User login
Hereditary hemochromatosis: Molecular genetic testing issues for the clinician
A 52-year-old man with excessive daytime sleepiness
Which is more effective for as-needed treatment of seasonal allergy symptoms: intranasal corticosteroids or oral antihistamines?
ABSTRACT
BACKGROUND: Symptoms resulting from early response to allergen exposure are histamine mediated, last a few minutes, and often cue patients to take medication. Hours later, the late response begins and typically leads to symptoms of congestion. The late-phase response is not histamine mediated; other studies have shown intranasal corticosteroids to inhibit the response. The researchers tested the hypothesis that intranasal steroids may be as beneficial as or superior to antihistamines for as-needed use because of their effect on the late response to environmental allergens.
POPULATION STUDIED: The 88 subjects, aged 18 to 48 years, had fall seasonal rhinitis for at least 2 ragweed seasons before enrollment and had a positive puncture skin test to ragweed antigen extract. The population was 52% male, 60% white and in general good health. Patients were excluded for nasal polyps, displaced septum, perennial rhinitis, and signs or symptoms of renal, hepatic, or cardiovascular disease. Patients were also excluded if they had received immunotherapy within 2 years before enrollment or had taken topical or systemic steroids, antihistamines, decongestants, or cromolyn sodium within 2 weeks before enrollment.
STUDY DESIGN AND VALIDITY: This is a randomized unblinded study. Patients were enrolled before or during the early part of the ragweed season. They were randomized to receive 100 μg/day fluticasone propionate per nostril or 10 mg loratadine once daily as needed for 4 weeks. Nasal lavage for eosinophil count and eosinophil cationic protein (ECP) and completion of the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ, a validated instrument) were performed initially, at 2 weeks, and at 4 weeks. Patients were instructed to record medication usage and symptom severity in a diary twice daily. Itchy eyes and 3 symptoms for each nostril (rhinorrhea, nasal congestion, and sneezing) were rated on a scale of 0 to 3, ranging from 0 = no symptoms to 3 = severe symptoms.
OUTCOMES MEASURED: The RQLQ score was the primary outcome. The symptom diary scores were evaluated by symptom; a total symptom score was calculated. Other outcomes included nasal lavage eosinophil count and ECP levels.
RESULTS: Patients used medication an average of 17 of 28 days in the fluticasone group, similar to the average of 18 of 28 days in the loratadine group. The RQLQ scores were similar in the 2 groups initially. Significant improvement in the fluticasone group over the loratadine group was seen at the second and third visits in the overall score and activity, sleep, practical, and nasal domains of the RQLQ (P < .05). Symptom diaries showed a median score of 7.0 out of 21 for the loratadine-treated group and 4.0 out of 21 for the steroid-treated group (P = .005). Eosinophil count and ECP showed significant decreases in the steroid group.
This study shows that for as-needed treatment of allergic rhinitis, fluticasone propionate appears to be superior to loratadine in both subjective and objective measurements. A double-blind design would have strengthened our confidence in these results. Regular use of intranasal steroids has also been demonstrated to provide better symptom control than antihistamines do. The clinician may consider prescribing as-needed antihistamines or intranasal steroids for first-line treatment of allergic rhinitis.
ABSTRACT
BACKGROUND: Symptoms resulting from early response to allergen exposure are histamine mediated, last a few minutes, and often cue patients to take medication. Hours later, the late response begins and typically leads to symptoms of congestion. The late-phase response is not histamine mediated; other studies have shown intranasal corticosteroids to inhibit the response. The researchers tested the hypothesis that intranasal steroids may be as beneficial as or superior to antihistamines for as-needed use because of their effect on the late response to environmental allergens.
POPULATION STUDIED: The 88 subjects, aged 18 to 48 years, had fall seasonal rhinitis for at least 2 ragweed seasons before enrollment and had a positive puncture skin test to ragweed antigen extract. The population was 52% male, 60% white and in general good health. Patients were excluded for nasal polyps, displaced septum, perennial rhinitis, and signs or symptoms of renal, hepatic, or cardiovascular disease. Patients were also excluded if they had received immunotherapy within 2 years before enrollment or had taken topical or systemic steroids, antihistamines, decongestants, or cromolyn sodium within 2 weeks before enrollment.
STUDY DESIGN AND VALIDITY: This is a randomized unblinded study. Patients were enrolled before or during the early part of the ragweed season. They were randomized to receive 100 μg/day fluticasone propionate per nostril or 10 mg loratadine once daily as needed for 4 weeks. Nasal lavage for eosinophil count and eosinophil cationic protein (ECP) and completion of the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ, a validated instrument) were performed initially, at 2 weeks, and at 4 weeks. Patients were instructed to record medication usage and symptom severity in a diary twice daily. Itchy eyes and 3 symptoms for each nostril (rhinorrhea, nasal congestion, and sneezing) were rated on a scale of 0 to 3, ranging from 0 = no symptoms to 3 = severe symptoms.
OUTCOMES MEASURED: The RQLQ score was the primary outcome. The symptom diary scores were evaluated by symptom; a total symptom score was calculated. Other outcomes included nasal lavage eosinophil count and ECP levels.
RESULTS: Patients used medication an average of 17 of 28 days in the fluticasone group, similar to the average of 18 of 28 days in the loratadine group. The RQLQ scores were similar in the 2 groups initially. Significant improvement in the fluticasone group over the loratadine group was seen at the second and third visits in the overall score and activity, sleep, practical, and nasal domains of the RQLQ (P < .05). Symptom diaries showed a median score of 7.0 out of 21 for the loratadine-treated group and 4.0 out of 21 for the steroid-treated group (P = .005). Eosinophil count and ECP showed significant decreases in the steroid group.
This study shows that for as-needed treatment of allergic rhinitis, fluticasone propionate appears to be superior to loratadine in both subjective and objective measurements. A double-blind design would have strengthened our confidence in these results. Regular use of intranasal steroids has also been demonstrated to provide better symptom control than antihistamines do. The clinician may consider prescribing as-needed antihistamines or intranasal steroids for first-line treatment of allergic rhinitis.
ABSTRACT
BACKGROUND: Symptoms resulting from early response to allergen exposure are histamine mediated, last a few minutes, and often cue patients to take medication. Hours later, the late response begins and typically leads to symptoms of congestion. The late-phase response is not histamine mediated; other studies have shown intranasal corticosteroids to inhibit the response. The researchers tested the hypothesis that intranasal steroids may be as beneficial as or superior to antihistamines for as-needed use because of their effect on the late response to environmental allergens.
POPULATION STUDIED: The 88 subjects, aged 18 to 48 years, had fall seasonal rhinitis for at least 2 ragweed seasons before enrollment and had a positive puncture skin test to ragweed antigen extract. The population was 52% male, 60% white and in general good health. Patients were excluded for nasal polyps, displaced septum, perennial rhinitis, and signs or symptoms of renal, hepatic, or cardiovascular disease. Patients were also excluded if they had received immunotherapy within 2 years before enrollment or had taken topical or systemic steroids, antihistamines, decongestants, or cromolyn sodium within 2 weeks before enrollment.
STUDY DESIGN AND VALIDITY: This is a randomized unblinded study. Patients were enrolled before or during the early part of the ragweed season. They were randomized to receive 100 μg/day fluticasone propionate per nostril or 10 mg loratadine once daily as needed for 4 weeks. Nasal lavage for eosinophil count and eosinophil cationic protein (ECP) and completion of the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ, a validated instrument) were performed initially, at 2 weeks, and at 4 weeks. Patients were instructed to record medication usage and symptom severity in a diary twice daily. Itchy eyes and 3 symptoms for each nostril (rhinorrhea, nasal congestion, and sneezing) were rated on a scale of 0 to 3, ranging from 0 = no symptoms to 3 = severe symptoms.
OUTCOMES MEASURED: The RQLQ score was the primary outcome. The symptom diary scores were evaluated by symptom; a total symptom score was calculated. Other outcomes included nasal lavage eosinophil count and ECP levels.
RESULTS: Patients used medication an average of 17 of 28 days in the fluticasone group, similar to the average of 18 of 28 days in the loratadine group. The RQLQ scores were similar in the 2 groups initially. Significant improvement in the fluticasone group over the loratadine group was seen at the second and third visits in the overall score and activity, sleep, practical, and nasal domains of the RQLQ (P < .05). Symptom diaries showed a median score of 7.0 out of 21 for the loratadine-treated group and 4.0 out of 21 for the steroid-treated group (P = .005). Eosinophil count and ECP showed significant decreases in the steroid group.
This study shows that for as-needed treatment of allergic rhinitis, fluticasone propionate appears to be superior to loratadine in both subjective and objective measurements. A double-blind design would have strengthened our confidence in these results. Regular use of intranasal steroids has also been demonstrated to provide better symptom control than antihistamines do. The clinician may consider prescribing as-needed antihistamines or intranasal steroids for first-line treatment of allergic rhinitis.
In children hospitalized for asthma exacerbations, does adding ipratropium bromide to albuterol and corticosteroids improve outcome?
ABSTRACT
BACKGROUND: Adding 2 to 3 doses of ipratropium bromide (Atrovent) to conventional therapy with inhaled β-agonists and systemic corticosteroids improves lung function and decreases hospital admissions when given in the emergency department (ED). This study evaluated whether ipratropium bromide administration improves outcomes in children who require subsequent hospitalization.
POPULATION STUDIED: The authors enrolled 80 children aged 1 to 18 years with a history of asthma admitted to the pediatric inpatient unit of a tertiary-care urban hospital. Children had to have moderate to severe symptoms upon admission, defined as requiring inhaled β2-agonists at least every 2 hours, having a forced expiratory volume in 1 second (FEV1) of 25% to 80% of predicted, or having a clinical asthma score of 3 to 9 out of a possible 10. The clinical asthma score is a total of 5 items—respiratory rate, wheezing, inspiratory–expiratory ratio, retracting, and observed dyspnea—scored on a 3-point scale. Excluded patients had coexisting cardiac, neurologic, immunosuppressive, or other chronic pulmonary disease, hypersensitivity to the study drugs, or known ocular abnormalities. Children were excluded if their asthma score was 10, if they needed airway intervention, or if more than 12 hours had elapsed between the first nebulizer treatment and admission.
STUDY DESIGN AND VALIDITY: This was a double-blind randomized controlled trial. Study patients received frequent nebulized albuterol at 0.15 mg/kg as well as either IV hydrocortisone at 4 to 6 mg/kg every 6 hours or oral prednisone 1 mg/kg once daily. Attending physicians determined nebulizer treatment frequency, ranging from 30 minutes to 4 hours. Subjects were randomized to receive either ipratropium bromide or normal saline, matched to the albuterol dosing interval. Participants were stratified by age (less than 5 years vs 5 years or more) and by the number of ipratropium bromide doses they received in the ED (3 or less vs more than 3). Investigators used an intention-to-treat analysis and allocation was concealed.
OUTCOMES MEASURED: The primary outcome was the clinical asthma score, measured at baseline and every 6 hours until discharge. The clinical score is reproducible, valid, and predictive. Secondary outcomes included oxygen saturation, FEV1, length of stay, time to a 4-hour albuterol dosing interval, and readmission to the hospital or ED within 72 hours of discharge.
RESULTS: Of the 212 patients assessed for the trial, only 99 were eligible. Of these, 84 parents consented to enroll their children (4 children were later determined not to meet inclusion criteria and were excluded). The ipratropium and placebo groups were essentially the same. There was no difference in the asthma score between treatment and control groups in 3 of the 4 subgroups. In one subgroup—those who had fewer than 3 doses of ipratropium bromide in the ED—ipratropium provided a slight benefit. The difference in change in scores was 0.5 on the clinical asthma score, a statistically but not clinically important change. There were no differences in the secondary outcomes. The average heart rate was 6 to 10 beats per minute greater in the ipratropium group. The authors noted no transient anisocoria, a potential adverse effect of ipratropium bromide in children.
Giving ipratropium bromide to children with moderate to severe asthma exacerbations reduces admissions and asthma symptoms when given with appropriate β-agonists and corticosteroids in the ED. Ipratropium bromide provides no further benefit for children who require hospitalization after receiving the drug in the ED; therefore, adding ipratropium bromide to standard in-hospital care is not beneficial.
ABSTRACT
BACKGROUND: Adding 2 to 3 doses of ipratropium bromide (Atrovent) to conventional therapy with inhaled β-agonists and systemic corticosteroids improves lung function and decreases hospital admissions when given in the emergency department (ED). This study evaluated whether ipratropium bromide administration improves outcomes in children who require subsequent hospitalization.
POPULATION STUDIED: The authors enrolled 80 children aged 1 to 18 years with a history of asthma admitted to the pediatric inpatient unit of a tertiary-care urban hospital. Children had to have moderate to severe symptoms upon admission, defined as requiring inhaled β2-agonists at least every 2 hours, having a forced expiratory volume in 1 second (FEV1) of 25% to 80% of predicted, or having a clinical asthma score of 3 to 9 out of a possible 10. The clinical asthma score is a total of 5 items—respiratory rate, wheezing, inspiratory–expiratory ratio, retracting, and observed dyspnea—scored on a 3-point scale. Excluded patients had coexisting cardiac, neurologic, immunosuppressive, or other chronic pulmonary disease, hypersensitivity to the study drugs, or known ocular abnormalities. Children were excluded if their asthma score was 10, if they needed airway intervention, or if more than 12 hours had elapsed between the first nebulizer treatment and admission.
STUDY DESIGN AND VALIDITY: This was a double-blind randomized controlled trial. Study patients received frequent nebulized albuterol at 0.15 mg/kg as well as either IV hydrocortisone at 4 to 6 mg/kg every 6 hours or oral prednisone 1 mg/kg once daily. Attending physicians determined nebulizer treatment frequency, ranging from 30 minutes to 4 hours. Subjects were randomized to receive either ipratropium bromide or normal saline, matched to the albuterol dosing interval. Participants were stratified by age (less than 5 years vs 5 years or more) and by the number of ipratropium bromide doses they received in the ED (3 or less vs more than 3). Investigators used an intention-to-treat analysis and allocation was concealed.
OUTCOMES MEASURED: The primary outcome was the clinical asthma score, measured at baseline and every 6 hours until discharge. The clinical score is reproducible, valid, and predictive. Secondary outcomes included oxygen saturation, FEV1, length of stay, time to a 4-hour albuterol dosing interval, and readmission to the hospital or ED within 72 hours of discharge.
RESULTS: Of the 212 patients assessed for the trial, only 99 were eligible. Of these, 84 parents consented to enroll their children (4 children were later determined not to meet inclusion criteria and were excluded). The ipratropium and placebo groups were essentially the same. There was no difference in the asthma score between treatment and control groups in 3 of the 4 subgroups. In one subgroup—those who had fewer than 3 doses of ipratropium bromide in the ED—ipratropium provided a slight benefit. The difference in change in scores was 0.5 on the clinical asthma score, a statistically but not clinically important change. There were no differences in the secondary outcomes. The average heart rate was 6 to 10 beats per minute greater in the ipratropium group. The authors noted no transient anisocoria, a potential adverse effect of ipratropium bromide in children.
Giving ipratropium bromide to children with moderate to severe asthma exacerbations reduces admissions and asthma symptoms when given with appropriate β-agonists and corticosteroids in the ED. Ipratropium bromide provides no further benefit for children who require hospitalization after receiving the drug in the ED; therefore, adding ipratropium bromide to standard in-hospital care is not beneficial.
ABSTRACT
BACKGROUND: Adding 2 to 3 doses of ipratropium bromide (Atrovent) to conventional therapy with inhaled β-agonists and systemic corticosteroids improves lung function and decreases hospital admissions when given in the emergency department (ED). This study evaluated whether ipratropium bromide administration improves outcomes in children who require subsequent hospitalization.
POPULATION STUDIED: The authors enrolled 80 children aged 1 to 18 years with a history of asthma admitted to the pediatric inpatient unit of a tertiary-care urban hospital. Children had to have moderate to severe symptoms upon admission, defined as requiring inhaled β2-agonists at least every 2 hours, having a forced expiratory volume in 1 second (FEV1) of 25% to 80% of predicted, or having a clinical asthma score of 3 to 9 out of a possible 10. The clinical asthma score is a total of 5 items—respiratory rate, wheezing, inspiratory–expiratory ratio, retracting, and observed dyspnea—scored on a 3-point scale. Excluded patients had coexisting cardiac, neurologic, immunosuppressive, or other chronic pulmonary disease, hypersensitivity to the study drugs, or known ocular abnormalities. Children were excluded if their asthma score was 10, if they needed airway intervention, or if more than 12 hours had elapsed between the first nebulizer treatment and admission.
STUDY DESIGN AND VALIDITY: This was a double-blind randomized controlled trial. Study patients received frequent nebulized albuterol at 0.15 mg/kg as well as either IV hydrocortisone at 4 to 6 mg/kg every 6 hours or oral prednisone 1 mg/kg once daily. Attending physicians determined nebulizer treatment frequency, ranging from 30 minutes to 4 hours. Subjects were randomized to receive either ipratropium bromide or normal saline, matched to the albuterol dosing interval. Participants were stratified by age (less than 5 years vs 5 years or more) and by the number of ipratropium bromide doses they received in the ED (3 or less vs more than 3). Investigators used an intention-to-treat analysis and allocation was concealed.
OUTCOMES MEASURED: The primary outcome was the clinical asthma score, measured at baseline and every 6 hours until discharge. The clinical score is reproducible, valid, and predictive. Secondary outcomes included oxygen saturation, FEV1, length of stay, time to a 4-hour albuterol dosing interval, and readmission to the hospital or ED within 72 hours of discharge.
RESULTS: Of the 212 patients assessed for the trial, only 99 were eligible. Of these, 84 parents consented to enroll their children (4 children were later determined not to meet inclusion criteria and were excluded). The ipratropium and placebo groups were essentially the same. There was no difference in the asthma score between treatment and control groups in 3 of the 4 subgroups. In one subgroup—those who had fewer than 3 doses of ipratropium bromide in the ED—ipratropium provided a slight benefit. The difference in change in scores was 0.5 on the clinical asthma score, a statistically but not clinically important change. There were no differences in the secondary outcomes. The average heart rate was 6 to 10 beats per minute greater in the ipratropium group. The authors noted no transient anisocoria, a potential adverse effect of ipratropium bromide in children.
Giving ipratropium bromide to children with moderate to severe asthma exacerbations reduces admissions and asthma symptoms when given with appropriate β-agonists and corticosteroids in the ED. Ipratropium bromide provides no further benefit for children who require hospitalization after receiving the drug in the ED; therefore, adding ipratropium bromide to standard in-hospital care is not beneficial.
How often is coughing the presenting complaint in patients with gastroesophageal reflux disease?
Frequent coughing is a concern for approximately 35% of those with typical gastroesophageal reflux disease (GERD) symptoms of heartburn and acid regurgitation as compared with 11% in those who do not have these symptoms. Among pulmonary clinic patients with complaints of chronic cough, GERD may be the underlying cause in 40%. (Grade of recommendation: C, based on extrapolation from cohort studies.) However, no studies directly address prevalence of coughing as a presenting complaint in patients with GERD.
Evidence summary
While many sources state that extraesophageal symptoms (eg, cough, chest pain, asthma) are reported by patients with GERD, only one study reported the frequency of associated symptoms.1 This population-based survey showed that symptoms of reflux and acid regurgitation are experienced by almost 60% of the population each year. The prevalence of frequent heartburn and acid reflux was approximately 20%. Bronchitis, defined as cough that occurs as often as 4 to 6 times per day on 4 or more days per week, was reported by more than 20% of those with frequent typical GERD symptoms (occurring at least weekly) and by 15% of those with infrequent GERD symptoms. Interestingly, bronchitis was reported by almost 11% of those without GERD. This study showed the association of cough with GERD but did not address whether the cough was the initial presenting complaint.
In as many as 40% of patients with cough, GERD is the underlying cause.2-7 Chronic cough may be triggered by more than one condition (eg, GERD, postnasal drip, or asthma) in 18% to 93% of patients.8 Among patients with cough caused by GERD, 50% to 75% do not have classic symptoms of reflux or regurgitation.9 Finally, cough may initiate GERD and start a cough–reflux cycle.9 These studies were conducted in pulmonary clinics. Patients with cough whose underlying GERD was easily diagnosed and treated by their primary physician were probably not referred for evaluation in a pulmonary clinic.
Recommendations from others
The American College of Chest Physicians issued a consensus statement in 1999 regarding the management of cough.10 According to the statement, GERD should be strongly suspected in coughing patients with upper GI symptoms or in those without GI symptoms who have normal chest radiographs, do not smoke, and do not take angiotensin-converting enzyme inhibitors. The statement reports that asthma, postnasal drip syndrome (PNDS), and GERD are the causes of cough in nearly 100% of these patients. The recommendation for evaluation of GERD is a 24-hour pH monitor or an empiric trial of antireflux medication after ruling out asthma and PNDS.
Les W. Hall, MD
Department of Internal Medicine University of Missouri Columbia
Most studies of patients with chronic cough find GERD to be among the top 3 causes of this condition. Although many of these patients report other symptoms of reflux, cough is the sole symptom in some. Monitoring of esophageal pH for 24 hours is considered the gold standard for diagnosis of GERD, but limited availability and variable patient acceptance diminish the universal application of this method. A trial of intensive antireflux therapy may represent a cost-effective and practical approach to such patients, since cough from GERD may take up to 3 months to improve under such a regimen.
1. Locke GR, III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ. Gastroenterology 1997;112:1448-56.
2. Irwin RS, Curley FJ, French CL. Am Rev Respir Dis 1990;141:640-7.
3. Irwin RS, Corrao WM, Pratter MR. Am Rev Respir Dis 1981;123:413-7.
4. Mello CJ, Irwin RS, Curley FJ. Arch Intern Med 1996;156:997-1003.
5. Poe RH, Israel RH, Utell MJ, Hall WJ. Am Rev Respir Dis 1982;126:160-2.
6. Poe RH, Harder RV, Israel RH, Kallay MC. Chest 1989;95:723-8.
7. Pratter MR, Bartter T, Akers S, Dubois J. Ann Intern Med 1993;119:977-83.
8. Irwin RS, Richter JE. Am J Gastroenterol 2000;95:S9-S14.
9. Ing AJ. Am J Med 1997;103:91S-96S.
10. Irwin RS, Boulet LP, Cloutier MM, et al. Chest 1998;114:133S-181S.
Frequent coughing is a concern for approximately 35% of those with typical gastroesophageal reflux disease (GERD) symptoms of heartburn and acid regurgitation as compared with 11% in those who do not have these symptoms. Among pulmonary clinic patients with complaints of chronic cough, GERD may be the underlying cause in 40%. (Grade of recommendation: C, based on extrapolation from cohort studies.) However, no studies directly address prevalence of coughing as a presenting complaint in patients with GERD.
Evidence summary
While many sources state that extraesophageal symptoms (eg, cough, chest pain, asthma) are reported by patients with GERD, only one study reported the frequency of associated symptoms.1 This population-based survey showed that symptoms of reflux and acid regurgitation are experienced by almost 60% of the population each year. The prevalence of frequent heartburn and acid reflux was approximately 20%. Bronchitis, defined as cough that occurs as often as 4 to 6 times per day on 4 or more days per week, was reported by more than 20% of those with frequent typical GERD symptoms (occurring at least weekly) and by 15% of those with infrequent GERD symptoms. Interestingly, bronchitis was reported by almost 11% of those without GERD. This study showed the association of cough with GERD but did not address whether the cough was the initial presenting complaint.
In as many as 40% of patients with cough, GERD is the underlying cause.2-7 Chronic cough may be triggered by more than one condition (eg, GERD, postnasal drip, or asthma) in 18% to 93% of patients.8 Among patients with cough caused by GERD, 50% to 75% do not have classic symptoms of reflux or regurgitation.9 Finally, cough may initiate GERD and start a cough–reflux cycle.9 These studies were conducted in pulmonary clinics. Patients with cough whose underlying GERD was easily diagnosed and treated by their primary physician were probably not referred for evaluation in a pulmonary clinic.
Recommendations from others
The American College of Chest Physicians issued a consensus statement in 1999 regarding the management of cough.10 According to the statement, GERD should be strongly suspected in coughing patients with upper GI symptoms or in those without GI symptoms who have normal chest radiographs, do not smoke, and do not take angiotensin-converting enzyme inhibitors. The statement reports that asthma, postnasal drip syndrome (PNDS), and GERD are the causes of cough in nearly 100% of these patients. The recommendation for evaluation of GERD is a 24-hour pH monitor or an empiric trial of antireflux medication after ruling out asthma and PNDS.
Les W. Hall, MD
Department of Internal Medicine University of Missouri Columbia
Most studies of patients with chronic cough find GERD to be among the top 3 causes of this condition. Although many of these patients report other symptoms of reflux, cough is the sole symptom in some. Monitoring of esophageal pH for 24 hours is considered the gold standard for diagnosis of GERD, but limited availability and variable patient acceptance diminish the universal application of this method. A trial of intensive antireflux therapy may represent a cost-effective and practical approach to such patients, since cough from GERD may take up to 3 months to improve under such a regimen.
Frequent coughing is a concern for approximately 35% of those with typical gastroesophageal reflux disease (GERD) symptoms of heartburn and acid regurgitation as compared with 11% in those who do not have these symptoms. Among pulmonary clinic patients with complaints of chronic cough, GERD may be the underlying cause in 40%. (Grade of recommendation: C, based on extrapolation from cohort studies.) However, no studies directly address prevalence of coughing as a presenting complaint in patients with GERD.
Evidence summary
While many sources state that extraesophageal symptoms (eg, cough, chest pain, asthma) are reported by patients with GERD, only one study reported the frequency of associated symptoms.1 This population-based survey showed that symptoms of reflux and acid regurgitation are experienced by almost 60% of the population each year. The prevalence of frequent heartburn and acid reflux was approximately 20%. Bronchitis, defined as cough that occurs as often as 4 to 6 times per day on 4 or more days per week, was reported by more than 20% of those with frequent typical GERD symptoms (occurring at least weekly) and by 15% of those with infrequent GERD symptoms. Interestingly, bronchitis was reported by almost 11% of those without GERD. This study showed the association of cough with GERD but did not address whether the cough was the initial presenting complaint.
In as many as 40% of patients with cough, GERD is the underlying cause.2-7 Chronic cough may be triggered by more than one condition (eg, GERD, postnasal drip, or asthma) in 18% to 93% of patients.8 Among patients with cough caused by GERD, 50% to 75% do not have classic symptoms of reflux or regurgitation.9 Finally, cough may initiate GERD and start a cough–reflux cycle.9 These studies were conducted in pulmonary clinics. Patients with cough whose underlying GERD was easily diagnosed and treated by their primary physician were probably not referred for evaluation in a pulmonary clinic.
Recommendations from others
The American College of Chest Physicians issued a consensus statement in 1999 regarding the management of cough.10 According to the statement, GERD should be strongly suspected in coughing patients with upper GI symptoms or in those without GI symptoms who have normal chest radiographs, do not smoke, and do not take angiotensin-converting enzyme inhibitors. The statement reports that asthma, postnasal drip syndrome (PNDS), and GERD are the causes of cough in nearly 100% of these patients. The recommendation for evaluation of GERD is a 24-hour pH monitor or an empiric trial of antireflux medication after ruling out asthma and PNDS.
Les W. Hall, MD
Department of Internal Medicine University of Missouri Columbia
Most studies of patients with chronic cough find GERD to be among the top 3 causes of this condition. Although many of these patients report other symptoms of reflux, cough is the sole symptom in some. Monitoring of esophageal pH for 24 hours is considered the gold standard for diagnosis of GERD, but limited availability and variable patient acceptance diminish the universal application of this method. A trial of intensive antireflux therapy may represent a cost-effective and practical approach to such patients, since cough from GERD may take up to 3 months to improve under such a regimen.
1. Locke GR, III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ. Gastroenterology 1997;112:1448-56.
2. Irwin RS, Curley FJ, French CL. Am Rev Respir Dis 1990;141:640-7.
3. Irwin RS, Corrao WM, Pratter MR. Am Rev Respir Dis 1981;123:413-7.
4. Mello CJ, Irwin RS, Curley FJ. Arch Intern Med 1996;156:997-1003.
5. Poe RH, Israel RH, Utell MJ, Hall WJ. Am Rev Respir Dis 1982;126:160-2.
6. Poe RH, Harder RV, Israel RH, Kallay MC. Chest 1989;95:723-8.
7. Pratter MR, Bartter T, Akers S, Dubois J. Ann Intern Med 1993;119:977-83.
8. Irwin RS, Richter JE. Am J Gastroenterol 2000;95:S9-S14.
9. Ing AJ. Am J Med 1997;103:91S-96S.
10. Irwin RS, Boulet LP, Cloutier MM, et al. Chest 1998;114:133S-181S.
1. Locke GR, III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ. Gastroenterology 1997;112:1448-56.
2. Irwin RS, Curley FJ, French CL. Am Rev Respir Dis 1990;141:640-7.
3. Irwin RS, Corrao WM, Pratter MR. Am Rev Respir Dis 1981;123:413-7.
4. Mello CJ, Irwin RS, Curley FJ. Arch Intern Med 1996;156:997-1003.
5. Poe RH, Israel RH, Utell MJ, Hall WJ. Am Rev Respir Dis 1982;126:160-2.
6. Poe RH, Harder RV, Israel RH, Kallay MC. Chest 1989;95:723-8.
7. Pratter MR, Bartter T, Akers S, Dubois J. Ann Intern Med 1993;119:977-83.
8. Irwin RS, Richter JE. Am J Gastroenterol 2000;95:S9-S14.
9. Ing AJ. Am J Med 1997;103:91S-96S.
10. Irwin RS, Boulet LP, Cloutier MM, et al. Chest 1998;114:133S-181S.
Evidence-based answers from the Family Physicians Inquiries Network
What to do if you—or a patient—is a victim of stalking
About 1.4 million people are stalked each year in the United States.1 Chances are you or one of your patients have been among that statistic.
In the U.S., 8% to 12 % of adult women and 2% to 4% of adult men have been stalked at some point in their lives.2 While celebrities and politicians tend to be high-profile targets, psychiatrists and other health-care professionals may find themselves subject to unwanted contact or obsessive pursuit; this may be because psychiatrists are perceived to be warm, caring, or nurturing. Also, mental health professionals regularly see patients who are particularly prone to engaging in stalking behaviors.
As a former forensic psychiatry fellow, I have studied the risks and patterns of stalking in an effort to help victims of stalkers protect themselves and use legal remedies when appropriate.
The objectives of this article are threefold:
- To identify the unique problem of a patient stalking a psychiatrist and how to cope.
- To address what every stalking victim (including a patient) can do to protect herself or himself.
- To provide basic definitions of stalking and to outline the current, most widely accepted clinical classification of stalkers and its relevance in predicting the stalker’s response to legal and/or mental health interventions. All 50 states and the District of Columbia have passed laws specifically criminalizing stalking.3
When a psychiatrist is stalked
In her book, I Know You Really Love Me,4 psychiatrist Doreen Orion, MD, recounts her experience as a stalking victim. Her victimization began in 1989, when she was on night call for a psychiatric hospital in Arizona. One of the patients she admitted that night was Fran, who developed the erotomanic delusion that Dr. Orion loved her. Despite all evidence to the contrary, Fran pursued Dr. Orion for nearly 8 years, even following her to another state.
