User login
Update on eating disorders: Binge-eating disorder
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
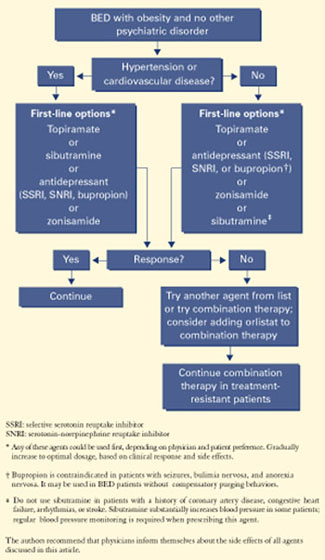
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
Figure 2 Medication options for BED with obesity and a mood disorder*

Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
Figure 2 Medication options for BED with obesity and a mood disorder*
Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
Figure 2 Medication options for BED with obesity and a mood disorder*
Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.
How effective are leukotriene inhibitors for asthma in children?
Evidence on the use of leukotriene inhibitors in children is insufficient to permit conclusions regarding efficacy. Given the proven efficacy of inhaled corticosteroids in asthma management, leukotriene inhibitors should not replace inhaled corticosteroids for maintenance of asthma in children (strength of recommendation: B).
Current guidelines that list leukotriene inhibitors as a potential addition or alternative to corticosteroid therapy in children with asthma appear to be based on scant studies and extrapolation from adult research.
Evidence summary
Asthma is characterized by inflammation of the bronchial airways. Leukotrienes are potent mediators of inflammation and are believed to contribute significantly to the inflammatory pathophysiology of asthma. Leukotriene inhibitors interfere with leukotriene production or leukotriene receptors and thus inhibit inflammation.1
Leukotriene inhibitors are administered orally, a significant advantage over inhalation in the pediatric population. For children, the theoretical corticosteroid-sparing effect of leukotriene inhibitors is appealing but has not been demonstrated.
In January 2002, Cochrane reviewers identified 3 studies of leukotriene inhibitor use in children that met their quality criteria for meta-analysis. Unfortunately, recent changes in asthma classification terminology make it difficult to precisely translate past studies into current practice. Based on these studies, the Cochrane reviewers concluded there is insufficient evidence to support the use of leukotriene inhibitors in children as monotherapy or as an addition to corticosteroids.1,2
One randomized, double-blind crossover study of 279 children with corticosteroid-dependent (persistent) asthma compared montelukast 5 mg (Singulair) once a day plus inhaled budesonide 200 μg (Pulmicort) twice a day with placebo plus budesonide (Rhinocort). Each study period lasted only 4 weeks, starting after a 4-week run-in period. Montelukast modestly improved asthma control over placebo. Compared with the placebo period, montelukast decreased the average use of beta-agonists by 1 puff per day. Asthma exacerbation days decreased by about 1 per month during montelukast treatment. The effects of montelukast and placebo on forced expiratory volume in 1 second (FEV1), quality of life, and adverse events did not differ significantly.3
One randomized, open-label crossover study of 124 children with “mild” asthma found that montelukast provided equivalent control and superior patient and parent satisfaction when compared with inhaled corticosteroids. Outcomes assessed were FEV1, school and work loss, medical resource utilization, safety, and patient and parent satisfaction. Children entering this study were self-selected to extend participation from a previous larger study that did not meet Cochrane quality criteria for inclusion in meta-analysis. The authors acknowledge the potential for selection bias.4
A randomized, double-blind, placebo-controlled study of 338 patients aged 12 years to adult compared zafirlukast (Accolate) with fluticasone propionate (Flovent) for control of persistent asthma. This study concluded that fluticasone was superior for all clinical outcomes measured including symptom scores, albuterol use, nighttime awakenings pulmonary function, and number of exacerbations requiring oral corticosteroids. Pooling of adult and adolescent cases in this study limits generalized application of these results to pediatric practice.5
Recommendations from others
The National Asthma Education and Prevention Program6 and the Global Initiative for Asthma7 guidelines conclude that inhaled corticosteroid, at the lowest effective dose, is the preferred therapy for children of all ages with persistent asthma whether mild, moderate, or severe.
