User login
Principal Investigations
What can you do with a quarter of a million dollars? In some places, that amount can buy a home that can shelter a family for decades. In other places, it is enough to pay annual malpractice insurance premiums for physicians practicing in high-risk specialties—with a little left over.
But if you wanted to use that money for an enduring healthcare project that would provide the most good for the most people, how would you do it? Hospitalists can look to the Agency for Healthcare Research and Quality (AHRQ) for stellar examples of well-invested dollars with excellent return.
AHRQ Funding
With a staff of approximately 300, the tiny AHRQ is the lead federal agency charged with improving the quality, safety, efficiency, and effectiveness of healthcare for all Americans. It creates a priority research agenda annually, and funds studies in areas where improvement is deemed most needed. These include patient safety, data development, pharmaceutical outcomes, and other areas described on its Web site (www.ahrq.gov/).
In 2005, AHRQ announced its Partnerships in Implementing Patient Safety (PIPS) and committed up to $9 million in total costs to fund new grants of less than $300,000 per year, lasting two years. AHRQ indicated that eligible safe practice intervention projects would be required to include “tool kits,” and a comprehensive implementation tool kit to help others overcome barriers and allay adoption concerns. AHRQ’s goal was and is to disseminate funded projects’ perfected tools widely for adaptation and/or adoption by diverse healthcare settings.
AHRQ asked that principal investigators (PIs) be experienced senior level individuals familiar with implementing change in healthcare settings. Their expectation was that PIs would devote at least 15% of their time to the project for its duration. Thus the competitive challenge to potential PIs was great:
- Select a worthy project from among the endless areas where healthcare needs improvement, and then plan specific, realistic, achievable interventions that could create measurable improvement over two years;
- Implement the program; and
- Develop a plan and tools so basic and user-friendly that they could feasibly be applied in not just the local practice setting, but in other healthcare settings.
Although the size and duration of the awards varied, many of the 17 projects they funded received slightly more than a quarter of a million dollars. Among the funded projects, two boast hospitalists as their PIs and address areas of obvious concern in most healthcare settings. Greg Maynard, MD, MS, at the University of California, San Diego, was funded to implement a venous thromboembolism (VTE) intervention program. And Mark V. Williams, MD, FACP, professor of medicine, Emory University School of Medicine, Atlanta, and editor of the Journal of Hospital Medicine, was funded to implement a discharge bundle of patient safety interventions respectively.
Stalking the Silent Killer
Dr. Maynard’s project, “Optimal Prevention of Hospital Acquired Venous Thromboembolism,” focuses on eliminating preventable hospital-acquired VTE at an academic healthcare facility that has a large population of Hispanic patients.
The project’s timeliness and utility is clear: Although the exact incidence of VTE is unknown, experts estimate that approximately 260,000 are clinically recognized annually in acutely hospitalized patients.1 Pulmonary embolism (PE) resulting from deep vein thrombosis (DVT) is the most common cause of preventable hospital death, the majority of hospitalized patients with risk factors for DVT receive no prophylaxis, and the rate of fatal PE more than doubles between age 50 and 80.2,3 The problem is easily recognizable, but “Getting people to do what they need to do to prevent VTE can be hard,” says Dr. Maynard.
This project was carefully planned. It used a rigorous quality improvement process, involving all appropriate clinicians, nurses, managers, and technical support personnel.
Dr. Maynard and his team anticipated roadblocks and negotiated in advance to reduce their effects. They accepted that when patients are hospitalized, things frequently happen that cause physicians to stop VTE prophylaxis: A hemoglobin or platelet count may fall, the patient may have difficulty taking the drug, or the patient’s status may change abruptly. Or the prophylaxis might be accidentally discontinued—perhaps when a patient is transferred.
The team also looked at other institutions’ solutions. Then, using a basic understanding of the ways in which their process was missing VTE prophylaxis opportunities, they built interventions.
This team considered logistics carefully because it was clear that the only intervention that could decrease risk would have to be repetitive in nature. “The process we ultimately selected is very, very quick, yet valid,” says Dr. Maynard, while acknowledging that presenting any intervention repeatedly has the potential to interfere with care. “Other models require the physician to use math and add points. This one does not, and takes only seconds.”
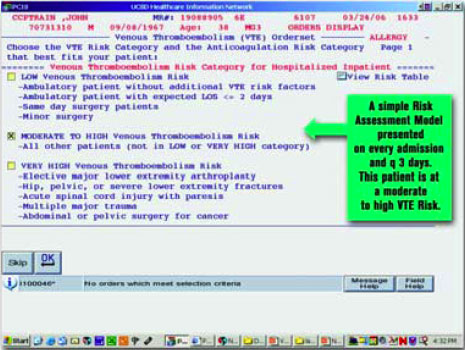
Beginning April 19, 2006, the University of California, San Diego (UCSD) will introduce an intervention that presents a VTE risk assessment screen on every patient who is admitted. This process inquires about the need for prophylaxis every three days for the duration of hospitalization, and physicians cannot skip the screen. If risk factors are present and bleeding risk is not, the screen presents appropriate VTE options.
For example, the system will suggest enoxaparin 40 mg daily, enoxaparin 30 mg twice daily, or appropriately dosed warfarin for a high-risk orthopedic surgery patient who has no bleeding risk. Every three days, the process repeats itself, making explicit decisions or suggestions about appropriate prophylaxis. (Figure 1, below, shows a sample screen for a patient with moderately high risk.
Much evidence about VTE is still being gathered. For example, opinions vary about when to start prophylaxis or how long to continue it. Dr. Maynard and his team also addressed real versus relative contraindications—another area of debate among clinicians. Many clinicians are uncertain about how soon after surgery to restart VTE prophylaxis. After orthopedic spine surgery, for example, some might start it on day five, while others may not restart prophylaxis even after day 10. At UCSD, clinical stakeholders in the process came to consensus, and now all restart by day seven.
The tool kit UCSD is developing recognizes that every institution is unique. Those that choose to implement a similar program must identify their baseline rate of VTE and monitor change over time to determine if progress is being made. Every institution must define adequate VTE prophylaxis and tailor the tools appropriately.
Wait? No Need
One compelling aspect of Dr. Maynard’s project is that some of UCSD’s VTE tools are already available on the SHM Web site in the “VTE Resource Room.” With or without AHRQ funding, UCSD planned to develop and implement a VTE awareness program. UCSD’s grant department provided the support Dr. Maynard and his colleagues needed to apply for the AHRQ funding, and Dr. Maynard says the funding they received helped UCSD “disseminate the program better and to carry it out with more rigor.”
UCSD worked with SHM to develop the tool kit. In return, SHM is providing and promoting the VTE tool kit at no charge to interested parties. Additionally, SHM recently received funding via an unrestricted sponsorship to create a mentored implementation project for the “VTE Resource Room.” Interested institutions will be mentored by UCSD staff who have experience with the tool kit.
Over time, Dr. Maynard will measure the effects of the intervention to ensure it is working. In addition to creating a malleable tool kit, UCSD research hospitalists will examine race, gender, and age to determine the effects of these on the likelihood of getting adequate prophylaxis.
Hospital Patient Safe-D(ischarge)
Dr. Williams and his colleagues at Emory University and the University of Ottawa received funding for “Hospital Patient Safe-D(ischarge): A Discharge Bundle for Patients,” a program that builds on previous AHRQ funding. This intervention implements a “discharge bundle” of patient safety interventions to improve patient transition from the hospital to home or another healthcare setting.
“We hope that every patient will undergo discharge, and of course the majority do, but the discharge process has almost been treated as an afterthought,” explains Dr. Williams. “Doctors spend a lot of time on diagnosis and treatment, but not on discharge. This process of transition from total care with a call button, lots of nursing attention, daily visits from the doctor, and delivered meals to greater independence, has not been well researched.”
What little research exists tends to indicate that discharge processes are very heterogeneous.
So far, Dr. Williams’ team’s examination of the process has produced only one surprise: The team has discovered that the discharge process is even more capricious than they suspected. As patients prepare to leave the hospital, what could and should be an orderly process that educates and prepares patients to assume responsibility for their own care in a new and better way is often interrupted or disjointed.
Preparing patients for discharge once fell to the nursing staff. As nursing faces staffing shortages and expanded roles, the discharge process often belongs to everyone and to no one. That physicians’ discharge visits pay much less than the time required to do it well also complicates the problem. The researchers were not surprised, however, to learn that many patients do not know their diagnosis or treatment plan as discharge is imminent. Their goal is to develop a consistent, comprehensive discharge process that will be a national model.
Here again, the precepts of continuous quality improvement are apparent. Dr. Williams’ team’s effort represents collaboration among physicians, pharmacists, nurses, and patients; involves SHM and several other professional organizations; and calls upon an advisory committee consisting of nationally recognized patient care and safety experts.
The discharge bundle of patient safety interventions—a concept advocated by the Joint Commission on Accreditation of Healthcare Organizations and other quality-promoting groups—adds a post-discharge continuity check to medication reconciliation and patient-centered education at discharge.
The four project phases—implement, evaluate, develop a tool, and disseminate the discharge bundle—overlap and ensure success.
Dr. Williams believes that the group of patients most likely to benefit from this intervention is the elderly. “The elderly bear the greatest burden of chronic disease and typically have several concurrent health problems,” he says.
Educating elders at the time of discharge should decrease the medication error rate and improve adherence to other treatments and recommended lifestyle changes. To gauge the appropriateness of the discharge bundle, John Banja, PhD, an expert in communication and safety, observes the discharge process directly. All communications must be patient-centered, and thus presented in a manner that patients will understand and appreciate. Banja relies on his background in patient safety and disability/rehabilitation to assess the discharge process.
Initial enrollment in this study seems successful. More than 50 patients have consented to participate, but Banja projects a need for 200 to complete the entire process. Recently, the team increased its planned maximum accrual to 300 to increase the statistical power of their findings. The participants like the program because most of them find discharge somewhat discomforting. Patients know they have knowledge gaps and appreciate clinicians’ efforts to fill those gaps seamlessly. A small investment of time can prevent problems after discharge.
Added Value
Clearly, the findings from these AHRQ-funded studies have the potential to reduce morbidity and mortality in a logarithmic manner as other institutions adapt these new tool kits. Dr. Williams indicates that recipients of PIPS funding receive more than just funding and the satisfaction of creating tools that will help all Americans.
“The AHRQ sponsors quarterly conference calls for all participants, regardless of their research topic, and an annual meeting in June to bring all investigators together,” he says.
The opportunity to learn how others address problems, plan interventions, and tackle hurdles proves invaluable. In addition, being privy to interim study results or learning how others handle research dilemmas helps hospitalists expand their skill sets.
Listening to Drs. Maynard and Williams is a not-so-subtle reminder that every hospital needs a well-structured quality improvement plan, and that hospitalists are essential in the plan’s success. Every hospitalist needs an understanding of the precepts these PIs used to earn this well-deserved funding: interdisciplinary and professional organization collaboration, good communication, realistic planning, managing change by measuring, and above all, sharing success. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
References
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991 May;151(5):933-938.
- Clagett GP, Anderson FA Jr, Heit J, et al. Prevention of venous thromboembolism. Chest. 1995 Oct;108(4 Suppl):312S-334S.
- Geerts WH, Heit JA, Clagett GP, et al. Prevention of venous thromboembolism. Chest. 2001;119(1 Suppl):132S-175S.
What can you do with a quarter of a million dollars? In some places, that amount can buy a home that can shelter a family for decades. In other places, it is enough to pay annual malpractice insurance premiums for physicians practicing in high-risk specialties—with a little left over.
But if you wanted to use that money for an enduring healthcare project that would provide the most good for the most people, how would you do it? Hospitalists can look to the Agency for Healthcare Research and Quality (AHRQ) for stellar examples of well-invested dollars with excellent return.
AHRQ Funding
With a staff of approximately 300, the tiny AHRQ is the lead federal agency charged with improving the quality, safety, efficiency, and effectiveness of healthcare for all Americans. It creates a priority research agenda annually, and funds studies in areas where improvement is deemed most needed. These include patient safety, data development, pharmaceutical outcomes, and other areas described on its Web site (www.ahrq.gov/).
In 2005, AHRQ announced its Partnerships in Implementing Patient Safety (PIPS) and committed up to $9 million in total costs to fund new grants of less than $300,000 per year, lasting two years. AHRQ indicated that eligible safe practice intervention projects would be required to include “tool kits,” and a comprehensive implementation tool kit to help others overcome barriers and allay adoption concerns. AHRQ’s goal was and is to disseminate funded projects’ perfected tools widely for adaptation and/or adoption by diverse healthcare settings.
AHRQ asked that principal investigators (PIs) be experienced senior level individuals familiar with implementing change in healthcare settings. Their expectation was that PIs would devote at least 15% of their time to the project for its duration. Thus the competitive challenge to potential PIs was great:
- Select a worthy project from among the endless areas where healthcare needs improvement, and then plan specific, realistic, achievable interventions that could create measurable improvement over two years;
- Implement the program; and
- Develop a plan and tools so basic and user-friendly that they could feasibly be applied in not just the local practice setting, but in other healthcare settings.
Although the size and duration of the awards varied, many of the 17 projects they funded received slightly more than a quarter of a million dollars. Among the funded projects, two boast hospitalists as their PIs and address areas of obvious concern in most healthcare settings. Greg Maynard, MD, MS, at the University of California, San Diego, was funded to implement a venous thromboembolism (VTE) intervention program. And Mark V. Williams, MD, FACP, professor of medicine, Emory University School of Medicine, Atlanta, and editor of the Journal of Hospital Medicine, was funded to implement a discharge bundle of patient safety interventions respectively.
Stalking the Silent Killer
Dr. Maynard’s project, “Optimal Prevention of Hospital Acquired Venous Thromboembolism,” focuses on eliminating preventable hospital-acquired VTE at an academic healthcare facility that has a large population of Hispanic patients.
The project’s timeliness and utility is clear: Although the exact incidence of VTE is unknown, experts estimate that approximately 260,000 are clinically recognized annually in acutely hospitalized patients.1 Pulmonary embolism (PE) resulting from deep vein thrombosis (DVT) is the most common cause of preventable hospital death, the majority of hospitalized patients with risk factors for DVT receive no prophylaxis, and the rate of fatal PE more than doubles between age 50 and 80.2,3 The problem is easily recognizable, but “Getting people to do what they need to do to prevent VTE can be hard,” says Dr. Maynard.
This project was carefully planned. It used a rigorous quality improvement process, involving all appropriate clinicians, nurses, managers, and technical support personnel.
Dr. Maynard and his team anticipated roadblocks and negotiated in advance to reduce their effects. They accepted that when patients are hospitalized, things frequently happen that cause physicians to stop VTE prophylaxis: A hemoglobin or platelet count may fall, the patient may have difficulty taking the drug, or the patient’s status may change abruptly. Or the prophylaxis might be accidentally discontinued—perhaps when a patient is transferred.
The team also looked at other institutions’ solutions. Then, using a basic understanding of the ways in which their process was missing VTE prophylaxis opportunities, they built interventions.
This team considered logistics carefully because it was clear that the only intervention that could decrease risk would have to be repetitive in nature. “The process we ultimately selected is very, very quick, yet valid,” says Dr. Maynard, while acknowledging that presenting any intervention repeatedly has the potential to interfere with care. “Other models require the physician to use math and add points. This one does not, and takes only seconds.”
Beginning April 19, 2006, the University of California, San Diego (UCSD) will introduce an intervention that presents a VTE risk assessment screen on every patient who is admitted. This process inquires about the need for prophylaxis every three days for the duration of hospitalization, and physicians cannot skip the screen. If risk factors are present and bleeding risk is not, the screen presents appropriate VTE options.
For example, the system will suggest enoxaparin 40 mg daily, enoxaparin 30 mg twice daily, or appropriately dosed warfarin for a high-risk orthopedic surgery patient who has no bleeding risk. Every three days, the process repeats itself, making explicit decisions or suggestions about appropriate prophylaxis. (Figure 1, below, shows a sample screen for a patient with moderately high risk.
Much evidence about VTE is still being gathered. For example, opinions vary about when to start prophylaxis or how long to continue it. Dr. Maynard and his team also addressed real versus relative contraindications—another area of debate among clinicians. Many clinicians are uncertain about how soon after surgery to restart VTE prophylaxis. After orthopedic spine surgery, for example, some might start it on day five, while others may not restart prophylaxis even after day 10. At UCSD, clinical stakeholders in the process came to consensus, and now all restart by day seven.
The tool kit UCSD is developing recognizes that every institution is unique. Those that choose to implement a similar program must identify their baseline rate of VTE and monitor change over time to determine if progress is being made. Every institution must define adequate VTE prophylaxis and tailor the tools appropriately.
Wait? No Need
One compelling aspect of Dr. Maynard’s project is that some of UCSD’s VTE tools are already available on the SHM Web site in the “VTE Resource Room.” With or without AHRQ funding, UCSD planned to develop and implement a VTE awareness program. UCSD’s grant department provided the support Dr. Maynard and his colleagues needed to apply for the AHRQ funding, and Dr. Maynard says the funding they received helped UCSD “disseminate the program better and to carry it out with more rigor.”
UCSD worked with SHM to develop the tool kit. In return, SHM is providing and promoting the VTE tool kit at no charge to interested parties. Additionally, SHM recently received funding via an unrestricted sponsorship to create a mentored implementation project for the “VTE Resource Room.” Interested institutions will be mentored by UCSD staff who have experience with the tool kit.
Over time, Dr. Maynard will measure the effects of the intervention to ensure it is working. In addition to creating a malleable tool kit, UCSD research hospitalists will examine race, gender, and age to determine the effects of these on the likelihood of getting adequate prophylaxis.
Hospital Patient Safe-D(ischarge)
Dr. Williams and his colleagues at Emory University and the University of Ottawa received funding for “Hospital Patient Safe-D(ischarge): A Discharge Bundle for Patients,” a program that builds on previous AHRQ funding. This intervention implements a “discharge bundle” of patient safety interventions to improve patient transition from the hospital to home or another healthcare setting.
“We hope that every patient will undergo discharge, and of course the majority do, but the discharge process has almost been treated as an afterthought,” explains Dr. Williams. “Doctors spend a lot of time on diagnosis and treatment, but not on discharge. This process of transition from total care with a call button, lots of nursing attention, daily visits from the doctor, and delivered meals to greater independence, has not been well researched.”
What little research exists tends to indicate that discharge processes are very heterogeneous.
So far, Dr. Williams’ team’s examination of the process has produced only one surprise: The team has discovered that the discharge process is even more capricious than they suspected. As patients prepare to leave the hospital, what could and should be an orderly process that educates and prepares patients to assume responsibility for their own care in a new and better way is often interrupted or disjointed.
Preparing patients for discharge once fell to the nursing staff. As nursing faces staffing shortages and expanded roles, the discharge process often belongs to everyone and to no one. That physicians’ discharge visits pay much less than the time required to do it well also complicates the problem. The researchers were not surprised, however, to learn that many patients do not know their diagnosis or treatment plan as discharge is imminent. Their goal is to develop a consistent, comprehensive discharge process that will be a national model.
Here again, the precepts of continuous quality improvement are apparent. Dr. Williams’ team’s effort represents collaboration among physicians, pharmacists, nurses, and patients; involves SHM and several other professional organizations; and calls upon an advisory committee consisting of nationally recognized patient care and safety experts.
The discharge bundle of patient safety interventions—a concept advocated by the Joint Commission on Accreditation of Healthcare Organizations and other quality-promoting groups—adds a post-discharge continuity check to medication reconciliation and patient-centered education at discharge.
The four project phases—implement, evaluate, develop a tool, and disseminate the discharge bundle—overlap and ensure success.
Dr. Williams believes that the group of patients most likely to benefit from this intervention is the elderly. “The elderly bear the greatest burden of chronic disease and typically have several concurrent health problems,” he says.
Educating elders at the time of discharge should decrease the medication error rate and improve adherence to other treatments and recommended lifestyle changes. To gauge the appropriateness of the discharge bundle, John Banja, PhD, an expert in communication and safety, observes the discharge process directly. All communications must be patient-centered, and thus presented in a manner that patients will understand and appreciate. Banja relies on his background in patient safety and disability/rehabilitation to assess the discharge process.
Initial enrollment in this study seems successful. More than 50 patients have consented to participate, but Banja projects a need for 200 to complete the entire process. Recently, the team increased its planned maximum accrual to 300 to increase the statistical power of their findings. The participants like the program because most of them find discharge somewhat discomforting. Patients know they have knowledge gaps and appreciate clinicians’ efforts to fill those gaps seamlessly. A small investment of time can prevent problems after discharge.
Added Value
Clearly, the findings from these AHRQ-funded studies have the potential to reduce morbidity and mortality in a logarithmic manner as other institutions adapt these new tool kits. Dr. Williams indicates that recipients of PIPS funding receive more than just funding and the satisfaction of creating tools that will help all Americans.
“The AHRQ sponsors quarterly conference calls for all participants, regardless of their research topic, and an annual meeting in June to bring all investigators together,” he says.
The opportunity to learn how others address problems, plan interventions, and tackle hurdles proves invaluable. In addition, being privy to interim study results or learning how others handle research dilemmas helps hospitalists expand their skill sets.
Listening to Drs. Maynard and Williams is a not-so-subtle reminder that every hospital needs a well-structured quality improvement plan, and that hospitalists are essential in the plan’s success. Every hospitalist needs an understanding of the precepts these PIs used to earn this well-deserved funding: interdisciplinary and professional organization collaboration, good communication, realistic planning, managing change by measuring, and above all, sharing success. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
References
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991 May;151(5):933-938.
- Clagett GP, Anderson FA Jr, Heit J, et al. Prevention of venous thromboembolism. Chest. 1995 Oct;108(4 Suppl):312S-334S.
- Geerts WH, Heit JA, Clagett GP, et al. Prevention of venous thromboembolism. Chest. 2001;119(1 Suppl):132S-175S.
What can you do with a quarter of a million dollars? In some places, that amount can buy a home that can shelter a family for decades. In other places, it is enough to pay annual malpractice insurance premiums for physicians practicing in high-risk specialties—with a little left over.
But if you wanted to use that money for an enduring healthcare project that would provide the most good for the most people, how would you do it? Hospitalists can look to the Agency for Healthcare Research and Quality (AHRQ) for stellar examples of well-invested dollars with excellent return.
AHRQ Funding
With a staff of approximately 300, the tiny AHRQ is the lead federal agency charged with improving the quality, safety, efficiency, and effectiveness of healthcare for all Americans. It creates a priority research agenda annually, and funds studies in areas where improvement is deemed most needed. These include patient safety, data development, pharmaceutical outcomes, and other areas described on its Web site (www.ahrq.gov/).
In 2005, AHRQ announced its Partnerships in Implementing Patient Safety (PIPS) and committed up to $9 million in total costs to fund new grants of less than $300,000 per year, lasting two years. AHRQ indicated that eligible safe practice intervention projects would be required to include “tool kits,” and a comprehensive implementation tool kit to help others overcome barriers and allay adoption concerns. AHRQ’s goal was and is to disseminate funded projects’ perfected tools widely for adaptation and/or adoption by diverse healthcare settings.
AHRQ asked that principal investigators (PIs) be experienced senior level individuals familiar with implementing change in healthcare settings. Their expectation was that PIs would devote at least 15% of their time to the project for its duration. Thus the competitive challenge to potential PIs was great:
- Select a worthy project from among the endless areas where healthcare needs improvement, and then plan specific, realistic, achievable interventions that could create measurable improvement over two years;
- Implement the program; and
- Develop a plan and tools so basic and user-friendly that they could feasibly be applied in not just the local practice setting, but in other healthcare settings.
Although the size and duration of the awards varied, many of the 17 projects they funded received slightly more than a quarter of a million dollars. Among the funded projects, two boast hospitalists as their PIs and address areas of obvious concern in most healthcare settings. Greg Maynard, MD, MS, at the University of California, San Diego, was funded to implement a venous thromboembolism (VTE) intervention program. And Mark V. Williams, MD, FACP, professor of medicine, Emory University School of Medicine, Atlanta, and editor of the Journal of Hospital Medicine, was funded to implement a discharge bundle of patient safety interventions respectively.
Stalking the Silent Killer
Dr. Maynard’s project, “Optimal Prevention of Hospital Acquired Venous Thromboembolism,” focuses on eliminating preventable hospital-acquired VTE at an academic healthcare facility that has a large population of Hispanic patients.
The project’s timeliness and utility is clear: Although the exact incidence of VTE is unknown, experts estimate that approximately 260,000 are clinically recognized annually in acutely hospitalized patients.1 Pulmonary embolism (PE) resulting from deep vein thrombosis (DVT) is the most common cause of preventable hospital death, the majority of hospitalized patients with risk factors for DVT receive no prophylaxis, and the rate of fatal PE more than doubles between age 50 and 80.2,3 The problem is easily recognizable, but “Getting people to do what they need to do to prevent VTE can be hard,” says Dr. Maynard.
This project was carefully planned. It used a rigorous quality improvement process, involving all appropriate clinicians, nurses, managers, and technical support personnel.
Dr. Maynard and his team anticipated roadblocks and negotiated in advance to reduce their effects. They accepted that when patients are hospitalized, things frequently happen that cause physicians to stop VTE prophylaxis: A hemoglobin or platelet count may fall, the patient may have difficulty taking the drug, or the patient’s status may change abruptly. Or the prophylaxis might be accidentally discontinued—perhaps when a patient is transferred.
The team also looked at other institutions’ solutions. Then, using a basic understanding of the ways in which their process was missing VTE prophylaxis opportunities, they built interventions.
This team considered logistics carefully because it was clear that the only intervention that could decrease risk would have to be repetitive in nature. “The process we ultimately selected is very, very quick, yet valid,” says Dr. Maynard, while acknowledging that presenting any intervention repeatedly has the potential to interfere with care. “Other models require the physician to use math and add points. This one does not, and takes only seconds.”
Beginning April 19, 2006, the University of California, San Diego (UCSD) will introduce an intervention that presents a VTE risk assessment screen on every patient who is admitted. This process inquires about the need for prophylaxis every three days for the duration of hospitalization, and physicians cannot skip the screen. If risk factors are present and bleeding risk is not, the screen presents appropriate VTE options.
For example, the system will suggest enoxaparin 40 mg daily, enoxaparin 30 mg twice daily, or appropriately dosed warfarin for a high-risk orthopedic surgery patient who has no bleeding risk. Every three days, the process repeats itself, making explicit decisions or suggestions about appropriate prophylaxis. (Figure 1, below, shows a sample screen for a patient with moderately high risk.
Much evidence about VTE is still being gathered. For example, opinions vary about when to start prophylaxis or how long to continue it. Dr. Maynard and his team also addressed real versus relative contraindications—another area of debate among clinicians. Many clinicians are uncertain about how soon after surgery to restart VTE prophylaxis. After orthopedic spine surgery, for example, some might start it on day five, while others may not restart prophylaxis even after day 10. At UCSD, clinical stakeholders in the process came to consensus, and now all restart by day seven.
The tool kit UCSD is developing recognizes that every institution is unique. Those that choose to implement a similar program must identify their baseline rate of VTE and monitor change over time to determine if progress is being made. Every institution must define adequate VTE prophylaxis and tailor the tools appropriately.
Wait? No Need
One compelling aspect of Dr. Maynard’s project is that some of UCSD’s VTE tools are already available on the SHM Web site in the “VTE Resource Room.” With or without AHRQ funding, UCSD planned to develop and implement a VTE awareness program. UCSD’s grant department provided the support Dr. Maynard and his colleagues needed to apply for the AHRQ funding, and Dr. Maynard says the funding they received helped UCSD “disseminate the program better and to carry it out with more rigor.”
UCSD worked with SHM to develop the tool kit. In return, SHM is providing and promoting the VTE tool kit at no charge to interested parties. Additionally, SHM recently received funding via an unrestricted sponsorship to create a mentored implementation project for the “VTE Resource Room.” Interested institutions will be mentored by UCSD staff who have experience with the tool kit.
Over time, Dr. Maynard will measure the effects of the intervention to ensure it is working. In addition to creating a malleable tool kit, UCSD research hospitalists will examine race, gender, and age to determine the effects of these on the likelihood of getting adequate prophylaxis.
Hospital Patient Safe-D(ischarge)
Dr. Williams and his colleagues at Emory University and the University of Ottawa received funding for “Hospital Patient Safe-D(ischarge): A Discharge Bundle for Patients,” a program that builds on previous AHRQ funding. This intervention implements a “discharge bundle” of patient safety interventions to improve patient transition from the hospital to home or another healthcare setting.
“We hope that every patient will undergo discharge, and of course the majority do, but the discharge process has almost been treated as an afterthought,” explains Dr. Williams. “Doctors spend a lot of time on diagnosis and treatment, but not on discharge. This process of transition from total care with a call button, lots of nursing attention, daily visits from the doctor, and delivered meals to greater independence, has not been well researched.”
What little research exists tends to indicate that discharge processes are very heterogeneous.
So far, Dr. Williams’ team’s examination of the process has produced only one surprise: The team has discovered that the discharge process is even more capricious than they suspected. As patients prepare to leave the hospital, what could and should be an orderly process that educates and prepares patients to assume responsibility for their own care in a new and better way is often interrupted or disjointed.
Preparing patients for discharge once fell to the nursing staff. As nursing faces staffing shortages and expanded roles, the discharge process often belongs to everyone and to no one. That physicians’ discharge visits pay much less than the time required to do it well also complicates the problem. The researchers were not surprised, however, to learn that many patients do not know their diagnosis or treatment plan as discharge is imminent. Their goal is to develop a consistent, comprehensive discharge process that will be a national model.
Here again, the precepts of continuous quality improvement are apparent. Dr. Williams’ team’s effort represents collaboration among physicians, pharmacists, nurses, and patients; involves SHM and several other professional organizations; and calls upon an advisory committee consisting of nationally recognized patient care and safety experts.
The discharge bundle of patient safety interventions—a concept advocated by the Joint Commission on Accreditation of Healthcare Organizations and other quality-promoting groups—adds a post-discharge continuity check to medication reconciliation and patient-centered education at discharge.
The four project phases—implement, evaluate, develop a tool, and disseminate the discharge bundle—overlap and ensure success.
Dr. Williams believes that the group of patients most likely to benefit from this intervention is the elderly. “The elderly bear the greatest burden of chronic disease and typically have several concurrent health problems,” he says.
Educating elders at the time of discharge should decrease the medication error rate and improve adherence to other treatments and recommended lifestyle changes. To gauge the appropriateness of the discharge bundle, John Banja, PhD, an expert in communication and safety, observes the discharge process directly. All communications must be patient-centered, and thus presented in a manner that patients will understand and appreciate. Banja relies on his background in patient safety and disability/rehabilitation to assess the discharge process.
Initial enrollment in this study seems successful. More than 50 patients have consented to participate, but Banja projects a need for 200 to complete the entire process. Recently, the team increased its planned maximum accrual to 300 to increase the statistical power of their findings. The participants like the program because most of them find discharge somewhat discomforting. Patients know they have knowledge gaps and appreciate clinicians’ efforts to fill those gaps seamlessly. A small investment of time can prevent problems after discharge.
Added Value
Clearly, the findings from these AHRQ-funded studies have the potential to reduce morbidity and mortality in a logarithmic manner as other institutions adapt these new tool kits. Dr. Williams indicates that recipients of PIPS funding receive more than just funding and the satisfaction of creating tools that will help all Americans.
“The AHRQ sponsors quarterly conference calls for all participants, regardless of their research topic, and an annual meeting in June to bring all investigators together,” he says.
The opportunity to learn how others address problems, plan interventions, and tackle hurdles proves invaluable. In addition, being privy to interim study results or learning how others handle research dilemmas helps hospitalists expand their skill sets.
Listening to Drs. Maynard and Williams is a not-so-subtle reminder that every hospital needs a well-structured quality improvement plan, and that hospitalists are essential in the plan’s success. Every hospitalist needs an understanding of the precepts these PIs used to earn this well-deserved funding: interdisciplinary and professional organization collaboration, good communication, realistic planning, managing change by measuring, and above all, sharing success. TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
References
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991 May;151(5):933-938.
- Clagett GP, Anderson FA Jr, Heit J, et al. Prevention of venous thromboembolism. Chest. 1995 Oct;108(4 Suppl):312S-334S.
- Geerts WH, Heit JA, Clagett GP, et al. Prevention of venous thromboembolism. Chest. 2001;119(1 Suppl):132S-175S.
Listen Between the Lines
When an elderly person is admitted to the hospital, Adrienne Green, MD, sees an opportunity for something beyond addressing the medical issues at hand.
“One of the key issues that is important for practical, everyday care is trying to figure out how the elderly are not functioning well at home,” says Dr. Green, an associate clinical professor of medicine at the University of California at San Francisco and a member of UCSF’s hospitalist group. “I think we do a great job of managing their diseases, but what we don’t do very well is helping them out with other things [such as coping with] their losses and the fact that they may be just barely hanging on at home in terms of their ability to care for themselves; and this hospitalization may really have set them back.”
Eva Chittenden, MD, an assistant clinical professor of medicine, also at UCSF, agrees. “Many hospitalists are so focused on the hospital that they’re not thinking about the ‘before the hospital’ and the ‘after the hospital,’” she says.
But after identifying the challenges that elderly patients face, communication itself may be challenging. Elderly individuals struggle with issues of control and allowing people to tell them what they need to change in their lives may not be an easy task. What are the best ways to communicate with hospitalized elderly patients to facilitate the best “whole-person” care?

—David Solie, MS, PA
Under the Radar Screen
The hospitalists interviewed for this article agreed that getting a broader picture of an elderly patient’s health and well-being involves discovering how they are really doing at home. Dr. Green asks simple questions, particularly about activities of daily living, such as whether they’re doing their own shopping and cooking. She also involves the family, “because very frequently the patient will say, ‘I’m doing fine,’ and the family member is in the background shaking their head.”
She also looks for clues about whether the patient needs more help at home, whether they are compliant with their medications, and if not, why (e.g., can they open their medicine bottles)?
“I frequently have the elderly patients evaluated for home care just to get someone into their house … ,” says Dr. Green. “I think that probably 80% of our patients who are over 80 who come into the hospital have things in their homes that are not safe, such as throw rugs.” Even if patients are basically doing OK, “if I can get some home care for them, I know we’ll uncover a ton [of things that can be improved],” she says. “These patients may have … kind of snuck under the radar screen of their families and their primary [care physician], and I think the hospitalization kind of opens that up in some ways.”
Facing Resistance
Even if issues are uncovered by means of interviews and home-health visits, however, many elderly patients present a particular communication challenge. This, says David Solie, MS, PA, author of How to Say It to Seniors: Closing the Communication Gap with Our Elders, is because of the difference in circumstances and current experiences between the elderly and their hospitalist providers.1 It is common knowledge that younger people go through stages of development, but the elderly do, too, says Solie, who is medical director and CEO of Second Opinion Insurance Services in Woodland Hills, Calif., a brokerage that specializes in the insurance needs of impaired-risk, elderly individuals.
The last human developmental stage compels elderly adults to work hard at maintaining control over their lives in the face of almost daily losses. A big part of the losses they experience involve their health and functioning, and the ways different patients cope with loss and the perceived stresses of healthcare have been analyzed and categorized.2-5
But in addition to loss of control, the elderly also face the daunting task of discovering what their legacy will be—what will live on after they die. “The way our elders communicate contains clues to the urgency they feel in trying to resolve these items on their agendas,” writes Solie. “In almost every conversation with older adults, control and legacy issues rise to the surface.”
A Matter of Loss
By the time a person is old (over 70) or old-old (over 85) their losses may have manifested in many areas: They’ve lost:
- Parents;
- Other relatives—perhaps including children;
- Friends;
- Places of residence (both homes and the familiarity of cities or towns);
- Possessions;
- Other relationships (sometimes other healthcare providers);
- Careers;
- Consultative authority (“ours is not a culture that values the wisdom of our elders,” writes Solie);
- Identity;
- Financial independence;
- Habits and pleasures;
- Physical space (the room at their son or daughter’s or in assisted living or the nursing home can’t compare to the homes, gardens, and expanses of view they may have had as younger people), and, of course; and
- Physical and mental capacities.
Sometimes the losses elders sustain occur in rapid-fire sequence, with little or no recovery time in between.1,6
It is no wonder that older adults, in one way or another, exhibit what we consider resistance to their changing lives. In terms of a hospitalization, this may mean saying “no” to medications, individual providers, tests, surgery, home-health visits, or something as small as being talked to or touched in what they perceive as a disturbing, overly familiar, or mechanized manner.
“Many patients are resistant to having people come into their homes and help them, and at the same time they are resistant to going to a skilled nursing care facility,” says Dr. Green, “and it has to do with their [feelings of the] loss of independence and control over their lives.”
“It’s very easy if you’re in medicine to normalize your context of the hospital,” says Solie. “In other words, the hospital seems familiar to you and you’re very comfortable moving around there, and mainly because you’re in control. You’re the doctor … and you move in the hospital in order to make things happen and you never feel all that threatened. But when you bring an older person who already has a heightened sensitivity toward losing control into the hospital—this complex, technological world of medicine—and they have the cumulative disadvantage of being sick,” says Solie, “it’s really important to remember that there will probably be no other state that they’ll be in, except maybe nursing home care, where they will feel so out of control.”
A good first step in communicating with older patients is to quickly develop a rapport with them and show them you recognize what they’re up against.7 “They really want to know whether or not I get it,” says Solie.
The way you communicate that you get it, he says, is fairly straightforward: When I’m first interacting with the patient, I say, “if you are like my [other] elderly patients … I’m sure you’re feeling a lot of anxiety over [not having much] control and, first of all, I want to assure you that I’m going to make sure you understand the choices and help you make all the decisions. And … I’m definitely going to … put everything in a language that you understand. But if I’m not successful, I’m going to employ someone from your family. We’re going to work together. Even though you’re hospitalized and even though you’re fighting this illness (or whatever the condition might be), you still [have] the right to make choices, and my goal is to partner with you. My expertise is medicine, but you have an expertise in your life.”
In other words, you are signaling that you recognize that control is the issue. Acknowledge the loss, ask about the value of the event or decision to the patient, ask what you can do to help them deal with their feelings or make up their minds. It also allows you to remind an older patient’s children that control is a big and normal concern for their mother or father.

—Eva Chittenden, MD
Hospitalists at a Different Time and Place
The elderly desperately need people who can serve them as natural healers, who are not constantly in a hurry, and who care what they are thinking and feeling. How can hospitalists relate to those who are in the midst of life review and who are hanging on to an escaping control? How can they serve their patients in a way that meets all needs?
