User login
Data Daze

As I write this column, our nation’s economy is looking pretty shaky. In early January, the labor market report showed a significant uptick in the unemployment rate. This led worried investors to sell stocks, and the Federal Reserve lowered the interest rate dramatically in response to the sudden fall in the stock market. Or at least that’s the version of events we’re being fed by most of the press.
Do investors overreact to job numbers? There is a lot of debate about the accuracy of job and unemployment statistics. Clearly they are valuable, but there are all kinds of problems with the way the labor surveys are conducted and the resulting data analyzed.
There may not be a better way to collect the data, so despite their flaws surveys may provide the best information on the labor market that we can get.
The real problem arises when investors—sort of like you and me but a lot richer—look at these data and fail to keep in mind all its strengths and weaknesses. There is a risk people will focus on a single number and overestimate its precision. This has been called the “salience bias.” Writing in The New Yorker, James Surowiecki says this salience bias can lead to “a hard-to-break feedback loop: The fact that traders act as if the jobs report were definitive makes it so. A little information can be a dangerous thing.”1
I discuss hospitalist survey data with people all the time. I’m struck by how often they seem misled by salience bias, among other things. With SHM’s release this month of its latest biannual survey of hospitalist productivity and compensation, now seems like a good time to discuss the strengths and weaknesses in the data—and cautions when interpreting it.
Understand the strengths and limitations of the survey. SHM’s “Bi-Annual Survey on the State of the Hospital Medicine Movement” is a self-reporting survey in which each practice leader (or his/her designee) completes the survey. The responses aren’t verified or audited, so some respondents might submit shoddy data. Perhaps a busy group leader might complete the survey from memory and estimate things like each doctor’s production of work-only relative value units (wRVUs). When I’ve looked at the raw data, I’ve wondered if some respondents are trying to “spin” their numbers higher or lower for a variety of reasons (e.g., to look unusually good or show how hard their doctors can work). And there may be a response bias: Those who think their practice is atypical might not respond to the survey.
This year, SHM worked to “scrub” the data. Outlier metrics were established for each question, and SHM staff followed up with the respondent to ensure he/she understood the question and provided accurate data. In fact, I completed the survey for the group I’m part of and got a call from a survey staffer questioning the productivity I reported for some members of the group (our nocturnists have lower wRVU productivity than others in the group—that is one reason they’re willing to work at night).
Remember that data are historical and should be “aged” to the time period you’re using it. The data in the 2008 SHM survey were collected from October through December.
Review the original questions asked in the survey. To make sense of the survey responses, you will need to clearly understand the question asked. Review the survey instrument and form your own conclusions about ways the questions were posed that might influence the responses. And don’t assume you understand what a particular term means—verify it by looking at the survey instrument. For example, I encounter a wide variety of opinions regarding what constitutes base salary, incentive pay, productivity compensation, bonus, and total compensation. The survey instrument spells these things out clearly.
It can be valuable to trend some data over successive surveys. For example, you may want to know the trend in the average hospitalist’s wRVU productivity over the past two surveys. You should look at the questions asked in both surveys to make sure there hasn’t been a change that could influence the responses. In the case of wRVUs you will need to understand how the January 2007 change in wRVUs values for many services provided by hospitalists was handled by the survey.
Pay attention to how data are lumped or split. Some data are appropriate for analysis of hospitalist groups, other data for individual hospitalists. If half of hospitalist groups use a shift-based schedule, that doesn’t mean half of individual hospitalists work such a schedule. Shift-based schedules are more common in larger groups, so even if half the groups in the country schedule by shifts, there may be 80% of individual hospitalists who use this schedule.
Salary incentives illustrate another way responses are lumped or split. As of the last survey (reported in 2006), most hospitalists had a variable component to their compensation—most often based on productivity or quality. There are relatively few ways hospitalists are paid on productivity (basing it on wRVUs is most common). But there are myriad quality incentives, based on things like Centers for Medicare and Medicaid Services core measures, and patient and referring physician satisfaction. Depending on how you aggregated these different categories in the 2006 survey, you might reach different conclusions about whether more hospitalists have productivity-based incentives or quality-based incentives (productivity was more common in the 2006 survey).
Drill down to respondent populations that most closely match your group. There is a real temptation to overemphasize the “headline” numbers in the survey like the average total salary for a hospitalist. Yet in many cases, it may be more useful to drill down to a population that matches your group. You might be most interested in compensation for hospital-employed hospitalists in non-teaching hospitals in the South (thereby excluding academicians and pediatric hospitalists from your comparison group). Just make sure to look at the resultant sample size (the “n”) reported for that subset of the data to make sure it is large enough to be meaningful.
Remember that the survey is not telling you what is right for your group. The survey simply describes a number of metrics relevant to hospitalist practice. It is not SHM’s position on the right compensation or productivity for a particular practice. It is the best source of national data regarding hospitalists. (See my column “Comp Close-Up” for a comparison between the SHM and Medical Group Management Association surveys [July 2007, p.73]). Things like the two other hospitalist practices in your town probably will have a lot more to do with influencing your group’s productivity and compensation metrics than any national data set.
While it’s tempting to reduce things to a single number (e.g., how much is the average hospitalist paid?) this is falling prey to salience bias. Try to grasp the stories behind the numbers by understanding the survey methods and looking at responses for different subsets of the survey population. And realize that the right or optimal compensation and productivity for a group might be quite different from the survey means and medians. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Surowiecki J. Running numbers. The New Yorker. January 21, 2008. Available online at www.newyorker.com/talk/financial/2008/01/21/080121ta_talk_surowiecki. Last accessed Feb. 7, 2008.
As I write this column, our nation’s economy is looking pretty shaky. In early January, the labor market report showed a significant uptick in the unemployment rate. This led worried investors to sell stocks, and the Federal Reserve lowered the interest rate dramatically in response to the sudden fall in the stock market. Or at least that’s the version of events we’re being fed by most of the press.
Do investors overreact to job numbers? There is a lot of debate about the accuracy of job and unemployment statistics. Clearly they are valuable, but there are all kinds of problems with the way the labor surveys are conducted and the resulting data analyzed.
There may not be a better way to collect the data, so despite their flaws surveys may provide the best information on the labor market that we can get.
The real problem arises when investors—sort of like you and me but a lot richer—look at these data and fail to keep in mind all its strengths and weaknesses. There is a risk people will focus on a single number and overestimate its precision. This has been called the “salience bias.” Writing in The New Yorker, James Surowiecki says this salience bias can lead to “a hard-to-break feedback loop: The fact that traders act as if the jobs report were definitive makes it so. A little information can be a dangerous thing.”1
I discuss hospitalist survey data with people all the time. I’m struck by how often they seem misled by salience bias, among other things. With SHM’s release this month of its latest biannual survey of hospitalist productivity and compensation, now seems like a good time to discuss the strengths and weaknesses in the data—and cautions when interpreting it.
Understand the strengths and limitations of the survey. SHM’s “Bi-Annual Survey on the State of the Hospital Medicine Movement” is a self-reporting survey in which each practice leader (or his/her designee) completes the survey. The responses aren’t verified or audited, so some respondents might submit shoddy data. Perhaps a busy group leader might complete the survey from memory and estimate things like each doctor’s production of work-only relative value units (wRVUs). When I’ve looked at the raw data, I’ve wondered if some respondents are trying to “spin” their numbers higher or lower for a variety of reasons (e.g., to look unusually good or show how hard their doctors can work). And there may be a response bias: Those who think their practice is atypical might not respond to the survey.
This year, SHM worked to “scrub” the data. Outlier metrics were established for each question, and SHM staff followed up with the respondent to ensure he/she understood the question and provided accurate data. In fact, I completed the survey for the group I’m part of and got a call from a survey staffer questioning the productivity I reported for some members of the group (our nocturnists have lower wRVU productivity than others in the group—that is one reason they’re willing to work at night).
Remember that data are historical and should be “aged” to the time period you’re using it. The data in the 2008 SHM survey were collected from October through December.
Review the original questions asked in the survey. To make sense of the survey responses, you will need to clearly understand the question asked. Review the survey instrument and form your own conclusions about ways the questions were posed that might influence the responses. And don’t assume you understand what a particular term means—verify it by looking at the survey instrument. For example, I encounter a wide variety of opinions regarding what constitutes base salary, incentive pay, productivity compensation, bonus, and total compensation. The survey instrument spells these things out clearly.
It can be valuable to trend some data over successive surveys. For example, you may want to know the trend in the average hospitalist’s wRVU productivity over the past two surveys. You should look at the questions asked in both surveys to make sure there hasn’t been a change that could influence the responses. In the case of wRVUs you will need to understand how the January 2007 change in wRVUs values for many services provided by hospitalists was handled by the survey.
Pay attention to how data are lumped or split. Some data are appropriate for analysis of hospitalist groups, other data for individual hospitalists. If half of hospitalist groups use a shift-based schedule, that doesn’t mean half of individual hospitalists work such a schedule. Shift-based schedules are more common in larger groups, so even if half the groups in the country schedule by shifts, there may be 80% of individual hospitalists who use this schedule.
Salary incentives illustrate another way responses are lumped or split. As of the last survey (reported in 2006), most hospitalists had a variable component to their compensation—most often based on productivity or quality. There are relatively few ways hospitalists are paid on productivity (basing it on wRVUs is most common). But there are myriad quality incentives, based on things like Centers for Medicare and Medicaid Services core measures, and patient and referring physician satisfaction. Depending on how you aggregated these different categories in the 2006 survey, you might reach different conclusions about whether more hospitalists have productivity-based incentives or quality-based incentives (productivity was more common in the 2006 survey).
Drill down to respondent populations that most closely match your group. There is a real temptation to overemphasize the “headline” numbers in the survey like the average total salary for a hospitalist. Yet in many cases, it may be more useful to drill down to a population that matches your group. You might be most interested in compensation for hospital-employed hospitalists in non-teaching hospitals in the South (thereby excluding academicians and pediatric hospitalists from your comparison group). Just make sure to look at the resultant sample size (the “n”) reported for that subset of the data to make sure it is large enough to be meaningful.
Remember that the survey is not telling you what is right for your group. The survey simply describes a number of metrics relevant to hospitalist practice. It is not SHM’s position on the right compensation or productivity for a particular practice. It is the best source of national data regarding hospitalists. (See my column “Comp Close-Up” for a comparison between the SHM and Medical Group Management Association surveys [July 2007, p.73]). Things like the two other hospitalist practices in your town probably will have a lot more to do with influencing your group’s productivity and compensation metrics than any national data set.
While it’s tempting to reduce things to a single number (e.g., how much is the average hospitalist paid?) this is falling prey to salience bias. Try to grasp the stories behind the numbers by understanding the survey methods and looking at responses for different subsets of the survey population. And realize that the right or optimal compensation and productivity for a group might be quite different from the survey means and medians. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Surowiecki J. Running numbers. The New Yorker. January 21, 2008. Available online at www.newyorker.com/talk/financial/2008/01/21/080121ta_talk_surowiecki. Last accessed Feb. 7, 2008.
As I write this column, our nation’s economy is looking pretty shaky. In early January, the labor market report showed a significant uptick in the unemployment rate. This led worried investors to sell stocks, and the Federal Reserve lowered the interest rate dramatically in response to the sudden fall in the stock market. Or at least that’s the version of events we’re being fed by most of the press.
Do investors overreact to job numbers? There is a lot of debate about the accuracy of job and unemployment statistics. Clearly they are valuable, but there are all kinds of problems with the way the labor surveys are conducted and the resulting data analyzed.
There may not be a better way to collect the data, so despite their flaws surveys may provide the best information on the labor market that we can get.
The real problem arises when investors—sort of like you and me but a lot richer—look at these data and fail to keep in mind all its strengths and weaknesses. There is a risk people will focus on a single number and overestimate its precision. This has been called the “salience bias.” Writing in The New Yorker, James Surowiecki says this salience bias can lead to “a hard-to-break feedback loop: The fact that traders act as if the jobs report were definitive makes it so. A little information can be a dangerous thing.”1
I discuss hospitalist survey data with people all the time. I’m struck by how often they seem misled by salience bias, among other things. With SHM’s release this month of its latest biannual survey of hospitalist productivity and compensation, now seems like a good time to discuss the strengths and weaknesses in the data—and cautions when interpreting it.
Understand the strengths and limitations of the survey. SHM’s “Bi-Annual Survey on the State of the Hospital Medicine Movement” is a self-reporting survey in which each practice leader (or his/her designee) completes the survey. The responses aren’t verified or audited, so some respondents might submit shoddy data. Perhaps a busy group leader might complete the survey from memory and estimate things like each doctor’s production of work-only relative value units (wRVUs). When I’ve looked at the raw data, I’ve wondered if some respondents are trying to “spin” their numbers higher or lower for a variety of reasons (e.g., to look unusually good or show how hard their doctors can work). And there may be a response bias: Those who think their practice is atypical might not respond to the survey.
This year, SHM worked to “scrub” the data. Outlier metrics were established for each question, and SHM staff followed up with the respondent to ensure he/she understood the question and provided accurate data. In fact, I completed the survey for the group I’m part of and got a call from a survey staffer questioning the productivity I reported for some members of the group (our nocturnists have lower wRVU productivity than others in the group—that is one reason they’re willing to work at night).
Remember that data are historical and should be “aged” to the time period you’re using it. The data in the 2008 SHM survey were collected from October through December.
Review the original questions asked in the survey. To make sense of the survey responses, you will need to clearly understand the question asked. Review the survey instrument and form your own conclusions about ways the questions were posed that might influence the responses. And don’t assume you understand what a particular term means—verify it by looking at the survey instrument. For example, I encounter a wide variety of opinions regarding what constitutes base salary, incentive pay, productivity compensation, bonus, and total compensation. The survey instrument spells these things out clearly.
It can be valuable to trend some data over successive surveys. For example, you may want to know the trend in the average hospitalist’s wRVU productivity over the past two surveys. You should look at the questions asked in both surveys to make sure there hasn’t been a change that could influence the responses. In the case of wRVUs you will need to understand how the January 2007 change in wRVUs values for many services provided by hospitalists was handled by the survey.
Pay attention to how data are lumped or split. Some data are appropriate for analysis of hospitalist groups, other data for individual hospitalists. If half of hospitalist groups use a shift-based schedule, that doesn’t mean half of individual hospitalists work such a schedule. Shift-based schedules are more common in larger groups, so even if half the groups in the country schedule by shifts, there may be 80% of individual hospitalists who use this schedule.
Salary incentives illustrate another way responses are lumped or split. As of the last survey (reported in 2006), most hospitalists had a variable component to their compensation—most often based on productivity or quality. There are relatively few ways hospitalists are paid on productivity (basing it on wRVUs is most common). But there are myriad quality incentives, based on things like Centers for Medicare and Medicaid Services core measures, and patient and referring physician satisfaction. Depending on how you aggregated these different categories in the 2006 survey, you might reach different conclusions about whether more hospitalists have productivity-based incentives or quality-based incentives (productivity was more common in the 2006 survey).
Drill down to respondent populations that most closely match your group. There is a real temptation to overemphasize the “headline” numbers in the survey like the average total salary for a hospitalist. Yet in many cases, it may be more useful to drill down to a population that matches your group. You might be most interested in compensation for hospital-employed hospitalists in non-teaching hospitals in the South (thereby excluding academicians and pediatric hospitalists from your comparison group). Just make sure to look at the resultant sample size (the “n”) reported for that subset of the data to make sure it is large enough to be meaningful.
Remember that the survey is not telling you what is right for your group. The survey simply describes a number of metrics relevant to hospitalist practice. It is not SHM’s position on the right compensation or productivity for a particular practice. It is the best source of national data regarding hospitalists. (See my column “Comp Close-Up” for a comparison between the SHM and Medical Group Management Association surveys [July 2007, p.73]). Things like the two other hospitalist practices in your town probably will have a lot more to do with influencing your group’s productivity and compensation metrics than any national data set.
While it’s tempting to reduce things to a single number (e.g., how much is the average hospitalist paid?) this is falling prey to salience bias. Try to grasp the stories behind the numbers by understanding the survey methods and looking at responses for different subsets of the survey population. And realize that the right or optimal compensation and productivity for a group might be quite different from the survey means and medians. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Surowiecki J. Running numbers. The New Yorker. January 21, 2008. Available online at www.newyorker.com/talk/financial/2008/01/21/080121ta_talk_surowiecki. Last accessed Feb. 7, 2008.
MySpace For Hospitalists

As I stared down the length of a limp, moderately deflated breakfast burrito, my thoughts meandered. I doubted about the ability of my little chylomicron-infused buddy to dust the cobwebs from a night in the Gaslamp Quarter that overemphasized wine and underemphasized sleep. I pondered the merit of showing up at 6:30 in the morning for this meeting.
I was shaken from my musings by a voice introducing himself as Bob Wachter. Clearly this apparition parading as one of the luminaries of the hospital medicine movement must be another manifestation of a night of overabundant revelry—and not my adviser for this SHM mentorship breakfast.
It turns out it was the real Dr. Wachter, and indeed he was there to provide an hour and a half of his undivided attention to mentor me as an early-career academic hospitalist. The year was 2003, the location San Diego, the event the sixth SHM Annual Meeting. The significance: This was my first SHM meeting.
Descending on San Diego five years later, I’ve had the chance to reflect on my growth as a hospitalist and the enzymatic role the society’s annual meeting has played in my development.
At the time I had been an academic hospitalist at the Denver Veterans Affairs Medical Center for three years. I’d come to San Diego to learn more about this group that was—until a name change announced at this meeting—calling itself the NAIP, or the National Association of Inpatient Physicians. I also came to present, for the first time, a research abstract.
The annual meeting represents many things to many people. For some it is a time to expand their clinical horizons. Indeed, the clinical content is top-notch and ensures that attendees stay current. The meeting also offers opportunities to learn a new skill such as how to build a hospital medicine program, become a top-notch educator, or develop procedural skills.
Others look to the meeting to present their research data to their peers. Still others attend to get away from the grind of their daily job and bathe in the rejuvenating energy of the annual meeting. Some even look to the meeting location as a vehicle to visit distant family or explore a new or favorite city.
I came to my first annual meeting to sample many of these offerings. What I found was something unexpected and powerful—a professional and social network.
This brings me back to my encounter with Bob. I had seen him speak the day prior at the “Building and Improving Hospitalist Programs” pre-course. Bob gave a rousing and edifying discourse about documenting the value of your hospitalist group. Our early morning gathering was part of the SHM mentorship breakfast, where an early-career hospitalist is paired with a more senior hospitalist in his/her area of interest for career counseling.
Meeting the man who coined the word “hospitalist” was, needless to say, a little nerve-wracking. However, Bob was disarming, engaging, and truly interested in helping me advance. We talked about the development of a hospitalist group at the University of Colorado, a new group I was to direct in three short months. Subsequent to our meeting, Bob was instrumental in helping me develop our group’s business plan, connecting frequently via e-mail and phone.
Later that morning as I was setting up my abstract poster, I looked up to find one of my medical school colleagues, Thomas McIlriath, perusing the aisles of posters.
Thomas, who directs the Mercy Medical Group’s hospitalist program in Sacramento, and I had been good friends in medical school but found our friendship sidetracked by the grind of residency training at different institutions. I had not seen or heard from him in seven years. I later stumbled upon another medical school colleague and quite enjoyed the opportunity to reconnect with such important figures from my past.
Over lunch I attended my first SHM research committee meeting. Not knowing what to expect, I found a group of early-career hospitalists interested in developing academic careers and a burgeoning SHM research infrastructure. I also met Andy Auerbach, MD, at the time a slightly younger but no less talented clinician-researcher at the University of California, San Francisco. Over the years I’ve had the chance to get to know Andy much better and have found him an inspiration, a collaborator, and an enjoyable person to reconnect with whenever serendipity offers us the chance.
Toward the end of the first day’s sessions I attended an innovations workshop that featured a presentation of an online billing tool I thought might be the answer to a research question that I had. Unbeknownst to me the presenter was Eric Siegal, MD, who had graduated from my residency the year before I started and had been a passing acquaintance.
In the end, the presentation was not the answer to my question. But connecting with Eric, now a regional director at Cogent Healthcare, was not only pleasurable but has led to a burgeoning professional bond and personal friendship that has resulted in a couple of co-written publications, hikes through the mountains of Montana, and too numerous to count phone calls seeking professional advice.
That evening I presented my data to my peers at the abstract session and found the feedback to be interesting and enlightening. I also found it another opportunity to discover like-minded people with common interests.
One of them was Ken Epstein, MD, with IPC-The Hospitalist Company. It turned out that Ken had access to data that could answer the research question that had brought me to the innovations session earlier in the day.
Since this encounter, Ken and I have published the answer to our research question and formed a friendship and collaboration that continues to grow today.
While I didn’t recognize it at the time, that span of 24 hours in early April 2003 was arguably the most important and productive day of my working career. I reconnected with old friends, developed new professional acquaintances, and, most important, forged several new and lasting friendships.
As I ready myself for another annual meeting in San Diego I excitedly ponder the opportunities that await me—not least of which is another go in the Gaslamp Quarter! TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I stared down the length of a limp, moderately deflated breakfast burrito, my thoughts meandered. I doubted about the ability of my little chylomicron-infused buddy to dust the cobwebs from a night in the Gaslamp Quarter that overemphasized wine and underemphasized sleep. I pondered the merit of showing up at 6:30 in the morning for this meeting.
I was shaken from my musings by a voice introducing himself as Bob Wachter. Clearly this apparition parading as one of the luminaries of the hospital medicine movement must be another manifestation of a night of overabundant revelry—and not my adviser for this SHM mentorship breakfast.
It turns out it was the real Dr. Wachter, and indeed he was there to provide an hour and a half of his undivided attention to mentor me as an early-career academic hospitalist. The year was 2003, the location San Diego, the event the sixth SHM Annual Meeting. The significance: This was my first SHM meeting.
Descending on San Diego five years later, I’ve had the chance to reflect on my growth as a hospitalist and the enzymatic role the society’s annual meeting has played in my development.
At the time I had been an academic hospitalist at the Denver Veterans Affairs Medical Center for three years. I’d come to San Diego to learn more about this group that was—until a name change announced at this meeting—calling itself the NAIP, or the National Association of Inpatient Physicians. I also came to present, for the first time, a research abstract.
The annual meeting represents many things to many people. For some it is a time to expand their clinical horizons. Indeed, the clinical content is top-notch and ensures that attendees stay current. The meeting also offers opportunities to learn a new skill such as how to build a hospital medicine program, become a top-notch educator, or develop procedural skills.
Others look to the meeting to present their research data to their peers. Still others attend to get away from the grind of their daily job and bathe in the rejuvenating energy of the annual meeting. Some even look to the meeting location as a vehicle to visit distant family or explore a new or favorite city.
I came to my first annual meeting to sample many of these offerings. What I found was something unexpected and powerful—a professional and social network.
This brings me back to my encounter with Bob. I had seen him speak the day prior at the “Building and Improving Hospitalist Programs” pre-course. Bob gave a rousing and edifying discourse about documenting the value of your hospitalist group. Our early morning gathering was part of the SHM mentorship breakfast, where an early-career hospitalist is paired with a more senior hospitalist in his/her area of interest for career counseling.
Meeting the man who coined the word “hospitalist” was, needless to say, a little nerve-wracking. However, Bob was disarming, engaging, and truly interested in helping me advance. We talked about the development of a hospitalist group at the University of Colorado, a new group I was to direct in three short months. Subsequent to our meeting, Bob was instrumental in helping me develop our group’s business plan, connecting frequently via e-mail and phone.
