User login
Observational hospital stays for HF linked to worse outcomes
NEW ORLEANS – The Centers for Medicare & Medicaid Services policy providing financial incentives for hospitals to readmit patients for heart failure for an observational stay rather than as an inpatient is antithetical to the patients’ best interests, according to data presented at the American Heart Association scientific sessions.
“We showed that if you get admitted under observation, the risk of you coming back is much higher than if you’re under an inpatient stay,” said Ahmad Masri, MBBS, of the University of Pittsburgh.
“Since CMS instituted this rule in 2013, there has been a surge in utilization of observational status versus inpatient status,” Dr. Masri noted.
That might make sense if the patients selected for in-hospital observation were less ill at the time than the heart failure patients admitted as inpatients, but that wasn’t the case in his large, retrospective study.
Dr. Masri reported on 21,339 patients with a total of 52,493 admissions for a primary diagnosis of heart failure during 2008-2015 in an 18-hospital health care system. After excluding admissions which involved cardiac surgery or in-hospital mortality, the total was 50,654 admissions.
Of these admissions, 5% were for in-hospital observation; 17% were inpatient admissions with discharge in less than 2 days. The two groups were similar in terms of age, comorbid conditions, and use of guideline-directed medications, although 36% of patients admitted under observation had a left ventricular ejection fraction below 40%, compared with 30% of those with an inpatient admission for less than 2 days.
The majority of patients in both groups were readmitted for heart failure within 1 year; however, the readmission rate was 23% lower in the group with an inpatient stay of less than 2 days, in an analysis adjusted for age, sex, ejection fraction, hypertension, diabetes, pneumonia, chronic obstructive pulmonary disease, liver disease, and renal failure.
Similarly, the group with an inpatient stay of less than 2 days’ duration was 24% less likely to have a cardiac readmission within 1 year than the group admitted for a penalty-free observational stay. The short inpatient stay group’s 1-year all-cause readmission rate was also 24% lower. All of these differences were statistically significant and clinically meaningful.
Yet 1-year all-cause mortality in the two groups was no different.
“This suggests that the difference between these two groups is more of an administrative distinction than a reflection of patient status at time of admission. It looks like it’s just random,” according to Dr. Masri. “There is a real need for a patient-centered, streamlined approach in evaluating and treating patients with heart failure, with a revised treatment-based algorithm and admission rules that guide physicians and shape health care policy.”
He reported having no financial conflicts of interest regarding this study.
NEW ORLEANS – The Centers for Medicare & Medicaid Services policy providing financial incentives for hospitals to readmit patients for heart failure for an observational stay rather than as an inpatient is antithetical to the patients’ best interests, according to data presented at the American Heart Association scientific sessions.
“We showed that if you get admitted under observation, the risk of you coming back is much higher than if you’re under an inpatient stay,” said Ahmad Masri, MBBS, of the University of Pittsburgh.
“Since CMS instituted this rule in 2013, there has been a surge in utilization of observational status versus inpatient status,” Dr. Masri noted.
That might make sense if the patients selected for in-hospital observation were less ill at the time than the heart failure patients admitted as inpatients, but that wasn’t the case in his large, retrospective study.
Dr. Masri reported on 21,339 patients with a total of 52,493 admissions for a primary diagnosis of heart failure during 2008-2015 in an 18-hospital health care system. After excluding admissions which involved cardiac surgery or in-hospital mortality, the total was 50,654 admissions.
Of these admissions, 5% were for in-hospital observation; 17% were inpatient admissions with discharge in less than 2 days. The two groups were similar in terms of age, comorbid conditions, and use of guideline-directed medications, although 36% of patients admitted under observation had a left ventricular ejection fraction below 40%, compared with 30% of those with an inpatient admission for less than 2 days.
The majority of patients in both groups were readmitted for heart failure within 1 year; however, the readmission rate was 23% lower in the group with an inpatient stay of less than 2 days, in an analysis adjusted for age, sex, ejection fraction, hypertension, diabetes, pneumonia, chronic obstructive pulmonary disease, liver disease, and renal failure.
Similarly, the group with an inpatient stay of less than 2 days’ duration was 24% less likely to have a cardiac readmission within 1 year than the group admitted for a penalty-free observational stay. The short inpatient stay group’s 1-year all-cause readmission rate was also 24% lower. All of these differences were statistically significant and clinically meaningful.
Yet 1-year all-cause mortality in the two groups was no different.
“This suggests that the difference between these two groups is more of an administrative distinction than a reflection of patient status at time of admission. It looks like it’s just random,” according to Dr. Masri. “There is a real need for a patient-centered, streamlined approach in evaluating and treating patients with heart failure, with a revised treatment-based algorithm and admission rules that guide physicians and shape health care policy.”
He reported having no financial conflicts of interest regarding this study.
NEW ORLEANS – The Centers for Medicare & Medicaid Services policy providing financial incentives for hospitals to readmit patients for heart failure for an observational stay rather than as an inpatient is antithetical to the patients’ best interests, according to data presented at the American Heart Association scientific sessions.
“We showed that if you get admitted under observation, the risk of you coming back is much higher than if you’re under an inpatient stay,” said Ahmad Masri, MBBS, of the University of Pittsburgh.
“Since CMS instituted this rule in 2013, there has been a surge in utilization of observational status versus inpatient status,” Dr. Masri noted.
That might make sense if the patients selected for in-hospital observation were less ill at the time than the heart failure patients admitted as inpatients, but that wasn’t the case in his large, retrospective study.
Dr. Masri reported on 21,339 patients with a total of 52,493 admissions for a primary diagnosis of heart failure during 2008-2015 in an 18-hospital health care system. After excluding admissions which involved cardiac surgery or in-hospital mortality, the total was 50,654 admissions.
Of these admissions, 5% were for in-hospital observation; 17% were inpatient admissions with discharge in less than 2 days. The two groups were similar in terms of age, comorbid conditions, and use of guideline-directed medications, although 36% of patients admitted under observation had a left ventricular ejection fraction below 40%, compared with 30% of those with an inpatient admission for less than 2 days.
The majority of patients in both groups were readmitted for heart failure within 1 year; however, the readmission rate was 23% lower in the group with an inpatient stay of less than 2 days, in an analysis adjusted for age, sex, ejection fraction, hypertension, diabetes, pneumonia, chronic obstructive pulmonary disease, liver disease, and renal failure.
Similarly, the group with an inpatient stay of less than 2 days’ duration was 24% less likely to have a cardiac readmission within 1 year than the group admitted for a penalty-free observational stay. The short inpatient stay group’s 1-year all-cause readmission rate was also 24% lower. All of these differences were statistically significant and clinically meaningful.
Yet 1-year all-cause mortality in the two groups was no different.
“This suggests that the difference between these two groups is more of an administrative distinction than a reflection of patient status at time of admission. It looks like it’s just random,” according to Dr. Masri. “There is a real need for a patient-centered, streamlined approach in evaluating and treating patients with heart failure, with a revised treatment-based algorithm and admission rules that guide physicians and shape health care policy.”
He reported having no financial conflicts of interest regarding this study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The 1-year rates of readmission for heart failure, cardiac readmission, and all-cause readmission were each 23%-24% lower in heart failure patients admitted for an inpatient stay of less than 2 days’ duration than if they were designated as being admitted under observation.
Data source: A retrospective analysis of more than 50,000 hospital admissions with a primary diagnosis of heart failure in 21,339 patients during 2008-2015.
Disclosures: The presenter reported having no financial conflicts of interest regarding the study.
Mixed findings on iron repletion in HF
NEW ORLEANS – Oral iron supplementation was declared ineffective for the treatment of iron deficiency in patients with heart failure with reduced ejection fraction in one major randomized trial while intravenous ferric carboxymaltose improved exercise capacity and quality of life in another study presented at the American Heart Association scientific sessions.
Iron deficiency is present in roughly half of patients with heart failure with reduced ejection fraction (HFrEF). In affected patients it’s associated with diminished functional capacity and poor quality of life, and is an independent predictor of mortality. Thus, it has emerged as a potential therapeutic target in HFrEF.

The IRONOUT HF (Oral Iron Repletion Effects on Oxygen UpTake in Heart Failure) trial was a multicenter, randomized, double-blind, placebo-controlled clinical trial conducted by the National Heart, Lung, and Blood Institute’s Clinical Heart Failure Network investigators. It included 225 patients with HFrEF and iron deficiency who were randomized to 16 weeks of oral iron polysaccharide at 150 mg b.i.d. or matching placebo.
The primary endpoint was change from baseline to 16 weeks in exercise capacity, as measured via peak oxygen uptake during cardiopulmonary exercise testing. The results were no better in the iron-supplemented group than in placebo-treated controls. Nor was there any benefit for oral iron therapy in terms of quality of life, as assessed by the Kansas City Cardiomyopathy Questionnaire or any of numerous other secondary endpoints, according to Dr. Lewis, head of the heart failure section and director of the cardiopulmonary exercise testing laboratory at Massachusetts General Hospital, Boston.
Participants’ mean baseline hemoglobin level was 12.6 g/dL, but whether patients were anemic at baseline or not made no difference in terms of outcomes. Rates of venous congestion and bleeding were low during the trial.
The problem, the investigators found, was that high-dose oral iron only minimally repleted iron stores. Transferrin saturation increased by a paltry absolute 3% after 16 weeks of twice-daily therapy. Serum ferritin levels increased only 1/20th as much as after intravenous iron ferric carboxymaltose therapy in the earlier positive FAIR-HF (Ferinject Assessment in Patients With Iron Deficiency and Chronic Heart Failure) trial (N Engl J Med. 2009 Dec 17;361:2436-48).
Levels of hepcidin were elevated in study participants. And the higher the level of hepcidin – which Dr. Lewis called “a massive regulator of iron bioavailability and absorption” – the more refractory patients were to oral iron repletion.
“Hepcidin was invented by nature to protect against iron from stimulating growth of bacteria. And when it’s elevated, taking iron orally just has no chance of success,” explained Dr. Anker, professor of cardiology at the University of Gottingen (Germany).
Dr. Anker, who chaired the positive FAIR-HF trial of intravenous iron, said IRONOUT HF was a very well-conducted and definitive clinical trial of oral iron supplementation in HFrEF.
“It’s very simple: Oral iron does not work in patients with chronic heart failure. That’s the take home message. It’s true for peak VO2 [oxygen consumption], for 6-minute walk distance, for symptoms, for quality of life, and even for surrogate markers like NT-proBNP [N-terminal pro b-type natriuretic peptide]. If iron doesn’t get into the body, it’s really difficult to [imagine] that the iron that doesn’t get into the body can exert an effect,” he said.
The primary endpoint in EFFECT-HF was assessor-blinded change in peak VO2 from baseline to week 24. The control group experienced a decrease in peak VO2 over time such that there was a significant difference of 1.0 mL/kg per minute between the two groups.
The ferric carboxymaltose recipients also did significantly better in terms of secondary endpoints including improvement in New York Heart Association functional class, self-reported Patient Global Assessment score, and quality-of-life measures, reported Dr. van Veldhuisen, professor and chairman of cardiology at University Medical Center Groningen (the Netherlands).
Session moderator Clyde Yancy, MD, commented that intravenous iron is not ready for prime time use in clinical practice for several reasons. The open-label EFFECT-HF trial, like the earlier positive double-blind FAIR-HF and CONFIRM-HF IV ferric carboxymaltose trials, was too modest in size to be convincing, especially since this is an expensive and intrusive therapy.
“The endpoint of peak VO2, although a very powerful endpoint, is still one for which there may be some subjectivity, and so we need a more definitive endpoint to be absolutely certain about the potential benefit of the administration of ferric carboxymaltose,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
Discussant Adrian Hernandez, MD, of the Duke Clinical Research Institute in Durham, N.C., said he considers peak VO2 an important endpoint.
“When you talk to patients, exercise capacity is an outcome that matters to them,” he said. “They often comment that what matters to them is living longer with a better quality of life, free of worsening heart failure, and having improvement in everyday functional status. So the cardiopulmonary exercise test is not just a surrogate endpoint; it’s a measure of functional outcome that matters to patients,” he said.
Still, like Dr. Yancy, Dr. Hernandez said he thinks it’s time to have larger, longer, definitive trials with clinical endpoints in order to understand the role of intravenous iron. Both cardiologists applauded Dr. Anker’s announcement that such a trial, known as FAIR-HF2, is now getting started.
The IRONOUT HF trial was funded by the National Institutes of Health. Dr. Lewis reported receiving research support from a handful of pharmaceutical and medical device companies. Dr. van Velduisen reported serving as a scientific adviser to Vifor Pharma, which sponsored the EFFECT-HF trial. Dr. Anker, who was an EFFECT-HF investigator, serves as a consultant to Vifor and several other companies. Dr. Hernandez was an IRONOUT HF investigator and reported receiving research grants from a handful of pharmaceutical companies.
NEW ORLEANS – Oral iron supplementation was declared ineffective for the treatment of iron deficiency in patients with heart failure with reduced ejection fraction in one major randomized trial while intravenous ferric carboxymaltose improved exercise capacity and quality of life in another study presented at the American Heart Association scientific sessions.
Iron deficiency is present in roughly half of patients with heart failure with reduced ejection fraction (HFrEF). In affected patients it’s associated with diminished functional capacity and poor quality of life, and is an independent predictor of mortality. Thus, it has emerged as a potential therapeutic target in HFrEF.
The IRONOUT HF (Oral Iron Repletion Effects on Oxygen UpTake in Heart Failure) trial was a multicenter, randomized, double-blind, placebo-controlled clinical trial conducted by the National Heart, Lung, and Blood Institute’s Clinical Heart Failure Network investigators. It included 225 patients with HFrEF and iron deficiency who were randomized to 16 weeks of oral iron polysaccharide at 150 mg b.i.d. or matching placebo.
The primary endpoint was change from baseline to 16 weeks in exercise capacity, as measured via peak oxygen uptake during cardiopulmonary exercise testing. The results were no better in the iron-supplemented group than in placebo-treated controls. Nor was there any benefit for oral iron therapy in terms of quality of life, as assessed by the Kansas City Cardiomyopathy Questionnaire or any of numerous other secondary endpoints, according to Dr. Lewis, head of the heart failure section and director of the cardiopulmonary exercise testing laboratory at Massachusetts General Hospital, Boston.
Participants’ mean baseline hemoglobin level was 12.6 g/dL, but whether patients were anemic at baseline or not made no difference in terms of outcomes. Rates of venous congestion and bleeding were low during the trial.
The problem, the investigators found, was that high-dose oral iron only minimally repleted iron stores. Transferrin saturation increased by a paltry absolute 3% after 16 weeks of twice-daily therapy. Serum ferritin levels increased only 1/20th as much as after intravenous iron ferric carboxymaltose therapy in the earlier positive FAIR-HF (Ferinject Assessment in Patients With Iron Deficiency and Chronic Heart Failure) trial (N Engl J Med. 2009 Dec 17;361:2436-48).
Levels of hepcidin were elevated in study participants. And the higher the level of hepcidin – which Dr. Lewis called “a massive regulator of iron bioavailability and absorption” – the more refractory patients were to oral iron repletion.
“Hepcidin was invented by nature to protect against iron from stimulating growth of bacteria. And when it’s elevated, taking iron orally just has no chance of success,” explained Dr. Anker, professor of cardiology at the University of Gottingen (Germany).
Dr. Anker, who chaired the positive FAIR-HF trial of intravenous iron, said IRONOUT HF was a very well-conducted and definitive clinical trial of oral iron supplementation in HFrEF.
“It’s very simple: Oral iron does not work in patients with chronic heart failure. That’s the take home message. It’s true for peak VO2 [oxygen consumption], for 6-minute walk distance, for symptoms, for quality of life, and even for surrogate markers like NT-proBNP [N-terminal pro b-type natriuretic peptide]. If iron doesn’t get into the body, it’s really difficult to [imagine] that the iron that doesn’t get into the body can exert an effect,” he said.
The primary endpoint in EFFECT-HF was assessor-blinded change in peak VO2 from baseline to week 24. The control group experienced a decrease in peak VO2 over time such that there was a significant difference of 1.0 mL/kg per minute between the two groups.
The ferric carboxymaltose recipients also did significantly better in terms of secondary endpoints including improvement in New York Heart Association functional class, self-reported Patient Global Assessment score, and quality-of-life measures, reported Dr. van Veldhuisen, professor and chairman of cardiology at University Medical Center Groningen (the Netherlands).
Session moderator Clyde Yancy, MD, commented that intravenous iron is not ready for prime time use in clinical practice for several reasons. The open-label EFFECT-HF trial, like the earlier positive double-blind FAIR-HF and CONFIRM-HF IV ferric carboxymaltose trials, was too modest in size to be convincing, especially since this is an expensive and intrusive therapy.
“The endpoint of peak VO2, although a very powerful endpoint, is still one for which there may be some subjectivity, and so we need a more definitive endpoint to be absolutely certain about the potential benefit of the administration of ferric carboxymaltose,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
Discussant Adrian Hernandez, MD, of the Duke Clinical Research Institute in Durham, N.C., said he considers peak VO2 an important endpoint.
“When you talk to patients, exercise capacity is an outcome that matters to them,” he said. “They often comment that what matters to them is living longer with a better quality of life, free of worsening heart failure, and having improvement in everyday functional status. So the cardiopulmonary exercise test is not just a surrogate endpoint; it’s a measure of functional outcome that matters to patients,” he said.
Still, like Dr. Yancy, Dr. Hernandez said he thinks it’s time to have larger, longer, definitive trials with clinical endpoints in order to understand the role of intravenous iron. Both cardiologists applauded Dr. Anker’s announcement that such a trial, known as FAIR-HF2, is now getting started.