Fighting—with denial or ignorance—the resistance that patients might put up will more than likely provoke them. A fight for control can undermine and sabotage the best intentions of the provider and the greatest wishes for the patient to experience comfort or regain health and well-being. Rather than justifying wresting control from elderly patients because it’s for their own good, advises Solie, what we must do instead is to “step back, hand them the control baton, and allow them to run with it.”1
A person’s admission to the hospital “might be such a huge crisis for them, whereas for us it’s our routine work,” says Dr. Chittenden, who practices as a hospitalist and also works on her institution’s inpatient palliative care service. “And many people who are hospitalists—who are even in their late 20s, 30s, 40s—have been totally healthy their whole life, so it is hard to relate to what it’s like to be older and to be losing function, losing friends who are also dying, losing their house … . I think that it can be very helpful for the hospitalist to take a little more time and explore some of those issues [of loss and legacy]. I try to meet the person where they’re at and try to understand what their goals, needs, ... and fears are [as well as] their functional status.”
Allowing older patients to engage with you about their lives and their pasts is a privilege for any healthcare provider. Engaging with them in a way that will help facilitate their loosening the reins on control may expedite and allow greater quality into their healthcare. It may provide an opening whereby you can order that home-health visit with less struggle.
Create Openings
“There are a lot of different ‘on-ramps’ to asking the life-review questions, which are extremely comforting,” says Solie. “For example, you might say, ‘Mary, I notice that you were born in Iowa. You know, my family on my father’s side came from Iowa. Where were you raised?’ And ‘Do you have a big family on your farm, because my aunt had cows.’”
Once you get a response that engages the patient, then you “are in the slipstream. Physicians have such a high experience curve, they see so many patients,” he says. “They don’t have to go very far into their inventory of experiences [to find one] that essentially matches up with that patient.”
Any kind of comment that will key you in to their background experience can help establish some kind of foundation for relationship. Another example: “You know, Mary, I was working with this woman who was about your age and she was raised in the Midwest and was dealing with some of these issues of congestive heart failure, and one of her big concerns was something that I didn’t appreciate until I understood what an impact it was having on her life.”
This kind of communication, says Solie, can help to relieve some of the patient’s control anxieties, “because she feels that if I ‘get it,’ she’s open to what I have to say, such as, ‘The first thing, we have to deal with is there is too much fluid going on in your body and it’s putting a big strain on your heart, so the first couple days all we did for that [other] woman was try to pull some fluid off and keep everything in balance.’”
You’ve communicated that you have a plan, that you can be trusted, and that you will help her to exercise as much control as possible. Creating and accessing those openings is also “the ideal way to weave the family into this whole life-review process, which is where the patient lives, psychologically and emotionally, when outside the hospital environment,” he says. “We become so myopic when we’re caught in the hospital environment that the world becomes a narrow tunnel and we forget the greater matrix outside that we’re all connected to.”
The Boon of Biology
Whereas the physiology and anatomy of humans deteriorate with time, some of the changes in mental processes in old age may actually enhance the ability to reflect and make informed judgments. Solie’s view is that what younger people may view as slow behavior, confusing speech patterns, and physical frailty don’t hinder the tasks that are before the elderly. On the contrary, they assist the fulfillment of their developmental agendas to feel in control when they’re losing control and to let go enough to reveal the legacy that will survive after they go.
Research on the aging brain indicates that changes in brain chemistry facilitate the life-review process.1,6 In general, reflection is the normal mode of existence for elderly adults and their primary focus. Thus, viewing them as diminished because they communicate differently than younger people do is doing them a disservice.
Those slowed mental processes, Dr. Chittenden concurs, “are conducive to reflection. Someone younger will pathologize it. … I agree that we don’t value the slowing down process, but I also think that when this population is in the hospital we are tending to look at loss of functional status or the quick mental traits that we value as opposed to [that which is] adaptive [and] that enables them to look at things differently and reflect.”
The key to connecting the dots of where they are and where they need to be (both medically and psychosocially), as well as how they occur to their providers and their families as opposed to how they occur to themselves, is to listen to and speak with them by making use of what you know about this stage of their life as it affects their communication. You can do this, says Solie, by invoking the “access code,” which is “to clearly understand that at the top of their agenda—no matter what else is happening—is the need for control and the need to develop and go after a legacy, and that means life review. If you know that, you will never lose your reference point with them.”
Communication Habits of the Elderly
Solie identifies some verbal behaviors that are common in older people. In many cases these behaviors may reveal something between the lines.
- Lack of urgency. Older people need more time to decide things. Accept that slower pace as normal. Don’t take it personally. Adjust your schedule to allow time to deliver news or ask for choices and then allow time for them to discuss with their families or contemplate on their own; return to them at a later time. Become expert at spontaneous facilitation. Use your access code to get their attention and gain their trust.
- Nonlinear conversations. Although older patients may appear to wander off topic, they may do so in the urge to ground themselves in what their priorities are, what their feelings are, what their choices will be. Signal you’re willing to listen and that you’re tuned in to the content, even if you don’t know where it is leading. (Obviously, someone who is demented or delirious presents a different scenario altogether, and depression is common and frequently overlooked.) Listen for patterns and themes. Nonlinear conversations can lead to spontaneous revelations and great insights for your patients and for yourself and can help patients revisit life dramas that test and clarify values. This, too, is a part of healthcare.
- Repetition and attention to details. In situations when dementia is ruled out, a patient’s repetition may indicate a means to emphasize an important point or value. Keep in mind, too, that as we age, we all repeat stories to some degree. Details in stories may be the means by which older adults connect to their pasts and may also serve as clues to what is important to these people. Don’t assume details demand any action on your part. You are only being asked to listen as the older person sorts things out.
- Uncoupling. Solie describes uncoupling as any time an older person appears to disconnect from you in the course of a conversation. For a professional, this can feel as if you are dismissed or ignored just when you think you’ve hit the mark with a comment or question. Go back and assess the information you’ve gathered by doing some verification. Rethink the objective: Any action that works against their maintaining control and discovering a legacy will produce uncoupling.
“I try to be aware of when I’m losing people,” says Dr. Chittenden of this phenomenon. “I would say, ‘I seem to be losing you and I’m wondering what you’re thinking right now.’ I would try to find out where they’re at and if it was something I said that didn’t gel with them, didn’t make sense to them, or wasn’t their priority.” This is something, she emphasizes, that a hospitalist needs to watch for with patients of all ages. “Whether you’re older or younger,” she says, the communication can be complicated because “you’re … in the hospital culture and the priorities of doctors are so often different from the priorities of patients.”
Conclusion
Older and especially old-old individuals in some ways live in an era other than the one traversed by the young and middle-aged.6 Their purposes, agendas, and mission are different and the slowing down of their functioning can facilitate their attempts to put their lives into perspective and manage what control they can still exercise or are still allowed. Viewing older patients with the utmost respect and acknowledging the challenges they face at these last phases of their lives can better help you to partner with them and their families in their care. TH
Andrea Sattinger also writes about the importance of apology in this issue.
References
- Solie D. How to Say it to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Chochinov HM, Cann BJ. Interventions to enhance the spiritual aspects of dying. J Palliat Med. 2005;8:Suppl 1:S103-115.
- Dennis KE. Patients' control and the information imperative: clarification and confirmation. Nurs Res. 1990;39(3):162-166.
- Kiesler DJ, Auerbach SM. Integrating measurement of control and affiliation in studies of physician-patient interaction: the interpersonal circumplex. Soc Sci Med. 2003;57(9):1707-1722.
- Breemhaar B, Visser AP, Kleijnen JG. Perceptions and behaviour among elderly hospital patients: description and explanation of age differences in satisfaction, knowledge, emotions and behaviour. Soc Sci Med. 1990;31(12):1377-1385.
- Pipher M. Another Country: Navigating the Emotional Terrain of Our Elders. New York: Riverhead Books; 1999.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
When an elderly person is admitted to the hospital, Adrienne Green, MD, sees an opportunity for something beyond addressing the medical issues at hand.
“One of the key issues that is important for practical, everyday care is trying to figure out how the elderly are not functioning well at home,” says Dr. Green, an associate clinical professor of medicine at the University of California at San Francisco and a member of UCSF’s hospitalist group. “I think we do a great job of managing their diseases, but what we don’t do very well is helping them out with other things [such as coping with] their losses and the fact that they may be just barely hanging on at home in terms of their ability to care for themselves; and this hospitalization may really have set them back.”
Eva Chittenden, MD, an assistant clinical professor of medicine, also at UCSF, agrees. “Many hospitalists are so focused on the hospital that they’re not thinking about the ‘before the hospital’ and the ‘after the hospital,’” she says.
But after identifying the challenges that elderly patients face, communication itself may be challenging. Elderly individuals struggle with issues of control and allowing people to tell them what they need to change in their lives may not be an easy task. What are the best ways to communicate with hospitalized elderly patients to facilitate the best “whole-person” care?
—David Solie, MS, PA
Under the Radar Screen
The hospitalists interviewed for this article agreed that getting a broader picture of an elderly patient’s health and well-being involves discovering how they are really doing at home. Dr. Green asks simple questions, particularly about activities of daily living, such as whether they’re doing their own shopping and cooking. She also involves the family, “because very frequently the patient will say, ‘I’m doing fine,’ and the family member is in the background shaking their head.”
She also looks for clues about whether the patient needs more help at home, whether they are compliant with their medications, and if not, why (e.g., can they open their medicine bottles)?
“I frequently have the elderly patients evaluated for home care just to get someone into their house … ,” says Dr. Green. “I think that probably 80% of our patients who are over 80 who come into the hospital have things in their homes that are not safe, such as throw rugs.” Even if patients are basically doing OK, “if I can get some home care for them, I know we’ll uncover a ton [of things that can be improved],” she says. “These patients may have … kind of snuck under the radar screen of their families and their primary [care physician], and I think the hospitalization kind of opens that up in some ways.”
Facing Resistance
Even if issues are uncovered by means of interviews and home-health visits, however, many elderly patients present a particular communication challenge. This, says David Solie, MS, PA, author of How to Say It to Seniors: Closing the Communication Gap with Our Elders, is because of the difference in circumstances and current experiences between the elderly and their hospitalist providers.1 It is common knowledge that younger people go through stages of development, but the elderly do, too, says Solie, who is medical director and CEO of Second Opinion Insurance Services in Woodland Hills, Calif., a brokerage that specializes in the insurance needs of impaired-risk, elderly individuals.
The last human developmental stage compels elderly adults to work hard at maintaining control over their lives in the face of almost daily losses. A big part of the losses they experience involve their health and functioning, and the ways different patients cope with loss and the perceived stresses of healthcare have been analyzed and categorized.2-5
But in addition to loss of control, the elderly also face the daunting task of discovering what their legacy will be—what will live on after they die. “The way our elders communicate contains clues to the urgency they feel in trying to resolve these items on their agendas,” writes Solie. “In almost every conversation with older adults, control and legacy issues rise to the surface.”
A Matter of Loss
By the time a person is old (over 70) or old-old (over 85) their losses may have manifested in many areas: They’ve lost:
- Parents;
- Other relatives—perhaps including children;
- Friends;
- Places of residence (both homes and the familiarity of cities or towns);
- Possessions;
- Other relationships (sometimes other healthcare providers);
- Careers;
- Consultative authority (“ours is not a culture that values the wisdom of our elders,” writes Solie);
- Identity;
- Financial independence;
- Habits and pleasures;
- Physical space (the room at their son or daughter’s or in assisted living or the nursing home can’t compare to the homes, gardens, and expanses of view they may have had as younger people), and, of course; and
- Physical and mental capacities.
Sometimes the losses elders sustain occur in rapid-fire sequence, with little or no recovery time in between.1,6
It is no wonder that older adults, in one way or another, exhibit what we consider resistance to their changing lives. In terms of a hospitalization, this may mean saying “no” to medications, individual providers, tests, surgery, home-health visits, or something as small as being talked to or touched in what they perceive as a disturbing, overly familiar, or mechanized manner.
“Many patients are resistant to having people come into their homes and help them, and at the same time they are resistant to going to a skilled nursing care facility,” says Dr. Green, “and it has to do with their [feelings of the] loss of independence and control over their lives.”
“It’s very easy if you’re in medicine to normalize your context of the hospital,” says Solie. “In other words, the hospital seems familiar to you and you’re very comfortable moving around there, and mainly because you’re in control. You’re the doctor … and you move in the hospital in order to make things happen and you never feel all that threatened. But when you bring an older person who already has a heightened sensitivity toward losing control into the hospital—this complex, technological world of medicine—and they have the cumulative disadvantage of being sick,” says Solie, “it’s really important to remember that there will probably be no other state that they’ll be in, except maybe nursing home care, where they will feel so out of control.”
A good first step in communicating with older patients is to quickly develop a rapport with them and show them you recognize what they’re up against.7 “They really want to know whether or not I get it,” says Solie.
The way you communicate that you get it, he says, is fairly straightforward: When I’m first interacting with the patient, I say, “if you are like my [other] elderly patients … I’m sure you’re feeling a lot of anxiety over [not having much] control and, first of all, I want to assure you that I’m going to make sure you understand the choices and help you make all the decisions. And … I’m definitely going to … put everything in a language that you understand. But if I’m not successful, I’m going to employ someone from your family. We’re going to work together. Even though you’re hospitalized and even though you’re fighting this illness (or whatever the condition might be), you still [have] the right to make choices, and my goal is to partner with you. My expertise is medicine, but you have an expertise in your life.”
In other words, you are signaling that you recognize that control is the issue. Acknowledge the loss, ask about the value of the event or decision to the patient, ask what you can do to help them deal with their feelings or make up their minds. It also allows you to remind an older patient’s children that control is a big and normal concern for their mother or father.
—Eva Chittenden, MD
Hospitalists at a Different Time and Place
The elderly desperately need people who can serve them as natural healers, who are not constantly in a hurry, and who care what they are thinking and feeling. How can hospitalists relate to those who are in the midst of life review and who are hanging on to an escaping control? How can they serve their patients in a way that meets all needs?
Fighting—with denial or ignorance—the resistance that patients might put up will more than likely provoke them. A fight for control can undermine and sabotage the best intentions of the provider and the greatest wishes for the patient to experience comfort or regain health and well-being. Rather than justifying wresting control from elderly patients because it’s for their own good, advises Solie, what we must do instead is to “step back, hand them the control baton, and allow them to run with it.”1
A person’s admission to the hospital “might be such a huge crisis for them, whereas for us it’s our routine work,” says Dr. Chittenden, who practices as a hospitalist and also works on her institution’s inpatient palliative care service. “And many people who are hospitalists—who are even in their late 20s, 30s, 40s—have been totally healthy their whole life, so it is hard to relate to what it’s like to be older and to be losing function, losing friends who are also dying, losing their house … . I think that it can be very helpful for the hospitalist to take a little more time and explore some of those issues [of loss and legacy]. I try to meet the person where they’re at and try to understand what their goals, needs, ... and fears are [as well as] their functional status.”
Allowing older patients to engage with you about their lives and their pasts is a privilege for any healthcare provider. Engaging with them in a way that will help facilitate their loosening the reins on control may expedite and allow greater quality into their healthcare. It may provide an opening whereby you can order that home-health visit with less struggle.
Create Openings
“There are a lot of different ‘on-ramps’ to asking the life-review questions, which are extremely comforting,” says Solie. “For example, you might say, ‘Mary, I notice that you were born in Iowa. You know, my family on my father’s side came from Iowa. Where were you raised?’ And ‘Do you have a big family on your farm, because my aunt had cows.’”
Once you get a response that engages the patient, then you “are in the slipstream. Physicians have such a high experience curve, they see so many patients,” he says. “They don’t have to go very far into their inventory of experiences [to find one] that essentially matches up with that patient.”
Any kind of comment that will key you in to their background experience can help establish some kind of foundation for relationship. Another example: “You know, Mary, I was working with this woman who was about your age and she was raised in the Midwest and was dealing with some of these issues of congestive heart failure, and one of her big concerns was something that I didn’t appreciate until I understood what an impact it was having on her life.”
This kind of communication, says Solie, can help to relieve some of the patient’s control anxieties, “because she feels that if I ‘get it,’ she’s open to what I have to say, such as, ‘The first thing, we have to deal with is there is too much fluid going on in your body and it’s putting a big strain on your heart, so the first couple days all we did for that [other] woman was try to pull some fluid off and keep everything in balance.’”
You’ve communicated that you have a plan, that you can be trusted, and that you will help her to exercise as much control as possible. Creating and accessing those openings is also “the ideal way to weave the family into this whole life-review process, which is where the patient lives, psychologically and emotionally, when outside the hospital environment,” he says. “We become so myopic when we’re caught in the hospital environment that the world becomes a narrow tunnel and we forget the greater matrix outside that we’re all connected to.”
The Boon of Biology
Whereas the physiology and anatomy of humans deteriorate with time, some of the changes in mental processes in old age may actually enhance the ability to reflect and make informed judgments. Solie’s view is that what younger people may view as slow behavior, confusing speech patterns, and physical frailty don’t hinder the tasks that are before the elderly. On the contrary, they assist the fulfillment of their developmental agendas to feel in control when they’re losing control and to let go enough to reveal the legacy that will survive after they go.
Research on the aging brain indicates that changes in brain chemistry facilitate the life-review process.1,6 In general, reflection is the normal mode of existence for elderly adults and their primary focus. Thus, viewing them as diminished because they communicate differently than younger people do is doing them a disservice.
Those slowed mental processes, Dr. Chittenden concurs, “are conducive to reflection. Someone younger will pathologize it. … I agree that we don’t value the slowing down process, but I also think that when this population is in the hospital we are tending to look at loss of functional status or the quick mental traits that we value as opposed to [that which is] adaptive [and] that enables them to look at things differently and reflect.”
The key to connecting the dots of where they are and where they need to be (both medically and psychosocially), as well as how they occur to their providers and their families as opposed to how they occur to themselves, is to listen to and speak with them by making use of what you know about this stage of their life as it affects their communication. You can do this, says Solie, by invoking the “access code,” which is “to clearly understand that at the top of their agenda—no matter what else is happening—is the need for control and the need to develop and go after a legacy, and that means life review. If you know that, you will never lose your reference point with them.”
Communication Habits of the Elderly
Solie identifies some verbal behaviors that are common in older people. In many cases these behaviors may reveal something between the lines.
- Lack of urgency. Older people need more time to decide things. Accept that slower pace as normal. Don’t take it personally. Adjust your schedule to allow time to deliver news or ask for choices and then allow time for them to discuss with their families or contemplate on their own; return to them at a later time. Become expert at spontaneous facilitation. Use your access code to get their attention and gain their trust.
- Nonlinear conversations. Although older patients may appear to wander off topic, they may do so in the urge to ground themselves in what their priorities are, what their feelings are, what their choices will be. Signal you’re willing to listen and that you’re tuned in to the content, even if you don’t know where it is leading. (Obviously, someone who is demented or delirious presents a different scenario altogether, and depression is common and frequently overlooked.) Listen for patterns and themes. Nonlinear conversations can lead to spontaneous revelations and great insights for your patients and for yourself and can help patients revisit life dramas that test and clarify values. This, too, is a part of healthcare.
- Repetition and attention to details. In situations when dementia is ruled out, a patient’s repetition may indicate a means to emphasize an important point or value. Keep in mind, too, that as we age, we all repeat stories to some degree. Details in stories may be the means by which older adults connect to their pasts and may also serve as clues to what is important to these people. Don’t assume details demand any action on your part. You are only being asked to listen as the older person sorts things out.
- Uncoupling. Solie describes uncoupling as any time an older person appears to disconnect from you in the course of a conversation. For a professional, this can feel as if you are dismissed or ignored just when you think you’ve hit the mark with a comment or question. Go back and assess the information you’ve gathered by doing some verification. Rethink the objective: Any action that works against their maintaining control and discovering a legacy will produce uncoupling.
“I try to be aware of when I’m losing people,” says Dr. Chittenden of this phenomenon. “I would say, ‘I seem to be losing you and I’m wondering what you’re thinking right now.’ I would try to find out where they’re at and if it was something I said that didn’t gel with them, didn’t make sense to them, or wasn’t their priority.” This is something, she emphasizes, that a hospitalist needs to watch for with patients of all ages. “Whether you’re older or younger,” she says, the communication can be complicated because “you’re … in the hospital culture and the priorities of doctors are so often different from the priorities of patients.”
Conclusion
Older and especially old-old individuals in some ways live in an era other than the one traversed by the young and middle-aged.6 Their purposes, agendas, and mission are different and the slowing down of their functioning can facilitate their attempts to put their lives into perspective and manage what control they can still exercise or are still allowed. Viewing older patients with the utmost respect and acknowledging the challenges they face at these last phases of their lives can better help you to partner with them and their families in their care. TH
Andrea Sattinger also writes about the importance of apology in this issue.
References
- Solie D. How to Say it to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Chochinov HM, Cann BJ. Interventions to enhance the spiritual aspects of dying. J Palliat Med. 2005;8:Suppl 1:S103-115.
- Dennis KE. Patients' control and the information imperative: clarification and confirmation. Nurs Res. 1990;39(3):162-166.
- Kiesler DJ, Auerbach SM. Integrating measurement of control and affiliation in studies of physician-patient interaction: the interpersonal circumplex. Soc Sci Med. 2003;57(9):1707-1722.
- Breemhaar B, Visser AP, Kleijnen JG. Perceptions and behaviour among elderly hospital patients: description and explanation of age differences in satisfaction, knowledge, emotions and behaviour. Soc Sci Med. 1990;31(12):1377-1385.
- Pipher M. Another Country: Navigating the Emotional Terrain of Our Elders. New York: Riverhead Books; 1999.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
When an elderly person is admitted to the hospital, Adrienne Green, MD, sees an opportunity for something beyond addressing the medical issues at hand.
“One of the key issues that is important for practical, everyday care is trying to figure out how the elderly are not functioning well at home,” says Dr. Green, an associate clinical professor of medicine at the University of California at San Francisco and a member of UCSF’s hospitalist group. “I think we do a great job of managing their diseases, but what we don’t do very well is helping them out with other things [such as coping with] their losses and the fact that they may be just barely hanging on at home in terms of their ability to care for themselves; and this hospitalization may really have set them back.”
Eva Chittenden, MD, an assistant clinical professor of medicine, also at UCSF, agrees. “Many hospitalists are so focused on the hospital that they’re not thinking about the ‘before the hospital’ and the ‘after the hospital,’” she says.
But after identifying the challenges that elderly patients face, communication itself may be challenging. Elderly individuals struggle with issues of control and allowing people to tell them what they need to change in their lives may not be an easy task. What are the best ways to communicate with hospitalized elderly patients to facilitate the best “whole-person” care?
—David Solie, MS, PA
Under the Radar Screen
The hospitalists interviewed for this article agreed that getting a broader picture of an elderly patient’s health and well-being involves discovering how they are really doing at home. Dr. Green asks simple questions, particularly about activities of daily living, such as whether they’re doing their own shopping and cooking. She also involves the family, “because very frequently the patient will say, ‘I’m doing fine,’ and the family member is in the background shaking their head.”
She also looks for clues about whether the patient needs more help at home, whether they are compliant with their medications, and if not, why (e.g., can they open their medicine bottles)?
“I frequently have the elderly patients evaluated for home care just to get someone into their house … ,” says Dr. Green. “I think that probably 80% of our patients who are over 80 who come into the hospital have things in their homes that are not safe, such as throw rugs.” Even if patients are basically doing OK, “if I can get some home care for them, I know we’ll uncover a ton [of things that can be improved],” she says. “These patients may have … kind of snuck under the radar screen of their families and their primary [care physician], and I think the hospitalization kind of opens that up in some ways.”
Facing Resistance
Even if issues are uncovered by means of interviews and home-health visits, however, many elderly patients present a particular communication challenge. This, says David Solie, MS, PA, author of How to Say It to Seniors: Closing the Communication Gap with Our Elders, is because of the difference in circumstances and current experiences between the elderly and their hospitalist providers.1 It is common knowledge that younger people go through stages of development, but the elderly do, too, says Solie, who is medical director and CEO of Second Opinion Insurance Services in Woodland Hills, Calif., a brokerage that specializes in the insurance needs of impaired-risk, elderly individuals.
The last human developmental stage compels elderly adults to work hard at maintaining control over their lives in the face of almost daily losses. A big part of the losses they experience involve their health and functioning, and the ways different patients cope with loss and the perceived stresses of healthcare have been analyzed and categorized.2-5
But in addition to loss of control, the elderly also face the daunting task of discovering what their legacy will be—what will live on after they die. “The way our elders communicate contains clues to the urgency they feel in trying to resolve these items on their agendas,” writes Solie. “In almost every conversation with older adults, control and legacy issues rise to the surface.”
A Matter of Loss
By the time a person is old (over 70) or old-old (over 85) their losses may have manifested in many areas: They’ve lost:
- Parents;
- Other relatives—perhaps including children;
- Friends;
- Places of residence (both homes and the familiarity of cities or towns);
- Possessions;
- Other relationships (sometimes other healthcare providers);
- Careers;
- Consultative authority (“ours is not a culture that values the wisdom of our elders,” writes Solie);
- Identity;
- Financial independence;
- Habits and pleasures;
- Physical space (the room at their son or daughter’s or in assisted living or the nursing home can’t compare to the homes, gardens, and expanses of view they may have had as younger people), and, of course; and
- Physical and mental capacities.
Sometimes the losses elders sustain occur in rapid-fire sequence, with little or no recovery time in between.1,6
It is no wonder that older adults, in one way or another, exhibit what we consider resistance to their changing lives. In terms of a hospitalization, this may mean saying “no” to medications, individual providers, tests, surgery, home-health visits, or something as small as being talked to or touched in what they perceive as a disturbing, overly familiar, or mechanized manner.
“Many patients are resistant to having people come into their homes and help them, and at the same time they are resistant to going to a skilled nursing care facility,” says Dr. Green, “and it has to do with their [feelings of the] loss of independence and control over their lives.”
“It’s very easy if you’re in medicine to normalize your context of the hospital,” says Solie. “In other words, the hospital seems familiar to you and you’re very comfortable moving around there, and mainly because you’re in control. You’re the doctor … and you move in the hospital in order to make things happen and you never feel all that threatened. But when you bring an older person who already has a heightened sensitivity toward losing control into the hospital—this complex, technological world of medicine—and they have the cumulative disadvantage of being sick,” says Solie, “it’s really important to remember that there will probably be no other state that they’ll be in, except maybe nursing home care, where they will feel so out of control.”
A good first step in communicating with older patients is to quickly develop a rapport with them and show them you recognize what they’re up against.7 “They really want to know whether or not I get it,” says Solie.
The way you communicate that you get it, he says, is fairly straightforward: When I’m first interacting with the patient, I say, “if you are like my [other] elderly patients … I’m sure you’re feeling a lot of anxiety over [not having much] control and, first of all, I want to assure you that I’m going to make sure you understand the choices and help you make all the decisions. And … I’m definitely going to … put everything in a language that you understand. But if I’m not successful, I’m going to employ someone from your family. We’re going to work together. Even though you’re hospitalized and even though you’re fighting this illness (or whatever the condition might be), you still [have] the right to make choices, and my goal is to partner with you. My expertise is medicine, but you have an expertise in your life.”
In other words, you are signaling that you recognize that control is the issue. Acknowledge the loss, ask about the value of the event or decision to the patient, ask what you can do to help them deal with their feelings or make up their minds. It also allows you to remind an older patient’s children that control is a big and normal concern for their mother or father.
—Eva Chittenden, MD
Hospitalists at a Different Time and Place
The elderly desperately need people who can serve them as natural healers, who are not constantly in a hurry, and who care what they are thinking and feeling. How can hospitalists relate to those who are in the midst of life review and who are hanging on to an escaping control? How can they serve their patients in a way that meets all needs?
Fighting—with denial or ignorance—the resistance that patients might put up will more than likely provoke them. A fight for control can undermine and sabotage the best intentions of the provider and the greatest wishes for the patient to experience comfort or regain health and well-being. Rather than justifying wresting control from elderly patients because it’s for their own good, advises Solie, what we must do instead is to “step back, hand them the control baton, and allow them to run with it.”1
A person’s admission to the hospital “might be such a huge crisis for them, whereas for us it’s our routine work,” says Dr. Chittenden, who practices as a hospitalist and also works on her institution’s inpatient palliative care service. “And many people who are hospitalists—who are even in their late 20s, 30s, 40s—have been totally healthy their whole life, so it is hard to relate to what it’s like to be older and to be losing function, losing friends who are also dying, losing their house … . I think that it can be very helpful for the hospitalist to take a little more time and explore some of those issues [of loss and legacy]. I try to meet the person where they’re at and try to understand what their goals, needs, ... and fears are [as well as] their functional status.”
Allowing older patients to engage with you about their lives and their pasts is a privilege for any healthcare provider. Engaging with them in a way that will help facilitate their loosening the reins on control may expedite and allow greater quality into their healthcare. It may provide an opening whereby you can order that home-health visit with less struggle.
Create Openings
“There are a lot of different ‘on-ramps’ to asking the life-review questions, which are extremely comforting,” says Solie. “For example, you might say, ‘Mary, I notice that you were born in Iowa. You know, my family on my father’s side came from Iowa. Where were you raised?’ And ‘Do you have a big family on your farm, because my aunt had cows.’”
Once you get a response that engages the patient, then you “are in the slipstream. Physicians have such a high experience curve, they see so many patients,” he says. “They don’t have to go very far into their inventory of experiences [to find one] that essentially matches up with that patient.”
Any kind of comment that will key you in to their background experience can help establish some kind of foundation for relationship. Another example: “You know, Mary, I was working with this woman who was about your age and she was raised in the Midwest and was dealing with some of these issues of congestive heart failure, and one of her big concerns was something that I didn’t appreciate until I understood what an impact it was having on her life.”
This kind of communication, says Solie, can help to relieve some of the patient’s control anxieties, “because she feels that if I ‘get it,’ she’s open to what I have to say, such as, ‘The first thing, we have to deal with is there is too much fluid going on in your body and it’s putting a big strain on your heart, so the first couple days all we did for that [other] woman was try to pull some fluid off and keep everything in balance.’”
You’ve communicated that you have a plan, that you can be trusted, and that you will help her to exercise as much control as possible. Creating and accessing those openings is also “the ideal way to weave the family into this whole life-review process, which is where the patient lives, psychologically and emotionally, when outside the hospital environment,” he says. “We become so myopic when we’re caught in the hospital environment that the world becomes a narrow tunnel and we forget the greater matrix outside that we’re all connected to.”
The Boon of Biology
Whereas the physiology and anatomy of humans deteriorate with time, some of the changes in mental processes in old age may actually enhance the ability to reflect and make informed judgments. Solie’s view is that what younger people may view as slow behavior, confusing speech patterns, and physical frailty don’t hinder the tasks that are before the elderly. On the contrary, they assist the fulfillment of their developmental agendas to feel in control when they’re losing control and to let go enough to reveal the legacy that will survive after they go.
Research on the aging brain indicates that changes in brain chemistry facilitate the life-review process.1,6 In general, reflection is the normal mode of existence for elderly adults and their primary focus. Thus, viewing them as diminished because they communicate differently than younger people do is doing them a disservice.
Those slowed mental processes, Dr. Chittenden concurs, “are conducive to reflection. Someone younger will pathologize it. … I agree that we don’t value the slowing down process, but I also think that when this population is in the hospital we are tending to look at loss of functional status or the quick mental traits that we value as opposed to [that which is] adaptive [and] that enables them to look at things differently and reflect.”
The key to connecting the dots of where they are and where they need to be (both medically and psychosocially), as well as how they occur to their providers and their families as opposed to how they occur to themselves, is to listen to and speak with them by making use of what you know about this stage of their life as it affects their communication. You can do this, says Solie, by invoking the “access code,” which is “to clearly understand that at the top of their agenda—no matter what else is happening—is the need for control and the need to develop and go after a legacy, and that means life review. If you know that, you will never lose your reference point with them.”
Communication Habits of the Elderly
Solie identifies some verbal behaviors that are common in older people. In many cases these behaviors may reveal something between the lines.
- Lack of urgency. Older people need more time to decide things. Accept that slower pace as normal. Don’t take it personally. Adjust your schedule to allow time to deliver news or ask for choices and then allow time for them to discuss with their families or contemplate on their own; return to them at a later time. Become expert at spontaneous facilitation. Use your access code to get their attention and gain their trust.
- Nonlinear conversations. Although older patients may appear to wander off topic, they may do so in the urge to ground themselves in what their priorities are, what their feelings are, what their choices will be. Signal you’re willing to listen and that you’re tuned in to the content, even if you don’t know where it is leading. (Obviously, someone who is demented or delirious presents a different scenario altogether, and depression is common and frequently overlooked.) Listen for patterns and themes. Nonlinear conversations can lead to spontaneous revelations and great insights for your patients and for yourself and can help patients revisit life dramas that test and clarify values. This, too, is a part of healthcare.
- Repetition and attention to details. In situations when dementia is ruled out, a patient’s repetition may indicate a means to emphasize an important point or value. Keep in mind, too, that as we age, we all repeat stories to some degree. Details in stories may be the means by which older adults connect to their pasts and may also serve as clues to what is important to these people. Don’t assume details demand any action on your part. You are only being asked to listen as the older person sorts things out.
- Uncoupling. Solie describes uncoupling as any time an older person appears to disconnect from you in the course of a conversation. For a professional, this can feel as if you are dismissed or ignored just when you think you’ve hit the mark with a comment or question. Go back and assess the information you’ve gathered by doing some verification. Rethink the objective: Any action that works against their maintaining control and discovering a legacy will produce uncoupling.
“I try to be aware of when I’m losing people,” says Dr. Chittenden of this phenomenon. “I would say, ‘I seem to be losing you and I’m wondering what you’re thinking right now.’ I would try to find out where they’re at and if it was something I said that didn’t gel with them, didn’t make sense to them, or wasn’t their priority.” This is something, she emphasizes, that a hospitalist needs to watch for with patients of all ages. “Whether you’re older or younger,” she says, the communication can be complicated because “you’re … in the hospital culture and the priorities of doctors are so often different from the priorities of patients.”
Conclusion
Older and especially old-old individuals in some ways live in an era other than the one traversed by the young and middle-aged.6 Their purposes, agendas, and mission are different and the slowing down of their functioning can facilitate their attempts to put their lives into perspective and manage what control they can still exercise or are still allowed. Viewing older patients with the utmost respect and acknowledging the challenges they face at these last phases of their lives can better help you to partner with them and their families in their care. TH
Andrea Sattinger also writes about the importance of apology in this issue.
References
- Solie D. How to Say it to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Chochinov HM, Cann BJ. Interventions to enhance the spiritual aspects of dying. J Palliat Med. 2005;8:Suppl 1:S103-115.
- Dennis KE. Patients' control and the information imperative: clarification and confirmation. Nurs Res. 1990;39(3):162-166.
- Kiesler DJ, Auerbach SM. Integrating measurement of control and affiliation in studies of physician-patient interaction: the interpersonal circumplex. Soc Sci Med. 2003;57(9):1707-1722.
- Breemhaar B, Visser AP, Kleijnen JG. Perceptions and behaviour among elderly hospital patients: description and explanation of age differences in satisfaction, knowledge, emotions and behaviour. Soc Sci Med. 1990;31(12):1377-1385.
- Pipher M. Another Country: Navigating the Emotional Terrain of Our Elders. New York: Riverhead Books; 1999.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
Conflict Conundrums
Contrary to popular belief, conflicts are not necessarily bad. In fact, conflicts can spark discussions that can lead to improved processes and quality care. They also can help open lines of communication among practitioners and between physicians and patients.
Of course, not all conflict is positive and discord can be detrimental to patients and to relationships in the hospital. It behooves hospitalists to understand how to resolve conflicts constructively and communicate effectively in emotionally charged and controversial situations.
Good Conflict
When resolved effectively, conflicts can lead to positive changes, process improvements, and enhanced quality, says Leonard Marcus, PhD, founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health (Boston). In fact, conflict sometimes is necessary because it:
- Raises and resolves problems;
- Focuses change efforts on the most urgent and appropriate issues;
- Motivates people to participate in efforts to create positive changes; and
- Helps people learn to benefit from and recognize their differences.
Conflict is problematic when it:
- Hampers productivity;
- Lowers morale and/or hurts relationships;
- Creates more and continued conflicts; and
- Causes inappropriate and/or dangerous behaviors.
Conflicts often arise from everyday occurrences. Poor communication is one of the most common causes of disputes. However, conflicts also may result from insufficient resources, personality clashes, and leadership problems (e.g., inconsistent, missing, dictatorial, or uninformed leadership).
—Peter Prendergast, MD
Anatomy of a Conflict
A primary care physician, Dr. X, tells a patient, Mrs. Y, that she needs to be admitted to the hospital. If the hospitalist examines Mrs. Y and agrees that admission is necessary, there is no conflict. However, if the hospitalist determines that Mrs. Y doesn’t need to be admitted, the potential for conflict is ripe.
“This can create real tension,” says James W. Leyhane, MD, hospitalist director at Auburn Memorial Hospital, N.Y. “The hospitalist can find himself facing a conflict with the patient or the physician—or both.”
These situations can be highly charged and difficult to resolve. “Sometimes the person is adamant that he or she wants to be admitted,” says Dr. Leyhane. “And the stronger the relationship the patient has with the primary care physician, the greater the resistance they may have to what you are saying.”
The most common approach Dr. Leyhane takes to such a situation is to get on the physician’s side. “I will say something like, ‘I understand why Dr. Jones thought you should be admitted. However, after further examination, we now realize that admission is unnecessary,’” he explains.
Once the hospitalist addresses any anger or frustrations patients feel, most are relieved to avoid a hospitalization. But sometimes this approach doesn’t work, and some patients still insist on being admitted. In those cases, Dr. Leyhane will appeal to their pocketbook instead of their emotions. “I will tell them that I can admit them if they insist,” he says. “However, someone else will review their chart for insurance purposes, and they will have to pay out-of-pocket for the stay because it is not medically necessary. This is very persuasive.”
When Hospitalists and Attendings Clash
When such situations create conflict with physicians, they must be addressed carefully and resolved promptly. Dr. Marcus suggests that such conflicts can be minimized or eliminated altogether when “physicians negotiate expectations of their relationships” up front. “It is best for attendings and hospitalists to be communicating on an ongoing basis and understand each other’s positions before situations occur,” he offers.
