User login
For patients with HBV, daily aspirin may reduce risk of liver cancer

Sixteen years of data showed that daily aspirin therapy reduced the risk of HBV-related HCC by 29%, reported lead author Teng-Yu Lee, MD, PhD, of Taichung (Taiwan) Veterans General Hospital and his colleagues. Analysis also showed that antiviral nucleos(t)ide analogue therapy and statin use were independently associated with reduced risk of HCC, whereas older age, cirrhosis, and male sex increased risk.
“Therapy with [nucleos(t)ide analogues] is associated with reductions in HCC risk, but the risk is not erased,” the investigators wrote in JAMA Internal Medicine. “Therefore, using only [nucleos(t)ide analogue] therapy may not be enough for HCC prevention. Antiviral therapy is not indicated in most HBV carriers, so another effective way of reducing HCC risk needs to be developed.”
Previous studies have shown that aspirin can reduce the risk of colorectal cancer; however, data supporting aspirin for HCC prevention are limited to a few animal models and human studies, the latter of which are statistically unreliable.
“Therefore, we conducted a nationwide cohort study to evaluate the association of daily aspirin therapy with HBV-related HCC,” the investigators wrote.
They screened 204,507 patients with HBV included in the Taiwanese National Health Insurance Research Database (NHIRD) between 1997 and 2012, first excluding any with confounding conditions, such as hepatitis C infection or alcoholic liver disease. Next, 2,123 patients were identified who had taken aspirin for 90 days or longer. Finally, these cases were randomly matched with 8,492 control patients with HBV who had never received antiplatelet therapy. The main measured outcome was diagnosis with HCC. Patients were followed until this diagnosis was made, death occurred, or the end of the study period.
Analysis showed that most patients were male (72.4%) and took aspirin for about 4 years, usually prescribed for cardiovascular disease risk factors. Almost all patients in the treatment group (98%) received an aspirin dose of 100 mg or less.
After 5 years, the cumulative incidence of HCC in the aspirin group was 5.20% versus 7.87% in the control group (P less than .001). Multivariable analysis revealed that daily aspirin was associated with a significant risk reduction of 29% (HR 0.71; P less than .001), as were nucleos(t)ide analogues and statins, which lowered risk by 46% and 38%, respectively. In contrast, risk increased with older age at the rate of 1% per year, male sex carried an additional risk of 75%, and liver cirrhosis was associated with a 2.89-fold risk increase.
“In the present study, we report that daily aspirin therapy was associated with a reduced incidence of HCC in patients with [chronic hepatitis B],” the investigators wrote. “Our findings may be of help in future efforts to further improve the chemoprevention of HBV-related HCC, and a proof-of-concept study is thus warranted.”
The investigators described several mechanisms that may have contribute to the possible risk reduction provided by aspirin. For one, aspirin inhibits platelet activation, which is associated with development of HBV-related liver disease. Additional benefit may come from induction of HCC cell apoptosis, control of tumor growth, reduced liver fibrosis, and increased liver regeneration, all of which have been associated with aspirin in rodent models.
“Hepatitis B virus–related HCC is generally a consequence of chronic inflammation due to hepatitis, fibrosis, dysplasia, and tumor growth,” the investigators wrote, suggesting that aspirin-related reductions in inflammation could also explain reduced neoplastic activity.
To assess for increased risk of peptic ulcers secondary to aspirin, the investigators performed a subanalysis of peptic ulcer bleeding. These results showed that rates of peptic ulcer bleeding, at around 5%-6%, were similar between the aspirin group and the control group. Among other variables, cirrhosis didn’t significantly affect rates of peptic ulcer bleeding, and aspirin users had similar rates of peptic ulcer bleeding regardless of HBV status. Because of the study design, however, the investigators cautioned that these analyses could underestimate ulcer risk because patients who could not tolerate aspirin for at least 90 days were excluded from the study.
Although statins stood out as another possible risk reducer, the investigators noted that “randomized clinical trials are required to confirm the chemopreventive effect of statins.”
Similarly, the investigators suggested that a prospective trial is needed before aspirin can be adopted as an HCC preventive.
The study was funded by the Ministry of Science and Technology, National Health Research Institutes, and Taichung (Taiwan) Veterans General Hospital, Taiwan. One author reported financial compensation from Gilead and Bristol-Myers Squibb.
SOURCE: Lee T-Y et al. JAMA Intern Med. 2019 Mar 18. doi:10.1001/jamainternmed.2018.8342.
Sixteen years of data showed that daily aspirin therapy reduced the risk of HBV-related HCC by 29%, reported lead author Teng-Yu Lee, MD, PhD, of Taichung (Taiwan) Veterans General Hospital and his colleagues. Analysis also showed that antiviral nucleos(t)ide analogue therapy and statin use were independently associated with reduced risk of HCC, whereas older age, cirrhosis, and male sex increased risk.
“Therapy with [nucleos(t)ide analogues] is associated with reductions in HCC risk, but the risk is not erased,” the investigators wrote in JAMA Internal Medicine. “Therefore, using only [nucleos(t)ide analogue] therapy may not be enough for HCC prevention. Antiviral therapy is not indicated in most HBV carriers, so another effective way of reducing HCC risk needs to be developed.”
Previous studies have shown that aspirin can reduce the risk of colorectal cancer; however, data supporting aspirin for HCC prevention are limited to a few animal models and human studies, the latter of which are statistically unreliable.
“Therefore, we conducted a nationwide cohort study to evaluate the association of daily aspirin therapy with HBV-related HCC,” the investigators wrote.
They screened 204,507 patients with HBV included in the Taiwanese National Health Insurance Research Database (NHIRD) between 1997 and 2012, first excluding any with confounding conditions, such as hepatitis C infection or alcoholic liver disease. Next, 2,123 patients were identified who had taken aspirin for 90 days or longer. Finally, these cases were randomly matched with 8,492 control patients with HBV who had never received antiplatelet therapy. The main measured outcome was diagnosis with HCC. Patients were followed until this diagnosis was made, death occurred, or the end of the study period.
Analysis showed that most patients were male (72.4%) and took aspirin for about 4 years, usually prescribed for cardiovascular disease risk factors. Almost all patients in the treatment group (98%) received an aspirin dose of 100 mg or less.
After 5 years, the cumulative incidence of HCC in the aspirin group was 5.20% versus 7.87% in the control group (P less than .001). Multivariable analysis revealed that daily aspirin was associated with a significant risk reduction of 29% (HR 0.71; P less than .001), as were nucleos(t)ide analogues and statins, which lowered risk by 46% and 38%, respectively. In contrast, risk increased with older age at the rate of 1% per year, male sex carried an additional risk of 75%, and liver cirrhosis was associated with a 2.89-fold risk increase.
“In the present study, we report that daily aspirin therapy was associated with a reduced incidence of HCC in patients with [chronic hepatitis B],” the investigators wrote. “Our findings may be of help in future efforts to further improve the chemoprevention of HBV-related HCC, and a proof-of-concept study is thus warranted.”
The investigators described several mechanisms that may have contribute to the possible risk reduction provided by aspirin. For one, aspirin inhibits platelet activation, which is associated with development of HBV-related liver disease. Additional benefit may come from induction of HCC cell apoptosis, control of tumor growth, reduced liver fibrosis, and increased liver regeneration, all of which have been associated with aspirin in rodent models.
“Hepatitis B virus–related HCC is generally a consequence of chronic inflammation due to hepatitis, fibrosis, dysplasia, and tumor growth,” the investigators wrote, suggesting that aspirin-related reductions in inflammation could also explain reduced neoplastic activity.
To assess for increased risk of peptic ulcers secondary to aspirin, the investigators performed a subanalysis of peptic ulcer bleeding. These results showed that rates of peptic ulcer bleeding, at around 5%-6%, were similar between the aspirin group and the control group. Among other variables, cirrhosis didn’t significantly affect rates of peptic ulcer bleeding, and aspirin users had similar rates of peptic ulcer bleeding regardless of HBV status. Because of the study design, however, the investigators cautioned that these analyses could underestimate ulcer risk because patients who could not tolerate aspirin for at least 90 days were excluded from the study.
Although statins stood out as another possible risk reducer, the investigators noted that “randomized clinical trials are required to confirm the chemopreventive effect of statins.”
Similarly, the investigators suggested that a prospective trial is needed before aspirin can be adopted as an HCC preventive.
The study was funded by the Ministry of Science and Technology, National Health Research Institutes, and Taichung (Taiwan) Veterans General Hospital, Taiwan. One author reported financial compensation from Gilead and Bristol-Myers Squibb.
SOURCE: Lee T-Y et al. JAMA Intern Med. 2019 Mar 18. doi:10.1001/jamainternmed.2018.8342.
Sixteen years of data showed that daily aspirin therapy reduced the risk of HBV-related HCC by 29%, reported lead author Teng-Yu Lee, MD, PhD, of Taichung (Taiwan) Veterans General Hospital and his colleagues. Analysis also showed that antiviral nucleos(t)ide analogue therapy and statin use were independently associated with reduced risk of HCC, whereas older age, cirrhosis, and male sex increased risk.
“Therapy with [nucleos(t)ide analogues] is associated with reductions in HCC risk, but the risk is not erased,” the investigators wrote in JAMA Internal Medicine. “Therefore, using only [nucleos(t)ide analogue] therapy may not be enough for HCC prevention. Antiviral therapy is not indicated in most HBV carriers, so another effective way of reducing HCC risk needs to be developed.”
Previous studies have shown that aspirin can reduce the risk of colorectal cancer; however, data supporting aspirin for HCC prevention are limited to a few animal models and human studies, the latter of which are statistically unreliable.
“Therefore, we conducted a nationwide cohort study to evaluate the association of daily aspirin therapy with HBV-related HCC,” the investigators wrote.
They screened 204,507 patients with HBV included in the Taiwanese National Health Insurance Research Database (NHIRD) between 1997 and 2012, first excluding any with confounding conditions, such as hepatitis C infection or alcoholic liver disease. Next, 2,123 patients were identified who had taken aspirin for 90 days or longer. Finally, these cases were randomly matched with 8,492 control patients with HBV who had never received antiplatelet therapy. The main measured outcome was diagnosis with HCC. Patients were followed until this diagnosis was made, death occurred, or the end of the study period.
Analysis showed that most patients were male (72.4%) and took aspirin for about 4 years, usually prescribed for cardiovascular disease risk factors. Almost all patients in the treatment group (98%) received an aspirin dose of 100 mg or less.
After 5 years, the cumulative incidence of HCC in the aspirin group was 5.20% versus 7.87% in the control group (P less than .001). Multivariable analysis revealed that daily aspirin was associated with a significant risk reduction of 29% (HR 0.71; P less than .001), as were nucleos(t)ide analogues and statins, which lowered risk by 46% and 38%, respectively. In contrast, risk increased with older age at the rate of 1% per year, male sex carried an additional risk of 75%, and liver cirrhosis was associated with a 2.89-fold risk increase.