The IRONOUT HF trial was funded by the National Institutes of Health. Dr. Lewis reported receiving research support from a handful of pharmaceutical and medical device companies. Dr. van Velduisen reported serving as a scientific adviser to Vifor Pharma, which sponsored the EFFECT-HF trial. Dr. Anker, who was an EFFECT-HF investigator, serves as a consultant to Vifor and several other companies. Dr. Hernandez was an IRONOUT HF investigator and reported receiving research grants from a handful of pharmaceutical companies.
NEW ORLEANS – Oral iron supplementation was declared ineffective for the treatment of iron deficiency in patients with heart failure with reduced ejection fraction in one major randomized trial while intravenous ferric carboxymaltose improved exercise capacity and quality of life in another study presented at the American Heart Association scientific sessions.
Iron deficiency is present in roughly half of patients with heart failure with reduced ejection fraction (HFrEF). In affected patients it’s associated with diminished functional capacity and poor quality of life, and is an independent predictor of mortality. Thus, it has emerged as a potential therapeutic target in HFrEF.
The IRONOUT HF (Oral Iron Repletion Effects on Oxygen UpTake in Heart Failure) trial was a multicenter, randomized, double-blind, placebo-controlled clinical trial conducted by the National Heart, Lung, and Blood Institute’s Clinical Heart Failure Network investigators. It included 225 patients with HFrEF and iron deficiency who were randomized to 16 weeks of oral iron polysaccharide at 150 mg b.i.d. or matching placebo.
The primary endpoint was change from baseline to 16 weeks in exercise capacity, as measured via peak oxygen uptake during cardiopulmonary exercise testing. The results were no better in the iron-supplemented group than in placebo-treated controls. Nor was there any benefit for oral iron therapy in terms of quality of life, as assessed by the Kansas City Cardiomyopathy Questionnaire or any of numerous other secondary endpoints, according to Dr. Lewis, head of the heart failure section and director of the cardiopulmonary exercise testing laboratory at Massachusetts General Hospital, Boston.
Participants’ mean baseline hemoglobin level was 12.6 g/dL, but whether patients were anemic at baseline or not made no difference in terms of outcomes. Rates of venous congestion and bleeding were low during the trial.
The problem, the investigators found, was that high-dose oral iron only minimally repleted iron stores. Transferrin saturation increased by a paltry absolute 3% after 16 weeks of twice-daily therapy. Serum ferritin levels increased only 1/20th as much as after intravenous iron ferric carboxymaltose therapy in the earlier positive FAIR-HF (Ferinject Assessment in Patients With Iron Deficiency and Chronic Heart Failure) trial (N Engl J Med. 2009 Dec 17;361:2436-48).
Levels of hepcidin were elevated in study participants. And the higher the level of hepcidin – which Dr. Lewis called “a massive regulator of iron bioavailability and absorption” – the more refractory patients were to oral iron repletion.
“Hepcidin was invented by nature to protect against iron from stimulating growth of bacteria. And when it’s elevated, taking iron orally just has no chance of success,” explained Dr. Anker, professor of cardiology at the University of Gottingen (Germany).
Dr. Anker, who chaired the positive FAIR-HF trial of intravenous iron, said IRONOUT HF was a very well-conducted and definitive clinical trial of oral iron supplementation in HFrEF.
“It’s very simple: Oral iron does not work in patients with chronic heart failure. That’s the take home message. It’s true for peak VO2 [oxygen consumption], for 6-minute walk distance, for symptoms, for quality of life, and even for surrogate markers like NT-proBNP [N-terminal pro b-type natriuretic peptide]. If iron doesn’t get into the body, it’s really difficult to [imagine] that the iron that doesn’t get into the body can exert an effect,” he said.
The primary endpoint in EFFECT-HF was assessor-blinded change in peak VO2 from baseline to week 24. The control group experienced a decrease in peak VO2 over time such that there was a significant difference of 1.0 mL/kg per minute between the two groups.
The ferric carboxymaltose recipients also did significantly better in terms of secondary endpoints including improvement in New York Heart Association functional class, self-reported Patient Global Assessment score, and quality-of-life measures, reported Dr. van Veldhuisen, professor and chairman of cardiology at University Medical Center Groningen (the Netherlands).
Session moderator Clyde Yancy, MD, commented that intravenous iron is not ready for prime time use in clinical practice for several reasons. The open-label EFFECT-HF trial, like the earlier positive double-blind FAIR-HF and CONFIRM-HF IV ferric carboxymaltose trials, was too modest in size to be convincing, especially since this is an expensive and intrusive therapy.
“The endpoint of peak VO2, although a very powerful endpoint, is still one for which there may be some subjectivity, and so we need a more definitive endpoint to be absolutely certain about the potential benefit of the administration of ferric carboxymaltose,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
Discussant Adrian Hernandez, MD, of the Duke Clinical Research Institute in Durham, N.C., said he considers peak VO2 an important endpoint.
“When you talk to patients, exercise capacity is an outcome that matters to them,” he said. “They often comment that what matters to them is living longer with a better quality of life, free of worsening heart failure, and having improvement in everyday functional status. So the cardiopulmonary exercise test is not just a surrogate endpoint; it’s a measure of functional outcome that matters to patients,” he said.
Still, like Dr. Yancy, Dr. Hernandez said he thinks it’s time to have larger, longer, definitive trials with clinical endpoints in order to understand the role of intravenous iron. Both cardiologists applauded Dr. Anker’s announcement that such a trial, known as FAIR-HF2, is now getting started.
The IRONOUT HF trial was funded by the National Institutes of Health. Dr. Lewis reported receiving research support from a handful of pharmaceutical and medical device companies. Dr. van Velduisen reported serving as a scientific adviser to Vifor Pharma, which sponsored the EFFECT-HF trial. Dr. Anker, who was an EFFECT-HF investigator, serves as a consultant to Vifor and several other companies. Dr. Hernandez was an IRONOUT HF investigator and reported receiving research grants from a handful of pharmaceutical companies.
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
Allogeneic stem cells show promise for treating nonischemic dilated cardiomyopathy
NEW ORLEANS – Allogeneic stem cells appear to be a safe treatment option for nonischemic dilated cardiomyopathy and show somewhat greater efficacy than autologous stem cells, according to the results of the randomized POSEIDON-DCM trial.
“Nonischemic dilated cardiomyopathy is an incurable condition with significant genetic and immunologic underpinnings,” noted lead investigator Joshua M. Hare, MD, director of the Interdisciplinary Stem Cell Institute and professor of medicine at the University of Miami. 
The phase I/II trial undertook a head-to-head comparison of allogeneic and autologous bone marrow–derived mesenchymal stem cells in 37 patients with nonischemic dilated cardiomyopathy.
Results presented at the American Heart Association scientific sessions and simultaneously published (J Am Coll Cardiol. 2016. doi: 10.1016/j.jacc.2016.11.009) showed that none of the patients in either group experienced a 30-day treatment-emergent serious adverse event, the trial’s primary endpoint.
The allogeneic group had a greater shift to a lesser inflammatory immune profile, and, at 12 months, a lower rate of major adverse cardiac events and more improvement in walk test distance. Additionally, half of patients in the allogeneic group no longer met the ejection fraction cutoff typically used to define dilated cardiomyopathy, compared with only about one-fifth of those in the autologous group.
“Immunomodulation may contribute to the efficacy of allogeneic human mesenchymal stem cells in nonischemic dilated cardiomyopathy, as we have shown suppression of immune activation to a greater degree with the allo versus auto cells,” Dr. Hare said.
“We argue that these data support the use of allogeneic mesenchymal stem cell therapy in future pivotal placebo-controlled clinical trials for this patient population, an important patient population with significant unmet need.”
Trial details
The patients enrolled in POSEIDON-DCM had left ventricular dysfunction due to nonischemic dilated cardiomyopathy and were randomized evenly to allogeneic or autologous stem cell therapy. Stem cells were delivered by transendocardial injection into 10 left ventricular sites using a catheter.
In the first 30 days after treatment, there were no treatment-emergent serious adverse events, defined as death, nonfatal myocardial infarction, stroke, hospitalization for worsening heart failure, cardiac perforation, pericardial tamponade, or sustained ventricular arrhythmias. “The 30-day safety and tolerability was excellent in both groups receiving either allogeneic or autologous therapy,” Dr. Hare said.
At 12 months, the allogeneic group had lower rates than the autologous group of major adverse cardiac events (20.3% vs. 57.1%, P = .0186) and all-cause rehospitalizations (28.2% vs. 70.0%, P = .0447).
In terms of efficacy, ejection fraction at 12 months had improved by a significant 8.0 Units in the allogeneic group and a nonsignificant 5.4 Units in the autologous group (P not significant for difference between groups). Roughly half of patients in the allogeneic group had achieved an ejection fraction of greater than 40%, compared with only two patients in the autologous group. “This is meaningful because the clinical definition of dilated cardiomyopathy typically uses an ejection fraction cutoff of 40%,” he noted.
The 6-minute walk test distance increased by a significant 37.0 m for the allogeneic group and by a nonsignificant 7.3 m for the autologous group (P = .0168 for difference between groups). Scores on the Minnesota Living With Heart Failure Questionnaire fell significantly in the former group and nonsignificantly in the latter group (P not significant for difference between groups).
Patients in the allogeneic group were more likely to have an improvement from baseline in New York Heart Association class (66.7% vs. 27.3%, P = .0527).
“An issue of concern in this field has been the formation of ectopic tissue with mesenchymal stem cells, so patients received whole-body CT scanning over 12 months,” Dr. Hare reported. “There was no ectopic tissue formation or tumor formation in any patient.”
In terms of biologic endpoints, two measures of endothelial function known to be suppressed in the setting of circulatory failure – endothelial progenitor cell colony-forming units and flow-mediated vasodilation – had increased significantly at 3 months in the allogeneic group only. Tumor necrosis factor–alpha levels fell by roughly 70% with allogeneic therapy versus 50% with autologous therapy (P = .05).
Both groups had a lessening of the immunosuppression that is common in heart failure, but benefit in several markers, such as the percentage of switched memory B cells, was greater with the allogeneic therapy. Additionally, there was a trend toward greater reduction of early T-cell activation in the allogeneic group.
“Of importance in the field of allogeneic cell therapy is [whether] the allogeneic cells mount a panel-reactive antigen [PRA],” commented Dr. Hare, who disclosed that he has an ownership interest in and is a consultant or advisory board member for Vestion.
Results showed that one patient in the allogeneic group developed a high-risk PRA, compared with none in the autologous group. Another four patients in the former group developed a moderate-risk PRA, compared with one in the latter group (P less than or equal to .05).
NEW ORLEANS – Allogeneic stem cells appear to be a safe treatment option for nonischemic dilated cardiomyopathy and show somewhat greater efficacy than autologous stem cells, according to the results of the randomized POSEIDON-DCM trial.
“Nonischemic dilated cardiomyopathy is an incurable condition with significant genetic and immunologic underpinnings,” noted lead investigator Joshua M. Hare, MD, director of the Interdisciplinary Stem Cell Institute and professor of medicine at the University of Miami.
The phase I/II trial undertook a head-to-head comparison of allogeneic and autologous bone marrow–derived mesenchymal stem cells in 37 patients with nonischemic dilated cardiomyopathy.
Results presented at the American Heart Association scientific sessions and simultaneously published (J Am Coll Cardiol. 2016. doi: 10.1016/j.jacc.2016.11.009) showed that none of the patients in either group experienced a 30-day treatment-emergent serious adverse event, the trial’s primary endpoint.
The allogeneic group had a greater shift to a lesser inflammatory immune profile, and, at 12 months, a lower rate of major adverse cardiac events and more improvement in walk test distance. Additionally, half of patients in the allogeneic group no longer met the ejection fraction cutoff typically used to define dilated cardiomyopathy, compared with only about one-fifth of those in the autologous group.
“Immunomodulation may contribute to the efficacy of allogeneic human mesenchymal stem cells in nonischemic dilated cardiomyopathy, as we have shown suppression of immune activation to a greater degree with the allo versus auto cells,” Dr. Hare said.
“We argue that these data support the use of allogeneic mesenchymal stem cell therapy in future pivotal placebo-controlled clinical trials for this patient population, an important patient population with significant unmet need.”
Trial details
The patients enrolled in POSEIDON-DCM had left ventricular dysfunction due to nonischemic dilated cardiomyopathy and were randomized evenly to allogeneic or autologous stem cell therapy. Stem cells were delivered by transendocardial injection into 10 left ventricular sites using a catheter.
In the first 30 days after treatment, there were no treatment-emergent serious adverse events, defined as death, nonfatal myocardial infarction, stroke, hospitalization for worsening heart failure, cardiac perforation, pericardial tamponade, or sustained ventricular arrhythmias. “The 30-day safety and tolerability was excellent in both groups receiving either allogeneic or autologous therapy,” Dr. Hare said.
At 12 months, the allogeneic group had lower rates than the autologous group of major adverse cardiac events (20.3% vs. 57.1%, P = .0186) and all-cause rehospitalizations (28.2% vs. 70.0%, P = .0447).
In terms of efficacy, ejection fraction at 12 months had improved by a significant 8.0 Units in the allogeneic group and a nonsignificant 5.4 Units in the autologous group (P not significant for difference between groups). Roughly half of patients in the allogeneic group had achieved an ejection fraction of greater than 40%, compared with only two patients in the autologous group. “This is meaningful because the clinical definition of dilated cardiomyopathy typically uses an ejection fraction cutoff of 40%,” he noted.
The 6-minute walk test distance increased by a significant 37.0 m for the allogeneic group and by a nonsignificant 7.3 m for the autologous group (P = .0168 for difference between groups). Scores on the Minnesota Living With Heart Failure Questionnaire fell significantly in the former group and nonsignificantly in the latter group (P not significant for difference between groups).
Patients in the allogeneic group were more likely to have an improvement from baseline in New York Heart Association class (66.7% vs. 27.3%, P = .0527).
“An issue of concern in this field has been the formation of ectopic tissue with mesenchymal stem cells, so patients received whole-body CT scanning over 12 months,” Dr. Hare reported. “There was no ectopic tissue formation or tumor formation in any patient.”
In terms of biologic endpoints, two measures of endothelial function known to be suppressed in the setting of circulatory failure – endothelial progenitor cell colony-forming units and flow-mediated vasodilation – had increased significantly at 3 months in the allogeneic group only. Tumor necrosis factor–alpha levels fell by roughly 70% with allogeneic therapy versus 50% with autologous therapy (P = .05).
Both groups had a lessening of the immunosuppression that is common in heart failure, but benefit in several markers, such as the percentage of switched memory B cells, was greater with the allogeneic therapy. Additionally, there was a trend toward greater reduction of early T-cell activation in the allogeneic group.
“Of importance in the field of allogeneic cell therapy is [whether] the allogeneic cells mount a panel-reactive antigen [PRA],” commented Dr. Hare, who disclosed that he has an ownership interest in and is a consultant or advisory board member for Vestion.
Results showed that one patient in the allogeneic group developed a high-risk PRA, compared with none in the autologous group. Another four patients in the former group developed a moderate-risk PRA, compared with one in the latter group (P less than or equal to .05).
NEW ORLEANS – Allogeneic stem cells appear to be a safe treatment option for nonischemic dilated cardiomyopathy and show somewhat greater efficacy than autologous stem cells, according to the results of the randomized POSEIDON-DCM trial.
“Nonischemic dilated cardiomyopathy is an incurable condition with significant genetic and immunologic underpinnings,” noted lead investigator Joshua M. Hare, MD, director of the Interdisciplinary Stem Cell Institute and professor of medicine at the University of Miami.
The phase I/II trial undertook a head-to-head comparison of allogeneic and autologous bone marrow–derived mesenchymal stem cells in 37 patients with nonischemic dilated cardiomyopathy.
Results presented at the American Heart Association scientific sessions and simultaneously published (J Am Coll Cardiol. 2016. doi: 10.1016/j.jacc.2016.11.009) showed that none of the patients in either group experienced a 30-day treatment-emergent serious adverse event, the trial’s primary endpoint.
The allogeneic group had a greater shift to a lesser inflammatory immune profile, and, at 12 months, a lower rate of major adverse cardiac events and more improvement in walk test distance. Additionally, half of patients in the allogeneic group no longer met the ejection fraction cutoff typically used to define dilated cardiomyopathy, compared with only about one-fifth of those in the autologous group.
“Immunomodulation may contribute to the efficacy of allogeneic human mesenchymal stem cells in nonischemic dilated cardiomyopathy, as we have shown suppression of immune activation to a greater degree with the allo versus auto cells,” Dr. Hare said.
“We argue that these data support the use of allogeneic mesenchymal stem cell therapy in future pivotal placebo-controlled clinical trials for this patient population, an important patient population with significant unmet need.”
Trial details
The patients enrolled in POSEIDON-DCM had left ventricular dysfunction due to nonischemic dilated cardiomyopathy and were randomized evenly to allogeneic or autologous stem cell therapy. Stem cells were delivered by transendocardial injection into 10 left ventricular sites using a catheter.
In the first 30 days after treatment, there were no treatment-emergent serious adverse events, defined as death, nonfatal myocardial infarction, stroke, hospitalization for worsening heart failure, cardiac perforation, pericardial tamponade, or sustained ventricular arrhythmias. “The 30-day safety and tolerability was excellent in both groups receiving either allogeneic or autologous therapy,” Dr. Hare said.