Both guidelines list leukotriene inhibitors as a potential adjunct to corticosteroids for moderate persistent asthma, as an alternative to corticosteroids plus long-acting beta2-agonist. The guidelines also list leukotriene inhibitors as an alternative treatment to inhaled corticosteroids for mild persistent asthma in patients aged >5 years. Montelukast (Singulair) is approved for use in children aged ≥12 months, zafirlukast (Accolate) is approved for children aged≥5 years, and zileuton (Zyflo) is approved only for children aged >12 years.
An inhaled corticosteroid controller should be the first step
Lawrence S. Slotnick, MD
Moses Cone Health System, Greensboro, NC
Until evidence supports a different conclusion, I think we should continue to follow current national and global guidelines. The most important concept in both is that once a child is diagnosed with persistent asthma, starting an inhaled corticosteroid controller should be the first step.
Leukotriene inhibitors should be considered as second or third choice as a controller. The main indications for using a leukotriene inhibitor are aspirin-sensitive, exerciseinduced, and nocturnal asthma. I would use a leukotriene inhibitor as a controller only if a patient could not comply with inhaled corticosteroids.
1. Ducharme F, Hicks G, Kakuma R. Addition of anti-leukotriene agents to inhaled corticosteriods for chronic asthma. Cochrane Database Syst Rev 2002;(1):CD003133.-
2. Ducharme FM, Hicks GC. Anti-leukotriene agents compared to inhaled coritcosteriods in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev 2002;(3):CD002314-
3. Simons FE, Villa JR, Lee BW G, et al. Montelukast added to budesonide in children with persistent asthma: a randomized, double-blind, crossover study. J Pediatr 2001;138:694-698.
4. Maspero JF, Duenas-Meza E, Volovitz B, et al. Oral montelukast versus inhaled beclamethasone in 6- to 11- year-old children with asthma: results of an open-label extension study evaluating long-term safety, satisfaction and adherence with therapy. Curr Med Res Opin. 2001;17:96-104.
5. Busse W, Wolfe J, Storms W, et al. Fluticasone propionate compared with zafirlukast in controlling persistent asthma: a randomized double-blind, placebo-controlled trial. J Fam Pract 2001;50:595-602.
6. National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma. 1997 (rev 2002). Available at: www.nhlbi.nih.gov/guidelines/asthma/. Accessed on March 5, 2004.
7. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Rockville, Md: National Heart, Lung, and Blood Institute. 1995 (revised 2002). Available at: www.ginasthma.com/wr.html. Accessed on March 5, 2004.
Evidence on the use of leukotriene inhibitors in children is insufficient to permit conclusions regarding efficacy. Given the proven efficacy of inhaled corticosteroids in asthma management, leukotriene inhibitors should not replace inhaled corticosteroids for maintenance of asthma in children (strength of recommendation: B).
Current guidelines that list leukotriene inhibitors as a potential addition or alternative to corticosteroid therapy in children with asthma appear to be based on scant studies and extrapolation from adult research.
Evidence summary
Asthma is characterized by inflammation of the bronchial airways. Leukotrienes are potent mediators of inflammation and are believed to contribute significantly to the inflammatory pathophysiology of asthma. Leukotriene inhibitors interfere with leukotriene production or leukotriene receptors and thus inhibit inflammation.1
Leukotriene inhibitors are administered orally, a significant advantage over inhalation in the pediatric population. For children, the theoretical corticosteroid-sparing effect of leukotriene inhibitors is appealing but has not been demonstrated.
