User login
Improve Glycemic Control in Inpatients
For most of recent history, it has been standard practice to tolerate hyperglycemia and expect some hypoglycemia when caring for diabetic patients in the hospital. This attitude stems from the many barriers to controlling glucose levels in hospitalized patients (e.g., the stress of acute illness and the changes in diet and medications that occur on admission to the hospital). In addition, most diabetic patients are hospitalized for illness other than their diabetes. In these situations, glycemic control may not be a priority, and fear of hypoglycemia may be prominent.
However, in recent years, there has been a change in attitude regarding glycemic control in the hospitalized patient. Recently, clinical studies have shown that hyperglycemia leads to poor outcomes in some hospitalized patients, prompting the American College of Endocrinology and the American Association of Clinical Endocrinologists to publish a position statement on inpatient diabetes and metabolic control.1 In addition, best practice strategies for controlling glucose levels in hospitalized patients have been recently reviewed.2
At the same time, hospitalists have emerged on the scene, bringing with them a new awareness of the gaps between the best practice and real practice. In real practice, both hyperglycemia and hypoglycemia are common, and insulin use in the hospital is often guided by strategies that are based on simplicity, instead of strategies that are based on established principles of diabetes management. There has been remarkably little attention given to the management of diabetes and hyperglycemia in noncritically ill hospitalized patients, and glucose levels are often far outside of the recommended range in this group.
SHM’s Glycemic Control Task Force
The Glycemic Control Task Force was assembled with the intent of improving glycemic control in hospitals nationally by providing hospitalists with an understanding of the best practice of glycemic control in the hospital, and by providing them with the tools and skills to make real changes in their own systems. With the assistance of a grant from Sanofi-Aventis, the Glycemic Control Summit was held on Oct. 20, 2005, in Chicago. A distinguished panel of experts attended, including hospitalists, endocrinologists, nurses, case managers, diabetes educators, and pharmacists. The goals of the meeting were as follows:
- To identify the currently available resources pertinent to glycemic control in the hospital (e.g., resources related to best practice, education, quality improvement, awareness, clinical tools, research, metrics/quality parameters);
- To identify the gaps in those resources; and
- To assemble several focused work groups to address the major gaps in the existing resources, and to determine specific interventions or products that could fill those gaps.
The meeting spawned several smaller work groups that will address the major barriers to improving glycemic control in hospitalized patients. These groups were formed in direct response to the gaps that were identified during the meeting. A description of each of the work groups is provided below, highlighting the major gaps that were identified and the strategies being considered to overcome them.
Education: This group will focus on creating case-based, educational materials that will provide physicians, nurses, and other providers with pragmatic examples illustrating the best practice of glycemic control and insulin management in the hospital and at the transition of care. In addition, this group will address patient education issues, educational metrics, and other issues.
Potential deliverables from this group include Web-based, case-based educational modules applicable to CME or to support quality improvement efforts at individual institutions and patient education materials.
Quality improvement process: This group will focus on formulating a how-to resource for performing quality improvement projects related to glycemic control. This group will attempt to provide hospitalists with a practical guideline to help them successfully implement changes in their own institutions. Topics will include forming and leading a multidisciplinary team, setting goals, defining metrics, and identifying process analysis and evaluation methods.
Deliverables from this group will likely include a glycemic control quality improvement workbook that will guide individuals through the complex process of performing robust quality improvement projects in their own hospitals. This workbook will be similar in format to one that is currently available in the “VTE Quality Improvement Resource Room” on the SHM Web site.
Clinical tools: This group will focus on compiling and appraising already existing clinical tools (e.g., standardized order sets, protocols) and identifying the key features of these tools and the differences among them. The emphasis will be on either compiling or creating ready-to-use clinical tools.
Potential deliverables from this group include a collection of tools that will have substantial built-in decision support and will be useful in a range of settings. These might include standardized order sets, protocols, and charting tools.
Metrics: This group will focus on defining useful metrics for performing glycemic control research and quality improvement projects. This group intends to define the best ways to measure glycemic control, balancing measures, process measures, and other specific outcomes. These metrics will allow hospitals to examine their current performance and to develop quality standards for inpatient glycemic control.
Care transitions: This group is charged with beginning to identify and address the many challenges that are faced when diabetic and/or hyperglycemic patients move from one care setting to another (e.g., ICU to general ward, hospital to outpatient setting). The work done by this group is likely to have an impact on all of the other groups.
Potential deliverables from this group include a set of standards that can be applied to care transitions. There may also be specific clinical tools developed to improve the process of these care transitions, such as checklists, order sets, and protocols.
Promotional: This group will focus on creating national awareness of the importance of glycemic control in hospitals, particularly at the administrative level. This may include efforts to partner with relevant medical societies, regulatory agencies, and other professional organizations focused on improving glycemic control.
Goals and Timelines
The three-month goal is for each of the focus groups is to further delineate the gaps in the existing resources, and to further refine the specific deliverables that they will produce. Each group will need to determine specific goals and timelines.
An intermediate-term goal is the formation of a white paper that will describe, in detail, the existing glycemic control resources, the gaps in these resources, and the need for additional work in these areas.
In addition, work on the glycemic control quality improvement workbook is under way, and this resource will be used in the “Quality Improvement Precourse” that will take place May 3, 2006, at the SHM Annual Meeting.
The work being done by this task force will lead to a collection of high-quality, user-friendly resources that will enhance awareness of the issue of inpatient glycemic control and facilitate the implementation of effective inpatient diabetes quality improvement across the nation. The longer term goal will be to bring about demonstration projects in the area of inpatient glycemic control and advance the science of diabetes care in the hospital.
References
- American College of Endocrinology Task Force on Inpatient Diabetes and Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Prac. 2004;10:77-82.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
Non-Physician Provider Task Force Progress
Annual meeting workshop plans, plus continued Web development
Shm’s Non-Physician Provider Task Force has continued to meet via conference calls on a regular basis. The task force now has representation from the ranks of nurse practitioners, physician assistants, hospitalist clinical care coordinators, health systems pharmacists, and hospitalist physicians. We realize that there are many other professionals vital to hospital medicine and plan to recruit more representatives from the SHM member ranks as qualified individuals are brought to our attention.
Task force members will provide important contributions to the annual meeting. The special interest forum on non-physician providers in hospital medicine has been growing each year. This forum is an important venue for exchanging ideas and meeting fellow professionals. It also gives the task force members a chance to make contact with individuals who want to get involved in Non-Physician Provider Task Force activities.
This year task force members Scarlett Blue, RNC, MSN, CNA, and Ryan Genzink, PAC, will lead the forum. Mitchell Wilson, MD, will lead a workshop, “Integrating Non-Physician Providers into Hospital Medicine Services.” National trends that include decreasing availability of generalist physicians, decreasing workloads for resident physicians, and the rapid growth in hospital medicine as a specialty will make this workshop vital to SHM members faced with these pressures.
The task force remains interested in developing a network for communication within the community of professionals in hospital medicine who have an interest in non-physician provider issues and practice. The Hub-and-Spoke initiative is intended to provide a network to allow more individuals to provide input to the task force. The forum at the annual meeting will be an opportunity to meet task force members, exchange e-mail addresses, and discuss how to become involved.
SHM’s Web site has a link for “Non-Physician Provider Resources,” and the task force has continued to work on the content of this site. The priorities for expansion include adding staffing models, billing and documentation resources, value added by non-physician providers, and FAQs. The task force welcomes SHM members to submit documents for posting to the resource center.
For most of recent history, it has been standard practice to tolerate hyperglycemia and expect some hypoglycemia when caring for diabetic patients in the hospital. This attitude stems from the many barriers to controlling glucose levels in hospitalized patients (e.g., the stress of acute illness and the changes in diet and medications that occur on admission to the hospital). In addition, most diabetic patients are hospitalized for illness other than their diabetes. In these situations, glycemic control may not be a priority, and fear of hypoglycemia may be prominent.