Later that morning as I was setting up my abstract poster, I looked up to find one of my medical school colleagues, Thomas McIlriath, perusing the aisles of posters.
Thomas, who directs the Mercy Medical Group’s hospitalist program in Sacramento, and I had been good friends in medical school but found our friendship sidetracked by the grind of residency training at different institutions. I had not seen or heard from him in seven years. I later stumbled upon another medical school colleague and quite enjoyed the opportunity to reconnect with such important figures from my past.
Over lunch I attended my first SHM research committee meeting. Not knowing what to expect, I found a group of early-career hospitalists interested in developing academic careers and a burgeoning SHM research infrastructure. I also met Andy Auerbach, MD, at the time a slightly younger but no less talented clinician-researcher at the University of California, San Francisco. Over the years I’ve had the chance to get to know Andy much better and have found him an inspiration, a collaborator, and an enjoyable person to reconnect with whenever serendipity offers us the chance.
Toward the end of the first day’s sessions I attended an innovations workshop that featured a presentation of an online billing tool I thought might be the answer to a research question that I had. Unbeknownst to me the presenter was Eric Siegal, MD, who had graduated from my residency the year before I started and had been a passing acquaintance.
In the end, the presentation was not the answer to my question. But connecting with Eric, now a regional director at Cogent Healthcare, was not only pleasurable but has led to a burgeoning professional bond and personal friendship that has resulted in a couple of co-written publications, hikes through the mountains of Montana, and too numerous to count phone calls seeking professional advice.
That evening I presented my data to my peers at the abstract session and found the feedback to be interesting and enlightening. I also found it another opportunity to discover like-minded people with common interests.
One of them was Ken Epstein, MD, with IPC-The Hospitalist Company. It turned out that Ken had access to data that could answer the research question that had brought me to the innovations session earlier in the day.
Since this encounter, Ken and I have published the answer to our research question and formed a friendship and collaboration that continues to grow today.
While I didn’t recognize it at the time, that span of 24 hours in early April 2003 was arguably the most important and productive day of my working career. I reconnected with old friends, developed new professional acquaintances, and, most important, forged several new and lasting friendships.
As I ready myself for another annual meeting in San Diego I excitedly ponder the opportunities that await me—not least of which is another go in the Gaslamp Quarter! TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I stared down the length of a limp, moderately deflated breakfast burrito, my thoughts meandered. I doubted about the ability of my little chylomicron-infused buddy to dust the cobwebs from a night in the Gaslamp Quarter that overemphasized wine and underemphasized sleep. I pondered the merit of showing up at 6:30 in the morning for this meeting.
I was shaken from my musings by a voice introducing himself as Bob Wachter. Clearly this apparition parading as one of the luminaries of the hospital medicine movement must be another manifestation of a night of overabundant revelry—and not my adviser for this SHM mentorship breakfast.
It turns out it was the real Dr. Wachter, and indeed he was there to provide an hour and a half of his undivided attention to mentor me as an early-career academic hospitalist. The year was 2003, the location San Diego, the event the sixth SHM Annual Meeting. The significance: This was my first SHM meeting.
Descending on San Diego five years later, I’ve had the chance to reflect on my growth as a hospitalist and the enzymatic role the society’s annual meeting has played in my development.
At the time I had been an academic hospitalist at the Denver Veterans Affairs Medical Center for three years. I’d come to San Diego to learn more about this group that was—until a name change announced at this meeting—calling itself the NAIP, or the National Association of Inpatient Physicians. I also came to present, for the first time, a research abstract.
The annual meeting represents many things to many people. For some it is a time to expand their clinical horizons. Indeed, the clinical content is top-notch and ensures that attendees stay current. The meeting also offers opportunities to learn a new skill such as how to build a hospital medicine program, become a top-notch educator, or develop procedural skills.
Others look to the meeting to present their research data to their peers. Still others attend to get away from the grind of their daily job and bathe in the rejuvenating energy of the annual meeting. Some even look to the meeting location as a vehicle to visit distant family or explore a new or favorite city.
I came to my first annual meeting to sample many of these offerings. What I found was something unexpected and powerful—a professional and social network.
This brings me back to my encounter with Bob. I had seen him speak the day prior at the “Building and Improving Hospitalist Programs” pre-course. Bob gave a rousing and edifying discourse about documenting the value of your hospitalist group. Our early morning gathering was part of the SHM mentorship breakfast, where an early-career hospitalist is paired with a more senior hospitalist in his/her area of interest for career counseling.
Meeting the man who coined the word “hospitalist” was, needless to say, a little nerve-wracking. However, Bob was disarming, engaging, and truly interested in helping me advance. We talked about the development of a hospitalist group at the University of Colorado, a new group I was to direct in three short months. Subsequent to our meeting, Bob was instrumental in helping me develop our group’s business plan, connecting frequently via e-mail and phone.
Later that morning as I was setting up my abstract poster, I looked up to find one of my medical school colleagues, Thomas McIlriath, perusing the aisles of posters.
Thomas, who directs the Mercy Medical Group’s hospitalist program in Sacramento, and I had been good friends in medical school but found our friendship sidetracked by the grind of residency training at different institutions. I had not seen or heard from him in seven years. I later stumbled upon another medical school colleague and quite enjoyed the opportunity to reconnect with such important figures from my past.
Over lunch I attended my first SHM research committee meeting. Not knowing what to expect, I found a group of early-career hospitalists interested in developing academic careers and a burgeoning SHM research infrastructure. I also met Andy Auerbach, MD, at the time a slightly younger but no less talented clinician-researcher at the University of California, San Francisco. Over the years I’ve had the chance to get to know Andy much better and have found him an inspiration, a collaborator, and an enjoyable person to reconnect with whenever serendipity offers us the chance.
Toward the end of the first day’s sessions I attended an innovations workshop that featured a presentation of an online billing tool I thought might be the answer to a research question that I had. Unbeknownst to me the presenter was Eric Siegal, MD, who had graduated from my residency the year before I started and had been a passing acquaintance.
In the end, the presentation was not the answer to my question. But connecting with Eric, now a regional director at Cogent Healthcare, was not only pleasurable but has led to a burgeoning professional bond and personal friendship that has resulted in a couple of co-written publications, hikes through the mountains of Montana, and too numerous to count phone calls seeking professional advice.
That evening I presented my data to my peers at the abstract session and found the feedback to be interesting and enlightening. I also found it another opportunity to discover like-minded people with common interests.
One of them was Ken Epstein, MD, with IPC-The Hospitalist Company. It turned out that Ken had access to data that could answer the research question that had brought me to the innovations session earlier in the day.
Since this encounter, Ken and I have published the answer to our research question and formed a friendship and collaboration that continues to grow today.
While I didn’t recognize it at the time, that span of 24 hours in early April 2003 was arguably the most important and productive day of my working career. I reconnected with old friends, developed new professional acquaintances, and, most important, forged several new and lasting friendships.
As I ready myself for another annual meeting in San Diego I excitedly ponder the opportunities that await me—not least of which is another go in the Gaslamp Quarter! TH
Dr. Glasheen is associate professor of medicine at the University of Colorado at Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
See Further

The rate of change within hospital medicine has been astounding over the past 11 years, and we have always tried to position SHM to remain nimble to respond to those changes. Racing legend Mario Andretti once said that if everything seems under control, you aren’t going fast enough.
Rapid responsiveness has become deeply ingrained within the culture of SHM. Every member should be proud because this is the result of the hard work and dedication of the many members who simply refuse to accept the status quo.
A few months ago, I met with a group of young hospitalists. We were discussing a variety of topics when one of the hospitalists asked in a frustrated tone, “When is the change going to stop?” Her program was experiencing rapid growth while still trying to recruit sufficient hospitalists. Yet at the same time, she was enjoying involvement in several quality improvement projects at her hospital.
I began to talk with her about schedules, smart growth, time management—all the management techniques I have picked up over time. But she pushed back: “No, when is it going to stop? I love my job, but all this change and push to see more patients and comply with increasing safety/quality mandates is really stressing me. I simply see no end in sight. Our program is going to end up admitting or consulting on almost every patient in this hospital. We can’t find enough hospitalists! When is it going to stop?”
Before answering her, I thought about all the accomplishments of hospital medicine, particularly those fostered by SHM. The list is numerous. I wondered whether, despite our nimbleness, we were still helping this frustrated hospitalist and her patients. She was asking what it’s going to take to move beyond the frustration despite 11 years of hospital medicine milestones.
My answer: It is not going to stop until we look beyond our current view. We have laid a great foundation at SHM and in hospital medicine, but we must embrace a different method of delivering care to our patients. Our long-term professional satisfaction demands it. Moreover, if we really want to deliver high-quality care to the many patients we are being asked to see, this change is an absolute necessity. It won’t come easily, but hospitalists are not alone in this; many other specialties must face it, as well.
During my 13 years as a hospitalist—half of which were spent in hospital medicine private practice—I have seen patients in 10 hospitals. These hospitals ranged from a 100-bed community hospital to a 600-bed academic medical center. Some have been for profit, some not for profit, and some government sponsored. What is interesting is that in each of these facilities, my ability to see patients was vastly different. In one hospital, I could comfortably see 25 to 30 patients a day. In another, I could barely see eight to 10. In some, the admission process took me 30 minutes, in another 90 minutes.
What is the difference in these hospitals? It usually isn’t much. Maybe it’s the fact the charts are always in one place. Maybe the electronic medical record is simply better, or the ward secretaries more helpful. Or maybe it’s several of these factors, and others. But the point is that it is possible to vastly improve things with some minor tweaks in the system. It usually happens when the hospital and physicians have communicated with each other to make these changes.
But what if the hospital and the hospital medicine group engage in a true partnership—a proactive joint venture in which each fully appreciates the other’s value proposition? What if each seeks to deliver something greater than the mere sum of hospital resources and hospitalist resources? Suppose the hospital embraces the idea of helping build structure and processes to maximize the number of patients seen by a hospitalist. Suppose the hospital medicine program embraces this but also embraces the goal of high-quality care in all its dimensions. What results is true synergy, where both parties benefit tremendously and the real winner is the patient. This won’t happen just by tweaking to make improvements at the edges; only wholesale change will take patient care delivery to a new level.
This will require hospitalists to embrace new methods of patient care. When I speak of this concept to hospitalists, I ask them to imagine doubling the amount of patients they currently see. If your census is 15 patients a day, imagine seeing 30. Most hospitalists immediately push back and say it isn’t possible because they can’t envision a new way of patient care. But what if by engaging in this partnership, the hospital brought to bear all its potential resources to help you—maybe a scribe, or several midlevel providers? What if there were zero barriers to finding data? What if the pharmacist took such a reliable medication history that you could fully depend on it? How about before you see a patient, a history and physical was already done so all you had to do was review the findings?
Many of you are still skeptical. Some of you struggle just getting approval for a part-time administrative person. You can’t ever imagine the hospital providing additional resources. Trust me when I tell you times are changing. One of the chief concerns all hospital executives have is the imperative to change the hospital-physician relationship. Much has been written on this topic, and the prevailing wisdom among hospital leaders is that the old medical staff leadership concept is dead. New types of leadership are necessary if hospitals and physicians are to survive.1
Because I am a hospitalist and a hospital executive, I feel the hospital part is the easy one. As chief medical officer, my main goal is to improve the quality of care delivered. The chief constraint I encounter is the number of engaged physicians. Much of my day is spent working with physicians to engage them in a hospital-physician partnership. The No. 1 thing preventing engagement is clinical workload. From the hospital perspective, I know I need to mobilize hospital resources to help physicians and remove time as the constraint. But for me to take them away from seeing patients may also hurt the hospital.
Now don’t misunderstand me. I am not advocating an improvement in efficiency just for the sake of it or just to improve our recruiting problems. The vision must be the delivery of higher quality care.
Change is not over. SHM’s responsiveness to change will greatly enhance your ability to promote change from within your hospital. Physician leadership is essential.2 We have much more to accomplish, but SHM is well positioned to continue to help you and your patients. We will continue to be nimble. We will continue to respond to the many changes on the road ahead. Even the road we can’t quite see yet. TH
Dr. Cawley is president of SHM.
References
- Petasnick WD. Hospital-physician relationships: imperative for clinical enterprise collaboration. Front Health Serv Manage. 2007;24(1):1:3-10.
- Porter M, Teisberg EO. How physicians can change the future of healthcare. JAMA. 2007;297(10):1103-1111.
The rate of change within hospital medicine has been astounding over the past 11 years, and we have always tried to position SHM to remain nimble to respond to those changes. Racing legend Mario Andretti once said that if everything seems under control, you aren’t going fast enough.
Rapid responsiveness has become deeply ingrained within the culture of SHM. Every member should be proud because this is the result of the hard work and dedication of the many members who simply refuse to accept the status quo.
A few months ago, I met with a group of young hospitalists. We were discussing a variety of topics when one of the hospitalists asked in a frustrated tone, “When is the change going to stop?” Her program was experiencing rapid growth while still trying to recruit sufficient hospitalists. Yet at the same time, she was enjoying involvement in several quality improvement projects at her hospital.
I began to talk with her about schedules, smart growth, time management—all the management techniques I have picked up over time. But she pushed back: “No, when is it going to stop? I love my job, but all this change and push to see more patients and comply with increasing safety/quality mandates is really stressing me. I simply see no end in sight. Our program is going to end up admitting or consulting on almost every patient in this hospital. We can’t find enough hospitalists! When is it going to stop?”
Before answering her, I thought about all the accomplishments of hospital medicine, particularly those fostered by SHM. The list is numerous. I wondered whether, despite our nimbleness, we were still helping this frustrated hospitalist and her patients. She was asking what it’s going to take to move beyond the frustration despite 11 years of hospital medicine milestones.
My answer: It is not going to stop until we look beyond our current view. We have laid a great foundation at SHM and in hospital medicine, but we must embrace a different method of delivering care to our patients. Our long-term professional satisfaction demands it. Moreover, if we really want to deliver high-quality care to the many patients we are being asked to see, this change is an absolute necessity. It won’t come easily, but hospitalists are not alone in this; many other specialties must face it, as well.
During my 13 years as a hospitalist—half of which were spent in hospital medicine private practice—I have seen patients in 10 hospitals. These hospitals ranged from a 100-bed community hospital to a 600-bed academic medical center. Some have been for profit, some not for profit, and some government sponsored. What is interesting is that in each of these facilities, my ability to see patients was vastly different. In one hospital, I could comfortably see 25 to 30 patients a day. In another, I could barely see eight to 10. In some, the admission process took me 30 minutes, in another 90 minutes.
What is the difference in these hospitals? It usually isn’t much. Maybe it’s the fact the charts are always in one place. Maybe the electronic medical record is simply better, or the ward secretaries more helpful. Or maybe it’s several of these factors, and others. But the point is that it is possible to vastly improve things with some minor tweaks in the system. It usually happens when the hospital and physicians have communicated with each other to make these changes.
But what if the hospital and the hospital medicine group engage in a true partnership—a proactive joint venture in which each fully appreciates the other’s value proposition? What if each seeks to deliver something greater than the mere sum of hospital resources and hospitalist resources? Suppose the hospital embraces the idea of helping build structure and processes to maximize the number of patients seen by a hospitalist. Suppose the hospital medicine program embraces this but also embraces the goal of high-quality care in all its dimensions. What results is true synergy, where both parties benefit tremendously and the real winner is the patient. This won’t happen just by tweaking to make improvements at the edges; only wholesale change will take patient care delivery to a new level.
This will require hospitalists to embrace new methods of patient care. When I speak of this concept to hospitalists, I ask them to imagine doubling the amount of patients they currently see. If your census is 15 patients a day, imagine seeing 30. Most hospitalists immediately push back and say it isn’t possible because they can’t envision a new way of patient care. But what if by engaging in this partnership, the hospital brought to bear all its potential resources to help you—maybe a scribe, or several midlevel providers? What if there were zero barriers to finding data? What if the pharmacist took such a reliable medication history that you could fully depend on it? How about before you see a patient, a history and physical was already done so all you had to do was review the findings?
Many of you are still skeptical. Some of you struggle just getting approval for a part-time administrative person. You can’t ever imagine the hospital providing additional resources. Trust me when I tell you times are changing. One of the chief concerns all hospital executives have is the imperative to change the hospital-physician relationship. Much has been written on this topic, and the prevailing wisdom among hospital leaders is that the old medical staff leadership concept is dead. New types of leadership are necessary if hospitals and physicians are to survive.1
Because I am a hospitalist and a hospital executive, I feel the hospital part is the easy one. As chief medical officer, my main goal is to improve the quality of care delivered. The chief constraint I encounter is the number of engaged physicians. Much of my day is spent working with physicians to engage them in a hospital-physician partnership. The No. 1 thing preventing engagement is clinical workload. From the hospital perspective, I know I need to mobilize hospital resources to help physicians and remove time as the constraint. But for me to take them away from seeing patients may also hurt the hospital.
Now don’t misunderstand me. I am not advocating an improvement in efficiency just for the sake of it or just to improve our recruiting problems. The vision must be the delivery of higher quality care.
Change is not over. SHM’s responsiveness to change will greatly enhance your ability to promote change from within your hospital. Physician leadership is essential.2 We have much more to accomplish, but SHM is well positioned to continue to help you and your patients. We will continue to be nimble. We will continue to respond to the many changes on the road ahead. Even the road we can’t quite see yet. TH
Dr. Cawley is president of SHM.
References
- Petasnick WD. Hospital-physician relationships: imperative for clinical enterprise collaboration. Front Health Serv Manage. 2007;24(1):1:3-10.
- Porter M, Teisberg EO. How physicians can change the future of healthcare. JAMA. 2007;297(10):1103-1111.
The rate of change within hospital medicine has been astounding over the past 11 years, and we have always tried to position SHM to remain nimble to respond to those changes. Racing legend Mario Andretti once said that if everything seems under control, you aren’t going fast enough.
Rapid responsiveness has become deeply ingrained within the culture of SHM. Every member should be proud because this is the result of the hard work and dedication of the many members who simply refuse to accept the status quo.
A few months ago, I met with a group of young hospitalists. We were discussing a variety of topics when one of the hospitalists asked in a frustrated tone, “When is the change going to stop?” Her program was experiencing rapid growth while still trying to recruit sufficient hospitalists. Yet at the same time, she was enjoying involvement in several quality improvement projects at her hospital.
I began to talk with her about schedules, smart growth, time management—all the management techniques I have picked up over time. But she pushed back: “No, when is it going to stop? I love my job, but all this change and push to see more patients and comply with increasing safety/quality mandates is really stressing me. I simply see no end in sight. Our program is going to end up admitting or consulting on almost every patient in this hospital. We can’t find enough hospitalists! When is it going to stop?”
Before answering her, I thought about all the accomplishments of hospital medicine, particularly those fostered by SHM. The list is numerous. I wondered whether, despite our nimbleness, we were still helping this frustrated hospitalist and her patients. She was asking what it’s going to take to move beyond the frustration despite 11 years of hospital medicine milestones.
My answer: It is not going to stop until we look beyond our current view. We have laid a great foundation at SHM and in hospital medicine, but we must embrace a different method of delivering care to our patients. Our long-term professional satisfaction demands it. Moreover, if we really want to deliver high-quality care to the many patients we are being asked to see, this change is an absolute necessity. It won’t come easily, but hospitalists are not alone in this; many other specialties must face it, as well.
During my 13 years as a hospitalist—half of which were spent in hospital medicine private practice—I have seen patients in 10 hospitals. These hospitals ranged from a 100-bed community hospital to a 600-bed academic medical center. Some have been for profit, some not for profit, and some government sponsored. What is interesting is that in each of these facilities, my ability to see patients was vastly different. In one hospital, I could comfortably see 25 to 30 patients a day. In another, I could barely see eight to 10. In some, the admission process took me 30 minutes, in another 90 minutes.
What is the difference in these hospitals? It usually isn’t much. Maybe it’s the fact the charts are always in one place. Maybe the electronic medical record is simply better, or the ward secretaries more helpful. Or maybe it’s several of these factors, and others. But the point is that it is possible to vastly improve things with some minor tweaks in the system. It usually happens when the hospital and physicians have communicated with each other to make these changes.
But what if the hospital and the hospital medicine group engage in a true partnership—a proactive joint venture in which each fully appreciates the other’s value proposition? What if each seeks to deliver something greater than the mere sum of hospital resources and hospitalist resources? Suppose the hospital embraces the idea of helping build structure and processes to maximize the number of patients seen by a hospitalist. Suppose the hospital medicine program embraces this but also embraces the goal of high-quality care in all its dimensions. What results is true synergy, where both parties benefit tremendously and the real winner is the patient. This won’t happen just by tweaking to make improvements at the edges; only wholesale change will take patient care delivery to a new level.
This will require hospitalists to embrace new methods of patient care. When I speak of this concept to hospitalists, I ask them to imagine doubling the amount of patients they currently see. If your census is 15 patients a day, imagine seeing 30. Most hospitalists immediately push back and say it isn’t possible because they can’t envision a new way of patient care. But what if by engaging in this partnership, the hospital brought to bear all its potential resources to help you—maybe a scribe, or several midlevel providers? What if there were zero barriers to finding data? What if the pharmacist took such a reliable medication history that you could fully depend on it? How about before you see a patient, a history and physical was already done so all you had to do was review the findings?
Many of you are still skeptical. Some of you struggle just getting approval for a part-time administrative person. You can’t ever imagine the hospital providing additional resources. Trust me when I tell you times are changing. One of the chief concerns all hospital executives have is the imperative to change the hospital-physician relationship. Much has been written on this topic, and the prevailing wisdom among hospital leaders is that the old medical staff leadership concept is dead. New types of leadership are necessary if hospitals and physicians are to survive.1
Because I am a hospitalist and a hospital executive, I feel the hospital part is the easy one. As chief medical officer, my main goal is to improve the quality of care delivered. The chief constraint I encounter is the number of engaged physicians. Much of my day is spent working with physicians to engage them in a hospital-physician partnership. The No. 1 thing preventing engagement is clinical workload. From the hospital perspective, I know I need to mobilize hospital resources to help physicians and remove time as the constraint. But for me to take them away from seeing patients may also hurt the hospital.
Now don’t misunderstand me. I am not advocating an improvement in efficiency just for the sake of it or just to improve our recruiting problems. The vision must be the delivery of higher quality care.
Change is not over. SHM’s responsiveness to change will greatly enhance your ability to promote change from within your hospital. Physician leadership is essential.2 We have much more to accomplish, but SHM is well positioned to continue to help you and your patients. We will continue to be nimble. We will continue to respond to the many changes on the road ahead. Even the road we can’t quite see yet. TH
Dr. Cawley is president of SHM.
References
- Petasnick WD. Hospital-physician relationships: imperative for clinical enterprise collaboration. Front Health Serv Manage. 2007;24(1):1:3-10.
- Porter M, Teisberg EO. How physicians can change the future of healthcare. JAMA. 2007;297(10):1103-1111.
Feedback Failures
On the evening of July 30, 1945, a U.S. battleship traveling from Guam to the Philippines was spotted in the Philippine Sea by a Japanese submarine crew. Six torpedoes sped across the black water with devastating effect.
Three hundred sailors died immediately as the stricken ship sank. Another 900 men were left floating in an oil slick in the shark-infested Pacific Ocean for four days.1
The events that led to the sinking represent a classic tale of systems failures. They ring familiar to any physician who has closely examined modern medical error.
The communication breakdown that prevented the ship’s captain from being aware of submarine activity on the same route four days before is no different than communication breakdowns in complex hospital systems. The bureaucratic decision by a remote administrator to withhold the safety measure of an escort to prevent such an attack on the grounds that it “lacked necessity” likely resonates with physicians who have struggled with getting authorization for care.
