User login
Low intensity bridging may be best path to CAR T in adult ALL
CHICAGO – A low intensity chemotherapy regimen may be the best approach to bridge patients waiting for chimeric antigen receptor (CAR) T-cell therapy, according to a retrospective analysis of adults with acute lymphoblastic leukemia (ALL).
Investigators found that high intensity bridging regimens provided no clear outcome benefit, but did produce a greater number of infections.
But the decision on the type of regimen is very much dependent on the individual patient, Karlo Perica, MD, PhD, of Memorial Sloan Kettering Cancer Center in New York, said at the annual meeting of the American Society of Clinical Oncology.
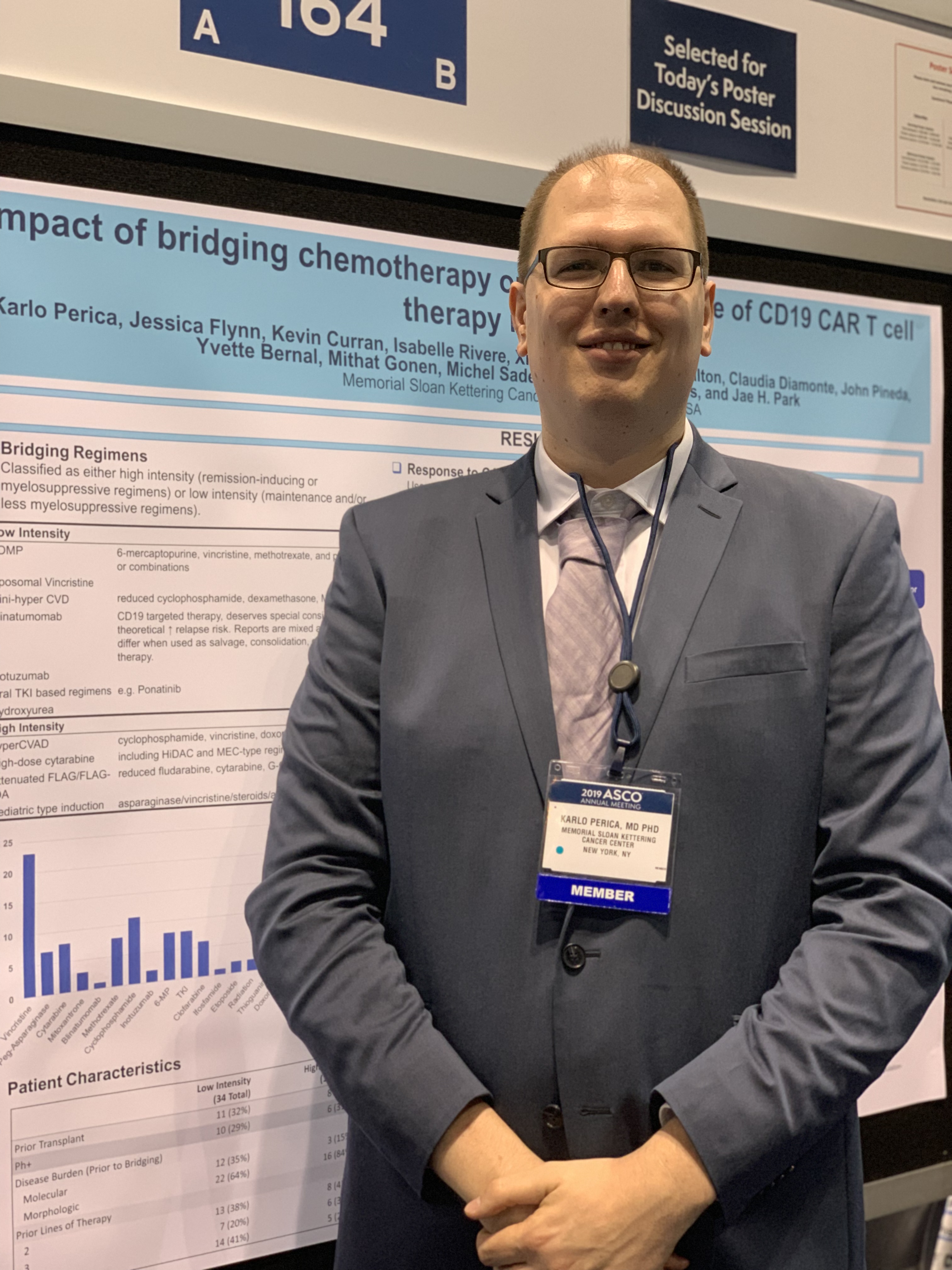
Dr. Perica and his colleagues at Memorial Sloan Kettering examined the effectiveness and toxicity of bridging therapies provided to relapsed or refractory ALL patients waiting to receive CD19 CAR T-cell therapy as part of a phase 1 trial (N Engl J Med. 2018 Feb 1;378[5]:449-59).
Bridging therapy was defined as any therapy given from leukapheresis to cell infusion.
The low-intensity regimens included POMP (6-mercaptopurine, vincristine, methotrexate, and prednisone, or combinations), liposomal vincristine, mini-hyper CVD (reduced cyclophosphamide, dexamethasone, methotrexate, Ara-C), blinatumomab, inotuzumab, oral tyrosine kinase inhibitor-based regimens, or hydroxyurea.
The high-intensity regimens included hyper-CVAD (cyclophosphamide, vincristine, doxorubicin, dexamethasone), high-dose cytarabine, attenuated FLAG/FLAG-IDA (reduced fludarabine, cytarabine, G-CSF plus or minus idarubicin), and pediatric-type induction.
Of the 53 patients who were ultimately infused with CAR T cells, 19 received some type of high intensity regimen, 29 received low intensity regimens, and 5 received no bridging treatment. The group overall was heavily pretreated. Nearly a third of the low intensity and no bridging patients and 42% of the high intensity patients had previously undergone transplant. More than 40% of the low intensity and no bridging patients and about a quarter of the high intensity bridging group had four or more prior lines of therapy.
The use of high intensity bridging therapy was not associated with improved overall response or relapse-free survival to CAR T-cell therapy, the investigators reported. In a subgroup with 23 high disease burden patients with greater than 20% blasts, there was no difference in MRD-negative complete response by intensity (75% versus 60%, Fisher’s P = .65).
High intensity bridging was also not associated with successful CAR T-cell infusion, versus low intensity regimens (63% versus 79%, P greater than .05) or a combined endpoint of CAR T-cell infusion plus transplant or alternative treatment (80% versus 86%, P greater than .05).
In terms of toxicity, the high intensity bridging regimens were associated with a higher rate of grade 3 or 4 infections – 15 versus 11 infections (Fisher’s P = .002). But there was no association with post-infusion grade 3 or 4 cytokine release syndrome or neurotoxicity.
Dr. Perica said the results reflect that the real goal of bridging is not to reduce disease burden but instead to successfully bring patients to the next phase of their treatment. “The goal of the bridging therapy is to get the patient to the CAR infusion,” he said.
Due to the retrospective nature of the study, Dr. Perica said he can’t recommend any single bridging regimen and he emphasized that the decisions are patient-specific.
The original study was funded by several foundations and Juno Therapeutics. Dr. Perica reported royalties from technology licensed to Neximmune.
SOURCE: Perica K et al. ASCO 2019, Abstract 2520.
CHICAGO – A low intensity chemotherapy regimen may be the best approach to bridge patients waiting for chimeric antigen receptor (CAR) T-cell therapy, according to a retrospective analysis of adults with acute lymphoblastic leukemia (ALL).
Investigators found that high intensity bridging regimens provided no clear outcome benefit, but did produce a greater number of infections.
But the decision on the type of regimen is very much dependent on the individual patient, Karlo Perica, MD, PhD, of Memorial Sloan Kettering Cancer Center in New York, said at the annual meeting of the American Society of Clinical Oncology.
Dr. Perica and his colleagues at Memorial Sloan Kettering examined the effectiveness and toxicity of bridging therapies provided to relapsed or refractory ALL patients waiting to receive CD19 CAR T-cell therapy as part of a phase 1 trial (N Engl J Med. 2018 Feb 1;378[5]:449-59).
Bridging therapy was defined as any therapy given from leukapheresis to cell infusion.
The low-intensity regimens included POMP (6-mercaptopurine, vincristine, methotrexate, and prednisone, or combinations), liposomal vincristine, mini-hyper CVD (reduced cyclophosphamide, dexamethasone, methotrexate, Ara-C), blinatumomab, inotuzumab, oral tyrosine kinase inhibitor-based regimens, or hydroxyurea.
The high-intensity regimens included hyper-CVAD (cyclophosphamide, vincristine, doxorubicin, dexamethasone), high-dose cytarabine, attenuated FLAG/FLAG-IDA (reduced fludarabine, cytarabine, G-CSF plus or minus idarubicin), and pediatric-type induction.
Of the 53 patients who were ultimately infused with CAR T cells, 19 received some type of high intensity regimen, 29 received low intensity regimens, and 5 received no bridging treatment. The group overall was heavily pretreated. Nearly a third of the low intensity and no bridging patients and 42% of the high intensity patients had previously undergone transplant. More than 40% of the low intensity and no bridging patients and about a quarter of the high intensity bridging group had four or more prior lines of therapy.
The use of high intensity bridging therapy was not associated with improved overall response or relapse-free survival to CAR T-cell therapy, the investigators reported. In a subgroup with 23 high disease burden patients with greater than 20% blasts, there was no difference in MRD-negative complete response by intensity (75% versus 60%, Fisher’s P = .65).
High intensity bridging was also not associated with successful CAR T-cell infusion, versus low intensity regimens (63% versus 79%, P greater than .05) or a combined endpoint of CAR T-cell infusion plus transplant or alternative treatment (80% versus 86%, P greater than .05).
In terms of toxicity, the high intensity bridging regimens were associated with a higher rate of grade 3 or 4 infections – 15 versus 11 infections (Fisher’s P = .002). But there was no association with post-infusion grade 3 or 4 cytokine release syndrome or neurotoxicity.
Dr. Perica said the results reflect that the real goal of bridging is not to reduce disease burden but instead to successfully bring patients to the next phase of their treatment. “The goal of the bridging therapy is to get the patient to the CAR infusion,” he said.
Due to the retrospective nature of the study, Dr. Perica said he can’t recommend any single bridging regimen and he emphasized that the decisions are patient-specific.
The original study was funded by several foundations and Juno Therapeutics. Dr. Perica reported royalties from technology licensed to Neximmune.
SOURCE: Perica K et al. ASCO 2019, Abstract 2520.
CHICAGO – A low intensity chemotherapy regimen may be the best approach to bridge patients waiting for chimeric antigen receptor (CAR) T-cell therapy, according to a retrospective analysis of adults with acute lymphoblastic leukemia (ALL).
Investigators found that high intensity bridging regimens provided no clear outcome benefit, but did produce a greater number of infections.
But the decision on the type of regimen is very much dependent on the individual patient, Karlo Perica, MD, PhD, of Memorial Sloan Kettering Cancer Center in New York, said at the annual meeting of the American Society of Clinical Oncology.
Dr. Perica and his colleagues at Memorial Sloan Kettering examined the effectiveness and toxicity of bridging therapies provided to relapsed or refractory ALL patients waiting to receive CD19 CAR T-cell therapy as part of a phase 1 trial (N Engl J Med. 2018 Feb 1;378[5]:449-59).
Bridging therapy was defined as any therapy given from leukapheresis to cell infusion.
The low-intensity regimens included POMP (6-mercaptopurine, vincristine, methotrexate, and prednisone, or combinations), liposomal vincristine, mini-hyper CVD (reduced cyclophosphamide, dexamethasone, methotrexate, Ara-C), blinatumomab, inotuzumab, oral tyrosine kinase inhibitor-based regimens, or hydroxyurea.
The high-intensity regimens included hyper-CVAD (cyclophosphamide, vincristine, doxorubicin, dexamethasone), high-dose cytarabine, attenuated FLAG/FLAG-IDA (reduced fludarabine, cytarabine, G-CSF plus or minus idarubicin), and pediatric-type induction.
Of the 53 patients who were ultimately infused with CAR T cells, 19 received some type of high intensity regimen, 29 received low intensity regimens, and 5 received no bridging treatment. The group overall was heavily pretreated. Nearly a third of the low intensity and no bridging patients and 42% of the high intensity patients had previously undergone transplant. More than 40% of the low intensity and no bridging patients and about a quarter of the high intensity bridging group had four or more prior lines of therapy.