However, in recent years, there has been a change in attitude regarding glycemic control in the hospitalized patient. Recently, clinical studies have shown that hyperglycemia leads to poor outcomes in some hospitalized patients, prompting the American College of Endocrinology and the American Association of Clinical Endocrinologists to publish a position statement on inpatient diabetes and metabolic control.1 In addition, best practice strategies for controlling glucose levels in hospitalized patients have been recently reviewed.2
At the same time, hospitalists have emerged on the scene, bringing with them a new awareness of the gaps between the best practice and real practice. In real practice, both hyperglycemia and hypoglycemia are common, and insulin use in the hospital is often guided by strategies that are based on simplicity, instead of strategies that are based on established principles of diabetes management. There has been remarkably little attention given to the management of diabetes and hyperglycemia in noncritically ill hospitalized patients, and glucose levels are often far outside of the recommended range in this group.
SHM’s Glycemic Control Task Force
The Glycemic Control Task Force was assembled with the intent of improving glycemic control in hospitals nationally by providing hospitalists with an understanding of the best practice of glycemic control in the hospital, and by providing them with the tools and skills to make real changes in their own systems. With the assistance of a grant from Sanofi-Aventis, the Glycemic Control Summit was held on Oct. 20, 2005, in Chicago. A distinguished panel of experts attended, including hospitalists, endocrinologists, nurses, case managers, diabetes educators, and pharmacists. The goals of the meeting were as follows:
- To identify the currently available resources pertinent to glycemic control in the hospital (e.g., resources related to best practice, education, quality improvement, awareness, clinical tools, research, metrics/quality parameters);
- To identify the gaps in those resources; and
- To assemble several focused work groups to address the major gaps in the existing resources, and to determine specific interventions or products that could fill those gaps.
The meeting spawned several smaller work groups that will address the major barriers to improving glycemic control in hospitalized patients. These groups were formed in direct response to the gaps that were identified during the meeting. A description of each of the work groups is provided below, highlighting the major gaps that were identified and the strategies being considered to overcome them.
Education: This group will focus on creating case-based, educational materials that will provide physicians, nurses, and other providers with pragmatic examples illustrating the best practice of glycemic control and insulin management in the hospital and at the transition of care. In addition, this group will address patient education issues, educational metrics, and other issues.
Potential deliverables from this group include Web-based, case-based educational modules applicable to CME or to support quality improvement efforts at individual institutions and patient education materials.
Quality improvement process: This group will focus on formulating a how-to resource for performing quality improvement projects related to glycemic control. This group will attempt to provide hospitalists with a practical guideline to help them successfully implement changes in their own institutions. Topics will include forming and leading a multidisciplinary team, setting goals, defining metrics, and identifying process analysis and evaluation methods.
Deliverables from this group will likely include a glycemic control quality improvement workbook that will guide individuals through the complex process of performing robust quality improvement projects in their own hospitals. This workbook will be similar in format to one that is currently available in the “VTE Quality Improvement Resource Room” on the SHM Web site.
Clinical tools: This group will focus on compiling and appraising already existing clinical tools (e.g., standardized order sets, protocols) and identifying the key features of these tools and the differences among them. The emphasis will be on either compiling or creating ready-to-use clinical tools.
Potential deliverables from this group include a collection of tools that will have substantial built-in decision support and will be useful in a range of settings. These might include standardized order sets, protocols, and charting tools.
Metrics: This group will focus on defining useful metrics for performing glycemic control research and quality improvement projects. This group intends to define the best ways to measure glycemic control, balancing measures, process measures, and other specific outcomes. These metrics will allow hospitals to examine their current performance and to develop quality standards for inpatient glycemic control.
Care transitions: This group is charged with beginning to identify and address the many challenges that are faced when diabetic and/or hyperglycemic patients move from one care setting to another (e.g., ICU to general ward, hospital to outpatient setting). The work done by this group is likely to have an impact on all of the other groups.
Potential deliverables from this group include a set of standards that can be applied to care transitions. There may also be specific clinical tools developed to improve the process of these care transitions, such as checklists, order sets, and protocols.
Promotional: This group will focus on creating national awareness of the importance of glycemic control in hospitals, particularly at the administrative level. This may include efforts to partner with relevant medical societies, regulatory agencies, and other professional organizations focused on improving glycemic control.
Goals and Timelines
The three-month goal is for each of the focus groups is to further delineate the gaps in the existing resources, and to further refine the specific deliverables that they will produce. Each group will need to determine specific goals and timelines.
An intermediate-term goal is the formation of a white paper that will describe, in detail, the existing glycemic control resources, the gaps in these resources, and the need for additional work in these areas.
In addition, work on the glycemic control quality improvement workbook is under way, and this resource will be used in the “Quality Improvement Precourse” that will take place May 3, 2006, at the SHM Annual Meeting.
The work being done by this task force will lead to a collection of high-quality, user-friendly resources that will enhance awareness of the issue of inpatient glycemic control and facilitate the implementation of effective inpatient diabetes quality improvement across the nation. The longer term goal will be to bring about demonstration projects in the area of inpatient glycemic control and advance the science of diabetes care in the hospital.
References
- American College of Endocrinology Task Force on Inpatient Diabetes and Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Prac. 2004;10:77-82.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
Non-Physician Provider Task Force Progress
Annual meeting workshop plans, plus continued Web development
Shm’s Non-Physician Provider Task Force has continued to meet via conference calls on a regular basis. The task force now has representation from the ranks of nurse practitioners, physician assistants, hospitalist clinical care coordinators, health systems pharmacists, and hospitalist physicians. We realize that there are many other professionals vital to hospital medicine and plan to recruit more representatives from the SHM member ranks as qualified individuals are brought to our attention.
Task force members will provide important contributions to the annual meeting. The special interest forum on non-physician providers in hospital medicine has been growing each year. This forum is an important venue for exchanging ideas and meeting fellow professionals. It also gives the task force members a chance to make contact with individuals who want to get involved in Non-Physician Provider Task Force activities.
This year task force members Scarlett Blue, RNC, MSN, CNA, and Ryan Genzink, PAC, will lead the forum. Mitchell Wilson, MD, will lead a workshop, “Integrating Non-Physician Providers into Hospital Medicine Services.” National trends that include decreasing availability of generalist physicians, decreasing workloads for resident physicians, and the rapid growth in hospital medicine as a specialty will make this workshop vital to SHM members faced with these pressures.
The task force remains interested in developing a network for communication within the community of professionals in hospital medicine who have an interest in non-physician provider issues and practice. The Hub-and-Spoke initiative is intended to provide a network to allow more individuals to provide input to the task force. The forum at the annual meeting will be an opportunity to meet task force members, exchange e-mail addresses, and discuss how to become involved.
SHM’s Web site has a link for “Non-Physician Provider Resources,” and the task force has continued to work on the content of this site. The priorities for expansion include adding staffing models, billing and documentation resources, value added by non-physician providers, and FAQs. The task force welcomes SHM members to submit documents for posting to the resource center.
For most of recent history, it has been standard practice to tolerate hyperglycemia and expect some hypoglycemia when caring for diabetic patients in the hospital. This attitude stems from the many barriers to controlling glucose levels in hospitalized patients (e.g., the stress of acute illness and the changes in diet and medications that occur on admission to the hospital). In addition, most diabetic patients are hospitalized for illness other than their diabetes. In these situations, glycemic control may not be a priority, and fear of hypoglycemia may be prominent.
However, in recent years, there has been a change in attitude regarding glycemic control in the hospitalized patient. Recently, clinical studies have shown that hyperglycemia leads to poor outcomes in some hospitalized patients, prompting the American College of Endocrinology and the American Association of Clinical Endocrinologists to publish a position statement on inpatient diabetes and metabolic control.1 In addition, best practice strategies for controlling glucose levels in hospitalized patients have been recently reviewed.2
At the same time, hospitalists have emerged on the scene, bringing with them a new awareness of the gaps between the best practice and real practice. In real practice, both hyperglycemia and hypoglycemia are common, and insulin use in the hospital is often guided by strategies that are based on simplicity, instead of strategies that are based on established principles of diabetes management. There has been remarkably little attention given to the management of diabetes and hyperglycemia in noncritically ill hospitalized patients, and glucose levels are often far outside of the recommended range in this group.
