User login
The SHM Fellow designation: Class of 2021
Spotlight on Tanisha Hamilton, MD, FHM
As we navigate a time unlike any other, it is clear that the value hospitalists provide is growing stronger as the hospital medicine field expands. Many Society of Hospital Medicine members look to its Fellows program as a worthwhile opportunity to distinguish themselves as leaders in the field and accelerate their careers in the specialty.

An active member of SHM since 2012 and member of its 2020 class of Fellows, Tanisha Hamilton, MD, FHM, is one of these ambitious individuals.
Dr. Hamilton is based at Baylor University Medical Center in Dallas, an affiliate of Baylor Scott & White Health. Known for personalized health and wellness care, Dr. Hamilton has more than 14 years of experience in the medical field.
Her love for the hospital medicine specialty is rooted in its diversity and complexity of patient cases – something that she knew would innately complement her personality. She says that an invaluable aspect of working in the field is the ability to interact and connect with people from all walks of life.
“My patients keep me motivated in this space. Learning from my patients and having the responsibility of serving as their advocate is incredibly rewarding,” Dr. Hamilton said. “I hope my patients feel like I’ve helped to make a difference in their lives, if only for just a moment.”
When reflecting on why she joined SHM 8 years ago, Dr. Hamilton said she was encouraged to do so because of its like-minded membership community and professional development opportunities, including the Fellows program.
“I applied to SHM’s Fellows program because I’m committed to the specialty. Hospital medicine is an ever-changing field loaded with opportunities to enhance personal and professional career growth,” said Dr. Hamilton. “To me, SHM’s Fellow in Hospital Medicine [FHM] designation demonstrates the ability to make a contribution to the field and to be an instrument for change.”
She credits receiving her designation as a distinction that has opened doors to other career-enhancing opportunities and networking resources, including an expansive global community, program development at her institution, and positions within SHM. Since earning her FHM designation, Dr. Hamilton has become an engaged member of the annual meeting committee and the North Central Texas Chapter.
“Since we are taking our annual conference virtual for SHM Converge in 2021, I’m excited to see how we can transform a meeting of more than 5,000 attendees into a full digital experience with interactive workshops, exhibits, research competitions, and more,” Dr. Hamilton said. “It’s certainly going to be a challenge, but I know that our meetings department and annual conference committee will make it a success!”
As Dr. Hamilton looks forward in her hospital medicine career, she is committed to making a positive impact on the field and for her patients.
In the future, Dr. Hamilton hopes to share curriculum she recently developed and sponsored around diversity, equity, and inclusion with her team at Baylor University Medical Center.
“Following the tragic deaths of numerous individuals, including Breonna Taylor, Ahmaud Abery, and George Floyd, and other people of color who have died because of COVID-19, I have felt compelled to educate my colleagues on how to curtail systemic racism, sexism, religious discrimination, and xenophobia in health care,” Dr. Hamilton said. “This curriculum includes courses on health disparities and cultural competencies, launching a lecture series, and other educational components.”
While 2020 has been a trying year, Dr. Hamilton remains hopeful for a prosperous future.
“When I think of the future of hospital medicine, I am hopeful that hospitalists will have a more prominent role in changing the direction of our health care system,” she said. “The pandemic has made the world realize the importance of hospital medicine. We, as hospitalists, are a critical part of its infrastructure and its success.”
If you would like to join Dr. Hamilton and other like-minded hospital medicine leaders in accelerating your career, SHM is currently recruiting for the Fellows and Senior Fellows class of 2021. Applications are open until Nov. 20, 2020. These designations are available across a variety of membership categories, including physicians, nurse practitioners, physician assistants, and qualified practice administrators. Dedicated to promoting excellence, innovation, and quality improvement in patient care, Fellows designations provide members with a distinguishing credential as established pioneers in the industry.
For more information and to review your eligibility, visit hospitalmedicine.org/fellows.
Ms. Cowan is a communications specialist at the Society of Hospital Medicine.
Spotlight on Tanisha Hamilton, MD, FHM
Spotlight on Tanisha Hamilton, MD, FHM
As we navigate a time unlike any other, it is clear that the value hospitalists provide is growing stronger as the hospital medicine field expands. Many Society of Hospital Medicine members look to its Fellows program as a worthwhile opportunity to distinguish themselves as leaders in the field and accelerate their careers in the specialty.
An active member of SHM since 2012 and member of its 2020 class of Fellows, Tanisha Hamilton, MD, FHM, is one of these ambitious individuals.
Dr. Hamilton is based at Baylor University Medical Center in Dallas, an affiliate of Baylor Scott & White Health. Known for personalized health and wellness care, Dr. Hamilton has more than 14 years of experience in the medical field.
Her love for the hospital medicine specialty is rooted in its diversity and complexity of patient cases – something that she knew would innately complement her personality. She says that an invaluable aspect of working in the field is the ability to interact and connect with people from all walks of life.
“My patients keep me motivated in this space. Learning from my patients and having the responsibility of serving as their advocate is incredibly rewarding,” Dr. Hamilton said. “I hope my patients feel like I’ve helped to make a difference in their lives, if only for just a moment.”
When reflecting on why she joined SHM 8 years ago, Dr. Hamilton said she was encouraged to do so because of its like-minded membership community and professional development opportunities, including the Fellows program.
“I applied to SHM’s Fellows program because I’m committed to the specialty. Hospital medicine is an ever-changing field loaded with opportunities to enhance personal and professional career growth,” said Dr. Hamilton. “To me, SHM’s Fellow in Hospital Medicine [FHM] designation demonstrates the ability to make a contribution to the field and to be an instrument for change.”
She credits receiving her designation as a distinction that has opened doors to other career-enhancing opportunities and networking resources, including an expansive global community, program development at her institution, and positions within SHM. Since earning her FHM designation, Dr. Hamilton has become an engaged member of the annual meeting committee and the North Central Texas Chapter.
“Since we are taking our annual conference virtual for SHM Converge in 2021, I’m excited to see how we can transform a meeting of more than 5,000 attendees into a full digital experience with interactive workshops, exhibits, research competitions, and more,” Dr. Hamilton said. “It’s certainly going to be a challenge, but I know that our meetings department and annual conference committee will make it a success!”
As Dr. Hamilton looks forward in her hospital medicine career, she is committed to making a positive impact on the field and for her patients.
In the future, Dr. Hamilton hopes to share curriculum she recently developed and sponsored around diversity, equity, and inclusion with her team at Baylor University Medical Center.
“Following the tragic deaths of numerous individuals, including Breonna Taylor, Ahmaud Abery, and George Floyd, and other people of color who have died because of COVID-19, I have felt compelled to educate my colleagues on how to curtail systemic racism, sexism, religious discrimination, and xenophobia in health care,” Dr. Hamilton said. “This curriculum includes courses on health disparities and cultural competencies, launching a lecture series, and other educational components.”
While 2020 has been a trying year, Dr. Hamilton remains hopeful for a prosperous future.
“When I think of the future of hospital medicine, I am hopeful that hospitalists will have a more prominent role in changing the direction of our health care system,” she said. “The pandemic has made the world realize the importance of hospital medicine. We, as hospitalists, are a critical part of its infrastructure and its success.”
If you would like to join Dr. Hamilton and other like-minded hospital medicine leaders in accelerating your career, SHM is currently recruiting for the Fellows and Senior Fellows class of 2021. Applications are open until Nov. 20, 2020. These designations are available across a variety of membership categories, including physicians, nurse practitioners, physician assistants, and qualified practice administrators. Dedicated to promoting excellence, innovation, and quality improvement in patient care, Fellows designations provide members with a distinguishing credential as established pioneers in the industry.
For more information and to review your eligibility, visit hospitalmedicine.org/fellows.
Ms. Cowan is a communications specialist at the Society of Hospital Medicine.
As we navigate a time unlike any other, it is clear that the value hospitalists provide is growing stronger as the hospital medicine field expands. Many Society of Hospital Medicine members look to its Fellows program as a worthwhile opportunity to distinguish themselves as leaders in the field and accelerate their careers in the specialty.
An active member of SHM since 2012 and member of its 2020 class of Fellows, Tanisha Hamilton, MD, FHM, is one of these ambitious individuals.
Dr. Hamilton is based at Baylor University Medical Center in Dallas, an affiliate of Baylor Scott & White Health. Known for personalized health and wellness care, Dr. Hamilton has more than 14 years of experience in the medical field.
Her love for the hospital medicine specialty is rooted in its diversity and complexity of patient cases – something that she knew would innately complement her personality. She says that an invaluable aspect of working in the field is the ability to interact and connect with people from all walks of life.
“My patients keep me motivated in this space. Learning from my patients and having the responsibility of serving as their advocate is incredibly rewarding,” Dr. Hamilton said. “I hope my patients feel like I’ve helped to make a difference in their lives, if only for just a moment.”
When reflecting on why she joined SHM 8 years ago, Dr. Hamilton said she was encouraged to do so because of its like-minded membership community and professional development opportunities, including the Fellows program.
“I applied to SHM’s Fellows program because I’m committed to the specialty. Hospital medicine is an ever-changing field loaded with opportunities to enhance personal and professional career growth,” said Dr. Hamilton. “To me, SHM’s Fellow in Hospital Medicine [FHM] designation demonstrates the ability to make a contribution to the field and to be an instrument for change.”
She credits receiving her designation as a distinction that has opened doors to other career-enhancing opportunities and networking resources, including an expansive global community, program development at her institution, and positions within SHM. Since earning her FHM designation, Dr. Hamilton has become an engaged member of the annual meeting committee and the North Central Texas Chapter.
“Since we are taking our annual conference virtual for SHM Converge in 2021, I’m excited to see how we can transform a meeting of more than 5,000 attendees into a full digital experience with interactive workshops, exhibits, research competitions, and more,” Dr. Hamilton said. “It’s certainly going to be a challenge, but I know that our meetings department and annual conference committee will make it a success!”
As Dr. Hamilton looks forward in her hospital medicine career, she is committed to making a positive impact on the field and for her patients.
In the future, Dr. Hamilton hopes to share curriculum she recently developed and sponsored around diversity, equity, and inclusion with her team at Baylor University Medical Center.
“Following the tragic deaths of numerous individuals, including Breonna Taylor, Ahmaud Abery, and George Floyd, and other people of color who have died because of COVID-19, I have felt compelled to educate my colleagues on how to curtail systemic racism, sexism, religious discrimination, and xenophobia in health care,” Dr. Hamilton said. “This curriculum includes courses on health disparities and cultural competencies, launching a lecture series, and other educational components.”
While 2020 has been a trying year, Dr. Hamilton remains hopeful for a prosperous future.
“When I think of the future of hospital medicine, I am hopeful that hospitalists will have a more prominent role in changing the direction of our health care system,” she said. “The pandemic has made the world realize the importance of hospital medicine. We, as hospitalists, are a critical part of its infrastructure and its success.”
If you would like to join Dr. Hamilton and other like-minded hospital medicine leaders in accelerating your career, SHM is currently recruiting for the Fellows and Senior Fellows class of 2021. Applications are open until Nov. 20, 2020. These designations are available across a variety of membership categories, including physicians, nurse practitioners, physician assistants, and qualified practice administrators. Dedicated to promoting excellence, innovation, and quality improvement in patient care, Fellows designations provide members with a distinguishing credential as established pioneers in the industry.
For more information and to review your eligibility, visit hospitalmedicine.org/fellows.
Ms. Cowan is a communications specialist at the Society of Hospital Medicine.
Burnout risk may be exacerbated by COVID crisis
New kinds of job stress multiply in unusual times
Clarissa Barnes, MD, a hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and until recently medical director of Avera’s LIGHT Program, a wellness-oriented service for doctors, nurse practitioners, and physician assistants, watched the COVID-19 crisis unfold up close in her community and her hospital. Sioux Falls traced its surge of COVID patients to an outbreak at a local meatpacking plant.

“In the beginning, we didn’t know much about the virus and its communicability, although we have since gotten a better handle on that,” she said. “We had questions: Should we give patients more fluids – or less? Steroids or not? In my experience as a hospitalist I never had patients die every day on my shift, but that was happening with COVID.” The crisis imposed serious stresses on frontline providers, and hospitalists were concerned about personal safety and exposure risk – not just for themselves but for their families.
“The first time I worked on the COVID unit, I moved into the guest room in our home, apart from my husband and our young children,” Dr. Barnes said. “Ultimately I caught the virus, although I have since recovered.” Her experience has highlighted how existing issues of job stress and burnout in hospital medicine have been exacerbated by COVID-19. Even physicians who consider themselves healthy may have little emotional reserve to draw upon in a crisis of this magnitude.
“We are social distancing at work, wearing masks, not eating together with our colleagues – with less camaraderie and social support than we used to have,” she said. “I feel exhausted and there’s no question that my colleagues and I have sacrificed a lot to deal with the pandemic.” Add to that the second front of the COVID-19 crisis, Dr. Barnes said, which is “fighting the medical information wars, trying to correct misinformation put out there by people. Physicians who have been on the front lines of the pandemic know how demoralizing it can be to have people negate your first-hand experience.”
The situation has gotten better in Sioux Falls, Dr. Barnes said, although cases have started rising in the state again. The stress, while not gone, is reduced. For some doctors, “COVID reminded us of why we do what we do. Some of the usual bureaucratic requirements were set aside and we could focus on what our patients needed and how to take care of them.”
Taking job stress seriously
Tiffani Panek, MA, SFHM, CLHM, administrator of the division of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, said job stress is a major issue for hospitalist groups.

“We take it seriously here, and use a survey tool to measure morale in our group annually,” she said. “So far, knock on wood, Baltimore has not been one of the big hot spots, but we’ve definitely had waves of COVID patients.”
The Bayview hospitalist group has a diversified set of leaders, including a wellness director. “They’re always checking up on our people, keeping an eye on those who are most vulnerable. One of the stressors we hadn’t thought about before was for our people who live alone. With the isolation and lockdown, they haven’t been able to socialize, so we’ve made direct outreach, asking people how they were doing,” Ms. Panek said. “People know we’ve got their back – professionally and personally. They know, if there’s something we can do to help, we will do it.”
Bayview Medical Center has COVID-specific units and non-COVID units, and has tried to rotate hospitalist assignments because more than a couple days in a row spent wearing full personal protective equipment (PPE) is exhausting, Ms. Panek said. The group also allocated a respite room just outside the biocontainment unit, with a computer and opportunities for providers to just sit and take a breather – with appropriate social distancing. “It’s not fancy, but you just have to wear a mask, not full PPE.”
The Hopkins hospitalist group’s wellness director, Catherine Washburn, MD, also a working hospitalist, said providers are exhausted, and trying to transition to the new normal is a moving target.
“It’s hard for anyone to say what our lives will look like in 6 months,” she said. “People in our group have lost family members to COVID, or postponed major life events, like weddings. We acknowledge losses together as a group, and celebrate things worth celebrating, like babies or birthdays.”
Greatest COVID caseload
Joshua Case, MD, hospitalist medical director for 16 acute care hospitals of Northwell Health serving metropolitan New York City and Long Island, said his group’s hospitalists and other staff worked incredibly hard during the surge of COVID-19 patients in New York. “Northwell likely cared for more COVID patients than any other health care system in the U.S., if not the world.

“It’s vastly different now. We went from a peak of thousands of cases per day down to about 70-90 new cases a day across our system. We’re lucky our system recognized that COVID could be an issue early on, with all of the multifaceted stressors on patient care,” Dr. Case said. “We’ve done whatever we could to give people time off, especially as the census started to come down. We freed up as many supportive mental health services as we could, working with the health system’s employee assistance program.”
Northwell gave out numbers for the psychiatry department, with clinicians available 24/7 for a confidential call, along with outside volunteers and a network of trauma psychologists. “Our system also provided emergency child care for staff, including hospitalists, wherever we could, drawing upon community resources,” Dr. Case added.
“We recognize that we’re all in the same foxhole. That’s been a helpful attitude – recognizing that it’s okay to be upset in a crisis and to have trouble dealing with what’s going on,” he said. “We need to acknowledge that some of us are suffering and try to encourage people to face it head on. For a lot of physicians, especially those who were redeployed here from other departments, it was important just to have us ask if they were doing okay.”
Brian Schroeder, MHA, FACHE, FHM, assistant vice president for hospital and emergency medicine for Atrium Health, based in Charlotte, N.C., said one of the biggest sources of stress on his staff has been the constant pace of change – whether local hospital protocols, state policies, or guidelines from the Centers for Disease Control and Prevention. “The updating is difficult to keep up with. A lot of our physicians get worried and anxious that they’re not following the latest guidelines or correctly doing what they should be doing to care for COVID patients. One thing we’ve done to alleviate some of that fear and anxiety is through weekly huddles with our hospital teams, focusing on changes relevant to their work. We also have weekly ‘all-hands’ meetings for our 250 providers across 13 acute and four postacute facilities.”
Before COVID, it was difficult to get everyone together as one big group from hospitals up to 5 hours apart, but with the Microsoft Teams platform, they can all meet together.
“At the height of the pandemic, we’d convene weekly and share national statistics, organizational statistics, testing updates, changes to protocols,” Mr. Schroeder said. As the pace of change has slowed, these meetings were cut back to monthly. “Our physicians feel we are passing on information as soon as we get it. They know we’ll always tell them what we know.”
Sarah Richards, MD, assistant professor of internal medicine at the University of Nebraska, Omaha, who heads the Society of Hospital Medicine’s Well-Being Task Force, formed to address staff stress in the COVID environment, said there are things that health care systems can do to help mitigate job stress and burnout. But broader issues may need to be addressed at a national level. “SHM is trying to understand work-related stress – and to identify resources that could support doctors, so they can spend more of their time doing what they enjoy most, which is taking care of patients,” she said.
“We also recognize that people have had very different experiences, depending on geography, and at the individual level stressors are experienced very differently,” Dr. Richard noted. “One of the most common stressors we’ve heard from doctors is the challenge of caring for patients who are lonely and isolated in their hospital rooms, suffering and dying in new ways. In low-incidence areas, doctors are expressing guilt because they aren’t under as much stress as their colleagues. In high-incidence areas, doctors are already experiencing posttraumatic stress disorder.”
SHM’s Well-Being Task Force is working on a tool to help normalize these stressors and encourage open conversations about mental health issues. A guide called “HM COVID Check-in Guide for Self & Peers” is designed to help hospitalists break the culture of silence around well-being and burnout during COVID-19 and how people are handling and processing the pandemic experience. It is expected to be completed later this year, Dr. Richards said. Other SHM projects and resources for staff support are also in the works.
The impact on women doctors
In a recent Journal of Hospital Medicine article entitled “Collateral Damage: How COVID-19 is Adversely Impacting Women Physicians,” hospitalist Yemisi Jones, MD, medical director of continuing medical education at Cincinnati Children’s Hospital Medical Center, and colleagues argue that preexisting gender inequities in compensation, academic rank and leadership positions for physicians have made the COVID-19 crisis even more burdensome on female hospitalists.1

“Increased childcare and schooling obligations, coupled with disproportionate household responsibilities and an inability to work from home, will likely result in female hospitalists struggling to meet family needs while pandemic-related work responsibilities are ramping up,” they write. COVID may intensify workplace inequalities, with a lack of recognition of the undue strain that group policies place on women.
“Often women suffer in silence,” said coauthor Jennifer O’Toole, MD, MEd, director of education in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center and program director of the internal medicine–pediatrics residency. “We are not always the best self-advocates, although many of us are working on that.”
When women in hospital medicine take leadership roles, these often tend to involve mutual support activities, taking care of colleagues, and promoting collaborative work environments, Dr. Jones added. The stereotypical example is the committee that organizes celebrations when group members get married or have babies.
These activities can take a lot of time, she said. “We need to pay attention to that kind of role in our groups, because it’s important to the cohesiveness of the group. But it often goes unrecognized and doesn’t translate into the currency of promotion and leadership in medicine. When women go for promotions in the future, how will what happened during the COVID crisis impact their opportunities?”
What is the answer to overcoming these systemic inequities? Start with making sure women are part of the leadership team, with responsibilities for group policies, schedules, and other important decisions. “Look at your group’s leadership – particularly the higher positions. If it’s not diverse, ask why. ‘What is it about the structure of our group?’ Make a more concerted effort in your recruitment and retention,” Dr. Jones said.
The JHM article also recommends closely monitoring the direct and indirect effects of COVID-19 on female hospitalists, inquiring specifically about the needs of women in the organization, and ensuring that diversity, inclusion, and equity efforts are not suspended during the pandemic. Gender-based disparities in pay also need a closer look, and not just one time but reviewed periodically and adjusted accordingly.
Mentoring for early career women is important, but more so is sponsorship – someone in a high-level leadership role in the group sponsoring women who are rising up the career ladder, Dr. O’Toole said. “Professional women tend to be overmentored and undersponsored.”
What are the answers?
Ultimately, listening is key to try to help people get through the pandemic, Dr. Washburn said. “People become burned out when they feel leadership doesn’t understand their needs or doesn’t hear their concerns. Our group leaders all do clinical work, so they are seen as one of us. They try very hard; they have listening ears. But listening is just the first step. Next step is to work creatively to get the identified needs met.”
A few years ago, Johns Hopkins developed training in enhanced communication in health care for all hospital providers, including nurses and doctors, encouraging them to get trained in how to actively listen and address their patients’ emotional and social experiences as well as disease, Dr. Washburn explained. Learning how to listen better to patients can enhance skills at listening to colleagues, and vice versa. “We recognize the importance of better communication – for reducing sentinel events in the hospital and also for preventing staff burnout.”
Dr. Barnes also does physician coaching, and says a lot of that work is helping people achieve clarity on their core values. “Healing patients is a core identify for physicians; we want to take care of people. But other things can get in the way of that, and hospitalist groups can work at minimizing those barriers. We also need to learn, as hospitalists, that we work in a group. You need to be creative in how you do your team building, especially now, when you can no longer get together for dinner. Whatever it is, how do we bring our team back together? The biggest source of support for many hospitalists, beyond their family, is the group.”
Dr. Case said there is a longer-term need to study the root causes of burnout in hospitalists and to identify the issues that cause job stress. “What is modifiable? How can we tackle it? I see that as big part of my job every day. Being a physician is hard enough as it is. Let’s work to resolve those issues that add needlessly to the stress.”
“I think the pandemic brought a magnifying glass to how important a concern staff stress is,” Ms. Panek said. Resilience is important.
“We were working in our group on creating a culture that values trust and transparency, and then the COVID crisis hit,” she said. “But you can still keep working on those things. We would not have been as good or as positive as we were in managing this crisis without that preexisting culture to draw upon. We always said it was important. Now we know that’s true.”
Reference
1. Jones Y et al. Collateral Damage: How COVID-19 Is Adversely Impacting Women Physicians. J Hosp Med. 2020 August;15(8):507-9.
New kinds of job stress multiply in unusual times
New kinds of job stress multiply in unusual times
Clarissa Barnes, MD, a hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and until recently medical director of Avera’s LIGHT Program, a wellness-oriented service for doctors, nurse practitioners, and physician assistants, watched the COVID-19 crisis unfold up close in her community and her hospital. Sioux Falls traced its surge of COVID patients to an outbreak at a local meatpacking plant.
“In the beginning, we didn’t know much about the virus and its communicability, although we have since gotten a better handle on that,” she said. “We had questions: Should we give patients more fluids – or less? Steroids or not? In my experience as a hospitalist I never had patients die every day on my shift, but that was happening with COVID.” The crisis imposed serious stresses on frontline providers, and hospitalists were concerned about personal safety and exposure risk – not just for themselves but for their families.
“The first time I worked on the COVID unit, I moved into the guest room in our home, apart from my husband and our young children,” Dr. Barnes said. “Ultimately I caught the virus, although I have since recovered.” Her experience has highlighted how existing issues of job stress and burnout in hospital medicine have been exacerbated by COVID-19. Even physicians who consider themselves healthy may have little emotional reserve to draw upon in a crisis of this magnitude.
“We are social distancing at work, wearing masks, not eating together with our colleagues – with less camaraderie and social support than we used to have,” she said. “I feel exhausted and there’s no question that my colleagues and I have sacrificed a lot to deal with the pandemic.” Add to that the second front of the COVID-19 crisis, Dr. Barnes said, which is “fighting the medical information wars, trying to correct misinformation put out there by people. Physicians who have been on the front lines of the pandemic know how demoralizing it can be to have people negate your first-hand experience.”
The situation has gotten better in Sioux Falls, Dr. Barnes said, although cases have started rising in the state again. The stress, while not gone, is reduced. For some doctors, “COVID reminded us of why we do what we do. Some of the usual bureaucratic requirements were set aside and we could focus on what our patients needed and how to take care of them.”
Taking job stress seriously
Tiffani Panek, MA, SFHM, CLHM, administrator of the division of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, said job stress is a major issue for hospitalist groups.
“We take it seriously here, and use a survey tool to measure morale in our group annually,” she said. “So far, knock on wood, Baltimore has not been one of the big hot spots, but we’ve definitely had waves of COVID patients.”
The Bayview hospitalist group has a diversified set of leaders, including a wellness director. “They’re always checking up on our people, keeping an eye on those who are most vulnerable. One of the stressors we hadn’t thought about before was for our people who live alone. With the isolation and lockdown, they haven’t been able to socialize, so we’ve made direct outreach, asking people how they were doing,” Ms. Panek said. “People know we’ve got their back – professionally and personally. They know, if there’s something we can do to help, we will do it.”
Bayview Medical Center has COVID-specific units and non-COVID units, and has tried to rotate hospitalist assignments because more than a couple days in a row spent wearing full personal protective equipment (PPE) is exhausting, Ms. Panek said. The group also allocated a respite room just outside the biocontainment unit, with a computer and opportunities for providers to just sit and take a breather – with appropriate social distancing. “It’s not fancy, but you just have to wear a mask, not full PPE.”
The Hopkins hospitalist group’s wellness director, Catherine Washburn, MD, also a working hospitalist, said providers are exhausted, and trying to transition to the new normal is a moving target.
“It’s hard for anyone to say what our lives will look like in 6 months,” she said. “People in our group have lost family members to COVID, or postponed major life events, like weddings. We acknowledge losses together as a group, and celebrate things worth celebrating, like babies or birthdays.”
Greatest COVID caseload
Joshua Case, MD, hospitalist medical director for 16 acute care hospitals of Northwell Health serving metropolitan New York City and Long Island, said his group’s hospitalists and other staff worked incredibly hard during the surge of COVID-19 patients in New York. “Northwell likely cared for more COVID patients than any other health care system in the U.S., if not the world.
“It’s vastly different now. We went from a peak of thousands of cases per day down to about 70-90 new cases a day across our system. We’re lucky our system recognized that COVID could be an issue early on, with all of the multifaceted stressors on patient care,” Dr. Case said. “We’ve done whatever we could to give people time off, especially as the census started to come down. We freed up as many supportive mental health services as we could, working with the health system’s employee assistance program.”
Northwell gave out numbers for the psychiatry department, with clinicians available 24/7 for a confidential call, along with outside volunteers and a network of trauma psychologists. “Our system also provided emergency child care for staff, including hospitalists, wherever we could, drawing upon community resources,” Dr. Case added.