Why did those sailors remain in the water four days before rescue? Despite being only a two-hour flight from the nearest base, they were not recovered—or even missed—for what must have seemed an endless amount of time.
In the end, slightly more than 300 men were alive when they were spotted by a plane that happened to fly past. The rest succumbed to dehydration, exposure, and sharks. The failure of the Navy to rescue the sailors offers lessons to the clinician trying to improve transitions of care more than a half a century later.
The Feedback Loop
Hospital discharge is a complex process initiated by physician orders on charts, prescription pads, and patient instructions. Most often, the things we assume will be done out of our direct view are carried out satisfactorily. However, any hospitalist can easily recount stories of tests or follow-up that didn’t happen as ordered. Patients who fall through the cracks at discharge—like the stranded sailors of the USS Indianapolis—are, in part, the story of a simple omitted step: the feedback loop.
A feedback loop occurs when the results or consequences of an action are returned as an input loop to the initiating step in order to modify subsequent actions. This fundamental engineering concept can keep complex systems on course. The feedback loop allows the lack of completion of a portion of a process to be recognized—and corrective measures taken—before additional harm occurs.
In Guam, the island base from which the USS Indianapolis departed, the marker indicating the ship on the plotting board was removed when the ship left. Later, the Philippine port of Leyte failed to note that the ship didn’t arrive. Policy at the time was that all ships that left port were presumed to have arrived at their destination unless a call indicating trouble was received. The junior officer who noticed that the ship hadn’t arrived assumed there had been an order to divert to an alternate port. The Navy had no feedback mechanism to communicate between the two ports and raise an alarm when a ship did not arrive. In fact, a Navy directive discouraged communicating the arrival of combat ships as a matter of military secrecy. As a result, no rescue mission was launched—and the sharks began to arrive.
A closer examination of usual hospitalist discharge practice reveals too much similarity for comfort. Similar to how the USS Indianapolis was removed from the plotting board on Guam, discharged patients are removed from the hospitalist’s census list. Follow-up becomes the responsibility of the patient and primary care physician.
Communication with the primary care provider is recognized as a best practice for discharge, but research suggests direct communication occurs less than 20% of the time.2 These dismal statistic suggests the “port of arrival” is unaware our patients are expected in a significant percentage of discharges. Outpatient physicians, like the junior port director in Leyte, may assume that patients who do not call or arrive for appointments have been readmitted, seen by another physician, or otherwise diverted.
Even a superficial review reveals significant deficits in the feedback provided by our current discharge practice. When patients don’t arrive at follow-up appointments, most hospitalists lack any ability to recognize this failure of their transition plan. The assumption in most hospitalist groups is that patients who leave the hospital will achieve follow-up as directed. This “presumption of success” is ill-founded and may expose the patient to potential harm—and the physician to liability.
The case of Shirk v. Kelsey offers parallels to discharge situations hospitalists commonly encounter.3 In this malpractice case, a procedure was unsuccessful in terminating a patient’s pregnancy. The performing physician left follow-up of the pathology results to the patient’s usual outpatient obstetrical provider. The patient’s lack of follow-up was not recognized by the discharging obstetrician. This provider—not the practitioner with whom follow-up was intended—was found liable.
The American Medical Association’s code of ethics states: “Once having undertaken a case, the physician should not neglect the patient.” Hospitalists form physician-patient relationships with hospitalized patients that usually terminate on discharge. Our duty to not abandon or neglect a patient diminishes significantly after discharge, when we are no longer responsible for ongoing hospital care or exchanging information with patients on a daily basis.
But our duty does not disappear. Certainly, the responsibility falls to the hospitalist to be aware of and ensure a follow-up plan for important results such as pathology reports that return after discharge.
Allegations of improper post-discharge communication or failure to pass along critical results that become available once the patient has left the hospital, are common in medical malpractice claims.
Most are settled out of court, and many do not find the physician liable for malpractice. However, legal consequences are far less relevant than the safety and quality of care compromised when patients are failed by a system that lacks feedback loops to ensure safe transitions.
The ultimate goal of medicine is to improve the health and quality of life of our patients. Whether or not a lawsuit results, we need to recognize the commonality of patients who have their care compromised, delayed, or mismanaged because of our inability to recognize a foundering transition plan. Instead of looking at this as a failure of individual physicians to communicate, the problem needs to be addressed by creating effective, reliable systems.
Solutions
Providers discharging patients with follow-up needs should have a mechanism to identify those at highest risk for problems with transition. For these patients, follow-up with a post-discharge telephone call may be an effective feedback step.
One study looking at post-discharge phone contact found that 20% of patients had not filled new discharge prescriptions. Another post-discharge study revealed that a quarter of patients had medication questions that required clarification.4,5 Other research indicates more than one in 10 patients had new or worsening symptoms in the first five days after leaving the hospital.6 Despite these symptoms, 39% of these patients did not have a follow-up appointment established.
An integrated informatics system that prompts hospitalists and primary care physicians when patients do not arrive at expected follow-up or when test results return after discharge would be optimal. But a simple phone call to identify problems can be effective. Some hospitalist groups have incorporated routine post-discharge telephone contact into their practice—but most have not. Research identifying which patients would benefit is needed to allow targeted use of resources.7
While it’s understood that not all patient discharges will go smoothly, just as not all battleships will arrive at port without incident, there is frequently an opportunity to recover when things begin to go awry. A change in the common attitude that hospitalist responsibility ends when the patient leaves the hospital is necessary.
An element of the solution lies in the creation of feedback loops to identify patients who are not obtaining follow-up as expected. This step requires a commitment of resources—something our fragmented medical system, with location-based reimbursement, does not provide incentives for.
Creation of a feedback loop may be as complex as integrated medical informatics systems, or as simple as a follow-up phone call, but it is incumbent on each hospitalist to examine the environment in which they practice and ensure this vital element of a safe and reliable system is being addressed. TH
Drs. Cumbler and Egan are assistant professors in the Section of Hospital Medicine at the University of Colorado at Denver.
References
- Stanton D. In harms way: the sinking of the USS Indianapolis and the extraordinary story of its survivors. New York, NY: Henry Holt and Company LLC; 2001.
- Kripalani S, LeFevre F, Phillips F, Williams M, Basaviah P, Baker D. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Alpers A. Key legal principles for hospitalists. Am J Med. 1999;111(9):5-9.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111:26S-30S.
- Boockvar K, LaCorte H, Giambanco V, Fridman B, Siu A. Medication reconciliation for reducing drug
- discrepancy adverse events. Am J Geriatr Pharmacother. 2006;4:236-243.
- Epstein K, Juarez E, Loya K, Gorman MJ, Singer A. Frequency of new or worsening symptoms in the posthospitalization period. JHM. 2007;2:58-68.
- Mistiaen P, Poot E. Telephone follow-up, initiated by a hospital-based health professional, for postdischarge problems in patients discharged from hospital to home. Cochrane Database of Systemic Reviews 2006; 4. Article No.:CD004510. DOI:10.1002/14651858.CD004510.pub3.
On the evening of July 30, 1945, a U.S. battleship traveling from Guam to the Philippines was spotted in the Philippine Sea by a Japanese submarine crew. Six torpedoes sped across the black water with devastating effect.
Three hundred sailors died immediately as the stricken ship sank. Another 900 men were left floating in an oil slick in the shark-infested Pacific Ocean for four days.1
The events that led to the sinking represent a classic tale of systems failures. They ring familiar to any physician who has closely examined modern medical error.
The communication breakdown that prevented the ship’s captain from being aware of submarine activity on the same route four days before is no different than communication breakdowns in complex hospital systems. The bureaucratic decision by a remote administrator to withhold the safety measure of an escort to prevent such an attack on the grounds that it “lacked necessity” likely resonates with physicians who have struggled with getting authorization for care.
Why did those sailors remain in the water four days before rescue? Despite being only a two-hour flight from the nearest base, they were not recovered—or even missed—for what must have seemed an endless amount of time.
In the end, slightly more than 300 men were alive when they were spotted by a plane that happened to fly past. The rest succumbed to dehydration, exposure, and sharks. The failure of the Navy to rescue the sailors offers lessons to the clinician trying to improve transitions of care more than a half a century later.
The Feedback Loop
Hospital discharge is a complex process initiated by physician orders on charts, prescription pads, and patient instructions. Most often, the things we assume will be done out of our direct view are carried out satisfactorily. However, any hospitalist can easily recount stories of tests or follow-up that didn’t happen as ordered. Patients who fall through the cracks at discharge—like the stranded sailors of the USS Indianapolis—are, in part, the story of a simple omitted step: the feedback loop.
A feedback loop occurs when the results or consequences of an action are returned as an input loop to the initiating step in order to modify subsequent actions. This fundamental engineering concept can keep complex systems on course. The feedback loop allows the lack of completion of a portion of a process to be recognized—and corrective measures taken—before additional harm occurs.
In Guam, the island base from which the USS Indianapolis departed, the marker indicating the ship on the plotting board was removed when the ship left. Later, the Philippine port of Leyte failed to note that the ship didn’t arrive. Policy at the time was that all ships that left port were presumed to have arrived at their destination unless a call indicating trouble was received. The junior officer who noticed that the ship hadn’t arrived assumed there had been an order to divert to an alternate port. The Navy had no feedback mechanism to communicate between the two ports and raise an alarm when a ship did not arrive. In fact, a Navy directive discouraged communicating the arrival of combat ships as a matter of military secrecy. As a result, no rescue mission was launched—and the sharks began to arrive.
A closer examination of usual hospitalist discharge practice reveals too much similarity for comfort. Similar to how the USS Indianapolis was removed from the plotting board on Guam, discharged patients are removed from the hospitalist’s census list. Follow-up becomes the responsibility of the patient and primary care physician.
Communication with the primary care provider is recognized as a best practice for discharge, but research suggests direct communication occurs less than 20% of the time.2 These dismal statistic suggests the “port of arrival” is unaware our patients are expected in a significant percentage of discharges. Outpatient physicians, like the junior port director in Leyte, may assume that patients who do not call or arrive for appointments have been readmitted, seen by another physician, or otherwise diverted.
Even a superficial review reveals significant deficits in the feedback provided by our current discharge practice. When patients don’t arrive at follow-up appointments, most hospitalists lack any ability to recognize this failure of their transition plan. The assumption in most hospitalist groups is that patients who leave the hospital will achieve follow-up as directed. This “presumption of success” is ill-founded and may expose the patient to potential harm—and the physician to liability.
The case of Shirk v. Kelsey offers parallels to discharge situations hospitalists commonly encounter.3 In this malpractice case, a procedure was unsuccessful in terminating a patient’s pregnancy. The performing physician left follow-up of the pathology results to the patient’s usual outpatient obstetrical provider. The patient’s lack of follow-up was not recognized by the discharging obstetrician. This provider—not the practitioner with whom follow-up was intended—was found liable.
The American Medical Association’s code of ethics states: “Once having undertaken a case, the physician should not neglect the patient.” Hospitalists form physician-patient relationships with hospitalized patients that usually terminate on discharge. Our duty to not abandon or neglect a patient diminishes significantly after discharge, when we are no longer responsible for ongoing hospital care or exchanging information with patients on a daily basis.
But our duty does not disappear. Certainly, the responsibility falls to the hospitalist to be aware of and ensure a follow-up plan for important results such as pathology reports that return after discharge.
Allegations of improper post-discharge communication or failure to pass along critical results that become available once the patient has left the hospital, are common in medical malpractice claims.
Most are settled out of court, and many do not find the physician liable for malpractice. However, legal consequences are far less relevant than the safety and quality of care compromised when patients are failed by a system that lacks feedback loops to ensure safe transitions.
The ultimate goal of medicine is to improve the health and quality of life of our patients. Whether or not a lawsuit results, we need to recognize the commonality of patients who have their care compromised, delayed, or mismanaged because of our inability to recognize a foundering transition plan. Instead of looking at this as a failure of individual physicians to communicate, the problem needs to be addressed by creating effective, reliable systems.
Solutions
Providers discharging patients with follow-up needs should have a mechanism to identify those at highest risk for problems with transition. For these patients, follow-up with a post-discharge telephone call may be an effective feedback step.
One study looking at post-discharge phone contact found that 20% of patients had not filled new discharge prescriptions. Another post-discharge study revealed that a quarter of patients had medication questions that required clarification.4,5 Other research indicates more than one in 10 patients had new or worsening symptoms in the first five days after leaving the hospital.6 Despite these symptoms, 39% of these patients did not have a follow-up appointment established.
An integrated informatics system that prompts hospitalists and primary care physicians when patients do not arrive at expected follow-up or when test results return after discharge would be optimal. But a simple phone call to identify problems can be effective. Some hospitalist groups have incorporated routine post-discharge telephone contact into their practice—but most have not. Research identifying which patients would benefit is needed to allow targeted use of resources.7
While it’s understood that not all patient discharges will go smoothly, just as not all battleships will arrive at port without incident, there is frequently an opportunity to recover when things begin to go awry. A change in the common attitude that hospitalist responsibility ends when the patient leaves the hospital is necessary.
An element of the solution lies in the creation of feedback loops to identify patients who are not obtaining follow-up as expected. This step requires a commitment of resources—something our fragmented medical system, with location-based reimbursement, does not provide incentives for.
Creation of a feedback loop may be as complex as integrated medical informatics systems, or as simple as a follow-up phone call, but it is incumbent on each hospitalist to examine the environment in which they practice and ensure this vital element of a safe and reliable system is being addressed. TH
Drs. Cumbler and Egan are assistant professors in the Section of Hospital Medicine at the University of Colorado at Denver.
References
- Stanton D. In harms way: the sinking of the USS Indianapolis and the extraordinary story of its survivors. New York, NY: Henry Holt and Company LLC; 2001.
- Kripalani S, LeFevre F, Phillips F, Williams M, Basaviah P, Baker D. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Alpers A. Key legal principles for hospitalists. Am J Med. 1999;111(9):5-9.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111:26S-30S.
- Boockvar K, LaCorte H, Giambanco V, Fridman B, Siu A. Medication reconciliation for reducing drug
- discrepancy adverse events. Am J Geriatr Pharmacother. 2006;4:236-243.
- Epstein K, Juarez E, Loya K, Gorman MJ, Singer A. Frequency of new or worsening symptoms in the posthospitalization period. JHM. 2007;2:58-68.
- Mistiaen P, Poot E. Telephone follow-up, initiated by a hospital-based health professional, for postdischarge problems in patients discharged from hospital to home. Cochrane Database of Systemic Reviews 2006; 4. Article No.:CD004510. DOI:10.1002/14651858.CD004510.pub3.
On the evening of July 30, 1945, a U.S. battleship traveling from Guam to the Philippines was spotted in the Philippine Sea by a Japanese submarine crew. Six torpedoes sped across the black water with devastating effect.
Three hundred sailors died immediately as the stricken ship sank. Another 900 men were left floating in an oil slick in the shark-infested Pacific Ocean for four days.1
The events that led to the sinking represent a classic tale of systems failures. They ring familiar to any physician who has closely examined modern medical error.
The communication breakdown that prevented the ship’s captain from being aware of submarine activity on the same route four days before is no different than communication breakdowns in complex hospital systems. The bureaucratic decision by a remote administrator to withhold the safety measure of an escort to prevent such an attack on the grounds that it “lacked necessity” likely resonates with physicians who have struggled with getting authorization for care.
Why did those sailors remain in the water four days before rescue? Despite being only a two-hour flight from the nearest base, they were not recovered—or even missed—for what must have seemed an endless amount of time.
In the end, slightly more than 300 men were alive when they were spotted by a plane that happened to fly past. The rest succumbed to dehydration, exposure, and sharks. The failure of the Navy to rescue the sailors offers lessons to the clinician trying to improve transitions of care more than a half a century later.
The Feedback Loop
Hospital discharge is a complex process initiated by physician orders on charts, prescription pads, and patient instructions. Most often, the things we assume will be done out of our direct view are carried out satisfactorily. However, any hospitalist can easily recount stories of tests or follow-up that didn’t happen as ordered. Patients who fall through the cracks at discharge—like the stranded sailors of the USS Indianapolis—are, in part, the story of a simple omitted step: the feedback loop.
A feedback loop occurs when the results or consequences of an action are returned as an input loop to the initiating step in order to modify subsequent actions. This fundamental engineering concept can keep complex systems on course. The feedback loop allows the lack of completion of a portion of a process to be recognized—and corrective measures taken—before additional harm occurs.
In Guam, the island base from which the USS Indianapolis departed, the marker indicating the ship on the plotting board was removed when the ship left. Later, the Philippine port of Leyte failed to note that the ship didn’t arrive. Policy at the time was that all ships that left port were presumed to have arrived at their destination unless a call indicating trouble was received. The junior officer who noticed that the ship hadn’t arrived assumed there had been an order to divert to an alternate port. The Navy had no feedback mechanism to communicate between the two ports and raise an alarm when a ship did not arrive. In fact, a Navy directive discouraged communicating the arrival of combat ships as a matter of military secrecy. As a result, no rescue mission was launched—and the sharks began to arrive.
A closer examination of usual hospitalist discharge practice reveals too much similarity for comfort. Similar to how the USS Indianapolis was removed from the plotting board on Guam, discharged patients are removed from the hospitalist’s census list. Follow-up becomes the responsibility of the patient and primary care physician.
Communication with the primary care provider is recognized as a best practice for discharge, but research suggests direct communication occurs less than 20% of the time.2 These dismal statistic suggests the “port of arrival” is unaware our patients are expected in a significant percentage of discharges. Outpatient physicians, like the junior port director in Leyte, may assume that patients who do not call or arrive for appointments have been readmitted, seen by another physician, or otherwise diverted.
Even a superficial review reveals significant deficits in the feedback provided by our current discharge practice. When patients don’t arrive at follow-up appointments, most hospitalists lack any ability to recognize this failure of their transition plan. The assumption in most hospitalist groups is that patients who leave the hospital will achieve follow-up as directed. This “presumption of success” is ill-founded and may expose the patient to potential harm—and the physician to liability.
The case of Shirk v. Kelsey offers parallels to discharge situations hospitalists commonly encounter.3 In this malpractice case, a procedure was unsuccessful in terminating a patient’s pregnancy. The performing physician left follow-up of the pathology results to the patient’s usual outpatient obstetrical provider. The patient’s lack of follow-up was not recognized by the discharging obstetrician. This provider—not the practitioner with whom follow-up was intended—was found liable.
The American Medical Association’s code of ethics states: “Once having undertaken a case, the physician should not neglect the patient.” Hospitalists form physician-patient relationships with hospitalized patients that usually terminate on discharge. Our duty to not abandon or neglect a patient diminishes significantly after discharge, when we are no longer responsible for ongoing hospital care or exchanging information with patients on a daily basis.
But our duty does not disappear. Certainly, the responsibility falls to the hospitalist to be aware of and ensure a follow-up plan for important results such as pathology reports that return after discharge.
Allegations of improper post-discharge communication or failure to pass along critical results that become available once the patient has left the hospital, are common in medical malpractice claims.
Most are settled out of court, and many do not find the physician liable for malpractice. However, legal consequences are far less relevant than the safety and quality of care compromised when patients are failed by a system that lacks feedback loops to ensure safe transitions.
The ultimate goal of medicine is to improve the health and quality of life of our patients. Whether or not a lawsuit results, we need to recognize the commonality of patients who have their care compromised, delayed, or mismanaged because of our inability to recognize a foundering transition plan. Instead of looking at this as a failure of individual physicians to communicate, the problem needs to be addressed by creating effective, reliable systems.
Solutions
Providers discharging patients with follow-up needs should have a mechanism to identify those at highest risk for problems with transition. For these patients, follow-up with a post-discharge telephone call may be an effective feedback step.
One study looking at post-discharge phone contact found that 20% of patients had not filled new discharge prescriptions. Another post-discharge study revealed that a quarter of patients had medication questions that required clarification.4,5 Other research indicates more than one in 10 patients had new or worsening symptoms in the first five days after leaving the hospital.6 Despite these symptoms, 39% of these patients did not have a follow-up appointment established.
An integrated informatics system that prompts hospitalists and primary care physicians when patients do not arrive at expected follow-up or when test results return after discharge would be optimal. But a simple phone call to identify problems can be effective. Some hospitalist groups have incorporated routine post-discharge telephone contact into their practice—but most have not. Research identifying which patients would benefit is needed to allow targeted use of resources.7
While it’s understood that not all patient discharges will go smoothly, just as not all battleships will arrive at port without incident, there is frequently an opportunity to recover when things begin to go awry. A change in the common attitude that hospitalist responsibility ends when the patient leaves the hospital is necessary.
An element of the solution lies in the creation of feedback loops to identify patients who are not obtaining follow-up as expected. This step requires a commitment of resources—something our fragmented medical system, with location-based reimbursement, does not provide incentives for.
Creation of a feedback loop may be as complex as integrated medical informatics systems, or as simple as a follow-up phone call, but it is incumbent on each hospitalist to examine the environment in which they practice and ensure this vital element of a safe and reliable system is being addressed. TH
Drs. Cumbler and Egan are assistant professors in the Section of Hospital Medicine at the University of Colorado at Denver.
References
- Stanton D. In harms way: the sinking of the USS Indianapolis and the extraordinary story of its survivors. New York, NY: Henry Holt and Company LLC; 2001.
- Kripalani S, LeFevre F, Phillips F, Williams M, Basaviah P, Baker D. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831-841.
- Alpers A. Key legal principles for hospitalists. Am J Med. 1999;111(9):5-9.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111:26S-30S.
- Boockvar K, LaCorte H, Giambanco V, Fridman B, Siu A. Medication reconciliation for reducing drug
- discrepancy adverse events. Am J Geriatr Pharmacother. 2006;4:236-243.
- Epstein K, Juarez E, Loya K, Gorman MJ, Singer A. Frequency of new or worsening symptoms in the posthospitalization period. JHM. 2007;2:58-68.
- Mistiaen P, Poot E. Telephone follow-up, initiated by a hospital-based health professional, for postdischarge problems in patients discharged from hospital to home. Cochrane Database of Systemic Reviews 2006; 4. Article No.:CD004510. DOI:10.1002/14651858.CD004510.pub3.
A Defining Night
It was just before 7:30 p.m. Feb. 7 when a huge explosion in the small Georgia town of Port Wentworth shook the community to its core.
It proved to be a night no one would soon forget. It also tested the young hospitalist program at Memorial University Medical Center (MUMC) in Savannah, a few miles from Port Wentworth.
At least 12 people were killed and more than 40 seriously or critically injured in the blast at the Imperial Sugar Refinery, better known to locals as the Dixie Crystal Sugar Refinery, a Savannah-area landmark for more than 100 years.
The Place to Go
MUMC is an academic medical center with a Level 1 trauma center that serves a 35-county area in southeast Georgia and southern South Carolina. It is often said that if a patient is in a serious accident, MUMC is the place to go.











We started a hospitalist program at MUMC in September 2006, with three hospitalists and an average census of four patients. We now have seven hospitalists, expanding to 10 in July, and an average census of 65. Though still a fledgling department, we grew a lot the night of Feb. 7 and played a significant role in helping disaster victims. Immediate response, flexibility, and focus were paramount in defining our reaction to the crisis. Here’s how events unfolded that difficult night:
7:30 p.m.
We got the call and mobilized all five hospitalists in the emergency department (ED) 20 minutes later. It was organized chaos as trauma surgeons and ED physicians attended to the rapidly increasing number of victims arriving by ambulance and helicopter. Before the blast, the ED waiting room was packed with about 45 patients who needed attention.
8:15 p.m.