SHM’s Glycemic Control Task Force
The Glycemic Control Task Force was assembled with the intent of improving glycemic control in hospitals nationally by providing hospitalists with an understanding of the best practice of glycemic control in the hospital, and by providing them with the tools and skills to make real changes in their own systems. With the assistance of a grant from Sanofi-Aventis, the Glycemic Control Summit was held on Oct. 20, 2005, in Chicago. A distinguished panel of experts attended, including hospitalists, endocrinologists, nurses, case managers, diabetes educators, and pharmacists. The goals of the meeting were as follows:
- To identify the currently available resources pertinent to glycemic control in the hospital (e.g., resources related to best practice, education, quality improvement, awareness, clinical tools, research, metrics/quality parameters);
- To identify the gaps in those resources; and
- To assemble several focused work groups to address the major gaps in the existing resources, and to determine specific interventions or products that could fill those gaps.
The meeting spawned several smaller work groups that will address the major barriers to improving glycemic control in hospitalized patients. These groups were formed in direct response to the gaps that were identified during the meeting. A description of each of the work groups is provided below, highlighting the major gaps that were identified and the strategies being considered to overcome them.
Education: This group will focus on creating case-based, educational materials that will provide physicians, nurses, and other providers with pragmatic examples illustrating the best practice of glycemic control and insulin management in the hospital and at the transition of care. In addition, this group will address patient education issues, educational metrics, and other issues.
Potential deliverables from this group include Web-based, case-based educational modules applicable to CME or to support quality improvement efforts at individual institutions and patient education materials.
Quality improvement process: This group will focus on formulating a how-to resource for performing quality improvement projects related to glycemic control. This group will attempt to provide hospitalists with a practical guideline to help them successfully implement changes in their own institutions. Topics will include forming and leading a multidisciplinary team, setting goals, defining metrics, and identifying process analysis and evaluation methods.
Deliverables from this group will likely include a glycemic control quality improvement workbook that will guide individuals through the complex process of performing robust quality improvement projects in their own hospitals. This workbook will be similar in format to one that is currently available in the “VTE Quality Improvement Resource Room” on the SHM Web site.
Clinical tools: This group will focus on compiling and appraising already existing clinical tools (e.g., standardized order sets, protocols) and identifying the key features of these tools and the differences among them. The emphasis will be on either compiling or creating ready-to-use clinical tools.
Potential deliverables from this group include a collection of tools that will have substantial built-in decision support and will be useful in a range of settings. These might include standardized order sets, protocols, and charting tools.
Metrics: This group will focus on defining useful metrics for performing glycemic control research and quality improvement projects. This group intends to define the best ways to measure glycemic control, balancing measures, process measures, and other specific outcomes. These metrics will allow hospitals to examine their current performance and to develop quality standards for inpatient glycemic control.
Care transitions: This group is charged with beginning to identify and address the many challenges that are faced when diabetic and/or hyperglycemic patients move from one care setting to another (e.g., ICU to general ward, hospital to outpatient setting). The work done by this group is likely to have an impact on all of the other groups.
Potential deliverables from this group include a set of standards that can be applied to care transitions. There may also be specific clinical tools developed to improve the process of these care transitions, such as checklists, order sets, and protocols.
Promotional: This group will focus on creating national awareness of the importance of glycemic control in hospitals, particularly at the administrative level. This may include efforts to partner with relevant medical societies, regulatory agencies, and other professional organizations focused on improving glycemic control.
Goals and Timelines
The three-month goal is for each of the focus groups is to further delineate the gaps in the existing resources, and to further refine the specific deliverables that they will produce. Each group will need to determine specific goals and timelines.
An intermediate-term goal is the formation of a white paper that will describe, in detail, the existing glycemic control resources, the gaps in these resources, and the need for additional work in these areas.
In addition, work on the glycemic control quality improvement workbook is under way, and this resource will be used in the “Quality Improvement Precourse” that will take place May 3, 2006, at the SHM Annual Meeting.
The work being done by this task force will lead to a collection of high-quality, user-friendly resources that will enhance awareness of the issue of inpatient glycemic control and facilitate the implementation of effective inpatient diabetes quality improvement across the nation. The longer term goal will be to bring about demonstration projects in the area of inpatient glycemic control and advance the science of diabetes care in the hospital.
References
- American College of Endocrinology Task Force on Inpatient Diabetes and Metabolic Control. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Prac. 2004;10:77-82.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
Non-Physician Provider Task Force Progress
Annual meeting workshop plans, plus continued Web development
Shm’s Non-Physician Provider Task Force has continued to meet via conference calls on a regular basis. The task force now has representation from the ranks of nurse practitioners, physician assistants, hospitalist clinical care coordinators, health systems pharmacists, and hospitalist physicians. We realize that there are many other professionals vital to hospital medicine and plan to recruit more representatives from the SHM member ranks as qualified individuals are brought to our attention.
Task force members will provide important contributions to the annual meeting. The special interest forum on non-physician providers in hospital medicine has been growing each year. This forum is an important venue for exchanging ideas and meeting fellow professionals. It also gives the task force members a chance to make contact with individuals who want to get involved in Non-Physician Provider Task Force activities.
This year task force members Scarlett Blue, RNC, MSN, CNA, and Ryan Genzink, PAC, will lead the forum. Mitchell Wilson, MD, will lead a workshop, “Integrating Non-Physician Providers into Hospital Medicine Services.” National trends that include decreasing availability of generalist physicians, decreasing workloads for resident physicians, and the rapid growth in hospital medicine as a specialty will make this workshop vital to SHM members faced with these pressures.
The task force remains interested in developing a network for communication within the community of professionals in hospital medicine who have an interest in non-physician provider issues and practice. The Hub-and-Spoke initiative is intended to provide a network to allow more individuals to provide input to the task force. The forum at the annual meeting will be an opportunity to meet task force members, exchange e-mail addresses, and discuss how to become involved.
SHM’s Web site has a link for “Non-Physician Provider Resources,” and the task force has continued to work on the content of this site. The priorities for expansion include adding staffing models, billing and documentation resources, value added by non-physician providers, and FAQs. The task force welcomes SHM members to submit documents for posting to the resource center.
Leading Roles
The 100 hospitalists who gathered in September at the Vail Cascade Hotel and Spa among Vail, Colorado’s high peaks for SHM’s second Hospitalist Medicine Leadership Academy showed their character early during a simulation led by David Javitch, PhD, a Harvard University instructor. The exercise usually goes like this: The leader auctions $1 bills, with bidders paying their highest bid whether they win or lose. Participants’ aggressive juices flow and someone usually pays $5 or $10 for the lone dollar. Then they realize that their irrational bidding behavior is fueled by their need to compete rather than to cooperate, and the leader discusses the value of cooperation over greed.
But the SHM Leadership Academy hospitalists played the game differently. Dr. Javitch earmarked the proceeds of the auction for a pediatric AIDS foundation. After early bids to $5, one Mississippi doctor who had worked in a hospital without water and electricity during Hurricane Katrina bid $100. The bidding ceased abruptly. Spontaneously, several groups took up collections to boost the donation’s size. This stopped the facilitator in his tracks.
Instead of giving the participants a lesson on the destructive power of greed and competition, the facilitator got a lesson about hospitalist altruism—a dedication to serving people that is transforming how patients are treated in America’s medical centers. This exercise revealed both the pros and the cons of hospitalists’ leadership tendencies.
The Academy Format
Working at round tables of 10, the hospitalists spent all four days in the same small group. Each group was led by a facilitator who guided its exercises, kept the discussion on track, and encouraged participation in feedback and Q&A sessions. The hospitalists were put through their paces by experts in various disciplines relating to hospital medicine, learning about the field’s leadership challenges, its business metrics, strategic planning, understanding various personality traits and communication styles, and managing change and transformation efforts.
