User login
Evaluation of Inherent Differences Between African American and White Skin Surface Properties Using Subjective and Objective Measures
After 62 years, her husband is a ‘stranger’
Presenting symptoms: Marital memories
Ms. A, age 83, has been experiencing increasing confusion, agitation, and memory loss across 4 to 5 years. Family members say her memory loss has become prominent within the last year. She can no longer cook, manage her finances, shop, or perform other basic activities. At times she does not recognize her husband of 62 years and needs help with bathing and grooming.
Ms. A’s Folstein Mini-Mental State Examination (MMSE) score is 18, indicating moderate dementia. She exhibits disorientation, diminished short-term memory, impaired attention including apraxia, and executive dysfunction. Her Geriatric Depression Scale (15-item short form) score indicates normal mood.
A neurologic exam reveals mild parkinsonism, including mild bilateral upper-extremity cogwheeltype rigidity and questionable frontal release signs including a possible mild bilateral grasp reflex. No snout reflex was seen.
This presentation suggests Ms. A has:
- Alzheimer’s disease
- Lewy body dementia
- or vascular dementia
The authors’ observations:
Differentiating among Alzheimer’s, Lewy body, and vascular dementias is important (Table 1), as their treatments and clinical courses differ.
The initial workup’s goal is to diagnose a reversible medical condition that may be hastening cognitive decline. Brain imaging (CT or MRI) can uncover cerebrovascular disease, subdural hematomas, normal-pressure hydrocephalus, tumors, or other cerebral diseases. Laboratory tests can reveal systemic conditions such as hypothyroidism, vitamin B12 deficiency, hypercalcemia, neurosyphilis, or HIV infection.1
Table 1
Differences in Alzheimer’s, Lewy body, and vascular dementias
| Alzheimer’s dementia | Lewy body dementia | Vascular dementia |
|---|---|---|
| Gradual onset and chronic cognitive decline Memory difficulty combined with apraxia, aphasia, agnosia, or executive dysfunction | Cognitive, memory changes with one or more of the following:
| Early findings often include depression or personality changes, plus incontinence and gait disorder |
| Psychosis common in middle to late stages | Visual hallucinations, other psychoses in early stages Periods of marked delirium, “sundowning” | Temporal relationship between stroke and dementia onset, but variability in course |
| Day-to-day cognitive performance stable | Cognitive performance fluctuates during early stages. | Day-to-day cognitive performance stable |
| Parkinsonism not apparent in early stages, may present in middle to late stages | Parkinsonism in early stages Tremor not common | Gait disorder and parkinsonism common, especially with basal ganglia infarcts |
| Neurologic signs present in late stages | Exquisite sensitivity to neuroleptic therapy | Increased sensitivity to neuroleptics |
| Cannot be explained as vascular or mixed-type dementia | Cannot be explained as vascular or mixed-type dementia | Imaging necessary to document cerebrovascular disease |
With a thorough history and laboratory testing, a diagnosis of “probable” AD can be as much as 85% accurate. Probable AD is characterized by progressive gradual decline of cognitive functions affecting memory and at least one other domain including executive dysfunction, apraxia, aphasia, and/or agnosia. These deficits must cause significant functional impairment.
Neurologic test results may support AD diagnosis after ruling out reversible causes of dementia. Neuropsychological testing can provide valuable early information when subtle findings cannot be ascertained on clinical screening. (For a listing of neuropsychological tests, see this article at currentpsychiatry.com.)
Diagnosis: An unpredictable patient
Ms. A received a CBC; comprehensive metabolic panel; urinalysis; screens for rapid plasma reagin, B12, folate, and homocysteine levels; and a brain MRI. Hemoglobin and serum albumin were mildly depressed, reflecting early malnutrition. MRI showed generalized cerebral atrophy. Significant vascular disease was not identified.
Ms. A was diagnosed as having probable Alzheimer’s-type dementia based on the test results and the fact that her cognition was steadily declining. Other explanatory mechanisms were absent. She did not exhibit hallucinatory psychosis or fluctuating consciousness, which would signal Lewy body dementia.
Table 2
Medications for treating agitation in Alzheimer’s dementia
| Drug | Supporting evidence | Recommended dosage (mg/d)* | Rationale | Drawbacks |
|---|---|---|---|---|
| Anticonvulsants | ||||
| Carbamazepine | Tariot et al2 | 200 to 1,200 mg/d in divided doses | Commonly used for impulse control disorders | Agranulocytosis, hyponatremia, liver toxicity (all rare) |
| Divalproex | Loy and Tariot3 | 250 to 2,000 mg/d | Increasing evidence points to neuroprotective qualities | Possible white blood cell suppression, liver toxicity, pancreatitis (all rare) |
| Gabapentin | Roane et al4 | 100 to 1,200 mg/d | Safe in patients with hepatic dysfunction | Scant data on use in Alzheimer’s disease |
| Lamotrigine | Tekin et al5 | Start at 25 mg/d; titrate slowly to 50 to 200 mg/d | Possibly neuroprotective via N-methyl-D-aspartate mechanism | Rapid titration may cause Stevens-Johnson syndrome |
| Atypical antipsychotics | ||||
| Olanzapine | Street et al6 | 2.5 to 10 mg/d | Sedating effects may aid sleep | Anticholinergic effects may increase confusion, compound cognitive deficit |
| Quetiapine | Tariot et al7 | 25 to 300 mg/d | Tolerable Sedating effects may aid sleep | Watch for orthostasis, especially at higher dosages |
| Risperidone | DeVane et al8 | 0.25 to 3 mg/d | Strong data support use | High orthostatic potential, possible extrapyramidal symptoms with higher dosages |
| Ziprasidone | None | Oral:20to80mgbid IM: 10 to 20 mg, maximum 40 mg over 24 hours | Effective in managing agitation | No controlled trials, case reports in AD-associated agitation |
| SSRIs | ||||
| Citalopram | Pollock et al9 | 10 to 40 mg/d | Minimal CYP-2D6 inhibition | Effect may take 2 to 4 weeks |
| Sertraline | Lyketsos et al10 | 25 to 200 mg/d | Minimal CYP-2D6 inhibition | Effect may take 2 to 4 weeks |
| * No specific, widely accepted dosing guidelines exist for patients age > 65, but this group often does not tolerate higher dosages. | ||||
| SSRI: Selective serotonin reuptake inhibitor | ||||
| IM: Intramuscula | ||||
The psychiatrist started galantamine, 4 mg bid, and vitamin E, 400 IU bid, to maximize her cognition and attempt to slow her functional decline. Ms. A, who was in an assisted living facility when we evaluated her, was transferred to the facility’s nursing section shortly afterward.
At follow-up 3 weeks later, Ms. A’s behavior improved moderately, but she remained unpredictable and intermittently agitated. Staff reported that she was physically assaulting caregivers two to three times weekly.
Which medication(s) would you use to control Ms. A’s agitation and paranoia?
- an SSRI
- a mood stabilizer
- an atypical antipsychotic
- a combination or two or more of these drug classes
The authors’ observations
Aside from controlling agitation, medication treatment in AD should slow cognitive decline, improve behavior, help the patient perform daily activities, and delay nursing home placement.
- Watch for drug-drug interactions. Many patients with AD also are taking medications for hypertension, hypercholesterolemia, diabetes, arthritis, and other medical comorbidities.
- Start low and go slow. Older patients generally do not tolerate rapid dos-ing adjustments as well as younger patients (Table 2).
SSRIS. Selective serotonin reuptake inhibitors increase serotonin at the synaptic terminal. Serotonin has long been associated with impulsivity and aggression, and decreased 5-hydroxyindole acetic acid, a metabolite of serotonin, has been found in violent criminals and in psychiatric patients who have demonstrated inward or outward aggression.11
SSRIs generally are tolerable, safe, effective, and have little cholinergic blockade. Citalopram and sertraline minimally inhibit the cytochrome P-450 2D6 isoenzyme and have lower proteinbinding affinities than fluoxetine or paroxetine. Thus, citalopram and sertraline are less likely to alter therapeutic levels of highly bound medications through displacement of either drug’s protein-bound portion.10
Anticonvulsants with mood-stabilizing effects are another option. Reasonably strong data support use of divalproex for managing agitation in AD, either as a first-line agent or as an adjunct after failed SSRI therapy. Unlike other anticonvulsants, divalproex also may be neuroprotective.3
Divalproex, however, is associated with white blood cell suppression, significant liver toxicity, and pancreatitis, although these effects are rare.13 Monitor white blood cell counts and liver enzymes early in treatment, even if divalproex blood levels below the standard reference range produce a response.14
Though not studied specifically for treating agitation in AD, carbamazepine has demonstrated significant short-term efficacy in treating dementia-related agitation and aggression.2 Scant data support use of gabapentin or lamotrigine in Alzheimer’s dementia, but these agents are often used to manage agitation in other disorders.
Atypical antipsychotics. Psychosis usually occurs in middle-to-late-stage AD but can occur at any point. If psychosis occurs early, rule out Lewy body dementia.15
Choose an atypical antipsychotic that exhibits rapid dopamine receptor dissociation constants to reduce the risk of extrapyramidal symptoms, tardive dyskinesia, and cognitive decline with prolonged use. Quetiapine has shown efficacy for treating behavioral problems in Alzheimer’s and Lewy body dementia,7 and its sedating effects may help regulate sleep-wake cycles.
Data support use of olanzapine for agitation in AD,6 but watch for anticholinergic effects including worsening of cognition. Fast-dissolving olanzapine and risperidone oral wafers may help circumvent dosing difficulties in patients who cannot swallow—or will not take—their medication. Intramuscular olanzapine and ziprasidone have shown efficacy in treating acute agitation, but no systematic studies have examined their use in agitation secondary to dementia.
Recent data suggest a modestly increased risk of cerebrovascular accidents in AD patients taking atypicals compared with placebo, but the absolute rate of such events remains low.
Treatment: 3 months of stability
Ms. A’s galantamine dosage was increased to 8 mg bid and sertraline—25 mg/d for 7 days, then 50 mg/d—was added in an effort to better control her agitation, but the behavior continued unabated for 2 weeks. Divalproex, 125 mg bid titrated over 4 weeks to 750 mg/d, was added. Still, her agitation persisted.
Over the next 4 to 6 weeks, Ms. A showed signs of psychosis, often talking to herself and occasionally reporting “people attacking me.” She became paranoid toward members of her church, who she said were “trying to hurt” her. The paranoia intensified her agitation and disrupted her sleep. Physical examination was unremarkable, as were chest X-ray and urinalysis.
Sertraline and divalproex were gradually discontinued. Quetiapine—25 mg nightly, titrated across 2 weeks to 150 mg nightly—was started. Ms. A’s agitation and psychosis decreased with quetiapine titration, and her sleep improved. Her paranoid delusions remained but no longer impeded functioning or prompted a violent reaction.
Then after remaining stable for about 3 months, Ms. A’s paranoid delusions worsened and her agitation increased.
What treatment options are available at this point?
The authors’ observations
Treating agitation and delaying nursing home placement for patients with AD is challenging. When faced with inadequate or no response, consider less-conventional alternatives.
Vitamin E and selegiline were found separately to postpone functional decline in ambulatory patients with moderately severe AD, but the agents given together were less effective than either agent alone.16
Use of methylphenidate,17 buspirone,18 clonazepam,19 zolpidem,20 and—most recently— memantine21 for AD-related agitation also has been described.
Continued treatment: Medication changes
Quetiapine was increased to 350 mg nightly across 4 weeks, resulting in mild to moderate improvement. The higher dosage did not significantly worsen rigidity or motor function, and Ms. A tolerated the increased dosage without clinical orthostasis.
Memantine was added to address Ms. A’s agitation and preserve function. The agent was started at 5 mg/d and titrated across 4 weeks to 10 mg bid.
On clinical exam, Ms. A was more calm and directable and required less intervention. Her paranoia also decreased, allowing improved interaction with family, caregivers, and others. Ms. A remains stable on memantine, 10 mg bid; galantamine, 8 mg; quetiapine, 350 mg nightly; and vitamin E, 400 IU bid. Her cognitive ability has gradually declined over the past 18 months, as evidenced by her most recent MMSE score of 16/30.
Related resources
- Cummings JL. Use of cholinesterase inhibitors in clinical practice: evidence-based recommendations. Am J Geriatr Psychiatry 2003; 11:131-45.
- Alzheimer’s Disease Education and Referral Center, a service of the National Institute on Aging. http://www.alzheimers.org.
- Paleacu D, Mazeh D, Mirecki I, et al. Donepezil for the treatment of behavioral symptoms in patients with Alzheimer’s disease. Clin Neuropharmacol 2002;25:313-7.
- Tariot PN, Loy R, Ryan JM, et al. Mood stabilizers in Alzheimer’s disease: symptomatic and neuroprotective rationales. Adv Drug Deliv Rev 2002;54:1567-77.
Drug brand names
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote, DepakoteER
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Galantamine • Reminyl
- Lamotrigine • Lamictal
- Memantine • Namenda
- Methylphenidate • Concerta, Ritalin
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone wafers • RisperdalM-Tabs
- Rivastigmine • Exelon
- Selegiline • Eldepryl
- Sertraline • Zoloft
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Goforth is a speaker for Pfizer Inc., Forest Pharmaceuticals, and BristolMyers Squibb Co., and has received grant support from Pfizer Inc. He has also received support from the Bristol-Myers Squibb Fellowship in Geriatric Psychiatry through the American Association of Geriatric Psychiatry.
Dr. Rao is a speaker for Pfizer Inc.
Drs. Raval and Ruth report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Askin-Edgar S, White KE, Cummings JL. Neuropsychiatric aspects of Alzheimer’s disease and other dementing illnesses. In: Textbook of neuropsychiatry and clinical neurosciences (4th ed). Washington, DC: American Psychiatric Publishing, 2002.
2. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155:54-61.
3. Loy R, Tariot PN. Neuroprotective properties of valproate: potential benefit for AD and tauopathies. J Mol Neurosci 2002;19:303-7.
4. Roane DM, Feinberg TE, Meckler L, et al. Treatment of dementiaassociated agitation with gabapentin. J Neuropsychiatry Clin Neurosci 2000;12:40-3.
5. Tekin S, Aykut-Bingol C, Tanridag T, Aktan S. Antiglutamatergic therapy in Alzheimer’s disease—effects of lamotrigine. J Neural Transm 1998;105:295-303.
6. Street JS, Clark WS, Kadam DL, et al. Long-term efficacy of olanzapine in the control of psychotic and behavioral symptoms in nursing home patients with Alzheimer’s dementia. Int J Geriatr Psychiatry 2001;16(suppl 1):S62-S70.
7. Tariot PN, Ismail MS. Use of quetiapine in elderly patients. J Clin Psychiatry 2002;63(suppl 13):21-6.
8. DeVane CL, Mintzer J. Risperidone in the management of psychiatric and neurodegenerative disease in the elderly: an update. Psychopharmacol Bull 2003;37:116-32.
9. Pollock BG, Mulsant BH, Rosen J, et al. Comparison of citalopram, perphenazine, and placebo for the acute treatment of psychosis and behavioral disturbances in hospitalized, demented patients. Am J Psychiatry 2002;159:460-5.
10. Lyketsos CG, DelCampo L, Steinberg M, et al. Treating depression in Alzheimer disease: efficacy and safety of sertraline therapy, and the benefits of depression reduction: the DIADS. Arch Gen Psychiatry 2003;60:737-46.
