User login
Speak Up
By putting a little time and effort into your presentation skills, you can become more persuasive and effective in your day-to-day job—and even advance your career and reputation.
For hospitalists, with their often-heavy committee load and frequent formal or informal teaching conversations, addressing groups is part of the job.
“At the end of the day, hospitalists are advocates—whether for quality improvement or patient-care issues,” says Jeffrey Wiese, MD, FACP, associate professor of medicine at Tulane University Health Sciences Center in New Orleans, associate chairman of medicine, director of the Tulane Internal Medicine Residency Program, and associate director of student programs, internal medicine. “And most of their advocacy efforts [are] going to be person-to-person, verbal discussions, where their passion and conviction can come through.”
Even if you’re never asked to present at a national meeting, you are likely to address a lot of committees, teams, and task forces in your career.
“It’s important to realize that people’s time is valuable in committee meetings,” stresses Dr. Wiese. “You have to be able to speak clearly, concisely, and to the point to make your case effectively.”
Learn by Listening
If you haven’t had much experience addressing groups or you feel your presentation skills are lacking, there are simple steps to become comfortable—even accomplished—at speaking.
“Most effective speakers are partly born but mostly made,” says Robert Wachter, MD, co-founder of SHM, frequent keynote speaker and professor and associate chairman of the Department of Medicine at the University of California, San Francisco.
Becoming an effective speaker may require formal training, perhaps from a course or a book. But one step every aspiring speaker can easily take is to listen to other speakers—a lot of them.
While working on his own presentation skills, Dr. Wachter says: “I learned to be a shameless mimic and thief. Even now, when I hear a good lecture, I always ask myself what that person did really well, and can I do that, too. And when I hear a crummy speaker, I wonder what I would tell them to them improve.”
Dr. Wiese does the same thing. “My strategy is to learn from every talk I sit in on,” he says. “Watch how the speaker is performing—not just at medical meetings, but also on TV. In this election year there are a lot of opportunities to listen to speeches. Note good speakers’ cadence, pitch and tone, and borrow from them.”
Simple Secrets
Effective speaking is built on some basic tenets. “There are fundamental skills that most speakers don’t use—you’d be surprised how basic these skills are,” says Dr. Wiese. These basics include:
Practice makes perfect: No matter how confident you are of your material, practice. Whether you’ll teach, speak to a quality-improvement committee or address a national group, make an outline and run through your speech. “There’s no talk I give without at least sitting down an hour beforehand to think through what I’m going to say,” says Dr. Wiese.
Give it all you’ve got: “When you’re asked to address a group, you have to convince yourself that this is the most important talk you’ve ever given,” stresses Dr. Wiese. “Your belief in this will give you the passion and commitment to your topic that comes out in how you speak.”
Start strong: Getting your audience’s interest and attention immediately is crucial.
“Engaging the audience successfully in the first one to three minutes is unbelievably important because unless you get them to care enough to listen at the outset, you’ve lost them for the rest of the talk,” he says. He believes only about one in 100 speakers do this well. “I assume the audience is not really with me and that I need to actively engage them—and I make sure they know enough to care about the topic. I start with the reasonable assumption that I know more and care more about my topic than they do. Make sure you give them enough background to get them started.”
Fledgling speakers can try capturing their audience’s attention by starting with a joke, story, dramatic anecdote, or shocking data. Starting your presentation with a bang, says Dr. Wachter, “is a learnable skill, and it’s a lot easier when you’re addressing a small group of people you know.”
Spice up dry information: If you’re stuck with a topic you fear is too boring to engage, find a “hook” to draw the audience in. Dr. Wachter suggests, “When you explain facts, use analogy and metaphors, and use graphics only when appropriate,” he suggests.
Find your voice: A tricky thing for new speakers is controlling their voice and using it to maintain interest. Avoid using a monotone—a common effect of reading from notes or slides.
“It’s important to work on your cadence and on the pitch and tone of your voice,” advises Dr. Wiese. “I think speaking is similar to music. Music has rest notes for a reason: to augment what you just said and to set up what you’re about to say. Try replacing the “ums” and “uhs” you use while you’re thinking about what to say next with silence. The audience will be riveted.”
Go easy on the PowerPoint: Don’t rely on your slides or flipchart to influence or engage your audience. Make eye contact with individuals and in a small group; touch a shoulder or two. “The truth is that most people use PowerPoint slides because they didn’t practice their talk,” says Dr. Wiese. “Turn away from your slides and talk person to person—you’ll be much more compelling.”
Speaking Opportunities
For an ambitious hospitalist, opportunities are abundant. “Find the residency director at the nearest program and tell them you’d like to give a conference for free,” Dr. Wiese recommends. “I guarantee this will get you 20 or 30 offers.”
He says national and regional organizations are great opportunities to get involved. “All it really takes is to attend the meetings, find the people doing the talks and tell them that you want an opportunity to hone your speaking skills,” he notes.
If you’re convinced that practicing your speaking skills will help you influence committees, enhance your reputation and improve your career possibilities, then take Dr. Wiese’s advice and get ready to launch your speaking career. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
By putting a little time and effort into your presentation skills, you can become more persuasive and effective in your day-to-day job—and even advance your career and reputation.
For hospitalists, with their often-heavy committee load and frequent formal or informal teaching conversations, addressing groups is part of the job.
“At the end of the day, hospitalists are advocates—whether for quality improvement or patient-care issues,” says Jeffrey Wiese, MD, FACP, associate professor of medicine at Tulane University Health Sciences Center in New Orleans, associate chairman of medicine, director of the Tulane Internal Medicine Residency Program, and associate director of student programs, internal medicine. “And most of their advocacy efforts [are] going to be person-to-person, verbal discussions, where their passion and conviction can come through.”
Even if you’re never asked to present at a national meeting, you are likely to address a lot of committees, teams, and task forces in your career.
“It’s important to realize that people’s time is valuable in committee meetings,” stresses Dr. Wiese. “You have to be able to speak clearly, concisely, and to the point to make your case effectively.”
Learn by Listening
If you haven’t had much experience addressing groups or you feel your presentation skills are lacking, there are simple steps to become comfortable—even accomplished—at speaking.
“Most effective speakers are partly born but mostly made,” says Robert Wachter, MD, co-founder of SHM, frequent keynote speaker and professor and associate chairman of the Department of Medicine at the University of California, San Francisco.
Becoming an effective speaker may require formal training, perhaps from a course or a book. But one step every aspiring speaker can easily take is to listen to other speakers—a lot of them.
While working on his own presentation skills, Dr. Wachter says: “I learned to be a shameless mimic and thief. Even now, when I hear a good lecture, I always ask myself what that person did really well, and can I do that, too. And when I hear a crummy speaker, I wonder what I would tell them to them improve.”
Dr. Wiese does the same thing. “My strategy is to learn from every talk I sit in on,” he says. “Watch how the speaker is performing—not just at medical meetings, but also on TV. In this election year there are a lot of opportunities to listen to speeches. Note good speakers’ cadence, pitch and tone, and borrow from them.”
Simple Secrets
Effective speaking is built on some basic tenets. “There are fundamental skills that most speakers don’t use—you’d be surprised how basic these skills are,” says Dr. Wiese. These basics include:
Practice makes perfect: No matter how confident you are of your material, practice. Whether you’ll teach, speak to a quality-improvement committee or address a national group, make an outline and run through your speech. “There’s no talk I give without at least sitting down an hour beforehand to think through what I’m going to say,” says Dr. Wiese.
Give it all you’ve got: “When you’re asked to address a group, you have to convince yourself that this is the most important talk you’ve ever given,” stresses Dr. Wiese. “Your belief in this will give you the passion and commitment to your topic that comes out in how you speak.”
Start strong: Getting your audience’s interest and attention immediately is crucial.
“Engaging the audience successfully in the first one to three minutes is unbelievably important because unless you get them to care enough to listen at the outset, you’ve lost them for the rest of the talk,” he says. He believes only about one in 100 speakers do this well. “I assume the audience is not really with me and that I need to actively engage them—and I make sure they know enough to care about the topic. I start with the reasonable assumption that I know more and care more about my topic than they do. Make sure you give them enough background to get them started.”
Fledgling speakers can try capturing their audience’s attention by starting with a joke, story, dramatic anecdote, or shocking data. Starting your presentation with a bang, says Dr. Wachter, “is a learnable skill, and it’s a lot easier when you’re addressing a small group of people you know.”
Spice up dry information: If you’re stuck with a topic you fear is too boring to engage, find a “hook” to draw the audience in. Dr. Wachter suggests, “When you explain facts, use analogy and metaphors, and use graphics only when appropriate,” he suggests.
Find your voice: A tricky thing for new speakers is controlling their voice and using it to maintain interest. Avoid using a monotone—a common effect of reading from notes or slides.
“It’s important to work on your cadence and on the pitch and tone of your voice,” advises Dr. Wiese. “I think speaking is similar to music. Music has rest notes for a reason: to augment what you just said and to set up what you’re about to say. Try replacing the “ums” and “uhs” you use while you’re thinking about what to say next with silence. The audience will be riveted.”
Go easy on the PowerPoint: Don’t rely on your slides or flipchart to influence or engage your audience. Make eye contact with individuals and in a small group; touch a shoulder or two. “The truth is that most people use PowerPoint slides because they didn’t practice their talk,” says Dr. Wiese. “Turn away from your slides and talk person to person—you’ll be much more compelling.”
Speaking Opportunities
For an ambitious hospitalist, opportunities are abundant. “Find the residency director at the nearest program and tell them you’d like to give a conference for free,” Dr. Wiese recommends. “I guarantee this will get you 20 or 30 offers.”
He says national and regional organizations are great opportunities to get involved. “All it really takes is to attend the meetings, find the people doing the talks and tell them that you want an opportunity to hone your speaking skills,” he notes.
If you’re convinced that practicing your speaking skills will help you influence committees, enhance your reputation and improve your career possibilities, then take Dr. Wiese’s advice and get ready to launch your speaking career. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
By putting a little time and effort into your presentation skills, you can become more persuasive and effective in your day-to-day job—and even advance your career and reputation.
For hospitalists, with their often-heavy committee load and frequent formal or informal teaching conversations, addressing groups is part of the job.
“At the end of the day, hospitalists are advocates—whether for quality improvement or patient-care issues,” says Jeffrey Wiese, MD, FACP, associate professor of medicine at Tulane University Health Sciences Center in New Orleans, associate chairman of medicine, director of the Tulane Internal Medicine Residency Program, and associate director of student programs, internal medicine. “And most of their advocacy efforts [are] going to be person-to-person, verbal discussions, where their passion and conviction can come through.”
Even if you’re never asked to present at a national meeting, you are likely to address a lot of committees, teams, and task forces in your career.
“It’s important to realize that people’s time is valuable in committee meetings,” stresses Dr. Wiese. “You have to be able to speak clearly, concisely, and to the point to make your case effectively.”
Learn by Listening
If you haven’t had much experience addressing groups or you feel your presentation skills are lacking, there are simple steps to become comfortable—even accomplished—at speaking.
“Most effective speakers are partly born but mostly made,” says Robert Wachter, MD, co-founder of SHM, frequent keynote speaker and professor and associate chairman of the Department of Medicine at the University of California, San Francisco.
Becoming an effective speaker may require formal training, perhaps from a course or a book. But one step every aspiring speaker can easily take is to listen to other speakers—a lot of them.
While working on his own presentation skills, Dr. Wachter says: “I learned to be a shameless mimic and thief. Even now, when I hear a good lecture, I always ask myself what that person did really well, and can I do that, too. And when I hear a crummy speaker, I wonder what I would tell them to them improve.”
Dr. Wiese does the same thing. “My strategy is to learn from every talk I sit in on,” he says. “Watch how the speaker is performing—not just at medical meetings, but also on TV. In this election year there are a lot of opportunities to listen to speeches. Note good speakers’ cadence, pitch and tone, and borrow from them.”
Simple Secrets
Effective speaking is built on some basic tenets. “There are fundamental skills that most speakers don’t use—you’d be surprised how basic these skills are,” says Dr. Wiese. These basics include:
Practice makes perfect: No matter how confident you are of your material, practice. Whether you’ll teach, speak to a quality-improvement committee or address a national group, make an outline and run through your speech. “There’s no talk I give without at least sitting down an hour beforehand to think through what I’m going to say,” says Dr. Wiese.
Give it all you’ve got: “When you’re asked to address a group, you have to convince yourself that this is the most important talk you’ve ever given,” stresses Dr. Wiese. “Your belief in this will give you the passion and commitment to your topic that comes out in how you speak.”
Start strong: Getting your audience’s interest and attention immediately is crucial.
“Engaging the audience successfully in the first one to three minutes is unbelievably important because unless you get them to care enough to listen at the outset, you’ve lost them for the rest of the talk,” he says. He believes only about one in 100 speakers do this well. “I assume the audience is not really with me and that I need to actively engage them—and I make sure they know enough to care about the topic. I start with the reasonable assumption that I know more and care more about my topic than they do. Make sure you give them enough background to get them started.”
Fledgling speakers can try capturing their audience’s attention by starting with a joke, story, dramatic anecdote, or shocking data. Starting your presentation with a bang, says Dr. Wachter, “is a learnable skill, and it’s a lot easier when you’re addressing a small group of people you know.”
Spice up dry information: If you’re stuck with a topic you fear is too boring to engage, find a “hook” to draw the audience in. Dr. Wachter suggests, “When you explain facts, use analogy and metaphors, and use graphics only when appropriate,” he suggests.
Find your voice: A tricky thing for new speakers is controlling their voice and using it to maintain interest. Avoid using a monotone—a common effect of reading from notes or slides.
“It’s important to work on your cadence and on the pitch and tone of your voice,” advises Dr. Wiese. “I think speaking is similar to music. Music has rest notes for a reason: to augment what you just said and to set up what you’re about to say. Try replacing the “ums” and “uhs” you use while you’re thinking about what to say next with silence. The audience will be riveted.”
Go easy on the PowerPoint: Don’t rely on your slides or flipchart to influence or engage your audience. Make eye contact with individuals and in a small group; touch a shoulder or two. “The truth is that most people use PowerPoint slides because they didn’t practice their talk,” says Dr. Wiese. “Turn away from your slides and talk person to person—you’ll be much more compelling.”
Speaking Opportunities
For an ambitious hospitalist, opportunities are abundant. “Find the residency director at the nearest program and tell them you’d like to give a conference for free,” Dr. Wiese recommends. “I guarantee this will get you 20 or 30 offers.”
He says national and regional organizations are great opportunities to get involved. “All it really takes is to attend the meetings, find the people doing the talks and tell them that you want an opportunity to hone your speaking skills,” he notes.
If you’re convinced that practicing your speaking skills will help you influence committees, enhance your reputation and improve your career possibilities, then take Dr. Wiese’s advice and get ready to launch your speaking career. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Drug Misuse Varies
Elderly inpatients’ risk of receiving potentially inappropriate medication (PIM) varies widely depending on where in the country they’re hospitalized and the specialty of their attending physicians, according to a study in the March-April edition of the Journal of Hospital Medicine.
Hospitalists may be encouraged by the fact that they, along with geriatricians, internists, and family physicians, were less likely than cardiologists to prescribe PIMs. Still, the major take-home message of the study is to “examine your individual practice and think about whether it’s appropriate to prescribe these medications,” says lead author Michael Rothberg, MD, assistant professor of medicine at Tufts University School of Medicine in Boston.
PIM use was highest in hospitals in the South. There, 55% of elderly patients received at least one PIM, compared with 34% of patients in Northeastern hospitals, where PIM use was lowest. The exact reason for this discrepancy is not known, but Dr. Rothberg hypothesizes that “we tend to prescribe like people in our hospital and like people in our region.” In other words, “it has to do with learning from the people around us.”
Most interesting to him is the wide variation in prescribing practices among individual doctors—even within the same specialty. “The decision to prescribe a drug is based on the individual provider and has to do with how you as a doctor feel about these drugs,” he explains. Although nearly half of all of the patients had received at least one PIM, there were seven hospitals in which those drugs never were prescribed. Somehow, “they found a way to care for people without [those medications],” he points out.
PIM use has been examined among elderly outpatients and nursing home residents, but only a handful of small studies have looked at the problem in hospital inpatients, says Dr. Rothberg. He and his coauthors used data from hospitals across the United States participating in Perspective, a database developed by Charlotte, N.C.-based Premier to measure quality and healthcare utilization.
The survey included patients 65 years or older admitted between Sept. 1, 2002, and June 30, 2005. Their principal diagnoses were acute myocardial infarction, chronic obstructive pulmonary disease, chest pain, community acquired pneumonia, congestive heart failure, ischemic stroke, or urinary tract infection. Surgical patients were excluded. Using the 2002 update of the Beers criteria for PIM use in older adults, the authors identified the total number of PIMs administered to each patient during his or her hospital stay. They further classified each PIM as high- or low-severity, based on the expert consensus expressed in the 1997 update of the Beers criteria.
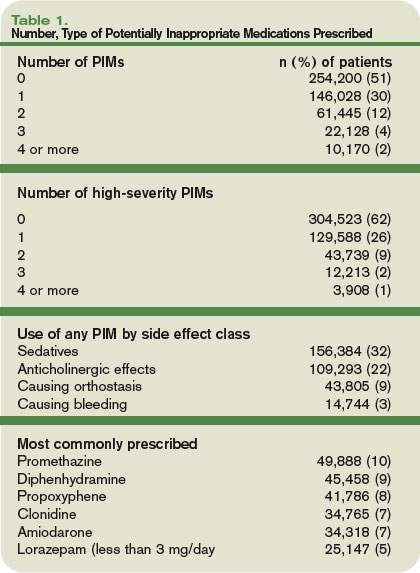
Data were available on 493,971 patients from 384 hospitals. Of those individuals, 49% received at least one PIM, and 6% received three or more. Thirty-eight percent of patients received at least one PIM with a high severity rating.
The three agents most likely to be prescribed were promethazine, diphenhydramine, and propoxyphene—probably because these drugs treat the problems most commonly encountered in hospitals, such as allergies, sleep problems, nausea, and pain, Dr. Rothberg says.
Hospital region emerged as the most important predictor of PIM use. Compared with patients in the Midwest, patients in the South had an odds ratio of 1.63 of receiving a high-severity PIM. The odds ratio for patients in the West was 1.43. Patients in the Northeast had an odds ratio of 0.85.
The median rate of prescribing high-severity PIMs was lowest among geriatricians, at 24%. Rates among hospitalists, internists, and family physicians were 33% to 36%. Cardiologists had the highest rate: 48% prescribed at least one high-severity PIM.
Interestingly, older patient age also was associated with a lower risk of PIM use. Of patients 85 or older, 42% received at least one PIM, compared with 53% of patients age 65 to 74 (p<0.0001). This suggests that “doctors are aware that the older patients are more frail and vulnerable” and take extra care to avoid prescribing PIMs to people in that age range, Dr. Rothberg says. A diagnosis of stroke or chronic obstructive pulmonary disease also was associated with a lower risk of receiving a PIM—further evidence that “doctors were, to some extent, taking patient factors into account” when prescribing medication.
PIM use among inpatients, as reported in this study, far exceeds the rates published for elders dwelling in the community or in nursing homes, writes Daniel S. Budnitz, MD, MPH, in an editorial accompanying the study.
The wide variation in prescribing practices means each facility must monitor its use of PIMs, just as individual hospitals monitor antibiotic use and resistance, advises Dr. Budnitz, a medical officer in the Division of Healthcare Quality Promotion at the Centers for Disease Control and Prevention. He also points out that the evidence that PIMs cause clinically significant adverse events is “weak and based largely on observational studies with inconsistent results.” The drugs in the Beers criteria are “potentially” inappropriate, he says, but some centers have recategorized them as “ ‘always avoid’ medications, ‘rarely acceptable’ medications, and medications which, indeed, have ‘some indications’ for use in older adults.” Thus, some variation among hospitals may be acceptable.