The SHM Leadership Academy, which limits attendance to 100, balances lectures with exercises, simulations, personality and communication inventories, and time for questions and sharing about professional issues. There was also time set aside for networking, including at a cocktail party hosted by IPC: The Hospitalist Company, North Hollywood, Calif., as well as sightseeing, biking, and visits to Vail Village to explore local shops and restaurants
Who Attended
The hospitalist attendees came to the Leadership Academy from diverse paths and at various stages of their careers. Some physicians started hospitalist programs fresh from residency, some worked in large teams, some had been in solo and group practice before becoming hospitalists, some were employed by hospitalist groups and health plans, and one started as a community-based solo practice hospitalist. They work in a wide range of settings, from rural and suburban community hospitals to academic medical centers, and in cities large and small.
Russell (“Rusty”) Holman, MD, and Cogent Healthcare’s, Irvine, Calif., national medical director, spelled out the Leadership Academy’s goals: for hospitalists to run their programs more efficiently, improve morale within their groups, maximize team efficiency, and identify critical drivers of success.
“Our goal at this conference is for you to learn new things, to improve your skills as leaders, and to learn how to continually demonstrate value to your CEOs and CFOs,” says Dr. Holman, who also led participants through the analytic steps of a strategic plan in their small groups.
Leadership Challenges
Laurence Wellikson, MD, SHM CEO, spelled out the challenges confronting hospital medicine.
“In a nation that spent $1.7 trillion on healthcare in 2003, or 15.3% of the nation’s GDP, with rising insurance premiums and out-of-pocket costs to consumers, hospitalists will be part of a systemic solution to controlling costs and providing high quality care,” says Dr. Wellikson.
He points out that hospitals are changing rapidly, requiring hospitalists to adapt to work environments in flux. The 20% annual turnover in nursing staffs, PCPs giving up inpatient care, subspecialists narrowing their hospital work, and overcrowded emergency departments all create both opportunities and challenges for hospitalists.
“Hospital medicine is growing rapidly and so are the demands on hospitalists,” adds Dr. Wellikson, who articulated SHM’s goal of helping hospitalists develop their leadership skills in a rapidly changing and complex field. He urges participants to transcend medicine’s “cult of uniqueness among individual doctors” and to lead teams that will reform hospitals internally and provide measurable improvements in patient care quality and reduce waste.
These trends are playing out in a healthcare system that’s forced to do more with less. Michael Guthrie, MD, MBA, executive in residence at the University of Colorado at Denver, points out that hospitalists must assume their CEOs and CFOs mindsets to understand the myriad challenges that arise from the swelling number of uninsured patients, the demands of aging baby boomers, malpractice liability, competition, rapid changes in technology, the need for new buildings, and the emphasis on patient satisfaction and safety. The rise of consumer-directed care resulting from employers shifting healthcare costs to employees has raised concerns about how “shopping around” among hospitals might affect clinical performance.
Dr. Guthrie stresses that value is in the eyes of the beholder and that the hospitalist’s work greatly affects other care team members’ satisfaction, relationships with other physicians, patient satisfaction and safety, and the hospital’s business interests.
“Hospitalists use their knowledge, ideas, skills, and expertise with process improvement to get things done with and through other people,” he explains. “When we understand what problems need to be solved and what our measures of success are we can have the rapture of accomplishment.”
Turmoil throughout the healthcare system and rapid growth of the hospitalist movement provided an apt backdrop for remarks Jack Silversin, DMD, DrPh, made in a session titled, “Leading and Managing Change.” Dr. Silversin is the president of Amicus Inc., a consultant firm based in Cambridge, Mass. He urges physicians to transcend their traditional roles as protectors of the status quo to become sponsors of change instead. Physicians as change agents publicly demonstrate their commitment to being leaders in several important ways.
“Change is definitely more work than maintaining the status quo,” says Dr. Silversin, “but organizations need doctors who sponsor change rather than resist it.”
Working through a simulation of a headstrong hospitalist trying to strong-arm her way to a 24/7 schedule for hospitalists rather than having the medical staff or moonlighters taking night call, participants developed their own insights into handling change.
“You’ve got to start small and gain credibility with little victories rather than doing something major right away,” said one attendee.
Trying to get non-hospitalists to support change was another idea: “Leadership doesn’t always have an MD credential attached to it,” added Dr. Silversin.
Being a change agent means looking inward as well as outward, and to that end attendees at the Leadership Academy spent time exploring their personal strengths and communication styles. Having completed a “Strength Deployment Inventory,” a self-scored test published by Personal Strength Publishing of Carlsbad, Calif., that measures an individual’s motives and values, prior to the conference, the hospitalists—led by Dr. Javitch—determined their strengths and weaknesses on altruism, assertiveness, and analysis. Small groups and dyads role-played situations where a colleague, an administrator, or a subordinate had a vastly different approach to problem-solving and decision-making.
“There are no right or wrong answers here, just a growing awareness of what our strengths are and things we need to guard against,” says Javitch.
Timothy Keogh, PhD, clinical associate professor of Managerial Communication at Tulane University, New Orleans, discussed that effective communication—both spoken and nonverbal—is a key tool skill mastered by good leaders. Explaining that everyone’s façade masks things that are hidden consciously or unconsciously, self-awareness can help us “enlarge our arena and tap into talents that can flower.” He also points out that 80% of our communication style is due to our personality and 20% to environment, and that it “costs us energy to flex.”
Dr. Keogh encouraged attendees to adapt to other communication styles so the listener can hear what is being said. For example, someone with a dominant communication style might be perceived as pushy by a one with a conscientious perfecting style. Completing the DiSC, a self-scored communication and personality style inventory from Inscape Publishing of Minneapolis, 22% of the hospitalists were predominantly creative, while 18% were perfectionists, and 12% inspirational communicators. Dr. Keogh says that this pattern is consistent with norms for physicians, and urged attendees to study how personality types can improve their handling of emotions, goals, values, fears, and judgments.
Throughout the sessions hospitalists raised issues, some of which mesh with others in the hospital, such as top administrators, and some of which don’t mesh. Many spoke candidly about their difficulties growing a hospitalist program beyond an admitting service into a full-blown inpatient medicine service—particularly with office-based colleagues waiting in the wings to be relieved of hospital work. Physician recruitment and retention were very much on their minds, as were rocky relationships with subspecialists, turnover in top administration that results in having to “resell” the hospitalist program to new leaders, and constant pressures to seek new ways to reduce average length of stay and emergency department throughput. Achieving a balance of patient care, committee responsibilities, and teaching and research for physicians interested in those areas were also mentioned.
Looking to the future, Mary Jo Gorman, MD, MD, SHM president-elect and chief medical officer of IPC: The Hospitalist Company, indicates her organizational vision: “It isn’t easy to build something brand new in only one year, so I plan to build on SHM’s momentum. My goal is to keep defining and building hospital medicine as a career rather than as an extension of the house officer path.”
Conclusion
With 100 hospitalists now armed with a new tool kit, Dr. Wellikson outlined SHM’s plans for upcoming Leadership Academies: “Our next Academy is Jan 9-12, 2006 in Tucson [Ariz.], and we’ve added a medical directors’ forum for managing burnout.” An advanced Leadership Academy is also planned for 2006. TH
The 100 hospitalists who gathered in September at the Vail Cascade Hotel and Spa among Vail, Colorado’s high peaks for SHM’s second Hospitalist Medicine Leadership Academy showed their character early during a simulation led by David Javitch, PhD, a Harvard University instructor. The exercise usually goes like this: The leader auctions $1 bills, with bidders paying their highest bid whether they win or lose. Participants’ aggressive juices flow and someone usually pays $5 or $10 for the lone dollar. Then they realize that their irrational bidding behavior is fueled by their need to compete rather than to cooperate, and the leader discusses the value of cooperation over greed.
But the SHM Leadership Academy hospitalists played the game differently. Dr. Javitch earmarked the proceeds of the auction for a pediatric AIDS foundation. After early bids to $5, one Mississippi doctor who had worked in a hospital without water and electricity during Hurricane Katrina bid $100. The bidding ceased abruptly. Spontaneously, several groups took up collections to boost the donation’s size. This stopped the facilitator in his tracks.
