User login
Current Concepts in Pelvic Anatomy and Reconstructive Surgery
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD
Preface: Sizing up the evolution of reconstructive pelvic surgery
Avian influenza: An emerging pandemic threat
A patient with acute flank pain
How long can my patient use intranasal steroid sprays?
Vacationing vs. abandoning
Hospitalized patient hangs himself; estate blames vacationing psychiatrist
Los Angeles County (CA) Superior Court
Police took a 34-year-old man to an inpatient psychiatric facility after they found him walking naked on a city street. The hospital admitted him on a 72-hour involuntary hold because of his suicidal thoughts, although the psychiatrist did not believe he intended to kill himself. The patient had never attempted suicide before. The psychiatrist ordered treatment with risperidone and monitoring every 30 minutes.
Two days later, at the beginning of the psychiatrist’s vacation, the hospital started a 14-day hold process. After 3 days, the on-call psychiatrist documented the patient’s refusal to communicate and take medication, but the patient denied suicidal thinking.
After 3 more days, staff discovered the patient sitting unconscious on the floor next to the toilet, with his pants wrapped around his neck and tied to a grab bar. Staff attempted cardiopulmonary resuscitation and called paramedics, but the patient was dead.
The patient’s estate claimed that the hospital and first treating psychiatrist did not take appropriate measures to prevent the suicide. It charged the hospital with negligence in failing to have a breakaway grab bar and claimed the original psychiatrist did not adequately communicate the patient’s status with the covering psychiatrist before leaving on vacation.
The defense claimed the patient was not at high risk for suicide and that the standard of care is to communicate information regarding high-risk patients to the covering psychiatrist. The original psychiatrist also claimed the patient was doing well when he left for vacation.
- The jury decided for the defense
Dr. Grant’s observations
Patients and their families may feel abandoned in their psychiatrists’ absence. But this absence does not legally constitute abandonment unless:
- a doctor-patient relationship exists
- the doctor terminates the relationship
- there is a need for continuing care
- termination lacks reasonable notice so arrangements for continuing care cannot be made.
- Ensure that a system for getting urgent information to covering psychiatrists is in place.
- Verify that the covering psychiatrist knows he or she is responsible for your patients in emergency distress—including interviewing, reviewing records, and documenting treatment. His or her role is not just to fill space until you return.
- Tell emergency-prone patients the dates you’ll be unavailable and give them the contact information for the covering psychiatrist.
- Inform the covering psychiatrist about patients at high risk for suicide, decompensation, or hospitalization.
While travel is at times necessary, psychiatrists must ensure that emergency-prone patients have access to care in their absence (Box). You can delegate this responsibility to a covering psychiatrist, but choose him or her wisely. Selecting a physician you know is incapable of providing sound treatment is considered negligent. The primary psychiatrist cannot be held responsible for a substitute psychiatrist’s negligence if the choice of substitute is viewed as a competent delegation.
Cases are selected by Current Psychiatry's editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Hospitalized patient hangs himself; estate blames vacationing psychiatrist
Los Angeles County (CA) Superior Court
Police took a 34-year-old man to an inpatient psychiatric facility after they found him walking naked on a city street. The hospital admitted him on a 72-hour involuntary hold because of his suicidal thoughts, although the psychiatrist did not believe he intended to kill himself. The patient had never attempted suicide before. The psychiatrist ordered treatment with risperidone and monitoring every 30 minutes.
Two days later, at the beginning of the psychiatrist’s vacation, the hospital started a 14-day hold process. After 3 days, the on-call psychiatrist documented the patient’s refusal to communicate and take medication, but the patient denied suicidal thinking.
After 3 more days, staff discovered the patient sitting unconscious on the floor next to the toilet, with his pants wrapped around his neck and tied to a grab bar. Staff attempted cardiopulmonary resuscitation and called paramedics, but the patient was dead.
The patient’s estate claimed that the hospital and first treating psychiatrist did not take appropriate measures to prevent the suicide. It charged the hospital with negligence in failing to have a breakaway grab bar and claimed the original psychiatrist did not adequately communicate the patient’s status with the covering psychiatrist before leaving on vacation.
The defense claimed the patient was not at high risk for suicide and that the standard of care is to communicate information regarding high-risk patients to the covering psychiatrist. The original psychiatrist also claimed the patient was doing well when he left for vacation.
- The jury decided for the defense
Dr. Grant’s observations
Patients and their families may feel abandoned in their psychiatrists’ absence. But this absence does not legally constitute abandonment unless:
- a doctor-patient relationship exists
- the doctor terminates the relationship
- there is a need for continuing care
- termination lacks reasonable notice so arrangements for continuing care cannot be made.
- Ensure that a system for getting urgent information to covering psychiatrists is in place.
- Verify that the covering psychiatrist knows he or she is responsible for your patients in emergency distress—including interviewing, reviewing records, and documenting treatment. His or her role is not just to fill space until you return.
- Tell emergency-prone patients the dates you’ll be unavailable and give them the contact information for the covering psychiatrist.
- Inform the covering psychiatrist about patients at high risk for suicide, decompensation, or hospitalization.
While travel is at times necessary, psychiatrists must ensure that emergency-prone patients have access to care in their absence (Box). You can delegate this responsibility to a covering psychiatrist, but choose him or her wisely. Selecting a physician you know is incapable of providing sound treatment is considered negligent. The primary psychiatrist cannot be held responsible for a substitute psychiatrist’s negligence if the choice of substitute is viewed as a competent delegation.
Hospitalized patient hangs himself; estate blames vacationing psychiatrist
Los Angeles County (CA) Superior Court
Police took a 34-year-old man to an inpatient psychiatric facility after they found him walking naked on a city street. The hospital admitted him on a 72-hour involuntary hold because of his suicidal thoughts, although the psychiatrist did not believe he intended to kill himself. The patient had never attempted suicide before. The psychiatrist ordered treatment with risperidone and monitoring every 30 minutes.
Two days later, at the beginning of the psychiatrist’s vacation, the hospital started a 14-day hold process. After 3 days, the on-call psychiatrist documented the patient’s refusal to communicate and take medication, but the patient denied suicidal thinking.
After 3 more days, staff discovered the patient sitting unconscious on the floor next to the toilet, with his pants wrapped around his neck and tied to a grab bar. Staff attempted cardiopulmonary resuscitation and called paramedics, but the patient was dead.
The patient’s estate claimed that the hospital and first treating psychiatrist did not take appropriate measures to prevent the suicide. It charged the hospital with negligence in failing to have a breakaway grab bar and claimed the original psychiatrist did not adequately communicate the patient’s status with the covering psychiatrist before leaving on vacation.
The defense claimed the patient was not at high risk for suicide and that the standard of care is to communicate information regarding high-risk patients to the covering psychiatrist. The original psychiatrist also claimed the patient was doing well when he left for vacation.
- The jury decided for the defense
Dr. Grant’s observations
Patients and their families may feel abandoned in their psychiatrists’ absence. But this absence does not legally constitute abandonment unless:
- a doctor-patient relationship exists
- the doctor terminates the relationship
- there is a need for continuing care
- termination lacks reasonable notice so arrangements for continuing care cannot be made.
- Ensure that a system for getting urgent information to covering psychiatrists is in place.
- Verify that the covering psychiatrist knows he or she is responsible for your patients in emergency distress—including interviewing, reviewing records, and documenting treatment. His or her role is not just to fill space until you return.
- Tell emergency-prone patients the dates you’ll be unavailable and give them the contact information for the covering psychiatrist.
- Inform the covering psychiatrist about patients at high risk for suicide, decompensation, or hospitalization.
While travel is at times necessary, psychiatrists must ensure that emergency-prone patients have access to care in their absence (Box). You can delegate this responsibility to a covering psychiatrist, but choose him or her wisely. Selecting a physician you know is incapable of providing sound treatment is considered negligent. The primary psychiatrist cannot be held responsible for a substitute psychiatrist’s negligence if the choice of substitute is viewed as a competent delegation.
Cases are selected by Current Psychiatry's editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Cases are selected by Current Psychiatry's editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
The Dangerous Season

It was a dreary cold, December day and I was on call. It had been slow, but that was about to change. An 82-year-old man was admitted to my service with diarrhea, vomiting, fever, and abdominal cramps. He had never had any gastrointestinal problems and was on no medications. The only pertinent history was that his grandson was sick with a similar illness, and his daughter had been sick three days earlier.
Moments later, I received a second call for a preop clearance on a man who had been electrocuted while decorating his house for the holidays. He had fallen and broken his hip. Before I put the phone down the pager went off again—a patient admitted with a glucose level of 820. The light bulb over my head went off: We had entered the Dangerous Season.
What is this season that bodes well for no one? This poorly understood clinical risk factor begins during Halloween and lasts through Christmas, New Year’s, Valentine’s Day, and—in some areas of the country—until Mardi Gras. And now they’re upon us again: the holidays. Our bodies shudder, increasingly deprived of sunlight and oversupplied with calories, as we begin our festive mode.

All Hallow’s Eve: The Dangerous Season starts with Halloween, a pagan ritual. What child would not want to stay up after dark, run around in a mask scaring people, and eat too much candy to commemorate the leprous dead?
Halloween is the most medical of holidays. Many costumes and traditions are related to medicine: Frankenstein’s monster was assembled from body parts obtained by anatomic grave robbers. Mummies are well-preserved corpses, and mummy powder was a traditional remedy for skin ailments for centuries. Vampires may have nutritional deficiencies, and werewolves porphyria. Spider web is a traditional therapy used cutaneously as a styptic and internally for asthma.
For diabetics—especially diabetic children—Halloween is a painful time. In addition, there’s no shortage of pumpkin seed-induced diverticulitis, not to mention the unfortunate periodic occurrence of poisoned candy. According to the American College of Emergency Physicians there’s also a serious increase in risk of injury from collisions with motor vehicles, eye injuries from sharp objects, and burns from flammable costumes.
Other Halloween problems include minor inconveniences such as lost fillings secondary to nougat, falls from trees while removing toilet paper, and the occasional rotten egg to the posterior occiput. In our household there appears to be a higher than usual incidence of emesis and general abdominal pain.
Turkey Day: Next comes Thanksgiving, a seemingly benign day of turkey consumption and family cheer. The greatest danger of this holiday remains Salmonella, though Campylobacter jejuni lurks somewhere nearby. Undercooked turkey is a potent source of this infection, as are uncooked eggs in cookie dough.
