User login
Moby Doc

Chapter 1: Loomings
Call me Dr. Ishmael. Some years ago—never mind how long precisely—having little or no money in my purse and nothing particular to interest me, I thought I would go to medical school. I wanted to feel an enlarged spleen and learn the circulation.
Chapter 2: A Bosom Friend
It was the evening before the start of a long rotation, and I had to find quarters. I had been assigned to share a call room with another student. It was late and I dimmed the lights and fell into a disturbed sleep. Suddenly the lights flashed on, and a sight unlike any I had imagined came before my bleary eyes. It was a huge man, covered in tattoos, with strange piercings and wires sticking from his ears.
“Nizetameetya,” he mumbled. He pulled off his shirt, and I could see a large caduceus motif filled the canvas of his back.
“Watchaheerfaw?” he asked. It was some time before I could translate his strange island dialect. His name was Queequeg and he was from the island of Long. Before the sun had risen, we were best of friends. Better yet, we had been assigned to the same medicine service.
Chapter 3: The Hospital
A strange old building was the Pequod Hospital, an outreach of the Nantucket General Hospital. It was a hospital of the old school. The wooden floors were shiny with use and the walls a dim yellow. It had the distinct odor of disinfectant with a trace of stale urine; it smelled like a hospital. The spirits of patients lingered in the air.
Chapter 4: The Warning
As we entered the lobby, a student in a short white coat stumbled by us. Bedraggled, he was splattered with nameless filth. His name tag read “ELISA.”
“Doing a rotation are you? At the Pequod? You on Ahab’s team are you? It’s not too late to switch services. Not too late. Too late,” he said as he staggered off.
Chapter 5: Two Squires
We entered the ward and met an intern, Dr. Flask. A short, ruddy young fellow. Very pugnacious concerning scut. He was bent over a patient’s arm prodding for a vessel. He looked at Queequeg.
“Oh lord what have we here, are you a medical student or a freak show?” he barked. Queequeg pushed him aside, pulled a needle from a loaded pocket, and without hesitation plunged it into the patient’s arm, hitting the vein instantly. He turned toward Flask, who was now smiling broadly.
Several minutes later, a second intern named Dr. Stubb walked in. A mellow dude, neither serious nor intense. He was calm in a code; fearless in the face of an angry family. He constantly twirled a drug company pen, revolving endlessly around the fingers of his left hand. During rounds, while taking a history, perhaps while asleep, that ballpoint spun continually on a journey nowhere. It was hypnotizing.
Chapter 6: A Knight
I smelled him before I saw him. It was a scent of the islands, of roasted beans and cinnamon. It was Dr. Starbuck. He held the largest cup of coffee I had ever seen.
He caught my eye and rightly read my thoughts. “It’s a triple soy latte with a twist,” he said between sips. I never saw him without a cup in his hand. Lattes, espressos, cappuccinos—cold or scalding, frothy or black, Kona or Colombian—these were his passions. It was only about the divine essence of the bean that I saw him show his true emotions.
Chapter 7: Rounds
And so the strange rotation began to take shape. We headed down the long old ward, the patient’s beds in groups of two. For those of you who never rounded in these days gone by, not corrupted by the mighty powers of Microsoft, it was an odd sight. A mass of physicians huddled around a chart rack. From this rack were pulled clipboards: long wood or plastic holders with strange colored papers barely held in place, waiting to fall out and flutter to the floor, their normal order destroyed. The rack was our lifeboat, our master, and our servant. We went from room to room to see patients, discuss them, make a diagnostic plan. Then the resident turned to the interns and began to grill them. And Lord help the student who could not withstand the devious pimpage.
Knight Starbuck was no exception to this rule. He would scour the physiology and pharmacologic depths of our souls between sips of Jamaican roast. When we did not know, he would turn to Flask or Stubb. Stubb would generally answer, his pen incessantly turning.
Something felt wrong about this service, though. Some foreboding. Some hint of disaster to come. I realized then we were a ship without a rudder, dismasted without our leader, our attending physician. We heard footsteps coming our way. I could not say precisely how, but the air seemed to become charged, as if before a storm.
Chapter 8: Enter Ahab
Dr. Ahab strode upon the ward. His whole broad form was bronzed from some strange ailment or weeks at the beach. A large scar ran along the anterior part of his neck, white against the dark skin. A mark of some desperate wound or endarterectomy. But it was not this that left me speechless in his presence; it was his great white coat.
Each of us, except Queequeg who rejected such formalities, wore a white coat. Mine was short (in measure to my educational rank), filled to the brim with anything I thought might be of value. I was not one to be found wanting when an item was needed. The residents wore longer versions, their pockets stuffed with their own totems of power.
But Ahab’s white coat was of another dimension entirely. To call it pristine would fall short of its purity: It was incandescent. A wrinkle would have expired of loneliness. It was starched and unbending, like Dr. Ahab himself. It went nearly to the floor, the tops of his wing tips barely visible beneath. It was his armor, his shield, it was Ahab.
“Do you know what I’m looking for team?” he asked each of us in turn, as the hair rose on the back of my neck. “It’s evidence I’m looking for. And not just any, but Grade A-1 that we’ll be seeking”
Chapter 9: The Chase for Evidence
And so rounds began again. Each patient in their turn was prodded and poked. The medicines were reviewed; the care plan discussed. With each case Ahab became more agitated. He demanded proof that our therapies were supported by the literature. He worshipfully spoke of articles and references like they had a life of their own, a hierarchy of existence.
As we came to the last patient, Ahab began to pace nervously. It was Stubb’s turn to present.
“The next patient is a morbidly obese 74-year-old with a DVT and PE, on heparin. We are starting Coumadin now,” began Stubb.
Suddenly Ahab erupted: “Why is this patient in the hospital? Why isn’t he on LMWH and home already?”
“I thought he needed heparinization, and I’m concerned about hypoxia,” stammered Stubb.
“Aye, but what’s your evidence that inpatient is better than outpatient treatment? Can you drive blindfolded? Are your thoughts and concerns worth the wasted resources?” hissed Ahab.
The pen fell from Stubb’s hand and lay lifeless on the floor.
Suddenly the nurse ran from the patient’s room, calling a code. We rushed into the room. The patient was a huge man—a leviathan—his flesh an off-white in the fluorescent light. Flask jumped on his chest and began to pump; Stubb intubated and bagged, while Starbuck sipped his coffee. Queequeg plunged a needle into the patient’s femoral artery for a blood gas and a central line in his subclavian before I could move my feet. A small jet of blood streamed out while Queequeg positioned the tubing. The patient was resuscitated and wheeled to the ICU. I stood helplessly, thinking about evidence.
I then noticed that Ahab, who seemed shaken, was rooted to the floor. He stared at his own chest, a streak of clotted blood across his perfect white coat.
“Oh, lonely stats of death and life. Toward thee I strive, thou all-consuming data. From a cohort’s heart I randomize thee; to the last I graph with thee; for evidence sake I control my last study.” He stumbled from the room.
Chapter 10: Epilogue
I watched Ahab head to the elevator, his perfect coat tinged now with red. He waved to me three times, beckoning me to follow. But I leaned against the chart rack; it was solid. It kept me afloat. I stood there until the other team came by and joined them for their teaching rounds. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Chapter 1: Loomings
Call me Dr. Ishmael. Some years ago—never mind how long precisely—having little or no money in my purse and nothing particular to interest me, I thought I would go to medical school. I wanted to feel an enlarged spleen and learn the circulation.
Chapter 2: A Bosom Friend
It was the evening before the start of a long rotation, and I had to find quarters. I had been assigned to share a call room with another student. It was late and I dimmed the lights and fell into a disturbed sleep. Suddenly the lights flashed on, and a sight unlike any I had imagined came before my bleary eyes. It was a huge man, covered in tattoos, with strange piercings and wires sticking from his ears.
“Nizetameetya,” he mumbled. He pulled off his shirt, and I could see a large caduceus motif filled the canvas of his back.
“Watchaheerfaw?” he asked. It was some time before I could translate his strange island dialect. His name was Queequeg and he was from the island of Long. Before the sun had risen, we were best of friends. Better yet, we had been assigned to the same medicine service.
Chapter 3: The Hospital
A strange old building was the Pequod Hospital, an outreach of the Nantucket General Hospital. It was a hospital of the old school. The wooden floors were shiny with use and the walls a dim yellow. It had the distinct odor of disinfectant with a trace of stale urine; it smelled like a hospital. The spirits of patients lingered in the air.
Chapter 4: The Warning
As we entered the lobby, a student in a short white coat stumbled by us. Bedraggled, he was splattered with nameless filth. His name tag read “ELISA.”
“Doing a rotation are you? At the Pequod? You on Ahab’s team are you? It’s not too late to switch services. Not too late. Too late,” he said as he staggered off.
Chapter 5: Two Squires
We entered the ward and met an intern, Dr. Flask. A short, ruddy young fellow. Very pugnacious concerning scut. He was bent over a patient’s arm prodding for a vessel. He looked at Queequeg.
“Oh lord what have we here, are you a medical student or a freak show?” he barked. Queequeg pushed him aside, pulled a needle from a loaded pocket, and without hesitation plunged it into the patient’s arm, hitting the vein instantly. He turned toward Flask, who was now smiling broadly.
Several minutes later, a second intern named Dr. Stubb walked in. A mellow dude, neither serious nor intense. He was calm in a code; fearless in the face of an angry family. He constantly twirled a drug company pen, revolving endlessly around the fingers of his left hand. During rounds, while taking a history, perhaps while asleep, that ballpoint spun continually on a journey nowhere. It was hypnotizing.
Chapter 6: A Knight
I smelled him before I saw him. It was a scent of the islands, of roasted beans and cinnamon. It was Dr. Starbuck. He held the largest cup of coffee I had ever seen.
He caught my eye and rightly read my thoughts. “It’s a triple soy latte with a twist,” he said between sips. I never saw him without a cup in his hand. Lattes, espressos, cappuccinos—cold or scalding, frothy or black, Kona or Colombian—these were his passions. It was only about the divine essence of the bean that I saw him show his true emotions.
Chapter 7: Rounds
And so the strange rotation began to take shape. We headed down the long old ward, the patient’s beds in groups of two. For those of you who never rounded in these days gone by, not corrupted by the mighty powers of Microsoft, it was an odd sight. A mass of physicians huddled around a chart rack. From this rack were pulled clipboards: long wood or plastic holders with strange colored papers barely held in place, waiting to fall out and flutter to the floor, their normal order destroyed. The rack was our lifeboat, our master, and our servant. We went from room to room to see patients, discuss them, make a diagnostic plan. Then the resident turned to the interns and began to grill them. And Lord help the student who could not withstand the devious pimpage.
Knight Starbuck was no exception to this rule. He would scour the physiology and pharmacologic depths of our souls between sips of Jamaican roast. When we did not know, he would turn to Flask or Stubb. Stubb would generally answer, his pen incessantly turning.
Something felt wrong about this service, though. Some foreboding. Some hint of disaster to come. I realized then we were a ship without a rudder, dismasted without our leader, our attending physician. We heard footsteps coming our way. I could not say precisely how, but the air seemed to become charged, as if before a storm.
Chapter 8: Enter Ahab
Dr. Ahab strode upon the ward. His whole broad form was bronzed from some strange ailment or weeks at the beach. A large scar ran along the anterior part of his neck, white against the dark skin. A mark of some desperate wound or endarterectomy. But it was not this that left me speechless in his presence; it was his great white coat.
Each of us, except Queequeg who rejected such formalities, wore a white coat. Mine was short (in measure to my educational rank), filled to the brim with anything I thought might be of value. I was not one to be found wanting when an item was needed. The residents wore longer versions, their pockets stuffed with their own totems of power.
But Ahab’s white coat was of another dimension entirely. To call it pristine would fall short of its purity: It was incandescent. A wrinkle would have expired of loneliness. It was starched and unbending, like Dr. Ahab himself. It went nearly to the floor, the tops of his wing tips barely visible beneath. It was his armor, his shield, it was Ahab.
“Do you know what I’m looking for team?” he asked each of us in turn, as the hair rose on the back of my neck. “It’s evidence I’m looking for. And not just any, but Grade A-1 that we’ll be seeking”
Chapter 9: The Chase for Evidence
And so rounds began again. Each patient in their turn was prodded and poked. The medicines were reviewed; the care plan discussed. With each case Ahab became more agitated. He demanded proof that our therapies were supported by the literature. He worshipfully spoke of articles and references like they had a life of their own, a hierarchy of existence.
As we came to the last patient, Ahab began to pace nervously. It was Stubb’s turn to present.
“The next patient is a morbidly obese 74-year-old with a DVT and PE, on heparin. We are starting Coumadin now,” began Stubb.
Suddenly Ahab erupted: “Why is this patient in the hospital? Why isn’t he on LMWH and home already?”
“I thought he needed heparinization, and I’m concerned about hypoxia,” stammered Stubb.
“Aye, but what’s your evidence that inpatient is better than outpatient treatment? Can you drive blindfolded? Are your thoughts and concerns worth the wasted resources?” hissed Ahab.
The pen fell from Stubb’s hand and lay lifeless on the floor.
Suddenly the nurse ran from the patient’s room, calling a code. We rushed into the room. The patient was a huge man—a leviathan—his flesh an off-white in the fluorescent light. Flask jumped on his chest and began to pump; Stubb intubated and bagged, while Starbuck sipped his coffee. Queequeg plunged a needle into the patient’s femoral artery for a blood gas and a central line in his subclavian before I could move my feet. A small jet of blood streamed out while Queequeg positioned the tubing. The patient was resuscitated and wheeled to the ICU. I stood helplessly, thinking about evidence.
I then noticed that Ahab, who seemed shaken, was rooted to the floor. He stared at his own chest, a streak of clotted blood across his perfect white coat.
“Oh, lonely stats of death and life. Toward thee I strive, thou all-consuming data. From a cohort’s heart I randomize thee; to the last I graph with thee; for evidence sake I control my last study.” He stumbled from the room.
Chapter 10: Epilogue
I watched Ahab head to the elevator, his perfect coat tinged now with red. He waved to me three times, beckoning me to follow. But I leaned against the chart rack; it was solid. It kept me afloat. I stood there until the other team came by and joined them for their teaching rounds. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Chapter 1: Loomings
Call me Dr. Ishmael. Some years ago—never mind how long precisely—having little or no money in my purse and nothing particular to interest me, I thought I would go to medical school. I wanted to feel an enlarged spleen and learn the circulation.
Chapter 2: A Bosom Friend
It was the evening before the start of a long rotation, and I had to find quarters. I had been assigned to share a call room with another student. It was late and I dimmed the lights and fell into a disturbed sleep. Suddenly the lights flashed on, and a sight unlike any I had imagined came before my bleary eyes. It was a huge man, covered in tattoos, with strange piercings and wires sticking from his ears.
“Nizetameetya,” he mumbled. He pulled off his shirt, and I could see a large caduceus motif filled the canvas of his back.
“Watchaheerfaw?” he asked. It was some time before I could translate his strange island dialect. His name was Queequeg and he was from the island of Long. Before the sun had risen, we were best of friends. Better yet, we had been assigned to the same medicine service.
Chapter 3: The Hospital
A strange old building was the Pequod Hospital, an outreach of the Nantucket General Hospital. It was a hospital of the old school. The wooden floors were shiny with use and the walls a dim yellow. It had the distinct odor of disinfectant with a trace of stale urine; it smelled like a hospital. The spirits of patients lingered in the air.
Chapter 4: The Warning
As we entered the lobby, a student in a short white coat stumbled by us. Bedraggled, he was splattered with nameless filth. His name tag read “ELISA.”
“Doing a rotation are you? At the Pequod? You on Ahab’s team are you? It’s not too late to switch services. Not too late. Too late,” he said as he staggered off.
Chapter 5: Two Squires
We entered the ward and met an intern, Dr. Flask. A short, ruddy young fellow. Very pugnacious concerning scut. He was bent over a patient’s arm prodding for a vessel. He looked at Queequeg.
“Oh lord what have we here, are you a medical student or a freak show?” he barked. Queequeg pushed him aside, pulled a needle from a loaded pocket, and without hesitation plunged it into the patient’s arm, hitting the vein instantly. He turned toward Flask, who was now smiling broadly.
Several minutes later, a second intern named Dr. Stubb walked in. A mellow dude, neither serious nor intense. He was calm in a code; fearless in the face of an angry family. He constantly twirled a drug company pen, revolving endlessly around the fingers of his left hand. During rounds, while taking a history, perhaps while asleep, that ballpoint spun continually on a journey nowhere. It was hypnotizing.
Chapter 6: A Knight
I smelled him before I saw him. It was a scent of the islands, of roasted beans and cinnamon. It was Dr. Starbuck. He held the largest cup of coffee I had ever seen.
He caught my eye and rightly read my thoughts. “It’s a triple soy latte with a twist,” he said between sips. I never saw him without a cup in his hand. Lattes, espressos, cappuccinos—cold or scalding, frothy or black, Kona or Colombian—these were his passions. It was only about the divine essence of the bean that I saw him show his true emotions.
Chapter 7: Rounds
And so the strange rotation began to take shape. We headed down the long old ward, the patient’s beds in groups of two. For those of you who never rounded in these days gone by, not corrupted by the mighty powers of Microsoft, it was an odd sight. A mass of physicians huddled around a chart rack. From this rack were pulled clipboards: long wood or plastic holders with strange colored papers barely held in place, waiting to fall out and flutter to the floor, their normal order destroyed. The rack was our lifeboat, our master, and our servant. We went from room to room to see patients, discuss them, make a diagnostic plan. Then the resident turned to the interns and began to grill them. And Lord help the student who could not withstand the devious pimpage.
Knight Starbuck was no exception to this rule. He would scour the physiology and pharmacologic depths of our souls between sips of Jamaican roast. When we did not know, he would turn to Flask or Stubb. Stubb would generally answer, his pen incessantly turning.
Something felt wrong about this service, though. Some foreboding. Some hint of disaster to come. I realized then we were a ship without a rudder, dismasted without our leader, our attending physician. We heard footsteps coming our way. I could not say precisely how, but the air seemed to become charged, as if before a storm.
Chapter 8: Enter Ahab
Dr. Ahab strode upon the ward. His whole broad form was bronzed from some strange ailment or weeks at the beach. A large scar ran along the anterior part of his neck, white against the dark skin. A mark of some desperate wound or endarterectomy. But it was not this that left me speechless in his presence; it was his great white coat.
Each of us, except Queequeg who rejected such formalities, wore a white coat. Mine was short (in measure to my educational rank), filled to the brim with anything I thought might be of value. I was not one to be found wanting when an item was needed. The residents wore longer versions, their pockets stuffed with their own totems of power.
But Ahab’s white coat was of another dimension entirely. To call it pristine would fall short of its purity: It was incandescent. A wrinkle would have expired of loneliness. It was starched and unbending, like Dr. Ahab himself. It went nearly to the floor, the tops of his wing tips barely visible beneath. It was his armor, his shield, it was Ahab.
“Do you know what I’m looking for team?” he asked each of us in turn, as the hair rose on the back of my neck. “It’s evidence I’m looking for. And not just any, but Grade A-1 that we’ll be seeking”
Chapter 9: The Chase for Evidence
And so rounds began again. Each patient in their turn was prodded and poked. The medicines were reviewed; the care plan discussed. With each case Ahab became more agitated. He demanded proof that our therapies were supported by the literature. He worshipfully spoke of articles and references like they had a life of their own, a hierarchy of existence.
As we came to the last patient, Ahab began to pace nervously. It was Stubb’s turn to present.
“The next patient is a morbidly obese 74-year-old with a DVT and PE, on heparin. We are starting Coumadin now,” began Stubb.
Suddenly Ahab erupted: “Why is this patient in the hospital? Why isn’t he on LMWH and home already?”
“I thought he needed heparinization, and I’m concerned about hypoxia,” stammered Stubb.
“Aye, but what’s your evidence that inpatient is better than outpatient treatment? Can you drive blindfolded? Are your thoughts and concerns worth the wasted resources?” hissed Ahab.
The pen fell from Stubb’s hand and lay lifeless on the floor.
Suddenly the nurse ran from the patient’s room, calling a code. We rushed into the room. The patient was a huge man—a leviathan—his flesh an off-white in the fluorescent light. Flask jumped on his chest and began to pump; Stubb intubated and bagged, while Starbuck sipped his coffee. Queequeg plunged a needle into the patient’s femoral artery for a blood gas and a central line in his subclavian before I could move my feet. A small jet of blood streamed out while Queequeg positioned the tubing. The patient was resuscitated and wheeled to the ICU. I stood helplessly, thinking about evidence.
I then noticed that Ahab, who seemed shaken, was rooted to the floor. He stared at his own chest, a streak of clotted blood across his perfect white coat.
“Oh, lonely stats of death and life. Toward thee I strive, thou all-consuming data. From a cohort’s heart I randomize thee; to the last I graph with thee; for evidence sake I control my last study.” He stumbled from the room.
Chapter 10: Epilogue
I watched Ahab head to the elevator, his perfect coat tinged now with red. He waved to me three times, beckoning me to follow. But I leaned against the chart rack; it was solid. It kept me afloat. I stood there until the other team came by and joined them for their teaching rounds. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, senior associate consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Help Me. I Can’t Speak.
Each week in the United States, child protective services and agencies receive reports of more than 50,000 suspected child abuse incidents. In 2002, 2.6 million incidents involving 4.5 million children were reported. Approximately four children die every day as a result of abuse or neglect.1 But numbers don’t tell the whole story. Behind every number is a child at risk.
“I can picture right now in my mind a young baby who was about six months of age with a belly that was protruded and distended,” says Erin R. Stucky, MD, a pediatric hospitalist at Children’s Hospital and Health Center San Diego, and an associate professor of pediatrics at the University of California San Diego. “[She had] no bowel sounds, and the arms and legs were so thin, had no fat whatsoever. The skin was rolling. The face looked dysmorphic, but it was simply because the eyes were so white, and there was no fat on the face at all. The baby had an irritated cry. The hair was thin. [She] had a look of anxiety, true anxiety [in her] eyes. It was impressive, as though this infant was saying, ‘Help me. I can’t speak.’ [She] was very socially engaged, but tired. If you had to qualify the look further, it would be something like, ‘I’m in pain. Protect me. Please don’t walk out the door.’
“The child had been admitted from the emergency department at an outside facility. They had been focused, appropriately to some extent, on the fact that the belly was distended and that the baby had no bowel sounds. They were focused on the fact that the parent’s history [of the child] was of vomiting during the day, but it clearly did not equate whatsoever with the way the child looked. It was immediately clear, simply looking at the baby while walking in the room, that something very bad was wrong and that the parents’ answers and explanations did not fit.”
What It Is
Child abuse manifests in many forms, including physical abuse, sexual abuse, emotional abuse, and neglect, with a “child” typically defined as a person under 18. Legal definitions of the forms of child abuse vary, but, in general, they reflect societal views of actions deemed improper and unacceptable because they place a child at risk of physical or emotional harm.2 The federal Child Abuse Prevention and Treatment Act (CAPTA) defines child abuse and neglect as:
- Any recent act or failure to act on the part of a parent or caretaker that results in death, serious physical or emotional harm, sexual abuse, or exploitation; or
- An act or failure to act that presents an imminent risk of serious harm.3
States must include these minimum standards in their statutes in order to receive federal funds.
Neglect is the most common form of child abuse.2 Although definitions of neglect vary by state, they share characteristics. Minnesota defines neglect as inadequate food, shelter, clothing, or medical care. California includes both overt acts and omissions in the definition of neglect, defining general neglect as a lack of food, clothing, or medical care and severe neglect as malnutrition, failure to thrive, or willfully putting a child in danger. And Rhode Island’s neglect definition goes even further, including the above acts and omissions as well as the failure to provide a minimum degree of care or proper supervision or guardianship due to unwillingness, social problems, mental incompetency, or the use of a drug, drugs or alcohol, desertion, or abandonment. Rhode Island also includes the failure to take financial responsibility for a child.4
According to Georgia Berrenberg, esq., deputy district attorney, Second Judicial District of New Mexico, sexual abuse is the most common type that goes to trial. Berrenberg, who has been a prosecutor since 1984 and was in the child abuse division from 1996–2005, estimates that approximately 70% of cases involve sexual abuse compared with 30% that involve physical abuse.
However, pediatric hospitalists will most commonly see neglect, presenting as malnutrition or failure to thrive, in a child admitted to the hospital.4
Recognize Abuse and Neglect
Pediatric hospitalists are in a unique position to recognize child abuse and neglect, intervene appropriately, and help families avoid ultimate tragedy. They are trained to consider the entire child—no matter the presenting condition—to look at general issues and to think about development and nutrition every time they examine a child.
“When someone says, ‘This child has pneumonia,’ my job is to not think pneumonia; my job is to think, ‘What’s causing this child to breathe fast?’ to make sure I don’t miss anything,” says Dr. Stucky. “If the history doesn’t fit the examination and my first, second, [and] third thoughts are child abuse/neglect. It’s my job to work on that, but it’s also my job to push my own buttons to make sure that it’s not anything else medically going on. The child that never has a bruise or fracture is the odd one out. The key [to recognizing abuse] is history.”
Don’t jump to conclusions. Hospitalists need to consider the history reported by the parent in light of the physical exam of the child. For example, if the parent tells you that the child fell headfirst off a tricycle and landed on his face, note the pattern of the bruising. If the child has bruising around the eye then that could be consistent with the history, but if the child’s eyelid is cut or bruised and there’s no bruising around the eye, that’s another matter. The eyebrow and cheekbone will protect the eye when you fall and land on your face.
“Pay attention to what you hear and see in those first few minutes and hours with that family because stories are going to change,” says Berrenberg. “Be very, very clear about the initial things that are said.”
Dealing with the medical issues that led to the admission is paramount, and it’s important for the hospitalist to communicate effectively with the parent to ensure that the child receives the most appropriate treatment. Asking open-ended questions while you take the history can be revealing:
- Can you tell me how long this has been happening?
- What do you think might be contributing to this?
- Can you tell me how you’ve been dealing with these issues at home?
- Run me through a typical day at home with your baby.
In addition to the history, consider the parent/child interaction. “Most kids, even when they’re stressed and in pain are very attentive to where their parents are,” says Dr. Stucky. “They want to be with them no matter what. They may be angry and battling. They may respond to pain differently, but that relationship is very important. As you watch it you can really get a good sense [of whether] this child’s anger outburst is because they’re in pain, they’re confused, they have autism, or they are really angry with their parent and this is the way they’re protecting themselves.”
The hospitalist has to be up front with the parent about what the next step in their child’s treatment is going to be. “It’s a delicate discussion, but an honest one,” says Dr. Stucky. “It’s important to say to the parent, overtly, ‘I’m very concerned about your baby’s weight loss. I’m very concerned that this has happened over the past several months and that it has taken this long for your baby to be seen by a doctor. I’m very concerned, and I want you to understand that your baby has a critical condition right now. It’s so malnourished that the body’s organs aren’t working properly. ... Because of this concern, I’m going to call social workers. Because of this concern I’ll use [work with] a team of people to help me to take care of your baby. They’ll ask a lot of questions, and it’s very important that you answer honestly so we can do the best for your baby and make sure that the whole family can get whatever help is needed to take care of the problem.’ ”
Reporting Requirements
In most states healthcare workers not only have a moral responsibility to report suspected abuse, they are required by law to do so. In fact, New Mexico’s statute requires anyone who suspects child abuse to report it and makes failure to do so a misdemeanor. Hospitalists should know in advance to whom to report the suspected abuse.
Consider making a call to a social worker your first step. “Social workers are invaluable,” says Dr. Stucky. “They’re there for the families. They ask the harder questions that allow us to have that medical relationship and continue to care for the child’s needs. They can look up information that we can’t. They can look up child protection history, whether the parent has been incarcerated, things that support the possibility of abuse. They can file the CPS report, allowing the hospitalist to continue caring medically for the child.”
According to Berrenberg, the police should be your second call.
Dealing with child abuse and neglect is a team effort. In addition to the police and a social worker, you need to involve the nutritionist and the primary care pediatrician (if they have one). If you’re lucky, your hospital may have a child abuse specialist on staff. “Be ready to deal with a whole variety of people who may or may not know what else has already happened,” says Berrenberg.
After the Hospital Stay
Although child abuse is all too common, most pediatric hospitalists won’t often see the inside of a courtroom. Dr. Stucky says that cases with which she’s been involved have gone to trial twice during her 10 years as a pediatric hospitalist. And Berrenberg says, “Failure to thrive is not something we charge very often. That’s a difficult thing to prove.”
That said, prepare for the possibility of being called as a fact witness. According to Berrenberg, physicians may be asked to report on not just their observations of the child, but also on statements made in their presence.
“Statements made to physicians and to healthcare personnel are critical—be it by parents, caretakers, or the child themselves in the case of sexual abuse,” she says. “If statements are made in the course of diagnosis and treatment, then those statements can come in under hearsay exceptions. ... The doctor can testify about those statements.”
Remember it’s the doctor/patient relationship that’s important. Your patient’s parents have no doctor/patient relationship.
Berrenberg offers the following advice for physicians preparing to testify: “Be patient. Read everything you have on your case. Expect everything to change. When you’re told that you’re going to trial on Monday, expect that to change. If you’ve testified before and there are transcripts available, expect the defense to know about that previous testimony. If you’re basing your opinion on literature, expect the defense attorney to have found that literature and be familiar with it.
“Work with your prosecutor. Know what they want you for. They might only want you for a limited piece; they might want you for the whole gamut. They will tell you what they’re going to expect of you. Spend as much time as you can with them, with the photos, with the file. It’s always what you don’t expect to come up that comes up.”
Pediatric hospitalists should also be prepared for old cases to come back. “We’ll bring you from wherever you are—even if you’re out of the country,” says Berrenberg. “We’ll bring you back if we need you to testify. We’ll find you. If you’re the one who saw the child and were the initial responder, so to speak, no one else can say what you saw.”
Conclusion
What happened to the six-month-old baby Dr. Stucky remembers so clearly?
“I only know what happened during the hospital stay,” she says. “This family clearly needed help and guidance. There was an overwhelming, clear [indication] that the mother had significant, major depression. She wasn’t feeding the baby. She was completely ignoring the child, and she acknowledged that. ... The father was at work and thought that perhaps this baby was just ill or sickly. He was told that the baby was being taken to the doctor, and that wasn’t happening. He was naive and innocent in thinking that things were being dealt with and thinking that their baby was simply a baby who cried a lot and wasn’t gaining weight well.
“Once this was all [addressed], he jumped at the opportunity to have the mother in therapy and on medications. The mother herself was completely willing to give up the care. ... In this case, the paternal grandmother took over the care of this child. The father would drop off the baby at her house during the day and pick up the baby at night. On weekends they would share the duties. That was the plan at discharge. ... I can’t guarantee it, but it’s my sense that this worked very well.”
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov/topics/prevention/index.cfm.
- “What Is Child Maltreatment?” From A Coordinated Response to Child Abuse and Neglect: The Foundation for Practice. National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov.
- Child Abuse Prevention and Treatment Act. Download the complete text from the Cornell University Legal Information Institute: www4.law.cornell.edu/uscode/42/ch67.html.
- “Monitoring Child Neglect.” Summary of discussions at a meeting co-sponsored by the Centers for Disease Control and Prevention (CDC) and Prevent Child Abuse America (PCA America), March 29, 2002.
PEDIATRIC SPECIAL SECTION
In the Literature
Optimizing Management of GERD: Medical therapy or surgical intervention?
Hassall E. Outcomes of fundoplication: causes for concern, newer options. Arch Dis Child. 2005;90:1047-1052.
Review by Ray Chan, MD
This narrative review provides a concise overview of gastroesophageal reflux disease (GERD) while specifically addressing surgical treatment. The author focuses on the potential complications of surgical treatment and cites several studies demonstrating a high rate of complications and patient dissatisfaction with their outcomes. In contrast, the review does cite several sources that concluded good outcomes; however, the article questions the conclusions of these studies due to study designs with poorly defined and subjective outcome measures.
In contrast to the discussion on fundoplication, the review offers a more favorable description of proton pump inhibitor therapy. In the concluding remarks Hassall argues that medical therapy options should be exhausted prior to surgical therapy. The author states that the risk of mortality and morbidity combined with less than desirable efficacy of fundoplication should caution clinicians from being too eager in recommending fundoplication.
Clinically significant GERD is a common inpatient problem. This article provides a good review of the pathophysiology of this disease and available treatment options. Unfortunately, this narrative review does not utilize a systematic method of identifying relevant studies nor does it include a systematic approach for critical appraisal of these studies. Nevertheless the caution it raises about fundoplication is a worthy one that should be explored further. It is interesting to note that prior to this review the author has received grant support and was a paid consultant for AstraZeneca and TAP Pharmaceutical Products Inc.
