User login
Note to Self: Document Wisely
One patient was as “fat as a whale,” according to his medical record. A patient who fell out of bed at night had “a nocturnal misadventure,” according to his chart, which provided no further information. Another medical record stated that a patient had been seen without the physician reviewing previous documentation. Yet another chart says the doctor referred the patient to a physician whose “credentials he was unsure of.”
Whether humorous or serious, medical records all too often include inappropriate information. While some of it may seem merely tasteless or silly, inappropriate remarks can cause serious problems—medical, legal, regulatory, and financial.
Because records are critical in so many areas of medical practice, hospitalists need to work harder to ensure they are accurate and appropriate. Experts say there should be more training in documentation.
“Doctors are trained to think about clinical and legal issues in documentation, but far less about the regulatory and billing aspects,” says David Grace, MD, area medical officer for The Schumacher Group, Hospital Medicine Division, in Lafayette, La., who saw the records of the obese patient and the one who fell at night.
As area medical officer, Dr. Grace reviews records and is developing a fellowship for Schumacher’s hospitalists in which documentation will be taught early on. “You have to teach doctors how to be hospitalists, and proper documentation is critical,” he says.
Patrick O’Rourke, an attorney for the University of Colorado, Denver, and legal columnist for The Hospitalist, also believes doctors need more training in documentation. He works with them on that in order to help them “stay out of court.”
The Courtroom
O’Rourke, who has worked on medical malpractice cases for his university’s Health Sciences Center and in private practice for 11 years, says the most common inappropriate wording he sees is back-handed denigration.
“Phrases like ‘hysterical’ or ‘oversensitive,’ ” he says. “Don’t question a patient’s mental condition when the presenting problem is physical. These kinds of comments can look very callous to a jury.”
O’Rourke also says while most physicians are good at documenting what they did or saw, they don’t usually do a lot to explain why. “Making clear your thought process is good in court, in part because doctors often don’t remember a lot years later in front of a jury.”
Documentation should reflect the process of differential diagnosis, O’Rourke says. “If a patient is having difficulty breathing, for example, it could be pneumonia, reactive airway disease, allergies, or a cold. The record should explain the basis for the doctor’s diagnosis and treatment actions.”
Never go back and change records—that undermines their credibility with juries, O’Rourke advises. “You have to make corrections with an addendum, the date and time, and reason for the change,” he says. “Since records go to insurers and other providers, they have to match. In court, the doctor really loses credibility when they don’t.”
It’s also risky to overuse medical abbreviations, says O’Rourke. “A recent study found that 5% of 30,000 medical errors were due to medical abbreviations.” He notes that the Institute for Safe Medication Practices has a list of error-prone abbreviations, symbols, and dose designations on its Web site (www.ismp.org/Tools/errorproneabbreviations.pdf).
Legibility
Another big problem with documentation is legibility, says O’Rourke, noting that many lawsuits have arisen from wrong medications and dosages. “Illegibility causes many medical errors that are preventable,” he says.
“Physicians must remember that just because they can read their writing doesn’t mean others can,” says O’Rourke. “Doctors think the records are their records, but they’re really the patients’ records. If other doctors, pharmacists, etc., can’t read them, why make them?”
Joseph Li, MD, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston, also says illegibility is a big problem. “Physician signatures must be legible,” he notes. “It’s critical to know who wrote the notes. If someone doesn’t know something or can’t read something, they can find out.”
Yet “just telling physicians to write legibly doesn’t work,” says Dr. Li, who is also an assistant professor at Harvard Medical School. “Doctors need to print their name beneath their signature.”
Dr. Li’s group uses templates for admission and progress notes. They include the names of each physician with a check box so they can indicate who wrote the notes. “This is how we comply with that guideline from the Joint Commission on Hospital Accreditation,” he says.
Robert Rohr, MD, vice president for medical affairs at Cortland Regional Medical Center in New York, has reviewed malpractice cases for hospitals and lawyers and in his current role focuses on deficiencies in documentation. He has seen numerous kinds of inappropriate information in medical records. Among his suggestions:
—Patrick O’Rourke, an attorney for the University of Colorado, Denver
Don’t try to settle a dispute in a chart. Dr. Rohr recalls a patient who had a leaking abdominal hernia. A resident wrote in the chart the patient should have surgery within six hours or he would die. The surgeon disagreed. The patient lived without having surgery within the six hours, but if the case had been litigated, the chart note could have been used against the surgeon. “Settle things face to face or on the phone. The medical record must only detail your best thinking about the patient,” says Dr. Rohr. “Don’t be speculative. Agree on a course of action with other physicians and make documentation represent the agreed-upon plan. Showing differences of opinions helps plaintiffs’ lawyers.”
Don’t use charts as note pads for drawings, doodles, or other extraneous markings. “Nothing should be on the record that doesn’t help the next physician care for the patient,” says Dr. Rohr. “It makes the chart look unprofessional. Not good in court or anywhere else.”
Don’t leave the impression that you haven’t done a complete exam. Dr. Rohr saw the documentation that says a patient was “seen without chart.” Instead, he says, doctors should collect as much history as possible. “There are other ways to get information,” he asserts. “Doctors should shy away from making statements in charts about what isn’t available. Instead, outline all the information that is.”
Don’t just run through standard descriptions. Give a specific description of what you have actually examined and then state that “no other abnormalities were seen.” Errors and inappropriate information often go into records within standard exam information, Dr. Rohr and others say.
Avoid controversy in the chart—or, in Dr. Rohr’s words, “Don’t confess to malpractice.” “Don’t put things in charts that indicate you haven’t given the patient your best,” he says, recalling the physician whose chart mentioned a referral to a physician with uncertain credentials.
Be careful in documentation about whether a patient can afford a treatment. Payment issues should be worked out elsewhere. “You are in jeopardy if you give a patient less treatment because they can’t pay for it,” he warns. “It would look bad to a jury. You can include that a patient refused a treatment, but you don’t have to say why.”
Be as complete as possible, including all pertinent detail of a patient’s history. “You need to be thorough for the medical professionals who will treat the patient after you and you need to note certain conditions accurately for appropriate payments to physicians and facilities.” That need to create records that serve regulatory and billing purposes is becoming increasingly important to physicians and hospitals. TH
Karla Feuer is a journalist based in New York.
One patient was as “fat as a whale,” according to his medical record. A patient who fell out of bed at night had “a nocturnal misadventure,” according to his chart, which provided no further information. Another medical record stated that a patient had been seen without the physician reviewing previous documentation. Yet another chart says the doctor referred the patient to a physician whose “credentials he was unsure of.”
Whether humorous or serious, medical records all too often include inappropriate information. While some of it may seem merely tasteless or silly, inappropriate remarks can cause serious problems—medical, legal, regulatory, and financial.
Because records are critical in so many areas of medical practice, hospitalists need to work harder to ensure they are accurate and appropriate. Experts say there should be more training in documentation.
“Doctors are trained to think about clinical and legal issues in documentation, but far less about the regulatory and billing aspects,” says David Grace, MD, area medical officer for The Schumacher Group, Hospital Medicine Division, in Lafayette, La., who saw the records of the obese patient and the one who fell at night.
As area medical officer, Dr. Grace reviews records and is developing a fellowship for Schumacher’s hospitalists in which documentation will be taught early on. “You have to teach doctors how to be hospitalists, and proper documentation is critical,” he says.
Patrick O’Rourke, an attorney for the University of Colorado, Denver, and legal columnist for The Hospitalist, also believes doctors need more training in documentation. He works with them on that in order to help them “stay out of court.”
The Courtroom
O’Rourke, who has worked on medical malpractice cases for his university’s Health Sciences Center and in private practice for 11 years, says the most common inappropriate wording he sees is back-handed denigration.
“Phrases like ‘hysterical’ or ‘oversensitive,’ ” he says. “Don’t question a patient’s mental condition when the presenting problem is physical. These kinds of comments can look very callous to a jury.”
O’Rourke also says while most physicians are good at documenting what they did or saw, they don’t usually do a lot to explain why. “Making clear your thought process is good in court, in part because doctors often don’t remember a lot years later in front of a jury.”
Documentation should reflect the process of differential diagnosis, O’Rourke says. “If a patient is having difficulty breathing, for example, it could be pneumonia, reactive airway disease, allergies, or a cold. The record should explain the basis for the doctor’s diagnosis and treatment actions.”
Never go back and change records—that undermines their credibility with juries, O’Rourke advises. “You have to make corrections with an addendum, the date and time, and reason for the change,” he says. “Since records go to insurers and other providers, they have to match. In court, the doctor really loses credibility when they don’t.”
It’s also risky to overuse medical abbreviations, says O’Rourke. “A recent study found that 5% of 30,000 medical errors were due to medical abbreviations.” He notes that the Institute for Safe Medication Practices has a list of error-prone abbreviations, symbols, and dose designations on its Web site (www.ismp.org/Tools/errorproneabbreviations.pdf).
Legibility
Another big problem with documentation is legibility, says O’Rourke, noting that many lawsuits have arisen from wrong medications and dosages. “Illegibility causes many medical errors that are preventable,” he says.
“Physicians must remember that just because they can read their writing doesn’t mean others can,” says O’Rourke. “Doctors think the records are their records, but they’re really the patients’ records. If other doctors, pharmacists, etc., can’t read them, why make them?”
Joseph Li, MD, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston, also says illegibility is a big problem. “Physician signatures must be legible,” he notes. “It’s critical to know who wrote the notes. If someone doesn’t know something or can’t read something, they can find out.”
Yet “just telling physicians to write legibly doesn’t work,” says Dr. Li, who is also an assistant professor at Harvard Medical School. “Doctors need to print their name beneath their signature.”
Dr. Li’s group uses templates for admission and progress notes. They include the names of each physician with a check box so they can indicate who wrote the notes. “This is how we comply with that guideline from the Joint Commission on Hospital Accreditation,” he says.
Robert Rohr, MD, vice president for medical affairs at Cortland Regional Medical Center in New York, has reviewed malpractice cases for hospitals and lawyers and in his current role focuses on deficiencies in documentation. He has seen numerous kinds of inappropriate information in medical records. Among his suggestions:
—Patrick O’Rourke, an attorney for the University of Colorado, Denver
Don’t try to settle a dispute in a chart. Dr. Rohr recalls a patient who had a leaking abdominal hernia. A resident wrote in the chart the patient should have surgery within six hours or he would die. The surgeon disagreed. The patient lived without having surgery within the six hours, but if the case had been litigated, the chart note could have been used against the surgeon. “Settle things face to face or on the phone. The medical record must only detail your best thinking about the patient,” says Dr. Rohr. “Don’t be speculative. Agree on a course of action with other physicians and make documentation represent the agreed-upon plan. Showing differences of opinions helps plaintiffs’ lawyers.”
Don’t use charts as note pads for drawings, doodles, or other extraneous markings. “Nothing should be on the record that doesn’t help the next physician care for the patient,” says Dr. Rohr. “It makes the chart look unprofessional. Not good in court or anywhere else.”
Don’t leave the impression that you haven’t done a complete exam. Dr. Rohr saw the documentation that says a patient was “seen without chart.” Instead, he says, doctors should collect as much history as possible. “There are other ways to get information,” he asserts. “Doctors should shy away from making statements in charts about what isn’t available. Instead, outline all the information that is.”
Don’t just run through standard descriptions. Give a specific description of what you have actually examined and then state that “no other abnormalities were seen.” Errors and inappropriate information often go into records within standard exam information, Dr. Rohr and others say.
Avoid controversy in the chart—or, in Dr. Rohr’s words, “Don’t confess to malpractice.” “Don’t put things in charts that indicate you haven’t given the patient your best,” he says, recalling the physician whose chart mentioned a referral to a physician with uncertain credentials.
Be careful in documentation about whether a patient can afford a treatment. Payment issues should be worked out elsewhere. “You are in jeopardy if you give a patient less treatment because they can’t pay for it,” he warns. “It would look bad to a jury. You can include that a patient refused a treatment, but you don’t have to say why.”
Be as complete as possible, including all pertinent detail of a patient’s history. “You need to be thorough for the medical professionals who will treat the patient after you and you need to note certain conditions accurately for appropriate payments to physicians and facilities.” That need to create records that serve regulatory and billing purposes is becoming increasingly important to physicians and hospitals. TH
Karla Feuer is a journalist based in New York.
One patient was as “fat as a whale,” according to his medical record. A patient who fell out of bed at night had “a nocturnal misadventure,” according to his chart, which provided no further information. Another medical record stated that a patient had been seen without the physician reviewing previous documentation. Yet another chart says the doctor referred the patient to a physician whose “credentials he was unsure of.”
Whether humorous or serious, medical records all too often include inappropriate information. While some of it may seem merely tasteless or silly, inappropriate remarks can cause serious problems—medical, legal, regulatory, and financial.
Because records are critical in so many areas of medical practice, hospitalists need to work harder to ensure they are accurate and appropriate. Experts say there should be more training in documentation.
“Doctors are trained to think about clinical and legal issues in documentation, but far less about the regulatory and billing aspects,” says David Grace, MD, area medical officer for The Schumacher Group, Hospital Medicine Division, in Lafayette, La., who saw the records of the obese patient and the one who fell at night.
As area medical officer, Dr. Grace reviews records and is developing a fellowship for Schumacher’s hospitalists in which documentation will be taught early on. “You have to teach doctors how to be hospitalists, and proper documentation is critical,” he says.
Patrick O’Rourke, an attorney for the University of Colorado, Denver, and legal columnist for The Hospitalist, also believes doctors need more training in documentation. He works with them on that in order to help them “stay out of court.”
The Courtroom
O’Rourke, who has worked on medical malpractice cases for his university’s Health Sciences Center and in private practice for 11 years, says the most common inappropriate wording he sees is back-handed denigration.
“Phrases like ‘hysterical’ or ‘oversensitive,’ ” he says. “Don’t question a patient’s mental condition when the presenting problem is physical. These kinds of comments can look very callous to a jury.”
O’Rourke also says while most physicians are good at documenting what they did or saw, they don’t usually do a lot to explain why. “Making clear your thought process is good in court, in part because doctors often don’t remember a lot years later in front of a jury.”
Documentation should reflect the process of differential diagnosis, O’Rourke says. “If a patient is having difficulty breathing, for example, it could be pneumonia, reactive airway disease, allergies, or a cold. The record should explain the basis for the doctor’s diagnosis and treatment actions.”
Never go back and change records—that undermines their credibility with juries, O’Rourke advises. “You have to make corrections with an addendum, the date and time, and reason for the change,” he says. “Since records go to insurers and other providers, they have to match. In court, the doctor really loses credibility when they don’t.”
It’s also risky to overuse medical abbreviations, says O’Rourke. “A recent study found that 5% of 30,000 medical errors were due to medical abbreviations.” He notes that the Institute for Safe Medication Practices has a list of error-prone abbreviations, symbols, and dose designations on its Web site (www.ismp.org/Tools/errorproneabbreviations.pdf).
Legibility
Another big problem with documentation is legibility, says O’Rourke, noting that many lawsuits have arisen from wrong medications and dosages. “Illegibility causes many medical errors that are preventable,” he says.
“Physicians must remember that just because they can read their writing doesn’t mean others can,” says O’Rourke. “Doctors think the records are their records, but they’re really the patients’ records. If other doctors, pharmacists, etc., can’t read them, why make them?”
Joseph Li, MD, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston, also says illegibility is a big problem. “Physician signatures must be legible,” he notes. “It’s critical to know who wrote the notes. If someone doesn’t know something or can’t read something, they can find out.”
Yet “just telling physicians to write legibly doesn’t work,” says Dr. Li, who is also an assistant professor at Harvard Medical School. “Doctors need to print their name beneath their signature.”
Dr. Li’s group uses templates for admission and progress notes. They include the names of each physician with a check box so they can indicate who wrote the notes. “This is how we comply with that guideline from the Joint Commission on Hospital Accreditation,” he says.
Robert Rohr, MD, vice president for medical affairs at Cortland Regional Medical Center in New York, has reviewed malpractice cases for hospitals and lawyers and in his current role focuses on deficiencies in documentation. He has seen numerous kinds of inappropriate information in medical records. Among his suggestions:
—Patrick O’Rourke, an attorney for the University of Colorado, Denver
Don’t try to settle a dispute in a chart. Dr. Rohr recalls a patient who had a leaking abdominal hernia. A resident wrote in the chart the patient should have surgery within six hours or he would die. The surgeon disagreed. The patient lived without having surgery within the six hours, but if the case had been litigated, the chart note could have been used against the surgeon. “Settle things face to face or on the phone. The medical record must only detail your best thinking about the patient,” says Dr. Rohr. “Don’t be speculative. Agree on a course of action with other physicians and make documentation represent the agreed-upon plan. Showing differences of opinions helps plaintiffs’ lawyers.”
Don’t use charts as note pads for drawings, doodles, or other extraneous markings. “Nothing should be on the record that doesn’t help the next physician care for the patient,” says Dr. Rohr. “It makes the chart look unprofessional. Not good in court or anywhere else.”
Don’t leave the impression that you haven’t done a complete exam. Dr. Rohr saw the documentation that says a patient was “seen without chart.” Instead, he says, doctors should collect as much history as possible. “There are other ways to get information,” he asserts. “Doctors should shy away from making statements in charts about what isn’t available. Instead, outline all the information that is.”
Don’t just run through standard descriptions. Give a specific description of what you have actually examined and then state that “no other abnormalities were seen.” Errors and inappropriate information often go into records within standard exam information, Dr. Rohr and others say.
Avoid controversy in the chart—or, in Dr. Rohr’s words, “Don’t confess to malpractice.” “Don’t put things in charts that indicate you haven’t given the patient your best,” he says, recalling the physician whose chart mentioned a referral to a physician with uncertain credentials.
Be careful in documentation about whether a patient can afford a treatment. Payment issues should be worked out elsewhere. “You are in jeopardy if you give a patient less treatment because they can’t pay for it,” he warns. “It would look bad to a jury. You can include that a patient refused a treatment, but you don’t have to say why.”
Be as complete as possible, including all pertinent detail of a patient’s history. “You need to be thorough for the medical professionals who will treat the patient after you and you need to note certain conditions accurately for appropriate payments to physicians and facilities.” That need to create records that serve regulatory and billing purposes is becoming increasingly important to physicians and hospitals. TH
Karla Feuer is a journalist based in New York.
Bill by Time Spent on Case
In my recent columns, I addressed documentation guidelines with respect to the three key components: history, exam, and medical decision-making. However, time is considered the fourth key component.
