User login
What I want people to know about the Chauvin verdict
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.

There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.
There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I woke up from a nap on Tuesday, April 20, to a barrage of text messages and social media alerts about the Derek Chauvin verdict. Messages varied in content, from “let’s celebrate,” to “just so exciting,” to “finally.” As I took in the sentiments of others, I could barely sense what, if any, sentiments I had of my own.
There I sat, a Black DEI [diversity, equity, and inclusion] consultant who calls herself a “psychiatrist-activist,” but slept through the landmark court decision for policing African Americans and felt almost nothing about it.
However, I did have feelings about other matters such as the slide decks due for my client, sending reassuring text messages about the hospitalization of a friend’s child, and the 2 weeks of patient notes on my to-do list. So why did I feel emotionally flatlined about an issue that should stimulate the opposite – emotional intensity?
The answer to “why” could be attributed to a number of psychological buzz words like trauma, grief, desensitization, dissociation, numbness, or my new favorite term, languishing.
Despite the applicability of any of the above, I think my emotional flattening has more to do with the fact that in addition to the guilty verdict, I also woke up to news that 16-year-old Ma’Khia Bryant had been shot by a police officer in Columbus, Ohio.
I asked myself: How can anyone find time to grieve, nevertheless celebrate when (young) Black people continue to be killed by the police?
While it hurts to see individuals who look like me being shot by police, or even emboldened citizens, my hurt likely pales in comparison to someone who grew up surrounded by police gun violence. I grew up solidly middle class, lived in a house at the end of a cul-de-sac in a semi-gated community, and have many years ahead of me to reach my earning potential as a physician in one of the most liberal cities in the nation. While I have the skin color that puts me at risk of being shot by police due to racism, I am in a cushy position compared to other Black people who live in cities or neighborhoods with more police shootings.
Given this line of thinking, it seems clearer to me why I do not feel like celebrating, but instead, feel grateful to be alive. Not only do I feel grateful to be alive, but alive with the emotional stamina to help White people understand their contributions to the widespread oppression that keeps our society rooted in white supremacy.
This brings me to my point of what I want people, especially physicians, to know about the guilty verdict of Derek Chauvin: Some of us cannot really celebrate until there is actual police reform. This is not to say that anyone is wrong to celebrate, as long as there is an understanding that .
Meanwhile, White men like Kyle Rittenhouse who are peaceably arrested after shooting a man with a semi-automatic weapon receive donations from a Virginia police lieutenant; a policeman who, in a possible world, could one day pull me over while driving through Virginia given its proximity to Washington D.C., where I currently live.
Black and Brown people cannot fully celebrate until there is actual police reform, and reform across American institutions like the health care system. Celebration comes when the leaders who run schools, hospitals, and courtrooms look more like the numbers actually reflected in U.S. racial demographics and look less like Derek Chauvin.
Until there are more doctors who look like the racial breakdown of the nation, Black and Brown patients can never fully trust their primary care doctors, orthopedic surgeons, and psychiatrists who are White. While this reality may sound harsh, it is the reality for many of us who are dealing with trauma, grief, desensitization, dissociation, emotional numbness, or languishment resulting from racist experiences.
People of color cannot and will not stop protesting in the streets, being the one who always brings up race in the meeting, or disagreeing that the new changes are “not enough” until there is actual anti-racist institutional reform. More importantly, the efforts of people of color can be made more powerful working collectively with White allies.
But we need White allies who recognize their tendency to perceive “progress” in racial equality. We need White allies who recognize that despite the passage of the Civil Rights Act, the two-time election of a Black president, and the guilty verdict of Derek Chauvin, there is still so much work to do.
Dr. Cyrus is assistant professor in the department of psychiatry at Johns Hopkins University, Baltimore. She reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Chauvin guilty verdict: Now it’s time to get to work
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.

In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.
As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.
In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.
As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
On Tuesday, April 20, the country braced for the impact of the trial verdict in death of George Floyd. Despite the case having what many would consider an overwhelming amount of evidence pointing toward conviction, if we’re completely honest, the country – and particularly the African American community – had significant doubts that the jury would render a guilty verdict.
In the hour leading up to the announcement, people and images dominated my thoughts; Tamir Rice, Breonna Taylor, Eric Garner, Rashard Brooks, and most recently, Daunte Wright. With the deaths of these Black Americans and many others as historical context, I took a stoic stance and held my breath as the verdict was read. Former Minneapolis Police Officer Derek Chauvin was found guilty of second-degree murder, third-degree murder, and second-degree manslaughter.
As Mr. Chauvin was remanded to custody and led away in handcuffs, it was clear there were no “winners” in this verdict. Mr. Floyd is still dead, and violent encounters experienced by Black Americans continue at a vastly disproportionate rate. The result is far from true justice, but what we as a country do have is a moment of accountability – and perhaps an opportunity for true system-level reform.
The final report of the President’s Task Force on 21st Century Policing, released in May 2015, recommended major policy changes at the federal level and developed key pillars aimed at promoting effective crime reduction while building public trust. Based on this report, four key takeaways are relevant to any discussion of police reform. All are vitally important, but two stand out as particularly relevant in the aftermath of the verdict. One of the key recommendations was “embracing a guardian – rather than a warrior mindset” in an effort to build trust and legitimacy. Another was ensuring that “peace officer and standards training (POST) boards include mandatory Crisis Intervention Training.”
As health professionals, we know that the ultimate effectiveness of any intervention is based upon the amount of shared trust and collaboration in the patient-physician relationship. As a consultation-liaison psychiatrist, I’ve been trained to recognize that, when requested to consult on a case, I’m frequently not making a medical diagnosis or delivering an intervention; I’m helping the team and patient reestablish trust in each other. Communication skills and techniques help start a dialogue, but you will ultimately fall short of shared understanding without trust. The underpinning of trust could begin with a commitment to procedural justice. Procedural justice, as described in The Justice Collaboratory of Yale Law School, “speaks to the idea of fair processes and how the quality of their experiences strongly impacts people’s perception of fairness.” There are four central tenets of procedural justice:
- Whether they were treated with dignity and respect.
- Whether they were given voice.
- Whether the decision-maker was neutral and transparent.
- Whether the decision-maker conveyed trustworthy motives.
These four tenets have been researched and shown to improve the trust and confidence a community has in police, and lay the foundation for creating a standard set of shared interests and values.
As health professionals, there are many aspects of procedural justice that we can and should embrace, particularly as we come to our reckoning with the use of restraints in medical settings.
Building on the work of the Task Force on 21st Century Policing, the National Initiative for Building Community Trust and Justice, from January 2015 through December 2018, implemented a six-city intervention aimed at generating measurable improvements in officer behavior, public safety, and community trust in police. The National Initiative was organized around three principal ideas: procedural justice, implicit bias training, and reconciliation and candid conversations about law enforcement’s historic role in racial tensions.
In addition to the recommendations of the federal government and independent institutions, national-level health policy organizations have made clear statements regarding police brutality and the need for systemic reform to address police brutality and systemic racism. In 2018, the American Psychiatric Association released a position statement on Police Brutality and Black Males. This was then followed in 2020 with a joint statement from the National Medical Association and the APA condemning systemic racism and police violence against Black Americans. Other health policy associations, including the American Medical Association and the American Association of Medical Colleges, have made clear statements condemning systemic racism and police brutality.
In the aftermath of the verdict, we also saw something very different. In our partisan country, there appeared to be uniform common ground. Statements were made acknowledging the importance of this historic moment, from police unions, and both political parties, and various invested grassroots organizations. In short, we may have true agreement and motivation to take the next hard steps in police reform for this country. There will be policy discussions and new mandates for training, and certainly a push to ban the use of lethal techniques, such as choke holds. While helpful, these will ultimately fall short unless we hold ourselves accountable for a true culture change.
The challenge of implementing procedural justice shouldn’t be just a law enforcement challenge, and it shouldn’t fall on the shoulders of communities with high crime areas. In other words, no single racial group should own it. Ultimately, procedural justice will need to be embraced by all of us.
On April 20, as I watched the verdict, my oldest daughter watched with me, and she asked, “What do you think, Dad?” I responded: “It’s accountability and an opportunity.” She nodded her head with resolve. She then grabbed her smartphone and jumped into social media and proclaimed in her very knowledgeable teenage voice, “See Dad, one voice is cool, but many voices in unison is better; time to get to work!” To Darnella Frazier, who captured the crime on video at age 17, and all in your generation who dare to hold us accountable, I salute you. I thank you for forcing us to look even when it was painful and not ignore the humanity of our fellow man. It is indeed time to get to work.
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.

PTSD linked to ischemic heart disease
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.
Adjunctive MDMA safe, effective for severe PTSD
Adding 3,4-methylenedioxymethamphetamine (MDMA) to integrative psychotherapy may significantly improve symptoms and well-being for patients with severe posttraumatic stress disorder, including those with the dissociative subtype, new research suggests.
MAPP1 is the first phase 3 randomized controlled trial of MDMA-assisted therapy in this population. Participants who received the active treatment showed greater improvement in PTSD symptoms, mood, and empathy in comparison with participants who received placebo.
MDMA was “extremely effective, particularly for a subpopulation that ordinarily does not respond well to conventional treatment,” study coinvestigator Bessel van der Kolk, MD, professor of psychiatry at Boston University School of Medicine, told delegates attending the virtual European Psychiatric Association (EPA) 2021 Congress.
Growing interest
, particularly because failure rates with most available evidence-based treatments have been relatively high.
As previously reported by this news organization, in 2017, the U.S. Food and Drug Administration approved the trial design of Dr. van der Kolk’s and colleagues’ MAPP1 study after granting MDMA breakthrough designation.
The MAPP1 investigators assessed 90 patients with PTSD (mean age, 41 years; 77% White; 66% women) from 50 sites. For the majority of patients (84%), trauma history was developmental. “In other words, trauma [occurred] very early in life, usually at the hands of their own caregivers,” Dr. van der Kolk noted.
In addition, 18% of the patients were veterans, and 12% had combat exposure. The average duration of PTSD before enrollment was 18 years. All patients underwent screening and three preparatory psychotherapy sessions at enrollment.
Participants were randomly assigned to receive MDMA 80 mg or 120 mg (n = 46) or placebo (n = 44) followed by three integrative psychotherapy sessions lasting a total of 8 hours. A supplemental dose of 40 or 60 mg of MDMA could be administered from 1.5 to 2 hours after the first dose.
The patients stayed in the laboratory on the evening of the treatment session and attended a debriefing the next morning. The session was repeated a month later and again a month after that. In between, patients had telephone contact with the raters, who were blinded to the treatment received.
Follow-up assessments were conducted 2 months after the third treatment session and again at 12 months. The primary outcome measure was change in Clinician Administered PTSD Scale for DSM 5 (CAPS-5) score from baseline.
‘Dramatic improvement’
Results showed that both the MDMA and placebo groups experienced a statistically significant improvement in PTSD symptoms, “but MDMA had a dramatically significant improvement, with an effect size of over 0.9,” Dr. van der Kolk said.
The MDMA group also reported enhanced mood and well-being, increased responsiveness to emotional and sensory stimuli, a greater sense of closeness to other people, and a greater feeling of empathy.
Patients also reported having heightened openness, “and clearly the issue of empathy for themselves and others was a very large part of the process,” said Dr. van der Kolk.
“But for me, the most interesting part of the study is that the Adverse Childhood Experiences scale had no effect,” he noted. In other words, “the amount of childhood adverse experiences did not predict outcomes, which was very surprising because usually those patients are very treatment resistant.”
Dr. van der Kolk added that the dissociative subtype of PTSD was first described in the DSM-5 and that patients are “notoriously unresponsive to most unconventional treatments.”
In the current study, 13 patients met the criteria for the subtype, and investigators found they “did better than people with classical PTSD,” Dr. van der Kolk said. He added that this is a “very, very important finding.”
Carefully controlled
Overall, 82% of patients reported a significant improvement by the end of the study; 56% reported that they no longer had PTSD.
In addition, 67% of patients no longer met diagnostic criteria for PTSD. These included patients who had crossed over to active treatment from the placebo group.
Eleven patients (12%) experienced relapse by 12 months; in nine of the cases, this was due to the presence of additional stressors.
There were “very few adverse side effects” during the study, Dr. van der Kolk noted. In addition, “there were really no serious mental side effects,” despite the patients’ “opening up so much very painful material,” he added.
The most common adverse events among the MDMA group were muscle tightness (63%), decreased appetite (52%), nausea (30%), hyperhidrosis (20%), and feeling cold (20%). These effects were “quite small [and] the sort of side effects you would expect in response to an amphetamine substance like MDMA,” said Dr. van der Kolk.
“An important reason why we think the side effect profile is so good is because the study was extremely carefully done, very carefully controlled,” he added. “There was a great deal of support, [and] we paid an enormous amount of attention to creating a very safe context in which this drug was being used.”
However, he expressed concern that “as people see the very good results, they may skimp a little bit on the creation of the context and not have as careful a psychotherapy protocol as we had here.”
‘On the right track’
Commenting on the findings for this news organization, David Nutt, MD, PhD, Edmond J. Safra Professor of Neuropsychopharmacology, Imperial College London, said the results are proof that the investigators’ “earlier smaller trials of MDMA were on the right track.”

“This larger and multicenter trial shows that MDMA therapy can be broadened into newer research groups, which augurs well for the much larger rollout that will be required once it gets a license,” said Dr. Nutt, who was not involved with the research.
He added, “the prior evidence of the safety of MDMA has [now] been confirmed.”
The study represents an “important step in the path to the clinical use of MDMA for PTSD,” Dr. Nutt said.
The study was sponsored by the Multidisciplinary Association for Psychedelic Studies. The investigators and Dr. Nutt have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adding 3,4-methylenedioxymethamphetamine (MDMA) to integrative psychotherapy may significantly improve symptoms and well-being for patients with severe posttraumatic stress disorder, including those with the dissociative subtype, new research suggests.
MAPP1 is the first phase 3 randomized controlled trial of MDMA-assisted therapy in this population. Participants who received the active treatment showed greater improvement in PTSD symptoms, mood, and empathy in comparison with participants who received placebo.
MDMA was “extremely effective, particularly for a subpopulation that ordinarily does not respond well to conventional treatment,” study coinvestigator Bessel van der Kolk, MD, professor of psychiatry at Boston University School of Medicine, told delegates attending the virtual European Psychiatric Association (EPA) 2021 Congress.
Growing interest
, particularly because failure rates with most available evidence-based treatments have been relatively high.
As previously reported by this news organization, in 2017, the U.S. Food and Drug Administration approved the trial design of Dr. van der Kolk’s and colleagues’ MAPP1 study after granting MDMA breakthrough designation.
The MAPP1 investigators assessed 90 patients with PTSD (mean age, 41 years; 77% White; 66% women) from 50 sites. For the majority of patients (84%), trauma history was developmental. “In other words, trauma [occurred] very early in life, usually at the hands of their own caregivers,” Dr. van der Kolk noted.
In addition, 18% of the patients were veterans, and 12% had combat exposure. The average duration of PTSD before enrollment was 18 years. All patients underwent screening and three preparatory psychotherapy sessions at enrollment.
Participants were randomly assigned to receive MDMA 80 mg or 120 mg (n = 46) or placebo (n = 44) followed by three integrative psychotherapy sessions lasting a total of 8 hours. A supplemental dose of 40 or 60 mg of MDMA could be administered from 1.5 to 2 hours after the first dose.
The patients stayed in the laboratory on the evening of the treatment session and attended a debriefing the next morning. The session was repeated a month later and again a month after that. In between, patients had telephone contact with the raters, who were blinded to the treatment received.
Follow-up assessments were conducted 2 months after the third treatment session and again at 12 months. The primary outcome measure was change in Clinician Administered PTSD Scale for DSM 5 (CAPS-5) score from baseline.
‘Dramatic improvement’
Results showed that both the MDMA and placebo groups experienced a statistically significant improvement in PTSD symptoms, “but MDMA had a dramatically significant improvement, with an effect size of over 0.9,” Dr. van der Kolk said.
The MDMA group also reported enhanced mood and well-being, increased responsiveness to emotional and sensory stimuli, a greater sense of closeness to other people, and a greater feeling of empathy.
Patients also reported having heightened openness, “and clearly the issue of empathy for themselves and others was a very large part of the process,” said Dr. van der Kolk.
“But for me, the most interesting part of the study is that the Adverse Childhood Experiences scale had no effect,” he noted. In other words, “the amount of childhood adverse experiences did not predict outcomes, which was very surprising because usually those patients are very treatment resistant.”
Dr. van der Kolk added that the dissociative subtype of PTSD was first described in the DSM-5 and that patients are “notoriously unresponsive to most unconventional treatments.”
In the current study, 13 patients met the criteria for the subtype, and investigators found they “did better than people with classical PTSD,” Dr. van der Kolk said. He added that this is a “very, very important finding.”
Carefully controlled
Overall, 82% of patients reported a significant improvement by the end of the study; 56% reported that they no longer had PTSD.
In addition, 67% of patients no longer met diagnostic criteria for PTSD. These included patients who had crossed over to active treatment from the placebo group.
Eleven patients (12%) experienced relapse by 12 months; in nine of the cases, this was due to the presence of additional stressors.
There were “very few adverse side effects” during the study, Dr. van der Kolk noted. In addition, “there were really no serious mental side effects,” despite the patients’ “opening up so much very painful material,” he added.
The most common adverse events among the MDMA group were muscle tightness (63%), decreased appetite (52%), nausea (30%), hyperhidrosis (20%), and feeling cold (20%). These effects were “quite small [and] the sort of side effects you would expect in response to an amphetamine substance like MDMA,” said Dr. van der Kolk.
“An important reason why we think the side effect profile is so good is because the study was extremely carefully done, very carefully controlled,” he added. “There was a great deal of support, [and] we paid an enormous amount of attention to creating a very safe context in which this drug was being used.”
However, he expressed concern that “as people see the very good results, they may skimp a little bit on the creation of the context and not have as careful a psychotherapy protocol as we had here.”
‘On the right track’
Commenting on the findings for this news organization, David Nutt, MD, PhD, Edmond J. Safra Professor of Neuropsychopharmacology, Imperial College London, said the results are proof that the investigators’ “earlier smaller trials of MDMA were on the right track.”
“This larger and multicenter trial shows that MDMA therapy can be broadened into newer research groups, which augurs well for the much larger rollout that will be required once it gets a license,” said Dr. Nutt, who was not involved with the research.
He added, “the prior evidence of the safety of MDMA has [now] been confirmed.”
The study represents an “important step in the path to the clinical use of MDMA for PTSD,” Dr. Nutt said.
The study was sponsored by the Multidisciplinary Association for Psychedelic Studies. The investigators and Dr. Nutt have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adding 3,4-methylenedioxymethamphetamine (MDMA) to integrative psychotherapy may significantly improve symptoms and well-being for patients with severe posttraumatic stress disorder, including those with the dissociative subtype, new research suggests.
MAPP1 is the first phase 3 randomized controlled trial of MDMA-assisted therapy in this population. Participants who received the active treatment showed greater improvement in PTSD symptoms, mood, and empathy in comparison with participants who received placebo.
MDMA was “extremely effective, particularly for a subpopulation that ordinarily does not respond well to conventional treatment,” study coinvestigator Bessel van der Kolk, MD, professor of psychiatry at Boston University School of Medicine, told delegates attending the virtual European Psychiatric Association (EPA) 2021 Congress.
Growing interest
, particularly because failure rates with most available evidence-based treatments have been relatively high.
As previously reported by this news organization, in 2017, the U.S. Food and Drug Administration approved the trial design of Dr. van der Kolk’s and colleagues’ MAPP1 study after granting MDMA breakthrough designation.
The MAPP1 investigators assessed 90 patients with PTSD (mean age, 41 years; 77% White; 66% women) from 50 sites. For the majority of patients (84%), trauma history was developmental. “In other words, trauma [occurred] very early in life, usually at the hands of their own caregivers,” Dr. van der Kolk noted.
In addition, 18% of the patients were veterans, and 12% had combat exposure. The average duration of PTSD before enrollment was 18 years. All patients underwent screening and three preparatory psychotherapy sessions at enrollment.
Participants were randomly assigned to receive MDMA 80 mg or 120 mg (n = 46) or placebo (n = 44) followed by three integrative psychotherapy sessions lasting a total of 8 hours. A supplemental dose of 40 or 60 mg of MDMA could be administered from 1.5 to 2 hours after the first dose.
The patients stayed in the laboratory on the evening of the treatment session and attended a debriefing the next morning. The session was repeated a month later and again a month after that. In between, patients had telephone contact with the raters, who were blinded to the treatment received.
Follow-up assessments were conducted 2 months after the third treatment session and again at 12 months. The primary outcome measure was change in Clinician Administered PTSD Scale for DSM 5 (CAPS-5) score from baseline.
‘Dramatic improvement’
Results showed that both the MDMA and placebo groups experienced a statistically significant improvement in PTSD symptoms, “but MDMA had a dramatically significant improvement, with an effect size of over 0.9,” Dr. van der Kolk said.
The MDMA group also reported enhanced mood and well-being, increased responsiveness to emotional and sensory stimuli, a greater sense of closeness to other people, and a greater feeling of empathy.
Patients also reported having heightened openness, “and clearly the issue of empathy for themselves and others was a very large part of the process,” said Dr. van der Kolk.
“But for me, the most interesting part of the study is that the Adverse Childhood Experiences scale had no effect,” he noted. In other words, “the amount of childhood adverse experiences did not predict outcomes, which was very surprising because usually those patients are very treatment resistant.”
Dr. van der Kolk added that the dissociative subtype of PTSD was first described in the DSM-5 and that patients are “notoriously unresponsive to most unconventional treatments.”
In the current study, 13 patients met the criteria for the subtype, and investigators found they “did better than people with classical PTSD,” Dr. van der Kolk said. He added that this is a “very, very important finding.”
Carefully controlled
Overall, 82% of patients reported a significant improvement by the end of the study; 56% reported that they no longer had PTSD.
In addition, 67% of patients no longer met diagnostic criteria for PTSD. These included patients who had crossed over to active treatment from the placebo group.
Eleven patients (12%) experienced relapse by 12 months; in nine of the cases, this was due to the presence of additional stressors.
There were “very few adverse side effects” during the study, Dr. van der Kolk noted. In addition, “there were really no serious mental side effects,” despite the patients’ “opening up so much very painful material,” he added.
The most common adverse events among the MDMA group were muscle tightness (63%), decreased appetite (52%), nausea (30%), hyperhidrosis (20%), and feeling cold (20%). These effects were “quite small [and] the sort of side effects you would expect in response to an amphetamine substance like MDMA,” said Dr. van der Kolk.
“An important reason why we think the side effect profile is so good is because the study was extremely carefully done, very carefully controlled,” he added. “There was a great deal of support, [and] we paid an enormous amount of attention to creating a very safe context in which this drug was being used.”
However, he expressed concern that “as people see the very good results, they may skimp a little bit on the creation of the context and not have as careful a psychotherapy protocol as we had here.”
‘On the right track’
Commenting on the findings for this news organization, David Nutt, MD, PhD, Edmond J. Safra Professor of Neuropsychopharmacology, Imperial College London, said the results are proof that the investigators’ “earlier smaller trials of MDMA were on the right track.”