The amount of time to properly thaw and cook a whole turkey, for example, is much longer than the standard-size poultry pieces and cuts of meat served year-round. When thawed correctly in the refrigerator or at a temperature of no more than 40 degrees F, a 20-pound turkey requires two to three days to thaw completely. Thawing the turkey completely before cooking is important. Otherwise, the outside of the turkey will be done before the inside.
To check a turkey for doneness, insert a food thermometer into the inner thigh area near the breast of the turkey (but not touching bone). The turkey is done when the temperature reaches 180 degrees F. If the turkey is stuffed, the temperature of the stuffing should be 165 degrees F. It is not unusual for whole families to fall ill after eating the Thanksgiving feast. Salmonella may be found in turkey, gravy, stuffing, pies, and other foods served at the Thanksgiving dinner.
Another danger of turkey consumption is its high L-tryptophan concentration. Excessive turkey consumption may lead to significant sleepiness, which when combined with substantial alcohol intake may lead to traffic accidents or, at minimum, falling asleep in front of the television. Of course Thanksgiving is not a healthy day for turkeys.
Perhaps the safest thing about Thanksgiving day is the cranberry sauce. If you can get real sauce and not canned, jellied sugar, you might prevent a urinary tract infection caused by E. coli by inhibiting the bacterial podocytes’ adherence to your bladder wall.

Christmas: Christmas can be a time of great stress, especially for the non-Christian members of our society, who are deluged with holiday images. There is an increased incident of suicide over the peri-Christmas timeframe, perhaps worsened by seasonal affective disorder, though there is no study showing higher suicide rates in this time period in the north.
For some unclear reason there’s a higher rate of deadly train collisions and other disasters over Christmas. The year 1910 was an especially bad year, with eight accidents in the United States, England, and France on Christmas Eve and Day with a total mortality of 56 lives.
As per Thanksgiving, the same dietary risks exist at Christmas, along with the addition of deadly bacterially infested homemade eggnog (best to drink the pasteurized variety). Fruitcake, a mysterious substance not currently listed on the periodic table, is used most frequently as a doorstop. In a limited survey of holiday revelers none of the subjects had actually ever eaten any. In all fairness to fruitcakes, Dec. 27 is National Fruitcake Day.
The most dangerous part of Christmas, besides paper cuts from wrapping presents and frustration from assembling bicycles, is the venerable Christmas tree. A tradition that likely started in 16th century Germany, Christmas trees only became accepted in the United States in the mid-1840s. Trees are a fire hazard and can fall, injuring children. The biggest problem, though, is electrocution from holiday lights placed on the tree and home.
In 1999 the New Zealand Ministry of Consumer Affairs’ Energy Safety Service warned consumers to cease using certain types of lights because of a danger of electrocution. Metal objects—especially tinsel—from a Christmas tree could come in contact with the adapter and act as a conductor. Perhaps Charlie Brown’s tree was best after all.
Both Hanukkah and Kwanzaa have candle-lighting ceremonies—the menorah and kinara, respectively—and carry an increased risk of burns and fires.
New Year’s and Valentine’s: New Year’s Eve (aka amateur night) is a chance for those who never stay up late drinking to do so. Other than vehicular manslaughter, a major risk of this evening is stray gunfire. The Los Angeles Police Department has launched a Citywide Gunfire Reduction Campaign for New Year’s because this has become a time to shoot guns. The best-known treatment for over-libation is the ever-popular menudo (a Mexican soup made with hominy and tripe—not the boy band).
Saint Valentine’s Day is another Hallmark bonanza, as well as an amateur day for lovers. There are many myths involving this saint. One legend contends that Valentine was a priest who served during the third century in Rome. When Emperor Claudius II decided that single men made better soldiers than those with wives and families, he outlawed marriage for young men—his crop of potential soldiers. Valentine, realizing the injustice of the decree, defied Claudius and continued to perform marriages for young lovers in secret. When Valentine’s actions were discovered, Claudius ordered that he be put to death.
A less likely version is that while in prison Valentine fell in love with a young girl—his jailer’s daughter—who visited him during his confinement. Before his death he allegedly wrote her a letter, which he signed “From your Valentine,” an expression still in use today.
The dangers of Valentine’s Day are so pervasive and hideous it is difficult to write about them all, so I won’t. Let it be said, though, that from herpes to HIV, lipstick on the collar to lymphogranuloma venereum, lust can kill.
In the South, Mardi Gras ends the dangerous season. Eye trauma from flying beads and sightings of flying monkeys are a constant threat. I have been to Mardi Gras, but this is all I can remember of it.
So ’tis the season to be jolly, to spend time with our loved ones, and to bask in the familial hearth. Bah, hum and bug. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
It was a dreary cold, December day and I was on call. It had been slow, but that was about to change. An 82-year-old man was admitted to my service with diarrhea, vomiting, fever, and abdominal cramps. He had never had any gastrointestinal problems and was on no medications. The only pertinent history was that his grandson was sick with a similar illness, and his daughter had been sick three days earlier.
Moments later, I received a second call for a preop clearance on a man who had been electrocuted while decorating his house for the holidays. He had fallen and broken his hip. Before I put the phone down the pager went off again—a patient admitted with a glucose level of 820. The light bulb over my head went off: We had entered the Dangerous Season.
What is this season that bodes well for no one? This poorly understood clinical risk factor begins during Halloween and lasts through Christmas, New Year’s, Valentine’s Day, and—in some areas of the country—until Mardi Gras. And now they’re upon us again: the holidays. Our bodies shudder, increasingly deprived of sunlight and oversupplied with calories, as we begin our festive mode.
All Hallow’s Eve: The Dangerous Season starts with Halloween, a pagan ritual. What child would not want to stay up after dark, run around in a mask scaring people, and eat too much candy to commemorate the leprous dead?
Halloween is the most medical of holidays. Many costumes and traditions are related to medicine: Frankenstein’s monster was assembled from body parts obtained by anatomic grave robbers. Mummies are well-preserved corpses, and mummy powder was a traditional remedy for skin ailments for centuries. Vampires may have nutritional deficiencies, and werewolves porphyria. Spider web is a traditional therapy used cutaneously as a styptic and internally for asthma.
For diabetics—especially diabetic children—Halloween is a painful time. In addition, there’s no shortage of pumpkin seed-induced diverticulitis, not to mention the unfortunate periodic occurrence of poisoned candy. According to the American College of Emergency Physicians there’s also a serious increase in risk of injury from collisions with motor vehicles, eye injuries from sharp objects, and burns from flammable costumes.
Other Halloween problems include minor inconveniences such as lost fillings secondary to nougat, falls from trees while removing toilet paper, and the occasional rotten egg to the posterior occiput. In our household there appears to be a higher than usual incidence of emesis and general abdominal pain.
Turkey Day: Next comes Thanksgiving, a seemingly benign day of turkey consumption and family cheer. The greatest danger of this holiday remains Salmonella, though Campylobacter jejuni lurks somewhere nearby. Undercooked turkey is a potent source of this infection, as are uncooked eggs in cookie dough.
The amount of time to properly thaw and cook a whole turkey, for example, is much longer than the standard-size poultry pieces and cuts of meat served year-round. When thawed correctly in the refrigerator or at a temperature of no more than 40 degrees F, a 20-pound turkey requires two to three days to thaw completely. Thawing the turkey completely before cooking is important. Otherwise, the outside of the turkey will be done before the inside.
To check a turkey for doneness, insert a food thermometer into the inner thigh area near the breast of the turkey (but not touching bone). The turkey is done when the temperature reaches 180 degrees F. If the turkey is stuffed, the temperature of the stuffing should be 165 degrees F. It is not unusual for whole families to fall ill after eating the Thanksgiving feast. Salmonella may be found in turkey, gravy, stuffing, pies, and other foods served at the Thanksgiving dinner.
Another danger of turkey consumption is its high L-tryptophan concentration. Excessive turkey consumption may lead to significant sleepiness, which when combined with substantial alcohol intake may lead to traffic accidents or, at minimum, falling asleep in front of the television. Of course Thanksgiving is not a healthy day for turkeys.
Perhaps the safest thing about Thanksgiving day is the cranberry sauce. If you can get real sauce and not canned, jellied sugar, you might prevent a urinary tract infection caused by E. coli by inhibiting the bacterial podocytes’ adherence to your bladder wall.
Christmas: Christmas can be a time of great stress, especially for the non-Christian members of our society, who are deluged with holiday images. There is an increased incident of suicide over the peri-Christmas timeframe, perhaps worsened by seasonal affective disorder, though there is no study showing higher suicide rates in this time period in the north.
For some unclear reason there’s a higher rate of deadly train collisions and other disasters over Christmas. The year 1910 was an especially bad year, with eight accidents in the United States, England, and France on Christmas Eve and Day with a total mortality of 56 lives.
As per Thanksgiving, the same dietary risks exist at Christmas, along with the addition of deadly bacterially infested homemade eggnog (best to drink the pasteurized variety). Fruitcake, a mysterious substance not currently listed on the periodic table, is used most frequently as a doorstop. In a limited survey of holiday revelers none of the subjects had actually ever eaten any. In all fairness to fruitcakes, Dec. 27 is National Fruitcake Day.
The most dangerous part of Christmas, besides paper cuts from wrapping presents and frustration from assembling bicycles, is the venerable Christmas tree. A tradition that likely started in 16th century Germany, Christmas trees only became accepted in the United States in the mid-1840s. Trees are a fire hazard and can fall, injuring children. The biggest problem, though, is electrocution from holiday lights placed on the tree and home.
In 1999 the New Zealand Ministry of Consumer Affairs’ Energy Safety Service warned consumers to cease using certain types of lights because of a danger of electrocution. Metal objects—especially tinsel—from a Christmas tree could come in contact with the adapter and act as a conductor. Perhaps Charlie Brown’s tree was best after all.
Both Hanukkah and Kwanzaa have candle-lighting ceremonies—the menorah and kinara, respectively—and carry an increased risk of burns and fires.
New Year’s and Valentine’s: New Year’s Eve (aka amateur night) is a chance for those who never stay up late drinking to do so. Other than vehicular manslaughter, a major risk of this evening is stray gunfire. The Los Angeles Police Department has launched a Citywide Gunfire Reduction Campaign for New Year’s because this has become a time to shoot guns. The best-known treatment for over-libation is the ever-popular menudo (a Mexican soup made with hominy and tripe—not the boy band).