Time-based billing places significant emphasis on the duration of the hospitalist-patient encounter more so than the detail or quality of the documentation. This month, I’ll focus on the guidelines for reporting inpatient hospital services based on time.
Counseling, Coordination
Hospitalists try to make their rounds as efficient as possible while still upholding a high standard of care. It is not unusual for a patient encounter to vary from the norm of updating the history, performing the necessary exam, and implementing the plan.
In fact, hospitalists often counsel patients with newly diagnosed conditions or when treatment options seem extensive and complicated. Based on these circumstances, physicians can document only a brief history and exam or none at all, since the bulk of the encounter focuses on medical decision-making, counseling, and coordination of care. Despite the minimal documentation compared with other physician services, it still is possible to report something more than the lowest service level (e.g., subsequent hospital care, 99231).
To use time as the determining factor for the visit level, more than 50% of the total visit time must involve counseling/coordination of care. The total visit time encompasses both the face-to-face time spent with the patient at the bedside and the additional time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers. Physicians providing care in academic settings cannot contribute teaching time toward the total visit time. Further, only the attending physician’s time counts.
Documentation
Hospitalists must document events during the patient encounter. There may be little or no history and an exam and counseling may dominate the entire visit.
Physicians must document both the counseling/coordination of care time and total visit time. The format may vary: “Total visit time = 25 minutes; more than 50% spent counseling/coordinating care,” or “20 of 25 minutes spent counseling/coordinating care.” Any given payer may prefer one documentation style over another. It always is best to query payers and review their documentation standards to determine the local preference.
In addition to the time, physicians must document the medical decision-making and details of the counseling/coordination of care. For example, patients with newly diagnosed diabetes need to be educated about their condition, lifestyle, and medication requirements. Physicians should include information regarding these factors in their progress notes as necessary.
Family Discussions
As noted in my previous article on critical care services (March 2008, p. 18), family discussions can contribute toward counseling/coordination of care time when:
- The patient is unable or clinically incompetent to participate in discussions;
- Time is spent on the unit/floor with family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; or
- The conversation bears directly on the management of the patient.
Prolonged Care
A physician makes his rounds in the morning. He cares for a 72-year-old female with diabetes, end-stage renal disease, and hypertension. In the afternoon, he returns to find the family waiting with questions. He spends an additional 30 minutes speaking at the bedside with the patient and family. The additional afternoon effort may be captured as prolonged care if both services are documented appropriately.
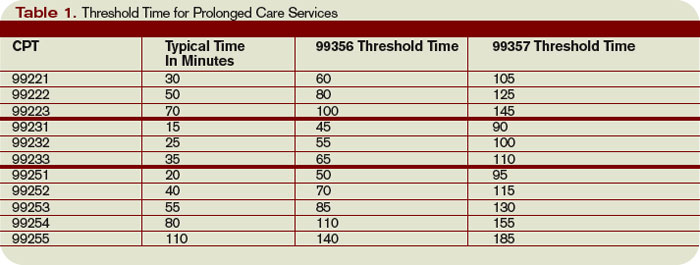
For inpatient services, CPT defines code 99356 as the first hour of prolonged physician services requiring face-to-face patient contact beyond the usual services (reportable after the initial 30 minutes). Code 99357 is used for each additional 30 minutes of prolonged care beyond the first hour (reportable after the first 15 minutes of each additional segment). Both codes are considered add-on codes and cannot be reported alone on a claim form; a primary code must be reported. Code 99357 must be used with 99356, and 99356 must be reported with one of the following inpatient service [primary] codes: 99221-99223, 99231-99233, or 99251-99255.
Prolonged care employs the concept of threshold time. This means total face-to-face physician visit time must exceed the time requirements associated with the primary codes by 30 minutes (e.g., 99232 plus 99356 = 25 minutes plus 30 minutes = 55 total face-to-face attending visit minutes). Accordingly, the physician must document the total face-to-face time spent during each portion of care in two separate notes or in one cumulative note. Be aware that this varies from the standard reporting of counseling and/or coordination of care time in that the physician must meet the threshold face-to-face-time requirements (see Table 1, left), making prolonged care services inefficient. When two providers from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service. To reiterate, 99356 must be reported on the same invoice as the primary visit code (e.g., 99232). Be sure once again to query payers, because most non-Medicare insurers do not recognize these codes. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
In my recent columns, I addressed documentation guidelines with respect to the three key components: history, exam, and medical decision-making. However, time is considered the fourth key component.
Time-based billing places significant emphasis on the duration of the hospitalist-patient encounter more so than the detail or quality of the documentation. This month, I’ll focus on the guidelines for reporting inpatient hospital services based on time.
Counseling, Coordination
Hospitalists try to make their rounds as efficient as possible while still upholding a high standard of care. It is not unusual for a patient encounter to vary from the norm of updating the history, performing the necessary exam, and implementing the plan.
In fact, hospitalists often counsel patients with newly diagnosed conditions or when treatment options seem extensive and complicated. Based on these circumstances, physicians can document only a brief history and exam or none at all, since the bulk of the encounter focuses on medical decision-making, counseling, and coordination of care. Despite the minimal documentation compared with other physician services, it still is possible to report something more than the lowest service level (e.g., subsequent hospital care, 99231).
To use time as the determining factor for the visit level, more than 50% of the total visit time must involve counseling/coordination of care. The total visit time encompasses both the face-to-face time spent with the patient at the bedside and the additional time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers. Physicians providing care in academic settings cannot contribute teaching time toward the total visit time. Further, only the attending physician’s time counts.
Documentation
Hospitalists must document events during the patient encounter. There may be little or no history and an exam and counseling may dominate the entire visit.
Physicians must document both the counseling/coordination of care time and total visit time. The format may vary: “Total visit time = 25 minutes; more than 50% spent counseling/coordinating care,” or “20 of 25 minutes spent counseling/coordinating care.” Any given payer may prefer one documentation style over another. It always is best to query payers and review their documentation standards to determine the local preference.
In addition to the time, physicians must document the medical decision-making and details of the counseling/coordination of care. For example, patients with newly diagnosed diabetes need to be educated about their condition, lifestyle, and medication requirements. Physicians should include information regarding these factors in their progress notes as necessary.
Family Discussions
As noted in my previous article on critical care services (March 2008, p. 18), family discussions can contribute toward counseling/coordination of care time when:
- The patient is unable or clinically incompetent to participate in discussions;
- Time is spent on the unit/floor with family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; or
- The conversation bears directly on the management of the patient.
Prolonged Care
A physician makes his rounds in the morning. He cares for a 72-year-old female with diabetes, end-stage renal disease, and hypertension. In the afternoon, he returns to find the family waiting with questions. He spends an additional 30 minutes speaking at the bedside with the patient and family. The additional afternoon effort may be captured as prolonged care if both services are documented appropriately.
For inpatient services, CPT defines code 99356 as the first hour of prolonged physician services requiring face-to-face patient contact beyond the usual services (reportable after the initial 30 minutes). Code 99357 is used for each additional 30 minutes of prolonged care beyond the first hour (reportable after the first 15 minutes of each additional segment). Both codes are considered add-on codes and cannot be reported alone on a claim form; a primary code must be reported. Code 99357 must be used with 99356, and 99356 must be reported with one of the following inpatient service [primary] codes: 99221-99223, 99231-99233, or 99251-99255.
Prolonged care employs the concept of threshold time. This means total face-to-face physician visit time must exceed the time requirements associated with the primary codes by 30 minutes (e.g., 99232 plus 99356 = 25 minutes plus 30 minutes = 55 total face-to-face attending visit minutes). Accordingly, the physician must document the total face-to-face time spent during each portion of care in two separate notes or in one cumulative note. Be aware that this varies from the standard reporting of counseling and/or coordination of care time in that the physician must meet the threshold face-to-face-time requirements (see Table 1, left), making prolonged care services inefficient. When two providers from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service. To reiterate, 99356 must be reported on the same invoice as the primary visit code (e.g., 99232). Be sure once again to query payers, because most non-Medicare insurers do not recognize these codes. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
In my recent columns, I addressed documentation guidelines with respect to the three key components: history, exam, and medical decision-making. However, time is considered the fourth key component.
Time-based billing places significant emphasis on the duration of the hospitalist-patient encounter more so than the detail or quality of the documentation. This month, I’ll focus on the guidelines for reporting inpatient hospital services based on time.
Counseling, Coordination
Hospitalists try to make their rounds as efficient as possible while still upholding a high standard of care. It is not unusual for a patient encounter to vary from the norm of updating the history, performing the necessary exam, and implementing the plan.
In fact, hospitalists often counsel patients with newly diagnosed conditions or when treatment options seem extensive and complicated. Based on these circumstances, physicians can document only a brief history and exam or none at all, since the bulk of the encounter focuses on medical decision-making, counseling, and coordination of care. Despite the minimal documentation compared with other physician services, it still is possible to report something more than the lowest service level (e.g., subsequent hospital care, 99231).
To use time as the determining factor for the visit level, more than 50% of the total visit time must involve counseling/coordination of care. The total visit time encompasses both the face-to-face time spent with the patient at the bedside and the additional time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers. Physicians providing care in academic settings cannot contribute teaching time toward the total visit time. Further, only the attending physician’s time counts.
Documentation
Hospitalists must document events during the patient encounter. There may be little or no history and an exam and counseling may dominate the entire visit.
Physicians must document both the counseling/coordination of care time and total visit time. The format may vary: “Total visit time = 25 minutes; more than 50% spent counseling/coordinating care,” or “20 of 25 minutes spent counseling/coordinating care.” Any given payer may prefer one documentation style over another. It always is best to query payers and review their documentation standards to determine the local preference.
In addition to the time, physicians must document the medical decision-making and details of the counseling/coordination of care. For example, patients with newly diagnosed diabetes need to be educated about their condition, lifestyle, and medication requirements. Physicians should include information regarding these factors in their progress notes as necessary.
Family Discussions
As noted in my previous article on critical care services (March 2008, p. 18), family discussions can contribute toward counseling/coordination of care time when:
- The patient is unable or clinically incompetent to participate in discussions;
- Time is spent on the unit/floor with family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; or
- The conversation bears directly on the management of the patient.
Prolonged Care
A physician makes his rounds in the morning. He cares for a 72-year-old female with diabetes, end-stage renal disease, and hypertension. In the afternoon, he returns to find the family waiting with questions. He spends an additional 30 minutes speaking at the bedside with the patient and family. The additional afternoon effort may be captured as prolonged care if both services are documented appropriately.
For inpatient services, CPT defines code 99356 as the first hour of prolonged physician services requiring face-to-face patient contact beyond the usual services (reportable after the initial 30 minutes). Code 99357 is used for each additional 30 minutes of prolonged care beyond the first hour (reportable after the first 15 minutes of each additional segment). Both codes are considered add-on codes and cannot be reported alone on a claim form; a primary code must be reported. Code 99357 must be used with 99356, and 99356 must be reported with one of the following inpatient service [primary] codes: 99221-99223, 99231-99233, or 99251-99255.
Prolonged care employs the concept of threshold time. This means total face-to-face physician visit time must exceed the time requirements associated with the primary codes by 30 minutes (e.g., 99232 plus 99356 = 25 minutes plus 30 minutes = 55 total face-to-face attending visit minutes). Accordingly, the physician must document the total face-to-face time spent during each portion of care in two separate notes or in one cumulative note. Be aware that this varies from the standard reporting of counseling and/or coordination of care time in that the physician must meet the threshold face-to-face-time requirements (see Table 1, left), making prolonged care services inefficient. When two providers from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service. To reiterate, 99356 must be reported on the same invoice as the primary visit code (e.g., 99232). Be sure once again to query payers, because most non-Medicare insurers do not recognize these codes. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Medicare too Costly?
In April, the Centers for Medicare and Medicaid (CMS) published its proposed Inpatient Prospective Payment System (IPPS) rule for fiscal year 2009. The rule contains many important components, including additional categories of hospital-acquired conditions (HACs) that no longer will earn higher Medicare payment.
The good news is that under the proposed rule, Medicare payments to hospitals would increase by nearly $4 billion. However, the requirements to earn that are causing concern among some individuals and organizations, including SHM.
This year, CMS announced it would begin withholding additional payments for eight specific HACs, including some “never events”—a practice that won’t take effect until October (May 2008, p. 25). Now, the agency proposes to add nine more. Why double these restrictions so soon?
—Gregory Maynard, MD, MSc, division chief of hospital medicine, University of California, San Diego
“I think it’s a combination of things,” says Gregory Maynard, MD, MSc, division chief of hospital medicine at the University of California, San Diego Medical Center. “Medicare is trying hard to find things that will improve quality and reduce costs, and there are many ways you can do both.”
CMS will pay the lesser Medicare Severity DRG (MS-DRG) amount if the complication was acquired at the hospital and the patient has no other complications or comorbidities.
“It’s not that Medicare won’t pay for the hospital stay—they won’t pay for that condition as a co-morbidity,” explains Dr. Maynard.
- The new HACs include:
- Surgical site infections following certain elective surgeries;
- Legionnaires’ disease;
- Glycemic control for diabetes;
- Iatrogenic pneumothorax;
- Delirium;
- Ventilator-associated pneumonia;
- Deep-vein thrombosis/pulmonary embolism (DVT/PE);
- Staphylococcus aureus septicemia; and
- Clostridium difficile-associated disease.
Unlike the original eight HACs, these proposed conditions are raising questions.
“The first round of conditions, such as objects left in during surgery, those are obvious and people can buy into them,” Dr. Maynard says. Regarding the proposed additions, he says, “Some of these are just out there.”
He singled out a couple of the new HACs. “DVT is a pet of mine, because we’ve done a lot of work in that area,’’ he notes. “We have good information about what patients are on when they develop DVTs or PEs, and we know that very, very few patients who do were neglected.”
As for C diff.-associated disease, he points out: “C diff.-associated diarrhea—that’s tough to totally avoid. In spite of a perfect process, it will still happen.”
SHM sent a letter to CMS regarding specific concerns with three HACs, stating: “SHM supports the CMS initiative to improve the quality of care for hospitalized patients by preventing avoidable hospital-acquired conditions as proposed in the Final Rule for fiscal year 2008. We have concerns about the conditions selected for FY 2009 and the potential for creating unintended consequences through the inclusion of these conditions.”
Dr. Maynard and others fear the new HACs will lead to the addition of processes and other expenses. “I can’t speak totally for SHM,” he says. “I know they support transparency—but you have to think carefully about the process of transparency. There are unintended consequences, like testing everyone who comes in the door for certain conditions, and even treating a condition that doesn’t need to be treated.”
In an April 28 post on his blog “Wachter’s World” (www.wachtersworld.org) Robert Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco, says: “This new list is a case of too far, too fast. … I can’t argue with the premise—many of the [adverse events] on this list are no doubt partly preventable with more religious implementation of certain safety practices (for example, for C diff., avoiding unnecessary antibiotics and adhering to strict infection control practices with suspected cases). But they are nowhere near ready for prime time. Adoption of this new list will lead to all kinds of gaming, [present on admission] shenanigans, wasted effort on preventive strategies with no supportive evidence, and nasty unintended consequences.”
Too Many Measures?
The proposed rule also will significantly increase quality data reporting requirements for hospitals. The rule adds 43 quality measures to the existing 30, so hospitals would need to report on 73 measures to qualify for a full update to their FY 2009 payment rates. The new measures include:
- Surgical Care Improvement Project (one new measure);
- Hospital readmissions (three new measures);
- Nursing care (four new measures);
- Patient safety indicators developed by the Agency for Healthcare Research and Quality (AHRQ) (five new measures);
- Inpatient quality indicators by AHRQ (four new measures);
- Venous thromboembolism (six new measures);
- Stroke measures (five new measures); and
- Cardiac surgery measures (15 new measures).
Critics of the rule believe reporting on 73 measures is unreasonable—and perhaps impossible for smaller hospitals. In a statement released by the American Hospital Association (AHA), Nancy Foster, the AHA’s vice president for quality and patient safety. says, “… we are dismayed that CMS has proposed to add a long and confusing list of measures to those on which hospitals must report to get their full update.” Foster recommends CMS only include measures endorsed by the National Quality Forum as appropriate national standards and adopted by the Hospital Quality Alliance as useful for public reporting on hospital quality of care.
In the Middle
As with previous CMS programs and rules, the increased reporting requirements will mean a continued role for hospitalists.
“This will put hospitalists in the middle even more than they are now,” predicts Dr. Maynard. “It could be good—increasing their role of communicating and training hospital staff and leading quality improvement initiatives—or it could come down to a blame game. Hospitalists are taking care of half the patients in the hospital these days, so if something goes wrong, it may be seen as their fault.”
Read more about the proposed rule online at www.cms.hhs.gov. CMS will respond to comments in a final rule to be issued by Aug 1. TH
Jane Jerrard is a medical writer based in Chicago.
In April, the Centers for Medicare and Medicaid (CMS) published its proposed Inpatient Prospective Payment System (IPPS) rule for fiscal year 2009. The rule contains many important components, including additional categories of hospital-acquired conditions (HACs) that no longer will earn higher Medicare payment.
The good news is that under the proposed rule, Medicare payments to hospitals would increase by nearly $4 billion. However, the requirements to earn that are causing concern among some individuals and organizations, including SHM.
This year, CMS announced it would begin withholding additional payments for eight specific HACs, including some “never events”—a practice that won’t take effect until October (May 2008, p. 25). Now, the agency proposes to add nine more. Why double these restrictions so soon?
—Gregory Maynard, MD, MSc, division chief of hospital medicine, University of California, San Diego
“I think it’s a combination of things,” says Gregory Maynard, MD, MSc, division chief of hospital medicine at the University of California, San Diego Medical Center. “Medicare is trying hard to find things that will improve quality and reduce costs, and there are many ways you can do both.”
CMS will pay the lesser Medicare Severity DRG (MS-DRG) amount if the complication was acquired at the hospital and the patient has no other complications or comorbidities.
“It’s not that Medicare won’t pay for the hospital stay—they won’t pay for that condition as a co-morbidity,” explains Dr. Maynard.
- The new HACs include:
- Surgical site infections following certain elective surgeries;
- Legionnaires’ disease;
- Glycemic control for diabetes;
- Iatrogenic pneumothorax;
- Delirium;
- Ventilator-associated pneumonia;
- Deep-vein thrombosis/pulmonary embolism (DVT/PE);
- Staphylococcus aureus septicemia; and
- Clostridium difficile-associated disease.