11. Swann AC. Neuroreceptor mechanisms of aggression and its treatment. J Clin Psychiatry 2003;64(suppl 4):26-35.
12. Olin JT, Schneider LS, Katz IR, et al. Provisional diagnostic criteria for depression of Alzheimer disease. Am J Geriatr Psychiatry 2002;10:125-8.
13. Physician’sdesk reference(58thed). Montvale, NJ:Thomson PDR,2004.
14. Porsteinsson AP, Tariot PN, Erb R, Gaile S. An open trial of valproate for agitation in geriatric neuropsychiatric disorders. Am J Geriatr Psychiatry 1997;5:344-51.
15. Assal F, Cummings JL. Neuropsychiatric symptoms in the dementias. Curr Opin Neurol 2002;15:445-50.
16. Sano M, Ernesto C, Thomas RG, et al. A controlled trial of selegiline, alpha-tocopherol, or both as treatment for Alzheimer’s disease. The Alzheimer’s Disease Cooperative Study. N Engl J Med 1997;336:1216-22.
17. Kittur S, Hauser P. Improvement of sleep and behavior by methylphenidate in Alzheimer’s disease. Am J Psychiatry 1999;156:1116-7.
18. Salzman C. Treatment of the agitation of late-life psychosis and Alzheimer’s disease. Eur Psychiatry 2001;16(suppl 1):25s-28s.
19. Ginsburg ML. Clonazepam for agitated patients with Alzheimer’s disease. Can J Psychiatry 1991;36:237-8.
20. Jackson CW, Pitner JK, Mintzer JE. Zolpidem for the treatment of agitation in elderly demented patients. J Clin Psychiatry 1996;57:372-3.
21. Reisberg B, Doody R, Stoffler A, et al. Memantine Study Group. Memantine in moderate-to-severe Alzheimer’s disease. N Engl J Med 2003;348:1333-41.
Presenting symptoms: Marital memories
Ms. A, age 83, has been experiencing increasing confusion, agitation, and memory loss across 4 to 5 years. Family members say her memory loss has become prominent within the last year. She can no longer cook, manage her finances, shop, or perform other basic activities. At times she does not recognize her husband of 62 years and needs help with bathing and grooming.
Ms. A’s Folstein Mini-Mental State Examination (MMSE) score is 18, indicating moderate dementia. She exhibits disorientation, diminished short-term memory, impaired attention including apraxia, and executive dysfunction. Her Geriatric Depression Scale (15-item short form) score indicates normal mood.
A neurologic exam reveals mild parkinsonism, including mild bilateral upper-extremity cogwheeltype rigidity and questionable frontal release signs including a possible mild bilateral grasp reflex. No snout reflex was seen.
This presentation suggests Ms. A has:
- Alzheimer’s disease
- Lewy body dementia
- or vascular dementia
The authors’ observations:
Differentiating among Alzheimer’s, Lewy body, and vascular dementias is important (Table 1), as their treatments and clinical courses differ.
The initial workup’s goal is to diagnose a reversible medical condition that may be hastening cognitive decline. Brain imaging (CT or MRI) can uncover cerebrovascular disease, subdural hematomas, normal-pressure hydrocephalus, tumors, or other cerebral diseases. Laboratory tests can reveal systemic conditions such as hypothyroidism, vitamin B12 deficiency, hypercalcemia, neurosyphilis, or HIV infection.1
Table 1
Differences in Alzheimer’s, Lewy body, and vascular dementias
| Alzheimer’s dementia | Lewy body dementia | Vascular dementia |
|---|---|---|
| Gradual onset and chronic cognitive decline Memory difficulty combined with apraxia, aphasia, agnosia, or executive dysfunction | Cognitive, memory changes with one or more of the following:
| Early findings often include depression or personality changes, plus incontinence and gait disorder |
| Psychosis common in middle to late stages | Visual hallucinations, other psychoses in early stages Periods of marked delirium, “sundowning” | Temporal relationship between stroke and dementia onset, but variability in course |
| Day-to-day cognitive performance stable | Cognitive performance fluctuates during early stages. | Day-to-day cognitive performance stable |
| Parkinsonism not apparent in early stages, may present in middle to late stages | Parkinsonism in early stages Tremor not common | Gait disorder and parkinsonism common, especially with basal ganglia infarcts |
| Neurologic signs present in late stages | Exquisite sensitivity to neuroleptic therapy | Increased sensitivity to neuroleptics |
| Cannot be explained as vascular or mixed-type dementia | Cannot be explained as vascular or mixed-type dementia | Imaging necessary to document cerebrovascular disease |
With a thorough history and laboratory testing, a diagnosis of “probable” AD can be as much as 85% accurate. Probable AD is characterized by progressive gradual decline of cognitive functions affecting memory and at least one other domain including executive dysfunction, apraxia, aphasia, and/or agnosia. These deficits must cause significant functional impairment.
Neurologic test results may support AD diagnosis after ruling out reversible causes of dementia. Neuropsychological testing can provide valuable early information when subtle findings cannot be ascertained on clinical screening. (For a listing of neuropsychological tests, see this article at currentpsychiatry.com.)
Diagnosis: An unpredictable patient
Ms. A received a CBC; comprehensive metabolic panel; urinalysis; screens for rapid plasma reagin, B12, folate, and homocysteine levels; and a brain MRI. Hemoglobin and serum albumin were mildly depressed, reflecting early malnutrition. MRI showed generalized cerebral atrophy. Significant vascular disease was not identified.
Ms. A was diagnosed as having probable Alzheimer’s-type dementia based on the test results and the fact that her cognition was steadily declining. Other explanatory mechanisms were absent. She did not exhibit hallucinatory psychosis or fluctuating consciousness, which would signal Lewy body dementia.
Table 2
Medications for treating agitation in Alzheimer’s dementia
| Drug | Supporting evidence | Recommended dosage (mg/d)* | Rationale | Drawbacks |
|---|---|---|---|---|
| Anticonvulsants | ||||
| Carbamazepine | Tariot et al2 | 200 to 1,200 mg/d in divided doses | Commonly used for impulse control disorders | Agranulocytosis, hyponatremia, liver toxicity (all rare) |
| Divalproex | Loy and Tariot3 | 250 to 2,000 mg/d | Increasing evidence points to neuroprotective qualities | Possible white blood cell suppression, liver toxicity, pancreatitis (all rare) |
| Gabapentin | Roane et al4 | 100 to 1,200 mg/d | Safe in patients with hepatic dysfunction | Scant data on use in Alzheimer’s disease |
| Lamotrigine | Tekin et al5 | Start at 25 mg/d; titrate slowly to 50 to 200 mg/d | Possibly neuroprotective via N-methyl-D-aspartate mechanism | Rapid titration may cause Stevens-Johnson syndrome |
| Atypical antipsychotics | ||||
| Olanzapine | Street et al6 | 2.5 to 10 mg/d | Sedating effects may aid sleep | Anticholinergic effects may increase confusion, compound cognitive deficit |
| Quetiapine | Tariot et al7 | 25 to 300 mg/d | Tolerable Sedating effects may aid sleep | Watch for orthostasis, especially at higher dosages |
| Risperidone | DeVane et al8 | 0.25 to 3 mg/d | Strong data support use | High orthostatic potential, possible extrapyramidal symptoms with higher dosages |
| Ziprasidone | None | Oral:20to80mgbid IM: 10 to 20 mg, maximum 40 mg over 24 hours | Effective in managing agitation | No controlled trials, case reports in AD-associated agitation |
| SSRIs | ||||
| Citalopram | Pollock et al9 | 10 to 40 mg/d | Minimal CYP-2D6 inhibition | Effect may take 2 to 4 weeks |
| Sertraline | Lyketsos et al10 | 25 to 200 mg/d | Minimal CYP-2D6 inhibition | Effect may take 2 to 4 weeks |
| * No specific, widely accepted dosing guidelines exist for patients age > 65, but this group often does not tolerate higher dosages. | ||||
| SSRI: Selective serotonin reuptake inhibitor | ||||
| IM: Intramuscula | ||||
The psychiatrist started galantamine, 4 mg bid, and vitamin E, 400 IU bid, to maximize her cognition and attempt to slow her functional decline. Ms. A, who was in an assisted living facility when we evaluated her, was transferred to the facility’s nursing section shortly afterward.
At follow-up 3 weeks later, Ms. A’s behavior improved moderately, but she remained unpredictable and intermittently agitated. Staff reported that she was physically assaulting caregivers two to three times weekly.
Which medication(s) would you use to control Ms. A’s agitation and paranoia?
- an SSRI
- a mood stabilizer
- an atypical antipsychotic
- a combination or two or more of these drug classes
The authors’ observations
Aside from controlling agitation, medication treatment in AD should slow cognitive decline, improve behavior, help the patient perform daily activities, and delay nursing home placement.
- Watch for drug-drug interactions. Many patients with AD also are taking medications for hypertension, hypercholesterolemia, diabetes, arthritis, and other medical comorbidities.
- Start low and go slow. Older patients generally do not tolerate rapid dos-ing adjustments as well as younger patients (Table 2).
SSRIS. Selective serotonin reuptake inhibitors increase serotonin at the synaptic terminal. Serotonin has long been associated with impulsivity and aggression, and decreased 5-hydroxyindole acetic acid, a metabolite of serotonin, has been found in violent criminals and in psychiatric patients who have demonstrated inward or outward aggression.11
SSRIs generally are tolerable, safe, effective, and have little cholinergic blockade. Citalopram and sertraline minimally inhibit the cytochrome P-450 2D6 isoenzyme and have lower proteinbinding affinities than fluoxetine or paroxetine. Thus, citalopram and sertraline are less likely to alter therapeutic levels of highly bound medications through displacement of either drug’s protein-bound portion.10
Anticonvulsants with mood-stabilizing effects are another option. Reasonably strong data support use of divalproex for managing agitation in AD, either as a first-line agent or as an adjunct after failed SSRI therapy. Unlike other anticonvulsants, divalproex also may be neuroprotective.3
Divalproex, however, is associated with white blood cell suppression, significant liver toxicity, and pancreatitis, although these effects are rare.13 Monitor white blood cell counts and liver enzymes early in treatment, even if divalproex blood levels below the standard reference range produce a response.14
Though not studied specifically for treating agitation in AD, carbamazepine has demonstrated significant short-term efficacy in treating dementia-related agitation and aggression.2 Scant data support use of gabapentin or lamotrigine in Alzheimer’s dementia, but these agents are often used to manage agitation in other disorders.
Atypical antipsychotics. Psychosis usually occurs in middle-to-late-stage AD but can occur at any point. If psychosis occurs early, rule out Lewy body dementia.15
Choose an atypical antipsychotic that exhibits rapid dopamine receptor dissociation constants to reduce the risk of extrapyramidal symptoms, tardive dyskinesia, and cognitive decline with prolonged use. Quetiapine has shown efficacy for treating behavioral problems in Alzheimer’s and Lewy body dementia,7 and its sedating effects may help regulate sleep-wake cycles.
Data support use of olanzapine for agitation in AD,6 but watch for anticholinergic effects including worsening of cognition. Fast-dissolving olanzapine and risperidone oral wafers may help circumvent dosing difficulties in patients who cannot swallow—or will not take—their medication. Intramuscular olanzapine and ziprasidone have shown efficacy in treating acute agitation, but no systematic studies have examined their use in agitation secondary to dementia.
Recent data suggest a modestly increased risk of cerebrovascular accidents in AD patients taking atypicals compared with placebo, but the absolute rate of such events remains low.
Treatment: 3 months of stability
Ms. A’s galantamine dosage was increased to 8 mg bid and sertraline—25 mg/d for 7 days, then 50 mg/d—was added in an effort to better control her agitation, but the behavior continued unabated for 2 weeks. Divalproex, 125 mg bid titrated over 4 weeks to 750 mg/d, was added. Still, her agitation persisted.
Over the next 4 to 6 weeks, Ms. A showed signs of psychosis, often talking to herself and occasionally reporting “people attacking me.” She became paranoid toward members of her church, who she said were “trying to hurt” her. The paranoia intensified her agitation and disrupted her sleep. Physical examination was unremarkable, as were chest X-ray and urinalysis.
Sertraline and divalproex were gradually discontinued. Quetiapine—25 mg nightly, titrated across 2 weeks to 150 mg nightly—was started. Ms. A’s agitation and psychosis decreased with quetiapine titration, and her sleep improved. Her paranoid delusions remained but no longer impeded functioning or prompted a violent reaction.
Then after remaining stable for about 3 months, Ms. A’s paranoid delusions worsened and her agitation increased.
What treatment options are available at this point?
The authors’ observations
Treating agitation and delaying nursing home placement for patients with AD is challenging. When faced with inadequate or no response, consider less-conventional alternatives.
Vitamin E and selegiline were found separately to postpone functional decline in ambulatory patients with moderately severe AD, but the agents given together were less effective than either agent alone.16
Use of methylphenidate,17 buspirone,18 clonazepam,19 zolpidem,20 and—most recently— memantine21 for AD-related agitation also has been described.
Continued treatment: Medication changes
Quetiapine was increased to 350 mg nightly across 4 weeks, resulting in mild to moderate improvement. The higher dosage did not significantly worsen rigidity or motor function, and Ms. A tolerated the increased dosage without clinical orthostasis.
Memantine was added to address Ms. A’s agitation and preserve function. The agent was started at 5 mg/d and titrated across 4 weeks to 10 mg bid.
On clinical exam, Ms. A was more calm and directable and required less intervention. Her paranoia also decreased, allowing improved interaction with family, caregivers, and others. Ms. A remains stable on memantine, 10 mg bid; galantamine, 8 mg; quetiapine, 350 mg nightly; and vitamin E, 400 IU bid. Her cognitive ability has gradually declined over the past 18 months, as evidenced by her most recent MMSE score of 16/30.
Related resources
- Cummings JL. Use of cholinesterase inhibitors in clinical practice: evidence-based recommendations. Am J Geriatr Psychiatry 2003; 11:131-45.
- Alzheimer’s Disease Education and Referral Center, a service of the National Institute on Aging. http://www.alzheimers.org.
- Paleacu D, Mazeh D, Mirecki I, et al. Donepezil for the treatment of behavioral symptoms in patients with Alzheimer’s disease. Clin Neuropharmacol 2002;25:313-7.
- Tariot PN, Loy R, Ryan JM, et al. Mood stabilizers in Alzheimer’s disease: symptomatic and neuroprotective rationales. Adv Drug Deliv Rev 2002;54:1567-77.
Drug brand names
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote, DepakoteER
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Galantamine • Reminyl
- Lamotrigine • Lamictal
- Memantine • Namenda
- Methylphenidate • Concerta, Ritalin
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone wafers • RisperdalM-Tabs
- Rivastigmine • Exelon
- Selegiline • Eldepryl
- Sertraline • Zoloft
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Goforth is a speaker for Pfizer Inc., Forest Pharmaceuticals, and BristolMyers Squibb Co., and has received grant support from Pfizer Inc. He has also received support from the Bristol-Myers Squibb Fellowship in Geriatric Psychiatry through the American Association of Geriatric Psychiatry.
Dr. Rao is a speaker for Pfizer Inc.