Saint Valentine’s Day is another Hallmark bonanza, as well as an amateur day for lovers. There are many myths involving this saint. One legend contends that Valentine was a priest who served during the third century in Rome. When Emperor Claudius II decided that single men made better soldiers than those with wives and families, he outlawed marriage for young men—his crop of potential soldiers. Valentine, realizing the injustice of the decree, defied Claudius and continued to perform marriages for young lovers in secret. When Valentine’s actions were discovered, Claudius ordered that he be put to death.
A less likely version is that while in prison Valentine fell in love with a young girl—his jailer’s daughter—who visited him during his confinement. Before his death he allegedly wrote her a letter, which he signed “From your Valentine,” an expression still in use today.
The dangers of Valentine’s Day are so pervasive and hideous it is difficult to write about them all, so I won’t. Let it be said, though, that from herpes to HIV, lipstick on the collar to lymphogranuloma venereum, lust can kill.
In the South, Mardi Gras ends the dangerous season. Eye trauma from flying beads and sightings of flying monkeys are a constant threat. I have been to Mardi Gras, but this is all I can remember of it.
So ’tis the season to be jolly, to spend time with our loved ones, and to bask in the familial hearth. Bah, hum and bug. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
It was a dreary cold, December day and I was on call. It had been slow, but that was about to change. An 82-year-old man was admitted to my service with diarrhea, vomiting, fever, and abdominal cramps. He had never had any gastrointestinal problems and was on no medications. The only pertinent history was that his grandson was sick with a similar illness, and his daughter had been sick three days earlier.
Moments later, I received a second call for a preop clearance on a man who had been electrocuted while decorating his house for the holidays. He had fallen and broken his hip. Before I put the phone down the pager went off again—a patient admitted with a glucose level of 820. The light bulb over my head went off: We had entered the Dangerous Season.
What is this season that bodes well for no one? This poorly understood clinical risk factor begins during Halloween and lasts through Christmas, New Year’s, Valentine’s Day, and—in some areas of the country—until Mardi Gras. And now they’re upon us again: the holidays. Our bodies shudder, increasingly deprived of sunlight and oversupplied with calories, as we begin our festive mode.
All Hallow’s Eve: The Dangerous Season starts with Halloween, a pagan ritual. What child would not want to stay up after dark, run around in a mask scaring people, and eat too much candy to commemorate the leprous dead?
Halloween is the most medical of holidays. Many costumes and traditions are related to medicine: Frankenstein’s monster was assembled from body parts obtained by anatomic grave robbers. Mummies are well-preserved corpses, and mummy powder was a traditional remedy for skin ailments for centuries. Vampires may have nutritional deficiencies, and werewolves porphyria. Spider web is a traditional therapy used cutaneously as a styptic and internally for asthma.
For diabetics—especially diabetic children—Halloween is a painful time. In addition, there’s no shortage of pumpkin seed-induced diverticulitis, not to mention the unfortunate periodic occurrence of poisoned candy. According to the American College of Emergency Physicians there’s also a serious increase in risk of injury from collisions with motor vehicles, eye injuries from sharp objects, and burns from flammable costumes.
Other Halloween problems include minor inconveniences such as lost fillings secondary to nougat, falls from trees while removing toilet paper, and the occasional rotten egg to the posterior occiput. In our household there appears to be a higher than usual incidence of emesis and general abdominal pain.
Turkey Day: Next comes Thanksgiving, a seemingly benign day of turkey consumption and family cheer. The greatest danger of this holiday remains Salmonella, though Campylobacter jejuni lurks somewhere nearby. Undercooked turkey is a potent source of this infection, as are uncooked eggs in cookie dough.
The amount of time to properly thaw and cook a whole turkey, for example, is much longer than the standard-size poultry pieces and cuts of meat served year-round. When thawed correctly in the refrigerator or at a temperature of no more than 40 degrees F, a 20-pound turkey requires two to three days to thaw completely. Thawing the turkey completely before cooking is important. Otherwise, the outside of the turkey will be done before the inside.
To check a turkey for doneness, insert a food thermometer into the inner thigh area near the breast of the turkey (but not touching bone). The turkey is done when the temperature reaches 180 degrees F. If the turkey is stuffed, the temperature of the stuffing should be 165 degrees F. It is not unusual for whole families to fall ill after eating the Thanksgiving feast. Salmonella may be found in turkey, gravy, stuffing, pies, and other foods served at the Thanksgiving dinner.
Another danger of turkey consumption is its high L-tryptophan concentration. Excessive turkey consumption may lead to significant sleepiness, which when combined with substantial alcohol intake may lead to traffic accidents or, at minimum, falling asleep in front of the television. Of course Thanksgiving is not a healthy day for turkeys.
Perhaps the safest thing about Thanksgiving day is the cranberry sauce. If you can get real sauce and not canned, jellied sugar, you might prevent a urinary tract infection caused by E. coli by inhibiting the bacterial podocytes’ adherence to your bladder wall.
Christmas: Christmas can be a time of great stress, especially for the non-Christian members of our society, who are deluged with holiday images. There is an increased incident of suicide over the peri-Christmas timeframe, perhaps worsened by seasonal affective disorder, though there is no study showing higher suicide rates in this time period in the north.
For some unclear reason there’s a higher rate of deadly train collisions and other disasters over Christmas. The year 1910 was an especially bad year, with eight accidents in the United States, England, and France on Christmas Eve and Day with a total mortality of 56 lives.
As per Thanksgiving, the same dietary risks exist at Christmas, along with the addition of deadly bacterially infested homemade eggnog (best to drink the pasteurized variety). Fruitcake, a mysterious substance not currently listed on the periodic table, is used most frequently as a doorstop. In a limited survey of holiday revelers none of the subjects had actually ever eaten any. In all fairness to fruitcakes, Dec. 27 is National Fruitcake Day.
The most dangerous part of Christmas, besides paper cuts from wrapping presents and frustration from assembling bicycles, is the venerable Christmas tree. A tradition that likely started in 16th century Germany, Christmas trees only became accepted in the United States in the mid-1840s. Trees are a fire hazard and can fall, injuring children. The biggest problem, though, is electrocution from holiday lights placed on the tree and home.
In 1999 the New Zealand Ministry of Consumer Affairs’ Energy Safety Service warned consumers to cease using certain types of lights because of a danger of electrocution. Metal objects—especially tinsel—from a Christmas tree could come in contact with the adapter and act as a conductor. Perhaps Charlie Brown’s tree was best after all.
Both Hanukkah and Kwanzaa have candle-lighting ceremonies—the menorah and kinara, respectively—and carry an increased risk of burns and fires.
New Year’s and Valentine’s: New Year’s Eve (aka amateur night) is a chance for those who never stay up late drinking to do so. Other than vehicular manslaughter, a major risk of this evening is stray gunfire. The Los Angeles Police Department has launched a Citywide Gunfire Reduction Campaign for New Year’s because this has become a time to shoot guns. The best-known treatment for over-libation is the ever-popular menudo (a Mexican soup made with hominy and tripe—not the boy band).
Saint Valentine’s Day is another Hallmark bonanza, as well as an amateur day for lovers. There are many myths involving this saint. One legend contends that Valentine was a priest who served during the third century in Rome. When Emperor Claudius II decided that single men made better soldiers than those with wives and families, he outlawed marriage for young men—his crop of potential soldiers. Valentine, realizing the injustice of the decree, defied Claudius and continued to perform marriages for young lovers in secret. When Valentine’s actions were discovered, Claudius ordered that he be put to death.
A less likely version is that while in prison Valentine fell in love with a young girl—his jailer’s daughter—who visited him during his confinement. Before his death he allegedly wrote her a letter, which he signed “From your Valentine,” an expression still in use today.
The dangers of Valentine’s Day are so pervasive and hideous it is difficult to write about them all, so I won’t. Let it be said, though, that from herpes to HIV, lipstick on the collar to lymphogranuloma venereum, lust can kill.
In the South, Mardi Gras ends the dangerous season. Eye trauma from flying beads and sightings of flying monkeys are a constant threat. I have been to Mardi Gras, but this is all I can remember of it.
So ’tis the season to be jolly, to spend time with our loved ones, and to bask in the familial hearth. Bah, hum and bug. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Postdischarge Test Results, Acute Renal Failure, Diagnosing PE
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
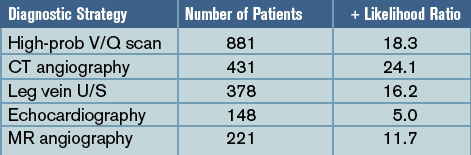
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
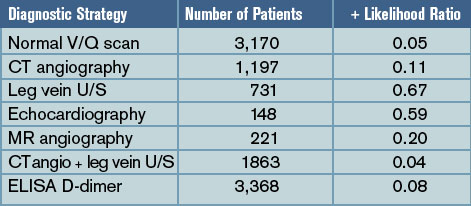
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
PEDIATRIC SPECIAL SECTION: Children’s National Medical Center’sHospitalist Division
Although pediatric resident graduates are well prepared to care for many ill children who require hospitalization, there are clinical, academic, and administrative skills that aren’t a standard part of residency, but are necessary for long-term academic success. The Children’s National Medical Center (CNMC) Hospitalist Fellowship program is structured over three years, through a combination of formal course work, seminars, clinical work, and mentored independent study.
Fellows work under the supervision of faculty in our 20-member Hospitalist Division, with inpatient pediatric services at five hospitals in Washington D.C., and suburban Maryland. A faculty appointment as a clinical instructor of the George Washington University (GWU) School of Medicine and Health Sciences qualifies the fellow to complete a Masters in Public Health, taking 15-18 credits per year. In addition to specific clinical, research, and didactic learning objectives, participation in committees and quality improvement and epidemiologic projects will facilitate study of hospital administration, budget, epidemiology and infection control.
The fellow must be a successful graduate of an American Council of Graduate Medical Education approved pediatric residency.
Clinical Training
Fellows spend approximately three months during the three year fellowship in the pediatric intensive care unit, two weeks in anesthesia, and two months in the emergency department to gain increased confidence, knowledge, and skill in airway management, placement of central lines, evaluation and management of the severely ill/injured child (respiratory failure and shock), conscious sedation, and pain management.
In addition, fellows spend 12 weeks per year on the CNMC hospitalist service. They co-attend with a CNMC hospitalist and lead a team of residents and students to practice an evidence-based approach to the acute evaluation and management of common inpatient problems such as bronchiolitis; asthma; gastroenteritis and dehydration; pneumonia; UTI; ALTE; common head, neck, skin and musculoskeletal infections; metabolic disorders; HIV infection; rheumatologic disease; and child abuse. Fellows also devote eight weeks per year to studying the process of providing coordinated care for the medically complex/technology dependent patients at CNMC and at rehab/subacute care hospital units that focus on improving care for children with multiorgan system disease. They also learn about complications associated with use of technology. Fellows’ elective clinical time may focus on delivery room management skills and well-baby teaching and management issues at one of our community hospital sites with 8,000 deliveries annually.