Many victims suffered serious burns from the explosion. Burn specialists from the Joseph M. Still Burn Center in Augusta arrived by helicopter. Space in the ED became desperately crowded with the seemingly endless number of victims, so we were all busily tending to the existing ED patients in every capacity possible to try and get them out of the ED. We sutured wounds, started and removed IVs, treated pregnant patients, triaged every medical patient, transported patients, and did whatever else was required. In about 90 minutes we had essentially cleared the entire ED. At this point, some of the trauma victims were moved upstairs to the intensive care unit (ICU).
9 p.m.
Victims were still arriving with burns over 40% to 80% of their bodies. After we’d cleared the ED as much as possible to make room for new patients, we focused on the immediate need for medical-surgical beds. MUMC was almost at capacity before the explosion, and suddenly a large number of patients were being emergently triaged out of the ICUs to make way for the burn victims.
The teamwork throughout the hospital was amazing to watch. From the ED to the medical floor, everyone worked together with precision as if this happened every day. Several patients were held in the ICU awaiting helicopter fight to the Augusta Burn Center; extra staff were assigned to those patients. Patient-care technicians began taking water and blankets to family members who had arrived at the hospital.
Our team began leading a massive effort to discharge and transfer noncritical patients from the medical floors. We called our coordinator Deborah Haywood, RN, BSN, who was at central command and told her we could use some of the nurses and case managers who were showing up to offer help. We took our census and identified patients who could possibly be discharged. We turned on televisions in patients’ rooms to show and explain to patients what was happening with the explosion. With the aid of arriving nurses we arranged discharge, follow-up, and transportation for every patient who could leave.
9:45 p.m.
Victims stopped arriving at the hospital. As the first of our patients from the floors began to leave, the internal medicine and family medicine residents came to offer help. We quickly went through the census and helped them figure out which patients could be discharged.
Amazingly, our coordinator located and directed case managers, psychiatric nurse managers, and intake personnel to us. They paired with the residents to help them transfer and discharge patients. We were fortunate that some of the smaller community hospitals opened their doors and accepted some of the less-critical patients in transfer.
10:30 p.m.
Several burn victims received emergent escharotomies. Helicopters transported the most severely burned to the Augusta burn center. Patients transferred from the ICU and holding areas around the ED began to occupy the medical-surgical beds we had created.
Clearly we needed more beds. We went back, reviewed the census on each floor, and found more patients willing and able to leave. Within two hours we discharged 22 patients. Our coordinator took their names, and patient relations called to ensure proper follow-up and thanks to the patients for helping in a time of crisis.
12:45 a.m.
When we finally got together and looked at the clock it was 12:45 a.m. The ED was clear and beds were available. Staff started to go home. Many of us had been working with minimal break time since 7 a.m.
We either went home or found a call room to rest in because we all knew the next day would be a long one. It had been a swift and busy night, but the true journey for the victims and our community had really just begun.
It was with tremendous sadness that we watched this event unfold on local and national news. None of us knew the extent of the damage done at the plant, and it was difficult to comprehend and empathize with what the victims had just suffered. Several victims were in such pain and emotional shock that it took them several days to describe to us what had happened.
It was also with a heightened sense of purpose that we went to work after this disaster. MUMC staff should be proud of the work, coordination, and precision with which such a large number of people came together and saved lives. The trauma teams, ED, and ICU staff, and countless others from every department at MUMC along with staff from the Joseph M. Still Burn Center in Augusta demonstrated competence and coordination.
As a group, MUMC Hospitalists played an important role, helping people in their hour of need. We believed in our team and our hospital’s ability to respond to an unforeseen crisis. We had defined our role instantly and spontaneously. We took a leadership position in a much-needed, albeit not so obvious, area.
We appreciated the fact that our relatively young hospitalist program was recognized for its contribution that night. We were part of the hospital’s debriefing and have become an integral part of the institution’s official disaster team.
While we certainly hope never to have to respond to such a devastating situation again, we know we are an important part of the team—and that our dedication and commitment will allow us to rise to any occasion. TH
The authors are members of Memorial Health Hospitalists, the hospitalist program at Memorial University Medical Center in Savannah, Ga.
It was just before 7:30 p.m. Feb. 7 when a huge explosion in the small Georgia town of Port Wentworth shook the community to its core.
It proved to be a night no one would soon forget. It also tested the young hospitalist program at Memorial University Medical Center (MUMC) in Savannah, a few miles from Port Wentworth.
At least 12 people were killed and more than 40 seriously or critically injured in the blast at the Imperial Sugar Refinery, better known to locals as the Dixie Crystal Sugar Refinery, a Savannah-area landmark for more than 100 years.
The Place to Go
MUMC is an academic medical center with a Level 1 trauma center that serves a 35-county area in southeast Georgia and southern South Carolina. It is often said that if a patient is in a serious accident, MUMC is the place to go.
We started a hospitalist program at MUMC in September 2006, with three hospitalists and an average census of four patients. We now have seven hospitalists, expanding to 10 in July, and an average census of 65. Though still a fledgling department, we grew a lot the night of Feb. 7 and played a significant role in helping disaster victims. Immediate response, flexibility, and focus were paramount in defining our reaction to the crisis. Here’s how events unfolded that difficult night:
7:30 p.m.
We got the call and mobilized all five hospitalists in the emergency department (ED) 20 minutes later. It was organized chaos as trauma surgeons and ED physicians attended to the rapidly increasing number of victims arriving by ambulance and helicopter. Before the blast, the ED waiting room was packed with about 45 patients who needed attention.
8:15 p.m.
Many victims suffered serious burns from the explosion. Burn specialists from the Joseph M. Still Burn Center in Augusta arrived by helicopter. Space in the ED became desperately crowded with the seemingly endless number of victims, so we were all busily tending to the existing ED patients in every capacity possible to try and get them out of the ED. We sutured wounds, started and removed IVs, treated pregnant patients, triaged every medical patient, transported patients, and did whatever else was required. In about 90 minutes we had essentially cleared the entire ED. At this point, some of the trauma victims were moved upstairs to the intensive care unit (ICU).
9 p.m.
Victims were still arriving with burns over 40% to 80% of their bodies. After we’d cleared the ED as much as possible to make room for new patients, we focused on the immediate need for medical-surgical beds. MUMC was almost at capacity before the explosion, and suddenly a large number of patients were being emergently triaged out of the ICUs to make way for the burn victims.
The teamwork throughout the hospital was amazing to watch. From the ED to the medical floor, everyone worked together with precision as if this happened every day. Several patients were held in the ICU awaiting helicopter fight to the Augusta Burn Center; extra staff were assigned to those patients. Patient-care technicians began taking water and blankets to family members who had arrived at the hospital.
Our team began leading a massive effort to discharge and transfer noncritical patients from the medical floors. We called our coordinator Deborah Haywood, RN, BSN, who was at central command and told her we could use some of the nurses and case managers who were showing up to offer help. We took our census and identified patients who could possibly be discharged. We turned on televisions in patients’ rooms to show and explain to patients what was happening with the explosion. With the aid of arriving nurses we arranged discharge, follow-up, and transportation for every patient who could leave.
9:45 p.m.
Victims stopped arriving at the hospital. As the first of our patients from the floors began to leave, the internal medicine and family medicine residents came to offer help. We quickly went through the census and helped them figure out which patients could be discharged.
Amazingly, our coordinator located and directed case managers, psychiatric nurse managers, and intake personnel to us. They paired with the residents to help them transfer and discharge patients. We were fortunate that some of the smaller community hospitals opened their doors and accepted some of the less-critical patients in transfer.
10:30 p.m.
Several burn victims received emergent escharotomies. Helicopters transported the most severely burned to the Augusta burn center. Patients transferred from the ICU and holding areas around the ED began to occupy the medical-surgical beds we had created.
Clearly we needed more beds. We went back, reviewed the census on each floor, and found more patients willing and able to leave. Within two hours we discharged 22 patients. Our coordinator took their names, and patient relations called to ensure proper follow-up and thanks to the patients for helping in a time of crisis.
12:45 a.m.
When we finally got together and looked at the clock it was 12:45 a.m. The ED was clear and beds were available. Staff started to go home. Many of us had been working with minimal break time since 7 a.m.
We either went home or found a call room to rest in because we all knew the next day would be a long one. It had been a swift and busy night, but the true journey for the victims and our community had really just begun.
It was with tremendous sadness that we watched this event unfold on local and national news. None of us knew the extent of the damage done at the plant, and it was difficult to comprehend and empathize with what the victims had just suffered. Several victims were in such pain and emotional shock that it took them several days to describe to us what had happened.
It was also with a heightened sense of purpose that we went to work after this disaster. MUMC staff should be proud of the work, coordination, and precision with which such a large number of people came together and saved lives. The trauma teams, ED, and ICU staff, and countless others from every department at MUMC along with staff from the Joseph M. Still Burn Center in Augusta demonstrated competence and coordination.
As a group, MUMC Hospitalists played an important role, helping people in their hour of need. We believed in our team and our hospital’s ability to respond to an unforeseen crisis. We had defined our role instantly and spontaneously. We took a leadership position in a much-needed, albeit not so obvious, area.
We appreciated the fact that our relatively young hospitalist program was recognized for its contribution that night. We were part of the hospital’s debriefing and have become an integral part of the institution’s official disaster team.
While we certainly hope never to have to respond to such a devastating situation again, we know we are an important part of the team—and that our dedication and commitment will allow us to rise to any occasion. TH
The authors are members of Memorial Health Hospitalists, the hospitalist program at Memorial University Medical Center in Savannah, Ga.
It was just before 7:30 p.m. Feb. 7 when a huge explosion in the small Georgia town of Port Wentworth shook the community to its core.
It proved to be a night no one would soon forget. It also tested the young hospitalist program at Memorial University Medical Center (MUMC) in Savannah, a few miles from Port Wentworth.
At least 12 people were killed and more than 40 seriously or critically injured in the blast at the Imperial Sugar Refinery, better known to locals as the Dixie Crystal Sugar Refinery, a Savannah-area landmark for more than 100 years.
The Place to Go
MUMC is an academic medical center with a Level 1 trauma center that serves a 35-county area in southeast Georgia and southern South Carolina. It is often said that if a patient is in a serious accident, MUMC is the place to go.
We started a hospitalist program at MUMC in September 2006, with three hospitalists and an average census of four patients. We now have seven hospitalists, expanding to 10 in July, and an average census of 65. Though still a fledgling department, we grew a lot the night of Feb. 7 and played a significant role in helping disaster victims. Immediate response, flexibility, and focus were paramount in defining our reaction to the crisis. Here’s how events unfolded that difficult night:
7:30 p.m.
We got the call and mobilized all five hospitalists in the emergency department (ED) 20 minutes later. It was organized chaos as trauma surgeons and ED physicians attended to the rapidly increasing number of victims arriving by ambulance and helicopter. Before the blast, the ED waiting room was packed with about 45 patients who needed attention.
8:15 p.m.
Many victims suffered serious burns from the explosion. Burn specialists from the Joseph M. Still Burn Center in Augusta arrived by helicopter. Space in the ED became desperately crowded with the seemingly endless number of victims, so we were all busily tending to the existing ED patients in every capacity possible to try and get them out of the ED. We sutured wounds, started and removed IVs, treated pregnant patients, triaged every medical patient, transported patients, and did whatever else was required. In about 90 minutes we had essentially cleared the entire ED. At this point, some of the trauma victims were moved upstairs to the intensive care unit (ICU).
9 p.m.
Victims were still arriving with burns over 40% to 80% of their bodies. After we’d cleared the ED as much as possible to make room for new patients, we focused on the immediate need for medical-surgical beds. MUMC was almost at capacity before the explosion, and suddenly a large number of patients were being emergently triaged out of the ICUs to make way for the burn victims.
The teamwork throughout the hospital was amazing to watch. From the ED to the medical floor, everyone worked together with precision as if this happened every day. Several patients were held in the ICU awaiting helicopter fight to the Augusta Burn Center; extra staff were assigned to those patients. Patient-care technicians began taking water and blankets to family members who had arrived at the hospital.
Our team began leading a massive effort to discharge and transfer noncritical patients from the medical floors. We called our coordinator Deborah Haywood, RN, BSN, who was at central command and told her we could use some of the nurses and case managers who were showing up to offer help. We took our census and identified patients who could possibly be discharged. We turned on televisions in patients’ rooms to show and explain to patients what was happening with the explosion. With the aid of arriving nurses we arranged discharge, follow-up, and transportation for every patient who could leave.
9:45 p.m.
Victims stopped arriving at the hospital. As the first of our patients from the floors began to leave, the internal medicine and family medicine residents came to offer help. We quickly went through the census and helped them figure out which patients could be discharged.
Amazingly, our coordinator located and directed case managers, psychiatric nurse managers, and intake personnel to us. They paired with the residents to help them transfer and discharge patients. We were fortunate that some of the smaller community hospitals opened their doors and accepted some of the less-critical patients in transfer.
10:30 p.m.
Several burn victims received emergent escharotomies. Helicopters transported the most severely burned to the Augusta burn center. Patients transferred from the ICU and holding areas around the ED began to occupy the medical-surgical beds we had created.
Clearly we needed more beds. We went back, reviewed the census on each floor, and found more patients willing and able to leave. Within two hours we discharged 22 patients. Our coordinator took their names, and patient relations called to ensure proper follow-up and thanks to the patients for helping in a time of crisis.
12:45 a.m.
When we finally got together and looked at the clock it was 12:45 a.m. The ED was clear and beds were available. Staff started to go home. Many of us had been working with minimal break time since 7 a.m.
We either went home or found a call room to rest in because we all knew the next day would be a long one. It had been a swift and busy night, but the true journey for the victims and our community had really just begun.
It was with tremendous sadness that we watched this event unfold on local and national news. None of us knew the extent of the damage done at the plant, and it was difficult to comprehend and empathize with what the victims had just suffered. Several victims were in such pain and emotional shock that it took them several days to describe to us what had happened.
It was also with a heightened sense of purpose that we went to work after this disaster. MUMC staff should be proud of the work, coordination, and precision with which such a large number of people came together and saved lives. The trauma teams, ED, and ICU staff, and countless others from every department at MUMC along with staff from the Joseph M. Still Burn Center in Augusta demonstrated competence and coordination.
As a group, MUMC Hospitalists played an important role, helping people in their hour of need. We believed in our team and our hospital’s ability to respond to an unforeseen crisis. We had defined our role instantly and spontaneously. We took a leadership position in a much-needed, albeit not so obvious, area.
We appreciated the fact that our relatively young hospitalist program was recognized for its contribution that night. We were part of the hospital’s debriefing and have become an integral part of the institution’s official disaster team.
While we certainly hope never to have to respond to such a devastating situation again, we know we are an important part of the team—and that our dedication and commitment will allow us to rise to any occasion. TH
The authors are members of Memorial Health Hospitalists, the hospitalist program at Memorial University Medical Center in Savannah, Ga.
What is the best method of treating acutely worsened chronic pain?
Case
A 69-year-old female with metastatic ovarian cancer and chronic pain syndrome presented to the hospital with seven days of progressively worsening abdominal pain. The pain had been similar to her chronic cancer pain but more severe. She has acute renal failure secondary to volume depletion from poor intake. A CT scan of the abdomen and pelvis reveal progression of her cancer with acute pathology. What is the best method of treating this patient’s pain?
Overview
Pain is pandemic. It is the most common reason patients seek healthcare.1 Almost one-third of Americans will experience severe chronic pain at some point in their lives. Every year, approximately 25 million Americans experience acute pain and 50 million experience chronic pain. Only one in four patients with pain receives appropriate therapy and control of their pain.
Pain is the most common symptom experienced by hospitalized adults.2 Acute or chronic pain can be particularly challenging to treat because these patients are frequently opioid dependent and have many psychosocial factors. No one method of pain control is superior to another. However, one method to gain rapid control of an acute pain crisis in a patient with chronic pain is to use patient-controlled analgesia (PCA).
Review of the Data
The first commercially available PCA pumps became available in 1976.3 They were created after studies in the 1960s demonstrated that small doses of opioids given intravenously provided more effective pain relief than conventional intramuscular injections.
The majority of studies on PCAs are in the postoperative patient, with cancer pain being next most commonly studied. PCAs utilize microprocessor-controlled infusion pumps that deliver a preprogrammed dose of opioid when the patient pushes the demand button. They allow programming of dose (demand dose), time between doses (lockout interval), background infusion rate (basal rate), and nurse-initiated dose (bolus dose).
The PCA paradigm is based on the opioid pharmacologic concept of minimum effective analgesic concentration (MEAC).4,5 The MEAC is the smallest serum opioid concentration at which pain is relieved. The dose-response curve to opioids is sigmoidal such that minimal analgesia is achieved until the MEAC is reached, after which minute increases in opioid concentrations produce analgesia, until further increases produce no significant increased analgesic effect.
PCAs allow individualized dosing and titration to achieve the MEAC, with small incremental doses administered whenever the serum concentration falls below the MEAC. A major goal of PCA technology is to regulate drug delivery to rapidly achieve and maintain the MEAC.
Advantages of PCAs
- More individual dosing and titration of pain medications to account for inter-individual and intra-individual variability in the response to opioids;
- Negative feedback control system, an added safety measure to avoid respiratory depression. As patients become too sedated from opioids, they are no longer able to push the button to receive further opioids;
- Higher patient satisfaction with pain control, a major determinant being personal control over the delivery of pain relief;6-8 and
- Greater analgesic efficacy vs. conventional analgesia.
Disadvantages of PCAs
Select patient populations: Not all patients are able to understand and retain the required instructions necessary to safely or effectively use self-administered opioids (e.g., cognitively impaired patients).
Potential for opioid dosing errors: These are related to equipment factors, medical personnel prescribing or programming errors.
Increased cost: PCAs have been shown to be more expensive in comparison with intramuscular (IM) injections, the prior standard of care.9-10
PCA Prescribing
The parameters programmed into the PCA machine include the basal rate, demand (or incremental) dose, lockout interval, nurse-initiated bolus dose, and choice of opioid.
Basal rate: The continuous infusion of opioid set at an hourly rate. Most studies that compare PCA use with and without basal rates (in postoperative patients) do not show improved pain relief or sleep with basal rates.11 Basal rates have been associated with increased risk of sedation and respiratory depression.12
The routine use of basal rates is not recommended initially, unless a patient is opioid-tolerant (i.e., on chronic opioid therapy). For patients on chronic opioids, their 24-hour total opioid requirement is converted by equianalgesic dosing to the basal rate. Steady state is not achieved for eight to 12 hours of continuous infusion; therefore, it is not recommended to change the basal rate more frequently than every eight hours.13
Demand dose: The dose patients provide themselves by pushing the button. Studies on opioid-naïve patients using morphine PCAs have shown that 1 mg IV morphine was the optimal starting dose, based on good pain relief without respiratory depression. Lower doses, such as 0.5 mg IV morphine, are generally used in the elderly as opioid requirements are known to decrease with patient age.14
For patients with a basal rate, the demand dose is often set at 50% to 100% of the basal rate. The demand dose is the parameter that should be titrated up for acute pain control. World Health Organization guidelines recommend increasing the dose by 25% to 50% for mild to moderate pain, and 50% to 100% for moderate to severe pain.15
Lockout interval: Minimal allowable time between demand doses. This time is based on the time to peak effect of IV opioids and can vary from five to 15 minutes. The effects of varying lockout intervals—seven to 11 minutes for morphine and five to eight minutes for fentanyl—had no effect on pain levels or side effects.16 Ten minutes is a standard lockout interval.
Bolus dose: The nurse-initiated dose that may be given initially to achieve pain control and later to counteract incidental pain (e.g., that caused by physical therapy, dressing changes, or radiology tests). A recommended dose is equivalent to the basal rate or twice the demand dose.
Choice of opioid: Morphine is the standard opioid because of its familiarity, cost, and years of study. Although inter-individual variability exists, there are no major differences in side effects among the different opioids. Renal and hepatic insufficiency can increase the effects of opioids. Morphine is especially troublesome in renal failure because it has an active metabolite—morphine-6-glucuronide—that can accumulate and increase the risk of sedation and respiratory depression.
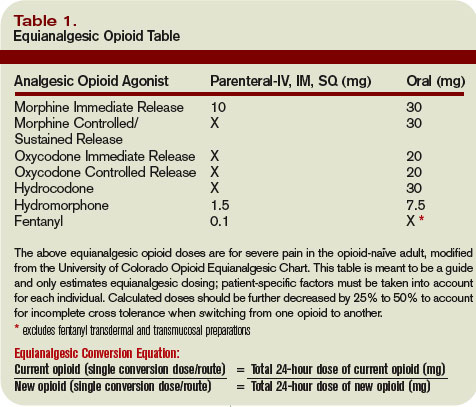
Other Concerns
PCA complications: The most well-studied adverse effects of PCAs are nausea and respiratory depression. There is no difference between PCAs and conventional analgesia in rates of nausea or respiratory depression.17
Nausea is the most common side effect in postoperative patients on PCAs. Patients rapidly develop tolerance to nausea over a period of days. However, many clinicians are concerned about respiratory depression and the risk of death. The overall incidence of respiratory depression with PCAs is less than 1% (range from 0.1 to 0.8%), similar to conventional analgesia. However, the incidence is significantly higher when basal rates are used, rising to 1.1 to 3.9%. Other factors predisposing a patient to increased risk of respiratory depression are older age, obstructive sleep apnea, hypovolemia, renal failure, and the concurrent use of other sedating medications.18
Medication errors are also common. The overall incidence of medication mishaps with PCAs is 1.2%.19 More than 50% of these occur because of operator-related errors (e.g., improper loading, programming errors, and documentation errors). Equipment malfunction is the next most common error.
Opioid equianalgesic dosing conversions: The equianalgesic dose ratio is the ratio of the dose of two opioids required to produce the same analgesic effect. (See Table 1, right.) For example, IV morphine is three times as potent as oral morphine, with an equianalgesic dose ratio of 1:3. Equianalgesic dose tables vary somewhat in their values, which have been largely determined by single-dose administration studies.20 The generalizability of these tables to chronic opioid administration is not well studied.
Incomplete cross tolerance: When switching from one opioid to another, lower doses can be used to control pain.21, 22 Tolerance to one opioid does not completely transfer to the new opioid. Starting at half to two-thirds of the new opioid dose is generally recommended to avoid opioid-specific tolerance and inter-individual variability.23,24
Back to the Case
Opioids are the mainstay of pharmacological management of moderate-to-severe cancer pain. Evaluation of the patient reveals that her acute increase in pain is likely due to progression of her cancer. She had been taking morphine (sustained-release, 90 mg oral) twice daily for her pain and had been using approximately five doses per day of immediate-release oral morphine 20 mg for breakthrough pain. This is equivalent to a total 24-hour opioid requirement of 280 mg oral morphine.
She should be started on a PCA for rapid pain control and titration. Hydromorphone (Dilaudid) is a better PCA choice than morphine because she has acute renal failure. The equianalgesic dose ratio of oral morphine to IV hydromorphone is approximately 30:1.5. The total 24-hour opioid dose of 280 mg oral morphine is equivalent to 14 mg IV hydromorphone ([280mg morphine per day ÷ 30] x 1.5 = 14).
After adjusting for 60% incomplete cross tolerance, the total 24-hour opioid dose is reduced to 8.4 mg IV hydromorphone (14 mg x 0.6 = 8.4 mg). This is approximately equivalent to 0.4 mg IV hydromorphone/hour (8.4 mg ÷ 24 hours), which is her initial basal rate. The demand dose should be set at 0.2 mg (50% the basal rate) with a lockout interval of 10 minutes.