“We recognize that we’re all in the same foxhole. That’s been a helpful attitude – recognizing that it’s okay to be upset in a crisis and to have trouble dealing with what’s going on,” he said. “We need to acknowledge that some of us are suffering and try to encourage people to face it head on. For a lot of physicians, especially those who were redeployed here from other departments, it was important just to have us ask if they were doing okay.”
Brian Schroeder, MHA, FACHE, FHM, assistant vice president for hospital and emergency medicine for Atrium Health, based in Charlotte, N.C., said one of the biggest sources of stress on his staff has been the constant pace of change – whether local hospital protocols, state policies, or guidelines from the Centers for Disease Control and Prevention. “The updating is difficult to keep up with. A lot of our physicians get worried and anxious that they’re not following the latest guidelines or correctly doing what they should be doing to care for COVID patients. One thing we’ve done to alleviate some of that fear and anxiety is through weekly huddles with our hospital teams, focusing on changes relevant to their work. We also have weekly ‘all-hands’ meetings for our 250 providers across 13 acute and four postacute facilities.”
Before COVID, it was difficult to get everyone together as one big group from hospitals up to 5 hours apart, but with the Microsoft Teams platform, they can all meet together.
“At the height of the pandemic, we’d convene weekly and share national statistics, organizational statistics, testing updates, changes to protocols,” Mr. Schroeder said. As the pace of change has slowed, these meetings were cut back to monthly. “Our physicians feel we are passing on information as soon as we get it. They know we’ll always tell them what we know.”
Sarah Richards, MD, assistant professor of internal medicine at the University of Nebraska, Omaha, who heads the Society of Hospital Medicine’s Well-Being Task Force, formed to address staff stress in the COVID environment, said there are things that health care systems can do to help mitigate job stress and burnout. But broader issues may need to be addressed at a national level. “SHM is trying to understand work-related stress – and to identify resources that could support doctors, so they can spend more of their time doing what they enjoy most, which is taking care of patients,” she said.
“We also recognize that people have had very different experiences, depending on geography, and at the individual level stressors are experienced very differently,” Dr. Richard noted. “One of the most common stressors we’ve heard from doctors is the challenge of caring for patients who are lonely and isolated in their hospital rooms, suffering and dying in new ways. In low-incidence areas, doctors are expressing guilt because they aren’t under as much stress as their colleagues. In high-incidence areas, doctors are already experiencing posttraumatic stress disorder.”
SHM’s Well-Being Task Force is working on a tool to help normalize these stressors and encourage open conversations about mental health issues. A guide called “HM COVID Check-in Guide for Self & Peers” is designed to help hospitalists break the culture of silence around well-being and burnout during COVID-19 and how people are handling and processing the pandemic experience. It is expected to be completed later this year, Dr. Richards said. Other SHM projects and resources for staff support are also in the works.
The impact on women doctors
In a recent Journal of Hospital Medicine article entitled “Collateral Damage: How COVID-19 is Adversely Impacting Women Physicians,” hospitalist Yemisi Jones, MD, medical director of continuing medical education at Cincinnati Children’s Hospital Medical Center, and colleagues argue that preexisting gender inequities in compensation, academic rank and leadership positions for physicians have made the COVID-19 crisis even more burdensome on female hospitalists.1
“Increased childcare and schooling obligations, coupled with disproportionate household responsibilities and an inability to work from home, will likely result in female hospitalists struggling to meet family needs while pandemic-related work responsibilities are ramping up,” they write. COVID may intensify workplace inequalities, with a lack of recognition of the undue strain that group policies place on women.
“Often women suffer in silence,” said coauthor Jennifer O’Toole, MD, MEd, director of education in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center and program director of the internal medicine–pediatrics residency. “We are not always the best self-advocates, although many of us are working on that.”
When women in hospital medicine take leadership roles, these often tend to involve mutual support activities, taking care of colleagues, and promoting collaborative work environments, Dr. Jones added. The stereotypical example is the committee that organizes celebrations when group members get married or have babies.
These activities can take a lot of time, she said. “We need to pay attention to that kind of role in our groups, because it’s important to the cohesiveness of the group. But it often goes unrecognized and doesn’t translate into the currency of promotion and leadership in medicine. When women go for promotions in the future, how will what happened during the COVID crisis impact their opportunities?”
What is the answer to overcoming these systemic inequities? Start with making sure women are part of the leadership team, with responsibilities for group policies, schedules, and other important decisions. “Look at your group’s leadership – particularly the higher positions. If it’s not diverse, ask why. ‘What is it about the structure of our group?’ Make a more concerted effort in your recruitment and retention,” Dr. Jones said.
The JHM article also recommends closely monitoring the direct and indirect effects of COVID-19 on female hospitalists, inquiring specifically about the needs of women in the organization, and ensuring that diversity, inclusion, and equity efforts are not suspended during the pandemic. Gender-based disparities in pay also need a closer look, and not just one time but reviewed periodically and adjusted accordingly.
Mentoring for early career women is important, but more so is sponsorship – someone in a high-level leadership role in the group sponsoring women who are rising up the career ladder, Dr. O’Toole said. “Professional women tend to be overmentored and undersponsored.”
What are the answers?
Ultimately, listening is key to try to help people get through the pandemic, Dr. Washburn said. “People become burned out when they feel leadership doesn’t understand their needs or doesn’t hear their concerns. Our group leaders all do clinical work, so they are seen as one of us. They try very hard; they have listening ears. But listening is just the first step. Next step is to work creatively to get the identified needs met.”
A few years ago, Johns Hopkins developed training in enhanced communication in health care for all hospital providers, including nurses and doctors, encouraging them to get trained in how to actively listen and address their patients’ emotional and social experiences as well as disease, Dr. Washburn explained. Learning how to listen better to patients can enhance skills at listening to colleagues, and vice versa. “We recognize the importance of better communication – for reducing sentinel events in the hospital and also for preventing staff burnout.”
Dr. Barnes also does physician coaching, and says a lot of that work is helping people achieve clarity on their core values. “Healing patients is a core identify for physicians; we want to take care of people. But other things can get in the way of that, and hospitalist groups can work at minimizing those barriers. We also need to learn, as hospitalists, that we work in a group. You need to be creative in how you do your team building, especially now, when you can no longer get together for dinner. Whatever it is, how do we bring our team back together? The biggest source of support for many hospitalists, beyond their family, is the group.”
Dr. Case said there is a longer-term need to study the root causes of burnout in hospitalists and to identify the issues that cause job stress. “What is modifiable? How can we tackle it? I see that as big part of my job every day. Being a physician is hard enough as it is. Let’s work to resolve those issues that add needlessly to the stress.”
“I think the pandemic brought a magnifying glass to how important a concern staff stress is,” Ms. Panek said. Resilience is important.
“We were working in our group on creating a culture that values trust and transparency, and then the COVID crisis hit,” she said. “But you can still keep working on those things. We would not have been as good or as positive as we were in managing this crisis without that preexisting culture to draw upon. We always said it was important. Now we know that’s true.”
Reference
1. Jones Y et al. Collateral Damage: How COVID-19 Is Adversely Impacting Women Physicians. J Hosp Med. 2020 August;15(8):507-9.
Clarissa Barnes, MD, a hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and until recently medical director of Avera’s LIGHT Program, a wellness-oriented service for doctors, nurse practitioners, and physician assistants, watched the COVID-19 crisis unfold up close in her community and her hospital. Sioux Falls traced its surge of COVID patients to an outbreak at a local meatpacking plant.
“In the beginning, we didn’t know much about the virus and its communicability, although we have since gotten a better handle on that,” she said. “We had questions: Should we give patients more fluids – or less? Steroids or not? In my experience as a hospitalist I never had patients die every day on my shift, but that was happening with COVID.” The crisis imposed serious stresses on frontline providers, and hospitalists were concerned about personal safety and exposure risk – not just for themselves but for their families.
“The first time I worked on the COVID unit, I moved into the guest room in our home, apart from my husband and our young children,” Dr. Barnes said. “Ultimately I caught the virus, although I have since recovered.” Her experience has highlighted how existing issues of job stress and burnout in hospital medicine have been exacerbated by COVID-19. Even physicians who consider themselves healthy may have little emotional reserve to draw upon in a crisis of this magnitude.
“We are social distancing at work, wearing masks, not eating together with our colleagues – with less camaraderie and social support than we used to have,” she said. “I feel exhausted and there’s no question that my colleagues and I have sacrificed a lot to deal with the pandemic.” Add to that the second front of the COVID-19 crisis, Dr. Barnes said, which is “fighting the medical information wars, trying to correct misinformation put out there by people. Physicians who have been on the front lines of the pandemic know how demoralizing it can be to have people negate your first-hand experience.”
The situation has gotten better in Sioux Falls, Dr. Barnes said, although cases have started rising in the state again. The stress, while not gone, is reduced. For some doctors, “COVID reminded us of why we do what we do. Some of the usual bureaucratic requirements were set aside and we could focus on what our patients needed and how to take care of them.”
Taking job stress seriously
Tiffani Panek, MA, SFHM, CLHM, administrator of the division of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, said job stress is a major issue for hospitalist groups.
“We take it seriously here, and use a survey tool to measure morale in our group annually,” she said. “So far, knock on wood, Baltimore has not been one of the big hot spots, but we’ve definitely had waves of COVID patients.”
The Bayview hospitalist group has a diversified set of leaders, including a wellness director. “They’re always checking up on our people, keeping an eye on those who are most vulnerable. One of the stressors we hadn’t thought about before was for our people who live alone. With the isolation and lockdown, they haven’t been able to socialize, so we’ve made direct outreach, asking people how they were doing,” Ms. Panek said. “People know we’ve got their back – professionally and personally. They know, if there’s something we can do to help, we will do it.”
Bayview Medical Center has COVID-specific units and non-COVID units, and has tried to rotate hospitalist assignments because more than a couple days in a row spent wearing full personal protective equipment (PPE) is exhausting, Ms. Panek said. The group also allocated a respite room just outside the biocontainment unit, with a computer and opportunities for providers to just sit and take a breather – with appropriate social distancing. “It’s not fancy, but you just have to wear a mask, not full PPE.”
The Hopkins hospitalist group’s wellness director, Catherine Washburn, MD, also a working hospitalist, said providers are exhausted, and trying to transition to the new normal is a moving target.
“It’s hard for anyone to say what our lives will look like in 6 months,” she said. “People in our group have lost family members to COVID, or postponed major life events, like weddings. We acknowledge losses together as a group, and celebrate things worth celebrating, like babies or birthdays.”
Greatest COVID caseload
Joshua Case, MD, hospitalist medical director for 16 acute care hospitals of Northwell Health serving metropolitan New York City and Long Island, said his group’s hospitalists and other staff worked incredibly hard during the surge of COVID-19 patients in New York. “Northwell likely cared for more COVID patients than any other health care system in the U.S., if not the world.
“It’s vastly different now. We went from a peak of thousands of cases per day down to about 70-90 new cases a day across our system. We’re lucky our system recognized that COVID could be an issue early on, with all of the multifaceted stressors on patient care,” Dr. Case said. “We’ve done whatever we could to give people time off, especially as the census started to come down. We freed up as many supportive mental health services as we could, working with the health system’s employee assistance program.”
Northwell gave out numbers for the psychiatry department, with clinicians available 24/7 for a confidential call, along with outside volunteers and a network of trauma psychologists. “Our system also provided emergency child care for staff, including hospitalists, wherever we could, drawing upon community resources,” Dr. Case added.
“We recognize that we’re all in the same foxhole. That’s been a helpful attitude – recognizing that it’s okay to be upset in a crisis and to have trouble dealing with what’s going on,” he said. “We need to acknowledge that some of us are suffering and try to encourage people to face it head on. For a lot of physicians, especially those who were redeployed here from other departments, it was important just to have us ask if they were doing okay.”
Brian Schroeder, MHA, FACHE, FHM, assistant vice president for hospital and emergency medicine for Atrium Health, based in Charlotte, N.C., said one of the biggest sources of stress on his staff has been the constant pace of change – whether local hospital protocols, state policies, or guidelines from the Centers for Disease Control and Prevention. “The updating is difficult to keep up with. A lot of our physicians get worried and anxious that they’re not following the latest guidelines or correctly doing what they should be doing to care for COVID patients. One thing we’ve done to alleviate some of that fear and anxiety is through weekly huddles with our hospital teams, focusing on changes relevant to their work. We also have weekly ‘all-hands’ meetings for our 250 providers across 13 acute and four postacute facilities.”
Before COVID, it was difficult to get everyone together as one big group from hospitals up to 5 hours apart, but with the Microsoft Teams platform, they can all meet together.
“At the height of the pandemic, we’d convene weekly and share national statistics, organizational statistics, testing updates, changes to protocols,” Mr. Schroeder said. As the pace of change has slowed, these meetings were cut back to monthly. “Our physicians feel we are passing on information as soon as we get it. They know we’ll always tell them what we know.”
Sarah Richards, MD, assistant professor of internal medicine at the University of Nebraska, Omaha, who heads the Society of Hospital Medicine’s Well-Being Task Force, formed to address staff stress in the COVID environment, said there are things that health care systems can do to help mitigate job stress and burnout. But broader issues may need to be addressed at a national level. “SHM is trying to understand work-related stress – and to identify resources that could support doctors, so they can spend more of their time doing what they enjoy most, which is taking care of patients,” she said.
“We also recognize that people have had very different experiences, depending on geography, and at the individual level stressors are experienced very differently,” Dr. Richard noted. “One of the most common stressors we’ve heard from doctors is the challenge of caring for patients who are lonely and isolated in their hospital rooms, suffering and dying in new ways. In low-incidence areas, doctors are expressing guilt because they aren’t under as much stress as their colleagues. In high-incidence areas, doctors are already experiencing posttraumatic stress disorder.”
SHM’s Well-Being Task Force is working on a tool to help normalize these stressors and encourage open conversations about mental health issues. A guide called “HM COVID Check-in Guide for Self & Peers” is designed to help hospitalists break the culture of silence around well-being and burnout during COVID-19 and how people are handling and processing the pandemic experience. It is expected to be completed later this year, Dr. Richards said. Other SHM projects and resources for staff support are also in the works.
The impact on women doctors
In a recent Journal of Hospital Medicine article entitled “Collateral Damage: How COVID-19 is Adversely Impacting Women Physicians,” hospitalist Yemisi Jones, MD, medical director of continuing medical education at Cincinnati Children’s Hospital Medical Center, and colleagues argue that preexisting gender inequities in compensation, academic rank and leadership positions for physicians have made the COVID-19 crisis even more burdensome on female hospitalists.1
“Increased childcare and schooling obligations, coupled with disproportionate household responsibilities and an inability to work from home, will likely result in female hospitalists struggling to meet family needs while pandemic-related work responsibilities are ramping up,” they write. COVID may intensify workplace inequalities, with a lack of recognition of the undue strain that group policies place on women.
“Often women suffer in silence,” said coauthor Jennifer O’Toole, MD, MEd, director of education in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center and program director of the internal medicine–pediatrics residency. “We are not always the best self-advocates, although many of us are working on that.”
When women in hospital medicine take leadership roles, these often tend to involve mutual support activities, taking care of colleagues, and promoting collaborative work environments, Dr. Jones added. The stereotypical example is the committee that organizes celebrations when group members get married or have babies.
These activities can take a lot of time, she said. “We need to pay attention to that kind of role in our groups, because it’s important to the cohesiveness of the group. But it often goes unrecognized and doesn’t translate into the currency of promotion and leadership in medicine. When women go for promotions in the future, how will what happened during the COVID crisis impact their opportunities?”
What is the answer to overcoming these systemic inequities? Start with making sure women are part of the leadership team, with responsibilities for group policies, schedules, and other important decisions. “Look at your group’s leadership – particularly the higher positions. If it’s not diverse, ask why. ‘What is it about the structure of our group?’ Make a more concerted effort in your recruitment and retention,” Dr. Jones said.
The JHM article also recommends closely monitoring the direct and indirect effects of COVID-19 on female hospitalists, inquiring specifically about the needs of women in the organization, and ensuring that diversity, inclusion, and equity efforts are not suspended during the pandemic. Gender-based disparities in pay also need a closer look, and not just one time but reviewed periodically and adjusted accordingly.
Mentoring for early career women is important, but more so is sponsorship – someone in a high-level leadership role in the group sponsoring women who are rising up the career ladder, Dr. O’Toole said. “Professional women tend to be overmentored and undersponsored.”
What are the answers?
Ultimately, listening is key to try to help people get through the pandemic, Dr. Washburn said. “People become burned out when they feel leadership doesn’t understand their needs or doesn’t hear their concerns. Our group leaders all do clinical work, so they are seen as one of us. They try very hard; they have listening ears. But listening is just the first step. Next step is to work creatively to get the identified needs met.”
A few years ago, Johns Hopkins developed training in enhanced communication in health care for all hospital providers, including nurses and doctors, encouraging them to get trained in how to actively listen and address their patients’ emotional and social experiences as well as disease, Dr. Washburn explained. Learning how to listen better to patients can enhance skills at listening to colleagues, and vice versa. “We recognize the importance of better communication – for reducing sentinel events in the hospital and also for preventing staff burnout.”
Dr. Barnes also does physician coaching, and says a lot of that work is helping people achieve clarity on their core values. “Healing patients is a core identify for physicians; we want to take care of people. But other things can get in the way of that, and hospitalist groups can work at minimizing those barriers. We also need to learn, as hospitalists, that we work in a group. You need to be creative in how you do your team building, especially now, when you can no longer get together for dinner. Whatever it is, how do we bring our team back together? The biggest source of support for many hospitalists, beyond their family, is the group.”
Dr. Case said there is a longer-term need to study the root causes of burnout in hospitalists and to identify the issues that cause job stress. “What is modifiable? How can we tackle it? I see that as big part of my job every day. Being a physician is hard enough as it is. Let’s work to resolve those issues that add needlessly to the stress.”
“I think the pandemic brought a magnifying glass to how important a concern staff stress is,” Ms. Panek said. Resilience is important.
“We were working in our group on creating a culture that values trust and transparency, and then the COVID crisis hit,” she said. “But you can still keep working on those things. We would not have been as good or as positive as we were in managing this crisis without that preexisting culture to draw upon. We always said it was important. Now we know that’s true.”
Reference
1. Jones Y et al. Collateral Damage: How COVID-19 Is Adversely Impacting Women Physicians. J Hosp Med. 2020 August;15(8):507-9.
The authority/accountability balance
Evaluating your career trajectory
I have had the pleasure of working on the Society of Hospital Medicine’s signature Leadership Academies since 2010, and I enjoy working with hospital medicine leaders from around the country every year. I started as a hospital medicine leader in 2000 and served during the unprecedented growth of the field when it was “the most rapidly growing specialty in the history of medicine.”
Most businesses dream of having a year of double-digit growth; my department grew an average of 15% annually for more than 10 years. These unique experiences have taught me many lessons and afforded me the opportunity to watch many stars of hospital medicine rise, as well as to learn from several less-scrupulous leaders about the darker side of hospital politics.
One of the lessons I learned the hard way about hospital politics is striking the “Authority/Accountability balance” in your career. I shared this perspective at the SHM annual conference in 2018, at speaking engagements on the West Coast, and with my leadership group at the academies. I am sharing it with you because the feedback I have received has been very positive.
The Authority/Accountability balance is a tool for evaluating your current career trajectory and measuring if it is set up for success or failure. The essence is that your Authority and Accountability need to be balanced for you to be successful in your career, regardless of your station. Everybody from the hospitalist fresh out of residency to the CEO needs to have Authority and Accountability in balance to be successful. And as you use the tool to measure your own potential for success or failure, learn to apply it to those who report to you.
I believe the rising tide lifts all boats and the success of your subordinates, through mentoring and support, will add to your success. There is another, more cynical view of subordinates that can be identified using the Authority/Accountability balance, which I will address.
Authority
In this construct, “Authority” has a much broader meaning than just the ability to tell people what to do. The ability to tell people what to do is important but not sufficient for success in hospital politics.
Financial resources are essential for a successful Authority/Accountability balance – not only the hardware such as computers, telephones, pagers, and so on, but also clerical support, technical support, and analytic support so that you are getting high-quality data on the performance of the members of your hospital medicine group (HMG). These “soft” resources (clerical, technical, and analytical) are often overlooked as needs that HMG leaders must advocate for; I speak with many HMG leaders who remain under-resourced with “soft” assets. However, being appropriately resourced in these areas can be transformational for a group. Hospitalists don’t like doing clerical work, and if you don’t like a menial job assigned to you, you probably won’t do it very well. Having an unlicensed person dedicated to these clerical activities not only will cost less, but will ensure the job is done better.
Reporting structure is critically important, often overlooked, and historically misaligned in HMGs. When hospital medicine was starting in the late 1990s and early 2000s, rapidly growing hospitalist groups were typically led by young, early-career physicians who had chosen hospital medicine as a career. The problem was that they often lacked the seniority and connections at the executive level to advocate for their HMG. All too often the hospitalist group was tucked in under another department or division which, in turn, reported HMG updates and issues to the board of directors and the CEO.
A common reporting structure in the early days was that a senior member of the medical staff, or group, had once worked in the hospital and therefore “understood” the issues and challenges that the hospitalists were facing. It was up to this physician with seniority and connections to advocate for the hospitalists as they saw fit. The problem was that the hospital landscape was, and is, constantly evolving in innumerable ways. These “once removed” reporting structures for HMGs failed to get the required information on the rapidly changing, and evolving, hospitalist landscape to the desks of executives who had the financial and structural control to address the challenges that the hospitalists in the trenches were facing.
Numerous HMGs failed in the early days of hospital medicine because of this type of misaligned reporting structure. This is a lesson that should not be forgotten: Make sure your HMG leader has a seat at the table where executive decisions are made, including but not limited to the board of directors. To be in balance, you have to be “in the room where it happens.”
Accountability
The outcomes that you are responsible for need to be explicit, appropriately resourced with Authority, and clearly spelled out in your job description. Your job description is a document you should know, own, and revisit regularly with whomever you report to, in order to ensure success.
Once you have the Authority side of the equation appropriately resourced, setting outcomes that are a stretch, but still realistic and achievable within the scope of your position, is critical to your success. It is good to think about short-, medium-, and long-term goals, especially if you are in a leadership role. For example, one expectation you will have, regardless of your station, is that you keep up on your email and answer your phone. These are short-term goals that will often be included in your job description. However, taking on a new hospital contract and making sure that it has 24/7 hospitalist coverage, that all the hospitalists are meeting the geometric mean length of stay, and that all the physicians are having 15 encounters per day doesn’t happen immediately. Long-term goals, such as taking on a new hospital contract, are the big-picture stuff that can make or break the career of an HMG leader. Long-term goals also need to be delineated in the job description, along with specific time stamps and the resources you need to accomplish big ticket items – which are spelled out in the Authority side (that is, physician recruiter, secretary, background checks, and so on).
One of the classic misuses of Accountability is the “Fall Guy” scenario. The Fall Guy scenario is often used by cynical hospital and medical group executives to expand their influence while limiting their liability. In the Fall Guy scenario, the executive is surrounded with junior partners who are underpowered with Authority, and then the executive makes decisions for which the junior partners are Accountable. This allows the senior executive to make risky decisions on behalf of the hospital or medical group without the liability of being held accountable when the decision-making process fails. When the risky, and often ill-informed, decision fails, the junior partner who lacked the Authority to make the decision – but held the Accountability for it – becomes the Fall Guy for the failed endeavor. This is a critical outcome that the Authority/Accountability balance can help you avoid, if you use it wisely and properly.
If you find yourself in the Fall Guy position, it is time for a change. The Authority, the Accountability, or both need to change so that they are in better balance. Or your employer needs to change. Changing employers is an outcome worth avoiding, if at all possible. I have scrutinized thousands of resumes in my career, and frequent job changes always wave a red flag to prospective employers. However, changing jobs remains a crucial option if you are being set up for failure when Authority and Accountability are out of balance.
If you are unable to negotiate for the balance that will allow you to be successful with your current group, remember that HMG leaders are a prized commodity and in short supply. Leaving a group that has been your career is hard, but it is better to leave than stay in a position where you are set up for failure as the Fall Guy. Further, the most effective time to expand your Authority is when you are negotiating the terms of a new position. Changing positions is the nuclear option. However, it is better than becoming the Fall Guy, and a change can create opportunities that will accelerate your career and influence, if done right.
When I talk about Authority/Accountability balance, I always counter the Fall Guy with an ignominious historical figure: General George B. McClellan. General McClellan was the commander of the Army of the Potomac during the early years of the American Civil War. General McClellan had the industrial might of the Union north at his beck and call, as well as extraordinary resources for recruiting and retaining soldiers for his army. At every encounter with General Robert E. Lee’s Army of Northern Virginia, General McClellan outnumbered them, sometimes by more than two to one. Yet General McClellan was outfoxed repeatedly for the same reason: He failed to take decisive action.
Every time that McClellan failed, he blamed insufficient resources and told President Lincoln that he needed more troops and more equipment to be successful. In summary, while the Fall Guy scenario needs to be avoided, once you are adequately resourced, success requires taking decisive and strategic action, or you will suffer as did General McClellan. Failing to act when you are appropriately resourced can be just as damaging to your career and credibility as allowing yourself to become the Fall Guy.
Job description
Everybody has somebody that they report to, no matter how high up on the executive ladder they have climbed. Even the CEO must report to the board of directors. And that reporting structure usually involves periodic formal reviews. Your formal review is a good time to go over your job description, note what is relevant, remove what is irrelevant, and add new elements that have evolved in importance since your last review.
Job descriptions take many forms, but they always include a list of qualifications. If you have the job, you have the qualifications, so that is not likely to change. You may become more qualified for a higher-level position, but that is an entirely different discussion. I like to think of a well-written job description as including short-term and long-term goals. Short-term goals are usually the daily stuff that keeps operations running smoothly but garners little attention. Examples would include staying current on your emails, answering your phone, organizing meetings, and regularly attending various committees. Even some of these short-term goals can and will change over time. I always enjoyed quality oversight in my department, but as the department and my responsibilities grew, I realized I couldn’t do everything that I wanted to do. I needed to focus on the things only I could do and delegate those things that could be done by someone else, even though I wanted to continue doing them myself. I created a position for a clinical quality officer, and quality oversight moved off of my job description.
Long-term goals are the aspirational items, such as increasing market share, decreasing readmissions, improving patient satisfaction, and the like. Effective leaders are often focused on these aspirational, long-term goals, but they still must effectively execute their short-term goals. Stephen Covey outlines the dilemma with the “time management matrix” in his seminal work “The 7 Habits of Highly Effective People.” An in-depth discussion is beyond the scope of this article, but the time management matrix places tasks into one of four categories based on urgency and importance, and provides strategies for staying up on short-term goals while continually moving long-term goals forward.If you show up at your review with a list of accomplishments as well as an understanding of how the “time management matrix” affects your responsibilities, your boss will be impressed. It is also worth mentioning that Covey’s first habit is “Proactivity.” He uses the term Proactivity in a much more nuanced form than we typically think of, however. Simply put, Proactivity is the opposite of Reactivity, and it is another invaluable tool for success with those long-term goals that will help you make a name for yourself.
When you show up for your review, be it annual, biannual, or other, be prepared. Not only should you bring your job description and recommendations for how it should be adapted in the changing environment, but also bring examples of your accomplishments since the last review.
