It’s about having a say in how clinical operations work and helping make them better. We want the delivery system to work better. This is an opportunity for us to do so.
Dr. Glatter: That translates into technology: obviously, generative artificial intelligence (AI) coming into the forefront, as we know, and changing care delivery models as you’re referring to, which is going to happen. It’s going to be a slow process. I think that the evolution is happening and will happen, as you accurately described.
Dr. Miller: The other thing that’s different now vs 20 years ago is that managed care is here, there, and everywhere, as Dr Seuss would say. You have utilization review and prior authorization, which I’ve experienced as a patient and a physician, and boy, is it not a fun process. There’s a large amount of friction that needs to be improved. If we’re worried about induced demand or inappropriate utilization, we have managed care right there to help police bad behavior.
Reforming Healthcare Systems and Restoring Patient-Centric Focus
Dr. Glatter: If you were to come up with, say, three bullet points of how we can work our way out of this current morass of where our healthcare systems exist, where do you see the solutions or how can we make and effect change?
Dr. Miller: I’d say there are a couple of things. One is, let business models compete fairly on an equal playing field. Let the physician-owned hospital compete with the tax-exempt hospital and the nonprofit hospital. Put them on an equal playing field. We have things like 340B, which favors tax-exempt hospitals. For-profit or tax-paying hospitals are not able to participate in that. That doesn’t make any sense just from a public policy perspective. Tax-paying hospitals and physician-owned hospitals pay taxes on investments, but tax-exempt hospitals don’t. I think, in public policy, we need to equalize the playing field between business models. Let the best business model win.
The other thing we need to do is to encourage the adoption of technology. The physician will eventually be an arbiter of tech-driven or AI-driven tools. In fact, at some point, the standard of care might be to use those tools. Not using those tools would be seen as negligence. If you think about placing a jugular or central venous catheter, to not use ultrasound would be considered insane. Thirty years ago, to use ultrasound would be considered novel. I think technology and AI will get us to that point of helping make care more efficient and more customized.
Those are the two biggest interventions, I would say. Third, every time we have a conversation in public policy, we need to remember what it is to be a patient. The decision should be driven not around any one industry’s profitability, but what it is to be a patient and how we can make that experience less burdensome, less expensive, or in plain English, suck less.
Dr. Glatter: Safety net hospitals and critical access hospitals are part of this discussion that, yes, we want everything to, in an ideal world, function more efficiently and effectively, with less cost and less red tape. The safety net of our nation is struggling.
Dr. Miller: I 100% agree. The Cook County hospitals of the world are deserving of our support and, frankly, our gratitude. Facilities like that have huge burdens of patients with Medicaid. We also still have millions of uninsured patients. The neighborhoods that they serve are also poorer. I think facilities like that are deserving of public support.
I also think we need to clearly define what those hospitals are. One of the challenges I’ve realized as I waded into this space is that market definitions of what a service market is for a hospital, its specialty type or what a safety net hospital is need to be more clearly defined because those facilities 100% are deserving of our support. We just need to be clear about what they are.
Regarding critical access hospitals, when you practice in a rural area, you have to think differently about care delivery. I’d say many of the rural systems are highly creative in how they structure clinical operations. Before the public health emergency, during the COVID pandemic, when we had a massive change in telehealth, rural hospitals were using — within the very narrow confines — as much telehealth as they could and should.
Rural hospitals also make greater use of nurse practitioners (NPs) and physician assistants (PAs). For many of the specialty services, I remember, your first call was an NP or a PA because the physician was downstairs doing procedures. They’d come up and assess the patient before the procedure, but most of your consult questions were answered by the NP or PA. I’m not saying that’s the model we should use nationwide, but that rural systems are highly innovative and creative; they’re deserving of our time, attention, and support, and frankly, we can learn from them.
Dr. Glatter: I want to thank you for your time and your expertise in this area. We’ll see how the congressional hearings affect the industry as a whole, how the needle moves, and whether the ban or moratorium on physician-owned hospitals continues to exist going forward.
Dr. Miller: I appreciate you having me. The hospital industry is one of the most important industries for health care. This is a time of inflection, right? We need to go back to the value of what it means to be a clinician and serve patients. Hospitals need to reorient themselves around that core concern. How do we help support clinicians — doctors, nurses, pharmacists, whomever it is — in serving patients? Hospitals have become too corporate, so I think that this is an expected pushback.
Dr. Glatter: Again, I want to thank you for your time. This was a very important discussion. Thank you for your expertise.
Robert D. Glatter, MD, is an assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. He is a medical advisor for Medscape and hosts the Hot Topics in EM series. He disclosed no relevant financial relationships.Brian J. Miller, MD, MBA, MPH, is a hospitalist and an assistant professor of medicine at the Johns Hopkins University School of Medicine. He is also a nonresident fellow at the American Enterprise Institute. From 2014 to 2017, Dr. Miller worked at four federal regulatory agencies: Federal Trade Commission (FTC), Federal Communications Commission (FCC), Centers for Medicare & Medicaid Services (CMS), and the Food & Drug Administration (FDA). Dr. Miller disclosed ties with the Medicare Payment Advisory Commission.
A version of this article appeared on Medscape.com.
Doctors Win $7 Million Settlement in EEOC Forced Retirement Case
In a victory for clinicians who fought to keep working regardless of age,
In a statement, the US Equal Employment Opportunity Commission (EEOC) said the settlement will resolve an age and disability discrimination charge filed against Scripps Clinic Medical Group. The medical group is part of Scripps Health, a major provider of medical services in the San Diego region that operates five local hospitals.
The EECO said it found “reasonable cause” that the medical group violated the Age Discrimination in Employment Act and the Americans with Disabilities Act.
US health systems are facing lawsuits that claim they’ve engaged in age discrimination by requiring physicians to take cognitive tests when they reach specific ages.
The Scripps medical group’s mandatory retirement policy began in 2016 and was consistent with California law, which specifically allows for mandatory retirement of physicians in medical groups at age 70, Scripps said in a statement, adding that it rescinded the policy in 2018.
“This policy was put in place to enhance patient safety,” Scripps said. “The EEOC took the position while such a policy is expressly legal under California law; it is not allowed under federal law.”
The Federal Age Discrimination in Employment Act, passed in 1967, states that employers may not “fail or refuse to hire or to discharge any individual or otherwise discriminate against any individual with respect to his compensation, terms, conditions, or privileges of employment because of such individual’s age.” There are exceptions, however, in cases of public safety for professions such as air traffic controllers.
California law has a similar provision banning age discrimination, but it makes an exception for “any employee who has attained 70 years of age and is a physician employed by a professional medical corporation, the articles or bylaws of which provide for compulsory retirement.”
In 2020, an estimated 12% of US licensed physicians were at least 70 years old — more than 120,000 in total — up from 9% in a 2010, according to a Federation of State Medical Boards 2021 report.
Scripps Clinic Medical Group settled with the EEOC “without any admission of fault or wrongdoing to avoid the continued expense and distraction of litigation,” its statement said. It agreed to pay $6.875 million to the affected physicians.
When asked about how many physicians were affected by the policy, a Scripps human resources official said, “this was disputed but very few. The policy was only in effect for 2 years, 2016 and 2017. Additionally, by age 75, most doctors have retired. And those who have not almost always have voluntarily limited their practice.”
The Scripps official didn’t respond to questions about the number of patients served by the medical group and how many physicians it employs.
According to the EEOC, the medical group has agreed to tell employees that the policy has been scrapped and must “clarify that the company does not have any policy in which age is a factor in making employment decisions, including termination, retirement, and terms and conditions of employment.”
Scripps Clinic Medical Group also agreed to require division and department heads, executive leadership, and human resources employees to be trained regarding the Age Discrimination in Employment Act and the Americans with Disabilities Act.
A version of this article appeared on Medscape.com.
In a victory for clinicians who fought to keep working regardless of age,
In a statement, the US Equal Employment Opportunity Commission (EEOC) said the settlement will resolve an age and disability discrimination charge filed against Scripps Clinic Medical Group. The medical group is part of Scripps Health, a major provider of medical services in the San Diego region that operates five local hospitals.
The EECO said it found “reasonable cause” that the medical group violated the Age Discrimination in Employment Act and the Americans with Disabilities Act.
US health systems are facing lawsuits that claim they’ve engaged in age discrimination by requiring physicians to take cognitive tests when they reach specific ages.
The Scripps medical group’s mandatory retirement policy began in 2016 and was consistent with California law, which specifically allows for mandatory retirement of physicians in medical groups at age 70, Scripps said in a statement, adding that it rescinded the policy in 2018.
“This policy was put in place to enhance patient safety,” Scripps said. “The EEOC took the position while such a policy is expressly legal under California law; it is not allowed under federal law.”
The Federal Age Discrimination in Employment Act, passed in 1967, states that employers may not “fail or refuse to hire or to discharge any individual or otherwise discriminate against any individual with respect to his compensation, terms, conditions, or privileges of employment because of such individual’s age.” There are exceptions, however, in cases of public safety for professions such as air traffic controllers.