Unlike the original eight HACs, these proposed conditions are raising questions.
“The first round of conditions, such as objects left in during surgery, those are obvious and people can buy into them,” Dr. Maynard says. Regarding the proposed additions, he says, “Some of these are just out there.”
He singled out a couple of the new HACs. “DVT is a pet of mine, because we’ve done a lot of work in that area,’’ he notes. “We have good information about what patients are on when they develop DVTs or PEs, and we know that very, very few patients who do were neglected.”
As for C diff.-associated disease, he points out: “C diff.-associated diarrhea—that’s tough to totally avoid. In spite of a perfect process, it will still happen.”
SHM sent a letter to CMS regarding specific concerns with three HACs, stating: “SHM supports the CMS initiative to improve the quality of care for hospitalized patients by preventing avoidable hospital-acquired conditions as proposed in the Final Rule for fiscal year 2008. We have concerns about the conditions selected for FY 2009 and the potential for creating unintended consequences through the inclusion of these conditions.”
Dr. Maynard and others fear the new HACs will lead to the addition of processes and other expenses. “I can’t speak totally for SHM,” he says. “I know they support transparency—but you have to think carefully about the process of transparency. There are unintended consequences, like testing everyone who comes in the door for certain conditions, and even treating a condition that doesn’t need to be treated.”
In an April 28 post on his blog “Wachter’s World” (www.wachtersworld.org) Robert Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco, says: “This new list is a case of too far, too fast. … I can’t argue with the premise—many of the [adverse events] on this list are no doubt partly preventable with more religious implementation of certain safety practices (for example, for C diff., avoiding unnecessary antibiotics and adhering to strict infection control practices with suspected cases). But they are nowhere near ready for prime time. Adoption of this new list will lead to all kinds of gaming, [present on admission] shenanigans, wasted effort on preventive strategies with no supportive evidence, and nasty unintended consequences.”
Too Many Measures?
The proposed rule also will significantly increase quality data reporting requirements for hospitals. The rule adds 43 quality measures to the existing 30, so hospitals would need to report on 73 measures to qualify for a full update to their FY 2009 payment rates. The new measures include:
- Surgical Care Improvement Project (one new measure);
- Hospital readmissions (three new measures);
- Nursing care (four new measures);
- Patient safety indicators developed by the Agency for Healthcare Research and Quality (AHRQ) (five new measures);
- Inpatient quality indicators by AHRQ (four new measures);
- Venous thromboembolism (six new measures);
- Stroke measures (five new measures); and
- Cardiac surgery measures (15 new measures).
Critics of the rule believe reporting on 73 measures is unreasonable—and perhaps impossible for smaller hospitals. In a statement released by the American Hospital Association (AHA), Nancy Foster, the AHA’s vice president for quality and patient safety. says, “… we are dismayed that CMS has proposed to add a long and confusing list of measures to those on which hospitals must report to get their full update.” Foster recommends CMS only include measures endorsed by the National Quality Forum as appropriate national standards and adopted by the Hospital Quality Alliance as useful for public reporting on hospital quality of care.
In the Middle
As with previous CMS programs and rules, the increased reporting requirements will mean a continued role for hospitalists.
“This will put hospitalists in the middle even more than they are now,” predicts Dr. Maynard. “It could be good—increasing their role of communicating and training hospital staff and leading quality improvement initiatives—or it could come down to a blame game. Hospitalists are taking care of half the patients in the hospital these days, so if something goes wrong, it may be seen as their fault.”
Read more about the proposed rule online at www.cms.hhs.gov. CMS will respond to comments in a final rule to be issued by Aug 1. TH
Jane Jerrard is a medical writer based in Chicago.
In April, the Centers for Medicare and Medicaid (CMS) published its proposed Inpatient Prospective Payment System (IPPS) rule for fiscal year 2009. The rule contains many important components, including additional categories of hospital-acquired conditions (HACs) that no longer will earn higher Medicare payment.
The good news is that under the proposed rule, Medicare payments to hospitals would increase by nearly $4 billion. However, the requirements to earn that are causing concern among some individuals and organizations, including SHM.
This year, CMS announced it would begin withholding additional payments for eight specific HACs, including some “never events”—a practice that won’t take effect until October (May 2008, p. 25). Now, the agency proposes to add nine more. Why double these restrictions so soon?
—Gregory Maynard, MD, MSc, division chief of hospital medicine, University of California, San Diego
“I think it’s a combination of things,” says Gregory Maynard, MD, MSc, division chief of hospital medicine at the University of California, San Diego Medical Center. “Medicare is trying hard to find things that will improve quality and reduce costs, and there are many ways you can do both.”
CMS will pay the lesser Medicare Severity DRG (MS-DRG) amount if the complication was acquired at the hospital and the patient has no other complications or comorbidities.
“It’s not that Medicare won’t pay for the hospital stay—they won’t pay for that condition as a co-morbidity,” explains Dr. Maynard.
- The new HACs include:
- Surgical site infections following certain elective surgeries;
- Legionnaires’ disease;
- Glycemic control for diabetes;
- Iatrogenic pneumothorax;
- Delirium;
- Ventilator-associated pneumonia;
- Deep-vein thrombosis/pulmonary embolism (DVT/PE);
- Staphylococcus aureus septicemia; and
- Clostridium difficile-associated disease.
Unlike the original eight HACs, these proposed conditions are raising questions.
“The first round of conditions, such as objects left in during surgery, those are obvious and people can buy into them,” Dr. Maynard says. Regarding the proposed additions, he says, “Some of these are just out there.”
He singled out a couple of the new HACs. “DVT is a pet of mine, because we’ve done a lot of work in that area,’’ he notes. “We have good information about what patients are on when they develop DVTs or PEs, and we know that very, very few patients who do were neglected.”
As for C diff.-associated disease, he points out: “C diff.-associated diarrhea—that’s tough to totally avoid. In spite of a perfect process, it will still happen.”
SHM sent a letter to CMS regarding specific concerns with three HACs, stating: “SHM supports the CMS initiative to improve the quality of care for hospitalized patients by preventing avoidable hospital-acquired conditions as proposed in the Final Rule for fiscal year 2008. We have concerns about the conditions selected for FY 2009 and the potential for creating unintended consequences through the inclusion of these conditions.”
Dr. Maynard and others fear the new HACs will lead to the addition of processes and other expenses. “I can’t speak totally for SHM,” he says. “I know they support transparency—but you have to think carefully about the process of transparency. There are unintended consequences, like testing everyone who comes in the door for certain conditions, and even treating a condition that doesn’t need to be treated.”
In an April 28 post on his blog “Wachter’s World” (www.wachtersworld.org) Robert Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco, says: “This new list is a case of too far, too fast. … I can’t argue with the premise—many of the [adverse events] on this list are no doubt partly preventable with more religious implementation of certain safety practices (for example, for C diff., avoiding unnecessary antibiotics and adhering to strict infection control practices with suspected cases). But they are nowhere near ready for prime time. Adoption of this new list will lead to all kinds of gaming, [present on admission] shenanigans, wasted effort on preventive strategies with no supportive evidence, and nasty unintended consequences.”
Too Many Measures?
The proposed rule also will significantly increase quality data reporting requirements for hospitals. The rule adds 43 quality measures to the existing 30, so hospitals would need to report on 73 measures to qualify for a full update to their FY 2009 payment rates. The new measures include:
- Surgical Care Improvement Project (one new measure);
- Hospital readmissions (three new measures);
- Nursing care (four new measures);
- Patient safety indicators developed by the Agency for Healthcare Research and Quality (AHRQ) (five new measures);
- Inpatient quality indicators by AHRQ (four new measures);
- Venous thromboembolism (six new measures);
- Stroke measures (five new measures); and
- Cardiac surgery measures (15 new measures).
Critics of the rule believe reporting on 73 measures is unreasonable—and perhaps impossible for smaller hospitals. In a statement released by the American Hospital Association (AHA), Nancy Foster, the AHA’s vice president for quality and patient safety. says, “… we are dismayed that CMS has proposed to add a long and confusing list of measures to those on which hospitals must report to get their full update.” Foster recommends CMS only include measures endorsed by the National Quality Forum as appropriate national standards and adopted by the Hospital Quality Alliance as useful for public reporting on hospital quality of care.
In the Middle
As with previous CMS programs and rules, the increased reporting requirements will mean a continued role for hospitalists.
“This will put hospitalists in the middle even more than they are now,” predicts Dr. Maynard. “It could be good—increasing their role of communicating and training hospital staff and leading quality improvement initiatives—or it could come down to a blame game. Hospitalists are taking care of half the patients in the hospital these days, so if something goes wrong, it may be seen as their fault.”
Read more about the proposed rule online at www.cms.hhs.gov. CMS will respond to comments in a final rule to be issued by Aug 1. TH
Jane Jerrard is a medical writer based in Chicago.
Change Jobs Wisely
In today’s wide-open job market, hospitalists can pick a plum position anywhere in the United States. With promising opportunities in sunny Hawaii, bustling New York City, and everywhere in between—likely including your own hometown—the temptation to move to a warmer climate, kid-friendly small town, or bigger paycheck may be irresistible.
Michael-Anthony Williams, MD, chief medical officer for the Rocky Mountain Region of Sound Inpatient Physicians, has hired hospitalists who come to Denver from across the country.
“Market competition [for hospitalists] is definitely fierce and will remain so,” he says. “But no matter where you’re looking or what you’re searching for, you need to get a sense of the group you’ll be joining.”
Sameer Badlani, MD, hospitalist and instructor at the University of Chicago, agrees location should come second to the job itself. “You have to do a lot of introspection and decide what you’re looking for,” he cautions. “If you’re unhappy, ask yourself why a new job would be different.”
After taking this advice into account, consider the challenges and opportunities of starting life anew somewhere else.
Reasons to Relocate
Why think about moving in the first place?
“Money might be the biggest reason,” speculates Dr. Badlani. “The only way to make significantly more money is to become a partner in the practice. I’d say if you’re a hospitalist who’s relocating, you should definitely try to become a partner.”
Another reason to consider moving might be family reasons. “If a spouse gets a job offer in a different city, it’s easy for the hospitalist to move there and find a job,” Dr. Badlani points out. “With the economy the way it is, I think that more and more you’ll see spouses’ jobs influencing where hospitalists relocate.”
Some hospitalists move because they are drawn to a certain region or lifestyle. Dr. Williams says. “We certainly see people who target geography as playing a big role in their job search.”
If you fall into this category, be careful to do your research to discover the realities of your dream location.
“I’d advise that you make more than one trip to a place if you’ve never lived there before,” Dr. Badlani says. “See exactly what it means to live there. Visit the hospital medicine group more than once. Go out with a real estate agent and look at houses.”
—Sameer Badlani, MD, hospitalist and instructor, University of Chicago
Timing Is Everything
Once you’ve decided you are interested in moving—or have to move—get started with your location scouting and your job search.
“You should start looking [for a job] even earlier when you’re relocating,” Dr. Badlani advises. “And be sure to tell your supervisor that you’re thinking of relocating. This seems like a bad idea to some people, but it will be worse if you wait and give two weeks’ notice. That is unfair to your employer and your colleagues who will have to cover your work, and you will end up burning your bridges.” He recommends telling your current employer while interviewing for next year. If you’re already deep into your search, that should be about six or seven months in advance, he says.
“Your current employer will appreciate it, and they may even try to make some changes in order to keep you,” Dr. Badlani says.
Try to negotiate to keep your transition dates flexible. Your plans to move may not go as smoothly as you’d like. “Recently, we’ve seen a couple of people have a tough time selling their house before they move,” Dr. Williams says. “If you live in a tough real estate market, you might want to see if your new employer can be flexible on your start date.”
Consider Cost of Living
As you compare compensation offered by hospital medicine practices in different parts of the country—or even different parts of the same county—consider cost of living in each area.
“If you make $150,000 in Tulsa, Oklahoma, (then you need to make) $210,000 in Chicago,” Dr. Badlani says, who has worked in both cities. Cost of living, he adds, “can be misleading. Do your research and find out housing costs for the area. Online calculators only give approximations; make sure you compare housing in desirable areas of the city, not across the board.”
In addition, Dr. Badlani says, “If you choose a smaller town, it’s likely that you can get paid more—because they need you more—and live in a cheaper place. And you’ll find more opportunities in a smaller town because there are fewer doctors.”
The biggest challenge when comparing jobs is assessing the work required to make that salary, Dr. Williams adds. “Find out how many shifts per month you’ll work to earn it, and how many patients you’ll see per shift,” he suggests.
Relocation, Negotiation
Before you start negotiating a new contract, Dr. Badlani advises you first look at your current one to see what you’re walking away from.
“Every place has a golden handcuff,” he says. “The University of Chicago gives you three years before you’re fully vested in your retirement benefits; I know an Oklahoma hospital where it takes seven years. Leave before you’re vested and you could lose thousands of dollars in employer contributions. You have to ask, will your new job help you recover that quickly? Can you get a signing bonus that’s equal to all or most of what you’re walking away from, or the promise of a partnership? Try to mitigate that loss with other opportunities.
“Places like Kaiser Permanente offer money to help with a down payment for a house—that’s their version of a golden handcuff. If you stay in the job long enough, that becomes a free loan.”
Dr. Williams adds: “Will the group cover your moving expenses? That’s a lot of money. Also check on the state’s licensing fees and how long it will take to get your license—it varies greatly from state to state.”
While you’re interviewing, keep the negotiation process in mind: “I would never tell a recruiter or prospective employer all the reasons why I’m moving,” Dr. Badlani says. “You don’t want to show how interested you are. It’s a game you have to play. Be sure to say you’re looking at other opportunities and other towns.”
Finally, weigh your options against the rest of the market—and against what your peers are getting in terms of compensation and benefits.
“Talk to your friends and try to figure out what the best deal is,” Dr. Badlani says.
Although you can choose a hospitalist position anywhere in the country, the most important thing to consider is the group you’re joining. If it is not a good fit for your values and personality, then the state you’ve decided to move to will be one of discontent. TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
In today’s wide-open job market, hospitalists can pick a plum position anywhere in the United States. With promising opportunities in sunny Hawaii, bustling New York City, and everywhere in between—likely including your own hometown—the temptation to move to a warmer climate, kid-friendly small town, or bigger paycheck may be irresistible.
Michael-Anthony Williams, MD, chief medical officer for the Rocky Mountain Region of Sound Inpatient Physicians, has hired hospitalists who come to Denver from across the country.
“Market competition [for hospitalists] is definitely fierce and will remain so,” he says. “But no matter where you’re looking or what you’re searching for, you need to get a sense of the group you’ll be joining.”
Sameer Badlani, MD, hospitalist and instructor at the University of Chicago, agrees location should come second to the job itself. “You have to do a lot of introspection and decide what you’re looking for,” he cautions. “If you’re unhappy, ask yourself why a new job would be different.”
After taking this advice into account, consider the challenges and opportunities of starting life anew somewhere else.
Reasons to Relocate
Why think about moving in the first place?
“Money might be the biggest reason,” speculates Dr. Badlani. “The only way to make significantly more money is to become a partner in the practice. I’d say if you’re a hospitalist who’s relocating, you should definitely try to become a partner.”
Another reason to consider moving might be family reasons. “If a spouse gets a job offer in a different city, it’s easy for the hospitalist to move there and find a job,” Dr. Badlani points out. “With the economy the way it is, I think that more and more you’ll see spouses’ jobs influencing where hospitalists relocate.”
Some hospitalists move because they are drawn to a certain region or lifestyle. Dr. Williams says. “We certainly see people who target geography as playing a big role in their job search.”
If you fall into this category, be careful to do your research to discover the realities of your dream location.
“I’d advise that you make more than one trip to a place if you’ve never lived there before,” Dr. Badlani says. “See exactly what it means to live there. Visit the hospital medicine group more than once. Go out with a real estate agent and look at houses.”
—Sameer Badlani, MD, hospitalist and instructor, University of Chicago
Timing Is Everything
Once you’ve decided you are interested in moving—or have to move—get started with your location scouting and your job search.
“You should start looking [for a job] even earlier when you’re relocating,” Dr. Badlani advises. “And be sure to tell your supervisor that you’re thinking of relocating. This seems like a bad idea to some people, but it will be worse if you wait and give two weeks’ notice. That is unfair to your employer and your colleagues who will have to cover your work, and you will end up burning your bridges.” He recommends telling your current employer while interviewing for next year. If you’re already deep into your search, that should be about six or seven months in advance, he says.
“Your current employer will appreciate it, and they may even try to make some changes in order to keep you,” Dr. Badlani says.
Try to negotiate to keep your transition dates flexible. Your plans to move may not go as smoothly as you’d like. “Recently, we’ve seen a couple of people have a tough time selling their house before they move,” Dr. Williams says. “If you live in a tough real estate market, you might want to see if your new employer can be flexible on your start date.”
Consider Cost of Living
As you compare compensation offered by hospital medicine practices in different parts of the country—or even different parts of the same county—consider cost of living in each area.
“If you make $150,000 in Tulsa, Oklahoma, (then you need to make) $210,000 in Chicago,” Dr. Badlani says, who has worked in both cities. Cost of living, he adds, “can be misleading. Do your research and find out housing costs for the area. Online calculators only give approximations; make sure you compare housing in desirable areas of the city, not across the board.”
In addition, Dr. Badlani says, “If you choose a smaller town, it’s likely that you can get paid more—because they need you more—and live in a cheaper place. And you’ll find more opportunities in a smaller town because there are fewer doctors.”
The biggest challenge when comparing jobs is assessing the work required to make that salary, Dr. Williams adds. “Find out how many shifts per month you’ll work to earn it, and how many patients you’ll see per shift,” he suggests.
Relocation, Negotiation
Before you start negotiating a new contract, Dr. Badlani advises you first look at your current one to see what you’re walking away from.
“Every place has a golden handcuff,” he says. “The University of Chicago gives you three years before you’re fully vested in your retirement benefits; I know an Oklahoma hospital where it takes seven years. Leave before you’re vested and you could lose thousands of dollars in employer contributions. You have to ask, will your new job help you recover that quickly? Can you get a signing bonus that’s equal to all or most of what you’re walking away from, or the promise of a partnership? Try to mitigate that loss with other opportunities.
“Places like Kaiser Permanente offer money to help with a down payment for a house—that’s their version of a golden handcuff. If you stay in the job long enough, that becomes a free loan.”
Dr. Williams adds: “Will the group cover your moving expenses? That’s a lot of money. Also check on the state’s licensing fees and how long it will take to get your license—it varies greatly from state to state.”