“In the present study, we report that daily aspirin therapy was associated with a reduced incidence of HCC in patients with [chronic hepatitis B],” the investigators wrote. “Our findings may be of help in future efforts to further improve the chemoprevention of HBV-related HCC, and a proof-of-concept study is thus warranted.”
The investigators described several mechanisms that may have contribute to the possible risk reduction provided by aspirin. For one, aspirin inhibits platelet activation, which is associated with development of HBV-related liver disease. Additional benefit may come from induction of HCC cell apoptosis, control of tumor growth, reduced liver fibrosis, and increased liver regeneration, all of which have been associated with aspirin in rodent models.
“Hepatitis B virus–related HCC is generally a consequence of chronic inflammation due to hepatitis, fibrosis, dysplasia, and tumor growth,” the investigators wrote, suggesting that aspirin-related reductions in inflammation could also explain reduced neoplastic activity.
To assess for increased risk of peptic ulcers secondary to aspirin, the investigators performed a subanalysis of peptic ulcer bleeding. These results showed that rates of peptic ulcer bleeding, at around 5%-6%, were similar between the aspirin group and the control group. Among other variables, cirrhosis didn’t significantly affect rates of peptic ulcer bleeding, and aspirin users had similar rates of peptic ulcer bleeding regardless of HBV status. Because of the study design, however, the investigators cautioned that these analyses could underestimate ulcer risk because patients who could not tolerate aspirin for at least 90 days were excluded from the study.
Although statins stood out as another possible risk reducer, the investigators noted that “randomized clinical trials are required to confirm the chemopreventive effect of statins.”
Similarly, the investigators suggested that a prospective trial is needed before aspirin can be adopted as an HCC preventive.
The study was funded by the Ministry of Science and Technology, National Health Research Institutes, and Taichung (Taiwan) Veterans General Hospital, Taiwan. One author reported financial compensation from Gilead and Bristol-Myers Squibb.
SOURCE: Lee T-Y et al. JAMA Intern Med. 2019 Mar 18. doi:10.1001/jamainternmed.2018.8342.
FROM JAMA INTERNAL MEDICINE
Tuesday’s Product Theaters
12:30 - 1:30 p.m., Product Theater 1
Reduction in the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation (NVAF)
Speaker: Charles J. Dow, MD, FACC, cardiologist, Harvard Medical School, Boston
Sponsored by Pfizer
12:30 - 1:30 p.m., Product Theater 2
Improving Outcomes for Hospitalized Patients with HFrEF: Looking Beyond Stabilization
Speaker: Jennifer Brown, MD
Medstar Cardiology Associates
Annapolis, MD
Sponsored by Novartis Pharmaceuticals Corp.
12:30 - 1:30 p.m., Product Theater 3
The Role of the Hospital Medicine Specialist in Managing Transitions of Care in Acute Coronary Syndrome
Speaker: John Venditto, MD, MBA, senior medical director, cardiovascular metabolic disease,
U.S. Medical Affairs – AstraZeneca
Sponsored by AstraZeneca Pharmaceuticals LP
12:30 - 1:30 p.m., Product Theater 1
Reduction in the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation (NVAF)
Speaker: Charles J. Dow, MD, FACC, cardiologist, Harvard Medical School, Boston
Sponsored by Pfizer
12:30 - 1:30 p.m., Product Theater 2
Improving Outcomes for Hospitalized Patients with HFrEF: Looking Beyond Stabilization
Speaker: Jennifer Brown, MD
Medstar Cardiology Associates
Annapolis, MD
Sponsored by Novartis Pharmaceuticals Corp.
12:30 - 1:30 p.m., Product Theater 3
The Role of the Hospital Medicine Specialist in Managing Transitions of Care in Acute Coronary Syndrome
Speaker: John Venditto, MD, MBA, senior medical director, cardiovascular metabolic disease,
U.S. Medical Affairs – AstraZeneca
Sponsored by AstraZeneca Pharmaceuticals LP
12:30 - 1:30 p.m., Product Theater 1
Reduction in the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation (NVAF)
Speaker: Charles J. Dow, MD, FACC, cardiologist, Harvard Medical School, Boston
Sponsored by Pfizer
12:30 - 1:30 p.m., Product Theater 2
Improving Outcomes for Hospitalized Patients with HFrEF: Looking Beyond Stabilization
Speaker: Jennifer Brown, MD
Medstar Cardiology Associates
Annapolis, MD
Sponsored by Novartis Pharmaceuticals Corp.
12:30 - 1:30 p.m., Product Theater 3
The Role of the Hospital Medicine Specialist in Managing Transitions of Care in Acute Coronary Syndrome
Speaker: John Venditto, MD, MBA, senior medical director, cardiovascular metabolic disease,
U.S. Medical Affairs – AstraZeneca
Sponsored by AstraZeneca Pharmaceuticals LP
Hospitalists get emergency airway management training
A patient is having a medical emergency and is having difficulty breathing. If the airway isn’t managed well, the consequences could be tragic. If asked to step in, would you? Could you?
More hospitalists are being faced with this situation, said Joshua Lenchus, DO, RPh, SFHM, chief medical officer at the Broward Health Medical Center in South Florida. But when they are, they tend to be hesitant – usually with good reason, since training is frequently lacking.
Dr. Lenchus and a group of five other physicians who are experienced in airway management led 25 hospitalists in emergent airway management training on Monday at HM19, a first-of-its-kind session at the annual conference.
“Not all facilities that hospitalists practice at would require or even ask a hospitalist to step into a situation like this,” said Dr. Lenchus, who oversaw the training. “But as you walk around the exhibit hall at SHM, you find that of the locum tenens companies that ask for hospitalists to perform procedures, airway management is very high on the list.”
The trainers were Armando Ariza Giammaria, MD, an anesthesiologist and clinical assistant professor at Tulane University, New Orleans; Jorge Cabrera, DO, an intensivist and assistant professor of medicine at the University of Miami; Alice Gallo de Moraes, MD, a pulmonary critical care doctor at Mayo Clinic, Rochester, Minn.; Fernando Caceres, MD, a pulmonary critical care specialist at the Billings (Mont.) Clinic; and Aldo Pavon Canseco, MD, a hospitalist and assistant professor of medicine at the University of Miami who was trained as a pediatric anesthesiologist.
Over 3 hours, hospitalists first heard tips for airway management, with words of caution, and then did hands-on work using manikins under the guidance of the faculty members with a low trainee-to-instructor ratio.
“Do the basics well and the scary things will become manageable,” Dr. Cabrera said in the session.
Instructors said it was vital to have a checklist in the form of a mnemonic device, and to have not just Plan A for clearing an airway, but Plans B and C, too.
Dr. Ariza told the learners not to focus too much on intubation — it’s not always necessary. In fact, he said he couldn’t over-emphasize the importance of mastering bag-mask ventilation, a go-to method when other approaches fail.
Participants learned about devices that can be deployed through the nose to keep the airway clear, those that can be used in the mouth but that might not go down quite as far as the lung, an inflatable bag that can be placed over patients’ mouths and squeezed to help with their breathing, and endotracheal tubes.
Dr. Lenchus said that more training would likely be needed for most clinicians – perhaps with other faculty at their own institutions – before they could be expected to employ these techniques in a real-life emergency situation.
A patient is having a medical emergency and is having difficulty breathing. If the airway isn’t managed well, the consequences could be tragic. If asked to step in, would you? Could you?
More hospitalists are being faced with this situation, said Joshua Lenchus, DO, RPh, SFHM, chief medical officer at the Broward Health Medical Center in South Florida. But when they are, they tend to be hesitant – usually with good reason, since training is frequently lacking.
Dr. Lenchus and a group of five other physicians who are experienced in airway management led 25 hospitalists in emergent airway management training on Monday at HM19, a first-of-its-kind session at the annual conference.
“Not all facilities that hospitalists practice at would require or even ask a hospitalist to step into a situation like this,” said Dr. Lenchus, who oversaw the training. “But as you walk around the exhibit hall at SHM, you find that of the locum tenens companies that ask for hospitalists to perform procedures, airway management is very high on the list.”
The trainers were Armando Ariza Giammaria, MD, an anesthesiologist and clinical assistant professor at Tulane University, New Orleans; Jorge Cabrera, DO, an intensivist and assistant professor of medicine at the University of Miami; Alice Gallo de Moraes, MD, a pulmonary critical care doctor at Mayo Clinic, Rochester, Minn.; Fernando Caceres, MD, a pulmonary critical care specialist at the Billings (Mont.) Clinic; and Aldo Pavon Canseco, MD, a hospitalist and assistant professor of medicine at the University of Miami who was trained as a pediatric anesthesiologist.
Over 3 hours, hospitalists first heard tips for airway management, with words of caution, and then did hands-on work using manikins under the guidance of the faculty members with a low trainee-to-instructor ratio.
“Do the basics well and the scary things will become manageable,” Dr. Cabrera said in the session.
Instructors said it was vital to have a checklist in the form of a mnemonic device, and to have not just Plan A for clearing an airway, but Plans B and C, too.
Dr. Ariza told the learners not to focus too much on intubation — it’s not always necessary. In fact, he said he couldn’t over-emphasize the importance of mastering bag-mask ventilation, a go-to method when other approaches fail.
Participants learned about devices that can be deployed through the nose to keep the airway clear, those that can be used in the mouth but that might not go down quite as far as the lung, an inflatable bag that can be placed over patients’ mouths and squeezed to help with their breathing, and endotracheal tubes.
Dr. Lenchus said that more training would likely be needed for most clinicians – perhaps with other faculty at their own institutions – before they could be expected to employ these techniques in a real-life emergency situation.
A patient is having a medical emergency and is having difficulty breathing. If the airway isn’t managed well, the consequences could be tragic. If asked to step in, would you? Could you?
More hospitalists are being faced with this situation, said Joshua Lenchus, DO, RPh, SFHM, chief medical officer at the Broward Health Medical Center in South Florida. But when they are, they tend to be hesitant – usually with good reason, since training is frequently lacking.
Dr. Lenchus and a group of five other physicians who are experienced in airway management led 25 hospitalists in emergent airway management training on Monday at HM19, a first-of-its-kind session at the annual conference.
“Not all facilities that hospitalists practice at would require or even ask a hospitalist to step into a situation like this,” said Dr. Lenchus, who oversaw the training. “But as you walk around the exhibit hall at SHM, you find that of the locum tenens companies that ask for hospitalists to perform procedures, airway management is very high on the list.”
The trainers were Armando Ariza Giammaria, MD, an anesthesiologist and clinical assistant professor at Tulane University, New Orleans; Jorge Cabrera, DO, an intensivist and assistant professor of medicine at the University of Miami; Alice Gallo de Moraes, MD, a pulmonary critical care doctor at Mayo Clinic, Rochester, Minn.; Fernando Caceres, MD, a pulmonary critical care specialist at the Billings (Mont.) Clinic; and Aldo Pavon Canseco, MD, a hospitalist and assistant professor of medicine at the University of Miami who was trained as a pediatric anesthesiologist.
