User login
Independent Study Confirms Higher Riata ICD Lead Failure Rate
BOSTON – An independent investigation by seven U.S. centers has shown that recently recalled Riata implantable cardioverter defibrillator leads are significantly more prone to failure than are leads made by a different manufacturer.
A retrospective study of all patients older than 18 years who received ICDs with either Riata or Riata ST leads (St. Jude Medical) showed a failure rate of 1.93% per patient-year for Riata leads, significantly more than the rate of 0.43% for the comparator lead, Quattro Secure (Medtronic) (P less than .0001). The failure rate for Riata ST leads was 0.50%, a nonsignificant difference, reported Dr. Raed Abdelhadi of the Minneapolis Heart Institute.

The Riata and Riata ST ICD leads are prone to inside-out and outside-in silicone insulation defects, which can cause lead malfunction and externalization (breach of the outer insulation, visible outside the lead body) of the conductor cables, but until this study, there were no independent, multicenter investigations into the rate of lead failure, failure signs, or clinical sequelae, he said.
"Without such data, it is not possible to design evidence-based management strategies or to advise Riata patients of their risks," he said at the annual meeting of the Heart Rhythm Society.
Investigators at the seven centers looked at all-cause failures and electrical malfunctions in 774 patients who received an 8-French Riata lead (mean follow-up, 4.2 years), and 307 patients who received a 7-French Riata ST lead (mean follow-up, 3.3 years). ICD leads with silicone-polyurethane copolymer insulation (RIATA ST Optim and Durata leads) were excluded.
For comparison, they obtained data on the Quattro Secure ICD leads from a three-center study of the longevity and risk factors for failure of Sprint Fidelis leads (Circulation 2011;123:358-63).
The investigators defined lead failure as either "abnormal impedance leading to replacement, electrical noise manifested by nonphysiologic signals, increase in pacing threshold or decline in R-wave amplitude necessitating lead placement, inability to provide effective therapy due to apparent lead abnormality, or externalized conductor, clearly demonstrated on fluoroscopy or x-ray ... even if the lead was functioning normally and electrically intact."
Neither functional abnormalities (for example, exit block and physiologic oversensing in the presence of an electrically intact lead) nor lead displacement (unless caused by a bad fixation mechanism) were considered to be failures.
Of the 1,081 Riata and Riata ST leads implanted, 712 (66%) were active and functioning normally at last follow-up. Of the 302 (28%) removals from service, 266 were owing to death, 10 to transplant, 5 to perforation, 4 to infection, and 17 to other causes.
In all, 10% of leads in the study were examined for externalized conductors, and 27 (25%) were found to have them. Of this group, seven (26%) leads were malfunctioning.
There were 65 Riata failures and 5 Riata ST failures, for a 6.2% incidence of all-cause failures. Of this group, 47 failures were due to electrical malfunctions, including seven from the externalized conductors contributing to the malfunction, as noted before. An additional 20 leads had externalized conductors with normal function, but met the study definition of failure.
In contrast, there were 23 lead failures among 1,668 patients with Quattro Secure leads (1.37%).
In univariate analysis, neither age, gender, primary or secondary indication for ICD implantation, ejection fraction, type of cardiac disease, nor lead placement location were significantly associated with risk for lead failure. The same was true when the Riata ST leads were subtracted from the equation.
Signs of failure included noise resulting in inappropriate therapy, elevated thresholds requiring lead replacement resulting in loss of capture and syncope, abnormal pacing impedance, abnormal high-voltage impedance, decline in R value requiring lead replacement, and failed defibrillation threshold testing with abnormal high-voltage impedance, requiring lead replacement.
Dr. Abdelhadi noted that the study was limited by its retrospective design, the fact that only 10% of leads were examined for externalized conductors, and the relatively short follow-up in the Riata ST group compared with the other two groups. In addition, most lead failures were not confirmed by returned-product analysis.

The study confirms what was already known and what many meeting attendees expected to hear, commented Dr. Hugh Calkins, professor of cardiology at the Johns Hopkins Heart and Vascular Institute, Baltimore, and vice president of the Heart Rhythm Society, in an interview.
"The bottom line is that it’s all about the patients, and how we take care of them, advise them, and whether we explant the leads. The whole international heart rhythm community is focused on this question and what to do so that there aren’t deaths that result from noise, that there aren’t deaths from unnecessary lead extractions," he said. Dr. Calkins was not involved in the study, but he moderated a media briefing where Dr. Abdelhadi presented the data.
Dr. Abdelhadi and Dr. Calkins reported having no current conflicts of interest to disclose.
BOSTON – An independent investigation by seven U.S. centers has shown that recently recalled Riata implantable cardioverter defibrillator leads are significantly more prone to failure than are leads made by a different manufacturer.
A retrospective study of all patients older than 18 years who received ICDs with either Riata or Riata ST leads (St. Jude Medical) showed a failure rate of 1.93% per patient-year for Riata leads, significantly more than the rate of 0.43% for the comparator lead, Quattro Secure (Medtronic) (P less than .0001). The failure rate for Riata ST leads was 0.50%, a nonsignificant difference, reported Dr. Raed Abdelhadi of the Minneapolis Heart Institute.
The Riata and Riata ST ICD leads are prone to inside-out and outside-in silicone insulation defects, which can cause lead malfunction and externalization (breach of the outer insulation, visible outside the lead body) of the conductor cables, but until this study, there were no independent, multicenter investigations into the rate of lead failure, failure signs, or clinical sequelae, he said.
"Without such data, it is not possible to design evidence-based management strategies or to advise Riata patients of their risks," he said at the annual meeting of the Heart Rhythm Society.
Investigators at the seven centers looked at all-cause failures and electrical malfunctions in 774 patients who received an 8-French Riata lead (mean follow-up, 4.2 years), and 307 patients who received a 7-French Riata ST lead (mean follow-up, 3.3 years). ICD leads with silicone-polyurethane copolymer insulation (RIATA ST Optim and Durata leads) were excluded.
For comparison, they obtained data on the Quattro Secure ICD leads from a three-center study of the longevity and risk factors for failure of Sprint Fidelis leads (Circulation 2011;123:358-63).
The investigators defined lead failure as either "abnormal impedance leading to replacement, electrical noise manifested by nonphysiologic signals, increase in pacing threshold or decline in R-wave amplitude necessitating lead placement, inability to provide effective therapy due to apparent lead abnormality, or externalized conductor, clearly demonstrated on fluoroscopy or x-ray ... even if the lead was functioning normally and electrically intact."
Neither functional abnormalities (for example, exit block and physiologic oversensing in the presence of an electrically intact lead) nor lead displacement (unless caused by a bad fixation mechanism) were considered to be failures.
Of the 1,081 Riata and Riata ST leads implanted, 712 (66%) were active and functioning normally at last follow-up. Of the 302 (28%) removals from service, 266 were owing to death, 10 to transplant, 5 to perforation, 4 to infection, and 17 to other causes.
In all, 10% of leads in the study were examined for externalized conductors, and 27 (25%) were found to have them. Of this group, seven (26%) leads were malfunctioning.
There were 65 Riata failures and 5 Riata ST failures, for a 6.2% incidence of all-cause failures. Of this group, 47 failures were due to electrical malfunctions, including seven from the externalized conductors contributing to the malfunction, as noted before. An additional 20 leads had externalized conductors with normal function, but met the study definition of failure.
In contrast, there were 23 lead failures among 1,668 patients with Quattro Secure leads (1.37%).
In univariate analysis, neither age, gender, primary or secondary indication for ICD implantation, ejection fraction, type of cardiac disease, nor lead placement location were significantly associated with risk for lead failure. The same was true when the Riata ST leads were subtracted from the equation.
Signs of failure included noise resulting in inappropriate therapy, elevated thresholds requiring lead replacement resulting in loss of capture and syncope, abnormal pacing impedance, abnormal high-voltage impedance, decline in R value requiring lead replacement, and failed defibrillation threshold testing with abnormal high-voltage impedance, requiring lead replacement.
Dr. Abdelhadi noted that the study was limited by its retrospective design, the fact that only 10% of leads were examined for externalized conductors, and the relatively short follow-up in the Riata ST group compared with the other two groups. In addition, most lead failures were not confirmed by returned-product analysis.
The study confirms what was already known and what many meeting attendees expected to hear, commented Dr. Hugh Calkins, professor of cardiology at the Johns Hopkins Heart and Vascular Institute, Baltimore, and vice president of the Heart Rhythm Society, in an interview.
"The bottom line is that it’s all about the patients, and how we take care of them, advise them, and whether we explant the leads. The whole international heart rhythm community is focused on this question and what to do so that there aren’t deaths that result from noise, that there aren’t deaths from unnecessary lead extractions," he said. Dr. Calkins was not involved in the study, but he moderated a media briefing where Dr. Abdelhadi presented the data.
Dr. Abdelhadi and Dr. Calkins reported having no current conflicts of interest to disclose.
BOSTON – An independent investigation by seven U.S. centers has shown that recently recalled Riata implantable cardioverter defibrillator leads are significantly more prone to failure than are leads made by a different manufacturer.
A retrospective study of all patients older than 18 years who received ICDs with either Riata or Riata ST leads (St. Jude Medical) showed a failure rate of 1.93% per patient-year for Riata leads, significantly more than the rate of 0.43% for the comparator lead, Quattro Secure (Medtronic) (P less than .0001). The failure rate for Riata ST leads was 0.50%, a nonsignificant difference, reported Dr. Raed Abdelhadi of the Minneapolis Heart Institute.
The Riata and Riata ST ICD leads are prone to inside-out and outside-in silicone insulation defects, which can cause lead malfunction and externalization (breach of the outer insulation, visible outside the lead body) of the conductor cables, but until this study, there were no independent, multicenter investigations into the rate of lead failure, failure signs, or clinical sequelae, he said.
"Without such data, it is not possible to design evidence-based management strategies or to advise Riata patients of their risks," he said at the annual meeting of the Heart Rhythm Society.
Investigators at the seven centers looked at all-cause failures and electrical malfunctions in 774 patients who received an 8-French Riata lead (mean follow-up, 4.2 years), and 307 patients who received a 7-French Riata ST lead (mean follow-up, 3.3 years). ICD leads with silicone-polyurethane copolymer insulation (RIATA ST Optim and Durata leads) were excluded.
For comparison, they obtained data on the Quattro Secure ICD leads from a three-center study of the longevity and risk factors for failure of Sprint Fidelis leads (Circulation 2011;123:358-63).
The investigators defined lead failure as either "abnormal impedance leading to replacement, electrical noise manifested by nonphysiologic signals, increase in pacing threshold or decline in R-wave amplitude necessitating lead placement, inability to provide effective therapy due to apparent lead abnormality, or externalized conductor, clearly demonstrated on fluoroscopy or x-ray ... even if the lead was functioning normally and electrically intact."
Neither functional abnormalities (for example, exit block and physiologic oversensing in the presence of an electrically intact lead) nor lead displacement (unless caused by a bad fixation mechanism) were considered to be failures.
Of the 1,081 Riata and Riata ST leads implanted, 712 (66%) were active and functioning normally at last follow-up. Of the 302 (28%) removals from service, 266 were owing to death, 10 to transplant, 5 to perforation, 4 to infection, and 17 to other causes.
In all, 10% of leads in the study were examined for externalized conductors, and 27 (25%) were found to have them. Of this group, seven (26%) leads were malfunctioning.
There were 65 Riata failures and 5 Riata ST failures, for a 6.2% incidence of all-cause failures. Of this group, 47 failures were due to electrical malfunctions, including seven from the externalized conductors contributing to the malfunction, as noted before. An additional 20 leads had externalized conductors with normal function, but met the study definition of failure.
In contrast, there were 23 lead failures among 1,668 patients with Quattro Secure leads (1.37%).
In univariate analysis, neither age, gender, primary or secondary indication for ICD implantation, ejection fraction, type of cardiac disease, nor lead placement location were significantly associated with risk for lead failure. The same was true when the Riata ST leads were subtracted from the equation.
Signs of failure included noise resulting in inappropriate therapy, elevated thresholds requiring lead replacement resulting in loss of capture and syncope, abnormal pacing impedance, abnormal high-voltage impedance, decline in R value requiring lead replacement, and failed defibrillation threshold testing with abnormal high-voltage impedance, requiring lead replacement.
Dr. Abdelhadi noted that the study was limited by its retrospective design, the fact that only 10% of leads were examined for externalized conductors, and the relatively short follow-up in the Riata ST group compared with the other two groups. In addition, most lead failures were not confirmed by returned-product analysis.
The study confirms what was already known and what many meeting attendees expected to hear, commented Dr. Hugh Calkins, professor of cardiology at the Johns Hopkins Heart and Vascular Institute, Baltimore, and vice president of the Heart Rhythm Society, in an interview.
"The bottom line is that it’s all about the patients, and how we take care of them, advise them, and whether we explant the leads. The whole international heart rhythm community is focused on this question and what to do so that there aren’t deaths that result from noise, that there aren’t deaths from unnecessary lead extractions," he said. Dr. Calkins was not involved in the study, but he moderated a media briefing where Dr. Abdelhadi presented the data.
Dr. Abdelhadi and Dr. Calkins reported having no current conflicts of interest to disclose.
FROM THE ANNUAL MEETING OF THE HEART RHYTHM SOCIETY
Stem Cell Therapy and Cardiac Function

Nearly a decade after the first in-man trial to test the efficacy and safety of using stem cells to treat acute myocardial infarction, and after numerous other small phase II clinical trials, we still don’t know which stem cell type to use, what patient population to target, or the most appropriate delivery approach.
Three recent studies characterize the rocky path this area of research has traveled.
First, the pooled results of a meta-analysis of 33 randomized clinical trials conducted to evaluate the safety and efficacy of bone marrow–derived intracardiac stem cell therapy for AMI involving 1,765 subjects showed that stem cell therapy significantly reduced infarct size, modestly improved left ventricular function, and reduced LV volume (Cochrane Database Syst. Rev. 2012 [doi: 10.1002/14651858.CD006536.pub3]). There was also a small reduction in mortality and morbidity in favor of stem cell therapy that did not reach statistical significance.
Second, the results of the CADUCEUS trial showed that intracoronary infusion of autologous cardiosphere-derived stem cells (resident myocardial stem cells derived from right ventricular biopsies) soon after an AMI was safe and feasible, and led to reduced scar size and to an increase in viable muscle mass. Clinically, patients in the stem cell group showed an increase in 6-minute walk distance, but had no improvements in MLHFQ (Minnesota Living With Heart Failure Questionnaire) compared with placebo and no improvement in LV ejection fraction at 6 months (Lancet 2012;379:895-904 [doi:10.1016/S0140-6736(12)60195-0]).
Third, the results of the FOCUS-CCTRN trial, which examined the effects of autologous bone marrow mononuclear cells on functional capacity, LV function, and perfusion in patients with chronic ischemic heart failure, failed to achieve its primary and secondary end points. Compared with placebo, delivery of bone marrow stem cells did not improve LV end-systolic volume, regional wall motion, maximal oxygen consumption, reversibility on SPECT, fixed defect size, or clinical status (JAMA 2012;307:1717-26 [doi: 10.1001/jama.2012.418]).
These reports paint differing scenarios, ranging from encouraging positive outcomes to outright failure. Nonetheless, the weight of evidence suggests that there is merit in pursuing stem cell therapy for the treatment of AMI and possibly its downstream consequences, namely heart failure. The scientific evidence gathered to date appears to support the "safety" side of this form of therapeutic intervention, but to a much lesser extent, the "efficacy" side. Modest improvements in LV function and remodeling are frequently uncovered with many forms of stem cell therapy, but these benefits fall short of positively influencing clinical outcome viewed in terms of mortality and morbidity.
In the case of stem cell therapy, the scientific medical community has deviated somewhat from its usual course of pursuing knowledge, filling in gaps, and only then bringing forward an appropriate "knowledge-based" therapeutic approach, and has instead pursued the path of least resistance.
After many years of trial-by-error experimentation, we can ask ourselves the following: Do we really know if adult cardiospheres are better stem cells than skeletal muscle myoblasts, or for that matter, bone marrow–derived stem cells or even embryonics? Can we confirm that stem cells delivered to the myocardium survive and are integrated into physiologic structures? Are we certain that cell regeneration takes place, and if so, how? Is the integration of exogenous stem cells into the cardiac structure the mediator of benefit or is it what the stem cells elaborate? If the latter, should we not spend more time understanding this "response process"? Is it time to redirect our efforts and treasure to fill in the knowledge gaps in this field if we expect to benefit from this discovery?
We are already paying the price of frequent failures with stem cell therapy just as we did in the recent past with gene therapy. Clinical trial failures have tempered the enthusiasm and suppressed the appetite of the investment community and the pharmaceutical industry for this line of research and its potential therapeutic value. It is time to go back to the basics, gain needed knowledge, and reemerge with better tools that capitalize on the enormous therapeutic potential of stem cell therapy.
Dr. Sabbah is director of cardiovascular research at Henry Ford Health System in Detroit. He disclosed that he is a named inventor on U.S. patents dealing with use of stem cell hypoxia-conditioned media for the treatment of heart failure licensed by Henry Ford Health System to LoneStar Heart.
Nearly a decade after the first in-man trial to test the efficacy and safety of using stem cells to treat acute myocardial infarction, and after numerous other small phase II clinical trials, we still don’t know which stem cell type to use, what patient population to target, or the most appropriate delivery approach.
Three recent studies characterize the rocky path this area of research has traveled.
First, the pooled results of a meta-analysis of 33 randomized clinical trials conducted to evaluate the safety and efficacy of bone marrow–derived intracardiac stem cell therapy for AMI involving 1,765 subjects showed that stem cell therapy significantly reduced infarct size, modestly improved left ventricular function, and reduced LV volume (Cochrane Database Syst. Rev. 2012 [doi: 10.1002/14651858.CD006536.pub3]). There was also a small reduction in mortality and morbidity in favor of stem cell therapy that did not reach statistical significance.
Second, the results of the CADUCEUS trial showed that intracoronary infusion of autologous cardiosphere-derived stem cells (resident myocardial stem cells derived from right ventricular biopsies) soon after an AMI was safe and feasible, and led to reduced scar size and to an increase in viable muscle mass. Clinically, patients in the stem cell group showed an increase in 6-minute walk distance, but had no improvements in MLHFQ (Minnesota Living With Heart Failure Questionnaire) compared with placebo and no improvement in LV ejection fraction at 6 months (Lancet 2012;379:895-904 [doi:10.1016/S0140-6736(12)60195-0]).
Third, the results of the FOCUS-CCTRN trial, which examined the effects of autologous bone marrow mononuclear cells on functional capacity, LV function, and perfusion in patients with chronic ischemic heart failure, failed to achieve its primary and secondary end points. Compared with placebo, delivery of bone marrow stem cells did not improve LV end-systolic volume, regional wall motion, maximal oxygen consumption, reversibility on SPECT, fixed defect size, or clinical status (JAMA 2012;307:1717-26 [doi: 10.1001/jama.2012.418]).
These reports paint differing scenarios, ranging from encouraging positive outcomes to outright failure. Nonetheless, the weight of evidence suggests that there is merit in pursuing stem cell therapy for the treatment of AMI and possibly its downstream consequences, namely heart failure. The scientific evidence gathered to date appears to support the "safety" side of this form of therapeutic intervention, but to a much lesser extent, the "efficacy" side. Modest improvements in LV function and remodeling are frequently uncovered with many forms of stem cell therapy, but these benefits fall short of positively influencing clinical outcome viewed in terms of mortality and morbidity.
In the case of stem cell therapy, the scientific medical community has deviated somewhat from its usual course of pursuing knowledge, filling in gaps, and only then bringing forward an appropriate "knowledge-based" therapeutic approach, and has instead pursued the path of least resistance.
After many years of trial-by-error experimentation, we can ask ourselves the following: Do we really know if adult cardiospheres are better stem cells than skeletal muscle myoblasts, or for that matter, bone marrow–derived stem cells or even embryonics? Can we confirm that stem cells delivered to the myocardium survive and are integrated into physiologic structures? Are we certain that cell regeneration takes place, and if so, how? Is the integration of exogenous stem cells into the cardiac structure the mediator of benefit or is it what the stem cells elaborate? If the latter, should we not spend more time understanding this "response process"? Is it time to redirect our efforts and treasure to fill in the knowledge gaps in this field if we expect to benefit from this discovery?
We are already paying the price of frequent failures with stem cell therapy just as we did in the recent past with gene therapy. Clinical trial failures have tempered the enthusiasm and suppressed the appetite of the investment community and the pharmaceutical industry for this line of research and its potential therapeutic value. It is time to go back to the basics, gain needed knowledge, and reemerge with better tools that capitalize on the enormous therapeutic potential of stem cell therapy.
Dr. Sabbah is director of cardiovascular research at Henry Ford Health System in Detroit. He disclosed that he is a named inventor on U.S. patents dealing with use of stem cell hypoxia-conditioned media for the treatment of heart failure licensed by Henry Ford Health System to LoneStar Heart.
Nearly a decade after the first in-man trial to test the efficacy and safety of using stem cells to treat acute myocardial infarction, and after numerous other small phase II clinical trials, we still don’t know which stem cell type to use, what patient population to target, or the most appropriate delivery approach.
Three recent studies characterize the rocky path this area of research has traveled.
First, the pooled results of a meta-analysis of 33 randomized clinical trials conducted to evaluate the safety and efficacy of bone marrow–derived intracardiac stem cell therapy for AMI involving 1,765 subjects showed that stem cell therapy significantly reduced infarct size, modestly improved left ventricular function, and reduced LV volume (Cochrane Database Syst. Rev. 2012 [doi: 10.1002/14651858.CD006536.pub3]). There was also a small reduction in mortality and morbidity in favor of stem cell therapy that did not reach statistical significance.
Second, the results of the CADUCEUS trial showed that intracoronary infusion of autologous cardiosphere-derived stem cells (resident myocardial stem cells derived from right ventricular biopsies) soon after an AMI was safe and feasible, and led to reduced scar size and to an increase in viable muscle mass. Clinically, patients in the stem cell group showed an increase in 6-minute walk distance, but had no improvements in MLHFQ (Minnesota Living With Heart Failure Questionnaire) compared with placebo and no improvement in LV ejection fraction at 6 months (Lancet 2012;379:895-904 [doi:10.1016/S0140-6736(12)60195-0]).
Third, the results of the FOCUS-CCTRN trial, which examined the effects of autologous bone marrow mononuclear cells on functional capacity, LV function, and perfusion in patients with chronic ischemic heart failure, failed to achieve its primary and secondary end points. Compared with placebo, delivery of bone marrow stem cells did not improve LV end-systolic volume, regional wall motion, maximal oxygen consumption, reversibility on SPECT, fixed defect size, or clinical status (JAMA 2012;307:1717-26 [doi: 10.1001/jama.2012.418]).