Dr. Orion’s book illustrates several issues of import, starting with a crucial failure to communicate. The following morning, Dr. Orion went to the psychiatric hospital to evaluate the patients she had admitted the night before. She contacted Fran’s treating psychiatrist, who angrily hung up on Dr. Orion because Fran had been admitted to the “wrong hospital.” He neglected to inform Dr. Orion that Fran had a history of same-sex stalking and erotomanic delusions. Had she been informed of Fran’s stalking patterns. Dr. Orion may have then simply transferred Fran’s care to a male colleague.
Ultimately, some of Dr. Orion’s colleagues viewed her as somehow inviting or being at fault for her stalking victimization. This classic “blaming the victim” aggravated a situation that was already maddening enough. (Eventually, after several legal and psychiatric evaluations, the stalking stopped.)
Dr. Orion’s book is a cautionary tale. Knowing the patient’s history by reviewing prior records and contacting former treating clinicians can uncover a past pattern of stalking. However, as we are well aware today, terrorists may not become known as such until their first terrorist act; with stalkers, a previous pattern may not be apparent in some cases.
It is important to recognize stalking behaviors for what they are and to act quickly. As psychiatrists, we may be more able than other clinicians to do this because we are trained to ask the patient questions, then simultaneously observe and monitor both the patient’s behavior and our reactions to it. Gavin DeBecker’s book, The Gift of Fear,5 details the survival properties of being in tune with one’s fear response as protective.
Typically, stalking has an insidious onset and may even seem initially harmless, perhaps noted as an erotic transference. But you must pay attention to the behavior and how it makes you feel. Be aware that it may escalate and be prepared to take measures to protect yourself.
Questions to ask yourself might include:
- What are your clinical impressions?
- Are axis I and/or axis II disorders present that may respond to treatment?
- Is your therapeutic relationship with the patient fairly new, or is this an established doctor-patient relationship?
- Is the patient an otherwise stable person who is under stress and engaging in uncharacteristic behavior?
Consider the answers carefully, bearing in mind the typology or typologies involved (Table 1). Stalking encompasses a continuum of unwanted behaviors, ranging from the innocuous to overt and harmful stalking. Your clinical decision-making depends on the typology and intensity of the behavior, as well as your own tolerance for such behaviors.
Table 1
STALKER CLASSIFICATION SYSTEM*
| Type | Features | Assault potential | Response to legal interventions | Response to mental health interventions |
|---|---|---|---|---|
| Rejected | Response to an unwelcome end to relationship Seeks to maintain the relationship Long duration | Along with Predatory, the most likely to assault | Will usually curb behaviors | Typically not responsive to therapy |
| Resentful | Response to a perceived insult Seeks vindication Self-righteous and self-pitying | Most likely to threaten, least likely to assault | Will usually stop behaviors | Difficult to engage in therapy Focus on ruminations that drive stalkers |
| Intimacy seeking | Belief that they are loved or will be loved by the victim Satisfies need for contact and feeds fantasies of eventual loving relationship | May assault | Impervious to legal interventions | If erotomanic delusions are present, they are resistive to change |
| Incompetent | Intellectually limited Socially incompetent Desires intimacy but lacks sufficient skills in courting rituals | Low assault potential | Will stop Typically has previous stalking victims Responsive to restraining orders | May benefit from basic social skills and courting rituals education |
| Predatory | Desire is for sexual gratification and control Rehearsal for violent sexual fantasies and satisfaction of voyeuristic and sadistic desires | High assault potential | Cannot determine before an attack | Poor candidate for therapy |
| *Mullen P, Pathe M, Purcell R, Stuart G. Study of Stalkers. Am J Psychiatry. 1999; 156:1244-1249. | ||||
Interestingly, a female patient also exhibited unwanted behavior toward Dr. Orion’s psychiatrist husband. This patient frequently parked in front of their home in the evenings. Unlike Fran, whose stalking behaviors became increasingly intrusive, frightening, and violent, this patient did not escalate her behavior. It was an unwanted intrusion, but he did not feel fearful or victimized by it. Therefore, it didn’t meet the clinical or legal definition of stalking—the unwanted behaviors must produce fear in the victim. Another psychiatrist, however, might consider the same scenario to be fearful.
Terminating the therapeutic relationship
Once you have reviewed the case with a colleague and/or a threat-assessment professional and determined that you feel uncomfortable and unsafe, it’s time to terminate the doctor-patient relationship.
Ethical and professional care dictates that you provide the patient with a reasonable written notice (e.g., 30 days) prior to termination. Three referral options with phone numbers are typically provided. This also protects you from a potential malpractice tort of abandonment while the patient still needs treatment. If you sense possibly imminent danger, however, you may need to abbreviate the 30-day notice.
Write a summary note in the patient’s chart that includes, in addition to the usual case summary components, the following:
- Your reason(s) for termination. Include discussion with colleagues and/or threat assessment or law enforcement professionals;
- Your diagnostic and treatment impressions, the treatment provided, and the patient’s response to treatment;
- Your referral choices and the rationale for those decisions, e.g., “female patient with schizophrenia and erotomanic delusions and a history of same-sex stalking referred to a male psychiatrist.” The referral should be made to an outside agency or system. (Once Dr. Orion realized that she was being stalked, she initially made the mistake of transferring her patient to a male colleague who shared her office suite, thus making it easy for Fran to continue to stalk Dr. Orion in her own office.)
- Documentation of your discussion with professionals to whom you are referring the patient, along with the patient’s release of information permitting you to do so.
- Documentation of your discussion with the patient. If applicable, include your statement that you feel it is in the patient’s best interest to continue psychiatric care.
- A copy of the termination letter.
If the stalking persists, the psychiatrist should follow guidelines for victims provided later in this article.
J.P. and his ‘ex-girlfriend’
J.P., 19, met Ms. T. when both were 16 and still in high school. Ms. T. was a “partying friend”; they smoked pot together and “hung out.” Although they never dated nor had a romantic relationship, J.P. found Ms. T. to be “pretty and fun,” and developed secret romantic feelings for her.
In their senior year, J.P. wrote Ms. T. a letter professing his love for her. She laughed at it, was dismissive of his feelings, and shared it with friends. He subsequently felt humiliated and rejected and, in retaliation, began spreading rumors that she was a “witch” and a “lesbian.”
After their graduation, they saw each other on a few occasions at parties, but rarely spoke. About a year and a half later, J.P. saw Ms T. with a man he had once fought. He regarded this man as “no good” and a poor choice on Ms. T.’s part. He obtained her phone number from one of their mutual high school acquaintances and called her. They spoke briefly; he accused her of “using drugs and dating an asshole.”
In Ohio, the legal definition of menacing by stalking* includes:
- Engaging in a pattern of conduct that knowingly causes another to believe that the offender will cause physical harm to the other person or cause mental distress to the other person
- A first-degree misdemeanor or fourth-degree felony
Clinical definitions of stalking include:
- The willful, malicious, and repeated following and harassing of another person that threatens his or her safety
- Repeated and persistent unwanted communications and/or approaches that produce fear in the victim
Unwanted communications or behaviors that a stalker might engage in:
- Sending letters
- Phone calls
- E-mails
- Appearing at victim’s home or workplace
- Destroying property
- Assault
- Murder
Typical profile of a stalker:
- Male
- Unemployed or underemployed
- Single or divorced
- Criminal, psychiatric, and drug abuse history
- High school or college education
- Significantly more intelligent than other criminals
- Suffered loss of primary caretaker in childhood
- Significant loss, usually of a job or relationship, within a year of the onset of stalking
*Ohio revised code. Sec. 2903.211
- Whether to change a phone line. One recommendation is to maintain the phone line with an answering machine turned down and let the stalker call it. The victim then obtains another phone line and gives the number only to select friends, colleagues, etc. This way the stalker has a venue for self-expression but the victim does not have to listen to it. Law enforcement can be given the tapes for review. By allowing the stalker continued access to the phone line, the stalker does not have to seek out other potentially more violent ways to pursue his or her victim.
- Whether to seek a restraining order. There is some disagreement on whether restraining orders are useful. In some cases, a restraining order may escalate the situation, such as with prior intimates. In other situations, it may give the victim a false sense of security and ultimately may be of little use if the stalker violates it. When the stalker violates a restraining order and experiences no significant painful consequences, this can increase his sense of power and correspondingly reduce that of the victim.
Source: www.stalkingassistance.com
Thus began a pattern of unwanted phone calls and letters left through the mail slot of her parents’ front door and on her car windshield. One letter featured a drawing of 2 tombstones, one with his name and one with hers, with R.I.P. (Rot In Pieces) scrawled below her tombstone. When asked how he thought she might respond to this, J.P. shrugged and explained it was “funny.” He claimed he was “just imitating Eminem,” a well-known “badboy” rapper who has a similar tattoo on his abdomen.
One letter indicated his desire to become a professional baseball player and his belief that if he had her love, he could succeed at this endeavor. He seemed unaffected by her lack of interest in him.
The situation escalated further when J.P. coincidentally showed up at a downtown club on a night when Ms. T. and her boyfriend were there. The boyfriend (the same one that J.P. had criticized Ms. T. for becoming involved with) hit J.P. A fight ensued; both men were thrown out of the club.
Complicating J.P.’s problems was his ongoing substance abuse including marijuana, alcohol, and weekend ecstasy (MDMA, a mixed hallucinogen/amphetaminelike drug). J.P. had also complained to a psychiatrist of attention-deficit/hyperactivity disorder-like symptoms and was placed on an amphetamine, which he also abused, according to his mother. Finally, the removal of his wisdom teeth necessitated a codeine prescription for pain, which he overused.
J.P. presented to the psychiatric emergency room with full-blown psychosis, about 2 months after he allegedly began stalking Ms. T. He reported paranoid ideations, i.e., communications through the TV and computer, male coworkers reading his mind, and thoughts of killing his “ex-girlfriend” (a misnomer describing Ms. T.).
J.P. was hospitalized and placed on antipsychotic and mood-stabilizing medications, quickly recompensated and was discharged. Diagnostically, he had a myriad of rule-outs at the time and was discharged on mood stabilizing and antipsychotic medications.
Mediation was attempted in an effort to end the stalking, but J.P. appeared “disorganized” and alarmed both Ms. T. and her parents. J.P. then was scheduled for a court trial and underwent a court-ordered psychiatric evaluation. He did not qualify to plead not guilty by reason of insanity as defined by Ohio statute.
J.P. was found guilty of menacing by stalking and was sentenced to a year probation. He was ordered to continue psychiatric treatment and was barred from any contact with the victim. To my knowledge, the stalking has stopped.
What this case illustrates
Stalking is not a new crime; it has been around for centuries.6 But what was once romanticized as a persistent and devoted lover’s pursuit is now considered intrusive and a violation of an individual’s basic right to be left alone.7 See Box 1 for legal and clinical definitions of stalking.
In the case vignette, Ms. T. made several good choices that are in line with current recommendations for stalking victims. She did:
List each event of stalking behavior, recording its nature according the keys indicated below. Make a copy of this record on a regular basis for a family member or trusted professional.
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:________________________________________________________________
Witnesses:_____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:_______________________________________________________________
Witnesses:____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:____________Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):__________________________________________________
Place:_________________________________________________________________
Witnesses:_____________________________________________________________
_____________________________________________________________________
Description:____________________________________________________________
_____________________________________________________________________
Stalking Behaviors Key:
Ph = Phone Calling PD = Property Damage L = Letters T = Threats F = Following K = Kidnapping
E = E-mail G = Gift NV = Non-Violent Threats A = Assault SV = Surveillance SL = Defamation/Slander
List Emergency Numbers:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
Source: www.stalkingbehavior.com
- Inform neighbors and friends and provide them a description of the stalker;
- Screen calls and block calls from his number (Box 2);
- Notify police and file an affidavit against him (Box 2);
- Buy new locks and secure her doors with deadbolts;
- Add exterior and motion-detector lighting;
- Document and record all incidents involving the stalker, and save all unwanted correspondence (e.g., letters) from him.
But Ms. T. also made some poor choices contrary to current recommendations. She did not:
- End all contact and communication with the stalker; instead she tried to be nice (after all, they were old high school friends) and to chat with him superficially. This encouraged his continued stalking behaviors.
- Refuse to attend the proposed mediation process. This illustrates a lack of understanding of stalking. Her attendance unwittingly reinforced the stalker and failed to curb his behaviors.
You must take into consideration the stalker’s typology, which will aid in predicting his or her likely response to legal intervention. Several stalker classification systems have been devised. The one created by Mullen et al (Table 1) is most widely accepted at this time. It is based on:
- The stalker’s motivation;
- His or her prior relationship with the victim;
- Whether the stalker is psychotic.
Knowing the typology can help determine the risk to victims and guide effective and protective victim responses. Typologies may overlap. Both psychotic and nonpsychotic stalkers are equally likely to threaten, but nonpsychotic stalkers are twice as likely to assault.
Restraining orders typically do not sway intimacy-seeking and delusional stalkers. In fact, stalkers may view restraining orders merely as obstacles they must overcome in order to achieve union with their beloved. A restraining order might work in some instances but it is wise to know the law in your state and what steps law enforcement will actually take if the order is violated. If the violation results in just a citation, not arrest or incarceration, it probably isn’t worth the trouble. Even if the law takes further steps, it is typically for a brief time and the action may ultimately enrage the stalker and escalate him to a violent act. Violent episodes are typically not preceded by a specific threat.8
Aside from law enforcement, publicly funded and private threat-assessment teams are located throughout the country. [See “Related resources,” below.] These can help you review the stalking situation in detail and arrive at the most effective response.
Finally, it is important to document the stalking behaviors in order to establish a pattern of conduct that could later be used to prosecute the stalker. Written documentation can be detailed in a log book (Box 3). Saving all physical evidence such as letters, gifts, objects, and e-mails can help establish a pattern of stalking behaviors.
- National Organization for Victim Assistance (NOVA) 1757 Park Rd., NW Washington, DC 20010 (800) 879-6682 or (202) 232-6682.
- National Center for Victims of Crime www.ncvc.org (703) 276-2880
- Stalking Behavior. www.stalkingbehavior.com
- The Stalking Assistance Site. www.stalkingassistance.com
- National Victim Center help guide for stalking victims http://www.ojp.usdoj.gov/ovc/assist/nvaa/ch21-2st.htm
1. The Stalking Assistance Site home page. www.stalkingassistance.com.
2. Tjaden P. The crime of stalking: how big is the problem? Washington, DC, U.S. Department of Justice, National Institute of Justice, Nov. 1977. Call The National Criminal Justice Reference Service at (800) 851-3420, ask for NCJ# FS 000186.
3. U.S. Department of Justice Report to Congress on Stalking and Domestic Violence, May 2001.
4. Orion D. I Know You Really Love Me: A Psychiatrist’s Account of Stalking and Obsessive Love. New York: Bantam Doubleday Dell Publishing Group, 1997.
5. deBecker G. The Gift of Fear (and Other Survival Strategies that Protect Us from Violence). Studio City, Calif: Gavin deBecker & Associates, www.gdbinc.com.
6. Meloy JR. Stalking: An old behavior, a new crime. Psychiatr Clin North Am. 1999;22(2):85-99.
7. Supreme Court Justice Brandeis, Olmstead v. United States, 227U.S.438 (1928).
8. Dietz P, Matthews D, et al. Threatening and otherwise inappropriate letters sent to members of the United States Congress. J Forensic Sci. 1991;36(5):1445-1468.
About 1.4 million people are stalked each year in the United States.1 Chances are you or one of your patients have been among that statistic.
In the U.S., 8% to 12 % of adult women and 2% to 4% of adult men have been stalked at some point in their lives.2 While celebrities and politicians tend to be high-profile targets, psychiatrists and other health-care professionals may find themselves subject to unwanted contact or obsessive pursuit; this may be because psychiatrists are perceived to be warm, caring, or nurturing. Also, mental health professionals regularly see patients who are particularly prone to engaging in stalking behaviors.
As a former forensic psychiatry fellow, I have studied the risks and patterns of stalking in an effort to help victims of stalkers protect themselves and use legal remedies when appropriate.
The objectives of this article are threefold:
- To identify the unique problem of a patient stalking a psychiatrist and how to cope.
- To address what every stalking victim (including a patient) can do to protect herself or himself.
- To provide basic definitions of stalking and to outline the current, most widely accepted clinical classification of stalkers and its relevance in predicting the stalker’s response to legal and/or mental health interventions. All 50 states and the District of Columbia have passed laws specifically criminalizing stalking.3
When a psychiatrist is stalked
In her book, I Know You Really Love Me,4 psychiatrist Doreen Orion, MD, recounts her experience as a stalking victim. Her victimization began in 1989, when she was on night call for a psychiatric hospital in Arizona. One of the patients she admitted that night was Fran, who developed the erotomanic delusion that Dr. Orion loved her. Despite all evidence to the contrary, Fran pursued Dr. Orion for nearly 8 years, even following her to another state.
Dr. Orion’s book illustrates several issues of import, starting with a crucial failure to communicate. The following morning, Dr. Orion went to the psychiatric hospital to evaluate the patients she had admitted the night before. She contacted Fran’s treating psychiatrist, who angrily hung up on Dr. Orion because Fran had been admitted to the “wrong hospital.” He neglected to inform Dr. Orion that Fran had a history of same-sex stalking and erotomanic delusions. Had she been informed of Fran’s stalking patterns. Dr. Orion may have then simply transferred Fran’s care to a male colleague.
Ultimately, some of Dr. Orion’s colleagues viewed her as somehow inviting or being at fault for her stalking victimization. This classic “blaming the victim” aggravated a situation that was already maddening enough. (Eventually, after several legal and psychiatric evaluations, the stalking stopped.)
Dr. Orion’s book is a cautionary tale. Knowing the patient’s history by reviewing prior records and contacting former treating clinicians can uncover a past pattern of stalking. However, as we are well aware today, terrorists may not become known as such until their first terrorist act; with stalkers, a previous pattern may not be apparent in some cases.
It is important to recognize stalking behaviors for what they are and to act quickly. As psychiatrists, we may be more able than other clinicians to do this because we are trained to ask the patient questions, then simultaneously observe and monitor both the patient’s behavior and our reactions to it. Gavin DeBecker’s book, The Gift of Fear,5 details the survival properties of being in tune with one’s fear response as protective.
Typically, stalking has an insidious onset and may even seem initially harmless, perhaps noted as an erotic transference. But you must pay attention to the behavior and how it makes you feel. Be aware that it may escalate and be prepared to take measures to protect yourself.
Questions to ask yourself might include:
- What are your clinical impressions?
- Are axis I and/or axis II disorders present that may respond to treatment?
- Is your therapeutic relationship with the patient fairly new, or is this an established doctor-patient relationship?
- Is the patient an otherwise stable person who is under stress and engaging in uncharacteristic behavior?
Consider the answers carefully, bearing in mind the typology or typologies involved (Table 1). Stalking encompasses a continuum of unwanted behaviors, ranging from the innocuous to overt and harmful stalking. Your clinical decision-making depends on the typology and intensity of the behavior, as well as your own tolerance for such behaviors.
Table 1
STALKER CLASSIFICATION SYSTEM*
| Type | Features | Assault potential | Response to legal interventions | Response to mental health interventions |
|---|---|---|---|---|
| Rejected | Response to an unwelcome end to relationship Seeks to maintain the relationship Long duration | Along with Predatory, the most likely to assault | Will usually curb behaviors | Typically not responsive to therapy |
| Resentful | Response to a perceived insult Seeks vindication Self-righteous and self-pitying | Most likely to threaten, least likely to assault | Will usually stop behaviors | Difficult to engage in therapy Focus on ruminations that drive stalkers |
| Intimacy seeking | Belief that they are loved or will be loved by the victim Satisfies need for contact and feeds fantasies of eventual loving relationship | May assault | Impervious to legal interventions | If erotomanic delusions are present, they are resistive to change |
| Incompetent | Intellectually limited Socially incompetent Desires intimacy but lacks sufficient skills in courting rituals | Low assault potential | Will stop Typically has previous stalking victims Responsive to restraining orders | May benefit from basic social skills and courting rituals education |
| Predatory | Desire is for sexual gratification and control Rehearsal for violent sexual fantasies and satisfaction of voyeuristic and sadistic desires | High assault potential | Cannot determine before an attack | Poor candidate for therapy |
| *Mullen P, Pathe M, Purcell R, Stuart G. Study of Stalkers. Am J Psychiatry. 1999; 156:1244-1249. | ||||
Interestingly, a female patient also exhibited unwanted behavior toward Dr. Orion’s psychiatrist husband. This patient frequently parked in front of their home in the evenings. Unlike Fran, whose stalking behaviors became increasingly intrusive, frightening, and violent, this patient did not escalate her behavior. It was an unwanted intrusion, but he did not feel fearful or victimized by it. Therefore, it didn’t meet the clinical or legal definition of stalking—the unwanted behaviors must produce fear in the victim. Another psychiatrist, however, might consider the same scenario to be fearful.
Terminating the therapeutic relationship
Once you have reviewed the case with a colleague and/or a threat-assessment professional and determined that you feel uncomfortable and unsafe, it’s time to terminate the doctor-patient relationship.
Ethical and professional care dictates that you provide the patient with a reasonable written notice (e.g., 30 days) prior to termination. Three referral options with phone numbers are typically provided. This also protects you from a potential malpractice tort of abandonment while the patient still needs treatment. If you sense possibly imminent danger, however, you may need to abbreviate the 30-day notice.
Write a summary note in the patient’s chart that includes, in addition to the usual case summary components, the following:
- Your reason(s) for termination. Include discussion with colleagues and/or threat assessment or law enforcement professionals;
- Your diagnostic and treatment impressions, the treatment provided, and the patient’s response to treatment;
- Your referral choices and the rationale for those decisions, e.g., “female patient with schizophrenia and erotomanic delusions and a history of same-sex stalking referred to a male psychiatrist.” The referral should be made to an outside agency or system. (Once Dr. Orion realized that she was being stalked, she initially made the mistake of transferring her patient to a male colleague who shared her office suite, thus making it easy for Fran to continue to stalk Dr. Orion in her own office.)
- Documentation of your discussion with professionals to whom you are referring the patient, along with the patient’s release of information permitting you to do so.
- Documentation of your discussion with the patient. If applicable, include your statement that you feel it is in the patient’s best interest to continue psychiatric care.
- A copy of the termination letter.
If the stalking persists, the psychiatrist should follow guidelines for victims provided later in this article.
J.P. and his ‘ex-girlfriend’
J.P., 19, met Ms. T. when both were 16 and still in high school. Ms. T. was a “partying friend”; they smoked pot together and “hung out.” Although they never dated nor had a romantic relationship, J.P. found Ms. T. to be “pretty and fun,” and developed secret romantic feelings for her.
In their senior year, J.P. wrote Ms. T. a letter professing his love for her. She laughed at it, was dismissive of his feelings, and shared it with friends. He subsequently felt humiliated and rejected and, in retaliation, began spreading rumors that she was a “witch” and a “lesbian.”
After their graduation, they saw each other on a few occasions at parties, but rarely spoke. About a year and a half later, J.P. saw Ms T. with a man he had once fought. He regarded this man as “no good” and a poor choice on Ms. T.’s part. He obtained her phone number from one of their mutual high school acquaintances and called her. They spoke briefly; he accused her of “using drugs and dating an asshole.”
In Ohio, the legal definition of menacing by stalking* includes:
- Engaging in a pattern of conduct that knowingly causes another to believe that the offender will cause physical harm to the other person or cause mental distress to the other person
- A first-degree misdemeanor or fourth-degree felony
Clinical definitions of stalking include:
- The willful, malicious, and repeated following and harassing of another person that threatens his or her safety
- Repeated and persistent unwanted communications and/or approaches that produce fear in the victim
Unwanted communications or behaviors that a stalker might engage in:
- Sending letters
- Phone calls
- E-mails
- Appearing at victim’s home or workplace
- Destroying property
- Assault
- Murder
Typical profile of a stalker:
- Male
- Unemployed or underemployed
- Single or divorced
- Criminal, psychiatric, and drug abuse history
- High school or college education
- Significantly more intelligent than other criminals
- Suffered loss of primary caretaker in childhood
- Significant loss, usually of a job or relationship, within a year of the onset of stalking
*Ohio revised code. Sec. 2903.211
- Whether to change a phone line. One recommendation is to maintain the phone line with an answering machine turned down and let the stalker call it. The victim then obtains another phone line and gives the number only to select friends, colleagues, etc. This way the stalker has a venue for self-expression but the victim does not have to listen to it. Law enforcement can be given the tapes for review. By allowing the stalker continued access to the phone line, the stalker does not have to seek out other potentially more violent ways to pursue his or her victim.
- Whether to seek a restraining order. There is some disagreement on whether restraining orders are useful. In some cases, a restraining order may escalate the situation, such as with prior intimates. In other situations, it may give the victim a false sense of security and ultimately may be of little use if the stalker violates it. When the stalker violates a restraining order and experiences no significant painful consequences, this can increase his sense of power and correspondingly reduce that of the victim.
Source: www.stalkingassistance.com
Thus began a pattern of unwanted phone calls and letters left through the mail slot of her parents’ front door and on her car windshield. One letter featured a drawing of 2 tombstones, one with his name and one with hers, with R.I.P. (Rot In Pieces) scrawled below her tombstone. When asked how he thought she might respond to this, J.P. shrugged and explained it was “funny.” He claimed he was “just imitating Eminem,” a well-known “badboy” rapper who has a similar tattoo on his abdomen.
One letter indicated his desire to become a professional baseball player and his belief that if he had her love, he could succeed at this endeavor. He seemed unaffected by her lack of interest in him.
The situation escalated further when J.P. coincidentally showed up at a downtown club on a night when Ms. T. and her boyfriend were there. The boyfriend (the same one that J.P. had criticized Ms. T. for becoming involved with) hit J.P. A fight ensued; both men were thrown out of the club.
Complicating J.P.’s problems was his ongoing substance abuse including marijuana, alcohol, and weekend ecstasy (MDMA, a mixed hallucinogen/amphetaminelike drug). J.P. had also complained to a psychiatrist of attention-deficit/hyperactivity disorder-like symptoms and was placed on an amphetamine, which he also abused, according to his mother. Finally, the removal of his wisdom teeth necessitated a codeine prescription for pain, which he overused.
J.P. presented to the psychiatric emergency room with full-blown psychosis, about 2 months after he allegedly began stalking Ms. T. He reported paranoid ideations, i.e., communications through the TV and computer, male coworkers reading his mind, and thoughts of killing his “ex-girlfriend” (a misnomer describing Ms. T.).
J.P. was hospitalized and placed on antipsychotic and mood-stabilizing medications, quickly recompensated and was discharged. Diagnostically, he had a myriad of rule-outs at the time and was discharged on mood stabilizing and antipsychotic medications.
Mediation was attempted in an effort to end the stalking, but J.P. appeared “disorganized” and alarmed both Ms. T. and her parents. J.P. then was scheduled for a court trial and underwent a court-ordered psychiatric evaluation. He did not qualify to plead not guilty by reason of insanity as defined by Ohio statute.
J.P. was found guilty of menacing by stalking and was sentenced to a year probation. He was ordered to continue psychiatric treatment and was barred from any contact with the victim. To my knowledge, the stalking has stopped.
What this case illustrates
Stalking is not a new crime; it has been around for centuries.6 But what was once romanticized as a persistent and devoted lover’s pursuit is now considered intrusive and a violation of an individual’s basic right to be left alone.7 See Box 1 for legal and clinical definitions of stalking.
In the case vignette, Ms. T. made several good choices that are in line with current recommendations for stalking victims. She did:
List each event of stalking behavior, recording its nature according the keys indicated below. Make a copy of this record on a regular basis for a family member or trusted professional.
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:________________________________________________________________
Witnesses:_____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:_______________________________________________________________
Witnesses:____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:____________Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):__________________________________________________
Place:_________________________________________________________________
Witnesses:_____________________________________________________________
_____________________________________________________________________
Description:____________________________________________________________
_____________________________________________________________________
Stalking Behaviors Key:
Ph = Phone Calling PD = Property Damage L = Letters T = Threats F = Following K = Kidnapping
E = E-mail G = Gift NV = Non-Violent Threats A = Assault SV = Surveillance SL = Defamation/Slander
List Emergency Numbers:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
Source: www.stalkingbehavior.com
- Inform neighbors and friends and provide them a description of the stalker;
- Screen calls and block calls from his number (Box 2);
- Notify police and file an affidavit against him (Box 2);
- Buy new locks and secure her doors with deadbolts;
- Add exterior and motion-detector lighting;
- Document and record all incidents involving the stalker, and save all unwanted correspondence (e.g., letters) from him.
But Ms. T. also made some poor choices contrary to current recommendations. She did not:
- End all contact and communication with the stalker; instead she tried to be nice (after all, they were old high school friends) and to chat with him superficially. This encouraged his continued stalking behaviors.
- Refuse to attend the proposed mediation process. This illustrates a lack of understanding of stalking. Her attendance unwittingly reinforced the stalker and failed to curb his behaviors.
You must take into consideration the stalker’s typology, which will aid in predicting his or her likely response to legal intervention. Several stalker classification systems have been devised. The one created by Mullen et al (Table 1) is most widely accepted at this time. It is based on:
- The stalker’s motivation;
- His or her prior relationship with the victim;
- Whether the stalker is psychotic.
Knowing the typology can help determine the risk to victims and guide effective and protective victim responses. Typologies may overlap. Both psychotic and nonpsychotic stalkers are equally likely to threaten, but nonpsychotic stalkers are twice as likely to assault.
Restraining orders typically do not sway intimacy-seeking and delusional stalkers. In fact, stalkers may view restraining orders merely as obstacles they must overcome in order to achieve union with their beloved. A restraining order might work in some instances but it is wise to know the law in your state and what steps law enforcement will actually take if the order is violated. If the violation results in just a citation, not arrest or incarceration, it probably isn’t worth the trouble. Even if the law takes further steps, it is typically for a brief time and the action may ultimately enrage the stalker and escalate him to a violent act. Violent episodes are typically not preceded by a specific threat.8
Aside from law enforcement, publicly funded and private threat-assessment teams are located throughout the country. [See “Related resources,” below.] These can help you review the stalking situation in detail and arrive at the most effective response.
Finally, it is important to document the stalking behaviors in order to establish a pattern of conduct that could later be used to prosecute the stalker. Written documentation can be detailed in a log book (Box 3). Saving all physical evidence such as letters, gifts, objects, and e-mails can help establish a pattern of stalking behaviors.
- National Organization for Victim Assistance (NOVA) 1757 Park Rd., NW Washington, DC 20010 (800) 879-6682 or (202) 232-6682.
- National Center for Victims of Crime www.ncvc.org (703) 276-2880
- Stalking Behavior. www.stalkingbehavior.com
- The Stalking Assistance Site. www.stalkingassistance.com
- National Victim Center help guide for stalking victims http://www.ojp.usdoj.gov/ovc/assist/nvaa/ch21-2st.htm
About 1.4 million people are stalked each year in the United States.1 Chances are you or one of your patients have been among that statistic.
In the U.S., 8% to 12 % of adult women and 2% to 4% of adult men have been stalked at some point in their lives.2 While celebrities and politicians tend to be high-profile targets, psychiatrists and other health-care professionals may find themselves subject to unwanted contact or obsessive pursuit; this may be because psychiatrists are perceived to be warm, caring, or nurturing. Also, mental health professionals regularly see patients who are particularly prone to engaging in stalking behaviors.
As a former forensic psychiatry fellow, I have studied the risks and patterns of stalking in an effort to help victims of stalkers protect themselves and use legal remedies when appropriate.
The objectives of this article are threefold:
- To identify the unique problem of a patient stalking a psychiatrist and how to cope.