Over 3 hours, hospitalists first heard tips for airway management, with words of caution, and then did hands-on work using manikins under the guidance of the faculty members with a low trainee-to-instructor ratio.
“Do the basics well and the scary things will become manageable,” Dr. Cabrera said in the session.
Instructors said it was vital to have a checklist in the form of a mnemonic device, and to have not just Plan A for clearing an airway, but Plans B and C, too.
Dr. Ariza told the learners not to focus too much on intubation — it’s not always necessary. In fact, he said he couldn’t over-emphasize the importance of mastering bag-mask ventilation, a go-to method when other approaches fail.
Participants learned about devices that can be deployed through the nose to keep the airway clear, those that can be used in the mouth but that might not go down quite as far as the lung, an inflatable bag that can be placed over patients’ mouths and squeezed to help with their breathing, and endotracheal tubes.
Dr. Lenchus said that more training would likely be needed for most clinicians – perhaps with other faculty at their own institutions – before they could be expected to employ these techniques in a real-life emergency situation.
Welcome to Day 2 of HM19!
Hospitalists, welcome to Day 2 of HM19 – the only meeting solely dedicated to the training and advancement of hospitalists.

What an exciting start to the meeting. Pre-Course Day on Sunday focused on some key skills essential to hospitalists – from ultrasound to practice management and palliative care, hospitalists mastered new expertise and forged new collaborations with colleagues. On Monday, Dr. Marc Harrison’s keynote address kicked us off, reminding us of the critical role we all play in population health management. I was thrilled to see the recognition of our new class of SHM Fellows, Senior Fellows, and Masters – a testament to the hard work and dedication of many providers who bear the name “hospitalist.”
Today, we have yet another energizing day of thought-provoking plenaries and educational sessions. Starting off with the Best of Research and Innovations in 2019, come and learn from our colleagues about advancements in hospital medicine. Next, we celebrate our hospitalists who have demonstrated exemplary contributions in teaching, clinical excellence, and service in our Awards of Excellence. The plenary will be led by Tait Shanafelt, MD, who will discuss “The High Cost of Clinician Burnout” and how we can ensure wellness and wellbeing in a dynamic health care environment with competing priorities and an ever-increasing demand for quality, volume, and patient satisfaction. Don’t miss out on the sessions and workshops scheduled at 11:00 a.m. to 12:30 p.m., on topics from nutritional counseling to “Things We Do for No Reason,” updates in acute coronary syndrome and heart failure, and telemedicine – you’re sure to find an engaging topic of interest.
After lunch, we have the highly anticipated and always entertaining “Update in Hospital Medicine” by Carrie Herzke, MD, SFHM, and Chris Moriates, MD, SFHM. Learn the latest and most high-impact published research influencing our practice. You can attend several sessions this afternoon, from a review of medical marijuana, being fe(male) in hospital medicine, dermatologic exam pearls, top new guidelines in hospital medicine, and understanding and addressing the educational needs of millennium learners.
Plan your evening around SHM’s exciting offerings and opportunities:
- Special Interest Forums: Connects hospitalists with a variety of interests from across the country and the globe.
- Top Pediatric Articles in 2018: Leverages the expertise of our leaders to highlight key areas of research advancement for the care of our pediatric patients.
- Solving Clinical and Cultural Conundrums in the Rubik’s Cube of NP/PA/MD/DO HM Practice: Discusses the key challenges we face in the day-to-day practice of hospital medicine and practice management.
- Mastering the Job Interview: Builds skills for our student and resident attendees.
Our heartfelt thank you to the amazing SHM staff who have worked tirelessly on HM19 – our gratitude to the Annual Conference Committee and all our faculty who have made this meeting a tremendous success. Enjoy Day 2!
Dr. Afsar is president of the Society of Hospital Medicine, and chief ambulatory officer and chief medical officer for accountable care organizations at UC Irvine Health.
Hospitalists, welcome to Day 2 of HM19 – the only meeting solely dedicated to the training and advancement of hospitalists.
What an exciting start to the meeting. Pre-Course Day on Sunday focused on some key skills essential to hospitalists – from ultrasound to practice management and palliative care, hospitalists mastered new expertise and forged new collaborations with colleagues. On Monday, Dr. Marc Harrison’s keynote address kicked us off, reminding us of the critical role we all play in population health management. I was thrilled to see the recognition of our new class of SHM Fellows, Senior Fellows, and Masters – a testament to the hard work and dedication of many providers who bear the name “hospitalist.”
Today, we have yet another energizing day of thought-provoking plenaries and educational sessions. Starting off with the Best of Research and Innovations in 2019, come and learn from our colleagues about advancements in hospital medicine. Next, we celebrate our hospitalists who have demonstrated exemplary contributions in teaching, clinical excellence, and service in our Awards of Excellence. The plenary will be led by Tait Shanafelt, MD, who will discuss “The High Cost of Clinician Burnout” and how we can ensure wellness and wellbeing in a dynamic health care environment with competing priorities and an ever-increasing demand for quality, volume, and patient satisfaction. Don’t miss out on the sessions and workshops scheduled at 11:00 a.m. to 12:30 p.m., on topics from nutritional counseling to “Things We Do for No Reason,” updates in acute coronary syndrome and heart failure, and telemedicine – you’re sure to find an engaging topic of interest.
After lunch, we have the highly anticipated and always entertaining “Update in Hospital Medicine” by Carrie Herzke, MD, SFHM, and Chris Moriates, MD, SFHM. Learn the latest and most high-impact published research influencing our practice. You can attend several sessions this afternoon, from a review of medical marijuana, being fe(male) in hospital medicine, dermatologic exam pearls, top new guidelines in hospital medicine, and understanding and addressing the educational needs of millennium learners.
Plan your evening around SHM’s exciting offerings and opportunities:
- Special Interest Forums: Connects hospitalists with a variety of interests from across the country and the globe.
- Top Pediatric Articles in 2018: Leverages the expertise of our leaders to highlight key areas of research advancement for the care of our pediatric patients.
- Solving Clinical and Cultural Conundrums in the Rubik’s Cube of NP/PA/MD/DO HM Practice: Discusses the key challenges we face in the day-to-day practice of hospital medicine and practice management.
- Mastering the Job Interview: Builds skills for our student and resident attendees.
Our heartfelt thank you to the amazing SHM staff who have worked tirelessly on HM19 – our gratitude to the Annual Conference Committee and all our faculty who have made this meeting a tremendous success. Enjoy Day 2!
Dr. Afsar is president of the Society of Hospital Medicine, and chief ambulatory officer and chief medical officer for accountable care organizations at UC Irvine Health.
Hospitalists, welcome to Day 2 of HM19 – the only meeting solely dedicated to the training and advancement of hospitalists.
What an exciting start to the meeting. Pre-Course Day on Sunday focused on some key skills essential to hospitalists – from ultrasound to practice management and palliative care, hospitalists mastered new expertise and forged new collaborations with colleagues. On Monday, Dr. Marc Harrison’s keynote address kicked us off, reminding us of the critical role we all play in population health management. I was thrilled to see the recognition of our new class of SHM Fellows, Senior Fellows, and Masters – a testament to the hard work and dedication of many providers who bear the name “hospitalist.”
Today, we have yet another energizing day of thought-provoking plenaries and educational sessions. Starting off with the Best of Research and Innovations in 2019, come and learn from our colleagues about advancements in hospital medicine. Next, we celebrate our hospitalists who have demonstrated exemplary contributions in teaching, clinical excellence, and service in our Awards of Excellence. The plenary will be led by Tait Shanafelt, MD, who will discuss “The High Cost of Clinician Burnout” and how we can ensure wellness and wellbeing in a dynamic health care environment with competing priorities and an ever-increasing demand for quality, volume, and patient satisfaction. Don’t miss out on the sessions and workshops scheduled at 11:00 a.m. to 12:30 p.m., on topics from nutritional counseling to “Things We Do for No Reason,” updates in acute coronary syndrome and heart failure, and telemedicine – you’re sure to find an engaging topic of interest.
After lunch, we have the highly anticipated and always entertaining “Update in Hospital Medicine” by Carrie Herzke, MD, SFHM, and Chris Moriates, MD, SFHM. Learn the latest and most high-impact published research influencing our practice. You can attend several sessions this afternoon, from a review of medical marijuana, being fe(male) in hospital medicine, dermatologic exam pearls, top new guidelines in hospital medicine, and understanding and addressing the educational needs of millennium learners.
Plan your evening around SHM’s exciting offerings and opportunities:
- Special Interest Forums: Connects hospitalists with a variety of interests from across the country and the globe.
- Top Pediatric Articles in 2018: Leverages the expertise of our leaders to highlight key areas of research advancement for the care of our pediatric patients.
- Solving Clinical and Cultural Conundrums in the Rubik’s Cube of NP/PA/MD/DO HM Practice: Discusses the key challenges we face in the day-to-day practice of hospital medicine and practice management.
- Mastering the Job Interview: Builds skills for our student and resident attendees.
Our heartfelt thank you to the amazing SHM staff who have worked tirelessly on HM19 – our gratitude to the Annual Conference Committee and all our faculty who have made this meeting a tremendous success. Enjoy Day 2!
Dr. Afsar is president of the Society of Hospital Medicine, and chief ambulatory officer and chief medical officer for accountable care organizations at UC Irvine Health.
Why did you choose to become a hospitalist? (VIDEO)
HM19 attendees explain why they became hospitalists.

HM19 attendees explain why they became hospitalists.
HM19 attendees explain why they became hospitalists.

SHM honors extraordinary leader, editor
When Andrew Auerbach, MD, MPH, SFHM, started as a hospitalist, his specialty didn’t have a name. His title was simply “medical director.” Now, 2 decades later, he is a professor of medicine at the University of California, San Francisco, and one of the most experienced and influential hospitalists in the field.
SHM will honor Dr. Auerbach and celebrate his achievements today at HM19, at the Awards plenary following the Chapter Awards of Excellence ceremony that begins at 8:30 a.m. SHM president Nasim Afsar, MD, SFHM, will present him with a plaque and review his contributions to the growth of the Journal of Hospital Medicine.
Throughout his career, even going back to the days he helped to found the Society of Hospital Medicine, Dr. Auerbach has played a crucial role in defining how a hospitalist works and thinks. Over the last 7 years, he led the Journal of Hospital Medicine through an extraordinary period of growth that has secured its reputation as a crucial resource for hospitalists and beyond.
“Andy Auerbach transformed the Journal of Hospital Medicine from the status of a ‘start-up’ Version 1.0 to a polished, efficient machine – Version 2.0. His efforts garnered the national respect that JHM deserves,” said Mark Williams, MD, MHM, University of Kentucky HealthCare hospital medicine division chief and tenured professor of medicine. Dr. Williams served as editor in chief of the journal immediately prior to Dr. Auerbach. “I hope Andy will be known as the editor who transformed an acceptable journal into a stellar example of what a medical journal can become.”