While you’re interviewing, keep the negotiation process in mind: “I would never tell a recruiter or prospective employer all the reasons why I’m moving,” Dr. Badlani says. “You don’t want to show how interested you are. It’s a game you have to play. Be sure to say you’re looking at other opportunities and other towns.”
Finally, weigh your options against the rest of the market—and against what your peers are getting in terms of compensation and benefits.
“Talk to your friends and try to figure out what the best deal is,” Dr. Badlani says.
Although you can choose a hospitalist position anywhere in the country, the most important thing to consider is the group you’re joining. If it is not a good fit for your values and personality, then the state you’ve decided to move to will be one of discontent. TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
In today’s wide-open job market, hospitalists can pick a plum position anywhere in the United States. With promising opportunities in sunny Hawaii, bustling New York City, and everywhere in between—likely including your own hometown—the temptation to move to a warmer climate, kid-friendly small town, or bigger paycheck may be irresistible.
Michael-Anthony Williams, MD, chief medical officer for the Rocky Mountain Region of Sound Inpatient Physicians, has hired hospitalists who come to Denver from across the country.
“Market competition [for hospitalists] is definitely fierce and will remain so,” he says. “But no matter where you’re looking or what you’re searching for, you need to get a sense of the group you’ll be joining.”
Sameer Badlani, MD, hospitalist and instructor at the University of Chicago, agrees location should come second to the job itself. “You have to do a lot of introspection and decide what you’re looking for,” he cautions. “If you’re unhappy, ask yourself why a new job would be different.”
After taking this advice into account, consider the challenges and opportunities of starting life anew somewhere else.
Reasons to Relocate
Why think about moving in the first place?
“Money might be the biggest reason,” speculates Dr. Badlani. “The only way to make significantly more money is to become a partner in the practice. I’d say if you’re a hospitalist who’s relocating, you should definitely try to become a partner.”
Another reason to consider moving might be family reasons. “If a spouse gets a job offer in a different city, it’s easy for the hospitalist to move there and find a job,” Dr. Badlani points out. “With the economy the way it is, I think that more and more you’ll see spouses’ jobs influencing where hospitalists relocate.”
Some hospitalists move because they are drawn to a certain region or lifestyle. Dr. Williams says. “We certainly see people who target geography as playing a big role in their job search.”
If you fall into this category, be careful to do your research to discover the realities of your dream location.
“I’d advise that you make more than one trip to a place if you’ve never lived there before,” Dr. Badlani says. “See exactly what it means to live there. Visit the hospital medicine group more than once. Go out with a real estate agent and look at houses.”
—Sameer Badlani, MD, hospitalist and instructor, University of Chicago
Timing Is Everything
Once you’ve decided you are interested in moving—or have to move—get started with your location scouting and your job search.
“You should start looking [for a job] even earlier when you’re relocating,” Dr. Badlani advises. “And be sure to tell your supervisor that you’re thinking of relocating. This seems like a bad idea to some people, but it will be worse if you wait and give two weeks’ notice. That is unfair to your employer and your colleagues who will have to cover your work, and you will end up burning your bridges.” He recommends telling your current employer while interviewing for next year. If you’re already deep into your search, that should be about six or seven months in advance, he says.
“Your current employer will appreciate it, and they may even try to make some changes in order to keep you,” Dr. Badlani says.
Try to negotiate to keep your transition dates flexible. Your plans to move may not go as smoothly as you’d like. “Recently, we’ve seen a couple of people have a tough time selling their house before they move,” Dr. Williams says. “If you live in a tough real estate market, you might want to see if your new employer can be flexible on your start date.”
Consider Cost of Living
As you compare compensation offered by hospital medicine practices in different parts of the country—or even different parts of the same county—consider cost of living in each area.
“If you make $150,000 in Tulsa, Oklahoma, (then you need to make) $210,000 in Chicago,” Dr. Badlani says, who has worked in both cities. Cost of living, he adds, “can be misleading. Do your research and find out housing costs for the area. Online calculators only give approximations; make sure you compare housing in desirable areas of the city, not across the board.”
In addition, Dr. Badlani says, “If you choose a smaller town, it’s likely that you can get paid more—because they need you more—and live in a cheaper place. And you’ll find more opportunities in a smaller town because there are fewer doctors.”
The biggest challenge when comparing jobs is assessing the work required to make that salary, Dr. Williams adds. “Find out how many shifts per month you’ll work to earn it, and how many patients you’ll see per shift,” he suggests.
Relocation, Negotiation
Before you start negotiating a new contract, Dr. Badlani advises you first look at your current one to see what you’re walking away from.
“Every place has a golden handcuff,” he says. “The University of Chicago gives you three years before you’re fully vested in your retirement benefits; I know an Oklahoma hospital where it takes seven years. Leave before you’re vested and you could lose thousands of dollars in employer contributions. You have to ask, will your new job help you recover that quickly? Can you get a signing bonus that’s equal to all or most of what you’re walking away from, or the promise of a partnership? Try to mitigate that loss with other opportunities.
“Places like Kaiser Permanente offer money to help with a down payment for a house—that’s their version of a golden handcuff. If you stay in the job long enough, that becomes a free loan.”
Dr. Williams adds: “Will the group cover your moving expenses? That’s a lot of money. Also check on the state’s licensing fees and how long it will take to get your license—it varies greatly from state to state.”
While you’re interviewing, keep the negotiation process in mind: “I would never tell a recruiter or prospective employer all the reasons why I’m moving,” Dr. Badlani says. “You don’t want to show how interested you are. It’s a game you have to play. Be sure to say you’re looking at other opportunities and other towns.”
Finally, weigh your options against the rest of the market—and against what your peers are getting in terms of compensation and benefits.
“Talk to your friends and try to figure out what the best deal is,” Dr. Badlani says.
Although you can choose a hospitalist position anywhere in the country, the most important thing to consider is the group you’re joining. If it is not a good fit for your values and personality, then the state you’ve decided to move to will be one of discontent. TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
SHM Rides to the Rescue

A few months ago SHM received an e-mail from SHM member Jennifer Bellino, MD, a hospitalist at William Backus Hospital in Norwich, Conn. She had gotten wind of a proposal flowing through the Public Health Committee at the Connecticut State Legislature that would mandate the frequency of communications between hospitalists and primary care physicians (PCPs). From her short e-mail SHM’s advocacy enterprise sprung into action.
Bill 5721 was being introduced to the Public Health Committee in the Connecticut Legislature, and it required the development of state regulations that would have governed the timing and frequency of communications between hospitalists and PCPs.
Laura Allendorf, SHM’s head of Governmental Affairs, engaged SHM’s Public Policy Committee to better understand the issues involved in this bill and to get a sense of whether this was a unique bill for Connecticut or whether it was being introduced in other state legislatures.
While the bill appeared to be isolated to Connecticut, the Public Policy Committee thought the issue was threatening enough to the practice of hospital medicine that local aggressive action was necessary.
Allendorf contacted the Connecticut State Medical Society and spoke to Ken Ferrucci, director of government relations, who was already aware of Bill 5721. The Connecticut State Medical Society (CSMS) was opposed to the bill as well, and Ferrucci proposed that SHM find a Connecticut hospitalist who could come to Hartford to speak against Bill 5721 at the Public Health Committee, which would hear testimony in just a few days.
Unfortunately, no one on the Public Policy Committee was from Connecticut. Fortunately, SHM was familiar with Bill Rifkin, MD, from Yale (New Haven) and Waterbury Hospital, who is active at SHM as a member of our Education Committee. Allendorf contacted Dr. Rifkin and explained the situation. He dropped everything on his calendar and changed his appointments and agreed to come to Hartford to fly the SHM banner and testify before the Public Health Committee.
Working together Allendorf, Eric Siegal, the Public Policy committee chair, and Dr. Rifkin crafted the testimony necessary to explain to the legislators just what hospital medicine is and what hospitalists do. In addition, they emphasized that hospitalists are working hard to be the experts in transitions of care and that mandates and regulations were not needed and, in fact, could be detrimental to the fundamental relationship between PCPs and hospitalists.
SHM then coordinated our approach with that of the Connecticut State Medical Society to create a unified front for maximum effectiveness. In the end Dr. Rifkin carried the day.
After Dr. Rifkin’s testimony, as well as testimony from the Connecticut State Medical Society, the bill died a quiet death. Eventually, a watered down amendment was made to another public health bill, which contained language that basically said hospitalists and PCPs should talk to each other. This amendment asked that the Quality of Care Advisory Committee, which advises the Department of Public Health, make recommendations to the department concerning best practices with respect to communications between a patient’s PCP and other providers involved in a patient’s care, including hospitalists and specialists.
Thanks to CSMS’ and SHM’s efforts, no regulations or mandates are currently planned in Connecticut.
It is unfortunate that some states, driven by a small vocal group of consumers or sometimes by just one legislator, can single out hospitalists for scrutiny and regulation. Dr. Rifkin found out how important and necessary it is to provide education to the involved legislators, as some professed knowing few of the details of the hospital medicine movement.
While you might be sitting in Texas or Minnesota or California and wondering what all of this has to do with you, know that a wildfire can start from a smoldering ember. SHM must vigilantly monitor the actions of local legislatures and regulators so that in their misunderstanding of hospital medicine or in their concerns for changes in the healthcare system they do not attempt to use the state or federal legislatures for their remedies.
Hospital medicine is new, and we are challenging the status quo. While we are driven by a goal of creating a more efficient healthcare system, driven by accountability and data, some will see the turbulence of change and attempt to rein this in. While some places have seen significant improvements, hospital medicine is still very much in its growth and evolutionary phase. This is the time to have the ability for flexibility and even experimentation in the best sense of the word. It is important not to be stifled by overregulation. At the same time, hospitalists need to be aware that we are no longer a boutique specialty off on the margins of healthcare. Hospital medicine is front and center at more than 2,000 hospitals and with 15,000 hospitalists nationwide too large to be ignored.
Expect more attempts to legislate how hospitalists practice. One SHM member’s e-mail brought the full strength of SHM to quash the wrong bill in Connecticut. We need your local eyes to let us know what is happening out in the real world. In the meantime SHM will work hard to develop the bench strength to be able to rise to your challenges. TH
Dr. Wellikson has been CEO of SHM since 2000.
A few months ago SHM received an e-mail from SHM member Jennifer Bellino, MD, a hospitalist at William Backus Hospital in Norwich, Conn. She had gotten wind of a proposal flowing through the Public Health Committee at the Connecticut State Legislature that would mandate the frequency of communications between hospitalists and primary care physicians (PCPs). From her short e-mail SHM’s advocacy enterprise sprung into action.
Bill 5721 was being introduced to the Public Health Committee in the Connecticut Legislature, and it required the development of state regulations that would have governed the timing and frequency of communications between hospitalists and PCPs.
Laura Allendorf, SHM’s head of Governmental Affairs, engaged SHM’s Public Policy Committee to better understand the issues involved in this bill and to get a sense of whether this was a unique bill for Connecticut or whether it was being introduced in other state legislatures.
While the bill appeared to be isolated to Connecticut, the Public Policy Committee thought the issue was threatening enough to the practice of hospital medicine that local aggressive action was necessary.
Allendorf contacted the Connecticut State Medical Society and spoke to Ken Ferrucci, director of government relations, who was already aware of Bill 5721. The Connecticut State Medical Society (CSMS) was opposed to the bill as well, and Ferrucci proposed that SHM find a Connecticut hospitalist who could come to Hartford to speak against Bill 5721 at the Public Health Committee, which would hear testimony in just a few days.
Unfortunately, no one on the Public Policy Committee was from Connecticut. Fortunately, SHM was familiar with Bill Rifkin, MD, from Yale (New Haven) and Waterbury Hospital, who is active at SHM as a member of our Education Committee. Allendorf contacted Dr. Rifkin and explained the situation. He dropped everything on his calendar and changed his appointments and agreed to come to Hartford to fly the SHM banner and testify before the Public Health Committee.
Working together Allendorf, Eric Siegal, the Public Policy committee chair, and Dr. Rifkin crafted the testimony necessary to explain to the legislators just what hospital medicine is and what hospitalists do. In addition, they emphasized that hospitalists are working hard to be the experts in transitions of care and that mandates and regulations were not needed and, in fact, could be detrimental to the fundamental relationship between PCPs and hospitalists.
SHM then coordinated our approach with that of the Connecticut State Medical Society to create a unified front for maximum effectiveness. In the end Dr. Rifkin carried the day.
After Dr. Rifkin’s testimony, as well as testimony from the Connecticut State Medical Society, the bill died a quiet death. Eventually, a watered down amendment was made to another public health bill, which contained language that basically said hospitalists and PCPs should talk to each other. This amendment asked that the Quality of Care Advisory Committee, which advises the Department of Public Health, make recommendations to the department concerning best practices with respect to communications between a patient’s PCP and other providers involved in a patient’s care, including hospitalists and specialists.
Thanks to CSMS’ and SHM’s efforts, no regulations or mandates are currently planned in Connecticut.
It is unfortunate that some states, driven by a small vocal group of consumers or sometimes by just one legislator, can single out hospitalists for scrutiny and regulation. Dr. Rifkin found out how important and necessary it is to provide education to the involved legislators, as some professed knowing few of the details of the hospital medicine movement.
While you might be sitting in Texas or Minnesota or California and wondering what all of this has to do with you, know that a wildfire can start from a smoldering ember. SHM must vigilantly monitor the actions of local legislatures and regulators so that in their misunderstanding of hospital medicine or in their concerns for changes in the healthcare system they do not attempt to use the state or federal legislatures for their remedies.
Hospital medicine is new, and we are challenging the status quo. While we are driven by a goal of creating a more efficient healthcare system, driven by accountability and data, some will see the turbulence of change and attempt to rein this in. While some places have seen significant improvements, hospital medicine is still very much in its growth and evolutionary phase. This is the time to have the ability for flexibility and even experimentation in the best sense of the word. It is important not to be stifled by overregulation. At the same time, hospitalists need to be aware that we are no longer a boutique specialty off on the margins of healthcare. Hospital medicine is front and center at more than 2,000 hospitals and with 15,000 hospitalists nationwide too large to be ignored.
Expect more attempts to legislate how hospitalists practice. One SHM member’s e-mail brought the full strength of SHM to quash the wrong bill in Connecticut. We need your local eyes to let us know what is happening out in the real world. In the meantime SHM will work hard to develop the bench strength to be able to rise to your challenges. TH
Dr. Wellikson has been CEO of SHM since 2000.
A few months ago SHM received an e-mail from SHM member Jennifer Bellino, MD, a hospitalist at William Backus Hospital in Norwich, Conn. She had gotten wind of a proposal flowing through the Public Health Committee at the Connecticut State Legislature that would mandate the frequency of communications between hospitalists and primary care physicians (PCPs). From her short e-mail SHM’s advocacy enterprise sprung into action.
Bill 5721 was being introduced to the Public Health Committee in the Connecticut Legislature, and it required the development of state regulations that would have governed the timing and frequency of communications between hospitalists and PCPs.
Laura Allendorf, SHM’s head of Governmental Affairs, engaged SHM’s Public Policy Committee to better understand the issues involved in this bill and to get a sense of whether this was a unique bill for Connecticut or whether it was being introduced in other state legislatures.
While the bill appeared to be isolated to Connecticut, the Public Policy Committee thought the issue was threatening enough to the practice of hospital medicine that local aggressive action was necessary.
Allendorf contacted the Connecticut State Medical Society and spoke to Ken Ferrucci, director of government relations, who was already aware of Bill 5721. The Connecticut State Medical Society (CSMS) was opposed to the bill as well, and Ferrucci proposed that SHM find a Connecticut hospitalist who could come to Hartford to speak against Bill 5721 at the Public Health Committee, which would hear testimony in just a few days.
Unfortunately, no one on the Public Policy Committee was from Connecticut. Fortunately, SHM was familiar with Bill Rifkin, MD, from Yale (New Haven) and Waterbury Hospital, who is active at SHM as a member of our Education Committee. Allendorf contacted Dr. Rifkin and explained the situation. He dropped everything on his calendar and changed his appointments and agreed to come to Hartford to fly the SHM banner and testify before the Public Health Committee.
Working together Allendorf, Eric Siegal, the Public Policy committee chair, and Dr. Rifkin crafted the testimony necessary to explain to the legislators just what hospital medicine is and what hospitalists do. In addition, they emphasized that hospitalists are working hard to be the experts in transitions of care and that mandates and regulations were not needed and, in fact, could be detrimental to the fundamental relationship between PCPs and hospitalists.
SHM then coordinated our approach with that of the Connecticut State Medical Society to create a unified front for maximum effectiveness. In the end Dr. Rifkin carried the day.
After Dr. Rifkin’s testimony, as well as testimony from the Connecticut State Medical Society, the bill died a quiet death. Eventually, a watered down amendment was made to another public health bill, which contained language that basically said hospitalists and PCPs should talk to each other. This amendment asked that the Quality of Care Advisory Committee, which advises the Department of Public Health, make recommendations to the department concerning best practices with respect to communications between a patient’s PCP and other providers involved in a patient’s care, including hospitalists and specialists.
Thanks to CSMS’ and SHM’s efforts, no regulations or mandates are currently planned in Connecticut.
It is unfortunate that some states, driven by a small vocal group of consumers or sometimes by just one legislator, can single out hospitalists for scrutiny and regulation. Dr. Rifkin found out how important and necessary it is to provide education to the involved legislators, as some professed knowing few of the details of the hospital medicine movement.
While you might be sitting in Texas or Minnesota or California and wondering what all of this has to do with you, know that a wildfire can start from a smoldering ember. SHM must vigilantly monitor the actions of local legislatures and regulators so that in their misunderstanding of hospital medicine or in their concerns for changes in the healthcare system they do not attempt to use the state or federal legislatures for their remedies.
Hospital medicine is new, and we are challenging the status quo. While we are driven by a goal of creating a more efficient healthcare system, driven by accountability and data, some will see the turbulence of change and attempt to rein this in. While some places have seen significant improvements, hospital medicine is still very much in its growth and evolutionary phase. This is the time to have the ability for flexibility and even experimentation in the best sense of the word. It is important not to be stifled by overregulation. At the same time, hospitalists need to be aware that we are no longer a boutique specialty off on the margins of healthcare. Hospital medicine is front and center at more than 2,000 hospitals and with 15,000 hospitalists nationwide too large to be ignored.