In January 2002, Cochrane reviewers identified 3 studies of leukotriene inhibitor use in children that met their quality criteria for meta-analysis. Unfortunately, recent changes in asthma classification terminology make it difficult to precisely translate past studies into current practice. Based on these studies, the Cochrane reviewers concluded there is insufficient evidence to support the use of leukotriene inhibitors in children as monotherapy or as an addition to corticosteroids.1,2
One randomized, double-blind crossover study of 279 children with corticosteroid-dependent (persistent) asthma compared montelukast 5 mg (Singulair) once a day plus inhaled budesonide 200 μg (Pulmicort) twice a day with placebo plus budesonide (Rhinocort). Each study period lasted only 4 weeks, starting after a 4-week run-in period. Montelukast modestly improved asthma control over placebo. Compared with the placebo period, montelukast decreased the average use of beta-agonists by 1 puff per day. Asthma exacerbation days decreased by about 1 per month during montelukast treatment. The effects of montelukast and placebo on forced expiratory volume in 1 second (FEV1), quality of life, and adverse events did not differ significantly.3
One randomized, open-label crossover study of 124 children with “mild” asthma found that montelukast provided equivalent control and superior patient and parent satisfaction when compared with inhaled corticosteroids. Outcomes assessed were FEV1, school and work loss, medical resource utilization, safety, and patient and parent satisfaction. Children entering this study were self-selected to extend participation from a previous larger study that did not meet Cochrane quality criteria for inclusion in meta-analysis. The authors acknowledge the potential for selection bias.4
A randomized, double-blind, placebo-controlled study of 338 patients aged 12 years to adult compared zafirlukast (Accolate) with fluticasone propionate (Flovent) for control of persistent asthma. This study concluded that fluticasone was superior for all clinical outcomes measured including symptom scores, albuterol use, nighttime awakenings pulmonary function, and number of exacerbations requiring oral corticosteroids. Pooling of adult and adolescent cases in this study limits generalized application of these results to pediatric practice.5
Recommendations from others
The National Asthma Education and Prevention Program6 and the Global Initiative for Asthma7 guidelines conclude that inhaled corticosteroid, at the lowest effective dose, is the preferred therapy for children of all ages with persistent asthma whether mild, moderate, or severe.
Both guidelines list leukotriene inhibitors as a potential adjunct to corticosteroids for moderate persistent asthma, as an alternative to corticosteroids plus long-acting beta2-agonist. The guidelines also list leukotriene inhibitors as an alternative treatment to inhaled corticosteroids for mild persistent asthma in patients aged >5 years. Montelukast (Singulair) is approved for use in children aged ≥12 months, zafirlukast (Accolate) is approved for children aged≥5 years, and zileuton (Zyflo) is approved only for children aged >12 years.
An inhaled corticosteroid controller should be the first step
Lawrence S. Slotnick, MD
Moses Cone Health System, Greensboro, NC
Until evidence supports a different conclusion, I think we should continue to follow current national and global guidelines. The most important concept in both is that once a child is diagnosed with persistent asthma, starting an inhaled corticosteroid controller should be the first step.
Leukotriene inhibitors should be considered as second or third choice as a controller. The main indications for using a leukotriene inhibitor are aspirin-sensitive, exerciseinduced, and nocturnal asthma. I would use a leukotriene inhibitor as a controller only if a patient could not comply with inhaled corticosteroids.
Evidence on the use of leukotriene inhibitors in children is insufficient to permit conclusions regarding efficacy. Given the proven efficacy of inhaled corticosteroids in asthma management, leukotriene inhibitors should not replace inhaled corticosteroids for maintenance of asthma in children (strength of recommendation: B).
Current guidelines that list leukotriene inhibitors as a potential addition or alternative to corticosteroid therapy in children with asthma appear to be based on scant studies and extrapolation from adult research.
Evidence summary
Asthma is characterized by inflammation of the bronchial airways. Leukotrienes are potent mediators of inflammation and are believed to contribute significantly to the inflammatory pathophysiology of asthma. Leukotriene inhibitors interfere with leukotriene production or leukotriene receptors and thus inhibit inflammation.1
Leukotriene inhibitors are administered orally, a significant advantage over inhalation in the pediatric population. For children, the theoretical corticosteroid-sparing effect of leukotriene inhibitors is appealing but has not been demonstrated.
