User login
The Hospital of the Future
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
Magic Bullets

Patients with acute stroke or transient ischemic attack (TIA) should be admitted to a hospital for initial care and assessment; however, a substantial number of these patients will never be seen by a neurologist because of the limited number of physicians in this specialty area. Currently there is only one neurologist per 26,000 people in the United States, and most neurologists prefer to practice in the outpatient setting.1 According to one study, only 11.3% of stroke patients are attended exclusively by a neurologist.2 Hospitalists play a vital role in overcoming this lack of specialized care for stroke patients.
Pharmacotherapy
A significant body of evidence supports secondary prevention as a critical intervention strategy in reducing stroke risk. Identifying specific risk factors remains pivotal to successful secondary prevention. Managing hypertension, diabetes, and hyperlipidemia serves as an effective preventive role; however, preventive management with antithrombotic agents is an important part of the drug regimen for secondary prevention of recurrent ischemic stroke (IS).3
The choice of pharmacologic agents is based on stroke etiology. Anticoagulants such as warfarin are restricted to patients with stroke due to a cardioembolic source, whereas antiplatelet agents are mainly used to treat noncardioembolic and lacunar strokes.4 Currently, four oral antiplatelet agents may be used as therapy to prevent secondary IS: aspirin (acetylsalicylic acid or ASA), ticlopidine, clopidogrel, and ASA plus extended-release dipyridamole.
Aspirin
ASA is the most widely used and cost-effective antiplatelet agent. A salicylate, it blocks platelet activation by inhibiting the cyclo-oxygenase enzymes (COX-1 and COX-2). In several primary prevention trials ASA was associated with a statistically significant reduction in risk of first myocardial infarction (MI). Neither overall cardiovascular mortality nor total number of strokes was reduced by long-term ASA prophylaxis, however.5
ASA was shown to be effective in secondary prevention of noncardioembolic stroke (offering equivalent or better efficacy compared with warfarin) in the Stroke Prevention in Reversible Ischemia Trial and the Warfarin-Aspirin Recurrent Stroke Study.6 The Swedish Aspirin Low-Dose Trial, Dutch TIA Trial, and United Kingdom Transient Ischaemic Attack Aspirin Trial consistently demonstrated the efficacy and reduced gastric toxicity of low-dose ASA.7 A meta-analysis of 197 randomized trials versus control and 90 randomized comparisons between antiplatelet regimens show risk reduction with ASA of approximately 23% in combined vascular events (MI, stroke, and vascular death).8
Ticlopidine
Ticlopidine hydrochloride (thienopyridine) blocks platelet activation by inhibiting adenosine diphosphate-induced fibrinogen binding.7 Ticlopidine was superior to placebo and high-dose ASA in reducing the occurrence of stroke, MI, or vascular death in patients of both genders who had recent cerebral ischemia. This was demonstrated in two major phase 3 multicenter trials: the Ticlopidine Aspirin Stroke Study and the Canadian American Ticlopidine Study.9 Despite ticlopidine’s efficacy in these trials, the drug has been associated with severe adverse effects, including life-threatening neutropenia (1%) and thrombocytopenic purpura (one per 1,600 to 5,000 patients treated).3
Clopidogrel
The ticlopidine analogue clopidogrel is a potent inhibitor of platelet aggregation induced by adenosine diphosphate.7 The efficacy and safety of clopidogrel was evaluated in a randomized, double-blind, multicenter study—the Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events trial, the largest clinical study of clopidogrel—of 19,000 patients with stroke, MI, or peripheral arterial disease.10
In this study, clopidogrel showed a more favorable safety and tolerability profile than ticlopidine; however, compared with ASA clopidogrel offered only a modest benefit of 8.7% for all cardiovascular events and showed no significant benefit over ASA for recurrent stroke.
Findings from two randomized trials—Clopidogrel in Unstable Angina to Prevent Recurrent Ischemic Events (CURE) and Clopidogrel for the Reduction of Events During Observation (CREDO)—have shown sustained benefits of clopidogrel for combined endpoints of MI, stroke, and vascular death.11-12 The incidence of stroke was very small and the risk of serious bleeding was significantly increased.
These trials provided the rationale to undertake the Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attack or Ischemic Stroke study (MATCH).13 This study was designed to determine whether the addition of ASA to clopidogrel would further reduce the risk of recurrent ischemic attacks in high-risk patients after recent IS or TIA, as was observed with coronary manifestations of atherothrombosis in the CURE and CREDO trials.
MATCH, a randomized, double-blind, placebo-controlled trial, involved 7,599 patients and compared clopidogrel with low-dose ASA plus clopidogrel. During an 18-month follow-up, no significant benefit was observed for ASA plus clopidogrel versus clopidogrel monotherapy; however, there was a significant increase in the risk of life-threatening bleeding in the group receiving combined therapy (2.6% versus 1.3%, respectively). Therefore, ASA plus clopidogrel is not a recommended option for prevention of secondary stroke in cerebrovascular patients.
STROKE
The scope of the problem

Stroke is one of the most significant health problems in the United States. Approximately 700,000 strokes and occur each year. Of these, 200,000 are recurrent strokes.18 Extensive studies have identified increasing age as the leading risk factor for stroke.16
Approximately 72% of stroke patients are older than 65; on average, patients with stroke tend to be older than patients with MI.4-19 Thus, the frequency of stroke will increase dramatically with lengthening of life expectancy and advancing age of our population.
A history of TIA poses another strong risk factor for stroke. Each year approximately 300,000 Americans suffer TIAs; about one-third of these people will develop a stroke.20-21 Risk factors include hypertension, cigarette smoking, diabetes mellitus, hyperlipidemia, obesity, and heart disease.—SS
ASA Plus Extended-Release Dipyridamole
The Second European Stroke Prevention Study (ESPS-2), a randomized trial with 2,500 patients, was conducted to compare the efficacy of ASA plus dipyridamole versus placebo. Dipyridamole is a pyrimidopyrimidine derivative from the papaverine family with antithrombotic properties and vasodilatory effects on cells and vasculature.14 It inhibits phosphodiesterases, resulting in increased concentration of cyclic adenosine monophosphate (cAMP) and cyclic guanine monophosphate (cGMP), which inhibits platelet activation and adhesion.14
ESPS-2 results showed a 38% relative reduction in risk of stroke for the combination versus placebo. The study did not include an ASA-only group. Results prompted reformulation of dipyridamole into a high-dose extended-release capsule combined with low-dose ASA. The higher dose and slower release of dipyridamole combined with ASA provides a more consistent plasma level and is less affected by stomach acidity or concomitant medications.
This combination was tested versus ASA alone in the ESPS-2 trial.15 ESPS-2, a randomized, double-blind, multicenter study, enrolled 6,602 patients with prior stroke or TIA. During the two-year follow-up ASA plus extended-release dipyridamole reduced the risk of recurrent stroke by 37% compared with placebo, and by 22% compared with ASA or dipyridamole alone. Adverse events associated with this combination are similar to those observed with low-dose ASA.
These results were further substantiated by a recent post hoc analysis conducted using data from the ESPS-2 trial. ASA plus extended-release dipyridamole had greater efficacy in preventing stroke than ASA; this difference in efficacy was more pronounced in high-risk patients.16
We need further studies that include direct comparisons to verify the most effective and safe antiplatelet agent for secondary stroke prevention. The Prospective Regimen for Effectively Avoiding Second Strokes (PRoFESS) is a head-to-head trial designed to compare the combination of ASA plus extended-release dipyridamole to clopidogrel in terms of efficacy and safety. This study includes 15,500 patients in more than 20 countries at approximately 600 sites.17
Conclusions
Stroke remains a major public health concern. Hospitalists play a central role in stroke management by improving the overall quality of hospital care for stroke patients. Still, most residency programs don’t provide sufficient stroke education. Therefore, comprehensive neurology educational programs should be provided for hospitalists so they can provide efficient inpatient care; initiate effective secondary prevention strategies tailored to the specific needs of the patients, starting with appropriate antiplatelet therapy; monitor patients at poststroke rehabilitation centers during recovery period; and educate stroke patients and their caregivers about the disease and its risk factors.
Hospitalists can also initiate effective communication with outpatient primary care providers at the time of discharge to help ensure that the secondary prevention strategies initiated in the hospital are not only continued but strengthened. TH
Dr. Sachdeva is lead hospitalist in the Stroke Program at the Swedish Medical Center, Seattle, and clinical instructor at the University of Washington, Seattle.
References
- Kmietowicz Z. United Kingdom needs to double the number of neurologists. BMJ. 2001;322:1508.
- Ringel SP. The neurologist’s role in stroke management. Stroke. 1996; 27(11):1935-1936.
- Weinberger J. Adverse effects and drug interactions of antithrombotic agents used in prevention of ischaemic stroke. Drugs. 2005;65(4):461-471.
- Weinberger J. Managing and preventing ischemic stroke: Part II—risk assessment and prevention of secondary ischemic stroke. Clin Geriatr. 2004;12(8):41-46.
- Patrono C, Coller B, Dalen JF. Platelet-active drugs: the relationship among dose, effectiveness and side effects. Chest. 2001:119(suppl):39S-63S.
- Fayad P, Singh SP. Anti-thrombotic therapy for the secondary prevention of ischemic stroke. Chest. 2004;126(3):483S-512S.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke. Chest. 2001;119(suppl):300S-320S.
- Antiplatelet Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;12;324(7329):71-86.
- Robert S, Miller AJ, Fagan SC. Ticlopidine: a new antiplatelet agent for cerebrovascular disease. Pharmacotherapy. 1991;11(4):317-322.
- CAPRIE Steering Committee. A randomized, blinded trial of clopidogrel versus aspirin in patients at risk for ischemic events. Lancet. 1996;348:1329-1339.
- Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345(7):494-502.
- Steinhubl SR, Berger PB, Mann JT 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288(19):2411-2420.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331-337.
- European Stroke Prevention Study. ESPS Group. Stroke. 1990;21(8):1122-1130.20
- Diener HC, Cunha L, Forbes C, et al. European stroke prevention study. 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143(1-2):1-13.
- Sacco RL, Sivenius J, Diener HC. Efficacy of aspirin plus extended-release dipyridamole in preventing recurrent stroke in high-risk populations. Arch Neurol. 2005;62:403-408.
- PRoFESS Web site. Available at: www.profess-study.com/com/Main/newscentre/news_040604.jsp. Last accessed July 18, 2005
- Weinberger J. Managing and preventing ischemic stroke: Part I—risk assessment and treatment of primary ischemic stroke. Clin Geriatr. 2004;12(7):48-53.
- Heart Disease and Stroke Statistics—2005 Update. Dallas, Texas. American Heart Association; Dallas. 2005
- Johnston SC, Gress DR, Browner WS, et al. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901-2906.
- Feinberg WM, Albers GW, Barnett H, et al. Guidelines for the management of transient ischemic attacks. Stroke. 1994;25:1320-1335.
Patients with acute stroke or transient ischemic attack (TIA) should be admitted to a hospital for initial care and assessment; however, a substantial number of these patients will never be seen by a neurologist because of the limited number of physicians in this specialty area. Currently there is only one neurologist per 26,000 people in the United States, and most neurologists prefer to practice in the outpatient setting.1 According to one study, only 11.3% of stroke patients are attended exclusively by a neurologist.2 Hospitalists play a vital role in overcoming this lack of specialized care for stroke patients.
Pharmacotherapy
A significant body of evidence supports secondary prevention as a critical intervention strategy in reducing stroke risk. Identifying specific risk factors remains pivotal to successful secondary prevention. Managing hypertension, diabetes, and hyperlipidemia serves as an effective preventive role; however, preventive management with antithrombotic agents is an important part of the drug regimen for secondary prevention of recurrent ischemic stroke (IS).3
The choice of pharmacologic agents is based on stroke etiology. Anticoagulants such as warfarin are restricted to patients with stroke due to a cardioembolic source, whereas antiplatelet agents are mainly used to treat noncardioembolic and lacunar strokes.4 Currently, four oral antiplatelet agents may be used as therapy to prevent secondary IS: aspirin (acetylsalicylic acid or ASA), ticlopidine, clopidogrel, and ASA plus extended-release dipyridamole.
Aspirin
ASA is the most widely used and cost-effective antiplatelet agent. A salicylate, it blocks platelet activation by inhibiting the cyclo-oxygenase enzymes (COX-1 and COX-2). In several primary prevention trials ASA was associated with a statistically significant reduction in risk of first myocardial infarction (MI). Neither overall cardiovascular mortality nor total number of strokes was reduced by long-term ASA prophylaxis, however.5
ASA was shown to be effective in secondary prevention of noncardioembolic stroke (offering equivalent or better efficacy compared with warfarin) in the Stroke Prevention in Reversible Ischemia Trial and the Warfarin-Aspirin Recurrent Stroke Study.6 The Swedish Aspirin Low-Dose Trial, Dutch TIA Trial, and United Kingdom Transient Ischaemic Attack Aspirin Trial consistently demonstrated the efficacy and reduced gastric toxicity of low-dose ASA.7 A meta-analysis of 197 randomized trials versus control and 90 randomized comparisons between antiplatelet regimens show risk reduction with ASA of approximately 23% in combined vascular events (MI, stroke, and vascular death).8
Ticlopidine
Ticlopidine hydrochloride (thienopyridine) blocks platelet activation by inhibiting adenosine diphosphate-induced fibrinogen binding.7 Ticlopidine was superior to placebo and high-dose ASA in reducing the occurrence of stroke, MI, or vascular death in patients of both genders who had recent cerebral ischemia. This was demonstrated in two major phase 3 multicenter trials: the Ticlopidine Aspirin Stroke Study and the Canadian American Ticlopidine Study.9 Despite ticlopidine’s efficacy in these trials, the drug has been associated with severe adverse effects, including life-threatening neutropenia (1%) and thrombocytopenic purpura (one per 1,600 to 5,000 patients treated).3
Clopidogrel
The ticlopidine analogue clopidogrel is a potent inhibitor of platelet aggregation induced by adenosine diphosphate.7 The efficacy and safety of clopidogrel was evaluated in a randomized, double-blind, multicenter study—the Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events trial, the largest clinical study of clopidogrel—of 19,000 patients with stroke, MI, or peripheral arterial disease.10
In this study, clopidogrel showed a more favorable safety and tolerability profile than ticlopidine; however, compared with ASA clopidogrel offered only a modest benefit of 8.7% for all cardiovascular events and showed no significant benefit over ASA for recurrent stroke.
Findings from two randomized trials—Clopidogrel in Unstable Angina to Prevent Recurrent Ischemic Events (CURE) and Clopidogrel for the Reduction of Events During Observation (CREDO)—have shown sustained benefits of clopidogrel for combined endpoints of MI, stroke, and vascular death.11-12 The incidence of stroke was very small and the risk of serious bleeding was significantly increased.
These trials provided the rationale to undertake the Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attack or Ischemic Stroke study (MATCH).13 This study was designed to determine whether the addition of ASA to clopidogrel would further reduce the risk of recurrent ischemic attacks in high-risk patients after recent IS or TIA, as was observed with coronary manifestations of atherothrombosis in the CURE and CREDO trials.
MATCH, a randomized, double-blind, placebo-controlled trial, involved 7,599 patients and compared clopidogrel with low-dose ASA plus clopidogrel. During an 18-month follow-up, no significant benefit was observed for ASA plus clopidogrel versus clopidogrel monotherapy; however, there was a significant increase in the risk of life-threatening bleeding in the group receiving combined therapy (2.6% versus 1.3%, respectively). Therefore, ASA plus clopidogrel is not a recommended option for prevention of secondary stroke in cerebrovascular patients.
STROKE
The scope of the problem
Stroke is one of the most significant health problems in the United States. Approximately 700,000 strokes and occur each year. Of these, 200,000 are recurrent strokes.18 Extensive studies have identified increasing age as the leading risk factor for stroke.16
Approximately 72% of stroke patients are older than 65; on average, patients with stroke tend to be older than patients with MI.4-19 Thus, the frequency of stroke will increase dramatically with lengthening of life expectancy and advancing age of our population.
A history of TIA poses another strong risk factor for stroke. Each year approximately 300,000 Americans suffer TIAs; about one-third of these people will develop a stroke.20-21 Risk factors include hypertension, cigarette smoking, diabetes mellitus, hyperlipidemia, obesity, and heart disease.—SS
ASA Plus Extended-Release Dipyridamole
The Second European Stroke Prevention Study (ESPS-2), a randomized trial with 2,500 patients, was conducted to compare the efficacy of ASA plus dipyridamole versus placebo. Dipyridamole is a pyrimidopyrimidine derivative from the papaverine family with antithrombotic properties and vasodilatory effects on cells and vasculature.14 It inhibits phosphodiesterases, resulting in increased concentration of cyclic adenosine monophosphate (cAMP) and cyclic guanine monophosphate (cGMP), which inhibits platelet activation and adhesion.14
ESPS-2 results showed a 38% relative reduction in risk of stroke for the combination versus placebo. The study did not include an ASA-only group. Results prompted reformulation of dipyridamole into a high-dose extended-release capsule combined with low-dose ASA. The higher dose and slower release of dipyridamole combined with ASA provides a more consistent plasma level and is less affected by stomach acidity or concomitant medications.
This combination was tested versus ASA alone in the ESPS-2 trial.15 ESPS-2, a randomized, double-blind, multicenter study, enrolled 6,602 patients with prior stroke or TIA. During the two-year follow-up ASA plus extended-release dipyridamole reduced the risk of recurrent stroke by 37% compared with placebo, and by 22% compared with ASA or dipyridamole alone. Adverse events associated with this combination are similar to those observed with low-dose ASA.
These results were further substantiated by a recent post hoc analysis conducted using data from the ESPS-2 trial. ASA plus extended-release dipyridamole had greater efficacy in preventing stroke than ASA; this difference in efficacy was more pronounced in high-risk patients.16
We need further studies that include direct comparisons to verify the most effective and safe antiplatelet agent for secondary stroke prevention. The Prospective Regimen for Effectively Avoiding Second Strokes (PRoFESS) is a head-to-head trial designed to compare the combination of ASA plus extended-release dipyridamole to clopidogrel in terms of efficacy and safety. This study includes 15,500 patients in more than 20 countries at approximately 600 sites.17
Conclusions
Stroke remains a major public health concern. Hospitalists play a central role in stroke management by improving the overall quality of hospital care for stroke patients. Still, most residency programs don’t provide sufficient stroke education. Therefore, comprehensive neurology educational programs should be provided for hospitalists so they can provide efficient inpatient care; initiate effective secondary prevention strategies tailored to the specific needs of the patients, starting with appropriate antiplatelet therapy; monitor patients at poststroke rehabilitation centers during recovery period; and educate stroke patients and their caregivers about the disease and its risk factors.
Hospitalists can also initiate effective communication with outpatient primary care providers at the time of discharge to help ensure that the secondary prevention strategies initiated in the hospital are not only continued but strengthened. TH
Dr. Sachdeva is lead hospitalist in the Stroke Program at the Swedish Medical Center, Seattle, and clinical instructor at the University of Washington, Seattle.
References
- Kmietowicz Z. United Kingdom needs to double the number of neurologists. BMJ. 2001;322:1508.
- Ringel SP. The neurologist’s role in stroke management. Stroke. 1996; 27(11):1935-1936.
- Weinberger J. Adverse effects and drug interactions of antithrombotic agents used in prevention of ischaemic stroke. Drugs. 2005;65(4):461-471.
- Weinberger J. Managing and preventing ischemic stroke: Part II—risk assessment and prevention of secondary ischemic stroke. Clin Geriatr. 2004;12(8):41-46.
- Patrono C, Coller B, Dalen JF. Platelet-active drugs: the relationship among dose, effectiveness and side effects. Chest. 2001:119(suppl):39S-63S.
- Fayad P, Singh SP. Anti-thrombotic therapy for the secondary prevention of ischemic stroke. Chest. 2004;126(3):483S-512S.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke. Chest. 2001;119(suppl):300S-320S.
- Antiplatelet Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;12;324(7329):71-86.
- Robert S, Miller AJ, Fagan SC. Ticlopidine: a new antiplatelet agent for cerebrovascular disease. Pharmacotherapy. 1991;11(4):317-322.
- CAPRIE Steering Committee. A randomized, blinded trial of clopidogrel versus aspirin in patients at risk for ischemic events. Lancet. 1996;348:1329-1339.
- Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345(7):494-502.
- Steinhubl SR, Berger PB, Mann JT 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288(19):2411-2420.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331-337.
- European Stroke Prevention Study. ESPS Group. Stroke. 1990;21(8):1122-1130.20
- Diener HC, Cunha L, Forbes C, et al. European stroke prevention study. 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143(1-2):1-13.
- Sacco RL, Sivenius J, Diener HC. Efficacy of aspirin plus extended-release dipyridamole in preventing recurrent stroke in high-risk populations. Arch Neurol. 2005;62:403-408.
- PRoFESS Web site. Available at: www.profess-study.com/com/Main/newscentre/news_040604.jsp. Last accessed July 18, 2005
- Weinberger J. Managing and preventing ischemic stroke: Part I—risk assessment and treatment of primary ischemic stroke. Clin Geriatr. 2004;12(7):48-53.
- Heart Disease and Stroke Statistics—2005 Update. Dallas, Texas. American Heart Association; Dallas. 2005
- Johnston SC, Gress DR, Browner WS, et al. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901-2906.
- Feinberg WM, Albers GW, Barnett H, et al. Guidelines for the management of transient ischemic attacks. Stroke. 1994;25:1320-1335.
Patients with acute stroke or transient ischemic attack (TIA) should be admitted to a hospital for initial care and assessment; however, a substantial number of these patients will never be seen by a neurologist because of the limited number of physicians in this specialty area. Currently there is only one neurologist per 26,000 people in the United States, and most neurologists prefer to practice in the outpatient setting.1 According to one study, only 11.3% of stroke patients are attended exclusively by a neurologist.2 Hospitalists play a vital role in overcoming this lack of specialized care for stroke patients.
Pharmacotherapy
A significant body of evidence supports secondary prevention as a critical intervention strategy in reducing stroke risk. Identifying specific risk factors remains pivotal to successful secondary prevention. Managing hypertension, diabetes, and hyperlipidemia serves as an effective preventive role; however, preventive management with antithrombotic agents is an important part of the drug regimen for secondary prevention of recurrent ischemic stroke (IS).3
The choice of pharmacologic agents is based on stroke etiology. Anticoagulants such as warfarin are restricted to patients with stroke due to a cardioembolic source, whereas antiplatelet agents are mainly used to treat noncardioembolic and lacunar strokes.4 Currently, four oral antiplatelet agents may be used as therapy to prevent secondary IS: aspirin (acetylsalicylic acid or ASA), ticlopidine, clopidogrel, and ASA plus extended-release dipyridamole.
Aspirin
ASA is the most widely used and cost-effective antiplatelet agent. A salicylate, it blocks platelet activation by inhibiting the cyclo-oxygenase enzymes (COX-1 and COX-2). In several primary prevention trials ASA was associated with a statistically significant reduction in risk of first myocardial infarction (MI). Neither overall cardiovascular mortality nor total number of strokes was reduced by long-term ASA prophylaxis, however.5
ASA was shown to be effective in secondary prevention of noncardioembolic stroke (offering equivalent or better efficacy compared with warfarin) in the Stroke Prevention in Reversible Ischemia Trial and the Warfarin-Aspirin Recurrent Stroke Study.6 The Swedish Aspirin Low-Dose Trial, Dutch TIA Trial, and United Kingdom Transient Ischaemic Attack Aspirin Trial consistently demonstrated the efficacy and reduced gastric toxicity of low-dose ASA.7 A meta-analysis of 197 randomized trials versus control and 90 randomized comparisons between antiplatelet regimens show risk reduction with ASA of approximately 23% in combined vascular events (MI, stroke, and vascular death).8
Ticlopidine
Ticlopidine hydrochloride (thienopyridine) blocks platelet activation by inhibiting adenosine diphosphate-induced fibrinogen binding.7 Ticlopidine was superior to placebo and high-dose ASA in reducing the occurrence of stroke, MI, or vascular death in patients of both genders who had recent cerebral ischemia. This was demonstrated in two major phase 3 multicenter trials: the Ticlopidine Aspirin Stroke Study and the Canadian American Ticlopidine Study.9 Despite ticlopidine’s efficacy in these trials, the drug has been associated with severe adverse effects, including life-threatening neutropenia (1%) and thrombocytopenic purpura (one per 1,600 to 5,000 patients treated).3
Clopidogrel
The ticlopidine analogue clopidogrel is a potent inhibitor of platelet aggregation induced by adenosine diphosphate.7 The efficacy and safety of clopidogrel was evaluated in a randomized, double-blind, multicenter study—the Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events trial, the largest clinical study of clopidogrel—of 19,000 patients with stroke, MI, or peripheral arterial disease.10
In this study, clopidogrel showed a more favorable safety and tolerability profile than ticlopidine; however, compared with ASA clopidogrel offered only a modest benefit of 8.7% for all cardiovascular events and showed no significant benefit over ASA for recurrent stroke.
Findings from two randomized trials—Clopidogrel in Unstable Angina to Prevent Recurrent Ischemic Events (CURE) and Clopidogrel for the Reduction of Events During Observation (CREDO)—have shown sustained benefits of clopidogrel for combined endpoints of MI, stroke, and vascular death.11-12 The incidence of stroke was very small and the risk of serious bleeding was significantly increased.
These trials provided the rationale to undertake the Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attack or Ischemic Stroke study (MATCH).13 This study was designed to determine whether the addition of ASA to clopidogrel would further reduce the risk of recurrent ischemic attacks in high-risk patients after recent IS or TIA, as was observed with coronary manifestations of atherothrombosis in the CURE and CREDO trials.
MATCH, a randomized, double-blind, placebo-controlled trial, involved 7,599 patients and compared clopidogrel with low-dose ASA plus clopidogrel. During an 18-month follow-up, no significant benefit was observed for ASA plus clopidogrel versus clopidogrel monotherapy; however, there was a significant increase in the risk of life-threatening bleeding in the group receiving combined therapy (2.6% versus 1.3%, respectively). Therefore, ASA plus clopidogrel is not a recommended option for prevention of secondary stroke in cerebrovascular patients.
STROKE
The scope of the problem
Stroke is one of the most significant health problems in the United States. Approximately 700,000 strokes and occur each year. Of these, 200,000 are recurrent strokes.18 Extensive studies have identified increasing age as the leading risk factor for stroke.16
Approximately 72% of stroke patients are older than 65; on average, patients with stroke tend to be older than patients with MI.4-19 Thus, the frequency of stroke will increase dramatically with lengthening of life expectancy and advancing age of our population.
A history of TIA poses another strong risk factor for stroke. Each year approximately 300,000 Americans suffer TIAs; about one-third of these people will develop a stroke.20-21 Risk factors include hypertension, cigarette smoking, diabetes mellitus, hyperlipidemia, obesity, and heart disease.—SS
ASA Plus Extended-Release Dipyridamole
The Second European Stroke Prevention Study (ESPS-2), a randomized trial with 2,500 patients, was conducted to compare the efficacy of ASA plus dipyridamole versus placebo. Dipyridamole is a pyrimidopyrimidine derivative from the papaverine family with antithrombotic properties and vasodilatory effects on cells and vasculature.14 It inhibits phosphodiesterases, resulting in increased concentration of cyclic adenosine monophosphate (cAMP) and cyclic guanine monophosphate (cGMP), which inhibits platelet activation and adhesion.14
ESPS-2 results showed a 38% relative reduction in risk of stroke for the combination versus placebo. The study did not include an ASA-only group. Results prompted reformulation of dipyridamole into a high-dose extended-release capsule combined with low-dose ASA. The higher dose and slower release of dipyridamole combined with ASA provides a more consistent plasma level and is less affected by stomach acidity or concomitant medications.
This combination was tested versus ASA alone in the ESPS-2 trial.15 ESPS-2, a randomized, double-blind, multicenter study, enrolled 6,602 patients with prior stroke or TIA. During the two-year follow-up ASA plus extended-release dipyridamole reduced the risk of recurrent stroke by 37% compared with placebo, and by 22% compared with ASA or dipyridamole alone. Adverse events associated with this combination are similar to those observed with low-dose ASA.