Expect more attempts to legislate how hospitalists practice. One SHM member’s e-mail brought the full strength of SHM to quash the wrong bill in Connecticut. We need your local eyes to let us know what is happening out in the real world. In the meantime SHM will work hard to develop the bench strength to be able to rise to your challenges. TH
Dr. Wellikson has been CEO of SHM since 2000.
The Specialist Advantage
The speed at which hospital medicine is growing is leaving many hospitalists in uncharted waters as they try to balance clinical practice and academic activities such as teaching, quality improvement, and research.
“Hospitalists often have great ideas but lack the resources to carry them out,” said Scott Flanders, MD, SHM president-elect, clinical associate professor of internal medicine, and director of the hospitalist program at the University of Michigan Health System, Ann Arbor.
Also, hospitalists do not always recognize the role of the subspecialist in diagnosing and treating complex patients—nor the advantages those specialists bring to designing and supporting clinical research. Given the nature of their education, specialists have a deeper understanding than hospitalists of the pathophysiologic concepts and scientific principles underlying important clinical questions, and are more likely to have had fellowship training that includes clinical research experience. They’re likely to be more adept at navigating outside bureaucracies to obtain grants for disease-based investigation.
All in all, specialist participation in hospital-based clinical research projects may improve project feasibility, increase the chances of obtaining money, and allow for wider dissemination of the results than if these projects had been undertaken by hospitalists alone.
“At large institutions, having hospitalists partner with clinical subspecialists could enhance patient enrollment and enhance funding opportunities, because subspecialists have a lot of credibility with funding agencies,” Dr. Flanders says.
Yet, clinical research programs performed by hospitalists and hospital medicine programs still are in an embryonic stage. In this month’s issue of the Journal of Hospital Medicine, he and his colleagues describe a new program for accelerating clinical and translational research by having hospitalists team with subspecialist physicians and other healthcare professionals to ask and answer novel research questions.
SHARP Solution
In the Specialist-Hospitalist Allied Research Program (SHARP), an academic hospitalist and an academic cardiologist serve as principle and co-principle investigators, respectively. Together, they direct a team of supporting personnel, including a hospitalist investigator, clinical research nurse, research associate, and clinical epidemiologist.
The program began in 2006, with the goal of facilitating multicenter, intervention-based clinical trials. Other aims include enhancing patient participation and supporting pilot projects that would generate enough data to attract money for more in-depth studies. The program is paid for three years by the department of internal medicine with revenues generated for the hospital medicine division.
Through SHARP, there will be “a pool of dollars to support a program and provide an infrastructure for a project,” Dr. Flanders says. “Otherwise, each new project would require a new team to find funding [and] perform data analysis.”
SHARP is, in part, an acknowledgment of the increasingly complex nature of clinical research, Dr. Flanders says. “Many big research projects involve more than one specialty, so there will always be a need to collaborate.”
In a sense, the program is an extension of what hospitalists do already. “Hospitalist work in general is often collaborative and team-based,” Dr. Flanders notes. “We frequently work with nurses and other hospital-based staff members.”
How it Works
A steering committee chaired by the two principle investigators and consisting of academic administrators from the University of Michigan will identify appropriate research projects, determine the best allocation of resources, and help the team overcome the bureaucratic hurdles that inevitably arise in any project that includes multiple departments and institutions.
The program has two opening projects. One is aimed at reducing the incidence of false-positive blood cultures. Right now, as many as half of all the blood cultures that test positive at the University of Michigan turn out to be contaminated. The SHARP team has started a randomized, controlled trial to compare the effects of several different skin antiseptics on the false-positive rate, and ultimately will test more than 12,000 blood culture sets. Other key outcomes will be the quantity of additional diagnostic testing generated by positive cultures, use of resources, and associated costs. Mortality and length of stay also will be examined as secondary outcomes.
The second study has been completed, and data analysis has begun. It examined the role of an inpatient clinical pharmacist in preventing medication errors related to hospital discharge among elderly patients.
“In our experience at the University of Michigan, patients frequently have medication-related adverse events after discharge because they do not understand what medications they should be taking, what they are used for, how to manage side effects, or whom to call with problems,” Dr. Flanders and his colleagues wrote. “In addition, predictable medication-related issues (such as ability to pay for a medicine or expected serum electrolyte changes with newly added medications) are not universally anticipated.”
The pharmacist divided his time between a non-resident hospitalist service and a resident general medicine service, focusing on high-risk patients older than 65. Those patients received pre-discharge counseling and post-discharge follow-up calls from the pharmacist within 72 hours and 30 days of leaving the hospital. The key outcomes include medication issues and actions taken by the pharmacist at or after discharge, as well as clinical outcomes such as emergency department visits, readmission rates, and healthcare-related costs.
So far, the biggest challenge faced by the hospitalists interested in SHARP simply has been finding enough hours in the day for it. One of the program’s goals is to generate grant money to hire supporting staff, but right now the doctors must participate on their own time. Nevertheless, says Dr. Flanders, the response to the program has been positive. “It facilitates the small, difficult steps [in funding and implementing research] along the way,” he says. “People have been pleasantly surprised that it works as well as it does.”TH
Norra MacReady is a medical writer based in California.
The speed at which hospital medicine is growing is leaving many hospitalists in uncharted waters as they try to balance clinical practice and academic activities such as teaching, quality improvement, and research.
“Hospitalists often have great ideas but lack the resources to carry them out,” said Scott Flanders, MD, SHM president-elect, clinical associate professor of internal medicine, and director of the hospitalist program at the University of Michigan Health System, Ann Arbor.
Also, hospitalists do not always recognize the role of the subspecialist in diagnosing and treating complex patients—nor the advantages those specialists bring to designing and supporting clinical research. Given the nature of their education, specialists have a deeper understanding than hospitalists of the pathophysiologic concepts and scientific principles underlying important clinical questions, and are more likely to have had fellowship training that includes clinical research experience. They’re likely to be more adept at navigating outside bureaucracies to obtain grants for disease-based investigation.
All in all, specialist participation in hospital-based clinical research projects may improve project feasibility, increase the chances of obtaining money, and allow for wider dissemination of the results than if these projects had been undertaken by hospitalists alone.
“At large institutions, having hospitalists partner with clinical subspecialists could enhance patient enrollment and enhance funding opportunities, because subspecialists have a lot of credibility with funding agencies,” Dr. Flanders says.
Yet, clinical research programs performed by hospitalists and hospital medicine programs still are in an embryonic stage. In this month’s issue of the Journal of Hospital Medicine, he and his colleagues describe a new program for accelerating clinical and translational research by having hospitalists team with subspecialist physicians and other healthcare professionals to ask and answer novel research questions.
SHARP Solution
In the Specialist-Hospitalist Allied Research Program (SHARP), an academic hospitalist and an academic cardiologist serve as principle and co-principle investigators, respectively. Together, they direct a team of supporting personnel, including a hospitalist investigator, clinical research nurse, research associate, and clinical epidemiologist.
The program began in 2006, with the goal of facilitating multicenter, intervention-based clinical trials. Other aims include enhancing patient participation and supporting pilot projects that would generate enough data to attract money for more in-depth studies. The program is paid for three years by the department of internal medicine with revenues generated for the hospital medicine division.
Through SHARP, there will be “a pool of dollars to support a program and provide an infrastructure for a project,” Dr. Flanders says. “Otherwise, each new project would require a new team to find funding [and] perform data analysis.”
SHARP is, in part, an acknowledgment of the increasingly complex nature of clinical research, Dr. Flanders says. “Many big research projects involve more than one specialty, so there will always be a need to collaborate.”
In a sense, the program is an extension of what hospitalists do already. “Hospitalist work in general is often collaborative and team-based,” Dr. Flanders notes. “We frequently work with nurses and other hospital-based staff members.”
How it Works
A steering committee chaired by the two principle investigators and consisting of academic administrators from the University of Michigan will identify appropriate research projects, determine the best allocation of resources, and help the team overcome the bureaucratic hurdles that inevitably arise in any project that includes multiple departments and institutions.
The program has two opening projects. One is aimed at reducing the incidence of false-positive blood cultures. Right now, as many as half of all the blood cultures that test positive at the University of Michigan turn out to be contaminated. The SHARP team has started a randomized, controlled trial to compare the effects of several different skin antiseptics on the false-positive rate, and ultimately will test more than 12,000 blood culture sets. Other key outcomes will be the quantity of additional diagnostic testing generated by positive cultures, use of resources, and associated costs. Mortality and length of stay also will be examined as secondary outcomes.
The second study has been completed, and data analysis has begun. It examined the role of an inpatient clinical pharmacist in preventing medication errors related to hospital discharge among elderly patients.
“In our experience at the University of Michigan, patients frequently have medication-related adverse events after discharge because they do not understand what medications they should be taking, what they are used for, how to manage side effects, or whom to call with problems,” Dr. Flanders and his colleagues wrote. “In addition, predictable medication-related issues (such as ability to pay for a medicine or expected serum electrolyte changes with newly added medications) are not universally anticipated.”
The pharmacist divided his time between a non-resident hospitalist service and a resident general medicine service, focusing on high-risk patients older than 65. Those patients received pre-discharge counseling and post-discharge follow-up calls from the pharmacist within 72 hours and 30 days of leaving the hospital. The key outcomes include medication issues and actions taken by the pharmacist at or after discharge, as well as clinical outcomes such as emergency department visits, readmission rates, and healthcare-related costs.
So far, the biggest challenge faced by the hospitalists interested in SHARP simply has been finding enough hours in the day for it. One of the program’s goals is to generate grant money to hire supporting staff, but right now the doctors must participate on their own time. Nevertheless, says Dr. Flanders, the response to the program has been positive. “It facilitates the small, difficult steps [in funding and implementing research] along the way,” he says. “People have been pleasantly surprised that it works as well as it does.”TH
Norra MacReady is a medical writer based in California.
The speed at which hospital medicine is growing is leaving many hospitalists in uncharted waters as they try to balance clinical practice and academic activities such as teaching, quality improvement, and research.
“Hospitalists often have great ideas but lack the resources to carry them out,” said Scott Flanders, MD, SHM president-elect, clinical associate professor of internal medicine, and director of the hospitalist program at the University of Michigan Health System, Ann Arbor.
Also, hospitalists do not always recognize the role of the subspecialist in diagnosing and treating complex patients—nor the advantages those specialists bring to designing and supporting clinical research. Given the nature of their education, specialists have a deeper understanding than hospitalists of the pathophysiologic concepts and scientific principles underlying important clinical questions, and are more likely to have had fellowship training that includes clinical research experience. They’re likely to be more adept at navigating outside bureaucracies to obtain grants for disease-based investigation.
All in all, specialist participation in hospital-based clinical research projects may improve project feasibility, increase the chances of obtaining money, and allow for wider dissemination of the results than if these projects had been undertaken by hospitalists alone.
“At large institutions, having hospitalists partner with clinical subspecialists could enhance patient enrollment and enhance funding opportunities, because subspecialists have a lot of credibility with funding agencies,” Dr. Flanders says.
Yet, clinical research programs performed by hospitalists and hospital medicine programs still are in an embryonic stage. In this month’s issue of the Journal of Hospital Medicine, he and his colleagues describe a new program for accelerating clinical and translational research by having hospitalists team with subspecialist physicians and other healthcare professionals to ask and answer novel research questions.
SHARP Solution
In the Specialist-Hospitalist Allied Research Program (SHARP), an academic hospitalist and an academic cardiologist serve as principle and co-principle investigators, respectively. Together, they direct a team of supporting personnel, including a hospitalist investigator, clinical research nurse, research associate, and clinical epidemiologist.
The program began in 2006, with the goal of facilitating multicenter, intervention-based clinical trials. Other aims include enhancing patient participation and supporting pilot projects that would generate enough data to attract money for more in-depth studies. The program is paid for three years by the department of internal medicine with revenues generated for the hospital medicine division.
Through SHARP, there will be “a pool of dollars to support a program and provide an infrastructure for a project,” Dr. Flanders says. “Otherwise, each new project would require a new team to find funding [and] perform data analysis.”
SHARP is, in part, an acknowledgment of the increasingly complex nature of clinical research, Dr. Flanders says. “Many big research projects involve more than one specialty, so there will always be a need to collaborate.”
In a sense, the program is an extension of what hospitalists do already. “Hospitalist work in general is often collaborative and team-based,” Dr. Flanders notes. “We frequently work with nurses and other hospital-based staff members.”
How it Works
A steering committee chaired by the two principle investigators and consisting of academic administrators from the University of Michigan will identify appropriate research projects, determine the best allocation of resources, and help the team overcome the bureaucratic hurdles that inevitably arise in any project that includes multiple departments and institutions.
The program has two opening projects. One is aimed at reducing the incidence of false-positive blood cultures. Right now, as many as half of all the blood cultures that test positive at the University of Michigan turn out to be contaminated. The SHARP team has started a randomized, controlled trial to compare the effects of several different skin antiseptics on the false-positive rate, and ultimately will test more than 12,000 blood culture sets. Other key outcomes will be the quantity of additional diagnostic testing generated by positive cultures, use of resources, and associated costs. Mortality and length of stay also will be examined as secondary outcomes.
The second study has been completed, and data analysis has begun. It examined the role of an inpatient clinical pharmacist in preventing medication errors related to hospital discharge among elderly patients.
“In our experience at the University of Michigan, patients frequently have medication-related adverse events after discharge because they do not understand what medications they should be taking, what they are used for, how to manage side effects, or whom to call with problems,” Dr. Flanders and his colleagues wrote. “In addition, predictable medication-related issues (such as ability to pay for a medicine or expected serum electrolyte changes with newly added medications) are not universally anticipated.”
The pharmacist divided his time between a non-resident hospitalist service and a resident general medicine service, focusing on high-risk patients older than 65. Those patients received pre-discharge counseling and post-discharge follow-up calls from the pharmacist within 72 hours and 30 days of leaving the hospital. The key outcomes include medication issues and actions taken by the pharmacist at or after discharge, as well as clinical outcomes such as emergency department visits, readmission rates, and healthcare-related costs.
So far, the biggest challenge faced by the hospitalists interested in SHARP simply has been finding enough hours in the day for it. One of the program’s goals is to generate grant money to hire supporting staff, but right now the doctors must participate on their own time. Nevertheless, says Dr. Flanders, the response to the program has been positive. “It facilitates the small, difficult steps [in funding and implementing research] along the way,” he says. “People have been pleasantly surprised that it works as well as it does.”TH
Norra MacReady is a medical writer based in California.
In the Literature
Literature at a Glance
A guide to this month’s studies.
- Survival of in-hospital cardiac arrest decreases during nights and weekends.
- C-reactive protein levels predict severity and complications in community-acquired pneumonia.
- Adherence to current guidelines improves outcome in treatment of prosthetic joint infection.
- Sodium phosphate bowel prep use is associated with a decline in GFR.
- Minimally interrupted cardiac resuscitation improves survival.
- Lower aPTT increases risk for future VTE.
- Warfarin combined with antiplatelet therapy increases hemorrhage rate.
- Creatinine rise during MI hospitalization is associated with long-term risk of death and ESRD.
- Communication improves patient adherence to beta-blockers after MI.
Does Time of Day Affect Survival of Cardiac Arrest Patients?
Background: In-hospital cardiac arrest is a major public health problem. Small studies have demonstrated survival after cardiac arrest is worse at night as compared with all other times. Multiple hypothesis are proffered for this decreased survival, including less effective detection and treatment of the warning signs of impending arrest during the night hours.
Study design: Prospective registry.
Setting: 507 hospitals participating through the National Registry of Cardiopulmonary Resuscitation.
Synopsis: 86,748 consecutive, inpatient cardiac arrests were reported from Jan. 1, 2000, through Feb. 1, 2007, including 58,593 cases during day/evening hours and 28,155 cases during night hours.
Rates of survival to discharge (14.7 % vs. 19.8%), survival at 24 hours (28.9% vs. 35.4%), and favorable neurological outcomes (11.0% vs. 15.2%) were substantially lower during the night compared with day/evening (all p values < 0.001). The first documented rhythm at night was more frequently asystole as opposed to ventricular fibrillation during the day/evening. There also was a higher survival rate with cardiac arrests during day/evening hours occurring on weekdays compared with weekends (odds ratio [OR] 1.15). There was no difference in survival rates between weekdays or weekends among cardiac arrests occurring during the night hours.
Bottom line: Survival rates for in-hospital cardiac arrest are lower during nights and weekends, which may relate to differential physician and hospital staffing patterns during these hours.
Citation: Peberdy MA, Ornato JP, Larkin GL et al. Survival from in-hospital cardiac arrest during nights and weekends. JAMA 2008;299:785-792.
Can CRP Identify Risk in CAP Patients?
Background: Small initial studies suggest an elevated C-reactive protein (CRP) is relatively nonspecific but may have a role in predicting disease severity in community-acquired pneumonia (CAP).
Study design: Prospective study.
Setting: Large academic center in the United Kingdom.
Synopsis: In this study of 570 patients over a two-year time period, all patients presenting to the hospital with a diagnosis of CAP and the absence of exclusion criteria were evaluated. CRP was measured on admission and repeated on day four of hospitalization.
Low CRP levels (less than 100 mg/L) were independently associated with a reduced risk of 30-day mortality (OR 0.18; p=0.03), need for invasive ventilation and/or inotropic support (OR 0.21; p=0.002), and complicated pneumonia (OR 0.05; p=0.003). In addition, the failure of CRP to fall by 50% or more at day four of hospitalization was associated with an increased risk of 30-day mortality (OR 24.5; p<0.0001), need for mechanical ventilation and/or inotropic support (OR 7.1; p<0.0001), and complicated pneumonia (OR 15.4; p<0.0001).
Patients with chronic lung disease, immunosuppression, active malignancy or hospital-acquired pneumonia were excluded from the study and the conclusions cannot be extrapolated to these higher risk populations.
Bottom line: C-reactive protein is an independent marker of severity in CAP, and low levels can be used as an adjunct to clinical judgment to help identify patients who may be safely discharged from the hospital.
Citation: Chalmers JD, Singanayagam A, Hill AT. C-reactive protein is an independent predictor of severity in community-acquired pneumonia. Am J of Med. 2008;121:219-225.
Do Aggressive Surgical Intervention and Antimicrobial Treatment Improve Outcomes in Patients Suffering PJI?
Background: Prosthetic joint infection (PJI) is a severe complication, causing significant morbidity and healthcare costs. A recent article put forth up to date guidelines for the management of PJI. The purpose of this current study was to evaluate the external clinical validity of these treatment recommendations.
Study design: Retrospective cohort analysis.