“This larger and multicenter trial shows that MDMA therapy can be broadened into newer research groups, which augurs well for the much larger rollout that will be required once it gets a license,” said Dr. Nutt, who was not involved with the research.
He added, “the prior evidence of the safety of MDMA has [now] been confirmed.”
The study represents an “important step in the path to the clinical use of MDMA for PTSD,” Dr. Nutt said.
The study was sponsored by the Multidisciplinary Association for Psychedelic Studies. The investigators and Dr. Nutt have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Gastrointestinal Symptoms and Lactic Acidosis in a Chronic Marijuana User
A 57-year-old woman with a history of traumatic brain injury, posttraumatic stress disorder, depression, migraines, hypothyroidism, and a hiatal hernia repair presented to the emergency department with a 1-day history of nausea, vomiting, and diffuse abdominal pain. She reported that her symptoms were relieved by hot showers. She also reported having similar symptoms and a previous gastric-emptying study that showed a slow-emptying stomach. Her history also consisted of frequent cannabis use for mood and appetite stimulation along with eliminating meat and fish from her diet, an increase in consumption of simple carbohydrates in the past year, and no alcohol use. Her medications included topiramate 100 mg and clonidine 0.3 mg nightly for migraines; levothyroxine 200 mcg daily for hypothyroidism; tizanidine 4 mg twice a day for muscle spasm; famotidine 40 mg twice a day as needed for gastric reflux; and bupropion 50 mg daily, citalopram 20 mg daily, and lamotrigine 25 mg nightly for mood.
The patient’s physical examination was notable for bradycardia (43 beats/min) and epigastric tenderness. Admission laboratory results were notable for an elevated lactic acid level of 4.8 (normal range, 0.50-2.20) mmol/L and a leukocytosis count of 10.8×109 cells/L. Serum alcohol level and blood cultures were negative. Liver function test, hemoglobin A1c, and lipase test were unremarkable. Her electrocardiogram showed an unchanged right bundle branch block. Chest X-ray, computed tomography (CT) of her abdomen/pelvis and echocardiogram were unremarkable.
What is your diagnosis?
How would you treat this patient?
This patient was diagnosed with gastrointestinal beriberi. Because of her dietary changes, lactic acidosis, and bradycardia, thiamine deficiency was suspected after ruling out other possibilities on the differential diagnosis (Table). The patient’s symptoms resolved after administration of high-dose IV thiamine 500 mg 3 times daily for 4 days. Her white blood cell count and lactic acid level normalized. Unfortunately, thiamine levels were not obtained for the patient before treatment was initiated. After administration of IV thiamine, her plasma thiamine level was > 1,200 (normal range, 8-30) nmol/L.
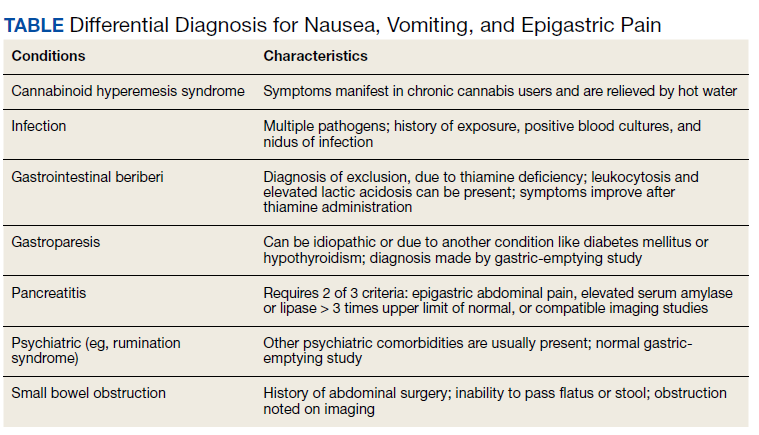
Her differential diagnosis included infectious etiology. Given her leukocytosis and lactic acidosis, vancomycin and piperacillin/tazobactam were started on admission. One day later, her leukocytosis count doubled to 20.7×109 cells/L. However, after 48 hours of negative blood cultures, antibiotics were discontinued.
Small bowel obstruction was suspected due to the patient’s history of abdominal surgery but was ruled out with CT imaging. Similarly, pancreatitis was ruled out based on negative CT imaging and the patient’s normal lipase level. Gastroparesis also was considered because of the patient’s history of hypothyroidism, tobacco use, and her prior gastric-emptying study. The patient was treated for gastroparesis with a course of metoclopramide and erythromycin without improvement in symptoms. Additionally, gastroparesis would not explain the patient’s leukocytosis.
Cannabinoid hyperemesis syndrome (CHS) was suspected because the patient’s symptoms improved with cannabis discontinuation and hot showers.1 In chronic users, however, tetrahydrocannabinol levels have a half-life of 5 to 13 days.2 Although lactic acidosis and leukocytosis have been previously reported with cannabis use, it is unlikely that the patient would have such significant improvement within the first 4 days after discontinuation.1,3,4 Although the patient had many psychiatric comorbidities with previous hospitalizations describing concern for somatization disorder, her leukocytosis and elevated lactic acid levels were suggestive of an organic rather than a psychiatric etiology of her symptoms.
Discussion
Gastrointestinal beriberi has been reported in chronic cannabis users who present with nausea, vomiting, epigastric pain, leukocytosis, and lactic acidosis; all these symptoms rapidly improve after thiamine administration.5,6 The patient’s dietary change also eliminated her intake of vitamin B12, which compounded her condition. Thiamine deficiency produces lactic acidosis by disrupting pyruvate metabolism.7 Bradycardia also can be a sign of thiamine deficiency, although the patient’s use of clonidine for migraines is a confounder.8
Chronically ill patients are prone to nutritional deficiencies, including deficiencies of thiamine.7,9 Many patients with chronic illnesses also use cannabis to ameliorate physical and neuropsychiatric symptoms.2 Recent reports suggest cannabis users are prone to gastrointestinal beriberi and Wernicke encephalopathy.5,10 Treating gastrointestinal symptoms in these patients can be challenging to diagnose because gastrointestinal beriberi and CHS share many clinical manifestations.
The patient’s presentation is likely multifactorial resulting from the combination of gastrointestinal beriberi and CHS. However, thiamine deficiency seems to play the dominant role.
There is no standard treatment regimen for thiamine deficiency with neurologic deficits, and patients only retain about 10 to 15% of intramuscular (IM) injections of cyanocobalamin.11,12 The British Committee for Standards in Haematology recommends IM injections of 1,000 mcg of cyanocobalamin 3 times a week for 2 weeks and then reassess the need for continued treatment.13 The British Columbia guidelines also recommend IM injections of 1,000 mcg daily for 1 to 5 days before transitioning to oral repletion.14 European Neurology guidelines for the treatment of Wernicke encephalopathy recommend IV cyanocobalamin 200 mg 3 times daily.15 Low-level evidence with observational studies informs these decisions and is why there is variation.
The patient’s serum lactate and leukocytosis normalized 1 day after the administration of thiamine. Thiamine deficiency classically causes Wernicke encephalopathy and wet beriberi.16 The patient did not present with Wernicke encephalopathy’s triad: ophthalmoplegia, ataxia, or confusion. She also was euvolemic without signs or symptoms of wet beriberi.
Conclusions
Thiamine deficiency is principally a clinical diagnosis. Thiamine laboratory testing may not be readily available in all medical centers, and confirming a diagnosis of thiamine deficiency should not delay treatment when thiamine deficiency is suspected. This patient’s thiamine levels resulted a week after collection. The administration of thiamine before sampling also can alter the result as it did in this case. Additionally, laboratories may offer whole blood and serum testing. Whole blood testing is more accurate because most bioactive thiamine is found in red blood cells.17
1. Price SL, Fisher C, Kumar R, Hilgerson A. Cannabinoid hyperemesis syndrome as the underlying cause of intractable nausea and vomiting. J Am Osteopath Assoc. 2011;111(3):166-169. doi:10.7556/jaoa.2011.111.3.166
2. Sharma P, Murthy P, Bharath MM. Chemistry, metabolism, and toxicology of cannabis: clinical implications. Iran J Psychiatry. 2012;7(4):149-156.
3. Antill T, Jakkoju A, Dieguez J, Laskhmiprasad L. Lactic acidosis: a rare manifestation of synthetic marijuana intoxication. J La State Med Soc. 2015;167(3):155.
4. Sullivan S. Cannabinoid hyperemesis. Can J Gastroenterol. 2010;24(5):284-285. doi:10.1155/2010/481940
5. Duca J, Lum CJ, Lo AM. Elevated lactate secondary to gastrointestinal beriberi. J Gen Intern Med. 2016;31(1):133-136. doi:10.1007/s11606-015-3326-2
6. Prakash S. Gastrointestinal beriberi: a forme fruste of Wernicke’s encephalopathy? BMJ Case Rep. 2018;bcr2018224841. doi:10.1136/bcr-2018-224841
7. Friedenberg AS, Brandoff DE, Schiffman FJ. Type B lactic acidosis as a severe metabolic complication in lymphoma and leukemia: a case series from a single institution and literature review. Medicine (Baltimore). 2007;86(4):225-232. doi:10.1097/MD.0b013e318125759a
8. Liang CC. Bradycardia in thiamin deficiency and the role of glyoxylate. J Nutrition Sci Vitaminology. 1977;23(1):1-6. doi:10.3177/jnsv.23.1
9. Attaluri P, Castillo A, Edriss H, Nugent K. Thiamine deficiency: an important consideration in critically ill patients. Am J Med Sci. 2018;356(4):382-390. doi:10.1016/j.amjms.2018.06.015
10. Chaudhari A, Li ZY, Long A, Afshinnik A. Heavy cannabis use associated with Wernicke’s encephalopathy. Cureus. 2019;11(7):e5109. doi:10.7759/cureus.5109
11. Stabler SP. Vitamin B12 deficiency. N Engl J Med. 2013;368(2):149-160. doi:10.1056/NEJMcp1113996
12. Green R, Allen LH, Bjørke-Monsen A-L, et al. Vitamin B12 deficiency. Nat Rev Dis Primers. 2017;3(1):17040. doi:10.1038/nrdp.2017.40
13. Devalia V, Hamilton MS, Molloy AM. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br J Haematol. 2014;166(4):496-513. doi:10.1111/bjh.12959
14. British Columbia Ministry of Health; Guidelines and Protocols and Advisory Committee. Guidelines and protocols cobalamin (vitamin B12) deficiency–investigation & management. Effective January 1, 2012. Revised May 1, 2013. Accessed March 10, 2021. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/vitamin-b12
15. Galvin R, Brathen G, Ivashynka A, Hillbom M, Tanasescu R, Leone MA. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur J Neurol. 2010;17(12):1408-1418. doi:10.1111/j.1468-1331.2010.03153.x
16. Wiley KD, Gupta M. Vitamin B1 thiamine deficiency (beriberi). In: StatPearls. StatPearls Publishing LLC; 2019.
17. Jenco J, Krcmova LK, Solichova D, Solich P. Recent trends in determination of thiamine and its derivatives in clinical practice. J Chromatogra A. 2017;1510:1-12. doi:10.1016/j.chroma.2017.06.048
A 57-year-old woman with a history of traumatic brain injury, posttraumatic stress disorder, depression, migraines, hypothyroidism, and a hiatal hernia repair presented to the emergency department with a 1-day history of nausea, vomiting, and diffuse abdominal pain. She reported that her symptoms were relieved by hot showers. She also reported having similar symptoms and a previous gastric-emptying study that showed a slow-emptying stomach. Her history also consisted of frequent cannabis use for mood and appetite stimulation along with eliminating meat and fish from her diet, an increase in consumption of simple carbohydrates in the past year, and no alcohol use. Her medications included topiramate 100 mg and clonidine 0.3 mg nightly for migraines; levothyroxine 200 mcg daily for hypothyroidism; tizanidine 4 mg twice a day for muscle spasm; famotidine 40 mg twice a day as needed for gastric reflux; and bupropion 50 mg daily, citalopram 20 mg daily, and lamotrigine 25 mg nightly for mood.
The patient’s physical examination was notable for bradycardia (43 beats/min) and epigastric tenderness. Admission laboratory results were notable for an elevated lactic acid level of 4.8 (normal range, 0.50-2.20) mmol/L and a leukocytosis count of 10.8×109 cells/L. Serum alcohol level and blood cultures were negative. Liver function test, hemoglobin A1c, and lipase test were unremarkable. Her electrocardiogram showed an unchanged right bundle branch block. Chest X-ray, computed tomography (CT) of her abdomen/pelvis and echocardiogram were unremarkable.
What is your diagnosis?
How would you treat this patient?
This patient was diagnosed with gastrointestinal beriberi. Because of her dietary changes, lactic acidosis, and bradycardia, thiamine deficiency was suspected after ruling out other possibilities on the differential diagnosis (Table). The patient’s symptoms resolved after administration of high-dose IV thiamine 500 mg 3 times daily for 4 days. Her white blood cell count and lactic acid level normalized. Unfortunately, thiamine levels were not obtained for the patient before treatment was initiated. After administration of IV thiamine, her plasma thiamine level was > 1,200 (normal range, 8-30) nmol/L.
Her differential diagnosis included infectious etiology. Given her leukocytosis and lactic acidosis, vancomycin and piperacillin/tazobactam were started on admission. One day later, her leukocytosis count doubled to 20.7×109 cells/L. However, after 48 hours of negative blood cultures, antibiotics were discontinued.
Small bowel obstruction was suspected due to the patient’s history of abdominal surgery but was ruled out with CT imaging. Similarly, pancreatitis was ruled out based on negative CT imaging and the patient’s normal lipase level. Gastroparesis also was considered because of the patient’s history of hypothyroidism, tobacco use, and her prior gastric-emptying study. The patient was treated for gastroparesis with a course of metoclopramide and erythromycin without improvement in symptoms. Additionally, gastroparesis would not explain the patient’s leukocytosis.
Cannabinoid hyperemesis syndrome (CHS) was suspected because the patient’s symptoms improved with cannabis discontinuation and hot showers.1 In chronic users, however, tetrahydrocannabinol levels have a half-life of 5 to 13 days.2 Although lactic acidosis and leukocytosis have been previously reported with cannabis use, it is unlikely that the patient would have such significant improvement within the first 4 days after discontinuation.1,3,4 Although the patient had many psychiatric comorbidities with previous hospitalizations describing concern for somatization disorder, her leukocytosis and elevated lactic acid levels were suggestive of an organic rather than a psychiatric etiology of her symptoms.
Discussion
Gastrointestinal beriberi has been reported in chronic cannabis users who present with nausea, vomiting, epigastric pain, leukocytosis, and lactic acidosis; all these symptoms rapidly improve after thiamine administration.5,6 The patient’s dietary change also eliminated her intake of vitamin B12, which compounded her condition. Thiamine deficiency produces lactic acidosis by disrupting pyruvate metabolism.7 Bradycardia also can be a sign of thiamine deficiency, although the patient’s use of clonidine for migraines is a confounder.8
Chronically ill patients are prone to nutritional deficiencies, including deficiencies of thiamine.7,9 Many patients with chronic illnesses also use cannabis to ameliorate physical and neuropsychiatric symptoms.2 Recent reports suggest cannabis users are prone to gastrointestinal beriberi and Wernicke encephalopathy.5,10 Treating gastrointestinal symptoms in these patients can be challenging to diagnose because gastrointestinal beriberi and CHS share many clinical manifestations.
The patient’s presentation is likely multifactorial resulting from the combination of gastrointestinal beriberi and CHS. However, thiamine deficiency seems to play the dominant role.
There is no standard treatment regimen for thiamine deficiency with neurologic deficits, and patients only retain about 10 to 15% of intramuscular (IM) injections of cyanocobalamin.11,12 The British Committee for Standards in Haematology recommends IM injections of 1,000 mcg of cyanocobalamin 3 times a week for 2 weeks and then reassess the need for continued treatment.13 The British Columbia guidelines also recommend IM injections of 1,000 mcg daily for 1 to 5 days before transitioning to oral repletion.14 European Neurology guidelines for the treatment of Wernicke encephalopathy recommend IV cyanocobalamin 200 mg 3 times daily.15 Low-level evidence with observational studies informs these decisions and is why there is variation.
The patient’s serum lactate and leukocytosis normalized 1 day after the administration of thiamine. Thiamine deficiency classically causes Wernicke encephalopathy and wet beriberi.16 The patient did not present with Wernicke encephalopathy’s triad: ophthalmoplegia, ataxia, or confusion. She also was euvolemic without signs or symptoms of wet beriberi.
Conclusions
Thiamine deficiency is principally a clinical diagnosis. Thiamine laboratory testing may not be readily available in all medical centers, and confirming a diagnosis of thiamine deficiency should not delay treatment when thiamine deficiency is suspected. This patient’s thiamine levels resulted a week after collection. The administration of thiamine before sampling also can alter the result as it did in this case. Additionally, laboratories may offer whole blood and serum testing. Whole blood testing is more accurate because most bioactive thiamine is found in red blood cells.17
A 57-year-old woman with a history of traumatic brain injury, posttraumatic stress disorder, depression, migraines, hypothyroidism, and a hiatal hernia repair presented to the emergency department with a 1-day history of nausea, vomiting, and diffuse abdominal pain. She reported that her symptoms were relieved by hot showers. She also reported having similar symptoms and a previous gastric-emptying study that showed a slow-emptying stomach. Her history also consisted of frequent cannabis use for mood and appetite stimulation along with eliminating meat and fish from her diet, an increase in consumption of simple carbohydrates in the past year, and no alcohol use. Her medications included topiramate 100 mg and clonidine 0.3 mg nightly for migraines; levothyroxine 200 mcg daily for hypothyroidism; tizanidine 4 mg twice a day for muscle spasm; famotidine 40 mg twice a day as needed for gastric reflux; and bupropion 50 mg daily, citalopram 20 mg daily, and lamotrigine 25 mg nightly for mood.
The patient’s physical examination was notable for bradycardia (43 beats/min) and epigastric tenderness. Admission laboratory results were notable for an elevated lactic acid level of 4.8 (normal range, 0.50-2.20) mmol/L and a leukocytosis count of 10.8×109 cells/L. Serum alcohol level and blood cultures were negative. Liver function test, hemoglobin A1c, and lipase test were unremarkable. Her electrocardiogram showed an unchanged right bundle branch block. Chest X-ray, computed tomography (CT) of her abdomen/pelvis and echocardiogram were unremarkable.
What is your diagnosis?
How would you treat this patient?
This patient was diagnosed with gastrointestinal beriberi. Because of her dietary changes, lactic acidosis, and bradycardia, thiamine deficiency was suspected after ruling out other possibilities on the differential diagnosis (Table). The patient’s symptoms resolved after administration of high-dose IV thiamine 500 mg 3 times daily for 4 days. Her white blood cell count and lactic acid level normalized. Unfortunately, thiamine levels were not obtained for the patient before treatment was initiated. After administration of IV thiamine, her plasma thiamine level was > 1,200 (normal range, 8-30) nmol/L.
Her differential diagnosis included infectious etiology. Given her leukocytosis and lactic acidosis, vancomycin and piperacillin/tazobactam were started on admission. One day later, her leukocytosis count doubled to 20.7×109 cells/L. However, after 48 hours of negative blood cultures, antibiotics were discontinued.
Small bowel obstruction was suspected due to the patient’s history of abdominal surgery but was ruled out with CT imaging. Similarly, pancreatitis was ruled out based on negative CT imaging and the patient’s normal lipase level. Gastroparesis also was considered because of the patient’s history of hypothyroidism, tobacco use, and her prior gastric-emptying study. The patient was treated for gastroparesis with a course of metoclopramide and erythromycin without improvement in symptoms. Additionally, gastroparesis would not explain the patient’s leukocytosis.
Cannabinoid hyperemesis syndrome (CHS) was suspected because the patient’s symptoms improved with cannabis discontinuation and hot showers.1 In chronic users, however, tetrahydrocannabinol levels have a half-life of 5 to 13 days.2 Although lactic acidosis and leukocytosis have been previously reported with cannabis use, it is unlikely that the patient would have such significant improvement within the first 4 days after discontinuation.1,3,4 Although the patient had many psychiatric comorbidities with previous hospitalizations describing concern for somatization disorder, her leukocytosis and elevated lactic acid levels were suggestive of an organic rather than a psychiatric etiology of her symptoms.
Discussion
Gastrointestinal beriberi has been reported in chronic cannabis users who present with nausea, vomiting, epigastric pain, leukocytosis, and lactic acidosis; all these symptoms rapidly improve after thiamine administration.5,6 The patient’s dietary change also eliminated her intake of vitamin B12, which compounded her condition. Thiamine deficiency produces lactic acidosis by disrupting pyruvate metabolism.7 Bradycardia also can be a sign of thiamine deficiency, although the patient’s use of clonidine for migraines is a confounder.8
Chronically ill patients are prone to nutritional deficiencies, including deficiencies of thiamine.7,9 Many patients with chronic illnesses also use cannabis to ameliorate physical and neuropsychiatric symptoms.2 Recent reports suggest cannabis users are prone to gastrointestinal beriberi and Wernicke encephalopathy.5,10 Treating gastrointestinal symptoms in these patients can be challenging to diagnose because gastrointestinal beriberi and CHS share many clinical manifestations.
The patient’s presentation is likely multifactorial resulting from the combination of gastrointestinal beriberi and CHS. However, thiamine deficiency seems to play the dominant role.
There is no standard treatment regimen for thiamine deficiency with neurologic deficits, and patients only retain about 10 to 15% of intramuscular (IM) injections of cyanocobalamin.11,12 The British Committee for Standards in Haematology recommends IM injections of 1,000 mcg of cyanocobalamin 3 times a week for 2 weeks and then reassess the need for continued treatment.13 The British Columbia guidelines also recommend IM injections of 1,000 mcg daily for 1 to 5 days before transitioning to oral repletion.14 European Neurology guidelines for the treatment of Wernicke encephalopathy recommend IV cyanocobalamin 200 mg 3 times daily.15 Low-level evidence with observational studies informs these decisions and is why there is variation.
The patient’s serum lactate and leukocytosis normalized 1 day after the administration of thiamine. Thiamine deficiency classically causes Wernicke encephalopathy and wet beriberi.16 The patient did not present with Wernicke encephalopathy’s triad: ophthalmoplegia, ataxia, or confusion. She also was euvolemic without signs or symptoms of wet beriberi.
Conclusions
Thiamine deficiency is principally a clinical diagnosis. Thiamine laboratory testing may not be readily available in all medical centers, and confirming a diagnosis of thiamine deficiency should not delay treatment when thiamine deficiency is suspected. This patient’s thiamine levels resulted a week after collection. The administration of thiamine before sampling also can alter the result as it did in this case. Additionally, laboratories may offer whole blood and serum testing. Whole blood testing is more accurate because most bioactive thiamine is found in red blood cells.17
1. Price SL, Fisher C, Kumar R, Hilgerson A. Cannabinoid hyperemesis syndrome as the underlying cause of intractable nausea and vomiting. J Am Osteopath Assoc. 2011;111(3):166-169. doi:10.7556/jaoa.2011.111.3.166
2. Sharma P, Murthy P, Bharath MM. Chemistry, metabolism, and toxicology of cannabis: clinical implications. Iran J Psychiatry. 2012;7(4):149-156.