Rather than concentrate on the Beers criteria, hospitalists should focus “on identifying and mitigating the most common and most severe adverse drug events occurring in their hospitals,” such as bleeding from anticoagulants, hypoglycemic events from insulin, and oversedation from opioid analgesics, Dr. Budnitz points out. TH
Norra MacReady is a medical writer based in California.
Elderly inpatients’ risk of receiving potentially inappropriate medication (PIM) varies widely depending on where in the country they’re hospitalized and the specialty of their attending physicians, according to a study in the March-April edition of the Journal of Hospital Medicine.
Hospitalists may be encouraged by the fact that they, along with geriatricians, internists, and family physicians, were less likely than cardiologists to prescribe PIMs. Still, the major take-home message of the study is to “examine your individual practice and think about whether it’s appropriate to prescribe these medications,” says lead author Michael Rothberg, MD, assistant professor of medicine at Tufts University School of Medicine in Boston.
PIM use was highest in hospitals in the South. There, 55% of elderly patients received at least one PIM, compared with 34% of patients in Northeastern hospitals, where PIM use was lowest. The exact reason for this discrepancy is not known, but Dr. Rothberg hypothesizes that “we tend to prescribe like people in our hospital and like people in our region.” In other words, “it has to do with learning from the people around us.”
Most interesting to him is the wide variation in prescribing practices among individual doctors—even within the same specialty. “The decision to prescribe a drug is based on the individual provider and has to do with how you as a doctor feel about these drugs,” he explains. Although nearly half of all of the patients had received at least one PIM, there were seven hospitals in which those drugs never were prescribed. Somehow, “they found a way to care for people without [those medications],” he points out.
PIM use has been examined among elderly outpatients and nursing home residents, but only a handful of small studies have looked at the problem in hospital inpatients, says Dr. Rothberg. He and his coauthors used data from hospitals across the United States participating in Perspective, a database developed by Charlotte, N.C.-based Premier to measure quality and healthcare utilization.
The survey included patients 65 years or older admitted between Sept. 1, 2002, and June 30, 2005. Their principal diagnoses were acute myocardial infarction, chronic obstructive pulmonary disease, chest pain, community acquired pneumonia, congestive heart failure, ischemic stroke, or urinary tract infection. Surgical patients were excluded. Using the 2002 update of the Beers criteria for PIM use in older adults, the authors identified the total number of PIMs administered to each patient during his or her hospital stay. They further classified each PIM as high- or low-severity, based on the expert consensus expressed in the 1997 update of the Beers criteria.
Data were available on 493,971 patients from 384 hospitals. Of those individuals, 49% received at least one PIM, and 6% received three or more. Thirty-eight percent of patients received at least one PIM with a high severity rating.
The three agents most likely to be prescribed were promethazine, diphenhydramine, and propoxyphene—probably because these drugs treat the problems most commonly encountered in hospitals, such as allergies, sleep problems, nausea, and pain, Dr. Rothberg says.
Hospital region emerged as the most important predictor of PIM use. Compared with patients in the Midwest, patients in the South had an odds ratio of 1.63 of receiving a high-severity PIM. The odds ratio for patients in the West was 1.43. Patients in the Northeast had an odds ratio of 0.85.
The median rate of prescribing high-severity PIMs was lowest among geriatricians, at 24%. Rates among hospitalists, internists, and family physicians were 33% to 36%. Cardiologists had the highest rate: 48% prescribed at least one high-severity PIM.
Interestingly, older patient age also was associated with a lower risk of PIM use. Of patients 85 or older, 42% received at least one PIM, compared with 53% of patients age 65 to 74 (p<0.0001). This suggests that “doctors are aware that the older patients are more frail and vulnerable” and take extra care to avoid prescribing PIMs to people in that age range, Dr. Rothberg says. A diagnosis of stroke or chronic obstructive pulmonary disease also was associated with a lower risk of receiving a PIM—further evidence that “doctors were, to some extent, taking patient factors into account” when prescribing medication.
PIM use among inpatients, as reported in this study, far exceeds the rates published for elders dwelling in the community or in nursing homes, writes Daniel S. Budnitz, MD, MPH, in an editorial accompanying the study.
The wide variation in prescribing practices means each facility must monitor its use of PIMs, just as individual hospitals monitor antibiotic use and resistance, advises Dr. Budnitz, a medical officer in the Division of Healthcare Quality Promotion at the Centers for Disease Control and Prevention. He also points out that the evidence that PIMs cause clinically significant adverse events is “weak and based largely on observational studies with inconsistent results.” The drugs in the Beers criteria are “potentially” inappropriate, he says, but some centers have recategorized them as “ ‘always avoid’ medications, ‘rarely acceptable’ medications, and medications which, indeed, have ‘some indications’ for use in older adults.” Thus, some variation among hospitals may be acceptable.
Rather than concentrate on the Beers criteria, hospitalists should focus “on identifying and mitigating the most common and most severe adverse drug events occurring in their hospitals,” such as bleeding from anticoagulants, hypoglycemic events from insulin, and oversedation from opioid analgesics, Dr. Budnitz points out. TH
Norra MacReady is a medical writer based in California.
Elderly inpatients’ risk of receiving potentially inappropriate medication (PIM) varies widely depending on where in the country they’re hospitalized and the specialty of their attending physicians, according to a study in the March-April edition of the Journal of Hospital Medicine.
Hospitalists may be encouraged by the fact that they, along with geriatricians, internists, and family physicians, were less likely than cardiologists to prescribe PIMs. Still, the major take-home message of the study is to “examine your individual practice and think about whether it’s appropriate to prescribe these medications,” says lead author Michael Rothberg, MD, assistant professor of medicine at Tufts University School of Medicine in Boston.
PIM use was highest in hospitals in the South. There, 55% of elderly patients received at least one PIM, compared with 34% of patients in Northeastern hospitals, where PIM use was lowest. The exact reason for this discrepancy is not known, but Dr. Rothberg hypothesizes that “we tend to prescribe like people in our hospital and like people in our region.” In other words, “it has to do with learning from the people around us.”
Most interesting to him is the wide variation in prescribing practices among individual doctors—even within the same specialty. “The decision to prescribe a drug is based on the individual provider and has to do with how you as a doctor feel about these drugs,” he explains. Although nearly half of all of the patients had received at least one PIM, there were seven hospitals in which those drugs never were prescribed. Somehow, “they found a way to care for people without [those medications],” he points out.
PIM use has been examined among elderly outpatients and nursing home residents, but only a handful of small studies have looked at the problem in hospital inpatients, says Dr. Rothberg. He and his coauthors used data from hospitals across the United States participating in Perspective, a database developed by Charlotte, N.C.-based Premier to measure quality and healthcare utilization.
The survey included patients 65 years or older admitted between Sept. 1, 2002, and June 30, 2005. Their principal diagnoses were acute myocardial infarction, chronic obstructive pulmonary disease, chest pain, community acquired pneumonia, congestive heart failure, ischemic stroke, or urinary tract infection. Surgical patients were excluded. Using the 2002 update of the Beers criteria for PIM use in older adults, the authors identified the total number of PIMs administered to each patient during his or her hospital stay. They further classified each PIM as high- or low-severity, based on the expert consensus expressed in the 1997 update of the Beers criteria.
Data were available on 493,971 patients from 384 hospitals. Of those individuals, 49% received at least one PIM, and 6% received three or more. Thirty-eight percent of patients received at least one PIM with a high severity rating.
The three agents most likely to be prescribed were promethazine, diphenhydramine, and propoxyphene—probably because these drugs treat the problems most commonly encountered in hospitals, such as allergies, sleep problems, nausea, and pain, Dr. Rothberg says.
Hospital region emerged as the most important predictor of PIM use. Compared with patients in the Midwest, patients in the South had an odds ratio of 1.63 of receiving a high-severity PIM. The odds ratio for patients in the West was 1.43. Patients in the Northeast had an odds ratio of 0.85.
The median rate of prescribing high-severity PIMs was lowest among geriatricians, at 24%. Rates among hospitalists, internists, and family physicians were 33% to 36%. Cardiologists had the highest rate: 48% prescribed at least one high-severity PIM.
Interestingly, older patient age also was associated with a lower risk of PIM use. Of patients 85 or older, 42% received at least one PIM, compared with 53% of patients age 65 to 74 (p<0.0001). This suggests that “doctors are aware that the older patients are more frail and vulnerable” and take extra care to avoid prescribing PIMs to people in that age range, Dr. Rothberg says. A diagnosis of stroke or chronic obstructive pulmonary disease also was associated with a lower risk of receiving a PIM—further evidence that “doctors were, to some extent, taking patient factors into account” when prescribing medication.
PIM use among inpatients, as reported in this study, far exceeds the rates published for elders dwelling in the community or in nursing homes, writes Daniel S. Budnitz, MD, MPH, in an editorial accompanying the study.
The wide variation in prescribing practices means each facility must monitor its use of PIMs, just as individual hospitals monitor antibiotic use and resistance, advises Dr. Budnitz, a medical officer in the Division of Healthcare Quality Promotion at the Centers for Disease Control and Prevention. He also points out that the evidence that PIMs cause clinically significant adverse events is “weak and based largely on observational studies with inconsistent results.” The drugs in the Beers criteria are “potentially” inappropriate, he says, but some centers have recategorized them as “ ‘always avoid’ medications, ‘rarely acceptable’ medications, and medications which, indeed, have ‘some indications’ for use in older adults.” Thus, some variation among hospitals may be acceptable.
Rather than concentrate on the Beers criteria, hospitalists should focus “on identifying and mitigating the most common and most severe adverse drug events occurring in their hospitals,” such as bleeding from anticoagulants, hypoglycemic events from insulin, and oversedation from opioid analgesics, Dr. Budnitz points out. TH
Norra MacReady is a medical writer based in California.
Vital VTE Interventions
Venous thromboembolism (VTE) affects more than 2 million Americans every year.1 Pulmonary embolism (PE) is one of the most common preventable causes of in-hospital deaths in the United States. Clinical manifestations of PE may be the first indication the patient has a VTE, and fatal PEs occur in at least 75% of hospitalized medical patients. More than 300,000 patients die from PE each year—an estimated incidence of 10%. This makes VTE prevention a top patient-safety goal in hospitals.2,3
Thromboprophylaxis can be accomplished with unfractionated heparin (UFH), low-molecular-weight heparin (LMWH; e.g., enoxaparin, dalteparin, tinzaparin) or heparinoid, or a selective factor Xa inhibitor (e.g., fondaparinux).4 For long-term treatment, oral warfarin is often used. Doses and duration of prophylaxis and treatment regimens vary.
Current guidelines should be reviewed for specific recommendations. Two current guidelines are the American College of Chest Physicians (ACCP) Seventh Conference on the Prevention of VTE and the American Society of Clinical Oncology (ASCO) Guideline for VTE prophylaxis and treatment in oncology patients. Although guidelines are available, thromboprophylaxis continues to baffle many healthcare providers. There are many advantages to thromboprophylaxis including the prevention of significant morbidity, prevention of PE, decreases in resource consumption, and decreases in the long-term clinical and economic sequelae.
The ACCP notes that most surgical patients will require thromboprophylaxis. Contraindications need to be evaluated prior to antithrombotic/anticoagulant use. Additionally, all trauma patients with at least one VTE risk factor should receive thromboprophylaxis. Acutely ill patients hospitalized with congestive heart failure or severe respiratory distress or who are confined to bed and have one or more additional risk factors, should receive VTE prophylaxis. Additionally, most patients upon admission to an intensive-care unit should be assessed for VTE risk and receive thromboprophylaxis as required.
VTE is a major complication in up to 20% of cancer patients, with hospitalized oncology patients and those undergoing treatment at the highest risk. Some of the newer drug treatments used in these patients have higher VTE rates (e.g., bevacizumab, thalidomide, lenalidomide). These patients need to be carefully evaluated for VTE prophylaxis and closely monitored.5
Generally, in hospitalized patients with cancer, VTE prophylaxis should be considered with UFH, LMWH, or fondaparinux, in the absence of bleeding or other contraindications to anticoagulation. Relative contraindications to anticoagulation include (but are not limited to):
- Active uncontrolled bleeding;
- Active cerebrovascular hemorrhage;
- Dissecting or cerebral aneurysm;
- Bacterial endocarditis;
- Pericarditis;
- Active peptic or gastrointestinal ulceration;
- Severe uncontrolled or malignant hypertension;
- Severe head trauma;
- Pregnancy (warfarin contraindication);
- Heparin-induced thrombocytopenia (heparin, LMWH); and
- Epidural catheter placement.
These same contraindications can be applied to the non-oncology patient, as well.
An important aspect of VTE management is the “Clinical Practice Guideline from the American Academy of Family Physicians and the American College of Physicians on the Diagnosis of VTE from the Annals of Family Medicine.” Consult this for a review of diagnostic tests for VTE.
Thromboprophylaxis is a necessity in a number of at-risk hospitalized patients. Knowing which patients will benefit, and the contraindications for use, will improve patient outcomes. Consult current guidelines for diagnosis recommendations as well as agents of choice, dosing regimens, and therapy duration. TH
Michele B. Kaufman is registered pharmacist based in New York City.
References
- DVT: Assess Your Patients’ Risk, Take Preventive Measures. ASHP Foundation Discoveries, Summer 2007;19(1):1,5. Available at www.ashpfoundation.org/MainMenuCategories/AboutUs/Newsletter/DiscoveriesSummer2007.aspx. Last accessed Nov. 26, 2007.
- Geertz WH, Pineo Graham F, Heit JA et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126:338-400.
- Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients, a meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167:1476-1486.
- Lyman GH, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34): 5490–5505.
- Qaseem A, Snow V, Barry P for the Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Vein Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
Venous thromboembolism (VTE) affects more than 2 million Americans every year.1 Pulmonary embolism (PE) is one of the most common preventable causes of in-hospital deaths in the United States. Clinical manifestations of PE may be the first indication the patient has a VTE, and fatal PEs occur in at least 75% of hospitalized medical patients. More than 300,000 patients die from PE each year—an estimated incidence of 10%. This makes VTE prevention a top patient-safety goal in hospitals.2,3
Thromboprophylaxis can be accomplished with unfractionated heparin (UFH), low-molecular-weight heparin (LMWH; e.g., enoxaparin, dalteparin, tinzaparin) or heparinoid, or a selective factor Xa inhibitor (e.g., fondaparinux).4 For long-term treatment, oral warfarin is often used. Doses and duration of prophylaxis and treatment regimens vary.
Current guidelines should be reviewed for specific recommendations. Two current guidelines are the American College of Chest Physicians (ACCP) Seventh Conference on the Prevention of VTE and the American Society of Clinical Oncology (ASCO) Guideline for VTE prophylaxis and treatment in oncology patients. Although guidelines are available, thromboprophylaxis continues to baffle many healthcare providers. There are many advantages to thromboprophylaxis including the prevention of significant morbidity, prevention of PE, decreases in resource consumption, and decreases in the long-term clinical and economic sequelae.
The ACCP notes that most surgical patients will require thromboprophylaxis. Contraindications need to be evaluated prior to antithrombotic/anticoagulant use. Additionally, all trauma patients with at least one VTE risk factor should receive thromboprophylaxis. Acutely ill patients hospitalized with congestive heart failure or severe respiratory distress or who are confined to bed and have one or more additional risk factors, should receive VTE prophylaxis. Additionally, most patients upon admission to an intensive-care unit should be assessed for VTE risk and receive thromboprophylaxis as required.
VTE is a major complication in up to 20% of cancer patients, with hospitalized oncology patients and those undergoing treatment at the highest risk. Some of the newer drug treatments used in these patients have higher VTE rates (e.g., bevacizumab, thalidomide, lenalidomide). These patients need to be carefully evaluated for VTE prophylaxis and closely monitored.5
Generally, in hospitalized patients with cancer, VTE prophylaxis should be considered with UFH, LMWH, or fondaparinux, in the absence of bleeding or other contraindications to anticoagulation. Relative contraindications to anticoagulation include (but are not limited to):
- Active uncontrolled bleeding;
- Active cerebrovascular hemorrhage;
- Dissecting or cerebral aneurysm;
- Bacterial endocarditis;
- Pericarditis;
- Active peptic or gastrointestinal ulceration;
- Severe uncontrolled or malignant hypertension;
- Severe head trauma;
- Pregnancy (warfarin contraindication);
- Heparin-induced thrombocytopenia (heparin, LMWH); and
- Epidural catheter placement.
These same contraindications can be applied to the non-oncology patient, as well.
An important aspect of VTE management is the “Clinical Practice Guideline from the American Academy of Family Physicians and the American College of Physicians on the Diagnosis of VTE from the Annals of Family Medicine.” Consult this for a review of diagnostic tests for VTE.
Thromboprophylaxis is a necessity in a number of at-risk hospitalized patients. Knowing which patients will benefit, and the contraindications for use, will improve patient outcomes. Consult current guidelines for diagnosis recommendations as well as agents of choice, dosing regimens, and therapy duration. TH
Michele B. Kaufman is registered pharmacist based in New York City.
References
- DVT: Assess Your Patients’ Risk, Take Preventive Measures. ASHP Foundation Discoveries, Summer 2007;19(1):1,5. Available at www.ashpfoundation.org/MainMenuCategories/AboutUs/Newsletter/DiscoveriesSummer2007.aspx. Last accessed Nov. 26, 2007.
- Geertz WH, Pineo Graham F, Heit JA et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126:338-400.
- Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients, a meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167:1476-1486.
- Lyman GH, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34): 5490–5505.
- Qaseem A, Snow V, Barry P for the Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Vein Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
Venous thromboembolism (VTE) affects more than 2 million Americans every year.1 Pulmonary embolism (PE) is one of the most common preventable causes of in-hospital deaths in the United States. Clinical manifestations of PE may be the first indication the patient has a VTE, and fatal PEs occur in at least 75% of hospitalized medical patients. More than 300,000 patients die from PE each year—an estimated incidence of 10%. This makes VTE prevention a top patient-safety goal in hospitals.2,3
Thromboprophylaxis can be accomplished with unfractionated heparin (UFH), low-molecular-weight heparin (LMWH; e.g., enoxaparin, dalteparin, tinzaparin) or heparinoid, or a selective factor Xa inhibitor (e.g., fondaparinux).4 For long-term treatment, oral warfarin is often used. Doses and duration of prophylaxis and treatment regimens vary.
Current guidelines should be reviewed for specific recommendations. Two current guidelines are the American College of Chest Physicians (ACCP) Seventh Conference on the Prevention of VTE and the American Society of Clinical Oncology (ASCO) Guideline for VTE prophylaxis and treatment in oncology patients. Although guidelines are available, thromboprophylaxis continues to baffle many healthcare providers. There are many advantages to thromboprophylaxis including the prevention of significant morbidity, prevention of PE, decreases in resource consumption, and decreases in the long-term clinical and economic sequelae.
The ACCP notes that most surgical patients will require thromboprophylaxis. Contraindications need to be evaluated prior to antithrombotic/anticoagulant use. Additionally, all trauma patients with at least one VTE risk factor should receive thromboprophylaxis. Acutely ill patients hospitalized with congestive heart failure or severe respiratory distress or who are confined to bed and have one or more additional risk factors, should receive VTE prophylaxis. Additionally, most patients upon admission to an intensive-care unit should be assessed for VTE risk and receive thromboprophylaxis as required.
VTE is a major complication in up to 20% of cancer patients, with hospitalized oncology patients and those undergoing treatment at the highest risk. Some of the newer drug treatments used in these patients have higher VTE rates (e.g., bevacizumab, thalidomide, lenalidomide). These patients need to be carefully evaluated for VTE prophylaxis and closely monitored.5
Generally, in hospitalized patients with cancer, VTE prophylaxis should be considered with UFH, LMWH, or fondaparinux, in the absence of bleeding or other contraindications to anticoagulation. Relative contraindications to anticoagulation include (but are not limited to):
- Active uncontrolled bleeding;
- Active cerebrovascular hemorrhage;
- Dissecting or cerebral aneurysm;
- Bacterial endocarditis;
- Pericarditis;
- Active peptic or gastrointestinal ulceration;
- Severe uncontrolled or malignant hypertension;
- Severe head trauma;
- Pregnancy (warfarin contraindication);
- Heparin-induced thrombocytopenia (heparin, LMWH); and
- Epidural catheter placement.