- To address what every stalking victim (including a patient) can do to protect herself or himself.
- To provide basic definitions of stalking and to outline the current, most widely accepted clinical classification of stalkers and its relevance in predicting the stalker’s response to legal and/or mental health interventions. All 50 states and the District of Columbia have passed laws specifically criminalizing stalking.3
When a psychiatrist is stalked
In her book, I Know You Really Love Me,4 psychiatrist Doreen Orion, MD, recounts her experience as a stalking victim. Her victimization began in 1989, when she was on night call for a psychiatric hospital in Arizona. One of the patients she admitted that night was Fran, who developed the erotomanic delusion that Dr. Orion loved her. Despite all evidence to the contrary, Fran pursued Dr. Orion for nearly 8 years, even following her to another state.
Dr. Orion’s book illustrates several issues of import, starting with a crucial failure to communicate. The following morning, Dr. Orion went to the psychiatric hospital to evaluate the patients she had admitted the night before. She contacted Fran’s treating psychiatrist, who angrily hung up on Dr. Orion because Fran had been admitted to the “wrong hospital.” He neglected to inform Dr. Orion that Fran had a history of same-sex stalking and erotomanic delusions. Had she been informed of Fran’s stalking patterns. Dr. Orion may have then simply transferred Fran’s care to a male colleague.
Ultimately, some of Dr. Orion’s colleagues viewed her as somehow inviting or being at fault for her stalking victimization. This classic “blaming the victim” aggravated a situation that was already maddening enough. (Eventually, after several legal and psychiatric evaluations, the stalking stopped.)
Dr. Orion’s book is a cautionary tale. Knowing the patient’s history by reviewing prior records and contacting former treating clinicians can uncover a past pattern of stalking. However, as we are well aware today, terrorists may not become known as such until their first terrorist act; with stalkers, a previous pattern may not be apparent in some cases.
It is important to recognize stalking behaviors for what they are and to act quickly. As psychiatrists, we may be more able than other clinicians to do this because we are trained to ask the patient questions, then simultaneously observe and monitor both the patient’s behavior and our reactions to it. Gavin DeBecker’s book, The Gift of Fear,5 details the survival properties of being in tune with one’s fear response as protective.
Typically, stalking has an insidious onset and may even seem initially harmless, perhaps noted as an erotic transference. But you must pay attention to the behavior and how it makes you feel. Be aware that it may escalate and be prepared to take measures to protect yourself.
Questions to ask yourself might include:
- What are your clinical impressions?
- Are axis I and/or axis II disorders present that may respond to treatment?
- Is your therapeutic relationship with the patient fairly new, or is this an established doctor-patient relationship?
- Is the patient an otherwise stable person who is under stress and engaging in uncharacteristic behavior?
Consider the answers carefully, bearing in mind the typology or typologies involved (Table 1). Stalking encompasses a continuum of unwanted behaviors, ranging from the innocuous to overt and harmful stalking. Your clinical decision-making depends on the typology and intensity of the behavior, as well as your own tolerance for such behaviors.
Table 1
STALKER CLASSIFICATION SYSTEM*
| Type | Features | Assault potential | Response to legal interventions | Response to mental health interventions |
|---|---|---|---|---|
| Rejected | Response to an unwelcome end to relationship Seeks to maintain the relationship Long duration | Along with Predatory, the most likely to assault | Will usually curb behaviors | Typically not responsive to therapy |
| Resentful | Response to a perceived insult Seeks vindication Self-righteous and self-pitying | Most likely to threaten, least likely to assault | Will usually stop behaviors | Difficult to engage in therapy Focus on ruminations that drive stalkers |
| Intimacy seeking | Belief that they are loved or will be loved by the victim Satisfies need for contact and feeds fantasies of eventual loving relationship | May assault | Impervious to legal interventions | If erotomanic delusions are present, they are resistive to change |
| Incompetent | Intellectually limited Socially incompetent Desires intimacy but lacks sufficient skills in courting rituals | Low assault potential | Will stop Typically has previous stalking victims Responsive to restraining orders | May benefit from basic social skills and courting rituals education |
| Predatory | Desire is for sexual gratification and control Rehearsal for violent sexual fantasies and satisfaction of voyeuristic and sadistic desires | High assault potential | Cannot determine before an attack | Poor candidate for therapy |
| *Mullen P, Pathe M, Purcell R, Stuart G. Study of Stalkers. Am J Psychiatry. 1999; 156:1244-1249. | ||||
Interestingly, a female patient also exhibited unwanted behavior toward Dr. Orion’s psychiatrist husband. This patient frequently parked in front of their home in the evenings. Unlike Fran, whose stalking behaviors became increasingly intrusive, frightening, and violent, this patient did not escalate her behavior. It was an unwanted intrusion, but he did not feel fearful or victimized by it. Therefore, it didn’t meet the clinical or legal definition of stalking—the unwanted behaviors must produce fear in the victim. Another psychiatrist, however, might consider the same scenario to be fearful.
Terminating the therapeutic relationship
Once you have reviewed the case with a colleague and/or a threat-assessment professional and determined that you feel uncomfortable and unsafe, it’s time to terminate the doctor-patient relationship.
Ethical and professional care dictates that you provide the patient with a reasonable written notice (e.g., 30 days) prior to termination. Three referral options with phone numbers are typically provided. This also protects you from a potential malpractice tort of abandonment while the patient still needs treatment. If you sense possibly imminent danger, however, you may need to abbreviate the 30-day notice.
Write a summary note in the patient’s chart that includes, in addition to the usual case summary components, the following:
- Your reason(s) for termination. Include discussion with colleagues and/or threat assessment or law enforcement professionals;
- Your diagnostic and treatment impressions, the treatment provided, and the patient’s response to treatment;
- Your referral choices and the rationale for those decisions, e.g., “female patient with schizophrenia and erotomanic delusions and a history of same-sex stalking referred to a male psychiatrist.” The referral should be made to an outside agency or system. (Once Dr. Orion realized that she was being stalked, she initially made the mistake of transferring her patient to a male colleague who shared her office suite, thus making it easy for Fran to continue to stalk Dr. Orion in her own office.)
- Documentation of your discussion with professionals to whom you are referring the patient, along with the patient’s release of information permitting you to do so.
- Documentation of your discussion with the patient. If applicable, include your statement that you feel it is in the patient’s best interest to continue psychiatric care.
- A copy of the termination letter.
If the stalking persists, the psychiatrist should follow guidelines for victims provided later in this article.
J.P. and his ‘ex-girlfriend’
J.P., 19, met Ms. T. when both were 16 and still in high school. Ms. T. was a “partying friend”; they smoked pot together and “hung out.” Although they never dated nor had a romantic relationship, J.P. found Ms. T. to be “pretty and fun,” and developed secret romantic feelings for her.
In their senior year, J.P. wrote Ms. T. a letter professing his love for her. She laughed at it, was dismissive of his feelings, and shared it with friends. He subsequently felt humiliated and rejected and, in retaliation, began spreading rumors that she was a “witch” and a “lesbian.”
After their graduation, they saw each other on a few occasions at parties, but rarely spoke. About a year and a half later, J.P. saw Ms T. with a man he had once fought. He regarded this man as “no good” and a poor choice on Ms. T.’s part. He obtained her phone number from one of their mutual high school acquaintances and called her. They spoke briefly; he accused her of “using drugs and dating an asshole.”
In Ohio, the legal definition of menacing by stalking* includes:
- Engaging in a pattern of conduct that knowingly causes another to believe that the offender will cause physical harm to the other person or cause mental distress to the other person
- A first-degree misdemeanor or fourth-degree felony
Clinical definitions of stalking include:
- The willful, malicious, and repeated following and harassing of another person that threatens his or her safety
- Repeated and persistent unwanted communications and/or approaches that produce fear in the victim
Unwanted communications or behaviors that a stalker might engage in:
- Sending letters
- Phone calls
- E-mails
- Appearing at victim’s home or workplace
- Destroying property
- Assault
- Murder
Typical profile of a stalker:
- Male
- Unemployed or underemployed
- Single or divorced
- Criminal, psychiatric, and drug abuse history
- High school or college education
- Significantly more intelligent than other criminals
- Suffered loss of primary caretaker in childhood
- Significant loss, usually of a job or relationship, within a year of the onset of stalking
*Ohio revised code. Sec. 2903.211
- Whether to change a phone line. One recommendation is to maintain the phone line with an answering machine turned down and let the stalker call it. The victim then obtains another phone line and gives the number only to select friends, colleagues, etc. This way the stalker has a venue for self-expression but the victim does not have to listen to it. Law enforcement can be given the tapes for review. By allowing the stalker continued access to the phone line, the stalker does not have to seek out other potentially more violent ways to pursue his or her victim.
- Whether to seek a restraining order. There is some disagreement on whether restraining orders are useful. In some cases, a restraining order may escalate the situation, such as with prior intimates. In other situations, it may give the victim a false sense of security and ultimately may be of little use if the stalker violates it. When the stalker violates a restraining order and experiences no significant painful consequences, this can increase his sense of power and correspondingly reduce that of the victim.
Source: www.stalkingassistance.com
Thus began a pattern of unwanted phone calls and letters left through the mail slot of her parents’ front door and on her car windshield. One letter featured a drawing of 2 tombstones, one with his name and one with hers, with R.I.P. (Rot In Pieces) scrawled below her tombstone. When asked how he thought she might respond to this, J.P. shrugged and explained it was “funny.” He claimed he was “just imitating Eminem,” a well-known “badboy” rapper who has a similar tattoo on his abdomen.
One letter indicated his desire to become a professional baseball player and his belief that if he had her love, he could succeed at this endeavor. He seemed unaffected by her lack of interest in him.
The situation escalated further when J.P. coincidentally showed up at a downtown club on a night when Ms. T. and her boyfriend were there. The boyfriend (the same one that J.P. had criticized Ms. T. for becoming involved with) hit J.P. A fight ensued; both men were thrown out of the club.
Complicating J.P.’s problems was his ongoing substance abuse including marijuana, alcohol, and weekend ecstasy (MDMA, a mixed hallucinogen/amphetaminelike drug). J.P. had also complained to a psychiatrist of attention-deficit/hyperactivity disorder-like symptoms and was placed on an amphetamine, which he also abused, according to his mother. Finally, the removal of his wisdom teeth necessitated a codeine prescription for pain, which he overused.
J.P. presented to the psychiatric emergency room with full-blown psychosis, about 2 months after he allegedly began stalking Ms. T. He reported paranoid ideations, i.e., communications through the TV and computer, male coworkers reading his mind, and thoughts of killing his “ex-girlfriend” (a misnomer describing Ms. T.).
J.P. was hospitalized and placed on antipsychotic and mood-stabilizing medications, quickly recompensated and was discharged. Diagnostically, he had a myriad of rule-outs at the time and was discharged on mood stabilizing and antipsychotic medications.
Mediation was attempted in an effort to end the stalking, but J.P. appeared “disorganized” and alarmed both Ms. T. and her parents. J.P. then was scheduled for a court trial and underwent a court-ordered psychiatric evaluation. He did not qualify to plead not guilty by reason of insanity as defined by Ohio statute.
J.P. was found guilty of menacing by stalking and was sentenced to a year probation. He was ordered to continue psychiatric treatment and was barred from any contact with the victim. To my knowledge, the stalking has stopped.
What this case illustrates
Stalking is not a new crime; it has been around for centuries.6 But what was once romanticized as a persistent and devoted lover’s pursuit is now considered intrusive and a violation of an individual’s basic right to be left alone.7 See Box 1 for legal and clinical definitions of stalking.
In the case vignette, Ms. T. made several good choices that are in line with current recommendations for stalking victims. She did:
List each event of stalking behavior, recording its nature according the keys indicated below. Make a copy of this record on a regular basis for a family member or trusted professional.
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:________________________________________________________________
Witnesses:_____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:_______________________________________________________________
Witnesses:____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:____________Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):__________________________________________________
Place:_________________________________________________________________
Witnesses:_____________________________________________________________
_____________________________________________________________________
Description:____________________________________________________________
_____________________________________________________________________
Stalking Behaviors Key:
Ph = Phone Calling PD = Property Damage L = Letters T = Threats F = Following K = Kidnapping
E = E-mail G = Gift NV = Non-Violent Threats A = Assault SV = Surveillance SL = Defamation/Slander
List Emergency Numbers:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
Source: www.stalkingbehavior.com
- Inform neighbors and friends and provide them a description of the stalker;
- Screen calls and block calls from his number (Box 2);
- Notify police and file an affidavit against him (Box 2);
- Buy new locks and secure her doors with deadbolts;
- Add exterior and motion-detector lighting;
- Document and record all incidents involving the stalker, and save all unwanted correspondence (e.g., letters) from him.
But Ms. T. also made some poor choices contrary to current recommendations. She did not:
- End all contact and communication with the stalker; instead she tried to be nice (after all, they were old high school friends) and to chat with him superficially. This encouraged his continued stalking behaviors.
- Refuse to attend the proposed mediation process. This illustrates a lack of understanding of stalking. Her attendance unwittingly reinforced the stalker and failed to curb his behaviors.
You must take into consideration the stalker’s typology, which will aid in predicting his or her likely response to legal intervention. Several stalker classification systems have been devised. The one created by Mullen et al (Table 1) is most widely accepted at this time. It is based on:
- The stalker’s motivation;
- His or her prior relationship with the victim;
- Whether the stalker is psychotic.
Knowing the typology can help determine the risk to victims and guide effective and protective victim responses. Typologies may overlap. Both psychotic and nonpsychotic stalkers are equally likely to threaten, but nonpsychotic stalkers are twice as likely to assault.
Restraining orders typically do not sway intimacy-seeking and delusional stalkers. In fact, stalkers may view restraining orders merely as obstacles they must overcome in order to achieve union with their beloved. A restraining order might work in some instances but it is wise to know the law in your state and what steps law enforcement will actually take if the order is violated. If the violation results in just a citation, not arrest or incarceration, it probably isn’t worth the trouble. Even if the law takes further steps, it is typically for a brief time and the action may ultimately enrage the stalker and escalate him to a violent act. Violent episodes are typically not preceded by a specific threat.8
Aside from law enforcement, publicly funded and private threat-assessment teams are located throughout the country. [See “Related resources,” below.] These can help you review the stalking situation in detail and arrive at the most effective response.
Finally, it is important to document the stalking behaviors in order to establish a pattern of conduct that could later be used to prosecute the stalker. Written documentation can be detailed in a log book (Box 3). Saving all physical evidence such as letters, gifts, objects, and e-mails can help establish a pattern of stalking behaviors.
- National Organization for Victim Assistance (NOVA) 1757 Park Rd., NW Washington, DC 20010 (800) 879-6682 or (202) 232-6682.
- National Center for Victims of Crime www.ncvc.org (703) 276-2880
- Stalking Behavior. www.stalkingbehavior.com
- The Stalking Assistance Site. www.stalkingassistance.com
- National Victim Center help guide for stalking victims http://www.ojp.usdoj.gov/ovc/assist/nvaa/ch21-2st.htm
1. The Stalking Assistance Site home page. www.stalkingassistance.com.
2. Tjaden P. The crime of stalking: how big is the problem? Washington, DC, U.S. Department of Justice, National Institute of Justice, Nov. 1977. Call The National Criminal Justice Reference Service at (800) 851-3420, ask for NCJ# FS 000186.
3. U.S. Department of Justice Report to Congress on Stalking and Domestic Violence, May 2001.
4. Orion D. I Know You Really Love Me: A Psychiatrist’s Account of Stalking and Obsessive Love. New York: Bantam Doubleday Dell Publishing Group, 1997.
5. deBecker G. The Gift of Fear (and Other Survival Strategies that Protect Us from Violence). Studio City, Calif: Gavin deBecker & Associates, www.gdbinc.com.
6. Meloy JR. Stalking: An old behavior, a new crime. Psychiatr Clin North Am. 1999;22(2):85-99.
7. Supreme Court Justice Brandeis, Olmstead v. United States, 227U.S.438 (1928).
8. Dietz P, Matthews D, et al. Threatening and otherwise inappropriate letters sent to members of the United States Congress. J Forensic Sci. 1991;36(5):1445-1468.
1. The Stalking Assistance Site home page. www.stalkingassistance.com.
2. Tjaden P. The crime of stalking: how big is the problem? Washington, DC, U.S. Department of Justice, National Institute of Justice, Nov. 1977. Call The National Criminal Justice Reference Service at (800) 851-3420, ask for NCJ# FS 000186.
3. U.S. Department of Justice Report to Congress on Stalking and Domestic Violence, May 2001.
4. Orion D. I Know You Really Love Me: A Psychiatrist’s Account of Stalking and Obsessive Love. New York: Bantam Doubleday Dell Publishing Group, 1997.
5. deBecker G. The Gift of Fear (and Other Survival Strategies that Protect Us from Violence). Studio City, Calif: Gavin deBecker & Associates, www.gdbinc.com.
6. Meloy JR. Stalking: An old behavior, a new crime. Psychiatr Clin North Am. 1999;22(2):85-99.
7. Supreme Court Justice Brandeis, Olmstead v. United States, 227U.S.438 (1928).
8. Dietz P, Matthews D, et al. Threatening and otherwise inappropriate letters sent to members of the United States Congress. J Forensic Sci. 1991;36(5):1445-1468.
What to do if you—or a patient—is a victim of stalking
About 1.4 million people are stalked each year in the United States.1 Chances are you or one of your patients have been among that statistic.
In the U.S., 8% to 12 % of adult women and 2% to 4% of adult men have been stalked at some point in their lives.2 While celebrities and politicians tend to be high-profile targets, psychiatrists and other health-care professionals may find themselves subject to unwanted contact or obsessive pursuit; this may be because psychiatrists are perceived to be warm, caring, or nurturing. Also, mental health professionals regularly see patients who are particularly prone to engaging in stalking behaviors.
As a former forensic psychiatry fellow, I have studied the risks and patterns of stalking in an effort to help victims of stalkers protect themselves and use legal remedies when appropriate.
The objectives of this article are threefold:
- To identify the unique problem of a patient stalking a psychiatrist and how to cope.
- To address what every stalking victim (including a patient) can do to protect herself or himself.
- To provide basic definitions of stalking and to outline the current, most widely accepted clinical classification of stalkers and its relevance in predicting the stalker’s response to legal and/or mental health interventions. All 50 states and the District of Columbia have passed laws specifically criminalizing stalking.3
When a psychiatrist is stalked
In her book, I Know You Really Love Me,4 psychiatrist Doreen Orion, MD, recounts her experience as a stalking victim. Her victimization began in 1989, when she was on night call for a psychiatric hospital in Arizona. One of the patients she admitted that night was Fran, who developed the erotomanic delusion that Dr. Orion loved her. Despite all evidence to the contrary, Fran pursued Dr. Orion for nearly 8 years, even following her to another state.
Dr. Orion’s book illustrates several issues of import, starting with a crucial failure to communicate. The following morning, Dr. Orion went to the psychiatric hospital to evaluate the patients she had admitted the night before. She contacted Fran’s treating psychiatrist, who angrily hung up on Dr. Orion because Fran had been admitted to the “wrong hospital.” He neglected to inform Dr. Orion that Fran had a history of same-sex stalking and erotomanic delusions. Had she been informed of Fran’s stalking patterns. Dr. Orion may have then simply transferred Fran’s care to a male colleague.
Ultimately, some of Dr. Orion’s colleagues viewed her as somehow inviting or being at fault for her stalking victimization. This classic “blaming the victim” aggravated a situation that was already maddening enough. (Eventually, after several legal and psychiatric evaluations, the stalking stopped.)
Dr. Orion’s book is a cautionary tale. Knowing the patient’s history by reviewing prior records and contacting former treating clinicians can uncover a past pattern of stalking. However, as we are well aware today, terrorists may not become known as such until their first terrorist act; with stalkers, a previous pattern may not be apparent in some cases.
It is important to recognize stalking behaviors for what they are and to act quickly. As psychiatrists, we may be more able than other clinicians to do this because we are trained to ask the patient questions, then simultaneously observe and monitor both the patient’s behavior and our reactions to it. Gavin DeBecker’s book, The Gift of Fear,5 details the survival properties of being in tune with one’s fear response as protective.
Typically, stalking has an insidious onset and may even seem initially harmless, perhaps noted as an erotic transference. But you must pay attention to the behavior and how it makes you feel. Be aware that it may escalate and be prepared to take measures to protect yourself.
Questions to ask yourself might include:
- What are your clinical impressions?
- Are axis I and/or axis II disorders present that may respond to treatment?
- Is your therapeutic relationship with the patient fairly new, or is this an established doctor-patient relationship?
- Is the patient an otherwise stable person who is under stress and engaging in uncharacteristic behavior?
Consider the answers carefully, bearing in mind the typology or typologies involved (Table 1). Stalking encompasses a continuum of unwanted behaviors, ranging from the innocuous to overt and harmful stalking. Your clinical decision-making depends on the typology and intensity of the behavior, as well as your own tolerance for such behaviors.
Table 1
STALKER CLASSIFICATION SYSTEM*
| Type | Features | Assault potential | Response to legal interventions | Response to mental health interventions |
|---|---|---|---|---|
| Rejected | Response to an unwelcome end to relationship Seeks to maintain the relationship Long duration | Along with Predatory, the most likely to assault | Will usually curb behaviors | Typically not responsive to therapy |
| Resentful | Response to a perceived insult Seeks vindication Self-righteous and self-pitying | Most likely to threaten, least likely to assault | Will usually stop behaviors | Difficult to engage in therapy Focus on ruminations that drive stalkers |
| Intimacy seeking | Belief that they are loved or will be loved by the victim Satisfies need for contact and feeds fantasies of eventual loving relationship | May assault | Impervious to legal interventions | If erotomanic delusions are present, they are resistive to change |
| Incompetent | Intellectually limited Socially incompetent Desires intimacy but lacks sufficient skills in courting rituals | Low assault potential | Will stop Typically has previous stalking victims Responsive to restraining orders | May benefit from basic social skills and courting rituals education |
| Predatory | Desire is for sexual gratification and control Rehearsal for violent sexual fantasies and satisfaction of voyeuristic and sadistic desires | High assault potential | Cannot determine before an attack | Poor candidate for therapy |
| *Mullen P, Pathe M, Purcell R, Stuart G. Study of Stalkers. Am J Psychiatry. 1999; 156:1244-1249. | ||||
Interestingly, a female patient also exhibited unwanted behavior toward Dr. Orion’s psychiatrist husband. This patient frequently parked in front of their home in the evenings. Unlike Fran, whose stalking behaviors became increasingly intrusive, frightening, and violent, this patient did not escalate her behavior. It was an unwanted intrusion, but he did not feel fearful or victimized by it. Therefore, it didn’t meet the clinical or legal definition of stalking—the unwanted behaviors must produce fear in the victim. Another psychiatrist, however, might consider the same scenario to be fearful.
Terminating the therapeutic relationship
Once you have reviewed the case with a colleague and/or a threat-assessment professional and determined that you feel uncomfortable and unsafe, it’s time to terminate the doctor-patient relationship.
Ethical and professional care dictates that you provide the patient with a reasonable written notice (e.g., 30 days) prior to termination. Three referral options with phone numbers are typically provided. This also protects you from a potential malpractice tort of abandonment while the patient still needs treatment. If you sense possibly imminent danger, however, you may need to abbreviate the 30-day notice.
Write a summary note in the patient’s chart that includes, in addition to the usual case summary components, the following:
- Your reason(s) for termination. Include discussion with colleagues and/or threat assessment or law enforcement professionals;
- Your diagnostic and treatment impressions, the treatment provided, and the patient’s response to treatment;
- Your referral choices and the rationale for those decisions, e.g., “female patient with schizophrenia and erotomanic delusions and a history of same-sex stalking referred to a male psychiatrist.” The referral should be made to an outside agency or system. (Once Dr. Orion realized that she was being stalked, she initially made the mistake of transferring her patient to a male colleague who shared her office suite, thus making it easy for Fran to continue to stalk Dr. Orion in her own office.)
- Documentation of your discussion with professionals to whom you are referring the patient, along with the patient’s release of information permitting you to do so.
- Documentation of your discussion with the patient. If applicable, include your statement that you feel it is in the patient’s best interest to continue psychiatric care.
- A copy of the termination letter.
If the stalking persists, the psychiatrist should follow guidelines for victims provided later in this article.
J.P. and his ‘ex-girlfriend’
J.P., 19, met Ms. T. when both were 16 and still in high school. Ms. T. was a “partying friend”; they smoked pot together and “hung out.” Although they never dated nor had a romantic relationship, J.P. found Ms. T. to be “pretty and fun,” and developed secret romantic feelings for her.
In their senior year, J.P. wrote Ms. T. a letter professing his love for her. She laughed at it, was dismissive of his feelings, and shared it with friends. He subsequently felt humiliated and rejected and, in retaliation, began spreading rumors that she was a “witch” and a “lesbian.”
After their graduation, they saw each other on a few occasions at parties, but rarely spoke. About a year and a half later, J.P. saw Ms T. with a man he had once fought. He regarded this man as “no good” and a poor choice on Ms. T.’s part. He obtained her phone number from one of their mutual high school acquaintances and called her. They spoke briefly; he accused her of “using drugs and dating an asshole.”
In Ohio, the legal definition of menacing by stalking* includes:
- Engaging in a pattern of conduct that knowingly causes another to believe that the offender will cause physical harm to the other person or cause mental distress to the other person
- A first-degree misdemeanor or fourth-degree felony
Clinical definitions of stalking include:
- The willful, malicious, and repeated following and harassing of another person that threatens his or her safety
- Repeated and persistent unwanted communications and/or approaches that produce fear in the victim
Unwanted communications or behaviors that a stalker might engage in:
- Sending letters
- Phone calls
- E-mails
- Appearing at victim’s home or workplace
- Destroying property
- Assault
- Murder
Typical profile of a stalker:
- Male
- Unemployed or underemployed
- Single or divorced
- Criminal, psychiatric, and drug abuse history
- High school or college education
- Significantly more intelligent than other criminals
- Suffered loss of primary caretaker in childhood
- Significant loss, usually of a job or relationship, within a year of the onset of stalking
*Ohio revised code. Sec. 2903.211
- Whether to change a phone line. One recommendation is to maintain the phone line with an answering machine turned down and let the stalker call it. The victim then obtains another phone line and gives the number only to select friends, colleagues, etc. This way the stalker has a venue for self-expression but the victim does not have to listen to it. Law enforcement can be given the tapes for review. By allowing the stalker continued access to the phone line, the stalker does not have to seek out other potentially more violent ways to pursue his or her victim.
- Whether to seek a restraining order. There is some disagreement on whether restraining orders are useful. In some cases, a restraining order may escalate the situation, such as with prior intimates. In other situations, it may give the victim a false sense of security and ultimately may be of little use if the stalker violates it. When the stalker violates a restraining order and experiences no significant painful consequences, this can increase his sense of power and correspondingly reduce that of the victim.
Source: www.stalkingassistance.com
Thus began a pattern of unwanted phone calls and letters left through the mail slot of her parents’ front door and on her car windshield. One letter featured a drawing of 2 tombstones, one with his name and one with hers, with R.I.P. (Rot In Pieces) scrawled below her tombstone. When asked how he thought she might respond to this, J.P. shrugged and explained it was “funny.” He claimed he was “just imitating Eminem,” a well-known “badboy” rapper who has a similar tattoo on his abdomen.
One letter indicated his desire to become a professional baseball player and his belief that if he had her love, he could succeed at this endeavor. He seemed unaffected by her lack of interest in him.
The situation escalated further when J.P. coincidentally showed up at a downtown club on a night when Ms. T. and her boyfriend were there. The boyfriend (the same one that J.P. had criticized Ms. T. for becoming involved with) hit J.P. A fight ensued; both men were thrown out of the club.
Complicating J.P.’s problems was his ongoing substance abuse including marijuana, alcohol, and weekend ecstasy (MDMA, a mixed hallucinogen/amphetaminelike drug). J.P. had also complained to a psychiatrist of attention-deficit/hyperactivity disorder-like symptoms and was placed on an amphetamine, which he also abused, according to his mother. Finally, the removal of his wisdom teeth necessitated a codeine prescription for pain, which he overused.
J.P. presented to the psychiatric emergency room with full-blown psychosis, about 2 months after he allegedly began stalking Ms. T. He reported paranoid ideations, i.e., communications through the TV and computer, male coworkers reading his mind, and thoughts of killing his “ex-girlfriend” (a misnomer describing Ms. T.).
J.P. was hospitalized and placed on antipsychotic and mood-stabilizing medications, quickly recompensated and was discharged. Diagnostically, he had a myriad of rule-outs at the time and was discharged on mood stabilizing and antipsychotic medications.
Mediation was attempted in an effort to end the stalking, but J.P. appeared “disorganized” and alarmed both Ms. T. and her parents. J.P. then was scheduled for a court trial and underwent a court-ordered psychiatric evaluation. He did not qualify to plead not guilty by reason of insanity as defined by Ohio statute.
J.P. was found guilty of menacing by stalking and was sentenced to a year probation. He was ordered to continue psychiatric treatment and was barred from any contact with the victim. To my knowledge, the stalking has stopped.
What this case illustrates
Stalking is not a new crime; it has been around for centuries.6 But what was once romanticized as a persistent and devoted lover’s pursuit is now considered intrusive and a violation of an individual’s basic right to be left alone.7 See Box 1 for legal and clinical definitions of stalking.
In the case vignette, Ms. T. made several good choices that are in line with current recommendations for stalking victims. She did:
List each event of stalking behavior, recording its nature according the keys indicated below. Make a copy of this record on a regular basis for a family member or trusted professional.
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:________________________________________________________________
Witnesses:_____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:_______________________________________________________________
Witnesses:____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:____________Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):__________________________________________________
Place:_________________________________________________________________
Witnesses:_____________________________________________________________
_____________________________________________________________________
Description:____________________________________________________________
_____________________________________________________________________
Stalking Behaviors Key:
Ph = Phone Calling PD = Property Damage L = Letters T = Threats F = Following K = Kidnapping
E = E-mail G = Gift NV = Non-Violent Threats A = Assault SV = Surveillance SL = Defamation/Slander
List Emergency Numbers:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
Source: www.stalkingbehavior.com
- Inform neighbors and friends and provide them a description of the stalker;
- Screen calls and block calls from his number (Box 2);
- Notify police and file an affidavit against him (Box 2);
- Buy new locks and secure her doors with deadbolts;
- Add exterior and motion-detector lighting;
- Document and record all incidents involving the stalker, and save all unwanted correspondence (e.g., letters) from him.
But Ms. T. also made some poor choices contrary to current recommendations. She did not:
- End all contact and communication with the stalker; instead she tried to be nice (after all, they were old high school friends) and to chat with him superficially. This encouraged his continued stalking behaviors.
- Refuse to attend the proposed mediation process. This illustrates a lack of understanding of stalking. Her attendance unwittingly reinforced the stalker and failed to curb his behaviors.
You must take into consideration the stalker’s typology, which will aid in predicting his or her likely response to legal intervention. Several stalker classification systems have been devised. The one created by Mullen et al (Table 1) is most widely accepted at this time. It is based on:
- The stalker’s motivation;
- His or her prior relationship with the victim;
- Whether the stalker is psychotic.
Knowing the typology can help determine the risk to victims and guide effective and protective victim responses. Typologies may overlap. Both psychotic and nonpsychotic stalkers are equally likely to threaten, but nonpsychotic stalkers are twice as likely to assault.