These reports paint differing scenarios, ranging from encouraging positive outcomes to outright failure. Nonetheless, the weight of evidence suggests that there is merit in pursuing stem cell therapy for the treatment of AMI and possibly its downstream consequences, namely heart failure. The scientific evidence gathered to date appears to support the "safety" side of this form of therapeutic intervention, but to a much lesser extent, the "efficacy" side. Modest improvements in LV function and remodeling are frequently uncovered with many forms of stem cell therapy, but these benefits fall short of positively influencing clinical outcome viewed in terms of mortality and morbidity.
In the case of stem cell therapy, the scientific medical community has deviated somewhat from its usual course of pursuing knowledge, filling in gaps, and only then bringing forward an appropriate "knowledge-based" therapeutic approach, and has instead pursued the path of least resistance.
After many years of trial-by-error experimentation, we can ask ourselves the following: Do we really know if adult cardiospheres are better stem cells than skeletal muscle myoblasts, or for that matter, bone marrow–derived stem cells or even embryonics? Can we confirm that stem cells delivered to the myocardium survive and are integrated into physiologic structures? Are we certain that cell regeneration takes place, and if so, how? Is the integration of exogenous stem cells into the cardiac structure the mediator of benefit or is it what the stem cells elaborate? If the latter, should we not spend more time understanding this "response process"? Is it time to redirect our efforts and treasure to fill in the knowledge gaps in this field if we expect to benefit from this discovery?
We are already paying the price of frequent failures with stem cell therapy just as we did in the recent past with gene therapy. Clinical trial failures have tempered the enthusiasm and suppressed the appetite of the investment community and the pharmaceutical industry for this line of research and its potential therapeutic value. It is time to go back to the basics, gain needed knowledge, and reemerge with better tools that capitalize on the enormous therapeutic potential of stem cell therapy.
Dr. Sabbah is director of cardiovascular research at Henry Ford Health System in Detroit. He disclosed that he is a named inventor on U.S. patents dealing with use of stem cell hypoxia-conditioned media for the treatment of heart failure licensed by Henry Ford Health System to LoneStar Heart.
Act 2 Opens for Stem-Cell Heart Treatments
Stem-cell treatment for cardiac disease recently launched into advanced clinical trials, as a flurry of early-phase studies over the last year collectively confirmed the treatment as safe but left its efficacy unresolved.
At least two phase III trials are now underway and others are possibly imminent. But until these pivotal studies begin to yield outcome results in about 4 years, stem-cell treatment remains a question mark – an appealing idea fueled by hints of effectiveness but also dogged by failures that prompt skepticism about its future.

The gush of recent early-phase studies also hint at possible explanations for the variability in the success of stem cell treatment. The studies examined a broad range of cell types and patients. (Click here to see a chart of the studies.) The results imply that select types of bone marrow cells may be more effective as therapy and that the number and potency of stem cells decrease with age.
Clinical testing of stem cells for heart disease has hit its stride more than a decade after the first-in-human report in 2001 of a patient treated following an acute myocardial infarction (Dtsch. Med. Wochenschr. 2001;126:932-8), which was followed by the first randomized clinical trial, also in myocardial infarction patients, reported in 2004 (Lancet 2004;364:141-8).
"So far, stem-cell treatment has been safe in all the areas where it’s been used. I’m very satisfied" with the progress, said Dr. Emerson C. Perin, an interventional cardiologist and medical director of the Stem Cell Center at the Texas Heart Institute and one of the U.S. researchers who has worked longest on stem-cell clinical studies. Those working on clinical investigations of stem cells "haven’t done anything stupid to kill it, and we’ve gone from a crawl to a walk," he said in an interview.
Development of stem cell therapies "has been on a normal track; each step takes time. It’s very similar to what happened with fibrinolytic therapy for treating acute myocardial infarctions" in the 1980s and 1990s, said Dr. Timothy D. Henry, an interventional cardiologist, director of research at the Minneapolis Heart Institute Foundation, and another very active stem cell researcher. "It was a good 10 years before we got lytics up and going. People want [stem cells] to be a magic bullet. I think some people have put unrealistic expectations on stem cells, but it’s like any other treatment. You need to do a trial and find out the relative risks and benefits, and that takes time," he said in an interview.

A different take on the past decade of stem-cell work came from another researcher in the field, Dr. Eduardo Marbán. "The pace of progress has been disappointingly slow, marked by numerous examples of clinical studies prematurely undertaken without benefit of adequate preclinical data. We are lucky that no one has been killed," said Dr. Marbán, professor and director of the Cedars-Sinai Heart Institute in Los Angeles. But despite whatever role luck may have played, Dr. Marbán agreed on the bottom line: "The major accomplishment of the 11-year experience has been the convincing demonstration that most forms of cell therapy are safe, if administered via the intracoronary route." Then he added the elephant in the room: "Efficacy is another matter.
record. Why subject patients to risk in receiving a cell product that has not been extensively validated in vitro and in small and large animals? Yet this has been done over and over again" by investigators running clinical trials of stem cells and other cells for heart disease, Dr. Marbán said in an interview.
Making It to Phase III: REPAIR-AMI/BAMI
The recent surge of study results, and the path to phase III may be best exemplified by the landmark phase II trial done by German investigators, the Reinfusion of Enriched Progenitor Cells and Infarct Remodeling in Acute Myocardial Infarction (REPAIR-AMI) trial (N. Engl. J. Med. 2006;355:1210-21). The multicenter German study randomized 204 patients an average of 4 days following an acute myocardial infarction (MI) to receive either an intracoronary infusion of autologous bone marrow cells processed to enrich for progenitor cells, or placebo.
Last November, at the annual Scientific Sessions of the American Heart Association, the group presented 5-year follow-up results for 200 of the 204 patients. Helped by the lengthy follow-up, the researchers found that the stem-cell treatment cut the cumulative rate of death, recurrent MI, or need for revascularization from 64% in the control arm to 42%, a statistically significant difference in a prespecified end point of the study.
This striking change in a very meaningful clinical outcome contrasted with the modest change in a surrogate end point at 4 months (first reported in the 2006 article), and led to the launch of the largest phase III study of stem cells for heart disease, the Effect of Intracoronary Reinfusion of Bone Marrow Derived Mononuclear Cells (BM-MNC) on All-Cause Mortality in Acute Myocardial Infarction (BAMI), a 3,000-patient, multi-center study funded by the European Union. The study will enroll patients within 3-6 days after reperfusion therapy of an acute MI if they have a left ventricular ejection fraction of 45% or less. The primary end point is a reduction in all-cause mortality, a design that will allow BAMI to use standard care as its control instead of a sham infusion.
"We discussed the end point with the EMA [European Medicines Agency], and they said that if you use only death as the end point we can do it with a state-of-the-art control. I think that is the proper way, because some people believe that intracoronary instrumentation by itself carries a risk that could also affect placebo groups," said Dr. Andreas M. Zeiher, professor and chairman of medicine at Goethe University in Frankfurt, Germany, speaking last November at the American Heart Association meeting.
Dr. Zeiher, who led the team that ran REPAIR-AMI and spearheaded organization of the BAMI trial, also stressed the need to avoid heparin when handling and administering autologous bone marrow cells to achieve optimal results. "Heparin interferes with a process that is absolutely crucial for these cells to extravasate during infusion to enter ischemic tissue," he said during a talk in March at the American College of Cardiology Scientific Session in Chicago. "Heparin in the syringe more or less completely abolishes the migratory capacity of the [bone-marrow] cells." Dr. Zeiher reviewed the methods and results of more than 20 stem-cell studies and found those that used heparin-treated bone-marrow cells had little clinical effect, when studies that avoided heparin or neutralized the drug with serum the cell treatments proved effective. REPAIR-AMI used serum to neutralize heparin, and BAMI will use bivalirudin as an anticoagulant and no heparin, he said.
In contrast to the success in REPAIR-AMI, no efficacy signal occurred in a Norwegian study of bone-marrow mononuclear cells injected into the hearts of 47 acute MI patients in the Autologous Stem-Cell Transplantation in Acute Myocardial Infarction (ASTAMI) study, which coincidently appeared in the same issue of The New England Journal of Medicine as the REPAIR-AMI report (N. Engl. J. Med. 2006;355:1199-209). The lack of success in ASTAMI juxtaposed against the efficacy signal in REPAIR-AMI (a signal later confirmed and strengthened by longer follow-up) provides an example in microcosm of the uneven road that stem cell therapy traversed over the past 11 years. Also worth noting: in ASTAMI the investigators used heparin.
"Heparin interferes with a process that is absolutely crucial for these cells to extravasate during infusion to enter ischemic tissuu," Dr. Andreas M. Zeiher said.
Dr. Zeiher’s heparin explanation for outcome differences among many stem-cell studies is "an interesting hypothesis," said Dr. Robert D. Simari, a cardiologist and professor of medicine at the Mayo Clinic in Rochester, Minn. There are likely several important differences" between the stem-cell trials that have been positive and those that have failed. Trials have differed in their design, patient populations, their stem cell products, and in the end points they have used to measure success, said Dr. Simari, who also chairs the steering committee of the Cardiovascular Cell Therapy Research Network (CCTRN), a research group of seven U.S. centers organized by the National Heart Lung and Blood Institute to run early-phase clinical trials with cell treatments.
Also in the Phase III Act: ACT34-CMI/RENEW
Another cell therapy success story now advancing to a phase III trial is led by Dr. Douglas W. Losordo using autologous CD34+ cells injected into the myocardium of patients with refractory angina. He and his associates published results last August from a phase II study with167 patients, the Double-blind, Prospective, Randomized, Placebo-controlled Study to Determine the Tolerability, Efficacy, Safety, and Dose Range of Intramyocardial Injections of G-CSF Mobilized Auto–CD34+ Cells for Reduction of Angina Episodes in Patients With Refractory Chronic Myocardial Ischemia (ACT34-CMI).
The researchers obtained the autologous cell preparation used in ACT34-CMI by first treating each patient with granulocyte colony stimulating factor daily for 4 or 5 days to mobilize their CD34+ cells. The day following the last dose of drug, each patient underwent leukopheresis to collect mononuclear cells. The cell material then underwent further ex vivo enrichment for CD34+ cells using a commercially-available magnetic cell selection device marketed by Baxter Healthcare. Patients received 100,000 CD34+ cells/kg, 500,000 CD34+ cells/kg, or placebo as intramyocardial injections at 10 sites identified by electromechanical endocardial mapping. Dr. Losordo and his associates said they used CD34+ cells because of evidence these cells, called endothelial progenitor cells, can stimulate neovascularization in ischemic tissue, and improved function in animal models of acute and chronic myocardial ischemia. The patients enrolled in ACT34-CMI all had Canadian Cardiovascular Society class III or IV chronic refractory angina despite optimal medial treatment.
The study, done at 26 U.S. centers, found that at 6 and 12 months after treatment, 54 patients who received the low-dose injections had significantly fewer angina episodes per week than the 53 patients who received placebo infections, the study’s primary end point. Patients who received the higher-dose injections also had fewer angina episodes than the controls, but the difference was not statistically significant at either 6- or 12-month follow-up. The low-dose patients also had statistically significant improvement in their total exercise time in an exercise tolerance test compared with the placebo patients; the high-dose patients also had better exercise times, but not significantly better than the controls.
Speaking at the American College of Cardiology meeting in Chicago in March, Dr. Losordo presented 2-year follow-up data on the patients in ACT34-CMI. At 2 years, the low-dose patients continued to have a significantly lower rate of weekly angina counts than control patients, while the high-dose patients continued to have a numerically lower rate that was not significantly different from the controls. The cumulative, 2-year rate of death, MI, or hospitalization for acute coronary syndrome was 30% in the control patients, 18% in the low-dose patients, and 14% in the high-dose patients. Although these between group differences were not statistically significant, the trends were "in the right direction," said Dr. Losordo, an interventional cardiologist at Northwestern University in Chicago, and vice president for new therapeutic development at Baxter International. Baxter sponsored ACT34-CMI, as well as the phase III study now starting based on the phase II results.
The phase III study, A Prospective, Randomized, Double-blinded, Active-control and Unblinded Standard of Care (SOC) Controlled Study to Determine the Efficacy and Safety of Targeted Intramyocardial Delivery of Autologous CD34+ Cells (Auto-CD34+ Cells) for Increasing Exercise Capacity During Standardized Exercise Testing in Subjects With Refractory Angina Pectoris and Chronic Myocardial Ischemia (RENEW), will enroll about 450 refractory angina patients at 50 U.S. sites, randomizing them to CD34+ treatment, placebo treatment, or no treatment and optimal standard care. The primary efficacy outcome will be change in total exercise time on an exercise tolerance test after 12 months.
Choosing the Right Cells
The success of the ACT34-CMI study, and the decision by Dr. Losordo and Baxter to move on to the phase III RENEW trial, highlights what may be a possible advantage to using selected stem and progenitor cells compared with the strategy of using an unselected cell population, such as the bone-marrow cells used in many of the studies of the past 11 years.
More evidence favoring cell selection came recently in results reported by Dr. Perin from the First Mononuclear Cells Injected in the United States Conducted by the Cardiovascular Cell Therapy Research Network (FOCUS-CCTRN) study, which he presented in March at the American College of Cardiology meeting in Chicago. The phase II study enrolled 92 patients with chronic heart failure and a left ventricular ejection fraction of 45% or less. Patients received a transendocardial injection of 100 million autologous bone-marrow cells or placebo. The primary end points were 6-month changes in left ventricular end systolic volume, in maximal oxygen consumption, and the extent of ischemic myocardial defects measured by single photon emission tomography. The results showed no statistically significant improvement for any of these three end points in the patients treated with bone-marrow cells compared with the controls, and were simultaneously reported in an article published online (JAMA 2012; March 24 [doi:10.1001/jama.2012.418]).
Despite the study’s failure for its prespecified end points, it also showed signals of efficacy and possibly highlighted some important lessons on how to best apply stem cell therapy in the future. On the efficacy side, the 61 patients who received bone-marrow cell injections had an average 1.4% improvement in their left ventricular ejection fraction, compared with an average 1.3% decline in the 31 placebo patients, an overall between-group difference of 2.7% that was statistically significant. Further analysis showed that patients who received bone-marrow cell preparations that had higher levels of either CD34+ cell or CD133+ cells had greater increases in their left ventricular ejection fractions. Also, when the researchers analyzed responses in subgroups divided by their age, patients 62 years old or younger (62 years old was the median age in the study) who received bone-marrow cells had a statistically significant, 4.7% improvement in their left ventricular ejection fraction after 6 months compared with placebo patients, while among patients greater than 62 years old treatment with autologous bone-marrow cells produced no significant improvement in ejection fraction compared with the controls.
"It could very well be that [unfractionated] bone marrow is a weaker product than using a specific cell type," said Dr. Perin. "Now we’ll start using parts of bone marrow, specific cells or cell combinations," he predicted, although he added that additional analysis of the FOCUS-CCTRN data must occur before he and his associates decide which cell types show the most promise. "Even though it’s not answered perfectly, the results definitely point us toward" using more selected types of bone marrow cells, he said.
"The most important lesson FOCUS-CCTRN showed was that as patients get older the number and potency of their stem cells decreases. It showed that if you give cells that aren’t potent they won’t work," said Dr. Henry, a co-investigator of the study and an active member of CCTRN. "That’s a really important insight, because if you treat patients with 100 mg of a beta blocker you get a consistent effect, but if you treat patients with autologous stem cells, every patient gets something different."
Development of stem cell therapies "has been on a normal track; each step takes time. It’s very similar to what happened with fibrinolytic therapy for treating acute myocardial infarctions" in the 1980s and 1990s, said Dr. Timothy D. Henry.
"The FOCUS results showed some evidence of an effect, but there are a number of ways to make it better," Dr. Henry said. One approach is to use selected cells, such as CD34+ cells. Another strategy is to deliver allogenic cells obtained initially from young and healthy donors, a way to avoid the issue of older patients and those with co-morbidities who may have compromised stem cells.
Administering selected or allogenic cells has another potential advantage: it opens the door to commercial involvement with a potentially saleable product, a strategy that can attract the interest of a company willing to shoulder the cost of a phase III trial.
"A challenge with [unprocessed] bone marrow is it’s too easy. Bone marrow is inexpensive, and anyone can do it," Dr. Henry noted. That’s one reason why it took several years for the REPAIR-AMI strategy to advance into a phase III trial, eventually moving forward when it received financial backing from the European Union. In contrast, the promising ACT34-CMI strategy quickly jumped to the phase III level, aided by financial support from Baxter.
But others cautioned against drawing too many inferences from FOCUS-CCTRN because it was a negative study and hence all its results must be considered suspect.
"I do not believe that post-hoc analysis of cell potency should be used to guide future trials. FOCUS was negative; the subgroup analyses and cell potency assays were attempts to glean some positivity from that study after the fact," said Dr. Marbán.
More Phase III Studies Coming, with Commercial Support
Another example of a selected, allogenic cell preparation with commercial support is the study of mesenchymal precursor cells (MPC), bone-marrow cells obtained from young, healthy donors and delivered by transendocardial injection to 45 patients with cardiomyopathy, New York Heart Association class II or III heart failure, and impaired left ventricular function in a phase II study presented by Dr. Perin last November at the American Heart Association’s Scientific Sessions in Orlando. The MPC preparation he and his associates tested was an "off-the-shelf" stem-cell product made by the Australian-based company Mesoblast.
The injections were safe, and the three different amounts of cells delivered showed various signs of efficacy. The lowest dose of cells tested showed a statistically significant improvement in left ventricular ejection fraction at 3 months compared with placebo; the highest cell dose tested showed a statistically significant improvement in left ventricular end-systolic volume at 12 months compared with the placebo control; and collectively, all three cell doses tested produced a statistically significant 20% reduction in the rate of major adverse coronary events compared with the placebo patients during a follow-up of up to 3 years, Dr. Perin reported last November.
"Given the very positive results we saw in the phase II trial, it would be logical to move on to a bigger trial," said Dr. Perin in an interview, but he added that he was unable to provide details about possible additional trials with this MPC product.
Another commercially-backed stem-cell product poised for a larger trial is cardiopoietic stem cells, made by a proprietary, patented method that uses a patient’s autologous bone-marrow stem cells and treats them in vitro to produce cells that are then injected into a patient’s myocardium where they produce new heart muscle. Researchers at the Mayo Clinic in Rochester, Minn. developed this process, and Mayo licensed it to a Belgian company, Cardio 3 BioSciences.

The company released results in November 2010 from the C-Cure study done in Belgium, Serbia, and Switzerland that enrolled 45-patients with severe ischemic heart failure. Six months after treatment, the 21 patients who received injections of the stem cells had an average 18% relative increase in their left ventricular ejection fraction compared with baseline, versus a 4% relative increase over baseline among 24 control patients. Speaking in March at the American College of Cardiology meeting, Dr. André Terzic, who led the study, provided a few more details from the results. Average ejection fraction in the actively-treated patients rose from 28% at baseline to 33%. The treatment was especially effective for the patients who entered the study with an ejection fraction below 28%, said Dr. Terzic, a professor of medicine and cardiology, and director of the Center for Regenerative Medicine at the Mayo Clinic. The 6-month results also showed other indications of benefit in the patients treated with the cardiopoietic stem cells, including significantly increased left ventricular end systolic volume, and reduced left ventricular mass index.
Cardio 3 Biosciences is now planning to start a "late phase II" or phase III trial with this material, said Dr. Simari, who is not directly involved in these studies.
What Comes Next?
Despite 11 years of work, "it’s still very early in the field. We’re still trying to figure out the cells and out targets," said Dr. Simari. "This is the haze of early days, of learning from groups of 10, 20, or 80 patients. Only in retrospect, and as we get to larger trials will the truth emerge. Right now, there is a lot of work needed and few headlines, and it will probably stay that way for awhile. This is not a game for people with short attention spans.
"The business model for autologous cells remains uncertain," he added. "For allogenic products that are generated from young, healthy donors and made into thousands of doses, the business model is different and the costs might be more reasonable. Hopefully, as our knowledge grows, we will develop treatments that end up costing less."
"I have no doubt that cell treatment is one of the great avenues of future medicine; it’s just a matter of figuring it out," said Dr. Perin. "Having phase III trials now starting is a step forward. Things are starting to come into focus. Unless something totally unforeseen happens, we will eventually have an approved product," he predicted.
Dr. Perin said that he has been a consultant to Amorcyte, Teva, Cytori, and Aldagen. Dr. Henry said that he has served on steering committees for and received research grants from Aastrom and Mesoblast. Dr. Marbán said that he is a founder of and holds equity in Capricor. Dr. Simari said that he had no disclosures. Dr. Zeiher said he is a cofounder of and scientific advisor to t2cure, a company set up to run the BAMI trial, sponsored by the European Union Dr. Losordo is an employee of Baxter International. Dr. Terzic said that he has received research grants from Cardio 3 BioSciences.
Stem-cell treatment for cardiac disease recently launched into advanced clinical trials, as a flurry of early-phase studies over the last year collectively confirmed the treatment as safe but left its efficacy unresolved.
At least two phase III trials are now underway and others are possibly imminent. But until these pivotal studies begin to yield outcome results in about 4 years, stem-cell treatment remains a question mark – an appealing idea fueled by hints of effectiveness but also dogged by failures that prompt skepticism about its future.
The gush of recent early-phase studies also hint at possible explanations for the variability in the success of stem cell treatment. The studies examined a broad range of cell types and patients. (Click here to see a chart of the studies.) The results imply that select types of bone marrow cells may be more effective as therapy and that the number and potency of stem cells decrease with age.
Clinical testing of stem cells for heart disease has hit its stride more than a decade after the first-in-human report in 2001 of a patient treated following an acute myocardial infarction (Dtsch. Med. Wochenschr. 2001;126:932-8), which was followed by the first randomized clinical trial, also in myocardial infarction patients, reported in 2004 (Lancet 2004;364:141-8).
"So far, stem-cell treatment has been safe in all the areas where it’s been used. I’m very satisfied" with the progress, said Dr. Emerson C. Perin, an interventional cardiologist and medical director of the Stem Cell Center at the Texas Heart Institute and one of the U.S. researchers who has worked longest on stem-cell clinical studies. Those working on clinical investigations of stem cells "haven’t done anything stupid to kill it, and we’ve gone from a crawl to a walk," he said in an interview.