In January 2002, Cochrane reviewers identified 3 studies of leukotriene inhibitor use in children that met their quality criteria for meta-analysis. Unfortunately, recent changes in asthma classification terminology make it difficult to precisely translate past studies into current practice. Based on these studies, the Cochrane reviewers concluded there is insufficient evidence to support the use of leukotriene inhibitors in children as monotherapy or as an addition to corticosteroids.1,2
One randomized, double-blind crossover study of 279 children with corticosteroid-dependent (persistent) asthma compared montelukast 5 mg (Singulair) once a day plus inhaled budesonide 200 μg (Pulmicort) twice a day with placebo plus budesonide (Rhinocort). Each study period lasted only 4 weeks, starting after a 4-week run-in period. Montelukast modestly improved asthma control over placebo. Compared with the placebo period, montelukast decreased the average use of beta-agonists by 1 puff per day. Asthma exacerbation days decreased by about 1 per month during montelukast treatment. The effects of montelukast and placebo on forced expiratory volume in 1 second (FEV1), quality of life, and adverse events did not differ significantly.3
One randomized, open-label crossover study of 124 children with “mild” asthma found that montelukast provided equivalent control and superior patient and parent satisfaction when compared with inhaled corticosteroids. Outcomes assessed were FEV1, school and work loss, medical resource utilization, safety, and patient and parent satisfaction. Children entering this study were self-selected to extend participation from a previous larger study that did not meet Cochrane quality criteria for inclusion in meta-analysis. The authors acknowledge the potential for selection bias.4
A randomized, double-blind, placebo-controlled study of 338 patients aged 12 years to adult compared zafirlukast (Accolate) with fluticasone propionate (Flovent) for control of persistent asthma. This study concluded that fluticasone was superior for all clinical outcomes measured including symptom scores, albuterol use, nighttime awakenings pulmonary function, and number of exacerbations requiring oral corticosteroids. Pooling of adult and adolescent cases in this study limits generalized application of these results to pediatric practice.5
Recommendations from others
The National Asthma Education and Prevention Program6 and the Global Initiative for Asthma7 guidelines conclude that inhaled corticosteroid, at the lowest effective dose, is the preferred therapy for children of all ages with persistent asthma whether mild, moderate, or severe.
Both guidelines list leukotriene inhibitors as a potential adjunct to corticosteroids for moderate persistent asthma, as an alternative to corticosteroids plus long-acting beta2-agonist. The guidelines also list leukotriene inhibitors as an alternative treatment to inhaled corticosteroids for mild persistent asthma in patients aged >5 years. Montelukast (Singulair) is approved for use in children aged ≥12 months, zafirlukast (Accolate) is approved for children aged≥5 years, and zileuton (Zyflo) is approved only for children aged >12 years.
An inhaled corticosteroid controller should be the first step
Lawrence S. Slotnick, MD
Moses Cone Health System, Greensboro, NC
Until evidence supports a different conclusion, I think we should continue to follow current national and global guidelines. The most important concept in both is that once a child is diagnosed with persistent asthma, starting an inhaled corticosteroid controller should be the first step.
Leukotriene inhibitors should be considered as second or third choice as a controller. The main indications for using a leukotriene inhibitor are aspirin-sensitive, exerciseinduced, and nocturnal asthma. I would use a leukotriene inhibitor as a controller only if a patient could not comply with inhaled corticosteroids.
1. Ducharme F, Hicks G, Kakuma R. Addition of anti-leukotriene agents to inhaled corticosteriods for chronic asthma. Cochrane Database Syst Rev 2002;(1):CD003133.-
2. Ducharme FM, Hicks GC. Anti-leukotriene agents compared to inhaled coritcosteriods in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev 2002;(3):CD002314-
3. Simons FE, Villa JR, Lee BW G, et al. Montelukast added to budesonide in children with persistent asthma: a randomized, double-blind, crossover study. J Pediatr 2001;138:694-698.