Samir S. Shah, MD, MSCE, MHM, who has replaced Dr. Auerbach as editor in chief of the journal, also has praise for his predecessor. “Andy has really invested in advancing scholarship in hospital medicine and ensuring that great work is broadly disseminated,” said Dr. Shah, chief of hospital medicine at Cincinnati Children’s Hospital Medical Center.
Dr. Auerbach said his interest in inpatient and perioperative care sparked his focus on hospital medicine. “My initial research was foundational for the field. I wanted to understand, refine, and improve our role: Do hospitalists improve care and outcomes? Do they affect patient perceptions of their doctors?”
At the time, hospital medicine felt like a 1990s dot-com startup, he recalled, but one that was destined to last. “It was clear that hospital medicine was going to take off, but the academic pursuits were taking longer to get going. We were starting from zero.”
Enter the Journal of Hospital Medicine. The publication received about 200 submissions a year when Dr. Auerbach took over as editor in chief. Now, it receives more than 800.
The higher number of submissions allows editors to be more selective about the papers that are published. At the same time, the growth in the journal’s profile and influence has allowed it to evolve into a more wide-ranging publication, Dr. Auerbach said.
“Geriatricians and nephrologists are sending us papers,” he said. “They believe our work is important, and they understand that we’re publishing research about topics such as acute kidney injury, delirium, inpatient safety issues, and transfer of care.”
According to Dr. Williams, his successor has played a crucial role in the journal’s success. “Andy improved the response rate of JHM, dramatically shortening the time for reviews while maintaining and even improving the quality of reviews,” he said. “This single act profoundly impacted author satisfaction and drove the increased number of article submissions.”
Dr. Auerbach also revolutionized the journal’s approach to technology. “Under his leadership, the journal pioneered the use of social media to engage readers in ways that were fundamentally different from established processes at the time,” said new editor in chief Dr. Shah. “For example, the journal has created roles for social media editors, and it routinely publishes visual abstracts to provide readers with a quick overview of journal research. We also hold regular dialogues with readers via our #JHMChat Twitter journal club to engage them in discussing the latest research published in JHM.”
Dr. Shah also noted that Dr. Auerbach boosted hospital medicine and the journal in other ways during his tenure. “He encouraged the team of editors to engage with our authors in meaningful and substantive ways. That meant encouraging thoughtful feedback and also reaching out to authors directly to provide additional guidance as they revised their manuscript and, oftentimes, as they prepared to submit their manuscript elsewhere,” he said.
In addition, Dr. Shah said that his colleague “also created the JHM editorial fellowship as a way to help develop the pipeline for academic leadership. This fellowship provides chief residents, academic hospital medicine fellows, and junior faculty an opportunity to learn about medical publishing, hone their skills in evaluating research and writing, and network with leaders in the field.”
For his part, Dr. Auerbach hopes his legacy at the journal will include an expansion, perhaps within a year or 2. “I’d love to see the journal come out twice a month,” he said. “There’s enough potential science out there, and I think it could be in that position soon.”
Awards of Excellence
Tuesday, 8:30 – 9:10 a.m.
Potomac ABCD
When Andrew Auerbach, MD, MPH, SFHM, started as a hospitalist, his specialty didn’t have a name. His title was simply “medical director.” Now, 2 decades later, he is a professor of medicine at the University of California, San Francisco, and one of the most experienced and influential hospitalists in the field.
SHM will honor Dr. Auerbach and celebrate his achievements today at HM19, at the Awards plenary following the Chapter Awards of Excellence ceremony that begins at 8:30 a.m. SHM president Nasim Afsar, MD, SFHM, will present him with a plaque and review his contributions to the growth of the Journal of Hospital Medicine.
Throughout his career, even going back to the days he helped to found the Society of Hospital Medicine, Dr. Auerbach has played a crucial role in defining how a hospitalist works and thinks. Over the last 7 years, he led the Journal of Hospital Medicine through an extraordinary period of growth that has secured its reputation as a crucial resource for hospitalists and beyond.
“Andy Auerbach transformed the Journal of Hospital Medicine from the status of a ‘start-up’ Version 1.0 to a polished, efficient machine – Version 2.0. His efforts garnered the national respect that JHM deserves,” said Mark Williams, MD, MHM, University of Kentucky HealthCare hospital medicine division chief and tenured professor of medicine. Dr. Williams served as editor in chief of the journal immediately prior to Dr. Auerbach. “I hope Andy will be known as the editor who transformed an acceptable journal into a stellar example of what a medical journal can become.”
Samir S. Shah, MD, MSCE, MHM, who has replaced Dr. Auerbach as editor in chief of the journal, also has praise for his predecessor. “Andy has really invested in advancing scholarship in hospital medicine and ensuring that great work is broadly disseminated,” said Dr. Shah, chief of hospital medicine at Cincinnati Children’s Hospital Medical Center.
Dr. Auerbach said his interest in inpatient and perioperative care sparked his focus on hospital medicine. “My initial research was foundational for the field. I wanted to understand, refine, and improve our role: Do hospitalists improve care and outcomes? Do they affect patient perceptions of their doctors?”
At the time, hospital medicine felt like a 1990s dot-com startup, he recalled, but one that was destined to last. “It was clear that hospital medicine was going to take off, but the academic pursuits were taking longer to get going. We were starting from zero.”
Enter the Journal of Hospital Medicine. The publication received about 200 submissions a year when Dr. Auerbach took over as editor in chief. Now, it receives more than 800.
The higher number of submissions allows editors to be more selective about the papers that are published. At the same time, the growth in the journal’s profile and influence has allowed it to evolve into a more wide-ranging publication, Dr. Auerbach said.
“Geriatricians and nephrologists are sending us papers,” he said. “They believe our work is important, and they understand that we’re publishing research about topics such as acute kidney injury, delirium, inpatient safety issues, and transfer of care.”
According to Dr. Williams, his successor has played a crucial role in the journal’s success. “Andy improved the response rate of JHM, dramatically shortening the time for reviews while maintaining and even improving the quality of reviews,” he said. “This single act profoundly impacted author satisfaction and drove the increased number of article submissions.”
Dr. Auerbach also revolutionized the journal’s approach to technology. “Under his leadership, the journal pioneered the use of social media to engage readers in ways that were fundamentally different from established processes at the time,” said new editor in chief Dr. Shah. “For example, the journal has created roles for social media editors, and it routinely publishes visual abstracts to provide readers with a quick overview of journal research. We also hold regular dialogues with readers via our #JHMChat Twitter journal club to engage them in discussing the latest research published in JHM.”
Dr. Shah also noted that Dr. Auerbach boosted hospital medicine and the journal in other ways during his tenure. “He encouraged the team of editors to engage with our authors in meaningful and substantive ways. That meant encouraging thoughtful feedback and also reaching out to authors directly to provide additional guidance as they revised their manuscript and, oftentimes, as they prepared to submit their manuscript elsewhere,” he said.
In addition, Dr. Shah said that his colleague “also created the JHM editorial fellowship as a way to help develop the pipeline for academic leadership. This fellowship provides chief residents, academic hospital medicine fellows, and junior faculty an opportunity to learn about medical publishing, hone their skills in evaluating research and writing, and network with leaders in the field.”
For his part, Dr. Auerbach hopes his legacy at the journal will include an expansion, perhaps within a year or 2. “I’d love to see the journal come out twice a month,” he said. “There’s enough potential science out there, and I think it could be in that position soon.”
Awards of Excellence
Tuesday, 8:30 – 9:10 a.m.
Potomac ABCD
When Andrew Auerbach, MD, MPH, SFHM, started as a hospitalist, his specialty didn’t have a name. His title was simply “medical director.” Now, 2 decades later, he is a professor of medicine at the University of California, San Francisco, and one of the most experienced and influential hospitalists in the field.
SHM will honor Dr. Auerbach and celebrate his achievements today at HM19, at the Awards plenary following the Chapter Awards of Excellence ceremony that begins at 8:30 a.m. SHM president Nasim Afsar, MD, SFHM, will present him with a plaque and review his contributions to the growth of the Journal of Hospital Medicine.
Throughout his career, even going back to the days he helped to found the Society of Hospital Medicine, Dr. Auerbach has played a crucial role in defining how a hospitalist works and thinks. Over the last 7 years, he led the Journal of Hospital Medicine through an extraordinary period of growth that has secured its reputation as a crucial resource for hospitalists and beyond.
“Andy Auerbach transformed the Journal of Hospital Medicine from the status of a ‘start-up’ Version 1.0 to a polished, efficient machine – Version 2.0. His efforts garnered the national respect that JHM deserves,” said Mark Williams, MD, MHM, University of Kentucky HealthCare hospital medicine division chief and tenured professor of medicine. Dr. Williams served as editor in chief of the journal immediately prior to Dr. Auerbach. “I hope Andy will be known as the editor who transformed an acceptable journal into a stellar example of what a medical journal can become.”
Samir S. Shah, MD, MSCE, MHM, who has replaced Dr. Auerbach as editor in chief of the journal, also has praise for his predecessor. “Andy has really invested in advancing scholarship in hospital medicine and ensuring that great work is broadly disseminated,” said Dr. Shah, chief of hospital medicine at Cincinnati Children’s Hospital Medical Center.
Dr. Auerbach said his interest in inpatient and perioperative care sparked his focus on hospital medicine. “My initial research was foundational for the field. I wanted to understand, refine, and improve our role: Do hospitalists improve care and outcomes? Do they affect patient perceptions of their doctors?”
At the time, hospital medicine felt like a 1990s dot-com startup, he recalled, but one that was destined to last. “It was clear that hospital medicine was going to take off, but the academic pursuits were taking longer to get going. We were starting from zero.”
Enter the Journal of Hospital Medicine. The publication received about 200 submissions a year when Dr. Auerbach took over as editor in chief. Now, it receives more than 800.
The higher number of submissions allows editors to be more selective about the papers that are published. At the same time, the growth in the journal’s profile and influence has allowed it to evolve into a more wide-ranging publication, Dr. Auerbach said.
“Geriatricians and nephrologists are sending us papers,” he said. “They believe our work is important, and they understand that we’re publishing research about topics such as acute kidney injury, delirium, inpatient safety issues, and transfer of care.”
According to Dr. Williams, his successor has played a crucial role in the journal’s success. “Andy improved the response rate of JHM, dramatically shortening the time for reviews while maintaining and even improving the quality of reviews,” he said. “This single act profoundly impacted author satisfaction and drove the increased number of article submissions.”
Dr. Auerbach also revolutionized the journal’s approach to technology. “Under his leadership, the journal pioneered the use of social media to engage readers in ways that were fundamentally different from established processes at the time,” said new editor in chief Dr. Shah. “For example, the journal has created roles for social media editors, and it routinely publishes visual abstracts to provide readers with a quick overview of journal research. We also hold regular dialogues with readers via our #JHMChat Twitter journal club to engage them in discussing the latest research published in JHM.”