Development of stem cell therapies "has been on a normal track; each step takes time. It’s very similar to what happened with fibrinolytic therapy for treating acute myocardial infarctions" in the 1980s and 1990s, said Dr. Timothy D. Henry, an interventional cardiologist, director of research at the Minneapolis Heart Institute Foundation, and another very active stem cell researcher. "It was a good 10 years before we got lytics up and going. People want [stem cells] to be a magic bullet. I think some people have put unrealistic expectations on stem cells, but it’s like any other treatment. You need to do a trial and find out the relative risks and benefits, and that takes time," he said in an interview.
A different take on the past decade of stem-cell work came from another researcher in the field, Dr. Eduardo Marbán. "The pace of progress has been disappointingly slow, marked by numerous examples of clinical studies prematurely undertaken without benefit of adequate preclinical data. We are lucky that no one has been killed," said Dr. Marbán, professor and director of the Cedars-Sinai Heart Institute in Los Angeles. But despite whatever role luck may have played, Dr. Marbán agreed on the bottom line: "The major accomplishment of the 11-year experience has been the convincing demonstration that most forms of cell therapy are safe, if administered via the intracoronary route." Then he added the elephant in the room: "Efficacy is another matter.
record. Why subject patients to risk in receiving a cell product that has not been extensively validated in vitro and in small and large animals? Yet this has been done over and over again" by investigators running clinical trials of stem cells and other cells for heart disease, Dr. Marbán said in an interview.
Making It to Phase III: REPAIR-AMI/BAMI
The recent surge of study results, and the path to phase III may be best exemplified by the landmark phase II trial done by German investigators, the Reinfusion of Enriched Progenitor Cells and Infarct Remodeling in Acute Myocardial Infarction (REPAIR-AMI) trial (N. Engl. J. Med. 2006;355:1210-21). The multicenter German study randomized 204 patients an average of 4 days following an acute myocardial infarction (MI) to receive either an intracoronary infusion of autologous bone marrow cells processed to enrich for progenitor cells, or placebo.
Last November, at the annual Scientific Sessions of the American Heart Association, the group presented 5-year follow-up results for 200 of the 204 patients. Helped by the lengthy follow-up, the researchers found that the stem-cell treatment cut the cumulative rate of death, recurrent MI, or need for revascularization from 64% in the control arm to 42%, a statistically significant difference in a prespecified end point of the study.
This striking change in a very meaningful clinical outcome contrasted with the modest change in a surrogate end point at 4 months (first reported in the 2006 article), and led to the launch of the largest phase III study of stem cells for heart disease, the Effect of Intracoronary Reinfusion of Bone Marrow Derived Mononuclear Cells (BM-MNC) on All-Cause Mortality in Acute Myocardial Infarction (BAMI), a 3,000-patient, multi-center study funded by the European Union. The study will enroll patients within 3-6 days after reperfusion therapy of an acute MI if they have a left ventricular ejection fraction of 45% or less. The primary end point is a reduction in all-cause mortality, a design that will allow BAMI to use standard care as its control instead of a sham infusion.
"We discussed the end point with the EMA [European Medicines Agency], and they said that if you use only death as the end point we can do it with a state-of-the-art control. I think that is the proper way, because some people believe that intracoronary instrumentation by itself carries a risk that could also affect placebo groups," said Dr. Andreas M. Zeiher, professor and chairman of medicine at Goethe University in Frankfurt, Germany, speaking last November at the American Heart Association meeting.
Dr. Zeiher, who led the team that ran REPAIR-AMI and spearheaded organization of the BAMI trial, also stressed the need to avoid heparin when handling and administering autologous bone marrow cells to achieve optimal results. "Heparin interferes with a process that is absolutely crucial for these cells to extravasate during infusion to enter ischemic tissue," he said during a talk in March at the American College of Cardiology Scientific Session in Chicago. "Heparin in the syringe more or less completely abolishes the migratory capacity of the [bone-marrow] cells." Dr. Zeiher reviewed the methods and results of more than 20 stem-cell studies and found those that used heparin-treated bone-marrow cells had little clinical effect, when studies that avoided heparin or neutralized the drug with serum the cell treatments proved effective. REPAIR-AMI used serum to neutralize heparin, and BAMI will use bivalirudin as an anticoagulant and no heparin, he said.
In contrast to the success in REPAIR-AMI, no efficacy signal occurred in a Norwegian study of bone-marrow mononuclear cells injected into the hearts of 47 acute MI patients in the Autologous Stem-Cell Transplantation in Acute Myocardial Infarction (ASTAMI) study, which coincidently appeared in the same issue of The New England Journal of Medicine as the REPAIR-AMI report (N. Engl. J. Med. 2006;355:1199-209). The lack of success in ASTAMI juxtaposed against the efficacy signal in REPAIR-AMI (a signal later confirmed and strengthened by longer follow-up) provides an example in microcosm of the uneven road that stem cell therapy traversed over the past 11 years. Also worth noting: in ASTAMI the investigators used heparin.
"Heparin interferes with a process that is absolutely crucial for these cells to extravasate during infusion to enter ischemic tissuu," Dr. Andreas M. Zeiher said.
Dr. Zeiher’s heparin explanation for outcome differences among many stem-cell studies is "an interesting hypothesis," said Dr. Robert D. Simari, a cardiologist and professor of medicine at the Mayo Clinic in Rochester, Minn. There are likely several important differences" between the stem-cell trials that have been positive and those that have failed. Trials have differed in their design, patient populations, their stem cell products, and in the end points they have used to measure success, said Dr. Simari, who also chairs the steering committee of the Cardiovascular Cell Therapy Research Network (CCTRN), a research group of seven U.S. centers organized by the National Heart Lung and Blood Institute to run early-phase clinical trials with cell treatments.
Also in the Phase III Act: ACT34-CMI/RENEW
Another cell therapy success story now advancing to a phase III trial is led by Dr. Douglas W. Losordo using autologous CD34+ cells injected into the myocardium of patients with refractory angina. He and his associates published results last August from a phase II study with167 patients, the Double-blind, Prospective, Randomized, Placebo-controlled Study to Determine the Tolerability, Efficacy, Safety, and Dose Range of Intramyocardial Injections of G-CSF Mobilized Auto–CD34+ Cells for Reduction of Angina Episodes in Patients With Refractory Chronic Myocardial Ischemia (ACT34-CMI).
The researchers obtained the autologous cell preparation used in ACT34-CMI by first treating each patient with granulocyte colony stimulating factor daily for 4 or 5 days to mobilize their CD34+ cells. The day following the last dose of drug, each patient underwent leukopheresis to collect mononuclear cells. The cell material then underwent further ex vivo enrichment for CD34+ cells using a commercially-available magnetic cell selection device marketed by Baxter Healthcare. Patients received 100,000 CD34+ cells/kg, 500,000 CD34+ cells/kg, or placebo as intramyocardial injections at 10 sites identified by electromechanical endocardial mapping. Dr. Losordo and his associates said they used CD34+ cells because of evidence these cells, called endothelial progenitor cells, can stimulate neovascularization in ischemic tissue, and improved function in animal models of acute and chronic myocardial ischemia. The patients enrolled in ACT34-CMI all had Canadian Cardiovascular Society class III or IV chronic refractory angina despite optimal medial treatment.
The study, done at 26 U.S. centers, found that at 6 and 12 months after treatment, 54 patients who received the low-dose injections had significantly fewer angina episodes per week than the 53 patients who received placebo infections, the study’s primary end point. Patients who received the higher-dose injections also had fewer angina episodes than the controls, but the difference was not statistically significant at either 6- or 12-month follow-up. The low-dose patients also had statistically significant improvement in their total exercise time in an exercise tolerance test compared with the placebo patients; the high-dose patients also had better exercise times, but not significantly better than the controls.
Speaking at the American College of Cardiology meeting in Chicago in March, Dr. Losordo presented 2-year follow-up data on the patients in ACT34-CMI. At 2 years, the low-dose patients continued to have a significantly lower rate of weekly angina counts than control patients, while the high-dose patients continued to have a numerically lower rate that was not significantly different from the controls. The cumulative, 2-year rate of death, MI, or hospitalization for acute coronary syndrome was 30% in the control patients, 18% in the low-dose patients, and 14% in the high-dose patients. Although these between group differences were not statistically significant, the trends were "in the right direction," said Dr. Losordo, an interventional cardiologist at Northwestern University in Chicago, and vice president for new therapeutic development at Baxter International. Baxter sponsored ACT34-CMI, as well as the phase III study now starting based on the phase II results.
The phase III study, A Prospective, Randomized, Double-blinded, Active-control and Unblinded Standard of Care (SOC) Controlled Study to Determine the Efficacy and Safety of Targeted Intramyocardial Delivery of Autologous CD34+ Cells (Auto-CD34+ Cells) for Increasing Exercise Capacity During Standardized Exercise Testing in Subjects With Refractory Angina Pectoris and Chronic Myocardial Ischemia (RENEW), will enroll about 450 refractory angina patients at 50 U.S. sites, randomizing them to CD34+ treatment, placebo treatment, or no treatment and optimal standard care. The primary efficacy outcome will be change in total exercise time on an exercise tolerance test after 12 months.
Choosing the Right Cells
The success of the ACT34-CMI study, and the decision by Dr. Losordo and Baxter to move on to the phase III RENEW trial, highlights what may be a possible advantage to using selected stem and progenitor cells compared with the strategy of using an unselected cell population, such as the bone-marrow cells used in many of the studies of the past 11 years.
More evidence favoring cell selection came recently in results reported by Dr. Perin from the First Mononuclear Cells Injected in the United States Conducted by the Cardiovascular Cell Therapy Research Network (FOCUS-CCTRN) study, which he presented in March at the American College of Cardiology meeting in Chicago. The phase II study enrolled 92 patients with chronic heart failure and a left ventricular ejection fraction of 45% or less. Patients received a transendocardial injection of 100 million autologous bone-marrow cells or placebo. The primary end points were 6-month changes in left ventricular end systolic volume, in maximal oxygen consumption, and the extent of ischemic myocardial defects measured by single photon emission tomography. The results showed no statistically significant improvement for any of these three end points in the patients treated with bone-marrow cells compared with the controls, and were simultaneously reported in an article published online (JAMA 2012; March 24 [doi:10.1001/jama.2012.418]).
Despite the study’s failure for its prespecified end points, it also showed signals of efficacy and possibly highlighted some important lessons on how to best apply stem cell therapy in the future. On the efficacy side, the 61 patients who received bone-marrow cell injections had an average 1.4% improvement in their left ventricular ejection fraction, compared with an average 1.3% decline in the 31 placebo patients, an overall between-group difference of 2.7% that was statistically significant. Further analysis showed that patients who received bone-marrow cell preparations that had higher levels of either CD34+ cell or CD133+ cells had greater increases in their left ventricular ejection fractions. Also, when the researchers analyzed responses in subgroups divided by their age, patients 62 years old or younger (62 years old was the median age in the study) who received bone-marrow cells had a statistically significant, 4.7% improvement in their left ventricular ejection fraction after 6 months compared with placebo patients, while among patients greater than 62 years old treatment with autologous bone-marrow cells produced no significant improvement in ejection fraction compared with the controls.
"It could very well be that [unfractionated] bone marrow is a weaker product than using a specific cell type," said Dr. Perin. "Now we’ll start using parts of bone marrow, specific cells or cell combinations," he predicted, although he added that additional analysis of the FOCUS-CCTRN data must occur before he and his associates decide which cell types show the most promise. "Even though it’s not answered perfectly, the results definitely point us toward" using more selected types of bone marrow cells, he said.
"The most important lesson FOCUS-CCTRN showed was that as patients get older the number and potency of their stem cells decreases. It showed that if you give cells that aren’t potent they won’t work," said Dr. Henry, a co-investigator of the study and an active member of CCTRN. "That’s a really important insight, because if you treat patients with 100 mg of a beta blocker you get a consistent effect, but if you treat patients with autologous stem cells, every patient gets something different."
Development of stem cell therapies "has been on a normal track; each step takes time. It’s very similar to what happened with fibrinolytic therapy for treating acute myocardial infarctions" in the 1980s and 1990s, said Dr. Timothy D. Henry.
"The FOCUS results showed some evidence of an effect, but there are a number of ways to make it better," Dr. Henry said. One approach is to use selected cells, such as CD34+ cells. Another strategy is to deliver allogenic cells obtained initially from young and healthy donors, a way to avoid the issue of older patients and those with co-morbidities who may have compromised stem cells.
Administering selected or allogenic cells has another potential advantage: it opens the door to commercial involvement with a potentially saleable product, a strategy that can attract the interest of a company willing to shoulder the cost of a phase III trial.
"A challenge with [unprocessed] bone marrow is it’s too easy. Bone marrow is inexpensive, and anyone can do it," Dr. Henry noted. That’s one reason why it took several years for the REPAIR-AMI strategy to advance into a phase III trial, eventually moving forward when it received financial backing from the European Union. In contrast, the promising ACT34-CMI strategy quickly jumped to the phase III level, aided by financial support from Baxter.
But others cautioned against drawing too many inferences from FOCUS-CCTRN because it was a negative study and hence all its results must be considered suspect.
"I do not believe that post-hoc analysis of cell potency should be used to guide future trials. FOCUS was negative; the subgroup analyses and cell potency assays were attempts to glean some positivity from that study after the fact," said Dr. Marbán.
More Phase III Studies Coming, with Commercial Support
Another example of a selected, allogenic cell preparation with commercial support is the study of mesenchymal precursor cells (MPC), bone-marrow cells obtained from young, healthy donors and delivered by transendocardial injection to 45 patients with cardiomyopathy, New York Heart Association class II or III heart failure, and impaired left ventricular function in a phase II study presented by Dr. Perin last November at the American Heart Association’s Scientific Sessions in Orlando. The MPC preparation he and his associates tested was an "off-the-shelf" stem-cell product made by the Australian-based company Mesoblast.
The injections were safe, and the three different amounts of cells delivered showed various signs of efficacy. The lowest dose of cells tested showed a statistically significant improvement in left ventricular ejection fraction at 3 months compared with placebo; the highest cell dose tested showed a statistically significant improvement in left ventricular end-systolic volume at 12 months compared with the placebo control; and collectively, all three cell doses tested produced a statistically significant 20% reduction in the rate of major adverse coronary events compared with the placebo patients during a follow-up of up to 3 years, Dr. Perin reported last November.
"Given the very positive results we saw in the phase II trial, it would be logical to move on to a bigger trial," said Dr. Perin in an interview, but he added that he was unable to provide details about possible additional trials with this MPC product.
Another commercially-backed stem-cell product poised for a larger trial is cardiopoietic stem cells, made by a proprietary, patented method that uses a patient’s autologous bone-marrow stem cells and treats them in vitro to produce cells that are then injected into a patient’s myocardium where they produce new heart muscle. Researchers at the Mayo Clinic in Rochester, Minn. developed this process, and Mayo licensed it to a Belgian company, Cardio 3 BioSciences.
The company released results in November 2010 from the C-Cure study done in Belgium, Serbia, and Switzerland that enrolled 45-patients with severe ischemic heart failure. Six months after treatment, the 21 patients who received injections of the stem cells had an average 18% relative increase in their left ventricular ejection fraction compared with baseline, versus a 4% relative increase over baseline among 24 control patients. Speaking in March at the American College of Cardiology meeting, Dr. André Terzic, who led the study, provided a few more details from the results. Average ejection fraction in the actively-treated patients rose from 28% at baseline to 33%. The treatment was especially effective for the patients who entered the study with an ejection fraction below 28%, said Dr. Terzic, a professor of medicine and cardiology, and director of the Center for Regenerative Medicine at the Mayo Clinic. The 6-month results also showed other indications of benefit in the patients treated with the cardiopoietic stem cells, including significantly increased left ventricular end systolic volume, and reduced left ventricular mass index.
Cardio 3 Biosciences is now planning to start a "late phase II" or phase III trial with this material, said Dr. Simari, who is not directly involved in these studies.
What Comes Next?
Despite 11 years of work, "it’s still very early in the field. We’re still trying to figure out the cells and out targets," said Dr. Simari. "This is the haze of early days, of learning from groups of 10, 20, or 80 patients. Only in retrospect, and as we get to larger trials will the truth emerge. Right now, there is a lot of work needed and few headlines, and it will probably stay that way for awhile. This is not a game for people with short attention spans.
"The business model for autologous cells remains uncertain," he added. "For allogenic products that are generated from young, healthy donors and made into thousands of doses, the business model is different and the costs might be more reasonable. Hopefully, as our knowledge grows, we will develop treatments that end up costing less."
"I have no doubt that cell treatment is one of the great avenues of future medicine; it’s just a matter of figuring it out," said Dr. Perin. "Having phase III trials now starting is a step forward. Things are starting to come into focus. Unless something totally unforeseen happens, we will eventually have an approved product," he predicted.
Dr. Perin said that he has been a consultant to Amorcyte, Teva, Cytori, and Aldagen. Dr. Henry said that he has served on steering committees for and received research grants from Aastrom and Mesoblast. Dr. Marbán said that he is a founder of and holds equity in Capricor. Dr. Simari said that he had no disclosures. Dr. Zeiher said he is a cofounder of and scientific advisor to t2cure, a company set up to run the BAMI trial, sponsored by the European Union Dr. Losordo is an employee of Baxter International. Dr. Terzic said that he has received research grants from Cardio 3 BioSciences.
Stem-cell treatment for cardiac disease recently launched into advanced clinical trials, as a flurry of early-phase studies over the last year collectively confirmed the treatment as safe but left its efficacy unresolved.
At least two phase III trials are now underway and others are possibly imminent. But until these pivotal studies begin to yield outcome results in about 4 years, stem-cell treatment remains a question mark – an appealing idea fueled by hints of effectiveness but also dogged by failures that prompt skepticism about its future.
The gush of recent early-phase studies also hint at possible explanations for the variability in the success of stem cell treatment. The studies examined a broad range of cell types and patients. (Click here to see a chart of the studies.) The results imply that select types of bone marrow cells may be more effective as therapy and that the number and potency of stem cells decrease with age.
Clinical testing of stem cells for heart disease has hit its stride more than a decade after the first-in-human report in 2001 of a patient treated following an acute myocardial infarction (Dtsch. Med. Wochenschr. 2001;126:932-8), which was followed by the first randomized clinical trial, also in myocardial infarction patients, reported in 2004 (Lancet 2004;364:141-8).
"So far, stem-cell treatment has been safe in all the areas where it’s been used. I’m very satisfied" with the progress, said Dr. Emerson C. Perin, an interventional cardiologist and medical director of the Stem Cell Center at the Texas Heart Institute and one of the U.S. researchers who has worked longest on stem-cell clinical studies. Those working on clinical investigations of stem cells "haven’t done anything stupid to kill it, and we’ve gone from a crawl to a walk," he said in an interview.
Development of stem cell therapies "has been on a normal track; each step takes time. It’s very similar to what happened with fibrinolytic therapy for treating acute myocardial infarctions" in the 1980s and 1990s, said Dr. Timothy D. Henry, an interventional cardiologist, director of research at the Minneapolis Heart Institute Foundation, and another very active stem cell researcher. "It was a good 10 years before we got lytics up and going. People want [stem cells] to be a magic bullet. I think some people have put unrealistic expectations on stem cells, but it’s like any other treatment. You need to do a trial and find out the relative risks and benefits, and that takes time," he said in an interview.
A different take on the past decade of stem-cell work came from another researcher in the field, Dr. Eduardo Marbán. "The pace of progress has been disappointingly slow, marked by numerous examples of clinical studies prematurely undertaken without benefit of adequate preclinical data. We are lucky that no one has been killed," said Dr. Marbán, professor and director of the Cedars-Sinai Heart Institute in Los Angeles. But despite whatever role luck may have played, Dr. Marbán agreed on the bottom line: "The major accomplishment of the 11-year experience has been the convincing demonstration that most forms of cell therapy are safe, if administered via the intracoronary route." Then he added the elephant in the room: "Efficacy is another matter.
record. Why subject patients to risk in receiving a cell product that has not been extensively validated in vitro and in small and large animals? Yet this has been done over and over again" by investigators running clinical trials of stem cells and other cells for heart disease, Dr. Marbán said in an interview.
Making It to Phase III: REPAIR-AMI/BAMI
The recent surge of study results, and the path to phase III may be best exemplified by the landmark phase II trial done by German investigators, the Reinfusion of Enriched Progenitor Cells and Infarct Remodeling in Acute Myocardial Infarction (REPAIR-AMI) trial (N. Engl. J. Med. 2006;355:1210-21). The multicenter German study randomized 204 patients an average of 4 days following an acute myocardial infarction (MI) to receive either an intracoronary infusion of autologous bone marrow cells processed to enrich for progenitor cells, or placebo.
Last November, at the annual Scientific Sessions of the American Heart Association, the group presented 5-year follow-up results for 200 of the 204 patients. Helped by the lengthy follow-up, the researchers found that the stem-cell treatment cut the cumulative rate of death, recurrent MI, or need for revascularization from 64% in the control arm to 42%, a statistically significant difference in a prespecified end point of the study.
This striking change in a very meaningful clinical outcome contrasted with the modest change in a surrogate end point at 4 months (first reported in the 2006 article), and led to the launch of the largest phase III study of stem cells for heart disease, the Effect of Intracoronary Reinfusion of Bone Marrow Derived Mononuclear Cells (BM-MNC) on All-Cause Mortality in Acute Myocardial Infarction (BAMI), a 3,000-patient, multi-center study funded by the European Union. The study will enroll patients within 3-6 days after reperfusion therapy of an acute MI if they have a left ventricular ejection fraction of 45% or less. The primary end point is a reduction in all-cause mortality, a design that will allow BAMI to use standard care as its control instead of a sham infusion.
"We discussed the end point with the EMA [European Medicines Agency], and they said that if you use only death as the end point we can do it with a state-of-the-art control. I think that is the proper way, because some people believe that intracoronary instrumentation by itself carries a risk that could also affect placebo groups," said Dr. Andreas M. Zeiher, professor and chairman of medicine at Goethe University in Frankfurt, Germany, speaking last November at the American Heart Association meeting.
Dr. Zeiher, who led the team that ran REPAIR-AMI and spearheaded organization of the BAMI trial, also stressed the need to avoid heparin when handling and administering autologous bone marrow cells to achieve optimal results. "Heparin interferes with a process that is absolutely crucial for these cells to extravasate during infusion to enter ischemic tissue," he said during a talk in March at the American College of Cardiology Scientific Session in Chicago. "Heparin in the syringe more or less completely abolishes the migratory capacity of the [bone-marrow] cells." Dr. Zeiher reviewed the methods and results of more than 20 stem-cell studies and found those that used heparin-treated bone-marrow cells had little clinical effect, when studies that avoided heparin or neutralized the drug with serum the cell treatments proved effective. REPAIR-AMI used serum to neutralize heparin, and BAMI will use bivalirudin as an anticoagulant and no heparin, he said.