Over a period of several days, the patient’s pain was controlled and her opioid requirements stabilized. She was on a basal rate of 1.4 mg/hour and a demand dose of 1 mg with a 10-minute lockout. Her total 24-hour opioid requirement was 44 mg of IV hydromorphone. As her renal function improved but did not completely normalize, oxycodone was chosen over morphine when converting her back to oral pain medications (less active renal metabolites). The equianalgesic dose ratio of oral oxycodone to IV hydromorphone is approximately 20:1.5. Her total 24-hour opioid dose of 44 mg IV hydromorphone is equivalent to 587 mg oral oxycodone (44 ÷ 1.5) x 20. After adjusting for 60% incomplete cross tolerance, the total 24-hour opioid dose is reduced to 352 mg oral oxycodone or 180 mg of sustained-release oxycodone twice daily (352 mg ÷ 2 ≈ 180 mg). For breakthrough pain she should receive 40 mg of immediate-release oxycodone every hour as needed (10% to 15% of the 24-hour opioid requirement). TH
Dr. Youngwerth is a hospitalist and instructor of medicine, University of Colorado at Denver, assistant director, Palliative Care Consult Service, associate director, Colorado Palliative Medicine Fellowship Program, and medical director, Hospice of Saint John.
References
- American Pain Society. Pain: Current understanding of assessment, management, and treatments. National Pharmaceutical Council 2006;1-79.
- Morrison RS, Meier DE, Fischberg D, et al. Improving the management of pain in hospitalized adults. Arch Intern Med. 2006;166:1033-1039.
- Grass JA. Patient-controlled analgesia. Anesth Analg. 2005;101:S44-S61.
- Etches RC. Patient-controlled analgesia. Surg Clinics N Amer. 1999;79:297-312.
- Nolan MF and Wilson M-C B. Patient-controlled analgesia: A method for the controlled self-administration of opioid pain medications. Phys Ther. 1995;75:374-379.
- Ballantyne JC, Carr DB, Chalmers TC, Dear KBG, Angelillo IF, Mosteller F. Postoperative patient-controlled analgesia: Meta-analyses of initial randomized control trials. J Clin Anesth. 1993;5:182-193.
- Hudcova J, McNicol E, Quah C, Lau J, Carr DB. Patient controlled opioid analgesia versus conventional opioid analgesia for postoperative pain. Cochrane Database of Systematic Reviews. 2006;4:1-10.
- Sidebotham D, Dijkhuizen MRJ, Schug SA. The safety and utilization of patient-controlled analgesia. J Pain Symptom Manage. 1997;14:202-209.
- Macintyre PE. Safety and efficacy of patient-controlled analgesia. Br J Anaesth. 2001;87:36-46.
- Manon C, Rittenhouse BE, Perreault S, et al. Efficacy and costs of patient-controlled analgesia versus regularly administered intramuscular opioid therapy. Amer Soc Anesth Inc. 1998;89:1377-1388.
- Krenn H, Oczenski W, Jellinek H, Krumpl-Ströher M, Schweitzer E, Fitzgerald RD. Nalbuphine by PCA-pump for analgesia following hysterectomy: Bolus application versus continuous infusion with bolus application. Eur J Pain. 2001;5:219-226.
- Lehmann KA. Recent developments in patient-controlled analgesia. J Pain Symptom Manage. 2005;29:S72-S89.
- American Pain Society. Principles of analgesic use in the treatment of acute pain and cancer pain. 5th ed. 2003:1-73.
- Macintyre PC, Jarvis DA. Age is the best predictor of postoperative morphine requirements. Pain. 1995;64:357-364.
- National Comprehensive Cancer Network. Clinical practice guidelines in oncology: Adult cancer pain. Version 2.2005:1-30.
- Ginsberg B, Gil KM, Muir M, Sullivan F, Williams DA, Glass PSA. The influence of lockout intervals and drug selection on patient-controlled analgesia following gynecological surgery. Pain. 1995;62:95-100.
- Walder B, Schafer M, Henzi I, Tramer MR. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain. Acta Anaesthesiol Scand. 2001;45:795-804.
- Etches RC. Respiratory depression associated with patient-controlled analgesia: a review of eight cases. Can J Anaesth. 1994;41:125-132.
- Oswalt KE, Shrewsbury P, Stanton-Hicks M. The incidence of medication mishaps in 3,299 PCA patients. Pain. 1990;S5;S152.
- Pereira J, Lawlor P, Vigano A, Dorgan M, Bruera E. Equianalgesic dose rations for opioids: A critical review and proposals for long-term dosing. J Pain Symptom Manage. 2001;22:672-687.
- Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med. 2003;349:1943-1953.
- Mercandante S. Opioid rotation for cancer pain. Cancer. 1999;86:1856-1866.
- Mehta V, Langford RM. Acute pain management for opioid dependent patients. Anaesthesia. 2006;61:269-276.
- Pasternak GW. Incomplete cross tolerance and multiple mu opioid peptide receptors. Trends Pharm Sciences. 2001;22:67-70.
Case
A 69-year-old female with metastatic ovarian cancer and chronic pain syndrome presented to the hospital with seven days of progressively worsening abdominal pain. The pain had been similar to her chronic cancer pain but more severe. She has acute renal failure secondary to volume depletion from poor intake. A CT scan of the abdomen and pelvis reveal progression of her cancer with acute pathology. What is the best method of treating this patient’s pain?
Overview
Pain is pandemic. It is the most common reason patients seek healthcare.1 Almost one-third of Americans will experience severe chronic pain at some point in their lives. Every year, approximately 25 million Americans experience acute pain and 50 million experience chronic pain. Only one in four patients with pain receives appropriate therapy and control of their pain.
Pain is the most common symptom experienced by hospitalized adults.2 Acute or chronic pain can be particularly challenging to treat because these patients are frequently opioid dependent and have many psychosocial factors. No one method of pain control is superior to another. However, one method to gain rapid control of an acute pain crisis in a patient with chronic pain is to use patient-controlled analgesia (PCA).
Review of the Data
The first commercially available PCA pumps became available in 1976.3 They were created after studies in the 1960s demonstrated that small doses of opioids given intravenously provided more effective pain relief than conventional intramuscular injections.
The majority of studies on PCAs are in the postoperative patient, with cancer pain being next most commonly studied. PCAs utilize microprocessor-controlled infusion pumps that deliver a preprogrammed dose of opioid when the patient pushes the demand button. They allow programming of dose (demand dose), time between doses (lockout interval), background infusion rate (basal rate), and nurse-initiated dose (bolus dose).
The PCA paradigm is based on the opioid pharmacologic concept of minimum effective analgesic concentration (MEAC).4,5 The MEAC is the smallest serum opioid concentration at which pain is relieved. The dose-response curve to opioids is sigmoidal such that minimal analgesia is achieved until the MEAC is reached, after which minute increases in opioid concentrations produce analgesia, until further increases produce no significant increased analgesic effect.
PCAs allow individualized dosing and titration to achieve the MEAC, with small incremental doses administered whenever the serum concentration falls below the MEAC. A major goal of PCA technology is to regulate drug delivery to rapidly achieve and maintain the MEAC.
Advantages of PCAs
- More individual dosing and titration of pain medications to account for inter-individual and intra-individual variability in the response to opioids;
- Negative feedback control system, an added safety measure to avoid respiratory depression. As patients become too sedated from opioids, they are no longer able to push the button to receive further opioids;
- Higher patient satisfaction with pain control, a major determinant being personal control over the delivery of pain relief;6-8 and
- Greater analgesic efficacy vs. conventional analgesia.
Disadvantages of PCAs
Select patient populations: Not all patients are able to understand and retain the required instructions necessary to safely or effectively use self-administered opioids (e.g., cognitively impaired patients).
Potential for opioid dosing errors: These are related to equipment factors, medical personnel prescribing or programming errors.
Increased cost: PCAs have been shown to be more expensive in comparison with intramuscular (IM) injections, the prior standard of care.9-10
PCA Prescribing
The parameters programmed into the PCA machine include the basal rate, demand (or incremental) dose, lockout interval, nurse-initiated bolus dose, and choice of opioid.
Basal rate: The continuous infusion of opioid set at an hourly rate. Most studies that compare PCA use with and without basal rates (in postoperative patients) do not show improved pain relief or sleep with basal rates.11 Basal rates have been associated with increased risk of sedation and respiratory depression.12
The routine use of basal rates is not recommended initially, unless a patient is opioid-tolerant (i.e., on chronic opioid therapy). For patients on chronic opioids, their 24-hour total opioid requirement is converted by equianalgesic dosing to the basal rate. Steady state is not achieved for eight to 12 hours of continuous infusion; therefore, it is not recommended to change the basal rate more frequently than every eight hours.13
Demand dose: The dose patients provide themselves by pushing the button. Studies on opioid-naïve patients using morphine PCAs have shown that 1 mg IV morphine was the optimal starting dose, based on good pain relief without respiratory depression. Lower doses, such as 0.5 mg IV morphine, are generally used in the elderly as opioid requirements are known to decrease with patient age.14
For patients with a basal rate, the demand dose is often set at 50% to 100% of the basal rate. The demand dose is the parameter that should be titrated up for acute pain control. World Health Organization guidelines recommend increasing the dose by 25% to 50% for mild to moderate pain, and 50% to 100% for moderate to severe pain.15
Lockout interval: Minimal allowable time between demand doses. This time is based on the time to peak effect of IV opioids and can vary from five to 15 minutes. The effects of varying lockout intervals—seven to 11 minutes for morphine and five to eight minutes for fentanyl—had no effect on pain levels or side effects.16 Ten minutes is a standard lockout interval.
Bolus dose: The nurse-initiated dose that may be given initially to achieve pain control and later to counteract incidental pain (e.g., that caused by physical therapy, dressing changes, or radiology tests). A recommended dose is equivalent to the basal rate or twice the demand dose.
Choice of opioid: Morphine is the standard opioid because of its familiarity, cost, and years of study. Although inter-individual variability exists, there are no major differences in side effects among the different opioids. Renal and hepatic insufficiency can increase the effects of opioids. Morphine is especially troublesome in renal failure because it has an active metabolite—morphine-6-glucuronide—that can accumulate and increase the risk of sedation and respiratory depression.
Other Concerns
PCA complications: The most well-studied adverse effects of PCAs are nausea and respiratory depression. There is no difference between PCAs and conventional analgesia in rates of nausea or respiratory depression.17
Nausea is the most common side effect in postoperative patients on PCAs. Patients rapidly develop tolerance to nausea over a period of days. However, many clinicians are concerned about respiratory depression and the risk of death. The overall incidence of respiratory depression with PCAs is less than 1% (range from 0.1 to 0.8%), similar to conventional analgesia. However, the incidence is significantly higher when basal rates are used, rising to 1.1 to 3.9%. Other factors predisposing a patient to increased risk of respiratory depression are older age, obstructive sleep apnea, hypovolemia, renal failure, and the concurrent use of other sedating medications.18
Medication errors are also common. The overall incidence of medication mishaps with PCAs is 1.2%.19 More than 50% of these occur because of operator-related errors (e.g., improper loading, programming errors, and documentation errors). Equipment malfunction is the next most common error.
Opioid equianalgesic dosing conversions: The equianalgesic dose ratio is the ratio of the dose of two opioids required to produce the same analgesic effect. (See Table 1, right.) For example, IV morphine is three times as potent as oral morphine, with an equianalgesic dose ratio of 1:3. Equianalgesic dose tables vary somewhat in their values, which have been largely determined by single-dose administration studies.20 The generalizability of these tables to chronic opioid administration is not well studied.
Incomplete cross tolerance: When switching from one opioid to another, lower doses can be used to control pain.21, 22 Tolerance to one opioid does not completely transfer to the new opioid. Starting at half to two-thirds of the new opioid dose is generally recommended to avoid opioid-specific tolerance and inter-individual variability.23,24
Back to the Case
Opioids are the mainstay of pharmacological management of moderate-to-severe cancer pain. Evaluation of the patient reveals that her acute increase in pain is likely due to progression of her cancer. She had been taking morphine (sustained-release, 90 mg oral) twice daily for her pain and had been using approximately five doses per day of immediate-release oral morphine 20 mg for breakthrough pain. This is equivalent to a total 24-hour opioid requirement of 280 mg oral morphine.
She should be started on a PCA for rapid pain control and titration. Hydromorphone (Dilaudid) is a better PCA choice than morphine because she has acute renal failure. The equianalgesic dose ratio of oral morphine to IV hydromorphone is approximately 30:1.5. The total 24-hour opioid dose of 280 mg oral morphine is equivalent to 14 mg IV hydromorphone ([280mg morphine per day ÷ 30] x 1.5 = 14).
After adjusting for 60% incomplete cross tolerance, the total 24-hour opioid dose is reduced to 8.4 mg IV hydromorphone (14 mg x 0.6 = 8.4 mg). This is approximately equivalent to 0.4 mg IV hydromorphone/hour (8.4 mg ÷ 24 hours), which is her initial basal rate. The demand dose should be set at 0.2 mg (50% the basal rate) with a lockout interval of 10 minutes.
Over a period of several days, the patient’s pain was controlled and her opioid requirements stabilized. She was on a basal rate of 1.4 mg/hour and a demand dose of 1 mg with a 10-minute lockout. Her total 24-hour opioid requirement was 44 mg of IV hydromorphone. As her renal function improved but did not completely normalize, oxycodone was chosen over morphine when converting her back to oral pain medications (less active renal metabolites). The equianalgesic dose ratio of oral oxycodone to IV hydromorphone is approximately 20:1.5. Her total 24-hour opioid dose of 44 mg IV hydromorphone is equivalent to 587 mg oral oxycodone (44 ÷ 1.5) x 20. After adjusting for 60% incomplete cross tolerance, the total 24-hour opioid dose is reduced to 352 mg oral oxycodone or 180 mg of sustained-release oxycodone twice daily (352 mg ÷ 2 ≈ 180 mg). For breakthrough pain she should receive 40 mg of immediate-release oxycodone every hour as needed (10% to 15% of the 24-hour opioid requirement). TH
Dr. Youngwerth is a hospitalist and instructor of medicine, University of Colorado at Denver, assistant director, Palliative Care Consult Service, associate director, Colorado Palliative Medicine Fellowship Program, and medical director, Hospice of Saint John.
References
- American Pain Society. Pain: Current understanding of assessment, management, and treatments. National Pharmaceutical Council 2006;1-79.
- Morrison RS, Meier DE, Fischberg D, et al. Improving the management of pain in hospitalized adults. Arch Intern Med. 2006;166:1033-1039.
- Grass JA. Patient-controlled analgesia. Anesth Analg. 2005;101:S44-S61.
- Etches RC. Patient-controlled analgesia. Surg Clinics N Amer. 1999;79:297-312.
- Nolan MF and Wilson M-C B. Patient-controlled analgesia: A method for the controlled self-administration of opioid pain medications. Phys Ther. 1995;75:374-379.
- Ballantyne JC, Carr DB, Chalmers TC, Dear KBG, Angelillo IF, Mosteller F. Postoperative patient-controlled analgesia: Meta-analyses of initial randomized control trials. J Clin Anesth. 1993;5:182-193.
- Hudcova J, McNicol E, Quah C, Lau J, Carr DB. Patient controlled opioid analgesia versus conventional opioid analgesia for postoperative pain. Cochrane Database of Systematic Reviews. 2006;4:1-10.
- Sidebotham D, Dijkhuizen MRJ, Schug SA. The safety and utilization of patient-controlled analgesia. J Pain Symptom Manage. 1997;14:202-209.
- Macintyre PE. Safety and efficacy of patient-controlled analgesia. Br J Anaesth. 2001;87:36-46.
- Manon C, Rittenhouse BE, Perreault S, et al. Efficacy and costs of patient-controlled analgesia versus regularly administered intramuscular opioid therapy. Amer Soc Anesth Inc. 1998;89:1377-1388.
- Krenn H, Oczenski W, Jellinek H, Krumpl-Ströher M, Schweitzer E, Fitzgerald RD. Nalbuphine by PCA-pump for analgesia following hysterectomy: Bolus application versus continuous infusion with bolus application. Eur J Pain. 2001;5:219-226.
- Lehmann KA. Recent developments in patient-controlled analgesia. J Pain Symptom Manage. 2005;29:S72-S89.
- American Pain Society. Principles of analgesic use in the treatment of acute pain and cancer pain. 5th ed. 2003:1-73.
- Macintyre PC, Jarvis DA. Age is the best predictor of postoperative morphine requirements. Pain. 1995;64:357-364.
- National Comprehensive Cancer Network. Clinical practice guidelines in oncology: Adult cancer pain. Version 2.2005:1-30.
- Ginsberg B, Gil KM, Muir M, Sullivan F, Williams DA, Glass PSA. The influence of lockout intervals and drug selection on patient-controlled analgesia following gynecological surgery. Pain. 1995;62:95-100.
- Walder B, Schafer M, Henzi I, Tramer MR. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain. Acta Anaesthesiol Scand. 2001;45:795-804.
- Etches RC. Respiratory depression associated with patient-controlled analgesia: a review of eight cases. Can J Anaesth. 1994;41:125-132.
- Oswalt KE, Shrewsbury P, Stanton-Hicks M. The incidence of medication mishaps in 3,299 PCA patients. Pain. 1990;S5;S152.
- Pereira J, Lawlor P, Vigano A, Dorgan M, Bruera E. Equianalgesic dose rations for opioids: A critical review and proposals for long-term dosing. J Pain Symptom Manage. 2001;22:672-687.
- Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med. 2003;349:1943-1953.
- Mercandante S. Opioid rotation for cancer pain. Cancer. 1999;86:1856-1866.
- Mehta V, Langford RM. Acute pain management for opioid dependent patients. Anaesthesia. 2006;61:269-276.
- Pasternak GW. Incomplete cross tolerance and multiple mu opioid peptide receptors. Trends Pharm Sciences. 2001;22:67-70.
Case
A 69-year-old female with metastatic ovarian cancer and chronic pain syndrome presented to the hospital with seven days of progressively worsening abdominal pain. The pain had been similar to her chronic cancer pain but more severe. She has acute renal failure secondary to volume depletion from poor intake. A CT scan of the abdomen and pelvis reveal progression of her cancer with acute pathology. What is the best method of treating this patient’s pain?
Overview
Pain is pandemic. It is the most common reason patients seek healthcare.1 Almost one-third of Americans will experience severe chronic pain at some point in their lives. Every year, approximately 25 million Americans experience acute pain and 50 million experience chronic pain. Only one in four patients with pain receives appropriate therapy and control of their pain.
Pain is the most common symptom experienced by hospitalized adults.2 Acute or chronic pain can be particularly challenging to treat because these patients are frequently opioid dependent and have many psychosocial factors. No one method of pain control is superior to another. However, one method to gain rapid control of an acute pain crisis in a patient with chronic pain is to use patient-controlled analgesia (PCA).
Review of the Data
The first commercially available PCA pumps became available in 1976.3 They were created after studies in the 1960s demonstrated that small doses of opioids given intravenously provided more effective pain relief than conventional intramuscular injections.
The majority of studies on PCAs are in the postoperative patient, with cancer pain being next most commonly studied. PCAs utilize microprocessor-controlled infusion pumps that deliver a preprogrammed dose of opioid when the patient pushes the demand button. They allow programming of dose (demand dose), time between doses (lockout interval), background infusion rate (basal rate), and nurse-initiated dose (bolus dose).
The PCA paradigm is based on the opioid pharmacologic concept of minimum effective analgesic concentration (MEAC).4,5 The MEAC is the smallest serum opioid concentration at which pain is relieved. The dose-response curve to opioids is sigmoidal such that minimal analgesia is achieved until the MEAC is reached, after which minute increases in opioid concentrations produce analgesia, until further increases produce no significant increased analgesic effect.
PCAs allow individualized dosing and titration to achieve the MEAC, with small incremental doses administered whenever the serum concentration falls below the MEAC. A major goal of PCA technology is to regulate drug delivery to rapidly achieve and maintain the MEAC.
Advantages of PCAs
- More individual dosing and titration of pain medications to account for inter-individual and intra-individual variability in the response to opioids;
- Negative feedback control system, an added safety measure to avoid respiratory depression. As patients become too sedated from opioids, they are no longer able to push the button to receive further opioids;
- Higher patient satisfaction with pain control, a major determinant being personal control over the delivery of pain relief;6-8 and
- Greater analgesic efficacy vs. conventional analgesia.
Disadvantages of PCAs
Select patient populations: Not all patients are able to understand and retain the required instructions necessary to safely or effectively use self-administered opioids (e.g., cognitively impaired patients).
Potential for opioid dosing errors: These are related to equipment factors, medical personnel prescribing or programming errors.
Increased cost: PCAs have been shown to be more expensive in comparison with intramuscular (IM) injections, the prior standard of care.9-10
PCA Prescribing
The parameters programmed into the PCA machine include the basal rate, demand (or incremental) dose, lockout interval, nurse-initiated bolus dose, and choice of opioid.
Basal rate: The continuous infusion of opioid set at an hourly rate. Most studies that compare PCA use with and without basal rates (in postoperative patients) do not show improved pain relief or sleep with basal rates.11 Basal rates have been associated with increased risk of sedation and respiratory depression.12
The routine use of basal rates is not recommended initially, unless a patient is opioid-tolerant (i.e., on chronic opioid therapy). For patients on chronic opioids, their 24-hour total opioid requirement is converted by equianalgesic dosing to the basal rate. Steady state is not achieved for eight to 12 hours of continuous infusion; therefore, it is not recommended to change the basal rate more frequently than every eight hours.13
Demand dose: The dose patients provide themselves by pushing the button. Studies on opioid-naïve patients using morphine PCAs have shown that 1 mg IV morphine was the optimal starting dose, based on good pain relief without respiratory depression. Lower doses, such as 0.5 mg IV morphine, are generally used in the elderly as opioid requirements are known to decrease with patient age.14
For patients with a basal rate, the demand dose is often set at 50% to 100% of the basal rate. The demand dose is the parameter that should be titrated up for acute pain control. World Health Organization guidelines recommend increasing the dose by 25% to 50% for mild to moderate pain, and 50% to 100% for moderate to severe pain.15
Lockout interval: Minimal allowable time between demand doses. This time is based on the time to peak effect of IV opioids and can vary from five to 15 minutes. The effects of varying lockout intervals—seven to 11 minutes for morphine and five to eight minutes for fentanyl—had no effect on pain levels or side effects.16 Ten minutes is a standard lockout interval.
Bolus dose: The nurse-initiated dose that may be given initially to achieve pain control and later to counteract incidental pain (e.g., that caused by physical therapy, dressing changes, or radiology tests). A recommended dose is equivalent to the basal rate or twice the demand dose.
Choice of opioid: Morphine is the standard opioid because of its familiarity, cost, and years of study. Although inter-individual variability exists, there are no major differences in side effects among the different opioids. Renal and hepatic insufficiency can increase the effects of opioids. Morphine is especially troublesome in renal failure because it has an active metabolite—morphine-6-glucuronide—that can accumulate and increase the risk of sedation and respiratory depression.
Other Concerns
PCA complications: The most well-studied adverse effects of PCAs are nausea and respiratory depression. There is no difference between PCAs and conventional analgesia in rates of nausea or respiratory depression.17
Nausea is the most common side effect in postoperative patients on PCAs. Patients rapidly develop tolerance to nausea over a period of days. However, many clinicians are concerned about respiratory depression and the risk of death. The overall incidence of respiratory depression with PCAs is less than 1% (range from 0.1 to 0.8%), similar to conventional analgesia. However, the incidence is significantly higher when basal rates are used, rising to 1.1 to 3.9%. Other factors predisposing a patient to increased risk of respiratory depression are older age, obstructive sleep apnea, hypovolemia, renal failure, and the concurrent use of other sedating medications.18
Medication errors are also common. The overall incidence of medication mishaps with PCAs is 1.2%.19 More than 50% of these occur because of operator-related errors (e.g., improper loading, programming errors, and documentation errors). Equipment malfunction is the next most common error.