I talk with leaders frequently who are hardworking and diligent and hate bragging about their achievements; I get that. At the same time, if you don’t inform your superiors about your successes, there is no guarantee that they will hear about them or understand them in the appropriate context. Bragging about how great you are in the physician’s lounge is annoying; telling your boss about your accomplishments since the last review is critical to maintaining the momentum of past accomplishments. If you are not willing to toot your own horn, there is a very good chance that your horn will remain silent. I don’t think self-promotion comes easily to anyone, and it has to be done with a degree of humility and sensitivity; but it has to be done, so prepare for it.
Look out for yourself and others
We talk about teamwork and collaboration as hospitalists, and SHM is always underscoring the importance of teamwork and highlighting examples of successful teamwork in its many conferences and publications. Most hospital executives are focused on their own careers, however, and many have no reservations about damaging your career (your brand) if they think it will promote theirs. You have to look out for yourself and size up every leadership position you get into.
Physicians can expect their careers to last decades. The average hospital CEO has a tenure of less than 3.5 years, however, and when a new CEO is hired, almost half of chief financial, chief operating, and chief information officers are fired within 9 months. You may be focused on the long-term success of your organization as you plan your career, but many hospital administrators are interested only in short-term gains. It is similar to some members of Congress who are interested only in what they need to do now to win the next election and not in the long-term needs of the country. You should understand this disconnect when dealing with hospital executives, and how you and your credibility can become cannon fodder in their quest for short-term self-preservation.
You have to look out for and take care of yourself as you promote your group. With a better understanding of the Authority/Accountability balance, you have new tools to assess your chances of success and to advocate for yourself so that you and your group can be successful.
Despite my cynicism toward executives in the medical field, I personally advocate for supporting the career development of those around you and advise against furthering your career at the expense of others. Many unscrupulous executives will use this approach, surrounding themselves with Fall Guys, but my experience shows that this is not a sustainable strategy for success. It can lead to short-term gains, but eventually the piper must be paid. Moreover, the most successful medical executives and leaders that I have encountered have been those who genuinely cared about their subordinates, looked out for them, and selflessly promoted their careers.
In the age of social media, tearing others down seems to be the fastest way to get more “likes.” However, I strongly believe that you can’t build up your group, and our profession, just by tearing people down. Lending a helping hand may bring you less attention in the short term, but such action raises your stature, creates loyalty, and leads to sustainable success for the long run.
Dr. McIlraith is the founding chairman of the Hospital Medicine Department at Mercy Medical Group in Sacramento, Calif. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016 and is currently a member of the SHM Practice Management and Awards Committees, as well as the SHM Critical Care Task Force.
Sources
Quinn R. HM Turns 20: A look at the evolution of hospital medicine. The Hospitalist. 2016 August. https://www.the-hospitalist.org/hospitalist/article/121525/hm-turns-20-look-evolution-hospital-medicine
Stephen R. Covey. The 7 Habits of Highly Effective People: Powerful Lessons in Personal Change. Simon & Schuster. 1989.
10 Statistics on CEO Turnover, Recruitment. Becker’s Hospital Review. 2020. https://www.beckershospitalreview.com/hospital-management-administration/10-statistics-on-ceo-turnover-recruitment.html
Evaluating your career trajectory
Evaluating your career trajectory
I have had the pleasure of working on the Society of Hospital Medicine’s signature Leadership Academies since 2010, and I enjoy working with hospital medicine leaders from around the country every year. I started as a hospital medicine leader in 2000 and served during the unprecedented growth of the field when it was “the most rapidly growing specialty in the history of medicine.”
Most businesses dream of having a year of double-digit growth; my department grew an average of 15% annually for more than 10 years. These unique experiences have taught me many lessons and afforded me the opportunity to watch many stars of hospital medicine rise, as well as to learn from several less-scrupulous leaders about the darker side of hospital politics.
One of the lessons I learned the hard way about hospital politics is striking the “Authority/Accountability balance” in your career. I shared this perspective at the SHM annual conference in 2018, at speaking engagements on the West Coast, and with my leadership group at the academies. I am sharing it with you because the feedback I have received has been very positive.
The Authority/Accountability balance is a tool for evaluating your current career trajectory and measuring if it is set up for success or failure. The essence is that your Authority and Accountability need to be balanced for you to be successful in your career, regardless of your station. Everybody from the hospitalist fresh out of residency to the CEO needs to have Authority and Accountability in balance to be successful. And as you use the tool to measure your own potential for success or failure, learn to apply it to those who report to you.
I believe the rising tide lifts all boats and the success of your subordinates, through mentoring and support, will add to your success. There is another, more cynical view of subordinates that can be identified using the Authority/Accountability balance, which I will address.
Authority
In this construct, “Authority” has a much broader meaning than just the ability to tell people what to do. The ability to tell people what to do is important but not sufficient for success in hospital politics.
Financial resources are essential for a successful Authority/Accountability balance – not only the hardware such as computers, telephones, pagers, and so on, but also clerical support, technical support, and analytic support so that you are getting high-quality data on the performance of the members of your hospital medicine group (HMG). These “soft” resources (clerical, technical, and analytical) are often overlooked as needs that HMG leaders must advocate for; I speak with many HMG leaders who remain under-resourced with “soft” assets. However, being appropriately resourced in these areas can be transformational for a group. Hospitalists don’t like doing clerical work, and if you don’t like a menial job assigned to you, you probably won’t do it very well. Having an unlicensed person dedicated to these clerical activities not only will cost less, but will ensure the job is done better.
Reporting structure is critically important, often overlooked, and historically misaligned in HMGs. When hospital medicine was starting in the late 1990s and early 2000s, rapidly growing hospitalist groups were typically led by young, early-career physicians who had chosen hospital medicine as a career. The problem was that they often lacked the seniority and connections at the executive level to advocate for their HMG. All too often the hospitalist group was tucked in under another department or division which, in turn, reported HMG updates and issues to the board of directors and the CEO.
A common reporting structure in the early days was that a senior member of the medical staff, or group, had once worked in the hospital and therefore “understood” the issues and challenges that the hospitalists were facing. It was up to this physician with seniority and connections to advocate for the hospitalists as they saw fit. The problem was that the hospital landscape was, and is, constantly evolving in innumerable ways. These “once removed” reporting structures for HMGs failed to get the required information on the rapidly changing, and evolving, hospitalist landscape to the desks of executives who had the financial and structural control to address the challenges that the hospitalists in the trenches were facing.
Numerous HMGs failed in the early days of hospital medicine because of this type of misaligned reporting structure. This is a lesson that should not be forgotten: Make sure your HMG leader has a seat at the table where executive decisions are made, including but not limited to the board of directors. To be in balance, you have to be “in the room where it happens.”
Accountability
The outcomes that you are responsible for need to be explicit, appropriately resourced with Authority, and clearly spelled out in your job description. Your job description is a document you should know, own, and revisit regularly with whomever you report to, in order to ensure success.
Once you have the Authority side of the equation appropriately resourced, setting outcomes that are a stretch, but still realistic and achievable within the scope of your position, is critical to your success. It is good to think about short-, medium-, and long-term goals, especially if you are in a leadership role. For example, one expectation you will have, regardless of your station, is that you keep up on your email and answer your phone. These are short-term goals that will often be included in your job description. However, taking on a new hospital contract and making sure that it has 24/7 hospitalist coverage, that all the hospitalists are meeting the geometric mean length of stay, and that all the physicians are having 15 encounters per day doesn’t happen immediately. Long-term goals, such as taking on a new hospital contract, are the big-picture stuff that can make or break the career of an HMG leader. Long-term goals also need to be delineated in the job description, along with specific time stamps and the resources you need to accomplish big ticket items – which are spelled out in the Authority side (that is, physician recruiter, secretary, background checks, and so on).
One of the classic misuses of Accountability is the “Fall Guy” scenario. The Fall Guy scenario is often used by cynical hospital and medical group executives to expand their influence while limiting their liability. In the Fall Guy scenario, the executive is surrounded with junior partners who are underpowered with Authority, and then the executive makes decisions for which the junior partners are Accountable. This allows the senior executive to make risky decisions on behalf of the hospital or medical group without the liability of being held accountable when the decision-making process fails. When the risky, and often ill-informed, decision fails, the junior partner who lacked the Authority to make the decision – but held the Accountability for it – becomes the Fall Guy for the failed endeavor. This is a critical outcome that the Authority/Accountability balance can help you avoid, if you use it wisely and properly.
If you find yourself in the Fall Guy position, it is time for a change. The Authority, the Accountability, or both need to change so that they are in better balance. Or your employer needs to change. Changing employers is an outcome worth avoiding, if at all possible. I have scrutinized thousands of resumes in my career, and frequent job changes always wave a red flag to prospective employers. However, changing jobs remains a crucial option if you are being set up for failure when Authority and Accountability are out of balance.
If you are unable to negotiate for the balance that will allow you to be successful with your current group, remember that HMG leaders are a prized commodity and in short supply. Leaving a group that has been your career is hard, but it is better to leave than stay in a position where you are set up for failure as the Fall Guy. Further, the most effective time to expand your Authority is when you are negotiating the terms of a new position. Changing positions is the nuclear option. However, it is better than becoming the Fall Guy, and a change can create opportunities that will accelerate your career and influence, if done right.
When I talk about Authority/Accountability balance, I always counter the Fall Guy with an ignominious historical figure: General George B. McClellan. General McClellan was the commander of the Army of the Potomac during the early years of the American Civil War. General McClellan had the industrial might of the Union north at his beck and call, as well as extraordinary resources for recruiting and retaining soldiers for his army. At every encounter with General Robert E. Lee’s Army of Northern Virginia, General McClellan outnumbered them, sometimes by more than two to one. Yet General McClellan was outfoxed repeatedly for the same reason: He failed to take decisive action.
Every time that McClellan failed, he blamed insufficient resources and told President Lincoln that he needed more troops and more equipment to be successful. In summary, while the Fall Guy scenario needs to be avoided, once you are adequately resourced, success requires taking decisive and strategic action, or you will suffer as did General McClellan. Failing to act when you are appropriately resourced can be just as damaging to your career and credibility as allowing yourself to become the Fall Guy.
Job description
Everybody has somebody that they report to, no matter how high up on the executive ladder they have climbed. Even the CEO must report to the board of directors. And that reporting structure usually involves periodic formal reviews. Your formal review is a good time to go over your job description, note what is relevant, remove what is irrelevant, and add new elements that have evolved in importance since your last review.
Job descriptions take many forms, but they always include a list of qualifications. If you have the job, you have the qualifications, so that is not likely to change. You may become more qualified for a higher-level position, but that is an entirely different discussion. I like to think of a well-written job description as including short-term and long-term goals. Short-term goals are usually the daily stuff that keeps operations running smoothly but garners little attention. Examples would include staying current on your emails, answering your phone, organizing meetings, and regularly attending various committees. Even some of these short-term goals can and will change over time. I always enjoyed quality oversight in my department, but as the department and my responsibilities grew, I realized I couldn’t do everything that I wanted to do. I needed to focus on the things only I could do and delegate those things that could be done by someone else, even though I wanted to continue doing them myself. I created a position for a clinical quality officer, and quality oversight moved off of my job description.
Long-term goals are the aspirational items, such as increasing market share, decreasing readmissions, improving patient satisfaction, and the like. Effective leaders are often focused on these aspirational, long-term goals, but they still must effectively execute their short-term goals. Stephen Covey outlines the dilemma with the “time management matrix” in his seminal work “The 7 Habits of Highly Effective People.” An in-depth discussion is beyond the scope of this article, but the time management matrix places tasks into one of four categories based on urgency and importance, and provides strategies for staying up on short-term goals while continually moving long-term goals forward.If you show up at your review with a list of accomplishments as well as an understanding of how the “time management matrix” affects your responsibilities, your boss will be impressed. It is also worth mentioning that Covey’s first habit is “Proactivity.” He uses the term Proactivity in a much more nuanced form than we typically think of, however. Simply put, Proactivity is the opposite of Reactivity, and it is another invaluable tool for success with those long-term goals that will help you make a name for yourself.
When you show up for your review, be it annual, biannual, or other, be prepared. Not only should you bring your job description and recommendations for how it should be adapted in the changing environment, but also bring examples of your accomplishments since the last review.
I talk with leaders frequently who are hardworking and diligent and hate bragging about their achievements; I get that. At the same time, if you don’t inform your superiors about your successes, there is no guarantee that they will hear about them or understand them in the appropriate context. Bragging about how great you are in the physician’s lounge is annoying; telling your boss about your accomplishments since the last review is critical to maintaining the momentum of past accomplishments. If you are not willing to toot your own horn, there is a very good chance that your horn will remain silent. I don’t think self-promotion comes easily to anyone, and it has to be done with a degree of humility and sensitivity; but it has to be done, so prepare for it.
Look out for yourself and others
We talk about teamwork and collaboration as hospitalists, and SHM is always underscoring the importance of teamwork and highlighting examples of successful teamwork in its many conferences and publications. Most hospital executives are focused on their own careers, however, and many have no reservations about damaging your career (your brand) if they think it will promote theirs. You have to look out for yourself and size up every leadership position you get into.
Physicians can expect their careers to last decades. The average hospital CEO has a tenure of less than 3.5 years, however, and when a new CEO is hired, almost half of chief financial, chief operating, and chief information officers are fired within 9 months. You may be focused on the long-term success of your organization as you plan your career, but many hospital administrators are interested only in short-term gains. It is similar to some members of Congress who are interested only in what they need to do now to win the next election and not in the long-term needs of the country. You should understand this disconnect when dealing with hospital executives, and how you and your credibility can become cannon fodder in their quest for short-term self-preservation.
You have to look out for and take care of yourself as you promote your group. With a better understanding of the Authority/Accountability balance, you have new tools to assess your chances of success and to advocate for yourself so that you and your group can be successful.
Despite my cynicism toward executives in the medical field, I personally advocate for supporting the career development of those around you and advise against furthering your career at the expense of others. Many unscrupulous executives will use this approach, surrounding themselves with Fall Guys, but my experience shows that this is not a sustainable strategy for success. It can lead to short-term gains, but eventually the piper must be paid. Moreover, the most successful medical executives and leaders that I have encountered have been those who genuinely cared about their subordinates, looked out for them, and selflessly promoted their careers.
In the age of social media, tearing others down seems to be the fastest way to get more “likes.” However, I strongly believe that you can’t build up your group, and our profession, just by tearing people down. Lending a helping hand may bring you less attention in the short term, but such action raises your stature, creates loyalty, and leads to sustainable success for the long run.
Dr. McIlraith is the founding chairman of the Hospital Medicine Department at Mercy Medical Group in Sacramento, Calif. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016 and is currently a member of the SHM Practice Management and Awards Committees, as well as the SHM Critical Care Task Force.
Sources
Quinn R. HM Turns 20: A look at the evolution of hospital medicine. The Hospitalist. 2016 August. https://www.the-hospitalist.org/hospitalist/article/121525/hm-turns-20-look-evolution-hospital-medicine
Stephen R. Covey. The 7 Habits of Highly Effective People: Powerful Lessons in Personal Change. Simon & Schuster. 1989.
10 Statistics on CEO Turnover, Recruitment. Becker’s Hospital Review. 2020. https://www.beckershospitalreview.com/hospital-management-administration/10-statistics-on-ceo-turnover-recruitment.html
I have had the pleasure of working on the Society of Hospital Medicine’s signature Leadership Academies since 2010, and I enjoy working with hospital medicine leaders from around the country every year. I started as a hospital medicine leader in 2000 and served during the unprecedented growth of the field when it was “the most rapidly growing specialty in the history of medicine.”
Most businesses dream of having a year of double-digit growth; my department grew an average of 15% annually for more than 10 years. These unique experiences have taught me many lessons and afforded me the opportunity to watch many stars of hospital medicine rise, as well as to learn from several less-scrupulous leaders about the darker side of hospital politics.
One of the lessons I learned the hard way about hospital politics is striking the “Authority/Accountability balance” in your career. I shared this perspective at the SHM annual conference in 2018, at speaking engagements on the West Coast, and with my leadership group at the academies. I am sharing it with you because the feedback I have received has been very positive.
The Authority/Accountability balance is a tool for evaluating your current career trajectory and measuring if it is set up for success or failure. The essence is that your Authority and Accountability need to be balanced for you to be successful in your career, regardless of your station. Everybody from the hospitalist fresh out of residency to the CEO needs to have Authority and Accountability in balance to be successful. And as you use the tool to measure your own potential for success or failure, learn to apply it to those who report to you.
I believe the rising tide lifts all boats and the success of your subordinates, through mentoring and support, will add to your success. There is another, more cynical view of subordinates that can be identified using the Authority/Accountability balance, which I will address.
Authority
In this construct, “Authority” has a much broader meaning than just the ability to tell people what to do. The ability to tell people what to do is important but not sufficient for success in hospital politics.
Financial resources are essential for a successful Authority/Accountability balance – not only the hardware such as computers, telephones, pagers, and so on, but also clerical support, technical support, and analytic support so that you are getting high-quality data on the performance of the members of your hospital medicine group (HMG). These “soft” resources (clerical, technical, and analytical) are often overlooked as needs that HMG leaders must advocate for; I speak with many HMG leaders who remain under-resourced with “soft” assets. However, being appropriately resourced in these areas can be transformational for a group. Hospitalists don’t like doing clerical work, and if you don’t like a menial job assigned to you, you probably won’t do it very well. Having an unlicensed person dedicated to these clerical activities not only will cost less, but will ensure the job is done better.
Reporting structure is critically important, often overlooked, and historically misaligned in HMGs. When hospital medicine was starting in the late 1990s and early 2000s, rapidly growing hospitalist groups were typically led by young, early-career physicians who had chosen hospital medicine as a career. The problem was that they often lacked the seniority and connections at the executive level to advocate for their HMG. All too often the hospitalist group was tucked in under another department or division which, in turn, reported HMG updates and issues to the board of directors and the CEO.
A common reporting structure in the early days was that a senior member of the medical staff, or group, had once worked in the hospital and therefore “understood” the issues and challenges that the hospitalists were facing. It was up to this physician with seniority and connections to advocate for the hospitalists as they saw fit. The problem was that the hospital landscape was, and is, constantly evolving in innumerable ways. These “once removed” reporting structures for HMGs failed to get the required information on the rapidly changing, and evolving, hospitalist landscape to the desks of executives who had the financial and structural control to address the challenges that the hospitalists in the trenches were facing.
Numerous HMGs failed in the early days of hospital medicine because of this type of misaligned reporting structure. This is a lesson that should not be forgotten: Make sure your HMG leader has a seat at the table where executive decisions are made, including but not limited to the board of directors. To be in balance, you have to be “in the room where it happens.”
Accountability
The outcomes that you are responsible for need to be explicit, appropriately resourced with Authority, and clearly spelled out in your job description. Your job description is a document you should know, own, and revisit regularly with whomever you report to, in order to ensure success.
Once you have the Authority side of the equation appropriately resourced, setting outcomes that are a stretch, but still realistic and achievable within the scope of your position, is critical to your success. It is good to think about short-, medium-, and long-term goals, especially if you are in a leadership role. For example, one expectation you will have, regardless of your station, is that you keep up on your email and answer your phone. These are short-term goals that will often be included in your job description. However, taking on a new hospital contract and making sure that it has 24/7 hospitalist coverage, that all the hospitalists are meeting the geometric mean length of stay, and that all the physicians are having 15 encounters per day doesn’t happen immediately. Long-term goals, such as taking on a new hospital contract, are the big-picture stuff that can make or break the career of an HMG leader. Long-term goals also need to be delineated in the job description, along with specific time stamps and the resources you need to accomplish big ticket items – which are spelled out in the Authority side (that is, physician recruiter, secretary, background checks, and so on).
One of the classic misuses of Accountability is the “Fall Guy” scenario. The Fall Guy scenario is often used by cynical hospital and medical group executives to expand their influence while limiting their liability. In the Fall Guy scenario, the executive is surrounded with junior partners who are underpowered with Authority, and then the executive makes decisions for which the junior partners are Accountable. This allows the senior executive to make risky decisions on behalf of the hospital or medical group without the liability of being held accountable when the decision-making process fails. When the risky, and often ill-informed, decision fails, the junior partner who lacked the Authority to make the decision – but held the Accountability for it – becomes the Fall Guy for the failed endeavor. This is a critical outcome that the Authority/Accountability balance can help you avoid, if you use it wisely and properly.
If you find yourself in the Fall Guy position, it is time for a change. The Authority, the Accountability, or both need to change so that they are in better balance. Or your employer needs to change. Changing employers is an outcome worth avoiding, if at all possible. I have scrutinized thousands of resumes in my career, and frequent job changes always wave a red flag to prospective employers. However, changing jobs remains a crucial option if you are being set up for failure when Authority and Accountability are out of balance.
If you are unable to negotiate for the balance that will allow you to be successful with your current group, remember that HMG leaders are a prized commodity and in short supply. Leaving a group that has been your career is hard, but it is better to leave than stay in a position where you are set up for failure as the Fall Guy. Further, the most effective time to expand your Authority is when you are negotiating the terms of a new position. Changing positions is the nuclear option. However, it is better than becoming the Fall Guy, and a change can create opportunities that will accelerate your career and influence, if done right.
When I talk about Authority/Accountability balance, I always counter the Fall Guy with an ignominious historical figure: General George B. McClellan. General McClellan was the commander of the Army of the Potomac during the early years of the American Civil War. General McClellan had the industrial might of the Union north at his beck and call, as well as extraordinary resources for recruiting and retaining soldiers for his army. At every encounter with General Robert E. Lee’s Army of Northern Virginia, General McClellan outnumbered them, sometimes by more than two to one. Yet General McClellan was outfoxed repeatedly for the same reason: He failed to take decisive action.
Every time that McClellan failed, he blamed insufficient resources and told President Lincoln that he needed more troops and more equipment to be successful. In summary, while the Fall Guy scenario needs to be avoided, once you are adequately resourced, success requires taking decisive and strategic action, or you will suffer as did General McClellan. Failing to act when you are appropriately resourced can be just as damaging to your career and credibility as allowing yourself to become the Fall Guy.
Job description
Everybody has somebody that they report to, no matter how high up on the executive ladder they have climbed. Even the CEO must report to the board of directors. And that reporting structure usually involves periodic formal reviews. Your formal review is a good time to go over your job description, note what is relevant, remove what is irrelevant, and add new elements that have evolved in importance since your last review.
Job descriptions take many forms, but they always include a list of qualifications. If you have the job, you have the qualifications, so that is not likely to change. You may become more qualified for a higher-level position, but that is an entirely different discussion. I like to think of a well-written job description as including short-term and long-term goals. Short-term goals are usually the daily stuff that keeps operations running smoothly but garners little attention. Examples would include staying current on your emails, answering your phone, organizing meetings, and regularly attending various committees. Even some of these short-term goals can and will change over time. I always enjoyed quality oversight in my department, but as the department and my responsibilities grew, I realized I couldn’t do everything that I wanted to do. I needed to focus on the things only I could do and delegate those things that could be done by someone else, even though I wanted to continue doing them myself. I created a position for a clinical quality officer, and quality oversight moved off of my job description.
Long-term goals are the aspirational items, such as increasing market share, decreasing readmissions, improving patient satisfaction, and the like. Effective leaders are often focused on these aspirational, long-term goals, but they still must effectively execute their short-term goals. Stephen Covey outlines the dilemma with the “time management matrix” in his seminal work “The 7 Habits of Highly Effective People.” An in-depth discussion is beyond the scope of this article, but the time management matrix places tasks into one of four categories based on urgency and importance, and provides strategies for staying up on short-term goals while continually moving long-term goals forward.If you show up at your review with a list of accomplishments as well as an understanding of how the “time management matrix” affects your responsibilities, your boss will be impressed. It is also worth mentioning that Covey’s first habit is “Proactivity.” He uses the term Proactivity in a much more nuanced form than we typically think of, however. Simply put, Proactivity is the opposite of Reactivity, and it is another invaluable tool for success with those long-term goals that will help you make a name for yourself.
When you show up for your review, be it annual, biannual, or other, be prepared. Not only should you bring your job description and recommendations for how it should be adapted in the changing environment, but also bring examples of your accomplishments since the last review.
I talk with leaders frequently who are hardworking and diligent and hate bragging about their achievements; I get that. At the same time, if you don’t inform your superiors about your successes, there is no guarantee that they will hear about them or understand them in the appropriate context. Bragging about how great you are in the physician’s lounge is annoying; telling your boss about your accomplishments since the last review is critical to maintaining the momentum of past accomplishments. If you are not willing to toot your own horn, there is a very good chance that your horn will remain silent. I don’t think self-promotion comes easily to anyone, and it has to be done with a degree of humility and sensitivity; but it has to be done, so prepare for it.
Look out for yourself and others
We talk about teamwork and collaboration as hospitalists, and SHM is always underscoring the importance of teamwork and highlighting examples of successful teamwork in its many conferences and publications. Most hospital executives are focused on their own careers, however, and many have no reservations about damaging your career (your brand) if they think it will promote theirs. You have to look out for yourself and size up every leadership position you get into.
Physicians can expect their careers to last decades. The average hospital CEO has a tenure of less than 3.5 years, however, and when a new CEO is hired, almost half of chief financial, chief operating, and chief information officers are fired within 9 months. You may be focused on the long-term success of your organization as you plan your career, but many hospital administrators are interested only in short-term gains. It is similar to some members of Congress who are interested only in what they need to do now to win the next election and not in the long-term needs of the country. You should understand this disconnect when dealing with hospital executives, and how you and your credibility can become cannon fodder in their quest for short-term self-preservation.
You have to look out for and take care of yourself as you promote your group. With a better understanding of the Authority/Accountability balance, you have new tools to assess your chances of success and to advocate for yourself so that you and your group can be successful.
Despite my cynicism toward executives in the medical field, I personally advocate for supporting the career development of those around you and advise against furthering your career at the expense of others. Many unscrupulous executives will use this approach, surrounding themselves with Fall Guys, but my experience shows that this is not a sustainable strategy for success. It can lead to short-term gains, but eventually the piper must be paid. Moreover, the most successful medical executives and leaders that I have encountered have been those who genuinely cared about their subordinates, looked out for them, and selflessly promoted their careers.
In the age of social media, tearing others down seems to be the fastest way to get more “likes.” However, I strongly believe that you can’t build up your group, and our profession, just by tearing people down. Lending a helping hand may bring you less attention in the short term, but such action raises your stature, creates loyalty, and leads to sustainable success for the long run.
Dr. McIlraith is the founding chairman of the Hospital Medicine Department at Mercy Medical Group in Sacramento, Calif. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016 and is currently a member of the SHM Practice Management and Awards Committees, as well as the SHM Critical Care Task Force.
Sources
Quinn R. HM Turns 20: A look at the evolution of hospital medicine. The Hospitalist. 2016 August. https://www.the-hospitalist.org/hospitalist/article/121525/hm-turns-20-look-evolution-hospital-medicine
Stephen R. Covey. The 7 Habits of Highly Effective People: Powerful Lessons in Personal Change. Simon & Schuster. 1989.