The use of high intensity bridging therapy was not associated with improved overall response or relapse-free survival to CAR T-cell therapy, the investigators reported. In a subgroup with 23 high disease burden patients with greater than 20% blasts, there was no difference in MRD-negative complete response by intensity (75% versus 60%, Fisher’s P = .65).
High intensity bridging was also not associated with successful CAR T-cell infusion, versus low intensity regimens (63% versus 79%, P greater than .05) or a combined endpoint of CAR T-cell infusion plus transplant or alternative treatment (80% versus 86%, P greater than .05).
In terms of toxicity, the high intensity bridging regimens were associated with a higher rate of grade 3 or 4 infections – 15 versus 11 infections (Fisher’s P = .002). But there was no association with post-infusion grade 3 or 4 cytokine release syndrome or neurotoxicity.
Dr. Perica said the results reflect that the real goal of bridging is not to reduce disease burden but instead to successfully bring patients to the next phase of their treatment. “The goal of the bridging therapy is to get the patient to the CAR infusion,” he said.
Due to the retrospective nature of the study, Dr. Perica said he can’t recommend any single bridging regimen and he emphasized that the decisions are patient-specific.
The original study was funded by several foundations and Juno Therapeutics. Dr. Perica reported royalties from technology licensed to Neximmune.
SOURCE: Perica K et al. ASCO 2019, Abstract 2520.
FROM ASCO 2019
Ribociclib plus endocrine therapy boosts survival of HR+/HER2- breast cancer
CHICAGO – Adding ribociclib to endocrine therapy significantly improved overall survival of premenopausal women with advanced hormone receptor positive, HER2-negative breast cancer, results of the randomized phase 3 MONALEESA-7 trial showed.
A landmark analysis performed at 42 months of follow-up showed that the overall survival (OS) rate for women randomized to receive endocrine therapy with either a nonsteroidal aromatase inhibitor (AI) or tamoxifen plus the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor ribociclib (Kisqali) was 70%, compared with 46% for women randomized to endocrine therapy plus placebo.
The trial is the first study to evaluate a CDK4/6 inhibitor exclusively in premenopausal women, and the first to show a statistically significant improvement in overall survival with a CDK4/6 inhibitor in combination with endocrine therapy in patients with HR-positive, HER2-negative advanced breast cancer.
In a video interview at the American Society of Clinical Oncology annual meeting, Sara A. Hurvitz, MD, from the University of California Los Angeles Jonsson Comprehensive Cancer Center, describes the significance of the MONALEESA-7 findings and the potential for improving on the study results with other agents or combinations.
The MONALEESA-7 trial is supported by Novartis. Dr. Hurvitz reported travel and accommodation expenses from Novartis.
CHICAGO – Adding ribociclib to endocrine therapy significantly improved overall survival of premenopausal women with advanced hormone receptor positive, HER2-negative breast cancer, results of the randomized phase 3 MONALEESA-7 trial showed.
A landmark analysis performed at 42 months of follow-up showed that the overall survival (OS) rate for women randomized to receive endocrine therapy with either a nonsteroidal aromatase inhibitor (AI) or tamoxifen plus the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor ribociclib (Kisqali) was 70%, compared with 46% for women randomized to endocrine therapy plus placebo.
The trial is the first study to evaluate a CDK4/6 inhibitor exclusively in premenopausal women, and the first to show a statistically significant improvement in overall survival with a CDK4/6 inhibitor in combination with endocrine therapy in patients with HR-positive, HER2-negative advanced breast cancer.
In a video interview at the American Society of Clinical Oncology annual meeting, Sara A. Hurvitz, MD, from the University of California Los Angeles Jonsson Comprehensive Cancer Center, describes the significance of the MONALEESA-7 findings and the potential for improving on the study results with other agents or combinations.
The MONALEESA-7 trial is supported by Novartis. Dr. Hurvitz reported travel and accommodation expenses from Novartis.
CHICAGO – Adding ribociclib to endocrine therapy significantly improved overall survival of premenopausal women with advanced hormone receptor positive, HER2-negative breast cancer, results of the randomized phase 3 MONALEESA-7 trial showed.
A landmark analysis performed at 42 months of follow-up showed that the overall survival (OS) rate for women randomized to receive endocrine therapy with either a nonsteroidal aromatase inhibitor (AI) or tamoxifen plus the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor ribociclib (Kisqali) was 70%, compared with 46% for women randomized to endocrine therapy plus placebo.
The trial is the first study to evaluate a CDK4/6 inhibitor exclusively in premenopausal women, and the first to show a statistically significant improvement in overall survival with a CDK4/6 inhibitor in combination with endocrine therapy in patients with HR-positive, HER2-negative advanced breast cancer.
In a video interview at the American Society of Clinical Oncology annual meeting, Sara A. Hurvitz, MD, from the University of California Los Angeles Jonsson Comprehensive Cancer Center, describes the significance of the MONALEESA-7 findings and the potential for improving on the study results with other agents or combinations.
The MONALEESA-7 trial is supported by Novartis. Dr. Hurvitz reported travel and accommodation expenses from Novartis.
REPORTING FROM ASCO 2019

Impetigo: Addressing Treatment Challenges and Burden of Disease

Over the past few decades there has been a shift in the bacteriology and resistance patterns associated with impetigo, making it difficult to identify the best treatment choice for this common bacterial skin infection. In this supplement to Dermatology News, Adelaide A. Hebert, MD and Linda F. Stein Gold, MD, review the current impetigo treatment landscape and the growing concern over methicillin-resistant S. aureus (MRSA).
Over the past few decades there has been a shift in the bacteriology and resistance patterns associated with impetigo, making it difficult to identify the best treatment choice for this common bacterial skin infection. In this supplement to Dermatology News, Adelaide A. Hebert, MD and Linda F. Stein Gold, MD, review the current impetigo treatment landscape and the growing concern over methicillin-resistant S. aureus (MRSA).
Over the past few decades there has been a shift in the bacteriology and resistance patterns associated with impetigo, making it difficult to identify the best treatment choice for this common bacterial skin infection. In this supplement to Dermatology News, Adelaide A. Hebert, MD and Linda F. Stein Gold, MD, review the current impetigo treatment landscape and the growing concern over methicillin-resistant S. aureus (MRSA).

Pembro with or without chemo superior to EXTREME for advanced HNSCC
CHICAGO – Pembrolizumab with and without chemotherapy proved superior for overall survival compared with the EXTREME regimen when used first line in certain subgroups of patients with recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC), according to “practice-changing” final results from the randomized phase 3 KEYNOTE-048 study.
Compared with 300 patients randomized to receive the EXTREME regimen (a certuximab loading dose followed by carboplatin or cisplatin and 5-fluorouracil), 281 who received pembrolizumab plus chemotherapy (P+C) had superior overall survival (OS) with comparable safety–including both those with programmed death-Ligand 1 (PD-L1) combined positive score (CPS) of 20 or greater (median 14.7 vs 11.0 months; hazard ratio, 0.60) and with CPS of 1 or greater (median, 13.6 vs. 10.4 months; HR, 0.65), Danny Rischin, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The differences were highly statistically significant, said Dr. Rischin, a professor and director of the Division of Cancer Medicine and head of the Department of Medical Oncology at Peter MacCallum Cancer Centre, Melbourne, Australia.
“And this benefit in overall survival in CPS greater than or equal to 20 and greater than or equal to 1 appeared to be present across all the subgroups that we looked at,” he added.
The response rates did not differ between P+C and EXTREME groups, but the median duration of response was significantly greater with P+C vs. EXTREME in both the CPS of 20 or greater and 1 or greater (7.1 vs. 4.2 months and 6.7 vs. 4.3 months, respectively).
Additionally, the final results of the study showed an OS benefit with P+C vs. EXTREME in the total population (13.0 vs. 10.7 months; HR, 0.72), Dr. Rischin said.
The difference between the groups with respect to progression-free survival (PFS), however, was not statistically significant and did not reach the superiority threshold, he noted.
In the 301 patients who received pembrolizumab alone, OS was superior in the CPS 20 or greater and 1 or greater populations (median, 14.8 vs. 10.7 months; HR, 0.58 and 12.4 vs. 10.3 months; HR, 0.74, respectively), compared with EXTREME, but was noninferior in the total population (median 11.5 vs. 10.7 months; HR, 0.83), and safety was favorable .
Again, PFS did not differ between the groups (median, 2.3 vs. 5.2 months; HR, 1.34), and while the overall response rates did not differ significantly, the median duration of response was substantially longer with pembrolizumab at 22.6 vs. 4.5 months with EXTREME, he said.
Study participants had locally incurable R/M HNSCC and no prior systemic therapy in the R/M setting. Those in he P+C arm received pembrolizumab at 200 mg plus 6 cycles of cisplatin at 100 mg/m2 or carboplatin AUC 5, and 5-fluorouracil at a dose of 1000 mg/m2/day for 4 days every 3 weeks; those in the pembrolizumab alone arm received 200 mg every 3 weeks for up to 35 cycles, and those in the EXTREME arm received certuximab at a 400 mg/m2 loading dose followed by 250 mg/m2 weekly with carboplatin AUC 5 or cisplatin at 100 mg/m2, and 5-FU at 1000 mg/m2/day for 4 days for 6 cycles.
“The data from KEYNOTE-048 support pembrolizumab plus platinum-based chemotherapy and pembrolizumab monotherapy as new standard of care monotherapies for recurrent/metastatic head and neck squamous cell carcinoma,” he concluded.
Discussant Vanita Noronha, MD, a professor in the Department of Medical Oncology at Tata Memorial Hospital in Mumbai, India, said that while the findings are practice changing, they also raise a number of questions, such as which patients should get pembrolizumab and which should get P+C, why there is a differential effect of pembrolizumab based on PD-L1 by CPS–and what about those with CPS of 0 or 1-20, and why the response rates and PFS rates were not improved in the pembrolizumab groups.
Other important questions include whether there are predictive biomarkers for response, and whether sequential therapy would be of benefit, she added.
While these and other questions remain to be addressed, the KEYNOTE-048 findings have implications for practice going forward; based on the current data, her approach to treating patients with R/M HNSCC not amenable to radical therapy is to treat with pembrolizumab alone in those with disease-free interval of 6 months or less, she said.
For those with disease-free interval greater than 6 months and good performance status who have controlled comorbidities, are platinum eligible, and for whom the treatment is reimbursable/affordable, treatment depends on symptom severity; she would treat those with mild/moderate symptoms and CPS of 20 or greater with pembrolizumab alone, those with CPS of 1 or greater with P+C or pembrolizumab alone, and those with CPS of 0 or unknown CPS with EXTREME or a similar regimen or with P+C, and she would treat those with severe symptoms with P+C.
“If the patient were a bit borderline, had multiple comorbidities, could not receive platinum, or had financial constraints, I would treat the patient with singe-agent intravenous chemotherapy or with oral metronomic chemotherapy, single-agent targeted therapy or with best supportive care,” she said.
Dr. Rischin has received research funding from Amgen, Bristol-Myers Squibb, Genentech/Roche, GSK, Merck, and Regeneron. Dr. Noronha has received research funding (to her institution) from Amgen,and Sanofi Aventis.
SOURCE: D Rischin et al., ASCO 2019: Abstract 6000.
CHICAGO – Pembrolizumab with and without chemotherapy proved superior for overall survival compared with the EXTREME regimen when used first line in certain subgroups of patients with recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC), according to “practice-changing” final results from the randomized phase 3 KEYNOTE-048 study.
Compared with 300 patients randomized to receive the EXTREME regimen (a certuximab loading dose followed by carboplatin or cisplatin and 5-fluorouracil), 281 who received pembrolizumab plus chemotherapy (P+C) had superior overall survival (OS) with comparable safety–including both those with programmed death-Ligand 1 (PD-L1) combined positive score (CPS) of 20 or greater (median 14.7 vs 11.0 months; hazard ratio, 0.60) and with CPS of 1 or greater (median, 13.6 vs. 10.4 months; HR, 0.65), Danny Rischin, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The differences were highly statistically significant, said Dr. Rischin, a professor and director of the Division of Cancer Medicine and head of the Department of Medical Oncology at Peter MacCallum Cancer Centre, Melbourne, Australia.
“And this benefit in overall survival in CPS greater than or equal to 20 and greater than or equal to 1 appeared to be present across all the subgroups that we looked at,” he added.