These results were further substantiated by a recent post hoc analysis conducted using data from the ESPS-2 trial. ASA plus extended-release dipyridamole had greater efficacy in preventing stroke than ASA; this difference in efficacy was more pronounced in high-risk patients.16
We need further studies that include direct comparisons to verify the most effective and safe antiplatelet agent for secondary stroke prevention. The Prospective Regimen for Effectively Avoiding Second Strokes (PRoFESS) is a head-to-head trial designed to compare the combination of ASA plus extended-release dipyridamole to clopidogrel in terms of efficacy and safety. This study includes 15,500 patients in more than 20 countries at approximately 600 sites.17
Conclusions
Stroke remains a major public health concern. Hospitalists play a central role in stroke management by improving the overall quality of hospital care for stroke patients. Still, most residency programs don’t provide sufficient stroke education. Therefore, comprehensive neurology educational programs should be provided for hospitalists so they can provide efficient inpatient care; initiate effective secondary prevention strategies tailored to the specific needs of the patients, starting with appropriate antiplatelet therapy; monitor patients at poststroke rehabilitation centers during recovery period; and educate stroke patients and their caregivers about the disease and its risk factors.
Hospitalists can also initiate effective communication with outpatient primary care providers at the time of discharge to help ensure that the secondary prevention strategies initiated in the hospital are not only continued but strengthened. TH
Dr. Sachdeva is lead hospitalist in the Stroke Program at the Swedish Medical Center, Seattle, and clinical instructor at the University of Washington, Seattle.
References
- Kmietowicz Z. United Kingdom needs to double the number of neurologists. BMJ. 2001;322:1508.
- Ringel SP. The neurologist’s role in stroke management. Stroke. 1996; 27(11):1935-1936.
- Weinberger J. Adverse effects and drug interactions of antithrombotic agents used in prevention of ischaemic stroke. Drugs. 2005;65(4):461-471.
- Weinberger J. Managing and preventing ischemic stroke: Part II—risk assessment and prevention of secondary ischemic stroke. Clin Geriatr. 2004;12(8):41-46.
- Patrono C, Coller B, Dalen JF. Platelet-active drugs: the relationship among dose, effectiveness and side effects. Chest. 2001:119(suppl):39S-63S.
- Fayad P, Singh SP. Anti-thrombotic therapy for the secondary prevention of ischemic stroke. Chest. 2004;126(3):483S-512S.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke. Chest. 2001;119(suppl):300S-320S.
- Antiplatelet Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;12;324(7329):71-86.
- Robert S, Miller AJ, Fagan SC. Ticlopidine: a new antiplatelet agent for cerebrovascular disease. Pharmacotherapy. 1991;11(4):317-322.
- CAPRIE Steering Committee. A randomized, blinded trial of clopidogrel versus aspirin in patients at risk for ischemic events. Lancet. 1996;348:1329-1339.
- Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345(7):494-502.
- Steinhubl SR, Berger PB, Mann JT 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288(19):2411-2420.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331-337.
- European Stroke Prevention Study. ESPS Group. Stroke. 1990;21(8):1122-1130.20
- Diener HC, Cunha L, Forbes C, et al. European stroke prevention study. 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143(1-2):1-13.
- Sacco RL, Sivenius J, Diener HC. Efficacy of aspirin plus extended-release dipyridamole in preventing recurrent stroke in high-risk populations. Arch Neurol. 2005;62:403-408.
- PRoFESS Web site. Available at: www.profess-study.com/com/Main/newscentre/news_040604.jsp. Last accessed July 18, 2005
- Weinberger J. Managing and preventing ischemic stroke: Part I—risk assessment and treatment of primary ischemic stroke. Clin Geriatr. 2004;12(7):48-53.
- Heart Disease and Stroke Statistics—2005 Update. Dallas, Texas. American Heart Association; Dallas. 2005
- Johnston SC, Gress DR, Browner WS, et al. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901-2906.
- Feinberg WM, Albers GW, Barnett H, et al. Guidelines for the management of transient ischemic attacks. Stroke. 1994;25:1320-1335.
The Case of the Nonhealing Wound

An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
2005 Election for SHM Board of Directors
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to nominations@hospitalmedicine.org or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at lhiggins@hospitalmedicine.org.
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at smckean@partners.org (Sylvia McKean, MD), tbw@medicine.wisc.edu (Tosha Wetterneck, MD), or wfwhit@comcast.net (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to nominations@hospitalmedicine.org or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at lhiggins@hospitalmedicine.org.
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at smckean@partners.org (Sylvia McKean, MD), tbw@medicine.wisc.edu (Tosha Wetterneck, MD), or wfwhit@comcast.net (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to nominations@hospitalmedicine.org or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at lhiggins@hospitalmedicine.org.
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at smckean@partners.org (Sylvia McKean, MD), tbw@medicine.wisc.edu (Tosha Wetterneck, MD), or wfwhit@comcast.net (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH
Hospitalists Stand Up at AMA and in D.C.

A week before the American Medical (AMA) Association House of Delegates met in Chicago this past June, the SHM leadership became aware of the AMA Board of Trustee’s Report 19 to be debated at the AMA meeting. The report, “Corporate Practice of Medicine,” and its recommendations included the following provision:
The Board of Trustees recommends that the following be adopted: That our AMA develop model legislation prohibiting lay corporations, including hospitals, from directly employing physicians, and make this model available to state and national medical societies.
Because more than 50% of hospitalists are currently either employed by hospitals, health systems, or corporations this policy—had it been enacted—would have adversely affected hospitalists.
Mobilize the Troops
Rewind to last June: As the clock ticked, SHM leadership sprang into action. SHM developed a letter (see “Letter from SHM to the AMA,” at right on p. 7) to the AMA president, chairman of the board of trustees, and the executive vice president, expressing strong opposition to this policy. SHM senior leaders also made direct, personal appeals to individuals on the AMA board.
In addition SHM sought the counsel and advice of the American College of Physicians (ACP), especially the ACP’s Washington, D.C., senior staff, including Bob Doherty, senior vice president of governmental affairs and public policy, and Jack Ginsburg, director of health policy analysis and research. SHM also consulted the leadership of the ACP delegation to the AMA. In this effort ACP allied with SHM to defeat this resolution.
SHM’s Tosha Wetterneck, an AMA delegate from Wisconsin and the Young Physicians Section, was prepared to give testimony against this report and recommendations at the AMA Reference Committee and, if necessary, on the floor of the AMA House of Delegates.
All this happened in a matter of days as delegates headed to Chicago for the AMA meeting.
The Decision
Through the efforts of SHM, ACP, and others, the AMA board wisely decided to withdraw the report and recommendations from the business of the House of Delegates and contacted SHM to thank us for our comments and participation.
Hospital medicine is a relatively new specialty, and SHM is a young organization compared with the AMA and the many specialty societies represented at AMA meetings. In addition, hospitalists tend to be generally younger physicians, who may feel that participation in national medical organizations such as ACP and AMA are not relevant to their professional lives.
In reality, though, the very turbulence and reinvention of the healthcare system in this country drives the growth of hospital medicine and may fuel a response from traditional professionals concerned about change and evolution. Because of the unique perspective of hospitalists and hospital medicine, SHM needs to be at the table. And we need to have thoughtful suggestions as we help to shape the future as well as send articulate responsible hospitalists to participate in these deliberations.
Public Policy Committee Leads the Way
The SHM Public Policy Committee (under the chairmanship of Eric Siegal and Laura Allendorf on SHM’s Washington D.C.-based staff) is taking the initial steps to be a player in healthcare advocacy. SHM has commissioned Health Policy Alternatives, a major Washington D.C. advisor on health policy, legislation, regulations, and policy making process, to develop a White Paper to better define the unique aspects of hospital medicine in a form that is understandable and meaningful to legislators and regulators, including the Centers for Medicare and Medicaid Services (CMS).
The Public Policy Committee will also formulate and recommend SHM policy on compensation reform and pay for performance. In consultation with the Hospital Quality and Patient Safety Committee, the Public Policy Committee will also develop policy on quality initiatives and safety standards.
To get hospitalists involved in the advocacy arena in a face-to-face, hands-on fashion, the Public Policy Committee plans to hold the first SHM Legislative Day on May 3, 2006, just prior to the SHM Annual Meeting in Washington, D.C. SHM will invite hospital medicine leaders to Washington to be educated on the key advocacy issues and how best to interact with their congressional representatives, senators, and their health staff. Appointments will be made for the hospitalist leaders to go to the Hill for meetings with their legislators on May 3. Check the SHM Web site (www.hospitalmedicine.org) and future issues of The Hospitalist for details about how you might participate in the SHM Legislative Day 2006.
Hospitalists Participate in Code Review
This year—2005—is the Five Year Review of all the billing codes by AMA’s Relative Value Update (or RUC) Committee with recommendations to CMS and the government. Most medical societies participate by having key members examine the work involved in performing specific functions described by the current procedural terminology (CPT) codes. The idea is to update the work and, therefore, the compensation for the work of healthcare.
SHM partnered with ACP in this effort, and more than 25 SHM members concentrated on a review of hospital admission, consultation, and daily visit codes. SHM appreciates the time spent by these hospitalists. We hope that as the relative values of visits and procedures are reconfigured this input will be helpful.
SHM continues its interest in developing an alternative to the current system that compensates physicians by the unit of the visit. We favor a shift to a broader management fee that better reflects the reality that current inpatient care requires multiple visits each day and a more in-depth approach than is currently captured in a one-visit-and-gone approach.
Medicare’s CCIP Initiative
The Chronic Care Improvement Program (CCIP) is a component of the Medicare Modernization Act of 2003. This program is the first large-scale chronic care improvement initiative under the Medicare fee-for-service program. CMS selected organizations that will offer self-care guidance and support to chronically ill beneficiaries. These organizations will help beneficiaries manage their health, adhere to their physicians’ plans of care, and ensure that they seek or obtain medical care as needed to reduce their health risks.
Performance-based contracting is one of the most important features of the CCIP design. The CCIPs will be paid based on achieving measurable improvements in clinical and financial outcomes, as well as satisfaction levels across their assigned populations. Payment is not based on services provided. CCIP organizations will be paid monthly fees, but those fees will be fully at risk. The organizations will be required to refund some or all of their fees to the federal government if they do not meet agreed-upon standards for quality improvement, savings to Medicare, and increased beneficiary satisfaction levels.
Phase I programs will be large-scale, collectively serving approximately 180,000 chronically ill beneficiaries. This is the phase currently under development. The programs are intended to help increase adherence to evidence-based care, reduce unnecessary hospital stays and emergency department visits, and help beneficiaries avoid costly and debilitating complications and comorbidities. With the attention to reducing hospital costs by reducing unnecessary stays and emergency department visits, hospitalists may play an important role in CCIPs.
Ten organizations in 10 states were awarded opportunities to pilot CCIP programs. SHM believes that hospitalists can play a key role in the CCIP programs and demonstrate efficient and effective care (i.e., better quality at a lower use of resources). SHM has developed a list of its members who are willing to work in the CCIP process and has contacted all of the CCIP awardees to discuss the role of hospitalists in quality improvement.
This is a tangible way that SHM can work with the government and its contractors as pilot programs are funded and developed to improve healthcare at the local level.
SHM: We’re Here for You
The healthcare landscape is changing before our eyes. Whether pay for performance or chronic care improvement or a reworking of the compensation system for healthcare, it’s important that hospital medicine be part of the discussion and decision-making process.
In the near future more than 30,000 hospitalists will practice nationwide, and virtually every hospital will have a hospital medicine program. Hospitalists will be asked to shape and implement the changes that are coming our way. This is our future, and with your help SHM will help you make it a better place for hospitalists, other health professionals, and the patients we serve. TH
Dr. Wellikson has been the CEO of SHM since 2000.
A week before the American Medical (AMA) Association House of Delegates met in Chicago this past June, the SHM leadership became aware of the AMA Board of Trustee’s Report 19 to be debated at the AMA meeting. The report, “Corporate Practice of Medicine,” and its recommendations included the following provision:
The Board of Trustees recommends that the following be adopted: That our AMA develop model legislation prohibiting lay corporations, including hospitals, from directly employing physicians, and make this model available to state and national medical societies.
Because more than 50% of hospitalists are currently either employed by hospitals, health systems, or corporations this policy—had it been enacted—would have adversely affected hospitalists.
Mobilize the Troops
Rewind to last June: As the clock ticked, SHM leadership sprang into action. SHM developed a letter (see “Letter from SHM to the AMA,” at right on p. 7) to the AMA president, chairman of the board of trustees, and the executive vice president, expressing strong opposition to this policy. SHM senior leaders also made direct, personal appeals to individuals on the AMA board.
In addition SHM sought the counsel and advice of the American College of Physicians (ACP), especially the ACP’s Washington, D.C., senior staff, including Bob Doherty, senior vice president of governmental affairs and public policy, and Jack Ginsburg, director of health policy analysis and research. SHM also consulted the leadership of the ACP delegation to the AMA. In this effort ACP allied with SHM to defeat this resolution.
SHM’s Tosha Wetterneck, an AMA delegate from Wisconsin and the Young Physicians Section, was prepared to give testimony against this report and recommendations at the AMA Reference Committee and, if necessary, on the floor of the AMA House of Delegates.
All this happened in a matter of days as delegates headed to Chicago for the AMA meeting.
The Decision
Through the efforts of SHM, ACP, and others, the AMA board wisely decided to withdraw the report and recommendations from the business of the House of Delegates and contacted SHM to thank us for our comments and participation.
Hospital medicine is a relatively new specialty, and SHM is a young organization compared with the AMA and the many specialty societies represented at AMA meetings. In addition, hospitalists tend to be generally younger physicians, who may feel that participation in national medical organizations such as ACP and AMA are not relevant to their professional lives.
In reality, though, the very turbulence and reinvention of the healthcare system in this country drives the growth of hospital medicine and may fuel a response from traditional professionals concerned about change and evolution. Because of the unique perspective of hospitalists and hospital medicine, SHM needs to be at the table. And we need to have thoughtful suggestions as we help to shape the future as well as send articulate responsible hospitalists to participate in these deliberations.
Public Policy Committee Leads the Way
The SHM Public Policy Committee (under the chairmanship of Eric Siegal and Laura Allendorf on SHM’s Washington D.C.-based staff) is taking the initial steps to be a player in healthcare advocacy. SHM has commissioned Health Policy Alternatives, a major Washington D.C. advisor on health policy, legislation, regulations, and policy making process, to develop a White Paper to better define the unique aspects of hospital medicine in a form that is understandable and meaningful to legislators and regulators, including the Centers for Medicare and Medicaid Services (CMS).
The Public Policy Committee will also formulate and recommend SHM policy on compensation reform and pay for performance. In consultation with the Hospital Quality and Patient Safety Committee, the Public Policy Committee will also develop policy on quality initiatives and safety standards.
To get hospitalists involved in the advocacy arena in a face-to-face, hands-on fashion, the Public Policy Committee plans to hold the first SHM Legislative Day on May 3, 2006, just prior to the SHM Annual Meeting in Washington, D.C. SHM will invite hospital medicine leaders to Washington to be educated on the key advocacy issues and how best to interact with their congressional representatives, senators, and their health staff. Appointments will be made for the hospitalist leaders to go to the Hill for meetings with their legislators on May 3. Check the SHM Web site (www.hospitalmedicine.org) and future issues of The Hospitalist for details about how you might participate in the SHM Legislative Day 2006.
Hospitalists Participate in Code Review
This year—2005—is the Five Year Review of all the billing codes by AMA’s Relative Value Update (or RUC) Committee with recommendations to CMS and the government. Most medical societies participate by having key members examine the work involved in performing specific functions described by the current procedural terminology (CPT) codes. The idea is to update the work and, therefore, the compensation for the work of healthcare.
SHM partnered with ACP in this effort, and more than 25 SHM members concentrated on a review of hospital admission, consultation, and daily visit codes. SHM appreciates the time spent by these hospitalists. We hope that as the relative values of visits and procedures are reconfigured this input will be helpful.
SHM continues its interest in developing an alternative to the current system that compensates physicians by the unit of the visit. We favor a shift to a broader management fee that better reflects the reality that current inpatient care requires multiple visits each day and a more in-depth approach than is currently captured in a one-visit-and-gone approach.
Medicare’s CCIP Initiative
The Chronic Care Improvement Program (CCIP) is a component of the Medicare Modernization Act of 2003. This program is the first large-scale chronic care improvement initiative under the Medicare fee-for-service program. CMS selected organizations that will offer self-care guidance and support to chronically ill beneficiaries. These organizations will help beneficiaries manage their health, adhere to their physicians’ plans of care, and ensure that they seek or obtain medical care as needed to reduce their health risks.
Performance-based contracting is one of the most important features of the CCIP design. The CCIPs will be paid based on achieving measurable improvements in clinical and financial outcomes, as well as satisfaction levels across their assigned populations. Payment is not based on services provided. CCIP organizations will be paid monthly fees, but those fees will be fully at risk. The organizations will be required to refund some or all of their fees to the federal government if they do not meet agreed-upon standards for quality improvement, savings to Medicare, and increased beneficiary satisfaction levels.
Phase I programs will be large-scale, collectively serving approximately 180,000 chronically ill beneficiaries. This is the phase currently under development. The programs are intended to help increase adherence to evidence-based care, reduce unnecessary hospital stays and emergency department visits, and help beneficiaries avoid costly and debilitating complications and comorbidities. With the attention to reducing hospital costs by reducing unnecessary stays and emergency department visits, hospitalists may play an important role in CCIPs.
Ten organizations in 10 states were awarded opportunities to pilot CCIP programs. SHM believes that hospitalists can play a key role in the CCIP programs and demonstrate efficient and effective care (i.e., better quality at a lower use of resources). SHM has developed a list of its members who are willing to work in the CCIP process and has contacted all of the CCIP awardees to discuss the role of hospitalists in quality improvement.
This is a tangible way that SHM can work with the government and its contractors as pilot programs are funded and developed to improve healthcare at the local level.
SHM: We’re Here for You
The healthcare landscape is changing before our eyes. Whether pay for performance or chronic care improvement or a reworking of the compensation system for healthcare, it’s important that hospital medicine be part of the discussion and decision-making process.
In the near future more than 30,000 hospitalists will practice nationwide, and virtually every hospital will have a hospital medicine program. Hospitalists will be asked to shape and implement the changes that are coming our way. This is our future, and with your help SHM will help you make it a better place for hospitalists, other health professionals, and the patients we serve. TH
Dr. Wellikson has been the CEO of SHM since 2000.
A week before the American Medical (AMA) Association House of Delegates met in Chicago this past June, the SHM leadership became aware of the AMA Board of Trustee’s Report 19 to be debated at the AMA meeting. The report, “Corporate Practice of Medicine,” and its recommendations included the following provision:
The Board of Trustees recommends that the following be adopted: That our AMA develop model legislation prohibiting lay corporations, including hospitals, from directly employing physicians, and make this model available to state and national medical societies.
Because more than 50% of hospitalists are currently either employed by hospitals, health systems, or corporations this policy—had it been enacted—would have adversely affected hospitalists.
Mobilize the Troops
Rewind to last June: As the clock ticked, SHM leadership sprang into action. SHM developed a letter (see “Letter from SHM to the AMA,” at right on p. 7) to the AMA president, chairman of the board of trustees, and the executive vice president, expressing strong opposition to this policy. SHM senior leaders also made direct, personal appeals to individuals on the AMA board.
In addition SHM sought the counsel and advice of the American College of Physicians (ACP), especially the ACP’s Washington, D.C., senior staff, including Bob Doherty, senior vice president of governmental affairs and public policy, and Jack Ginsburg, director of health policy analysis and research. SHM also consulted the leadership of the ACP delegation to the AMA. In this effort ACP allied with SHM to defeat this resolution.
SHM’s Tosha Wetterneck, an AMA delegate from Wisconsin and the Young Physicians Section, was prepared to give testimony against this report and recommendations at the AMA Reference Committee and, if necessary, on the floor of the AMA House of Delegates.
All this happened in a matter of days as delegates headed to Chicago for the AMA meeting.
The Decision
Through the efforts of SHM, ACP, and others, the AMA board wisely decided to withdraw the report and recommendations from the business of the House of Delegates and contacted SHM to thank us for our comments and participation.
Hospital medicine is a relatively new specialty, and SHM is a young organization compared with the AMA and the many specialty societies represented at AMA meetings. In addition, hospitalists tend to be generally younger physicians, who may feel that participation in national medical organizations such as ACP and AMA are not relevant to their professional lives.
In reality, though, the very turbulence and reinvention of the healthcare system in this country drives the growth of hospital medicine and may fuel a response from traditional professionals concerned about change and evolution. Because of the unique perspective of hospitalists and hospital medicine, SHM needs to be at the table. And we need to have thoughtful suggestions as we help to shape the future as well as send articulate responsible hospitalists to participate in these deliberations.
Public Policy Committee Leads the Way
The SHM Public Policy Committee (under the chairmanship of Eric Siegal and Laura Allendorf on SHM’s Washington D.C.-based staff) is taking the initial steps to be a player in healthcare advocacy. SHM has commissioned Health Policy Alternatives, a major Washington D.C. advisor on health policy, legislation, regulations, and policy making process, to develop a White Paper to better define the unique aspects of hospital medicine in a form that is understandable and meaningful to legislators and regulators, including the Centers for Medicare and Medicaid Services (CMS).
The Public Policy Committee will also formulate and recommend SHM policy on compensation reform and pay for performance. In consultation with the Hospital Quality and Patient Safety Committee, the Public Policy Committee will also develop policy on quality initiatives and safety standards.
To get hospitalists involved in the advocacy arena in a face-to-face, hands-on fashion, the Public Policy Committee plans to hold the first SHM Legislative Day on May 3, 2006, just prior to the SHM Annual Meeting in Washington, D.C. SHM will invite hospital medicine leaders to Washington to be educated on the key advocacy issues and how best to interact with their congressional representatives, senators, and their health staff. Appointments will be made for the hospitalist leaders to go to the Hill for meetings with their legislators on May 3. Check the SHM Web site (www.hospitalmedicine.org) and future issues of The Hospitalist for details about how you might participate in the SHM Legislative Day 2006.
Hospitalists Participate in Code Review
This year—2005—is the Five Year Review of all the billing codes by AMA’s Relative Value Update (or RUC) Committee with recommendations to CMS and the government. Most medical societies participate by having key members examine the work involved in performing specific functions described by the current procedural terminology (CPT) codes. The idea is to update the work and, therefore, the compensation for the work of healthcare.
SHM partnered with ACP in this effort, and more than 25 SHM members concentrated on a review of hospital admission, consultation, and daily visit codes. SHM appreciates the time spent by these hospitalists. We hope that as the relative values of visits and procedures are reconfigured this input will be helpful.
SHM continues its interest in developing an alternative to the current system that compensates physicians by the unit of the visit. We favor a shift to a broader management fee that better reflects the reality that current inpatient care requires multiple visits each day and a more in-depth approach than is currently captured in a one-visit-and-gone approach.
Medicare’s CCIP Initiative
The Chronic Care Improvement Program (CCIP) is a component of the Medicare Modernization Act of 2003. This program is the first large-scale chronic care improvement initiative under the Medicare fee-for-service program. CMS selected organizations that will offer self-care guidance and support to chronically ill beneficiaries. These organizations will help beneficiaries manage their health, adhere to their physicians’ plans of care, and ensure that they seek or obtain medical care as needed to reduce their health risks.
Performance-based contracting is one of the most important features of the CCIP design. The CCIPs will be paid based on achieving measurable improvements in clinical and financial outcomes, as well as satisfaction levels across their assigned populations. Payment is not based on services provided. CCIP organizations will be paid monthly fees, but those fees will be fully at risk. The organizations will be required to refund some or all of their fees to the federal government if they do not meet agreed-upon standards for quality improvement, savings to Medicare, and increased beneficiary satisfaction levels.
Phase I programs will be large-scale, collectively serving approximately 180,000 chronically ill beneficiaries. This is the phase currently under development. The programs are intended to help increase adherence to evidence-based care, reduce unnecessary hospital stays and emergency department visits, and help beneficiaries avoid costly and debilitating complications and comorbidities. With the attention to reducing hospital costs by reducing unnecessary stays and emergency department visits, hospitalists may play an important role in CCIPs.
Ten organizations in 10 states were awarded opportunities to pilot CCIP programs. SHM believes that hospitalists can play a key role in the CCIP programs and demonstrate efficient and effective care (i.e., better quality at a lower use of resources). SHM has developed a list of its members who are willing to work in the CCIP process and has contacted all of the CCIP awardees to discuss the role of hospitalists in quality improvement.
This is a tangible way that SHM can work with the government and its contractors as pilot programs are funded and developed to improve healthcare at the local level.
SHM: We’re Here for You
The healthcare landscape is changing before our eyes. Whether pay for performance or chronic care improvement or a reworking of the compensation system for healthcare, it’s important that hospital medicine be part of the discussion and decision-making process.
In the near future more than 30,000 hospitalists will practice nationwide, and virtually every hospital will have a hospital medicine program. Hospitalists will be asked to shape and implement the changes that are coming our way. This is our future, and with your help SHM will help you make it a better place for hospitalists, other health professionals, and the patients we serve. TH
Dr. Wellikson has been the CEO of SHM since 2000.
The New and the Timeless

I recently picked up volume 1, number 1 of The Hospitalist, which was edited by John Nelson and Win Whitcomb and published in spring 1997. The Hospitalist was six pages long and had five articles and three job advertisements. The articles included one by Bob Wachter about how hospitalists represent “without a doubt … a bona fide new specialty in American medicine,” and one by Richard Slataper about how hospitalists improve quality of care.
As I compare volume 1, number 1 with the current volume, I marvel at how much things have changed—and how much they have stayed the same. The change is obvious just by looking at The Hospitalist. The similarities are evident by reading the content. We still talk about how hospital medicine is emerging as a new specialty and is taking important strides in that direction. Quality is still the key metric by which we measure our practice.
With this volume, we enter a new, exciting era for The Hospitalist with a new format, new editorial staff leadership, and a new publisher—but the same commitment to excellence and dedication to addressing key issues in the field of hospital medicine. I thank Jim Pile for his outstanding job as the previous editor of The Hospitalist. Jamie Newman assumes the role of physician editor with this issue, and I am excited to have his energy and creative ideas to lead the new phase of this important publication.
It has been said that half of what you learn in medical school is obsolete five years after you graduate. The trouble is you can’t know which half that will be until five years later. I remember being warned as an intern never to give a beta-blocker to a patient with heart failure. We now know that beta-blockers are lifesaving for people with heart failure. We are fortunate to practice in a world where scientific discoveries enhance our ability to help our patients and where the pace of discovery is growing by leaps and bounds. I wish I could list everything we do today that will be obsolete in five years, but my crystal ball is not that clear. Because I cannot predict what will change in medicine, I have instead thought about what does not change. As we celebrate the new with this volume of The Hospitalist I want to remember what is timeless in our profession.
Cornerstones of Diagnosis
With so much technology it is easy to believe that technology makes the diagnosis and heals the patient. But despite all of the new and amazing tests at our disposal, the patient history and physical examination remain the cornerstones of diagnosis.
It has been said that in more than 90% of cases the correct diagnosis appears on the differential after the history and physical. The tests merely help to confirm or rule out diagnoses. As technology races ahead the importance of sitting at the bedside, talking with the patient, and hearing her story stays constant.
One of my mentors says, “Don’t just do something, sit there.” When I’m confused about what is going on with a patient, my best aid in figuring things out is to pull up a chair and have the patient tell me his story from the beginning. What I like so much about being a hospitalist is that I have the ability to spend that kind of time when I need to. Unlike the outpatient setting where patients are scheduled every 15 minutes regardless of the reason for the visit, in the hospital I can be more flexible about how I allocate my time. I can spend time sitting and listening.
There is an apocryphal story I like that says that if you sit down in the patient’s room the patient will experience your visit as having lasted longer than if you stand for the same amount of time. I say apocryphal because I have searched for this study but have never found it; however, I believe it. Patients also like telling their story. There is healing in the telling and in knowing that you have been heard. As so much of medicine changes, sitting with the patient and hearing her story remains timeless.
Reach Out and Touch
Another part of medicine that has not changed over the millennia is the power of touch. During my second year of residency I realized that in many situations the physical examination just didn’t add much to my care of the patient. Perhaps this fact reflected my physical examination skills, but I believe it was more a function of realizing that in the absence of complaints in the chest I was unlikely to discover something on lung exam.
The great symbolism and importance of touching and examining the patient goes beyond discovering the unexpected finding. The laying on of hands creates a physical connection to the patient and can heal. I now make it a point to physically examine every patient every day. I examine patients not just to support billing and not just because there just may be a new finding, but because there is power and healing in touch. I want the patient to benefit from this power and I want to connect to it for myself. As a hospitalist I feel privileged to be able to be at the bedside with patients.
Identify with the Patient
Another timeless part of patient care is empathy. Many patients simply want someone to walk alongside them and understand their experience of illness. Empathy makes this possible.
As I talk with patients I use myself as a guide for understanding the patient’s emotional experience and try to reflect that back. More than simply taking the history or laying my hands on the patient, I try to understand what the patient is feeling and going through. The fear and loneliness of illness can be greatly relieved by knowing that another person understands your experience and is walking with you. Our patients’ need and desire for empathy has not changed despite all of our technological innovations.