In contrast to the success in REPAIR-AMI, no efficacy signal occurred in a Norwegian study of bone-marrow mononuclear cells injected into the hearts of 47 acute MI patients in the Autologous Stem-Cell Transplantation in Acute Myocardial Infarction (ASTAMI) study, which coincidently appeared in the same issue of The New England Journal of Medicine as the REPAIR-AMI report (N. Engl. J. Med. 2006;355:1199-209). The lack of success in ASTAMI juxtaposed against the efficacy signal in REPAIR-AMI (a signal later confirmed and strengthened by longer follow-up) provides an example in microcosm of the uneven road that stem cell therapy traversed over the past 11 years. Also worth noting: in ASTAMI the investigators used heparin.
"Heparin interferes with a process that is absolutely crucial for these cells to extravasate during infusion to enter ischemic tissuu," Dr. Andreas M. Zeiher said.
Dr. Zeiher’s heparin explanation for outcome differences among many stem-cell studies is "an interesting hypothesis," said Dr. Robert D. Simari, a cardiologist and professor of medicine at the Mayo Clinic in Rochester, Minn. There are likely several important differences" between the stem-cell trials that have been positive and those that have failed. Trials have differed in their design, patient populations, their stem cell products, and in the end points they have used to measure success, said Dr. Simari, who also chairs the steering committee of the Cardiovascular Cell Therapy Research Network (CCTRN), a research group of seven U.S. centers organized by the National Heart Lung and Blood Institute to run early-phase clinical trials with cell treatments.
Also in the Phase III Act: ACT34-CMI/RENEW
Another cell therapy success story now advancing to a phase III trial is led by Dr. Douglas W. Losordo using autologous CD34+ cells injected into the myocardium of patients with refractory angina. He and his associates published results last August from a phase II study with167 patients, the Double-blind, Prospective, Randomized, Placebo-controlled Study to Determine the Tolerability, Efficacy, Safety, and Dose Range of Intramyocardial Injections of G-CSF Mobilized Auto–CD34+ Cells for Reduction of Angina Episodes in Patients With Refractory Chronic Myocardial Ischemia (ACT34-CMI).
The researchers obtained the autologous cell preparation used in ACT34-CMI by first treating each patient with granulocyte colony stimulating factor daily for 4 or 5 days to mobilize their CD34+ cells. The day following the last dose of drug, each patient underwent leukopheresis to collect mononuclear cells. The cell material then underwent further ex vivo enrichment for CD34+ cells using a commercially-available magnetic cell selection device marketed by Baxter Healthcare. Patients received 100,000 CD34+ cells/kg, 500,000 CD34+ cells/kg, or placebo as intramyocardial injections at 10 sites identified by electromechanical endocardial mapping. Dr. Losordo and his associates said they used CD34+ cells because of evidence these cells, called endothelial progenitor cells, can stimulate neovascularization in ischemic tissue, and improved function in animal models of acute and chronic myocardial ischemia. The patients enrolled in ACT34-CMI all had Canadian Cardiovascular Society class III or IV chronic refractory angina despite optimal medial treatment.
The study, done at 26 U.S. centers, found that at 6 and 12 months after treatment, 54 patients who received the low-dose injections had significantly fewer angina episodes per week than the 53 patients who received placebo infections, the study’s primary end point. Patients who received the higher-dose injections also had fewer angina episodes than the controls, but the difference was not statistically significant at either 6- or 12-month follow-up. The low-dose patients also had statistically significant improvement in their total exercise time in an exercise tolerance test compared with the placebo patients; the high-dose patients also had better exercise times, but not significantly better than the controls.
Speaking at the American College of Cardiology meeting in Chicago in March, Dr. Losordo presented 2-year follow-up data on the patients in ACT34-CMI. At 2 years, the low-dose patients continued to have a significantly lower rate of weekly angina counts than control patients, while the high-dose patients continued to have a numerically lower rate that was not significantly different from the controls. The cumulative, 2-year rate of death, MI, or hospitalization for acute coronary syndrome was 30% in the control patients, 18% in the low-dose patients, and 14% in the high-dose patients. Although these between group differences were not statistically significant, the trends were "in the right direction," said Dr. Losordo, an interventional cardiologist at Northwestern University in Chicago, and vice president for new therapeutic development at Baxter International. Baxter sponsored ACT34-CMI, as well as the phase III study now starting based on the phase II results.
The phase III study, A Prospective, Randomized, Double-blinded, Active-control and Unblinded Standard of Care (SOC) Controlled Study to Determine the Efficacy and Safety of Targeted Intramyocardial Delivery of Autologous CD34+ Cells (Auto-CD34+ Cells) for Increasing Exercise Capacity During Standardized Exercise Testing in Subjects With Refractory Angina Pectoris and Chronic Myocardial Ischemia (RENEW), will enroll about 450 refractory angina patients at 50 U.S. sites, randomizing them to CD34+ treatment, placebo treatment, or no treatment and optimal standard care. The primary efficacy outcome will be change in total exercise time on an exercise tolerance test after 12 months.
Choosing the Right Cells
The success of the ACT34-CMI study, and the decision by Dr. Losordo and Baxter to move on to the phase III RENEW trial, highlights what may be a possible advantage to using selected stem and progenitor cells compared with the strategy of using an unselected cell population, such as the bone-marrow cells used in many of the studies of the past 11 years.
More evidence favoring cell selection came recently in results reported by Dr. Perin from the First Mononuclear Cells Injected in the United States Conducted by the Cardiovascular Cell Therapy Research Network (FOCUS-CCTRN) study, which he presented in March at the American College of Cardiology meeting in Chicago. The phase II study enrolled 92 patients with chronic heart failure and a left ventricular ejection fraction of 45% or less. Patients received a transendocardial injection of 100 million autologous bone-marrow cells or placebo. The primary end points were 6-month changes in left ventricular end systolic volume, in maximal oxygen consumption, and the extent of ischemic myocardial defects measured by single photon emission tomography. The results showed no statistically significant improvement for any of these three end points in the patients treated with bone-marrow cells compared with the controls, and were simultaneously reported in an article published online (JAMA 2012; March 24 [doi:10.1001/jama.2012.418]).
Despite the study’s failure for its prespecified end points, it also showed signals of efficacy and possibly highlighted some important lessons on how to best apply stem cell therapy in the future. On the efficacy side, the 61 patients who received bone-marrow cell injections had an average 1.4% improvement in their left ventricular ejection fraction, compared with an average 1.3% decline in the 31 placebo patients, an overall between-group difference of 2.7% that was statistically significant. Further analysis showed that patients who received bone-marrow cell preparations that had higher levels of either CD34+ cell or CD133+ cells had greater increases in their left ventricular ejection fractions. Also, when the researchers analyzed responses in subgroups divided by their age, patients 62 years old or younger (62 years old was the median age in the study) who received bone-marrow cells had a statistically significant, 4.7% improvement in their left ventricular ejection fraction after 6 months compared with placebo patients, while among patients greater than 62 years old treatment with autologous bone-marrow cells produced no significant improvement in ejection fraction compared with the controls.
"It could very well be that [unfractionated] bone marrow is a weaker product than using a specific cell type," said Dr. Perin. "Now we’ll start using parts of bone marrow, specific cells or cell combinations," he predicted, although he added that additional analysis of the FOCUS-CCTRN data must occur before he and his associates decide which cell types show the most promise. "Even though it’s not answered perfectly, the results definitely point us toward" using more selected types of bone marrow cells, he said.
"The most important lesson FOCUS-CCTRN showed was that as patients get older the number and potency of their stem cells decreases. It showed that if you give cells that aren’t potent they won’t work," said Dr. Henry, a co-investigator of the study and an active member of CCTRN. "That’s a really important insight, because if you treat patients with 100 mg of a beta blocker you get a consistent effect, but if you treat patients with autologous stem cells, every patient gets something different."
Development of stem cell therapies "has been on a normal track; each step takes time. It’s very similar to what happened with fibrinolytic therapy for treating acute myocardial infarctions" in the 1980s and 1990s, said Dr. Timothy D. Henry.
"The FOCUS results showed some evidence of an effect, but there are a number of ways to make it better," Dr. Henry said. One approach is to use selected cells, such as CD34+ cells. Another strategy is to deliver allogenic cells obtained initially from young and healthy donors, a way to avoid the issue of older patients and those with co-morbidities who may have compromised stem cells.
Administering selected or allogenic cells has another potential advantage: it opens the door to commercial involvement with a potentially saleable product, a strategy that can attract the interest of a company willing to shoulder the cost of a phase III trial.
"A challenge with [unprocessed] bone marrow is it’s too easy. Bone marrow is inexpensive, and anyone can do it," Dr. Henry noted. That’s one reason why it took several years for the REPAIR-AMI strategy to advance into a phase III trial, eventually moving forward when it received financial backing from the European Union. In contrast, the promising ACT34-CMI strategy quickly jumped to the phase III level, aided by financial support from Baxter.
But others cautioned against drawing too many inferences from FOCUS-CCTRN because it was a negative study and hence all its results must be considered suspect.
"I do not believe that post-hoc analysis of cell potency should be used to guide future trials. FOCUS was negative; the subgroup analyses and cell potency assays were attempts to glean some positivity from that study after the fact," said Dr. Marbán.
More Phase III Studies Coming, with Commercial Support
Another example of a selected, allogenic cell preparation with commercial support is the study of mesenchymal precursor cells (MPC), bone-marrow cells obtained from young, healthy donors and delivered by transendocardial injection to 45 patients with cardiomyopathy, New York Heart Association class II or III heart failure, and impaired left ventricular function in a phase II study presented by Dr. Perin last November at the American Heart Association’s Scientific Sessions in Orlando. The MPC preparation he and his associates tested was an "off-the-shelf" stem-cell product made by the Australian-based company Mesoblast.
The injections were safe, and the three different amounts of cells delivered showed various signs of efficacy. The lowest dose of cells tested showed a statistically significant improvement in left ventricular ejection fraction at 3 months compared with placebo; the highest cell dose tested showed a statistically significant improvement in left ventricular end-systolic volume at 12 months compared with the placebo control; and collectively, all three cell doses tested produced a statistically significant 20% reduction in the rate of major adverse coronary events compared with the placebo patients during a follow-up of up to 3 years, Dr. Perin reported last November.
"Given the very positive results we saw in the phase II trial, it would be logical to move on to a bigger trial," said Dr. Perin in an interview, but he added that he was unable to provide details about possible additional trials with this MPC product.
Another commercially-backed stem-cell product poised for a larger trial is cardiopoietic stem cells, made by a proprietary, patented method that uses a patient’s autologous bone-marrow stem cells and treats them in vitro to produce cells that are then injected into a patient’s myocardium where they produce new heart muscle. Researchers at the Mayo Clinic in Rochester, Minn. developed this process, and Mayo licensed it to a Belgian company, Cardio 3 BioSciences.
The company released results in November 2010 from the C-Cure study done in Belgium, Serbia, and Switzerland that enrolled 45-patients with severe ischemic heart failure. Six months after treatment, the 21 patients who received injections of the stem cells had an average 18% relative increase in their left ventricular ejection fraction compared with baseline, versus a 4% relative increase over baseline among 24 control patients. Speaking in March at the American College of Cardiology meeting, Dr. André Terzic, who led the study, provided a few more details from the results. Average ejection fraction in the actively-treated patients rose from 28% at baseline to 33%. The treatment was especially effective for the patients who entered the study with an ejection fraction below 28%, said Dr. Terzic, a professor of medicine and cardiology, and director of the Center for Regenerative Medicine at the Mayo Clinic. The 6-month results also showed other indications of benefit in the patients treated with the cardiopoietic stem cells, including significantly increased left ventricular end systolic volume, and reduced left ventricular mass index.
Cardio 3 Biosciences is now planning to start a "late phase II" or phase III trial with this material, said Dr. Simari, who is not directly involved in these studies.
What Comes Next?
Despite 11 years of work, "it’s still very early in the field. We’re still trying to figure out the cells and out targets," said Dr. Simari. "This is the haze of early days, of learning from groups of 10, 20, or 80 patients. Only in retrospect, and as we get to larger trials will the truth emerge. Right now, there is a lot of work needed and few headlines, and it will probably stay that way for awhile. This is not a game for people with short attention spans.
"The business model for autologous cells remains uncertain," he added. "For allogenic products that are generated from young, healthy donors and made into thousands of doses, the business model is different and the costs might be more reasonable. Hopefully, as our knowledge grows, we will develop treatments that end up costing less."
"I have no doubt that cell treatment is one of the great avenues of future medicine; it’s just a matter of figuring it out," said Dr. Perin. "Having phase III trials now starting is a step forward. Things are starting to come into focus. Unless something totally unforeseen happens, we will eventually have an approved product," he predicted.
Dr. Perin said that he has been a consultant to Amorcyte, Teva, Cytori, and Aldagen. Dr. Henry said that he has served on steering committees for and received research grants from Aastrom and Mesoblast. Dr. Marbán said that he is a founder of and holds equity in Capricor. Dr. Simari said that he had no disclosures. Dr. Zeiher said he is a cofounder of and scientific advisor to t2cure, a company set up to run the BAMI trial, sponsored by the European Union Dr. Losordo is an employee of Baxter International. Dr. Terzic said that he has received research grants from Cardio 3 BioSciences.
FDA Advisers Endorse Subcutaneous ICD
GAITHERSBURG, MD. – The results of a clinical trial of a cardioverter defibrillator that is implanted subcutaneously and does not require transvenous leads support the approval of the device as a treatment for ventricular tachyarrhythmias, the majority of a Food and Drug Administration Advisory panel agreed at a meeting on April 26.
The FDA’s Circulatory System Devices Panel voted 7-1 that the benefits of the subcutaneous implantable cardioverter defibrillator (S-ICD) system outweighed its risks in patients who meet the criteria in the indication proposed by the manufacturer, Cameron Health: to provide "defibrillation therapy for the treatment of life-threatening ventricular tachyarrhythmias in patients who do not have symptomatic bradycardia; incessant ventricular tachycardia; or spontaneous, frequently recurring ventricular tachycardia that is reliably terminated with antitachycardia pacing."

The components of the S-ICD system include a pulse generator, which is implanted subcutaneously in the lateral thoracic region and is connected to an electrode, with a defibrillation coil that is subcutaneously implanted along the rib margin to the sternum, without radiographic guidance, according to the company. The device has the capacity to deliver more than 100 shocks; with typical usage, it is expected to last a little more than 5 years.
Although they agreed that further follow-up of the safety and effectiveness of the device was needed and pointed out the importance of proper physician training and patient selection, the panel unanimously voted that there was "reasonable assurance" that the device was safe, and voted 7-1 that there was "reasonable assurance" that it was effective for this group of patients.
Panelists voting in favor of the risk-benefit profile said that the S-ICD would be a useful addition to the transvenous ICDs that are currently available. They agreed that the inappropriate shock rate in the clinical trial was comparable to the rates seen with currently available transvenous ICDs.
"This device is a substantial additional adjunctive tool for electrophysiologists to manage patients who are at high risk for sudden cardiac death," said Dr. Ralph Brindis, senior advisor for cardiovascular disease at Kaiser Permanente in Oakland, Calif. The availability of a device "in particular to manage patients who have infections of transvenous systems is a very important adjunct in the armamentarium." he added.
The dissenting panelist, Dr. David Milan, an electrophysiologist at Massachusetts General Hospital, Boston, said that it was important to balance enthusiasm for the device with "a cautious approach," noting that the standard for efficacy was quite high for the transvenous devices.
His concerns included whether the clinical effectiveness of the device was up to par with currently available devices, which he noted could not be assuaged by the number of patients and relatively short follow-up of patients in the pivotal trial.
The primary and safety effectiveness end points were met in the pivotal study, a prospective single arm study of 330 people with a class I, IIa, or IIb ICD indication, including patients who needed a replacement ICD, conducted in the United States, Europe, and New Zealand from January 2010 through May 2011, to evaluate the device in treating life-threatening ventricular arrhythmias. Their mean age was 52 years, which was younger than other contemporary ICD studies, but 60% were older than 50 years. In all, 74% were male; 65% were white and 24% were black; about 85% were on a beta-blocker; and about 8% were on antiarrhythmic drugs. More than half (61%) had heart failure, predominantly NYHA class II.
Among the 304 evaluable patients, the device was 98.8% effective in converting acute induced ventricular fibrillation, with 95% of the events treated in less than 21 seconds and 88% in less than 18 seconds. During the study, there were 109 spontaneous episodes of VT/VF. Of the 68 for which evaluable recorded data were available, all were successfully converted with the S-ICD, except for one case that terminated spontaneously and another case of VT/VF storm that required an external shock, according to the FDA. There were about 18 infections, of which 5 required surgical treatment, including four explants. The device was explanted in another seven patients for reasons that included repositioning, and a depleted battery. None of the eight deaths in the study was attributed to the device.
The S-ICD is distributed in 10 other countries, and so far, more than 1,200 patients have been implanted worldwide, according to Cameron Health.
The company has proposed a postmarketing study, a prospective multicenter observational registry to evaluate the long-term safety of the device.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
GAITHERSBURG, MD. – The results of a clinical trial of a cardioverter defibrillator that is implanted subcutaneously and does not require transvenous leads support the approval of the device as a treatment for ventricular tachyarrhythmias, the majority of a Food and Drug Administration Advisory panel agreed at a meeting on April 26.
The FDA’s Circulatory System Devices Panel voted 7-1 that the benefits of the subcutaneous implantable cardioverter defibrillator (S-ICD) system outweighed its risks in patients who meet the criteria in the indication proposed by the manufacturer, Cameron Health: to provide "defibrillation therapy for the treatment of life-threatening ventricular tachyarrhythmias in patients who do not have symptomatic bradycardia; incessant ventricular tachycardia; or spontaneous, frequently recurring ventricular tachycardia that is reliably terminated with antitachycardia pacing."
The components of the S-ICD system include a pulse generator, which is implanted subcutaneously in the lateral thoracic region and is connected to an electrode, with a defibrillation coil that is subcutaneously implanted along the rib margin to the sternum, without radiographic guidance, according to the company. The device has the capacity to deliver more than 100 shocks; with typical usage, it is expected to last a little more than 5 years.
Although they agreed that further follow-up of the safety and effectiveness of the device was needed and pointed out the importance of proper physician training and patient selection, the panel unanimously voted that there was "reasonable assurance" that the device was safe, and voted 7-1 that there was "reasonable assurance" that it was effective for this group of patients.
Panelists voting in favor of the risk-benefit profile said that the S-ICD would be a useful addition to the transvenous ICDs that are currently available. They agreed that the inappropriate shock rate in the clinical trial was comparable to the rates seen with currently available transvenous ICDs.
"This device is a substantial additional adjunctive tool for electrophysiologists to manage patients who are at high risk for sudden cardiac death," said Dr. Ralph Brindis, senior advisor for cardiovascular disease at Kaiser Permanente in Oakland, Calif. The availability of a device "in particular to manage patients who have infections of transvenous systems is a very important adjunct in the armamentarium." he added.
The dissenting panelist, Dr. David Milan, an electrophysiologist at Massachusetts General Hospital, Boston, said that it was important to balance enthusiasm for the device with "a cautious approach," noting that the standard for efficacy was quite high for the transvenous devices.
His concerns included whether the clinical effectiveness of the device was up to par with currently available devices, which he noted could not be assuaged by the number of patients and relatively short follow-up of patients in the pivotal trial.
The primary and safety effectiveness end points were met in the pivotal study, a prospective single arm study of 330 people with a class I, IIa, or IIb ICD indication, including patients who needed a replacement ICD, conducted in the United States, Europe, and New Zealand from January 2010 through May 2011, to evaluate the device in treating life-threatening ventricular arrhythmias. Their mean age was 52 years, which was younger than other contemporary ICD studies, but 60% were older than 50 years. In all, 74% were male; 65% were white and 24% were black; about 85% were on a beta-blocker; and about 8% were on antiarrhythmic drugs. More than half (61%) had heart failure, predominantly NYHA class II.
Among the 304 evaluable patients, the device was 98.8% effective in converting acute induced ventricular fibrillation, with 95% of the events treated in less than 21 seconds and 88% in less than 18 seconds. During the study, there were 109 spontaneous episodes of VT/VF. Of the 68 for which evaluable recorded data were available, all were successfully converted with the S-ICD, except for one case that terminated spontaneously and another case of VT/VF storm that required an external shock, according to the FDA. There were about 18 infections, of which 5 required surgical treatment, including four explants. The device was explanted in another seven patients for reasons that included repositioning, and a depleted battery. None of the eight deaths in the study was attributed to the device.
The S-ICD is distributed in 10 other countries, and so far, more than 1,200 patients have been implanted worldwide, according to Cameron Health.
The company has proposed a postmarketing study, a prospective multicenter observational registry to evaluate the long-term safety of the device.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
GAITHERSBURG, MD. – The results of a clinical trial of a cardioverter defibrillator that is implanted subcutaneously and does not require transvenous leads support the approval of the device as a treatment for ventricular tachyarrhythmias, the majority of a Food and Drug Administration Advisory panel agreed at a meeting on April 26.
The FDA’s Circulatory System Devices Panel voted 7-1 that the benefits of the subcutaneous implantable cardioverter defibrillator (S-ICD) system outweighed its risks in patients who meet the criteria in the indication proposed by the manufacturer, Cameron Health: to provide "defibrillation therapy for the treatment of life-threatening ventricular tachyarrhythmias in patients who do not have symptomatic bradycardia; incessant ventricular tachycardia; or spontaneous, frequently recurring ventricular tachycardia that is reliably terminated with antitachycardia pacing."
The components of the S-ICD system include a pulse generator, which is implanted subcutaneously in the lateral thoracic region and is connected to an electrode, with a defibrillation coil that is subcutaneously implanted along the rib margin to the sternum, without radiographic guidance, according to the company. The device has the capacity to deliver more than 100 shocks; with typical usage, it is expected to last a little more than 5 years.
Although they agreed that further follow-up of the safety and effectiveness of the device was needed and pointed out the importance of proper physician training and patient selection, the panel unanimously voted that there was "reasonable assurance" that the device was safe, and voted 7-1 that there was "reasonable assurance" that it was effective for this group of patients.
Panelists voting in favor of the risk-benefit profile said that the S-ICD would be a useful addition to the transvenous ICDs that are currently available. They agreed that the inappropriate shock rate in the clinical trial was comparable to the rates seen with currently available transvenous ICDs.