Dr. Shah also noted that Dr. Auerbach boosted hospital medicine and the journal in other ways during his tenure. “He encouraged the team of editors to engage with our authors in meaningful and substantive ways. That meant encouraging thoughtful feedback and also reaching out to authors directly to provide additional guidance as they revised their manuscript and, oftentimes, as they prepared to submit their manuscript elsewhere,” he said.
In addition, Dr. Shah said that his colleague “also created the JHM editorial fellowship as a way to help develop the pipeline for academic leadership. This fellowship provides chief residents, academic hospital medicine fellows, and junior faculty an opportunity to learn about medical publishing, hone their skills in evaluating research and writing, and network with leaders in the field.”
For his part, Dr. Auerbach hopes his legacy at the journal will include an expansion, perhaps within a year or 2. “I’d love to see the journal come out twice a month,” he said. “There’s enough potential science out there, and I think it could be in that position soon.”
Awards of Excellence
Tuesday, 8:30 – 9:10 a.m.
Potomac ABCD
Cancer researchers take home AACR honors
The American Association for Cancer Research (AACR) has granted 14 awards and lectureships to cancer researchers and plans to recognize the recipients at the annual meeting of the American Association for Cancer Research.
Emil J. Freireich, MD, of the University of Texas MD Anderson Cancer Center in Houston, has won the 16th AACR Award for Lifetime Achievement in Cancer Research. AACR cited Dr. Freireich’s contributions related to leukocyte and allogeneic platelet transfusions, engraftment of peripheral blood stem cells, and combination chemotherapy approaches in the treatment of childhood leukemia. Dr. Freireich will receive the award during the opening ceremony of the meeting on March 31.
Another award to be given at the opening ceremony is the 13th Margaret Foti Award for Leadership and Extraordinary Achievements in Cancer Research. Raymond N. DuBois, MD, PhD, of the Medical University of South Carolina in Charleston, will receive the award for his contributions to the “early detection, interception, and prevention of colorectal cancer.” This includes elucidating the role of prostaglandins and cyclooxygenase in colon cancer tumorigenesis and pioneering the use of nonsteroidal anti-inflammatory mediators for cancer prevention. Dr. DuBois will deliver the lecture “Inflammation and Inflammatory Mediators as Potential Targets for Cancer Prevention or Interception” on April 1.

Jennifer R. Grandis, MD, of the University of California, San Francisco, has won the 22nd AACR–Women in Cancer Research Charlotte Friend Memorial Lectureship. Dr. Grandis characterized the role of EGFR, STAT3, and other signaling pathways in head and neck squamous cell carcinoma and used the findings to uncover new treatment options. Dr. Grandis will deliver her award lecture, “Leveraging Biologic Insights to Prevent and Treat Head and Neck Cancer,” on March 30.![]()
John M. Carethers, MD, of the University of Michigan in Ann Arbor, has won the 14th AACR–Minorities in Cancer Research Jane Cooke Wright Memorial Lectureship. Dr. Carethers is being recognized for his work related to DNA mismatch repair, tumor resistance, inflammation, and health disparities in colorectal cancer patients. He will deliver his award lecture, “A Role for Inflammation-Induced DNA Mismatch Repair Deficits in Racial Outcomes from Advanced Colorectal Cancer,” on March 31.
Susan L. Cohn, MD, of the University of Chicago, has won the 24th AACR–Joseph H. Burchenal Memorial Award for Outstanding Achievement in Clinical Cancer Research (supported by Bristol-Myers Squibb). She won this award for her work in refining pediatric cancer risk-group classification, making discoveries that changed treatment strategies, and creating computational frameworks that enabled data collection and sharing. Dr. Cohn will deliver her award lecture, “Advancing Treatment Through Collaboration: A Pediatric Oncology Paradigm,” on April 2.
Another awardee to be recognized at the meeting is Alberto Mantovani, MD, a professor at Humanitas University in Milan, Italy, who won the 22nd Pezcoller Foundation–AACR International Award for Extraordinary Achievement in Cancer Research (supported by the Pezcoller Foundation).
Jeffrey A. Bluestone, PhD, of the University of California, San Francisco, won the 15th AACR–Irving Weinstein Foundation Distinguished Lecture (supported by the Irving Weinstein Foundation).
Andrew T. Chan, MD, of Massachusetts General Hospital in Boston, won the Third AACR–Waun Ki Hong Award for Outstanding Achievement in Translational and Clinical Cancer Research.
Elaine Fuchs, PhD, of Rockefeller University in New York, won the 59th AACR G.H.A. Clowes Memorial Award (supported by Lilly Oncology).
Charles L. Sawyers, MD, of the Memorial Sloan Kettering Cancer Center in New York, won the 13th AACR Princess Takamatsu Memorial Lectureship (supported by the Princess Takamatsu Cancer Research Fund).
Michael E. Jung, PhD, of the University of California, Los Angeles, won the 13th AACR Award for Outstanding Achievement in Chemistry in Cancer Research.
Cornelis J.M. Melief, MD, PhD, of Leiden (the Netherlands) University Medical Center and ISA Pharmaceuticals, also in Leiden, won the Seventh AACR–Cancer Research Institute Lloyd J. Old Award in Cancer Immunology (supported by the Cancer Research Institute).
Edward L. Giovannucci, MD, of the Harvard T.H. Chan School of Public Health in Boston, won the 28th AACR-American Cancer Society Award for Research Excellence in Cancer Epidemiology and Prevention (supported by the American Cancer Society).
Melissa M. Hudson, MD, and 15 other researchers from St. Jude Children’s Research Hospital in Memphis won the 13th AACR Team Science Award (supported by Lilly Oncology).
Movers in Medicine highlights career moves and personal achievements by hematologists and oncologists. Did you switch jobs, take on a new role, climb a mountain? Tell us all about it at hematologynews@mdedge.com, and you could be featured in Movers in Medicine.
The American Association for Cancer Research (AACR) has granted 14 awards and lectureships to cancer researchers and plans to recognize the recipients at the annual meeting of the American Association for Cancer Research.
Emil J. Freireich, MD, of the University of Texas MD Anderson Cancer Center in Houston, has won the 16th AACR Award for Lifetime Achievement in Cancer Research. AACR cited Dr. Freireich’s contributions related to leukocyte and allogeneic platelet transfusions, engraftment of peripheral blood stem cells, and combination chemotherapy approaches in the treatment of childhood leukemia. Dr. Freireich will receive the award during the opening ceremony of the meeting on March 31.
Another award to be given at the opening ceremony is the 13th Margaret Foti Award for Leadership and Extraordinary Achievements in Cancer Research. Raymond N. DuBois, MD, PhD, of the Medical University of South Carolina in Charleston, will receive the award for his contributions to the “early detection, interception, and prevention of colorectal cancer.” This includes elucidating the role of prostaglandins and cyclooxygenase in colon cancer tumorigenesis and pioneering the use of nonsteroidal anti-inflammatory mediators for cancer prevention. Dr. DuBois will deliver the lecture “Inflammation and Inflammatory Mediators as Potential Targets for Cancer Prevention or Interception” on April 1.
Jennifer R. Grandis, MD, of the University of California, San Francisco, has won the 22nd AACR–Women in Cancer Research Charlotte Friend Memorial Lectureship. Dr. Grandis characterized the role of EGFR, STAT3, and other signaling pathways in head and neck squamous cell carcinoma and used the findings to uncover new treatment options. Dr. Grandis will deliver her award lecture, “Leveraging Biologic Insights to Prevent and Treat Head and Neck Cancer,” on March 30.![]()
John M. Carethers, MD, of the University of Michigan in Ann Arbor, has won the 14th AACR–Minorities in Cancer Research Jane Cooke Wright Memorial Lectureship. Dr. Carethers is being recognized for his work related to DNA mismatch repair, tumor resistance, inflammation, and health disparities in colorectal cancer patients. He will deliver his award lecture, “A Role for Inflammation-Induced DNA Mismatch Repair Deficits in Racial Outcomes from Advanced Colorectal Cancer,” on March 31.
Susan L. Cohn, MD, of the University of Chicago, has won the 24th AACR–Joseph H. Burchenal Memorial Award for Outstanding Achievement in Clinical Cancer Research (supported by Bristol-Myers Squibb). She won this award for her work in refining pediatric cancer risk-group classification, making discoveries that changed treatment strategies, and creating computational frameworks that enabled data collection and sharing. Dr. Cohn will deliver her award lecture, “Advancing Treatment Through Collaboration: A Pediatric Oncology Paradigm,” on April 2.
Another awardee to be recognized at the meeting is Alberto Mantovani, MD, a professor at Humanitas University in Milan, Italy, who won the 22nd Pezcoller Foundation–AACR International Award for Extraordinary Achievement in Cancer Research (supported by the Pezcoller Foundation).
Jeffrey A. Bluestone, PhD, of the University of California, San Francisco, won the 15th AACR–Irving Weinstein Foundation Distinguished Lecture (supported by the Irving Weinstein Foundation).
Andrew T. Chan, MD, of Massachusetts General Hospital in Boston, won the Third AACR–Waun Ki Hong Award for Outstanding Achievement in Translational and Clinical Cancer Research.
Elaine Fuchs, PhD, of Rockefeller University in New York, won the 59th AACR G.H.A. Clowes Memorial Award (supported by Lilly Oncology).
Charles L. Sawyers, MD, of the Memorial Sloan Kettering Cancer Center in New York, won the 13th AACR Princess Takamatsu Memorial Lectureship (supported by the Princess Takamatsu Cancer Research Fund).
Michael E. Jung, PhD, of the University of California, Los Angeles, won the 13th AACR Award for Outstanding Achievement in Chemistry in Cancer Research.
Cornelis J.M. Melief, MD, PhD, of Leiden (the Netherlands) University Medical Center and ISA Pharmaceuticals, also in Leiden, won the Seventh AACR–Cancer Research Institute Lloyd J. Old Award in Cancer Immunology (supported by the Cancer Research Institute).
Edward L. Giovannucci, MD, of the Harvard T.H. Chan School of Public Health in Boston, won the 28th AACR-American Cancer Society Award for Research Excellence in Cancer Epidemiology and Prevention (supported by the American Cancer Society).
Melissa M. Hudson, MD, and 15 other researchers from St. Jude Children’s Research Hospital in Memphis won the 13th AACR Team Science Award (supported by Lilly Oncology).
Movers in Medicine highlights career moves and personal achievements by hematologists and oncologists. Did you switch jobs, take on a new role, climb a mountain? Tell us all about it at hematologynews@mdedge.com, and you could be featured in Movers in Medicine.
The American Association for Cancer Research (AACR) has granted 14 awards and lectureships to cancer researchers and plans to recognize the recipients at the annual meeting of the American Association for Cancer Research.