Support for Bag UA Screening During Evaluation for UTI
McGillivray D, Mok E, Mulrooney E, et al. A head-to-head comparison: “clean-void” bag versus catheter urinalysis in the diagnosis of urinary tract infection in young children. J Pediatr. 2005;147(4):451-456.
Review by Jenny Geheb, RN, CPNP
Early detection of urinary tract infection (UTI) can be especially important in children. This study uses a cross-sectional design to compare the validity of the urinalysis on clean-voided bag versus catheter urine specimens using the catheter culture as the “gold” standard. This study looked at 303 non-toilet-trained children under age three at risk for UTI who presented to a children’s hospital emergency department. Paired bag and catheter specimens were obtained from each child and sent for dipstick and microscopic urinalysis. Sensitivity and specificity were compared using McNemar’s [chi]2 test for paired specimens and the ordinary [chi]2 test for unpaired comparisons.
The study, which was conducted at the Montreal Children’s Hospital, found that the bag dipstick was more sensitive than the catheter dipstick for the entire study sample: 0.85 (95% confidence interval [CI] = 0.78 to 0.93) versus 0.71 (95% CI= 0.95 to 0.99), respectively. Both bag and catheter dipstick sensitivities were lower in infants <90 days old. Specificity was consistently lower for the bag specimens than for the catheter specimens.
A child at high risk for UTI (previous history of UTI, anatomic abnormalities, immunosuppressed, or presence of urinary symptoms) should be catheterized to obtain both a UA and culture; however, in children older than 90 days with fever without source and at low risk for UTI, a “selective catheterization” approach, as outlined in the American Academy of Pediatrics practice parameter, appears to be reasonable.
In low-risk children, serious consequences of infection are less likely, and the authors propose that the risks of missing a UTI are likely to be outweighed by the risks of catheterization, including pain, false-positive result, trauma, introduction of infection, test resistance by staff, and parental concern.
In summary, the provider may choose to use a bag urine screening strategy to reduce the number of unnecessary catheterizations in children who are considered low risk and over 90 days old. Further studies are needed to analyze the cost-benefit ratio of this approach as well as to confirm these findings with larger populations.
Short-Course Antibiotic Treatment for Streptococcal Pharyngitis
Casey JR, Pichichero ME. Meta-analysis of short course antibiotic treatment for group A streptococcal tonsillopharyngitis. Ped Infect Dis J. 2005;24(10):909-917.
Review by Jenny Geheb, RN, CPNP
Group A streptococcal (GAS) tonsillopharyngitis is a common cause for antibiotic treatment in children. Researchers at the University of Rochester Medical Center (N.Y.) performed a meta-analysis of current data to compare bacterial and clinical cure rates in patients with GAS tonsillopharyngitis treated with short course antibiotic treatment with oral [beta]-lactam or macrolide antibiotics for four to five days with standard 10-day treatment courses. Medline, Embase, reference lists, and abstract searches were all used to identify applicable publications. Trials were included if there was bacteriologic confirmation of GAS tonsillopharyngitis, random assignment to antibiotic therapy for a [beta]-lactam or macrolide antibiotic of shortened course versus a 10-day course, and assessment of bacteriologic outcome using a throat culture.
Twenty-two trials involving 7,470 patients were included in four separate analyses. Trials were grouped by a short course of cephalosporins (n=14), macrolides (other than azithromycin) (n=6), penicillin (n=2), and amoxicillin (n=2). Cephalosporin trials were further grouped by penicillin (n=12) or the same cephalosporin (n=3). Five trials were conducted in the United States with the remainder conducted in Europe.
Meta-analysis showed that short course cephalosporin treatment was superior for bacterial cure rate compared with 10 days of penicillin (OR 1.47; 95% CI, 1.06-2.03). Short-course penicillin therapy was inferior in achieving bacterial cure versus 10 days of penicillin. Clinical cure rate mirrored the bacterial cure rate results. Small sample size limited the statistical power and conclusions of the short course macrolide trials as well as trials of four or five days of cephalosporin therapy compared with 10 days of the same.
This meta-analysis shows that short-course treatment of GAS tonsillopharyngitis can be more effective when prescribing four or five days of cefdinir, cefpodoxime, or cefuroxime treatment than standard 10-day treatment of penicillin. In the United States cefdinir, cefpodoxime, and azithromycin are indicated for short-course treatment. As prescribing practitioners, it is important for us to consider the advantages of shortened antibiotic courses, including improved patient compliance, fewer adverse effects, and reduced impact on development of antibiotic resistance and nasopharyngeal colonization with resistant bacteria. However, the authors emphasize that caution must be used in interpretation of the results of this meta-analysis.
For example, the trials were grouped according to class of antibiotics so that the cephalosporin group included seven different cephalosporins (one first generation, two second generation, and four third generation). In addition, there was much variability in the quality and design of compared studies, which makes it difficult to make strong conclusions. Repeat studies are needed, especially in regard to short-course macrolide or amoxicillin treatment.
Each week in the United States, child protective services and agencies receive reports of more than 50,000 suspected child abuse incidents. In 2002, 2.6 million incidents involving 4.5 million children were reported. Approximately four children die every day as a result of abuse or neglect.1 But numbers don’t tell the whole story. Behind every number is a child at risk.
“I can picture right now in my mind a young baby who was about six months of age with a belly that was protruded and distended,” says Erin R. Stucky, MD, a pediatric hospitalist at Children’s Hospital and Health Center San Diego, and an associate professor of pediatrics at the University of California San Diego. “[She had] no bowel sounds, and the arms and legs were so thin, had no fat whatsoever. The skin was rolling. The face looked dysmorphic, but it was simply because the eyes were so white, and there was no fat on the face at all. The baby had an irritated cry. The hair was thin. [She] had a look of anxiety, true anxiety [in her] eyes. It was impressive, as though this infant was saying, ‘Help me. I can’t speak.’ [She] was very socially engaged, but tired. If you had to qualify the look further, it would be something like, ‘I’m in pain. Protect me. Please don’t walk out the door.’
“The child had been admitted from the emergency department at an outside facility. They had been focused, appropriately to some extent, on the fact that the belly was distended and that the baby had no bowel sounds. They were focused on the fact that the parent’s history [of the child] was of vomiting during the day, but it clearly did not equate whatsoever with the way the child looked. It was immediately clear, simply looking at the baby while walking in the room, that something very bad was wrong and that the parents’ answers and explanations did not fit.”
What It Is
Child abuse manifests in many forms, including physical abuse, sexual abuse, emotional abuse, and neglect, with a “child” typically defined as a person under 18. Legal definitions of the forms of child abuse vary, but, in general, they reflect societal views of actions deemed improper and unacceptable because they place a child at risk of physical or emotional harm.2 The federal Child Abuse Prevention and Treatment Act (CAPTA) defines child abuse and neglect as:
- Any recent act or failure to act on the part of a parent or caretaker that results in death, serious physical or emotional harm, sexual abuse, or exploitation; or
- An act or failure to act that presents an imminent risk of serious harm.3
States must include these minimum standards in their statutes in order to receive federal funds.
Neglect is the most common form of child abuse.2 Although definitions of neglect vary by state, they share characteristics. Minnesota defines neglect as inadequate food, shelter, clothing, or medical care. California includes both overt acts and omissions in the definition of neglect, defining general neglect as a lack of food, clothing, or medical care and severe neglect as malnutrition, failure to thrive, or willfully putting a child in danger. And Rhode Island’s neglect definition goes even further, including the above acts and omissions as well as the failure to provide a minimum degree of care or proper supervision or guardianship due to unwillingness, social problems, mental incompetency, or the use of a drug, drugs or alcohol, desertion, or abandonment. Rhode Island also includes the failure to take financial responsibility for a child.4
According to Georgia Berrenberg, esq., deputy district attorney, Second Judicial District of New Mexico, sexual abuse is the most common type that goes to trial. Berrenberg, who has been a prosecutor since 1984 and was in the child abuse division from 1996–2005, estimates that approximately 70% of cases involve sexual abuse compared with 30% that involve physical abuse.
However, pediatric hospitalists will most commonly see neglect, presenting as malnutrition or failure to thrive, in a child admitted to the hospital.4
Recognize Abuse and Neglect
Pediatric hospitalists are in a unique position to recognize child abuse and neglect, intervene appropriately, and help families avoid ultimate tragedy. They are trained to consider the entire child—no matter the presenting condition—to look at general issues and to think about development and nutrition every time they examine a child.
“When someone says, ‘This child has pneumonia,’ my job is to not think pneumonia; my job is to think, ‘What’s causing this child to breathe fast?’ to make sure I don’t miss anything,” says Dr. Stucky. “If the history doesn’t fit the examination and my first, second, [and] third thoughts are child abuse/neglect. It’s my job to work on that, but it’s also my job to push my own buttons to make sure that it’s not anything else medically going on. The child that never has a bruise or fracture is the odd one out. The key [to recognizing abuse] is history.”
Don’t jump to conclusions. Hospitalists need to consider the history reported by the parent in light of the physical exam of the child. For example, if the parent tells you that the child fell headfirst off a tricycle and landed on his face, note the pattern of the bruising. If the child has bruising around the eye then that could be consistent with the history, but if the child’s eyelid is cut or bruised and there’s no bruising around the eye, that’s another matter. The eyebrow and cheekbone will protect the eye when you fall and land on your face.
“Pay attention to what you hear and see in those first few minutes and hours with that family because stories are going to change,” says Berrenberg. “Be very, very clear about the initial things that are said.”
Dealing with the medical issues that led to the admission is paramount, and it’s important for the hospitalist to communicate effectively with the parent to ensure that the child receives the most appropriate treatment. Asking open-ended questions while you take the history can be revealing:
- Can you tell me how long this has been happening?
- What do you think might be contributing to this?
- Can you tell me how you’ve been dealing with these issues at home?
- Run me through a typical day at home with your baby.
In addition to the history, consider the parent/child interaction. “Most kids, even when they’re stressed and in pain are very attentive to where their parents are,” says Dr. Stucky. “They want to be with them no matter what. They may be angry and battling. They may respond to pain differently, but that relationship is very important. As you watch it you can really get a good sense [of whether] this child’s anger outburst is because they’re in pain, they’re confused, they have autism, or they are really angry with their parent and this is the way they’re protecting themselves.”
The hospitalist has to be up front with the parent about what the next step in their child’s treatment is going to be. “It’s a delicate discussion, but an honest one,” says Dr. Stucky. “It’s important to say to the parent, overtly, ‘I’m very concerned about your baby’s weight loss. I’m very concerned that this has happened over the past several months and that it has taken this long for your baby to be seen by a doctor. I’m very concerned, and I want you to understand that your baby has a critical condition right now. It’s so malnourished that the body’s organs aren’t working properly. ... Because of this concern, I’m going to call social workers. Because of this concern I’ll use [work with] a team of people to help me to take care of your baby. They’ll ask a lot of questions, and it’s very important that you answer honestly so we can do the best for your baby and make sure that the whole family can get whatever help is needed to take care of the problem.’ ”
Reporting Requirements
In most states healthcare workers not only have a moral responsibility to report suspected abuse, they are required by law to do so. In fact, New Mexico’s statute requires anyone who suspects child abuse to report it and makes failure to do so a misdemeanor. Hospitalists should know in advance to whom to report the suspected abuse.
Consider making a call to a social worker your first step. “Social workers are invaluable,” says Dr. Stucky. “They’re there for the families. They ask the harder questions that allow us to have that medical relationship and continue to care for the child’s needs. They can look up information that we can’t. They can look up child protection history, whether the parent has been incarcerated, things that support the possibility of abuse. They can file the CPS report, allowing the hospitalist to continue caring medically for the child.”
According to Berrenberg, the police should be your second call.
Dealing with child abuse and neglect is a team effort. In addition to the police and a social worker, you need to involve the nutritionist and the primary care pediatrician (if they have one). If you’re lucky, your hospital may have a child abuse specialist on staff. “Be ready to deal with a whole variety of people who may or may not know what else has already happened,” says Berrenberg.
After the Hospital Stay
Although child abuse is all too common, most pediatric hospitalists won’t often see the inside of a courtroom. Dr. Stucky says that cases with which she’s been involved have gone to trial twice during her 10 years as a pediatric hospitalist. And Berrenberg says, “Failure to thrive is not something we charge very often. That’s a difficult thing to prove.”
That said, prepare for the possibility of being called as a fact witness. According to Berrenberg, physicians may be asked to report on not just their observations of the child, but also on statements made in their presence.
“Statements made to physicians and to healthcare personnel are critical—be it by parents, caretakers, or the child themselves in the case of sexual abuse,” she says. “If statements are made in the course of diagnosis and treatment, then those statements can come in under hearsay exceptions. ... The doctor can testify about those statements.”
Remember it’s the doctor/patient relationship that’s important. Your patient’s parents have no doctor/patient relationship.
Berrenberg offers the following advice for physicians preparing to testify: “Be patient. Read everything you have on your case. Expect everything to change. When you’re told that you’re going to trial on Monday, expect that to change. If you’ve testified before and there are transcripts available, expect the defense to know about that previous testimony. If you’re basing your opinion on literature, expect the defense attorney to have found that literature and be familiar with it.
“Work with your prosecutor. Know what they want you for. They might only want you for a limited piece; they might want you for the whole gamut. They will tell you what they’re going to expect of you. Spend as much time as you can with them, with the photos, with the file. It’s always what you don’t expect to come up that comes up.”
Pediatric hospitalists should also be prepared for old cases to come back. “We’ll bring you from wherever you are—even if you’re out of the country,” says Berrenberg. “We’ll bring you back if we need you to testify. We’ll find you. If you’re the one who saw the child and were the initial responder, so to speak, no one else can say what you saw.”
Conclusion
What happened to the six-month-old baby Dr. Stucky remembers so clearly?
“I only know what happened during the hospital stay,” she says. “This family clearly needed help and guidance. There was an overwhelming, clear [indication] that the mother had significant, major depression. She wasn’t feeding the baby. She was completely ignoring the child, and she acknowledged that. ... The father was at work and thought that perhaps this baby was just ill or sickly. He was told that the baby was being taken to the doctor, and that wasn’t happening. He was naive and innocent in thinking that things were being dealt with and thinking that their baby was simply a baby who cried a lot and wasn’t gaining weight well.
“Once this was all [addressed], he jumped at the opportunity to have the mother in therapy and on medications. The mother herself was completely willing to give up the care. ... In this case, the paternal grandmother took over the care of this child. The father would drop off the baby at her house during the day and pick up the baby at night. On weekends they would share the duties. That was the plan at discharge. ... I can’t guarantee it, but it’s my sense that this worked very well.”
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov/topics/prevention/index.cfm.
- “What Is Child Maltreatment?” From A Coordinated Response to Child Abuse and Neglect: The Foundation for Practice. National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov.
- Child Abuse Prevention and Treatment Act. Download the complete text from the Cornell University Legal Information Institute: www4.law.cornell.edu/uscode/42/ch67.html.
- “Monitoring Child Neglect.” Summary of discussions at a meeting co-sponsored by the Centers for Disease Control and Prevention (CDC) and Prevent Child Abuse America (PCA America), March 29, 2002.
PEDIATRIC SPECIAL SECTION
In the Literature
Optimizing Management of GERD: Medical therapy or surgical intervention?
Hassall E. Outcomes of fundoplication: causes for concern, newer options. Arch Dis Child. 2005;90:1047-1052.
Review by Ray Chan, MD
This narrative review provides a concise overview of gastroesophageal reflux disease (GERD) while specifically addressing surgical treatment. The author focuses on the potential complications of surgical treatment and cites several studies demonstrating a high rate of complications and patient dissatisfaction with their outcomes. In contrast, the review does cite several sources that concluded good outcomes; however, the article questions the conclusions of these studies due to study designs with poorly defined and subjective outcome measures.
In contrast to the discussion on fundoplication, the review offers a more favorable description of proton pump inhibitor therapy. In the concluding remarks Hassall argues that medical therapy options should be exhausted prior to surgical therapy. The author states that the risk of mortality and morbidity combined with less than desirable efficacy of fundoplication should caution clinicians from being too eager in recommending fundoplication.
Clinically significant GERD is a common inpatient problem. This article provides a good review of the pathophysiology of this disease and available treatment options. Unfortunately, this narrative review does not utilize a systematic method of identifying relevant studies nor does it include a systematic approach for critical appraisal of these studies. Nevertheless the caution it raises about fundoplication is a worthy one that should be explored further. It is interesting to note that prior to this review the author has received grant support and was a paid consultant for AstraZeneca and TAP Pharmaceutical Products Inc.
Support for Bag UA Screening During Evaluation for UTI
McGillivray D, Mok E, Mulrooney E, et al. A head-to-head comparison: “clean-void” bag versus catheter urinalysis in the diagnosis of urinary tract infection in young children. J Pediatr. 2005;147(4):451-456.
Review by Jenny Geheb, RN, CPNP
Early detection of urinary tract infection (UTI) can be especially important in children. This study uses a cross-sectional design to compare the validity of the urinalysis on clean-voided bag versus catheter urine specimens using the catheter culture as the “gold” standard. This study looked at 303 non-toilet-trained children under age three at risk for UTI who presented to a children’s hospital emergency department. Paired bag and catheter specimens were obtained from each child and sent for dipstick and microscopic urinalysis. Sensitivity and specificity were compared using McNemar’s [chi]2 test for paired specimens and the ordinary [chi]2 test for unpaired comparisons.
The study, which was conducted at the Montreal Children’s Hospital, found that the bag dipstick was more sensitive than the catheter dipstick for the entire study sample: 0.85 (95% confidence interval [CI] = 0.78 to 0.93) versus 0.71 (95% CI= 0.95 to 0.99), respectively. Both bag and catheter dipstick sensitivities were lower in infants <90 days old. Specificity was consistently lower for the bag specimens than for the catheter specimens.
A child at high risk for UTI (previous history of UTI, anatomic abnormalities, immunosuppressed, or presence of urinary symptoms) should be catheterized to obtain both a UA and culture; however, in children older than 90 days with fever without source and at low risk for UTI, a “selective catheterization” approach, as outlined in the American Academy of Pediatrics practice parameter, appears to be reasonable.
In low-risk children, serious consequences of infection are less likely, and the authors propose that the risks of missing a UTI are likely to be outweighed by the risks of catheterization, including pain, false-positive result, trauma, introduction of infection, test resistance by staff, and parental concern.
In summary, the provider may choose to use a bag urine screening strategy to reduce the number of unnecessary catheterizations in children who are considered low risk and over 90 days old. Further studies are needed to analyze the cost-benefit ratio of this approach as well as to confirm these findings with larger populations.
Short-Course Antibiotic Treatment for Streptococcal Pharyngitis
Casey JR, Pichichero ME. Meta-analysis of short course antibiotic treatment for group A streptococcal tonsillopharyngitis. Ped Infect Dis J. 2005;24(10):909-917.
Review by Jenny Geheb, RN, CPNP
Group A streptococcal (GAS) tonsillopharyngitis is a common cause for antibiotic treatment in children. Researchers at the University of Rochester Medical Center (N.Y.) performed a meta-analysis of current data to compare bacterial and clinical cure rates in patients with GAS tonsillopharyngitis treated with short course antibiotic treatment with oral [beta]-lactam or macrolide antibiotics for four to five days with standard 10-day treatment courses. Medline, Embase, reference lists, and abstract searches were all used to identify applicable publications. Trials were included if there was bacteriologic confirmation of GAS tonsillopharyngitis, random assignment to antibiotic therapy for a [beta]-lactam or macrolide antibiotic of shortened course versus a 10-day course, and assessment of bacteriologic outcome using a throat culture.
Twenty-two trials involving 7,470 patients were included in four separate analyses. Trials were grouped by a short course of cephalosporins (n=14), macrolides (other than azithromycin) (n=6), penicillin (n=2), and amoxicillin (n=2). Cephalosporin trials were further grouped by penicillin (n=12) or the same cephalosporin (n=3). Five trials were conducted in the United States with the remainder conducted in Europe.
Meta-analysis showed that short course cephalosporin treatment was superior for bacterial cure rate compared with 10 days of penicillin (OR 1.47; 95% CI, 1.06-2.03). Short-course penicillin therapy was inferior in achieving bacterial cure versus 10 days of penicillin. Clinical cure rate mirrored the bacterial cure rate results. Small sample size limited the statistical power and conclusions of the short course macrolide trials as well as trials of four or five days of cephalosporin therapy compared with 10 days of the same.
This meta-analysis shows that short-course treatment of GAS tonsillopharyngitis can be more effective when prescribing four or five days of cefdinir, cefpodoxime, or cefuroxime treatment than standard 10-day treatment of penicillin. In the United States cefdinir, cefpodoxime, and azithromycin are indicated for short-course treatment. As prescribing practitioners, it is important for us to consider the advantages of shortened antibiotic courses, including improved patient compliance, fewer adverse effects, and reduced impact on development of antibiotic resistance and nasopharyngeal colonization with resistant bacteria. However, the authors emphasize that caution must be used in interpretation of the results of this meta-analysis.
For example, the trials were grouped according to class of antibiotics so that the cephalosporin group included seven different cephalosporins (one first generation, two second generation, and four third generation). In addition, there was much variability in the quality and design of compared studies, which makes it difficult to make strong conclusions. Repeat studies are needed, especially in regard to short-course macrolide or amoxicillin treatment.
Each week in the United States, child protective services and agencies receive reports of more than 50,000 suspected child abuse incidents. In 2002, 2.6 million incidents involving 4.5 million children were reported. Approximately four children die every day as a result of abuse or neglect.1 But numbers don’t tell the whole story. Behind every number is a child at risk.
“I can picture right now in my mind a young baby who was about six months of age with a belly that was protruded and distended,” says Erin R. Stucky, MD, a pediatric hospitalist at Children’s Hospital and Health Center San Diego, and an associate professor of pediatrics at the University of California San Diego. “[She had] no bowel sounds, and the arms and legs were so thin, had no fat whatsoever. The skin was rolling. The face looked dysmorphic, but it was simply because the eyes were so white, and there was no fat on the face at all. The baby had an irritated cry. The hair was thin. [She] had a look of anxiety, true anxiety [in her] eyes. It was impressive, as though this infant was saying, ‘Help me. I can’t speak.’ [She] was very socially engaged, but tired. If you had to qualify the look further, it would be something like, ‘I’m in pain. Protect me. Please don’t walk out the door.’
“The child had been admitted from the emergency department at an outside facility. They had been focused, appropriately to some extent, on the fact that the belly was distended and that the baby had no bowel sounds. They were focused on the fact that the parent’s history [of the child] was of vomiting during the day, but it clearly did not equate whatsoever with the way the child looked. It was immediately clear, simply looking at the baby while walking in the room, that something very bad was wrong and that the parents’ answers and explanations did not fit.”
What It Is
Child abuse manifests in many forms, including physical abuse, sexual abuse, emotional abuse, and neglect, with a “child” typically defined as a person under 18. Legal definitions of the forms of child abuse vary, but, in general, they reflect societal views of actions deemed improper and unacceptable because they place a child at risk of physical or emotional harm.2 The federal Child Abuse Prevention and Treatment Act (CAPTA) defines child abuse and neglect as:
- Any recent act or failure to act on the part of a parent or caretaker that results in death, serious physical or emotional harm, sexual abuse, or exploitation; or
- An act or failure to act that presents an imminent risk of serious harm.3
States must include these minimum standards in their statutes in order to receive federal funds.
Neglect is the most common form of child abuse.2 Although definitions of neglect vary by state, they share characteristics. Minnesota defines neglect as inadequate food, shelter, clothing, or medical care. California includes both overt acts and omissions in the definition of neglect, defining general neglect as a lack of food, clothing, or medical care and severe neglect as malnutrition, failure to thrive, or willfully putting a child in danger. And Rhode Island’s neglect definition goes even further, including the above acts and omissions as well as the failure to provide a minimum degree of care or proper supervision or guardianship due to unwillingness, social problems, mental incompetency, or the use of a drug, drugs or alcohol, desertion, or abandonment. Rhode Island also includes the failure to take financial responsibility for a child.4
According to Georgia Berrenberg, esq., deputy district attorney, Second Judicial District of New Mexico, sexual abuse is the most common type that goes to trial. Berrenberg, who has been a prosecutor since 1984 and was in the child abuse division from 1996–2005, estimates that approximately 70% of cases involve sexual abuse compared with 30% that involve physical abuse.
However, pediatric hospitalists will most commonly see neglect, presenting as malnutrition or failure to thrive, in a child admitted to the hospital.4
Recognize Abuse and Neglect
Pediatric hospitalists are in a unique position to recognize child abuse and neglect, intervene appropriately, and help families avoid ultimate tragedy. They are trained to consider the entire child—no matter the presenting condition—to look at general issues and to think about development and nutrition every time they examine a child.
“When someone says, ‘This child has pneumonia,’ my job is to not think pneumonia; my job is to think, ‘What’s causing this child to breathe fast?’ to make sure I don’t miss anything,” says Dr. Stucky. “If the history doesn’t fit the examination and my first, second, [and] third thoughts are child abuse/neglect. It’s my job to work on that, but it’s also my job to push my own buttons to make sure that it’s not anything else medically going on. The child that never has a bruise or fracture is the odd one out. The key [to recognizing abuse] is history.”
Don’t jump to conclusions. Hospitalists need to consider the history reported by the parent in light of the physical exam of the child. For example, if the parent tells you that the child fell headfirst off a tricycle and landed on his face, note the pattern of the bruising. If the child has bruising around the eye then that could be consistent with the history, but if the child’s eyelid is cut or bruised and there’s no bruising around the eye, that’s another matter. The eyebrow and cheekbone will protect the eye when you fall and land on your face.
“Pay attention to what you hear and see in those first few minutes and hours with that family because stories are going to change,” says Berrenberg. “Be very, very clear about the initial things that are said.”
Dealing with the medical issues that led to the admission is paramount, and it’s important for the hospitalist to communicate effectively with the parent to ensure that the child receives the most appropriate treatment. Asking open-ended questions while you take the history can be revealing:
- Can you tell me how long this has been happening?
- What do you think might be contributing to this?
- Can you tell me how you’ve been dealing with these issues at home?
- Run me through a typical day at home with your baby.
In addition to the history, consider the parent/child interaction. “Most kids, even when they’re stressed and in pain are very attentive to where their parents are,” says Dr. Stucky. “They want to be with them no matter what. They may be angry and battling. They may respond to pain differently, but that relationship is very important. As you watch it you can really get a good sense [of whether] this child’s anger outburst is because they’re in pain, they’re confused, they have autism, or they are really angry with their parent and this is the way they’re protecting themselves.”
The hospitalist has to be up front with the parent about what the next step in their child’s treatment is going to be. “It’s a delicate discussion, but an honest one,” says Dr. Stucky. “It’s important to say to the parent, overtly, ‘I’m very concerned about your baby’s weight loss. I’m very concerned that this has happened over the past several months and that it has taken this long for your baby to be seen by a doctor. I’m very concerned, and I want you to understand that your baby has a critical condition right now. It’s so malnourished that the body’s organs aren’t working properly. ... Because of this concern, I’m going to call social workers. Because of this concern I’ll use [work with] a team of people to help me to take care of your baby. They’ll ask a lot of questions, and it’s very important that you answer honestly so we can do the best for your baby and make sure that the whole family can get whatever help is needed to take care of the problem.’ ”
Reporting Requirements
In most states healthcare workers not only have a moral responsibility to report suspected abuse, they are required by law to do so. In fact, New Mexico’s statute requires anyone who suspects child abuse to report it and makes failure to do so a misdemeanor. Hospitalists should know in advance to whom to report the suspected abuse.
Consider making a call to a social worker your first step. “Social workers are invaluable,” says Dr. Stucky. “They’re there for the families. They ask the harder questions that allow us to have that medical relationship and continue to care for the child’s needs. They can look up information that we can’t. They can look up child protection history, whether the parent has been incarcerated, things that support the possibility of abuse. They can file the CPS report, allowing the hospitalist to continue caring medically for the child.”
According to Berrenberg, the police should be your second call.
Dealing with child abuse and neglect is a team effort. In addition to the police and a social worker, you need to involve the nutritionist and the primary care pediatrician (if they have one). If you’re lucky, your hospital may have a child abuse specialist on staff. “Be ready to deal with a whole variety of people who may or may not know what else has already happened,” says Berrenberg.
After the Hospital Stay
Although child abuse is all too common, most pediatric hospitalists won’t often see the inside of a courtroom. Dr. Stucky says that cases with which she’s been involved have gone to trial twice during her 10 years as a pediatric hospitalist. And Berrenberg says, “Failure to thrive is not something we charge very often. That’s a difficult thing to prove.”
That said, prepare for the possibility of being called as a fact witness. According to Berrenberg, physicians may be asked to report on not just their observations of the child, but also on statements made in their presence.
“Statements made to physicians and to healthcare personnel are critical—be it by parents, caretakers, or the child themselves in the case of sexual abuse,” she says. “If statements are made in the course of diagnosis and treatment, then those statements can come in under hearsay exceptions. ... The doctor can testify about those statements.”
Remember it’s the doctor/patient relationship that’s important. Your patient’s parents have no doctor/patient relationship.
Berrenberg offers the following advice for physicians preparing to testify: “Be patient. Read everything you have on your case. Expect everything to change. When you’re told that you’re going to trial on Monday, expect that to change. If you’ve testified before and there are transcripts available, expect the defense to know about that previous testimony. If you’re basing your opinion on literature, expect the defense attorney to have found that literature and be familiar with it.
“Work with your prosecutor. Know what they want you for. They might only want you for a limited piece; they might want you for the whole gamut. They will tell you what they’re going to expect of you. Spend as much time as you can with them, with the photos, with the file. It’s always what you don’t expect to come up that comes up.”
Pediatric hospitalists should also be prepared for old cases to come back. “We’ll bring you from wherever you are—even if you’re out of the country,” says Berrenberg. “We’ll bring you back if we need you to testify. We’ll find you. If you’re the one who saw the child and were the initial responder, so to speak, no one else can say what you saw.”
Conclusion
What happened to the six-month-old baby Dr. Stucky remembers so clearly?
“I only know what happened during the hospital stay,” she says. “This family clearly needed help and guidance. There was an overwhelming, clear [indication] that the mother had significant, major depression. She wasn’t feeding the baby. She was completely ignoring the child, and she acknowledged that. ... The father was at work and thought that perhaps this baby was just ill or sickly. He was told that the baby was being taken to the doctor, and that wasn’t happening. He was naive and innocent in thinking that things were being dealt with and thinking that their baby was simply a baby who cried a lot and wasn’t gaining weight well.
“Once this was all [addressed], he jumped at the opportunity to have the mother in therapy and on medications. The mother herself was completely willing to give up the care. ... In this case, the paternal grandmother took over the care of this child. The father would drop off the baby at her house during the day and pick up the baby at night. On weekends they would share the duties. That was the plan at discharge. ... I can’t guarantee it, but it’s my sense that this worked very well.”
Keri Losavio is a medical journalist with more than 10 years’ experience.
References
- National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov/topics/prevention/index.cfm.
- “What Is Child Maltreatment?” From A Coordinated Response to Child Abuse and Neglect: The Foundation for Practice. National Clearinghouse on Child Abuse and Neglect Information: http://nccanch.acf.hhs.gov.
- Child Abuse Prevention and Treatment Act. Download the complete text from the Cornell University Legal Information Institute: www4.law.cornell.edu/uscode/42/ch67.html.
- “Monitoring Child Neglect.” Summary of discussions at a meeting co-sponsored by the Centers for Disease Control and Prevention (CDC) and Prevent Child Abuse America (PCA America), March 29, 2002.
PEDIATRIC SPECIAL SECTION
In the Literature
Optimizing Management of GERD: Medical therapy or surgical intervention?
Hassall E. Outcomes of fundoplication: causes for concern, newer options. Arch Dis Child. 2005;90:1047-1052.
Review by Ray Chan, MD
This narrative review provides a concise overview of gastroesophageal reflux disease (GERD) while specifically addressing surgical treatment. The author focuses on the potential complications of surgical treatment and cites several studies demonstrating a high rate of complications and patient dissatisfaction with their outcomes. In contrast, the review does cite several sources that concluded good outcomes; however, the article questions the conclusions of these studies due to study designs with poorly defined and subjective outcome measures.
In contrast to the discussion on fundoplication, the review offers a more favorable description of proton pump inhibitor therapy. In the concluding remarks Hassall argues that medical therapy options should be exhausted prior to surgical therapy. The author states that the risk of mortality and morbidity combined with less than desirable efficacy of fundoplication should caution clinicians from being too eager in recommending fundoplication.
Clinically significant GERD is a common inpatient problem. This article provides a good review of the pathophysiology of this disease and available treatment options. Unfortunately, this narrative review does not utilize a systematic method of identifying relevant studies nor does it include a systematic approach for critical appraisal of these studies. Nevertheless the caution it raises about fundoplication is a worthy one that should be explored further. It is interesting to note that prior to this review the author has received grant support and was a paid consultant for AstraZeneca and TAP Pharmaceutical Products Inc.