The response rates did not differ between P+C and EXTREME groups, but the median duration of response was significantly greater with P+C vs. EXTREME in both the CPS of 20 or greater and 1 or greater (7.1 vs. 4.2 months and 6.7 vs. 4.3 months, respectively).
Additionally, the final results of the study showed an OS benefit with P+C vs. EXTREME in the total population (13.0 vs. 10.7 months; HR, 0.72), Dr. Rischin said.
The difference between the groups with respect to progression-free survival (PFS), however, was not statistically significant and did not reach the superiority threshold, he noted.
In the 301 patients who received pembrolizumab alone, OS was superior in the CPS 20 or greater and 1 or greater populations (median, 14.8 vs. 10.7 months; HR, 0.58 and 12.4 vs. 10.3 months; HR, 0.74, respectively), compared with EXTREME, but was noninferior in the total population (median 11.5 vs. 10.7 months; HR, 0.83), and safety was favorable .
Again, PFS did not differ between the groups (median, 2.3 vs. 5.2 months; HR, 1.34), and while the overall response rates did not differ significantly, the median duration of response was substantially longer with pembrolizumab at 22.6 vs. 4.5 months with EXTREME, he said.
Study participants had locally incurable R/M HNSCC and no prior systemic therapy in the R/M setting. Those in he P+C arm received pembrolizumab at 200 mg plus 6 cycles of cisplatin at 100 mg/m2 or carboplatin AUC 5, and 5-fluorouracil at a dose of 1000 mg/m2/day for 4 days every 3 weeks; those in the pembrolizumab alone arm received 200 mg every 3 weeks for up to 35 cycles, and those in the EXTREME arm received certuximab at a 400 mg/m2 loading dose followed by 250 mg/m2 weekly with carboplatin AUC 5 or cisplatin at 100 mg/m2, and 5-FU at 1000 mg/m2/day for 4 days for 6 cycles.
“The data from KEYNOTE-048 support pembrolizumab plus platinum-based chemotherapy and pembrolizumab monotherapy as new standard of care monotherapies for recurrent/metastatic head and neck squamous cell carcinoma,” he concluded.
Discussant Vanita Noronha, MD, a professor in the Department of Medical Oncology at Tata Memorial Hospital in Mumbai, India, said that while the findings are practice changing, they also raise a number of questions, such as which patients should get pembrolizumab and which should get P+C, why there is a differential effect of pembrolizumab based on PD-L1 by CPS–and what about those with CPS of 0 or 1-20, and why the response rates and PFS rates were not improved in the pembrolizumab groups.
Other important questions include whether there are predictive biomarkers for response, and whether sequential therapy would be of benefit, she added.
While these and other questions remain to be addressed, the KEYNOTE-048 findings have implications for practice going forward; based on the current data, her approach to treating patients with R/M HNSCC not amenable to radical therapy is to treat with pembrolizumab alone in those with disease-free interval of 6 months or less, she said.
For those with disease-free interval greater than 6 months and good performance status who have controlled comorbidities, are platinum eligible, and for whom the treatment is reimbursable/affordable, treatment depends on symptom severity; she would treat those with mild/moderate symptoms and CPS of 20 or greater with pembrolizumab alone, those with CPS of 1 or greater with P+C or pembrolizumab alone, and those with CPS of 0 or unknown CPS with EXTREME or a similar regimen or with P+C, and she would treat those with severe symptoms with P+C.
“If the patient were a bit borderline, had multiple comorbidities, could not receive platinum, or had financial constraints, I would treat the patient with singe-agent intravenous chemotherapy or with oral metronomic chemotherapy, single-agent targeted therapy or with best supportive care,” she said.
Dr. Rischin has received research funding from Amgen, Bristol-Myers Squibb, Genentech/Roche, GSK, Merck, and Regeneron. Dr. Noronha has received research funding (to her institution) from Amgen,and Sanofi Aventis.
SOURCE: D Rischin et al., ASCO 2019: Abstract 6000.
CHICAGO – Pembrolizumab with and without chemotherapy proved superior for overall survival compared with the EXTREME regimen when used first line in certain subgroups of patients with recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC), according to “practice-changing” final results from the randomized phase 3 KEYNOTE-048 study.
Compared with 300 patients randomized to receive the EXTREME regimen (a certuximab loading dose followed by carboplatin or cisplatin and 5-fluorouracil), 281 who received pembrolizumab plus chemotherapy (P+C) had superior overall survival (OS) with comparable safety–including both those with programmed death-Ligand 1 (PD-L1) combined positive score (CPS) of 20 or greater (median 14.7 vs 11.0 months; hazard ratio, 0.60) and with CPS of 1 or greater (median, 13.6 vs. 10.4 months; HR, 0.65), Danny Rischin, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The differences were highly statistically significant, said Dr. Rischin, a professor and director of the Division of Cancer Medicine and head of the Department of Medical Oncology at Peter MacCallum Cancer Centre, Melbourne, Australia.
“And this benefit in overall survival in CPS greater than or equal to 20 and greater than or equal to 1 appeared to be present across all the subgroups that we looked at,” he added.
The response rates did not differ between P+C and EXTREME groups, but the median duration of response was significantly greater with P+C vs. EXTREME in both the CPS of 20 or greater and 1 or greater (7.1 vs. 4.2 months and 6.7 vs. 4.3 months, respectively).
Additionally, the final results of the study showed an OS benefit with P+C vs. EXTREME in the total population (13.0 vs. 10.7 months; HR, 0.72), Dr. Rischin said.
The difference between the groups with respect to progression-free survival (PFS), however, was not statistically significant and did not reach the superiority threshold, he noted.
In the 301 patients who received pembrolizumab alone, OS was superior in the CPS 20 or greater and 1 or greater populations (median, 14.8 vs. 10.7 months; HR, 0.58 and 12.4 vs. 10.3 months; HR, 0.74, respectively), compared with EXTREME, but was noninferior in the total population (median 11.5 vs. 10.7 months; HR, 0.83), and safety was favorable .
Again, PFS did not differ between the groups (median, 2.3 vs. 5.2 months; HR, 1.34), and while the overall response rates did not differ significantly, the median duration of response was substantially longer with pembrolizumab at 22.6 vs. 4.5 months with EXTREME, he said.
Study participants had locally incurable R/M HNSCC and no prior systemic therapy in the R/M setting. Those in he P+C arm received pembrolizumab at 200 mg plus 6 cycles of cisplatin at 100 mg/m2 or carboplatin AUC 5, and 5-fluorouracil at a dose of 1000 mg/m2/day for 4 days every 3 weeks; those in the pembrolizumab alone arm received 200 mg every 3 weeks for up to 35 cycles, and those in the EXTREME arm received certuximab at a 400 mg/m2 loading dose followed by 250 mg/m2 weekly with carboplatin AUC 5 or cisplatin at 100 mg/m2, and 5-FU at 1000 mg/m2/day for 4 days for 6 cycles.
“The data from KEYNOTE-048 support pembrolizumab plus platinum-based chemotherapy and pembrolizumab monotherapy as new standard of care monotherapies for recurrent/metastatic head and neck squamous cell carcinoma,” he concluded.
Discussant Vanita Noronha, MD, a professor in the Department of Medical Oncology at Tata Memorial Hospital in Mumbai, India, said that while the findings are practice changing, they also raise a number of questions, such as which patients should get pembrolizumab and which should get P+C, why there is a differential effect of pembrolizumab based on PD-L1 by CPS–and what about those with CPS of 0 or 1-20, and why the response rates and PFS rates were not improved in the pembrolizumab groups.
Other important questions include whether there are predictive biomarkers for response, and whether sequential therapy would be of benefit, she added.
While these and other questions remain to be addressed, the KEYNOTE-048 findings have implications for practice going forward; based on the current data, her approach to treating patients with R/M HNSCC not amenable to radical therapy is to treat with pembrolizumab alone in those with disease-free interval of 6 months or less, she said.
For those with disease-free interval greater than 6 months and good performance status who have controlled comorbidities, are platinum eligible, and for whom the treatment is reimbursable/affordable, treatment depends on symptom severity; she would treat those with mild/moderate symptoms and CPS of 20 or greater with pembrolizumab alone, those with CPS of 1 or greater with P+C or pembrolizumab alone, and those with CPS of 0 or unknown CPS with EXTREME or a similar regimen or with P+C, and she would treat those with severe symptoms with P+C.
“If the patient were a bit borderline, had multiple comorbidities, could not receive platinum, or had financial constraints, I would treat the patient with singe-agent intravenous chemotherapy or with oral metronomic chemotherapy, single-agent targeted therapy or with best supportive care,” she said.
Dr. Rischin has received research funding from Amgen, Bristol-Myers Squibb, Genentech/Roche, GSK, Merck, and Regeneron. Dr. Noronha has received research funding (to her institution) from Amgen,and Sanofi Aventis.
SOURCE: D Rischin et al., ASCO 2019: Abstract 6000.
REPORTING FROM ASCO 2019
Short-term ADT improves radiation salvage after prostatectomy
CHICAGO – Adding short-term androgen deprivation therapy (ADT) to radiotherapy as salvage treatment after radical prostatectomy was associated with significantly better metastasis-free survival at nearly 10 years compared with salvage radiation alone, long-term results of a randomized phase 3 trial show.

After a median follow-up of 112 months (9.3 years), the metastasis-free survival (MFS) rate for 369 patients assigned to receive salvage radiation and short-term goserelin was 75%, compared with 69% for 374 patients randomized to radiation alone (P = .034), reported Nicolas Magné, MD, from Jean Monnet Saint Etienne University in Saint-Priest en Jarez, France.
“We can conclude and do believe that short ADT, only two injections at 3-month intervals, could increase MFS at 10 years compared to radiation alone in patients with rising PSA after initial prostatectomy,“ he said at the annual meeting of the American Society of Clinical Oncology.
There was no significant difference, however, in the secondary endpoint of overall survival at 10 years.
Dr. Magné and co-investigators in the GETUG-AFU 16 trial had previously reported that after a median follow-up of 5.3 years, patients assigned to radiation plus goserelin were significantly more likely to be free of biochemical or clinical progression at 5 years than patients assigned to radiotherapy alone (80% vs, 62%, hazard ratio [HR] 0.50, P less than .0001).
The open-label trial enrolled men 18 or older from 43 French centers who had been treated for a histologically confirmed adenocarcinoma of the prostate but had not received prior androgen deprivation therapy (ADT) or pelvic radiation. The patients had either stage pT2 or pT3 cancers, or stage pT4a with invasive disease limited to the bladder neck. The patients all had biochemical failure, defined as a rising prostate-specific antigen (PSA) of 0.2 to 2.0 mcg/L following radical prostatectomy, with no clinically evident disease.
The patients were randomly assigned to receive standard salvage radiotherapy either alone or with hormonal therapy. Randomization was stratified by investigational site, radiotherapy modality, and prognosis.
Radiotherapy consisted of either 3-D conformal radiotherapy or intensity modulated radiotherapy, delivered in 66 Gy doses divided into 33 fractions of 2 Gy each 5 days a week for 7 weeks.
Patients assigned to hormonal therapy in addition to radiation received one subcutaneous injection of goserelin 10.8 mg on the first day of radiation, and a second injection 3 months later.
Progression-free survival (PFS), the primary endpoint, was significantly better with the combination than with radiation alone for both low-risk patients (HR 0.47, 95% confidence interval [CI] 0.28-0.80), and high-risk patients (HR 0.56, CI 0.44-0.83).
As noted before, metastasis-free survival was also significantly better in the combination arm ( HR, 0.73, P = .034) at 10 years.
Invited discussant Daniel Spratt, MD, from the University of Michigan in Ann Arbor, commented that the study results “do show, just like they did in 2016, that bicochemical control is improved, which is linked to their primary endpoint of PFS, but I always caution that this alone will always be improved with testosterone suppression.”

He noted that if you give ADT to patients with low-risk prostate cancer “that we don’t usually even treat today,” adding hormonal therapy will produce a nearly identical improvement in biochemical control, suggesting more of a signal than a clinical benefit.
The improvement in MFS, however, is indeed a clinical benefit, “but it is a small difference, and one thing to note is that when you give these patients about 6 months of hormonal therapy, depending on the age of the patient, it can be about 6 months until they recover testosterone, and at their median follow-up, you can see that the delay in MFS, which is usually the trigger to start hormone therapy, is about 12 months. So it’s important when you counsel these patients that [for] about potentially 6 months to a year of symptoms you may delay the need for hormone therapy by about 12 months,” he said.