At 12 months, the allogeneic group had lower rates than the autologous group of major adverse cardiac events (20.3% vs. 57.1%, P = .0186) and all-cause rehospitalizations (28.2% vs. 70.0%, P = .0447).
In terms of efficacy, ejection fraction at 12 months had improved by a significant 8.0 Units in the allogeneic group and a nonsignificant 5.4 Units in the autologous group (P not significant for difference between groups). Roughly half of patients in the allogeneic group had achieved an ejection fraction of greater than 40%, compared with only two patients in the autologous group. “This is meaningful because the clinical definition of dilated cardiomyopathy typically uses an ejection fraction cutoff of 40%,” he noted.
The 6-minute walk test distance increased by a significant 37.0 m for the allogeneic group and by a nonsignificant 7.3 m for the autologous group (P = .0168 for difference between groups). Scores on the Minnesota Living With Heart Failure Questionnaire fell significantly in the former group and nonsignificantly in the latter group (P not significant for difference between groups).
Patients in the allogeneic group were more likely to have an improvement from baseline in New York Heart Association class (66.7% vs. 27.3%, P = .0527).
“An issue of concern in this field has been the formation of ectopic tissue with mesenchymal stem cells, so patients received whole-body CT scanning over 12 months,” Dr. Hare reported. “There was no ectopic tissue formation or tumor formation in any patient.”
In terms of biologic endpoints, two measures of endothelial function known to be suppressed in the setting of circulatory failure – endothelial progenitor cell colony-forming units and flow-mediated vasodilation – had increased significantly at 3 months in the allogeneic group only. Tumor necrosis factor–alpha levels fell by roughly 70% with allogeneic therapy versus 50% with autologous therapy (P = .05).
Both groups had a lessening of the immunosuppression that is common in heart failure, but benefit in several markers, such as the percentage of switched memory B cells, was greater with the allogeneic therapy. Additionally, there was a trend toward greater reduction of early T-cell activation in the allogeneic group.
“Of importance in the field of allogeneic cell therapy is [whether] the allogeneic cells mount a panel-reactive antigen [PRA],” commented Dr. Hare, who disclosed that he has an ownership interest in and is a consultant or advisory board member for Vestion.
Results showed that one patient in the allogeneic group developed a high-risk PRA, compared with none in the autologous group. Another four patients in the former group developed a moderate-risk PRA, compared with one in the latter group (P less than or equal to .05).
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: At 12 months, the allogeneic group had lower rates than the autologous group of major adverse cardiac events (20.3% vs. 57.1%, P = .0186) and all-cause rehospitalizations (28.2% vs. 70.0%, P = .0447).
Data source: A randomized phase I/II trial among 37 patients with nonischemic dilated cardiomyopathy (POSEIDON-DCM trial).
Disclosures: Dr. Hare disclosed that he has an ownership interest in and is a consultant or advisory board member for Vestion.
TRUE-AHF: Urgent vasodilator therapy in acute HF provides no long-term benefit
NEW ORLEANS – An investigational synthetic natriuretic peptide given early during hospitalization for acute decompensated heart failure didn’t produce any of the hoped-for intermediate- or long-term clinical benefits in the phase III TRUE-AHF study, Milton Packer, MD, reported at the American Heart Association scientific sessions.
The failure of this investigational vasodilator, ularitide, to influence downstream cardiovascular mortality or early readmission for heart failure closes the door on the once-promising hypothesis that myocardial microinjury occurring during ADHF is due to ventricular distension, observed Dr. Packer, the Distinguished Scholar in Cardiovascular Science at Baylor University Medical Center, Dallas. “Ularitide did exactly what we expected it to do while we were giving it: we caused intravascular decompression, we reduced cardiac wall stress, but we did not affect cardiac microinjury, and we didn’t change long-term cardiovascular mortality or any of our secondary endpoints, including and in particular the 30-day risk of rehospitalization for heart failure,” he said.
During a median follow-up of 15 months there were 236 cardiovascular deaths in the ularitide group and 225 in the control group, a nonsignificant difference. Nor were there any differences between the two groups in secondary endpoints including length of stay in the ICU during the index hospitalization, rehospitalization for ADHF within 30 days of discharge, or the composite of all-cause mortality or cardiovascular hospitalization within 6 months, which occurred in 40.7% of the ularitide group and 37.2% of controls.
The explanation for this lack of long-term benefit lies in the finding that myocardial microinjury wasn’t prevented by the rapid reduction of cardiac distension produced by ularitide. This was evident in the therapy’s inability to dampen the rise in high-sensitivity cardiac troponin T which occurred in the initial 48 hours of the study.
“The trial demonstrated the effects and safety of ularitide. However, to gain long-term benefits on hospitalizations and death in patients following a hospital admission for heart failure, physicians must focus on the drugs that patients take as an outpatient rather than the drugs they receive as an inpatient,” Dr. Packer concluded.
“Readmission rates remain stubbornly at 20% within 30 days and near 50% at 6 months. Acute decompensation is an inflection point in the natural history of heart failure with subsequent 1-year mortality rates consistently approximating 25%. Clearly there is something about the hospitalization that is a herald event which speaks to much worse outcomes, compared with chronic ambulatory heart failure,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
He agreed with Dr. Packer that in light of the TRUE-AHF results, what Dr. Yancy termed “the early injury hypothesis” isn’t worth further pursuit.
Ularitide thus joins a long list of failed therapies for ADHF. Treatments that have convincingly been shown to have no significant impact on mortality and at best only modest impact on morbidity include continuous IV infusion of loop diuretics in the DOSE trial; the arginine vasopressin antagonists, which failed to impress in EVEREST, SECRET, and TACTICS; nesiritide (Natrecor) in the ASCEND-HF trial; and levosimendan (Simdax), which proved disappointing in the SURVIVE and REVIVE II studies, according to Dr. Yancy.
The jury is still out on serelaxin, he added. The drug showed a favorable signal in the RELAX-AHF trial. The results of RELAX II are awaited with interest.
“Today we still don’t have an effective single intervention for acute decompensated heart failure other than process-of-care improvement,” the cardiologist noted.
What holds promise for improved long-term outcomes in ADHF at this point? Dr. Yancy said sacubitril/valsartan (Entresto) is intriguing based upon the results of the PARADIGM-HF trial (N Engl J Med. 2014;371:993-1004). But the drug needs to be studied prospectively in patients in the throes of ADHF before it can appropriately be recommended for the purpose of changing the natural history of this disorder, Dr. Yancy stressed.
Devices such as the implantable pulmonary catheter are under study as a promising means of altering the natural history of ADHF by identifying actionable signals of impending decompensation weeks beforehand, he added.
The TRUE-AHF trial was sponsored by Cardiorentis. Dr. Packer reported serving as a consultant to that company and more than a dozen other pharmaceutical and medical device companies.
bjancin@frontlinemedcom.com
NEW ORLEANS – An investigational synthetic natriuretic peptide given early during hospitalization for acute decompensated heart failure didn’t produce any of the hoped-for intermediate- or long-term clinical benefits in the phase III TRUE-AHF study, Milton Packer, MD, reported at the American Heart Association scientific sessions.
The failure of this investigational vasodilator, ularitide, to influence downstream cardiovascular mortality or early readmission for heart failure closes the door on the once-promising hypothesis that myocardial microinjury occurring during ADHF is due to ventricular distension, observed Dr. Packer, the Distinguished Scholar in Cardiovascular Science at Baylor University Medical Center, Dallas. “Ularitide did exactly what we expected it to do while we were giving it: we caused intravascular decompression, we reduced cardiac wall stress, but we did not affect cardiac microinjury, and we didn’t change long-term cardiovascular mortality or any of our secondary endpoints, including and in particular the 30-day risk of rehospitalization for heart failure,” he said.
During a median follow-up of 15 months there were 236 cardiovascular deaths in the ularitide group and 225 in the control group, a nonsignificant difference. Nor were there any differences between the two groups in secondary endpoints including length of stay in the ICU during the index hospitalization, rehospitalization for ADHF within 30 days of discharge, or the composite of all-cause mortality or cardiovascular hospitalization within 6 months, which occurred in 40.7% of the ularitide group and 37.2% of controls.
The explanation for this lack of long-term benefit lies in the finding that myocardial microinjury wasn’t prevented by the rapid reduction of cardiac distension produced by ularitide. This was evident in the therapy’s inability to dampen the rise in high-sensitivity cardiac troponin T which occurred in the initial 48 hours of the study.
“The trial demonstrated the effects and safety of ularitide. However, to gain long-term benefits on hospitalizations and death in patients following a hospital admission for heart failure, physicians must focus on the drugs that patients take as an outpatient rather than the drugs they receive as an inpatient,” Dr. Packer concluded.
“Readmission rates remain stubbornly at 20% within 30 days and near 50% at 6 months. Acute decompensation is an inflection point in the natural history of heart failure with subsequent 1-year mortality rates consistently approximating 25%. Clearly there is something about the hospitalization that is a herald event which speaks to much worse outcomes, compared with chronic ambulatory heart failure,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
He agreed with Dr. Packer that in light of the TRUE-AHF results, what Dr. Yancy termed “the early injury hypothesis” isn’t worth further pursuit.
Ularitide thus joins a long list of failed therapies for ADHF. Treatments that have convincingly been shown to have no significant impact on mortality and at best only modest impact on morbidity include continuous IV infusion of loop diuretics in the DOSE trial; the arginine vasopressin antagonists, which failed to impress in EVEREST, SECRET, and TACTICS; nesiritide (Natrecor) in the ASCEND-HF trial; and levosimendan (Simdax), which proved disappointing in the SURVIVE and REVIVE II studies, according to Dr. Yancy.
The jury is still out on serelaxin, he added. The drug showed a favorable signal in the RELAX-AHF trial. The results of RELAX II are awaited with interest.
“Today we still don’t have an effective single intervention for acute decompensated heart failure other than process-of-care improvement,” the cardiologist noted.
What holds promise for improved long-term outcomes in ADHF at this point? Dr. Yancy said sacubitril/valsartan (Entresto) is intriguing based upon the results of the PARADIGM-HF trial (N Engl J Med. 2014;371:993-1004). But the drug needs to be studied prospectively in patients in the throes of ADHF before it can appropriately be recommended for the purpose of changing the natural history of this disorder, Dr. Yancy stressed.
Devices such as the implantable pulmonary catheter are under study as a promising means of altering the natural history of ADHF by identifying actionable signals of impending decompensation weeks beforehand, he added.
The TRUE-AHF trial was sponsored by Cardiorentis. Dr. Packer reported serving as a consultant to that company and more than a dozen other pharmaceutical and medical device companies.
bjancin@frontlinemedcom.com
NEW ORLEANS – An investigational synthetic natriuretic peptide given early during hospitalization for acute decompensated heart failure didn’t produce any of the hoped-for intermediate- or long-term clinical benefits in the phase III TRUE-AHF study, Milton Packer, MD, reported at the American Heart Association scientific sessions.
The failure of this investigational vasodilator, ularitide, to influence downstream cardiovascular mortality or early readmission for heart failure closes the door on the once-promising hypothesis that myocardial microinjury occurring during ADHF is due to ventricular distension, observed Dr. Packer, the Distinguished Scholar in Cardiovascular Science at Baylor University Medical Center, Dallas. “Ularitide did exactly what we expected it to do while we were giving it: we caused intravascular decompression, we reduced cardiac wall stress, but we did not affect cardiac microinjury, and we didn’t change long-term cardiovascular mortality or any of our secondary endpoints, including and in particular the 30-day risk of rehospitalization for heart failure,” he said.
During a median follow-up of 15 months there were 236 cardiovascular deaths in the ularitide group and 225 in the control group, a nonsignificant difference. Nor were there any differences between the two groups in secondary endpoints including length of stay in the ICU during the index hospitalization, rehospitalization for ADHF within 30 days of discharge, or the composite of all-cause mortality or cardiovascular hospitalization within 6 months, which occurred in 40.7% of the ularitide group and 37.2% of controls.
The explanation for this lack of long-term benefit lies in the finding that myocardial microinjury wasn’t prevented by the rapid reduction of cardiac distension produced by ularitide. This was evident in the therapy’s inability to dampen the rise in high-sensitivity cardiac troponin T which occurred in the initial 48 hours of the study.
“The trial demonstrated the effects and safety of ularitide. However, to gain long-term benefits on hospitalizations and death in patients following a hospital admission for heart failure, physicians must focus on the drugs that patients take as an outpatient rather than the drugs they receive as an inpatient,” Dr. Packer concluded.
“Readmission rates remain stubbornly at 20% within 30 days and near 50% at 6 months. Acute decompensation is an inflection point in the natural history of heart failure with subsequent 1-year mortality rates consistently approximating 25%. Clearly there is something about the hospitalization that is a herald event which speaks to much worse outcomes, compared with chronic ambulatory heart failure,” said Dr. Yancy, professor of medicine and chief of cardiology at Northwestern University in Chicago.
He agreed with Dr. Packer that in light of the TRUE-AHF results, what Dr. Yancy termed “the early injury hypothesis” isn’t worth further pursuit.
Ularitide thus joins a long list of failed therapies for ADHF. Treatments that have convincingly been shown to have no significant impact on mortality and at best only modest impact on morbidity include continuous IV infusion of loop diuretics in the DOSE trial; the arginine vasopressin antagonists, which failed to impress in EVEREST, SECRET, and TACTICS; nesiritide (Natrecor) in the ASCEND-HF trial; and levosimendan (Simdax), which proved disappointing in the SURVIVE and REVIVE II studies, according to Dr. Yancy.
The jury is still out on serelaxin, he added. The drug showed a favorable signal in the RELAX-AHF trial. The results of RELAX II are awaited with interest.
“Today we still don’t have an effective single intervention for acute decompensated heart failure other than process-of-care improvement,” the cardiologist noted.
What holds promise for improved long-term outcomes in ADHF at this point? Dr. Yancy said sacubitril/valsartan (Entresto) is intriguing based upon the results of the PARADIGM-HF trial (N Engl J Med. 2014;371:993-1004). But the drug needs to be studied prospectively in patients in the throes of ADHF before it can appropriately be recommended for the purpose of changing the natural history of this disorder, Dr. Yancy stressed.
Devices such as the implantable pulmonary catheter are under study as a promising means of altering the natural history of ADHF by identifying actionable signals of impending decompensation weeks beforehand, he added.
The TRUE-AHF trial was sponsored by Cardiorentis. Dr. Packer reported serving as a consultant to that company and more than a dozen other pharmaceutical and medical device companies.
bjancin@frontlinemedcom.com
Key clinical point:
Major finding: Early administration of ularitide during hospitalization for acute decompensated heart failure failed to achieve any long-term clinical benefits.
Data source: The TRUE-AHF trial was a double-blind, placebo-controlled, randomized trial including 2,157 patients hospitalized for acute decompensated heart failure at 156 centers in 23 countries.
Disclosures: The study was sponsored by Cardiorentis. The presenter reported serving as a consultant to that company and more than a dozen other pharmaceutical and medical device companies.
Interatrial shunt benefits sustained for 1 year in HFpEF patients
NEW ORLEANS – An interatrial septal shunt device continued to provide “sustained and meaningful clinical benefit” at 1-year follow-up for 64 patients who had heart failure with preserved ejection fraction (HFpEF), David M. Kaye, MD, PhD, reported at the American Heart Association scientific sessions.
The device is implanted via cardiac catheterization and is intended to reduce elevated left atrial pressure, particularly that associated with exertion, by allowing a small amount but not excessive left-to-right shunting. Patients showed improvements in 6-minute walk distance, New York Heart Association class, and HF-related quality of life scores at 6 months, and those effects persisted at the most recent (12-month) follow-up, he said in a presentation that was simultaneously published online in Circulation (2016 Nov 16).
Overall survival at 1 year was 95%. Three patients died (one from combined pneumonia and renal failure, one from a fatal stroke, and one from an undetermined cause) and one was lost to follow-up. Thirteen patients required 17 hospitalizations for heart failure.
Six-minute walk distance improved from 331 meters at baseline to 363 meters. NYHA classification improved dramatically, as did quality of life scores as assessed by the Minnesota Living with HF questionnaire.
All 48 devices that were evaluable on echocardiographic imaging remained patent, showing continued left-to-right shunting. Left ventricular ejection fraction remained unchanged while right ventricular ejection fraction was significantly elevated over baseline levels. “In conjunction, there were modest but stable reductions in LV end-diastolic volume index with a concomitant rise in RV end-diastolic index,” he said.
A subset of 18 study participants underwent heart catheterization during both rest and exercise so that hemodynamics could be assessed. Exercise time increased significantly, from 8.2 minutes at baseline to 9.7 minutes at 6 months and to 10.4 minutes at 1 year. Similarly, peak work capacity during supine cycling increased from 48 watts at baseline to 60 watts at 6 months and 55 watts at 1 year. These benefits occurred without any increase in pulmonary capillary wedge pressure.
Systemic blood pressure did not change over time, either at rest or during exercise. Left and right atrial volumes also remained unchanged.
Perhaps most importantly, Dr. Kaye said, right-sided cardiac output increased significantly, while left-sided cardiac output remained unchanged. There was no evidence of increased pulmonary pressure or pulmonary vascular resistance. This meant that patients could do more physical activity for a given level of left atrial pressure, he said.
Furthermore, 1-year mortality was lower in this trial, at 4.6%, than in the placebo groups of the I-PRESERVE trial in irbesartan (5.2%) and the U.S. group of the TOPCAT trial in spironolactone (7.7%), said Dr. Kaye, professor and chief of cardiology at the University of Arizona, Tuscon.