"This device is a substantial additional adjunctive tool for electrophysiologists to manage patients who are at high risk for sudden cardiac death," said Dr. Ralph Brindis, senior advisor for cardiovascular disease at Kaiser Permanente in Oakland, Calif. The availability of a device "in particular to manage patients who have infections of transvenous systems is a very important adjunct in the armamentarium." he added.
The dissenting panelist, Dr. David Milan, an electrophysiologist at Massachusetts General Hospital, Boston, said that it was important to balance enthusiasm for the device with "a cautious approach," noting that the standard for efficacy was quite high for the transvenous devices.
His concerns included whether the clinical effectiveness of the device was up to par with currently available devices, which he noted could not be assuaged by the number of patients and relatively short follow-up of patients in the pivotal trial.
The primary and safety effectiveness end points were met in the pivotal study, a prospective single arm study of 330 people with a class I, IIa, or IIb ICD indication, including patients who needed a replacement ICD, conducted in the United States, Europe, and New Zealand from January 2010 through May 2011, to evaluate the device in treating life-threatening ventricular arrhythmias. Their mean age was 52 years, which was younger than other contemporary ICD studies, but 60% were older than 50 years. In all, 74% were male; 65% were white and 24% were black; about 85% were on a beta-blocker; and about 8% were on antiarrhythmic drugs. More than half (61%) had heart failure, predominantly NYHA class II.
Among the 304 evaluable patients, the device was 98.8% effective in converting acute induced ventricular fibrillation, with 95% of the events treated in less than 21 seconds and 88% in less than 18 seconds. During the study, there were 109 spontaneous episodes of VT/VF. Of the 68 for which evaluable recorded data were available, all were successfully converted with the S-ICD, except for one case that terminated spontaneously and another case of VT/VF storm that required an external shock, according to the FDA. There were about 18 infections, of which 5 required surgical treatment, including four explants. The device was explanted in another seven patients for reasons that included repositioning, and a depleted battery. None of the eight deaths in the study was attributed to the device.
The S-ICD is distributed in 10 other countries, and so far, more than 1,200 patients have been implanted worldwide, according to Cameron Health.
The company has proposed a postmarketing study, a prospective multicenter observational registry to evaluate the long-term safety of the device.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
FROM A MEETING OF THE FDA'S CIRCULATORY SYSTEM DEVICES PANEL
FDA Panel Backs HeartWare VAS Despite Safety Concerns
GAITHERBURG, MD. – Despite problems with the quality of the safety data in the pivotal trial, the majority of a Food and Drug Administration advisory panel supported approval of the HeartWare left ventricular assist device as a bridge-to-transplant in people with end-stage heart failure at an April 25 meeting of the FDA’s Circulatory System Devices Panel.
At the meeting, the panel voted 9-2 that the benefits of the HeartWare Ventricular Assist System (VAS) outweighed its risks for use as a bridge to cardiac transplantation in patients at risk of death from refractory end-stage heart failure, the indication proposed for approval by the manufacturer, HeartWare.
The HeartWare VAS is a small, lightweight, continuous-flow pump that is implanted entirely in the pericardial space via a median sternotomy; it is the first magnetically levitated left ventricular assist device (LVAD) pump, providing flows of up to 10 L/min; it is connected to an external controller via a 4.2 diameter percutaneous driveline. It is intended for use inside and outside of the hospital and is contraindicated in patients with a body surface area (BSA) of less than 1.2 m2, in patients who cannot tolerate anticoagulation therapy, and in pregnant women.
If approved, it would be the first LVAD that does not require an abdominal incision and creation of an abdominal pump pocket.
The panel voted unanimously that based on the available data, there was "reasonable assurance" that the device was effective for this group of patients, and voted 8-3 that there was "reasonable assurance" that it was safe.
The panelists raised issues about the quality of the safety data, which were described as a "mess" and having "more holes ... than Swiss cheese."
But the majority agreed the data supported its effectiveness, particularly when considering the alternatives for this group of patients with end-stage heart failure. The panel chair, Dr. Richard Page, chair of the department of medicine at the University of Wisconsin, Madison, said that despite the safety issues, the bar for efficacy had been met and that the device "represents a real advance in technology" that will make a difference for many patients. Panelist Dr. David Slotwiner, of Long Island Jewish Medical Center, New Hyde Park, N.Y., said that despite flaws in the safety data, he described it as "a novel device for a desperate population."
In the pivotal trial, the ADVANCE (Evaluation of the HeartWare LVAD System for the Treatment of Advanced Heart Failure) trial, a U.S. prospective, multicenter, nonrandomized study, 140 patients with New York Heart Association class IV heart failure, who were on a list for a transplant, received the HeartWare VAS as a bridge to transplant. Their outcomes were compared with 499 patients in a National Institute of Health–sponsored U.S. registry tracking outcomes in recipients of commercially available LVADs, INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support). More than 90% of those in INTERMACS have received Thoratec’s HeartMate II LVAD. This was the first LVAD study where data from INTERMACS have been used as a contemporaneous control.
The study met the primary end point, which was a success rate at 180 days (defined as remaining on the original device, transplanted, or explanted for recovery) at 180 days among the HeartWare VAD recipients (90.7%) that was noninferior to the success rate in the INTERMACs control group (90.1%).
Safety data from INTERMACS were not available for the safety analysis, so safety data on LVADs from the literature were used for comparison.
Although the trial met the prespecified primary end point, FDA reviewers raised concerns about the comparability of the two groups, and the thrombosis rates, the need to exchange devices, and ischemic strokes in recipients of the HeartWare VAS. Within 180 days, the observed ischemic stroke rate was 8% (11 patients), and the observed hemorrhagic stroke rate was 3% (4 patients). Of the ischemic stroke patients, 27% died or were considered ineligible for transplant because of the stroke; all of the hemorrhagic stroke patients died or became ineligible for transplant.
The panel agreed that while the strokes are a concern, the rates seen in the study did not appear to be substantially different than the rates reported in the literature, although they all agreed that better safety data were needed.
Within 180 days of implantation, seven HVAD pumps were exchanged in seven patients, all of which were associated with signs and symptoms of intraventricular/pump thrombosis, according to the FDA’s analysis. Panelists said that while these cases raised some concerns, it was difficult to make any conclusions without a control group, and one panelist said that in his view, the risks of pump thrombosis were outweighed by the potential benefits.
If approved, the manufacturer’s postmarketing plans include a study that will continue to evaluate patients in the ADVANCE trial. The HeartWare VAS was approved in the European Union in 2009. It is also being studied as destination therapy, comparing it to the HeartMate II.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
GAITHERBURG, MD. – Despite problems with the quality of the safety data in the pivotal trial, the majority of a Food and Drug Administration advisory panel supported approval of the HeartWare left ventricular assist device as a bridge-to-transplant in people with end-stage heart failure at an April 25 meeting of the FDA’s Circulatory System Devices Panel.
At the meeting, the panel voted 9-2 that the benefits of the HeartWare Ventricular Assist System (VAS) outweighed its risks for use as a bridge to cardiac transplantation in patients at risk of death from refractory end-stage heart failure, the indication proposed for approval by the manufacturer, HeartWare.
The HeartWare VAS is a small, lightweight, continuous-flow pump that is implanted entirely in the pericardial space via a median sternotomy; it is the first magnetically levitated left ventricular assist device (LVAD) pump, providing flows of up to 10 L/min; it is connected to an external controller via a 4.2 diameter percutaneous driveline. It is intended for use inside and outside of the hospital and is contraindicated in patients with a body surface area (BSA) of less than 1.2 m2, in patients who cannot tolerate anticoagulation therapy, and in pregnant women.
If approved, it would be the first LVAD that does not require an abdominal incision and creation of an abdominal pump pocket.
The panel voted unanimously that based on the available data, there was "reasonable assurance" that the device was effective for this group of patients, and voted 8-3 that there was "reasonable assurance" that it was safe.
The panelists raised issues about the quality of the safety data, which were described as a "mess" and having "more holes ... than Swiss cheese."
But the majority agreed the data supported its effectiveness, particularly when considering the alternatives for this group of patients with end-stage heart failure. The panel chair, Dr. Richard Page, chair of the department of medicine at the University of Wisconsin, Madison, said that despite the safety issues, the bar for efficacy had been met and that the device "represents a real advance in technology" that will make a difference for many patients. Panelist Dr. David Slotwiner, of Long Island Jewish Medical Center, New Hyde Park, N.Y., said that despite flaws in the safety data, he described it as "a novel device for a desperate population."
In the pivotal trial, the ADVANCE (Evaluation of the HeartWare LVAD System for the Treatment of Advanced Heart Failure) trial, a U.S. prospective, multicenter, nonrandomized study, 140 patients with New York Heart Association class IV heart failure, who were on a list for a transplant, received the HeartWare VAS as a bridge to transplant. Their outcomes were compared with 499 patients in a National Institute of Health–sponsored U.S. registry tracking outcomes in recipients of commercially available LVADs, INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support). More than 90% of those in INTERMACS have received Thoratec’s HeartMate II LVAD. This was the first LVAD study where data from INTERMACS have been used as a contemporaneous control.
The study met the primary end point, which was a success rate at 180 days (defined as remaining on the original device, transplanted, or explanted for recovery) at 180 days among the HeartWare VAD recipients (90.7%) that was noninferior to the success rate in the INTERMACs control group (90.1%).
Safety data from INTERMACS were not available for the safety analysis, so safety data on LVADs from the literature were used for comparison.
Although the trial met the prespecified primary end point, FDA reviewers raised concerns about the comparability of the two groups, and the thrombosis rates, the need to exchange devices, and ischemic strokes in recipients of the HeartWare VAS. Within 180 days, the observed ischemic stroke rate was 8% (11 patients), and the observed hemorrhagic stroke rate was 3% (4 patients). Of the ischemic stroke patients, 27% died or were considered ineligible for transplant because of the stroke; all of the hemorrhagic stroke patients died or became ineligible for transplant.
The panel agreed that while the strokes are a concern, the rates seen in the study did not appear to be substantially different than the rates reported in the literature, although they all agreed that better safety data were needed.
Within 180 days of implantation, seven HVAD pumps were exchanged in seven patients, all of which were associated with signs and symptoms of intraventricular/pump thrombosis, according to the FDA’s analysis. Panelists said that while these cases raised some concerns, it was difficult to make any conclusions without a control group, and one panelist said that in his view, the risks of pump thrombosis were outweighed by the potential benefits.
If approved, the manufacturer’s postmarketing plans include a study that will continue to evaluate patients in the ADVANCE trial. The HeartWare VAS was approved in the European Union in 2009. It is also being studied as destination therapy, comparing it to the HeartMate II.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
GAITHERBURG, MD. – Despite problems with the quality of the safety data in the pivotal trial, the majority of a Food and Drug Administration advisory panel supported approval of the HeartWare left ventricular assist device as a bridge-to-transplant in people with end-stage heart failure at an April 25 meeting of the FDA’s Circulatory System Devices Panel.
At the meeting, the panel voted 9-2 that the benefits of the HeartWare Ventricular Assist System (VAS) outweighed its risks for use as a bridge to cardiac transplantation in patients at risk of death from refractory end-stage heart failure, the indication proposed for approval by the manufacturer, HeartWare.
The HeartWare VAS is a small, lightweight, continuous-flow pump that is implanted entirely in the pericardial space via a median sternotomy; it is the first magnetically levitated left ventricular assist device (LVAD) pump, providing flows of up to 10 L/min; it is connected to an external controller via a 4.2 diameter percutaneous driveline. It is intended for use inside and outside of the hospital and is contraindicated in patients with a body surface area (BSA) of less than 1.2 m2, in patients who cannot tolerate anticoagulation therapy, and in pregnant women.
If approved, it would be the first LVAD that does not require an abdominal incision and creation of an abdominal pump pocket.
The panel voted unanimously that based on the available data, there was "reasonable assurance" that the device was effective for this group of patients, and voted 8-3 that there was "reasonable assurance" that it was safe.
The panelists raised issues about the quality of the safety data, which were described as a "mess" and having "more holes ... than Swiss cheese."
But the majority agreed the data supported its effectiveness, particularly when considering the alternatives for this group of patients with end-stage heart failure. The panel chair, Dr. Richard Page, chair of the department of medicine at the University of Wisconsin, Madison, said that despite the safety issues, the bar for efficacy had been met and that the device "represents a real advance in technology" that will make a difference for many patients. Panelist Dr. David Slotwiner, of Long Island Jewish Medical Center, New Hyde Park, N.Y., said that despite flaws in the safety data, he described it as "a novel device for a desperate population."
In the pivotal trial, the ADVANCE (Evaluation of the HeartWare LVAD System for the Treatment of Advanced Heart Failure) trial, a U.S. prospective, multicenter, nonrandomized study, 140 patients with New York Heart Association class IV heart failure, who were on a list for a transplant, received the HeartWare VAS as a bridge to transplant. Their outcomes were compared with 499 patients in a National Institute of Health–sponsored U.S. registry tracking outcomes in recipients of commercially available LVADs, INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support). More than 90% of those in INTERMACS have received Thoratec’s HeartMate II LVAD. This was the first LVAD study where data from INTERMACS have been used as a contemporaneous control.
The study met the primary end point, which was a success rate at 180 days (defined as remaining on the original device, transplanted, or explanted for recovery) at 180 days among the HeartWare VAD recipients (90.7%) that was noninferior to the success rate in the INTERMACs control group (90.1%).
Safety data from INTERMACS were not available for the safety analysis, so safety data on LVADs from the literature were used for comparison.
Although the trial met the prespecified primary end point, FDA reviewers raised concerns about the comparability of the two groups, and the thrombosis rates, the need to exchange devices, and ischemic strokes in recipients of the HeartWare VAS. Within 180 days, the observed ischemic stroke rate was 8% (11 patients), and the observed hemorrhagic stroke rate was 3% (4 patients). Of the ischemic stroke patients, 27% died or were considered ineligible for transplant because of the stroke; all of the hemorrhagic stroke patients died or became ineligible for transplant.
The panel agreed that while the strokes are a concern, the rates seen in the study did not appear to be substantially different than the rates reported in the literature, although they all agreed that better safety data were needed.
Within 180 days of implantation, seven HVAD pumps were exchanged in seven patients, all of which were associated with signs and symptoms of intraventricular/pump thrombosis, according to the FDA’s analysis. Panelists said that while these cases raised some concerns, it was difficult to make any conclusions without a control group, and one panelist said that in his view, the risks of pump thrombosis were outweighed by the potential benefits.
If approved, the manufacturer’s postmarketing plans include a study that will continue to evaluate patients in the ADVANCE trial. The HeartWare VAS was approved in the European Union in 2009. It is also being studied as destination therapy, comparing it to the HeartMate II.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
FROM A MEETING OF THE FDA'S CIRCULATORY SYSTEM DEVICES PANEL
Updated Measures Assess Heart Failure Care
A set of nine performance measures aimed at assessing whether adults with heart failure are receiving the best care was issued by the American College of Cardiology Foundation, the American Heart Association, and the American Medical Association’s Physician Consortium for Performance Improvement.
The measure set, which was published April 23 in the Journal of the American College of Cardiology, includes three new performance measures and six revised measures. The new measure set was drafted by a panel of physicians, pharmacists, and patient advocates (J. Am. Coll. Cardiol. April 23, 2012;doi:10.1016/j.jacc.2012.03.013). The performance measures were last revised in 2005.
The measure set includes two performance metrics for inpatient care, five that address care in the outpatient setting, and two measures that apply to care in both settings. The idea, according to the sponsors, was to stress the need to measure quality over time and across providers, not in silos.
"To be successful as quality improvement tools, the heart failure performance measures need to be integrated as routine components of patient care across various care settings, with particular attention to transitions of care from inpatient to outpatient environments," Dr. Robert O. Bonow, cochair of the work group that developed the measure set and director of the center for cardiovascular innovation at Northwestern University, Chicago, said in a statement.
Improving care transitions is likely to be a major focus for physicians in and out of the hospital as officials at the Centers for Medicare and Medicaid Services begin to test a series of alternative payment and care delivery models, from Accountable Care Organizations to bundled payments. Adding to that pressure, this October, the CMS will begin cutting Medicare payments to hospitals whose heart failure and acute myocardial infarction readmission rates are considered too high.
The updated measure set will help prepare physicians for the payment and care delivery changes, Dr. Kathleen Blake, a member of the measure work group and a senior research director at the Center for Medical Technology Policy in Baltimore, said in an interview.
Performance measures, by definition, address areas where there are gaps in care, said Dr. Blake, who is a cardiologist. So physicians can take the updated heart failure measure set and embed it in their care, like a checklist, to ensure that patients are being considered for all appropriate evidence-based treatments.
"We are inundated with medical literature these days. This basically distills it into a measure set," she said.
The work group considered the ACCF/AHA 2009 practice guidelines on heart failure as well as existing heart failure performance measures from the Joint Commission, the CMS, and the Agency for Healthcare Research and Quality in putting together the updated set of measures. Along with the new and revised measures, they retired eight performance measures from the 2005 list.
The updated measure set includes:
1. Left Ventricular Ejection Fraction (LVEF) assessment in the outpatient setting.
2. LVEF in the inpatient setting.
3. Symptom and activity assessment in the outpatient setting.
4. NEW: Symptom management in the outpatient setting (for quality improvement only).
5. Patient self-care education in the outpatient setting (for quality improvement only).
6. Beta-blocker therapy for left ventricular systolic dysfunction in the outpatient and inpatient settings.
7. ACE inhibitor for angiotensin receptor blocker therapy for left ventricular systolic dysfunction in the inpatient and outpatient setting.
8. NEW: Counseling regarding implantable cardioverter-defibrillator (ICD) implantation for patients with left ventricular systolic dysfunction combination medical therapy in the outpatient setting (for quality improvement only).
9. NEW: Postdischarge appointment for heart failure patients in the inpatient setting.
One of the significant changes in the updated measure set, according to the ACCF, is the expansion of the beta-blocker measure to the inpatient setting. In the 2005 set, the measure was only recommended for outpatient care. The panel sought to expand its use based on inpatient care information in the 2009 ACCF-AHA heart failure guidelines.
The work group also recommended that measures 6 and 7, which call for the use of beta-blockers, and ACE and ARB therapy, respectively, should be used together.
Another change in the updated measure set is the addition of a measure calling for a postdischarge appointment to be in place at the time of discharge from the hospital.
While most of the measures are considered appropriate for use in pay-for-performance programs, physician rankings, and public reporting, the writing panel recommended that the measures related to symptom management, patient self-care education, and counseling for ICD implantation be used only for internal quality improvement purposes.
Dr. Blake said these are areas where the work group wanted to give physicians time to collect data. In the case of the ICD counseling measure, they wanted to include a quality improvement measure that would serve as a reminder to physicians to discuss this option with eligible patients. "It doesn’t mean the patient should receive the device," she said. "It means that it should be a topic for discussion as part of a comprehensive review of the patient. It’s also an opportunity to discern what their goals and objectives are."
Dr. Bonow and Dr. Blake disclosed that they had no relationships with industry.
A set of nine performance measures aimed at assessing whether adults with heart failure are receiving the best care was issued by the American College of Cardiology Foundation, the American Heart Association, and the American Medical Association’s Physician Consortium for Performance Improvement.
The measure set, which was published April 23 in the Journal of the American College of Cardiology, includes three new performance measures and six revised measures. The new measure set was drafted by a panel of physicians, pharmacists, and patient advocates (J. Am. Coll. Cardiol. April 23, 2012;doi:10.1016/j.jacc.2012.03.013). The performance measures were last revised in 2005.
The measure set includes two performance metrics for inpatient care, five that address care in the outpatient setting, and two measures that apply to care in both settings. The idea, according to the sponsors, was to stress the need to measure quality over time and across providers, not in silos.
"To be successful as quality improvement tools, the heart failure performance measures need to be integrated as routine components of patient care across various care settings, with particular attention to transitions of care from inpatient to outpatient environments," Dr. Robert O. Bonow, cochair of the work group that developed the measure set and director of the center for cardiovascular innovation at Northwestern University, Chicago, said in a statement.
Improving care transitions is likely to be a major focus for physicians in and out of the hospital as officials at the Centers for Medicare and Medicaid Services begin to test a series of alternative payment and care delivery models, from Accountable Care Organizations to bundled payments. Adding to that pressure, this October, the CMS will begin cutting Medicare payments to hospitals whose heart failure and acute myocardial infarction readmission rates are considered too high.
The updated measure set will help prepare physicians for the payment and care delivery changes, Dr. Kathleen Blake, a member of the measure work group and a senior research director at the Center for Medical Technology Policy in Baltimore, said in an interview.
Performance measures, by definition, address areas where there are gaps in care, said Dr. Blake, who is a cardiologist. So physicians can take the updated heart failure measure set and embed it in their care, like a checklist, to ensure that patients are being considered for all appropriate evidence-based treatments.
"We are inundated with medical literature these days. This basically distills it into a measure set," she said.
The work group considered the ACCF/AHA 2009 practice guidelines on heart failure as well as existing heart failure performance measures from the Joint Commission, the CMS, and the Agency for Healthcare Research and Quality in putting together the updated set of measures. Along with the new and revised measures, they retired eight performance measures from the 2005 list.
The updated measure set includes:
1. Left Ventricular Ejection Fraction (LVEF) assessment in the outpatient setting.
2. LVEF in the inpatient setting.
3. Symptom and activity assessment in the outpatient setting.
4. NEW: Symptom management in the outpatient setting (for quality improvement only).
5. Patient self-care education in the outpatient setting (for quality improvement only).
6. Beta-blocker therapy for left ventricular systolic dysfunction in the outpatient and inpatient settings.
7. ACE inhibitor for angiotensin receptor blocker therapy for left ventricular systolic dysfunction in the inpatient and outpatient setting.
8. NEW: Counseling regarding implantable cardioverter-defibrillator (ICD) implantation for patients with left ventricular systolic dysfunction combination medical therapy in the outpatient setting (for quality improvement only).
9. NEW: Postdischarge appointment for heart failure patients in the inpatient setting.
One of the significant changes in the updated measure set, according to the ACCF, is the expansion of the beta-blocker measure to the inpatient setting. In the 2005 set, the measure was only recommended for outpatient care. The panel sought to expand its use based on inpatient care information in the 2009 ACCF-AHA heart failure guidelines.
The work group also recommended that measures 6 and 7, which call for the use of beta-blockers, and ACE and ARB therapy, respectively, should be used together.
Another change in the updated measure set is the addition of a measure calling for a postdischarge appointment to be in place at the time of discharge from the hospital.
While most of the measures are considered appropriate for use in pay-for-performance programs, physician rankings, and public reporting, the writing panel recommended that the measures related to symptom management, patient self-care education, and counseling for ICD implantation be used only for internal quality improvement purposes.