The study was supported by UNICANCER and AstraZeneca. Dr. Magné reported no relevant disclosures. Dr. Spratt reported amconsulting or advisory role with Blue Earth Diagnostics and Janssen Oncology.
SOURCE: Magn é D et al. ASCO 2019. Abstract 5001.
CHICAGO – Adding short-term androgen deprivation therapy (ADT) to radiotherapy as salvage treatment after radical prostatectomy was associated with significantly better metastasis-free survival at nearly 10 years compared with salvage radiation alone, long-term results of a randomized phase 3 trial show.
After a median follow-up of 112 months (9.3 years), the metastasis-free survival (MFS) rate for 369 patients assigned to receive salvage radiation and short-term goserelin was 75%, compared with 69% for 374 patients randomized to radiation alone (P = .034), reported Nicolas Magné, MD, from Jean Monnet Saint Etienne University in Saint-Priest en Jarez, France.
“We can conclude and do believe that short ADT, only two injections at 3-month intervals, could increase MFS at 10 years compared to radiation alone in patients with rising PSA after initial prostatectomy,“ he said at the annual meeting of the American Society of Clinical Oncology.
There was no significant difference, however, in the secondary endpoint of overall survival at 10 years.
Dr. Magné and co-investigators in the GETUG-AFU 16 trial had previously reported that after a median follow-up of 5.3 years, patients assigned to radiation plus goserelin were significantly more likely to be free of biochemical or clinical progression at 5 years than patients assigned to radiotherapy alone (80% vs, 62%, hazard ratio [HR] 0.50, P less than .0001).
The open-label trial enrolled men 18 or older from 43 French centers who had been treated for a histologically confirmed adenocarcinoma of the prostate but had not received prior androgen deprivation therapy (ADT) or pelvic radiation. The patients had either stage pT2 or pT3 cancers, or stage pT4a with invasive disease limited to the bladder neck. The patients all had biochemical failure, defined as a rising prostate-specific antigen (PSA) of 0.2 to 2.0 mcg/L following radical prostatectomy, with no clinically evident disease.
The patients were randomly assigned to receive standard salvage radiotherapy either alone or with hormonal therapy. Randomization was stratified by investigational site, radiotherapy modality, and prognosis.
Radiotherapy consisted of either 3-D conformal radiotherapy or intensity modulated radiotherapy, delivered in 66 Gy doses divided into 33 fractions of 2 Gy each 5 days a week for 7 weeks.
Patients assigned to hormonal therapy in addition to radiation received one subcutaneous injection of goserelin 10.8 mg on the first day of radiation, and a second injection 3 months later.
Progression-free survival (PFS), the primary endpoint, was significantly better with the combination than with radiation alone for both low-risk patients (HR 0.47, 95% confidence interval [CI] 0.28-0.80), and high-risk patients (HR 0.56, CI 0.44-0.83).
As noted before, metastasis-free survival was also significantly better in the combination arm ( HR, 0.73, P = .034) at 10 years.
Invited discussant Daniel Spratt, MD, from the University of Michigan in Ann Arbor, commented that the study results “do show, just like they did in 2016, that bicochemical control is improved, which is linked to their primary endpoint of PFS, but I always caution that this alone will always be improved with testosterone suppression.”
He noted that if you give ADT to patients with low-risk prostate cancer “that we don’t usually even treat today,” adding hormonal therapy will produce a nearly identical improvement in biochemical control, suggesting more of a signal than a clinical benefit.
The improvement in MFS, however, is indeed a clinical benefit, “but it is a small difference, and one thing to note is that when you give these patients about 6 months of hormonal therapy, depending on the age of the patient, it can be about 6 months until they recover testosterone, and at their median follow-up, you can see that the delay in MFS, which is usually the trigger to start hormone therapy, is about 12 months. So it’s important when you counsel these patients that [for] about potentially 6 months to a year of symptoms you may delay the need for hormone therapy by about 12 months,” he said.
The study was supported by UNICANCER and AstraZeneca. Dr. Magné reported no relevant disclosures. Dr. Spratt reported amconsulting or advisory role with Blue Earth Diagnostics and Janssen Oncology.
SOURCE: Magn é D et al. ASCO 2019. Abstract 5001.
CHICAGO – Adding short-term androgen deprivation therapy (ADT) to radiotherapy as salvage treatment after radical prostatectomy was associated with significantly better metastasis-free survival at nearly 10 years compared with salvage radiation alone, long-term results of a randomized phase 3 trial show.
After a median follow-up of 112 months (9.3 years), the metastasis-free survival (MFS) rate for 369 patients assigned to receive salvage radiation and short-term goserelin was 75%, compared with 69% for 374 patients randomized to radiation alone (P = .034), reported Nicolas Magné, MD, from Jean Monnet Saint Etienne University in Saint-Priest en Jarez, France.
“We can conclude and do believe that short ADT, only two injections at 3-month intervals, could increase MFS at 10 years compared to radiation alone in patients with rising PSA after initial prostatectomy,“ he said at the annual meeting of the American Society of Clinical Oncology.
There was no significant difference, however, in the secondary endpoint of overall survival at 10 years.
Dr. Magné and co-investigators in the GETUG-AFU 16 trial had previously reported that after a median follow-up of 5.3 years, patients assigned to radiation plus goserelin were significantly more likely to be free of biochemical or clinical progression at 5 years than patients assigned to radiotherapy alone (80% vs, 62%, hazard ratio [HR] 0.50, P less than .0001).
The open-label trial enrolled men 18 or older from 43 French centers who had been treated for a histologically confirmed adenocarcinoma of the prostate but had not received prior androgen deprivation therapy (ADT) or pelvic radiation. The patients had either stage pT2 or pT3 cancers, or stage pT4a with invasive disease limited to the bladder neck. The patients all had biochemical failure, defined as a rising prostate-specific antigen (PSA) of 0.2 to 2.0 mcg/L following radical prostatectomy, with no clinically evident disease.
The patients were randomly assigned to receive standard salvage radiotherapy either alone or with hormonal therapy. Randomization was stratified by investigational site, radiotherapy modality, and prognosis.
Radiotherapy consisted of either 3-D conformal radiotherapy or intensity modulated radiotherapy, delivered in 66 Gy doses divided into 33 fractions of 2 Gy each 5 days a week for 7 weeks.
Patients assigned to hormonal therapy in addition to radiation received one subcutaneous injection of goserelin 10.8 mg on the first day of radiation, and a second injection 3 months later.
Progression-free survival (PFS), the primary endpoint, was significantly better with the combination than with radiation alone for both low-risk patients (HR 0.47, 95% confidence interval [CI] 0.28-0.80), and high-risk patients (HR 0.56, CI 0.44-0.83).
As noted before, metastasis-free survival was also significantly better in the combination arm ( HR, 0.73, P = .034) at 10 years.
Invited discussant Daniel Spratt, MD, from the University of Michigan in Ann Arbor, commented that the study results “do show, just like they did in 2016, that bicochemical control is improved, which is linked to their primary endpoint of PFS, but I always caution that this alone will always be improved with testosterone suppression.”
He noted that if you give ADT to patients with low-risk prostate cancer “that we don’t usually even treat today,” adding hormonal therapy will produce a nearly identical improvement in biochemical control, suggesting more of a signal than a clinical benefit.
The improvement in MFS, however, is indeed a clinical benefit, “but it is a small difference, and one thing to note is that when you give these patients about 6 months of hormonal therapy, depending on the age of the patient, it can be about 6 months until they recover testosterone, and at their median follow-up, you can see that the delay in MFS, which is usually the trigger to start hormone therapy, is about 12 months. So it’s important when you counsel these patients that [for] about potentially 6 months to a year of symptoms you may delay the need for hormone therapy by about 12 months,” he said.
The study was supported by UNICANCER and AstraZeneca. Dr. Magné reported no relevant disclosures. Dr. Spratt reported amconsulting or advisory role with Blue Earth Diagnostics and Janssen Oncology.
SOURCE: Magn é D et al. ASCO 2019. Abstract 5001.
REPORTING FROM ASCO 2019
Antibodies may have role in ‘TKI world’ of EGFR-mutant NSCLC
CHICAGO – While tyrosine kinase inhibitors (TKIs) have long dominated treatment approaches for EGFR-driven advanced non-small cell lung cancer, a few newer antibodies are showing early promise as potential new strategies to use after progression, recent reports show.
Both JNJ-372, an EGFR and MET bispecific antibody, and U3-1402, a HER3-directed antibody-drug conjugate (ADC), demonstrated manageable safety profiles and preliminary antitumor activity in phase 1 study results presented here at the annual meeting of the American Society of Clinical Oncology.
“There is definitely a role to play for antibodies in the TKI world,” said Jessica Ruth Bauman, MD, of Fox Chase Cancer Center, Philadelphia, Pa., a discussant on both abstracts.
These two antibodies harness new mechanisms of action that are not specific to a resistance mechanism, which may lead to broad applicability, according to Dr. Bauman.
“Mechanisms of acquired resistance have been the Achilles heel of EGFR TKI treatment,” she said.
The JNJ-372 bispecific antibody has preclinical data consistent with several proposed mechanisms of action, including inhibition of EGFR and cMet signaling, receptor degradation, and antibody-dependent cellular cytotoxicity, said investigator Eric B. Haura, MD, of H. Lee Moffitt Cancer Center & Research Institute, Tampa, Fla.
In the phase 1 study, which included patients with diverse EGFR mutations, 32 out of 108 patients (30%) had a best response of partial response (PR) after treatment with JNJ-372, Dr. Haura reported in an oral abstract presentation.
Responses were seen in patients with mutations that represent areas of high unmet need, including those with EGFR C797S-mediated or cMet-mediated resistance to the third-generation TKI osimertinib, and those with TKI-naïve EGFR exon 20 insertions, he emphasized in his presentation.
The safety profile was “manageable” and consistent with EGFR inhibition, he said, with a low (9%) rate of grade 3 or greater toxicities and frequent infusion-related reactions, mostly after the first dose.
Enrollment of patients with high unmet need is ongoing, according to Dr. Haura.
U3-1402, the antibody-drug conjugate that may have a place in the TKI world, consists of a fully human HER3-targeted antibody linked to a topoisomerase I inhibitor payload.
“Targeting HER3 with U3-1402 may be a practical approach to treat EGFR-mutant NSCLC with diverse mechanisms of resistance to EGFR TKIs,” said investigator Pasi A. Jänne, MD, PhD, of Dana-Farber Cancer Institute, Boston, Mass.
That’s because mechanisms of resistance to TKIs in EGFR-mutant NSCLC are turning out to be so diverse, that trying to combat each individual resistance mechanism is likely “impractical,” Dr. Jänne said.
Targeting HER3, the perhaps lesser-known of the four members of the EGFR tyrosine kinase family, may address multiple resistance mechanisms, and 57% to 67% of EGFR-mutant NSCLCs have at least some level of HER3 expression, according to the presenter.
In the phase 1 study data reported at the meeting, the response rate following U3-1402 treatment was about 31%, or 5 out of 16 patients, including 4 confirmed partial responses. Most treatment-emergent adverse events were grade 1 or 2, and only one patient discontinued due to an adverse event, according to Dr. Jänne, who said the study is ongoing.
Taken together, findings for U3-1402 and JNJ-372 show that there may be room for other approaches beyond TKIs to address the need for new therapies to overcome resistance, Dr. Bauman said in her commentary on these studies.
“Additional research will enable us to determine who will benefit from these compounds, what biomarkers are predictive, and novel combinations to consider,” she added.
Dr. Bauman reported a consulting or advisory role with Pfizer. Dr. Haura provided disclosures related to Bristol-Myers Squibb; Janssen Oncology, Boehringer Ingelheim, FORMA Therapeutics, Ignyta, Janssen, Lilly, and Ventana, plus a patent pending on technology related to kinase inhibitor sensitivity biomarkers. Dr. Jänne reported disclosures related to Gatekeeper Pharmaceuticals, Loxo, Araxes Pharma, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Lilly, and others.
SOURCE: Haura EB, et al. ASCO 2019. Abstract 9009, Jänne PA, et al. ASCO 2019. Abstract 9010.