Device therapy could have an enormous impact in carefully selected patients with HFpEF, for whom there are no medical treatments, despite the nonrandomized nature of the trial.
REDUCE LAP-HF was funded by Corvia Medical, maker of the shunt device. Dr. Kaye is an unpaid member of Corvia’s scientific advisory group. Dr. Sweitzer is an investigator in the ongoing randomized trial of the interatrial shunt.
NEW ORLEANS – An interatrial septal shunt device continued to provide “sustained and meaningful clinical benefit” at 1-year follow-up for 64 patients who had heart failure with preserved ejection fraction (HFpEF), David M. Kaye, MD, PhD, reported at the American Heart Association scientific sessions.
The device is implanted via cardiac catheterization and is intended to reduce elevated left atrial pressure, particularly that associated with exertion, by allowing a small amount but not excessive left-to-right shunting. Patients showed improvements in 6-minute walk distance, New York Heart Association class, and HF-related quality of life scores at 6 months, and those effects persisted at the most recent (12-month) follow-up, he said in a presentation that was simultaneously published online in Circulation (2016 Nov 16).
Overall survival at 1 year was 95%. Three patients died (one from combined pneumonia and renal failure, one from a fatal stroke, and one from an undetermined cause) and one was lost to follow-up. Thirteen patients required 17 hospitalizations for heart failure.
Six-minute walk distance improved from 331 meters at baseline to 363 meters. NYHA classification improved dramatically, as did quality of life scores as assessed by the Minnesota Living with HF questionnaire.
All 48 devices that were evaluable on echocardiographic imaging remained patent, showing continued left-to-right shunting. Left ventricular ejection fraction remained unchanged while right ventricular ejection fraction was significantly elevated over baseline levels. “In conjunction, there were modest but stable reductions in LV end-diastolic volume index with a concomitant rise in RV end-diastolic index,” he said.
A subset of 18 study participants underwent heart catheterization during both rest and exercise so that hemodynamics could be assessed. Exercise time increased significantly, from 8.2 minutes at baseline to 9.7 minutes at 6 months and to 10.4 minutes at 1 year. Similarly, peak work capacity during supine cycling increased from 48 watts at baseline to 60 watts at 6 months and 55 watts at 1 year. These benefits occurred without any increase in pulmonary capillary wedge pressure.
Systemic blood pressure did not change over time, either at rest or during exercise. Left and right atrial volumes also remained unchanged.
Perhaps most importantly, Dr. Kaye said, right-sided cardiac output increased significantly, while left-sided cardiac output remained unchanged. There was no evidence of increased pulmonary pressure or pulmonary vascular resistance. This meant that patients could do more physical activity for a given level of left atrial pressure, he said.
Furthermore, 1-year mortality was lower in this trial, at 4.6%, than in the placebo groups of the I-PRESERVE trial in irbesartan (5.2%) and the U.S. group of the TOPCAT trial in spironolactone (7.7%), said Dr. Kaye, professor and chief of cardiology at the University of Arizona, Tuscon.
Device therapy could have an enormous impact in carefully selected patients with HFpEF, for whom there are no medical treatments, despite the nonrandomized nature of the trial.
REDUCE LAP-HF was funded by Corvia Medical, maker of the shunt device. Dr. Kaye is an unpaid member of Corvia’s scientific advisory group. Dr. Sweitzer is an investigator in the ongoing randomized trial of the interatrial shunt.
NEW ORLEANS – An interatrial septal shunt device continued to provide “sustained and meaningful clinical benefit” at 1-year follow-up for 64 patients who had heart failure with preserved ejection fraction (HFpEF), David M. Kaye, MD, PhD, reported at the American Heart Association scientific sessions.
The device is implanted via cardiac catheterization and is intended to reduce elevated left atrial pressure, particularly that associated with exertion, by allowing a small amount but not excessive left-to-right shunting. Patients showed improvements in 6-minute walk distance, New York Heart Association class, and HF-related quality of life scores at 6 months, and those effects persisted at the most recent (12-month) follow-up, he said in a presentation that was simultaneously published online in Circulation (2016 Nov 16).
Overall survival at 1 year was 95%. Three patients died (one from combined pneumonia and renal failure, one from a fatal stroke, and one from an undetermined cause) and one was lost to follow-up. Thirteen patients required 17 hospitalizations for heart failure.
Six-minute walk distance improved from 331 meters at baseline to 363 meters. NYHA classification improved dramatically, as did quality of life scores as assessed by the Minnesota Living with HF questionnaire.
All 48 devices that were evaluable on echocardiographic imaging remained patent, showing continued left-to-right shunting. Left ventricular ejection fraction remained unchanged while right ventricular ejection fraction was significantly elevated over baseline levels. “In conjunction, there were modest but stable reductions in LV end-diastolic volume index with a concomitant rise in RV end-diastolic index,” he said.
A subset of 18 study participants underwent heart catheterization during both rest and exercise so that hemodynamics could be assessed. Exercise time increased significantly, from 8.2 minutes at baseline to 9.7 minutes at 6 months and to 10.4 minutes at 1 year. Similarly, peak work capacity during supine cycling increased from 48 watts at baseline to 60 watts at 6 months and 55 watts at 1 year. These benefits occurred without any increase in pulmonary capillary wedge pressure.
Systemic blood pressure did not change over time, either at rest or during exercise. Left and right atrial volumes also remained unchanged.
Perhaps most importantly, Dr. Kaye said, right-sided cardiac output increased significantly, while left-sided cardiac output remained unchanged. There was no evidence of increased pulmonary pressure or pulmonary vascular resistance. This meant that patients could do more physical activity for a given level of left atrial pressure, he said.
Furthermore, 1-year mortality was lower in this trial, at 4.6%, than in the placebo groups of the I-PRESERVE trial in irbesartan (5.2%) and the U.S. group of the TOPCAT trial in spironolactone (7.7%), said Dr. Kaye, professor and chief of cardiology at the University of Arizona, Tuscon.
Device therapy could have an enormous impact in carefully selected patients with HFpEF, for whom there are no medical treatments, despite the nonrandomized nature of the trial.
REDUCE LAP-HF was funded by Corvia Medical, maker of the shunt device. Dr. Kaye is an unpaid member of Corvia’s scientific advisory group. Dr. Sweitzer is an investigator in the ongoing randomized trial of the interatrial shunt.
AT THE AHA SCIENTIFIC SESSIONS 2016
Key clinical point: An interatrial septal shunt device continued to provide sustained and meaningful clinical benefit at 1-year follow-up for 64 patients who had heart failure with preserved ejection fraction.
Major finding: Six-minute walk distance improved from 331 meters at baseline to 363 meters at 1 year, NYHA classification improved dramatically, and HF-related quality of life scores also improved.
Data source: REDUCE LAP-HF, a multicenter, prospective, open-label study involving 64 patients followed for 1 year after transcatheter implantation of a shunt device.
Disclosures: REDUCE LAP-HF was funded by Corvia Medical, maker of the shunt device. Dr. Kaye is an unpaid member of Corvia’s scientific advisory group.
VIDEO: Bariatric surgery may protect against heart failure
NEW ORLEANS – Results of a new 40,000-patient Swedish observational study provide the strongest evidence to date suggesting a causal relationship between bariatric surgery and reduced risk of heart failure, according to Johan Sundström, MD.
The study, which included patients drawn from two large Swedish national registries, demonstrated that bariatric surgery was associated with a 46% reduction in the incidence of heart failure during a median 4.1 years of follow-up, compared with an intensive lifestyle modification program for weight loss.
“These are observational data, but it’s a very large study population – and probably there will never be a large randomized trial of bariatric surgery versus weight loss through intensive lifestyle modification as a means of reducing the risk of heart failure,” Dr. Sundström, professor of epidemiology and a cardiologist at Uppsala (Sweden) University, said at the American Heart Association scientific sessions.
The study included 25,804 bariatric surgery patients in SOReg, the Scandinavian Obesity Surgery Registry, and a matched comparator group of 13,701 participants in a Swedish national registry of obese participants in a commercial Sweden-based intensive structural lifestyle modification program for weight loss called Itrim. The two groups were matched for baseline body mass index, which was a mean of 41.5 kg, and numerous other demographic factors and comorbid conditions. Participants weighed an average of 119 kg at baseline. None of the subjects had a history of heart failure.
The bariatric surgery group lost substantially more weight than did the lifestyle modification group: an average loss of about 35 kg after 1 year, which was 18.8 kg more than in the lifestyle modification group. After 2 years, the bariatric surgery group had an average of 22.6 kg more weight loss than did the comparison group.
The primary outcome was hospitalization for new-onset heart failure during a median 4.1 years of follow-up. Subjects were well below the age range when the incidence of heart failure accelerates – they averaged 41 years of age – but 73 of them did develop heart failure during follow-up. The incidence was 46% lower in the bariatric surgery patients. This supports the study hypothesis that bariatric surgery leads to a low incidence of new-onset heart failure, compared with intensive lifestyle modification because of its larger weight loss effect.
When Dr. Sundström and his coinvestigators combined the two study groups, they found that a 10-kg weight loss at 1 year was associated with a 23% reduction in the risk of heart failure during follow-up, irrespective of whether the weight loss was achieved surgically or through the lifestyle program.
“A great way of studying causality is to take away the exposure and note what happens to the outcome. If there’s a causal link, then if you take away the risk factor – in this case, obesity – the disease should go away,” he explained in a video interview.
The reduced risk of heart failure in the bariatric surgery patients wasn’t because of fewer acute MIs. Indeed, their acute MI rate during follow-up was similar to that of the lifestyle modification group. But bariatric surgery was associated with relative risk reductions of 35%-37% for atrial fibrillation or need for diabetes or blood pressure–lowering medications at 1 year – and atrial fibrillation, diabetes, and hypertension are all established risk factors for heart failure, Dr. Sundström noted.
The Itrim intensive lifestyle modification program entailed an initial very-low-energy diet for the first 3 months in order to achieve massive weight loss, followed by a 9-month maintenance program involving motivational counseling, exercise, behavioral therapy, and a restricted diet.
Dr. Sundström said he and his coinvestigators plan to continue the study and expand it to look at differences in additional cardiovascular endpoints as patients age.
The study was funded by the U.S. National Institute of Diabetes and Digestive and Kidney Diseases, Uppsala University, the Karolinska Institute, and the Swedish Research Council. Dr. Sundström reported serving as a scientific advisor to Itrim.
NEW ORLEANS – Results of a new 40,000-patient Swedish observational study provide the strongest evidence to date suggesting a causal relationship between bariatric surgery and reduced risk of heart failure, according to Johan Sundström, MD.
The study, which included patients drawn from two large Swedish national registries, demonstrated that bariatric surgery was associated with a 46% reduction in the incidence of heart failure during a median 4.1 years of follow-up, compared with an intensive lifestyle modification program for weight loss.
“These are observational data, but it’s a very large study population – and probably there will never be a large randomized trial of bariatric surgery versus weight loss through intensive lifestyle modification as a means of reducing the risk of heart failure,” Dr. Sundström, professor of epidemiology and a cardiologist at Uppsala (Sweden) University, said at the American Heart Association scientific sessions.
The study included 25,804 bariatric surgery patients in SOReg, the Scandinavian Obesity Surgery Registry, and a matched comparator group of 13,701 participants in a Swedish national registry of obese participants in a commercial Sweden-based intensive structural lifestyle modification program for weight loss called Itrim. The two groups were matched for baseline body mass index, which was a mean of 41.5 kg, and numerous other demographic factors and comorbid conditions. Participants weighed an average of 119 kg at baseline. None of the subjects had a history of heart failure.
The bariatric surgery group lost substantially more weight than did the lifestyle modification group: an average loss of about 35 kg after 1 year, which was 18.8 kg more than in the lifestyle modification group. After 2 years, the bariatric surgery group had an average of 22.6 kg more weight loss than did the comparison group.
The primary outcome was hospitalization for new-onset heart failure during a median 4.1 years of follow-up. Subjects were well below the age range when the incidence of heart failure accelerates – they averaged 41 years of age – but 73 of them did develop heart failure during follow-up. The incidence was 46% lower in the bariatric surgery patients. This supports the study hypothesis that bariatric surgery leads to a low incidence of new-onset heart failure, compared with intensive lifestyle modification because of its larger weight loss effect.
When Dr. Sundström and his coinvestigators combined the two study groups, they found that a 10-kg weight loss at 1 year was associated with a 23% reduction in the risk of heart failure during follow-up, irrespective of whether the weight loss was achieved surgically or through the lifestyle program.
“A great way of studying causality is to take away the exposure and note what happens to the outcome. If there’s a causal link, then if you take away the risk factor – in this case, obesity – the disease should go away,” he explained in a video interview.
The reduced risk of heart failure in the bariatric surgery patients wasn’t because of fewer acute MIs. Indeed, their acute MI rate during follow-up was similar to that of the lifestyle modification group. But bariatric surgery was associated with relative risk reductions of 35%-37% for atrial fibrillation or need for diabetes or blood pressure–lowering medications at 1 year – and atrial fibrillation, diabetes, and hypertension are all established risk factors for heart failure, Dr. Sundström noted.
The Itrim intensive lifestyle modification program entailed an initial very-low-energy diet for the first 3 months in order to achieve massive weight loss, followed by a 9-month maintenance program involving motivational counseling, exercise, behavioral therapy, and a restricted diet.
Dr. Sundström said he and his coinvestigators plan to continue the study and expand it to look at differences in additional cardiovascular endpoints as patients age.
The study was funded by the U.S. National Institute of Diabetes and Digestive and Kidney Diseases, Uppsala University, the Karolinska Institute, and the Swedish Research Council. Dr. Sundström reported serving as a scientific advisor to Itrim.
NEW ORLEANS – Results of a new 40,000-patient Swedish observational study provide the strongest evidence to date suggesting a causal relationship between bariatric surgery and reduced risk of heart failure, according to Johan Sundström, MD.
The study, which included patients drawn from two large Swedish national registries, demonstrated that bariatric surgery was associated with a 46% reduction in the incidence of heart failure during a median 4.1 years of follow-up, compared with an intensive lifestyle modification program for weight loss.
“These are observational data, but it’s a very large study population – and probably there will never be a large randomized trial of bariatric surgery versus weight loss through intensive lifestyle modification as a means of reducing the risk of heart failure,” Dr. Sundström, professor of epidemiology and a cardiologist at Uppsala (Sweden) University, said at the American Heart Association scientific sessions.
The study included 25,804 bariatric surgery patients in SOReg, the Scandinavian Obesity Surgery Registry, and a matched comparator group of 13,701 participants in a Swedish national registry of obese participants in a commercial Sweden-based intensive structural lifestyle modification program for weight loss called Itrim. The two groups were matched for baseline body mass index, which was a mean of 41.5 kg, and numerous other demographic factors and comorbid conditions. Participants weighed an average of 119 kg at baseline. None of the subjects had a history of heart failure.
The bariatric surgery group lost substantially more weight than did the lifestyle modification group: an average loss of about 35 kg after 1 year, which was 18.8 kg more than in the lifestyle modification group. After 2 years, the bariatric surgery group had an average of 22.6 kg more weight loss than did the comparison group.
The primary outcome was hospitalization for new-onset heart failure during a median 4.1 years of follow-up. Subjects were well below the age range when the incidence of heart failure accelerates – they averaged 41 years of age – but 73 of them did develop heart failure during follow-up. The incidence was 46% lower in the bariatric surgery patients. This supports the study hypothesis that bariatric surgery leads to a low incidence of new-onset heart failure, compared with intensive lifestyle modification because of its larger weight loss effect.
When Dr. Sundström and his coinvestigators combined the two study groups, they found that a 10-kg weight loss at 1 year was associated with a 23% reduction in the risk of heart failure during follow-up, irrespective of whether the weight loss was achieved surgically or through the lifestyle program.
“A great way of studying causality is to take away the exposure and note what happens to the outcome. If there’s a causal link, then if you take away the risk factor – in this case, obesity – the disease should go away,” he explained in a video interview.
The reduced risk of heart failure in the bariatric surgery patients wasn’t because of fewer acute MIs. Indeed, their acute MI rate during follow-up was similar to that of the lifestyle modification group. But bariatric surgery was associated with relative risk reductions of 35%-37% for atrial fibrillation or need for diabetes or blood pressure–lowering medications at 1 year – and atrial fibrillation, diabetes, and hypertension are all established risk factors for heart failure, Dr. Sundström noted.
The Itrim intensive lifestyle modification program entailed an initial very-low-energy diet for the first 3 months in order to achieve massive weight loss, followed by a 9-month maintenance program involving motivational counseling, exercise, behavioral therapy, and a restricted diet.
Dr. Sundström said he and his coinvestigators plan to continue the study and expand it to look at differences in additional cardiovascular endpoints as patients age.
The study was funded by the U.S. National Institute of Diabetes and Digestive and Kidney Diseases, Uppsala University, the Karolinska Institute, and the Swedish Research Council. Dr. Sundström reported serving as a scientific advisor to Itrim.
AT THE AHA SCIENTIFIC SESSIONS 2016
Key clinical point:
Major finding: The incidence of new-onset heart failure was 46% lower during follow-up after bariatric surgery than among participants in an intensive lifestyle modification program for weight loss.
Data source: This observational registry study followed nearly 26,000 Swedish bariatric surgery patients and 14,000 matched participants in a commercial intensive lifestyle modification program for a median of 4.1 years.
Disclosures: The study was funded by the U.S. National Institutes of Diabetes and Digestive and Kidney Diseases, Uppsala University, the Karolinska Institute, and the Swedish Research Council. The presenter reported serving as a scientific advisor to Itrim.