Dr. Blake said these are areas where the work group wanted to give physicians time to collect data. In the case of the ICD counseling measure, they wanted to include a quality improvement measure that would serve as a reminder to physicians to discuss this option with eligible patients. "It doesn’t mean the patient should receive the device," she said. "It means that it should be a topic for discussion as part of a comprehensive review of the patient. It’s also an opportunity to discern what their goals and objectives are."
Dr. Bonow and Dr. Blake disclosed that they had no relationships with industry.
A set of nine performance measures aimed at assessing whether adults with heart failure are receiving the best care was issued by the American College of Cardiology Foundation, the American Heart Association, and the American Medical Association’s Physician Consortium for Performance Improvement.
The measure set, which was published April 23 in the Journal of the American College of Cardiology, includes three new performance measures and six revised measures. The new measure set was drafted by a panel of physicians, pharmacists, and patient advocates (J. Am. Coll. Cardiol. April 23, 2012;doi:10.1016/j.jacc.2012.03.013). The performance measures were last revised in 2005.
The measure set includes two performance metrics for inpatient care, five that address care in the outpatient setting, and two measures that apply to care in both settings. The idea, according to the sponsors, was to stress the need to measure quality over time and across providers, not in silos.
"To be successful as quality improvement tools, the heart failure performance measures need to be integrated as routine components of patient care across various care settings, with particular attention to transitions of care from inpatient to outpatient environments," Dr. Robert O. Bonow, cochair of the work group that developed the measure set and director of the center for cardiovascular innovation at Northwestern University, Chicago, said in a statement.
Improving care transitions is likely to be a major focus for physicians in and out of the hospital as officials at the Centers for Medicare and Medicaid Services begin to test a series of alternative payment and care delivery models, from Accountable Care Organizations to bundled payments. Adding to that pressure, this October, the CMS will begin cutting Medicare payments to hospitals whose heart failure and acute myocardial infarction readmission rates are considered too high.
The updated measure set will help prepare physicians for the payment and care delivery changes, Dr. Kathleen Blake, a member of the measure work group and a senior research director at the Center for Medical Technology Policy in Baltimore, said in an interview.
Performance measures, by definition, address areas where there are gaps in care, said Dr. Blake, who is a cardiologist. So physicians can take the updated heart failure measure set and embed it in their care, like a checklist, to ensure that patients are being considered for all appropriate evidence-based treatments.
"We are inundated with medical literature these days. This basically distills it into a measure set," she said.
The work group considered the ACCF/AHA 2009 practice guidelines on heart failure as well as existing heart failure performance measures from the Joint Commission, the CMS, and the Agency for Healthcare Research and Quality in putting together the updated set of measures. Along with the new and revised measures, they retired eight performance measures from the 2005 list.
The updated measure set includes:
1. Left Ventricular Ejection Fraction (LVEF) assessment in the outpatient setting.
2. LVEF in the inpatient setting.
3. Symptom and activity assessment in the outpatient setting.
4. NEW: Symptom management in the outpatient setting (for quality improvement only).
5. Patient self-care education in the outpatient setting (for quality improvement only).
6. Beta-blocker therapy for left ventricular systolic dysfunction in the outpatient and inpatient settings.
7. ACE inhibitor for angiotensin receptor blocker therapy for left ventricular systolic dysfunction in the inpatient and outpatient setting.
8. NEW: Counseling regarding implantable cardioverter-defibrillator (ICD) implantation for patients with left ventricular systolic dysfunction combination medical therapy in the outpatient setting (for quality improvement only).
9. NEW: Postdischarge appointment for heart failure patients in the inpatient setting.
One of the significant changes in the updated measure set, according to the ACCF, is the expansion of the beta-blocker measure to the inpatient setting. In the 2005 set, the measure was only recommended for outpatient care. The panel sought to expand its use based on inpatient care information in the 2009 ACCF-AHA heart failure guidelines.
The work group also recommended that measures 6 and 7, which call for the use of beta-blockers, and ACE and ARB therapy, respectively, should be used together.
Another change in the updated measure set is the addition of a measure calling for a postdischarge appointment to be in place at the time of discharge from the hospital.
While most of the measures are considered appropriate for use in pay-for-performance programs, physician rankings, and public reporting, the writing panel recommended that the measures related to symptom management, patient self-care education, and counseling for ICD implantation be used only for internal quality improvement purposes.
Dr. Blake said these are areas where the work group wanted to give physicians time to collect data. In the case of the ICD counseling measure, they wanted to include a quality improvement measure that would serve as a reminder to physicians to discuss this option with eligible patients. "It doesn’t mean the patient should receive the device," she said. "It means that it should be a topic for discussion as part of a comprehensive review of the patient. It’s also an opportunity to discern what their goals and objectives are."
Dr. Bonow and Dr. Blake disclosed that they had no relationships with industry.
Why 30-Day Readmissions Are High
Once a month, a "dream team" of community and hospital physicians and nurses meets at the University of Connecticut, Farmington. Their goal: To improve the transition out of the hospital for patients with heart failure. Their progress: Since the group’s first meeting in 2008, the hospital’s 30-day, all-cause readmission rates for heart failure have fallen from 27% to less than 19%, according to figures tracked by the Connecticut Hospital Association.
"That’s a significant drop and puts the hospital below the state average of 25%. "We’re pretty proud of that," said Dr. Jason Ryan, a cardiologist and codirector of the Heart Failure Center at the university.

Dr. Ryan attributes the "dream team’s" successes to intensive patient education in the hospital, a mandatory follow-up visit with a physician at 7 days after discharge, and better communication between clinicians in the hospital and those in the community.
But possibly the biggest factor in their success has been physician commitment to keeping patients with preventable readmissions out of the hospital.
In the UConn program, the cardiologists have made a point of getting patients immediate clinic appointments to evaluate whether they are having a minor issue that can be dealt with in an outpatient setting or if they have a more serious concern that requires readmission to the hospital.
"Some of our patients call us with complaints that I could easily over the phone say, ‘Well, you need to go to the emergency room for that,’ " Dr. Ryan said. "If you’ve got a group of physicians who are not interested in this work, it’s very easy to send people to the emergency room."
The UConn program could end up being a model for other hospitals that are looking to reduce their readmission rates for heart failure and acute myocardial infarction ahead of financial penalties coming down the pike this fall from the Medicare program.
But can hospitals that serve diverse communities meaningfully enact such programs and expect similar successes?
And what will be the impact of the penalties on safety net hospitals that lack the money to undertake a major overhaul of their discharge and care coordination systems?
Even after the data are risk adjusted for their sicker patients, safety net hospitals could still end up with higher than average readmissions. If CMS penalizes them with lower reimbursements due to their excessive readmission rates, they could be left with even fewer resource to care for sicker patients.
Medicare Turns Up the Heat
Starting in October, the Centers for Medicare and Medicaid Services will begin cutting Medicare payments to hospitals whose acute MI and heart failure readmission rates are considered too high.
It’s still unclear exactly what the cutoff point will be. CMS will use readmission data from July 2008 through June 2011 to determine excessive rates and penalties for fiscal year 2013, which begins this October.
CMS is defining all-cause readmission as occurring when a patient is discharged from a hospital and then admitted to the same hospital or another acute care hospital within 30 days.
Recent, risk-adjusted data from CMS offer a glimpse of where the country is in terms of reducing readmission rates.
For acute MI, the national rate for 30-day all-cause readmissions has dropped slightly, going from 19.9% from 2006 through 2009 to 19.8% from 2007 through 2010. During the same time period, readmissions for heart failure rose slightly, creeping up from 24.5% to 24.8%.
The data show the similar trends for mortality during the two reporting periods. The acute MI rates fell from 16.2% to 15.9%, while heart failure mortality rose from 11.2% to 11.3%.
Blaming Length of Stay
A study published earlier this year paints a gloomy picture about how U.S. hospitals stack up against other countries in readmission for ST-elevation MI. The study found that 30-day readmission rates were on average 14.5% in the United States vs. 9.9% among the other countries studied (JAMA 2012;307:66-74). The study included patients in the United States, Canada, Australia, New Zealand, and 13 European countries.

At the same time, the median length of stay was shortest in the United States at 3 days. The longest median length of stay noted in the study was 8 days in Germany.
The study investigators pointed to the shorter length of stay in U.S. hospitals as a possible driver of the country’s higher rate of readmissions. But other experts say there are more complex factors at work, such as gaps in the discharge planning process and a lack of resources for patients once they leave the hospital.
There weren’t a lot of patients who were readmitted 2 days later for the same condition, which might indicate that they had been discharged too soon, Dr. Ryan said. More often, patients return to the hospital a week or several days later with a new problem. That tends to indicate that their medications may not have been adjusted correctly or that they were unable to access services in the outpatient world, he said.
There is very little evidence to support the idea that a longer initial length of stay would lead to either better use of evidence-based therapies or produce better clinical outcomes, said Dr. Gregg C. Fonarow, director of the Cardiomyopathy Center at the University of California, Los Angeles. Though there’s plenty of evidence to show that more time in the hospital increases patients’ risk for hospital-acquired infection, he added.
Over the last 2 decades, readmissions for heart failure patients have gone up as length of stay has decreased. But, Dr. Fonarow points out, during that same time the total number of days patients spent in the hospital has actually gone down, along with mortality. So from a global resource utilization perspective, patients are spending less time in the hospital and having better outcomes, he said.
"It’s important to have appropriate comparisons," he said.
Dr. Fonarow cautioned that there aren’t simple solutions to this problem. While there are many opportunities to improve readmission rates, there are also many rehospitalizations that are unavoidable or unrelated to the cardiovascular condition responsible for the initial hospitalization. Many patients hospitalized with acute MI, and to an even greater degree with heart failure, have multiple other cardiovascular and noncardiovascular comorbid conditions, he said.
"Efforts to try and reduce preventable readmissions have to go well beyond even the primary disease state that led to the hospitalization," Dr. Fonarow said. "They need to involve multiple components of care that go beyond just treating the single acute condition and focus on the multiple comorbid conditions that exist within that patient."
To make it even more complicated, patients who are hospitalized with heart failure tend to be older and to have multiple comorbid conditions. These individuals may face other challenges such as cognitive impairment, frailty, and poor socioeconomic support.
"It’s really a complex problem," he said.

Ensuring Needed Care
The looming Medicare readmission penalties have caused many hospital administrators, and in turn physicians, to look closely at the factors behind readmissions for the first time over the last few years.
"Everyone’s trying to figure this out because they do see the shift coming in the payment system," said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
And the payment cuts for excessive readmissions aren’t the only way that CMS is focusing on the issue, Dr. Rumsfeld said. Readmissions are also at the heart of pilot projects Medicare is launching for Accountable Care Organizations and bundled payments.
Dr. Rumsfeld said he’s concerned that physicians are getting the message that all readmissions are bad. "This is a potentially dangerous message for clinical care," he said.
The conversation needs to shift to unnecessary or potentially preventable readmissions, he said. It’s often underappreciated, Dr. Rumsfeld said, that patients who are having recurrent chest pain or severe shortness of breath after an acute MI should be admitted to the hospital for care. "There shouldn’t be anything in the system that disincentivizes that," he said.
Dr. Clyde W. Yancy, Chief of the Division of Cardiology at Northwestern University and Associate Director of the Bluhm Cardiovascular Institute at Northwestern Memorial Hospital in Chicago, agrees.
"We’re beating the drum about this problem mostly because it’s a health care utilization problem," Dr. Yancy said. "In the process of beating the drum, we have to have enough wherewithal as clinicians and administrators to realize that there are those – and not a small number – who should in fact be readmitted because their disease is unstable, or it’s advanced, or it requires that attention."
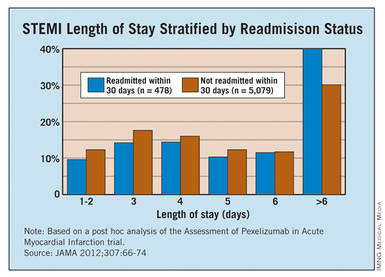
The fate of safety net hospitals is also a concern. Safety net hospitals are unlikely to have the money to undertake a major overhaul of their discharge and care coordination systems, which could leave them with higher than average readmissions, even after the data is risk adjusted for their sicker patients, Dr. Yancy said. Then, if CMS cuts their reimbursement due to their excessive readmission rates, they will be left to care for sicker patients with even fewer resources.
"There has to be a point in this whole process where reasonable people sit back and look at how the landscape is truly impacted by this focus on readmissions," he said. "We can’t allow our safety net hospitals to be further disadvantaged."
Dr. Vincent Bufalino, Senior Vice President and Senior Medical Director of Cardiology at Advocate Health Care, a 100-physician cardiology group serving 10 hospitals in the Chicago area, said he thinks the readmission rates are a bit deceptive. While the numbers are high, especially in heart failure, these are also very sick patients, he said. "I’m not so disturbed with the readmission rate, although there are obviously opportunities for us to do better," Dr. Bufalino said.
One of those opportunities is in home health. Many heart failure and acute MI patients who could benefit from home health care after discharge aren’t getting it, he said, and it’s mostly because of a paperwork burden. Physicians aren’t making the referrals for home health because the paperwork required by CMS is so daunting.
While there are plenty of areas where physicians and hospitals can do a better job at care coordination, it’s important not to set unrealistic targets that force patients to be sent home when they should be admitted, Dr. Bufalino said.
"If someone is sick and they need to be readmitted, readmit them," he said.
Lessons Learned in Heart Failure
Physicians looking to make a dent in their readmission rates for heart failure can take some cues from successful programs around the country.
While the implementation varies from place to place, programs that have been able to cut their readmissions stress the need for patients to see a physician or nurse practitioner shortly after discharge. Another essential element for success is improving the communication between providers in the hospital and those who will be caring for patients after discharge.

At the University of Connecticut Heart Failure Center, where the all-cause 30-day readmission rates for heart failure patients dropped from 27% in 2008 to under 19% in 2011, patients don’t leave the hospital without an appointment to see a physician within 7 days of discharge.
The appointment might be with a primary care physician, a cardiologist, or a physician or nurse practitioner at the university’s heart failure clinic.
"If we can’t get them in with someone else, we will always make room for them and see them," said Dr. Jason Ryan, codirector of the Heart Failure Center at the University of Connecticut, Farmington.
While patients are still in the hospital, they also meet with nurses who train them in taking their medications and monitoring for heart failure symptoms. Patients also meet with social workers who ensure they have transportation to their appointments and a way to pick up their medicines. And they spend time with a pharmacist who reviews their medications.
The other element they have employed at the University of Connecticut is community outreach. Before the push to reduce readmissions, physicians at the hospital didn’t know anyone at the nursing homes or visiting nurse organizations. Now they hold a monthly meeting with physicians and other providers who work outside the hospital. They have gone from not knowing each other’s names to exchanging cell phone numbers, Dr. Ryan said.
"So when our patients are out there we can communicate a lot more easily when problems crop up," he said.
At the University of California, San Francisco’s Medical Center, they have used similar strategies to cut their readmission rates.
The UCSF Heart Failure Readmission Reduction Program began in 2008 with a 2-year, $575,000 grant aimed at rapidly bringing down readmissions. Now in its fourth year, the nurse-run program has been a success. The 30-day all-cause readmission rates for heart failure patients age 65 and older was around 24% in 2009 but had dropped to less than 10% at the beginning of this year.
But the program couldn’t run without its two nurse coordinators, said Karen Rago, a nurse and executive director of Service Line Administration at UCSF.
"They own this population," she said. "If you don’t have a single point that owns it, there are so many things that fall through the cracks."
The nurses at the UCSF heart failure program spent the first year working with the Institute for Healthcare Improvement to learn the principles in their readmissions toolkit: teach-back, follow-up phone calls at 7 and 14 days, an appointment with a physician or heart failure nurse practitioner within 7 days, and medication reconciliation.
The nurse coordinators also serve as a bridge to providers in the outpatient setting, Ms. Rago said. During the second year of the program, they began making site visits to skilled nursing facilities and reaching out to primary care physicians, cardiologists, and home health agencies from outside of the hospital.
They created an e-mail group for each patient’s care team that includes physicians, nurses, home care, social work, and pharmacy, depending on the services the patient needed. An email goes out to the team at the time of admission and it provides a way to update everyone virtually in real-time about the care of the patient.
Having a closer relationship with the skilled nursing facilities has been a big help, Ms. Rago said. During one of the site visits, the nurses discovered that one of the facilities didn’t offer a low-salt diet. That helped explain why so many patients from that facility were being readmitted to the hospital and they were able to quickly address it, she said.
What physicians need to keep in mind is that while many of these solutions are common sense, there’s no one-size-fits-all approach to readmissions, said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
"It’s different in each community, so you can’t be prescriptive," he said.
The American College of Cardiology offers resources for reducing readmissions as part of a joint effort with the Institute for Healthcare Improvement called the Hospital to Home initiative.
Unlike other areas of care, such as getting a faster angioplasty, there aren’t six key steps for physicians to implement, Dr. Rumsfeld said. Instead, Hospital to Home is a place for physicians to share best practices based on their individual experiences. So far, more than 1,100 hospitals around the country have signed up.
Once a month, a "dream team" of community and hospital physicians and nurses meets at the University of Connecticut, Farmington. Their goal: To improve the transition out of the hospital for patients with heart failure. Their progress: Since the group’s first meeting in 2008, the hospital’s 30-day, all-cause readmission rates for heart failure have fallen from 27% to less than 19%, according to figures tracked by the Connecticut Hospital Association.
"That’s a significant drop and puts the hospital below the state average of 25%. "We’re pretty proud of that," said Dr. Jason Ryan, a cardiologist and codirector of the Heart Failure Center at the university.
Dr. Ryan attributes the "dream team’s" successes to intensive patient education in the hospital, a mandatory follow-up visit with a physician at 7 days after discharge, and better communication between clinicians in the hospital and those in the community.
But possibly the biggest factor in their success has been physician commitment to keeping patients with preventable readmissions out of the hospital.
In the UConn program, the cardiologists have made a point of getting patients immediate clinic appointments to evaluate whether they are having a minor issue that can be dealt with in an outpatient setting or if they have a more serious concern that requires readmission to the hospital.
"Some of our patients call us with complaints that I could easily over the phone say, ‘Well, you need to go to the emergency room for that,’ " Dr. Ryan said. "If you’ve got a group of physicians who are not interested in this work, it’s very easy to send people to the emergency room."
The UConn program could end up being a model for other hospitals that are looking to reduce their readmission rates for heart failure and acute myocardial infarction ahead of financial penalties coming down the pike this fall from the Medicare program.
But can hospitals that serve diverse communities meaningfully enact such programs and expect similar successes?
And what will be the impact of the penalties on safety net hospitals that lack the money to undertake a major overhaul of their discharge and care coordination systems?
Even after the data are risk adjusted for their sicker patients, safety net hospitals could still end up with higher than average readmissions. If CMS penalizes them with lower reimbursements due to their excessive readmission rates, they could be left with even fewer resource to care for sicker patients.
Medicare Turns Up the Heat
Starting in October, the Centers for Medicare and Medicaid Services will begin cutting Medicare payments to hospitals whose acute MI and heart failure readmission rates are considered too high.
It’s still unclear exactly what the cutoff point will be. CMS will use readmission data from July 2008 through June 2011 to determine excessive rates and penalties for fiscal year 2013, which begins this October.
CMS is defining all-cause readmission as occurring when a patient is discharged from a hospital and then admitted to the same hospital or another acute care hospital within 30 days.
Recent, risk-adjusted data from CMS offer a glimpse of where the country is in terms of reducing readmission rates.
For acute MI, the national rate for 30-day all-cause readmissions has dropped slightly, going from 19.9% from 2006 through 2009 to 19.8% from 2007 through 2010. During the same time period, readmissions for heart failure rose slightly, creeping up from 24.5% to 24.8%.
The data show the similar trends for mortality during the two reporting periods. The acute MI rates fell from 16.2% to 15.9%, while heart failure mortality rose from 11.2% to 11.3%.
Blaming Length of Stay
A study published earlier this year paints a gloomy picture about how U.S. hospitals stack up against other countries in readmission for ST-elevation MI. The study found that 30-day readmission rates were on average 14.5% in the United States vs. 9.9% among the other countries studied (JAMA 2012;307:66-74). The study included patients in the United States, Canada, Australia, New Zealand, and 13 European countries.
At the same time, the median length of stay was shortest in the United States at 3 days. The longest median length of stay noted in the study was 8 days in Germany.
The study investigators pointed to the shorter length of stay in U.S. hospitals as a possible driver of the country’s higher rate of readmissions. But other experts say there are more complex factors at work, such as gaps in the discharge planning process and a lack of resources for patients once they leave the hospital.
There weren’t a lot of patients who were readmitted 2 days later for the same condition, which might indicate that they had been discharged too soon, Dr. Ryan said. More often, patients return to the hospital a week or several days later with a new problem. That tends to indicate that their medications may not have been adjusted correctly or that they were unable to access services in the outpatient world, he said.
There is very little evidence to support the idea that a longer initial length of stay would lead to either better use of evidence-based therapies or produce better clinical outcomes, said Dr. Gregg C. Fonarow, director of the Cardiomyopathy Center at the University of California, Los Angeles. Though there’s plenty of evidence to show that more time in the hospital increases patients’ risk for hospital-acquired infection, he added.
Over the last 2 decades, readmissions for heart failure patients have gone up as length of stay has decreased. But, Dr. Fonarow points out, during that same time the total number of days patients spent in the hospital has actually gone down, along with mortality. So from a global resource utilization perspective, patients are spending less time in the hospital and having better outcomes, he said.
"It’s important to have appropriate comparisons," he said.
Dr. Fonarow cautioned that there aren’t simple solutions to this problem. While there are many opportunities to improve readmission rates, there are also many rehospitalizations that are unavoidable or unrelated to the cardiovascular condition responsible for the initial hospitalization. Many patients hospitalized with acute MI, and to an even greater degree with heart failure, have multiple other cardiovascular and noncardiovascular comorbid conditions, he said.
"Efforts to try and reduce preventable readmissions have to go well beyond even the primary disease state that led to the hospitalization," Dr. Fonarow said. "They need to involve multiple components of care that go beyond just treating the single acute condition and focus on the multiple comorbid conditions that exist within that patient."
To make it even more complicated, patients who are hospitalized with heart failure tend to be older and to have multiple comorbid conditions. These individuals may face other challenges such as cognitive impairment, frailty, and poor socioeconomic support.
"It’s really a complex problem," he said.
Ensuring Needed Care
The looming Medicare readmission penalties have caused many hospital administrators, and in turn physicians, to look closely at the factors behind readmissions for the first time over the last few years.