10 Statistics on CEO Turnover, Recruitment. Becker’s Hospital Review. 2020. https://www.beckershospitalreview.com/hospital-management-administration/10-statistics-on-ceo-turnover-recruitment.html
Establishing a strong and lasting mentor/mentee relationship
I. Finding a mentor
Case
You are a 27-year-old first-year resident who is seeking mentorship. You are halfway through the year and are thinking about your goals and future. You have a general interest in hematology/oncology but have limited experience and would like to gain more experience with clinically relevant scholarship. However, you do not know anyone in the field and are not sure who to ask for guidance.
Stage 1: Seeking the right mentor

Start first with your area of interest and then look broadly. In this case the resident is interested in heme/onc. The first place to look is on the heme/onc department website or in the faculty directory. It can be helpful to look at what the potential mentor has published recently and/or look at a version of their CV on the faculty directory or website. This can help determine how productive they are and help assess whether you share similar interests, and whether they have worked with many learners in the past.
It is also important to do some background work and ask around about potential mentors. Often resident colleagues and fellows have a good sense of current projects and which faculty work well with learners. Lastly, it is important to also look at non–heme/onc physicians as there may be internal medicine physicians or surgeons who are doing hematology or oncology research that more align with your interests.
After you have assessed whether you think this person would be a strong mentor for you, it is time to reach out. People are flattered to be asked and part of their promotion criteria is their ability to mentor. Do not assume that a potential mentor is too busy! Let him or her make that decision. Remember the worst a mentor can say is “no.” Even if they do not have time or the need for a mentee at the present time, they generally will offer some assistance or direction on who to ask.
Start with a straightforward, but pleasant email. Waiting up to 2 weeks for a response is reasonable. If after 2 weeks you have not received word, feel free to reach out again asking politely if he or she would be willing to work with you. Do not be afraid to ask bluntly for their guidance and mentorship and have a specific project or area of research that you would like their assistance with.
II. Optimizing the mentor/mentee relationship
Case continued
Success! Your email was received with interest by a hematologist who has done several projects, comes highly recommended by other residents, and worked with students and residents in the past. The project involves anticoagulation on the inpatient service. You are set to meet with her next month.
Stage 2: Establishing expectations and goals
Now comes the hard work in establishing an excellent mentor/mentee relationship. Before you meet with your mentor, brainstorm first. What do you want out of the relationship? A publication? Career advice? Attaining a fellowship position? You should feel empowered in knowing that you as the mentee are in the driver seat, but this relationship should be mutually beneficial. Consider basing the relationship and initial discussions on these key questions:
1. My goals
- What are my goals? It is okay not to know but be ready to communicate some information to your mentor.
- Remember to also ask your mentor what their goals are for you as well.
2. Outcome
- What type of outcome are both you and your mentor looking for from the relationship?
3. Expectations
- What mentorship expectations do you have?
- What are your mentor’s expectations of you?
Once you feel you have a sense of what you are looking for out of the relationship, it is important to communicate this with the mentor to establish congruent expectations of one another. For example, think about asking your mentor if the two of you can establish a mentor/mentee contract. This is a written document that can be found online and establishes a mutual agreement of roles, responsibilities, and expectations of one another for the relationship. It can further help to open a line for honest and consistent feedback. This can also give you a formalized endpoint and agreed upon scope for the mentoring relationship. Having a check-in preestablished in a contract reduces any potentially awkward conversations about redefining the relationship down the road. (For example, what if our case resident decides to pursue GI? It could happen.)
Stage 3: Establishing a common goal
After you have determined the goals and expectations of the relationship together (remember, this is a relationship), it is time to start exploring possible projects and establishing goals for those projects. Having a quality improvement or research project will determine a common goal to work towards and help establish and define the relationship.
Once you have delineated broadly what the project(s) should be, develop smaller SMART (specific, measurable, achievable, relevant, time-bound) goals to move the project forward. These goals determine stopping points for evaluation and feedback, which further establish the relationship and keep the project(s) progressing. For example, one goal could be to write the first draft of the proposal for your quality improvement project within 3 weeks.
Stage 4: Continued communication
With any project it is important to stay on the same page as your mentor and be clear to establish “who is doing what by when.” Do not expect accountability to be the mentor’s job. Remember that you are in the driver’s seat and that you should propose how often you need to meet and what those meetings look like by developing an agenda. You can have an open discussion and allow your mentor to help determine a reasonable timeline. Remember, the more you communicate your goals, the better your mentor will be able to address them.
One pro tip is to always exceed your mentor’s expectations – if you think you need 2 weeks to complete a task, ask for 3-4 weeks. This gives you extra padding in case of unforeseen circumstances and makes you look like a “rockstar” if you hit a deadline 1-2 weeks earlier than planned.
III. Ending and/or redefining the relationship
Case continued
You are now a senior resident who’s published multiple articles in the past year, and have completed an anticoagulation project for inpatients with pulmonary emboli. You look back on your experience and what stands out is the extent of your gratitude and appreciation for your incredible mentor. Not only do you feel that your mentor has guided you in your career and with your scholarship, but you feel that he or she has shaped your character and talent set. At this point your mentor is both a teacher and guide, but now also a friend. While you feel there is always more that you can learn from her, you are ready to explore new interests. How do you effectively end or redefine this relationship?
Stage 5: Redefining your mentoring relationship
First, go back to the expectations or contract established early in the relationship. The check-in is a key time in the relationship to reevaluate goals and priorities. At this point you may decide to amicably end the relationship or project, or move on to a new project with a change in your role. For example, the quality improvement project may change to research, or you as the mentee have a change in focus (e.g., change in specialty or scholarly focus).
In summary, the interaction between you and your mentor should be a relationship. And the keys to a great relationship are:
1. Establish clear expectations from the beginning. This clarifies the relationship and helps the mentee and mentor to become more successful.
2. Maintain clear and open communication throughout the relationship.3. Define your goals and discuss them with your mentor early. (Have we mentioned the importance of goals enough?) After all, your goal is the reason you started pursuing this relationship in the first place.
In clinical training having guidance can greatly enhance your experience and direct your future career in unexpected ways. We hope that using these tools will guide you towards forging a strong mentor/mentee relationship.
Dr. Zimmerberg-Helms is a resident physician at the University of New Mexico, Albuquerque. Dr. Rendon is an attending hospitalist at the University of New Mexico.
I. Finding a mentor
Case
You are a 27-year-old first-year resident who is seeking mentorship. You are halfway through the year and are thinking about your goals and future. You have a general interest in hematology/oncology but have limited experience and would like to gain more experience with clinically relevant scholarship. However, you do not know anyone in the field and are not sure who to ask for guidance.
Stage 1: Seeking the right mentor
Start first with your area of interest and then look broadly. In this case the resident is interested in heme/onc. The first place to look is on the heme/onc department website or in the faculty directory. It can be helpful to look at what the potential mentor has published recently and/or look at a version of their CV on the faculty directory or website. This can help determine how productive they are and help assess whether you share similar interests, and whether they have worked with many learners in the past.
It is also important to do some background work and ask around about potential mentors. Often resident colleagues and fellows have a good sense of current projects and which faculty work well with learners. Lastly, it is important to also look at non–heme/onc physicians as there may be internal medicine physicians or surgeons who are doing hematology or oncology research that more align with your interests.
After you have assessed whether you think this person would be a strong mentor for you, it is time to reach out. People are flattered to be asked and part of their promotion criteria is their ability to mentor. Do not assume that a potential mentor is too busy! Let him or her make that decision. Remember the worst a mentor can say is “no.” Even if they do not have time or the need for a mentee at the present time, they generally will offer some assistance or direction on who to ask.
Start with a straightforward, but pleasant email. Waiting up to 2 weeks for a response is reasonable. If after 2 weeks you have not received word, feel free to reach out again asking politely if he or she would be willing to work with you. Do not be afraid to ask bluntly for their guidance and mentorship and have a specific project or area of research that you would like their assistance with.
II. Optimizing the mentor/mentee relationship
Case continued
Success! Your email was received with interest by a hematologist who has done several projects, comes highly recommended by other residents, and worked with students and residents in the past. The project involves anticoagulation on the inpatient service. You are set to meet with her next month.
Stage 2: Establishing expectations and goals
Now comes the hard work in establishing an excellent mentor/mentee relationship. Before you meet with your mentor, brainstorm first. What do you want out of the relationship? A publication? Career advice? Attaining a fellowship position? You should feel empowered in knowing that you as the mentee are in the driver seat, but this relationship should be mutually beneficial. Consider basing the relationship and initial discussions on these key questions:
1. My goals
- What are my goals? It is okay not to know but be ready to communicate some information to your mentor.
- Remember to also ask your mentor what their goals are for you as well.
2. Outcome
- What type of outcome are both you and your mentor looking for from the relationship?
3. Expectations
- What mentorship expectations do you have?
- What are your mentor’s expectations of you?
Once you feel you have a sense of what you are looking for out of the relationship, it is important to communicate this with the mentor to establish congruent expectations of one another. For example, think about asking your mentor if the two of you can establish a mentor/mentee contract. This is a written document that can be found online and establishes a mutual agreement of roles, responsibilities, and expectations of one another for the relationship. It can further help to open a line for honest and consistent feedback. This can also give you a formalized endpoint and agreed upon scope for the mentoring relationship. Having a check-in preestablished in a contract reduces any potentially awkward conversations about redefining the relationship down the road. (For example, what if our case resident decides to pursue GI? It could happen.)
Stage 3: Establishing a common goal
After you have determined the goals and expectations of the relationship together (remember, this is a relationship), it is time to start exploring possible projects and establishing goals for those projects. Having a quality improvement or research project will determine a common goal to work towards and help establish and define the relationship.
Once you have delineated broadly what the project(s) should be, develop smaller SMART (specific, measurable, achievable, relevant, time-bound) goals to move the project forward. These goals determine stopping points for evaluation and feedback, which further establish the relationship and keep the project(s) progressing. For example, one goal could be to write the first draft of the proposal for your quality improvement project within 3 weeks.
Stage 4: Continued communication
With any project it is important to stay on the same page as your mentor and be clear to establish “who is doing what by when.” Do not expect accountability to be the mentor’s job. Remember that you are in the driver’s seat and that you should propose how often you need to meet and what those meetings look like by developing an agenda. You can have an open discussion and allow your mentor to help determine a reasonable timeline. Remember, the more you communicate your goals, the better your mentor will be able to address them.
One pro tip is to always exceed your mentor’s expectations – if you think you need 2 weeks to complete a task, ask for 3-4 weeks. This gives you extra padding in case of unforeseen circumstances and makes you look like a “rockstar” if you hit a deadline 1-2 weeks earlier than planned.
III. Ending and/or redefining the relationship
Case continued
You are now a senior resident who’s published multiple articles in the past year, and have completed an anticoagulation project for inpatients with pulmonary emboli. You look back on your experience and what stands out is the extent of your gratitude and appreciation for your incredible mentor. Not only do you feel that your mentor has guided you in your career and with your scholarship, but you feel that he or she has shaped your character and talent set. At this point your mentor is both a teacher and guide, but now also a friend. While you feel there is always more that you can learn from her, you are ready to explore new interests. How do you effectively end or redefine this relationship?
Stage 5: Redefining your mentoring relationship
First, go back to the expectations or contract established early in the relationship. The check-in is a key time in the relationship to reevaluate goals and priorities. At this point you may decide to amicably end the relationship or project, or move on to a new project with a change in your role. For example, the quality improvement project may change to research, or you as the mentee have a change in focus (e.g., change in specialty or scholarly focus).
In summary, the interaction between you and your mentor should be a relationship. And the keys to a great relationship are:
1. Establish clear expectations from the beginning. This clarifies the relationship and helps the mentee and mentor to become more successful.
2. Maintain clear and open communication throughout the relationship.3. Define your goals and discuss them with your mentor early. (Have we mentioned the importance of goals enough?) After all, your goal is the reason you started pursuing this relationship in the first place.
In clinical training having guidance can greatly enhance your experience and direct your future career in unexpected ways. We hope that using these tools will guide you towards forging a strong mentor/mentee relationship.
Dr. Zimmerberg-Helms is a resident physician at the University of New Mexico, Albuquerque. Dr. Rendon is an attending hospitalist at the University of New Mexico.
I. Finding a mentor
Case
You are a 27-year-old first-year resident who is seeking mentorship. You are halfway through the year and are thinking about your goals and future. You have a general interest in hematology/oncology but have limited experience and would like to gain more experience with clinically relevant scholarship. However, you do not know anyone in the field and are not sure who to ask for guidance.
Stage 1: Seeking the right mentor
Start first with your area of interest and then look broadly. In this case the resident is interested in heme/onc. The first place to look is on the heme/onc department website or in the faculty directory. It can be helpful to look at what the potential mentor has published recently and/or look at a version of their CV on the faculty directory or website. This can help determine how productive they are and help assess whether you share similar interests, and whether they have worked with many learners in the past.
It is also important to do some background work and ask around about potential mentors. Often resident colleagues and fellows have a good sense of current projects and which faculty work well with learners. Lastly, it is important to also look at non–heme/onc physicians as there may be internal medicine physicians or surgeons who are doing hematology or oncology research that more align with your interests.
After you have assessed whether you think this person would be a strong mentor for you, it is time to reach out. People are flattered to be asked and part of their promotion criteria is their ability to mentor. Do not assume that a potential mentor is too busy! Let him or her make that decision. Remember the worst a mentor can say is “no.” Even if they do not have time or the need for a mentee at the present time, they generally will offer some assistance or direction on who to ask.
Start with a straightforward, but pleasant email. Waiting up to 2 weeks for a response is reasonable. If after 2 weeks you have not received word, feel free to reach out again asking politely if he or she would be willing to work with you. Do not be afraid to ask bluntly for their guidance and mentorship and have a specific project or area of research that you would like their assistance with.
II. Optimizing the mentor/mentee relationship
Case continued
Success! Your email was received with interest by a hematologist who has done several projects, comes highly recommended by other residents, and worked with students and residents in the past. The project involves anticoagulation on the inpatient service. You are set to meet with her next month.
Stage 2: Establishing expectations and goals
Now comes the hard work in establishing an excellent mentor/mentee relationship. Before you meet with your mentor, brainstorm first. What do you want out of the relationship? A publication? Career advice? Attaining a fellowship position? You should feel empowered in knowing that you as the mentee are in the driver seat, but this relationship should be mutually beneficial. Consider basing the relationship and initial discussions on these key questions:
1. My goals
- What are my goals? It is okay not to know but be ready to communicate some information to your mentor.
- Remember to also ask your mentor what their goals are for you as well.
2. Outcome
- What type of outcome are both you and your mentor looking for from the relationship?
3. Expectations
- What mentorship expectations do you have?
- What are your mentor’s expectations of you?
Once you feel you have a sense of what you are looking for out of the relationship, it is important to communicate this with the mentor to establish congruent expectations of one another. For example, think about asking your mentor if the two of you can establish a mentor/mentee contract. This is a written document that can be found online and establishes a mutual agreement of roles, responsibilities, and expectations of one another for the relationship. It can further help to open a line for honest and consistent feedback. This can also give you a formalized endpoint and agreed upon scope for the mentoring relationship. Having a check-in preestablished in a contract reduces any potentially awkward conversations about redefining the relationship down the road. (For example, what if our case resident decides to pursue GI? It could happen.)
Stage 3: Establishing a common goal
After you have determined the goals and expectations of the relationship together (remember, this is a relationship), it is time to start exploring possible projects and establishing goals for those projects. Having a quality improvement or research project will determine a common goal to work towards and help establish and define the relationship.
Once you have delineated broadly what the project(s) should be, develop smaller SMART (specific, measurable, achievable, relevant, time-bound) goals to move the project forward. These goals determine stopping points for evaluation and feedback, which further establish the relationship and keep the project(s) progressing. For example, one goal could be to write the first draft of the proposal for your quality improvement project within 3 weeks.
Stage 4: Continued communication
With any project it is important to stay on the same page as your mentor and be clear to establish “who is doing what by when.” Do not expect accountability to be the mentor’s job. Remember that you are in the driver’s seat and that you should propose how often you need to meet and what those meetings look like by developing an agenda. You can have an open discussion and allow your mentor to help determine a reasonable timeline. Remember, the more you communicate your goals, the better your mentor will be able to address them.
One pro tip is to always exceed your mentor’s expectations – if you think you need 2 weeks to complete a task, ask for 3-4 weeks. This gives you extra padding in case of unforeseen circumstances and makes you look like a “rockstar” if you hit a deadline 1-2 weeks earlier than planned.
III. Ending and/or redefining the relationship
Case continued
You are now a senior resident who’s published multiple articles in the past year, and have completed an anticoagulation project for inpatients with pulmonary emboli. You look back on your experience and what stands out is the extent of your gratitude and appreciation for your incredible mentor. Not only do you feel that your mentor has guided you in your career and with your scholarship, but you feel that he or she has shaped your character and talent set. At this point your mentor is both a teacher and guide, but now also a friend. While you feel there is always more that you can learn from her, you are ready to explore new interests. How do you effectively end or redefine this relationship?
Stage 5: Redefining your mentoring relationship
First, go back to the expectations or contract established early in the relationship. The check-in is a key time in the relationship to reevaluate goals and priorities. At this point you may decide to amicably end the relationship or project, or move on to a new project with a change in your role. For example, the quality improvement project may change to research, or you as the mentee have a change in focus (e.g., change in specialty or scholarly focus).
In summary, the interaction between you and your mentor should be a relationship. And the keys to a great relationship are:
1. Establish clear expectations from the beginning. This clarifies the relationship and helps the mentee and mentor to become more successful.
2. Maintain clear and open communication throughout the relationship.3. Define your goals and discuss them with your mentor early. (Have we mentioned the importance of goals enough?) After all, your goal is the reason you started pursuing this relationship in the first place.
In clinical training having guidance can greatly enhance your experience and direct your future career in unexpected ways. We hope that using these tools will guide you towards forging a strong mentor/mentee relationship.
Dr. Zimmerberg-Helms is a resident physician at the University of New Mexico, Albuquerque. Dr. Rendon is an attending hospitalist at the University of New Mexico.
Increasing racial diversity in hospital medicine’s leadership ranks
Have you ever done something where you’re not quite sure why you did it at the time, but later on you realize it was part of some larger cosmic purpose, and you go, “Ahhh, now I understand…that’s why!”? Call it a fortuitous coincidence. Or a subconscious act of anticipation. Maybe a little push from God.

Last summer, as SHM’s Practice Analysis Committee was planning the State of Hospital Medicine survey for 2020, we received a request from SHM’s Diversity, Equity & Inclusion (DEI) Special Interest Group (SIG) to include a series of questions related to hospitalist gender, race and ethnic distribution in the new survey. We’ve generally resisted doing things like this because the SoHM is designed to capture data at the group level, not the individual level – and honestly, it’s as much as a lot of groups can do to tell us reliably how many FTEs they have, much less provide details about individual providers. In addition, the survey is already really long, and we are always looking for ways to make it shorter and easier for participants while still collecting the information report users care most about.
But we wanted to take the asks from the DEI SIG seriously, and as we considered their request, we realized that though it wasn’t practical to collect this information for individual hospital medicine group (HMG) members, we could collect it for group leaders. Little did we know last summer that issues of gender and racial diversity and equity would be so front-and-center right now, as we prepare to release the 2020 SoHM Report in early September. Ahhh, now I understand…that’s why – with the prompting of the DEI SIG – we so fortuitously chose to include those questions this year!
Here’s a sneak preview of what we learned. Among SoHM respondents, 57.1% reported that the highest-ranking leader in their HMG is White, and 23.5% of highest-ranking leaders are Asian. Only 5.5% of HMG leaders were Black/African American. Ethnicity was a separate question, and only 2.2% of HMG leaders were reported as Hispanic/Latino.
I have been profoundly moved by the wretched deaths of George Floyd and other people of color at the hands of police in recent months, and by the subsequent protests and our growing national reckoning over issues of racial equity and justice. In my efforts to understand more about race in America, I have been challenged by my friend Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., and others to go beyond just learning about these issues. I want to use my voice to advocate for change, and my actions to participate in effecting change, within the context of my sphere of influence.
So, what does that have to do with the SoHM data on HMG leader demographics? Well, it’s clear that Black and brown people are woefully underrepresented in the ranks of hospital medicine leadership.
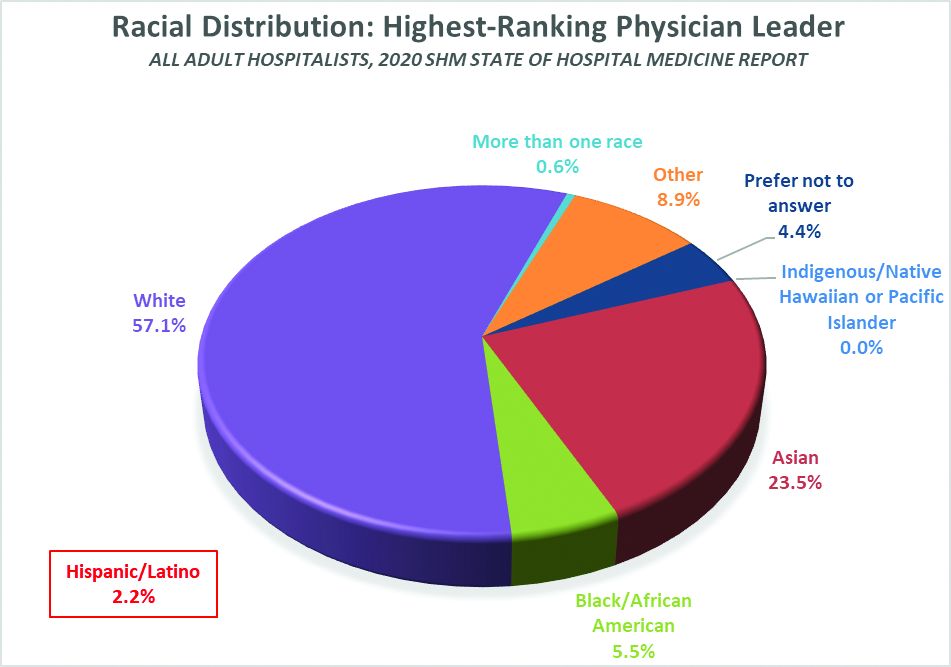
Unfortunately, we don’t have good information on racial diversity for hospitalists as a specialty, though I understand that SHM is working on plans to update membership profiles to begin collecting this information. In searching the Internet, I found a 2018 paper from the Journal of Health Care for the Poor and Underserved that studied racial and ethnic distribution of U.S. primary care physicians (doi: 10.1353/hpu.2018.0036). It reported that, in 2012, 7.8% of general internists were Black, along with 5.8% of family medicine/general practice physicians and 6.8% of pediatricians. A separate data set issued by the Association of American Medical Colleges reported that, in 2019, 6.4% of all actively practicing general internal medicine doctors were Black (5.5% of male IM physicians and 7.9% of female IM physicians). While this doesn’t mean hospitalists have the same racial and ethnic distribution, this is probably the best proxy we can come up with.
At first glance, having 5.5% of HMG leaders who are Black doesn’t seem terribly out of line with the reported range of 6.4 to 7.8% in the general population of internal medicine physicians (apologies to the family medicine and pediatric hospitalists reading this, but I’ll confine my discussion to internists for ease and brevity, since they represent the vast majority of the nation’s hospitalists). But do the math. It means Black hospitalists are likely underrepresented in HMG leadership ranks by something like 14% to 29% compared to their likely presence among hospitalists in general.
The real problem, of course, is that according the U.S. Census Bureau, 13.4% of the U.S. population is Black. So even if the racial distribution of HMG leaders catches up to the general hospitalist population, hospital medicine is still woefully underrepresenting the racial and ethnic distribution of our patient population.
The disconnect between the ethnic distribution of HMG leaders vs. hospitalists (based on general internal medicine distribution) is even more pronounced for Latinos. The JHCPU paper reported that, in 2012, 5.6% of general internists were Hispanic. The AAMC data set reported 5.8% of IM doctors were Hispanic/Latino. But only 2.2% of SoHM respondent HMGs reported a Hispanic/Latino leader, which means Latinos are underrepresented by somewhere around 61% or so relative to the likely hospitalist population, and by a whole lot more considering the fact that Latinos make up about 18.5% of the U.S. population.
I’m not saying that a White or Asian doctor can’t provide skilled, compassionate care to a Black or Latino patient, or vice-versa. It happens every day. I guess what I am saying is that we as a country and in the medical profession need to do a better job of creating pathways and promoting careers in medicine for people of color. A JAMA paper from 2019 reported that while the numbers and proportions of minority medical school matriculants has slowly been increasing from 2002 to 2017, the rate of increase was “slower than their age-matched counterparts in the U.S. population, resulting in increased underrepresentation” (doi:10.1001/jamanetworkopen.2019.10490). This means we’re falling behind, not catching up.
We need to make sure that people like Dr. Ryan Brown aren’t discouraged from pursuing medicine by teachers or school counselors because of their skin color or accent, or their gender or sexual orientation. And among those who become doctors, we need to promote hospital medicine as a desirable specialty for people of color and actively invite them in.
In my view, much of this starts with creating more and better paths to leadership within hospital medicine for people of color. Hospital medicine group leaders wield enormous – and increasing – influence, not only within their HMGs and within SHM, but within their institutions and health care systems. We need their voices and their influence to promote diversity within their groups, their institutions, within hospital medicine, and within medicine and the U.S. health care system more broadly.
The Society of Hospital Medicine is already taking steps to promote diversity, equity and inclusion. These include issuing a formal Diversity and Inclusion Statement, creating the DEI SIG, and the recent formation of a Board-designated DEI task force charged with making recommendations to promote DEI within SHM and in hospital medicine more broadly. But I want to challenge SHM to do more, particularly with regard to promoting diversity in leadership. Here are a few ideas to consider:
- Create and sponsor a mentoring program in which hospitalists volunteer to mentor minority junior high and high school students and help them prepare to pursue a career in medicine.
- Develop a formal, structured advocacy or collaboration effort with organizations like AAMC and the Accreditation Council for Graduate Medical Education designed to promote meaningful increases in the proportion of medical school students and residents who are people of color, and in the proportion who choose primary care – and ultimately, hospital medicine.
- Work hard to collect reliable racial, ethnic and gender information about SHM members and consider collaborating with MGMA to incorporate demographic questions into its survey tool for individual hospitalist compensation and productivity data. Challenge us on the Practice Analysis Committee who are responsible for the SoHM survey to continue surveying leadership demographics, and to consider how we can expand our collection of DEI information in 2022.
- Undertake a public relations campaign to highlight to health systems and other employers the under-representation of Black and Latino hospitalists in leadership positions, and to promote conscious efforts to increase those ranks.
- Create scholarships for hospitalists from underrepresented racial and ethnic groups to attend SHM-sponsored leadership development programs such as Leadership Academy, Academic Hospitalist Academy, and Quality and Safety Educators Academy, with the goal of increasing their ranks in positions of influence throughout healthcare. A scholarship program might even include raising funds to help minority hospitalists pursue Master’s-level programs such as an MBA, MHA, or MMM.
- Develop an educational track, mentoring program, or other support initiative for early-career hospitalist leaders and those interested in developing leadership skills, and ensure it gives specific attention to strategies for increasing the proportion of hospitalists of color in leadership positions.