Heart failure readmission metric not linked to care quality
Metrics used by the Centers for Medicare & Medicaid Services to determine penalties for heart failure hospital readmissions are not associated with quality of care or overall clinical outcomes, according to data presented at the annual scientific sessions of the American Heart Association.
Ambarish Pandey, MD, of the University of Texas Southwestern Medical Center in Dallas, and his colleagues analyzed data from centers participating in the American Heart Association’s Get With The Guidelines-Heart Failure (GWTG-HF) registry linked to Medicare claims from July 2008 to June 2011. Centers were stratified as having low risk-adjusted readmission rates and high risk-adjusted readmission rates based on publicly available data from 2013.
The study included 171 centers with 43,143 patients. Centers were almost evenly split between low- and high-risk–adjusted 30-day readmission rates, with just a few more (51%) falling in the low-risk–adjusted category.
Performance was nearly equal (95.7% for centers with a low risk-adjusted readmission rate vs. 96.5% for those with high risk-adjusted rate) for median adherence to all performance measures, as was the case for median percentage of defect-free care (90.0% vs. 91.1%, respectively) and composite 1-year outcome of death or all-cause readmission rates (median 62.9% vs. 65.3%, respectively). The higher readmission group had higher 1-year all-cause readmission rates (median, 59.1% vs. 54.7%), Dr. Pandey and his colleagues reported in the study that was published simultaneously in JACC: Heart Failure (2016 Nov 15. doi. org/10.1016/j.jchf.2016). One-year mortality rates were lower in the higher readmission group with a trend toward statistical significance (median, 28.2% vs. 31.7%; P = 0.07).
Taken together, the findings suggest the 30-day readmission metrics currently used by CMS to determine readmission penalties are not associated with quality of care or overall clinical outcomes, Dr. Pandey and his colleagues wrote. Results showing higher 30-day readmissions do not necessarily reflect poor quality of care and may be related to other factors.
“These findings question the usefulness of the [hospital readmission reduction program] metric in identifying and penalizing hospitals with low quality of care,” Dr. Pandey wrote, adding that the findings were consistent with previous studies that have demonstrated a lack of association between in-hospital quality of care and 30-day readmission rates.
CMS implemented the federal Hospital Readmissions Reduction Program (HRRP) in 2012 to provide financial incentives for hospitals to reduce readmissions. Under the program, CMS uses claims data to determine whether readmission rates for heart failure, acute myocardial infarction, and pneumonia at eligible hospitals are higher than would be predicted by CMS models. Centers with higher than expected readmission rates face up to a 3% reimbursement penalty.
agallegos@frontlinemedcom.com
On Twitter @legal_med
These authors add to a chorus of voices expressing concern regarding the appropriateness and validity of the 30-day readmission metric. Arguably, this metric has driven our entire provider workforce to construct machinery designed to reduce short-term posthospitalization utilization, while doing little to improve quality for the 5.7 million (and counting) Americans with heart failure.

Marvin A. Konstam, MD, of Tufts University, Boston, made these comments in an accompanying editorial (JACC: Heart Fail. 2016 Nov 15. doi: 10.1016/j.jchf.2016.10.004). He reported no relevant disclosures.
These authors add to a chorus of voices expressing concern regarding the appropriateness and validity of the 30-day readmission metric. Arguably, this metric has driven our entire provider workforce to construct machinery designed to reduce short-term posthospitalization utilization, while doing little to improve quality for the 5.7 million (and counting) Americans with heart failure.
Marvin A. Konstam, MD, of Tufts University, Boston, made these comments in an accompanying editorial (JACC: Heart Fail. 2016 Nov 15. doi: 10.1016/j.jchf.2016.10.004). He reported no relevant disclosures.
These authors add to a chorus of voices expressing concern regarding the appropriateness and validity of the 30-day readmission metric. Arguably, this metric has driven our entire provider workforce to construct machinery designed to reduce short-term posthospitalization utilization, while doing little to improve quality for the 5.7 million (and counting) Americans with heart failure.
Marvin A. Konstam, MD, of Tufts University, Boston, made these comments in an accompanying editorial (JACC: Heart Fail. 2016 Nov 15. doi: 10.1016/j.jchf.2016.10.004). He reported no relevant disclosures.
Metrics used by the Centers for Medicare & Medicaid Services to determine penalties for heart failure hospital readmissions are not associated with quality of care or overall clinical outcomes, according to data presented at the annual scientific sessions of the American Heart Association.
Ambarish Pandey, MD, of the University of Texas Southwestern Medical Center in Dallas, and his colleagues analyzed data from centers participating in the American Heart Association’s Get With The Guidelines-Heart Failure (GWTG-HF) registry linked to Medicare claims from July 2008 to June 2011. Centers were stratified as having low risk-adjusted readmission rates and high risk-adjusted readmission rates based on publicly available data from 2013.
The study included 171 centers with 43,143 patients. Centers were almost evenly split between low- and high-risk–adjusted 30-day readmission rates, with just a few more (51%) falling in the low-risk–adjusted category.
Performance was nearly equal (95.7% for centers with a low risk-adjusted readmission rate vs. 96.5% for those with high risk-adjusted rate) for median adherence to all performance measures, as was the case for median percentage of defect-free care (90.0% vs. 91.1%, respectively) and composite 1-year outcome of death or all-cause readmission rates (median 62.9% vs. 65.3%, respectively). The higher readmission group had higher 1-year all-cause readmission rates (median, 59.1% vs. 54.7%), Dr. Pandey and his colleagues reported in the study that was published simultaneously in JACC: Heart Failure (2016 Nov 15. doi. org/10.1016/j.jchf.2016). One-year mortality rates were lower in the higher readmission group with a trend toward statistical significance (median, 28.2% vs. 31.7%; P = 0.07).
Taken together, the findings suggest the 30-day readmission metrics currently used by CMS to determine readmission penalties are not associated with quality of care or overall clinical outcomes, Dr. Pandey and his colleagues wrote. Results showing higher 30-day readmissions do not necessarily reflect poor quality of care and may be related to other factors.
“These findings question the usefulness of the [hospital readmission reduction program] metric in identifying and penalizing hospitals with low quality of care,” Dr. Pandey wrote, adding that the findings were consistent with previous studies that have demonstrated a lack of association between in-hospital quality of care and 30-day readmission rates.
CMS implemented the federal Hospital Readmissions Reduction Program (HRRP) in 2012 to provide financial incentives for hospitals to reduce readmissions. Under the program, CMS uses claims data to determine whether readmission rates for heart failure, acute myocardial infarction, and pneumonia at eligible hospitals are higher than would be predicted by CMS models. Centers with higher than expected readmission rates face up to a 3% reimbursement penalty.
agallegos@frontlinemedcom.com
On Twitter @legal_med
Metrics used by the Centers for Medicare & Medicaid Services to determine penalties for heart failure hospital readmissions are not associated with quality of care or overall clinical outcomes, according to data presented at the annual scientific sessions of the American Heart Association.
Ambarish Pandey, MD, of the University of Texas Southwestern Medical Center in Dallas, and his colleagues analyzed data from centers participating in the American Heart Association’s Get With The Guidelines-Heart Failure (GWTG-HF) registry linked to Medicare claims from July 2008 to June 2011. Centers were stratified as having low risk-adjusted readmission rates and high risk-adjusted readmission rates based on publicly available data from 2013.
The study included 171 centers with 43,143 patients. Centers were almost evenly split between low- and high-risk–adjusted 30-day readmission rates, with just a few more (51%) falling in the low-risk–adjusted category.
Performance was nearly equal (95.7% for centers with a low risk-adjusted readmission rate vs. 96.5% for those with high risk-adjusted rate) for median adherence to all performance measures, as was the case for median percentage of defect-free care (90.0% vs. 91.1%, respectively) and composite 1-year outcome of death or all-cause readmission rates (median 62.9% vs. 65.3%, respectively). The higher readmission group had higher 1-year all-cause readmission rates (median, 59.1% vs. 54.7%), Dr. Pandey and his colleagues reported in the study that was published simultaneously in JACC: Heart Failure (2016 Nov 15. doi. org/10.1016/j.jchf.2016). One-year mortality rates were lower in the higher readmission group with a trend toward statistical significance (median, 28.2% vs. 31.7%; P = 0.07).
Taken together, the findings suggest the 30-day readmission metrics currently used by CMS to determine readmission penalties are not associated with quality of care or overall clinical outcomes, Dr. Pandey and his colleagues wrote. Results showing higher 30-day readmissions do not necessarily reflect poor quality of care and may be related to other factors.
“These findings question the usefulness of the [hospital readmission reduction program] metric in identifying and penalizing hospitals with low quality of care,” Dr. Pandey wrote, adding that the findings were consistent with previous studies that have demonstrated a lack of association between in-hospital quality of care and 30-day readmission rates.
CMS implemented the federal Hospital Readmissions Reduction Program (HRRP) in 2012 to provide financial incentives for hospitals to reduce readmissions. Under the program, CMS uses claims data to determine whether readmission rates for heart failure, acute myocardial infarction, and pneumonia at eligible hospitals are higher than would be predicted by CMS models. Centers with higher than expected readmission rates face up to a 3% reimbursement penalty.
agallegos@frontlinemedcom.com
On Twitter @legal_med
FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Performance was nearly equal (95.7% for centers with a low risk-adjusted readmission rate vs. 96.5% for those with high risk-adjusted rate) for median adherence to all performance measures.
Data source: Analysis of publicly available data reported to the CMS Hospital Readmission Reduction program.
Disclosures: No relevant conflicts of interest.
AHA Late-Breaking Clinical Trials preview
The emphasis on this year’s American Heart Association Scientific Sessions in New Orleans is bigness: “Big science, big technology, and big networking opportunities,” the AHA 16 website says.
And so the 19 abstracts out of thousands submitted that got the biggest score from program committee for AHA 2016, led by Frank Sellke, MD, were chosen for presentation at four Late-Breaking Clinical Trials session previewed the late-breaking science.
Big trials for big questions
The first late-breaker session, on Sunday, Nov. 13, at 3:45 p.m., CT, is titled will, as its title says present the long-awaited results of four trials with large enrollment and long-term outcomes.
EUCLID (A Study Comparing Cardiovascular Effects of Ticagrelor and Clopidogrel in Patients With Peripheral Artery Disease) randomized an estimated 16,000 patients with symptomatic PAD to long-term antiplatelet monotherapy with either ticagrelor or clopidogrel to see which one would be superior in preventing the composite of cardiovascular death, myocardial infarction and ischemic stroke up to 40 months. Secondarily, it looked at acute limb ischemia, need for revascularization, and disease progression. “This could have tremendous implications for patients treat for pad trying to prevent CV disease,” Dr. Sellke said.
PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs Ibuprofen or Naproxen) harks back to 2005, when the Food and Drug Administration, wrestling with the growing evidence that NSAIDs were linked with cardiovascular events, asked for a large, cardiovascular outcomes trial. PRECISION, sponsored by Pfizer but run by an academic-led steering committee led by Steven Nissen, MD, now chief of cardiovascular medicine at the Cleveland Clinic, randomized some 20,000 arthritis patients with or at risk for cardiovascular disease to long-term pain treatment with celecoxib, naproxen, or ibuprofen for a planned follow-up of 2 years. The primary endpoint is a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. Dr. Sellke noted that the results will be important for many physicians and patients wanting to minimize the risks associated with NSAIDs.
HOPE 3 (Heart Outcomes Evaluation 3), presented in April this year at the American College of Cardiology meeting in Chicago, showed the combination of rosuvastatin plus candesartan and hydrochlorothiazide reduced cardiovascular events in intermediate-risk patients with hypertension, regardless of their baseline LDL cholesterol and inflammatory biomarker levels. The analysis to be presented at AHA will show whether the combination has any effect on cognitive function. As evidence builds of the cardiovascular benefit of aggressive treatment of hypertension, as in the SPRINT trial, the results could be tremendously important, Dr. Sellke said.
TRUE AHF (Efficacy and Safety of Ularitide for the Treatment of Acute Decompensated Heart Failure) randomized about 2,150 patients with acute decompensated heart failure to receive a 48-hour intravenous infusion of the natriuretic peptide ularitide or placebo. The primary outcome is a composite of 48-hour improved in-hospital worsening or unchanged clinical conditions, as well as long-term cardiovascular mortality with a median follow-up of 7 months. Because there are no effective treatments for acute systolic heart failure, the results of TRUE AHF could be of tremendous benefit, Dr. Sellke said.
Pioneering the Future of HeART Interventions
The trials with the greatest impact for practice to be presented at AHA 2015, according to the Dr. Sellke’s admitted bias as a cardiothoracic surgeon, will all be presented in this second of the late-breaker sessions, on Monday, Nov. 14, at 10:45 a.m., CT.
ART (Arterial Revascularization Trial) was a comparison of single vs. bilateral internal mammary artery grafting in more than 3,000 randomized patients undergoing coronary artery bypass surgery (CABG). The outcomes of mortality, stroke, MI, and repeat revascularization were published in 2010, showing no differences between groups. The 5-year results to be presented on Monday may resolve some of the controversy surrounding the two methods, as surgeons and cardiologists are strongly divided on the benefits and risks of single, compared with double, internal mammary artery grafting.
FUTURE (Functional Testing Underlying Coronary Revascularization) compared fractional flow reserve–guided management with conventional management in roughly 900 patients undergoing revascularization with multivessel coronary artery disease. The primary outcome is a composite of death, MI, coronary revascularization, and stroke. FFR has received a lot of attention recently, Dr. Sellke said, because it looks at the physiologic, rather than the anatomic, effects of lesion on catheterization. The results will show whether there’s clinical benefit to adding FFR to angiography that will offset the additional time it takes to perform before PCI or CABG.
PIONEER AF-PCI (An Open-label, Randomized, Controlled, Multicenter Study Exploring Two Treatment Strategies of Rivaroxaban and a Dose-Adjusted Oral Vitamin K Antagonist Treatment Strategy in Subjects With Atrial Fibrillation Who Undergo Percutaneous Coronary Intervention) addressed the conundrum of treating anticoagulated patients with atrial fibrillation who are undergoing PCI with adequate dual-antiplatelet therapy – and avoiding bleeding events. About 2,000 patients were randomized to varying combinations of rivaroxaban or warfarin plus aspirin, ticagrelor prasugrel, and/or clopidogrel for 1 year. The primary outcome is significant bleeding. Dr. Sellke said that because drug-eluting stents require at least a year of DAPT, the PIONEER AF-PCI results will add knowledge in an important and controversial area.
GERMANY is a report from the German Aortic Valve Registry (GARY) on the 1-year outcomes of patients with intermediate-risk severe aortic stenosis who underwent either transcatheter or surgical aortic replacement on the efficacy and outcomes of the two approaches. Dr. Sellke noted that these results will be important because the patients in this registry were not at high risk or ineligible for surgical aortic replacement.
Insights from New Therapeutic Trials for Lipids
Of the five trials presented in this session on Tuesday, Nov. 15, at 10:45 a.m., CT, only one is in an approved treatment for lowering lipids. That is GLAGOV (Global Assessment of Plaque Regression With a PCSK9 Antibody as Measured by Intravascular Ultrasound), is looking at whether LDL lowering with the PCSK9 inhibitor evolocumab reduces atheroma volume in almost 1,000 patients.
Guiding the Momentum to Effect HF Outcomes – Ironing Out the Wrinkles
Two of the six heart failure trials presented in this session on Wednesday, Nov. 16, at 10:45 a.m., CT, study cardiorespiratory effects of iron, thus the title, Dr. Sellke said.
REDUCE LAP HF (A Study to Evaluate the DC Devices, Inc. IASD System II to REDUCE Elevated Left Atrial Pressure in Patients With Heart Failure). The primary outcome is a composite of death, stroke, MI, or a systemic embolic event at 6 months. The trial evaluated a transcatheter interatrial shunt device to left atrial pressure in patients with heart failure with preserved ejection fraction (HFpEF). In this type of diastolic heart failure in which patients’ hearts cannot relax, there is really no treatment, Dr. Sellke said. So although this treatment seems “hokey,” a positive result could be important.
ATHENA HF (Aldosterone Targeted Neurohormonal Combined with Natriuresis Therapy in Heart Failure) tested the diuretic spironolactone in heart failure. The investigators randomized 360 patients to high-dose spironolactone or usual care to see whether they could provide greater reductions of n-terminal prohormone of brain natriuretic peptide (NT-proBNP) levels within 96 hours. There’s evidence that spironolactone can provide symptomatic relief for patients with heart failure, so these results could be important, Dr. Sellke said.
IRONOUT HF (Oral Iron Repletion Effects on Oxygen Up Take in Heart Failure) randomized heart failure patients with iron deficiency to oral iron supplementation or placebo and measured peak oxygen uptake at 16 weeks.
EFFECT-HF (Effect of Ferric Carboxymaltose on Exercise Capacity in Patients with Iron Deficiency and Chronic Heart Failure) also studied the effect of iron supplementation, intravenous in this case, on exercise capacity in heart failure patients at 24 weeks. Iron depletion is a hallmark of heart failure, Dr. Sellke pointed out, so iron repletion could be a simple way to improve functional capacity.
MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HM3) evaluated the safety and effectiveness of the Thoratec HeartMate 3 left-ventricular assist device employing MagLev technology, which is said to facilitate the free flow of blood through the device. Roughly 1,000 patients with advanced, refractory heart failure were randomized to receive either the investigational HeartMate 3 or the HeartMate 2. The primary outcomes included short- and long-term survival and freedom from debilitating stroke. Trials such as this are very important, Dr. Sellke said, because the need for donor hearts far exceeds demand and better, cheaper LVADs that last longer could extend the lives of many thousands of patients every year.