California law has a similar provision banning age discrimination, but it makes an exception for “any employee who has attained 70 years of age and is a physician employed by a professional medical corporation, the articles or bylaws of which provide for compulsory retirement.”
In 2020, an estimated 12% of US licensed physicians were at least 70 years old — more than 120,000 in total — up from 9% in a 2010, according to a Federation of State Medical Boards 2021 report.
Scripps Clinic Medical Group settled with the EEOC “without any admission of fault or wrongdoing to avoid the continued expense and distraction of litigation,” its statement said. It agreed to pay $6.875 million to the affected physicians.
When asked about how many physicians were affected by the policy, a Scripps human resources official said, “this was disputed but very few. The policy was only in effect for 2 years, 2016 and 2017. Additionally, by age 75, most doctors have retired. And those who have not almost always have voluntarily limited their practice.”
The Scripps official didn’t respond to questions about the number of patients served by the medical group and how many physicians it employs.
According to the EEOC, the medical group has agreed to tell employees that the policy has been scrapped and must “clarify that the company does not have any policy in which age is a factor in making employment decisions, including termination, retirement, and terms and conditions of employment.”
Scripps Clinic Medical Group also agreed to require division and department heads, executive leadership, and human resources employees to be trained regarding the Age Discrimination in Employment Act and the Americans with Disabilities Act.
A version of this article appeared on Medscape.com.
In a victory for clinicians who fought to keep working regardless of age,
In a statement, the US Equal Employment Opportunity Commission (EEOC) said the settlement will resolve an age and disability discrimination charge filed against Scripps Clinic Medical Group. The medical group is part of Scripps Health, a major provider of medical services in the San Diego region that operates five local hospitals.
The EECO said it found “reasonable cause” that the medical group violated the Age Discrimination in Employment Act and the Americans with Disabilities Act.
US health systems are facing lawsuits that claim they’ve engaged in age discrimination by requiring physicians to take cognitive tests when they reach specific ages.
The Scripps medical group’s mandatory retirement policy began in 2016 and was consistent with California law, which specifically allows for mandatory retirement of physicians in medical groups at age 70, Scripps said in a statement, adding that it rescinded the policy in 2018.
“This policy was put in place to enhance patient safety,” Scripps said. “The EEOC took the position while such a policy is expressly legal under California law; it is not allowed under federal law.”
The Federal Age Discrimination in Employment Act, passed in 1967, states that employers may not “fail or refuse to hire or to discharge any individual or otherwise discriminate against any individual with respect to his compensation, terms, conditions, or privileges of employment because of such individual’s age.” There are exceptions, however, in cases of public safety for professions such as air traffic controllers.
California law has a similar provision banning age discrimination, but it makes an exception for “any employee who has attained 70 years of age and is a physician employed by a professional medical corporation, the articles or bylaws of which provide for compulsory retirement.”
In 2020, an estimated 12% of US licensed physicians were at least 70 years old — more than 120,000 in total — up from 9% in a 2010, according to a Federation of State Medical Boards 2021 report.
Scripps Clinic Medical Group settled with the EEOC “without any admission of fault or wrongdoing to avoid the continued expense and distraction of litigation,” its statement said. It agreed to pay $6.875 million to the affected physicians.
When asked about how many physicians were affected by the policy, a Scripps human resources official said, “this was disputed but very few. The policy was only in effect for 2 years, 2016 and 2017. Additionally, by age 75, most doctors have retired. And those who have not almost always have voluntarily limited their practice.”
The Scripps official didn’t respond to questions about the number of patients served by the medical group and how many physicians it employs.
According to the EEOC, the medical group has agreed to tell employees that the policy has been scrapped and must “clarify that the company does not have any policy in which age is a factor in making employment decisions, including termination, retirement, and terms and conditions of employment.”
Scripps Clinic Medical Group also agreed to require division and department heads, executive leadership, and human resources employees to be trained regarding the Age Discrimination in Employment Act and the Americans with Disabilities Act.
A version of this article appeared on Medscape.com.
From Mentee to Mentor
Mentoring is universally recognized as a key contributor to a successful career in academic medicine. Most of those who recently transitioned from fellow to faculty got to their current positions with the help of one or more mentors. While many will still need mentoring, coaching, and sponsoring, many are also eager to give back and wonder when and how to make that transition from mentee to mentor.
Dr. Lok: Senior Mentor’s Perspective
I (ASL) completed my hepatology fellowship training in London under Professor Dame Sheila Sherlock. I did not realize how fortunate I was until Dame Sheila’s retirement celebration (2 months before the end of my fellowship) when more than 200 former mentees flew in from all over the world to express their appreciation. Dame Sheila had always embraced all of us as part of the Sherlock family. I benefited tremendously not only from clinical and research training with Dame Sheila and her motherly love that continued well after I completed my fellowship but also the connections and support from my “siblings” who were the Who’s Who in Hepatology.

My transition from mentee to mentor occurred insidiously after my return to Hong Kong, coaching and collaborating with residents, fellows, and early career faculty in their research projects. A key tip I shared with them was the importance of establishing a robust database and sample repository — a vital element to success as a clinical investigator. Working in a busy clinical environment with no protected time and limited resources, we began by identifying clinical dilemmas that we faced in clinics each day and determined which ones were “solvable” if we dove deep. Through keen observations, protocolized clinical care, and robust data recording, we published in Gastroenterology one of the first prospective studies of hepatitis B reactivation in patients receiving chemotherapy, and it continues to be cited. Many principles in mentoring apply universally. Indeed, one of my most accomplished mentees in Hong Kong is a nephrologist with whom I continue to coauthor topics in UpToDate. This is an example of how mentee-mentor relationship can evolve and last, and how each can learn from the other to provide guidance on multi-disciplinary care of complex medical problems.
I became more involved in mentoring after I moved to the United States. I was first hired as Hepatology Program Director at Tulane University and then at the University of Michigan. These roles gave me a sense of responsibility not just to mentor one resident, fellow, or faculty on a research project but to have a holistic approach, providing the necessary guidance and support to help mentees make the best of their potentials and build successful careers, which in turn allows me to build a world-class program.
Over the years, I have mentored more than 60 trainees from all over the world, some of whom have now become division chiefs, department chairs, and chief medical officers of hospitals. Every mentor has a different style, and I had been criticized for being a “Tiger Mom.” I have mellowed over the years, and I hope I am no longer perceived as a “tiger,” though tough love is crucial in mentoring. I hope I am still considered a “mom,” because I see the role of a mentor as that of a parent, providing unconditional love and support with the only expectation that the mentees try to do their best to maximize their potentials and reach their goals. Mentoring is a time investment. It can be exhausting, frustrating, and heart-breaking. It is rarely recognized, and the time and effort rarely compensated. Thus, one should take on mentoring as a calling, a desire to pay it forward, and an understanding that problems can be solved only when generations of physicians and researchers continue to work on them.
A mentor, just like a parent, helps mentees recognize their potentials — passion, strengths, and weaknesses — and to set ambitious yet realistic goals. A very important role of a mentor is to help mentees determine their short- and long-term goals by guiding them to leverage their strengths and passion toward areas and niches that are important and attainable.
Each goal must be accompanied by a plan on how to get there based on resources available. Here is where tough love comes into play. Because there are so many distractions in life, mentees can veer off and be lost. Research projects (and life) never go exactly as planned, and it is difficult to keep going when projects hit a roadblock and papers and grants are rejected. A mentor must help mentees accept and learn from failures and persevere with renewed commitment or find an alternative path (when it is clear the original path is doomed). The most important role of the mentor is to continue to believe in the mentee. Project failure must not be equated to mentee failure though there are times when it is clear some mentees have their interests and talents in other areas. Helping mentees find an alternative path to success and fulfillment can be a blessing. Indeed, two of my mentees who were successful researchers during their early careers have now become successful chief medical officers of major hospitals. They are happy, and I am very proud of them. Times have changed, so my coauthor, who has been faculty for 3.5 years, will share his journey from mentee to mentor.
Dr. Chen: Early Mentor’s Perspective
I (VLC) completed training in 2020 and have mentored only people who are early in their careers, i.e., medical students, residents, and fellows. My transition from mentee to mentor was primarily motivated by gratitude to my past mentors. Watching my own former trainees move on to the next stages of their careers has been hugely fulfilling. It is important that mentee-mentor relationships are mutually beneficial, and I offer a few points to junior faculty considering taking on trainees as mentees.

Taking on a mentee is a commitment. Take it seriously. While a mentee’s success is ultimately their responsibility, mentors are implicitly agreeing to give them opportunities commensurate to their skills and motivation. If you are not in a position to offer such opportunities, do not accept mentees.
Mentorship takes time. Explaining and reviewing research protocols, reading abstract or manuscript drafts, and meeting with mentees to plan for next steps take more time than one might expect.