4. Maspero JF, Duenas-Meza E, Volovitz B, et al. Oral montelukast versus inhaled beclamethasone in 6- to 11- year-old children with asthma: results of an open-label extension study evaluating long-term safety, satisfaction and adherence with therapy. Curr Med Res Opin. 2001;17:96-104.
5. Busse W, Wolfe J, Storms W, et al. Fluticasone propionate compared with zafirlukast in controlling persistent asthma: a randomized double-blind, placebo-controlled trial. J Fam Pract 2001;50:595-602.
6. National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma. 1997 (rev 2002). Available at: www.nhlbi.nih.gov/guidelines/asthma/. Accessed on March 5, 2004.
7. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Rockville, Md: National Heart, Lung, and Blood Institute. 1995 (revised 2002). Available at: www.ginasthma.com/wr.html. Accessed on March 5, 2004.
1. Ducharme F, Hicks G, Kakuma R. Addition of anti-leukotriene agents to inhaled corticosteriods for chronic asthma. Cochrane Database Syst Rev 2002;(1):CD003133.-
2. Ducharme FM, Hicks GC. Anti-leukotriene agents compared to inhaled coritcosteriods in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev 2002;(3):CD002314-
3. Simons FE, Villa JR, Lee BW G, et al. Montelukast added to budesonide in children with persistent asthma: a randomized, double-blind, crossover study. J Pediatr 2001;138:694-698.
4. Maspero JF, Duenas-Meza E, Volovitz B, et al. Oral montelukast versus inhaled beclamethasone in 6- to 11- year-old children with asthma: results of an open-label extension study evaluating long-term safety, satisfaction and adherence with therapy. Curr Med Res Opin. 2001;17:96-104.
5. Busse W, Wolfe J, Storms W, et al. Fluticasone propionate compared with zafirlukast in controlling persistent asthma: a randomized double-blind, placebo-controlled trial. J Fam Pract 2001;50:595-602.
6. National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma. 1997 (rev 2002). Available at: www.nhlbi.nih.gov/guidelines/asthma/. Accessed on March 5, 2004.
7. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Rockville, Md: National Heart, Lung, and Blood Institute. 1995 (revised 2002). Available at: www.ginasthma.com/wr.html. Accessed on March 5, 2004.
Evidence-based answers from the Family Physicians Inquiries Network
Help night shift workers get enough sleep
Shift work sleep disorder is common among persons whose working hours fall between 6 PM and 7 AM. Some night or overnight shift workers cannot stay alert at work or sleep well when off duty, endangering others on the job or while driving.
When shift work sleep disorder is suspected, find out:
- Is the patient getting enough sleep? The average rotating shift worker sleeps 6 hours nightly1 while working the night shift.
- Is another sleep disorder present? Obstructive sleep apnea, restless legs syndrome, or other common comorbidities may also be disrupting sleep.
- Is an unrecognized comorbid psychiatric disorder present? Not surprisingly, major depression, chemical dependency, and other untreated psychiatric disorders impede adherence to a sleep schedule.
- Is caffeine being used appropriately? Shift workers can effectively use caffeine as an alerting agent but should only use it within 4 to 6 hours after arising. Advise patients against consuming beverages or foods containing caffeine within 8 to 10 hours of bedtime.
Promoting sleep
To help the patient get ample sleep, encourage him or her to:
- find time for uninterrupted sleep. Family time, social events, and errands must be scheduled so that they do not interfere.
- maintain a consistent sleep schedule when possible. Workers with long night shifts should try to stay awake all night and sleep during the day, even on days off.
- use bright lights during waking hours to promote alertness and prevent sleep disruption. Bright light has been shown to influence the human circadian clock.2
Some workplaces are installing artificial lights to increase light exposure during night work. Night shift workers traveling home in the morning should wear sunglasses to limit light exposure.
Also consider prescribing:
- a short-acting hypnotic. Although not specifically FDA-approved for shift work sleep disorder, medications such as zaleplon or zolpidem can reduce time to falling asleep and increase sleep without producing a hangover effect.