- Review and revise existing SHM documents such as The Key Principles and Characteristics of an Effective Hospital Medicine Group, the Core Competencies in Hospital Medicine, and various white papers and position statements to ensure they address diversity, equity and inclusion – both with regard to the hospital medicine workforce and leadership, and with regard to patient care and eliminating health disparities.
I’m sure there are plenty of other similar actions we can take that I haven’t thought of. But we need to start the conversation about concrete steps our Society, and the medical specialty we represent, can take to foster real change. And then, we need to follow our words up with actions.
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Conference Committees and helps to coordinate SHM’s biannual State of Hospital Medicine survey.
Have you ever done something where you’re not quite sure why you did it at the time, but later on you realize it was part of some larger cosmic purpose, and you go, “Ahhh, now I understand…that’s why!”? Call it a fortuitous coincidence. Or a subconscious act of anticipation. Maybe a little push from God.
Last summer, as SHM’s Practice Analysis Committee was planning the State of Hospital Medicine survey for 2020, we received a request from SHM’s Diversity, Equity & Inclusion (DEI) Special Interest Group (SIG) to include a series of questions related to hospitalist gender, race and ethnic distribution in the new survey. We’ve generally resisted doing things like this because the SoHM is designed to capture data at the group level, not the individual level – and honestly, it’s as much as a lot of groups can do to tell us reliably how many FTEs they have, much less provide details about individual providers. In addition, the survey is already really long, and we are always looking for ways to make it shorter and easier for participants while still collecting the information report users care most about.
But we wanted to take the asks from the DEI SIG seriously, and as we considered their request, we realized that though it wasn’t practical to collect this information for individual hospital medicine group (HMG) members, we could collect it for group leaders. Little did we know last summer that issues of gender and racial diversity and equity would be so front-and-center right now, as we prepare to release the 2020 SoHM Report in early September. Ahhh, now I understand…that’s why – with the prompting of the DEI SIG – we so fortuitously chose to include those questions this year!
Here’s a sneak preview of what we learned. Among SoHM respondents, 57.1% reported that the highest-ranking leader in their HMG is White, and 23.5% of highest-ranking leaders are Asian. Only 5.5% of HMG leaders were Black/African American. Ethnicity was a separate question, and only 2.2% of HMG leaders were reported as Hispanic/Latino.
I have been profoundly moved by the wretched deaths of George Floyd and other people of color at the hands of police in recent months, and by the subsequent protests and our growing national reckoning over issues of racial equity and justice. In my efforts to understand more about race in America, I have been challenged by my friend Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., and others to go beyond just learning about these issues. I want to use my voice to advocate for change, and my actions to participate in effecting change, within the context of my sphere of influence.
So, what does that have to do with the SoHM data on HMG leader demographics? Well, it’s clear that Black and brown people are woefully underrepresented in the ranks of hospital medicine leadership.
Unfortunately, we don’t have good information on racial diversity for hospitalists as a specialty, though I understand that SHM is working on plans to update membership profiles to begin collecting this information. In searching the Internet, I found a 2018 paper from the Journal of Health Care for the Poor and Underserved that studied racial and ethnic distribution of U.S. primary care physicians (doi: 10.1353/hpu.2018.0036). It reported that, in 2012, 7.8% of general internists were Black, along with 5.8% of family medicine/general practice physicians and 6.8% of pediatricians. A separate data set issued by the Association of American Medical Colleges reported that, in 2019, 6.4% of all actively practicing general internal medicine doctors were Black (5.5% of male IM physicians and 7.9% of female IM physicians). While this doesn’t mean hospitalists have the same racial and ethnic distribution, this is probably the best proxy we can come up with.
At first glance, having 5.5% of HMG leaders who are Black doesn’t seem terribly out of line with the reported range of 6.4 to 7.8% in the general population of internal medicine physicians (apologies to the family medicine and pediatric hospitalists reading this, but I’ll confine my discussion to internists for ease and brevity, since they represent the vast majority of the nation’s hospitalists). But do the math. It means Black hospitalists are likely underrepresented in HMG leadership ranks by something like 14% to 29% compared to their likely presence among hospitalists in general.
The real problem, of course, is that according the U.S. Census Bureau, 13.4% of the U.S. population is Black. So even if the racial distribution of HMG leaders catches up to the general hospitalist population, hospital medicine is still woefully underrepresenting the racial and ethnic distribution of our patient population.
The disconnect between the ethnic distribution of HMG leaders vs. hospitalists (based on general internal medicine distribution) is even more pronounced for Latinos. The JHCPU paper reported that, in 2012, 5.6% of general internists were Hispanic. The AAMC data set reported 5.8% of IM doctors were Hispanic/Latino. But only 2.2% of SoHM respondent HMGs reported a Hispanic/Latino leader, which means Latinos are underrepresented by somewhere around 61% or so relative to the likely hospitalist population, and by a whole lot more considering the fact that Latinos make up about 18.5% of the U.S. population.
I’m not saying that a White or Asian doctor can’t provide skilled, compassionate care to a Black or Latino patient, or vice-versa. It happens every day. I guess what I am saying is that we as a country and in the medical profession need to do a better job of creating pathways and promoting careers in medicine for people of color. A JAMA paper from 2019 reported that while the numbers and proportions of minority medical school matriculants has slowly been increasing from 2002 to 2017, the rate of increase was “slower than their age-matched counterparts in the U.S. population, resulting in increased underrepresentation” (doi:10.1001/jamanetworkopen.2019.10490). This means we’re falling behind, not catching up.
We need to make sure that people like Dr. Ryan Brown aren’t discouraged from pursuing medicine by teachers or school counselors because of their skin color or accent, or their gender or sexual orientation. And among those who become doctors, we need to promote hospital medicine as a desirable specialty for people of color and actively invite them in.
In my view, much of this starts with creating more and better paths to leadership within hospital medicine for people of color. Hospital medicine group leaders wield enormous – and increasing – influence, not only within their HMGs and within SHM, but within their institutions and health care systems. We need their voices and their influence to promote diversity within their groups, their institutions, within hospital medicine, and within medicine and the U.S. health care system more broadly.
The Society of Hospital Medicine is already taking steps to promote diversity, equity and inclusion. These include issuing a formal Diversity and Inclusion Statement, creating the DEI SIG, and the recent formation of a Board-designated DEI task force charged with making recommendations to promote DEI within SHM and in hospital medicine more broadly. But I want to challenge SHM to do more, particularly with regard to promoting diversity in leadership. Here are a few ideas to consider:
- Create and sponsor a mentoring program in which hospitalists volunteer to mentor minority junior high and high school students and help them prepare to pursue a career in medicine.
- Develop a formal, structured advocacy or collaboration effort with organizations like AAMC and the Accreditation Council for Graduate Medical Education designed to promote meaningful increases in the proportion of medical school students and residents who are people of color, and in the proportion who choose primary care – and ultimately, hospital medicine.
- Work hard to collect reliable racial, ethnic and gender information about SHM members and consider collaborating with MGMA to incorporate demographic questions into its survey tool for individual hospitalist compensation and productivity data. Challenge us on the Practice Analysis Committee who are responsible for the SoHM survey to continue surveying leadership demographics, and to consider how we can expand our collection of DEI information in 2022.
- Undertake a public relations campaign to highlight to health systems and other employers the under-representation of Black and Latino hospitalists in leadership positions, and to promote conscious efforts to increase those ranks.
- Create scholarships for hospitalists from underrepresented racial and ethnic groups to attend SHM-sponsored leadership development programs such as Leadership Academy, Academic Hospitalist Academy, and Quality and Safety Educators Academy, with the goal of increasing their ranks in positions of influence throughout healthcare. A scholarship program might even include raising funds to help minority hospitalists pursue Master’s-level programs such as an MBA, MHA, or MMM.
- Develop an educational track, mentoring program, or other support initiative for early-career hospitalist leaders and those interested in developing leadership skills, and ensure it gives specific attention to strategies for increasing the proportion of hospitalists of color in leadership positions.
- Review and revise existing SHM documents such as The Key Principles and Characteristics of an Effective Hospital Medicine Group, the Core Competencies in Hospital Medicine, and various white papers and position statements to ensure they address diversity, equity and inclusion – both with regard to the hospital medicine workforce and leadership, and with regard to patient care and eliminating health disparities.
I’m sure there are plenty of other similar actions we can take that I haven’t thought of. But we need to start the conversation about concrete steps our Society, and the medical specialty we represent, can take to foster real change. And then, we need to follow our words up with actions.
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Conference Committees and helps to coordinate SHM’s biannual State of Hospital Medicine survey.
Have you ever done something where you’re not quite sure why you did it at the time, but later on you realize it was part of some larger cosmic purpose, and you go, “Ahhh, now I understand…that’s why!”? Call it a fortuitous coincidence. Or a subconscious act of anticipation. Maybe a little push from God.
Last summer, as SHM’s Practice Analysis Committee was planning the State of Hospital Medicine survey for 2020, we received a request from SHM’s Diversity, Equity & Inclusion (DEI) Special Interest Group (SIG) to include a series of questions related to hospitalist gender, race and ethnic distribution in the new survey. We’ve generally resisted doing things like this because the SoHM is designed to capture data at the group level, not the individual level – and honestly, it’s as much as a lot of groups can do to tell us reliably how many FTEs they have, much less provide details about individual providers. In addition, the survey is already really long, and we are always looking for ways to make it shorter and easier for participants while still collecting the information report users care most about.
But we wanted to take the asks from the DEI SIG seriously, and as we considered their request, we realized that though it wasn’t practical to collect this information for individual hospital medicine group (HMG) members, we could collect it for group leaders. Little did we know last summer that issues of gender and racial diversity and equity would be so front-and-center right now, as we prepare to release the 2020 SoHM Report in early September. Ahhh, now I understand…that’s why – with the prompting of the DEI SIG – we so fortuitously chose to include those questions this year!
Here’s a sneak preview of what we learned. Among SoHM respondents, 57.1% reported that the highest-ranking leader in their HMG is White, and 23.5% of highest-ranking leaders are Asian. Only 5.5% of HMG leaders were Black/African American. Ethnicity was a separate question, and only 2.2% of HMG leaders were reported as Hispanic/Latino.
I have been profoundly moved by the wretched deaths of George Floyd and other people of color at the hands of police in recent months, and by the subsequent protests and our growing national reckoning over issues of racial equity and justice. In my efforts to understand more about race in America, I have been challenged by my friend Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., and others to go beyond just learning about these issues. I want to use my voice to advocate for change, and my actions to participate in effecting change, within the context of my sphere of influence.
So, what does that have to do with the SoHM data on HMG leader demographics? Well, it’s clear that Black and brown people are woefully underrepresented in the ranks of hospital medicine leadership.
Unfortunately, we don’t have good information on racial diversity for hospitalists as a specialty, though I understand that SHM is working on plans to update membership profiles to begin collecting this information. In searching the Internet, I found a 2018 paper from the Journal of Health Care for the Poor and Underserved that studied racial and ethnic distribution of U.S. primary care physicians (doi: 10.1353/hpu.2018.0036). It reported that, in 2012, 7.8% of general internists were Black, along with 5.8% of family medicine/general practice physicians and 6.8% of pediatricians. A separate data set issued by the Association of American Medical Colleges reported that, in 2019, 6.4% of all actively practicing general internal medicine doctors were Black (5.5% of male IM physicians and 7.9% of female IM physicians). While this doesn’t mean hospitalists have the same racial and ethnic distribution, this is probably the best proxy we can come up with.
At first glance, having 5.5% of HMG leaders who are Black doesn’t seem terribly out of line with the reported range of 6.4 to 7.8% in the general population of internal medicine physicians (apologies to the family medicine and pediatric hospitalists reading this, but I’ll confine my discussion to internists for ease and brevity, since they represent the vast majority of the nation’s hospitalists). But do the math. It means Black hospitalists are likely underrepresented in HMG leadership ranks by something like 14% to 29% compared to their likely presence among hospitalists in general.
The real problem, of course, is that according the U.S. Census Bureau, 13.4% of the U.S. population is Black. So even if the racial distribution of HMG leaders catches up to the general hospitalist population, hospital medicine is still woefully underrepresenting the racial and ethnic distribution of our patient population.
The disconnect between the ethnic distribution of HMG leaders vs. hospitalists (based on general internal medicine distribution) is even more pronounced for Latinos. The JHCPU paper reported that, in 2012, 5.6% of general internists were Hispanic. The AAMC data set reported 5.8% of IM doctors were Hispanic/Latino. But only 2.2% of SoHM respondent HMGs reported a Hispanic/Latino leader, which means Latinos are underrepresented by somewhere around 61% or so relative to the likely hospitalist population, and by a whole lot more considering the fact that Latinos make up about 18.5% of the U.S. population.
I’m not saying that a White or Asian doctor can’t provide skilled, compassionate care to a Black or Latino patient, or vice-versa. It happens every day. I guess what I am saying is that we as a country and in the medical profession need to do a better job of creating pathways and promoting careers in medicine for people of color. A JAMA paper from 2019 reported that while the numbers and proportions of minority medical school matriculants has slowly been increasing from 2002 to 2017, the rate of increase was “slower than their age-matched counterparts in the U.S. population, resulting in increased underrepresentation” (doi:10.1001/jamanetworkopen.2019.10490). This means we’re falling behind, not catching up.
We need to make sure that people like Dr. Ryan Brown aren’t discouraged from pursuing medicine by teachers or school counselors because of their skin color or accent, or their gender or sexual orientation. And among those who become doctors, we need to promote hospital medicine as a desirable specialty for people of color and actively invite them in.
In my view, much of this starts with creating more and better paths to leadership within hospital medicine for people of color. Hospital medicine group leaders wield enormous – and increasing – influence, not only within their HMGs and within SHM, but within their institutions and health care systems. We need their voices and their influence to promote diversity within their groups, their institutions, within hospital medicine, and within medicine and the U.S. health care system more broadly.
The Society of Hospital Medicine is already taking steps to promote diversity, equity and inclusion. These include issuing a formal Diversity and Inclusion Statement, creating the DEI SIG, and the recent formation of a Board-designated DEI task force charged with making recommendations to promote DEI within SHM and in hospital medicine more broadly. But I want to challenge SHM to do more, particularly with regard to promoting diversity in leadership. Here are a few ideas to consider:
- Create and sponsor a mentoring program in which hospitalists volunteer to mentor minority junior high and high school students and help them prepare to pursue a career in medicine.
- Develop a formal, structured advocacy or collaboration effort with organizations like AAMC and the Accreditation Council for Graduate Medical Education designed to promote meaningful increases in the proportion of medical school students and residents who are people of color, and in the proportion who choose primary care – and ultimately, hospital medicine.
- Work hard to collect reliable racial, ethnic and gender information about SHM members and consider collaborating with MGMA to incorporate demographic questions into its survey tool for individual hospitalist compensation and productivity data. Challenge us on the Practice Analysis Committee who are responsible for the SoHM survey to continue surveying leadership demographics, and to consider how we can expand our collection of DEI information in 2022.
- Undertake a public relations campaign to highlight to health systems and other employers the under-representation of Black and Latino hospitalists in leadership positions, and to promote conscious efforts to increase those ranks.
- Create scholarships for hospitalists from underrepresented racial and ethnic groups to attend SHM-sponsored leadership development programs such as Leadership Academy, Academic Hospitalist Academy, and Quality and Safety Educators Academy, with the goal of increasing their ranks in positions of influence throughout healthcare. A scholarship program might even include raising funds to help minority hospitalists pursue Master’s-level programs such as an MBA, MHA, or MMM.
- Develop an educational track, mentoring program, or other support initiative for early-career hospitalist leaders and those interested in developing leadership skills, and ensure it gives specific attention to strategies for increasing the proportion of hospitalists of color in leadership positions.
- Review and revise existing SHM documents such as The Key Principles and Characteristics of an Effective Hospital Medicine Group, the Core Competencies in Hospital Medicine, and various white papers and position statements to ensure they address diversity, equity and inclusion – both with regard to the hospital medicine workforce and leadership, and with regard to patient care and eliminating health disparities.
I’m sure there are plenty of other similar actions we can take that I haven’t thought of. But we need to start the conversation about concrete steps our Society, and the medical specialty we represent, can take to foster real change. And then, we need to follow our words up with actions.
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Conference Committees and helps to coordinate SHM’s biannual State of Hospital Medicine survey.
SHM Chapter innovations: A provider exchange program
The SHM Annual Conference is more than an educational event. It also provides an opportunity to collaborate, network and create innovative ideas to improve the quality of inpatient care.

During the 2019 Annual Conference (HM19) – the last “in-person” Annual Conference before the COVID pandemic – SHM chapter leaders from the New Mexico chapter (Krystle Apodaca) and the Wiregrass chapter (Amith Skandhan), which covers the counties of Southern Alabama and the Panhandle of Florida, met during a networking event.
As we talked, we realized the unique differences and similarities our practice settings shared. We debated the role of clinician wellbeing, quality of medical education, and faculty development on individual hospital medicine group (HMG) practice styles.
Clinician well-being is the prerequisite to the Triple Aim of improving the health of populations, enhancing the patient experience, and reducing the cost of care. Engagement in local SHM chapter activities promotes the efficiency of practice, a culture of wellness, and personal resilience. Each HMG faces similar challenges but approaches to solving them vary. Professional challenges can affect the well-being of individual clinicians. During our discussion we realized that an interinstitutional exchange programs could provide a platform to exchange ideas and establish mentors.
The quality of medical education is directly linked to the quality of faculty development. Improving the quality of medical education requires a multifaceted approach by highly developed faculty. The complex factors affecting medical education and faculty development are further complicated by geographic location, patient characteristics, and professional growth opportunities.
Overcoming these obstacles requires an innovative and collaborative approach. Although faculty exchanges are common in academic medicine, they are not commonly attempted with HMGs. Hospitalists are responsible for a significant part of inpatient training for residents, medical students, and nurse practitioners/physician assistants (NPs/PAs) but their faculty training can vary based on location.
As a young specialty, hospital medicine is still evolving and incorporating NPs/PAs and physician hospitalists in varied practice models. Each HMG addresses common obstacles differently based on their culture and practice styles. As chapter leaders we determined that an exchange program would afford the opportunity for visiting faculty members to experience these differences.
We shared the idea of a chapter-level exchange with SHM’s Chapter Development Committee and obtained chapter development funds to execute the event. We also requested that an SHM national board member visit during the exchange to provide insight and feedback. We researched the characteristics of individual academic HMGs and structured a faculty exchange involving physicians and NPs/PAs. During the exchange program planning, the visiting faculty itinerary was tailored to a well-planned agenda for one week, with separate tracks for physicians and NPs/PAs, giving increased access to their individual peer practice styles. Additionally, the visiting faculty had meetings and discussions with the HMG and hospital leadership, to specifically address the visiting faculty’s institutional challenges.
The overall goal of the exchange program was to promote cross-institutional collaboration, increase engagement, improve medical education through faculty development and improve the quality of care. The focus of the exchange program was to share ideas and innovation, and learn the approaches to unique challenges at each institution. Out of this also grew collaboration and mentoring opportunities.
SHM’s New Mexico chapter is based in Albuquerque, a city in the desert Southwest with an ethnically diverse population of 545,000, The chapter leadership works at the University of New Mexico (UNM), a 553-bed medical center. UNM has a well-established internal medicine residency program, an academic hospitalist program, and an NP/PA fellowship program embedded within the hospital medicine department. At the time of the exchange, the HMG at UNM has 26 physicians and 9 NP/PA’s.
The SHM Wiregrass chapter is located in Dothan, Ala., a town of 80,000 near the Gulf of Mexico. Chapter leadership works at Southeast Health, a tertiary care facility with 420 beds, an affiliated medical school, and an internal medicine residency program. At the time of the exchange, the HMG at SEH has 28 physicians and 5 NP/PA’s.
These are two similarly sized hospital medicine programs, located in different geographic regions, and serving different populations. SHM board member Howard Epstein, MD, SFHM, vice president and chief medical officer of Presbyterian Healthcare Services in Albuquerque, participated on behalf of the Society when SEH faculty visited UNM. Kris Rehm, MD, SFHM, a pediatric hospitalist and the vice chair of outreach medicine at Vanderbilt University Medical Center, Nashville, came to Dothan during the faculty visit by UNM.
Two SEH faculty members, a physician and an NP, visited the University of New Mexico Hospital for one week. They participated as observers, rounding with the teams and meeting the UNM HMG leadership. The focus of the discussions included faculty education, a curriculum for quality improvement, and ways to address practice challenges. The SEH faculty also presented a QI project from their institution, and established collaborative relationships.
During the second part of the exchange, three UNM faculty members, including one physician and two NPs, visited SEH for one week. During the visit, they observed NP/PA hospitalist team models, discussed innovations, established mentoring relationships with leadership, and discussed QI projects at SEH. Additionally, the visiting UNM faculty participated in Women In Medicine events and participated as judges for a poster competition. They also had an opportunity to explore the rural landscape and visit the beach.
The evaluation process after the exchanges involved interviews, a survey, and the establishment of shared QI projects in mutual areas of challenge. The survey provided feedback, lessons learned from the exchange, and areas to be improved. Collaborative QI projects currently underway as a result of the exchange include paging etiquette, quality of sleep for hospitalized patients, and onboarding of NPs/PAs in HMGs.
This innovation changed our thinking as medical educators by addressing faculty development and medical education via clinician well-being. The physician and NP/PA Faculty Exchange program was an essential and meaningful innovation that resulted in increased SHM member engagement, crossinstitutional collaboration, networking, and mentorship.
This event created opportunities for faculty collaboration and expanded the professional network of participating institutions. The costs of the exchange were minimal given support from SHM. We believe that once the COVID pandemic has ended, this initiative has the potential to expand facilitated exchanges nationally and internationally, enhance faculty development, and improve medical education.
Dr. Apodaca is assistant professor and nurse practitioner hospitalist at the University of New Mexico. She serves as codirector of the UNM APP Hospital Medicine Fellowship and director of the APP Hospital Medicine Team. Dr. Skandhan is a hospitalist and member of the Core Faculty for the Internal Medicine Residency Program at Southeast Health (SEH), Dothan Ala., and an assistant professor at the Alabama College of Osteopathic Medicine. He serves as the medical director/physician liaison for the Clinical Documentation Program at SEH and also as the director for physician integration for Southeast Health Statera Network, an Accountable Care Organization.
The SHM Annual Conference is more than an educational event. It also provides an opportunity to collaborate, network and create innovative ideas to improve the quality of inpatient care.
During the 2019 Annual Conference (HM19) – the last “in-person” Annual Conference before the COVID pandemic – SHM chapter leaders from the New Mexico chapter (Krystle Apodaca) and the Wiregrass chapter (Amith Skandhan), which covers the counties of Southern Alabama and the Panhandle of Florida, met during a networking event.
As we talked, we realized the unique differences and similarities our practice settings shared. We debated the role of clinician wellbeing, quality of medical education, and faculty development on individual hospital medicine group (HMG) practice styles.
Clinician well-being is the prerequisite to the Triple Aim of improving the health of populations, enhancing the patient experience, and reducing the cost of care. Engagement in local SHM chapter activities promotes the efficiency of practice, a culture of wellness, and personal resilience. Each HMG faces similar challenges but approaches to solving them vary. Professional challenges can affect the well-being of individual clinicians. During our discussion we realized that an interinstitutional exchange programs could provide a platform to exchange ideas and establish mentors.
The quality of medical education is directly linked to the quality of faculty development. Improving the quality of medical education requires a multifaceted approach by highly developed faculty. The complex factors affecting medical education and faculty development are further complicated by geographic location, patient characteristics, and professional growth opportunities.
Overcoming these obstacles requires an innovative and collaborative approach. Although faculty exchanges are common in academic medicine, they are not commonly attempted with HMGs. Hospitalists are responsible for a significant part of inpatient training for residents, medical students, and nurse practitioners/physician assistants (NPs/PAs) but their faculty training can vary based on location.
As a young specialty, hospital medicine is still evolving and incorporating NPs/PAs and physician hospitalists in varied practice models. Each HMG addresses common obstacles differently based on their culture and practice styles. As chapter leaders we determined that an exchange program would afford the opportunity for visiting faculty members to experience these differences.
We shared the idea of a chapter-level exchange with SHM’s Chapter Development Committee and obtained chapter development funds to execute the event. We also requested that an SHM national board member visit during the exchange to provide insight and feedback. We researched the characteristics of individual academic HMGs and structured a faculty exchange involving physicians and NPs/PAs. During the exchange program planning, the visiting faculty itinerary was tailored to a well-planned agenda for one week, with separate tracks for physicians and NPs/PAs, giving increased access to their individual peer practice styles. Additionally, the visiting faculty had meetings and discussions with the HMG and hospital leadership, to specifically address the visiting faculty’s institutional challenges.
The overall goal of the exchange program was to promote cross-institutional collaboration, increase engagement, improve medical education through faculty development and improve the quality of care. The focus of the exchange program was to share ideas and innovation, and learn the approaches to unique challenges at each institution. Out of this also grew collaboration and mentoring opportunities.
SHM’s New Mexico chapter is based in Albuquerque, a city in the desert Southwest with an ethnically diverse population of 545,000, The chapter leadership works at the University of New Mexico (UNM), a 553-bed medical center. UNM has a well-established internal medicine residency program, an academic hospitalist program, and an NP/PA fellowship program embedded within the hospital medicine department. At the time of the exchange, the HMG at UNM has 26 physicians and 9 NP/PA’s.
The SHM Wiregrass chapter is located in Dothan, Ala., a town of 80,000 near the Gulf of Mexico. Chapter leadership works at Southeast Health, a tertiary care facility with 420 beds, an affiliated medical school, and an internal medicine residency program. At the time of the exchange, the HMG at SEH has 28 physicians and 5 NP/PA’s.
These are two similarly sized hospital medicine programs, located in different geographic regions, and serving different populations. SHM board member Howard Epstein, MD, SFHM, vice president and chief medical officer of Presbyterian Healthcare Services in Albuquerque, participated on behalf of the Society when SEH faculty visited UNM. Kris Rehm, MD, SFHM, a pediatric hospitalist and the vice chair of outreach medicine at Vanderbilt University Medical Center, Nashville, came to Dothan during the faculty visit by UNM.
Two SEH faculty members, a physician and an NP, visited the University of New Mexico Hospital for one week. They participated as observers, rounding with the teams and meeting the UNM HMG leadership. The focus of the discussions included faculty education, a curriculum for quality improvement, and ways to address practice challenges. The SEH faculty also presented a QI project from their institution, and established collaborative relationships.
During the second part of the exchange, three UNM faculty members, including one physician and two NPs, visited SEH for one week. During the visit, they observed NP/PA hospitalist team models, discussed innovations, established mentoring relationships with leadership, and discussed QI projects at SEH. Additionally, the visiting UNM faculty participated in Women In Medicine events and participated as judges for a poster competition. They also had an opportunity to explore the rural landscape and visit the beach.
The evaluation process after the exchanges involved interviews, a survey, and the establishment of shared QI projects in mutual areas of challenge. The survey provided feedback, lessons learned from the exchange, and areas to be improved. Collaborative QI projects currently underway as a result of the exchange include paging etiquette, quality of sleep for hospitalized patients, and onboarding of NPs/PAs in HMGs.
This innovation changed our thinking as medical educators by addressing faculty development and medical education via clinician well-being. The physician and NP/PA Faculty Exchange program was an essential and meaningful innovation that resulted in increased SHM member engagement, crossinstitutional collaboration, networking, and mentorship.
