User login
gambling
compulsive behaviors
ammunition
assault rifle
black jack
Boko Haram
bondage
child abuse
cocaine
Daech
drug paraphernalia
explosion
gun
human trafficking
ISIL
ISIS
Islamic caliphate
Islamic state
mixed martial arts
MMA
molestation
national rifle association
NRA
nsfw
pedophile
pedophilia
poker
porn
pornography
psychedelic drug
recreational drug
sex slave rings
slot machine
terrorism
terrorist
Texas hold 'em
UFC
substance abuse
abuseed
abuseer
abusees
abuseing
abusely
abuses
aeolus
aeolused
aeoluser
aeoluses
aeolusing
aeolusly
aeoluss
ahole
aholeed
aholeer
aholees
aholeing
aholely
aholes
alcohol
alcoholed
alcoholer
alcoholes
alcoholing
alcoholly
alcohols
allman
allmaned
allmaner
allmanes
allmaning
allmanly
allmans
alted
altes
alting
altly
alts
analed
analer
anales
analing
anally
analprobe
analprobeed
analprobeer
analprobees
analprobeing
analprobely
analprobes
anals
anilingus
anilingused
anilinguser
anilinguses
anilingusing
anilingusly
anilinguss
anus
anused
anuser
anuses
anusing
anusly
anuss
areola
areolaed
areolaer
areolaes
areolaing
areolaly
areolas
areole
areoleed
areoleer
areolees
areoleing
areolely
areoles
arian
arianed
arianer
arianes
arianing
arianly
arians
aryan
aryaned
aryaner
aryanes
aryaning
aryanly
aryans
asiaed
asiaer
asiaes
asiaing
asialy
asias
ass
ass hole
ass lick
ass licked
ass licker
ass lickes
ass licking
ass lickly
ass licks
assbang
assbanged
assbangeded
assbangeder
assbangedes
assbangeding
assbangedly
assbangeds
assbanger
assbanges
assbanging
assbangly
assbangs
assbangsed
assbangser
assbangses
assbangsing
assbangsly
assbangss
assed
asser
asses
assesed
asseser
asseses
assesing
assesly
assess
assfuck
assfucked
assfucker
assfuckered
assfuckerer
assfuckeres
assfuckering
assfuckerly
assfuckers
assfuckes
assfucking
assfuckly
assfucks
asshat
asshated
asshater
asshates
asshating
asshatly
asshats
assholeed
assholeer
assholees
assholeing
assholely
assholes
assholesed
assholeser
assholeses
assholesing
assholesly
assholess
assing
assly
assmaster
assmastered
assmasterer
assmasteres
assmastering
assmasterly
assmasters
assmunch
assmunched
assmuncher
assmunches
assmunching
assmunchly
assmunchs
asss
asswipe
asswipeed
asswipeer
asswipees
asswipeing
asswipely
asswipes
asswipesed
asswipeser
asswipeses
asswipesing
asswipesly
asswipess
azz
azzed
azzer
azzes
azzing
azzly
azzs
babeed
babeer
babees
babeing
babely
babes
babesed
babeser
babeses
babesing
babesly
babess
ballsac
ballsaced
ballsacer
ballsaces
ballsacing
ballsack
ballsacked
ballsacker
ballsackes
ballsacking
ballsackly
ballsacks
ballsacly
ballsacs
ballsed
ballser
ballses
ballsing
ballsly
ballss
barf
barfed
barfer
barfes
barfing
barfly
barfs
bastard
bastarded
bastarder
bastardes
bastarding
bastardly
bastards
bastardsed
bastardser
bastardses
bastardsing
bastardsly
bastardss
bawdy
bawdyed
bawdyer
bawdyes
bawdying
bawdyly
bawdys
beaner
beanered
beanerer
beaneres
beanering
beanerly
beaners
beardedclam
beardedclamed
beardedclamer
beardedclames
beardedclaming
beardedclamly
beardedclams
beastiality
beastialityed
beastialityer
beastialityes
beastialitying
beastialityly
beastialitys
beatch
beatched
beatcher
beatches
beatching
beatchly
beatchs
beater
beatered
beaterer
beateres
beatering
beaterly
beaters
beered
beerer
beeres
beering
beerly
beeyotch
beeyotched
beeyotcher
beeyotches
beeyotching
beeyotchly
beeyotchs
beotch
beotched
beotcher
beotches
beotching
beotchly
beotchs
biatch
biatched
biatcher
biatches
biatching
biatchly
biatchs
big tits
big titsed
big titser
big titses
big titsing
big titsly
big titss
bigtits
bigtitsed
bigtitser
bigtitses
bigtitsing
bigtitsly
bigtitss
bimbo
bimboed
bimboer
bimboes
bimboing
bimboly
bimbos
bisexualed
bisexualer
bisexuales
bisexualing
bisexually
bisexuals
bitch
bitched
bitcheded
bitcheder
bitchedes
bitcheding
bitchedly
bitcheds
bitcher
bitches
bitchesed
bitcheser
bitcheses
bitchesing
bitchesly
bitchess
bitching
bitchly
bitchs
bitchy
bitchyed
bitchyer
bitchyes
bitchying
bitchyly
bitchys
bleached
bleacher
bleaches
bleaching
bleachly
bleachs
blow job
blow jobed
blow jober
blow jobes
blow jobing
blow jobly
blow jobs
blowed
blower
blowes
blowing
blowjob
blowjobed
blowjober
blowjobes
blowjobing
blowjobly
blowjobs
blowjobsed
blowjobser
blowjobses
blowjobsing
blowjobsly
blowjobss
blowly
blows
boink
boinked
boinker
boinkes
boinking
boinkly
boinks
bollock
bollocked
bollocker
bollockes
bollocking
bollockly
bollocks
bollocksed
bollockser
bollockses
bollocksing
bollocksly
bollockss
bollok
bolloked
bolloker
bollokes
bolloking
bollokly
bolloks
boner
bonered
bonerer
boneres
bonering
bonerly
boners
bonersed
bonerser
bonerses
bonersing
bonersly
bonerss
bong
bonged
bonger
bonges
bonging
bongly
bongs
boob
boobed
boober
boobes
boobies
boobiesed
boobieser
boobieses
boobiesing
boobiesly
boobiess
boobing
boobly
boobs
boobsed
boobser
boobses
boobsing
boobsly
boobss
booby
boobyed
boobyer
boobyes
boobying
boobyly
boobys
booger
boogered
boogerer
boogeres
boogering
boogerly
boogers
bookie
bookieed
bookieer
bookiees
bookieing
bookiely
bookies
bootee
booteeed
booteeer
booteees
booteeing
booteely
bootees
bootie
bootieed
bootieer
bootiees
bootieing
bootiely
booties
booty
bootyed
bootyer
bootyes
bootying
bootyly
bootys
boozeed
boozeer
boozees
boozeing
boozely
boozer
boozered
boozerer
boozeres
boozering
boozerly
boozers
boozes
boozy
boozyed
boozyer
boozyes
boozying
boozyly
boozys
bosomed
bosomer
bosomes
bosoming
bosomly
bosoms
bosomy
bosomyed
bosomyer
bosomyes
bosomying
bosomyly
bosomys
bugger
buggered
buggerer
buggeres
buggering
buggerly
buggers
bukkake
bukkakeed
bukkakeer
bukkakees
bukkakeing
bukkakely
bukkakes
bull shit
bull shited
bull shiter
bull shites
bull shiting
bull shitly
bull shits
bullshit
bullshited
bullshiter
bullshites
bullshiting
bullshitly
bullshits
bullshitsed
bullshitser
bullshitses
bullshitsing
bullshitsly
bullshitss
bullshitted
bullshitteded
bullshitteder
bullshittedes
bullshitteding
bullshittedly
bullshitteds
bullturds
bullturdsed
bullturdser
bullturdses
bullturdsing
bullturdsly
bullturdss
bung
bunged
bunger
bunges
bunging
bungly
bungs
busty
bustyed
bustyer
bustyes
bustying
bustyly
bustys
butt
butt fuck
butt fucked
butt fucker
butt fuckes
butt fucking
butt fuckly
butt fucks
butted
buttes
buttfuck
buttfucked
buttfucker
buttfuckered
buttfuckerer
buttfuckeres
buttfuckering
buttfuckerly
buttfuckers
buttfuckes
buttfucking
buttfuckly
buttfucks
butting
buttly
buttplug
buttpluged
buttpluger
buttpluges
buttpluging
buttplugly
buttplugs
butts
caca
cacaed
cacaer
cacaes
cacaing
cacaly
cacas
cahone
cahoneed
cahoneer
cahonees
cahoneing
cahonely
cahones
cameltoe
cameltoeed
cameltoeer
cameltoees
cameltoeing
cameltoely
cameltoes
carpetmuncher
carpetmunchered
carpetmuncherer
carpetmuncheres
carpetmunchering
carpetmuncherly
carpetmunchers
cawk
cawked
cawker
cawkes
cawking
cawkly
cawks
chinc
chinced
chincer
chinces
chincing
chincly
chincs
chincsed
chincser
chincses
chincsing
chincsly
chincss
chink
chinked
chinker
chinkes
chinking
chinkly
chinks
chode
chodeed
chodeer
chodees
chodeing
chodely
chodes
chodesed
chodeser
chodeses
chodesing
chodesly
chodess
clit
clited
cliter
clites
cliting
clitly
clitoris
clitorised
clitoriser
clitorises
clitorising
clitorisly
clitoriss
clitorus
clitorused
clitoruser
clitoruses
clitorusing
clitorusly
clitoruss
clits
clitsed
clitser
clitses
clitsing
clitsly
clitss
clitty
clittyed
clittyer
clittyes
clittying
clittyly
clittys
cocain
cocaine
cocained
cocaineed
cocaineer
cocainees
cocaineing
cocainely
cocainer
cocaines
cocaining
cocainly
cocains
cock
cock sucker
cock suckered
cock suckerer
cock suckeres
cock suckering
cock suckerly
cock suckers
cockblock
cockblocked
cockblocker
cockblockes
cockblocking
cockblockly
cockblocks
cocked
cocker
cockes
cockholster
cockholstered
cockholsterer
cockholsteres
cockholstering
cockholsterly
cockholsters
cocking
cockknocker
cockknockered
cockknockerer
cockknockeres
cockknockering
cockknockerly
cockknockers
cockly
cocks
cocksed
cockser
cockses
cocksing
cocksly
cocksmoker
cocksmokered
cocksmokerer
cocksmokeres
cocksmokering
cocksmokerly
cocksmokers
cockss
cocksucker
cocksuckered
cocksuckerer
cocksuckeres
cocksuckering
cocksuckerly
cocksuckers
coital
coitaled
coitaler
coitales
coitaling
coitally
coitals
commie
commieed
commieer
commiees
commieing
commiely
commies
condomed
condomer
condomes
condoming
condomly
condoms
coon
cooned
cooner
coones
cooning
coonly
coons
coonsed
coonser
coonses
coonsing
coonsly
coonss
corksucker
corksuckered
corksuckerer
corksuckeres
corksuckering
corksuckerly
corksuckers
cracked
crackwhore
crackwhoreed
crackwhoreer
crackwhorees
crackwhoreing
crackwhorely
crackwhores
crap
craped
craper
crapes
craping
craply
crappy
crappyed
crappyer
crappyes
crappying
crappyly
crappys
cum
cumed
cumer
cumes
cuming
cumly
cummin
cummined
cumminer
cummines
cumming
cumminged
cumminger
cumminges
cumminging
cummingly
cummings
cummining
cumminly
cummins
cums
cumshot
cumshoted
cumshoter
cumshotes
cumshoting
cumshotly
cumshots
cumshotsed
cumshotser
cumshotses
cumshotsing
cumshotsly
cumshotss
cumslut
cumsluted
cumsluter
cumslutes
cumsluting
cumslutly
cumsluts
cumstain
cumstained
cumstainer
cumstaines
cumstaining
cumstainly
cumstains
cunilingus
cunilingused
cunilinguser
cunilinguses
cunilingusing
cunilingusly
cunilinguss
cunnilingus
cunnilingused
cunnilinguser
cunnilinguses
cunnilingusing
cunnilingusly
cunnilinguss
cunny
cunnyed
cunnyer
cunnyes
cunnying
cunnyly
cunnys
cunt
cunted
cunter
cuntes
cuntface
cuntfaceed
cuntfaceer
cuntfacees
cuntfaceing
cuntfacely
cuntfaces
cunthunter
cunthuntered
cunthunterer
cunthunteres
cunthuntering
cunthunterly
cunthunters
cunting
cuntlick
cuntlicked
cuntlicker
cuntlickered
cuntlickerer
cuntlickeres
cuntlickering
cuntlickerly
cuntlickers
cuntlickes
cuntlicking
cuntlickly
cuntlicks
cuntly
cunts
cuntsed
cuntser
cuntses
cuntsing
cuntsly
cuntss
dago
dagoed
dagoer
dagoes
dagoing
dagoly
dagos
dagosed
dagoser
dagoses
dagosing
dagosly
dagoss
dammit
dammited
dammiter
dammites
dammiting
dammitly
dammits
damn
damned
damneded
damneder
damnedes
damneding
damnedly
damneds
damner
damnes
damning
damnit
damnited
damniter
damnites
damniting
damnitly
damnits
damnly
damns
dick
dickbag
dickbaged
dickbager
dickbages
dickbaging
dickbagly
dickbags
dickdipper
dickdippered
dickdipperer
dickdipperes
dickdippering
dickdipperly
dickdippers
dicked
dicker
dickes
dickface
dickfaceed
dickfaceer
dickfacees
dickfaceing
dickfacely
dickfaces
dickflipper
dickflippered
dickflipperer
dickflipperes
dickflippering
dickflipperly
dickflippers
dickhead
dickheaded
dickheader
dickheades
dickheading
dickheadly
dickheads
dickheadsed
dickheadser
dickheadses
dickheadsing
dickheadsly
dickheadss
dicking
dickish
dickished
dickisher
dickishes
dickishing
dickishly
dickishs
dickly
dickripper
dickrippered
dickripperer
dickripperes
dickrippering
dickripperly
dickrippers
dicks
dicksipper
dicksippered
dicksipperer
dicksipperes
dicksippering
dicksipperly
dicksippers
dickweed
dickweeded
dickweeder
dickweedes
dickweeding
dickweedly
dickweeds
dickwhipper
dickwhippered
dickwhipperer
dickwhipperes
dickwhippering
dickwhipperly
dickwhippers
dickzipper
dickzippered
dickzipperer
dickzipperes
dickzippering
dickzipperly
dickzippers
diddle
diddleed
diddleer
diddlees
diddleing
diddlely
diddles
dike
dikeed
dikeer
dikees
dikeing
dikely
dikes
dildo
dildoed
dildoer
dildoes
dildoing
dildoly
dildos
dildosed
dildoser
dildoses
dildosing
dildosly
dildoss
diligaf
diligafed
diligafer
diligafes
diligafing
diligafly
diligafs
dillweed
dillweeded
dillweeder
dillweedes
dillweeding
dillweedly
dillweeds
dimwit
dimwited
dimwiter
dimwites
dimwiting
dimwitly
dimwits
dingle
dingleed
dingleer
dinglees
dingleing
dinglely
dingles
dipship
dipshiped
dipshiper
dipshipes
dipshiping
dipshiply
dipships
dizzyed
dizzyer
dizzyes
dizzying
dizzyly
dizzys
doggiestyleed
doggiestyleer
doggiestylees
doggiestyleing
doggiestylely
doggiestyles
doggystyleed
doggystyleer
doggystylees
doggystyleing
doggystylely
doggystyles
dong
donged
donger
donges
donging
dongly
dongs
doofus
doofused
doofuser
doofuses
doofusing
doofusly
doofuss
doosh
dooshed
doosher
dooshes
dooshing
dooshly
dooshs
dopeyed
dopeyer
dopeyes
dopeying
dopeyly
dopeys
douchebag
douchebaged
douchebager
douchebages
douchebaging
douchebagly
douchebags
douchebagsed
douchebagser
douchebagses
douchebagsing
douchebagsly
douchebagss
doucheed
doucheer
douchees
doucheing
douchely
douches
douchey
doucheyed
doucheyer
doucheyes
doucheying
doucheyly
doucheys
drunk
drunked
drunker
drunkes
drunking
drunkly
drunks
dumass
dumassed
dumasser
dumasses
dumassing
dumassly
dumasss
dumbass
dumbassed
dumbasser
dumbasses
dumbassesed
dumbasseser
dumbasseses
dumbassesing
dumbassesly
dumbassess
dumbassing
dumbassly
dumbasss
dummy
dummyed
dummyer
dummyes
dummying
dummyly
dummys
dyke
dykeed
dykeer
dykees
dykeing
dykely
dykes
dykesed
dykeser
dykeses
dykesing
dykesly
dykess
erotic
eroticed
eroticer
erotices
eroticing
eroticly
erotics
extacy
extacyed
extacyer
extacyes
extacying
extacyly
extacys
extasy
extasyed
extasyer
extasyes
extasying
extasyly
extasys
fack
facked
facker
fackes
facking
fackly
facks
fag
faged
fager
fages
fagg
fagged
faggeded
faggeder
faggedes
faggeding
faggedly
faggeds
fagger
fagges
fagging
faggit
faggited
faggiter
faggites
faggiting
faggitly
faggits
faggly
faggot
faggoted
faggoter
faggotes
faggoting
faggotly
faggots
faggs
faging
fagly
fagot
fagoted
fagoter
fagotes
fagoting
fagotly
fagots
fags
fagsed
fagser
fagses
fagsing
fagsly
fagss
faig
faiged
faiger
faiges
faiging
faigly
faigs
faigt
faigted
faigter
faigtes
faigting
faigtly
faigts
fannybandit
fannybandited
fannybanditer
fannybandites
fannybanditing
fannybanditly
fannybandits
farted
farter
fartes
farting
fartknocker
fartknockered
fartknockerer
fartknockeres
fartknockering
fartknockerly
fartknockers
fartly
farts
felch
felched
felcher
felchered
felcherer
felcheres
felchering
felcherly
felchers
felches
felching
felchinged
felchinger
felchinges
felchinging
felchingly
felchings
felchly
felchs
fellate
fellateed
fellateer
fellatees
fellateing
fellately
fellates
fellatio
fellatioed
fellatioer
fellatioes
fellatioing
fellatioly
fellatios
feltch
feltched
feltcher
feltchered
feltcherer
feltcheres
feltchering
feltcherly
feltchers
feltches
feltching
feltchly
feltchs
feom
feomed
feomer
feomes
feoming
feomly
feoms
fisted
fisteded
fisteder
fistedes
fisteding
fistedly
fisteds
fisting
fistinged
fistinger
fistinges
fistinging
fistingly
fistings
fisty
fistyed
fistyer
fistyes
fistying
fistyly
fistys
floozy
floozyed
floozyer
floozyes
floozying
floozyly
floozys
foad
foaded
foader
foades
foading
foadly
foads
fondleed
fondleer
fondlees
fondleing
fondlely
fondles
foobar
foobared
foobarer
foobares
foobaring
foobarly
foobars
freex
freexed
freexer
freexes
freexing
freexly
freexs
frigg
frigga
friggaed
friggaer
friggaes
friggaing
friggaly
friggas
frigged
frigger
frigges
frigging
friggly
friggs
fubar
fubared
fubarer
fubares
fubaring
fubarly
fubars
fuck
fuckass
fuckassed
fuckasser
fuckasses
fuckassing
fuckassly
fuckasss
fucked
fuckeded
fuckeder
fuckedes
fuckeding
fuckedly
fuckeds
fucker
fuckered
fuckerer
fuckeres
fuckering
fuckerly
fuckers
fuckes
fuckface
fuckfaceed
fuckfaceer
fuckfacees
fuckfaceing
fuckfacely
fuckfaces
fuckin
fuckined
fuckiner
fuckines
fucking
fuckinged
fuckinger
fuckinges
fuckinging
fuckingly
fuckings
fuckining
fuckinly
fuckins
fuckly
fucknugget
fucknuggeted
fucknuggeter
fucknuggetes
fucknuggeting
fucknuggetly
fucknuggets
fucknut
fucknuted
fucknuter
fucknutes
fucknuting
fucknutly
fucknuts
fuckoff
fuckoffed
fuckoffer
fuckoffes
fuckoffing
fuckoffly
fuckoffs
fucks
fucksed
fuckser
fuckses
fucksing
fucksly
fuckss
fucktard
fucktarded
fucktarder
fucktardes
fucktarding
fucktardly
fucktards
fuckup
fuckuped
fuckuper
fuckupes
fuckuping
fuckuply
fuckups
fuckwad
fuckwaded
fuckwader
fuckwades
fuckwading
fuckwadly
fuckwads
fuckwit
fuckwited
fuckwiter
fuckwites
fuckwiting
fuckwitly
fuckwits
fudgepacker
fudgepackered
fudgepackerer
fudgepackeres
fudgepackering
fudgepackerly
fudgepackers
fuk
fuked
fuker
fukes
fuking
fukly
fuks
fvck
fvcked
fvcker
fvckes
fvcking
fvckly
fvcks
fxck
fxcked
fxcker
fxckes
fxcking
fxckly
fxcks
gae
gaeed
gaeer
gaees
gaeing
gaely
gaes
gai
gaied
gaier
gaies
gaiing
gaily
gais
ganja
ganjaed
ganjaer
ganjaes
ganjaing
ganjaly
ganjas
gayed
gayer
gayes
gaying
gayly
gays
gaysed
gayser
gayses
gaysing
gaysly
gayss
gey
geyed
geyer
geyes
geying
geyly
geys
gfc
gfced
gfcer
gfces
gfcing
gfcly
gfcs
gfy
gfyed
gfyer
gfyes
gfying
gfyly
gfys
ghay
ghayed
ghayer
ghayes
ghaying
ghayly
ghays
ghey
gheyed
gheyer
gheyes
gheying
gheyly
gheys
gigolo
gigoloed
gigoloer
gigoloes
gigoloing
gigololy
gigolos
goatse
goatseed
goatseer
goatsees
goatseing
goatsely
goatses
godamn
godamned
godamner
godamnes
godamning
godamnit
godamnited
godamniter
godamnites
godamniting
godamnitly
godamnits
godamnly
godamns
goddam
goddamed
goddamer
goddames
goddaming
goddamly
goddammit
goddammited
goddammiter
goddammites
goddammiting
goddammitly
goddammits
goddamn
goddamned
goddamner
goddamnes
goddamning
goddamnly
goddamns
goddams
goldenshower
goldenshowered
goldenshowerer
goldenshoweres
goldenshowering
goldenshowerly
goldenshowers
gonad
gonaded
gonader
gonades
gonading
gonadly
gonads
gonadsed
gonadser
gonadses
gonadsing
gonadsly
gonadss
gook
gooked
gooker
gookes
gooking
gookly
gooks
gooksed
gookser
gookses
gooksing
gooksly
gookss
gringo
gringoed
gringoer
gringoes
gringoing
gringoly
gringos
gspot
gspoted
gspoter
gspotes
gspoting
gspotly
gspots
gtfo
gtfoed
gtfoer
gtfoes
gtfoing
gtfoly
gtfos
guido
guidoed
guidoer
guidoes
guidoing
guidoly
guidos
handjob
handjobed
handjober
handjobes
handjobing
handjobly
handjobs
hard on
hard oned
hard oner
hard ones
hard oning
hard only
hard ons
hardknight
hardknighted
hardknighter
hardknightes
hardknighting
hardknightly
hardknights
hebe
hebeed
hebeer
hebees
hebeing
hebely
hebes
heeb
heebed
heeber
heebes
heebing
heebly
heebs
hell
helled
heller
helles
helling
hellly
hells
hemp
hemped
hemper
hempes
hemping
hemply
hemps
heroined
heroiner
heroines
heroining
heroinly
heroins
herp
herped
herper
herpes
herpesed
herpeser
herpeses
herpesing
herpesly
herpess
herping
herply
herps
herpy
herpyed
herpyer
herpyes
herpying
herpyly
herpys
hitler
hitlered
hitlerer
hitleres
hitlering
hitlerly
hitlers
hived
hiver
hives
hiving
hivly
hivs
hobag
hobaged
hobager
hobages
hobaging
hobagly
hobags
homey
homeyed
homeyer
homeyes
homeying
homeyly
homeys
homo
homoed
homoer
homoes
homoey
homoeyed
homoeyer
homoeyes
homoeying
homoeyly
homoeys
homoing
homoly
homos
honky
honkyed
honkyer
honkyes
honkying
honkyly
honkys
hooch
hooched
hoocher
hooches
hooching
hoochly
hoochs
hookah
hookahed
hookaher
hookahes
hookahing
hookahly
hookahs
hooker
hookered
hookerer
hookeres
hookering
hookerly
hookers
hoor
hoored
hoorer
hoores
hooring
hoorly
hoors
hootch
hootched
hootcher
hootches
hootching
hootchly
hootchs
hooter
hootered
hooterer
hooteres
hootering
hooterly
hooters
hootersed
hooterser
hooterses
hootersing
hootersly
hooterss
horny
hornyed
hornyer
hornyes
hornying
hornyly
hornys
houstoned
houstoner
houstones
houstoning
houstonly
houstons
hump
humped
humpeded
humpeder
humpedes
humpeding
humpedly
humpeds
humper
humpes
humping
humpinged
humpinger
humpinges
humpinging
humpingly
humpings
humply
humps
husbanded
husbander
husbandes
husbanding
husbandly
husbands
hussy
hussyed
hussyer
hussyes
hussying
hussyly
hussys
hymened
hymener
hymenes
hymening
hymenly
hymens
inbred
inbreded
inbreder
inbredes
inbreding
inbredly
inbreds
incest
incested
incester
incestes
incesting
incestly
incests
injun
injuned
injuner
injunes
injuning
injunly
injuns
jackass
jackassed
jackasser
jackasses
jackassing
jackassly
jackasss
jackhole
jackholeed
jackholeer
jackholees
jackholeing
jackholely
jackholes
jackoff
jackoffed
jackoffer
jackoffes
jackoffing
jackoffly
jackoffs
jap
japed
japer
japes
japing
japly
japs
japsed
japser
japses
japsing
japsly
japss
jerkoff
jerkoffed
jerkoffer
jerkoffes
jerkoffing
jerkoffly
jerkoffs
jerks
jism
jismed
jismer
jismes
jisming
jismly
jisms
jiz
jized
jizer
jizes
jizing
jizly
jizm
jizmed
jizmer
jizmes
jizming
jizmly
jizms
jizs
jizz
jizzed
jizzeded
jizzeder
jizzedes
jizzeding
jizzedly
jizzeds
jizzer
jizzes
jizzing
jizzly
jizzs
junkie
junkieed
junkieer
junkiees
junkieing
junkiely
junkies
junky
junkyed
junkyer
junkyes
junkying
junkyly
junkys
kike
kikeed
kikeer
kikees
kikeing
kikely
kikes
kikesed
kikeser
kikeses
kikesing
kikesly
kikess
killed
killer
killes
killing
killly
kills
kinky
kinkyed
kinkyer
kinkyes
kinkying
kinkyly
kinkys
kkk
kkked
kkker
kkkes
kkking
kkkly
kkks
klan
klaned
klaner
klanes
klaning
klanly
klans
knobend
knobended
knobender
knobendes
knobending
knobendly
knobends
kooch
kooched
koocher
kooches
koochesed
koocheser
koocheses
koochesing
koochesly
koochess
kooching
koochly
koochs
kootch
kootched
kootcher
kootches
kootching
kootchly
kootchs
kraut
krauted
krauter
krautes
krauting
krautly
krauts
kyke
kykeed
kykeer
kykees
kykeing
kykely
kykes
lech
leched
lecher
leches
leching
lechly
lechs
leper
lepered
leperer
leperes
lepering
leperly
lepers
lesbiansed
lesbianser
lesbianses
lesbiansing
lesbiansly
lesbianss
lesbo
lesboed
lesboer
lesboes
lesboing
lesboly
lesbos
lesbosed
lesboser
lesboses
lesbosing
lesbosly
lesboss
lez
lezbianed
lezbianer
lezbianes
lezbianing
lezbianly
lezbians
lezbiansed
lezbianser
lezbianses
lezbiansing
lezbiansly
lezbianss
lezbo
lezboed
lezboer
lezboes
lezboing
lezboly
lezbos
lezbosed
lezboser
lezboses
lezbosing
lezbosly
lezboss
lezed
lezer
lezes
lezing
lezly
lezs
lezzie
lezzieed
lezzieer
lezziees
lezzieing
lezziely
lezzies