Restraining orders typically do not sway intimacy-seeking and delusional stalkers. In fact, stalkers may view restraining orders merely as obstacles they must overcome in order to achieve union with their beloved. A restraining order might work in some instances but it is wise to know the law in your state and what steps law enforcement will actually take if the order is violated. If the violation results in just a citation, not arrest or incarceration, it probably isn’t worth the trouble. Even if the law takes further steps, it is typically for a brief time and the action may ultimately enrage the stalker and escalate him to a violent act. Violent episodes are typically not preceded by a specific threat.8
Aside from law enforcement, publicly funded and private threat-assessment teams are located throughout the country. [See “Related resources,” below.] These can help you review the stalking situation in detail and arrive at the most effective response.
Finally, it is important to document the stalking behaviors in order to establish a pattern of conduct that could later be used to prosecute the stalker. Written documentation can be detailed in a log book (Box 3). Saving all physical evidence such as letters, gifts, objects, and e-mails can help establish a pattern of stalking behaviors.
- National Organization for Victim Assistance (NOVA) 1757 Park Rd., NW Washington, DC 20010 (800) 879-6682 or (202) 232-6682.
- National Center for Victims of Crime www.ncvc.org (703) 276-2880
- Stalking Behavior. www.stalkingbehavior.com
- The Stalking Assistance Site. www.stalkingassistance.com
- National Victim Center help guide for stalking victims http://www.ojp.usdoj.gov/ovc/assist/nvaa/ch21-2st.htm
1. The Stalking Assistance Site home page. www.stalkingassistance.com.
2. Tjaden P. The crime of stalking: how big is the problem? Washington, DC, U.S. Department of Justice, National Institute of Justice, Nov. 1977. Call The National Criminal Justice Reference Service at (800) 851-3420, ask for NCJ# FS 000186.
3. U.S. Department of Justice Report to Congress on Stalking and Domestic Violence, May 2001.
4. Orion D. I Know You Really Love Me: A Psychiatrist’s Account of Stalking and Obsessive Love. New York: Bantam Doubleday Dell Publishing Group, 1997.
5. deBecker G. The Gift of Fear (and Other Survival Strategies that Protect Us from Violence). Studio City, Calif: Gavin deBecker & Associates, www.gdbinc.com.
6. Meloy JR. Stalking: An old behavior, a new crime. Psychiatr Clin North Am. 1999;22(2):85-99.
7. Supreme Court Justice Brandeis, Olmstead v. United States, 227U.S.438 (1928).
8. Dietz P, Matthews D, et al. Threatening and otherwise inappropriate letters sent to members of the United States Congress. J Forensic Sci. 1991;36(5):1445-1468.
About 1.4 million people are stalked each year in the United States.1 Chances are you or one of your patients have been among that statistic.
In the U.S., 8% to 12 % of adult women and 2% to 4% of adult men have been stalked at some point in their lives.2 While celebrities and politicians tend to be high-profile targets, psychiatrists and other health-care professionals may find themselves subject to unwanted contact or obsessive pursuit; this may be because psychiatrists are perceived to be warm, caring, or nurturing. Also, mental health professionals regularly see patients who are particularly prone to engaging in stalking behaviors.
As a former forensic psychiatry fellow, I have studied the risks and patterns of stalking in an effort to help victims of stalkers protect themselves and use legal remedies when appropriate.
The objectives of this article are threefold:
- To identify the unique problem of a patient stalking a psychiatrist and how to cope.
- To address what every stalking victim (including a patient) can do to protect herself or himself.
- To provide basic definitions of stalking and to outline the current, most widely accepted clinical classification of stalkers and its relevance in predicting the stalker’s response to legal and/or mental health interventions. All 50 states and the District of Columbia have passed laws specifically criminalizing stalking.3
When a psychiatrist is stalked
In her book, I Know You Really Love Me,4 psychiatrist Doreen Orion, MD, recounts her experience as a stalking victim. Her victimization began in 1989, when she was on night call for a psychiatric hospital in Arizona. One of the patients she admitted that night was Fran, who developed the erotomanic delusion that Dr. Orion loved her. Despite all evidence to the contrary, Fran pursued Dr. Orion for nearly 8 years, even following her to another state.
Dr. Orion’s book illustrates several issues of import, starting with a crucial failure to communicate. The following morning, Dr. Orion went to the psychiatric hospital to evaluate the patients she had admitted the night before. She contacted Fran’s treating psychiatrist, who angrily hung up on Dr. Orion because Fran had been admitted to the “wrong hospital.” He neglected to inform Dr. Orion that Fran had a history of same-sex stalking and erotomanic delusions. Had she been informed of Fran’s stalking patterns. Dr. Orion may have then simply transferred Fran’s care to a male colleague.
Ultimately, some of Dr. Orion’s colleagues viewed her as somehow inviting or being at fault for her stalking victimization. This classic “blaming the victim” aggravated a situation that was already maddening enough. (Eventually, after several legal and psychiatric evaluations, the stalking stopped.)
Dr. Orion’s book is a cautionary tale. Knowing the patient’s history by reviewing prior records and contacting former treating clinicians can uncover a past pattern of stalking. However, as we are well aware today, terrorists may not become known as such until their first terrorist act; with stalkers, a previous pattern may not be apparent in some cases.
It is important to recognize stalking behaviors for what they are and to act quickly. As psychiatrists, we may be more able than other clinicians to do this because we are trained to ask the patient questions, then simultaneously observe and monitor both the patient’s behavior and our reactions to it. Gavin DeBecker’s book, The Gift of Fear,5 details the survival properties of being in tune with one’s fear response as protective.
Typically, stalking has an insidious onset and may even seem initially harmless, perhaps noted as an erotic transference. But you must pay attention to the behavior and how it makes you feel. Be aware that it may escalate and be prepared to take measures to protect yourself.
Questions to ask yourself might include:
- What are your clinical impressions?
- Are axis I and/or axis II disorders present that may respond to treatment?
- Is your therapeutic relationship with the patient fairly new, or is this an established doctor-patient relationship?
- Is the patient an otherwise stable person who is under stress and engaging in uncharacteristic behavior?
Consider the answers carefully, bearing in mind the typology or typologies involved (Table 1). Stalking encompasses a continuum of unwanted behaviors, ranging from the innocuous to overt and harmful stalking. Your clinical decision-making depends on the typology and intensity of the behavior, as well as your own tolerance for such behaviors.
Table 1
STALKER CLASSIFICATION SYSTEM*
| Type | Features | Assault potential | Response to legal interventions | Response to mental health interventions |
|---|---|---|---|---|
| Rejected | Response to an unwelcome end to relationship Seeks to maintain the relationship Long duration | Along with Predatory, the most likely to assault | Will usually curb behaviors | Typically not responsive to therapy |
| Resentful | Response to a perceived insult Seeks vindication Self-righteous and self-pitying | Most likely to threaten, least likely to assault | Will usually stop behaviors | Difficult to engage in therapy Focus on ruminations that drive stalkers |
| Intimacy seeking | Belief that they are loved or will be loved by the victim Satisfies need for contact and feeds fantasies of eventual loving relationship | May assault | Impervious to legal interventions | If erotomanic delusions are present, they are resistive to change |
| Incompetent | Intellectually limited Socially incompetent Desires intimacy but lacks sufficient skills in courting rituals | Low assault potential | Will stop Typically has previous stalking victims Responsive to restraining orders | May benefit from basic social skills and courting rituals education |
| Predatory | Desire is for sexual gratification and control Rehearsal for violent sexual fantasies and satisfaction of voyeuristic and sadistic desires | High assault potential | Cannot determine before an attack | Poor candidate for therapy |
| *Mullen P, Pathe M, Purcell R, Stuart G. Study of Stalkers. Am J Psychiatry. 1999; 156:1244-1249. | ||||
Interestingly, a female patient also exhibited unwanted behavior toward Dr. Orion’s psychiatrist husband. This patient frequently parked in front of their home in the evenings. Unlike Fran, whose stalking behaviors became increasingly intrusive, frightening, and violent, this patient did not escalate her behavior. It was an unwanted intrusion, but he did not feel fearful or victimized by it. Therefore, it didn’t meet the clinical or legal definition of stalking—the unwanted behaviors must produce fear in the victim. Another psychiatrist, however, might consider the same scenario to be fearful.
Terminating the therapeutic relationship
Once you have reviewed the case with a colleague and/or a threat-assessment professional and determined that you feel uncomfortable and unsafe, it’s time to terminate the doctor-patient relationship.
Ethical and professional care dictates that you provide the patient with a reasonable written notice (e.g., 30 days) prior to termination. Three referral options with phone numbers are typically provided. This also protects you from a potential malpractice tort of abandonment while the patient still needs treatment. If you sense possibly imminent danger, however, you may need to abbreviate the 30-day notice.
Write a summary note in the patient’s chart that includes, in addition to the usual case summary components, the following:
- Your reason(s) for termination. Include discussion with colleagues and/or threat assessment or law enforcement professionals;
- Your diagnostic and treatment impressions, the treatment provided, and the patient’s response to treatment;
- Your referral choices and the rationale for those decisions, e.g., “female patient with schizophrenia and erotomanic delusions and a history of same-sex stalking referred to a male psychiatrist.” The referral should be made to an outside agency or system. (Once Dr. Orion realized that she was being stalked, she initially made the mistake of transferring her patient to a male colleague who shared her office suite, thus making it easy for Fran to continue to stalk Dr. Orion in her own office.)
- Documentation of your discussion with professionals to whom you are referring the patient, along with the patient’s release of information permitting you to do so.
- Documentation of your discussion with the patient. If applicable, include your statement that you feel it is in the patient’s best interest to continue psychiatric care.
- A copy of the termination letter.
If the stalking persists, the psychiatrist should follow guidelines for victims provided later in this article.
J.P. and his ‘ex-girlfriend’
J.P., 19, met Ms. T. when both were 16 and still in high school. Ms. T. was a “partying friend”; they smoked pot together and “hung out.” Although they never dated nor had a romantic relationship, J.P. found Ms. T. to be “pretty and fun,” and developed secret romantic feelings for her.
In their senior year, J.P. wrote Ms. T. a letter professing his love for her. She laughed at it, was dismissive of his feelings, and shared it with friends. He subsequently felt humiliated and rejected and, in retaliation, began spreading rumors that she was a “witch” and a “lesbian.”
After their graduation, they saw each other on a few occasions at parties, but rarely spoke. About a year and a half later, J.P. saw Ms T. with a man he had once fought. He regarded this man as “no good” and a poor choice on Ms. T.’s part. He obtained her phone number from one of their mutual high school acquaintances and called her. They spoke briefly; he accused her of “using drugs and dating an asshole.”
In Ohio, the legal definition of menacing by stalking* includes:
- Engaging in a pattern of conduct that knowingly causes another to believe that the offender will cause physical harm to the other person or cause mental distress to the other person
- A first-degree misdemeanor or fourth-degree felony
Clinical definitions of stalking include:
- The willful, malicious, and repeated following and harassing of another person that threatens his or her safety
- Repeated and persistent unwanted communications and/or approaches that produce fear in the victim
Unwanted communications or behaviors that a stalker might engage in:
- Sending letters
- Phone calls
- E-mails
- Appearing at victim’s home or workplace
- Destroying property
- Assault
- Murder
Typical profile of a stalker:
- Male
- Unemployed or underemployed
- Single or divorced
- Criminal, psychiatric, and drug abuse history
- High school or college education
- Significantly more intelligent than other criminals
- Suffered loss of primary caretaker in childhood
- Significant loss, usually of a job or relationship, within a year of the onset of stalking
*Ohio revised code. Sec. 2903.211
- Whether to change a phone line. One recommendation is to maintain the phone line with an answering machine turned down and let the stalker call it. The victim then obtains another phone line and gives the number only to select friends, colleagues, etc. This way the stalker has a venue for self-expression but the victim does not have to listen to it. Law enforcement can be given the tapes for review. By allowing the stalker continued access to the phone line, the stalker does not have to seek out other potentially more violent ways to pursue his or her victim.
- Whether to seek a restraining order. There is some disagreement on whether restraining orders are useful. In some cases, a restraining order may escalate the situation, such as with prior intimates. In other situations, it may give the victim a false sense of security and ultimately may be of little use if the stalker violates it. When the stalker violates a restraining order and experiences no significant painful consequences, this can increase his sense of power and correspondingly reduce that of the victim.
Source: www.stalkingassistance.com
Thus began a pattern of unwanted phone calls and letters left through the mail slot of her parents’ front door and on her car windshield. One letter featured a drawing of 2 tombstones, one with his name and one with hers, with R.I.P. (Rot In Pieces) scrawled below her tombstone. When asked how he thought she might respond to this, J.P. shrugged and explained it was “funny.” He claimed he was “just imitating Eminem,” a well-known “badboy” rapper who has a similar tattoo on his abdomen.
One letter indicated his desire to become a professional baseball player and his belief that if he had her love, he could succeed at this endeavor. He seemed unaffected by her lack of interest in him.
The situation escalated further when J.P. coincidentally showed up at a downtown club on a night when Ms. T. and her boyfriend were there. The boyfriend (the same one that J.P. had criticized Ms. T. for becoming involved with) hit J.P. A fight ensued; both men were thrown out of the club.
Complicating J.P.’s problems was his ongoing substance abuse including marijuana, alcohol, and weekend ecstasy (MDMA, a mixed hallucinogen/amphetaminelike drug). J.P. had also complained to a psychiatrist of attention-deficit/hyperactivity disorder-like symptoms and was placed on an amphetamine, which he also abused, according to his mother. Finally, the removal of his wisdom teeth necessitated a codeine prescription for pain, which he overused.
J.P. presented to the psychiatric emergency room with full-blown psychosis, about 2 months after he allegedly began stalking Ms. T. He reported paranoid ideations, i.e., communications through the TV and computer, male coworkers reading his mind, and thoughts of killing his “ex-girlfriend” (a misnomer describing Ms. T.).
J.P. was hospitalized and placed on antipsychotic and mood-stabilizing medications, quickly recompensated and was discharged. Diagnostically, he had a myriad of rule-outs at the time and was discharged on mood stabilizing and antipsychotic medications.
Mediation was attempted in an effort to end the stalking, but J.P. appeared “disorganized” and alarmed both Ms. T. and her parents. J.P. then was scheduled for a court trial and underwent a court-ordered psychiatric evaluation. He did not qualify to plead not guilty by reason of insanity as defined by Ohio statute.
J.P. was found guilty of menacing by stalking and was sentenced to a year probation. He was ordered to continue psychiatric treatment and was barred from any contact with the victim. To my knowledge, the stalking has stopped.
What this case illustrates
Stalking is not a new crime; it has been around for centuries.6 But what was once romanticized as a persistent and devoted lover’s pursuit is now considered intrusive and a violation of an individual’s basic right to be left alone.7 See Box 1 for legal and clinical definitions of stalking.
In the case vignette, Ms. T. made several good choices that are in line with current recommendations for stalking victims. She did:
List each event of stalking behavior, recording its nature according the keys indicated below. Make a copy of this record on a regular basis for a family member or trusted professional.
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:________________________________________________________________
Witnesses:_____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:_______________________________________________________________
Witnesses:____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:____________Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):__________________________________________________
Place:_________________________________________________________________
Witnesses:_____________________________________________________________
_____________________________________________________________________
Description:____________________________________________________________
_____________________________________________________________________
Stalking Behaviors Key:
Ph = Phone Calling PD = Property Damage L = Letters T = Threats F = Following K = Kidnapping
E = E-mail G = Gift NV = Non-Violent Threats A = Assault SV = Surveillance SL = Defamation/Slander
List Emergency Numbers:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
Source: www.stalkingbehavior.com
- Inform neighbors and friends and provide them a description of the stalker;
- Screen calls and block calls from his number (Box 2);
- Notify police and file an affidavit against him (Box 2);
- Buy new locks and secure her doors with deadbolts;
- Add exterior and motion-detector lighting;
- Document and record all incidents involving the stalker, and save all unwanted correspondence (e.g., letters) from him.
But Ms. T. also made some poor choices contrary to current recommendations. She did not:
- End all contact and communication with the stalker; instead she tried to be nice (after all, they were old high school friends) and to chat with him superficially. This encouraged his continued stalking behaviors.
- Refuse to attend the proposed mediation process. This illustrates a lack of understanding of stalking. Her attendance unwittingly reinforced the stalker and failed to curb his behaviors.
You must take into consideration the stalker’s typology, which will aid in predicting his or her likely response to legal intervention. Several stalker classification systems have been devised. The one created by Mullen et al (Table 1) is most widely accepted at this time. It is based on:
- The stalker’s motivation;
- His or her prior relationship with the victim;
- Whether the stalker is psychotic.
Knowing the typology can help determine the risk to victims and guide effective and protective victim responses. Typologies may overlap. Both psychotic and nonpsychotic stalkers are equally likely to threaten, but nonpsychotic stalkers are twice as likely to assault.
Restraining orders typically do not sway intimacy-seeking and delusional stalkers. In fact, stalkers may view restraining orders merely as obstacles they must overcome in order to achieve union with their beloved. A restraining order might work in some instances but it is wise to know the law in your state and what steps law enforcement will actually take if the order is violated. If the violation results in just a citation, not arrest or incarceration, it probably isn’t worth the trouble. Even if the law takes further steps, it is typically for a brief time and the action may ultimately enrage the stalker and escalate him to a violent act. Violent episodes are typically not preceded by a specific threat.8
Aside from law enforcement, publicly funded and private threat-assessment teams are located throughout the country. [See “Related resources,” below.] These can help you review the stalking situation in detail and arrive at the most effective response.
Finally, it is important to document the stalking behaviors in order to establish a pattern of conduct that could later be used to prosecute the stalker. Written documentation can be detailed in a log book (Box 3). Saving all physical evidence such as letters, gifts, objects, and e-mails can help establish a pattern of stalking behaviors.
- National Organization for Victim Assistance (NOVA) 1757 Park Rd., NW Washington, DC 20010 (800) 879-6682 or (202) 232-6682.
- National Center for Victims of Crime www.ncvc.org (703) 276-2880
- Stalking Behavior. www.stalkingbehavior.com
- The Stalking Assistance Site. www.stalkingassistance.com
- National Victim Center help guide for stalking victims http://www.ojp.usdoj.gov/ovc/assist/nvaa/ch21-2st.htm
About 1.4 million people are stalked each year in the United States.1 Chances are you or one of your patients have been among that statistic.
In the U.S., 8% to 12 % of adult women and 2% to 4% of adult men have been stalked at some point in their lives.2 While celebrities and politicians tend to be high-profile targets, psychiatrists and other health-care professionals may find themselves subject to unwanted contact or obsessive pursuit; this may be because psychiatrists are perceived to be warm, caring, or nurturing. Also, mental health professionals regularly see patients who are particularly prone to engaging in stalking behaviors.
As a former forensic psychiatry fellow, I have studied the risks and patterns of stalking in an effort to help victims of stalkers protect themselves and use legal remedies when appropriate.
The objectives of this article are threefold:
- To identify the unique problem of a patient stalking a psychiatrist and how to cope.
- To address what every stalking victim (including a patient) can do to protect herself or himself.
- To provide basic definitions of stalking and to outline the current, most widely accepted clinical classification of stalkers and its relevance in predicting the stalker’s response to legal and/or mental health interventions. All 50 states and the District of Columbia have passed laws specifically criminalizing stalking.3
When a psychiatrist is stalked
In her book, I Know You Really Love Me,4 psychiatrist Doreen Orion, MD, recounts her experience as a stalking victim. Her victimization began in 1989, when she was on night call for a psychiatric hospital in Arizona. One of the patients she admitted that night was Fran, who developed the erotomanic delusion that Dr. Orion loved her. Despite all evidence to the contrary, Fran pursued Dr. Orion for nearly 8 years, even following her to another state.
Dr. Orion’s book illustrates several issues of import, starting with a crucial failure to communicate. The following morning, Dr. Orion went to the psychiatric hospital to evaluate the patients she had admitted the night before. She contacted Fran’s treating psychiatrist, who angrily hung up on Dr. Orion because Fran had been admitted to the “wrong hospital.” He neglected to inform Dr. Orion that Fran had a history of same-sex stalking and erotomanic delusions. Had she been informed of Fran’s stalking patterns. Dr. Orion may have then simply transferred Fran’s care to a male colleague.
Ultimately, some of Dr. Orion’s colleagues viewed her as somehow inviting or being at fault for her stalking victimization. This classic “blaming the victim” aggravated a situation that was already maddening enough. (Eventually, after several legal and psychiatric evaluations, the stalking stopped.)
Dr. Orion’s book is a cautionary tale. Knowing the patient’s history by reviewing prior records and contacting former treating clinicians can uncover a past pattern of stalking. However, as we are well aware today, terrorists may not become known as such until their first terrorist act; with stalkers, a previous pattern may not be apparent in some cases.
It is important to recognize stalking behaviors for what they are and to act quickly. As psychiatrists, we may be more able than other clinicians to do this because we are trained to ask the patient questions, then simultaneously observe and monitor both the patient’s behavior and our reactions to it. Gavin DeBecker’s book, The Gift of Fear,5 details the survival properties of being in tune with one’s fear response as protective.
Typically, stalking has an insidious onset and may even seem initially harmless, perhaps noted as an erotic transference. But you must pay attention to the behavior and how it makes you feel. Be aware that it may escalate and be prepared to take measures to protect yourself.
Questions to ask yourself might include:
- What are your clinical impressions?
- Are axis I and/or axis II disorders present that may respond to treatment?
- Is your therapeutic relationship with the patient fairly new, or is this an established doctor-patient relationship?
- Is the patient an otherwise stable person who is under stress and engaging in uncharacteristic behavior?
Consider the answers carefully, bearing in mind the typology or typologies involved (Table 1). Stalking encompasses a continuum of unwanted behaviors, ranging from the innocuous to overt and harmful stalking. Your clinical decision-making depends on the typology and intensity of the behavior, as well as your own tolerance for such behaviors.
Table 1
STALKER CLASSIFICATION SYSTEM*
| Type | Features | Assault potential | Response to legal interventions | Response to mental health interventions |
|---|---|---|---|---|
| Rejected | Response to an unwelcome end to relationship Seeks to maintain the relationship Long duration | Along with Predatory, the most likely to assault | Will usually curb behaviors | Typically not responsive to therapy |
| Resentful | Response to a perceived insult Seeks vindication Self-righteous and self-pitying | Most likely to threaten, least likely to assault | Will usually stop behaviors | Difficult to engage in therapy Focus on ruminations that drive stalkers |
| Intimacy seeking | Belief that they are loved or will be loved by the victim Satisfies need for contact and feeds fantasies of eventual loving relationship | May assault | Impervious to legal interventions | If erotomanic delusions are present, they are resistive to change |
| Incompetent | Intellectually limited Socially incompetent Desires intimacy but lacks sufficient skills in courting rituals | Low assault potential | Will stop Typically has previous stalking victims Responsive to restraining orders | May benefit from basic social skills and courting rituals education |
| Predatory | Desire is for sexual gratification and control Rehearsal for violent sexual fantasies and satisfaction of voyeuristic and sadistic desires | High assault potential | Cannot determine before an attack | Poor candidate for therapy |
| *Mullen P, Pathe M, Purcell R, Stuart G. Study of Stalkers. Am J Psychiatry. 1999; 156:1244-1249. | ||||
Interestingly, a female patient also exhibited unwanted behavior toward Dr. Orion’s psychiatrist husband. This patient frequently parked in front of their home in the evenings. Unlike Fran, whose stalking behaviors became increasingly intrusive, frightening, and violent, this patient did not escalate her behavior. It was an unwanted intrusion, but he did not feel fearful or victimized by it. Therefore, it didn’t meet the clinical or legal definition of stalking—the unwanted behaviors must produce fear in the victim. Another psychiatrist, however, might consider the same scenario to be fearful.
Terminating the therapeutic relationship
Once you have reviewed the case with a colleague and/or a threat-assessment professional and determined that you feel uncomfortable and unsafe, it’s time to terminate the doctor-patient relationship.
Ethical and professional care dictates that you provide the patient with a reasonable written notice (e.g., 30 days) prior to termination. Three referral options with phone numbers are typically provided. This also protects you from a potential malpractice tort of abandonment while the patient still needs treatment. If you sense possibly imminent danger, however, you may need to abbreviate the 30-day notice.
Write a summary note in the patient’s chart that includes, in addition to the usual case summary components, the following:
- Your reason(s) for termination. Include discussion with colleagues and/or threat assessment or law enforcement professionals;
- Your diagnostic and treatment impressions, the treatment provided, and the patient’s response to treatment;
- Your referral choices and the rationale for those decisions, e.g., “female patient with schizophrenia and erotomanic delusions and a history of same-sex stalking referred to a male psychiatrist.” The referral should be made to an outside agency or system. (Once Dr. Orion realized that she was being stalked, she initially made the mistake of transferring her patient to a male colleague who shared her office suite, thus making it easy for Fran to continue to stalk Dr. Orion in her own office.)
- Documentation of your discussion with professionals to whom you are referring the patient, along with the patient’s release of information permitting you to do so.
- Documentation of your discussion with the patient. If applicable, include your statement that you feel it is in the patient’s best interest to continue psychiatric care.
- A copy of the termination letter.
If the stalking persists, the psychiatrist should follow guidelines for victims provided later in this article.
J.P. and his ‘ex-girlfriend’
J.P., 19, met Ms. T. when both were 16 and still in high school. Ms. T. was a “partying friend”; they smoked pot together and “hung out.” Although they never dated nor had a romantic relationship, J.P. found Ms. T. to be “pretty and fun,” and developed secret romantic feelings for her.
In their senior year, J.P. wrote Ms. T. a letter professing his love for her. She laughed at it, was dismissive of his feelings, and shared it with friends. He subsequently felt humiliated and rejected and, in retaliation, began spreading rumors that she was a “witch” and a “lesbian.”
After their graduation, they saw each other on a few occasions at parties, but rarely spoke. About a year and a half later, J.P. saw Ms T. with a man he had once fought. He regarded this man as “no good” and a poor choice on Ms. T.’s part. He obtained her phone number from one of their mutual high school acquaintances and called her. They spoke briefly; he accused her of “using drugs and dating an asshole.”
In Ohio, the legal definition of menacing by stalking* includes:
- Engaging in a pattern of conduct that knowingly causes another to believe that the offender will cause physical harm to the other person or cause mental distress to the other person
- A first-degree misdemeanor or fourth-degree felony
Clinical definitions of stalking include:
- The willful, malicious, and repeated following and harassing of another person that threatens his or her safety
- Repeated and persistent unwanted communications and/or approaches that produce fear in the victim
Unwanted communications or behaviors that a stalker might engage in:
- Sending letters
- Phone calls
- E-mails
- Appearing at victim’s home or workplace
- Destroying property
- Assault
- Murder
Typical profile of a stalker:
- Male
- Unemployed or underemployed
- Single or divorced
- Criminal, psychiatric, and drug abuse history
- High school or college education
- Significantly more intelligent than other criminals
- Suffered loss of primary caretaker in childhood
- Significant loss, usually of a job or relationship, within a year of the onset of stalking
*Ohio revised code. Sec. 2903.211
- Whether to change a phone line. One recommendation is to maintain the phone line with an answering machine turned down and let the stalker call it. The victim then obtains another phone line and gives the number only to select friends, colleagues, etc. This way the stalker has a venue for self-expression but the victim does not have to listen to it. Law enforcement can be given the tapes for review. By allowing the stalker continued access to the phone line, the stalker does not have to seek out other potentially more violent ways to pursue his or her victim.
- Whether to seek a restraining order. There is some disagreement on whether restraining orders are useful. In some cases, a restraining order may escalate the situation, such as with prior intimates. In other situations, it may give the victim a false sense of security and ultimately may be of little use if the stalker violates it. When the stalker violates a restraining order and experiences no significant painful consequences, this can increase his sense of power and correspondingly reduce that of the victim.
Source: www.stalkingassistance.com
Thus began a pattern of unwanted phone calls and letters left through the mail slot of her parents’ front door and on her car windshield. One letter featured a drawing of 2 tombstones, one with his name and one with hers, with R.I.P. (Rot In Pieces) scrawled below her tombstone. When asked how he thought she might respond to this, J.P. shrugged and explained it was “funny.” He claimed he was “just imitating Eminem,” a well-known “badboy” rapper who has a similar tattoo on his abdomen.
One letter indicated his desire to become a professional baseball player and his belief that if he had her love, he could succeed at this endeavor. He seemed unaffected by her lack of interest in him.
The situation escalated further when J.P. coincidentally showed up at a downtown club on a night when Ms. T. and her boyfriend were there. The boyfriend (the same one that J.P. had criticized Ms. T. for becoming involved with) hit J.P. A fight ensued; both men were thrown out of the club.
Complicating J.P.’s problems was his ongoing substance abuse including marijuana, alcohol, and weekend ecstasy (MDMA, a mixed hallucinogen/amphetaminelike drug). J.P. had also complained to a psychiatrist of attention-deficit/hyperactivity disorder-like symptoms and was placed on an amphetamine, which he also abused, according to his mother. Finally, the removal of his wisdom teeth necessitated a codeine prescription for pain, which he overused.
J.P. presented to the psychiatric emergency room with full-blown psychosis, about 2 months after he allegedly began stalking Ms. T. He reported paranoid ideations, i.e., communications through the TV and computer, male coworkers reading his mind, and thoughts of killing his “ex-girlfriend” (a misnomer describing Ms. T.).
J.P. was hospitalized and placed on antipsychotic and mood-stabilizing medications, quickly recompensated and was discharged. Diagnostically, he had a myriad of rule-outs at the time and was discharged on mood stabilizing and antipsychotic medications.
Mediation was attempted in an effort to end the stalking, but J.P. appeared “disorganized” and alarmed both Ms. T. and her parents. J.P. then was scheduled for a court trial and underwent a court-ordered psychiatric evaluation. He did not qualify to plead not guilty by reason of insanity as defined by Ohio statute.
J.P. was found guilty of menacing by stalking and was sentenced to a year probation. He was ordered to continue psychiatric treatment and was barred from any contact with the victim. To my knowledge, the stalking has stopped.
What this case illustrates
Stalking is not a new crime; it has been around for centuries.6 But what was once romanticized as a persistent and devoted lover’s pursuit is now considered intrusive and a violation of an individual’s basic right to be left alone.7 See Box 1 for legal and clinical definitions of stalking.
In the case vignette, Ms. T. made several good choices that are in line with current recommendations for stalking victims. She did:
List each event of stalking behavior, recording its nature according the keys indicated below. Make a copy of this record on a regular basis for a family member or trusted professional.
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:________________________________________________________________
Witnesses:_____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:___________ Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):_________________________________________________
Place:_______________________________________________________________
Witnesses:____________________________________________________________
____________________________________________________________________
Description:___________________________________________________________
____________________________________________________________________
Date:____________Time: From______________am/pm To_________________am/pm
Stalking Behavior Key(s):__________________________________________________
Place:_________________________________________________________________
Witnesses:_____________________________________________________________
_____________________________________________________________________
Description:____________________________________________________________
_____________________________________________________________________
Stalking Behaviors Key:
Ph = Phone Calling PD = Property Damage L = Letters T = Threats F = Following K = Kidnapping
E = E-mail G = Gift NV = Non-Violent Threats A = Assault SV = Surveillance SL = Defamation/Slander
List Emergency Numbers:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
Source: www.stalkingbehavior.com
- Inform neighbors and friends and provide them a description of the stalker;
- Screen calls and block calls from his number (Box 2);
- Notify police and file an affidavit against him (Box 2);
- Buy new locks and secure her doors with deadbolts;
- Add exterior and motion-detector lighting;
- Document and record all incidents involving the stalker, and save all unwanted correspondence (e.g., letters) from him.