As hospitalists we meet people at their sickest and most vulnerable. They enter the foreign world of the hospital where they are often alone and where they have little to no control over what happens to them. Patients typically can’t even dictate the basics of life in the hospital like when or what they can eat. Even if we imagine the ideal hospital of the future built around the patient and that affords maximum control to the patient, the hospital will still be foreign. The power of empathy and the human interaction it represents will remain as important in this ideal hospital as it is today and as it always has been.
Education Never Ends
The other certainty in medicine is that science and technology will advance, bringing new and better ways to diagnose and treat illness. Thus the final constant in medicine is the need to always be learning. As an attending I had to learn that beta-blockers were good for people with heart failure and saved lives. I have learned many more new things since residency and understand the need to continue to learn.
Another wonderful aspect of being a hospitalist is the continuous progress of medical care and the ability to apply it to help patients. Advances in diagnosis and treatment, changes to systems that ensure that all patients receive this care, and attention to patient safety, quality, and palliative care all help ensure that patients receive the best possible care. Hospitalists are at the forefront of all of these activities.
In Conclusion
I delight in the new and celebrate progress that this era for The Hospitalist represents. I’m proud of the The Hospitalist and look forward to it continuing the tradition of quality while it expands and grows in new ways. In the same way I’m excited about medical advances but try always to remember what is timeless. Sitting with patients, listening to them, touching them, and being empathic reap great rewards for patients and for us.
As hospitalists we care for people at their most vulnerable moments. At those times our humanity, our gentle, caring touch, and our empathy matter most. In addition to bringing to bear the best that modern medicine has to offer in medications, diagnostic tests, and interventions let us remember the power to heal that we bring to the bedside when we bring ourselves—open to being with the patient and not just doing something but sitting there. TH
Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
I recently picked up volume 1, number 1 of The Hospitalist, which was edited by John Nelson and Win Whitcomb and published in spring 1997. The Hospitalist was six pages long and had five articles and three job advertisements. The articles included one by Bob Wachter about how hospitalists represent “without a doubt … a bona fide new specialty in American medicine,” and one by Richard Slataper about how hospitalists improve quality of care.
As I compare volume 1, number 1 with the current volume, I marvel at how much things have changed—and how much they have stayed the same. The change is obvious just by looking at The Hospitalist. The similarities are evident by reading the content. We still talk about how hospital medicine is emerging as a new specialty and is taking important strides in that direction. Quality is still the key metric by which we measure our practice.
With this volume, we enter a new, exciting era for The Hospitalist with a new format, new editorial staff leadership, and a new publisher—but the same commitment to excellence and dedication to addressing key issues in the field of hospital medicine. I thank Jim Pile for his outstanding job as the previous editor of The Hospitalist. Jamie Newman assumes the role of physician editor with this issue, and I am excited to have his energy and creative ideas to lead the new phase of this important publication.
It has been said that half of what you learn in medical school is obsolete five years after you graduate. The trouble is you can’t know which half that will be until five years later. I remember being warned as an intern never to give a beta-blocker to a patient with heart failure. We now know that beta-blockers are lifesaving for people with heart failure. We are fortunate to practice in a world where scientific discoveries enhance our ability to help our patients and where the pace of discovery is growing by leaps and bounds. I wish I could list everything we do today that will be obsolete in five years, but my crystal ball is not that clear. Because I cannot predict what will change in medicine, I have instead thought about what does not change. As we celebrate the new with this volume of The Hospitalist I want to remember what is timeless in our profession.
Cornerstones of Diagnosis
With so much technology it is easy to believe that technology makes the diagnosis and heals the patient. But despite all of the new and amazing tests at our disposal, the patient history and physical examination remain the cornerstones of diagnosis.
It has been said that in more than 90% of cases the correct diagnosis appears on the differential after the history and physical. The tests merely help to confirm or rule out diagnoses. As technology races ahead the importance of sitting at the bedside, talking with the patient, and hearing her story stays constant.
One of my mentors says, “Don’t just do something, sit there.” When I’m confused about what is going on with a patient, my best aid in figuring things out is to pull up a chair and have the patient tell me his story from the beginning. What I like so much about being a hospitalist is that I have the ability to spend that kind of time when I need to. Unlike the outpatient setting where patients are scheduled every 15 minutes regardless of the reason for the visit, in the hospital I can be more flexible about how I allocate my time. I can spend time sitting and listening.
There is an apocryphal story I like that says that if you sit down in the patient’s room the patient will experience your visit as having lasted longer than if you stand for the same amount of time. I say apocryphal because I have searched for this study but have never found it; however, I believe it. Patients also like telling their story. There is healing in the telling and in knowing that you have been heard. As so much of medicine changes, sitting with the patient and hearing her story remains timeless.
Reach Out and Touch
Another part of medicine that has not changed over the millennia is the power of touch. During my second year of residency I realized that in many situations the physical examination just didn’t add much to my care of the patient. Perhaps this fact reflected my physical examination skills, but I believe it was more a function of realizing that in the absence of complaints in the chest I was unlikely to discover something on lung exam.
The great symbolism and importance of touching and examining the patient goes beyond discovering the unexpected finding. The laying on of hands creates a physical connection to the patient and can heal. I now make it a point to physically examine every patient every day. I examine patients not just to support billing and not just because there just may be a new finding, but because there is power and healing in touch. I want the patient to benefit from this power and I want to connect to it for myself. As a hospitalist I feel privileged to be able to be at the bedside with patients.
Identify with the Patient
Another timeless part of patient care is empathy. Many patients simply want someone to walk alongside them and understand their experience of illness. Empathy makes this possible.
As I talk with patients I use myself as a guide for understanding the patient’s emotional experience and try to reflect that back. More than simply taking the history or laying my hands on the patient, I try to understand what the patient is feeling and going through. The fear and loneliness of illness can be greatly relieved by knowing that another person understands your experience and is walking with you. Our patients’ need and desire for empathy has not changed despite all of our technological innovations.
As hospitalists we meet people at their sickest and most vulnerable. They enter the foreign world of the hospital where they are often alone and where they have little to no control over what happens to them. Patients typically can’t even dictate the basics of life in the hospital like when or what they can eat. Even if we imagine the ideal hospital of the future built around the patient and that affords maximum control to the patient, the hospital will still be foreign. The power of empathy and the human interaction it represents will remain as important in this ideal hospital as it is today and as it always has been.
Education Never Ends
The other certainty in medicine is that science and technology will advance, bringing new and better ways to diagnose and treat illness. Thus the final constant in medicine is the need to always be learning. As an attending I had to learn that beta-blockers were good for people with heart failure and saved lives. I have learned many more new things since residency and understand the need to continue to learn.
Another wonderful aspect of being a hospitalist is the continuous progress of medical care and the ability to apply it to help patients. Advances in diagnosis and treatment, changes to systems that ensure that all patients receive this care, and attention to patient safety, quality, and palliative care all help ensure that patients receive the best possible care. Hospitalists are at the forefront of all of these activities.
In Conclusion
I delight in the new and celebrate progress that this era for The Hospitalist represents. I’m proud of the The Hospitalist and look forward to it continuing the tradition of quality while it expands and grows in new ways. In the same way I’m excited about medical advances but try always to remember what is timeless. Sitting with patients, listening to them, touching them, and being empathic reap great rewards for patients and for us.
As hospitalists we care for people at their most vulnerable moments. At those times our humanity, our gentle, caring touch, and our empathy matter most. In addition to bringing to bear the best that modern medicine has to offer in medications, diagnostic tests, and interventions let us remember the power to heal that we bring to the bedside when we bring ourselves—open to being with the patient and not just doing something but sitting there. TH
Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
I recently picked up volume 1, number 1 of The Hospitalist, which was edited by John Nelson and Win Whitcomb and published in spring 1997. The Hospitalist was six pages long and had five articles and three job advertisements. The articles included one by Bob Wachter about how hospitalists represent “without a doubt … a bona fide new specialty in American medicine,” and one by Richard Slataper about how hospitalists improve quality of care.
As I compare volume 1, number 1 with the current volume, I marvel at how much things have changed—and how much they have stayed the same. The change is obvious just by looking at The Hospitalist. The similarities are evident by reading the content. We still talk about how hospital medicine is emerging as a new specialty and is taking important strides in that direction. Quality is still the key metric by which we measure our practice.
With this volume, we enter a new, exciting era for The Hospitalist with a new format, new editorial staff leadership, and a new publisher—but the same commitment to excellence and dedication to addressing key issues in the field of hospital medicine. I thank Jim Pile for his outstanding job as the previous editor of The Hospitalist. Jamie Newman assumes the role of physician editor with this issue, and I am excited to have his energy and creative ideas to lead the new phase of this important publication.
It has been said that half of what you learn in medical school is obsolete five years after you graduate. The trouble is you can’t know which half that will be until five years later. I remember being warned as an intern never to give a beta-blocker to a patient with heart failure. We now know that beta-blockers are lifesaving for people with heart failure. We are fortunate to practice in a world where scientific discoveries enhance our ability to help our patients and where the pace of discovery is growing by leaps and bounds. I wish I could list everything we do today that will be obsolete in five years, but my crystal ball is not that clear. Because I cannot predict what will change in medicine, I have instead thought about what does not change. As we celebrate the new with this volume of The Hospitalist I want to remember what is timeless in our profession.
Cornerstones of Diagnosis
With so much technology it is easy to believe that technology makes the diagnosis and heals the patient. But despite all of the new and amazing tests at our disposal, the patient history and physical examination remain the cornerstones of diagnosis.
It has been said that in more than 90% of cases the correct diagnosis appears on the differential after the history and physical. The tests merely help to confirm or rule out diagnoses. As technology races ahead the importance of sitting at the bedside, talking with the patient, and hearing her story stays constant.
One of my mentors says, “Don’t just do something, sit there.” When I’m confused about what is going on with a patient, my best aid in figuring things out is to pull up a chair and have the patient tell me his story from the beginning. What I like so much about being a hospitalist is that I have the ability to spend that kind of time when I need to. Unlike the outpatient setting where patients are scheduled every 15 minutes regardless of the reason for the visit, in the hospital I can be more flexible about how I allocate my time. I can spend time sitting and listening.
There is an apocryphal story I like that says that if you sit down in the patient’s room the patient will experience your visit as having lasted longer than if you stand for the same amount of time. I say apocryphal because I have searched for this study but have never found it; however, I believe it. Patients also like telling their story. There is healing in the telling and in knowing that you have been heard. As so much of medicine changes, sitting with the patient and hearing her story remains timeless.
Reach Out and Touch
Another part of medicine that has not changed over the millennia is the power of touch. During my second year of residency I realized that in many situations the physical examination just didn’t add much to my care of the patient. Perhaps this fact reflected my physical examination skills, but I believe it was more a function of realizing that in the absence of complaints in the chest I was unlikely to discover something on lung exam.
The great symbolism and importance of touching and examining the patient goes beyond discovering the unexpected finding. The laying on of hands creates a physical connection to the patient and can heal. I now make it a point to physically examine every patient every day. I examine patients not just to support billing and not just because there just may be a new finding, but because there is power and healing in touch. I want the patient to benefit from this power and I want to connect to it for myself. As a hospitalist I feel privileged to be able to be at the bedside with patients.
Identify with the Patient
Another timeless part of patient care is empathy. Many patients simply want someone to walk alongside them and understand their experience of illness. Empathy makes this possible.
As I talk with patients I use myself as a guide for understanding the patient’s emotional experience and try to reflect that back. More than simply taking the history or laying my hands on the patient, I try to understand what the patient is feeling and going through. The fear and loneliness of illness can be greatly relieved by knowing that another person understands your experience and is walking with you. Our patients’ need and desire for empathy has not changed despite all of our technological innovations.
As hospitalists we meet people at their sickest and most vulnerable. They enter the foreign world of the hospital where they are often alone and where they have little to no control over what happens to them. Patients typically can’t even dictate the basics of life in the hospital like when or what they can eat. Even if we imagine the ideal hospital of the future built around the patient and that affords maximum control to the patient, the hospital will still be foreign. The power of empathy and the human interaction it represents will remain as important in this ideal hospital as it is today and as it always has been.
Education Never Ends
The other certainty in medicine is that science and technology will advance, bringing new and better ways to diagnose and treat illness. Thus the final constant in medicine is the need to always be learning. As an attending I had to learn that beta-blockers were good for people with heart failure and saved lives. I have learned many more new things since residency and understand the need to continue to learn.
Another wonderful aspect of being a hospitalist is the continuous progress of medical care and the ability to apply it to help patients. Advances in diagnosis and treatment, changes to systems that ensure that all patients receive this care, and attention to patient safety, quality, and palliative care all help ensure that patients receive the best possible care. Hospitalists are at the forefront of all of these activities.
In Conclusion
I delight in the new and celebrate progress that this era for The Hospitalist represents. I’m proud of the The Hospitalist and look forward to it continuing the tradition of quality while it expands and grows in new ways. In the same way I’m excited about medical advances but try always to remember what is timeless. Sitting with patients, listening to them, touching them, and being empathic reap great rewards for patients and for us.
As hospitalists we care for people at their most vulnerable moments. At those times our humanity, our gentle, caring touch, and our empathy matter most. In addition to bringing to bear the best that modern medicine has to offer in medications, diagnostic tests, and interventions let us remember the power to heal that we bring to the bedside when we bring ourselves—open to being with the patient and not just doing something but sitting there. TH
Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
Are You Culturally Competent?
As the diversity of the U.S. population increases, so do the challenges for hospitalists, as they seek to deliver truly patient-centered care in the 21st century. The March 2002 Institute of Medicine report, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care,” concluded that, while some care inequities can be attributed to access and linguistic barriers, healthcare providers themselves may contribute to disparities in care for their minority patients.1
How can hospitalists ensure that they bridge the cultural divide between themselves and their patients from different racial, ethnic, and cultural backgrounds and avoid potential missteps in care delivery?
An Open Mind
Experts in cultural competency interviewed for this article explained that hospitalists can readily acquire the knowledge and skills necessary to effectively provide patient-centered care for all their patients. (See “Resource List,” p. 27.) But the most critical element in culturally competent healthcare delivery is the attitude with which the provider approaches his or her patients.
“I don’t think we can teach attitude,” says Alicia Fernandez, MD, assistant clinical professor of medicine, Division of General Internal Medicine, University of California, San Francisco, a nationally known researcher on language barriers and former full-time hospitalist. “But I think that any doctor who’s trying to do the best he or she can by their individual patients has the right attitude, which is to remain open to practicing patient-centered care.”

—Jack Percelay, MD
Physicians must be able to approach each patient on his or her own terms, and to acknowledge that members of different racial and ethnic groups hold beliefs about health and illness that diverge from those of Western medicine.
“You really need to have the capacity to empathize, and turn off all of your own belief systems, in some cases, to listen,” says Stacy Goldsholl, MD, a hospitalist based in Wilmington, N.C., and an SHM Board member.
Dr. Goldsholl recalls one situation involving a patient who was a Jehovah’s Witness who entered the hospital with a gastrointestinal bleed. Because of religious proscriptions, the patient refused a blood transfusion.
“It was extremely difficult as a scientist-trained physician, to watch someone bleed to a hemoglobin of 5, knowing that a simple transfusion would save this patient,” recalls Dr. Goldsholl.
The patient later underwent surgery without a transfusion and survived, but Dr. Goldsholl believes this case illustrates that delivering patient-centered care requires the practice not just of the science—but the art—of medicine.
“I think the real message is, you have to think outside of your own box,” she offers. “In addition, the cultural issues become much more pronounced when you start to approach end-of-life issues that take on more of a cultural, ethnic. and spiritual dimension.”
Awareness and Knowledge
Mitchell D. Wilson, MD, believes “the average American tends to be very ethnocentric. We are not taught cultural awareness in recognizing our own inherent biases, so we are unable to take the next step and recognize that there is a gap between our culture and another person’s culture that would require us to take a different approach.”
Dr. Wilson is associate professor of medicine, medical director and physician advisor, Department of Clinical Care Management, University of North Carolina (UNC) Hospitals, and section chief of hospital medicine and medical director, FirstHealth of the Carolinas Hospitalist Services, UNC School of Medicine, Chapel Hill. He is also an SHM Board member.
Dr. Wilson says that his own cultural awareness emanated from participation in a spirituality and medicine program for student doctors and nurses at the medical school where he trained and was later on faculty.
“I was able to function both as a small group facilitator and a large group panelist, and we used a case-based format for creating awareness of spirituality in medicine,” he explains.
Dr. Wilson notes that he later drew on these experiences when, as a hospitalist at a regional medical center, he was called to admit a woman to the hospital from the emergency department. She was dressed in traditional Muslim clothing and spoke no English. Knowing that it is offensive for traditional Islamic women to be examined by a man, Dr. Wilson asked through the woman’s friends who had accompanied the woman whether she would prefer a woman doctor and whether she would be comfortable at least with his taking her history. She answered “yes” to both questions.
Dr. Wilson prevailed upon a female doctor in a competing practice to perform the examination and also made a special effort to admit the patient to the female physician in his own group who would be working the next day.
“It’s not that I’ve been trained in cultural awareness,” he says, “but this case points out the importance of recognizing other traditions, so that you can deliver care that is effective and culturally sensitive.”
Earning Trust
Maren Grainger-Monsen, MD, senior research scholar and director of the Biomedical Ethics in Film Program at the Stanford University Center for Biomedical Ethics (Calif.), has produced several award-winning films about patients from different racial and ethnic groups and their interface with the healthcare delivery system. In the process of filming patients with their families, she has realized that as a physician she often mistook respect for trust.
Patients, she says, “would be respectful and polite and seeming to agree with me, but as I have worked on these films and spent time with families, I realize that they approach the physician and the hospital system with more caution and they wait to see if the people are trustworthy.”
Jack Percelay, MD, chair, American Academy of Pediatrics Section on Hospital Medicine and SHM Board member, notes that “hospitalists face more difficulty with some cultural issues than primary care providers because we’re thrust into a situation of an acute illness, whereas the primary care provider at least gets an opportunity to establish a relationship. In pediatric hospital medicine, we need to be very careful and cognizant of this, make sure we employ translation resources and social workers, and be hesitant to judge someone else’s value system, while still advocating for the patient.”
While it can be important to acquire a baseline of knowledge about dominant cultural and religious groups (especially if a group comprises a sizable percentage of patients seen at one’s institution), Dr. Fernandez cautions against using a laundry list approach to cultural competency.
“It’s helpful to know, for instance, that many Vietnamese here came as a result of the Vietnam War,” she says. “On the other hand, it is not that helpful to say [something like], ‘Don’t shake hands with Vietnamese.’ Our patients are forgiving of whether we shake hands or don’t shake hands. They are less forgiving when we appear not to listen to them.”
Lost in Translation
Nearly 14% of people who live in the United States speak a language other than English in their homes, according to the U.S. Census Bureau’s Census 2000 estimates.2 When a person with limited English proficiency (LEP) enters the healthcare system, the potential for medical error increases if language barriers are not addressed. Indeed, healthcare institutions that receive federal healthcare dollars (Medicare, Medicaid) are obligated under Title VI of the Civil Rights Act of 1964 to provide access to interpreter services—free of charge—to LEP patients.
Those interviewed for this article advised that physicians should avail themselves of trained medical interpreters whenever possible. These professionals are trained to translate providers’ and patients’ communications verbatim—without editing—and are conversant with medical terminology.
However, such resources may not be available in rural hospitals. Such is the case for William D. Atchley, Jr., MD, medical director of the Hospitalist Service at Sentara Careplex Hospital in Hampton, Va., who recently used a cafeteria staff person to translate while he examined and admitted a Mexico-born patient with rhabdomyolysis that resulted from heat exhaustion. Dr. Atchley, an SHM Board member, has also used family members as translators. He notes, though, that “trying to get an understanding of what is going on can be difficult at times because the one family member who may act as a translator may not have as good a command of English [as a trained medical interpreter]. You are always fearful that something could get lost in translation.”
Even large institutions that have medical interpreters on staff may not have 24-hour coverage. In that case, telephone interpreters through AT&T’s Language Line service can be another option (www.languageline.com). Physicians can also work with ad-hoc interpreters, defined as family members or friends who act as interpreters, but are not professionally trained, says Dr. Fernandez.
“It can pay off to first take a few minutes to explain to these interpreters that you want them to repeat everything they hear as much word for word as they can,” she explains. “Tell them that you will give them time to participate in the conversation—as a family member—later on. First, you want them to play this narrow role as interpreter, and later you will let them add information as the family member because their contribution is also valuable.”
Young people, including teenage children, should not be used to interpret unless the situation is immediately life-threatening. “There has been a lot of research,” says Dr. Fernandez, “showing that [using children as interpreters] distorts family roles and makes the children uncomfortable.”
For example, says Dr. Grainger-Monsen, it would be completely inappropriate for a child to translate while a physician asks his mother about her past sexual history or vaginal bleeding.

The Time It Takes
At San Francisco General Hospital, where Dr. Fernandez is an attending physician, there are 140 languages spoken each month. She says the variety of patient backgrounds presents a challenge even for someone like herself, who has conducted extensive research on barriers to minority healthcare. She admits that she sometimes experiences an “internal groan” when she notices that the next patient in her busy clinic day is someone who speaks a language that she doesn’t. Like many of the hospitalists interviewed for this article, Dr. Fernandez notes that because using medical interpreters is time-consuming, she experiences initial resistance to the process.
A 2004 Canadian study examined the relationship between length of stay and LEP in the ambulatory care setting. It found that LEP patients stayed in the hospital longer for conditions, such as unstable coronary syndromes and chest pain, stroke, diabetes, and elective hip replacement.3
Issues about cultural competency are “fairly complex,” notes Alpesh Amin, MD, MBA, FACP, executive director Hospitalist Program and vice chair for clinical affairs, Department of Medicine at the University of California, Irvine, and SHM Board member. Sorting through issues surrounding patients’ beliefs toward healthcare, as well as their family values and dynamics, “takes time to resolve, and if I really want to understand your personal beliefs, I’ve got to be willing to sit down and talk about it. But, I’m not going to get paid for that time. This is not a reimbursable expense for the physician.”
Still, taking time to explore a patient’s preferences could also shorten length of stay if, for instance, the patient indicated that prescribed management indicated after an expensive test would not be his choice of care, says Dr. Amin.
Understanding what beliefs and experiences patients bring to the table, as well as their past health behaviors, does involve a time investment, agrees Minn.-based Russell Holman, MD, national medical director for Cogent Healthcare, Inc. and SHM Board member. But that investment “can only help efficiency,” he maintains. “We’ve invested ourselves tremendously in terms of identifying what are best practices for a patient with heart failure, or pneumonia, or heart attack, but the cultural competency dimension of healthcare has been largely overlooked.”
Training in cultural competency is piecemeal at best, notes Dr. Holman, and often acquired on the job. He recalls a situation in which he learned first-hand the profound effect that culture has on health. While working with a Hmong man who was in a coma and on a ventilator, Dr. Holman initially attempted to seek decision-making from the patient’s wife.
“I found out that was not the appropriate decision-making process for their culture,” says Dr. Holman. The discussion was initiated in the patient’s room, and was moved to a lecture-style classroom to accommodate the 37 members of the man’s clan who came to discuss his condition.
“The fascinating thing to me was that the patient’s wife and the other women sat in the back of the classroom and did not speak the entire time,” explains Dr. Holman. “The decisions were largely conducted by the clan elders. I also found out that my patient was the clan leader, and the elders had very clear goals in mind. The goal was to keep this individual alive, because he was so important as a figure in the clan. I learned that their culture had a profound impact on their expectations of me as a physician and a provider—how I conducted myself in terms of family and clan communications, what resources I brought to bear to try and stabilize and improve his health, and how I worked with specialists. I also learned that although some clan and family members were fluent in English, even modest miscommunications, if I were to use them as translators, could result in significant setbacks.”
Prior to his current position with Cogent Healthcare, Dr. Holman managed a group of 30 hospitalists at HealthPartners Medical Group in Minnesota and in partnership with the Center for International Health developed a cultural competency curriculum for their group and for the University of Minnesota residents in training at Regions Hospital in St. Paul.
“When you are busy working in the hospital, you need to be able to quickly access some resources to be able to give you a ‘just in time’ amount of information and awareness” with which to approach your patient, he says.
Agents for Change?
In addition to Title VI compliance, hospitals are now surveyed by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and are evaluated on their ability to provide language services.
“This is a changing area,” notes Dr. Fernandez, “and I think it is important for hospitalists to be on the forefront of that change, part of the process that says, ‘Yes, we need to be able to provide more efficient, more patient-centered, and safer care.’ Language barriers, as one example, are inefficient, are dangerous, and are clearly associated with increased medical error.”
Dr. Percelay believes that dealing with patients from different backgrounds involves using “common sense, being respectful and legitimately curious, and avoiding shortcuts in terms of translation issues. I think if people have an inherent respect for diversity, and are open to it, it can enrich your practice.”
Dr. Fernandez agrees. “Practicing medicine in a patient-centered way is ultimately a more rewarding way to work and live,” she says. “There also needs to be reform at a national level that allows physicians and hospitalists to be appropriately compensated for much of the conversation and bedside work that we do.” TH
Writer Gretchen Henkel lives in California and writes regularly about healthcare.
References
- Unequal Treatment: Understanding Racial and Ethnic Disparities in Health Care. Institute of Medicine, National Academy of Sciences. 2002. Available from the National Academy Press Available at http://books.nap.edu/catalog/11036.html. Last accessed July 27, 2005; and Unequal Treatment: What Healthcare Providers Need to Know about Racial and Ethnic Disparities in Healthcare. Institute of Medicine, National Academy of Sciences. Available at www.nap.edu/catalog/10260.html. Last accessed July 27, 2005.
- Shin HB, Bruno R. Language use and English-speaking ability: a Census 2000 brief. U.S. Census Bureau, 2003. Available online at www.census.gov/population/www/cen2000/briefs.html. Last accessed July 27, 2005.
- John-Baptiste A, Naglie G, Tomlinson G, et al. The effect of English language proficiency on length of stay and in-hospital mortality. J Gen Intern Med. March 2004;19(3):221-228.
As the diversity of the U.S. population increases, so do the challenges for hospitalists, as they seek to deliver truly patient-centered care in the 21st century. The March 2002 Institute of Medicine report, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care,” concluded that, while some care inequities can be attributed to access and linguistic barriers, healthcare providers themselves may contribute to disparities in care for their minority patients.1
How can hospitalists ensure that they bridge the cultural divide between themselves and their patients from different racial, ethnic, and cultural backgrounds and avoid potential missteps in care delivery?
An Open Mind
Experts in cultural competency interviewed for this article explained that hospitalists can readily acquire the knowledge and skills necessary to effectively provide patient-centered care for all their patients. (See “Resource List,” p. 27.) But the most critical element in culturally competent healthcare delivery is the attitude with which the provider approaches his or her patients.
“I don’t think we can teach attitude,” says Alicia Fernandez, MD, assistant clinical professor of medicine, Division of General Internal Medicine, University of California, San Francisco, a nationally known researcher on language barriers and former full-time hospitalist. “But I think that any doctor who’s trying to do the best he or she can by their individual patients has the right attitude, which is to remain open to practicing patient-centered care.”
—Jack Percelay, MD
Physicians must be able to approach each patient on his or her own terms, and to acknowledge that members of different racial and ethnic groups hold beliefs about health and illness that diverge from those of Western medicine.
“You really need to have the capacity to empathize, and turn off all of your own belief systems, in some cases, to listen,” says Stacy Goldsholl, MD, a hospitalist based in Wilmington, N.C., and an SHM Board member.
Dr. Goldsholl recalls one situation involving a patient who was a Jehovah’s Witness who entered the hospital with a gastrointestinal bleed. Because of religious proscriptions, the patient refused a blood transfusion.
“It was extremely difficult as a scientist-trained physician, to watch someone bleed to a hemoglobin of 5, knowing that a simple transfusion would save this patient,” recalls Dr. Goldsholl.
The patient later underwent surgery without a transfusion and survived, but Dr. Goldsholl believes this case illustrates that delivering patient-centered care requires the practice not just of the science—but the art—of medicine.
“I think the real message is, you have to think outside of your own box,” she offers. “In addition, the cultural issues become much more pronounced when you start to approach end-of-life issues that take on more of a cultural, ethnic. and spiritual dimension.”
Awareness and Knowledge
Mitchell D. Wilson, MD, believes “the average American tends to be very ethnocentric. We are not taught cultural awareness in recognizing our own inherent biases, so we are unable to take the next step and recognize that there is a gap between our culture and another person’s culture that would require us to take a different approach.”