Understand what potential mentees want. Most trainees are looking for help making it to the next stage of their career (college to medical school, residency to fellowship, etc.) and need abstracts and/or publications to get there. When I work with residents applying to GI fellowship, the goal is that by the time fellowship applications are submitted (early in third year of residency), they have at a minimum presented an abstract at Digestive Diseases Week (DDW) in their second year and submitted an abstract to the American College of Gastroenterology and/or American Association for the Study of Liver Diseases meetings in their third year. This requires planning to ensure they start working early enough to meet conference abstract deadlines. In my opinion, it is reasonable to give the trainee a less ambitious project or a piece of a larger project (i.e., middle authorship on a paper).
By contrast, for trainees who are seriously interested in a research career, the goal is not superfluous abstracts. Rather it is crucial to ensure that the trainee leads a meaningful project that will be a steppingstone to their future career and/or provide preliminary data to support grant applications. Similarly, training in research methodology should be more rigorous for these mentees.
Recognize the limitations of your circumstances. Early-stage faculty often operate on a shoestring budget and little protected time. Even those with 50% or more protected research time and excellent nursing support will find that the time they spend on patient care extends far beyond the time spent in endoscopy units and clinics. Time management and discipline — including not getting bogged down on low-impact research studies — are essential skills.
Be (slightly) selfish. Make sure that you get something out of the mentee as well. Ask yourself:
Do I have work they can help me with? Avoid creating projects simply to give a trainee something to do. It is much better to have them work on a project that you want to do anyway.
How do the trainee’s skills fit in with the type of work that I do? A trainee with no background in statistics may not be able to conduct analyses but may be able to do chart reviews.
Consider “testing” a potential mentee by assigning a limited, straightforward task. If the mentee completes this quickly and to a high standard, then move on to progressively more important or high-stakes projects.
Set concrete and realistic expectations, keeping in mind that trainees have other commitments such as classes and clinical rotations.
Serving as a mentor to the next generation of gastroenterologists is a privilege that junior faculty should not take lightly, and an opportunity for a symbiotic relationship.
Dr. Chen and Dr. Lok are with the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan. They have no financial conflicts related to this article.
Mentoring is universally recognized as a key contributor to a successful career in academic medicine. Most of those who recently transitioned from fellow to faculty got to their current positions with the help of one or more mentors. While many will still need mentoring, coaching, and sponsoring, many are also eager to give back and wonder when and how to make that transition from mentee to mentor.
Dr. Lok: Senior Mentor’s Perspective
I (ASL) completed my hepatology fellowship training in London under Professor Dame Sheila Sherlock. I did not realize how fortunate I was until Dame Sheila’s retirement celebration (2 months before the end of my fellowship) when more than 200 former mentees flew in from all over the world to express their appreciation. Dame Sheila had always embraced all of us as part of the Sherlock family. I benefited tremendously not only from clinical and research training with Dame Sheila and her motherly love that continued well after I completed my fellowship but also the connections and support from my “siblings” who were the Who’s Who in Hepatology.
My transition from mentee to mentor occurred insidiously after my return to Hong Kong, coaching and collaborating with residents, fellows, and early career faculty in their research projects. A key tip I shared with them was the importance of establishing a robust database and sample repository — a vital element to success as a clinical investigator. Working in a busy clinical environment with no protected time and limited resources, we began by identifying clinical dilemmas that we faced in clinics each day and determined which ones were “solvable” if we dove deep. Through keen observations, protocolized clinical care, and robust data recording, we published in Gastroenterology one of the first prospective studies of hepatitis B reactivation in patients receiving chemotherapy, and it continues to be cited. Many principles in mentoring apply universally. Indeed, one of my most accomplished mentees in Hong Kong is a nephrologist with whom I continue to coauthor topics in UpToDate. This is an example of how mentee-mentor relationship can evolve and last, and how each can learn from the other to provide guidance on multi-disciplinary care of complex medical problems.
I became more involved in mentoring after I moved to the United States. I was first hired as Hepatology Program Director at Tulane University and then at the University of Michigan. These roles gave me a sense of responsibility not just to mentor one resident, fellow, or faculty on a research project but to have a holistic approach, providing the necessary guidance and support to help mentees make the best of their potentials and build successful careers, which in turn allows me to build a world-class program.
Over the years, I have mentored more than 60 trainees from all over the world, some of whom have now become division chiefs, department chairs, and chief medical officers of hospitals. Every mentor has a different style, and I had been criticized for being a “Tiger Mom.” I have mellowed over the years, and I hope I am no longer perceived as a “tiger,” though tough love is crucial in mentoring. I hope I am still considered a “mom,” because I see the role of a mentor as that of a parent, providing unconditional love and support with the only expectation that the mentees try to do their best to maximize their potentials and reach their goals. Mentoring is a time investment. It can be exhausting, frustrating, and heart-breaking. It is rarely recognized, and the time and effort rarely compensated. Thus, one should take on mentoring as a calling, a desire to pay it forward, and an understanding that problems can be solved only when generations of physicians and researchers continue to work on them.
A mentor, just like a parent, helps mentees recognize their potentials — passion, strengths, and weaknesses — and to set ambitious yet realistic goals. A very important role of a mentor is to help mentees determine their short- and long-term goals by guiding them to leverage their strengths and passion toward areas and niches that are important and attainable.
Each goal must be accompanied by a plan on how to get there based on resources available. Here is where tough love comes into play. Because there are so many distractions in life, mentees can veer off and be lost. Research projects (and life) never go exactly as planned, and it is difficult to keep going when projects hit a roadblock and papers and grants are rejected. A mentor must help mentees accept and learn from failures and persevere with renewed commitment or find an alternative path (when it is clear the original path is doomed). The most important role of the mentor is to continue to believe in the mentee. Project failure must not be equated to mentee failure though there are times when it is clear some mentees have their interests and talents in other areas. Helping mentees find an alternative path to success and fulfillment can be a blessing. Indeed, two of my mentees who were successful researchers during their early careers have now become successful chief medical officers of major hospitals. They are happy, and I am very proud of them. Times have changed, so my coauthor, who has been faculty for 3.5 years, will share his journey from mentee to mentor.
Dr. Chen: Early Mentor’s Perspective
I (VLC) completed training in 2020 and have mentored only people who are early in their careers, i.e., medical students, residents, and fellows. My transition from mentee to mentor was primarily motivated by gratitude to my past mentors. Watching my own former trainees move on to the next stages of their careers has been hugely fulfilling. It is important that mentee-mentor relationships are mutually beneficial, and I offer a few points to junior faculty considering taking on trainees as mentees.
Taking on a mentee is a commitment. Take it seriously. While a mentee’s success is ultimately their responsibility, mentors are implicitly agreeing to give them opportunities commensurate to their skills and motivation. If you are not in a position to offer such opportunities, do not accept mentees.
Mentorship takes time. Explaining and reviewing research protocols, reading abstract or manuscript drafts, and meeting with mentees to plan for next steps take more time than one might expect.
Understand what potential mentees want. Most trainees are looking for help making it to the next stage of their career (college to medical school, residency to fellowship, etc.) and need abstracts and/or publications to get there. When I work with residents applying to GI fellowship, the goal is that by the time fellowship applications are submitted (early in third year of residency), they have at a minimum presented an abstract at Digestive Diseases Week (DDW) in their second year and submitted an abstract to the American College of Gastroenterology and/or American Association for the Study of Liver Diseases meetings in their third year. This requires planning to ensure they start working early enough to meet conference abstract deadlines. In my opinion, it is reasonable to give the trainee a less ambitious project or a piece of a larger project (i.e., middle authorship on a paper).
By contrast, for trainees who are seriously interested in a research career, the goal is not superfluous abstracts. Rather it is crucial to ensure that the trainee leads a meaningful project that will be a steppingstone to their future career and/or provide preliminary data to support grant applications. Similarly, training in research methodology should be more rigorous for these mentees.
Recognize the limitations of your circumstances. Early-stage faculty often operate on a shoestring budget and little protected time. Even those with 50% or more protected research time and excellent nursing support will find that the time they spend on patient care extends far beyond the time spent in endoscopy units and clinics. Time management and discipline — including not getting bogged down on low-impact research studies — are essential skills.
Be (slightly) selfish. Make sure that you get something out of the mentee as well. Ask yourself:
Do I have work they can help me with? Avoid creating projects simply to give a trainee something to do. It is much better to have them work on a project that you want to do anyway.
How do the trainee’s skills fit in with the type of work that I do? A trainee with no background in statistics may not be able to conduct analyses but may be able to do chart reviews.
Consider “testing” a potential mentee by assigning a limited, straightforward task. If the mentee completes this quickly and to a high standard, then move on to progressively more important or high-stakes projects.
Set concrete and realistic expectations, keeping in mind that trainees have other commitments such as classes and clinical rotations.
Serving as a mentor to the next generation of gastroenterologists is a privilege that junior faculty should not take lightly, and an opportunity for a symbiotic relationship.
Dr. Chen and Dr. Lok are with the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan. They have no financial conflicts related to this article.
Mentoring is universally recognized as a key contributor to a successful career in academic medicine. Most of those who recently transitioned from fellow to faculty got to their current positions with the help of one or more mentors. While many will still need mentoring, coaching, and sponsoring, many are also eager to give back and wonder when and how to make that transition from mentee to mentor.