These same contraindications can be applied to the non-oncology patient, as well.
An important aspect of VTE management is the “Clinical Practice Guideline from the American Academy of Family Physicians and the American College of Physicians on the Diagnosis of VTE from the Annals of Family Medicine.” Consult this for a review of diagnostic tests for VTE.
Thromboprophylaxis is a necessity in a number of at-risk hospitalized patients. Knowing which patients will benefit, and the contraindications for use, will improve patient outcomes. Consult current guidelines for diagnosis recommendations as well as agents of choice, dosing regimens, and therapy duration. TH
Michele B. Kaufman is registered pharmacist based in New York City.
References
- DVT: Assess Your Patients’ Risk, Take Preventive Measures. ASHP Foundation Discoveries, Summer 2007;19(1):1,5. Available at www.ashpfoundation.org/MainMenuCategories/AboutUs/Newsletter/DiscoveriesSummer2007.aspx. Last accessed Nov. 26, 2007.
- Geertz WH, Pineo Graham F, Heit JA et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126:338-400.
- Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients, a meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167:1476-1486.
- Lyman GH, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25(34): 5490–5505.
- Qaseem A, Snow V, Barry P for the Joint American Academy of Family Physicians/American College of Physicians Panel on Deep Vein Thrombosis/Pulmonary Embolism. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2007;5:57-62.
In the Literature
Literature at a Glance
A guide to this month’s abstracts
- Steroids reduce mortality only in patients with confirmed bacterial meningitis.
- Probiotics can be useful in the treatment of acute diarrhea in children.
- CT pulmonary angiography is not inferior to V/Q scanning for exclusion of PE.
- Hospitalist care results in shorter LOS compared with care by traditional general internists and family practice physicians.
- The early risk of stroke after TIA is approximately 15% to 20% at 90 days after the sentinel event.
- Different anti-thrombotic strategies produce no difference in outcomes of early acute coronary syndromes.
- The risk of fatal PE is highest in the first year after medication is stopped.
- Beers criteria medications are associated with fewer ED visits by elderly patients compared with warfarin, digoxin, and insulin.
Do Steroids Affect the Outcome in Patients with Meningitis?
Background: Pyogenic (bacterial) meningitis has high morbidity and mortality. Studies suggest some benefit of steroids in children but provide limited evidence for adult use.
Study design: Intention-to-treat, randomized control trial.
Setting: Single hospital in Vietnam.
Synopsis: Of 435 patients older than 14 with suspected meningitis all received lumbar puncture with randomization to IV dexamethasone or placebo for four days. Results showed 69% of patients had definite meningitis, 28.3% were probable, and 2.8% had an alternative diagnosis based on culture results.
The primary outcome was death after one month, which did not differ among groups (risk ratio [RR] 0.79, confidence interval [CI] 0.45-1.39).
Predefined subgroup analysis of patients with definitive meningitis showed a significant reduction in mortality at one month (RR 0.43, CI 0.2-0.94) and death/disability at six months (odds ratio [OR] 0.56, CI 0.32-0.98).
In patients with probable meningitis, those who received steroids demonstrated a trend toward harm (OR 2.65, CI 0.73-9.63).
Probable versus definite meningitis was determined retrospectively based on cultures. The most common isolate was Streptococcus suis.
Bottom line: This study provides some evidence for using steroids in adults with confirmed bacterial meningitis. Clinical application is limited by bacterial epidemiology and the difficulty of prospectively separating patients who would benefit from those who might be harmed.
Citation: Nguyen TH, Tran TH, Thwaites G, et. al. Dexamethasone in Vietnamese adolescents and adults with bacterial meningitis. N Engl J Med. 2007;357:2431-2439.
Which Probiotic Preparations Best Reduce the Duration of Acute Diarrhea in Children?
Background: Probiotics have been suggested as an adjunctive therapy to reduce the severity and duration of acute diarrhea in children. However, there are no clear data to suggest if specific probiotic agents are superior to others.
Study design: Prospective single-blind, randomized, controlled trial.
Setting: Outpatient primary care in Naples, Italy.
Synopsis: This study compared five commercially available probiotic preparations (mix of Lactobacillus delbrueckii var bulgaricus/Streptococcus thermophilus/L. acidophilus/ Bifido-bacterium bifidum; L. rhamnosus strain GG; Saccharomyces boulardii; Bacillus clausii; or Enterococcus faecium SF68) and a control group in the treatment of outpatient acute diarrhea in 571 children age 3 months to 36 months.
The primary outcomes were the duration of diarrhea and the number and consistency of stools. The groups receiving Lactobacillus GG and the mixture had a shorter total duration of diarrhea (78.5 and 70 hours, respectively), decreased total number of stools, and improved stool consistency when compared with the control (115.5 hours). The other therapies showed no improvement over the control group. These data report on products commercially available in Italy, which may differ greatly from products available locally.
Bottom line: Probiotic preparations for the treatment of acute diarrhea in children should be chosen based on effectiveness data.
Citation: Canani RB, Cirillo P, Terrin G, et al. Probiotics for treatment of acute diarrhoea in children: randomised clinical trial of five different preparations. BMJ 2007;335:340-345.
Is CTPA a Reliable Alternative to V/Q Scan for Diagnosing PE?
Background: Computed tomography pulmonary angiogram (CTPA) has replaced ventilation/perfusion (V/Q) scanning at many hospitals as the test of choice for ruling out pulmonary embolism (PE). But limited clinical data compare CTPA with V/Q scanning in those suspected of having venous thromboembolism (VTE).
Study design: Randomized, investigator blinded, controlled trial.
Setting: The emergency departments (ED), inpatient wards, and outpatient clinics of five academic centers.
Synopsis: In the study, 1,411 patients were enrolled from five medical centers. Of 694 patients randomized to CTPA, 133 (19.2%) were diagnosed with VTE in the initial evaluation period, while 101 of 712 patients (14.2%) receiving a V/Q scan were diagnosed with VTE.
Patients not initially diagnosed with VTE were monitored. At three-month follow-up, 0.4% of the CTPA group and 1.0% of the V/Q group had a diagnosed VTE.
The overall rate of VTE found in the initial diagnostic period was significantly greater in patients randomized to CTPA (19.2% vs. 14.2%; difference, 5.0%; 95% CI; 1.1% to 8.9% p=.01). This suggests CTPA has a higher false positive rate or detects clinically insignificant thrombi.
Bottom line: CTPA was not inferior to V/Q scanning for excluding clinically meaningful PE, but CTPA diagnosed about 30% more patients with VTE than did V/Q scanning.
Citation: Anderson DR, Kahn SR, Rodger MA, et al. Computed tomographic pulmonary angiography vs. ventilation-perfusion lung scanning in patients with suspected pulmonary embolism: a randomized controlled trial. JAMA. 2007;298(23):2743-2753.
Does the Hospitalist Model Improve Length of Stay, Quality, and Cost of Care?
Background: The hospitalist model, with increased physician availability and expertise but greater discontinuity of care, is becoming more prevalent in U.S. medicine. What little is known about how this model will affect patient care is derived from a number of small studies.
Study design: Retrospective cohort study.
Setting: 45 small to midsize, predominantly nonteaching hospitals throughout the U.S.
Synopsis: Using the Premier Healthcare Informatics database, this study examined information on 76,926 patients admitted for seven common diagnoses to one of three services: hospitalist, general internist, or family physician. Analysis showed that patients on a hospitalist service had a 0.4-day shorter length of stay (p<0.001) compared with those on a general internist or family physician service.
The cost to patients cared for by a hospitalist was lower than the cost of family physicians ($125 less, p=0.33) and internists ($268 less, p=0.02). There was no difference found in death rate or 14-day readmission rate among the three services.
Given the retrospective design of this study, no causal relationship can be deduced. This study is further limited by its lack of specific data on the physicians categorized into one of the three groups solely by administrative data. The authors had concerns that the biases inherent to the retrospective nature of their work accounted for the significant difference found between hospitalists and internists.
Bottom line: The hospitalist model is associated with modest improvements in length of stay as compared with traditional inpatient approaches.
Citation: Lindenauer PK, Rothberg MB, Pekow PS, et. al. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007;357:2589-2600.
What Is the Stroke Risk Soon after TIA, and What Factors Drive the Variability of Previous Findings?
Background: Many studies have attempted to estimate the risk of stroke in the early period after a transient ischemic attack (TIA). These studies vary widely in their calculation of the estimated risk. Further, the clinical and methodological factors underlying this variability are unclear.
Study design: Systematic review and meta-analysis.
Setting: Community and hospital.
Synopsis: Searching the Cochrane review database, MEDLINE, EMBASE, CINAHL, and BIOSIS, 11 studies from 1973 to 2006 were included for meta-analysis, selected from 694 potential candidate studies identified on initial screening. The studies ranged in size from 62 to 2,285 patients.
The pooled estimate of risk for stroke following TIA was found to be 3.5%, 8%, and 9.2% at two, 30, and 90 days following TIA, respectively. However, there was significant heterogeneity for all periods considered (p<0.001).
Outcome ascertainment was identified as a major source of methodological heterogeneity. When risk of stroke at follow-up was determined by passive ascertainment (e.g., administrative documentation) the early risk of stroke was 3.1% two days after TIA, 6.4% at 30 days, and 8.7% at 90 days. But active ascertainment (e.g., direct, personal contact with study participants) determined stroke risk to be 9.9%, 13.4%, and 17.4% at two, 30, and 90 days after TIA, respectively.
Bottom line: Based on analysis of completed studies that included directly observed follow-up of study participants, the early risk of stroke after TIA is approximately 15% to 20% at 90 days following the sentinel event.
Citation: Wu CM, McLaughlin K, Lorenzetti DL, Hill MD, Manns BJ, Ghali WA. Early risk of stroke after transient ischemic attack. Arch Intern Med. 2007;167:2417-2422.
What Is the 1-year Ischemia and Mortality Rate for Three Anti-thrombotic Therapies for Early Invasive Management of ACS?
Background: Early interventional or surgical revascularization has improved morbidity and mortality in patients with acute coronary syndrome (ACS). The optimal anti-thrombotic regimen to reduce late ischemic and death rates has not been determined.
Study design: Prospective, open-label randomized control trial.
Setting: 450 academic and community-based institutions in 17 countries.
Synopsis: A total of 13,819 patients were enrolled between August 2003 and December 2005. They were assigned to heparin plus glycoprotein (GP) IIb/IIIa inhibitors (n=4,603), bivalirudin (Angiomax) plus IIb/IIIa inhibitors (n=4,604), or bivalirudin monotherapy (n=4,612).
For patients receiving GP IIb/IIIa inhibitors, a 2x2 factorial design assigned half the heparin and bivalirudin groups to routine upstream GP inhibitor administration (4,605 patients). The other half received selective GP IIb/IIIa inhibitors administration if PCI was indicated (4,602 patients).
At one year, there was no statistically significant difference in ischemia or mortality rate among the three therapy groups. No difference in ischemia rate was detected between the two GP IIb/IIIa inhibitor utilization strategies.
Since the hypotheses and the power for the one-year analysis in this trial were not prospectively determined, the results are considered to be exploratory and hypothesis generating.
Bottom line: At one year, there is no statistically significant difference in ischemia or mortality rate for the three antithrombotic regiments and the two glycoprotein utilization strategies.
Citation: Stone GW, Ware JH, Bertrand ME, et. al. Antithrombotic strategies in patients with acute coronary syndromes undergoing early invasive management. One-year results from the ACUITY trial. JAMA 2007;298:2497-2505.
What Is the PE Risk after Discontinuing Anticoagulation in Patients with Symptomatic VTE?
Background: The natural history of patients with symptomatic VTE who have completed anticoagulation is not well understood.
Study design: Inception cohort using pooled data from a prospective cohort study and one arm of an open-label randomized trial.
Setting: Academic medical centers in Canada, Sweden, and Italy.
Synopsis: Using pooled data from two previous studies, 2,052 patients with a first diagnosis of symptomatic VTE (lower-extremity deep-vein thrombosis [DVT], PE, or both) were evaluated for fatal PE after a standard course of therapy (mean of six months) with a vitamin K antagonist.
Patients were followed for up to 120 months. The investigators found an annual event risk of 0.19-0.49 per 100 person-years for fatal PE. Patients with prolonged immobility, active cancer, and thrombophilia were excluded, as were those with recurrent acute DVT.
Secondary analysis revealed an incidence of any fatal, definite or probable PE within the first year of discontinuing therapy of 0.35%-0.81%.
After the first year, the annual event risk ranged from 0.15-0.40 events per 100 person-years. Patients with advanced age, idiopathic VTE as well as those presenting with PE had higher rates of fatal PE.
Bottom line: There is a real though small (less than 1%) risk of fatal PE in the first year following discontinuation of anticoagulation for the first VTE episode. The optimal course of treatment for patients with idiopathic VTE is yet to be determined.
Citation: Douketis JD, Gu CS, Schulman S, et al. The risk for fatal pulmonary embolism after discontinuing anticoagulant therapy for venous thromboembolism. Ann Intern Med. 2007;147(11):766-774.
Do the Beers Criteria Predict ED Visits Associated with Adverse Drug Events?
Background: Adverse drug events are common in the elderly. The Beers criteria are a consensus-based list of 41 medications that are considered inappropriate for use in older adults and often lead to poor outcomes.
Study design: Retrospective medical record review and data analysis.
Setting: Three nationally representative, U.S. public health surveillance systems: the National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance System (NEISS-CADES), 2004-2005; the National Ambulatory Medical Care Survey (NAMCS), 2004; and National Hospital Ambulatory Medical Care Survey (NHAMCS), 2004.
Synopsis: Using data collected from ED visits at 58 hospitals in the NEISS-CADES system, this study estimated that 177,504 visits for adverse drug events occur annually in the United States. Only 8.8% of such visits were attributable to the 41 medications included in the Beers criteria. Three drug classes (anticoagulant and antiplatelet agents, antidiabetic agents, and narrow therapeutic index agents) accounted for nearly half of all such ED visits. Warfarin (17.3%), insulin (13%), and digoxin (3.2%) were the most commonly implicated medications, collectively accounting for 33% of visits (CI, 27.8% to 38.7%).
This study suggests that because of the common use and high risk of adverse events associated with these three drugs, interventions targeting their use may prevent ED visits for adverse drug events in the elderly, compared with interventions aimed at reducing the use of medications identified in the Beers criteria.
This study only included adverse drug events identified in the ED and relied on the diagnosis and documentation of such events by the ED physician.
Bottom line: Beers criteria medications, although considered inappropriate for use in the elderly, were associated with significantly fewer ED visits for adverse events compared with warfarin, digoxin, and insulin.
Citation: Budnitz DS, Shehab N, Kegler SR, et. al. Medication use leading to emergency department visits for adverse drug events in older adults. Ann Intern Med. 2007;147:755-765. TH
Literature at a Glance
A guide to this month’s abstracts
- Steroids reduce mortality only in patients with confirmed bacterial meningitis.
- Probiotics can be useful in the treatment of acute diarrhea in children.
- CT pulmonary angiography is not inferior to V/Q scanning for exclusion of PE.
- Hospitalist care results in shorter LOS compared with care by traditional general internists and family practice physicians.
- The early risk of stroke after TIA is approximately 15% to 20% at 90 days after the sentinel event.
- Different anti-thrombotic strategies produce no difference in outcomes of early acute coronary syndromes.
- The risk of fatal PE is highest in the first year after medication is stopped.
- Beers criteria medications are associated with fewer ED visits by elderly patients compared with warfarin, digoxin, and insulin.
Do Steroids Affect the Outcome in Patients with Meningitis?
Background: Pyogenic (bacterial) meningitis has high morbidity and mortality. Studies suggest some benefit of steroids in children but provide limited evidence for adult use.
Study design: Intention-to-treat, randomized control trial.
Setting: Single hospital in Vietnam.
Synopsis: Of 435 patients older than 14 with suspected meningitis all received lumbar puncture with randomization to IV dexamethasone or placebo for four days. Results showed 69% of patients had definite meningitis, 28.3% were probable, and 2.8% had an alternative diagnosis based on culture results.
The primary outcome was death after one month, which did not differ among groups (risk ratio [RR] 0.79, confidence interval [CI] 0.45-1.39).
Predefined subgroup analysis of patients with definitive meningitis showed a significant reduction in mortality at one month (RR 0.43, CI 0.2-0.94) and death/disability at six months (odds ratio [OR] 0.56, CI 0.32-0.98).
In patients with probable meningitis, those who received steroids demonstrated a trend toward harm (OR 2.65, CI 0.73-9.63).
Probable versus definite meningitis was determined retrospectively based on cultures. The most common isolate was Streptococcus suis.
Bottom line: This study provides some evidence for using steroids in adults with confirmed bacterial meningitis. Clinical application is limited by bacterial epidemiology and the difficulty of prospectively separating patients who would benefit from those who might be harmed.
Citation: Nguyen TH, Tran TH, Thwaites G, et. al. Dexamethasone in Vietnamese adolescents and adults with bacterial meningitis. N Engl J Med. 2007;357:2431-2439.
Which Probiotic Preparations Best Reduce the Duration of Acute Diarrhea in Children?
Background: Probiotics have been suggested as an adjunctive therapy to reduce the severity and duration of acute diarrhea in children. However, there are no clear data to suggest if specific probiotic agents are superior to others.
Study design: Prospective single-blind, randomized, controlled trial.
Setting: Outpatient primary care in Naples, Italy.
Synopsis: This study compared five commercially available probiotic preparations (mix of Lactobacillus delbrueckii var bulgaricus/Streptococcus thermophilus/L. acidophilus/ Bifido-bacterium bifidum; L. rhamnosus strain GG; Saccharomyces boulardii; Bacillus clausii; or Enterococcus faecium SF68) and a control group in the treatment of outpatient acute diarrhea in 571 children age 3 months to 36 months.
The primary outcomes were the duration of diarrhea and the number and consistency of stools. The groups receiving Lactobacillus GG and the mixture had a shorter total duration of diarrhea (78.5 and 70 hours, respectively), decreased total number of stools, and improved stool consistency when compared with the control (115.5 hours). The other therapies showed no improvement over the control group. These data report on products commercially available in Italy, which may differ greatly from products available locally.
Bottom line: Probiotic preparations for the treatment of acute diarrhea in children should be chosen based on effectiveness data.
Citation: Canani RB, Cirillo P, Terrin G, et al. Probiotics for treatment of acute diarrhoea in children: randomised clinical trial of five different preparations. BMJ 2007;335:340-345.
Is CTPA a Reliable Alternative to V/Q Scan for Diagnosing PE?
Background: Computed tomography pulmonary angiogram (CTPA) has replaced ventilation/perfusion (V/Q) scanning at many hospitals as the test of choice for ruling out pulmonary embolism (PE). But limited clinical data compare CTPA with V/Q scanning in those suspected of having venous thromboembolism (VTE).
Study design: Randomized, investigator blinded, controlled trial.
Setting: The emergency departments (ED), inpatient wards, and outpatient clinics of five academic centers.
Synopsis: In the study, 1,411 patients were enrolled from five medical centers. Of 694 patients randomized to CTPA, 133 (19.2%) were diagnosed with VTE in the initial evaluation period, while 101 of 712 patients (14.2%) receiving a V/Q scan were diagnosed with VTE.
Patients not initially diagnosed with VTE were monitored. At three-month follow-up, 0.4% of the CTPA group and 1.0% of the V/Q group had a diagnosed VTE.
The overall rate of VTE found in the initial diagnostic period was significantly greater in patients randomized to CTPA (19.2% vs. 14.2%; difference, 5.0%; 95% CI; 1.1% to 8.9% p=.01). This suggests CTPA has a higher false positive rate or detects clinically insignificant thrombi.