lezziesed
lezzieser
lezzieses
lezziesing
lezziesly
lezziess
lezzy
lezzyed
lezzyer
lezzyes
lezzying
lezzyly
lezzys
lmaoed
lmaoer
lmaoes
lmaoing
lmaoly
lmaos
lmfao
lmfaoed
lmfaoer
lmfaoes
lmfaoing
lmfaoly
lmfaos
loined
loiner
loines
loining
loinly
loins
loinsed
loinser
loinses
loinsing
loinsly
loinss
lubeed
lubeer
lubees
lubeing
lubely
lubes
lusty
lustyed
lustyer
lustyes
lustying
lustyly
lustys
massa
massaed
massaer
massaes
massaing
massaly
massas
masterbate
masterbateed
masterbateer
masterbatees
masterbateing
masterbately
masterbates
masterbating
masterbatinged
masterbatinger
masterbatinges
masterbatinging
masterbatingly
masterbatings
masterbation
masterbationed
masterbationer
masterbationes
masterbationing
masterbationly
masterbations
masturbate
masturbateed
masturbateer
masturbatees
masturbateing
masturbately
masturbates
masturbating
masturbatinged
masturbatinger
masturbatinges
masturbatinging
masturbatingly
masturbatings
masturbation
masturbationed
masturbationer
masturbationes
masturbationing
masturbationly
masturbations
methed
mether
methes
mething
methly
meths
militaryed
militaryer
militaryes
militarying
militaryly
militarys
mofo
mofoed
mofoer
mofoes
mofoing
mofoly
mofos
molest
molested
molester
molestes
molesting
molestly
molests
moolie
moolieed
moolieer
mooliees
moolieing
mooliely
moolies
moron
moroned
moroner
morones
moroning
moronly
morons
motherfucka
motherfuckaed
motherfuckaer
motherfuckaes
motherfuckaing
motherfuckaly
motherfuckas
motherfucker
motherfuckered
motherfuckerer
motherfuckeres
motherfuckering
motherfuckerly
motherfuckers
motherfucking
motherfuckinged
motherfuckinger
motherfuckinges
motherfuckinging
motherfuckingly
motherfuckings
mtherfucker
mtherfuckered
mtherfuckerer
mtherfuckeres
mtherfuckering
mtherfuckerly
mtherfuckers
mthrfucker
mthrfuckered
mthrfuckerer
mthrfuckeres
mthrfuckering
mthrfuckerly
mthrfuckers
mthrfucking
mthrfuckinged
mthrfuckinger
mthrfuckinges
mthrfuckinging
mthrfuckingly
mthrfuckings
muff
muffdiver
muffdivered
muffdiverer
muffdiveres
muffdivering
muffdiverly
muffdivers
muffed
muffer
muffes
muffing
muffly
muffs
murdered
murderer
murderes
murdering
murderly
murders
muthafuckaz
muthafuckazed
muthafuckazer
muthafuckazes
muthafuckazing
muthafuckazly
muthafuckazs
muthafucker
muthafuckered
muthafuckerer
muthafuckeres
muthafuckering
muthafuckerly
muthafuckers
mutherfucker
mutherfuckered
mutherfuckerer
mutherfuckeres
mutherfuckering
mutherfuckerly
mutherfuckers
mutherfucking
mutherfuckinged
mutherfuckinger
mutherfuckinges
mutherfuckinging
mutherfuckingly
mutherfuckings
muthrfucking
muthrfuckinged
muthrfuckinger
muthrfuckinges
muthrfuckinging
muthrfuckingly
muthrfuckings
nad
naded
nader
nades
nading
nadly
nads
nadsed
nadser
nadses
nadsing
nadsly
nadss
nakeded
nakeder
nakedes
nakeding
nakedly
nakeds
napalm
napalmed
napalmer
napalmes
napalming
napalmly
napalms
nappy
nappyed
nappyer
nappyes
nappying
nappyly
nappys
nazi
nazied
nazier
nazies
naziing
nazily
nazis
nazism
nazismed
nazismer
nazismes
nazisming
nazismly
nazisms
negro
negroed
negroer
negroes
negroing
negroly
negros
nigga
niggaed
niggaer
niggaes
niggah
niggahed
niggaher
niggahes
niggahing
niggahly
niggahs
niggaing
niggaly
niggas
niggased
niggaser
niggases
niggasing
niggasly
niggass
niggaz
niggazed
niggazer
niggazes
niggazing
niggazly
niggazs
nigger
niggered
niggerer
niggeres
niggering
niggerly
niggers
niggersed
niggerser
niggerses
niggersing
niggersly
niggerss
niggle
niggleed
niggleer
nigglees
niggleing
nigglely
niggles
niglet
nigleted
nigleter
nigletes
nigleting
nigletly
niglets
nimrod
nimroded
nimroder
nimrodes
nimroding
nimrodly
nimrods
ninny
ninnyed
ninnyer
ninnyes
ninnying
ninnyly
ninnys
nooky
nookyed
nookyer
nookyes
nookying
nookyly
nookys
nuccitelli
nuccitellied
nuccitellier
nuccitellies
nuccitelliing
nuccitellily
nuccitellis
nympho
nymphoed
nymphoer
nymphoes
nymphoing
nympholy
nymphos
opium
opiumed
opiumer
opiumes
opiuming
opiumly
opiums
orgies
orgiesed
orgieser
orgieses
orgiesing
orgiesly
orgiess
orgy
orgyed
orgyer
orgyes
orgying
orgyly
orgys
paddy
paddyed
paddyer
paddyes
paddying
paddyly
paddys
paki
pakied
pakier
pakies
pakiing
pakily
pakis
pantie
pantieed
pantieer
pantiees
pantieing
pantiely
panties
pantiesed
pantieser
pantieses
pantiesing
pantiesly
pantiess
panty
pantyed
pantyer
pantyes
pantying
pantyly
pantys
pastie
pastieed
pastieer
pastiees
pastieing
pastiely
pasties
pasty
pastyed
pastyer
pastyes
pastying
pastyly
pastys
pecker
peckered
peckerer
peckeres
peckering
peckerly
peckers
pedo
pedoed
pedoer
pedoes
pedoing
pedoly
pedophile
pedophileed
pedophileer
pedophilees
pedophileing
pedophilely
pedophiles
pedophilia
pedophiliac
pedophiliaced
pedophiliacer
pedophiliaces
pedophiliacing
pedophiliacly
pedophiliacs
pedophiliaed
pedophiliaer
pedophiliaes
pedophiliaing
pedophilialy
pedophilias
pedos
penial
penialed
penialer
peniales
penialing
penially
penials
penile
penileed
penileer
penilees
penileing
penilely
peniles
penis
penised
peniser
penises
penising
penisly
peniss
perversion
perversioned
perversioner
perversiones
perversioning
perversionly
perversions
peyote
peyoteed
peyoteer
peyotees
peyoteing
peyotely
peyotes
phuck
phucked
phucker
phuckes
phucking
phuckly
phucks
pillowbiter
pillowbitered
pillowbiterer
pillowbiteres
pillowbitering
pillowbiterly
pillowbiters
pimp
pimped
pimper
pimpes
pimping
pimply
pimps
pinko
pinkoed
pinkoer
pinkoes
pinkoing
pinkoly
pinkos
pissed
pisseded
pisseder
pissedes
pisseding
pissedly
pisseds
pisser
pisses
pissing
pissly
pissoff
pissoffed
pissoffer
pissoffes
pissoffing
pissoffly
pissoffs
pisss
polack
polacked
polacker
polackes
polacking
polackly
polacks
pollock
pollocked
pollocker
pollockes
pollocking
pollockly
pollocks
poon
pooned
pooner
poones
pooning
poonly
poons
poontang
poontanged
poontanger
poontanges
poontanging
poontangly
poontangs
porn
porned
porner
pornes
porning
pornly
porno
pornoed
pornoer
pornoes
pornography
pornographyed
pornographyer
pornographyes
pornographying
pornographyly
pornographys
pornoing
pornoly
pornos
porns
prick
pricked
pricker
prickes
pricking
prickly
pricks
prig
priged
priger
priges
priging
prigly
prigs
prostitute
prostituteed
prostituteer
prostitutees
prostituteing
prostitutely
prostitutes
prude
prudeed
prudeer
prudees
prudeing
prudely
prudes
punkass
punkassed
punkasser
punkasses
punkassing
punkassly
punkasss
punky
punkyed
punkyer
punkyes
punkying
punkyly
punkys
puss
pussed
pusser
pusses
pussies
pussiesed
pussieser
pussieses
pussiesing
pussiesly
pussiess
pussing
pussly
pusss
pussy
pussyed
pussyer
pussyes
pussying
pussyly
pussypounder
pussypoundered
pussypounderer
pussypounderes
pussypoundering
pussypounderly
pussypounders
pussys
puto
putoed
putoer
putoes
putoing
putoly
putos
queaf
queafed
queafer
queafes
queafing
queafly
queafs
queef
queefed
queefer
queefes
queefing
queefly
queefs
queer
queered
queerer
queeres
queering
queerly
queero
queeroed
queeroer
queeroes
queeroing
queeroly
queeros
queers
queersed
queerser
queerses
queersing
queersly
queerss
quicky
quickyed
quickyer
quickyes
quickying
quickyly
quickys
quim
quimed
quimer
quimes
quiming
quimly
quims
racy
racyed
racyer
racyes
racying
racyly
racys
rape
raped
rapeded
rapeder
rapedes
rapeding
rapedly
rapeds
rapeed
rapeer
rapees
rapeing
rapely
raper
rapered
raperer
raperes
rapering
raperly
rapers
rapes
rapist
rapisted
rapister
rapistes
rapisting
rapistly
rapists
raunch
raunched
rauncher
raunches
raunching
raunchly
raunchs
rectus
rectused
rectuser
rectuses
rectusing
rectusly
rectuss
reefer
reefered
reeferer
reeferes
reefering
reeferly
reefers
reetard
reetarded
reetarder
reetardes
reetarding
reetardly
reetards
reich
reiched
reicher
reiches
reiching
reichly
reichs
retard
retarded
retardeded
retardeder
retardedes
retardeding
retardedly
retardeds
retarder
retardes
retarding
retardly
retards
rimjob
rimjobed
rimjober
rimjobes
rimjobing
rimjobly
rimjobs
ritard
ritarded
ritarder
ritardes
ritarding
ritardly
ritards
rtard
rtarded
rtarder
rtardes
rtarding
rtardly
rtards
rum
rumed
rumer
rumes
ruming
rumly
rump
rumped
rumper
rumpes
rumping
rumply
rumprammer
rumprammered
rumprammerer
rumprammeres
rumprammering
rumprammerly
rumprammers
rumps
rums
ruski
ruskied
ruskier
ruskies
ruskiing
ruskily
ruskis
sadism
sadismed
sadismer
sadismes
sadisming
sadismly
sadisms
sadist
sadisted
sadister
sadistes
sadisting
sadistly
sadists
scag
scaged
scager
scages
scaging
scagly
scags
scantily
scantilyed
scantilyer
scantilyes
scantilying
scantilyly
scantilys
schlong
schlonged
schlonger
schlonges
schlonging
schlongly
schlongs
scrog
scroged
scroger
scroges
scroging
scrogly
scrogs
scrot
scrote
scroted
scroteed
scroteer
scrotees
scroteing
scrotely
scroter
scrotes
scroting
scrotly
scrots
scrotum
scrotumed
scrotumer
scrotumes
scrotuming
scrotumly
scrotums
scrud
scruded
scruder
scrudes
scruding
scrudly
scruds
scum
scumed
scumer
scumes
scuming
scumly
scums
seaman
seamaned
seamaner
seamanes
seamaning
seamanly
seamans
seamen
seamened
seamener
seamenes
seamening
seamenly
seamens
seduceed
seduceer
seducees
seduceing
seducely
seduces
semen
semened
semener
semenes
semening
semenly
semens
shamedame
shamedameed
shamedameer
shamedamees
shamedameing
shamedamely
shamedames
shit
shite
shiteater
shiteatered
shiteaterer
shiteateres
shiteatering
shiteaterly
shiteaters
shited
shiteed
shiteer
shitees
shiteing
shitely
shiter
shites
shitface
shitfaceed
shitfaceer
shitfacees
shitfaceing
shitfacely
shitfaces
shithead
shitheaded
shitheader
shitheades
shitheading
shitheadly
shitheads
shithole
shitholeed
shitholeer
shitholees
shitholeing
shitholely
shitholes
shithouse
shithouseed
shithouseer
shithousees
shithouseing
shithousely
shithouses
shiting
shitly
shits
shitsed
shitser
shitses
shitsing
shitsly
shitss
shitt
shitted
shitteded
shitteder
shittedes
shitteding
shittedly
shitteds
shitter
shittered
shitterer
shitteres
shittering
shitterly
shitters
shittes
shitting
shittly
shitts
shitty
shittyed
shittyer
shittyes
shittying
shittyly
shittys
shiz
shized
shizer
shizes
shizing
shizly
shizs
shooted
shooter
shootes
shooting
shootly
shoots
sissy
sissyed
sissyer
sissyes
sissying
sissyly
sissys
skag
skaged
skager
skages
skaging
skagly
skags
skank
skanked
skanker
skankes
skanking
skankly
skanks
slave
slaveed
slaveer
slavees
slaveing
slavely
slaves
sleaze
sleazeed
sleazeer
sleazees
sleazeing
sleazely
sleazes
sleazy
sleazyed
sleazyer
sleazyes
sleazying
sleazyly
sleazys
slut
slutdumper
slutdumpered
slutdumperer
slutdumperes
slutdumpering
slutdumperly
slutdumpers
sluted
sluter
slutes
sluting
slutkiss
slutkissed
slutkisser
slutkisses
slutkissing
slutkissly
slutkisss
slutly
sluts
slutsed
slutser
slutses
slutsing
slutsly
slutss
smegma
smegmaed
smegmaer
smegmaes
smegmaing
smegmaly
smegmas
smut
smuted
smuter
smutes
smuting
smutly
smuts
smutty
smuttyed
smuttyer
smuttyes
smuttying
smuttyly
smuttys
snatch
snatched
snatcher
snatches
snatching
snatchly
snatchs
sniper
snipered
sniperer
sniperes
snipering
sniperly
snipers
snort
snorted
snorter
snortes
snorting
snortly
snorts
snuff
snuffed
snuffer
snuffes
snuffing
snuffly
snuffs
sodom
sodomed
sodomer
sodomes
sodoming
sodomly
sodoms
spic
spiced
spicer
spices
spicing
spick
spicked
spicker
spickes
spicking
spickly
spicks
spicly
spics
spik
spoof
spoofed
spoofer
spoofes
spoofing
spoofly
spoofs
spooge
spoogeed
spoogeer
spoogees
spoogeing
spoogely
spooges
spunk
spunked
spunker
spunkes
spunking
spunkly
spunks
steamyed
steamyer
steamyes
steamying
steamyly
steamys
stfu
stfued
stfuer
stfues
stfuing
stfuly
stfus
stiffy
stiffyed
stiffyer
stiffyes
stiffying
stiffyly
stiffys
stoneded
stoneder
stonedes
stoneding
stonedly
stoneds
stupided
stupider
stupides
stupiding
stupidly
stupids
suckeded
suckeder
suckedes
suckeding
suckedly
suckeds
sucker
suckes
sucking
suckinged
suckinger
suckinges
suckinging
suckingly
suckings
suckly
sucks
sumofabiatch
sumofabiatched
sumofabiatcher
sumofabiatches
sumofabiatching
sumofabiatchly
sumofabiatchs
tard
tarded
tarder
tardes
tarding
tardly
tards
tawdry
tawdryed
tawdryer
tawdryes
tawdrying
tawdryly
tawdrys
teabagging
teabagginged
teabagginger
teabagginges
teabagginging
teabaggingly
teabaggings
terd
terded
terder
terdes
terding
terdly
terds
teste
testee
testeed
testeeed
testeeer
testeees
testeeing
testeely
testeer
testees
testeing
testely
testes
testesed
testeser
testeses
testesing
testesly
testess
testicle
testicleed
testicleer
testiclees
testicleing
testiclely
testicles
testis
testised
testiser
testises
testising
testisly
testiss
thrusted
thruster
thrustes
thrusting
thrustly
thrusts
thug
thuged
thuger
thuges
thuging
thugly
thugs
tinkle
tinkleed
tinkleer
tinklees
tinkleing
tinklely
tinkles
tit
tited
titer
tites
titfuck
titfucked
titfucker
titfuckes
titfucking
titfuckly
titfucks
titi
titied
titier
tities
titiing
titily
titing
titis
titly
tits
titsed
titser
titses
titsing
titsly
titss
tittiefucker
tittiefuckered
tittiefuckerer
tittiefuckeres
tittiefuckering
tittiefuckerly
tittiefuckers
titties
tittiesed
tittieser
tittieses
tittiesing
tittiesly
tittiess
titty
tittyed
tittyer
tittyes
tittyfuck
tittyfucked
tittyfucker
tittyfuckered
tittyfuckerer
tittyfuckeres
tittyfuckering
tittyfuckerly
tittyfuckers
tittyfuckes
tittyfucking
tittyfuckly
tittyfucks
tittying
tittyly
tittys
toke
tokeed
tokeer
tokees
tokeing
tokely
tokes
toots
tootsed
tootser
tootses
tootsing
tootsly
tootss
tramp
tramped
tramper
trampes
tramping
tramply
tramps
transsexualed
transsexualer
transsexuales
transsexualing
transsexually
transsexuals
trashy
trashyed
trashyer
trashyes
trashying
trashyly
trashys
tubgirl
tubgirled
tubgirler
tubgirles
tubgirling
tubgirlly
tubgirls
turd
turded
turder
turdes
turding
turdly
turds
tush
tushed
tusher
tushes
tushing
tushly
tushs
twat
twated
twater
twates
twating
twatly
twats
twatsed
twatser
twatses
twatsing
twatsly
twatss
undies
undiesed
undieser
undieses
undiesing
undiesly
undiess
unweded
unweder
unwedes
unweding
unwedly
unweds
uzi
uzied
uzier
uzies
uziing
uzily
uzis
vag
vaged
vager
vages
vaging
vagly
vags
valium
valiumed
valiumer
valiumes
valiuming
valiumly
valiums
venous
virgined
virginer
virgines
virgining
virginly
virgins
vixen
vixened
vixener
vixenes
vixening
vixenly
vixens
vodkaed
vodkaer
vodkaes
vodkaing
vodkaly
vodkas
voyeur
voyeured
voyeurer
voyeures
voyeuring
voyeurly
voyeurs
vulgar
vulgared
vulgarer
vulgares
vulgaring
vulgarly
vulgars
wang
wanged
wanger
wanges
wanging
wangly
wangs
wank
wanked
wanker
wankered
wankerer
wankeres
wankering
wankerly
wankers
wankes
wanking
wankly
wanks
wazoo
wazooed
wazooer
wazooes
wazooing
wazooly
wazoos
wedgie
wedgieed
wedgieer
wedgiees
wedgieing
wedgiely
wedgies
weeded
weeder
weedes
weeding
weedly
weeds
weenie
weenieed
weenieer
weeniees
weenieing
weeniely
weenies
weewee
weeweeed
weeweeer
weeweees
weeweeing
weeweely
weewees
weiner
weinered
weinerer
weineres
weinering
weinerly
weiners
weirdo
weirdoed
weirdoer
weirdoes
weirdoing
weirdoly
weirdos
wench
wenched
wencher
wenches
wenching
wenchly
wenchs
wetback
wetbacked
wetbacker
wetbackes
wetbacking
wetbackly
wetbacks
whitey
whiteyed
whiteyer
whiteyes
whiteying
whiteyly
whiteys
whiz
whized
whizer
whizes
whizing
whizly
whizs
whoralicious
whoralicioused
whoraliciouser
whoraliciouses
whoraliciousing
whoraliciously
whoraliciouss
whore
whorealicious
whorealicioused
whorealiciouser
whorealiciouses
whorealiciousing
whorealiciously
whorealiciouss
whored
whoreded
whoreder
whoredes
whoreding
whoredly
whoreds
whoreed
whoreer
whorees
whoreface
whorefaceed
whorefaceer
whorefacees
whorefaceing
whorefacely
whorefaces
whorehopper
whorehoppered
whorehopperer
whorehopperes
whorehoppering
whorehopperly
whorehoppers
whorehouse
whorehouseed
whorehouseer
whorehousees
whorehouseing
whorehousely
whorehouses
whoreing
whorely
whores
whoresed
whoreser
whoreses
whoresing
whoresly
whoress
whoring
whoringed
whoringer
whoringes
whoringing
whoringly
whorings
wigger
wiggered
wiggerer
wiggeres
wiggering
wiggerly
wiggers
woody
woodyed
woodyer
woodyes
woodying
woodyly
woodys
wop
woped
woper
wopes
woping
woply
wops
wtf
wtfed
wtfer
wtfes
wtfing
wtfly
wtfs
xxx
xxxed
xxxer
xxxes
xxxing
xxxly
xxxs
yeasty
yeastyed
yeastyer
yeastyes
yeastying
yeastyly
yeastys
yobbo
yobboed
yobboer
yobboes
yobboing
yobboly
yobbos
zoophile
zoophileed
zoophileer
zoophilees
zoophileing
zoophilely
zoophiles
anal
ass
ass lick
balls
ballsac
bisexual
bleach
causas
cheap
cost of miracles
cunt
display network stats
fart
fda and death
fda AND warn
fda AND warning
fda AND warns
feom
fuck
gfc
humira AND expensive
illegal
madvocate
masturbation
nuccitelli
overdose
porn
shit
snort
texarkana
effective for the treatment of a baby
effective for the treatment of a boy
effective for the treatment of a child
effective for the treatment of a female
effective for the treatment of a girl
effective for the treatment of a kid
effective for the treatment of a minor
effective for the treatment of a newborn
effective for the treatment of a teen
effective for the treatment of a teenager
effective for the treatment of a toddler
effective for the treatment of a woman
effective for the treatment of adolescents
effective for the treatment of an adolescent
effective for the treatment of an infant
effective for the treatment of babies
effective for the treatment of baby
effective for the treatment of body building
effective for the treatment of boys
effective for the treatment of breast feeding
effective for the treatment of children
effective for the treatment of females
effective for the treatment of fetus
effective for the treatment of girls
effective for the treatment of infants
effective for the treatment of kids
effective for the treatment of minors
effective for the treatment of newborn
effective for the treatment of pediatric
effective for the treatment of pregnancy
effective for the treatment of pregnant
effective for the treatment of teenagers
effective for the treatment of teens
effective for the treatment of toddlers
effective for the treatment of women
effective for the treatment of youths
for the relief of a baby
for the relief of a boy
for the relief of a child
for the relief of a female
for the relief of a girl
for the relief of a kid
for the relief of a minor
for the relief of a newborn
for the relief of a teen
for the relief of a teenager
for the relief of a toddler
for the relief of a woman
for the relief of adolescents
for the relief of an adolescent
for the relief of an infant
for the relief of babies
for the relief of baby
for the relief of body building
for the relief of boys
for the relief of breast feeding
for the relief of children
for the relief of females
for the relief of fetus
for the relief of girls
for the relief of infants
for the relief of kids
for the relief of minors
for the relief of newborn
for the relief of pediatric
for the relief of pregnancy
for the relief of pregnant
for the relief of teenagers
for the relief of teens
for the relief of toddlers
for the relief of women
for the relief of youths
medicating a baby
medicating a boy
medicating a child
medicating a female
medicating a girl
medicating a kid
medicating a minor
medicating a newborn
medicating a teen
medicating a teenager
medicating a toddler
medicating a woman
medicating adolescents
medicating an adolescent
medicating an infant
medicating babies
medicating baby
medicating body building
medicating boys
medicating breast feeding
medicating children
medicating females
medicating fetus
medicating girls
medicating infants
medicating kids
medicating minors
medicating newborn
medicating pediatric
medicating pregnancy
medicating pregnant
medicating teenagers
medicating teens
medicating toddlers
medicating women
medicating youths
at risk for a baby
at risk for a boy
at risk for a child
at risk for a female
at risk for a girl
at risk for a kid
at risk for a minor
at risk for a newborn
at risk for a teen
at risk for a teenager
at risk for a toddler
at risk for a woman
at risk for adolescents
at risk for an adolescent
at risk for an infant
at risk for babies
at risk for baby
at risk for body building
at risk for boys
at risk for breast feeding
at risk for children
at risk for females
at risk for fetus
at risk for girls
at risk for infants
at risk for kids
at risk for minors
at risk for newborn
at risk for pediatric
at risk for pregnancy
at risk for pregnant
at risk for teenagers
at risk for teens
at risk for toddlers
at risk for women
at risk for youths
treating a baby
treating a boy
treating a child
treating a female
treating a girl
treating a kid
treating a minor
treating a newborn
treating a teen
treating a teenager
treating a toddler
treating a woman
treating adolescents
treating an adolescent
treating an infant
treating babies
treating baby
treating body building
treating boys
treating breast feeding
treating children
treating females
treating fetus
treating girls
treating infants
treating kids
treating minors
treating newborn
treating pediatric
treating pregnancy
treating pregnant
treating teenagers
treating teens
treating toddlers
treating women
treating youths
treatment for a baby
treatment for a boy
treatment for a child
treatment for a female
treatment for a girl
treatment for a kid
treatment for a minor
treatment for a newborn
treatment for a teen
treatment for a teenager
treatment for a toddler
treatment for a woman
treatment for adolescents
treatment for an adolescent
treatment for an infant
treatment for babies
treatment for baby
treatment for body building
treatment for boys
treatment for breast feeding
treatment for children
treatment for females
treatment for fetus
treatment for girls
treatment for infants
treatment for kids