CHICAGO – While tyrosine kinase inhibitors (TKIs) have long dominated treatment approaches for EGFR-driven advanced non-small cell lung cancer, a few newer antibodies are showing early promise as potential new strategies to use after progression, recent reports show.
Both JNJ-372, an EGFR and MET bispecific antibody, and U3-1402, a HER3-directed antibody-drug conjugate (ADC), demonstrated manageable safety profiles and preliminary antitumor activity in phase 1 study results presented here at the annual meeting of the American Society of Clinical Oncology.
“There is definitely a role to play for antibodies in the TKI world,” said Jessica Ruth Bauman, MD, of Fox Chase Cancer Center, Philadelphia, Pa., a discussant on both abstracts.
These two antibodies harness new mechanisms of action that are not specific to a resistance mechanism, which may lead to broad applicability, according to Dr. Bauman.
“Mechanisms of acquired resistance have been the Achilles heel of EGFR TKI treatment,” she said.
The JNJ-372 bispecific antibody has preclinical data consistent with several proposed mechanisms of action, including inhibition of EGFR and cMet signaling, receptor degradation, and antibody-dependent cellular cytotoxicity, said investigator Eric B. Haura, MD, of H. Lee Moffitt Cancer Center & Research Institute, Tampa, Fla.
In the phase 1 study, which included patients with diverse EGFR mutations, 32 out of 108 patients (30%) had a best response of partial response (PR) after treatment with JNJ-372, Dr. Haura reported in an oral abstract presentation.
Responses were seen in patients with mutations that represent areas of high unmet need, including those with EGFR C797S-mediated or cMet-mediated resistance to the third-generation TKI osimertinib, and those with TKI-naïve EGFR exon 20 insertions, he emphasized in his presentation.
The safety profile was “manageable” and consistent with EGFR inhibition, he said, with a low (9%) rate of grade 3 or greater toxicities and frequent infusion-related reactions, mostly after the first dose.
Enrollment of patients with high unmet need is ongoing, according to Dr. Haura.
U3-1402, the antibody-drug conjugate that may have a place in the TKI world, consists of a fully human HER3-targeted antibody linked to a topoisomerase I inhibitor payload.
“Targeting HER3 with U3-1402 may be a practical approach to treat EGFR-mutant NSCLC with diverse mechanisms of resistance to EGFR TKIs,” said investigator Pasi A. Jänne, MD, PhD, of Dana-Farber Cancer Institute, Boston, Mass.
That’s because mechanisms of resistance to TKIs in EGFR-mutant NSCLC are turning out to be so diverse, that trying to combat each individual resistance mechanism is likely “impractical,” Dr. Jänne said.
Targeting HER3, the perhaps lesser-known of the four members of the EGFR tyrosine kinase family, may address multiple resistance mechanisms, and 57% to 67% of EGFR-mutant NSCLCs have at least some level of HER3 expression, according to the presenter.
In the phase 1 study data reported at the meeting, the response rate following U3-1402 treatment was about 31%, or 5 out of 16 patients, including 4 confirmed partial responses. Most treatment-emergent adverse events were grade 1 or 2, and only one patient discontinued due to an adverse event, according to Dr. Jänne, who said the study is ongoing.
Taken together, findings for U3-1402 and JNJ-372 show that there may be room for other approaches beyond TKIs to address the need for new therapies to overcome resistance, Dr. Bauman said in her commentary on these studies.
“Additional research will enable us to determine who will benefit from these compounds, what biomarkers are predictive, and novel combinations to consider,” she added.
Dr. Bauman reported a consulting or advisory role with Pfizer. Dr. Haura provided disclosures related to Bristol-Myers Squibb; Janssen Oncology, Boehringer Ingelheim, FORMA Therapeutics, Ignyta, Janssen, Lilly, and Ventana, plus a patent pending on technology related to kinase inhibitor sensitivity biomarkers. Dr. Jänne reported disclosures related to Gatekeeper Pharmaceuticals, Loxo, Araxes Pharma, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Lilly, and others.
SOURCE: Haura EB, et al. ASCO 2019. Abstract 9009, Jänne PA, et al. ASCO 2019. Abstract 9010.
CHICAGO – While tyrosine kinase inhibitors (TKIs) have long dominated treatment approaches for EGFR-driven advanced non-small cell lung cancer, a few newer antibodies are showing early promise as potential new strategies to use after progression, recent reports show.
Both JNJ-372, an EGFR and MET bispecific antibody, and U3-1402, a HER3-directed antibody-drug conjugate (ADC), demonstrated manageable safety profiles and preliminary antitumor activity in phase 1 study results presented here at the annual meeting of the American Society of Clinical Oncology.
“There is definitely a role to play for antibodies in the TKI world,” said Jessica Ruth Bauman, MD, of Fox Chase Cancer Center, Philadelphia, Pa., a discussant on both abstracts.
These two antibodies harness new mechanisms of action that are not specific to a resistance mechanism, which may lead to broad applicability, according to Dr. Bauman.
“Mechanisms of acquired resistance have been the Achilles heel of EGFR TKI treatment,” she said.
The JNJ-372 bispecific antibody has preclinical data consistent with several proposed mechanisms of action, including inhibition of EGFR and cMet signaling, receptor degradation, and antibody-dependent cellular cytotoxicity, said investigator Eric B. Haura, MD, of H. Lee Moffitt Cancer Center & Research Institute, Tampa, Fla.
In the phase 1 study, which included patients with diverse EGFR mutations, 32 out of 108 patients (30%) had a best response of partial response (PR) after treatment with JNJ-372, Dr. Haura reported in an oral abstract presentation.
Responses were seen in patients with mutations that represent areas of high unmet need, including those with EGFR C797S-mediated or cMet-mediated resistance to the third-generation TKI osimertinib, and those with TKI-naïve EGFR exon 20 insertions, he emphasized in his presentation.
The safety profile was “manageable” and consistent with EGFR inhibition, he said, with a low (9%) rate of grade 3 or greater toxicities and frequent infusion-related reactions, mostly after the first dose.
Enrollment of patients with high unmet need is ongoing, according to Dr. Haura.
U3-1402, the antibody-drug conjugate that may have a place in the TKI world, consists of a fully human HER3-targeted antibody linked to a topoisomerase I inhibitor payload.
“Targeting HER3 with U3-1402 may be a practical approach to treat EGFR-mutant NSCLC with diverse mechanisms of resistance to EGFR TKIs,” said investigator Pasi A. Jänne, MD, PhD, of Dana-Farber Cancer Institute, Boston, Mass.
That’s because mechanisms of resistance to TKIs in EGFR-mutant NSCLC are turning out to be so diverse, that trying to combat each individual resistance mechanism is likely “impractical,” Dr. Jänne said.
Targeting HER3, the perhaps lesser-known of the four members of the EGFR tyrosine kinase family, may address multiple resistance mechanisms, and 57% to 67% of EGFR-mutant NSCLCs have at least some level of HER3 expression, according to the presenter.
In the phase 1 study data reported at the meeting, the response rate following U3-1402 treatment was about 31%, or 5 out of 16 patients, including 4 confirmed partial responses. Most treatment-emergent adverse events were grade 1 or 2, and only one patient discontinued due to an adverse event, according to Dr. Jänne, who said the study is ongoing.
Taken together, findings for U3-1402 and JNJ-372 show that there may be room for other approaches beyond TKIs to address the need for new therapies to overcome resistance, Dr. Bauman said in her commentary on these studies.
“Additional research will enable us to determine who will benefit from these compounds, what biomarkers are predictive, and novel combinations to consider,” she added.
Dr. Bauman reported a consulting or advisory role with Pfizer. Dr. Haura provided disclosures related to Bristol-Myers Squibb; Janssen Oncology, Boehringer Ingelheim, FORMA Therapeutics, Ignyta, Janssen, Lilly, and Ventana, plus a patent pending on technology related to kinase inhibitor sensitivity biomarkers. Dr. Jänne reported disclosures related to Gatekeeper Pharmaceuticals, Loxo, Araxes Pharma, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Lilly, and others.
SOURCE: Haura EB, et al. ASCO 2019. Abstract 9009, Jänne PA, et al. ASCO 2019. Abstract 9010.
REPORTING FROM ASCO 2019
Combo produces ‘best response rate’ after first relapse in kids with AML
CHICAGO – Administering CPX-351 prior to a three-drug regimen produced a high response rate in pediatric patients with acute myeloid leukemia (AML) in first relapse.

In a phase 1/2 trial, CPX-351 followed by fludarabine, cytarabine, and filgrastim (FLAG) produced an overall response rate of 81%, and 70% of responders had their best response while receiving CPX-351.
“This is the best response rate published in North America for those [pediatric AML patients] in first relapse,” said Todd Cooper, DO, of Seattle Children’s Hospital in Washington.
Dr. Cooper presented results from the phase 1/2 AAML1421 trial (NCT02642965) at the annual meeting of the American Society of Clinical Oncology.
The primary objective of phase 1 was to determine the recommended phase 2 dose and toxicities of CPX-351, a liposomal preparation of cytarabine and daunorubicin. The primary objective of phase 2 was to assess the best response in patients who received CPX-351 in cycle 1 and FLAG in cycle 2.
The trial enrolled 38 AML patients, 6 in the dose-finding phase and 32 in the efficacy phase. The patients’ median age at study entry was 11.91 years (range, 1.81-21.5). Most patients (88.9%) had CNS 1 disease, and most (73.7%) had not received a transplant.
Half of patients had a first complete response (CR) that lasted 180 to 365 days, 13.2% had a first CR lasting less than 180 days, and 36.8% had a first CR lasting more than 1 year.
Dosing and toxicity
During the dose-finding portion of the study, the first dose level of CPX-351 was 135 units/m2 on days 1, 3, and 5. There was one dose-limiting toxicity — grade 3 decrease in ejection fraction — so 135 units/m2 was deemed the recommended phase 2 dose.
The most common grade 3 or higher adverse events observed with CPX-351 in cycle 1 were infections and infestations (47.4%), febrile neutropenia (44.7%), maculopapular rash (39.5%), and prolonged QT interval (18.4%).
The most common grade 3 or higher adverse events observed with FLAG in cycle 2 were febrile neutropenia (23.1%), prolonged QT interval (23.1%), and infections and infestations (19.2%).
Response and survival
There were 37 patients evaluable for response. The overall response rate was defined as CR plus CR without platelet recovery (CRp) plus CR with incomplete hematologic recovery (CRi).
The overall response rate was 81.1% (n = 30), which included 20 CRs (54.1%), 5 CRps (13.5%), and 5 CRis (13.5%). Five patients had a partial response (13.5%), and two patients had treatment failure (5.4%).
During CPX-351 treatment (n = 37), the CR rate was 37.8% (n = 14), the CRp rate was 5.4% (n = 2), and the CRi rate was 32.4% (n = 12).
During FLAG treatment (n = 27), the CR rate was 48.1% (n = 13), the CRp rate was 25.9% (n = 7), and the CRi rate was 7.4% (n = 2).
Of the 25 patients who achieved a CR or CRp at any time, 21 (84%) were minimal residual disease negative by flow cytometry. Twelve patients were minimal residual disease negative after cycle 1.
Most patients who achieved a CRi or better (83.3%) went on to hematopoietic stem cell transplant.
The 2-year overall survival was 47% for all patients and 60% for responders. None of the non-responders were still alive 2 years after therapy.
“The results certainly warrant a phase 3 study of CPX-351,” Dr. Cooper said. “In fact, it is the lead molecule that’s going to be incorporated into the next COG phase 3 study.”
AAML1421 was sponsored by the Children’s Oncology Group in collaboration with the National Cancer Institute. Dr. Cooper disclosed relationships with Juno Therapeutics and Celgene.
SOURCE: Cooper TM et al. ASCO 2019. Abstract 10003.
CHICAGO – Administering CPX-351 prior to a three-drug regimen produced a high response rate in pediatric patients with acute myeloid leukemia (AML) in first relapse.
In a phase 1/2 trial, CPX-351 followed by fludarabine, cytarabine, and filgrastim (FLAG) produced an overall response rate of 81%, and 70% of responders had their best response while receiving CPX-351.
“This is the best response rate published in North America for those [pediatric AML patients] in first relapse,” said Todd Cooper, DO, of Seattle Children’s Hospital in Washington.
Dr. Cooper presented results from the phase 1/2 AAML1421 trial (NCT02642965) at the annual meeting of the American Society of Clinical Oncology.