Bottom line: CTPA was not inferior to V/Q scanning for excluding clinically meaningful PE, but CTPA diagnosed about 30% more patients with VTE than did V/Q scanning.
Citation: Anderson DR, Kahn SR, Rodger MA, et al. Computed tomographic pulmonary angiography vs. ventilation-perfusion lung scanning in patients with suspected pulmonary embolism: a randomized controlled trial. JAMA. 2007;298(23):2743-2753.
Does the Hospitalist Model Improve Length of Stay, Quality, and Cost of Care?
Background: The hospitalist model, with increased physician availability and expertise but greater discontinuity of care, is becoming more prevalent in U.S. medicine. What little is known about how this model will affect patient care is derived from a number of small studies.
Study design: Retrospective cohort study.
Setting: 45 small to midsize, predominantly nonteaching hospitals throughout the U.S.
Synopsis: Using the Premier Healthcare Informatics database, this study examined information on 76,926 patients admitted for seven common diagnoses to one of three services: hospitalist, general internist, or family physician. Analysis showed that patients on a hospitalist service had a 0.4-day shorter length of stay (p<0.001) compared with those on a general internist or family physician service.
The cost to patients cared for by a hospitalist was lower than the cost of family physicians ($125 less, p=0.33) and internists ($268 less, p=0.02). There was no difference found in death rate or 14-day readmission rate among the three services.
Given the retrospective design of this study, no causal relationship can be deduced. This study is further limited by its lack of specific data on the physicians categorized into one of the three groups solely by administrative data. The authors had concerns that the biases inherent to the retrospective nature of their work accounted for the significant difference found between hospitalists and internists.
Bottom line: The hospitalist model is associated with modest improvements in length of stay as compared with traditional inpatient approaches.
Citation: Lindenauer PK, Rothberg MB, Pekow PS, et. al. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007;357:2589-2600.
What Is the Stroke Risk Soon after TIA, and What Factors Drive the Variability of Previous Findings?
Background: Many studies have attempted to estimate the risk of stroke in the early period after a transient ischemic attack (TIA). These studies vary widely in their calculation of the estimated risk. Further, the clinical and methodological factors underlying this variability are unclear.
Study design: Systematic review and meta-analysis.
Setting: Community and hospital.
Synopsis: Searching the Cochrane review database, MEDLINE, EMBASE, CINAHL, and BIOSIS, 11 studies from 1973 to 2006 were included for meta-analysis, selected from 694 potential candidate studies identified on initial screening. The studies ranged in size from 62 to 2,285 patients.
The pooled estimate of risk for stroke following TIA was found to be 3.5%, 8%, and 9.2% at two, 30, and 90 days following TIA, respectively. However, there was significant heterogeneity for all periods considered (p<0.001).
Outcome ascertainment was identified as a major source of methodological heterogeneity. When risk of stroke at follow-up was determined by passive ascertainment (e.g., administrative documentation) the early risk of stroke was 3.1% two days after TIA, 6.4% at 30 days, and 8.7% at 90 days. But active ascertainment (e.g., direct, personal contact with study participants) determined stroke risk to be 9.9%, 13.4%, and 17.4% at two, 30, and 90 days after TIA, respectively.
Bottom line: Based on analysis of completed studies that included directly observed follow-up of study participants, the early risk of stroke after TIA is approximately 15% to 20% at 90 days following the sentinel event.
Citation: Wu CM, McLaughlin K, Lorenzetti DL, Hill MD, Manns BJ, Ghali WA. Early risk of stroke after transient ischemic attack. Arch Intern Med. 2007;167:2417-2422.
What Is the 1-year Ischemia and Mortality Rate for Three Anti-thrombotic Therapies for Early Invasive Management of ACS?
Background: Early interventional or surgical revascularization has improved morbidity and mortality in patients with acute coronary syndrome (ACS). The optimal anti-thrombotic regimen to reduce late ischemic and death rates has not been determined.
Study design: Prospective, open-label randomized control trial.
Setting: 450 academic and community-based institutions in 17 countries.
Synopsis: A total of 13,819 patients were enrolled between August 2003 and December 2005. They were assigned to heparin plus glycoprotein (GP) IIb/IIIa inhibitors (n=4,603), bivalirudin (Angiomax) plus IIb/IIIa inhibitors (n=4,604), or bivalirudin monotherapy (n=4,612).
For patients receiving GP IIb/IIIa inhibitors, a 2x2 factorial design assigned half the heparin and bivalirudin groups to routine upstream GP inhibitor administration (4,605 patients). The other half received selective GP IIb/IIIa inhibitors administration if PCI was indicated (4,602 patients).
At one year, there was no statistically significant difference in ischemia or mortality rate among the three therapy groups. No difference in ischemia rate was detected between the two GP IIb/IIIa inhibitor utilization strategies.
Since the hypotheses and the power for the one-year analysis in this trial were not prospectively determined, the results are considered to be exploratory and hypothesis generating.
Bottom line: At one year, there is no statistically significant difference in ischemia or mortality rate for the three antithrombotic regiments and the two glycoprotein utilization strategies.
Citation: Stone GW, Ware JH, Bertrand ME, et. al. Antithrombotic strategies in patients with acute coronary syndromes undergoing early invasive management. One-year results from the ACUITY trial. JAMA 2007;298:2497-2505.
What Is the PE Risk after Discontinuing Anticoagulation in Patients with Symptomatic VTE?
Background: The natural history of patients with symptomatic VTE who have completed anticoagulation is not well understood.
Study design: Inception cohort using pooled data from a prospective cohort study and one arm of an open-label randomized trial.
Setting: Academic medical centers in Canada, Sweden, and Italy.
Synopsis: Using pooled data from two previous studies, 2,052 patients with a first diagnosis of symptomatic VTE (lower-extremity deep-vein thrombosis [DVT], PE, or both) were evaluated for fatal PE after a standard course of therapy (mean of six months) with a vitamin K antagonist.
Patients were followed for up to 120 months. The investigators found an annual event risk of 0.19-0.49 per 100 person-years for fatal PE. Patients with prolonged immobility, active cancer, and thrombophilia were excluded, as were those with recurrent acute DVT.
Secondary analysis revealed an incidence of any fatal, definite or probable PE within the first year of discontinuing therapy of 0.35%-0.81%.
After the first year, the annual event risk ranged from 0.15-0.40 events per 100 person-years. Patients with advanced age, idiopathic VTE as well as those presenting with PE had higher rates of fatal PE.
Bottom line: There is a real though small (less than 1%) risk of fatal PE in the first year following discontinuation of anticoagulation for the first VTE episode. The optimal course of treatment for patients with idiopathic VTE is yet to be determined.
Citation: Douketis JD, Gu CS, Schulman S, et al. The risk for fatal pulmonary embolism after discontinuing anticoagulant therapy for venous thromboembolism. Ann Intern Med. 2007;147(11):766-774.
Do the Beers Criteria Predict ED Visits Associated with Adverse Drug Events?
Background: Adverse drug events are common in the elderly. The Beers criteria are a consensus-based list of 41 medications that are considered inappropriate for use in older adults and often lead to poor outcomes.
Study design: Retrospective medical record review and data analysis.
Setting: Three nationally representative, U.S. public health surveillance systems: the National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance System (NEISS-CADES), 2004-2005; the National Ambulatory Medical Care Survey (NAMCS), 2004; and National Hospital Ambulatory Medical Care Survey (NHAMCS), 2004.
Synopsis: Using data collected from ED visits at 58 hospitals in the NEISS-CADES system, this study estimated that 177,504 visits for adverse drug events occur annually in the United States. Only 8.8% of such visits were attributable to the 41 medications included in the Beers criteria. Three drug classes (anticoagulant and antiplatelet agents, antidiabetic agents, and narrow therapeutic index agents) accounted for nearly half of all such ED visits. Warfarin (17.3%), insulin (13%), and digoxin (3.2%) were the most commonly implicated medications, collectively accounting for 33% of visits (CI, 27.8% to 38.7%).
This study suggests that because of the common use and high risk of adverse events associated with these three drugs, interventions targeting their use may prevent ED visits for adverse drug events in the elderly, compared with interventions aimed at reducing the use of medications identified in the Beers criteria.
This study only included adverse drug events identified in the ED and relied on the diagnosis and documentation of such events by the ED physician.
Bottom line: Beers criteria medications, although considered inappropriate for use in the elderly, were associated with significantly fewer ED visits for adverse events compared with warfarin, digoxin, and insulin.
Citation: Budnitz DS, Shehab N, Kegler SR, et. al. Medication use leading to emergency department visits for adverse drug events in older adults. Ann Intern Med. 2007;147:755-765. TH
Literature at a Glance
A guide to this month’s abstracts
- Steroids reduce mortality only in patients with confirmed bacterial meningitis.
- Probiotics can be useful in the treatment of acute diarrhea in children.
- CT pulmonary angiography is not inferior to V/Q scanning for exclusion of PE.
- Hospitalist care results in shorter LOS compared with care by traditional general internists and family practice physicians.
- The early risk of stroke after TIA is approximately 15% to 20% at 90 days after the sentinel event.
- Different anti-thrombotic strategies produce no difference in outcomes of early acute coronary syndromes.
- The risk of fatal PE is highest in the first year after medication is stopped.
- Beers criteria medications are associated with fewer ED visits by elderly patients compared with warfarin, digoxin, and insulin.
Do Steroids Affect the Outcome in Patients with Meningitis?
Background: Pyogenic (bacterial) meningitis has high morbidity and mortality. Studies suggest some benefit of steroids in children but provide limited evidence for adult use.
Study design: Intention-to-treat, randomized control trial.
Setting: Single hospital in Vietnam.
Synopsis: Of 435 patients older than 14 with suspected meningitis all received lumbar puncture with randomization to IV dexamethasone or placebo for four days. Results showed 69% of patients had definite meningitis, 28.3% were probable, and 2.8% had an alternative diagnosis based on culture results.
The primary outcome was death after one month, which did not differ among groups (risk ratio [RR] 0.79, confidence interval [CI] 0.45-1.39).
Predefined subgroup analysis of patients with definitive meningitis showed a significant reduction in mortality at one month (RR 0.43, CI 0.2-0.94) and death/disability at six months (odds ratio [OR] 0.56, CI 0.32-0.98).
In patients with probable meningitis, those who received steroids demonstrated a trend toward harm (OR 2.65, CI 0.73-9.63).
Probable versus definite meningitis was determined retrospectively based on cultures. The most common isolate was Streptococcus suis.
Bottom line: This study provides some evidence for using steroids in adults with confirmed bacterial meningitis. Clinical application is limited by bacterial epidemiology and the difficulty of prospectively separating patients who would benefit from those who might be harmed.
Citation: Nguyen TH, Tran TH, Thwaites G, et. al. Dexamethasone in Vietnamese adolescents and adults with bacterial meningitis. N Engl J Med. 2007;357:2431-2439.
Which Probiotic Preparations Best Reduce the Duration of Acute Diarrhea in Children?
Background: Probiotics have been suggested as an adjunctive therapy to reduce the severity and duration of acute diarrhea in children. However, there are no clear data to suggest if specific probiotic agents are superior to others.
Study design: Prospective single-blind, randomized, controlled trial.
Setting: Outpatient primary care in Naples, Italy.
Synopsis: This study compared five commercially available probiotic preparations (mix of Lactobacillus delbrueckii var bulgaricus/Streptococcus thermophilus/L. acidophilus/ Bifido-bacterium bifidum; L. rhamnosus strain GG; Saccharomyces boulardii; Bacillus clausii; or Enterococcus faecium SF68) and a control group in the treatment of outpatient acute diarrhea in 571 children age 3 months to 36 months.
The primary outcomes were the duration of diarrhea and the number and consistency of stools. The groups receiving Lactobacillus GG and the mixture had a shorter total duration of diarrhea (78.5 and 70 hours, respectively), decreased total number of stools, and improved stool consistency when compared with the control (115.5 hours). The other therapies showed no improvement over the control group. These data report on products commercially available in Italy, which may differ greatly from products available locally.
Bottom line: Probiotic preparations for the treatment of acute diarrhea in children should be chosen based on effectiveness data.
Citation: Canani RB, Cirillo P, Terrin G, et al. Probiotics for treatment of acute diarrhoea in children: randomised clinical trial of five different preparations. BMJ 2007;335:340-345.
Is CTPA a Reliable Alternative to V/Q Scan for Diagnosing PE?
Background: Computed tomography pulmonary angiogram (CTPA) has replaced ventilation/perfusion (V/Q) scanning at many hospitals as the test of choice for ruling out pulmonary embolism (PE). But limited clinical data compare CTPA with V/Q scanning in those suspected of having venous thromboembolism (VTE).
Study design: Randomized, investigator blinded, controlled trial.
Setting: The emergency departments (ED), inpatient wards, and outpatient clinics of five academic centers.
Synopsis: In the study, 1,411 patients were enrolled from five medical centers. Of 694 patients randomized to CTPA, 133 (19.2%) were diagnosed with VTE in the initial evaluation period, while 101 of 712 patients (14.2%) receiving a V/Q scan were diagnosed with VTE.
Patients not initially diagnosed with VTE were monitored. At three-month follow-up, 0.4% of the CTPA group and 1.0% of the V/Q group had a diagnosed VTE.
The overall rate of VTE found in the initial diagnostic period was significantly greater in patients randomized to CTPA (19.2% vs. 14.2%; difference, 5.0%; 95% CI; 1.1% to 8.9% p=.01). This suggests CTPA has a higher false positive rate or detects clinically insignificant thrombi.
Bottom line: CTPA was not inferior to V/Q scanning for excluding clinically meaningful PE, but CTPA diagnosed about 30% more patients with VTE than did V/Q scanning.
Citation: Anderson DR, Kahn SR, Rodger MA, et al. Computed tomographic pulmonary angiography vs. ventilation-perfusion lung scanning in patients with suspected pulmonary embolism: a randomized controlled trial. JAMA. 2007;298(23):2743-2753.
Does the Hospitalist Model Improve Length of Stay, Quality, and Cost of Care?
Background: The hospitalist model, with increased physician availability and expertise but greater discontinuity of care, is becoming more prevalent in U.S. medicine. What little is known about how this model will affect patient care is derived from a number of small studies.
Study design: Retrospective cohort study.
Setting: 45 small to midsize, predominantly nonteaching hospitals throughout the U.S.
Synopsis: Using the Premier Healthcare Informatics database, this study examined information on 76,926 patients admitted for seven common diagnoses to one of three services: hospitalist, general internist, or family physician. Analysis showed that patients on a hospitalist service had a 0.4-day shorter length of stay (p<0.001) compared with those on a general internist or family physician service.
The cost to patients cared for by a hospitalist was lower than the cost of family physicians ($125 less, p=0.33) and internists ($268 less, p=0.02). There was no difference found in death rate or 14-day readmission rate among the three services.
Given the retrospective design of this study, no causal relationship can be deduced. This study is further limited by its lack of specific data on the physicians categorized into one of the three groups solely by administrative data. The authors had concerns that the biases inherent to the retrospective nature of their work accounted for the significant difference found between hospitalists and internists.
Bottom line: The hospitalist model is associated with modest improvements in length of stay as compared with traditional inpatient approaches.
Citation: Lindenauer PK, Rothberg MB, Pekow PS, et. al. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007;357:2589-2600.
What Is the Stroke Risk Soon after TIA, and What Factors Drive the Variability of Previous Findings?
Background: Many studies have attempted to estimate the risk of stroke in the early period after a transient ischemic attack (TIA). These studies vary widely in their calculation of the estimated risk. Further, the clinical and methodological factors underlying this variability are unclear.
Study design: Systematic review and meta-analysis.
Setting: Community and hospital.
Synopsis: Searching the Cochrane review database, MEDLINE, EMBASE, CINAHL, and BIOSIS, 11 studies from 1973 to 2006 were included for meta-analysis, selected from 694 potential candidate studies identified on initial screening. The studies ranged in size from 62 to 2,285 patients.
The pooled estimate of risk for stroke following TIA was found to be 3.5%, 8%, and 9.2% at two, 30, and 90 days following TIA, respectively. However, there was significant heterogeneity for all periods considered (p<0.001).
Outcome ascertainment was identified as a major source of methodological heterogeneity. When risk of stroke at follow-up was determined by passive ascertainment (e.g., administrative documentation) the early risk of stroke was 3.1% two days after TIA, 6.4% at 30 days, and 8.7% at 90 days. But active ascertainment (e.g., direct, personal contact with study participants) determined stroke risk to be 9.9%, 13.4%, and 17.4% at two, 30, and 90 days after TIA, respectively.
Bottom line: Based on analysis of completed studies that included directly observed follow-up of study participants, the early risk of stroke after TIA is approximately 15% to 20% at 90 days following the sentinel event.
Citation: Wu CM, McLaughlin K, Lorenzetti DL, Hill MD, Manns BJ, Ghali WA. Early risk of stroke after transient ischemic attack. Arch Intern Med. 2007;167:2417-2422.
What Is the 1-year Ischemia and Mortality Rate for Three Anti-thrombotic Therapies for Early Invasive Management of ACS?
Background: Early interventional or surgical revascularization has improved morbidity and mortality in patients with acute coronary syndrome (ACS). The optimal anti-thrombotic regimen to reduce late ischemic and death rates has not been determined.
Study design: Prospective, open-label randomized control trial.
Setting: 450 academic and community-based institutions in 17 countries.
Synopsis: A total of 13,819 patients were enrolled between August 2003 and December 2005. They were assigned to heparin plus glycoprotein (GP) IIb/IIIa inhibitors (n=4,603), bivalirudin (Angiomax) plus IIb/IIIa inhibitors (n=4,604), or bivalirudin monotherapy (n=4,612).
For patients receiving GP IIb/IIIa inhibitors, a 2x2 factorial design assigned half the heparin and bivalirudin groups to routine upstream GP inhibitor administration (4,605 patients). The other half received selective GP IIb/IIIa inhibitors administration if PCI was indicated (4,602 patients).
At one year, there was no statistically significant difference in ischemia or mortality rate among the three therapy groups. No difference in ischemia rate was detected between the two GP IIb/IIIa inhibitor utilization strategies.
Since the hypotheses and the power for the one-year analysis in this trial were not prospectively determined, the results are considered to be exploratory and hypothesis generating.
Bottom line: At one year, there is no statistically significant difference in ischemia or mortality rate for the three antithrombotic regiments and the two glycoprotein utilization strategies.
Citation: Stone GW, Ware JH, Bertrand ME, et. al. Antithrombotic strategies in patients with acute coronary syndromes undergoing early invasive management. One-year results from the ACUITY trial. JAMA 2007;298:2497-2505.
What Is the PE Risk after Discontinuing Anticoagulation in Patients with Symptomatic VTE?
Background: The natural history of patients with symptomatic VTE who have completed anticoagulation is not well understood.
Study design: Inception cohort using pooled data from a prospective cohort study and one arm of an open-label randomized trial.
Setting: Academic medical centers in Canada, Sweden, and Italy.
Synopsis: Using pooled data from two previous studies, 2,052 patients with a first diagnosis of symptomatic VTE (lower-extremity deep-vein thrombosis [DVT], PE, or both) were evaluated for fatal PE after a standard course of therapy (mean of six months) with a vitamin K antagonist.
Patients were followed for up to 120 months. The investigators found an annual event risk of 0.19-0.49 per 100 person-years for fatal PE. Patients with prolonged immobility, active cancer, and thrombophilia were excluded, as were those with recurrent acute DVT.
Secondary analysis revealed an incidence of any fatal, definite or probable PE within the first year of discontinuing therapy of 0.35%-0.81%.
After the first year, the annual event risk ranged from 0.15-0.40 events per 100 person-years. Patients with advanced age, idiopathic VTE as well as those presenting with PE had higher rates of fatal PE.
Bottom line: There is a real though small (less than 1%) risk of fatal PE in the first year following discontinuation of anticoagulation for the first VTE episode. The optimal course of treatment for patients with idiopathic VTE is yet to be determined.