Opioid equianalgesic dosing conversions: The equianalgesic dose ratio is the ratio of the dose of two opioids required to produce the same analgesic effect. (See Table 1, right.) For example, IV morphine is three times as potent as oral morphine, with an equianalgesic dose ratio of 1:3. Equianalgesic dose tables vary somewhat in their values, which have been largely determined by single-dose administration studies.20 The generalizability of these tables to chronic opioid administration is not well studied.
Incomplete cross tolerance: When switching from one opioid to another, lower doses can be used to control pain.21, 22 Tolerance to one opioid does not completely transfer to the new opioid. Starting at half to two-thirds of the new opioid dose is generally recommended to avoid opioid-specific tolerance and inter-individual variability.23,24
Back to the Case
Opioids are the mainstay of pharmacological management of moderate-to-severe cancer pain. Evaluation of the patient reveals that her acute increase in pain is likely due to progression of her cancer. She had been taking morphine (sustained-release, 90 mg oral) twice daily for her pain and had been using approximately five doses per day of immediate-release oral morphine 20 mg for breakthrough pain. This is equivalent to a total 24-hour opioid requirement of 280 mg oral morphine.
She should be started on a PCA for rapid pain control and titration. Hydromorphone (Dilaudid) is a better PCA choice than morphine because she has acute renal failure. The equianalgesic dose ratio of oral morphine to IV hydromorphone is approximately 30:1.5. The total 24-hour opioid dose of 280 mg oral morphine is equivalent to 14 mg IV hydromorphone ([280mg morphine per day ÷ 30] x 1.5 = 14).
After adjusting for 60% incomplete cross tolerance, the total 24-hour opioid dose is reduced to 8.4 mg IV hydromorphone (14 mg x 0.6 = 8.4 mg). This is approximately equivalent to 0.4 mg IV hydromorphone/hour (8.4 mg ÷ 24 hours), which is her initial basal rate. The demand dose should be set at 0.2 mg (50% the basal rate) with a lockout interval of 10 minutes.
Over a period of several days, the patient’s pain was controlled and her opioid requirements stabilized. She was on a basal rate of 1.4 mg/hour and a demand dose of 1 mg with a 10-minute lockout. Her total 24-hour opioid requirement was 44 mg of IV hydromorphone. As her renal function improved but did not completely normalize, oxycodone was chosen over morphine when converting her back to oral pain medications (less active renal metabolites). The equianalgesic dose ratio of oral oxycodone to IV hydromorphone is approximately 20:1.5. Her total 24-hour opioid dose of 44 mg IV hydromorphone is equivalent to 587 mg oral oxycodone (44 ÷ 1.5) x 20. After adjusting for 60% incomplete cross tolerance, the total 24-hour opioid dose is reduced to 352 mg oral oxycodone or 180 mg of sustained-release oxycodone twice daily (352 mg ÷ 2 ≈ 180 mg). For breakthrough pain she should receive 40 mg of immediate-release oxycodone every hour as needed (10% to 15% of the 24-hour opioid requirement). TH
Dr. Youngwerth is a hospitalist and instructor of medicine, University of Colorado at Denver, assistant director, Palliative Care Consult Service, associate director, Colorado Palliative Medicine Fellowship Program, and medical director, Hospice of Saint John.
References
- American Pain Society. Pain: Current understanding of assessment, management, and treatments. National Pharmaceutical Council 2006;1-79.
- Morrison RS, Meier DE, Fischberg D, et al. Improving the management of pain in hospitalized adults. Arch Intern Med. 2006;166:1033-1039.
- Grass JA. Patient-controlled analgesia. Anesth Analg. 2005;101:S44-S61.
- Etches RC. Patient-controlled analgesia. Surg Clinics N Amer. 1999;79:297-312.
- Nolan MF and Wilson M-C B. Patient-controlled analgesia: A method for the controlled self-administration of opioid pain medications. Phys Ther. 1995;75:374-379.
- Ballantyne JC, Carr DB, Chalmers TC, Dear KBG, Angelillo IF, Mosteller F. Postoperative patient-controlled analgesia: Meta-analyses of initial randomized control trials. J Clin Anesth. 1993;5:182-193.
- Hudcova J, McNicol E, Quah C, Lau J, Carr DB. Patient controlled opioid analgesia versus conventional opioid analgesia for postoperative pain. Cochrane Database of Systematic Reviews. 2006;4:1-10.
- Sidebotham D, Dijkhuizen MRJ, Schug SA. The safety and utilization of patient-controlled analgesia. J Pain Symptom Manage. 1997;14:202-209.
- Macintyre PE. Safety and efficacy of patient-controlled analgesia. Br J Anaesth. 2001;87:36-46.
- Manon C, Rittenhouse BE, Perreault S, et al. Efficacy and costs of patient-controlled analgesia versus regularly administered intramuscular opioid therapy. Amer Soc Anesth Inc. 1998;89:1377-1388.
- Krenn H, Oczenski W, Jellinek H, Krumpl-Ströher M, Schweitzer E, Fitzgerald RD. Nalbuphine by PCA-pump for analgesia following hysterectomy: Bolus application versus continuous infusion with bolus application. Eur J Pain. 2001;5:219-226.
- Lehmann KA. Recent developments in patient-controlled analgesia. J Pain Symptom Manage. 2005;29:S72-S89.
- American Pain Society. Principles of analgesic use in the treatment of acute pain and cancer pain. 5th ed. 2003:1-73.
- Macintyre PC, Jarvis DA. Age is the best predictor of postoperative morphine requirements. Pain. 1995;64:357-364.
- National Comprehensive Cancer Network. Clinical practice guidelines in oncology: Adult cancer pain. Version 2.2005:1-30.
- Ginsberg B, Gil KM, Muir M, Sullivan F, Williams DA, Glass PSA. The influence of lockout intervals and drug selection on patient-controlled analgesia following gynecological surgery. Pain. 1995;62:95-100.
- Walder B, Schafer M, Henzi I, Tramer MR. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain. Acta Anaesthesiol Scand. 2001;45:795-804.
- Etches RC. Respiratory depression associated with patient-controlled analgesia: a review of eight cases. Can J Anaesth. 1994;41:125-132.
- Oswalt KE, Shrewsbury P, Stanton-Hicks M. The incidence of medication mishaps in 3,299 PCA patients. Pain. 1990;S5;S152.
- Pereira J, Lawlor P, Vigano A, Dorgan M, Bruera E. Equianalgesic dose rations for opioids: A critical review and proposals for long-term dosing. J Pain Symptom Manage. 2001;22:672-687.
- Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med. 2003;349:1943-1953.
- Mercandante S. Opioid rotation for cancer pain. Cancer. 1999;86:1856-1866.
- Mehta V, Langford RM. Acute pain management for opioid dependent patients. Anaesthesia. 2006;61:269-276.
- Pasternak GW. Incomplete cross tolerance and multiple mu opioid peptide receptors. Trends Pharm Sciences. 2001;22:67-70.
Secrets of Supervision
Little information is available on how teaching outcomes involving academic hospitalists and resident physicians affect patient safety and error rates—particularly under duty-hour restrictions on residents by the Accreditation Council for Graduate Medical Education (ACGME).
But data show that when medical errors occur they are often connected with residents’ errors in judgment, lack of technical competence, inadequate supervision by senior physicians, and a breakdown in teamwork.1 In a study of 889 cases resulting in error and injury, 240 involved trainees with at least a “moderately important” role. Among the findings:
- Residents were involved in 208 of those 240 cases;
- 168 of the cases occurred in the inpatient setting;
- 80 of the cases involved obstetrics-gynecology residents, and 45 involved general surgery residents;
- Trainees “lacked technical competence or knowledge” of diagnosis in 67 cases; and
- Attending physicians were involved in 106 supervision failures.
Based on this information, how can academic hospitalists best supervise residents to reduce errors and optimize patient safety and treatment while enhancing residents’ training and satisfaction? Academic hospitalists across the United States grapple with this question daily. And a few have come up with ways that meet the needs of patients and residents.
—Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis.
Oversight vs. Hindsight
Reflecting on his residency, Eric Siegal, MD, a regional medical director with Cogent Healthcare in Madison, Wis., and chair of SHM’s Public Policy Committee, says he recalls times when he did not receive sufficient oversight from senior physicians. Consequently, he and his patients suffered, he says.
“We were thrown into things with little or no supervision, and we were told to sink or swim,” he says. “The good news is that we learned a ton on our own. The bad news is we hurt people in the process. So, the question is how do you walk a line of creating house staff who are autonomous and competent while protecting the patient?”
As an attending physician at the University of Wisconsin, Dr. Siegal says he gave his residents autonomy to make decisions. But there were things he did not let them do alone or without first asking. “The obvious thing was procedures,” he notes. “When residents did procedures, I was standing right there next to them. The extent to which I got involved was entirely dependent on the extent to which the resident was competent.”
Likewise, Alpesh Amin, MD, MBA, professor and chief, division of general internal medicine and executive director of the hospitalist program at the University of California, Irvine, says he gives residents oversight but doesn’t hover. “Otherwise they’re not learning from experience by only doing what someone else tells them to do,” he says. “But without oversight, you don’t prevent errors.”
Dr. Amin, a member of SHM’s Board of Directors, says that as an attending he begins the month with an orientation, reviewing items that help prevent hospital errors. For example, he urges residents before giving medicine to think about possible renal insufficiency and drug interactions. He says he also stresses the importance of preventive techniques.
Developing a system that allows residents to feel comfortable approaching their attending with questions is also vital, says Dr. Amin. Meanwhile, the attending needs to feel he can ask residents pointed questions, yet allow them to think things through.
Dr. Siegal maintained a dialogue with residents regarding the degree of supervision they needed. “A week into the rotation, I asked them how they felt,” he recalls. “Are you getting enough supervision? Too much? Most residents have a reasonable sense of what their deficiencies and discomforts are.”
Joseph Li, MD, director of the hospital medicine program at Boston’s Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, and Kenneth Epstein, MD, MBA, a hospitalist and director of medical affairs and clinical research at IPC-The Hospitalist Company, agree. Dr. Li, also an SHM board member, says not only are residents seeking the right amount of supervision, they’re also seeking the right type of supervision based on their strengths and weaknesses. He says residents also are looking for something else—a medical model. “I think they look for someone to model themselves after,” he suggests. “I think all of us do throughout life, sometimes on purpose but also without intending to do so to better ourselves and learn how to do things.”
Culture Change
Once an atmosphere rife with assigning blame for medical errors, teaching hospitals are changing how errors are found and disclosed, says Michael Lukela, MD, director of the pediatrics program at the University of Michigan and assistant professor of internal medicine and pediatrics.
“The focus is now on patient safety and looking more broadly at how medical errors come about,” he says. “The focus is shifting away from the individual while not overlooking the personal responsibility. There should be safeguards in place, which should prevent errors from occurring, so errors are not just about one person.
“Trainees want to know about the culture. What if they do make an error? Who should they talk with? Their attending? Many are fearful, but these fears don’t have basis. It’s based on what they experience in medical school, saw on TV, and learned from observing others.”
Instead, Dr. Lukela says residents should be saying: “ ‘I don’t understand how my patient got this wrong medication. How can we prevent that?’ It’s up to us as educators to step back and say, ‘That’s a great question’ and get them to think about why errors happen.”
Residents want to focus on the big picture—to learn the art of practicing medicine and get support to do what they need to do, says Dr. Amin. And attendings are looking for residents motivated to learn. “It takes time, energy, and motivation to teach—just like it takes time, energy, and motivation to take care of patients,” he says. “And the hospitalist is in the perfect position to do that.”
Hand-Off Errors
Although hand-offs long have been a part of hospital medicine, the ACGME’s recent resident work-hour limit has raised questions concerning its benefits and drawbacks.
“The concept of 80 hours [a week] is a very good one, but practically it has meant increasing the number of hand-offs,” says Dr. Lukela. “And when you’re increasing the number of handoffs, there’s an increased potential in increasing errors.”
To prevent errors, Dr. Amin says it’s essential to develop a culture around proper hand-offs. “Taking care of patients is not just about getting a history and giving patients drugs or doing surgery,” he cautions. “It’s also thinking about potential errors that can occur and minimizing them through the process of care.”
Dr. Lukela agrees, saying the key part of the hand-off that affects efficiency, quality of care, and error reduction is the thought process of the physician handing off. What is the patient’s history? What tests are pending? What is the action plan? And from day one in the hospital, he says, there needs to be a discharge plan so residents know what direction the patient is going in.
Residents also need to learn that information needs to be meticulously transmitted when there is a transition of care from hospital to nursing facility or from hospital to home. “Residents may view life in the academic center as a vacuum from the outside primary care world,” says Dr. Epstein. “The residents may see the care as what they did in the hospital, but the care is part of a continuum from the primary care, the person’s doctor,” he says.
Team Approach
For hospitalist Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison, teamwork coupled with redundancy has proven an effective method of teaching residents while delivering first-rate patient care.
“I structure the learning environment so that each person knows what level of responsibility he has within the healthcare team,” she says.
Dr. Wright requires that medical students learn how wards work, that interns learn more about diagnosis and management, and that residents learn how to assign responsibility to the patient team while taking responsibility for patient care. Meanwhile, the attending makes sure the proper diagnosis has been made, and the treatment plan has been carried out.
This arrangement she finds helps her teach and helps prevent errors. “What happens is that there’s some duplication of effort within the medical team,” says Dr. Wright. “But you want more than one person checking to make sure things are getting done, and that way it’s not only excellent care for the patient, but it’s a learning environment.”
The Bottom Line
Dr. Wright says she favors training residents by teaching them about each patient being cared for and that patient’s particular manifestation of a disease. “This method fits in very well with the whole idea of how each one of us is working to help this patient with this condition. I like to pool information and actually take care of the patient as we talk about a condition: helping that patient improve, helping make the diagnosis, helping decide on a treatment. The bottom line is the patient, getting the patient excellent care,” says Dr. Wright.
“As teachers, we try to teach with emotions,” says Dr. Li. “When we teach trainees to care for patients we try to think about how to make it memorable for them—and you remember something that’s emotional,” “So, despite some of the challenges we face, I think we’re at a better place than we were 10 years ago, having hospitalists on the wards. And I think 10 years from now, we’re going to be in an even better place. We’ll have the luxury of 10 more years of clinical experience and emotional experience to impart to trainees.” TH
Robin Tricoles is a medical writer based in New Jersey.
Reference
- Singh H, Thomas EJ, Peterson LA, et al. Medical errors involving trainees. A study of closed malpractice claims from 5 insurers. Arch Intern Med. 2007 Oct;167(19):2030-2036.
Little information is available on how teaching outcomes involving academic hospitalists and resident physicians affect patient safety and error rates—particularly under duty-hour restrictions on residents by the Accreditation Council for Graduate Medical Education (ACGME).
But data show that when medical errors occur they are often connected with residents’ errors in judgment, lack of technical competence, inadequate supervision by senior physicians, and a breakdown in teamwork.1 In a study of 889 cases resulting in error and injury, 240 involved trainees with at least a “moderately important” role. Among the findings:
- Residents were involved in 208 of those 240 cases;
- 168 of the cases occurred in the inpatient setting;
- 80 of the cases involved obstetrics-gynecology residents, and 45 involved general surgery residents;
- Trainees “lacked technical competence or knowledge” of diagnosis in 67 cases; and
- Attending physicians were involved in 106 supervision failures.
Based on this information, how can academic hospitalists best supervise residents to reduce errors and optimize patient safety and treatment while enhancing residents’ training and satisfaction? Academic hospitalists across the United States grapple with this question daily. And a few have come up with ways that meet the needs of patients and residents.
—Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis.
Oversight vs. Hindsight
Reflecting on his residency, Eric Siegal, MD, a regional medical director with Cogent Healthcare in Madison, Wis., and chair of SHM’s Public Policy Committee, says he recalls times when he did not receive sufficient oversight from senior physicians. Consequently, he and his patients suffered, he says.
“We were thrown into things with little or no supervision, and we were told to sink or swim,” he says. “The good news is that we learned a ton on our own. The bad news is we hurt people in the process. So, the question is how do you walk a line of creating house staff who are autonomous and competent while protecting the patient?”
As an attending physician at the University of Wisconsin, Dr. Siegal says he gave his residents autonomy to make decisions. But there were things he did not let them do alone or without first asking. “The obvious thing was procedures,” he notes. “When residents did procedures, I was standing right there next to them. The extent to which I got involved was entirely dependent on the extent to which the resident was competent.”
Likewise, Alpesh Amin, MD, MBA, professor and chief, division of general internal medicine and executive director of the hospitalist program at the University of California, Irvine, says he gives residents oversight but doesn’t hover. “Otherwise they’re not learning from experience by only doing what someone else tells them to do,” he says. “But without oversight, you don’t prevent errors.”
Dr. Amin, a member of SHM’s Board of Directors, says that as an attending he begins the month with an orientation, reviewing items that help prevent hospital errors. For example, he urges residents before giving medicine to think about possible renal insufficiency and drug interactions. He says he also stresses the importance of preventive techniques.
Developing a system that allows residents to feel comfortable approaching their attending with questions is also vital, says Dr. Amin. Meanwhile, the attending needs to feel he can ask residents pointed questions, yet allow them to think things through.
Dr. Siegal maintained a dialogue with residents regarding the degree of supervision they needed. “A week into the rotation, I asked them how they felt,” he recalls. “Are you getting enough supervision? Too much? Most residents have a reasonable sense of what their deficiencies and discomforts are.”
Joseph Li, MD, director of the hospital medicine program at Boston’s Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, and Kenneth Epstein, MD, MBA, a hospitalist and director of medical affairs and clinical research at IPC-The Hospitalist Company, agree. Dr. Li, also an SHM board member, says not only are residents seeking the right amount of supervision, they’re also seeking the right type of supervision based on their strengths and weaknesses. He says residents also are looking for something else—a medical model. “I think they look for someone to model themselves after,” he suggests. “I think all of us do throughout life, sometimes on purpose but also without intending to do so to better ourselves and learn how to do things.”
Culture Change
Once an atmosphere rife with assigning blame for medical errors, teaching hospitals are changing how errors are found and disclosed, says Michael Lukela, MD, director of the pediatrics program at the University of Michigan and assistant professor of internal medicine and pediatrics.
“The focus is now on patient safety and looking more broadly at how medical errors come about,” he says. “The focus is shifting away from the individual while not overlooking the personal responsibility. There should be safeguards in place, which should prevent errors from occurring, so errors are not just about one person.
“Trainees want to know about the culture. What if they do make an error? Who should they talk with? Their attending? Many are fearful, but these fears don’t have basis. It’s based on what they experience in medical school, saw on TV, and learned from observing others.”
Instead, Dr. Lukela says residents should be saying: “ ‘I don’t understand how my patient got this wrong medication. How can we prevent that?’ It’s up to us as educators to step back and say, ‘That’s a great question’ and get them to think about why errors happen.”
Residents want to focus on the big picture—to learn the art of practicing medicine and get support to do what they need to do, says Dr. Amin. And attendings are looking for residents motivated to learn. “It takes time, energy, and motivation to teach—just like it takes time, energy, and motivation to take care of patients,” he says. “And the hospitalist is in the perfect position to do that.”
Hand-Off Errors
Although hand-offs long have been a part of hospital medicine, the ACGME’s recent resident work-hour limit has raised questions concerning its benefits and drawbacks.
“The concept of 80 hours [a week] is a very good one, but practically it has meant increasing the number of hand-offs,” says Dr. Lukela. “And when you’re increasing the number of handoffs, there’s an increased potential in increasing errors.”
To prevent errors, Dr. Amin says it’s essential to develop a culture around proper hand-offs. “Taking care of patients is not just about getting a history and giving patients drugs or doing surgery,” he cautions. “It’s also thinking about potential errors that can occur and minimizing them through the process of care.”
Dr. Lukela agrees, saying the key part of the hand-off that affects efficiency, quality of care, and error reduction is the thought process of the physician handing off. What is the patient’s history? What tests are pending? What is the action plan? And from day one in the hospital, he says, there needs to be a discharge plan so residents know what direction the patient is going in.
Residents also need to learn that information needs to be meticulously transmitted when there is a transition of care from hospital to nursing facility or from hospital to home. “Residents may view life in the academic center as a vacuum from the outside primary care world,” says Dr. Epstein. “The residents may see the care as what they did in the hospital, but the care is part of a continuum from the primary care, the person’s doctor,” he says.
Team Approach
For hospitalist Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison, teamwork coupled with redundancy has proven an effective method of teaching residents while delivering first-rate patient care.
“I structure the learning environment so that each person knows what level of responsibility he has within the healthcare team,” she says.
Dr. Wright requires that medical students learn how wards work, that interns learn more about diagnosis and management, and that residents learn how to assign responsibility to the patient team while taking responsibility for patient care. Meanwhile, the attending makes sure the proper diagnosis has been made, and the treatment plan has been carried out.
This arrangement she finds helps her teach and helps prevent errors. “What happens is that there’s some duplication of effort within the medical team,” says Dr. Wright. “But you want more than one person checking to make sure things are getting done, and that way it’s not only excellent care for the patient, but it’s a learning environment.”
The Bottom Line
Dr. Wright says she favors training residents by teaching them about each patient being cared for and that patient’s particular manifestation of a disease. “This method fits in very well with the whole idea of how each one of us is working to help this patient with this condition. I like to pool information and actually take care of the patient as we talk about a condition: helping that patient improve, helping make the diagnosis, helping decide on a treatment. The bottom line is the patient, getting the patient excellent care,” says Dr. Wright.
“As teachers, we try to teach with emotions,” says Dr. Li. “When we teach trainees to care for patients we try to think about how to make it memorable for them—and you remember something that’s emotional,” “So, despite some of the challenges we face, I think we’re at a better place than we were 10 years ago, having hospitalists on the wards. And I think 10 years from now, we’re going to be in an even better place. We’ll have the luxury of 10 more years of clinical experience and emotional experience to impart to trainees.” TH
Robin Tricoles is a medical writer based in New Jersey.
Reference
- Singh H, Thomas EJ, Peterson LA, et al. Medical errors involving trainees. A study of closed malpractice claims from 5 insurers. Arch Intern Med. 2007 Oct;167(19):2030-2036.
Little information is available on how teaching outcomes involving academic hospitalists and resident physicians affect patient safety and error rates—particularly under duty-hour restrictions on residents by the Accreditation Council for Graduate Medical Education (ACGME).
But data show that when medical errors occur they are often connected with residents’ errors in judgment, lack of technical competence, inadequate supervision by senior physicians, and a breakdown in teamwork.1 In a study of 889 cases resulting in error and injury, 240 involved trainees with at least a “moderately important” role. Among the findings:
- Residents were involved in 208 of those 240 cases;
- 168 of the cases occurred in the inpatient setting;
- 80 of the cases involved obstetrics-gynecology residents, and 45 involved general surgery residents;
- Trainees “lacked technical competence or knowledge” of diagnosis in 67 cases; and
- Attending physicians were involved in 106 supervision failures.
Based on this information, how can academic hospitalists best supervise residents to reduce errors and optimize patient safety and treatment while enhancing residents’ training and satisfaction? Academic hospitalists across the United States grapple with this question daily. And a few have come up with ways that meet the needs of patients and residents.
—Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis.