This event created opportunities for faculty collaboration and expanded the professional network of participating institutions. The costs of the exchange were minimal given support from SHM. We believe that once the COVID pandemic has ended, this initiative has the potential to expand facilitated exchanges nationally and internationally, enhance faculty development, and improve medical education.
Dr. Apodaca is assistant professor and nurse practitioner hospitalist at the University of New Mexico. She serves as codirector of the UNM APP Hospital Medicine Fellowship and director of the APP Hospital Medicine Team. Dr. Skandhan is a hospitalist and member of the Core Faculty for the Internal Medicine Residency Program at Southeast Health (SEH), Dothan Ala., and an assistant professor at the Alabama College of Osteopathic Medicine. He serves as the medical director/physician liaison for the Clinical Documentation Program at SEH and also as the director for physician integration for Southeast Health Statera Network, an Accountable Care Organization.
The SHM Annual Conference is more than an educational event. It also provides an opportunity to collaborate, network and create innovative ideas to improve the quality of inpatient care.
During the 2019 Annual Conference (HM19) – the last “in-person” Annual Conference before the COVID pandemic – SHM chapter leaders from the New Mexico chapter (Krystle Apodaca) and the Wiregrass chapter (Amith Skandhan), which covers the counties of Southern Alabama and the Panhandle of Florida, met during a networking event.
As we talked, we realized the unique differences and similarities our practice settings shared. We debated the role of clinician wellbeing, quality of medical education, and faculty development on individual hospital medicine group (HMG) practice styles.
Clinician well-being is the prerequisite to the Triple Aim of improving the health of populations, enhancing the patient experience, and reducing the cost of care. Engagement in local SHM chapter activities promotes the efficiency of practice, a culture of wellness, and personal resilience. Each HMG faces similar challenges but approaches to solving them vary. Professional challenges can affect the well-being of individual clinicians. During our discussion we realized that an interinstitutional exchange programs could provide a platform to exchange ideas and establish mentors.
The quality of medical education is directly linked to the quality of faculty development. Improving the quality of medical education requires a multifaceted approach by highly developed faculty. The complex factors affecting medical education and faculty development are further complicated by geographic location, patient characteristics, and professional growth opportunities.
Overcoming these obstacles requires an innovative and collaborative approach. Although faculty exchanges are common in academic medicine, they are not commonly attempted with HMGs. Hospitalists are responsible for a significant part of inpatient training for residents, medical students, and nurse practitioners/physician assistants (NPs/PAs) but their faculty training can vary based on location.
As a young specialty, hospital medicine is still evolving and incorporating NPs/PAs and physician hospitalists in varied practice models. Each HMG addresses common obstacles differently based on their culture and practice styles. As chapter leaders we determined that an exchange program would afford the opportunity for visiting faculty members to experience these differences.
We shared the idea of a chapter-level exchange with SHM’s Chapter Development Committee and obtained chapter development funds to execute the event. We also requested that an SHM national board member visit during the exchange to provide insight and feedback. We researched the characteristics of individual academic HMGs and structured a faculty exchange involving physicians and NPs/PAs. During the exchange program planning, the visiting faculty itinerary was tailored to a well-planned agenda for one week, with separate tracks for physicians and NPs/PAs, giving increased access to their individual peer practice styles. Additionally, the visiting faculty had meetings and discussions with the HMG and hospital leadership, to specifically address the visiting faculty’s institutional challenges.
The overall goal of the exchange program was to promote cross-institutional collaboration, increase engagement, improve medical education through faculty development and improve the quality of care. The focus of the exchange program was to share ideas and innovation, and learn the approaches to unique challenges at each institution. Out of this also grew collaboration and mentoring opportunities.
SHM’s New Mexico chapter is based in Albuquerque, a city in the desert Southwest with an ethnically diverse population of 545,000, The chapter leadership works at the University of New Mexico (UNM), a 553-bed medical center. UNM has a well-established internal medicine residency program, an academic hospitalist program, and an NP/PA fellowship program embedded within the hospital medicine department. At the time of the exchange, the HMG at UNM has 26 physicians and 9 NP/PA’s.
The SHM Wiregrass chapter is located in Dothan, Ala., a town of 80,000 near the Gulf of Mexico. Chapter leadership works at Southeast Health, a tertiary care facility with 420 beds, an affiliated medical school, and an internal medicine residency program. At the time of the exchange, the HMG at SEH has 28 physicians and 5 NP/PA’s.
These are two similarly sized hospital medicine programs, located in different geographic regions, and serving different populations. SHM board member Howard Epstein, MD, SFHM, vice president and chief medical officer of Presbyterian Healthcare Services in Albuquerque, participated on behalf of the Society when SEH faculty visited UNM. Kris Rehm, MD, SFHM, a pediatric hospitalist and the vice chair of outreach medicine at Vanderbilt University Medical Center, Nashville, came to Dothan during the faculty visit by UNM.
Two SEH faculty members, a physician and an NP, visited the University of New Mexico Hospital for one week. They participated as observers, rounding with the teams and meeting the UNM HMG leadership. The focus of the discussions included faculty education, a curriculum for quality improvement, and ways to address practice challenges. The SEH faculty also presented a QI project from their institution, and established collaborative relationships.
During the second part of the exchange, three UNM faculty members, including one physician and two NPs, visited SEH for one week. During the visit, they observed NP/PA hospitalist team models, discussed innovations, established mentoring relationships with leadership, and discussed QI projects at SEH. Additionally, the visiting UNM faculty participated in Women In Medicine events and participated as judges for a poster competition. They also had an opportunity to explore the rural landscape and visit the beach.
The evaluation process after the exchanges involved interviews, a survey, and the establishment of shared QI projects in mutual areas of challenge. The survey provided feedback, lessons learned from the exchange, and areas to be improved. Collaborative QI projects currently underway as a result of the exchange include paging etiquette, quality of sleep for hospitalized patients, and onboarding of NPs/PAs in HMGs.
This innovation changed our thinking as medical educators by addressing faculty development and medical education via clinician well-being. The physician and NP/PA Faculty Exchange program was an essential and meaningful innovation that resulted in increased SHM member engagement, crossinstitutional collaboration, networking, and mentorship.
This event created opportunities for faculty collaboration and expanded the professional network of participating institutions. The costs of the exchange were minimal given support from SHM. We believe that once the COVID pandemic has ended, this initiative has the potential to expand facilitated exchanges nationally and internationally, enhance faculty development, and improve medical education.
Dr. Apodaca is assistant professor and nurse practitioner hospitalist at the University of New Mexico. She serves as codirector of the UNM APP Hospital Medicine Fellowship and director of the APP Hospital Medicine Team. Dr. Skandhan is a hospitalist and member of the Core Faculty for the Internal Medicine Residency Program at Southeast Health (SEH), Dothan Ala., and an assistant professor at the Alabama College of Osteopathic Medicine. He serves as the medical director/physician liaison for the Clinical Documentation Program at SEH and also as the director for physician integration for Southeast Health Statera Network, an Accountable Care Organization.
Medicine and the meritocracy
Addressing systemic bias, gender inequity and discrimination
There are many challenges facing modern medicine today. Recent events have highlighted important issues affecting our society as a whole – systemic racism, sexism, and implicit bias. In medicine, we have seen a renewed focus on health equity, health disparities and the implicit systemic bias that affect those who work in the field. It is truly troubling that it has taken the continued loss of black lives to police brutality and a pandemic for this conversation to happen at every level in society.

Systemic bias is present throughout corporate America, and it is no different within the physician workforce. Overall, there has been gradual interest in promoting and teaching diversity. Institutions have been slowly creating policies and administrative positions focused on inclusion and diversity over the last decade. So has diversity training objectively increased representation and advancement of women and minority groups? Do traditionally marginalized groups have better access to health? And are women and people of color (POC) represented equally in leadership positions in medicine?
Clearly, the answers are not straightforward.
Diving into the data
A guilty pleasure of mine is to assess how diverse and inclusive an institution is by looking at the wall of pictures recognizing top leadership in hospitals. Despite women accounting for 47.9% of graduates from medical school in 2018-2019, I still see very few women or POC elevated to this level. Of the total women graduates, 22.6% were Asian, 8% were Black and 5.4% were Hispanic.
Being of Indian descent, I am a woman of color (albeit one who may not be as profoundly affected by racism in medicine as my less represented colleagues). It is especially rare for me to see someone I can identify with in the ranks of top leadership. I find encouragement in seeing any woman on any leadership board because to me, it means that there is hope. The literature seems to support this degree of disparity as well. For example, a recent analysis shows that presidential leadership in medical societies are predominantly held by men (82.6% male vs. 17.4% female). Other datasets demonstrate that only 15% of deans and interim deans are women and AAMC’s report shows that women account for only 18% of all department chairs.
Growing up, my parents fueled my interest to pursue medicine. They described it as a noble profession that rewarded true merit and dedication to the cause. However, those that have been traditionally elevated in medicine are men. If merit knows no gender, why does a gender gap exist? If merit is blind to race, why are minorities so poorly represented in the workforce (much less in leadership)? My view of the wall leaves me wondering about the role of both sexism and racism in medicine.
These visual representations of the medical culture reinforce the acceptable norms and values – white and masculine – in medicine. The feminist movement over the last several decades has increased awareness about the need for equality of the sexes. However, it was not until the concept of intersectionality was introduced by Black feminist Professor Kimberle Crenshaw, that feminism become a more inclusive term. Professor Crenshaw’s paper details how every individual has intersecting factors – race, gender, sexual identity, socioeconomic status – that create the sum of their experience be it privilege, oppression, or discrimination.
For example, a White woman has privileges that a woman of color does not. Among non-white women, race and sexual identity are confounding factors – a Black woman, a Black LGBTQ woman, and an Asian woman, for example, will not experience discrimination in the same way. The farther you deviate from the accepted norms and values, the harder it is for you to obtain support and achieve recognition.
Addressing the patriarchal structure and systemic bias in medicine
Why do patriarchal structures still exist in medicine? How do we resolve systemic bias? Addressing them in isolation – race or gender or sexual identity – is unlikely to create long-lasting change. For change to occur, organizations and individuals need to be intrinsically motivated. Creating awareness and challenging the status quo is the first step.
Over the last decade, implicit bias training and diversity training have become mandatory in various industries and states. Diversity training has grown to be a multi-billion-dollar industry that corporate America has embraced over the last several years. And yet, research shows that mandating such training may not be the most effective. To get results, organizations need to implement programs that “spark engagement, increase contact between different groups and draw on people’s desire to look good to others.”
Historically, the medical curriculum has not included a discourse on feminist theories and the advancement of women in medicine. Cultural competency training is typically offered on an annual basis once we are in the workforce, but in my experience, it focuses more on our interactions with patients and other health care colleagues, and less with regards to our physician peers and leadership. Is this enough to change deep rooted beliefs and traditions?
We can take our cue from non-medical organizations and consider changing this culture of no culture in medicine – introducing diversity task forces that hold departments accountable for recruiting and promoting women and minorities; employing diversity managers; voluntary training; cross-training to increase contact among different groups and mentoring programs that match senior leadership to women and POC. While some medical institutions have implemented some of these principles, changing century-old traditions will require embracing concepts of organizational change and every available effective tool.
Committing to change
Change is especially hard when the target outcome is not accurately quantifiable – even if you can measure attitudes, values, and beliefs, these are subject to reporting bias and tokenism. At the organizational level, change management involves employing a systematic approach to change organizational values, goals, policies, and processes.
Individual change, self-reflection, and personal growth are key components in changing culture. Reflexivity is being aware of your own values, norms, position, and power – an important concept to understand and apply in our everyday interactions. Believing that one’s class, gender, race and sexual orientation are irrelevant to their practice of medicine would not foster the change that we direly need in medicine. Rather, identifying how your own values and professional identity are shaped by your medical training, your organization and the broader cultural context are critically important to developing a greater empathic sense to motivate systemic change.
There has been valuable discussion on bottom-up changes to ensure women and POC have support, encouragement and a pathway to advance in an organization. Some of these include policy and process changes including providing flexible working conditions for women and sponsorship of women and minorities to help them navigate the barriers and microaggressions they encounter at work. While technical (policy) changes form the foundation for any organizational change, it is important to remember that the people side of change – the resistance that you encounter for any change effort in an organization – is equally important to address at the organizational level. A top-down approach is also vital to ensure that change is permanent in an organization and does not end when the individuals responsible for the change leave the organization.
Lewin’s three-stage change management model provides a framework for structural and organizational change in hospital systems. The three-stages of this model are: unfreezing, changing, and refreezing. Unfreezing is the process of determining what needs to change and obtaining leadership support. The actual change process involves getting people on board, empowering them to change and communicating with them frequently. Refreezing cements this change into the organization’s culture by providing support and training to sustain changes. Research has shown that Lewin’s change management model has applicability in the hospital setting.
Industry research in change management methodologies in the business sector has identified sponsorship by CEOs/senior management of an organization and having a structured implementation model for change management as two important factors for ensuring that change efforts are successful and sustainable.
This can be extrapolated to health care organizations – top leadership committed to changing the status quo should solidify organizational commitment by incorporating new attainable and measurable goals into their vision for the organization. Designing a phased implementation of change management methodologies should follow an open discussion to identify an organization’s weaknesses, strengths, capacity, and readiness for change. Lastly, helping busy professionals adapt to change requires innovative and continuous improvement strategies using formal, systematic tools for organization-wide strategic deployment.
Without a concrete commitment at the organizational level, programs such as diversity training may end up being band-aids on wounds that run deep.
I believe that the combination of both individual and organizational commitment to change systemic bias in medicine can be quite powerful. One without the other will fail to permanently change the system. The work to true equality – regardless of the intersecting factors of discrimination – starts with a commitment to change. We may all have different opportunities because of the inequality that is apparent in our systems today, but if we unite around the goal of a bias-free, merit-based equality, it gives us the strength we need to overcome challenges that we once thought insurmountable.
Each one of us is a leader in our own right. Speaking up for those with less power or opportunity than us and supporting talent and hard work solidifies medicine as a meritocracy. Even if the magnitude of change that we fight for may not be realized during our time in medical practice, our commitment to eradicate sexism, racism and discrimination will shape the future of medicine.
Just as our children are a legacy that we leave behind, our work in correcting bias in medicine will pave the path for a better future for the doctors of tomorrow. After all, when I think that my young daughter will be affected by what I do or do not do to address the discrimination, there is no better motivation for me to break down every barrier for her success.
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany Medical College in Albany, NY. This article first appeared on The Hospital Leader, the official blog of SHM.
Addressing systemic bias, gender inequity and discrimination
Addressing systemic bias, gender inequity and discrimination
There are many challenges facing modern medicine today. Recent events have highlighted important issues affecting our society as a whole – systemic racism, sexism, and implicit bias. In medicine, we have seen a renewed focus on health equity, health disparities and the implicit systemic bias that affect those who work in the field. It is truly troubling that it has taken the continued loss of black lives to police brutality and a pandemic for this conversation to happen at every level in society.
Systemic bias is present throughout corporate America, and it is no different within the physician workforce. Overall, there has been gradual interest in promoting and teaching diversity. Institutions have been slowly creating policies and administrative positions focused on inclusion and diversity over the last decade. So has diversity training objectively increased representation and advancement of women and minority groups? Do traditionally marginalized groups have better access to health? And are women and people of color (POC) represented equally in leadership positions in medicine?
Clearly, the answers are not straightforward.
Diving into the data
A guilty pleasure of mine is to assess how diverse and inclusive an institution is by looking at the wall of pictures recognizing top leadership in hospitals. Despite women accounting for 47.9% of graduates from medical school in 2018-2019, I still see very few women or POC elevated to this level. Of the total women graduates, 22.6% were Asian, 8% were Black and 5.4% were Hispanic.
Being of Indian descent, I am a woman of color (albeit one who may not be as profoundly affected by racism in medicine as my less represented colleagues). It is especially rare for me to see someone I can identify with in the ranks of top leadership. I find encouragement in seeing any woman on any leadership board because to me, it means that there is hope. The literature seems to support this degree of disparity as well. For example, a recent analysis shows that presidential leadership in medical societies are predominantly held by men (82.6% male vs. 17.4% female). Other datasets demonstrate that only 15% of deans and interim deans are women and AAMC’s report shows that women account for only 18% of all department chairs.
Growing up, my parents fueled my interest to pursue medicine. They described it as a noble profession that rewarded true merit and dedication to the cause. However, those that have been traditionally elevated in medicine are men. If merit knows no gender, why does a gender gap exist? If merit is blind to race, why are minorities so poorly represented in the workforce (much less in leadership)? My view of the wall leaves me wondering about the role of both sexism and racism in medicine.
These visual representations of the medical culture reinforce the acceptable norms and values – white and masculine – in medicine. The feminist movement over the last several decades has increased awareness about the need for equality of the sexes. However, it was not until the concept of intersectionality was introduced by Black feminist Professor Kimberle Crenshaw, that feminism become a more inclusive term. Professor Crenshaw’s paper details how every individual has intersecting factors – race, gender, sexual identity, socioeconomic status – that create the sum of their experience be it privilege, oppression, or discrimination.
For example, a White woman has privileges that a woman of color does not. Among non-white women, race and sexual identity are confounding factors – a Black woman, a Black LGBTQ woman, and an Asian woman, for example, will not experience discrimination in the same way. The farther you deviate from the accepted norms and values, the harder it is for you to obtain support and achieve recognition.
Addressing the patriarchal structure and systemic bias in medicine
Why do patriarchal structures still exist in medicine? How do we resolve systemic bias? Addressing them in isolation – race or gender or sexual identity – is unlikely to create long-lasting change. For change to occur, organizations and individuals need to be intrinsically motivated. Creating awareness and challenging the status quo is the first step.
Over the last decade, implicit bias training and diversity training have become mandatory in various industries and states. Diversity training has grown to be a multi-billion-dollar industry that corporate America has embraced over the last several years. And yet, research shows that mandating such training may not be the most effective. To get results, organizations need to implement programs that “spark engagement, increase contact between different groups and draw on people’s desire to look good to others.”
Historically, the medical curriculum has not included a discourse on feminist theories and the advancement of women in medicine. Cultural competency training is typically offered on an annual basis once we are in the workforce, but in my experience, it focuses more on our interactions with patients and other health care colleagues, and less with regards to our physician peers and leadership. Is this enough to change deep rooted beliefs and traditions?
We can take our cue from non-medical organizations and consider changing this culture of no culture in medicine – introducing diversity task forces that hold departments accountable for recruiting and promoting women and minorities; employing diversity managers; voluntary training; cross-training to increase contact among different groups and mentoring programs that match senior leadership to women and POC. While some medical institutions have implemented some of these principles, changing century-old traditions will require embracing concepts of organizational change and every available effective tool.
Committing to change
Change is especially hard when the target outcome is not accurately quantifiable – even if you can measure attitudes, values, and beliefs, these are subject to reporting bias and tokenism. At the organizational level, change management involves employing a systematic approach to change organizational values, goals, policies, and processes.
Individual change, self-reflection, and personal growth are key components in changing culture. Reflexivity is being aware of your own values, norms, position, and power – an important concept to understand and apply in our everyday interactions. Believing that one’s class, gender, race and sexual orientation are irrelevant to their practice of medicine would not foster the change that we direly need in medicine. Rather, identifying how your own values and professional identity are shaped by your medical training, your organization and the broader cultural context are critically important to developing a greater empathic sense to motivate systemic change.
There has been valuable discussion on bottom-up changes to ensure women and POC have support, encouragement and a pathway to advance in an organization. Some of these include policy and process changes including providing flexible working conditions for women and sponsorship of women and minorities to help them navigate the barriers and microaggressions they encounter at work. While technical (policy) changes form the foundation for any organizational change, it is important to remember that the people side of change – the resistance that you encounter for any change effort in an organization – is equally important to address at the organizational level. A top-down approach is also vital to ensure that change is permanent in an organization and does not end when the individuals responsible for the change leave the organization.
Lewin’s three-stage change management model provides a framework for structural and organizational change in hospital systems. The three-stages of this model are: unfreezing, changing, and refreezing. Unfreezing is the process of determining what needs to change and obtaining leadership support. The actual change process involves getting people on board, empowering them to change and communicating with them frequently. Refreezing cements this change into the organization’s culture by providing support and training to sustain changes. Research has shown that Lewin’s change management model has applicability in the hospital setting.
Industry research in change management methodologies in the business sector has identified sponsorship by CEOs/senior management of an organization and having a structured implementation model for change management as two important factors for ensuring that change efforts are successful and sustainable.
This can be extrapolated to health care organizations – top leadership committed to changing the status quo should solidify organizational commitment by incorporating new attainable and measurable goals into their vision for the organization. Designing a phased implementation of change management methodologies should follow an open discussion to identify an organization’s weaknesses, strengths, capacity, and readiness for change. Lastly, helping busy professionals adapt to change requires innovative and continuous improvement strategies using formal, systematic tools for organization-wide strategic deployment.
Without a concrete commitment at the organizational level, programs such as diversity training may end up being band-aids on wounds that run deep.
I believe that the combination of both individual and organizational commitment to change systemic bias in medicine can be quite powerful. One without the other will fail to permanently change the system. The work to true equality – regardless of the intersecting factors of discrimination – starts with a commitment to change. We may all have different opportunities because of the inequality that is apparent in our systems today, but if we unite around the goal of a bias-free, merit-based equality, it gives us the strength we need to overcome challenges that we once thought insurmountable.
Each one of us is a leader in our own right. Speaking up for those with less power or opportunity than us and supporting talent and hard work solidifies medicine as a meritocracy. Even if the magnitude of change that we fight for may not be realized during our time in medical practice, our commitment to eradicate sexism, racism and discrimination will shape the future of medicine.
Just as our children are a legacy that we leave behind, our work in correcting bias in medicine will pave the path for a better future for the doctors of tomorrow. After all, when I think that my young daughter will be affected by what I do or do not do to address the discrimination, there is no better motivation for me to break down every barrier for her success.
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany Medical College in Albany, NY. This article first appeared on The Hospital Leader, the official blog of SHM.
There are many challenges facing modern medicine today. Recent events have highlighted important issues affecting our society as a whole – systemic racism, sexism, and implicit bias. In medicine, we have seen a renewed focus on health equity, health disparities and the implicit systemic bias that affect those who work in the field. It is truly troubling that it has taken the continued loss of black lives to police brutality and a pandemic for this conversation to happen at every level in society.
Systemic bias is present throughout corporate America, and it is no different within the physician workforce. Overall, there has been gradual interest in promoting and teaching diversity. Institutions have been slowly creating policies and administrative positions focused on inclusion and diversity over the last decade. So has diversity training objectively increased representation and advancement of women and minority groups? Do traditionally marginalized groups have better access to health? And are women and people of color (POC) represented equally in leadership positions in medicine?
Clearly, the answers are not straightforward.
Diving into the data
A guilty pleasure of mine is to assess how diverse and inclusive an institution is by looking at the wall of pictures recognizing top leadership in hospitals. Despite women accounting for 47.9% of graduates from medical school in 2018-2019, I still see very few women or POC elevated to this level. Of the total women graduates, 22.6% were Asian, 8% were Black and 5.4% were Hispanic.
Being of Indian descent, I am a woman of color (albeit one who may not be as profoundly affected by racism in medicine as my less represented colleagues). It is especially rare for me to see someone I can identify with in the ranks of top leadership. I find encouragement in seeing any woman on any leadership board because to me, it means that there is hope. The literature seems to support this degree of disparity as well. For example, a recent analysis shows that presidential leadership in medical societies are predominantly held by men (82.6% male vs. 17.4% female). Other datasets demonstrate that only 15% of deans and interim deans are women and AAMC’s report shows that women account for only 18% of all department chairs.
Growing up, my parents fueled my interest to pursue medicine. They described it as a noble profession that rewarded true merit and dedication to the cause. However, those that have been traditionally elevated in medicine are men. If merit knows no gender, why does a gender gap exist? If merit is blind to race, why are minorities so poorly represented in the workforce (much less in leadership)? My view of the wall leaves me wondering about the role of both sexism and racism in medicine.
These visual representations of the medical culture reinforce the acceptable norms and values – white and masculine – in medicine. The feminist movement over the last several decades has increased awareness about the need for equality of the sexes. However, it was not until the concept of intersectionality was introduced by Black feminist Professor Kimberle Crenshaw, that feminism become a more inclusive term. Professor Crenshaw’s paper details how every individual has intersecting factors – race, gender, sexual identity, socioeconomic status – that create the sum of their experience be it privilege, oppression, or discrimination.
For example, a White woman has privileges that a woman of color does not. Among non-white women, race and sexual identity are confounding factors – a Black woman, a Black LGBTQ woman, and an Asian woman, for example, will not experience discrimination in the same way. The farther you deviate from the accepted norms and values, the harder it is for you to obtain support and achieve recognition.
Addressing the patriarchal structure and systemic bias in medicine
Why do patriarchal structures still exist in medicine? How do we resolve systemic bias? Addressing them in isolation – race or gender or sexual identity – is unlikely to create long-lasting change. For change to occur, organizations and individuals need to be intrinsically motivated. Creating awareness and challenging the status quo is the first step.
Over the last decade, implicit bias training and diversity training have become mandatory in various industries and states. Diversity training has grown to be a multi-billion-dollar industry that corporate America has embraced over the last several years. And yet, research shows that mandating such training may not be the most effective. To get results, organizations need to implement programs that “spark engagement, increase contact between different groups and draw on people’s desire to look good to others.”
Historically, the medical curriculum has not included a discourse on feminist theories and the advancement of women in medicine. Cultural competency training is typically offered on an annual basis once we are in the workforce, but in my experience, it focuses more on our interactions with patients and other health care colleagues, and less with regards to our physician peers and leadership. Is this enough to change deep rooted beliefs and traditions?
We can take our cue from non-medical organizations and consider changing this culture of no culture in medicine – introducing diversity task forces that hold departments accountable for recruiting and promoting women and minorities; employing diversity managers; voluntary training; cross-training to increase contact among different groups and mentoring programs that match senior leadership to women and POC. While some medical institutions have implemented some of these principles, changing century-old traditions will require embracing concepts of organizational change and every available effective tool.
Committing to change
Change is especially hard when the target outcome is not accurately quantifiable – even if you can measure attitudes, values, and beliefs, these are subject to reporting bias and tokenism. At the organizational level, change management involves employing a systematic approach to change organizational values, goals, policies, and processes.
Individual change, self-reflection, and personal growth are key components in changing culture. Reflexivity is being aware of your own values, norms, position, and power – an important concept to understand and apply in our everyday interactions. Believing that one’s class, gender, race and sexual orientation are irrelevant to their practice of medicine would not foster the change that we direly need in medicine. Rather, identifying how your own values and professional identity are shaped by your medical training, your organization and the broader cultural context are critically important to developing a greater empathic sense to motivate systemic change.
There has been valuable discussion on bottom-up changes to ensure women and POC have support, encouragement and a pathway to advance in an organization. Some of these include policy and process changes including providing flexible working conditions for women and sponsorship of women and minorities to help them navigate the barriers and microaggressions they encounter at work. While technical (policy) changes form the foundation for any organizational change, it is important to remember that the people side of change – the resistance that you encounter for any change effort in an organization – is equally important to address at the organizational level. A top-down approach is also vital to ensure that change is permanent in an organization and does not end when the individuals responsible for the change leave the organization.