Support for Bag UA Screening During Evaluation for UTI
McGillivray D, Mok E, Mulrooney E, et al. A head-to-head comparison: “clean-void” bag versus catheter urinalysis in the diagnosis of urinary tract infection in young children. J Pediatr. 2005;147(4):451-456.
Review by Jenny Geheb, RN, CPNP
Early detection of urinary tract infection (UTI) can be especially important in children. This study uses a cross-sectional design to compare the validity of the urinalysis on clean-voided bag versus catheter urine specimens using the catheter culture as the “gold” standard. This study looked at 303 non-toilet-trained children under age three at risk for UTI who presented to a children’s hospital emergency department. Paired bag and catheter specimens were obtained from each child and sent for dipstick and microscopic urinalysis. Sensitivity and specificity were compared using McNemar’s [chi]2 test for paired specimens and the ordinary [chi]2 test for unpaired comparisons.
The study, which was conducted at the Montreal Children’s Hospital, found that the bag dipstick was more sensitive than the catheter dipstick for the entire study sample: 0.85 (95% confidence interval [CI] = 0.78 to 0.93) versus 0.71 (95% CI= 0.95 to 0.99), respectively. Both bag and catheter dipstick sensitivities were lower in infants <90 days old. Specificity was consistently lower for the bag specimens than for the catheter specimens.
A child at high risk for UTI (previous history of UTI, anatomic abnormalities, immunosuppressed, or presence of urinary symptoms) should be catheterized to obtain both a UA and culture; however, in children older than 90 days with fever without source and at low risk for UTI, a “selective catheterization” approach, as outlined in the American Academy of Pediatrics practice parameter, appears to be reasonable.
In low-risk children, serious consequences of infection are less likely, and the authors propose that the risks of missing a UTI are likely to be outweighed by the risks of catheterization, including pain, false-positive result, trauma, introduction of infection, test resistance by staff, and parental concern.
In summary, the provider may choose to use a bag urine screening strategy to reduce the number of unnecessary catheterizations in children who are considered low risk and over 90 days old. Further studies are needed to analyze the cost-benefit ratio of this approach as well as to confirm these findings with larger populations.
Short-Course Antibiotic Treatment for Streptococcal Pharyngitis
Casey JR, Pichichero ME. Meta-analysis of short course antibiotic treatment for group A streptococcal tonsillopharyngitis. Ped Infect Dis J. 2005;24(10):909-917.
Review by Jenny Geheb, RN, CPNP
Group A streptococcal (GAS) tonsillopharyngitis is a common cause for antibiotic treatment in children. Researchers at the University of Rochester Medical Center (N.Y.) performed a meta-analysis of current data to compare bacterial and clinical cure rates in patients with GAS tonsillopharyngitis treated with short course antibiotic treatment with oral [beta]-lactam or macrolide antibiotics for four to five days with standard 10-day treatment courses. Medline, Embase, reference lists, and abstract searches were all used to identify applicable publications. Trials were included if there was bacteriologic confirmation of GAS tonsillopharyngitis, random assignment to antibiotic therapy for a [beta]-lactam or macrolide antibiotic of shortened course versus a 10-day course, and assessment of bacteriologic outcome using a throat culture.
Twenty-two trials involving 7,470 patients were included in four separate analyses. Trials were grouped by a short course of cephalosporins (n=14), macrolides (other than azithromycin) (n=6), penicillin (n=2), and amoxicillin (n=2). Cephalosporin trials were further grouped by penicillin (n=12) or the same cephalosporin (n=3). Five trials were conducted in the United States with the remainder conducted in Europe.
Meta-analysis showed that short course cephalosporin treatment was superior for bacterial cure rate compared with 10 days of penicillin (OR 1.47; 95% CI, 1.06-2.03). Short-course penicillin therapy was inferior in achieving bacterial cure versus 10 days of penicillin. Clinical cure rate mirrored the bacterial cure rate results. Small sample size limited the statistical power and conclusions of the short course macrolide trials as well as trials of four or five days of cephalosporin therapy compared with 10 days of the same.
This meta-analysis shows that short-course treatment of GAS tonsillopharyngitis can be more effective when prescribing four or five days of cefdinir, cefpodoxime, or cefuroxime treatment than standard 10-day treatment of penicillin. In the United States cefdinir, cefpodoxime, and azithromycin are indicated for short-course treatment. As prescribing practitioners, it is important for us to consider the advantages of shortened antibiotic courses, including improved patient compliance, fewer adverse effects, and reduced impact on development of antibiotic resistance and nasopharyngeal colonization with resistant bacteria. However, the authors emphasize that caution must be used in interpretation of the results of this meta-analysis.
For example, the trials were grouped according to class of antibiotics so that the cephalosporin group included seven different cephalosporins (one first generation, two second generation, and four third generation). In addition, there was much variability in the quality and design of compared studies, which makes it difficult to make strong conclusions. Repeat studies are needed, especially in regard to short-course macrolide or amoxicillin treatment.
Top PICS
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.


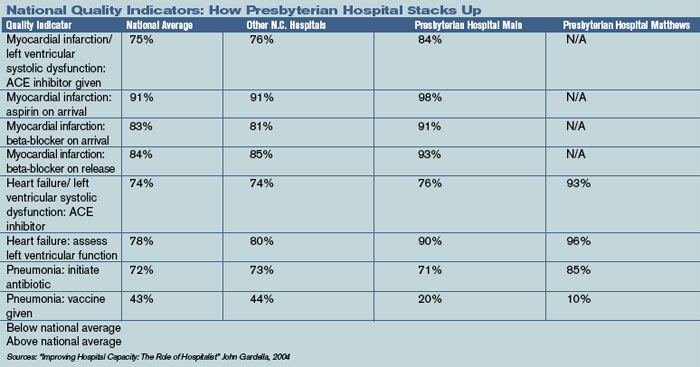
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
E-Prescribing is E-Slow
Health information technology, including e-prescribing, is “truly on the national marquee,” according to Carolyn M. Clancy, MD, director of the Agency for Healthcare Research and Technology (AHRQ). Speaking at the Annual Conference of the Healthcare Information and Management Systems Society earlier this year, she said, “Americans are quickly coming to understand how much we have to gain from health information technology (HIT). And one thing about Americans—we don’t like to wait.”
Clancy and other government officials have been pushing for widespread implementation and use of e-prescribing and other HIT in hospitals and other care settings. In 2003 the Medicare Modernization Act included a provision offering grants to physicians who implement e-prescribing systems. While all of the talk and action have stopped short of mandating the use of this technology, the handwriting is clearly on the wall. Like it or not, e-prescribing is part of healthcare’s future.
Yet despite all of these efforts on behalf of HIT few physicians are jumping on the e-prescribing bandwagon. Current estimates show that only between 5% and 18% of physicians and other clinicians use e-prescribing.
Nonetheless, while few physicians use these systems, they clearly see their value. In one survey, 78% of physicians say they believe that within the next seven years e-prescribing will account for more than half of the prescriptions written; and 75% cited reduced medication errors and time savings as two benefits of this technology.1 Another survey showed that while only 5% of physicians say they use their handheld computers for prescribing, 100% say that they use their PDAs for drug information.2
Despite the technology’s benefits, there are many reasons hospitalists and other physicians have resisted the call of e-prescribing. However, it behooves these practitioners to know about e-prescribing, consider how they might implement various technologies in their prescribing practices, and become involved in HIT initiatives at their facilities.
Money Matters: Costs Can Keep Hospitalists from E-Prescribing
E-prescribing is not widespread among hospitalists and other physicians, suggests Philip Strong, MD, IT physician liaison at El Camino Hospital and a hospitalist with the El Camino Medical Center in Mountain View, Calif.
Mark Zielzinski, chief information officer at El Camino, says that e-prescribing doesn’t really fit well with what hospitalists do.
E-prescribing is “wonderful in the physician’s office,” he explains. This is because the community-based physician writes many prescriptions every day and needs to communicate prescription information to a wide array of facilities and pharmacies.
“Hospitalists write far fewer prescriptions than attending physicians,” says Ronald Newman, MD, medical director of the hospitalist program at Beverly Hospital in Beverly, Mass. “I don’t write more than five a day.” An e-prescribing system simply isn’t practical for him.
Dr. Strong suggests, however, that the lack of enthusiasm for e-prescribing has more “to do with dollars. Systems are fairly expensive,” he says because a good system could cost as much as $150,000.
Why so much? “For a system to make sense and create more work for hospitalists, it has to interface with whatever system a hospital is using for pharmacies in the area,” explains Dr. Strong. And this can be expensive.
The cost for an individual physician or a small practice to implement e-prescribing seems much more reasonable. However, Dr. Zielzinski says that this represents only about 20% of the total cost of new technology.
“Think of what you spend when you get a home computer,” he says. “Say you spend $1,000 for the PC itself. Then you have to buy software, Internet access, a printer, and other accessories. Then you have to take the time to learn to use it all. Consider everything you spend in five years, and that $1,000 is a drop in the bucket.”
Dr. Zielzinski emphasizes that it’s not just the money that keeps hospitalists and other physicians from using e-prescribing. “Physicians have an intrinsic sociological resistance to change. After all, they are accustomed to evidence-based care and they are expected to have evidence to back up their decisions and actions,” he says, adding that “it takes a new clinical technique, theory, or practice an average of 17 years to get into mainstream practice. So how can we expect to accept new technology just like that?”

—Philip Strong, MD
Practical Protests: When Systems Hinder Efficiency
Another barrier to hospitalist acceptance of e-prescribing and other technology is that it sometimes takes longer to use, especially at the beginning.
“I’m part of an eight-hospitalist team, and we could use an e-prescribing system that our medical group has deployed, but we don’t,” admits Dr. Strong. “To use e-prescribing would require an extra step of work for us. We already have to dictate discharge notes and handwrite prescriptions. We don’t have the ability to substitute e-prescribing; it would just be an additional tool—and an additional step that would slow down our discharges.”
Dr. Newman agrees that physicians won’t use time-consuming technology. “Many systems take a lot of time to learn to use efficiently and effectively,” he says. “Physicians are afraid that these systems, such as e-prescribing, will slow them down and hurt their efficiency.”
He says hospitals are concerned about this and are waiting to implement systems they know physicians will use.
Eric Reines, MD, vice president of North Suburban Hospitalists PC and a hospitalist at Beverly Hospital, confesses to being a techie who enjoys this stuff. He says, however, that “most of the e-prescribing systems I’ve seen have been very poor. I like technology, but I won’t use a clunky system.”
Ease of use is essential for hospitalist acceptance of e-prescribing systems. “You can’t have a system with boxes popping up all over the screen and small black and white type that you can’t read,” says Dr. Reines. “Hospitalists and other physicians just won’t use these.”
Implementing systems that physicians don’t like is a worry that IT developers at hospitals think about about continually, confesses Dr. Zielzinski. “The biggest thing that keeps me awake at night is worrying that physicians will say, ‘This takes too long,’ ” he says, emphasizing that it’s important to educate physicians about how to use systems to make the most of their features and maximize efficiency.
While hospitals are concerned about how physicians will react to the implementation of technology, physicians’ general resistance to using e-prescribing actually could be a boon for hospitalists.
“Attending physicians aren’t likely to leave hospitals because they are required to use e-prescribing or other technology, but they might be more inclined to turn patients over to hospitalists at these facilities so that they don’t have to use these systems,” says Dr. Newman.
Vendor Vexation
Physicians often face the challenge of finding systems and software that integrate successfully with other systems and settings. Dr. Reines says vendors don’t always make widespread system compatibility a priority during product development.
Some data further suggest that e-prescribing products don’t always meet users’ needs. A report commissioned by the California Health Care Foundation evaluated 19 e-prescribing product vendors and found only four offer practical alternatives to more costly and complex prescription writing solutions.
CPOE First … Then E-Prescribing
Before you jump into e-prescribing, Dr. Strong suggests that more hospitals need to implement computerized physician order entry systems (CPOE). CPOE goes beyond prescriptions and enables physicians to electronically order everything from laboratory tests and dietary interventions to nursing care.
CPOE isn’t new; El Camino has used such a system for 30 years. “We are big-time believers in CPOE,” says Dr. Zielzinski. “It has enabled us to reduce a lot of errors.”
Dr. Strong adds that “these systems are better for overall patient through-put. The routing happens as soon as I input the order. There are no faxes, no paperwork, and no delays.”
Other groups also have long promoted the benefits of CPOE. For example, the Leapfrog Group, an organization of large healthcare purchasers, has suggested standards for CPOE systems that can intercept 50% or more of common serious prescribing errors. At the same time, a number of studies have been published documenting the value of CPOE in reducing medication errors and preventable adverse drug events.
Despite the benefits of CPOE, hospitals have been slow to implement it and many physicians oppose its use. “It’s high time we got over that,” says Dr. Strong. “We need to embrace CPOE now. If we do, e-prescribing won’t be such a shock when it comes down the pike.”
When e-prescribing piggybacks a good CPOE system, it will make more sense. “And when e-prescribing is done well, it will make more sense for physicians to embrace it,” he says. “Until then, it doesn’t make sense for most common situations.”
Dr. Zielzinski agrees that physicians and others need to get over their fear of CPOE. “I think you’ll find that CMS, JCAHO, the Leapfrog Group, and others will push more and more for this to happen. It’s the right thing to do.”
When Hospitalists Embrace High Tech
It is important to emphasize that many hospitalists and other physicians embrace technology. “The reality is that physicians come [to El Camino] because of our technology—it’s part of our culture,” says Dr. Zielzinski. When hospitalists join the El Camino staff, they go through a high-tech orientation with a physician trainer.
Pediatric Hospitalist Bettina Ackerman, MD, uses e-prescribing at her facility, Children’s Hospital of Pittsburgh (Pa.), and she likes the system. She admits that certain aspects of the technology can be cumbersome.
For example, “it’s much easier to handwrite certain information, such as complicated dosing instructions that require a lot of text,” she says. Nonetheless, she has seen the benefits as well. “It has drastically reduced medication errors in our hospital. And there is an efficiency that wasn’t there before.”
Dr. Reines stated that hospitalists are like other physicians: Some of them like e-prescribing and other technology, while others don’t. Age isn’t always a predictor, he emphasizes, noting that he is “the oldest physician in his group but I’m also the most interested in technology.” However, he suggested that hospitalists who are “fresh out of training are more used to technology such as e-prescribing. They kind of expect to use it.”
The Hospitalist’s Role … Starting Now
Dr. Strong suggests that hospitalists need to be part of the IT solution. In fact, they already are actively involved in his facility. “It is important for hospitalists to know what HIT their facilities are using and considering for purchase,” he says.
Dr. Reines agrees that physicians need to be active in IT decisions at their hospitals. “I’m on the tech committee at my facility, as are several physicians,” he explains, adding that they have strong opinions and specific input on what they want HIT programs and systems to do, what information they need, and how they expect technology to work to enhance their efficiency and benefit their patients.
Hospitalists who work at teaching hospitals can have a role in educating students about technology. “We need to look at learning opportunities that involve technology,” says Dr. Reines. “And we should encourage people not to be afraid of technology or change.”
Why Bother?
If there are so many barriers to e-prescribing and so many contraindications to its use, why should hospitalists bother with this technology?
While there is much disagreement about the use, benefits, and drawbacks of e-prescribing, there is little doubt that government agencies, regulatory bodies, and third-party payers will continue to push for the widespread implementation of such technology in the coming years.
For example, JCAHO’s establishment of the medication reconciliation process, whereby hospitals and other healthcare providers are expected to compile and use medication lists whenever patients move to a new setting will make e-prescribing more important and practical for hospitalists.
“The need to reconcile our patients’ medications at admission, during their stay, and at discharge will spur a greater need for e-prescribing,” says Dr. Zielzinski.
Dr. Ackerman urges her colleagues to learn about e-prescribing and other systems now. However, she also encourages “the powers that be” to provide more specific guidance on HIT to help physicians and others make the best use of it.
Although he doesn’t use or have a real need for e-prescribing, “I certainly think we will be seeing more hospitalists and hospitals using these systems in the coming years,” says Dr. Newman. “The opportunity—however small—to prevent certain types of errors will make it worthwhile eventually in most settings.” TH
Writer Joanne Kaldy is based in Maryland.
References
- iHealthbeat. Survey: few docs use PDAs for e-prescribing. Sept. 8, 2005. Available at ihealthbeat.org. Last accessed Sept. 14, 2005.
- Mobile Village. Docs embrace handheld e-prescribing to save time, prevent errors. Mobile & Wireless News. Feb. 7, 2003.
Health information technology, including e-prescribing, is “truly on the national marquee,” according to Carolyn M. Clancy, MD, director of the Agency for Healthcare Research and Technology (AHRQ). Speaking at the Annual Conference of the Healthcare Information and Management Systems Society earlier this year, she said, “Americans are quickly coming to understand how much we have to gain from health information technology (HIT). And one thing about Americans—we don’t like to wait.”
Clancy and other government officials have been pushing for widespread implementation and use of e-prescribing and other HIT in hospitals and other care settings. In 2003 the Medicare Modernization Act included a provision offering grants to physicians who implement e-prescribing systems. While all of the talk and action have stopped short of mandating the use of this technology, the handwriting is clearly on the wall. Like it or not, e-prescribing is part of healthcare’s future.
Yet despite all of these efforts on behalf of HIT few physicians are jumping on the e-prescribing bandwagon. Current estimates show that only between 5% and 18% of physicians and other clinicians use e-prescribing.
Nonetheless, while few physicians use these systems, they clearly see their value. In one survey, 78% of physicians say they believe that within the next seven years e-prescribing will account for more than half of the prescriptions written; and 75% cited reduced medication errors and time savings as two benefits of this technology.1 Another survey showed that while only 5% of physicians say they use their handheld computers for prescribing, 100% say that they use their PDAs for drug information.2
Despite the technology’s benefits, there are many reasons hospitalists and other physicians have resisted the call of e-prescribing. However, it behooves these practitioners to know about e-prescribing, consider how they might implement various technologies in their prescribing practices, and become involved in HIT initiatives at their facilities.
Money Matters: Costs Can Keep Hospitalists from E-Prescribing
E-prescribing is not widespread among hospitalists and other physicians, suggests Philip Strong, MD, IT physician liaison at El Camino Hospital and a hospitalist with the El Camino Medical Center in Mountain View, Calif.
Mark Zielzinski, chief information officer at El Camino, says that e-prescribing doesn’t really fit well with what hospitalists do.
E-prescribing is “wonderful in the physician’s office,” he explains. This is because the community-based physician writes many prescriptions every day and needs to communicate prescription information to a wide array of facilities and pharmacies.
“Hospitalists write far fewer prescriptions than attending physicians,” says Ronald Newman, MD, medical director of the hospitalist program at Beverly Hospital in Beverly, Mass. “I don’t write more than five a day.” An e-prescribing system simply isn’t practical for him.
Dr. Strong suggests, however, that the lack of enthusiasm for e-prescribing has more “to do with dollars. Systems are fairly expensive,” he says because a good system could cost as much as $150,000.
Why so much? “For a system to make sense and create more work for hospitalists, it has to interface with whatever system a hospital is using for pharmacies in the area,” explains Dr. Strong. And this can be expensive.
The cost for an individual physician or a small practice to implement e-prescribing seems much more reasonable. However, Dr. Zielzinski says that this represents only about 20% of the total cost of new technology.
“Think of what you spend when you get a home computer,” he says. “Say you spend $1,000 for the PC itself. Then you have to buy software, Internet access, a printer, and other accessories. Then you have to take the time to learn to use it all. Consider everything you spend in five years, and that $1,000 is a drop in the bucket.”
Dr. Zielzinski emphasizes that it’s not just the money that keeps hospitalists and other physicians from using e-prescribing. “Physicians have an intrinsic sociological resistance to change. After all, they are accustomed to evidence-based care and they are expected to have evidence to back up their decisions and actions,” he says, adding that “it takes a new clinical technique, theory, or practice an average of 17 years to get into mainstream practice. So how can we expect to accept new technology just like that?”
—Philip Strong, MD
Practical Protests: When Systems Hinder Efficiency
Another barrier to hospitalist acceptance of e-prescribing and other technology is that it sometimes takes longer to use, especially at the beginning.
“I’m part of an eight-hospitalist team, and we could use an e-prescribing system that our medical group has deployed, but we don’t,” admits Dr. Strong. “To use e-prescribing would require an extra step of work for us. We already have to dictate discharge notes and handwrite prescriptions. We don’t have the ability to substitute e-prescribing; it would just be an additional tool—and an additional step that would slow down our discharges.”
Dr. Newman agrees that physicians won’t use time-consuming technology. “Many systems take a lot of time to learn to use efficiently and effectively,” he says. “Physicians are afraid that these systems, such as e-prescribing, will slow them down and hurt their efficiency.”
He says hospitals are concerned about this and are waiting to implement systems they know physicians will use.
Eric Reines, MD, vice president of North Suburban Hospitalists PC and a hospitalist at Beverly Hospital, confesses to being a techie who enjoys this stuff. He says, however, that “most of the e-prescribing systems I’ve seen have been very poor. I like technology, but I won’t use a clunky system.”
Ease of use is essential for hospitalist acceptance of e-prescribing systems. “You can’t have a system with boxes popping up all over the screen and small black and white type that you can’t read,” says Dr. Reines. “Hospitalists and other physicians just won’t use these.”
Implementing systems that physicians don’t like is a worry that IT developers at hospitals think about about continually, confesses Dr. Zielzinski. “The biggest thing that keeps me awake at night is worrying that physicians will say, ‘This takes too long,’ ” he says, emphasizing that it’s important to educate physicians about how to use systems to make the most of their features and maximize efficiency.
While hospitals are concerned about how physicians will react to the implementation of technology, physicians’ general resistance to using e-prescribing actually could be a boon for hospitalists.
“Attending physicians aren’t likely to leave hospitals because they are required to use e-prescribing or other technology, but they might be more inclined to turn patients over to hospitalists at these facilities so that they don’t have to use these systems,” says Dr. Newman.
Vendor Vexation
Physicians often face the challenge of finding systems and software that integrate successfully with other systems and settings. Dr. Reines says vendors don’t always make widespread system compatibility a priority during product development.
Some data further suggest that e-prescribing products don’t always meet users’ needs. A report commissioned by the California Health Care Foundation evaluated 19 e-prescribing product vendors and found only four offer practical alternatives to more costly and complex prescription writing solutions.
CPOE First … Then E-Prescribing
Before you jump into e-prescribing, Dr. Strong suggests that more hospitals need to implement computerized physician order entry systems (CPOE). CPOE goes beyond prescriptions and enables physicians to electronically order everything from laboratory tests and dietary interventions to nursing care.
CPOE isn’t new; El Camino has used such a system for 30 years. “We are big-time believers in CPOE,” says Dr. Zielzinski. “It has enabled us to reduce a lot of errors.”
Dr. Strong adds that “these systems are better for overall patient through-put. The routing happens as soon as I input the order. There are no faxes, no paperwork, and no delays.”
Other groups also have long promoted the benefits of CPOE. For example, the Leapfrog Group, an organization of large healthcare purchasers, has suggested standards for CPOE systems that can intercept 50% or more of common serious prescribing errors. At the same time, a number of studies have been published documenting the value of CPOE in reducing medication errors and preventable adverse drug events.
Despite the benefits of CPOE, hospitals have been slow to implement it and many physicians oppose its use. “It’s high time we got over that,” says Dr. Strong. “We need to embrace CPOE now. If we do, e-prescribing won’t be such a shock when it comes down the pike.”
When e-prescribing piggybacks a good CPOE system, it will make more sense. “And when e-prescribing is done well, it will make more sense for physicians to embrace it,” he says. “Until then, it doesn’t make sense for most common situations.”
Dr. Zielzinski agrees that physicians and others need to get over their fear of CPOE. “I think you’ll find that CMS, JCAHO, the Leapfrog Group, and others will push more and more for this to happen. It’s the right thing to do.”
When Hospitalists Embrace High Tech
It is important to emphasize that many hospitalists and other physicians embrace technology. “The reality is that physicians come [to El Camino] because of our technology—it’s part of our culture,” says Dr. Zielzinski. When hospitalists join the El Camino staff, they go through a high-tech orientation with a physician trainer.
Pediatric Hospitalist Bettina Ackerman, MD, uses e-prescribing at her facility, Children’s Hospital of Pittsburgh (Pa.), and she likes the system. She admits that certain aspects of the technology can be cumbersome.
For example, “it’s much easier to handwrite certain information, such as complicated dosing instructions that require a lot of text,” she says. Nonetheless, she has seen the benefits as well. “It has drastically reduced medication errors in our hospital. And there is an efficiency that wasn’t there before.”
Dr. Reines stated that hospitalists are like other physicians: Some of them like e-prescribing and other technology, while others don’t. Age isn’t always a predictor, he emphasizes, noting that he is “the oldest physician in his group but I’m also the most interested in technology.” However, he suggested that hospitalists who are “fresh out of training are more used to technology such as e-prescribing. They kind of expect to use it.”
The Hospitalist’s Role … Starting Now
Dr. Strong suggests that hospitalists need to be part of the IT solution. In fact, they already are actively involved in his facility. “It is important for hospitalists to know what HIT their facilities are using and considering for purchase,” he says.
Dr. Reines agrees that physicians need to be active in IT decisions at their hospitals. “I’m on the tech committee at my facility, as are several physicians,” he explains, adding that they have strong opinions and specific input on what they want HIT programs and systems to do, what information they need, and how they expect technology to work to enhance their efficiency and benefit their patients.
Hospitalists who work at teaching hospitals can have a role in educating students about technology. “We need to look at learning opportunities that involve technology,” says Dr. Reines. “And we should encourage people not to be afraid of technology or change.”
Why Bother?
If there are so many barriers to e-prescribing and so many contraindications to its use, why should hospitalists bother with this technology?
While there is much disagreement about the use, benefits, and drawbacks of e-prescribing, there is little doubt that government agencies, regulatory bodies, and third-party payers will continue to push for the widespread implementation of such technology in the coming years.
For example, JCAHO’s establishment of the medication reconciliation process, whereby hospitals and other healthcare providers are expected to compile and use medication lists whenever patients move to a new setting will make e-prescribing more important and practical for hospitalists.
“The need to reconcile our patients’ medications at admission, during their stay, and at discharge will spur a greater need for e-prescribing,” says Dr. Zielzinski.
Dr. Ackerman urges her colleagues to learn about e-prescribing and other systems now. However, she also encourages “the powers that be” to provide more specific guidance on HIT to help physicians and others make the best use of it.
Although he doesn’t use or have a real need for e-prescribing, “I certainly think we will be seeing more hospitalists and hospitals using these systems in the coming years,” says Dr. Newman. “The opportunity—however small—to prevent certain types of errors will make it worthwhile eventually in most settings.” TH
Writer Joanne Kaldy is based in Maryland.
References
- iHealthbeat. Survey: few docs use PDAs for e-prescribing. Sept. 8, 2005. Available at ihealthbeat.org. Last accessed Sept. 14, 2005.
- Mobile Village. Docs embrace handheld e-prescribing to save time, prevent errors. Mobile & Wireless News. Feb. 7, 2003.
Health information technology, including e-prescribing, is “truly on the national marquee,” according to Carolyn M. Clancy, MD, director of the Agency for Healthcare Research and Technology (AHRQ). Speaking at the Annual Conference of the Healthcare Information and Management Systems Society earlier this year, she said, “Americans are quickly coming to understand how much we have to gain from health information technology (HIT). And one thing about Americans—we don’t like to wait.”
Clancy and other government officials have been pushing for widespread implementation and use of e-prescribing and other HIT in hospitals and other care settings. In 2003 the Medicare Modernization Act included a provision offering grants to physicians who implement e-prescribing systems. While all of the talk and action have stopped short of mandating the use of this technology, the handwriting is clearly on the wall. Like it or not, e-prescribing is part of healthcare’s future.
Yet despite all of these efforts on behalf of HIT few physicians are jumping on the e-prescribing bandwagon. Current estimates show that only between 5% and 18% of physicians and other clinicians use e-prescribing.
Nonetheless, while few physicians use these systems, they clearly see their value. In one survey, 78% of physicians say they believe that within the next seven years e-prescribing will account for more than half of the prescriptions written; and 75% cited reduced medication errors and time savings as two benefits of this technology.1 Another survey showed that while only 5% of physicians say they use their handheld computers for prescribing, 100% say that they use their PDAs for drug information.2
Despite the technology’s benefits, there are many reasons hospitalists and other physicians have resisted the call of e-prescribing. However, it behooves these practitioners to know about e-prescribing, consider how they might implement various technologies in their prescribing practices, and become involved in HIT initiatives at their facilities.
Money Matters: Costs Can Keep Hospitalists from E-Prescribing
E-prescribing is not widespread among hospitalists and other physicians, suggests Philip Strong, MD, IT physician liaison at El Camino Hospital and a hospitalist with the El Camino Medical Center in Mountain View, Calif.
Mark Zielzinski, chief information officer at El Camino, says that e-prescribing doesn’t really fit well with what hospitalists do.
E-prescribing is “wonderful in the physician’s office,” he explains. This is because the community-based physician writes many prescriptions every day and needs to communicate prescription information to a wide array of facilities and pharmacies.
“Hospitalists write far fewer prescriptions than attending physicians,” says Ronald Newman, MD, medical director of the hospitalist program at Beverly Hospital in Beverly, Mass. “I don’t write more than five a day.” An e-prescribing system simply isn’t practical for him.
Dr. Strong suggests, however, that the lack of enthusiasm for e-prescribing has more “to do with dollars. Systems are fairly expensive,” he says because a good system could cost as much as $150,000.
Why so much? “For a system to make sense and create more work for hospitalists, it has to interface with whatever system a hospital is using for pharmacies in the area,” explains Dr. Strong. And this can be expensive.
The cost for an individual physician or a small practice to implement e-prescribing seems much more reasonable. However, Dr. Zielzinski says that this represents only about 20% of the total cost of new technology.
“Think of what you spend when you get a home computer,” he says. “Say you spend $1,000 for the PC itself. Then you have to buy software, Internet access, a printer, and other accessories. Then you have to take the time to learn to use it all. Consider everything you spend in five years, and that $1,000 is a drop in the bucket.”
Dr. Zielzinski emphasizes that it’s not just the money that keeps hospitalists and other physicians from using e-prescribing. “Physicians have an intrinsic sociological resistance to change. After all, they are accustomed to evidence-based care and they are expected to have evidence to back up their decisions and actions,” he says, adding that “it takes a new clinical technique, theory, or practice an average of 17 years to get into mainstream practice. So how can we expect to accept new technology just like that?”
—Philip Strong, MD
Practical Protests: When Systems Hinder Efficiency
Another barrier to hospitalist acceptance of e-prescribing and other technology is that it sometimes takes longer to use, especially at the beginning.
“I’m part of an eight-hospitalist team, and we could use an e-prescribing system that our medical group has deployed, but we don’t,” admits Dr. Strong. “To use e-prescribing would require an extra step of work for us. We already have to dictate discharge notes and handwrite prescriptions. We don’t have the ability to substitute e-prescribing; it would just be an additional tool—and an additional step that would slow down our discharges.”
Dr. Newman agrees that physicians won’t use time-consuming technology. “Many systems take a lot of time to learn to use efficiently and effectively,” he says. “Physicians are afraid that these systems, such as e-prescribing, will slow them down and hurt their efficiency.”
He says hospitals are concerned about this and are waiting to implement systems they know physicians will use.
Eric Reines, MD, vice president of North Suburban Hospitalists PC and a hospitalist at Beverly Hospital, confesses to being a techie who enjoys this stuff. He says, however, that “most of the e-prescribing systems I’ve seen have been very poor. I like technology, but I won’t use a clunky system.”
Ease of use is essential for hospitalist acceptance of e-prescribing systems. “You can’t have a system with boxes popping up all over the screen and small black and white type that you can’t read,” says Dr. Reines. “Hospitalists and other physicians just won’t use these.”
Implementing systems that physicians don’t like is a worry that IT developers at hospitals think about about continually, confesses Dr. Zielzinski. “The biggest thing that keeps me awake at night is worrying that physicians will say, ‘This takes too long,’ ” he says, emphasizing that it’s important to educate physicians about how to use systems to make the most of their features and maximize efficiency.
While hospitals are concerned about how physicians will react to the implementation of technology, physicians’ general resistance to using e-prescribing actually could be a boon for hospitalists.
“Attending physicians aren’t likely to leave hospitals because they are required to use e-prescribing or other technology, but they might be more inclined to turn patients over to hospitalists at these facilities so that they don’t have to use these systems,” says Dr. Newman.
Vendor Vexation
Physicians often face the challenge of finding systems and software that integrate successfully with other systems and settings. Dr. Reines says vendors don’t always make widespread system compatibility a priority during product development.
Some data further suggest that e-prescribing products don’t always meet users’ needs. A report commissioned by the California Health Care Foundation evaluated 19 e-prescribing product vendors and found only four offer practical alternatives to more costly and complex prescription writing solutions.