- a wakefulness-promoting agent. The FDA recently approved modafinil for reducing excessive daytime sleepiness in shift work sleep disorder. Patients take modafinil, 200 mg/d, shortly after arising to increase alertness at work. Be sure to advise patients that the medication is not a substitute for getting adequate sleep.
1. Colligan M, Tepas D. The stress of hours at work. Am Ind Hyg Assoc J 1986;47:686-95.
2. Horowitz TS, Tanigawa T. Circadian-based new technologies for night workers. Ind Health 2002;40(3):223-36.
Dr. Krahn is chair, department of psychiatry and psychology, Mayo Clinic, Scottsdale, AZ, and associate professor, Mayo Clinic College of Medicine. She is an Associate Editor of CURRENT PSYCHIATRY.
Shift work sleep disorder is common among persons whose working hours fall between 6 PM and 7 AM. Some night or overnight shift workers cannot stay alert at work or sleep well when off duty, endangering others on the job or while driving.
When shift work sleep disorder is suspected, find out:
- Is the patient getting enough sleep? The average rotating shift worker sleeps 6 hours nightly1 while working the night shift.
- Is another sleep disorder present? Obstructive sleep apnea, restless legs syndrome, or other common comorbidities may also be disrupting sleep.
- Is an unrecognized comorbid psychiatric disorder present? Not surprisingly, major depression, chemical dependency, and other untreated psychiatric disorders impede adherence to a sleep schedule.
- Is caffeine being used appropriately? Shift workers can effectively use caffeine as an alerting agent but should only use it within 4 to 6 hours after arising. Advise patients against consuming beverages or foods containing caffeine within 8 to 10 hours of bedtime.
Promoting sleep
To help the patient get ample sleep, encourage him or her to:
- find time for uninterrupted sleep. Family time, social events, and errands must be scheduled so that they do not interfere.
- maintain a consistent sleep schedule when possible. Workers with long night shifts should try to stay awake all night and sleep during the day, even on days off.
- use bright lights during waking hours to promote alertness and prevent sleep disruption. Bright light has been shown to influence the human circadian clock.2
Some workplaces are installing artificial lights to increase light exposure during night work. Night shift workers traveling home in the morning should wear sunglasses to limit light exposure.
Also consider prescribing:
- a short-acting hypnotic. Although not specifically FDA-approved for shift work sleep disorder, medications such as zaleplon or zolpidem can reduce time to falling asleep and increase sleep without producing a hangover effect.
- a wakefulness-promoting agent. The FDA recently approved modafinil for reducing excessive daytime sleepiness in shift work sleep disorder. Patients take modafinil, 200 mg/d, shortly after arising to increase alertness at work. Be sure to advise patients that the medication is not a substitute for getting adequate sleep.
Shift work sleep disorder is common among persons whose working hours fall between 6 PM and 7 AM. Some night or overnight shift workers cannot stay alert at work or sleep well when off duty, endangering others on the job or while driving.
When shift work sleep disorder is suspected, find out:
- Is the patient getting enough sleep? The average rotating shift worker sleeps 6 hours nightly1 while working the night shift.
- Is another sleep disorder present? Obstructive sleep apnea, restless legs syndrome, or other common comorbidities may also be disrupting sleep.
- Is an unrecognized comorbid psychiatric disorder present? Not surprisingly, major depression, chemical dependency, and other untreated psychiatric disorders impede adherence to a sleep schedule.
- Is caffeine being used appropriately? Shift workers can effectively use caffeine as an alerting agent but should only use it within 4 to 6 hours after arising. Advise patients against consuming beverages or foods containing caffeine within 8 to 10 hours of bedtime.
Promoting sleep
To help the patient get ample sleep, encourage him or her to:
- find time for uninterrupted sleep. Family time, social events, and errands must be scheduled so that they do not interfere.
- maintain a consistent sleep schedule when possible. Workers with long night shifts should try to stay awake all night and sleep during the day, even on days off.