treatment for minors
treatment for newborn
treatment for pediatric
treatment for pregnancy
treatment for pregnant
treatment for teenagers
treatment for teens
treatment for toddlers
treatment for women
treatment for youths
treatments for a baby
treatments for a boy
treatments for a child
treatments for a female
treatments for a girl
treatments for a kid
treatments for a minor
treatments for a newborn
treatments for a teen
treatments for a teenager
treatments for a toddler
treatments for a woman
treatments for adolescents
treatments for an adolescent
treatments for an infant
treatments for babies
treatments for baby
treatments for body building
treatments for boys
treatments for breast feeding
treatments for children
treatments for females
treatments for fetus
treatments for girls
treatments for infants
treatments for kids
treatments for minors
treatments for newborn
treatments for pediatric
treatments for pregnancy
treatments for pregnant
treatments for teenagers
treatments for teens
treatments for toddlers
treatments for women
treatments for youths
diagnosing a baby
diagnosing a boy
diagnosing a child
diagnosing a female
diagnosing a girl
diagnosing a kid
diagnosing a minor
diagnosing a newborn
diagnosing a teen
diagnosing a teenager
diagnosing a toddler
diagnosing a woman
diagnosing adolescents
diagnosing an adolescent
diagnosing an infant
diagnosing babies
diagnosing baby
diagnosing body building
diagnosing boys
diagnosing breast feeding
diagnosing children
diagnosing females
diagnosing fetus
diagnosing girls
diagnosing infants
diagnosing kids
diagnosing minors
diagnosing newborn
diagnosing pediatric
diagnosing pregnancy
diagnosing pregnant
diagnosing teenagers
diagnosing teens
diagnosing toddlers
diagnosing women
diagnosing youths
indicated for a baby
indicated for a boy
indicated for a child
indicated for a female
indicated for a girl
indicated for a kid
indicated for a minor
indicated for a newborn
indicated for a teen
indicated for a teenager
indicated for a toddler
indicated for a woman
indicated for adolescents
indicated for an adolescent
indicated for an infant
indicated for babies
indicated for baby
indicated for body building
indicated for boys
indicated for breast feeding
indicated for children
indicated for females
indicated for fetus
indicated for girls
indicated for infants
indicated for kids
indicated for minors
indicated for newborn
indicated for pediatric
indicated for pregnancy
indicated for pregnant
indicated for teenagers
indicated for teens
indicated for toddlers
indicated for women
indicated for youths
useful for a baby
useful for a boy
useful for a child
useful for a female
useful for a girl
useful for a kid
useful for a minor
useful for a newborn
useful for a teen
useful for a teenager
useful for a toddler
useful for a woman
useful for adolescents
useful for an adolescent
useful for an infant
useful for babies
useful for baby
useful for body building
useful for boys
useful for breast feeding
useful for children
useful for females
useful for fetus
useful for girls
useful for infants
useful for kids
useful for minors
useful for newborn
useful for pediatric
useful for pregnancy
useful for pregnant
useful for teenagers
useful for teens
useful for toddlers
useful for women
useful for youths
effective for a baby
effective for a boy
effective for a child
effective for a female
effective for a girl
effective for a kid
effective for a minor
effective for a newborn
effective for a teen
effective for a teenager
effective for a toddler
effective for a woman
effective for adolescents
effective for an adolescent
effective for an infant
effective for babies
effective for baby
effective for body building
effective for boys
effective for breast feeding
effective for children
effective for females
effective for fetus
effective for girls
effective for infants
effective for kids
effective for minors
effective for newborn
effective for pediatric
effective for pregnancy
effective for pregnant
effective for teenagers
effective for teens
effective for toddlers
effective for women
effective for youths
cures for a baby
cures for a boy
cures for a child
cures for a female
cures for a girl
cures for a kid
cures for a minor
cures for a newborn
cures for a teen
cures for a teenager
cures for a toddler
cures for a woman
cures for adolescents
cures for an adolescent
cures for an infant
cures for babies
cures for baby
cures for body building
cures for boys
cures for breast feeding
cures for children
cures for females
cures for fetus
cures for girls
cures for infants
cures for kids
cures for minors
cures for newborn
cures for pediatric
cures for pregnancy
cures for pregnant
cures for teenagers
cures for teens
cures for toddlers
cures for women
cures for youths
use in a baby
use in a boy
use in a child
use in a female
use in a girl
use in a kid
use in a minor
use in a newborn
use in a teen
use in a teenager
use in a toddler
use in a woman
use in adolescents
use in an adolescent
use in an infant
use in babies
use in baby
use in body building
use in boys
use in breast feeding
use in children
use in females
use in fetus
use in girls
use in infants
use in kids
use in minors
use in newborn
use in pediatric
use in pregnancy
use in pregnant
use in teenagers
use in teens
use in toddlers
use in women
use in youths
use in patients with a baby
use in patients with a boy
use in patients with a child
use in patients with a female
use in patients with a girl
use in patients with a kid
use in patients with a minor
use in patients with a newborn
use in patients with a teen
use in patients with a teenager
use in patients with a toddler
use in patients with a woman
use in patients with adolescents
use in patients with an adolescent
use in patients with an infant
use in patients with babies
use in patients with baby
use in patients with body building
use in patients with boys
use in patients with breast feeding
use in patients with children
use in patients with females
use in patients with fetus
use in patients with girls
use in patients with infants
use in patients with kids
use in patients with minors
use in patients with newborn
use in patients with pediatric
use in patients with pregnancy
use in patients with pregnant
use in patients with teenagers
use in patients with teens
use in patients with toddlers
use in patients with women
use in patients with youths
a baby diagnosis
a boy diagnosis
a child diagnosis
a female diagnosis
a girl diagnosis
a kid diagnosis
a minor diagnosis
a newborn diagnosis
a teen diagnosis
a teenager diagnosis
a toddler diagnosis
a woman diagnosis
adolescents diagnosis
an adolescent diagnosis
an infant diagnosis
babies diagnosis
baby diagnosis
body building diagnosis
boys diagnosis
breast feeding diagnosis
children diagnosis
females diagnosis
fetus diagnosis
girls diagnosis
infants diagnosis
kids diagnosis
minors diagnosis
newborn diagnosis
pediatric diagnosis
pregnancy diagnosis
pregnant diagnosis
teenagers diagnosis
teens diagnosis
toddlers diagnosis
women diagnosis
youths diagnosis
a baby medication
a boy medication
a child medication
a female medication
a girl medication
a kid medication
a minor medication
a newborn medication
a teen medication
a teenager medication
a toddler medication
a woman medication
adolescents medication
an adolescent medication
an infant medication
babies medication
baby medication
body building medication
boys medication
breast feeding medication
children medication
females medication
fetus medication
girls medication
infants medication
kids medication
minors medication
newborn medication
pediatric medication
pregnancy medication
pregnant medication
teenagers medication
teens medication
toddlers medication
women medication
youths medication
a baby therapy
a boy therapy
a child therapy
a female therapy
a girl therapy
a kid therapy
a minor therapy
a newborn therapy
a teen therapy
a teenager therapy
a toddler therapy
a woman therapy
adolescents therapy
an adolescent therapy
an infant therapy
babies therapy
baby therapy
body building therapy
boys therapy
breast feeding therapy
children therapy
females therapy
fetus therapy
girls therapy
infants therapy
kids therapy
minors therapy
newborn therapy
pediatric therapy
pregnancy therapy
pregnant therapy
teenagers therapy
teens therapy
toddlers therapy
women therapy
youths therapy
a baby treatment
a boy treatment
a child treatment
a female treatment
a girl treatment
a kid treatment
a minor treatment
a newborn treatment
a teen treatment
a teenager treatment
a toddler treatment
a woman treatment
adolescents treatment
an adolescent treatment
an infant treatment
babies treatment
baby treatment
body building treatment
boys treatment
breast feeding treatment
children treatment
females treatment
fetus treatment
girls treatment
infants treatment
kids treatment
minors treatment
newborn treatment
pediatric treatment
pregnancy treatment
pregnant treatment
teenagers treatment
teens treatment
toddlers treatment
women treatment
youths treatment
a baby cure
a boy cure
a child cure
a female cure
a girl cure
a kid cure
a minor cure
a newborn cure
a teen cure
a teenager cure
a toddler cure
a woman cure
adolescents cure
an adolescent cure
an infant cure
babies cure
baby cure
body building cure
boys cure
breast feeding cure
children cure
females cure
fetus cure
girls cure
infants cure
kids cure
minors cure
newborn cure
pediatric cure
pregnancy cure
pregnant cure
teenagers cure
teens cure
toddlers cure
women cure
youths cure
a baby symptoms
a boy symptoms
a child symptoms
a female symptoms
a girl symptoms
a kid symptoms
a minor symptoms
a newborn symptoms
a teen symptoms
a teenager symptoms
a toddler symptoms
a woman symptoms
adolescents symptoms
an adolescent symptoms
an infant symptoms
babies symptoms
baby symptoms
body building symptoms
boys symptoms
breast feeding symptoms
children symptoms
females symptoms
fetus symptoms
girls symptoms
infants symptoms
kids symptoms
minors symptoms
newborn symptoms
pediatric symptoms
pregnancy symptoms
pregnant symptoms
teenagers symptoms
teens symptoms
toddlers symptoms
women symptoms
youths symptoms
a baby medicine
a boy medicine
a child medicine
a female medicine
a girl medicine
a kid medicine
a minor medicine
a newborn medicine
a teen medicine
a teenager medicine
a toddler medicine
a woman medicine
adolescents medicine
an adolescent medicine
an infant medicine
babies medicine
baby medicine
body building medicine
boys medicine
breast feeding medicine
children medicine
females medicine
fetus medicine
girls medicine
infants medicine
kids medicine
minors medicine
newborn medicine
pediatric medicine
pregnancy medicine
pregnant medicine
teenagers medicine
teens medicine
toddlers medicine
women medicine
youths medicine
a baby usage
a boy usage
a child usage
a female usage
a girl usage
a kid usage
a minor usage
a newborn usage
a teen usage
a teenager usage
a toddler usage
a woman usage
adolescents usage
an adolescent usage
an infant usage
babies usage
baby usage
body building usage
boys usage
breast feeding usage
children usage
females usage
fetus usage
girls usage
infants usage
kids usage
minors usage
newborn usage
pediatric usage
pregnancy usage
pregnant usage
teenagers usage
teens usage
toddlers usage
women usage
youths usage
a baby remedy
a boy remedy
a child remedy
a female remedy
a girl remedy
a kid remedy
a minor remedy
a newborn remedy
a teen remedy
a teenager remedy
a toddler remedy
a woman remedy
adolescents remedy
an adolescent remedy
an infant remedy
babies remedy
baby remedy
body building remedy
boys remedy
breast feeding remedy
children remedy
females remedy
fetus remedy
girls remedy
infants remedy
kids remedy
minors remedy
newborn remedy
pediatric remedy
pregnancy remedy
pregnant remedy
teenagers remedy
teens remedy
toddlers remedy
women remedy
youths remedy
a baby prescription
a boy prescription
a child prescription
a female prescription
a girl prescription
a kid prescription
a minor prescription
a newborn prescription
a teen prescription
a teenager prescription
a toddler prescription
a woman prescription
adolescents prescription
an adolescent prescription
an infant prescription
babies prescription
baby prescription
body building prescription
boys prescription
breast feeding prescription
children prescription
females prescription
fetus prescription
girls prescription
infants prescription
kids prescription
minors prescription
newborn prescription
pediatric prescription
pregnancy prescription
pregnant prescription
teenagers prescription
teens prescription
toddlers prescription
women prescription
youths prescription
a baby pill
a boy pill
a child pill
a female pill
a girl pill
a kid pill
a minor pill
a newborn pill
a teen pill
a teenager pill
a toddler pill
a woman pill
adolescents pill
an adolescent pill
an infant pill
babies pill
baby pill
body building pill
boys pill
breast feeding pill
children pill
females pill
fetus pill
girls pill
infants pill
kids pill
minors pill
newborn pill
pediatric pill
pregnancy pill
pregnant pill
teenagers pill
teens pill
toddlers pill
women pill
youths pill
a baby drug
a boy drug
a child drug
a female drug
a girl drug
a kid drug
a minor drug
a newborn drug
a teen drug
a teenager drug
a toddler drug
a woman drug
adolescents drug
an adolescent drug
an infant drug
babies drug
baby drug
body building drug
boys drug
breast feeding drug
children drug
females drug
fetus drug
girls drug
infants drug
kids drug
minors drug
newborn drug
pediatric drug
pregnancy drug
pregnant drug
teenagers drug
teens drug
toddlers drug
women drug
youths drug
a baby tablet
a boy tablet
a child tablet
a female tablet
a girl tablet
a kid tablet
a minor tablet
a newborn tablet
a teen tablet
a teenager tablet
a toddler tablet
a woman tablet
adolescents tablet
an adolescent tablet
an infant tablet
babies tablet
baby tablet
body building tablet
boys tablet
breast feeding tablet
children tablet
females tablet
fetus tablet
girls tablet
infants tablet
kids tablet
minors tablet
newborn tablet
pediatric tablet
pregnancy tablet
pregnant tablet
teenagers tablet
teens tablet
toddlers tablet
women tablet
youths tablet
a baby management
a boy management
a child management
a female management
a girl management
a kid management
a minor management
a newborn management
a teen management
a teenager management
a toddler management
a woman management
adolescents management
an adolescent management
an infant management
babies management
baby management
body building management
boys management
breast feeding management
children management
females management
fetus management
girls management
infants management
kids management
minors management
newborn management
pediatric management
pregnancy management
pregnant management
teenagers management
teens management
toddlers management
women management
youths management
a baby indication
a boy indication
a child indication
a female indication
a girl indication
a kid indication
a minor indication
a newborn indication
a teen indication
a teenager indication
a toddler indication
a woman indication
adolescents indication
an adolescent indication
an infant indication
babies indication
baby indication
body building indication
boys indication
breast feeding indication
children indication
females indication
fetus indication
girls indication
infants indication
kids indication
minors indication
newborn indication
pediatric indication
pregnancy indication
pregnant indication
teenagers indication
teens indication
toddlers indication
women indication
youths indication
breast cancer a baby
breast cancer a boy
breast cancer a child
breast cancer a female
breast cancer a girl
breast cancer a kid
breast cancer a minor
breast cancer a newborn
breast cancer a teen
breast cancer a teenager
breast cancer a toddler
breast cancer a woman
breast cancer adolescents
breast cancer an adolescent
breast cancer an infant
breast cancer babies
breast cancer baby
breast cancer body building
breast cancer boys
breast cancer breast feeding
breast cancer children
breast cancer females
breast cancer fetus
breast cancer girls
breast cancer infants
breast cancer kids
breast cancer minors
breast cancer newborn
breast cancer pediatric
breast cancer pregnancy
breast cancer pregnant
breast cancer teenagers
breast cancer teens
breast cancer toddlers
breast cancer women
breast cancer youths
prostate cancer a baby
prostate cancer a boy
prostate cancer a child
prostate cancer a female
prostate cancer a girl
prostate cancer a kid
prostate cancer a minor
prostate cancer a newborn
prostate cancer a teen
prostate cancer a teenager
prostate cancer a toddler
prostate cancer a woman
prostate cancer adolescents
prostate cancer an adolescent
prostate cancer an infant
prostate cancer babies
prostate cancer baby
prostate cancer body building
prostate cancer boys
prostate cancer breast feeding
prostate cancer children
prostate cancer females
prostate cancer fetus
prostate cancer girls
prostate cancer infants
prostate cancer kids
prostate cancer minors
prostate cancer newborn
prostate cancer pediatric
prostate cancer pregnancy
prostate cancer pregnant
prostate cancer teenagers
prostate cancer teens
prostate cancer toddlers
prostate cancer women
prostate cancer youths
steroid a baby
steroid a boy
steroid a child
steroid a female
steroid a girl
steroid a kid
steroid a minor
steroid a newborn
steroid a teen
steroid a teenager
steroid a toddler
steroid a woman
steroid adolescents
steroid an adolescent
steroid an infant
steroid babies
steroid baby
steroid body building
steroid boys
steroid breast feeding
steroid children
steroid females
steroid fetus
steroid girls
steroid infants
steroid kids
steroid minors
steroid newborn
steroid pediatric
steroid pregnancy
steroid pregnant
steroid teenagers
steroid teens
steroid toddlers
steroid women
steroid youths
steroids a baby
steroids a boy
steroids a child
steroids a female
steroids a girl
steroids a kid
steroids a minor
steroids a newborn
steroids a teen
steroids a teenager
steroids a toddler
steroids a woman
steroids adolescents
steroids an adolescent
steroids an infant
steroids babies
steroids baby
steroids body building
steroids boys
steroids breast feeding
steroids children
steroids females
steroids fetus
steroids girls
steroids infants
steroids kids
steroids minors
steroids newborn
steroids pediatric
steroids pregnancy
steroids pregnant
steroids teenagers
steroids teens
steroids toddlers
steroids women
steroids youths
abbvie
AbbVie
acid
addicted
addiction
adolescent
adult sites
Advocacy
advocacy
agitated states
AJO, postsurgical analgesic, knee, replacement, surgery
alcohol
amphetamine
androgen
antibody
apple cider vinegar
assistance
Assistance
association
at home
attorney
audit
ayurvedic
baby
ban
baricitinib
bed bugs
best
bible
bisexual
black
bleach
blog
bulimia nervosa
buy
cannabis
certificate
certification
certified
cervical cancer, concurrent chemoradiotherapy, intravoxel incoherent motion magnetic resonance imaging, MRI, IVIM, diffusion-weighted MRI, DWI
charlie sheen
cheap
cheapest
child
childhood
childlike
children
chronic fatigue syndrome
Cladribine Tablets
cocaine
cock
combination therapies, synergistic antitumor efficacy, pertuzumab, trastuzumab, ipilimumab, nivolumab, palbociclib, letrozole, lapatinib, docetaxel, trametinib, dabrafenib, carflzomib, lenalidomide
contagious
Cortical Lesions
cream
creams
crime
criminal
cure
dangerous
dangers
dasabuvir
Dasabuvir
dead
deadly
death
dementia
dependence
dependent
depression
dermatillomania
die
diet
Disability
Discount
discount
dog
drink
drug abuse
drug-induced
dying
eastern medicine
eat
ect
eczema
electroconvulsive therapy
electromagnetic therapy
electrotherapy
epa
epilepsy
erectile dysfunction
explosive disorder
fake
Fake-ovir
fatal
fatalities
fatality
fibromyalgia
financial
Financial
fish oil
food
foods
foundation
free
Gabriel Pardo
gaston
general hospital
genetic
geriatric
Giancarlo Comi
gilead
Gilead
glaucoma
Glenn S. Williams
Glenn Williams
Gloria Dalla Costa
gonorrhea
Greedy
greedy
guns
hallucinations
harvoni
Harvoni
herbal
herbs
heroin
herpes
Hidradenitis Suppurativa
holistic
home
home remedies
home remedy
homeopathic
homeopathy
hydrocortisone
ice
image
images
job
kid
kids
kill
killer
laser
lawsuit
lawyer
ledipasvir
Ledipasvir
lesbian
lesions
lights
liver
lupus
marijuana
melancholic
memory loss
menopausal
mental retardation
military
milk
moisturizers
monoamine oxidase inhibitor drugs
MRI
MS
murder
national
natural
natural cure
natural cures
natural medications
natural medicine
natural medicines
natural remedies
natural remedy
natural treatment
natural treatments
naturally
Needy
needy
Neurology Reviews
neuropathic
nightclub massacre
nightclub shooting
nude
nudity
nutraceuticals
OASIS
oasis
off label
ombitasvir
Ombitasvir
ombitasvir/paritaprevir/ritonavir with dasabuvir
orlando shooting
overactive thyroid gland
overdose
overdosed
Paolo Preziosa
paritaprevir
Paritaprevir
pediatric
pedophile
photo
photos
picture
post partum
postnatal
pregnancy
pregnant
prenatal
prepartum
prison
program
Program
Protest
protest
psychedelics
pulse nightclub
puppy
purchase
purchasing
rape
recall
recreational drug
Rehabilitation
Retinal Measurements
retrograde ejaculation
risperdal
ritonavir
Ritonavir
ritonavir with dasabuvir
robin williams
sales
sasquatch
schizophrenia
seizure
seizures
sex
sexual
sexy
shock treatment
silver
sleep disorders
smoking
sociopath
sofosbuvir
Sofosbuvir
sovaldi
ssri
store
sue
suicidal
suicide
supplements
support