The primary objective of phase 1 was to determine the recommended phase 2 dose and toxicities of CPX-351, a liposomal preparation of cytarabine and daunorubicin. The primary objective of phase 2 was to assess the best response in patients who received CPX-351 in cycle 1 and FLAG in cycle 2.
The trial enrolled 38 AML patients, 6 in the dose-finding phase and 32 in the efficacy phase. The patients’ median age at study entry was 11.91 years (range, 1.81-21.5). Most patients (88.9%) had CNS 1 disease, and most (73.7%) had not received a transplant.
Half of patients had a first complete response (CR) that lasted 180 to 365 days, 13.2% had a first CR lasting less than 180 days, and 36.8% had a first CR lasting more than 1 year.
Dosing and toxicity
During the dose-finding portion of the study, the first dose level of CPX-351 was 135 units/m2 on days 1, 3, and 5. There was one dose-limiting toxicity — grade 3 decrease in ejection fraction — so 135 units/m2 was deemed the recommended phase 2 dose.
The most common grade 3 or higher adverse events observed with CPX-351 in cycle 1 were infections and infestations (47.4%), febrile neutropenia (44.7%), maculopapular rash (39.5%), and prolonged QT interval (18.4%).
The most common grade 3 or higher adverse events observed with FLAG in cycle 2 were febrile neutropenia (23.1%), prolonged QT interval (23.1%), and infections and infestations (19.2%).
Response and survival
There were 37 patients evaluable for response. The overall response rate was defined as CR plus CR without platelet recovery (CRp) plus CR with incomplete hematologic recovery (CRi).
The overall response rate was 81.1% (n = 30), which included 20 CRs (54.1%), 5 CRps (13.5%), and 5 CRis (13.5%). Five patients had a partial response (13.5%), and two patients had treatment failure (5.4%).
During CPX-351 treatment (n = 37), the CR rate was 37.8% (n = 14), the CRp rate was 5.4% (n = 2), and the CRi rate was 32.4% (n = 12).
During FLAG treatment (n = 27), the CR rate was 48.1% (n = 13), the CRp rate was 25.9% (n = 7), and the CRi rate was 7.4% (n = 2).
Of the 25 patients who achieved a CR or CRp at any time, 21 (84%) were minimal residual disease negative by flow cytometry. Twelve patients were minimal residual disease negative after cycle 1.
Most patients who achieved a CRi or better (83.3%) went on to hematopoietic stem cell transplant.
The 2-year overall survival was 47% for all patients and 60% for responders. None of the non-responders were still alive 2 years after therapy.
“The results certainly warrant a phase 3 study of CPX-351,” Dr. Cooper said. “In fact, it is the lead molecule that’s going to be incorporated into the next COG phase 3 study.”
AAML1421 was sponsored by the Children’s Oncology Group in collaboration with the National Cancer Institute. Dr. Cooper disclosed relationships with Juno Therapeutics and Celgene.
SOURCE: Cooper TM et al. ASCO 2019. Abstract 10003.
CHICAGO – Administering CPX-351 prior to a three-drug regimen produced a high response rate in pediatric patients with acute myeloid leukemia (AML) in first relapse.
In a phase 1/2 trial, CPX-351 followed by fludarabine, cytarabine, and filgrastim (FLAG) produced an overall response rate of 81%, and 70% of responders had their best response while receiving CPX-351.
“This is the best response rate published in North America for those [pediatric AML patients] in first relapse,” said Todd Cooper, DO, of Seattle Children’s Hospital in Washington.
Dr. Cooper presented results from the phase 1/2 AAML1421 trial (NCT02642965) at the annual meeting of the American Society of Clinical Oncology.
The primary objective of phase 1 was to determine the recommended phase 2 dose and toxicities of CPX-351, a liposomal preparation of cytarabine and daunorubicin. The primary objective of phase 2 was to assess the best response in patients who received CPX-351 in cycle 1 and FLAG in cycle 2.
The trial enrolled 38 AML patients, 6 in the dose-finding phase and 32 in the efficacy phase. The patients’ median age at study entry was 11.91 years (range, 1.81-21.5). Most patients (88.9%) had CNS 1 disease, and most (73.7%) had not received a transplant.
Half of patients had a first complete response (CR) that lasted 180 to 365 days, 13.2% had a first CR lasting less than 180 days, and 36.8% had a first CR lasting more than 1 year.
Dosing and toxicity
During the dose-finding portion of the study, the first dose level of CPX-351 was 135 units/m2 on days 1, 3, and 5. There was one dose-limiting toxicity — grade 3 decrease in ejection fraction — so 135 units/m2 was deemed the recommended phase 2 dose.
The most common grade 3 or higher adverse events observed with CPX-351 in cycle 1 were infections and infestations (47.4%), febrile neutropenia (44.7%), maculopapular rash (39.5%), and prolonged QT interval (18.4%).
The most common grade 3 or higher adverse events observed with FLAG in cycle 2 were febrile neutropenia (23.1%), prolonged QT interval (23.1%), and infections and infestations (19.2%).
Response and survival
There were 37 patients evaluable for response. The overall response rate was defined as CR plus CR without platelet recovery (CRp) plus CR with incomplete hematologic recovery (CRi).
The overall response rate was 81.1% (n = 30), which included 20 CRs (54.1%), 5 CRps (13.5%), and 5 CRis (13.5%). Five patients had a partial response (13.5%), and two patients had treatment failure (5.4%).
During CPX-351 treatment (n = 37), the CR rate was 37.8% (n = 14), the CRp rate was 5.4% (n = 2), and the CRi rate was 32.4% (n = 12).
During FLAG treatment (n = 27), the CR rate was 48.1% (n = 13), the CRp rate was 25.9% (n = 7), and the CRi rate was 7.4% (n = 2).
Of the 25 patients who achieved a CR or CRp at any time, 21 (84%) were minimal residual disease negative by flow cytometry. Twelve patients were minimal residual disease negative after cycle 1.
Most patients who achieved a CRi or better (83.3%) went on to hematopoietic stem cell transplant.
The 2-year overall survival was 47% for all patients and 60% for responders. None of the non-responders were still alive 2 years after therapy.
“The results certainly warrant a phase 3 study of CPX-351,” Dr. Cooper said. “In fact, it is the lead molecule that’s going to be incorporated into the next COG phase 3 study.”
AAML1421 was sponsored by the Children’s Oncology Group in collaboration with the National Cancer Institute. Dr. Cooper disclosed relationships with Juno Therapeutics and Celgene.
SOURCE: Cooper TM et al. ASCO 2019. Abstract 10003.
REPORTING FROM ASCO 2019
Timed perfectly
When I entered the examination room, I saw his alma mater’s logo on his wristwatch. He was a retired physician with a new diagnosis of leukemia who drove to see me, even though he lived closer to his beloved medical school where he had practiced his entire career.

As is frequently the case, he came to see me because he could not get the appointment he wanted in his university’s clinic for another 6 months. He called us on Friday, and 3 days later, he and I were meeting. He is still an ardent supporter of his institution, but I am now his hematologist.
As it turned out, his leukemia was asymptomatic, indolent, and required no treatment. He could have waited 6 months to be seen. But, no; he couldn’t.
This story repeats itself over and over again. A sick patient calls to be seen and is told there is no availability for weeks or months. I do not understand how health care facilities, my own included, find this acceptable.
My father was very proud of his policy to see every patient in his waiting room no matter how long his office needed to stay open. He felt that access was of primary importance to his patients and to his practice. If he didn’t see them, somebody else would. Those of us working in large academic centers do not always feel the financial consequences of patients lost because of poor service.
Luckily, I work in a large cancer center that values access as much as a small practice would. When a patient calls us with a hematologic problem, we see them in less than 7 days, unless the patient prefers a different time frame. We monitor the time it takes to see patients and proactively assess upcoming appointments to ensure insurance coverage and the availability of records. If an obstruction is identified, the case is escalated to administrative leadership to be addressed and resolved. We are very proud of this work.
However, our focus on access does not end there. Once seen, we expedite patient evaluation by assessing workflows to obtain all necessary testing as quickly as possible. By doing so, we accelerate the time it takes from diagnosis to the time we start treating (time to treat). We have always tried to reduce time to treat for acute leukemia and we have applied those lessons to patients with lymphoma and solid tumors, resulting in a 33% improvement over the last 5 years.
We not only lessen the anxiety that comes with a scary diagnosis, emerging data indicate outcomes are improved with faster treatment, too (PLoS One. 2019 Mar 1;14(3):e0213209. doi: 10.1371/journal.pone.0213209).

These efforts will be criticized by those who feel the delivery of medical care should be structured more around the physician than the patient. Certainly, the system has developed to support a mindset of “physician first.” Not only do patients have to make an appointment for the privilege of seeing us, they have to navigate significant geographic and financial hurdles for that privilege.
Once at the appointment, physicians have historically been the provider giving the “orders” while others correct them, carry them out, follow-up on the results, manage phone calls, and schedule follow-up. This hierarchy has served physicians very well, but the pyramidal structure of health care is on the verge of being upended.
Too few physicians for an increasing demand for medical attention has led to the rise of advanced practice providers (APPs), who often serve as the only provider a patient may have, particularly in rural areas. In our center, we evolved from thinking of APPs as similar to house-staff who saw patients with us and did most of the work, but could not bill, to independent providers who work with us, do most of the work, and bill for their efforts. This slow transformation of our practice will soon seem quaint as we face the rapid disruption coming to our current conception of the health care delivery system.
Technologically savvy patients already demand immediate access to unlimited supplies of consumer goods, video, audio, books, magazines, and just about anything else you can think of. Immediate access to health care at a time convenient to the patient also will become an expectation because plenty of health care delivery models already are providing it. The local pharmacy or retail store may have a physician or APP right there ready to see a patient at any time. Some physicians are already online ready for an electronic interaction. See MDLIVE and Teladoc as examples.
The nimble cancer center that embraces these trends to become more patient-centric will be the center that captures national – if not international – market share, as insurance companies and governments adjust their reimbursement models to include these services. With blood work obtained just about anywhere, what would keep a patient with immune thrombocytopenic purpura from consulting with any online hematologist she chooses, whenever she chooses?
If first impressions are important, then patient access is important. Refrains of “I don’t have clinic that day,” “the pathology has not yet been reviewed,” and “that is not a disease I take care of,” ring as hollow to me as I suspect they do to our patients. When someone in my family has a significant illness, I want them to be seen now, not later. I believe we all would want prompt, efficient service.
We should strive to provide the same level of care to our patients as we expect for our family. Patients do not know that chronic leukemia is not an emergency. Time may not be critical to us, but it is to them. The perfect time to meet their needs is now.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematology and medical oncology at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
When I entered the examination room, I saw his alma mater’s logo on his wristwatch. He was a retired physician with a new diagnosis of leukemia who drove to see me, even though he lived closer to his beloved medical school where he had practiced his entire career.
As is frequently the case, he came to see me because he could not get the appointment he wanted in his university’s clinic for another 6 months. He called us on Friday, and 3 days later, he and I were meeting. He is still an ardent supporter of his institution, but I am now his hematologist.
As it turned out, his leukemia was asymptomatic, indolent, and required no treatment. He could have waited 6 months to be seen. But, no; he couldn’t.
This story repeats itself over and over again. A sick patient calls to be seen and is told there is no availability for weeks or months. I do not understand how health care facilities, my own included, find this acceptable.
My father was very proud of his policy to see every patient in his waiting room no matter how long his office needed to stay open. He felt that access was of primary importance to his patients and to his practice. If he didn’t see them, somebody else would. Those of us working in large academic centers do not always feel the financial consequences of patients lost because of poor service.
Luckily, I work in a large cancer center that values access as much as a small practice would. When a patient calls us with a hematologic problem, we see them in less than 7 days, unless the patient prefers a different time frame. We monitor the time it takes to see patients and proactively assess upcoming appointments to ensure insurance coverage and the availability of records. If an obstruction is identified, the case is escalated to administrative leadership to be addressed and resolved. We are very proud of this work.
However, our focus on access does not end there. Once seen, we expedite patient evaluation by assessing workflows to obtain all necessary testing as quickly as possible. By doing so, we accelerate the time it takes from diagnosis to the time we start treating (time to treat). We have always tried to reduce time to treat for acute leukemia and we have applied those lessons to patients with lymphoma and solid tumors, resulting in a 33% improvement over the last 5 years.