- use bright lights during waking hours to promote alertness and prevent sleep disruption. Bright light has been shown to influence the human circadian clock.2
Some workplaces are installing artificial lights to increase light exposure during night work. Night shift workers traveling home in the morning should wear sunglasses to limit light exposure.
Also consider prescribing:
- a short-acting hypnotic. Although not specifically FDA-approved for shift work sleep disorder, medications such as zaleplon or zolpidem can reduce time to falling asleep and increase sleep without producing a hangover effect.
- a wakefulness-promoting agent. The FDA recently approved modafinil for reducing excessive daytime sleepiness in shift work sleep disorder. Patients take modafinil, 200 mg/d, shortly after arising to increase alertness at work. Be sure to advise patients that the medication is not a substitute for getting adequate sleep.
1. Colligan M, Tepas D. The stress of hours at work. Am Ind Hyg Assoc J 1986;47:686-95.
2. Horowitz TS, Tanigawa T. Circadian-based new technologies for night workers. Ind Health 2002;40(3):223-36.
Dr. Krahn is chair, department of psychiatry and psychology, Mayo Clinic, Scottsdale, AZ, and associate professor, Mayo Clinic College of Medicine. She is an Associate Editor of CURRENT PSYCHIATRY.
1. Colligan M, Tepas D. The stress of hours at work. Am Ind Hyg Assoc J 1986;47:686-95.
2. Horowitz TS, Tanigawa T. Circadian-based new technologies for night workers. Ind Health 2002;40(3):223-36.
Dr. Krahn is chair, department of psychiatry and psychology, Mayo Clinic, Scottsdale, AZ, and associate professor, Mayo Clinic College of Medicine. She is an Associate Editor of CURRENT PSYCHIATRY.
Donepezil minimally effective for patients with vascular dementia
Donepezil (Aricept—a potent acetylcholin-esterase inhibitor) had small effects on mentation for patients with mild to moderate vascular dementia as measured by validated instruments of cognition.
Donepezil’s side effects are similar to placebo at 5 mg but double at 10 mg, with no improvement in the patient’s cognition. Even though this medication was minimally effective, there are no other highly effective medical treatments for vascular dementia. Therefore, if a patient chooses a trial of donepezil, the lower, 5-mg dose should be offered.
The medication’s effect is likely a class effect and not an individual drug effect; therefore, rivastigmine (Exelon) and galantamine(Reminyl) are 2 other acetylcholinesterase inhibitors that should also be considered. Cost is similar for all 3 drugs at about $130.00 per month.
Donepezil (Aricept—a potent acetylcholin-esterase inhibitor) had small effects on mentation for patients with mild to moderate vascular dementia as measured by validated instruments of cognition.
Donepezil’s side effects are similar to placebo at 5 mg but double at 10 mg, with no improvement in the patient’s cognition. Even though this medication was minimally effective, there are no other highly effective medical treatments for vascular dementia. Therefore, if a patient chooses a trial of donepezil, the lower, 5-mg dose should be offered.
The medication’s effect is likely a class effect and not an individual drug effect; therefore, rivastigmine (Exelon) and galantamine(Reminyl) are 2 other acetylcholinesterase inhibitors that should also be considered. Cost is similar for all 3 drugs at about $130.00 per month.
Donepezil (Aricept—a potent acetylcholin-esterase inhibitor) had small effects on mentation for patients with mild to moderate vascular dementia as measured by validated instruments of cognition.
Donepezil’s side effects are similar to placebo at 5 mg but double at 10 mg, with no improvement in the patient’s cognition. Even though this medication was minimally effective, there are no other highly effective medical treatments for vascular dementia. Therefore, if a patient chooses a trial of donepezil, the lower, 5-mg dose should be offered.
The medication’s effect is likely a class effect and not an individual drug effect; therefore, rivastigmine (Exelon) and galantamine(Reminyl) are 2 other acetylcholinesterase inhibitors that should also be considered. Cost is similar for all 3 drugs at about $130.00 per month.