Setting: 1,000-bed tertiary care center in Switzerland.
Synopsis: 68 consecutive episodes of PJI from January 1995 through December 2004 were reviewed. Patients with polymicrobial infections and with treatment failures prior to referral to this center were included.
The success rate for treatment of PJI was highest (67%) when the surgical strategy met current recommendations and antimicrobial treatment was adequate or partially adequate. The preferred surgical strategy was a two-stage exchange. The risk of treatment failure was higher for PJI treated with a surgical strategy other than that recommended (hazard ratio [HR] 2.34, p=0.01) and for PJIs treated with antibiotics not corresponding to recommendations (HR 3.45, p=0.002).
This study was limited by its small sample size and retrospective nature. Patients were not randomized, and cure rates for PJI were significantly lower than in prior published studies.
Bottom line: Treatment of PJI in higher risk populations in accordance with currently recommended surgical and antimicrobial treatment recommendations is associated with better outcomes and cure rates.
Citation: Betsch BY, Eggli S, Siebenrock KA, Tauber MG, Muhlemann K. Treatment of joint prosthesis infection in accordance with current recommendations improves outcome. Clin Infect Dis. 2008;46:1221-1226.
Do Oral Sodium Phosphate Drugs in Large Bowel Prep for Endoscopy Worsen Renal Function?
Background: Proper bowel preparation is essential for adequate colonoscopy and flexible sigmoidoscopy. Oral agents that are most commonly used for bowel preparation are sodium phosphate drugs, polyethylglycol and magnesium citrate. Sodium phosphate drugs are often preferred because of the decreased amount of fluid necessary for bowel preparation.
Study design: Retrospective study.
Setting: Scott and White Clinic, Temple, Texas.
Synopsis: Researchers compared 286 patients receiving an oral sodium phosphate solution for colonoscopy bowel preparation with 125 patients with similar comorbidities who received a non-sodium phosphate solution for bowel preparation. All patients had normal baseline creatinine levels.
The baseline, six-month, and one-year glomerular filtration rates (GFR) were compared between the two groups. GFR declined from 79 to 73 to 71 ml/min/1.73 m2 in the study group vs. 76 to 74 to 74 ml/min/1.73 m2 in the control group for the baseline, six-month, and one-year time periods, respectively.
This is an observational study and thus limited by its non-randomized nature. Sodium phosphate has a black-box warning in stage four and five chronic kidney disease because of its deleterious effect on renal function and the potential for inducing electrolyte abnormalities. Given the findings of this study and the availability of other effective preps alternative regimens should be considered for colonic preparation.
Bottom line: Oral sodium phosphate drugs may cause an acute and chronic decline in renal function as measured by the GFR.
Citation: Khurana A, McLean L, Atkinson S, Foulks C. The effect of oral sodium phosphate drug products on renal function in adults is undergoing bowel endoscopy. Arch Intern Med. 2008; 168(6):593-597.
Does MICR Improve Survival-to-hospital Discharge vs. Traditional CPR and ACLS in Cardiac Arrest Outside the Hospital?
Background: Minimally interrupted cardiac resuscitation (MICR), also known as cardiocerebral resuscitation, is hypothesized to increase survival compared with traditional CPR and advanced cardiac life support (ACLS) in out-of-hospital cardiac arrest. In MICR, 200 “pre-shock” chest compressions (100 compressions/minute) are initially given. The rhythm is then analyzed, with a single shock given if indicated.
Study design: Prospective study.
Setting: Two cities in Arizona.
Synopsis: Using data in the Save Heart in Arizona Registry and Education (SHARE) program, outcomes of 218 individuals with cardiac arrest receiving traditional CPR/ACLS were compared to 668 individuals after MICR training was instituted in the same two metropolitan cities. Survival-to-hospital discharge increased from 1.8% (4/218) before MICR training to 5.4% (36/668) after MICR training. The authors then compared the outcomes of 1,799 individuals with cardiac arrest resuscitated by emergency medical services (EMS) who did not receive training in MICR to 661 individuals who received MICR training over the same period. Survival-to-hospital discharge was 9.1% (60/601) in the patients cared from by EMS that received MICR training versus 3.8% (69/1730) in their non-MICR trained colleagues.
This study is limited by its observational nature and lack of randomization. Surprisingly, more individuals were intubated in the MICR groups. For hospitalists, the results could have a dramatic affect on cardiac arrest survival and lead to future changes to CPR/ACLS protocols.
Bottom line: MICR has a significant impact on survival in out-of-hospital cardiac arrest as compared with traditional CPR and ACLS.
Citation: Bobrow B, Clark L, Ewy G, et al. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. JAMA. 2008;299(10):1158-1165.
Does Lower aPTT Increase Future VTE Independent of Other Pro-coagulant Factors?
Background: Certain factors, such as obesity, D-dimer levels, and factor V Leiden gene mutations, increase the risk of future venous thromboembolism (VTE) events. This study sought to determine whether lower baseline levels of activated partial thromboplastin time aPTT also increase this risk.
Study design: Prospective multicenter cohort study.
Setting: Longitudinal Investigation of Thromboembolism Etiology research study (Atherosclerosis Risk in Communities portion) in four U.S. communities.
Synopsis: 13,880 individuals with baseline aPTT measurements were followed for 13 years for future VTE events. Of those, 260 developed a VTE of which 111 were described as idiopathic. Individuals in the lowest two quartiles of aPTT compared with the highest fourth quartile had a 2.4-fold and 1.9-fold increase in the risk of VTE, respectively. A lower aPTT further increased the risk of VTE when associated with obesity, elevated D-dimer level, and particularly factor V Leiden.
This study was limited by the relatively small number of VTE events. It also did not clarify whether aPTT measurements in high-risk groups such as those with positive family history of VTE were useful for predicting risk of future VTE. For hospitalists, patients with a lower initial aPTT may warrant more aggressive inpatient DVT prophylaxis.
Bottom line: aPTT below the median level increases the risk of future VTE events, especially if associated with obesity, elevated D-dimer levels, and/or factor V Leiden.
Citation: Zakai NA, Ohira T, White R, Folsom A, Cushman M. Activated partial thromboplastin time and risk of future venous thromboembolism. Am J of Med. 2008;121:231-238.
What Bleeding Outcomes are Associated with Using Warfarin with Antiplatelet Agents?
Background: Despite a high prevalence of combining antiplatelet and warfarin therapy, the timing, safety, and efficacy of this strategy remain controversial.
Study design: Retrospective cohort study.
Setting: Kaiser Permanente Colorado.
Synopsis: Using a pharmacy database, the authors identified 2,560 patients receiving warfarin alone (monotherapy cohort) and 1,623 patients receiving warfarin combined with antiplatelet agents (combination therapy cohort).
In the combination therapy cohort, aspirin was the most common antiplatelet agent (37%) followed by clopidogrel (13%) and dipyridamole (2%). During a six-month period, the combination therapy cohort had a 4.2% risk of hemorrhage and a 2.0% risk of major hemorrhage. Warfarin monotherapy was associated with a 2% risk of hemorrhage and 0.9% risk of major hemorrhage.
At baseline, the combination therapy patients were twice as likely to have diabetes or congestive heart failure and four times as likely to have coronary artery disease. In both cohorts, the most common reason for warfarin therapy was atrial fibrillation.
Since this was a retrospective investigation, hospitalists should be careful about drawing conclusions from this study alone, but are reminded to discuss risks carefully and engage in shared decision-making with patients when using combined warfarin and antiplatelet therapy.
Bottom line: Warfarin use in combination with antiplatelet therapy is associated with more than double the risk of bleeding compared with warfarin monotherapy.
Citation: Johnson SG, Rogers K, Delate T, Witt DM. Outcomes associated with combined antiplatelet and anticoagulant therapy. Chest. 2008;133:948-954.
Does a Rise in Serum Creatinine Affect Post-hospitalization Mortality and ESRD in Elderly MI Patients?
Background: Previous studies found an association between small changes in serum creatinine during hospitalization and short-term mortality. Data has shown patients experiencing a rise in creatinine at the time of CABG have increased in-hospital and long-term follow-up mortality.
Study design: Retrospective cohort study
Setting: Nationwide Medicare database of acute MI hospitalizations.
Synopsis: The authors reviewed outcomes data for 87,094 patients hospitalized for acute myocardial infarction (MI) from 1994-1995 with follow-up data through 2004. Patients were classified into groups with no rise in creatinine during hospitalization and those with rises of 0.1 mg/dL, 0.2 mg/dL, 0.3-0.5 mg/dL, and 0.6-3 mg/dL.
Compared with patients with no rise in creatinine, a rise of 0.1 mg/dL was associated with an adjusted hazard ratio of 1.45 for end-stage renal disease (ESRD) and 1.14 for post-hospitalization death during long-term follow-up. An incremental increase in poor outcomes was seen with more dramatic increases in creatinine, with patients in the group with a 0.6-3 mg/dL rise in creatinine having an adjusted hazard ratio of 3.26 for ESRD and 1.39 for post-hospitalization death. Among patients with a creatinine rise, the absolute risk of mortality (15% annually) was greater than that of ESRD (0.3% annually).
Hospitalists should note limitations of this retrospective study, including its restriction to hospitalized elderly patients.
Bottom line: Even small rises in serum creatinine during acute hospitalization for MI are associated with long-term risk for death and ESRD in elderly patients.
Citation: Newsome BB, Warnock DG, McClellan WM, et al. Long-term risk of mortality and end-stage renal disease among the elderly after small increases in serum creatinine level during hospitalization for acute myocardial infarction. Arch Intern Med. 2008;168(6):609-616.
Does Direct-to-patient Communication Improve Adherence to Beta-blocker Therapy Following an MI?
Background: The joint American Heart Association and American College of Cardiology guidelines have specific treatment recommendations regarding care of a patient post-myocardial infarction (MI). A key component of this regimen is beta-blocker therapy. Beta-blockers routinely are prescribed at hospital discharge following MI; however, patient adherence has been shown to decline substantially over time.
Study design: Cluster randomized control trial.
Setting: Four health maintenance organizations in Boston, Minneapolis, Atlanta, and Portland, Ore.
Synopsis: 836 post-MI patients were given a beta-blocker prescription upon discharge from the hospital. The intervention group received two mailed communications. The first was a personalized, simply worded letter from a health plan physician-administrator, followed two months later by a similar letter with a brochure. Mailers were low cost and easily replicable; they addressed the importance of these medications, the risks of non-adherence, and adverse effects.
The primary outcome measure was beta-blocker adherence. Medication adherence was analyzed as a continuous measure and as a monthly proportion of days covered (PDC) of 80% or greater. Across all months of follow-up, a mean of 64.8% of intervention patients had a PDC of more than 80% compared with 58.5% of control group patients (number needed to treat=16). The intervention group was 17% more likely to have a PDC of 80% or greater over the entire post-intervention period.
These interventions were studied in a prepaid integrated care delivery system—limiting generalization to other insurance types. Nevertheless, finding ways to improve patient compliance and decrease recurrent cardiac events is liking to result in cost saving to any healthcare plan.
Bottom line: A low-cost direct-to-patient communication effort can have a positive effect on beta-blocker adherence following MI.
Citation: Smith DH, Kramer JM, Perrin N, et al. A randomized trial of direct-to-patient communication to enhance adherence to beta-blocker therapy following myocardial infarction. Arch Intern Med. 2008;168(5):477-483. TH
Literature at a Glance
A guide to this month’s studies.
- Survival of in-hospital cardiac arrest decreases during nights and weekends.
- C-reactive protein levels predict severity and complications in community-acquired pneumonia.
- Adherence to current guidelines improves outcome in treatment of prosthetic joint infection.
- Sodium phosphate bowel prep use is associated with a decline in GFR.
- Minimally interrupted cardiac resuscitation improves survival.
- Lower aPTT increases risk for future VTE.
- Warfarin combined with antiplatelet therapy increases hemorrhage rate.
- Creatinine rise during MI hospitalization is associated with long-term risk of death and ESRD.
- Communication improves patient adherence to beta-blockers after MI.
Does Time of Day Affect Survival of Cardiac Arrest Patients?
Background: In-hospital cardiac arrest is a major public health problem. Small studies have demonstrated survival after cardiac arrest is worse at night as compared with all other times. Multiple hypothesis are proffered for this decreased survival, including less effective detection and treatment of the warning signs of impending arrest during the night hours.
Study design: Prospective registry.
Setting: 507 hospitals participating through the National Registry of Cardiopulmonary Resuscitation.
Synopsis: 86,748 consecutive, inpatient cardiac arrests were reported from Jan. 1, 2000, through Feb. 1, 2007, including 58,593 cases during day/evening hours and 28,155 cases during night hours.
Rates of survival to discharge (14.7 % vs. 19.8%), survival at 24 hours (28.9% vs. 35.4%), and favorable neurological outcomes (11.0% vs. 15.2%) were substantially lower during the night compared with day/evening (all p values < 0.001). The first documented rhythm at night was more frequently asystole as opposed to ventricular fibrillation during the day/evening. There also was a higher survival rate with cardiac arrests during day/evening hours occurring on weekdays compared with weekends (odds ratio [OR] 1.15). There was no difference in survival rates between weekdays or weekends among cardiac arrests occurring during the night hours.
Bottom line: Survival rates for in-hospital cardiac arrest are lower during nights and weekends, which may relate to differential physician and hospital staffing patterns during these hours.
Citation: Peberdy MA, Ornato JP, Larkin GL et al. Survival from in-hospital cardiac arrest during nights and weekends. JAMA 2008;299:785-792.
Can CRP Identify Risk in CAP Patients?
Background: Small initial studies suggest an elevated C-reactive protein (CRP) is relatively nonspecific but may have a role in predicting disease severity in community-acquired pneumonia (CAP).
Study design: Prospective study.
Setting: Large academic center in the United Kingdom.
Synopsis: In this study of 570 patients over a two-year time period, all patients presenting to the hospital with a diagnosis of CAP and the absence of exclusion criteria were evaluated. CRP was measured on admission and repeated on day four of hospitalization.
Low CRP levels (less than 100 mg/L) were independently associated with a reduced risk of 30-day mortality (OR 0.18; p=0.03), need for invasive ventilation and/or inotropic support (OR 0.21; p=0.002), and complicated pneumonia (OR 0.05; p=0.003). In addition, the failure of CRP to fall by 50% or more at day four of hospitalization was associated with an increased risk of 30-day mortality (OR 24.5; p<0.0001), need for mechanical ventilation and/or inotropic support (OR 7.1; p<0.0001), and complicated pneumonia (OR 15.4; p<0.0001).
Patients with chronic lung disease, immunosuppression, active malignancy or hospital-acquired pneumonia were excluded from the study and the conclusions cannot be extrapolated to these higher risk populations.
Bottom line: C-reactive protein is an independent marker of severity in CAP, and low levels can be used as an adjunct to clinical judgment to help identify patients who may be safely discharged from the hospital.
Citation: Chalmers JD, Singanayagam A, Hill AT. C-reactive protein is an independent predictor of severity in community-acquired pneumonia. Am J of Med. 2008;121:219-225.
Do Aggressive Surgical Intervention and Antimicrobial Treatment Improve Outcomes in Patients Suffering PJI?
Background: Prosthetic joint infection (PJI) is a severe complication, causing significant morbidity and healthcare costs. A recent article put forth up to date guidelines for the management of PJI. The purpose of this current study was to evaluate the external clinical validity of these treatment recommendations.
Study design: Retrospective cohort analysis.
Setting: 1,000-bed tertiary care center in Switzerland.
Synopsis: 68 consecutive episodes of PJI from January 1995 through December 2004 were reviewed. Patients with polymicrobial infections and with treatment failures prior to referral to this center were included.
The success rate for treatment of PJI was highest (67%) when the surgical strategy met current recommendations and antimicrobial treatment was adequate or partially adequate. The preferred surgical strategy was a two-stage exchange. The risk of treatment failure was higher for PJI treated with a surgical strategy other than that recommended (hazard ratio [HR] 2.34, p=0.01) and for PJIs treated with antibiotics not corresponding to recommendations (HR 3.45, p=0.002).
This study was limited by its small sample size and retrospective nature. Patients were not randomized, and cure rates for PJI were significantly lower than in prior published studies.
Bottom line: Treatment of PJI in higher risk populations in accordance with currently recommended surgical and antimicrobial treatment recommendations is associated with better outcomes and cure rates.
Citation: Betsch BY, Eggli S, Siebenrock KA, Tauber MG, Muhlemann K. Treatment of joint prosthesis infection in accordance with current recommendations improves outcome. Clin Infect Dis. 2008;46:1221-1226.
Do Oral Sodium Phosphate Drugs in Large Bowel Prep for Endoscopy Worsen Renal Function?
Background: Proper bowel preparation is essential for adequate colonoscopy and flexible sigmoidoscopy. Oral agents that are most commonly used for bowel preparation are sodium phosphate drugs, polyethylglycol and magnesium citrate. Sodium phosphate drugs are often preferred because of the decreased amount of fluid necessary for bowel preparation.
Study design: Retrospective study.
Setting: Scott and White Clinic, Temple, Texas.
Synopsis: Researchers compared 286 patients receiving an oral sodium phosphate solution for colonoscopy bowel preparation with 125 patients with similar comorbidities who received a non-sodium phosphate solution for bowel preparation. All patients had normal baseline creatinine levels.
The baseline, six-month, and one-year glomerular filtration rates (GFR) were compared between the two groups. GFR declined from 79 to 73 to 71 ml/min/1.73 m2 in the study group vs. 76 to 74 to 74 ml/min/1.73 m2 in the control group for the baseline, six-month, and one-year time periods, respectively.
This is an observational study and thus limited by its non-randomized nature. Sodium phosphate has a black-box warning in stage four and five chronic kidney disease because of its deleterious effect on renal function and the potential for inducing electrolyte abnormalities. Given the findings of this study and the availability of other effective preps alternative regimens should be considered for colonic preparation.
Bottom line: Oral sodium phosphate drugs may cause an acute and chronic decline in renal function as measured by the GFR.
Citation: Khurana A, McLean L, Atkinson S, Foulks C. The effect of oral sodium phosphate drug products on renal function in adults is undergoing bowel endoscopy. Arch Intern Med. 2008; 168(6):593-597.
Does MICR Improve Survival-to-hospital Discharge vs. Traditional CPR and ACLS in Cardiac Arrest Outside the Hospital?