Peter Prendergast, MD, chief hospitalist at St. Joseph’s Hospital and associate professor of Medicine at SUNY Upstate Medicine Center in Syracuse, New York, suggests that conflicts with physicians in these situations are not common. “Physicians overwhelmingly understand that we have more information by which to make admitting decisions,” says Dr. Prendergast. “We just need to make sure the patient understands that the physician makes the best possible decision with the data set he or she has and that we have access to more information and assessment tools and may draw a different conclusion.”
Nonetheless, Dr. Prendergast acknowledges that there are other situations that present the potential for attending-hospitalist conflict. “You may run into a problem with the primary care physician when the patient presents with a medical problem that previously was treated in the hospital that now is treated on an outpatient basis,” he notes.
Dr. Leyhane offers another common conflict with attendings. “Sometimes the physician will order a test or procedure that will not be reimbursed because it is unrelated to the patient’s reason for admission,” he says. “When this happens and the patient gets the bill, he or she is unhappy with the hospital and not the attending physician.”
These situations generally occur because the physician doesn’t realize that a service isn’t reimbursable or that a protocol has changed, Dr. Prendergast stresses, and not because the practitioner is being stubborn or contrary. Nonetheless, it presents a conflict.
“You need to let the physician know that there has been a change in treatment standards or that there is a reimbursement issue. Once he or she has the facts, you aren’t likely to have another problem,” says Dr. Prendergast. “The physician needs to get a phone call or at least a note in a timely manner.”
Dr. Marcus actually advises that hospitalists talk with the physician before communicating any information to the patient that conflicts with what the doctor has told him or her. “Otherwise,” he observes, “the conflict already has escalated.” Physicians, he says, don’t want to hear about a difference of opinion after the fact.
Hospitalist-Patient Conflicts
Roger Gildersleeve, MD, administrative hospitalist at Augusta Medical Center, Fishersville, Va., says conflicts with patients or family members are common situations for the hospitalist. “You may see conflicts when there is a disconnect between the patient’s or family’s expectations and the realities of the patient’s prognosis and outcomes,” he says. “We spend a lot of time trying to bring these two things closer together.”
One key to resolving these problems is to make a quick study of the situation. “You usually can read patients and families—by their body language and facial expressions—when you enter the room,” says Dr. Gildersleeve, “and you can detect tension and hostility.”
Dr. Prendergast agrees. “When you see patients and families in certain situations—such as 2 a.m. in the ER—you can make some reasonable assumptions about what they are thinking or feeling,” he says. “You can predict what these people’s concerns are, and you can address them even before they ask. Acknowledging their position and concerns is important.”
When possible, preparing for family and/or patient encounters can make a difference. “Before seeing a new patient, I try to learn as much as I can about him or her,” says Dr. Gildersleeve. “We have a good computer system, so it’s pretty easy. I use some of what I’ve learned in my opening comments, and this gives patients and families more confidence in me and my ability to deal with them as individuals.”
This is especially important for hospitalists, who have to establish patient relationships in a relatively short period of time.
Resolving Conflicts
Of course, it is impossible to prevent or avoid all conflicts. “To some degree, conflicts are inevitable,” says Dr. Marcus. “It’s the nature of medical practice.”
When conflicts occur, many of them can—and should—be resolved before they escalate into a dangerous confrontation or litigation. Listening is key to resolving conflicts quickly. “By listening, you can prevent a lot of conflicts from escalating or even starting,” says Dr. Prendergast. “We teach our physicians to listen, then repeat back what they heard—‘I’m hearing that you’re upset because … .’ If you get it right, the person knows that you are listening and that you understand their concerns. If you miss, they are likely to state their concern directly.”
Dr. Marcus believes conflict resolution may be particularly effective and satisfying when interest-based negotiation (IBN) is employed. IBN is a problem-solving strategy that focuses on satisfying as many interests or needs as possible for all involved parties. Because this technique addresses people’s needs and interests and separates people from the problem, it enables the parties to reach an integrative solution rather than creating a win-lose situation.
IBN enables those involved in a conflict to work together to reach a mutually satisfactory conclusion. The technique commonly results in creative and durable solutions, as well as enhanced relationships.
Conflict resolution efforts are more likely to fail, says Dr. Marcus, when the physicians and others involved apply position-based negotiations. With this conflict-management method, the parties argue only their positions, and their underlying interests may never be stated explicitly or understood. People are more likely to reach an impasse when they employ position-based negotiations, and they are more likely to see the situation as having a clear-cut winner and a loser.
“When you negotiate based on positions,” explains Dr. Marcus, “that is when situations are likely to escalate.”
While clear hospital policies and procedures can help resolve or prevent some conflicts involving physicians, more layers of policy are not necessarily the answer. “I think the time it would take to establish these policies would be better spent developing pathways for easier and better communication,” says Dr. Gildersleeve. “You see few of these hospitalist-physician conflicts when there is good communication between all the players.”
Professional mediator Pat Costello suggests that policy changes actually can help resolve some disputes. “Continued conflicts might suggest a need for a policy change or a new policy,” says Costello. “I have mediated a lot of situations that were resolved by policy changes.”
15 Seconds to Make an Impression
Hospitalists must remain cognizant of mistakes they can make that actually exacerbate conflicts with patients and families. “When physicians use an overbearing approach, they can’t accomplish as much,” says Dr. Marcus. “You have to take care to treat patients and families with care and concern and the same respect they afford their colleagues.”
It is important for hospitalists to be aware of how they come across to others, stressed Carole Houk, Esq., president of Carole Houk International, Alexandria, Va.
“You make a snap judgment of whether or not you like someone in about 15 seconds,” says Houk. “Studies show that physicians who use a dominant tone of voice are more likely to be sued than those who don’t.
“Explain what happens and why—and put a lot of focus on your tone of voice,” she says. “Rather than coming down imperiously, reach out to patients in a compassionate way. You need to be seen as someone with a heart and not a gatekeeper for the insurance company.”
When Hospitalists Can’t Resolve a Conflict
Unfortunately, some conflicts can’t be resolved easily. While hospitalists require some conflict resolution skills, they must also be willing and able to recognize when they need assistance. For example, suggests Houk, “We have ombudsmen in some hospitals who serve as conflict coaches. They are trained for this purpose. Hospitalists and others can go to these people for help resolving conflicts.”
Elsewhere, she notes, “We are training risk managers on conflict skills so that they can help resolve disputes in their hospitals and serve as informal mediators.”
On rare occasions, it may be necessary to seek the involvement of an independent professional mediator. Mediator Costello says this might be necessary in instances where there is an ongoing and escalating lack of communication, repeated conflicts (despite attempts to resolve them), physical altercations or threats of violence, and/or imminent risk to a patent’s safety.
While there may be conflicts that hospitalists cannot resolve, overall they are well equipped to communicate effectively in a way that minimizes disputes. “Many of us were attracted to this profession because of the opportunities and challenges of working with a wide range of situations and colleagues,” says Dr. Leyhane. “We know that communication skills are important, and we get a lot of practice during our interactions with physicians, families, patients, administrators, and ancillary staff.”
Houk agrees: “This field seems to attract people with big hearts. They understand the importance of understanding and acknowledging the needs and feelings of others.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Contrary to popular belief, conflicts are not necessarily bad. In fact, conflicts can spark discussions that can lead to improved processes and quality care. They also can help open lines of communication among practitioners and between physicians and patients.
Of course, not all conflict is positive and discord can be detrimental to patients and to relationships in the hospital. It behooves hospitalists to understand how to resolve conflicts constructively and communicate effectively in emotionally charged and controversial situations.
Good Conflict
When resolved effectively, conflicts can lead to positive changes, process improvements, and enhanced quality, says Leonard Marcus, PhD, founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health (Boston). In fact, conflict sometimes is necessary because it:
- Raises and resolves problems;
- Focuses change efforts on the most urgent and appropriate issues;
- Motivates people to participate in efforts to create positive changes; and
- Helps people learn to benefit from and recognize their differences.
Conflict is problematic when it:
- Hampers productivity;
- Lowers morale and/or hurts relationships;
- Creates more and continued conflicts; and
- Causes inappropriate and/or dangerous behaviors.
Conflicts often arise from everyday occurrences. Poor communication is one of the most common causes of disputes. However, conflicts also may result from insufficient resources, personality clashes, and leadership problems (e.g., inconsistent, missing, dictatorial, or uninformed leadership).
—Peter Prendergast, MD
Anatomy of a Conflict
A primary care physician, Dr. X, tells a patient, Mrs. Y, that she needs to be admitted to the hospital. If the hospitalist examines Mrs. Y and agrees that admission is necessary, there is no conflict. However, if the hospitalist determines that Mrs. Y doesn’t need to be admitted, the potential for conflict is ripe.
“This can create real tension,” says James W. Leyhane, MD, hospitalist director at Auburn Memorial Hospital, N.Y. “The hospitalist can find himself facing a conflict with the patient or the physician—or both.”
These situations can be highly charged and difficult to resolve. “Sometimes the person is adamant that he or she wants to be admitted,” says Dr. Leyhane. “And the stronger the relationship the patient has with the primary care physician, the greater the resistance they may have to what you are saying.”
The most common approach Dr. Leyhane takes to such a situation is to get on the physician’s side. “I will say something like, ‘I understand why Dr. Jones thought you should be admitted. However, after further examination, we now realize that admission is unnecessary,’” he explains.
Once the hospitalist addresses any anger or frustrations patients feel, most are relieved to avoid a hospitalization. But sometimes this approach doesn’t work, and some patients still insist on being admitted. In those cases, Dr. Leyhane will appeal to their pocketbook instead of their emotions. “I will tell them that I can admit them if they insist,” he says. “However, someone else will review their chart for insurance purposes, and they will have to pay out-of-pocket for the stay because it is not medically necessary. This is very persuasive.”
When Hospitalists and Attendings Clash
When such situations create conflict with physicians, they must be addressed carefully and resolved promptly. Dr. Marcus suggests that such conflicts can be minimized or eliminated altogether when “physicians negotiate expectations of their relationships” up front. “It is best for attendings and hospitalists to be communicating on an ongoing basis and understand each other’s positions before situations occur,” he offers.
Peter Prendergast, MD, chief hospitalist at St. Joseph’s Hospital and associate professor of Medicine at SUNY Upstate Medicine Center in Syracuse, New York, suggests that conflicts with physicians in these situations are not common. “Physicians overwhelmingly understand that we have more information by which to make admitting decisions,” says Dr. Prendergast. “We just need to make sure the patient understands that the physician makes the best possible decision with the data set he or she has and that we have access to more information and assessment tools and may draw a different conclusion.”
Nonetheless, Dr. Prendergast acknowledges that there are other situations that present the potential for attending-hospitalist conflict. “You may run into a problem with the primary care physician when the patient presents with a medical problem that previously was treated in the hospital that now is treated on an outpatient basis,” he notes.
Dr. Leyhane offers another common conflict with attendings. “Sometimes the physician will order a test or procedure that will not be reimbursed because it is unrelated to the patient’s reason for admission,” he says. “When this happens and the patient gets the bill, he or she is unhappy with the hospital and not the attending physician.”
These situations generally occur because the physician doesn’t realize that a service isn’t reimbursable or that a protocol has changed, Dr. Prendergast stresses, and not because the practitioner is being stubborn or contrary. Nonetheless, it presents a conflict.
“You need to let the physician know that there has been a change in treatment standards or that there is a reimbursement issue. Once he or she has the facts, you aren’t likely to have another problem,” says Dr. Prendergast. “The physician needs to get a phone call or at least a note in a timely manner.”
Dr. Marcus actually advises that hospitalists talk with the physician before communicating any information to the patient that conflicts with what the doctor has told him or her. “Otherwise,” he observes, “the conflict already has escalated.” Physicians, he says, don’t want to hear about a difference of opinion after the fact.
Hospitalist-Patient Conflicts
Roger Gildersleeve, MD, administrative hospitalist at Augusta Medical Center, Fishersville, Va., says conflicts with patients or family members are common situations for the hospitalist. “You may see conflicts when there is a disconnect between the patient’s or family’s expectations and the realities of the patient’s prognosis and outcomes,” he says. “We spend a lot of time trying to bring these two things closer together.”
One key to resolving these problems is to make a quick study of the situation. “You usually can read patients and families—by their body language and facial expressions—when you enter the room,” says Dr. Gildersleeve, “and you can detect tension and hostility.”
Dr. Prendergast agrees. “When you see patients and families in certain situations—such as 2 a.m. in the ER—you can make some reasonable assumptions about what they are thinking or feeling,” he says. “You can predict what these people’s concerns are, and you can address them even before they ask. Acknowledging their position and concerns is important.”
When possible, preparing for family and/or patient encounters can make a difference. “Before seeing a new patient, I try to learn as much as I can about him or her,” says Dr. Gildersleeve. “We have a good computer system, so it’s pretty easy. I use some of what I’ve learned in my opening comments, and this gives patients and families more confidence in me and my ability to deal with them as individuals.”
This is especially important for hospitalists, who have to establish patient relationships in a relatively short period of time.
Resolving Conflicts
Of course, it is impossible to prevent or avoid all conflicts. “To some degree, conflicts are inevitable,” says Dr. Marcus. “It’s the nature of medical practice.”
When conflicts occur, many of them can—and should—be resolved before they escalate into a dangerous confrontation or litigation. Listening is key to resolving conflicts quickly. “By listening, you can prevent a lot of conflicts from escalating or even starting,” says Dr. Prendergast. “We teach our physicians to listen, then repeat back what they heard—‘I’m hearing that you’re upset because … .’ If you get it right, the person knows that you are listening and that you understand their concerns. If you miss, they are likely to state their concern directly.”
Dr. Marcus believes conflict resolution may be particularly effective and satisfying when interest-based negotiation (IBN) is employed. IBN is a problem-solving strategy that focuses on satisfying as many interests or needs as possible for all involved parties. Because this technique addresses people’s needs and interests and separates people from the problem, it enables the parties to reach an integrative solution rather than creating a win-lose situation.
IBN enables those involved in a conflict to work together to reach a mutually satisfactory conclusion. The technique commonly results in creative and durable solutions, as well as enhanced relationships.
Conflict resolution efforts are more likely to fail, says Dr. Marcus, when the physicians and others involved apply position-based negotiations. With this conflict-management method, the parties argue only their positions, and their underlying interests may never be stated explicitly or understood. People are more likely to reach an impasse when they employ position-based negotiations, and they are more likely to see the situation as having a clear-cut winner and a loser.
“When you negotiate based on positions,” explains Dr. Marcus, “that is when situations are likely to escalate.”
While clear hospital policies and procedures can help resolve or prevent some conflicts involving physicians, more layers of policy are not necessarily the answer. “I think the time it would take to establish these policies would be better spent developing pathways for easier and better communication,” says Dr. Gildersleeve. “You see few of these hospitalist-physician conflicts when there is good communication between all the players.”
Professional mediator Pat Costello suggests that policy changes actually can help resolve some disputes. “Continued conflicts might suggest a need for a policy change or a new policy,” says Costello. “I have mediated a lot of situations that were resolved by policy changes.”
15 Seconds to Make an Impression
Hospitalists must remain cognizant of mistakes they can make that actually exacerbate conflicts with patients and families. “When physicians use an overbearing approach, they can’t accomplish as much,” says Dr. Marcus. “You have to take care to treat patients and families with care and concern and the same respect they afford their colleagues.”
It is important for hospitalists to be aware of how they come across to others, stressed Carole Houk, Esq., president of Carole Houk International, Alexandria, Va.
“You make a snap judgment of whether or not you like someone in about 15 seconds,” says Houk. “Studies show that physicians who use a dominant tone of voice are more likely to be sued than those who don’t.
“Explain what happens and why—and put a lot of focus on your tone of voice,” she says. “Rather than coming down imperiously, reach out to patients in a compassionate way. You need to be seen as someone with a heart and not a gatekeeper for the insurance company.”
When Hospitalists Can’t Resolve a Conflict
Unfortunately, some conflicts can’t be resolved easily. While hospitalists require some conflict resolution skills, they must also be willing and able to recognize when they need assistance. For example, suggests Houk, “We have ombudsmen in some hospitals who serve as conflict coaches. They are trained for this purpose. Hospitalists and others can go to these people for help resolving conflicts.”
Elsewhere, she notes, “We are training risk managers on conflict skills so that they can help resolve disputes in their hospitals and serve as informal mediators.”
On rare occasions, it may be necessary to seek the involvement of an independent professional mediator. Mediator Costello says this might be necessary in instances where there is an ongoing and escalating lack of communication, repeated conflicts (despite attempts to resolve them), physical altercations or threats of violence, and/or imminent risk to a patent’s safety.
While there may be conflicts that hospitalists cannot resolve, overall they are well equipped to communicate effectively in a way that minimizes disputes. “Many of us were attracted to this profession because of the opportunities and challenges of working with a wide range of situations and colleagues,” says Dr. Leyhane. “We know that communication skills are important, and we get a lot of practice during our interactions with physicians, families, patients, administrators, and ancillary staff.”
Houk agrees: “This field seems to attract people with big hearts. They understand the importance of understanding and acknowledging the needs and feelings of others.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Contrary to popular belief, conflicts are not necessarily bad. In fact, conflicts can spark discussions that can lead to improved processes and quality care. They also can help open lines of communication among practitioners and between physicians and patients.
Of course, not all conflict is positive and discord can be detrimental to patients and to relationships in the hospital. It behooves hospitalists to understand how to resolve conflicts constructively and communicate effectively in emotionally charged and controversial situations.
Good Conflict
When resolved effectively, conflicts can lead to positive changes, process improvements, and enhanced quality, says Leonard Marcus, PhD, founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health (Boston). In fact, conflict sometimes is necessary because it:
- Raises and resolves problems;
- Focuses change efforts on the most urgent and appropriate issues;
- Motivates people to participate in efforts to create positive changes; and
- Helps people learn to benefit from and recognize their differences.
Conflict is problematic when it:
- Hampers productivity;
- Lowers morale and/or hurts relationships;
- Creates more and continued conflicts; and
- Causes inappropriate and/or dangerous behaviors.
Conflicts often arise from everyday occurrences. Poor communication is one of the most common causes of disputes. However, conflicts also may result from insufficient resources, personality clashes, and leadership problems (e.g., inconsistent, missing, dictatorial, or uninformed leadership).
—Peter Prendergast, MD
Anatomy of a Conflict
A primary care physician, Dr. X, tells a patient, Mrs. Y, that she needs to be admitted to the hospital. If the hospitalist examines Mrs. Y and agrees that admission is necessary, there is no conflict. However, if the hospitalist determines that Mrs. Y doesn’t need to be admitted, the potential for conflict is ripe.
“This can create real tension,” says James W. Leyhane, MD, hospitalist director at Auburn Memorial Hospital, N.Y. “The hospitalist can find himself facing a conflict with the patient or the physician—or both.”
These situations can be highly charged and difficult to resolve. “Sometimes the person is adamant that he or she wants to be admitted,” says Dr. Leyhane. “And the stronger the relationship the patient has with the primary care physician, the greater the resistance they may have to what you are saying.”
The most common approach Dr. Leyhane takes to such a situation is to get on the physician’s side. “I will say something like, ‘I understand why Dr. Jones thought you should be admitted. However, after further examination, we now realize that admission is unnecessary,’” he explains.
Once the hospitalist addresses any anger or frustrations patients feel, most are relieved to avoid a hospitalization. But sometimes this approach doesn’t work, and some patients still insist on being admitted. In those cases, Dr. Leyhane will appeal to their pocketbook instead of their emotions. “I will tell them that I can admit them if they insist,” he says. “However, someone else will review their chart for insurance purposes, and they will have to pay out-of-pocket for the stay because it is not medically necessary. This is very persuasive.”
When Hospitalists and Attendings Clash
When such situations create conflict with physicians, they must be addressed carefully and resolved promptly. Dr. Marcus suggests that such conflicts can be minimized or eliminated altogether when “physicians negotiate expectations of their relationships” up front. “It is best for attendings and hospitalists to be communicating on an ongoing basis and understand each other’s positions before situations occur,” he offers.
Peter Prendergast, MD, chief hospitalist at St. Joseph’s Hospital and associate professor of Medicine at SUNY Upstate Medicine Center in Syracuse, New York, suggests that conflicts with physicians in these situations are not common. “Physicians overwhelmingly understand that we have more information by which to make admitting decisions,” says Dr. Prendergast. “We just need to make sure the patient understands that the physician makes the best possible decision with the data set he or she has and that we have access to more information and assessment tools and may draw a different conclusion.”
Nonetheless, Dr. Prendergast acknowledges that there are other situations that present the potential for attending-hospitalist conflict. “You may run into a problem with the primary care physician when the patient presents with a medical problem that previously was treated in the hospital that now is treated on an outpatient basis,” he notes.
Dr. Leyhane offers another common conflict with attendings. “Sometimes the physician will order a test or procedure that will not be reimbursed because it is unrelated to the patient’s reason for admission,” he says. “When this happens and the patient gets the bill, he or she is unhappy with the hospital and not the attending physician.”
These situations generally occur because the physician doesn’t realize that a service isn’t reimbursable or that a protocol has changed, Dr. Prendergast stresses, and not because the practitioner is being stubborn or contrary. Nonetheless, it presents a conflict.
“You need to let the physician know that there has been a change in treatment standards or that there is a reimbursement issue. Once he or she has the facts, you aren’t likely to have another problem,” says Dr. Prendergast. “The physician needs to get a phone call or at least a note in a timely manner.”
Dr. Marcus actually advises that hospitalists talk with the physician before communicating any information to the patient that conflicts with what the doctor has told him or her. “Otherwise,” he observes, “the conflict already has escalated.” Physicians, he says, don’t want to hear about a difference of opinion after the fact.
Hospitalist-Patient Conflicts
Roger Gildersleeve, MD, administrative hospitalist at Augusta Medical Center, Fishersville, Va., says conflicts with patients or family members are common situations for the hospitalist. “You may see conflicts when there is a disconnect between the patient’s or family’s expectations and the realities of the patient’s prognosis and outcomes,” he says. “We spend a lot of time trying to bring these two things closer together.”
One key to resolving these problems is to make a quick study of the situation. “You usually can read patients and families—by their body language and facial expressions—when you enter the room,” says Dr. Gildersleeve, “and you can detect tension and hostility.”
Dr. Prendergast agrees. “When you see patients and families in certain situations—such as 2 a.m. in the ER—you can make some reasonable assumptions about what they are thinking or feeling,” he says. “You can predict what these people’s concerns are, and you can address them even before they ask. Acknowledging their position and concerns is important.”
When possible, preparing for family and/or patient encounters can make a difference. “Before seeing a new patient, I try to learn as much as I can about him or her,” says Dr. Gildersleeve. “We have a good computer system, so it’s pretty easy. I use some of what I’ve learned in my opening comments, and this gives patients and families more confidence in me and my ability to deal with them as individuals.”
This is especially important for hospitalists, who have to establish patient relationships in a relatively short period of time.
Resolving Conflicts
Of course, it is impossible to prevent or avoid all conflicts. “To some degree, conflicts are inevitable,” says Dr. Marcus. “It’s the nature of medical practice.”
When conflicts occur, many of them can—and should—be resolved before they escalate into a dangerous confrontation or litigation. Listening is key to resolving conflicts quickly. “By listening, you can prevent a lot of conflicts from escalating or even starting,” says Dr. Prendergast. “We teach our physicians to listen, then repeat back what they heard—‘I’m hearing that you’re upset because … .’ If you get it right, the person knows that you are listening and that you understand their concerns. If you miss, they are likely to state their concern directly.”
Dr. Marcus believes conflict resolution may be particularly effective and satisfying when interest-based negotiation (IBN) is employed. IBN is a problem-solving strategy that focuses on satisfying as many interests or needs as possible for all involved parties. Because this technique addresses people’s needs and interests and separates people from the problem, it enables the parties to reach an integrative solution rather than creating a win-lose situation.
IBN enables those involved in a conflict to work together to reach a mutually satisfactory conclusion. The technique commonly results in creative and durable solutions, as well as enhanced relationships.
Conflict resolution efforts are more likely to fail, says Dr. Marcus, when the physicians and others involved apply position-based negotiations. With this conflict-management method, the parties argue only their positions, and their underlying interests may never be stated explicitly or understood. People are more likely to reach an impasse when they employ position-based negotiations, and they are more likely to see the situation as having a clear-cut winner and a loser.
“When you negotiate based on positions,” explains Dr. Marcus, “that is when situations are likely to escalate.”
While clear hospital policies and procedures can help resolve or prevent some conflicts involving physicians, more layers of policy are not necessarily the answer. “I think the time it would take to establish these policies would be better spent developing pathways for easier and better communication,” says Dr. Gildersleeve. “You see few of these hospitalist-physician conflicts when there is good communication between all the players.”
Professional mediator Pat Costello suggests that policy changes actually can help resolve some disputes. “Continued conflicts might suggest a need for a policy change or a new policy,” says Costello. “I have mediated a lot of situations that were resolved by policy changes.”
15 Seconds to Make an Impression
Hospitalists must remain cognizant of mistakes they can make that actually exacerbate conflicts with patients and families. “When physicians use an overbearing approach, they can’t accomplish as much,” says Dr. Marcus. “You have to take care to treat patients and families with care and concern and the same respect they afford their colleagues.”
It is important for hospitalists to be aware of how they come across to others, stressed Carole Houk, Esq., president of Carole Houk International, Alexandria, Va.
“You make a snap judgment of whether or not you like someone in about 15 seconds,” says Houk. “Studies show that physicians who use a dominant tone of voice are more likely to be sued than those who don’t.
“Explain what happens and why—and put a lot of focus on your tone of voice,” she says. “Rather than coming down imperiously, reach out to patients in a compassionate way. You need to be seen as someone with a heart and not a gatekeeper for the insurance company.”
When Hospitalists Can’t Resolve a Conflict
Unfortunately, some conflicts can’t be resolved easily. While hospitalists require some conflict resolution skills, they must also be willing and able to recognize when they need assistance. For example, suggests Houk, “We have ombudsmen in some hospitals who serve as conflict coaches. They are trained for this purpose. Hospitalists and others can go to these people for help resolving conflicts.”
Elsewhere, she notes, “We are training risk managers on conflict skills so that they can help resolve disputes in their hospitals and serve as informal mediators.”
On rare occasions, it may be necessary to seek the involvement of an independent professional mediator. Mediator Costello says this might be necessary in instances where there is an ongoing and escalating lack of communication, repeated conflicts (despite attempts to resolve them), physical altercations or threats of violence, and/or imminent risk to a patent’s safety.
While there may be conflicts that hospitalists cannot resolve, overall they are well equipped to communicate effectively in a way that minimizes disputes. “Many of us were attracted to this profession because of the opportunities and challenges of working with a wide range of situations and colleagues,” says Dr. Leyhane. “We know that communication skills are important, and we get a lot of practice during our interactions with physicians, families, patients, administrators, and ancillary staff.”
Houk agrees: “This field seems to attract people with big hearts. They understand the importance of understanding and acknowledging the needs and feelings of others.” TH
Joanne Kaldy writes regularly for The Hospitalist.
I'm Sorry
Apologizing to a patient is the right thing to do,” says Michael S. Woods, MD, a general surgeon at St. Vincent’s Regional Medical Center in Santa Fe, N.M. “It is the respectful thing in any relationship in terms of trust whenever there is a violation, whether it is real or perceived.” Dr. Woods, the author of Healing Words: The Power of Apology in Medicine, teaches and consults with corporations around the country about apology as well as physician leadership.1-2 In fact, his study of apology stemmed from examining the subject of physician leadership, and he and other experts consider the vital components of leadership to be effective communication, integrity, honesty, and respectful treatment of other individuals.3,4
Dr. Woods also works with Doug Wojcieszak, a public relations consultant whose victims’ rights group proposed “Sorry Works!” This program recommends apologies and settlements when medical mistakes occur. (See “A History of Sorry Works!” p. 26.) Dr. Woods says Wojcieszak comes from an interesting angle that he supports. “Something I increasingly try to hammer home when I speak is that one of the most important components of the apology law has nothing to do with the backhand of the reduction of litigation as much as the fact that it gives the physician the green light to say ‘I’m sorry,’” says Dr. Woods.
The Benefit of Healing
Providers may be less than open when things go terribly wrong because of feelings of fear, shame, and guilt regarding the consequences to the patient as well as to themselves.1,3 Apology heals by restoring the patient’s dignity and self-respect, providing assurance of shared values, and assuring patients that they are not at fault, they are now safe, and that the caregiver shares their suffering.4,7
Two Senses of Apology
There are circumstances other than when errors occur in which a physician’s apology may carry the power to improve patient care. Peter Barnett, MD, MPH, a clinical associate professor of medicine at the University of New Mexico in Albuquerque, says that in general there are two senses of apology.
“The first sense of apology regards the situation,” he says. For example, you might say, ‘I’m sorry you have cancer,’ or ‘I’m sorry that our system doesn’t allow your family doctor to be taking care of you in the hospital.’ It’s an expression of sympathy, but I think apology works better.”
The other sense of apology regards responsibility, says Dr. Barnett, citing the example, “I’m sorry I gave you the wrong drug.”
Situational needs for apology include when patients have been waiting a long time, such as when a hospitalist meets them in the emergency department. “In those cases you would say, ‘I’m sorry that you had to wait so long,’” says Dr. Barnett. “It’s not my fault, but I really am sorry.”
Bridging the Gap
Dr. Barnett, who practices hospital medicine part-time along with his major focus in addiction medicine, was formerly the director of the UNM hospitalist team. He explains that one of the primary reasons hospitalists may need to apologize to patients is that the hospitalist and patient have no prior relationship that could serve as a foundation for interpreting each other’s behavior.8
He believes apologizing for the delays and inconveniences that happen in the hospital “can help bridge the relationship gap in hospital medicine. Because what people believe about their primary care physicians is that they know and care about them,” he says. “To minimize their anxiety about you, show them that you do care about them by getting to know them well, and apology is the one of the best ways of doing that.”
When asked to elaborate what he means by “getting to know them well,” Dr. Barnett says, “I might tell someone, ‘I’d like to get to know you better; what can you tell me about yourself that would help bring me up to speed?’” It’s open-ended, he says, and you let the patient choose the topic. “Most people will say something. … It’s empathic inquiry with really good reflective listening; that is probably the simplest way of summarizing what it takes.”
Dr. Barnett suggests this kind of inquiry can mitigate the gaps in relationships that may lead to misunderstandings, edgy situations, and errors that may later call for apology. He recommends asking or saying some of the following to patients:
- What do you know about your illness?
- What do you believe about your illness?
- What are your feelings, values, beliefs, and preferences about/for your treatment?
- What can you tell me about your experiences in the hospital?
For patients who have been ill many times and have had a lot of medical experience, you could ask:
- Could you tell me about your doctors?
- What do you like about doctors?
- What don’t you like about your doctors?
These questions can help you discern who they are as a patient, and it gives patients the opportunity to be candid with you.
“It’s not about finding information that’s embarrassing or critical to your predecessor physicians, but it allows you to not make the same mistakes inadvertently,” says Dr. Barnett, who considers it concrete information. “I want them to have good medical care. I don’t want to make them unhappy. I want to avoid pitfalls. I think the two of us—the patient and I—should avoid pitfalls together.”
Asking the patient in a straightforward way what they want and don’t want gives the patient an opportunity to give the physician advice on how to stay out of trouble with them.
Apology When Disclosing Errors
The matter of assuming responsibility for errors is more complicated as it pertains to the use of apology, but it is an “idea whose time has come.”9 Although it is hard to quantify, plenty of evidence shows that apologizing for errors reduces the number of lawsuits and may reduce the settlement value of malpractice claims.3,5-7,10-26 Although there is not always agreement about the specifics of full disclosure, above all patients have the right to know what happens during their medical care and, therefore, restricting the information that is given to a patient can have legal ramifications.
Beyond this, writes Lucian Leape, MD, adjunct professor of health policy at the Harvard School of Public Health and an internationally recognized leader in the patient safety movement, wrote in the March-April issue of Physician Executive that apology is a “therapeutic necessity” that allows the patient to recognize a physician’s humanity and fallibility as well as his or her remorse at having caused harm.9 In the long run, apologizing to patients defuses more situations than it aggravates, and it pays off emotionally, financially, and in practice morale.5,6,9
Data from studies of medical practices that issue apologies in circumstances where accountability is clearly established show that litigation claims are reduced. In one 1992 study, 24% of people who sued physicians said they did so because the doctor was dishonest and withheld information. Nineteen percent said that they either sued to deter subsequent malpractice or for revenge.11,12 In each case of legal action, the investigators hypothesized that the doctor could have avoided the lawsuit by taking responsibility and apologizing up front and making amends at that time. It has been estimated that more than half of claims relegated to litigation could be avoided with use of prudent disclosure and apology.3,21
“My mantra, if you will,” says Dr. Woods, “is that [when] you apologize because it’s the right thing to do, all the benefits naturally ensue.”
Anticipating Apology
The issue of complications, adverse events, and errors carries its own protocol in terms of whether and how apology is offered. “Hopefully some of these have been anticipated,” says Dr. Barnett. “For instance, when you spoke with the patient about their pneumonia, you’ve said something about the possibility that pneumonias could become complicated, and [they] might have some kind of complications; or if they’ve had a heart attack, [you mentioned that] they might have some complications. So you’re actually already warning people about what could happen and you’ve said you’re going to try to prevent it, but it could [still happen].”
Apology can be appropriately offered when those events do occur and you genuinely express disappointment that you and the patient share.
“There are some quite complicated systematic problems [related to apology and hospital medicine],” says Dr. Barnett. “Some are communication aspects and some are legal ones. What I have heard from the attorneys is that you want to keep the apology relatively simple, … and it shouldn’t include any statements about other people who may have been involved, such as pharmacy or nurses.”
The other important issue related to hospitalists and apology, says Dr. Barnett, is that because of the lack of relationship, the severity of illness of the patients you are treating, and the strangeness of systems, people come to the hospital expecting errors. They expect them and may be afraid of them. In particular, when a medication error is made, they expect those errors to be disclosed to them.7,27 Dr. Barnett believes patients are waiting and watching, and hoping that nothing happens to them. Complicating the issue, he says, is that “many hospitalists are fairly guarded in this respect. The emotional deck is sort of stacked against everybody, so if the hospitalist is sensitive about the situation, that tends actually to make the situation worse. If you can apologize sincerely and simply, the patient may be reassured that you’re not trying to conceal anything, you’re honest, you’re on top of it, and you’ll do your best to deal with it,” he says, adding, “they know that that stuff happens; they hope that it is not hidden, ignored, or mismanaged.”
Start Early and Let It Flow
Dr. Woods’ advice is to offer apology earlier rather than later and to widen the spectrum of those to whom you wish to show your empathy, sympathy, respect, and compassion.
“What I promote to organizations is that they drive this into the consciousness of the organization by getting people to apologize for the least infraction—not waiting for the grave errors.” He interprets this as apologizing “when you’re running 30 minutes late, apologize when you’ve interrupted the patient or the family when they’re speaking. These are the things we would do for our spouse or our significant other or our family members; why is it any different at work?”
He also believes it is inherent for doctors as leaders to “apologize to your staff members, apologize to the nurses.” Because the image you express serves as a role model in this regard and will permeate your practice culture. Drive respectful treatment as a basic common social courtesy into the organizational consciousness, says Dr. Woods, and then in any circumstance where an apology is offered, it is perceived as authentic.
Conclusion
Hospitalists may find a need to apologize to patients and families for situations and circumstances in the hospital environment as well as the gap in relationship that exists when hospitalists and patients first encounter each other. Apologizing early rather than later as well as simply and authentically goes a long way to help achieve the ethical and business objectives held by most hospital physicians. TH
Andrea Sattinger wrote about error reporting in the May issue.
References
- Woods MS, Star JI. Healing Words: The Power of Apology in Medicine. Santa Fe, N.M.: Doctors in Touch; 2004.
- Woods MS. Applying Personal Leadership Principles to Health Care: The DEPO Principle. Orlando, Fl.: American College of Physician Executives; 2001.
- Leape LL. National Patient Safety Foundation. Understanding the power of apology: how saying “I’m sorry" helps heal patients and caregivers. Focus on Patient Safety. 2005;8:1-3.
- Lazare A. On Apology. Oxford, U.K.: Oxford University Press; 2004.
- Boothman RC. Apologies and a strong defense at the University of Michigan Health System. Physician Exec. 2006 Mar-Apr; 32(2):7-10.
- Weber DO. Who’s sorry now? Special report: patient trust and safety. Physician Exec. 2006 Mar-Apr:32(2)6-14.
- When Things Go Wrong: Responding to Adverse Events. A Consensus Statement of the Harvard Hospitals. Burlington, Massachusetts: Massachusetts Coalition for the Prevention of Medical Errors; 2006.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
- Leape LL. Full disclosure and apology—an idea whose time has come. Physician Exec. Mar-Apr 2006 32:16-18.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. Jun 27 1994;154(12):1365-1370.
- Cohen JR. Apology and organizations: Exploring an example from medical practice. Fordham Urban Law J. 2000;27(5):1447-1482.
- Cohen JR. Advising clients to apologize. South Calif Law Rev. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care. JAMA. 1994 Nov 23-30;272(20):1588-1591.
- Gesensway D. Hospitalists and the malpractice insurance crisis. The Hospitalist. 2002Jul/Aug;11-13.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997 Feb19;227(7):553-559.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002 Apr;48(4):281-290.
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003 Jun 5;348(23):2281-2284.
- Shapiro RS, Simpson DE, Lawrence SL, et al. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989 Oct;149(10):2190-2196.
- Zimmerman R. Doctors' new tool to fight lawsuits: saying 'I'm sorry.' Malpractice insurers find owning up to errors soothes patient anger. 'The risks are extraordinary.' J Okla State Med Assoc. 2004 Jun;97(6):245-247.
- Ambady N, LaPlante D, Nguyen T, et al. Surgeons' tone of voice: a clue to malpractice history. Surgery. 2002 Jul;132(1):5-9.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999 Dec 21;131(12):970-972.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation. N Engl J Med. 1996 Dec;335(26):1963-1967.
- Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002 Jun 12;287(22):2951-1957.
- Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005 Oct;118(10):1126-1133.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005 Feb;20(2):101-107.
- Harris Interactive(R). Telephone survey conducted for the American Academy on Physician and Patient, March 3-6, 2006.