3. Antill T, Jakkoju A, Dieguez J, Laskhmiprasad L. Lactic acidosis: a rare manifestation of synthetic marijuana intoxication. J La State Med Soc. 2015;167(3):155.
4. Sullivan S. Cannabinoid hyperemesis. Can J Gastroenterol. 2010;24(5):284-285. doi:10.1155/2010/481940
5. Duca J, Lum CJ, Lo AM. Elevated lactate secondary to gastrointestinal beriberi. J Gen Intern Med. 2016;31(1):133-136. doi:10.1007/s11606-015-3326-2
6. Prakash S. Gastrointestinal beriberi: a forme fruste of Wernicke’s encephalopathy? BMJ Case Rep. 2018;bcr2018224841. doi:10.1136/bcr-2018-224841
7. Friedenberg AS, Brandoff DE, Schiffman FJ. Type B lactic acidosis as a severe metabolic complication in lymphoma and leukemia: a case series from a single institution and literature review. Medicine (Baltimore). 2007;86(4):225-232. doi:10.1097/MD.0b013e318125759a
8. Liang CC. Bradycardia in thiamin deficiency and the role of glyoxylate. J Nutrition Sci Vitaminology. 1977;23(1):1-6. doi:10.3177/jnsv.23.1
9. Attaluri P, Castillo A, Edriss H, Nugent K. Thiamine deficiency: an important consideration in critically ill patients. Am J Med Sci. 2018;356(4):382-390. doi:10.1016/j.amjms.2018.06.015
10. Chaudhari A, Li ZY, Long A, Afshinnik A. Heavy cannabis use associated with Wernicke’s encephalopathy. Cureus. 2019;11(7):e5109. doi:10.7759/cureus.5109
11. Stabler SP. Vitamin B12 deficiency. N Engl J Med. 2013;368(2):149-160. doi:10.1056/NEJMcp1113996
12. Green R, Allen LH, Bjørke-Monsen A-L, et al. Vitamin B12 deficiency. Nat Rev Dis Primers. 2017;3(1):17040. doi:10.1038/nrdp.2017.40
13. Devalia V, Hamilton MS, Molloy AM. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br J Haematol. 2014;166(4):496-513. doi:10.1111/bjh.12959
14. British Columbia Ministry of Health; Guidelines and Protocols and Advisory Committee. Guidelines and protocols cobalamin (vitamin B12) deficiency–investigation & management. Effective January 1, 2012. Revised May 1, 2013. Accessed March 10, 2021. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/vitamin-b12
15. Galvin R, Brathen G, Ivashynka A, Hillbom M, Tanasescu R, Leone MA. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur J Neurol. 2010;17(12):1408-1418. doi:10.1111/j.1468-1331.2010.03153.x
16. Wiley KD, Gupta M. Vitamin B1 thiamine deficiency (beriberi). In: StatPearls. StatPearls Publishing LLC; 2019.
17. Jenco J, Krcmova LK, Solichova D, Solich P. Recent trends in determination of thiamine and its derivatives in clinical practice. J Chromatogra A. 2017;1510:1-12. doi:10.1016/j.chroma.2017.06.048
1. Price SL, Fisher C, Kumar R, Hilgerson A. Cannabinoid hyperemesis syndrome as the underlying cause of intractable nausea and vomiting. J Am Osteopath Assoc. 2011;111(3):166-169. doi:10.7556/jaoa.2011.111.3.166
2. Sharma P, Murthy P, Bharath MM. Chemistry, metabolism, and toxicology of cannabis: clinical implications. Iran J Psychiatry. 2012;7(4):149-156.
3. Antill T, Jakkoju A, Dieguez J, Laskhmiprasad L. Lactic acidosis: a rare manifestation of synthetic marijuana intoxication. J La State Med Soc. 2015;167(3):155.
4. Sullivan S. Cannabinoid hyperemesis. Can J Gastroenterol. 2010;24(5):284-285. doi:10.1155/2010/481940
5. Duca J, Lum CJ, Lo AM. Elevated lactate secondary to gastrointestinal beriberi. J Gen Intern Med. 2016;31(1):133-136. doi:10.1007/s11606-015-3326-2
6. Prakash S. Gastrointestinal beriberi: a forme fruste of Wernicke’s encephalopathy? BMJ Case Rep. 2018;bcr2018224841. doi:10.1136/bcr-2018-224841
7. Friedenberg AS, Brandoff DE, Schiffman FJ. Type B lactic acidosis as a severe metabolic complication in lymphoma and leukemia: a case series from a single institution and literature review. Medicine (Baltimore). 2007;86(4):225-232. doi:10.1097/MD.0b013e318125759a
8. Liang CC. Bradycardia in thiamin deficiency and the role of glyoxylate. J Nutrition Sci Vitaminology. 1977;23(1):1-6. doi:10.3177/jnsv.23.1
9. Attaluri P, Castillo A, Edriss H, Nugent K. Thiamine deficiency: an important consideration in critically ill patients. Am J Med Sci. 2018;356(4):382-390. doi:10.1016/j.amjms.2018.06.015
10. Chaudhari A, Li ZY, Long A, Afshinnik A. Heavy cannabis use associated with Wernicke’s encephalopathy. Cureus. 2019;11(7):e5109. doi:10.7759/cureus.5109
11. Stabler SP. Vitamin B12 deficiency. N Engl J Med. 2013;368(2):149-160. doi:10.1056/NEJMcp1113996
12. Green R, Allen LH, Bjørke-Monsen A-L, et al. Vitamin B12 deficiency. Nat Rev Dis Primers. 2017;3(1):17040. doi:10.1038/nrdp.2017.40
13. Devalia V, Hamilton MS, Molloy AM. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br J Haematol. 2014;166(4):496-513. doi:10.1111/bjh.12959
14. British Columbia Ministry of Health; Guidelines and Protocols and Advisory Committee. Guidelines and protocols cobalamin (vitamin B12) deficiency–investigation & management. Effective January 1, 2012. Revised May 1, 2013. Accessed March 10, 2021. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/vitamin-b12
15. Galvin R, Brathen G, Ivashynka A, Hillbom M, Tanasescu R, Leone MA. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur J Neurol. 2010;17(12):1408-1418. doi:10.1111/j.1468-1331.2010.03153.x
16. Wiley KD, Gupta M. Vitamin B1 thiamine deficiency (beriberi). In: StatPearls. StatPearls Publishing LLC; 2019.
17. Jenco J, Krcmova LK, Solichova D, Solich P. Recent trends in determination of thiamine and its derivatives in clinical practice. J Chromatogra A. 2017;1510:1-12. doi:10.1016/j.chroma.2017.06.048
Reflections on George Floyd, Derek Chauvin, and racism in America
Exhaustion, numbness, dissociation, and most notably, anger are my emotional response when viewing the video of George Floyd’s death. The homicide trial of former Minneapolis police officer Derek Chauvin activates the shared stress of those who experienced intergenerational trauma and the legacy of racism in the United States of America.
On May 25, 2020, Mr. Floyd died after Derek Chauvin used a lethal maneuver and placed his knee on Mr. Floyd’s neck for 9 minutes and 29 seconds. Mr. Floyd has died physically, but his death is replayed through high-definition social media daily, if not hourly, as I write this article and think of the generational legacy of trauma that African Americans must cope with on an everyday basis. I struggle daily to explain this legacy to my daughters, students, residents, and colleagues. I hope to share with you some of my perspectives on the current trial and give you some insight as to how my training and personal life experience have affected my views on police brutality and the use of lethal force toward African American men.
My earliest recollection of public video-recorded images of police brutality occurred when Rodney King was beaten and assaulted by the Los Angeles Police Department on March 3, 1991. At that time, I was a senior in high school, and the world was different. My clear expectation was that any attempt to resist police arrest would be met with overwhelming and potentially lethal force. This was simply a matter of my daily reality, so, while witnessing the assault of Mr. King, the 17-year-old child didn’t expect much, if any, real change to come about in regard to police brutality. At that time, my mother kept me focused on one singular goal – becoming a physician – and protected me as best she could from the effects of intergenerational trauma woven into the African American experience.
The issue of police brutality and police-involved deaths has been recognized as a significant public health concern for some time. Over the 3 decades since the assault on Mr. King, several researchers have examined these issues. A review of all the research is beyond the scope of this opinion piece. Still, I will highlight a study that I believe illustrates some conclusions scholars have come to regarding police use of lethal force and subsequent mortality in African American men. A recent study by Frank Edwards, PhD, and colleagues, published in the Proceedings of the National Academy of Sciences, showed that Black men were 2.5 times more likely to be killed by police over their life course than White men.
The researchers also developed predictive models that about 1 in 1,000 Black men and boys will be killed by police over their life course, and that among all age groups Black men and boys face the highest lifetime risk. The authors concluded that “Our analysis shows that the risk of being killed by police is jointly patterned by one’s race, gender, and age. Police violence is a leading cause of death for young men, and young men of color face an exceptionally high risk of being killed by police. Inequalities in risk are pronounced throughout the life course. This study reinforces calls to treat police violence as a public health issue.”
Research such as this helps validate on a visceral level what I already was taught: “As a Black male, encounters with police can quickly become deadly, and you must remain calm, or you could die.” This thought process informed much of my thinking whenever I heard about a Black male being fatally shot by police. My first response was to ask, “Was he resisting arrest?” At this time, my naive impression was that “if you don’t resist or conflict, you’ll live.” It wasn’t until my training in psychiatry that I realized that the duty to calm, support, and most importantly, protect was the responsibility of the person who is given the trust of the public. As a psychiatrist, I am humbled by the trust the public places in physicians to restrain patients and take part in their involuntary hospitalizations. Over the years, I learned from my attending physicians, colleagues in security, social work, nursing, assertive community treatment (ACT) teams, and many other allied health professions that the responsibility to show restraint, calm, and compassion lies with those who have the power and trust of the public.
Mostly, I learned from my patients. They taught me to meet distress with compassion and humanity and not simply with force. With those lessons in mind, I now fast forward to July 17, 2014, and the death of Eric Garner. On July 17, New York Police Department officers approached Mr. Garner on the suspicion that he was selling loose cigarettes. Amid this encounter, Mr. Garner was subjected to a chokehold, and his face was pinned to the ground while he can be heard saying, “I can’t breathe.” At this time in my professional career, I had just become a dean of student affairs at the George Washington School of Medicine and Health Sciences. I can still remember the response of my minority students, and the sense of pain and anguish they felt watching the video of a chokehold being used on a man stating, “I can’t breathe.” At this point, my training would not allow me to see this as anything other than an unnecessary use of lethal force that would subsequently be ruled a homicide. I hoped that we as a nation had reached a “reckoning “ because of Mr. Garner’s death and Michael Brown Jr.’s subsequent death in Ferguson, Mo., in St. Louis County, on Aug. 9, 2014. I hoped we were ready to finally address police brutality and excessive use of force that had disproportionately affected Black men. I was utterly wrong. Black men such as Alton Sterling, Jamar Clark, and many others would die in fatal police encounters. So would Tamir Rice, who was 12 years old when he was shot and killed by a police officer.
This brings me back to the death of Mr. Floyd. As I listened to the witnesses’ testimony, it triggered an emotional response from sadness, fear, shock, but mostly anger. Some would consider it progress that the Minneapolis Police Department’s top homicide detective testified that kneeling on Mr. Floyd’s neck after he had been restrained was “unnecessary.” The officer stated, “If your knee is on someone’s neck, that could kill him.” While I acknowledge this is a form of progress, we must ultimately address the other “substantial causal factor of death” for Mr. Floyd. Namely, the systemic racism present in a criminal justice system in the form of policies and procedures that allow for continued racial disparities and inequities.
There will be coverage of the court proceedings and a detailed dissection of the legal arguments. Questions regarding Mr. Floyd’s physical health and struggle with opiate use disorder will be raised by the defense. The debate about the substantial causal factor will be played out in the court and the media. Ultimately, we, as health professionals, need to ask ourselves, “Who has the power and the duty to do no harm?”
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
Exhaustion, numbness, dissociation, and most notably, anger are my emotional response when viewing the video of George Floyd’s death. The homicide trial of former Minneapolis police officer Derek Chauvin activates the shared stress of those who experienced intergenerational trauma and the legacy of racism in the United States of America.
On May 25, 2020, Mr. Floyd died after Derek Chauvin used a lethal maneuver and placed his knee on Mr. Floyd’s neck for 9 minutes and 29 seconds. Mr. Floyd has died physically, but his death is replayed through high-definition social media daily, if not hourly, as I write this article and think of the generational legacy of trauma that African Americans must cope with on an everyday basis. I struggle daily to explain this legacy to my daughters, students, residents, and colleagues. I hope to share with you some of my perspectives on the current trial and give you some insight as to how my training and personal life experience have affected my views on police brutality and the use of lethal force toward African American men.
My earliest recollection of public video-recorded images of police brutality occurred when Rodney King was beaten and assaulted by the Los Angeles Police Department on March 3, 1991. At that time, I was a senior in high school, and the world was different. My clear expectation was that any attempt to resist police arrest would be met with overwhelming and potentially lethal force. This was simply a matter of my daily reality, so, while witnessing the assault of Mr. King, the 17-year-old child didn’t expect much, if any, real change to come about in regard to police brutality. At that time, my mother kept me focused on one singular goal – becoming a physician – and protected me as best she could from the effects of intergenerational trauma woven into the African American experience.
The issue of police brutality and police-involved deaths has been recognized as a significant public health concern for some time. Over the 3 decades since the assault on Mr. King, several researchers have examined these issues. A review of all the research is beyond the scope of this opinion piece. Still, I will highlight a study that I believe illustrates some conclusions scholars have come to regarding police use of lethal force and subsequent mortality in African American men. A recent study by Frank Edwards, PhD, and colleagues, published in the Proceedings of the National Academy of Sciences, showed that Black men were 2.5 times more likely to be killed by police over their life course than White men.
The researchers also developed predictive models that about 1 in 1,000 Black men and boys will be killed by police over their life course, and that among all age groups Black men and boys face the highest lifetime risk. The authors concluded that “Our analysis shows that the risk of being killed by police is jointly patterned by one’s race, gender, and age. Police violence is a leading cause of death for young men, and young men of color face an exceptionally high risk of being killed by police. Inequalities in risk are pronounced throughout the life course. This study reinforces calls to treat police violence as a public health issue.”
Research such as this helps validate on a visceral level what I already was taught: “As a Black male, encounters with police can quickly become deadly, and you must remain calm, or you could die.” This thought process informed much of my thinking whenever I heard about a Black male being fatally shot by police. My first response was to ask, “Was he resisting arrest?” At this time, my naive impression was that “if you don’t resist or conflict, you’ll live.” It wasn’t until my training in psychiatry that I realized that the duty to calm, support, and most importantly, protect was the responsibility of the person who is given the trust of the public. As a psychiatrist, I am humbled by the trust the public places in physicians to restrain patients and take part in their involuntary hospitalizations. Over the years, I learned from my attending physicians, colleagues in security, social work, nursing, assertive community treatment (ACT) teams, and many other allied health professions that the responsibility to show restraint, calm, and compassion lies with those who have the power and trust of the public.
Mostly, I learned from my patients. They taught me to meet distress with compassion and humanity and not simply with force. With those lessons in mind, I now fast forward to July 17, 2014, and the death of Eric Garner. On July 17, New York Police Department officers approached Mr. Garner on the suspicion that he was selling loose cigarettes. Amid this encounter, Mr. Garner was subjected to a chokehold, and his face was pinned to the ground while he can be heard saying, “I can’t breathe.” At this time in my professional career, I had just become a dean of student affairs at the George Washington School of Medicine and Health Sciences. I can still remember the response of my minority students, and the sense of pain and anguish they felt watching the video of a chokehold being used on a man stating, “I can’t breathe.” At this point, my training would not allow me to see this as anything other than an unnecessary use of lethal force that would subsequently be ruled a homicide. I hoped that we as a nation had reached a “reckoning “ because of Mr. Garner’s death and Michael Brown Jr.’s subsequent death in Ferguson, Mo., in St. Louis County, on Aug. 9, 2014. I hoped we were ready to finally address police brutality and excessive use of force that had disproportionately affected Black men. I was utterly wrong. Black men such as Alton Sterling, Jamar Clark, and many others would die in fatal police encounters. So would Tamir Rice, who was 12 years old when he was shot and killed by a police officer.
This brings me back to the death of Mr. Floyd. As I listened to the witnesses’ testimony, it triggered an emotional response from sadness, fear, shock, but mostly anger. Some would consider it progress that the Minneapolis Police Department’s top homicide detective testified that kneeling on Mr. Floyd’s neck after he had been restrained was “unnecessary.” The officer stated, “If your knee is on someone’s neck, that could kill him.” While I acknowledge this is a form of progress, we must ultimately address the other “substantial causal factor of death” for Mr. Floyd. Namely, the systemic racism present in a criminal justice system in the form of policies and procedures that allow for continued racial disparities and inequities.
There will be coverage of the court proceedings and a detailed dissection of the legal arguments. Questions regarding Mr. Floyd’s physical health and struggle with opiate use disorder will be raised by the defense. The debate about the substantial causal factor will be played out in the court and the media. Ultimately, we, as health professionals, need to ask ourselves, “Who has the power and the duty to do no harm?”
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
Exhaustion, numbness, dissociation, and most notably, anger are my emotional response when viewing the video of George Floyd’s death. The homicide trial of former Minneapolis police officer Derek Chauvin activates the shared stress of those who experienced intergenerational trauma and the legacy of racism in the United States of America.
On May 25, 2020, Mr. Floyd died after Derek Chauvin used a lethal maneuver and placed his knee on Mr. Floyd’s neck for 9 minutes and 29 seconds. Mr. Floyd has died physically, but his death is replayed through high-definition social media daily, if not hourly, as I write this article and think of the generational legacy of trauma that African Americans must cope with on an everyday basis. I struggle daily to explain this legacy to my daughters, students, residents, and colleagues. I hope to share with you some of my perspectives on the current trial and give you some insight as to how my training and personal life experience have affected my views on police brutality and the use of lethal force toward African American men.
My earliest recollection of public video-recorded images of police brutality occurred when Rodney King was beaten and assaulted by the Los Angeles Police Department on March 3, 1991. At that time, I was a senior in high school, and the world was different. My clear expectation was that any attempt to resist police arrest would be met with overwhelming and potentially lethal force. This was simply a matter of my daily reality, so, while witnessing the assault of Mr. King, the 17-year-old child didn’t expect much, if any, real change to come about in regard to police brutality. At that time, my mother kept me focused on one singular goal – becoming a physician – and protected me as best she could from the effects of intergenerational trauma woven into the African American experience.
The issue of police brutality and police-involved deaths has been recognized as a significant public health concern for some time. Over the 3 decades since the assault on Mr. King, several researchers have examined these issues. A review of all the research is beyond the scope of this opinion piece. Still, I will highlight a study that I believe illustrates some conclusions scholars have come to regarding police use of lethal force and subsequent mortality in African American men. A recent study by Frank Edwards, PhD, and colleagues, published in the Proceedings of the National Academy of Sciences, showed that Black men were 2.5 times more likely to be killed by police over their life course than White men.
The researchers also developed predictive models that about 1 in 1,000 Black men and boys will be killed by police over their life course, and that among all age groups Black men and boys face the highest lifetime risk. The authors concluded that “Our analysis shows that the risk of being killed by police is jointly patterned by one’s race, gender, and age. Police violence is a leading cause of death for young men, and young men of color face an exceptionally high risk of being killed by police. Inequalities in risk are pronounced throughout the life course. This study reinforces calls to treat police violence as a public health issue.”
Research such as this helps validate on a visceral level what I already was taught: “As a Black male, encounters with police can quickly become deadly, and you must remain calm, or you could die.” This thought process informed much of my thinking whenever I heard about a Black male being fatally shot by police. My first response was to ask, “Was he resisting arrest?” At this time, my naive impression was that “if you don’t resist or conflict, you’ll live.” It wasn’t until my training in psychiatry that I realized that the duty to calm, support, and most importantly, protect was the responsibility of the person who is given the trust of the public. As a psychiatrist, I am humbled by the trust the public places in physicians to restrain patients and take part in their involuntary hospitalizations. Over the years, I learned from my attending physicians, colleagues in security, social work, nursing, assertive community treatment (ACT) teams, and many other allied health professions that the responsibility to show restraint, calm, and compassion lies with those who have the power and trust of the public.
Mostly, I learned from my patients. They taught me to meet distress with compassion and humanity and not simply with force. With those lessons in mind, I now fast forward to July 17, 2014, and the death of Eric Garner. On July 17, New York Police Department officers approached Mr. Garner on the suspicion that he was selling loose cigarettes. Amid this encounter, Mr. Garner was subjected to a chokehold, and his face was pinned to the ground while he can be heard saying, “I can’t breathe.” At this time in my professional career, I had just become a dean of student affairs at the George Washington School of Medicine and Health Sciences. I can still remember the response of my minority students, and the sense of pain and anguish they felt watching the video of a chokehold being used on a man stating, “I can’t breathe.” At this point, my training would not allow me to see this as anything other than an unnecessary use of lethal force that would subsequently be ruled a homicide. I hoped that we as a nation had reached a “reckoning “ because of Mr. Garner’s death and Michael Brown Jr.’s subsequent death in Ferguson, Mo., in St. Louis County, on Aug. 9, 2014. I hoped we were ready to finally address police brutality and excessive use of force that had disproportionately affected Black men. I was utterly wrong. Black men such as Alton Sterling, Jamar Clark, and many others would die in fatal police encounters. So would Tamir Rice, who was 12 years old when he was shot and killed by a police officer.
This brings me back to the death of Mr. Floyd. As I listened to the witnesses’ testimony, it triggered an emotional response from sadness, fear, shock, but mostly anger. Some would consider it progress that the Minneapolis Police Department’s top homicide detective testified that kneeling on Mr. Floyd’s neck after he had been restrained was “unnecessary.” The officer stated, “If your knee is on someone’s neck, that could kill him.” While I acknowledge this is a form of progress, we must ultimately address the other “substantial causal factor of death” for Mr. Floyd. Namely, the systemic racism present in a criminal justice system in the form of policies and procedures that allow for continued racial disparities and inequities.
There will be coverage of the court proceedings and a detailed dissection of the legal arguments. Questions regarding Mr. Floyd’s physical health and struggle with opiate use disorder will be raised by the defense. The debate about the substantial causal factor will be played out in the court and the media. Ultimately, we, as health professionals, need to ask ourselves, “Who has the power and the duty to do no harm?”
Dr. Norris is associate dean of student affairs and administration at George Washington University, Washington. He has no disclosures.
An international trip: Global experts weigh in on psychedelics
In 1967, when the United Nations Convention on Drugs classified psychedelics as schedule I substances, it effectively ended research into these agents as potential therapeutics for psychiatric disorders.

Psychedelics induce altered states of perception. They bind to the 5-hydroxytryptamine 2A (5-HT2A) receptor and include psilocybin, which is derived from “magic mushrooms”; N,N-dimethyltryptamine (DMT), a component of ayahuasca and mescaline (peyote cactus); and the synthesized compound D-lysergic acid diethylamide (LSD). Other agents, such as ketamine and 3,4-methylenedioxymethamphetamine (MDMA), also known as ecstasy, are sometimes considered psychedelics as well.