But Ms. T. also made some poor choices contrary to current recommendations. She did not:
- End all contact and communication with the stalker; instead she tried to be nice (after all, they were old high school friends) and to chat with him superficially. This encouraged his continued stalking behaviors.
- Refuse to attend the proposed mediation process. This illustrates a lack of understanding of stalking. Her attendance unwittingly reinforced the stalker and failed to curb his behaviors.
You must take into consideration the stalker’s typology, which will aid in predicting his or her likely response to legal intervention. Several stalker classification systems have been devised. The one created by Mullen et al (Table 1) is most widely accepted at this time. It is based on:
- The stalker’s motivation;
- His or her prior relationship with the victim;
- Whether the stalker is psychotic.
Knowing the typology can help determine the risk to victims and guide effective and protective victim responses. Typologies may overlap. Both psychotic and nonpsychotic stalkers are equally likely to threaten, but nonpsychotic stalkers are twice as likely to assault.
Restraining orders typically do not sway intimacy-seeking and delusional stalkers. In fact, stalkers may view restraining orders merely as obstacles they must overcome in order to achieve union with their beloved. A restraining order might work in some instances but it is wise to know the law in your state and what steps law enforcement will actually take if the order is violated. If the violation results in just a citation, not arrest or incarceration, it probably isn’t worth the trouble. Even if the law takes further steps, it is typically for a brief time and the action may ultimately enrage the stalker and escalate him to a violent act. Violent episodes are typically not preceded by a specific threat.8
Aside from law enforcement, publicly funded and private threat-assessment teams are located throughout the country. [See “Related resources,” below.] These can help you review the stalking situation in detail and arrive at the most effective response.
Finally, it is important to document the stalking behaviors in order to establish a pattern of conduct that could later be used to prosecute the stalker. Written documentation can be detailed in a log book (Box 3). Saving all physical evidence such as letters, gifts, objects, and e-mails can help establish a pattern of stalking behaviors.
- National Organization for Victim Assistance (NOVA) 1757 Park Rd., NW Washington, DC 20010 (800) 879-6682 or (202) 232-6682.
- National Center for Victims of Crime www.ncvc.org (703) 276-2880
- Stalking Behavior. www.stalkingbehavior.com
- The Stalking Assistance Site. www.stalkingassistance.com
- National Victim Center help guide for stalking victims http://www.ojp.usdoj.gov/ovc/assist/nvaa/ch21-2st.htm
1. The Stalking Assistance Site home page. www.stalkingassistance.com.
2. Tjaden P. The crime of stalking: how big is the problem? Washington, DC, U.S. Department of Justice, National Institute of Justice, Nov. 1977. Call The National Criminal Justice Reference Service at (800) 851-3420, ask for NCJ# FS 000186.
3. U.S. Department of Justice Report to Congress on Stalking and Domestic Violence, May 2001.
4. Orion D. I Know You Really Love Me: A Psychiatrist’s Account of Stalking and Obsessive Love. New York: Bantam Doubleday Dell Publishing Group, 1997.
5. deBecker G. The Gift of Fear (and Other Survival Strategies that Protect Us from Violence). Studio City, Calif: Gavin deBecker & Associates, www.gdbinc.com.
6. Meloy JR. Stalking: An old behavior, a new crime. Psychiatr Clin North Am. 1999;22(2):85-99.
7. Supreme Court Justice Brandeis, Olmstead v. United States, 227U.S.438 (1928).
8. Dietz P, Matthews D, et al. Threatening and otherwise inappropriate letters sent to members of the United States Congress. J Forensic Sci. 1991;36(5):1445-1468.
1. The Stalking Assistance Site home page. www.stalkingassistance.com.
2. Tjaden P. The crime of stalking: how big is the problem? Washington, DC, U.S. Department of Justice, National Institute of Justice, Nov. 1977. Call The National Criminal Justice Reference Service at (800) 851-3420, ask for NCJ# FS 000186.
3. U.S. Department of Justice Report to Congress on Stalking and Domestic Violence, May 2001.
4. Orion D. I Know You Really Love Me: A Psychiatrist’s Account of Stalking and Obsessive Love. New York: Bantam Doubleday Dell Publishing Group, 1997.
5. deBecker G. The Gift of Fear (and Other Survival Strategies that Protect Us from Violence). Studio City, Calif: Gavin deBecker & Associates, www.gdbinc.com.
6. Meloy JR. Stalking: An old behavior, a new crime. Psychiatr Clin North Am. 1999;22(2):85-99.
7. Supreme Court Justice Brandeis, Olmstead v. United States, 227U.S.438 (1928).
8. Dietz P, Matthews D, et al. Threatening and otherwise inappropriate letters sent to members of the United States Congress. J Forensic Sci. 1991;36(5):1445-1468.
When does shyness become a disorder?
Social phobia was accorded official psychiatric diagnostic status in the United States less than 20 years ago, but has been described in the medical literature for centuries. Hippocrates described such a patient: “He dare not come in company for fear he should be misused, disgraced, overshoot himself in gestures or speeches or be sick; he thinks every man observes him.”1
This observation was made more than 2,000 years ago. Yet social anxiety disorder (SAD) was left largely unstudied until the mid-1980s.2 An estimated 20 million people in the U.S. suffer from this disorder.
What causes some people to break into a cold sweat at the thought of the most casual encounter with a checkout clerk, a coworker, or an acquaintance? Limited evidence points to underlying biological abnormalities in SAD, but there have been no conclusive findings.
Two main subtypes of SAD exist (Box 1). Roughly 25% of sufferers have discrete or nongeneralized SAD, that is, circumscribed social fears limited to one or two situations, such as speaking in public or performing before an audience. The remaining 75% suffer from generalized SAD, the more severe subtype in which all or nearly all interpersonal interactions are difficult.
Generalized SAD often begins early in life, with a mean onset at about age 15, but 35% of the time SAD occurs in individuals before age 10.3 This subtype appears to run in families, while the nongeneralized subtype does not, suggesting that a genetic inheritance is possible. From an etiological perspective, the possible effects of parenting styles of socially anxious parents, or acquisition of social anxiety conditioned by experiencing extreme embarrassment, may also contribute to the development of SAD in some people. Approximately twice as many females as males are affected, and almost all are affected before age 25.3,4 When social fears interfere with social, occupational, or family life, the affected individual is not suffering from normal "shyness," but rather a treatable anxiety disorder.
–Toastmasters slogan
Generalized
- Most social interactions
- Early onset
- Social skills deficit
- High comorbidity
- Lower achievement
- Remission rare
Nongeneralized
- Limited fears
- Later onset
- Social skills normal
- Less comorbidity
- Less Impairment
- Remits often
The National Comorbidity Survey (NCS) estimated lifetime prevalence of SAD at 13.3% and 12-month prevalence at 7.6%, making it the third most common psychiatric disorder, following only major depression and alcohol abuse/dependence.5 Despite this high rate, SAD remains woefully underdiagnosed.
Anyone who has had to speak in public, play a musical instrument at a recital, or perform in some way under the watchful expectation of an audience has experienced anxiety as he or she anticipates the "big moment” (Box 2). Once the performance is under way, the anxiety usually lessens to a more manageable level for most people. In fact, nearly one in three Americans will admit to moderate or great fear of speaking in public.

Mr. L, a 40-year-old eighth-grade teacher, consulted a psychiatrist because he was scheduled to be evaluated by a state education accreditation committee while teaching class. Though he had always passed these before, he had been worried sick for weeks and was experiencing panic attacks each time he thought about the accreditation visit.
He lived with his mother, had never dated, and had few friends. He was extremely inhibited outside the classroom, brought cash to stores to avoid being observed while writing a check or signing credit card slips, and avoided social gatherings outside of his church, which he attended with his mother and tolerated with distress.
Further history revealed that he had quit medical school during his third year because he had so much difficulty presenting cases to the attending on ward rounds that he chose to leave the profession in order to avoid feeling sick each morning and afternoon.
Enough people encounter the fear of public speaking to support the weekly Toastmasters meetings in most U.S. cities. Many people overcome their social anxiety about public speaking or performing with continued practice. However, those with nongeneralized SAD, who are among the most severely affected, may remain so fearful of speaking or performing under scrutiny that they avoid it at any cost—even if it means passing up a job or promotion or even choosing to change professions.
The majority (75%) of those with SAD—representing approximately 15 million individuals in the U.S.—suffer from generalized SAD, a much more severe, potentially disabling subtype. These unfortunate individuals fear and avoid most or all social interactions outside their home except those with family or close friends. When they encounter or even anticipate entering feared social situations, individuals with generalized SAD experience severe anxiety. Blushing, tremulousness, and sweating can be noticed by others, and thus are particularly distressing to those with SAD.
Recovery without treatment is rare. The typically early age at onset of generalized SAD3,4 imposes greater limitations on development of social competence than on those who develop more discrete fear of public speaking or performing later in life—after socialization skills have already developed.
Individuals with SAD frequently suffer from comorbid psychiatric disorders, mostly depression and/or other anxiety disorders.6Figure 1 shows that individuals with SAD are at significantly increased risk for depression, other anxiety disorders, and alcohol and drug abuse. Since generalized SAD usually appears at an earlier age than other anxiety disorders, it represents a risk factor for subsequent depression. The level of functional impairment caused by SAD is similar to that caused by major depression7 (Figure 2).
As more comorbid psychiatric disorders accrue, impairment and increased risk for additional disorders may occur. Further, the risk of suicide is increased in those with comorbid SAD vs. those with SAD only. The findings suggest that if social anxiety were detected and treated effectively at an early age, it might be possible to prevent other psychiatric disorders—particularly depression—as well as the predictable morbidity and mortality that accompanies untreated SAD. Given the estimated $44 billion annual cost of anxiety disorders in the U.S.,8 research targeted at testing this hypothesis would appear to be a good investment.
Figure 1 HOW PREVALENT IS LIFETIME COMORBIDITY IN SAD?
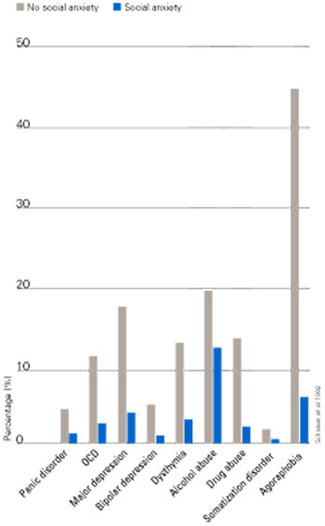
- Inherent avoidance of scrutiny, (e.g., evaluation)
- Uncertain diagnostic threshold
- Acceptance of pathological shyness as ‘just my personality’
- Lack of understanding by professionals, family, friends
- Coping strategies that mask disability
- Comorbid psychiatric disorders that mask SAD
Figure 2 QUALITY OF LIFE IN PATIENTS WITH SOCIAL ANXIETY DISORDER
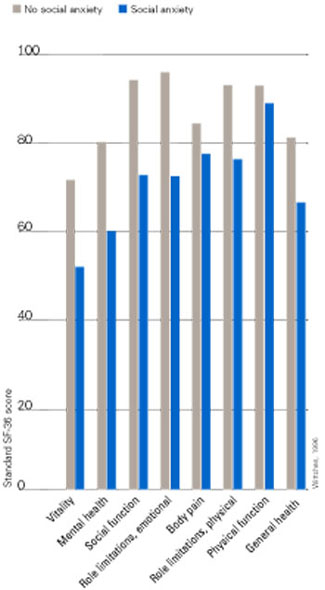
Seeing the unseen: making the diagnosis quickly
Although SAD is extremely common, a variety of factors may contribute to the low rate of recognition of the disorder (Box 3). Because of their intense discomfort toward scrutiny by authority figures such as their physician, individuals with SAD may not be willing to discuss their fears. Studies estimating the prevalence in primary care suggest that these individuals visit their referring physicians at about the same rate as the general population.6,9-11 Affected individuals are unlikely to seek psychiatric treatment unless they have a comorbid depression or anxiety.6,7
Table 1
DIFFERENTIAL DIAGNOSIS FOR SOCIAL ANXIETY DISORDER
| Condition | Diagnostic features |
|---|---|
| Posttraumatic stress disorder | Temporally follows traumatic event; cues related to trauma, not exclusively to social situations |
| Panic disorder | Unexpected panic attacks, not exclusively socially mediated anxiety |
| Agoraphobia | Fearful avoidance of situations in which panic attacks may occur, not limited to social situations |
| Major depression or atypical depression | Social withdrawal temporally related to mood disturbance, not to fear of humiliation or embarrassment; atypical depression with rejection sensitivity associated with other symptoms (e.g., hypersomnia, hyperphagia, anergy, mood reactivity) |
| Generalized anxiety disorder | Focus of worry not limited to social situations; social discomfort or avoidance not a key feature |
| Body dysmorphic disorder | Avoidance of social activity focused on concern over perceived ugliness |
| Avoidant personality disorder | Often present in generalized social anxiety disorder; may represent more severe end of social anxiety disorder spectrum; social activity desired but avoided |
| Schizotypal/schizoid personality disorders | Avoidance of social situations is preferred by individual and is not due to fear of embarrassment or humiliation |
| Normal shyness | Minimal or no interference with social, occupational, or family functioning |
| Adapted from Lydiard RB. Social anxiety disorder: comorbidity and its implications. J Clin Psychiatry.2001;62(suppl 1):17-23. | |
SAD can be difficult to tease apart from other coexisting conditions. Individuals who present for treatment of other anxiety disorders, depression, or substance abuse disorders should be considered at risk for current but undetected SAD. Many of the symptoms overlap (Table 1). The key diagnostic feature, which leads to the diagnosis of SAD, is that the fear and avoidance specifically are related to being in or anticipating a feared social situation (Box 4).
Social
- Attending parties, weddings etc.
- Conversing in a group
- Speaking on the telephone
- Interacting with authority figure (e.g., teacher or boss)
- Making eye contact
- Ordering in a restaurant
Performance
- Public speaking
- Eating in public
- Writing a check
- Using a public toilet
- Taking a test
- Trying on clothes in a store
- Speaking up at a meeting
Many clinicians mistake social anxiety for panic disorder, since panic attacks in people with SAD are often cued by social situations. There can be up to a 40% overlap of SAD with panic disorder.4 Without probing carefully into the focus on fear and avoidance, SAD can be easily overlooked. Individuals with panic disorder experience unexpected attacks and are terrified at the prospect of additional attacks, while those with SAD experience attacks linked to social situations and fear scrutiny and embarrassment more than the attacks themselves.
SAD and major depression frequently coexist,4,11,12 challenging clinicians to distinguish social reticence and withdrawal accompanying depression from the fearful avoidance that typifies SAD. SAD usually precedes depression. Asking if the patient experienced social anxiety prior to the onset of depression can help identify SAD with comorbid depression.
Alcohol-related disorders are twice as likely to occur in those affected by SAD as in those not affected. The risk for females increases more than it does for males.2-4 SAD most often precedes alcohol abuse. Studies show that about 30% of patients receiving treatment for alcohol abuse/dependence have SAD. If it remains undetected, the risk of rapid relapse is high. That’s because patients are highly unlikely to participate in psychosocial treatments that help sustain post-treatment abstinence, such as the Alcoholics Anonymous 12-step program. A recent study found that both social anxiety and alcohol abuse disorders improve when SAD in alcoholics is treated.13
A substantially higher percentage of adults with SAD, especially women, have histories of prior childhood sexual and/or physical abuse than the general population.14 Recent studies both in women following rape and in combat veterans with posttraumatic stress disorder (PTSD) suggest that those with perceived life-threatening events are at higher risk for developing secondary SAD than are individuals who experience less severe trauma.15,16 We do not yet know if secondary SAD in trauma victims is different in character or response to treatment.
Individuals with certain medical conditions can develop symptoms resembling SAD. These include stuttering, benign essential tremor,17 Parkinson’s disease, disfiguring burn injuries, and possibly irritable bowel syndrome. Such patients are technically excluded from being diagnosed with SAD, though they would meet criteria if the diagnostic rules were suspended. A limited body of literature and clinical experience suggests that symptoms secondary to physical conditions may respond to the same treatment as SAD in medically healthy persons. A treatment trial for selected patients with SAD symptoms associated with medical conditions may provide significant benefits. Clearly more research is needed in this area.
- “Being embarrassed or looking stupid are among my worst fears.”
- “Fear of embarrassment causes me to avoid doing things or speaking to people.”
- “I avoid activities in which I am the center of attention.”
Connor et al, Depress Anxiety 2001;14:137
A recently developed self-rating scale, the Social Phobia Inventory (SPIN), assesses the spectrum of cognitive, behavioral, and physiological symptoms associated with SAD.18 Three of the 17 SPIN items have been found to identify generalized SAD with a high degree of sensitivity (Box 5).
The 3 main goals of SAD treatment are
- Acute reduction and control of pathological anxiety and related phobic avoidance;
- Adequate treatment of depression or other comorbid conditions;
- Long-term management of the social phobia.
Significant advances in treatment have emerged over the past 2 decades. We now know that cognitive behavioral therapy (CBT), medication, and their combination are efficacious.
Social situations involving speaking or performance are usually predictable, and nongeneralized SAD is thus amenable to use of a beta-blocker or benzodiazepine (Box 6). Beta-blockers are often adequate for control of tremor and increased heart rate. Some patients may also benefit more from judicious use of a benzodiazepine prior to the event.
In contrast, generalized SAD is less predictable, and continual treatment is recommended. Ideally, a medication regimen would be easily tolerated long-term, and would have antidepressant effects and a broad spectrum of efficacy against commonly coexisting disorders. Because of the significant risk for depression in individuals with SAD, first-line antidepressant treatment is preferred when possible over other medications.
The selective serotonin reuptake inhibitors (SSRIs) are now considered the first-line pharmacological treatment for social phobia. Paroxetine was the first to receive FDA approval for generalized SAD.19 Large multicenter studies supporting the efficacy of two other SSRIs—sertraline and fluvoxamine—have been reported.12 The SSRIs also appear to work against the other psychiatric disorders with which SAD commonly co-occurs, such as panic disorder, major depression, generalized anxiety disorder, and PTSD.
The empirical database is very limited, but it appears that SSRI treatment for a significant percentage of patients with SAD may require higher doses (up to twice the amount) than are usually needed for depression.10 Approximately 50% to 65% of patients with generalized SAD respond to any given SSRI. In our experience, failure to respond to one SSRI does not preclude response to a second SSRI.
The irreversible monoamine oxidase (MAO) inhibitor phenelzine was the first antidepressant shown to be useful for SAD. Tranylcypromine is less well studied, but also appears to be effective. The significant side effects (weight gain, orthostatic hypotension, insomnia) and inconvenience of administration have reduced use of these agents.
Nongeneralized
- PRN treatment
- Beta-blockers
- Benzodiazepines
Generalized
- Continuous treatment
- Broad-spectrum antidepressants
- Benzodiazepines
- MAOIs
- Antiepileptic agents
The tricyclic antidepressants are probably not effective, with the exception of clomipramine (also a potent inhibitor of serotonin reuptake).12 Clomipramine, while an effective anxiolytic and antidepressant, causes prohibitive side effects in many patients (e.g., sexual dysfunction and weight gain).
Key elements for individual or group setting
- Cognitive “restructuring”
- Social skills enhancement
The newer antidepressants venlafaxine and nefazodone are less well studied than the SSRIs, but show promise as potential broad-spectrum agents. Bupropion, a novel antidepressant, and the azapirone anxiolytic buspirone do not appear to work against SAD.
The main role of the benzodiazepines in SAD treatment is adjunctive to antidepressants or in some patients intolerant of, or unresponsive to, other treatments. Clonazepam, alprazolam, and probably others are effective for SAD, but they may not effectively treat or prevent depression or other commonly associated disorders.
The anticonvulsant gabapentin has been shown in one controlled study to be effective in treating SAD.20 This agent may be particularly useful for complicated patients such as those with a history of alcohol-related disorders, bipolar-spectrum disorder, or intolerance to SSRIs.
In parallel with the development of effective psychopharmacological treatments, several types of behavioral and cognitive behavioral treatments have been investigated, including imaginal flooding, graduated exposure, social skills training, cognitive-behavior approaches, and combined cognitive restructuring and graduated exposure.21 These treatments involve similar elements targeted at the cognitive distortions and avoidance behaviors, which represent core features of SAD (Box 7).
Many clinicians believe that combined pharmacotherapy and CBT treatment are superior to either modality alone for treating SAD. The little empirical information available indicates that acute treatment differences between drug alone and drug in combination with CBT are not impressive. However, there appears to be a lower rate of relapse following CBT than after medication discontinuation.
Despite our ability to treat this disorder, only a small fraction of sufferers get treatment. If untreated, the risk of comorbidity is extremely high. Routine screening for SAD, especially in younger individuals, could provide for early detection and treatment. Psychiatrists can play an important role in early detection and treatment by educating consumers, teachers, school nurses, psychologists, and pediatricians.
Related resources
- Lydiard, R.B. Social anxiety disorder comorbidity and its implications J. Clin. Psychiatry. 2001;62(suppl):17-23.
- American Psychiatric Association, http://www.psych.org
- American Psychological Association, http://www.apa.org
- National Institute for Mental Health: Anxiety Disorders, http://www.nimh.nih.gov/anxiety/
- Anxiety Disorders Associations of America, http://www.adaa.org/
Drug brand names
- Alprazolam • Xanax
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lorazepam • Ativan
- Nefazodone • Serzone
- Paroxetine • Paxil
- Phenelzine • Nardil
- Propranolol • Inderal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor
Disclosure
The author reports that he has received grant/research support and has served as a consultant to and on the speaker's bureau of Bristol-Myers Squibb Co., GlaxoSmithKline, Pfizer Inc., Eli Lilly and Co., Parke-Davis, and Solvay Pharmaceuticals. He also has received grant/research support and served as a consultant for Forest Pharmaceuticals, Wyeth-Ayerst Pharmaceuticals, and Roche; received grant/research support from Sanofi-Synthelabo; and has served as consultant for Dupont Pharmaceuticals and AstraZeneca.
1. Burton R. The Anatomy of Melancholy, vol. 1, 11th ed. London, England. Thomas Tegg, Cheapside; 1845.
2. Liebowitz MR, Gorman JM, Fyer AJ, Klein DF. Social phobia: review of a neglected anxiety disorder. Arch Gen Psychiatry. 1985;42:729-736.
3. Magee WJ, Eaton WW, Wittchen HU, et al. Agoraphobia, simple phobia, and social phobia in the National Comorbidity Survey. Arch Gen Psychiatry. 1996;53:159-168.
4. Schneier FR, Johnson J, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282-288.
5. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8-19.
6. Goldenberg IM, et al. The infrequency of “pure culture” diagnosis among the anxiety disorders. J Clin Psychiatry. 1996;57:528-533.
7. Wittchen HU, Beloch E. The impact of social phobia on quality of life. Int Clin Psychopharmacol. 1996;11(suppl):15-23.
8. Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999;60:427-435.
9. Weiller E, Bisserbe JC, Boyer P, et al. Social phobia in general health care. Br J Psychiatry. 1996;168:169-174.
10. Katzelnick DJ, Greist JH. Social anxiety disorder: an unrecognized problem in primary care. J Clin Psychiatry. 2001;62:11.-
11. Davidson J. Social anxiety disorder under scrutiny. Depress Anxiety. 2000;11:93-98.
12. Lydiard RB. Social anxiety disorder: treatment role of the SSRIs. In Montgomery SA, den Boer JA (eds). SSRIs in Depression and Anxiety Perspectives in Psychiatry ,vol 8. NY: Wiley, Chichester, 129-150, 2001.
13. Randall CL, et al. Paroxetine improves both social anxiety and alcohol use in dually-diagnosed patients at the American College of Neuropsychopharmacology. San Juan, Puerto Rico. Dec 10-15, 2000.
14. Stein MB, Walker JR, Anderson G, et al. Childhood physical and sexual abuse in patients with anxiety disorders and in a community sample. Am J Psychiatry. 1996;153:275-277.
15. Boudreaux E, Kilpatrick DG, Resnick HS, et al. Criminal victimization, posttraumatic stress disorder, and comorbid psychopathology among a community sample of women. J Trauma Stress. 1998;11:665-678.
16. Orsillo SM, Heimberg RG, Juster HR, Garrett J. Social phobia and PTSD in Vietnam veterans. J Trauma Stress. 1996;9:235-252.
17. George MS, Lydiard RB. Social phobia secondary to physical disability: a review of benign essential tremor (BET) and stuttering. Psychosomatics. 1994;35:520-523.
18. Connor KM, et al. Mini-SPIN: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety. 2001;14:137-140.
19. Stein MB, Liebowitz MR, Lydiard RB, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial. JAMA. 1998;280:708-713.
20. Pande AC, Davidson JR, Jefferson JW, et al. Treatment of social phobia with gabapentin: a placebo-controlled study. J Clin Psychopharmacol. 1999;19:341-348.
21. Heimberg RG. Specific issues in the cognitive behavioral treatment of social phobia. J Clin Psychiatry. 1993;54(suppl 12):36-45.
Social phobia was accorded official psychiatric diagnostic status in the United States less than 20 years ago, but has been described in the medical literature for centuries. Hippocrates described such a patient: “He dare not come in company for fear he should be misused, disgraced, overshoot himself in gestures or speeches or be sick; he thinks every man observes him.”1
This observation was made more than 2,000 years ago. Yet social anxiety disorder (SAD) was left largely unstudied until the mid-1980s.2 An estimated 20 million people in the U.S. suffer from this disorder.
What causes some people to break into a cold sweat at the thought of the most casual encounter with a checkout clerk, a coworker, or an acquaintance? Limited evidence points to underlying biological abnormalities in SAD, but there have been no conclusive findings.
Two main subtypes of SAD exist (Box 1). Roughly 25% of sufferers have discrete or nongeneralized SAD, that is, circumscribed social fears limited to one or two situations, such as speaking in public or performing before an audience. The remaining 75% suffer from generalized SAD, the more severe subtype in which all or nearly all interpersonal interactions are difficult.
Generalized SAD often begins early in life, with a mean onset at about age 15, but 35% of the time SAD occurs in individuals before age 10.3 This subtype appears to run in families, while the nongeneralized subtype does not, suggesting that a genetic inheritance is possible. From an etiological perspective, the possible effects of parenting styles of socially anxious parents, or acquisition of social anxiety conditioned by experiencing extreme embarrassment, may also contribute to the development of SAD in some people. Approximately twice as many females as males are affected, and almost all are affected before age 25.3,4 When social fears interfere with social, occupational, or family life, the affected individual is not suffering from normal "shyness," but rather a treatable anxiety disorder.
–Toastmasters slogan
Generalized
- Most social interactions
- Early onset
- Social skills deficit
- High comorbidity
- Lower achievement
- Remission rare
Nongeneralized
- Limited fears
- Later onset
- Social skills normal
- Less comorbidity
- Less Impairment
- Remits often
The National Comorbidity Survey (NCS) estimated lifetime prevalence of SAD at 13.3% and 12-month prevalence at 7.6%, making it the third most common psychiatric disorder, following only major depression and alcohol abuse/dependence.5 Despite this high rate, SAD remains woefully underdiagnosed.
Anyone who has had to speak in public, play a musical instrument at a recital, or perform in some way under the watchful expectation of an audience has experienced anxiety as he or she anticipates the "big moment” (Box 2). Once the performance is under way, the anxiety usually lessens to a more manageable level for most people. In fact, nearly one in three Americans will admit to moderate or great fear of speaking in public.
Mr. L, a 40-year-old eighth-grade teacher, consulted a psychiatrist because he was scheduled to be evaluated by a state education accreditation committee while teaching class. Though he had always passed these before, he had been worried sick for weeks and was experiencing panic attacks each time he thought about the accreditation visit.
He lived with his mother, had never dated, and had few friends. He was extremely inhibited outside the classroom, brought cash to stores to avoid being observed while writing a check or signing credit card slips, and avoided social gatherings outside of his church, which he attended with his mother and tolerated with distress.
Further history revealed that he had quit medical school during his third year because he had so much difficulty presenting cases to the attending on ward rounds that he chose to leave the profession in order to avoid feeling sick each morning and afternoon.
Enough people encounter the fear of public speaking to support the weekly Toastmasters meetings in most U.S. cities. Many people overcome their social anxiety about public speaking or performing with continued practice. However, those with nongeneralized SAD, who are among the most severely affected, may remain so fearful of speaking or performing under scrutiny that they avoid it at any cost—even if it means passing up a job or promotion or even choosing to change professions.
The majority (75%) of those with SAD—representing approximately 15 million individuals in the U.S.—suffer from generalized SAD, a much more severe, potentially disabling subtype. These unfortunate individuals fear and avoid most or all social interactions outside their home except those with family or close friends. When they encounter or even anticipate entering feared social situations, individuals with generalized SAD experience severe anxiety. Blushing, tremulousness, and sweating can be noticed by others, and thus are particularly distressing to those with SAD.
Recovery without treatment is rare. The typically early age at onset of generalized SAD3,4 imposes greater limitations on development of social competence than on those who develop more discrete fear of public speaking or performing later in life—after socialization skills have already developed.
Individuals with SAD frequently suffer from comorbid psychiatric disorders, mostly depression and/or other anxiety disorders.6Figure 1 shows that individuals with SAD are at significantly increased risk for depression, other anxiety disorders, and alcohol and drug abuse. Since generalized SAD usually appears at an earlier age than other anxiety disorders, it represents a risk factor for subsequent depression. The level of functional impairment caused by SAD is similar to that caused by major depression7 (Figure 2).
As more comorbid psychiatric disorders accrue, impairment and increased risk for additional disorders may occur. Further, the risk of suicide is increased in those with comorbid SAD vs. those with SAD only. The findings suggest that if social anxiety were detected and treated effectively at an early age, it might be possible to prevent other psychiatric disorders—particularly depression—as well as the predictable morbidity and mortality that accompanies untreated SAD. Given the estimated $44 billion annual cost of anxiety disorders in the U.S.,8 research targeted at testing this hypothesis would appear to be a good investment.
Figure 1 HOW PREVALENT IS LIFETIME COMORBIDITY IN SAD?