Apologizing to a patient is the right thing to do,” says Michael S. Woods, MD, a general surgeon at St. Vincent’s Regional Medical Center in Santa Fe, N.M. “It is the respectful thing in any relationship in terms of trust whenever there is a violation, whether it is real or perceived.” Dr. Woods, the author of Healing Words: The Power of Apology in Medicine, teaches and consults with corporations around the country about apology as well as physician leadership.1-2 In fact, his study of apology stemmed from examining the subject of physician leadership, and he and other experts consider the vital components of leadership to be effective communication, integrity, honesty, and respectful treatment of other individuals.3,4
Dr. Woods also works with Doug Wojcieszak, a public relations consultant whose victims’ rights group proposed “Sorry Works!” This program recommends apologies and settlements when medical mistakes occur. (See “A History of Sorry Works!” p. 26.) Dr. Woods says Wojcieszak comes from an interesting angle that he supports. “Something I increasingly try to hammer home when I speak is that one of the most important components of the apology law has nothing to do with the backhand of the reduction of litigation as much as the fact that it gives the physician the green light to say ‘I’m sorry,’” says Dr. Woods.
The Benefit of Healing
Providers may be less than open when things go terribly wrong because of feelings of fear, shame, and guilt regarding the consequences to the patient as well as to themselves.1,3 Apology heals by restoring the patient’s dignity and self-respect, providing assurance of shared values, and assuring patients that they are not at fault, they are now safe, and that the caregiver shares their suffering.4,7
Two Senses of Apology
There are circumstances other than when errors occur in which a physician’s apology may carry the power to improve patient care. Peter Barnett, MD, MPH, a clinical associate professor of medicine at the University of New Mexico in Albuquerque, says that in general there are two senses of apology.
“The first sense of apology regards the situation,” he says. For example, you might say, ‘I’m sorry you have cancer,’ or ‘I’m sorry that our system doesn’t allow your family doctor to be taking care of you in the hospital.’ It’s an expression of sympathy, but I think apology works better.”
The other sense of apology regards responsibility, says Dr. Barnett, citing the example, “I’m sorry I gave you the wrong drug.”
Situational needs for apology include when patients have been waiting a long time, such as when a hospitalist meets them in the emergency department. “In those cases you would say, ‘I’m sorry that you had to wait so long,’” says Dr. Barnett. “It’s not my fault, but I really am sorry.”
Bridging the Gap
Dr. Barnett, who practices hospital medicine part-time along with his major focus in addiction medicine, was formerly the director of the UNM hospitalist team. He explains that one of the primary reasons hospitalists may need to apologize to patients is that the hospitalist and patient have no prior relationship that could serve as a foundation for interpreting each other’s behavior.8
He believes apologizing for the delays and inconveniences that happen in the hospital “can help bridge the relationship gap in hospital medicine. Because what people believe about their primary care physicians is that they know and care about them,” he says. “To minimize their anxiety about you, show them that you do care about them by getting to know them well, and apology is the one of the best ways of doing that.”
When asked to elaborate what he means by “getting to know them well,” Dr. Barnett says, “I might tell someone, ‘I’d like to get to know you better; what can you tell me about yourself that would help bring me up to speed?’” It’s open-ended, he says, and you let the patient choose the topic. “Most people will say something. … It’s empathic inquiry with really good reflective listening; that is probably the simplest way of summarizing what it takes.”
Dr. Barnett suggests this kind of inquiry can mitigate the gaps in relationships that may lead to misunderstandings, edgy situations, and errors that may later call for apology. He recommends asking or saying some of the following to patients:
- What do you know about your illness?
- What do you believe about your illness?
- What are your feelings, values, beliefs, and preferences about/for your treatment?
- What can you tell me about your experiences in the hospital?
For patients who have been ill many times and have had a lot of medical experience, you could ask:
- Could you tell me about your doctors?
- What do you like about doctors?
- What don’t you like about your doctors?
These questions can help you discern who they are as a patient, and it gives patients the opportunity to be candid with you.
“It’s not about finding information that’s embarrassing or critical to your predecessor physicians, but it allows you to not make the same mistakes inadvertently,” says Dr. Barnett, who considers it concrete information. “I want them to have good medical care. I don’t want to make them unhappy. I want to avoid pitfalls. I think the two of us—the patient and I—should avoid pitfalls together.”
Asking the patient in a straightforward way what they want and don’t want gives the patient an opportunity to give the physician advice on how to stay out of trouble with them.
Apology When Disclosing Errors
The matter of assuming responsibility for errors is more complicated as it pertains to the use of apology, but it is an “idea whose time has come.”9 Although it is hard to quantify, plenty of evidence shows that apologizing for errors reduces the number of lawsuits and may reduce the settlement value of malpractice claims.3,5-7,10-26 Although there is not always agreement about the specifics of full disclosure, above all patients have the right to know what happens during their medical care and, therefore, restricting the information that is given to a patient can have legal ramifications.
Beyond this, writes Lucian Leape, MD, adjunct professor of health policy at the Harvard School of Public Health and an internationally recognized leader in the patient safety movement, wrote in the March-April issue of Physician Executive that apology is a “therapeutic necessity” that allows the patient to recognize a physician’s humanity and fallibility as well as his or her remorse at having caused harm.9 In the long run, apologizing to patients defuses more situations than it aggravates, and it pays off emotionally, financially, and in practice morale.5,6,9
Data from studies of medical practices that issue apologies in circumstances where accountability is clearly established show that litigation claims are reduced. In one 1992 study, 24% of people who sued physicians said they did so because the doctor was dishonest and withheld information. Nineteen percent said that they either sued to deter subsequent malpractice or for revenge.11,12 In each case of legal action, the investigators hypothesized that the doctor could have avoided the lawsuit by taking responsibility and apologizing up front and making amends at that time. It has been estimated that more than half of claims relegated to litigation could be avoided with use of prudent disclosure and apology.3,21
“My mantra, if you will,” says Dr. Woods, “is that [when] you apologize because it’s the right thing to do, all the benefits naturally ensue.”
Anticipating Apology
The issue of complications, adverse events, and errors carries its own protocol in terms of whether and how apology is offered. “Hopefully some of these have been anticipated,” says Dr. Barnett. “For instance, when you spoke with the patient about their pneumonia, you’ve said something about the possibility that pneumonias could become complicated, and [they] might have some kind of complications; or if they’ve had a heart attack, [you mentioned that] they might have some complications. So you’re actually already warning people about what could happen and you’ve said you’re going to try to prevent it, but it could [still happen].”
Apology can be appropriately offered when those events do occur and you genuinely express disappointment that you and the patient share.
“There are some quite complicated systematic problems [related to apology and hospital medicine],” says Dr. Barnett. “Some are communication aspects and some are legal ones. What I have heard from the attorneys is that you want to keep the apology relatively simple, … and it shouldn’t include any statements about other people who may have been involved, such as pharmacy or nurses.”
The other important issue related to hospitalists and apology, says Dr. Barnett, is that because of the lack of relationship, the severity of illness of the patients you are treating, and the strangeness of systems, people come to the hospital expecting errors. They expect them and may be afraid of them. In particular, when a medication error is made, they expect those errors to be disclosed to them.7,27 Dr. Barnett believes patients are waiting and watching, and hoping that nothing happens to them. Complicating the issue, he says, is that “many hospitalists are fairly guarded in this respect. The emotional deck is sort of stacked against everybody, so if the hospitalist is sensitive about the situation, that tends actually to make the situation worse. If you can apologize sincerely and simply, the patient may be reassured that you’re not trying to conceal anything, you’re honest, you’re on top of it, and you’ll do your best to deal with it,” he says, adding, “they know that that stuff happens; they hope that it is not hidden, ignored, or mismanaged.”
Start Early and Let It Flow
Dr. Woods’ advice is to offer apology earlier rather than later and to widen the spectrum of those to whom you wish to show your empathy, sympathy, respect, and compassion.
“What I promote to organizations is that they drive this into the consciousness of the organization by getting people to apologize for the least infraction—not waiting for the grave errors.” He interprets this as apologizing “when you’re running 30 minutes late, apologize when you’ve interrupted the patient or the family when they’re speaking. These are the things we would do for our spouse or our significant other or our family members; why is it any different at work?”
He also believes it is inherent for doctors as leaders to “apologize to your staff members, apologize to the nurses.” Because the image you express serves as a role model in this regard and will permeate your practice culture. Drive respectful treatment as a basic common social courtesy into the organizational consciousness, says Dr. Woods, and then in any circumstance where an apology is offered, it is perceived as authentic.
Conclusion
Hospitalists may find a need to apologize to patients and families for situations and circumstances in the hospital environment as well as the gap in relationship that exists when hospitalists and patients first encounter each other. Apologizing early rather than later as well as simply and authentically goes a long way to help achieve the ethical and business objectives held by most hospital physicians. TH
Andrea Sattinger wrote about error reporting in the May issue.
References
- Woods MS, Star JI. Healing Words: The Power of Apology in Medicine. Santa Fe, N.M.: Doctors in Touch; 2004.
- Woods MS. Applying Personal Leadership Principles to Health Care: The DEPO Principle. Orlando, Fl.: American College of Physician Executives; 2001.
- Leape LL. National Patient Safety Foundation. Understanding the power of apology: how saying “I’m sorry" helps heal patients and caregivers. Focus on Patient Safety. 2005;8:1-3.
- Lazare A. On Apology. Oxford, U.K.: Oxford University Press; 2004.
- Boothman RC. Apologies and a strong defense at the University of Michigan Health System. Physician Exec. 2006 Mar-Apr; 32(2):7-10.
- Weber DO. Who’s sorry now? Special report: patient trust and safety. Physician Exec. 2006 Mar-Apr:32(2)6-14.
- When Things Go Wrong: Responding to Adverse Events. A Consensus Statement of the Harvard Hospitals. Burlington, Massachusetts: Massachusetts Coalition for the Prevention of Medical Errors; 2006.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
- Leape LL. Full disclosure and apology—an idea whose time has come. Physician Exec. Mar-Apr 2006 32:16-18.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. Jun 27 1994;154(12):1365-1370.
- Cohen JR. Apology and organizations: Exploring an example from medical practice. Fordham Urban Law J. 2000;27(5):1447-1482.
- Cohen JR. Advising clients to apologize. South Calif Law Rev. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care. JAMA. 1994 Nov 23-30;272(20):1588-1591.
- Gesensway D. Hospitalists and the malpractice insurance crisis. The Hospitalist. 2002Jul/Aug;11-13.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997 Feb19;227(7):553-559.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002 Apr;48(4):281-290.
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003 Jun 5;348(23):2281-2284.
- Shapiro RS, Simpson DE, Lawrence SL, et al. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989 Oct;149(10):2190-2196.
- Zimmerman R. Doctors' new tool to fight lawsuits: saying 'I'm sorry.' Malpractice insurers find owning up to errors soothes patient anger. 'The risks are extraordinary.' J Okla State Med Assoc. 2004 Jun;97(6):245-247.
- Ambady N, LaPlante D, Nguyen T, et al. Surgeons' tone of voice: a clue to malpractice history. Surgery. 2002 Jul;132(1):5-9.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999 Dec 21;131(12):970-972.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation. N Engl J Med. 1996 Dec;335(26):1963-1967.
- Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002 Jun 12;287(22):2951-1957.
- Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005 Oct;118(10):1126-1133.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005 Feb;20(2):101-107.
- Harris Interactive(R). Telephone survey conducted for the American Academy on Physician and Patient, March 3-6, 2006.
Apologizing to a patient is the right thing to do,” says Michael S. Woods, MD, a general surgeon at St. Vincent’s Regional Medical Center in Santa Fe, N.M. “It is the respectful thing in any relationship in terms of trust whenever there is a violation, whether it is real or perceived.” Dr. Woods, the author of Healing Words: The Power of Apology in Medicine, teaches and consults with corporations around the country about apology as well as physician leadership.1-2 In fact, his study of apology stemmed from examining the subject of physician leadership, and he and other experts consider the vital components of leadership to be effective communication, integrity, honesty, and respectful treatment of other individuals.3,4
Dr. Woods also works with Doug Wojcieszak, a public relations consultant whose victims’ rights group proposed “Sorry Works!” This program recommends apologies and settlements when medical mistakes occur. (See “A History of Sorry Works!” p. 26.) Dr. Woods says Wojcieszak comes from an interesting angle that he supports. “Something I increasingly try to hammer home when I speak is that one of the most important components of the apology law has nothing to do with the backhand of the reduction of litigation as much as the fact that it gives the physician the green light to say ‘I’m sorry,’” says Dr. Woods.
The Benefit of Healing
Providers may be less than open when things go terribly wrong because of feelings of fear, shame, and guilt regarding the consequences to the patient as well as to themselves.1,3 Apology heals by restoring the patient’s dignity and self-respect, providing assurance of shared values, and assuring patients that they are not at fault, they are now safe, and that the caregiver shares their suffering.4,7
Two Senses of Apology
There are circumstances other than when errors occur in which a physician’s apology may carry the power to improve patient care. Peter Barnett, MD, MPH, a clinical associate professor of medicine at the University of New Mexico in Albuquerque, says that in general there are two senses of apology.
“The first sense of apology regards the situation,” he says. For example, you might say, ‘I’m sorry you have cancer,’ or ‘I’m sorry that our system doesn’t allow your family doctor to be taking care of you in the hospital.’ It’s an expression of sympathy, but I think apology works better.”
The other sense of apology regards responsibility, says Dr. Barnett, citing the example, “I’m sorry I gave you the wrong drug.”
Situational needs for apology include when patients have been waiting a long time, such as when a hospitalist meets them in the emergency department. “In those cases you would say, ‘I’m sorry that you had to wait so long,’” says Dr. Barnett. “It’s not my fault, but I really am sorry.”
Bridging the Gap
Dr. Barnett, who practices hospital medicine part-time along with his major focus in addiction medicine, was formerly the director of the UNM hospitalist team. He explains that one of the primary reasons hospitalists may need to apologize to patients is that the hospitalist and patient have no prior relationship that could serve as a foundation for interpreting each other’s behavior.8
He believes apologizing for the delays and inconveniences that happen in the hospital “can help bridge the relationship gap in hospital medicine. Because what people believe about their primary care physicians is that they know and care about them,” he says. “To minimize their anxiety about you, show them that you do care about them by getting to know them well, and apology is the one of the best ways of doing that.”
When asked to elaborate what he means by “getting to know them well,” Dr. Barnett says, “I might tell someone, ‘I’d like to get to know you better; what can you tell me about yourself that would help bring me up to speed?’” It’s open-ended, he says, and you let the patient choose the topic. “Most people will say something. … It’s empathic inquiry with really good reflective listening; that is probably the simplest way of summarizing what it takes.”
Dr. Barnett suggests this kind of inquiry can mitigate the gaps in relationships that may lead to misunderstandings, edgy situations, and errors that may later call for apology. He recommends asking or saying some of the following to patients:
- What do you know about your illness?
- What do you believe about your illness?
- What are your feelings, values, beliefs, and preferences about/for your treatment?
- What can you tell me about your experiences in the hospital?
For patients who have been ill many times and have had a lot of medical experience, you could ask:
- Could you tell me about your doctors?
- What do you like about doctors?
- What don’t you like about your doctors?
These questions can help you discern who they are as a patient, and it gives patients the opportunity to be candid with you.
“It’s not about finding information that’s embarrassing or critical to your predecessor physicians, but it allows you to not make the same mistakes inadvertently,” says Dr. Barnett, who considers it concrete information. “I want them to have good medical care. I don’t want to make them unhappy. I want to avoid pitfalls. I think the two of us—the patient and I—should avoid pitfalls together.”
Asking the patient in a straightforward way what they want and don’t want gives the patient an opportunity to give the physician advice on how to stay out of trouble with them.
Apology When Disclosing Errors
The matter of assuming responsibility for errors is more complicated as it pertains to the use of apology, but it is an “idea whose time has come.”9 Although it is hard to quantify, plenty of evidence shows that apologizing for errors reduces the number of lawsuits and may reduce the settlement value of malpractice claims.3,5-7,10-26 Although there is not always agreement about the specifics of full disclosure, above all patients have the right to know what happens during their medical care and, therefore, restricting the information that is given to a patient can have legal ramifications.
Beyond this, writes Lucian Leape, MD, adjunct professor of health policy at the Harvard School of Public Health and an internationally recognized leader in the patient safety movement, wrote in the March-April issue of Physician Executive that apology is a “therapeutic necessity” that allows the patient to recognize a physician’s humanity and fallibility as well as his or her remorse at having caused harm.9 In the long run, apologizing to patients defuses more situations than it aggravates, and it pays off emotionally, financially, and in practice morale.5,6,9
Data from studies of medical practices that issue apologies in circumstances where accountability is clearly established show that litigation claims are reduced. In one 1992 study, 24% of people who sued physicians said they did so because the doctor was dishonest and withheld information. Nineteen percent said that they either sued to deter subsequent malpractice or for revenge.11,12 In each case of legal action, the investigators hypothesized that the doctor could have avoided the lawsuit by taking responsibility and apologizing up front and making amends at that time. It has been estimated that more than half of claims relegated to litigation could be avoided with use of prudent disclosure and apology.3,21
“My mantra, if you will,” says Dr. Woods, “is that [when] you apologize because it’s the right thing to do, all the benefits naturally ensue.”
Anticipating Apology
The issue of complications, adverse events, and errors carries its own protocol in terms of whether and how apology is offered. “Hopefully some of these have been anticipated,” says Dr. Barnett. “For instance, when you spoke with the patient about their pneumonia, you’ve said something about the possibility that pneumonias could become complicated, and [they] might have some kind of complications; or if they’ve had a heart attack, [you mentioned that] they might have some complications. So you’re actually already warning people about what could happen and you’ve said you’re going to try to prevent it, but it could [still happen].”
Apology can be appropriately offered when those events do occur and you genuinely express disappointment that you and the patient share.
“There are some quite complicated systematic problems [related to apology and hospital medicine],” says Dr. Barnett. “Some are communication aspects and some are legal ones. What I have heard from the attorneys is that you want to keep the apology relatively simple, … and it shouldn’t include any statements about other people who may have been involved, such as pharmacy or nurses.”
The other important issue related to hospitalists and apology, says Dr. Barnett, is that because of the lack of relationship, the severity of illness of the patients you are treating, and the strangeness of systems, people come to the hospital expecting errors. They expect them and may be afraid of them. In particular, when a medication error is made, they expect those errors to be disclosed to them.7,27 Dr. Barnett believes patients are waiting and watching, and hoping that nothing happens to them. Complicating the issue, he says, is that “many hospitalists are fairly guarded in this respect. The emotional deck is sort of stacked against everybody, so if the hospitalist is sensitive about the situation, that tends actually to make the situation worse. If you can apologize sincerely and simply, the patient may be reassured that you’re not trying to conceal anything, you’re honest, you’re on top of it, and you’ll do your best to deal with it,” he says, adding, “they know that that stuff happens; they hope that it is not hidden, ignored, or mismanaged.”
Start Early and Let It Flow
Dr. Woods’ advice is to offer apology earlier rather than later and to widen the spectrum of those to whom you wish to show your empathy, sympathy, respect, and compassion.
“What I promote to organizations is that they drive this into the consciousness of the organization by getting people to apologize for the least infraction—not waiting for the grave errors.” He interprets this as apologizing “when you’re running 30 minutes late, apologize when you’ve interrupted the patient or the family when they’re speaking. These are the things we would do for our spouse or our significant other or our family members; why is it any different at work?”
He also believes it is inherent for doctors as leaders to “apologize to your staff members, apologize to the nurses.” Because the image you express serves as a role model in this regard and will permeate your practice culture. Drive respectful treatment as a basic common social courtesy into the organizational consciousness, says Dr. Woods, and then in any circumstance where an apology is offered, it is perceived as authentic.
Conclusion
Hospitalists may find a need to apologize to patients and families for situations and circumstances in the hospital environment as well as the gap in relationship that exists when hospitalists and patients first encounter each other. Apologizing early rather than later as well as simply and authentically goes a long way to help achieve the ethical and business objectives held by most hospital physicians. TH
Andrea Sattinger wrote about error reporting in the May issue.
References
- Woods MS, Star JI. Healing Words: The Power of Apology in Medicine. Santa Fe, N.M.: Doctors in Touch; 2004.
- Woods MS. Applying Personal Leadership Principles to Health Care: The DEPO Principle. Orlando, Fl.: American College of Physician Executives; 2001.
- Leape LL. National Patient Safety Foundation. Understanding the power of apology: how saying “I’m sorry" helps heal patients and caregivers. Focus on Patient Safety. 2005;8:1-3.
- Lazare A. On Apology. Oxford, U.K.: Oxford University Press; 2004.
- Boothman RC. Apologies and a strong defense at the University of Michigan Health System. Physician Exec. 2006 Mar-Apr; 32(2):7-10.
- Weber DO. Who’s sorry now? Special report: patient trust and safety. Physician Exec. 2006 Mar-Apr:32(2)6-14.
- When Things Go Wrong: Responding to Adverse Events. A Consensus Statement of the Harvard Hospitals. Burlington, Massachusetts: Massachusetts Coalition for the Prevention of Medical Errors; 2006.
- Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111:31S-35S.
- Leape LL. Full disclosure and apology—an idea whose time has come. Physician Exec. Mar-Apr 2006 32:16-18.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. Jun 27 1994;154(12):1365-1370.
- Cohen JR. Apology and organizations: Exploring an example from medical practice. Fordham Urban Law J. 2000;27(5):1447-1482.
- Cohen JR. Advising clients to apologize. South Calif Law Rev. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care. JAMA. 1994 Nov 23-30;272(20):1588-1591.
- Gesensway D. Hospitalists and the malpractice insurance crisis. The Hospitalist. 2002Jul/Aug;11-13.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997 Feb19;227(7):553-559.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002 Apr;48(4):281-290.
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003 Jun 5;348(23):2281-2284.
- Shapiro RS, Simpson DE, Lawrence SL, et al. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989 Oct;149(10):2190-2196.
- Zimmerman R. Doctors' new tool to fight lawsuits: saying 'I'm sorry.' Malpractice insurers find owning up to errors soothes patient anger. 'The risks are extraordinary.' J Okla State Med Assoc. 2004 Jun;97(6):245-247.
- Ambady N, LaPlante D, Nguyen T, et al. Surgeons' tone of voice: a clue to malpractice history. Surgery. 2002 Jul;132(1):5-9.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999 Dec 21;131(12):970-972.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation. N Engl J Med. 1996 Dec;335(26):1963-1967.
- Hickson GB, Federspiel CF, Pichert JW, et al. Patient complaints and malpractice risk. JAMA. 2002 Jun 12;287(22):2951-1957.
- Stelfox HT, Gandhi TK, Orav EJ, et al. The relation of patient satisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005 Oct;118(10):1126-1133.
- Pham HH, Devers KJ, Kuo S, et al. Health care market trends and the evolution of hospitalist use and roles. J Gen Intern Med. 2005 Feb;20(2):101-107.
- Harris Interactive(R). Telephone survey conducted for the American Academy on Physician and Patient, March 3-6, 2006.
A Case of Palpebral Purpura and Trouble Swallowing
A48-year-old female was admitted to the hospital with atrial fibrillation. Her medical history was significant for systemic lupus erythematosus (SLE) diagnosed 28 years ago, with low dose prednisone treatment for the past 15 years.
In the past year, the patient had experienced progressive difficulty swallowing and often choked on her food, resulting in a 35-pound weight loss. She also mentioned that she had been bruising easily.
On examination, the patient had bruising around her eyes and a thick, enlarged tongue with clear marks of her teeth visible on the surface.

Which test will most likely lead to a diagnosis?
- Magnetic resonance imaging (MRI) of pituitary gland;
- Abdominal fat pad biopsy;
- Thyroid stimulating hormone (TSH) level;
- Serum Angiotensin converting enzyme (ACE) levels
- Tongue biopsy
Discussion
The answer is B: abdominal fat pad biopsy. Macroglossia, especially in adults, is a rare clinical finding and is most often associated with amyloidosis.1 It has also been rarely described in association with acromegaly, hypothyroidism, and sarcoidosis. In children, macroglossia may be seen in a variety of conditions including cretinism, Down syndrome, Beckwith-Wiedemann syndrome, and various storage diseases.2 Lymphangioma of the tongue may also present with macroglossia.3
Another finding classically seen in amyloidosis is palpebral purpura.4 The occurrence of these two physical findings together in this patient strongly suggests the diagnosis of amyloidosis. The amyloidoses are now considered a group of diseases characterized by extracellular deposition of insoluble fibrillar proteins in various organs secondary to misfolding of proteins.
They include not only primary and secondary amyloidosis but also Alzheimer’s, prion diseases, many other neurodegenerative disorders, and some types of cystic fibroses.5
Traditionally, amyloidosis was described as one of three types: primary, secondary, and heritable. Primary amyloidosis is the most common type and results from deposition of fragments of light chain immunoglobulin deposits. It is most frequently associated with plasma cell dyscrasias. Secondary, or AA, amyloidosis occurs in association with inflammatory conditions and results from deposition of fragments of the acute phase reactant serum amyloid A. Familial amyloidoses or the ATTR amyloidoses are a fairly heterogeneous group with different proteins associated with different disorders.5
The typical findings seen in this case are associated with primary amyloidosis.4 The presence of primary amyloidosis was confirmed in this case by a bone marrow biopsy. This patient had SLE, but SLE is usually not complicated by the development of amyloidosis, although rare cases in literature have been described.6 Also, as mentioned above, secondary amyloidosis is usually characterized by AA rather than AL amyloidosis.
The diagnosis of amyloidosis is made pathologically when an involved organ is biopsied. When clinical suspicion is high and no organ has been biopsied, the simplest procedure is to obtain an abdominal fat pad biopsy and stain it with Congo red. This test is 85% sensitive in patients with primary amyloidosis.4 TH
References
- Xavier SD, Bussoloti IF, Muller H. Macroglossia secondary to systemic amyloidosis: case report and literature review. Ear Nose Throat J. 2005 Jun;84(6):358-361.
- Wolford LM, Cottrell DA. Diagnosis of macroglossia and indications for reduction glossectomy. Am J Orthod Dentofacial Orthop. 1996 Aug;110:170-177.
- Gulemann M, Katz J. Macroglossia combined with lymphangioma: a case report. J Clin Pediatr Dent. 2003 Winter;27(2):167-169.
- Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses. N Engl J Med 1997; 337: 898-909.
- Merlini G, Bellotti V. Mechanisms of disease: molecular mechanisms of amyloidosis. N Engl J Med. 2003; 349:583-596.
- Al-Hoqail I, Naddaf H, Al-Rikabi A, et al. Systemic lupus erythematosus and amyloidosis. Clin Rheumatol. 1997 Jun;16(4):422-424.on.
A48-year-old female was admitted to the hospital with atrial fibrillation. Her medical history was significant for systemic lupus erythematosus (SLE) diagnosed 28 years ago, with low dose prednisone treatment for the past 15 years.
In the past year, the patient had experienced progressive difficulty swallowing and often choked on her food, resulting in a 35-pound weight loss. She also mentioned that she had been bruising easily.
On examination, the patient had bruising around her eyes and a thick, enlarged tongue with clear marks of her teeth visible on the surface.
Which test will most likely lead to a diagnosis?
- Magnetic resonance imaging (MRI) of pituitary gland;
- Abdominal fat pad biopsy;
- Thyroid stimulating hormone (TSH) level;
- Serum Angiotensin converting enzyme (ACE) levels
- Tongue biopsy
Discussion
The answer is B: abdominal fat pad biopsy. Macroglossia, especially in adults, is a rare clinical finding and is most often associated with amyloidosis.1 It has also been rarely described in association with acromegaly, hypothyroidism, and sarcoidosis. In children, macroglossia may be seen in a variety of conditions including cretinism, Down syndrome, Beckwith-Wiedemann syndrome, and various storage diseases.2 Lymphangioma of the tongue may also present with macroglossia.3
Another finding classically seen in amyloidosis is palpebral purpura.4 The occurrence of these two physical findings together in this patient strongly suggests the diagnosis of amyloidosis. The amyloidoses are now considered a group of diseases characterized by extracellular deposition of insoluble fibrillar proteins in various organs secondary to misfolding of proteins.
They include not only primary and secondary amyloidosis but also Alzheimer’s, prion diseases, many other neurodegenerative disorders, and some types of cystic fibroses.5
Traditionally, amyloidosis was described as one of three types: primary, secondary, and heritable. Primary amyloidosis is the most common type and results from deposition of fragments of light chain immunoglobulin deposits. It is most frequently associated with plasma cell dyscrasias. Secondary, or AA, amyloidosis occurs in association with inflammatory conditions and results from deposition of fragments of the acute phase reactant serum amyloid A. Familial amyloidoses or the ATTR amyloidoses are a fairly heterogeneous group with different proteins associated with different disorders.5
The typical findings seen in this case are associated with primary amyloidosis.4 The presence of primary amyloidosis was confirmed in this case by a bone marrow biopsy. This patient had SLE, but SLE is usually not complicated by the development of amyloidosis, although rare cases in literature have been described.6 Also, as mentioned above, secondary amyloidosis is usually characterized by AA rather than AL amyloidosis.
The diagnosis of amyloidosis is made pathologically when an involved organ is biopsied. When clinical suspicion is high and no organ has been biopsied, the simplest procedure is to obtain an abdominal fat pad biopsy and stain it with Congo red. This test is 85% sensitive in patients with primary amyloidosis.4 TH
References
- Xavier SD, Bussoloti IF, Muller H. Macroglossia secondary to systemic amyloidosis: case report and literature review. Ear Nose Throat J. 2005 Jun;84(6):358-361.
- Wolford LM, Cottrell DA. Diagnosis of macroglossia and indications for reduction glossectomy. Am J Orthod Dentofacial Orthop. 1996 Aug;110:170-177.
- Gulemann M, Katz J. Macroglossia combined with lymphangioma: a case report. J Clin Pediatr Dent. 2003 Winter;27(2):167-169.
- Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses. N Engl J Med 1997; 337: 898-909.
- Merlini G, Bellotti V. Mechanisms of disease: molecular mechanisms of amyloidosis. N Engl J Med. 2003; 349:583-596.
- Al-Hoqail I, Naddaf H, Al-Rikabi A, et al. Systemic lupus erythematosus and amyloidosis. Clin Rheumatol. 1997 Jun;16(4):422-424.on.
A48-year-old female was admitted to the hospital with atrial fibrillation. Her medical history was significant for systemic lupus erythematosus (SLE) diagnosed 28 years ago, with low dose prednisone treatment for the past 15 years.
In the past year, the patient had experienced progressive difficulty swallowing and often choked on her food, resulting in a 35-pound weight loss. She also mentioned that she had been bruising easily.
On examination, the patient had bruising around her eyes and a thick, enlarged tongue with clear marks of her teeth visible on the surface.
Which test will most likely lead to a diagnosis?
- Magnetic resonance imaging (MRI) of pituitary gland;
- Abdominal fat pad biopsy;
- Thyroid stimulating hormone (TSH) level;
- Serum Angiotensin converting enzyme (ACE) levels
- Tongue biopsy
Discussion
The answer is B: abdominal fat pad biopsy. Macroglossia, especially in adults, is a rare clinical finding and is most often associated with amyloidosis.1 It has also been rarely described in association with acromegaly, hypothyroidism, and sarcoidosis. In children, macroglossia may be seen in a variety of conditions including cretinism, Down syndrome, Beckwith-Wiedemann syndrome, and various storage diseases.2 Lymphangioma of the tongue may also present with macroglossia.3
Another finding classically seen in amyloidosis is palpebral purpura.4 The occurrence of these two physical findings together in this patient strongly suggests the diagnosis of amyloidosis. The amyloidoses are now considered a group of diseases characterized by extracellular deposition of insoluble fibrillar proteins in various organs secondary to misfolding of proteins.
They include not only primary and secondary amyloidosis but also Alzheimer’s, prion diseases, many other neurodegenerative disorders, and some types of cystic fibroses.5
Traditionally, amyloidosis was described as one of three types: primary, secondary, and heritable. Primary amyloidosis is the most common type and results from deposition of fragments of light chain immunoglobulin deposits. It is most frequently associated with plasma cell dyscrasias. Secondary, or AA, amyloidosis occurs in association with inflammatory conditions and results from deposition of fragments of the acute phase reactant serum amyloid A. Familial amyloidoses or the ATTR amyloidoses are a fairly heterogeneous group with different proteins associated with different disorders.5
The typical findings seen in this case are associated with primary amyloidosis.4 The presence of primary amyloidosis was confirmed in this case by a bone marrow biopsy. This patient had SLE, but SLE is usually not complicated by the development of amyloidosis, although rare cases in literature have been described.6 Also, as mentioned above, secondary amyloidosis is usually characterized by AA rather than AL amyloidosis.
The diagnosis of amyloidosis is made pathologically when an involved organ is biopsied. When clinical suspicion is high and no organ has been biopsied, the simplest procedure is to obtain an abdominal fat pad biopsy and stain it with Congo red. This test is 85% sensitive in patients with primary amyloidosis.4 TH
References
- Xavier SD, Bussoloti IF, Muller H. Macroglossia secondary to systemic amyloidosis: case report and literature review. Ear Nose Throat J. 2005 Jun;84(6):358-361.
- Wolford LM, Cottrell DA. Diagnosis of macroglossia and indications for reduction glossectomy. Am J Orthod Dentofacial Orthop. 1996 Aug;110:170-177.
- Gulemann M, Katz J. Macroglossia combined with lymphangioma: a case report. J Clin Pediatr Dent. 2003 Winter;27(2):167-169.
- Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses. N Engl J Med 1997; 337: 898-909.
- Merlini G, Bellotti V. Mechanisms of disease: molecular mechanisms of amyloidosis. N Engl J Med. 2003; 349:583-596.
- Al-Hoqail I, Naddaf H, Al-Rikabi A, et al. Systemic lupus erythematosus and amyloidosis. Clin Rheumatol. 1997 Jun;16(4):422-424.on.
Show us the Money
At a hefty 291 pages, SHM’s 2005-2006 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” contains a wealth of detail about hospitalists and their working conditions. Most readers will probably first refer to the compensation and benefits package statistics. But take a closer look: The survey’s chapters and tables yield a depth of even more helpful information.
After reviewing the survey’s “Executive Summary” (available online at the SHM Web site, www.hospitalmedicine.org), Charlene Carroll Clark, MD, a hospitalist at Inpatient Care Service at Good Samaritan Regional Medical Center in Corvallis, Ore., says “I think knowledge is always a good thing. Just knowing what is going on in other locations helps us. We can see that we fit right in with the median compensation, and that we are competitive as we recruit.”
It is reassuring, other sources concurred, to see that their hospitalist groups compare favorably with national median salaries and benefits packages. However, some group leaders caution that hospitalists should not benchmark their groups’ professional viability using only compensation and benefits medians. The real worth of the survey’s statistics, they say, will be realized when hospitalists utilize the document as a tool for improving management and care processes at their own institutions.
Indeed, in conversations with SHM leaders and with hospitalists across the country, it becomes clear that the survey has multiple uses, depending on its readers’ specific characteristics. And that’s just what SHM intends, says Joe Miller, SHM senior vice president, who was in charge of the survey project. “Our role was to create more of an almanac and a reference, rather than furnish an interpretation,” says Miller. “I think the real value for people will be in finding the metrics that are descriptive of their particular program.”
Survey Participation Increases
Miller is gratified by the increase in participation since the 2003-2004 SHM survey. Two years ago approximately 300 hospital medicine group (HMG) leaders participated in the survey. This time 396 HMG leaders participated—a 32% increase. Individual hospitalists completing the survey increased by more than 500 over the previous survey to a total of 2,550 individual hospitalist respondents.
“Given the magnitude of this survey, I think we’ve got very impressive representation of the industry,” says Miller. For instance, the regional representation of respondents was almost equally divided: 24% from the East, 26% from the South, 27% from the Midwest, and 22% from the West.
Miller attributes the greater participation to a variety of factors: conducting a multifaceted communication campaign, targeting every SHM board member and committee member, and extending the survey deadline.
An Eclectic and Thriving Group
According to Miller, the survey reveals many characteristics about hospitalists and the profession in general. While some of the results may not be surprising, they serve to corroborate (with real numbers) what many have perceived anecdotally about the hospital medicine movement. For instance:
- The hospital medicine movement is diverse. The survey documents six different models for hospital medicine programs. Currently, 34% of hospitalists are employed by hospitals or hospital corporations, and 12% are employed by local hospitalist-only groups. Multistate hospitalist-only groups or management companies employ 19%, while multi-specialty groups employ 14% of hospitalists. Academic hospital medicine programs employ 20%, and another 2% are employed by emergency or critical care physician groups.
- Hospitalists provide documented value for their hospitals, including around-the-clock patient care (51% of HMGs have on-site providers at night, and 41% of programs provide hospitalists on call), and participation in quality improvement (86%), hospital committees (92%), and other value-added activities, such as implementing information technology (54%).
- Other trends emerge when comparing 2003-2004 survey results with the current survey, including an increase in HMGs that now use a hybrid coverage schedule (a combination of shift and call schedules; an increase to 35% from 27%); more groups being paid using a mixed compensation model (a combination of salary and productive/performance-based compensation; up to 67% from 47% in 2003-2004); and a slight increase in hospitalists employed by academic institutions—up to 20% from a prior 16%.
Value Added


The survey also underscores hospitalists’ roles as change leaders in their institutions. In the “non-clinical activities” section of Chapter 3, “The Work of Hospital Medicine Groups,” results reveal high participation in hospital committees (92%), in quality improvement initiatives (86%); and other activities, such as generating practice guidelines, teaching, planning, and research.
John A. Bolinger, DO, FACP, medical director of the hospitalist program at Terre Haute (Ind.) Regional Hospital, serves on multiple committees at his hospital: critical care, pharmacy therapeutics, patient safety, credentials (as chair), and the executive committee. He and his hospital’s clinical pharmacist have developed standardized order sets, a new IV insulin protocol, and a new DVT prophylaxis protocol.
“I think participation in non-clinical activities is a plus for the hospitalist profession,” he says. In addition, “every hospital with a hospitalist involved in practice sees a tremendous benefit from that very thing.”
The Devil’s in the Details
John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, and cofounder and past president of SHM, was one of three panelists at the recent annual meeting where survey results were presented. Dr. Nelson believes that the statistics “can be a kind of starting point for thinking about whether your workload and compensation are typical. However,” he cautions, “the mistake I see so often is that people tend to think the average compensation, the average workload, are right for a given practice. Well, there are very few practices that are average. The variation is dramatic, and there’s no reason you should be average.”
Dr. Nelson advises hospitalists and group leaders not to interpret the compensation medians in the survey as a “final authority” for what hospitalists should be earning. Rather, he says, “what you could do is look at the big picture of an average practice—in terms of compensation, productivity, and other factors, such as location, whether your practice is primary adult or pediatric—and then compare your practice to see how you differ.