Research Training
CNMC fellows learn to plan, implement, analyze, and present results of a research study to answer a question relevant to hospitalists. By the end of the fellowship the fellows have an article accepted for publication in a peer-reviewed journal and present findings at a national meeting. To gain knowledge and skill needed to conduct an independent research project the fellows complete coursework in the School of Public Health at GWU and work under faculty mentors at CNMC.
Didactic Training
Four faculty members of our Hospitalist Division have completed the CNMC Master Teacher Certificate program with the GWU School of Education. In seminars taught by master teachers, fellows learn to lead, teach, and develop educational programs effectively. Faculty observe the fellow’s teaching skills in a variety of settings and provide feedback. Fellows have the opportunity to participate and develop computerized and standardized patient simulations to assess residents’ and students’ ability to care for pediatric inpatients.
PEDIATRIC SPECIAL SECTION
In the Literature
Formula Supplementation Prophylaxis for Jaundice in Breastfed Newborns
Gourley GR, Li Z, Kreamer BL, et al. A controlled, randomized, double-blind trial of prophylaxis against jaundice among breastfed newborns. Pediatrics. 2005;116(2):385-391.
Question: In breastfed newborns does oral beta-glucuronidase inhibitors during the first week after birth increase fecal bilirubin excretion and reduce jaundice without affecting breastfeeding deleteriously?
Design: Randomized (randomization table), double-blinded (supplements were prepared by a third party and labeled by a code) controlled trial.
Setting: Clinic.
Patients: 69 newborns, Caucasian, >37 week of gestation who were exclusively breastfed.
Intervention: Patients were randomly assigned to four groups: breastfeeding only (control), L-aspartic acid supplementation (L-aspartic), enzymatically hydrolyzed casein (EHC), and whey/casein-supplement without beta-glucuronidase inhibitor (W/C).
Main outcome measure: Daily transcutaneous and fecal bilirubin levels were obtained. Long-term follow-up assessments included age at first formula feeding, breastfeeding cessation age, and mother’s subjective impression of study.
Main results: Infants in all supplementation groups had significantly lower transcutaneous bilirubin levels in the first week of life than the nonsupplemented infants. The EHC and W/C groups both excreted more bilirubin diglucuronide and bilirubin monoglucuronide than the control group, and the L-aspartic acid had increased bilirubin monoglucuronide excretion compared with the control group. No negative effects from the supplementations were noted.
Conclusions: There is a significant reduction in transcutaneous bilirubin levels, with no negative effects on breastfeeding through the administration of specific supplements that are currently found in infant formulas.
Conflict of interest: None declared.
Commentary: The study describes a possible method of reducing hyperbilirubinemia associated with breastfeeding that employs small-volume supplementations of ingredients found in common infant formulas. The study did not reveal any negative effects on breastfeeding. Though the study was described as blinded the authors do not comment on how the exclusively breastfed infant group was blinded from the researchers and family.
The other control group (W/C) not fed a supplement without a beta-glucuronidase inhibitor yielded the unexpected significant reduction in transcutaneous bilirubin level compared with the control. This may mean that there is at least one other mechanism for the reduction of bilirubin in formula-fed infants than initially proposed by the authors.
In their conclusion, the authors pose a hypothesis explaining this result. They also correctly point out that due to this small study population, larger studies are needed to confirm these results.
This study used transcutaneous bilirubin measurements raising the question of reliability of this method compared to serum bilirubin measurements. A search of Medline using the terms “bilirubin and transcutaneous” produced a technical report.1 One section of this article reviewed available studies on the accuracy of transcutaneous bilirubin measurements concluding that the transcutaneous measurement has a linear correlation to serum bilirubin and its use for hyperbilirubinemia screening is reliable.
Reference
Ip S, Chung M, Kulig J, et al. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. An evidence-based review of important issues concerning neonatal hyperbilirubinemia. Pediatrics. 2004;Jul;114(1):e130-153.
Comparing Controllers: Montelukast and Fluticasone in Mild Persistent Asthma
Garcia Garcia ML, Wahn U, Gilles L, et al. Montelukast, compared with fluticasone, for control of asthma among 6- to 14-year-old patients with mild asthma: the MOSAIC study. Pediatrics. 2005;116(2):360-369.
Question: In children with mild asthma is the use of an antileukotriene medication as effective as an anti-inflammatory agent in maintaining number of days without the need of a rescue medication or utilization of asthma-related health resources?
Design: Multicenter, double-blind, double-dummy, randomized, parallel-group study. A four-week, single-blind, placebo run-in period was done prior to the initiation of the double-blind portion of the study. This run-in period included three clinic visits. During this time all participants discontinued any asthma controller medications and received image-matching, single-blind, montelukast and fluticasone. A short acting beta-agonist medication (open label) was also provided. Medication usage teaching was done during this time period. There was no placebo control group.
Setting: 104 study sites in 24 countries.
Patients: Patients (six-14 years of age) with mild persistent asthma as defined by the Global Initiative for Asthma (GINA) guidelines and otherwise in good health. Patients were required to have a FEV1 of ≥80% while the beta-receptor agonist was withheld for more than six hours in the first two visits and ≥70% on the third visit of the run-in period.
Intervention: Patients were randomized to receive either montelukast (5 mg oral before bedtime or 10 mg for patients ≥15) or fluticasone (100 mcg through MDI twice a day) and the appropriate placeboes.
Main outcome measures: Percentage of asthma rescue-free days (RFD).
RFD was defined as a day without:
- The use of a rescue medication: defined as any day during which a beta-receptor agonist, a systemic corticosteroid, or other rescue medications were used; and
- The use of an asthma health resource: defined as an unscheduled visit to a physician, an urgent/emergency care center or a hospital.
Main results: The number of RFDs were statistically similar between both groups. Mean percentage of RFD was 84% in the montelukast group and 86.7% in the fluticasone group.
Conflict of interest: Two of the study authors were employees of Merck and Company, which markets montelukast.
Commentary: This is an extensive study with multiple outcome measures. The study mimics actual clinical experience by using clinically relevant end points as primary outcomes. The study does not have a placebo control group. Overall the study showed that there is no significant difference between montelukast and fluticasone with regard to the primary outcome of RFDs, but there were some differences favoring fluticasone in secondary outcome measures, including number of days of beta-receptor agonist use and improvement of the average score of the control domain of the Pediatric Asthma Therapy Assessment Questionnaire.
K. Kingae Causes Osteomyelitis/Septic Arthritis
Kiang KM, Ogunmodede F, Juni BA, et al. Outbreak of osteomyelitis/septic arthritis caused by Kingella kingae among child care center attendees. Pediatrics. 2005;116;e206-213.
Review by Julia Simmons, MD
Kingella kingae (K. kingae), a gram-negative organism known to colonize the oropharynx, may cause invasive diseases, such as septic arthritis and osteomyelitis in children who were previously healthy. In this article, the authors describe the first reported outbreak of K. kingae causing osteomyelitis/septic arthritis.
In October 2003 the Minnesota Department of Health was notified of an outbreak of K. kingae at a daycare facility. There were two culture positive cases and one culture negative but clinically presumed to be secondary to K. kingae. The children were all in the same classroom (toddler classroom 1) and were between the ages of 17 and 21 months. The previously healthy children presented with fever and limp.
In this cohort study, the authors investigated risk factors for invasive disease and for colonization with K. kingae. They also determined the prevalence of asymptomatic colonization at the daycare involving the confirmed cases and at a second daycare facility, which served as the control. Culture samples were analyzed at the Minnesota Department of Health Public Health Laboratory. The laboratory performed confirmation, pulsed-field gel electrophoresis, DNA sequencing, and antimicrobial testing specifically with rifampin, penicillin, and azithromycin.
At the study facility 115/122 (94%) children and 28/29 (97%) adult staff members were cultured. Fifteen (13 %) of the children were colonized. The prevalence of colonization was 45% (9 children) in the toddler 1 classroom, which is the classroom of the confirmed cases. The three case patients had negative oropharyngeal cultures; however, all three had been pretreated with antibiotic therapy. The pulsed-field gel electrophoresis was indistinguishable in the confirmed cases and the colonized students. The authors did not discover any risk factors for invasive disease. This information was gathered from a list of questions regarding past medical history, which the parents discussed on the telephone with the investigators. Rifampin, penicillin, and azithromycin all had low MICs
At the control care center, 45/118 (38%) of people were cultured from the oropharynx. Seven (16%) were colonized. The pulsed-field gel electrophoresis was the same for the control care facility, but varied from the electrophoresis pattern at the study facility.
In conclusion, the authors summarized the findings of K. kingae osteomyelitis/septic arthritis in a daycare facility. There were no identifiable risk factors for invasive disease or for asymptomatic carrier state. It is important to remember that up to 50% of culture negative cases of septic arthritis in patients less than two years of age may be attributed to K. kingae. Thus, the clinician must maintain a high index of suspicion and relay this information to the laboratory so that appropriate measures are taken to ensure the optimal growth environment for the bacteria.
Although the study size was small, the investigators provide initial documentation regarding outbreaks of invasive K. kingae infections. Further studies will be useful to clarify the exact mode of transmission and appropriate duration of antimicrobial therapy.
Systematic Review of Therapy for Pediatric Migraine
Damen L, Bruijn JKJ, Verhagen AP, et al. Symptomatic treatment of migraine in children: a systematic review of medication trials. Pediatrics. 2005;116(2):295-302.
Migraines affect 3%-5% of prepubescent children. The symptoms frequently include unilateral throbbing headache associated with nausea and vomiting. If poorly controlled, the headaches can cause students to miss school and have a decreased quality of life. Symptomatic pharmacologic interventions involve analgesics, triptans, and antiemetics. Nonpharmacologic interventions include dietary changes, biofeedback, and exercise. Treatment is tailored to the patient; however, there are limited studies providing evidence describing the most efficacious pharmacologic treatment for managing symptomatic migraines.