CPOE First … Then E-Prescribing
Before you jump into e-prescribing, Dr. Strong suggests that more hospitals need to implement computerized physician order entry systems (CPOE). CPOE goes beyond prescriptions and enables physicians to electronically order everything from laboratory tests and dietary interventions to nursing care.
CPOE isn’t new; El Camino has used such a system for 30 years. “We are big-time believers in CPOE,” says Dr. Zielzinski. “It has enabled us to reduce a lot of errors.”
Dr. Strong adds that “these systems are better for overall patient through-put. The routing happens as soon as I input the order. There are no faxes, no paperwork, and no delays.”
Other groups also have long promoted the benefits of CPOE. For example, the Leapfrog Group, an organization of large healthcare purchasers, has suggested standards for CPOE systems that can intercept 50% or more of common serious prescribing errors. At the same time, a number of studies have been published documenting the value of CPOE in reducing medication errors and preventable adverse drug events.
Despite the benefits of CPOE, hospitals have been slow to implement it and many physicians oppose its use. “It’s high time we got over that,” says Dr. Strong. “We need to embrace CPOE now. If we do, e-prescribing won’t be such a shock when it comes down the pike.”
When e-prescribing piggybacks a good CPOE system, it will make more sense. “And when e-prescribing is done well, it will make more sense for physicians to embrace it,” he says. “Until then, it doesn’t make sense for most common situations.”
Dr. Zielzinski agrees that physicians and others need to get over their fear of CPOE. “I think you’ll find that CMS, JCAHO, the Leapfrog Group, and others will push more and more for this to happen. It’s the right thing to do.”
When Hospitalists Embrace High Tech
It is important to emphasize that many hospitalists and other physicians embrace technology. “The reality is that physicians come [to El Camino] because of our technology—it’s part of our culture,” says Dr. Zielzinski. When hospitalists join the El Camino staff, they go through a high-tech orientation with a physician trainer.
Pediatric Hospitalist Bettina Ackerman, MD, uses e-prescribing at her facility, Children’s Hospital of Pittsburgh (Pa.), and she likes the system. She admits that certain aspects of the technology can be cumbersome.
For example, “it’s much easier to handwrite certain information, such as complicated dosing instructions that require a lot of text,” she says. Nonetheless, she has seen the benefits as well. “It has drastically reduced medication errors in our hospital. And there is an efficiency that wasn’t there before.”
Dr. Reines stated that hospitalists are like other physicians: Some of them like e-prescribing and other technology, while others don’t. Age isn’t always a predictor, he emphasizes, noting that he is “the oldest physician in his group but I’m also the most interested in technology.” However, he suggested that hospitalists who are “fresh out of training are more used to technology such as e-prescribing. They kind of expect to use it.”
The Hospitalist’s Role … Starting Now
Dr. Strong suggests that hospitalists need to be part of the IT solution. In fact, they already are actively involved in his facility. “It is important for hospitalists to know what HIT their facilities are using and considering for purchase,” he says.
Dr. Reines agrees that physicians need to be active in IT decisions at their hospitals. “I’m on the tech committee at my facility, as are several physicians,” he explains, adding that they have strong opinions and specific input on what they want HIT programs and systems to do, what information they need, and how they expect technology to work to enhance their efficiency and benefit their patients.
Hospitalists who work at teaching hospitals can have a role in educating students about technology. “We need to look at learning opportunities that involve technology,” says Dr. Reines. “And we should encourage people not to be afraid of technology or change.”
Why Bother?
If there are so many barriers to e-prescribing and so many contraindications to its use, why should hospitalists bother with this technology?
While there is much disagreement about the use, benefits, and drawbacks of e-prescribing, there is little doubt that government agencies, regulatory bodies, and third-party payers will continue to push for the widespread implementation of such technology in the coming years.
For example, JCAHO’s establishment of the medication reconciliation process, whereby hospitals and other healthcare providers are expected to compile and use medication lists whenever patients move to a new setting will make e-prescribing more important and practical for hospitalists.
“The need to reconcile our patients’ medications at admission, during their stay, and at discharge will spur a greater need for e-prescribing,” says Dr. Zielzinski.
Dr. Ackerman urges her colleagues to learn about e-prescribing and other systems now. However, she also encourages “the powers that be” to provide more specific guidance on HIT to help physicians and others make the best use of it.
Although he doesn’t use or have a real need for e-prescribing, “I certainly think we will be seeing more hospitalists and hospitals using these systems in the coming years,” says Dr. Newman. “The opportunity—however small—to prevent certain types of errors will make it worthwhile eventually in most settings.” TH
Writer Joanne Kaldy is based in Maryland.
References
- iHealthbeat. Survey: few docs use PDAs for e-prescribing. Sept. 8, 2005. Available at ihealthbeat.org. Last accessed Sept. 14, 2005.
- Mobile Village. Docs embrace handheld e-prescribing to save time, prevent errors. Mobile & Wireless News. Feb. 7, 2003.
Evidence Based Medicine for The Hospitalist Installment #4
The previous installments in this series have discussed how to ask answerable clinical questions and then search for the best evidence addressing those questions. Not all evidence is of high enough quality to provide meaningful information for patient care, however, and it is important to evaluate all studies with a critical eye toward study design and analysis.
A study can be flawed in many ways, and while many flaws still allow us to apply study results to patients, we need to understand these limitations. It is also insufficient to trust factors such as a medical journal’s impact factor or prestige: Many examples of suboptimal evidence come from higher-tier journals, and it has been estimated that even in the top internal medicine journals up to 50% of papers contain significant design and analysis errors.
While the growth of EBM has directed increasing attention to these issues, the onus remains on the literature consumer to critically appraise the evidence in order to make treatment decisions in as informed a manner as is possible.
Study Validity
Results from a valid study can be expected to be unbiased. In other words, these results should portray the true underlying effect of interest. There are many threats to a study’s validity. Such factors must be evaluated to ensure that they do not systematically affect results and therefore alter the correct interpretation of study findings.
The primary goal of any unbiased study design is to make the comparison groups as similar as possible for all factors potentially affecting the outcome of interest—except for the intervention or exposure of interest. If the only difference between groups’ histories, comorbidities, study experiences, and so on is the intervention or exposure, we can be more confident that any observed outcome differences are due to the exposure rather than other confounding variables.
For example, consider a trial of treatment options for esophageal cancer in which twice as many control group patients smoked as in the intervention group. If the intervention group had better outcomes, we would not know whether this was due to the intervention or to the lower smoking rates in the treatment arm of the study. A well-designed, valid study will make every effort to minimize such problems. This principle applies to all study designs, including observational designs such as case-control and cohort studies, and experimental designs such as the classic randomized controlled trial. We will briefly present a few of the key threats to study validity in this segment of the series. We will focus on clinical trial designs, but the same principles apply to observational designs as well.
Minimize Bias and Protect Study Validity
Randomization: If we wish to make study groups similar on all variables other than the exposure of interest, and we can assign interventions such as in a clinical trial, we can maximize validity by appropriately randomizing patients to intervention groups. Randomization has the effect of balancing comparison groups with respect to both recognized and unrecognized factors that may affect outcomes.
A key feature to look for in a randomization procedure is that the randomization algorithm is in fact completely random. It should be impossible to predict for any study subject to which group they will be randomized. Therefore, for example, procedures systematically alternating subject assignments among groups (A-B-A-B- … ) are not truly random and do not confer the validity benefits of true randomization. It is also important that the randomization process be separate from all other aspects of the study, so that no other factors may influence group assignment. This is closely related to the concept of blinding.
Blinding: If patients, providers, or anybody else involved in a research study are aware of treatment assignments, conscious or subconscious differences in the experience of study participants can be introduced. This is important at all stages of a study, from randomization as described previously through to data analysis at the conclusion of a study. This is also important for all participants in a study. Practically speaking, it may not be possible to blind everybody involved in a study to the assigned treatment group (consider a study of surgical versus medical therapy, where a sham incision may not be desirable or ethical). However, blinding of patients and outcome assessors is desirable whenever feasible. Again, the goal is to treat all study subjects the same way throughout the study, so that the only difference between groups is the intervention of interest.
Intention-to-treat analysis: An intention-to-treat analysis attributes all patients to the group to which they were originally randomized. This further ensures that we are measuring the effect of the intervention of interest rather than imbalances across other factors that might impact whether patients complete the intended treatment program. This has become a well-accepted procedure in clinical trial practice.
Complete follow-up: Loss to follow-up and missing data in general can lead to bias if patients with missing data systematically differ from study completers. No statistical technique can fully compensate for missing data, and there are no general rules regarding acceptable amounts of missing data.
Unfortunately, it is essentially impossible to entirely eliminate missing data, but sensitivity analyses can be helpful in judging whether the degree of missing data is likely to change study findings. In these analyses, study outcomes for different possible missing data results are reviewed. If the conclusions of the study are consistent across the range of possible missing data points, we have good evidence that the amount of missing data is unlikely to be a major limitation of the study.
Validity for Observational Study Designs
The biases to which case-control and cohort studies are prone differ from those of prospective clinical trials, but identical general principles apply. We will not review these biases in detail. The important point is that the goal remains to keep the groups similar on all variables apart from the explanatory variable of interest.
For example, recall bias, in which cases may often be more likely than controls to recall an exposure, can result in associations between exposure and outcome that may be due either to the exposure itself or to the likelihood of recalling an exposure. This can be a serious validity concern for case-control studies, or any design requiring a retrospective recollection of past experiences. Additional information on many other common biases may be found in the recommended reading sources.
Summary
Once an article addressing your clinical question has been identified, the quality of the evidence must be critically appraised. The first central feature of this appraisal is an evaluation of the validity, or lack of bias, of the reported results. Only a valid unbiased study can be trusted to accurately represent a true underlying effect. The goal of techniques to protect validity is to isolate the intervention or exposure of interest as the only varying factor, so that any observed findings can be attributed to the exposure rather than explained by other variables. Once we have reassured ourselves that a study is reasonably valid, we need to be able to interpret the results and determine whether we can apply the results to the care of our patients. We will address these aspects of critical appraisal in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
The previous installments in this series have discussed how to ask answerable clinical questions and then search for the best evidence addressing those questions. Not all evidence is of high enough quality to provide meaningful information for patient care, however, and it is important to evaluate all studies with a critical eye toward study design and analysis.
A study can be flawed in many ways, and while many flaws still allow us to apply study results to patients, we need to understand these limitations. It is also insufficient to trust factors such as a medical journal’s impact factor or prestige: Many examples of suboptimal evidence come from higher-tier journals, and it has been estimated that even in the top internal medicine journals up to 50% of papers contain significant design and analysis errors.
While the growth of EBM has directed increasing attention to these issues, the onus remains on the literature consumer to critically appraise the evidence in order to make treatment decisions in as informed a manner as is possible.
Study Validity
Results from a valid study can be expected to be unbiased. In other words, these results should portray the true underlying effect of interest. There are many threats to a study’s validity. Such factors must be evaluated to ensure that they do not systematically affect results and therefore alter the correct interpretation of study findings.
The primary goal of any unbiased study design is to make the comparison groups as similar as possible for all factors potentially affecting the outcome of interest—except for the intervention or exposure of interest. If the only difference between groups’ histories, comorbidities, study experiences, and so on is the intervention or exposure, we can be more confident that any observed outcome differences are due to the exposure rather than other confounding variables.
For example, consider a trial of treatment options for esophageal cancer in which twice as many control group patients smoked as in the intervention group. If the intervention group had better outcomes, we would not know whether this was due to the intervention or to the lower smoking rates in the treatment arm of the study. A well-designed, valid study will make every effort to minimize such problems. This principle applies to all study designs, including observational designs such as case-control and cohort studies, and experimental designs such as the classic randomized controlled trial. We will briefly present a few of the key threats to study validity in this segment of the series. We will focus on clinical trial designs, but the same principles apply to observational designs as well.
Minimize Bias and Protect Study Validity
Randomization: If we wish to make study groups similar on all variables other than the exposure of interest, and we can assign interventions such as in a clinical trial, we can maximize validity by appropriately randomizing patients to intervention groups. Randomization has the effect of balancing comparison groups with respect to both recognized and unrecognized factors that may affect outcomes.
A key feature to look for in a randomization procedure is that the randomization algorithm is in fact completely random. It should be impossible to predict for any study subject to which group they will be randomized. Therefore, for example, procedures systematically alternating subject assignments among groups (A-B-A-B- … ) are not truly random and do not confer the validity benefits of true randomization. It is also important that the randomization process be separate from all other aspects of the study, so that no other factors may influence group assignment. This is closely related to the concept of blinding.
Blinding: If patients, providers, or anybody else involved in a research study are aware of treatment assignments, conscious or subconscious differences in the experience of study participants can be introduced. This is important at all stages of a study, from randomization as described previously through to data analysis at the conclusion of a study. This is also important for all participants in a study. Practically speaking, it may not be possible to blind everybody involved in a study to the assigned treatment group (consider a study of surgical versus medical therapy, where a sham incision may not be desirable or ethical). However, blinding of patients and outcome assessors is desirable whenever feasible. Again, the goal is to treat all study subjects the same way throughout the study, so that the only difference between groups is the intervention of interest.
Intention-to-treat analysis: An intention-to-treat analysis attributes all patients to the group to which they were originally randomized. This further ensures that we are measuring the effect of the intervention of interest rather than imbalances across other factors that might impact whether patients complete the intended treatment program. This has become a well-accepted procedure in clinical trial practice.
Complete follow-up: Loss to follow-up and missing data in general can lead to bias if patients with missing data systematically differ from study completers. No statistical technique can fully compensate for missing data, and there are no general rules regarding acceptable amounts of missing data.
Unfortunately, it is essentially impossible to entirely eliminate missing data, but sensitivity analyses can be helpful in judging whether the degree of missing data is likely to change study findings. In these analyses, study outcomes for different possible missing data results are reviewed. If the conclusions of the study are consistent across the range of possible missing data points, we have good evidence that the amount of missing data is unlikely to be a major limitation of the study.
Validity for Observational Study Designs
The biases to which case-control and cohort studies are prone differ from those of prospective clinical trials, but identical general principles apply. We will not review these biases in detail. The important point is that the goal remains to keep the groups similar on all variables apart from the explanatory variable of interest.
For example, recall bias, in which cases may often be more likely than controls to recall an exposure, can result in associations between exposure and outcome that may be due either to the exposure itself or to the likelihood of recalling an exposure. This can be a serious validity concern for case-control studies, or any design requiring a retrospective recollection of past experiences. Additional information on many other common biases may be found in the recommended reading sources.
Summary
Once an article addressing your clinical question has been identified, the quality of the evidence must be critically appraised. The first central feature of this appraisal is an evaluation of the validity, or lack of bias, of the reported results. Only a valid unbiased study can be trusted to accurately represent a true underlying effect. The goal of techniques to protect validity is to isolate the intervention or exposure of interest as the only varying factor, so that any observed findings can be attributed to the exposure rather than explained by other variables. Once we have reassured ourselves that a study is reasonably valid, we need to be able to interpret the results and determine whether we can apply the results to the care of our patients. We will address these aspects of critical appraisal in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
The previous installments in this series have discussed how to ask answerable clinical questions and then search for the best evidence addressing those questions. Not all evidence is of high enough quality to provide meaningful information for patient care, however, and it is important to evaluate all studies with a critical eye toward study design and analysis.
A study can be flawed in many ways, and while many flaws still allow us to apply study results to patients, we need to understand these limitations. It is also insufficient to trust factors such as a medical journal’s impact factor or prestige: Many examples of suboptimal evidence come from higher-tier journals, and it has been estimated that even in the top internal medicine journals up to 50% of papers contain significant design and analysis errors.
While the growth of EBM has directed increasing attention to these issues, the onus remains on the literature consumer to critically appraise the evidence in order to make treatment decisions in as informed a manner as is possible.
Study Validity
Results from a valid study can be expected to be unbiased. In other words, these results should portray the true underlying effect of interest. There are many threats to a study’s validity. Such factors must be evaluated to ensure that they do not systematically affect results and therefore alter the correct interpretation of study findings.
The primary goal of any unbiased study design is to make the comparison groups as similar as possible for all factors potentially affecting the outcome of interest—except for the intervention or exposure of interest. If the only difference between groups’ histories, comorbidities, study experiences, and so on is the intervention or exposure, we can be more confident that any observed outcome differences are due to the exposure rather than other confounding variables.
For example, consider a trial of treatment options for esophageal cancer in which twice as many control group patients smoked as in the intervention group. If the intervention group had better outcomes, we would not know whether this was due to the intervention or to the lower smoking rates in the treatment arm of the study. A well-designed, valid study will make every effort to minimize such problems. This principle applies to all study designs, including observational designs such as case-control and cohort studies, and experimental designs such as the classic randomized controlled trial. We will briefly present a few of the key threats to study validity in this segment of the series. We will focus on clinical trial designs, but the same principles apply to observational designs as well.
Minimize Bias and Protect Study Validity
Randomization: If we wish to make study groups similar on all variables other than the exposure of interest, and we can assign interventions such as in a clinical trial, we can maximize validity by appropriately randomizing patients to intervention groups. Randomization has the effect of balancing comparison groups with respect to both recognized and unrecognized factors that may affect outcomes.
A key feature to look for in a randomization procedure is that the randomization algorithm is in fact completely random. It should be impossible to predict for any study subject to which group they will be randomized. Therefore, for example, procedures systematically alternating subject assignments among groups (A-B-A-B- … ) are not truly random and do not confer the validity benefits of true randomization. It is also important that the randomization process be separate from all other aspects of the study, so that no other factors may influence group assignment. This is closely related to the concept of blinding.
Blinding: If patients, providers, or anybody else involved in a research study are aware of treatment assignments, conscious or subconscious differences in the experience of study participants can be introduced. This is important at all stages of a study, from randomization as described previously through to data analysis at the conclusion of a study. This is also important for all participants in a study. Practically speaking, it may not be possible to blind everybody involved in a study to the assigned treatment group (consider a study of surgical versus medical therapy, where a sham incision may not be desirable or ethical). However, blinding of patients and outcome assessors is desirable whenever feasible. Again, the goal is to treat all study subjects the same way throughout the study, so that the only difference between groups is the intervention of interest.
Intention-to-treat analysis: An intention-to-treat analysis attributes all patients to the group to which they were originally randomized. This further ensures that we are measuring the effect of the intervention of interest rather than imbalances across other factors that might impact whether patients complete the intended treatment program. This has become a well-accepted procedure in clinical trial practice.
Complete follow-up: Loss to follow-up and missing data in general can lead to bias if patients with missing data systematically differ from study completers. No statistical technique can fully compensate for missing data, and there are no general rules regarding acceptable amounts of missing data.
Unfortunately, it is essentially impossible to entirely eliminate missing data, but sensitivity analyses can be helpful in judging whether the degree of missing data is likely to change study findings. In these analyses, study outcomes for different possible missing data results are reviewed. If the conclusions of the study are consistent across the range of possible missing data points, we have good evidence that the amount of missing data is unlikely to be a major limitation of the study.
Validity for Observational Study Designs
The biases to which case-control and cohort studies are prone differ from those of prospective clinical trials, but identical general principles apply. We will not review these biases in detail. The important point is that the goal remains to keep the groups similar on all variables apart from the explanatory variable of interest.
For example, recall bias, in which cases may often be more likely than controls to recall an exposure, can result in associations between exposure and outcome that may be due either to the exposure itself or to the likelihood of recalling an exposure. This can be a serious validity concern for case-control studies, or any design requiring a retrospective recollection of past experiences. Additional information on many other common biases may be found in the recommended reading sources.
Summary
Once an article addressing your clinical question has been identified, the quality of the evidence must be critically appraised. The first central feature of this appraisal is an evaluation of the validity, or lack of bias, of the reported results. Only a valid unbiased study can be trusted to accurately represent a true underlying effect. The goal of techniques to protect validity is to isolate the intervention or exposure of interest as the only varying factor, so that any observed findings can be attributed to the exposure rather than explained by other variables. Once we have reassured ourselves that a study is reasonably valid, we need to be able to interpret the results and determine whether we can apply the results to the care of our patients. We will address these aspects of critical appraisal in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
A Granary Becomes a Hospital
California gained statehood in 1850. Two months later Navy Secretary William Graham wrote to President Fillmore that “a new empire has, as by magic, sprung into existence. San Francisco promises, at no distant time, to become another New York.” He went on to say that “a Navy yard is very much needed in California, and no time will be lost in accomplishing the work.”
A three-officer commission was soon dispatched to choose a suitable site, and they decided on one protected inside San Francisco Bay at Mare Island. Commander David G. Farragut (of “Damn the torpedoes! Full speed ahead!” fame, a Civil War hero and the first admiral of the U.S. Navy) arrived at the remote place in 1854.
Within two days of his arrival at the California site, Farragut ordered the sloop-of-war over from Sausalito. This ship, soon to be replaced by the much larger USS Independence, served as the first naval medical facility on the West Coast. Ambulatory care was given in the ship’s sick bay, and the “hospitalized” were cared for from wooden bed frames suspended from the sick bay overhead or from their own hammocks. The average inpatient load was 10 sailors or civilian Navy yard workers.

The limitations of care aboard ship are made clear in a note from the yard surgeon in 1863; he wrote, “The frigate Independence, particularly in the winter season, is a very unsuitable place to treat the sick. It is cold, wet, and open to every wind that blows.”
Navy officials, while sympathetic to the plight of men serving in the tiny Pacific squadron, did little to correct the situation—likely because their attentions were focused on prosecuting the Civil War and not on a little Navy yard in far away California. Taking the situation into their own hands, surgeon Bishop and the commandant of the Navy yard submitted plans for a temporary facility—to be fashioned from an unused granary. The plans provided for a 25' x 25' ward on the first floor and a 24' x 40'9" ward space above, and called for a large cistern for year-round water supply, an attached bath approached from outside, and a nearby outdoor privy.
Still, Washington resisted, recommending that sick sailors be sent to the Marine (Public Health) Hospital in San Francisco, 25 miles away. This suggestion was met by stiff resistance both by local Naval authorities who feared desertion by sailors not under their direct observation and by the sailors themselves, who didn’t cotton to being hospitalized with merchant mariners.
Permission from Washington finally came through in July 1863. Work completed, the “Temporary Hospital” at Mare Island Navy Yard opened on Feb. 23, 1864.
The hospital carried an average inpatient load of 30, cared for by a surgeon and a surgeon’s steward, until the first permanent hospital—palatial by comparison—opened in 1871. TH
Dr. Snyder is a retired captain of the U.S. Naval Reserves’ Medical Corps. He writes regularly about naval medicine.
California gained statehood in 1850. Two months later Navy Secretary William Graham wrote to President Fillmore that “a new empire has, as by magic, sprung into existence. San Francisco promises, at no distant time, to become another New York.” He went on to say that “a Navy yard is very much needed in California, and no time will be lost in accomplishing the work.”
A three-officer commission was soon dispatched to choose a suitable site, and they decided on one protected inside San Francisco Bay at Mare Island. Commander David G. Farragut (of “Damn the torpedoes! Full speed ahead!” fame, a Civil War hero and the first admiral of the U.S. Navy) arrived at the remote place in 1854.
Within two days of his arrival at the California site, Farragut ordered the sloop-of-war over from Sausalito. This ship, soon to be replaced by the much larger USS Independence, served as the first naval medical facility on the West Coast. Ambulatory care was given in the ship’s sick bay, and the “hospitalized” were cared for from wooden bed frames suspended from the sick bay overhead or from their own hammocks. The average inpatient load was 10 sailors or civilian Navy yard workers.
The limitations of care aboard ship are made clear in a note from the yard surgeon in 1863; he wrote, “The frigate Independence, particularly in the winter season, is a very unsuitable place to treat the sick. It is cold, wet, and open to every wind that blows.”
Navy officials, while sympathetic to the plight of men serving in the tiny Pacific squadron, did little to correct the situation—likely because their attentions were focused on prosecuting the Civil War and not on a little Navy yard in far away California. Taking the situation into their own hands, surgeon Bishop and the commandant of the Navy yard submitted plans for a temporary facility—to be fashioned from an unused granary. The plans provided for a 25' x 25' ward on the first floor and a 24' x 40'9" ward space above, and called for a large cistern for year-round water supply, an attached bath approached from outside, and a nearby outdoor privy.
Still, Washington resisted, recommending that sick sailors be sent to the Marine (Public Health) Hospital in San Francisco, 25 miles away. This suggestion was met by stiff resistance both by local Naval authorities who feared desertion by sailors not under their direct observation and by the sailors themselves, who didn’t cotton to being hospitalized with merchant mariners.
Permission from Washington finally came through in July 1863. Work completed, the “Temporary Hospital” at Mare Island Navy Yard opened on Feb. 23, 1864.
The hospital carried an average inpatient load of 30, cared for by a surgeon and a surgeon’s steward, until the first permanent hospital—palatial by comparison—opened in 1871. TH
Dr. Snyder is a retired captain of the U.S. Naval Reserves’ Medical Corps. He writes regularly about naval medicine.
California gained statehood in 1850. Two months later Navy Secretary William Graham wrote to President Fillmore that “a new empire has, as by magic, sprung into existence. San Francisco promises, at no distant time, to become another New York.” He went on to say that “a Navy yard is very much needed in California, and no time will be lost in accomplishing the work.”
A three-officer commission was soon dispatched to choose a suitable site, and they decided on one protected inside San Francisco Bay at Mare Island. Commander David G. Farragut (of “Damn the torpedoes! Full speed ahead!” fame, a Civil War hero and the first admiral of the U.S. Navy) arrived at the remote place in 1854.
Within two days of his arrival at the California site, Farragut ordered the sloop-of-war over from Sausalito. This ship, soon to be replaced by the much larger USS Independence, served as the first naval medical facility on the West Coast. Ambulatory care was given in the ship’s sick bay, and the “hospitalized” were cared for from wooden bed frames suspended from the sick bay overhead or from their own hammocks. The average inpatient load was 10 sailors or civilian Navy yard workers.
The limitations of care aboard ship are made clear in a note from the yard surgeon in 1863; he wrote, “The frigate Independence, particularly in the winter season, is a very unsuitable place to treat the sick. It is cold, wet, and open to every wind that blows.”
Navy officials, while sympathetic to the plight of men serving in the tiny Pacific squadron, did little to correct the situation—likely because their attentions were focused on prosecuting the Civil War and not on a little Navy yard in far away California. Taking the situation into their own hands, surgeon Bishop and the commandant of the Navy yard submitted plans for a temporary facility—to be fashioned from an unused granary. The plans provided for a 25' x 25' ward on the first floor and a 24' x 40'9" ward space above, and called for a large cistern for year-round water supply, an attached bath approached from outside, and a nearby outdoor privy.
Still, Washington resisted, recommending that sick sailors be sent to the Marine (Public Health) Hospital in San Francisco, 25 miles away. This suggestion was met by stiff resistance both by local Naval authorities who feared desertion by sailors not under their direct observation and by the sailors themselves, who didn’t cotton to being hospitalized with merchant mariners.
Permission from Washington finally came through in July 1863. Work completed, the “Temporary Hospital” at Mare Island Navy Yard opened on Feb. 23, 1864.
The hospital carried an average inpatient load of 30, cared for by a surgeon and a surgeon’s steward, until the first permanent hospital—palatial by comparison—opened in 1871. TH
Dr. Snyder is a retired captain of the U.S. Naval Reserves’ Medical Corps. He writes regularly about naval medicine.
Limits for Disaster Responders
Most healthcare providers are inexperienced in caring for people in disasters. However, in a national disaster that hinders mobility both into and out of an affected area, available skilled personnel are limited. A disaster response asks more of the scarce manpower: Providers must work longer hours and extend their customary scope of expertise to aid the largest number of victims. While these mandates are designed to maximize the care provided, the emotional and physical burdens on providers and victims in these circumstances are significant, and it is important that we remember the fundamental duty to prevent unnecessary harm in the provision of healthcare.
Should healthcare providers be held to different standards in times of disaster? If so, what are acceptable limits to disaster care, and what ethical dilemmas result during such exceptional times?
Unique Circumstances Call for Unique Standards of Care
Standards in a variety of areas differ in the face of a large-scale disaster, but the fact that standards must change to accommodate the circumstances does not mean that they cease to exist entirely. In the event of a large-scale disaster where populations become isolated and no new resources will arrive in the immediate future, the risks of inaction are magnified and we accept a higher risk resulting from relief action. When only one doctor is available, that doctor is obligated to provide whatever care he or she can to whoever is in need.
When the alternative is that no help will be given, any able doctor should provide whatever help they can. However, there are limits to this responsibility. Greater risks may be justified, and standards may be different, but physicians’ fundamental duties to patients are unchanged and avoidable mistakes causing injuries still need to be prevented. The basic duties of beneficence and non-malfeasance must still guide physician behavior, and the reality of the circumstances in disaster response favors pre-emptive determination on the safety limits that physicians should observe in providing disaster assistance.
Disasters inherently influence doctors to both continue to provide care when they are impaired by sleep or grief and to provide care that under other circumstances they would consider their experience inadequate to undertake. These are realities of disaster response, and all skilled personnel can and should exceed the limits that normally exist in a fully functional system with adequate resources. However, at some point a doctor becomes too impaired or too inexperienced to provide care to patients—even if no one else is available. Doctors are neither trained nor encouraged to weigh the global risks and benefits in this manner; in fact, we are trained to push ourselves beyond our reasonable limits even when absolute scarcity of resources isn’t an issue. People are quite willing to compromise their own comfort and safety in the event of a disaster, but there comes a point at which they may do more harm than good.
There is extensive evidence that sleep deprivation impairs judgment and performance in the medical setting.1-2 Despite the fact that standards change in emergencies and greater risk must be undertaken by both providers and victims, there must still be safety limits. At some point a doctor becomes so sleep deprived that he or she is more dangerous providing care than leaving people entirely without a provider, and further may have impaired judgment on the severity of the various conditions they are facing and the reasonable limits on their expertise. This problem is inherent to the setting. How much risk should doctors subject patients to? In the face of a life-threatening condition should a completely inexperienced physician undertake care? What if the doctor is mistaken as to the severity of the illness or the proper response to it?
In response to Hurricane Katrina, state and national regulatory agencies had to create emergency exceptions to licensing regulations and to HIPAA and EMTALA requirements in order to facilitate patient care.3 Both the Model State Emergency Health Powers Act (legislation designed to serve as template for states to use to create emergency health response mechanisms) and the Louisiana legislation that governed provision of medical care in a state of emergency limit liability of any provider assisting in an emergency.4-5 Providers assisting in an emergency will not be held liable for any injury resulting from action or inaction except for intentional or grossly negligent acts or omissions. Such limitation of liability is essential to ensure that all available resources are utilized in an emergency. However, given that patients will have limited remedies for injuries caused, it is increasingly important to proactively define limitations on provider activity during emergencies. Because other remedies and regulatory structures are relaxed, ethical self-regulation becomes increasingly important.
The first priority in emergency disaster response must be ensuring that providers are available and do not encounter unnecessary barriers to providing care to ill or injured patients. However, a secondary goal must be ensuring that the safest and most effective care is provided under the circumstances. As with many things in disaster response, once the disaster has occurred there is little time for contemplation. Therefore, disaster response plans should include guidelines for providers on how to ensure safety in the care they provide.
Disaster response issues must be dealt with proactively because resources cannot be diverted to these issues in the thick of emergency response. Some organizations and providers have experience with disaster response and can provide guidance. A major goal of medical relief organizations is to provide relief for fatigued providers. When relief is not available and not likely to arrive soon, providers should be encouraged to self-impose sleep periods despite the apparent urgency of the situations they face. Urging providers to ensure that they eat at least twice and sleep for two to four hours in any 24-hour period is a reasonable limit on the physical activity of providers.
Providers and patients need to understand that this is essential to ensure that providers are capable of giving safe care in a sustained fashion. Emergency responders must maintain adequate perspective on their own abilities and patients’ needs to ensure that unnecessary risks are not undertaken nor avoidable injures inflicted. Importantly, these limitations should not be legislated or imposed externally, but should be defined by the profession and self-enforced by providers.
There have been significant discussion of what aspects of the U.S. system of response to large-scale disasters need to be improved. The Katrina disaster has given us the opportunity to enhance essential response mechanisms, whether the cause of the disaster is natural, infectious, or terrorist. A good disaster plan takes steps to ensure availability of care, but also to ensure that the care is as ethical, safe and effective as possible.
References
- Arnedt JT, Owens J, Crouch M, Stahl J, Carskadon MA. Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. JAMA. 2005;294(9):1025-1033.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns' work hours on serious medical errors in intensive care units. N Eng J Med. 2004;351(18):1838-1848.
- Hyland, et al. Federal, State Regulations Relaxed for Providers Affected by Hurricane. BNA Health Law Reporter. 2005;15(36):1190-1191.