- Inherent avoidance of scrutiny, (e.g., evaluation)
- Uncertain diagnostic threshold
- Acceptance of pathological shyness as ‘just my personality’
- Lack of understanding by professionals, family, friends
- Coping strategies that mask disability
- Comorbid psychiatric disorders that mask SAD
Figure 2 QUALITY OF LIFE IN PATIENTS WITH SOCIAL ANXIETY DISORDER
Seeing the unseen: making the diagnosis quickly
Although SAD is extremely common, a variety of factors may contribute to the low rate of recognition of the disorder (Box 3). Because of their intense discomfort toward scrutiny by authority figures such as their physician, individuals with SAD may not be willing to discuss their fears. Studies estimating the prevalence in primary care suggest that these individuals visit their referring physicians at about the same rate as the general population.6,9-11 Affected individuals are unlikely to seek psychiatric treatment unless they have a comorbid depression or anxiety.6,7
Table 1
DIFFERENTIAL DIAGNOSIS FOR SOCIAL ANXIETY DISORDER
| Condition | Diagnostic features |
|---|---|
| Posttraumatic stress disorder | Temporally follows traumatic event; cues related to trauma, not exclusively to social situations |
| Panic disorder | Unexpected panic attacks, not exclusively socially mediated anxiety |
| Agoraphobia | Fearful avoidance of situations in which panic attacks may occur, not limited to social situations |
| Major depression or atypical depression | Social withdrawal temporally related to mood disturbance, not to fear of humiliation or embarrassment; atypical depression with rejection sensitivity associated with other symptoms (e.g., hypersomnia, hyperphagia, anergy, mood reactivity) |
| Generalized anxiety disorder | Focus of worry not limited to social situations; social discomfort or avoidance not a key feature |
| Body dysmorphic disorder | Avoidance of social activity focused on concern over perceived ugliness |
| Avoidant personality disorder | Often present in generalized social anxiety disorder; may represent more severe end of social anxiety disorder spectrum; social activity desired but avoided |
| Schizotypal/schizoid personality disorders | Avoidance of social situations is preferred by individual and is not due to fear of embarrassment or humiliation |
| Normal shyness | Minimal or no interference with social, occupational, or family functioning |
| Adapted from Lydiard RB. Social anxiety disorder: comorbidity and its implications. J Clin Psychiatry.2001;62(suppl 1):17-23. | |
SAD can be difficult to tease apart from other coexisting conditions. Individuals who present for treatment of other anxiety disorders, depression, or substance abuse disorders should be considered at risk for current but undetected SAD. Many of the symptoms overlap (Table 1). The key diagnostic feature, which leads to the diagnosis of SAD, is that the fear and avoidance specifically are related to being in or anticipating a feared social situation (Box 4).
Social
- Attending parties, weddings etc.
- Conversing in a group
- Speaking on the telephone
- Interacting with authority figure (e.g., teacher or boss)
- Making eye contact
- Ordering in a restaurant
Performance
- Public speaking
- Eating in public
- Writing a check
- Using a public toilet
- Taking a test
- Trying on clothes in a store
- Speaking up at a meeting
Many clinicians mistake social anxiety for panic disorder, since panic attacks in people with SAD are often cued by social situations. There can be up to a 40% overlap of SAD with panic disorder.4 Without probing carefully into the focus on fear and avoidance, SAD can be easily overlooked. Individuals with panic disorder experience unexpected attacks and are terrified at the prospect of additional attacks, while those with SAD experience attacks linked to social situations and fear scrutiny and embarrassment more than the attacks themselves.
SAD and major depression frequently coexist,4,11,12 challenging clinicians to distinguish social reticence and withdrawal accompanying depression from the fearful avoidance that typifies SAD. SAD usually precedes depression. Asking if the patient experienced social anxiety prior to the onset of depression can help identify SAD with comorbid depression.
Alcohol-related disorders are twice as likely to occur in those affected by SAD as in those not affected. The risk for females increases more than it does for males.2-4 SAD most often precedes alcohol abuse. Studies show that about 30% of patients receiving treatment for alcohol abuse/dependence have SAD. If it remains undetected, the risk of rapid relapse is high. That’s because patients are highly unlikely to participate in psychosocial treatments that help sustain post-treatment abstinence, such as the Alcoholics Anonymous 12-step program. A recent study found that both social anxiety and alcohol abuse disorders improve when SAD in alcoholics is treated.13
A substantially higher percentage of adults with SAD, especially women, have histories of prior childhood sexual and/or physical abuse than the general population.14 Recent studies both in women following rape and in combat veterans with posttraumatic stress disorder (PTSD) suggest that those with perceived life-threatening events are at higher risk for developing secondary SAD than are individuals who experience less severe trauma.15,16 We do not yet know if secondary SAD in trauma victims is different in character or response to treatment.
Individuals with certain medical conditions can develop symptoms resembling SAD. These include stuttering, benign essential tremor,17 Parkinson’s disease, disfiguring burn injuries, and possibly irritable bowel syndrome. Such patients are technically excluded from being diagnosed with SAD, though they would meet criteria if the diagnostic rules were suspended. A limited body of literature and clinical experience suggests that symptoms secondary to physical conditions may respond to the same treatment as SAD in medically healthy persons. A treatment trial for selected patients with SAD symptoms associated with medical conditions may provide significant benefits. Clearly more research is needed in this area.
- “Being embarrassed or looking stupid are among my worst fears.”
- “Fear of embarrassment causes me to avoid doing things or speaking to people.”
- “I avoid activities in which I am the center of attention.”
Connor et al, Depress Anxiety 2001;14:137
A recently developed self-rating scale, the Social Phobia Inventory (SPIN), assesses the spectrum of cognitive, behavioral, and physiological symptoms associated with SAD.18 Three of the 17 SPIN items have been found to identify generalized SAD with a high degree of sensitivity (Box 5).
The 3 main goals of SAD treatment are
- Acute reduction and control of pathological anxiety and related phobic avoidance;
- Adequate treatment of depression or other comorbid conditions;
- Long-term management of the social phobia.
Significant advances in treatment have emerged over the past 2 decades. We now know that cognitive behavioral therapy (CBT), medication, and their combination are efficacious.
Social situations involving speaking or performance are usually predictable, and nongeneralized SAD is thus amenable to use of a beta-blocker or benzodiazepine (Box 6). Beta-blockers are often adequate for control of tremor and increased heart rate. Some patients may also benefit more from judicious use of a benzodiazepine prior to the event.
In contrast, generalized SAD is less predictable, and continual treatment is recommended. Ideally, a medication regimen would be easily tolerated long-term, and would have antidepressant effects and a broad spectrum of efficacy against commonly coexisting disorders. Because of the significant risk for depression in individuals with SAD, first-line antidepressant treatment is preferred when possible over other medications.
The selective serotonin reuptake inhibitors (SSRIs) are now considered the first-line pharmacological treatment for social phobia. Paroxetine was the first to receive FDA approval for generalized SAD.19 Large multicenter studies supporting the efficacy of two other SSRIs—sertraline and fluvoxamine—have been reported.12 The SSRIs also appear to work against the other psychiatric disorders with which SAD commonly co-occurs, such as panic disorder, major depression, generalized anxiety disorder, and PTSD.
The empirical database is very limited, but it appears that SSRI treatment for a significant percentage of patients with SAD may require higher doses (up to twice the amount) than are usually needed for depression.10 Approximately 50% to 65% of patients with generalized SAD respond to any given SSRI. In our experience, failure to respond to one SSRI does not preclude response to a second SSRI.
The irreversible monoamine oxidase (MAO) inhibitor phenelzine was the first antidepressant shown to be useful for SAD. Tranylcypromine is less well studied, but also appears to be effective. The significant side effects (weight gain, orthostatic hypotension, insomnia) and inconvenience of administration have reduced use of these agents.
Nongeneralized
- PRN treatment
- Beta-blockers
- Benzodiazepines
Generalized
- Continuous treatment
- Broad-spectrum antidepressants
- Benzodiazepines
- MAOIs
- Antiepileptic agents
The tricyclic antidepressants are probably not effective, with the exception of clomipramine (also a potent inhibitor of serotonin reuptake).12 Clomipramine, while an effective anxiolytic and antidepressant, causes prohibitive side effects in many patients (e.g., sexual dysfunction and weight gain).
Key elements for individual or group setting
- Cognitive “restructuring”
- Social skills enhancement
The newer antidepressants venlafaxine and nefazodone are less well studied than the SSRIs, but show promise as potential broad-spectrum agents. Bupropion, a novel antidepressant, and the azapirone anxiolytic buspirone do not appear to work against SAD.
The main role of the benzodiazepines in SAD treatment is adjunctive to antidepressants or in some patients intolerant of, or unresponsive to, other treatments. Clonazepam, alprazolam, and probably others are effective for SAD, but they may not effectively treat or prevent depression or other commonly associated disorders.
The anticonvulsant gabapentin has been shown in one controlled study to be effective in treating SAD.20 This agent may be particularly useful for complicated patients such as those with a history of alcohol-related disorders, bipolar-spectrum disorder, or intolerance to SSRIs.
In parallel with the development of effective psychopharmacological treatments, several types of behavioral and cognitive behavioral treatments have been investigated, including imaginal flooding, graduated exposure, social skills training, cognitive-behavior approaches, and combined cognitive restructuring and graduated exposure.21 These treatments involve similar elements targeted at the cognitive distortions and avoidance behaviors, which represent core features of SAD (Box 7).
Many clinicians believe that combined pharmacotherapy and CBT treatment are superior to either modality alone for treating SAD. The little empirical information available indicates that acute treatment differences between drug alone and drug in combination with CBT are not impressive. However, there appears to be a lower rate of relapse following CBT than after medication discontinuation.
Despite our ability to treat this disorder, only a small fraction of sufferers get treatment. If untreated, the risk of comorbidity is extremely high. Routine screening for SAD, especially in younger individuals, could provide for early detection and treatment. Psychiatrists can play an important role in early detection and treatment by educating consumers, teachers, school nurses, psychologists, and pediatricians.
Related resources
- Lydiard, R.B. Social anxiety disorder comorbidity and its implications J. Clin. Psychiatry. 2001;62(suppl):17-23.
- American Psychiatric Association, http://www.psych.org
- American Psychological Association, http://www.apa.org
- National Institute for Mental Health: Anxiety Disorders, http://www.nimh.nih.gov/anxiety/
- Anxiety Disorders Associations of America, http://www.adaa.org/
Drug brand names
- Alprazolam • Xanax
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lorazepam • Ativan
- Nefazodone • Serzone
- Paroxetine • Paxil
- Phenelzine • Nardil
- Propranolol • Inderal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor
Disclosure
The author reports that he has received grant/research support and has served as a consultant to and on the speaker's bureau of Bristol-Myers Squibb Co., GlaxoSmithKline, Pfizer Inc., Eli Lilly and Co., Parke-Davis, and Solvay Pharmaceuticals. He also has received grant/research support and served as a consultant for Forest Pharmaceuticals, Wyeth-Ayerst Pharmaceuticals, and Roche; received grant/research support from Sanofi-Synthelabo; and has served as consultant for Dupont Pharmaceuticals and AstraZeneca.
Social phobia was accorded official psychiatric diagnostic status in the United States less than 20 years ago, but has been described in the medical literature for centuries. Hippocrates described such a patient: “He dare not come in company for fear he should be misused, disgraced, overshoot himself in gestures or speeches or be sick; he thinks every man observes him.”1
This observation was made more than 2,000 years ago. Yet social anxiety disorder (SAD) was left largely unstudied until the mid-1980s.2 An estimated 20 million people in the U.S. suffer from this disorder.
What causes some people to break into a cold sweat at the thought of the most casual encounter with a checkout clerk, a coworker, or an acquaintance? Limited evidence points to underlying biological abnormalities in SAD, but there have been no conclusive findings.
Two main subtypes of SAD exist (Box 1). Roughly 25% of sufferers have discrete or nongeneralized SAD, that is, circumscribed social fears limited to one or two situations, such as speaking in public or performing before an audience. The remaining 75% suffer from generalized SAD, the more severe subtype in which all or nearly all interpersonal interactions are difficult.
Generalized SAD often begins early in life, with a mean onset at about age 15, but 35% of the time SAD occurs in individuals before age 10.3 This subtype appears to run in families, while the nongeneralized subtype does not, suggesting that a genetic inheritance is possible. From an etiological perspective, the possible effects of parenting styles of socially anxious parents, or acquisition of social anxiety conditioned by experiencing extreme embarrassment, may also contribute to the development of SAD in some people. Approximately twice as many females as males are affected, and almost all are affected before age 25.3,4 When social fears interfere with social, occupational, or family life, the affected individual is not suffering from normal "shyness," but rather a treatable anxiety disorder.
–Toastmasters slogan
Generalized
- Most social interactions
- Early onset
- Social skills deficit
- High comorbidity
- Lower achievement
- Remission rare
Nongeneralized
- Limited fears
- Later onset
- Social skills normal
- Less comorbidity
- Less Impairment
- Remits often
The National Comorbidity Survey (NCS) estimated lifetime prevalence of SAD at 13.3% and 12-month prevalence at 7.6%, making it the third most common psychiatric disorder, following only major depression and alcohol abuse/dependence.5 Despite this high rate, SAD remains woefully underdiagnosed.
Anyone who has had to speak in public, play a musical instrument at a recital, or perform in some way under the watchful expectation of an audience has experienced anxiety as he or she anticipates the "big moment” (Box 2). Once the performance is under way, the anxiety usually lessens to a more manageable level for most people. In fact, nearly one in three Americans will admit to moderate or great fear of speaking in public.
Mr. L, a 40-year-old eighth-grade teacher, consulted a psychiatrist because he was scheduled to be evaluated by a state education accreditation committee while teaching class. Though he had always passed these before, he had been worried sick for weeks and was experiencing panic attacks each time he thought about the accreditation visit.
He lived with his mother, had never dated, and had few friends. He was extremely inhibited outside the classroom, brought cash to stores to avoid being observed while writing a check or signing credit card slips, and avoided social gatherings outside of his church, which he attended with his mother and tolerated with distress.
Further history revealed that he had quit medical school during his third year because he had so much difficulty presenting cases to the attending on ward rounds that he chose to leave the profession in order to avoid feeling sick each morning and afternoon.
Enough people encounter the fear of public speaking to support the weekly Toastmasters meetings in most U.S. cities. Many people overcome their social anxiety about public speaking or performing with continued practice. However, those with nongeneralized SAD, who are among the most severely affected, may remain so fearful of speaking or performing under scrutiny that they avoid it at any cost—even if it means passing up a job or promotion or even choosing to change professions.
The majority (75%) of those with SAD—representing approximately 15 million individuals in the U.S.—suffer from generalized SAD, a much more severe, potentially disabling subtype. These unfortunate individuals fear and avoid most or all social interactions outside their home except those with family or close friends. When they encounter or even anticipate entering feared social situations, individuals with generalized SAD experience severe anxiety. Blushing, tremulousness, and sweating can be noticed by others, and thus are particularly distressing to those with SAD.
Recovery without treatment is rare. The typically early age at onset of generalized SAD3,4 imposes greater limitations on development of social competence than on those who develop more discrete fear of public speaking or performing later in life—after socialization skills have already developed.
Individuals with SAD frequently suffer from comorbid psychiatric disorders, mostly depression and/or other anxiety disorders.6Figure 1 shows that individuals with SAD are at significantly increased risk for depression, other anxiety disorders, and alcohol and drug abuse. Since generalized SAD usually appears at an earlier age than other anxiety disorders, it represents a risk factor for subsequent depression. The level of functional impairment caused by SAD is similar to that caused by major depression7 (Figure 2).
As more comorbid psychiatric disorders accrue, impairment and increased risk for additional disorders may occur. Further, the risk of suicide is increased in those with comorbid SAD vs. those with SAD only. The findings suggest that if social anxiety were detected and treated effectively at an early age, it might be possible to prevent other psychiatric disorders—particularly depression—as well as the predictable morbidity and mortality that accompanies untreated SAD. Given the estimated $44 billion annual cost of anxiety disorders in the U.S.,8 research targeted at testing this hypothesis would appear to be a good investment.
Figure 1 HOW PREVALENT IS LIFETIME COMORBIDITY IN SAD?
- Inherent avoidance of scrutiny, (e.g., evaluation)
- Uncertain diagnostic threshold
- Acceptance of pathological shyness as ‘just my personality’
- Lack of understanding by professionals, family, friends
- Coping strategies that mask disability
- Comorbid psychiatric disorders that mask SAD
Figure 2 QUALITY OF LIFE IN PATIENTS WITH SOCIAL ANXIETY DISORDER
Seeing the unseen: making the diagnosis quickly
Although SAD is extremely common, a variety of factors may contribute to the low rate of recognition of the disorder (Box 3). Because of their intense discomfort toward scrutiny by authority figures such as their physician, individuals with SAD may not be willing to discuss their fears. Studies estimating the prevalence in primary care suggest that these individuals visit their referring physicians at about the same rate as the general population.6,9-11 Affected individuals are unlikely to seek psychiatric treatment unless they have a comorbid depression or anxiety.6,7
Table 1
DIFFERENTIAL DIAGNOSIS FOR SOCIAL ANXIETY DISORDER
| Condition | Diagnostic features |
|---|---|
| Posttraumatic stress disorder | Temporally follows traumatic event; cues related to trauma, not exclusively to social situations |
| Panic disorder | Unexpected panic attacks, not exclusively socially mediated anxiety |
| Agoraphobia | Fearful avoidance of situations in which panic attacks may occur, not limited to social situations |
| Major depression or atypical depression | Social withdrawal temporally related to mood disturbance, not to fear of humiliation or embarrassment; atypical depression with rejection sensitivity associated with other symptoms (e.g., hypersomnia, hyperphagia, anergy, mood reactivity) |
| Generalized anxiety disorder | Focus of worry not limited to social situations; social discomfort or avoidance not a key feature |
| Body dysmorphic disorder | Avoidance of social activity focused on concern over perceived ugliness |
| Avoidant personality disorder | Often present in generalized social anxiety disorder; may represent more severe end of social anxiety disorder spectrum; social activity desired but avoided |
| Schizotypal/schizoid personality disorders | Avoidance of social situations is preferred by individual and is not due to fear of embarrassment or humiliation |
| Normal shyness | Minimal or no interference with social, occupational, or family functioning |
| Adapted from Lydiard RB. Social anxiety disorder: comorbidity and its implications. J Clin Psychiatry.2001;62(suppl 1):17-23. | |
SAD can be difficult to tease apart from other coexisting conditions. Individuals who present for treatment of other anxiety disorders, depression, or substance abuse disorders should be considered at risk for current but undetected SAD. Many of the symptoms overlap (Table 1). The key diagnostic feature, which leads to the diagnosis of SAD, is that the fear and avoidance specifically are related to being in or anticipating a feared social situation (Box 4).
Social
- Attending parties, weddings etc.
- Conversing in a group
- Speaking on the telephone
- Interacting with authority figure (e.g., teacher or boss)
- Making eye contact
- Ordering in a restaurant
Performance
- Public speaking
- Eating in public
- Writing a check
- Using a public toilet
- Taking a test
- Trying on clothes in a store
- Speaking up at a meeting
Many clinicians mistake social anxiety for panic disorder, since panic attacks in people with SAD are often cued by social situations. There can be up to a 40% overlap of SAD with panic disorder.4 Without probing carefully into the focus on fear and avoidance, SAD can be easily overlooked. Individuals with panic disorder experience unexpected attacks and are terrified at the prospect of additional attacks, while those with SAD experience attacks linked to social situations and fear scrutiny and embarrassment more than the attacks themselves.
SAD and major depression frequently coexist,4,11,12 challenging clinicians to distinguish social reticence and withdrawal accompanying depression from the fearful avoidance that typifies SAD. SAD usually precedes depression. Asking if the patient experienced social anxiety prior to the onset of depression can help identify SAD with comorbid depression.
Alcohol-related disorders are twice as likely to occur in those affected by SAD as in those not affected. The risk for females increases more than it does for males.2-4 SAD most often precedes alcohol abuse. Studies show that about 30% of patients receiving treatment for alcohol abuse/dependence have SAD. If it remains undetected, the risk of rapid relapse is high. That’s because patients are highly unlikely to participate in psychosocial treatments that help sustain post-treatment abstinence, such as the Alcoholics Anonymous 12-step program. A recent study found that both social anxiety and alcohol abuse disorders improve when SAD in alcoholics is treated.13
A substantially higher percentage of adults with SAD, especially women, have histories of prior childhood sexual and/or physical abuse than the general population.14 Recent studies both in women following rape and in combat veterans with posttraumatic stress disorder (PTSD) suggest that those with perceived life-threatening events are at higher risk for developing secondary SAD than are individuals who experience less severe trauma.15,16 We do not yet know if secondary SAD in trauma victims is different in character or response to treatment.
Individuals with certain medical conditions can develop symptoms resembling SAD. These include stuttering, benign essential tremor,17 Parkinson’s disease, disfiguring burn injuries, and possibly irritable bowel syndrome. Such patients are technically excluded from being diagnosed with SAD, though they would meet criteria if the diagnostic rules were suspended. A limited body of literature and clinical experience suggests that symptoms secondary to physical conditions may respond to the same treatment as SAD in medically healthy persons. A treatment trial for selected patients with SAD symptoms associated with medical conditions may provide significant benefits. Clearly more research is needed in this area.
- “Being embarrassed or looking stupid are among my worst fears.”
- “Fear of embarrassment causes me to avoid doing things or speaking to people.”
- “I avoid activities in which I am the center of attention.”
Connor et al, Depress Anxiety 2001;14:137
A recently developed self-rating scale, the Social Phobia Inventory (SPIN), assesses the spectrum of cognitive, behavioral, and physiological symptoms associated with SAD.18 Three of the 17 SPIN items have been found to identify generalized SAD with a high degree of sensitivity (Box 5).
The 3 main goals of SAD treatment are
- Acute reduction and control of pathological anxiety and related phobic avoidance;
- Adequate treatment of depression or other comorbid conditions;
- Long-term management of the social phobia.
Significant advances in treatment have emerged over the past 2 decades. We now know that cognitive behavioral therapy (CBT), medication, and their combination are efficacious.
Social situations involving speaking or performance are usually predictable, and nongeneralized SAD is thus amenable to use of a beta-blocker or benzodiazepine (Box 6). Beta-blockers are often adequate for control of tremor and increased heart rate. Some patients may also benefit more from judicious use of a benzodiazepine prior to the event.
In contrast, generalized SAD is less predictable, and continual treatment is recommended. Ideally, a medication regimen would be easily tolerated long-term, and would have antidepressant effects and a broad spectrum of efficacy against commonly coexisting disorders. Because of the significant risk for depression in individuals with SAD, first-line antidepressant treatment is preferred when possible over other medications.
The selective serotonin reuptake inhibitors (SSRIs) are now considered the first-line pharmacological treatment for social phobia. Paroxetine was the first to receive FDA approval for generalized SAD.19 Large multicenter studies supporting the efficacy of two other SSRIs—sertraline and fluvoxamine—have been reported.12 The SSRIs also appear to work against the other psychiatric disorders with which SAD commonly co-occurs, such as panic disorder, major depression, generalized anxiety disorder, and PTSD.
The empirical database is very limited, but it appears that SSRI treatment for a significant percentage of patients with SAD may require higher doses (up to twice the amount) than are usually needed for depression.10 Approximately 50% to 65% of patients with generalized SAD respond to any given SSRI. In our experience, failure to respond to one SSRI does not preclude response to a second SSRI.
The irreversible monoamine oxidase (MAO) inhibitor phenelzine was the first antidepressant shown to be useful for SAD. Tranylcypromine is less well studied, but also appears to be effective. The significant side effects (weight gain, orthostatic hypotension, insomnia) and inconvenience of administration have reduced use of these agents.
Nongeneralized
- PRN treatment
- Beta-blockers
- Benzodiazepines
Generalized
- Continuous treatment
- Broad-spectrum antidepressants
- Benzodiazepines
- MAOIs
- Antiepileptic agents
The tricyclic antidepressants are probably not effective, with the exception of clomipramine (also a potent inhibitor of serotonin reuptake).12 Clomipramine, while an effective anxiolytic and antidepressant, causes prohibitive side effects in many patients (e.g., sexual dysfunction and weight gain).
Key elements for individual or group setting
- Cognitive “restructuring”
- Social skills enhancement
The newer antidepressants venlafaxine and nefazodone are less well studied than the SSRIs, but show promise as potential broad-spectrum agents. Bupropion, a novel antidepressant, and the azapirone anxiolytic buspirone do not appear to work against SAD.
The main role of the benzodiazepines in SAD treatment is adjunctive to antidepressants or in some patients intolerant of, or unresponsive to, other treatments. Clonazepam, alprazolam, and probably others are effective for SAD, but they may not effectively treat or prevent depression or other commonly associated disorders.
The anticonvulsant gabapentin has been shown in one controlled study to be effective in treating SAD.20 This agent may be particularly useful for complicated patients such as those with a history of alcohol-related disorders, bipolar-spectrum disorder, or intolerance to SSRIs.
In parallel with the development of effective psychopharmacological treatments, several types of behavioral and cognitive behavioral treatments have been investigated, including imaginal flooding, graduated exposure, social skills training, cognitive-behavior approaches, and combined cognitive restructuring and graduated exposure.21 These treatments involve similar elements targeted at the cognitive distortions and avoidance behaviors, which represent core features of SAD (Box 7).
Many clinicians believe that combined pharmacotherapy and CBT treatment are superior to either modality alone for treating SAD. The little empirical information available indicates that acute treatment differences between drug alone and drug in combination with CBT are not impressive. However, there appears to be a lower rate of relapse following CBT than after medication discontinuation.
Despite our ability to treat this disorder, only a small fraction of sufferers get treatment. If untreated, the risk of comorbidity is extremely high. Routine screening for SAD, especially in younger individuals, could provide for early detection and treatment. Psychiatrists can play an important role in early detection and treatment by educating consumers, teachers, school nurses, psychologists, and pediatricians.
Related resources
- Lydiard, R.B. Social anxiety disorder comorbidity and its implications J. Clin. Psychiatry. 2001;62(suppl):17-23.
- American Psychiatric Association, http://www.psych.org
- American Psychological Association, http://www.apa.org
- National Institute for Mental Health: Anxiety Disorders, http://www.nimh.nih.gov/anxiety/
- Anxiety Disorders Associations of America, http://www.adaa.org/
Drug brand names
- Alprazolam • Xanax
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lorazepam • Ativan
- Nefazodone • Serzone
- Paroxetine • Paxil
- Phenelzine • Nardil
- Propranolol • Inderal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor
Disclosure
The author reports that he has received grant/research support and has served as a consultant to and on the speaker's bureau of Bristol-Myers Squibb Co., GlaxoSmithKline, Pfizer Inc., Eli Lilly and Co., Parke-Davis, and Solvay Pharmaceuticals. He also has received grant/research support and served as a consultant for Forest Pharmaceuticals, Wyeth-Ayerst Pharmaceuticals, and Roche; received grant/research support from Sanofi-Synthelabo; and has served as consultant for Dupont Pharmaceuticals and AstraZeneca.
1. Burton R. The Anatomy of Melancholy, vol. 1, 11th ed. London, England. Thomas Tegg, Cheapside; 1845.
2. Liebowitz MR, Gorman JM, Fyer AJ, Klein DF. Social phobia: review of a neglected anxiety disorder. Arch Gen Psychiatry. 1985;42:729-736.
3. Magee WJ, Eaton WW, Wittchen HU, et al. Agoraphobia, simple phobia, and social phobia in the National Comorbidity Survey. Arch Gen Psychiatry. 1996;53:159-168.
4. Schneier FR, Johnson J, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282-288.
5. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8-19.
6. Goldenberg IM, et al. The infrequency of “pure culture” diagnosis among the anxiety disorders. J Clin Psychiatry. 1996;57:528-533.
7. Wittchen HU, Beloch E. The impact of social phobia on quality of life. Int Clin Psychopharmacol. 1996;11(suppl):15-23.
8. Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999;60:427-435.
9. Weiller E, Bisserbe JC, Boyer P, et al. Social phobia in general health care. Br J Psychiatry. 1996;168:169-174.
10. Katzelnick DJ, Greist JH. Social anxiety disorder: an unrecognized problem in primary care. J Clin Psychiatry. 2001;62:11.-
11. Davidson J. Social anxiety disorder under scrutiny. Depress Anxiety. 2000;11:93-98.
12. Lydiard RB. Social anxiety disorder: treatment role of the SSRIs. In Montgomery SA, den Boer JA (eds). SSRIs in Depression and Anxiety Perspectives in Psychiatry ,vol 8. NY: Wiley, Chichester, 129-150, 2001.
13. Randall CL, et al. Paroxetine improves both social anxiety and alcohol use in dually-diagnosed patients at the American College of Neuropsychopharmacology. San Juan, Puerto Rico. Dec 10-15, 2000.
14. Stein MB, Walker JR, Anderson G, et al. Childhood physical and sexual abuse in patients with anxiety disorders and in a community sample. Am J Psychiatry. 1996;153:275-277.
15. Boudreaux E, Kilpatrick DG, Resnick HS, et al. Criminal victimization, posttraumatic stress disorder, and comorbid psychopathology among a community sample of women. J Trauma Stress. 1998;11:665-678.
16. Orsillo SM, Heimberg RG, Juster HR, Garrett J. Social phobia and PTSD in Vietnam veterans. J Trauma Stress. 1996;9:235-252.
17. George MS, Lydiard RB. Social phobia secondary to physical disability: a review of benign essential tremor (BET) and stuttering. Psychosomatics. 1994;35:520-523.
18. Connor KM, et al. Mini-SPIN: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety. 2001;14:137-140.
19. Stein MB, Liebowitz MR, Lydiard RB, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial. JAMA. 1998;280:708-713.
20. Pande AC, Davidson JR, Jefferson JW, et al. Treatment of social phobia with gabapentin: a placebo-controlled study. J Clin Psychopharmacol. 1999;19:341-348.
21. Heimberg RG. Specific issues in the cognitive behavioral treatment of social phobia. J Clin Psychiatry. 1993;54(suppl 12):36-45.
1. Burton R. The Anatomy of Melancholy, vol. 1, 11th ed. London, England. Thomas Tegg, Cheapside; 1845.
2. Liebowitz MR, Gorman JM, Fyer AJ, Klein DF. Social phobia: review of a neglected anxiety disorder. Arch Gen Psychiatry. 1985;42:729-736.
3. Magee WJ, Eaton WW, Wittchen HU, et al. Agoraphobia, simple phobia, and social phobia in the National Comorbidity Survey. Arch Gen Psychiatry. 1996;53:159-168.
4. Schneier FR, Johnson J, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282-288.
5. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8-19.
6. Goldenberg IM, et al. The infrequency of “pure culture” diagnosis among the anxiety disorders. J Clin Psychiatry. 1996;57:528-533.
7. Wittchen HU, Beloch E. The impact of social phobia on quality of life. Int Clin Psychopharmacol. 1996;11(suppl):15-23.
8. Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999;60:427-435.
9. Weiller E, Bisserbe JC, Boyer P, et al. Social phobia in general health care. Br J Psychiatry. 1996;168:169-174.
10. Katzelnick DJ, Greist JH. Social anxiety disorder: an unrecognized problem in primary care. J Clin Psychiatry. 2001;62:11.-
11. Davidson J. Social anxiety disorder under scrutiny. Depress Anxiety. 2000;11:93-98.
12. Lydiard RB. Social anxiety disorder: treatment role of the SSRIs. In Montgomery SA, den Boer JA (eds). SSRIs in Depression and Anxiety Perspectives in Psychiatry ,vol 8. NY: Wiley, Chichester, 129-150, 2001.
13. Randall CL, et al. Paroxetine improves both social anxiety and alcohol use in dually-diagnosed patients at the American College of Neuropsychopharmacology. San Juan, Puerto Rico. Dec 10-15, 2000.
14. Stein MB, Walker JR, Anderson G, et al. Childhood physical and sexual abuse in patients with anxiety disorders and in a community sample. Am J Psychiatry. 1996;153:275-277.
15. Boudreaux E, Kilpatrick DG, Resnick HS, et al. Criminal victimization, posttraumatic stress disorder, and comorbid psychopathology among a community sample of women. J Trauma Stress. 1998;11:665-678.
16. Orsillo SM, Heimberg RG, Juster HR, Garrett J. Social phobia and PTSD in Vietnam veterans. J Trauma Stress. 1996;9:235-252.
17. George MS, Lydiard RB. Social phobia secondary to physical disability: a review of benign essential tremor (BET) and stuttering. Psychosomatics. 1994;35:520-523.