When and how is it appropriate to terminate the physician-patient relationship?
The Psychological Aspects of Vitiligo
Update on eating disorders Anorexia nervosa: Dual therapy can bring patients back from the brink
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
Epilepsy in Women
Supplement Editors:
Nancy Foldvary-Schaefer, DO, and Martha J. Morrell, MD
Contents
Introduction
Nancy Foldvary-Schaefer, DO, and Martha J. Morrell, MD
Cellular and molecular effects of steroid hormones on CNS excitability
Sheryl S. Smith, PhD, and Catherine S. Woolley, PhD
Hormones and seizures
Nancy Foldvary-Schaefer, DO; Cynthia Harden, MD; Andrew Herzog, MD; and Tommaso Falcone, MD
Reproductive disturbances in patients with epilepsy
Martha J. Morrell, MD, and Georgia D. Montouris, MD
Risks and management of pregnancy in women with epilepsy
Mark S. Yerby, MD, MPH; Peter Kaplan, MB; and Teresa Tran, MD
Neurodevelopmental outcomes of children born to mothers with epilepsy
Kimford J. Meador, MD, and Mary L. Zupanc, MD
Bone disease associated with antiepileptic drugs
Alison M. Pack, MD; Barry Gidal, PharmD; and Blanca Vazquez, MD
Recommendations for the care of women with epilepsy
Patricia E. Penovich, MD; Karen E. Eck, MS, FNP; and Vasiliki V. Economou, MD
Supplement Editors:
Nancy Foldvary-Schaefer, DO, and Martha J. Morrell, MD
Contents
Introduction
Nancy Foldvary-Schaefer, DO, and Martha J. Morrell, MD
Cellular and molecular effects of steroid hormones on CNS excitability
Sheryl S. Smith, PhD, and Catherine S. Woolley, PhD
Hormones and seizures
Nancy Foldvary-Schaefer, DO; Cynthia Harden, MD; Andrew Herzog, MD; and Tommaso Falcone, MD
Reproductive disturbances in patients with epilepsy
Martha J. Morrell, MD, and Georgia D. Montouris, MD
Risks and management of pregnancy in women with epilepsy
Mark S. Yerby, MD, MPH; Peter Kaplan, MB; and Teresa Tran, MD
Neurodevelopmental outcomes of children born to mothers with epilepsy
Kimford J. Meador, MD, and Mary L. Zupanc, MD
Bone disease associated with antiepileptic drugs
Alison M. Pack, MD; Barry Gidal, PharmD; and Blanca Vazquez, MD
Recommendations for the care of women with epilepsy
Patricia E. Penovich, MD; Karen E. Eck, MS, FNP; and Vasiliki V. Economou, MD
Supplement Editors:
Nancy Foldvary-Schaefer, DO, and Martha J. Morrell, MD
Contents
Introduction
Nancy Foldvary-Schaefer, DO, and Martha J. Morrell, MD
Cellular and molecular effects of steroid hormones on CNS excitability
Sheryl S. Smith, PhD, and Catherine S. Woolley, PhD
Hormones and seizures
Nancy Foldvary-Schaefer, DO; Cynthia Harden, MD; Andrew Herzog, MD; and Tommaso Falcone, MD
Reproductive disturbances in patients with epilepsy
Martha J. Morrell, MD, and Georgia D. Montouris, MD
Risks and management of pregnancy in women with epilepsy
Mark S. Yerby, MD, MPH; Peter Kaplan, MB; and Teresa Tran, MD
Neurodevelopmental outcomes of children born to mothers with epilepsy
Kimford J. Meador, MD, and Mary L. Zupanc, MD
Bone disease associated with antiepileptic drugs
Alison M. Pack, MD; Barry Gidal, PharmD; and Blanca Vazquez, MD
Recommendations for the care of women with epilepsy
Patricia E. Penovich, MD; Karen E. Eck, MS, FNP; and Vasiliki V. Economou, MD