Dr. Lok: Senior Mentor’s Perspective
I (ASL) completed my hepatology fellowship training in London under Professor Dame Sheila Sherlock. I did not realize how fortunate I was until Dame Sheila’s retirement celebration (2 months before the end of my fellowship) when more than 200 former mentees flew in from all over the world to express their appreciation. Dame Sheila had always embraced all of us as part of the Sherlock family. I benefited tremendously not only from clinical and research training with Dame Sheila and her motherly love that continued well after I completed my fellowship but also the connections and support from my “siblings” who were the Who’s Who in Hepatology.
My transition from mentee to mentor occurred insidiously after my return to Hong Kong, coaching and collaborating with residents, fellows, and early career faculty in their research projects. A key tip I shared with them was the importance of establishing a robust database and sample repository — a vital element to success as a clinical investigator. Working in a busy clinical environment with no protected time and limited resources, we began by identifying clinical dilemmas that we faced in clinics each day and determined which ones were “solvable” if we dove deep. Through keen observations, protocolized clinical care, and robust data recording, we published in Gastroenterology one of the first prospective studies of hepatitis B reactivation in patients receiving chemotherapy, and it continues to be cited. Many principles in mentoring apply universally. Indeed, one of my most accomplished mentees in Hong Kong is a nephrologist with whom I continue to coauthor topics in UpToDate. This is an example of how mentee-mentor relationship can evolve and last, and how each can learn from the other to provide guidance on multi-disciplinary care of complex medical problems.
I became more involved in mentoring after I moved to the United States. I was first hired as Hepatology Program Director at Tulane University and then at the University of Michigan. These roles gave me a sense of responsibility not just to mentor one resident, fellow, or faculty on a research project but to have a holistic approach, providing the necessary guidance and support to help mentees make the best of their potentials and build successful careers, which in turn allows me to build a world-class program.
Over the years, I have mentored more than 60 trainees from all over the world, some of whom have now become division chiefs, department chairs, and chief medical officers of hospitals. Every mentor has a different style, and I had been criticized for being a “Tiger Mom.” I have mellowed over the years, and I hope I am no longer perceived as a “tiger,” though tough love is crucial in mentoring. I hope I am still considered a “mom,” because I see the role of a mentor as that of a parent, providing unconditional love and support with the only expectation that the mentees try to do their best to maximize their potentials and reach their goals. Mentoring is a time investment. It can be exhausting, frustrating, and heart-breaking. It is rarely recognized, and the time and effort rarely compensated. Thus, one should take on mentoring as a calling, a desire to pay it forward, and an understanding that problems can be solved only when generations of physicians and researchers continue to work on them.
A mentor, just like a parent, helps mentees recognize their potentials — passion, strengths, and weaknesses — and to set ambitious yet realistic goals. A very important role of a mentor is to help mentees determine their short- and long-term goals by guiding them to leverage their strengths and passion toward areas and niches that are important and attainable.
Each goal must be accompanied by a plan on how to get there based on resources available. Here is where tough love comes into play. Because there are so many distractions in life, mentees can veer off and be lost. Research projects (and life) never go exactly as planned, and it is difficult to keep going when projects hit a roadblock and papers and grants are rejected. A mentor must help mentees accept and learn from failures and persevere with renewed commitment or find an alternative path (when it is clear the original path is doomed). The most important role of the mentor is to continue to believe in the mentee. Project failure must not be equated to mentee failure though there are times when it is clear some mentees have their interests and talents in other areas. Helping mentees find an alternative path to success and fulfillment can be a blessing. Indeed, two of my mentees who were successful researchers during their early careers have now become successful chief medical officers of major hospitals. They are happy, and I am very proud of them. Times have changed, so my coauthor, who has been faculty for 3.5 years, will share his journey from mentee to mentor.
Dr. Chen: Early Mentor’s Perspective
I (VLC) completed training in 2020 and have mentored only people who are early in their careers, i.e., medical students, residents, and fellows. My transition from mentee to mentor was primarily motivated by gratitude to my past mentors. Watching my own former trainees move on to the next stages of their careers has been hugely fulfilling. It is important that mentee-mentor relationships are mutually beneficial, and I offer a few points to junior faculty considering taking on trainees as mentees.
Taking on a mentee is a commitment. Take it seriously. While a mentee’s success is ultimately their responsibility, mentors are implicitly agreeing to give them opportunities commensurate to their skills and motivation. If you are not in a position to offer such opportunities, do not accept mentees.
Mentorship takes time. Explaining and reviewing research protocols, reading abstract or manuscript drafts, and meeting with mentees to plan for next steps take more time than one might expect.
Understand what potential mentees want. Most trainees are looking for help making it to the next stage of their career (college to medical school, residency to fellowship, etc.) and need abstracts and/or publications to get there. When I work with residents applying to GI fellowship, the goal is that by the time fellowship applications are submitted (early in third year of residency), they have at a minimum presented an abstract at Digestive Diseases Week (DDW) in their second year and submitted an abstract to the American College of Gastroenterology and/or American Association for the Study of Liver Diseases meetings in their third year. This requires planning to ensure they start working early enough to meet conference abstract deadlines. In my opinion, it is reasonable to give the trainee a less ambitious project or a piece of a larger project (i.e., middle authorship on a paper).
By contrast, for trainees who are seriously interested in a research career, the goal is not superfluous abstracts. Rather it is crucial to ensure that the trainee leads a meaningful project that will be a steppingstone to their future career and/or provide preliminary data to support grant applications. Similarly, training in research methodology should be more rigorous for these mentees.
Recognize the limitations of your circumstances. Early-stage faculty often operate on a shoestring budget and little protected time. Even those with 50% or more protected research time and excellent nursing support will find that the time they spend on patient care extends far beyond the time spent in endoscopy units and clinics. Time management and discipline — including not getting bogged down on low-impact research studies — are essential skills.
Be (slightly) selfish. Make sure that you get something out of the mentee as well. Ask yourself:
Do I have work they can help me with? Avoid creating projects simply to give a trainee something to do. It is much better to have them work on a project that you want to do anyway.
How do the trainee’s skills fit in with the type of work that I do? A trainee with no background in statistics may not be able to conduct analyses but may be able to do chart reviews.
Consider “testing” a potential mentee by assigning a limited, straightforward task. If the mentee completes this quickly and to a high standard, then move on to progressively more important or high-stakes projects.
Set concrete and realistic expectations, keeping in mind that trainees have other commitments such as classes and clinical rotations.
Serving as a mentor to the next generation of gastroenterologists is a privilege that junior faculty should not take lightly, and an opportunity for a symbiotic relationship.
Dr. Chen and Dr. Lok are with the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan. They have no financial conflicts related to this article.
Tax Questions Frequently Asked by Physicians
Physicians spend years of their lives in education and training. There are countless hours devoted to studying, researching, and clinical training, not to mention residency and possible fellowships. Then literally overnight, they transition out of a resident salary into a full-time attending pay with little to no education around what to do with this significant increase in salary.
Every job position is unique in terms of benefits, how compensation is earned, job expectations, etc. But they all share one thing in common — taxes. Increased income comes with increased taxes. 
FAQ 1. What is the difference between W2 income and 1099 income?
A: If you are a W2 employee, your employer is responsible for paying half of your Social Security and Medicare taxes. You, as the employee, are then responsible only for the remaining half of your Social Security and Medicare taxes. Additionally, your employer will withhold these taxes, along with federal income taxes, from your paycheck each pay period. You are not responsible for remitting any taxes to the IRS or state agencies, as your employer will do this for you. As a W2 employee, you are not able to deduct any employee expenses against your income.

As a 1099 contractor, you are considered self-employed and are responsible for the employer and employee portion of the Social Security and Medicare taxes. You are also responsible for remitting these taxes, as well as quarterly estimated federal withholding, to the IRS and state agencies. You can deduct work-related expenses against your 1099 income.
Both types of income have pros and cons. Either of these can be more beneficial to a specific situation.
FAQ 2. How do I know if I am withholding enough taxes?
A: This is a very common issue I see, especially with physicians who are transitioning out of training into their full-time attending salary. Because this transition happens mid-year, often the first half of the year you are withholding at a rate much lower than what you will be earning as an attending and end up with a tax surprise at filing. One way to remedy this is to look at how much taxes are being withheld from your paycheck and compare this to what tax bracket you anticipate to be in, depending on filing status (Figure 1). If you do this and realize you are not withholding enough taxes, you can submit an amended form W4 to your employer to have additional withholding taken out each pay period.