“Do you work harder and make less? In that case, you might want to fix it. If you work less and make more, you might want to be quiet!” he quips.
Brian Bossard, MD, medical director of Inpatient Physician Associates, a group of 15 hospitalists and two nurse coordinators that contracts with Bryan LGH hospital in Lincoln, Neb., to provide hospitalist services, agrees with Dr. Nelson’s characterization of the survey results as “a starting point.” While Dr. Bossard declined to state specifics about his group’s compensation figures, he did say that the median total compensation for non-leader physician hospitalists ($168,000 per year) was “about what I would expect it to be if you combine all hospitalists.”
He says that the numbers listed for HMG leaders was more reliable because leader roles are not quite as variable as non-leader roles. The survey shows that HMG leaders typically make $12,000 more annually than non-leader hospitalists, and that they tend to do less clinical work.
“It is also important to caution everyone in this area, too: This survey has not established the correct salary for a group leader—it varies tremendously,” reiterates Dr. Nelson.
In his role as HMG director, Dr. Bossard finds the survey’s work hours and work productivity data more valuable than compensation medians. “The number of hours per shift [median, 10.8] is very useful as a guide, I think, for someone who is starting a program or for someone like me, who knows what my numbers are,” he explains. “That—the median of 187 shifts per year; 10.8 hours per shift—provides an excellent target for new or established groups.”
Dr. Clark says that, in terms of pertinent data, the average number of encounters per hour was high on her list. Although that information is not highlighted in the survey’s “Executive Summary,” it is contained in Chapter 8, “Hospitalist Productivity.” Dr. Clark says this issue engenders an ongoing discussion with hospital administration.
“There are only so many patients you can see and provide excellent care, but there is a pull [from the administrative side] that they would like that number to be more,” she explains. “It’s nice to know what the average number of encounters is and what the society considers reasonable. I think it’s one of those things that we’re going to have to emphasize since the trade-off for seeing increased numbers of patients is to sacrifice quality patient care.”
Walter Bohnenblust, MD, is medical director of a hospitalist group at The Reading Hospital and Medical Center in West Reading, Pa. “What I like most about the survey is that productivity is represented not just with total billing, but with encounters and RVUs [relative value units]. We are in a low reimbursement area here, so if the survey included only gross charges and gross collections and not encounters plus RVUs, it would be more difficult in our market to justify to administration how hard we’re working. It’s uncanny how our group fits right in with the median in terms of productivity,” he says. “This gives me a baseline and more leverage with the administration, when they say we should be doing twice as many encounters as I think is reasonable.
“Like it or not, when someone is paying a subsidy for your service, they will try to get more out of you,” continues Dr. Bohnenblust. “It’s their job to try and get more out of the nurses and more out of the doctors. It’s not just us they’re picking on—the ER docs at our hospital have the same pressure. It’s good to have these numbers to go back and say, ‘Look, we are right where we should be [in terms of work productivity]. If you try and work us harder, you may lose some people and also not get out of the program what you wish.’”
Work productivity data provides an additional tool for recruitment, adds Dr. Bohnenblust, although he has not had much problem attracting new staff: “People are smart enough now to not only look at what [the prospective hospitalist group] income is, but how many patients they will have to see and what the work hours are.”
Uses of the Survey
Chapter 3, “The Work of Hospital Medicine Groups,” devotes attention to the types of non-clinical activities in which hospitalists participate. The section, say several sources, can also be a valuable negotiating tool with hospital administrators because it quantifies the amount of time hospitalists spend in such endeavors.
“One of the things that hospitalists add to inpatient care is that they have a greater presence all throughout the day in that facility,” says Timothy Bode, MD, medical director of Hospital Physician Services of Central Alabama. “And they’re a lot more involved with the medical staff, serving on committees, and involved in new processes and changes.
“To be able to see what kind of numbers are represented nationally, with hospitalists’ involvement in non-clinical activities, helps me with the hospitalists in my group,” he continues. “I can use these numbers to say, ‘This is a national trend. We need to be involved and we need to be leaders here as well, because that’s really the core of what we do.’ ”
Dr. Clark sees another important aspect of the hospitalist role: “ … participating on committees and QI initiatives and developing order sets, [which] can be additional and/or non-paid time. I think this needs to be recognized by hospitals in general, and physicians have to advocate for their value in this regard.”
The section on participation in non-clinical activities also drew praise from Dr. Bossard. “I don’t think this [percentage of time in non-clinical activities] would be necessary in terms of negotiating with the hospital, but it would be a very useful gauge for assessing where an individual program is relative to the rest of the programs, to see whether you are overdoing or under-representing yourself on committees.
“These surveys are just fabulous,” he says. “I’ve used the prior surveys to present information to the hospitals and identify how hard we’re working relative to our own region, and I present results to my hospitalist group in terms of pay and benefits. The survey is a wonderful tool.”
Academic Hospitalists Weigh In
Robert Wachter, MD, FACP, professor and associate chairman of the department of medicine at the University of California, San Francisco, and past president of SHM, also participated in the survey panel discussion and addresses issues specific to academic hospitalists. The growth in academic hospitalists shown in the current survey—while not surprising—confirms his impression that the field has grown in the last couple of years. The evidence of growth furnishes useful information for him as a hospitalist group leader in an academic institution.
“Unlike seven or eight years ago when I would be competing against only a handful of other academic programs for good people, I am now going to be competing against dozens and dozens of different groups,” he explains. “That changes the dynamic of my recruiting strategy.”
In addition, Dr. Wachter says he will make use of specific tables addressing concerns of academic hospitalists. “There are certain issues that are very different in an academic program, as compared to a community-based program,” he notes. “For instance, in my environment, burnout issues—or ‘dissatisfiers’—may relate to income or schedules or the abilities of support staff, but they may also relate to the teaching role or the research infrastructure—things that may be irrelevant to other people [in community programs] answering the surveys.”
Healthy Signs, Troubling Signs
Dr. Nelson summarizes his main points from the panel discussion about the survey: “It seems to show that incomes are rising faster than could be explained by inflation. There is also a rise in productivity, so incomes are up in part due to that.”
Another healthy trend, he says, is that in the last several surveys there has been a significant decline in hospitalists paid a fixed salary and an increase in those paid a combination of a base salary with a variable component, such as productivity. “I think getting away from fixed salaries is a good idea,” he notes.
Mary Jo Gorman, MD, MBA, SHM president and chief medical officer of IPC—The Hospitalist Company, was also a presenter during the survey’s debut in panel discussion. “Sustainability,” she says, is “very important for the field of hospital medicine. What this [survey] shows is that physicians are making a living, doing better than the average internist, and apparently getting career longevity out of this. Each year, the percentage of people who are staying in hospital medicine is increasing. New people are coming to the field, but other people are also staying. It’s not all about money and hours worked, but it’s some magical mixture of that.”
Dr. Bolinger agrees: “I definitely think that hospital medicine will sustain itself because we’re constantly setting the standard, and we’re showing the way it should be, the way it can be. As a profession, and as physicians, we are constantly striving to improve our quality of care. I think we are setting the mark for evidence-based medicine, and trying to encourage more evidence-based research.”
Dr. Bossard, who is based in Lincoln, Neb., found the 9% program turnover rate to be a relatively healthy sign, as did Dr. Wachter. “The turnover rates do not strike me as being incredibly high, given the portability of the field,” says Dr. Wachter. “We know very well that it is easier for hospitalists to pick up and leave their institutions for another one. In a primary care practice, changing practices involves a fair amount of work and a moderate amount of angst: You’re saying goodbye to all your patients and changing practice structure and style.”
One statistic did strike Dr. Bossard as potentially troubling, however: the increase in the percentage of hospitalists employed by multi-state hospitalist-only group or management companies from 9% in the 2003-2004 survey to 19% in the current survey.
“I think we’re seeing larger entities infiltrating markets and I’m not sure it’s a healthy trend for the hospitalist movement,” he says. “If you bring in physicians who do things a certain way, who may not have a commitment to a certain community, then I think you potentially lose some of the benefit of hospitalist programs. I think the finances will change. There will be a profit issue: Neither the hospital systems nor the hospitalist will see [that profit], and that’s a concerning trend to me.”
A Service to Members
Dr. Bohnenblust believes SHM truly serves its members by conducting the survey. The particular work environments and conditions of hospitalists can only be appreciated by a survey this specific, he says: “I applaud them for this [survey]. This is exactly what SHM needs to do to keep us viable as a profession.”
Dr. Wachter also believes the surveys are an invaluable tool.
“ … [Because we work in a] still-new field, we [hospitalists] are operating in a complex marketplace,” he says. “We are trying to figure out the best practices across all dimensions: schedules, organization structure, reporting relationships, funding. These kinds of surveys do not necessarily tell you the best practices, but they tell you about the prevalent practices. And I think that often is helpful in examining your own system and seeing whether it’s organized in the way you want to organize it. Having the society be the source of such information is a useful thing to do. It also helps the society design programs.”
The survey highlights many of the strengths of the growing hospital medicine movement. “I think in medicine in general there has been a frustration with having so much to do in so little time that it brings on stress,” says Dr. Bode. “When you can have a practice that devotes itself to one area, like the hospital, when you’re not running back and forth from the office to the hospital, you feel that you can really do a good job.
“I think most of the general population has no idea how the [healthcare] system works,” he continues. “To have a few minutes to spend telling patients how it works and how their care is flowing along is neat. You don’t feel that you have got to rush in and rush out all the time. The system can be so complex and frustrating for patients. When you can dive into the middle of it and try to streamline and demystify it, it’s really exciting.”
Conclusion
All survey participants received a free CD of the survey results. Copies of the CD as well as a booklet are available for purchase.
For more information on ordering “The Authoritative Source on the State of the Hospital Medicine Movement,” contact SHM at (800) 843-3360. TH
Gretchen Henkel writes regularly for The Hospitalist.
At a hefty 291 pages, SHM’s 2005-2006 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” contains a wealth of detail about hospitalists and their working conditions. Most readers will probably first refer to the compensation and benefits package statistics. But take a closer look: The survey’s chapters and tables yield a depth of even more helpful information.
After reviewing the survey’s “Executive Summary” (available online at the SHM Web site, www.hospitalmedicine.org), Charlene Carroll Clark, MD, a hospitalist at Inpatient Care Service at Good Samaritan Regional Medical Center in Corvallis, Ore., says “I think knowledge is always a good thing. Just knowing what is going on in other locations helps us. We can see that we fit right in with the median compensation, and that we are competitive as we recruit.”
It is reassuring, other sources concurred, to see that their hospitalist groups compare favorably with national median salaries and benefits packages. However, some group leaders caution that hospitalists should not benchmark their groups’ professional viability using only compensation and benefits medians. The real worth of the survey’s statistics, they say, will be realized when hospitalists utilize the document as a tool for improving management and care processes at their own institutions.
Indeed, in conversations with SHM leaders and with hospitalists across the country, it becomes clear that the survey has multiple uses, depending on its readers’ specific characteristics. And that’s just what SHM intends, says Joe Miller, SHM senior vice president, who was in charge of the survey project. “Our role was to create more of an almanac and a reference, rather than furnish an interpretation,” says Miller. “I think the real value for people will be in finding the metrics that are descriptive of their particular program.”
Survey Participation Increases
Miller is gratified by the increase in participation since the 2003-2004 SHM survey. Two years ago approximately 300 hospital medicine group (HMG) leaders participated in the survey. This time 396 HMG leaders participated—a 32% increase. Individual hospitalists completing the survey increased by more than 500 over the previous survey to a total of 2,550 individual hospitalist respondents.
“Given the magnitude of this survey, I think we’ve got very impressive representation of the industry,” says Miller. For instance, the regional representation of respondents was almost equally divided: 24% from the East, 26% from the South, 27% from the Midwest, and 22% from the West.
Miller attributes the greater participation to a variety of factors: conducting a multifaceted communication campaign, targeting every SHM board member and committee member, and extending the survey deadline.
An Eclectic and Thriving Group
According to Miller, the survey reveals many characteristics about hospitalists and the profession in general. While some of the results may not be surprising, they serve to corroborate (with real numbers) what many have perceived anecdotally about the hospital medicine movement. For instance:
- The hospital medicine movement is diverse. The survey documents six different models for hospital medicine programs. Currently, 34% of hospitalists are employed by hospitals or hospital corporations, and 12% are employed by local hospitalist-only groups. Multistate hospitalist-only groups or management companies employ 19%, while multi-specialty groups employ 14% of hospitalists. Academic hospital medicine programs employ 20%, and another 2% are employed by emergency or critical care physician groups.
- Hospitalists provide documented value for their hospitals, including around-the-clock patient care (51% of HMGs have on-site providers at night, and 41% of programs provide hospitalists on call), and participation in quality improvement (86%), hospital committees (92%), and other value-added activities, such as implementing information technology (54%).
- Other trends emerge when comparing 2003-2004 survey results with the current survey, including an increase in HMGs that now use a hybrid coverage schedule (a combination of shift and call schedules; an increase to 35% from 27%); more groups being paid using a mixed compensation model (a combination of salary and productive/performance-based compensation; up to 67% from 47% in 2003-2004); and a slight increase in hospitalists employed by academic institutions—up to 20% from a prior 16%.
Value Added
The survey also underscores hospitalists’ roles as change leaders in their institutions. In the “non-clinical activities” section of Chapter 3, “The Work of Hospital Medicine Groups,” results reveal high participation in hospital committees (92%), in quality improvement initiatives (86%); and other activities, such as generating practice guidelines, teaching, planning, and research.
John A. Bolinger, DO, FACP, medical director of the hospitalist program at Terre Haute (Ind.) Regional Hospital, serves on multiple committees at his hospital: critical care, pharmacy therapeutics, patient safety, credentials (as chair), and the executive committee. He and his hospital’s clinical pharmacist have developed standardized order sets, a new IV insulin protocol, and a new DVT prophylaxis protocol.
“I think participation in non-clinical activities is a plus for the hospitalist profession,” he says. In addition, “every hospital with a hospitalist involved in practice sees a tremendous benefit from that very thing.”
The Devil’s in the Details
John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, and cofounder and past president of SHM, was one of three panelists at the recent annual meeting where survey results were presented. Dr. Nelson believes that the statistics “can be a kind of starting point for thinking about whether your workload and compensation are typical. However,” he cautions, “the mistake I see so often is that people tend to think the average compensation, the average workload, are right for a given practice. Well, there are very few practices that are average. The variation is dramatic, and there’s no reason you should be average.”
Dr. Nelson advises hospitalists and group leaders not to interpret the compensation medians in the survey as a “final authority” for what hospitalists should be earning. Rather, he says, “what you could do is look at the big picture of an average practice—in terms of compensation, productivity, and other factors, such as location, whether your practice is primary adult or pediatric—and then compare your practice to see how you differ.
“Do you work harder and make less? In that case, you might want to fix it. If you work less and make more, you might want to be quiet!” he quips.
Brian Bossard, MD, medical director of Inpatient Physician Associates, a group of 15 hospitalists and two nurse coordinators that contracts with Bryan LGH hospital in Lincoln, Neb., to provide hospitalist services, agrees with Dr. Nelson’s characterization of the survey results as “a starting point.” While Dr. Bossard declined to state specifics about his group’s compensation figures, he did say that the median total compensation for non-leader physician hospitalists ($168,000 per year) was “about what I would expect it to be if you combine all hospitalists.”
He says that the numbers listed for HMG leaders was more reliable because leader roles are not quite as variable as non-leader roles. The survey shows that HMG leaders typically make $12,000 more annually than non-leader hospitalists, and that they tend to do less clinical work.
“It is also important to caution everyone in this area, too: This survey has not established the correct salary for a group leader—it varies tremendously,” reiterates Dr. Nelson.
In his role as HMG director, Dr. Bossard finds the survey’s work hours and work productivity data more valuable than compensation medians. “The number of hours per shift [median, 10.8] is very useful as a guide, I think, for someone who is starting a program or for someone like me, who knows what my numbers are,” he explains. “That—the median of 187 shifts per year; 10.8 hours per shift—provides an excellent target for new or established groups.”
Dr. Clark says that, in terms of pertinent data, the average number of encounters per hour was high on her list. Although that information is not highlighted in the survey’s “Executive Summary,” it is contained in Chapter 8, “Hospitalist Productivity.” Dr. Clark says this issue engenders an ongoing discussion with hospital administration.
“There are only so many patients you can see and provide excellent care, but there is a pull [from the administrative side] that they would like that number to be more,” she explains. “It’s nice to know what the average number of encounters is and what the society considers reasonable. I think it’s one of those things that we’re going to have to emphasize since the trade-off for seeing increased numbers of patients is to sacrifice quality patient care.”
Walter Bohnenblust, MD, is medical director of a hospitalist group at The Reading Hospital and Medical Center in West Reading, Pa. “What I like most about the survey is that productivity is represented not just with total billing, but with encounters and RVUs [relative value units]. We are in a low reimbursement area here, so if the survey included only gross charges and gross collections and not encounters plus RVUs, it would be more difficult in our market to justify to administration how hard we’re working. It’s uncanny how our group fits right in with the median in terms of productivity,” he says. “This gives me a baseline and more leverage with the administration, when they say we should be doing twice as many encounters as I think is reasonable.
“Like it or not, when someone is paying a subsidy for your service, they will try to get more out of you,” continues Dr. Bohnenblust. “It’s their job to try and get more out of the nurses and more out of the doctors. It’s not just us they’re picking on—the ER docs at our hospital have the same pressure. It’s good to have these numbers to go back and say, ‘Look, we are right where we should be [in terms of work productivity]. If you try and work us harder, you may lose some people and also not get out of the program what you wish.’”
Work productivity data provides an additional tool for recruitment, adds Dr. Bohnenblust, although he has not had much problem attracting new staff: “People are smart enough now to not only look at what [the prospective hospitalist group] income is, but how many patients they will have to see and what the work hours are.”
Uses of the Survey
Chapter 3, “The Work of Hospital Medicine Groups,” devotes attention to the types of non-clinical activities in which hospitalists participate. The section, say several sources, can also be a valuable negotiating tool with hospital administrators because it quantifies the amount of time hospitalists spend in such endeavors.
“One of the things that hospitalists add to inpatient care is that they have a greater presence all throughout the day in that facility,” says Timothy Bode, MD, medical director of Hospital Physician Services of Central Alabama. “And they’re a lot more involved with the medical staff, serving on committees, and involved in new processes and changes.
“To be able to see what kind of numbers are represented nationally, with hospitalists’ involvement in non-clinical activities, helps me with the hospitalists in my group,” he continues. “I can use these numbers to say, ‘This is a national trend. We need to be involved and we need to be leaders here as well, because that’s really the core of what we do.’ ”
Dr. Clark sees another important aspect of the hospitalist role: “ … participating on committees and QI initiatives and developing order sets, [which] can be additional and/or non-paid time. I think this needs to be recognized by hospitals in general, and physicians have to advocate for their value in this regard.”
The section on participation in non-clinical activities also drew praise from Dr. Bossard. “I don’t think this [percentage of time in non-clinical activities] would be necessary in terms of negotiating with the hospital, but it would be a very useful gauge for assessing where an individual program is relative to the rest of the programs, to see whether you are overdoing or under-representing yourself on committees.
“These surveys are just fabulous,” he says. “I’ve used the prior surveys to present information to the hospitals and identify how hard we’re working relative to our own region, and I present results to my hospitalist group in terms of pay and benefits. The survey is a wonderful tool.”
Academic Hospitalists Weigh In
Robert Wachter, MD, FACP, professor and associate chairman of the department of medicine at the University of California, San Francisco, and past president of SHM, also participated in the survey panel discussion and addresses issues specific to academic hospitalists. The growth in academic hospitalists shown in the current survey—while not surprising—confirms his impression that the field has grown in the last couple of years. The evidence of growth furnishes useful information for him as a hospitalist group leader in an academic institution.
“Unlike seven or eight years ago when I would be competing against only a handful of other academic programs for good people, I am now going to be competing against dozens and dozens of different groups,” he explains. “That changes the dynamic of my recruiting strategy.”
In addition, Dr. Wachter says he will make use of specific tables addressing concerns of academic hospitalists. “There are certain issues that are very different in an academic program, as compared to a community-based program,” he notes. “For instance, in my environment, burnout issues—or ‘dissatisfiers’—may relate to income or schedules or the abilities of support staff, but they may also relate to the teaching role or the research infrastructure—things that may be irrelevant to other people [in community programs] answering the surveys.”
Healthy Signs, Troubling Signs
Dr. Nelson summarizes his main points from the panel discussion about the survey: “It seems to show that incomes are rising faster than could be explained by inflation. There is also a rise in productivity, so incomes are up in part due to that.”
Another healthy trend, he says, is that in the last several surveys there has been a significant decline in hospitalists paid a fixed salary and an increase in those paid a combination of a base salary with a variable component, such as productivity. “I think getting away from fixed salaries is a good idea,” he notes.
Mary Jo Gorman, MD, MBA, SHM president and chief medical officer of IPC—The Hospitalist Company, was also a presenter during the survey’s debut in panel discussion. “Sustainability,” she says, is “very important for the field of hospital medicine. What this [survey] shows is that physicians are making a living, doing better than the average internist, and apparently getting career longevity out of this. Each year, the percentage of people who are staying in hospital medicine is increasing. New people are coming to the field, but other people are also staying. It’s not all about money and hours worked, but it’s some magical mixture of that.”
Dr. Bolinger agrees: “I definitely think that hospital medicine will sustain itself because we’re constantly setting the standard, and we’re showing the way it should be, the way it can be. As a profession, and as physicians, we are constantly striving to improve our quality of care. I think we are setting the mark for evidence-based medicine, and trying to encourage more evidence-based research.”
Dr. Bossard, who is based in Lincoln, Neb., found the 9% program turnover rate to be a relatively healthy sign, as did Dr. Wachter. “The turnover rates do not strike me as being incredibly high, given the portability of the field,” says Dr. Wachter. “We know very well that it is easier for hospitalists to pick up and leave their institutions for another one. In a primary care practice, changing practices involves a fair amount of work and a moderate amount of angst: You’re saying goodbye to all your patients and changing practice structure and style.”
One statistic did strike Dr. Bossard as potentially troubling, however: the increase in the percentage of hospitalists employed by multi-state hospitalist-only group or management companies from 9% in the 2003-2004 survey to 19% in the current survey.
“I think we’re seeing larger entities infiltrating markets and I’m not sure it’s a healthy trend for the hospitalist movement,” he says. “If you bring in physicians who do things a certain way, who may not have a commitment to a certain community, then I think you potentially lose some of the benefit of hospitalist programs. I think the finances will change. There will be a profit issue: Neither the hospital systems nor the hospitalist will see [that profit], and that’s a concerning trend to me.”
A Service to Members
Dr. Bohnenblust believes SHM truly serves its members by conducting the survey. The particular work environments and conditions of hospitalists can only be appreciated by a survey this specific, he says: “I applaud them for this [survey]. This is exactly what SHM needs to do to keep us viable as a profession.”
Dr. Wachter also believes the surveys are an invaluable tool.
“ … [Because we work in a] still-new field, we [hospitalists] are operating in a complex marketplace,” he says. “We are trying to figure out the best practices across all dimensions: schedules, organization structure, reporting relationships, funding. These kinds of surveys do not necessarily tell you the best practices, but they tell you about the prevalent practices. And I think that often is helpful in examining your own system and seeing whether it’s organized in the way you want to organize it. Having the society be the source of such information is a useful thing to do. It also helps the society design programs.”
The survey highlights many of the strengths of the growing hospital medicine movement. “I think in medicine in general there has been a frustration with having so much to do in so little time that it brings on stress,” says Dr. Bode. “When you can have a practice that devotes itself to one area, like the hospital, when you’re not running back and forth from the office to the hospital, you feel that you can really do a good job.
“I think most of the general population has no idea how the [healthcare] system works,” he continues. “To have a few minutes to spend telling patients how it works and how their care is flowing along is neat. You don’t feel that you have got to rush in and rush out all the time. The system can be so complex and frustrating for patients. When you can dive into the middle of it and try to streamline and demystify it, it’s really exciting.”
Conclusion
All survey participants received a free CD of the survey results. Copies of the CD as well as a booklet are available for purchase.
For more information on ordering “The Authoritative Source on the State of the Hospital Medicine Movement,” contact SHM at (800) 843-3360. TH
Gretchen Henkel writes regularly for The Hospitalist.
At a hefty 291 pages, SHM’s 2005-2006 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” contains a wealth of detail about hospitalists and their working conditions. Most readers will probably first refer to the compensation and benefits package statistics. But take a closer look: The survey’s chapters and tables yield a depth of even more helpful information.
After reviewing the survey’s “Executive Summary” (available online at the SHM Web site, www.hospitalmedicine.org), Charlene Carroll Clark, MD, a hospitalist at Inpatient Care Service at Good Samaritan Regional Medical Center in Corvallis, Ore., says “I think knowledge is always a good thing. Just knowing what is going on in other locations helps us. We can see that we fit right in with the median compensation, and that we are competitive as we recruit.”
It is reassuring, other sources concurred, to see that their hospitalist groups compare favorably with national median salaries and benefits packages. However, some group leaders caution that hospitalists should not benchmark their groups’ professional viability using only compensation and benefits medians. The real worth of the survey’s statistics, they say, will be realized when hospitalists utilize the document as a tool for improving management and care processes at their own institutions.
Indeed, in conversations with SHM leaders and with hospitalists across the country, it becomes clear that the survey has multiple uses, depending on its readers’ specific characteristics. And that’s just what SHM intends, says Joe Miller, SHM senior vice president, who was in charge of the survey project. “Our role was to create more of an almanac and a reference, rather than furnish an interpretation,” says Miller. “I think the real value for people will be in finding the metrics that are descriptive of their particular program.”
Survey Participation Increases
Miller is gratified by the increase in participation since the 2003-2004 SHM survey. Two years ago approximately 300 hospital medicine group (HMG) leaders participated in the survey. This time 396 HMG leaders participated—a 32% increase. Individual hospitalists completing the survey increased by more than 500 over the previous survey to a total of 2,550 individual hospitalist respondents.
“Given the magnitude of this survey, I think we’ve got very impressive representation of the industry,” says Miller. For instance, the regional representation of respondents was almost equally divided: 24% from the East, 26% from the South, 27% from the Midwest, and 22% from the West.
Miller attributes the greater participation to a variety of factors: conducting a multifaceted communication campaign, targeting every SHM board member and committee member, and extending the survey deadline.
An Eclectic and Thriving Group
According to Miller, the survey reveals many characteristics about hospitalists and the profession in general. While some of the results may not be surprising, they serve to corroborate (with real numbers) what many have perceived anecdotally about the hospital medicine movement. For instance:
- The hospital medicine movement is diverse. The survey documents six different models for hospital medicine programs. Currently, 34% of hospitalists are employed by hospitals or hospital corporations, and 12% are employed by local hospitalist-only groups. Multistate hospitalist-only groups or management companies employ 19%, while multi-specialty groups employ 14% of hospitalists. Academic hospital medicine programs employ 20%, and another 2% are employed by emergency or critical care physician groups.
- Hospitalists provide documented value for their hospitals, including around-the-clock patient care (51% of HMGs have on-site providers at night, and 41% of programs provide hospitalists on call), and participation in quality improvement (86%), hospital committees (92%), and other value-added activities, such as implementing information technology (54%).
- Other trends emerge when comparing 2003-2004 survey results with the current survey, including an increase in HMGs that now use a hybrid coverage schedule (a combination of shift and call schedules; an increase to 35% from 27%); more groups being paid using a mixed compensation model (a combination of salary and productive/performance-based compensation; up to 67% from 47% in 2003-2004); and a slight increase in hospitalists employed by academic institutions—up to 20% from a prior 16%.
Value Added
The survey also underscores hospitalists’ roles as change leaders in their institutions. In the “non-clinical activities” section of Chapter 3, “The Work of Hospital Medicine Groups,” results reveal high participation in hospital committees (92%), in quality improvement initiatives (86%); and other activities, such as generating practice guidelines, teaching, planning, and research.
John A. Bolinger, DO, FACP, medical director of the hospitalist program at Terre Haute (Ind.) Regional Hospital, serves on multiple committees at his hospital: critical care, pharmacy therapeutics, patient safety, credentials (as chair), and the executive committee. He and his hospital’s clinical pharmacist have developed standardized order sets, a new IV insulin protocol, and a new DVT prophylaxis protocol.
“I think participation in non-clinical activities is a plus for the hospitalist profession,” he says. In addition, “every hospital with a hospitalist involved in practice sees a tremendous benefit from that very thing.”
The Devil’s in the Details
John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, and cofounder and past president of SHM, was one of three panelists at the recent annual meeting where survey results were presented. Dr. Nelson believes that the statistics “can be a kind of starting point for thinking about whether your workload and compensation are typical. However,” he cautions, “the mistake I see so often is that people tend to think the average compensation, the average workload, are right for a given practice. Well, there are very few practices that are average. The variation is dramatic, and there’s no reason you should be average.”
Dr. Nelson advises hospitalists and group leaders not to interpret the compensation medians in the survey as a “final authority” for what hospitalists should be earning. Rather, he says, “what you could do is look at the big picture of an average practice—in terms of compensation, productivity, and other factors, such as location, whether your practice is primary adult or pediatric—and then compare your practice to see how you differ.
“Do you work harder and make less? In that case, you might want to fix it. If you work less and make more, you might want to be quiet!” he quips.
Brian Bossard, MD, medical director of Inpatient Physician Associates, a group of 15 hospitalists and two nurse coordinators that contracts with Bryan LGH hospital in Lincoln, Neb., to provide hospitalist services, agrees with Dr. Nelson’s characterization of the survey results as “a starting point.” While Dr. Bossard declined to state specifics about his group’s compensation figures, he did say that the median total compensation for non-leader physician hospitalists ($168,000 per year) was “about what I would expect it to be if you combine all hospitalists.”
He says that the numbers listed for HMG leaders was more reliable because leader roles are not quite as variable as non-leader roles. The survey shows that HMG leaders typically make $12,000 more annually than non-leader hospitalists, and that they tend to do less clinical work.
“It is also important to caution everyone in this area, too: This survey has not established the correct salary for a group leader—it varies tremendously,” reiterates Dr. Nelson.
In his role as HMG director, Dr. Bossard finds the survey’s work hours and work productivity data more valuable than compensation medians. “The number of hours per shift [median, 10.8] is very useful as a guide, I think, for someone who is starting a program or for someone like me, who knows what my numbers are,” he explains. “That—the median of 187 shifts per year; 10.8 hours per shift—provides an excellent target for new or established groups.”
Dr. Clark says that, in terms of pertinent data, the average number of encounters per hour was high on her list. Although that information is not highlighted in the survey’s “Executive Summary,” it is contained in Chapter 8, “Hospitalist Productivity.” Dr. Clark says this issue engenders an ongoing discussion with hospital administration.
“There are only so many patients you can see and provide excellent care, but there is a pull [from the administrative side] that they would like that number to be more,” she explains. “It’s nice to know what the average number of encounters is and what the society considers reasonable. I think it’s one of those things that we’re going to have to emphasize since the trade-off for seeing increased numbers of patients is to sacrifice quality patient care.”
Walter Bohnenblust, MD, is medical director of a hospitalist group at The Reading Hospital and Medical Center in West Reading, Pa. “What I like most about the survey is that productivity is represented not just with total billing, but with encounters and RVUs [relative value units]. We are in a low reimbursement area here, so if the survey included only gross charges and gross collections and not encounters plus RVUs, it would be more difficult in our market to justify to administration how hard we’re working. It’s uncanny how our group fits right in with the median in terms of productivity,” he says. “This gives me a baseline and more leverage with the administration, when they say we should be doing twice as many encounters as I think is reasonable.
“Like it or not, when someone is paying a subsidy for your service, they will try to get more out of you,” continues Dr. Bohnenblust. “It’s their job to try and get more out of the nurses and more out of the doctors. It’s not just us they’re picking on—the ER docs at our hospital have the same pressure. It’s good to have these numbers to go back and say, ‘Look, we are right where we should be [in terms of work productivity]. If you try and work us harder, you may lose some people and also not get out of the program what you wish.’”
Work productivity data provides an additional tool for recruitment, adds Dr. Bohnenblust, although he has not had much problem attracting new staff: “People are smart enough now to not only look at what [the prospective hospitalist group] income is, but how many patients they will have to see and what the work hours are.”
Uses of the Survey
Chapter 3, “The Work of Hospital Medicine Groups,” devotes attention to the types of non-clinical activities in which hospitalists participate. The section, say several sources, can also be a valuable negotiating tool with hospital administrators because it quantifies the amount of time hospitalists spend in such endeavors.
“One of the things that hospitalists add to inpatient care is that they have a greater presence all throughout the day in that facility,” says Timothy Bode, MD, medical director of Hospital Physician Services of Central Alabama. “And they’re a lot more involved with the medical staff, serving on committees, and involved in new processes and changes.
“To be able to see what kind of numbers are represented nationally, with hospitalists’ involvement in non-clinical activities, helps me with the hospitalists in my group,” he continues. “I can use these numbers to say, ‘This is a national trend. We need to be involved and we need to be leaders here as well, because that’s really the core of what we do.’ ”
Dr. Clark sees another important aspect of the hospitalist role: “ … participating on committees and QI initiatives and developing order sets, [which] can be additional and/or non-paid time. I think this needs to be recognized by hospitals in general, and physicians have to advocate for their value in this regard.”
The section on participation in non-clinical activities also drew praise from Dr. Bossard. “I don’t think this [percentage of time in non-clinical activities] would be necessary in terms of negotiating with the hospital, but it would be a very useful gauge for assessing where an individual program is relative to the rest of the programs, to see whether you are overdoing or under-representing yourself on committees.
“These surveys are just fabulous,” he says. “I’ve used the prior surveys to present information to the hospitals and identify how hard we’re working relative to our own region, and I present results to my hospitalist group in terms of pay and benefits. The survey is a wonderful tool.”
Academic Hospitalists Weigh In
Robert Wachter, MD, FACP, professor and associate chairman of the department of medicine at the University of California, San Francisco, and past president of SHM, also participated in the survey panel discussion and addresses issues specific to academic hospitalists. The growth in academic hospitalists shown in the current survey—while not surprising—confirms his impression that the field has grown in the last couple of years. The evidence of growth furnishes useful information for him as a hospitalist group leader in an academic institution.
“Unlike seven or eight years ago when I would be competing against only a handful of other academic programs for good people, I am now going to be competing against dozens and dozens of different groups,” he explains. “That changes the dynamic of my recruiting strategy.”
In addition, Dr. Wachter says he will make use of specific tables addressing concerns of academic hospitalists. “There are certain issues that are very different in an academic program, as compared to a community-based program,” he notes. “For instance, in my environment, burnout issues—or ‘dissatisfiers’—may relate to income or schedules or the abilities of support staff, but they may also relate to the teaching role or the research infrastructure—things that may be irrelevant to other people [in community programs] answering the surveys.”
Healthy Signs, Troubling Signs
Dr. Nelson summarizes his main points from the panel discussion about the survey: “It seems to show that incomes are rising faster than could be explained by inflation. There is also a rise in productivity, so incomes are up in part due to that.”
Another healthy trend, he says, is that in the last several surveys there has been a significant decline in hospitalists paid a fixed salary and an increase in those paid a combination of a base salary with a variable component, such as productivity. “I think getting away from fixed salaries is a good idea,” he notes.
Mary Jo Gorman, MD, MBA, SHM president and chief medical officer of IPC—The Hospitalist Company, was also a presenter during the survey’s debut in panel discussion. “Sustainability,” she says, is “very important for the field of hospital medicine. What this [survey] shows is that physicians are making a living, doing better than the average internist, and apparently getting career longevity out of this. Each year, the percentage of people who are staying in hospital medicine is increasing. New people are coming to the field, but other people are also staying. It’s not all about money and hours worked, but it’s some magical mixture of that.”
Dr. Bolinger agrees: “I definitely think that hospital medicine will sustain itself because we’re constantly setting the standard, and we’re showing the way it should be, the way it can be. As a profession, and as physicians, we are constantly striving to improve our quality of care. I think we are setting the mark for evidence-based medicine, and trying to encourage more evidence-based research.”
Dr. Bossard, who is based in Lincoln, Neb., found the 9% program turnover rate to be a relatively healthy sign, as did Dr. Wachter. “The turnover rates do not strike me as being incredibly high, given the portability of the field,” says Dr. Wachter. “We know very well that it is easier for hospitalists to pick up and leave their institutions for another one. In a primary care practice, changing practices involves a fair amount of work and a moderate amount of angst: You’re saying goodbye to all your patients and changing practice structure and style.”
One statistic did strike Dr. Bossard as potentially troubling, however: the increase in the percentage of hospitalists employed by multi-state hospitalist-only group or management companies from 9% in the 2003-2004 survey to 19% in the current survey.
“I think we’re seeing larger entities infiltrating markets and I’m not sure it’s a healthy trend for the hospitalist movement,” he says. “If you bring in physicians who do things a certain way, who may not have a commitment to a certain community, then I think you potentially lose some of the benefit of hospitalist programs. I think the finances will change. There will be a profit issue: Neither the hospital systems nor the hospitalist will see [that profit], and that’s a concerning trend to me.”
A Service to Members
Dr. Bohnenblust believes SHM truly serves its members by conducting the survey. The particular work environments and conditions of hospitalists can only be appreciated by a survey this specific, he says: “I applaud them for this [survey]. This is exactly what SHM needs to do to keep us viable as a profession.”
Dr. Wachter also believes the surveys are an invaluable tool.
“ … [Because we work in a] still-new field, we [hospitalists] are operating in a complex marketplace,” he says. “We are trying to figure out the best practices across all dimensions: schedules, organization structure, reporting relationships, funding. These kinds of surveys do not necessarily tell you the best practices, but they tell you about the prevalent practices. And I think that often is helpful in examining your own system and seeing whether it’s organized in the way you want to organize it. Having the society be the source of such information is a useful thing to do. It also helps the society design programs.”
The survey highlights many of the strengths of the growing hospital medicine movement. “I think in medicine in general there has been a frustration with having so much to do in so little time that it brings on stress,” says Dr. Bode. “When you can have a practice that devotes itself to one area, like the hospital, when you’re not running back and forth from the office to the hospital, you feel that you can really do a good job.
“I think most of the general population has no idea how the [healthcare] system works,” he continues. “To have a few minutes to spend telling patients how it works and how their care is flowing along is neat. You don’t feel that you have got to rush in and rush out all the time. The system can be so complex and frustrating for patients. When you can dive into the middle of it and try to streamline and demystify it, it’s really exciting.”