Oversight vs. Hindsight
Reflecting on his residency, Eric Siegal, MD, a regional medical director with Cogent Healthcare in Madison, Wis., and chair of SHM’s Public Policy Committee, says he recalls times when he did not receive sufficient oversight from senior physicians. Consequently, he and his patients suffered, he says.
“We were thrown into things with little or no supervision, and we were told to sink or swim,” he says. “The good news is that we learned a ton on our own. The bad news is we hurt people in the process. So, the question is how do you walk a line of creating house staff who are autonomous and competent while protecting the patient?”
As an attending physician at the University of Wisconsin, Dr. Siegal says he gave his residents autonomy to make decisions. But there were things he did not let them do alone or without first asking. “The obvious thing was procedures,” he notes. “When residents did procedures, I was standing right there next to them. The extent to which I got involved was entirely dependent on the extent to which the resident was competent.”
Likewise, Alpesh Amin, MD, MBA, professor and chief, division of general internal medicine and executive director of the hospitalist program at the University of California, Irvine, says he gives residents oversight but doesn’t hover. “Otherwise they’re not learning from experience by only doing what someone else tells them to do,” he says. “But without oversight, you don’t prevent errors.”
Dr. Amin, a member of SHM’s Board of Directors, says that as an attending he begins the month with an orientation, reviewing items that help prevent hospital errors. For example, he urges residents before giving medicine to think about possible renal insufficiency and drug interactions. He says he also stresses the importance of preventive techniques.
Developing a system that allows residents to feel comfortable approaching their attending with questions is also vital, says Dr. Amin. Meanwhile, the attending needs to feel he can ask residents pointed questions, yet allow them to think things through.
Dr. Siegal maintained a dialogue with residents regarding the degree of supervision they needed. “A week into the rotation, I asked them how they felt,” he recalls. “Are you getting enough supervision? Too much? Most residents have a reasonable sense of what their deficiencies and discomforts are.”
Joseph Li, MD, director of the hospital medicine program at Boston’s Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, and Kenneth Epstein, MD, MBA, a hospitalist and director of medical affairs and clinical research at IPC-The Hospitalist Company, agree. Dr. Li, also an SHM board member, says not only are residents seeking the right amount of supervision, they’re also seeking the right type of supervision based on their strengths and weaknesses. He says residents also are looking for something else—a medical model. “I think they look for someone to model themselves after,” he suggests. “I think all of us do throughout life, sometimes on purpose but also without intending to do so to better ourselves and learn how to do things.”
Culture Change
Once an atmosphere rife with assigning blame for medical errors, teaching hospitals are changing how errors are found and disclosed, says Michael Lukela, MD, director of the pediatrics program at the University of Michigan and assistant professor of internal medicine and pediatrics.
“The focus is now on patient safety and looking more broadly at how medical errors come about,” he says. “The focus is shifting away from the individual while not overlooking the personal responsibility. There should be safeguards in place, which should prevent errors from occurring, so errors are not just about one person.
“Trainees want to know about the culture. What if they do make an error? Who should they talk with? Their attending? Many are fearful, but these fears don’t have basis. It’s based on what they experience in medical school, saw on TV, and learned from observing others.”
Instead, Dr. Lukela says residents should be saying: “ ‘I don’t understand how my patient got this wrong medication. How can we prevent that?’ It’s up to us as educators to step back and say, ‘That’s a great question’ and get them to think about why errors happen.”
Residents want to focus on the big picture—to learn the art of practicing medicine and get support to do what they need to do, says Dr. Amin. And attendings are looking for residents motivated to learn. “It takes time, energy, and motivation to teach—just like it takes time, energy, and motivation to take care of patients,” he says. “And the hospitalist is in the perfect position to do that.”
Hand-Off Errors
Although hand-offs long have been a part of hospital medicine, the ACGME’s recent resident work-hour limit has raised questions concerning its benefits and drawbacks.
“The concept of 80 hours [a week] is a very good one, but practically it has meant increasing the number of hand-offs,” says Dr. Lukela. “And when you’re increasing the number of handoffs, there’s an increased potential in increasing errors.”
To prevent errors, Dr. Amin says it’s essential to develop a culture around proper hand-offs. “Taking care of patients is not just about getting a history and giving patients drugs or doing surgery,” he cautions. “It’s also thinking about potential errors that can occur and minimizing them through the process of care.”
Dr. Lukela agrees, saying the key part of the hand-off that affects efficiency, quality of care, and error reduction is the thought process of the physician handing off. What is the patient’s history? What tests are pending? What is the action plan? And from day one in the hospital, he says, there needs to be a discharge plan so residents know what direction the patient is going in.
Residents also need to learn that information needs to be meticulously transmitted when there is a transition of care from hospital to nursing facility or from hospital to home. “Residents may view life in the academic center as a vacuum from the outside primary care world,” says Dr. Epstein. “The residents may see the care as what they did in the hospital, but the care is part of a continuum from the primary care, the person’s doctor,” he says.
Team Approach
For hospitalist Julia Wright, MD, associate clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison, teamwork coupled with redundancy has proven an effective method of teaching residents while delivering first-rate patient care.
“I structure the learning environment so that each person knows what level of responsibility he has within the healthcare team,” she says.
Dr. Wright requires that medical students learn how wards work, that interns learn more about diagnosis and management, and that residents learn how to assign responsibility to the patient team while taking responsibility for patient care. Meanwhile, the attending makes sure the proper diagnosis has been made, and the treatment plan has been carried out.
This arrangement she finds helps her teach and helps prevent errors. “What happens is that there’s some duplication of effort within the medical team,” says Dr. Wright. “But you want more than one person checking to make sure things are getting done, and that way it’s not only excellent care for the patient, but it’s a learning environment.”
The Bottom Line
Dr. Wright says she favors training residents by teaching them about each patient being cared for and that patient’s particular manifestation of a disease. “This method fits in very well with the whole idea of how each one of us is working to help this patient with this condition. I like to pool information and actually take care of the patient as we talk about a condition: helping that patient improve, helping make the diagnosis, helping decide on a treatment. The bottom line is the patient, getting the patient excellent care,” says Dr. Wright.
“As teachers, we try to teach with emotions,” says Dr. Li. “When we teach trainees to care for patients we try to think about how to make it memorable for them—and you remember something that’s emotional,” “So, despite some of the challenges we face, I think we’re at a better place than we were 10 years ago, having hospitalists on the wards. And I think 10 years from now, we’re going to be in an even better place. We’ll have the luxury of 10 more years of clinical experience and emotional experience to impart to trainees.” TH
Robin Tricoles is a medical writer based in New Jersey.
Reference
- Singh H, Thomas EJ, Peterson LA, et al. Medical errors involving trainees. A study of closed malpractice claims from 5 insurers. Arch Intern Med. 2007 Oct;167(19):2030-2036.
All Hands on Deck
As hospitalist groups evolve, they seek ways to make the best use of support staff to improve patient care and efficiency.
A look at hospitalist groups around the country shows there is no one perfect formula for putting together the best support staff. Rather, the choices groups make are tailored to their specific needs and their relationship with their hospitals.
Support staff members can include secretaries, clerical workers, case managers, social workers, administrators and administrative assistants, office managers, nurses, nurse practitioners, and physician’s assistants.
New Approaches
One trend is the use of registered nurses in hybrid nursing/administrative roles that require medical knowledge and hospital savvy.
Brian Bossard, MD, created a nurse coordinator role in 2003 to provide support to the 18 hospitalists he directs at Inpatient Physician Associates, a group that provides care to patients at BryanLGH Medical Center in Lincoln, Neb.
The group’s three nurse coordinators serve as liaisons with patients and their families and with the hospital’s nursing staff and ancillary staff. The nurse coordinators expedite discharge management by initiating discharge orders, justifying medications, and fielding any questions or issues that need to be discussed with doctors. They keep track of the group’s 18 hospitalists and determine who is available to take on new admissions. It’s an often-complex process of knowing who’s where on rounds and whether they’re busy with difficult cases.
Before the nurse coordinator roles were established, physicians were in charge of figuring out who would take the next patient. “That physician would take all the information, but that may not be the physician available to take care of the patient,” says Dr. Bossard. “That physician would have to call another physician and give the same information—which occupied our doctors’ time. The nurse coordinators are really a time-saving feature.”
At the hospital medicine program at Temple University School of Medicine in Philadelphia, six clinical care coordinators, all trained RNs, play a similar role for the program’s 23 hospitalists.
William Ford, MD, medical director for Cogent Healthcare directing the program at Temple University, credits the clinical care coordinators, who help maintain communication with patients’ primary care physician during and after discharge, for cutting the hospital’s 30-day and 72-hour readmission rate in half within a year’s time. He says coordinators have played a significant role in boosting the group’s overall efficiency. “Our doctors can see three to five more patients a day because of the time the clinical care coordinators save them,” he says.
Some companies providing hospitalist services have relied mainly on office manager-type staff members to take care of clerical tasks and ensure the flow of information between hospitalists and primary care physicians. “Practice coordinators” play this role at the seven hospitalist groups run by The Schumacher Group’s Hospital Medicine Division of Lafayette, La.
David Grace, MD, area medical officer for Schumacher’s hospital medicine division, says practice coordinators are also in charge of collecting data on patients’ length of stay and level of satisfaction and ensuring accuracy in coding and documentation of diagnoses.
Practice coordinators are not required to have nursing degrees, as the job doesn’t include direct patient care. But he looks for applicants with a background in healthcare and an understanding of medical terminology. “Although practice coordinators don’t provide clinical care, the position improves the care delivered by the hospitalists,” he says.
Strike a Balance
One trap hospitalist groups fall into is hiring more support staff than they need, says John Nelson, MD, a principal in Nelson/Flores, a hospitalist management consulting firm, and the medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash.
In his consulting work, Dr. Nelson has seen secretaries file huge volumes of reports and spend their time creating charts and spreadsheets no one will look at again. “It’s very unusual for a hospitalist group to need any sort of medical records kept separately from the hospital,” he says. “So support staff may be doing busy work that doesn’t benefit the practice.”
His advice? “Think critically about whether adding that person is really likely to make the practice better. Challenge yourself to justify any support person you’re considering adding. Make sure every element of the job description contributes to the practice.”
The need for support staff often depends on the hospitalist group’s working relationship to the hospital. Julia Wright, MD, is director of hospital medicine at the University of Wisconsin Hospitals and Clinics (UWHC) in Madison, an academic hospital medicine group of 11 physicians and one advanced practice nurse practitioner. She says the group is assisted by support staff working within the Department of Medicine.
Her part-time program assistant, who tends to secretarial duties such as setting up meetings and assisting with policy development and scheduling, is employed by the primary care department. “We have a benevolent arrangement with the hospital,” she says. “It allows us to do more research and teaching. When we want to put forward an initiative, we usually have the person power and interest and the support to do it.”
Another trend in hiring among hospitalist groups is employing midlevel practitioners, such as nurse practitioners and physician’s assistants. Dr. Ford worked with a physician’s assistant when he was a hospitalist at Union Hospital, a 120-bed community hospital in Elkton, Md. He called midlevel practitioners, who make $70,000 to $90,000 a year —about half the average pay for a hospitalist—a “windfall.”
“They see less-acute patients,” he says. “Patients with stable pneumonia still generate the same billing code as a sicker patient who takes more time and expertise, so midlevels can be more efficient providers from that aspect.”
But this strategy can backfire, according to Dr. Nelson. “On paper, giving nurse practitioners patients who are less sick is logical,” he says. “But in practice, it’s hard to divide up the responsibilities efficiently every day, and there is often a lot of inefficient or unnecessary overlap in work done by the MD and the NP.”
At UWHC, Dr. Wright has found it useful to create a specific definition of the advanced practice nurse practitioner’s role, using feedback from the nurse practitioner and the group’s hospitalists. “We came up with a document that looked at patient complexity, diagnoses, patient volume, and the nondirect patient care issues she is able to help with,” Dr. Wright says. “It’s posted so everyone can remember what kinds of things she can do.”
Sometimes, hospitalist groups can’t make full use of nurse practitioners and other midlevel providers because of hospital regulations. Matthew Szvetecz, MD, head of the hospitalist program at Kadlec Medical Center in Richland, Wash., says he would like to hire nurse practitioners, but hospital bylaws prevent nurse practitioners from writing orders. “If we have to give that kind of direct level of supervision, we might as well take care of them ourselves,” he says.
Dr. Szvetecz’s program has 13 adult hospitalists, four intensivists, and four pediatric physicians. Support staff members include a coordinator in charge of secretarial and administrative assistant duties, a coder who helps with billing, a nurse coordinator, and an executive director. He says the support staff helps contain costs and prevents physicians from spending too much time on administrative duties.
But as a group, “it’s understood that we may not break even or generate positive cash flow,” he says. “Like most hospitalist groups, we have to be subsidized as far as the upfront cash flow, but there are benefits on the back end as far as reduced lengths of stay and better documentation.”
Caveats
Dr. Bossard cautions against letting support staff take over certain duties. The group has avoided letting anyone but physicians take calls from referring primary care physicians, or make calls to primary care physicians at the time of discharge.
“We want to market ourselves as service oriented and felt that placing an intermediary in the communications process isn’t a good thing to do,” he says. “We don’t think it’s good to have secretaries triage calls from physicians. It takes a lot of the physicians’ time, but that’s time well spent.”
Dr. Wright says efficiency and cost containment can improve according to how well the hospitalist group works with the hospital infrastructure and how invested hospitalists and support staff feel in the success of their program. “If they know they’re valued and they feel like they have a say in the work they do, they’ll be more invested in the work they do,” she says. “That usually leads to more efficiency, in my experience.”
Though it’s important for hospitalist groups to work closely with hospitals, Dr. Nelson warns hospitalists not to copy the administrative structures and systems they see in hospitals. “It’s too easy for practices to make mistakes based on what is going on in hospitals,” he says. “They need to critically think about what’s needed in their practice.” TH
Lisa Phillips is a medical writer based in New York.
As hospitalist groups evolve, they seek ways to make the best use of support staff to improve patient care and efficiency.
A look at hospitalist groups around the country shows there is no one perfect formula for putting together the best support staff. Rather, the choices groups make are tailored to their specific needs and their relationship with their hospitals.
Support staff members can include secretaries, clerical workers, case managers, social workers, administrators and administrative assistants, office managers, nurses, nurse practitioners, and physician’s assistants.
New Approaches
One trend is the use of registered nurses in hybrid nursing/administrative roles that require medical knowledge and hospital savvy.
Brian Bossard, MD, created a nurse coordinator role in 2003 to provide support to the 18 hospitalists he directs at Inpatient Physician Associates, a group that provides care to patients at BryanLGH Medical Center in Lincoln, Neb.
The group’s three nurse coordinators serve as liaisons with patients and their families and with the hospital’s nursing staff and ancillary staff. The nurse coordinators expedite discharge management by initiating discharge orders, justifying medications, and fielding any questions or issues that need to be discussed with doctors. They keep track of the group’s 18 hospitalists and determine who is available to take on new admissions. It’s an often-complex process of knowing who’s where on rounds and whether they’re busy with difficult cases.
Before the nurse coordinator roles were established, physicians were in charge of figuring out who would take the next patient. “That physician would take all the information, but that may not be the physician available to take care of the patient,” says Dr. Bossard. “That physician would have to call another physician and give the same information—which occupied our doctors’ time. The nurse coordinators are really a time-saving feature.”
At the hospital medicine program at Temple University School of Medicine in Philadelphia, six clinical care coordinators, all trained RNs, play a similar role for the program’s 23 hospitalists.
William Ford, MD, medical director for Cogent Healthcare directing the program at Temple University, credits the clinical care coordinators, who help maintain communication with patients’ primary care physician during and after discharge, for cutting the hospital’s 30-day and 72-hour readmission rate in half within a year’s time. He says coordinators have played a significant role in boosting the group’s overall efficiency. “Our doctors can see three to five more patients a day because of the time the clinical care coordinators save them,” he says.
Some companies providing hospitalist services have relied mainly on office manager-type staff members to take care of clerical tasks and ensure the flow of information between hospitalists and primary care physicians. “Practice coordinators” play this role at the seven hospitalist groups run by The Schumacher Group’s Hospital Medicine Division of Lafayette, La.
David Grace, MD, area medical officer for Schumacher’s hospital medicine division, says practice coordinators are also in charge of collecting data on patients’ length of stay and level of satisfaction and ensuring accuracy in coding and documentation of diagnoses.
Practice coordinators are not required to have nursing degrees, as the job doesn’t include direct patient care. But he looks for applicants with a background in healthcare and an understanding of medical terminology. “Although practice coordinators don’t provide clinical care, the position improves the care delivered by the hospitalists,” he says.
Strike a Balance
One trap hospitalist groups fall into is hiring more support staff than they need, says John Nelson, MD, a principal in Nelson/Flores, a hospitalist management consulting firm, and the medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash.
In his consulting work, Dr. Nelson has seen secretaries file huge volumes of reports and spend their time creating charts and spreadsheets no one will look at again. “It’s very unusual for a hospitalist group to need any sort of medical records kept separately from the hospital,” he says. “So support staff may be doing busy work that doesn’t benefit the practice.”
His advice? “Think critically about whether adding that person is really likely to make the practice better. Challenge yourself to justify any support person you’re considering adding. Make sure every element of the job description contributes to the practice.”
The need for support staff often depends on the hospitalist group’s working relationship to the hospital. Julia Wright, MD, is director of hospital medicine at the University of Wisconsin Hospitals and Clinics (UWHC) in Madison, an academic hospital medicine group of 11 physicians and one advanced practice nurse practitioner. She says the group is assisted by support staff working within the Department of Medicine.
Her part-time program assistant, who tends to secretarial duties such as setting up meetings and assisting with policy development and scheduling, is employed by the primary care department. “We have a benevolent arrangement with the hospital,” she says. “It allows us to do more research and teaching. When we want to put forward an initiative, we usually have the person power and interest and the support to do it.”
Another trend in hiring among hospitalist groups is employing midlevel practitioners, such as nurse practitioners and physician’s assistants. Dr. Ford worked with a physician’s assistant when he was a hospitalist at Union Hospital, a 120-bed community hospital in Elkton, Md. He called midlevel practitioners, who make $70,000 to $90,000 a year —about half the average pay for a hospitalist—a “windfall.”
“They see less-acute patients,” he says. “Patients with stable pneumonia still generate the same billing code as a sicker patient who takes more time and expertise, so midlevels can be more efficient providers from that aspect.”
But this strategy can backfire, according to Dr. Nelson. “On paper, giving nurse practitioners patients who are less sick is logical,” he says. “But in practice, it’s hard to divide up the responsibilities efficiently every day, and there is often a lot of inefficient or unnecessary overlap in work done by the MD and the NP.”
At UWHC, Dr. Wright has found it useful to create a specific definition of the advanced practice nurse practitioner’s role, using feedback from the nurse practitioner and the group’s hospitalists. “We came up with a document that looked at patient complexity, diagnoses, patient volume, and the nondirect patient care issues she is able to help with,” Dr. Wright says. “It’s posted so everyone can remember what kinds of things she can do.”
Sometimes, hospitalist groups can’t make full use of nurse practitioners and other midlevel providers because of hospital regulations. Matthew Szvetecz, MD, head of the hospitalist program at Kadlec Medical Center in Richland, Wash., says he would like to hire nurse practitioners, but hospital bylaws prevent nurse practitioners from writing orders. “If we have to give that kind of direct level of supervision, we might as well take care of them ourselves,” he says.
Dr. Szvetecz’s program has 13 adult hospitalists, four intensivists, and four pediatric physicians. Support staff members include a coordinator in charge of secretarial and administrative assistant duties, a coder who helps with billing, a nurse coordinator, and an executive director. He says the support staff helps contain costs and prevents physicians from spending too much time on administrative duties.
But as a group, “it’s understood that we may not break even or generate positive cash flow,” he says. “Like most hospitalist groups, we have to be subsidized as far as the upfront cash flow, but there are benefits on the back end as far as reduced lengths of stay and better documentation.”
Caveats
Dr. Bossard cautions against letting support staff take over certain duties. The group has avoided letting anyone but physicians take calls from referring primary care physicians, or make calls to primary care physicians at the time of discharge.
“We want to market ourselves as service oriented and felt that placing an intermediary in the communications process isn’t a good thing to do,” he says. “We don’t think it’s good to have secretaries triage calls from physicians. It takes a lot of the physicians’ time, but that’s time well spent.”
Dr. Wright says efficiency and cost containment can improve according to how well the hospitalist group works with the hospital infrastructure and how invested hospitalists and support staff feel in the success of their program. “If they know they’re valued and they feel like they have a say in the work they do, they’ll be more invested in the work they do,” she says. “That usually leads to more efficiency, in my experience.”
Though it’s important for hospitalist groups to work closely with hospitals, Dr. Nelson warns hospitalists not to copy the administrative structures and systems they see in hospitals. “It’s too easy for practices to make mistakes based on what is going on in hospitals,” he says. “They need to critically think about what’s needed in their practice.” TH
Lisa Phillips is a medical writer based in New York.
As hospitalist groups evolve, they seek ways to make the best use of support staff to improve patient care and efficiency.
A look at hospitalist groups around the country shows there is no one perfect formula for putting together the best support staff. Rather, the choices groups make are tailored to their specific needs and their relationship with their hospitals.
Support staff members can include secretaries, clerical workers, case managers, social workers, administrators and administrative assistants, office managers, nurses, nurse practitioners, and physician’s assistants.
New Approaches
One trend is the use of registered nurses in hybrid nursing/administrative roles that require medical knowledge and hospital savvy.
Brian Bossard, MD, created a nurse coordinator role in 2003 to provide support to the 18 hospitalists he directs at Inpatient Physician Associates, a group that provides care to patients at BryanLGH Medical Center in Lincoln, Neb.
The group’s three nurse coordinators serve as liaisons with patients and their families and with the hospital’s nursing staff and ancillary staff. The nurse coordinators expedite discharge management by initiating discharge orders, justifying medications, and fielding any questions or issues that need to be discussed with doctors. They keep track of the group’s 18 hospitalists and determine who is available to take on new admissions. It’s an often-complex process of knowing who’s where on rounds and whether they’re busy with difficult cases.
Before the nurse coordinator roles were established, physicians were in charge of figuring out who would take the next patient. “That physician would take all the information, but that may not be the physician available to take care of the patient,” says Dr. Bossard. “That physician would have to call another physician and give the same information—which occupied our doctors’ time. The nurse coordinators are really a time-saving feature.”
At the hospital medicine program at Temple University School of Medicine in Philadelphia, six clinical care coordinators, all trained RNs, play a similar role for the program’s 23 hospitalists.
William Ford, MD, medical director for Cogent Healthcare directing the program at Temple University, credits the clinical care coordinators, who help maintain communication with patients’ primary care physician during and after discharge, for cutting the hospital’s 30-day and 72-hour readmission rate in half within a year’s time. He says coordinators have played a significant role in boosting the group’s overall efficiency. “Our doctors can see three to five more patients a day because of the time the clinical care coordinators save them,” he says.
Some companies providing hospitalist services have relied mainly on office manager-type staff members to take care of clerical tasks and ensure the flow of information between hospitalists and primary care physicians. “Practice coordinators” play this role at the seven hospitalist groups run by The Schumacher Group’s Hospital Medicine Division of Lafayette, La.
David Grace, MD, area medical officer for Schumacher’s hospital medicine division, says practice coordinators are also in charge of collecting data on patients’ length of stay and level of satisfaction and ensuring accuracy in coding and documentation of diagnoses.