Support
Support Path
teen
teenage
teenagers
Telerehabilitation
testosterone
Th17
Th17:FoxP3+Treg cell ratio
Th22
toxic
toxin
tragedy
treatment resistant
V Pak
vagina
velpatasvir
Viekira Pa
Viekira Pak
viekira pak
violence
virgin
vitamin
VPak
weight loss
withdrawal
wrinkles
xxx
young adult
young adults
zoloft
financial
sofosbuvir
ritonavir with dasabuvir
discount
support path
program
ritonavir
greedy
ledipasvir
assistance
viekira pak
vpak
advocacy
needy
protest
abbvie
paritaprevir
ombitasvir
direct-acting antivirals
dasabuvir
gilead
fake-ovir
support
v pak
oasis
harvoni
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-imn')]
div[contains(@class, 'pane-pub-home-imn')]
div[contains(@class, 'pane-pub-topic-imn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Study Helps Define Patient-Centered Definition of Atopic Dermatitis Flares
TOPLINE:
, which most agreed would help when communicating with their healthcare providers (HCPs).
METHODOLOGY:
- To develop a patient-centered definition of AD flare, researchers used a modified eDelphi method, which involved a focus group and survey to reach consensus on key aspects of an AD flare.
- The focus group included 26 US adults aged ≥ 18 years with AD who had experienced a flare within the past 12 months. The survey was conducted among 631 adults with AD to validate the identified concepts and assess their agreement with the consensus statements.
- Participants rated 98 statements on a scale from 1 to 9, with consensus defined as at least 70% rating a statement as 7-9 and less than 15% rating it as 1-3.
- In focus groups, participants identified six key concepts for a patient-centered definition of flare, including changes from baseline, mental and emotional consequences, and physical changes in skin.
TAKEAWAY:
- The focus group reached consensus on 15 statements, and survey participants reached consensus on 12 of those statements defining an AD flare, with the highest agreement on symptoms taking more attention than normal, worsening of physical symptoms associated with AD, and worsening of itching associated with AD.
- The statement “acute worsening of symptoms of AD” was ranked as the most important, while “a worsening of physical symptoms” was ranked the least important.
- Most participants (79.7%) reported that prior definitions of AD flare did not resonate with them.
- More than half (52.9%) agreed with their HCP on what constitutes an AD flare, and the majority (77.6%) indicated that a patient-centered definition would be useful for communication with their HCP and for self-management.
IN PRACTICE:
“In this consensus survey study, we identified statements that are critical to the definition of an AD flare from the patient perspective,” the authors wrote. These findings, they added, “may be useful in clinical practice to improve communication between patients and HCPs who may be using the term flare without a mutual understanding of its meaning” and “may also be applied to the development of outcome measures focused on AD flares, which is an important treatment outcome for people with AD.”
SOURCE:
The study was led by Aaron M. Drucker, MD, ScM, of the Division of Dermatology, Department of Medicine, University of Toronto, Ontario, Canada, and was published online September 11 in JAMA Dermatology.
LIMITATIONS:
Participants had higher-than-average knowledge about AD, and the study’s findings may not be generalizable to all people with AD. The study included a higher proportion of moderate to severe AD cases than the general population, which may introduce responder bias. The findings may not be applicable to children, caregivers, or individuals in other countries.
DISCLOSURES:
This work was supported by a grant to the National Eczema Association from Pfizer. Dr. Drucker disclosed received compensation from the British Journal of Dermatology, American Academy of Dermatology, and Canadian Dermatology Today, and consultant fees from the National Eczema Association and Canadian Agency for Drugs and Technologies in Health. Another author reported receiving personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
, which most agreed would help when communicating with their healthcare providers (HCPs).
METHODOLOGY:
- To develop a patient-centered definition of AD flare, researchers used a modified eDelphi method, which involved a focus group and survey to reach consensus on key aspects of an AD flare.
- The focus group included 26 US adults aged ≥ 18 years with AD who had experienced a flare within the past 12 months. The survey was conducted among 631 adults with AD to validate the identified concepts and assess their agreement with the consensus statements.
- Participants rated 98 statements on a scale from 1 to 9, with consensus defined as at least 70% rating a statement as 7-9 and less than 15% rating it as 1-3.
- In focus groups, participants identified six key concepts for a patient-centered definition of flare, including changes from baseline, mental and emotional consequences, and physical changes in skin.
TAKEAWAY:
- The focus group reached consensus on 15 statements, and survey participants reached consensus on 12 of those statements defining an AD flare, with the highest agreement on symptoms taking more attention than normal, worsening of physical symptoms associated with AD, and worsening of itching associated with AD.
- The statement “acute worsening of symptoms of AD” was ranked as the most important, while “a worsening of physical symptoms” was ranked the least important.
- Most participants (79.7%) reported that prior definitions of AD flare did not resonate with them.
- More than half (52.9%) agreed with their HCP on what constitutes an AD flare, and the majority (77.6%) indicated that a patient-centered definition would be useful for communication with their HCP and for self-management.
IN PRACTICE:
“In this consensus survey study, we identified statements that are critical to the definition of an AD flare from the patient perspective,” the authors wrote. These findings, they added, “may be useful in clinical practice to improve communication between patients and HCPs who may be using the term flare without a mutual understanding of its meaning” and “may also be applied to the development of outcome measures focused on AD flares, which is an important treatment outcome for people with AD.”
SOURCE:
The study was led by Aaron M. Drucker, MD, ScM, of the Division of Dermatology, Department of Medicine, University of Toronto, Ontario, Canada, and was published online September 11 in JAMA Dermatology.
LIMITATIONS:
Participants had higher-than-average knowledge about AD, and the study’s findings may not be generalizable to all people with AD. The study included a higher proportion of moderate to severe AD cases than the general population, which may introduce responder bias. The findings may not be applicable to children, caregivers, or individuals in other countries.
DISCLOSURES:
This work was supported by a grant to the National Eczema Association from Pfizer. Dr. Drucker disclosed received compensation from the British Journal of Dermatology, American Academy of Dermatology, and Canadian Dermatology Today, and consultant fees from the National Eczema Association and Canadian Agency for Drugs and Technologies in Health. Another author reported receiving personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
, which most agreed would help when communicating with their healthcare providers (HCPs).
METHODOLOGY:
- To develop a patient-centered definition of AD flare, researchers used a modified eDelphi method, which involved a focus group and survey to reach consensus on key aspects of an AD flare.
- The focus group included 26 US adults aged ≥ 18 years with AD who had experienced a flare within the past 12 months. The survey was conducted among 631 adults with AD to validate the identified concepts and assess their agreement with the consensus statements.
- Participants rated 98 statements on a scale from 1 to 9, with consensus defined as at least 70% rating a statement as 7-9 and less than 15% rating it as 1-3.
- In focus groups, participants identified six key concepts for a patient-centered definition of flare, including changes from baseline, mental and emotional consequences, and physical changes in skin.
TAKEAWAY:
- The focus group reached consensus on 15 statements, and survey participants reached consensus on 12 of those statements defining an AD flare, with the highest agreement on symptoms taking more attention than normal, worsening of physical symptoms associated with AD, and worsening of itching associated with AD.
- The statement “acute worsening of symptoms of AD” was ranked as the most important, while “a worsening of physical symptoms” was ranked the least important.
- Most participants (79.7%) reported that prior definitions of AD flare did not resonate with them.
- More than half (52.9%) agreed with their HCP on what constitutes an AD flare, and the majority (77.6%) indicated that a patient-centered definition would be useful for communication with their HCP and for self-management.
IN PRACTICE:
“In this consensus survey study, we identified statements that are critical to the definition of an AD flare from the patient perspective,” the authors wrote. These findings, they added, “may be useful in clinical practice to improve communication between patients and HCPs who may be using the term flare without a mutual understanding of its meaning” and “may also be applied to the development of outcome measures focused on AD flares, which is an important treatment outcome for people with AD.”
SOURCE:
The study was led by Aaron M. Drucker, MD, ScM, of the Division of Dermatology, Department of Medicine, University of Toronto, Ontario, Canada, and was published online September 11 in JAMA Dermatology.
LIMITATIONS:
Participants had higher-than-average knowledge about AD, and the study’s findings may not be generalizable to all people with AD. The study included a higher proportion of moderate to severe AD cases than the general population, which may introduce responder bias. The findings may not be applicable to children, caregivers, or individuals in other countries.
DISCLOSURES:
This work was supported by a grant to the National Eczema Association from Pfizer. Dr. Drucker disclosed received compensation from the British Journal of Dermatology, American Academy of Dermatology, and Canadian Dermatology Today, and consultant fees from the National Eczema Association and Canadian Agency for Drugs and Technologies in Health. Another author reported receiving personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Imaging Tool Helps Identify Features of Nail Disorders
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Short Steroid Treatment May Raise Diabetes Risk: Study
People who received systemic glucocorticoids during short hospital stays were more than twice as likely to develop new onset diabetes than those who didn’t, reported the authors of a large study that analyzed more than a decade’s worth of patient records.
Rajna Golubic, MD, PhD, of the diabetes trials unit at the University of Oxford, United Kingdom, and colleagues did an observational cohort study, using data from electronic healthcare records of more than patients admitted between January 1, 2013, and October 1, 2023.
They looked for patients who didn’t have a diabetes diagnosis at the time of admission and who were not taking a steroid. Their research was presented this month at the 2024 annual meeting of the European Association for the Study of Diabetes (EASD) in Madrid, Spain.
About 1.8%, of 316, of the 17,258 patients who received systemic glucocorticoids (tablets, injections, or infusions) during their hospital stay developed new-onset diabetes, while this happened to only 0.8%, or 3450, of the 434,348 who did not get these drugs, according to an abstract of the EASD presentation.
The median length of stay was 3 days (2-8) for the group of patients who took steroids, compared with 1 day (1-3) in those who did not. Further analysis showed that, when age and sex were factored in, patients receiving systemic glucocorticoids were more than twice as likely (2.6 times) to develop diabetes as those not receiving the treatment, Dr. Golubic said.
This research builds on previous studies that looked at smaller groups of patients and the diabetes risk in patients with specific conditions, including rheumatoid arthritis, Dr. Golubic said. It may prove helpful for clinicians considering when to employ steroids, which are useful medications for managing inflammation associated with many conditions.
“This gives them a very good estimate of how much more likely people treated with systemic glucocorticoids are to develop new-onset diabetes,” Dr. Golubic said.
Glucocorticoids have for decades been used for managing acute and chronic inflammatory diseases. The link to diabetes has been previously reported in smaller studies and in ones linked to specific conditions such as respiratory disease and rheumatoid arthritis.
Carolyn Cummins, PhD, an associate professor at the University of Toronto, Canada, who was not part of this study, told this news organization she was pleased to see a study of diabetes and steroids done with the scope that Dr. Golubic and colleagues undertook. Dr. Cummins in 2022 published an article titled “Fresh insights into glucocorticoid-induced diabetes mellitus and new therapeutic directions” in Nature Reviews Endocrinology.
“We know that this is an issue, but we didn’t necessarily know numerically how significant it was,” Dr. Cummins said. “I would say it wasn’t a surprising finding, but it’s nice to actually have the numbers from a large study.”
Dr. Golubic and Dr. Cummins reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
People who received systemic glucocorticoids during short hospital stays were more than twice as likely to develop new onset diabetes than those who didn’t, reported the authors of a large study that analyzed more than a decade’s worth of patient records.
Rajna Golubic, MD, PhD, of the diabetes trials unit at the University of Oxford, United Kingdom, and colleagues did an observational cohort study, using data from electronic healthcare records of more than patients admitted between January 1, 2013, and October 1, 2023.
They looked for patients who didn’t have a diabetes diagnosis at the time of admission and who were not taking a steroid. Their research was presented this month at the 2024 annual meeting of the European Association for the Study of Diabetes (EASD) in Madrid, Spain.
About 1.8%, of 316, of the 17,258 patients who received systemic glucocorticoids (tablets, injections, or infusions) during their hospital stay developed new-onset diabetes, while this happened to only 0.8%, or 3450, of the 434,348 who did not get these drugs, according to an abstract of the EASD presentation.
The median length of stay was 3 days (2-8) for the group of patients who took steroids, compared with 1 day (1-3) in those who did not. Further analysis showed that, when age and sex were factored in, patients receiving systemic glucocorticoids were more than twice as likely (2.6 times) to develop diabetes as those not receiving the treatment, Dr. Golubic said.
This research builds on previous studies that looked at smaller groups of patients and the diabetes risk in patients with specific conditions, including rheumatoid arthritis, Dr. Golubic said. It may prove helpful for clinicians considering when to employ steroids, which are useful medications for managing inflammation associated with many conditions.
“This gives them a very good estimate of how much more likely people treated with systemic glucocorticoids are to develop new-onset diabetes,” Dr. Golubic said.
Glucocorticoids have for decades been used for managing acute and chronic inflammatory diseases. The link to diabetes has been previously reported in smaller studies and in ones linked to specific conditions such as respiratory disease and rheumatoid arthritis.
Carolyn Cummins, PhD, an associate professor at the University of Toronto, Canada, who was not part of this study, told this news organization she was pleased to see a study of diabetes and steroids done with the scope that Dr. Golubic and colleagues undertook. Dr. Cummins in 2022 published an article titled “Fresh insights into glucocorticoid-induced diabetes mellitus and new therapeutic directions” in Nature Reviews Endocrinology.
“We know that this is an issue, but we didn’t necessarily know numerically how significant it was,” Dr. Cummins said. “I would say it wasn’t a surprising finding, but it’s nice to actually have the numbers from a large study.”
Dr. Golubic and Dr. Cummins reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
People who received systemic glucocorticoids during short hospital stays were more than twice as likely to develop new onset diabetes than those who didn’t, reported the authors of a large study that analyzed more than a decade’s worth of patient records.
Rajna Golubic, MD, PhD, of the diabetes trials unit at the University of Oxford, United Kingdom, and colleagues did an observational cohort study, using data from electronic healthcare records of more than patients admitted between January 1, 2013, and October 1, 2023.
They looked for patients who didn’t have a diabetes diagnosis at the time of admission and who were not taking a steroid. Their research was presented this month at the 2024 annual meeting of the European Association for the Study of Diabetes (EASD) in Madrid, Spain.
About 1.8%, of 316, of the 17,258 patients who received systemic glucocorticoids (tablets, injections, or infusions) during their hospital stay developed new-onset diabetes, while this happened to only 0.8%, or 3450, of the 434,348 who did not get these drugs, according to an abstract of the EASD presentation.
The median length of stay was 3 days (2-8) for the group of patients who took steroids, compared with 1 day (1-3) in those who did not. Further analysis showed that, when age and sex were factored in, patients receiving systemic glucocorticoids were more than twice as likely (2.6 times) to develop diabetes as those not receiving the treatment, Dr. Golubic said.
This research builds on previous studies that looked at smaller groups of patients and the diabetes risk in patients with specific conditions, including rheumatoid arthritis, Dr. Golubic said. It may prove helpful for clinicians considering when to employ steroids, which are useful medications for managing inflammation associated with many conditions.
“This gives them a very good estimate of how much more likely people treated with systemic glucocorticoids are to develop new-onset diabetes,” Dr. Golubic said.
Glucocorticoids have for decades been used for managing acute and chronic inflammatory diseases. The link to diabetes has been previously reported in smaller studies and in ones linked to specific conditions such as respiratory disease and rheumatoid arthritis.
Carolyn Cummins, PhD, an associate professor at the University of Toronto, Canada, who was not part of this study, told this news organization she was pleased to see a study of diabetes and steroids done with the scope that Dr. Golubic and colleagues undertook. Dr. Cummins in 2022 published an article titled “Fresh insights into glucocorticoid-induced diabetes mellitus and new therapeutic directions” in Nature Reviews Endocrinology.
“We know that this is an issue, but we didn’t necessarily know numerically how significant it was,” Dr. Cummins said. “I would say it wasn’t a surprising finding, but it’s nice to actually have the numbers from a large study.”
Dr. Golubic and Dr. Cummins reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EASD 2024
When You and Your Malpractice Insurer Disagree on Your Case
You’ve been sued for medical malpractice. If you are a physician in the United States, that is not an unlikely scenario.
An analysis by the American Medical Association shows that almost half of all physicians are sued by the time they reach 54. In some specialties, such as ob.gyn., one is almost guaranteed to be sued at some point.
But that’s what medical malpractice insurance is for, right? Your medical malpractice insurer will assign an attorney to take care of you and help you through this situation. Won’t they?
Maybe so, but the attorney and the claims representative your insurer assigns to your case may have a different idea about how to proceed than you do. Though the defense attorney assigned to you represents you, he or she gets paid by the insurance carrier.
This can create a conflict when your defense counsel and your insurance claims representative aim to take your case in a direction you don’t like.
Disagreements might include:
- Choice of expert witnesses
- Tactical decisions related to trial strategy
- Public relations considerations
- Admissions of liability
- Allocation of resources
To Settle or Not?
One of the most challenging — and common — disagreements is whether to settle the case.
Sometimes a malpractice insurer wants to settle the case against the defendant doctor’s wishes. Or the doctor wants to settle but is pushed into going to trial. In the following case, one doctor had to face the consequences of a decision he didn’t even make.