We not only lessen the anxiety that comes with a scary diagnosis, emerging data indicate outcomes are improved with faster treatment, too (PLoS One. 2019 Mar 1;14(3):e0213209. doi: 10.1371/journal.pone.0213209).
These efforts will be criticized by those who feel the delivery of medical care should be structured more around the physician than the patient. Certainly, the system has developed to support a mindset of “physician first.” Not only do patients have to make an appointment for the privilege of seeing us, they have to navigate significant geographic and financial hurdles for that privilege.
Once at the appointment, physicians have historically been the provider giving the “orders” while others correct them, carry them out, follow-up on the results, manage phone calls, and schedule follow-up. This hierarchy has served physicians very well, but the pyramidal structure of health care is on the verge of being upended.
Too few physicians for an increasing demand for medical attention has led to the rise of advanced practice providers (APPs), who often serve as the only provider a patient may have, particularly in rural areas. In our center, we evolved from thinking of APPs as similar to house-staff who saw patients with us and did most of the work, but could not bill, to independent providers who work with us, do most of the work, and bill for their efforts. This slow transformation of our practice will soon seem quaint as we face the rapid disruption coming to our current conception of the health care delivery system.
Technologically savvy patients already demand immediate access to unlimited supplies of consumer goods, video, audio, books, magazines, and just about anything else you can think of. Immediate access to health care at a time convenient to the patient also will become an expectation because plenty of health care delivery models already are providing it. The local pharmacy or retail store may have a physician or APP right there ready to see a patient at any time. Some physicians are already online ready for an electronic interaction. See MDLIVE and Teladoc as examples.
The nimble cancer center that embraces these trends to become more patient-centric will be the center that captures national – if not international – market share, as insurance companies and governments adjust their reimbursement models to include these services. With blood work obtained just about anywhere, what would keep a patient with immune thrombocytopenic purpura from consulting with any online hematologist she chooses, whenever she chooses?
If first impressions are important, then patient access is important. Refrains of “I don’t have clinic that day,” “the pathology has not yet been reviewed,” and “that is not a disease I take care of,” ring as hollow to me as I suspect they do to our patients. When someone in my family has a significant illness, I want them to be seen now, not later. I believe we all would want prompt, efficient service.
We should strive to provide the same level of care to our patients as we expect for our family. Patients do not know that chronic leukemia is not an emergency. Time may not be critical to us, but it is to them. The perfect time to meet their needs is now.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematology and medical oncology at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
When I entered the examination room, I saw his alma mater’s logo on his wristwatch. He was a retired physician with a new diagnosis of leukemia who drove to see me, even though he lived closer to his beloved medical school where he had practiced his entire career.
As is frequently the case, he came to see me because he could not get the appointment he wanted in his university’s clinic for another 6 months. He called us on Friday, and 3 days later, he and I were meeting. He is still an ardent supporter of his institution, but I am now his hematologist.
As it turned out, his leukemia was asymptomatic, indolent, and required no treatment. He could have waited 6 months to be seen. But, no; he couldn’t.
This story repeats itself over and over again. A sick patient calls to be seen and is told there is no availability for weeks or months. I do not understand how health care facilities, my own included, find this acceptable.
My father was very proud of his policy to see every patient in his waiting room no matter how long his office needed to stay open. He felt that access was of primary importance to his patients and to his practice. If he didn’t see them, somebody else would. Those of us working in large academic centers do not always feel the financial consequences of patients lost because of poor service.
Luckily, I work in a large cancer center that values access as much as a small practice would. When a patient calls us with a hematologic problem, we see them in less than 7 days, unless the patient prefers a different time frame. We monitor the time it takes to see patients and proactively assess upcoming appointments to ensure insurance coverage and the availability of records. If an obstruction is identified, the case is escalated to administrative leadership to be addressed and resolved. We are very proud of this work.
However, our focus on access does not end there. Once seen, we expedite patient evaluation by assessing workflows to obtain all necessary testing as quickly as possible. By doing so, we accelerate the time it takes from diagnosis to the time we start treating (time to treat). We have always tried to reduce time to treat for acute leukemia and we have applied those lessons to patients with lymphoma and solid tumors, resulting in a 33% improvement over the last 5 years.
We not only lessen the anxiety that comes with a scary diagnosis, emerging data indicate outcomes are improved with faster treatment, too (PLoS One. 2019 Mar 1;14(3):e0213209. doi: 10.1371/journal.pone.0213209).
These efforts will be criticized by those who feel the delivery of medical care should be structured more around the physician than the patient. Certainly, the system has developed to support a mindset of “physician first.” Not only do patients have to make an appointment for the privilege of seeing us, they have to navigate significant geographic and financial hurdles for that privilege.
Once at the appointment, physicians have historically been the provider giving the “orders” while others correct them, carry them out, follow-up on the results, manage phone calls, and schedule follow-up. This hierarchy has served physicians very well, but the pyramidal structure of health care is on the verge of being upended.
Too few physicians for an increasing demand for medical attention has led to the rise of advanced practice providers (APPs), who often serve as the only provider a patient may have, particularly in rural areas. In our center, we evolved from thinking of APPs as similar to house-staff who saw patients with us and did most of the work, but could not bill, to independent providers who work with us, do most of the work, and bill for their efforts. This slow transformation of our practice will soon seem quaint as we face the rapid disruption coming to our current conception of the health care delivery system.
Technologically savvy patients already demand immediate access to unlimited supplies of consumer goods, video, audio, books, magazines, and just about anything else you can think of. Immediate access to health care at a time convenient to the patient also will become an expectation because plenty of health care delivery models already are providing it. The local pharmacy or retail store may have a physician or APP right there ready to see a patient at any time. Some physicians are already online ready for an electronic interaction. See MDLIVE and Teladoc as examples.
The nimble cancer center that embraces these trends to become more patient-centric will be the center that captures national – if not international – market share, as insurance companies and governments adjust their reimbursement models to include these services. With blood work obtained just about anywhere, what would keep a patient with immune thrombocytopenic purpura from consulting with any online hematologist she chooses, whenever she chooses?
If first impressions are important, then patient access is important. Refrains of “I don’t have clinic that day,” “the pathology has not yet been reviewed,” and “that is not a disease I take care of,” ring as hollow to me as I suspect they do to our patients. When someone in my family has a significant illness, I want them to be seen now, not later. I believe we all would want prompt, efficient service.
We should strive to provide the same level of care to our patients as we expect for our family. Patients do not know that chronic leukemia is not an emergency. Time may not be critical to us, but it is to them. The perfect time to meet their needs is now.
Dr. Kalaycio is editor in chief of Hematology News. He chairs the department of hematology and medical oncology at Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.

Leadership and Professional Development: TIME’S UP for Hospital Medicine
“If it is true that the full humanity of women is not our culture, then we can and must make it our culture.”
—Chimamanda Ngozi Adichie
A young boy is on the way home from soccer when a driver hits his car head-on. His father dies immediately, but the boy survives. The boy is transported to the hospital and immediately rushed into the OR. The surgeon takes one look at him and says, “I can’t operate on this patient. He’s my son!” The riddle asks: If the father is dead, who is the surgeon?
Struggling to realize that the surgeon is a mom highlights the depth of gender bias in medicine. Gender bias leads to inequities which are magnified when compounded with differences in race, ethnicity, sexual orientation, gender identity and/or socioeconomic status. The recent National Academies report described the toll of gender inequities, including sexual harassment, and their impact on women in medicine.1 But like this riddle, the focus was directed towards those at the top of the hierarchy: physicians. It is undeniable that women physicians suffer the effects of inequities, but why exclude other women in healthcare? For example, over 90% of nurses are female, yet male nurses make higher salaries with lower degrees.2 If we only focus on physicians, we risk ignoring a problem faced by the entirety of our workforce.
Healthcare is a team sport. The practice of hospital medicine is a prime example of how each team member brings critical value. One would never be able to run an effective code without excellent nursing or successfully intubate a patient without a skilled respiratory therapist. Yet, when it comes to conversations about gender bias and sexual harassment, we rarely work together. The work of equity in healthcare must therefore become more like a lattice than a ladder, with many of us advocating for or with one another.
As hospital medicine has grown, hospitalists have become genuine agents of change. Therefore, this change too, must begin with hospitalists. As leaders in healthcare, we must advocate for equity for all, from the lab technician to the CEO. We must engage and respond when direct care workers (often minorities), face gender or racial bias. In short, if we see something, we must say something.
To create a culture of inclusivity and intersectionality in healthcare, we suggest the following:
- Unite healthcare workers across fields. View your fellow healthcare worker as a team member, not as a subordinate or ancillary staff. Ask them what their experiences regarding inequity have been. See things from their perspective.
- Be a champion for those affected by harassment and inequity. Offer direct support to anyone affected by harassment or inequity. Accompany them to human resources or use your influence to advocate for gender-based salary audits.
- Raise awareness and knowledge. Know the resources in your institution and share them with others. Encourage teams to discuss the impact of microaggressions and implicit bias together as opposed to in role-specific groups. Use communication to lend allyship and support. If you see microaggressions based on gender or race, inquire by asking “I’m curious...why would you say that?” or share the impact a statement has on you by noting “The comment doesn’t just affect one person, it affects all of us.”
People create culture. Meaningful cultural change must be inclusive and intersectional. Historically, movements focused on equity have failed to be inclusive, leading to certain groups feeling marginalized. The time has come to affect change in healthcare across all differences. Whether in the role of physician, nurse, advanced practice provider, or paramedical staff, it’s time to stand together and say: “time is up.”
Disclosures
Dr Kass and Dr. Acholonu are founding members of TIME’S UP Healthcare
1. National Academies of Sciences, Engineering, and Medicine. Sexual harassment of women: climate, culture, and consequences in academic sciences, engineering, and medicine. Washington, DC: National Academies Press, August 2018. (https://www.nap.edu/catalog/24994/sexual-harassment-of-women-climate-culture-and-consequences-in-academic). Accessed March 1, 2019.
2. 2018 Nurse.com. Nursing Salary Research Report. http://mediakit.nurse.com/wp-content/uploads/2018/06/2018-Nurse.com-Salary-Research-Report.pdf. Accessed March 1, 2019.
“If it is true that the full humanity of women is not our culture, then we can and must make it our culture.”
—Chimamanda Ngozi Adichie
A young boy is on the way home from soccer when a driver hits his car head-on. His father dies immediately, but the boy survives. The boy is transported to the hospital and immediately rushed into the OR. The surgeon takes one look at him and says, “I can’t operate on this patient. He’s my son!” The riddle asks: If the father is dead, who is the surgeon?
Struggling to realize that the surgeon is a mom highlights the depth of gender bias in medicine. Gender bias leads to inequities which are magnified when compounded with differences in race, ethnicity, sexual orientation, gender identity and/or socioeconomic status. The recent National Academies report described the toll of gender inequities, including sexual harassment, and their impact on women in medicine.1 But like this riddle, the focus was directed towards those at the top of the hierarchy: physicians. It is undeniable that women physicians suffer the effects of inequities, but why exclude other women in healthcare? For example, over 90% of nurses are female, yet male nurses make higher salaries with lower degrees.2 If we only focus on physicians, we risk ignoring a problem faced by the entirety of our workforce.
Healthcare is a team sport. The practice of hospital medicine is a prime example of how each team member brings critical value. One would never be able to run an effective code without excellent nursing or successfully intubate a patient without a skilled respiratory therapist. Yet, when it comes to conversations about gender bias and sexual harassment, we rarely work together. The work of equity in healthcare must therefore become more like a lattice than a ladder, with many of us advocating for or with one another.
As hospital medicine has grown, hospitalists have become genuine agents of change. Therefore, this change too, must begin with hospitalists. As leaders in healthcare, we must advocate for equity for all, from the lab technician to the CEO. We must engage and respond when direct care workers (often minorities), face gender or racial bias. In short, if we see something, we must say something.
To create a culture of inclusivity and intersectionality in healthcare, we suggest the following:
- Unite healthcare workers across fields. View your fellow healthcare worker as a team member, not as a subordinate or ancillary staff. Ask them what their experiences regarding inequity have been. See things from their perspective.
- Be a champion for those affected by harassment and inequity. Offer direct support to anyone affected by harassment or inequity. Accompany them to human resources or use your influence to advocate for gender-based salary audits.