Dr. Wilson is associate professor of medicine, medical director and physician advisor, Department of Clinical Care Management, University of North Carolina (UNC) Hospitals, and section chief of hospital medicine and medical director, FirstHealth of the Carolinas Hospitalist Services, UNC School of Medicine, Chapel Hill. He is also an SHM Board member.
Dr. Wilson says that his own cultural awareness emanated from participation in a spirituality and medicine program for student doctors and nurses at the medical school where he trained and was later on faculty.
“I was able to function both as a small group facilitator and a large group panelist, and we used a case-based format for creating awareness of spirituality in medicine,” he explains.
Dr. Wilson notes that he later drew on these experiences when, as a hospitalist at a regional medical center, he was called to admit a woman to the hospital from the emergency department. She was dressed in traditional Muslim clothing and spoke no English. Knowing that it is offensive for traditional Islamic women to be examined by a man, Dr. Wilson asked through the woman’s friends who had accompanied the woman whether she would prefer a woman doctor and whether she would be comfortable at least with his taking her history. She answered “yes” to both questions.
Dr. Wilson prevailed upon a female doctor in a competing practice to perform the examination and also made a special effort to admit the patient to the female physician in his own group who would be working the next day.
“It’s not that I’ve been trained in cultural awareness,” he says, “but this case points out the importance of recognizing other traditions, so that you can deliver care that is effective and culturally sensitive.”
Earning Trust
Maren Grainger-Monsen, MD, senior research scholar and director of the Biomedical Ethics in Film Program at the Stanford University Center for Biomedical Ethics (Calif.), has produced several award-winning films about patients from different racial and ethnic groups and their interface with the healthcare delivery system. In the process of filming patients with their families, she has realized that as a physician she often mistook respect for trust.
Patients, she says, “would be respectful and polite and seeming to agree with me, but as I have worked on these films and spent time with families, I realize that they approach the physician and the hospital system with more caution and they wait to see if the people are trustworthy.”
Jack Percelay, MD, chair, American Academy of Pediatrics Section on Hospital Medicine and SHM Board member, notes that “hospitalists face more difficulty with some cultural issues than primary care providers because we’re thrust into a situation of an acute illness, whereas the primary care provider at least gets an opportunity to establish a relationship. In pediatric hospital medicine, we need to be very careful and cognizant of this, make sure we employ translation resources and social workers, and be hesitant to judge someone else’s value system, while still advocating for the patient.”
While it can be important to acquire a baseline of knowledge about dominant cultural and religious groups (especially if a group comprises a sizable percentage of patients seen at one’s institution), Dr. Fernandez cautions against using a laundry list approach to cultural competency.
“It’s helpful to know, for instance, that many Vietnamese here came as a result of the Vietnam War,” she says. “On the other hand, it is not that helpful to say [something like], ‘Don’t shake hands with Vietnamese.’ Our patients are forgiving of whether we shake hands or don’t shake hands. They are less forgiving when we appear not to listen to them.”
Lost in Translation
Nearly 14% of people who live in the United States speak a language other than English in their homes, according to the U.S. Census Bureau’s Census 2000 estimates.2 When a person with limited English proficiency (LEP) enters the healthcare system, the potential for medical error increases if language barriers are not addressed. Indeed, healthcare institutions that receive federal healthcare dollars (Medicare, Medicaid) are obligated under Title VI of the Civil Rights Act of 1964 to provide access to interpreter services—free of charge—to LEP patients.
Those interviewed for this article advised that physicians should avail themselves of trained medical interpreters whenever possible. These professionals are trained to translate providers’ and patients’ communications verbatim—without editing—and are conversant with medical terminology.
However, such resources may not be available in rural hospitals. Such is the case for William D. Atchley, Jr., MD, medical director of the Hospitalist Service at Sentara Careplex Hospital in Hampton, Va., who recently used a cafeteria staff person to translate while he examined and admitted a Mexico-born patient with rhabdomyolysis that resulted from heat exhaustion. Dr. Atchley, an SHM Board member, has also used family members as translators. He notes, though, that “trying to get an understanding of what is going on can be difficult at times because the one family member who may act as a translator may not have as good a command of English [as a trained medical interpreter]. You are always fearful that something could get lost in translation.”
Even large institutions that have medical interpreters on staff may not have 24-hour coverage. In that case, telephone interpreters through AT&T’s Language Line service can be another option (www.languageline.com). Physicians can also work with ad-hoc interpreters, defined as family members or friends who act as interpreters, but are not professionally trained, says Dr. Fernandez.
“It can pay off to first take a few minutes to explain to these interpreters that you want them to repeat everything they hear as much word for word as they can,” she explains. “Tell them that you will give them time to participate in the conversation—as a family member—later on. First, you want them to play this narrow role as interpreter, and later you will let them add information as the family member because their contribution is also valuable.”
Young people, including teenage children, should not be used to interpret unless the situation is immediately life-threatening. “There has been a lot of research,” says Dr. Fernandez, “showing that [using children as interpreters] distorts family roles and makes the children uncomfortable.”
For example, says Dr. Grainger-Monsen, it would be completely inappropriate for a child to translate while a physician asks his mother about her past sexual history or vaginal bleeding.
The Time It Takes
At San Francisco General Hospital, where Dr. Fernandez is an attending physician, there are 140 languages spoken each month. She says the variety of patient backgrounds presents a challenge even for someone like herself, who has conducted extensive research on barriers to minority healthcare. She admits that she sometimes experiences an “internal groan” when she notices that the next patient in her busy clinic day is someone who speaks a language that she doesn’t. Like many of the hospitalists interviewed for this article, Dr. Fernandez notes that because using medical interpreters is time-consuming, she experiences initial resistance to the process.
A 2004 Canadian study examined the relationship between length of stay and LEP in the ambulatory care setting. It found that LEP patients stayed in the hospital longer for conditions, such as unstable coronary syndromes and chest pain, stroke, diabetes, and elective hip replacement.3
Issues about cultural competency are “fairly complex,” notes Alpesh Amin, MD, MBA, FACP, executive director Hospitalist Program and vice chair for clinical affairs, Department of Medicine at the University of California, Irvine, and SHM Board member. Sorting through issues surrounding patients’ beliefs toward healthcare, as well as their family values and dynamics, “takes time to resolve, and if I really want to understand your personal beliefs, I’ve got to be willing to sit down and talk about it. But, I’m not going to get paid for that time. This is not a reimbursable expense for the physician.”
Still, taking time to explore a patient’s preferences could also shorten length of stay if, for instance, the patient indicated that prescribed management indicated after an expensive test would not be his choice of care, says Dr. Amin.
Understanding what beliefs and experiences patients bring to the table, as well as their past health behaviors, does involve a time investment, agrees Minn.-based Russell Holman, MD, national medical director for Cogent Healthcare, Inc. and SHM Board member. But that investment “can only help efficiency,” he maintains. “We’ve invested ourselves tremendously in terms of identifying what are best practices for a patient with heart failure, or pneumonia, or heart attack, but the cultural competency dimension of healthcare has been largely overlooked.”
Training in cultural competency is piecemeal at best, notes Dr. Holman, and often acquired on the job. He recalls a situation in which he learned first-hand the profound effect that culture has on health. While working with a Hmong man who was in a coma and on a ventilator, Dr. Holman initially attempted to seek decision-making from the patient’s wife.
“I found out that was not the appropriate decision-making process for their culture,” says Dr. Holman. The discussion was initiated in the patient’s room, and was moved to a lecture-style classroom to accommodate the 37 members of the man’s clan who came to discuss his condition.
“The fascinating thing to me was that the patient’s wife and the other women sat in the back of the classroom and did not speak the entire time,” explains Dr. Holman. “The decisions were largely conducted by the clan elders. I also found out that my patient was the clan leader, and the elders had very clear goals in mind. The goal was to keep this individual alive, because he was so important as a figure in the clan. I learned that their culture had a profound impact on their expectations of me as a physician and a provider—how I conducted myself in terms of family and clan communications, what resources I brought to bear to try and stabilize and improve his health, and how I worked with specialists. I also learned that although some clan and family members were fluent in English, even modest miscommunications, if I were to use them as translators, could result in significant setbacks.”
Prior to his current position with Cogent Healthcare, Dr. Holman managed a group of 30 hospitalists at HealthPartners Medical Group in Minnesota and in partnership with the Center for International Health developed a cultural competency curriculum for their group and for the University of Minnesota residents in training at Regions Hospital in St. Paul.
“When you are busy working in the hospital, you need to be able to quickly access some resources to be able to give you a ‘just in time’ amount of information and awareness” with which to approach your patient, he says.
Agents for Change?
In addition to Title VI compliance, hospitals are now surveyed by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and are evaluated on their ability to provide language services.
“This is a changing area,” notes Dr. Fernandez, “and I think it is important for hospitalists to be on the forefront of that change, part of the process that says, ‘Yes, we need to be able to provide more efficient, more patient-centered, and safer care.’ Language barriers, as one example, are inefficient, are dangerous, and are clearly associated with increased medical error.”
Dr. Percelay believes that dealing with patients from different backgrounds involves using “common sense, being respectful and legitimately curious, and avoiding shortcuts in terms of translation issues. I think if people have an inherent respect for diversity, and are open to it, it can enrich your practice.”
Dr. Fernandez agrees. “Practicing medicine in a patient-centered way is ultimately a more rewarding way to work and live,” she says. “There also needs to be reform at a national level that allows physicians and hospitalists to be appropriately compensated for much of the conversation and bedside work that we do.” TH
Writer Gretchen Henkel lives in California and writes regularly about healthcare.
References
- Unequal Treatment: Understanding Racial and Ethnic Disparities in Health Care. Institute of Medicine, National Academy of Sciences. 2002. Available from the National Academy Press Available at http://books.nap.edu/catalog/11036.html. Last accessed July 27, 2005; and Unequal Treatment: What Healthcare Providers Need to Know about Racial and Ethnic Disparities in Healthcare. Institute of Medicine, National Academy of Sciences. Available at www.nap.edu/catalog/10260.html. Last accessed July 27, 2005.
- Shin HB, Bruno R. Language use and English-speaking ability: a Census 2000 brief. U.S. Census Bureau, 2003. Available online at www.census.gov/population/www/cen2000/briefs.html. Last accessed July 27, 2005.
- John-Baptiste A, Naglie G, Tomlinson G, et al. The effect of English language proficiency on length of stay and in-hospital mortality. J Gen Intern Med. March 2004;19(3):221-228.
As the diversity of the U.S. population increases, so do the challenges for hospitalists, as they seek to deliver truly patient-centered care in the 21st century. The March 2002 Institute of Medicine report, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care,” concluded that, while some care inequities can be attributed to access and linguistic barriers, healthcare providers themselves may contribute to disparities in care for their minority patients.1
How can hospitalists ensure that they bridge the cultural divide between themselves and their patients from different racial, ethnic, and cultural backgrounds and avoid potential missteps in care delivery?
An Open Mind
Experts in cultural competency interviewed for this article explained that hospitalists can readily acquire the knowledge and skills necessary to effectively provide patient-centered care for all their patients. (See “Resource List,” p. 27.) But the most critical element in culturally competent healthcare delivery is the attitude with which the provider approaches his or her patients.
“I don’t think we can teach attitude,” says Alicia Fernandez, MD, assistant clinical professor of medicine, Division of General Internal Medicine, University of California, San Francisco, a nationally known researcher on language barriers and former full-time hospitalist. “But I think that any doctor who’s trying to do the best he or she can by their individual patients has the right attitude, which is to remain open to practicing patient-centered care.”
—Jack Percelay, MD
Physicians must be able to approach each patient on his or her own terms, and to acknowledge that members of different racial and ethnic groups hold beliefs about health and illness that diverge from those of Western medicine.
“You really need to have the capacity to empathize, and turn off all of your own belief systems, in some cases, to listen,” says Stacy Goldsholl, MD, a hospitalist based in Wilmington, N.C., and an SHM Board member.
Dr. Goldsholl recalls one situation involving a patient who was a Jehovah’s Witness who entered the hospital with a gastrointestinal bleed. Because of religious proscriptions, the patient refused a blood transfusion.
“It was extremely difficult as a scientist-trained physician, to watch someone bleed to a hemoglobin of 5, knowing that a simple transfusion would save this patient,” recalls Dr. Goldsholl.
The patient later underwent surgery without a transfusion and survived, but Dr. Goldsholl believes this case illustrates that delivering patient-centered care requires the practice not just of the science—but the art—of medicine.
“I think the real message is, you have to think outside of your own box,” she offers. “In addition, the cultural issues become much more pronounced when you start to approach end-of-life issues that take on more of a cultural, ethnic. and spiritual dimension.”
Awareness and Knowledge
Mitchell D. Wilson, MD, believes “the average American tends to be very ethnocentric. We are not taught cultural awareness in recognizing our own inherent biases, so we are unable to take the next step and recognize that there is a gap between our culture and another person’s culture that would require us to take a different approach.”
Dr. Wilson is associate professor of medicine, medical director and physician advisor, Department of Clinical Care Management, University of North Carolina (UNC) Hospitals, and section chief of hospital medicine and medical director, FirstHealth of the Carolinas Hospitalist Services, UNC School of Medicine, Chapel Hill. He is also an SHM Board member.
Dr. Wilson says that his own cultural awareness emanated from participation in a spirituality and medicine program for student doctors and nurses at the medical school where he trained and was later on faculty.
“I was able to function both as a small group facilitator and a large group panelist, and we used a case-based format for creating awareness of spirituality in medicine,” he explains.
Dr. Wilson notes that he later drew on these experiences when, as a hospitalist at a regional medical center, he was called to admit a woman to the hospital from the emergency department. She was dressed in traditional Muslim clothing and spoke no English. Knowing that it is offensive for traditional Islamic women to be examined by a man, Dr. Wilson asked through the woman’s friends who had accompanied the woman whether she would prefer a woman doctor and whether she would be comfortable at least with his taking her history. She answered “yes” to both questions.
Dr. Wilson prevailed upon a female doctor in a competing practice to perform the examination and also made a special effort to admit the patient to the female physician in his own group who would be working the next day.
“It’s not that I’ve been trained in cultural awareness,” he says, “but this case points out the importance of recognizing other traditions, so that you can deliver care that is effective and culturally sensitive.”
Earning Trust
Maren Grainger-Monsen, MD, senior research scholar and director of the Biomedical Ethics in Film Program at the Stanford University Center for Biomedical Ethics (Calif.), has produced several award-winning films about patients from different racial and ethnic groups and their interface with the healthcare delivery system. In the process of filming patients with their families, she has realized that as a physician she often mistook respect for trust.
Patients, she says, “would be respectful and polite and seeming to agree with me, but as I have worked on these films and spent time with families, I realize that they approach the physician and the hospital system with more caution and they wait to see if the people are trustworthy.”
Jack Percelay, MD, chair, American Academy of Pediatrics Section on Hospital Medicine and SHM Board member, notes that “hospitalists face more difficulty with some cultural issues than primary care providers because we’re thrust into a situation of an acute illness, whereas the primary care provider at least gets an opportunity to establish a relationship. In pediatric hospital medicine, we need to be very careful and cognizant of this, make sure we employ translation resources and social workers, and be hesitant to judge someone else’s value system, while still advocating for the patient.”
While it can be important to acquire a baseline of knowledge about dominant cultural and religious groups (especially if a group comprises a sizable percentage of patients seen at one’s institution), Dr. Fernandez cautions against using a laundry list approach to cultural competency.
“It’s helpful to know, for instance, that many Vietnamese here came as a result of the Vietnam War,” she says. “On the other hand, it is not that helpful to say [something like], ‘Don’t shake hands with Vietnamese.’ Our patients are forgiving of whether we shake hands or don’t shake hands. They are less forgiving when we appear not to listen to them.”
Lost in Translation
Nearly 14% of people who live in the United States speak a language other than English in their homes, according to the U.S. Census Bureau’s Census 2000 estimates.2 When a person with limited English proficiency (LEP) enters the healthcare system, the potential for medical error increases if language barriers are not addressed. Indeed, healthcare institutions that receive federal healthcare dollars (Medicare, Medicaid) are obligated under Title VI of the Civil Rights Act of 1964 to provide access to interpreter services—free of charge—to LEP patients.
Those interviewed for this article advised that physicians should avail themselves of trained medical interpreters whenever possible. These professionals are trained to translate providers’ and patients’ communications verbatim—without editing—and are conversant with medical terminology.
However, such resources may not be available in rural hospitals. Such is the case for William D. Atchley, Jr., MD, medical director of the Hospitalist Service at Sentara Careplex Hospital in Hampton, Va., who recently used a cafeteria staff person to translate while he examined and admitted a Mexico-born patient with rhabdomyolysis that resulted from heat exhaustion. Dr. Atchley, an SHM Board member, has also used family members as translators. He notes, though, that “trying to get an understanding of what is going on can be difficult at times because the one family member who may act as a translator may not have as good a command of English [as a trained medical interpreter]. You are always fearful that something could get lost in translation.”
Even large institutions that have medical interpreters on staff may not have 24-hour coverage. In that case, telephone interpreters through AT&T’s Language Line service can be another option (www.languageline.com). Physicians can also work with ad-hoc interpreters, defined as family members or friends who act as interpreters, but are not professionally trained, says Dr. Fernandez.
“It can pay off to first take a few minutes to explain to these interpreters that you want them to repeat everything they hear as much word for word as they can,” she explains. “Tell them that you will give them time to participate in the conversation—as a family member—later on. First, you want them to play this narrow role as interpreter, and later you will let them add information as the family member because their contribution is also valuable.”
Young people, including teenage children, should not be used to interpret unless the situation is immediately life-threatening. “There has been a lot of research,” says Dr. Fernandez, “showing that [using children as interpreters] distorts family roles and makes the children uncomfortable.”
For example, says Dr. Grainger-Monsen, it would be completely inappropriate for a child to translate while a physician asks his mother about her past sexual history or vaginal bleeding.
The Time It Takes
At San Francisco General Hospital, where Dr. Fernandez is an attending physician, there are 140 languages spoken each month. She says the variety of patient backgrounds presents a challenge even for someone like herself, who has conducted extensive research on barriers to minority healthcare. She admits that she sometimes experiences an “internal groan” when she notices that the next patient in her busy clinic day is someone who speaks a language that she doesn’t. Like many of the hospitalists interviewed for this article, Dr. Fernandez notes that because using medical interpreters is time-consuming, she experiences initial resistance to the process.
A 2004 Canadian study examined the relationship between length of stay and LEP in the ambulatory care setting. It found that LEP patients stayed in the hospital longer for conditions, such as unstable coronary syndromes and chest pain, stroke, diabetes, and elective hip replacement.3
Issues about cultural competency are “fairly complex,” notes Alpesh Amin, MD, MBA, FACP, executive director Hospitalist Program and vice chair for clinical affairs, Department of Medicine at the University of California, Irvine, and SHM Board member. Sorting through issues surrounding patients’ beliefs toward healthcare, as well as their family values and dynamics, “takes time to resolve, and if I really want to understand your personal beliefs, I’ve got to be willing to sit down and talk about it. But, I’m not going to get paid for that time. This is not a reimbursable expense for the physician.”
Still, taking time to explore a patient’s preferences could also shorten length of stay if, for instance, the patient indicated that prescribed management indicated after an expensive test would not be his choice of care, says Dr. Amin.
Understanding what beliefs and experiences patients bring to the table, as well as their past health behaviors, does involve a time investment, agrees Minn.-based Russell Holman, MD, national medical director for Cogent Healthcare, Inc. and SHM Board member. But that investment “can only help efficiency,” he maintains. “We’ve invested ourselves tremendously in terms of identifying what are best practices for a patient with heart failure, or pneumonia, or heart attack, but the cultural competency dimension of healthcare has been largely overlooked.”
Training in cultural competency is piecemeal at best, notes Dr. Holman, and often acquired on the job. He recalls a situation in which he learned first-hand the profound effect that culture has on health. While working with a Hmong man who was in a coma and on a ventilator, Dr. Holman initially attempted to seek decision-making from the patient’s wife.
“I found out that was not the appropriate decision-making process for their culture,” says Dr. Holman. The discussion was initiated in the patient’s room, and was moved to a lecture-style classroom to accommodate the 37 members of the man’s clan who came to discuss his condition.
“The fascinating thing to me was that the patient’s wife and the other women sat in the back of the classroom and did not speak the entire time,” explains Dr. Holman. “The decisions were largely conducted by the clan elders. I also found out that my patient was the clan leader, and the elders had very clear goals in mind. The goal was to keep this individual alive, because he was so important as a figure in the clan. I learned that their culture had a profound impact on their expectations of me as a physician and a provider—how I conducted myself in terms of family and clan communications, what resources I brought to bear to try and stabilize and improve his health, and how I worked with specialists. I also learned that although some clan and family members were fluent in English, even modest miscommunications, if I were to use them as translators, could result in significant setbacks.”
Prior to his current position with Cogent Healthcare, Dr. Holman managed a group of 30 hospitalists at HealthPartners Medical Group in Minnesota and in partnership with the Center for International Health developed a cultural competency curriculum for their group and for the University of Minnesota residents in training at Regions Hospital in St. Paul.
“When you are busy working in the hospital, you need to be able to quickly access some resources to be able to give you a ‘just in time’ amount of information and awareness” with which to approach your patient, he says.
Agents for Change?
In addition to Title VI compliance, hospitals are now surveyed by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and are evaluated on their ability to provide language services.
“This is a changing area,” notes Dr. Fernandez, “and I think it is important for hospitalists to be on the forefront of that change, part of the process that says, ‘Yes, we need to be able to provide more efficient, more patient-centered, and safer care.’ Language barriers, as one example, are inefficient, are dangerous, and are clearly associated with increased medical error.”
Dr. Percelay believes that dealing with patients from different backgrounds involves using “common sense, being respectful and legitimately curious, and avoiding shortcuts in terms of translation issues. I think if people have an inherent respect for diversity, and are open to it, it can enrich your practice.”
Dr. Fernandez agrees. “Practicing medicine in a patient-centered way is ultimately a more rewarding way to work and live,” she says. “There also needs to be reform at a national level that allows physicians and hospitalists to be appropriately compensated for much of the conversation and bedside work that we do.” TH
Writer Gretchen Henkel lives in California and writes regularly about healthcare.
References
- Unequal Treatment: Understanding Racial and Ethnic Disparities in Health Care. Institute of Medicine, National Academy of Sciences. 2002. Available from the National Academy Press Available at http://books.nap.edu/catalog/11036.html. Last accessed July 27, 2005; and Unequal Treatment: What Healthcare Providers Need to Know about Racial and Ethnic Disparities in Healthcare. Institute of Medicine, National Academy of Sciences. Available at www.nap.edu/catalog/10260.html. Last accessed July 27, 2005.
- Shin HB, Bruno R. Language use and English-speaking ability: a Census 2000 brief. U.S. Census Bureau, 2003. Available online at www.census.gov/population/www/cen2000/briefs.html. Last accessed July 27, 2005.
- John-Baptiste A, Naglie G, Tomlinson G, et al. The effect of English language proficiency on length of stay and in-hospital mortality. J Gen Intern Med. March 2004;19(3):221-228.
Community-Acquired Pneumonia: Implications for the Hospitalized Child
Pneumonia is associated with as many as 2 million annual deaths among children globally and 19% of all deaths in children less than 5 years of age (1). It is one of the most common diagnoses made in the acutely ill child, with an annual incidence of 34 to 40 cases per 1,000 children in Europe and North America.
In the past, viral pathogens were estimated to cause as many as 80% of cases. Streptococcus pneumoniae was generally regarded as the most frequent bacterial cause of community-acquired pneumonia (CAP), especially in cases with complicated parapneumonic effusions. Infectious etiologies are age specific, with bacterial etiologies predominating in the very young infant and viral pathogens in the older infant and adult (Table 1). Knowledge of the most likely pathogen, the prevailing susceptibilities of these infecting pathogens, and the severity of the illness will help guide antibiotic and other treatment decision making.
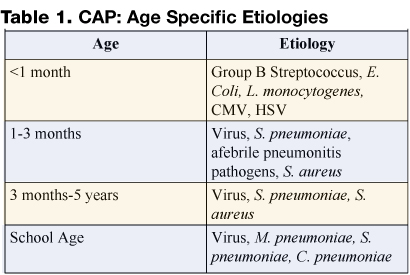
Most children do not require hospital admission, and mildly ill children who likely have a viral illness do not need antibiotics. The following guideline will attempt to help the practitioner identify those who do require hospitalization and provide an approach to management of those with complicated infection.
Recognition of the Patient with CAP
The first obstacle is to identify the patient with pneumonia. In managing the child with CAP, it is important to distinguish those with other underlying pathology, including asthma, RSV, or other confirmed viral etiology. It is important to remember that pathogens in the compromised host, cystic fibrosis patient, or patient with other chronic pulmonary pathology are different from typical CAP pathogens and include a wide differential. Most patients with CAP have an acute illness associated with fever (>38°C), cough, and evidence of lower respiratory tract symptoms/signs. Chest radiograph typically shows pulmonary infiltrate. Whether this is patchy infiltrate or lobar in appearance can assist the practitioner in treatment decision making in that the latter is much more likely to be associated with a bacterial etiology.
Once the diagnosis is considered, further assessment should focus on hydration status, hemodynamic parameters, and oxygenation. A careful assessment should identify other associated foci (i.e., meningitis or bacteremia) on examination and laboratory evaluation.
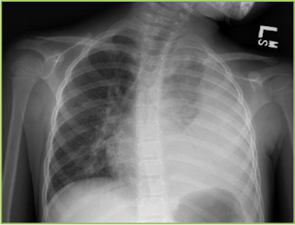
Identification of the Patient Requiring Hospitalization
Consider hospital admission for the toxic patient, those with altered mental status, significant dehydration, hypoxemia, dyspnea, grunting respirations, or retractions, and any patient with hemodynamic instability. Chest radiograph showing a significant pleural effusion should also be considered an indicator for hospital admission.
Bacterial pathogens are more likely in the severely ill patient, patients with a rapidly progressive process, and those with radiographic evidence of lobar consolidation or pleural effusion. Some children with viral processes may require admission for supportive care.
Prompt Recognition of the Patient with Empyema
For the patient with pneumonia and parapneumonic effusion, distinction between a free-flowing effusion and pleural empyema is critical. Standard plain film can identify pulmonary infiltrate and often effusion and lateral decubitus films can help identify free flowing effusion (Figure 1). While CT scan more effectively identifies pleural fibrinous adhesions that may entrap lung, ultrasound most effectively identifies complex fluid collections with loculation and septation, and it can be utilized to guide thoracentesis.
Empyema is defined as pus in the pleural space and is estimated to occur in 10–40% of patients with pneumonia. Empyema may also result from causes other than a complication of bacterial pneumonia, such as thoracic trauma or postsurgical complication, rupture of lung abscess, esophageal tear, or complication of indwelling catheter. It generally occurs in stages including acute (early-cloudy fluid), fibrino-purulent (thicker, multiloculated fluid), and organized (late with thick pleural peel and entrapment of lung).
Pleural fluid evaluation is important both in diagnosis and in guiding treatment in such cases. Pleural fluid collections are defined as transudative or exudative based on biochemical evaluation. Evaluation includes cell type and differential, pH, glucose, protein and LDH. Gram-stained smear needs to be performed on all specimens at the time of culture. Empyema is exudative, typically with low glucose and high LDH (Table 2 on page 64) (2).
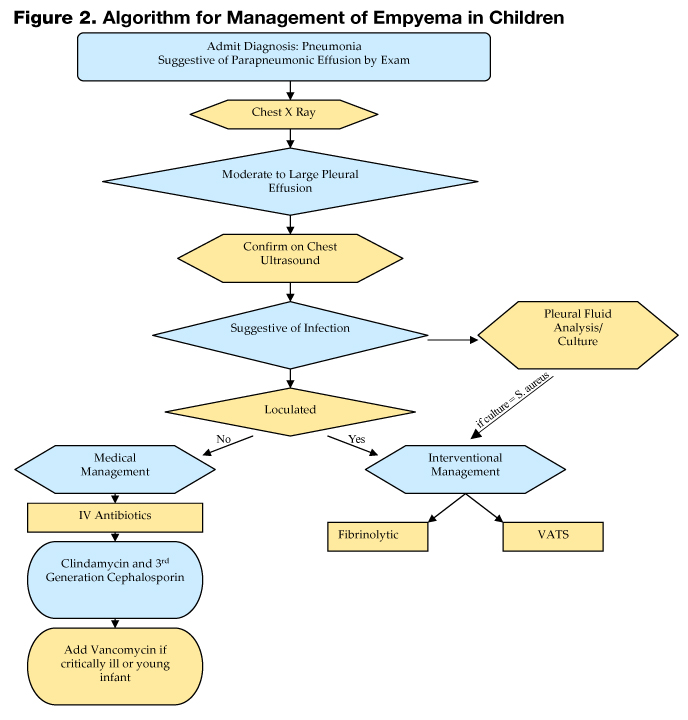
Changing Epidemiology and Antibiotic Decision Making
Data presented by Finland and Barnes in 1978 confirmed that S. pneumoniae, group A streptococcus (GAS), and Staphylococcus aureus were the most commonly identified pathogens in empyema cases in 1935, with S. aureus emerging in the 1950s (3). Most literature from the 1960–1980s detailing etiology of pneumonia with pleural empyema continued to emphasize the role of S. aureus in such cases. In all reviews, staphylococcal pneumonia is noted primarily to be a disease of infants. In 1 review of 100 cases of staphylococcal pneumonia, the median age was 5 months, 78 patients being below 1 year of age (4). Chartrand and McCracken analyzed 79 cases of staphylococcal pneumonia and noted that in about 75% of cases, staphylococcal pneumonia was a primary pneumonia in infants with a median age of 6 months. In this study, older children were more likely to have pulmonary involvement as a secondary finding in the setting of disseminated staphylococcal disease. A pleural effusion was found in 80% of infants with primary pneumonia and in 61% of those with secondary disease, thus providing the tip-off of a more serious process to the clinician (5). A high index of suspicion for S. aureus in the young infant with pneumonia is important, as physicians need to expect a rapidly progressive clinical course. Those infants frequently require ventilatory support, alteration in antibiotic choice, and the prompt recognition of pleural complications including pneumothoraces and pneumatoceles.