Emil J. Freireich, MD, of the University of Texas MD Anderson Cancer Center in Houston, has won the 16th AACR Award for Lifetime Achievement in Cancer Research. AACR cited Dr. Freireich’s contributions related to leukocyte and allogeneic platelet transfusions, engraftment of peripheral blood stem cells, and combination chemotherapy approaches in the treatment of childhood leukemia. Dr. Freireich will receive the award during the opening ceremony of the meeting on March 31.
Another award to be given at the opening ceremony is the 13th Margaret Foti Award for Leadership and Extraordinary Achievements in Cancer Research. Raymond N. DuBois, MD, PhD, of the Medical University of South Carolina in Charleston, will receive the award for his contributions to the “early detection, interception, and prevention of colorectal cancer.” This includes elucidating the role of prostaglandins and cyclooxygenase in colon cancer tumorigenesis and pioneering the use of nonsteroidal anti-inflammatory mediators for cancer prevention. Dr. DuBois will deliver the lecture “Inflammation and Inflammatory Mediators as Potential Targets for Cancer Prevention or Interception” on April 1.
Jennifer R. Grandis, MD, of the University of California, San Francisco, has won the 22nd AACR–Women in Cancer Research Charlotte Friend Memorial Lectureship. Dr. Grandis characterized the role of EGFR, STAT3, and other signaling pathways in head and neck squamous cell carcinoma and used the findings to uncover new treatment options. Dr. Grandis will deliver her award lecture, “Leveraging Biologic Insights to Prevent and Treat Head and Neck Cancer,” on March 30.![]()
John M. Carethers, MD, of the University of Michigan in Ann Arbor, has won the 14th AACR–Minorities in Cancer Research Jane Cooke Wright Memorial Lectureship. Dr. Carethers is being recognized for his work related to DNA mismatch repair, tumor resistance, inflammation, and health disparities in colorectal cancer patients. He will deliver his award lecture, “A Role for Inflammation-Induced DNA Mismatch Repair Deficits in Racial Outcomes from Advanced Colorectal Cancer,” on March 31.
Susan L. Cohn, MD, of the University of Chicago, has won the 24th AACR–Joseph H. Burchenal Memorial Award for Outstanding Achievement in Clinical Cancer Research (supported by Bristol-Myers Squibb). She won this award for her work in refining pediatric cancer risk-group classification, making discoveries that changed treatment strategies, and creating computational frameworks that enabled data collection and sharing. Dr. Cohn will deliver her award lecture, “Advancing Treatment Through Collaboration: A Pediatric Oncology Paradigm,” on April 2.
Another awardee to be recognized at the meeting is Alberto Mantovani, MD, a professor at Humanitas University in Milan, Italy, who won the 22nd Pezcoller Foundation–AACR International Award for Extraordinary Achievement in Cancer Research (supported by the Pezcoller Foundation).
Jeffrey A. Bluestone, PhD, of the University of California, San Francisco, won the 15th AACR–Irving Weinstein Foundation Distinguished Lecture (supported by the Irving Weinstein Foundation).
Andrew T. Chan, MD, of Massachusetts General Hospital in Boston, won the Third AACR–Waun Ki Hong Award for Outstanding Achievement in Translational and Clinical Cancer Research.
Elaine Fuchs, PhD, of Rockefeller University in New York, won the 59th AACR G.H.A. Clowes Memorial Award (supported by Lilly Oncology).
Charles L. Sawyers, MD, of the Memorial Sloan Kettering Cancer Center in New York, won the 13th AACR Princess Takamatsu Memorial Lectureship (supported by the Princess Takamatsu Cancer Research Fund).
Michael E. Jung, PhD, of the University of California, Los Angeles, won the 13th AACR Award for Outstanding Achievement in Chemistry in Cancer Research.
Cornelis J.M. Melief, MD, PhD, of Leiden (the Netherlands) University Medical Center and ISA Pharmaceuticals, also in Leiden, won the Seventh AACR–Cancer Research Institute Lloyd J. Old Award in Cancer Immunology (supported by the Cancer Research Institute).
Edward L. Giovannucci, MD, of the Harvard T.H. Chan School of Public Health in Boston, won the 28th AACR-American Cancer Society Award for Research Excellence in Cancer Epidemiology and Prevention (supported by the American Cancer Society).
Melissa M. Hudson, MD, and 15 other researchers from St. Jude Children’s Research Hospital in Memphis won the 13th AACR Team Science Award (supported by Lilly Oncology).
Movers in Medicine highlights career moves and personal achievements by hematologists and oncologists. Did you switch jobs, take on a new role, climb a mountain? Tell us all about it at hematologynews@mdedge.com, and you could be featured in Movers in Medicine.
United States now over 300 measles cases for the year
Despite those 46 new cases, the number of states with reported cases remains at 15, the CDC reported March 25.
For the fifth consecutive week the busiest outbreak was in Brooklyn, N.Y., which added 23 new cases. New York’s Rockland County, which is just north of New York City and has 46 confirmed cases for the year, is home to another of the six current outbreaks in the country, with the other four located in Washington (74 total cases for the state), Texas (14 cases), California (7 cases), and Illinois (6 cases). Other states with cases are Arizona, Colorado, Connecticut, Georgia, Kentucky, Missouri, New Hampshire, New Jersey, and Oregon, reported the CDC.
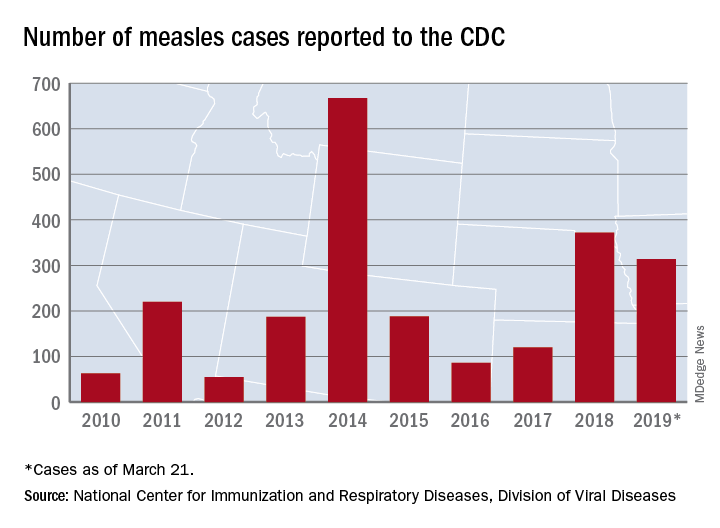
This year’s case total through less than 3 months is nearing the 372 that occurred in 2018, which was the second-worst year for measles in the last decade, but is still well off the 10-year high of 667 reported in 2014, the CDC said.
Despite those 46 new cases, the number of states with reported cases remains at 15, the CDC reported March 25.
For the fifth consecutive week the busiest outbreak was in Brooklyn, N.Y., which added 23 new cases. New York’s Rockland County, which is just north of New York City and has 46 confirmed cases for the year, is home to another of the six current outbreaks in the country, with the other four located in Washington (74 total cases for the state), Texas (14 cases), California (7 cases), and Illinois (6 cases). Other states with cases are Arizona, Colorado, Connecticut, Georgia, Kentucky, Missouri, New Hampshire, New Jersey, and Oregon, reported the CDC.
This year’s case total through less than 3 months is nearing the 372 that occurred in 2018, which was the second-worst year for measles in the last decade, but is still well off the 10-year high of 667 reported in 2014, the CDC said.
Despite those 46 new cases, the number of states with reported cases remains at 15, the CDC reported March 25.
For the fifth consecutive week the busiest outbreak was in Brooklyn, N.Y., which added 23 new cases. New York’s Rockland County, which is just north of New York City and has 46 confirmed cases for the year, is home to another of the six current outbreaks in the country, with the other four located in Washington (74 total cases for the state), Texas (14 cases), California (7 cases), and Illinois (6 cases). Other states with cases are Arizona, Colorado, Connecticut, Georgia, Kentucky, Missouri, New Hampshire, New Jersey, and Oregon, reported the CDC.
This year’s case total through less than 3 months is nearing the 372 that occurred in 2018, which was the second-worst year for measles in the last decade, but is still well off the 10-year high of 667 reported in 2014, the CDC said.
Hospitalists ‘in exactly the right place’ to move to value-based care
Hospitalists are uniquely positioned to be agents of change in the health care system, helping to care for very sick patients as well as identifying cost-efficient ways to keep them well, Marc Harrison, MD, said in his keynote presentation Monday at HM19.

“You’re in exactly the right place in exactly the right specialty to make an enormous difference for our country, which desperately needs an upgrade in terms of how we approach keeping people well and then taking care of people when they’re sick in a superefficient as well as independent fashion,” said Dr. Harrison, president and CEO of Intermountain Healthcare, based in Salt Lake City.
Hospital medicine, hospitalists, and the health care system in general are at an inflection point, and leading change in a positive fashion is the “single core competency” attendees need as health care transitions toward value-based care. This means moving away from a volume-based care model and asking hard questions about whether providers are doing the right things for patients, said Dr. Harrison at the Annual Conference of the Society of Hospital Medicine.
“It’s going to require humility, risk taking, and a desire to truly serve others if we’re going to change the paradigm for health care delivery,” he added.
About one-third of health care that providers deliver is redundant, which costs the United States approximately $1 trillion per year, Dr. Harrison noted. “There’s plenty of money in American health care; it’s just being misspent.”
Health care is “expensive, not consumer centric, and provides uneven quality,” which has spurred businesses like Google and Amazon to try to change the model. Other trends in the health care industry are an increased focus on mergers and acquisitions, negative growth outlook for hospitals, rural hospitals facing closure, and consumers increasingly demanding transparency in health care in such places as their hospital bills.
“We need to be on our front foot” to adapt to these changes, said Dr. Harrison, which means changing how money is spent in U.S. health care. There is currently a disparity: 10% of a person’s health care comes from hospitals and clinics, while 90% of money spent in U.S. health care is on that 10%. Spending should instead be inverted, focused on population-based health initiatives such as addressing social issues surrounding housing, transportation, and food security.
A crisis is coming for providers and health systems that continue to focus on volume-based care models instead of making hard changes to value-based care, said Dr. Harrison. Population-based health initiatives that should be implemented include lowering the cost of care by shifting to outpatient care models and lowering insurance premiums.
“It doesn’t matter how technically good you are if people can’t afford what you’re doing,” he said.
Population-based health initiatives also should be modernized to care upstream, fixing the cause of health problems rather than treating the symptoms. The goal, said Dr. Harrison, is a system with end-to-end seamless care, in which providers understand patients’ goals, are intentional about keeping their patients well, and can “ensure seamless handoff” to other caregivers.
Dr. Harrison said the future of hospital medicine is providing acute care in this way, and attendees are uniquely suited to take care of patients not only in the hospital but also at home, as well as providing consultations with colleagues in care environments without hospitalist programs.