Instead of giving the participants a lesson on the destructive power of greed and competition, the facilitator got a lesson about hospitalist altruism—a dedication to serving people that is transforming how patients are treated in America’s medical centers. This exercise revealed both the pros and the cons of hospitalists’ leadership tendencies.
The Academy Format
Working at round tables of 10, the hospitalists spent all four days in the same small group. Each group was led by a facilitator who guided its exercises, kept the discussion on track, and encouraged participation in feedback and Q&A sessions. The hospitalists were put through their paces by experts in various disciplines relating to hospital medicine, learning about the field’s leadership challenges, its business metrics, strategic planning, understanding various personality traits and communication styles, and managing change and transformation efforts.
The SHM Leadership Academy, which limits attendance to 100, balances lectures with exercises, simulations, personality and communication inventories, and time for questions and sharing about professional issues. There was also time set aside for networking, including at a cocktail party hosted by IPC: The Hospitalist Company, North Hollywood, Calif., as well as sightseeing, biking, and visits to Vail Village to explore local shops and restaurants
Who Attended
The hospitalist attendees came to the Leadership Academy from diverse paths and at various stages of their careers. Some physicians started hospitalist programs fresh from residency, some worked in large teams, some had been in solo and group practice before becoming hospitalists, some were employed by hospitalist groups and health plans, and one started as a community-based solo practice hospitalist. They work in a wide range of settings, from rural and suburban community hospitals to academic medical centers, and in cities large and small.
Russell (“Rusty”) Holman, MD, and Cogent Healthcare’s, Irvine, Calif., national medical director, spelled out the Leadership Academy’s goals: for hospitalists to run their programs more efficiently, improve morale within their groups, maximize team efficiency, and identify critical drivers of success.
“Our goal at this conference is for you to learn new things, to improve your skills as leaders, and to learn how to continually demonstrate value to your CEOs and CFOs,” says Dr. Holman, who also led participants through the analytic steps of a strategic plan in their small groups.
Leadership Challenges
Laurence Wellikson, MD, SHM CEO, spelled out the challenges confronting hospital medicine.
“In a nation that spent $1.7 trillion on healthcare in 2003, or 15.3% of the nation’s GDP, with rising insurance premiums and out-of-pocket costs to consumers, hospitalists will be part of a systemic solution to controlling costs and providing high quality care,” says Dr. Wellikson.
He points out that hospitals are changing rapidly, requiring hospitalists to adapt to work environments in flux. The 20% annual turnover in nursing staffs, PCPs giving up inpatient care, subspecialists narrowing their hospital work, and overcrowded emergency departments all create both opportunities and challenges for hospitalists.
“Hospital medicine is growing rapidly and so are the demands on hospitalists,” adds Dr. Wellikson, who articulated SHM’s goal of helping hospitalists develop their leadership skills in a rapidly changing and complex field. He urges participants to transcend medicine’s “cult of uniqueness among individual doctors” and to lead teams that will reform hospitals internally and provide measurable improvements in patient care quality and reduce waste.
These trends are playing out in a healthcare system that’s forced to do more with less. Michael Guthrie, MD, MBA, executive in residence at the University of Colorado at Denver, points out that hospitalists must assume their CEOs and CFOs mindsets to understand the myriad challenges that arise from the swelling number of uninsured patients, the demands of aging baby boomers, malpractice liability, competition, rapid changes in technology, the need for new buildings, and the emphasis on patient satisfaction and safety. The rise of consumer-directed care resulting from employers shifting healthcare costs to employees has raised concerns about how “shopping around” among hospitals might affect clinical performance.
Dr. Guthrie stresses that value is in the eyes of the beholder and that the hospitalist’s work greatly affects other care team members’ satisfaction, relationships with other physicians, patient satisfaction and safety, and the hospital’s business interests.
“Hospitalists use their knowledge, ideas, skills, and expertise with process improvement to get things done with and through other people,” he explains. “When we understand what problems need to be solved and what our measures of success are we can have the rapture of accomplishment.”
Turmoil throughout the healthcare system and rapid growth of the hospitalist movement provided an apt backdrop for remarks Jack Silversin, DMD, DrPh, made in a session titled, “Leading and Managing Change.” Dr. Silversin is the president of Amicus Inc., a consultant firm based in Cambridge, Mass. He urges physicians to transcend their traditional roles as protectors of the status quo to become sponsors of change instead. Physicians as change agents publicly demonstrate their commitment to being leaders in several important ways.
“Change is definitely more work than maintaining the status quo,” says Dr. Silversin, “but organizations need doctors who sponsor change rather than resist it.”
Working through a simulation of a headstrong hospitalist trying to strong-arm her way to a 24/7 schedule for hospitalists rather than having the medical staff or moonlighters taking night call, participants developed their own insights into handling change.
“You’ve got to start small and gain credibility with little victories rather than doing something major right away,” said one attendee.
Trying to get non-hospitalists to support change was another idea: “Leadership doesn’t always have an MD credential attached to it,” added Dr. Silversin.
Being a change agent means looking inward as well as outward, and to that end attendees at the Leadership Academy spent time exploring their personal strengths and communication styles. Having completed a “Strength Deployment Inventory,” a self-scored test published by Personal Strength Publishing of Carlsbad, Calif., that measures an individual’s motives and values, prior to the conference, the hospitalists—led by Dr. Javitch—determined their strengths and weaknesses on altruism, assertiveness, and analysis. Small groups and dyads role-played situations where a colleague, an administrator, or a subordinate had a vastly different approach to problem-solving and decision-making.
“There are no right or wrong answers here, just a growing awareness of what our strengths are and things we need to guard against,” says Javitch.
Timothy Keogh, PhD, clinical associate professor of Managerial Communication at Tulane University, New Orleans, discussed that effective communication—both spoken and nonverbal—is a key tool skill mastered by good leaders. Explaining that everyone’s façade masks things that are hidden consciously or unconsciously, self-awareness can help us “enlarge our arena and tap into talents that can flower.” He also points out that 80% of our communication style is due to our personality and 20% to environment, and that it “costs us energy to flex.”
Dr. Keogh encouraged attendees to adapt to other communication styles so the listener can hear what is being said. For example, someone with a dominant communication style might be perceived as pushy by a one with a conscientious perfecting style. Completing the DiSC, a self-scored communication and personality style inventory from Inscape Publishing of Minneapolis, 22% of the hospitalists were predominantly creative, while 18% were perfectionists, and 12% inspirational communicators. Dr. Keogh says that this pattern is consistent with norms for physicians, and urged attendees to study how personality types can improve their handling of emotions, goals, values, fears, and judgments.
Throughout the sessions hospitalists raised issues, some of which mesh with others in the hospital, such as top administrators, and some of which don’t mesh. Many spoke candidly about their difficulties growing a hospitalist program beyond an admitting service into a full-blown inpatient medicine service—particularly with office-based colleagues waiting in the wings to be relieved of hospital work. Physician recruitment and retention were very much on their minds, as were rocky relationships with subspecialists, turnover in top administration that results in having to “resell” the hospitalist program to new leaders, and constant pressures to seek new ways to reduce average length of stay and emergency department throughput. Achieving a balance of patient care, committee responsibilities, and teaching and research for physicians interested in those areas were also mentioned.
Looking to the future, Mary Jo Gorman, MD, MD, SHM president-elect and chief medical officer of IPC: The Hospitalist Company, indicates her organizational vision: “It isn’t easy to build something brand new in only one year, so I plan to build on SHM’s momentum. My goal is to keep defining and building hospital medicine as a career rather than as an extension of the house officer path.”
Conclusion
With 100 hospitalists now armed with a new tool kit, Dr. Wellikson outlined SHM’s plans for upcoming Leadership Academies: “Our next Academy is Jan 9-12, 2006 in Tucson [Ariz.], and we’ve added a medical directors’ forum for managing burnout.” An advanced Leadership Academy is also planned for 2006. TH
The 100 hospitalists who gathered in September at the Vail Cascade Hotel and Spa among Vail, Colorado’s high peaks for SHM’s second Hospitalist Medicine Leadership Academy showed their character early during a simulation led by David Javitch, PhD, a Harvard University instructor. The exercise usually goes like this: The leader auctions $1 bills, with bidders paying their highest bid whether they win or lose. Participants’ aggressive juices flow and someone usually pays $5 or $10 for the lone dollar. Then they realize that their irrational bidding behavior is fueled by their need to compete rather than to cooperate, and the leader discusses the value of cooperation over greed.