The authors conducted a retrospective literature review to evaluate the evidence from randomized controlled trials (RCT) and clinical controlled trials (CCT) regarding the treatment of symptomatic migraine in children younger than 18. The primary outcome measure was headache clinical improvement defined as a headache decline by >50%. Secondary measures included headache intensity, frequency, duration, and headache index. The authors searched Medline, Embase, PsychInfo, Web of Science, and Cinahl from the start of the databases to June 2004. They used appropriate search terms including “headache,” “migraine,” “child” and variations thereof. Further, they searched reference lists of the articles and the included studies. Two authors independently reviewed the titles and abstracts to determine acceptability in the study. They also used the Delphi list to assess the methodologic quality of the included trials.
Of 3,492 relevant studies, 10 met the inclusion criteria specified by the authors. There were a total of 1,575 patients with a mean age of 11.7 +/- 2.2 years included in the study. A mean of 19.8% of subjects did not complete participation in their respective studies. Overall, the percentage of male and female participants was equal. Six studies were considered to be of high quality by the authors. They found moderate evidence that ibuprofen and acetaminophen were more effective in decreasing headache symptoms one and two hours after ingestion in comparison with a placebo. Further, the nasal spray sumatriptan was more efficacious in diminishing headache than placebo; however, it was associated with more side effects. Intravenous prochlorperazine was more effective than intravenous ketorolac in diminishing symptoms one hour after intake.
While accomplishing a sound systematic review of the available controlled trials, the authors conclude that there are insufficient trials of adequate quality to fully elucidate the most efficacious symptomatic pharmacologic therapy for pediatric patients suffering from migraine headaches. A large randomized prospective trial comparing analgesics, triptans, and antiemetics against placebo is needed. TH
Although pediatric resident graduates are well prepared to care for many ill children who require hospitalization, there are clinical, academic, and administrative skills that aren’t a standard part of residency, but are necessary for long-term academic success. The Children’s National Medical Center (CNMC) Hospitalist Fellowship program is structured over three years, through a combination of formal course work, seminars, clinical work, and mentored independent study.
Fellows work under the supervision of faculty in our 20-member Hospitalist Division, with inpatient pediatric services at five hospitals in Washington D.C., and suburban Maryland. A faculty appointment as a clinical instructor of the George Washington University (GWU) School of Medicine and Health Sciences qualifies the fellow to complete a Masters in Public Health, taking 15-18 credits per year. In addition to specific clinical, research, and didactic learning objectives, participation in committees and quality improvement and epidemiologic projects will facilitate study of hospital administration, budget, epidemiology and infection control.
The fellow must be a successful graduate of an American Council of Graduate Medical Education approved pediatric residency.
Clinical Training
Fellows spend approximately three months during the three year fellowship in the pediatric intensive care unit, two weeks in anesthesia, and two months in the emergency department to gain increased confidence, knowledge, and skill in airway management, placement of central lines, evaluation and management of the severely ill/injured child (respiratory failure and shock), conscious sedation, and pain management.
In addition, fellows spend 12 weeks per year on the CNMC hospitalist service. They co-attend with a CNMC hospitalist and lead a team of residents and students to practice an evidence-based approach to the acute evaluation and management of common inpatient problems such as bronchiolitis; asthma; gastroenteritis and dehydration; pneumonia; UTI; ALTE; common head, neck, skin and musculoskeletal infections; metabolic disorders; HIV infection; rheumatologic disease; and child abuse. Fellows also devote eight weeks per year to studying the process of providing coordinated care for the medically complex/technology dependent patients at CNMC and at rehab/subacute care hospital units that focus on improving care for children with multiorgan system disease. They also learn about complications associated with use of technology. Fellows’ elective clinical time may focus on delivery room management skills and well-baby teaching and management issues at one of our community hospital sites with 8,000 deliveries annually.
Research Training
CNMC fellows learn to plan, implement, analyze, and present results of a research study to answer a question relevant to hospitalists. By the end of the fellowship the fellows have an article accepted for publication in a peer-reviewed journal and present findings at a national meeting. To gain knowledge and skill needed to conduct an independent research project the fellows complete coursework in the School of Public Health at GWU and work under faculty mentors at CNMC.
Didactic Training
Four faculty members of our Hospitalist Division have completed the CNMC Master Teacher Certificate program with the GWU School of Education. In seminars taught by master teachers, fellows learn to lead, teach, and develop educational programs effectively. Faculty observe the fellow’s teaching skills in a variety of settings and provide feedback. Fellows have the opportunity to participate and develop computerized and standardized patient simulations to assess residents’ and students’ ability to care for pediatric inpatients.
PEDIATRIC SPECIAL SECTION
In the Literature
Formula Supplementation Prophylaxis for Jaundice in Breastfed Newborns
Gourley GR, Li Z, Kreamer BL, et al. A controlled, randomized, double-blind trial of prophylaxis against jaundice among breastfed newborns. Pediatrics. 2005;116(2):385-391.
Question: In breastfed newborns does oral beta-glucuronidase inhibitors during the first week after birth increase fecal bilirubin excretion and reduce jaundice without affecting breastfeeding deleteriously?
Design: Randomized (randomization table), double-blinded (supplements were prepared by a third party and labeled by a code) controlled trial.
Setting: Clinic.
Patients: 69 newborns, Caucasian, >37 week of gestation who were exclusively breastfed.
Intervention: Patients were randomly assigned to four groups: breastfeeding only (control), L-aspartic acid supplementation (L-aspartic), enzymatically hydrolyzed casein (EHC), and whey/casein-supplement without beta-glucuronidase inhibitor (W/C).
Main outcome measure: Daily transcutaneous and fecal bilirubin levels were obtained. Long-term follow-up assessments included age at first formula feeding, breastfeeding cessation age, and mother’s subjective impression of study.
Main results: Infants in all supplementation groups had significantly lower transcutaneous bilirubin levels in the first week of life than the nonsupplemented infants. The EHC and W/C groups both excreted more bilirubin diglucuronide and bilirubin monoglucuronide than the control group, and the L-aspartic acid had increased bilirubin monoglucuronide excretion compared with the control group. No negative effects from the supplementations were noted.
Conclusions: There is a significant reduction in transcutaneous bilirubin levels, with no negative effects on breastfeeding through the administration of specific supplements that are currently found in infant formulas.
Conflict of interest: None declared.
Commentary: The study describes a possible method of reducing hyperbilirubinemia associated with breastfeeding that employs small-volume supplementations of ingredients found in common infant formulas. The study did not reveal any negative effects on breastfeeding. Though the study was described as blinded the authors do not comment on how the exclusively breastfed infant group was blinded from the researchers and family.
The other control group (W/C) not fed a supplement without a beta-glucuronidase inhibitor yielded the unexpected significant reduction in transcutaneous bilirubin level compared with the control. This may mean that there is at least one other mechanism for the reduction of bilirubin in formula-fed infants than initially proposed by the authors.
In their conclusion, the authors pose a hypothesis explaining this result. They also correctly point out that due to this small study population, larger studies are needed to confirm these results.
This study used transcutaneous bilirubin measurements raising the question of reliability of this method compared to serum bilirubin measurements. A search of Medline using the terms “bilirubin and transcutaneous” produced a technical report.1 One section of this article reviewed available studies on the accuracy of transcutaneous bilirubin measurements concluding that the transcutaneous measurement has a linear correlation to serum bilirubin and its use for hyperbilirubinemia screening is reliable.
Reference
Ip S, Chung M, Kulig J, et al. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. An evidence-based review of important issues concerning neonatal hyperbilirubinemia. Pediatrics. 2004;Jul;114(1):e130-153.
Comparing Controllers: Montelukast and Fluticasone in Mild Persistent Asthma
Garcia Garcia ML, Wahn U, Gilles L, et al. Montelukast, compared with fluticasone, for control of asthma among 6- to 14-year-old patients with mild asthma: the MOSAIC study. Pediatrics. 2005;116(2):360-369.
Question: In children with mild asthma is the use of an antileukotriene medication as effective as an anti-inflammatory agent in maintaining number of days without the need of a rescue medication or utilization of asthma-related health resources?
Design: Multicenter, double-blind, double-dummy, randomized, parallel-group study. A four-week, single-blind, placebo run-in period was done prior to the initiation of the double-blind portion of the study. This run-in period included three clinic visits. During this time all participants discontinued any asthma controller medications and received image-matching, single-blind, montelukast and fluticasone. A short acting beta-agonist medication (open label) was also provided. Medication usage teaching was done during this time period. There was no placebo control group.
Setting: 104 study sites in 24 countries.
Patients: Patients (six-14 years of age) with mild persistent asthma as defined by the Global Initiative for Asthma (GINA) guidelines and otherwise in good health. Patients were required to have a FEV1 of ≥80% while the beta-receptor agonist was withheld for more than six hours in the first two visits and ≥70% on the third visit of the run-in period.
Intervention: Patients were randomized to receive either montelukast (5 mg oral before bedtime or 10 mg for patients ≥15) or fluticasone (100 mcg through MDI twice a day) and the appropriate placeboes.
Main outcome measures: Percentage of asthma rescue-free days (RFD).
RFD was defined as a day without:
- The use of a rescue medication: defined as any day during which a beta-receptor agonist, a systemic corticosteroid, or other rescue medications were used; and
- The use of an asthma health resource: defined as an unscheduled visit to a physician, an urgent/emergency care center or a hospital.
Main results: The number of RFDs were statistically similar between both groups. Mean percentage of RFD was 84% in the montelukast group and 86.7% in the fluticasone group.
Conflict of interest: Two of the study authors were employees of Merck and Company, which markets montelukast.
Commentary: This is an extensive study with multiple outcome measures. The study mimics actual clinical experience by using clinically relevant end points as primary outcomes. The study does not have a placebo control group. Overall the study showed that there is no significant difference between montelukast and fluticasone with regard to the primary outcome of RFDs, but there were some differences favoring fluticasone in secondary outcome measures, including number of days of beta-receptor agonist use and improvement of the average score of the control domain of the Pediatric Asthma Therapy Assessment Questionnaire.
K. Kingae Causes Osteomyelitis/Septic Arthritis
Kiang KM, Ogunmodede F, Juni BA, et al. Outbreak of osteomyelitis/septic arthritis caused by Kingella kingae among child care center attendees. Pediatrics. 2005;116;e206-213.
Review by Julia Simmons, MD
Kingella kingae (K. kingae), a gram-negative organism known to colonize the oropharynx, may cause invasive diseases, such as septic arthritis and osteomyelitis in children who were previously healthy. In this article, the authors describe the first reported outbreak of K. kingae causing osteomyelitis/septic arthritis.