"Everyone’s trying to figure this out because they do see the shift coming in the payment system," said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
And the payment cuts for excessive readmissions aren’t the only way that CMS is focusing on the issue, Dr. Rumsfeld said. Readmissions are also at the heart of pilot projects Medicare is launching for Accountable Care Organizations and bundled payments.
Dr. Rumsfeld said he’s concerned that physicians are getting the message that all readmissions are bad. "This is a potentially dangerous message for clinical care," he said.
The conversation needs to shift to unnecessary or potentially preventable readmissions, he said. It’s often underappreciated, Dr. Rumsfeld said, that patients who are having recurrent chest pain or severe shortness of breath after an acute MI should be admitted to the hospital for care. "There shouldn’t be anything in the system that disincentivizes that," he said.
Dr. Clyde W. Yancy, Chief of the Division of Cardiology at Northwestern University and Associate Director of the Bluhm Cardiovascular Institute at Northwestern Memorial Hospital in Chicago, agrees.
"We’re beating the drum about this problem mostly because it’s a health care utilization problem," Dr. Yancy said. "In the process of beating the drum, we have to have enough wherewithal as clinicians and administrators to realize that there are those – and not a small number – who should in fact be readmitted because their disease is unstable, or it’s advanced, or it requires that attention."
The fate of safety net hospitals is also a concern. Safety net hospitals are unlikely to have the money to undertake a major overhaul of their discharge and care coordination systems, which could leave them with higher than average readmissions, even after the data is risk adjusted for their sicker patients, Dr. Yancy said. Then, if CMS cuts their reimbursement due to their excessive readmission rates, they will be left to care for sicker patients with even fewer resources.
"There has to be a point in this whole process where reasonable people sit back and look at how the landscape is truly impacted by this focus on readmissions," he said. "We can’t allow our safety net hospitals to be further disadvantaged."
Dr. Vincent Bufalino, Senior Vice President and Senior Medical Director of Cardiology at Advocate Health Care, a 100-physician cardiology group serving 10 hospitals in the Chicago area, said he thinks the readmission rates are a bit deceptive. While the numbers are high, especially in heart failure, these are also very sick patients, he said. "I’m not so disturbed with the readmission rate, although there are obviously opportunities for us to do better," Dr. Bufalino said.
One of those opportunities is in home health. Many heart failure and acute MI patients who could benefit from home health care after discharge aren’t getting it, he said, and it’s mostly because of a paperwork burden. Physicians aren’t making the referrals for home health because the paperwork required by CMS is so daunting.
While there are plenty of areas where physicians and hospitals can do a better job at care coordination, it’s important not to set unrealistic targets that force patients to be sent home when they should be admitted, Dr. Bufalino said.
"If someone is sick and they need to be readmitted, readmit them," he said.
Lessons Learned in Heart Failure
Physicians looking to make a dent in their readmission rates for heart failure can take some cues from successful programs around the country.
While the implementation varies from place to place, programs that have been able to cut their readmissions stress the need for patients to see a physician or nurse practitioner shortly after discharge. Another essential element for success is improving the communication between providers in the hospital and those who will be caring for patients after discharge.
At the University of Connecticut Heart Failure Center, where the all-cause 30-day readmission rates for heart failure patients dropped from 27% in 2008 to under 19% in 2011, patients don’t leave the hospital without an appointment to see a physician within 7 days of discharge.
The appointment might be with a primary care physician, a cardiologist, or a physician or nurse practitioner at the university’s heart failure clinic.
"If we can’t get them in with someone else, we will always make room for them and see them," said Dr. Jason Ryan, codirector of the Heart Failure Center at the University of Connecticut, Farmington.
While patients are still in the hospital, they also meet with nurses who train them in taking their medications and monitoring for heart failure symptoms. Patients also meet with social workers who ensure they have transportation to their appointments and a way to pick up their medicines. And they spend time with a pharmacist who reviews their medications.
The other element they have employed at the University of Connecticut is community outreach. Before the push to reduce readmissions, physicians at the hospital didn’t know anyone at the nursing homes or visiting nurse organizations. Now they hold a monthly meeting with physicians and other providers who work outside the hospital. They have gone from not knowing each other’s names to exchanging cell phone numbers, Dr. Ryan said.
"So when our patients are out there we can communicate a lot more easily when problems crop up," he said.
At the University of California, San Francisco’s Medical Center, they have used similar strategies to cut their readmission rates.
The UCSF Heart Failure Readmission Reduction Program began in 2008 with a 2-year, $575,000 grant aimed at rapidly bringing down readmissions. Now in its fourth year, the nurse-run program has been a success. The 30-day all-cause readmission rates for heart failure patients age 65 and older was around 24% in 2009 but had dropped to less than 10% at the beginning of this year.
But the program couldn’t run without its two nurse coordinators, said Karen Rago, a nurse and executive director of Service Line Administration at UCSF.
"They own this population," she said. "If you don’t have a single point that owns it, there are so many things that fall through the cracks."
The nurses at the UCSF heart failure program spent the first year working with the Institute for Healthcare Improvement to learn the principles in their readmissions toolkit: teach-back, follow-up phone calls at 7 and 14 days, an appointment with a physician or heart failure nurse practitioner within 7 days, and medication reconciliation.
The nurse coordinators also serve as a bridge to providers in the outpatient setting, Ms. Rago said. During the second year of the program, they began making site visits to skilled nursing facilities and reaching out to primary care physicians, cardiologists, and home health agencies from outside of the hospital.
They created an e-mail group for each patient’s care team that includes physicians, nurses, home care, social work, and pharmacy, depending on the services the patient needed. An email goes out to the team at the time of admission and it provides a way to update everyone virtually in real-time about the care of the patient.
Having a closer relationship with the skilled nursing facilities has been a big help, Ms. Rago said. During one of the site visits, the nurses discovered that one of the facilities didn’t offer a low-salt diet. That helped explain why so many patients from that facility were being readmitted to the hospital and they were able to quickly address it, she said.
What physicians need to keep in mind is that while many of these solutions are common sense, there’s no one-size-fits-all approach to readmissions, said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
"It’s different in each community, so you can’t be prescriptive," he said.
The American College of Cardiology offers resources for reducing readmissions as part of a joint effort with the Institute for Healthcare Improvement called the Hospital to Home initiative.
Unlike other areas of care, such as getting a faster angioplasty, there aren’t six key steps for physicians to implement, Dr. Rumsfeld said. Instead, Hospital to Home is a place for physicians to share best practices based on their individual experiences. So far, more than 1,100 hospitals around the country have signed up.
Once a month, a "dream team" of community and hospital physicians and nurses meets at the University of Connecticut, Farmington. Their goal: To improve the transition out of the hospital for patients with heart failure. Their progress: Since the group’s first meeting in 2008, the hospital’s 30-day, all-cause readmission rates for heart failure have fallen from 27% to less than 19%, according to figures tracked by the Connecticut Hospital Association.
"That’s a significant drop and puts the hospital below the state average of 25%. "We’re pretty proud of that," said Dr. Jason Ryan, a cardiologist and codirector of the Heart Failure Center at the university.
Dr. Ryan attributes the "dream team’s" successes to intensive patient education in the hospital, a mandatory follow-up visit with a physician at 7 days after discharge, and better communication between clinicians in the hospital and those in the community.
But possibly the biggest factor in their success has been physician commitment to keeping patients with preventable readmissions out of the hospital.
In the UConn program, the cardiologists have made a point of getting patients immediate clinic appointments to evaluate whether they are having a minor issue that can be dealt with in an outpatient setting or if they have a more serious concern that requires readmission to the hospital.
"Some of our patients call us with complaints that I could easily over the phone say, ‘Well, you need to go to the emergency room for that,’ " Dr. Ryan said. "If you’ve got a group of physicians who are not interested in this work, it’s very easy to send people to the emergency room."
The UConn program could end up being a model for other hospitals that are looking to reduce their readmission rates for heart failure and acute myocardial infarction ahead of financial penalties coming down the pike this fall from the Medicare program.
But can hospitals that serve diverse communities meaningfully enact such programs and expect similar successes?
And what will be the impact of the penalties on safety net hospitals that lack the money to undertake a major overhaul of their discharge and care coordination systems?
Even after the data are risk adjusted for their sicker patients, safety net hospitals could still end up with higher than average readmissions. If CMS penalizes them with lower reimbursements due to their excessive readmission rates, they could be left with even fewer resource to care for sicker patients.
Medicare Turns Up the Heat
Starting in October, the Centers for Medicare and Medicaid Services will begin cutting Medicare payments to hospitals whose acute MI and heart failure readmission rates are considered too high.
It’s still unclear exactly what the cutoff point will be. CMS will use readmission data from July 2008 through June 2011 to determine excessive rates and penalties for fiscal year 2013, which begins this October.
CMS is defining all-cause readmission as occurring when a patient is discharged from a hospital and then admitted to the same hospital or another acute care hospital within 30 days.
Recent, risk-adjusted data from CMS offer a glimpse of where the country is in terms of reducing readmission rates.
For acute MI, the national rate for 30-day all-cause readmissions has dropped slightly, going from 19.9% from 2006 through 2009 to 19.8% from 2007 through 2010. During the same time period, readmissions for heart failure rose slightly, creeping up from 24.5% to 24.8%.
The data show the similar trends for mortality during the two reporting periods. The acute MI rates fell from 16.2% to 15.9%, while heart failure mortality rose from 11.2% to 11.3%.
Blaming Length of Stay
A study published earlier this year paints a gloomy picture about how U.S. hospitals stack up against other countries in readmission for ST-elevation MI. The study found that 30-day readmission rates were on average 14.5% in the United States vs. 9.9% among the other countries studied (JAMA 2012;307:66-74). The study included patients in the United States, Canada, Australia, New Zealand, and 13 European countries.
At the same time, the median length of stay was shortest in the United States at 3 days. The longest median length of stay noted in the study was 8 days in Germany.
The study investigators pointed to the shorter length of stay in U.S. hospitals as a possible driver of the country’s higher rate of readmissions. But other experts say there are more complex factors at work, such as gaps in the discharge planning process and a lack of resources for patients once they leave the hospital.
There weren’t a lot of patients who were readmitted 2 days later for the same condition, which might indicate that they had been discharged too soon, Dr. Ryan said. More often, patients return to the hospital a week or several days later with a new problem. That tends to indicate that their medications may not have been adjusted correctly or that they were unable to access services in the outpatient world, he said.
There is very little evidence to support the idea that a longer initial length of stay would lead to either better use of evidence-based therapies or produce better clinical outcomes, said Dr. Gregg C. Fonarow, director of the Cardiomyopathy Center at the University of California, Los Angeles. Though there’s plenty of evidence to show that more time in the hospital increases patients’ risk for hospital-acquired infection, he added.
Over the last 2 decades, readmissions for heart failure patients have gone up as length of stay has decreased. But, Dr. Fonarow points out, during that same time the total number of days patients spent in the hospital has actually gone down, along with mortality. So from a global resource utilization perspective, patients are spending less time in the hospital and having better outcomes, he said.
"It’s important to have appropriate comparisons," he said.
Dr. Fonarow cautioned that there aren’t simple solutions to this problem. While there are many opportunities to improve readmission rates, there are also many rehospitalizations that are unavoidable or unrelated to the cardiovascular condition responsible for the initial hospitalization. Many patients hospitalized with acute MI, and to an even greater degree with heart failure, have multiple other cardiovascular and noncardiovascular comorbid conditions, he said.
"Efforts to try and reduce preventable readmissions have to go well beyond even the primary disease state that led to the hospitalization," Dr. Fonarow said. "They need to involve multiple components of care that go beyond just treating the single acute condition and focus on the multiple comorbid conditions that exist within that patient."
To make it even more complicated, patients who are hospitalized with heart failure tend to be older and to have multiple comorbid conditions. These individuals may face other challenges such as cognitive impairment, frailty, and poor socioeconomic support.
"It’s really a complex problem," he said.
Ensuring Needed Care
The looming Medicare readmission penalties have caused many hospital administrators, and in turn physicians, to look closely at the factors behind readmissions for the first time over the last few years.
"Everyone’s trying to figure this out because they do see the shift coming in the payment system," said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
And the payment cuts for excessive readmissions aren’t the only way that CMS is focusing on the issue, Dr. Rumsfeld said. Readmissions are also at the heart of pilot projects Medicare is launching for Accountable Care Organizations and bundled payments.
Dr. Rumsfeld said he’s concerned that physicians are getting the message that all readmissions are bad. "This is a potentially dangerous message for clinical care," he said.
The conversation needs to shift to unnecessary or potentially preventable readmissions, he said. It’s often underappreciated, Dr. Rumsfeld said, that patients who are having recurrent chest pain or severe shortness of breath after an acute MI should be admitted to the hospital for care. "There shouldn’t be anything in the system that disincentivizes that," he said.
Dr. Clyde W. Yancy, Chief of the Division of Cardiology at Northwestern University and Associate Director of the Bluhm Cardiovascular Institute at Northwestern Memorial Hospital in Chicago, agrees.
"We’re beating the drum about this problem mostly because it’s a health care utilization problem," Dr. Yancy said. "In the process of beating the drum, we have to have enough wherewithal as clinicians and administrators to realize that there are those – and not a small number – who should in fact be readmitted because their disease is unstable, or it’s advanced, or it requires that attention."
The fate of safety net hospitals is also a concern. Safety net hospitals are unlikely to have the money to undertake a major overhaul of their discharge and care coordination systems, which could leave them with higher than average readmissions, even after the data is risk adjusted for their sicker patients, Dr. Yancy said. Then, if CMS cuts their reimbursement due to their excessive readmission rates, they will be left to care for sicker patients with even fewer resources.
"There has to be a point in this whole process where reasonable people sit back and look at how the landscape is truly impacted by this focus on readmissions," he said. "We can’t allow our safety net hospitals to be further disadvantaged."
Dr. Vincent Bufalino, Senior Vice President and Senior Medical Director of Cardiology at Advocate Health Care, a 100-physician cardiology group serving 10 hospitals in the Chicago area, said he thinks the readmission rates are a bit deceptive. While the numbers are high, especially in heart failure, these are also very sick patients, he said. "I’m not so disturbed with the readmission rate, although there are obviously opportunities for us to do better," Dr. Bufalino said.
One of those opportunities is in home health. Many heart failure and acute MI patients who could benefit from home health care after discharge aren’t getting it, he said, and it’s mostly because of a paperwork burden. Physicians aren’t making the referrals for home health because the paperwork required by CMS is so daunting.
While there are plenty of areas where physicians and hospitals can do a better job at care coordination, it’s important not to set unrealistic targets that force patients to be sent home when they should be admitted, Dr. Bufalino said.
"If someone is sick and they need to be readmitted, readmit them," he said.
Lessons Learned in Heart Failure
Physicians looking to make a dent in their readmission rates for heart failure can take some cues from successful programs around the country.
While the implementation varies from place to place, programs that have been able to cut their readmissions stress the need for patients to see a physician or nurse practitioner shortly after discharge. Another essential element for success is improving the communication between providers in the hospital and those who will be caring for patients after discharge.
At the University of Connecticut Heart Failure Center, where the all-cause 30-day readmission rates for heart failure patients dropped from 27% in 2008 to under 19% in 2011, patients don’t leave the hospital without an appointment to see a physician within 7 days of discharge.
The appointment might be with a primary care physician, a cardiologist, or a physician or nurse practitioner at the university’s heart failure clinic.
"If we can’t get them in with someone else, we will always make room for them and see them," said Dr. Jason Ryan, codirector of the Heart Failure Center at the University of Connecticut, Farmington.
While patients are still in the hospital, they also meet with nurses who train them in taking their medications and monitoring for heart failure symptoms. Patients also meet with social workers who ensure they have transportation to their appointments and a way to pick up their medicines. And they spend time with a pharmacist who reviews their medications.
The other element they have employed at the University of Connecticut is community outreach. Before the push to reduce readmissions, physicians at the hospital didn’t know anyone at the nursing homes or visiting nurse organizations. Now they hold a monthly meeting with physicians and other providers who work outside the hospital. They have gone from not knowing each other’s names to exchanging cell phone numbers, Dr. Ryan said.
"So when our patients are out there we can communicate a lot more easily when problems crop up," he said.
At the University of California, San Francisco’s Medical Center, they have used similar strategies to cut their readmission rates.
The UCSF Heart Failure Readmission Reduction Program began in 2008 with a 2-year, $575,000 grant aimed at rapidly bringing down readmissions. Now in its fourth year, the nurse-run program has been a success. The 30-day all-cause readmission rates for heart failure patients age 65 and older was around 24% in 2009 but had dropped to less than 10% at the beginning of this year.
But the program couldn’t run without its two nurse coordinators, said Karen Rago, a nurse and executive director of Service Line Administration at UCSF.
"They own this population," she said. "If you don’t have a single point that owns it, there are so many things that fall through the cracks."
The nurses at the UCSF heart failure program spent the first year working with the Institute for Healthcare Improvement to learn the principles in their readmissions toolkit: teach-back, follow-up phone calls at 7 and 14 days, an appointment with a physician or heart failure nurse practitioner within 7 days, and medication reconciliation.
The nurse coordinators also serve as a bridge to providers in the outpatient setting, Ms. Rago said. During the second year of the program, they began making site visits to skilled nursing facilities and reaching out to primary care physicians, cardiologists, and home health agencies from outside of the hospital.
They created an e-mail group for each patient’s care team that includes physicians, nurses, home care, social work, and pharmacy, depending on the services the patient needed. An email goes out to the team at the time of admission and it provides a way to update everyone virtually in real-time about the care of the patient.
Having a closer relationship with the skilled nursing facilities has been a big help, Ms. Rago said. During one of the site visits, the nurses discovered that one of the facilities didn’t offer a low-salt diet. That helped explain why so many patients from that facility were being readmitted to the hospital and they were able to quickly address it, she said.
What physicians need to keep in mind is that while many of these solutions are common sense, there’s no one-size-fits-all approach to readmissions, said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
"It’s different in each community, so you can’t be prescriptive," he said.
The American College of Cardiology offers resources for reducing readmissions as part of a joint effort with the Institute for Healthcare Improvement called the Hospital to Home initiative.
Unlike other areas of care, such as getting a faster angioplasty, there aren’t six key steps for physicians to implement, Dr. Rumsfeld said. Instead, Hospital to Home is a place for physicians to share best practices based on their individual experiences. So far, more than 1,100 hospitals around the country have signed up.
Routine Oxygen at End of Life Typically Unhelpful
DENVER – The routine administration of oxygen to terminally ill patients who are near death is unwarranted, according to the results of a randomized, double-blind trial.
"I would suggest that we always use the patient in respiratory distress as their own control in an n-of-1 trial of oxygen. If oxygen does reduce their distress, then that patient should have oxygen, but if it does not – if there’s no change in patient distress – then that oxygen can be discontinued, or certainly not initiated in the first place," Mary L. Campbell, Ph.D., declared at the annual meeting of the American Academy of Hospice and Palliative Care Medicine.
Oxygen has well-established benefits in hypoxemic patients with acute or chronic exacerbations of an underlying pulmonary condition, but without ever having been subjected to scientific scrutiny, oxygen administration has become routine for patients who are near death, asserted Dr. Campbell of Wayne State University, Detroit.
"Oxygen has become almost an iconic intervention at the end of life – as common as golf clubs on a Wednesday afternoon," she said.
And oxygen support is not a benign intervention. It’s expensive, particularly in home care, where it requires additional personnel and materials in the home, including a noisy, intrusive concentrator at the bedside. It also causes nasal drying and nosebleeds as well as feelings of suffocation, Dr. Campbell said.
["Comfort Seldom Comes from Cannula" -- Commentary, Hospitalist News, 4/6/12]
To assess the value of routine oxygen administration, she conducted a double-blind, randomized, crossover study involving 32 terminally ill patients. None was in respiratory distress at baseline, but all were at high risk for distress because of underlying COPD, heart failure, pneumonia, or lung cancer. All participants had a Palliative Performance Scale score of 30 or less, which is associated with a median 9- to 14-day survival.
Each patient received a capnoline – that is, a nasal cannula with a piece of plastic hanging down over the patient’s mouth to capture exhaled carbon dioxide. Next, randomly alternating 10-minute intervals of oxygen, medical air, and no flow were administered for 90 minutes.
The key finding: 29 of 32 patients experienced no distress during the 90-minute protocol, indicating that they didn’t need the oxygen. Yet, at enrollment, 27 patients had oxygen flowing, reflecting this widespread clinical practice at the end of life, Dr. Campbell said.
The remaining three patients rapidly became hypoxemic and distressed when crossed over from oxygen to no flow. They were returned to baseline oxygen and respiratory comfort.
As many of the study participants were unconscious or cognitively impaired and couldn’t self report their distress, the Respiratory Distress Observation Scale was assessed at baseline and for 10 minutes after every flow change. A score of 4 or less on the 0-16 scale indicates little or no distress; the average baseline score was 1.47, and it didn’t vary significantly during the different flow conditions, she reported.
The average oxygen saturation at baseline was 93.6%, and it didn’t change significantly during the 90-minute protocol.
Dr. Campbell said that she determines the need for oxygen in an end-of-life patient by taking the patient off oxygen for 10 minutes and watching for distress.
Several audience members predicted that the patient’s family is likely to object to this approach because oxygen has become an expected part of end-of-life care. Dr. Campbell responded that the solution to that problem is simply good communication.
"I think if you explain to families that this is a treatment that can be helpful but has side effects, and we always take away the things that aren’t helping when they’re no longer helping, you won’t have pushback from family members," she said.
Dr. Campbell’s study was funded by the Blue Cross/Blue Shield of Michigan Foundation. She reported having no financial conflicts.
DENVER – The routine administration of oxygen to terminally ill patients who are near death is unwarranted, according to the results of a randomized, double-blind trial.
"I would suggest that we always use the patient in respiratory distress as their own control in an n-of-1 trial of oxygen. If oxygen does reduce their distress, then that patient should have oxygen, but if it does not – if there’s no change in patient distress – then that oxygen can be discontinued, or certainly not initiated in the first place," Mary L. Campbell, Ph.D., declared at the annual meeting of the American Academy of Hospice and Palliative Care Medicine.
Oxygen has well-established benefits in hypoxemic patients with acute or chronic exacerbations of an underlying pulmonary condition, but without ever having been subjected to scientific scrutiny, oxygen administration has become routine for patients who are near death, asserted Dr. Campbell of Wayne State University, Detroit.
"Oxygen has become almost an iconic intervention at the end of life – as common as golf clubs on a Wednesday afternoon," she said.
And oxygen support is not a benign intervention. It’s expensive, particularly in home care, where it requires additional personnel and materials in the home, including a noisy, intrusive concentrator at the bedside. It also causes nasal drying and nosebleeds as well as feelings of suffocation, Dr. Campbell said.