But the SHM Leadership Academy hospitalists played the game differently. Dr. Javitch earmarked the proceeds of the auction for a pediatric AIDS foundation. After early bids to $5, one Mississippi doctor who had worked in a hospital without water and electricity during Hurricane Katrina bid $100. The bidding ceased abruptly. Spontaneously, several groups took up collections to boost the donation’s size. This stopped the facilitator in his tracks.
Instead of giving the participants a lesson on the destructive power of greed and competition, the facilitator got a lesson about hospitalist altruism—a dedication to serving people that is transforming how patients are treated in America’s medical centers. This exercise revealed both the pros and the cons of hospitalists’ leadership tendencies.
The Academy Format
Working at round tables of 10, the hospitalists spent all four days in the same small group. Each group was led by a facilitator who guided its exercises, kept the discussion on track, and encouraged participation in feedback and Q&A sessions. The hospitalists were put through their paces by experts in various disciplines relating to hospital medicine, learning about the field’s leadership challenges, its business metrics, strategic planning, understanding various personality traits and communication styles, and managing change and transformation efforts.
The SHM Leadership Academy, which limits attendance to 100, balances lectures with exercises, simulations, personality and communication inventories, and time for questions and sharing about professional issues. There was also time set aside for networking, including at a cocktail party hosted by IPC: The Hospitalist Company, North Hollywood, Calif., as well as sightseeing, biking, and visits to Vail Village to explore local shops and restaurants
Who Attended
The hospitalist attendees came to the Leadership Academy from diverse paths and at various stages of their careers. Some physicians started hospitalist programs fresh from residency, some worked in large teams, some had been in solo and group practice before becoming hospitalists, some were employed by hospitalist groups and health plans, and one started as a community-based solo practice hospitalist. They work in a wide range of settings, from rural and suburban community hospitals to academic medical centers, and in cities large and small.
Russell (“Rusty”) Holman, MD, and Cogent Healthcare’s, Irvine, Calif., national medical director, spelled out the Leadership Academy’s goals: for hospitalists to run their programs more efficiently, improve morale within their groups, maximize team efficiency, and identify critical drivers of success.
“Our goal at this conference is for you to learn new things, to improve your skills as leaders, and to learn how to continually demonstrate value to your CEOs and CFOs,” says Dr. Holman, who also led participants through the analytic steps of a strategic plan in their small groups.
Leadership Challenges
Laurence Wellikson, MD, SHM CEO, spelled out the challenges confronting hospital medicine.
“In a nation that spent $1.7 trillion on healthcare in 2003, or 15.3% of the nation’s GDP, with rising insurance premiums and out-of-pocket costs to consumers, hospitalists will be part of a systemic solution to controlling costs and providing high quality care,” says Dr. Wellikson.
He points out that hospitals are changing rapidly, requiring hospitalists to adapt to work environments in flux. The 20% annual turnover in nursing staffs, PCPs giving up inpatient care, subspecialists narrowing their hospital work, and overcrowded emergency departments all create both opportunities and challenges for hospitalists.
“Hospital medicine is growing rapidly and so are the demands on hospitalists,” adds Dr. Wellikson, who articulated SHM’s goal of helping hospitalists develop their leadership skills in a rapidly changing and complex field. He urges participants to transcend medicine’s “cult of uniqueness among individual doctors” and to lead teams that will reform hospitals internally and provide measurable improvements in patient care quality and reduce waste.
These trends are playing out in a healthcare system that’s forced to do more with less. Michael Guthrie, MD, MBA, executive in residence at the University of Colorado at Denver, points out that hospitalists must assume their CEOs and CFOs mindsets to understand the myriad challenges that arise from the swelling number of uninsured patients, the demands of aging baby boomers, malpractice liability, competition, rapid changes in technology, the need for new buildings, and the emphasis on patient satisfaction and safety. The rise of consumer-directed care resulting from employers shifting healthcare costs to employees has raised concerns about how “shopping around” among hospitals might affect clinical performance.
Dr. Guthrie stresses that value is in the eyes of the beholder and that the hospitalist’s work greatly affects other care team members’ satisfaction, relationships with other physicians, patient satisfaction and safety, and the hospital’s business interests.
“Hospitalists use their knowledge, ideas, skills, and expertise with process improvement to get things done with and through other people,” he explains. “When we understand what problems need to be solved and what our measures of success are we can have the rapture of accomplishment.”
Turmoil throughout the healthcare system and rapid growth of the hospitalist movement provided an apt backdrop for remarks Jack Silversin, DMD, DrPh, made in a session titled, “Leading and Managing Change.” Dr. Silversin is the president of Amicus Inc., a consultant firm based in Cambridge, Mass. He urges physicians to transcend their traditional roles as protectors of the status quo to become sponsors of change instead. Physicians as change agents publicly demonstrate their commitment to being leaders in several important ways.
“Change is definitely more work than maintaining the status quo,” says Dr. Silversin, “but organizations need doctors who sponsor change rather than resist it.”
Working through a simulation of a headstrong hospitalist trying to strong-arm her way to a 24/7 schedule for hospitalists rather than having the medical staff or moonlighters taking night call, participants developed their own insights into handling change.
“You’ve got to start small and gain credibility with little victories rather than doing something major right away,” said one attendee.
Trying to get non-hospitalists to support change was another idea: “Leadership doesn’t always have an MD credential attached to it,” added Dr. Silversin.
Being a change agent means looking inward as well as outward, and to that end attendees at the Leadership Academy spent time exploring their personal strengths and communication styles. Having completed a “Strength Deployment Inventory,” a self-scored test published by Personal Strength Publishing of Carlsbad, Calif., that measures an individual’s motives and values, prior to the conference, the hospitalists—led by Dr. Javitch—determined their strengths and weaknesses on altruism, assertiveness, and analysis. Small groups and dyads role-played situations where a colleague, an administrator, or a subordinate had a vastly different approach to problem-solving and decision-making.
“There are no right or wrong answers here, just a growing awareness of what our strengths are and things we need to guard against,” says Javitch.
Timothy Keogh, PhD, clinical associate professor of Managerial Communication at Tulane University, New Orleans, discussed that effective communication—both spoken and nonverbal—is a key tool skill mastered by good leaders. Explaining that everyone’s façade masks things that are hidden consciously or unconsciously, self-awareness can help us “enlarge our arena and tap into talents that can flower.” He also points out that 80% of our communication style is due to our personality and 20% to environment, and that it “costs us energy to flex.”
Dr. Keogh encouraged attendees to adapt to other communication styles so the listener can hear what is being said. For example, someone with a dominant communication style might be perceived as pushy by a one with a conscientious perfecting style. Completing the DiSC, a self-scored communication and personality style inventory from Inscape Publishing of Minneapolis, 22% of the hospitalists were predominantly creative, while 18% were perfectionists, and 12% inspirational communicators. Dr. Keogh says that this pattern is consistent with norms for physicians, and urged attendees to study how personality types can improve their handling of emotions, goals, values, fears, and judgments.
Throughout the sessions hospitalists raised issues, some of which mesh with others in the hospital, such as top administrators, and some of which don’t mesh. Many spoke candidly about their difficulties growing a hospitalist program beyond an admitting service into a full-blown inpatient medicine service—particularly with office-based colleagues waiting in the wings to be relieved of hospital work. Physician recruitment and retention were very much on their minds, as were rocky relationships with subspecialists, turnover in top administration that results in having to “resell” the hospitalist program to new leaders, and constant pressures to seek new ways to reduce average length of stay and emergency department throughput. Achieving a balance of patient care, committee responsibilities, and teaching and research for physicians interested in those areas were also mentioned.