Background: Minimally interrupted cardiac resuscitation (MICR), also known as cardiocerebral resuscitation, is hypothesized to increase survival compared with traditional CPR and advanced cardiac life support (ACLS) in out-of-hospital cardiac arrest. In MICR, 200 “pre-shock” chest compressions (100 compressions/minute) are initially given. The rhythm is then analyzed, with a single shock given if indicated.
Study design: Prospective study.
Setting: Two cities in Arizona.
Synopsis: Using data in the Save Heart in Arizona Registry and Education (SHARE) program, outcomes of 218 individuals with cardiac arrest receiving traditional CPR/ACLS were compared to 668 individuals after MICR training was instituted in the same two metropolitan cities. Survival-to-hospital discharge increased from 1.8% (4/218) before MICR training to 5.4% (36/668) after MICR training. The authors then compared the outcomes of 1,799 individuals with cardiac arrest resuscitated by emergency medical services (EMS) who did not receive training in MICR to 661 individuals who received MICR training over the same period. Survival-to-hospital discharge was 9.1% (60/601) in the patients cared from by EMS that received MICR training versus 3.8% (69/1730) in their non-MICR trained colleagues.
This study is limited by its observational nature and lack of randomization. Surprisingly, more individuals were intubated in the MICR groups. For hospitalists, the results could have a dramatic affect on cardiac arrest survival and lead to future changes to CPR/ACLS protocols.
Bottom line: MICR has a significant impact on survival in out-of-hospital cardiac arrest as compared with traditional CPR and ACLS.
Citation: Bobrow B, Clark L, Ewy G, et al. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. JAMA. 2008;299(10):1158-1165.
Does Lower aPTT Increase Future VTE Independent of Other Pro-coagulant Factors?
Background: Certain factors, such as obesity, D-dimer levels, and factor V Leiden gene mutations, increase the risk of future venous thromboembolism (VTE) events. This study sought to determine whether lower baseline levels of activated partial thromboplastin time aPTT also increase this risk.
Study design: Prospective multicenter cohort study.
Setting: Longitudinal Investigation of Thromboembolism Etiology research study (Atherosclerosis Risk in Communities portion) in four U.S. communities.
Synopsis: 13,880 individuals with baseline aPTT measurements were followed for 13 years for future VTE events. Of those, 260 developed a VTE of which 111 were described as idiopathic. Individuals in the lowest two quartiles of aPTT compared with the highest fourth quartile had a 2.4-fold and 1.9-fold increase in the risk of VTE, respectively. A lower aPTT further increased the risk of VTE when associated with obesity, elevated D-dimer level, and particularly factor V Leiden.
This study was limited by the relatively small number of VTE events. It also did not clarify whether aPTT measurements in high-risk groups such as those with positive family history of VTE were useful for predicting risk of future VTE. For hospitalists, patients with a lower initial aPTT may warrant more aggressive inpatient DVT prophylaxis.
Bottom line: aPTT below the median level increases the risk of future VTE events, especially if associated with obesity, elevated D-dimer levels, and/or factor V Leiden.
Citation: Zakai NA, Ohira T, White R, Folsom A, Cushman M. Activated partial thromboplastin time and risk of future venous thromboembolism. Am J of Med. 2008;121:231-238.
What Bleeding Outcomes are Associated with Using Warfarin with Antiplatelet Agents?
Background: Despite a high prevalence of combining antiplatelet and warfarin therapy, the timing, safety, and efficacy of this strategy remain controversial.
Study design: Retrospective cohort study.
Setting: Kaiser Permanente Colorado.
Synopsis: Using a pharmacy database, the authors identified 2,560 patients receiving warfarin alone (monotherapy cohort) and 1,623 patients receiving warfarin combined with antiplatelet agents (combination therapy cohort).
In the combination therapy cohort, aspirin was the most common antiplatelet agent (37%) followed by clopidogrel (13%) and dipyridamole (2%). During a six-month period, the combination therapy cohort had a 4.2% risk of hemorrhage and a 2.0% risk of major hemorrhage. Warfarin monotherapy was associated with a 2% risk of hemorrhage and 0.9% risk of major hemorrhage.
At baseline, the combination therapy patients were twice as likely to have diabetes or congestive heart failure and four times as likely to have coronary artery disease. In both cohorts, the most common reason for warfarin therapy was atrial fibrillation.
Since this was a retrospective investigation, hospitalists should be careful about drawing conclusions from this study alone, but are reminded to discuss risks carefully and engage in shared decision-making with patients when using combined warfarin and antiplatelet therapy.
Bottom line: Warfarin use in combination with antiplatelet therapy is associated with more than double the risk of bleeding compared with warfarin monotherapy.
Citation: Johnson SG, Rogers K, Delate T, Witt DM. Outcomes associated with combined antiplatelet and anticoagulant therapy. Chest. 2008;133:948-954.
Does a Rise in Serum Creatinine Affect Post-hospitalization Mortality and ESRD in Elderly MI Patients?
Background: Previous studies found an association between small changes in serum creatinine during hospitalization and short-term mortality. Data has shown patients experiencing a rise in creatinine at the time of CABG have increased in-hospital and long-term follow-up mortality.
Study design: Retrospective cohort study
Setting: Nationwide Medicare database of acute MI hospitalizations.
Synopsis: The authors reviewed outcomes data for 87,094 patients hospitalized for acute myocardial infarction (MI) from 1994-1995 with follow-up data through 2004. Patients were classified into groups with no rise in creatinine during hospitalization and those with rises of 0.1 mg/dL, 0.2 mg/dL, 0.3-0.5 mg/dL, and 0.6-3 mg/dL.
Compared with patients with no rise in creatinine, a rise of 0.1 mg/dL was associated with an adjusted hazard ratio of 1.45 for end-stage renal disease (ESRD) and 1.14 for post-hospitalization death during long-term follow-up. An incremental increase in poor outcomes was seen with more dramatic increases in creatinine, with patients in the group with a 0.6-3 mg/dL rise in creatinine having an adjusted hazard ratio of 3.26 for ESRD and 1.39 for post-hospitalization death. Among patients with a creatinine rise, the absolute risk of mortality (15% annually) was greater than that of ESRD (0.3% annually).
Hospitalists should note limitations of this retrospective study, including its restriction to hospitalized elderly patients.
Bottom line: Even small rises in serum creatinine during acute hospitalization for MI are associated with long-term risk for death and ESRD in elderly patients.
Citation: Newsome BB, Warnock DG, McClellan WM, et al. Long-term risk of mortality and end-stage renal disease among the elderly after small increases in serum creatinine level during hospitalization for acute myocardial infarction. Arch Intern Med. 2008;168(6):609-616.
Does Direct-to-patient Communication Improve Adherence to Beta-blocker Therapy Following an MI?
Background: The joint American Heart Association and American College of Cardiology guidelines have specific treatment recommendations regarding care of a patient post-myocardial infarction (MI). A key component of this regimen is beta-blocker therapy. Beta-blockers routinely are prescribed at hospital discharge following MI; however, patient adherence has been shown to decline substantially over time.
Study design: Cluster randomized control trial.
Setting: Four health maintenance organizations in Boston, Minneapolis, Atlanta, and Portland, Ore.
Synopsis: 836 post-MI patients were given a beta-blocker prescription upon discharge from the hospital. The intervention group received two mailed communications. The first was a personalized, simply worded letter from a health plan physician-administrator, followed two months later by a similar letter with a brochure. Mailers were low cost and easily replicable; they addressed the importance of these medications, the risks of non-adherence, and adverse effects.
The primary outcome measure was beta-blocker adherence. Medication adherence was analyzed as a continuous measure and as a monthly proportion of days covered (PDC) of 80% or greater. Across all months of follow-up, a mean of 64.8% of intervention patients had a PDC of more than 80% compared with 58.5% of control group patients (number needed to treat=16). The intervention group was 17% more likely to have a PDC of 80% or greater over the entire post-intervention period.
These interventions were studied in a prepaid integrated care delivery system—limiting generalization to other insurance types. Nevertheless, finding ways to improve patient compliance and decrease recurrent cardiac events is liking to result in cost saving to any healthcare plan.
Bottom line: A low-cost direct-to-patient communication effort can have a positive effect on beta-blocker adherence following MI.
Citation: Smith DH, Kramer JM, Perrin N, et al. A randomized trial of direct-to-patient communication to enhance adherence to beta-blocker therapy following myocardial infarction. Arch Intern Med. 2008;168(5):477-483. TH
Literature at a Glance
A guide to this month’s studies.
- Survival of in-hospital cardiac arrest decreases during nights and weekends.
- C-reactive protein levels predict severity and complications in community-acquired pneumonia.
- Adherence to current guidelines improves outcome in treatment of prosthetic joint infection.
- Sodium phosphate bowel prep use is associated with a decline in GFR.
- Minimally interrupted cardiac resuscitation improves survival.
- Lower aPTT increases risk for future VTE.
- Warfarin combined with antiplatelet therapy increases hemorrhage rate.
- Creatinine rise during MI hospitalization is associated with long-term risk of death and ESRD.
- Communication improves patient adherence to beta-blockers after MI.
Does Time of Day Affect Survival of Cardiac Arrest Patients?
Background: In-hospital cardiac arrest is a major public health problem. Small studies have demonstrated survival after cardiac arrest is worse at night as compared with all other times. Multiple hypothesis are proffered for this decreased survival, including less effective detection and treatment of the warning signs of impending arrest during the night hours.
Study design: Prospective registry.
Setting: 507 hospitals participating through the National Registry of Cardiopulmonary Resuscitation.
Synopsis: 86,748 consecutive, inpatient cardiac arrests were reported from Jan. 1, 2000, through Feb. 1, 2007, including 58,593 cases during day/evening hours and 28,155 cases during night hours.
Rates of survival to discharge (14.7 % vs. 19.8%), survival at 24 hours (28.9% vs. 35.4%), and favorable neurological outcomes (11.0% vs. 15.2%) were substantially lower during the night compared with day/evening (all p values < 0.001). The first documented rhythm at night was more frequently asystole as opposed to ventricular fibrillation during the day/evening. There also was a higher survival rate with cardiac arrests during day/evening hours occurring on weekdays compared with weekends (odds ratio [OR] 1.15). There was no difference in survival rates between weekdays or weekends among cardiac arrests occurring during the night hours.
Bottom line: Survival rates for in-hospital cardiac arrest are lower during nights and weekends, which may relate to differential physician and hospital staffing patterns during these hours.
Citation: Peberdy MA, Ornato JP, Larkin GL et al. Survival from in-hospital cardiac arrest during nights and weekends. JAMA 2008;299:785-792.
Can CRP Identify Risk in CAP Patients?
Background: Small initial studies suggest an elevated C-reactive protein (CRP) is relatively nonspecific but may have a role in predicting disease severity in community-acquired pneumonia (CAP).
Study design: Prospective study.
Setting: Large academic center in the United Kingdom.
Synopsis: In this study of 570 patients over a two-year time period, all patients presenting to the hospital with a diagnosis of CAP and the absence of exclusion criteria were evaluated. CRP was measured on admission and repeated on day four of hospitalization.
Low CRP levels (less than 100 mg/L) were independently associated with a reduced risk of 30-day mortality (OR 0.18; p=0.03), need for invasive ventilation and/or inotropic support (OR 0.21; p=0.002), and complicated pneumonia (OR 0.05; p=0.003). In addition, the failure of CRP to fall by 50% or more at day four of hospitalization was associated with an increased risk of 30-day mortality (OR 24.5; p<0.0001), need for mechanical ventilation and/or inotropic support (OR 7.1; p<0.0001), and complicated pneumonia (OR 15.4; p<0.0001).
Patients with chronic lung disease, immunosuppression, active malignancy or hospital-acquired pneumonia were excluded from the study and the conclusions cannot be extrapolated to these higher risk populations.
Bottom line: C-reactive protein is an independent marker of severity in CAP, and low levels can be used as an adjunct to clinical judgment to help identify patients who may be safely discharged from the hospital.
Citation: Chalmers JD, Singanayagam A, Hill AT. C-reactive protein is an independent predictor of severity in community-acquired pneumonia. Am J of Med. 2008;121:219-225.
Do Aggressive Surgical Intervention and Antimicrobial Treatment Improve Outcomes in Patients Suffering PJI?
Background: Prosthetic joint infection (PJI) is a severe complication, causing significant morbidity and healthcare costs. A recent article put forth up to date guidelines for the management of PJI. The purpose of this current study was to evaluate the external clinical validity of these treatment recommendations.
Study design: Retrospective cohort analysis.
Setting: 1,000-bed tertiary care center in Switzerland.
Synopsis: 68 consecutive episodes of PJI from January 1995 through December 2004 were reviewed. Patients with polymicrobial infections and with treatment failures prior to referral to this center were included.
The success rate for treatment of PJI was highest (67%) when the surgical strategy met current recommendations and antimicrobial treatment was adequate or partially adequate. The preferred surgical strategy was a two-stage exchange. The risk of treatment failure was higher for PJI treated with a surgical strategy other than that recommended (hazard ratio [HR] 2.34, p=0.01) and for PJIs treated with antibiotics not corresponding to recommendations (HR 3.45, p=0.002).
This study was limited by its small sample size and retrospective nature. Patients were not randomized, and cure rates for PJI were significantly lower than in prior published studies.
Bottom line: Treatment of PJI in higher risk populations in accordance with currently recommended surgical and antimicrobial treatment recommendations is associated with better outcomes and cure rates.
Citation: Betsch BY, Eggli S, Siebenrock KA, Tauber MG, Muhlemann K. Treatment of joint prosthesis infection in accordance with current recommendations improves outcome. Clin Infect Dis. 2008;46:1221-1226.
Do Oral Sodium Phosphate Drugs in Large Bowel Prep for Endoscopy Worsen Renal Function?
Background: Proper bowel preparation is essential for adequate colonoscopy and flexible sigmoidoscopy. Oral agents that are most commonly used for bowel preparation are sodium phosphate drugs, polyethylglycol and magnesium citrate. Sodium phosphate drugs are often preferred because of the decreased amount of fluid necessary for bowel preparation.
Study design: Retrospective study.
Setting: Scott and White Clinic, Temple, Texas.
Synopsis: Researchers compared 286 patients receiving an oral sodium phosphate solution for colonoscopy bowel preparation with 125 patients with similar comorbidities who received a non-sodium phosphate solution for bowel preparation. All patients had normal baseline creatinine levels.
The baseline, six-month, and one-year glomerular filtration rates (GFR) were compared between the two groups. GFR declined from 79 to 73 to 71 ml/min/1.73 m2 in the study group vs. 76 to 74 to 74 ml/min/1.73 m2 in the control group for the baseline, six-month, and one-year time periods, respectively.
This is an observational study and thus limited by its non-randomized nature. Sodium phosphate has a black-box warning in stage four and five chronic kidney disease because of its deleterious effect on renal function and the potential for inducing electrolyte abnormalities. Given the findings of this study and the availability of other effective preps alternative regimens should be considered for colonic preparation.
Bottom line: Oral sodium phosphate drugs may cause an acute and chronic decline in renal function as measured by the GFR.
Citation: Khurana A, McLean L, Atkinson S, Foulks C. The effect of oral sodium phosphate drug products on renal function in adults is undergoing bowel endoscopy. Arch Intern Med. 2008; 168(6):593-597.
Does MICR Improve Survival-to-hospital Discharge vs. Traditional CPR and ACLS in Cardiac Arrest Outside the Hospital?
Background: Minimally interrupted cardiac resuscitation (MICR), also known as cardiocerebral resuscitation, is hypothesized to increase survival compared with traditional CPR and advanced cardiac life support (ACLS) in out-of-hospital cardiac arrest. In MICR, 200 “pre-shock” chest compressions (100 compressions/minute) are initially given. The rhythm is then analyzed, with a single shock given if indicated.
Study design: Prospective study.
Setting: Two cities in Arizona.
Synopsis: Using data in the Save Heart in Arizona Registry and Education (SHARE) program, outcomes of 218 individuals with cardiac arrest receiving traditional CPR/ACLS were compared to 668 individuals after MICR training was instituted in the same two metropolitan cities. Survival-to-hospital discharge increased from 1.8% (4/218) before MICR training to 5.4% (36/668) after MICR training. The authors then compared the outcomes of 1,799 individuals with cardiac arrest resuscitated by emergency medical services (EMS) who did not receive training in MICR to 661 individuals who received MICR training over the same period. Survival-to-hospital discharge was 9.1% (60/601) in the patients cared from by EMS that received MICR training versus 3.8% (69/1730) in their non-MICR trained colleagues.
This study is limited by its observational nature and lack of randomization. Surprisingly, more individuals were intubated in the MICR groups. For hospitalists, the results could have a dramatic affect on cardiac arrest survival and lead to future changes to CPR/ACLS protocols.
Bottom line: MICR has a significant impact on survival in out-of-hospital cardiac arrest as compared with traditional CPR and ACLS.
Citation: Bobrow B, Clark L, Ewy G, et al. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. JAMA. 2008;299(10):1158-1165.
Does Lower aPTT Increase Future VTE Independent of Other Pro-coagulant Factors?
Background: Certain factors, such as obesity, D-dimer levels, and factor V Leiden gene mutations, increase the risk of future venous thromboembolism (VTE) events. This study sought to determine whether lower baseline levels of activated partial thromboplastin time aPTT also increase this risk.
Study design: Prospective multicenter cohort study.
Setting: Longitudinal Investigation of Thromboembolism Etiology research study (Atherosclerosis Risk in Communities portion) in four U.S. communities.
Synopsis: 13,880 individuals with baseline aPTT measurements were followed for 13 years for future VTE events. Of those, 260 developed a VTE of which 111 were described as idiopathic. Individuals in the lowest two quartiles of aPTT compared with the highest fourth quartile had a 2.4-fold and 1.9-fold increase in the risk of VTE, respectively. A lower aPTT further increased the risk of VTE when associated with obesity, elevated D-dimer level, and particularly factor V Leiden.
This study was limited by the relatively small number of VTE events. It also did not clarify whether aPTT measurements in high-risk groups such as those with positive family history of VTE were useful for predicting risk of future VTE. For hospitalists, patients with a lower initial aPTT may warrant more aggressive inpatient DVT prophylaxis.
Bottom line: aPTT below the median level increases the risk of future VTE events, especially if associated with obesity, elevated D-dimer levels, and/or factor V Leiden.
Citation: Zakai NA, Ohira T, White R, Folsom A, Cushman M. Activated partial thromboplastin time and risk of future venous thromboembolism. Am J of Med. 2008;121:231-238.
What Bleeding Outcomes are Associated with Using Warfarin with Antiplatelet Agents?