In October 2003 the Minnesota Department of Health was notified of an outbreak of K. kingae at a daycare facility. There were two culture positive cases and one culture negative but clinically presumed to be secondary to K. kingae. The children were all in the same classroom (toddler classroom 1) and were between the ages of 17 and 21 months. The previously healthy children presented with fever and limp.
In this cohort study, the authors investigated risk factors for invasive disease and for colonization with K. kingae. They also determined the prevalence of asymptomatic colonization at the daycare involving the confirmed cases and at a second daycare facility, which served as the control. Culture samples were analyzed at the Minnesota Department of Health Public Health Laboratory. The laboratory performed confirmation, pulsed-field gel electrophoresis, DNA sequencing, and antimicrobial testing specifically with rifampin, penicillin, and azithromycin.
At the study facility 115/122 (94%) children and 28/29 (97%) adult staff members were cultured. Fifteen (13 %) of the children were colonized. The prevalence of colonization was 45% (9 children) in the toddler 1 classroom, which is the classroom of the confirmed cases. The three case patients had negative oropharyngeal cultures; however, all three had been pretreated with antibiotic therapy. The pulsed-field gel electrophoresis was indistinguishable in the confirmed cases and the colonized students. The authors did not discover any risk factors for invasive disease. This information was gathered from a list of questions regarding past medical history, which the parents discussed on the telephone with the investigators. Rifampin, penicillin, and azithromycin all had low MICs
At the control care center, 45/118 (38%) of people were cultured from the oropharynx. Seven (16%) were colonized. The pulsed-field gel electrophoresis was the same for the control care facility, but varied from the electrophoresis pattern at the study facility.
In conclusion, the authors summarized the findings of K. kingae osteomyelitis/septic arthritis in a daycare facility. There were no identifiable risk factors for invasive disease or for asymptomatic carrier state. It is important to remember that up to 50% of culture negative cases of septic arthritis in patients less than two years of age may be attributed to K. kingae. Thus, the clinician must maintain a high index of suspicion and relay this information to the laboratory so that appropriate measures are taken to ensure the optimal growth environment for the bacteria.
Although the study size was small, the investigators provide initial documentation regarding outbreaks of invasive K. kingae infections. Further studies will be useful to clarify the exact mode of transmission and appropriate duration of antimicrobial therapy.
Systematic Review of Therapy for Pediatric Migraine
Damen L, Bruijn JKJ, Verhagen AP, et al. Symptomatic treatment of migraine in children: a systematic review of medication trials. Pediatrics. 2005;116(2):295-302.
Migraines affect 3%-5% of prepubescent children. The symptoms frequently include unilateral throbbing headache associated with nausea and vomiting. If poorly controlled, the headaches can cause students to miss school and have a decreased quality of life. Symptomatic pharmacologic interventions involve analgesics, triptans, and antiemetics. Nonpharmacologic interventions include dietary changes, biofeedback, and exercise. Treatment is tailored to the patient; however, there are limited studies providing evidence describing the most efficacious pharmacologic treatment for managing symptomatic migraines.
The authors conducted a retrospective literature review to evaluate the evidence from randomized controlled trials (RCT) and clinical controlled trials (CCT) regarding the treatment of symptomatic migraine in children younger than 18. The primary outcome measure was headache clinical improvement defined as a headache decline by >50%. Secondary measures included headache intensity, frequency, duration, and headache index. The authors searched Medline, Embase, PsychInfo, Web of Science, and Cinahl from the start of the databases to June 2004. They used appropriate search terms including “headache,” “migraine,” “child” and variations thereof. Further, they searched reference lists of the articles and the included studies. Two authors independently reviewed the titles and abstracts to determine acceptability in the study. They also used the Delphi list to assess the methodologic quality of the included trials.
Of 3,492 relevant studies, 10 met the inclusion criteria specified by the authors. There were a total of 1,575 patients with a mean age of 11.7 +/- 2.2 years included in the study. A mean of 19.8% of subjects did not complete participation in their respective studies. Overall, the percentage of male and female participants was equal. Six studies were considered to be of high quality by the authors. They found moderate evidence that ibuprofen and acetaminophen were more effective in decreasing headache symptoms one and two hours after ingestion in comparison with a placebo. Further, the nasal spray sumatriptan was more efficacious in diminishing headache than placebo; however, it was associated with more side effects. Intravenous prochlorperazine was more effective than intravenous ketorolac in diminishing symptoms one hour after intake.
While accomplishing a sound systematic review of the available controlled trials, the authors conclude that there are insufficient trials of adequate quality to fully elucidate the most efficacious symptomatic pharmacologic therapy for pediatric patients suffering from migraine headaches. A large randomized prospective trial comparing analgesics, triptans, and antiemetics against placebo is needed. TH
Although pediatric resident graduates are well prepared to care for many ill children who require hospitalization, there are clinical, academic, and administrative skills that aren’t a standard part of residency, but are necessary for long-term academic success. The Children’s National Medical Center (CNMC) Hospitalist Fellowship program is structured over three years, through a combination of formal course work, seminars, clinical work, and mentored independent study.
Fellows work under the supervision of faculty in our 20-member Hospitalist Division, with inpatient pediatric services at five hospitals in Washington D.C., and suburban Maryland. A faculty appointment as a clinical instructor of the George Washington University (GWU) School of Medicine and Health Sciences qualifies the fellow to complete a Masters in Public Health, taking 15-18 credits per year. In addition to specific clinical, research, and didactic learning objectives, participation in committees and quality improvement and epidemiologic projects will facilitate study of hospital administration, budget, epidemiology and infection control.
The fellow must be a successful graduate of an American Council of Graduate Medical Education approved pediatric residency.
Clinical Training
Fellows spend approximately three months during the three year fellowship in the pediatric intensive care unit, two weeks in anesthesia, and two months in the emergency department to gain increased confidence, knowledge, and skill in airway management, placement of central lines, evaluation and management of the severely ill/injured child (respiratory failure and shock), conscious sedation, and pain management.
In addition, fellows spend 12 weeks per year on the CNMC hospitalist service. They co-attend with a CNMC hospitalist and lead a team of residents and students to practice an evidence-based approach to the acute evaluation and management of common inpatient problems such as bronchiolitis; asthma; gastroenteritis and dehydration; pneumonia; UTI; ALTE; common head, neck, skin and musculoskeletal infections; metabolic disorders; HIV infection; rheumatologic disease; and child abuse. Fellows also devote eight weeks per year to studying the process of providing coordinated care for the medically complex/technology dependent patients at CNMC and at rehab/subacute care hospital units that focus on improving care for children with multiorgan system disease. They also learn about complications associated with use of technology. Fellows’ elective clinical time may focus on delivery room management skills and well-baby teaching and management issues at one of our community hospital sites with 8,000 deliveries annually.
Research Training
CNMC fellows learn to plan, implement, analyze, and present results of a research study to answer a question relevant to hospitalists. By the end of the fellowship the fellows have an article accepted for publication in a peer-reviewed journal and present findings at a national meeting. To gain knowledge and skill needed to conduct an independent research project the fellows complete coursework in the School of Public Health at GWU and work under faculty mentors at CNMC.
Didactic Training
Four faculty members of our Hospitalist Division have completed the CNMC Master Teacher Certificate program with the GWU School of Education. In seminars taught by master teachers, fellows learn to lead, teach, and develop educational programs effectively. Faculty observe the fellow’s teaching skills in a variety of settings and provide feedback. Fellows have the opportunity to participate and develop computerized and standardized patient simulations to assess residents’ and students’ ability to care for pediatric inpatients.
PEDIATRIC SPECIAL SECTION
In the Literature
Formula Supplementation Prophylaxis for Jaundice in Breastfed Newborns
Gourley GR, Li Z, Kreamer BL, et al. A controlled, randomized, double-blind trial of prophylaxis against jaundice among breastfed newborns. Pediatrics. 2005;116(2):385-391.
Question: In breastfed newborns does oral beta-glucuronidase inhibitors during the first week after birth increase fecal bilirubin excretion and reduce jaundice without affecting breastfeeding deleteriously?
Design: Randomized (randomization table), double-blinded (supplements were prepared by a third party and labeled by a code) controlled trial.
Setting: Clinic.
Patients: 69 newborns, Caucasian, >37 week of gestation who were exclusively breastfed.
Intervention: Patients were randomly assigned to four groups: breastfeeding only (control), L-aspartic acid supplementation (L-aspartic), enzymatically hydrolyzed casein (EHC), and whey/casein-supplement without beta-glucuronidase inhibitor (W/C).
Main outcome measure: Daily transcutaneous and fecal bilirubin levels were obtained. Long-term follow-up assessments included age at first formula feeding, breastfeeding cessation age, and mother’s subjective impression of study.
Main results: Infants in all supplementation groups had significantly lower transcutaneous bilirubin levels in the first week of life than the nonsupplemented infants. The EHC and W/C groups both excreted more bilirubin diglucuronide and bilirubin monoglucuronide than the control group, and the L-aspartic acid had increased bilirubin monoglucuronide excretion compared with the control group. No negative effects from the supplementations were noted.
Conclusions: There is a significant reduction in transcutaneous bilirubin levels, with no negative effects on breastfeeding through the administration of specific supplements that are currently found in infant formulas.
Conflict of interest: None declared.
Commentary: The study describes a possible method of reducing hyperbilirubinemia associated with breastfeeding that employs small-volume supplementations of ingredients found in common infant formulas. The study did not reveal any negative effects on breastfeeding. Though the study was described as blinded the authors do not comment on how the exclusively breastfed infant group was blinded from the researchers and family.
The other control group (W/C) not fed a supplement without a beta-glucuronidase inhibitor yielded the unexpected significant reduction in transcutaneous bilirubin level compared with the control. This may mean that there is at least one other mechanism for the reduction of bilirubin in formula-fed infants than initially proposed by the authors.
In their conclusion, the authors pose a hypothesis explaining this result. They also correctly point out that due to this small study population, larger studies are needed to confirm these results.
This study used transcutaneous bilirubin measurements raising the question of reliability of this method compared to serum bilirubin measurements. A search of Medline using the terms “bilirubin and transcutaneous” produced a technical report.1 One section of this article reviewed available studies on the accuracy of transcutaneous bilirubin measurements concluding that the transcutaneous measurement has a linear correlation to serum bilirubin and its use for hyperbilirubinemia screening is reliable.
Reference
Ip S, Chung M, Kulig J, et al. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. An evidence-based review of important issues concerning neonatal hyperbilirubinemia. Pediatrics. 2004;Jul;114(1):e130-153.