Looking to the future, Mary Jo Gorman, MD, MD, SHM president-elect and chief medical officer of IPC: The Hospitalist Company, indicates her organizational vision: “It isn’t easy to build something brand new in only one year, so I plan to build on SHM’s momentum. My goal is to keep defining and building hospital medicine as a career rather than as an extension of the house officer path.”
Conclusion
With 100 hospitalists now armed with a new tool kit, Dr. Wellikson outlined SHM’s plans for upcoming Leadership Academies: “Our next Academy is Jan 9-12, 2006 in Tucson [Ariz.], and we’ve added a medical directors’ forum for managing burnout.” An advanced Leadership Academy is also planned for 2006. TH
Come Together

Has the time come for a major overhaul of internal medicine training to better prepare new physicians for the reality of medical practice they will face in the 21st century? Has hospital medicine’s rapid growth been one indication that the roles internists are being asked to perform are in many ways different from just a decade earlier? Are these concerns just as applicable for young family practitioners and pediatricians?
On Dec. 2, 2005, the Alliance for Academic Internal Medicine (AAIM) and the American Board of Internal Medicine (ABIM) brought together more than 40 of the key opinion leaders in internal medicine to look into these very issues. This watershed meeting included the top leaders at ABIM, the American College of Physicians (ACP), the Association of Program Directors in Internal Medicine (APDIM), the Association of Professors of Medicine (APM), all of the medical subspecialty societies, the American Medical Association (AMA), the AMA/Specialty Society RVS Update Committee (RUC), and the American Association of Medical Colleges (AAMC). And, yes, SHM, was well represented.
In addition to agreeing that an overhaul of internal medicine residency training is long overdue, part of this meeting was also devoted to potential changes in the maintenance of certification process to allow for formal recognition of expertise in hospital medicine and ambulatory internal medicine. More about that later.
APDIM and APM, representing the collective organizations in AAIM, presented a plan for revision in training that would identify a core of internal medicine that could form the basis for the front end of training (e.g., possibly the first two years) and allow for a concentration in the later stages of internal medicine residencies. This might take the form of a third year with an emphasis in hospital medicine, ambulatory medicine, traditional internal medicine, or one of the medical subspecialties.
Amazingly, this approach was almost universally accepted by the attendees at the Dec. 2 meeting. With this broad support, AAIM plans to push forward in the coming months, disseminating details of their plan with an opportunity for a broader comment on just what would constitute the “core” of internal medicine. APM and APDIM then plan to take this input and come back by midyear with a more fleshed out proposal.
Of interest is that SHM is publishing the Core Competencies in Hospital Medicine as a supplement to the first issue of the Journal of Hospital Medicine. The work hospitalist thought leaders have put into defining these core competencies over the last few years should be helpful in providing the hospital medicine slant on the core of internal medicine as well as forming the basis for the curriculum with concentration in hospital medicine in the third year of training.
While the goal is to allow training to reflect the career choices of today’s internists and to better prepare them for their professional lives, the devil is truly in the details. Besides serving as a platform for education, internal medicine residency has evolved into a major service load supporting many health systems. Any revision to internal medicine residency needs to accommodate for the service load. In addition, any changes need to be blended into subspecialty fellowship training.
Weaved into this entire discussion was the evolving reshaping of internal medicine. At one time the well-trained general internist was the consummate well-rounded physician serving as a consultant on many diseases to surgeons and other physicians. The last quarter of the 20th century saw the blossoming of many subspecialties in internal medicine and in the last decade a further sub-subspecialization with endoscopists, electrophysiologists, and the like. As the complexity and demands increased in recent years in both the hospital and the outpatient arena, some internists chose to limit their practice to the hospital or the office, and hospital medicine grew and its competencies became more defined.
As internists further refined their skills and narrowed their professional focus, their expectations of their certification and especially their maintenance of certification (MOC) by the ABIM became an issue. Is the MOC process relevant to what they feel they do and should know?
In addition, many subspecialty societies have concerns about how maintaining a basis in internal medicine fits in with MOC in their subspecialties. At this meeting it became clear that many subspecialists feel there is a core of internal medicine they should continue to know and be evaluated on without being expected to know everything a practicing hospitalist or ambulatory internist knows. For example, a cardiologist may be expected to know when their diabetic patients are getting into trouble and need consultation but may not need to know the intricacies of managing extremes in glycemic control.
Many at this meeting felt that the time is now here for using the MOC process to offer those initially credentialed in general internal medicine to have their MOC evaluation tailored to their real-life practice as a hospitalist or an internist with an ambulatory practice and to allow for them to be identified as having expertise in hospital or ambulatory medicine. This was a recognition that these aspects of what have traditionally been lumped together as general internal medicine have key defined skills and knowledge and needs to be recognized as more than just an internist who is not a subspecialist.
Once again there is still much work to be done. SHM, ACP, SGIM, and others will need to work with ABIM and RUC and others to define the skills and the competencies that would form the basis for the training and evaluation of new and improved internists in the 21st century.
The good news from the Dec. 2, 2005, meeting in Dallas is that the national leadership in internal medicine recognizes the need to change internal medicine residency training and to have an MOC process that is relevant to all internists—general internists, subspecialists, and hospitalists. There was also a sense that this process needs to move forward with reasoned speed. We don’t need to write another white paper and declare victory. Today’s and tomorrow’s internists and our patients need us to provide the leadership to produce the best trained and motivated internists and subspecialists to meet the increasing needs of a sophisticated and aging population.
As always SHM will be there, playing an active role. Whatever we come up with for internal medicine I hope can be applicable to family practice and pediatrics as well. Because this is the professional world you will live in, we will continue to invite your input and ideas. TH
Dr. Wellikson has been CEO of SHM since 2000.
Has the time come for a major overhaul of internal medicine training to better prepare new physicians for the reality of medical practice they will face in the 21st century? Has hospital medicine’s rapid growth been one indication that the roles internists are being asked to perform are in many ways different from just a decade earlier? Are these concerns just as applicable for young family practitioners and pediatricians?
On Dec. 2, 2005, the Alliance for Academic Internal Medicine (AAIM) and the American Board of Internal Medicine (ABIM) brought together more than 40 of the key opinion leaders in internal medicine to look into these very issues. This watershed meeting included the top leaders at ABIM, the American College of Physicians (ACP), the Association of Program Directors in Internal Medicine (APDIM), the Association of Professors of Medicine (APM), all of the medical subspecialty societies, the American Medical Association (AMA), the AMA/Specialty Society RVS Update Committee (RUC), and the American Association of Medical Colleges (AAMC). And, yes, SHM, was well represented.
In addition to agreeing that an overhaul of internal medicine residency training is long overdue, part of this meeting was also devoted to potential changes in the maintenance of certification process to allow for formal recognition of expertise in hospital medicine and ambulatory internal medicine. More about that later.
APDIM and APM, representing the collective organizations in AAIM, presented a plan for revision in training that would identify a core of internal medicine that could form the basis for the front end of training (e.g., possibly the first two years) and allow for a concentration in the later stages of internal medicine residencies. This might take the form of a third year with an emphasis in hospital medicine, ambulatory medicine, traditional internal medicine, or one of the medical subspecialties.
Amazingly, this approach was almost universally accepted by the attendees at the Dec. 2 meeting. With this broad support, AAIM plans to push forward in the coming months, disseminating details of their plan with an opportunity for a broader comment on just what would constitute the “core” of internal medicine. APM and APDIM then plan to take this input and come back by midyear with a more fleshed out proposal.
Of interest is that SHM is publishing the Core Competencies in Hospital Medicine as a supplement to the first issue of the Journal of Hospital Medicine. The work hospitalist thought leaders have put into defining these core competencies over the last few years should be helpful in providing the hospital medicine slant on the core of internal medicine as well as forming the basis for the curriculum with concentration in hospital medicine in the third year of training.
While the goal is to allow training to reflect the career choices of today’s internists and to better prepare them for their professional lives, the devil is truly in the details. Besides serving as a platform for education, internal medicine residency has evolved into a major service load supporting many health systems. Any revision to internal medicine residency needs to accommodate for the service load. In addition, any changes need to be blended into subspecialty fellowship training.