Before they were classified as schedule I agents, psychedelics had been shown to be particularly beneficial for patients with treatment-resistant conditions, including depression and posttraumatic stress disorder (PTSD), especially when administered in a supportive, therapeutic setting.
Now, after a hiatus of almost 50 years, there is renewed global interest in the scientific investigation of psychedelics. The attention was spurred in part by several exploratory studies of DMT in humans conducted in the 1990s by Rick Strassman, MD, and colleagues at the University of New Mexico, Albuquerque.
Around the same time, Franz X. Vollenweider, MD, and colleagues at the University of Zürich began researching psilocybin and its effects on human behavior. However, it was a 2006 study of psilocybin by a team of researchers at Johns Hopkins University, Baltimore, that is widely cited as a catalyst for the current renaissance in psychedelic research.
To provide a broad-based, international perspective on these agents, including their current legal status and indications, treatment regimens, safety, efficacy, and future considerations, this news organization interviewed nine expert researchers from around the globe.
Global legal status
In most, if not all, countries, it is still illegal to prescribe psychedelics in other than a research setting.
They can be used in research, but only with approval from the Food and Drug Administration under licensure from the Drug Enforcement Administration.
France lists all synthetic hallucinogens and hallucinogenic mushrooms as narcotic. As a result, possession, use, transportation, and collection are subject to criminal sanctions.
In France, NMDA antagonists such as ketamine and nitrous oxide are regarded as psychedelic molecules and can be used off label for various conditions or as part of research protocols authorized by the French public health code.
Although psychedelics are illegal under Mexican law, they are commonly used in indigenous communities as part of traditional rituals.
“The line between traditional consumption and psychedelic tourism is very thin,” José J. Mendoza Velásquez, MD, professor in the department of mental health, National Autonomous University of Mexico, Mexico City, said in an interview.
Psychedelics also are illegal in the United Kingdom, although government agencies have recently allowed research groups to investigate them. Psychedelics cannot be prescribed in Germany, Spain, or Italy. However, investigators in these countries can request permission from regulatory agencies to conduct research.
Brazil allows psychedelic substances to be researched, particularly ayahuasca, which has long traditional and religious roots in the country.
However, as in other countries, none of the classic psychedelics is regulated for therapeutic use in Brazil. It is widely expected that the Brazilian government will approve MDMA sometime in 2024 for use in the treatment of PTSD.
Potential indications
Psychedelics are currently under investigation as potential treatments for major depression, treatment-resistant depression, PTSD, pain management, and anorexia, among other conditions.
In France, Florian Ferreri, MD, PhD, at Hospital Saint-Antoine, Paris, is researching ketamine for treatment of patients with suicidal crisis/ideation and treatment-resistant depression.
In the United Kingdom, David Nutt, FMedSci, Edmond J. Safra Professor of Neuropsychopharmacology at Imperial College London, and his team have conducted studies of the use of psychedelics in conjunction with psychological support for patients with treatment-resistant depression, and they are currently exploring their use in the treatment of anorexia and various pain syndromes.
In Germany, Gerhard Gründer, MD, professor of psychiatry at the Central Institute of Mental Health, in Mannheim, noted that a study of psilocybin for treatment-resistant depression will launch sometime in 2021. In Italy, current research is focusing on MDMA and ketamine in the laboratory environment and in animal models for treating depression and drug abuse.
Researcher Helen Dolengevich-Segal, MD, a psychiatrist at Hospital Universitario del Henares, Madrid, noted that although research on esketamine for the treatment of severe depressive disorder with suicidal thoughts is underway, there is very limited published research from that country into the use of classic psychedelics for various psychiatric disorders, given their current illegal status.
Mexico’s Dr. Velásquez noted that although he is prohibited from prescribing psychedelics, he does have patients who take the drugs to augment medical treatment. For instance, he said, his patients frequently use psilocybin to help with severe depression, pain, and insomnia.
Environment is key
Most researchers agree that for psychedelics to be safe and effective, patient education and administration in a controlled environment by experienced clinicians are key to successful treatment.
Roland R. Griffiths, PhD, director of the Center for Psychedelic and Consciousness Research at Johns Hopkins, said that ongoing U.S. psilocybin research – primarily in major depressive disorder and psychological distress associated with life-threatening illness, drug addiction, anorexia nervosa, obsessive-compulsive disorder, and headache – generally includes one or two treatment sessions, each of which lasts 6-8 hours.
Such sessions typically involve oral administration of a moderately high dose of a psychedelic under what he characterizes as “psychologically supported conditions.”
For Dr. Griffiths, there are serious potential risks associated with the use of psilocybin and other psychedelics outside such environments.
“When taken in uncontrolled conditions, classic psychedelics can produce confusion and disorientation resulting in behavior dangerous to the participant and others, including life-threatening risk,” he said.
Dr. Gründer agreed.
“At the moment, I cannot imagine that you would go to the pharmacy with a prescription for psilocybin and get yourself a pill and then take it in a quiet little room,” he said. Dr. Dolengevich-Segal and Dr. Velásquez echoed these sentiments, noting the optimal location for administration is one that is quiet and secure and where patients feel safe.
Luís Fernando Tófoli, MD, PhD, professor of medical psychology and psychiatry at the University of Campinas, and Eduardo Schenberg, PhD, founder and CEO of Instituto Phaneros in São Paulo, Brazil, said more research is needed to determine the optimal therapeutic environment for individual agents.
“Most studies have a low number of participants (around 20 or 30), especially in neuroimaging, with high unblinding rates,” Dr. Schenberg said. “Therefore, novel methodological approaches are also necessary, as these substances do not easily fit into the traditional pharmacology epistemic model.”
Risks, abuse potential
The abuse potential of psychedelics is an ongoing concern for the public, researchers, and regulators, but the consensus among nearly all of these experts is that when administered by medical professionals in controlled settings, these drugs are associated with extremely low risk.
It is recreational use that presents an abuse concern, said Dr. Ferreri, but with the low doses used in psychiatry, the risk is “very limited or even nonexistent.”
Dr. Nutt said the abuse potential of psychedelics is so low that they can be used to treat addiction.
“Functionally, psychedelics are antiaddictive,” Dr. Nutt said. “The fact is, if you take them repeatedly, you develop tolerance, and the effect disappears. You can’t overcome it. But everyone believes they’re addictive because they’re scheduled drugs.”
Dr. Velásquez is something of an outlier. He believes the abuse potential with psychedelics is poorly understood and that some patients may develop tolerance, which is a potential gateway to dependence.
“Such is the case with LSD,” he said, “where this substance also favors tolerance to other psychedelic drugs such as psilocybin.”
Dosing also seems to play a key role in mitigating potential abuse, said Luca Pani, MD, professor of pharmacology and psychiatry at the University of Modena, Italy. Dr. Pani explained that with low doses and microdoses of psychedelics, the potential for abuse is eliminated.
Dr. Nutt, Dr. Pani, and Dr. Ferreri also noted the importance of medical supervision. For instance, said Dr. Ferreri, when administering ketamine, his team closely monitors both mental and physical parameters – heart rate and blood pressure, in particular – because the drug can have hypertensive effects.
Dr. Schenberg noted that ibogaine, a naturally occurring psychedelic frequently used by traditional communities in Africa in rituals and for healing purposes, could cause potentially fatal arrhythmias, so it’s critical that the treatment is administered in a hospital setting that has a cardiac unit.
Dr. Pani said there is a need for more research, especially regarding the molecular mechanisms behind the behavioral effects of low-dose psychedelic therapy and the potential risks of multiple treatments with the drugs.
“Although extensive toxicology has been conducted on a single active dose of psilocybin, which has been proven to be safe, further research is required to understand better the possible health risks, especially in relation to cardiac and lung tissue,” he said.
Psychologically challenging
The experts note that given the relative lack of experience with psychedelic therapy, preparing patients for potential adverse effects is paramount. This is particularly relevant in the research setting and highlights the need for adequate patient screening and aftercare.
Dr. Gründer and Dr. Dolengevich-Segal emphasized the importance of having qualified personnel available in the event that patients experience adverse psychological events during treatment.
For Dr. Gründer, the potential for psilocybin to cause patients to lose control, experience psychotic symptoms, or become paranoid warrants considerable preparation by treating physicians.
Patients occasionally experience fear and anxiety during treatment, though it’s usually short-lived, said Dr. Griffiths. Nevertheless, these experiences may open the door to greater insight. “A number of people report that these psychologically challenging states are a valuable part of the overall experience,” he said.
The situation is similar in Spain, where Dr. Dolengevich-Segal noted that typical treatment regimens have a strong focus on the patient’s experience as a therapeutic tool. As in the United Kingdom and the United States, her team guides patients to what they call a “peak experience,” which allows them to gain a better understanding of the trauma underlying their mental health problems.
Dr. Nutt said that in the United Kingdom, they haven’t seen adverse reactions in patients receiving psychedelic therapy, although sedatives such as benzodiazepines could be used to manage them. He added that at his center, two therapists are present at every treatment session, and all personnel are “trained medics or psychologists.”
Patient education
Preparing and educating patients about the therapy are critical, said Dr. Gründer, especially given the intense response psychedelic treatment often invokes.
Echoing Dr. Gründer, Dr. Tófoli said explaining the nature of psychedelic treatment to potential patients helps ease anxiety.
Dr. Griffiths noted that in the United States, study participants are not only educated about the potential effects of psychedelic agents but also undergo several hours of psychological preparation in advance of their first treatment session and are provided with psychological support after treatment.
There is also a strong emphasis on patient preparation and education in the United Kingdom, where patients meet with therapists before and after treatment. During these posttreatment debriefings, clinicians use the patients’ experience with psychedelics to help them gain insight into the underlying cause of their depression.
Dr. Schenberg noted that at his institution in São Paulo, there are online courses to teach clinicians about psychedelic therapy for psychiatric disorders. Next year, he added, a new training program in MDMA-assisted psychotherapy will begin.
Working out treatment protocols
Treatment protocols for psychedelics vary by agent and indication from country to country. For instance, Dr. Pani noted that current psychedelic research in Italy predominantly focuses more on microdosing, which involves administering 1% of the pharmacologically active dose to a maximum of 100 mcg, in contrast to low dosing or full dosing.
Therapeutic regimens in Brazil, said Dr. Schenberg, also differ by agent but share common elements. For instance, psychedelics are always administered in a research setting, and sessions include concomitant psychotherapy.
In Germany, investigators are working to determine optimal treatment regimen for psilocybin for resistant depression in a randomized three-arm study planned for 2021.
For Mexico’s Dr. Velásquez, treatment regimens are complex and varied. Either way, he said, patients always require long-term follow-up.
With ketamine therapy, Dr. Ferreri said his team administers the drug in 45- to 60-minute intravenous infusion sessions in a hospital room without light or sound stimulation. Regardless of the drug’s immediate effect, he said, the protocol is repeated within a 6-month period.
The question of the duration of treatment effect is important. Dr. Griffiths said research suggests that the positive effects of psilocybin are long lasting and that most individuals report positive changes in mood, attitude, and behavior that endure for months or even years after the session.
“Our research has shown that the benefits of these experiences can last as long as 14 months, often longer, and that many participants characterize their psilocybin experience as among the most profound and personally meaningful experiences of their lives,” said Dr. Griffiths.
Dr. Nutt agreed, noting that a single intense “trip” can improve mood for weeks, months, or even years. Nevertheless, he said, in his experience, approximately three-quarters of patients treated with psychedelics for major depression relapse within 3-9 months.
“Most get better,” he said, “but the majority of depression comes back over a period of months.”
Given the current illegal status of the drugs, he said it’s nearly impossible to provide patients with regular, subsequent treatment with psychedelics over time.
“My suspicion is that you might well have to dose four or five times over a couple of years to get people to escape from very severe depression,” said Dr. Nutt. “The longer they’ve been depressed, the harder it is for them to make a full recovery, because it’s more entrenched in the brain.”
All experts agree that exciting times are ahead for psychedelics as therapeutics for a wide range of psychiatric disorders.
“We can look forward to continued growth and expansion of this research,” said Dr. Griffiths, “including the refinement of protocols for a variety of therapeutic indications and to the development of a variety of new classic psychedelic compounds.”
A version of this article first appeared on Medscape.com.
In 1967, when the United Nations Convention on Drugs classified psychedelics as schedule I substances, it effectively ended research into these agents as potential therapeutics for psychiatric disorders.
Psychedelics induce altered states of perception. They bind to the 5-hydroxytryptamine 2A (5-HT2A) receptor and include psilocybin, which is derived from “magic mushrooms”; N,N-dimethyltryptamine (DMT), a component of ayahuasca and mescaline (peyote cactus); and the synthesized compound D-lysergic acid diethylamide (LSD). Other agents, such as ketamine and 3,4-methylenedioxymethamphetamine (MDMA), also known as ecstasy, are sometimes considered psychedelics as well.
Before they were classified as schedule I agents, psychedelics had been shown to be particularly beneficial for patients with treatment-resistant conditions, including depression and posttraumatic stress disorder (PTSD), especially when administered in a supportive, therapeutic setting.
Now, after a hiatus of almost 50 years, there is renewed global interest in the scientific investigation of psychedelics. The attention was spurred in part by several exploratory studies of DMT in humans conducted in the 1990s by Rick Strassman, MD, and colleagues at the University of New Mexico, Albuquerque.
Around the same time, Franz X. Vollenweider, MD, and colleagues at the University of Zürich began researching psilocybin and its effects on human behavior. However, it was a 2006 study of psilocybin by a team of researchers at Johns Hopkins University, Baltimore, that is widely cited as a catalyst for the current renaissance in psychedelic research.
To provide a broad-based, international perspective on these agents, including their current legal status and indications, treatment regimens, safety, efficacy, and future considerations, this news organization interviewed nine expert researchers from around the globe.
Global legal status
In most, if not all, countries, it is still illegal to prescribe psychedelics in other than a research setting.
They can be used in research, but only with approval from the Food and Drug Administration under licensure from the Drug Enforcement Administration.
France lists all synthetic hallucinogens and hallucinogenic mushrooms as narcotic. As a result, possession, use, transportation, and collection are subject to criminal sanctions.
In France, NMDA antagonists such as ketamine and nitrous oxide are regarded as psychedelic molecules and can be used off label for various conditions or as part of research protocols authorized by the French public health code.
Although psychedelics are illegal under Mexican law, they are commonly used in indigenous communities as part of traditional rituals.
“The line between traditional consumption and psychedelic tourism is very thin,” José J. Mendoza Velásquez, MD, professor in the department of mental health, National Autonomous University of Mexico, Mexico City, said in an interview.
Psychedelics also are illegal in the United Kingdom, although government agencies have recently allowed research groups to investigate them. Psychedelics cannot be prescribed in Germany, Spain, or Italy. However, investigators in these countries can request permission from regulatory agencies to conduct research.
Brazil allows psychedelic substances to be researched, particularly ayahuasca, which has long traditional and religious roots in the country.
However, as in other countries, none of the classic psychedelics is regulated for therapeutic use in Brazil. It is widely expected that the Brazilian government will approve MDMA sometime in 2024 for use in the treatment of PTSD.
Potential indications
Psychedelics are currently under investigation as potential treatments for major depression, treatment-resistant depression, PTSD, pain management, and anorexia, among other conditions.
In France, Florian Ferreri, MD, PhD, at Hospital Saint-Antoine, Paris, is researching ketamine for treatment of patients with suicidal crisis/ideation and treatment-resistant depression.
In the United Kingdom, David Nutt, FMedSci, Edmond J. Safra Professor of Neuropsychopharmacology at Imperial College London, and his team have conducted studies of the use of psychedelics in conjunction with psychological support for patients with treatment-resistant depression, and they are currently exploring their use in the treatment of anorexia and various pain syndromes.
In Germany, Gerhard Gründer, MD, professor of psychiatry at the Central Institute of Mental Health, in Mannheim, noted that a study of psilocybin for treatment-resistant depression will launch sometime in 2021. In Italy, current research is focusing on MDMA and ketamine in the laboratory environment and in animal models for treating depression and drug abuse.
Researcher Helen Dolengevich-Segal, MD, a psychiatrist at Hospital Universitario del Henares, Madrid, noted that although research on esketamine for the treatment of severe depressive disorder with suicidal thoughts is underway, there is very limited published research from that country into the use of classic psychedelics for various psychiatric disorders, given their current illegal status.
Mexico’s Dr. Velásquez noted that although he is prohibited from prescribing psychedelics, he does have patients who take the drugs to augment medical treatment. For instance, he said, his patients frequently use psilocybin to help with severe depression, pain, and insomnia.
Environment is key
Most researchers agree that for psychedelics to be safe and effective, patient education and administration in a controlled environment by experienced clinicians are key to successful treatment.
Roland R. Griffiths, PhD, director of the Center for Psychedelic and Consciousness Research at Johns Hopkins, said that ongoing U.S. psilocybin research – primarily in major depressive disorder and psychological distress associated with life-threatening illness, drug addiction, anorexia nervosa, obsessive-compulsive disorder, and headache – generally includes one or two treatment sessions, each of which lasts 6-8 hours.
Such sessions typically involve oral administration of a moderately high dose of a psychedelic under what he characterizes as “psychologically supported conditions.”
For Dr. Griffiths, there are serious potential risks associated with the use of psilocybin and other psychedelics outside such environments.
“When taken in uncontrolled conditions, classic psychedelics can produce confusion and disorientation resulting in behavior dangerous to the participant and others, including life-threatening risk,” he said.
Dr. Gründer agreed.
“At the moment, I cannot imagine that you would go to the pharmacy with a prescription for psilocybin and get yourself a pill and then take it in a quiet little room,” he said. Dr. Dolengevich-Segal and Dr. Velásquez echoed these sentiments, noting the optimal location for administration is one that is quiet and secure and where patients feel safe.
Luís Fernando Tófoli, MD, PhD, professor of medical psychology and psychiatry at the University of Campinas, and Eduardo Schenberg, PhD, founder and CEO of Instituto Phaneros in São Paulo, Brazil, said more research is needed to determine the optimal therapeutic environment for individual agents.
“Most studies have a low number of participants (around 20 or 30), especially in neuroimaging, with high unblinding rates,” Dr. Schenberg said. “Therefore, novel methodological approaches are also necessary, as these substances do not easily fit into the traditional pharmacology epistemic model.”
Risks, abuse potential
The abuse potential of psychedelics is an ongoing concern for the public, researchers, and regulators, but the consensus among nearly all of these experts is that when administered by medical professionals in controlled settings, these drugs are associated with extremely low risk.
It is recreational use that presents an abuse concern, said Dr. Ferreri, but with the low doses used in psychiatry, the risk is “very limited or even nonexistent.”
Dr. Nutt said the abuse potential of psychedelics is so low that they can be used to treat addiction.
“Functionally, psychedelics are antiaddictive,” Dr. Nutt said. “The fact is, if you take them repeatedly, you develop tolerance, and the effect disappears. You can’t overcome it. But everyone believes they’re addictive because they’re scheduled drugs.”
Dr. Velásquez is something of an outlier. He believes the abuse potential with psychedelics is poorly understood and that some patients may develop tolerance, which is a potential gateway to dependence.
“Such is the case with LSD,” he said, “where this substance also favors tolerance to other psychedelic drugs such as psilocybin.”
Dosing also seems to play a key role in mitigating potential abuse, said Luca Pani, MD, professor of pharmacology and psychiatry at the University of Modena, Italy. Dr. Pani explained that with low doses and microdoses of psychedelics, the potential for abuse is eliminated.
Dr. Nutt, Dr. Pani, and Dr. Ferreri also noted the importance of medical supervision. For instance, said Dr. Ferreri, when administering ketamine, his team closely monitors both mental and physical parameters – heart rate and blood pressure, in particular – because the drug can have hypertensive effects.
Dr. Schenberg noted that ibogaine, a naturally occurring psychedelic frequently used by traditional communities in Africa in rituals and for healing purposes, could cause potentially fatal arrhythmias, so it’s critical that the treatment is administered in a hospital setting that has a cardiac unit.
Dr. Pani said there is a need for more research, especially regarding the molecular mechanisms behind the behavioral effects of low-dose psychedelic therapy and the potential risks of multiple treatments with the drugs.
“Although extensive toxicology has been conducted on a single active dose of psilocybin, which has been proven to be safe, further research is required to understand better the possible health risks, especially in relation to cardiac and lung tissue,” he said.
Psychologically challenging
The experts note that given the relative lack of experience with psychedelic therapy, preparing patients for potential adverse effects is paramount. This is particularly relevant in the research setting and highlights the need for adequate patient screening and aftercare.
Dr. Gründer and Dr. Dolengevich-Segal emphasized the importance of having qualified personnel available in the event that patients experience adverse psychological events during treatment.
For Dr. Gründer, the potential for psilocybin to cause patients to lose control, experience psychotic symptoms, or become paranoid warrants considerable preparation by treating physicians.
Patients occasionally experience fear and anxiety during treatment, though it’s usually short-lived, said Dr. Griffiths. Nevertheless, these experiences may open the door to greater insight. “A number of people report that these psychologically challenging states are a valuable part of the overall experience,” he said.
The situation is similar in Spain, where Dr. Dolengevich-Segal noted that typical treatment regimens have a strong focus on the patient’s experience as a therapeutic tool. As in the United Kingdom and the United States, her team guides patients to what they call a “peak experience,” which allows them to gain a better understanding of the trauma underlying their mental health problems.
Dr. Nutt said that in the United Kingdom, they haven’t seen adverse reactions in patients receiving psychedelic therapy, although sedatives such as benzodiazepines could be used to manage them. He added that at his center, two therapists are present at every treatment session, and all personnel are “trained medics or psychologists.”
Patient education
Preparing and educating patients about the therapy are critical, said Dr. Gründer, especially given the intense response psychedelic treatment often invokes.
Echoing Dr. Gründer, Dr. Tófoli said explaining the nature of psychedelic treatment to potential patients helps ease anxiety.
Dr. Griffiths noted that in the United States, study participants are not only educated about the potential effects of psychedelic agents but also undergo several hours of psychological preparation in advance of their first treatment session and are provided with psychological support after treatment.
There is also a strong emphasis on patient preparation and education in the United Kingdom, where patients meet with therapists before and after treatment. During these posttreatment debriefings, clinicians use the patients’ experience with psychedelics to help them gain insight into the underlying cause of their depression.
Dr. Schenberg noted that at his institution in São Paulo, there are online courses to teach clinicians about psychedelic therapy for psychiatric disorders. Next year, he added, a new training program in MDMA-assisted psychotherapy will begin.
Working out treatment protocols
Treatment protocols for psychedelics vary by agent and indication from country to country. For instance, Dr. Pani noted that current psychedelic research in Italy predominantly focuses more on microdosing, which involves administering 1% of the pharmacologically active dose to a maximum of 100 mcg, in contrast to low dosing or full dosing.
Therapeutic regimens in Brazil, said Dr. Schenberg, also differ by agent but share common elements. For instance, psychedelics are always administered in a research setting, and sessions include concomitant psychotherapy.
In Germany, investigators are working to determine optimal treatment regimen for psilocybin for resistant depression in a randomized three-arm study planned for 2021.
For Mexico’s Dr. Velásquez, treatment regimens are complex and varied. Either way, he said, patients always require long-term follow-up.