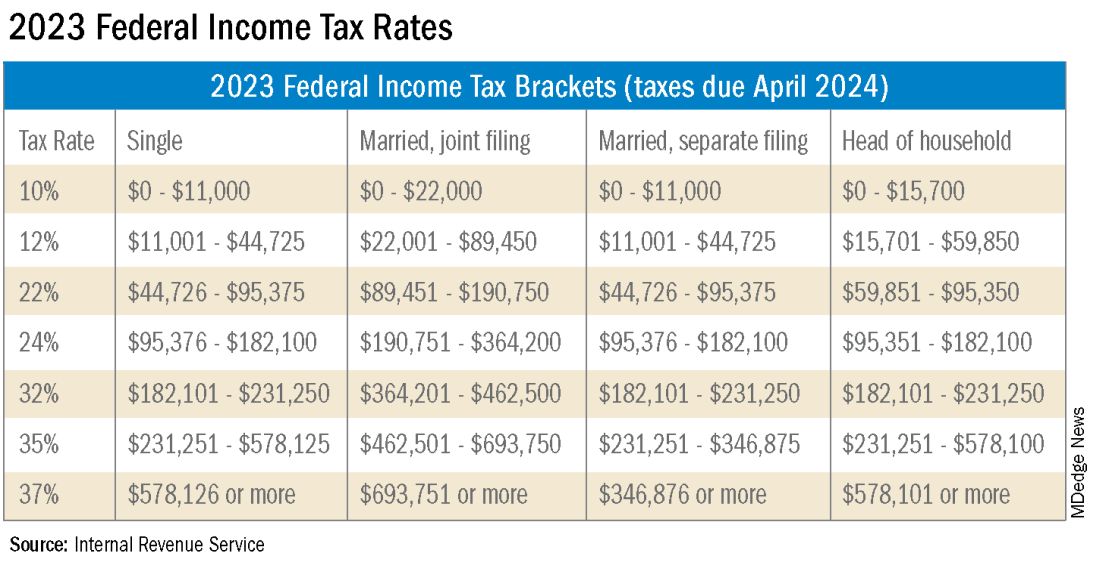
FAQ 3. I am a 1099 contractor; do I need a PLLC, and should I file as an S-Corporation?
A: The term “S-Corp” gets mentioned often related to 1099 contractors and can be extremely beneficial from a tax savings perspective. Often physicians may moonlight — in addition to working in their W2 positions — and would receive this compensation as a 1099 contractor rather than an employee. This is an example of when a Professional Limited Liability Company (PLLC) might be advisable. A PLLC is created at a state level and helps shield owners from potential litigation. The owner of a PLLC pays Social Security and Medicare taxes on all income earned from the entity, and the PLLC is included in the owner’s individual income tax return.
A Small-Corporation (S-Corporation) is a tax classification that passes income through to the owners. The PLLC is now taxed as an S-Corporation, rather than a disregarded entity. The shareholders of the S-Corporation are required to pay a reasonable salary (W2 income). The remaining income passes through to the owner and is not subject to Social Security and Medicare taxes, only federal income tax. This taxation status requires an additional tax return and payroll service. Because there are additional expenses with being taxed as an S-Corporation, a cost-benefit analysis should be done before changing the tax classification to confirm that the tax savings are greater than the additional costs.
FAQ 4. What is the ‘backdoor Roth’ strategy? Should I implement it?
A: A Roth IRA is a specific type of Individual Retirement Account (IRA) that is funded with after-tax dollars. The contributions and growth in a Roth IRA can be withdrawn at retirement, tax free. As physicians who are typically high earners, you are not able to contribute directly to a Roth IRA because of income limitations. This is where the Roth conversion strategy — the backdoor Roth — comes into play. This strategy allows you to make a nondeductible traditional IRA contribution and then convert those dollars into a Roth IRA. In 2023, you can contribute up to $6,500 into this type of account. There are many additional considerations that must be made before implementing this strategy. Discussion with a financial advisor or CPA is recommended.
FAQ 5. I’ve always done my own taxes. Do I need to hire a CPA?
A: For many physicians, especially during training, your tax situation may not warrant the need for a Certified Public Accountant (CPA). However, as your income and tax complexity increase, working with a CPA not only decreases your risk for error, but also helps ensure you are not overpaying in taxes. There are many different types of services that a CPA can offer, the most basic being tax preparation. This is simply compiling your tax return based on the circumstances that occurred in the prior year. Tax planning is an additional level of service that may not be included in tax preparation cost. Tax planning is a proactive approach to taxes and helps maximize tax savings opportunities before return preparation. When interviewing a potential CPA, you can ask what level of services are included in the fees quoted.
These are just a few of the questions I regularly answer related to physicians’ taxation. The tax code is complex and ever changing. Recommendations that are made today might not be applicable or advisable in the future to any given situation. Working with a professional can ensure you have the most up-to-date and accurate information related to your taxes.
Ms. Anderson is with Physician’s Resource Services and is on Instagram @physiciansrs . Dr. Anderson is a CA-1 Resident in Anesthesia at Baylor Scott and White Health. The authors have no conflicts of interest.
Physicians spend years of their lives in education and training. There are countless hours devoted to studying, researching, and clinical training, not to mention residency and possible fellowships. Then literally overnight, they transition out of a resident salary into a full-time attending pay with little to no education around what to do with this significant increase in salary.
Every job position is unique in terms of benefits, how compensation is earned, job expectations, etc. But they all share one thing in common — taxes. Increased income comes with increased taxes.
FAQ 1. What is the difference between W2 income and 1099 income?
A: If you are a W2 employee, your employer is responsible for paying half of your Social Security and Medicare taxes. You, as the employee, are then responsible only for the remaining half of your Social Security and Medicare taxes. Additionally, your employer will withhold these taxes, along with federal income taxes, from your paycheck each pay period. You are not responsible for remitting any taxes to the IRS or state agencies, as your employer will do this for you. As a W2 employee, you are not able to deduct any employee expenses against your income.
As a 1099 contractor, you are considered self-employed and are responsible for the employer and employee portion of the Social Security and Medicare taxes. You are also responsible for remitting these taxes, as well as quarterly estimated federal withholding, to the IRS and state agencies. You can deduct work-related expenses against your 1099 income.
Both types of income have pros and cons. Either of these can be more beneficial to a specific situation.
FAQ 2. How do I know if I am withholding enough taxes?
A: This is a very common issue I see, especially with physicians who are transitioning out of training into their full-time attending salary. Because this transition happens mid-year, often the first half of the year you are withholding at a rate much lower than what you will be earning as an attending and end up with a tax surprise at filing. One way to remedy this is to look at how much taxes are being withheld from your paycheck and compare this to what tax bracket you anticipate to be in, depending on filing status (Figure 1). If you do this and realize you are not withholding enough taxes, you can submit an amended form W4 to your employer to have additional withholding taken out each pay period.
FAQ 3. I am a 1099 contractor; do I need a PLLC, and should I file as an S-Corporation?
A: The term “S-Corp” gets mentioned often related to 1099 contractors and can be extremely beneficial from a tax savings perspective. Often physicians may moonlight — in addition to working in their W2 positions — and would receive this compensation as a 1099 contractor rather than an employee. This is an example of when a Professional Limited Liability Company (PLLC) might be advisable. A PLLC is created at a state level and helps shield owners from potential litigation. The owner of a PLLC pays Social Security and Medicare taxes on all income earned from the entity, and the PLLC is included in the owner’s individual income tax return.
A Small-Corporation (S-Corporation) is a tax classification that passes income through to the owners. The PLLC is now taxed as an S-Corporation, rather than a disregarded entity. The shareholders of the S-Corporation are required to pay a reasonable salary (W2 income). The remaining income passes through to the owner and is not subject to Social Security and Medicare taxes, only federal income tax. This taxation status requires an additional tax return and payroll service. Because there are additional expenses with being taxed as an S-Corporation, a cost-benefit analysis should be done before changing the tax classification to confirm that the tax savings are greater than the additional costs.
FAQ 4. What is the ‘backdoor Roth’ strategy? Should I implement it?
A: A Roth IRA is a specific type of Individual Retirement Account (IRA) that is funded with after-tax dollars. The contributions and growth in a Roth IRA can be withdrawn at retirement, tax free. As physicians who are typically high earners, you are not able to contribute directly to a Roth IRA because of income limitations. This is where the Roth conversion strategy — the backdoor Roth — comes into play. This strategy allows you to make a nondeductible traditional IRA contribution and then convert those dollars into a Roth IRA. In 2023, you can contribute up to $6,500 into this type of account. There are many additional considerations that must be made before implementing this strategy. Discussion with a financial advisor or CPA is recommended.
FAQ 5. I’ve always done my own taxes. Do I need to hire a CPA?
A: For many physicians, especially during training, your tax situation may not warrant the need for a Certified Public Accountant (CPA). However, as your income and tax complexity increase, working with a CPA not only decreases your risk for error, but also helps ensure you are not overpaying in taxes. There are many different types of services that a CPA can offer, the most basic being tax preparation. This is simply compiling your tax return based on the circumstances that occurred in the prior year. Tax planning is an additional level of service that may not be included in tax preparation cost. Tax planning is a proactive approach to taxes and helps maximize tax savings opportunities before return preparation. When interviewing a potential CPA, you can ask what level of services are included in the fees quoted.
These are just a few of the questions I regularly answer related to physicians’ taxation. The tax code is complex and ever changing. Recommendations that are made today might not be applicable or advisable in the future to any given situation. Working with a professional can ensure you have the most up-to-date and accurate information related to your taxes.