Comparing Controllers: Montelukast and Fluticasone in Mild Persistent Asthma
Garcia Garcia ML, Wahn U, Gilles L, et al. Montelukast, compared with fluticasone, for control of asthma among 6- to 14-year-old patients with mild asthma: the MOSAIC study. Pediatrics. 2005;116(2):360-369.
Question: In children with mild asthma is the use of an antileukotriene medication as effective as an anti-inflammatory agent in maintaining number of days without the need of a rescue medication or utilization of asthma-related health resources?
Design: Multicenter, double-blind, double-dummy, randomized, parallel-group study. A four-week, single-blind, placebo run-in period was done prior to the initiation of the double-blind portion of the study. This run-in period included three clinic visits. During this time all participants discontinued any asthma controller medications and received image-matching, single-blind, montelukast and fluticasone. A short acting beta-agonist medication (open label) was also provided. Medication usage teaching was done during this time period. There was no placebo control group.
Setting: 104 study sites in 24 countries.
Patients: Patients (six-14 years of age) with mild persistent asthma as defined by the Global Initiative for Asthma (GINA) guidelines and otherwise in good health. Patients were required to have a FEV1 of ≥80% while the beta-receptor agonist was withheld for more than six hours in the first two visits and ≥70% on the third visit of the run-in period.
Intervention: Patients were randomized to receive either montelukast (5 mg oral before bedtime or 10 mg for patients ≥15) or fluticasone (100 mcg through MDI twice a day) and the appropriate placeboes.
Main outcome measures: Percentage of asthma rescue-free days (RFD).
RFD was defined as a day without:
- The use of a rescue medication: defined as any day during which a beta-receptor agonist, a systemic corticosteroid, or other rescue medications were used; and
- The use of an asthma health resource: defined as an unscheduled visit to a physician, an urgent/emergency care center or a hospital.
Main results: The number of RFDs were statistically similar between both groups. Mean percentage of RFD was 84% in the montelukast group and 86.7% in the fluticasone group.
Conflict of interest: Two of the study authors were employees of Merck and Company, which markets montelukast.
Commentary: This is an extensive study with multiple outcome measures. The study mimics actual clinical experience by using clinically relevant end points as primary outcomes. The study does not have a placebo control group. Overall the study showed that there is no significant difference between montelukast and fluticasone with regard to the primary outcome of RFDs, but there were some differences favoring fluticasone in secondary outcome measures, including number of days of beta-receptor agonist use and improvement of the average score of the control domain of the Pediatric Asthma Therapy Assessment Questionnaire.
K. Kingae Causes Osteomyelitis/Septic Arthritis
Kiang KM, Ogunmodede F, Juni BA, et al. Outbreak of osteomyelitis/septic arthritis caused by Kingella kingae among child care center attendees. Pediatrics. 2005;116;e206-213.
Review by Julia Simmons, MD
Kingella kingae (K. kingae), a gram-negative organism known to colonize the oropharynx, may cause invasive diseases, such as septic arthritis and osteomyelitis in children who were previously healthy. In this article, the authors describe the first reported outbreak of K. kingae causing osteomyelitis/septic arthritis.
In October 2003 the Minnesota Department of Health was notified of an outbreak of K. kingae at a daycare facility. There were two culture positive cases and one culture negative but clinically presumed to be secondary to K. kingae. The children were all in the same classroom (toddler classroom 1) and were between the ages of 17 and 21 months. The previously healthy children presented with fever and limp.
In this cohort study, the authors investigated risk factors for invasive disease and for colonization with K. kingae. They also determined the prevalence of asymptomatic colonization at the daycare involving the confirmed cases and at a second daycare facility, which served as the control. Culture samples were analyzed at the Minnesota Department of Health Public Health Laboratory. The laboratory performed confirmation, pulsed-field gel electrophoresis, DNA sequencing, and antimicrobial testing specifically with rifampin, penicillin, and azithromycin.
At the study facility 115/122 (94%) children and 28/29 (97%) adult staff members were cultured. Fifteen (13 %) of the children were colonized. The prevalence of colonization was 45% (9 children) in the toddler 1 classroom, which is the classroom of the confirmed cases. The three case patients had negative oropharyngeal cultures; however, all three had been pretreated with antibiotic therapy. The pulsed-field gel electrophoresis was indistinguishable in the confirmed cases and the colonized students. The authors did not discover any risk factors for invasive disease. This information was gathered from a list of questions regarding past medical history, which the parents discussed on the telephone with the investigators. Rifampin, penicillin, and azithromycin all had low MICs
At the control care center, 45/118 (38%) of people were cultured from the oropharynx. Seven (16%) were colonized. The pulsed-field gel electrophoresis was the same for the control care facility, but varied from the electrophoresis pattern at the study facility.
In conclusion, the authors summarized the findings of K. kingae osteomyelitis/septic arthritis in a daycare facility. There were no identifiable risk factors for invasive disease or for asymptomatic carrier state. It is important to remember that up to 50% of culture negative cases of septic arthritis in patients less than two years of age may be attributed to K. kingae. Thus, the clinician must maintain a high index of suspicion and relay this information to the laboratory so that appropriate measures are taken to ensure the optimal growth environment for the bacteria.
Although the study size was small, the investigators provide initial documentation regarding outbreaks of invasive K. kingae infections. Further studies will be useful to clarify the exact mode of transmission and appropriate duration of antimicrobial therapy.
Systematic Review of Therapy for Pediatric Migraine
Damen L, Bruijn JKJ, Verhagen AP, et al. Symptomatic treatment of migraine in children: a systematic review of medication trials. Pediatrics. 2005;116(2):295-302.
Migraines affect 3%-5% of prepubescent children. The symptoms frequently include unilateral throbbing headache associated with nausea and vomiting. If poorly controlled, the headaches can cause students to miss school and have a decreased quality of life. Symptomatic pharmacologic interventions involve analgesics, triptans, and antiemetics. Nonpharmacologic interventions include dietary changes, biofeedback, and exercise. Treatment is tailored to the patient; however, there are limited studies providing evidence describing the most efficacious pharmacologic treatment for managing symptomatic migraines.
The authors conducted a retrospective literature review to evaluate the evidence from randomized controlled trials (RCT) and clinical controlled trials (CCT) regarding the treatment of symptomatic migraine in children younger than 18. The primary outcome measure was headache clinical improvement defined as a headache decline by >50%. Secondary measures included headache intensity, frequency, duration, and headache index. The authors searched Medline, Embase, PsychInfo, Web of Science, and Cinahl from the start of the databases to June 2004. They used appropriate search terms including “headache,” “migraine,” “child” and variations thereof. Further, they searched reference lists of the articles and the included studies. Two authors independently reviewed the titles and abstracts to determine acceptability in the study. They also used the Delphi list to assess the methodologic quality of the included trials.
Of 3,492 relevant studies, 10 met the inclusion criteria specified by the authors. There were a total of 1,575 patients with a mean age of 11.7 +/- 2.2 years included in the study. A mean of 19.8% of subjects did not complete participation in their respective studies. Overall, the percentage of male and female participants was equal. Six studies were considered to be of high quality by the authors. They found moderate evidence that ibuprofen and acetaminophen were more effective in decreasing headache symptoms one and two hours after ingestion in comparison with a placebo. Further, the nasal spray sumatriptan was more efficacious in diminishing headache than placebo; however, it was associated with more side effects. Intravenous prochlorperazine was more effective than intravenous ketorolac in diminishing symptoms one hour after intake.
While accomplishing a sound systematic review of the available controlled trials, the authors conclude that there are insufficient trials of adequate quality to fully elucidate the most efficacious symptomatic pharmacologic therapy for pediatric patients suffering from migraine headaches. A large randomized prospective trial comparing analgesics, triptans, and antiemetics against placebo is needed. TH
Evidence Based Medicine for The Hospitalist
Each of us asks dozens of clinical questions every day. Sometimes the answers are clear: If our question is “Which statin is on formulary?” the answer will be provided to us by a patient’s insurance plan or by our own hospital pharmacy. Many times, however, the answers to our questions aren’t so well defined. Further, these are often the questions that most affect patient care: This is precisely why we ask them in the first place. Many of us give little thought to how we state our questions, but the format of a question can have a dramatic effect on whether or not we will be able to locate an answer. There is an art to asking clinical questions in a manner that maximizes our ability to find a meaningful answer in an efficient way.
Consider an example: We are seeing a 72-year-old man newly diagnosed with a stage II (T2M0N0) renal cell carcinoma. We are curious about treatment options, so we might ask, “Should all cancer patients receive chemotherapy?” It is intuitively clear that the answer to this question depends on a multitude of variables not clarified in the question.
For example, different types of cancer respond differently to chemotherapy and there are innumerable chemotherapy regimens, each having differing mechanisms of action. The patient’s age and gender may matter, and the patient’s medical history will almost certainly affect treatment options. As stated the question is essentially impossible to answer.
A better question might be, “Among men over age 65 with stage II renal cell carcinoma, does post-resection chemotherapy prolong survival compared with nephrectomy alone?” This question is far more specific and therefore more relevant to our individual patient. It is also more likely to yield an answer when we search for one. The point of this somewhat extreme example is that a clear, focused clinical question will usually lead to more precise answers. A vague question will often lead only to frustration.
Construct an Effective Clinical Question
How, then, can we phrase questions to optimize our chances of obtaining clinically helpful answers? One approach is to adopt the PICO or PICOT format. (See “Illustration of PICOT Approach to Clinical Questions,” p. 32.) This format provides a structure for question formation that emphasizes the elements most questions are designed to address: the patients of interest, the intervention in question, what it will be compared with, and what outcome we wish to assess.
The first element (P) represents the patient or population of interest. The aim is to define a group of patients similar to the one prompting the question. For example, our patient is a 72-year-old man with stage II renal cell carcinoma, so we would like to find information on patients that at least approximately fit this description.
The second element (I) represents the intervention, which is usually fairly straightforward to determine if the question relates to a choice of treatments. However, this can also be the prognostic factor or exposure of interest, depending on the type of study and specific question. In our example, the intervention is post-resection chemotherapy, and our clinical question needs to incorporate this information.
The third element (C) is the comparison of interest, if appropriate. For some questions there may not be a comparison, such as when we simply want to know how often a certain side effect occurs. In our example, though, the comparison group is patients treated with surgical resection alone.
The final element (O) is the outcome. The aim here is to define the specific result you are interested in. This will be patient survival in many cases, but it can also be incidence of side effects, correct diagnosis of disease, or any number of other possibilities. In the example, the outcome of interest is survival. We might wish to further refine this by imposing a time at which we would like to assess survival, leading us to look at five-year survival rates, for instance.