With ketamine therapy, Dr. Ferreri said his team administers the drug in 45- to 60-minute intravenous infusion sessions in a hospital room without light or sound stimulation. Regardless of the drug’s immediate effect, he said, the protocol is repeated within a 6-month period.
The question of the duration of treatment effect is important. Dr. Griffiths said research suggests that the positive effects of psilocybin are long lasting and that most individuals report positive changes in mood, attitude, and behavior that endure for months or even years after the session.
“Our research has shown that the benefits of these experiences can last as long as 14 months, often longer, and that many participants characterize their psilocybin experience as among the most profound and personally meaningful experiences of their lives,” said Dr. Griffiths.
Dr. Nutt agreed, noting that a single intense “trip” can improve mood for weeks, months, or even years. Nevertheless, he said, in his experience, approximately three-quarters of patients treated with psychedelics for major depression relapse within 3-9 months.
“Most get better,” he said, “but the majority of depression comes back over a period of months.”
Given the current illegal status of the drugs, he said it’s nearly impossible to provide patients with regular, subsequent treatment with psychedelics over time.
“My suspicion is that you might well have to dose four or five times over a couple of years to get people to escape from very severe depression,” said Dr. Nutt. “The longer they’ve been depressed, the harder it is for them to make a full recovery, because it’s more entrenched in the brain.”
All experts agree that exciting times are ahead for psychedelics as therapeutics for a wide range of psychiatric disorders.
“We can look forward to continued growth and expansion of this research,” said Dr. Griffiths, “including the refinement of protocols for a variety of therapeutic indications and to the development of a variety of new classic psychedelic compounds.”
A version of this article first appeared on Medscape.com.
In 1967, when the United Nations Convention on Drugs classified psychedelics as schedule I substances, it effectively ended research into these agents as potential therapeutics for psychiatric disorders.
Psychedelics induce altered states of perception. They bind to the 5-hydroxytryptamine 2A (5-HT2A) receptor and include psilocybin, which is derived from “magic mushrooms”; N,N-dimethyltryptamine (DMT), a component of ayahuasca and mescaline (peyote cactus); and the synthesized compound D-lysergic acid diethylamide (LSD). Other agents, such as ketamine and 3,4-methylenedioxymethamphetamine (MDMA), also known as ecstasy, are sometimes considered psychedelics as well.
Before they were classified as schedule I agents, psychedelics had been shown to be particularly beneficial for patients with treatment-resistant conditions, including depression and posttraumatic stress disorder (PTSD), especially when administered in a supportive, therapeutic setting.
Now, after a hiatus of almost 50 years, there is renewed global interest in the scientific investigation of psychedelics. The attention was spurred in part by several exploratory studies of DMT in humans conducted in the 1990s by Rick Strassman, MD, and colleagues at the University of New Mexico, Albuquerque.
Around the same time, Franz X. Vollenweider, MD, and colleagues at the University of Zürich began researching psilocybin and its effects on human behavior. However, it was a 2006 study of psilocybin by a team of researchers at Johns Hopkins University, Baltimore, that is widely cited as a catalyst for the current renaissance in psychedelic research.
To provide a broad-based, international perspective on these agents, including their current legal status and indications, treatment regimens, safety, efficacy, and future considerations, this news organization interviewed nine expert researchers from around the globe.
Global legal status
In most, if not all, countries, it is still illegal to prescribe psychedelics in other than a research setting.
They can be used in research, but only with approval from the Food and Drug Administration under licensure from the Drug Enforcement Administration.
France lists all synthetic hallucinogens and hallucinogenic mushrooms as narcotic. As a result, possession, use, transportation, and collection are subject to criminal sanctions.
In France, NMDA antagonists such as ketamine and nitrous oxide are regarded as psychedelic molecules and can be used off label for various conditions or as part of research protocols authorized by the French public health code.
Although psychedelics are illegal under Mexican law, they are commonly used in indigenous communities as part of traditional rituals.
“The line between traditional consumption and psychedelic tourism is very thin,” José J. Mendoza Velásquez, MD, professor in the department of mental health, National Autonomous University of Mexico, Mexico City, said in an interview.
Psychedelics also are illegal in the United Kingdom, although government agencies have recently allowed research groups to investigate them. Psychedelics cannot be prescribed in Germany, Spain, or Italy. However, investigators in these countries can request permission from regulatory agencies to conduct research.
Brazil allows psychedelic substances to be researched, particularly ayahuasca, which has long traditional and religious roots in the country.
However, as in other countries, none of the classic psychedelics is regulated for therapeutic use in Brazil. It is widely expected that the Brazilian government will approve MDMA sometime in 2024 for use in the treatment of PTSD.
Potential indications
Psychedelics are currently under investigation as potential treatments for major depression, treatment-resistant depression, PTSD, pain management, and anorexia, among other conditions.
In France, Florian Ferreri, MD, PhD, at Hospital Saint-Antoine, Paris, is researching ketamine for treatment of patients with suicidal crisis/ideation and treatment-resistant depression.
In the United Kingdom, David Nutt, FMedSci, Edmond J. Safra Professor of Neuropsychopharmacology at Imperial College London, and his team have conducted studies of the use of psychedelics in conjunction with psychological support for patients with treatment-resistant depression, and they are currently exploring their use in the treatment of anorexia and various pain syndromes.
In Germany, Gerhard Gründer, MD, professor of psychiatry at the Central Institute of Mental Health, in Mannheim, noted that a study of psilocybin for treatment-resistant depression will launch sometime in 2021. In Italy, current research is focusing on MDMA and ketamine in the laboratory environment and in animal models for treating depression and drug abuse.
Researcher Helen Dolengevich-Segal, MD, a psychiatrist at Hospital Universitario del Henares, Madrid, noted that although research on esketamine for the treatment of severe depressive disorder with suicidal thoughts is underway, there is very limited published research from that country into the use of classic psychedelics for various psychiatric disorders, given their current illegal status.
Mexico’s Dr. Velásquez noted that although he is prohibited from prescribing psychedelics, he does have patients who take the drugs to augment medical treatment. For instance, he said, his patients frequently use psilocybin to help with severe depression, pain, and insomnia.
Environment is key
Most researchers agree that for psychedelics to be safe and effective, patient education and administration in a controlled environment by experienced clinicians are key to successful treatment.
Roland R. Griffiths, PhD, director of the Center for Psychedelic and Consciousness Research at Johns Hopkins, said that ongoing U.S. psilocybin research – primarily in major depressive disorder and psychological distress associated with life-threatening illness, drug addiction, anorexia nervosa, obsessive-compulsive disorder, and headache – generally includes one or two treatment sessions, each of which lasts 6-8 hours.
Such sessions typically involve oral administration of a moderately high dose of a psychedelic under what he characterizes as “psychologically supported conditions.”
For Dr. Griffiths, there are serious potential risks associated with the use of psilocybin and other psychedelics outside such environments.
“When taken in uncontrolled conditions, classic psychedelics can produce confusion and disorientation resulting in behavior dangerous to the participant and others, including life-threatening risk,” he said.
Dr. Gründer agreed.
“At the moment, I cannot imagine that you would go to the pharmacy with a prescription for psilocybin and get yourself a pill and then take it in a quiet little room,” he said. Dr. Dolengevich-Segal and Dr. Velásquez echoed these sentiments, noting the optimal location for administration is one that is quiet and secure and where patients feel safe.
Luís Fernando Tófoli, MD, PhD, professor of medical psychology and psychiatry at the University of Campinas, and Eduardo Schenberg, PhD, founder and CEO of Instituto Phaneros in São Paulo, Brazil, said more research is needed to determine the optimal therapeutic environment for individual agents.
“Most studies have a low number of participants (around 20 or 30), especially in neuroimaging, with high unblinding rates,” Dr. Schenberg said. “Therefore, novel methodological approaches are also necessary, as these substances do not easily fit into the traditional pharmacology epistemic model.”
Risks, abuse potential
The abuse potential of psychedelics is an ongoing concern for the public, researchers, and regulators, but the consensus among nearly all of these experts is that when administered by medical professionals in controlled settings, these drugs are associated with extremely low risk.
It is recreational use that presents an abuse concern, said Dr. Ferreri, but with the low doses used in psychiatry, the risk is “very limited or even nonexistent.”
Dr. Nutt said the abuse potential of psychedelics is so low that they can be used to treat addiction.
“Functionally, psychedelics are antiaddictive,” Dr. Nutt said. “The fact is, if you take them repeatedly, you develop tolerance, and the effect disappears. You can’t overcome it. But everyone believes they’re addictive because they’re scheduled drugs.”
Dr. Velásquez is something of an outlier. He believes the abuse potential with psychedelics is poorly understood and that some patients may develop tolerance, which is a potential gateway to dependence.
“Such is the case with LSD,” he said, “where this substance also favors tolerance to other psychedelic drugs such as psilocybin.”
Dosing also seems to play a key role in mitigating potential abuse, said Luca Pani, MD, professor of pharmacology and psychiatry at the University of Modena, Italy. Dr. Pani explained that with low doses and microdoses of psychedelics, the potential for abuse is eliminated.
Dr. Nutt, Dr. Pani, and Dr. Ferreri also noted the importance of medical supervision. For instance, said Dr. Ferreri, when administering ketamine, his team closely monitors both mental and physical parameters – heart rate and blood pressure, in particular – because the drug can have hypertensive effects.
Dr. Schenberg noted that ibogaine, a naturally occurring psychedelic frequently used by traditional communities in Africa in rituals and for healing purposes, could cause potentially fatal arrhythmias, so it’s critical that the treatment is administered in a hospital setting that has a cardiac unit.
Dr. Pani said there is a need for more research, especially regarding the molecular mechanisms behind the behavioral effects of low-dose psychedelic therapy and the potential risks of multiple treatments with the drugs.
“Although extensive toxicology has been conducted on a single active dose of psilocybin, which has been proven to be safe, further research is required to understand better the possible health risks, especially in relation to cardiac and lung tissue,” he said.
Psychologically challenging
The experts note that given the relative lack of experience with psychedelic therapy, preparing patients for potential adverse effects is paramount. This is particularly relevant in the research setting and highlights the need for adequate patient screening and aftercare.
Dr. Gründer and Dr. Dolengevich-Segal emphasized the importance of having qualified personnel available in the event that patients experience adverse psychological events during treatment.
For Dr. Gründer, the potential for psilocybin to cause patients to lose control, experience psychotic symptoms, or become paranoid warrants considerable preparation by treating physicians.
Patients occasionally experience fear and anxiety during treatment, though it’s usually short-lived, said Dr. Griffiths. Nevertheless, these experiences may open the door to greater insight. “A number of people report that these psychologically challenging states are a valuable part of the overall experience,” he said.
The situation is similar in Spain, where Dr. Dolengevich-Segal noted that typical treatment regimens have a strong focus on the patient’s experience as a therapeutic tool. As in the United Kingdom and the United States, her team guides patients to what they call a “peak experience,” which allows them to gain a better understanding of the trauma underlying their mental health problems.
Dr. Nutt said that in the United Kingdom, they haven’t seen adverse reactions in patients receiving psychedelic therapy, although sedatives such as benzodiazepines could be used to manage them. He added that at his center, two therapists are present at every treatment session, and all personnel are “trained medics or psychologists.”
Patient education
Preparing and educating patients about the therapy are critical, said Dr. Gründer, especially given the intense response psychedelic treatment often invokes.
Echoing Dr. Gründer, Dr. Tófoli said explaining the nature of psychedelic treatment to potential patients helps ease anxiety.
Dr. Griffiths noted that in the United States, study participants are not only educated about the potential effects of psychedelic agents but also undergo several hours of psychological preparation in advance of their first treatment session and are provided with psychological support after treatment.
There is also a strong emphasis on patient preparation and education in the United Kingdom, where patients meet with therapists before and after treatment. During these posttreatment debriefings, clinicians use the patients’ experience with psychedelics to help them gain insight into the underlying cause of their depression.
Dr. Schenberg noted that at his institution in São Paulo, there are online courses to teach clinicians about psychedelic therapy for psychiatric disorders. Next year, he added, a new training program in MDMA-assisted psychotherapy will begin.
Working out treatment protocols
Treatment protocols for psychedelics vary by agent and indication from country to country. For instance, Dr. Pani noted that current psychedelic research in Italy predominantly focuses more on microdosing, which involves administering 1% of the pharmacologically active dose to a maximum of 100 mcg, in contrast to low dosing or full dosing.
Therapeutic regimens in Brazil, said Dr. Schenberg, also differ by agent but share common elements. For instance, psychedelics are always administered in a research setting, and sessions include concomitant psychotherapy.
In Germany, investigators are working to determine optimal treatment regimen for psilocybin for resistant depression in a randomized three-arm study planned for 2021.
For Mexico’s Dr. Velásquez, treatment regimens are complex and varied. Either way, he said, patients always require long-term follow-up.
With ketamine therapy, Dr. Ferreri said his team administers the drug in 45- to 60-minute intravenous infusion sessions in a hospital room without light or sound stimulation. Regardless of the drug’s immediate effect, he said, the protocol is repeated within a 6-month period.
The question of the duration of treatment effect is important. Dr. Griffiths said research suggests that the positive effects of psilocybin are long lasting and that most individuals report positive changes in mood, attitude, and behavior that endure for months or even years after the session.
“Our research has shown that the benefits of these experiences can last as long as 14 months, often longer, and that many participants characterize their psilocybin experience as among the most profound and personally meaningful experiences of their lives,” said Dr. Griffiths.
Dr. Nutt agreed, noting that a single intense “trip” can improve mood for weeks, months, or even years. Nevertheless, he said, in his experience, approximately three-quarters of patients treated with psychedelics for major depression relapse within 3-9 months.
“Most get better,” he said, “but the majority of depression comes back over a period of months.”
Given the current illegal status of the drugs, he said it’s nearly impossible to provide patients with regular, subsequent treatment with psychedelics over time.
“My suspicion is that you might well have to dose four or five times over a couple of years to get people to escape from very severe depression,” said Dr. Nutt. “The longer they’ve been depressed, the harder it is for them to make a full recovery, because it’s more entrenched in the brain.”
All experts agree that exciting times are ahead for psychedelics as therapeutics for a wide range of psychiatric disorders.
“We can look forward to continued growth and expansion of this research,” said Dr. Griffiths, “including the refinement of protocols for a variety of therapeutic indications and to the development of a variety of new classic psychedelic compounds.”
A version of this article first appeared on Medscape.com.

New data on worldwide mental health impact of COVID-19
A new survey that assessed the mental health impact of COVID-19 across the globe shows high rates of trauma and clinical mood disorders related to the pandemic.

The survey, carried out by Sapien Labs, was conducted in eight English-speaking countries and included 49,000 adults. It showed that 57% of respondents experienced some COVID-19–related adversity or trauma.
Roughly one-quarter showed clinical signs of or were at risk for a mood disorder, and 40% described themselves as “succeeding or thriving.”
Those who reported the poorest mental health were young adults and individuals who experienced financial adversity or were unable to receive care for other medical conditions. Nonbinary gender and not getting enough sleep, exercise, or face-to-face socialization also increased the risk for poorer mental well-being.
“The data suggest that there will be long-term fallout from the pandemic on the mental health front,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, said in a press release.
Novel initiative
Dr. Thiagarajan said in an interview that she was running a company that provided microloans to 30,000 villages in India. The company included a research group the goal of which was to understand what predicts success in an individual and in a particular ecosystem, she said – “Why did some villages succeed and others didn’t?”
Dr. Thiagarajan and associates thought that “something big is happening in our life circumstances that causes changes in our brain and felt that we need to understand what they are and how they affect humanity. This was the impetus for founding Sapien Labs. “
The survey, which is part of the company’s Mental Health Million project, is an ongoing research initiative that makes data freely available to other researchers.
The investigators developed a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability,” said Dr. Thiagarajan.
The MHQ consists of 47 “elements of mental well-being.” Respondents’ MHQ scores ranged from –100 to +200. Negative scores indicate poorer mental well-being. Respondents were categorized as clinical, at risk, enduring, managing, succeeding, and thriving.
MHQ scores were computed for six “broad dimensions” of mental health: Core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
Participants were recruited through advertising on Google and Facebook in eight English-speaking countries – Canada, the United States, the United Kingdom, South Africa, Singapore, Australia, New Zealand, and India. The researchers collected demographic information, including age, education, and gender.
First step
The assessment was completed by 48,808 respondents between April 8 and Dec. 31, 2020.
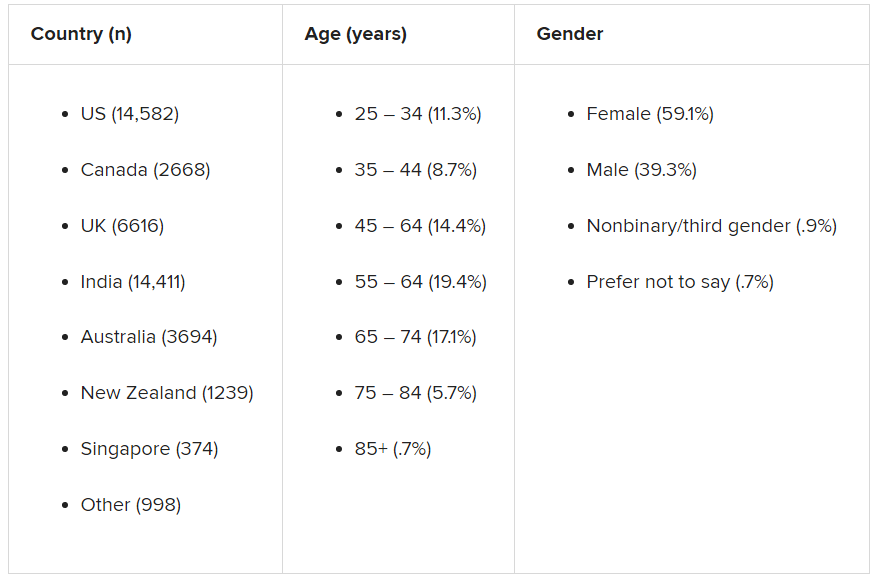
A smaller sample of 2,000 people from the same countries who were polled by the investigators in 2019 was used as a comparator.
Taken together, the overall mental well-being score for 2020 was 8% lower than the score obtained in 2019 from the same countries, and the percentage of respondents who fell into the “clinical” category increased from 14% in 2009 to 26% in 2020.
Residents of Singapore had the highest MHQ score, followed by residents of the United States. At the other extreme, respondents from the United Kingdom and South Africa had the poorest MHQ scores.
“It is important to keep in mind that the English-speaking, Internet-enabled populace is not necessarily representative of each country as a whole,” the authors noted.
Youth hardest hit
whose average MHQ score was 29% lower than those aged at least 65 years.
Worldwide, 70% of respondents aged at least 65 years fell into the categories of “succeeding” or “thriving,” compared with just 17% of those aged 18-24 years.
“We saw a massive trend of diminishing mental well-being in younger individuals, suggesting that some societal force is at play that we need to get to the bottom of,” said Dr. Thiagarajan.
“Young people are still learning how to calibrate themselves in the world, and with age comes maturity, leading to a difference in emotional resilience,” she said.
Highest risk group
Mental well-being was poorest among nonbinary/third-gender respondents. Among those persons, more than 50% were classified as being at clinical risk, in comparison with males and females combined, and their MHQ scores were about 47 points lower.
Nonbinary individuals “are universally doing very poorly, relative to males or females,” said Dr. Thiagarajan. “This is a demographic at very high risk with a lot of suicidal thoughts.”
Respondents who had insufficient sleep, who lacked social interaction, and whose level of exercise was insufficient had lower MHQ scores of an “unexpected magnitude,” compared with their counterparts who had sufficient sleep, more social interaction, and more exercise (a discrepancy of 82, 66, and 46 points, respectively).
Only 3.9% of respondents reported having had COVID-19; 0.7% reported having had a severe case. Yet 57% of respondents reported that the pandemic had had negative consequences with regard to their health or their finances or social situation.
Those who were unable to get care for their other health conditions because of the pandemic (2% of all respondents) reported the worst mental well-being, followed by those who struggled for basic necessities (1.4%).
Reduced household income was associated with a 4% lower score but affected a higher percentage of people (17%). Social isolation was associated with a score of about 20 less. Higher rates of lifetime traumas and adversities were likewise associated with lower scores for mental well-being.
Creative, generous approach
Commenting on the survey results, Ken Duckworth, MD, clinical professor at Harvard Medical School, Boston, and chief medical officer of the National Alliance of Mental Illness, noted that the findings were similar to findings from studies in the United States, which showed disproportionately higher rates of mental health problems in younger individuals. Dr. Duckworth was not involved with the survey.

“The idea that this is an international phenomenon and the broad-stroke finding that younger people are suffering across nations is compelling and important for policymakers to look at,” he said.
Dr. Duckworth noted that although the findings are not “representative” of entire populations in a given country, the report is a “first step in a long journey.”
He described the report as “extremely brilliant, creative, and generous, allowing any academician to get access to the data.”
He saw it “less as a definitive report and more as a directionally informative survey that will yield great fruit over time.”
In a comment, Joshua Morganstein, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, said: “One of the important things a document like this highlights is the importance of understanding more where risk [for mental health disorders] is concentrated and what things have occurred or might occur that can buffer against that risk or protect us from it. We see that each nation has similar but also different challenges.”
Dr. Thiagarajan is the founder and chief scientist of Sapien Labs. Her coauthors are employees of Sapien Labs. Dr. Duckworth and Dr. Morganstein disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new survey that assessed the mental health impact of COVID-19 across the globe shows high rates of trauma and clinical mood disorders related to the pandemic.
The survey, carried out by Sapien Labs, was conducted in eight English-speaking countries and included 49,000 adults. It showed that 57% of respondents experienced some COVID-19–related adversity or trauma.
Roughly one-quarter showed clinical signs of or were at risk for a mood disorder, and 40% described themselves as “succeeding or thriving.”
Those who reported the poorest mental health were young adults and individuals who experienced financial adversity or were unable to receive care for other medical conditions. Nonbinary gender and not getting enough sleep, exercise, or face-to-face socialization also increased the risk for poorer mental well-being.
“The data suggest that there will be long-term fallout from the pandemic on the mental health front,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, said in a press release.
Novel initiative
Dr. Thiagarajan said in an interview that she was running a company that provided microloans to 30,000 villages in India. The company included a research group the goal of which was to understand what predicts success in an individual and in a particular ecosystem, she said – “Why did some villages succeed and others didn’t?”
Dr. Thiagarajan and associates thought that “something big is happening in our life circumstances that causes changes in our brain and felt that we need to understand what they are and how they affect humanity. This was the impetus for founding Sapien Labs. “
The survey, which is part of the company’s Mental Health Million project, is an ongoing research initiative that makes data freely available to other researchers.
The investigators developed a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability,” said Dr. Thiagarajan.
The MHQ consists of 47 “elements of mental well-being.” Respondents’ MHQ scores ranged from –100 to +200. Negative scores indicate poorer mental well-being. Respondents were categorized as clinical, at risk, enduring, managing, succeeding, and thriving.
MHQ scores were computed for six “broad dimensions” of mental health: Core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
Participants were recruited through advertising on Google and Facebook in eight English-speaking countries – Canada, the United States, the United Kingdom, South Africa, Singapore, Australia, New Zealand, and India. The researchers collected demographic information, including age, education, and gender.