Ms. Anderson is with Physician’s Resource Services and is on Instagram @physiciansrs . Dr. Anderson is a CA-1 Resident in Anesthesia at Baylor Scott and White Health. The authors have no conflicts of interest.
Physicians spend years of their lives in education and training. There are countless hours devoted to studying, researching, and clinical training, not to mention residency and possible fellowships. Then literally overnight, they transition out of a resident salary into a full-time attending pay with little to no education around what to do with this significant increase in salary.
Every job position is unique in terms of benefits, how compensation is earned, job expectations, etc. But they all share one thing in common — taxes. Increased income comes with increased taxes.
FAQ 1. What is the difference between W2 income and 1099 income?
A: If you are a W2 employee, your employer is responsible for paying half of your Social Security and Medicare taxes. You, as the employee, are then responsible only for the remaining half of your Social Security and Medicare taxes. Additionally, your employer will withhold these taxes, along with federal income taxes, from your paycheck each pay period. You are not responsible for remitting any taxes to the IRS or state agencies, as your employer will do this for you. As a W2 employee, you are not able to deduct any employee expenses against your income.
As a 1099 contractor, you are considered self-employed and are responsible for the employer and employee portion of the Social Security and Medicare taxes. You are also responsible for remitting these taxes, as well as quarterly estimated federal withholding, to the IRS and state agencies. You can deduct work-related expenses against your 1099 income.
Both types of income have pros and cons. Either of these can be more beneficial to a specific situation.
FAQ 2. How do I know if I am withholding enough taxes?
A: This is a very common issue I see, especially with physicians who are transitioning out of training into their full-time attending salary. Because this transition happens mid-year, often the first half of the year you are withholding at a rate much lower than what you will be earning as an attending and end up with a tax surprise at filing. One way to remedy this is to look at how much taxes are being withheld from your paycheck and compare this to what tax bracket you anticipate to be in, depending on filing status (Figure 1). If you do this and realize you are not withholding enough taxes, you can submit an amended form W4 to your employer to have additional withholding taken out each pay period.
FAQ 3. I am a 1099 contractor; do I need a PLLC, and should I file as an S-Corporation?
A: The term “S-Corp” gets mentioned often related to 1099 contractors and can be extremely beneficial from a tax savings perspective. Often physicians may moonlight — in addition to working in their W2 positions — and would receive this compensation as a 1099 contractor rather than an employee. This is an example of when a Professional Limited Liability Company (PLLC) might be advisable. A PLLC is created at a state level and helps shield owners from potential litigation. The owner of a PLLC pays Social Security and Medicare taxes on all income earned from the entity, and the PLLC is included in the owner’s individual income tax return.
A Small-Corporation (S-Corporation) is a tax classification that passes income through to the owners. The PLLC is now taxed as an S-Corporation, rather than a disregarded entity. The shareholders of the S-Corporation are required to pay a reasonable salary (W2 income). The remaining income passes through to the owner and is not subject to Social Security and Medicare taxes, only federal income tax. This taxation status requires an additional tax return and payroll service. Because there are additional expenses with being taxed as an S-Corporation, a cost-benefit analysis should be done before changing the tax classification to confirm that the tax savings are greater than the additional costs.
FAQ 4. What is the ‘backdoor Roth’ strategy? Should I implement it?
A: A Roth IRA is a specific type of Individual Retirement Account (IRA) that is funded with after-tax dollars. The contributions and growth in a Roth IRA can be withdrawn at retirement, tax free. As physicians who are typically high earners, you are not able to contribute directly to a Roth IRA because of income limitations. This is where the Roth conversion strategy — the backdoor Roth — comes into play. This strategy allows you to make a nondeductible traditional IRA contribution and then convert those dollars into a Roth IRA. In 2023, you can contribute up to $6,500 into this type of account. There are many additional considerations that must be made before implementing this strategy. Discussion with a financial advisor or CPA is recommended.
FAQ 5. I’ve always done my own taxes. Do I need to hire a CPA?
A: For many physicians, especially during training, your tax situation may not warrant the need for a Certified Public Accountant (CPA). However, as your income and tax complexity increase, working with a CPA not only decreases your risk for error, but also helps ensure you are not overpaying in taxes. There are many different types of services that a CPA can offer, the most basic being tax preparation. This is simply compiling your tax return based on the circumstances that occurred in the prior year. Tax planning is an additional level of service that may not be included in tax preparation cost. Tax planning is a proactive approach to taxes and helps maximize tax savings opportunities before return preparation. When interviewing a potential CPA, you can ask what level of services are included in the fees quoted.
These are just a few of the questions I regularly answer related to physicians’ taxation. The tax code is complex and ever changing. Recommendations that are made today might not be applicable or advisable in the future to any given situation. Working with a professional can ensure you have the most up-to-date and accurate information related to your taxes.
Ms. Anderson is with Physician’s Resource Services and is on Instagram @physiciansrs . Dr. Anderson is a CA-1 Resident in Anesthesia at Baylor Scott and White Health. The authors have no conflicts of interest.
Survival-Toxicity Trade-off With T-DM1 in HER+ Breast Cancer
SAN ANTONIO — in older patients with advanced human epidermal growth factor receptor 2–positive (HER2+) breast cancer, although toxicity is much lower, results from the HERB TEA study show.
Overall, the standard-of-care triple regimen of monoclonal antibodies pertuzumab and trastuzumab plus docetaxel remains the “first-line treatment for HER2-positive advanced breast cancer, regardless of age,” said study author Akihiko Shimomura, MD, PhD, who presented the findings (abstract RF02-04) on December 7 at the San Antonio Breast Cancer Symposium.
However, he noted that the standard-of-care regimen appears to be “intolerable mentally and physically” in those older than 65 years, and “impairs” quality of life.
Therefore a “new standard treatment with less toxicity and noninferior efficacy for older patients is needed,” said Dr. Shimomura, Department of Breast and Medical Oncology, National Center for Global Health and Medicine, Tokyo.
Dr. Shimomura and colleagues recruited patients aged 65 years or older with advanced HER2+ breast cancer who had received no prior chemotherapy for metastatic breast cancer and had a good performance status.
Patients were randomly assigned to either pertuzumab and trastuzumab plus docetaxel or T-DM1 until disease progression. The planned sample size was 250 patients, but the study was terminated after 148 participants were recruited because an interim analysis showed that T-DM1 failed to show noninferiority.
Among 75 patients assigned to the standard-of-care regimen, the mean age was 71 years, with 64% aged 65-74 years. Sixty-five percent had stage IV disease, and 35% had relapsed. These baseline characteristics were similar among the 73 patients given T-DM1.
At the data cutoff of June 15, 2023, the median progression-free survival was comparable between the two groups, at 15.6 months with the triple therapy vs 11.3 months with T-DM1 (hazard ratio [HR], 1.358; P =.1236).
There was also no significant difference in overall survival between the two groups (HR, 1.263; P =.95322).
However, T-DM1 failed to meet its primary endpoint of noninferiority to pertuzumab and trastuzumab plus docetaxel, defined as a hazard ratio for overall survival of 1.35.
Nevertheless, T-DM1 was associated with significantly less toxicity than the standard-of care-regimen, with rates of grade 3 or worse adverse events of 36.1% vs 56.8%, Shimomura reported.
The most common hematologic adverse events with the triple therapy were leukopenia (34.2%) and neutropenia (52.0%), whereas thrombocytopenia was the most common event with T-DM1 (16.7%).
Liver toxicities were also increased with the antibody-drug conjugate, whereas fatigue, diarrhea, and appetite loss were more frequently seen with the standard-of-care regimen.
Although T-DM1 did not achieve noninferiority, given its lower toxicity profile, a “detailed analysis, including geriatric assessment, is needed to identify the patient population for whom T-DM1 may be used as first line treatment,” said Shimomura.
Virginia Kaklamani, MD, codirector of the SABCS and leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center, Texas, said in an interview that the trial shows T-DM1 could be “a good alternative to our first line therapy in HER2+ metastatic breast cancer” for some patients.
“It is, however, unlikely to change the standard of care due to several changes in the field including the results from the KATHERINE trial and the DESTINY-Breast trials,” she said.
The study was funded by the Japanese National Cancer Center. Dr. Shimomura declares relationships with Daiichi Sankyo, Pfizer, AstraZeneca K.K., Chugai Pharmaceutical Co. Ltd, Eli Lilly Japan K.K., MSD Co. Ltd, Eisai Co. Ltd, Gilead Sciences, and Taiho Pharmaceutical Co. Ltd.
A version of this article appeared on Medscape.com.
SAN ANTONIO — in older patients with advanced human epidermal growth factor receptor 2–positive (HER2+) breast cancer, although toxicity is much lower, results from the HERB TEA study show.
Overall, the standard-of-care triple regimen of monoclonal antibodies pertuzumab and trastuzumab plus docetaxel remains the “first-line treatment for HER2-positive advanced breast cancer, regardless of age,” said study author Akihiko Shimomura, MD, PhD, who presented the findings (abstract RF02-04) on December 7 at the San Antonio Breast Cancer Symposium.