The Underlying Medical Malpractice Case
Dr. D was sued by a patient who had allegedly called Dr. D’s office six times in 2 days complaining of intermittent chest pain.
Dr. D had been swamped with patients and couldn’t squeeze this patient in for an office visit, but he did call back. The patient later claimed that during the call he told the doctor he was suffering from chest pain. The doctor recalled that the patient had complained of abdominal discomfort that began after he had exercised.
The physician wrote a prescription for an ECG at the local hospital and called to ensure that the patient could just walk in. The ECG was allegedly abnormal but was not read as representing an impending or current heart attack. Later that evening, however, the patient went to the emergency department of another hospital where it was confirmed that he had suffered a heart attack. The patient underwent cardiac catheterization and stent placement to address a blockage in his left anterior descending artery.
The patient subsequently sued Dr. D and the hospital where he had the original ECG. Dr. D contacted his medical malpractice insurance company. The insurance company assigned an attorney to represent Dr. D. Discovery in the case began.
The plaintiff’s own medical expert testified in a deposition that there was no way for the heart attack to have been prevented and that the treatment would have been the same either way. But Dr. D could not find a record of the phone calls with the patient, and he had not noted his conversation the patient in their medical records.
Dr. D held a policy for $1 million, and his state had a fund that would kick in an additional $1 million. But the plaintiffs demanded $4 million to settle.
A month before trial, the plaintiff’s attorney sent a threatening letter to Dr. D’s attorney warning him that Dr. D was underinsured and suggesting that it would be in the physician’s best interests to settle.
“I want to stress to you that it is not my desire to harm your client’s reputation or to destroy his business,” wrote the plaintiff’s attorney. “However, now is the time to avoid consequences such as these by making a good faith effort to get this case resolved.”
The letter went on to note that the defense attorney should give Dr. D a copy of the letter so that everyone would be aware of the potential consequences of an award against Dr. D in excess of his limits of insurance coverage. The plaintiff’s attorney even suggested that Dr. D should retain personal counsel.
Dr. D’s defense attorney downplayed the letter and assured him that there was no reason to worry.
Meanwhile the case inched closer to trial.
The codefendant hospital settled with the plaintiff on the night before jury selection, leaving Dr. D in the uncomfortable position of being the only defendant in the case. At this point, Dr. D decided he would like to settle, and he sent his attorney an email telling him so. But the attorney instead referred him to an insurance company claims.
Just days before the trial was to start, Dr. D repeatedly told the claims representative assigned to his claim that he did not want to go to trial but rather wanted to settle. The representative told Dr. D that he had no choice in whether the action settled.
A committee at the insurance company had decided to proceed with the trial rather than settle.
The trial proved a painful debacle for Dr. D. His attorney’s idea of showing a “gotcha” video of the allegedly permanently injured plaintiff carrying a large, heavy box backfired when the jury was shown by the plaintiff that the box actually contained ice cream cones and weighed very little.
Prior to trial, the plaintiff offered to settle for $1 million. On the first day of trial, they lowered that amount to $750,000, yet the defense attorney did not settle the case, and it proceeded to a jury verdict. The jury awarded the plaintiff over $4 million — well in excess of Dr. D’s policy limits.
The Follow-up
Dr. D was horrified, but the insurance company claims representative said the insurer would promptly offer $2 million in available insurance coverage to settle the case post verdict. This did not happen. Instead, the insurer chose to appeal the verdict against Dr. D’s wishes.
Ultimately, Dr. D was forced to hire his own lawyer. He ultimately sued the insurance company for breach of contract and bad faith.
The insurance company eventually attempted to settle with the plaintiffs’ counsel, but the plaintiff refused to accept the available insurance coverage. The insurance carrier still has not posted the entire appeal bond. The case is still pending.
Protecting Yourself
The lesson from Dr. D’s experience: Understand that the insurance company is not your friend. It’s a business looking out for its own interests.
The plaintiff’s attorney was absolutely correct in suggesting that Dr. D retain his own attorney to represent his own interests. You should hire your own lawyer when:
- You disagree with your insurer on how to proceed in a case.
- You receive a demand that exceeds your available insurance coverage or for damages that may not be covered by your policy, such as punitive damages.
- Your insurance carrier attempts to deny insurance coverage for your claim or sends you a letter stating that it is “reserving its rights” not to cover or to limit coverage for your claim.
Retaining independent counsel protects your interests, not those of your insurance company.
Independent counsel can give you a second opinion on the strengths and weaknesses of your claim, help you prepare for your deposition, and attend court dates with you to ensure that you are completely protected.
Independent counsel can challenge your insurance company’s decision to deny or limit your insurance coverage and ensure that you receive all of the benefits to which you are entitled under your insurance policy. Some policies may include an independent lawyer to be paid for by your insurance carrier in case of a conflicts.
The most important takeaway? Your medical malpractice insurance carrier is not your friend, so act accordingly in times of conflict.
A version of this article first appeared on Medscape.com.
You’ve been sued for medical malpractice. If you are a physician in the United States, that is not an unlikely scenario.
An analysis by the American Medical Association shows that almost half of all physicians are sued by the time they reach 54. In some specialties, such as ob.gyn., one is almost guaranteed to be sued at some point.
But that’s what medical malpractice insurance is for, right? Your medical malpractice insurer will assign an attorney to take care of you and help you through this situation. Won’t they?
Maybe so, but the attorney and the claims representative your insurer assigns to your case may have a different idea about how to proceed than you do. Though the defense attorney assigned to you represents you, he or she gets paid by the insurance carrier.
This can create a conflict when your defense counsel and your insurance claims representative aim to take your case in a direction you don’t like.
Disagreements might include:
- Choice of expert witnesses
- Tactical decisions related to trial strategy
- Public relations considerations
- Admissions of liability
- Allocation of resources
To Settle or Not?
One of the most challenging — and common — disagreements is whether to settle the case.
Sometimes a malpractice insurer wants to settle the case against the defendant doctor’s wishes. Or the doctor wants to settle but is pushed into going to trial. In the following case, one doctor had to face the consequences of a decision he didn’t even make.
The Underlying Medical Malpractice Case
Dr. D was sued by a patient who had allegedly called Dr. D’s office six times in 2 days complaining of intermittent chest pain.
Dr. D had been swamped with patients and couldn’t squeeze this patient in for an office visit, but he did call back. The patient later claimed that during the call he told the doctor he was suffering from chest pain. The doctor recalled that the patient had complained of abdominal discomfort that began after he had exercised.
The physician wrote a prescription for an ECG at the local hospital and called to ensure that the patient could just walk in. The ECG was allegedly abnormal but was not read as representing an impending or current heart attack. Later that evening, however, the patient went to the emergency department of another hospital where it was confirmed that he had suffered a heart attack. The patient underwent cardiac catheterization and stent placement to address a blockage in his left anterior descending artery.
The patient subsequently sued Dr. D and the hospital where he had the original ECG. Dr. D contacted his medical malpractice insurance company. The insurance company assigned an attorney to represent Dr. D. Discovery in the case began.
The plaintiff’s own medical expert testified in a deposition that there was no way for the heart attack to have been prevented and that the treatment would have been the same either way. But Dr. D could not find a record of the phone calls with the patient, and he had not noted his conversation the patient in their medical records.
Dr. D held a policy for $1 million, and his state had a fund that would kick in an additional $1 million. But the plaintiffs demanded $4 million to settle.
A month before trial, the plaintiff’s attorney sent a threatening letter to Dr. D’s attorney warning him that Dr. D was underinsured and suggesting that it would be in the physician’s best interests to settle.
“I want to stress to you that it is not my desire to harm your client’s reputation or to destroy his business,” wrote the plaintiff’s attorney. “However, now is the time to avoid consequences such as these by making a good faith effort to get this case resolved.”
The letter went on to note that the defense attorney should give Dr. D a copy of the letter so that everyone would be aware of the potential consequences of an award against Dr. D in excess of his limits of insurance coverage. The plaintiff’s attorney even suggested that Dr. D should retain personal counsel.
Dr. D’s defense attorney downplayed the letter and assured him that there was no reason to worry.
Meanwhile the case inched closer to trial.
The codefendant hospital settled with the plaintiff on the night before jury selection, leaving Dr. D in the uncomfortable position of being the only defendant in the case. At this point, Dr. D decided he would like to settle, and he sent his attorney an email telling him so. But the attorney instead referred him to an insurance company claims.
Just days before the trial was to start, Dr. D repeatedly told the claims representative assigned to his claim that he did not want to go to trial but rather wanted to settle. The representative told Dr. D that he had no choice in whether the action settled.
A committee at the insurance company had decided to proceed with the trial rather than settle.
The trial proved a painful debacle for Dr. D. His attorney’s idea of showing a “gotcha” video of the allegedly permanently injured plaintiff carrying a large, heavy box backfired when the jury was shown by the plaintiff that the box actually contained ice cream cones and weighed very little.
Prior to trial, the plaintiff offered to settle for $1 million. On the first day of trial, they lowered that amount to $750,000, yet the defense attorney did not settle the case, and it proceeded to a jury verdict. The jury awarded the plaintiff over $4 million — well in excess of Dr. D’s policy limits.
The Follow-up
Dr. D was horrified, but the insurance company claims representative said the insurer would promptly offer $2 million in available insurance coverage to settle the case post verdict. This did not happen. Instead, the insurer chose to appeal the verdict against Dr. D’s wishes.
Ultimately, Dr. D was forced to hire his own lawyer. He ultimately sued the insurance company for breach of contract and bad faith.
The insurance company eventually attempted to settle with the plaintiffs’ counsel, but the plaintiff refused to accept the available insurance coverage. The insurance carrier still has not posted the entire appeal bond. The case is still pending.
Protecting Yourself
The lesson from Dr. D’s experience: Understand that the insurance company is not your friend. It’s a business looking out for its own interests.
The plaintiff’s attorney was absolutely correct in suggesting that Dr. D retain his own attorney to represent his own interests. You should hire your own lawyer when:
- You disagree with your insurer on how to proceed in a case.
- You receive a demand that exceeds your available insurance coverage or for damages that may not be covered by your policy, such as punitive damages.
- Your insurance carrier attempts to deny insurance coverage for your claim or sends you a letter stating that it is “reserving its rights” not to cover or to limit coverage for your claim.
Retaining independent counsel protects your interests, not those of your insurance company.
Independent counsel can give you a second opinion on the strengths and weaknesses of your claim, help you prepare for your deposition, and attend court dates with you to ensure that you are completely protected.
Independent counsel can challenge your insurance company’s decision to deny or limit your insurance coverage and ensure that you receive all of the benefits to which you are entitled under your insurance policy. Some policies may include an independent lawyer to be paid for by your insurance carrier in case of a conflicts.
The most important takeaway? Your medical malpractice insurance carrier is not your friend, so act accordingly in times of conflict.
A version of this article first appeared on Medscape.com.
You’ve been sued for medical malpractice. If you are a physician in the United States, that is not an unlikely scenario.
An analysis by the American Medical Association shows that almost half of all physicians are sued by the time they reach 54. In some specialties, such as ob.gyn., one is almost guaranteed to be sued at some point.
But that’s what medical malpractice insurance is for, right? Your medical malpractice insurer will assign an attorney to take care of you and help you through this situation. Won’t they?
Maybe so, but the attorney and the claims representative your insurer assigns to your case may have a different idea about how to proceed than you do. Though the defense attorney assigned to you represents you, he or she gets paid by the insurance carrier.
This can create a conflict when your defense counsel and your insurance claims representative aim to take your case in a direction you don’t like.
Disagreements might include:
- Choice of expert witnesses
- Tactical decisions related to trial strategy
- Public relations considerations
- Admissions of liability
- Allocation of resources
To Settle or Not?
One of the most challenging — and common — disagreements is whether to settle the case.
Sometimes a malpractice insurer wants to settle the case against the defendant doctor’s wishes. Or the doctor wants to settle but is pushed into going to trial. In the following case, one doctor had to face the consequences of a decision he didn’t even make.
The Underlying Medical Malpractice Case
Dr. D was sued by a patient who had allegedly called Dr. D’s office six times in 2 days complaining of intermittent chest pain.
Dr. D had been swamped with patients and couldn’t squeeze this patient in for an office visit, but he did call back. The patient later claimed that during the call he told the doctor he was suffering from chest pain. The doctor recalled that the patient had complained of abdominal discomfort that began after he had exercised.
The physician wrote a prescription for an ECG at the local hospital and called to ensure that the patient could just walk in. The ECG was allegedly abnormal but was not read as representing an impending or current heart attack. Later that evening, however, the patient went to the emergency department of another hospital where it was confirmed that he had suffered a heart attack. The patient underwent cardiac catheterization and stent placement to address a blockage in his left anterior descending artery.
The patient subsequently sued Dr. D and the hospital where he had the original ECG. Dr. D contacted his medical malpractice insurance company. The insurance company assigned an attorney to represent Dr. D. Discovery in the case began.
The plaintiff’s own medical expert testified in a deposition that there was no way for the heart attack to have been prevented and that the treatment would have been the same either way. But Dr. D could not find a record of the phone calls with the patient, and he had not noted his conversation the patient in their medical records.
Dr. D held a policy for $1 million, and his state had a fund that would kick in an additional $1 million. But the plaintiffs demanded $4 million to settle.
A month before trial, the plaintiff’s attorney sent a threatening letter to Dr. D’s attorney warning him that Dr. D was underinsured and suggesting that it would be in the physician’s best interests to settle.
“I want to stress to you that it is not my desire to harm your client’s reputation or to destroy his business,” wrote the plaintiff’s attorney. “However, now is the time to avoid consequences such as these by making a good faith effort to get this case resolved.”
The letter went on to note that the defense attorney should give Dr. D a copy of the letter so that everyone would be aware of the potential consequences of an award against Dr. D in excess of his limits of insurance coverage. The plaintiff’s attorney even suggested that Dr. D should retain personal counsel.
Dr. D’s defense attorney downplayed the letter and assured him that there was no reason to worry.
Meanwhile the case inched closer to trial.
The codefendant hospital settled with the plaintiff on the night before jury selection, leaving Dr. D in the uncomfortable position of being the only defendant in the case. At this point, Dr. D decided he would like to settle, and he sent his attorney an email telling him so. But the attorney instead referred him to an insurance company claims.
Just days before the trial was to start, Dr. D repeatedly told the claims representative assigned to his claim that he did not want to go to trial but rather wanted to settle. The representative told Dr. D that he had no choice in whether the action settled.
A committee at the insurance company had decided to proceed with the trial rather than settle.
The trial proved a painful debacle for Dr. D. His attorney’s idea of showing a “gotcha” video of the allegedly permanently injured plaintiff carrying a large, heavy box backfired when the jury was shown by the plaintiff that the box actually contained ice cream cones and weighed very little.
Prior to trial, the plaintiff offered to settle for $1 million. On the first day of trial, they lowered that amount to $750,000, yet the defense attorney did not settle the case, and it proceeded to a jury verdict. The jury awarded the plaintiff over $4 million — well in excess of Dr. D’s policy limits.
The Follow-up
Dr. D was horrified, but the insurance company claims representative said the insurer would promptly offer $2 million in available insurance coverage to settle the case post verdict. This did not happen. Instead, the insurer chose to appeal the verdict against Dr. D’s wishes.
Ultimately, Dr. D was forced to hire his own lawyer. He ultimately sued the insurance company for breach of contract and bad faith.
The insurance company eventually attempted to settle with the plaintiffs’ counsel, but the plaintiff refused to accept the available insurance coverage. The insurance carrier still has not posted the entire appeal bond. The case is still pending.
Protecting Yourself
The lesson from Dr. D’s experience: Understand that the insurance company is not your friend. It’s a business looking out for its own interests.
The plaintiff’s attorney was absolutely correct in suggesting that Dr. D retain his own attorney to represent his own interests. You should hire your own lawyer when:
- You disagree with your insurer on how to proceed in a case.
- You receive a demand that exceeds your available insurance coverage or for damages that may not be covered by your policy, such as punitive damages.
- Your insurance carrier attempts to deny insurance coverage for your claim or sends you a letter stating that it is “reserving its rights” not to cover or to limit coverage for your claim.
Retaining independent counsel protects your interests, not those of your insurance company.
Independent counsel can give you a second opinion on the strengths and weaknesses of your claim, help you prepare for your deposition, and attend court dates with you to ensure that you are completely protected.
Independent counsel can challenge your insurance company’s decision to deny or limit your insurance coverage and ensure that you receive all of the benefits to which you are entitled under your insurance policy. Some policies may include an independent lawyer to be paid for by your insurance carrier in case of a conflicts.
The most important takeaway? Your medical malpractice insurance carrier is not your friend, so act accordingly in times of conflict.
A version of this article first appeared on Medscape.com.
First Combined Face and Eye Transplant Performed
In a groundbreaking procedure, a team of surgeons from New York University Langone Health successfully performed the first combined face and eye transplant on a patient with extensive craniofacial tissue loss after an electrical accident.
The highly complex surgery lasted for 21 hours and involved more than 140 surgeons, nurses, and other healthcare professionals under the leadership of Eduardo D. Rodriguez. MD. It not only restored the patient’s facial features, but also integrated a functional eyeball, potentially setting a new standard for future treatments in similar cases.
The transplant took place in May 2023, and the case report was published on September 5 this year in JAMA.
The 46-year-old man lost a large part of his craniofacial tissue and his left eyeball. The approach was highly specialized. Advanced microsurgical techniques such as anastomoses of microscopic vessels and delicate suturing techniques were crucial for the transplant’s success.
Moreover, customized surgical devices, specific implants, and tissue manipulation tools were developed specifically for this case, thus ensuring the viability of the transplant and adequate perfusion of the transplanted ocular tissue.
The initial results are encouraging. Retinal arterial perfusion has been maintained, and retinal architecture has been preserved, as demonstrated by optical coherence tomography. Electroretinography confirmed retinal responses to light, suggesting that the transplanted eye may eventually contribute to the patient’s visual perception. These results are comparable to those of previous facial tissue transplants, but with the significant addition of ocular functionality, which is a notable advance.
“The successful revascularization of the transplanted eye achieved in this study may serve as a step toward the goal of globe transplant for restoration of vision,” wrote the authors.
The complexity of the combined transplant required a deep understanding of facial and ocular anatomy, as well as tissue preservation techniques. The surgical team reported significant challenges, including the need to align delicate anatomical structures and ensure immunological compatibility between the donor and recipient. Meticulous planning from donor selection to postoperative follow-up was considered essential to maximize the likelihood of success and minimize the risk for allograft rejection.
The patient will now be continuously monitored and receive treatment with immunosuppressants such as tacrolimus and prednisone, adjusted according to his response to the transplant. According to the researchers, further studies will be needed to assess the long-term functionality of the transplanted eye and its integration with the central nervous system.
Despite being the fifth facial transplant surgery performed under Dr. Rodriguez’s leadership, this is the first record of a whole-eye transplant. “The mere fact that we have successfully performed the first whole-eye transplant along with a face transplant is a tremendous achievement that many believed to be impossible,” the doctor said in a statement. “We have taken a giant step forward and paved the way for the next chapter in vision restoration.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
In a groundbreaking procedure, a team of surgeons from New York University Langone Health successfully performed the first combined face and eye transplant on a patient with extensive craniofacial tissue loss after an electrical accident.
The highly complex surgery lasted for 21 hours and involved more than 140 surgeons, nurses, and other healthcare professionals under the leadership of Eduardo D. Rodriguez. MD. It not only restored the patient’s facial features, but also integrated a functional eyeball, potentially setting a new standard for future treatments in similar cases.
The transplant took place in May 2023, and the case report was published on September 5 this year in JAMA.
The 46-year-old man lost a large part of his craniofacial tissue and his left eyeball. The approach was highly specialized. Advanced microsurgical techniques such as anastomoses of microscopic vessels and delicate suturing techniques were crucial for the transplant’s success.
Moreover, customized surgical devices, specific implants, and tissue manipulation tools were developed specifically for this case, thus ensuring the viability of the transplant and adequate perfusion of the transplanted ocular tissue.
The initial results are encouraging. Retinal arterial perfusion has been maintained, and retinal architecture has been preserved, as demonstrated by optical coherence tomography. Electroretinography confirmed retinal responses to light, suggesting that the transplanted eye may eventually contribute to the patient’s visual perception. These results are comparable to those of previous facial tissue transplants, but with the significant addition of ocular functionality, which is a notable advance.
“The successful revascularization of the transplanted eye achieved in this study may serve as a step toward the goal of globe transplant for restoration of vision,” wrote the authors.
The complexity of the combined transplant required a deep understanding of facial and ocular anatomy, as well as tissue preservation techniques. The surgical team reported significant challenges, including the need to align delicate anatomical structures and ensure immunological compatibility between the donor and recipient. Meticulous planning from donor selection to postoperative follow-up was considered essential to maximize the likelihood of success and minimize the risk for allograft rejection.
The patient will now be continuously monitored and receive treatment with immunosuppressants such as tacrolimus and prednisone, adjusted according to his response to the transplant. According to the researchers, further studies will be needed to assess the long-term functionality of the transplanted eye and its integration with the central nervous system.
Despite being the fifth facial transplant surgery performed under Dr. Rodriguez’s leadership, this is the first record of a whole-eye transplant. “The mere fact that we have successfully performed the first whole-eye transplant along with a face transplant is a tremendous achievement that many believed to be impossible,” the doctor said in a statement. “We have taken a giant step forward and paved the way for the next chapter in vision restoration.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
In a groundbreaking procedure, a team of surgeons from New York University Langone Health successfully performed the first combined face and eye transplant on a patient with extensive craniofacial tissue loss after an electrical accident.
The highly complex surgery lasted for 21 hours and involved more than 140 surgeons, nurses, and other healthcare professionals under the leadership of Eduardo D. Rodriguez. MD. It not only restored the patient’s facial features, but also integrated a functional eyeball, potentially setting a new standard for future treatments in similar cases.
The transplant took place in May 2023, and the case report was published on September 5 this year in JAMA.
The 46-year-old man lost a large part of his craniofacial tissue and his left eyeball. The approach was highly specialized. Advanced microsurgical techniques such as anastomoses of microscopic vessels and delicate suturing techniques were crucial for the transplant’s success.
Moreover, customized surgical devices, specific implants, and tissue manipulation tools were developed specifically for this case, thus ensuring the viability of the transplant and adequate perfusion of the transplanted ocular tissue.
The initial results are encouraging. Retinal arterial perfusion has been maintained, and retinal architecture has been preserved, as demonstrated by optical coherence tomography. Electroretinography confirmed retinal responses to light, suggesting that the transplanted eye may eventually contribute to the patient’s visual perception. These results are comparable to those of previous facial tissue transplants, but with the significant addition of ocular functionality, which is a notable advance.
“The successful revascularization of the transplanted eye achieved in this study may serve as a step toward the goal of globe transplant for restoration of vision,” wrote the authors.