Conclusion
All survey participants received a free CD of the survey results. Copies of the CD as well as a booklet are available for purchase.
For more information on ordering “The Authoritative Source on the State of the Hospital Medicine Movement,” contact SHM at (800) 843-3360. TH
Gretchen Henkel writes regularly for The Hospitalist.
Historic Puzzler II

Jacques Cartier was in Newfoundland with his men in 1534, when the following occurred: “In December we understood the pestilence had come to the people of Stadacona … whereupon we charged them neither to come near our Fort, nor our ships. The said unknowen sickness began to spread itselfe amongst us after the strangest sort that ever was eyther heard of or seene, insomuch as some did lose all their strength, and could not stand on their feete, then their legges did swell. Others had all their skins spotted with spots of blood of a purple colour; then it did ascend up to ther ankels, knees, and thighs. Their mouth became stincking, their gummes so rotten, that all the flesh did fall off.”
What was the diagnosis and with what was it treated? Can you make the diagnosis based on the information provided? If so, e-mail your diagnosis to Physician Editor Jamie Newman at newman.james@mayo.edu. The deadline is Wednesday, July 5. We’ll publish the winner’s response in a future issue of The Hospitalist. TH
Jacques Cartier was in Newfoundland with his men in 1534, when the following occurred: “In December we understood the pestilence had come to the people of Stadacona … whereupon we charged them neither to come near our Fort, nor our ships. The said unknowen sickness began to spread itselfe amongst us after the strangest sort that ever was eyther heard of or seene, insomuch as some did lose all their strength, and could not stand on their feete, then their legges did swell. Others had all their skins spotted with spots of blood of a purple colour; then it did ascend up to ther ankels, knees, and thighs. Their mouth became stincking, their gummes so rotten, that all the flesh did fall off.”
What was the diagnosis and with what was it treated? Can you make the diagnosis based on the information provided? If so, e-mail your diagnosis to Physician Editor Jamie Newman at newman.james@mayo.edu. The deadline is Wednesday, July 5. We’ll publish the winner’s response in a future issue of The Hospitalist. TH
Jacques Cartier was in Newfoundland with his men in 1534, when the following occurred: “In December we understood the pestilence had come to the people of Stadacona … whereupon we charged them neither to come near our Fort, nor our ships. The said unknowen sickness began to spread itselfe amongst us after the strangest sort that ever was eyther heard of or seene, insomuch as some did lose all their strength, and could not stand on their feete, then their legges did swell. Others had all their skins spotted with spots of blood of a purple colour; then it did ascend up to ther ankels, knees, and thighs. Their mouth became stincking, their gummes so rotten, that all the flesh did fall off.”
What was the diagnosis and with what was it treated? Can you make the diagnosis based on the information provided? If so, e-mail your diagnosis to Physician Editor Jamie Newman at newman.james@mayo.edu. The deadline is Wednesday, July 5. We’ll publish the winner’s response in a future issue of The Hospitalist. TH
Add Mentoring to Your Hospitalist Mix
Providing a mentoring program that pairs newly hired hospitalists with more experienced ones is beneficial for several reasons. Mentors can boost the comfort level of new hospitalists and improve likelihood of retention. They can also add continuity of culture and processes to a hospital medicine program.
This month we look at how—and why—Cogent Healthcare maintains its system-wide mentoring program. “Mentoring provides an added dimension to a traditional management structure,” explains Russell L. Holman, MD, senior vice president and national medical director, Cogent Healthcare, and president-elect of SHM. “Mentors can put a very personal, subjective, human element to learning. There’s almost an emotional component, as opposed to being more didactic.”
Case Study in Brief
Cogent’s mentoring program has evolved over time, but the organization tries to keep the program’s structure loose and informal. “In the world of mentoring research—which is largely the business world, not the healthcare world—it’s clear that mentoring relationships that develop naturally are more effective than those that are assigned,” says Dr. Holman.
Cogent teams mentor new programs, rather than individual hospitalists. However, their broad outline of the mentor/mentee relationship can be applied to a one-on-one scenario. At Cogent, an experienced hospitalist will visit a new facility at set times.
“With all programs, we schedule visits at certain intervals,” says Dr. Holman. “But there’s a fair amount of informal contact with the mentors on an as-needed basis.”
Each site visit lasts one to two days. “When a mentor is on-site, their only responsibility is to spend time with the physicians,” explains Dr. Holman. “And typically, at the end of each visit we look forward to evaluating it, getting feedback from the physicians as well as the mentor.”
During the site visit, all physicians in the program have complete, open access to the mentor. “It’s a group dynamic, but there’s as much one-on-one time as possible,” says Dr. Holman.
The intervals at which a mentor visits a program are standard, as are the topics covered—at least at first. “We look at critical phases in the life cycle of our programs,” says Dr. Holman. “When a program first starts, people are concerned with the nuts and bolts of operations, such as the use of guidelines, information systems, decision support tools, coding/billing, and even scheduling suggestions. A mentorship visit at this stage provides useful tips on operational implementation that are highly pragmatic.”
The next visit takes place within three to six months of the program’s implementation. At this point, says Dr. Holman, “there’s a comfortable workflow established but it’s likely that none of the physicians have worked together before. A mentor can talk about teamwork, including tips to bring consistency to the practice style.”
Next, after the program has been up and running for nine to 12 months, Dr. Holman says, “there’s enough experience in the program to speak more specifically to efficiency issues. An experienced hospitalist can provide focused mentorship on time-management skills, ways to extend your clinical reach, and ways to expand the number of patients you’re caring for. Most hospitalists are relatively young—many are within a year or two of completing their residency—so they’re still building these skills.”
At 12 months and beyond, the mentoring becomes much more customized to the specific needs of the individual program. “Maybe a program is trying to establish good working relationships with key departments within the hospital … or they want advanced clinical tools,” speculates Dr. Holman. “It may be that our hospitalists have been asked to lead an initiative, and they don’t have experience in leading hospital-wide initiatives. At this point, mentorship can reach a new level.”
Meet the Mentors
A mentor should be well versed in organizational processes, have clinical expertise and—if not an experienced teacher—should have well-honed people skills.
“Our mentors come from a profile of different folks, including the founding group of Cogent, a large practice in Los Angeles comprised of experienced hospitalists,” explains Dr. Holman. “Another group of mentors is our entire slate of medical directors, who have individual expertise in different areas. When mentors go on site visits, there’s no direct reporting, but they bring their expertise and facilitate networking.”
Cogent continues to widen its pool of available mentors, and is working to include physicians with special expertise. “We’re trying to build a diverse team [of mentors],” says Dr. Holman. “We look for clinical expertise in physicians who may not necessarily hold leadership roles. We try to predetermine which available mentor we think will be the best fit for a program, including personality, culture, and expertise.”
You Can Introduce Mentoring
You many not have the resources or number of physicians that Cogent has, but you can still start your own mentoring program. “Any program can look at a variety of resources to build a stable of mentors, or at least have a couple of mentors they can draw on,” insists Dr. Holman. “Look at other members of the medical staff that are experienced and role models for desirable qualities. Mentors can be within the healthcare field, but they don’t have to be physicians. One of my personal mentors for years was a director of human resources. You can even look outside healthcare.
“SHM is constantly looking at how to facilitate mentorship through venues like the Mentorship Breakfast at the Annual Meeting, and I still keep in touch with people I’ve met there,” he continues. “The SHM Annual Meeting is a terrific venue in general if you’re looking to connect members of your group (or yourself) with others from around the country.”
Implementing and maintaining a mentoring program may add to your workload, but it will pay off immediately. Just remember not to plan it out too carefully. “Mentoring is a constant work in progress,” concludes Dr. Holman. “We never want to see it as a static or inflexible entity. It’s a dynamic process driven by physician needs.” TH
Jane Jerrard writes “Career Development” each month for The Hospitalist
Providing a mentoring program that pairs newly hired hospitalists with more experienced ones is beneficial for several reasons. Mentors can boost the comfort level of new hospitalists and improve likelihood of retention. They can also add continuity of culture and processes to a hospital medicine program.
This month we look at how—and why—Cogent Healthcare maintains its system-wide mentoring program. “Mentoring provides an added dimension to a traditional management structure,” explains Russell L. Holman, MD, senior vice president and national medical director, Cogent Healthcare, and president-elect of SHM. “Mentors can put a very personal, subjective, human element to learning. There’s almost an emotional component, as opposed to being more didactic.”
Case Study in Brief
Cogent’s mentoring program has evolved over time, but the organization tries to keep the program’s structure loose and informal. “In the world of mentoring research—which is largely the business world, not the healthcare world—it’s clear that mentoring relationships that develop naturally are more effective than those that are assigned,” says Dr. Holman.
Cogent teams mentor new programs, rather than individual hospitalists. However, their broad outline of the mentor/mentee relationship can be applied to a one-on-one scenario. At Cogent, an experienced hospitalist will visit a new facility at set times.
“With all programs, we schedule visits at certain intervals,” says Dr. Holman. “But there’s a fair amount of informal contact with the mentors on an as-needed basis.”
Each site visit lasts one to two days. “When a mentor is on-site, their only responsibility is to spend time with the physicians,” explains Dr. Holman. “And typically, at the end of each visit we look forward to evaluating it, getting feedback from the physicians as well as the mentor.”
During the site visit, all physicians in the program have complete, open access to the mentor. “It’s a group dynamic, but there’s as much one-on-one time as possible,” says Dr. Holman.
The intervals at which a mentor visits a program are standard, as are the topics covered—at least at first. “We look at critical phases in the life cycle of our programs,” says Dr. Holman. “When a program first starts, people are concerned with the nuts and bolts of operations, such as the use of guidelines, information systems, decision support tools, coding/billing, and even scheduling suggestions. A mentorship visit at this stage provides useful tips on operational implementation that are highly pragmatic.”
The next visit takes place within three to six months of the program’s implementation. At this point, says Dr. Holman, “there’s a comfortable workflow established but it’s likely that none of the physicians have worked together before. A mentor can talk about teamwork, including tips to bring consistency to the practice style.”
Next, after the program has been up and running for nine to 12 months, Dr. Holman says, “there’s enough experience in the program to speak more specifically to efficiency issues. An experienced hospitalist can provide focused mentorship on time-management skills, ways to extend your clinical reach, and ways to expand the number of patients you’re caring for. Most hospitalists are relatively young—many are within a year or two of completing their residency—so they’re still building these skills.”
At 12 months and beyond, the mentoring becomes much more customized to the specific needs of the individual program. “Maybe a program is trying to establish good working relationships with key departments within the hospital … or they want advanced clinical tools,” speculates Dr. Holman. “It may be that our hospitalists have been asked to lead an initiative, and they don’t have experience in leading hospital-wide initiatives. At this point, mentorship can reach a new level.”
Meet the Mentors
A mentor should be well versed in organizational processes, have clinical expertise and—if not an experienced teacher—should have well-honed people skills.
“Our mentors come from a profile of different folks, including the founding group of Cogent, a large practice in Los Angeles comprised of experienced hospitalists,” explains Dr. Holman. “Another group of mentors is our entire slate of medical directors, who have individual expertise in different areas. When mentors go on site visits, there’s no direct reporting, but they bring their expertise and facilitate networking.”
Cogent continues to widen its pool of available mentors, and is working to include physicians with special expertise. “We’re trying to build a diverse team [of mentors],” says Dr. Holman. “We look for clinical expertise in physicians who may not necessarily hold leadership roles. We try to predetermine which available mentor we think will be the best fit for a program, including personality, culture, and expertise.”
You Can Introduce Mentoring
You many not have the resources or number of physicians that Cogent has, but you can still start your own mentoring program. “Any program can look at a variety of resources to build a stable of mentors, or at least have a couple of mentors they can draw on,” insists Dr. Holman. “Look at other members of the medical staff that are experienced and role models for desirable qualities. Mentors can be within the healthcare field, but they don’t have to be physicians. One of my personal mentors for years was a director of human resources. You can even look outside healthcare.
“SHM is constantly looking at how to facilitate mentorship through venues like the Mentorship Breakfast at the Annual Meeting, and I still keep in touch with people I’ve met there,” he continues. “The SHM Annual Meeting is a terrific venue in general if you’re looking to connect members of your group (or yourself) with others from around the country.”
Implementing and maintaining a mentoring program may add to your workload, but it will pay off immediately. Just remember not to plan it out too carefully. “Mentoring is a constant work in progress,” concludes Dr. Holman. “We never want to see it as a static or inflexible entity. It’s a dynamic process driven by physician needs.” TH
Jane Jerrard writes “Career Development” each month for The Hospitalist
Providing a mentoring program that pairs newly hired hospitalists with more experienced ones is beneficial for several reasons. Mentors can boost the comfort level of new hospitalists and improve likelihood of retention. They can also add continuity of culture and processes to a hospital medicine program.
This month we look at how—and why—Cogent Healthcare maintains its system-wide mentoring program. “Mentoring provides an added dimension to a traditional management structure,” explains Russell L. Holman, MD, senior vice president and national medical director, Cogent Healthcare, and president-elect of SHM. “Mentors can put a very personal, subjective, human element to learning. There’s almost an emotional component, as opposed to being more didactic.”
Case Study in Brief
Cogent’s mentoring program has evolved over time, but the organization tries to keep the program’s structure loose and informal. “In the world of mentoring research—which is largely the business world, not the healthcare world—it’s clear that mentoring relationships that develop naturally are more effective than those that are assigned,” says Dr. Holman.
Cogent teams mentor new programs, rather than individual hospitalists. However, their broad outline of the mentor/mentee relationship can be applied to a one-on-one scenario. At Cogent, an experienced hospitalist will visit a new facility at set times.
“With all programs, we schedule visits at certain intervals,” says Dr. Holman. “But there’s a fair amount of informal contact with the mentors on an as-needed basis.”
Each site visit lasts one to two days. “When a mentor is on-site, their only responsibility is to spend time with the physicians,” explains Dr. Holman. “And typically, at the end of each visit we look forward to evaluating it, getting feedback from the physicians as well as the mentor.”
During the site visit, all physicians in the program have complete, open access to the mentor. “It’s a group dynamic, but there’s as much one-on-one time as possible,” says Dr. Holman.
The intervals at which a mentor visits a program are standard, as are the topics covered—at least at first. “We look at critical phases in the life cycle of our programs,” says Dr. Holman. “When a program first starts, people are concerned with the nuts and bolts of operations, such as the use of guidelines, information systems, decision support tools, coding/billing, and even scheduling suggestions. A mentorship visit at this stage provides useful tips on operational implementation that are highly pragmatic.”
The next visit takes place within three to six months of the program’s implementation. At this point, says Dr. Holman, “there’s a comfortable workflow established but it’s likely that none of the physicians have worked together before. A mentor can talk about teamwork, including tips to bring consistency to the practice style.”
Next, after the program has been up and running for nine to 12 months, Dr. Holman says, “there’s enough experience in the program to speak more specifically to efficiency issues. An experienced hospitalist can provide focused mentorship on time-management skills, ways to extend your clinical reach, and ways to expand the number of patients you’re caring for. Most hospitalists are relatively young—many are within a year or two of completing their residency—so they’re still building these skills.”
At 12 months and beyond, the mentoring becomes much more customized to the specific needs of the individual program. “Maybe a program is trying to establish good working relationships with key departments within the hospital … or they want advanced clinical tools,” speculates Dr. Holman. “It may be that our hospitalists have been asked to lead an initiative, and they don’t have experience in leading hospital-wide initiatives. At this point, mentorship can reach a new level.”
Meet the Mentors
A mentor should be well versed in organizational processes, have clinical expertise and—if not an experienced teacher—should have well-honed people skills.
“Our mentors come from a profile of different folks, including the founding group of Cogent, a large practice in Los Angeles comprised of experienced hospitalists,” explains Dr. Holman. “Another group of mentors is our entire slate of medical directors, who have individual expertise in different areas. When mentors go on site visits, there’s no direct reporting, but they bring their expertise and facilitate networking.”
Cogent continues to widen its pool of available mentors, and is working to include physicians with special expertise. “We’re trying to build a diverse team [of mentors],” says Dr. Holman. “We look for clinical expertise in physicians who may not necessarily hold leadership roles. We try to predetermine which available mentor we think will be the best fit for a program, including personality, culture, and expertise.”
You Can Introduce Mentoring
You many not have the resources or number of physicians that Cogent has, but you can still start your own mentoring program. “Any program can look at a variety of resources to build a stable of mentors, or at least have a couple of mentors they can draw on,” insists Dr. Holman. “Look at other members of the medical staff that are experienced and role models for desirable qualities. Mentors can be within the healthcare field, but they don’t have to be physicians. One of my personal mentors for years was a director of human resources. You can even look outside healthcare.
“SHM is constantly looking at how to facilitate mentorship through venues like the Mentorship Breakfast at the Annual Meeting, and I still keep in touch with people I’ve met there,” he continues. “The SHM Annual Meeting is a terrific venue in general if you’re looking to connect members of your group (or yourself) with others from around the country.”
Implementing and maintaining a mentoring program may add to your workload, but it will pay off immediately. Just remember not to plan it out too carefully. “Mentoring is a constant work in progress,” concludes Dr. Holman. “We never want to see it as a static or inflexible entity. It’s a dynamic process driven by physician needs.” TH
Jane Jerrard writes “Career Development” each month for The Hospitalist
What's Up with Voluntary Reporting? - Part 2
This article is the second in a two-part series on the CMS Physician Voluntary Reporting Program. Part one appeared on p. 11 of the May 2006 issue.
Changes in Medicare reporting and payment are coming, and they’re coming fast. Regardless of whether you agree with where Medicare is heading or plan to participate in the first stage of these changes, you’re better off knowing what’s in store.
The first part of this article provided an overview of the Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid (CMS) initiated at the beginning of 2006, including how the reported quality measures apply—or don’t apply—to hospitalists.
Benefits of Reporting
Eric Siegal, MD, chair of SHM’s Public Policy Committee, is convinced that hospitalists should participate in PVRP, although he stresses that he does not speak for SHM on the matter.
“Hospital medicine has positioned itself as a champion of quality improvement,” he points out. “We talk the talk, so now we need to walk the walk [with voluntary reporting]. As a group of physicians who live and breathe this issue, we’ll have that much more credibility for supporting this program.”
Dr. Siegal not only believes hospitalists should report through PVRP, he thinks they will excel at doing so: “Because we’re already used to being measured, I have a suspicion that our adherence to these metrics is going to look very good. This will serve to bolster the argument that hospitalists add value to the care of hospitalized patients.”
Potential Problem Areas for Hospitalists
Hospitalists who participate in PVRP may face a bumpy road. “There are small problems,” admits Dr. Siegal. One of those is the disconnect between the 16 quality measures that physicians can report on and the role that hospitalists play.
“Of the 16 metrics in the starter set, maybe seven apply to hospitalists,” he explains.
Hospitalists may face another unique problem in meeting those measures: “We may have dilemmas over responsibility and reporting,” predicts Dr. Siegal. “For instance, we’re increasingly co-managing patients with surgeons. If a hospitalist wants to comply with a metric, but the surgeon disagrees, does the hospitalist take the hit? The same is true with something like administering aspirin on arrival for acute myocardial infarction. Is that my responsibility or the emergency physician’s?”
Another issue is the Healthcare Common Procedure Coding System (HCPCS) codes—or G-codes—that comprise each of the current PVRP’s 16 quality measures.
“The G-codes are cumbersome,” says Dr. Siegal. “There are G-codes for each measure, and there is talk about changing to a different system. So you may set up to report G-codes only to have the system change. But get used to it—this is a dynamic process that is definitely going to evolve.”
PVRP Is the Future
Dr. Siegal—and many others—believe that the PVRP will evolve into a broader reporting program and will ultimately transform into a mandatory pay-for-performance system for CMS. This may happen faster than CMS usually moves.
“Eventually there will be money tied to this,” he says. “Rumors are that payment modifiers may be tied to reporting as early as the fourth quarter of this year. As things go in the federal government, the evolution to value-based purchasing is moving at a lightning-fast pace—CMS is actually getting pushback from medical groups for moving too fast.”
Dr. Siegal adds that, “CMS is very interested in engaging physician organizations for their input. [CMS Administrator Mark B.] McClellan has done an admirable job of making this an interactive process.”
As PRVP evolves, it is likely to become more applicable to hospitalists.
“This is all part of a larger evolutionary trend in medicine,” explains Dr. Siegal. “Currently, hospitals and physicians are treated separately by CMS, and paid and incentivized differently. There’s growing realization that with rising costs and increased need for quality improvement hospitals and physicians need to have their incentives aligned. Things are going to change and it will take a long time for this to shake out.”
Because PVRP is the wave of the future for CMS payment, Dr. Siegal believes that hospitalists will be better off if they join in now. Voluntary reporting requires hospitalists to develop a new reporting infrastructure, and, as he says, “It’s better to do that now, with only 16 measures, than to have to do it later when there are 36 or 42.”
Dr. Siegal is convinced that hospitalists should support PVRP now, in its first stage. He also believes that SHM will begin to get involved. “We clearly need to be at this table,” he emphasizes. “Hospitalists are going to be the dominant providers of care to hospitalized Medicare patients. That said, SHM is still a relatively small society, and we don’t have the resources to engage every aspect of this debate. This is a huge and complex issue and SHM needs to use its limited resources wisely.”
SHM’s Public Policy Committee will continue to monitor what happens with PVRP and CMS, and SHM may eventually pursue membership in the national quality forums that are developing new metrics.
CMS provides details on the PVRP, including instructions on how to sign up, on their Web site at www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
This article is the second in a two-part series on the CMS Physician Voluntary Reporting Program. Part one appeared on p. 11 of the May 2006 issue.
Changes in Medicare reporting and payment are coming, and they’re coming fast. Regardless of whether you agree with where Medicare is heading or plan to participate in the first stage of these changes, you’re better off knowing what’s in store.
The first part of this article provided an overview of the Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid (CMS) initiated at the beginning of 2006, including how the reported quality measures apply—or don’t apply—to hospitalists.
Benefits of Reporting
Eric Siegal, MD, chair of SHM’s Public Policy Committee, is convinced that hospitalists should participate in PVRP, although he stresses that he does not speak for SHM on the matter.
“Hospital medicine has positioned itself as a champion of quality improvement,” he points out. “We talk the talk, so now we need to walk the walk [with voluntary reporting]. As a group of physicians who live and breathe this issue, we’ll have that much more credibility for supporting this program.”
Dr. Siegal not only believes hospitalists should report through PVRP, he thinks they will excel at doing so: “Because we’re already used to being measured, I have a suspicion that our adherence to these metrics is going to look very good. This will serve to bolster the argument that hospitalists add value to the care of hospitalized patients.”
Potential Problem Areas for Hospitalists
Hospitalists who participate in PVRP may face a bumpy road. “There are small problems,” admits Dr. Siegal. One of those is the disconnect between the 16 quality measures that physicians can report on and the role that hospitalists play.
“Of the 16 metrics in the starter set, maybe seven apply to hospitalists,” he explains.
Hospitalists may face another unique problem in meeting those measures: “We may have dilemmas over responsibility and reporting,” predicts Dr. Siegal. “For instance, we’re increasingly co-managing patients with surgeons. If a hospitalist wants to comply with a metric, but the surgeon disagrees, does the hospitalist take the hit? The same is true with something like administering aspirin on arrival for acute myocardial infarction. Is that my responsibility or the emergency physician’s?”
Another issue is the Healthcare Common Procedure Coding System (HCPCS) codes—or G-codes—that comprise each of the current PVRP’s 16 quality measures.
“The G-codes are cumbersome,” says Dr. Siegal. “There are G-codes for each measure, and there is talk about changing to a different system. So you may set up to report G-codes only to have the system change. But get used to it—this is a dynamic process that is definitely going to evolve.”
PVRP Is the Future
Dr. Siegal—and many others—believe that the PVRP will evolve into a broader reporting program and will ultimately transform into a mandatory pay-for-performance system for CMS. This may happen faster than CMS usually moves.
“Eventually there will be money tied to this,” he says. “Rumors are that payment modifiers may be tied to reporting as early as the fourth quarter of this year. As things go in the federal government, the evolution to value-based purchasing is moving at a lightning-fast pace—CMS is actually getting pushback from medical groups for moving too fast.”
Dr. Siegal adds that, “CMS is very interested in engaging physician organizations for their input. [CMS Administrator Mark B.] McClellan has done an admirable job of making this an interactive process.”
As PRVP evolves, it is likely to become more applicable to hospitalists.
“This is all part of a larger evolutionary trend in medicine,” explains Dr. Siegal. “Currently, hospitals and physicians are treated separately by CMS, and paid and incentivized differently. There’s growing realization that with rising costs and increased need for quality improvement hospitals and physicians need to have their incentives aligned. Things are going to change and it will take a long time for this to shake out.”
Because PVRP is the wave of the future for CMS payment, Dr. Siegal believes that hospitalists will be better off if they join in now. Voluntary reporting requires hospitalists to develop a new reporting infrastructure, and, as he says, “It’s better to do that now, with only 16 measures, than to have to do it later when there are 36 or 42.”
Dr. Siegal is convinced that hospitalists should support PVRP now, in its first stage. He also believes that SHM will begin to get involved. “We clearly need to be at this table,” he emphasizes. “Hospitalists are going to be the dominant providers of care to hospitalized Medicare patients. That said, SHM is still a relatively small society, and we don’t have the resources to engage every aspect of this debate. This is a huge and complex issue and SHM needs to use its limited resources wisely.”
SHM’s Public Policy Committee will continue to monitor what happens with PVRP and CMS, and SHM may eventually pursue membership in the national quality forums that are developing new metrics.
CMS provides details on the PVRP, including instructions on how to sign up, on their Web site at www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
This article is the second in a two-part series on the CMS Physician Voluntary Reporting Program. Part one appeared on p. 11 of the May 2006 issue.
Changes in Medicare reporting and payment are coming, and they’re coming fast. Regardless of whether you agree with where Medicare is heading or plan to participate in the first stage of these changes, you’re better off knowing what’s in store.
The first part of this article provided an overview of the Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid (CMS) initiated at the beginning of 2006, including how the reported quality measures apply—or don’t apply—to hospitalists.
Benefits of Reporting
Eric Siegal, MD, chair of SHM’s Public Policy Committee, is convinced that hospitalists should participate in PVRP, although he stresses that he does not speak for SHM on the matter.
“Hospital medicine has positioned itself as a champion of quality improvement,” he points out. “We talk the talk, so now we need to walk the walk [with voluntary reporting]. As a group of physicians who live and breathe this issue, we’ll have that much more credibility for supporting this program.”
Dr. Siegal not only believes hospitalists should report through PVRP, he thinks they will excel at doing so: “Because we’re already used to being measured, I have a suspicion that our adherence to these metrics is going to look very good. This will serve to bolster the argument that hospitalists add value to the care of hospitalized patients.”
Potential Problem Areas for Hospitalists
Hospitalists who participate in PVRP may face a bumpy road. “There are small problems,” admits Dr. Siegal. One of those is the disconnect between the 16 quality measures that physicians can report on and the role that hospitalists play.
“Of the 16 metrics in the starter set, maybe seven apply to hospitalists,” he explains.
Hospitalists may face another unique problem in meeting those measures: “We may have dilemmas over responsibility and reporting,” predicts Dr. Siegal. “For instance, we’re increasingly co-managing patients with surgeons. If a hospitalist wants to comply with a metric, but the surgeon disagrees, does the hospitalist take the hit? The same is true with something like administering aspirin on arrival for acute myocardial infarction. Is that my responsibility or the emergency physician’s?”
Another issue is the Healthcare Common Procedure Coding System (HCPCS) codes—or G-codes—that comprise each of the current PVRP’s 16 quality measures.
“The G-codes are cumbersome,” says Dr. Siegal. “There are G-codes for each measure, and there is talk about changing to a different system. So you may set up to report G-codes only to have the system change. But get used to it—this is a dynamic process that is definitely going to evolve.”
PVRP Is the Future
Dr. Siegal—and many others—believe that the PVRP will evolve into a broader reporting program and will ultimately transform into a mandatory pay-for-performance system for CMS. This may happen faster than CMS usually moves.
“Eventually there will be money tied to this,” he says. “Rumors are that payment modifiers may be tied to reporting as early as the fourth quarter of this year. As things go in the federal government, the evolution to value-based purchasing is moving at a lightning-fast pace—CMS is actually getting pushback from medical groups for moving too fast.”
Dr. Siegal adds that, “CMS is very interested in engaging physician organizations for their input. [CMS Administrator Mark B.] McClellan has done an admirable job of making this an interactive process.”
As PRVP evolves, it is likely to become more applicable to hospitalists.
“This is all part of a larger evolutionary trend in medicine,” explains Dr. Siegal. “Currently, hospitals and physicians are treated separately by CMS, and paid and incentivized differently. There’s growing realization that with rising costs and increased need for quality improvement hospitals and physicians need to have their incentives aligned. Things are going to change and it will take a long time for this to shake out.”
Because PVRP is the wave of the future for CMS payment, Dr. Siegal believes that hospitalists will be better off if they join in now. Voluntary reporting requires hospitalists to develop a new reporting infrastructure, and, as he says, “It’s better to do that now, with only 16 measures, than to have to do it later when there are 36 or 42.”
Dr. Siegal is convinced that hospitalists should support PVRP now, in its first stage. He also believes that SHM will begin to get involved. “We clearly need to be at this table,” he emphasizes. “Hospitalists are going to be the dominant providers of care to hospitalized Medicare patients. That said, SHM is still a relatively small society, and we don’t have the resources to engage every aspect of this debate. This is a huge and complex issue and SHM needs to use its limited resources wisely.”
SHM’s Public Policy Committee will continue to monitor what happens with PVRP and CMS, and SHM may eventually pursue membership in the national quality forums that are developing new metrics.
CMS provides details on the PVRP, including instructions on how to sign up, on their Web site at www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
Changing of the Guard
Each year a new team of SHM officers is elected to lend their wisdom, time, experience, and skills in a collaborative effort to help manage the business of our organization, drive new initiatives, and support the society’s mission. At this year’s annual meeting in Washington, D.C., we again witnessed that familiar changing of the guard with the following inductions:
- President Mary Jo Gorman, MD, MBA;
- President-Elect Russell Holman, MD;
- Treasurer Patrick Cawley, MD; and
- Secretary Jack Percelay, MD, MPH.
“Hospitalists are squarely in the spotlight today on key issues affecting patient care, quality of hospital care, hospital leadership, and other concerns. So it is important that we have a strong, hands-on leadership team that is committed to continuing the positive momentum SHM has generated for hospitalists,” says Larry Wellikson, MD, FACP, CEO of SHM. “I couldn’t be more thrilled with our slate of newly appointed officers. Time and again through the years Mary Jo, Rusty, Pat, and Jack have proven that they are active participants, and that they are leaders who will rise to the occasion to help us meet our objectives.”

Dr. Gorman, a charter member of SHM, has been a practicing hospitalist since 1997, when she founded the first hospitalist practice in St. Louis. In early 1999, her group merged into IPC—The Hospitalist Company and grew to become the dominant hospitalist group in the city. In 2001, Dr. Gorman was promoted to vice-president of medical affairs for IPC, responsible for the design and implementation of company-wide programs involving business development, recruitment, physician training, and operations in all of IPC’s markets. In 2003, she was named chief medical officer and today works with more than 300 physicians nationwide to develop programs and strategies that enhance clinical performance and drive the delivery system towards more efficient care and greater patient satisfaction. She also oversees IPC’s physician training, mentoring and retention programs, as well as IPC’s call center nurses, healthcare services and clinical studies.
A cum laude graduate of St. Louis University, Dr. Gorman earned a BA in Chemistry/Biology in 1981, then went on to earn her MD in 1984 from Southern Illinois University School of Medicine in Springfield. In 1996, she earned a MBA from Washington University, Olin School of Business, in St. Louis.

SHM’s new President-Elect Dr. Holman is senior vice president and national medical director for Cogent Healthcare, an organization that manages hospital medicine programs throughout the country. He is responsible for program implementation and management, quality systems reporting and auditing, physician leadership development, and data systems integration. Formerly, Dr. Holman was the medical director of Hospital Services for HealthPartners Medical Group & Clinics, part of HealthPartners, Inc. in Minnesota. There he also was the founder and director of the HPMG Fellowship Program in Hospital Medicine.
A long-time member of SHM, Dr. Holman served on the Board of Directors as treasurer from 2004-2005. He was previously chair of the Leadership Development Committee, chair of the Midwest Council, course director of the SHM Leadership Academy, and a member of the Public Policy Committee. In February 2006 he co-authored the “Update in Hospital Medicine,” which appeared in Annals of Internal Medicine. In 2002, he received the SHM Award for Outstanding Service in Hospital Medicine.
Through the years, Dr. Holman’s commitment to hospital medicine has helped produce nationally recognized standards in the areas of quality improvement activities, models of medical education, observation units, communication systems, compensation plans, case management, surgical co-management collaborations, and patient flow initiatives. Dr. Holman serves on two national editorial boards for medical publications and is currently co-authoring a comprehensive textbook and electronic decision support tool in hospital medicine.
Dr. Holman earned his MD from Washington University School of Medicine in St. Louis and trained as a resident and chief medical resident at the University of Minnesota in Minneapolis.

New Treasurer Dr. Cawley is a hospitalist at the Medical University of South Carolina in Charleston, where he currently serves as interim executive medical director of MUSC Medical Center. He previously served as the chief of the Section of Hospital Medicine, vice chairman of clinical affairs in the Department of Medicine, and associate executive medical director at MUSC Medical Center.
A charter member of SHM, Dr. Cawley has served on numerous committees and was previously secretary of the Board for the 2004-2005 term. He has worked in both academic and nonacademic hospitals and has served as a consultant to numerous hospitals in the development of hospital medicine programs.
Dr. Cawley received his Bachelor of Science in 1988 from the University of Scranton (Pa.) and his MD from Georgetown University School of Medicine in Washington, D.C. He completed an internal medicine residency at Duke University in Durham, N.C. Later this year, he will complete his MBA from the University of Massachusetts-Amherst.

SHM’s new secretary is Dr. Percelay. He is director of Virtua Inpatient Pediatrics, a large pediatric hospital medicine group in Southern New Jersey with 14 full-time hospitalists covering two hospitals. Since 1991, Dr. Percelay has worked in a variety of community-based settings including the general pediatric ward, pediatric sub-specialty units, pediatric intensive care unit (PICU), neonatal intensive care unit (NICU), and the emergency department.
A charter member of SHM and one of the nation’s first pediatric hospitalists, Dr. Percelay currently holds the Pediatric Seat on the SHM Board, in addition to serving on the Public Policy Committee and co-chairing the Pediatric Committee. He has been intimately involved in collaborative Pediatric hospital medicine projects such as the PRIS research network and the Denver 2005 and 2007 Pediatric Hospital Medicine conferences.
Dr. Percelay is also the founding chairperson and immediate past chair of the American Academy of Pediatrics Section on Hospital Medicine and co-authored the AAP policy statement on pediatric hospitalists. He completed his medical school and pediatric training at the University of California at San Francisco, along with an MPH at the University of California at Berkeley.
SHM congratulates these new officers and thanks our 2005 officers (Steve Pantilat, MD, president, William Atchley, MD, FACP, treasurer, and Lisa Kettering, MD, FACP, secretary) for their exemplary work.
Annual Meeting e-Community a Success
If the feedback from attendees at this year’s Annual Meeting was any indication, the inaugural launch of SHM’s Annual Meeting e-Community was a success.
Each year, SHM’s Annual Meeting provides an opportunity for hospital medicine professionals to network with colleagues and take advantage of more than 40 educational sessions during the course of three days.
While the location for the meeting changes regularly, there is a constant desire within the Annual Meeting planning committee (a group of volunteer members) to improve the attendee experience. The Annual Meeting e-Community (AMeC) was designed with that in mind.
The AMeC effectively extended the reach of the annual meeting both before and after the event. Since early April, attendees have been able to access the handouts for the presentations that were given at the event and network with colleagues thanks to dedicated discussion communities. There are also listings of exhibitors scheduled to be in attendance and general information about Washington, D.C., on the AMeC.
Because of the positive feedback received, the e-Community will stay online through early July, giving attendees the chance to download presentations from sessions that they didn’t attend and make contact with colleagues they met while in Washington, D.C.
Attendees appreciated the ability to access meeting materials prior to the event. “The Annual Meeting e-Community gave me a great opportunity to really plan out the sessions that I wanted to attend prior to the meeting,” says William Rifkin, MD, a hospitalist from the Yale School of Medicine.
According to Joy Wittnebert, AMeC project manager, the site was launched in response to feedback from past annual meetings. “Attendees have been consistently telling us that they want to be able to customize their experience and have more opportunities to network with colleagues before and after the event,” she says.
In the coming months, SHM staff will work with the Annual Meeting Committee to analyze additional feedback and begin making plans for the 2007 version of the site.
SHM Education Committee Launches 18-Month Strategic Plan
Helping our members and the hospital medicine community advance in professional growth and development has been on center stage as seen in the SHM Education Committee’s recent completion of an 18-month strategic plan. The plan is a framework designed to guide staff and volunteer leadership as they work to expand the society’s current slate of educational offerings. Inherent in the framework’s design is a focus on taking advantage of the myriad new channels that have come online for delivering educational content.
The plan is rooted primarily in the recently released Core Competencies in Hospital Medicine. The Core Competencies are a benchmark for the development of curricula within the hospital medicine specialty.
“One of the most exciting parts of this plan is its connection to the Core Competencies,” says Geri Barnes, SHM’s director of education and quality initiatives. “The connection means that this is one of the strongest educational plans that the society has put forward.”
A driving force in the creation of this plan was the committee’s desire to expand SHM’s educational offerings through a variety of technologic venues. “In the coming year, our educational offerings will truly become multi-dimensional,” says Scott Johnson, SHM’s director of information services. “As we expand into audio CDs, podcasts, and Web-based offerings, more hospitalists will be able to take advantage of these learning opportunities, which will have profound effects on the hospital medicine movement.”
With the education plan approved by SHM’s Board of Directors at its recent meeting, the Education Committee, chaired by Preetha Basaviah, MD, from Stanford University, will turn its attention to the first stage of implementation—a complete needs analysis. Some research has already taken place as part of SHM’s ongoing internal quality improvement processes.
“The key to the success of our plan is that we will be integrating feedback from hospitalists throughout North America as we move forward,” says Dr. Basaviah. “Ultimately, this kind of communication will ensure that we reach our primary goal: to provide tools and resources that help hospital medicine professionals improve the quality of care that they provide.”