Drs. Raval and Ruth report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Presenting symptoms: Marital memories
Ms. A, age 83, has been experiencing increasing confusion, agitation, and memory loss across 4 to 5 years. Family members say her memory loss has become prominent within the last year. She can no longer cook, manage her finances, shop, or perform other basic activities. At times she does not recognize her husband of 62 years and needs help with bathing and grooming.
Ms. A’s Folstein Mini-Mental State Examination (MMSE) score is 18, indicating moderate dementia. She exhibits disorientation, diminished short-term memory, impaired attention including apraxia, and executive dysfunction. Her Geriatric Depression Scale (15-item short form) score indicates normal mood.
A neurologic exam reveals mild parkinsonism, including mild bilateral upper-extremity cogwheeltype rigidity and questionable frontal release signs including a possible mild bilateral grasp reflex. No snout reflex was seen.
This presentation suggests Ms. A has:
- Alzheimer’s disease
- Lewy body dementia
- or vascular dementia
The authors’ observations:
Differentiating among Alzheimer’s, Lewy body, and vascular dementias is important (Table 1), as their treatments and clinical courses differ.
The initial workup’s goal is to diagnose a reversible medical condition that may be hastening cognitive decline. Brain imaging (CT or MRI) can uncover cerebrovascular disease, subdural hematomas, normal-pressure hydrocephalus, tumors, or other cerebral diseases. Laboratory tests can reveal systemic conditions such as hypothyroidism, vitamin B12 deficiency, hypercalcemia, neurosyphilis, or HIV infection.1
Table 1
Differences in Alzheimer’s, Lewy body, and vascular dementias
| Alzheimer’s dementia | Lewy body dementia | Vascular dementia |
|---|---|---|
| Gradual onset and chronic cognitive decline Memory difficulty combined with apraxia, aphasia, agnosia, or executive dysfunction | Cognitive, memory changes with one or more of the following:
| Early findings often include depression or personality changes, plus incontinence and gait disorder |
| Psychosis common in middle to late stages | Visual hallucinations, other psychoses in early stages Periods of marked delirium, “sundowning” | Temporal relationship between stroke and dementia onset, but variability in course |
| Day-to-day cognitive performance stable | Cognitive performance fluctuates during early stages. | Day-to-day cognitive performance stable |
| Parkinsonism not apparent in early stages, may present in middle to late stages | Parkinsonism in early stages Tremor not common | Gait disorder and parkinsonism common, especially with basal ganglia infarcts |
| Neurologic signs present in late stages | Exquisite sensitivity to neuroleptic therapy | Increased sensitivity to neuroleptics |
| Cannot be explained as vascular or mixed-type dementia | Cannot be explained as vascular or mixed-type dementia | Imaging necessary to document cerebrovascular disease |
With a thorough history and laboratory testing, a diagnosis of “probable” AD can be as much as 85% accurate. Probable AD is characterized by progressive gradual decline of cognitive functions affecting memory and at least one other domain including executive dysfunction, apraxia, aphasia, and/or agnosia. These deficits must cause significant functional impairment.
Neurologic test results may support AD diagnosis after ruling out reversible causes of dementia. Neuropsychological testing can provide valuable early information when subtle findings cannot be ascertained on clinical screening. (For a listing of neuropsychological tests, see this article at currentpsychiatry.com.)
Diagnosis: An unpredictable patient
Ms. A received a CBC; comprehensive metabolic panel; urinalysis; screens for rapid plasma reagin, B12, folate, and homocysteine levels; and a brain MRI. Hemoglobin and serum albumin were mildly depressed, reflecting early malnutrition. MRI showed generalized cerebral atrophy. Significant vascular disease was not identified.
Ms. A was diagnosed as having probable Alzheimer’s-type dementia based on the test results and the fact that her cognition was steadily declining. Other explanatory mechanisms were absent. She did not exhibit hallucinatory psychosis or fluctuating consciousness, which would signal Lewy body dementia.
Table 2
Medications for treating agitation in Alzheimer’s dementia
| Drug | Supporting evidence | Recommended dosage (mg/d)* | Rationale | Drawbacks |
|---|---|---|---|---|
| Anticonvulsants | ||||
| Carbamazepine | Tariot et al2 | 200 to 1,200 mg/d in divided doses | Commonly used for impulse control disorders | Agranulocytosis, hyponatremia, liver toxicity (all rare) |
| Divalproex | Loy and Tariot3 | 250 to 2,000 mg/d | Increasing evidence points to neuroprotective qualities | Possible white blood cell suppression, liver toxicity, pancreatitis (all rare) |
| Gabapentin | Roane et al4 | 100 to 1,200 mg/d | Safe in patients with hepatic dysfunction | Scant data on use in Alzheimer’s disease |
| Lamotrigine | Tekin et al5 | Start at 25 mg/d; titrate slowly to 50 to 200 mg/d | Possibly neuroprotective via N-methyl-D-aspartate mechanism | Rapid titration may cause Stevens-Johnson syndrome |
| Atypical antipsychotics | ||||
| Olanzapine | Street et al6 | 2.5 to 10 mg/d | Sedating effects may aid sleep | Anticholinergic effects may increase confusion, compound cognitive deficit |
| Quetiapine | Tariot et al7 | 25 to 300 mg/d | Tolerable Sedating effects may aid sleep | Watch for orthostasis, especially at higher dosages |
| Risperidone | DeVane et al8 | 0.25 to 3 mg/d | Strong data support use | High orthostatic potential, possible extrapyramidal symptoms with higher dosages |
| Ziprasidone | None | Oral:20to80mgbid IM: 10 to 20 mg, maximum 40 mg over 24 hours | Effective in managing agitation | No controlled trials, case reports in AD-associated agitation |
| SSRIs | ||||
| Citalopram | Pollock et al9 | 10 to 40 mg/d | Minimal CYP-2D6 inhibition | Effect may take 2 to 4 weeks |
| Sertraline | Lyketsos et al10 | 25 to 200 mg/d | Minimal CYP-2D6 inhibition | Effect may take 2 to 4 weeks |
| * No specific, widely accepted dosing guidelines exist for patients age > 65, but this group often does not tolerate higher dosages. | ||||
| SSRI: Selective serotonin reuptake inhibitor | ||||
| IM: Intramuscula | ||||
The psychiatrist started galantamine, 4 mg bid, and vitamin E, 400 IU bid, to maximize her cognition and attempt to slow her functional decline. Ms. A, who was in an assisted living facility when we evaluated her, was transferred to the facility’s nursing section shortly afterward.
At follow-up 3 weeks later, Ms. A’s behavior improved moderately, but she remained unpredictable and intermittently agitated. Staff reported that she was physically assaulting caregivers two to three times weekly.
Which medication(s) would you use to control Ms. A’s agitation and paranoia?
- an SSRI
- a mood stabilizer
- an atypical antipsychotic
- a combination or two or more of these drug classes
The authors’ observations
Aside from controlling agitation, medication treatment in AD should slow cognitive decline, improve behavior, help the patient perform daily activities, and delay nursing home placement.
- Watch for drug-drug interactions. Many patients with AD also are taking medications for hypertension, hypercholesterolemia, diabetes, arthritis, and other medical comorbidities.
- Start low and go slow. Older patients generally do not tolerate rapid dos-ing adjustments as well as younger patients (Table 2).
SSRIS. Selective serotonin reuptake inhibitors increase serotonin at the synaptic terminal. Serotonin has long been associated with impulsivity and aggression, and decreased 5-hydroxyindole acetic acid, a metabolite of serotonin, has been found in violent criminals and in psychiatric patients who have demonstrated inward or outward aggression.11
SSRIs generally are tolerable, safe, effective, and have little cholinergic blockade. Citalopram and sertraline minimally inhibit the cytochrome P-450 2D6 isoenzyme and have lower proteinbinding affinities than fluoxetine or paroxetine. Thus, citalopram and sertraline are less likely to alter therapeutic levels of highly bound medications through displacement of either drug’s protein-bound portion.10
Anticonvulsants with mood-stabilizing effects are another option. Reasonably strong data support use of divalproex for managing agitation in AD, either as a first-line agent or as an adjunct after failed SSRI therapy. Unlike other anticonvulsants, divalproex also may be neuroprotective.3
Divalproex, however, is associated with white blood cell suppression, significant liver toxicity, and pancreatitis, although these effects are rare.13 Monitor white blood cell counts and liver enzymes early in treatment, even if divalproex blood levels below the standard reference range produce a response.14
Though not studied specifically for treating agitation in AD, carbamazepine has demonstrated significant short-term efficacy in treating dementia-related agitation and aggression.2 Scant data support use of gabapentin or lamotrigine in Alzheimer’s dementia, but these agents are often used to manage agitation in other disorders.
Atypical antipsychotics. Psychosis usually occurs in middle-to-late-stage AD but can occur at any point. If psychosis occurs early, rule out Lewy body dementia.15
Choose an atypical antipsychotic that exhibits rapid dopamine receptor dissociation constants to reduce the risk of extrapyramidal symptoms, tardive dyskinesia, and cognitive decline with prolonged use. Quetiapine has shown efficacy for treating behavioral problems in Alzheimer’s and Lewy body dementia,7 and its sedating effects may help regulate sleep-wake cycles.
Data support use of olanzapine for agitation in AD,6 but watch for anticholinergic effects including worsening of cognition. Fast-dissolving olanzapine and risperidone oral wafers may help circumvent dosing difficulties in patients who cannot swallow—or will not take—their medication. Intramuscular olanzapine and ziprasidone have shown efficacy in treating acute agitation, but no systematic studies have examined their use in agitation secondary to dementia.
Recent data suggest a modestly increased risk of cerebrovascular accidents in AD patients taking atypicals compared with placebo, but the absolute rate of such events remains low.
Treatment: 3 months of stability
Ms. A’s galantamine dosage was increased to 8 mg bid and sertraline—25 mg/d for 7 days, then 50 mg/d—was added in an effort to better control her agitation, but the behavior continued unabated for 2 weeks. Divalproex, 125 mg bid titrated over 4 weeks to 750 mg/d, was added. Still, her agitation persisted.
Over the next 4 to 6 weeks, Ms. A showed signs of psychosis, often talking to herself and occasionally reporting “people attacking me.” She became paranoid toward members of her church, who she said were “trying to hurt” her. The paranoia intensified her agitation and disrupted her sleep. Physical examination was unremarkable, as were chest X-ray and urinalysis.
Sertraline and divalproex were gradually discontinued. Quetiapine—25 mg nightly, titrated across 2 weeks to 150 mg nightly—was started. Ms. A’s agitation and psychosis decreased with quetiapine titration, and her sleep improved. Her paranoid delusions remained but no longer impeded functioning or prompted a violent reaction.
Then after remaining stable for about 3 months, Ms. A’s paranoid delusions worsened and her agitation increased.
What treatment options are available at this point?
The authors’ observations
Treating agitation and delaying nursing home placement for patients with AD is challenging. When faced with inadequate or no response, consider less-conventional alternatives.
Vitamin E and selegiline were found separately to postpone functional decline in ambulatory patients with moderately severe AD, but the agents given together were less effective than either agent alone.16
Use of methylphenidate,17 buspirone,18 clonazepam,19 zolpidem,20 and—most recently— memantine21 for AD-related agitation also has been described.
Continued treatment: Medication changes
Quetiapine was increased to 350 mg nightly across 4 weeks, resulting in mild to moderate improvement. The higher dosage did not significantly worsen rigidity or motor function, and Ms. A tolerated the increased dosage without clinical orthostasis.
Memantine was added to address Ms. A’s agitation and preserve function. The agent was started at 5 mg/d and titrated across 4 weeks to 10 mg bid.
On clinical exam, Ms. A was more calm and directable and required less intervention. Her paranoia also decreased, allowing improved interaction with family, caregivers, and others. Ms. A remains stable on memantine, 10 mg bid; galantamine, 8 mg; quetiapine, 350 mg nightly; and vitamin E, 400 IU bid. Her cognitive ability has gradually declined over the past 18 months, as evidenced by her most recent MMSE score of 16/30.
Related resources
- Cummings JL. Use of cholinesterase inhibitors in clinical practice: evidence-based recommendations. Am J Geriatr Psychiatry 2003; 11:131-45.
- Alzheimer’s Disease Education and Referral Center, a service of the National Institute on Aging. http://www.alzheimers.org.
- Paleacu D, Mazeh D, Mirecki I, et al. Donepezil for the treatment of behavioral symptoms in patients with Alzheimer’s disease. Clin Neuropharmacol 2002;25:313-7.
- Tariot PN, Loy R, Ryan JM, et al. Mood stabilizers in Alzheimer’s disease: symptomatic and neuroprotective rationales. Adv Drug Deliv Rev 2002;54:1567-77.
Drug brand names
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Divalproex • Depakote, DepakoteER
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Galantamine • Reminyl
- Lamotrigine • Lamictal
- Memantine • Namenda
- Methylphenidate • Concerta, Ritalin
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone wafers • RisperdalM-Tabs
- Rivastigmine • Exelon
- Selegiline • Eldepryl
- Sertraline • Zoloft
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Goforth is a speaker for Pfizer Inc., Forest Pharmaceuticals, and BristolMyers Squibb Co., and has received grant support from Pfizer Inc. He has also received support from the Bristol-Myers Squibb Fellowship in Geriatric Psychiatry through the American Association of Geriatric Psychiatry.
Dr. Rao is a speaker for Pfizer Inc.
Drs. Raval and Ruth report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Askin-Edgar S, White KE, Cummings JL. Neuropsychiatric aspects of Alzheimer’s disease and other dementing illnesses. In: Textbook of neuropsychiatry and clinical neurosciences (4th ed). Washington, DC: American Psychiatric Publishing, 2002.
2. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155:54-61.
3. Loy R, Tariot PN. Neuroprotective properties of valproate: potential benefit for AD and tauopathies. J Mol Neurosci 2002;19:303-7.
4. Roane DM, Feinberg TE, Meckler L, et al. Treatment of dementiaassociated agitation with gabapentin. J Neuropsychiatry Clin Neurosci 2000;12:40-3.
5. Tekin S, Aykut-Bingol C, Tanridag T, Aktan S. Antiglutamatergic therapy in Alzheimer’s disease—effects of lamotrigine. J Neural Transm 1998;105:295-303.
6. Street JS, Clark WS, Kadam DL, et al. Long-term efficacy of olanzapine in the control of psychotic and behavioral symptoms in nursing home patients with Alzheimer’s dementia. Int J Geriatr Psychiatry 2001;16(suppl 1):S62-S70.
7. Tariot PN, Ismail MS. Use of quetiapine in elderly patients. J Clin Psychiatry 2002;63(suppl 13):21-6.
8. DeVane CL, Mintzer J. Risperidone in the management of psychiatric and neurodegenerative disease in the elderly: an update. Psychopharmacol Bull 2003;37:116-32.
9. Pollock BG, Mulsant BH, Rosen J, et al. Comparison of citalopram, perphenazine, and placebo for the acute treatment of psychosis and behavioral disturbances in hospitalized, demented patients. Am J Psychiatry 2002;159:460-5.
10. Lyketsos CG, DelCampo L, Steinberg M, et al. Treating depression in Alzheimer disease: efficacy and safety of sertraline therapy, and the benefits of depression reduction: the DIADS. Arch Gen Psychiatry 2003;60:737-46.