However, he noted that the standard-of-care regimen appears to be “intolerable mentally and physically” in those older than 65 years, and “impairs” quality of life.
Therefore a “new standard treatment with less toxicity and noninferior efficacy for older patients is needed,” said Dr. Shimomura, Department of Breast and Medical Oncology, National Center for Global Health and Medicine, Tokyo.
Dr. Shimomura and colleagues recruited patients aged 65 years or older with advanced HER2+ breast cancer who had received no prior chemotherapy for metastatic breast cancer and had a good performance status.
Patients were randomly assigned to either pertuzumab and trastuzumab plus docetaxel or T-DM1 until disease progression. The planned sample size was 250 patients, but the study was terminated after 148 participants were recruited because an interim analysis showed that T-DM1 failed to show noninferiority.
Among 75 patients assigned to the standard-of-care regimen, the mean age was 71 years, with 64% aged 65-74 years. Sixty-five percent had stage IV disease, and 35% had relapsed. These baseline characteristics were similar among the 73 patients given T-DM1.
At the data cutoff of June 15, 2023, the median progression-free survival was comparable between the two groups, at 15.6 months with the triple therapy vs 11.3 months with T-DM1 (hazard ratio [HR], 1.358; P =.1236).
There was also no significant difference in overall survival between the two groups (HR, 1.263; P =.95322).
However, T-DM1 failed to meet its primary endpoint of noninferiority to pertuzumab and trastuzumab plus docetaxel, defined as a hazard ratio for overall survival of 1.35.
Nevertheless, T-DM1 was associated with significantly less toxicity than the standard-of care-regimen, with rates of grade 3 or worse adverse events of 36.1% vs 56.8%, Shimomura reported.
The most common hematologic adverse events with the triple therapy were leukopenia (34.2%) and neutropenia (52.0%), whereas thrombocytopenia was the most common event with T-DM1 (16.7%).
Liver toxicities were also increased with the antibody-drug conjugate, whereas fatigue, diarrhea, and appetite loss were more frequently seen with the standard-of-care regimen.
Although T-DM1 did not achieve noninferiority, given its lower toxicity profile, a “detailed analysis, including geriatric assessment, is needed to identify the patient population for whom T-DM1 may be used as first line treatment,” said Shimomura.
Virginia Kaklamani, MD, codirector of the SABCS and leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center, Texas, said in an interview that the trial shows T-DM1 could be “a good alternative to our first line therapy in HER2+ metastatic breast cancer” for some patients.
“It is, however, unlikely to change the standard of care due to several changes in the field including the results from the KATHERINE trial and the DESTINY-Breast trials,” she said.
The study was funded by the Japanese National Cancer Center. Dr. Shimomura declares relationships with Daiichi Sankyo, Pfizer, AstraZeneca K.K., Chugai Pharmaceutical Co. Ltd, Eli Lilly Japan K.K., MSD Co. Ltd, Eisai Co. Ltd, Gilead Sciences, and Taiho Pharmaceutical Co. Ltd.
A version of this article appeared on Medscape.com.
SAN ANTONIO — in older patients with advanced human epidermal growth factor receptor 2–positive (HER2+) breast cancer, although toxicity is much lower, results from the HERB TEA study show.
Overall, the standard-of-care triple regimen of monoclonal antibodies pertuzumab and trastuzumab plus docetaxel remains the “first-line treatment for HER2-positive advanced breast cancer, regardless of age,” said study author Akihiko Shimomura, MD, PhD, who presented the findings (abstract RF02-04) on December 7 at the San Antonio Breast Cancer Symposium.
However, he noted that the standard-of-care regimen appears to be “intolerable mentally and physically” in those older than 65 years, and “impairs” quality of life.
Therefore a “new standard treatment with less toxicity and noninferior efficacy for older patients is needed,” said Dr. Shimomura, Department of Breast and Medical Oncology, National Center for Global Health and Medicine, Tokyo.
Dr. Shimomura and colleagues recruited patients aged 65 years or older with advanced HER2+ breast cancer who had received no prior chemotherapy for metastatic breast cancer and had a good performance status.
Patients were randomly assigned to either pertuzumab and trastuzumab plus docetaxel or T-DM1 until disease progression. The planned sample size was 250 patients, but the study was terminated after 148 participants were recruited because an interim analysis showed that T-DM1 failed to show noninferiority.
Among 75 patients assigned to the standard-of-care regimen, the mean age was 71 years, with 64% aged 65-74 years. Sixty-five percent had stage IV disease, and 35% had relapsed. These baseline characteristics were similar among the 73 patients given T-DM1.
At the data cutoff of June 15, 2023, the median progression-free survival was comparable between the two groups, at 15.6 months with the triple therapy vs 11.3 months with T-DM1 (hazard ratio [HR], 1.358; P =.1236).
There was also no significant difference in overall survival between the two groups (HR, 1.263; P =.95322).
However, T-DM1 failed to meet its primary endpoint of noninferiority to pertuzumab and trastuzumab plus docetaxel, defined as a hazard ratio for overall survival of 1.35.
Nevertheless, T-DM1 was associated with significantly less toxicity than the standard-of care-regimen, with rates of grade 3 or worse adverse events of 36.1% vs 56.8%, Shimomura reported.
The most common hematologic adverse events with the triple therapy were leukopenia (34.2%) and neutropenia (52.0%), whereas thrombocytopenia was the most common event with T-DM1 (16.7%).
Liver toxicities were also increased with the antibody-drug conjugate, whereas fatigue, diarrhea, and appetite loss were more frequently seen with the standard-of-care regimen.
Although T-DM1 did not achieve noninferiority, given its lower toxicity profile, a “detailed analysis, including geriatric assessment, is needed to identify the patient population for whom T-DM1 may be used as first line treatment,” said Shimomura.
Virginia Kaklamani, MD, codirector of the SABCS and leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center, Texas, said in an interview that the trial shows T-DM1 could be “a good alternative to our first line therapy in HER2+ metastatic breast cancer” for some patients.
“It is, however, unlikely to change the standard of care due to several changes in the field including the results from the KATHERINE trial and the DESTINY-Breast trials,” she said.
The study was funded by the Japanese National Cancer Center. Dr. Shimomura declares relationships with Daiichi Sankyo, Pfizer, AstraZeneca K.K., Chugai Pharmaceutical Co. Ltd, Eli Lilly Japan K.K., MSD Co. Ltd, Eisai Co. Ltd, Gilead Sciences, and Taiho Pharmaceutical Co. Ltd.
A version of this article appeared on Medscape.com.
AT SABCS 2023
10% of US physicians work for or under UnitedHealth. Is that a problem?
as more payers and private equity firms pursue medical practice acquisitions.
The company added 20,000 physicians in the last year alone, including a previously physician-owned multispecialty group practice of 400 doctors in New York. They join the growing web of doctors — about 90,000 of the 950,000 active US physicians — working for the UnitedHealth Group subsidiary, Optum Health, providing primary, specialty, urgent, and surgical care. Amar Desai, MD, chief executive officer of Optum Health, shared the updated workforce numbers during the health care conglomerate’s annual investor conference.
Health care mergers and consolidations have become more common as physician groups struggle to stay afloat amid dwindling payer reimbursements. Although private equity and health systems often acquire practices, payers like UHC are increasingly doing so as part of their model to advance value-based care.
Yashaswini Singh, PhD, health care economist and assistant professor of health services, policy, and practice at Brown University, says such moves mirror the broader trend in corporate consolidation of physician practices. She said in an interview that the integrated models could possibly enhance care coordination and improve outcomes, but the impact of payer-led consolidation has not been extensively studied.
Meanwhile, evidence considering private equity ownership is just emerging. In a 2022 study published in JAMA Health Forum, with Dr. Singh as lead author, findings showed that private equity involvement increased healthcare spending through higher prices and utilization.
Consolidation can also raise anti-trust concerns. “If payers incentivize referral patterns of their employed physicians to favor other physicians employed by the payer, it can reduce competition by restricting consumer choice,” said Dr. Singh.
A potential merger between Cigna and Humana that could happen by the end of the year will likely face intense scrutiny as it would create a company that rivals the size of UnitedHealth Group or CVS Health. If it goes through, the duo could streamline its insurance offerings and leverage each other’s care delivery platforms, clinics, and provider workforce.
The Biden Administration has sought to strengthen anti-trust statutes to prevent industry monopolies and consumer harm, and the US Department of Justice and Federal Trade Commission have proposed new merger guidelines that have yet to be finalized.
According to Dr. Singh, some of Optum’s medical practice purchases may bypass anti-trust statutes since most prospective mergers and acquisitions are reviewed only if they exceed a specific value ($101 million for 2023). Limited transparency in ownership structures further complicates matters. Plus, Dr. Singh said instances where physicians are hired instead of acquired through mergers would not be subject to current anti-trust laws.
The ‘corporatization’ of health care is not good for patients or physicians, said Robert McNamara, MD, chief medical officer of the American Academy of Emergency Medicine Physician Group and cofounder of Take Medicine Back, a physician group advocating to remove corporate interests from health care.