First step
The assessment was completed by 48,808 respondents between April 8 and Dec. 31, 2020.
A smaller sample of 2,000 people from the same countries who were polled by the investigators in 2019 was used as a comparator.
Taken together, the overall mental well-being score for 2020 was 8% lower than the score obtained in 2019 from the same countries, and the percentage of respondents who fell into the “clinical” category increased from 14% in 2009 to 26% in 2020.
Residents of Singapore had the highest MHQ score, followed by residents of the United States. At the other extreme, respondents from the United Kingdom and South Africa had the poorest MHQ scores.
“It is important to keep in mind that the English-speaking, Internet-enabled populace is not necessarily representative of each country as a whole,” the authors noted.
Youth hardest hit
whose average MHQ score was 29% lower than those aged at least 65 years.
Worldwide, 70% of respondents aged at least 65 years fell into the categories of “succeeding” or “thriving,” compared with just 17% of those aged 18-24 years.
“We saw a massive trend of diminishing mental well-being in younger individuals, suggesting that some societal force is at play that we need to get to the bottom of,” said Dr. Thiagarajan.
“Young people are still learning how to calibrate themselves in the world, and with age comes maturity, leading to a difference in emotional resilience,” she said.
Highest risk group
Mental well-being was poorest among nonbinary/third-gender respondents. Among those persons, more than 50% were classified as being at clinical risk, in comparison with males and females combined, and their MHQ scores were about 47 points lower.
Nonbinary individuals “are universally doing very poorly, relative to males or females,” said Dr. Thiagarajan. “This is a demographic at very high risk with a lot of suicidal thoughts.”
Respondents who had insufficient sleep, who lacked social interaction, and whose level of exercise was insufficient had lower MHQ scores of an “unexpected magnitude,” compared with their counterparts who had sufficient sleep, more social interaction, and more exercise (a discrepancy of 82, 66, and 46 points, respectively).
Only 3.9% of respondents reported having had COVID-19; 0.7% reported having had a severe case. Yet 57% of respondents reported that the pandemic had had negative consequences with regard to their health or their finances or social situation.
Those who were unable to get care for their other health conditions because of the pandemic (2% of all respondents) reported the worst mental well-being, followed by those who struggled for basic necessities (1.4%).
Reduced household income was associated with a 4% lower score but affected a higher percentage of people (17%). Social isolation was associated with a score of about 20 less. Higher rates of lifetime traumas and adversities were likewise associated with lower scores for mental well-being.
Creative, generous approach
Commenting on the survey results, Ken Duckworth, MD, clinical professor at Harvard Medical School, Boston, and chief medical officer of the National Alliance of Mental Illness, noted that the findings were similar to findings from studies in the United States, which showed disproportionately higher rates of mental health problems in younger individuals. Dr. Duckworth was not involved with the survey.
“The idea that this is an international phenomenon and the broad-stroke finding that younger people are suffering across nations is compelling and important for policymakers to look at,” he said.
Dr. Duckworth noted that although the findings are not “representative” of entire populations in a given country, the report is a “first step in a long journey.”
He described the report as “extremely brilliant, creative, and generous, allowing any academician to get access to the data.”
He saw it “less as a definitive report and more as a directionally informative survey that will yield great fruit over time.”
In a comment, Joshua Morganstein, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, said: “One of the important things a document like this highlights is the importance of understanding more where risk [for mental health disorders] is concentrated and what things have occurred or might occur that can buffer against that risk or protect us from it. We see that each nation has similar but also different challenges.”
Dr. Thiagarajan is the founder and chief scientist of Sapien Labs. Her coauthors are employees of Sapien Labs. Dr. Duckworth and Dr. Morganstein disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new survey that assessed the mental health impact of COVID-19 across the globe shows high rates of trauma and clinical mood disorders related to the pandemic.
The survey, carried out by Sapien Labs, was conducted in eight English-speaking countries and included 49,000 adults. It showed that 57% of respondents experienced some COVID-19–related adversity or trauma.
Roughly one-quarter showed clinical signs of or were at risk for a mood disorder, and 40% described themselves as “succeeding or thriving.”
Those who reported the poorest mental health were young adults and individuals who experienced financial adversity or were unable to receive care for other medical conditions. Nonbinary gender and not getting enough sleep, exercise, or face-to-face socialization also increased the risk for poorer mental well-being.
“The data suggest that there will be long-term fallout from the pandemic on the mental health front,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, said in a press release.
Novel initiative
Dr. Thiagarajan said in an interview that she was running a company that provided microloans to 30,000 villages in India. The company included a research group the goal of which was to understand what predicts success in an individual and in a particular ecosystem, she said – “Why did some villages succeed and others didn’t?”
Dr. Thiagarajan and associates thought that “something big is happening in our life circumstances that causes changes in our brain and felt that we need to understand what they are and how they affect humanity. This was the impetus for founding Sapien Labs. “
The survey, which is part of the company’s Mental Health Million project, is an ongoing research initiative that makes data freely available to other researchers.
The investigators developed a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability,” said Dr. Thiagarajan.
The MHQ consists of 47 “elements of mental well-being.” Respondents’ MHQ scores ranged from –100 to +200. Negative scores indicate poorer mental well-being. Respondents were categorized as clinical, at risk, enduring, managing, succeeding, and thriving.
MHQ scores were computed for six “broad dimensions” of mental health: Core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
Participants were recruited through advertising on Google and Facebook in eight English-speaking countries – Canada, the United States, the United Kingdom, South Africa, Singapore, Australia, New Zealand, and India. The researchers collected demographic information, including age, education, and gender.
First step
The assessment was completed by 48,808 respondents between April 8 and Dec. 31, 2020.
A smaller sample of 2,000 people from the same countries who were polled by the investigators in 2019 was used as a comparator.
Taken together, the overall mental well-being score for 2020 was 8% lower than the score obtained in 2019 from the same countries, and the percentage of respondents who fell into the “clinical” category increased from 14% in 2009 to 26% in 2020.
Residents of Singapore had the highest MHQ score, followed by residents of the United States. At the other extreme, respondents from the United Kingdom and South Africa had the poorest MHQ scores.
“It is important to keep in mind that the English-speaking, Internet-enabled populace is not necessarily representative of each country as a whole,” the authors noted.
Youth hardest hit
whose average MHQ score was 29% lower than those aged at least 65 years.
Worldwide, 70% of respondents aged at least 65 years fell into the categories of “succeeding” or “thriving,” compared with just 17% of those aged 18-24 years.
“We saw a massive trend of diminishing mental well-being in younger individuals, suggesting that some societal force is at play that we need to get to the bottom of,” said Dr. Thiagarajan.
“Young people are still learning how to calibrate themselves in the world, and with age comes maturity, leading to a difference in emotional resilience,” she said.
Highest risk group
Mental well-being was poorest among nonbinary/third-gender respondents. Among those persons, more than 50% were classified as being at clinical risk, in comparison with males and females combined, and their MHQ scores were about 47 points lower.
Nonbinary individuals “are universally doing very poorly, relative to males or females,” said Dr. Thiagarajan. “This is a demographic at very high risk with a lot of suicidal thoughts.”
Respondents who had insufficient sleep, who lacked social interaction, and whose level of exercise was insufficient had lower MHQ scores of an “unexpected magnitude,” compared with their counterparts who had sufficient sleep, more social interaction, and more exercise (a discrepancy of 82, 66, and 46 points, respectively).
Only 3.9% of respondents reported having had COVID-19; 0.7% reported having had a severe case. Yet 57% of respondents reported that the pandemic had had negative consequences with regard to their health or their finances or social situation.
Those who were unable to get care for their other health conditions because of the pandemic (2% of all respondents) reported the worst mental well-being, followed by those who struggled for basic necessities (1.4%).
Reduced household income was associated with a 4% lower score but affected a higher percentage of people (17%). Social isolation was associated with a score of about 20 less. Higher rates of lifetime traumas and adversities were likewise associated with lower scores for mental well-being.
Creative, generous approach
Commenting on the survey results, Ken Duckworth, MD, clinical professor at Harvard Medical School, Boston, and chief medical officer of the National Alliance of Mental Illness, noted that the findings were similar to findings from studies in the United States, which showed disproportionately higher rates of mental health problems in younger individuals. Dr. Duckworth was not involved with the survey.
“The idea that this is an international phenomenon and the broad-stroke finding that younger people are suffering across nations is compelling and important for policymakers to look at,” he said.
Dr. Duckworth noted that although the findings are not “representative” of entire populations in a given country, the report is a “first step in a long journey.”
He described the report as “extremely brilliant, creative, and generous, allowing any academician to get access to the data.”
He saw it “less as a definitive report and more as a directionally informative survey that will yield great fruit over time.”
In a comment, Joshua Morganstein, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, said: “One of the important things a document like this highlights is the importance of understanding more where risk [for mental health disorders] is concentrated and what things have occurred or might occur that can buffer against that risk or protect us from it. We see that each nation has similar but also different challenges.”
Dr. Thiagarajan is the founder and chief scientist of Sapien Labs. Her coauthors are employees of Sapien Labs. Dr. Duckworth and Dr. Morganstein disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The lasting effects of childhood trauma
Childhood trauma, which is also called adverse childhood experiences (ACEs), can have lasting detrimental effects on individuals as they grow and mature into adulthood. ACEs may occur in children age ≤18 years if they experience abuse or neglect, violence, or other traumatic losses. More than 60% of people experience at least 1 ACE, and 1 in 6 individuals reported that they had experienced ≥4 ACEs.1 Subsequent additional ACEs have a cumulative deteriorating impact on the brain. This predisposes individuals to mental health disorders, substance use disorders, and other psychosocial problems. The efficacy of current therapeutic approaches provides only partial symptom resolution. For such individuals, the illness load and health care costs typically remain high across the lifespan.1,2
In this article, we discuss types of ACEs, protective factors and risk factors that influence the development of posttraumatic stress disorder (PTSD) in individuals who experience ACEs, how ACEs can negatively impact mental health in adulthood, and approaches to prevent or treat PTSD and other symptoms.
Types of trauma and correlation with PTSD
ACEs can be indexed as neglect or emotional, physical, or sexual abuse. Physical and sexual abuse strongly correlate with an increased risk of PTSD.3 Although neglect and emotional abuse do not directly predict the development of PTSD, these experiences foretell high rates of lifelong trauma exposure and are indirectly related to late PTSD symptoms.4,5 ACEs can impede an individual’s cognitive, social, and emotional development, diminish quality of life, and lead to an early death.6 The lifetime prevalence of PTSD is 6.1% to 9.2%.7 Compared with men, women are 4 times more likely to develop PTSD following a traumatic event.7
The development of PTSD is influenced by the nature, duration, and degree of trauma, and age at the time of exposure to trauma. Children who survive complex trauma (≥2 types of trauma) have a higher likelihood of developing PTSD.8 Prolonged trauma exposure has a more substantial negative impact than a one-time occurrence. However, it is an erroneous oversimplification to assume that each type of ACE has an equally traumatic effect.6
Factors that protect against PTSD
Factors that can protect against developing PTSD are listed in Table 1.7 Two of these are resilience and hope.

Resilience is defined as an individual’s strength to cope with difficulties in life.9 Resilience has internal psychological characteristics and external factors that aid in protecting against childhood adversities.10,11 The Brief Resilience Scale is a self-assessment that measures innate abilities to cope, including optimism, self-efficacy, patience, faith, and humor.12,13 External factors associated with resilience are family, friends, and community support.11,13
Hope can help in surmounting ACEs. The Adult Hope Scale has been used in many studies to assess this construct in individuals who have survived trauma.13 Some studies have found decreased hope in individuals who sustained early trauma and were diagnosed with PTSD in adulthood.14 A study examining children exposed to domestic violence found that children who showed high hope, endurance, and curiosity were better able to cope with adversities.15
Continue to: PTSD risk factors
PTSD risk factors
Many individual and societal risk factors can influence the likelihood of developing PTSD. Some of these factors are outlined in Table 1.7
Pathophysiology of PTSD
Multiple brain regions, pathways, and neurotransmitters are involved in the development of PTSD. Neuroimaging has identified volume and activity changes of the hippocampus, prefrontal cortex, and amygdala in patients with early trauma and PTSD. Some researchers have suggested a gross reduction in locus coeruleus neuronal volume in war veterans with a likely diagnosis of PTSD compared with controls.16,17 In other studies, chronic stress exposure has been found to cause neuronal cell death and affect neuronal plasticity in the limbic area of the brain.18
Diagnosing PTSD
More than 30% of individuals who experience ACEs develop PTSD.19 The DSM-5 diagnostic criteria for PTSD are outlined in Table 2.20 Several instruments are used to determine the diagnosis and assess the severity of PTSD. These include the Clinician-Administered PTSD Scale for DSM-5,21 which is a 30-item structured interview that can be administered in 45 to 60 minutes; the PTSD Symptom Scale Self-Report Version, which is a 17-item, Likert scale, self-report questionnaire; and the Structured Clinical Interview: PTSD Module, which is a semi-structured interview that can take up to several hours to administer.21

Other disorders. In addition to PTSD, individuals with ACEs are at high risk for other mental health issues throughout their lifetime. Individuals with ACE often experience depressive symptoms (approximately 40%); anxiety (approximately 30%); anger; guilt or shame; negative self-cognition; interpersonal difficulties; rumination; and thoughts of self-harm and suicide.22 Epidemiological studies suggest that patients who experience childhood sexual abuse are more likely to develop mood, anxiety, and substance use disorders in adulthood.23,24
Psychotherapeutic treatments for PTSD
Cognitive-behavioral therapy (CBT) addresses the relationship between an individual’s thoughts, emotions, and behaviors. CBT can be used to treat adults and children with PTSD. Before starting CBT, assess the patient’s current safety to ensure that they have the coping skills to manage distress related to their ACEs, and address any coexisting substance use.25
Continue to: According to the American Psychological Association...
According to the American Psychological Association, several CBT-based psychotherapies are recommended for treating PTSD26:
Trauma-focused–CBT includes psychoeducation, trauma narrative, processing, exposure, and relaxation skills training. It consists of approximately 12 to 16 sessions and incorporates elements of family therapy.
Cognitive processing therapy (CPT) focuses on helping patients develop adaptive cognitive domains about the self, the people around them, and the world. CPT therapists assist in information processing by accessing the traumatic memory and trying to eliminate emotions tied to it.25,27 CPT consists of 12 to 16 structured individual, group, or combined sessions.
Prolonged exposure (PE) targets fear-related emotions and works on the principles of habituation to extinguish trauma and fear response to the trigger. This increases self-reliance and competence and decreases the generalization of anxiety to innocuous triggers. PE typically consists of 9 to 12 sessions. PE alone or in combination with cognitive restructuring is successful in treating patients with PTSD, but cognitive restructuring has limited utility in young children.25,27
Cognitive exposure can be individual or group therapy delivered over 3 months, where negative self-evaluation and traumatic memories are challenged with the goal of interrupting maladaptive behaviors and thoughts.27
Continue to: Stress inoculation training
Stress inoculation training (SIT) provides psychoeducation, skills training, role-playing, deep muscle relaxation, paced breathing, and thought stopping. Emphasis is on coaching skills to alleviate anxiety, fear, and symptoms of depression associated with trauma. In SIT, exposures to traumatic memories are indirect (eg, role play), compared with PE, where the exposures are direct.25
The American Psychological Association conditionally recommended several other forms for psychotherapy for treating patients with PTSD26:
Brief eclectic psychotherapy uses CBT and psychodynamic approaches to target feelings of guilt and shame in 16 sessions.27
Narrative exposure therapy consists of 4 to 10 group sessions in which individuals provide detailed narration of the events; the focus is on self-respect and personal rights.27
Eye movement desensitization and reprocessing (EMDR) is a 6- to 12-session, 8-phase treatment that uses principles of accelerated information processing to target nonverbal expression of trauma and dissociative experiences. Patients with PTSD are suggested to have disrupted rapid eye movements. In EMDR, patients follow rhythmic movements of the therapist’s hands or flashed light. This is designed to decrease stress associated with accessing trauma memories, the emotional/physiologic response from the memories, and negative cognitive distortions about self, and to replace negative cognition distortions with positive thoughts about self.25,27
Continue to: Accelerated resolution therapy
Accelerated resolution therapy is a derivative of EMDR. It helps to reconsolidate the emotional and physical experiences associated with distressing memories by replacing them with positive ones or decreasing physiological arousal and anxiety related to the recall of traumatic memories.28
Pharmacologic treatments
Selective serotonin reuptake inhibitors (SSRIs). Multiple studies using different scales have found that paroxetine, sertraline, and fluoxetine can decrease PTSD symptoms. Approximately 60% of patients treated with SSRIs experience partial remission of symptoms, and 20% to 30% experience complete symptom resolution.29 Davidson et al30 found that 22% of patients with PTSD who received fluoxetine had a relapse of symptoms, compared with 50% of patients who received placebo.
Serotonin-norepinephrine reuptake inhibitors (SNRIs) and other antidepressants. The SNRIs venlafaxine and duloxetine can help reduce hyperarousal symptoms and improve mood, anxiety, and sleep.26 Mirtazapine, an alpha 2A/2C adrenoceptor antagonist/5-HT 2A/2C/3 antagonist, can address PTSD symptoms from both serotonergic pathways and increase norepinephrine release by blocking autoreceptors and enhancing alpha-1 receptor activity. This alleviates hyperarousal symptoms and promotes sleep.29 In addition to having monoaminergic effects, antidepressant medications also regulate the hypothalamic–pituitary–adrenal (HPA) axis response to stress and promote neurogenesis in the hippocampal region.29
Adrenergic agents
Adrenergic receptor antagonists. Prazosin, an alpha-1 adrenoceptor antagonist, decreases hyperarousal symptoms, improves sleep, and decreases nightmares related to PTSD by decreasing noradrenergic hyperactivity.29
Beta-blockers such as propranolol can decrease physiological response to trauma but have mixed results in the prevention or improvement of PTSD symptoms.29,31
Continue to: Glucocorticoid receptor agonists
Glucocorticoid receptor agonists. In a very small study, low-dose cortisol decreased the severity of traumatic memory (consolidation phase).32 Glucocorticoid receptor agonists can also diminish memory retrieval (reconsolidation phase) through intrusive thoughts and flashbacks.29
Anticonvulsants, benzodiazepines, and antipsychotics
These medications have had a limited role in the treatment of PTSD.26,29
Future directions: Preventive treatments
Because PTSD has a profound impact on an individual’s quality of life and the development of other illnesses, there is strong interest in finding treatments that can prevent PTSD. Based on limited evidence primarily from animal studies, some researchers have suggested that certain agents may someday be helpful for PTSD prevention29:
Glucocorticoid antagonists such as corticotropin-releasing factor 1 (CRF1) antagonists or cholecystokinin 2 (CCK2) receptor antagonists might promote resilience to stress by inhibiting the HPA axis and influencing the amygdala by decreasing fear conditioning, as observed in animal models. Similarly, in animal models, CRF1 and CCK2 are predicted to decrease memory consolidation in response to exposure to stress.
Adrenoceptor antagonists and agonists also might have a role in preventive treatment, but the evidence is scarce. Prazosin, an alpha-1 adrenoceptor antagonist, was ineffective in animal models.29,31 Propranolol, a beta-adrenoceptor blocker, has had mixed results but can decrease trauma-induced physiological arousal when administered soon after exposure.29
Continue to: N-methyl-
N-methyl-
Bottom Line
Adverse childhood experiences (ACEs) are strong predictors for the development of posttraumatic stress disorder (PTSD) and other mental health or medical issues in late adolescence and adulthood. Experiencing a higher number of ACEs increases the risk of developing PTSD as an adult. Timely psychotherapeutic and pharmacologic interventions can help limit symptoms and reduce the severity of PTSD.
Related Resources
- Smith P, Dalglesih T, Meiser-Stedman R. Practitioner review: posttraumatic stress disorder and its treatment in children and adolescents. J Child Psychol Psychiatry. 2019;60(5):500-515.
- North CS, Hong BA, Downs DL. PTSD: a systematic approach to diagnosis and treatment. Current Psychiatry 2018;17(4):35-43.
Drug Brand Names
Duloxetine • Cymbalta
Fluoxetine • Prozac
Mirtazapine • Remeron
Paroxetine • Paxil
Prazosin • Minipress
Propranolol • Inderal, Pronol
Sertraline • Zoloft
Venlafaxine • Effexor
1. Centers for Disease Control and Prevention. Preventing adverse childhood experiences. Published April 3, 2020. Accessed January 26, 2021. https://www.cdc.gov/violenceprevention/childabuseandneglect/aces/fastfact.html
2. Kessler RC, McLaughlin KA, Green JG, et al. Childhood adversities and adult psychopathology in the WHO world mental health surveys. Br J Psychiatry. 2010;197:378-385.
3. Norman RE, Byambaa M, De R, et al. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine. 2012;9(11):e1001349. doi: 10.1371/journal.pmed.1001349
4. Spertus IL, Yehuda R, Wong CM, et al. Childhood emotional abuse and neglect as predictors of psychological and physical symptoms in women presenting to a primary care practice. Child Abuse Negl. 2003;27(11):1247-1258.
5. Glück TM, Knefel M, Lueger-Schuster B. A network analysis of anger, shame, proposed ICD-11 post-traumatic stress disorder, and different types of childhood trauma in foster care settings in a sample of adult survivors. Eur J Psychotraumatol. 2017;8(suppl 3):1372543. doi: 10.1080/20008198.2017.1372543
6. Edwards VJ, Holden GW, Felitti VJ, et al. Relationship between multiple forms of childhood maltreatment and adult mental health in community respondents: results from the adverse childhood experiences study. Am J Psychiatry. 2003;160:1453-1460.
7. Sareen J. Posttraumatic stress disorder in adults: epidemiology, pathophysiology, clinical manifestations, course, assessment, and diagnosis. UpToDate. Updated December 3, 2020. Accessed January 26, 2021. https://www.uptodate.com/contents/posttraumatic-stress-disorder-in-adults-epidemiology-pathophysiology-clinical-manifestations-course-assessment-and-diagnosis
8. Widom CS. Posttraumatic stress disorder in abused and neglected children grown up. Am J Psychiatry. 1999:156;1223-1229.
9. Rutter M. Psychosocial resilience and protective mechanisms. Am J Orthopsychiatry. 1987;57(3):316-331.
10. Ahern NR, Kiehl EM, Sole ML, et al. A review of instruments measuring resilience. Issues Compr Pediatr Nurs. 2006;29(2):103-125.
11. Zimmerman MA. Resiliency theory: a strengths-based approach to research and practice for adolescent health. Health Educ Behav. 2013;40(4):381-383.
12. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76-82.
13. Munoz RT, Hanks H, Hellman CM. Hope and resilience as distinct contributors to psychological flourishing among childhood trauma survivors. Traumatology. 2020;26(2):177-184.
14. Baxter MA, Hemming EJ, McIntosh HC, et al. Exploring the relationship between adverse childhood experiences and hope. J Child Sex Abus. 2017;26(8):948-956.
15. Hellman CM, Gwinn C. Camp HOPE as an intervention for children exposed to domestic violence: a program evaluation of hope, and strength of character. Child Adolesc Soc Work J. 2017;34:269-276.