Data in the 1990s emphasized the role of multidrug resistant pneumococcus as a pathogen in empyema. In a recent review of cases in the postpneumococcal conjugate disease era, pneumococcus remained the most commonly confirmed etiologic agent, with other gram-positive pathogens, including GAS and S. aureus, also documented (6). Despite widespread implementation of pneumococcal conjugate vaccine (PCV), and a population based surveillance study in the US that suggested that adding PCV to the childhood immunization schedule was associated with a 10-fold greater reduction in pneumonia (7), serious pneumonia caused by S. pneumoniae continued to be reported. The prevalence of serotype 1 and 3 as the etiologies of such infections may limit the utility of the current vaccine. One study from Greece demonstrated that the most common serotypes causing bacteremic pneumonia were 14, 6B, 1 and 19F (8). Childhood empyema in the UK is noted to be increasing, and a recent study of 47 empyema cases confirmed pneumococcus as the major pathogen, with over half caused by serotype 1 (9).
More recent data suggest yet another change to the epidemiology of empyema. Schultz et al. from Houston, TX, reviewed a decade of experience from 1993–2002, and while they identified a decrease in total cases of empyema, the emergence of methicillin-resistant S. aureus (MRSA) infection was noted (10).
While MRSA has long been considered an important pathogen in the etiology of healthcare-associated infection, experience in our institution also confirms the appearance of an increasing number of cases of community-acquired MRSA disease. Vancomycin is clearly part of the treatment regimen in the child at risk for staphylococcal pneumonia, though many have utilized clindamycin for the non–critically ill patient. The increase in such cases clearly has important implications for treatment decisions, as MRSA with inducible clindamycin resistance is not yet recognized in every facility. Data are not available to confirm the utility of trimethoprim-sulfamethoxazole in serious community-aquired MRSA infections, and the role for newer antibiotics, such as linezolid, has not been clearly defined.
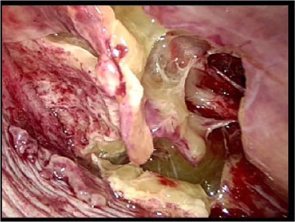
Management: Antibiotics and the Role of Pleural Drainage Procedures
Figure 2 on page 58 shows an algorithm that guides clinical management of the empyema patient. Once a diagnosis is made, attention should be directed to fluid and electrolyte correction, hemodynamic stabilization, and respiratory support (i.e., oxygenation and ventilation). Antibiotics should be initiated and the choice is based on severity of illness and age of the child.
Drainage of the pleural pus has long been recognized as integral to the success in treatment of pneumonia with empyema. Recently, there has been much debate concerning which modality to use and when.
Intrapleural fibrinolytic therapy has been shown in multiple studies to decrease length of stay without increased risk. Data compiled in the Cochrane database comparing fibrinolytic therapy vs. more conservative management suggests that intrapleural fibrinolytic therapy confers significant benefit when compared with normal saline control; however, a definitive statement was not made, given that the trial numbers were too small (11). More recent data from the Cochrane database and a systematic review suggest that video-assisted thoracostomy (VATS) performed early in the disease course is associated with better outcome than chest tube drainage with streptokinase with regard to duration of chest tube placement and hospital stay. However there are questions about validity, and this study is also too small to draw conclusions (12,13). Figure 3 shows the typical findings encountered at VATS in a child with empyema.
A retrospective chart review from our institution from December 2000 to March 2004, excluding immunocompromised hosts, found 96 cases of radiographic pneumonia with pleural effusion. Thirty-four met criteria for empyema, including ultrasound and/or chest CT showing pleural fluid loculation and septation, or purulent fluid/positive culture. Average age was 5 years, and pathogens were defined in 38% of patients. Length of stay averaged 9 days, with a range of 5–23 days. Two had no intervention and had a stay of 8 days, 14 had tube thoracostomy and had an average stay of 11.5 days with 6 failures, 10 had thoracostomy and fibrinolytic therapy with an average stay of 7 days, 3 had early VATS with an average stay of 7 days, and 5 had late VATS with an average stay of 10.4 days. In our institution, among invasive interventions, tube thoracostomy alone had longer LOS and more failures. Early VATS and intrapleural fibrinolysis have shorter stays and are on the lower end of the cost scale: $25,549 vs. $21,062 respectively (Figure 4).
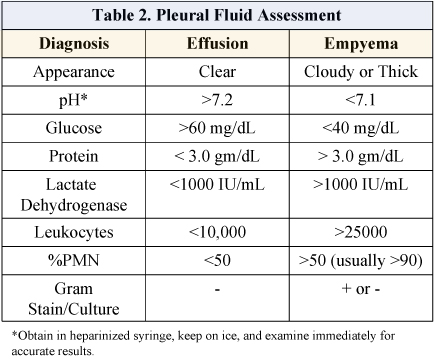
The decision for interventional management of empyema will likely be institutionally variable in the absence of large randomized controlled studies. Institutions with aggressive interventional radiologists may favor thoracostomy tube with fibrinolysis. Those with surgeons skilled in video-scopic surgery may provide early VATS. Data on interventions clearly show benefit beyond that provided by routine chest tube placement. The key becomes prompt diagnosis of empyema with early use of ultrasound, knowledge of local antibiotic susceptibilities, and clear guidelines set up by each institution to guide interventional management.
The Future
Increasing the accuracy of diagnostic testing for children with CAP would likely lead to decreased morbidity, mortality, and total cost of care. The use of PCR is becoming more widespread and could be utilized to more rapidly confirm the diagnosis of both chlamydophila pneumoniae, mycoplasma pneumoniae, and Influenza A virus (14). Influenza A is well known to cause serious morbidity and mortality and may be the most common virus causing CAP, with a comparable clinical burden to viruses such as respiratory syneytial virus. This is further evidence supporting universal childhood influenza immunization. Expansion of the serotypes included in pneumococcal conjugate vaccines (PCV) is to include serotypes 1 and 3, both currently non-PCV strains in the U.S. vaccine, is underway.
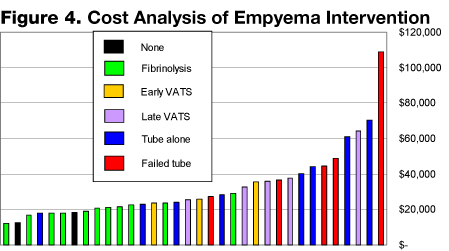
As the epidemiology of CAP continues to evolve, practitioners need to be aware of the prevalent pathogens in their region. In the age of continuing antimicrobial resistance of bacterial pathogens, it is important to know the local antimicrobial susceptibility patterns to appropriately choose empiric therapy when a bacterial process is suspected. Local laboratories can commonly provide this data.
Whatever the future holds, we continue to need the collaboration and expertise of the inpatient practitioner, the infectious disease specialist, and the surgeon/interventionalist. All are necessary to ensure the prompt recognition of empyema and the need for timely medical and surgical intervention for these patients.
References
- Bryce J, Boschi-Pinto C, Shibuya K, Black RE; WHO Child Health Epidemiology Reference Group. WHO estimates of the causes of death in children. Lancet. 2005;365:1147-52.
- Wheeler JG, Jacobs RF. Pleural effusions and empyema. In: Feigin RD, Cherry JD, Demmler GJ, Kaplan SL, eds. Textbook of Pediatric Infectious Diseases. 5th ed. Philadelphia, Pa: Saunders;2004:320-30.
- Finland M, Barnes MW. Changing ecology of acute bacterial empyema: occurrence and mortality at Boston City Hospital during 12 selected years from 1935 to 1972. J Infect Dis. 1978;137:274-91.
- Goel A, Bamford L, Hanslo D, Hussey G. Primary staphylococcal pneumonia in young children: a review of 100 cases. J Trop Pediatr. 1999;45:233-6.
- Chartrand SA, McCracken GH Jr. Staphylococcal pneumonia in infants and children Pediatr Infect Dis. 1982;1:19-23.
- Buckingham SC, King MD, Miller ML. Incidence and etiologies of complicated parapneumonic effusions in children, 1996 to 2001. Pediatr Infect Dis J. 2003;22:499-504.
- Poehling KA, Lafleur BJ, Szilagyi PG, et al. Populationbased impact of pneumococcal conjugate vaccine in young children. Pediatrics. 2004;114:755-61.
- Syriopoulou V, Daikos GL, Soulis K, et al. Epidemiology of invasive childhood pneumococcal infections in Greece. Acta Paediatr Suppl. 2000;89:30-4.
- Eastham KM, Freeman R, Kearns AM, et al. Clinical features, aetiology and outcome of empyema in children in the north east of England. Thorax. 2004;59:522-5.
- Schultz KD, Fan LL, Pinsky J, et al. The changing face of pleural empyemas in children: epidemiology and management. Pediatrics. 2004;113:1735-40.
- Cameron R, Davies HR. Intra-pleural fibrinolytic therapy versus conservative management in the treatment of para-pneumonic effusions and empyema. Cochrane Database Syst Rev. 2004:CD002312. Review.
- Coote N. Surgical versus non-surgical management of pleural empyema. Cochrane Database Syst Rev. 2002:CD001956. Review.
- Gates RL, Caniano DA, Hayes JR, Arca MJ. Does VATS provide optimal treatment of empyema in children? A systematic review. J Pediatr Surg. 2004;39:381-6. Review.
- Laundy M, Ajayi-Obe E, Hawrami K, Aitken C, Breuer J, Booy R. Influenza A community-acquired pneumonia in East London infants and young children. Pediatr Infect Dis J. 2003;22(Suppl):S223-7.
Pneumonia is associated with as many as 2 million annual deaths among children globally and 19% of all deaths in children less than 5 years of age (1). It is one of the most common diagnoses made in the acutely ill child, with an annual incidence of 34 to 40 cases per 1,000 children in Europe and North America.
In the past, viral pathogens were estimated to cause as many as 80% of cases. Streptococcus pneumoniae was generally regarded as the most frequent bacterial cause of community-acquired pneumonia (CAP), especially in cases with complicated parapneumonic effusions. Infectious etiologies are age specific, with bacterial etiologies predominating in the very young infant and viral pathogens in the older infant and adult (Table 1). Knowledge of the most likely pathogen, the prevailing susceptibilities of these infecting pathogens, and the severity of the illness will help guide antibiotic and other treatment decision making.
Most children do not require hospital admission, and mildly ill children who likely have a viral illness do not need antibiotics. The following guideline will attempt to help the practitioner identify those who do require hospitalization and provide an approach to management of those with complicated infection.
Recognition of the Patient with CAP
The first obstacle is to identify the patient with pneumonia. In managing the child with CAP, it is important to distinguish those with other underlying pathology, including asthma, RSV, or other confirmed viral etiology. It is important to remember that pathogens in the compromised host, cystic fibrosis patient, or patient with other chronic pulmonary pathology are different from typical CAP pathogens and include a wide differential. Most patients with CAP have an acute illness associated with fever (>38°C), cough, and evidence of lower respiratory tract symptoms/signs. Chest radiograph typically shows pulmonary infiltrate. Whether this is patchy infiltrate or lobar in appearance can assist the practitioner in treatment decision making in that the latter is much more likely to be associated with a bacterial etiology.
Once the diagnosis is considered, further assessment should focus on hydration status, hemodynamic parameters, and oxygenation. A careful assessment should identify other associated foci (i.e., meningitis or bacteremia) on examination and laboratory evaluation.
Identification of the Patient Requiring Hospitalization
Consider hospital admission for the toxic patient, those with altered mental status, significant dehydration, hypoxemia, dyspnea, grunting respirations, or retractions, and any patient with hemodynamic instability. Chest radiograph showing a significant pleural effusion should also be considered an indicator for hospital admission.
Bacterial pathogens are more likely in the severely ill patient, patients with a rapidly progressive process, and those with radiographic evidence of lobar consolidation or pleural effusion. Some children with viral processes may require admission for supportive care.
Prompt Recognition of the Patient with Empyema
For the patient with pneumonia and parapneumonic effusion, distinction between a free-flowing effusion and pleural empyema is critical. Standard plain film can identify pulmonary infiltrate and often effusion and lateral decubitus films can help identify free flowing effusion (Figure 1). While CT scan more effectively identifies pleural fibrinous adhesions that may entrap lung, ultrasound most effectively identifies complex fluid collections with loculation and septation, and it can be utilized to guide thoracentesis.
Empyema is defined as pus in the pleural space and is estimated to occur in 10–40% of patients with pneumonia. Empyema may also result from causes other than a complication of bacterial pneumonia, such as thoracic trauma or postsurgical complication, rupture of lung abscess, esophageal tear, or complication of indwelling catheter. It generally occurs in stages including acute (early-cloudy fluid), fibrino-purulent (thicker, multiloculated fluid), and organized (late with thick pleural peel and entrapment of lung).
Pleural fluid evaluation is important both in diagnosis and in guiding treatment in such cases. Pleural fluid collections are defined as transudative or exudative based on biochemical evaluation. Evaluation includes cell type and differential, pH, glucose, protein and LDH. Gram-stained smear needs to be performed on all specimens at the time of culture. Empyema is exudative, typically with low glucose and high LDH (Table 2 on page 64) (2).
Changing Epidemiology and Antibiotic Decision Making
Data presented by Finland and Barnes in 1978 confirmed that S. pneumoniae, group A streptococcus (GAS), and Staphylococcus aureus were the most commonly identified pathogens in empyema cases in 1935, with S. aureus emerging in the 1950s (3). Most literature from the 1960–1980s detailing etiology of pneumonia with pleural empyema continued to emphasize the role of S. aureus in such cases. In all reviews, staphylococcal pneumonia is noted primarily to be a disease of infants. In 1 review of 100 cases of staphylococcal pneumonia, the median age was 5 months, 78 patients being below 1 year of age (4). Chartrand and McCracken analyzed 79 cases of staphylococcal pneumonia and noted that in about 75% of cases, staphylococcal pneumonia was a primary pneumonia in infants with a median age of 6 months. In this study, older children were more likely to have pulmonary involvement as a secondary finding in the setting of disseminated staphylococcal disease. A pleural effusion was found in 80% of infants with primary pneumonia and in 61% of those with secondary disease, thus providing the tip-off of a more serious process to the clinician (5). A high index of suspicion for S. aureus in the young infant with pneumonia is important, as physicians need to expect a rapidly progressive clinical course. Those infants frequently require ventilatory support, alteration in antibiotic choice, and the prompt recognition of pleural complications including pneumothoraces and pneumatoceles.
Data in the 1990s emphasized the role of multidrug resistant pneumococcus as a pathogen in empyema. In a recent review of cases in the postpneumococcal conjugate disease era, pneumococcus remained the most commonly confirmed etiologic agent, with other gram-positive pathogens, including GAS and S. aureus, also documented (6). Despite widespread implementation of pneumococcal conjugate vaccine (PCV), and a population based surveillance study in the US that suggested that adding PCV to the childhood immunization schedule was associated with a 10-fold greater reduction in pneumonia (7), serious pneumonia caused by S. pneumoniae continued to be reported. The prevalence of serotype 1 and 3 as the etiologies of such infections may limit the utility of the current vaccine. One study from Greece demonstrated that the most common serotypes causing bacteremic pneumonia were 14, 6B, 1 and 19F (8). Childhood empyema in the UK is noted to be increasing, and a recent study of 47 empyema cases confirmed pneumococcus as the major pathogen, with over half caused by serotype 1 (9).
More recent data suggest yet another change to the epidemiology of empyema. Schultz et al. from Houston, TX, reviewed a decade of experience from 1993–2002, and while they identified a decrease in total cases of empyema, the emergence of methicillin-resistant S. aureus (MRSA) infection was noted (10).
While MRSA has long been considered an important pathogen in the etiology of healthcare-associated infection, experience in our institution also confirms the appearance of an increasing number of cases of community-acquired MRSA disease. Vancomycin is clearly part of the treatment regimen in the child at risk for staphylococcal pneumonia, though many have utilized clindamycin for the non–critically ill patient. The increase in such cases clearly has important implications for treatment decisions, as MRSA with inducible clindamycin resistance is not yet recognized in every facility. Data are not available to confirm the utility of trimethoprim-sulfamethoxazole in serious community-aquired MRSA infections, and the role for newer antibiotics, such as linezolid, has not been clearly defined.
Management: Antibiotics and the Role of Pleural Drainage Procedures
Figure 2 on page 58 shows an algorithm that guides clinical management of the empyema patient. Once a diagnosis is made, attention should be directed to fluid and electrolyte correction, hemodynamic stabilization, and respiratory support (i.e., oxygenation and ventilation). Antibiotics should be initiated and the choice is based on severity of illness and age of the child.
Drainage of the pleural pus has long been recognized as integral to the success in treatment of pneumonia with empyema. Recently, there has been much debate concerning which modality to use and when.
Intrapleural fibrinolytic therapy has been shown in multiple studies to decrease length of stay without increased risk. Data compiled in the Cochrane database comparing fibrinolytic therapy vs. more conservative management suggests that intrapleural fibrinolytic therapy confers significant benefit when compared with normal saline control; however, a definitive statement was not made, given that the trial numbers were too small (11). More recent data from the Cochrane database and a systematic review suggest that video-assisted thoracostomy (VATS) performed early in the disease course is associated with better outcome than chest tube drainage with streptokinase with regard to duration of chest tube placement and hospital stay. However there are questions about validity, and this study is also too small to draw conclusions (12,13). Figure 3 shows the typical findings encountered at VATS in a child with empyema.
A retrospective chart review from our institution from December 2000 to March 2004, excluding immunocompromised hosts, found 96 cases of radiographic pneumonia with pleural effusion. Thirty-four met criteria for empyema, including ultrasound and/or chest CT showing pleural fluid loculation and septation, or purulent fluid/positive culture. Average age was 5 years, and pathogens were defined in 38% of patients. Length of stay averaged 9 days, with a range of 5–23 days. Two had no intervention and had a stay of 8 days, 14 had tube thoracostomy and had an average stay of 11.5 days with 6 failures, 10 had thoracostomy and fibrinolytic therapy with an average stay of 7 days, 3 had early VATS with an average stay of 7 days, and 5 had late VATS with an average stay of 10.4 days. In our institution, among invasive interventions, tube thoracostomy alone had longer LOS and more failures. Early VATS and intrapleural fibrinolysis have shorter stays and are on the lower end of the cost scale: $25,549 vs. $21,062 respectively (Figure 4).
The decision for interventional management of empyema will likely be institutionally variable in the absence of large randomized controlled studies. Institutions with aggressive interventional radiologists may favor thoracostomy tube with fibrinolysis. Those with surgeons skilled in video-scopic surgery may provide early VATS. Data on interventions clearly show benefit beyond that provided by routine chest tube placement. The key becomes prompt diagnosis of empyema with early use of ultrasound, knowledge of local antibiotic susceptibilities, and clear guidelines set up by each institution to guide interventional management.
The Future
Increasing the accuracy of diagnostic testing for children with CAP would likely lead to decreased morbidity, mortality, and total cost of care. The use of PCR is becoming more widespread and could be utilized to more rapidly confirm the diagnosis of both chlamydophila pneumoniae, mycoplasma pneumoniae, and Influenza A virus (14). Influenza A is well known to cause serious morbidity and mortality and may be the most common virus causing CAP, with a comparable clinical burden to viruses such as respiratory syneytial virus. This is further evidence supporting universal childhood influenza immunization. Expansion of the serotypes included in pneumococcal conjugate vaccines (PCV) is to include serotypes 1 and 3, both currently non-PCV strains in the U.S. vaccine, is underway.
As the epidemiology of CAP continues to evolve, practitioners need to be aware of the prevalent pathogens in their region. In the age of continuing antimicrobial resistance of bacterial pathogens, it is important to know the local antimicrobial susceptibility patterns to appropriately choose empiric therapy when a bacterial process is suspected. Local laboratories can commonly provide this data.
Whatever the future holds, we continue to need the collaboration and expertise of the inpatient practitioner, the infectious disease specialist, and the surgeon/interventionalist. All are necessary to ensure the prompt recognition of empyema and the need for timely medical and surgical intervention for these patients.
References
- Bryce J, Boschi-Pinto C, Shibuya K, Black RE; WHO Child Health Epidemiology Reference Group. WHO estimates of the causes of death in children. Lancet. 2005;365:1147-52.
- Wheeler JG, Jacobs RF. Pleural effusions and empyema. In: Feigin RD, Cherry JD, Demmler GJ, Kaplan SL, eds. Textbook of Pediatric Infectious Diseases. 5th ed. Philadelphia, Pa: Saunders;2004:320-30.
- Finland M, Barnes MW. Changing ecology of acute bacterial empyema: occurrence and mortality at Boston City Hospital during 12 selected years from 1935 to 1972. J Infect Dis. 1978;137:274-91.
- Goel A, Bamford L, Hanslo D, Hussey G. Primary staphylococcal pneumonia in young children: a review of 100 cases. J Trop Pediatr. 1999;45:233-6.
- Chartrand SA, McCracken GH Jr. Staphylococcal pneumonia in infants and children Pediatr Infect Dis. 1982;1:19-23.
- Buckingham SC, King MD, Miller ML. Incidence and etiologies of complicated parapneumonic effusions in children, 1996 to 2001. Pediatr Infect Dis J. 2003;22:499-504.
- Poehling KA, Lafleur BJ, Szilagyi PG, et al. Populationbased impact of pneumococcal conjugate vaccine in young children. Pediatrics. 2004;114:755-61.
- Syriopoulou V, Daikos GL, Soulis K, et al. Epidemiology of invasive childhood pneumococcal infections in Greece. Acta Paediatr Suppl. 2000;89:30-4.
- Eastham KM, Freeman R, Kearns AM, et al. Clinical features, aetiology and outcome of empyema in children in the north east of England. Thorax. 2004;59:522-5.
- Schultz KD, Fan LL, Pinsky J, et al. The changing face of pleural empyemas in children: epidemiology and management. Pediatrics. 2004;113:1735-40.
- Cameron R, Davies HR. Intra-pleural fibrinolytic therapy versus conservative management in the treatment of para-pneumonic effusions and empyema. Cochrane Database Syst Rev. 2004:CD002312. Review.
- Coote N. Surgical versus non-surgical management of pleural empyema. Cochrane Database Syst Rev. 2002:CD001956. Review.
- Gates RL, Caniano DA, Hayes JR, Arca MJ. Does VATS provide optimal treatment of empyema in children? A systematic review. J Pediatr Surg. 2004;39:381-6. Review.
- Laundy M, Ajayi-Obe E, Hawrami K, Aitken C, Breuer J, Booy R. Influenza A community-acquired pneumonia in East London infants and young children. Pediatr Infect Dis J. 2003;22(Suppl):S223-7.
Pneumonia is associated with as many as 2 million annual deaths among children globally and 19% of all deaths in children less than 5 years of age (1). It is one of the most common diagnoses made in the acutely ill child, with an annual incidence of 34 to 40 cases per 1,000 children in Europe and North America.
In the past, viral pathogens were estimated to cause as many as 80% of cases. Streptococcus pneumoniae was generally regarded as the most frequent bacterial cause of community-acquired pneumonia (CAP), especially in cases with complicated parapneumonic effusions. Infectious etiologies are age specific, with bacterial etiologies predominating in the very young infant and viral pathogens in the older infant and adult (Table 1). Knowledge of the most likely pathogen, the prevailing susceptibilities of these infecting pathogens, and the severity of the illness will help guide antibiotic and other treatment decision making.
Most children do not require hospital admission, and mildly ill children who likely have a viral illness do not need antibiotics. The following guideline will attempt to help the practitioner identify those who do require hospitalization and provide an approach to management of those with complicated infection.
Recognition of the Patient with CAP
The first obstacle is to identify the patient with pneumonia. In managing the child with CAP, it is important to distinguish those with other underlying pathology, including asthma, RSV, or other confirmed viral etiology. It is important to remember that pathogens in the compromised host, cystic fibrosis patient, or patient with other chronic pulmonary pathology are different from typical CAP pathogens and include a wide differential. Most patients with CAP have an acute illness associated with fever (>38°C), cough, and evidence of lower respiratory tract symptoms/signs. Chest radiograph typically shows pulmonary infiltrate. Whether this is patchy infiltrate or lobar in appearance can assist the practitioner in treatment decision making in that the latter is much more likely to be associated with a bacterial etiology.
Once the diagnosis is considered, further assessment should focus on hydration status, hemodynamic parameters, and oxygenation. A careful assessment should identify other associated foci (i.e., meningitis or bacteremia) on examination and laboratory evaluation.
Identification of the Patient Requiring Hospitalization
Consider hospital admission for the toxic patient, those with altered mental status, significant dehydration, hypoxemia, dyspnea, grunting respirations, or retractions, and any patient with hemodynamic instability. Chest radiograph showing a significant pleural effusion should also be considered an indicator for hospital admission.
Bacterial pathogens are more likely in the severely ill patient, patients with a rapidly progressive process, and those with radiographic evidence of lobar consolidation or pleural effusion. Some children with viral processes may require admission for supportive care.
Prompt Recognition of the Patient with Empyema
For the patient with pneumonia and parapneumonic effusion, distinction between a free-flowing effusion and pleural empyema is critical. Standard plain film can identify pulmonary infiltrate and often effusion and lateral decubitus films can help identify free flowing effusion (Figure 1). While CT scan more effectively identifies pleural fibrinous adhesions that may entrap lung, ultrasound most effectively identifies complex fluid collections with loculation and septation, and it can be utilized to guide thoracentesis.
Empyema is defined as pus in the pleural space and is estimated to occur in 10–40% of patients with pneumonia. Empyema may also result from causes other than a complication of bacterial pneumonia, such as thoracic trauma or postsurgical complication, rupture of lung abscess, esophageal tear, or complication of indwelling catheter. It generally occurs in stages including acute (early-cloudy fluid), fibrino-purulent (thicker, multiloculated fluid), and organized (late with thick pleural peel and entrapment of lung).
Pleural fluid evaluation is important both in diagnosis and in guiding treatment in such cases. Pleural fluid collections are defined as transudative or exudative based on biochemical evaluation. Evaluation includes cell type and differential, pH, glucose, protein and LDH. Gram-stained smear needs to be performed on all specimens at the time of culture. Empyema is exudative, typically with low glucose and high LDH (Table 2 on page 64) (2).
Changing Epidemiology and Antibiotic Decision Making
Data presented by Finland and Barnes in 1978 confirmed that S. pneumoniae, group A streptococcus (GAS), and Staphylococcus aureus were the most commonly identified pathogens in empyema cases in 1935, with S. aureus emerging in the 1950s (3). Most literature from the 1960–1980s detailing etiology of pneumonia with pleural empyema continued to emphasize the role of S. aureus in such cases. In all reviews, staphylococcal pneumonia is noted primarily to be a disease of infants. In 1 review of 100 cases of staphylococcal pneumonia, the median age was 5 months, 78 patients being below 1 year of age (4). Chartrand and McCracken analyzed 79 cases of staphylococcal pneumonia and noted that in about 75% of cases, staphylococcal pneumonia was a primary pneumonia in infants with a median age of 6 months. In this study, older children were more likely to have pulmonary involvement as a secondary finding in the setting of disseminated staphylococcal disease. A pleural effusion was found in 80% of infants with primary pneumonia and in 61% of those with secondary disease, thus providing the tip-off of a more serious process to the clinician (5). A high index of suspicion for S. aureus in the young infant with pneumonia is important, as physicians need to expect a rapidly progressive clinical course. Those infants frequently require ventilatory support, alteration in antibiotic choice, and the prompt recognition of pleural complications including pneumothoraces and pneumatoceles.