“If you ask a physician what causes them the most moral conflict, they’ll tell you it’s the insurance companies denying something they want to do for their patients,” he said. “To have the doctors now working for the insurance industry conflicts with a physician’s duty to put the patient first.”
Dr. McNamara, chair of emergency medicine at Temple University’s Katz School of Medicine, said in an interview that more than half the states in the United States have laws or court rulings that support protecting physician autonomy from corporate interests. Still, he hopes a federal prohibition on private equity’s involvement in healthcare can soon gain traction. In November, Take Medicine Back raised a resolution at the American Medical Association’s interim House of Delegates meeting, which he said was subsequently referred to a committee.
Emergency medicine was among the first specialties to succumb to private equity firms, but Dr. McNamara said that all types of health care providers and entities — from cardiology and urology to addiction treatment centers and nursing homes — are being swallowed up by larger organizations, including payers.
UHC was named in a class action suit recently for allegedly shirking doctors’ orders and relying on a flawed algorithm to determine the length of skilled nursing facility stays for Medicare Advantage policyholders.
At the investor meeting, Dr. Desai reiterated Optum’s desire to continue expanding care delivery options, especially in its pharmacy and behavioral health business lines, and focus on adopting value-based care. He credited the rapid growth to developing strong relationships with providers and standardizing technology and clinical systems.
A version of this article appeared on Medscape.com.
as more payers and private equity firms pursue medical practice acquisitions.
The company added 20,000 physicians in the last year alone, including a previously physician-owned multispecialty group practice of 400 doctors in New York. They join the growing web of doctors — about 90,000 of the 950,000 active US physicians — working for the UnitedHealth Group subsidiary, Optum Health, providing primary, specialty, urgent, and surgical care. Amar Desai, MD, chief executive officer of Optum Health, shared the updated workforce numbers during the health care conglomerate’s annual investor conference.
Health care mergers and consolidations have become more common as physician groups struggle to stay afloat amid dwindling payer reimbursements. Although private equity and health systems often acquire practices, payers like UHC are increasingly doing so as part of their model to advance value-based care.
Yashaswini Singh, PhD, health care economist and assistant professor of health services, policy, and practice at Brown University, says such moves mirror the broader trend in corporate consolidation of physician practices. She said in an interview that the integrated models could possibly enhance care coordination and improve outcomes, but the impact of payer-led consolidation has not been extensively studied.
Meanwhile, evidence considering private equity ownership is just emerging. In a 2022 study published in JAMA Health Forum, with Dr. Singh as lead author, findings showed that private equity involvement increased healthcare spending through higher prices and utilization.
Consolidation can also raise anti-trust concerns. “If payers incentivize referral patterns of their employed physicians to favor other physicians employed by the payer, it can reduce competition by restricting consumer choice,” said Dr. Singh.
A potential merger between Cigna and Humana that could happen by the end of the year will likely face intense scrutiny as it would create a company that rivals the size of UnitedHealth Group or CVS Health. If it goes through, the duo could streamline its insurance offerings and leverage each other’s care delivery platforms, clinics, and provider workforce.
The Biden Administration has sought to strengthen anti-trust statutes to prevent industry monopolies and consumer harm, and the US Department of Justice and Federal Trade Commission have proposed new merger guidelines that have yet to be finalized.
According to Dr. Singh, some of Optum’s medical practice purchases may bypass anti-trust statutes since most prospective mergers and acquisitions are reviewed only if they exceed a specific value ($101 million for 2023). Limited transparency in ownership structures further complicates matters. Plus, Dr. Singh said instances where physicians are hired instead of acquired through mergers would not be subject to current anti-trust laws.
The ‘corporatization’ of health care is not good for patients or physicians, said Robert McNamara, MD, chief medical officer of the American Academy of Emergency Medicine Physician Group and cofounder of Take Medicine Back, a physician group advocating to remove corporate interests from health care.
“If you ask a physician what causes them the most moral conflict, they’ll tell you it’s the insurance companies denying something they want to do for their patients,” he said. “To have the doctors now working for the insurance industry conflicts with a physician’s duty to put the patient first.”
Dr. McNamara, chair of emergency medicine at Temple University’s Katz School of Medicine, said in an interview that more than half the states in the United States have laws or court rulings that support protecting physician autonomy from corporate interests. Still, he hopes a federal prohibition on private equity’s involvement in healthcare can soon gain traction. In November, Take Medicine Back raised a resolution at the American Medical Association’s interim House of Delegates meeting, which he said was subsequently referred to a committee.
Emergency medicine was among the first specialties to succumb to private equity firms, but Dr. McNamara said that all types of health care providers and entities — from cardiology and urology to addiction treatment centers and nursing homes — are being swallowed up by larger organizations, including payers.
UHC was named in a class action suit recently for allegedly shirking doctors’ orders and relying on a flawed algorithm to determine the length of skilled nursing facility stays for Medicare Advantage policyholders.
At the investor meeting, Dr. Desai reiterated Optum’s desire to continue expanding care delivery options, especially in its pharmacy and behavioral health business lines, and focus on adopting value-based care. He credited the rapid growth to developing strong relationships with providers and standardizing technology and clinical systems.
A version of this article appeared on Medscape.com.
as more payers and private equity firms pursue medical practice acquisitions.
The company added 20,000 physicians in the last year alone, including a previously physician-owned multispecialty group practice of 400 doctors in New York. They join the growing web of doctors — about 90,000 of the 950,000 active US physicians — working for the UnitedHealth Group subsidiary, Optum Health, providing primary, specialty, urgent, and surgical care. Amar Desai, MD, chief executive officer of Optum Health, shared the updated workforce numbers during the health care conglomerate’s annual investor conference.
Health care mergers and consolidations have become more common as physician groups struggle to stay afloat amid dwindling payer reimbursements. Although private equity and health systems often acquire practices, payers like UHC are increasingly doing so as part of their model to advance value-based care.
Yashaswini Singh, PhD, health care economist and assistant professor of health services, policy, and practice at Brown University, says such moves mirror the broader trend in corporate consolidation of physician practices. She said in an interview that the integrated models could possibly enhance care coordination and improve outcomes, but the impact of payer-led consolidation has not been extensively studied.
Meanwhile, evidence considering private equity ownership is just emerging. In a 2022 study published in JAMA Health Forum, with Dr. Singh as lead author, findings showed that private equity involvement increased healthcare spending through higher prices and utilization.
Consolidation can also raise anti-trust concerns. “If payers incentivize referral patterns of their employed physicians to favor other physicians employed by the payer, it can reduce competition by restricting consumer choice,” said Dr. Singh.
A potential merger between Cigna and Humana that could happen by the end of the year will likely face intense scrutiny as it would create a company that rivals the size of UnitedHealth Group or CVS Health. If it goes through, the duo could streamline its insurance offerings and leverage each other’s care delivery platforms, clinics, and provider workforce.
The Biden Administration has sought to strengthen anti-trust statutes to prevent industry monopolies and consumer harm, and the US Department of Justice and Federal Trade Commission have proposed new merger guidelines that have yet to be finalized.
According to Dr. Singh, some of Optum’s medical practice purchases may bypass anti-trust statutes since most prospective mergers and acquisitions are reviewed only if they exceed a specific value ($101 million for 2023). Limited transparency in ownership structures further complicates matters. Plus, Dr. Singh said instances where physicians are hired instead of acquired through mergers would not be subject to current anti-trust laws.
The ‘corporatization’ of health care is not good for patients or physicians, said Robert McNamara, MD, chief medical officer of the American Academy of Emergency Medicine Physician Group and cofounder of Take Medicine Back, a physician group advocating to remove corporate interests from health care.
“If you ask a physician what causes them the most moral conflict, they’ll tell you it’s the insurance companies denying something they want to do for their patients,” he said. “To have the doctors now working for the insurance industry conflicts with a physician’s duty to put the patient first.”
Dr. McNamara, chair of emergency medicine at Temple University’s Katz School of Medicine, said in an interview that more than half the states in the United States have laws or court rulings that support protecting physician autonomy from corporate interests. Still, he hopes a federal prohibition on private equity’s involvement in healthcare can soon gain traction. In November, Take Medicine Back raised a resolution at the American Medical Association’s interim House of Delegates meeting, which he said was subsequently referred to a committee.
Emergency medicine was among the first specialties to succumb to private equity firms, but Dr. McNamara said that all types of health care providers and entities — from cardiology and urology to addiction treatment centers and nursing homes — are being swallowed up by larger organizations, including payers.
UHC was named in a class action suit recently for allegedly shirking doctors’ orders and relying on a flawed algorithm to determine the length of skilled nursing facility stays for Medicare Advantage policyholders.
At the investor meeting, Dr. Desai reiterated Optum’s desire to continue expanding care delivery options, especially in its pharmacy and behavioral health business lines, and focus on adopting value-based care. He credited the rapid growth to developing strong relationships with providers and standardizing technology and clinical systems.
A version of this article appeared on Medscape.com.