Citation: Douketis JD, Gu CS, Schulman S, et al. The risk for fatal pulmonary embolism after discontinuing anticoagulant therapy for venous thromboembolism. Ann Intern Med. 2007;147(11):766-774.
Do the Beers Criteria Predict ED Visits Associated with Adverse Drug Events?
Background: Adverse drug events are common in the elderly. The Beers criteria are a consensus-based list of 41 medications that are considered inappropriate for use in older adults and often lead to poor outcomes.
Study design: Retrospective medical record review and data analysis.
Setting: Three nationally representative, U.S. public health surveillance systems: the National Electronic Injury Surveillance System-Cooperative Adverse Drug Event Surveillance System (NEISS-CADES), 2004-2005; the National Ambulatory Medical Care Survey (NAMCS), 2004; and National Hospital Ambulatory Medical Care Survey (NHAMCS), 2004.
Synopsis: Using data collected from ED visits at 58 hospitals in the NEISS-CADES system, this study estimated that 177,504 visits for adverse drug events occur annually in the United States. Only 8.8% of such visits were attributable to the 41 medications included in the Beers criteria. Three drug classes (anticoagulant and antiplatelet agents, antidiabetic agents, and narrow therapeutic index agents) accounted for nearly half of all such ED visits. Warfarin (17.3%), insulin (13%), and digoxin (3.2%) were the most commonly implicated medications, collectively accounting for 33% of visits (CI, 27.8% to 38.7%).
This study suggests that because of the common use and high risk of adverse events associated with these three drugs, interventions targeting their use may prevent ED visits for adverse drug events in the elderly, compared with interventions aimed at reducing the use of medications identified in the Beers criteria.
This study only included adverse drug events identified in the ED and relied on the diagnosis and documentation of such events by the ED physician.
Bottom line: Beers criteria medications, although considered inappropriate for use in the elderly, were associated with significantly fewer ED visits for adverse events compared with warfarin, digoxin, and insulin.
Citation: Budnitz DS, Shehab N, Kegler SR, et. al. Medication use leading to emergency department visits for adverse drug events in older adults. Ann Intern Med. 2007;147:755-765. TH
Research Committee Chair Reflects

Before Andy Auerbach, MD, MPH, concludes a four-year term as chair of SHM’s Research Committee, I talked with him about his perspective on hospital medicine research. Dr. Auerbach is an associate professor of medicine at the University of California, San Francisco.
He received a career development award from the National Institutes of Health (NIH) early in his career and is the principal investigator of an R01 research project grant from the NHLBI titled “Improving use of perioperative beta-blockers through a multidimensional QI program.”
He is also a co-author of “Outcomes of Patients Treated by Hospitalists, General Internists, and Family Physicians” in the December 2007 New England Journal of Medicine, which found statistically significant differences in length of stay and cost. He received his medical degree from Dartmouth Medical School in Hanover, N.H., and did his residency training in internal medicine at Yale New Haven Hospital in Connecticut. He completed an MPH in clinical epidemiology at the Harvard School of Public Health in Boston in 1998.
Q: So, is academia as glamorous as it sounds?
Dr. Auerbach: Way more glamorous—you should see my office. And yes, we are in a white tower.
Q: How did you get your start in research?
Dr. Auerbach: I actually started out my research fellowship wanting to be a cardiologist and go into the cath lab while developing the skills to participate in and teach research methods. I found I really enjoyed the work, particularly the creative and entrepreneurial aspects of developing a project or grant and seeing it through to completion.
Q: What are the research options for hospitalists practicing in nonteaching settings?
Dr. Auerbach: I think the most straightforward way to participate in research is to partner with a clinical research organization to help enroll patients in their trials. While you don’t get the opportunity to design the study, you do get to get a feel for consent/enrollment and internal review board [IRB] processes.
The next best way to get involved with research is to partner with a researcher—and this need not be a hospitalist—at your site or very near by. Many QI projects are close to being research-ready and may provide an opportunity to make that work count twice. But it will require you to learn about analytic methods.
I’d also be remiss if I didn’t mention the value of other very useful academic products—rigorous reports of a QI intervention (think of both success and failure stories) and patient case reports. If well referenced and used as teaching documents, these can be very useful ways to advance knowledge.
Q: Are there any particular prerequisites in terms of training that you find especially helpful as you conduct your research?
Dr. Auerbach: It is hard to be a capital-R “Researcher” and compete for career development grants and NIH funding without some advanced [degrees] and a clinical research fellowship. I hesitate to call these prerequisites, but they are nearly so.
Q: What do you like best about your career as a hospitalist?
Dr. Auerbach: I really like acute care medicine, but didn’t want to subspecialize—otherwise I’d be wearing lead in a cath lab now. I also like the questions and processes in the hospital a bit more than the clinic setting.
Q: Who are your mentors and how did you find them?
Dr. Auerbach: I’ve had a remarkable set of mentors from fellowship [Mary Beth Hamel, Roger Davis, Russ Phillips] through my early career [Lee Goldman, Bob Wachter, Ralph Gonzales]. Now that I am early-mid career, I’m trying to pass their teaching on.
Q: Any advice for hospitalists interested in research but daunted by the prospect of starting their own studies?
Dr. Auerbach: If you want to do a scholarly/academic project to round out your personal/career satisfaction, I think the daunting nature of research can be overcome with the right questions and right support—and by defining what these are well before you actually dive into a dataset or implementation project. You also have to decide how much satisfaction you will get from the project in the end compared to the incremental nights/weekends you will spend to plan and execute your project—not to mention publish.
If you are thinking of research as a career, be aware of what makes you happy. If you like to write, enjoy the process of hypothesis generating/testing, and take rejection well you may be happy as a researcher. There are still plenty of nights/weekends to be spent, though.
Making a switch from full-time clinical or administrative work to research means making a very big commitment to going back to get the skills as part of a fellowship.
Q: Do researchers interested in quality improvement questions still have to run their work past the IRB?
Dr. Auerbach: Unfortunately this is now an area of uncertainty for people—unnecessarily so. Until recent events, IRBs have not required approval for QI projects that seek to enhance care according to an evidence-based standard, especially if that standard is endorsed by the institution. If you plan to publish your findings—particularly if you talk to or touch patients, or collect personal health information—I think it is nearly always wise to at least call your local IRB to ask for how you can or should conduct the study. This is best done before you start the project, obviously.
If you want to publish your results using deidentified data after the project is done, our IRB would say that is exempt from review [e.g., no need for approval]. But I think even this case would be worth a phone call to ensure your IRB feels similarly.
Whether or not you get IRB approval, be very aware of how and where you store data. TH
Before Andy Auerbach, MD, MPH, concludes a four-year term as chair of SHM’s Research Committee, I talked with him about his perspective on hospital medicine research. Dr. Auerbach is an associate professor of medicine at the University of California, San Francisco.
He received a career development award from the National Institutes of Health (NIH) early in his career and is the principal investigator of an R01 research project grant from the NHLBI titled “Improving use of perioperative beta-blockers through a multidimensional QI program.”
He is also a co-author of “Outcomes of Patients Treated by Hospitalists, General Internists, and Family Physicians” in the December 2007 New England Journal of Medicine, which found statistically significant differences in length of stay and cost. He received his medical degree from Dartmouth Medical School in Hanover, N.H., and did his residency training in internal medicine at Yale New Haven Hospital in Connecticut. He completed an MPH in clinical epidemiology at the Harvard School of Public Health in Boston in 1998.
Q: So, is academia as glamorous as it sounds?
Dr. Auerbach: Way more glamorous—you should see my office. And yes, we are in a white tower.
Q: How did you get your start in research?
Dr. Auerbach: I actually started out my research fellowship wanting to be a cardiologist and go into the cath lab while developing the skills to participate in and teach research methods. I found I really enjoyed the work, particularly the creative and entrepreneurial aspects of developing a project or grant and seeing it through to completion.
Q: What are the research options for hospitalists practicing in nonteaching settings?
Dr. Auerbach: I think the most straightforward way to participate in research is to partner with a clinical research organization to help enroll patients in their trials. While you don’t get the opportunity to design the study, you do get to get a feel for consent/enrollment and internal review board [IRB] processes.
The next best way to get involved with research is to partner with a researcher—and this need not be a hospitalist—at your site or very near by. Many QI projects are close to being research-ready and may provide an opportunity to make that work count twice. But it will require you to learn about analytic methods.
I’d also be remiss if I didn’t mention the value of other very useful academic products—rigorous reports of a QI intervention (think of both success and failure stories) and patient case reports. If well referenced and used as teaching documents, these can be very useful ways to advance knowledge.
Q: Are there any particular prerequisites in terms of training that you find especially helpful as you conduct your research?
Dr. Auerbach: It is hard to be a capital-R “Researcher” and compete for career development grants and NIH funding without some advanced [degrees] and a clinical research fellowship. I hesitate to call these prerequisites, but they are nearly so.
Q: What do you like best about your career as a hospitalist?
Dr. Auerbach: I really like acute care medicine, but didn’t want to subspecialize—otherwise I’d be wearing lead in a cath lab now. I also like the questions and processes in the hospital a bit more than the clinic setting.
Q: Who are your mentors and how did you find them?
Dr. Auerbach: I’ve had a remarkable set of mentors from fellowship [Mary Beth Hamel, Roger Davis, Russ Phillips] through my early career [Lee Goldman, Bob Wachter, Ralph Gonzales]. Now that I am early-mid career, I’m trying to pass their teaching on.
Q: Any advice for hospitalists interested in research but daunted by the prospect of starting their own studies?
Dr. Auerbach: If you want to do a scholarly/academic project to round out your personal/career satisfaction, I think the daunting nature of research can be overcome with the right questions and right support—and by defining what these are well before you actually dive into a dataset or implementation project. You also have to decide how much satisfaction you will get from the project in the end compared to the incremental nights/weekends you will spend to plan and execute your project—not to mention publish.
If you are thinking of research as a career, be aware of what makes you happy. If you like to write, enjoy the process of hypothesis generating/testing, and take rejection well you may be happy as a researcher. There are still plenty of nights/weekends to be spent, though.
Making a switch from full-time clinical or administrative work to research means making a very big commitment to going back to get the skills as part of a fellowship.
Q: Do researchers interested in quality improvement questions still have to run their work past the IRB?
Dr. Auerbach: Unfortunately this is now an area of uncertainty for people—unnecessarily so. Until recent events, IRBs have not required approval for QI projects that seek to enhance care according to an evidence-based standard, especially if that standard is endorsed by the institution. If you plan to publish your findings—particularly if you talk to or touch patients, or collect personal health information—I think it is nearly always wise to at least call your local IRB to ask for how you can or should conduct the study. This is best done before you start the project, obviously.
If you want to publish your results using deidentified data after the project is done, our IRB would say that is exempt from review [e.g., no need for approval]. But I think even this case would be worth a phone call to ensure your IRB feels similarly.
Whether or not you get IRB approval, be very aware of how and where you store data. TH
Before Andy Auerbach, MD, MPH, concludes a four-year term as chair of SHM’s Research Committee, I talked with him about his perspective on hospital medicine research. Dr. Auerbach is an associate professor of medicine at the University of California, San Francisco.
He received a career development award from the National Institutes of Health (NIH) early in his career and is the principal investigator of an R01 research project grant from the NHLBI titled “Improving use of perioperative beta-blockers through a multidimensional QI program.”
He is also a co-author of “Outcomes of Patients Treated by Hospitalists, General Internists, and Family Physicians” in the December 2007 New England Journal of Medicine, which found statistically significant differences in length of stay and cost. He received his medical degree from Dartmouth Medical School in Hanover, N.H., and did his residency training in internal medicine at Yale New Haven Hospital in Connecticut. He completed an MPH in clinical epidemiology at the Harvard School of Public Health in Boston in 1998.
Q: So, is academia as glamorous as it sounds?
Dr. Auerbach: Way more glamorous—you should see my office. And yes, we are in a white tower.
Q: How did you get your start in research?
Dr. Auerbach: I actually started out my research fellowship wanting to be a cardiologist and go into the cath lab while developing the skills to participate in and teach research methods. I found I really enjoyed the work, particularly the creative and entrepreneurial aspects of developing a project or grant and seeing it through to completion.
Q: What are the research options for hospitalists practicing in nonteaching settings?
Dr. Auerbach: I think the most straightforward way to participate in research is to partner with a clinical research organization to help enroll patients in their trials. While you don’t get the opportunity to design the study, you do get to get a feel for consent/enrollment and internal review board [IRB] processes.
The next best way to get involved with research is to partner with a researcher—and this need not be a hospitalist—at your site or very near by. Many QI projects are close to being research-ready and may provide an opportunity to make that work count twice. But it will require you to learn about analytic methods.
I’d also be remiss if I didn’t mention the value of other very useful academic products—rigorous reports of a QI intervention (think of both success and failure stories) and patient case reports. If well referenced and used as teaching documents, these can be very useful ways to advance knowledge.
Q: Are there any particular prerequisites in terms of training that you find especially helpful as you conduct your research?
Dr. Auerbach: It is hard to be a capital-R “Researcher” and compete for career development grants and NIH funding without some advanced [degrees] and a clinical research fellowship. I hesitate to call these prerequisites, but they are nearly so.
Q: What do you like best about your career as a hospitalist?
Dr. Auerbach: I really like acute care medicine, but didn’t want to subspecialize—otherwise I’d be wearing lead in a cath lab now. I also like the questions and processes in the hospital a bit more than the clinic setting.
Q: Who are your mentors and how did you find them?
Dr. Auerbach: I’ve had a remarkable set of mentors from fellowship [Mary Beth Hamel, Roger Davis, Russ Phillips] through my early career [Lee Goldman, Bob Wachter, Ralph Gonzales]. Now that I am early-mid career, I’m trying to pass their teaching on.
Q: Any advice for hospitalists interested in research but daunted by the prospect of starting their own studies?
Dr. Auerbach: If you want to do a scholarly/academic project to round out your personal/career satisfaction, I think the daunting nature of research can be overcome with the right questions and right support—and by defining what these are well before you actually dive into a dataset or implementation project. You also have to decide how much satisfaction you will get from the project in the end compared to the incremental nights/weekends you will spend to plan and execute your project—not to mention publish.
If you are thinking of research as a career, be aware of what makes you happy. If you like to write, enjoy the process of hypothesis generating/testing, and take rejection well you may be happy as a researcher. There are still plenty of nights/weekends to be spent, though.
Making a switch from full-time clinical or administrative work to research means making a very big commitment to going back to get the skills as part of a fellowship.
Q: Do researchers interested in quality improvement questions still have to run their work past the IRB?
Dr. Auerbach: Unfortunately this is now an area of uncertainty for people—unnecessarily so. Until recent events, IRBs have not required approval for QI projects that seek to enhance care according to an evidence-based standard, especially if that standard is endorsed by the institution. If you plan to publish your findings—particularly if you talk to or touch patients, or collect personal health information—I think it is nearly always wise to at least call your local IRB to ask for how you can or should conduct the study. This is best done before you start the project, obviously.
If you want to publish your results using deidentified data after the project is done, our IRB would say that is exempt from review [e.g., no need for approval]. But I think even this case would be worth a phone call to ensure your IRB feels similarly.
Whether or not you get IRB approval, be very aware of how and where you store data. TH
Satisfaction Is Job No. 1
The Career Satisfaction Task Force has focused on two key areas this year to build upon the work that resulted in last year’s white paper “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction.”
The paper outlined a framework for hospital medicine program leaders and hospitalists to identify important components of matching individuals and programs for the best job fit.
This year, the task force is working to bring the white paper to life and moving it from a conceptual framework to demonstrating how to use it to solve real issues facing programs and individuals.
The first of these projects was a Webinar led by SHM Senior Vice President Joe Miller, Sylvia McKean, MD (course director of Hospital Medicine 2008), and Win Whitcomb, MD (a co-founder of SHM). Each of them has held leadership roles on this task force. About 80 people participated in the December event, and more than three-fourths of attendees rated it highly.
At last year’s Annual Meeting in Dallas, the white paper was presented in a task force workshop. In keeping with our aim to bring the framework to life, this year’s workshop will use real case studies to demonstrate how to use bring the concepts to solutions. The workshop will be facilitated by Chad Whelan, MD, assistant professor of medicine and director of the Hospitalists Scholars Training Program, University of Chicago. Discussing key concepts will be Doug Carlson, MD, associate professor, Pediatrics Division, Washington University School of Medicine in St. Louis, and Tosha Wetterneck, MD, University of Wisconsin Hospital/Clinics, Madison. Drs. Carlson and Wetterneck made significant contributions to the white paper. In this highly interactive workshop, case studies that demonstrate challenges with workload/scheduling and autonomy will be discussed. Drs. Carlson and Wetterneck will lead the participants through discussions aimed at identifying the root causes of struggle and potential solutions for the program.
In the coming months, we hope to develop a series of articles to be published in The Hospitalist addressing the issues of greatest importance for career satisfaction.
The task force realizes there may be opportunities to add knowledge about career satisfaction and provide a valuable service to SHM member. We are in the early stages of developing a survey geared to further clarifying the most important factors in making satisfying career matches as well as providing detailed feedback about programs to their leaders. We are seeking funding to enable us to begin this exciting work.
The Career Satisfaction Task Force has focused on two key areas this year to build upon the work that resulted in last year’s white paper “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction.”
The paper outlined a framework for hospital medicine program leaders and hospitalists to identify important components of matching individuals and programs for the best job fit.
This year, the task force is working to bring the white paper to life and moving it from a conceptual framework to demonstrating how to use it to solve real issues facing programs and individuals.
The first of these projects was a Webinar led by SHM Senior Vice President Joe Miller, Sylvia McKean, MD (course director of Hospital Medicine 2008), and Win Whitcomb, MD (a co-founder of SHM). Each of them has held leadership roles on this task force. About 80 people participated in the December event, and more than three-fourths of attendees rated it highly.
At last year’s Annual Meeting in Dallas, the white paper was presented in a task force workshop. In keeping with our aim to bring the framework to life, this year’s workshop will use real case studies to demonstrate how to use bring the concepts to solutions. The workshop will be facilitated by Chad Whelan, MD, assistant professor of medicine and director of the Hospitalists Scholars Training Program, University of Chicago. Discussing key concepts will be Doug Carlson, MD, associate professor, Pediatrics Division, Washington University School of Medicine in St. Louis, and Tosha Wetterneck, MD, University of Wisconsin Hospital/Clinics, Madison. Drs. Carlson and Wetterneck made significant contributions to the white paper. In this highly interactive workshop, case studies that demonstrate challenges with workload/scheduling and autonomy will be discussed. Drs. Carlson and Wetterneck will lead the participants through discussions aimed at identifying the root causes of struggle and potential solutions for the program.
In the coming months, we hope to develop a series of articles to be published in The Hospitalist addressing the issues of greatest importance for career satisfaction.
The task force realizes there may be opportunities to add knowledge about career satisfaction and provide a valuable service to SHM member. We are in the early stages of developing a survey geared to further clarifying the most important factors in making satisfying career matches as well as providing detailed feedback about programs to their leaders. We are seeking funding to enable us to begin this exciting work.
The Career Satisfaction Task Force has focused on two key areas this year to build upon the work that resulted in last year’s white paper “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction.”
The paper outlined a framework for hospital medicine program leaders and hospitalists to identify important components of matching individuals and programs for the best job fit.
This year, the task force is working to bring the white paper to life and moving it from a conceptual framework to demonstrating how to use it to solve real issues facing programs and individuals.
The first of these projects was a Webinar led by SHM Senior Vice President Joe Miller, Sylvia McKean, MD (course director of Hospital Medicine 2008), and Win Whitcomb, MD (a co-founder of SHM). Each of them has held leadership roles on this task force. About 80 people participated in the December event, and more than three-fourths of attendees rated it highly.