Data in the 1990s emphasized the role of multidrug resistant pneumococcus as a pathogen in empyema. In a recent review of cases in the postpneumococcal conjugate disease era, pneumococcus remained the most commonly confirmed etiologic agent, with other gram-positive pathogens, including GAS and S. aureus, also documented (6). Despite widespread implementation of pneumococcal conjugate vaccine (PCV), and a population based surveillance study in the US that suggested that adding PCV to the childhood immunization schedule was associated with a 10-fold greater reduction in pneumonia (7), serious pneumonia caused by S. pneumoniae continued to be reported. The prevalence of serotype 1 and 3 as the etiologies of such infections may limit the utility of the current vaccine. One study from Greece demonstrated that the most common serotypes causing bacteremic pneumonia were 14, 6B, 1 and 19F (8). Childhood empyema in the UK is noted to be increasing, and a recent study of 47 empyema cases confirmed pneumococcus as the major pathogen, with over half caused by serotype 1 (9).
More recent data suggest yet another change to the epidemiology of empyema. Schultz et al. from Houston, TX, reviewed a decade of experience from 1993–2002, and while they identified a decrease in total cases of empyema, the emergence of methicillin-resistant S. aureus (MRSA) infection was noted (10).
While MRSA has long been considered an important pathogen in the etiology of healthcare-associated infection, experience in our institution also confirms the appearance of an increasing number of cases of community-acquired MRSA disease. Vancomycin is clearly part of the treatment regimen in the child at risk for staphylococcal pneumonia, though many have utilized clindamycin for the non–critically ill patient. The increase in such cases clearly has important implications for treatment decisions, as MRSA with inducible clindamycin resistance is not yet recognized in every facility. Data are not available to confirm the utility of trimethoprim-sulfamethoxazole in serious community-aquired MRSA infections, and the role for newer antibiotics, such as linezolid, has not been clearly defined.
Management: Antibiotics and the Role of Pleural Drainage Procedures
Figure 2 on page 58 shows an algorithm that guides clinical management of the empyema patient. Once a diagnosis is made, attention should be directed to fluid and electrolyte correction, hemodynamic stabilization, and respiratory support (i.e., oxygenation and ventilation). Antibiotics should be initiated and the choice is based on severity of illness and age of the child.
Drainage of the pleural pus has long been recognized as integral to the success in treatment of pneumonia with empyema. Recently, there has been much debate concerning which modality to use and when.
Intrapleural fibrinolytic therapy has been shown in multiple studies to decrease length of stay without increased risk. Data compiled in the Cochrane database comparing fibrinolytic therapy vs. more conservative management suggests that intrapleural fibrinolytic therapy confers significant benefit when compared with normal saline control; however, a definitive statement was not made, given that the trial numbers were too small (11). More recent data from the Cochrane database and a systematic review suggest that video-assisted thoracostomy (VATS) performed early in the disease course is associated with better outcome than chest tube drainage with streptokinase with regard to duration of chest tube placement and hospital stay. However there are questions about validity, and this study is also too small to draw conclusions (12,13). Figure 3 shows the typical findings encountered at VATS in a child with empyema.
A retrospective chart review from our institution from December 2000 to March 2004, excluding immunocompromised hosts, found 96 cases of radiographic pneumonia with pleural effusion. Thirty-four met criteria for empyema, including ultrasound and/or chest CT showing pleural fluid loculation and septation, or purulent fluid/positive culture. Average age was 5 years, and pathogens were defined in 38% of patients. Length of stay averaged 9 days, with a range of 5–23 days. Two had no intervention and had a stay of 8 days, 14 had tube thoracostomy and had an average stay of 11.5 days with 6 failures, 10 had thoracostomy and fibrinolytic therapy with an average stay of 7 days, 3 had early VATS with an average stay of 7 days, and 5 had late VATS with an average stay of 10.4 days. In our institution, among invasive interventions, tube thoracostomy alone had longer LOS and more failures. Early VATS and intrapleural fibrinolysis have shorter stays and are on the lower end of the cost scale: $25,549 vs. $21,062 respectively (Figure 4).
The decision for interventional management of empyema will likely be institutionally variable in the absence of large randomized controlled studies. Institutions with aggressive interventional radiologists may favor thoracostomy tube with fibrinolysis. Those with surgeons skilled in video-scopic surgery may provide early VATS. Data on interventions clearly show benefit beyond that provided by routine chest tube placement. The key becomes prompt diagnosis of empyema with early use of ultrasound, knowledge of local antibiotic susceptibilities, and clear guidelines set up by each institution to guide interventional management.
The Future
Increasing the accuracy of diagnostic testing for children with CAP would likely lead to decreased morbidity, mortality, and total cost of care. The use of PCR is becoming more widespread and could be utilized to more rapidly confirm the diagnosis of both chlamydophila pneumoniae, mycoplasma pneumoniae, and Influenza A virus (14). Influenza A is well known to cause serious morbidity and mortality and may be the most common virus causing CAP, with a comparable clinical burden to viruses such as respiratory syneytial virus. This is further evidence supporting universal childhood influenza immunization. Expansion of the serotypes included in pneumococcal conjugate vaccines (PCV) is to include serotypes 1 and 3, both currently non-PCV strains in the U.S. vaccine, is underway.
As the epidemiology of CAP continues to evolve, practitioners need to be aware of the prevalent pathogens in their region. In the age of continuing antimicrobial resistance of bacterial pathogens, it is important to know the local antimicrobial susceptibility patterns to appropriately choose empiric therapy when a bacterial process is suspected. Local laboratories can commonly provide this data.
Whatever the future holds, we continue to need the collaboration and expertise of the inpatient practitioner, the infectious disease specialist, and the surgeon/interventionalist. All are necessary to ensure the prompt recognition of empyema and the need for timely medical and surgical intervention for these patients.
References
- Bryce J, Boschi-Pinto C, Shibuya K, Black RE; WHO Child Health Epidemiology Reference Group. WHO estimates of the causes of death in children. Lancet. 2005;365:1147-52.
- Wheeler JG, Jacobs RF. Pleural effusions and empyema. In: Feigin RD, Cherry JD, Demmler GJ, Kaplan SL, eds. Textbook of Pediatric Infectious Diseases. 5th ed. Philadelphia, Pa: Saunders;2004:320-30.
- Finland M, Barnes MW. Changing ecology of acute bacterial empyema: occurrence and mortality at Boston City Hospital during 12 selected years from 1935 to 1972. J Infect Dis. 1978;137:274-91.
- Goel A, Bamford L, Hanslo D, Hussey G. Primary staphylococcal pneumonia in young children: a review of 100 cases. J Trop Pediatr. 1999;45:233-6.
- Chartrand SA, McCracken GH Jr. Staphylococcal pneumonia in infants and children Pediatr Infect Dis. 1982;1:19-23.
- Buckingham SC, King MD, Miller ML. Incidence and etiologies of complicated parapneumonic effusions in children, 1996 to 2001. Pediatr Infect Dis J. 2003;22:499-504.
- Poehling KA, Lafleur BJ, Szilagyi PG, et al. Populationbased impact of pneumococcal conjugate vaccine in young children. Pediatrics. 2004;114:755-61.
- Syriopoulou V, Daikos GL, Soulis K, et al. Epidemiology of invasive childhood pneumococcal infections in Greece. Acta Paediatr Suppl. 2000;89:30-4.
- Eastham KM, Freeman R, Kearns AM, et al. Clinical features, aetiology and outcome of empyema in children in the north east of England. Thorax. 2004;59:522-5.
- Schultz KD, Fan LL, Pinsky J, et al. The changing face of pleural empyemas in children: epidemiology and management. Pediatrics. 2004;113:1735-40.
- Cameron R, Davies HR. Intra-pleural fibrinolytic therapy versus conservative management in the treatment of para-pneumonic effusions and empyema. Cochrane Database Syst Rev. 2004:CD002312. Review.
- Coote N. Surgical versus non-surgical management of pleural empyema. Cochrane Database Syst Rev. 2002:CD001956. Review.
- Gates RL, Caniano DA, Hayes JR, Arca MJ. Does VATS provide optimal treatment of empyema in children? A systematic review. J Pediatr Surg. 2004;39:381-6. Review.
- Laundy M, Ajayi-Obe E, Hawrami K, Aitken C, Breuer J, Booy R. Influenza A community-acquired pneumonia in East London infants and young children. Pediatr Infect Dis J. 2003;22(Suppl):S223-7.
Hospitalists Recognize and Reward Value
Hospital medicine has arrived at just the right moment for a healthcare delivery system in need of change. Medical errors and cost escalation continue to dominate the headlines. With regard to quality the National Quality Foundation is attempting to define standards and health plans are creating incentives through Pay for Performance programs. With regard to costs, there are expectations that they will rise even higher as the baby boomer population ages.
Providing high-quality, cost-effective care to acutely ill patients in the hospital is becoming more complex. It requires physicians who can focus on inpatient care, allowing primary care physicians, surgeons, and subspecialists to concentrate on what they do best. Providing the best care available to the hospitalized patients can no longer be done by one health professional acting alone, no matter how wise and well meaning. Hospitalists have dedicated their professional careers to providing team-based, patient-centered care that achieves cost-effective, quality outcomes.
As the specialty society for hospital medicine, SHM provides a vehicle to define this new specialty. We are doing this with our surveys of hospitalist productivity and compensation, by articles that appear in the medical and lay press, and by the Core Curriculum for Hospital Medicine that will be published in the coming months.
Hospitalists provide significant value to their healthcare communities and to patients, physicians, other health professionals, and administrators well beyond the benefits of direct patient care. This supplement to The Hospitalist, the official publication of SHM, is a compendium of papers designed to further define the full range of benefits provided by the specialty of hospital medicine.
Physician Methods of Payment Outdated
As the American healthcare system is reshaped, we must recognize that part of the problem is the outdated way in which we pay for medical services. Physicians are rewarded as piece workers by the unit of the visit or the procedure. This has led to a culture of doing more things for one individual patient rather than attempting to make the hospital work better for all patients. In addition, this unit-based payment does not reward efficiency or effectiveness.
Hospitalists are, in many ways, change agents in the inpatient environment. Hospitalists can spend as much as 50% of their professional time improving the entire enterprise by taking on the responsibilities of other physicians, developing plans to improve quality educating hospital staff or medical trainees, addressing efficiencies through earlier discharge or improved throughput in the ED or ICU, creating teams of health professionals, or being available around the clock.
The diverse work that hospitalizes perform is very important and time consuming. However, the traditional payment scheme for physicians does not provide a direct way to compensate the hospitalist for this skill and expertise.
Hospitals have realized that these hospitalist skills bring real value to their health communities. And hospitals have been willing to invest their own funds to grow and support their hospital medicine groups to the tune of $75,000 or more per hospitalist per year. This is not a hand-out or a subsidy. This is true commerce. Hospitals continue to get significant benefits from their hospitalists.
In fact, when confronted with the choice of whether to ask the hospitalists to ''just see patients'' to generate more direct patient fees or to continue to improve the effectiveness and efficiency of their health communities, enlightened hospital executives vote with their money and ask the hospitalists to improve quality, build teams, reduce LOS, improve throughput, educate their staff, and generally build the hospital of the future.
With regard to paying physicians, SHM believes that the Pay for Performance movement is an important step in the right direction. Hospitalists welcome a reimbursement scheme that rewards institutions that follow best practices and achieve superior outcomes.
Audiences for this Supplement
This supplement, How Hospitalists Add Value, has two major audiences. First, hospitalists need to categorize what they can and will do for their hospitals and healthcare communities. They need to understand that this is not voluntary work to be done in their spare time. The provision of these services provides strategic and market benefits to their hospital.
Second, there are hospital administrators and leaders at 1,500 hospitals who have been crucial to growing hospital medicine to more than 12,000 hospitalists. They recognize that hospitalists are core to their future. This supplement will further confirm and document the ways in which hospitalists can help their organizations. The facts put forth in these papers can create a rationale for continued support with dollars and manpower, not as a subsidy but as an intelligent investment for the hospital.
Hospitalists Add Value
- Hospitalists can provide measurable quality improvement through setting standards and compliance.
- Hospitalists can save money and resources by reducing LOS and achieving better utilization.
- Hospitalists can improve the efficiency of the hospital by early discharge, better throughput in the ED, and the opening up of ICU beds.
- Hospitalists can create a seamless continuity from inpatient to outpatient care, from the ED to the floor, and from the ICU to the floor.
- Hospitalists can make other physicians' lives better and help hospitals to recruit and retain PCPs, surgeons, and specialists.
- Hospitalists can do things other physicians have given up by admitting patients without health insurance or by serving on hospital committees.
- Hospitalists can be instrumental in creating teams of healthcare professionals that make better use of the talent at the hospital and create a better working environment for nurses and others.
- Hospitalists can have a leading role in educating nurses, other hospital staff, and physicals in training.
- And hospitalizes can take care of the acutely ill complex hospitalized patients.
Add it all up and it is clear that hospitalists are a resource to hospitals in meeting the complex challenges of their healthcare communities. Hopefully, this set of important papers will define these issues more clearly and assist hospitalists and their hospital leaders in creating a stable and supportive environment for collaboration that can lead to better healthcare for our patients.
Hospital medicine has arrived at just the right moment for a healthcare delivery system in need of change. Medical errors and cost escalation continue to dominate the headlines. With regard to quality the National Quality Foundation is attempting to define standards and health plans are creating incentives through Pay for Performance programs. With regard to costs, there are expectations that they will rise even higher as the baby boomer population ages.
Providing high-quality, cost-effective care to acutely ill patients in the hospital is becoming more complex. It requires physicians who can focus on inpatient care, allowing primary care physicians, surgeons, and subspecialists to concentrate on what they do best. Providing the best care available to the hospitalized patients can no longer be done by one health professional acting alone, no matter how wise and well meaning. Hospitalists have dedicated their professional careers to providing team-based, patient-centered care that achieves cost-effective, quality outcomes.
As the specialty society for hospital medicine, SHM provides a vehicle to define this new specialty. We are doing this with our surveys of hospitalist productivity and compensation, by articles that appear in the medical and lay press, and by the Core Curriculum for Hospital Medicine that will be published in the coming months.
Hospitalists provide significant value to their healthcare communities and to patients, physicians, other health professionals, and administrators well beyond the benefits of direct patient care. This supplement to The Hospitalist, the official publication of SHM, is a compendium of papers designed to further define the full range of benefits provided by the specialty of hospital medicine.
Physician Methods of Payment Outdated
As the American healthcare system is reshaped, we must recognize that part of the problem is the outdated way in which we pay for medical services. Physicians are rewarded as piece workers by the unit of the visit or the procedure. This has led to a culture of doing more things for one individual patient rather than attempting to make the hospital work better for all patients. In addition, this unit-based payment does not reward efficiency or effectiveness.
Hospitalists are, in many ways, change agents in the inpatient environment. Hospitalists can spend as much as 50% of their professional time improving the entire enterprise by taking on the responsibilities of other physicians, developing plans to improve quality educating hospital staff or medical trainees, addressing efficiencies through earlier discharge or improved throughput in the ED or ICU, creating teams of health professionals, or being available around the clock.
The diverse work that hospitalizes perform is very important and time consuming. However, the traditional payment scheme for physicians does not provide a direct way to compensate the hospitalist for this skill and expertise.
Hospitals have realized that these hospitalist skills bring real value to their health communities. And hospitals have been willing to invest their own funds to grow and support their hospital medicine groups to the tune of $75,000 or more per hospitalist per year. This is not a hand-out or a subsidy. This is true commerce. Hospitals continue to get significant benefits from their hospitalists.
In fact, when confronted with the choice of whether to ask the hospitalists to ''just see patients'' to generate more direct patient fees or to continue to improve the effectiveness and efficiency of their health communities, enlightened hospital executives vote with their money and ask the hospitalists to improve quality, build teams, reduce LOS, improve throughput, educate their staff, and generally build the hospital of the future.
With regard to paying physicians, SHM believes that the Pay for Performance movement is an important step in the right direction. Hospitalists welcome a reimbursement scheme that rewards institutions that follow best practices and achieve superior outcomes.
Audiences for this Supplement
This supplement, How Hospitalists Add Value, has two major audiences. First, hospitalists need to categorize what they can and will do for their hospitals and healthcare communities. They need to understand that this is not voluntary work to be done in their spare time. The provision of these services provides strategic and market benefits to their hospital.
Second, there are hospital administrators and leaders at 1,500 hospitals who have been crucial to growing hospital medicine to more than 12,000 hospitalists. They recognize that hospitalists are core to their future. This supplement will further confirm and document the ways in which hospitalists can help their organizations. The facts put forth in these papers can create a rationale for continued support with dollars and manpower, not as a subsidy but as an intelligent investment for the hospital.
Hospitalists Add Value
- Hospitalists can provide measurable quality improvement through setting standards and compliance.
- Hospitalists can save money and resources by reducing LOS and achieving better utilization.
- Hospitalists can improve the efficiency of the hospital by early discharge, better throughput in the ED, and the opening up of ICU beds.
- Hospitalists can create a seamless continuity from inpatient to outpatient care, from the ED to the floor, and from the ICU to the floor.
- Hospitalists can make other physicians' lives better and help hospitals to recruit and retain PCPs, surgeons, and specialists.
- Hospitalists can do things other physicians have given up by admitting patients without health insurance or by serving on hospital committees.
- Hospitalists can be instrumental in creating teams of healthcare professionals that make better use of the talent at the hospital and create a better working environment for nurses and others.
- Hospitalists can have a leading role in educating nurses, other hospital staff, and physicals in training.
- And hospitalizes can take care of the acutely ill complex hospitalized patients.
Add it all up and it is clear that hospitalists are a resource to hospitals in meeting the complex challenges of their healthcare communities. Hopefully, this set of important papers will define these issues more clearly and assist hospitalists and their hospital leaders in creating a stable and supportive environment for collaboration that can lead to better healthcare for our patients.
Hospital medicine has arrived at just the right moment for a healthcare delivery system in need of change. Medical errors and cost escalation continue to dominate the headlines. With regard to quality the National Quality Foundation is attempting to define standards and health plans are creating incentives through Pay for Performance programs. With regard to costs, there are expectations that they will rise even higher as the baby boomer population ages.
Providing high-quality, cost-effective care to acutely ill patients in the hospital is becoming more complex. It requires physicians who can focus on inpatient care, allowing primary care physicians, surgeons, and subspecialists to concentrate on what they do best. Providing the best care available to the hospitalized patients can no longer be done by one health professional acting alone, no matter how wise and well meaning. Hospitalists have dedicated their professional careers to providing team-based, patient-centered care that achieves cost-effective, quality outcomes.
As the specialty society for hospital medicine, SHM provides a vehicle to define this new specialty. We are doing this with our surveys of hospitalist productivity and compensation, by articles that appear in the medical and lay press, and by the Core Curriculum for Hospital Medicine that will be published in the coming months.
Hospitalists provide significant value to their healthcare communities and to patients, physicians, other health professionals, and administrators well beyond the benefits of direct patient care. This supplement to The Hospitalist, the official publication of SHM, is a compendium of papers designed to further define the full range of benefits provided by the specialty of hospital medicine.
Physician Methods of Payment Outdated
As the American healthcare system is reshaped, we must recognize that part of the problem is the outdated way in which we pay for medical services. Physicians are rewarded as piece workers by the unit of the visit or the procedure. This has led to a culture of doing more things for one individual patient rather than attempting to make the hospital work better for all patients. In addition, this unit-based payment does not reward efficiency or effectiveness.
Hospitalists are, in many ways, change agents in the inpatient environment. Hospitalists can spend as much as 50% of their professional time improving the entire enterprise by taking on the responsibilities of other physicians, developing plans to improve quality educating hospital staff or medical trainees, addressing efficiencies through earlier discharge or improved throughput in the ED or ICU, creating teams of health professionals, or being available around the clock.
The diverse work that hospitalizes perform is very important and time consuming. However, the traditional payment scheme for physicians does not provide a direct way to compensate the hospitalist for this skill and expertise.
Hospitals have realized that these hospitalist skills bring real value to their health communities. And hospitals have been willing to invest their own funds to grow and support their hospital medicine groups to the tune of $75,000 or more per hospitalist per year. This is not a hand-out or a subsidy. This is true commerce. Hospitals continue to get significant benefits from their hospitalists.
In fact, when confronted with the choice of whether to ask the hospitalists to ''just see patients'' to generate more direct patient fees or to continue to improve the effectiveness and efficiency of their health communities, enlightened hospital executives vote with their money and ask the hospitalists to improve quality, build teams, reduce LOS, improve throughput, educate their staff, and generally build the hospital of the future.
With regard to paying physicians, SHM believes that the Pay for Performance movement is an important step in the right direction. Hospitalists welcome a reimbursement scheme that rewards institutions that follow best practices and achieve superior outcomes.
Audiences for this Supplement
This supplement, How Hospitalists Add Value, has two major audiences. First, hospitalists need to categorize what they can and will do for their hospitals and healthcare communities. They need to understand that this is not voluntary work to be done in their spare time. The provision of these services provides strategic and market benefits to their hospital.
Second, there are hospital administrators and leaders at 1,500 hospitals who have been crucial to growing hospital medicine to more than 12,000 hospitalists. They recognize that hospitalists are core to their future. This supplement will further confirm and document the ways in which hospitalists can help their organizations. The facts put forth in these papers can create a rationale for continued support with dollars and manpower, not as a subsidy but as an intelligent investment for the hospital.
Hospitalists Add Value
- Hospitalists can provide measurable quality improvement through setting standards and compliance.
- Hospitalists can save money and resources by reducing LOS and achieving better utilization.
- Hospitalists can improve the efficiency of the hospital by early discharge, better throughput in the ED, and the opening up of ICU beds.
- Hospitalists can create a seamless continuity from inpatient to outpatient care, from the ED to the floor, and from the ICU to the floor.
- Hospitalists can make other physicians' lives better and help hospitals to recruit and retain PCPs, surgeons, and specialists.
- Hospitalists can do things other physicians have given up by admitting patients without health insurance or by serving on hospital committees.
- Hospitalists can be instrumental in creating teams of healthcare professionals that make better use of the talent at the hospital and create a better working environment for nurses and others.
- Hospitalists can have a leading role in educating nurses, other hospital staff, and physicals in training.
- And hospitalizes can take care of the acutely ill complex hospitalized patients.
Add it all up and it is clear that hospitalists are a resource to hospitals in meeting the complex challenges of their healthcare communities. Hopefully, this set of important papers will define these issues more clearly and assist hospitalists and their hospital leaders in creating a stable and supportive environment for collaboration that can lead to better healthcare for our patients.
Clostridium difficile–Associated Diarrhea and Colitis: A Significant Cause of Nosocomial Infection
Introduction
Clostridium difficile–associated diarrhea (CDAD) has been recognized with increased frequency as a cause of nosocomial illness. The frequency and incidence of CDAD varies widely, and is influenced by multiple factors including nosocomial outbreaks, patterns of antimicrobial use, and individual susceptibility. There are no reports of prospective studies by hospitals tracking positive toxin A or A/B and the outcomes of CDAD and its complications.
The Centers for Disease Control and Prevention (CDC) has analyzed secular trends in the incidence of CDAD, and it reported a steady increase from 1987 to 2001 (1). In this report, 30% of 440 infectious disease physicians who participated in a Web-based poll reported that they are seeing higher rates of CDAD, more severe CDAD, and more relapsing CDAD than in the past. There is an overall impression that there has been an increase in the proportion of cases with severe and fatal complications, and an increase in the relapse rate among affected patients.
In addition to morbidity and mortality, the economic burden of C. difficile infection in terms of delayed discharge and other hospital costs is considerable.
Epidemiology
The frequency and incidence of CDAD varies between hospitals and within a given institution over time. The risk for disease increases in patients with antibiotic exposure, gastrointestinal surgery, increasing length of stay in healthcare settings, serious underlying illness, immuno-compromising conditions, and advanced age.
C. difficile is shed in feces. Any surface, device, or material (e.g., commode, bathing tub, and electronic rectal thermometer) that becomes contaminated with feces may serve as a reservoir for C. difficile spores. Spores are transferred to patients mainly via the hands of healthcare personnel who have touched a contaminated surface or item (2-6).
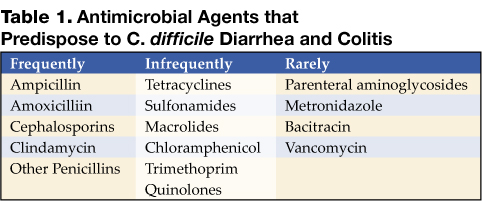
The Organism and Pathophysiology of C. difficile Diarrhea
C. difficile is a gram-positive, anaerobic, spore-forming bacillus that is responsible for the development of antibiotic-associated diarrhea and colitis. C. difficile was first described in 1935 as a component of the fecal flora of healthy newborns and was initially not thought to be pathogenic (7). The bacillus was named difficile because it grows slowly and is difficult to culture. C. difficile is presently responsible for nearly all causes of pseudomembranous colitis and as many as 20% of cases of antibiotic-associated diarrhea without colitis. Although found in the stool of only 5% of the general population, as many as 21% of adults become colonized with this organism while hospitalized (2,6).
An alteration of the normal colonic microflora, usually caused by antibiotic therapy, is the main factor that predisposes to infection with C. difficile. Almost all antibiotics have been associated with C. difficile diarrhea and colitis. The antibiotics most frequently associated include clindamycin, cephalosporins, ampicillin, and amoxicillin (Table 1) (8).
In addition to antibiotic therapy, older age and severity of underlying disease are important risk factors for C. difficile infection. Other risk factors include the presence of a nasogastric tube, gastrointestinal procedures, acid antisecretory medications, intensive care unit stay, and duration of hospitalization (9).
C. difficile diarrhea is caused primarily by the elaboration of toxins A and B produced by bacterial multiplication within the intestinal lumen. These toxins bind to the colonic mucosa and exert their deleterious effects upon it. The organism rarely damages the colon by direct invasion, and diarrhea is caused by the effects of toxins produced within the intestinal lumen that adhere to the mucosal surface. Most toxigenic isolates produce both toxins, and about 5–25% of isolates produce neither toxin A nor B, and do not cause colitis or diarrhea (3-5).
Clinical Manifestations
Infection with C. difficile may produce a wide range of clinical manifestations, including asymptomatic carriage, mild-to-moderate diarrhea, and fulminant disease with pseudomembranous colitis (10). In patients who develop CDAD, symptoms usually begin soon after colonization. Colonization may occur during antibiotic treatment or up to several weeks after a course of antibiotics. CDAD typically is associated with the passage of frequent, loose bowel movements consistent with proctocolitis. Mucus or occult blood may be present, but visible blood is rare.
Diagnosis
The diagnosis of CDAD is based on a history of recent or current antibiotic therapy, development of diarrhea or other evidence of acute colitis, and demonstration of infection by toxigenic C. difficile, usually by detection of toxin A or toxin B in stool sample.
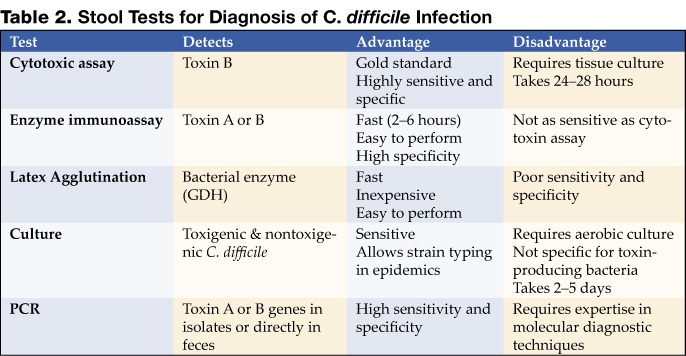
Practical Guidelines for Diagnosis of C. difficile Diarrheal Syndromes
- The diagnosis should be suspected in anyone with diarrhea who has received antibiotics within the previous 2 months and/or whose diarrhea begins 72 hours or more after hospitalization.
- When the diagnosis is suspected, a single stool specimen should be sent to the laboratory for testing for the presence of C. difficile and/or its toxins.
- When diarrhea persists despite a negative stool toxin result, one or two additional samples may be sent for testing with the same or different tests (4). Endoscopy is reserved for special situations, such as when a rapid diagnosis is needed and test results are delayed or the test is not highly sensitive, when the patient has ileus and stool is not available, or when other colonic diseases are also a consideration.
There is as yet no simple, inexpensive, rapid, sensitive and specific test for diagnosing C. difficile diarrhea and colitis, nor are all the available tests suitable for adoption by every laboratory (Table 2) (11).