- Gostin, LO, Model State Emergency Health Powers Act, §608 Licensing and Appointment of Health Care Personnel, December 21, 2001. Available at www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Last accessed Dec. 1, 2005.
- La. R.S. 29:656 (2005).
FROM THE PUBLIC POLICY COMMITTEE
Make a Positive Difference in the Politics of Healthcare
SHM to sponsor Legislative Advocacy Day on May 3
By Eric Siegal, MD, committee chair
“The stakes are too high for government to be a spectator sport.”
—Barbara Jordan, former U.S. Congresswoman
SHM is taking advantage of its 2006 annual meeting location in Washington, D.C., and sponsoring its first Legislative Advocacy Day on May 3. The Public Policy Committee is excited about the opportunity this initiative presents for hospitalists to learn more about how government really works and to speak with members of Congress about issues that are vital to patient care and clinical practice.
Are you concerned about continued Medicare cuts? Worried about how pending pay-for-performance legislation will affect hospitalists? SHM members registering for Advocacy Day will meet with their members of Congress and staff to discuss these and other important issues affecting hospital medicine.
I encourage you to register for Advocacy Day. There is no better way to influence how health policy is made in Washington than by meeting directly with your elected officials and their staffs. Lawmakers need constituent input to be effective legislators. Whether your legislator is a newly elected representative or a veteran senator with years of experience, he or she wants—and needs—to hear what you have to say about issues under consideration by the U.S. Congress, particularly in an election year. Input from their constituents always receives attention and consideration and can frequently make the difference in the way a lawmaker votes. Who better to educate members of Congress on changes to Medicare than the physicians directly involved in caring for the program’s beneficiaries?
We will give you the tools and information you need to make the most of your meetings on Capitol Hill. Legislative appointments will be scheduled by SHM as part of the registration process. SHM members will be grouped together by congressional district for House meetings and by state for Senate meetings and each registrant will have a minimum of three Hill appointments. To familiarize you with SHM’s legislative objectives for the second session of the 109th Congress, Laura Allendorf, SHM’s Washington representative, and I will conduct a pre-visit breakfast briefing from 7 a.m. to 8:30 a.m. on May 3. This briefing will cover procedural tips on how to have a successful meeting and update you on the status of the key health issues you will be discussing while on Capitol Hill. These meetings will take place from 9 a.m. to 5 p.m. that day.
Join us on May 3 and help educate members of Congress about the unique role hospitalists play in the delivery of medical care in our nation’s hospitals. We hope Advocacy Day will be the start of regular contact by hospitalists with their elected representatives in Washington.
FROM THE PEDIATRICS COMMITTEE
CME, Pediatric Core Curriculum on the Horizon
Multiple initiatives keep committee active
The Pediatric Committee at SHM is both the center of pediatric activity within SHM and a clearinghouse for SHM committee and task force activity as it relates to pediatrics.
The major pediatric activity in SHM continues to be CME activities and the Pediatric Core Curriculum. The dramatic success of the Pediatric Hospital Medicine Meeting was documented in the October issue of The Hospitalist (p. 33.)
Evaluations of the meeting overwhelmingly favored staging a three- to four-day Pediatric Hospital Medicine meeting on an annual basis during the late summer as a stand-alone meeting, with sponsorship rotating among SHM, the AAP, and the APA. There was insufficient lead time to offer a comprehensive meeting in 2006, but a meeting is scheduled for 2007 sponsored by AAP, with SHM taking the lead in 2008. More information to follow both in the SHM online discussion communities and through these committee reports.
The Pediatric Core Curriculum is nearly complete and should be at the review stage by early 2006. This curriculum is modeled after the adult core curriculum. It will serve as a framework for residency and fellowship directors, as well as a basis for the topics addressed at the Pediatric Hospital Medicine Meetings. Thanks to Tim Cornell, MD, Dan Rauch, MD, and all the authors and editors who have contributed to this work.
We will offer a full pediatric track in May at the SHM Annual Meeting in Washington, D.C., as we have in prior years. Registration is available online. Meetings of both the Pediatric Committee and the Pediatric Forum will be held during the meeting. This year’s meeting immediately precedes the PAS Meetings in San Francisco, and we encourage you to plan early so that at least one member of your program is able to attend the SHM Meeting. Once the Pediatric Hospital Medicine Meetings are held on an annual basis, we will need to decide how to balance SHM meeting offerings between the summer stand-alone Denver meeting and the SHM Annual Meeting.
The second function of Pediatric Committee involves having pediatric representatives on the various SHM committees and task forces report on their individual group’s activities, particularly as it relates to pediatrics. This keeps the broader group of pediatric leadership within SHM informed about the society’s global picture. SHM is committed to having a pediatric representative on each committee. You never know when or where an important issue for pediatricians may arise. Even geriatrics overlaps with pediatrics with regard to both family-centered care and proxy decision-makers.
Major endeavors at this point include the activities of the Benchmark and Career Satisfaction groups. SHM continues to make a strong effort to collect and generate data for workload and compensation, and to provide specific “pediatric only” subsets. Efforts regarding credentialing, sub-specialty designation/certification, and board re-certification are an active focus of SHM for adult hospitalists with ongoing discussions with the Board of Internal Medicine. We pediatricians stand on the sidelines of this battle, with the expectation that once the adults figure out how to do it, we can modify their approach with lower casualties on both sides.
The clinical Resource Rooms on the SHM Web site are clearly targeted toward adult topics. We intend to develop similar resources for pediatrics and are exploring possibilities of doing this collaboratively with the AAP and the APA. Sub-committees on pediatric hospital medicine topics are developing under a loose and shared structure with the AAP’s Section on Hospital Medicine. For example, SHM has taken the lead on a palliative care task force. Maggie Hood is the pediatric representative to this task force and wants to involve other interested pediatric hospitalists in a sub-committee on this topic. The AAP’s Karen Kingry has taken the lead on developing a sub-committee for community (pediatric) hospitalists; membership on her committee is open to SHM members. Expect other topics to develop as well.
If you have any comments, feedback or suggestions for the SHM Pediatric Committee, please contact co-chairs, David Zipes (dgzipes@indy.rr.com) or Jack Percelay (JPercelayMD@yahoo.com). TH
Most healthcare providers are inexperienced in caring for people in disasters. However, in a national disaster that hinders mobility both into and out of an affected area, available skilled personnel are limited. A disaster response asks more of the scarce manpower: Providers must work longer hours and extend their customary scope of expertise to aid the largest number of victims. While these mandates are designed to maximize the care provided, the emotional and physical burdens on providers and victims in these circumstances are significant, and it is important that we remember the fundamental duty to prevent unnecessary harm in the provision of healthcare.
Should healthcare providers be held to different standards in times of disaster? If so, what are acceptable limits to disaster care, and what ethical dilemmas result during such exceptional times?
Unique Circumstances Call for Unique Standards of Care
Standards in a variety of areas differ in the face of a large-scale disaster, but the fact that standards must change to accommodate the circumstances does not mean that they cease to exist entirely. In the event of a large-scale disaster where populations become isolated and no new resources will arrive in the immediate future, the risks of inaction are magnified and we accept a higher risk resulting from relief action. When only one doctor is available, that doctor is obligated to provide whatever care he or she can to whoever is in need.
When the alternative is that no help will be given, any able doctor should provide whatever help they can. However, there are limits to this responsibility. Greater risks may be justified, and standards may be different, but physicians’ fundamental duties to patients are unchanged and avoidable mistakes causing injuries still need to be prevented. The basic duties of beneficence and non-malfeasance must still guide physician behavior, and the reality of the circumstances in disaster response favors pre-emptive determination on the safety limits that physicians should observe in providing disaster assistance.
Disasters inherently influence doctors to both continue to provide care when they are impaired by sleep or grief and to provide care that under other circumstances they would consider their experience inadequate to undertake. These are realities of disaster response, and all skilled personnel can and should exceed the limits that normally exist in a fully functional system with adequate resources. However, at some point a doctor becomes too impaired or too inexperienced to provide care to patients—even if no one else is available. Doctors are neither trained nor encouraged to weigh the global risks and benefits in this manner; in fact, we are trained to push ourselves beyond our reasonable limits even when absolute scarcity of resources isn’t an issue. People are quite willing to compromise their own comfort and safety in the event of a disaster, but there comes a point at which they may do more harm than good.
There is extensive evidence that sleep deprivation impairs judgment and performance in the medical setting.1-2 Despite the fact that standards change in emergencies and greater risk must be undertaken by both providers and victims, there must still be safety limits. At some point a doctor becomes so sleep deprived that he or she is more dangerous providing care than leaving people entirely without a provider, and further may have impaired judgment on the severity of the various conditions they are facing and the reasonable limits on their expertise. This problem is inherent to the setting. How much risk should doctors subject patients to? In the face of a life-threatening condition should a completely inexperienced physician undertake care? What if the doctor is mistaken as to the severity of the illness or the proper response to it?
In response to Hurricane Katrina, state and national regulatory agencies had to create emergency exceptions to licensing regulations and to HIPAA and EMTALA requirements in order to facilitate patient care.3 Both the Model State Emergency Health Powers Act (legislation designed to serve as template for states to use to create emergency health response mechanisms) and the Louisiana legislation that governed provision of medical care in a state of emergency limit liability of any provider assisting in an emergency.4-5 Providers assisting in an emergency will not be held liable for any injury resulting from action or inaction except for intentional or grossly negligent acts or omissions. Such limitation of liability is essential to ensure that all available resources are utilized in an emergency. However, given that patients will have limited remedies for injuries caused, it is increasingly important to proactively define limitations on provider activity during emergencies. Because other remedies and regulatory structures are relaxed, ethical self-regulation becomes increasingly important.
The first priority in emergency disaster response must be ensuring that providers are available and do not encounter unnecessary barriers to providing care to ill or injured patients. However, a secondary goal must be ensuring that the safest and most effective care is provided under the circumstances. As with many things in disaster response, once the disaster has occurred there is little time for contemplation. Therefore, disaster response plans should include guidelines for providers on how to ensure safety in the care they provide.
Disaster response issues must be dealt with proactively because resources cannot be diverted to these issues in the thick of emergency response. Some organizations and providers have experience with disaster response and can provide guidance. A major goal of medical relief organizations is to provide relief for fatigued providers. When relief is not available and not likely to arrive soon, providers should be encouraged to self-impose sleep periods despite the apparent urgency of the situations they face. Urging providers to ensure that they eat at least twice and sleep for two to four hours in any 24-hour period is a reasonable limit on the physical activity of providers.
Providers and patients need to understand that this is essential to ensure that providers are capable of giving safe care in a sustained fashion. Emergency responders must maintain adequate perspective on their own abilities and patients’ needs to ensure that unnecessary risks are not undertaken nor avoidable injures inflicted. Importantly, these limitations should not be legislated or imposed externally, but should be defined by the profession and self-enforced by providers.
There have been significant discussion of what aspects of the U.S. system of response to large-scale disasters need to be improved. The Katrina disaster has given us the opportunity to enhance essential response mechanisms, whether the cause of the disaster is natural, infectious, or terrorist. A good disaster plan takes steps to ensure availability of care, but also to ensure that the care is as ethical, safe and effective as possible.
References
- Arnedt JT, Owens J, Crouch M, Stahl J, Carskadon MA. Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. JAMA. 2005;294(9):1025-1033.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns' work hours on serious medical errors in intensive care units. N Eng J Med. 2004;351(18):1838-1848.
- Hyland, et al. Federal, State Regulations Relaxed for Providers Affected by Hurricane. BNA Health Law Reporter. 2005;15(36):1190-1191.
- Gostin, LO, Model State Emergency Health Powers Act, §608 Licensing and Appointment of Health Care Personnel, December 21, 2001. Available at www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Last accessed Dec. 1, 2005.
- La. R.S. 29:656 (2005).
FROM THE PUBLIC POLICY COMMITTEE
Make a Positive Difference in the Politics of Healthcare
SHM to sponsor Legislative Advocacy Day on May 3
By Eric Siegal, MD, committee chair
“The stakes are too high for government to be a spectator sport.”
—Barbara Jordan, former U.S. Congresswoman
SHM is taking advantage of its 2006 annual meeting location in Washington, D.C., and sponsoring its first Legislative Advocacy Day on May 3. The Public Policy Committee is excited about the opportunity this initiative presents for hospitalists to learn more about how government really works and to speak with members of Congress about issues that are vital to patient care and clinical practice.
Are you concerned about continued Medicare cuts? Worried about how pending pay-for-performance legislation will affect hospitalists? SHM members registering for Advocacy Day will meet with their members of Congress and staff to discuss these and other important issues affecting hospital medicine.
I encourage you to register for Advocacy Day. There is no better way to influence how health policy is made in Washington than by meeting directly with your elected officials and their staffs. Lawmakers need constituent input to be effective legislators. Whether your legislator is a newly elected representative or a veteran senator with years of experience, he or she wants—and needs—to hear what you have to say about issues under consideration by the U.S. Congress, particularly in an election year. Input from their constituents always receives attention and consideration and can frequently make the difference in the way a lawmaker votes. Who better to educate members of Congress on changes to Medicare than the physicians directly involved in caring for the program’s beneficiaries?
We will give you the tools and information you need to make the most of your meetings on Capitol Hill. Legislative appointments will be scheduled by SHM as part of the registration process. SHM members will be grouped together by congressional district for House meetings and by state for Senate meetings and each registrant will have a minimum of three Hill appointments. To familiarize you with SHM’s legislative objectives for the second session of the 109th Congress, Laura Allendorf, SHM’s Washington representative, and I will conduct a pre-visit breakfast briefing from 7 a.m. to 8:30 a.m. on May 3. This briefing will cover procedural tips on how to have a successful meeting and update you on the status of the key health issues you will be discussing while on Capitol Hill. These meetings will take place from 9 a.m. to 5 p.m. that day.
Join us on May 3 and help educate members of Congress about the unique role hospitalists play in the delivery of medical care in our nation’s hospitals. We hope Advocacy Day will be the start of regular contact by hospitalists with their elected representatives in Washington.
FROM THE PEDIATRICS COMMITTEE
CME, Pediatric Core Curriculum on the Horizon
Multiple initiatives keep committee active
The Pediatric Committee at SHM is both the center of pediatric activity within SHM and a clearinghouse for SHM committee and task force activity as it relates to pediatrics.
The major pediatric activity in SHM continues to be CME activities and the Pediatric Core Curriculum. The dramatic success of the Pediatric Hospital Medicine Meeting was documented in the October issue of The Hospitalist (p. 33.)
Evaluations of the meeting overwhelmingly favored staging a three- to four-day Pediatric Hospital Medicine meeting on an annual basis during the late summer as a stand-alone meeting, with sponsorship rotating among SHM, the AAP, and the APA. There was insufficient lead time to offer a comprehensive meeting in 2006, but a meeting is scheduled for 2007 sponsored by AAP, with SHM taking the lead in 2008. More information to follow both in the SHM online discussion communities and through these committee reports.
The Pediatric Core Curriculum is nearly complete and should be at the review stage by early 2006. This curriculum is modeled after the adult core curriculum. It will serve as a framework for residency and fellowship directors, as well as a basis for the topics addressed at the Pediatric Hospital Medicine Meetings. Thanks to Tim Cornell, MD, Dan Rauch, MD, and all the authors and editors who have contributed to this work.
We will offer a full pediatric track in May at the SHM Annual Meeting in Washington, D.C., as we have in prior years. Registration is available online. Meetings of both the Pediatric Committee and the Pediatric Forum will be held during the meeting. This year’s meeting immediately precedes the PAS Meetings in San Francisco, and we encourage you to plan early so that at least one member of your program is able to attend the SHM Meeting. Once the Pediatric Hospital Medicine Meetings are held on an annual basis, we will need to decide how to balance SHM meeting offerings between the summer stand-alone Denver meeting and the SHM Annual Meeting.
The second function of Pediatric Committee involves having pediatric representatives on the various SHM committees and task forces report on their individual group’s activities, particularly as it relates to pediatrics. This keeps the broader group of pediatric leadership within SHM informed about the society’s global picture. SHM is committed to having a pediatric representative on each committee. You never know when or where an important issue for pediatricians may arise. Even geriatrics overlaps with pediatrics with regard to both family-centered care and proxy decision-makers.
Major endeavors at this point include the activities of the Benchmark and Career Satisfaction groups. SHM continues to make a strong effort to collect and generate data for workload and compensation, and to provide specific “pediatric only” subsets. Efforts regarding credentialing, sub-specialty designation/certification, and board re-certification are an active focus of SHM for adult hospitalists with ongoing discussions with the Board of Internal Medicine. We pediatricians stand on the sidelines of this battle, with the expectation that once the adults figure out how to do it, we can modify their approach with lower casualties on both sides.
The clinical Resource Rooms on the SHM Web site are clearly targeted toward adult topics. We intend to develop similar resources for pediatrics and are exploring possibilities of doing this collaboratively with the AAP and the APA. Sub-committees on pediatric hospital medicine topics are developing under a loose and shared structure with the AAP’s Section on Hospital Medicine. For example, SHM has taken the lead on a palliative care task force. Maggie Hood is the pediatric representative to this task force and wants to involve other interested pediatric hospitalists in a sub-committee on this topic. The AAP’s Karen Kingry has taken the lead on developing a sub-committee for community (pediatric) hospitalists; membership on her committee is open to SHM members. Expect other topics to develop as well.
If you have any comments, feedback or suggestions for the SHM Pediatric Committee, please contact co-chairs, David Zipes (dgzipes@indy.rr.com) or Jack Percelay (JPercelayMD@yahoo.com). TH
Most healthcare providers are inexperienced in caring for people in disasters. However, in a national disaster that hinders mobility both into and out of an affected area, available skilled personnel are limited. A disaster response asks more of the scarce manpower: Providers must work longer hours and extend their customary scope of expertise to aid the largest number of victims. While these mandates are designed to maximize the care provided, the emotional and physical burdens on providers and victims in these circumstances are significant, and it is important that we remember the fundamental duty to prevent unnecessary harm in the provision of healthcare.
Should healthcare providers be held to different standards in times of disaster? If so, what are acceptable limits to disaster care, and what ethical dilemmas result during such exceptional times?
Unique Circumstances Call for Unique Standards of Care
Standards in a variety of areas differ in the face of a large-scale disaster, but the fact that standards must change to accommodate the circumstances does not mean that they cease to exist entirely. In the event of a large-scale disaster where populations become isolated and no new resources will arrive in the immediate future, the risks of inaction are magnified and we accept a higher risk resulting from relief action. When only one doctor is available, that doctor is obligated to provide whatever care he or she can to whoever is in need.
When the alternative is that no help will be given, any able doctor should provide whatever help they can. However, there are limits to this responsibility. Greater risks may be justified, and standards may be different, but physicians’ fundamental duties to patients are unchanged and avoidable mistakes causing injuries still need to be prevented. The basic duties of beneficence and non-malfeasance must still guide physician behavior, and the reality of the circumstances in disaster response favors pre-emptive determination on the safety limits that physicians should observe in providing disaster assistance.
Disasters inherently influence doctors to both continue to provide care when they are impaired by sleep or grief and to provide care that under other circumstances they would consider their experience inadequate to undertake. These are realities of disaster response, and all skilled personnel can and should exceed the limits that normally exist in a fully functional system with adequate resources. However, at some point a doctor becomes too impaired or too inexperienced to provide care to patients—even if no one else is available. Doctors are neither trained nor encouraged to weigh the global risks and benefits in this manner; in fact, we are trained to push ourselves beyond our reasonable limits even when absolute scarcity of resources isn’t an issue. People are quite willing to compromise their own comfort and safety in the event of a disaster, but there comes a point at which they may do more harm than good.
There is extensive evidence that sleep deprivation impairs judgment and performance in the medical setting.1-2 Despite the fact that standards change in emergencies and greater risk must be undertaken by both providers and victims, there must still be safety limits. At some point a doctor becomes so sleep deprived that he or she is more dangerous providing care than leaving people entirely without a provider, and further may have impaired judgment on the severity of the various conditions they are facing and the reasonable limits on their expertise. This problem is inherent to the setting. How much risk should doctors subject patients to? In the face of a life-threatening condition should a completely inexperienced physician undertake care? What if the doctor is mistaken as to the severity of the illness or the proper response to it?
In response to Hurricane Katrina, state and national regulatory agencies had to create emergency exceptions to licensing regulations and to HIPAA and EMTALA requirements in order to facilitate patient care.3 Both the Model State Emergency Health Powers Act (legislation designed to serve as template for states to use to create emergency health response mechanisms) and the Louisiana legislation that governed provision of medical care in a state of emergency limit liability of any provider assisting in an emergency.4-5 Providers assisting in an emergency will not be held liable for any injury resulting from action or inaction except for intentional or grossly negligent acts or omissions. Such limitation of liability is essential to ensure that all available resources are utilized in an emergency. However, given that patients will have limited remedies for injuries caused, it is increasingly important to proactively define limitations on provider activity during emergencies. Because other remedies and regulatory structures are relaxed, ethical self-regulation becomes increasingly important.
The first priority in emergency disaster response must be ensuring that providers are available and do not encounter unnecessary barriers to providing care to ill or injured patients. However, a secondary goal must be ensuring that the safest and most effective care is provided under the circumstances. As with many things in disaster response, once the disaster has occurred there is little time for contemplation. Therefore, disaster response plans should include guidelines for providers on how to ensure safety in the care they provide.
Disaster response issues must be dealt with proactively because resources cannot be diverted to these issues in the thick of emergency response. Some organizations and providers have experience with disaster response and can provide guidance. A major goal of medical relief organizations is to provide relief for fatigued providers. When relief is not available and not likely to arrive soon, providers should be encouraged to self-impose sleep periods despite the apparent urgency of the situations they face. Urging providers to ensure that they eat at least twice and sleep for two to four hours in any 24-hour period is a reasonable limit on the physical activity of providers.
Providers and patients need to understand that this is essential to ensure that providers are capable of giving safe care in a sustained fashion. Emergency responders must maintain adequate perspective on their own abilities and patients’ needs to ensure that unnecessary risks are not undertaken nor avoidable injures inflicted. Importantly, these limitations should not be legislated or imposed externally, but should be defined by the profession and self-enforced by providers.
There have been significant discussion of what aspects of the U.S. system of response to large-scale disasters need to be improved. The Katrina disaster has given us the opportunity to enhance essential response mechanisms, whether the cause of the disaster is natural, infectious, or terrorist. A good disaster plan takes steps to ensure availability of care, but also to ensure that the care is as ethical, safe and effective as possible.
References
- Arnedt JT, Owens J, Crouch M, Stahl J, Carskadon MA. Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. JAMA. 2005;294(9):1025-1033.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns' work hours on serious medical errors in intensive care units. N Eng J Med. 2004;351(18):1838-1848.
- Hyland, et al. Federal, State Regulations Relaxed for Providers Affected by Hurricane. BNA Health Law Reporter. 2005;15(36):1190-1191.
- Gostin, LO, Model State Emergency Health Powers Act, §608 Licensing and Appointment of Health Care Personnel, December 21, 2001. Available at www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Last accessed Dec. 1, 2005.
- La. R.S. 29:656 (2005).
FROM THE PUBLIC POLICY COMMITTEE
Make a Positive Difference in the Politics of Healthcare
SHM to sponsor Legislative Advocacy Day on May 3
By Eric Siegal, MD, committee chair
“The stakes are too high for government to be a spectator sport.”
—Barbara Jordan, former U.S. Congresswoman
SHM is taking advantage of its 2006 annual meeting location in Washington, D.C., and sponsoring its first Legislative Advocacy Day on May 3. The Public Policy Committee is excited about the opportunity this initiative presents for hospitalists to learn more about how government really works and to speak with members of Congress about issues that are vital to patient care and clinical practice.
Are you concerned about continued Medicare cuts? Worried about how pending pay-for-performance legislation will affect hospitalists? SHM members registering for Advocacy Day will meet with their members of Congress and staff to discuss these and other important issues affecting hospital medicine.
I encourage you to register for Advocacy Day. There is no better way to influence how health policy is made in Washington than by meeting directly with your elected officials and their staffs. Lawmakers need constituent input to be effective legislators. Whether your legislator is a newly elected representative or a veteran senator with years of experience, he or she wants—and needs—to hear what you have to say about issues under consideration by the U.S. Congress, particularly in an election year. Input from their constituents always receives attention and consideration and can frequently make the difference in the way a lawmaker votes. Who better to educate members of Congress on changes to Medicare than the physicians directly involved in caring for the program’s beneficiaries?
We will give you the tools and information you need to make the most of your meetings on Capitol Hill. Legislative appointments will be scheduled by SHM as part of the registration process. SHM members will be grouped together by congressional district for House meetings and by state for Senate meetings and each registrant will have a minimum of three Hill appointments. To familiarize you with SHM’s legislative objectives for the second session of the 109th Congress, Laura Allendorf, SHM’s Washington representative, and I will conduct a pre-visit breakfast briefing from 7 a.m. to 8:30 a.m. on May 3. This briefing will cover procedural tips on how to have a successful meeting and update you on the status of the key health issues you will be discussing while on Capitol Hill. These meetings will take place from 9 a.m. to 5 p.m. that day.
Join us on May 3 and help educate members of Congress about the unique role hospitalists play in the delivery of medical care in our nation’s hospitals. We hope Advocacy Day will be the start of regular contact by hospitalists with their elected representatives in Washington.
FROM THE PEDIATRICS COMMITTEE
CME, Pediatric Core Curriculum on the Horizon
Multiple initiatives keep committee active
The Pediatric Committee at SHM is both the center of pediatric activity within SHM and a clearinghouse for SHM committee and task force activity as it relates to pediatrics.
The major pediatric activity in SHM continues to be CME activities and the Pediatric Core Curriculum. The dramatic success of the Pediatric Hospital Medicine Meeting was documented in the October issue of The Hospitalist (p. 33.)
Evaluations of the meeting overwhelmingly favored staging a three- to four-day Pediatric Hospital Medicine meeting on an annual basis during the late summer as a stand-alone meeting, with sponsorship rotating among SHM, the AAP, and the APA. There was insufficient lead time to offer a comprehensive meeting in 2006, but a meeting is scheduled for 2007 sponsored by AAP, with SHM taking the lead in 2008. More information to follow both in the SHM online discussion communities and through these committee reports.
The Pediatric Core Curriculum is nearly complete and should be at the review stage by early 2006. This curriculum is modeled after the adult core curriculum. It will serve as a framework for residency and fellowship directors, as well as a basis for the topics addressed at the Pediatric Hospital Medicine Meetings. Thanks to Tim Cornell, MD, Dan Rauch, MD, and all the authors and editors who have contributed to this work.
We will offer a full pediatric track in May at the SHM Annual Meeting in Washington, D.C., as we have in prior years. Registration is available online. Meetings of both the Pediatric Committee and the Pediatric Forum will be held during the meeting. This year’s meeting immediately precedes the PAS Meetings in San Francisco, and we encourage you to plan early so that at least one member of your program is able to attend the SHM Meeting. Once the Pediatric Hospital Medicine Meetings are held on an annual basis, we will need to decide how to balance SHM meeting offerings between the summer stand-alone Denver meeting and the SHM Annual Meeting.
The second function of Pediatric Committee involves having pediatric representatives on the various SHM committees and task forces report on their individual group’s activities, particularly as it relates to pediatrics. This keeps the broader group of pediatric leadership within SHM informed about the society’s global picture. SHM is committed to having a pediatric representative on each committee. You never know when or where an important issue for pediatricians may arise. Even geriatrics overlaps with pediatrics with regard to both family-centered care and proxy decision-makers.
Major endeavors at this point include the activities of the Benchmark and Career Satisfaction groups. SHM continues to make a strong effort to collect and generate data for workload and compensation, and to provide specific “pediatric only” subsets. Efforts regarding credentialing, sub-specialty designation/certification, and board re-certification are an active focus of SHM for adult hospitalists with ongoing discussions with the Board of Internal Medicine. We pediatricians stand on the sidelines of this battle, with the expectation that once the adults figure out how to do it, we can modify their approach with lower casualties on both sides.
The clinical Resource Rooms on the SHM Web site are clearly targeted toward adult topics. We intend to develop similar resources for pediatrics and are exploring possibilities of doing this collaboratively with the AAP and the APA. Sub-committees on pediatric hospital medicine topics are developing under a loose and shared structure with the AAP’s Section on Hospital Medicine. For example, SHM has taken the lead on a palliative care task force. Maggie Hood is the pediatric representative to this task force and wants to involve other interested pediatric hospitalists in a sub-committee on this topic. The AAP’s Karen Kingry has taken the lead on developing a sub-committee for community (pediatric) hospitalists; membership on her committee is open to SHM members. Expect other topics to develop as well.
If you have any comments, feedback or suggestions for the SHM Pediatric Committee, please contact co-chairs, David Zipes (dgzipes@indy.rr.com) or Jack Percelay (JPercelayMD@yahoo.com). TH
Core Visionaries
If you want something done, the saying goes, ask a busy person to do it. That was precisely the situation when SHM’s Core Competencies Task Force editorial board was formed in May 2003. Charged with producing the society’s first-ever curriculum guidance document, the editorial team faced a daunting task: solicit, organize, and edit chapters for the competencies framework on topics from specific clinical conditions to ethical issues. Over the next two and a half years, each of the physician members contributed hundreds of hours of uncompensated time to the project, juggling work, family, and other professional obligations.
Because they are so involved with their own institutions and the future of hospital medicine, the physicians tapped to guide the core competencies to reality were the right pick.
“Working with the four of them was phenomenal,” says SHM staff member Tina Budnitz, MPH, who serves on both the Education Committee and the Core Competencies Task Force. “They are all incredibly hard working, driven, and intelligent. I think the hardest thing was just the logistics of coordinating schedules, since this was a volunteer activity for them.” Budnitz points out that the original target date for completion of the core competencies was early 2005. Instead, the sheer bulk of editing work pushed the deadline back to early 2006, when release of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development by the Society of Hospital Medicine coincides with the premiere of the Journal of Hospital Medicine.
Recently, The Hospitalist caught up with each of the editorial board members, who divulged some of their personal motivations for participating in the ambitious core competencies project. They also discussed the workings of the editorial board and assessed the success of their efforts.
—Daniel D. Dressler, MD, MSc
Genesis and Vision
During a July 2002 Educational Summit the SHM Education Committee and Board of Directors determined that one element necessary to evolve SHM’s educational offerings would be a framework to guide and prioritize their efforts. A parallel conversation within the Education Committee, according to Budnitz, revolved around the need to better define hospital medicine. “We’re frequently asked, ‘what differentiates a hospitalist from other general internists? What exactly should the expectations be for a practicing hospitalist?’ ” she explains.
The Editorial Board
Michael J. Pistoria, DO, FACP, associate program director, Internal Medicine Residency, and medical director of both the Hospitalist Services and the Express Admission Unit at Lehigh Valley Hospital in Allentown, Pa., began his journey as chair of the Core Competencies Task Force shortly after SHM’s September 2002 Education Summit retreat.
Dr. Pistoria also serves on SHM’s Education Committee and admits that his allegiance to the field was a strong motivation for agreeing to participate in generating the Core Competencies.
“In my mind, hospital medicine is one of the neatest things in medicine to come along in a long time,” says Dr. Pistoria. “Hospital medicine has the potential to make a significant, positive difference in the way healthcare is delivered in the United States. And to have the opportunity to be a part of a process that helps define hospital medicine, to me, was just something almost too good to be true.”
A very active SHM member, Alpesh Amin, MD, MBA, FACP, is the associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California Irvine (UCI), where he also founded the UCI hospitalist program in 1998. His role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his key role in the Core Competencies Task Force editorial board.
“It was one of my goals—while chairing the Education Committee—for our society to put together the core competencies for hospital medicine,” says Dr. Amin. “I felt that if we had core competencies, this would be the next step to move us toward defining the field of hospital medicine.”
Accordingly, Dr. Amin was instrumental during the first and second SHM Education Summits in securing both committee and SHM Board of Directors’ buy-in of such a project.
For Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine, involvement with SHM’s (and formerly NAIP’s) Education Committee was a natural extension of his own interests in medical education. At Emory University Hospital, Dr. Dressler conducts a hospital medicine elective for house staff, “to give them a better understanding of what hospital medicine is and what we do, both in the community setting and in the academic setting.”
“I thought that [development of core competencies] was something that hospitalists as a group needed to do in order to a) become recognized and b) to clarify our own understanding and expectations of hospitalist physicians around the country,” he says.

—Tina Budnitz, MPH
Like her colleagues on the editorial board, Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist (BWF) Service (Boston), attended the 2002 SHM Education Summit and subsequently joined the Core Competencies Task Force. She is also co-chair of the society’s Career Satisfaction Task Force and views this role as linked to the missions of core competencies and education because education is a key component of professional advancement and engagement in the field. The Career Satisfaction Task Force, she notes, examines what components contribute to a long and satisfying career in hospital medicine.