Lewin’s three-stage change management model provides a framework for structural and organizational change in hospital systems. The three-stages of this model are: unfreezing, changing, and refreezing. Unfreezing is the process of determining what needs to change and obtaining leadership support. The actual change process involves getting people on board, empowering them to change and communicating with them frequently. Refreezing cements this change into the organization’s culture by providing support and training to sustain changes. Research has shown that Lewin’s change management model has applicability in the hospital setting.
Industry research in change management methodologies in the business sector has identified sponsorship by CEOs/senior management of an organization and having a structured implementation model for change management as two important factors for ensuring that change efforts are successful and sustainable.
This can be extrapolated to health care organizations – top leadership committed to changing the status quo should solidify organizational commitment by incorporating new attainable and measurable goals into their vision for the organization. Designing a phased implementation of change management methodologies should follow an open discussion to identify an organization’s weaknesses, strengths, capacity, and readiness for change. Lastly, helping busy professionals adapt to change requires innovative and continuous improvement strategies using formal, systematic tools for organization-wide strategic deployment.
Without a concrete commitment at the organizational level, programs such as diversity training may end up being band-aids on wounds that run deep.
I believe that the combination of both individual and organizational commitment to change systemic bias in medicine can be quite powerful. One without the other will fail to permanently change the system. The work to true equality – regardless of the intersecting factors of discrimination – starts with a commitment to change. We may all have different opportunities because of the inequality that is apparent in our systems today, but if we unite around the goal of a bias-free, merit-based equality, it gives us the strength we need to overcome challenges that we once thought insurmountable.
Each one of us is a leader in our own right. Speaking up for those with less power or opportunity than us and supporting talent and hard work solidifies medicine as a meritocracy. Even if the magnitude of change that we fight for may not be realized during our time in medical practice, our commitment to eradicate sexism, racism and discrimination will shape the future of medicine.
Just as our children are a legacy that we leave behind, our work in correcting bias in medicine will pave the path for a better future for the doctors of tomorrow. After all, when I think that my young daughter will be affected by what I do or do not do to address the discrimination, there is no better motivation for me to break down every barrier for her success.
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany Medical College in Albany, NY. This article first appeared on The Hospital Leader, the official blog of SHM.
Hospital leadership lessons in the era of COVID-19
The year 2020 has brought the COVID-19 pandemic and civil unrest and protests, which have resulted in unprecedented health care challenges to hospitals and clinics. The daunting prospect of a fall influenza season has hospital staff and administrators looking ahead to still greater challenges.

This year of crisis has put even greater emphasis on leadership in hospitals, as patients, clinicians, and staff look for direction in the face of uncertainty and stress. But hospital leaders often arrive at their positions unprepared for their roles, according to Leonard Marcus, PhD, director of the Program for Health Care Negotiation and Conflict Resolution at Harvard T.H. Chan School of Public Health, Boston.
“Many times what happens in medicine is that someone with the greatest technical skills or greatest clinical skills emerges to be leader of a department, or a group, or a hospital, without having really paid attention to how they can build their leadership skills,” Dr. Marcus said during the 2020 Society of Hospital Medicine Leadership Virtual Seminar, held online Sept. 16-17.
Over 2 days, Dr. Marcus discussed the complex environments faced by hospital leaders, and some of the tools and strategies that can be used to maintain calm, problem-solve, and chart a course ahead.
He emphasized that hospitals and medical systems are complex, nonlinear organizations, which could be swept up by change in the form of mergers, financial policies, patient surges due to local emergencies, or pandemics.
“Complexity has to be central to how you think about leadership. If you think you can control everything, that doesn’t work that well,” said Dr. Marcus.
Most think of leadership as hierarchical, with a boss on top and underlings below, though this is starting to change. Dr. Marcus suggested a different view. Instead of just “leading down” to those who report to them, leaders should consider “leading up” to their own bosses or oversight committees, and across to other departments or even beyond to interlinked organizations such as nursing homes.
“Being able to build that connectivity not only within your hospital, but beyond your hospital, lets you see the chain that goes through the experience of any patient. You are looking at the problem from a much wider lens. We call this meta-leadership,” Dr. Marcus said.
A key focus of meta-leadership is to create a culture where individuals are working together to help one another succeed. Leadership in hospitals is often dominated by egos, with individual leaders battling one another in a win-lose effort, and this gets in the way of incorporating different perspectives into problem-solving.
Dr. Marcus used an example from previous seminars in which he instructed participants to arm wrestle the person sitting next to them. The goal was to attain as many pins as possible in 30 seconds. About half would fight as hard as they could, and achieve a few victories. The other half worked cooperatively, letting one person win, then the other, so that they could have 30 or 40 wins each. Dr. Marcus told the story of a young nurse who was paired up with a much stronger surgeon. She let him win twice, and when he asked her why she wasn’t resisting, she took his arm and placed it in a winning position, then a losing position, and then a winning position again, and he instantly understood that the cooperative approach could be more effective. Why didn’t she just tell him? She told Dr. Marcus that she knew he wouldn’t take instruction, so she let him win and then demonstrated an alternative. “We nurses learned how to do that a long time ago,” she told Dr. Marcus.
The idea is collaborative problem-solving. “How do you orient people looking to you for leadership so that we’re in this together and we can accomplish a whole lot more in 30 seconds if we’re working together instead of always battling one another? If we’re always battling one another, we’re putting all of our effort into the contest,” said Dr. Marcus. This sort of approach is all the more important when facing the complexity experienced by hospital systems, especially during crises such as COVID-19.
A critical element of meta-leadership is emotional intelligence, which includes elements such as self-awareness, self-regulation, empathy, determining motivation of yourself and others, and the social skills to portray yourself as caring, open, and interested.
Emotional intelligence also can help recognize when you’ve entered survival mode in reaction to a crisis or incident, or something as simple as losing your car keys – what Dr. Marcus terms “going to the basement.” Responses revolve around freeze, fight, or flight. It’s helpful in the wake of a car accident, but not when trying to make managerial decisions or respond to a complex situation. It’s vital for leaders to quickly get themselves out of the basement, said Dr. Marcus, and that they help other members of the team get out as well.
He recommended protocols designed in advance, both to recognize when you’re in the basement, and to lift yourself out. Dr. Marcus uses a trigger script, telling himself “I can do this,” and then when he’s working with other people, “we can do this.” He also speaks slowly, measuring every word. Whatever you do, “it has to be a pivot you do to get yourself out of the basement,” he said. It can be helpful to predict the kinds of situations that send you “to the basement” to help recognize it when it has happened.
It’s very important not to lead, negotiate, or make important decisions while in the basement, according to Dr. Marcus. If one thinks about some of the things they’ve said to others while under duress, they are often some of the statements they regret most.
Practical leadership skills
On the second day of the Leadership Seminar, Dr. Marcus moved his focus to using leadership skills and techniques. One important technique is to incorporate multiple perspectives. He gave the example of an opaque cube with a cone inside it, with a window on the side and one on top. Viewers from the side see the cone in profile, and see it as a triangle. Viewers from the top see an aerial perspective that looks like the circular base of the cone. The two groups could argue about what’s inside the cube, but they can only identify the object if they work together.
“When dealing with complex reality, you oftentimes find there are different people with different perspectives on a problem. They may have different experiences of what the problem is, and what often happens is that people get into an adversarial fight. Looking at the problem from different perspectives actually allows a much richer and more comprehensive view,” said Dr. Marcus.
The metaphor comes from a study of the tragic events at the Twin Towers in Manhattan on Sept. 11, 2001. The New York Fire Department had a command center at the base of the building, while the police had a helicopter flying around the buildings. The helicopter could see the steel girders beginning to melt and predicted a collapse, and therefore ordered their personnel out of the buildings. But they were unable to convey that information to the firefighters, who continued to send personnel into the buildings. In all, 343 firefighters lost their lives. The police force lost 32.
To best understand a problem, a key element is the “unknown knowns.” That is, information that is available, that someone has, but is unknown to you. It takes some imagination to conceive of what “unknown knowns” might be out there, but it’s worth the effort to identify possible knowledge sources. It’s vital to seek out this information, because a common leadership mistake is to assume you know something when you really don’t.
“In many ways what you’re doing is looking for obstacles. It could be you don’t have access to the information, that it’s beyond some sort of curtain you need to overcome, or it could be people in your own department who have the information and they’re not sharing it with you,” Dr. Marcus said.
He outlined a tool called the POP-DOC loop, which is a 6-step exercise designed to analyze problems and implement solutions. Step 1 is Perceiving the situation, determining knowns and unknowns, and incorporating multiple perspectives, emotions, and politics. Step 2 is to Orient oneself: examine patterns and how they may replicate themselves as long as conditions don’t change. For example, during COVID-19, physicians have begun to learn how the virus transmits and how it affects the immune system. Step 3, based on those patterns is to make Predictions. With COVID-19, it’s predictable that people who assemble without wearing masks are vulnerable to transmission. Step 4 is to use the predictions to begin to make Decisions. Step 5 is to begin Operationalizing those decisions, and step 6 is to Communicate those decisions effectively.
Dr. Marcus emphasized that POP-DOC is not a one-time exercise. Once decisions have been made and implemented, if they aren’t having the planned effect, it’s important to incorporate the results of those actions and start right back at the beginning of the POP-DOC loop.
“The POP side of the loop is perceiving, analysis. You get out of the basement and understand the situation that surrounds you. On the DOC side, you lead down, lead up, lead across and lead beyond. You’re bringing people into the action to get things done,” Dr. Marcus said.
Another tool Dr. Marcus described, aimed at problem-solving and negotiation, is the “Walk in the Woods.” The idea is to bring two parties together to help each other succeed. The first step is Self-Interest, where both parties articulate their objectives, perspectives, and fears. The second step, Enlarged Interests, requires each party to list their points of agreement, and only then should they focus on and list their points of disagreement. During conflict, people tend to focus on their disagreements. The parties often find that they agree on more than they realize, and this can frame the disagreements as more manageable. The third step, Enlightened Interest, is a free thinking period where both parties come up with potential solutions that had not been previously considered. In step 4, Aligned Interests, the parties discuss some of those ideas that can be explored further.
The Walk in the Woods is applicable to a wide range of situations, and negotiation is central to being a leader. “Being a clinician is all about negotiating – with patients, family members, with other clinicians, with the institution,” Dr. Marcus said. “We all want the patient to have the best possible care, and in the course of those conversations if we can better understand people, have empathy, and if there are new ideas or ways we can individualize our care, let’s do it, and then at the end of the day combine our motivations so that we’re providing the best possible care.”
In the end, meta-leadership is about creating a culture where individuals strive to help each other succeed, said Dr. Marcus. “That’s the essence: involving people, making them part of the solution, and if it’s a solution they’ve created together, everyone wants to make that solution a success.”
For more information, see the book “You’re It,” coauthored by Dr. Marcus, and available on Amazon for $16.99 in hardback, or $3.99 in Kindle format.
The year 2020 has brought the COVID-19 pandemic and civil unrest and protests, which have resulted in unprecedented health care challenges to hospitals and clinics. The daunting prospect of a fall influenza season has hospital staff and administrators looking ahead to still greater challenges.
This year of crisis has put even greater emphasis on leadership in hospitals, as patients, clinicians, and staff look for direction in the face of uncertainty and stress. But hospital leaders often arrive at their positions unprepared for their roles, according to Leonard Marcus, PhD, director of the Program for Health Care Negotiation and Conflict Resolution at Harvard T.H. Chan School of Public Health, Boston.
“Many times what happens in medicine is that someone with the greatest technical skills or greatest clinical skills emerges to be leader of a department, or a group, or a hospital, without having really paid attention to how they can build their leadership skills,” Dr. Marcus said during the 2020 Society of Hospital Medicine Leadership Virtual Seminar, held online Sept. 16-17.
Over 2 days, Dr. Marcus discussed the complex environments faced by hospital leaders, and some of the tools and strategies that can be used to maintain calm, problem-solve, and chart a course ahead.
He emphasized that hospitals and medical systems are complex, nonlinear organizations, which could be swept up by change in the form of mergers, financial policies, patient surges due to local emergencies, or pandemics.
“Complexity has to be central to how you think about leadership. If you think you can control everything, that doesn’t work that well,” said Dr. Marcus.
Most think of leadership as hierarchical, with a boss on top and underlings below, though this is starting to change. Dr. Marcus suggested a different view. Instead of just “leading down” to those who report to them, leaders should consider “leading up” to their own bosses or oversight committees, and across to other departments or even beyond to interlinked organizations such as nursing homes.
“Being able to build that connectivity not only within your hospital, but beyond your hospital, lets you see the chain that goes through the experience of any patient. You are looking at the problem from a much wider lens. We call this meta-leadership,” Dr. Marcus said.
A key focus of meta-leadership is to create a culture where individuals are working together to help one another succeed. Leadership in hospitals is often dominated by egos, with individual leaders battling one another in a win-lose effort, and this gets in the way of incorporating different perspectives into problem-solving.
Dr. Marcus used an example from previous seminars in which he instructed participants to arm wrestle the person sitting next to them. The goal was to attain as many pins as possible in 30 seconds. About half would fight as hard as they could, and achieve a few victories. The other half worked cooperatively, letting one person win, then the other, so that they could have 30 or 40 wins each. Dr. Marcus told the story of a young nurse who was paired up with a much stronger surgeon. She let him win twice, and when he asked her why she wasn’t resisting, she took his arm and placed it in a winning position, then a losing position, and then a winning position again, and he instantly understood that the cooperative approach could be more effective. Why didn’t she just tell him? She told Dr. Marcus that she knew he wouldn’t take instruction, so she let him win and then demonstrated an alternative. “We nurses learned how to do that a long time ago,” she told Dr. Marcus.
The idea is collaborative problem-solving. “How do you orient people looking to you for leadership so that we’re in this together and we can accomplish a whole lot more in 30 seconds if we’re working together instead of always battling one another? If we’re always battling one another, we’re putting all of our effort into the contest,” said Dr. Marcus. This sort of approach is all the more important when facing the complexity experienced by hospital systems, especially during crises such as COVID-19.
A critical element of meta-leadership is emotional intelligence, which includes elements such as self-awareness, self-regulation, empathy, determining motivation of yourself and others, and the social skills to portray yourself as caring, open, and interested.
Emotional intelligence also can help recognize when you’ve entered survival mode in reaction to a crisis or incident, or something as simple as losing your car keys – what Dr. Marcus terms “going to the basement.” Responses revolve around freeze, fight, or flight. It’s helpful in the wake of a car accident, but not when trying to make managerial decisions or respond to a complex situation. It’s vital for leaders to quickly get themselves out of the basement, said Dr. Marcus, and that they help other members of the team get out as well.
He recommended protocols designed in advance, both to recognize when you’re in the basement, and to lift yourself out. Dr. Marcus uses a trigger script, telling himself “I can do this,” and then when he’s working with other people, “we can do this.” He also speaks slowly, measuring every word. Whatever you do, “it has to be a pivot you do to get yourself out of the basement,” he said. It can be helpful to predict the kinds of situations that send you “to the basement” to help recognize it when it has happened.
It’s very important not to lead, negotiate, or make important decisions while in the basement, according to Dr. Marcus. If one thinks about some of the things they’ve said to others while under duress, they are often some of the statements they regret most.
Practical leadership skills
On the second day of the Leadership Seminar, Dr. Marcus moved his focus to using leadership skills and techniques. One important technique is to incorporate multiple perspectives. He gave the example of an opaque cube with a cone inside it, with a window on the side and one on top. Viewers from the side see the cone in profile, and see it as a triangle. Viewers from the top see an aerial perspective that looks like the circular base of the cone. The two groups could argue about what’s inside the cube, but they can only identify the object if they work together.
“When dealing with complex reality, you oftentimes find there are different people with different perspectives on a problem. They may have different experiences of what the problem is, and what often happens is that people get into an adversarial fight. Looking at the problem from different perspectives actually allows a much richer and more comprehensive view,” said Dr. Marcus.
The metaphor comes from a study of the tragic events at the Twin Towers in Manhattan on Sept. 11, 2001. The New York Fire Department had a command center at the base of the building, while the police had a helicopter flying around the buildings. The helicopter could see the steel girders beginning to melt and predicted a collapse, and therefore ordered their personnel out of the buildings. But they were unable to convey that information to the firefighters, who continued to send personnel into the buildings. In all, 343 firefighters lost their lives. The police force lost 32.
To best understand a problem, a key element is the “unknown knowns.” That is, information that is available, that someone has, but is unknown to you. It takes some imagination to conceive of what “unknown knowns” might be out there, but it’s worth the effort to identify possible knowledge sources. It’s vital to seek out this information, because a common leadership mistake is to assume you know something when you really don’t.
“In many ways what you’re doing is looking for obstacles. It could be you don’t have access to the information, that it’s beyond some sort of curtain you need to overcome, or it could be people in your own department who have the information and they’re not sharing it with you,” Dr. Marcus said.
He outlined a tool called the POP-DOC loop, which is a 6-step exercise designed to analyze problems and implement solutions. Step 1 is Perceiving the situation, determining knowns and unknowns, and incorporating multiple perspectives, emotions, and politics. Step 2 is to Orient oneself: examine patterns and how they may replicate themselves as long as conditions don’t change. For example, during COVID-19, physicians have begun to learn how the virus transmits and how it affects the immune system. Step 3, based on those patterns is to make Predictions. With COVID-19, it’s predictable that people who assemble without wearing masks are vulnerable to transmission. Step 4 is to use the predictions to begin to make Decisions. Step 5 is to begin Operationalizing those decisions, and step 6 is to Communicate those decisions effectively.
Dr. Marcus emphasized that POP-DOC is not a one-time exercise. Once decisions have been made and implemented, if they aren’t having the planned effect, it’s important to incorporate the results of those actions and start right back at the beginning of the POP-DOC loop.
“The POP side of the loop is perceiving, analysis. You get out of the basement and understand the situation that surrounds you. On the DOC side, you lead down, lead up, lead across and lead beyond. You’re bringing people into the action to get things done,” Dr. Marcus said.
Another tool Dr. Marcus described, aimed at problem-solving and negotiation, is the “Walk in the Woods.” The idea is to bring two parties together to help each other succeed. The first step is Self-Interest, where both parties articulate their objectives, perspectives, and fears. The second step, Enlarged Interests, requires each party to list their points of agreement, and only then should they focus on and list their points of disagreement. During conflict, people tend to focus on their disagreements. The parties often find that they agree on more than they realize, and this can frame the disagreements as more manageable. The third step, Enlightened Interest, is a free thinking period where both parties come up with potential solutions that had not been previously considered. In step 4, Aligned Interests, the parties discuss some of those ideas that can be explored further.
The Walk in the Woods is applicable to a wide range of situations, and negotiation is central to being a leader. “Being a clinician is all about negotiating – with patients, family members, with other clinicians, with the institution,” Dr. Marcus said. “We all want the patient to have the best possible care, and in the course of those conversations if we can better understand people, have empathy, and if there are new ideas or ways we can individualize our care, let’s do it, and then at the end of the day combine our motivations so that we’re providing the best possible care.”
In the end, meta-leadership is about creating a culture where individuals strive to help each other succeed, said Dr. Marcus. “That’s the essence: involving people, making them part of the solution, and if it’s a solution they’ve created together, everyone wants to make that solution a success.”
For more information, see the book “You’re It,” coauthored by Dr. Marcus, and available on Amazon for $16.99 in hardback, or $3.99 in Kindle format.
The year 2020 has brought the COVID-19 pandemic and civil unrest and protests, which have resulted in unprecedented health care challenges to hospitals and clinics. The daunting prospect of a fall influenza season has hospital staff and administrators looking ahead to still greater challenges.
This year of crisis has put even greater emphasis on leadership in hospitals, as patients, clinicians, and staff look for direction in the face of uncertainty and stress. But hospital leaders often arrive at their positions unprepared for their roles, according to Leonard Marcus, PhD, director of the Program for Health Care Negotiation and Conflict Resolution at Harvard T.H. Chan School of Public Health, Boston.
“Many times what happens in medicine is that someone with the greatest technical skills or greatest clinical skills emerges to be leader of a department, or a group, or a hospital, without having really paid attention to how they can build their leadership skills,” Dr. Marcus said during the 2020 Society of Hospital Medicine Leadership Virtual Seminar, held online Sept. 16-17.
Over 2 days, Dr. Marcus discussed the complex environments faced by hospital leaders, and some of the tools and strategies that can be used to maintain calm, problem-solve, and chart a course ahead.
He emphasized that hospitals and medical systems are complex, nonlinear organizations, which could be swept up by change in the form of mergers, financial policies, patient surges due to local emergencies, or pandemics.
“Complexity has to be central to how you think about leadership. If you think you can control everything, that doesn’t work that well,” said Dr. Marcus.
Most think of leadership as hierarchical, with a boss on top and underlings below, though this is starting to change. Dr. Marcus suggested a different view. Instead of just “leading down” to those who report to them, leaders should consider “leading up” to their own bosses or oversight committees, and across to other departments or even beyond to interlinked organizations such as nursing homes.
“Being able to build that connectivity not only within your hospital, but beyond your hospital, lets you see the chain that goes through the experience of any patient. You are looking at the problem from a much wider lens. We call this meta-leadership,” Dr. Marcus said.
A key focus of meta-leadership is to create a culture where individuals are working together to help one another succeed. Leadership in hospitals is often dominated by egos, with individual leaders battling one another in a win-lose effort, and this gets in the way of incorporating different perspectives into problem-solving.
Dr. Marcus used an example from previous seminars in which he instructed participants to arm wrestle the person sitting next to them. The goal was to attain as many pins as possible in 30 seconds. About half would fight as hard as they could, and achieve a few victories. The other half worked cooperatively, letting one person win, then the other, so that they could have 30 or 40 wins each. Dr. Marcus told the story of a young nurse who was paired up with a much stronger surgeon. She let him win twice, and when he asked her why she wasn’t resisting, she took his arm and placed it in a winning position, then a losing position, and then a winning position again, and he instantly understood that the cooperative approach could be more effective. Why didn’t she just tell him? She told Dr. Marcus that she knew he wouldn’t take instruction, so she let him win and then demonstrated an alternative. “We nurses learned how to do that a long time ago,” she told Dr. Marcus.
The idea is collaborative problem-solving. “How do you orient people looking to you for leadership so that we’re in this together and we can accomplish a whole lot more in 30 seconds if we’re working together instead of always battling one another? If we’re always battling one another, we’re putting all of our effort into the contest,” said Dr. Marcus. This sort of approach is all the more important when facing the complexity experienced by hospital systems, especially during crises such as COVID-19.
A critical element of meta-leadership is emotional intelligence, which includes elements such as self-awareness, self-regulation, empathy, determining motivation of yourself and others, and the social skills to portray yourself as caring, open, and interested.
Emotional intelligence also can help recognize when you’ve entered survival mode in reaction to a crisis or incident, or something as simple as losing your car keys – what Dr. Marcus terms “going to the basement.” Responses revolve around freeze, fight, or flight. It’s helpful in the wake of a car accident, but not when trying to make managerial decisions or respond to a complex situation. It’s vital for leaders to quickly get themselves out of the basement, said Dr. Marcus, and that they help other members of the team get out as well.
He recommended protocols designed in advance, both to recognize when you’re in the basement, and to lift yourself out. Dr. Marcus uses a trigger script, telling himself “I can do this,” and then when he’s working with other people, “we can do this.” He also speaks slowly, measuring every word. Whatever you do, “it has to be a pivot you do to get yourself out of the basement,” he said. It can be helpful to predict the kinds of situations that send you “to the basement” to help recognize it when it has happened.
It’s very important not to lead, negotiate, or make important decisions while in the basement, according to Dr. Marcus. If one thinks about some of the things they’ve said to others while under duress, they are often some of the statements they regret most.
Practical leadership skills
On the second day of the Leadership Seminar, Dr. Marcus moved his focus to using leadership skills and techniques. One important technique is to incorporate multiple perspectives. He gave the example of an opaque cube with a cone inside it, with a window on the side and one on top. Viewers from the side see the cone in profile, and see it as a triangle. Viewers from the top see an aerial perspective that looks like the circular base of the cone. The two groups could argue about what’s inside the cube, but they can only identify the object if they work together.
“When dealing with complex reality, you oftentimes find there are different people with different perspectives on a problem. They may have different experiences of what the problem is, and what often happens is that people get into an adversarial fight. Looking at the problem from different perspectives actually allows a much richer and more comprehensive view,” said Dr. Marcus.
The metaphor comes from a study of the tragic events at the Twin Towers in Manhattan on Sept. 11, 2001. The New York Fire Department had a command center at the base of the building, while the police had a helicopter flying around the buildings. The helicopter could see the steel girders beginning to melt and predicted a collapse, and therefore ordered their personnel out of the buildings. But they were unable to convey that information to the firefighters, who continued to send personnel into the buildings. In all, 343 firefighters lost their lives. The police force lost 32.
To best understand a problem, a key element is the “unknown knowns.” That is, information that is available, that someone has, but is unknown to you. It takes some imagination to conceive of what “unknown knowns” might be out there, but it’s worth the effort to identify possible knowledge sources. It’s vital to seek out this information, because a common leadership mistake is to assume you know something when you really don’t.
“In many ways what you’re doing is looking for obstacles. It could be you don’t have access to the information, that it’s beyond some sort of curtain you need to overcome, or it could be people in your own department who have the information and they’re not sharing it with you,” Dr. Marcus said.
He outlined a tool called the POP-DOC loop, which is a 6-step exercise designed to analyze problems and implement solutions. Step 1 is Perceiving the situation, determining knowns and unknowns, and incorporating multiple perspectives, emotions, and politics. Step 2 is to Orient oneself: examine patterns and how they may replicate themselves as long as conditions don’t change. For example, during COVID-19, physicians have begun to learn how the virus transmits and how it affects the immune system. Step 3, based on those patterns is to make Predictions. With COVID-19, it’s predictable that people who assemble without wearing masks are vulnerable to transmission. Step 4 is to use the predictions to begin to make Decisions. Step 5 is to begin Operationalizing those decisions, and step 6 is to Communicate those decisions effectively.
Dr. Marcus emphasized that POP-DOC is not a one-time exercise. Once decisions have been made and implemented, if they aren’t having the planned effect, it’s important to incorporate the results of those actions and start right back at the beginning of the POP-DOC loop.
“The POP side of the loop is perceiving, analysis. You get out of the basement and understand the situation that surrounds you. On the DOC side, you lead down, lead up, lead across and lead beyond. You’re bringing people into the action to get things done,” Dr. Marcus said.
Another tool Dr. Marcus described, aimed at problem-solving and negotiation, is the “Walk in the Woods.” The idea is to bring two parties together to help each other succeed. The first step is Self-Interest, where both parties articulate their objectives, perspectives, and fears. The second step, Enlarged Interests, requires each party to list their points of agreement, and only then should they focus on and list their points of disagreement. During conflict, people tend to focus on their disagreements. The parties often find that they agree on more than they realize, and this can frame the disagreements as more manageable. The third step, Enlightened Interest, is a free thinking period where both parties come up with potential solutions that had not been previously considered. In step 4, Aligned Interests, the parties discuss some of those ideas that can be explored further.