Endoscopic Diagnosis of C. difficile Diarrhea and Colitis
Sigmoidoscopy and colonoscopy are not indicated for most patients with CDAD (10,12). Endoscopy is helpful, however, in special situations, such as when the diagnosis is in doubt or the clinical situation demands rapid diagnosis. The results of endoscopic examination may be normal in patients with mild diarrhea or may show nonspecific colitis in moderate cases. The finding of colonic pseudomembranes in a patient with antibiotic-associated diarrhea is virtually pathognomonic for C. difficile colitis. A few patients without any diagnostic features in the rectosigmoid have pseudomembranes in the more proximal areas of the colon (13). Other endoscopic findings include erythema, edema, friability, and nonspecific colitis with small ulcerations or erosions.
Treatment
The first step in the management of C. difficile diarrhea and colitis is to discontinue the precipitating antibiotics if possible (10,12). Diarrhea resolves in approximately 15–25% of patients without specific anti–C. difficile therapy (14,15). Conservative management alone may not be indicated, however, in patients who are systemically ill or who have multiple medical problems, since it is difficult to predict which patients will improve spontaneously. If it is not possible to discontinue the precipitating antibiotic because of other active infections, the patient’s antibiotic regimen should be altered if possible to make use of agents less likely to cause CDAD (e.g., aminoglycosides, trimethoprim, rifampin, or a quinolone).
Antiperistaltic agents, such as diphenoxylate plus atropine (Lomotil), or loperamide (Imodium), and narcotic analgesics should be avoided because they may delay clearance of toxins from the colon and thereby exacerbate toxin-induced colonic injury or precipitate ileus and toxic dilatation (12,16). Specific therapy to eradicate C. difficile should be used in patients with initially severe symptoms and in patients whose symptoms persist despite discontinuation of antibiotic treatment. Although the diagnosis of C. difficile colitis should ideally be established before antimicrobial therapy is implemented, current ACG guidelines recommend that empiric therapy should be initiated in highly suggestive cases of severely ill patients (Table 3 on page 54) (12).
Currently, oral vancomycin or metronidazole, used for 7 to 10 days, are considered first-line therapy by most authors and current guidelines. Metronidazole at a dose of 250 mg 4 times daily is recommended by most authors and ACG guidelines as the drug of choice for the initial treatment of C. difficile colitis (12). These recommendations are largely based on efficacy, lower costs, and concerns about the development of vancomycin-resistant strains. Major disadvantages of metronidazole include a less desirable drug profile and contraindications in children and pregnant women.
Vancomycin, on the other hand, at a dose of 125 mg 4 times daily, is safe and well tolerated and achieves stool levels 20 times the required minimal inhibitory concentration for the treatment of C. difficile. Drawbacks to the use of vancomycin are cost and potential development of vancomycin-resistant strains. The current ACG guidelines consider vancomycin the drug of choice in severely ill patients and in cases in which the use of metronidazole is precluded.
Controlled clinical trials are lacking for patients with fulminant colitis who may not tolerate oral therapy. Administration of metronidazole intravenously or administration of vancomycin by nasogastric tube or rectal enema has been described in small case series (17-20). Intravenous administration of vancomycin is not recommended, because the drug is not excreted in the colon (17).
Management of Recurrent C. difficile Diarrhea
Despite successful initial treatment of CDAD, 15–20% of patients have recurrence of diarrhea in association with a positive stool test for C. difficile toxin. Symptomatic recurrence is rarely due to treatment failure or antimicrobial resistance to metronidazole or vancomycin. Approaches to management include conservative therapy (however, many patients are elderly and infirm and unable to tolerate diarrhea), therapy with specific anti–C. difficile antibiotics, the use of anion-binding resins, therapy with microorganisms (probiotics), and immunoglobulin therapy.
The most common therapy for recurrent C. difficile diarrhea is a second course of the same antibiotic used to treat the initial episode (12). In a large observational study in the United States, 92% of patients with recurrent CDAD responded successfully to a single repeated course of therapy, usually with metronidazole or vancomycin (14). There is evidence to suggest that patients with a history of recurrence have a high risk of further episodes of CDAD after antibiotic therapy is discontinued. There are no data to suggest that sequential episodes become progressively more severe or complicated (21). A variety of treatment schedules have been suggested for patients with multiple recurrences of C. difficile diarrhea. One approach is to give a prolonged course of vancomycin (or metronidazole) using a decreasing dosage schedule followed by pulse therapy (Table 4).
Cholestyramine, an anionexchange resin administered at a dose of 4 grams 3 or 4 times daily for 1 to 2 weeks, binds C. difficile toxins and may be used in conjunction with antibiotics to treat repeated relapses. Because cholestyramine may bind vancomycin as well as toxins, it should be taken at least 2 to 3 hours apart from the vancomycin.
Severe C. difficile Colitis
The incidence of fulminant C. difficile colitis has been reported to be 1.6–3.2% (22). Although recent precise figures from other centers are lacking, it is being recognized as an increasing cause of complications and death. The clinical syndrome of fulminant C. difficile colitis can be recognized with a proper knowledge of the spectrum of disease presentation.
A. Diarrhea: Although diarrhea is the hallmark of C. difficile colitis, it is not invariably present, and its absence may lead to diagnostic confusion. When diarrhea is absent, this appears to be secondary to severe colonic dysmotility. Even when present, diarrhea may be perceived to be a minor component of a nonspecific septic picture.

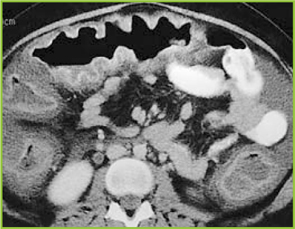
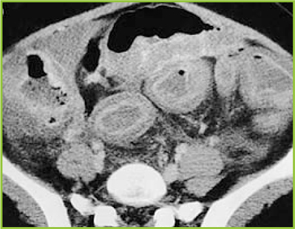
B. Severe Disease: Fulminant colitis is an unusual form of C. difficile infection, occurring in only 3% of patients but accounting for virtually all serious complications. Patients with more severe forms of the disease may present with or without diarrhea. When patients develop colitis localized to the cecum and right side of the colon, diarrhea may be minimal or absent. In the absence of diarrhea, the only clues to diagnosis may be systemic signs of toxicity (fever, tachycardia, leukocytosis, and/or volume depletion).
An elevated white blood cell count may be an important clue to impending fulminant C. difficile colitis. The rapid elevation of the peripheral white cell count (commonly as high as 30,000 to 50,000) with a significant excess of bands and sometimes more immature forms often precedes hemodynamic instability and the development of organ dysfunction. Even in patients who are mildly symptomatic for an extended period, sudden and unexpected progression to shock may occur. It is difficult to predict those patients who may not respond to medical treatment. Hence, early warning signs such as a leukemoid reaction may be invaluable.
Hypotension is a late finding and can be resistant to vasopressor support. Abdominal signs range from distention to generalized tenderness with guarding. Colonic perforation is usually accompanied by abdominal rigidity, involuntary guarding, rebound tenderness, and absent bowel sounds. Free air may be revealed on abdominal radiographs. Any suspicion of perforation in this setting should prompt immediate surgical consultation. Death generally occurs before free air and perforation can occur. In one study, contrary to most other literature, perforation was found to be rare (22).
Abdominal radiography may reveal a dilated colon (>7 cm in its greatest diameter), consistent with toxic megacolon. Patients with megacolon may have an associated small bowel ileus with dilated small intestine on plain abdominal radiographs, with air-fluid levels mimicking small intestinal obstruction or ischemia. CT without contrast and endoscopy can quickly diagnose or at least strongly suggest fulminant C.difficile colitis. CT scan findings include evidence of ascites, colonic wall thickening and/or dilatation. These findings may prove helpful in categorizing the severity of the colitis.
More aggressive intervention in medically unresponsive patients, including rapid identification of patients failing to respond to medical therapy, is crucial to a positive outcome, and early surgical intervention should be done in this group (Figures 1-3).
It is important that everyone involved with patient care in hospitals, nursing homes, and skilled nursing facilities be educated about the organism and its epidemiology, rational approaches to the treatment and care of patients with C. difficile diarrhea, the importance of hand washing between contact with patients, the use of gloves when caring for a patient with C. difficile diarrhea, and the avoidance of the unnecessary use of antimicrobials.
Conclusion
Recent years have raised concerns over rising incidence and serious complication rates of CDAD in North American hospitals (22,23). The Canadian Medical Association journal published a report in 2004 detailing an outbreak of CDAD involving several hospitals in Montreal. The introduction of new hypervirulent and highly transmissible strains of C. difficile has been postulated as the possible cause for the outbreak (24). A deteriorating infrastructure, inadequate infection control practices, the increasing number of debilitated patients, an aging population, and hypervirulent strains were all felt to be likely contributors to recent outbreaks in Canada (25).
Two epidemiological investigations in the United States and Canada (24,26) independently examined samples of C. difficile and found that a mutated version of the “wild” strain was responsible for outbreaks in Quebec and increased rates of CDAD in hospitals in the United States recently (22,23). Clinical epidemiologists at the CDC investigated C. difficile isolates from hospitals in the United States with recent (i.e., 2001–2004) CDAD outbreaks (22,23). The report indicates the emergence of a new epidemic strain, “BI” (distinct from the “J” strain of 1989–1992), which may be responsible for the recent increase in rates and apparent severity of CDAD (26).
CDAD and colitis in most cases can be treated by the administration of metronidazole or vancomycin. In some patients severe life-threatening toxicity develops despite appropriate and timely medical treatment, and surgical intervention is necessary. Systemic symptoms of infection with C. difficile are reported not to derive from bacteremia, colonic perforation or ischemia, but from toxin-induced inflammatory mediators released from the colon (27-29). Early surgical intervention should be employed in refractory cases of severe disease. Surgical intervention is far from ideal, however, and carries a very high rate of complications and significant risk of mortality (22). The future clinical approach to the treatment of nosocomial C. difficile colitis may eventually involve specific antitoxin hyperimmunoglobulins and inhibitors of the inflammatory cascade (28,30,31).
References
- Archibald LK, Banerjee SN, Jarvis WR. Secular trend in hospital-acquired Clostridium difficile disease in the United States; 1987-2001. J Infect Dis. 2004;189:1585-9.
- Fekety R. Antibiotic-associated colitis. In: Mandell G, Bennet JE, Dolin R, eds. Principles and Practice of Infectious Diseases. 4th ed. New York: Churchill Livingston; 1996:978-806.
- Mitty RD, LaMont T. Clostridium difficile diarrhea: Pathogenesis, epidemiology, and treatment. Gastroenterologist. 1994;2:61-9.
- Bartlett JG. Clostridium difficile: History of its role as an enteric pathogen and the current state of knowledge about the organism. Clin Infect Dis. 1994;18(Suppl 4):265-72.
- Johnson S, Gerding D. Clostridium difficile. In: Mayhall CG, ed. Hospital Epidemiology and Infection Control. Baltimore, Md: Williams & Wilkins; 1996:99-408.
- Mcfarland LV, Mulligan ME, Kwok RY, Stamm WE. Nosocomial acquisition of Clostridium difficile. N Engl J Med. 1989;320:204-10.
- Hall IC, O Toole E. Intestinal Flora in new-born infants: With a description of a new pathogenic anaerobe, Bacillus difficile. Am J Dis Child. 1935;49:390-402.
- Kelly CP, LaMont JT. Treatment of Clostridium difficile diarrhea and colitis. In: Wolfe MM, ed. Gastrointestinal Pharmacotherapy. Philadelphia, Pa.: WB Saunders; 1993:199-212.
- Bignardi GE. Risk factors for Clostridium difficile infection. J Hosp Infect. 1998;40:1-15.
- Kelly CP, Pothoulakas C, LaMont JT. Clostridium difficile colitis. N Engl J Med. 1994;330:257-62.
- Linevsky JK, Kelly CP. Clostridium difficile colitis. In: Lamont JT, ed. Gastrointestinal Infections: Diagnosis and Management. New York: Marcel Dekker; 1997:293-325.
- Fekety R. Guidelines for the diagnosis and management of Clostridium difficile associated diarrhea and colitis. American College of Gastroenetrology, Practice Parameters Committee. Am J Gastroenterol. 1997;92:739-50.
- Tedesco FJ, Corless JK, Brownstein RE. Rectal sparing in antibiotic-associated pseudomembranous colitis: A prospective study. Gastroenterology. 1982;83:1259-60.
- Olson MM, Shanholtzer CJ, Lee JT Jr, Gerding DN. Ten years of prospective Clostridium difficile-associated disease surveillance and treatment at the Minneapolis VA Medical Center, 1982-1991. Infect Control Hosp Epidemiol. 1994;15: 371-81.
- Teasley DG, Gerding DN, Olson MM, et al. Prospective randomized trial of metronidazole versus vancomycin for Clostridium-difficile-associated diarrhoea and colitis. Lancet. 1983;2:1043-6.
- Walley T, Milson D. Loperamide-related toxic megacolon in Clostridium difficile colitis. Postgrad Med J. 1990;66:582.
- Malnick SD, Zimhony O. Treatment of Clostridium difficile associated diarrhea. Ann Pharmacother. 2002;36:1767-75.
- Sehgal M, Kyne L. Clostridium difficile disease. Curr Treatment Options Infect Dis. 2002;4:201-10.
- Apisarnthanarak A, Razavi B, Mundy LM. Adjunctive intracolonic vancomycin for severe Clostridium difficile colitis: case series and review of the literature. Clin Infect Dis. 2002;35:690-6.
- Friendenberg F, Fernandez A, Kaul V, Niami P, Levine GM. Intravenous metronidazole for the treatment of Clostridium difficile colitis. Dis Colon Rectum. 2001;44:1176-80.
- Fekety R, McFarland LV, Surawicz CMGreenberg, RN, Elmer GW, Mulligan ME. Recurrent Clostridium difficile diarrhea: characteristics of and risk factors for patients enrolled in a prospective, randomized, double-blind trial. Clin Infect Dis. 1997;24:324-33.
- Dallal RM, Harbrecht BG, Boujoukas AJ, et al. Fulminant Clostridium difficile: an underappreciated and increasing cause of death and complications. Ann Surg. 2002;235:363-72.
- Morris AM, Jobe BA, Sontey, M, Sheppard BC, Deveney CW, Deveney KE. Clostridium difficile colitis: an increasingly aggressive iatrogenic disease? Arch Surg. 2002;137:1096-100.
- Eggerston L, Sibbald B. Hospitals battling outbreaks of C. difficile. CMAJ. 2004;171:19-21.
- Valiquette L, Low DE, Pepin J, McGeer A. Clostridium difficile infection in hospitals: a brewing storm. CMAJ. 2004;171:27-9.
- McDonald LC, Killgore GE, Thompson A, et al. Emergence of an epidemic strain of Clostridium difficile in the United States, 2001-4: Potential role for virulence factors and antimicrobial resistance traits. Infectious Diseases Society of America 42th Annual Meeting. Boston, MA, September 30 – October 3, 2004. Abstract # LB-2.
- Flegel W, Muller F, Daubener W, Fischer HG, Hadding U, Northoff H. Cytokine response by human monocytes to Clostridium difficile toxin A and toxin B. Infect Immun. 1991;59:3659-66.
- Castagliuolo I, Keates A, Qiu B, et al. Increased substance P responses in dorsal root ganglia, intestinal macrophages during Clostridium difficile toxin A enteritis in rats. Proc Natl Acad Sci U S A. 1997;94:4788-93.
- Castagliuolo I, Keates A, Wang C, et al. Clostridium difficile toxin A stimulates macrophage-inflammatory protein-2 production in rat intestinal epithelial cells. J Immunol. 1998;160:6039-45.
- Kelly C, Chetham S, Keates S, et al. Survival of anti-Clostridium difficile bovine immunoglobulin concentrate in the human gastrointestinal tract. Antimicrob Agents Chemother. 1997;41:236-41.
- Salcedo J, Keates S, Pothoulakis C, et. al. Intravenous immunoglobulin therapy for severe Clostridium difficile colitis. Gut. 1997;41:366-70.
General References
- Shea Position Paper Gerding DN,Johnson S, Peterson LR, Mulligan ME Silva J. SHEA Position Paper:Clostridium difficile-associated diarrhea and colitis; Infect Control Hosp Epidemiol 1995, 16:459-77
- Kyne L, Farrell RJ, Kelly CP. Clostridium difficile. Gastroenterol Clin North Am 2001; 30:753-77.
Introduction
Clostridium difficile–associated diarrhea (CDAD) has been recognized with increased frequency as a cause of nosocomial illness. The frequency and incidence of CDAD varies widely, and is influenced by multiple factors including nosocomial outbreaks, patterns of antimicrobial use, and individual susceptibility. There are no reports of prospective studies by hospitals tracking positive toxin A or A/B and the outcomes of CDAD and its complications.
The Centers for Disease Control and Prevention (CDC) has analyzed secular trends in the incidence of CDAD, and it reported a steady increase from 1987 to 2001 (1). In this report, 30% of 440 infectious disease physicians who participated in a Web-based poll reported that they are seeing higher rates of CDAD, more severe CDAD, and more relapsing CDAD than in the past. There is an overall impression that there has been an increase in the proportion of cases with severe and fatal complications, and an increase in the relapse rate among affected patients.
In addition to morbidity and mortality, the economic burden of C. difficile infection in terms of delayed discharge and other hospital costs is considerable.
Epidemiology
The frequency and incidence of CDAD varies between hospitals and within a given institution over time. The risk for disease increases in patients with antibiotic exposure, gastrointestinal surgery, increasing length of stay in healthcare settings, serious underlying illness, immuno-compromising conditions, and advanced age.
C. difficile is shed in feces. Any surface, device, or material (e.g., commode, bathing tub, and electronic rectal thermometer) that becomes contaminated with feces may serve as a reservoir for C. difficile spores. Spores are transferred to patients mainly via the hands of healthcare personnel who have touched a contaminated surface or item (2-6).
The Organism and Pathophysiology of C. difficile Diarrhea
C. difficile is a gram-positive, anaerobic, spore-forming bacillus that is responsible for the development of antibiotic-associated diarrhea and colitis. C. difficile was first described in 1935 as a component of the fecal flora of healthy newborns and was initially not thought to be pathogenic (7). The bacillus was named difficile because it grows slowly and is difficult to culture. C. difficile is presently responsible for nearly all causes of pseudomembranous colitis and as many as 20% of cases of antibiotic-associated diarrhea without colitis. Although found in the stool of only 5% of the general population, as many as 21% of adults become colonized with this organism while hospitalized (2,6).
An alteration of the normal colonic microflora, usually caused by antibiotic therapy, is the main factor that predisposes to infection with C. difficile. Almost all antibiotics have been associated with C. difficile diarrhea and colitis. The antibiotics most frequently associated include clindamycin, cephalosporins, ampicillin, and amoxicillin (Table 1) (8).
In addition to antibiotic therapy, older age and severity of underlying disease are important risk factors for C. difficile infection. Other risk factors include the presence of a nasogastric tube, gastrointestinal procedures, acid antisecretory medications, intensive care unit stay, and duration of hospitalization (9).
C. difficile diarrhea is caused primarily by the elaboration of toxins A and B produced by bacterial multiplication within the intestinal lumen. These toxins bind to the colonic mucosa and exert their deleterious effects upon it. The organism rarely damages the colon by direct invasion, and diarrhea is caused by the effects of toxins produced within the intestinal lumen that adhere to the mucosal surface. Most toxigenic isolates produce both toxins, and about 5–25% of isolates produce neither toxin A nor B, and do not cause colitis or diarrhea (3-5).
Clinical Manifestations
Infection with C. difficile may produce a wide range of clinical manifestations, including asymptomatic carriage, mild-to-moderate diarrhea, and fulminant disease with pseudomembranous colitis (10). In patients who develop CDAD, symptoms usually begin soon after colonization. Colonization may occur during antibiotic treatment or up to several weeks after a course of antibiotics. CDAD typically is associated with the passage of frequent, loose bowel movements consistent with proctocolitis. Mucus or occult blood may be present, but visible blood is rare.
Diagnosis
The diagnosis of CDAD is based on a history of recent or current antibiotic therapy, development of diarrhea or other evidence of acute colitis, and demonstration of infection by toxigenic C. difficile, usually by detection of toxin A or toxin B in stool sample.
Practical Guidelines for Diagnosis of C. difficile Diarrheal Syndromes
- The diagnosis should be suspected in anyone with diarrhea who has received antibiotics within the previous 2 months and/or whose diarrhea begins 72 hours or more after hospitalization.
- When the diagnosis is suspected, a single stool specimen should be sent to the laboratory for testing for the presence of C. difficile and/or its toxins.
- When diarrhea persists despite a negative stool toxin result, one or two additional samples may be sent for testing with the same or different tests (4). Endoscopy is reserved for special situations, such as when a rapid diagnosis is needed and test results are delayed or the test is not highly sensitive, when the patient has ileus and stool is not available, or when other colonic diseases are also a consideration.
There is as yet no simple, inexpensive, rapid, sensitive and specific test for diagnosing C. difficile diarrhea and colitis, nor are all the available tests suitable for adoption by every laboratory (Table 2) (11).
Endoscopic Diagnosis of C. difficile Diarrhea and Colitis
Sigmoidoscopy and colonoscopy are not indicated for most patients with CDAD (10,12). Endoscopy is helpful, however, in special situations, such as when the diagnosis is in doubt or the clinical situation demands rapid diagnosis. The results of endoscopic examination may be normal in patients with mild diarrhea or may show nonspecific colitis in moderate cases. The finding of colonic pseudomembranes in a patient with antibiotic-associated diarrhea is virtually pathognomonic for C. difficile colitis. A few patients without any diagnostic features in the rectosigmoid have pseudomembranes in the more proximal areas of the colon (13). Other endoscopic findings include erythema, edema, friability, and nonspecific colitis with small ulcerations or erosions.
Treatment
The first step in the management of C. difficile diarrhea and colitis is to discontinue the precipitating antibiotics if possible (10,12). Diarrhea resolves in approximately 15–25% of patients without specific anti–C. difficile therapy (14,15). Conservative management alone may not be indicated, however, in patients who are systemically ill or who have multiple medical problems, since it is difficult to predict which patients will improve spontaneously. If it is not possible to discontinue the precipitating antibiotic because of other active infections, the patient’s antibiotic regimen should be altered if possible to make use of agents less likely to cause CDAD (e.g., aminoglycosides, trimethoprim, rifampin, or a quinolone).
Antiperistaltic agents, such as diphenoxylate plus atropine (Lomotil), or loperamide (Imodium), and narcotic analgesics should be avoided because they may delay clearance of toxins from the colon and thereby exacerbate toxin-induced colonic injury or precipitate ileus and toxic dilatation (12,16). Specific therapy to eradicate C. difficile should be used in patients with initially severe symptoms and in patients whose symptoms persist despite discontinuation of antibiotic treatment. Although the diagnosis of C. difficile colitis should ideally be established before antimicrobial therapy is implemented, current ACG guidelines recommend that empiric therapy should be initiated in highly suggestive cases of severely ill patients (Table 3 on page 54) (12).
Currently, oral vancomycin or metronidazole, used for 7 to 10 days, are considered first-line therapy by most authors and current guidelines. Metronidazole at a dose of 250 mg 4 times daily is recommended by most authors and ACG guidelines as the drug of choice for the initial treatment of C. difficile colitis (12). These recommendations are largely based on efficacy, lower costs, and concerns about the development of vancomycin-resistant strains. Major disadvantages of metronidazole include a less desirable drug profile and contraindications in children and pregnant women.
Vancomycin, on the other hand, at a dose of 125 mg 4 times daily, is safe and well tolerated and achieves stool levels 20 times the required minimal inhibitory concentration for the treatment of C. difficile. Drawbacks to the use of vancomycin are cost and potential development of vancomycin-resistant strains. The current ACG guidelines consider vancomycin the drug of choice in severely ill patients and in cases in which the use of metronidazole is precluded.
Controlled clinical trials are lacking for patients with fulminant colitis who may not tolerate oral therapy. Administration of metronidazole intravenously or administration of vancomycin by nasogastric tube or rectal enema has been described in small case series (17-20). Intravenous administration of vancomycin is not recommended, because the drug is not excreted in the colon (17).
Management of Recurrent C. difficile Diarrhea
Despite successful initial treatment of CDAD, 15–20% of patients have recurrence of diarrhea in association with a positive stool test for C. difficile toxin. Symptomatic recurrence is rarely due to treatment failure or antimicrobial resistance to metronidazole or vancomycin. Approaches to management include conservative therapy (however, many patients are elderly and infirm and unable to tolerate diarrhea), therapy with specific anti–C. difficile antibiotics, the use of anion-binding resins, therapy with microorganisms (probiotics), and immunoglobulin therapy.
The most common therapy for recurrent C. difficile diarrhea is a second course of the same antibiotic used to treat the initial episode (12). In a large observational study in the United States, 92% of patients with recurrent CDAD responded successfully to a single repeated course of therapy, usually with metronidazole or vancomycin (14). There is evidence to suggest that patients with a history of recurrence have a high risk of further episodes of CDAD after antibiotic therapy is discontinued. There are no data to suggest that sequential episodes become progressively more severe or complicated (21). A variety of treatment schedules have been suggested for patients with multiple recurrences of C. difficile diarrhea. One approach is to give a prolonged course of vancomycin (or metronidazole) using a decreasing dosage schedule followed by pulse therapy (Table 4).
Cholestyramine, an anionexchange resin administered at a dose of 4 grams 3 or 4 times daily for 1 to 2 weeks, binds C. difficile toxins and may be used in conjunction with antibiotics to treat repeated relapses. Because cholestyramine may bind vancomycin as well as toxins, it should be taken at least 2 to 3 hours apart from the vancomycin.
Severe C. difficile Colitis
The incidence of fulminant C. difficile colitis has been reported to be 1.6–3.2% (22). Although recent precise figures from other centers are lacking, it is being recognized as an increasing cause of complications and death. The clinical syndrome of fulminant C. difficile colitis can be recognized with a proper knowledge of the spectrum of disease presentation.
A. Diarrhea: Although diarrhea is the hallmark of C. difficile colitis, it is not invariably present, and its absence may lead to diagnostic confusion. When diarrhea is absent, this appears to be secondary to severe colonic dysmotility. Even when present, diarrhea may be perceived to be a minor component of a nonspecific septic picture.
B. Severe Disease: Fulminant colitis is an unusual form of C. difficile infection, occurring in only 3% of patients but accounting for virtually all serious complications. Patients with more severe forms of the disease may present with or without diarrhea. When patients develop colitis localized to the cecum and right side of the colon, diarrhea may be minimal or absent. In the absence of diarrhea, the only clues to diagnosis may be systemic signs of toxicity (fever, tachycardia, leukocytosis, and/or volume depletion).
An elevated white blood cell count may be an important clue to impending fulminant C. difficile colitis. The rapid elevation of the peripheral white cell count (commonly as high as 30,000 to 50,000) with a significant excess of bands and sometimes more immature forms often precedes hemodynamic instability and the development of organ dysfunction. Even in patients who are mildly symptomatic for an extended period, sudden and unexpected progression to shock may occur. It is difficult to predict those patients who may not respond to medical treatment. Hence, early warning signs such as a leukemoid reaction may be invaluable.
Hypotension is a late finding and can be resistant to vasopressor support. Abdominal signs range from distention to generalized tenderness with guarding. Colonic perforation is usually accompanied by abdominal rigidity, involuntary guarding, rebound tenderness, and absent bowel sounds. Free air may be revealed on abdominal radiographs. Any suspicion of perforation in this setting should prompt immediate surgical consultation. Death generally occurs before free air and perforation can occur. In one study, contrary to most other literature, perforation was found to be rare (22).
Abdominal radiography may reveal a dilated colon (>7 cm in its greatest diameter), consistent with toxic megacolon. Patients with megacolon may have an associated small bowel ileus with dilated small intestine on plain abdominal radiographs, with air-fluid levels mimicking small intestinal obstruction or ischemia. CT without contrast and endoscopy can quickly diagnose or at least strongly suggest fulminant C.difficile colitis. CT scan findings include evidence of ascites, colonic wall thickening and/or dilatation. These findings may prove helpful in categorizing the severity of the colitis.
More aggressive intervention in medically unresponsive patients, including rapid identification of patients failing to respond to medical therapy, is crucial to a positive outcome, and early surgical intervention should be done in this group (Figures 1-3).
It is important that everyone involved with patient care in hospitals, nursing homes, and skilled nursing facilities be educated about the organism and its epidemiology, rational approaches to the treatment and care of patients with C. difficile diarrhea, the importance of hand washing between contact with patients, the use of gloves when caring for a patient with C. difficile diarrhea, and the avoidance of the unnecessary use of antimicrobials.