18. Connor KM, et al. Mini-SPIN: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety. 2001;14:137-140.
19. Stein MB, Liebowitz MR, Lydiard RB, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial. JAMA. 1998;280:708-713.
20. Pande AC, Davidson JR, Jefferson JW, et al. Treatment of social phobia with gabapentin: a placebo-controlled study. J Clin Psychopharmacol. 1999;19:341-348.
21. Heimberg RG. Specific issues in the cognitive behavioral treatment of social phobia. J Clin Psychiatry. 1993;54(suppl 12):36-45.
Cognitive enhancers for dementia: Do they work?
No psychiatrist likes to see the month-by-month deterioration in an Alzheimer’s patient—the losses in cognition, the declining ability to function, the behavioral aberrations that upset family and friends.
The problem will accelerate in the decades ahead as the proportion of elderly in the population increase. More than 4 million people in the United States are afflicted with this disorder. Prevalence rates as high as 10% have been estimated for individuals older than 65. Patients with the disease have estimated direct costs of $20,000 to $61,000 per year if the duration lasts 7 to 8 years.1
Although behavioral and functional deficits account for the high costs associated with Alzheimer’s disease (AD), the disorder is defined by cognitive criteria (Box 1). The majority of medication trials have been aimed at symptomatic treatment. More recently, studies have been designed to prevent or delay the onset of AD. Early on, initial therapies directed toward AD were aimed at reversing the cholinergic deficit (Box 2). Clinical trials utilizing lecithin (25-100 g/d) and choline (<16 g/d) as precursors of acetylcholine did not lead to significant benefit.6 Augmenting central cholinergic levels with acetylcholinesterase (AChE) inhibitors has consistently detected symptomatic improvement.
In recent years, the Food and Drug Administration has approved 4 AChE inhibitors—tacrine, donepezil, rivastigmine, and galantamine—for the treatment of AD. I will discuss only the latter 3, since tacrine, the first to Nshow benefit, has a high rate of adverse effects and is of limited use.7 The AChE inhibitors may improve cognition and behavioral symptoms and delay progression of the illness. They can also have beneficial effects on activities of daily living (ADL) and can reduce costs and improve caregiver burden.8
- The development of multiple cognitive deficits manifested by both:
- Memory impairment (impaired ability to learn new information or to recall previously learned information) and
- One (or more) of the following cognitive disturbances:
- Aphasia (language disturbance)
- Apraxia (impaired ability to carry out motor activities despite intact motor function)
- Agnosia (failure to recognize or identify objects despite intact sensory function)
- Disturbance in executive functioning (i.e., planning, organization, sequencing, abstracting)
- The cognitive deficits in Criteria A1 and A2 each cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning.
- The course is characterized by gradual onset and continuing cognitive decline.
Source: American Psychatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington DC: American Psychiatric Press., 1994.
The three AChE inhibitors have unique basic properties (Box 3). In order to maximize and prolong positive drug effects, it is important to start early and adjust dosage during the treatment9 (Table 1). Side effects are tolerable; the most common include nausea, vomiting, and diarrhea. Titrating the dosage slowly can reduce these. The cholinergic quality of these medications dictate that they be prescribed with caution in patients with bradycardic arrhythmias such as sick sinus syndrome, asthma, or chronic obstructive pulmonary disease.10
Effects on cognition and global assessments
Numerous efficacy studies examining cognition and global assessments in AD patients have been performed with the AChE inhibitors. Their major therapeutic effect is to maintain cognitive function at a constant level during a 6- to 12-month period of treatment, as compared to placebo. Comparison of clinical effects of all 3 agents demonstrates a similar magnitude of improvement. For some drugs, this may represent an upper limit, whereas for others it may still be possible to further increase the benefit.
The pathophysiologic processes implicated in Alzheimer’s disease (AD)include amyloid precursor protein metabolism, tau phosphorylation, apolipoprotein E, inflammation, oxidative stress, and apoptosis. Neuropathological features include amyloid plaques, neurofibrillary tangles, neuronal and synaptic loss, microgliosis, and astrocytosis. The resulting clinical syndrome of dementia is associated with neurotransmitter deficits and intracortical disconnection.
The central cholinergic neurotransmitter system is impaired in AD. This system is involved in learning and memory. The limbic system and neocortex receive projections from the cholinergic system in the septal nuclei and substantia innominata. This includes the medial septal nucleus, diagonal band, and nucleus basalis.2 Literature on animals has demonstrated that basal forebrain lesions impair learning and memory. Cholinergic agonists can improve this. Furthermore, cholinergic antagonists such as scopolamine and atropine can impair learning and memory in humans and animals.3 In AD, a 58% to 93% reduction in choline acetyltransferase levels (and other cholinergic markers) in the cortex and hippocampus can be observed and this correlates with dementia severity.4 Early AD is characterized by neuronal loss and tangles in the cholinergic nucleus basalis of Meynert.5
Results of 4 double-blind, placebo-controlled clinical trials of donepezil, involving more than 1,900 individuals with mild to moderate AD, have been published recently. In all, significant improvements in cognition were observed consistently for both therapeutic doses of donepezil (5 mg/d and 10 mg/d), relative to placebo. Similar benefits were reported for global functioning.
The long-term clinical efficacy and safety of donepezil versus placebo across 1 year in patients with mild to moderate AD was investigated.14 The Gottfries-Brane-Steen global assessment for rating dementia symptoms demonstrated the benefit of donepezil over placebo at weeks 24, 36, and 52, and at the study end point. Advantages of donepezil were also observed in cognition and ADL.
Donepezil also appears to work for patients with moderate to severe AD. In a recent 24-week study,15 patients receiving donepezil showed benefits on the Clinician’s Interview-Based Impression of Change with Caregiver Input (CIBIC+), compared with placebo, at all visits up to week 24 and at the study’s end point. All other secondary measures showed significant differences between the groups in favor of donepezil at the end of the study. These data suggest that donepezil’s benefits extend into more advanced stages of AD than those previously investigated, with good tolerability.
Clinical trials of rivastigmine (1.5-6 mg twice daily PO) have also demonstrated benefits on cognitive and global measures.16 The efficacy of rivastigmine tartrate (ENA 713) in patients with mild to moderately severe Alzheimer’s disease was evaluated in a 26-week open-label extension of a 26-week, double-blind, placebo-controlled study. By 52 weeks, patients originally treated with rivastigmine 6 to 12 mg/d had significantly better cognitive function than did patients originally treated with placebo.17- 19
Donepezil is a second-generation, piperidine-class, selective and reversible acetylcholinesterase (AChE) inhibitor. It is structurally dissimilar from other established AChE inhibitors.
Experimentally, donepezil inhibits AChE activity in human erythrocytes and increases extracellular acetylcholine levels in the cerebral cortex and the hippocampus of the rat. Pharmacologically, donepezil has a half-life of approximately 70h, lending itself to once-daily administration.11
Rivastigmine (ENA 713, or carbamoylatine) is an AChE inhibitor with brain-region selectivity and a long duration of action. Both preclinical studies and studies in human volunteers have shown that rivastigmine induces substantially greater inhibition of AChE in the central nervous system compartment than it does in the periphery (40% inhibition of central AChE compared with 10% inhibition of plasma butylcholinesterase in healthy volunteers). Rivastigmine also preferentially inhibits the G1 enzymatic form of AChE, which predominates in the brains of patients with Alzheimer’s disease (AD).
Evidence from animal studies also suggests that rivastigmine is a more potent inhibitor of AChE in the cortex and hippocampus, the brain regions most affected by AD. The principal metabolite of rivastigmine has at least 10-fold lower activity against AChE compared with the parent drug.
Rivastigmine is completely metabolized; the major route of elimination of the metabolites is renal. Rivastigmine is inactivated during the process of interacting with and inhibiting AChE, and, in contrast to other AChE inhibitors, the hepatic cytochrome P-450 (CYP-450) system is not involved in the metabolism of rivastigmine.12
Galantamine is an allosterically potentiating ligand that modulates nicotinic cholinergic receptors (nAChR) to increase acetylcholine release as well as acting as an AChE inhibitor. In preclinical experiments, the drug significantly improves learning, reduces AChE levels, and increases nicotinic receptor binding. Action of galantamine is on the most abundant nAChR in the human brain, the alpha4/beta2subtype.13
Clinical trials of galantamine (4-12 mg/bid PO) have demonstrated similar benefits.20 Following a 4-week placebo run-in, patients were randomized to 1 of 4 treatment arms: placebo or galantamine escalated to final maintenance dosages of 8, 16, or 24 mg/d for a 5-month treatment phase. At study’s end, the galantamine-place-bo differences on the cognitive subscale of the AD Assessment Scale were 3.3 points for the 16 mg/d group and 3.6 points for the 24 mg/d group. Treatment discontinuations due to adverse events were low in all galantamine groups (6% to 10%) and comparable with that in the placebo group (7%). The incidence of adverse events in the galantamine groups, notably gastrointestinal symptoms, was low and most adverse events were mild.
Other studies examining galantamine have demonstrated similar clinical benefits.8, 21
When using AChE inhibitors, the slope of cognitive decline is similar in treated and untreated patients after the initial improvement. These drugs essentially do not reverse the disorder’s course but shift upward the curve describing the time course of cognitive decline. This applies also to behavioral and functional benefits. Thus the benefit obtained is symptomatic and not neuroprotective, and is lost after discontinuing the medications.
Effects on functioning and behavior
In a 24-week multinational clinical trial, patients receiving donepezil (10 mg/d) were more able than placebo-treated patients to perform complex daily functioning tasks.22 Similar effects have been observed with rivastigmine and galantamine.16, 20
All 3 AChE inhibitors have demonstrated improvements in the behavioral changes associated with AD. Cummings et al23 tested the hypothesis that behavioral disturbances are reported at significantly lower rates by caregivers of AD patients receiving donepezil, compared with a group of patients not receiving a drug for treatment of dementia. Donepezil patients were described as significantly less likely to be threatening, destroy property, and talk loudly, and significantly fewer were treated with sedatives.
Table 1
COMPARING THEAChE INHIBITORS
| Donepezil | Rivastigmine | Galantamine | |
|---|---|---|---|
| Chemical class | Piperidine | Carbamate | Phenanthrene alkaloid |
| AChE inhibitor | Yes | Yes | Yes |
| BuChE inhibitor | Small | Yes | Small |
| Nicotinic modulation | No | No | Yes |
| Elimination half-life | 50-70 h | 0.6-2 h | 5-7 h |
| Administration | Once daily | Twice daily | Twice daily |
| Starting dosage | 5 mg/d | 1.5 mg bid | 4 mg bid |
| Total recommended dosage | 5-10 mg/d | 6-12 mg/d | 16-24 mg/d |
| Adapted from Conn DK. Cholinesterase inhibitors: Comparing the options for mild-to-moderate dementia. Geriatrics56: 56-57, 2001. | |||
An open-label study by Weiner et al24 examined the effects of donepezil on emotional and behavioral symptoms using the CERAD Behavior Rating Scale for Dementia and its subscales. In a group of 25 AD patients treated with donepezil, scores returned to baseline levels at 12 months. In contrast, the scores of the reference group worsened minimally.
Galantamine has also proved effective in treating behavioral symptoms associated with AD. In the Tariot et al20 study, galantamine at 16 mg/d and 24 mg/d had a significantly better outcome on CIBIC+, ADL, and behavioral symptoms versus placebo.
Rosler et al25 assessed the ability of rivastigmine to improve behavioral symptoms in AD. Using the behavioral component of the CIBIC+, results showed that long-term treatment with rivastigmine could slow the progression of symptoms. Symptoms showing stabilization included aggressiveness, activity disturbances, hallucinations, and paranoid features. The results also suggest that patients treated earlier with rivastigmine may attain a greater benefit than those whose treatment is delayed 6 months.
Rivastigmine also has significant effects on controlling behavioral symptoms in patients with Lewy body dementia.26 A placebo-controlled, double-blind, multicenter study was performed in 120 patients with Lewy body dementia. Individuals were given up to 12 mg/d rivastigmine or placebo for 20 weeks, followed by 3 weeks rest. Assessment by neuropsychiatric inventory was made at baseline, and again at weeks 12, 20, and 23.
Patients taking rivastigmine were significantly less apathetic and anxious than those on placebo, and had fewer delusions and hallucinations. Almost twice as many patients on rivastigmine as on placebo (37, 63% versus 18, 30%) showed at least a 30% improvement from baseline. In a computerized cognitive assessment system and neuropsychological tests, patients were significantly faster and better than those on placebo, particularly when performing tasks with a substantial attentional component.
Cost effectiveness
Numerous studies have demonstrated that AChE inhibitors are cost savers in AD treatment. Fillit et al27 examined the impact of donepezil in a multisite managed care organization for 2 years using claims data for 70 individuals with AD and related dementias. The median per diem medical costs were $1.22 lower post treatment than they were in the pretreatment phase. Moreover, posttreatment costs were reduced in 6 of 7 service settings, with median per diem savings of $0.77 in outpatient care and $0.65 in office visits.
Neumann et al28 utilized cost-effectiveness analysis to predict that for mild AD, donepezil would pay for itself in cost offsets if the drug’s effect exceeds 2 years. Donepezil costs were partially offset by a reduction in the costs of care due to enhanced cognitive functioning and the delay in placing the patient in more costly disease stages and settings.
One study used the disease-progression model to estimate potential per-patient savings resulting from the treatment of AD in Canada.29 Rivastigmine was estimated to delay the transition to more severe stages of AD by up to 188 days for patients with mild AD after 2 years of treatment. For patients with mild-to-moderate and moderate disease, this delay was estimated to be 106 and 44 days, respectively.
The Assessment of Health Economics in Alzheimer’s Disease model uses algorithms to predict the time until patients with AD require full-time care. A study, performed in Canada, compared treatment with galantamine to treatment without pharmacological interventions.30 Galantamine was predicted to reduce the duration of full-time care by almost 10%. Approximately 5.6 patients with mild-to-moderate disease must be placed on treatment to avoid 1 year of full-time care, resulting in savings averaging $528 per patient. For patients with moderate disease, 3.9 patients must be placed on treatment to avoid 1 year of full-time care, with savings predicted at $2,533 per patient.
Caregiving burden
Fillit et al addressed caregiver well-being in a self-administered, nationwide survey of AD caregivers. Caregivers of patients treated with donepezil (n = 274) were compared with caregivers of patients not treated with donepezil (n = 274).31 The Caregiver Burden Scale measured time demands and distress linked to commonly performed caregiving tasks. Donepezil caregivers reported significantly lower scores on difficulty of caregiving. Similar findings have been observed with galantamine.32
Related resources
- Bullock R. New drugs for Alzheimer’s disease and other dementias. Br J Psychiatry. 2002;180(2):135-139.
- Brodaty H, Ames D, et al. Pharmacological treatment of cognitive deficits in Alzheimer’s disease. Med J Aust. 2001;175(6):324-329.
- Ahmed MB. Alzheimer’s disease: recent advances in etiology, diagnosis, and management. Tex Med. 2001;97(12):50-58.
- Frisoni GB. Treatment of Alzheimer’s disease with acetyl-cholinesterase inhibitors: bridging the gap between evidence and practice. J Neurol. 2001;248(7):551-7.
Drug brand names
- Tacrine • Cognex
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl
Disclosure
The author reports that he receives grant/research support from, serves as a consultant to, and is on the speaker’s bureau of Janssen Pharmaceutica and Pfizer Inc., and serves as consultant to and is on the speaker’s bureau of Novartis Pharmaceuticals Corp.
1. Irizarry M, Hyman B. Alzheimer’s disease. In: Principles of neuroepidemiology. Batchelor T, Cudkowicz M, eds. Boston: Butterworth-Heinemann, 2001:69-98.
2. Mesulam MM, Mufson EJ, Levey AI, Warner BH. Cholinergic innervation of cortex by the basal forebrain: Cytochemistry and cortical connections of the septal area, diagonal band nuclei, nucleus basalis (substantia innominata), and hypothalamus in the rhesus monkey. J Comp Neurol. 1983a;214:170-197.
3. Drachman DA, Leavitt J. Human memory and the cholinergic system. A relationship to aging? Arch Neurol. 1974;30:113-121.
4. Davies P, Maloney AJ. Selective loss of central cholinergic neurons in Alzheimer’s disease. Lancet. 1976;2:1403.-
5. Whitehouse PJ, Price DL, Clark AW, Coyle JT, DeLong MR. Alzheimer disease: evidence for selective loss of cholinergic neurons in the nucleus basalis. Ann Neurol. 1981;10:122-126.
6. Higgins JPT, Flicker L. Lecithin and cognitive impairment. The Cochrane Database of Systematic Reviews. 2001.;
7. Knapp MJ, Knopman DS, Solomon PR, Pendlebury WW, Davis CS, Gracon SI. A 30-week randomized controlled trial of high-dose tacrine in patients with Alzheimer’s disease. The Tacrine Study Group. JAMA. 1994;271:985-991.
8. Raskind MA, Peskind ER, Wessel T, Yuan W. Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month extension. The Galantamine USA-1 Study Group. Neurology. 2000;54:2262-2268.
9. Giacobini E. Cholinesterase inhibitors stabilize Alzheimer’s disease. Methods Find Exp Clin Pharmacol. 2000;22:609-613.
10. Irizarry MC, Hyman BT. Alzhemier Disease Therapeutics. J Neuropathology Exp Neurology. 2001;60:923-928.
11. Wilkinson DG. The pharmacology of donepezil: a new treatment of Alzheimer’s disease. Expert Opin Pharmacother. 1999;1:121-135.
12. Polinsky RJ. Clinical pharmacology of rivastigmine: a new-generation acetyl-cholinesterase inhibitor for the treatment of Alzheimer’s disease. Clin Ther. 1998;20:634-647.
13. Samochocki M, Zerlin M, Jostock R, et al. Galantamine is an allosterically potentiating ligand of the human alpha4/beta2 nAChR. Acta Neurol Scand. 2000(Suppl);;176:68-73.
14. Winblad B, Engedal K, Soininen H, Verhey F, et al. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology. 2001;57:489-495.
15. Feldman H, Gauthier S, Hecker J, et al. Donepezil MSAD Study Investigators Group.A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Neurology. 2001;57:613-620.
16. Farlow M, Anand R, Messina J, Jr, Hartman R, Veach J. A 52-week study of the efficacy of rivastigmine in patients with mild to moderately severe Alzheimer’s disease. Eur Neurol. 2000;44:236-241.
17. Rogers S, Friedhoff L. Donepezil Study Group.The efficacy and safety of donepezil in patients with Alzhemier’s disease. Dementia. 1996;7:293-303.
18. Rogers S, Farlow M, Doody R, Morris R, Friedhoff L. A 24-week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer’s disease. Donepezil Study Group. Neurology. 1998;50:136-145.
19. Rosler M, Anand R, Cicin-Sain A, Gauthier S, Agid Y, DalBianco P, Stahelin HB, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: International randomized controlled trial. BMJ. 1999;318:633-638.
20. Tariot PN, Solomon PR, Morris JC, Kershaw P, Lilienfeld S, Ding C. A 5-month, randomized, placebo-controlled trial of galantamine in AD. The Galantamine USA-10 Study Group. Neurology. 2000;54:2269-2276.
21. Wilcock GK, Lilienfeld S, Gaens E. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: Multicentre randomized controlled trial. Galantamine International - 1 Study Group. BMJ. 2000;321:1445-1449.
22. Knopman DS. Management of cognition and function: new results from the clinical trials programme of Aricept (R) (donepezil Hcl). Int J Neuropsychopharmacol. 2000;3:13-20.
23. Cummings JL, Donohue JA, Brooks RL. The relationship between donepezil and behavioral disturbances in patients with Alzheimer’s disease. Am J Geriatr Psychiatry. 2000;8:134-140.
24. Weiner MF, Martin-Cook K, Foster BM, Saine K, et al. Effects of donepezil on emotional/behavioral symptoms in Alzheimer’s disease patients. J Clin Psychiatry. 2000;487-492.
25. Rosler M, Retz W, Retz-Junginger P, Dennler HJ. Effects of two-year treatment with the cholinesterase inhibitor rivastigmine on behavioural symptoms in Alzheimer’s disease. Behav Neurol. 1998;11:211-216.
26. McKeith I, Del Ser T, Spano P, Emre M, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
27. Fillit H, Gutterman EM, Lewis B. Donepezil use in managed Medicare: effect on health care costs and utilization. Clin Ther. 1999;21:2173-2185.
28. Neumann PJ, Hermann RC, Kuntz KM, Araki SS, Duff SB, Leon J, Berenbaum PA, et al. Cost-effectiveness of donepezil in the treatment of mild or moderate Alzheimer’s disease. Neurology. 1999;52:1115-1116.
29. Hauber AB, Gnanasakthy A, Mauskopf JA. Savings in the cost of caring for patients with Alzheimer’s disease in Canada: an analysis of treatment with rivastigmine. Clin Ther. 2000;22:439-451.
30. Getsios D, Caro JJ, Caro G, Ishak K. The AHEAD Study Group. Assessment of health economics in Alzheimer’s disease (AHEAD): galantamine treatment in Canada. Neurology. 2001;57:972-978.
31. Fillit HM, Gutterman EM, Brooks RL. Impact of donepezil on caregiving burden for patients with Alzheimer’s disease. Int Psychogeriatr. 2000;12(3):389-401.
32. Blesa R. Galantamine: therapeutic effects beyond cognition. Dement Geriatr Cogn Disord. 2000;11(Suppl)1:28-34.
No psychiatrist likes to see the month-by-month deterioration in an Alzheimer’s patient—the losses in cognition, the declining ability to function, the behavioral aberrations that upset family and friends.
The problem will accelerate in the decades ahead as the proportion of elderly in the population increase. More than 4 million people in the United States are afflicted with this disorder. Prevalence rates as high as 10% have been estimated for individuals older than 65. Patients with the disease have estimated direct costs of $20,000 to $61,000 per year if the duration lasts 7 to 8 years.1
Although behavioral and functional deficits account for the high costs associated with Alzheimer’s disease (AD), the disorder is defined by cognitive criteria (Box 1). The majority of medication trials have been aimed at symptomatic treatment. More recently, studies have been designed to prevent or delay the onset of AD. Early on, initial therapies directed toward AD were aimed at reversing the cholinergic deficit (Box 2). Clinical trials utilizing lecithin (25-100 g/d) and choline (<16 g/d) as precursors of acetylcholine did not lead to significant benefit.6 Augmenting central cholinergic levels with acetylcholinesterase (AChE) inhibitors has consistently detected symptomatic improvement.
In recent years, the Food and Drug Administration has approved 4 AChE inhibitors—tacrine, donepezil, rivastigmine, and galantamine—for the treatment of AD. I will discuss only the latter 3, since tacrine, the first to Nshow benefit, has a high rate of adverse effects and is of limited use.7 The AChE inhibitors may improve cognition and behavioral symptoms and delay progression of the illness. They can also have beneficial effects on activities of daily living (ADL) and can reduce costs and improve caregiver burden.8
- The development of multiple cognitive deficits manifested by both:
- Memory impairment (impaired ability to learn new information or to recall previously learned information) and
- One (or more) of the following cognitive disturbances:
- Aphasia (language disturbance)
- Apraxia (impaired ability to carry out motor activities despite intact motor function)
- Agnosia (failure to recognize or identify objects despite intact sensory function)
- Disturbance in executive functioning (i.e., planning, organization, sequencing, abstracting)
- The cognitive deficits in Criteria A1 and A2 each cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning.
- The course is characterized by gradual onset and continuing cognitive decline.
Source: American Psychatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington DC: American Psychiatric Press., 1994.
The three AChE inhibitors have unique basic properties (Box 3). In order to maximize and prolong positive drug effects, it is important to start early and adjust dosage during the treatment9 (Table 1). Side effects are tolerable; the most common include nausea, vomiting, and diarrhea. Titrating the dosage slowly can reduce these. The cholinergic quality of these medications dictate that they be prescribed with caution in patients with bradycardic arrhythmias such as sick sinus syndrome, asthma, or chronic obstructive pulmonary disease.10
Effects on cognition and global assessments
Numerous efficacy studies examining cognition and global assessments in AD patients have been performed with the AChE inhibitors. Their major therapeutic effect is to maintain cognitive function at a constant level during a 6- to 12-month period of treatment, as compared to placebo. Comparison of clinical effects of all 3 agents demonstrates a similar magnitude of improvement. For some drugs, this may represent an upper limit, whereas for others it may still be possible to further increase the benefit.
The pathophysiologic processes implicated in Alzheimer’s disease (AD)include amyloid precursor protein metabolism, tau phosphorylation, apolipoprotein E, inflammation, oxidative stress, and apoptosis. Neuropathological features include amyloid plaques, neurofibrillary tangles, neuronal and synaptic loss, microgliosis, and astrocytosis. The resulting clinical syndrome of dementia is associated with neurotransmitter deficits and intracortical disconnection.
The central cholinergic neurotransmitter system is impaired in AD. This system is involved in learning and memory. The limbic system and neocortex receive projections from the cholinergic system in the septal nuclei and substantia innominata. This includes the medial septal nucleus, diagonal band, and nucleus basalis.2 Literature on animals has demonstrated that basal forebrain lesions impair learning and memory. Cholinergic agonists can improve this. Furthermore, cholinergic antagonists such as scopolamine and atropine can impair learning and memory in humans and animals.3 In AD, a 58% to 93% reduction in choline acetyltransferase levels (and other cholinergic markers) in the cortex and hippocampus can be observed and this correlates with dementia severity.4 Early AD is characterized by neuronal loss and tangles in the cholinergic nucleus basalis of Meynert.5
Results of 4 double-blind, placebo-controlled clinical trials of donepezil, involving more than 1,900 individuals with mild to moderate AD, have been published recently. In all, significant improvements in cognition were observed consistently for both therapeutic doses of donepezil (5 mg/d and 10 mg/d), relative to placebo. Similar benefits were reported for global functioning.
The long-term clinical efficacy and safety of donepezil versus placebo across 1 year in patients with mild to moderate AD was investigated.14 The Gottfries-Brane-Steen global assessment for rating dementia symptoms demonstrated the benefit of donepezil over placebo at weeks 24, 36, and 52, and at the study end point. Advantages of donepezil were also observed in cognition and ADL.
Donepezil also appears to work for patients with moderate to severe AD. In a recent 24-week study,15 patients receiving donepezil showed benefits on the Clinician’s Interview-Based Impression of Change with Caregiver Input (CIBIC+), compared with placebo, at all visits up to week 24 and at the study’s end point. All other secondary measures showed significant differences between the groups in favor of donepezil at the end of the study. These data suggest that donepezil’s benefits extend into more advanced stages of AD than those previously investigated, with good tolerability.
Clinical trials of rivastigmine (1.5-6 mg twice daily PO) have also demonstrated benefits on cognitive and global measures.16 The efficacy of rivastigmine tartrate (ENA 713) in patients with mild to moderately severe Alzheimer’s disease was evaluated in a 26-week open-label extension of a 26-week, double-blind, placebo-controlled study. By 52 weeks, patients originally treated with rivastigmine 6 to 12 mg/d had significantly better cognitive function than did patients originally treated with placebo.17- 19
Donepezil is a second-generation, piperidine-class, selective and reversible acetylcholinesterase (AChE) inhibitor. It is structurally dissimilar from other established AChE inhibitors.
Experimentally, donepezil inhibits AChE activity in human erythrocytes and increases extracellular acetylcholine levels in the cerebral cortex and the hippocampus of the rat. Pharmacologically, donepezil has a half-life of approximately 70h, lending itself to once-daily administration.11
Rivastigmine (ENA 713, or carbamoylatine) is an AChE inhibitor with brain-region selectivity and a long duration of action. Both preclinical studies and studies in human volunteers have shown that rivastigmine induces substantially greater inhibition of AChE in the central nervous system compartment than it does in the periphery (40% inhibition of central AChE compared with 10% inhibition of plasma butylcholinesterase in healthy volunteers). Rivastigmine also preferentially inhibits the G1 enzymatic form of AChE, which predominates in the brains of patients with Alzheimer’s disease (AD).
Evidence from animal studies also suggests that rivastigmine is a more potent inhibitor of AChE in the cortex and hippocampus, the brain regions most affected by AD. The principal metabolite of rivastigmine has at least 10-fold lower activity against AChE compared with the parent drug.
Rivastigmine is completely metabolized; the major route of elimination of the metabolites is renal. Rivastigmine is inactivated during the process of interacting with and inhibiting AChE, and, in contrast to other AChE inhibitors, the hepatic cytochrome P-450 (CYP-450) system is not involved in the metabolism of rivastigmine.12
Galantamine is an allosterically potentiating ligand that modulates nicotinic cholinergic receptors (nAChR) to increase acetylcholine release as well as acting as an AChE inhibitor. In preclinical experiments, the drug significantly improves learning, reduces AChE levels, and increases nicotinic receptor binding. Action of galantamine is on the most abundant nAChR in the human brain, the alpha4/beta2subtype.13
Clinical trials of galantamine (4-12 mg/bid PO) have demonstrated similar benefits.20 Following a 4-week placebo run-in, patients were randomized to 1 of 4 treatment arms: placebo or galantamine escalated to final maintenance dosages of 8, 16, or 24 mg/d for a 5-month treatment phase. At study’s end, the galantamine-place-bo differences on the cognitive subscale of the AD Assessment Scale were 3.3 points for the 16 mg/d group and 3.6 points for the 24 mg/d group. Treatment discontinuations due to adverse events were low in all galantamine groups (6% to 10%) and comparable with that in the placebo group (7%). The incidence of adverse events in the galantamine groups, notably gastrointestinal symptoms, was low and most adverse events were mild.
Other studies examining galantamine have demonstrated similar clinical benefits.8, 21
When using AChE inhibitors, the slope of cognitive decline is similar in treated and untreated patients after the initial improvement. These drugs essentially do not reverse the disorder’s course but shift upward the curve describing the time course of cognitive decline. This applies also to behavioral and functional benefits. Thus the benefit obtained is symptomatic and not neuroprotective, and is lost after discontinuing the medications.
Effects on functioning and behavior
In a 24-week multinational clinical trial, patients receiving donepezil (10 mg/d) were more able than placebo-treated patients to perform complex daily functioning tasks.22 Similar effects have been observed with rivastigmine and galantamine.16, 20
All 3 AChE inhibitors have demonstrated improvements in the behavioral changes associated with AD. Cummings et al23 tested the hypothesis that behavioral disturbances are reported at significantly lower rates by caregivers of AD patients receiving donepezil, compared with a group of patients not receiving a drug for treatment of dementia. Donepezil patients were described as significantly less likely to be threatening, destroy property, and talk loudly, and significantly fewer were treated with sedatives.
Table 1
COMPARING THEAChE INHIBITORS
| Donepezil | Rivastigmine | Galantamine | |
|---|---|---|---|
| Chemical class | Piperidine | Carbamate | Phenanthrene alkaloid |
| AChE inhibitor | Yes | Yes | Yes |
| BuChE inhibitor | Small | Yes | Small |
| Nicotinic modulation | No | No | Yes |
| Elimination half-life | 50-70 h | 0.6-2 h | 5-7 h |
| Administration | Once daily | Twice daily | Twice daily |
| Starting dosage | 5 mg/d | 1.5 mg bid | 4 mg bid |
| Total recommended dosage | 5-10 mg/d | 6-12 mg/d | 16-24 mg/d |
| Adapted from Conn DK. Cholinesterase inhibitors: Comparing the options for mild-to-moderate dementia. Geriatrics56: 56-57, 2001. | |||
An open-label study by Weiner et al24 examined the effects of donepezil on emotional and behavioral symptoms using the CERAD Behavior Rating Scale for Dementia and its subscales. In a group of 25 AD patients treated with donepezil, scores returned to baseline levels at 12 months. In contrast, the scores of the reference group worsened minimally.