MultiSENSE (Evaluation of Multisensor Data in Heart Failure Patients With Implanted Devices) collected information taken from sensors in an implanted cardiac synchronization therapy device in 1,000 patients to develop algorithms that would detect worsening heart failure. Multiple readmissions for heart failure are frequent and ineffective, and detecting the onset of worsening heart failure has the potential to bring those admissions way down, Dr. Sellke said.
The emphasis on this year’s American Heart Association Scientific Sessions in New Orleans is bigness: “Big science, big technology, and big networking opportunities,” the AHA 16 website says.
And so the 19 abstracts out of thousands submitted that got the biggest score from program committee for AHA 2016, led by Frank Sellke, MD, were chosen for presentation at four Late-Breaking Clinical Trials session previewed the late-breaking science.
Big trials for big questions
The first late-breaker session, on Sunday, Nov. 13, at 3:45 p.m., CT, is titled will, as its title says present the long-awaited results of four trials with large enrollment and long-term outcomes.
EUCLID (A Study Comparing Cardiovascular Effects of Ticagrelor and Clopidogrel in Patients With Peripheral Artery Disease) randomized an estimated 16,000 patients with symptomatic PAD to long-term antiplatelet monotherapy with either ticagrelor or clopidogrel to see which one would be superior in preventing the composite of cardiovascular death, myocardial infarction and ischemic stroke up to 40 months. Secondarily, it looked at acute limb ischemia, need for revascularization, and disease progression. “This could have tremendous implications for patients treat for pad trying to prevent CV disease,” Dr. Sellke said.
PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs Ibuprofen or Naproxen) harks back to 2005, when the Food and Drug Administration, wrestling with the growing evidence that NSAIDs were linked with cardiovascular events, asked for a large, cardiovascular outcomes trial. PRECISION, sponsored by Pfizer but run by an academic-led steering committee led by Steven Nissen, MD, now chief of cardiovascular medicine at the Cleveland Clinic, randomized some 20,000 arthritis patients with or at risk for cardiovascular disease to long-term pain treatment with celecoxib, naproxen, or ibuprofen for a planned follow-up of 2 years. The primary endpoint is a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. Dr. Sellke noted that the results will be important for many physicians and patients wanting to minimize the risks associated with NSAIDs.
HOPE 3 (Heart Outcomes Evaluation 3), presented in April this year at the American College of Cardiology meeting in Chicago, showed the combination of rosuvastatin plus candesartan and hydrochlorothiazide reduced cardiovascular events in intermediate-risk patients with hypertension, regardless of their baseline LDL cholesterol and inflammatory biomarker levels. The analysis to be presented at AHA will show whether the combination has any effect on cognitive function. As evidence builds of the cardiovascular benefit of aggressive treatment of hypertension, as in the SPRINT trial, the results could be tremendously important, Dr. Sellke said.
TRUE AHF (Efficacy and Safety of Ularitide for the Treatment of Acute Decompensated Heart Failure) randomized about 2,150 patients with acute decompensated heart failure to receive a 48-hour intravenous infusion of the natriuretic peptide ularitide or placebo. The primary outcome is a composite of 48-hour improved in-hospital worsening or unchanged clinical conditions, as well as long-term cardiovascular mortality with a median follow-up of 7 months. Because there are no effective treatments for acute systolic heart failure, the results of TRUE AHF could be of tremendous benefit, Dr. Sellke said.
Pioneering the Future of HeART Interventions
The trials with the greatest impact for practice to be presented at AHA 2015, according to the Dr. Sellke’s admitted bias as a cardiothoracic surgeon, will all be presented in this second of the late-breaker sessions, on Monday, Nov. 14, at 10:45 a.m., CT.
ART (Arterial Revascularization Trial) was a comparison of single vs. bilateral internal mammary artery grafting in more than 3,000 randomized patients undergoing coronary artery bypass surgery (CABG). The outcomes of mortality, stroke, MI, and repeat revascularization were published in 2010, showing no differences between groups. The 5-year results to be presented on Monday may resolve some of the controversy surrounding the two methods, as surgeons and cardiologists are strongly divided on the benefits and risks of single, compared with double, internal mammary artery grafting.
FUTURE (Functional Testing Underlying Coronary Revascularization) compared fractional flow reserve–guided management with conventional management in roughly 900 patients undergoing revascularization with multivessel coronary artery disease. The primary outcome is a composite of death, MI, coronary revascularization, and stroke. FFR has received a lot of attention recently, Dr. Sellke said, because it looks at the physiologic, rather than the anatomic, effects of lesion on catheterization. The results will show whether there’s clinical benefit to adding FFR to angiography that will offset the additional time it takes to perform before PCI or CABG.
PIONEER AF-PCI (An Open-label, Randomized, Controlled, Multicenter Study Exploring Two Treatment Strategies of Rivaroxaban and a Dose-Adjusted Oral Vitamin K Antagonist Treatment Strategy in Subjects With Atrial Fibrillation Who Undergo Percutaneous Coronary Intervention) addressed the conundrum of treating anticoagulated patients with atrial fibrillation who are undergoing PCI with adequate dual-antiplatelet therapy – and avoiding bleeding events. About 2,000 patients were randomized to varying combinations of rivaroxaban or warfarin plus aspirin, ticagrelor prasugrel, and/or clopidogrel for 1 year. The primary outcome is significant bleeding. Dr. Sellke said that because drug-eluting stents require at least a year of DAPT, the PIONEER AF-PCI results will add knowledge in an important and controversial area.
GERMANY is a report from the German Aortic Valve Registry (GARY) on the 1-year outcomes of patients with intermediate-risk severe aortic stenosis who underwent either transcatheter or surgical aortic replacement on the efficacy and outcomes of the two approaches. Dr. Sellke noted that these results will be important because the patients in this registry were not at high risk or ineligible for surgical aortic replacement.
Insights from New Therapeutic Trials for Lipids
Of the five trials presented in this session on Tuesday, Nov. 15, at 10:45 a.m., CT, only one is in an approved treatment for lowering lipids. That is GLAGOV (Global Assessment of Plaque Regression With a PCSK9 Antibody as Measured by Intravascular Ultrasound), is looking at whether LDL lowering with the PCSK9 inhibitor evolocumab reduces atheroma volume in almost 1,000 patients.
Guiding the Momentum to Effect HF Outcomes – Ironing Out the Wrinkles
Two of the six heart failure trials presented in this session on Wednesday, Nov. 16, at 10:45 a.m., CT, study cardiorespiratory effects of iron, thus the title, Dr. Sellke said.
REDUCE LAP HF (A Study to Evaluate the DC Devices, Inc. IASD System II to REDUCE Elevated Left Atrial Pressure in Patients With Heart Failure). The primary outcome is a composite of death, stroke, MI, or a systemic embolic event at 6 months. The trial evaluated a transcatheter interatrial shunt device to left atrial pressure in patients with heart failure with preserved ejection fraction (HFpEF). In this type of diastolic heart failure in which patients’ hearts cannot relax, there is really no treatment, Dr. Sellke said. So although this treatment seems “hokey,” a positive result could be important.
ATHENA HF (Aldosterone Targeted Neurohormonal Combined with Natriuresis Therapy in Heart Failure) tested the diuretic spironolactone in heart failure. The investigators randomized 360 patients to high-dose spironolactone or usual care to see whether they could provide greater reductions of n-terminal prohormone of brain natriuretic peptide (NT-proBNP) levels within 96 hours. There’s evidence that spironolactone can provide symptomatic relief for patients with heart failure, so these results could be important, Dr. Sellke said.
IRONOUT HF (Oral Iron Repletion Effects on Oxygen Up Take in Heart Failure) randomized heart failure patients with iron deficiency to oral iron supplementation or placebo and measured peak oxygen uptake at 16 weeks.
EFFECT-HF (Effect of Ferric Carboxymaltose on Exercise Capacity in Patients with Iron Deficiency and Chronic Heart Failure) also studied the effect of iron supplementation, intravenous in this case, on exercise capacity in heart failure patients at 24 weeks. Iron depletion is a hallmark of heart failure, Dr. Sellke pointed out, so iron repletion could be a simple way to improve functional capacity.
MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HM3) evaluated the safety and effectiveness of the Thoratec HeartMate 3 left-ventricular assist device employing MagLev technology, which is said to facilitate the free flow of blood through the device. Roughly 1,000 patients with advanced, refractory heart failure were randomized to receive either the investigational HeartMate 3 or the HeartMate 2. The primary outcomes included short- and long-term survival and freedom from debilitating stroke. Trials such as this are very important, Dr. Sellke said, because the need for donor hearts far exceeds demand and better, cheaper LVADs that last longer could extend the lives of many thousands of patients every year.
MultiSENSE (Evaluation of Multisensor Data in Heart Failure Patients With Implanted Devices) collected information taken from sensors in an implanted cardiac synchronization therapy device in 1,000 patients to develop algorithms that would detect worsening heart failure. Multiple readmissions for heart failure are frequent and ineffective, and detecting the onset of worsening heart failure has the potential to bring those admissions way down, Dr. Sellke said.
The emphasis on this year’s American Heart Association Scientific Sessions in New Orleans is bigness: “Big science, big technology, and big networking opportunities,” the AHA 16 website says.
And so the 19 abstracts out of thousands submitted that got the biggest score from program committee for AHA 2016, led by Frank Sellke, MD, were chosen for presentation at four Late-Breaking Clinical Trials session previewed the late-breaking science.
Big trials for big questions
The first late-breaker session, on Sunday, Nov. 13, at 3:45 p.m., CT, is titled will, as its title says present the long-awaited results of four trials with large enrollment and long-term outcomes.
EUCLID (A Study Comparing Cardiovascular Effects of Ticagrelor and Clopidogrel in Patients With Peripheral Artery Disease) randomized an estimated 16,000 patients with symptomatic PAD to long-term antiplatelet monotherapy with either ticagrelor or clopidogrel to see which one would be superior in preventing the composite of cardiovascular death, myocardial infarction and ischemic stroke up to 40 months. Secondarily, it looked at acute limb ischemia, need for revascularization, and disease progression. “This could have tremendous implications for patients treat for pad trying to prevent CV disease,” Dr. Sellke said.
PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs Ibuprofen or Naproxen) harks back to 2005, when the Food and Drug Administration, wrestling with the growing evidence that NSAIDs were linked with cardiovascular events, asked for a large, cardiovascular outcomes trial. PRECISION, sponsored by Pfizer but run by an academic-led steering committee led by Steven Nissen, MD, now chief of cardiovascular medicine at the Cleveland Clinic, randomized some 20,000 arthritis patients with or at risk for cardiovascular disease to long-term pain treatment with celecoxib, naproxen, or ibuprofen for a planned follow-up of 2 years. The primary endpoint is a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. Dr. Sellke noted that the results will be important for many physicians and patients wanting to minimize the risks associated with NSAIDs.
HOPE 3 (Heart Outcomes Evaluation 3), presented in April this year at the American College of Cardiology meeting in Chicago, showed the combination of rosuvastatin plus candesartan and hydrochlorothiazide reduced cardiovascular events in intermediate-risk patients with hypertension, regardless of their baseline LDL cholesterol and inflammatory biomarker levels. The analysis to be presented at AHA will show whether the combination has any effect on cognitive function. As evidence builds of the cardiovascular benefit of aggressive treatment of hypertension, as in the SPRINT trial, the results could be tremendously important, Dr. Sellke said.
TRUE AHF (Efficacy and Safety of Ularitide for the Treatment of Acute Decompensated Heart Failure) randomized about 2,150 patients with acute decompensated heart failure to receive a 48-hour intravenous infusion of the natriuretic peptide ularitide or placebo. The primary outcome is a composite of 48-hour improved in-hospital worsening or unchanged clinical conditions, as well as long-term cardiovascular mortality with a median follow-up of 7 months. Because there are no effective treatments for acute systolic heart failure, the results of TRUE AHF could be of tremendous benefit, Dr. Sellke said.
Pioneering the Future of HeART Interventions
The trials with the greatest impact for practice to be presented at AHA 2015, according to the Dr. Sellke’s admitted bias as a cardiothoracic surgeon, will all be presented in this second of the late-breaker sessions, on Monday, Nov. 14, at 10:45 a.m., CT.
ART (Arterial Revascularization Trial) was a comparison of single vs. bilateral internal mammary artery grafting in more than 3,000 randomized patients undergoing coronary artery bypass surgery (CABG). The outcomes of mortality, stroke, MI, and repeat revascularization were published in 2010, showing no differences between groups. The 5-year results to be presented on Monday may resolve some of the controversy surrounding the two methods, as surgeons and cardiologists are strongly divided on the benefits and risks of single, compared with double, internal mammary artery grafting.
FUTURE (Functional Testing Underlying Coronary Revascularization) compared fractional flow reserve–guided management with conventional management in roughly 900 patients undergoing revascularization with multivessel coronary artery disease. The primary outcome is a composite of death, MI, coronary revascularization, and stroke. FFR has received a lot of attention recently, Dr. Sellke said, because it looks at the physiologic, rather than the anatomic, effects of lesion on catheterization. The results will show whether there’s clinical benefit to adding FFR to angiography that will offset the additional time it takes to perform before PCI or CABG.
PIONEER AF-PCI (An Open-label, Randomized, Controlled, Multicenter Study Exploring Two Treatment Strategies of Rivaroxaban and a Dose-Adjusted Oral Vitamin K Antagonist Treatment Strategy in Subjects With Atrial Fibrillation Who Undergo Percutaneous Coronary Intervention) addressed the conundrum of treating anticoagulated patients with atrial fibrillation who are undergoing PCI with adequate dual-antiplatelet therapy – and avoiding bleeding events. About 2,000 patients were randomized to varying combinations of rivaroxaban or warfarin plus aspirin, ticagrelor prasugrel, and/or clopidogrel for 1 year. The primary outcome is significant bleeding. Dr. Sellke said that because drug-eluting stents require at least a year of DAPT, the PIONEER AF-PCI results will add knowledge in an important and controversial area.
GERMANY is a report from the German Aortic Valve Registry (GARY) on the 1-year outcomes of patients with intermediate-risk severe aortic stenosis who underwent either transcatheter or surgical aortic replacement on the efficacy and outcomes of the two approaches. Dr. Sellke noted that these results will be important because the patients in this registry were not at high risk or ineligible for surgical aortic replacement.
Insights from New Therapeutic Trials for Lipids
Of the five trials presented in this session on Tuesday, Nov. 15, at 10:45 a.m., CT, only one is in an approved treatment for lowering lipids. That is GLAGOV (Global Assessment of Plaque Regression With a PCSK9 Antibody as Measured by Intravascular Ultrasound), is looking at whether LDL lowering with the PCSK9 inhibitor evolocumab reduces atheroma volume in almost 1,000 patients.
Guiding the Momentum to Effect HF Outcomes – Ironing Out the Wrinkles
Two of the six heart failure trials presented in this session on Wednesday, Nov. 16, at 10:45 a.m., CT, study cardiorespiratory effects of iron, thus the title, Dr. Sellke said.
REDUCE LAP HF (A Study to Evaluate the DC Devices, Inc. IASD System II to REDUCE Elevated Left Atrial Pressure in Patients With Heart Failure). The primary outcome is a composite of death, stroke, MI, or a systemic embolic event at 6 months. The trial evaluated a transcatheter interatrial shunt device to left atrial pressure in patients with heart failure with preserved ejection fraction (HFpEF). In this type of diastolic heart failure in which patients’ hearts cannot relax, there is really no treatment, Dr. Sellke said. So although this treatment seems “hokey,” a positive result could be important.
ATHENA HF (Aldosterone Targeted Neurohormonal Combined with Natriuresis Therapy in Heart Failure) tested the diuretic spironolactone in heart failure. The investigators randomized 360 patients to high-dose spironolactone or usual care to see whether they could provide greater reductions of n-terminal prohormone of brain natriuretic peptide (NT-proBNP) levels within 96 hours. There’s evidence that spironolactone can provide symptomatic relief for patients with heart failure, so these results could be important, Dr. Sellke said.
IRONOUT HF (Oral Iron Repletion Effects on Oxygen Up Take in Heart Failure) randomized heart failure patients with iron deficiency to oral iron supplementation or placebo and measured peak oxygen uptake at 16 weeks.
EFFECT-HF (Effect of Ferric Carboxymaltose on Exercise Capacity in Patients with Iron Deficiency and Chronic Heart Failure) also studied the effect of iron supplementation, intravenous in this case, on exercise capacity in heart failure patients at 24 weeks. Iron depletion is a hallmark of heart failure, Dr. Sellke pointed out, so iron repletion could be a simple way to improve functional capacity.
MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HM3) evaluated the safety and effectiveness of the Thoratec HeartMate 3 left-ventricular assist device employing MagLev technology, which is said to facilitate the free flow of blood through the device. Roughly 1,000 patients with advanced, refractory heart failure were randomized to receive either the investigational HeartMate 3 or the HeartMate 2. The primary outcomes included short- and long-term survival and freedom from debilitating stroke. Trials such as this are very important, Dr. Sellke said, because the need for donor hearts far exceeds demand and better, cheaper LVADs that last longer could extend the lives of many thousands of patients every year.
MultiSENSE (Evaluation of Multisensor Data in Heart Failure Patients With Implanted Devices) collected information taken from sensors in an implanted cardiac synchronization therapy device in 1,000 patients to develop algorithms that would detect worsening heart failure. Multiple readmissions for heart failure are frequent and ineffective, and detecting the onset of worsening heart failure has the potential to bring those admissions way down, Dr. Sellke said.