At last year’s Annual Meeting in Dallas, the white paper was presented in a task force workshop. In keeping with our aim to bring the framework to life, this year’s workshop will use real case studies to demonstrate how to use bring the concepts to solutions. The workshop will be facilitated by Chad Whelan, MD, assistant professor of medicine and director of the Hospitalists Scholars Training Program, University of Chicago. Discussing key concepts will be Doug Carlson, MD, associate professor, Pediatrics Division, Washington University School of Medicine in St. Louis, and Tosha Wetterneck, MD, University of Wisconsin Hospital/Clinics, Madison. Drs. Carlson and Wetterneck made significant contributions to the white paper. In this highly interactive workshop, case studies that demonstrate challenges with workload/scheduling and autonomy will be discussed. Drs. Carlson and Wetterneck will lead the participants through discussions aimed at identifying the root causes of struggle and potential solutions for the program.
In the coming months, we hope to develop a series of articles to be published in The Hospitalist addressing the issues of greatest importance for career satisfaction.
The task force realizes there may be opportunities to add knowledge about career satisfaction and provide a valuable service to SHM member. We are in the early stages of developing a survey geared to further clarifying the most important factors in making satisfying career matches as well as providing detailed feedback about programs to their leaders. We are seeking funding to enable us to begin this exciting work.
Hospital Medicine Continues to Make Inroads Overseas
Attendees at this year’s SHM Annual Meeting in San Diego brought with them exciting news of international developments that might broaden the scope of the specialty.
For example, Efren Manjarrez, MD, director of clinical operations for the division of hospital medicine of the Leonard M. Miller School of Medicine at the University of Miami, recently discovered a 500-plus-bed facility at the Universidad de Navarra during his trip to Pamplona, Spain.
Because Dr. Manjarrez is bilingual, past SHM President Mark Williams, MD, professor and chief of the division of hospital medicine at the Northwestern University Feinberg School of Medicine in Chicago, asked him to give a lecture.
“[The Universidad de Navarra] has one of the top two medical schools in Spain and they had the very first symposium on the management of the hospitalized patient,” Dr. Manjarrez says. “They had the very first hospitalist conference in Spain and quite possibly in Europe.”
While in Spain, Dr. Manjarrez realized hospitalists there were “at the grassroots level, where we were about 10 to 12 years ago,” just starting to have a few hospital medical units. The clinic in at the Universidad de Navarra had about five units, and there was a small hospitalist group near Valencia, as well.

Dr. Manjarrez is highly complimentary of the university’s “top-flight medical school,” where he said doctors perform liver transplants.
“They could compete favorably with any city in the United States,” he notes. “They’re interested in organizing hospitalists like Mark Williams and what people ahead of me did for SHM.”
Dr. Manjarrez and Dr. Williams have discussed what will happen with the hospital medicine movement internationally. They forecast that the work begun in the U.S. will globalize fairly soon.
“The Spaniards are very, very on the ball to ask us over there to see what’s going on to get a jump on it,” Dr. Manjarrez says. “SHM needs to start thinking ahead and have an international chapter and plan international meetings abroad to have SHM’s message spread globally. The time is ripe to export what SHM and hospital medicine is doing here”
Dr. Manjarrez notes that Argentina has small pockets of hospitalists. And, Guilherme Brauner Barcellos MD, specialist in internal medicine and intensive care at the Nossa Senhora de Conceicao Hospital in Brazil, is excited about the establishment of a hospital medicine program there. He finds the attempts to develop the specialty in his country “fascinating and challenging.”
“The implementation of hospital medicine, especially those aspects that involve more than just having a general medicine physician dealing with inpatient care, is brand new in Brazil,” Dr. Barcellos says. “We understand there is a long journey ahead.”
Dr. Barcellos is president of the recently formed Brazilian Society of Hospital Medicine and became a member of SHM last year, attending May’s meeting in Dallas. He says the number of hospitalists in Brazil is limited, but “a rapid expansion is predicted.”
“As in the U.S. several years ago, the case for hospitalists in Brazil is still being made,” he notes. “We did a hospital medicine meeting last October, and it led to the formation of the Brazilian Society of Hospital Medicine. We definitely fostered the discussion about the specialty and the model in Brazil.”
He hopes more people will talk about the topic through the new group’s Web site (www.medicinahospitalar.com.br) and in hospitals throughout the country.
“Before the year of 2005, the majority of people here didn’t know about the hospitalists,” he explains. “After that, we had a period in which people were confused, thinking hospitalists were the same as doctors who work in the rapid response teams only. Currently, everybody at least knows about hospital medicine.”
Dr. Williams notes that hospital medicine organizations are forming in Chile, Argentina, Australia, and New Zealand.
Dr. Barcellos believes hospitals across his country “will awake to hospital medicine” when they realize that traditional models aren’t property servicing hospitalized patients anymore. “Much of what is present is wrong, obsolete or out of time, and we should try new attempts to create a different organization,” he says. TH
Molly R. Okeon is a journalist based in California.
Attendees at this year’s SHM Annual Meeting in San Diego brought with them exciting news of international developments that might broaden the scope of the specialty.
For example, Efren Manjarrez, MD, director of clinical operations for the division of hospital medicine of the Leonard M. Miller School of Medicine at the University of Miami, recently discovered a 500-plus-bed facility at the Universidad de Navarra during his trip to Pamplona, Spain.
Because Dr. Manjarrez is bilingual, past SHM President Mark Williams, MD, professor and chief of the division of hospital medicine at the Northwestern University Feinberg School of Medicine in Chicago, asked him to give a lecture.
“[The Universidad de Navarra] has one of the top two medical schools in Spain and they had the very first symposium on the management of the hospitalized patient,” Dr. Manjarrez says. “They had the very first hospitalist conference in Spain and quite possibly in Europe.”
While in Spain, Dr. Manjarrez realized hospitalists there were “at the grassroots level, where we were about 10 to 12 years ago,” just starting to have a few hospital medical units. The clinic in at the Universidad de Navarra had about five units, and there was a small hospitalist group near Valencia, as well.
Dr. Manjarrez is highly complimentary of the university’s “top-flight medical school,” where he said doctors perform liver transplants.
“They could compete favorably with any city in the United States,” he notes. “They’re interested in organizing hospitalists like Mark Williams and what people ahead of me did for SHM.”
Dr. Manjarrez and Dr. Williams have discussed what will happen with the hospital medicine movement internationally. They forecast that the work begun in the U.S. will globalize fairly soon.
“The Spaniards are very, very on the ball to ask us over there to see what’s going on to get a jump on it,” Dr. Manjarrez says. “SHM needs to start thinking ahead and have an international chapter and plan international meetings abroad to have SHM’s message spread globally. The time is ripe to export what SHM and hospital medicine is doing here”
Dr. Manjarrez notes that Argentina has small pockets of hospitalists. And, Guilherme Brauner Barcellos MD, specialist in internal medicine and intensive care at the Nossa Senhora de Conceicao Hospital in Brazil, is excited about the establishment of a hospital medicine program there. He finds the attempts to develop the specialty in his country “fascinating and challenging.”
“The implementation of hospital medicine, especially those aspects that involve more than just having a general medicine physician dealing with inpatient care, is brand new in Brazil,” Dr. Barcellos says. “We understand there is a long journey ahead.”
Dr. Barcellos is president of the recently formed Brazilian Society of Hospital Medicine and became a member of SHM last year, attending May’s meeting in Dallas. He says the number of hospitalists in Brazil is limited, but “a rapid expansion is predicted.”
“As in the U.S. several years ago, the case for hospitalists in Brazil is still being made,” he notes. “We did a hospital medicine meeting last October, and it led to the formation of the Brazilian Society of Hospital Medicine. We definitely fostered the discussion about the specialty and the model in Brazil.”
He hopes more people will talk about the topic through the new group’s Web site (www.medicinahospitalar.com.br) and in hospitals throughout the country.
“Before the year of 2005, the majority of people here didn’t know about the hospitalists,” he explains. “After that, we had a period in which people were confused, thinking hospitalists were the same as doctors who work in the rapid response teams only. Currently, everybody at least knows about hospital medicine.”
Dr. Williams notes that hospital medicine organizations are forming in Chile, Argentina, Australia, and New Zealand.
Dr. Barcellos believes hospitals across his country “will awake to hospital medicine” when they realize that traditional models aren’t property servicing hospitalized patients anymore. “Much of what is present is wrong, obsolete or out of time, and we should try new attempts to create a different organization,” he says. TH
Molly R. Okeon is a journalist based in California.
Attendees at this year’s SHM Annual Meeting in San Diego brought with them exciting news of international developments that might broaden the scope of the specialty.
For example, Efren Manjarrez, MD, director of clinical operations for the division of hospital medicine of the Leonard M. Miller School of Medicine at the University of Miami, recently discovered a 500-plus-bed facility at the Universidad de Navarra during his trip to Pamplona, Spain.
Because Dr. Manjarrez is bilingual, past SHM President Mark Williams, MD, professor and chief of the division of hospital medicine at the Northwestern University Feinberg School of Medicine in Chicago, asked him to give a lecture.
“[The Universidad de Navarra] has one of the top two medical schools in Spain and they had the very first symposium on the management of the hospitalized patient,” Dr. Manjarrez says. “They had the very first hospitalist conference in Spain and quite possibly in Europe.”
While in Spain, Dr. Manjarrez realized hospitalists there were “at the grassroots level, where we were about 10 to 12 years ago,” just starting to have a few hospital medical units. The clinic in at the Universidad de Navarra had about five units, and there was a small hospitalist group near Valencia, as well.
Dr. Manjarrez is highly complimentary of the university’s “top-flight medical school,” where he said doctors perform liver transplants.
“They could compete favorably with any city in the United States,” he notes. “They’re interested in organizing hospitalists like Mark Williams and what people ahead of me did for SHM.”
Dr. Manjarrez and Dr. Williams have discussed what will happen with the hospital medicine movement internationally. They forecast that the work begun in the U.S. will globalize fairly soon.
“The Spaniards are very, very on the ball to ask us over there to see what’s going on to get a jump on it,” Dr. Manjarrez says. “SHM needs to start thinking ahead and have an international chapter and plan international meetings abroad to have SHM’s message spread globally. The time is ripe to export what SHM and hospital medicine is doing here”
Dr. Manjarrez notes that Argentina has small pockets of hospitalists. And, Guilherme Brauner Barcellos MD, specialist in internal medicine and intensive care at the Nossa Senhora de Conceicao Hospital in Brazil, is excited about the establishment of a hospital medicine program there. He finds the attempts to develop the specialty in his country “fascinating and challenging.”
“The implementation of hospital medicine, especially those aspects that involve more than just having a general medicine physician dealing with inpatient care, is brand new in Brazil,” Dr. Barcellos says. “We understand there is a long journey ahead.”
Dr. Barcellos is president of the recently formed Brazilian Society of Hospital Medicine and became a member of SHM last year, attending May’s meeting in Dallas. He says the number of hospitalists in Brazil is limited, but “a rapid expansion is predicted.”
“As in the U.S. several years ago, the case for hospitalists in Brazil is still being made,” he notes. “We did a hospital medicine meeting last October, and it led to the formation of the Brazilian Society of Hospital Medicine. We definitely fostered the discussion about the specialty and the model in Brazil.”
He hopes more people will talk about the topic through the new group’s Web site (www.medicinahospitalar.com.br) and in hospitals throughout the country.
“Before the year of 2005, the majority of people here didn’t know about the hospitalists,” he explains. “After that, we had a period in which people were confused, thinking hospitalists were the same as doctors who work in the rapid response teams only. Currently, everybody at least knows about hospital medicine.”
Dr. Williams notes that hospital medicine organizations are forming in Chile, Argentina, Australia, and New Zealand.
Dr. Barcellos believes hospitals across his country “will awake to hospital medicine” when they realize that traditional models aren’t property servicing hospitalized patients anymore. “Much of what is present is wrong, obsolete or out of time, and we should try new attempts to create a different organization,” he says. TH
Molly R. Okeon is a journalist based in California.
Research Riddle
The recent uproar over the Office of Human Research Protections (OHRP) ordering a multicenter study of a Michigan ICU checklist to halt data collection has left quality improvement (QI) researchers, ethicists, and legal experts scratching their heads.
Even before the Michigan debacle, there was considerable confusion about how patient privacy rules included in the Health Insurance Portability and Accountability Act of 1996 (HIPAA) affected QI studies. No one was really sure when institutional review board (IRBs) needed to be involved and when patients needed to be officially consented.
The HIPAA contains specific language addressing how patients and patient data should be handled by researchers. And experts say that’s a good thing—in theory.
But a 2007 study in the Journal of the American Medical Association found that many epidemiologists feel the rules have adversely affected research and done little to improve patient privacy.1
The situation for QI researchers is even more confusing. Many see studies examining the effect of QI interventions as fundamentally different from “human subjects research.” And because of this many were shocked when the OHRP halted data collection from the Michigan care-checklist program.
In that case, the OHRP argued that because the study was prospective, it wasn’t simply QI, but rather “human subjects research.” The OHRP demanded that researchers run their plans by the IRBs of every one of the 103 hospitals involved in the research before relenting Feb. 15 and letting the study resume. (Initial results of the study were published in the New England Journal of Medicine in 2006.2)
Many medical experts view the intervention being studied in Michigan—a simple checklist aimed at reminding physicians to follow some common-sense procedures designed to lower the infection rate associated with central lines—as a straightforward attempt at QI. They argued the study should be exempt from some of the rules regarding human research subjects.
Experts say the OHRP’s initial ruling made what was already a confusing subject into an impossibly muddled morass that may have a chilling effect on the publication of QI studies.
Some say the OHRP has extended HIPAA too far. First of all, legal experts say, it must be understood that HIPAA’s rules don’t apply equally to everyone. For example, public health authorities are allowed to gather patient data without consent if they are trying to prevent the spread of disease. And hospitals are allowed to use data to improve the quality of healthcare, says James G. Hodge Jr. an associate professor at the Johns Hopkins School of Public Health in Baltimore, and executive director of the Centers for Law and the Public’s Health at Johns Hopkins.
One key to resolving the issue may be for healthcare experts to come up with a definition of what constitutes “human subjects research.”
“This is where issues keep coming up,” Hodge says. “Is QI just an extension of clinical care or is it research? The answer to that question will tell you whether it implicates the rule or not.”
Researchers, ethicists, and legal experts hotly debate these issues. No one appears to know exactly where to draw the line that divides human subjects research from QI studies.
Even before the checklist controversy arose, HIPAA was already having a deleterious impact on the exchange of QI information, says Mary Ann Baily, PhD, an associate for ethics and health policy at the Hastings Center in Garrison, N.Y.
Loathe to run afoul of the OHRP, at least one of the larger managed-care providers decided against publishing results of its QI studies, Dr. Baily says. “They’re just trying to stay out of the OHRP’s way,” she explains. “At a recent workshop, researchers said, ‘We don’t publish our data. We make our own system work better and keep our heads down. That way we don’t run into any problems. It’s safer that way.’ ”
This means nobody benefits from that company’s research. “What a waste that is,” Dr. Baily asserts.
Not everyone has taken such a defensive position. But there is a wide range of opinions among QI researchers around the country.
“Certainly as someone who is involved in QI research on an operational level and who is also interested in conducting research looking at the effects of QI interventions I struggle with this regularly,” says Peter Lindenauer, MD, MSC, associate professor of medicine at the Tufts University School of Medicine in Boston and associate medical director, Division of Healthcare Quality, at Baystate Medical Center.
“QI officers don’t look at the work they do as being research,” Dr. Lindenauer notes. “They’re often translating research into practice and implementing and developing strategies designed to improve care. So, when you think about it in those terms, it would never dawn on a typical QI officer to seek IRB approval or to get consent from patients to participate.”
Some researchers avoid the issue by looking only at data with patient identifiers stripped. The assumption is that HIPAA rules apply only to medical records with identifiers intact.
Under that assumption, Lakshmi Halasyamani, MD, has performed two heart failure studies without getting into issues of patient consent. But she sees potential problems with future research.
“Because we were looking at the impact of interventions across the whole population of heart failure patients, it wasn’t a problem,” says Dr. Halasyamani, vice chair for the department of medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich., and a member of SHM’s Board of Directors. “So long as you’re looking at global outcomes, the regulations don’t have much impact.”
But Dr. Halasyamani and her colleagues may want to start looking at the benefits of interventions on subgroups. And this is where things can get messy, she says.
Healthcare professionals really need to figure out a working definition for what constitutes research—and they need to do it soon, Dr. Halasyamani says. Without a good definition, Dr. Halasyamani can see a slowdown of QI research and the possibility of researchers using a QI loophole to get around IRBs. “I could see where some researchers might be tempted to call their studies QI to avoid bureaucratic hassles and IRB oversight,” she says.
Some experts think the minute you decide to publish, by definition you’re doing research.
“I believe you have an ethical obligation to share what you learn with other hospitals,” says Dr. Lindenauer. “So, of course, you want to write it up. But once you start to talk about publication and sharing you start to get to the point where you’re crossing the line —where you’re creating generalizable knowledge.”
And that is precisely when government organizations like the OHRP think you’ve crossed over into research, Dr. Lindenauer says. “It’s a tricky question,” he adds.
Ethicist Baily agrees that experts need to work on coming up with a practical definition of research. Right now, the situation is impossible, she says. Take, for example, a medical plan that wants to send postcards to encourage patients to show up for an annual physical. If researchers want to learn whether that technique works, do they need to send a postcard, prior to the reminder postcard, to let patients know that they’re going to be part of a study, she asks.
And even more important, with all the staff cuts at medical institutions around the country, shouldn’t QI officers study whether these cost-cutting measures adversely affect patient care, she asks. TH
Linda Carroll is a medical journalist based in New Jersey.
References
- Ness RB, Joint Policy Committee, Societies of Epidemiology. Influence of the HIPAA Privacy Rule on health research. JAMA. 2007 Nov 14;298(18):2164-2170.
- Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725-2732. Erratum in: N Engl J Med. 2007 Jun 21;356(25):2660.
The recent uproar over the Office of Human Research Protections (OHRP) ordering a multicenter study of a Michigan ICU checklist to halt data collection has left quality improvement (QI) researchers, ethicists, and legal experts scratching their heads.
Even before the Michigan debacle, there was considerable confusion about how patient privacy rules included in the Health Insurance Portability and Accountability Act of 1996 (HIPAA) affected QI studies. No one was really sure when institutional review board (IRBs) needed to be involved and when patients needed to be officially consented.
The HIPAA contains specific language addressing how patients and patient data should be handled by researchers. And experts say that’s a good thing—in theory.
But a 2007 study in the Journal of the American Medical Association found that many epidemiologists feel the rules have adversely affected research and done little to improve patient privacy.1
The situation for QI researchers is even more confusing. Many see studies examining the effect of QI interventions as fundamentally different from “human subjects research.” And because of this many were shocked when the OHRP halted data collection from the Michigan care-checklist program.
In that case, the OHRP argued that because the study was prospective, it wasn’t simply QI, but rather “human subjects research.” The OHRP demanded that researchers run their plans by the IRBs of every one of the 103 hospitals involved in the research before relenting Feb. 15 and letting the study resume. (Initial results of the study were published in the New England Journal of Medicine in 2006.2)
Many medical experts view the intervention being studied in Michigan—a simple checklist aimed at reminding physicians to follow some common-sense procedures designed to lower the infection rate associated with central lines—as a straightforward attempt at QI. They argued the study should be exempt from some of the rules regarding human research subjects.
Experts say the OHRP’s initial ruling made what was already a confusing subject into an impossibly muddled morass that may have a chilling effect on the publication of QI studies.
Some say the OHRP has extended HIPAA too far. First of all, legal experts say, it must be understood that HIPAA’s rules don’t apply equally to everyone. For example, public health authorities are allowed to gather patient data without consent if they are trying to prevent the spread of disease. And hospitals are allowed to use data to improve the quality of healthcare, says James G. Hodge Jr. an associate professor at the Johns Hopkins School of Public Health in Baltimore, and executive director of the Centers for Law and the Public’s Health at Johns Hopkins.
One key to resolving the issue may be for healthcare experts to come up with a definition of what constitutes “human subjects research.”