11. Swann AC. Neuroreceptor mechanisms of aggression and its treatment. J Clin Psychiatry 2003;64(suppl 4):26-35.
12. Olin JT, Schneider LS, Katz IR, et al. Provisional diagnostic criteria for depression of Alzheimer disease. Am J Geriatr Psychiatry 2002;10:125-8.
13. Physician’sdesk reference(58thed). Montvale, NJ:Thomson PDR,2004.
14. Porsteinsson AP, Tariot PN, Erb R, Gaile S. An open trial of valproate for agitation in geriatric neuropsychiatric disorders. Am J Geriatr Psychiatry 1997;5:344-51.
15. Assal F, Cummings JL. Neuropsychiatric symptoms in the dementias. Curr Opin Neurol 2002;15:445-50.
16. Sano M, Ernesto C, Thomas RG, et al. A controlled trial of selegiline, alpha-tocopherol, or both as treatment for Alzheimer’s disease. The Alzheimer’s Disease Cooperative Study. N Engl J Med 1997;336:1216-22.
17. Kittur S, Hauser P. Improvement of sleep and behavior by methylphenidate in Alzheimer’s disease. Am J Psychiatry 1999;156:1116-7.
18. Salzman C. Treatment of the agitation of late-life psychosis and Alzheimer’s disease. Eur Psychiatry 2001;16(suppl 1):25s-28s.
19. Ginsburg ML. Clonazepam for agitated patients with Alzheimer’s disease. Can J Psychiatry 1991;36:237-8.
20. Jackson CW, Pitner JK, Mintzer JE. Zolpidem for the treatment of agitation in elderly demented patients. J Clin Psychiatry 1996;57:372-3.
21. Reisberg B, Doody R, Stoffler A, et al. Memantine Study Group. Memantine in moderate-to-severe Alzheimer’s disease. N Engl J Med 2003;348:1333-41.
1. Askin-Edgar S, White KE, Cummings JL. Neuropsychiatric aspects of Alzheimer’s disease and other dementing illnesses. In: Textbook of neuropsychiatry and clinical neurosciences (4th ed). Washington, DC: American Psychiatric Publishing, 2002.
2. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155:54-61.
3. Loy R, Tariot PN. Neuroprotective properties of valproate: potential benefit for AD and tauopathies. J Mol Neurosci 2002;19:303-7.
4. Roane DM, Feinberg TE, Meckler L, et al. Treatment of dementiaassociated agitation with gabapentin. J Neuropsychiatry Clin Neurosci 2000;12:40-3.
5. Tekin S, Aykut-Bingol C, Tanridag T, Aktan S. Antiglutamatergic therapy in Alzheimer’s disease—effects of lamotrigine. J Neural Transm 1998;105:295-303.
6. Street JS, Clark WS, Kadam DL, et al. Long-term efficacy of olanzapine in the control of psychotic and behavioral symptoms in nursing home patients with Alzheimer’s dementia. Int J Geriatr Psychiatry 2001;16(suppl 1):S62-S70.
7. Tariot PN, Ismail MS. Use of quetiapine in elderly patients. J Clin Psychiatry 2002;63(suppl 13):21-6.
8. DeVane CL, Mintzer J. Risperidone in the management of psychiatric and neurodegenerative disease in the elderly: an update. Psychopharmacol Bull 2003;37:116-32.
9. Pollock BG, Mulsant BH, Rosen J, et al. Comparison of citalopram, perphenazine, and placebo for the acute treatment of psychosis and behavioral disturbances in hospitalized, demented patients. Am J Psychiatry 2002;159:460-5.
10. Lyketsos CG, DelCampo L, Steinberg M, et al. Treating depression in Alzheimer disease: efficacy and safety of sertraline therapy, and the benefits of depression reduction: the DIADS. Arch Gen Psychiatry 2003;60:737-46.
11. Swann AC. Neuroreceptor mechanisms of aggression and its treatment. J Clin Psychiatry 2003;64(suppl 4):26-35.
12. Olin JT, Schneider LS, Katz IR, et al. Provisional diagnostic criteria for depression of Alzheimer disease. Am J Geriatr Psychiatry 2002;10:125-8.
13. Physician’sdesk reference(58thed). Montvale, NJ:Thomson PDR,2004.
14. Porsteinsson AP, Tariot PN, Erb R, Gaile S. An open trial of valproate for agitation in geriatric neuropsychiatric disorders. Am J Geriatr Psychiatry 1997;5:344-51.
15. Assal F, Cummings JL. Neuropsychiatric symptoms in the dementias. Curr Opin Neurol 2002;15:445-50.
16. Sano M, Ernesto C, Thomas RG, et al. A controlled trial of selegiline, alpha-tocopherol, or both as treatment for Alzheimer’s disease. The Alzheimer’s Disease Cooperative Study. N Engl J Med 1997;336:1216-22.
17. Kittur S, Hauser P. Improvement of sleep and behavior by methylphenidate in Alzheimer’s disease. Am J Psychiatry 1999;156:1116-7.
18. Salzman C. Treatment of the agitation of late-life psychosis and Alzheimer’s disease. Eur Psychiatry 2001;16(suppl 1):25s-28s.
19. Ginsburg ML. Clonazepam for agitated patients with Alzheimer’s disease. Can J Psychiatry 1991;36:237-8.
20. Jackson CW, Pitner JK, Mintzer JE. Zolpidem for the treatment of agitation in elderly demented patients. J Clin Psychiatry 1996;57:372-3.
21. Reisberg B, Doody R, Stoffler A, et al. Memantine Study Group. Memantine in moderate-to-severe Alzheimer’s disease. N Engl J Med 2003;348:1333-41.
Flight, then fight

“Psychological first aid: emergency care for terrorism and disaster survivors” (Current Psychiatry, May 2004) touches on flight, fight, and fright as human reactions to disaster.
Since the Sept. 11, 2001 terrorist attacks, medical professionals have become much more interested in the immediate adverse effects of extreme acute stress and humans’ instinctual response to disaster. “Fight or flight,” a widely used catchphrase, has influenced the understanding and expectations of clinicians and patients for decades.
“Fight or flight,” however, does not reflect the many advances in understanding acute response to stress that have occurred since the phrase was coined in 1929.1 Indeed, as we note in two soon-to-be-published articles,2,3 the phrase is no longer accurate.
Gray described the correct sequence of universal hardwired responses to extreme stress caused by a life-threatening situation.4 Ethologists working with nonhuman primates have clearly established that sequence.
In all mammalian species studied, the urge to flee is the first normative fear response. If fleeing is not an option, the impulse to fight follows. Male and female mammals have demonstrated this response sequence. The belief that man’s first instinct is to fight is probably a misconception.
Thus, “flight or fight” is the proper order of responses. Recognizing this order may help us more effectively treat acute stress in emergency and other clinical settings. Understanding these responses as instinct might also help us ameliorate the guilt that plagues many military veterans who wonder why they fled rather than put up a fight.
H. Stefan Bracha, MD; Tyler C. Ralston, MA; Jennifer M. Matsukawa, MA
Department of Veterans Affairs
Pacific Islands Health Care System
Spark M. Matsunaga Medical Center, Honolulu, HI
Andrew E. Williams, MA
Department of psychology
University of Hawaii at Manoa, Honolulu, HI
Amnona B. Miller, NP
Emergency department
New York-Presbyterian Medical Center
New York, NY
- Cannon WB. Bodily changes in pain, hunger, fear and rage: An account of recent research into the function of emotional excitement (2nd ed). New York: Appleton-Century-Crofts, 1929.
- Bracha HS. Freeze-flight-fight-fright-faint: Adaptationist perspective on the acute stress response spectrum. CNS Spectrums 2004. In press.
- Bracha HS, Williams AE, Ralston TC, et al. “Fight or flight”: Does this 75 year-old term need updating? Psychosomatics 2004. In press.
- Gray JA. The psychology of fear and stress (2nd ed). New York: Cambridge University Press, 1988.
“Psychological first aid: emergency care for terrorism and disaster survivors” (Current Psychiatry, May 2004) touches on flight, fight, and fright as human reactions to disaster.
Since the Sept. 11, 2001 terrorist attacks, medical professionals have become much more interested in the immediate adverse effects of extreme acute stress and humans’ instinctual response to disaster. “Fight or flight,” a widely used catchphrase, has influenced the understanding and expectations of clinicians and patients for decades.
“Fight or flight,” however, does not reflect the many advances in understanding acute response to stress that have occurred since the phrase was coined in 1929.1 Indeed, as we note in two soon-to-be-published articles,2,3 the phrase is no longer accurate.
Gray described the correct sequence of universal hardwired responses to extreme stress caused by a life-threatening situation.4 Ethologists working with nonhuman primates have clearly established that sequence.
In all mammalian species studied, the urge to flee is the first normative fear response. If fleeing is not an option, the impulse to fight follows. Male and female mammals have demonstrated this response sequence. The belief that man’s first instinct is to fight is probably a misconception.
Thus, “flight or fight” is the proper order of responses. Recognizing this order may help us more effectively treat acute stress in emergency and other clinical settings. Understanding these responses as instinct might also help us ameliorate the guilt that plagues many military veterans who wonder why they fled rather than put up a fight.
H. Stefan Bracha, MD; Tyler C. Ralston, MA; Jennifer M. Matsukawa, MA
Department of Veterans Affairs
Pacific Islands Health Care System
Spark M. Matsunaga Medical Center, Honolulu, HI
Andrew E. Williams, MA
Department of psychology
University of Hawaii at Manoa, Honolulu, HI
Amnona B. Miller, NP
Emergency department
New York-Presbyterian Medical Center
New York, NY
- Cannon WB. Bodily changes in pain, hunger, fear and rage: An account of recent research into the function of emotional excitement (2nd ed). New York: Appleton-Century-Crofts, 1929.
- Bracha HS. Freeze-flight-fight-fright-faint: Adaptationist perspective on the acute stress response spectrum. CNS Spectrums 2004. In press.
- Bracha HS, Williams AE, Ralston TC, et al. “Fight or flight”: Does this 75 year-old term need updating? Psychosomatics 2004. In press.
- Gray JA. The psychology of fear and stress (2nd ed). New York: Cambridge University Press, 1988.
“Psychological first aid: emergency care for terrorism and disaster survivors” (Current Psychiatry, May 2004) touches on flight, fight, and fright as human reactions to disaster.
Since the Sept. 11, 2001 terrorist attacks, medical professionals have become much more interested in the immediate adverse effects of extreme acute stress and humans’ instinctual response to disaster. “Fight or flight,” a widely used catchphrase, has influenced the understanding and expectations of clinicians and patients for decades.
“Fight or flight,” however, does not reflect the many advances in understanding acute response to stress that have occurred since the phrase was coined in 1929.1 Indeed, as we note in two soon-to-be-published articles,2,3 the phrase is no longer accurate.
Gray described the correct sequence of universal hardwired responses to extreme stress caused by a life-threatening situation.4 Ethologists working with nonhuman primates have clearly established that sequence.
In all mammalian species studied, the urge to flee is the first normative fear response. If fleeing is not an option, the impulse to fight follows. Male and female mammals have demonstrated this response sequence. The belief that man’s first instinct is to fight is probably a misconception.
Thus, “flight or fight” is the proper order of responses. Recognizing this order may help us more effectively treat acute stress in emergency and other clinical settings. Understanding these responses as instinct might also help us ameliorate the guilt that plagues many military veterans who wonder why they fled rather than put up a fight.
H. Stefan Bracha, MD; Tyler C. Ralston, MA; Jennifer M. Matsukawa, MA
Department of Veterans Affairs
Pacific Islands Health Care System
Spark M. Matsunaga Medical Center, Honolulu, HI
Andrew E. Williams, MA
Department of psychology
University of Hawaii at Manoa, Honolulu, HI
Amnona B. Miller, NP
Emergency department
New York-Presbyterian Medical Center
New York, NY
- Cannon WB. Bodily changes in pain, hunger, fear and rage: An account of recent research into the function of emotional excitement (2nd ed). New York: Appleton-Century-Crofts, 1929.
- Bracha HS. Freeze-flight-fight-fright-faint: Adaptationist perspective on the acute stress response spectrum. CNS Spectrums 2004. In press.
- Bracha HS, Williams AE, Ralston TC, et al. “Fight or flight”: Does this 75 year-old term need updating? Psychosomatics 2004. In press.
- Gray JA. The psychology of fear and stress (2nd ed). New York: Cambridge University Press, 1988.
When a patient threatens harm to a presidential candidate
Mr. K, age 52, has Asperger’s disorder and attention-deficit/hyperactivity disorder. Recently he sent an e-mail to President Bush, Vice President Cheney, Homeland Security Secretary Tom Ridge, television news commentator Wolf Blitzer, and numerous government agencies. Mr. K’s psychiatrist also received a copy.
In his message, Mr. K expressed intense personal offense at his belief that U.S. Sen. John Kerry had called his “beloved president” a liar, and challenged the presidential candidate to a duel. If Kerry refused, Mr. K wrote, he would “take other effective measures” to avenge this “insult to me, my family, and all loyal Americans.”
Immediately after seeing the note, the psychiatrist called the Secret Service. Ninety minutes later, agents interviewed Mr. K, searched his apartment, and found weapons and travel documents that strongly suggested Mr. K planned to follow Kerry. The patient was taken into custody and admitted to a secure psychiatric facility.
Patients with Asperger’s disorder often become fixated on a person or incident. Such patients’ social judgment is severely impaired, and they tend to view the world in absolute terms with no gray areas. In a presidential election year, that fixation can manifest as a verbal or written threat against the president, vice president, or a presidential candidate.
As doctors, we have both a civic duty and sworn obligation under state standard-of-practice codes to immediately inform the Secret Service of such a threat. Call the Secret Service even if you are unsure whether the patient will carry it out.
How to reach the Secret Service
- Find the phone number for the local Secret Service headquarters in the phone book’s U.S. government listings—usually under “frequently called numbers.”
- Tell the operator you are a psychiatrist reporting an imminent threat to the president’s or a candidate’s life. An agent will come on the line immediately.
If there is no Secret Service office in your area, contact the regional long-distance operator and demand to be connected with the nearest Secret Service headquarters.
When reporting a threat, insist on speaking to a live agent immediately. If you cannot reach the Secret Service, call the FBI at once.
Do not contact the patient once you have called authorities. The Secret Service will direct the investigation independent of your point of view.
Dr. Clark is a practicing psychiatrist and medical director, ADD Clinic Inc., Las Vegas, NV
Mr. K, age 52, has Asperger’s disorder and attention-deficit/hyperactivity disorder. Recently he sent an e-mail to President Bush, Vice President Cheney, Homeland Security Secretary Tom Ridge, television news commentator Wolf Blitzer, and numerous government agencies. Mr. K’s psychiatrist also received a copy.
In his message, Mr. K expressed intense personal offense at his belief that U.S. Sen. John Kerry had called his “beloved president” a liar, and challenged the presidential candidate to a duel. If Kerry refused, Mr. K wrote, he would “take other effective measures” to avenge this “insult to me, my family, and all loyal Americans.”
Immediately after seeing the note, the psychiatrist called the Secret Service. Ninety minutes later, agents interviewed Mr. K, searched his apartment, and found weapons and travel documents that strongly suggested Mr. K planned to follow Kerry. The patient was taken into custody and admitted to a secure psychiatric facility.