The complexity of the combined transplant required a deep understanding of facial and ocular anatomy, as well as tissue preservation techniques. The surgical team reported significant challenges, including the need to align delicate anatomical structures and ensure immunological compatibility between the donor and recipient. Meticulous planning from donor selection to postoperative follow-up was considered essential to maximize the likelihood of success and minimize the risk for allograft rejection.
The patient will now be continuously monitored and receive treatment with immunosuppressants such as tacrolimus and prednisone, adjusted according to his response to the transplant. According to the researchers, further studies will be needed to assess the long-term functionality of the transplanted eye and its integration with the central nervous system.
Despite being the fifth facial transplant surgery performed under Dr. Rodriguez’s leadership, this is the first record of a whole-eye transplant. “The mere fact that we have successfully performed the first whole-eye transplant along with a face transplant is a tremendous achievement that many believed to be impossible,” the doctor said in a statement. “We have taken a giant step forward and paved the way for the next chapter in vision restoration.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Coffee’s ‘Sweet Spot’: Daily Consumption and Cardiometabolic Risk
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.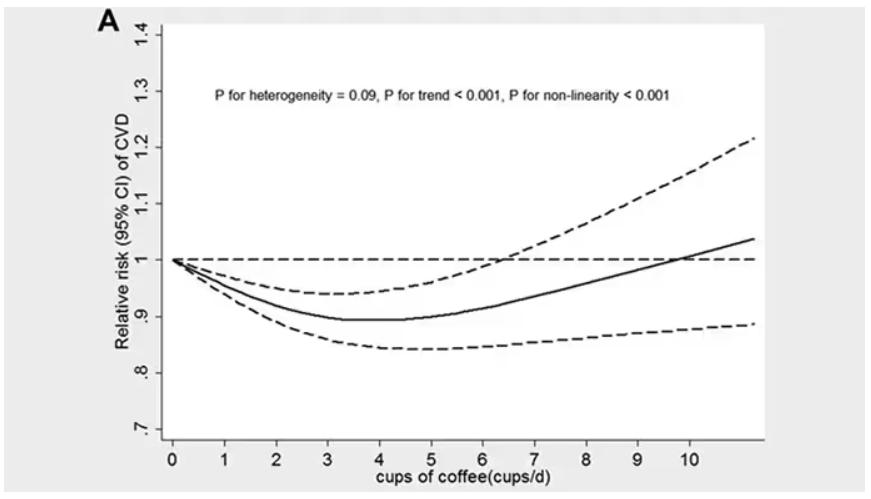
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.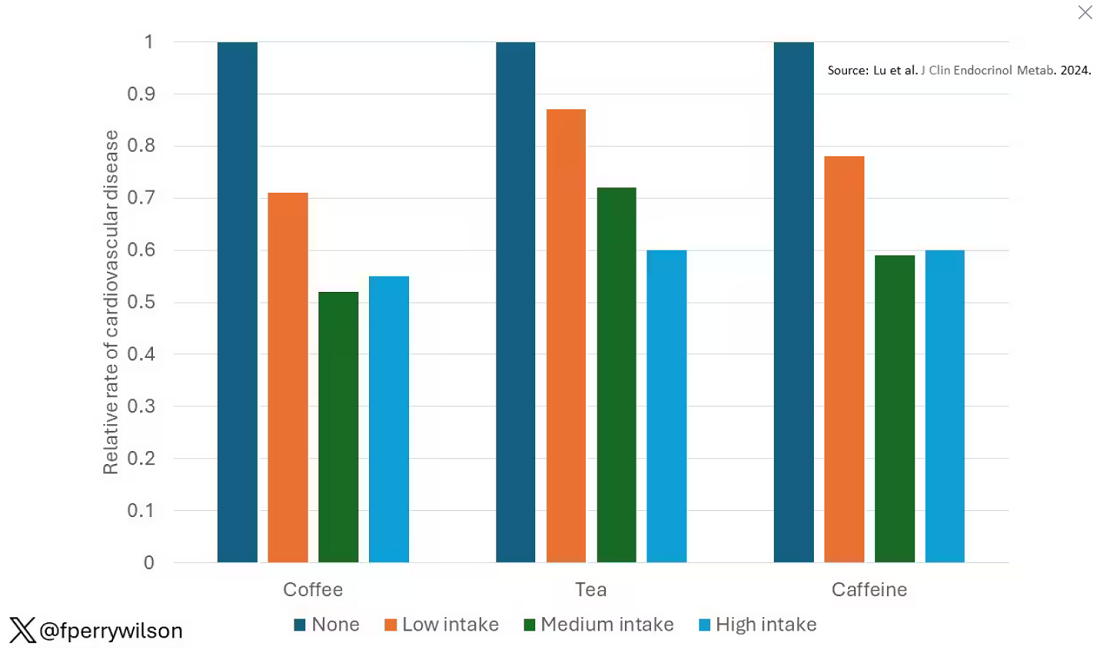
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine. 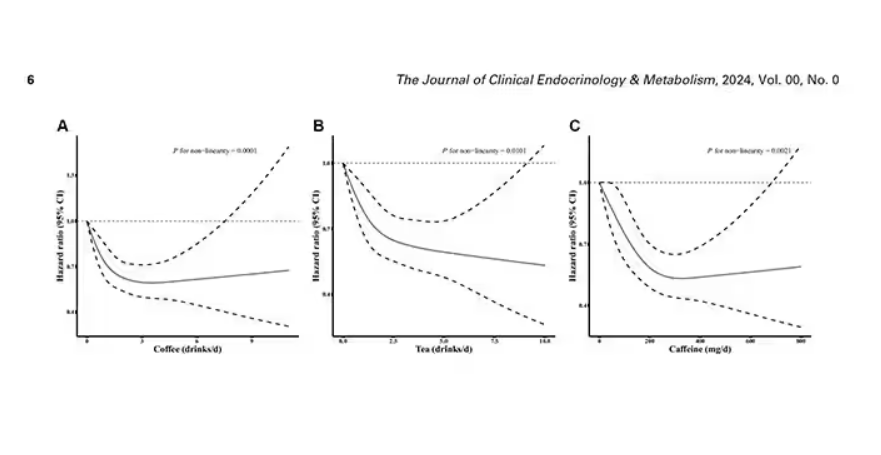
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated. 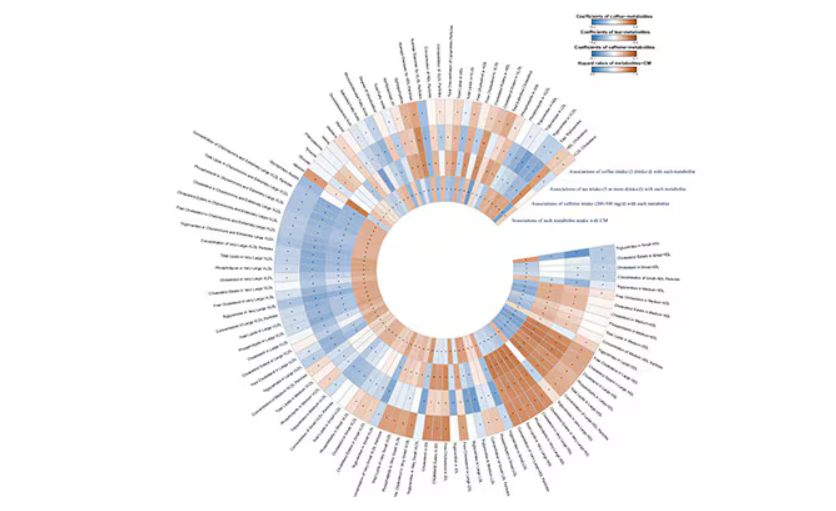
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.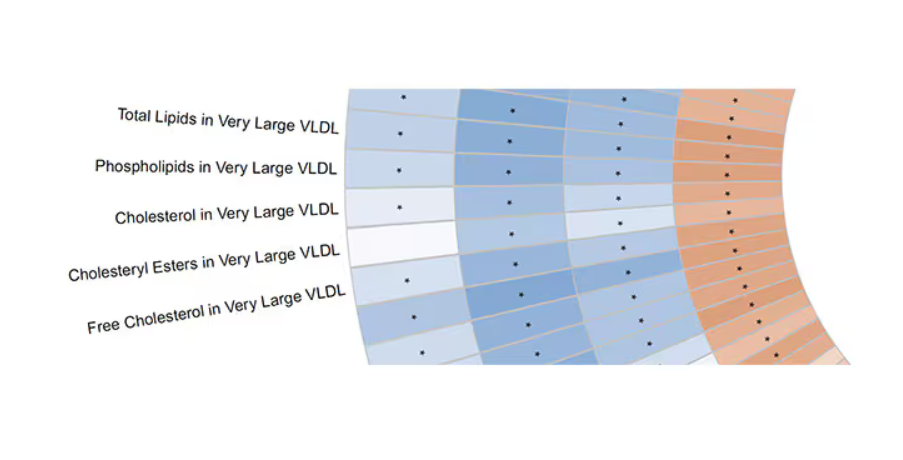
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine.
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated.
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine.
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated.
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Will New Obesity Drugs Make Bariatric Surgery Obsolete?
MADRID — In spirited presentations at the annual meeting of the European Association for the Study of Diabetes, Louis J. Aronne, MD, of Weill Cornell Medicine in New York City, made a compelling case that the next generation of obesity medications will make bariatric surgery obsolete, and Francesco Rubino, MD, of King’s College London in England, made an equally compelling case that they will not.
In fact, Dr. Rubino predicted that “metabolic” surgery — new nomenclature reflecting the power of surgery to reduce not only obesity, but also other metabolic conditions, over the long term — will continue and could even increase in years to come.
‘Medical Treatment Will Dominate’
“Obesity treatment is the superhero of treating metabolic disease because it can defeat all of the bad guys at once, not just one, like the other treatments,” Dr. Aronne told meeting attendees. “If you treat somebody’s cholesterol, you’re just treating their cholesterol, and you may actually increase their risk of developing type 2 diabetes (T2D). You treat their blood pressure, you don’t treat their glucose and you don’t treat their lipids — the list goes on and on and on. But by treating obesity, if you can get enough weight loss, you can get all those things at once.”
He pointed to the SELECT trial, which showed that treating obesity with a glucagon-like peptide 1 receptor agonist reduced major adverse cardiovascular events as well as death from any cause, results in line with those from other modes of treatment for cardiovascular disease (CVD) or lipid lowering, he said. “But we get much more with these drugs, including positive effects on heart failure, chronic kidney disease, and a 73% reduction in T2D. So, we’re now on the verge of a major change in the way we manage metabolic disease.”
Dr. Aronne drew a parallel between treating obesity and the historic way of treating hypertension. Years ago, he said, “we waited too long to treat people. We waited until they had severe hypertension that in many cases was irreversible. What would you prefer to do now for obesity — have the patient lose weight with a medicine that is proven to reduce complications or wait until they develop diabetes, high blood pressure, heart disease and then have them undergo surgery to treat that?”
Looking ahead, “the trend could be to treat obesity before it gets out of hand,” he suggested. Treatment might start in people with a body mass index (BMI) of 27 kg/m2, who would be treated to a target BMI of 25. “That’s only a 10% or so change, but our goal would be to keep them in the normal range so they never go above that target. In fact, I think we’re going to be looking at people with severe obesity in a few years and saying, ‘I can’t believe someone didn’t treat that guy earlier.’ What’s going to happen to bariatric surgery if no one gets to a higher weight?”
The plethora of current weight-loss drugs and the large group on the horizon mean that if someone doesn’t respond to one drug, there will be plenty of other choices, Dr. Aronne continued. People will be referred for surgery, but possibly only after they’ve not responded to medical treatment — or just the opposite. “In the United States, it’s much cheaper to have surgery, and I bet the insurance companies are going to make people have surgery before they can get the medicines,” he acknowledged.
A recent report from Morgan Stanley suggests that the global market for the newer weight-loss drugs could increase by 15-fold over the next 5 years as their benefits expand beyond weight loss and that as much as 9% of the US population will be taking the drugs by 2035, Dr. Aronne said, adding that he thinks 9% is an underestimate. By contrast, the number of patients treated by his team’s surgical program is down about 20%.
“I think it’s very clear that medical treatment is going to dominate,” he concluded. “But, it’s also possible that surgery could go up because so many people are going to be coming for medical therapy that we may wind up referring more for surgical therapy.”
‘Surgery Is Saving Lives’
Dr. Rubino is convinced that anti-obesity drugs will not make surgery obsolete, “but it will not be business as usual,” he told meeting attendees. “In fact, I think these drugs will expedite a process that is already ongoing — a transformation of bariatric into metabolic surgery.”
“Bariatric surgery will go down in history as one of the biggest missed opportunities that we, as medical professionals, have seen over the past many years,” he said. “It has been shown beyond any doubt to reduce all-cause mortality — in other words, it saves lives,” and it’s also cost effective and improves quality of life. Yet, fewer than 1% of people globally who meet the criteria actually get the surgery.
Many clinicians don’t inform patients about the treatment and don’t refer them for it, he said. “That would be equivalent to having surgery for CVD [cardiovascular disease], cancer, or other important diseases available but not being accessed as they should be.”
A big reason for the dearth of procedures is that people have unrealistic expectations about diet and exercise interventions for weight loss, he said. His team’s survey, presented at the 26th World Congress of the International Federation for the Surgery of Obesity and Metabolic Disorders, showed that 43% of respondents believed diet and exercise was the best treatment for severe obesity (BMI > 35). A more recent survey asked which among several choices was the most effective weight-loss intervention, and again a large proportion “believed wrongly that diet and exercise is most effective — more so than drugs or surgery — despite plenty of evidence that this is not the case.”
In this context, he said, “any surgery, no matter how safe or effective, would never be very popular.” If obesity is viewed as a modifiable risk factor, patients may say they’ll think about it for 6 months. In contrast, “nobody will tell you ‘I will think about it’ if you tell them they need gallbladder surgery to get rid of gallstone pain.”
Although drugs are available to treat obesity, none of them are curative, and if they’re stopped, the weight comes back, Dr. Rubino pointed out. “Efficacy of drugs is measured in weeks or months, whereas efficacy of surgery is measured in decades of durability — in the case of bariatric surgery, 10-20 years. That’s why bariatric surgery will remain an option,” he said. “It’s not just preventing disease, it’s resolving ongoing disease.”
Furthermore, bariatric surgery is showing value for people with established T2D, whereas in the past, it was mainly considered to be a weight-loss intervention for younger, healthier patients, he said. “In my practice, we’re operating more often in people with T2D, even those at higher risk for anesthesia and surgery — eg, patients with heart failure, chronic kidney disease, on dialysis — and we’re still able to maintain the same safety with minimally invasive laparoscopic surgery that we had with healthier patients.”
A vote held at the end of the session revealed that the audience was split about half and half in favor of drugs making bariatric surgery obsolete or not.
“I think we may have to duke it out now,” Dr. Aronne quipped.
Dr. Aronne disclosed being a consultant, speaker, and adviser for and receiving research support from Altimmune, Amgen, AstraZeneca, Eli Lilly, Intellihealth, Janssen, Novo Nordisk, Pfizer, Senda, UnitedHealth Group, Versanis, and others; he has ownership interests in ERX, Intellihealth, Jamieson, Kallyope, Skye Bioscience, Veru, and others; and he is on the board of directors of ERX, Jamieson Wellness, and Intellihealth/FlyteHealth. Dr. Rubino disclosed receiving research and educational grants from Novo Nordisk, Ethicon, and Medtronic; he is on the scientific advisory board/data safety advisory board for Keyron, Morphic Medical, and GT Metabolic Solutions; he receives speaking honoraria from Medtronic, Ethicon, Novo Nordisk, and Eli Lilly; and he is president of the nonprofit Metabolic Health Institute.
A version of this article first appeared on Medscape.com.
MADRID — In spirited presentations at the annual meeting of the European Association for the Study of Diabetes, Louis J. Aronne, MD, of Weill Cornell Medicine in New York City, made a compelling case that the next generation of obesity medications will make bariatric surgery obsolete, and Francesco Rubino, MD, of King’s College London in England, made an equally compelling case that they will not.
In fact, Dr. Rubino predicted that “metabolic” surgery — new nomenclature reflecting the power of surgery to reduce not only obesity, but also other metabolic conditions, over the long term — will continue and could even increase in years to come.
‘Medical Treatment Will Dominate’
“Obesity treatment is the superhero of treating metabolic disease because it can defeat all of the bad guys at once, not just one, like the other treatments,” Dr. Aronne told meeting attendees. “If you treat somebody’s cholesterol, you’re just treating their cholesterol, and you may actually increase their risk of developing type 2 diabetes (T2D). You treat their blood pressure, you don’t treat their glucose and you don’t treat their lipids — the list goes on and on and on. But by treating obesity, if you can get enough weight loss, you can get all those things at once.”
He pointed to the SELECT trial, which showed that treating obesity with a glucagon-like peptide 1 receptor agonist reduced major adverse cardiovascular events as well as death from any cause, results in line with those from other modes of treatment for cardiovascular disease (CVD) or lipid lowering, he said. “But we get much more with these drugs, including positive effects on heart failure, chronic kidney disease, and a 73% reduction in T2D. So, we’re now on the verge of a major change in the way we manage metabolic disease.”
Dr. Aronne drew a parallel between treating obesity and the historic way of treating hypertension. Years ago, he said, “we waited too long to treat people. We waited until they had severe hypertension that in many cases was irreversible. What would you prefer to do now for obesity — have the patient lose weight with a medicine that is proven to reduce complications or wait until they develop diabetes, high blood pressure, heart disease and then have them undergo surgery to treat that?”
Looking ahead, “the trend could be to treat obesity before it gets out of hand,” he suggested. Treatment might start in people with a body mass index (BMI) of 27 kg/m2, who would be treated to a target BMI of 25. “That’s only a 10% or so change, but our goal would be to keep them in the normal range so they never go above that target. In fact, I think we’re going to be looking at people with severe obesity in a few years and saying, ‘I can’t believe someone didn’t treat that guy earlier.’ What’s going to happen to bariatric surgery if no one gets to a higher weight?”
The plethora of current weight-loss drugs and the large group on the horizon mean that if someone doesn’t respond to one drug, there will be plenty of other choices, Dr. Aronne continued. People will be referred for surgery, but possibly only after they’ve not responded to medical treatment — or just the opposite. “In the United States, it’s much cheaper to have surgery, and I bet the insurance companies are going to make people have surgery before they can get the medicines,” he acknowledged.
A recent report from Morgan Stanley suggests that the global market for the newer weight-loss drugs could increase by 15-fold over the next 5 years as their benefits expand beyond weight loss and that as much as 9% of the US population will be taking the drugs by 2035, Dr. Aronne said, adding that he thinks 9% is an underestimate. By contrast, the number of patients treated by his team’s surgical program is down about 20%.
“I think it’s very clear that medical treatment is going to dominate,” he concluded. “But, it’s also possible that surgery could go up because so many people are going to be coming for medical therapy that we may wind up referring more for surgical therapy.”
‘Surgery Is Saving Lives’
Dr. Rubino is convinced that anti-obesity drugs will not make surgery obsolete, “but it will not be business as usual,” he told meeting attendees. “In fact, I think these drugs will expedite a process that is already ongoing — a transformation of bariatric into metabolic surgery.”
“Bariatric surgery will go down in history as one of the biggest missed opportunities that we, as medical professionals, have seen over the past many years,” he said. “It has been shown beyond any doubt to reduce all-cause mortality — in other words, it saves lives,” and it’s also cost effective and improves quality of life. Yet, fewer than 1% of people globally who meet the criteria actually get the surgery.
Many clinicians don’t inform patients about the treatment and don’t refer them for it, he said. “That would be equivalent to having surgery for CVD [cardiovascular disease], cancer, or other important diseases available but not being accessed as they should be.”
A big reason for the dearth of procedures is that people have unrealistic expectations about diet and exercise interventions for weight loss, he said. His team’s survey, presented at the 26th World Congress of the International Federation for the Surgery of Obesity and Metabolic Disorders, showed that 43% of respondents believed diet and exercise was the best treatment for severe obesity (BMI > 35). A more recent survey asked which among several choices was the most effective weight-loss intervention, and again a large proportion “believed wrongly that diet and exercise is most effective — more so than drugs or surgery — despite plenty of evidence that this is not the case.”
In this context, he said, “any surgery, no matter how safe or effective, would never be very popular.” If obesity is viewed as a modifiable risk factor, patients may say they’ll think about it for 6 months. In contrast, “nobody will tell you ‘I will think about it’ if you tell them they need gallbladder surgery to get rid of gallstone pain.”
Although drugs are available to treat obesity, none of them are curative, and if they’re stopped, the weight comes back, Dr. Rubino pointed out. “Efficacy of drugs is measured in weeks or months, whereas efficacy of surgery is measured in decades of durability — in the case of bariatric surgery, 10-20 years. That’s why bariatric surgery will remain an option,” he said. “It’s not just preventing disease, it’s resolving ongoing disease.”
Furthermore, bariatric surgery is showing value for people with established T2D, whereas in the past, it was mainly considered to be a weight-loss intervention for younger, healthier patients, he said. “In my practice, we’re operating more often in people with T2D, even those at higher risk for anesthesia and surgery — eg, patients with heart failure, chronic kidney disease, on dialysis — and we’re still able to maintain the same safety with minimally invasive laparoscopic surgery that we had with healthier patients.”
A vote held at the end of the session revealed that the audience was split about half and half in favor of drugs making bariatric surgery obsolete or not.
“I think we may have to duke it out now,” Dr. Aronne quipped.
Dr. Aronne disclosed being a consultant, speaker, and adviser for and receiving research support from Altimmune, Amgen, AstraZeneca, Eli Lilly, Intellihealth, Janssen, Novo Nordisk, Pfizer, Senda, UnitedHealth Group, Versanis, and others; he has ownership interests in ERX, Intellihealth, Jamieson, Kallyope, Skye Bioscience, Veru, and others; and he is on the board of directors of ERX, Jamieson Wellness, and Intellihealth/FlyteHealth. Dr. Rubino disclosed receiving research and educational grants from Novo Nordisk, Ethicon, and Medtronic; he is on the scientific advisory board/data safety advisory board for Keyron, Morphic Medical, and GT Metabolic Solutions; he receives speaking honoraria from Medtronic, Ethicon, Novo Nordisk, and Eli Lilly; and he is president of the nonprofit Metabolic Health Institute.
A version of this article first appeared on Medscape.com.
MADRID — In spirited presentations at the annual meeting of the European Association for the Study of Diabetes, Louis J. Aronne, MD, of Weill Cornell Medicine in New York City, made a compelling case that the next generation of obesity medications will make bariatric surgery obsolete, and Francesco Rubino, MD, of King’s College London in England, made an equally compelling case that they will not.
In fact, Dr. Rubino predicted that “metabolic” surgery — new nomenclature reflecting the power of surgery to reduce not only obesity, but also other metabolic conditions, over the long term — will continue and could even increase in years to come.