Dr. McKean’s personal motivation for participation on the Core Competencies Task Force relates directly to her love of teaching. Having developed two hospitalist programs (one with physicians Andy Halpert, former chief of medicine for Harvard Vanguard Associations and subsequently the BWF program in 1998) she has seen firsthand that “people right out of residency do not have all the skills that they need in order to be effective hospitalists.”
As medical director of the BWF Hospitalist Service, Dr. McKean developed a weekly Harvard Medical School CME conference Update in Hospital Medicine for members of the hospitalist service, as well a medical consultation syllabus for the newest members of the hospitalist service to distribute to residents.
“I identified what the newest members of our service right out of residency didn’t learn during their residency training and tried to make sure that we would have people come in and teach them about hospital medicine,” she explains.
As the hospitalist service matured, hospitalists developed significant expertise in these topics and frequently participate in this didactic series of lectures.
“Initially,” recounts Dr. McKean, “I was the only senior physician with experience in hospital medicine, but now my job is much easier, as I continue to learn from other hospitalists in our program.”

—Sylvia C.W. McKean, MD, FACP
A Framework, Not a Text
“We have a great team,” says Dr. Amin of the Task Force editorial board. “I think our goals were clear. We wanted to develop a set of competencies that would be unique and offer 1) an opportunity to define the space that we, as hospitalists, lead in system-based practice; and 2) a framework that would cross over the span of time, so that others could use that framework to develop future curricula.
“Once you write a book, the context is fixed. We thought this [framework for curriculum development] was a creative way of facilitating future projects and ideas,” he continues. “It becomes more of a bible for competencies in hospital medicine.”
Budnitz says the idea was to develop an enduring, flexible blueprint. “We set out to develop a guide that would serve as a blueprint for curricular development in hospital medicine,” she explains. “We wanted to standardize the expectations for learning outcomes but still allow curriculum developers to add their expertise of content and context. Each chapter of the guide is written as a set of learning objectives. We crafted these objectives to clearly indicate a proficiency level.
“For example,” says Budnitz, “it is a different expectation that someone can list the drugs that they might order for a particular condition, versus analyzing the benefits and limitations of different therapeutic approaches. And in both scenarios we have left it up to the content and curriculum developers to determine the precise list of therapeutic agents that are included in curricula and the educational approach that will most likely yield the intended learning outcome.”
Dr. Dressler elaborates on his colleagues’ characterizations of the document: “We weren’t planning on this being an overarching, comprehensive text on hospital medicine. We were not trying to develop or even provide content.”
Instead, he says, the aim was to provide medical educators with a relatively generic framework that would retain flexibility for change. “For instance,” he explains, “if a new drug comes out that is useful for [treating] heart failure, the expectation is that hospitalists should be able to explain and utilize the new and useful medications, but that we were not going to list every drug in the Core Competencies compendium.”
“The one idea that we kept coming back to is that we wanted to design a set of competencies,” said Dr. Pistoria. “We didn’t want to publish a textbook; we didn’t want to come up with a curriculum per se. We wanted to come up with a framework that someone could use to develop their own hospitalist program in their own institution.”
Soliciting Input
The Core Competencies Task Force developed an initial organizational structure for the guide and a list of chapter topics. The resulting chapter list was turned into a survey and sent to the SHM Board of Directors, Core Competencies Task Force, and Education Committee. The survey was also sent to a sample of members within each SHM region or chapter via its chapter or region director. A review of core competencies generated by other medical specialties and allied health professional societies followed.
Then, the task force put out a call for nominations of chapter contributors. Budnitz judges that there were between 150-200 responses for potential contributors. Reviewing all the nominations was no small task. In some cases the editorial board deemed it necessary to recruit non-hospitalist content experts to generate some chapters, such as those dealing with medical-legal issues. In those instances, the “outside expert” was often paired with a hospitalist to ensure that the hospitalist perspective was included.
Strategies for Content Inclusion
Dr. Amin points out that the task force “went as broad and as wide as we could to get feedback on the content for the Core Competencies.” However, it was simply not possible—nor was it the editorial board’s intent—to compile an exhaustive list of all the hundreds of diagnoses that hospitalists may see on a regular basis. The editorial board identified common diagnoses from the top 15-20 DRGs from the Medicare database. The task was then to communicate the most important aspects of what hospitalists do, in the domains of knowledge, skills, and attitudes.
To manage the sheer bulk of solicited CVs and potential chapter authors, the editorial board used a divide-and-conquer strategy. Even so, says Dr. Pistoria, this process took a fair amount of time. When chapters began arriving and the task force was reduced to the core editorial board, “the homework started kicking up, with a lot of home editing time, telephone and e-mail editing, and some face-to-face meetings to ensure that chapters were standardized and had the same format.”
Once the editorial board began its work, it was relatively easy to decide that majority rule would be the best process for resolving differences of opinion, “but honestly,” says Dr. McKean, “only a handful of issues were generated. If we didn’t develop a consensus or if we were not all in agreement, then we sometimes looked for feedback from experts outside of the task force and the editorial board.”
Keeping with the ethos of inclusion, most board members consulted with other experts at their institution about key elements to include in the document.
Regarding the “majority rules” process, “Everyone had the chance during the editorial process to voice their opinions,” says Dr. Pistoria. “If they had concerns and were able to persuade enough people, the appropriate change would be made. I think, in the end, that everyone in the core editorial group felt that their opinions were heard, and I think that lends itself to the pride that we all feel in the final product.”

—Alpesh Amin, MD, MBA, FACP
A Work in Progress
Budnitz contributed critical guidance when the board generated writing guidelines for chapter authors. Each received a template for their chapter: a document instructing them how to write a competency, and a letter indicating the intent for their particular chapter. The template went through several iterations, she says, as early chapters were returned and the board began their editing.
For example, each clinical condition is discussed through the domains of knowledge, skills, and attitudes. It was the board’s job to ensure that concepts consistently appeared in the same domain across chapters with a similar degree of specificity and in the same order. “Partway through the process, we refined our template and made it more specific,” reports Budnitz. “We were able to give the second round of contributors a little more guidance as a result.
“We originally thought the document would be ready in early 2005,” she explains. “I think we were under the misimpression that the chapters would come back, that we’d read through them in a month or two, and it would be done. It turns out that just the sheer logistics of editing four or five versions of 70 chapters was quite a process.”
“I think [the Core Competencies] is something that SHM can be proud of,” said Dr. Pistoria of the group’s efforts. “But this is by no means the end of the project – it’s only the beginning. It is a work in progress.”
Dr. Dressler agreed with Dr. Pistoria’s characterization of the Core Competencies as a work in progress.
“I am pretty satisfied with what we’ve accomplished,” says Dr. Dressler. “By no means do I feel that this is the end-all, be-all for hospital medicine, or even for education in hospital medicine. It’s a start. We expect comment. We expect criticism. Being hospitalists, we are all open and aware and willing to make changes. And so we make a start, our initial best effort to get something out there that hospitalists can look at, utilize, and then offer feedback. Our primary goal is to provide a structure for consistency in practice and consistency in expectations. We would like to make [the Core Competencies] something that hospitalists and hospitalist educators feel is useful and that can change with the needs of our specialty.”

—Michael Pistoria, DO, FACP
Concluding Thoughts
“[Working on the Core Competencies] was an exciting project,” says Dr. Amin. “It took a lot of time. We had to spend a fair amount of time learning before we could actually define what we wanted from our chapter authors. But it was a good process. It was a four-year process to develop a document that would be worthwhile and hopefully stand the test of time in defining the core aspects of the field of hospital medicine. It was great to be chairing [the] education [committee] and seeing the value of helping to facilitate this project, and now looking more broadly across how to apply this project to future educational efforts.”
The project certainly had its challenges, most of which were related to time constraints.
“All of us were working very hard in our respective programs,” notes Dr. McKean, “and we were doing this on a volunteer basis. I think we had 10 face-to-face meetings, and sat at our computers on Saturday afternoons for conference calls using a Web-based editing program.”
For her part, Dr. McKean found working on the core competencies “very satisfying. I think I learned a lot from other people on this task force, editorial board, and the organization of the Society of Hospital Medicine. This project helped me reflect upon skills that I should try to obtain, and to think about more global issues than the day-to-day hospital politics in which I was involved. I did more strategic planning and thinking about retreats. So, it was a learning experience for me, and I also felt that I was contributing to something worthwhile. It was a chance to make a difference.
“From my own professional experience, the development process has helped me here, at Brigham and Women’s Hospital, so I hope that anyone who wants to apply the core competencies would feel free to e-mail us or contact us if they have any questions at all,” she says.
Dr. Pistoria agrees with Dr. McKean’s observations. “Working on the Core Competencies had a really big impact on me, both personally and professionally,” he says. “The process helped me mature in how I deal with running a project like this because I have been given the opportunity to do some similar things at my institution. Some of the ideas that we hit upon as we were editing and developing these competencies make one think, ‘We need to do this at our institution.’ Let’s take a strong look at, say, discharge processes, get a group together, and generate some recommendations that we can then institute.”
Other editorial board members also acknowledged that their participation gave them new insights into their own practice of hospital medicine.
“It’s easy to have in your head what you think is the right thing to do,” notes Dr. Dressler, “But until you actually have to try to develop consistency in wording and expectations, to put a process together that can result in a protocol, you realize that sometimes some elements get left out—for instance, the importance of family communication in the setting of DVT.”
Regarding the board members’ hard work, Budnitz remarks, “I can’t say enough about the dedication of the editorial board. They volunteered a tremendous amount of time and stuck with the project for three years. Since the board lived in multiple time zones, we often had calls where people would be participating at 6 a.m. or 9 p.m. We convened on weekends in multiple cities across the U.S. I sincerely enjoyed the opportunity to be a part of this project and hopefully impact the future of medical education.
“I think the document makes a bold statement. It defines the hospitalist as the captain of the ship—and calls on hospitalists to lead multidisciplinary teams to improve the quality of care. I hope it sparks interest and debate about how we recruit, train, prepare, and certify physicians in hospital medicine.”
Dr. Pistoria believes that the Core Competencies will advance hospitalist programs. In fact, he says, hospitalists around the country have already affected improvements in care coordination. The hospitalist movement in general furnishes hospitals with physicians who say, “ ‘I’m going to take ownership of what happens within the four walls of this hospital,’ ” says Dr. Pistoria. “Previous to that, people obviously cared about what happened in the hospital, but they also worried about their office practices. This is our office practice. We want it to work as well as it can for our patients, for us, for our nursing colleagues, for our janitors—everybody needs to, and should, benefit from this.” TH
Writer Gretchen Henkel wrote about cultural competency in the September issue of The Hospitalist.
If you want something done, the saying goes, ask a busy person to do it. That was precisely the situation when SHM’s Core Competencies Task Force editorial board was formed in May 2003. Charged with producing the society’s first-ever curriculum guidance document, the editorial team faced a daunting task: solicit, organize, and edit chapters for the competencies framework on topics from specific clinical conditions to ethical issues. Over the next two and a half years, each of the physician members contributed hundreds of hours of uncompensated time to the project, juggling work, family, and other professional obligations.
Because they are so involved with their own institutions and the future of hospital medicine, the physicians tapped to guide the core competencies to reality were the right pick.
“Working with the four of them was phenomenal,” says SHM staff member Tina Budnitz, MPH, who serves on both the Education Committee and the Core Competencies Task Force. “They are all incredibly hard working, driven, and intelligent. I think the hardest thing was just the logistics of coordinating schedules, since this was a volunteer activity for them.” Budnitz points out that the original target date for completion of the core competencies was early 2005. Instead, the sheer bulk of editing work pushed the deadline back to early 2006, when release of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development by the Society of Hospital Medicine coincides with the premiere of the Journal of Hospital Medicine.
Recently, The Hospitalist caught up with each of the editorial board members, who divulged some of their personal motivations for participating in the ambitious core competencies project. They also discussed the workings of the editorial board and assessed the success of their efforts.
—Daniel D. Dressler, MD, MSc
Genesis and Vision
During a July 2002 Educational Summit the SHM Education Committee and Board of Directors determined that one element necessary to evolve SHM’s educational offerings would be a framework to guide and prioritize their efforts. A parallel conversation within the Education Committee, according to Budnitz, revolved around the need to better define hospital medicine. “We’re frequently asked, ‘what differentiates a hospitalist from other general internists? What exactly should the expectations be for a practicing hospitalist?’ ” she explains.
The Editorial Board
Michael J. Pistoria, DO, FACP, associate program director, Internal Medicine Residency, and medical director of both the Hospitalist Services and the Express Admission Unit at Lehigh Valley Hospital in Allentown, Pa., began his journey as chair of the Core Competencies Task Force shortly after SHM’s September 2002 Education Summit retreat.
Dr. Pistoria also serves on SHM’s Education Committee and admits that his allegiance to the field was a strong motivation for agreeing to participate in generating the Core Competencies.
“In my mind, hospital medicine is one of the neatest things in medicine to come along in a long time,” says Dr. Pistoria. “Hospital medicine has the potential to make a significant, positive difference in the way healthcare is delivered in the United States. And to have the opportunity to be a part of a process that helps define hospital medicine, to me, was just something almost too good to be true.”
A very active SHM member, Alpesh Amin, MD, MBA, FACP, is the associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California Irvine (UCI), where he also founded the UCI hospitalist program in 1998. His role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his key role in the Core Competencies Task Force editorial board.
“It was one of my goals—while chairing the Education Committee—for our society to put together the core competencies for hospital medicine,” says Dr. Amin. “I felt that if we had core competencies, this would be the next step to move us toward defining the field of hospital medicine.”
Accordingly, Dr. Amin was instrumental during the first and second SHM Education Summits in securing both committee and SHM Board of Directors’ buy-in of such a project.
For Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine, involvement with SHM’s (and formerly NAIP’s) Education Committee was a natural extension of his own interests in medical education. At Emory University Hospital, Dr. Dressler conducts a hospital medicine elective for house staff, “to give them a better understanding of what hospital medicine is and what we do, both in the community setting and in the academic setting.”
“I thought that [development of core competencies] was something that hospitalists as a group needed to do in order to a) become recognized and b) to clarify our own understanding and expectations of hospitalist physicians around the country,” he says.
—Tina Budnitz, MPH
Like her colleagues on the editorial board, Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist (BWF) Service (Boston), attended the 2002 SHM Education Summit and subsequently joined the Core Competencies Task Force. She is also co-chair of the society’s Career Satisfaction Task Force and views this role as linked to the missions of core competencies and education because education is a key component of professional advancement and engagement in the field. The Career Satisfaction Task Force, she notes, examines what components contribute to a long and satisfying career in hospital medicine.
Dr. McKean’s personal motivation for participation on the Core Competencies Task Force relates directly to her love of teaching. Having developed two hospitalist programs (one with physicians Andy Halpert, former chief of medicine for Harvard Vanguard Associations and subsequently the BWF program in 1998) she has seen firsthand that “people right out of residency do not have all the skills that they need in order to be effective hospitalists.”
As medical director of the BWF Hospitalist Service, Dr. McKean developed a weekly Harvard Medical School CME conference Update in Hospital Medicine for members of the hospitalist service, as well a medical consultation syllabus for the newest members of the hospitalist service to distribute to residents.
“I identified what the newest members of our service right out of residency didn’t learn during their residency training and tried to make sure that we would have people come in and teach them about hospital medicine,” she explains.
As the hospitalist service matured, hospitalists developed significant expertise in these topics and frequently participate in this didactic series of lectures.
“Initially,” recounts Dr. McKean, “I was the only senior physician with experience in hospital medicine, but now my job is much easier, as I continue to learn from other hospitalists in our program.”
—Sylvia C.W. McKean, MD, FACP
A Framework, Not a Text
“We have a great team,” says Dr. Amin of the Task Force editorial board. “I think our goals were clear. We wanted to develop a set of competencies that would be unique and offer 1) an opportunity to define the space that we, as hospitalists, lead in system-based practice; and 2) a framework that would cross over the span of time, so that others could use that framework to develop future curricula.
“Once you write a book, the context is fixed. We thought this [framework for curriculum development] was a creative way of facilitating future projects and ideas,” he continues. “It becomes more of a bible for competencies in hospital medicine.”
Budnitz says the idea was to develop an enduring, flexible blueprint. “We set out to develop a guide that would serve as a blueprint for curricular development in hospital medicine,” she explains. “We wanted to standardize the expectations for learning outcomes but still allow curriculum developers to add their expertise of content and context. Each chapter of the guide is written as a set of learning objectives. We crafted these objectives to clearly indicate a proficiency level.
“For example,” says Budnitz, “it is a different expectation that someone can list the drugs that they might order for a particular condition, versus analyzing the benefits and limitations of different therapeutic approaches. And in both scenarios we have left it up to the content and curriculum developers to determine the precise list of therapeutic agents that are included in curricula and the educational approach that will most likely yield the intended learning outcome.”
Dr. Dressler elaborates on his colleagues’ characterizations of the document: “We weren’t planning on this being an overarching, comprehensive text on hospital medicine. We were not trying to develop or even provide content.”
Instead, he says, the aim was to provide medical educators with a relatively generic framework that would retain flexibility for change. “For instance,” he explains, “if a new drug comes out that is useful for [treating] heart failure, the expectation is that hospitalists should be able to explain and utilize the new and useful medications, but that we were not going to list every drug in the Core Competencies compendium.”
“The one idea that we kept coming back to is that we wanted to design a set of competencies,” said Dr. Pistoria. “We didn’t want to publish a textbook; we didn’t want to come up with a curriculum per se. We wanted to come up with a framework that someone could use to develop their own hospitalist program in their own institution.”
Soliciting Input
The Core Competencies Task Force developed an initial organizational structure for the guide and a list of chapter topics. The resulting chapter list was turned into a survey and sent to the SHM Board of Directors, Core Competencies Task Force, and Education Committee. The survey was also sent to a sample of members within each SHM region or chapter via its chapter or region director. A review of core competencies generated by other medical specialties and allied health professional societies followed.
Then, the task force put out a call for nominations of chapter contributors. Budnitz judges that there were between 150-200 responses for potential contributors. Reviewing all the nominations was no small task. In some cases the editorial board deemed it necessary to recruit non-hospitalist content experts to generate some chapters, such as those dealing with medical-legal issues. In those instances, the “outside expert” was often paired with a hospitalist to ensure that the hospitalist perspective was included.
Strategies for Content Inclusion
Dr. Amin points out that the task force “went as broad and as wide as we could to get feedback on the content for the Core Competencies.” However, it was simply not possible—nor was it the editorial board’s intent—to compile an exhaustive list of all the hundreds of diagnoses that hospitalists may see on a regular basis. The editorial board identified common diagnoses from the top 15-20 DRGs from the Medicare database. The task was then to communicate the most important aspects of what hospitalists do, in the domains of knowledge, skills, and attitudes.
To manage the sheer bulk of solicited CVs and potential chapter authors, the editorial board used a divide-and-conquer strategy. Even so, says Dr. Pistoria, this process took a fair amount of time. When chapters began arriving and the task force was reduced to the core editorial board, “the homework started kicking up, with a lot of home editing time, telephone and e-mail editing, and some face-to-face meetings to ensure that chapters were standardized and had the same format.”
Once the editorial board began its work, it was relatively easy to decide that majority rule would be the best process for resolving differences of opinion, “but honestly,” says Dr. McKean, “only a handful of issues were generated. If we didn’t develop a consensus or if we were not all in agreement, then we sometimes looked for feedback from experts outside of the task force and the editorial board.”
Keeping with the ethos of inclusion, most board members consulted with other experts at their institution about key elements to include in the document.
Regarding the “majority rules” process, “Everyone had the chance during the editorial process to voice their opinions,” says Dr. Pistoria. “If they had concerns and were able to persuade enough people, the appropriate change would be made. I think, in the end, that everyone in the core editorial group felt that their opinions were heard, and I think that lends itself to the pride that we all feel in the final product.”
—Alpesh Amin, MD, MBA, FACP
A Work in Progress
Budnitz contributed critical guidance when the board generated writing guidelines for chapter authors. Each received a template for their chapter: a document instructing them how to write a competency, and a letter indicating the intent for their particular chapter. The template went through several iterations, she says, as early chapters were returned and the board began their editing.
For example, each clinical condition is discussed through the domains of knowledge, skills, and attitudes. It was the board’s job to ensure that concepts consistently appeared in the same domain across chapters with a similar degree of specificity and in the same order. “Partway through the process, we refined our template and made it more specific,” reports Budnitz. “We were able to give the second round of contributors a little more guidance as a result.
“We originally thought the document would be ready in early 2005,” she explains. “I think we were under the misimpression that the chapters would come back, that we’d read through them in a month or two, and it would be done. It turns out that just the sheer logistics of editing four or five versions of 70 chapters was quite a process.”
“I think [the Core Competencies] is something that SHM can be proud of,” said Dr. Pistoria of the group’s efforts. “But this is by no means the end of the project – it’s only the beginning. It is a work in progress.”
Dr. Dressler agreed with Dr. Pistoria’s characterization of the Core Competencies as a work in progress.
“I am pretty satisfied with what we’ve accomplished,” says Dr. Dressler. “By no means do I feel that this is the end-all, be-all for hospital medicine, or even for education in hospital medicine. It’s a start. We expect comment. We expect criticism. Being hospitalists, we are all open and aware and willing to make changes. And so we make a start, our initial best effort to get something out there that hospitalists can look at, utilize, and then offer feedback. Our primary goal is to provide a structure for consistency in practice and consistency in expectations. We would like to make [the Core Competencies] something that hospitalists and hospitalist educators feel is useful and that can change with the needs of our specialty.”
—Michael Pistoria, DO, FACP
Concluding Thoughts
“[Working on the Core Competencies] was an exciting project,” says Dr. Amin. “It took a lot of time. We had to spend a fair amount of time learning before we could actually define what we wanted from our chapter authors. But it was a good process. It was a four-year process to develop a document that would be worthwhile and hopefully stand the test of time in defining the core aspects of the field of hospital medicine. It was great to be chairing [the] education [committee] and seeing the value of helping to facilitate this project, and now looking more broadly across how to apply this project to future educational efforts.”
The project certainly had its challenges, most of which were related to time constraints.
“All of us were working very hard in our respective programs,” notes Dr. McKean, “and we were doing this on a volunteer basis. I think we had 10 face-to-face meetings, and sat at our computers on Saturday afternoons for conference calls using a Web-based editing program.”
For her part, Dr. McKean found working on the core competencies “very satisfying. I think I learned a lot from other people on this task force, editorial board, and the organization of the Society of Hospital Medicine. This project helped me reflect upon skills that I should try to obtain, and to think about more global issues than the day-to-day hospital politics in which I was involved. I did more strategic planning and thinking about retreats. So, it was a learning experience for me, and I also felt that I was contributing to something worthwhile. It was a chance to make a difference.
“From my own professional experience, the development process has helped me here, at Brigham and Women’s Hospital, so I hope that anyone who wants to apply the core competencies would feel free to e-mail us or contact us if they have any questions at all,” she says.
Dr. Pistoria agrees with Dr. McKean’s observations. “Working on the Core Competencies had a really big impact on me, both personally and professionally,” he says. “The process helped me mature in how I deal with running a project like this because I have been given the opportunity to do some similar things at my institution. Some of the ideas that we hit upon as we were editing and developing these competencies make one think, ‘We need to do this at our institution.’ Let’s take a strong look at, say, discharge processes, get a group together, and generate some recommendations that we can then institute.”
Other editorial board members also acknowledged that their participation gave them new insights into their own practice of hospital medicine.
“It’s easy to have in your head what you think is the right thing to do,” notes Dr. Dressler, “But until you actually have to try to develop consistency in wording and expectations, to put a process together that can result in a protocol, you realize that sometimes some elements get left out—for instance, the importance of family communication in the setting of DVT.”
Regarding the board members’ hard work, Budnitz remarks, “I can’t say enough about the dedication of the editorial board. They volunteered a tremendous amount of time and stuck with the project for three years. Since the board lived in multiple time zones, we often had calls where people would be participating at 6 a.m. or 9 p.m. We convened on weekends in multiple cities across the U.S. I sincerely enjoyed the opportunity to be a part of this project and hopefully impact the future of medical education.
“I think the document makes a bold statement. It defines the hospitalist as the captain of the ship—and calls on hospitalists to lead multidisciplinary teams to improve the quality of care. I hope it sparks interest and debate about how we recruit, train, prepare, and certify physicians in hospital medicine.”
Dr. Pistoria believes that the Core Competencies will advance hospitalist programs. In fact, he says, hospitalists around the country have already affected improvements in care coordination. The hospitalist movement in general furnishes hospitals with physicians who say, “ ‘I’m going to take ownership of what happens within the four walls of this hospital,’ ” says Dr. Pistoria. “Previous to that, people obviously cared about what happened in the hospital, but they also worried about their office practices. This is our office practice. We want it to work as well as it can for our patients, for us, for our nursing colleagues, for our janitors—everybody needs to, and should, benefit from this.” TH
Writer Gretchen Henkel wrote about cultural competency in the September issue of The Hospitalist.
If you want something done, the saying goes, ask a busy person to do it. That was precisely the situation when SHM’s Core Competencies Task Force editorial board was formed in May 2003. Charged with producing the society’s first-ever curriculum guidance document, the editorial team faced a daunting task: solicit, organize, and edit chapters for the competencies framework on topics from specific clinical conditions to ethical issues. Over the next two and a half years, each of the physician members contributed hundreds of hours of uncompensated time to the project, juggling work, family, and other professional obligations.
Because they are so involved with their own institutions and the future of hospital medicine, the physicians tapped to guide the core competencies to reality were the right pick.
“Working with the four of them was phenomenal,” says SHM staff member Tina Budnitz, MPH, who serves on both the Education Committee and the Core Competencies Task Force. “They are all incredibly hard working, driven, and intelligent. I think the hardest thing was just the logistics of coordinating schedules, since this was a volunteer activity for them.” Budnitz points out that the original target date for completion of the core competencies was early 2005. Instead, the sheer bulk of editing work pushed the deadline back to early 2006, when release of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development by the Society of Hospital Medicine coincides with the premiere of the Journal of Hospital Medicine.
Recently, The Hospitalist caught up with each of the editorial board members, who divulged some of their personal motivations for participating in the ambitious core competencies project. They also discussed the workings of the editorial board and assessed the success of their efforts.
—Daniel D. Dressler, MD, MSc
Genesis and Vision
During a July 2002 Educational Summit the SHM Education Committee and Board of Directors determined that one element necessary to evolve SHM’s educational offerings would be a framework to guide and prioritize their efforts. A parallel conversation within the Education Committee, according to Budnitz, revolved around the need to better define hospital medicine. “We’re frequently asked, ‘what differentiates a hospitalist from other general internists? What exactly should the expectations be for a practicing hospitalist?’ ” she explains.
The Editorial Board
Michael J. Pistoria, DO, FACP, associate program director, Internal Medicine Residency, and medical director of both the Hospitalist Services and the Express Admission Unit at Lehigh Valley Hospital in Allentown, Pa., began his journey as chair of the Core Competencies Task Force shortly after SHM’s September 2002 Education Summit retreat.
Dr. Pistoria also serves on SHM’s Education Committee and admits that his allegiance to the field was a strong motivation for agreeing to participate in generating the Core Competencies.
“In my mind, hospital medicine is one of the neatest things in medicine to come along in a long time,” says Dr. Pistoria. “Hospital medicine has the potential to make a significant, positive difference in the way healthcare is delivered in the United States. And to have the opportunity to be a part of a process that helps define hospital medicine, to me, was just something almost too good to be true.”
A very active SHM member, Alpesh Amin, MD, MBA, FACP, is the associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California Irvine (UCI), where he also founded the UCI hospitalist program in 1998. His role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his key role in the Core Competencies Task Force editorial board.
“It was one of my goals—while chairing the Education Committee—for our society to put together the core competencies for hospital medicine,” says Dr. Amin. “I felt that if we had core competencies, this would be the next step to move us toward defining the field of hospital medicine.”
Accordingly, Dr. Amin was instrumental during the first and second SHM Education Summits in securing both committee and SHM Board of Directors’ buy-in of such a project.
For Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine, involvement with SHM’s (and formerly NAIP’s) Education Committee was a natural extension of his own interests in medical education. At Emory University Hospital, Dr. Dressler conducts a hospital medicine elective for house staff, “to give them a better understanding of what hospital medicine is and what we do, both in the community setting and in the academic setting.”
“I thought that [development of core competencies] was something that hospitalists as a group needed to do in order to a) become recognized and b) to clarify our own understanding and expectations of hospitalist physicians around the country,” he says.
—Tina Budnitz, MPH
Like her colleagues on the editorial board, Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist (BWF) Service (Boston), attended the 2002 SHM Education Summit and subsequently joined the Core Competencies Task Force. She is also co-chair of the society’s Career Satisfaction Task Force and views this role as linked to the missions of core competencies and education because education is a key component of professional advancement and engagement in the field. The Career Satisfaction Task Force, she notes, examines what components contribute to a long and satisfying career in hospital medicine.
Dr. McKean’s personal motivation for participation on the Core Competencies Task Force relates directly to her love of teaching. Having developed two hospitalist programs (one with physicians Andy Halpert, former chief of medicine for Harvard Vanguard Associations and subsequently the BWF program in 1998) she has seen firsthand that “people right out of residency do not have all the skills that they need in order to be effective hospitalists.”
As medical director of the BWF Hospitalist Service, Dr. McKean developed a weekly Harvard Medical School CME conference Update in Hospital Medicine for members of the hospitalist service, as well a medical consultation syllabus for the newest members of the hospitalist service to distribute to residents.
“I identified what the newest members of our service right out of residency didn’t learn during their residency training and tried to make sure that we would have people come in and teach them about hospital medicine,” she explains.
As the hospitalist service matured, hospitalists developed significant expertise in these topics and frequently participate in this didactic series of lectures.
“Initially,” recounts Dr. McKean, “I was the only senior physician with experience in hospital medicine, but now my job is much easier, as I continue to learn from other hospitalists in our program.”
—Sylvia C.W. McKean, MD, FACP
A Framework, Not a Text
“We have a great team,” says Dr. Amin of the Task Force editorial board. “I think our goals were clear. We wanted to develop a set of competencies that would be unique and offer 1) an opportunity to define the space that we, as hospitalists, lead in system-based practice; and 2) a framework that would cross over the span of time, so that others could use that framework to develop future curricula.
“Once you write a book, the context is fixed. We thought this [framework for curriculum development] was a creative way of facilitating future projects and ideas,” he continues. “It becomes more of a bible for competencies in hospital medicine.”
Budnitz says the idea was to develop an enduring, flexible blueprint. “We set out to develop a guide that would serve as a blueprint for curricular development in hospital medicine,” she explains. “We wanted to standardize the expectations for learning outcomes but still allow curriculum developers to add their expertise of content and context. Each chapter of the guide is written as a set of learning objectives. We crafted these objectives to clearly indicate a proficiency level.
“For example,” says Budnitz, “it is a different expectation that someone can list the drugs that they might order for a particular condition, versus analyzing the benefits and limitations of different therapeutic approaches. And in both scenarios we have left it up to the content and curriculum developers to determine the precise list of therapeutic agents that are included in curricula and the educational approach that will most likely yield the intended learning outcome.”
Dr. Dressler elaborates on his colleagues’ characterizations of the document: “We weren’t planning on this being an overarching, comprehensive text on hospital medicine. We were not trying to develop or even provide content.”
Instead, he says, the aim was to provide medical educators with a relatively generic framework that would retain flexibility for change. “For instance,” he explains, “if a new drug comes out that is useful for [treating] heart failure, the expectation is that hospitalists should be able to explain and utilize the new and useful medications, but that we were not going to list every drug in the Core Competencies compendium.”
“The one idea that we kept coming back to is that we wanted to design a set of competencies,” said Dr. Pistoria. “We didn’t want to publish a textbook; we didn’t want to come up with a curriculum per se. We wanted to come up with a framework that someone could use to develop their own hospitalist program in their own institution.”
Soliciting Input
The Core Competencies Task Force developed an initial organizational structure for the guide and a list of chapter topics. The resulting chapter list was turned into a survey and sent to the SHM Board of Directors, Core Competencies Task Force, and Education Committee. The survey was also sent to a sample of members within each SHM region or chapter via its chapter or region director. A review of core competencies generated by other medical specialties and allied health professional societies followed.
Then, the task force put out a call for nominations of chapter contributors. Budnitz judges that there were between 150-200 responses for potential contributors. Reviewing all the nominations was no small task. In some cases the editorial board deemed it necessary to recruit non-hospitalist content experts to generate some chapters, such as those dealing with medical-legal issues. In those instances, the “outside expert” was often paired with a hospitalist to ensure that the hospitalist perspective was included.