An additional element that can be helpful to consider at this stage of the EBM process is what type (T) of question you are asking or what type of study would answer your question. Questions regarding treatment interventions are often questions of therapy and may suggest a search for randomized controlled trials or meta-analyses. Questions regarding the most appropriate diagnostic tests will be best answered by different types of studies. There are many possible types of questions and quite a few types of studies (the Guyatt and Rennie text in “Recommended Reading”(this page, top left) provides many excellent examples), but taking a moment to consider your options can further refine your subsequent search strategy and is well worth the time.
Advantages of the PICOT Question Format
The PICOT approach to constructing clinical questions focuses questions, allowing us to clarify exactly what we hope to answer. This format also provides insight into possible sources that may yield the answers we seek. For example, the question, “How are the stages of renal cell carcinoma defined?” This is a so-called background medical knowledge question and may be answerable by simply reviewing a textbook rather than conducting a complex and exhaustive literature search.
On the other hand, the more specific foreground question outlined in “Illustration of PICOT Approach to Clinical Questions” will likely require a more detailed search of the latest clinical trials.
Finally, this format facilitates the terms we will actually use when conducting the literature search. In many cases, the search terms may be lifted directly from the clinical question, and the PICOT approach typically suggests multiple search terms that can narrow your search. We will explore this further in the next entry of this series.
Summary
Constructing effective clinical questions is an important step in the EBM process. The well-built question makes searching for answers simpler, saving time and effort. The PICOT approach provides a structure flexible enough to accommodate almost any question, and leads directly to more effective search strategies. We will explore search strategies further in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
Each of us asks dozens of clinical questions every day. Sometimes the answers are clear: If our question is “Which statin is on formulary?” the answer will be provided to us by a patient’s insurance plan or by our own hospital pharmacy. Many times, however, the answers to our questions aren’t so well defined. Further, these are often the questions that most affect patient care: This is precisely why we ask them in the first place. Many of us give little thought to how we state our questions, but the format of a question can have a dramatic effect on whether or not we will be able to locate an answer. There is an art to asking clinical questions in a manner that maximizes our ability to find a meaningful answer in an efficient way.
Consider an example: We are seeing a 72-year-old man newly diagnosed with a stage II (T2M0N0) renal cell carcinoma. We are curious about treatment options, so we might ask, “Should all cancer patients receive chemotherapy?” It is intuitively clear that the answer to this question depends on a multitude of variables not clarified in the question.
For example, different types of cancer respond differently to chemotherapy and there are innumerable chemotherapy regimens, each having differing mechanisms of action. The patient’s age and gender may matter, and the patient’s medical history will almost certainly affect treatment options. As stated the question is essentially impossible to answer.
A better question might be, “Among men over age 65 with stage II renal cell carcinoma, does post-resection chemotherapy prolong survival compared with nephrectomy alone?” This question is far more specific and therefore more relevant to our individual patient. It is also more likely to yield an answer when we search for one. The point of this somewhat extreme example is that a clear, focused clinical question will usually lead to more precise answers. A vague question will often lead only to frustration.
Construct an Effective Clinical Question
How, then, can we phrase questions to optimize our chances of obtaining clinically helpful answers? One approach is to adopt the PICO or PICOT format. (See “Illustration of PICOT Approach to Clinical Questions,” p. 32.) This format provides a structure for question formation that emphasizes the elements most questions are designed to address: the patients of interest, the intervention in question, what it will be compared with, and what outcome we wish to assess.
The first element (P) represents the patient or population of interest. The aim is to define a group of patients similar to the one prompting the question. For example, our patient is a 72-year-old man with stage II renal cell carcinoma, so we would like to find information on patients that at least approximately fit this description.
The second element (I) represents the intervention, which is usually fairly straightforward to determine if the question relates to a choice of treatments. However, this can also be the prognostic factor or exposure of interest, depending on the type of study and specific question. In our example, the intervention is post-resection chemotherapy, and our clinical question needs to incorporate this information.
The third element (C) is the comparison of interest, if appropriate. For some questions there may not be a comparison, such as when we simply want to know how often a certain side effect occurs. In our example, though, the comparison group is patients treated with surgical resection alone.
The final element (O) is the outcome. The aim here is to define the specific result you are interested in. This will be patient survival in many cases, but it can also be incidence of side effects, correct diagnosis of disease, or any number of other possibilities. In the example, the outcome of interest is survival. We might wish to further refine this by imposing a time at which we would like to assess survival, leading us to look at five-year survival rates, for instance.
An additional element that can be helpful to consider at this stage of the EBM process is what type (T) of question you are asking or what type of study would answer your question. Questions regarding treatment interventions are often questions of therapy and may suggest a search for randomized controlled trials or meta-analyses. Questions regarding the most appropriate diagnostic tests will be best answered by different types of studies. There are many possible types of questions and quite a few types of studies (the Guyatt and Rennie text in “Recommended Reading”(this page, top left) provides many excellent examples), but taking a moment to consider your options can further refine your subsequent search strategy and is well worth the time.
Advantages of the PICOT Question Format
The PICOT approach to constructing clinical questions focuses questions, allowing us to clarify exactly what we hope to answer. This format also provides insight into possible sources that may yield the answers we seek. For example, the question, “How are the stages of renal cell carcinoma defined?” This is a so-called background medical knowledge question and may be answerable by simply reviewing a textbook rather than conducting a complex and exhaustive literature search.
On the other hand, the more specific foreground question outlined in “Illustration of PICOT Approach to Clinical Questions” will likely require a more detailed search of the latest clinical trials.
Finally, this format facilitates the terms we will actually use when conducting the literature search. In many cases, the search terms may be lifted directly from the clinical question, and the PICOT approach typically suggests multiple search terms that can narrow your search. We will explore this further in the next entry of this series.
Summary
Constructing effective clinical questions is an important step in the EBM process. The well-built question makes searching for answers simpler, saving time and effort. The PICOT approach provides a structure flexible enough to accommodate almost any question, and leads directly to more effective search strategies. We will explore search strategies further in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
Each of us asks dozens of clinical questions every day. Sometimes the answers are clear: If our question is “Which statin is on formulary?” the answer will be provided to us by a patient’s insurance plan or by our own hospital pharmacy. Many times, however, the answers to our questions aren’t so well defined. Further, these are often the questions that most affect patient care: This is precisely why we ask them in the first place. Many of us give little thought to how we state our questions, but the format of a question can have a dramatic effect on whether or not we will be able to locate an answer. There is an art to asking clinical questions in a manner that maximizes our ability to find a meaningful answer in an efficient way.
Consider an example: We are seeing a 72-year-old man newly diagnosed with a stage II (T2M0N0) renal cell carcinoma. We are curious about treatment options, so we might ask, “Should all cancer patients receive chemotherapy?” It is intuitively clear that the answer to this question depends on a multitude of variables not clarified in the question.
For example, different types of cancer respond differently to chemotherapy and there are innumerable chemotherapy regimens, each having differing mechanisms of action. The patient’s age and gender may matter, and the patient’s medical history will almost certainly affect treatment options. As stated the question is essentially impossible to answer.
A better question might be, “Among men over age 65 with stage II renal cell carcinoma, does post-resection chemotherapy prolong survival compared with nephrectomy alone?” This question is far more specific and therefore more relevant to our individual patient. It is also more likely to yield an answer when we search for one. The point of this somewhat extreme example is that a clear, focused clinical question will usually lead to more precise answers. A vague question will often lead only to frustration.
Construct an Effective Clinical Question
How, then, can we phrase questions to optimize our chances of obtaining clinically helpful answers? One approach is to adopt the PICO or PICOT format. (See “Illustration of PICOT Approach to Clinical Questions,” p. 32.) This format provides a structure for question formation that emphasizes the elements most questions are designed to address: the patients of interest, the intervention in question, what it will be compared with, and what outcome we wish to assess.
The first element (P) represents the patient or population of interest. The aim is to define a group of patients similar to the one prompting the question. For example, our patient is a 72-year-old man with stage II renal cell carcinoma, so we would like to find information on patients that at least approximately fit this description.
The second element (I) represents the intervention, which is usually fairly straightforward to determine if the question relates to a choice of treatments. However, this can also be the prognostic factor or exposure of interest, depending on the type of study and specific question. In our example, the intervention is post-resection chemotherapy, and our clinical question needs to incorporate this information.
The third element (C) is the comparison of interest, if appropriate. For some questions there may not be a comparison, such as when we simply want to know how often a certain side effect occurs. In our example, though, the comparison group is patients treated with surgical resection alone.
The final element (O) is the outcome. The aim here is to define the specific result you are interested in. This will be patient survival in many cases, but it can also be incidence of side effects, correct diagnosis of disease, or any number of other possibilities. In the example, the outcome of interest is survival. We might wish to further refine this by imposing a time at which we would like to assess survival, leading us to look at five-year survival rates, for instance.
An additional element that can be helpful to consider at this stage of the EBM process is what type (T) of question you are asking or what type of study would answer your question. Questions regarding treatment interventions are often questions of therapy and may suggest a search for randomized controlled trials or meta-analyses. Questions regarding the most appropriate diagnostic tests will be best answered by different types of studies. There are many possible types of questions and quite a few types of studies (the Guyatt and Rennie text in “Recommended Reading”(this page, top left) provides many excellent examples), but taking a moment to consider your options can further refine your subsequent search strategy and is well worth the time.
Advantages of the PICOT Question Format
The PICOT approach to constructing clinical questions focuses questions, allowing us to clarify exactly what we hope to answer. This format also provides insight into possible sources that may yield the answers we seek. For example, the question, “How are the stages of renal cell carcinoma defined?” This is a so-called background medical knowledge question and may be answerable by simply reviewing a textbook rather than conducting a complex and exhaustive literature search.
On the other hand, the more specific foreground question outlined in “Illustration of PICOT Approach to Clinical Questions” will likely require a more detailed search of the latest clinical trials.
Finally, this format facilitates the terms we will actually use when conducting the literature search. In many cases, the search terms may be lifted directly from the clinical question, and the PICOT approach typically suggests multiple search terms that can narrow your search. We will explore this further in the next entry of this series.
Summary
Constructing effective clinical questions is an important step in the EBM process. The well-built question makes searching for answers simpler, saving time and effort. The PICOT approach provides a structure flexible enough to accommodate almost any question, and leads directly to more effective search strategies. We will explore search strategies further in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.