16. Bracha HS, Garcia-Rill E, Mrak RE, et al. Postmortem locus coeruleus neuron count in three American veterans with probable or possible war-related PTSD. J Neuropsychiatry Clin Neurosci. 2005;17(4):503-9.
17. de Lange GM. Understanding the cellular and molecular alterations in PTSD brains: the necessity of post-mortem brain tissue. Eur J Psychotraumatol. 2017;8(1):1341824. doi: 10.1080/20008198.2017.1341824
18. Zunszain PA, Anacker C, Cattaneo A, et al. Glucocorticoids, cytokines and brain abnormalities in depression. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(3):722-729.
19. Greeson JKP, Briggs EC, Kisiel CL, et al. Complex trauma and mental health in children and adolescents placed in foster care: findings from the national child traumatic stress network. Child Welfare. 2011;90(6):91-108.
20. Diagnostic and statistical manual of mental disorders, 5th ed. American Psychiatric Association; 2013.
21. American Psychological Association. PTSD assessment instruments. Updated September 26, 2018. Accessed January 27, 2021. https://www.apa.org/ptsd-guideline/assessment/
22. Bellis MA, Hughes K, Ford K, et al. Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: a systematic review and meta-analysis. Lancet Public Health. 2019;4(10):e517-e528. doi: 10.1016/S2468-2667(19)30145-8
23. Mullen PE, Martin JL, Anderson JC, et al. Childhood sexual abuse and mental health in adult life. Br J Psychiatry. 1993;163:721-732.
24. Kendler KS, Bulik CM, Silberg J, et al. Childhood sexual abuse and adult psychiatric and substance use disorders in women. An epidemiological and cotwin control analysis. Arch Gen Psychiatry. 2000;57(10):953-959.
25. Chard KM, Gilman R. Counseling trauma victims: 4 brief therapies meet the test. Current Psychiatry. 2005;4(8):50,55-58,61-62.
26. Guideline Development Panel for the Treatment of PTSD in Adults, American Psychological Association. Summary of the clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults. American Psychol. 2019;74(5):596-607.
27. American Psychological Association. Clinical practice guideline for the treatment of posttraumatic stress disorder. PTSD treatments. Updated June 2020. Accessed January 27, 2021. https://www.apa.org/ptsd-guideline/treatments/
28. Kip KE, Elk CA, Sullivan KL, et al. Brief treatment of symptoms of post-traumatic stress disorder (PTSD) by use of accelerated resolution therapy (ART(®)). Behav Sci (Basel). 2012;2(2):115-134.
29. Steckler T, Risbrough V. Pharmacological treatment of PTSD - established and new approaches. Neuropharmacology. 2012;62(2):617-627.
30. Davidson JR, Connor KM, Hertzberg MA, et al. Maintenance therapy with fluoxetine in posttraumatic stress disorder: a placebo-controlled discontinuation study. J Clin Psychopharmacol. 2005;25(2):166-169.
31. Benedek DM, Friedman MJ, Zatzick D, et al. Guideline watch (March 2009): Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Focus. 2009;7(2):204-213.
32. Aerni A, Traber R, Hock C, et al. Low-dose cortisol for symptoms of posttraumatic stress disorder. Am J Psychiat. 2004;161(8):1488-1490.
33. McGhee LL, Maani CV, Garza TH, et al. The correlation between ketamine and posttraumatic stress disorder in burned service members. J Trauma. 2008;64(2 suppl):S195-S198. doi: 10.1097/TA.0b013e318160ba1d
Childhood trauma, which is also called adverse childhood experiences (ACEs), can have lasting detrimental effects on individuals as they grow and mature into adulthood. ACEs may occur in children age ≤18 years if they experience abuse or neglect, violence, or other traumatic losses. More than 60% of people experience at least 1 ACE, and 1 in 6 individuals reported that they had experienced ≥4 ACEs.1 Subsequent additional ACEs have a cumulative deteriorating impact on the brain. This predisposes individuals to mental health disorders, substance use disorders, and other psychosocial problems. The efficacy of current therapeutic approaches provides only partial symptom resolution. For such individuals, the illness load and health care costs typically remain high across the lifespan.1,2
In this article, we discuss types of ACEs, protective factors and risk factors that influence the development of posttraumatic stress disorder (PTSD) in individuals who experience ACEs, how ACEs can negatively impact mental health in adulthood, and approaches to prevent or treat PTSD and other symptoms.
Types of trauma and correlation with PTSD
ACEs can be indexed as neglect or emotional, physical, or sexual abuse. Physical and sexual abuse strongly correlate with an increased risk of PTSD.3 Although neglect and emotional abuse do not directly predict the development of PTSD, these experiences foretell high rates of lifelong trauma exposure and are indirectly related to late PTSD symptoms.4,5 ACEs can impede an individual’s cognitive, social, and emotional development, diminish quality of life, and lead to an early death.6 The lifetime prevalence of PTSD is 6.1% to 9.2%.7 Compared with men, women are 4 times more likely to develop PTSD following a traumatic event.7
The development of PTSD is influenced by the nature, duration, and degree of trauma, and age at the time of exposure to trauma. Children who survive complex trauma (≥2 types of trauma) have a higher likelihood of developing PTSD.8 Prolonged trauma exposure has a more substantial negative impact than a one-time occurrence. However, it is an erroneous oversimplification to assume that each type of ACE has an equally traumatic effect.6
Factors that protect against PTSD
Factors that can protect against developing PTSD are listed in Table 1.7 Two of these are resilience and hope.
Resilience is defined as an individual’s strength to cope with difficulties in life.9 Resilience has internal psychological characteristics and external factors that aid in protecting against childhood adversities.10,11 The Brief Resilience Scale is a self-assessment that measures innate abilities to cope, including optimism, self-efficacy, patience, faith, and humor.12,13 External factors associated with resilience are family, friends, and community support.11,13
Hope can help in surmounting ACEs. The Adult Hope Scale has been used in many studies to assess this construct in individuals who have survived trauma.13 Some studies have found decreased hope in individuals who sustained early trauma and were diagnosed with PTSD in adulthood.14 A study examining children exposed to domestic violence found that children who showed high hope, endurance, and curiosity were better able to cope with adversities.15
Continue to: PTSD risk factors
PTSD risk factors
Many individual and societal risk factors can influence the likelihood of developing PTSD. Some of these factors are outlined in Table 1.7
Pathophysiology of PTSD
Multiple brain regions, pathways, and neurotransmitters are involved in the development of PTSD. Neuroimaging has identified volume and activity changes of the hippocampus, prefrontal cortex, and amygdala in patients with early trauma and PTSD. Some researchers have suggested a gross reduction in locus coeruleus neuronal volume in war veterans with a likely diagnosis of PTSD compared with controls.16,17 In other studies, chronic stress exposure has been found to cause neuronal cell death and affect neuronal plasticity in the limbic area of the brain.18
Diagnosing PTSD
More than 30% of individuals who experience ACEs develop PTSD.19 The DSM-5 diagnostic criteria for PTSD are outlined in Table 2.20 Several instruments are used to determine the diagnosis and assess the severity of PTSD. These include the Clinician-Administered PTSD Scale for DSM-5,21 which is a 30-item structured interview that can be administered in 45 to 60 minutes; the PTSD Symptom Scale Self-Report Version, which is a 17-item, Likert scale, self-report questionnaire; and the Structured Clinical Interview: PTSD Module, which is a semi-structured interview that can take up to several hours to administer.21
Other disorders. In addition to PTSD, individuals with ACEs are at high risk for other mental health issues throughout their lifetime. Individuals with ACE often experience depressive symptoms (approximately 40%); anxiety (approximately 30%); anger; guilt or shame; negative self-cognition; interpersonal difficulties; rumination; and thoughts of self-harm and suicide.22 Epidemiological studies suggest that patients who experience childhood sexual abuse are more likely to develop mood, anxiety, and substance use disorders in adulthood.23,24
Psychotherapeutic treatments for PTSD
Cognitive-behavioral therapy (CBT) addresses the relationship between an individual’s thoughts, emotions, and behaviors. CBT can be used to treat adults and children with PTSD. Before starting CBT, assess the patient’s current safety to ensure that they have the coping skills to manage distress related to their ACEs, and address any coexisting substance use.25
Continue to: According to the American Psychological Association...
According to the American Psychological Association, several CBT-based psychotherapies are recommended for treating PTSD26:
Trauma-focused–CBT includes psychoeducation, trauma narrative, processing, exposure, and relaxation skills training. It consists of approximately 12 to 16 sessions and incorporates elements of family therapy.
Cognitive processing therapy (CPT) focuses on helping patients develop adaptive cognitive domains about the self, the people around them, and the world. CPT therapists assist in information processing by accessing the traumatic memory and trying to eliminate emotions tied to it.25,27 CPT consists of 12 to 16 structured individual, group, or combined sessions.
Prolonged exposure (PE) targets fear-related emotions and works on the principles of habituation to extinguish trauma and fear response to the trigger. This increases self-reliance and competence and decreases the generalization of anxiety to innocuous triggers. PE typically consists of 9 to 12 sessions. PE alone or in combination with cognitive restructuring is successful in treating patients with PTSD, but cognitive restructuring has limited utility in young children.25,27
Cognitive exposure can be individual or group therapy delivered over 3 months, where negative self-evaluation and traumatic memories are challenged with the goal of interrupting maladaptive behaviors and thoughts.27
Continue to: Stress inoculation training
Stress inoculation training (SIT) provides psychoeducation, skills training, role-playing, deep muscle relaxation, paced breathing, and thought stopping. Emphasis is on coaching skills to alleviate anxiety, fear, and symptoms of depression associated with trauma. In SIT, exposures to traumatic memories are indirect (eg, role play), compared with PE, where the exposures are direct.25
The American Psychological Association conditionally recommended several other forms for psychotherapy for treating patients with PTSD26:
Brief eclectic psychotherapy uses CBT and psychodynamic approaches to target feelings of guilt and shame in 16 sessions.27
Narrative exposure therapy consists of 4 to 10 group sessions in which individuals provide detailed narration of the events; the focus is on self-respect and personal rights.27
Eye movement desensitization and reprocessing (EMDR) is a 6- to 12-session, 8-phase treatment that uses principles of accelerated information processing to target nonverbal expression of trauma and dissociative experiences. Patients with PTSD are suggested to have disrupted rapid eye movements. In EMDR, patients follow rhythmic movements of the therapist’s hands or flashed light. This is designed to decrease stress associated with accessing trauma memories, the emotional/physiologic response from the memories, and negative cognitive distortions about self, and to replace negative cognition distortions with positive thoughts about self.25,27
Continue to: Accelerated resolution therapy
Accelerated resolution therapy is a derivative of EMDR. It helps to reconsolidate the emotional and physical experiences associated with distressing memories by replacing them with positive ones or decreasing physiological arousal and anxiety related to the recall of traumatic memories.28
Pharmacologic treatments
Selective serotonin reuptake inhibitors (SSRIs). Multiple studies using different scales have found that paroxetine, sertraline, and fluoxetine can decrease PTSD symptoms. Approximately 60% of patients treated with SSRIs experience partial remission of symptoms, and 20% to 30% experience complete symptom resolution.29 Davidson et al30 found that 22% of patients with PTSD who received fluoxetine had a relapse of symptoms, compared with 50% of patients who received placebo.
Serotonin-norepinephrine reuptake inhibitors (SNRIs) and other antidepressants. The SNRIs venlafaxine and duloxetine can help reduce hyperarousal symptoms and improve mood, anxiety, and sleep.26 Mirtazapine, an alpha 2A/2C adrenoceptor antagonist/5-HT 2A/2C/3 antagonist, can address PTSD symptoms from both serotonergic pathways and increase norepinephrine release by blocking autoreceptors and enhancing alpha-1 receptor activity. This alleviates hyperarousal symptoms and promotes sleep.29 In addition to having monoaminergic effects, antidepressant medications also regulate the hypothalamic–pituitary–adrenal (HPA) axis response to stress and promote neurogenesis in the hippocampal region.29
Adrenergic agents
Adrenergic receptor antagonists. Prazosin, an alpha-1 adrenoceptor antagonist, decreases hyperarousal symptoms, improves sleep, and decreases nightmares related to PTSD by decreasing noradrenergic hyperactivity.29
Beta-blockers such as propranolol can decrease physiological response to trauma but have mixed results in the prevention or improvement of PTSD symptoms.29,31
Continue to: Glucocorticoid receptor agonists
Glucocorticoid receptor agonists. In a very small study, low-dose cortisol decreased the severity of traumatic memory (consolidation phase).32 Glucocorticoid receptor agonists can also diminish memory retrieval (reconsolidation phase) through intrusive thoughts and flashbacks.29
Anticonvulsants, benzodiazepines, and antipsychotics
These medications have had a limited role in the treatment of PTSD.26,29
Future directions: Preventive treatments
Because PTSD has a profound impact on an individual’s quality of life and the development of other illnesses, there is strong interest in finding treatments that can prevent PTSD. Based on limited evidence primarily from animal studies, some researchers have suggested that certain agents may someday be helpful for PTSD prevention29:
Glucocorticoid antagonists such as corticotropin-releasing factor 1 (CRF1) antagonists or cholecystokinin 2 (CCK2) receptor antagonists might promote resilience to stress by inhibiting the HPA axis and influencing the amygdala by decreasing fear conditioning, as observed in animal models. Similarly, in animal models, CRF1 and CCK2 are predicted to decrease memory consolidation in response to exposure to stress.
Adrenoceptor antagonists and agonists also might have a role in preventive treatment, but the evidence is scarce. Prazosin, an alpha-1 adrenoceptor antagonist, was ineffective in animal models.29,31 Propranolol, a beta-adrenoceptor blocker, has had mixed results but can decrease trauma-induced physiological arousal when administered soon after exposure.29
Continue to: N-methyl-
N-methyl-
Bottom Line
Adverse childhood experiences (ACEs) are strong predictors for the development of posttraumatic stress disorder (PTSD) and other mental health or medical issues in late adolescence and adulthood. Experiencing a higher number of ACEs increases the risk of developing PTSD as an adult. Timely psychotherapeutic and pharmacologic interventions can help limit symptoms and reduce the severity of PTSD.
Related Resources
- Smith P, Dalglesih T, Meiser-Stedman R. Practitioner review: posttraumatic stress disorder and its treatment in children and adolescents. J Child Psychol Psychiatry. 2019;60(5):500-515.
- North CS, Hong BA, Downs DL. PTSD: a systematic approach to diagnosis and treatment. Current Psychiatry 2018;17(4):35-43.
Drug Brand Names
Duloxetine • Cymbalta
Fluoxetine • Prozac
Mirtazapine • Remeron
Paroxetine • Paxil
Prazosin • Minipress
Propranolol • Inderal, Pronol
Sertraline • Zoloft
Venlafaxine • Effexor
Childhood trauma, which is also called adverse childhood experiences (ACEs), can have lasting detrimental effects on individuals as they grow and mature into adulthood. ACEs may occur in children age ≤18 years if they experience abuse or neglect, violence, or other traumatic losses. More than 60% of people experience at least 1 ACE, and 1 in 6 individuals reported that they had experienced ≥4 ACEs.1 Subsequent additional ACEs have a cumulative deteriorating impact on the brain. This predisposes individuals to mental health disorders, substance use disorders, and other psychosocial problems. The efficacy of current therapeutic approaches provides only partial symptom resolution. For such individuals, the illness load and health care costs typically remain high across the lifespan.1,2
In this article, we discuss types of ACEs, protective factors and risk factors that influence the development of posttraumatic stress disorder (PTSD) in individuals who experience ACEs, how ACEs can negatively impact mental health in adulthood, and approaches to prevent or treat PTSD and other symptoms.
Types of trauma and correlation with PTSD
ACEs can be indexed as neglect or emotional, physical, or sexual abuse. Physical and sexual abuse strongly correlate with an increased risk of PTSD.3 Although neglect and emotional abuse do not directly predict the development of PTSD, these experiences foretell high rates of lifelong trauma exposure and are indirectly related to late PTSD symptoms.4,5 ACEs can impede an individual’s cognitive, social, and emotional development, diminish quality of life, and lead to an early death.6 The lifetime prevalence of PTSD is 6.1% to 9.2%.7 Compared with men, women are 4 times more likely to develop PTSD following a traumatic event.7
The development of PTSD is influenced by the nature, duration, and degree of trauma, and age at the time of exposure to trauma. Children who survive complex trauma (≥2 types of trauma) have a higher likelihood of developing PTSD.8 Prolonged trauma exposure has a more substantial negative impact than a one-time occurrence. However, it is an erroneous oversimplification to assume that each type of ACE has an equally traumatic effect.6
Factors that protect against PTSD
Factors that can protect against developing PTSD are listed in Table 1.7 Two of these are resilience and hope.
Resilience is defined as an individual’s strength to cope with difficulties in life.9 Resilience has internal psychological characteristics and external factors that aid in protecting against childhood adversities.10,11 The Brief Resilience Scale is a self-assessment that measures innate abilities to cope, including optimism, self-efficacy, patience, faith, and humor.12,13 External factors associated with resilience are family, friends, and community support.11,13
Hope can help in surmounting ACEs. The Adult Hope Scale has been used in many studies to assess this construct in individuals who have survived trauma.13 Some studies have found decreased hope in individuals who sustained early trauma and were diagnosed with PTSD in adulthood.14 A study examining children exposed to domestic violence found that children who showed high hope, endurance, and curiosity were better able to cope with adversities.15
Continue to: PTSD risk factors
PTSD risk factors
Many individual and societal risk factors can influence the likelihood of developing PTSD. Some of these factors are outlined in Table 1.7
Pathophysiology of PTSD
Multiple brain regions, pathways, and neurotransmitters are involved in the development of PTSD. Neuroimaging has identified volume and activity changes of the hippocampus, prefrontal cortex, and amygdala in patients with early trauma and PTSD. Some researchers have suggested a gross reduction in locus coeruleus neuronal volume in war veterans with a likely diagnosis of PTSD compared with controls.16,17 In other studies, chronic stress exposure has been found to cause neuronal cell death and affect neuronal plasticity in the limbic area of the brain.18
Diagnosing PTSD
More than 30% of individuals who experience ACEs develop PTSD.19 The DSM-5 diagnostic criteria for PTSD are outlined in Table 2.20 Several instruments are used to determine the diagnosis and assess the severity of PTSD. These include the Clinician-Administered PTSD Scale for DSM-5,21 which is a 30-item structured interview that can be administered in 45 to 60 minutes; the PTSD Symptom Scale Self-Report Version, which is a 17-item, Likert scale, self-report questionnaire; and the Structured Clinical Interview: PTSD Module, which is a semi-structured interview that can take up to several hours to administer.21
Other disorders. In addition to PTSD, individuals with ACEs are at high risk for other mental health issues throughout their lifetime. Individuals with ACE often experience depressive symptoms (approximately 40%); anxiety (approximately 30%); anger; guilt or shame; negative self-cognition; interpersonal difficulties; rumination; and thoughts of self-harm and suicide.22 Epidemiological studies suggest that patients who experience childhood sexual abuse are more likely to develop mood, anxiety, and substance use disorders in adulthood.23,24
Psychotherapeutic treatments for PTSD
Cognitive-behavioral therapy (CBT) addresses the relationship between an individual’s thoughts, emotions, and behaviors. CBT can be used to treat adults and children with PTSD. Before starting CBT, assess the patient’s current safety to ensure that they have the coping skills to manage distress related to their ACEs, and address any coexisting substance use.25
Continue to: According to the American Psychological Association...
According to the American Psychological Association, several CBT-based psychotherapies are recommended for treating PTSD26:
Trauma-focused–CBT includes psychoeducation, trauma narrative, processing, exposure, and relaxation skills training. It consists of approximately 12 to 16 sessions and incorporates elements of family therapy.
Cognitive processing therapy (CPT) focuses on helping patients develop adaptive cognitive domains about the self, the people around them, and the world. CPT therapists assist in information processing by accessing the traumatic memory and trying to eliminate emotions tied to it.25,27 CPT consists of 12 to 16 structured individual, group, or combined sessions.
Prolonged exposure (PE) targets fear-related emotions and works on the principles of habituation to extinguish trauma and fear response to the trigger. This increases self-reliance and competence and decreases the generalization of anxiety to innocuous triggers. PE typically consists of 9 to 12 sessions. PE alone or in combination with cognitive restructuring is successful in treating patients with PTSD, but cognitive restructuring has limited utility in young children.25,27
Cognitive exposure can be individual or group therapy delivered over 3 months, where negative self-evaluation and traumatic memories are challenged with the goal of interrupting maladaptive behaviors and thoughts.27
Continue to: Stress inoculation training
Stress inoculation training (SIT) provides psychoeducation, skills training, role-playing, deep muscle relaxation, paced breathing, and thought stopping. Emphasis is on coaching skills to alleviate anxiety, fear, and symptoms of depression associated with trauma. In SIT, exposures to traumatic memories are indirect (eg, role play), compared with PE, where the exposures are direct.25
The American Psychological Association conditionally recommended several other forms for psychotherapy for treating patients with PTSD26:
Brief eclectic psychotherapy uses CBT and psychodynamic approaches to target feelings of guilt and shame in 16 sessions.27
Narrative exposure therapy consists of 4 to 10 group sessions in which individuals provide detailed narration of the events; the focus is on self-respect and personal rights.27
Eye movement desensitization and reprocessing (EMDR) is a 6- to 12-session, 8-phase treatment that uses principles of accelerated information processing to target nonverbal expression of trauma and dissociative experiences. Patients with PTSD are suggested to have disrupted rapid eye movements. In EMDR, patients follow rhythmic movements of the therapist’s hands or flashed light. This is designed to decrease stress associated with accessing trauma memories, the emotional/physiologic response from the memories, and negative cognitive distortions about self, and to replace negative cognition distortions with positive thoughts about self.25,27
Continue to: Accelerated resolution therapy
Accelerated resolution therapy is a derivative of EMDR. It helps to reconsolidate the emotional and physical experiences associated with distressing memories by replacing them with positive ones or decreasing physiological arousal and anxiety related to the recall of traumatic memories.28
Pharmacologic treatments
Selective serotonin reuptake inhibitors (SSRIs). Multiple studies using different scales have found that paroxetine, sertraline, and fluoxetine can decrease PTSD symptoms. Approximately 60% of patients treated with SSRIs experience partial remission of symptoms, and 20% to 30% experience complete symptom resolution.29 Davidson et al30 found that 22% of patients with PTSD who received fluoxetine had a relapse of symptoms, compared with 50% of patients who received placebo.