“This is where issues keep coming up,” Hodge says. “Is QI just an extension of clinical care or is it research? The answer to that question will tell you whether it implicates the rule or not.”
Researchers, ethicists, and legal experts hotly debate these issues. No one appears to know exactly where to draw the line that divides human subjects research from QI studies.
Even before the checklist controversy arose, HIPAA was already having a deleterious impact on the exchange of QI information, says Mary Ann Baily, PhD, an associate for ethics and health policy at the Hastings Center in Garrison, N.Y.
Loathe to run afoul of the OHRP, at least one of the larger managed-care providers decided against publishing results of its QI studies, Dr. Baily says. “They’re just trying to stay out of the OHRP’s way,” she explains. “At a recent workshop, researchers said, ‘We don’t publish our data. We make our own system work better and keep our heads down. That way we don’t run into any problems. It’s safer that way.’ ”
This means nobody benefits from that company’s research. “What a waste that is,” Dr. Baily asserts.
Not everyone has taken such a defensive position. But there is a wide range of opinions among QI researchers around the country.
“Certainly as someone who is involved in QI research on an operational level and who is also interested in conducting research looking at the effects of QI interventions I struggle with this regularly,” says Peter Lindenauer, MD, MSC, associate professor of medicine at the Tufts University School of Medicine in Boston and associate medical director, Division of Healthcare Quality, at Baystate Medical Center.
“QI officers don’t look at the work they do as being research,” Dr. Lindenauer notes. “They’re often translating research into practice and implementing and developing strategies designed to improve care. So, when you think about it in those terms, it would never dawn on a typical QI officer to seek IRB approval or to get consent from patients to participate.”
Some researchers avoid the issue by looking only at data with patient identifiers stripped. The assumption is that HIPAA rules apply only to medical records with identifiers intact.
Under that assumption, Lakshmi Halasyamani, MD, has performed two heart failure studies without getting into issues of patient consent. But she sees potential problems with future research.
“Because we were looking at the impact of interventions across the whole population of heart failure patients, it wasn’t a problem,” says Dr. Halasyamani, vice chair for the department of medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich., and a member of SHM’s Board of Directors. “So long as you’re looking at global outcomes, the regulations don’t have much impact.”
But Dr. Halasyamani and her colleagues may want to start looking at the benefits of interventions on subgroups. And this is where things can get messy, she says.
Healthcare professionals really need to figure out a working definition for what constitutes research—and they need to do it soon, Dr. Halasyamani says. Without a good definition, Dr. Halasyamani can see a slowdown of QI research and the possibility of researchers using a QI loophole to get around IRBs. “I could see where some researchers might be tempted to call their studies QI to avoid bureaucratic hassles and IRB oversight,” she says.
Some experts think the minute you decide to publish, by definition you’re doing research.
“I believe you have an ethical obligation to share what you learn with other hospitals,” says Dr. Lindenauer. “So, of course, you want to write it up. But once you start to talk about publication and sharing you start to get to the point where you’re crossing the line —where you’re creating generalizable knowledge.”
And that is precisely when government organizations like the OHRP think you’ve crossed over into research, Dr. Lindenauer says. “It’s a tricky question,” he adds.
Ethicist Baily agrees that experts need to work on coming up with a practical definition of research. Right now, the situation is impossible, she says. Take, for example, a medical plan that wants to send postcards to encourage patients to show up for an annual physical. If researchers want to learn whether that technique works, do they need to send a postcard, prior to the reminder postcard, to let patients know that they’re going to be part of a study, she asks.
And even more important, with all the staff cuts at medical institutions around the country, shouldn’t QI officers study whether these cost-cutting measures adversely affect patient care, she asks. TH
Linda Carroll is a medical journalist based in New Jersey.
References
- Ness RB, Joint Policy Committee, Societies of Epidemiology. Influence of the HIPAA Privacy Rule on health research. JAMA. 2007 Nov 14;298(18):2164-2170.
- Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725-2732. Erratum in: N Engl J Med. 2007 Jun 21;356(25):2660.
The recent uproar over the Office of Human Research Protections (OHRP) ordering a multicenter study of a Michigan ICU checklist to halt data collection has left quality improvement (QI) researchers, ethicists, and legal experts scratching their heads.
Even before the Michigan debacle, there was considerable confusion about how patient privacy rules included in the Health Insurance Portability and Accountability Act of 1996 (HIPAA) affected QI studies. No one was really sure when institutional review board (IRBs) needed to be involved and when patients needed to be officially consented.
The HIPAA contains specific language addressing how patients and patient data should be handled by researchers. And experts say that’s a good thing—in theory.
But a 2007 study in the Journal of the American Medical Association found that many epidemiologists feel the rules have adversely affected research and done little to improve patient privacy.1
The situation for QI researchers is even more confusing. Many see studies examining the effect of QI interventions as fundamentally different from “human subjects research.” And because of this many were shocked when the OHRP halted data collection from the Michigan care-checklist program.
In that case, the OHRP argued that because the study was prospective, it wasn’t simply QI, but rather “human subjects research.” The OHRP demanded that researchers run their plans by the IRBs of every one of the 103 hospitals involved in the research before relenting Feb. 15 and letting the study resume. (Initial results of the study were published in the New England Journal of Medicine in 2006.2)
Many medical experts view the intervention being studied in Michigan—a simple checklist aimed at reminding physicians to follow some common-sense procedures designed to lower the infection rate associated with central lines—as a straightforward attempt at QI. They argued the study should be exempt from some of the rules regarding human research subjects.
Experts say the OHRP’s initial ruling made what was already a confusing subject into an impossibly muddled morass that may have a chilling effect on the publication of QI studies.
Some say the OHRP has extended HIPAA too far. First of all, legal experts say, it must be understood that HIPAA’s rules don’t apply equally to everyone. For example, public health authorities are allowed to gather patient data without consent if they are trying to prevent the spread of disease. And hospitals are allowed to use data to improve the quality of healthcare, says James G. Hodge Jr. an associate professor at the Johns Hopkins School of Public Health in Baltimore, and executive director of the Centers for Law and the Public’s Health at Johns Hopkins.
One key to resolving the issue may be for healthcare experts to come up with a definition of what constitutes “human subjects research.”
“This is where issues keep coming up,” Hodge says. “Is QI just an extension of clinical care or is it research? The answer to that question will tell you whether it implicates the rule or not.”
Researchers, ethicists, and legal experts hotly debate these issues. No one appears to know exactly where to draw the line that divides human subjects research from QI studies.
Even before the checklist controversy arose, HIPAA was already having a deleterious impact on the exchange of QI information, says Mary Ann Baily, PhD, an associate for ethics and health policy at the Hastings Center in Garrison, N.Y.
Loathe to run afoul of the OHRP, at least one of the larger managed-care providers decided against publishing results of its QI studies, Dr. Baily says. “They’re just trying to stay out of the OHRP’s way,” she explains. “At a recent workshop, researchers said, ‘We don’t publish our data. We make our own system work better and keep our heads down. That way we don’t run into any problems. It’s safer that way.’ ”
This means nobody benefits from that company’s research. “What a waste that is,” Dr. Baily asserts.
Not everyone has taken such a defensive position. But there is a wide range of opinions among QI researchers around the country.
“Certainly as someone who is involved in QI research on an operational level and who is also interested in conducting research looking at the effects of QI interventions I struggle with this regularly,” says Peter Lindenauer, MD, MSC, associate professor of medicine at the Tufts University School of Medicine in Boston and associate medical director, Division of Healthcare Quality, at Baystate Medical Center.
“QI officers don’t look at the work they do as being research,” Dr. Lindenauer notes. “They’re often translating research into practice and implementing and developing strategies designed to improve care. So, when you think about it in those terms, it would never dawn on a typical QI officer to seek IRB approval or to get consent from patients to participate.”
Some researchers avoid the issue by looking only at data with patient identifiers stripped. The assumption is that HIPAA rules apply only to medical records with identifiers intact.
Under that assumption, Lakshmi Halasyamani, MD, has performed two heart failure studies without getting into issues of patient consent. But she sees potential problems with future research.
“Because we were looking at the impact of interventions across the whole population of heart failure patients, it wasn’t a problem,” says Dr. Halasyamani, vice chair for the department of medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich., and a member of SHM’s Board of Directors. “So long as you’re looking at global outcomes, the regulations don’t have much impact.”
But Dr. Halasyamani and her colleagues may want to start looking at the benefits of interventions on subgroups. And this is where things can get messy, she says.
Healthcare professionals really need to figure out a working definition for what constitutes research—and they need to do it soon, Dr. Halasyamani says. Without a good definition, Dr. Halasyamani can see a slowdown of QI research and the possibility of researchers using a QI loophole to get around IRBs. “I could see where some researchers might be tempted to call their studies QI to avoid bureaucratic hassles and IRB oversight,” she says.
Some experts think the minute you decide to publish, by definition you’re doing research.
“I believe you have an ethical obligation to share what you learn with other hospitals,” says Dr. Lindenauer. “So, of course, you want to write it up. But once you start to talk about publication and sharing you start to get to the point where you’re crossing the line —where you’re creating generalizable knowledge.”
And that is precisely when government organizations like the OHRP think you’ve crossed over into research, Dr. Lindenauer says. “It’s a tricky question,” he adds.
Ethicist Baily agrees that experts need to work on coming up with a practical definition of research. Right now, the situation is impossible, she says. Take, for example, a medical plan that wants to send postcards to encourage patients to show up for an annual physical. If researchers want to learn whether that technique works, do they need to send a postcard, prior to the reminder postcard, to let patients know that they’re going to be part of a study, she asks.
And even more important, with all the staff cuts at medical institutions around the country, shouldn’t QI officers study whether these cost-cutting measures adversely affect patient care, she asks. TH
Linda Carroll is a medical journalist based in New Jersey.
References
- Ness RB, Joint Policy Committee, Societies of Epidemiology. Influence of the HIPAA Privacy Rule on health research. JAMA. 2007 Nov 14;298(18):2164-2170.
- Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725-2732. Erratum in: N Engl J Med. 2007 Jun 21;356(25):2660.
SHM Joins D.C. Session on Value-Based Purchasing
SHM had a seat at the table at a high-level roundtable meeting March 6 in Washington, D.C., to discuss Medicare’s value-based purchasing of hospital care.
SHM President Russell Holman, MD, chief operating officer for Cogent Healthcare, Nashville, participated in the roundtable convened by Senate Finance Committee Chairman Max Baucus, D-Mont., and ranking member Chuck Grassley, R-Iowa. The roundtable included representatives from 22 public and private healthcare organizations, including SHM, the American Hospital Association, and National Quality Forum.
“SHM was one of only two physician organizations participating,” points out Laura Allendorf, SHM’s senior adviser for advocacy and government affairs. “That is very significant. I think [our inclusion] is a testament to our growing presence, our advocacy efforts and our willingness to help representatives with healthcare issues like value-based purchasing.”
The Proposed Plan
At the roundtable, representatives from the Centers for Medicare and Medicaid Services (CMS), the Medicare Payment Advisory Commission (MedPAC), and the Government Accountability Office (GAO) presented an overview of the report that CMS submitted to Congress in November, which outlines a hospital value-based purchasing program. The plan is designed to meet CMS’ objective of “transforming Medicare from a passive payer of claims to an active purchaser of care.” It builds on the existing framework of the current pay-for-reporting program, Reporting Hospital Quality Data for Annual Payment Update, but more closely links hospital Medicare payments to performance.
Dr. Holman is well versed in the plan; he and members of SHM’s Public Policy Committee, who were in Washington for annual visits to Capitol Hill, had just met with CMS’s Chief Medical Officer Tom Valuck, MD.
“That same morning, Tom Valuck had spent an hour and a half briefing Public Policy Committee members on Medicare’s value-based purchasing plan,” says Allendorf. “I’d lined up that meeting before the roundtable was set up.”
A transition to CMS’s proposed value-based purchasing plan, or VBP, would probably occur over three years. Under the plan, a percentage of the hospital’s diagnosis related group (DRG) payment would rely on the hospital’s performance on a specific set of measures. Although the report is comprehensive, details on implementation, incentives, and more must be made final.
Public reporting of quality measures remains a key part of the plan; quality of care information would be available to patients through the CMS Hospital Compare site at www.medicare.gov. A PDF of the CMS report to Congress is available at www.cms.hhs.gov/center/hospital.asp.
Support For Harmonization
After the formal presentation on the VBP plan, roundtable moderator John Inglehart, founding editor of Health Affairs, asked a series of questions directed at specific segments of the group, targeting issues surrounding the plan’s quality measures, performance standards, incentives, and plan implementation.
Dr. Holman was asked to comment on how CMS could ensure that hospital measures and physician measures become more aligned.
“The measures that each party are asked to report in terms of Part B of Medicare are somewhat different and can lead to confusion and people working at cross purposes,” Dr. Holman explains. “This adds complexity to a system that’s already too complex. In my statement, I said that what we call harmonization [of reporting measures] is a very important step for CMS to take, so that physicians and hospitals are required to measure and report the same thing. The more we can move toward outcome measures, as well as efficiency and patient experience measures, the more harmonization we’ll have. Focusing on outcomes creates a common goal.”
Dr. Holman continued his comments to the roundtable by using an example of harmonization at the heart of hospital medicine: transitions of care. “I let the group know that SHM is working on a number of initiatives regarding care transitions,” he says. “Transitions of care require the whole system to come together; it’s a great way to help galvanize all the stakeholders toward that shared goal.”
In his written statement, Dr. Holman elaborated on SHM’s efforts regarding transitions of care and pushed for an alignment of CMS quality measures and incentives for physicians with those for hospitals.
Air of Excitement
Although they had many concerns about implementation, the roundtable participants were enthusiastic about the plan. “There was a fabulous give-and-take on issues regarding implementation,” says Allendorf.
Dr. Holman stayed after the meeting to discuss the proceedings with other participants. “All in all, the informal comments I heard after the meeting were that this was the most exciting moment they’d had in 30-plus years in healthcare,” he notes. “This marks a substantial change in the payment system, which has always been seen as a barrier to quality.”
What’s Next
The ball is now in the court of Sens. Baucus and Grassley, who will use the roundtable input to draft legislation that would make the necessary statutory changes in time for CMS to implement the plan by fiscal year 2009, or Oct. 1, as mandated by the Deficit Reduction Act (DRA) of 2005.
“I think they’ll be back in touch with [SHM] as they develop the plan,” Allendorf predicts. After the legislation has been submitted, it’s up to Congress to act. “Everything depends on whether any Medicare legislation moves this year, and no one know whether that will happen,” she says.
Whatever final form the CMS plan takes, the future looks bright for value-based purchasing—and for SHM’s continued involvement.
“This roundtable was an excellent opportunity for SHM to develop a relationship with CMS, and to link to the Senate Finance Committee,” Dr. Holman asserts. “My hope is that those relationships will bear fruit over time, and that we can continue to work with those entities, as well as the other roundtable participants, to propose and develop measures over time, and to bring alignment between hospital measures and physician measures.”
Jane Jerrard is a medical writer based in Chicago.
Read More Online
For more information on the roundtable, including Dr. Holman’s written statement and others, as well as a recorded Webcast, visit Sen. Baucus’ Web site at www.senate.gov/~finance/sitepages/VBProundtable030408.htm. TH
SHM had a seat at the table at a high-level roundtable meeting March 6 in Washington, D.C., to discuss Medicare’s value-based purchasing of hospital care.
SHM President Russell Holman, MD, chief operating officer for Cogent Healthcare, Nashville, participated in the roundtable convened by Senate Finance Committee Chairman Max Baucus, D-Mont., and ranking member Chuck Grassley, R-Iowa. The roundtable included representatives from 22 public and private healthcare organizations, including SHM, the American Hospital Association, and National Quality Forum.
“SHM was one of only two physician organizations participating,” points out Laura Allendorf, SHM’s senior adviser for advocacy and government affairs. “That is very significant. I think [our inclusion] is a testament to our growing presence, our advocacy efforts and our willingness to help representatives with healthcare issues like value-based purchasing.”
The Proposed Plan
At the roundtable, representatives from the Centers for Medicare and Medicaid Services (CMS), the Medicare Payment Advisory Commission (MedPAC), and the Government Accountability Office (GAO) presented an overview of the report that CMS submitted to Congress in November, which outlines a hospital value-based purchasing program. The plan is designed to meet CMS’ objective of “transforming Medicare from a passive payer of claims to an active purchaser of care.” It builds on the existing framework of the current pay-for-reporting program, Reporting Hospital Quality Data for Annual Payment Update, but more closely links hospital Medicare payments to performance.
Dr. Holman is well versed in the plan; he and members of SHM’s Public Policy Committee, who were in Washington for annual visits to Capitol Hill, had just met with CMS’s Chief Medical Officer Tom Valuck, MD.
“That same morning, Tom Valuck had spent an hour and a half briefing Public Policy Committee members on Medicare’s value-based purchasing plan,” says Allendorf. “I’d lined up that meeting before the roundtable was set up.”
A transition to CMS’s proposed value-based purchasing plan, or VBP, would probably occur over three years. Under the plan, a percentage of the hospital’s diagnosis related group (DRG) payment would rely on the hospital’s performance on a specific set of measures. Although the report is comprehensive, details on implementation, incentives, and more must be made final.
Public reporting of quality measures remains a key part of the plan; quality of care information would be available to patients through the CMS Hospital Compare site at www.medicare.gov. A PDF of the CMS report to Congress is available at www.cms.hhs.gov/center/hospital.asp.
Support For Harmonization
After the formal presentation on the VBP plan, roundtable moderator John Inglehart, founding editor of Health Affairs, asked a series of questions directed at specific segments of the group, targeting issues surrounding the plan’s quality measures, performance standards, incentives, and plan implementation.
Dr. Holman was asked to comment on how CMS could ensure that hospital measures and physician measures become more aligned.
“The measures that each party are asked to report in terms of Part B of Medicare are somewhat different and can lead to confusion and people working at cross purposes,” Dr. Holman explains. “This adds complexity to a system that’s already too complex. In my statement, I said that what we call harmonization [of reporting measures] is a very important step for CMS to take, so that physicians and hospitals are required to measure and report the same thing. The more we can move toward outcome measures, as well as efficiency and patient experience measures, the more harmonization we’ll have. Focusing on outcomes creates a common goal.”
Dr. Holman continued his comments to the roundtable by using an example of harmonization at the heart of hospital medicine: transitions of care. “I let the group know that SHM is working on a number of initiatives regarding care transitions,” he says. “Transitions of care require the whole system to come together; it’s a great way to help galvanize all the stakeholders toward that shared goal.”
In his written statement, Dr. Holman elaborated on SHM’s efforts regarding transitions of care and pushed for an alignment of CMS quality measures and incentives for physicians with those for hospitals.
Air of Excitement
Although they had many concerns about implementation, the roundtable participants were enthusiastic about the plan. “There was a fabulous give-and-take on issues regarding implementation,” says Allendorf.
Dr. Holman stayed after the meeting to discuss the proceedings with other participants. “All in all, the informal comments I heard after the meeting were that this was the most exciting moment they’d had in 30-plus years in healthcare,” he notes. “This marks a substantial change in the payment system, which has always been seen as a barrier to quality.”
What’s Next
The ball is now in the court of Sens. Baucus and Grassley, who will use the roundtable input to draft legislation that would make the necessary statutory changes in time for CMS to implement the plan by fiscal year 2009, or Oct. 1, as mandated by the Deficit Reduction Act (DRA) of 2005.
“I think they’ll be back in touch with [SHM] as they develop the plan,” Allendorf predicts. After the legislation has been submitted, it’s up to Congress to act. “Everything depends on whether any Medicare legislation moves this year, and no one know whether that will happen,” she says.
Whatever final form the CMS plan takes, the future looks bright for value-based purchasing—and for SHM’s continued involvement.
“This roundtable was an excellent opportunity for SHM to develop a relationship with CMS, and to link to the Senate Finance Committee,” Dr. Holman asserts. “My hope is that those relationships will bear fruit over time, and that we can continue to work with those entities, as well as the other roundtable participants, to propose and develop measures over time, and to bring alignment between hospital measures and physician measures.”