Diabetes drugs with cardiovascular benefits broaden cardiology’s turf
The dramatic reduction in cardiovascular death and heart failure hospitalization seen during treatment with empagliflozin (Jardiance) in the EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients) trial, for example, has prompted some cardiologists in the year since the first EMPA-REG report to become active prescribers of the drug to their patients who have type 2 diabetes and cardiovascular disease. The same evidence has driven other cardiologists who may not feel fully comfortable prescribing an antidiabetic drug on their own to enter into active partnerships with endocrinologists to work as a team to put diabetes patients with cardiovascular disease on empagliflozin.
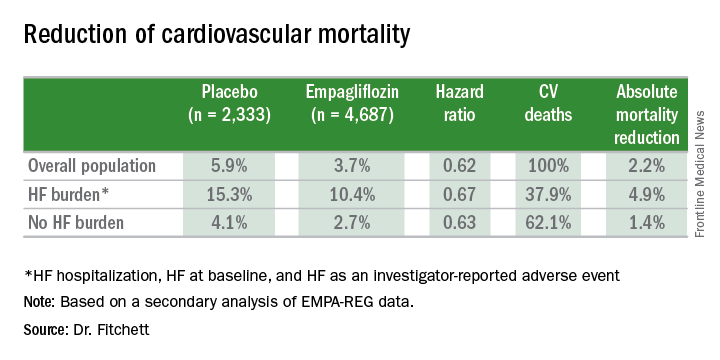
In Dr. Fitchett’s practice, “if a patient with type 2 diabetes has an endocrinologist, then I will send a letter to that physician saying I think the patient should be on one of these drugs,” empagliflozin or liraglutide, he said. “If the patient is being treated by a primary care physician, then I will prescribe empagliflozin myself because most primary care physicians are not willing to prescribe it. I think more and more cardiologists are doing this. The great thing about empagliflozin and liraglutide is that they do not cause hypoglycemia and the adverse effect profiles are relatively good. As long as drug cost is not an issue, then as cardiologists we need to adjust glycemia control with cardiovascular benefit as we did years ago with statin treatment,” explained Dr. Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a senior collaborator and coauthor on the EMPA-REG study.
When results from the 4S [Scandinavian Simvastatin Survival Study] came out in 1994, proving that long-term statin treatment was both safe and increased survival in patients with coronary heart disease, “cardiologists took over lipid management from endocrinologists,” he recalled. “We now have a safe and simple treatment for glucose lowering that also cuts cardiovascular disease events, so cardiologists have to also be involved, at least to some extent. Their degree of involvement depends on their practice and who provides a patient’s primary diabetes care,” he said.
Cardiologists vary on empagliflozin
Other cardiologists are mixed in their take on personally prescribing antidiabetic drugs to high-risk patients with type 2 diabetes. Greg C. Fonarow, MD, has also aggressively taken to empagliflozin over the past year, especially for his patients with heart failure or at high risk for developing heart failure. The EMPA-REG results showed that empagliflozin’s potent impact on reducing cardiovascular death in patients linked closely with a reduction in heart failure hospitalizations. In his recent experience, endocrinologists as well as other physicians who care for patients with type 2 diabetes “are often reluctant to make any changes [in a patient’s hypoglycemic regimen], and in general they have not gravitated toward the treatments that have been shown to improve cardiovascular outcomes and instead focus solely on a patient’s hemoglobin A1c,” Dr. Fonarow said in an interview at the recent annual meeting of the Heart Failure Society of America.
He said he prescribes empagliflozin to patients with type 2 diabetes if they are hospitalized for heart failure or as outpatients, and he targets it to patients diagnosed with heart failure – including heart failure with preserved ejection fraction – as well as to patients with other forms of cardiovascular disease, closely following the EMPA-REG enrollment criteria. It’s too early in the experience with empagliflozin to use it preferentially in diabetes patients without cardiovascular disease or patients who in any other way fall outside the enrollment criteria for EMPA-REG, he said.
“I am happy to consult with their endocrinologist, or I tell patients to discuss this treatment with their endocrinologist. If the endocrinologist prescribes empagliflozin, great; if not, I feel an obligation to provide the best care I can to my patients. This is not a hard medication to use. The safety profile is good. Treatment with empagliflozin obviously has renal-function considerations, but that’s true for many drugs. The biggest challenge is what is covered by the patient’s insurance. We often need preauthorization.
“So far I have seen excellent responses in patients for both metabolic control and clinical responses in patients with heart failure. Their symptoms seem to improve,” said Dr. Fonarow, professor of medicine and co-chief of cardiology at the University of Southern California , Los Angeles.
While Dr. Fonarow cautioned that he also would not start empagliflozin in a patient with a HbA1c below 7%, he would seriously consider swapping out a patient’s drug for empagliflozin if it were a sulfonylurea or a dipeptidyl peptidase-4 inhibitor. He stopped short of suggesting a substitution of empagliflozin for metformin. In Dr. Fonarow’s opinion, the evidence for empagliflozin is also “more robust” than it has been for liraglutide or semaglutide. With what’s now known about the clinical impact of these drugs, he foresees a time when a combination between a SGLT-2 inhibitor, with its effect on heart failure, and a GLP-1 analogue, with its effect on atherosclerotic disease, may seem an ideal initial drug pairing for patients with type 2 diabetes and significant cardiovascular disease risk, with metformin relegated to a second-line role.
Other cardiologists endorsed a more collaborative approach to prescribing empagliflozin and liraglutide.
Another team-approach advocate is Robert O. Bonow, MD, cardiologist and professor of medicine at Northwestern University in Chicago. “Cardiologists are comfortable prescribing metformin and telling patients about lifestyle, but when it comes to newer antidiabetic drugs, that’s a new field, and a team approach may be best,” he said in an interview. “If possible, a cardiologist should have a friendly partnership with a diabetologist or endocrinologist who is expert in treating diabetes.” Many cardiologists now work in and for hospitals, and easy access to an endocrinologist is probably available, he noted.
But new analyses of the EMPA-REG data reported by Dr. Fitchett at the ESC congress showed that empagliflozin treatment exerted a similar benefit of reduced cardiovascular death regardless of whether patients had prevalent heart failure at entry into the study, incident heart failure during follow-up, or no heart failure of any sort.
Impact of heart failure in EMPA-REG
Roughly 10% of the 7,020 patients enrolled in EMPA-REG had heart failure at the time they entered the trial. During a median follow-up of just over 3 years, the incidence of new-onset heart failure – tallied as either a new heart failure hospitalization or a clinical episode deemed to be heart failure by an investigator – occurred in 4.6% of patients on empagliflozin and in 6.5% of patients in the placebo arm, a 1.9-percentage-point difference and a 30% relative risk reduction linked with empagliflozin use, Dr. Fitchett reported.
The main EMPA-REG outcome was a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. This positive outcome in favor of empagliflozin treatment was primarily driven by a difference in the rate of cardiovascular death. In the new analysis, the relative reduction in cardiovascular deaths with empagliflozin compared with placebo was 29% among patients with prevalent heart failure at baseline, 35% among those who had an incident heart failure hospitalization during follow-up, 27% among patients with an incident heart failure episode diagnosed by an investigator during follow-up, 33% among the combined group of trial patients with any form of heart failure at trial entry or during the trial (those with prevalent heart failure at baseline plus those with an incident event), and 37% among the large number of patients in the trial who remained free from any indication of heart failure during follow-up.
In short, treatment with empagliflozin “reduced cardiovascular mortality by the same relative amount” regardless of whether patients did or did not have heart failure during the trial,” Dr. Fitchett concluded.
Additional secondary analyses from EMPA-REG reported at the ESC congress in August also documented that the benefit from empagliflozin treatment was roughly the same regardless of the age of patients enrolled in the trial and regardless of patients’ blood level of LDL cholesterol at entry into the study. These findings provide “confidence in the consistency of the effect” by empagliflozin, Dr. Fitchett said.
The endocrinologists’ view

“Most cardiologists are not thoroughly familiar with the full palette of medications for hyperglycemia. Selection of medication should not be made solely on the basis of results from a cardiovascular outcomes trial,” said Helena W. Rodbard, MD, a clinical endocrinologist in Rockville, Md.
“The EMPA-REG OUTCOMES and LEADER results are very exciting and encouraging. When all other factors are equal, the cardiovascular results could sway the decision about which medication to use. But an endocrinologist is in the best position to balance the many factors when choosing combination therapy and to set a target level for HbA1c, fasting blood glucose, and postprandial glucose, and to adjust therapy to minimize the risk of hypoglycemia,” Dr. Rodbard said in an interview.
He called empagliflozin a drug with “interesting promise,” especially for patients with incipient heart failure. The extra cardiovascular benefit from the GLP-1 analogues is “less settled,” although the liraglutide and semaglutide trial results are important and mean these drugs need more consideration and study. The EMPA-REG results were more clearly positive, he said.
“Metformin is still the initial drug” for most patients with type 2 diabetes, echoed Dr. Levy. Drugs like empagliflozin and liraglutide are usually used in combination with metformin.
“Like many endocrinologists, I have for some time used the oral SGLT-2 inhibitors and GLP-1 analogues in combination with metformin. It made sense before the recent cardiovascular data appeared, and it makes even more sense now,” said Dr. Jellinger, professor of clinical medicine and an endocrinologist at the University of Miami.
“Endocrinologists and diabetologists are aware that cardiologists have been taking a larger role in the care of patients with diabetes,” noted Dr. Rodbard. “I favor cardiologists and endocrinologists working in concert to improve the care of patients with diabetes.”
“Over the next few years, we will need to decide whether to treat patients with type 2 diabetes with an agent with proven benefits,” said Dr. Fitchett. “Until the results from EMPA-REG and the LEADER trial came out, there was no specific glucose-lowering agent that also reduced cardiovascular events. Some cardiologists might ask when they should get involved in managing patients with type 2 diabetes. What I would do for patients with a history of cardiovascular disease who develop new type 2 diabetes is start empagliflozin as their first drug,” Dr. Fitchett said, though he admitted that no evidence yet exists to back that approach.
The EMPA-REG trial was sponsored by Boehringer Ingelheim and by Eli Lilly, the companies that market empagliflozin. The LEADER trial was sponsored in part by Novo Nordisk, the company that markets liraglutide. Dr. Fitchett and Dr. Mentz were both researchers for EMPA-REG. Dr. Fitchett has been a consultant to AstraZeneca, Merck, and Amgen. Dr. Mentz has been an adviser to Boehringer Ingelheim. Dr. Fonarow has been an adviser to Amgen, Janssen, Novartis, and ZS Pharma. Dr. Bozkurt had no disclosures. Dr. Bonow has been a consultant to Gilead. Dr. Jellinger has been a speaker on behalf of Boehringer-Ingelheim, Novo Nordisk, Merck, and Janssen. Dr. Rodbard has been a consultant to or speaker for several drug companies including Boehringer-Ingelheim, Eli Lilly, and Novo Nordisk. Dr. Levy has been a speaker on behalf of Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and AstraZeneca. Dr. Hellman had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
The dramatic reduction in cardiovascular death and heart failure hospitalization seen during treatment with empagliflozin (Jardiance) in the EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients) trial, for example, has prompted some cardiologists in the year since the first EMPA-REG report to become active prescribers of the drug to their patients who have type 2 diabetes and cardiovascular disease. The same evidence has driven other cardiologists who may not feel fully comfortable prescribing an antidiabetic drug on their own to enter into active partnerships with endocrinologists to work as a team to put diabetes patients with cardiovascular disease on empagliflozin.
In Dr. Fitchett’s practice, “if a patient with type 2 diabetes has an endocrinologist, then I will send a letter to that physician saying I think the patient should be on one of these drugs,” empagliflozin or liraglutide, he said. “If the patient is being treated by a primary care physician, then I will prescribe empagliflozin myself because most primary care physicians are not willing to prescribe it. I think more and more cardiologists are doing this. The great thing about empagliflozin and liraglutide is that they do not cause hypoglycemia and the adverse effect profiles are relatively good. As long as drug cost is not an issue, then as cardiologists we need to adjust glycemia control with cardiovascular benefit as we did years ago with statin treatment,” explained Dr. Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a senior collaborator and coauthor on the EMPA-REG study.
When results from the 4S [Scandinavian Simvastatin Survival Study] came out in 1994, proving that long-term statin treatment was both safe and increased survival in patients with coronary heart disease, “cardiologists took over lipid management from endocrinologists,” he recalled. “We now have a safe and simple treatment for glucose lowering that also cuts cardiovascular disease events, so cardiologists have to also be involved, at least to some extent. Their degree of involvement depends on their practice and who provides a patient’s primary diabetes care,” he said.
Cardiologists vary on empagliflozin
Other cardiologists are mixed in their take on personally prescribing antidiabetic drugs to high-risk patients with type 2 diabetes. Greg C. Fonarow, MD, has also aggressively taken to empagliflozin over the past year, especially for his patients with heart failure or at high risk for developing heart failure. The EMPA-REG results showed that empagliflozin’s potent impact on reducing cardiovascular death in patients linked closely with a reduction in heart failure hospitalizations. In his recent experience, endocrinologists as well as other physicians who care for patients with type 2 diabetes “are often reluctant to make any changes [in a patient’s hypoglycemic regimen], and in general they have not gravitated toward the treatments that have been shown to improve cardiovascular outcomes and instead focus solely on a patient’s hemoglobin A1c,” Dr. Fonarow said in an interview at the recent annual meeting of the Heart Failure Society of America.
He said he prescribes empagliflozin to patients with type 2 diabetes if they are hospitalized for heart failure or as outpatients, and he targets it to patients diagnosed with heart failure – including heart failure with preserved ejection fraction – as well as to patients with other forms of cardiovascular disease, closely following the EMPA-REG enrollment criteria. It’s too early in the experience with empagliflozin to use it preferentially in diabetes patients without cardiovascular disease or patients who in any other way fall outside the enrollment criteria for EMPA-REG, he said.
“I am happy to consult with their endocrinologist, or I tell patients to discuss this treatment with their endocrinologist. If the endocrinologist prescribes empagliflozin, great; if not, I feel an obligation to provide the best care I can to my patients. This is not a hard medication to use. The safety profile is good. Treatment with empagliflozin obviously has renal-function considerations, but that’s true for many drugs. The biggest challenge is what is covered by the patient’s insurance. We often need preauthorization.
“So far I have seen excellent responses in patients for both metabolic control and clinical responses in patients with heart failure. Their symptoms seem to improve,” said Dr. Fonarow, professor of medicine and co-chief of cardiology at the University of Southern California , Los Angeles.
While Dr. Fonarow cautioned that he also would not start empagliflozin in a patient with a HbA1c below 7%, he would seriously consider swapping out a patient’s drug for empagliflozin if it were a sulfonylurea or a dipeptidyl peptidase-4 inhibitor. He stopped short of suggesting a substitution of empagliflozin for metformin. In Dr. Fonarow’s opinion, the evidence for empagliflozin is also “more robust” than it has been for liraglutide or semaglutide. With what’s now known about the clinical impact of these drugs, he foresees a time when a combination between a SGLT-2 inhibitor, with its effect on heart failure, and a GLP-1 analogue, with its effect on atherosclerotic disease, may seem an ideal initial drug pairing for patients with type 2 diabetes and significant cardiovascular disease risk, with metformin relegated to a second-line role.
Other cardiologists endorsed a more collaborative approach to prescribing empagliflozin and liraglutide.
Another team-approach advocate is Robert O. Bonow, MD, cardiologist and professor of medicine at Northwestern University in Chicago. “Cardiologists are comfortable prescribing metformin and telling patients about lifestyle, but when it comes to newer antidiabetic drugs, that’s a new field, and a team approach may be best,” he said in an interview. “If possible, a cardiologist should have a friendly partnership with a diabetologist or endocrinologist who is expert in treating diabetes.” Many cardiologists now work in and for hospitals, and easy access to an endocrinologist is probably available, he noted.
But new analyses of the EMPA-REG data reported by Dr. Fitchett at the ESC congress showed that empagliflozin treatment exerted a similar benefit of reduced cardiovascular death regardless of whether patients had prevalent heart failure at entry into the study, incident heart failure during follow-up, or no heart failure of any sort.
Impact of heart failure in EMPA-REG
Roughly 10% of the 7,020 patients enrolled in EMPA-REG had heart failure at the time they entered the trial. During a median follow-up of just over 3 years, the incidence of new-onset heart failure – tallied as either a new heart failure hospitalization or a clinical episode deemed to be heart failure by an investigator – occurred in 4.6% of patients on empagliflozin and in 6.5% of patients in the placebo arm, a 1.9-percentage-point difference and a 30% relative risk reduction linked with empagliflozin use, Dr. Fitchett reported.
The main EMPA-REG outcome was a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. This positive outcome in favor of empagliflozin treatment was primarily driven by a difference in the rate of cardiovascular death. In the new analysis, the relative reduction in cardiovascular deaths with empagliflozin compared with placebo was 29% among patients with prevalent heart failure at baseline, 35% among those who had an incident heart failure hospitalization during follow-up, 27% among patients with an incident heart failure episode diagnosed by an investigator during follow-up, 33% among the combined group of trial patients with any form of heart failure at trial entry or during the trial (those with prevalent heart failure at baseline plus those with an incident event), and 37% among the large number of patients in the trial who remained free from any indication of heart failure during follow-up.
In short, treatment with empagliflozin “reduced cardiovascular mortality by the same relative amount” regardless of whether patients did or did not have heart failure during the trial,” Dr. Fitchett concluded.