Strategies for Content Inclusion
Dr. Amin points out that the task force “went as broad and as wide as we could to get feedback on the content for the Core Competencies.” However, it was simply not possible—nor was it the editorial board’s intent—to compile an exhaustive list of all the hundreds of diagnoses that hospitalists may see on a regular basis. The editorial board identified common diagnoses from the top 15-20 DRGs from the Medicare database. The task was then to communicate the most important aspects of what hospitalists do, in the domains of knowledge, skills, and attitudes.
To manage the sheer bulk of solicited CVs and potential chapter authors, the editorial board used a divide-and-conquer strategy. Even so, says Dr. Pistoria, this process took a fair amount of time. When chapters began arriving and the task force was reduced to the core editorial board, “the homework started kicking up, with a lot of home editing time, telephone and e-mail editing, and some face-to-face meetings to ensure that chapters were standardized and had the same format.”
Once the editorial board began its work, it was relatively easy to decide that majority rule would be the best process for resolving differences of opinion, “but honestly,” says Dr. McKean, “only a handful of issues were generated. If we didn’t develop a consensus or if we were not all in agreement, then we sometimes looked for feedback from experts outside of the task force and the editorial board.”
Keeping with the ethos of inclusion, most board members consulted with other experts at their institution about key elements to include in the document.
Regarding the “majority rules” process, “Everyone had the chance during the editorial process to voice their opinions,” says Dr. Pistoria. “If they had concerns and were able to persuade enough people, the appropriate change would be made. I think, in the end, that everyone in the core editorial group felt that their opinions were heard, and I think that lends itself to the pride that we all feel in the final product.”
—Alpesh Amin, MD, MBA, FACP
A Work in Progress
Budnitz contributed critical guidance when the board generated writing guidelines for chapter authors. Each received a template for their chapter: a document instructing them how to write a competency, and a letter indicating the intent for their particular chapter. The template went through several iterations, she says, as early chapters were returned and the board began their editing.
For example, each clinical condition is discussed through the domains of knowledge, skills, and attitudes. It was the board’s job to ensure that concepts consistently appeared in the same domain across chapters with a similar degree of specificity and in the same order. “Partway through the process, we refined our template and made it more specific,” reports Budnitz. “We were able to give the second round of contributors a little more guidance as a result.
“We originally thought the document would be ready in early 2005,” she explains. “I think we were under the misimpression that the chapters would come back, that we’d read through them in a month or two, and it would be done. It turns out that just the sheer logistics of editing four or five versions of 70 chapters was quite a process.”
“I think [the Core Competencies] is something that SHM can be proud of,” said Dr. Pistoria of the group’s efforts. “But this is by no means the end of the project – it’s only the beginning. It is a work in progress.”
Dr. Dressler agreed with Dr. Pistoria’s characterization of the Core Competencies as a work in progress.
“I am pretty satisfied with what we’ve accomplished,” says Dr. Dressler. “By no means do I feel that this is the end-all, be-all for hospital medicine, or even for education in hospital medicine. It’s a start. We expect comment. We expect criticism. Being hospitalists, we are all open and aware and willing to make changes. And so we make a start, our initial best effort to get something out there that hospitalists can look at, utilize, and then offer feedback. Our primary goal is to provide a structure for consistency in practice and consistency in expectations. We would like to make [the Core Competencies] something that hospitalists and hospitalist educators feel is useful and that can change with the needs of our specialty.”
—Michael Pistoria, DO, FACP
Concluding Thoughts
“[Working on the Core Competencies] was an exciting project,” says Dr. Amin. “It took a lot of time. We had to spend a fair amount of time learning before we could actually define what we wanted from our chapter authors. But it was a good process. It was a four-year process to develop a document that would be worthwhile and hopefully stand the test of time in defining the core aspects of the field of hospital medicine. It was great to be chairing [the] education [committee] and seeing the value of helping to facilitate this project, and now looking more broadly across how to apply this project to future educational efforts.”
The project certainly had its challenges, most of which were related to time constraints.
“All of us were working very hard in our respective programs,” notes Dr. McKean, “and we were doing this on a volunteer basis. I think we had 10 face-to-face meetings, and sat at our computers on Saturday afternoons for conference calls using a Web-based editing program.”
For her part, Dr. McKean found working on the core competencies “very satisfying. I think I learned a lot from other people on this task force, editorial board, and the organization of the Society of Hospital Medicine. This project helped me reflect upon skills that I should try to obtain, and to think about more global issues than the day-to-day hospital politics in which I was involved. I did more strategic planning and thinking about retreats. So, it was a learning experience for me, and I also felt that I was contributing to something worthwhile. It was a chance to make a difference.
“From my own professional experience, the development process has helped me here, at Brigham and Women’s Hospital, so I hope that anyone who wants to apply the core competencies would feel free to e-mail us or contact us if they have any questions at all,” she says.
Dr. Pistoria agrees with Dr. McKean’s observations. “Working on the Core Competencies had a really big impact on me, both personally and professionally,” he says. “The process helped me mature in how I deal with running a project like this because I have been given the opportunity to do some similar things at my institution. Some of the ideas that we hit upon as we were editing and developing these competencies make one think, ‘We need to do this at our institution.’ Let’s take a strong look at, say, discharge processes, get a group together, and generate some recommendations that we can then institute.”
Other editorial board members also acknowledged that their participation gave them new insights into their own practice of hospital medicine.
“It’s easy to have in your head what you think is the right thing to do,” notes Dr. Dressler, “But until you actually have to try to develop consistency in wording and expectations, to put a process together that can result in a protocol, you realize that sometimes some elements get left out—for instance, the importance of family communication in the setting of DVT.”
Regarding the board members’ hard work, Budnitz remarks, “I can’t say enough about the dedication of the editorial board. They volunteered a tremendous amount of time and stuck with the project for three years. Since the board lived in multiple time zones, we often had calls where people would be participating at 6 a.m. or 9 p.m. We convened on weekends in multiple cities across the U.S. I sincerely enjoyed the opportunity to be a part of this project and hopefully impact the future of medical education.
“I think the document makes a bold statement. It defines the hospitalist as the captain of the ship—and calls on hospitalists to lead multidisciplinary teams to improve the quality of care. I hope it sparks interest and debate about how we recruit, train, prepare, and certify physicians in hospital medicine.”
Dr. Pistoria believes that the Core Competencies will advance hospitalist programs. In fact, he says, hospitalists around the country have already affected improvements in care coordination. The hospitalist movement in general furnishes hospitals with physicians who say, “ ‘I’m going to take ownership of what happens within the four walls of this hospital,’ ” says Dr. Pistoria. “Previous to that, people obviously cared about what happened in the hospital, but they also worried about their office practices. This is our office practice. We want it to work as well as it can for our patients, for us, for our nursing colleagues, for our janitors—everybody needs to, and should, benefit from this.” TH
Writer Gretchen Henkel wrote about cultural competency in the September issue of The Hospitalist.
Make a Difference

Welcome to 2006 and another coming-out party for SHM and hospitalists. In just a few short months more than a thousand hospitalists will come together in our nation’s capitol for the SHM Annual Meeting May 3-5, 2006. In addition to the largest convention of hospitalists, hundreds of other stakeholders in hospital medicine will gather for what has become the centerpiece of their year.
In addition to the opportunity to hear our nation’s experts talk about the up-to-date, state-of-the art medical knowledge for hospitalists, the SHM Annual Meeting is the place to find your next job, reconnect with colleagues from around the country, express your own opinions and vision for hospital medicine at the Special Interest Forums, and so much more.
SHM will be literally in the center of our nation’s capitol. It will be an opportunity for hospitalists to not only see the power center for our country, but with SHM’s help, a time for hospitalists to engage our legislators about issues important to hospitalists and our patients.
Taking advantage of the location of this year’s Annual Meeting, SHM’s Public Policy Committee has organized the first SHM Legislative Day on May 3, 2006. SHM meeting attendees can voluntarily sign up to meet with their congressmen and senators and their staffs.
SHM will make all the appointments for these Congressional visits. In addition, May 3 will kick off with a Washington overview and practical sessions on how best to approach your legislators to get your message across.
In addition, SHM has been working with HPA, a nationally recognized information resource in D.C. to put together a “Hospital Medicine White Paper” to concisely describe the emerging specialty of hospital medicine and how our perspectives and ideas are important to the healthcare debate.
The white paper will be a useful document to leave with your legislator and to use as a reference for your discussions. It will also contain some suggested policy recommendations supported by the SHM Board that can form the basis of what we would like to see move forward in Congress and on the Hill.
I have participated in many of these Legislative Days in my time on the ASIM and ACP Boards. I have found the legislators and their staffs interested in hearing from a passionate, informed part of their constituencies. Often these conversations were informal and personal and led to an ongoing relationship that continued when we were back home. I looked forward to coming back to Washington to renew our discussions.
And there can be real tangible changes as a result of these Congressional visits. I have seen changes in Medicare scope of benefits and reimbursement and methodologies based on messages I carried with the support of my professional medical societies.
Hospitalists are in a unique position to influence the current and future medical debates in Washington. We are young (average age 37) with a long professional career ahead of us. Hospitalists are at the center of many issues and initiatives that affect hospitals and the acutely ill patients they treat. Hospitalists measure and improve inpatient healthcare in an era of decreasing resources and increasing expectations.
Right now there is significant activity in pay for performance and in developing quality performance measures. There is also debate on gain-sharing and discussions of reducing and reshaping reimbursement for physicians. There are discussions on how to fund medical education and how to make sure all Americans get healthcare—even the 45 million without any insurance coverage. There are issues of access and limitations of crowded emergency departments and hospitals running at capacity.
There is no shortage of ideas and proposals, and most of these will affect hospitalists and the patients we treat and the hospitals we work in. In many ways these issues will shape our professional futures and determine how satisfying a career as a physician and specifically as a hospitalist will be.
Hospitalists and SHM must be part of the dialogue. We must clearly state where we stand and be prepared to back this up with data and to propose realistic solutions we are prepared to implement.
So clear your schedules May 3-5, 2006, and come to Washington, D.C., to join more than a thousand of your hospitalist colleagues as we take our first determined steps at the power center of our country. SHM will provide the support and materials for your success. But you must supply the voice and the presence. We owe no less to our profession and our patients now and in the future. TH
Dr. Wellikson has been CEO of SHM since 2000.
Welcome to 2006 and another coming-out party for SHM and hospitalists. In just a few short months more than a thousand hospitalists will come together in our nation’s capitol for the SHM Annual Meeting May 3-5, 2006. In addition to the largest convention of hospitalists, hundreds of other stakeholders in hospital medicine will gather for what has become the centerpiece of their year.
In addition to the opportunity to hear our nation’s experts talk about the up-to-date, state-of-the art medical knowledge for hospitalists, the SHM Annual Meeting is the place to find your next job, reconnect with colleagues from around the country, express your own opinions and vision for hospital medicine at the Special Interest Forums, and so much more.
SHM will be literally in the center of our nation’s capitol. It will be an opportunity for hospitalists to not only see the power center for our country, but with SHM’s help, a time for hospitalists to engage our legislators about issues important to hospitalists and our patients.
Taking advantage of the location of this year’s Annual Meeting, SHM’s Public Policy Committee has organized the first SHM Legislative Day on May 3, 2006. SHM meeting attendees can voluntarily sign up to meet with their congressmen and senators and their staffs.
SHM will make all the appointments for these Congressional visits. In addition, May 3 will kick off with a Washington overview and practical sessions on how best to approach your legislators to get your message across.
In addition, SHM has been working with HPA, a nationally recognized information resource in D.C. to put together a “Hospital Medicine White Paper” to concisely describe the emerging specialty of hospital medicine and how our perspectives and ideas are important to the healthcare debate.
The white paper will be a useful document to leave with your legislator and to use as a reference for your discussions. It will also contain some suggested policy recommendations supported by the SHM Board that can form the basis of what we would like to see move forward in Congress and on the Hill.
I have participated in many of these Legislative Days in my time on the ASIM and ACP Boards. I have found the legislators and their staffs interested in hearing from a passionate, informed part of their constituencies. Often these conversations were informal and personal and led to an ongoing relationship that continued when we were back home. I looked forward to coming back to Washington to renew our discussions.
And there can be real tangible changes as a result of these Congressional visits. I have seen changes in Medicare scope of benefits and reimbursement and methodologies based on messages I carried with the support of my professional medical societies.
Hospitalists are in a unique position to influence the current and future medical debates in Washington. We are young (average age 37) with a long professional career ahead of us. Hospitalists are at the center of many issues and initiatives that affect hospitals and the acutely ill patients they treat. Hospitalists measure and improve inpatient healthcare in an era of decreasing resources and increasing expectations.
Right now there is significant activity in pay for performance and in developing quality performance measures. There is also debate on gain-sharing and discussions of reducing and reshaping reimbursement for physicians. There are discussions on how to fund medical education and how to make sure all Americans get healthcare—even the 45 million without any insurance coverage. There are issues of access and limitations of crowded emergency departments and hospitals running at capacity.
There is no shortage of ideas and proposals, and most of these will affect hospitalists and the patients we treat and the hospitals we work in. In many ways these issues will shape our professional futures and determine how satisfying a career as a physician and specifically as a hospitalist will be.
Hospitalists and SHM must be part of the dialogue. We must clearly state where we stand and be prepared to back this up with data and to propose realistic solutions we are prepared to implement.
So clear your schedules May 3-5, 2006, and come to Washington, D.C., to join more than a thousand of your hospitalist colleagues as we take our first determined steps at the power center of our country. SHM will provide the support and materials for your success. But you must supply the voice and the presence. We owe no less to our profession and our patients now and in the future. TH
Dr. Wellikson has been CEO of SHM since 2000.
Welcome to 2006 and another coming-out party for SHM and hospitalists. In just a few short months more than a thousand hospitalists will come together in our nation’s capitol for the SHM Annual Meeting May 3-5, 2006. In addition to the largest convention of hospitalists, hundreds of other stakeholders in hospital medicine will gather for what has become the centerpiece of their year.
In addition to the opportunity to hear our nation’s experts talk about the up-to-date, state-of-the art medical knowledge for hospitalists, the SHM Annual Meeting is the place to find your next job, reconnect with colleagues from around the country, express your own opinions and vision for hospital medicine at the Special Interest Forums, and so much more.
SHM will be literally in the center of our nation’s capitol. It will be an opportunity for hospitalists to not only see the power center for our country, but with SHM’s help, a time for hospitalists to engage our legislators about issues important to hospitalists and our patients.
Taking advantage of the location of this year’s Annual Meeting, SHM’s Public Policy Committee has organized the first SHM Legislative Day on May 3, 2006. SHM meeting attendees can voluntarily sign up to meet with their congressmen and senators and their staffs.
SHM will make all the appointments for these Congressional visits. In addition, May 3 will kick off with a Washington overview and practical sessions on how best to approach your legislators to get your message across.
In addition, SHM has been working with HPA, a nationally recognized information resource in D.C. to put together a “Hospital Medicine White Paper” to concisely describe the emerging specialty of hospital medicine and how our perspectives and ideas are important to the healthcare debate.
The white paper will be a useful document to leave with your legislator and to use as a reference for your discussions. It will also contain some suggested policy recommendations supported by the SHM Board that can form the basis of what we would like to see move forward in Congress and on the Hill.
I have participated in many of these Legislative Days in my time on the ASIM and ACP Boards. I have found the legislators and their staffs interested in hearing from a passionate, informed part of their constituencies. Often these conversations were informal and personal and led to an ongoing relationship that continued when we were back home. I looked forward to coming back to Washington to renew our discussions.
And there can be real tangible changes as a result of these Congressional visits. I have seen changes in Medicare scope of benefits and reimbursement and methodologies based on messages I carried with the support of my professional medical societies.
Hospitalists are in a unique position to influence the current and future medical debates in Washington. We are young (average age 37) with a long professional career ahead of us. Hospitalists are at the center of many issues and initiatives that affect hospitals and the acutely ill patients they treat. Hospitalists measure and improve inpatient healthcare in an era of decreasing resources and increasing expectations.
Right now there is significant activity in pay for performance and in developing quality performance measures. There is also debate on gain-sharing and discussions of reducing and reshaping reimbursement for physicians. There are discussions on how to fund medical education and how to make sure all Americans get healthcare—even the 45 million without any insurance coverage. There are issues of access and limitations of crowded emergency departments and hospitals running at capacity.
There is no shortage of ideas and proposals, and most of these will affect hospitalists and the patients we treat and the hospitals we work in. In many ways these issues will shape our professional futures and determine how satisfying a career as a physician and specifically as a hospitalist will be.
Hospitalists and SHM must be part of the dialogue. We must clearly state where we stand and be prepared to back this up with data and to propose realistic solutions we are prepared to implement.
So clear your schedules May 3-5, 2006, and come to Washington, D.C., to join more than a thousand of your hospitalist colleagues as we take our first determined steps at the power center of our country. SHM will provide the support and materials for your success. But you must supply the voice and the presence. We owe no less to our profession and our patients now and in the future. TH
Dr. Wellikson has been CEO of SHM since 2000.
Afghan Revival
Editors’ note: During 2006 we will publish coverage of hospital practices in other countries. This is the first article in that effort.
Over the past two decades Afghanistan became known to many for its invasion by the Soviets (the war the mujahideen fought against its occupiers), the bloody infighting that followed the Soviet withdrawal, and the horrific rule of the Taliban. The expulsion of the Taliban in 2001 by coalition forces and Afghanistan’s recent steps toward democracy have made it the focus of much world attention.
Afghanistan’s health situation is among the worst in the world.1 The data that emerged in 2002 after the fall of the Taliban reported a maternal mortality ratio of 1,600 per 100,000 women, which translates into a lifetime risk that one in six women will die of complications of pregnancy and delivery.2-3 The same study showed severe inequities in mortality rates between rural and urban areas: Kabul’s maternal mortality ratio is 400 per 100,000, whereas in rural Badakhshan province it is 6,500 per 100,000—the highest recorded rate in the world in modern times.2 Afghanistan is the only country in the world where men outlive women. Twenty-five percent of children die before age five—most of treatable diseases such as diarrhea and pneumonia, and preventable diseases such as measles and pertussis. Children, women, and men face risks from communicable diseases that are among the highest in the world, as well as the risk of death or serious injury from landmines and other unexploded ordnance.
In this setting, the Ministry of Public Health made two major decisions in 2002: All health services would be contracted to nongovernmental organizations and the Ministry would be the steward of the health system, setting policies and regulating services; and the Basic Package of Health Services would be the main policy that all service providers would follow.4-5 This package defines specific services focused on women’s and children’s needs by level and by appropriate intervention.6 The Basic Package also stresses equity by giving priority to rural over urban areas and to women’s participation over men’s. A related policy on hospitals limits spending on hospitals to 40% of the national health budget, with the remaining 60% to be spent on basic health services.7
State of Hospitals
Many health facilities—especially hospitals—had been damaged or destroyed. A survey of all health facilities in the country by Management Sciences for Health (MSH) in 2002, with funding from the U.S. Agency for International Development and other donors, found that 35% of the facilities were severely damaged due to war or natural disasters, and the rest failed to meet current World Health Organization standards.8 A second major concern was the lack of health professionals, many of whom had fled the country during the war years. Finally, the staff remaining, especially physicians, lacked good clinical training and continuing education, which compromised quality of care. The Rural Expansion of Afghanistan’s Community-based Healthcare (REACH) was designed to address all these issues. REACH is a program funded by the U.S. Agency for International Development and implemented by MSH and the Afghan Ministry of Public Health. Partners include the Academy for Educational Development; JHPIEGO (an international health organization affiliated with Johns Hopkins University); Technical Assistance, Inc., and the University of Massachusetts/Amherst.
Hospitals are a critical element of the Afghan health system because they are part of the referral system that plays an essential role in reducing high maternal and early childhood mortality rates. In addition, hospitals use many of the most skilled health workers and the financial resources of the health system. Dramatic improvements in hospital management are needed so hospitals can use these scarce resources effectively and efficiently.9

Challenges
In brief, the key issues facing hospitals in the Afghan health system are:
- Maldistribution of hospitals and hospital beds throughout the country, which means a lack of equitable access to hospital care. People in urban areas have access but semi-urban and rural populations have limited access. For example, Kabul has 1.28 beds per 1,000 people while the provinces have only .22 per 1,000;
- Lack of standards for clinical patient care, resulting in poor quality of care; and
- Lack of hospital management skills, which results in inefficiently run hospitals, poorly managed staff, lack of supplies, and inoperable equipment due to lack of maintenance.10
Response: The Hospital Management Improvement Initiative
REACH began helping to rebuild the health sector in 2003. Initial efforts focused on expanding basic services, and in two years we have moved from 5% to 77% coverage of the population of Afghanistan. In 2004, the contract was amended to include the hospital sector, with a focus on provincial hospitals. REACH developed the Hospital Management Improvement Initiative to build the clinical and management capacity of hospitals so that:
- Health services are delivered more efficiently;
- The quality of services are improved;
- The population has increased access to hospital services; and
- There is a positive impact on health status—especially on the morbidity and mortality of women and children.
Introducing clinical and management improvements, combined with appropriate resources, will improve quality of care, increase access to hospital services, and streamline hospital operations. These improvements will ultimately result in achievement of the goals of improved health status, improved patient and community satisfaction with hospitals, and an improved referral system for Afghanistan.
Although the need was great, it was not possible to train the management team at each hospital in Afghanistan. Instead, clinical and management capacities at the provincial and central hospitals were strengthened through training, mentoring, networking and modeling, and provision of resources.

Areas of Standards for Hospitals in Afghanistan Governance
- Hospital community board*
Clinical Services
- Internal medicine
- General surgery *
- Anesthesia*
- Obstetrics and gynecology*
- Pediatrics*
- Emergency care*
- Outpatient department
- Infection prevention*
Diagnostic/Ancillary Services
- Laboratory
- Blood transfusion/blood bank*
- Radiology/x-ray
- Pharmacy*
Nursing Services
- Nursing care in patient wards
- Central service/sterilization
- Operating theater
Administration and Support Services
- Medical records
- Human resource (personnel) management*
- Housekeeping
- Catering/food service
- Laundry
- Facilities and equipment maintenance*
- Purchasing/medical stores
- Business office and administration
*=Standards developed and implemented at five provincial hospitals as of Sept. 2005.
Training
The Standards Based Management/Performance Quality Improvement approach that JHPIEGO has successfully developed and used to improve the quality of reproductive health services in many resource-poor settings has been expanded and adapted by REACH into a comprehensive approach to improve hospital management in Afghanistan. This process includes all clinical services (surgery, anesthesia, emergency care, pediatrics, infection prevention, and blood transfusion and blood banks) and management systems (governance, facilities and equipment management, pharmacy management, human resource systems) for general hospitals.
Standards were developed in each of these areas, and training modules developed. Eight workshops have been held to train key staff from each hospital, who return to their hospitals to introduce the standards to their medical and administrative staff. Each workshop produces a plan for implementing the standards according to the circumstances of each hospital. The training is incremental. For instance, rather than doing a one- to two-week workshop presenting all the training modules, two modules on standards (usually one clinical and one management area) are presented. Two new modules are presented quarterly thereafter, to prevent information overload, allow trainees to integrate what they have learned with real day-to-day management, and avoid the problem of hospitals being left without leadership for an extended period.
Mentoring
A skilled hospital management advisor visits the hospitals regularly so managers have the opportunity to work with a mentor to apply what they have learned to their hospitals. This practical experience involves applying principles to real-life situations with someone experienced enough to help overcome obstacles not anticipated in the workshops. Mentors from REACH and the Ministry of Public Health visit the provincial hospitals to discuss problems, review progress, talk about problems that prevented achievement of goals, and set goals for the next three-month period.
The first four provincial hospitals selected for this intervention are all in areas formerly controlled by the Taliban, and security issues have added other challenges to this program because of repeated terrorist attacks on non-governmental organizations and people employed by international organizations. The mentors involved must speak Pashto, the local language, and integrate into the culture so they do not attract attention or create local opposition. Mentoring is a necessary but dangerous activity for the success of the program.
Networking and Modeling
As more hospital managers and senior clinicians are trained through this program, networking becomes another important tool. The network uses meetings twice a year for two days in a participating hospital to provide an opportunity for hospital managers to discuss common issues and develop system-wide solutions. Between these meetings, hospital managers in the same region exchange visits to learn from each other. REACH facilitates this networking using e-mail (some of the provincial hospitals have Internet access, which has dramatically increased their participation in evidence-based approaches), dissemination of reports, and passing on requests for communication between hospitals. These formal meetings and informal exchanges permit hospital managers to interact about common problems and learn how other hospitals have solved those problems. This networking will slowly expand to cover more provincial hospitals and will assist in expanding the number of trainers and mentors.
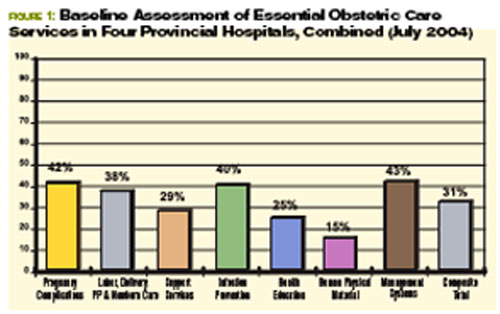
Modeling means trying new systems and methods generated by the trainees to address their self-identified problems. Improvements in five provincial hospitals (in Khost, Paktika, Paktia, Ghazni, and Badakhshan) will provide a model that demonstrates to the public that hospitals can be well run and serve the community. These hospitals can also be used as training grounds for other hospital managers from around the country as the initiative expands to more of the remaining 28 provincial hospitals. The goal is to develop optimism and creativity because one of the main barriers in training is that some managers have difficulty imagining things being different because they feel the system “has always been broken.” When trainees see that other hospitals have successfully tried new approaches, they will consider a broader range of possibilities for their own hospitals.
Resources
Along with the management improvements achieved through training, mentoring, and networking, additional resources are needed to improve hospital services. REACH has been the conduit for U.S. government funding, providing $2.6 million in critical resources to drive improvements in the five provincial hospitals. These funds are channeled through the contracted nongovernmental organizations, which hire staff and pay decent salaries.
The average hospital physician in the Ministry of Public Health is paid $50 a month. In this setting “under-the-table” charges for clinical services are common, and physicians usually leave the hospital by lunch to attend to their private clinics. This initiative pays physicians up to $500 a month with the expectations that they will work a full day, provide 24-hour emergency coverage, and not charge patients. Eighteen months of experience suggest that these expectations are being met. Resources are also used for remodeling facilities, purchasing equipment and supplies, and providing essential medicines. The management standards developed are designed to make rational use of these scarce resources.
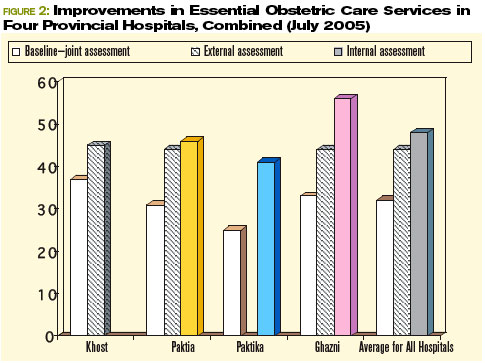
Prerequisites for the Initiative
Two key prerequisites for starting the Hospital Management Initiative were:
- Identifying where standards had to be developed: REACH has assisted the Ministry of Public Health to identify the standards that must be developed: responsibilities of hospitals to the community, patient care (clinical care), human resource management, management systems, environmental health, and leadership and management.10 “Areas of Standards for Hospitals in Afghanistan” shows the standards that have been or are to be developed. (See sidebar at left.)
- Essential Package of Hospital Services: To ensure that donor support does not stimulate a proliferation of hospitals and high-tech equipment that are not appropriate or sustainable for Afghanistan, REACH has been helping the Ministry of Public Health define the levels of hospitals (district, provincial, regional), the populations they serve, the services they offer, and the equipment, staff, supplies, and pharmaceuticals they need. The result was the publication of the Essential Package of Hospital Services, which defines these for each of the three levels of hospitals in the country, in 2005. This package will provide guidance for Afghanistan’s hospitals for the coming decade, much as the Basic Package of Health Services has done for primary healthcare services. The hospital package will also support long-term planning and help the Ministry make the best use of donor assistance for redeveloping the hospital sector.
Developing and Implementing Standards
Standards-based management begins by identifying existing clinical guidelines and standards developed by American or international specialty societies. Specialist consultants in each clinical area with many years’ experience in Afghanistan (some of them Afghan-American physicians) are contracted to develop these standards and then adapt them to the Afghan context, in consultation with physicians in Afghanistan.
For example, standards for acute abdominal pain had to be adapted to a situation where CAT scans and ultrasounds are not readily available, and the lack of electrolyte laboratory capacity in hospitals stimulated physicians to adapt standards for shock, and fluid and electrolyte balance that do not rely on knowing electrolyte levels. The standards development teams aimed to raise the standards of Afghan hospitals to a realistic extent but not set the bar so high that improvement was unattainable.
After the standards were developed, clinicians from Afghan hospitals reviewed and revised the standards to ensure that they were appropriate. This review also served as a means of training because the participants were able and eager to question the contracted expert about the standards in developed countries and the evidence supporting those standards. Once the standards are revised, a workshop is held to introduce them to hospital staff. The hospital teams then develop an action plan for introducing the standards into their facilities.
Quality improvement teams at each of the five hospitals take responsibility for shepherding the action plans through implementation. An advisor visits each hospital quarterly to review progress, assess barriers, and help hospital staff develop ways to overcome problems and accelerate standards implementation. During the mentor’s first visit after new standards have been introduced, he performs a baseline assessment of the hospital’s current compliance with the standards. This serves as a benchmark for future measurement of progress in meeting the standards.
The Results
The hospitals have been enthusiastic about this process and the gains they have seen in the quality of care at their facilities. “We have made more progress in four months of the Hospital Management Improvement Initiative than we made in the previous five years with many other donors because this methodology is sound and appropriate for Afghanistan,” said Dr. Mohammed Ismael, the director of Ghazni Provincial Hospital.
One example of the process and results was the first area in which standards were developed—essential obstetric care. Physicians examined seven components of the quality of emergency obstetric care: handling of pregnancy complications; labor, delivery, and postpartum and newborn care; support services; infection prevention; health education given to families and mothers; human, physical, and material resources; and management systems in the obstetrics/gynecology department. After the standards were established, the first step was to find out where each hospital stood in meeting them. (For the combined results of that first baseline assessment for four hospitals, see Figure 1, p. 20.)
The changes in standards for emergency obstetric care at the hospitals from July 2004 to July 2005 have been impressive. The overall composite scores for emergency obstetric care for the four hospitals have improved from 31% at the baseline assessment to 47%. Here are the average improvements in the same four hospitals over one year:
Lessons Learned
The principal lesson learned through this hospital management improvement initiative is that combining clinical and management improvements can create innovation in a developing country. Improvements are made throughout a hospital—not just in one clinical area. Second, mentoring has proven essential as a follow-up to training. The training alone will not bring about significant positive changes. Only with on-site visitation is there the opportunity to integrate new knowledge with practical implementation issues that have proven troublesome to overcome. Third, setting standards is key to the sustainability of improvements. Training individuals in skills is helpful but is not sustainable if those trained staff depart. Using hospital teams and common standards throughout different hospitals leads to institutionalization of the process.
Staff motivation has also proven to be essential to sustainability. Staff have been motivated because they see that many positive changes are within their control; they do not have to wait for someone else to make an improvement before they can introduce positive change. An ethic of continuous quality improvement is achieved through staff who are proud of the changes they have introduced. The iterative nature of this process has been essential to quality improvement: The standards are continually revisited and revised as needed. At times, new standards for other areas are developed when the hospitals need them. Finally, providing resources to pay adequate salaries, renovate facilities, buy equipment and supplies, and provide essential medicines are all important elements of this success.
This method has proven successful in such a short time that the Minister of Public Health, Dr. Mohammad Amin Fatimie, has expressed his desire to extend it to many other hospitals in the country in an effort to improve the quality of hospital care throughout Afghani-stan. The U.S. Agency for International Development and MSH have agreed to support this request, and the program will expand in future years. TH


Dr. Hartman, is a family physician with subspecialty training in infectious diseases, epidemiology, and public health. He serves as the technical director and deputy chief of party of the REACH Project, based in Kabul. Dr. Newbrander is a health economist who has served in Afghanistan since 2002 as a senior advisor to the Ministry of Health. He is currently Health Financing and Hospital Management Advisor for the USAID-funded REACH Project.
Acknowledgment: Funding for this article was provided by the United States Agency for International Development under the REACH Project, contract number EEE-C-00-03-00015-00. The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID.
References
- Newbrander W, Ickx P, Leitch GH. Addressing the immediate and long-term health needs in Afghanistan. Harvard Health Pol Rev. 2003;4.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA), US Centers for Disease Control and Prevention, United Nations Children’s Fund. Maternal mortality in Afghanistan: magnitude, causes, risk factors and preventability. Kabul: TISA; 2002.
- Bartlett LA, Mawji S, Whitehead S, et al. Where giving birth is a forecast of death: maternal mortality in four districts of Afghanistan, 1999-2002. Lancet. 2005;365:864-870.