Stay tuned to The Hospitalist for updates on the committee’s progress and an advanced look at new educational products.
Palliative Care: a Core Competency for Hospitalists
By Theresa Kristopaitis, MD, with input from Howard Epstein, MD, and the SHM Palliative Care Task Force
Palliative care is focused on the relief of suffering and support for the best quality of life for patients facing serious, life-threatening, or advanced illness, as well as their families. Palliative care is a general approach to healthcare that should be routinely integrated with disease modifying therapies. It is also a growing practice specialty for appropriately trained healthcare professionals dedicating their practice to the delivery of palliative care services.1
Optimally palliative care is delivered through an interdisciplinary team consisting of physicians, nurses, chaplains, social workers, pharmacists, as well as other disciplines as patient/family needs warrant. Models of palliative care delivery include hospital-based inpatient consultation services, inpatient palliative care units, outpatient and home-based consultation services, and ambulatory clinics. Hospitalists are ideally positioned to start inpatient palliative care services and reap the professional and institutional benefits that palliative care offers. Tools to develop a program can be obtained through the Center to Advance Palliative Care (www.capc.org).
A Core Competency
The skills gained from developing expertise in palliative care are indispensable to hospitalists—even if they don’t formally work with a palliative care team. Palliative care itself is identified as a healthcare systems core competency of hospital medicine.2 In addition, other hospital medicine competencies overlap with those key to palliative care: pain management, care of the elderly patient and vulnerable populations, communication, hospitalist as consultant, team approach and multidisciplinary care, transitions of care, and medical ethics.3 For some of the most challenging, yet common, inpatient clinical scenarios, palliative care and hospital practice can become indistinguishable.
Inpatient Scenarios: How Can Palliative Care Help?
Scenario 1: A patient on chronic long-acting opiate therapy is admitted to the hospital with complaints of pain, nausea, and vomiting.
The appropriate assessment and management of pain is a patient’s right and an institution’s responsibility, yet it is often inadequate.4 Many barriers to effective pain management have been identified, including limited physician undergraduate and graduate training.4,5 A fundamental goal of palliative care is pain relief. In turn, expertise in the pathophysiology of pain and safe prescribing of opioid, non-opioid, and adjuvant analgesics is critical for palliative care physicians. Palliative care training and resources focus on principles of analgesic pharmacology, equianalgesia, changing routes of administration, control of continuous and breakthrough pain, opioid rotation, and adverse effects of analgesics. A comprehensive introduction to the fundamentals of pain management can be obtained via Education on Palliative and End of Life Care (www.epec.net.) Pain Management Module.
Non-pain symptoms can be as troubling for patients with advanced illness as pain. The formal assessment, reassessment, and management of common symptoms, including nausea, vomiting, dyspnea, constipation, fatigue, and delirium, are a primary domain of palliative medicine. Nausea and vomiting, for example, can become a demoralizing symptom complex. Stimuli to the vomiting center can arise from the cerebral cortex, vestibular apparatus, chemoreceptor zone, and gastrointestinal tract resulting in a broad etiologic differential diagnosis.
With a solid understanding of its pathogenesis and pharmacologic and non-pharmacologic therapeutic principles, nausea and vomiting can be treated in the vast majority of patients. Multiple agents addressing multiple mechanisms may be required. Even the nausea associated with complete bowel obstruction often can be successfully palliated, without the use of nasogastric tubes or surgery.6 The End of Life/Palliative Education Resource Center (www.eperc.mcw.edu) is one of many resources with tools to improve a hospitalist’s evaluation and treatment of non-pain physical symptoms.
Scenario 2: A patient with advanced heart failure and his family are overwhelmed by differing consultant opinions on the appropriateness of implantable cardioverter defibrillator (ICD) insertion.
Effective communication with patients is a core responsibility of both hospitalists and palliative care physicians. A complementary—and at times challenging—skill is the ability to promote communication and consensus about care among multiple specialist consultants. Ripamonti and colleagues write, “Almost invariably, the act of communication is an important part of therapy: Occasionally it is the only constituent. It usually requires greater thought and planning than a drug prescription, and unfortunately it is commonly administered in subtherapeutic doses.”6
The American Academy of Hospice and Palliative Medicine UNIPAC series is a resource for physicians to hone their general communication skills, as well as those more specific to palliative care, such as sharing news (often bad) with patients and families and engaging in therapeutic dialogue.8
Palliative care begins with establishing the goals of care with a patient.9 All physicians bring great value to patient care when they are skilled at negotiating goals of care. There are numerous possible goals of care, from prevention, to cure, to prolongation of life, to achieving a good death. Ideally, goals of care should be discussed with patients and families as early as possible in the course of a serious, life-threatening illness. Establishing realistic and attainable goals of care assumes increased importance in the setting of advanced disease, where treatments intended to prolong life may become more burdensome than beneficial.9
As the reader may have experienced, too often these discussions have not taken place or are held late in the trajectory of illness, such as when patients are hospitalized for severe progressive disease or are facing imminent death.10 In the scenario of potential ICD insertion, conversations with patients to clarify device-specific goals are best accomplished before they are placed and in the context of a broader discussion of the patient’s general medical condition and overall goals for care.11 This type of discussion ultimately improves the informed consent process for ICDs and other technologies. ICD recipients should be guided to periodically revisit their goals, particularly when their health status significantly changes.11 Unlike for initial ICD placement, there are no guidelines for disabling already implanted ICDs. The opportunity to discuss this issue with a patient before a crisis or before they lose decision-making capacity is frequently lost and occurs all too often at life’s end.12
Scenario 3: An elderly debilitated woman with advanced cervical cancer has been hospitalized six times in the past two months. She is cared for at home. Her family is tired but they are doing “the best they can.” She is brought to the emergency department again with weakness.
Effective implementation of care management strategies for patients with life-threatening and advanced disease requires assessment of their physical, social, emotional, and spiritual concerns.1 Similarly, family caregivers have their own—often unvoiced—biopsychosocial stressors.13 Physicians directing patient care must appreciate the significance of these multiple issues, even if they are not comfortable or are ill-equipped to handle them on their own. The power of the interdisciplinary palliative care model is that team members evaluate the patient from different perspectives and pool their expertise in addressing the complex needs of their patients and families.8
In some multidisciplinary models, the onus may lie on the physician to recognize the patient and family needs and mobilize the appropriate resources. Coordination of care at home for patients in the later stages of chronic illness may seem daunting during hospital stays. However, by employing measures utilized by palliative care teams, such as reviewing the goals of care, introducing community resources to help patients and families manage at home, providing anticipatory grief and bereavement support, and considering hospice referral, discharge planning and transitions in care can be much more sustainable.14 With these interventions, patients, families, physicians, and hospitals all benefit.
Conclusion
Hospital-based palliative care programs are growing exponentially.15 Hospitalists are in a unique position to continue their development. Even if the time or circumstances are not yet right for you to become a part of a formal palliative care program, there are daily opportunities to reap rewards from the knowledge, attitudes, and skills that palliative care training offers.
References
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available at www.nationalconsensusproject.org. Last accessed April 28, 2006.
- Pistoria MJ, Amin AN, Dressler DD, et al. The core competencies in hospital medicine. J Hosp Med. 2006;1:2(S1).
- American Board of Hospice and Palliative Medicine. Available at www.abhpm.org. Last accessed April 28, 2006.
- Phillips DM. JCAHO pain management standards unveiled. JAMA. 2000;284:428-429.
- Sullivan AM, Lakoma MD, Block SD. The status of medical education in end-of-life care: a national report. J Gen Intern Med. 2003;18:685-695.
- Ripamonti C, De Conno F, Ventafridda V, et al. Management of bowel obstruction in advanced and terminal cancer patients. Ann Oncol. 1993 Jan;4(1):15-21.
- Buckman R. Communication in palliative care: a practical guide. In: Doyle D, Hanks GWC, MacDonald N, eds. Oxford Textbook of Palliative Medicine. New York: Oxford Community Press; 1993:47-61.
- Storey P, Knight CF. UNIPAC five—caring for the terminally ill—communication and the physician’s role in the interdisciplinary team. In: Hospice/Palliative Care Training for Physicians—A Self Study Program. New York: Mary Ann Liebert; 2003:1-147.
- Morrison RS, Meier DE. Palliative care. NEJM. 2004;350:2582-2590.
- Quill TE. Initiating end of life discussion with seriously ill patients: addressing the “elephant in the room.” JAMA. 2000;284:2502-2507.
- Berger, JT. The ethics of deactivating implanted cardioverter defibrillators. Ann Intern Med. 2005;142:631-634.
- Goldstein NE, Lampert R, Bradely E, et al. Management of implantable cardioverter defibrillators in end-of-life care. Ann Intern Med. 2004;141:835-838.
- Levine C. The loneliness of the long-term caregiver. NEJM. 1999;340:1587-1590.
- Meier D. Palliative care in hospitals. J Hosp Med. 2006;1:21-28.
- Morrison RS, et al. The growth of palliative care programs in United States hospitals. J Pall Med. 2006; 8 (6):1127-1133.
Get a Job!
SHM Launches the first-ever career Web site exclusively for hospitalists
By Jeannette Wick
Job boards—Internet sites designed to allow employers and prospective employees to find each other electronically—are among the most active Internet sites. For many job seekers Monster.com, CareerBuilder.com, and Indeed.com (among others) have become essential job search tools. Until now, however, no site has catered to healthcare professionals in general—much less to hospitalists in particular.
Thanks to the new SHM Career Center (http://hospitalmedicine.org/careercenter), though, things are about to change. The Career Center is part of a comprehensive, “cradle-to-grave” approach SHM is taking to assist hospital medicine professionals in their career development pursuits. The site offers numerous advantages over traditional job-hunting tools, such as classified advertisements, personal contacts, and randomly mailing resumes to interesting employers—advantages such as the ability to post your resume in a searchable database, a database of open positions across North America that you can search using a variety of variables and the opportunity to receive a notification when a job that matches your criteria is posted online.
The Career Center also represents an improvement over general job boards because the pool of positions offered and solicited on the site is restricted to those only for hospital medicine professionals. The site is free for all, although SHM members are able to take advantage of certain “members-only” functionality (resume posting, e-mail notification of new job postings). “Career opportunists,” or hospitalists who are gainfully employed but constantly curious about what else is available, will enjoy this site, too.
The Way it Works
SHM’s Career Center matches applicants and jobs using search features that allow applicants to tailor their search. As an applicant, you enter your job preferences as you would when searching for an article in PubMed or when looking online for a board-certified specialist in a specific geographic region when referring a patient. The boxes prompt you to provide the minimum information necessary for an acceptable search. For example, you need to provide geographical preferences, the type of position you’re looking for, and the specialty area you’re interested in to best tailor your search.
Visitors can browse all jobs by specialty or state—or view the complete list of jobs. The advanced search option augments the specialty and state fields with the ability to specify keywords (see “Hospitalists and Keywords,” p. 10), specialty, employment type (full time, moonlighting, and so on), and the announcement opening date. (The latter is important to applicants who believe older announcements raise a red flag indicating conditions that make it unattractive to candidates.)
The advanced search option also allows you to look at job summaries with the results. So instead of receiving a simple list of the job title, the location, and the announcement date, the summary includes a short description of the position. But visitor beware: You have to click a box to make this happen. Otherwise, your search will create a simple list of jobs, and clicking on any individual job will bring up the job summary. The information is accessible either way.
Get Started
Most job seekers will find the site quite easy to navigate, although a few may be impeded by cookies. (For more information, see “Got Cookies,” p. 10.) The FAQ area is a site strength and will help you eliminate hurdles, from inability to navigate the site, to figuring out how to be notified electronically when new jobs are added.
Once you enter your search criteria, a list of jobs displays. Then click on a specific job to open another page describing the position in great detail. After seeing the array of positions available, SHM non-members are likely to join the society just to have access to the full functionality of the Career Center.
Your next step is to create an account; doing so allows you to apply for positions with just a click. Once you establish an account (a process that takes just a few minutes), click on “Edit My Profile.” In this area, you’ll establish your profile.
Meat and Potatoes: Post Your Resume
The Career Center’s features are state-of-the-art. You can create a resume and a cover letter. To post your resume in “My Account,” for example, select “Post My Resume,” then “Document Management,” and then “Resume.” You’ll need to open a plain text version (no bold, underlining, italics, or bullets) of your current resume on your computer, and then copy your resume to the clipboard.
Never done this before? Here again, you can open a guidance window or a printable FAQ to walk you through the process. Two minor system limitations appear here: You must click a box to make the text wrap automatically, and the site has no spell-check function. You have to spell check your cover letter and resume before you copy and paste. If you edit your text at any time while in the Career Center boxes, then be sure to proofread to ensure you haven’t introduced any errors. After you create your resume, you can open a text version (a file that ends in the suffix .txt) to see how employers will view it.
In the past, hospital medicine applicants could stand out with a well-formatted resume on quality paper. Online documents force every applicant’s information into the same mold, and this often concerns applicants. Will a skilled, tri-lingual, well-published hospitalist look like every other applicant when an employer is looking at a simple text version of your resume?
The Career Center allows you to upload up to three formatted documents that can be attached to applications. If you are unable to upload your documents, you may e-mail them to the site, which will then attach them to your account. Some applicants find it useful to have two specific types of resumes on hand: a traditional reverse chronological resume that emphasizes experience, and a less structured functional resume that describes transferable skills.
Depending on your computer savvy, the time it takes to set up your account and load your resume will vary. Hospitalists with robust skills may be able to load a resume in fewer than 30 minutes, but it may take longer for others. Regardless, the return on investment is large because the information you enter will form the foundation of your materials that a perspective employer will review. Once your resume is loaded, applying for a position only requires a few clicks.
Benefits That Make Your Search Sizzle
If you are an SHM member, the “Job Agent” functionality allows you to receive weekly updates of new jobs added that match your search criteria. (Note: You can join SHM online through the Career Center or by visiting www.joinshm.org) This function is located in your account. It allows you to specify the date you would like to stop receiving notification e-mails. Your account also tracks applications submitted.
After you log in, click “Job Applications” to display any jobs you have applied for and the date that the application was submitted. When a job posting expires (according to a pre-established date set by the employer) a strikethrough line will appear through the job application. Applications remain in your account for 90 days from the submission date. Clicking on the “Apply for this Job” icon opens a new screen, and it allows applicants to edit applications even after you’ve sent it and until the job posting closes. Once the job posting is closed, no application changes can be made.
Employers post their vacancies for 30 days at a time, and they can select packages that include print advertisements in The Hospitalist and/or the Journal of Hospital Medicine. Approximately 85% of employers who advertise in print media also advertise on the Career Center, although a few advertise only on the Career Center. To cover your bases, look in all three places.
Just as some applicants prefer anonymity, some companies choose to list their ads confidentially. In these cases, you will submit your online application, and the employer will contact you via the system with more information if you are a good match.
Employer responses will be forwarded to your e-mail account through the Career Center. Once you begin talking with a prospective employer, it is up to you to use good research and interview skills to ensure that this is indeed a good match. When you find a position, you can remove your resume from circulation. Or, you can store it in the Career Center database for future opportunities by clicking “No, do not post my resume.”
Alternatively, you can remove your information from the database permanently: Go to “My Account” and select “Delete Account.”
What the Future Holds
SHM’s information services team will keep tabs on the recently launched SHM Career Center Web site and invites user feedback—specifically any demographic information that will help them build the most practical, useful career site for hospitalists.
With the average age of a hospitalist about 37, SHM expects that visitors and users to comprise a youthful, computer savvy group. Eventually, SHM wants to expand the site so it tells you more than just what jobs are available (e.g., how to create a resume, interview techniques, and how to build desirable hospital medicine skill sets). They will also track how many employer-employee matches are made using the Career Center.
Conclusion
When unemployment is low, as it most certainly is for hospitalists, leverage rests with job seekers, not employers. While employers are looking for talent and availability, career opportunists crave convenience. The SHM Career Center represents the most comprehensive collection of hospitalist opportunities available on the Internet.
Users will find site navigation easy, and prompts and cues offered by the site designers clear and accurate. Traffic on the site is expected to grow quickly as it becomes what SHM hopes is the most indispensable tool for hospitalists conducting job searches.TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
SHM: BEHIND THE SCENES
Membership: Listen, Then Act
By Todd Von Deak

As I write this column, there are only seven days left before the start of this year’s annual meeting. At last check, more 1,100 hospital medicine professionals were registered to join us in Washington, D.C., for the most important meeting in hospital medicine. Our office is abuzz with activity and last minute preparations. I’m sure there’s something else that I’m supposed to be doing right now, but I need the break.
While I take my break and write, I can’t help but think, “what’s next,” once the Annual Meeting is over? SHM is fast approaching the start of a new fiscal year, and, like any membership director, I am eager to hit the ground running.
The more I reflect on what’s next, the more I realize that part of my answer lies within the pages of The Hospitalist. Our research continues to show that you consider The Hospitalist to be one of the most valuable benefits of membership.
What strikes me as I read through past issues is that we have another story to tell. So this month we’re launching “SHM: Behind the Scenes.”
There are many reasons why we need to share this story. Key to those reasons is the fact that our sole purpose is to serve the hospital medicine community. You entrust us with your dues and meeting registrations to provide resources that will enable you to better serve your patients and grow your careers in the process. So it’s important that we, the staff, tell you firsthand what we are doing with your investment, and how we plan on continuing to earn your trust in the years to come.
Each month a different member of our senior staff will take turns writing this column. During the coming year you’ll hear from the heads of education and quality initiatives, business operations, membership, information services, marketing, legislative affairs, and research. In each column you’ll find a mix of current news, future plans, and tips for maximizing the value of your membership. If we do our jobs correctly, each month you will have a clearer picture on the true return of your membership investment.
We want you to clearly understand why—if you only belong to one organization—it has to be SHM.
This month I’ll focus on membership and our plans for the coming year. (See below.) Next month you’ll hear from Scott Johnson, SHM’s director of information services. Scott is our chief technologist in many ways and is leading the charge to use today’s latest technology to expand the reach of our educational products and enhance your membership investment as well.
Each year, membership departments at non-profit organizations write their strategic plans for the coming year. SHM is no exception.
For most, these strategic plans are based on a set of assumptions. In more offices than you’d like to believe, the staff just sits around and makes their best guesses in order to answer critical questions, including “what do members want to get out of their membership?”
Based on these guesses, the staff then plots their course expansion and enhances the benefits and services that the organization offers. These organizations are doomed to mediocrity.
Successful organizations, including SHM, actively seek to better understand their membership and use a variety of media to get to the heart of the questions that matter. I am proud to say that SHM is among the second group.
Building on previous efforts, the SHM Membership Department has been actively engaged in a “listening tour.” Our goal is to not rely on assumptions but rather to use your feedback in formulating our plans for the coming year.
Here’s some of what we’ve identified.
Top reasons for being a member:
- Education and quality improvement resources;
- The ability to affect the hospital medicine movement; and
- Subscriptions to The Hospitalist and Journal of Hospital Medicine.
Your main goals as a member:
- To learn from educational and quality improvement resources;
- Take advantage of networking opportunities; and
- Gain exposure for career advancement.
The benefits of membership that matter most:
- Information on www.hospitalmedicine.org;
- Access to results from SHM’s “Authoritative Source on the State of the Hospital Medicine Movement;” and
- The Hospitalist.
We’re already using this data, along with other information that we’ve gathered, to enhance the SHM experience and increase the return on your investment. Just look at the new SHM Career Center (www.hospitalmedicine.org/careercenter).
Like any good membership department, we realize that our data collection has just begun. So I’d like to pose a couple of questions:
- Do you agree with our findings?
- Should we offer a new benefit of membership?
- What can we do to enhance your SHM experience?
I’d love to hear your thoughts. Send them to me via e-mail at tvondeak@hospitalmedicine.org. Anyone who e-mails will be entered in a prize drawing.
In my next column, I will share a selection of the responses I receive and tell you the concrete steps we’re taking to improve communication with you and other members.
Von Deak is SHM’s director of membership and marketing.
Each year a new team of SHM officers is elected to lend their wisdom, time, experience, and skills in a collaborative effort to help manage the business of our organization, drive new initiatives, and support the society’s mission. At this year’s annual meeting in Washington, D.C., we again witnessed that familiar changing of the guard with the following inductions:
- President Mary Jo Gorman, MD, MBA;
- President-Elect Russell Holman, MD;
- Treasurer Patrick Cawley, MD; and
- Secretary Jack Percelay, MD, MPH.
“Hospitalists are squarely in the spotlight today on key issues affecting patient care, quality of hospital care, hospital leadership, and other concerns. So it is important that we have a strong, hands-on leadership team that is committed to continuing the positive momentum SHM has generated for hospitalists,” says Larry Wellikson, MD, FACP, CEO of SHM. “I couldn’t be more thrilled with our slate of newly appointed officers. Time and again through the years Mary Jo, Rusty, Pat, and Jack have proven that they are active participants, and that they are leaders who will rise to the occasion to help us meet our objectives.”
Dr. Gorman, a charter member of SHM, has been a practicing hospitalist since 1997, when she founded the first hospitalist practice in St. Louis. In early 1999, her group merged into IPC—The Hospitalist Company and grew to become the dominant hospitalist group in the city. In 2001, Dr. Gorman was promoted to vice-president of medical affairs for IPC, responsible for the design and implementation of company-wide programs involving business development, recruitment, physician training, and operations in all of IPC’s markets. In 2003, she was named chief medical officer and today works with more than 300 physicians nationwide to develop programs and strategies that enhance clinical performance and drive the delivery system towards more efficient care and greater patient satisfaction. She also oversees IPC’s physician training, mentoring and retention programs, as well as IPC’s call center nurses, healthcare services and clinical studies.
A cum laude graduate of St. Louis University, Dr. Gorman earned a BA in Chemistry/Biology in 1981, then went on to earn her MD in 1984 from Southern Illinois University School of Medicine in Springfield. In 1996, she earned a MBA from Washington University, Olin School of Business, in St. Louis.
SHM’s new President-Elect Dr. Holman is senior vice president and national medical director for Cogent Healthcare, an organization that manages hospital medicine programs throughout the country. He is responsible for program implementation and management, quality systems reporting and auditing, physician leadership development, and data systems integration. Formerly, Dr. Holman was the medical director of Hospital Services for HealthPartners Medical Group & Clinics, part of HealthPartners, Inc. in Minnesota. There he also was the founder and director of the HPMG Fellowship Program in Hospital Medicine.
A long-time member of SHM, Dr. Holman served on the Board of Directors as treasurer from 2004-2005. He was previously chair of the Leadership Development Committee, chair of the Midwest Council, course director of the SHM Leadership Academy, and a member of the Public Policy Committee. In February 2006 he co-authored the “Update in Hospital Medicine,” which appeared in Annals of Internal Medicine. In 2002, he received the SHM Award for Outstanding Service in Hospital Medicine.
Through the years, Dr. Holman’s commitment to hospital medicine has helped produce nationally recognized standards in the areas of quality improvement activities, models of medical education, observation units, communication systems, compensation plans, case management, surgical co-management collaborations, and patient flow initiatives. Dr. Holman serves on two national editorial boards for medical publications and is currently co-authoring a comprehensive textbook and electronic decision support tool in hospital medicine.
Dr. Holman earned his MD from Washington University School of Medicine in St. Louis and trained as a resident and chief medical resident at the University of Minnesota in Minneapolis.
New Treasurer Dr. Cawley is a hospitalist at the Medical University of South Carolina in Charleston, where he currently serves as interim executive medical director of MUSC Medical Center. He previously served as the chief of the Section of Hospital Medicine, vice chairman of clinical affairs in the Department of Medicine, and associate executive medical director at MUSC Medical Center.
A charter member of SHM, Dr. Cawley has served on numerous committees and was previously secretary of the Board for the 2004-2005 term. He has worked in both academic and nonacademic hospitals and has served as a consultant to numerous hospitals in the development of hospital medicine programs.
Dr. Cawley received his Bachelor of Science in 1988 from the University of Scranton (Pa.) and his MD from Georgetown University School of Medicine in Washington, D.C. He completed an internal medicine residency at Duke University in Durham, N.C. Later this year, he will complete his MBA from the University of Massachusetts-Amherst.
SHM’s new secretary is Dr. Percelay. He is director of Virtua Inpatient Pediatrics, a large pediatric hospital medicine group in Southern New Jersey with 14 full-time hospitalists covering two hospitals. Since 1991, Dr. Percelay has worked in a variety of community-based settings including the general pediatric ward, pediatric sub-specialty units, pediatric intensive care unit (PICU), neonatal intensive care unit (NICU), and the emergency department.
A charter member of SHM and one of the nation’s first pediatric hospitalists, Dr. Percelay currently holds the Pediatric Seat on the SHM Board, in addition to serving on the Public Policy Committee and co-chairing the Pediatric Committee. He has been intimately involved in collaborative Pediatric hospital medicine projects such as the PRIS research network and the Denver 2005 and 2007 Pediatric Hospital Medicine conferences.
Dr. Percelay is also the founding chairperson and immediate past chair of the American Academy of Pediatrics Section on Hospital Medicine and co-authored the AAP policy statement on pediatric hospitalists. He completed his medical school and pediatric training at the University of California at San Francisco, along with an MPH at the University of California at Berkeley.
SHM congratulates these new officers and thanks our 2005 officers (Steve Pantilat, MD, president, William Atchley, MD, FACP, treasurer, and Lisa Kettering, MD, FACP, secretary) for their exemplary work.
Annual Meeting e-Community a Success
If the feedback from attendees at this year’s Annual Meeting was any indication, the inaugural launch of SHM’s Annual Meeting e-Community was a success.
Each year, SHM’s Annual Meeting provides an opportunity for hospital medicine professionals to network with colleagues and take advantage of more than 40 educational sessions during the course of three days.
While the location for the meeting changes regularly, there is a constant desire within the Annual Meeting planning committee (a group of volunteer members) to improve the attendee experience. The Annual Meeting e-Community (AMeC) was designed with that in mind.
The AMeC effectively extended the reach of the annual meeting both before and after the event. Since early April, attendees have been able to access the handouts for the presentations that were given at the event and network with colleagues thanks to dedicated discussion communities. There are also listings of exhibitors scheduled to be in attendance and general information about Washington, D.C., on the AMeC.
Because of the positive feedback received, the e-Community will stay online through early July, giving attendees the chance to download presentations from sessions that they didn’t attend and make contact with colleagues they met while in Washington, D.C.
Attendees appreciated the ability to access meeting materials prior to the event. “The Annual Meeting e-Community gave me a great opportunity to really plan out the sessions that I wanted to attend prior to the meeting,” says William Rifkin, MD, a hospitalist from the Yale School of Medicine.
According to Joy Wittnebert, AMeC project manager, the site was launched in response to feedback from past annual meetings. “Attendees have been consistently telling us that they want to be able to customize their experience and have more opportunities to network with colleagues before and after the event,” she says.
In the coming months, SHM staff will work with the Annual Meeting Committee to analyze additional feedback and begin making plans for the 2007 version of the site.
SHM Education Committee Launches 18-Month Strategic Plan
Helping our members and the hospital medicine community advance in professional growth and development has been on center stage as seen in the SHM Education Committee’s recent completion of an 18-month strategic plan. The plan is a framework designed to guide staff and volunteer leadership as they work to expand the society’s current slate of educational offerings. Inherent in the framework’s design is a focus on taking advantage of the myriad new channels that have come online for delivering educational content.
The plan is rooted primarily in the recently released Core Competencies in Hospital Medicine. The Core Competencies are a benchmark for the development of curricula within the hospital medicine specialty.
“One of the most exciting parts of this plan is its connection to the Core Competencies,” says Geri Barnes, SHM’s director of education and quality initiatives. “The connection means that this is one of the strongest educational plans that the society has put forward.”
A driving force in the creation of this plan was the committee’s desire to expand SHM’s educational offerings through a variety of technologic venues. “In the coming year, our educational offerings will truly become multi-dimensional,” says Scott Johnson, SHM’s director of information services. “As we expand into audio CDs, podcasts, and Web-based offerings, more hospitalists will be able to take advantage of these learning opportunities, which will have profound effects on the hospital medicine movement.”
With the education plan approved by SHM’s Board of Directors at its recent meeting, the Education Committee, chaired by Preetha Basaviah, MD, from Stanford University, will turn its attention to the first stage of implementation—a complete needs analysis. Some research has already taken place as part of SHM’s ongoing internal quality improvement processes.
“The key to the success of our plan is that we will be integrating feedback from hospitalists throughout North America as we move forward,” says Dr. Basaviah. “Ultimately, this kind of communication will ensure that we reach our primary goal: to provide tools and resources that help hospital medicine professionals improve the quality of care that they provide.”
Stay tuned to The Hospitalist for updates on the committee’s progress and an advanced look at new educational products.
Palliative Care: a Core Competency for Hospitalists
By Theresa Kristopaitis, MD, with input from Howard Epstein, MD, and the SHM Palliative Care Task Force
Palliative care is focused on the relief of suffering and support for the best quality of life for patients facing serious, life-threatening, or advanced illness, as well as their families. Palliative care is a general approach to healthcare that should be routinely integrated with disease modifying therapies. It is also a growing practice specialty for appropriately trained healthcare professionals dedicating their practice to the delivery of palliative care services.1
Optimally palliative care is delivered through an interdisciplinary team consisting of physicians, nurses, chaplains, social workers, pharmacists, as well as other disciplines as patient/family needs warrant. Models of palliative care delivery include hospital-based inpatient consultation services, inpatient palliative care units, outpatient and home-based consultation services, and ambulatory clinics. Hospitalists are ideally positioned to start inpatient palliative care services and reap the professional and institutional benefits that palliative care offers. Tools to develop a program can be obtained through the Center to Advance Palliative Care (www.capc.org).
A Core Competency
The skills gained from developing expertise in palliative care are indispensable to hospitalists—even if they don’t formally work with a palliative care team. Palliative care itself is identified as a healthcare systems core competency of hospital medicine.2 In addition, other hospital medicine competencies overlap with those key to palliative care: pain management, care of the elderly patient and vulnerable populations, communication, hospitalist as consultant, team approach and multidisciplinary care, transitions of care, and medical ethics.3 For some of the most challenging, yet common, inpatient clinical scenarios, palliative care and hospital practice can become indistinguishable.
Inpatient Scenarios: How Can Palliative Care Help?
Scenario 1: A patient on chronic long-acting opiate therapy is admitted to the hospital with complaints of pain, nausea, and vomiting.
The appropriate assessment and management of pain is a patient’s right and an institution’s responsibility, yet it is often inadequate.4 Many barriers to effective pain management have been identified, including limited physician undergraduate and graduate training.4,5 A fundamental goal of palliative care is pain relief. In turn, expertise in the pathophysiology of pain and safe prescribing of opioid, non-opioid, and adjuvant analgesics is critical for palliative care physicians. Palliative care training and resources focus on principles of analgesic pharmacology, equianalgesia, changing routes of administration, control of continuous and breakthrough pain, opioid rotation, and adverse effects of analgesics. A comprehensive introduction to the fundamentals of pain management can be obtained via Education on Palliative and End of Life Care (www.epec.net.) Pain Management Module.
Non-pain symptoms can be as troubling for patients with advanced illness as pain. The formal assessment, reassessment, and management of common symptoms, including nausea, vomiting, dyspnea, constipation, fatigue, and delirium, are a primary domain of palliative medicine. Nausea and vomiting, for example, can become a demoralizing symptom complex. Stimuli to the vomiting center can arise from the cerebral cortex, vestibular apparatus, chemoreceptor zone, and gastrointestinal tract resulting in a broad etiologic differential diagnosis.
With a solid understanding of its pathogenesis and pharmacologic and non-pharmacologic therapeutic principles, nausea and vomiting can be treated in the vast majority of patients. Multiple agents addressing multiple mechanisms may be required. Even the nausea associated with complete bowel obstruction often can be successfully palliated, without the use of nasogastric tubes or surgery.6 The End of Life/Palliative Education Resource Center (www.eperc.mcw.edu) is one of many resources with tools to improve a hospitalist’s evaluation and treatment of non-pain physical symptoms.
Scenario 2: A patient with advanced heart failure and his family are overwhelmed by differing consultant opinions on the appropriateness of implantable cardioverter defibrillator (ICD) insertion.
Effective communication with patients is a core responsibility of both hospitalists and palliative care physicians. A complementary—and at times challenging—skill is the ability to promote communication and consensus about care among multiple specialist consultants. Ripamonti and colleagues write, “Almost invariably, the act of communication is an important part of therapy: Occasionally it is the only constituent. It usually requires greater thought and planning than a drug prescription, and unfortunately it is commonly administered in subtherapeutic doses.”6
The American Academy of Hospice and Palliative Medicine UNIPAC series is a resource for physicians to hone their general communication skills, as well as those more specific to palliative care, such as sharing news (often bad) with patients and families and engaging in therapeutic dialogue.8
Palliative care begins with establishing the goals of care with a patient.9 All physicians bring great value to patient care when they are skilled at negotiating goals of care. There are numerous possible goals of care, from prevention, to cure, to prolongation of life, to achieving a good death. Ideally, goals of care should be discussed with patients and families as early as possible in the course of a serious, life-threatening illness. Establishing realistic and attainable goals of care assumes increased importance in the setting of advanced disease, where treatments intended to prolong life may become more burdensome than beneficial.9
As the reader may have experienced, too often these discussions have not taken place or are held late in the trajectory of illness, such as when patients are hospitalized for severe progressive disease or are facing imminent death.10 In the scenario of potential ICD insertion, conversations with patients to clarify device-specific goals are best accomplished before they are placed and in the context of a broader discussion of the patient’s general medical condition and overall goals for care.11 This type of discussion ultimately improves the informed consent process for ICDs and other technologies. ICD recipients should be guided to periodically revisit their goals, particularly when their health status significantly changes.11 Unlike for initial ICD placement, there are no guidelines for disabling already implanted ICDs. The opportunity to discuss this issue with a patient before a crisis or before they lose decision-making capacity is frequently lost and occurs all too often at life’s end.12
Scenario 3: An elderly debilitated woman with advanced cervical cancer has been hospitalized six times in the past two months. She is cared for at home. Her family is tired but they are doing “the best they can.” She is brought to the emergency department again with weakness.
Effective implementation of care management strategies for patients with life-threatening and advanced disease requires assessment of their physical, social, emotional, and spiritual concerns.1 Similarly, family caregivers have their own—often unvoiced—biopsychosocial stressors.13 Physicians directing patient care must appreciate the significance of these multiple issues, even if they are not comfortable or are ill-equipped to handle them on their own. The power of the interdisciplinary palliative care model is that team members evaluate the patient from different perspectives and pool their expertise in addressing the complex needs of their patients and families.8
In some multidisciplinary models, the onus may lie on the physician to recognize the patient and family needs and mobilize the appropriate resources. Coordination of care at home for patients in the later stages of chronic illness may seem daunting during hospital stays. However, by employing measures utilized by palliative care teams, such as reviewing the goals of care, introducing community resources to help patients and families manage at home, providing anticipatory grief and bereavement support, and considering hospice referral, discharge planning and transitions in care can be much more sustainable.14 With these interventions, patients, families, physicians, and hospitals all benefit.
Conclusion
Hospital-based palliative care programs are growing exponentially.15 Hospitalists are in a unique position to continue their development. Even if the time or circumstances are not yet right for you to become a part of a formal palliative care program, there are daily opportunities to reap rewards from the knowledge, attitudes, and skills that palliative care training offers.
References
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available at www.nationalconsensusproject.org. Last accessed April 28, 2006.
- Pistoria MJ, Amin AN, Dressler DD, et al. The core competencies in hospital medicine. J Hosp Med. 2006;1:2(S1).
- American Board of Hospice and Palliative Medicine. Available at www.abhpm.org. Last accessed April 28, 2006.
- Phillips DM. JCAHO pain management standards unveiled. JAMA. 2000;284:428-429.
- Sullivan AM, Lakoma MD, Block SD. The status of medical education in end-of-life care: a national report. J Gen Intern Med. 2003;18:685-695.
- Ripamonti C, De Conno F, Ventafridda V, et al. Management of bowel obstruction in advanced and terminal cancer patients. Ann Oncol. 1993 Jan;4(1):15-21.
- Buckman R. Communication in palliative care: a practical guide. In: Doyle D, Hanks GWC, MacDonald N, eds. Oxford Textbook of Palliative Medicine. New York: Oxford Community Press; 1993:47-61.
- Storey P, Knight CF. UNIPAC five—caring for the terminally ill—communication and the physician’s role in the interdisciplinary team. In: Hospice/Palliative Care Training for Physicians—A Self Study Program. New York: Mary Ann Liebert; 2003:1-147.
- Morrison RS, Meier DE. Palliative care. NEJM. 2004;350:2582-2590.
- Quill TE. Initiating end of life discussion with seriously ill patients: addressing the “elephant in the room.” JAMA. 2000;284:2502-2507.
- Berger, JT. The ethics of deactivating implanted cardioverter defibrillators. Ann Intern Med. 2005;142:631-634.
- Goldstein NE, Lampert R, Bradely E, et al. Management of implantable cardioverter defibrillators in end-of-life care. Ann Intern Med. 2004;141:835-838.
- Levine C. The loneliness of the long-term caregiver. NEJM. 1999;340:1587-1590.
- Meier D. Palliative care in hospitals. J Hosp Med. 2006;1:21-28.
- Morrison RS, et al. The growth of palliative care programs in United States hospitals. J Pall Med. 2006; 8 (6):1127-1133.
Get a Job!
SHM Launches the first-ever career Web site exclusively for hospitalists
By Jeannette Wick
Job boards—Internet sites designed to allow employers and prospective employees to find each other electronically—are among the most active Internet sites. For many job seekers Monster.com, CareerBuilder.com, and Indeed.com (among others) have become essential job search tools. Until now, however, no site has catered to healthcare professionals in general—much less to hospitalists in particular.
Thanks to the new SHM Career Center (http://hospitalmedicine.org/careercenter), though, things are about to change. The Career Center is part of a comprehensive, “cradle-to-grave” approach SHM is taking to assist hospital medicine professionals in their career development pursuits. The site offers numerous advantages over traditional job-hunting tools, such as classified advertisements, personal contacts, and randomly mailing resumes to interesting employers—advantages such as the ability to post your resume in a searchable database, a database of open positions across North America that you can search using a variety of variables and the opportunity to receive a notification when a job that matches your criteria is posted online.