Background: Despite a high prevalence of combining antiplatelet and warfarin therapy, the timing, safety, and efficacy of this strategy remain controversial.
Study design: Retrospective cohort study.
Setting: Kaiser Permanente Colorado.
Synopsis: Using a pharmacy database, the authors identified 2,560 patients receiving warfarin alone (monotherapy cohort) and 1,623 patients receiving warfarin combined with antiplatelet agents (combination therapy cohort).
In the combination therapy cohort, aspirin was the most common antiplatelet agent (37%) followed by clopidogrel (13%) and dipyridamole (2%). During a six-month period, the combination therapy cohort had a 4.2% risk of hemorrhage and a 2.0% risk of major hemorrhage. Warfarin monotherapy was associated with a 2% risk of hemorrhage and 0.9% risk of major hemorrhage.
At baseline, the combination therapy patients were twice as likely to have diabetes or congestive heart failure and four times as likely to have coronary artery disease. In both cohorts, the most common reason for warfarin therapy was atrial fibrillation.
Since this was a retrospective investigation, hospitalists should be careful about drawing conclusions from this study alone, but are reminded to discuss risks carefully and engage in shared decision-making with patients when using combined warfarin and antiplatelet therapy.
Bottom line: Warfarin use in combination with antiplatelet therapy is associated with more than double the risk of bleeding compared with warfarin monotherapy.
Citation: Johnson SG, Rogers K, Delate T, Witt DM. Outcomes associated with combined antiplatelet and anticoagulant therapy. Chest. 2008;133:948-954.
Does a Rise in Serum Creatinine Affect Post-hospitalization Mortality and ESRD in Elderly MI Patients?
Background: Previous studies found an association between small changes in serum creatinine during hospitalization and short-term mortality. Data has shown patients experiencing a rise in creatinine at the time of CABG have increased in-hospital and long-term follow-up mortality.
Study design: Retrospective cohort study
Setting: Nationwide Medicare database of acute MI hospitalizations.
Synopsis: The authors reviewed outcomes data for 87,094 patients hospitalized for acute myocardial infarction (MI) from 1994-1995 with follow-up data through 2004. Patients were classified into groups with no rise in creatinine during hospitalization and those with rises of 0.1 mg/dL, 0.2 mg/dL, 0.3-0.5 mg/dL, and 0.6-3 mg/dL.
Compared with patients with no rise in creatinine, a rise of 0.1 mg/dL was associated with an adjusted hazard ratio of 1.45 for end-stage renal disease (ESRD) and 1.14 for post-hospitalization death during long-term follow-up. An incremental increase in poor outcomes was seen with more dramatic increases in creatinine, with patients in the group with a 0.6-3 mg/dL rise in creatinine having an adjusted hazard ratio of 3.26 for ESRD and 1.39 for post-hospitalization death. Among patients with a creatinine rise, the absolute risk of mortality (15% annually) was greater than that of ESRD (0.3% annually).
Hospitalists should note limitations of this retrospective study, including its restriction to hospitalized elderly patients.
Bottom line: Even small rises in serum creatinine during acute hospitalization for MI are associated with long-term risk for death and ESRD in elderly patients.
Citation: Newsome BB, Warnock DG, McClellan WM, et al. Long-term risk of mortality and end-stage renal disease among the elderly after small increases in serum creatinine level during hospitalization for acute myocardial infarction. Arch Intern Med. 2008;168(6):609-616.
Does Direct-to-patient Communication Improve Adherence to Beta-blocker Therapy Following an MI?
Background: The joint American Heart Association and American College of Cardiology guidelines have specific treatment recommendations regarding care of a patient post-myocardial infarction (MI). A key component of this regimen is beta-blocker therapy. Beta-blockers routinely are prescribed at hospital discharge following MI; however, patient adherence has been shown to decline substantially over time.
Study design: Cluster randomized control trial.
Setting: Four health maintenance organizations in Boston, Minneapolis, Atlanta, and Portland, Ore.
Synopsis: 836 post-MI patients were given a beta-blocker prescription upon discharge from the hospital. The intervention group received two mailed communications. The first was a personalized, simply worded letter from a health plan physician-administrator, followed two months later by a similar letter with a brochure. Mailers were low cost and easily replicable; they addressed the importance of these medications, the risks of non-adherence, and adverse effects.
The primary outcome measure was beta-blocker adherence. Medication adherence was analyzed as a continuous measure and as a monthly proportion of days covered (PDC) of 80% or greater. Across all months of follow-up, a mean of 64.8% of intervention patients had a PDC of more than 80% compared with 58.5% of control group patients (number needed to treat=16). The intervention group was 17% more likely to have a PDC of 80% or greater over the entire post-intervention period.
These interventions were studied in a prepaid integrated care delivery system—limiting generalization to other insurance types. Nevertheless, finding ways to improve patient compliance and decrease recurrent cardiac events is liking to result in cost saving to any healthcare plan.
Bottom line: A low-cost direct-to-patient communication effort can have a positive effect on beta-blocker adherence following MI.
Citation: Smith DH, Kramer JM, Perrin N, et al. A randomized trial of direct-to-patient communication to enhance adherence to beta-blocker therapy following myocardial infarction. Arch Intern Med. 2008;168(5):477-483. TH
SHM Explores Social Networks
Dear John Q. Hospitalist,
Recently, a pair of college students in our office presented an impressive summary of Web 2.0, including Facebook.com and LinkedIn.com, to the rest of the SHM staff.
As I listened to their presentation and heard the energy in their voices, I couldn’t help but think about my initial experience and excitement with the World Wide Web. Instead of doing homework, I spent many late nights searching the Internet looking for more information to help me create my first Web page. After countless hours of coding and debugging, as well as throwing the keyboard a time or two, I published my Web page and became a part of the Internet. I was hooked.
After listening to these students I was inspired to check out LinkedIn.com and create my own LinkedIn profile. While I did not stay up until the very early morning sending invites or completing every part of my profile, I found connections to old colleagues, college friends, high school buddies, and family members. Today, I eagerly await the flood of e-mail from people accepting me as a friend in their network, some of them members of SHM. I am hooked again.
Seeing SHM members on LinkedIn got me thinking about how SHM might use social networking technology. I think there is an opportunity here to create an interactive resource that will empower hospitalists to find other hospitalists, make connections, and build their own networks. I’m interested in getting your perspective. Do you think our members will use this type of an online resource?
Many social networking sites on the Internet grew out of individuals in an academic setting trying to find ways to connect with each other. I would imagine many of our student and resident members already are using social networking sites. Do you think this is the case? If so, what features and functions of a social networking tool do you think are most important? Is that different from a third-year resident, or a hospitalist who has been practicing hospital medicine for a number of years?

I know I have thrown a bunch of questions at you, so let me share with you some ideas and maybe we can begin a dialogue that will help SHM find ways in which we can leverage social networking and other Web 2.0 tools.
One of the tasks in creating a LinkedIn account is selecting the college or institution you attended and the years in which you attended. Immediately after setting up my account I was able to see the names of other alumni who attended my university during my four years and invite old friends to join my network. I can envision a scenario where an SHM member indicates which medical school he or she attended and is able to see a list of other colleagues who attended at the same time.
For the general member, someone who hasn’t attended a meeting, participated in a committee, or been more actively engaged in SHM, an online network might be a first step to increased involvement with SHM. Members could use this site to connect with other hospitalists in their area and share their interests and experience with others.
Along the way, they might learn about an SHM initiative they are interested in and connect with another hospitalist who working on this project and begin to have a dialogue. Throughout time, this person builds their network and establishes new connections. When it’s time to register for next year’s SHM Annual Meeting in Chicago, they already know a few faces in the crowd—and maybe a couple of them have become friends.
These are just a couple of ways I think SHM and our members might benefit from social networking. I am confident there are many, many more ways this technology can help our members and the hospital medicine community. What do you think? I would love to hear your thoughts and ideas. E-mail me at sjohnson@hospitalmedicine.org. TH
Dear John Q. Hospitalist,
Recently, a pair of college students in our office presented an impressive summary of Web 2.0, including Facebook.com and LinkedIn.com, to the rest of the SHM staff.
As I listened to their presentation and heard the energy in their voices, I couldn’t help but think about my initial experience and excitement with the World Wide Web. Instead of doing homework, I spent many late nights searching the Internet looking for more information to help me create my first Web page. After countless hours of coding and debugging, as well as throwing the keyboard a time or two, I published my Web page and became a part of the Internet. I was hooked.
After listening to these students I was inspired to check out LinkedIn.com and create my own LinkedIn profile. While I did not stay up until the very early morning sending invites or completing every part of my profile, I found connections to old colleagues, college friends, high school buddies, and family members. Today, I eagerly await the flood of e-mail from people accepting me as a friend in their network, some of them members of SHM. I am hooked again.
Seeing SHM members on LinkedIn got me thinking about how SHM might use social networking technology. I think there is an opportunity here to create an interactive resource that will empower hospitalists to find other hospitalists, make connections, and build their own networks. I’m interested in getting your perspective. Do you think our members will use this type of an online resource?
Many social networking sites on the Internet grew out of individuals in an academic setting trying to find ways to connect with each other. I would imagine many of our student and resident members already are using social networking sites. Do you think this is the case? If so, what features and functions of a social networking tool do you think are most important? Is that different from a third-year resident, or a hospitalist who has been practicing hospital medicine for a number of years?
I know I have thrown a bunch of questions at you, so let me share with you some ideas and maybe we can begin a dialogue that will help SHM find ways in which we can leverage social networking and other Web 2.0 tools.
One of the tasks in creating a LinkedIn account is selecting the college or institution you attended and the years in which you attended. Immediately after setting up my account I was able to see the names of other alumni who attended my university during my four years and invite old friends to join my network. I can envision a scenario where an SHM member indicates which medical school he or she attended and is able to see a list of other colleagues who attended at the same time.
For the general member, someone who hasn’t attended a meeting, participated in a committee, or been more actively engaged in SHM, an online network might be a first step to increased involvement with SHM. Members could use this site to connect with other hospitalists in their area and share their interests and experience with others.
Along the way, they might learn about an SHM initiative they are interested in and connect with another hospitalist who working on this project and begin to have a dialogue. Throughout time, this person builds their network and establishes new connections. When it’s time to register for next year’s SHM Annual Meeting in Chicago, they already know a few faces in the crowd—and maybe a couple of them have become friends.
These are just a couple of ways I think SHM and our members might benefit from social networking. I am confident there are many, many more ways this technology can help our members and the hospital medicine community. What do you think? I would love to hear your thoughts and ideas. E-mail me at sjohnson@hospitalmedicine.org. TH
Dear John Q. Hospitalist,
Recently, a pair of college students in our office presented an impressive summary of Web 2.0, including Facebook.com and LinkedIn.com, to the rest of the SHM staff.
As I listened to their presentation and heard the energy in their voices, I couldn’t help but think about my initial experience and excitement with the World Wide Web. Instead of doing homework, I spent many late nights searching the Internet looking for more information to help me create my first Web page. After countless hours of coding and debugging, as well as throwing the keyboard a time or two, I published my Web page and became a part of the Internet. I was hooked.
After listening to these students I was inspired to check out LinkedIn.com and create my own LinkedIn profile. While I did not stay up until the very early morning sending invites or completing every part of my profile, I found connections to old colleagues, college friends, high school buddies, and family members. Today, I eagerly await the flood of e-mail from people accepting me as a friend in their network, some of them members of SHM. I am hooked again.
Seeing SHM members on LinkedIn got me thinking about how SHM might use social networking technology. I think there is an opportunity here to create an interactive resource that will empower hospitalists to find other hospitalists, make connections, and build their own networks. I’m interested in getting your perspective. Do you think our members will use this type of an online resource?
Many social networking sites on the Internet grew out of individuals in an academic setting trying to find ways to connect with each other. I would imagine many of our student and resident members already are using social networking sites. Do you think this is the case? If so, what features and functions of a social networking tool do you think are most important? Is that different from a third-year resident, or a hospitalist who has been practicing hospital medicine for a number of years?
I know I have thrown a bunch of questions at you, so let me share with you some ideas and maybe we can begin a dialogue that will help SHM find ways in which we can leverage social networking and other Web 2.0 tools.
One of the tasks in creating a LinkedIn account is selecting the college or institution you attended and the years in which you attended. Immediately after setting up my account I was able to see the names of other alumni who attended my university during my four years and invite old friends to join my network. I can envision a scenario where an SHM member indicates which medical school he or she attended and is able to see a list of other colleagues who attended at the same time.
For the general member, someone who hasn’t attended a meeting, participated in a committee, or been more actively engaged in SHM, an online network might be a first step to increased involvement with SHM. Members could use this site to connect with other hospitalists in their area and share their interests and experience with others.
Along the way, they might learn about an SHM initiative they are interested in and connect with another hospitalist who working on this project and begin to have a dialogue. Throughout time, this person builds their network and establishes new connections. When it’s time to register for next year’s SHM Annual Meeting in Chicago, they already know a few faces in the crowd—and maybe a couple of them have become friends.
These are just a couple of ways I think SHM and our members might benefit from social networking. I am confident there are many, many more ways this technology can help our members and the hospital medicine community. What do you think? I would love to hear your thoughts and ideas. E-mail me at sjohnson@hospitalmedicine.org. TH
Fellow in HM
One of the best things about working in the membership department is seeing the passion and commitment our members have for the success of our specialty. You also get to hear about what is needed to elevate our field to the next level.
Throughout the past 10 years, hospitalists have been asking for a unique designation that clearly identifies those physicians whose career is committed to hospital medicine. SHM wants you to know that we have heard you and have responded to this need by creating a Fellowship in Hospital Medicine (FHM) program.
Hospitalists who earn their FHM designation will have a demonstrated commitment to hospital medicine, systems change, and quality improvement principals. There will be three designations available, each with increasingly more challenging selection criteria:
- Fellow in Hospital Medicine (FHM);
- Senior Fellow in Hospital Medicine (SFHM); and
- Master in Hospital Medicine (MHM).
Application requirements include:
- Five years as a practicing hospitalist;
- Demonstration of competencies tied to the SHM Core Competencies in Hospital Medicine, including systems improvement, quality initiatives, and clinical excellence; and
- Endorsement by two active SHM members.
Applications for Fellow in Hospital Medicine will be available this fall, and the first class will be inducted at Hospital Medicine 2009 in Chicago.
One of the best things about working in the membership department is seeing the passion and commitment our members have for the success of our specialty. You also get to hear about what is needed to elevate our field to the next level.
Throughout the past 10 years, hospitalists have been asking for a unique designation that clearly identifies those physicians whose career is committed to hospital medicine. SHM wants you to know that we have heard you and have responded to this need by creating a Fellowship in Hospital Medicine (FHM) program.
Hospitalists who earn their FHM designation will have a demonstrated commitment to hospital medicine, systems change, and quality improvement principals. There will be three designations available, each with increasingly more challenging selection criteria:
- Fellow in Hospital Medicine (FHM);
- Senior Fellow in Hospital Medicine (SFHM); and
- Master in Hospital Medicine (MHM).
Application requirements include:
- Five years as a practicing hospitalist;
- Demonstration of competencies tied to the SHM Core Competencies in Hospital Medicine, including systems improvement, quality initiatives, and clinical excellence; and
- Endorsement by two active SHM members.
Applications for Fellow in Hospital Medicine will be available this fall, and the first class will be inducted at Hospital Medicine 2009 in Chicago.
One of the best things about working in the membership department is seeing the passion and commitment our members have for the success of our specialty. You also get to hear about what is needed to elevate our field to the next level.
Throughout the past 10 years, hospitalists have been asking for a unique designation that clearly identifies those physicians whose career is committed to hospital medicine. SHM wants you to know that we have heard you and have responded to this need by creating a Fellowship in Hospital Medicine (FHM) program.
Hospitalists who earn their FHM designation will have a demonstrated commitment to hospital medicine, systems change, and quality improvement principals. There will be three designations available, each with increasingly more challenging selection criteria:
- Fellow in Hospital Medicine (FHM);
- Senior Fellow in Hospital Medicine (SFHM); and
- Master in Hospital Medicine (MHM).
Application requirements include:
- Five years as a practicing hospitalist;
- Demonstration of competencies tied to the SHM Core Competencies in Hospital Medicine, including systems improvement, quality initiatives, and clinical excellence; and
- Endorsement by two active SHM members.
Applications for Fellow in Hospital Medicine will be available this fall, and the first class will be inducted at Hospital Medicine 2009 in Chicago.
Hyperuricemia and Gout
Supplement Editor:
Brian F. Mandell, MD, PhD
Contents
Despite its treatability, gout remains a problem: Confessions of a goutophile
Brian F. Mandell, MD, PhD
The pathogenesis of gout
H. Ralph Schumacher, Jr, MD
Clinical manifestations of hyperuricemia and gout
Brian F. Mandell, MD, PhD
Epidemiology of gout
Arthur L. Weaver, MD, MS
The role of hyperuricemia and gout in kidney and cardiovascular disease
N. Lawrence Edwards, MD
The gout diagnosis
Robin K. Dore, MD
The practical management of gout
H. Ralph Schumacher, Jr, MD, and Lan X. Chen, MD, PhD
Supplement Editor:
Brian F. Mandell, MD, PhD
Contents
Despite its treatability, gout remains a problem: Confessions of a goutophile
Brian F. Mandell, MD, PhD
The pathogenesis of gout
H. Ralph Schumacher, Jr, MD
Clinical manifestations of hyperuricemia and gout
Brian F. Mandell, MD, PhD
Epidemiology of gout
Arthur L. Weaver, MD, MS
The role of hyperuricemia and gout in kidney and cardiovascular disease
N. Lawrence Edwards, MD
The gout diagnosis
Robin K. Dore, MD
The practical management of gout
H. Ralph Schumacher, Jr, MD, and Lan X. Chen, MD, PhD
Supplement Editor:
Brian F. Mandell, MD, PhD
Contents
Despite its treatability, gout remains a problem: Confessions of a goutophile
Brian F. Mandell, MD, PhD
The pathogenesis of gout
H. Ralph Schumacher, Jr, MD
Clinical manifestations of hyperuricemia and gout
Brian F. Mandell, MD, PhD
Epidemiology of gout
Arthur L. Weaver, MD, MS
The role of hyperuricemia and gout in kidney and cardiovascular disease
N. Lawrence Edwards, MD
The gout diagnosis
Robin K. Dore, MD
The practical management of gout
H. Ralph Schumacher, Jr, MD, and Lan X. Chen, MD, PhD