“You’re in the absolute perfect place to keep patients in the least-restrictive, least-expensive environment where they can receive superb care,” he said.
Hospitalists are uniquely positioned to be agents of change in the health care system, helping to care for very sick patients as well as identifying cost-efficient ways to keep them well, Marc Harrison, MD, said in his keynote presentation Monday at HM19.
“You’re in exactly the right place in exactly the right specialty to make an enormous difference for our country, which desperately needs an upgrade in terms of how we approach keeping people well and then taking care of people when they’re sick in a superefficient as well as independent fashion,” said Dr. Harrison, president and CEO of Intermountain Healthcare, based in Salt Lake City.
Hospital medicine, hospitalists, and the health care system in general are at an inflection point, and leading change in a positive fashion is the “single core competency” attendees need as health care transitions toward value-based care. This means moving away from a volume-based care model and asking hard questions about whether providers are doing the right things for patients, said Dr. Harrison at the Annual Conference of the Society of Hospital Medicine.
“It’s going to require humility, risk taking, and a desire to truly serve others if we’re going to change the paradigm for health care delivery,” he added.
About one-third of health care that providers deliver is redundant, which costs the United States approximately $1 trillion per year, Dr. Harrison noted. “There’s plenty of money in American health care; it’s just being misspent.”
Health care is “expensive, not consumer centric, and provides uneven quality,” which has spurred businesses like Google and Amazon to try to change the model. Other trends in the health care industry are an increased focus on mergers and acquisitions, negative growth outlook for hospitals, rural hospitals facing closure, and consumers increasingly demanding transparency in health care in such places as their hospital bills.
“We need to be on our front foot” to adapt to these changes, said Dr. Harrison, which means changing how money is spent in U.S. health care. There is currently a disparity: 10% of a person’s health care comes from hospitals and clinics, while 90% of money spent in U.S. health care is on that 10%. Spending should instead be inverted, focused on population-based health initiatives such as addressing social issues surrounding housing, transportation, and food security.
A crisis is coming for providers and health systems that continue to focus on volume-based care models instead of making hard changes to value-based care, said Dr. Harrison. Population-based health initiatives that should be implemented include lowering the cost of care by shifting to outpatient care models and lowering insurance premiums.
“It doesn’t matter how technically good you are if people can’t afford what you’re doing,” he said.
Population-based health initiatives also should be modernized to care upstream, fixing the cause of health problems rather than treating the symptoms. The goal, said Dr. Harrison, is a system with end-to-end seamless care, in which providers understand patients’ goals, are intentional about keeping their patients well, and can “ensure seamless handoff” to other caregivers.
Dr. Harrison said the future of hospital medicine is providing acute care in this way, and attendees are uniquely suited to take care of patients not only in the hospital but also at home, as well as providing consultations with colleagues in care environments without hospitalist programs.
“You’re in the absolute perfect place to keep patients in the least-restrictive, least-expensive environment where they can receive superb care,” he said.
Hospitalists are uniquely positioned to be agents of change in the health care system, helping to care for very sick patients as well as identifying cost-efficient ways to keep them well, Marc Harrison, MD, said in his keynote presentation Monday at HM19.
“You’re in exactly the right place in exactly the right specialty to make an enormous difference for our country, which desperately needs an upgrade in terms of how we approach keeping people well and then taking care of people when they’re sick in a superefficient as well as independent fashion,” said Dr. Harrison, president and CEO of Intermountain Healthcare, based in Salt Lake City.
Hospital medicine, hospitalists, and the health care system in general are at an inflection point, and leading change in a positive fashion is the “single core competency” attendees need as health care transitions toward value-based care. This means moving away from a volume-based care model and asking hard questions about whether providers are doing the right things for patients, said Dr. Harrison at the Annual Conference of the Society of Hospital Medicine.
“It’s going to require humility, risk taking, and a desire to truly serve others if we’re going to change the paradigm for health care delivery,” he added.
About one-third of health care that providers deliver is redundant, which costs the United States approximately $1 trillion per year, Dr. Harrison noted. “There’s plenty of money in American health care; it’s just being misspent.”
Health care is “expensive, not consumer centric, and provides uneven quality,” which has spurred businesses like Google and Amazon to try to change the model. Other trends in the health care industry are an increased focus on mergers and acquisitions, negative growth outlook for hospitals, rural hospitals facing closure, and consumers increasingly demanding transparency in health care in such places as their hospital bills.
“We need to be on our front foot” to adapt to these changes, said Dr. Harrison, which means changing how money is spent in U.S. health care. There is currently a disparity: 10% of a person’s health care comes from hospitals and clinics, while 90% of money spent in U.S. health care is on that 10%. Spending should instead be inverted, focused on population-based health initiatives such as addressing social issues surrounding housing, transportation, and food security.
A crisis is coming for providers and health systems that continue to focus on volume-based care models instead of making hard changes to value-based care, said Dr. Harrison. Population-based health initiatives that should be implemented include lowering the cost of care by shifting to outpatient care models and lowering insurance premiums.
“It doesn’t matter how technically good you are if people can’t afford what you’re doing,” he said.
Population-based health initiatives also should be modernized to care upstream, fixing the cause of health problems rather than treating the symptoms. The goal, said Dr. Harrison, is a system with end-to-end seamless care, in which providers understand patients’ goals, are intentional about keeping their patients well, and can “ensure seamless handoff” to other caregivers.
Dr. Harrison said the future of hospital medicine is providing acute care in this way, and attendees are uniquely suited to take care of patients not only in the hospital but also at home, as well as providing consultations with colleagues in care environments without hospitalist programs.
“You’re in the absolute perfect place to keep patients in the least-restrictive, least-expensive environment where they can receive superb care,” he said.
Can intraputamenal infusions of GDNF treat Parkinson’s disease?
researchers reported. The investigational therapy, delivered through a skull-mounted port, was well tolerated in a 40-week, randomized, controlled trial and a 40-week, open-label extension.
Neither study met its primary endpoint, but post hoc analyses suggest possible clinical benefits. In addition, PET imaging after the 40-week, randomized trial found significantly increased 18F-DOPA uptake in patients who received GDNF. The randomized trial was published in the March 2019 issue of Brain; data from the open-label extension were published online ahead of print Feb. 26, 2019, in the Journal of Parkinson’s Disease.
“The spatial and relative magnitude of the improvement in the brain scans is beyond anything seen previously in trials of surgically delivered growth-factor treatments for Parkinson’s [disease],” said principal investigator Alan L. Whone, MBChB, PhD, of the University of Bristol (England) and North Bristol National Health Service Trust. “This represents some of the most compelling evidence yet that we may have a means to possibly reawaken and restore the dopamine brain cells that are gradually destroyed in Parkinson’s [disease].”
Nevertheless, the trial did not confirm clinical benefits. The hypothesis that growth factors can benefit patients with Parkinson’s disease may be incorrect, the researchers acknowledged. It also is possible that the hypothesis is valid and that a trial with a higher GDNF dose, longer treatment duration, patients with an earlier disease stage, or different outcome measures would yield positive results. GDNF warrants further study, they wrote.
The findings could have implications for other neurologic disorders as well.
“This trial has shown that we can safely and repeatedly infuse drugs directly into patients’ brains over months or years. This is a significant breakthrough in our ability to treat neurologic conditions ... because most drugs that might work cannot cross from the bloodstream into the brain,” said Steven Gill, MB, MS. Mr. Gill, of the North Bristol NHS Trust and the U.K.-based engineering firm Renishaw, designed the convection-enhanced delivery system used in the studies.
A neurotrophic protein
GDNF has neurorestorative and neuroprotective effects in animal models of Parkinson’s disease. In open-label studies, continuous, low-rate intraputamenal administration of GDNF has shown signs of potential efficacy, but a placebo-controlled trial did not replicate clinical benefits. In the present studies, the researchers assessed intermittent GDNF administration using convection-enhanced delivery, which can achieve wider and more even distribution of GDNF, compared with the previous approach.
The researchers conducted a single-center, randomized, double-blind, placebo-controlled trial to study this novel administration approach. Patients were aged 35-75 years, had motor symptoms for at least 5 years, and had moderate disease severity in the off state (that is, Hoehn and Yahr stage 2-3 and Unified Parkinson’s Disease Rating Scale motor score–part III [UPDRS-III] of 25-45).
In a pilot stage of the trial, six patients were randomized 2:1 to receive GDNF (120 mcg per putamen) or placebo. In the primary stage, another 35 patients were randomized 1:1 to GDNF or placebo. The primary outcome was the percentage change from baseline to week 40 in the off-state UPDRS-III among patients from the primary stage of the trial. Further analyses included all 41 patients from the pilot and primary stages.
Patients in the primary analysis had a mean age of 56.4 years and mean disease duration of 10.9 years. About half were female.
Results on primary and secondary clinical endpoints did not significantly differ between the groups. Average off state UPDRS motor score decreased by 17.3 in the active treatment group, compared with 11.8 in the placebo group.
A post hoc analysis, however, found that nine patients (43%) in the active-treatment group had a large, clinically important motor improvement of 10 or more points in the off state, whereas no placebo patients did. These “10-point responders in the GDNF group are a potential focus of interest; however, as this is a post hoc finding we would not wish to overinterpret its meaning,” Dr. Whone and his colleagues wrote. Among patients who received GDNF, PET imaging demonstrated significantly increased 18F-DOPA uptake throughout the putamen, ranging from a 25% increase in the left anterior putamen to a 100% increase in both posterior putamena, whereas patients who received placebo did not have significantly increased uptake.
No drug-related serious adverse events were reported. “The majority of device-related adverse events were port site associated, most commonly local hypertrophic scarring or infections, amenable to antibiotics,” the investigators wrote. “The frequency of these declined during the trial as surgical and device handling experience improved.”
Open-label extension
By week 80, when all participants had received GDNF, both groups showed moderate to large improvement in symptoms, compared with baseline. From baseline to week 80, percentage change in UPDRS motor score in the off state did not significantly differ between patients who received GDNF for 80 weeks and patients who received placebo followed by GDNF (26.7% vs. 27.6%). Secondary endpoints also did not differ between the groups. Treatment compliance was 97.8%; no patients discontinued the study.
The trials were funded by Parkinson’s UK with support from the Cure Parkinson’s Trust and in association with the North Bristol NHS Trust. GDNF and additional resources and funding were provided by MedGenesis Therapeutix, which owns the license for GDNF and received funding from the Michael J. Fox Foundation for Parkinson’s Research. Renishaw manufactured the convection-enhanced delivery device on behalf of North Bristol NHS Trust. The Gatsby Foundation provided a 3T MRI scanner. Some study authors are employed by and have shares or share options with MedGenesis Therapeutix. Other authors are employees of Renishaw. Dr. Gill is Renishaw’s medical director and may have a future royalty share from the drug delivery system that he invented.