["Comfort Seldom Comes from Cannula" -- Commentary, Hospitalist News, 4/6/12]
To assess the value of routine oxygen administration, she conducted a double-blind, randomized, crossover study involving 32 terminally ill patients. None was in respiratory distress at baseline, but all were at high risk for distress because of underlying COPD, heart failure, pneumonia, or lung cancer. All participants had a Palliative Performance Scale score of 30 or less, which is associated with a median 9- to 14-day survival.
Each patient received a capnoline – that is, a nasal cannula with a piece of plastic hanging down over the patient’s mouth to capture exhaled carbon dioxide. Next, randomly alternating 10-minute intervals of oxygen, medical air, and no flow were administered for 90 minutes.
The key finding: 29 of 32 patients experienced no distress during the 90-minute protocol, indicating that they didn’t need the oxygen. Yet, at enrollment, 27 patients had oxygen flowing, reflecting this widespread clinical practice at the end of life, Dr. Campbell said.
The remaining three patients rapidly became hypoxemic and distressed when crossed over from oxygen to no flow. They were returned to baseline oxygen and respiratory comfort.
As many of the study participants were unconscious or cognitively impaired and couldn’t self report their distress, the Respiratory Distress Observation Scale was assessed at baseline and for 10 minutes after every flow change. A score of 4 or less on the 0-16 scale indicates little or no distress; the average baseline score was 1.47, and it didn’t vary significantly during the different flow conditions, she reported.
The average oxygen saturation at baseline was 93.6%, and it didn’t change significantly during the 90-minute protocol.
Dr. Campbell said that she determines the need for oxygen in an end-of-life patient by taking the patient off oxygen for 10 minutes and watching for distress.
Several audience members predicted that the patient’s family is likely to object to this approach because oxygen has become an expected part of end-of-life care. Dr. Campbell responded that the solution to that problem is simply good communication.
"I think if you explain to families that this is a treatment that can be helpful but has side effects, and we always take away the things that aren’t helping when they’re no longer helping, you won’t have pushback from family members," she said.
Dr. Campbell’s study was funded by the Blue Cross/Blue Shield of Michigan Foundation. She reported having no financial conflicts.
DENVER – The routine administration of oxygen to terminally ill patients who are near death is unwarranted, according to the results of a randomized, double-blind trial.
"I would suggest that we always use the patient in respiratory distress as their own control in an n-of-1 trial of oxygen. If oxygen does reduce their distress, then that patient should have oxygen, but if it does not – if there’s no change in patient distress – then that oxygen can be discontinued, or certainly not initiated in the first place," Mary L. Campbell, Ph.D., declared at the annual meeting of the American Academy of Hospice and Palliative Care Medicine.
Oxygen has well-established benefits in hypoxemic patients with acute or chronic exacerbations of an underlying pulmonary condition, but without ever having been subjected to scientific scrutiny, oxygen administration has become routine for patients who are near death, asserted Dr. Campbell of Wayne State University, Detroit.
"Oxygen has become almost an iconic intervention at the end of life – as common as golf clubs on a Wednesday afternoon," she said.
And oxygen support is not a benign intervention. It’s expensive, particularly in home care, where it requires additional personnel and materials in the home, including a noisy, intrusive concentrator at the bedside. It also causes nasal drying and nosebleeds as well as feelings of suffocation, Dr. Campbell said.
["Comfort Seldom Comes from Cannula" -- Commentary, Hospitalist News, 4/6/12]
To assess the value of routine oxygen administration, she conducted a double-blind, randomized, crossover study involving 32 terminally ill patients. None was in respiratory distress at baseline, but all were at high risk for distress because of underlying COPD, heart failure, pneumonia, or lung cancer. All participants had a Palliative Performance Scale score of 30 or less, which is associated with a median 9- to 14-day survival.
Each patient received a capnoline – that is, a nasal cannula with a piece of plastic hanging down over the patient’s mouth to capture exhaled carbon dioxide. Next, randomly alternating 10-minute intervals of oxygen, medical air, and no flow were administered for 90 minutes.
The key finding: 29 of 32 patients experienced no distress during the 90-minute protocol, indicating that they didn’t need the oxygen. Yet, at enrollment, 27 patients had oxygen flowing, reflecting this widespread clinical practice at the end of life, Dr. Campbell said.
The remaining three patients rapidly became hypoxemic and distressed when crossed over from oxygen to no flow. They were returned to baseline oxygen and respiratory comfort.
As many of the study participants were unconscious or cognitively impaired and couldn’t self report their distress, the Respiratory Distress Observation Scale was assessed at baseline and for 10 minutes after every flow change. A score of 4 or less on the 0-16 scale indicates little or no distress; the average baseline score was 1.47, and it didn’t vary significantly during the different flow conditions, she reported.
The average oxygen saturation at baseline was 93.6%, and it didn’t change significantly during the 90-minute protocol.
Dr. Campbell said that she determines the need for oxygen in an end-of-life patient by taking the patient off oxygen for 10 minutes and watching for distress.
Several audience members predicted that the patient’s family is likely to object to this approach because oxygen has become an expected part of end-of-life care. Dr. Campbell responded that the solution to that problem is simply good communication.
"I think if you explain to families that this is a treatment that can be helpful but has side effects, and we always take away the things that aren’t helping when they’re no longer helping, you won’t have pushback from family members," she said.
Dr. Campbell’s study was funded by the Blue Cross/Blue Shield of Michigan Foundation. She reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF HOSPICE AND PALLIATIVE CARE MEDICINE
Hemodialysis, Injection Drug Users Vulnerable to Recurrent Endocarditis
LONDON – Hemodialysis and injection drug use were major risk factors for recurrent episodes of infective endocarditis among patients enrolled in a large international prospective study.
Repeat infective endocarditis (IE) is a serious complication of patients who survive an initial episode. In previous studies, the incidence has ranged from 2% to 31%. "Repeat IE is associated with significant mortality. It is an uncommon complication but can be highly relevant among specific groups of patients," Dr. Laura Alagna of San Raffaele Hospital, Milan, said at the European Congress of Clinical Microbiology and Infectious Diseases.
The findings come from The International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS), a contemporary cohort of more than 5,000 patients with infective endocarditis (IE) from 64 centers in 28 countries worldwide. Patients included in the current analysis were those enrolled from June 2000 to December 2006, with a diagnosis of definite IE on native or prosthetic valves who had at least a 1-year follow-up.
Of 1,857 patients who met inclusion criteria, 1,783 had one episode of IE and 91 (5%) had a repeat IE. Of those, 17 had a presumed relapse, defined clinically as infection with the same pathogen isolated within 6 months of the initial episode. The other 74 had a presumed new infection, defined clinically as a repeat episode with a different pathogen or the same pathogen isolated greater than 6 months from the initial episode.
On bivariate analysis, being from North America, infection with Staphylococcus aureus, hemodialysis dependence, intravenous drug use (IDU), HIV infection, history of previous IE, and non-nosocomial health care as a presumed source of infection were all associated with repeat IE. However, on multivariate analysis, only four independent risk factors emerged: North American location (odds ratio, 1.96), hemodialysis (OR, 2.54), IDU (OR, 2.89), and history of previous IE (2.76).
At 1-year follow-up, survival was significantly lower for those with repeat IE, 80% compared to 91% for those with only one episode (P = .0034), Dr. Alagna reported.
Molecular analysis with pulsed-gel electrophoresis performed in 12 of the repeat IE patients demonstrated concordance with the clinical definition in 10, including eight confirmed relapses and two confirmed new infections. Of the other two patients, one had S. aureus with the same molecular pattern isolated more than a year after the first episode. That patient was hemodialysis-dependent and had other risk factors. In the other discordant patient, S. bovis with the same molecular pattern was isolated after nearly 9 months. In that patient, a cardiac device had not been removed during the first episode, she explained.
"The clinical classification of repeat IE is satisfactory, but can be improved with molecular analysis," she concluded.
Dr. Alagna stated that she had no disclosures.
LONDON – Hemodialysis and injection drug use were major risk factors for recurrent episodes of infective endocarditis among patients enrolled in a large international prospective study.
Repeat infective endocarditis (IE) is a serious complication of patients who survive an initial episode. In previous studies, the incidence has ranged from 2% to 31%. "Repeat IE is associated with significant mortality. It is an uncommon complication but can be highly relevant among specific groups of patients," Dr. Laura Alagna of San Raffaele Hospital, Milan, said at the European Congress of Clinical Microbiology and Infectious Diseases.
The findings come from The International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS), a contemporary cohort of more than 5,000 patients with infective endocarditis (IE) from 64 centers in 28 countries worldwide. Patients included in the current analysis were those enrolled from June 2000 to December 2006, with a diagnosis of definite IE on native or prosthetic valves who had at least a 1-year follow-up.
Of 1,857 patients who met inclusion criteria, 1,783 had one episode of IE and 91 (5%) had a repeat IE. Of those, 17 had a presumed relapse, defined clinically as infection with the same pathogen isolated within 6 months of the initial episode. The other 74 had a presumed new infection, defined clinically as a repeat episode with a different pathogen or the same pathogen isolated greater than 6 months from the initial episode.
On bivariate analysis, being from North America, infection with Staphylococcus aureus, hemodialysis dependence, intravenous drug use (IDU), HIV infection, history of previous IE, and non-nosocomial health care as a presumed source of infection were all associated with repeat IE. However, on multivariate analysis, only four independent risk factors emerged: North American location (odds ratio, 1.96), hemodialysis (OR, 2.54), IDU (OR, 2.89), and history of previous IE (2.76).
At 1-year follow-up, survival was significantly lower for those with repeat IE, 80% compared to 91% for those with only one episode (P = .0034), Dr. Alagna reported.
Molecular analysis with pulsed-gel electrophoresis performed in 12 of the repeat IE patients demonstrated concordance with the clinical definition in 10, including eight confirmed relapses and two confirmed new infections. Of the other two patients, one had S. aureus with the same molecular pattern isolated more than a year after the first episode. That patient was hemodialysis-dependent and had other risk factors. In the other discordant patient, S. bovis with the same molecular pattern was isolated after nearly 9 months. In that patient, a cardiac device had not been removed during the first episode, she explained.
"The clinical classification of repeat IE is satisfactory, but can be improved with molecular analysis," she concluded.
Dr. Alagna stated that she had no disclosures.
LONDON – Hemodialysis and injection drug use were major risk factors for recurrent episodes of infective endocarditis among patients enrolled in a large international prospective study.
Repeat infective endocarditis (IE) is a serious complication of patients who survive an initial episode. In previous studies, the incidence has ranged from 2% to 31%. "Repeat IE is associated with significant mortality. It is an uncommon complication but can be highly relevant among specific groups of patients," Dr. Laura Alagna of San Raffaele Hospital, Milan, said at the European Congress of Clinical Microbiology and Infectious Diseases.
The findings come from The International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS), a contemporary cohort of more than 5,000 patients with infective endocarditis (IE) from 64 centers in 28 countries worldwide. Patients included in the current analysis were those enrolled from June 2000 to December 2006, with a diagnosis of definite IE on native or prosthetic valves who had at least a 1-year follow-up.
Of 1,857 patients who met inclusion criteria, 1,783 had one episode of IE and 91 (5%) had a repeat IE. Of those, 17 had a presumed relapse, defined clinically as infection with the same pathogen isolated within 6 months of the initial episode. The other 74 had a presumed new infection, defined clinically as a repeat episode with a different pathogen or the same pathogen isolated greater than 6 months from the initial episode.
On bivariate analysis, being from North America, infection with Staphylococcus aureus, hemodialysis dependence, intravenous drug use (IDU), HIV infection, history of previous IE, and non-nosocomial health care as a presumed source of infection were all associated with repeat IE. However, on multivariate analysis, only four independent risk factors emerged: North American location (odds ratio, 1.96), hemodialysis (OR, 2.54), IDU (OR, 2.89), and history of previous IE (2.76).
At 1-year follow-up, survival was significantly lower for those with repeat IE, 80% compared to 91% for those with only one episode (P = .0034), Dr. Alagna reported.
Molecular analysis with pulsed-gel electrophoresis performed in 12 of the repeat IE patients demonstrated concordance with the clinical definition in 10, including eight confirmed relapses and two confirmed new infections. Of the other two patients, one had S. aureus with the same molecular pattern isolated more than a year after the first episode. That patient was hemodialysis-dependent and had other risk factors. In the other discordant patient, S. bovis with the same molecular pattern was isolated after nearly 9 months. In that patient, a cardiac device had not been removed during the first episode, she explained.
"The clinical classification of repeat IE is satisfactory, but can be improved with molecular analysis," she concluded.
Dr. Alagna stated that she had no disclosures.
FROM THE EUROPEAN CONGRESS OF CLINICAL MICROBIOLOGY AND INFECTIOUS DISEASES
Major Finding: On multivariate analysis, independent risk factors for repeat infective endocarditis were North American location (odds ratio, 1.96), hemodialysis (OR, 2.54), IDU (OR, 2.89), and history of previous IE (2.76).
Data Source: The findings come from The International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS), a contemporary cohort of more than 5,000 patients with infective endocarditis (IE) from 64 centers in 28 countries worldwide. Patients included in the current analysis were those enrolled from June 2000 to December 2006, with a diagnosis of definite IE on native or prosthetic valves who had at least a 1-year follow-up.
Disclosures: Dr. Alagna stated that she had no disclosures.
Benzodiazepines Improve Dyspnea in Palliative Care Patients
DENVER – Low-dose adjunctive benzodiazepines are effective in combination with opioids for dyspnea in palliative care patients who don’t respond to opioids alone, according to Dr. Patama Gomutbutra.
When opioids alone aren’t bringing significant improvement, adding a benzodiazepine is worthwhile, she said. The question of whether benzodiazepines alone are effective in the management of dyspnea must await answers from randomized clinical trials.
Dr. Gomutbutra conducted a retrospective chart review of 303 inpatients with dyspnea evaluated by members of the University of California, San Francisco, palliative care program. These were seriously ill patients: Twenty-three percent had primary lung cancer, 32% had cancer outside the lung, 12% had heart failure, and 7% had chronic obstructive pulmonary disease. Of these patients, 47% died in the hospital and 25% were discharged to hospice.
At baseline, physicians rated dyspnea as severe in 19% of patients, moderate in 28%, and mild in 53%. At baseline, 49% of patients were already on opioids at a median dose of 52 mg/day; 87% of these patients remained on opioids at 24 hours, with a bump up in dose to a median of 60 mg/day. Of the patients not initially taking an opioid, 41% were placed on the medication at a median dose of 22 mg/day.
"Our results should not dissuade people from using opioids as the first-line treatment."
At baseline, 17% of patients were on a benzodiazepine at a median dose of 1 mg/day of oral lorazepam or its equivalent. At 24 hours, 24% of patients were on a benzodiazepine, again at a median daily dose of 1 mg.
At follow-up 24 hours after adjustment of dosages or addition of an opioid or a benzodiazepine, the population with severe dyspnea had fallen from 19% to 4%. Dyspnea was rated moderate in 18% and mild in 44%, and was absent in 34%.
Overall, 57% of patients had a clinically meaningful improvement in dyspnea of one severity grade or more, 37% remained the same, and the rest became worse, according to Dr. Gomutbutra of Chiang Mai (Thailand) University.
Taking an opioid and a benzodiazepine at follow-up was independently associated with a 2.1-fold increased likelihood of significant improvement in dyspnea. Having moderate or severe dyspnea at baseline was associated with 4.1- and 4.5-fold increased likelihoods of improvement, respectively.
Surprisingly, being on an opioid at baseline wasn’t associated with significant improvement at follow-up, even though opioids are guideline-recommended therapy for dyspnea.
Dr. Gomutbutra cautioned against overinterpretation of this finding, given that her study was retrospective and thus vulnerable to confounding. For example, she noted, the respiratory rate typically slows near death, so affected patients may not have received continued or increased doses of opioids.
"Our results should not dissuade people from using opioids as the first-line treatment," Dr. Gomutbutra emphasized.
Dr. Gomutbutra carried out this study after observing big differences in how dyspnea is managed in palliative care settings in the United States, compared with Thailand. While the median daily dose of opioids at baseline in the San Francisco study was 52 mg/day, a typical dose in Thailand would be 6 mg/day. And benzodiazepines are far more widely used in treating dyspnea there, she added.
She reported having no financial conflicts.
DENVER – Low-dose adjunctive benzodiazepines are effective in combination with opioids for dyspnea in palliative care patients who don’t respond to opioids alone, according to Dr. Patama Gomutbutra.
When opioids alone aren’t bringing significant improvement, adding a benzodiazepine is worthwhile, she said. The question of whether benzodiazepines alone are effective in the management of dyspnea must await answers from randomized clinical trials.
Dr. Gomutbutra conducted a retrospective chart review of 303 inpatients with dyspnea evaluated by members of the University of California, San Francisco, palliative care program. These were seriously ill patients: Twenty-three percent had primary lung cancer, 32% had cancer outside the lung, 12% had heart failure, and 7% had chronic obstructive pulmonary disease. Of these patients, 47% died in the hospital and 25% were discharged to hospice.
At baseline, physicians rated dyspnea as severe in 19% of patients, moderate in 28%, and mild in 53%. At baseline, 49% of patients were already on opioids at a median dose of 52 mg/day; 87% of these patients remained on opioids at 24 hours, with a bump up in dose to a median of 60 mg/day. Of the patients not initially taking an opioid, 41% were placed on the medication at a median dose of 22 mg/day.
"Our results should not dissuade people from using opioids as the first-line treatment."
At baseline, 17% of patients were on a benzodiazepine at a median dose of 1 mg/day of oral lorazepam or its equivalent. At 24 hours, 24% of patients were on a benzodiazepine, again at a median daily dose of 1 mg.
At follow-up 24 hours after adjustment of dosages or addition of an opioid or a benzodiazepine, the population with severe dyspnea had fallen from 19% to 4%. Dyspnea was rated moderate in 18% and mild in 44%, and was absent in 34%.
Overall, 57% of patients had a clinically meaningful improvement in dyspnea of one severity grade or more, 37% remained the same, and the rest became worse, according to Dr. Gomutbutra of Chiang Mai (Thailand) University.
Taking an opioid and a benzodiazepine at follow-up was independently associated with a 2.1-fold increased likelihood of significant improvement in dyspnea. Having moderate or severe dyspnea at baseline was associated with 4.1- and 4.5-fold increased likelihoods of improvement, respectively.
Surprisingly, being on an opioid at baseline wasn’t associated with significant improvement at follow-up, even though opioids are guideline-recommended therapy for dyspnea.
Dr. Gomutbutra cautioned against overinterpretation of this finding, given that her study was retrospective and thus vulnerable to confounding. For example, she noted, the respiratory rate typically slows near death, so affected patients may not have received continued or increased doses of opioids.
"Our results should not dissuade people from using opioids as the first-line treatment," Dr. Gomutbutra emphasized.
Dr. Gomutbutra carried out this study after observing big differences in how dyspnea is managed in palliative care settings in the United States, compared with Thailand. While the median daily dose of opioids at baseline in the San Francisco study was 52 mg/day, a typical dose in Thailand would be 6 mg/day. And benzodiazepines are far more widely used in treating dyspnea there, she added.
She reported having no financial conflicts.
DENVER – Low-dose adjunctive benzodiazepines are effective in combination with opioids for dyspnea in palliative care patients who don’t respond to opioids alone, according to Dr. Patama Gomutbutra.
When opioids alone aren’t bringing significant improvement, adding a benzodiazepine is worthwhile, she said. The question of whether benzodiazepines alone are effective in the management of dyspnea must await answers from randomized clinical trials.
Dr. Gomutbutra conducted a retrospective chart review of 303 inpatients with dyspnea evaluated by members of the University of California, San Francisco, palliative care program. These were seriously ill patients: Twenty-three percent had primary lung cancer, 32% had cancer outside the lung, 12% had heart failure, and 7% had chronic obstructive pulmonary disease. Of these patients, 47% died in the hospital and 25% were discharged to hospice.
At baseline, physicians rated dyspnea as severe in 19% of patients, moderate in 28%, and mild in 53%. At baseline, 49% of patients were already on opioids at a median dose of 52 mg/day; 87% of these patients remained on opioids at 24 hours, with a bump up in dose to a median of 60 mg/day. Of the patients not initially taking an opioid, 41% were placed on the medication at a median dose of 22 mg/day.
"Our results should not dissuade people from using opioids as the first-line treatment."
At baseline, 17% of patients were on a benzodiazepine at a median dose of 1 mg/day of oral lorazepam or its equivalent. At 24 hours, 24% of patients were on a benzodiazepine, again at a median daily dose of 1 mg.
At follow-up 24 hours after adjustment of dosages or addition of an opioid or a benzodiazepine, the population with severe dyspnea had fallen from 19% to 4%. Dyspnea was rated moderate in 18% and mild in 44%, and was absent in 34%.
Overall, 57% of patients had a clinically meaningful improvement in dyspnea of one severity grade or more, 37% remained the same, and the rest became worse, according to Dr. Gomutbutra of Chiang Mai (Thailand) University.
Taking an opioid and a benzodiazepine at follow-up was independently associated with a 2.1-fold increased likelihood of significant improvement in dyspnea. Having moderate or severe dyspnea at baseline was associated with 4.1- and 4.5-fold increased likelihoods of improvement, respectively.
Surprisingly, being on an opioid at baseline wasn’t associated with significant improvement at follow-up, even though opioids are guideline-recommended therapy for dyspnea.
Dr. Gomutbutra cautioned against overinterpretation of this finding, given that her study was retrospective and thus vulnerable to confounding. For example, she noted, the respiratory rate typically slows near death, so affected patients may not have received continued or increased doses of opioids.
"Our results should not dissuade people from using opioids as the first-line treatment," Dr. Gomutbutra emphasized.
Dr. Gomutbutra carried out this study after observing big differences in how dyspnea is managed in palliative care settings in the United States, compared with Thailand. While the median daily dose of opioids at baseline in the San Francisco study was 52 mg/day, a typical dose in Thailand would be 6 mg/day. And benzodiazepines are far more widely used in treating dyspnea there, she added.
She reported having no financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF HOSPICE AND PALLIATIVE CARE MEDICINE
Major Finding: At follow-up 24 hours after adjustment of dosages or addition of an opioid or a benzodiazepine, the population with severe dyspnea had fallen from 19% to 4%. Dyspnea was rated moderate in 18% and mild in 44%, and was absent in 34%.
Data Source: Data were taken from a retrospective chart review of 303 inpatients with dyspnea evaluated by members of the University of California, San Francisco, palliative care program.
Disclosures: Dr. Gomutbutra reported having no financial conflicts.