‘Medical Treatment Will Dominate’
“Obesity treatment is the superhero of treating metabolic disease because it can defeat all of the bad guys at once, not just one, like the other treatments,” Dr. Aronne told meeting attendees. “If you treat somebody’s cholesterol, you’re just treating their cholesterol, and you may actually increase their risk of developing type 2 diabetes (T2D). You treat their blood pressure, you don’t treat their glucose and you don’t treat their lipids — the list goes on and on and on. But by treating obesity, if you can get enough weight loss, you can get all those things at once.”
He pointed to the SELECT trial, which showed that treating obesity with a glucagon-like peptide 1 receptor agonist reduced major adverse cardiovascular events as well as death from any cause, results in line with those from other modes of treatment for cardiovascular disease (CVD) or lipid lowering, he said. “But we get much more with these drugs, including positive effects on heart failure, chronic kidney disease, and a 73% reduction in T2D. So, we’re now on the verge of a major change in the way we manage metabolic disease.”
Dr. Aronne drew a parallel between treating obesity and the historic way of treating hypertension. Years ago, he said, “we waited too long to treat people. We waited until they had severe hypertension that in many cases was irreversible. What would you prefer to do now for obesity — have the patient lose weight with a medicine that is proven to reduce complications or wait until they develop diabetes, high blood pressure, heart disease and then have them undergo surgery to treat that?”
Looking ahead, “the trend could be to treat obesity before it gets out of hand,” he suggested. Treatment might start in people with a body mass index (BMI) of 27 kg/m2, who would be treated to a target BMI of 25. “That’s only a 10% or so change, but our goal would be to keep them in the normal range so they never go above that target. In fact, I think we’re going to be looking at people with severe obesity in a few years and saying, ‘I can’t believe someone didn’t treat that guy earlier.’ What’s going to happen to bariatric surgery if no one gets to a higher weight?”
The plethora of current weight-loss drugs and the large group on the horizon mean that if someone doesn’t respond to one drug, there will be plenty of other choices, Dr. Aronne continued. People will be referred for surgery, but possibly only after they’ve not responded to medical treatment — or just the opposite. “In the United States, it’s much cheaper to have surgery, and I bet the insurance companies are going to make people have surgery before they can get the medicines,” he acknowledged.
A recent report from Morgan Stanley suggests that the global market for the newer weight-loss drugs could increase by 15-fold over the next 5 years as their benefits expand beyond weight loss and that as much as 9% of the US population will be taking the drugs by 2035, Dr. Aronne said, adding that he thinks 9% is an underestimate. By contrast, the number of patients treated by his team’s surgical program is down about 20%.
“I think it’s very clear that medical treatment is going to dominate,” he concluded. “But, it’s also possible that surgery could go up because so many people are going to be coming for medical therapy that we may wind up referring more for surgical therapy.”
‘Surgery Is Saving Lives’
Dr. Rubino is convinced that anti-obesity drugs will not make surgery obsolete, “but it will not be business as usual,” he told meeting attendees. “In fact, I think these drugs will expedite a process that is already ongoing — a transformation of bariatric into metabolic surgery.”
“Bariatric surgery will go down in history as one of the biggest missed opportunities that we, as medical professionals, have seen over the past many years,” he said. “It has been shown beyond any doubt to reduce all-cause mortality — in other words, it saves lives,” and it’s also cost effective and improves quality of life. Yet, fewer than 1% of people globally who meet the criteria actually get the surgery.
Many clinicians don’t inform patients about the treatment and don’t refer them for it, he said. “That would be equivalent to having surgery for CVD [cardiovascular disease], cancer, or other important diseases available but not being accessed as they should be.”
A big reason for the dearth of procedures is that people have unrealistic expectations about diet and exercise interventions for weight loss, he said. His team’s survey, presented at the 26th World Congress of the International Federation for the Surgery of Obesity and Metabolic Disorders, showed that 43% of respondents believed diet and exercise was the best treatment for severe obesity (BMI > 35). A more recent survey asked which among several choices was the most effective weight-loss intervention, and again a large proportion “believed wrongly that diet and exercise is most effective — more so than drugs or surgery — despite plenty of evidence that this is not the case.”
In this context, he said, “any surgery, no matter how safe or effective, would never be very popular.” If obesity is viewed as a modifiable risk factor, patients may say they’ll think about it for 6 months. In contrast, “nobody will tell you ‘I will think about it’ if you tell them they need gallbladder surgery to get rid of gallstone pain.”
Although drugs are available to treat obesity, none of them are curative, and if they’re stopped, the weight comes back, Dr. Rubino pointed out. “Efficacy of drugs is measured in weeks or months, whereas efficacy of surgery is measured in decades of durability — in the case of bariatric surgery, 10-20 years. That’s why bariatric surgery will remain an option,” he said. “It’s not just preventing disease, it’s resolving ongoing disease.”
Furthermore, bariatric surgery is showing value for people with established T2D, whereas in the past, it was mainly considered to be a weight-loss intervention for younger, healthier patients, he said. “In my practice, we’re operating more often in people with T2D, even those at higher risk for anesthesia and surgery — eg, patients with heart failure, chronic kidney disease, on dialysis — and we’re still able to maintain the same safety with minimally invasive laparoscopic surgery that we had with healthier patients.”
A vote held at the end of the session revealed that the audience was split about half and half in favor of drugs making bariatric surgery obsolete or not.
“I think we may have to duke it out now,” Dr. Aronne quipped.
Dr. Aronne disclosed being a consultant, speaker, and adviser for and receiving research support from Altimmune, Amgen, AstraZeneca, Eli Lilly, Intellihealth, Janssen, Novo Nordisk, Pfizer, Senda, UnitedHealth Group, Versanis, and others; he has ownership interests in ERX, Intellihealth, Jamieson, Kallyope, Skye Bioscience, Veru, and others; and he is on the board of directors of ERX, Jamieson Wellness, and Intellihealth/FlyteHealth. Dr. Rubino disclosed receiving research and educational grants from Novo Nordisk, Ethicon, and Medtronic; he is on the scientific advisory board/data safety advisory board for Keyron, Morphic Medical, and GT Metabolic Solutions; he receives speaking honoraria from Medtronic, Ethicon, Novo Nordisk, and Eli Lilly; and he is president of the nonprofit Metabolic Health Institute.
A version of this article first appeared on Medscape.com.
FROM EASD 2024
Locally Acquired Dengue Case Confirmed in California
A case of locally acquired dengue fever has been confirmed in a resident of Baldwin Park, California, according to a press release from the Los Angeles County Department of Public Health.
“Dengue is the most common insect-borne viral infection in the world, with a wide geographic spread; we know that we have mosquitoes capable of carrying and transmitting the virus in the United States already, and Los Angeles county is a major epicenter for international travel and trade,” James Lawler, MD, associate director for International Programs and Innovation at the Global Center for Health Security and professor in the Infectious Diseases Division at the University of Nebraska Medical Center, Omaha, Nebraska, said in an interview.
Although the patient had no known history of travel to a dengue-endemic area, the potential risk for widespread transmission of the virus in the Los Angeles County area remains low, and no additional suspected cases of locally acquired dengue have been identified, according to the release. However, the recent cases highlight the need for vigilance on the part of the public to reduce transmission of mosquito-borne infections, the public health department noted.
Most cases of dengue occur in people who have traveled to areas where the disease is more common, mainly tropical and subtropical areas, according to the press release. However, the types of mosquitoes that spread dengue exist in parts of the United States, so locally acquired infections can occur.
The Centers for Disease Control and Prevention (CDC) issued an official health advisory in June 2024 about an increased risk for dengue infections in the United States. According to the advisory, 745 cases of dengue were identified in US travelers to endemic areas between January 1, 2024, and June 24, 2024.
The CDC advises clinicians to maintain a high level of suspicion for dengue among individuals with fever and recent travel to areas with frequent dengue transmission, but also to consider locally acquired disease in areas of mosquito vectors.
In clinical practice, dengue may be difficult to differentiate from other febrile systemic infections, Dr. Lawler noted. “Joint pain, low back pain, and headache (often retro-orbital) are common and can be severe, and a rash often appears several days into illness,” he noted.
Do not delay treatment in suspected cases while waiting for test results, the CDC emphasized in the advisory. Food and Drug Administration–approved tests for dengue include RT-PCR and IgM antibody tests or NS1 and IgM antibody tests.
“Severe dengue can be life-threatening and progress to a hemorrhagic fever-like syndrome, and patients with severe dengue should be cared for on a high-acuity or intensive care setting, with close monitoring of labs and fluid status,” Dr. Lawler told this news organization.
The World Health Organization has published guidelines for the management of dengue, which Dr. Lawler strongly recommends to clinicians in the rare event that they are facing a severe case. The treatment for dengue is supportive care, according to the CDC; a vaccine that was deemed safe and effective is no longer being manufactured because of low demand.
Most symptoms last for 2-7 days, and most patients recover within a week, but approximately 1 in 20 may develop severe disease, according to the Los Angeles County Department of Public Health.
Approximately one quarter of dengue infections are symptomatic, and clinicians should know the signs of progression to severe disease, which include abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy or restlessness, and liver enlargement, according to the CDC.
Local Dengue Not Unexpected
“Sadly, I am not surprised at another locally acquired case of dengue fever in the United States,” said Dr. Lawler. “We also have seen a trend of more historically tropical, insect-borne diseases popping up with locally acquired cases in the United States,” he noted.
Dr. Lawler suggested that “the erosion of state and local public health” is a major contributor to the increase in dengue cases. For more than 100 years, activities of state and local public health officials had significantly curtailed mosquito-borne diseases through aggressive control programs, “but we seem to be losing ground over the last several years,” he said.
“Locally acquired dengue cases are still rare in the United States,” he added. “However, people can protect themselves against dengue and more common arthropod-borne infections by taking precautions to cover up and wear insect repellent while outdoors.”
In addition, the Los Angeles County Department of Public Health emphasized in its press release that local residents reduce their risk for contact with mosquitoes by removing areas of standing water on their property and ensuring well-fitted screens on doors and windows.
Dr. Lawler had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
A case of locally acquired dengue fever has been confirmed in a resident of Baldwin Park, California, according to a press release from the Los Angeles County Department of Public Health.
“Dengue is the most common insect-borne viral infection in the world, with a wide geographic spread; we know that we have mosquitoes capable of carrying and transmitting the virus in the United States already, and Los Angeles county is a major epicenter for international travel and trade,” James Lawler, MD, associate director for International Programs and Innovation at the Global Center for Health Security and professor in the Infectious Diseases Division at the University of Nebraska Medical Center, Omaha, Nebraska, said in an interview.
Although the patient had no known history of travel to a dengue-endemic area, the potential risk for widespread transmission of the virus in the Los Angeles County area remains low, and no additional suspected cases of locally acquired dengue have been identified, according to the release. However, the recent cases highlight the need for vigilance on the part of the public to reduce transmission of mosquito-borne infections, the public health department noted.
Most cases of dengue occur in people who have traveled to areas where the disease is more common, mainly tropical and subtropical areas, according to the press release. However, the types of mosquitoes that spread dengue exist in parts of the United States, so locally acquired infections can occur.
The Centers for Disease Control and Prevention (CDC) issued an official health advisory in June 2024 about an increased risk for dengue infections in the United States. According to the advisory, 745 cases of dengue were identified in US travelers to endemic areas between January 1, 2024, and June 24, 2024.
The CDC advises clinicians to maintain a high level of suspicion for dengue among individuals with fever and recent travel to areas with frequent dengue transmission, but also to consider locally acquired disease in areas of mosquito vectors.
In clinical practice, dengue may be difficult to differentiate from other febrile systemic infections, Dr. Lawler noted. “Joint pain, low back pain, and headache (often retro-orbital) are common and can be severe, and a rash often appears several days into illness,” he noted.
Do not delay treatment in suspected cases while waiting for test results, the CDC emphasized in the advisory. Food and Drug Administration–approved tests for dengue include RT-PCR and IgM antibody tests or NS1 and IgM antibody tests.
“Severe dengue can be life-threatening and progress to a hemorrhagic fever-like syndrome, and patients with severe dengue should be cared for on a high-acuity or intensive care setting, with close monitoring of labs and fluid status,” Dr. Lawler told this news organization.
The World Health Organization has published guidelines for the management of dengue, which Dr. Lawler strongly recommends to clinicians in the rare event that they are facing a severe case. The treatment for dengue is supportive care, according to the CDC; a vaccine that was deemed safe and effective is no longer being manufactured because of low demand.
Most symptoms last for 2-7 days, and most patients recover within a week, but approximately 1 in 20 may develop severe disease, according to the Los Angeles County Department of Public Health.
Approximately one quarter of dengue infections are symptomatic, and clinicians should know the signs of progression to severe disease, which include abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy or restlessness, and liver enlargement, according to the CDC.
Local Dengue Not Unexpected
“Sadly, I am not surprised at another locally acquired case of dengue fever in the United States,” said Dr. Lawler. “We also have seen a trend of more historically tropical, insect-borne diseases popping up with locally acquired cases in the United States,” he noted.
Dr. Lawler suggested that “the erosion of state and local public health” is a major contributor to the increase in dengue cases. For more than 100 years, activities of state and local public health officials had significantly curtailed mosquito-borne diseases through aggressive control programs, “but we seem to be losing ground over the last several years,” he said.
“Locally acquired dengue cases are still rare in the United States,” he added. “However, people can protect themselves against dengue and more common arthropod-borne infections by taking precautions to cover up and wear insect repellent while outdoors.”
In addition, the Los Angeles County Department of Public Health emphasized in its press release that local residents reduce their risk for contact with mosquitoes by removing areas of standing water on their property and ensuring well-fitted screens on doors and windows.
Dr. Lawler had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
A case of locally acquired dengue fever has been confirmed in a resident of Baldwin Park, California, according to a press release from the Los Angeles County Department of Public Health.
“Dengue is the most common insect-borne viral infection in the world, with a wide geographic spread; we know that we have mosquitoes capable of carrying and transmitting the virus in the United States already, and Los Angeles county is a major epicenter for international travel and trade,” James Lawler, MD, associate director for International Programs and Innovation at the Global Center for Health Security and professor in the Infectious Diseases Division at the University of Nebraska Medical Center, Omaha, Nebraska, said in an interview.
Although the patient had no known history of travel to a dengue-endemic area, the potential risk for widespread transmission of the virus in the Los Angeles County area remains low, and no additional suspected cases of locally acquired dengue have been identified, according to the release. However, the recent cases highlight the need for vigilance on the part of the public to reduce transmission of mosquito-borne infections, the public health department noted.
Most cases of dengue occur in people who have traveled to areas where the disease is more common, mainly tropical and subtropical areas, according to the press release. However, the types of mosquitoes that spread dengue exist in parts of the United States, so locally acquired infections can occur.
The Centers for Disease Control and Prevention (CDC) issued an official health advisory in June 2024 about an increased risk for dengue infections in the United States. According to the advisory, 745 cases of dengue were identified in US travelers to endemic areas between January 1, 2024, and June 24, 2024.
The CDC advises clinicians to maintain a high level of suspicion for dengue among individuals with fever and recent travel to areas with frequent dengue transmission, but also to consider locally acquired disease in areas of mosquito vectors.
In clinical practice, dengue may be difficult to differentiate from other febrile systemic infections, Dr. Lawler noted. “Joint pain, low back pain, and headache (often retro-orbital) are common and can be severe, and a rash often appears several days into illness,” he noted.
Do not delay treatment in suspected cases while waiting for test results, the CDC emphasized in the advisory. Food and Drug Administration–approved tests for dengue include RT-PCR and IgM antibody tests or NS1 and IgM antibody tests.
“Severe dengue can be life-threatening and progress to a hemorrhagic fever-like syndrome, and patients with severe dengue should be cared for on a high-acuity or intensive care setting, with close monitoring of labs and fluid status,” Dr. Lawler told this news organization.
The World Health Organization has published guidelines for the management of dengue, which Dr. Lawler strongly recommends to clinicians in the rare event that they are facing a severe case. The treatment for dengue is supportive care, according to the CDC; a vaccine that was deemed safe and effective is no longer being manufactured because of low demand.
Most symptoms last for 2-7 days, and most patients recover within a week, but approximately 1 in 20 may develop severe disease, according to the Los Angeles County Department of Public Health.
Approximately one quarter of dengue infections are symptomatic, and clinicians should know the signs of progression to severe disease, which include abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy or restlessness, and liver enlargement, according to the CDC.
Local Dengue Not Unexpected
“Sadly, I am not surprised at another locally acquired case of dengue fever in the United States,” said Dr. Lawler. “We also have seen a trend of more historically tropical, insect-borne diseases popping up with locally acquired cases in the United States,” he noted.
Dr. Lawler suggested that “the erosion of state and local public health” is a major contributor to the increase in dengue cases. For more than 100 years, activities of state and local public health officials had significantly curtailed mosquito-borne diseases through aggressive control programs, “but we seem to be losing ground over the last several years,” he said.
“Locally acquired dengue cases are still rare in the United States,” he added. “However, people can protect themselves against dengue and more common arthropod-borne infections by taking precautions to cover up and wear insect repellent while outdoors.”
In addition, the Los Angeles County Department of Public Health emphasized in its press release that local residents reduce their risk for contact with mosquitoes by removing areas of standing water on their property and ensuring well-fitted screens on doors and windows.
Dr. Lawler had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Should Genetic Testing Be Routine for Breast Cancer?
TOPLINE:
METHODOLOGY:
- Traditional risk-based criteria, including family history and ancestry, are used to guide genetic testing decisions in women with breast cancer. However, these criteria may overlook patients with actionable genetic variants, particularly those outside the typical risk profile.
- To assess the efficacy of universal genetic testing, researchers conducted a cross-sectional study that included 729 women (median age at diagnosis, 53 years; 65.4% White women) newly diagnosed with invasive breast cancer between September 2019 and April 2022 at three Canadian institutions.
- All patients received genetic counseling followed by testing for the presence of germline pathogenic variants in 17 breast cancer susceptibility genes. The primary gene panel included screening for BRCA1, BRCA2, and PALB2, and the optional secondary panel included 14 additional breast cancer susceptibility genes.
- Of the participants, 659 (90.4%) were tested for both primary and secondary gene panels, whereas 70 (9.6%) underwent testing for only the primary panel. The majority of the cohort (66.8) were diagnosed with estrogen receptor–positive breast cancer, while 15.4% had triple-negative breast cancer.
TAKEAWAY:
- The prevalence of germline pathogenic variants was 7.3% (53 patients) — 5.3% for the primary gene panel and 2.1% for the secondary panel.
- Younger age (< 40 years; odds ratio [OR], 6.83), family history of ovarian cancer (OR, 9.75), high-grade disease (OR, 1.68), and triple-negative breast cancer (OR, 3.19) were independently associated with the presence of pathogenic genetic variants in BRCA1, BRCA2, or PALB2.
- Overall, 34.3% of patients with germline pathogenic variants in BRCA1, BRCA2, or PALB2, and 85.7% of carriers of secondary panel variants would not have qualified for traditional genetic testing according to the current risk factors.
- A total of 13 patients with BRCA1, BRCA2, or PALB2 variants had confirmed pathogenic mutations and were eligible for poly(adenosine diphosphate–ribose) polymerase (PARP) inhibitors.
IN PRACTICE:
These findings have “informed our clinical practice, and we now offer mainstream, oncology-led genetic testing to all women diagnosed with incident invasive breast cancer younger than 50 years of age, those with triple-negative breast cancer and/or bilateral breast cancer, those potentially eligible for PARP inhibitors,” as well as to men with breast cancer, the authors wrote.
SOURCE:
The study was led by Zoulikha Rezoug, MSc, Lady Davis Institute of the Jewish General Hospital, McGill University in Montreal, Québec, Canada. It was published online on September 3, 2024, in JAMA Network Open.
LIMITATIONS:
The COVID-19 pandemic resulted in a 6-month recruitment pause. Adjustments in recruitment criteria, focus on younger patients and those with triple-negative breast cancer could have overestimated prevalence of genetic pathogenic variants among women aged ≥ 70 years.
DISCLOSURES:
The study was supported by grants from the Jewish General Hospital Foundation and the Québec Breast Cancer Foundation, as well as an award from the Fonds de Recherche du Québec - Santé. Two authors reported receiving grants or personal fees from various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Traditional risk-based criteria, including family history and ancestry, are used to guide genetic testing decisions in women with breast cancer. However, these criteria may overlook patients with actionable genetic variants, particularly those outside the typical risk profile.
- To assess the efficacy of universal genetic testing, researchers conducted a cross-sectional study that included 729 women (median age at diagnosis, 53 years; 65.4% White women) newly diagnosed with invasive breast cancer between September 2019 and April 2022 at three Canadian institutions.
- All patients received genetic counseling followed by testing for the presence of germline pathogenic variants in 17 breast cancer susceptibility genes. The primary gene panel included screening for BRCA1, BRCA2, and PALB2, and the optional secondary panel included 14 additional breast cancer susceptibility genes.
- Of the participants, 659 (90.4%) were tested for both primary and secondary gene panels, whereas 70 (9.6%) underwent testing for only the primary panel. The majority of the cohort (66.8) were diagnosed with estrogen receptor–positive breast cancer, while 15.4% had triple-negative breast cancer.
TAKEAWAY:
- The prevalence of germline pathogenic variants was 7.3% (53 patients) — 5.3% for the primary gene panel and 2.1% for the secondary panel.
- Younger age (< 40 years; odds ratio [OR], 6.83), family history of ovarian cancer (OR, 9.75), high-grade disease (OR, 1.68), and triple-negative breast cancer (OR, 3.19) were independently associated with the presence of pathogenic genetic variants in BRCA1, BRCA2, or PALB2.
- Overall, 34.3% of patients with germline pathogenic variants in BRCA1, BRCA2, or PALB2, and 85.7% of carriers of secondary panel variants would not have qualified for traditional genetic testing according to the current risk factors.
- A total of 13 patients with BRCA1, BRCA2, or PALB2 variants had confirmed pathogenic mutations and were eligible for poly(adenosine diphosphate–ribose) polymerase (PARP) inhibitors.
IN PRACTICE:
These findings have “informed our clinical practice, and we now offer mainstream, oncology-led genetic testing to all women diagnosed with incident invasive breast cancer younger than 50 years of age, those with triple-negative breast cancer and/or bilateral breast cancer, those potentially eligible for PARP inhibitors,” as well as to men with breast cancer, the authors wrote.
SOURCE:
The study was led by Zoulikha Rezoug, MSc, Lady Davis Institute of the Jewish General Hospital, McGill University in Montreal, Québec, Canada. It was published online on September 3, 2024, in JAMA Network Open.
LIMITATIONS:
The COVID-19 pandemic resulted in a 6-month recruitment pause. Adjustments in recruitment criteria, focus on younger patients and those with triple-negative breast cancer could have overestimated prevalence of genetic pathogenic variants among women aged ≥ 70 years.