The Career Center also represents an improvement over general job boards because the pool of positions offered and solicited on the site is restricted to those only for hospital medicine professionals. The site is free for all, although SHM members are able to take advantage of certain “members-only” functionality (resume posting, e-mail notification of new job postings). “Career opportunists,” or hospitalists who are gainfully employed but constantly curious about what else is available, will enjoy this site, too.
The Way it Works
SHM’s Career Center matches applicants and jobs using search features that allow applicants to tailor their search. As an applicant, you enter your job preferences as you would when searching for an article in PubMed or when looking online for a board-certified specialist in a specific geographic region when referring a patient. The boxes prompt you to provide the minimum information necessary for an acceptable search. For example, you need to provide geographical preferences, the type of position you’re looking for, and the specialty area you’re interested in to best tailor your search.
Visitors can browse all jobs by specialty or state—or view the complete list of jobs. The advanced search option augments the specialty and state fields with the ability to specify keywords (see “Hospitalists and Keywords,” p. 10), specialty, employment type (full time, moonlighting, and so on), and the announcement opening date. (The latter is important to applicants who believe older announcements raise a red flag indicating conditions that make it unattractive to candidates.)
The advanced search option also allows you to look at job summaries with the results. So instead of receiving a simple list of the job title, the location, and the announcement date, the summary includes a short description of the position. But visitor beware: You have to click a box to make this happen. Otherwise, your search will create a simple list of jobs, and clicking on any individual job will bring up the job summary. The information is accessible either way.
Get Started
Most job seekers will find the site quite easy to navigate, although a few may be impeded by cookies. (For more information, see “Got Cookies,” p. 10.) The FAQ area is a site strength and will help you eliminate hurdles, from inability to navigate the site, to figuring out how to be notified electronically when new jobs are added.
Once you enter your search criteria, a list of jobs displays. Then click on a specific job to open another page describing the position in great detail. After seeing the array of positions available, SHM non-members are likely to join the society just to have access to the full functionality of the Career Center.
Your next step is to create an account; doing so allows you to apply for positions with just a click. Once you establish an account (a process that takes just a few minutes), click on “Edit My Profile.” In this area, you’ll establish your profile.
Meat and Potatoes: Post Your Resume
The Career Center’s features are state-of-the-art. You can create a resume and a cover letter. To post your resume in “My Account,” for example, select “Post My Resume,” then “Document Management,” and then “Resume.” You’ll need to open a plain text version (no bold, underlining, italics, or bullets) of your current resume on your computer, and then copy your resume to the clipboard.
Never done this before? Here again, you can open a guidance window or a printable FAQ to walk you through the process. Two minor system limitations appear here: You must click a box to make the text wrap automatically, and the site has no spell-check function. You have to spell check your cover letter and resume before you copy and paste. If you edit your text at any time while in the Career Center boxes, then be sure to proofread to ensure you haven’t introduced any errors. After you create your resume, you can open a text version (a file that ends in the suffix .txt) to see how employers will view it.
In the past, hospital medicine applicants could stand out with a well-formatted resume on quality paper. Online documents force every applicant’s information into the same mold, and this often concerns applicants. Will a skilled, tri-lingual, well-published hospitalist look like every other applicant when an employer is looking at a simple text version of your resume?
The Career Center allows you to upload up to three formatted documents that can be attached to applications. If you are unable to upload your documents, you may e-mail them to the site, which will then attach them to your account. Some applicants find it useful to have two specific types of resumes on hand: a traditional reverse chronological resume that emphasizes experience, and a less structured functional resume that describes transferable skills.
Depending on your computer savvy, the time it takes to set up your account and load your resume will vary. Hospitalists with robust skills may be able to load a resume in fewer than 30 minutes, but it may take longer for others. Regardless, the return on investment is large because the information you enter will form the foundation of your materials that a perspective employer will review. Once your resume is loaded, applying for a position only requires a few clicks.
Benefits That Make Your Search Sizzle
If you are an SHM member, the “Job Agent” functionality allows you to receive weekly updates of new jobs added that match your search criteria. (Note: You can join SHM online through the Career Center or by visiting www.joinshm.org) This function is located in your account. It allows you to specify the date you would like to stop receiving notification e-mails. Your account also tracks applications submitted.
After you log in, click “Job Applications” to display any jobs you have applied for and the date that the application was submitted. When a job posting expires (according to a pre-established date set by the employer) a strikethrough line will appear through the job application. Applications remain in your account for 90 days from the submission date. Clicking on the “Apply for this Job” icon opens a new screen, and it allows applicants to edit applications even after you’ve sent it and until the job posting closes. Once the job posting is closed, no application changes can be made.
Employers post their vacancies for 30 days at a time, and they can select packages that include print advertisements in The Hospitalist and/or the Journal of Hospital Medicine. Approximately 85% of employers who advertise in print media also advertise on the Career Center, although a few advertise only on the Career Center. To cover your bases, look in all three places.
Just as some applicants prefer anonymity, some companies choose to list their ads confidentially. In these cases, you will submit your online application, and the employer will contact you via the system with more information if you are a good match.
Employer responses will be forwarded to your e-mail account through the Career Center. Once you begin talking with a prospective employer, it is up to you to use good research and interview skills to ensure that this is indeed a good match. When you find a position, you can remove your resume from circulation. Or, you can store it in the Career Center database for future opportunities by clicking “No, do not post my resume.”
Alternatively, you can remove your information from the database permanently: Go to “My Account” and select “Delete Account.”
What the Future Holds
SHM’s information services team will keep tabs on the recently launched SHM Career Center Web site and invites user feedback—specifically any demographic information that will help them build the most practical, useful career site for hospitalists.
With the average age of a hospitalist about 37, SHM expects that visitors and users to comprise a youthful, computer savvy group. Eventually, SHM wants to expand the site so it tells you more than just what jobs are available (e.g., how to create a resume, interview techniques, and how to build desirable hospital medicine skill sets). They will also track how many employer-employee matches are made using the Career Center.
Conclusion
When unemployment is low, as it most certainly is for hospitalists, leverage rests with job seekers, not employers. While employers are looking for talent and availability, career opportunists crave convenience. The SHM Career Center represents the most comprehensive collection of hospitalist opportunities available on the Internet.
Users will find site navigation easy, and prompts and cues offered by the site designers clear and accurate. Traffic on the site is expected to grow quickly as it becomes what SHM hopes is the most indispensable tool for hospitalists conducting job searches.TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
SHM: BEHIND THE SCENES
Membership: Listen, Then Act
By Todd Von Deak
As I write this column, there are only seven days left before the start of this year’s annual meeting. At last check, more 1,100 hospital medicine professionals were registered to join us in Washington, D.C., for the most important meeting in hospital medicine. Our office is abuzz with activity and last minute preparations. I’m sure there’s something else that I’m supposed to be doing right now, but I need the break.
While I take my break and write, I can’t help but think, “what’s next,” once the Annual Meeting is over? SHM is fast approaching the start of a new fiscal year, and, like any membership director, I am eager to hit the ground running.
The more I reflect on what’s next, the more I realize that part of my answer lies within the pages of The Hospitalist. Our research continues to show that you consider The Hospitalist to be one of the most valuable benefits of membership.
What strikes me as I read through past issues is that we have another story to tell. So this month we’re launching “SHM: Behind the Scenes.”
There are many reasons why we need to share this story. Key to those reasons is the fact that our sole purpose is to serve the hospital medicine community. You entrust us with your dues and meeting registrations to provide resources that will enable you to better serve your patients and grow your careers in the process. So it’s important that we, the staff, tell you firsthand what we are doing with your investment, and how we plan on continuing to earn your trust in the years to come.
Each month a different member of our senior staff will take turns writing this column. During the coming year you’ll hear from the heads of education and quality initiatives, business operations, membership, information services, marketing, legislative affairs, and research. In each column you’ll find a mix of current news, future plans, and tips for maximizing the value of your membership. If we do our jobs correctly, each month you will have a clearer picture on the true return of your membership investment.
We want you to clearly understand why—if you only belong to one organization—it has to be SHM.
This month I’ll focus on membership and our plans for the coming year. (See below.) Next month you’ll hear from Scott Johnson, SHM’s director of information services. Scott is our chief technologist in many ways and is leading the charge to use today’s latest technology to expand the reach of our educational products and enhance your membership investment as well.
Each year, membership departments at non-profit organizations write their strategic plans for the coming year. SHM is no exception.
For most, these strategic plans are based on a set of assumptions. In more offices than you’d like to believe, the staff just sits around and makes their best guesses in order to answer critical questions, including “what do members want to get out of their membership?”
Based on these guesses, the staff then plots their course expansion and enhances the benefits and services that the organization offers. These organizations are doomed to mediocrity.
Successful organizations, including SHM, actively seek to better understand their membership and use a variety of media to get to the heart of the questions that matter. I am proud to say that SHM is among the second group.
Building on previous efforts, the SHM Membership Department has been actively engaged in a “listening tour.” Our goal is to not rely on assumptions but rather to use your feedback in formulating our plans for the coming year.
Here’s some of what we’ve identified.
Top reasons for being a member:
- Education and quality improvement resources;
- The ability to affect the hospital medicine movement; and
- Subscriptions to The Hospitalist and Journal of Hospital Medicine.
Your main goals as a member:
- To learn from educational and quality improvement resources;
- Take advantage of networking opportunities; and
- Gain exposure for career advancement.
The benefits of membership that matter most:
- Information on www.hospitalmedicine.org;
- Access to results from SHM’s “Authoritative Source on the State of the Hospital Medicine Movement;” and
- The Hospitalist.
We’re already using this data, along with other information that we’ve gathered, to enhance the SHM experience and increase the return on your investment. Just look at the new SHM Career Center (www.hospitalmedicine.org/careercenter).
Like any good membership department, we realize that our data collection has just begun. So I’d like to pose a couple of questions:
- Do you agree with our findings?
- Should we offer a new benefit of membership?
- What can we do to enhance your SHM experience?
I’d love to hear your thoughts. Send them to me via e-mail at tvondeak@hospitalmedicine.org. Anyone who e-mails will be entered in a prize drawing.
In my next column, I will share a selection of the responses I receive and tell you the concrete steps we’re taking to improve communication with you and other members.
Von Deak is SHM’s director of membership and marketing.
Each year a new team of SHM officers is elected to lend their wisdom, time, experience, and skills in a collaborative effort to help manage the business of our organization, drive new initiatives, and support the society’s mission. At this year’s annual meeting in Washington, D.C., we again witnessed that familiar changing of the guard with the following inductions:
- President Mary Jo Gorman, MD, MBA;
- President-Elect Russell Holman, MD;
- Treasurer Patrick Cawley, MD; and
- Secretary Jack Percelay, MD, MPH.
“Hospitalists are squarely in the spotlight today on key issues affecting patient care, quality of hospital care, hospital leadership, and other concerns. So it is important that we have a strong, hands-on leadership team that is committed to continuing the positive momentum SHM has generated for hospitalists,” says Larry Wellikson, MD, FACP, CEO of SHM. “I couldn’t be more thrilled with our slate of newly appointed officers. Time and again through the years Mary Jo, Rusty, Pat, and Jack have proven that they are active participants, and that they are leaders who will rise to the occasion to help us meet our objectives.”
Dr. Gorman, a charter member of SHM, has been a practicing hospitalist since 1997, when she founded the first hospitalist practice in St. Louis. In early 1999, her group merged into IPC—The Hospitalist Company and grew to become the dominant hospitalist group in the city. In 2001, Dr. Gorman was promoted to vice-president of medical affairs for IPC, responsible for the design and implementation of company-wide programs involving business development, recruitment, physician training, and operations in all of IPC’s markets. In 2003, she was named chief medical officer and today works with more than 300 physicians nationwide to develop programs and strategies that enhance clinical performance and drive the delivery system towards more efficient care and greater patient satisfaction. She also oversees IPC’s physician training, mentoring and retention programs, as well as IPC’s call center nurses, healthcare services and clinical studies.
A cum laude graduate of St. Louis University, Dr. Gorman earned a BA in Chemistry/Biology in 1981, then went on to earn her MD in 1984 from Southern Illinois University School of Medicine in Springfield. In 1996, she earned a MBA from Washington University, Olin School of Business, in St. Louis.
SHM’s new President-Elect Dr. Holman is senior vice president and national medical director for Cogent Healthcare, an organization that manages hospital medicine programs throughout the country. He is responsible for program implementation and management, quality systems reporting and auditing, physician leadership development, and data systems integration. Formerly, Dr. Holman was the medical director of Hospital Services for HealthPartners Medical Group & Clinics, part of HealthPartners, Inc. in Minnesota. There he also was the founder and director of the HPMG Fellowship Program in Hospital Medicine.
A long-time member of SHM, Dr. Holman served on the Board of Directors as treasurer from 2004-2005. He was previously chair of the Leadership Development Committee, chair of the Midwest Council, course director of the SHM Leadership Academy, and a member of the Public Policy Committee. In February 2006 he co-authored the “Update in Hospital Medicine,” which appeared in Annals of Internal Medicine. In 2002, he received the SHM Award for Outstanding Service in Hospital Medicine.
Through the years, Dr. Holman’s commitment to hospital medicine has helped produce nationally recognized standards in the areas of quality improvement activities, models of medical education, observation units, communication systems, compensation plans, case management, surgical co-management collaborations, and patient flow initiatives. Dr. Holman serves on two national editorial boards for medical publications and is currently co-authoring a comprehensive textbook and electronic decision support tool in hospital medicine.
Dr. Holman earned his MD from Washington University School of Medicine in St. Louis and trained as a resident and chief medical resident at the University of Minnesota in Minneapolis.
New Treasurer Dr. Cawley is a hospitalist at the Medical University of South Carolina in Charleston, where he currently serves as interim executive medical director of MUSC Medical Center. He previously served as the chief of the Section of Hospital Medicine, vice chairman of clinical affairs in the Department of Medicine, and associate executive medical director at MUSC Medical Center.
A charter member of SHM, Dr. Cawley has served on numerous committees and was previously secretary of the Board for the 2004-2005 term. He has worked in both academic and nonacademic hospitals and has served as a consultant to numerous hospitals in the development of hospital medicine programs.
Dr. Cawley received his Bachelor of Science in 1988 from the University of Scranton (Pa.) and his MD from Georgetown University School of Medicine in Washington, D.C. He completed an internal medicine residency at Duke University in Durham, N.C. Later this year, he will complete his MBA from the University of Massachusetts-Amherst.
SHM’s new secretary is Dr. Percelay. He is director of Virtua Inpatient Pediatrics, a large pediatric hospital medicine group in Southern New Jersey with 14 full-time hospitalists covering two hospitals. Since 1991, Dr. Percelay has worked in a variety of community-based settings including the general pediatric ward, pediatric sub-specialty units, pediatric intensive care unit (PICU), neonatal intensive care unit (NICU), and the emergency department.
A charter member of SHM and one of the nation’s first pediatric hospitalists, Dr. Percelay currently holds the Pediatric Seat on the SHM Board, in addition to serving on the Public Policy Committee and co-chairing the Pediatric Committee. He has been intimately involved in collaborative Pediatric hospital medicine projects such as the PRIS research network and the Denver 2005 and 2007 Pediatric Hospital Medicine conferences.
Dr. Percelay is also the founding chairperson and immediate past chair of the American Academy of Pediatrics Section on Hospital Medicine and co-authored the AAP policy statement on pediatric hospitalists. He completed his medical school and pediatric training at the University of California at San Francisco, along with an MPH at the University of California at Berkeley.
SHM congratulates these new officers and thanks our 2005 officers (Steve Pantilat, MD, president, William Atchley, MD, FACP, treasurer, and Lisa Kettering, MD, FACP, secretary) for their exemplary work.
Annual Meeting e-Community a Success
If the feedback from attendees at this year’s Annual Meeting was any indication, the inaugural launch of SHM’s Annual Meeting e-Community was a success.
Each year, SHM’s Annual Meeting provides an opportunity for hospital medicine professionals to network with colleagues and take advantage of more than 40 educational sessions during the course of three days.
While the location for the meeting changes regularly, there is a constant desire within the Annual Meeting planning committee (a group of volunteer members) to improve the attendee experience. The Annual Meeting e-Community (AMeC) was designed with that in mind.
The AMeC effectively extended the reach of the annual meeting both before and after the event. Since early April, attendees have been able to access the handouts for the presentations that were given at the event and network with colleagues thanks to dedicated discussion communities. There are also listings of exhibitors scheduled to be in attendance and general information about Washington, D.C., on the AMeC.
Because of the positive feedback received, the e-Community will stay online through early July, giving attendees the chance to download presentations from sessions that they didn’t attend and make contact with colleagues they met while in Washington, D.C.
Attendees appreciated the ability to access meeting materials prior to the event. “The Annual Meeting e-Community gave me a great opportunity to really plan out the sessions that I wanted to attend prior to the meeting,” says William Rifkin, MD, a hospitalist from the Yale School of Medicine.
According to Joy Wittnebert, AMeC project manager, the site was launched in response to feedback from past annual meetings. “Attendees have been consistently telling us that they want to be able to customize their experience and have more opportunities to network with colleagues before and after the event,” she says.
In the coming months, SHM staff will work with the Annual Meeting Committee to analyze additional feedback and begin making plans for the 2007 version of the site.
SHM Education Committee Launches 18-Month Strategic Plan
Helping our members and the hospital medicine community advance in professional growth and development has been on center stage as seen in the SHM Education Committee’s recent completion of an 18-month strategic plan. The plan is a framework designed to guide staff and volunteer leadership as they work to expand the society’s current slate of educational offerings. Inherent in the framework’s design is a focus on taking advantage of the myriad new channels that have come online for delivering educational content.
The plan is rooted primarily in the recently released Core Competencies in Hospital Medicine. The Core Competencies are a benchmark for the development of curricula within the hospital medicine specialty.
“One of the most exciting parts of this plan is its connection to the Core Competencies,” says Geri Barnes, SHM’s director of education and quality initiatives. “The connection means that this is one of the strongest educational plans that the society has put forward.”
A driving force in the creation of this plan was the committee’s desire to expand SHM’s educational offerings through a variety of technologic venues. “In the coming year, our educational offerings will truly become multi-dimensional,” says Scott Johnson, SHM’s director of information services. “As we expand into audio CDs, podcasts, and Web-based offerings, more hospitalists will be able to take advantage of these learning opportunities, which will have profound effects on the hospital medicine movement.”
With the education plan approved by SHM’s Board of Directors at its recent meeting, the Education Committee, chaired by Preetha Basaviah, MD, from Stanford University, will turn its attention to the first stage of implementation—a complete needs analysis. Some research has already taken place as part of SHM’s ongoing internal quality improvement processes.
“The key to the success of our plan is that we will be integrating feedback from hospitalists throughout North America as we move forward,” says Dr. Basaviah. “Ultimately, this kind of communication will ensure that we reach our primary goal: to provide tools and resources that help hospital medicine professionals improve the quality of care that they provide.”
Stay tuned to The Hospitalist for updates on the committee’s progress and an advanced look at new educational products.
Palliative Care: a Core Competency for Hospitalists
By Theresa Kristopaitis, MD, with input from Howard Epstein, MD, and the SHM Palliative Care Task Force
Palliative care is focused on the relief of suffering and support for the best quality of life for patients facing serious, life-threatening, or advanced illness, as well as their families. Palliative care is a general approach to healthcare that should be routinely integrated with disease modifying therapies. It is also a growing practice specialty for appropriately trained healthcare professionals dedicating their practice to the delivery of palliative care services.1
Optimally palliative care is delivered through an interdisciplinary team consisting of physicians, nurses, chaplains, social workers, pharmacists, as well as other disciplines as patient/family needs warrant. Models of palliative care delivery include hospital-based inpatient consultation services, inpatient palliative care units, outpatient and home-based consultation services, and ambulatory clinics. Hospitalists are ideally positioned to start inpatient palliative care services and reap the professional and institutional benefits that palliative care offers. Tools to develop a program can be obtained through the Center to Advance Palliative Care (www.capc.org).
A Core Competency
The skills gained from developing expertise in palliative care are indispensable to hospitalists—even if they don’t formally work with a palliative care team. Palliative care itself is identified as a healthcare systems core competency of hospital medicine.2 In addition, other hospital medicine competencies overlap with those key to palliative care: pain management, care of the elderly patient and vulnerable populations, communication, hospitalist as consultant, team approach and multidisciplinary care, transitions of care, and medical ethics.3 For some of the most challenging, yet common, inpatient clinical scenarios, palliative care and hospital practice can become indistinguishable.
Inpatient Scenarios: How Can Palliative Care Help?
Scenario 1: A patient on chronic long-acting opiate therapy is admitted to the hospital with complaints of pain, nausea, and vomiting.
The appropriate assessment and management of pain is a patient’s right and an institution’s responsibility, yet it is often inadequate.4 Many barriers to effective pain management have been identified, including limited physician undergraduate and graduate training.4,5 A fundamental goal of palliative care is pain relief. In turn, expertise in the pathophysiology of pain and safe prescribing of opioid, non-opioid, and adjuvant analgesics is critical for palliative care physicians. Palliative care training and resources focus on principles of analgesic pharmacology, equianalgesia, changing routes of administration, control of continuous and breakthrough pain, opioid rotation, and adverse effects of analgesics. A comprehensive introduction to the fundamentals of pain management can be obtained via Education on Palliative and End of Life Care (www.epec.net.) Pain Management Module.
Non-pain symptoms can be as troubling for patients with advanced illness as pain. The formal assessment, reassessment, and management of common symptoms, including nausea, vomiting, dyspnea, constipation, fatigue, and delirium, are a primary domain of palliative medicine. Nausea and vomiting, for example, can become a demoralizing symptom complex. Stimuli to the vomiting center can arise from the cerebral cortex, vestibular apparatus, chemoreceptor zone, and gastrointestinal tract resulting in a broad etiologic differential diagnosis.
With a solid understanding of its pathogenesis and pharmacologic and non-pharmacologic therapeutic principles, nausea and vomiting can be treated in the vast majority of patients. Multiple agents addressing multiple mechanisms may be required. Even the nausea associated with complete bowel obstruction often can be successfully palliated, without the use of nasogastric tubes or surgery.6 The End of Life/Palliative Education Resource Center (www.eperc.mcw.edu) is one of many resources with tools to improve a hospitalist’s evaluation and treatment of non-pain physical symptoms.
Scenario 2: A patient with advanced heart failure and his family are overwhelmed by differing consultant opinions on the appropriateness of implantable cardioverter defibrillator (ICD) insertion.
Effective communication with patients is a core responsibility of both hospitalists and palliative care physicians. A complementary—and at times challenging—skill is the ability to promote communication and consensus about care among multiple specialist consultants. Ripamonti and colleagues write, “Almost invariably, the act of communication is an important part of therapy: Occasionally it is the only constituent. It usually requires greater thought and planning than a drug prescription, and unfortunately it is commonly administered in subtherapeutic doses.”6
The American Academy of Hospice and Palliative Medicine UNIPAC series is a resource for physicians to hone their general communication skills, as well as those more specific to palliative care, such as sharing news (often bad) with patients and families and engaging in therapeutic dialogue.8
Palliative care begins with establishing the goals of care with a patient.9 All physicians bring great value to patient care when they are skilled at negotiating goals of care. There are numerous possible goals of care, from prevention, to cure, to prolongation of life, to achieving a good death. Ideally, goals of care should be discussed with patients and families as early as possible in the course of a serious, life-threatening illness. Establishing realistic and attainable goals of care assumes increased importance in the setting of advanced disease, where treatments intended to prolong life may become more burdensome than beneficial.9
As the reader may have experienced, too often these discussions have not taken place or are held late in the trajectory of illness, such as when patients are hospitalized for severe progressive disease or are facing imminent death.10 In the scenario of potential ICD insertion, conversations with patients to clarify device-specific goals are best accomplished before they are placed and in the context of a broader discussion of the patient’s general medical condition and overall goals for care.11 This type of discussion ultimately improves the informed consent process for ICDs and other technologies. ICD recipients should be guided to periodically revisit their goals, particularly when their health status significantly changes.11 Unlike for initial ICD placement, there are no guidelines for disabling already implanted ICDs. The opportunity to discuss this issue with a patient before a crisis or before they lose decision-making capacity is frequently lost and occurs all too often at life’s end.12
Scenario 3: An elderly debilitated woman with advanced cervical cancer has been hospitalized six times in the past two months. She is cared for at home. Her family is tired but they are doing “the best they can.” She is brought to the emergency department again with weakness.
Effective implementation of care management strategies for patients with life-threatening and advanced disease requires assessment of their physical, social, emotional, and spiritual concerns.1 Similarly, family caregivers have their own—often unvoiced—biopsychosocial stressors.13 Physicians directing patient care must appreciate the significance of these multiple issues, even if they are not comfortable or are ill-equipped to handle them on their own. The power of the interdisciplinary palliative care model is that team members evaluate the patient from different perspectives and pool their expertise in addressing the complex needs of their patients and families.8
In some multidisciplinary models, the onus may lie on the physician to recognize the patient and family needs and mobilize the appropriate resources. Coordination of care at home for patients in the later stages of chronic illness may seem daunting during hospital stays. However, by employing measures utilized by palliative care teams, such as reviewing the goals of care, introducing community resources to help patients and families manage at home, providing anticipatory grief and bereavement support, and considering hospice referral, discharge planning and transitions in care can be much more sustainable.14 With these interventions, patients, families, physicians, and hospitals all benefit.
Conclusion
Hospital-based palliative care programs are growing exponentially.15 Hospitalists are in a unique position to continue their development. Even if the time or circumstances are not yet right for you to become a part of a formal palliative care program, there are daily opportunities to reap rewards from the knowledge, attitudes, and skills that palliative care training offers.
References
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available at www.nationalconsensusproject.org. Last accessed April 28, 2006.
- Pistoria MJ, Amin AN, Dressler DD, et al. The core competencies in hospital medicine. J Hosp Med. 2006;1:2(S1).
- American Board of Hospice and Palliative Medicine. Available at www.abhpm.org. Last accessed April 28, 2006.
- Phillips DM. JCAHO pain management standards unveiled. JAMA. 2000;284:428-429.
- Sullivan AM, Lakoma MD, Block SD. The status of medical education in end-of-life care: a national report. J Gen Intern Med. 2003;18:685-695.
- Ripamonti C, De Conno F, Ventafridda V, et al. Management of bowel obstruction in advanced and terminal cancer patients. Ann Oncol. 1993 Jan;4(1):15-21.
- Buckman R. Communication in palliative care: a practical guide. In: Doyle D, Hanks GWC, MacDonald N, eds. Oxford Textbook of Palliative Medicine. New York: Oxford Community Press; 1993:47-61.
- Storey P, Knight CF. UNIPAC five—caring for the terminally ill—communication and the physician’s role in the interdisciplinary team. In: Hospice/Palliative Care Training for Physicians—A Self Study Program. New York: Mary Ann Liebert; 2003:1-147.
- Morrison RS, Meier DE. Palliative care. NEJM. 2004;350:2582-2590.
- Quill TE. Initiating end of life discussion with seriously ill patients: addressing the “elephant in the room.” JAMA. 2000;284:2502-2507.
- Berger, JT. The ethics of deactivating implanted cardioverter defibrillators. Ann Intern Med. 2005;142:631-634.
- Goldstein NE, Lampert R, Bradely E, et al. Management of implantable cardioverter defibrillators in end-of-life care. Ann Intern Med. 2004;141:835-838.
- Levine C. The loneliness of the long-term caregiver. NEJM. 1999;340:1587-1590.
- Meier D. Palliative care in hospitals. J Hosp Med. 2006;1:21-28.
- Morrison RS, et al. The growth of palliative care programs in United States hospitals. J Pall Med. 2006; 8 (6):1127-1133.
Get a Job!
SHM Launches the first-ever career Web site exclusively for hospitalists
By Jeannette Wick
Job boards—Internet sites designed to allow employers and prospective employees to find each other electronically—are among the most active Internet sites. For many job seekers Monster.com, CareerBuilder.com, and Indeed.com (among others) have become essential job search tools. Until now, however, no site has catered to healthcare professionals in general—much less to hospitalists in particular.
Thanks to the new SHM Career Center (http://hospitalmedicine.org/careercenter), though, things are about to change. The Career Center is part of a comprehensive, “cradle-to-grave” approach SHM is taking to assist hospital medicine professionals in their career development pursuits. The site offers numerous advantages over traditional job-hunting tools, such as classified advertisements, personal contacts, and randomly mailing resumes to interesting employers—advantages such as the ability to post your resume in a searchable database, a database of open positions across North America that you can search using a variety of variables and the opportunity to receive a notification when a job that matches your criteria is posted online.
The Career Center also represents an improvement over general job boards because the pool of positions offered and solicited on the site is restricted to those only for hospital medicine professionals. The site is free for all, although SHM members are able to take advantage of certain “members-only” functionality (resume posting, e-mail notification of new job postings). “Career opportunists,” or hospitalists who are gainfully employed but constantly curious about what else is available, will enjoy this site, too.
The Way it Works
SHM’s Career Center matches applicants and jobs using search features that allow applicants to tailor their search. As an applicant, you enter your job preferences as you would when searching for an article in PubMed or when looking online for a board-certified specialist in a specific geographic region when referring a patient. The boxes prompt you to provide the minimum information necessary for an acceptable search. For example, you need to provide geographical preferences, the type of position you’re looking for, and the specialty area you’re interested in to best tailor your search.
Visitors can browse all jobs by specialty or state—or view the complete list of jobs. The advanced search option augments the specialty and state fields with the ability to specify keywords (see “Hospitalists and Keywords,” p. 10), specialty, employment type (full time, moonlighting, and so on), and the announcement opening date. (The latter is important to applicants who believe older announcements raise a red flag indicating conditions that make it unattractive to candidates.)
The advanced search option also allows you to look at job summaries with the results. So instead of receiving a simple list of the job title, the location, and the announcement date, the summary includes a short description of the position. But visitor beware: You have to click a box to make this happen. Otherwise, your search will create a simple list of jobs, and clicking on any individual job will bring up the job summary. The information is accessible either way.
Get Started
Most job seekers will find the site quite easy to navigate, although a few may be impeded by cookies. (For more information, see “Got Cookies,” p. 10.) The FAQ area is a site strength and will help you eliminate hurdles, from inability to navigate the site, to figuring out how to be notified electronically when new jobs are added.
Once you enter your search criteria, a list of jobs displays. Then click on a specific job to open another page describing the position in great detail. After seeing the array of positions available, SHM non-members are likely to join the society just to have access to the full functionality of the Career Center.
Your next step is to create an account; doing so allows you to apply for positions with just a click. Once you establish an account (a process that takes just a few minutes), click on “Edit My Profile.” In this area, you’ll establish your profile.
Meat and Potatoes: Post Your Resume
The Career Center’s features are state-of-the-art. You can create a resume and a cover letter. To post your resume in “My Account,” for example, select “Post My Resume,” then “Document Management,” and then “Resume.” You’ll need to open a plain text version (no bold, underlining, italics, or bullets) of your current resume on your computer, and then copy your resume to the clipboard.
Never done this before? Here again, you can open a guidance window or a printable FAQ to walk you through the process. Two minor system limitations appear here: You must click a box to make the text wrap automatically, and the site has no spell-check function. You have to spell check your cover letter and resume before you copy and paste. If you edit your text at any time while in the Career Center boxes, then be sure to proofread to ensure you haven’t introduced any errors. After you create your resume, you can open a text version (a file that ends in the suffix .txt) to see how employers will view it.
In the past, hospital medicine applicants could stand out with a well-formatted resume on quality paper. Online documents force every applicant’s information into the same mold, and this often concerns applicants. Will a skilled, tri-lingual, well-published hospitalist look like every other applicant when an employer is looking at a simple text version of your resume?
The Career Center allows you to upload up to three formatted documents that can be attached to applications. If you are unable to upload your documents, you may e-mail them to the site, which will then attach them to your account. Some applicants find it useful to have two specific types of resumes on hand: a traditional reverse chronological resume that emphasizes experience, and a less structured functional resume that describes transferable skills.
Depending on your computer savvy, the time it takes to set up your account and load your resume will vary. Hospitalists with robust skills may be able to load a resume in fewer than 30 minutes, but it may take longer for others. Regardless, the return on investment is large because the information you enter will form the foundation of your materials that a perspective employer will review. Once your resume is loaded, applying for a position only requires a few clicks.
Benefits That Make Your Search Sizzle
If you are an SHM member, the “Job Agent” functionality allows you to receive weekly updates of new jobs added that match your search criteria. (Note: You can join SHM online through the Career Center or by visiting www.joinshm.org) This function is located in your account. It allows you to specify the date you would like to stop receiving notification e-mails. Your account also tracks applications submitted.
After you log in, click “Job Applications” to display any jobs you have applied for and the date that the application was submitted. When a job posting expires (according to a pre-established date set by the employer) a strikethrough line will appear through the job application. Applications remain in your account for 90 days from the submission date. Clicking on the “Apply for this Job” icon opens a new screen, and it allows applicants to edit applications even after you’ve sent it and until the job posting closes. Once the job posting is closed, no application changes can be made.
Employers post their vacancies for 30 days at a time, and they can select packages that include print advertisements in The Hospitalist and/or the Journal of Hospital Medicine. Approximately 85% of employers who advertise in print media also advertise on the Career Center, although a few advertise only on the Career Center. To cover your bases, look in all three places.
Just as some applicants prefer anonymity, some companies choose to list their ads confidentially. In these cases, you will submit your online application, and the employer will contact you via the system with more information if you are a good match.
Employer responses will be forwarded to your e-mail account through the Career Center. Once you begin talking with a prospective employer, it is up to you to use good research and interview skills to ensure that this is indeed a good match. When you find a position, you can remove your resume from circulation. Or, you can store it in the Career Center database for future opportunities by clicking “No, do not post my resume.”
Alternatively, you can remove your information from the database permanently: Go to “My Account” and select “Delete Account.”
What the Future Holds
SHM’s information services team will keep tabs on the recently launched SHM Career Center Web site and invites user feedback—specifically any demographic information that will help them build the most practical, useful career site for hospitalists.
With the average age of a hospitalist about 37, SHM expects that visitors and users to comprise a youthful, computer savvy group. Eventually, SHM wants to expand the site so it tells you more than just what jobs are available (e.g., how to create a resume, interview techniques, and how to build desirable hospital medicine skill sets). They will also track how many employer-employee matches are made using the Career Center.
Conclusion
When unemployment is low, as it most certainly is for hospitalists, leverage rests with job seekers, not employers. While employers are looking for talent and availability, career opportunists crave convenience. The SHM Career Center represents the most comprehensive collection of hospitalist opportunities available on the Internet.
Users will find site navigation easy, and prompts and cues offered by the site designers clear and accurate. Traffic on the site is expected to grow quickly as it becomes what SHM hopes is the most indispensable tool for hospitalists conducting job searches.TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
SHM: BEHIND THE SCENES
Membership: Listen, Then Act
By Todd Von Deak
As I write this column, there are only seven days left before the start of this year’s annual meeting. At last check, more 1,100 hospital medicine professionals were registered to join us in Washington, D.C., for the most important meeting in hospital medicine. Our office is abuzz with activity and last minute preparations. I’m sure there’s something else that I’m supposed to be doing right now, but I need the break.
While I take my break and write, I can’t help but think, “what’s next,” once the Annual Meeting is over? SHM is fast approaching the start of a new fiscal year, and, like any membership director, I am eager to hit the ground running.
The more I reflect on what’s next, the more I realize that part of my answer lies within the pages of The Hospitalist. Our research continues to show that you consider The Hospitalist to be one of the most valuable benefits of membership.
What strikes me as I read through past issues is that we have another story to tell. So this month we’re launching “SHM: Behind the Scenes.”
There are many reasons why we need to share this story. Key to those reasons is the fact that our sole purpose is to serve the hospital medicine community. You entrust us with your dues and meeting registrations to provide resources that will enable you to better serve your patients and grow your careers in the process. So it’s important that we, the staff, tell you firsthand what we are doing with your investment, and how we plan on continuing to earn your trust in the years to come.
Each month a different member of our senior staff will take turns writing this column. During the coming year you’ll hear from the heads of education and quality initiatives, business operations, membership, information services, marketing, legislative affairs, and research. In each column you’ll find a mix of current news, future plans, and tips for maximizing the value of your membership. If we do our jobs correctly, each month you will have a clearer picture on the true return of your membership investment.
We want you to clearly understand why—if you only belong to one organization—it has to be SHM.
This month I’ll focus on membership and our plans for the coming year. (See below.) Next month you’ll hear from Scott Johnson, SHM’s director of information services. Scott is our chief technologist in many ways and is leading the charge to use today’s latest technology to expand the reach of our educational products and enhance your membership investment as well.
Each year, membership departments at non-profit organizations write their strategic plans for the coming year. SHM is no exception.
For most, these strategic plans are based on a set of assumptions. In more offices than you’d like to believe, the staff just sits around and makes their best guesses in order to answer critical questions, including “what do members want to get out of their membership?”
Based on these guesses, the staff then plots their course expansion and enhances the benefits and services that the organization offers. These organizations are doomed to mediocrity.
Successful organizations, including SHM, actively seek to better understand their membership and use a variety of media to get to the heart of the questions that matter. I am proud to say that SHM is among the second group.
Building on previous efforts, the SHM Membership Department has been actively engaged in a “listening tour.” Our goal is to not rely on assumptions but rather to use your feedback in formulating our plans for the coming year.
Here’s some of what we’ve identified.
Top reasons for being a member:
- Education and quality improvement resources;
- The ability to affect the hospital medicine movement; and
- Subscriptions to The Hospitalist and Journal of Hospital Medicine.
Your main goals as a member:
- To learn from educational and quality improvement resources;
- Take advantage of networking opportunities; and
- Gain exposure for career advancement.
The benefits of membership that matter most:
- Information on www.hospitalmedicine.org;
- Access to results from SHM’s “Authoritative Source on the State of the Hospital Medicine Movement;” and
- The Hospitalist.
We’re already using this data, along with other information that we’ve gathered, to enhance the SHM experience and increase the return on your investment. Just look at the new SHM Career Center (www.hospitalmedicine.org/careercenter).
Like any good membership department, we realize that our data collection has just begun. So I’d like to pose a couple of questions:
- Do you agree with our findings?
- Should we offer a new benefit of membership?
- What can we do to enhance your SHM experience?
I’d love to hear your thoughts. Send them to me via e-mail at tvondeak@hospitalmedicine.org. Anyone who e-mails will be entered in a prize drawing.
In my next column, I will share a selection of the responses I receive and tell you the concrete steps we’re taking to improve communication with you and other members.
Von Deak is SHM’s director of membership and marketing.