Patients with Asperger’s disorder often become fixated on a person or incident. Such patients’ social judgment is severely impaired, and they tend to view the world in absolute terms with no gray areas. In a presidential election year, that fixation can manifest as a verbal or written threat against the president, vice president, or a presidential candidate.
As doctors, we have both a civic duty and sworn obligation under state standard-of-practice codes to immediately inform the Secret Service of such a threat. Call the Secret Service even if you are unsure whether the patient will carry it out.
How to reach the Secret Service
- Find the phone number for the local Secret Service headquarters in the phone book’s U.S. government listings—usually under “frequently called numbers.”
- Tell the operator you are a psychiatrist reporting an imminent threat to the president’s or a candidate’s life. An agent will come on the line immediately.
If there is no Secret Service office in your area, contact the regional long-distance operator and demand to be connected with the nearest Secret Service headquarters.
When reporting a threat, insist on speaking to a live agent immediately. If you cannot reach the Secret Service, call the FBI at once.
Do not contact the patient once you have called authorities. The Secret Service will direct the investigation independent of your point of view.
Mr. K, age 52, has Asperger’s disorder and attention-deficit/hyperactivity disorder. Recently he sent an e-mail to President Bush, Vice President Cheney, Homeland Security Secretary Tom Ridge, television news commentator Wolf Blitzer, and numerous government agencies. Mr. K’s psychiatrist also received a copy.
In his message, Mr. K expressed intense personal offense at his belief that U.S. Sen. John Kerry had called his “beloved president” a liar, and challenged the presidential candidate to a duel. If Kerry refused, Mr. K wrote, he would “take other effective measures” to avenge this “insult to me, my family, and all loyal Americans.”
Immediately after seeing the note, the psychiatrist called the Secret Service. Ninety minutes later, agents interviewed Mr. K, searched his apartment, and found weapons and travel documents that strongly suggested Mr. K planned to follow Kerry. The patient was taken into custody and admitted to a secure psychiatric facility.
Patients with Asperger’s disorder often become fixated on a person or incident. Such patients’ social judgment is severely impaired, and they tend to view the world in absolute terms with no gray areas. In a presidential election year, that fixation can manifest as a verbal or written threat against the president, vice president, or a presidential candidate.
As doctors, we have both a civic duty and sworn obligation under state standard-of-practice codes to immediately inform the Secret Service of such a threat. Call the Secret Service even if you are unsure whether the patient will carry it out.
How to reach the Secret Service
- Find the phone number for the local Secret Service headquarters in the phone book’s U.S. government listings—usually under “frequently called numbers.”
- Tell the operator you are a psychiatrist reporting an imminent threat to the president’s or a candidate’s life. An agent will come on the line immediately.
If there is no Secret Service office in your area, contact the regional long-distance operator and demand to be connected with the nearest Secret Service headquarters.
When reporting a threat, insist on speaking to a live agent immediately. If you cannot reach the Secret Service, call the FBI at once.
Do not contact the patient once you have called authorities. The Secret Service will direct the investigation independent of your point of view.
Dr. Clark is a practicing psychiatrist and medical director, ADD Clinic Inc., Las Vegas, NV
Dr. Clark is a practicing psychiatrist and medical director, ADD Clinic Inc., Las Vegas, NV
Optimizing Adherence to Therapy in Hepatitis C
Supplement Editor:
Zobair M. Younossi, MD, MPH
Contents
Foreword
Zobair M. Younossi, MD, MPH
The evolving treatment of chronic hepatitis C: Where we stand a decade out
Sherif Saadeh, MD, and Gary L. Davis, MD
Initial treatment for chronic hepatitis C: Current therapies and their optimal dosing and duration
Keyur Patel, MD, and John G. McHutchison, MD
Retreatment of patients who do not respond to initial therapy for chronic hepatitis C
Mitchell L. Shiffman, MD
Managing the hematologic side effects of antiviral therapy for chronic hepatitis C: Anemia, neutropenia, and thrombocytopenia
Janus P. Ong, MD, and Zobair M. Younossi, MD, MPH
The role of hematopoietic growth factors in special populations with chronic hepatitis C: Patients with HIV coinfection, end-stage renal disease, or liver transplantation
Stevan A. Gonzalez, MD, and Ira M. Jacobson, MD
Managing the neuropsychiatric side effects of interferon-based therapy for hepatitis C
Catherine C. Crone, MD; Geoffrey M. Gabriel, MD; and Thomas N. Wise, MD
The role of physician extenders in managing patients with chronic hepatitis C
Harpreet Gujral, RN, MSN, CRNP; Carla Viscomi, RN, BSN; and Rochelle Collantes, MD, MPH
Supplement Editor:
Zobair M. Younossi, MD, MPH
Contents
Foreword
Zobair M. Younossi, MD, MPH
The evolving treatment of chronic hepatitis C: Where we stand a decade out
Sherif Saadeh, MD, and Gary L. Davis, MD
Initial treatment for chronic hepatitis C: Current therapies and their optimal dosing and duration
Keyur Patel, MD, and John G. McHutchison, MD
Retreatment of patients who do not respond to initial therapy for chronic hepatitis C
Mitchell L. Shiffman, MD
Managing the hematologic side effects of antiviral therapy for chronic hepatitis C: Anemia, neutropenia, and thrombocytopenia
Janus P. Ong, MD, and Zobair M. Younossi, MD, MPH
The role of hematopoietic growth factors in special populations with chronic hepatitis C: Patients with HIV coinfection, end-stage renal disease, or liver transplantation
Stevan A. Gonzalez, MD, and Ira M. Jacobson, MD
Managing the neuropsychiatric side effects of interferon-based therapy for hepatitis C
Catherine C. Crone, MD; Geoffrey M. Gabriel, MD; and Thomas N. Wise, MD
The role of physician extenders in managing patients with chronic hepatitis C
Harpreet Gujral, RN, MSN, CRNP; Carla Viscomi, RN, BSN; and Rochelle Collantes, MD, MPH
Supplement Editor:
Zobair M. Younossi, MD, MPH
Contents
Foreword
Zobair M. Younossi, MD, MPH
The evolving treatment of chronic hepatitis C: Where we stand a decade out
Sherif Saadeh, MD, and Gary L. Davis, MD
Initial treatment for chronic hepatitis C: Current therapies and their optimal dosing and duration
Keyur Patel, MD, and John G. McHutchison, MD
Retreatment of patients who do not respond to initial therapy for chronic hepatitis C
Mitchell L. Shiffman, MD
Managing the hematologic side effects of antiviral therapy for chronic hepatitis C: Anemia, neutropenia, and thrombocytopenia
Janus P. Ong, MD, and Zobair M. Younossi, MD, MPH
The role of hematopoietic growth factors in special populations with chronic hepatitis C: Patients with HIV coinfection, end-stage renal disease, or liver transplantation
Stevan A. Gonzalez, MD, and Ira M. Jacobson, MD
Managing the neuropsychiatric side effects of interferon-based therapy for hepatitis C
Catherine C. Crone, MD; Geoffrey M. Gabriel, MD; and Thomas N. Wise, MD
The role of physician extenders in managing patients with chronic hepatitis C
Harpreet Gujral, RN, MSN, CRNP; Carla Viscomi, RN, BSN; and Rochelle Collantes, MD, MPH
Foreword
Shared medical appointments: Increasing patient access without increasing physician hours
Recurrent, Localized Urticaria and Erythema Multiforme: A Review and Management of Cutaneous Anthrax Vaccine–Related Events
The October 2001 domestic anthrax attacks affected 22 people, resulting in 5 fatalities. The added global terrorist threats have created an increasing need for homeland protection, as well as protection of our widely deployed forces battling terrorism. It is now relevant for physicians to be familiar with both clinical anthrax and adverse vaccine-related events associated with the resumption of the anthrax vaccine program. Dermatologists played a lead role in the initial response to the anthrax attack. We must be the lead providers most familiar with the cutaneous reactions that may be seen with the preventive vaccination. This article reviews the latest recommended evaluation and management of anthrax vaccine adverse events.
Case Reports Patient 1—A 36-year-old white male active duty military fighter pilot developed recurrent, localized urticaria after receiving his sixth anthrax vaccination (Figure 1). Results of a skin biopsy showed a superficial perivascular dermatitis with eosinophils consistent with urticaria. The urticaria continues to recur 21/2 years after his last vaccination and remains localized to the vaccinated arm.
Patient 2—A 33-year-old black male military member developed erythema multiforme one day after receiving his fifth anthrax vaccination. He had been treated for pharyngitis with a 10-day course of oral penicillin, which had been completed 2 days prior to receiving the vaccination. Target lesions were present on both arms and hands but were more prominent on the arm that received the vaccination (Figure 2). Results of a skin biopsy revealed a superficial perivascular and interface lymphocytic dermatitis, with vacuolar changes along the dermoepidermal junction compatible with erythema multiforme.
Patient 3—A 28-year-old white male military member presented with a pruritic rash that had developed on his face approximately 12 hours after receiving his fifth anthrax vaccination. The rash had spread to his torso (Figure 3) and lower extremities. Results of a punch biopsy revealed a superficial and deep lymphocytic infiltrate with interface changes and some extravasated red blood cells, findings felt to be consistent with an erythema multiforme reaction (Figure 4). The patient was treated with a 2-week course of prednisone and intramuscular diphenhydramine (Benadryl®), and clearing of symptoms was noted within 10 days.
Comment
The threat of anthrax is deadly and real, as shown by the domestic attacks via the US Postal Service in October 2001. In all, there were 11 confirmed cases of inhalation anthrax, resulting in 5 fatalities. In addition, there were 7 confirmed cases and 4 suspected cases of cutaneous anthrax. Twenty of the 22 cases were unquestionably linked to mail contaminated with a single strain of Bacillus anthracis.1 Anthrax is easy and cheap to produce and can be stored for prolonged periods, with spores survivable for decades in ambient conditions.2 The spores are resistant to dryness, heat, UV light, gamma radiation, and many disinfectants.3 In addition, anthrax is odorless, colorless, tasteless, and difficult to detect, thus making it a likely choice for future biological attacks. After the first gulf war, Iraq admitted to producing and deploying weaponized anthrax in missiles.4 The Sverdlovsk anthrax outbreak in the former Soviet Union occurred after the accidental release of aerosolized anthrax spores from a bioweapons facility and resulted in as many as 250 cases with 100 deaths.2 Fortunately, we have a vaccine that has been judged safe and effective by the US Food and Drug Administration (FDA), Centers for Disease Control and Prevention, and National Academy of Sciences. Protecting the health of US military forces who defend our vital interests is a national obligation.5 The trade-off for force protection of our military personnel involves a small incidence of vaccine-related adverse events (AEs), the most common being local type injection site reactions or skin reactions.
Natural cutaneous anthrax manifests within a few days as a painless, pruritic papule that progresses to a blister and evolves to a painless ulcer, with a black central eschar and surrounding local edema. In contrast, vaccine-related events manifest differently, and the vaccine cannot cause clinical anthrax infections. An algorithm for the evaluation of suspected cutaneous anthrax has been published by the American Academy of Dermatology Ad Hoc Task Force on Bioterrorism.6 Additional guidelines for clinical and laboratory diagnoses, specimen handling, and postexposure prophylaxis are available from the US Centers for Disease Control and Prevention.7
The vaccine itself is made from a noninfectious, cell-free sterile filtrate of an attenuated, nonencapsulated, nonproteolytic strain of B anthracis.8 It is considered an inactivated vaccine and is unable to cause infection. The anthrax vaccine has been approved by the FDA since 1970 and is safely administered to veterinarians, laboratory workers, woolen mill workers, and livestock handlers.8 In 1997, it was mandated that all US military personnel receive it. Full protection requires a schedule of 6 injections over 18 months (specifically, at 0, 2, and 4 weeks and 6, 12, and 18 months), with an annual booster thereafter. In the event of anthrax exposure, the vaccine also can be offered as postexposure prophylaxis with 3 doses at 2-week intervals, along with postexposure antibiotics.2 Contraindications to the anthrax vaccine include hypersensitivity reaction to a prior dose or vaccine component, human immunodeficiency virus positivity or immune suppression (active corticosteroid or other immunosuppressive treatment), any active infection or acute illness, pregnancy (confirmed or suspected), and age younger than 18 years or older than 65 years.
Efficacy and Safety
The vaccine's efficacy against aerosolized anthrax was shown in studies on nonhuman primates. Sixty-two (95%) of the 65 primates vaccinated with the anthrax vaccine adsorbed (AVA) survived a lethal aerosol challenge, whereas all 18 unvaccinated controls died.8 In actively monitored studies on the safety of AVA, mild local reactions occurred in 3% to 20% of doses, moderate reactions in 1% to 3% of doses, and severe reactions in less than 1% of doses.8 Acute systemic reactions were reported in 0.06% of doses and consisted of transient symptoms of fever, chills, nausea, and general body aches.8
The current system for reporting AEs is the Vaccine Adverse Event Reporting System (VAERS), and the FDA reviews 100% of these reports. In addition, a US Department of Defense directive requires its military providers to initiate a report for any event following AVA that results in hospitalization, any loss of duty of more than 24 hours, or for suspected vaccine contamination.9 Reporting of other reactions suspected because of vaccination is encouraged, especially those that are clinically significant or unusual. The form can be obtained on the Web at http://www.vaers.org or via telephone at 800-822-7967. Electronic reporting is available on the Web at http://secure.vaers.org/VaersDataEntryintro.htm. The VAERS is a passive surveillance system, and determining causal associations between vaccines and AEs is not always possible.10 Other concurrent infections or exposures may precipitate a given symptom that may simply coincide with the receipt of a vaccine.11 For example, patient 2 may have had vaccine-associated erythema multiforme but because he had recently completed a course of penicillin, we cannot exclude the possibility of a concurrent antibiotic association.
The Anthrax Vaccine Expert Committee reviewed 602 VAERS reports filed from 1998 through 1999.12 Nearly one half of reports noted a local injection site AE, 33% of which were noted to be moderate to large. A subcutaneous nodule was cited in 5.3% of reports. Although three fourths of reports noted a "systemic" AE, these covered a broad spectrum, with 34 types cited at a frequency of more than 1%. The most common AEs, in declining order of incidence, were flulike symptoms, 20.8%; malaise, 13.3%; rash, 14.2%; arthralgia, 12%; headache, 10.1%; with the remainder of AEs all affecting fewer than 10% of patients. Among the reported 45 total "serious or medically important AEs," one report of each of the following was noted: systemic lupus erythematosus, angioedema, anaphylactoid reaction, and toxic epidermal necrolysis. None of these AEs were judged to be causally (defined as likely, certain, or probable) related to the vaccine itself.12 According to Friedlander et al,8 the "FDA continues to view the anthrax vaccine as safe and effective for individuals at risk of exposure to anthrax."
Management of Adverse Events
Adverse reactions after vaccination can be divided into local and systemic.
Cutaneous Reactions—The cutaneous manifestations and the latest recommendations from the Walter Reed National Vaccine healthcare center network9 are summarized partially in Tables 1 and 2.
Local reactions involve the injection site or have contiguous spread and are graded based on the measured size of the local redness or swelling (Table 1). Most local anthrax vaccine reactions require no treatment and resolve within 72 hours, though topical or oral steroids and oral antihistamines can be used to help manage symptoms. Unless the local reaction is very large or complicated, the patient can usually proceed with subsequent doses. Although some of these reactions may mimic cellulitis, antibiotic therapy for postvaccination inflammation is not warranted. Allergy consultation is recommended for a large or complicated reaction, especially if this occurs after the second dose. In this instance, the patient may be immune (a hyperresponder) and may not require further series (with the exception of the yearly booster).9 When a significant local type reaction has occurred, pretreatment to help prevent future large local reactions is indicated.