The Walk in the Woods is applicable to a wide range of situations, and negotiation is central to being a leader. “Being a clinician is all about negotiating – with patients, family members, with other clinicians, with the institution,” Dr. Marcus said. “We all want the patient to have the best possible care, and in the course of those conversations if we can better understand people, have empathy, and if there are new ideas or ways we can individualize our care, let’s do it, and then at the end of the day combine our motivations so that we’re providing the best possible care.”
In the end, meta-leadership is about creating a culture where individuals strive to help each other succeed, said Dr. Marcus. “That’s the essence: involving people, making them part of the solution, and if it’s a solution they’ve created together, everyone wants to make that solution a success.”
For more information, see the book “You’re It,” coauthored by Dr. Marcus, and available on Amazon for $16.99 in hardback, or $3.99 in Kindle format.
FROM THE SHM LEADERSHIP SEMINAR
The path to leadership
It was 6 a.m. on a rainy, cold Pacific Northwest morning as I walked from my apartment to the hospital, dodging puddles and dreaming of the mediocre-yet-hot physician-lounge coffee. Another long day full of clinical and administrative tasks awaited me.
I was 6 months’ pregnant with our first child and working my sixth 12-hour shift in a row. We had recently lost our medical director, and the C-suite had offered me the role. The day ahead seemed like an enormous mountain to climb.
I felt tired and more than a little overwhelmed. But I whispered to myself: “Today is going to be a fantastic day. I will not fail my team. I will not fail my patients!”
Physician leadership starts with a decision
The timing of this call to leadership had not been ideal. There’s probably never a perfect time to step into a medical director role. And my situation was no exception.
In addition to the baby on the way, my husband was traveling a lot for work. Also, the job of a medical director seemed a little daunting – especially to a young physician leading a team for the first time.
But I knew that leadership was my calling. While I didn’t yet have decades of experience, I had been selected as the chief resident in internal medicine, completed a nephrology fellowship, and mentored several medical students and residents along my career path.
I also knew that I was passionate about supporting my patients and hospitalist team. I’d previously served as associate medical director in charge of quality, readmission reduction, and patient experience. Having achieved the highest patient satisfaction scores on the team for 2 consecutive years, I was specially tasked to improve our team’s HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores.
These experiences taught me that coaching with positive reinforcement was in my blood. This gave me the courage to face my tallest mountain yet.
No one climbs a mountain alone
I also stepped into my new physician leadership role with amazing support. Our outgoing medical director had recommended me, and my entire team was rooting for me. My spouse was 100% behind the idea.
What’s more, I had received amazing feedback from patients throughout my 3 years at the hospital. I had papered an entire office wall with their thank-you notes. I even had a quilt that an 85-year-old patient’s wife made to thank me for my compassionate care.
As I weighed my decision, I realized that I had a higher calling to be a true advocate for my patients. I loved what I did. Each day, I resolved to bring my best and most authentic self for them – no matter how drained I felt.
My team and patients needed me now, not at some more convenient time down the road. A medical director job was the natural next step for me. And so, I resolved to climb the mountain.
Climbing through storms
Stepping into a medical director job forced me to grow into a completely new person. So maybe starting that role during pregnancy was a great metaphor!
Each day, there was immense pressure to perform, to deliver quality outcomes, and to simultaneously meet expectations of the C-suite as well as my hospitalist team. There was no room for failure, because too much was at stake.
Looking back today, I wouldn’t trade the experience for anything. The medical director role was one of the most gratifying experiences in my life, and I am truly thankful for it.
A leader’s role truly boils down to working tirelessly to collaborate with different care teams. It’s important to care not only about our patients but also about our fellow hospitalists. We can do this by truly leading by example – be it picking up extra shifts, covering holidays so team members can be with family, or coming in at 10 p.m. to round with your night team.
I was also able to bring a unique perspective to the hospital C-suite meetings as a woman, an immigrant, and a true “mama bear” – not only of my infant son but also of my team.
My first year as a medical director required more commitment and heart than I could have imagined. But all this hard work paid off when our hospitalist group received the coveted Best Team Award for most improved quality outcomes, financial performance, and patient experience.
The summit is the beginning
My first medical director job fueled my passion for patient satisfaction even further. I now serve as the director of patient experience for the more than 4,200 clinicians at Vituity. Together we care for more than 6.5 million lives a year across the country.
In 2019, I coached 300 physicians and hospital leaders on communication, collaboration, and service recovery skills, leading to significant improvement in their HCAHPS scores. I was delighted to receive the Vituity Distinguished Service Award for my contributions. It’s such an honor to be instrumental in impacting patient care at a larger scale.
This year, I was invited to serve as vice chair of the Society for Hospital Medicine’s patient experience committee and to join the executive board of the SHM San Francisco chapter. Together, we have created a COVID-19 patient communication resource and reached out to our hospitalists to provide them with a space to share their stories during this pandemic. I am so excited to share my knowledge and passion with clinicians across the country given the wide reach of Vituity & SHM!
Many hospitalists shy away from leadership roles. The mountain is tough to scale, but the view from the top is worth it. The key is to start, even if you don’t feel ready. I am here to tell you it can be done!
Dr. Mehta is a hospitalist and director of quality & performance and patient experience at Vituity in Emeryville, Calif. She is vice chair of the SHM patient experience committee and executive board member of the SHM San Francisco Bay Area chapter.
It was 6 a.m. on a rainy, cold Pacific Northwest morning as I walked from my apartment to the hospital, dodging puddles and dreaming of the mediocre-yet-hot physician-lounge coffee. Another long day full of clinical and administrative tasks awaited me.
I was 6 months’ pregnant with our first child and working my sixth 12-hour shift in a row. We had recently lost our medical director, and the C-suite had offered me the role. The day ahead seemed like an enormous mountain to climb.
I felt tired and more than a little overwhelmed. But I whispered to myself: “Today is going to be a fantastic day. I will not fail my team. I will not fail my patients!”
Physician leadership starts with a decision
The timing of this call to leadership had not been ideal. There’s probably never a perfect time to step into a medical director role. And my situation was no exception.
In addition to the baby on the way, my husband was traveling a lot for work. Also, the job of a medical director seemed a little daunting – especially to a young physician leading a team for the first time.
But I knew that leadership was my calling. While I didn’t yet have decades of experience, I had been selected as the chief resident in internal medicine, completed a nephrology fellowship, and mentored several medical students and residents along my career path.
I also knew that I was passionate about supporting my patients and hospitalist team. I’d previously served as associate medical director in charge of quality, readmission reduction, and patient experience. Having achieved the highest patient satisfaction scores on the team for 2 consecutive years, I was specially tasked to improve our team’s HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores.
These experiences taught me that coaching with positive reinforcement was in my blood. This gave me the courage to face my tallest mountain yet.
No one climbs a mountain alone
I also stepped into my new physician leadership role with amazing support. Our outgoing medical director had recommended me, and my entire team was rooting for me. My spouse was 100% behind the idea.
What’s more, I had received amazing feedback from patients throughout my 3 years at the hospital. I had papered an entire office wall with their thank-you notes. I even had a quilt that an 85-year-old patient’s wife made to thank me for my compassionate care.
As I weighed my decision, I realized that I had a higher calling to be a true advocate for my patients. I loved what I did. Each day, I resolved to bring my best and most authentic self for them – no matter how drained I felt.
My team and patients needed me now, not at some more convenient time down the road. A medical director job was the natural next step for me. And so, I resolved to climb the mountain.
Climbing through storms
Stepping into a medical director job forced me to grow into a completely new person. So maybe starting that role during pregnancy was a great metaphor!
Each day, there was immense pressure to perform, to deliver quality outcomes, and to simultaneously meet expectations of the C-suite as well as my hospitalist team. There was no room for failure, because too much was at stake.
Looking back today, I wouldn’t trade the experience for anything. The medical director role was one of the most gratifying experiences in my life, and I am truly thankful for it.
A leader’s role truly boils down to working tirelessly to collaborate with different care teams. It’s important to care not only about our patients but also about our fellow hospitalists. We can do this by truly leading by example – be it picking up extra shifts, covering holidays so team members can be with family, or coming in at 10 p.m. to round with your night team.
I was also able to bring a unique perspective to the hospital C-suite meetings as a woman, an immigrant, and a true “mama bear” – not only of my infant son but also of my team.
My first year as a medical director required more commitment and heart than I could have imagined. But all this hard work paid off when our hospitalist group received the coveted Best Team Award for most improved quality outcomes, financial performance, and patient experience.
The summit is the beginning
My first medical director job fueled my passion for patient satisfaction even further. I now serve as the director of patient experience for the more than 4,200 clinicians at Vituity. Together we care for more than 6.5 million lives a year across the country.
In 2019, I coached 300 physicians and hospital leaders on communication, collaboration, and service recovery skills, leading to significant improvement in their HCAHPS scores. I was delighted to receive the Vituity Distinguished Service Award for my contributions. It’s such an honor to be instrumental in impacting patient care at a larger scale.
This year, I was invited to serve as vice chair of the Society for Hospital Medicine’s patient experience committee and to join the executive board of the SHM San Francisco chapter. Together, we have created a COVID-19 patient communication resource and reached out to our hospitalists to provide them with a space to share their stories during this pandemic. I am so excited to share my knowledge and passion with clinicians across the country given the wide reach of Vituity & SHM!
Many hospitalists shy away from leadership roles. The mountain is tough to scale, but the view from the top is worth it. The key is to start, even if you don’t feel ready. I am here to tell you it can be done!
Dr. Mehta is a hospitalist and director of quality & performance and patient experience at Vituity in Emeryville, Calif. She is vice chair of the SHM patient experience committee and executive board member of the SHM San Francisco Bay Area chapter.
It was 6 a.m. on a rainy, cold Pacific Northwest morning as I walked from my apartment to the hospital, dodging puddles and dreaming of the mediocre-yet-hot physician-lounge coffee. Another long day full of clinical and administrative tasks awaited me.
I was 6 months’ pregnant with our first child and working my sixth 12-hour shift in a row. We had recently lost our medical director, and the C-suite had offered me the role. The day ahead seemed like an enormous mountain to climb.
I felt tired and more than a little overwhelmed. But I whispered to myself: “Today is going to be a fantastic day. I will not fail my team. I will not fail my patients!”
Physician leadership starts with a decision
The timing of this call to leadership had not been ideal. There’s probably never a perfect time to step into a medical director role. And my situation was no exception.
In addition to the baby on the way, my husband was traveling a lot for work. Also, the job of a medical director seemed a little daunting – especially to a young physician leading a team for the first time.
But I knew that leadership was my calling. While I didn’t yet have decades of experience, I had been selected as the chief resident in internal medicine, completed a nephrology fellowship, and mentored several medical students and residents along my career path.
I also knew that I was passionate about supporting my patients and hospitalist team. I’d previously served as associate medical director in charge of quality, readmission reduction, and patient experience. Having achieved the highest patient satisfaction scores on the team for 2 consecutive years, I was specially tasked to improve our team’s HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores.
These experiences taught me that coaching with positive reinforcement was in my blood. This gave me the courage to face my tallest mountain yet.
No one climbs a mountain alone
I also stepped into my new physician leadership role with amazing support. Our outgoing medical director had recommended me, and my entire team was rooting for me. My spouse was 100% behind the idea.
What’s more, I had received amazing feedback from patients throughout my 3 years at the hospital. I had papered an entire office wall with their thank-you notes. I even had a quilt that an 85-year-old patient’s wife made to thank me for my compassionate care.
As I weighed my decision, I realized that I had a higher calling to be a true advocate for my patients. I loved what I did. Each day, I resolved to bring my best and most authentic self for them – no matter how drained I felt.
My team and patients needed me now, not at some more convenient time down the road. A medical director job was the natural next step for me. And so, I resolved to climb the mountain.
Climbing through storms
Stepping into a medical director job forced me to grow into a completely new person. So maybe starting that role during pregnancy was a great metaphor!
Each day, there was immense pressure to perform, to deliver quality outcomes, and to simultaneously meet expectations of the C-suite as well as my hospitalist team. There was no room for failure, because too much was at stake.
Looking back today, I wouldn’t trade the experience for anything. The medical director role was one of the most gratifying experiences in my life, and I am truly thankful for it.
A leader’s role truly boils down to working tirelessly to collaborate with different care teams. It’s important to care not only about our patients but also about our fellow hospitalists. We can do this by truly leading by example – be it picking up extra shifts, covering holidays so team members can be with family, or coming in at 10 p.m. to round with your night team.
I was also able to bring a unique perspective to the hospital C-suite meetings as a woman, an immigrant, and a true “mama bear” – not only of my infant son but also of my team.
My first year as a medical director required more commitment and heart than I could have imagined. But all this hard work paid off when our hospitalist group received the coveted Best Team Award for most improved quality outcomes, financial performance, and patient experience.
The summit is the beginning
My first medical director job fueled my passion for patient satisfaction even further. I now serve as the director of patient experience for the more than 4,200 clinicians at Vituity. Together we care for more than 6.5 million lives a year across the country.
In 2019, I coached 300 physicians and hospital leaders on communication, collaboration, and service recovery skills, leading to significant improvement in their HCAHPS scores. I was delighted to receive the Vituity Distinguished Service Award for my contributions. It’s such an honor to be instrumental in impacting patient care at a larger scale.
This year, I was invited to serve as vice chair of the Society for Hospital Medicine’s patient experience committee and to join the executive board of the SHM San Francisco chapter. Together, we have created a COVID-19 patient communication resource and reached out to our hospitalists to provide them with a space to share their stories during this pandemic. I am so excited to share my knowledge and passion with clinicians across the country given the wide reach of Vituity & SHM!
Many hospitalists shy away from leadership roles. The mountain is tough to scale, but the view from the top is worth it. The key is to start, even if you don’t feel ready. I am here to tell you it can be done!
Dr. Mehta is a hospitalist and director of quality & performance and patient experience at Vituity in Emeryville, Calif. She is vice chair of the SHM patient experience committee and executive board member of the SHM San Francisco Bay Area chapter.
Defining excellence with Dr. Kimberly Manning
2020 SHM Award of Excellence winner: Diversity Leadership
Each year, the Society of Hospital Medicine celebrates the exemplary actions and successes of its members through the Awards of Excellence program. Nominations open every fall, providing the SHM community with the opportunity to nominate a peer, or themselves, to receive an esteemed award of excellence in an array of categories including Teaching, Outstanding Service in Hospital Medicine, Research, and so many others.
While the program and its Awards Committee review nominations with a predetermined set of criteria, excellence is not a ‘one-size-fits-all’ defined term.

Kimberly D. Manning, MD, FACP, FAAP, is a professor of medicine and associate vice chair of Diversity, Equity and Inclusion at the Emory University School of Medicine and a hospitalist at Grady Memorial Hospital, both in Atlanta. She believes that every single person contributes something uniquely meaningful, and that it is up to each person to decide how to use their influence to make an impact.
“To me, being excellent is about discovering your mission and pushing yourself to explore ways to be the best steward of that mission,” Dr. Manning said. “My mission is focused on serving underserved populations, humanizing patients, and amplifying voices of those who have traditionally been silenced.”
Dr. Manning has challenged herself to be the best steward of her evolving mission for equity, representation, and accessibility in medical education and health care innovation for many years. An active member of SHM for 14 years and an inspiring social impact–driven hospitalist of 20 years, Dr. Manning is known for her extensive work in the diversity, equity, and inclusion (DEI) space.
In 2020, Dr. Manning was nominated for and received SHM’s inaugural Excellence in Diversity Leadership Award by her peer and colleague, Dr. Daniel Dressler of Emory University School of Medicine.
She was honored for her commitment to improving the care of underrepresented patient populations, increasing awareness of DEI necessity, and building inclusive communities. In addition to these noteworthy achievements, she demonstrated scholarship on diversity, equity, and inclusion.
One way that Dr. Manning is fusing her love for diversity, equity, and inclusion with innovation is through her role as associate vice chair of the DEI department of Emory University’s School of Medicine. Within the department’s programs, resources and affinity groups, Dr. Manning leads a Virtual Visiting Clerkship Program for underrepresented medical students interested in pursuing a career in internal medicine.
“It includes coaching, mentorship, and diagnostic reasoning in an intimate and personal way,” she explained. “It makes me wish I were a medical student!”
In addition to her patient-centric and student-focused initiatives in Atlanta, Dr. Manning is an active contributor to SHM’s publications, including the Journal of Hospital Medicine and The Hospital Leader blog, in speaking out about racism in medicine, and other social inequities in health care. She even helped to lead a #JHMchat discussion on Twitter around these topics.
In fact, beyond being presented with the Diversity Leadership Award, she says that SHM and JHM have really demonstrated a strong commitment to diversity, equity, and inclusion.
“If you are a person with a lived experience or a person who is underrepresented in medicine, a lot of this work in diversity, equity, and inclusion never really had a name. It was called survival and looking out for each other,” Dr. Manning explained. “It’s exciting to be in this space now where there is focused, professional attention being given to something so important in our clinical and learning environments.”
SHM continues to reaffirm its longstanding commitment to diversity and inclusion and is dedicated to supporting and learning from its diverse member community. While SHM’s new Excellence in Diversity Leadership award is symbolic of a step in the right direction of change, Dr. Manning says that it is also an honor to be recognized for her areas of expertise and passion.
But that recognition moves far beyond this award. With so many more ways to connect with one another, Dr. Manning, a self-proclaimed optimist, says that one of the most exciting changes is centered on communication.
“For us to move the needle on anti-racism and representation, and to do more for our patients and colleagues, it must be a shared conversation. I feel particularly optimistic that I’m able to be more transparent than ever. I’m saying things to people whom I would have been too scared to say them to in the past.
“We’re hungry to grow and learn together,” she continued. “People are interacting in a more positive and constructive way. I’m so glad that we’re pushing diversity and you can see that a lot of people want to see us do better with this. We can continue to do better with this.”
SHM’s 2020-2021 Awards of Excellence nominations are now open with nine unique categories, including Excellence in Diversity, Equity, and Inclusion Leadership. If you have a peer or colleague in mind, like Dr. Manning, who has made exceptional contributions to DEI, or another important domain in hospital medicine, submit your nomination by Sept. 28, 2020.
“I have a feeling that this year has provided a lot of opportunity for people to emerge. The Committee is going to have a very, very tough job,” Dr. Manning said. “They are going to have some exciting nominations on their hands!”
Ms. Cowan is the marketing communications specialist at the Society of Hospital Medicine.
2020 SHM Award of Excellence winner: Diversity Leadership
2020 SHM Award of Excellence winner: Diversity Leadership
Each year, the Society of Hospital Medicine celebrates the exemplary actions and successes of its members through the Awards of Excellence program. Nominations open every fall, providing the SHM community with the opportunity to nominate a peer, or themselves, to receive an esteemed award of excellence in an array of categories including Teaching, Outstanding Service in Hospital Medicine, Research, and so many others.
While the program and its Awards Committee review nominations with a predetermined set of criteria, excellence is not a ‘one-size-fits-all’ defined term.
Kimberly D. Manning, MD, FACP, FAAP, is a professor of medicine and associate vice chair of Diversity, Equity and Inclusion at the Emory University School of Medicine and a hospitalist at Grady Memorial Hospital, both in Atlanta. She believes that every single person contributes something uniquely meaningful, and that it is up to each person to decide how to use their influence to make an impact.
“To me, being excellent is about discovering your mission and pushing yourself to explore ways to be the best steward of that mission,” Dr. Manning said. “My mission is focused on serving underserved populations, humanizing patients, and amplifying voices of those who have traditionally been silenced.”
Dr. Manning has challenged herself to be the best steward of her evolving mission for equity, representation, and accessibility in medical education and health care innovation for many years. An active member of SHM for 14 years and an inspiring social impact–driven hospitalist of 20 years, Dr. Manning is known for her extensive work in the diversity, equity, and inclusion (DEI) space.
In 2020, Dr. Manning was nominated for and received SHM’s inaugural Excellence in Diversity Leadership Award by her peer and colleague, Dr. Daniel Dressler of Emory University School of Medicine.
She was honored for her commitment to improving the care of underrepresented patient populations, increasing awareness of DEI necessity, and building inclusive communities. In addition to these noteworthy achievements, she demonstrated scholarship on diversity, equity, and inclusion.
One way that Dr. Manning is fusing her love for diversity, equity, and inclusion with innovation is through her role as associate vice chair of the DEI department of Emory University’s School of Medicine. Within the department’s programs, resources and affinity groups, Dr. Manning leads a Virtual Visiting Clerkship Program for underrepresented medical students interested in pursuing a career in internal medicine.
“It includes coaching, mentorship, and diagnostic reasoning in an intimate and personal way,” she explained. “It makes me wish I were a medical student!”
In addition to her patient-centric and student-focused initiatives in Atlanta, Dr. Manning is an active contributor to SHM’s publications, including the Journal of Hospital Medicine and The Hospital Leader blog, in speaking out about racism in medicine, and other social inequities in health care. She even helped to lead a #JHMchat discussion on Twitter around these topics.
In fact, beyond being presented with the Diversity Leadership Award, she says that SHM and JHM have really demonstrated a strong commitment to diversity, equity, and inclusion.
“If you are a person with a lived experience or a person who is underrepresented in medicine, a lot of this work in diversity, equity, and inclusion never really had a name. It was called survival and looking out for each other,” Dr. Manning explained. “It’s exciting to be in this space now where there is focused, professional attention being given to something so important in our clinical and learning environments.”
SHM continues to reaffirm its longstanding commitment to diversity and inclusion and is dedicated to supporting and learning from its diverse member community. While SHM’s new Excellence in Diversity Leadership award is symbolic of a step in the right direction of change, Dr. Manning says that it is also an honor to be recognized for her areas of expertise and passion.
But that recognition moves far beyond this award. With so many more ways to connect with one another, Dr. Manning, a self-proclaimed optimist, says that one of the most exciting changes is centered on communication.
“For us to move the needle on anti-racism and representation, and to do more for our patients and colleagues, it must be a shared conversation. I feel particularly optimistic that I’m able to be more transparent than ever. I’m saying things to people whom I would have been too scared to say them to in the past.
“We’re hungry to grow and learn together,” she continued. “People are interacting in a more positive and constructive way. I’m so glad that we’re pushing diversity and you can see that a lot of people want to see us do better with this. We can continue to do better with this.”
SHM’s 2020-2021 Awards of Excellence nominations are now open with nine unique categories, including Excellence in Diversity, Equity, and Inclusion Leadership. If you have a peer or colleague in mind, like Dr. Manning, who has made exceptional contributions to DEI, or another important domain in hospital medicine, submit your nomination by Sept. 28, 2020.
“I have a feeling that this year has provided a lot of opportunity for people to emerge. The Committee is going to have a very, very tough job,” Dr. Manning said. “They are going to have some exciting nominations on their hands!”
Ms. Cowan is the marketing communications specialist at the Society of Hospital Medicine.
Each year, the Society of Hospital Medicine celebrates the exemplary actions and successes of its members through the Awards of Excellence program. Nominations open every fall, providing the SHM community with the opportunity to nominate a peer, or themselves, to receive an esteemed award of excellence in an array of categories including Teaching, Outstanding Service in Hospital Medicine, Research, and so many others.
While the program and its Awards Committee review nominations with a predetermined set of criteria, excellence is not a ‘one-size-fits-all’ defined term.
Kimberly D. Manning, MD, FACP, FAAP, is a professor of medicine and associate vice chair of Diversity, Equity and Inclusion at the Emory University School of Medicine and a hospitalist at Grady Memorial Hospital, both in Atlanta. She believes that every single person contributes something uniquely meaningful, and that it is up to each person to decide how to use their influence to make an impact.
“To me, being excellent is about discovering your mission and pushing yourself to explore ways to be the best steward of that mission,” Dr. Manning said. “My mission is focused on serving underserved populations, humanizing patients, and amplifying voices of those who have traditionally been silenced.”
Dr. Manning has challenged herself to be the best steward of her evolving mission for equity, representation, and accessibility in medical education and health care innovation for many years. An active member of SHM for 14 years and an inspiring social impact–driven hospitalist of 20 years, Dr. Manning is known for her extensive work in the diversity, equity, and inclusion (DEI) space.
In 2020, Dr. Manning was nominated for and received SHM’s inaugural Excellence in Diversity Leadership Award by her peer and colleague, Dr. Daniel Dressler of Emory University School of Medicine.
She was honored for her commitment to improving the care of underrepresented patient populations, increasing awareness of DEI necessity, and building inclusive communities. In addition to these noteworthy achievements, she demonstrated scholarship on diversity, equity, and inclusion.
One way that Dr. Manning is fusing her love for diversity, equity, and inclusion with innovation is through her role as associate vice chair of the DEI department of Emory University’s School of Medicine. Within the department’s programs, resources and affinity groups, Dr. Manning leads a Virtual Visiting Clerkship Program for underrepresented medical students interested in pursuing a career in internal medicine.
“It includes coaching, mentorship, and diagnostic reasoning in an intimate and personal way,” she explained. “It makes me wish I were a medical student!”
In addition to her patient-centric and student-focused initiatives in Atlanta, Dr. Manning is an active contributor to SHM’s publications, including the Journal of Hospital Medicine and The Hospital Leader blog, in speaking out about racism in medicine, and other social inequities in health care. She even helped to lead a #JHMchat discussion on Twitter around these topics.
In fact, beyond being presented with the Diversity Leadership Award, she says that SHM and JHM have really demonstrated a strong commitment to diversity, equity, and inclusion.
“If you are a person with a lived experience or a person who is underrepresented in medicine, a lot of this work in diversity, equity, and inclusion never really had a name. It was called survival and looking out for each other,” Dr. Manning explained. “It’s exciting to be in this space now where there is focused, professional attention being given to something so important in our clinical and learning environments.”
SHM continues to reaffirm its longstanding commitment to diversity and inclusion and is dedicated to supporting and learning from its diverse member community. While SHM’s new Excellence in Diversity Leadership award is symbolic of a step in the right direction of change, Dr. Manning says that it is also an honor to be recognized for her areas of expertise and passion.
But that recognition moves far beyond this award. With so many more ways to connect with one another, Dr. Manning, a self-proclaimed optimist, says that one of the most exciting changes is centered on communication.
“For us to move the needle on anti-racism and representation, and to do more for our patients and colleagues, it must be a shared conversation. I feel particularly optimistic that I’m able to be more transparent than ever. I’m saying things to people whom I would have been too scared to say them to in the past.
“We’re hungry to grow and learn together,” she continued. “People are interacting in a more positive and constructive way. I’m so glad that we’re pushing diversity and you can see that a lot of people want to see us do better with this. We can continue to do better with this.”
SHM’s 2020-2021 Awards of Excellence nominations are now open with nine unique categories, including Excellence in Diversity, Equity, and Inclusion Leadership. If you have a peer or colleague in mind, like Dr. Manning, who has made exceptional contributions to DEI, or another important domain in hospital medicine, submit your nomination by Sept. 28, 2020.
“I have a feeling that this year has provided a lot of opportunity for people to emerge. The Committee is going to have a very, very tough job,” Dr. Manning said. “They are going to have some exciting nominations on their hands!”
Ms. Cowan is the marketing communications specialist at the Society of Hospital Medicine.