Additional secondary analyses from EMPA-REG reported at the ESC congress in August also documented that the benefit from empagliflozin treatment was roughly the same regardless of the age of patients enrolled in the trial and regardless of patients’ blood level of LDL cholesterol at entry into the study. These findings provide “confidence in the consistency of the effect” by empagliflozin, Dr. Fitchett said.
The endocrinologists’ view
“Most cardiologists are not thoroughly familiar with the full palette of medications for hyperglycemia. Selection of medication should not be made solely on the basis of results from a cardiovascular outcomes trial,” said Helena W. Rodbard, MD, a clinical endocrinologist in Rockville, Md.
“The EMPA-REG OUTCOMES and LEADER results are very exciting and encouraging. When all other factors are equal, the cardiovascular results could sway the decision about which medication to use. But an endocrinologist is in the best position to balance the many factors when choosing combination therapy and to set a target level for HbA1c, fasting blood glucose, and postprandial glucose, and to adjust therapy to minimize the risk of hypoglycemia,” Dr. Rodbard said in an interview.
He called empagliflozin a drug with “interesting promise,” especially for patients with incipient heart failure. The extra cardiovascular benefit from the GLP-1 analogues is “less settled,” although the liraglutide and semaglutide trial results are important and mean these drugs need more consideration and study. The EMPA-REG results were more clearly positive, he said.
“Metformin is still the initial drug” for most patients with type 2 diabetes, echoed Dr. Levy. Drugs like empagliflozin and liraglutide are usually used in combination with metformin.
“Like many endocrinologists, I have for some time used the oral SGLT-2 inhibitors and GLP-1 analogues in combination with metformin. It made sense before the recent cardiovascular data appeared, and it makes even more sense now,” said Dr. Jellinger, professor of clinical medicine and an endocrinologist at the University of Miami.
“Endocrinologists and diabetologists are aware that cardiologists have been taking a larger role in the care of patients with diabetes,” noted Dr. Rodbard. “I favor cardiologists and endocrinologists working in concert to improve the care of patients with diabetes.”
“Over the next few years, we will need to decide whether to treat patients with type 2 diabetes with an agent with proven benefits,” said Dr. Fitchett. “Until the results from EMPA-REG and the LEADER trial came out, there was no specific glucose-lowering agent that also reduced cardiovascular events. Some cardiologists might ask when they should get involved in managing patients with type 2 diabetes. What I would do for patients with a history of cardiovascular disease who develop new type 2 diabetes is start empagliflozin as their first drug,” Dr. Fitchett said, though he admitted that no evidence yet exists to back that approach.
The EMPA-REG trial was sponsored by Boehringer Ingelheim and by Eli Lilly, the companies that market empagliflozin. The LEADER trial was sponsored in part by Novo Nordisk, the company that markets liraglutide. Dr. Fitchett and Dr. Mentz were both researchers for EMPA-REG. Dr. Fitchett has been a consultant to AstraZeneca, Merck, and Amgen. Dr. Mentz has been an adviser to Boehringer Ingelheim. Dr. Fonarow has been an adviser to Amgen, Janssen, Novartis, and ZS Pharma. Dr. Bozkurt had no disclosures. Dr. Bonow has been a consultant to Gilead. Dr. Jellinger has been a speaker on behalf of Boehringer-Ingelheim, Novo Nordisk, Merck, and Janssen. Dr. Rodbard has been a consultant to or speaker for several drug companies including Boehringer-Ingelheim, Eli Lilly, and Novo Nordisk. Dr. Levy has been a speaker on behalf of Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and AstraZeneca. Dr. Hellman had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
The dramatic reduction in cardiovascular death and heart failure hospitalization seen during treatment with empagliflozin (Jardiance) in the EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients) trial, for example, has prompted some cardiologists in the year since the first EMPA-REG report to become active prescribers of the drug to their patients who have type 2 diabetes and cardiovascular disease. The same evidence has driven other cardiologists who may not feel fully comfortable prescribing an antidiabetic drug on their own to enter into active partnerships with endocrinologists to work as a team to put diabetes patients with cardiovascular disease on empagliflozin.
In Dr. Fitchett’s practice, “if a patient with type 2 diabetes has an endocrinologist, then I will send a letter to that physician saying I think the patient should be on one of these drugs,” empagliflozin or liraglutide, he said. “If the patient is being treated by a primary care physician, then I will prescribe empagliflozin myself because most primary care physicians are not willing to prescribe it. I think more and more cardiologists are doing this. The great thing about empagliflozin and liraglutide is that they do not cause hypoglycemia and the adverse effect profiles are relatively good. As long as drug cost is not an issue, then as cardiologists we need to adjust glycemia control with cardiovascular benefit as we did years ago with statin treatment,” explained Dr. Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a senior collaborator and coauthor on the EMPA-REG study.
When results from the 4S [Scandinavian Simvastatin Survival Study] came out in 1994, proving that long-term statin treatment was both safe and increased survival in patients with coronary heart disease, “cardiologists took over lipid management from endocrinologists,” he recalled. “We now have a safe and simple treatment for glucose lowering that also cuts cardiovascular disease events, so cardiologists have to also be involved, at least to some extent. Their degree of involvement depends on their practice and who provides a patient’s primary diabetes care,” he said.
Cardiologists vary on empagliflozin
Other cardiologists are mixed in their take on personally prescribing antidiabetic drugs to high-risk patients with type 2 diabetes. Greg C. Fonarow, MD, has also aggressively taken to empagliflozin over the past year, especially for his patients with heart failure or at high risk for developing heart failure. The EMPA-REG results showed that empagliflozin’s potent impact on reducing cardiovascular death in patients linked closely with a reduction in heart failure hospitalizations. In his recent experience, endocrinologists as well as other physicians who care for patients with type 2 diabetes “are often reluctant to make any changes [in a patient’s hypoglycemic regimen], and in general they have not gravitated toward the treatments that have been shown to improve cardiovascular outcomes and instead focus solely on a patient’s hemoglobin A1c,” Dr. Fonarow said in an interview at the recent annual meeting of the Heart Failure Society of America.
He said he prescribes empagliflozin to patients with type 2 diabetes if they are hospitalized for heart failure or as outpatients, and he targets it to patients diagnosed with heart failure – including heart failure with preserved ejection fraction – as well as to patients with other forms of cardiovascular disease, closely following the EMPA-REG enrollment criteria. It’s too early in the experience with empagliflozin to use it preferentially in diabetes patients without cardiovascular disease or patients who in any other way fall outside the enrollment criteria for EMPA-REG, he said.
“I am happy to consult with their endocrinologist, or I tell patients to discuss this treatment with their endocrinologist. If the endocrinologist prescribes empagliflozin, great; if not, I feel an obligation to provide the best care I can to my patients. This is not a hard medication to use. The safety profile is good. Treatment with empagliflozin obviously has renal-function considerations, but that’s true for many drugs. The biggest challenge is what is covered by the patient’s insurance. We often need preauthorization.
“So far I have seen excellent responses in patients for both metabolic control and clinical responses in patients with heart failure. Their symptoms seem to improve,” said Dr. Fonarow, professor of medicine and co-chief of cardiology at the University of Southern California , Los Angeles.
While Dr. Fonarow cautioned that he also would not start empagliflozin in a patient with a HbA1c below 7%, he would seriously consider swapping out a patient’s drug for empagliflozin if it were a sulfonylurea or a dipeptidyl peptidase-4 inhibitor. He stopped short of suggesting a substitution of empagliflozin for metformin. In Dr. Fonarow’s opinion, the evidence for empagliflozin is also “more robust” than it has been for liraglutide or semaglutide. With what’s now known about the clinical impact of these drugs, he foresees a time when a combination between a SGLT-2 inhibitor, with its effect on heart failure, and a GLP-1 analogue, with its effect on atherosclerotic disease, may seem an ideal initial drug pairing for patients with type 2 diabetes and significant cardiovascular disease risk, with metformin relegated to a second-line role.
Other cardiologists endorsed a more collaborative approach to prescribing empagliflozin and liraglutide.
Another team-approach advocate is Robert O. Bonow, MD, cardiologist and professor of medicine at Northwestern University in Chicago. “Cardiologists are comfortable prescribing metformin and telling patients about lifestyle, but when it comes to newer antidiabetic drugs, that’s a new field, and a team approach may be best,” he said in an interview. “If possible, a cardiologist should have a friendly partnership with a diabetologist or endocrinologist who is expert in treating diabetes.” Many cardiologists now work in and for hospitals, and easy access to an endocrinologist is probably available, he noted.
But new analyses of the EMPA-REG data reported by Dr. Fitchett at the ESC congress showed that empagliflozin treatment exerted a similar benefit of reduced cardiovascular death regardless of whether patients had prevalent heart failure at entry into the study, incident heart failure during follow-up, or no heart failure of any sort.
Impact of heart failure in EMPA-REG
Roughly 10% of the 7,020 patients enrolled in EMPA-REG had heart failure at the time they entered the trial. During a median follow-up of just over 3 years, the incidence of new-onset heart failure – tallied as either a new heart failure hospitalization or a clinical episode deemed to be heart failure by an investigator – occurred in 4.6% of patients on empagliflozin and in 6.5% of patients in the placebo arm, a 1.9-percentage-point difference and a 30% relative risk reduction linked with empagliflozin use, Dr. Fitchett reported.
The main EMPA-REG outcome was a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. This positive outcome in favor of empagliflozin treatment was primarily driven by a difference in the rate of cardiovascular death. In the new analysis, the relative reduction in cardiovascular deaths with empagliflozin compared with placebo was 29% among patients with prevalent heart failure at baseline, 35% among those who had an incident heart failure hospitalization during follow-up, 27% among patients with an incident heart failure episode diagnosed by an investigator during follow-up, 33% among the combined group of trial patients with any form of heart failure at trial entry or during the trial (those with prevalent heart failure at baseline plus those with an incident event), and 37% among the large number of patients in the trial who remained free from any indication of heart failure during follow-up.
In short, treatment with empagliflozin “reduced cardiovascular mortality by the same relative amount” regardless of whether patients did or did not have heart failure during the trial,” Dr. Fitchett concluded.
Additional secondary analyses from EMPA-REG reported at the ESC congress in August also documented that the benefit from empagliflozin treatment was roughly the same regardless of the age of patients enrolled in the trial and regardless of patients’ blood level of LDL cholesterol at entry into the study. These findings provide “confidence in the consistency of the effect” by empagliflozin, Dr. Fitchett said.
The endocrinologists’ view
“Most cardiologists are not thoroughly familiar with the full palette of medications for hyperglycemia. Selection of medication should not be made solely on the basis of results from a cardiovascular outcomes trial,” said Helena W. Rodbard, MD, a clinical endocrinologist in Rockville, Md.
“The EMPA-REG OUTCOMES and LEADER results are very exciting and encouraging. When all other factors are equal, the cardiovascular results could sway the decision about which medication to use. But an endocrinologist is in the best position to balance the many factors when choosing combination therapy and to set a target level for HbA1c, fasting blood glucose, and postprandial glucose, and to adjust therapy to minimize the risk of hypoglycemia,” Dr. Rodbard said in an interview.
He called empagliflozin a drug with “interesting promise,” especially for patients with incipient heart failure. The extra cardiovascular benefit from the GLP-1 analogues is “less settled,” although the liraglutide and semaglutide trial results are important and mean these drugs need more consideration and study. The EMPA-REG results were more clearly positive, he said.
“Metformin is still the initial drug” for most patients with type 2 diabetes, echoed Dr. Levy. Drugs like empagliflozin and liraglutide are usually used in combination with metformin.
“Like many endocrinologists, I have for some time used the oral SGLT-2 inhibitors and GLP-1 analogues in combination with metformin. It made sense before the recent cardiovascular data appeared, and it makes even more sense now,” said Dr. Jellinger, professor of clinical medicine and an endocrinologist at the University of Miami.
“Endocrinologists and diabetologists are aware that cardiologists have been taking a larger role in the care of patients with diabetes,” noted Dr. Rodbard. “I favor cardiologists and endocrinologists working in concert to improve the care of patients with diabetes.”
“Over the next few years, we will need to decide whether to treat patients with type 2 diabetes with an agent with proven benefits,” said Dr. Fitchett. “Until the results from EMPA-REG and the LEADER trial came out, there was no specific glucose-lowering agent that also reduced cardiovascular events. Some cardiologists might ask when they should get involved in managing patients with type 2 diabetes. What I would do for patients with a history of cardiovascular disease who develop new type 2 diabetes is start empagliflozin as their first drug,” Dr. Fitchett said, though he admitted that no evidence yet exists to back that approach.
The EMPA-REG trial was sponsored by Boehringer Ingelheim and by Eli Lilly, the companies that market empagliflozin. The LEADER trial was sponsored in part by Novo Nordisk, the company that markets liraglutide. Dr. Fitchett and Dr. Mentz were both researchers for EMPA-REG. Dr. Fitchett has been a consultant to AstraZeneca, Merck, and Amgen. Dr. Mentz has been an adviser to Boehringer Ingelheim. Dr. Fonarow has been an adviser to Amgen, Janssen, Novartis, and ZS Pharma. Dr. Bozkurt had no disclosures. Dr. Bonow has been a consultant to Gilead. Dr. Jellinger has been a speaker on behalf of Boehringer-Ingelheim, Novo Nordisk, Merck, and Janssen. Dr. Rodbard has been a consultant to or speaker for several drug companies including Boehringer-Ingelheim, Eli Lilly, and Novo Nordisk. Dr. Levy has been a speaker on behalf of Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and AstraZeneca. Dr. Hellman had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Rheumatoid arthritis increases heart failure risk
ROME – Rheumatoid arthritis is associated with a significantly increased risk of hospitalization for heart failure, according to a nationwide Danish study, Usman Khalid, MD, reported at the annual congress of the European Society of Cardiology.
As a chronic systemic inflammatory disease, rheumatoid arthritis (RA) has been associated with increased risk of a variety of comorbid conditions, including cardiovascular disease. But RA’s relationship specifically with heart failure hasn’t previously been looked at in the comprehensive way that’s possible in Denmark, where linked national registries enable researchers to follow health issues in the entire population from birth to death, noted Dr. Khalid of the University of Copenhagen.
In an analysis adjusted for age, sex, and calendar year, individuals with RA were 83% more likely to be hospitalized for heart failure than were the non-RA Danish population. In a fully adjusted analysis that controlled for those potential confounders as well as comorbid conditions, smoking, alcohol intake, socioeconomic status, and prescription medications, patients with RA remained at a statistically significant and clinically meaningful 38% increased risk of heart failure hospitalization.
Further studies are planned to determine the underlying mechanisms of this association, Dr. Khalid added.
He reported having no financial conflicts of interest regarding this study, which was supported by an unrestricted grant from Leo Pharma.
ROME – Rheumatoid arthritis is associated with a significantly increased risk of hospitalization for heart failure, according to a nationwide Danish study, Usman Khalid, MD, reported at the annual congress of the European Society of Cardiology.
As a chronic systemic inflammatory disease, rheumatoid arthritis (RA) has been associated with increased risk of a variety of comorbid conditions, including cardiovascular disease. But RA’s relationship specifically with heart failure hasn’t previously been looked at in the comprehensive way that’s possible in Denmark, where linked national registries enable researchers to follow health issues in the entire population from birth to death, noted Dr. Khalid of the University of Copenhagen.
In an analysis adjusted for age, sex, and calendar year, individuals with RA were 83% more likely to be hospitalized for heart failure than were the non-RA Danish population. In a fully adjusted analysis that controlled for those potential confounders as well as comorbid conditions, smoking, alcohol intake, socioeconomic status, and prescription medications, patients with RA remained at a statistically significant and clinically meaningful 38% increased risk of heart failure hospitalization.
Further studies are planned to determine the underlying mechanisms of this association, Dr. Khalid added.
He reported having no financial conflicts of interest regarding this study, which was supported by an unrestricted grant from Leo Pharma.
ROME – Rheumatoid arthritis is associated with a significantly increased risk of hospitalization for heart failure, according to a nationwide Danish study, Usman Khalid, MD, reported at the annual congress of the European Society of Cardiology.
As a chronic systemic inflammatory disease, rheumatoid arthritis (RA) has been associated with increased risk of a variety of comorbid conditions, including cardiovascular disease. But RA’s relationship specifically with heart failure hasn’t previously been looked at in the comprehensive way that’s possible in Denmark, where linked national registries enable researchers to follow health issues in the entire population from birth to death, noted Dr. Khalid of the University of Copenhagen.
In an analysis adjusted for age, sex, and calendar year, individuals with RA were 83% more likely to be hospitalized for heart failure than were the non-RA Danish population. In a fully adjusted analysis that controlled for those potential confounders as well as comorbid conditions, smoking, alcohol intake, socioeconomic status, and prescription medications, patients with RA remained at a statistically significant and clinically meaningful 38% increased risk of heart failure hospitalization.
Further studies are planned to determine the underlying mechanisms of this association, Dr. Khalid added.
He reported having no financial conflicts of interest regarding this study, which was supported by an unrestricted grant from Leo Pharma.
AT THE ESC CONGRESS 2016
Key clinical point:
Major finding: The incidence rate for heart failure hospitalization was 7.37 per 1,000 person-years in Danish adults with rheumatoid arthritis, compared with 2.45 per 1,000 in the general population.
Data source: This study utilized Danish comprehensive national registries to determine the rate at which 13,800 Danes with rheumatoid arthritis and no baseline history of heart failure were hospitalized for heart failure during 15 years of follow-up.
Disclosures: The study was supported by an unrestricted grant from Leo Pharma. The presenter reported having no financial conflicts of interest.