Galantamine has also proved effective in treating behavioral symptoms associated with AD. In the Tariot et al20 study, galantamine at 16 mg/d and 24 mg/d had a significantly better outcome on CIBIC+, ADL, and behavioral symptoms versus placebo.
Rosler et al25 assessed the ability of rivastigmine to improve behavioral symptoms in AD. Using the behavioral component of the CIBIC+, results showed that long-term treatment with rivastigmine could slow the progression of symptoms. Symptoms showing stabilization included aggressiveness, activity disturbances, hallucinations, and paranoid features. The results also suggest that patients treated earlier with rivastigmine may attain a greater benefit than those whose treatment is delayed 6 months.
Rivastigmine also has significant effects on controlling behavioral symptoms in patients with Lewy body dementia.26 A placebo-controlled, double-blind, multicenter study was performed in 120 patients with Lewy body dementia. Individuals were given up to 12 mg/d rivastigmine or placebo for 20 weeks, followed by 3 weeks rest. Assessment by neuropsychiatric inventory was made at baseline, and again at weeks 12, 20, and 23.
Patients taking rivastigmine were significantly less apathetic and anxious than those on placebo, and had fewer delusions and hallucinations. Almost twice as many patients on rivastigmine as on placebo (37, 63% versus 18, 30%) showed at least a 30% improvement from baseline. In a computerized cognitive assessment system and neuropsychological tests, patients were significantly faster and better than those on placebo, particularly when performing tasks with a substantial attentional component.
Cost effectiveness
Numerous studies have demonstrated that AChE inhibitors are cost savers in AD treatment. Fillit et al27 examined the impact of donepezil in a multisite managed care organization for 2 years using claims data for 70 individuals with AD and related dementias. The median per diem medical costs were $1.22 lower post treatment than they were in the pretreatment phase. Moreover, posttreatment costs were reduced in 6 of 7 service settings, with median per diem savings of $0.77 in outpatient care and $0.65 in office visits.
Neumann et al28 utilized cost-effectiveness analysis to predict that for mild AD, donepezil would pay for itself in cost offsets if the drug’s effect exceeds 2 years. Donepezil costs were partially offset by a reduction in the costs of care due to enhanced cognitive functioning and the delay in placing the patient in more costly disease stages and settings.
One study used the disease-progression model to estimate potential per-patient savings resulting from the treatment of AD in Canada.29 Rivastigmine was estimated to delay the transition to more severe stages of AD by up to 188 days for patients with mild AD after 2 years of treatment. For patients with mild-to-moderate and moderate disease, this delay was estimated to be 106 and 44 days, respectively.
The Assessment of Health Economics in Alzheimer’s Disease model uses algorithms to predict the time until patients with AD require full-time care. A study, performed in Canada, compared treatment with galantamine to treatment without pharmacological interventions.30 Galantamine was predicted to reduce the duration of full-time care by almost 10%. Approximately 5.6 patients with mild-to-moderate disease must be placed on treatment to avoid 1 year of full-time care, resulting in savings averaging $528 per patient. For patients with moderate disease, 3.9 patients must be placed on treatment to avoid 1 year of full-time care, with savings predicted at $2,533 per patient.
Caregiving burden
Fillit et al addressed caregiver well-being in a self-administered, nationwide survey of AD caregivers. Caregivers of patients treated with donepezil (n = 274) were compared with caregivers of patients not treated with donepezil (n = 274).31 The Caregiver Burden Scale measured time demands and distress linked to commonly performed caregiving tasks. Donepezil caregivers reported significantly lower scores on difficulty of caregiving. Similar findings have been observed with galantamine.32
Related resources
- Bullock R. New drugs for Alzheimer’s disease and other dementias. Br J Psychiatry. 2002;180(2):135-139.
- Brodaty H, Ames D, et al. Pharmacological treatment of cognitive deficits in Alzheimer’s disease. Med J Aust. 2001;175(6):324-329.
- Ahmed MB. Alzheimer’s disease: recent advances in etiology, diagnosis, and management. Tex Med. 2001;97(12):50-58.
- Frisoni GB. Treatment of Alzheimer’s disease with acetyl-cholinesterase inhibitors: bridging the gap between evidence and practice. J Neurol. 2001;248(7):551-7.
Drug brand names
- Tacrine • Cognex
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl
Disclosure
The author reports that he receives grant/research support from, serves as a consultant to, and is on the speaker’s bureau of Janssen Pharmaceutica and Pfizer Inc., and serves as consultant to and is on the speaker’s bureau of Novartis Pharmaceuticals Corp.
No psychiatrist likes to see the month-by-month deterioration in an Alzheimer’s patient—the losses in cognition, the declining ability to function, the behavioral aberrations that upset family and friends.
The problem will accelerate in the decades ahead as the proportion of elderly in the population increase. More than 4 million people in the United States are afflicted with this disorder. Prevalence rates as high as 10% have been estimated for individuals older than 65. Patients with the disease have estimated direct costs of $20,000 to $61,000 per year if the duration lasts 7 to 8 years.1
Although behavioral and functional deficits account for the high costs associated with Alzheimer’s disease (AD), the disorder is defined by cognitive criteria (Box 1). The majority of medication trials have been aimed at symptomatic treatment. More recently, studies have been designed to prevent or delay the onset of AD. Early on, initial therapies directed toward AD were aimed at reversing the cholinergic deficit (Box 2). Clinical trials utilizing lecithin (25-100 g/d) and choline (<16 g/d) as precursors of acetylcholine did not lead to significant benefit.6 Augmenting central cholinergic levels with acetylcholinesterase (AChE) inhibitors has consistently detected symptomatic improvement.
In recent years, the Food and Drug Administration has approved 4 AChE inhibitors—tacrine, donepezil, rivastigmine, and galantamine—for the treatment of AD. I will discuss only the latter 3, since tacrine, the first to Nshow benefit, has a high rate of adverse effects and is of limited use.7 The AChE inhibitors may improve cognition and behavioral symptoms and delay progression of the illness. They can also have beneficial effects on activities of daily living (ADL) and can reduce costs and improve caregiver burden.8
- The development of multiple cognitive deficits manifested by both:
- Memory impairment (impaired ability to learn new information or to recall previously learned information) and
- One (or more) of the following cognitive disturbances:
- Aphasia (language disturbance)
- Apraxia (impaired ability to carry out motor activities despite intact motor function)
- Agnosia (failure to recognize or identify objects despite intact sensory function)
- Disturbance in executive functioning (i.e., planning, organization, sequencing, abstracting)
- The cognitive deficits in Criteria A1 and A2 each cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning.
- The course is characterized by gradual onset and continuing cognitive decline.
Source: American Psychatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington DC: American Psychiatric Press., 1994.
The three AChE inhibitors have unique basic properties (Box 3). In order to maximize and prolong positive drug effects, it is important to start early and adjust dosage during the treatment9 (Table 1). Side effects are tolerable; the most common include nausea, vomiting, and diarrhea. Titrating the dosage slowly can reduce these. The cholinergic quality of these medications dictate that they be prescribed with caution in patients with bradycardic arrhythmias such as sick sinus syndrome, asthma, or chronic obstructive pulmonary disease.10
Effects on cognition and global assessments
Numerous efficacy studies examining cognition and global assessments in AD patients have been performed with the AChE inhibitors. Their major therapeutic effect is to maintain cognitive function at a constant level during a 6- to 12-month period of treatment, as compared to placebo. Comparison of clinical effects of all 3 agents demonstrates a similar magnitude of improvement. For some drugs, this may represent an upper limit, whereas for others it may still be possible to further increase the benefit.
The pathophysiologic processes implicated in Alzheimer’s disease (AD)include amyloid precursor protein metabolism, tau phosphorylation, apolipoprotein E, inflammation, oxidative stress, and apoptosis. Neuropathological features include amyloid plaques, neurofibrillary tangles, neuronal and synaptic loss, microgliosis, and astrocytosis. The resulting clinical syndrome of dementia is associated with neurotransmitter deficits and intracortical disconnection.
The central cholinergic neurotransmitter system is impaired in AD. This system is involved in learning and memory. The limbic system and neocortex receive projections from the cholinergic system in the septal nuclei and substantia innominata. This includes the medial septal nucleus, diagonal band, and nucleus basalis.2 Literature on animals has demonstrated that basal forebrain lesions impair learning and memory. Cholinergic agonists can improve this. Furthermore, cholinergic antagonists such as scopolamine and atropine can impair learning and memory in humans and animals.3 In AD, a 58% to 93% reduction in choline acetyltransferase levels (and other cholinergic markers) in the cortex and hippocampus can be observed and this correlates with dementia severity.4 Early AD is characterized by neuronal loss and tangles in the cholinergic nucleus basalis of Meynert.5
Results of 4 double-blind, placebo-controlled clinical trials of donepezil, involving more than 1,900 individuals with mild to moderate AD, have been published recently. In all, significant improvements in cognition were observed consistently for both therapeutic doses of donepezil (5 mg/d and 10 mg/d), relative to placebo. Similar benefits were reported for global functioning.
The long-term clinical efficacy and safety of donepezil versus placebo across 1 year in patients with mild to moderate AD was investigated.14 The Gottfries-Brane-Steen global assessment for rating dementia symptoms demonstrated the benefit of donepezil over placebo at weeks 24, 36, and 52, and at the study end point. Advantages of donepezil were also observed in cognition and ADL.
Donepezil also appears to work for patients with moderate to severe AD. In a recent 24-week study,15 patients receiving donepezil showed benefits on the Clinician’s Interview-Based Impression of Change with Caregiver Input (CIBIC+), compared with placebo, at all visits up to week 24 and at the study’s end point. All other secondary measures showed significant differences between the groups in favor of donepezil at the end of the study. These data suggest that donepezil’s benefits extend into more advanced stages of AD than those previously investigated, with good tolerability.
Clinical trials of rivastigmine (1.5-6 mg twice daily PO) have also demonstrated benefits on cognitive and global measures.16 The efficacy of rivastigmine tartrate (ENA 713) in patients with mild to moderately severe Alzheimer’s disease was evaluated in a 26-week open-label extension of a 26-week, double-blind, placebo-controlled study. By 52 weeks, patients originally treated with rivastigmine 6 to 12 mg/d had significantly better cognitive function than did patients originally treated with placebo.17- 19
Donepezil is a second-generation, piperidine-class, selective and reversible acetylcholinesterase (AChE) inhibitor. It is structurally dissimilar from other established AChE inhibitors.
Experimentally, donepezil inhibits AChE activity in human erythrocytes and increases extracellular acetylcholine levels in the cerebral cortex and the hippocampus of the rat. Pharmacologically, donepezil has a half-life of approximately 70h, lending itself to once-daily administration.11
Rivastigmine (ENA 713, or carbamoylatine) is an AChE inhibitor with brain-region selectivity and a long duration of action. Both preclinical studies and studies in human volunteers have shown that rivastigmine induces substantially greater inhibition of AChE in the central nervous system compartment than it does in the periphery (40% inhibition of central AChE compared with 10% inhibition of plasma butylcholinesterase in healthy volunteers). Rivastigmine also preferentially inhibits the G1 enzymatic form of AChE, which predominates in the brains of patients with Alzheimer’s disease (AD).
Evidence from animal studies also suggests that rivastigmine is a more potent inhibitor of AChE in the cortex and hippocampus, the brain regions most affected by AD. The principal metabolite of rivastigmine has at least 10-fold lower activity against AChE compared with the parent drug.
Rivastigmine is completely metabolized; the major route of elimination of the metabolites is renal. Rivastigmine is inactivated during the process of interacting with and inhibiting AChE, and, in contrast to other AChE inhibitors, the hepatic cytochrome P-450 (CYP-450) system is not involved in the metabolism of rivastigmine.12
Galantamine is an allosterically potentiating ligand that modulates nicotinic cholinergic receptors (nAChR) to increase acetylcholine release as well as acting as an AChE inhibitor. In preclinical experiments, the drug significantly improves learning, reduces AChE levels, and increases nicotinic receptor binding. Action of galantamine is on the most abundant nAChR in the human brain, the alpha4/beta2subtype.13
Clinical trials of galantamine (4-12 mg/bid PO) have demonstrated similar benefits.20 Following a 4-week placebo run-in, patients were randomized to 1 of 4 treatment arms: placebo or galantamine escalated to final maintenance dosages of 8, 16, or 24 mg/d for a 5-month treatment phase. At study’s end, the galantamine-place-bo differences on the cognitive subscale of the AD Assessment Scale were 3.3 points for the 16 mg/d group and 3.6 points for the 24 mg/d group. Treatment discontinuations due to adverse events were low in all galantamine groups (6% to 10%) and comparable with that in the placebo group (7%). The incidence of adverse events in the galantamine groups, notably gastrointestinal symptoms, was low and most adverse events were mild.
Other studies examining galantamine have demonstrated similar clinical benefits.8, 21
When using AChE inhibitors, the slope of cognitive decline is similar in treated and untreated patients after the initial improvement. These drugs essentially do not reverse the disorder’s course but shift upward the curve describing the time course of cognitive decline. This applies also to behavioral and functional benefits. Thus the benefit obtained is symptomatic and not neuroprotective, and is lost after discontinuing the medications.
Effects on functioning and behavior
In a 24-week multinational clinical trial, patients receiving donepezil (10 mg/d) were more able than placebo-treated patients to perform complex daily functioning tasks.22 Similar effects have been observed with rivastigmine and galantamine.16, 20
All 3 AChE inhibitors have demonstrated improvements in the behavioral changes associated with AD. Cummings et al23 tested the hypothesis that behavioral disturbances are reported at significantly lower rates by caregivers of AD patients receiving donepezil, compared with a group of patients not receiving a drug for treatment of dementia. Donepezil patients were described as significantly less likely to be threatening, destroy property, and talk loudly, and significantly fewer were treated with sedatives.
Table 1
COMPARING THEAChE INHIBITORS
| Donepezil | Rivastigmine | Galantamine | |
|---|---|---|---|
| Chemical class | Piperidine | Carbamate | Phenanthrene alkaloid |
| AChE inhibitor | Yes | Yes | Yes |
| BuChE inhibitor | Small | Yes | Small |
| Nicotinic modulation | No | No | Yes |
| Elimination half-life | 50-70 h | 0.6-2 h | 5-7 h |
| Administration | Once daily | Twice daily | Twice daily |
| Starting dosage | 5 mg/d | 1.5 mg bid | 4 mg bid |
| Total recommended dosage | 5-10 mg/d | 6-12 mg/d | 16-24 mg/d |
| Adapted from Conn DK. Cholinesterase inhibitors: Comparing the options for mild-to-moderate dementia. Geriatrics56: 56-57, 2001. | |||
An open-label study by Weiner et al24 examined the effects of donepezil on emotional and behavioral symptoms using the CERAD Behavior Rating Scale for Dementia and its subscales. In a group of 25 AD patients treated with donepezil, scores returned to baseline levels at 12 months. In contrast, the scores of the reference group worsened minimally.
Galantamine has also proved effective in treating behavioral symptoms associated with AD. In the Tariot et al20 study, galantamine at 16 mg/d and 24 mg/d had a significantly better outcome on CIBIC+, ADL, and behavioral symptoms versus placebo.
Rosler et al25 assessed the ability of rivastigmine to improve behavioral symptoms in AD. Using the behavioral component of the CIBIC+, results showed that long-term treatment with rivastigmine could slow the progression of symptoms. Symptoms showing stabilization included aggressiveness, activity disturbances, hallucinations, and paranoid features. The results also suggest that patients treated earlier with rivastigmine may attain a greater benefit than those whose treatment is delayed 6 months.
Rivastigmine also has significant effects on controlling behavioral symptoms in patients with Lewy body dementia.26 A placebo-controlled, double-blind, multicenter study was performed in 120 patients with Lewy body dementia. Individuals were given up to 12 mg/d rivastigmine or placebo for 20 weeks, followed by 3 weeks rest. Assessment by neuropsychiatric inventory was made at baseline, and again at weeks 12, 20, and 23.
Patients taking rivastigmine were significantly less apathetic and anxious than those on placebo, and had fewer delusions and hallucinations. Almost twice as many patients on rivastigmine as on placebo (37, 63% versus 18, 30%) showed at least a 30% improvement from baseline. In a computerized cognitive assessment system and neuropsychological tests, patients were significantly faster and better than those on placebo, particularly when performing tasks with a substantial attentional component.
Cost effectiveness
Numerous studies have demonstrated that AChE inhibitors are cost savers in AD treatment. Fillit et al27 examined the impact of donepezil in a multisite managed care organization for 2 years using claims data for 70 individuals with AD and related dementias. The median per diem medical costs were $1.22 lower post treatment than they were in the pretreatment phase. Moreover, posttreatment costs were reduced in 6 of 7 service settings, with median per diem savings of $0.77 in outpatient care and $0.65 in office visits.
Neumann et al28 utilized cost-effectiveness analysis to predict that for mild AD, donepezil would pay for itself in cost offsets if the drug’s effect exceeds 2 years. Donepezil costs were partially offset by a reduction in the costs of care due to enhanced cognitive functioning and the delay in placing the patient in more costly disease stages and settings.
One study used the disease-progression model to estimate potential per-patient savings resulting from the treatment of AD in Canada.29 Rivastigmine was estimated to delay the transition to more severe stages of AD by up to 188 days for patients with mild AD after 2 years of treatment. For patients with mild-to-moderate and moderate disease, this delay was estimated to be 106 and 44 days, respectively.
The Assessment of Health Economics in Alzheimer’s Disease model uses algorithms to predict the time until patients with AD require full-time care. A study, performed in Canada, compared treatment with galantamine to treatment without pharmacological interventions.30 Galantamine was predicted to reduce the duration of full-time care by almost 10%. Approximately 5.6 patients with mild-to-moderate disease must be placed on treatment to avoid 1 year of full-time care, resulting in savings averaging $528 per patient. For patients with moderate disease, 3.9 patients must be placed on treatment to avoid 1 year of full-time care, with savings predicted at $2,533 per patient.
Caregiving burden
Fillit et al addressed caregiver well-being in a self-administered, nationwide survey of AD caregivers. Caregivers of patients treated with donepezil (n = 274) were compared with caregivers of patients not treated with donepezil (n = 274).31 The Caregiver Burden Scale measured time demands and distress linked to commonly performed caregiving tasks. Donepezil caregivers reported significantly lower scores on difficulty of caregiving. Similar findings have been observed with galantamine.32
Related resources
- Bullock R. New drugs for Alzheimer’s disease and other dementias. Br J Psychiatry. 2002;180(2):135-139.
- Brodaty H, Ames D, et al. Pharmacological treatment of cognitive deficits in Alzheimer’s disease. Med J Aust. 2001;175(6):324-329.
- Ahmed MB. Alzheimer’s disease: recent advances in etiology, diagnosis, and management. Tex Med. 2001;97(12):50-58.
- Frisoni GB. Treatment of Alzheimer’s disease with acetyl-cholinesterase inhibitors: bridging the gap between evidence and practice. J Neurol. 2001;248(7):551-7.
Drug brand names
- Tacrine • Cognex
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl
Disclosure
The author reports that he receives grant/research support from, serves as a consultant to, and is on the speaker’s bureau of Janssen Pharmaceutica and Pfizer Inc., and serves as consultant to and is on the speaker’s bureau of Novartis Pharmaceuticals Corp.
1. Irizarry M, Hyman B. Alzheimer’s disease. In: Principles of neuroepidemiology. Batchelor T, Cudkowicz M, eds. Boston: Butterworth-Heinemann, 2001:69-98.
2. Mesulam MM, Mufson EJ, Levey AI, Warner BH. Cholinergic innervation of cortex by the basal forebrain: Cytochemistry and cortical connections of the septal area, diagonal band nuclei, nucleus basalis (substantia innominata), and hypothalamus in the rhesus monkey. J Comp Neurol. 1983a;214:170-197.
3. Drachman DA, Leavitt J. Human memory and the cholinergic system. A relationship to aging? Arch Neurol. 1974;30:113-121.
4. Davies P, Maloney AJ. Selective loss of central cholinergic neurons in Alzheimer’s disease. Lancet. 1976;2:1403.-
5. Whitehouse PJ, Price DL, Clark AW, Coyle JT, DeLong MR. Alzheimer disease: evidence for selective loss of cholinergic neurons in the nucleus basalis. Ann Neurol. 1981;10:122-126.
6. Higgins JPT, Flicker L. Lecithin and cognitive impairment. The Cochrane Database of Systematic Reviews. 2001.;
7. Knapp MJ, Knopman DS, Solomon PR, Pendlebury WW, Davis CS, Gracon SI. A 30-week randomized controlled trial of high-dose tacrine in patients with Alzheimer’s disease. The Tacrine Study Group. JAMA. 1994;271:985-991.
8. Raskind MA, Peskind ER, Wessel T, Yuan W. Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month extension. The Galantamine USA-1 Study Group. Neurology. 2000;54:2262-2268.
9. Giacobini E. Cholinesterase inhibitors stabilize Alzheimer’s disease. Methods Find Exp Clin Pharmacol. 2000;22:609-613.
10. Irizarry MC, Hyman BT. Alzhemier Disease Therapeutics. J Neuropathology Exp Neurology. 2001;60:923-928.
11. Wilkinson DG. The pharmacology of donepezil: a new treatment of Alzheimer’s disease. Expert Opin Pharmacother. 1999;1:121-135.
12. Polinsky RJ. Clinical pharmacology of rivastigmine: a new-generation acetyl-cholinesterase inhibitor for the treatment of Alzheimer’s disease. Clin Ther. 1998;20:634-647.
13. Samochocki M, Zerlin M, Jostock R, et al. Galantamine is an allosterically potentiating ligand of the human alpha4/beta2 nAChR. Acta Neurol Scand. 2000(Suppl);;176:68-73.
14. Winblad B, Engedal K, Soininen H, Verhey F, et al. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology. 2001;57:489-495.
15. Feldman H, Gauthier S, Hecker J, et al. Donepezil MSAD Study Investigators Group.A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Neurology. 2001;57:613-620.
16. Farlow M, Anand R, Messina J, Jr, Hartman R, Veach J. A 52-week study of the efficacy of rivastigmine in patients with mild to moderately severe Alzheimer’s disease. Eur Neurol. 2000;44:236-241.
17. Rogers S, Friedhoff L. Donepezil Study Group.The efficacy and safety of donepezil in patients with Alzhemier’s disease. Dementia. 1996;7:293-303.
18. Rogers S, Farlow M, Doody R, Morris R, Friedhoff L. A 24-week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer’s disease. Donepezil Study Group. Neurology. 1998;50:136-145.
19. Rosler M, Anand R, Cicin-Sain A, Gauthier S, Agid Y, DalBianco P, Stahelin HB, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: International randomized controlled trial. BMJ. 1999;318:633-638.
20. Tariot PN, Solomon PR, Morris JC, Kershaw P, Lilienfeld S, Ding C. A 5-month, randomized, placebo-controlled trial of galantamine in AD. The Galantamine USA-10 Study Group. Neurology. 2000;54:2269-2276.
21. Wilcock GK, Lilienfeld S, Gaens E. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: Multicentre randomized controlled trial. Galantamine International - 1 Study Group. BMJ. 2000;321:1445-1449.
22. Knopman DS. Management of cognition and function: new results from the clinical trials programme of Aricept (R) (donepezil Hcl). Int J Neuropsychopharmacol. 2000;3:13-20.
23. Cummings JL, Donohue JA, Brooks RL. The relationship between donepezil and behavioral disturbances in patients with Alzheimer’s disease. Am J Geriatr Psychiatry. 2000;8:134-140.
24. Weiner MF, Martin-Cook K, Foster BM, Saine K, et al. Effects of donepezil on emotional/behavioral symptoms in Alzheimer’s disease patients. J Clin Psychiatry. 2000;487-492.
25. Rosler M, Retz W, Retz-Junginger P, Dennler HJ. Effects of two-year treatment with the cholinesterase inhibitor rivastigmine on behavioural symptoms in Alzheimer’s disease. Behav Neurol. 1998;11:211-216.
26. McKeith I, Del Ser T, Spano P, Emre M, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
27. Fillit H, Gutterman EM, Lewis B. Donepezil use in managed Medicare: effect on health care costs and utilization. Clin Ther. 1999;21:2173-2185.
28. Neumann PJ, Hermann RC, Kuntz KM, Araki SS, Duff SB, Leon J, Berenbaum PA, et al. Cost-effectiveness of donepezil in the treatment of mild or moderate Alzheimer’s disease. Neurology. 1999;52:1115-1116.
29. Hauber AB, Gnanasakthy A, Mauskopf JA. Savings in the cost of caring for patients with Alzheimer’s disease in Canada: an analysis of treatment with rivastigmine. Clin Ther. 2000;22:439-451.
30. Getsios D, Caro JJ, Caro G, Ishak K. The AHEAD Study Group. Assessment of health economics in Alzheimer’s disease (AHEAD): galantamine treatment in Canada. Neurology. 2001;57:972-978.
31. Fillit HM, Gutterman EM, Brooks RL. Impact of donepezil on caregiving burden for patients with Alzheimer’s disease. Int Psychogeriatr. 2000;12(3):389-401.
32. Blesa R. Galantamine: therapeutic effects beyond cognition. Dement Geriatr Cogn Disord. 2000;11(Suppl)1:28-34.
1. Irizarry M, Hyman B. Alzheimer’s disease. In: Principles of neuroepidemiology. Batchelor T, Cudkowicz M, eds. Boston: Butterworth-Heinemann, 2001:69-98.
2. Mesulam MM, Mufson EJ, Levey AI, Warner BH. Cholinergic innervation of cortex by the basal forebrain: Cytochemistry and cortical connections of the septal area, diagonal band nuclei, nucleus basalis (substantia innominata), and hypothalamus in the rhesus monkey. J Comp Neurol. 1983a;214:170-197.
3. Drachman DA, Leavitt J. Human memory and the cholinergic system. A relationship to aging? Arch Neurol. 1974;30:113-121.
4. Davies P, Maloney AJ. Selective loss of central cholinergic neurons in Alzheimer’s disease. Lancet. 1976;2:1403.-
5. Whitehouse PJ, Price DL, Clark AW, Coyle JT, DeLong MR. Alzheimer disease: evidence for selective loss of cholinergic neurons in the nucleus basalis. Ann Neurol. 1981;10:122-126.
6. Higgins JPT, Flicker L. Lecithin and cognitive impairment. The Cochrane Database of Systematic Reviews. 2001.;
7. Knapp MJ, Knopman DS, Solomon PR, Pendlebury WW, Davis CS, Gracon SI. A 30-week randomized controlled trial of high-dose tacrine in patients with Alzheimer’s disease. The Tacrine Study Group. JAMA. 1994;271:985-991.
8. Raskind MA, Peskind ER, Wessel T, Yuan W. Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month extension. The Galantamine USA-1 Study Group. Neurology. 2000;54:2262-2268.
9. Giacobini E. Cholinesterase inhibitors stabilize Alzheimer’s disease. Methods Find Exp Clin Pharmacol. 2000;22:609-613.
10. Irizarry MC, Hyman BT. Alzhemier Disease Therapeutics. J Neuropathology Exp Neurology. 2001;60:923-928.
11. Wilkinson DG. The pharmacology of donepezil: a new treatment of Alzheimer’s disease. Expert Opin Pharmacother. 1999;1:121-135.
12. Polinsky RJ. Clinical pharmacology of rivastigmine: a new-generation acetyl-cholinesterase inhibitor for the treatment of Alzheimer’s disease. Clin Ther. 1998;20:634-647.
13. Samochocki M, Zerlin M, Jostock R, et al. Galantamine is an allosterically potentiating ligand of the human alpha4/beta2 nAChR. Acta Neurol Scand. 2000(Suppl);;176:68-73.
14. Winblad B, Engedal K, Soininen H, Verhey F, et al. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology. 2001;57:489-495.
15. Feldman H, Gauthier S, Hecker J, et al. Donepezil MSAD Study Investigators Group.A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Neurology. 2001;57:613-620.
16. Farlow M, Anand R, Messina J, Jr, Hartman R, Veach J. A 52-week study of the efficacy of rivastigmine in patients with mild to moderately severe Alzheimer’s disease. Eur Neurol. 2000;44:236-241.
17. Rogers S, Friedhoff L. Donepezil Study Group.The efficacy and safety of donepezil in patients with Alzhemier’s disease. Dementia. 1996;7:293-303.
18. Rogers S, Farlow M, Doody R, Morris R, Friedhoff L. A 24-week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer’s disease. Donepezil Study Group. Neurology. 1998;50:136-145.
19. Rosler M, Anand R, Cicin-Sain A, Gauthier S, Agid Y, DalBianco P, Stahelin HB, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: International randomized controlled trial. BMJ. 1999;318:633-638.
20. Tariot PN, Solomon PR, Morris JC, Kershaw P, Lilienfeld S, Ding C. A 5-month, randomized, placebo-controlled trial of galantamine in AD. The Galantamine USA-10 Study Group. Neurology. 2000;54:2269-2276.
21. Wilcock GK, Lilienfeld S, Gaens E. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: Multicentre randomized controlled trial. Galantamine International - 1 Study Group. BMJ. 2000;321:1445-1449.
22. Knopman DS. Management of cognition and function: new results from the clinical trials programme of Aricept (R) (donepezil Hcl). Int J Neuropsychopharmacol. 2000;3:13-20.
23. Cummings JL, Donohue JA, Brooks RL. The relationship between donepezil and behavioral disturbances in patients with Alzheimer’s disease. Am J Geriatr Psychiatry. 2000;8:134-140.
24. Weiner MF, Martin-Cook K, Foster BM, Saine K, et al. Effects of donepezil on emotional/behavioral symptoms in Alzheimer’s disease patients. J Clin Psychiatry. 2000;487-492.
25. Rosler M, Retz W, Retz-Junginger P, Dennler HJ. Effects of two-year treatment with the cholinesterase inhibitor rivastigmine on behavioural symptoms in Alzheimer’s disease. Behav Neurol. 1998;11:211-216.
26. McKeith I, Del Ser T, Spano P, Emre M, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
27. Fillit H, Gutterman EM, Lewis B. Donepezil use in managed Medicare: effect on health care costs and utilization. Clin Ther. 1999;21:2173-2185.
28. Neumann PJ, Hermann RC, Kuntz KM, Araki SS, Duff SB, Leon J, Berenbaum PA, et al. Cost-effectiveness of donepezil in the treatment of mild or moderate Alzheimer’s disease. Neurology. 1999;52:1115-1116.
29. Hauber AB, Gnanasakthy A, Mauskopf JA. Savings in the cost of caring for patients with Alzheimer’s disease in Canada: an analysis of treatment with rivastigmine. Clin Ther. 2000;22:439-451.
30. Getsios D, Caro JJ, Caro G, Ishak K. The AHEAD Study Group. Assessment of health economics in Alzheimer’s disease (AHEAD): galantamine treatment in Canada. Neurology. 2001;57:972-978.
31. Fillit HM, Gutterman EM, Brooks RL. Impact of donepezil on caregiving burden for patients with Alzheimer’s disease. Int Psychogeriatr. 2000;12(3):389-401.
32. Blesa R. Galantamine: therapeutic effects beyond cognition. Dement Geriatr Cogn Disord. 2000;11(Suppl)1:28-34.