- Raise awareness and knowledge. Know the resources in your institution and share them with others. Encourage teams to discuss the impact of microaggressions and implicit bias together as opposed to in role-specific groups. Use communication to lend allyship and support. If you see microaggressions based on gender or race, inquire by asking “I’m curious...why would you say that?” or share the impact a statement has on you by noting “The comment doesn’t just affect one person, it affects all of us.”
People create culture. Meaningful cultural change must be inclusive and intersectional. Historically, movements focused on equity have failed to be inclusive, leading to certain groups feeling marginalized. The time has come to affect change in healthcare across all differences. Whether in the role of physician, nurse, advanced practice provider, or paramedical staff, it’s time to stand together and say: “time is up.”
Disclosures
Dr Kass and Dr. Acholonu are founding members of TIME’S UP Healthcare
“If it is true that the full humanity of women is not our culture, then we can and must make it our culture.”
—Chimamanda Ngozi Adichie
A young boy is on the way home from soccer when a driver hits his car head-on. His father dies immediately, but the boy survives. The boy is transported to the hospital and immediately rushed into the OR. The surgeon takes one look at him and says, “I can’t operate on this patient. He’s my son!” The riddle asks: If the father is dead, who is the surgeon?
Struggling to realize that the surgeon is a mom highlights the depth of gender bias in medicine. Gender bias leads to inequities which are magnified when compounded with differences in race, ethnicity, sexual orientation, gender identity and/or socioeconomic status. The recent National Academies report described the toll of gender inequities, including sexual harassment, and their impact on women in medicine.1 But like this riddle, the focus was directed towards those at the top of the hierarchy: physicians. It is undeniable that women physicians suffer the effects of inequities, but why exclude other women in healthcare? For example, over 90% of nurses are female, yet male nurses make higher salaries with lower degrees.2 If we only focus on physicians, we risk ignoring a problem faced by the entirety of our workforce.
Healthcare is a team sport. The practice of hospital medicine is a prime example of how each team member brings critical value. One would never be able to run an effective code without excellent nursing or successfully intubate a patient without a skilled respiratory therapist. Yet, when it comes to conversations about gender bias and sexual harassment, we rarely work together. The work of equity in healthcare must therefore become more like a lattice than a ladder, with many of us advocating for or with one another.
As hospital medicine has grown, hospitalists have become genuine agents of change. Therefore, this change too, must begin with hospitalists. As leaders in healthcare, we must advocate for equity for all, from the lab technician to the CEO. We must engage and respond when direct care workers (often minorities), face gender or racial bias. In short, if we see something, we must say something.
To create a culture of inclusivity and intersectionality in healthcare, we suggest the following:
- Unite healthcare workers across fields. View your fellow healthcare worker as a team member, not as a subordinate or ancillary staff. Ask them what their experiences regarding inequity have been. See things from their perspective.
- Be a champion for those affected by harassment and inequity. Offer direct support to anyone affected by harassment or inequity. Accompany them to human resources or use your influence to advocate for gender-based salary audits.
- Raise awareness and knowledge. Know the resources in your institution and share them with others. Encourage teams to discuss the impact of microaggressions and implicit bias together as opposed to in role-specific groups. Use communication to lend allyship and support. If you see microaggressions based on gender or race, inquire by asking “I’m curious...why would you say that?” or share the impact a statement has on you by noting “The comment doesn’t just affect one person, it affects all of us.”
People create culture. Meaningful cultural change must be inclusive and intersectional. Historically, movements focused on equity have failed to be inclusive, leading to certain groups feeling marginalized. The time has come to affect change in healthcare across all differences. Whether in the role of physician, nurse, advanced practice provider, or paramedical staff, it’s time to stand together and say: “time is up.”
Disclosures
Dr Kass and Dr. Acholonu are founding members of TIME’S UP Healthcare
1. National Academies of Sciences, Engineering, and Medicine. Sexual harassment of women: climate, culture, and consequences in academic sciences, engineering, and medicine. Washington, DC: National Academies Press, August 2018. (https://www.nap.edu/catalog/24994/sexual-harassment-of-women-climate-culture-and-consequences-in-academic). Accessed March 1, 2019.
2. 2018 Nurse.com. Nursing Salary Research Report. http://mediakit.nurse.com/wp-content/uploads/2018/06/2018-Nurse.com-Salary-Research-Report.pdf. Accessed March 1, 2019.
1. National Academies of Sciences, Engineering, and Medicine. Sexual harassment of women: climate, culture, and consequences in academic sciences, engineering, and medicine. Washington, DC: National Academies Press, August 2018. (https://www.nap.edu/catalog/24994/sexual-harassment-of-women-climate-culture-and-consequences-in-academic). Accessed March 1, 2019.
2. 2018 Nurse.com. Nursing Salary Research Report. http://mediakit.nurse.com/wp-content/uploads/2018/06/2018-Nurse.com-Salary-Research-Report.pdf. Accessed March 1, 2019.
© 2019 Society of Hospital Medicine
In Response to “In Reference to: ‘Preventing Hypoglycemia Following Treatment of Hyperkalemia in Hospitalized Patients’”
We appreciate the comments and interest of Al-Sharefi and colleagues who highlight the use of glucose-only infusion in the management of hyperkalemia.1 The incidence of hypoglycemia following hyperkalemia treatment with insulin/dextrose is high and measures to reduce this should be pursued.2 However, evidence of the efficacy of glucose-only infusions on lowering potassium in heterogeneous inpatient populations is lacking. The small study by Chothia et al demonstrated potassium lowering efficacy in ten clinically stable patients without diabetes receiving chronic hemodialysis.3 In contrast, multiple observational studies consistently show a clinically significant effect of insulin/dextrose on potassium lowering across different populations.4
Importantly, inpatient hyperglycemia is associated with increased morbidity and mortality and occurs in those with preexisting diabetes and also those without, due to stress hyperglycemia from acute illness, medication or nutrition support.5 Determining intact insulin sensitivity during acute illness is not straightforward and deciding on the appropriateness of glucose-only hyperkalemia treatment compared with insulin/dextrose would be challenging. With the rising prevalence of diabetes in the inpatient setting (>30% in our study), the number of eligible individuals for glucose-only treatment would be small and does not justify the use of two separate hyperkalemia treatment protocols.
Given the potential life-threatening consequences of hyperkalemia, rapid potassium lowering is a priority. For glucose-only infusions to be applied, there n
Disclosures
The authors have nothing to disclose.
1. Al Sharefi A, Quinton R, Roberts G. In Reference to: “Preventing Hypoglycemia Following Treatment of Hyperkalemia in Hospitalized Patients “. J Hosp Med. 2019;14(6):387. doi: 10.12788/jhm.3209.
2. Boughton CK, Dixon D, Goble E, Burridge A, Cox A, Noble-Bell G, et al. Preventing hypoglycemia following treatment of hyperkalemia in hospitalized patients. J Hosp Med. 2019;14(5):284-287. doi: 10.12788/jhm.3145. PubMed
3. Chothia MY, Halperin ML, Rensburg MA, Hassan MS, Davids MR. Bolus administration of intravenous glucose in the treatment of hyperkalemia: a randomized controlled trial. Nephron Physiol. 2014;126(1):1-8. doi: 10.1159/000358836. PubMed
4. Harel Z, Kamel KS. Optimal dose and method of administration of intravenous insulin in the management of emergency hyperkalemia: a systematic review. PLoS One. 2016;11(5):e0154963. doi: 10.1371/journal.pone.0154963. e PubMed
5. Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):978-982. doi: 10.1210/jcem.87.3.8341. PubMed
We appreciate the comments and interest of Al-Sharefi and colleagues who highlight the use of glucose-only infusion in the management of hyperkalemia.1 The incidence of hypoglycemia following hyperkalemia treatment with insulin/dextrose is high and measures to reduce this should be pursued.2 However, evidence of the efficacy of glucose-only infusions on lowering potassium in heterogeneous inpatient populations is lacking. The small study by Chothia et al demonstrated potassium lowering efficacy in ten clinically stable patients without diabetes receiving chronic hemodialysis.3 In contrast, multiple observational studies consistently show a clinically significant effect of insulin/dextrose on potassium lowering across different populations.4
Importantly, inpatient hyperglycemia is associated with increased morbidity and mortality and occurs in those with preexisting diabetes and also those without, due to stress hyperglycemia from acute illness, medication or nutrition support.5 Determining intact insulin sensitivity during acute illness is not straightforward and deciding on the appropriateness of glucose-only hyperkalemia treatment compared with insulin/dextrose would be challenging. With the rising prevalence of diabetes in the inpatient setting (>30% in our study), the number of eligible individuals for glucose-only treatment would be small and does not justify the use of two separate hyperkalemia treatment protocols.
Given the potential life-threatening consequences of hyperkalemia, rapid potassium lowering is a priority. For glucose-only infusions to be applied, there n
Disclosures
The authors have nothing to disclose.
We appreciate the comments and interest of Al-Sharefi and colleagues who highlight the use of glucose-only infusion in the management of hyperkalemia.1 The incidence of hypoglycemia following hyperkalemia treatment with insulin/dextrose is high and measures to reduce this should be pursued.2 However, evidence of the efficacy of glucose-only infusions on lowering potassium in heterogeneous inpatient populations is lacking. The small study by Chothia et al demonstrated potassium lowering efficacy in ten clinically stable patients without diabetes receiving chronic hemodialysis.3 In contrast, multiple observational studies consistently show a clinically significant effect of insulin/dextrose on potassium lowering across different populations.4
Importantly, inpatient hyperglycemia is associated with increased morbidity and mortality and occurs in those with preexisting diabetes and also those without, due to stress hyperglycemia from acute illness, medication or nutrition support.5 Determining intact insulin sensitivity during acute illness is not straightforward and deciding on the appropriateness of glucose-only hyperkalemia treatment compared with insulin/dextrose would be challenging. With the rising prevalence of diabetes in the inpatient setting (>30% in our study), the number of eligible individuals for glucose-only treatment would be small and does not justify the use of two separate hyperkalemia treatment protocols.
Given the potential life-threatening consequences of hyperkalemia, rapid potassium lowering is a priority. For glucose-only infusions to be applied, there n
Disclosures
The authors have nothing to disclose.
1. Al Sharefi A, Quinton R, Roberts G. In Reference to: “Preventing Hypoglycemia Following Treatment of Hyperkalemia in Hospitalized Patients “. J Hosp Med. 2019;14(6):387. doi: 10.12788/jhm.3209.
2. Boughton CK, Dixon D, Goble E, Burridge A, Cox A, Noble-Bell G, et al. Preventing hypoglycemia following treatment of hyperkalemia in hospitalized patients. J Hosp Med. 2019;14(5):284-287. doi: 10.12788/jhm.3145. PubMed
3. Chothia MY, Halperin ML, Rensburg MA, Hassan MS, Davids MR. Bolus administration of intravenous glucose in the treatment of hyperkalemia: a randomized controlled trial. Nephron Physiol. 2014;126(1):1-8. doi: 10.1159/000358836. PubMed
4. Harel Z, Kamel KS. Optimal dose and method of administration of intravenous insulin in the management of emergency hyperkalemia: a systematic review. PLoS One. 2016;11(5):e0154963. doi: 10.1371/journal.pone.0154963. e PubMed
5. Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):978-982. doi: 10.1210/jcem.87.3.8341. PubMed
1. Al Sharefi A, Quinton R, Roberts G. In Reference to: “Preventing Hypoglycemia Following Treatment of Hyperkalemia in Hospitalized Patients “. J Hosp Med. 2019;14(6):387. doi: 10.12788/jhm.3209.
2. Boughton CK, Dixon D, Goble E, Burridge A, Cox A, Noble-Bell G, et al. Preventing hypoglycemia following treatment of hyperkalemia in hospitalized patients. J Hosp Med. 2019;14(5):284-287. doi: 10.12788/jhm.3145. PubMed
3. Chothia MY, Halperin ML, Rensburg MA, Hassan MS, Davids MR. Bolus administration of intravenous glucose in the treatment of hyperkalemia: a randomized controlled trial. Nephron Physiol. 2014;126(1):1-8. doi: 10.1159/000358836. PubMed
4. Harel Z, Kamel KS. Optimal dose and method of administration of intravenous insulin in the management of emergency hyperkalemia: a systematic review. PLoS One. 2016;11(5):e0154963. doi: 10.1371/journal.pone.0154963. e PubMed
5. Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):978-982. doi: 10.1210/jcem.87.3.8341. PubMed
© 2019 Society of Hospital Medicine