- Strong L, Wali A, Sondorp E. Health Policy in Afghanistan: Two Years of Rapid Change: A Review of the Process from 2001 to 2003. London: London School of Hygiene and Tropical Medicine; 2005.
- Afghanistan’s health challenge. Lancet. 2003;362:841.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA). The Basic Package of Health Services for Afghanistan. Kabul: TISA; 2003.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA). Hospital Policy for Afghanistan’s Health System. Kabul: TISA; 2004.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA), Management Sciences for Health. Afghanistan national health resources assessment: Preliminary results. Kabul: TISA; 2002.
- A crucial time for Afghanistan’s fledgling health system. Lancet. 2005; 365:819-820.
- Ministry of Public Health (MOPH) Islamic Republic of Afghanistan. The Essential Package of Hospital Services for Afghanistan. Kabul: MOPH; 2005.
Editors’ note: During 2006 we will publish coverage of hospital practices in other countries. This is the first article in that effort.
Over the past two decades Afghanistan became known to many for its invasion by the Soviets (the war the mujahideen fought against its occupiers), the bloody infighting that followed the Soviet withdrawal, and the horrific rule of the Taliban. The expulsion of the Taliban in 2001 by coalition forces and Afghanistan’s recent steps toward democracy have made it the focus of much world attention.
Afghanistan’s health situation is among the worst in the world.1 The data that emerged in 2002 after the fall of the Taliban reported a maternal mortality ratio of 1,600 per 100,000 women, which translates into a lifetime risk that one in six women will die of complications of pregnancy and delivery.2-3 The same study showed severe inequities in mortality rates between rural and urban areas: Kabul’s maternal mortality ratio is 400 per 100,000, whereas in rural Badakhshan province it is 6,500 per 100,000—the highest recorded rate in the world in modern times.2 Afghanistan is the only country in the world where men outlive women. Twenty-five percent of children die before age five—most of treatable diseases such as diarrhea and pneumonia, and preventable diseases such as measles and pertussis. Children, women, and men face risks from communicable diseases that are among the highest in the world, as well as the risk of death or serious injury from landmines and other unexploded ordnance.
In this setting, the Ministry of Public Health made two major decisions in 2002: All health services would be contracted to nongovernmental organizations and the Ministry would be the steward of the health system, setting policies and regulating services; and the Basic Package of Health Services would be the main policy that all service providers would follow.4-5 This package defines specific services focused on women’s and children’s needs by level and by appropriate intervention.6 The Basic Package also stresses equity by giving priority to rural over urban areas and to women’s participation over men’s. A related policy on hospitals limits spending on hospitals to 40% of the national health budget, with the remaining 60% to be spent on basic health services.7
State of Hospitals
Many health facilities—especially hospitals—had been damaged or destroyed. A survey of all health facilities in the country by Management Sciences for Health (MSH) in 2002, with funding from the U.S. Agency for International Development and other donors, found that 35% of the facilities were severely damaged due to war or natural disasters, and the rest failed to meet current World Health Organization standards.8 A second major concern was the lack of health professionals, many of whom had fled the country during the war years. Finally, the staff remaining, especially physicians, lacked good clinical training and continuing education, which compromised quality of care. The Rural Expansion of Afghanistan’s Community-based Healthcare (REACH) was designed to address all these issues. REACH is a program funded by the U.S. Agency for International Development and implemented by MSH and the Afghan Ministry of Public Health. Partners include the Academy for Educational Development; JHPIEGO (an international health organization affiliated with Johns Hopkins University); Technical Assistance, Inc., and the University of Massachusetts/Amherst.
Hospitals are a critical element of the Afghan health system because they are part of the referral system that plays an essential role in reducing high maternal and early childhood mortality rates. In addition, hospitals use many of the most skilled health workers and the financial resources of the health system. Dramatic improvements in hospital management are needed so hospitals can use these scarce resources effectively and efficiently.9
Challenges
In brief, the key issues facing hospitals in the Afghan health system are:
- Maldistribution of hospitals and hospital beds throughout the country, which means a lack of equitable access to hospital care. People in urban areas have access but semi-urban and rural populations have limited access. For example, Kabul has 1.28 beds per 1,000 people while the provinces have only .22 per 1,000;
- Lack of standards for clinical patient care, resulting in poor quality of care; and
- Lack of hospital management skills, which results in inefficiently run hospitals, poorly managed staff, lack of supplies, and inoperable equipment due to lack of maintenance.10
Response: The Hospital Management Improvement Initiative
REACH began helping to rebuild the health sector in 2003. Initial efforts focused on expanding basic services, and in two years we have moved from 5% to 77% coverage of the population of Afghanistan. In 2004, the contract was amended to include the hospital sector, with a focus on provincial hospitals. REACH developed the Hospital Management Improvement Initiative to build the clinical and management capacity of hospitals so that:
- Health services are delivered more efficiently;
- The quality of services are improved;
- The population has increased access to hospital services; and
- There is a positive impact on health status—especially on the morbidity and mortality of women and children.
Introducing clinical and management improvements, combined with appropriate resources, will improve quality of care, increase access to hospital services, and streamline hospital operations. These improvements will ultimately result in achievement of the goals of improved health status, improved patient and community satisfaction with hospitals, and an improved referral system for Afghanistan.
Although the need was great, it was not possible to train the management team at each hospital in Afghanistan. Instead, clinical and management capacities at the provincial and central hospitals were strengthened through training, mentoring, networking and modeling, and provision of resources.
Areas of Standards for Hospitals in Afghanistan Governance
- Hospital community board*
Clinical Services
- Internal medicine
- General surgery *
- Anesthesia*
- Obstetrics and gynecology*
- Pediatrics*
- Emergency care*
- Outpatient department
- Infection prevention*
Diagnostic/Ancillary Services
- Laboratory
- Blood transfusion/blood bank*
- Radiology/x-ray
- Pharmacy*
Nursing Services
- Nursing care in patient wards
- Central service/sterilization
- Operating theater
Administration and Support Services
- Medical records
- Human resource (personnel) management*
- Housekeeping
- Catering/food service
- Laundry
- Facilities and equipment maintenance*
- Purchasing/medical stores
- Business office and administration
*=Standards developed and implemented at five provincial hospitals as of Sept. 2005.
Training
The Standards Based Management/Performance Quality Improvement approach that JHPIEGO has successfully developed and used to improve the quality of reproductive health services in many resource-poor settings has been expanded and adapted by REACH into a comprehensive approach to improve hospital management in Afghanistan. This process includes all clinical services (surgery, anesthesia, emergency care, pediatrics, infection prevention, and blood transfusion and blood banks) and management systems (governance, facilities and equipment management, pharmacy management, human resource systems) for general hospitals.
Standards were developed in each of these areas, and training modules developed. Eight workshops have been held to train key staff from each hospital, who return to their hospitals to introduce the standards to their medical and administrative staff. Each workshop produces a plan for implementing the standards according to the circumstances of each hospital. The training is incremental. For instance, rather than doing a one- to two-week workshop presenting all the training modules, two modules on standards (usually one clinical and one management area) are presented. Two new modules are presented quarterly thereafter, to prevent information overload, allow trainees to integrate what they have learned with real day-to-day management, and avoid the problem of hospitals being left without leadership for an extended period.
Mentoring
A skilled hospital management advisor visits the hospitals regularly so managers have the opportunity to work with a mentor to apply what they have learned to their hospitals. This practical experience involves applying principles to real-life situations with someone experienced enough to help overcome obstacles not anticipated in the workshops. Mentors from REACH and the Ministry of Public Health visit the provincial hospitals to discuss problems, review progress, talk about problems that prevented achievement of goals, and set goals for the next three-month period.
The first four provincial hospitals selected for this intervention are all in areas formerly controlled by the Taliban, and security issues have added other challenges to this program because of repeated terrorist attacks on non-governmental organizations and people employed by international organizations. The mentors involved must speak Pashto, the local language, and integrate into the culture so they do not attract attention or create local opposition. Mentoring is a necessary but dangerous activity for the success of the program.
Networking and Modeling
As more hospital managers and senior clinicians are trained through this program, networking becomes another important tool. The network uses meetings twice a year for two days in a participating hospital to provide an opportunity for hospital managers to discuss common issues and develop system-wide solutions. Between these meetings, hospital managers in the same region exchange visits to learn from each other. REACH facilitates this networking using e-mail (some of the provincial hospitals have Internet access, which has dramatically increased their participation in evidence-based approaches), dissemination of reports, and passing on requests for communication between hospitals. These formal meetings and informal exchanges permit hospital managers to interact about common problems and learn how other hospitals have solved those problems. This networking will slowly expand to cover more provincial hospitals and will assist in expanding the number of trainers and mentors.
Modeling means trying new systems and methods generated by the trainees to address their self-identified problems. Improvements in five provincial hospitals (in Khost, Paktika, Paktia, Ghazni, and Badakhshan) will provide a model that demonstrates to the public that hospitals can be well run and serve the community. These hospitals can also be used as training grounds for other hospital managers from around the country as the initiative expands to more of the remaining 28 provincial hospitals. The goal is to develop optimism and creativity because one of the main barriers in training is that some managers have difficulty imagining things being different because they feel the system “has always been broken.” When trainees see that other hospitals have successfully tried new approaches, they will consider a broader range of possibilities for their own hospitals.
Resources
Along with the management improvements achieved through training, mentoring, and networking, additional resources are needed to improve hospital services. REACH has been the conduit for U.S. government funding, providing $2.6 million in critical resources to drive improvements in the five provincial hospitals. These funds are channeled through the contracted nongovernmental organizations, which hire staff and pay decent salaries.
The average hospital physician in the Ministry of Public Health is paid $50 a month. In this setting “under-the-table” charges for clinical services are common, and physicians usually leave the hospital by lunch to attend to their private clinics. This initiative pays physicians up to $500 a month with the expectations that they will work a full day, provide 24-hour emergency coverage, and not charge patients. Eighteen months of experience suggest that these expectations are being met. Resources are also used for remodeling facilities, purchasing equipment and supplies, and providing essential medicines. The management standards developed are designed to make rational use of these scarce resources.
Prerequisites for the Initiative
Two key prerequisites for starting the Hospital Management Initiative were:
- Identifying where standards had to be developed: REACH has assisted the Ministry of Public Health to identify the standards that must be developed: responsibilities of hospitals to the community, patient care (clinical care), human resource management, management systems, environmental health, and leadership and management.10 “Areas of Standards for Hospitals in Afghanistan” shows the standards that have been or are to be developed. (See sidebar at left.)
- Essential Package of Hospital Services: To ensure that donor support does not stimulate a proliferation of hospitals and high-tech equipment that are not appropriate or sustainable for Afghanistan, REACH has been helping the Ministry of Public Health define the levels of hospitals (district, provincial, regional), the populations they serve, the services they offer, and the equipment, staff, supplies, and pharmaceuticals they need. The result was the publication of the Essential Package of Hospital Services, which defines these for each of the three levels of hospitals in the country, in 2005. This package will provide guidance for Afghanistan’s hospitals for the coming decade, much as the Basic Package of Health Services has done for primary healthcare services. The hospital package will also support long-term planning and help the Ministry make the best use of donor assistance for redeveloping the hospital sector.
Developing and Implementing Standards
Standards-based management begins by identifying existing clinical guidelines and standards developed by American or international specialty societies. Specialist consultants in each clinical area with many years’ experience in Afghanistan (some of them Afghan-American physicians) are contracted to develop these standards and then adapt them to the Afghan context, in consultation with physicians in Afghanistan.
For example, standards for acute abdominal pain had to be adapted to a situation where CAT scans and ultrasounds are not readily available, and the lack of electrolyte laboratory capacity in hospitals stimulated physicians to adapt standards for shock, and fluid and electrolyte balance that do not rely on knowing electrolyte levels. The standards development teams aimed to raise the standards of Afghan hospitals to a realistic extent but not set the bar so high that improvement was unattainable.
After the standards were developed, clinicians from Afghan hospitals reviewed and revised the standards to ensure that they were appropriate. This review also served as a means of training because the participants were able and eager to question the contracted expert about the standards in developed countries and the evidence supporting those standards. Once the standards are revised, a workshop is held to introduce them to hospital staff. The hospital teams then develop an action plan for introducing the standards into their facilities.
Quality improvement teams at each of the five hospitals take responsibility for shepherding the action plans through implementation. An advisor visits each hospital quarterly to review progress, assess barriers, and help hospital staff develop ways to overcome problems and accelerate standards implementation. During the mentor’s first visit after new standards have been introduced, he performs a baseline assessment of the hospital’s current compliance with the standards. This serves as a benchmark for future measurement of progress in meeting the standards.
The Results
The hospitals have been enthusiastic about this process and the gains they have seen in the quality of care at their facilities. “We have made more progress in four months of the Hospital Management Improvement Initiative than we made in the previous five years with many other donors because this methodology is sound and appropriate for Afghanistan,” said Dr. Mohammed Ismael, the director of Ghazni Provincial Hospital.
One example of the process and results was the first area in which standards were developed—essential obstetric care. Physicians examined seven components of the quality of emergency obstetric care: handling of pregnancy complications; labor, delivery, and postpartum and newborn care; support services; infection prevention; health education given to families and mothers; human, physical, and material resources; and management systems in the obstetrics/gynecology department. After the standards were established, the first step was to find out where each hospital stood in meeting them. (For the combined results of that first baseline assessment for four hospitals, see Figure 1, p. 20.)
The changes in standards for emergency obstetric care at the hospitals from July 2004 to July 2005 have been impressive. The overall composite scores for emergency obstetric care for the four hospitals have improved from 31% at the baseline assessment to 47%. Here are the average improvements in the same four hospitals over one year:
Lessons Learned
The principal lesson learned through this hospital management improvement initiative is that combining clinical and management improvements can create innovation in a developing country. Improvements are made throughout a hospital—not just in one clinical area. Second, mentoring has proven essential as a follow-up to training. The training alone will not bring about significant positive changes. Only with on-site visitation is there the opportunity to integrate new knowledge with practical implementation issues that have proven troublesome to overcome. Third, setting standards is key to the sustainability of improvements. Training individuals in skills is helpful but is not sustainable if those trained staff depart. Using hospital teams and common standards throughout different hospitals leads to institutionalization of the process.
Staff motivation has also proven to be essential to sustainability. Staff have been motivated because they see that many positive changes are within their control; they do not have to wait for someone else to make an improvement before they can introduce positive change. An ethic of continuous quality improvement is achieved through staff who are proud of the changes they have introduced. The iterative nature of this process has been essential to quality improvement: The standards are continually revisited and revised as needed. At times, new standards for other areas are developed when the hospitals need them. Finally, providing resources to pay adequate salaries, renovate facilities, buy equipment and supplies, and provide essential medicines are all important elements of this success.
This method has proven successful in such a short time that the Minister of Public Health, Dr. Mohammad Amin Fatimie, has expressed his desire to extend it to many other hospitals in the country in an effort to improve the quality of hospital care throughout Afghani-stan. The U.S. Agency for International Development and MSH have agreed to support this request, and the program will expand in future years. TH
Dr. Hartman, is a family physician with subspecialty training in infectious diseases, epidemiology, and public health. He serves as the technical director and deputy chief of party of the REACH Project, based in Kabul. Dr. Newbrander is a health economist who has served in Afghanistan since 2002 as a senior advisor to the Ministry of Health. He is currently Health Financing and Hospital Management Advisor for the USAID-funded REACH Project.
Acknowledgment: Funding for this article was provided by the United States Agency for International Development under the REACH Project, contract number EEE-C-00-03-00015-00. The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID.
References
- Newbrander W, Ickx P, Leitch GH. Addressing the immediate and long-term health needs in Afghanistan. Harvard Health Pol Rev. 2003;4.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA), US Centers for Disease Control and Prevention, United Nations Children’s Fund. Maternal mortality in Afghanistan: magnitude, causes, risk factors and preventability. Kabul: TISA; 2002.
- Bartlett LA, Mawji S, Whitehead S, et al. Where giving birth is a forecast of death: maternal mortality in four districts of Afghanistan, 1999-2002. Lancet. 2005;365:864-870.
- Strong L, Wali A, Sondorp E. Health Policy in Afghanistan: Two Years of Rapid Change: A Review of the Process from 2001 to 2003. London: London School of Hygiene and Tropical Medicine; 2005.
- Afghanistan’s health challenge. Lancet. 2003;362:841.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA). The Basic Package of Health Services for Afghanistan. Kabul: TISA; 2003.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA). Hospital Policy for Afghanistan’s Health System. Kabul: TISA; 2004.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA), Management Sciences for Health. Afghanistan national health resources assessment: Preliminary results. Kabul: TISA; 2002.
- A crucial time for Afghanistan’s fledgling health system. Lancet. 2005; 365:819-820.
- Ministry of Public Health (MOPH) Islamic Republic of Afghanistan. The Essential Package of Hospital Services for Afghanistan. Kabul: MOPH; 2005.
Editors’ note: During 2006 we will publish coverage of hospital practices in other countries. This is the first article in that effort.
Over the past two decades Afghanistan became known to many for its invasion by the Soviets (the war the mujahideen fought against its occupiers), the bloody infighting that followed the Soviet withdrawal, and the horrific rule of the Taliban. The expulsion of the Taliban in 2001 by coalition forces and Afghanistan’s recent steps toward democracy have made it the focus of much world attention.
Afghanistan’s health situation is among the worst in the world.1 The data that emerged in 2002 after the fall of the Taliban reported a maternal mortality ratio of 1,600 per 100,000 women, which translates into a lifetime risk that one in six women will die of complications of pregnancy and delivery.2-3 The same study showed severe inequities in mortality rates between rural and urban areas: Kabul’s maternal mortality ratio is 400 per 100,000, whereas in rural Badakhshan province it is 6,500 per 100,000—the highest recorded rate in the world in modern times.2 Afghanistan is the only country in the world where men outlive women. Twenty-five percent of children die before age five—most of treatable diseases such as diarrhea and pneumonia, and preventable diseases such as measles and pertussis. Children, women, and men face risks from communicable diseases that are among the highest in the world, as well as the risk of death or serious injury from landmines and other unexploded ordnance.
In this setting, the Ministry of Public Health made two major decisions in 2002: All health services would be contracted to nongovernmental organizations and the Ministry would be the steward of the health system, setting policies and regulating services; and the Basic Package of Health Services would be the main policy that all service providers would follow.4-5 This package defines specific services focused on women’s and children’s needs by level and by appropriate intervention.6 The Basic Package also stresses equity by giving priority to rural over urban areas and to women’s participation over men’s. A related policy on hospitals limits spending on hospitals to 40% of the national health budget, with the remaining 60% to be spent on basic health services.7
State of Hospitals
Many health facilities—especially hospitals—had been damaged or destroyed. A survey of all health facilities in the country by Management Sciences for Health (MSH) in 2002, with funding from the U.S. Agency for International Development and other donors, found that 35% of the facilities were severely damaged due to war or natural disasters, and the rest failed to meet current World Health Organization standards.8 A second major concern was the lack of health professionals, many of whom had fled the country during the war years. Finally, the staff remaining, especially physicians, lacked good clinical training and continuing education, which compromised quality of care. The Rural Expansion of Afghanistan’s Community-based Healthcare (REACH) was designed to address all these issues. REACH is a program funded by the U.S. Agency for International Development and implemented by MSH and the Afghan Ministry of Public Health. Partners include the Academy for Educational Development; JHPIEGO (an international health organization affiliated with Johns Hopkins University); Technical Assistance, Inc., and the University of Massachusetts/Amherst.
Hospitals are a critical element of the Afghan health system because they are part of the referral system that plays an essential role in reducing high maternal and early childhood mortality rates. In addition, hospitals use many of the most skilled health workers and the financial resources of the health system. Dramatic improvements in hospital management are needed so hospitals can use these scarce resources effectively and efficiently.9
Challenges
In brief, the key issues facing hospitals in the Afghan health system are:
- Maldistribution of hospitals and hospital beds throughout the country, which means a lack of equitable access to hospital care. People in urban areas have access but semi-urban and rural populations have limited access. For example, Kabul has 1.28 beds per 1,000 people while the provinces have only .22 per 1,000;
- Lack of standards for clinical patient care, resulting in poor quality of care; and
- Lack of hospital management skills, which results in inefficiently run hospitals, poorly managed staff, lack of supplies, and inoperable equipment due to lack of maintenance.10
Response: The Hospital Management Improvement Initiative
REACH began helping to rebuild the health sector in 2003. Initial efforts focused on expanding basic services, and in two years we have moved from 5% to 77% coverage of the population of Afghanistan. In 2004, the contract was amended to include the hospital sector, with a focus on provincial hospitals. REACH developed the Hospital Management Improvement Initiative to build the clinical and management capacity of hospitals so that:
- Health services are delivered more efficiently;
- The quality of services are improved;
- The population has increased access to hospital services; and
- There is a positive impact on health status—especially on the morbidity and mortality of women and children.
Introducing clinical and management improvements, combined with appropriate resources, will improve quality of care, increase access to hospital services, and streamline hospital operations. These improvements will ultimately result in achievement of the goals of improved health status, improved patient and community satisfaction with hospitals, and an improved referral system for Afghanistan.
Although the need was great, it was not possible to train the management team at each hospital in Afghanistan. Instead, clinical and management capacities at the provincial and central hospitals were strengthened through training, mentoring, networking and modeling, and provision of resources.
Areas of Standards for Hospitals in Afghanistan Governance
- Hospital community board*
Clinical Services
- Internal medicine
- General surgery *
- Anesthesia*
- Obstetrics and gynecology*
- Pediatrics*
- Emergency care*
- Outpatient department
- Infection prevention*
Diagnostic/Ancillary Services
- Laboratory
- Blood transfusion/blood bank*
- Radiology/x-ray
- Pharmacy*
Nursing Services
- Nursing care in patient wards
- Central service/sterilization
- Operating theater
Administration and Support Services
- Medical records
- Human resource (personnel) management*
- Housekeeping
- Catering/food service
- Laundry
- Facilities and equipment maintenance*
- Purchasing/medical stores
- Business office and administration
*=Standards developed and implemented at five provincial hospitals as of Sept. 2005.
Training
The Standards Based Management/Performance Quality Improvement approach that JHPIEGO has successfully developed and used to improve the quality of reproductive health services in many resource-poor settings has been expanded and adapted by REACH into a comprehensive approach to improve hospital management in Afghanistan. This process includes all clinical services (surgery, anesthesia, emergency care, pediatrics, infection prevention, and blood transfusion and blood banks) and management systems (governance, facilities and equipment management, pharmacy management, human resource systems) for general hospitals.
Standards were developed in each of these areas, and training modules developed. Eight workshops have been held to train key staff from each hospital, who return to their hospitals to introduce the standards to their medical and administrative staff. Each workshop produces a plan for implementing the standards according to the circumstances of each hospital. The training is incremental. For instance, rather than doing a one- to two-week workshop presenting all the training modules, two modules on standards (usually one clinical and one management area) are presented. Two new modules are presented quarterly thereafter, to prevent information overload, allow trainees to integrate what they have learned with real day-to-day management, and avoid the problem of hospitals being left without leadership for an extended period.
Mentoring
A skilled hospital management advisor visits the hospitals regularly so managers have the opportunity to work with a mentor to apply what they have learned to their hospitals. This practical experience involves applying principles to real-life situations with someone experienced enough to help overcome obstacles not anticipated in the workshops. Mentors from REACH and the Ministry of Public Health visit the provincial hospitals to discuss problems, review progress, talk about problems that prevented achievement of goals, and set goals for the next three-month period.
The first four provincial hospitals selected for this intervention are all in areas formerly controlled by the Taliban, and security issues have added other challenges to this program because of repeated terrorist attacks on non-governmental organizations and people employed by international organizations. The mentors involved must speak Pashto, the local language, and integrate into the culture so they do not attract attention or create local opposition. Mentoring is a necessary but dangerous activity for the success of the program.
Networking and Modeling
As more hospital managers and senior clinicians are trained through this program, networking becomes another important tool. The network uses meetings twice a year for two days in a participating hospital to provide an opportunity for hospital managers to discuss common issues and develop system-wide solutions. Between these meetings, hospital managers in the same region exchange visits to learn from each other. REACH facilitates this networking using e-mail (some of the provincial hospitals have Internet access, which has dramatically increased their participation in evidence-based approaches), dissemination of reports, and passing on requests for communication between hospitals. These formal meetings and informal exchanges permit hospital managers to interact about common problems and learn how other hospitals have solved those problems. This networking will slowly expand to cover more provincial hospitals and will assist in expanding the number of trainers and mentors.
Modeling means trying new systems and methods generated by the trainees to address their self-identified problems. Improvements in five provincial hospitals (in Khost, Paktika, Paktia, Ghazni, and Badakhshan) will provide a model that demonstrates to the public that hospitals can be well run and serve the community. These hospitals can also be used as training grounds for other hospital managers from around the country as the initiative expands to more of the remaining 28 provincial hospitals. The goal is to develop optimism and creativity because one of the main barriers in training is that some managers have difficulty imagining things being different because they feel the system “has always been broken.” When trainees see that other hospitals have successfully tried new approaches, they will consider a broader range of possibilities for their own hospitals.
Resources
Along with the management improvements achieved through training, mentoring, and networking, additional resources are needed to improve hospital services. REACH has been the conduit for U.S. government funding, providing $2.6 million in critical resources to drive improvements in the five provincial hospitals. These funds are channeled through the contracted nongovernmental organizations, which hire staff and pay decent salaries.
The average hospital physician in the Ministry of Public Health is paid $50 a month. In this setting “under-the-table” charges for clinical services are common, and physicians usually leave the hospital by lunch to attend to their private clinics. This initiative pays physicians up to $500 a month with the expectations that they will work a full day, provide 24-hour emergency coverage, and not charge patients. Eighteen months of experience suggest that these expectations are being met. Resources are also used for remodeling facilities, purchasing equipment and supplies, and providing essential medicines. The management standards developed are designed to make rational use of these scarce resources.
Prerequisites for the Initiative
Two key prerequisites for starting the Hospital Management Initiative were:
- Identifying where standards had to be developed: REACH has assisted the Ministry of Public Health to identify the standards that must be developed: responsibilities of hospitals to the community, patient care (clinical care), human resource management, management systems, environmental health, and leadership and management.10 “Areas of Standards for Hospitals in Afghanistan” shows the standards that have been or are to be developed. (See sidebar at left.)
- Essential Package of Hospital Services: To ensure that donor support does not stimulate a proliferation of hospitals and high-tech equipment that are not appropriate or sustainable for Afghanistan, REACH has been helping the Ministry of Public Health define the levels of hospitals (district, provincial, regional), the populations they serve, the services they offer, and the equipment, staff, supplies, and pharmaceuticals they need. The result was the publication of the Essential Package of Hospital Services, which defines these for each of the three levels of hospitals in the country, in 2005. This package will provide guidance for Afghanistan’s hospitals for the coming decade, much as the Basic Package of Health Services has done for primary healthcare services. The hospital package will also support long-term planning and help the Ministry make the best use of donor assistance for redeveloping the hospital sector.
Developing and Implementing Standards
Standards-based management begins by identifying existing clinical guidelines and standards developed by American or international specialty societies. Specialist consultants in each clinical area with many years’ experience in Afghanistan (some of them Afghan-American physicians) are contracted to develop these standards and then adapt them to the Afghan context, in consultation with physicians in Afghanistan.
For example, standards for acute abdominal pain had to be adapted to a situation where CAT scans and ultrasounds are not readily available, and the lack of electrolyte laboratory capacity in hospitals stimulated physicians to adapt standards for shock, and fluid and electrolyte balance that do not rely on knowing electrolyte levels. The standards development teams aimed to raise the standards of Afghan hospitals to a realistic extent but not set the bar so high that improvement was unattainable.
After the standards were developed, clinicians from Afghan hospitals reviewed and revised the standards to ensure that they were appropriate. This review also served as a means of training because the participants were able and eager to question the contracted expert about the standards in developed countries and the evidence supporting those standards. Once the standards are revised, a workshop is held to introduce them to hospital staff. The hospital teams then develop an action plan for introducing the standards into their facilities.
Quality improvement teams at each of the five hospitals take responsibility for shepherding the action plans through implementation. An advisor visits each hospital quarterly to review progress, assess barriers, and help hospital staff develop ways to overcome problems and accelerate standards implementation. During the mentor’s first visit after new standards have been introduced, he performs a baseline assessment of the hospital’s current compliance with the standards. This serves as a benchmark for future measurement of progress in meeting the standards.
The Results
The hospitals have been enthusiastic about this process and the gains they have seen in the quality of care at their facilities. “We have made more progress in four months of the Hospital Management Improvement Initiative than we made in the previous five years with many other donors because this methodology is sound and appropriate for Afghanistan,” said Dr. Mohammed Ismael, the director of Ghazni Provincial Hospital.
One example of the process and results was the first area in which standards were developed—essential obstetric care. Physicians examined seven components of the quality of emergency obstetric care: handling of pregnancy complications; labor, delivery, and postpartum and newborn care; support services; infection prevention; health education given to families and mothers; human, physical, and material resources; and management systems in the obstetrics/gynecology department. After the standards were established, the first step was to find out where each hospital stood in meeting them. (For the combined results of that first baseline assessment for four hospitals, see Figure 1, p. 20.)
The changes in standards for emergency obstetric care at the hospitals from July 2004 to July 2005 have been impressive. The overall composite scores for emergency obstetric care for the four hospitals have improved from 31% at the baseline assessment to 47%. Here are the average improvements in the same four hospitals over one year:
Lessons Learned
The principal lesson learned through this hospital management improvement initiative is that combining clinical and management improvements can create innovation in a developing country. Improvements are made throughout a hospital—not just in one clinical area. Second, mentoring has proven essential as a follow-up to training. The training alone will not bring about significant positive changes. Only with on-site visitation is there the opportunity to integrate new knowledge with practical implementation issues that have proven troublesome to overcome. Third, setting standards is key to the sustainability of improvements. Training individuals in skills is helpful but is not sustainable if those trained staff depart. Using hospital teams and common standards throughout different hospitals leads to institutionalization of the process.
Staff motivation has also proven to be essential to sustainability. Staff have been motivated because they see that many positive changes are within their control; they do not have to wait for someone else to make an improvement before they can introduce positive change. An ethic of continuous quality improvement is achieved through staff who are proud of the changes they have introduced. The iterative nature of this process has been essential to quality improvement: The standards are continually revisited and revised as needed. At times, new standards for other areas are developed when the hospitals need them. Finally, providing resources to pay adequate salaries, renovate facilities, buy equipment and supplies, and provide essential medicines are all important elements of this success.
This method has proven successful in such a short time that the Minister of Public Health, Dr. Mohammad Amin Fatimie, has expressed his desire to extend it to many other hospitals in the country in an effort to improve the quality of hospital care throughout Afghani-stan. The U.S. Agency for International Development and MSH have agreed to support this request, and the program will expand in future years. TH
Dr. Hartman, is a family physician with subspecialty training in infectious diseases, epidemiology, and public health. He serves as the technical director and deputy chief of party of the REACH Project, based in Kabul. Dr. Newbrander is a health economist who has served in Afghanistan since 2002 as a senior advisor to the Ministry of Health. He is currently Health Financing and Hospital Management Advisor for the USAID-funded REACH Project.
Acknowledgment: Funding for this article was provided by the United States Agency for International Development under the REACH Project, contract number EEE-C-00-03-00015-00. The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID.
References
- Newbrander W, Ickx P, Leitch GH. Addressing the immediate and long-term health needs in Afghanistan. Harvard Health Pol Rev. 2003;4.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA), US Centers for Disease Control and Prevention, United Nations Children’s Fund. Maternal mortality in Afghanistan: magnitude, causes, risk factors and preventability. Kabul: TISA; 2002.
- Bartlett LA, Mawji S, Whitehead S, et al. Where giving birth is a forecast of death: maternal mortality in four districts of Afghanistan, 1999-2002. Lancet. 2005;365:864-870.
- Strong L, Wali A, Sondorp E. Health Policy in Afghanistan: Two Years of Rapid Change: A Review of the Process from 2001 to 2003. London: London School of Hygiene and Tropical Medicine; 2005.
- Afghanistan’s health challenge. Lancet. 2003;362:841.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA). The Basic Package of Health Services for Afghanistan. Kabul: TISA; 2003.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA). Hospital Policy for Afghanistan’s Health System. Kabul: TISA; 2004.
- Ministry of Health Transitional Islamic Government of Afghanistan (TISA), Management Sciences for Health. Afghanistan national health resources assessment: Preliminary results. Kabul: TISA; 2002.
- A crucial time for Afghanistan’s fledgling health system. Lancet. 2005; 365:819-820.
- Ministry of Public Health (MOPH) Islamic Republic of Afghanistan. The Essential Package of Hospital Services for Afghanistan. Kabul: MOPH; 2005.