Practice coordinators are not required to have nursing degrees, as the job doesn’t include direct patient care. But he looks for applicants with a background in healthcare and an understanding of medical terminology. “Although practice coordinators don’t provide clinical care, the position improves the care delivered by the hospitalists,” he says.
Strike a Balance
One trap hospitalist groups fall into is hiring more support staff than they need, says John Nelson, MD, a principal in Nelson/Flores, a hospitalist management consulting firm, and the medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash.
In his consulting work, Dr. Nelson has seen secretaries file huge volumes of reports and spend their time creating charts and spreadsheets no one will look at again. “It’s very unusual for a hospitalist group to need any sort of medical records kept separately from the hospital,” he says. “So support staff may be doing busy work that doesn’t benefit the practice.”
His advice? “Think critically about whether adding that person is really likely to make the practice better. Challenge yourself to justify any support person you’re considering adding. Make sure every element of the job description contributes to the practice.”
The need for support staff often depends on the hospitalist group’s working relationship to the hospital. Julia Wright, MD, is director of hospital medicine at the University of Wisconsin Hospitals and Clinics (UWHC) in Madison, an academic hospital medicine group of 11 physicians and one advanced practice nurse practitioner. She says the group is assisted by support staff working within the Department of Medicine.
Her part-time program assistant, who tends to secretarial duties such as setting up meetings and assisting with policy development and scheduling, is employed by the primary care department. “We have a benevolent arrangement with the hospital,” she says. “It allows us to do more research and teaching. When we want to put forward an initiative, we usually have the person power and interest and the support to do it.”
Another trend in hiring among hospitalist groups is employing midlevel practitioners, such as nurse practitioners and physician’s assistants. Dr. Ford worked with a physician’s assistant when he was a hospitalist at Union Hospital, a 120-bed community hospital in Elkton, Md. He called midlevel practitioners, who make $70,000 to $90,000 a year —about half the average pay for a hospitalist—a “windfall.”
“They see less-acute patients,” he says. “Patients with stable pneumonia still generate the same billing code as a sicker patient who takes more time and expertise, so midlevels can be more efficient providers from that aspect.”
But this strategy can backfire, according to Dr. Nelson. “On paper, giving nurse practitioners patients who are less sick is logical,” he says. “But in practice, it’s hard to divide up the responsibilities efficiently every day, and there is often a lot of inefficient or unnecessary overlap in work done by the MD and the NP.”
At UWHC, Dr. Wright has found it useful to create a specific definition of the advanced practice nurse practitioner’s role, using feedback from the nurse practitioner and the group’s hospitalists. “We came up with a document that looked at patient complexity, diagnoses, patient volume, and the nondirect patient care issues she is able to help with,” Dr. Wright says. “It’s posted so everyone can remember what kinds of things she can do.”
Sometimes, hospitalist groups can’t make full use of nurse practitioners and other midlevel providers because of hospital regulations. Matthew Szvetecz, MD, head of the hospitalist program at Kadlec Medical Center in Richland, Wash., says he would like to hire nurse practitioners, but hospital bylaws prevent nurse practitioners from writing orders. “If we have to give that kind of direct level of supervision, we might as well take care of them ourselves,” he says.
Dr. Szvetecz’s program has 13 adult hospitalists, four intensivists, and four pediatric physicians. Support staff members include a coordinator in charge of secretarial and administrative assistant duties, a coder who helps with billing, a nurse coordinator, and an executive director. He says the support staff helps contain costs and prevents physicians from spending too much time on administrative duties.
But as a group, “it’s understood that we may not break even or generate positive cash flow,” he says. “Like most hospitalist groups, we have to be subsidized as far as the upfront cash flow, but there are benefits on the back end as far as reduced lengths of stay and better documentation.”
Caveats
Dr. Bossard cautions against letting support staff take over certain duties. The group has avoided letting anyone but physicians take calls from referring primary care physicians, or make calls to primary care physicians at the time of discharge.
“We want to market ourselves as service oriented and felt that placing an intermediary in the communications process isn’t a good thing to do,” he says. “We don’t think it’s good to have secretaries triage calls from physicians. It takes a lot of the physicians’ time, but that’s time well spent.”
Dr. Wright says efficiency and cost containment can improve according to how well the hospitalist group works with the hospital infrastructure and how invested hospitalists and support staff feel in the success of their program. “If they know they’re valued and they feel like they have a say in the work they do, they’ll be more invested in the work they do,” she says. “That usually leads to more efficiency, in my experience.”
Though it’s important for hospitalist groups to work closely with hospitals, Dr. Nelson warns hospitalists not to copy the administrative structures and systems they see in hospitals. “It’s too easy for practices to make mistakes based on what is going on in hospitals,” he says. “They need to critically think about what’s needed in their practice.” TH
Lisa Phillips is a medical writer based in New York.
Watch and Earn
With recent changes in Medicare rules making reimbursement even trickier for patients who aren’t well enough to be sent home quickly but aren’t sick enough to move to an inpatient bed, hospitalists are increasingly being tapped to set up observation units at medical centers around the country.
These patients, experts say, are the ones hospitals are most likely to lose money on. That’s because the Centers for Medicare and Medicaid Services (CMS) won’t pay unless a patient meets stringent guidelines for admission to the hospital. And while recently rewritten rules allow payment for 24 hours of observation, they also can also lead to denial of claims when patients aren’t considered sick enough to have been admitted.
—Jason Napolitano, MD, medical director of the observation unit, University of California at Los Angeles Medical Center
When they’re well run, observation units can even help cover losses from emergency departments (ED) that have trouble collecting on bills because most of their patient population is uninsured or underinsured.
But the drive to create observation units isn’t just about money, says Frank W. Peacock, MD, vice chair of the emergency department at the Cleveland Clinic in Ohio. Studies have shown that death rates drop when hospitals add observation units, Dr. Peacock says.
Despite these clear benefits, experts estimate that a mere 20% of medical centers around the nation have observation units.
This may in part be because creating such a unit—also known as clinical decision unit—takes a lot of planning to start up, says William T. Ford, MD, medical director for Nashville, Tenn.-based Cogent Healthcare and chief of the section of hospital medicine at Temple University in Philadelphia. Without proper planning, observation units can fail to flourish—or just fail.
That’s what happened at Temple, Dr. Ford says. “The original observation unit got bogged down in its own infrastructure,” he explains. “It wasn’t cost effective.”
After that first attempt failed, Temple reached out to Cogent and Dr. Ford for help in developing an observation unit that would be financially viable.
Observation Origins
Classically, Dr. Ford says, observation units were developed and staffed by emergency department physicians. But these days, the units are increasingly being designed and run by hospitalists, he says, adding that this change makes a lot of sense.
“Emergency department physicians don’t have the time or the resources to monitor patients for long periods of time,” Dr. Ford says. “That’s why I think some of the early ones failed—they didn’t work as efficiently and were staffed by the wrong people.”
Hospitalist Jason Napolitano, MD, agrees with the choice to staff observation units with hospitalists. “We want our emergency department physicians to be able to focus on life-or-death issues and on the stabilization of very sick patients,” says Dr. Napolitano, medical director of the observation unit at the University of California at Los Angeles Medical Center. “These are things that ED physicians do spectacularly well. But when it gets down to management and reassessment of patients over time, we wanted a dedicated staff of hospitalists who were trained in internal medicine.”
It made sense that many of the early observation units were staffed by ED doctors, says Mark Flitcraft, a nurse and unit director of nursing at UCLA. That’s because the units were originally adjuncts to the ED. These early units were initially seen as a way to take the pressure off overcrowded, overworked EDs, Flitcraft says. “They were a way for hospitals to avoid [diverting patients] as the beds in the ED started filing up,” he adds.
Avoiding such diversions is still one of the main justifications for adding an observation unit, Dr. Ford says. “The observation unit helps increase throughput time.”
Still, he says, if you’re going to create an observation unit staffed by hospitalists, “you need to make sure that the emergency department buys in to the concept. They should be your best friends. Go over and meet with them. If they don’t buy into the idea, then you’re going to have problems.”
Time Is of the Essence
For an observation unit to work well, the staff needs to think about time in a different way, Flitcraft says.
“It’s more of an outpatient designation from a Medicare standpoint,” he explains. “The focus has to be hours rather than days. You really need to know that the clock is ticking and work on rapid turnaround.” Take discharge, for example, Flitcraft says. Normally a hospitalist would wait for morning to send a patient home. “But there are patients we might discharge at 10 p.m.,” he says. “When they are stable they go home.”
In the observation unit, staff members always have the end in sight, agrees Robin J. Trupp, a grad student at Ohio State University, expert on observation units, and president of The American Association of Heart Failure Nurses. “You know what your goal is,” she adds. “There’s a 24-hour clock and it’s always ticking. At the end of 24 hours you have to make a treatment decision: admit the patient or send him home.”
Because observation units are generally limited to treating a select group of medical conditions, they can be more efficient. Some observation units are limited to only one or two diagnoses (e.g., chest pain and heart failure). Others see a slightly broader spectrum of illnesses, including asthma, stomach pain, and pneumonia.
One byproduct of limiting the number of conditions treated in the unit is ending up with a staff that can become specialized in treating those ailments, experts say.
“In the observation unit you’re not looking at urinary tract infections or doing stitches,” Trupp says. “You’re just working on this population. You become an expert on how it’s treated and managed.”
And that offers another advantage: the possibility of doing more patient education.
She points to the example of a unit dedicated to treating heart failure patients.
“You can take advantage of the fact that at this moment, the patient can clearly see cause and effect and maybe you’ll have a chance at getting some behavior changes,” Trupp says. “It’s the case of having put their hand in the fire and feeling and having learned it’s hot; they’ll learn not to do it again. They might learn that the symptoms that landed them in the ED came from excess salt load due to eating Chinese food or chips and salsa.”
Ultimately, for certain conditions, observation units can provide better care. Studies have shown that in the three months following a visit to the hospital, heart failure patients are far less likely to return if they’ve been seen in the observation unit rather than being treated as inpatients.
And if that weren’t enough of an inducement to administrators to create observation units, Dr. Peacock offers one other: The units can do more than pay for themselves.
“We are in an urban environment, and our patient population is not well insured,” he says. “There are years when the ED loses money. The observation unit never loses money. In fact, it’s saved us a few times. That was a pleasant surprise.” TH
Linda Carroll is a medical writer based in New Jersey.
With recent changes in Medicare rules making reimbursement even trickier for patients who aren’t well enough to be sent home quickly but aren’t sick enough to move to an inpatient bed, hospitalists are increasingly being tapped to set up observation units at medical centers around the country.
These patients, experts say, are the ones hospitals are most likely to lose money on. That’s because the Centers for Medicare and Medicaid Services (CMS) won’t pay unless a patient meets stringent guidelines for admission to the hospital. And while recently rewritten rules allow payment for 24 hours of observation, they also can also lead to denial of claims when patients aren’t considered sick enough to have been admitted.
—Jason Napolitano, MD, medical director of the observation unit, University of California at Los Angeles Medical Center
When they’re well run, observation units can even help cover losses from emergency departments (ED) that have trouble collecting on bills because most of their patient population is uninsured or underinsured.
But the drive to create observation units isn’t just about money, says Frank W. Peacock, MD, vice chair of the emergency department at the Cleveland Clinic in Ohio. Studies have shown that death rates drop when hospitals add observation units, Dr. Peacock says.
Despite these clear benefits, experts estimate that a mere 20% of medical centers around the nation have observation units.
This may in part be because creating such a unit—also known as clinical decision unit—takes a lot of planning to start up, says William T. Ford, MD, medical director for Nashville, Tenn.-based Cogent Healthcare and chief of the section of hospital medicine at Temple University in Philadelphia. Without proper planning, observation units can fail to flourish—or just fail.
That’s what happened at Temple, Dr. Ford says. “The original observation unit got bogged down in its own infrastructure,” he explains. “It wasn’t cost effective.”
After that first attempt failed, Temple reached out to Cogent and Dr. Ford for help in developing an observation unit that would be financially viable.
Observation Origins
Classically, Dr. Ford says, observation units were developed and staffed by emergency department physicians. But these days, the units are increasingly being designed and run by hospitalists, he says, adding that this change makes a lot of sense.
“Emergency department physicians don’t have the time or the resources to monitor patients for long periods of time,” Dr. Ford says. “That’s why I think some of the early ones failed—they didn’t work as efficiently and were staffed by the wrong people.”
Hospitalist Jason Napolitano, MD, agrees with the choice to staff observation units with hospitalists. “We want our emergency department physicians to be able to focus on life-or-death issues and on the stabilization of very sick patients,” says Dr. Napolitano, medical director of the observation unit at the University of California at Los Angeles Medical Center. “These are things that ED physicians do spectacularly well. But when it gets down to management and reassessment of patients over time, we wanted a dedicated staff of hospitalists who were trained in internal medicine.”
It made sense that many of the early observation units were staffed by ED doctors, says Mark Flitcraft, a nurse and unit director of nursing at UCLA. That’s because the units were originally adjuncts to the ED. These early units were initially seen as a way to take the pressure off overcrowded, overworked EDs, Flitcraft says. “They were a way for hospitals to avoid [diverting patients] as the beds in the ED started filing up,” he adds.
Avoiding such diversions is still one of the main justifications for adding an observation unit, Dr. Ford says. “The observation unit helps increase throughput time.”
Still, he says, if you’re going to create an observation unit staffed by hospitalists, “you need to make sure that the emergency department buys in to the concept. They should be your best friends. Go over and meet with them. If they don’t buy into the idea, then you’re going to have problems.”
Time Is of the Essence
For an observation unit to work well, the staff needs to think about time in a different way, Flitcraft says.
“It’s more of an outpatient designation from a Medicare standpoint,” he explains. “The focus has to be hours rather than days. You really need to know that the clock is ticking and work on rapid turnaround.” Take discharge, for example, Flitcraft says. Normally a hospitalist would wait for morning to send a patient home. “But there are patients we might discharge at 10 p.m.,” he says. “When they are stable they go home.”
In the observation unit, staff members always have the end in sight, agrees Robin J. Trupp, a grad student at Ohio State University, expert on observation units, and president of The American Association of Heart Failure Nurses. “You know what your goal is,” she adds. “There’s a 24-hour clock and it’s always ticking. At the end of 24 hours you have to make a treatment decision: admit the patient or send him home.”
Because observation units are generally limited to treating a select group of medical conditions, they can be more efficient. Some observation units are limited to only one or two diagnoses (e.g., chest pain and heart failure). Others see a slightly broader spectrum of illnesses, including asthma, stomach pain, and pneumonia.
One byproduct of limiting the number of conditions treated in the unit is ending up with a staff that can become specialized in treating those ailments, experts say.
“In the observation unit you’re not looking at urinary tract infections or doing stitches,” Trupp says. “You’re just working on this population. You become an expert on how it’s treated and managed.”
And that offers another advantage: the possibility of doing more patient education.
She points to the example of a unit dedicated to treating heart failure patients.
“You can take advantage of the fact that at this moment, the patient can clearly see cause and effect and maybe you’ll have a chance at getting some behavior changes,” Trupp says. “It’s the case of having put their hand in the fire and feeling and having learned it’s hot; they’ll learn not to do it again. They might learn that the symptoms that landed them in the ED came from excess salt load due to eating Chinese food or chips and salsa.”
Ultimately, for certain conditions, observation units can provide better care. Studies have shown that in the three months following a visit to the hospital, heart failure patients are far less likely to return if they’ve been seen in the observation unit rather than being treated as inpatients.
And if that weren’t enough of an inducement to administrators to create observation units, Dr. Peacock offers one other: The units can do more than pay for themselves.
“We are in an urban environment, and our patient population is not well insured,” he says. “There are years when the ED loses money. The observation unit never loses money. In fact, it’s saved us a few times. That was a pleasant surprise.” TH
Linda Carroll is a medical writer based in New Jersey.
With recent changes in Medicare rules making reimbursement even trickier for patients who aren’t well enough to be sent home quickly but aren’t sick enough to move to an inpatient bed, hospitalists are increasingly being tapped to set up observation units at medical centers around the country.
These patients, experts say, are the ones hospitals are most likely to lose money on. That’s because the Centers for Medicare and Medicaid Services (CMS) won’t pay unless a patient meets stringent guidelines for admission to the hospital. And while recently rewritten rules allow payment for 24 hours of observation, they also can also lead to denial of claims when patients aren’t considered sick enough to have been admitted.
—Jason Napolitano, MD, medical director of the observation unit, University of California at Los Angeles Medical Center
When they’re well run, observation units can even help cover losses from emergency departments (ED) that have trouble collecting on bills because most of their patient population is uninsured or underinsured.
But the drive to create observation units isn’t just about money, says Frank W. Peacock, MD, vice chair of the emergency department at the Cleveland Clinic in Ohio. Studies have shown that death rates drop when hospitals add observation units, Dr. Peacock says.
Despite these clear benefits, experts estimate that a mere 20% of medical centers around the nation have observation units.
This may in part be because creating such a unit—also known as clinical decision unit—takes a lot of planning to start up, says William T. Ford, MD, medical director for Nashville, Tenn.-based Cogent Healthcare and chief of the section of hospital medicine at Temple University in Philadelphia. Without proper planning, observation units can fail to flourish—or just fail.
That’s what happened at Temple, Dr. Ford says. “The original observation unit got bogged down in its own infrastructure,” he explains. “It wasn’t cost effective.”
After that first attempt failed, Temple reached out to Cogent and Dr. Ford for help in developing an observation unit that would be financially viable.
Observation Origins
Classically, Dr. Ford says, observation units were developed and staffed by emergency department physicians. But these days, the units are increasingly being designed and run by hospitalists, he says, adding that this change makes a lot of sense.
“Emergency department physicians don’t have the time or the resources to monitor patients for long periods of time,” Dr. Ford says. “That’s why I think some of the early ones failed—they didn’t work as efficiently and were staffed by the wrong people.”
Hospitalist Jason Napolitano, MD, agrees with the choice to staff observation units with hospitalists. “We want our emergency department physicians to be able to focus on life-or-death issues and on the stabilization of very sick patients,” says Dr. Napolitano, medical director of the observation unit at the University of California at Los Angeles Medical Center. “These are things that ED physicians do spectacularly well. But when it gets down to management and reassessment of patients over time, we wanted a dedicated staff of hospitalists who were trained in internal medicine.”
It made sense that many of the early observation units were staffed by ED doctors, says Mark Flitcraft, a nurse and unit director of nursing at UCLA. That’s because the units were originally adjuncts to the ED. These early units were initially seen as a way to take the pressure off overcrowded, overworked EDs, Flitcraft says. “They were a way for hospitals to avoid [diverting patients] as the beds in the ED started filing up,” he adds.
Avoiding such diversions is still one of the main justifications for adding an observation unit, Dr. Ford says. “The observation unit helps increase throughput time.”
Still, he says, if you’re going to create an observation unit staffed by hospitalists, “you need to make sure that the emergency department buys in to the concept. They should be your best friends. Go over and meet with them. If they don’t buy into the idea, then you’re going to have problems.”
Time Is of the Essence
For an observation unit to work well, the staff needs to think about time in a different way, Flitcraft says.
“It’s more of an outpatient designation from a Medicare standpoint,” he explains. “The focus has to be hours rather than days. You really need to know that the clock is ticking and work on rapid turnaround.” Take discharge, for example, Flitcraft says. Normally a hospitalist would wait for morning to send a patient home. “But there are patients we might discharge at 10 p.m.,” he says. “When they are stable they go home.”
In the observation unit, staff members always have the end in sight, agrees Robin J. Trupp, a grad student at Ohio State University, expert on observation units, and president of The American Association of Heart Failure Nurses. “You know what your goal is,” she adds. “There’s a 24-hour clock and it’s always ticking. At the end of 24 hours you have to make a treatment decision: admit the patient or send him home.”
Because observation units are generally limited to treating a select group of medical conditions, they can be more efficient. Some observation units are limited to only one or two diagnoses (e.g., chest pain and heart failure). Others see a slightly broader spectrum of illnesses, including asthma, stomach pain, and pneumonia.
One byproduct of limiting the number of conditions treated in the unit is ending up with a staff that can become specialized in treating those ailments, experts say.
“In the observation unit you’re not looking at urinary tract infections or doing stitches,” Trupp says. “You’re just working on this population. You become an expert on how it’s treated and managed.”
And that offers another advantage: the possibility of doing more patient education.
She points to the example of a unit dedicated to treating heart failure patients.
“You can take advantage of the fact that at this moment, the patient can clearly see cause and effect and maybe you’ll have a chance at getting some behavior changes,” Trupp says. “It’s the case of having put their hand in the fire and feeling and having learned it’s hot; they’ll learn not to do it again. They might learn that the symptoms that landed them in the ED came from excess salt load due to eating Chinese food or chips and salsa.”
Ultimately, for certain conditions, observation units can provide better care. Studies have shown that in the three months following a visit to the hospital, heart failure patients are far less likely to return if they’ve been seen in the observation unit rather than being treated as inpatients.
And if that weren’t enough of an inducement to administrators to create observation units, Dr. Peacock offers one other: The units can do more than pay for themselves.
“We are in an urban environment, and our patient population is not well insured,” he says. “There are years when the ED loses money. The observation unit never loses money. In fact, it’s saved us a few times. That was a pleasant surprise.” TH
Linda Carroll is a medical writer based in New Jersey.
Preventing Venous Thromboembolism Throughout the Continuum of Care
Supplement Editor:
Amir K. Jaffer, MD
Contents
An overview of venous thromboembolism: Impact, risks, and issues in prophylaxis
A.K. Jaffer
Prevention of venous thromboembolism in the hospitalized medical patient
A.K. Jaffer, A.N. Amin, D.J. Brotman, S.B. Deitelzweig, S.C. McKean, A.C. Spyropoulos
Prevention of venous thromboembolism in the cancer surgery patient
A.C. Spyropoulos, D.J. Brotman, A.N. Amin, S.B. Deitelzweig, A.K. Jaffer, S.C. McKean
Prevention of venous thromboembolism in the orthopedic surgery patient
S.B. Deitelzweig, S.C. McKean, A.N. Amin, D.J. Brotman, A.K. Jaffer, A.C. Spyropoulos
Supplement Editor:
Amir K. Jaffer, MD
Contents
An overview of venous thromboembolism: Impact, risks, and issues in prophylaxis
A.K. Jaffer
Prevention of venous thromboembolism in the hospitalized medical patient
A.K. Jaffer, A.N. Amin, D.J. Brotman, S.B. Deitelzweig, S.C. McKean, A.C. Spyropoulos
Prevention of venous thromboembolism in the cancer surgery patient
A.C. Spyropoulos, D.J. Brotman, A.N. Amin, S.B. Deitelzweig, A.K. Jaffer, S.C. McKean
Prevention of venous thromboembolism in the orthopedic surgery patient
S.B. Deitelzweig, S.C. McKean, A.N. Amin, D.J. Brotman, A.K. Jaffer, A.C. Spyropoulos
Supplement Editor:
Amir K. Jaffer, MD
Contents
An overview of venous thromboembolism: Impact, risks, and issues in prophylaxis
A.K. Jaffer
Prevention of venous thromboembolism in the hospitalized medical patient
A.K. Jaffer, A.N. Amin, D.J. Brotman, S.B. Deitelzweig, S.C. McKean, A.C. Spyropoulos
Prevention of venous thromboembolism in the cancer surgery patient
A.C. Spyropoulos, D.J. Brotman, A.N. Amin, S.B. Deitelzweig, A.K. Jaffer, S.C. McKean
Prevention of venous thromboembolism in the orthopedic surgery patient
S.B. Deitelzweig, S.C. McKean, A.N. Amin, D.J. Brotman, A.K. Jaffer, A.C. Spyropoulos