SOURCES: Whone AL et al. Brain. 2019 Feb 26. doi: 10.1093/brain/awz023; Whone AL et al. J Parkinsons Dis. 2019 Feb 26. doi: 10.3233/JPD-191576.
researchers reported. The investigational therapy, delivered through a skull-mounted port, was well tolerated in a 40-week, randomized, controlled trial and a 40-week, open-label extension.
Neither study met its primary endpoint, but post hoc analyses suggest possible clinical benefits. In addition, PET imaging after the 40-week, randomized trial found significantly increased 18F-DOPA uptake in patients who received GDNF. The randomized trial was published in the March 2019 issue of Brain; data from the open-label extension were published online ahead of print Feb. 26, 2019, in the Journal of Parkinson’s Disease.
“The spatial and relative magnitude of the improvement in the brain scans is beyond anything seen previously in trials of surgically delivered growth-factor treatments for Parkinson’s [disease],” said principal investigator Alan L. Whone, MBChB, PhD, of the University of Bristol (England) and North Bristol National Health Service Trust. “This represents some of the most compelling evidence yet that we may have a means to possibly reawaken and restore the dopamine brain cells that are gradually destroyed in Parkinson’s [disease].”
Nevertheless, the trial did not confirm clinical benefits. The hypothesis that growth factors can benefit patients with Parkinson’s disease may be incorrect, the researchers acknowledged. It also is possible that the hypothesis is valid and that a trial with a higher GDNF dose, longer treatment duration, patients with an earlier disease stage, or different outcome measures would yield positive results. GDNF warrants further study, they wrote.
The findings could have implications for other neurologic disorders as well.
“This trial has shown that we can safely and repeatedly infuse drugs directly into patients’ brains over months or years. This is a significant breakthrough in our ability to treat neurologic conditions ... because most drugs that might work cannot cross from the bloodstream into the brain,” said Steven Gill, MB, MS. Mr. Gill, of the North Bristol NHS Trust and the U.K.-based engineering firm Renishaw, designed the convection-enhanced delivery system used in the studies.
A neurotrophic protein
GDNF has neurorestorative and neuroprotective effects in animal models of Parkinson’s disease. In open-label studies, continuous, low-rate intraputamenal administration of GDNF has shown signs of potential efficacy, but a placebo-controlled trial did not replicate clinical benefits. In the present studies, the researchers assessed intermittent GDNF administration using convection-enhanced delivery, which can achieve wider and more even distribution of GDNF, compared with the previous approach.
The researchers conducted a single-center, randomized, double-blind, placebo-controlled trial to study this novel administration approach. Patients were aged 35-75 years, had motor symptoms for at least 5 years, and had moderate disease severity in the off state (that is, Hoehn and Yahr stage 2-3 and Unified Parkinson’s Disease Rating Scale motor score–part III [UPDRS-III] of 25-45).
In a pilot stage of the trial, six patients were randomized 2:1 to receive GDNF (120 mcg per putamen) or placebo. In the primary stage, another 35 patients were randomized 1:1 to GDNF or placebo. The primary outcome was the percentage change from baseline to week 40 in the off-state UPDRS-III among patients from the primary stage of the trial. Further analyses included all 41 patients from the pilot and primary stages.
Patients in the primary analysis had a mean age of 56.4 years and mean disease duration of 10.9 years. About half were female.
Results on primary and secondary clinical endpoints did not significantly differ between the groups. Average off state UPDRS motor score decreased by 17.3 in the active treatment group, compared with 11.8 in the placebo group.
A post hoc analysis, however, found that nine patients (43%) in the active-treatment group had a large, clinically important motor improvement of 10 or more points in the off state, whereas no placebo patients did. These “10-point responders in the GDNF group are a potential focus of interest; however, as this is a post hoc finding we would not wish to overinterpret its meaning,” Dr. Whone and his colleagues wrote. Among patients who received GDNF, PET imaging demonstrated significantly increased 18F-DOPA uptake throughout the putamen, ranging from a 25% increase in the left anterior putamen to a 100% increase in both posterior putamena, whereas patients who received placebo did not have significantly increased uptake.
No drug-related serious adverse events were reported. “The majority of device-related adverse events were port site associated, most commonly local hypertrophic scarring or infections, amenable to antibiotics,” the investigators wrote. “The frequency of these declined during the trial as surgical and device handling experience improved.”
Open-label extension
By week 80, when all participants had received GDNF, both groups showed moderate to large improvement in symptoms, compared with baseline. From baseline to week 80, percentage change in UPDRS motor score in the off state did not significantly differ between patients who received GDNF for 80 weeks and patients who received placebo followed by GDNF (26.7% vs. 27.6%). Secondary endpoints also did not differ between the groups. Treatment compliance was 97.8%; no patients discontinued the study.
The trials were funded by Parkinson’s UK with support from the Cure Parkinson’s Trust and in association with the North Bristol NHS Trust. GDNF and additional resources and funding were provided by MedGenesis Therapeutix, which owns the license for GDNF and received funding from the Michael J. Fox Foundation for Parkinson’s Research. Renishaw manufactured the convection-enhanced delivery device on behalf of North Bristol NHS Trust. The Gatsby Foundation provided a 3T MRI scanner. Some study authors are employed by and have shares or share options with MedGenesis Therapeutix. Other authors are employees of Renishaw. Dr. Gill is Renishaw’s medical director and may have a future royalty share from the drug delivery system that he invented.
SOURCES: Whone AL et al. Brain. 2019 Feb 26. doi: 10.1093/brain/awz023; Whone AL et al. J Parkinsons Dis. 2019 Feb 26. doi: 10.3233/JPD-191576.
researchers reported. The investigational therapy, delivered through a skull-mounted port, was well tolerated in a 40-week, randomized, controlled trial and a 40-week, open-label extension.
Neither study met its primary endpoint, but post hoc analyses suggest possible clinical benefits. In addition, PET imaging after the 40-week, randomized trial found significantly increased 18F-DOPA uptake in patients who received GDNF. The randomized trial was published in the March 2019 issue of Brain; data from the open-label extension were published online ahead of print Feb. 26, 2019, in the Journal of Parkinson’s Disease.
“The spatial and relative magnitude of the improvement in the brain scans is beyond anything seen previously in trials of surgically delivered growth-factor treatments for Parkinson’s [disease],” said principal investigator Alan L. Whone, MBChB, PhD, of the University of Bristol (England) and North Bristol National Health Service Trust. “This represents some of the most compelling evidence yet that we may have a means to possibly reawaken and restore the dopamine brain cells that are gradually destroyed in Parkinson’s [disease].”
Nevertheless, the trial did not confirm clinical benefits. The hypothesis that growth factors can benefit patients with Parkinson’s disease may be incorrect, the researchers acknowledged. It also is possible that the hypothesis is valid and that a trial with a higher GDNF dose, longer treatment duration, patients with an earlier disease stage, or different outcome measures would yield positive results. GDNF warrants further study, they wrote.
The findings could have implications for other neurologic disorders as well.
“This trial has shown that we can safely and repeatedly infuse drugs directly into patients’ brains over months or years. This is a significant breakthrough in our ability to treat neurologic conditions ... because most drugs that might work cannot cross from the bloodstream into the brain,” said Steven Gill, MB, MS. Mr. Gill, of the North Bristol NHS Trust and the U.K.-based engineering firm Renishaw, designed the convection-enhanced delivery system used in the studies.
A neurotrophic protein
GDNF has neurorestorative and neuroprotective effects in animal models of Parkinson’s disease. In open-label studies, continuous, low-rate intraputamenal administration of GDNF has shown signs of potential efficacy, but a placebo-controlled trial did not replicate clinical benefits. In the present studies, the researchers assessed intermittent GDNF administration using convection-enhanced delivery, which can achieve wider and more even distribution of GDNF, compared with the previous approach.
The researchers conducted a single-center, randomized, double-blind, placebo-controlled trial to study this novel administration approach. Patients were aged 35-75 years, had motor symptoms for at least 5 years, and had moderate disease severity in the off state (that is, Hoehn and Yahr stage 2-3 and Unified Parkinson’s Disease Rating Scale motor score–part III [UPDRS-III] of 25-45).
In a pilot stage of the trial, six patients were randomized 2:1 to receive GDNF (120 mcg per putamen) or placebo. In the primary stage, another 35 patients were randomized 1:1 to GDNF or placebo. The primary outcome was the percentage change from baseline to week 40 in the off-state UPDRS-III among patients from the primary stage of the trial. Further analyses included all 41 patients from the pilot and primary stages.
Patients in the primary analysis had a mean age of 56.4 years and mean disease duration of 10.9 years. About half were female.
Results on primary and secondary clinical endpoints did not significantly differ between the groups. Average off state UPDRS motor score decreased by 17.3 in the active treatment group, compared with 11.8 in the placebo group.
A post hoc analysis, however, found that nine patients (43%) in the active-treatment group had a large, clinically important motor improvement of 10 or more points in the off state, whereas no placebo patients did. These “10-point responders in the GDNF group are a potential focus of interest; however, as this is a post hoc finding we would not wish to overinterpret its meaning,” Dr. Whone and his colleagues wrote. Among patients who received GDNF, PET imaging demonstrated significantly increased 18F-DOPA uptake throughout the putamen, ranging from a 25% increase in the left anterior putamen to a 100% increase in both posterior putamena, whereas patients who received placebo did not have significantly increased uptake.
No drug-related serious adverse events were reported. “The majority of device-related adverse events were port site associated, most commonly local hypertrophic scarring or infections, amenable to antibiotics,” the investigators wrote. “The frequency of these declined during the trial as surgical and device handling experience improved.”
Open-label extension
By week 80, when all participants had received GDNF, both groups showed moderate to large improvement in symptoms, compared with baseline. From baseline to week 80, percentage change in UPDRS motor score in the off state did not significantly differ between patients who received GDNF for 80 weeks and patients who received placebo followed by GDNF (26.7% vs. 27.6%). Secondary endpoints also did not differ between the groups. Treatment compliance was 97.8%; no patients discontinued the study.
The trials were funded by Parkinson’s UK with support from the Cure Parkinson’s Trust and in association with the North Bristol NHS Trust. GDNF and additional resources and funding were provided by MedGenesis Therapeutix, which owns the license for GDNF and received funding from the Michael J. Fox Foundation for Parkinson’s Research. Renishaw manufactured the convection-enhanced delivery device on behalf of North Bristol NHS Trust. The Gatsby Foundation provided a 3T MRI scanner. Some study authors are employed by and have shares or share options with MedGenesis Therapeutix. Other authors are employees of Renishaw. Dr. Gill is Renishaw’s medical director and may have a future royalty share from the drug delivery system that he invented.
SOURCES: Whone AL et al. Brain. 2019 Feb 26. doi: 10.1093/brain/awz023; Whone AL et al. J Parkinsons Dis. 2019 Feb 26. doi: 10.3233/JPD-191576.