Systemic Reactions—These commonly include flulike symptoms, such as fever, anorexia, nausea, arthralgia, myalgia, or malaise. Treatment of mild to moderate systemic events is symptomatic (Table 2). Pretreatment also may be given with the next vaccine in patients who have had these symptoms on prior AVA vaccinations. If symptoms are clinically consistent with serum sickness or are severe and prolonged, the patient may benefit from a short course of oral prednisone. Vaccine-related AEs may warrant temporary delay from the schedule. When resumed, this does not require starting over but rather simply continuing from the last dose.9
For a generalized maculopapular rash or target lesions, a skin biopsy should be performed, especially if the rash is suggestive of early erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis. In these cases, temporary exemption from further vaccinations and VAERS reporting are indicated. The possibility exists that additional doses may result in a more serious skin reaction and should be given with caution only after expert evaluation and consideration of the risk:benefit ratio. The dermatologist should provide a clinical histopathologic diagnosis to help the allergist or expert in the vaccination program decide the best course for continuation or exemption from the full anthrax series. These cases may warrant permanent exemption from further vaccination series. No apparent safety data for challenge dosing or desensitization in these potentially life-threatening skin reactions exist. In patient 2 with erythema multiforme, further vaccinations for anthrax were waived permanently. Similarly, deferral from further anthrax vaccinations was recommended in patient 3.
In those cases of severe urticaria or angioedema, temporary exemption may be granted while requesting allergy consultation. Additional doses should be given with caution only after expert evaluation and consideration of the risk:benefit ratio. Permanent exemption may be required for those with anaphylaxis or sudden onset angioedema. In patient 1 with recurrent localized urticaria, the allergist recommended that a formal skin-prick test to future vaccine lots be performed before he received any further vaccine in the series. Although this local allergic-type reaction may be due to some component of the vaccine, we are unable to define the specific cause at this time. This is a rather unusual manifestation, with recurrence of the urticaria still persisting 21/2 years later and restricted only to the vaccinated arm.
Conclusion
There are ongoing studies to evaluate whether a reduced number of anthrax vaccinations will provide the same immunity. In addition, other ongoing studies are comparing intramuscular administration versus the current usual subcutaneous route. Preliminary reports have shown that local reactions are less common in patients who received the vaccine via the intramuscular route than in those who received the vaccine via the subcutaneous route.13 This change in route of administration could reduce the number of adverse cutaneous reactions in the future. For further expert advice or clinical consultations, contact the Walter Reed National Vaccine Healthcare Center via telephone: 202-782-0411; fax: 202-782-4658; or e-mail: askVHC@amedd.army.mil.
Since the domestic anthrax attacks in October 2001 and in the presence of continued worldwide threats to our armed forces, force protection remains a top priority. As dermatologists, we should be familiar with the current anthrax vaccine
program and be able to recognize and treat anthrax vaccine–related AEs.
- Bartlett JG, Inglesby TV, Borio L. Management of anthrax. Clin Infect Dis. 2002;35:851-858.
- Inglesby TV, O'Toole T, Henderson DA, et al. Anthrax as a biological weapon, 2002: updated recommendations for management. JAMA. 2002;287:2236-2252.
- Dixon TC, Meselson M, Guillemin J, et al. Anthrax. N Engl J Med. 1999;341:815-826.
- Swartz MN. Recognition and management of anthrax—an update. N Engl J Med. 2001;345:1621-1626.
- Mazzuchi JF, Claypool RG, Hyams KC, et al. Protecting the health of U.S. military forces: a national obligation. Aviat Space Environ Med. 2000;71:260-265.
- Carucci JA, McGovern TW, Norton SA, et al. Cutaneous anthrax management algorithm. J Am Acad Dermatol. 2002;47:766-769.
- Centers for Disease Control and Prevention. Guidelines for comprehensive procedures for collecting environmental samples for culturing Bacillus anthracis (revised April 2002) and anthrax: exposure management/prophylaxis (preventing transmission). Atlanta, Ga: Centers for Disease Control and Prevention Web sites. Available at: http://www.bt.cdc.gov. Accessed August 18, 2003.
- Friedlander AM, Pittman PR, Parker GW. Anthrax vaccine: evidence for safety and efficacy against inhalational anthrax. JAMA. 1999;282:2104-2106.
- Clinical guidelines for the management of adverse events after vaccination (official AVIP version). August 2002 Web site. Available at: http://www.deploymenthealth.mil/VHC/providers_management.htm. Accessed August 18, 2003.
- Centers for Disease Control and Prevention. Surveillance for safety after immunization: Vaccine Adverse Event Reporting System (VAERS)—United States, 1991-2000. MMWR Morb Mortal Wkly Rep. 2003;52:1-19.
- Halsey NA. Anthrax vaccine and causality assessment from individual case reports. Pharmacoepidemiol Drug Saf. 2002;11:185-187.
- Sever JL, Brenner AI, Gale AD, et al. Safety of anthrax vaccine: a review by the Anthrax Vaccine Expert Committee (AVEC) of adverse events reported to the Vaccine Adverse Event Reporting System (VAERS). Pharmacoepidemiol Drug Saf. 2002;11:189-202.
- Use of anthrax vaccine in the United States. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2000;49:1-20.
The October 2001 domestic anthrax attacks affected 22 people, resulting in 5 fatalities. The added global terrorist threats have created an increasing need for homeland protection, as well as protection of our widely deployed forces battling terrorism. It is now relevant for physicians to be familiar with both clinical anthrax and adverse vaccine-related events associated with the resumption of the anthrax vaccine program. Dermatologists played a lead role in the initial response to the anthrax attack. We must be the lead providers most familiar with the cutaneous reactions that may be seen with the preventive vaccination. This article reviews the latest recommended evaluation and management of anthrax vaccine adverse events.
Case Reports Patient 1—A 36-year-old white male active duty military fighter pilot developed recurrent, localized urticaria after receiving his sixth anthrax vaccination (Figure 1). Results of a skin biopsy showed a superficial perivascular dermatitis with eosinophils consistent with urticaria. The urticaria continues to recur 21/2 years after his last vaccination and remains localized to the vaccinated arm.
Patient 2—A 33-year-old black male military member developed erythema multiforme one day after receiving his fifth anthrax vaccination. He had been treated for pharyngitis with a 10-day course of oral penicillin, which had been completed 2 days prior to receiving the vaccination. Target lesions were present on both arms and hands but were more prominent on the arm that received the vaccination (Figure 2). Results of a skin biopsy revealed a superficial perivascular and interface lymphocytic dermatitis, with vacuolar changes along the dermoepidermal junction compatible with erythema multiforme.
Patient 3—A 28-year-old white male military member presented with a pruritic rash that had developed on his face approximately 12 hours after receiving his fifth anthrax vaccination. The rash had spread to his torso (Figure 3) and lower extremities. Results of a punch biopsy revealed a superficial and deep lymphocytic infiltrate with interface changes and some extravasated red blood cells, findings felt to be consistent with an erythema multiforme reaction (Figure 4). The patient was treated with a 2-week course of prednisone and intramuscular diphenhydramine (Benadryl®), and clearing of symptoms was noted within 10 days.
Comment
The threat of anthrax is deadly and real, as shown by the domestic attacks via the US Postal Service in October 2001. In all, there were 11 confirmed cases of inhalation anthrax, resulting in 5 fatalities. In addition, there were 7 confirmed cases and 4 suspected cases of cutaneous anthrax. Twenty of the 22 cases were unquestionably linked to mail contaminated with a single strain of Bacillus anthracis.1 Anthrax is easy and cheap to produce and can be stored for prolonged periods, with spores survivable for decades in ambient conditions.2 The spores are resistant to dryness, heat, UV light, gamma radiation, and many disinfectants.3 In addition, anthrax is odorless, colorless, tasteless, and difficult to detect, thus making it a likely choice for future biological attacks. After the first gulf war, Iraq admitted to producing and deploying weaponized anthrax in missiles.4 The Sverdlovsk anthrax outbreak in the former Soviet Union occurred after the accidental release of aerosolized anthrax spores from a bioweapons facility and resulted in as many as 250 cases with 100 deaths.2 Fortunately, we have a vaccine that has been judged safe and effective by the US Food and Drug Administration (FDA), Centers for Disease Control and Prevention, and National Academy of Sciences. Protecting the health of US military forces who defend our vital interests is a national obligation.5 The trade-off for force protection of our military personnel involves a small incidence of vaccine-related adverse events (AEs), the most common being local type injection site reactions or skin reactions.
Natural cutaneous anthrax manifests within a few days as a painless, pruritic papule that progresses to a blister and evolves to a painless ulcer, with a black central eschar and surrounding local edema. In contrast, vaccine-related events manifest differently, and the vaccine cannot cause clinical anthrax infections. An algorithm for the evaluation of suspected cutaneous anthrax has been published by the American Academy of Dermatology Ad Hoc Task Force on Bioterrorism.6 Additional guidelines for clinical and laboratory diagnoses, specimen handling, and postexposure prophylaxis are available from the US Centers for Disease Control and Prevention.7
The vaccine itself is made from a noninfectious, cell-free sterile filtrate of an attenuated, nonencapsulated, nonproteolytic strain of B anthracis.8 It is considered an inactivated vaccine and is unable to cause infection. The anthrax vaccine has been approved by the FDA since 1970 and is safely administered to veterinarians, laboratory workers, woolen mill workers, and livestock handlers.8 In 1997, it was mandated that all US military personnel receive it. Full protection requires a schedule of 6 injections over 18 months (specifically, at 0, 2, and 4 weeks and 6, 12, and 18 months), with an annual booster thereafter. In the event of anthrax exposure, the vaccine also can be offered as postexposure prophylaxis with 3 doses at 2-week intervals, along with postexposure antibiotics.2 Contraindications to the anthrax vaccine include hypersensitivity reaction to a prior dose or vaccine component, human immunodeficiency virus positivity or immune suppression (active corticosteroid or other immunosuppressive treatment), any active infection or acute illness, pregnancy (confirmed or suspected), and age younger than 18 years or older than 65 years.
Efficacy and Safety
The vaccine's efficacy against aerosolized anthrax was shown in studies on nonhuman primates. Sixty-two (95%) of the 65 primates vaccinated with the anthrax vaccine adsorbed (AVA) survived a lethal aerosol challenge, whereas all 18 unvaccinated controls died.8 In actively monitored studies on the safety of AVA, mild local reactions occurred in 3% to 20% of doses, moderate reactions in 1% to 3% of doses, and severe reactions in less than 1% of doses.8 Acute systemic reactions were reported in 0.06% of doses and consisted of transient symptoms of fever, chills, nausea, and general body aches.8
The current system for reporting AEs is the Vaccine Adverse Event Reporting System (VAERS), and the FDA reviews 100% of these reports. In addition, a US Department of Defense directive requires its military providers to initiate a report for any event following AVA that results in hospitalization, any loss of duty of more than 24 hours, or for suspected vaccine contamination.9 Reporting of other reactions suspected because of vaccination is encouraged, especially those that are clinically significant or unusual. The form can be obtained on the Web at http://www.vaers.org or via telephone at 800-822-7967. Electronic reporting is available on the Web at http://secure.vaers.org/VaersDataEntryintro.htm. The VAERS is a passive surveillance system, and determining causal associations between vaccines and AEs is not always possible.10 Other concurrent infections or exposures may precipitate a given symptom that may simply coincide with the receipt of a vaccine.11 For example, patient 2 may have had vaccine-associated erythema multiforme but because he had recently completed a course of penicillin, we cannot exclude the possibility of a concurrent antibiotic association.
The Anthrax Vaccine Expert Committee reviewed 602 VAERS reports filed from 1998 through 1999.12 Nearly one half of reports noted a local injection site AE, 33% of which were noted to be moderate to large. A subcutaneous nodule was cited in 5.3% of reports. Although three fourths of reports noted a "systemic" AE, these covered a broad spectrum, with 34 types cited at a frequency of more than 1%. The most common AEs, in declining order of incidence, were flulike symptoms, 20.8%; malaise, 13.3%; rash, 14.2%; arthralgia, 12%; headache, 10.1%; with the remainder of AEs all affecting fewer than 10% of patients. Among the reported 45 total "serious or medically important AEs," one report of each of the following was noted: systemic lupus erythematosus, angioedema, anaphylactoid reaction, and toxic epidermal necrolysis. None of these AEs were judged to be causally (defined as likely, certain, or probable) related to the vaccine itself.12 According to Friedlander et al,8 the "FDA continues to view the anthrax vaccine as safe and effective for individuals at risk of exposure to anthrax."
Management of Adverse Events
Adverse reactions after vaccination can be divided into local and systemic.
Cutaneous Reactions—The cutaneous manifestations and the latest recommendations from the Walter Reed National Vaccine healthcare center network9 are summarized partially in Tables 1 and 2.
Local reactions involve the injection site or have contiguous spread and are graded based on the measured size of the local redness or swelling (Table 1). Most local anthrax vaccine reactions require no treatment and resolve within 72 hours, though topical or oral steroids and oral antihistamines can be used to help manage symptoms. Unless the local reaction is very large or complicated, the patient can usually proceed with subsequent doses. Although some of these reactions may mimic cellulitis, antibiotic therapy for postvaccination inflammation is not warranted. Allergy consultation is recommended for a large or complicated reaction, especially if this occurs after the second dose. In this instance, the patient may be immune (a hyperresponder) and may not require further series (with the exception of the yearly booster).9 When a significant local type reaction has occurred, pretreatment to help prevent future large local reactions is indicated.
Systemic Reactions—These commonly include flulike symptoms, such as fever, anorexia, nausea, arthralgia, myalgia, or malaise. Treatment of mild to moderate systemic events is symptomatic (Table 2). Pretreatment also may be given with the next vaccine in patients who have had these symptoms on prior AVA vaccinations. If symptoms are clinically consistent with serum sickness or are severe and prolonged, the patient may benefit from a short course of oral prednisone. Vaccine-related AEs may warrant temporary delay from the schedule. When resumed, this does not require starting over but rather simply continuing from the last dose.9
For a generalized maculopapular rash or target lesions, a skin biopsy should be performed, especially if the rash is suggestive of early erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis. In these cases, temporary exemption from further vaccinations and VAERS reporting are indicated. The possibility exists that additional doses may result in a more serious skin reaction and should be given with caution only after expert evaluation and consideration of the risk:benefit ratio. The dermatologist should provide a clinical histopathologic diagnosis to help the allergist or expert in the vaccination program decide the best course for continuation or exemption from the full anthrax series. These cases may warrant permanent exemption from further vaccination series. No apparent safety data for challenge dosing or desensitization in these potentially life-threatening skin reactions exist. In patient 2 with erythema multiforme, further vaccinations for anthrax were waived permanently. Similarly, deferral from further anthrax vaccinations was recommended in patient 3.