DISCLOSURES:
The study was supported by grants from the Jewish General Hospital Foundation and the Québec Breast Cancer Foundation, as well as an award from the Fonds de Recherche du Québec - Santé. Two authors reported receiving grants or personal fees from various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Traditional risk-based criteria, including family history and ancestry, are used to guide genetic testing decisions in women with breast cancer. However, these criteria may overlook patients with actionable genetic variants, particularly those outside the typical risk profile.
- To assess the efficacy of universal genetic testing, researchers conducted a cross-sectional study that included 729 women (median age at diagnosis, 53 years; 65.4% White women) newly diagnosed with invasive breast cancer between September 2019 and April 2022 at three Canadian institutions.
- All patients received genetic counseling followed by testing for the presence of germline pathogenic variants in 17 breast cancer susceptibility genes. The primary gene panel included screening for BRCA1, BRCA2, and PALB2, and the optional secondary panel included 14 additional breast cancer susceptibility genes.
- Of the participants, 659 (90.4%) were tested for both primary and secondary gene panels, whereas 70 (9.6%) underwent testing for only the primary panel. The majority of the cohort (66.8) were diagnosed with estrogen receptor–positive breast cancer, while 15.4% had triple-negative breast cancer.
TAKEAWAY:
- The prevalence of germline pathogenic variants was 7.3% (53 patients) — 5.3% for the primary gene panel and 2.1% for the secondary panel.
- Younger age (< 40 years; odds ratio [OR], 6.83), family history of ovarian cancer (OR, 9.75), high-grade disease (OR, 1.68), and triple-negative breast cancer (OR, 3.19) were independently associated with the presence of pathogenic genetic variants in BRCA1, BRCA2, or PALB2.
- Overall, 34.3% of patients with germline pathogenic variants in BRCA1, BRCA2, or PALB2, and 85.7% of carriers of secondary panel variants would not have qualified for traditional genetic testing according to the current risk factors.
- A total of 13 patients with BRCA1, BRCA2, or PALB2 variants had confirmed pathogenic mutations and were eligible for poly(adenosine diphosphate–ribose) polymerase (PARP) inhibitors.
IN PRACTICE:
These findings have “informed our clinical practice, and we now offer mainstream, oncology-led genetic testing to all women diagnosed with incident invasive breast cancer younger than 50 years of age, those with triple-negative breast cancer and/or bilateral breast cancer, those potentially eligible for PARP inhibitors,” as well as to men with breast cancer, the authors wrote.
SOURCE:
The study was led by Zoulikha Rezoug, MSc, Lady Davis Institute of the Jewish General Hospital, McGill University in Montreal, Québec, Canada. It was published online on September 3, 2024, in JAMA Network Open.
LIMITATIONS:
The COVID-19 pandemic resulted in a 6-month recruitment pause. Adjustments in recruitment criteria, focus on younger patients and those with triple-negative breast cancer could have overestimated prevalence of genetic pathogenic variants among women aged ≥ 70 years.
DISCLOSURES:
The study was supported by grants from the Jewish General Hospital Foundation and the Québec Breast Cancer Foundation, as well as an award from the Fonds de Recherche du Québec - Santé. Two authors reported receiving grants or personal fees from various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
‘Reform School’ for Pharmacy Benefit Managers: How Might Legislation Help Patients?
The term “reform school” is a bit outdated. It used to refer to institutions where young offenders were sent instead of prison. Some argue that pharmacy benefit managers (PBMs) should bypass reform school and go straight to prison. “PBM reform” has become a ubiquitous term, encompassing any legislative or regulatory efforts aimed at curbing PBMs’ bad behavior. When discussing PBM reform, it’s crucial to understand the various segments of the healthcare system affected by PBMs. This complexity often makes it challenging to determine what these reform packages would actually achieve and who they would benefit.
Pharmacists have long been vocal critics of PBMs, and while their issues are extremely important, it is essential to remember that the ultimate victims of PBM misconduct, in terms of access to care, are patients. At some point, we will all be patients, making this issue universally relevant. It has been quite challenging to follow federal legislation on this topic as these packages attempt to address a number of bad behaviors by PBMs affecting a variety of victims. This discussion will examine those reforms that would directly improve patient’s access to available and affordable medications.
Policy Categories of PBM Reform
There are five policy categories of PBM reform legislation overall, including three that have the greatest potential to directly address patient needs. The first is patient access to medications (utilization management, copay assistance, prior authorization, etc.), followed by delinking drug list prices from PBM income and pass-through of price concessions from the manufacturer. The remaining two categories involve transparency and pharmacy-facing reform, both of which are very important. However, this discussion will revolve around the first three categories. It should be noted that many of the legislation packages addressing the categories of patient access, delinking, and pass-through also include transparency issues, particularly as they relate to pharmacy-facing issues.
Patient Access to Medications — Step Therapy Legislation
One of the major obstacles to patient access to medications is the use of PBM utilization management tools such as step therapy (“fail first”), prior authorizations, nonmedical switching, and formulary exclusions. These tools dictate when patients can obtain necessary medications and for how long patients who are stable on their current treatments can remain on them.

While many states have enacted step therapy reforms to prevent stable patients from being whip-sawed between medications that maximize PBM profits (often labeled as “savings”), these state protections apply only to state-regulated health plans. These include fully insured health plans and those offered through the Affordable Care Act’s Health Insurance Marketplace. It also includes state employees, state corrections, and, in some cases, state labor unions. State legislation does not extend to patients covered by employer self-insured health plans, called ERISA plans for the federal law that governs employee benefit plans, the Employee Retirement Income Security Act. These ERISA plans include nearly 35 million people nationwide.
This is where the Safe Step Act (S.652/H.R.2630) becomes crucial, as it allows employees to request exceptions to harmful fail-first protocols. The bill has gained significant momentum, having been reported out of the Senate HELP Committee and discussed in House markups. The Safe Step Act would mandate that an exception to a step therapy protocol must be granted if:
- The required treatment has been ineffective
- The treatment is expected to be ineffective, and delaying effective treatment would lead to irreversible consequences
- The treatment will cause or is likely to cause an adverse reaction
- The treatment is expected to prevent the individual from performing daily activities or occupational responsibilities
- The individual is stable on their current prescription drugs
- There are other circumstances as determined by the Employee Benefits Security Administration
This legislation is vital for ensuring that patients have timely access to the medications they need without unnecessary delays or disruptions.
Patient Access to Medications — Prior Authorizations
Another significant issue affecting patient access to medications is prior authorizations (PAs). According to an American Medical Association survey, nearly one in four physicians (24%) report that a PA has led to a serious adverse event for a patient in their care. In rheumatology, PAs often result in delays in care (even for those initially approved) and a significant increase in steroid usage. In particular, PAs in Medicare Advantage (MA) plans are harmful to Medicare beneficiaries.
The Improving Seniors’ Timely Access to Care Act (H.R.8702 / S.4532) aims to reform PAs used in MA plans, making the process more efficient and transparent to improve access to care for seniors. Unfortunately, it does not cover Part D drugs and may only cover Part B drugs depending on the MA plan’s benefit package. Here are the key provisions of the act:
- Electronic PA: Implementing real-time decisions for routinely approved items and services.
- Transparency: Requiring annual publication of PA information, such as the percentage of requests approved and the average response time.
- Quality and Timeliness Standards: The Centers for Medicare & Medicaid Services (CMS) will set standards for the quality and timeliness of PA determinations.
- Streamlining Approvals: Simplifying the approval process and reducing the time allowed for health plans to consider PA requests.
This bill passed the House in September 2022 but stalled in the Senate because of an unfavorable Congressional Budget Office score. CMS has since finalized portions of this bill via regulation, zeroing out the CBO score and increasing the chances of its passage.
Delinking Drug Prices from PBM Income and Pass-Through of Price Concessions
Affordability is a crucial aspect of accessibility, especially when it comes to medications. Over the years, we’ve learned that PBMs often favor placing the highest list price drugs on formularies because the rebates and various fees they receive from manufacturers are based on a percentage of the list price. In other words, the higher the medication’s price, the more money the PBM makes.
This practice is evident in both commercial and government formularies, where brand-name drugs are often preferred, while lower-priced generics are either excluded or placed on higher tiers. As a result, while major PBMs benefit from these rebates and fees, patients continue to pay their cost share based on the list price of the medication.
To improve the affordability of medications, a key aspect of PBM reform should be to disincentivize PBMs from selecting higher-priced medications and/or require the pass-through of manufacturer price concessions to patients.
Several major PBM reform bills are currently being considered that address either the delinking of price concessions from the list price of the drug or some form of pass-through of these concessions. These reforms are essential to ensure that patients can access affordable medications without being burdened by inflated costs.
The legislation includes the Pharmacy Benefit Manager Reform Act (S.1339); the Modernizing & Ensuring PBM Accountability Act (S.2973); the Better Mental Health Care, Lower Cost Drugs, and Extenders Act (S.3430); the Protecting Patients Against PBM Abuses Act (H.R. 2880); the DRUG Act (S.2474 / H.R.6283); and the Share the Savings with Seniors Act (S.2474 / H.R.5376).
As with all legislation, there are limitations and compromises in each of these. However, these bills are a good first step in addressing PBM remuneration (rebates and fees) based on the list price of the drug and/or passing through to the patient the benefit of manufacturer price concessions. By focusing on key areas like utilization management, delinking drug prices from PBM income, and allowing patients to directly benefit from manufacturer price concessions, we can work toward a more equitable and efficient healthcare system. Reigning in PBM bad behavior is a challenge, but the potential benefits for patient care and access make it a crucial fight worth pursuing.
Please help in efforts to improve patients’ access to available and affordable medications by contacting your representatives in Congress to impart to them the importance of passing legislation. The CSRO’s legislative map tool can help to inform you of the latest information on these and other bills and assist you in engaging with your representatives on them.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s vice president of Advocacy and Government Affairs and its immediate past president, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. She has no relevant conflicts of interest to disclose. You can reach her at rhnews@mdedge.com.
The term “reform school” is a bit outdated. It used to refer to institutions where young offenders were sent instead of prison. Some argue that pharmacy benefit managers (PBMs) should bypass reform school and go straight to prison. “PBM reform” has become a ubiquitous term, encompassing any legislative or regulatory efforts aimed at curbing PBMs’ bad behavior. When discussing PBM reform, it’s crucial to understand the various segments of the healthcare system affected by PBMs. This complexity often makes it challenging to determine what these reform packages would actually achieve and who they would benefit.
Pharmacists have long been vocal critics of PBMs, and while their issues are extremely important, it is essential to remember that the ultimate victims of PBM misconduct, in terms of access to care, are patients. At some point, we will all be patients, making this issue universally relevant. It has been quite challenging to follow federal legislation on this topic as these packages attempt to address a number of bad behaviors by PBMs affecting a variety of victims. This discussion will examine those reforms that would directly improve patient’s access to available and affordable medications.
Policy Categories of PBM Reform
There are five policy categories of PBM reform legislation overall, including three that have the greatest potential to directly address patient needs. The first is patient access to medications (utilization management, copay assistance, prior authorization, etc.), followed by delinking drug list prices from PBM income and pass-through of price concessions from the manufacturer. The remaining two categories involve transparency and pharmacy-facing reform, both of which are very important. However, this discussion will revolve around the first three categories. It should be noted that many of the legislation packages addressing the categories of patient access, delinking, and pass-through also include transparency issues, particularly as they relate to pharmacy-facing issues.
Patient Access to Medications — Step Therapy Legislation
One of the major obstacles to patient access to medications is the use of PBM utilization management tools such as step therapy (“fail first”), prior authorizations, nonmedical switching, and formulary exclusions. These tools dictate when patients can obtain necessary medications and for how long patients who are stable on their current treatments can remain on them.
While many states have enacted step therapy reforms to prevent stable patients from being whip-sawed between medications that maximize PBM profits (often labeled as “savings”), these state protections apply only to state-regulated health plans. These include fully insured health plans and those offered through the Affordable Care Act’s Health Insurance Marketplace. It also includes state employees, state corrections, and, in some cases, state labor unions. State legislation does not extend to patients covered by employer self-insured health plans, called ERISA plans for the federal law that governs employee benefit plans, the Employee Retirement Income Security Act. These ERISA plans include nearly 35 million people nationwide.
This is where the Safe Step Act (S.652/H.R.2630) becomes crucial, as it allows employees to request exceptions to harmful fail-first protocols. The bill has gained significant momentum, having been reported out of the Senate HELP Committee and discussed in House markups. The Safe Step Act would mandate that an exception to a step therapy protocol must be granted if:
- The required treatment has been ineffective
- The treatment is expected to be ineffective, and delaying effective treatment would lead to irreversible consequences
- The treatment will cause or is likely to cause an adverse reaction
- The treatment is expected to prevent the individual from performing daily activities or occupational responsibilities
- The individual is stable on their current prescription drugs
- There are other circumstances as determined by the Employee Benefits Security Administration
This legislation is vital for ensuring that patients have timely access to the medications they need without unnecessary delays or disruptions.
Patient Access to Medications — Prior Authorizations
Another significant issue affecting patient access to medications is prior authorizations (PAs). According to an American Medical Association survey, nearly one in four physicians (24%) report that a PA has led to a serious adverse event for a patient in their care. In rheumatology, PAs often result in delays in care (even for those initially approved) and a significant increase in steroid usage. In particular, PAs in Medicare Advantage (MA) plans are harmful to Medicare beneficiaries.
The Improving Seniors’ Timely Access to Care Act (H.R.8702 / S.4532) aims to reform PAs used in MA plans, making the process more efficient and transparent to improve access to care for seniors. Unfortunately, it does not cover Part D drugs and may only cover Part B drugs depending on the MA plan’s benefit package. Here are the key provisions of the act:
- Electronic PA: Implementing real-time decisions for routinely approved items and services.
- Transparency: Requiring annual publication of PA information, such as the percentage of requests approved and the average response time.
- Quality and Timeliness Standards: The Centers for Medicare & Medicaid Services (CMS) will set standards for the quality and timeliness of PA determinations.
- Streamlining Approvals: Simplifying the approval process and reducing the time allowed for health plans to consider PA requests.
This bill passed the House in September 2022 but stalled in the Senate because of an unfavorable Congressional Budget Office score. CMS has since finalized portions of this bill via regulation, zeroing out the CBO score and increasing the chances of its passage.
Delinking Drug Prices from PBM Income and Pass-Through of Price Concessions
Affordability is a crucial aspect of accessibility, especially when it comes to medications. Over the years, we’ve learned that PBMs often favor placing the highest list price drugs on formularies because the rebates and various fees they receive from manufacturers are based on a percentage of the list price. In other words, the higher the medication’s price, the more money the PBM makes.
This practice is evident in both commercial and government formularies, where brand-name drugs are often preferred, while lower-priced generics are either excluded or placed on higher tiers. As a result, while major PBMs benefit from these rebates and fees, patients continue to pay their cost share based on the list price of the medication.
To improve the affordability of medications, a key aspect of PBM reform should be to disincentivize PBMs from selecting higher-priced medications and/or require the pass-through of manufacturer price concessions to patients.
Several major PBM reform bills are currently being considered that address either the delinking of price concessions from the list price of the drug or some form of pass-through of these concessions. These reforms are essential to ensure that patients can access affordable medications without being burdened by inflated costs.
The legislation includes the Pharmacy Benefit Manager Reform Act (S.1339); the Modernizing & Ensuring PBM Accountability Act (S.2973); the Better Mental Health Care, Lower Cost Drugs, and Extenders Act (S.3430); the Protecting Patients Against PBM Abuses Act (H.R. 2880); the DRUG Act (S.2474 / H.R.6283); and the Share the Savings with Seniors Act (S.2474 / H.R.5376).
As with all legislation, there are limitations and compromises in each of these. However, these bills are a good first step in addressing PBM remuneration (rebates and fees) based on the list price of the drug and/or passing through to the patient the benefit of manufacturer price concessions. By focusing on key areas like utilization management, delinking drug prices from PBM income, and allowing patients to directly benefit from manufacturer price concessions, we can work toward a more equitable and efficient healthcare system. Reigning in PBM bad behavior is a challenge, but the potential benefits for patient care and access make it a crucial fight worth pursuing.
Please help in efforts to improve patients’ access to available and affordable medications by contacting your representatives in Congress to impart to them the importance of passing legislation. The CSRO’s legislative map tool can help to inform you of the latest information on these and other bills and assist you in engaging with your representatives on them.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s vice president of Advocacy and Government Affairs and its immediate past president, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. She has no relevant conflicts of interest to disclose. You can reach her at rhnews@mdedge.com.
The term “reform school” is a bit outdated. It used to refer to institutions where young offenders were sent instead of prison. Some argue that pharmacy benefit managers (PBMs) should bypass reform school and go straight to prison. “PBM reform” has become a ubiquitous term, encompassing any legislative or regulatory efforts aimed at curbing PBMs’ bad behavior. When discussing PBM reform, it’s crucial to understand the various segments of the healthcare system affected by PBMs. This complexity often makes it challenging to determine what these reform packages would actually achieve and who they would benefit.
Pharmacists have long been vocal critics of PBMs, and while their issues are extremely important, it is essential to remember that the ultimate victims of PBM misconduct, in terms of access to care, are patients. At some point, we will all be patients, making this issue universally relevant. It has been quite challenging to follow federal legislation on this topic as these packages attempt to address a number of bad behaviors by PBMs affecting a variety of victims. This discussion will examine those reforms that would directly improve patient’s access to available and affordable medications.
Policy Categories of PBM Reform
There are five policy categories of PBM reform legislation overall, including three that have the greatest potential to directly address patient needs. The first is patient access to medications (utilization management, copay assistance, prior authorization, etc.), followed by delinking drug list prices from PBM income and pass-through of price concessions from the manufacturer. The remaining two categories involve transparency and pharmacy-facing reform, both of which are very important. However, this discussion will revolve around the first three categories. It should be noted that many of the legislation packages addressing the categories of patient access, delinking, and pass-through also include transparency issues, particularly as they relate to pharmacy-facing issues.
Patient Access to Medications — Step Therapy Legislation
One of the major obstacles to patient access to medications is the use of PBM utilization management tools such as step therapy (“fail first”), prior authorizations, nonmedical switching, and formulary exclusions. These tools dictate when patients can obtain necessary medications and for how long patients who are stable on their current treatments can remain on them.
While many states have enacted step therapy reforms to prevent stable patients from being whip-sawed between medications that maximize PBM profits (often labeled as “savings”), these state protections apply only to state-regulated health plans. These include fully insured health plans and those offered through the Affordable Care Act’s Health Insurance Marketplace. It also includes state employees, state corrections, and, in some cases, state labor unions. State legislation does not extend to patients covered by employer self-insured health plans, called ERISA plans for the federal law that governs employee benefit plans, the Employee Retirement Income Security Act. These ERISA plans include nearly 35 million people nationwide.
This is where the Safe Step Act (S.652/H.R.2630) becomes crucial, as it allows employees to request exceptions to harmful fail-first protocols. The bill has gained significant momentum, having been reported out of the Senate HELP Committee and discussed in House markups. The Safe Step Act would mandate that an exception to a step therapy protocol must be granted if:
- The required treatment has been ineffective
- The treatment is expected to be ineffective, and delaying effective treatment would lead to irreversible consequences
- The treatment will cause or is likely to cause an adverse reaction
- The treatment is expected to prevent the individual from performing daily activities or occupational responsibilities
- The individual is stable on their current prescription drugs
- There are other circumstances as determined by the Employee Benefits Security Administration
This legislation is vital for ensuring that patients have timely access to the medications they need without unnecessary delays or disruptions.
Patient Access to Medications — Prior Authorizations
Another significant issue affecting patient access to medications is prior authorizations (PAs). According to an American Medical Association survey, nearly one in four physicians (24%) report that a PA has led to a serious adverse event for a patient in their care. In rheumatology, PAs often result in delays in care (even for those initially approved) and a significant increase in steroid usage. In particular, PAs in Medicare Advantage (MA) plans are harmful to Medicare beneficiaries.
The Improving Seniors’ Timely Access to Care Act (H.R.8702 / S.4532) aims to reform PAs used in MA plans, making the process more efficient and transparent to improve access to care for seniors. Unfortunately, it does not cover Part D drugs and may only cover Part B drugs depending on the MA plan’s benefit package. Here are the key provisions of the act:
- Electronic PA: Implementing real-time decisions for routinely approved items and services.
- Transparency: Requiring annual publication of PA information, such as the percentage of requests approved and the average response time.
- Quality and Timeliness Standards: The Centers for Medicare & Medicaid Services (CMS) will set standards for the quality and timeliness of PA determinations.
- Streamlining Approvals: Simplifying the approval process and reducing the time allowed for health plans to consider PA requests.
This bill passed the House in September 2022 but stalled in the Senate because of an unfavorable Congressional Budget Office score. CMS has since finalized portions of this bill via regulation, zeroing out the CBO score and increasing the chances of its passage.
Delinking Drug Prices from PBM Income and Pass-Through of Price Concessions
Affordability is a crucial aspect of accessibility, especially when it comes to medications. Over the years, we’ve learned that PBMs often favor placing the highest list price drugs on formularies because the rebates and various fees they receive from manufacturers are based on a percentage of the list price. In other words, the higher the medication’s price, the more money the PBM makes.
This practice is evident in both commercial and government formularies, where brand-name drugs are often preferred, while lower-priced generics are either excluded or placed on higher tiers. As a result, while major PBMs benefit from these rebates and fees, patients continue to pay their cost share based on the list price of the medication.
To improve the affordability of medications, a key aspect of PBM reform should be to disincentivize PBMs from selecting higher-priced medications and/or require the pass-through of manufacturer price concessions to patients.
Several major PBM reform bills are currently being considered that address either the delinking of price concessions from the list price of the drug or some form of pass-through of these concessions. These reforms are essential to ensure that patients can access affordable medications without being burdened by inflated costs.
The legislation includes the Pharmacy Benefit Manager Reform Act (S.1339); the Modernizing & Ensuring PBM Accountability Act (S.2973); the Better Mental Health Care, Lower Cost Drugs, and Extenders Act (S.3430); the Protecting Patients Against PBM Abuses Act (H.R. 2880); the DRUG Act (S.2474 / H.R.6283); and the Share the Savings with Seniors Act (S.2474 / H.R.5376).
As with all legislation, there are limitations and compromises in each of these. However, these bills are a good first step in addressing PBM remuneration (rebates and fees) based on the list price of the drug and/or passing through to the patient the benefit of manufacturer price concessions. By focusing on key areas like utilization management, delinking drug prices from PBM income, and allowing patients to directly benefit from manufacturer price concessions, we can work toward a more equitable and efficient healthcare system. Reigning in PBM bad behavior is a challenge, but the potential benefits for patient care and access make it a crucial fight worth pursuing.
Please help in efforts to improve patients’ access to available and affordable medications by contacting your representatives in Congress to impart to them the importance of passing legislation. The CSRO’s legislative map tool can help to inform you of the latest information on these and other bills and assist you in engaging with your representatives on them.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s vice president of Advocacy and Government Affairs and its immediate past president, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. She has no relevant conflicts of interest to disclose. You can reach her at rhnews@mdedge.com.