Serotonin-norepinephrine reuptake inhibitors (SNRIs) and other antidepressants. The SNRIs venlafaxine and duloxetine can help reduce hyperarousal symptoms and improve mood, anxiety, and sleep.26 Mirtazapine, an alpha 2A/2C adrenoceptor antagonist/5-HT 2A/2C/3 antagonist, can address PTSD symptoms from both serotonergic pathways and increase norepinephrine release by blocking autoreceptors and enhancing alpha-1 receptor activity. This alleviates hyperarousal symptoms and promotes sleep.29 In addition to having monoaminergic effects, antidepressant medications also regulate the hypothalamic–pituitary–adrenal (HPA) axis response to stress and promote neurogenesis in the hippocampal region.29
Adrenergic agents
Adrenergic receptor antagonists. Prazosin, an alpha-1 adrenoceptor antagonist, decreases hyperarousal symptoms, improves sleep, and decreases nightmares related to PTSD by decreasing noradrenergic hyperactivity.29
Beta-blockers such as propranolol can decrease physiological response to trauma but have mixed results in the prevention or improvement of PTSD symptoms.29,31
Continue to: Glucocorticoid receptor agonists
Glucocorticoid receptor agonists. In a very small study, low-dose cortisol decreased the severity of traumatic memory (consolidation phase).32 Glucocorticoid receptor agonists can also diminish memory retrieval (reconsolidation phase) through intrusive thoughts and flashbacks.29
Anticonvulsants, benzodiazepines, and antipsychotics
These medications have had a limited role in the treatment of PTSD.26,29
Future directions: Preventive treatments
Because PTSD has a profound impact on an individual’s quality of life and the development of other illnesses, there is strong interest in finding treatments that can prevent PTSD. Based on limited evidence primarily from animal studies, some researchers have suggested that certain agents may someday be helpful for PTSD prevention29:
Glucocorticoid antagonists such as corticotropin-releasing factor 1 (CRF1) antagonists or cholecystokinin 2 (CCK2) receptor antagonists might promote resilience to stress by inhibiting the HPA axis and influencing the amygdala by decreasing fear conditioning, as observed in animal models. Similarly, in animal models, CRF1 and CCK2 are predicted to decrease memory consolidation in response to exposure to stress.
Adrenoceptor antagonists and agonists also might have a role in preventive treatment, but the evidence is scarce. Prazosin, an alpha-1 adrenoceptor antagonist, was ineffective in animal models.29,31 Propranolol, a beta-adrenoceptor blocker, has had mixed results but can decrease trauma-induced physiological arousal when administered soon after exposure.29
Continue to: N-methyl-
N-methyl-
Bottom Line
Adverse childhood experiences (ACEs) are strong predictors for the development of posttraumatic stress disorder (PTSD) and other mental health or medical issues in late adolescence and adulthood. Experiencing a higher number of ACEs increases the risk of developing PTSD as an adult. Timely psychotherapeutic and pharmacologic interventions can help limit symptoms and reduce the severity of PTSD.
Related Resources
- Smith P, Dalglesih T, Meiser-Stedman R. Practitioner review: posttraumatic stress disorder and its treatment in children and adolescents. J Child Psychol Psychiatry. 2019;60(5):500-515.
- North CS, Hong BA, Downs DL. PTSD: a systematic approach to diagnosis and treatment. Current Psychiatry 2018;17(4):35-43.
Drug Brand Names
Duloxetine • Cymbalta
Fluoxetine • Prozac
Mirtazapine • Remeron
Paroxetine • Paxil
Prazosin • Minipress
Propranolol • Inderal, Pronol
Sertraline • Zoloft
Venlafaxine • Effexor
1. Centers for Disease Control and Prevention. Preventing adverse childhood experiences. Published April 3, 2020. Accessed January 26, 2021. https://www.cdc.gov/violenceprevention/childabuseandneglect/aces/fastfact.html
2. Kessler RC, McLaughlin KA, Green JG, et al. Childhood adversities and adult psychopathology in the WHO world mental health surveys. Br J Psychiatry. 2010;197:378-385.
3. Norman RE, Byambaa M, De R, et al. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine. 2012;9(11):e1001349. doi: 10.1371/journal.pmed.1001349
4. Spertus IL, Yehuda R, Wong CM, et al. Childhood emotional abuse and neglect as predictors of psychological and physical symptoms in women presenting to a primary care practice. Child Abuse Negl. 2003;27(11):1247-1258.
5. Glück TM, Knefel M, Lueger-Schuster B. A network analysis of anger, shame, proposed ICD-11 post-traumatic stress disorder, and different types of childhood trauma in foster care settings in a sample of adult survivors. Eur J Psychotraumatol. 2017;8(suppl 3):1372543. doi: 10.1080/20008198.2017.1372543
6. Edwards VJ, Holden GW, Felitti VJ, et al. Relationship between multiple forms of childhood maltreatment and adult mental health in community respondents: results from the adverse childhood experiences study. Am J Psychiatry. 2003;160:1453-1460.
7. Sareen J. Posttraumatic stress disorder in adults: epidemiology, pathophysiology, clinical manifestations, course, assessment, and diagnosis. UpToDate. Updated December 3, 2020. Accessed January 26, 2021. https://www.uptodate.com/contents/posttraumatic-stress-disorder-in-adults-epidemiology-pathophysiology-clinical-manifestations-course-assessment-and-diagnosis
8. Widom CS. Posttraumatic stress disorder in abused and neglected children grown up. Am J Psychiatry. 1999:156;1223-1229.
9. Rutter M. Psychosocial resilience and protective mechanisms. Am J Orthopsychiatry. 1987;57(3):316-331.
10. Ahern NR, Kiehl EM, Sole ML, et al. A review of instruments measuring resilience. Issues Compr Pediatr Nurs. 2006;29(2):103-125.
11. Zimmerman MA. Resiliency theory: a strengths-based approach to research and practice for adolescent health. Health Educ Behav. 2013;40(4):381-383.
12. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76-82.
13. Munoz RT, Hanks H, Hellman CM. Hope and resilience as distinct contributors to psychological flourishing among childhood trauma survivors. Traumatology. 2020;26(2):177-184.
14. Baxter MA, Hemming EJ, McIntosh HC, et al. Exploring the relationship between adverse childhood experiences and hope. J Child Sex Abus. 2017;26(8):948-956.
15. Hellman CM, Gwinn C. Camp HOPE as an intervention for children exposed to domestic violence: a program evaluation of hope, and strength of character. Child Adolesc Soc Work J. 2017;34:269-276.
16. Bracha HS, Garcia-Rill E, Mrak RE, et al. Postmortem locus coeruleus neuron count in three American veterans with probable or possible war-related PTSD. J Neuropsychiatry Clin Neurosci. 2005;17(4):503-9.
17. de Lange GM. Understanding the cellular and molecular alterations in PTSD brains: the necessity of post-mortem brain tissue. Eur J Psychotraumatol. 2017;8(1):1341824. doi: 10.1080/20008198.2017.1341824
18. Zunszain PA, Anacker C, Cattaneo A, et al. Glucocorticoids, cytokines and brain abnormalities in depression. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(3):722-729.
19. Greeson JKP, Briggs EC, Kisiel CL, et al. Complex trauma and mental health in children and adolescents placed in foster care: findings from the national child traumatic stress network. Child Welfare. 2011;90(6):91-108.
20. Diagnostic and statistical manual of mental disorders, 5th ed. American Psychiatric Association; 2013.
21. American Psychological Association. PTSD assessment instruments. Updated September 26, 2018. Accessed January 27, 2021. https://www.apa.org/ptsd-guideline/assessment/
22. Bellis MA, Hughes K, Ford K, et al. Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: a systematic review and meta-analysis. Lancet Public Health. 2019;4(10):e517-e528. doi: 10.1016/S2468-2667(19)30145-8
23. Mullen PE, Martin JL, Anderson JC, et al. Childhood sexual abuse and mental health in adult life. Br J Psychiatry. 1993;163:721-732.
24. Kendler KS, Bulik CM, Silberg J, et al. Childhood sexual abuse and adult psychiatric and substance use disorders in women. An epidemiological and cotwin control analysis. Arch Gen Psychiatry. 2000;57(10):953-959.
25. Chard KM, Gilman R. Counseling trauma victims: 4 brief therapies meet the test. Current Psychiatry. 2005;4(8):50,55-58,61-62.
26. Guideline Development Panel for the Treatment of PTSD in Adults, American Psychological Association. Summary of the clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults. American Psychol. 2019;74(5):596-607.
27. American Psychological Association. Clinical practice guideline for the treatment of posttraumatic stress disorder. PTSD treatments. Updated June 2020. Accessed January 27, 2021. https://www.apa.org/ptsd-guideline/treatments/
28. Kip KE, Elk CA, Sullivan KL, et al. Brief treatment of symptoms of post-traumatic stress disorder (PTSD) by use of accelerated resolution therapy (ART(®)). Behav Sci (Basel). 2012;2(2):115-134.
29. Steckler T, Risbrough V. Pharmacological treatment of PTSD - established and new approaches. Neuropharmacology. 2012;62(2):617-627.
30. Davidson JR, Connor KM, Hertzberg MA, et al. Maintenance therapy with fluoxetine in posttraumatic stress disorder: a placebo-controlled discontinuation study. J Clin Psychopharmacol. 2005;25(2):166-169.
31. Benedek DM, Friedman MJ, Zatzick D, et al. Guideline watch (March 2009): Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Focus. 2009;7(2):204-213.
32. Aerni A, Traber R, Hock C, et al. Low-dose cortisol for symptoms of posttraumatic stress disorder. Am J Psychiat. 2004;161(8):1488-1490.
33. McGhee LL, Maani CV, Garza TH, et al. The correlation between ketamine and posttraumatic stress disorder in burned service members. J Trauma. 2008;64(2 suppl):S195-S198. doi: 10.1097/TA.0b013e318160ba1d
1. Centers for Disease Control and Prevention. Preventing adverse childhood experiences. Published April 3, 2020. Accessed January 26, 2021. https://www.cdc.gov/violenceprevention/childabuseandneglect/aces/fastfact.html
2. Kessler RC, McLaughlin KA, Green JG, et al. Childhood adversities and adult psychopathology in the WHO world mental health surveys. Br J Psychiatry. 2010;197:378-385.
3. Norman RE, Byambaa M, De R, et al. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine. 2012;9(11):e1001349. doi: 10.1371/journal.pmed.1001349
4. Spertus IL, Yehuda R, Wong CM, et al. Childhood emotional abuse and neglect as predictors of psychological and physical symptoms in women presenting to a primary care practice. Child Abuse Negl. 2003;27(11):1247-1258.
5. Glück TM, Knefel M, Lueger-Schuster B. A network analysis of anger, shame, proposed ICD-11 post-traumatic stress disorder, and different types of childhood trauma in foster care settings in a sample of adult survivors. Eur J Psychotraumatol. 2017;8(suppl 3):1372543. doi: 10.1080/20008198.2017.1372543
6. Edwards VJ, Holden GW, Felitti VJ, et al. Relationship between multiple forms of childhood maltreatment and adult mental health in community respondents: results from the adverse childhood experiences study. Am J Psychiatry. 2003;160:1453-1460.
7. Sareen J. Posttraumatic stress disorder in adults: epidemiology, pathophysiology, clinical manifestations, course, assessment, and diagnosis. UpToDate. Updated December 3, 2020. Accessed January 26, 2021. https://www.uptodate.com/contents/posttraumatic-stress-disorder-in-adults-epidemiology-pathophysiology-clinical-manifestations-course-assessment-and-diagnosis
8. Widom CS. Posttraumatic stress disorder in abused and neglected children grown up. Am J Psychiatry. 1999:156;1223-1229.
9. Rutter M. Psychosocial resilience and protective mechanisms. Am J Orthopsychiatry. 1987;57(3):316-331.
10. Ahern NR, Kiehl EM, Sole ML, et al. A review of instruments measuring resilience. Issues Compr Pediatr Nurs. 2006;29(2):103-125.
11. Zimmerman MA. Resiliency theory: a strengths-based approach to research and practice for adolescent health. Health Educ Behav. 2013;40(4):381-383.
12. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76-82.
13. Munoz RT, Hanks H, Hellman CM. Hope and resilience as distinct contributors to psychological flourishing among childhood trauma survivors. Traumatology. 2020;26(2):177-184.
14. Baxter MA, Hemming EJ, McIntosh HC, et al. Exploring the relationship between adverse childhood experiences and hope. J Child Sex Abus. 2017;26(8):948-956.
15. Hellman CM, Gwinn C. Camp HOPE as an intervention for children exposed to domestic violence: a program evaluation of hope, and strength of character. Child Adolesc Soc Work J. 2017;34:269-276.
16. Bracha HS, Garcia-Rill E, Mrak RE, et al. Postmortem locus coeruleus neuron count in three American veterans with probable or possible war-related PTSD. J Neuropsychiatry Clin Neurosci. 2005;17(4):503-9.
17. de Lange GM. Understanding the cellular and molecular alterations in PTSD brains: the necessity of post-mortem brain tissue. Eur J Psychotraumatol. 2017;8(1):1341824. doi: 10.1080/20008198.2017.1341824
18. Zunszain PA, Anacker C, Cattaneo A, et al. Glucocorticoids, cytokines and brain abnormalities in depression. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(3):722-729.
19. Greeson JKP, Briggs EC, Kisiel CL, et al. Complex trauma and mental health in children and adolescents placed in foster care: findings from the national child traumatic stress network. Child Welfare. 2011;90(6):91-108.
20. Diagnostic and statistical manual of mental disorders, 5th ed. American Psychiatric Association; 2013.
21. American Psychological Association. PTSD assessment instruments. Updated September 26, 2018. Accessed January 27, 2021. https://www.apa.org/ptsd-guideline/assessment/
22. Bellis MA, Hughes K, Ford K, et al. Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: a systematic review and meta-analysis. Lancet Public Health. 2019;4(10):e517-e528. doi: 10.1016/S2468-2667(19)30145-8
23. Mullen PE, Martin JL, Anderson JC, et al. Childhood sexual abuse and mental health in adult life. Br J Psychiatry. 1993;163:721-732.
24. Kendler KS, Bulik CM, Silberg J, et al. Childhood sexual abuse and adult psychiatric and substance use disorders in women. An epidemiological and cotwin control analysis. Arch Gen Psychiatry. 2000;57(10):953-959.
25. Chard KM, Gilman R. Counseling trauma victims: 4 brief therapies meet the test. Current Psychiatry. 2005;4(8):50,55-58,61-62.
26. Guideline Development Panel for the Treatment of PTSD in Adults, American Psychological Association. Summary of the clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults. American Psychol. 2019;74(5):596-607.
27. American Psychological Association. Clinical practice guideline for the treatment of posttraumatic stress disorder. PTSD treatments. Updated June 2020. Accessed January 27, 2021. https://www.apa.org/ptsd-guideline/treatments/
28. Kip KE, Elk CA, Sullivan KL, et al. Brief treatment of symptoms of post-traumatic stress disorder (PTSD) by use of accelerated resolution therapy (ART(®)). Behav Sci (Basel). 2012;2(2):115-134.
29. Steckler T, Risbrough V. Pharmacological treatment of PTSD - established and new approaches. Neuropharmacology. 2012;62(2):617-627.
30. Davidson JR, Connor KM, Hertzberg MA, et al. Maintenance therapy with fluoxetine in posttraumatic stress disorder: a placebo-controlled discontinuation study. J Clin Psychopharmacol. 2005;25(2):166-169.
31. Benedek DM, Friedman MJ, Zatzick D, et al. Guideline watch (March 2009): Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Focus. 2009;7(2):204-213.
32. Aerni A, Traber R, Hock C, et al. Low-dose cortisol for symptoms of posttraumatic stress disorder. Am J Psychiat. 2004;161(8):1488-1490.
33. McGhee LL, Maani CV, Garza TH, et al. The correlation between ketamine and posttraumatic stress disorder in burned service members. J Trauma. 2008;64(2 suppl):S195-S198. doi: 10.1097/TA.0b013e318160ba1d

PTSD prevalent in survivors of severe COVID-19
Posttraumatic stress disorder may occur in up to a third of patients who recover from severe COVID-19 infection, new research suggests.
A study of more than 300 patients who presented to the emergency department with the virus showed a 30.2% prevalence for PTSD 30-120 days after COVID recovery.
or having persistent medical symptoms after hospitalization.
Additional diagnoses, such as depressive and hypomanic episodes and generalized anxiety disorder (GAD), were also present in some of the survivors.
“Previous coronavirus epidemics were associated with PTSD diagnoses in postillness stages, with meta-analytic findings indicating a prevalence of 32.2%,” write the investigators, led by Delfina Janiri, MD, department of psychiatry, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome.
However, data focused specifically on COVID-19 have been “piecemeal,” they add.
The findings were published online Feb. 18 in a research letter in JAMA Psychiatry.
A traumatic event
From April to October 2020, the researchers assessed 381 consecutive patients (100% white; 56.4% men; mean age, 55.3 years) who presented to the ED and subsequently participated in a health check at the Fondazione Policlinico Universitario Agostino Gemelli.
The mean length of stay for the 309 patients hospitalized with severe COVID-19 was 18.4 days.
Results showed that 115 participants (30.2%) had PTSD, based on DSM-5 criteria, and 55.7% of the women had the disorder. Additional diagnoses found in the full patient population included:
- Depressive episodes (17.3%).
- GAD (7%).
- Hypomanic episodes (0.7%).
- Psychotic disorders (0.2%).
Patients with PTSD had higher rates than those without PTSD of a previous history of psychiatric disorders (34.8% vs. 20.7%; P = .003) and of delirium or agitation during hospitalization, as assessed with the Confusion Assessment Method (16.5% vs. 6.4%; P = .002).
In addition, 62.6% of those with PTSD had three or more persistent COVID-19 symptoms vs. 37.2% of their counterparts without PTSD (P < .001).
After logistic regression analyses, significant factors associated with a PTSD diagnosis were persistent medical symptoms (P = .002), delirium or agitation (P = .02), and being female (P = .02).
The investigators note that their results are “in line” with findings reported in research examining other traumatic events. This includes about 30% of Hurricane Katrina survivors who experienced PTSD, as did around 25% of survivors of the 2011 “Great Japan Earthquake and Tsunami.”
Study limitations cited include the “relatively small” size of the patient population, that it focused on only one participating center, and that it didn’t include a control group of non-COVID patients who reported to the ED.
“Further longitudinal studies are needed to tailor therapeutic interventions and prevention strategies,” the researchers write.
Dr. Janiri and four of the five other authors have disclosed no relevant financial relationships. The other author, Gabriele Sani, MD, reported having received personal fees from Angelini Spa, Janssen, and Lundbeck outside the submitted work.
A version of this article first appeared on Medscape.com.
Posttraumatic stress disorder may occur in up to a third of patients who recover from severe COVID-19 infection, new research suggests.
A study of more than 300 patients who presented to the emergency department with the virus showed a 30.2% prevalence for PTSD 30-120 days after COVID recovery.
or having persistent medical symptoms after hospitalization.
Additional diagnoses, such as depressive and hypomanic episodes and generalized anxiety disorder (GAD), were also present in some of the survivors.
“Previous coronavirus epidemics were associated with PTSD diagnoses in postillness stages, with meta-analytic findings indicating a prevalence of 32.2%,” write the investigators, led by Delfina Janiri, MD, department of psychiatry, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome.
However, data focused specifically on COVID-19 have been “piecemeal,” they add.
The findings were published online Feb. 18 in a research letter in JAMA Psychiatry.
A traumatic event
From April to October 2020, the researchers assessed 381 consecutive patients (100% white; 56.4% men; mean age, 55.3 years) who presented to the ED and subsequently participated in a health check at the Fondazione Policlinico Universitario Agostino Gemelli.
The mean length of stay for the 309 patients hospitalized with severe COVID-19 was 18.4 days.
Results showed that 115 participants (30.2%) had PTSD, based on DSM-5 criteria, and 55.7% of the women had the disorder. Additional diagnoses found in the full patient population included:
- Depressive episodes (17.3%).
- GAD (7%).
- Hypomanic episodes (0.7%).
- Psychotic disorders (0.2%).
Patients with PTSD had higher rates than those without PTSD of a previous history of psychiatric disorders (34.8% vs. 20.7%; P = .003) and of delirium or agitation during hospitalization, as assessed with the Confusion Assessment Method (16.5% vs. 6.4%; P = .002).
In addition, 62.6% of those with PTSD had three or more persistent COVID-19 symptoms vs. 37.2% of their counterparts without PTSD (P < .001).
After logistic regression analyses, significant factors associated with a PTSD diagnosis were persistent medical symptoms (P = .002), delirium or agitation (P = .02), and being female (P = .02).
The investigators note that their results are “in line” with findings reported in research examining other traumatic events. This includes about 30% of Hurricane Katrina survivors who experienced PTSD, as did around 25% of survivors of the 2011 “Great Japan Earthquake and Tsunami.”
Study limitations cited include the “relatively small” size of the patient population, that it focused on only one participating center, and that it didn’t include a control group of non-COVID patients who reported to the ED.
“Further longitudinal studies are needed to tailor therapeutic interventions and prevention strategies,” the researchers write.
Dr. Janiri and four of the five other authors have disclosed no relevant financial relationships. The other author, Gabriele Sani, MD, reported having received personal fees from Angelini Spa, Janssen, and Lundbeck outside the submitted work.
A version of this article first appeared on Medscape.com.
Posttraumatic stress disorder may occur in up to a third of patients who recover from severe COVID-19 infection, new research suggests.
A study of more than 300 patients who presented to the emergency department with the virus showed a 30.2% prevalence for PTSD 30-120 days after COVID recovery.
or having persistent medical symptoms after hospitalization.
Additional diagnoses, such as depressive and hypomanic episodes and generalized anxiety disorder (GAD), were also present in some of the survivors.
“Previous coronavirus epidemics were associated with PTSD diagnoses in postillness stages, with meta-analytic findings indicating a prevalence of 32.2%,” write the investigators, led by Delfina Janiri, MD, department of psychiatry, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome.
However, data focused specifically on COVID-19 have been “piecemeal,” they add.
The findings were published online Feb. 18 in a research letter in JAMA Psychiatry.
A traumatic event
From April to October 2020, the researchers assessed 381 consecutive patients (100% white; 56.4% men; mean age, 55.3 years) who presented to the ED and subsequently participated in a health check at the Fondazione Policlinico Universitario Agostino Gemelli.
The mean length of stay for the 309 patients hospitalized with severe COVID-19 was 18.4 days.
Results showed that 115 participants (30.2%) had PTSD, based on DSM-5 criteria, and 55.7% of the women had the disorder. Additional diagnoses found in the full patient population included:
- Depressive episodes (17.3%).
- GAD (7%).
- Hypomanic episodes (0.7%).
- Psychotic disorders (0.2%).
Patients with PTSD had higher rates than those without PTSD of a previous history of psychiatric disorders (34.8% vs. 20.7%; P = .003) and of delirium or agitation during hospitalization, as assessed with the Confusion Assessment Method (16.5% vs. 6.4%; P = .002).
In addition, 62.6% of those with PTSD had three or more persistent COVID-19 symptoms vs. 37.2% of their counterparts without PTSD (P < .001).
After logistic regression analyses, significant factors associated with a PTSD diagnosis were persistent medical symptoms (P = .002), delirium or agitation (P = .02), and being female (P = .02).
The investigators note that their results are “in line” with findings reported in research examining other traumatic events. This includes about 30% of Hurricane Katrina survivors who experienced PTSD, as did around 25% of survivors of the 2011 “Great Japan Earthquake and Tsunami.”
Study limitations cited include the “relatively small” size of the patient population, that it focused on only one participating center, and that it didn’t include a control group of non-COVID patients who reported to the ED.
“Further longitudinal studies are needed to tailor therapeutic interventions and prevention strategies,” the researchers write.
Dr. Janiri and four of the five other authors have disclosed no relevant financial relationships. The other author, Gabriele Sani, MD, reported having received personal fees from Angelini Spa, Janssen, and Lundbeck outside the submitted work.
A version of this article first appeared on Medscape.com.