In those cases of severe urticaria or angioedema, temporary exemption may be granted while requesting allergy consultation. Additional doses should be given with caution only after expert evaluation and consideration of the risk:benefit ratio. Permanent exemption may be required for those with anaphylaxis or sudden onset angioedema. In patient 1 with recurrent localized urticaria, the allergist recommended that a formal skin-prick test to future vaccine lots be performed before he received any further vaccine in the series. Although this local allergic-type reaction may be due to some component of the vaccine, we are unable to define the specific cause at this time. This is a rather unusual manifestation, with recurrence of the urticaria still persisting 21/2 years later and restricted only to the vaccinated arm.
Conclusion
There are ongoing studies to evaluate whether a reduced number of anthrax vaccinations will provide the same immunity. In addition, other ongoing studies are comparing intramuscular administration versus the current usual subcutaneous route. Preliminary reports have shown that local reactions are less common in patients who received the vaccine via the intramuscular route than in those who received the vaccine via the subcutaneous route.13 This change in route of administration could reduce the number of adverse cutaneous reactions in the future. For further expert advice or clinical consultations, contact the Walter Reed National Vaccine Healthcare Center via telephone: 202-782-0411; fax: 202-782-4658; or e-mail: askVHC@amedd.army.mil.
Since the domestic anthrax attacks in October 2001 and in the presence of continued worldwide threats to our armed forces, force protection remains a top priority. As dermatologists, we should be familiar with the current anthrax vaccine
program and be able to recognize and treat anthrax vaccine–related AEs.
The October 2001 domestic anthrax attacks affected 22 people, resulting in 5 fatalities. The added global terrorist threats have created an increasing need for homeland protection, as well as protection of our widely deployed forces battling terrorism. It is now relevant for physicians to be familiar with both clinical anthrax and adverse vaccine-related events associated with the resumption of the anthrax vaccine program. Dermatologists played a lead role in the initial response to the anthrax attack. We must be the lead providers most familiar with the cutaneous reactions that may be seen with the preventive vaccination. This article reviews the latest recommended evaluation and management of anthrax vaccine adverse events.
Case Reports Patient 1—A 36-year-old white male active duty military fighter pilot developed recurrent, localized urticaria after receiving his sixth anthrax vaccination (Figure 1). Results of a skin biopsy showed a superficial perivascular dermatitis with eosinophils consistent with urticaria. The urticaria continues to recur 21/2 years after his last vaccination and remains localized to the vaccinated arm.
Patient 2—A 33-year-old black male military member developed erythema multiforme one day after receiving his fifth anthrax vaccination. He had been treated for pharyngitis with a 10-day course of oral penicillin, which had been completed 2 days prior to receiving the vaccination. Target lesions were present on both arms and hands but were more prominent on the arm that received the vaccination (Figure 2). Results of a skin biopsy revealed a superficial perivascular and interface lymphocytic dermatitis, with vacuolar changes along the dermoepidermal junction compatible with erythema multiforme.
Patient 3—A 28-year-old white male military member presented with a pruritic rash that had developed on his face approximately 12 hours after receiving his fifth anthrax vaccination. The rash had spread to his torso (Figure 3) and lower extremities. Results of a punch biopsy revealed a superficial and deep lymphocytic infiltrate with interface changes and some extravasated red blood cells, findings felt to be consistent with an erythema multiforme reaction (Figure 4). The patient was treated with a 2-week course of prednisone and intramuscular diphenhydramine (Benadryl®), and clearing of symptoms was noted within 10 days.
Comment
The threat of anthrax is deadly and real, as shown by the domestic attacks via the US Postal Service in October 2001. In all, there were 11 confirmed cases of inhalation anthrax, resulting in 5 fatalities. In addition, there were 7 confirmed cases and 4 suspected cases of cutaneous anthrax. Twenty of the 22 cases were unquestionably linked to mail contaminated with a single strain of Bacillus anthracis.1 Anthrax is easy and cheap to produce and can be stored for prolonged periods, with spores survivable for decades in ambient conditions.2 The spores are resistant to dryness, heat, UV light, gamma radiation, and many disinfectants.3 In addition, anthrax is odorless, colorless, tasteless, and difficult to detect, thus making it a likely choice for future biological attacks. After the first gulf war, Iraq admitted to producing and deploying weaponized anthrax in missiles.4 The Sverdlovsk anthrax outbreak in the former Soviet Union occurred after the accidental release of aerosolized anthrax spores from a bioweapons facility and resulted in as many as 250 cases with 100 deaths.2 Fortunately, we have a vaccine that has been judged safe and effective by the US Food and Drug Administration (FDA), Centers for Disease Control and Prevention, and National Academy of Sciences. Protecting the health of US military forces who defend our vital interests is a national obligation.5 The trade-off for force protection of our military personnel involves a small incidence of vaccine-related adverse events (AEs), the most common being local type injection site reactions or skin reactions.
Natural cutaneous anthrax manifests within a few days as a painless, pruritic papule that progresses to a blister and evolves to a painless ulcer, with a black central eschar and surrounding local edema. In contrast, vaccine-related events manifest differently, and the vaccine cannot cause clinical anthrax infections. An algorithm for the evaluation of suspected cutaneous anthrax has been published by the American Academy of Dermatology Ad Hoc Task Force on Bioterrorism.6 Additional guidelines for clinical and laboratory diagnoses, specimen handling, and postexposure prophylaxis are available from the US Centers for Disease Control and Prevention.7
The vaccine itself is made from a noninfectious, cell-free sterile filtrate of an attenuated, nonencapsulated, nonproteolytic strain of B anthracis.8 It is considered an inactivated vaccine and is unable to cause infection. The anthrax vaccine has been approved by the FDA since 1970 and is safely administered to veterinarians, laboratory workers, woolen mill workers, and livestock handlers.8 In 1997, it was mandated that all US military personnel receive it. Full protection requires a schedule of 6 injections over 18 months (specifically, at 0, 2, and 4 weeks and 6, 12, and 18 months), with an annual booster thereafter. In the event of anthrax exposure, the vaccine also can be offered as postexposure prophylaxis with 3 doses at 2-week intervals, along with postexposure antibiotics.2 Contraindications to the anthrax vaccine include hypersensitivity reaction to a prior dose or vaccine component, human immunodeficiency virus positivity or immune suppression (active corticosteroid or other immunosuppressive treatment), any active infection or acute illness, pregnancy (confirmed or suspected), and age younger than 18 years or older than 65 years.
Efficacy and Safety
The vaccine's efficacy against aerosolized anthrax was shown in studies on nonhuman primates. Sixty-two (95%) of the 65 primates vaccinated with the anthrax vaccine adsorbed (AVA) survived a lethal aerosol challenge, whereas all 18 unvaccinated controls died.8 In actively monitored studies on the safety of AVA, mild local reactions occurred in 3% to 20% of doses, moderate reactions in 1% to 3% of doses, and severe reactions in less than 1% of doses.8 Acute systemic reactions were reported in 0.06% of doses and consisted of transient symptoms of fever, chills, nausea, and general body aches.8
The current system for reporting AEs is the Vaccine Adverse Event Reporting System (VAERS), and the FDA reviews 100% of these reports. In addition, a US Department of Defense directive requires its military providers to initiate a report for any event following AVA that results in hospitalization, any loss of duty of more than 24 hours, or for suspected vaccine contamination.9 Reporting of other reactions suspected because of vaccination is encouraged, especially those that are clinically significant or unusual. The form can be obtained on the Web at http://www.vaers.org or via telephone at 800-822-7967. Electronic reporting is available on the Web at http://secure.vaers.org/VaersDataEntryintro.htm. The VAERS is a passive surveillance system, and determining causal associations between vaccines and AEs is not always possible.10 Other concurrent infections or exposures may precipitate a given symptom that may simply coincide with the receipt of a vaccine.11 For example, patient 2 may have had vaccine-associated erythema multiforme but because he had recently completed a course of penicillin, we cannot exclude the possibility of a concurrent antibiotic association.
The Anthrax Vaccine Expert Committee reviewed 602 VAERS reports filed from 1998 through 1999.12 Nearly one half of reports noted a local injection site AE, 33% of which were noted to be moderate to large. A subcutaneous nodule was cited in 5.3% of reports. Although three fourths of reports noted a "systemic" AE, these covered a broad spectrum, with 34 types cited at a frequency of more than 1%. The most common AEs, in declining order of incidence, were flulike symptoms, 20.8%; malaise, 13.3%; rash, 14.2%; arthralgia, 12%; headache, 10.1%; with the remainder of AEs all affecting fewer than 10% of patients. Among the reported 45 total "serious or medically important AEs," one report of each of the following was noted: systemic lupus erythematosus, angioedema, anaphylactoid reaction, and toxic epidermal necrolysis. None of these AEs were judged to be causally (defined as likely, certain, or probable) related to the vaccine itself.12 According to Friedlander et al,8 the "FDA continues to view the anthrax vaccine as safe and effective for individuals at risk of exposure to anthrax."
Management of Adverse Events
Adverse reactions after vaccination can be divided into local and systemic.
Cutaneous Reactions—The cutaneous manifestations and the latest recommendations from the Walter Reed National Vaccine healthcare center network9 are summarized partially in Tables 1 and 2.
Local reactions involve the injection site or have contiguous spread and are graded based on the measured size of the local redness or swelling (Table 1). Most local anthrax vaccine reactions require no treatment and resolve within 72 hours, though topical or oral steroids and oral antihistamines can be used to help manage symptoms. Unless the local reaction is very large or complicated, the patient can usually proceed with subsequent doses. Although some of these reactions may mimic cellulitis, antibiotic therapy for postvaccination inflammation is not warranted. Allergy consultation is recommended for a large or complicated reaction, especially if this occurs after the second dose. In this instance, the patient may be immune (a hyperresponder) and may not require further series (with the exception of the yearly booster).9 When a significant local type reaction has occurred, pretreatment to help prevent future large local reactions is indicated.
Systemic Reactions—These commonly include flulike symptoms, such as fever, anorexia, nausea, arthralgia, myalgia, or malaise. Treatment of mild to moderate systemic events is symptomatic (Table 2). Pretreatment also may be given with the next vaccine in patients who have had these symptoms on prior AVA vaccinations. If symptoms are clinically consistent with serum sickness or are severe and prolonged, the patient may benefit from a short course of oral prednisone. Vaccine-related AEs may warrant temporary delay from the schedule. When resumed, this does not require starting over but rather simply continuing from the last dose.9
For a generalized maculopapular rash or target lesions, a skin biopsy should be performed, especially if the rash is suggestive of early erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis. In these cases, temporary exemption from further vaccinations and VAERS reporting are indicated. The possibility exists that additional doses may result in a more serious skin reaction and should be given with caution only after expert evaluation and consideration of the risk:benefit ratio. The dermatologist should provide a clinical histopathologic diagnosis to help the allergist or expert in the vaccination program decide the best course for continuation or exemption from the full anthrax series. These cases may warrant permanent exemption from further vaccination series. No apparent safety data for challenge dosing or desensitization in these potentially life-threatening skin reactions exist. In patient 2 with erythema multiforme, further vaccinations for anthrax were waived permanently. Similarly, deferral from further anthrax vaccinations was recommended in patient 3.
In those cases of severe urticaria or angioedema, temporary exemption may be granted while requesting allergy consultation. Additional doses should be given with caution only after expert evaluation and consideration of the risk:benefit ratio. Permanent exemption may be required for those with anaphylaxis or sudden onset angioedema. In patient 1 with recurrent localized urticaria, the allergist recommended that a formal skin-prick test to future vaccine lots be performed before he received any further vaccine in the series. Although this local allergic-type reaction may be due to some component of the vaccine, we are unable to define the specific cause at this time. This is a rather unusual manifestation, with recurrence of the urticaria still persisting 21/2 years later and restricted only to the vaccinated arm.
Conclusion
There are ongoing studies to evaluate whether a reduced number of anthrax vaccinations will provide the same immunity. In addition, other ongoing studies are comparing intramuscular administration versus the current usual subcutaneous route. Preliminary reports have shown that local reactions are less common in patients who received the vaccine via the intramuscular route than in those who received the vaccine via the subcutaneous route.13 This change in route of administration could reduce the number of adverse cutaneous reactions in the future. For further expert advice or clinical consultations, contact the Walter Reed National Vaccine Healthcare Center via telephone: 202-782-0411; fax: 202-782-4658; or e-mail: askVHC@amedd.army.mil.
Since the domestic anthrax attacks in October 2001 and in the presence of continued worldwide threats to our armed forces, force protection remains a top priority. As dermatologists, we should be familiar with the current anthrax vaccine
program and be able to recognize and treat anthrax vaccine–related AEs.
- Bartlett JG, Inglesby TV, Borio L. Management of anthrax. Clin Infect Dis. 2002;35:851-858.
- Inglesby TV, O'Toole T, Henderson DA, et al. Anthrax as a biological weapon, 2002: updated recommendations for management. JAMA. 2002;287:2236-2252.
- Dixon TC, Meselson M, Guillemin J, et al. Anthrax. N Engl J Med. 1999;341:815-826.
- Swartz MN. Recognition and management of anthrax—an update. N Engl J Med. 2001;345:1621-1626.
- Mazzuchi JF, Claypool RG, Hyams KC, et al. Protecting the health of U.S. military forces: a national obligation. Aviat Space Environ Med. 2000;71:260-265.
- Carucci JA, McGovern TW, Norton SA, et al. Cutaneous anthrax management algorithm. J Am Acad Dermatol. 2002;47:766-769.
- Centers for Disease Control and Prevention. Guidelines for comprehensive procedures for collecting environmental samples for culturing Bacillus anthracis (revised April 2002) and anthrax: exposure management/prophylaxis (preventing transmission). Atlanta, Ga: Centers for Disease Control and Prevention Web sites. Available at: http://www.bt.cdc.gov. Accessed August 18, 2003.
- Friedlander AM, Pittman PR, Parker GW. Anthrax vaccine: evidence for safety and efficacy against inhalational anthrax. JAMA. 1999;282:2104-2106.
- Clinical guidelines for the management of adverse events after vaccination (official AVIP version). August 2002 Web site. Available at: http://www.deploymenthealth.mil/VHC/providers_management.htm. Accessed August 18, 2003.
- Centers for Disease Control and Prevention. Surveillance for safety after immunization: Vaccine Adverse Event Reporting System (VAERS)—United States, 1991-2000. MMWR Morb Mortal Wkly Rep. 2003;52:1-19.
- Halsey NA. Anthrax vaccine and causality assessment from individual case reports. Pharmacoepidemiol Drug Saf. 2002;11:185-187.
- Sever JL, Brenner AI, Gale AD, et al. Safety of anthrax vaccine: a review by the Anthrax Vaccine Expert Committee (AVEC) of adverse events reported to the Vaccine Adverse Event Reporting System (VAERS). Pharmacoepidemiol Drug Saf. 2002;11:189-202.
- Use of anthrax vaccine in the United States. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2000;49:1-20.
- Bartlett JG, Inglesby TV, Borio L. Management of anthrax. Clin Infect Dis. 2002;35:851-858.
- Inglesby TV, O'Toole T, Henderson DA, et al. Anthrax as a biological weapon, 2002: updated recommendations for management. JAMA. 2002;287:2236-2252.
- Dixon TC, Meselson M, Guillemin J, et al. Anthrax. N Engl J Med. 1999;341:815-826.
- Swartz MN. Recognition and management of anthrax—an update. N Engl J Med. 2001;345:1621-1626.