Conclusion
Recent years have raised concerns over rising incidence and serious complication rates of CDAD in North American hospitals (22,23). The Canadian Medical Association journal published a report in 2004 detailing an outbreak of CDAD involving several hospitals in Montreal. The introduction of new hypervirulent and highly transmissible strains of C. difficile has been postulated as the possible cause for the outbreak (24). A deteriorating infrastructure, inadequate infection control practices, the increasing number of debilitated patients, an aging population, and hypervirulent strains were all felt to be likely contributors to recent outbreaks in Canada (25).
Two epidemiological investigations in the United States and Canada (24,26) independently examined samples of C. difficile and found that a mutated version of the “wild” strain was responsible for outbreaks in Quebec and increased rates of CDAD in hospitals in the United States recently (22,23). Clinical epidemiologists at the CDC investigated C. difficile isolates from hospitals in the United States with recent (i.e., 2001–2004) CDAD outbreaks (22,23). The report indicates the emergence of a new epidemic strain, “BI” (distinct from the “J” strain of 1989–1992), which may be responsible for the recent increase in rates and apparent severity of CDAD (26).
CDAD and colitis in most cases can be treated by the administration of metronidazole or vancomycin. In some patients severe life-threatening toxicity develops despite appropriate and timely medical treatment, and surgical intervention is necessary. Systemic symptoms of infection with C. difficile are reported not to derive from bacteremia, colonic perforation or ischemia, but from toxin-induced inflammatory mediators released from the colon (27-29). Early surgical intervention should be employed in refractory cases of severe disease. Surgical intervention is far from ideal, however, and carries a very high rate of complications and significant risk of mortality (22). The future clinical approach to the treatment of nosocomial C. difficile colitis may eventually involve specific antitoxin hyperimmunoglobulins and inhibitors of the inflammatory cascade (28,30,31).
References
- Archibald LK, Banerjee SN, Jarvis WR. Secular trend in hospital-acquired Clostridium difficile disease in the United States; 1987-2001. J Infect Dis. 2004;189:1585-9.
- Fekety R. Antibiotic-associated colitis. In: Mandell G, Bennet JE, Dolin R, eds. Principles and Practice of Infectious Diseases. 4th ed. New York: Churchill Livingston; 1996:978-806.
- Mitty RD, LaMont T. Clostridium difficile diarrhea: Pathogenesis, epidemiology, and treatment. Gastroenterologist. 1994;2:61-9.
- Bartlett JG. Clostridium difficile: History of its role as an enteric pathogen and the current state of knowledge about the organism. Clin Infect Dis. 1994;18(Suppl 4):265-72.
- Johnson S, Gerding D. Clostridium difficile. In: Mayhall CG, ed. Hospital Epidemiology and Infection Control. Baltimore, Md: Williams & Wilkins; 1996:99-408.
- Mcfarland LV, Mulligan ME, Kwok RY, Stamm WE. Nosocomial acquisition of Clostridium difficile. N Engl J Med. 1989;320:204-10.
- Hall IC, O Toole E. Intestinal Flora in new-born infants: With a description of a new pathogenic anaerobe, Bacillus difficile. Am J Dis Child. 1935;49:390-402.
- Kelly CP, LaMont JT. Treatment of Clostridium difficile diarrhea and colitis. In: Wolfe MM, ed. Gastrointestinal Pharmacotherapy. Philadelphia, Pa.: WB Saunders; 1993:199-212.
- Bignardi GE. Risk factors for Clostridium difficile infection. J Hosp Infect. 1998;40:1-15.
- Kelly CP, Pothoulakas C, LaMont JT. Clostridium difficile colitis. N Engl J Med. 1994;330:257-62.
- Linevsky JK, Kelly CP. Clostridium difficile colitis. In: Lamont JT, ed. Gastrointestinal Infections: Diagnosis and Management. New York: Marcel Dekker; 1997:293-325.
- Fekety R. Guidelines for the diagnosis and management of Clostridium difficile associated diarrhea and colitis. American College of Gastroenetrology, Practice Parameters Committee. Am J Gastroenterol. 1997;92:739-50.
- Tedesco FJ, Corless JK, Brownstein RE. Rectal sparing in antibiotic-associated pseudomembranous colitis: A prospective study. Gastroenterology. 1982;83:1259-60.
- Olson MM, Shanholtzer CJ, Lee JT Jr, Gerding DN. Ten years of prospective Clostridium difficile-associated disease surveillance and treatment at the Minneapolis VA Medical Center, 1982-1991. Infect Control Hosp Epidemiol. 1994;15: 371-81.
- Teasley DG, Gerding DN, Olson MM, et al. Prospective randomized trial of metronidazole versus vancomycin for Clostridium-difficile-associated diarrhoea and colitis. Lancet. 1983;2:1043-6.
- Walley T, Milson D. Loperamide-related toxic megacolon in Clostridium difficile colitis. Postgrad Med J. 1990;66:582.
- Malnick SD, Zimhony O. Treatment of Clostridium difficile associated diarrhea. Ann Pharmacother. 2002;36:1767-75.
- Sehgal M, Kyne L. Clostridium difficile disease. Curr Treatment Options Infect Dis. 2002;4:201-10.
- Apisarnthanarak A, Razavi B, Mundy LM. Adjunctive intracolonic vancomycin for severe Clostridium difficile colitis: case series and review of the literature. Clin Infect Dis. 2002;35:690-6.
- Friendenberg F, Fernandez A, Kaul V, Niami P, Levine GM. Intravenous metronidazole for the treatment of Clostridium difficile colitis. Dis Colon Rectum. 2001;44:1176-80.
- Fekety R, McFarland LV, Surawicz CMGreenberg, RN, Elmer GW, Mulligan ME. Recurrent Clostridium difficile diarrhea: characteristics of and risk factors for patients enrolled in a prospective, randomized, double-blind trial. Clin Infect Dis. 1997;24:324-33.
- Dallal RM, Harbrecht BG, Boujoukas AJ, et al. Fulminant Clostridium difficile: an underappreciated and increasing cause of death and complications. Ann Surg. 2002;235:363-72.
- Morris AM, Jobe BA, Sontey, M, Sheppard BC, Deveney CW, Deveney KE. Clostridium difficile colitis: an increasingly aggressive iatrogenic disease? Arch Surg. 2002;137:1096-100.
- Eggerston L, Sibbald B. Hospitals battling outbreaks of C. difficile. CMAJ. 2004;171:19-21.
- Valiquette L, Low DE, Pepin J, McGeer A. Clostridium difficile infection in hospitals: a brewing storm. CMAJ. 2004;171:27-9.
- McDonald LC, Killgore GE, Thompson A, et al. Emergence of an epidemic strain of Clostridium difficile in the United States, 2001-4: Potential role for virulence factors and antimicrobial resistance traits. Infectious Diseases Society of America 42th Annual Meeting. Boston, MA, September 30 – October 3, 2004. Abstract # LB-2.
- Flegel W, Muller F, Daubener W, Fischer HG, Hadding U, Northoff H. Cytokine response by human monocytes to Clostridium difficile toxin A and toxin B. Infect Immun. 1991;59:3659-66.
- Castagliuolo I, Keates A, Qiu B, et al. Increased substance P responses in dorsal root ganglia, intestinal macrophages during Clostridium difficile toxin A enteritis in rats. Proc Natl Acad Sci U S A. 1997;94:4788-93.
- Castagliuolo I, Keates A, Wang C, et al. Clostridium difficile toxin A stimulates macrophage-inflammatory protein-2 production in rat intestinal epithelial cells. J Immunol. 1998;160:6039-45.
- Kelly C, Chetham S, Keates S, et al. Survival of anti-Clostridium difficile bovine immunoglobulin concentrate in the human gastrointestinal tract. Antimicrob Agents Chemother. 1997;41:236-41.
- Salcedo J, Keates S, Pothoulakis C, et. al. Intravenous immunoglobulin therapy for severe Clostridium difficile colitis. Gut. 1997;41:366-70.
General References
- Shea Position Paper Gerding DN,Johnson S, Peterson LR, Mulligan ME Silva J. SHEA Position Paper:Clostridium difficile-associated diarrhea and colitis; Infect Control Hosp Epidemiol 1995, 16:459-77
- Kyne L, Farrell RJ, Kelly CP. Clostridium difficile. Gastroenterol Clin North Am 2001; 30:753-77.
Introduction
Clostridium difficile–associated diarrhea (CDAD) has been recognized with increased frequency as a cause of nosocomial illness. The frequency and incidence of CDAD varies widely, and is influenced by multiple factors including nosocomial outbreaks, patterns of antimicrobial use, and individual susceptibility. There are no reports of prospective studies by hospitals tracking positive toxin A or A/B and the outcomes of CDAD and its complications.
The Centers for Disease Control and Prevention (CDC) has analyzed secular trends in the incidence of CDAD, and it reported a steady increase from 1987 to 2001 (1). In this report, 30% of 440 infectious disease physicians who participated in a Web-based poll reported that they are seeing higher rates of CDAD, more severe CDAD, and more relapsing CDAD than in the past. There is an overall impression that there has been an increase in the proportion of cases with severe and fatal complications, and an increase in the relapse rate among affected patients.
In addition to morbidity and mortality, the economic burden of C. difficile infection in terms of delayed discharge and other hospital costs is considerable.
Epidemiology
The frequency and incidence of CDAD varies between hospitals and within a given institution over time. The risk for disease increases in patients with antibiotic exposure, gastrointestinal surgery, increasing length of stay in healthcare settings, serious underlying illness, immuno-compromising conditions, and advanced age.
C. difficile is shed in feces. Any surface, device, or material (e.g., commode, bathing tub, and electronic rectal thermometer) that becomes contaminated with feces may serve as a reservoir for C. difficile spores. Spores are transferred to patients mainly via the hands of healthcare personnel who have touched a contaminated surface or item (2-6).
The Organism and Pathophysiology of C. difficile Diarrhea
C. difficile is a gram-positive, anaerobic, spore-forming bacillus that is responsible for the development of antibiotic-associated diarrhea and colitis. C. difficile was first described in 1935 as a component of the fecal flora of healthy newborns and was initially not thought to be pathogenic (7). The bacillus was named difficile because it grows slowly and is difficult to culture. C. difficile is presently responsible for nearly all causes of pseudomembranous colitis and as many as 20% of cases of antibiotic-associated diarrhea without colitis. Although found in the stool of only 5% of the general population, as many as 21% of adults become colonized with this organism while hospitalized (2,6).
An alteration of the normal colonic microflora, usually caused by antibiotic therapy, is the main factor that predisposes to infection with C. difficile. Almost all antibiotics have been associated with C. difficile diarrhea and colitis. The antibiotics most frequently associated include clindamycin, cephalosporins, ampicillin, and amoxicillin (Table 1) (8).
In addition to antibiotic therapy, older age and severity of underlying disease are important risk factors for C. difficile infection. Other risk factors include the presence of a nasogastric tube, gastrointestinal procedures, acid antisecretory medications, intensive care unit stay, and duration of hospitalization (9).
C. difficile diarrhea is caused primarily by the elaboration of toxins A and B produced by bacterial multiplication within the intestinal lumen. These toxins bind to the colonic mucosa and exert their deleterious effects upon it. The organism rarely damages the colon by direct invasion, and diarrhea is caused by the effects of toxins produced within the intestinal lumen that adhere to the mucosal surface. Most toxigenic isolates produce both toxins, and about 5–25% of isolates produce neither toxin A nor B, and do not cause colitis or diarrhea (3-5).
Clinical Manifestations
Infection with C. difficile may produce a wide range of clinical manifestations, including asymptomatic carriage, mild-to-moderate diarrhea, and fulminant disease with pseudomembranous colitis (10). In patients who develop CDAD, symptoms usually begin soon after colonization. Colonization may occur during antibiotic treatment or up to several weeks after a course of antibiotics. CDAD typically is associated with the passage of frequent, loose bowel movements consistent with proctocolitis. Mucus or occult blood may be present, but visible blood is rare.
Diagnosis
The diagnosis of CDAD is based on a history of recent or current antibiotic therapy, development of diarrhea or other evidence of acute colitis, and demonstration of infection by toxigenic C. difficile, usually by detection of toxin A or toxin B in stool sample.
Practical Guidelines for Diagnosis of C. difficile Diarrheal Syndromes
- The diagnosis should be suspected in anyone with diarrhea who has received antibiotics within the previous 2 months and/or whose diarrhea begins 72 hours or more after hospitalization.
- When the diagnosis is suspected, a single stool specimen should be sent to the laboratory for testing for the presence of C. difficile and/or its toxins.
- When diarrhea persists despite a negative stool toxin result, one or two additional samples may be sent for testing with the same or different tests (4). Endoscopy is reserved for special situations, such as when a rapid diagnosis is needed and test results are delayed or the test is not highly sensitive, when the patient has ileus and stool is not available, or when other colonic diseases are also a consideration.
There is as yet no simple, inexpensive, rapid, sensitive and specific test for diagnosing C. difficile diarrhea and colitis, nor are all the available tests suitable for adoption by every laboratory (Table 2) (11).
Endoscopic Diagnosis of C. difficile Diarrhea and Colitis
Sigmoidoscopy and colonoscopy are not indicated for most patients with CDAD (10,12). Endoscopy is helpful, however, in special situations, such as when the diagnosis is in doubt or the clinical situation demands rapid diagnosis. The results of endoscopic examination may be normal in patients with mild diarrhea or may show nonspecific colitis in moderate cases. The finding of colonic pseudomembranes in a patient with antibiotic-associated diarrhea is virtually pathognomonic for C. difficile colitis. A few patients without any diagnostic features in the rectosigmoid have pseudomembranes in the more proximal areas of the colon (13). Other endoscopic findings include erythema, edema, friability, and nonspecific colitis with small ulcerations or erosions.
Treatment
The first step in the management of C. difficile diarrhea and colitis is to discontinue the precipitating antibiotics if possible (10,12). Diarrhea resolves in approximately 15–25% of patients without specific anti–C. difficile therapy (14,15). Conservative management alone may not be indicated, however, in patients who are systemically ill or who have multiple medical problems, since it is difficult to predict which patients will improve spontaneously. If it is not possible to discontinue the precipitating antibiotic because of other active infections, the patient’s antibiotic regimen should be altered if possible to make use of agents less likely to cause CDAD (e.g., aminoglycosides, trimethoprim, rifampin, or a quinolone).
Antiperistaltic agents, such as diphenoxylate plus atropine (Lomotil), or loperamide (Imodium), and narcotic analgesics should be avoided because they may delay clearance of toxins from the colon and thereby exacerbate toxin-induced colonic injury or precipitate ileus and toxic dilatation (12,16). Specific therapy to eradicate C. difficile should be used in patients with initially severe symptoms and in patients whose symptoms persist despite discontinuation of antibiotic treatment. Although the diagnosis of C. difficile colitis should ideally be established before antimicrobial therapy is implemented, current ACG guidelines recommend that empiric therapy should be initiated in highly suggestive cases of severely ill patients (Table 3 on page 54) (12).
Currently, oral vancomycin or metronidazole, used for 7 to 10 days, are considered first-line therapy by most authors and current guidelines. Metronidazole at a dose of 250 mg 4 times daily is recommended by most authors and ACG guidelines as the drug of choice for the initial treatment of C. difficile colitis (12). These recommendations are largely based on efficacy, lower costs, and concerns about the development of vancomycin-resistant strains. Major disadvantages of metronidazole include a less desirable drug profile and contraindications in children and pregnant women.
Vancomycin, on the other hand, at a dose of 125 mg 4 times daily, is safe and well tolerated and achieves stool levels 20 times the required minimal inhibitory concentration for the treatment of C. difficile. Drawbacks to the use of vancomycin are cost and potential development of vancomycin-resistant strains. The current ACG guidelines consider vancomycin the drug of choice in severely ill patients and in cases in which the use of metronidazole is precluded.
Controlled clinical trials are lacking for patients with fulminant colitis who may not tolerate oral therapy. Administration of metronidazole intravenously or administration of vancomycin by nasogastric tube or rectal enema has been described in small case series (17-20). Intravenous administration of vancomycin is not recommended, because the drug is not excreted in the colon (17).
Management of Recurrent C. difficile Diarrhea
Despite successful initial treatment of CDAD, 15–20% of patients have recurrence of diarrhea in association with a positive stool test for C. difficile toxin. Symptomatic recurrence is rarely due to treatment failure or antimicrobial resistance to metronidazole or vancomycin. Approaches to management include conservative therapy (however, many patients are elderly and infirm and unable to tolerate diarrhea), therapy with specific anti–C. difficile antibiotics, the use of anion-binding resins, therapy with microorganisms (probiotics), and immunoglobulin therapy.
The most common therapy for recurrent C. difficile diarrhea is a second course of the same antibiotic used to treat the initial episode (12). In a large observational study in the United States, 92% of patients with recurrent CDAD responded successfully to a single repeated course of therapy, usually with metronidazole or vancomycin (14). There is evidence to suggest that patients with a history of recurrence have a high risk of further episodes of CDAD after antibiotic therapy is discontinued. There are no data to suggest that sequential episodes become progressively more severe or complicated (21). A variety of treatment schedules have been suggested for patients with multiple recurrences of C. difficile diarrhea. One approach is to give a prolonged course of vancomycin (or metronidazole) using a decreasing dosage schedule followed by pulse therapy (Table 4).
Cholestyramine, an anionexchange resin administered at a dose of 4 grams 3 or 4 times daily for 1 to 2 weeks, binds C. difficile toxins and may be used in conjunction with antibiotics to treat repeated relapses. Because cholestyramine may bind vancomycin as well as toxins, it should be taken at least 2 to 3 hours apart from the vancomycin.
Severe C. difficile Colitis
The incidence of fulminant C. difficile colitis has been reported to be 1.6–3.2% (22). Although recent precise figures from other centers are lacking, it is being recognized as an increasing cause of complications and death. The clinical syndrome of fulminant C. difficile colitis can be recognized with a proper knowledge of the spectrum of disease presentation.
A. Diarrhea: Although diarrhea is the hallmark of C. difficile colitis, it is not invariably present, and its absence may lead to diagnostic confusion. When diarrhea is absent, this appears to be secondary to severe colonic dysmotility. Even when present, diarrhea may be perceived to be a minor component of a nonspecific septic picture.
B. Severe Disease: Fulminant colitis is an unusual form of C. difficile infection, occurring in only 3% of patients but accounting for virtually all serious complications. Patients with more severe forms of the disease may present with or without diarrhea. When patients develop colitis localized to the cecum and right side of the colon, diarrhea may be minimal or absent. In the absence of diarrhea, the only clues to diagnosis may be systemic signs of toxicity (fever, tachycardia, leukocytosis, and/or volume depletion).
An elevated white blood cell count may be an important clue to impending fulminant C. difficile colitis. The rapid elevation of the peripheral white cell count (commonly as high as 30,000 to 50,000) with a significant excess of bands and sometimes more immature forms often precedes hemodynamic instability and the development of organ dysfunction. Even in patients who are mildly symptomatic for an extended period, sudden and unexpected progression to shock may occur. It is difficult to predict those patients who may not respond to medical treatment. Hence, early warning signs such as a leukemoid reaction may be invaluable.
Hypotension is a late finding and can be resistant to vasopressor support. Abdominal signs range from distention to generalized tenderness with guarding. Colonic perforation is usually accompanied by abdominal rigidity, involuntary guarding, rebound tenderness, and absent bowel sounds. Free air may be revealed on abdominal radiographs. Any suspicion of perforation in this setting should prompt immediate surgical consultation. Death generally occurs before free air and perforation can occur. In one study, contrary to most other literature, perforation was found to be rare (22).
Abdominal radiography may reveal a dilated colon (>7 cm in its greatest diameter), consistent with toxic megacolon. Patients with megacolon may have an associated small bowel ileus with dilated small intestine on plain abdominal radiographs, with air-fluid levels mimicking small intestinal obstruction or ischemia. CT without contrast and endoscopy can quickly diagnose or at least strongly suggest fulminant C.difficile colitis. CT scan findings include evidence of ascites, colonic wall thickening and/or dilatation. These findings may prove helpful in categorizing the severity of the colitis.
More aggressive intervention in medically unresponsive patients, including rapid identification of patients failing to respond to medical therapy, is crucial to a positive outcome, and early surgical intervention should be done in this group (Figures 1-3).
It is important that everyone involved with patient care in hospitals, nursing homes, and skilled nursing facilities be educated about the organism and its epidemiology, rational approaches to the treatment and care of patients with C. difficile diarrhea, the importance of hand washing between contact with patients, the use of gloves when caring for a patient with C. difficile diarrhea, and the avoidance of the unnecessary use of antimicrobials.
Conclusion
Recent years have raised concerns over rising incidence and serious complication rates of CDAD in North American hospitals (22,23). The Canadian Medical Association journal published a report in 2004 detailing an outbreak of CDAD involving several hospitals in Montreal. The introduction of new hypervirulent and highly transmissible strains of C. difficile has been postulated as the possible cause for the outbreak (24). A deteriorating infrastructure, inadequate infection control practices, the increasing number of debilitated patients, an aging population, and hypervirulent strains were all felt to be likely contributors to recent outbreaks in Canada (25).
Two epidemiological investigations in the United States and Canada (24,26) independently examined samples of C. difficile and found that a mutated version of the “wild” strain was responsible for outbreaks in Quebec and increased rates of CDAD in hospitals in the United States recently (22,23). Clinical epidemiologists at the CDC investigated C. difficile isolates from hospitals in the United States with recent (i.e., 2001–2004) CDAD outbreaks (22,23). The report indicates the emergence of a new epidemic strain, “BI” (distinct from the “J” strain of 1989–1992), which may be responsible for the recent increase in rates and apparent severity of CDAD (26).
CDAD and colitis in most cases can be treated by the administration of metronidazole or vancomycin. In some patients severe life-threatening toxicity develops despite appropriate and timely medical treatment, and surgical intervention is necessary. Systemic symptoms of infection with C. difficile are reported not to derive from bacteremia, colonic perforation or ischemia, but from toxin-induced inflammatory mediators released from the colon (27-29). Early surgical intervention should be employed in refractory cases of severe disease. Surgical intervention is far from ideal, however, and carries a very high rate of complications and significant risk of mortality (22). The future clinical approach to the treatment of nosocomial C. difficile colitis may eventually involve specific antitoxin hyperimmunoglobulins and inhibitors of the inflammatory cascade (28,30,31).
References
- Archibald LK, Banerjee SN, Jarvis WR. Secular trend in hospital-acquired Clostridium difficile disease in the United States; 1987-2001. J Infect Dis. 2004;189:1585-9.
- Fekety R. Antibiotic-associated colitis. In: Mandell G, Bennet JE, Dolin R, eds. Principles and Practice of Infectious Diseases. 4th ed. New York: Churchill Livingston; 1996:978-806.
- Mitty RD, LaMont T. Clostridium difficile diarrhea: Pathogenesis, epidemiology, and treatment. Gastroenterologist. 1994;2:61-9.
- Bartlett JG. Clostridium difficile: History of its role as an enteric pathogen and the current state of knowledge about the organism. Clin Infect Dis. 1994;18(Suppl 4):265-72.
- Johnson S, Gerding D. Clostridium difficile. In: Mayhall CG, ed. Hospital Epidemiology and Infection Control. Baltimore, Md: Williams & Wilkins; 1996:99-408.
- Mcfarland LV, Mulligan ME, Kwok RY, Stamm WE. Nosocomial acquisition of Clostridium difficile. N Engl J Med. 1989;320:204-10.
- Hall IC, O Toole E. Intestinal Flora in new-born infants: With a description of a new pathogenic anaerobe, Bacillus difficile. Am J Dis Child. 1935;49:390-402.
- Kelly CP, LaMont JT. Treatment of Clostridium difficile diarrhea and colitis. In: Wolfe MM, ed. Gastrointestinal Pharmacotherapy. Philadelphia, Pa.: WB Saunders; 1993:199-212.
- Bignardi GE. Risk factors for Clostridium difficile infection. J Hosp Infect. 1998;40:1-15.
- Kelly CP, Pothoulakas C, LaMont JT. Clostridium difficile colitis. N Engl J Med. 1994;330:257-62.
- Linevsky JK, Kelly CP. Clostridium difficile colitis. In: Lamont JT, ed. Gastrointestinal Infections: Diagnosis and Management. New York: Marcel Dekker; 1997:293-325.
- Fekety R. Guidelines for the diagnosis and management of Clostridium difficile associated diarrhea and colitis. American College of Gastroenetrology, Practice Parameters Committee. Am J Gastroenterol. 1997;92:739-50.
- Tedesco FJ, Corless JK, Brownstein RE. Rectal sparing in antibiotic-associated pseudomembranous colitis: A prospective study. Gastroenterology. 1982;83:1259-60.
- Olson MM, Shanholtzer CJ, Lee JT Jr, Gerding DN. Ten years of prospective Clostridium difficile-associated disease surveillance and treatment at the Minneapolis VA Medical Center, 1982-1991. Infect Control Hosp Epidemiol. 1994;15: 371-81.
- Teasley DG, Gerding DN, Olson MM, et al. Prospective randomized trial of metronidazole versus vancomycin for Clostridium-difficile-associated diarrhoea and colitis. Lancet. 1983;2:1043-6.
- Walley T, Milson D. Loperamide-related toxic megacolon in Clostridium difficile colitis. Postgrad Med J. 1990;66:582.
- Malnick SD, Zimhony O. Treatment of Clostridium difficile associated diarrhea. Ann Pharmacother. 2002;36:1767-75.
- Sehgal M, Kyne L. Clostridium difficile disease. Curr Treatment Options Infect Dis. 2002;4:201-10.
- Apisarnthanarak A, Razavi B, Mundy LM. Adjunctive intracolonic vancomycin for severe Clostridium difficile colitis: case series and review of the literature. Clin Infect Dis. 2002;35:690-6.
- Friendenberg F, Fernandez A, Kaul V, Niami P, Levine GM. Intravenous metronidazole for the treatment of Clostridium difficile colitis. Dis Colon Rectum. 2001;44:1176-80.
- Fekety R, McFarland LV, Surawicz CMGreenberg, RN, Elmer GW, Mulligan ME. Recurrent Clostridium difficile diarrhea: characteristics of and risk factors for patients enrolled in a prospective, randomized, double-blind trial. Clin Infect Dis. 1997;24:324-33.
- Dallal RM, Harbrecht BG, Boujoukas AJ, et al. Fulminant Clostridium difficile: an underappreciated and increasing cause of death and complications. Ann Surg. 2002;235:363-72.
- Morris AM, Jobe BA, Sontey, M, Sheppard BC, Deveney CW, Deveney KE. Clostridium difficile colitis: an increasingly aggressive iatrogenic disease? Arch Surg. 2002;137:1096-100.
- Eggerston L, Sibbald B. Hospitals battling outbreaks of C. difficile. CMAJ. 2004;171:19-21.
- Valiquette L, Low DE, Pepin J, McGeer A. Clostridium difficile infection in hospitals: a brewing storm. CMAJ. 2004;171:27-9.
- McDonald LC, Killgore GE, Thompson A, et al. Emergence of an epidemic strain of Clostridium difficile in the United States, 2001-4: Potential role for virulence factors and antimicrobial resistance traits. Infectious Diseases Society of America 42th Annual Meeting. Boston, MA, September 30 – October 3, 2004. Abstract # LB-2.
- Flegel W, Muller F, Daubener W, Fischer HG, Hadding U, Northoff H. Cytokine response by human monocytes to Clostridium difficile toxin A and toxin B. Infect Immun. 1991;59:3659-66.
- Castagliuolo I, Keates A, Qiu B, et al. Increased substance P responses in dorsal root ganglia, intestinal macrophages during Clostridium difficile toxin A enteritis in rats. Proc Natl Acad Sci U S A. 1997;94:4788-93.
- Castagliuolo I, Keates A, Wang C, et al. Clostridium difficile toxin A stimulates macrophage-inflammatory protein-2 production in rat intestinal epithelial cells. J Immunol. 1998;160:6039-45.
- Kelly C, Chetham S, Keates S, et al. Survival of anti-Clostridium difficile bovine immunoglobulin concentrate in the human gastrointestinal tract. Antimicrob Agents Chemother. 1997;41:236-41.
- Salcedo J, Keates S, Pothoulakis C, et. al. Intravenous immunoglobulin therapy for severe Clostridium difficile colitis. Gut. 1997;41:366-70.
General References
- Shea Position Paper Gerding DN,Johnson S, Peterson LR, Mulligan ME Silva J. SHEA Position Paper:Clostridium difficile-associated diarrhea and colitis; Infect Control Hosp Epidemiol 1995, 16:459-77
- Kyne L, Farrell RJ, Kelly CP. Clostridium difficile. Gastroenterol Clin North Am 2001; 30:753-77.