Jane Jerrard is a medical writer based in Chicago.
Read More Online
For more information on the roundtable, including Dr. Holman’s written statement and others, as well as a recorded Webcast, visit Sen. Baucus’ Web site at www.senate.gov/~finance/sitepages/VBProundtable030408.htm. TH
SHM had a seat at the table at a high-level roundtable meeting March 6 in Washington, D.C., to discuss Medicare’s value-based purchasing of hospital care.
SHM President Russell Holman, MD, chief operating officer for Cogent Healthcare, Nashville, participated in the roundtable convened by Senate Finance Committee Chairman Max Baucus, D-Mont., and ranking member Chuck Grassley, R-Iowa. The roundtable included representatives from 22 public and private healthcare organizations, including SHM, the American Hospital Association, and National Quality Forum.
“SHM was one of only two physician organizations participating,” points out Laura Allendorf, SHM’s senior adviser for advocacy and government affairs. “That is very significant. I think [our inclusion] is a testament to our growing presence, our advocacy efforts and our willingness to help representatives with healthcare issues like value-based purchasing.”
The Proposed Plan
At the roundtable, representatives from the Centers for Medicare and Medicaid Services (CMS), the Medicare Payment Advisory Commission (MedPAC), and the Government Accountability Office (GAO) presented an overview of the report that CMS submitted to Congress in November, which outlines a hospital value-based purchasing program. The plan is designed to meet CMS’ objective of “transforming Medicare from a passive payer of claims to an active purchaser of care.” It builds on the existing framework of the current pay-for-reporting program, Reporting Hospital Quality Data for Annual Payment Update, but more closely links hospital Medicare payments to performance.
Dr. Holman is well versed in the plan; he and members of SHM’s Public Policy Committee, who were in Washington for annual visits to Capitol Hill, had just met with CMS’s Chief Medical Officer Tom Valuck, MD.
“That same morning, Tom Valuck had spent an hour and a half briefing Public Policy Committee members on Medicare’s value-based purchasing plan,” says Allendorf. “I’d lined up that meeting before the roundtable was set up.”
A transition to CMS’s proposed value-based purchasing plan, or VBP, would probably occur over three years. Under the plan, a percentage of the hospital’s diagnosis related group (DRG) payment would rely on the hospital’s performance on a specific set of measures. Although the report is comprehensive, details on implementation, incentives, and more must be made final.
Public reporting of quality measures remains a key part of the plan; quality of care information would be available to patients through the CMS Hospital Compare site at www.medicare.gov. A PDF of the CMS report to Congress is available at www.cms.hhs.gov/center/hospital.asp.
Support For Harmonization
After the formal presentation on the VBP plan, roundtable moderator John Inglehart, founding editor of Health Affairs, asked a series of questions directed at specific segments of the group, targeting issues surrounding the plan’s quality measures, performance standards, incentives, and plan implementation.
Dr. Holman was asked to comment on how CMS could ensure that hospital measures and physician measures become more aligned.
“The measures that each party are asked to report in terms of Part B of Medicare are somewhat different and can lead to confusion and people working at cross purposes,” Dr. Holman explains. “This adds complexity to a system that’s already too complex. In my statement, I said that what we call harmonization [of reporting measures] is a very important step for CMS to take, so that physicians and hospitals are required to measure and report the same thing. The more we can move toward outcome measures, as well as efficiency and patient experience measures, the more harmonization we’ll have. Focusing on outcomes creates a common goal.”
Dr. Holman continued his comments to the roundtable by using an example of harmonization at the heart of hospital medicine: transitions of care. “I let the group know that SHM is working on a number of initiatives regarding care transitions,” he says. “Transitions of care require the whole system to come together; it’s a great way to help galvanize all the stakeholders toward that shared goal.”
In his written statement, Dr. Holman elaborated on SHM’s efforts regarding transitions of care and pushed for an alignment of CMS quality measures and incentives for physicians with those for hospitals.
Air of Excitement
Although they had many concerns about implementation, the roundtable participants were enthusiastic about the plan. “There was a fabulous give-and-take on issues regarding implementation,” says Allendorf.
Dr. Holman stayed after the meeting to discuss the proceedings with other participants. “All in all, the informal comments I heard after the meeting were that this was the most exciting moment they’d had in 30-plus years in healthcare,” he notes. “This marks a substantial change in the payment system, which has always been seen as a barrier to quality.”
What’s Next
The ball is now in the court of Sens. Baucus and Grassley, who will use the roundtable input to draft legislation that would make the necessary statutory changes in time for CMS to implement the plan by fiscal year 2009, or Oct. 1, as mandated by the Deficit Reduction Act (DRA) of 2005.
“I think they’ll be back in touch with [SHM] as they develop the plan,” Allendorf predicts. After the legislation has been submitted, it’s up to Congress to act. “Everything depends on whether any Medicare legislation moves this year, and no one know whether that will happen,” she says.
Whatever final form the CMS plan takes, the future looks bright for value-based purchasing—and for SHM’s continued involvement.
“This roundtable was an excellent opportunity for SHM to develop a relationship with CMS, and to link to the Senate Finance Committee,” Dr. Holman asserts. “My hope is that those relationships will bear fruit over time, and that we can continue to work with those entities, as well as the other roundtable participants, to propose and develop measures over time, and to bring alignment between hospital measures and physician measures.”
Jane Jerrard is a medical writer based in Chicago.
Read More Online
For more information on the roundtable, including Dr. Holman’s written statement and others, as well as a recorded Webcast, visit Sen. Baucus’ Web site at www.senate.gov/~finance/sitepages/VBProundtable030408.htm. TH
Consult for an HMG

Consult for an HMG
Question: We are an established hospitalist group going on two years. We started with two full-time physicians and now have five. We obviously have room for improvement and growth. Are there any hospitalist physician consultants who would be able to spend a couple of days with us to evaluate our program and review our systems?
Montell Hutchison,
Business Development Specialist,
Marietta Memorial Hospital,
Marietta, Ohio
Dr. Hospitalist responds: Since the term hospitalist was coined in 1996, the field has grown rapidly. The majority of hospitalist programs are less than five years old. Many hospitalist programs, having grown rapidly over the past few years, are planning to evaluate and improve their performance.
There are a number of options available to help programs benchmark themselves to industry standards. Hiring a consultant is certainly a reasonable choice. SHM has been a particularly valuable resource to help leaders understand how to evaluate their program.
On the Practice Resource section of its Web site (www.hospitalmedicine.org), SHM provides the names and descriptions of several practice management consultants. Also on the site is the downloadable dashboard white paper “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards,” developed by the SHM Benchmarks Committee.
The white paper discusses “issues related to developing, reporting and interpreting performance data.” SHM has also developed the practice management course “Best Practices in Managing a Hospital Medicine Program” and published the book Hospitalists: A Guide to Building and Sustaining a Successful Career to assist those interested in evaluating and improving their hospitalist program.
Lastly, SHM surveys hospitalists every other year to gather productivity and compensation date. The results of the latest “Bi-Annual Survey on the State of the Hospital Medicine Movement” will be released at the SHM Annual Meeting in San Diego April 3-5. Survey information will be available on its Web site shortly thereafter.
Lend A Hand
Question: I am a certified diabetes educator with 20 years’ experience in diabetes. I’m about to graduate as an adult nurse practitioner (ANP). My goal is to work with management of inpatient diabetes. Are you aware of any models of ANPs working for or with hospitalists?
Potential Team Member, Ohio
Dr. Hospitalist responds: There are about 20,000 hospitalists in the country. SHM believes that number could grow to 40,000. I am not surprised by the size of that estimate. Just about every hospital I know wants to develop or expand its hospitalist program.
Hospital medicine has filled its ranks over the past decade largely at the expense of primary care. Many physicians have left primary care for hospital medicine. At the same time, many graduates of internal medicine and family medicine training programs have chosen employment in hospital medicine instead of outpatient medicine.
Despite this trend, we are still short of hospitalists. The long-term solution is to expand the numbers of trainees who choose hospital medicine as a career. We are unlikely to see that occur rapidly over the short term. Another potential solution is to increase hospitalist efficiency.
Many in the field are working to redesign systems in the hospital to increase hospitalist efficiency and productivity. Again, these efforts will take time. Adding non-physician providers as care extenders is another viable option many programs are exploring. The results of the latest SHM productivity and compensation survey “Bi-Annual Survey on the State of the Hospital Medicine Movement” being released in April will give a sense of how many midlevel providers (nurse practitioners and physicians’ assistants) are working in hospitalist programs. It will not, however, fully describe their roles and responsibilities. I suspect more hospitalist programs are employing midlevel providers, but the majority of programs do not have midlevel providers among their staff.
For hospitalist programs entertaining the notion of hiring a midlevel provider (and for those midlevel providers interested in joining a hospitalist program), there are barriers to such a relationship. One inherent problem is that most hospitalists do not understand how to work with midlevel providers. Many hospitalists are unaware of the midlevel providers’ education and training.
I am not surprised. Most hospitalists did not work with midlevel providers during their training. There are not only differences in education and training among nurse practitioners (NPs) and physicians’ assistants (PAs), but many state licensing boards also limit their scopes of practice in a different manner. I find that many hospitalists want their midlevel providers to do the scut work hospitalists don’t want to do or feel they don’t have time to do.
I feel this is an expensive way to hire someone to do discharge summaries, put in orders, and make follow-up appointments. One does not need a midlevel education and training to perform those tasks. I suspect most midlevel providers—like hospitalists—find these tasks unsatisfying if it is the majority of their job description. Hospitalist programs would be better served if they involved midlevel providers in the care of patients. But this will require additional training to help hospitalist understand the level of supervision that is necessary for midlevel providers.
For hospitalists who work with midlevel providers, I find too often that many provide too much or too little supervision. Neither is appropriate. Another barrier in some parts of the country relates to the compensation of hospitalists and midlevel providers.
In the Northeast and on the West Coast, for example, we find smaller differences between hospitalist and NP salaries. Since NPs bill at 85% of physician billing, it may not necessarily make financial sense to hire NPs when one can hire a physician at slightly higher cost.
I hope I have not dissuaded you from pursuing a job in hospital medicine. I believe the development of roles for midlevel providers in hospital medicine is critical to the continued expansion of hospital medicine in this country.
I implore hospitalists and midlevel providers to work together to explore and establish models of care that will provide sustainable career opportunities for midlevel providers in hospital medicine. TH
Consult for an HMG
Question: We are an established hospitalist group going on two years. We started with two full-time physicians and now have five. We obviously have room for improvement and growth. Are there any hospitalist physician consultants who would be able to spend a couple of days with us to evaluate our program and review our systems?
Montell Hutchison,
Business Development Specialist,
Marietta Memorial Hospital,
Marietta, Ohio
Dr. Hospitalist responds: Since the term hospitalist was coined in 1996, the field has grown rapidly. The majority of hospitalist programs are less than five years old. Many hospitalist programs, having grown rapidly over the past few years, are planning to evaluate and improve their performance.
There are a number of options available to help programs benchmark themselves to industry standards. Hiring a consultant is certainly a reasonable choice. SHM has been a particularly valuable resource to help leaders understand how to evaluate their program.
On the Practice Resource section of its Web site (www.hospitalmedicine.org), SHM provides the names and descriptions of several practice management consultants. Also on the site is the downloadable dashboard white paper “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards,” developed by the SHM Benchmarks Committee.
The white paper discusses “issues related to developing, reporting and interpreting performance data.” SHM has also developed the practice management course “Best Practices in Managing a Hospital Medicine Program” and published the book Hospitalists: A Guide to Building and Sustaining a Successful Career to assist those interested in evaluating and improving their hospitalist program.
Lastly, SHM surveys hospitalists every other year to gather productivity and compensation date. The results of the latest “Bi-Annual Survey on the State of the Hospital Medicine Movement” will be released at the SHM Annual Meeting in San Diego April 3-5. Survey information will be available on its Web site shortly thereafter.
Lend A Hand
Question: I am a certified diabetes educator with 20 years’ experience in diabetes. I’m about to graduate as an adult nurse practitioner (ANP). My goal is to work with management of inpatient diabetes. Are you aware of any models of ANPs working for or with hospitalists?
Potential Team Member, Ohio
Dr. Hospitalist responds: There are about 20,000 hospitalists in the country. SHM believes that number could grow to 40,000. I am not surprised by the size of that estimate. Just about every hospital I know wants to develop or expand its hospitalist program.
Hospital medicine has filled its ranks over the past decade largely at the expense of primary care. Many physicians have left primary care for hospital medicine. At the same time, many graduates of internal medicine and family medicine training programs have chosen employment in hospital medicine instead of outpatient medicine.
Despite this trend, we are still short of hospitalists. The long-term solution is to expand the numbers of trainees who choose hospital medicine as a career. We are unlikely to see that occur rapidly over the short term. Another potential solution is to increase hospitalist efficiency.
Many in the field are working to redesign systems in the hospital to increase hospitalist efficiency and productivity. Again, these efforts will take time. Adding non-physician providers as care extenders is another viable option many programs are exploring. The results of the latest SHM productivity and compensation survey “Bi-Annual Survey on the State of the Hospital Medicine Movement” being released in April will give a sense of how many midlevel providers (nurse practitioners and physicians’ assistants) are working in hospitalist programs. It will not, however, fully describe their roles and responsibilities. I suspect more hospitalist programs are employing midlevel providers, but the majority of programs do not have midlevel providers among their staff.
For hospitalist programs entertaining the notion of hiring a midlevel provider (and for those midlevel providers interested in joining a hospitalist program), there are barriers to such a relationship. One inherent problem is that most hospitalists do not understand how to work with midlevel providers. Many hospitalists are unaware of the midlevel providers’ education and training.
I am not surprised. Most hospitalists did not work with midlevel providers during their training. There are not only differences in education and training among nurse practitioners (NPs) and physicians’ assistants (PAs), but many state licensing boards also limit their scopes of practice in a different manner. I find that many hospitalists want their midlevel providers to do the scut work hospitalists don’t want to do or feel they don’t have time to do.
I feel this is an expensive way to hire someone to do discharge summaries, put in orders, and make follow-up appointments. One does not need a midlevel education and training to perform those tasks. I suspect most midlevel providers—like hospitalists—find these tasks unsatisfying if it is the majority of their job description. Hospitalist programs would be better served if they involved midlevel providers in the care of patients. But this will require additional training to help hospitalist understand the level of supervision that is necessary for midlevel providers.
For hospitalists who work with midlevel providers, I find too often that many provide too much or too little supervision. Neither is appropriate. Another barrier in some parts of the country relates to the compensation of hospitalists and midlevel providers.
In the Northeast and on the West Coast, for example, we find smaller differences between hospitalist and NP salaries. Since NPs bill at 85% of physician billing, it may not necessarily make financial sense to hire NPs when one can hire a physician at slightly higher cost.
I hope I have not dissuaded you from pursuing a job in hospital medicine. I believe the development of roles for midlevel providers in hospital medicine is critical to the continued expansion of hospital medicine in this country.
I implore hospitalists and midlevel providers to work together to explore and establish models of care that will provide sustainable career opportunities for midlevel providers in hospital medicine. TH
Consult for an HMG
Question: We are an established hospitalist group going on two years. We started with two full-time physicians and now have five. We obviously have room for improvement and growth. Are there any hospitalist physician consultants who would be able to spend a couple of days with us to evaluate our program and review our systems?
Montell Hutchison,
Business Development Specialist,
Marietta Memorial Hospital,
Marietta, Ohio
Dr. Hospitalist responds: Since the term hospitalist was coined in 1996, the field has grown rapidly. The majority of hospitalist programs are less than five years old. Many hospitalist programs, having grown rapidly over the past few years, are planning to evaluate and improve their performance.
There are a number of options available to help programs benchmark themselves to industry standards. Hiring a consultant is certainly a reasonable choice. SHM has been a particularly valuable resource to help leaders understand how to evaluate their program.
On the Practice Resource section of its Web site (www.hospitalmedicine.org), SHM provides the names and descriptions of several practice management consultants. Also on the site is the downloadable dashboard white paper “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards,” developed by the SHM Benchmarks Committee.
The white paper discusses “issues related to developing, reporting and interpreting performance data.” SHM has also developed the practice management course “Best Practices in Managing a Hospital Medicine Program” and published the book Hospitalists: A Guide to Building and Sustaining a Successful Career to assist those interested in evaluating and improving their hospitalist program.
Lastly, SHM surveys hospitalists every other year to gather productivity and compensation date. The results of the latest “Bi-Annual Survey on the State of the Hospital Medicine Movement” will be released at the SHM Annual Meeting in San Diego April 3-5. Survey information will be available on its Web site shortly thereafter.
Lend A Hand
Question: I am a certified diabetes educator with 20 years’ experience in diabetes. I’m about to graduate as an adult nurse practitioner (ANP). My goal is to work with management of inpatient diabetes. Are you aware of any models of ANPs working for or with hospitalists?
Potential Team Member, Ohio
Dr. Hospitalist responds: There are about 20,000 hospitalists in the country. SHM believes that number could grow to 40,000. I am not surprised by the size of that estimate. Just about every hospital I know wants to develop or expand its hospitalist program.
Hospital medicine has filled its ranks over the past decade largely at the expense of primary care. Many physicians have left primary care for hospital medicine. At the same time, many graduates of internal medicine and family medicine training programs have chosen employment in hospital medicine instead of outpatient medicine.
Despite this trend, we are still short of hospitalists. The long-term solution is to expand the numbers of trainees who choose hospital medicine as a career. We are unlikely to see that occur rapidly over the short term. Another potential solution is to increase hospitalist efficiency.
Many in the field are working to redesign systems in the hospital to increase hospitalist efficiency and productivity. Again, these efforts will take time. Adding non-physician providers as care extenders is another viable option many programs are exploring. The results of the latest SHM productivity and compensation survey “Bi-Annual Survey on the State of the Hospital Medicine Movement” being released in April will give a sense of how many midlevel providers (nurse practitioners and physicians’ assistants) are working in hospitalist programs. It will not, however, fully describe their roles and responsibilities. I suspect more hospitalist programs are employing midlevel providers, but the majority of programs do not have midlevel providers among their staff.
For hospitalist programs entertaining the notion of hiring a midlevel provider (and for those midlevel providers interested in joining a hospitalist program), there are barriers to such a relationship. One inherent problem is that most hospitalists do not understand how to work with midlevel providers. Many hospitalists are unaware of the midlevel providers’ education and training.
I am not surprised. Most hospitalists did not work with midlevel providers during their training. There are not only differences in education and training among nurse practitioners (NPs) and physicians’ assistants (PAs), but many state licensing boards also limit their scopes of practice in a different manner. I find that many hospitalists want their midlevel providers to do the scut work hospitalists don’t want to do or feel they don’t have time to do.
I feel this is an expensive way to hire someone to do discharge summaries, put in orders, and make follow-up appointments. One does not need a midlevel education and training to perform those tasks. I suspect most midlevel providers—like hospitalists—find these tasks unsatisfying if it is the majority of their job description. Hospitalist programs would be better served if they involved midlevel providers in the care of patients. But this will require additional training to help hospitalist understand the level of supervision that is necessary for midlevel providers.
For hospitalists who work with midlevel providers, I find too often that many provide too much or too little supervision. Neither is appropriate. Another barrier in some parts of the country relates to the compensation of hospitalists and midlevel providers.
In the Northeast and on the West Coast, for example, we find smaller differences between hospitalist and NP salaries. Since NPs bill at 85% of physician billing, it may not necessarily make financial sense to hire NPs when one can hire a physician at slightly higher cost.
I hope I have not dissuaded you from pursuing a job in hospital medicine. I believe the development of roles for midlevel providers in hospital medicine is critical to the continued expansion of hospital medicine in this country.
I implore hospitalists and midlevel providers to work together to explore and establish models of care that will provide sustainable career opportunities for midlevel providers in hospital medicine. TH