- Mazzuchi JF, Claypool RG, Hyams KC, et al. Protecting the health of U.S. military forces: a national obligation. Aviat Space Environ Med. 2000;71:260-265.
- Carucci JA, McGovern TW, Norton SA, et al. Cutaneous anthrax management algorithm. J Am Acad Dermatol. 2002;47:766-769.
- Centers for Disease Control and Prevention. Guidelines for comprehensive procedures for collecting environmental samples for culturing Bacillus anthracis (revised April 2002) and anthrax: exposure management/prophylaxis (preventing transmission). Atlanta, Ga: Centers for Disease Control and Prevention Web sites. Available at: http://www.bt.cdc.gov. Accessed August 18, 2003.
- Friedlander AM, Pittman PR, Parker GW. Anthrax vaccine: evidence for safety and efficacy against inhalational anthrax. JAMA. 1999;282:2104-2106.
- Clinical guidelines for the management of adverse events after vaccination (official AVIP version). August 2002 Web site. Available at: http://www.deploymenthealth.mil/VHC/providers_management.htm. Accessed August 18, 2003.
- Centers for Disease Control and Prevention. Surveillance for safety after immunization: Vaccine Adverse Event Reporting System (VAERS)—United States, 1991-2000. MMWR Morb Mortal Wkly Rep. 2003;52:1-19.
- Halsey NA. Anthrax vaccine and causality assessment from individual case reports. Pharmacoepidemiol Drug Saf. 2002;11:185-187.
- Sever JL, Brenner AI, Gale AD, et al. Safety of anthrax vaccine: a review by the Anthrax Vaccine Expert Committee (AVEC) of adverse events reported to the Vaccine Adverse Event Reporting System (VAERS). Pharmacoepidemiol Drug Saf. 2002;11:189-202.
- Use of anthrax vaccine in the United States. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2000;49:1-20.
Posttraumatic stress disorder: Nature and nurture?
Posttraumatic stress disorder (PTSD) can be one of the most frustrating anxiety disorders for both the patient and clinician. Asymptomatic persons become haunted by an experience they can’t forget. Their resulting anxiety can sour what were once healthy relationships or disable someone who previously was productive.
In some cases, despite aggressive psychopharmacology and psychotherapy, the patient remains incapacitated by inappropriate and unremitting fear. The trauma seems to have broken something—changed something inside the brain—that can’t be fixed.
Brain imaging studies of patients with PTSD—combat veterans and women with histories of childhood sexual abuse—have shown smaller hippocampal volumes compared with patients without PTSD.1,2 This finding has led to speculation that stress hormones (glucocorticoids) adversely affect the hippocampus (Figure 1).
This line of reasoning suggests that prolonged stress causes increased production of glucocorticoids that are neurotoxic to the hippocampus, resulting in hippocampal atrophy.3 Studies of rodents and patients with Cushing’s syndrome support this hypothesis. The hippocampus, therefore, may have been irreversibly damaged in patients with severe PTSD.
Figure 1
The hippocampus, a specialized type of cortex, is key to memory and emotion. As this medial view shows, it extends along the lateral ventricle floor on each side of the brain.
Illustration for Current Psychiatry by Marcia Hartsock, CMI Hippocampus
Intuitively, this theory makes sense, as the hippocampus is crucial for memory and emotion. However, a recent study of identical twins raises doubts.
Surprising evidence
Gilbertson et al recruited 40 pairs of twins, in which one was a Vietnam combat veteran and the other stayed home.4 Using MRI, the researchers measured hippocampal volume in each twin and assessed the presence and severity of PTSD in the combat-exposed twin.
Consistent with earlier reports, the authors found smaller hippocampal volumes in combat-exposed individuals diagnosed with PTSD. However, they found an almost identical correlation between the noncombat-exposed twin’s hippocampal volume and the combat-exposed twin’s PTSD score (Figure 2). In other words, the twin’s hippocampus size was a better predictor of the veteran’s hippocampus size than was the veteran’s trauma exposure or PTSD symptoms.
This finding puts a new spin on the association between small hippocampal volume and PTSD. The authors stated, “these data indicate that smaller hippocampi in PTSD represents a pre-existing, familial vulnerability factor rather than the neurotoxic product of trauma exposure per se.” Put another way, the small hippocampus is not created by stress and trauma but is a preexisting condition. Further, this study suggests that a larger hippocampus may protect a person from developing PTSD.
This study may help explain why different individuals exposed to the same trauma are frequently left with different symptoms.5,6 PTSD would seem to be an excellent example of the combined effects of nature (small hippocampus) and nurture (traumatic experience).
Figure 2 Hippocampal volume correlates with posttraumatic symptoms
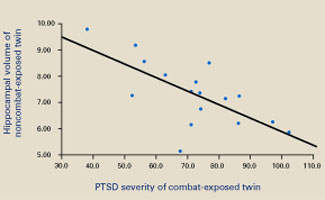
Smaller hippocampal volume in identical twins not exposed to combat was related to more-severe PTSD symptoms in their combat-exposed brothers (P = 0.002). Symptom severity was measured using Clinician-Administered PTSD Scale (CAPS) total scores.
Source: Reprinted with permission from Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nature Neurosci 2002;5:1242-7.
1. Bremner JD, Randall P, Scott TM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 1995;152:973-81.
2. Bremner JD, Vythilingam M, Vermetten E, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry 2003;160:924-32.
3. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
4. Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci 2002;5:1242-7.
5. Macklin ML, Metzger LJ, Litz BT, et al. Lower precombat intelligence is a risk factor for posttraumatic stress disorder. J Consult Clin Psychol 1998;66:323-6.
6. Schlenger WE, Caddell JM, Ebert L, et al. Psychological reactions to terrorist attacks: findings from the National Study of Americans’ Reactions to September 11. JAMA 2002;288:581-8.
Posttraumatic stress disorder (PTSD) can be one of the most frustrating anxiety disorders for both the patient and clinician. Asymptomatic persons become haunted by an experience they can’t forget. Their resulting anxiety can sour what were once healthy relationships or disable someone who previously was productive.
In some cases, despite aggressive psychopharmacology and psychotherapy, the patient remains incapacitated by inappropriate and unremitting fear. The trauma seems to have broken something—changed something inside the brain—that can’t be fixed.
Brain imaging studies of patients with PTSD—combat veterans and women with histories of childhood sexual abuse—have shown smaller hippocampal volumes compared with patients without PTSD.1,2 This finding has led to speculation that stress hormones (glucocorticoids) adversely affect the hippocampus (Figure 1).
This line of reasoning suggests that prolonged stress causes increased production of glucocorticoids that are neurotoxic to the hippocampus, resulting in hippocampal atrophy.3 Studies of rodents and patients with Cushing’s syndrome support this hypothesis. The hippocampus, therefore, may have been irreversibly damaged in patients with severe PTSD.
Figure 1
The hippocampus, a specialized type of cortex, is key to memory and emotion. As this medial view shows, it extends along the lateral ventricle floor on each side of the brain.
Illustration for Current Psychiatry by Marcia Hartsock, CMI Hippocampus
Intuitively, this theory makes sense, as the hippocampus is crucial for memory and emotion. However, a recent study of identical twins raises doubts.
Surprising evidence
Gilbertson et al recruited 40 pairs of twins, in which one was a Vietnam combat veteran and the other stayed home.4 Using MRI, the researchers measured hippocampal volume in each twin and assessed the presence and severity of PTSD in the combat-exposed twin.
Consistent with earlier reports, the authors found smaller hippocampal volumes in combat-exposed individuals diagnosed with PTSD. However, they found an almost identical correlation between the noncombat-exposed twin’s hippocampal volume and the combat-exposed twin’s PTSD score (Figure 2). In other words, the twin’s hippocampus size was a better predictor of the veteran’s hippocampus size than was the veteran’s trauma exposure or PTSD symptoms.
This finding puts a new spin on the association between small hippocampal volume and PTSD. The authors stated, “these data indicate that smaller hippocampi in PTSD represents a pre-existing, familial vulnerability factor rather than the neurotoxic product of trauma exposure per se.” Put another way, the small hippocampus is not created by stress and trauma but is a preexisting condition. Further, this study suggests that a larger hippocampus may protect a person from developing PTSD.
This study may help explain why different individuals exposed to the same trauma are frequently left with different symptoms.5,6 PTSD would seem to be an excellent example of the combined effects of nature (small hippocampus) and nurture (traumatic experience).
Figure 2 Hippocampal volume correlates with posttraumatic symptoms
Smaller hippocampal volume in identical twins not exposed to combat was related to more-severe PTSD symptoms in their combat-exposed brothers (P = 0.002). Symptom severity was measured using Clinician-Administered PTSD Scale (CAPS) total scores.
Source: Reprinted with permission from Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nature Neurosci 2002;5:1242-7.
Posttraumatic stress disorder (PTSD) can be one of the most frustrating anxiety disorders for both the patient and clinician. Asymptomatic persons become haunted by an experience they can’t forget. Their resulting anxiety can sour what were once healthy relationships or disable someone who previously was productive.
In some cases, despite aggressive psychopharmacology and psychotherapy, the patient remains incapacitated by inappropriate and unremitting fear. The trauma seems to have broken something—changed something inside the brain—that can’t be fixed.
Brain imaging studies of patients with PTSD—combat veterans and women with histories of childhood sexual abuse—have shown smaller hippocampal volumes compared with patients without PTSD.1,2 This finding has led to speculation that stress hormones (glucocorticoids) adversely affect the hippocampus (Figure 1).
This line of reasoning suggests that prolonged stress causes increased production of glucocorticoids that are neurotoxic to the hippocampus, resulting in hippocampal atrophy.3 Studies of rodents and patients with Cushing’s syndrome support this hypothesis. The hippocampus, therefore, may have been irreversibly damaged in patients with severe PTSD.
Figure 1
The hippocampus, a specialized type of cortex, is key to memory and emotion. As this medial view shows, it extends along the lateral ventricle floor on each side of the brain.
Illustration for Current Psychiatry by Marcia Hartsock, CMI Hippocampus
Intuitively, this theory makes sense, as the hippocampus is crucial for memory and emotion. However, a recent study of identical twins raises doubts.
Surprising evidence
Gilbertson et al recruited 40 pairs of twins, in which one was a Vietnam combat veteran and the other stayed home.4 Using MRI, the researchers measured hippocampal volume in each twin and assessed the presence and severity of PTSD in the combat-exposed twin.
Consistent with earlier reports, the authors found smaller hippocampal volumes in combat-exposed individuals diagnosed with PTSD. However, they found an almost identical correlation between the noncombat-exposed twin’s hippocampal volume and the combat-exposed twin’s PTSD score (Figure 2). In other words, the twin’s hippocampus size was a better predictor of the veteran’s hippocampus size than was the veteran’s trauma exposure or PTSD symptoms.
This finding puts a new spin on the association between small hippocampal volume and PTSD. The authors stated, “these data indicate that smaller hippocampi in PTSD represents a pre-existing, familial vulnerability factor rather than the neurotoxic product of trauma exposure per se.” Put another way, the small hippocampus is not created by stress and trauma but is a preexisting condition. Further, this study suggests that a larger hippocampus may protect a person from developing PTSD.
This study may help explain why different individuals exposed to the same trauma are frequently left with different symptoms.5,6 PTSD would seem to be an excellent example of the combined effects of nature (small hippocampus) and nurture (traumatic experience).
Figure 2 Hippocampal volume correlates with posttraumatic symptoms
Smaller hippocampal volume in identical twins not exposed to combat was related to more-severe PTSD symptoms in their combat-exposed brothers (P = 0.002). Symptom severity was measured using Clinician-Administered PTSD Scale (CAPS) total scores.
Source: Reprinted with permission from Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nature Neurosci 2002;5:1242-7.
1. Bremner JD, Randall P, Scott TM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 1995;152:973-81.
2. Bremner JD, Vythilingam M, Vermetten E, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry 2003;160:924-32.
3. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
4. Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci 2002;5:1242-7.
5. Macklin ML, Metzger LJ, Litz BT, et al. Lower precombat intelligence is a risk factor for posttraumatic stress disorder. J Consult Clin Psychol 1998;66:323-6.
6. Schlenger WE, Caddell JM, Ebert L, et al. Psychological reactions to terrorist attacks: findings from the National Study of Americans’ Reactions to September 11. JAMA 2002;288:581-8.
1. Bremner JD, Randall P, Scott TM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 1995;152:973-81.
2. Bremner JD, Vythilingam M, Vermetten E, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry 2003;160:924-32.
3. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
4. Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci 2002;5:1242-7.
5. Macklin ML, Metzger LJ, Litz BT, et al. Lower precombat intelligence is a risk factor for posttraumatic stress disorder. J Consult Clin Psychol 1998;66:323-6.
6. Schlenger WE, Caddell JM, Ebert L, et al. Psychological reactions to terrorist attacks: findings from the National Study of Americans’ Reactions to September 11. JAMA 2002;288:581-8.
Skin picking: one teenager’s struggle
I am most grateful for “Captive of the mirror” (Current Psychiatry, December 2003) by Drs. Jon Grant and Katharine Phillips.
I am a 19-year-old female college student who has been diagnosed with depression, anxiety, and trichotillomania. I have bitten my nails all my life, have been taking SSRIs since age 12, and have had numerous problems related to skin-picking. Since adolescence I have obsessively picked and squeezed at acne and miniscule bumps on my face, causing redness, bruising and—in some cases—bleeding. I would then hide from the world, sometimes for days, until the wounds healed.
Until now, I didn’t know skin picking was a recognized disorder, let alone common. Your article is a detailed, clear, evidence-based summary of the problem and possible treatments, most of which I never knew existed. After having tried many things with limited success, I am taking the article to a psychiatrist so that I can discuss options. For the first time in months, I am filled with hope.
I am most grateful for “Captive of the mirror” (Current Psychiatry, December 2003) by Drs. Jon Grant and Katharine Phillips.
I am a 19-year-old female college student who has been diagnosed with depression, anxiety, and trichotillomania. I have bitten my nails all my life, have been taking SSRIs since age 12, and have had numerous problems related to skin-picking. Since adolescence I have obsessively picked and squeezed at acne and miniscule bumps on my face, causing redness, bruising and—in some cases—bleeding. I would then hide from the world, sometimes for days, until the wounds healed.
Until now, I didn’t know skin picking was a recognized disorder, let alone common. Your article is a detailed, clear, evidence-based summary of the problem and possible treatments, most of which I never knew existed. After having tried many things with limited success, I am taking the article to a psychiatrist so that I can discuss options. For the first time in months, I am filled with hope.
I am most grateful for “Captive of the mirror” (Current Psychiatry, December 2003) by Drs. Jon Grant and Katharine Phillips.
I am a 19-year-old female college student who has been diagnosed with depression, anxiety, and trichotillomania. I have bitten my nails all my life, have been taking SSRIs since age 12, and have had numerous problems related to skin-picking. Since adolescence I have obsessively picked and squeezed at acne and miniscule bumps on my face, causing redness, bruising and—in some cases—bleeding. I would then hide from the world, sometimes for days, until the wounds healed.
Until now, I didn’t know skin picking was a recognized disorder, let alone common. Your article is a detailed, clear, evidence-based summary of the problem and possible treatments, most of which I never knew existed. After having tried many things with limited success, I am taking the article to a psychiatrist so that I can discuss options. For the first time in months, I am filled with hope.