Weaved into this entire discussion was the evolving reshaping of internal medicine. At one time the well-trained general internist was the consummate well-rounded physician serving as a consultant on many diseases to surgeons and other physicians. The last quarter of the 20th century saw the blossoming of many subspecialties in internal medicine and in the last decade a further sub-subspecialization with endoscopists, electrophysiologists, and the like. As the complexity and demands increased in recent years in both the hospital and the outpatient arena, some internists chose to limit their practice to the hospital or the office, and hospital medicine grew and its competencies became more defined.
As internists further refined their skills and narrowed their professional focus, their expectations of their certification and especially their maintenance of certification (MOC) by the ABIM became an issue. Is the MOC process relevant to what they feel they do and should know?
In addition, many subspecialty societies have concerns about how maintaining a basis in internal medicine fits in with MOC in their subspecialties. At this meeting it became clear that many subspecialists feel there is a core of internal medicine they should continue to know and be evaluated on without being expected to know everything a practicing hospitalist or ambulatory internist knows. For example, a cardiologist may be expected to know when their diabetic patients are getting into trouble and need consultation but may not need to know the intricacies of managing extremes in glycemic control.
Many at this meeting felt that the time is now here for using the MOC process to offer those initially credentialed in general internal medicine to have their MOC evaluation tailored to their real-life practice as a hospitalist or an internist with an ambulatory practice and to allow for them to be identified as having expertise in hospital or ambulatory medicine. This was a recognition that these aspects of what have traditionally been lumped together as general internal medicine have key defined skills and knowledge and needs to be recognized as more than just an internist who is not a subspecialist.
Once again there is still much work to be done. SHM, ACP, SGIM, and others will need to work with ABIM and RUC and others to define the skills and the competencies that would form the basis for the training and evaluation of new and improved internists in the 21st century.
The good news from the Dec. 2, 2005, meeting in Dallas is that the national leadership in internal medicine recognizes the need to change internal medicine residency training and to have an MOC process that is relevant to all internists—general internists, subspecialists, and hospitalists. There was also a sense that this process needs to move forward with reasoned speed. We don’t need to write another white paper and declare victory. Today’s and tomorrow’s internists and our patients need us to provide the leadership to produce the best trained and motivated internists and subspecialists to meet the increasing needs of a sophisticated and aging population.
As always SHM will be there, playing an active role. Whatever we come up with for internal medicine I hope can be applicable to family practice and pediatrics as well. Because this is the professional world you will live in, we will continue to invite your input and ideas. TH
Dr. Wellikson has been CEO of SHM since 2000.
Has the time come for a major overhaul of internal medicine training to better prepare new physicians for the reality of medical practice they will face in the 21st century? Has hospital medicine’s rapid growth been one indication that the roles internists are being asked to perform are in many ways different from just a decade earlier? Are these concerns just as applicable for young family practitioners and pediatricians?
On Dec. 2, 2005, the Alliance for Academic Internal Medicine (AAIM) and the American Board of Internal Medicine (ABIM) brought together more than 40 of the key opinion leaders in internal medicine to look into these very issues. This watershed meeting included the top leaders at ABIM, the American College of Physicians (ACP), the Association of Program Directors in Internal Medicine (APDIM), the Association of Professors of Medicine (APM), all of the medical subspecialty societies, the American Medical Association (AMA), the AMA/Specialty Society RVS Update Committee (RUC), and the American Association of Medical Colleges (AAMC). And, yes, SHM, was well represented.
In addition to agreeing that an overhaul of internal medicine residency training is long overdue, part of this meeting was also devoted to potential changes in the maintenance of certification process to allow for formal recognition of expertise in hospital medicine and ambulatory internal medicine. More about that later.
APDIM and APM, representing the collective organizations in AAIM, presented a plan for revision in training that would identify a core of internal medicine that could form the basis for the front end of training (e.g., possibly the first two years) and allow for a concentration in the later stages of internal medicine residencies. This might take the form of a third year with an emphasis in hospital medicine, ambulatory medicine, traditional internal medicine, or one of the medical subspecialties.
Amazingly, this approach was almost universally accepted by the attendees at the Dec. 2 meeting. With this broad support, AAIM plans to push forward in the coming months, disseminating details of their plan with an opportunity for a broader comment on just what would constitute the “core” of internal medicine. APM and APDIM then plan to take this input and come back by midyear with a more fleshed out proposal.
Of interest is that SHM is publishing the Core Competencies in Hospital Medicine as a supplement to the first issue of the Journal of Hospital Medicine. The work hospitalist thought leaders have put into defining these core competencies over the last few years should be helpful in providing the hospital medicine slant on the core of internal medicine as well as forming the basis for the curriculum with concentration in hospital medicine in the third year of training.
While the goal is to allow training to reflect the career choices of today’s internists and to better prepare them for their professional lives, the devil is truly in the details. Besides serving as a platform for education, internal medicine residency has evolved into a major service load supporting many health systems. Any revision to internal medicine residency needs to accommodate for the service load. In addition, any changes need to be blended into subspecialty fellowship training.
Weaved into this entire discussion was the evolving reshaping of internal medicine. At one time the well-trained general internist was the consummate well-rounded physician serving as a consultant on many diseases to surgeons and other physicians. The last quarter of the 20th century saw the blossoming of many subspecialties in internal medicine and in the last decade a further sub-subspecialization with endoscopists, electrophysiologists, and the like. As the complexity and demands increased in recent years in both the hospital and the outpatient arena, some internists chose to limit their practice to the hospital or the office, and hospital medicine grew and its competencies became more defined.
As internists further refined their skills and narrowed their professional focus, their expectations of their certification and especially their maintenance of certification (MOC) by the ABIM became an issue. Is the MOC process relevant to what they feel they do and should know?
In addition, many subspecialty societies have concerns about how maintaining a basis in internal medicine fits in with MOC in their subspecialties. At this meeting it became clear that many subspecialists feel there is a core of internal medicine they should continue to know and be evaluated on without being expected to know everything a practicing hospitalist or ambulatory internist knows. For example, a cardiologist may be expected to know when their diabetic patients are getting into trouble and need consultation but may not need to know the intricacies of managing extremes in glycemic control.
Many at this meeting felt that the time is now here for using the MOC process to offer those initially credentialed in general internal medicine to have their MOC evaluation tailored to their real-life practice as a hospitalist or an internist with an ambulatory practice and to allow for them to be identified as having expertise in hospital or ambulatory medicine. This was a recognition that these aspects of what have traditionally been lumped together as general internal medicine have key defined skills and knowledge and needs to be recognized as more than just an internist who is not a subspecialist.
Once again there is still much work to be done. SHM, ACP, SGIM, and others will need to work with ABIM and RUC and others to define the skills and the competencies that would form the basis for the training and evaluation of new and improved internists in the 21st century.
The good news from the Dec. 2, 2005, meeting in Dallas is that the national leadership in internal medicine recognizes the need to change internal medicine residency training and to have an MOC process that is relevant to all internists—general internists, subspecialists, and hospitalists. There was also a sense that this process needs to move forward with reasoned speed. We don’t need to write another white paper and declare victory. Today’s and tomorrow’s internists and our patients need us to provide the leadership to produce the best trained and motivated internists and subspecialists to meet the increasing needs of a sophisticated and aging population.
As always SHM will be there, playing an active role. Whatever we come up with for internal medicine I hope can be applicable to family practice and pediatrics as well. Because this is the professional world you will live in, we will continue to invite your input and ideas. TH
Dr. Wellikson has been CEO of SHM since 2000.
What Is a Hospitalist?

When I meet new people, I’m commonly asked, “So what do you do?” The first answer is easy: “I’m a doctor.” It’s the follow-up question that’s tricky: “What kind of doctor?”
“I’m a hospitalist,” I say.
“What’s that?”
I imagine that each of us faces similar questions almost daily from friends, family, patients, or strangers we meet. This tells me people are still learning who we are and what we are. I also imagine each of us has developed a standard way of answering that second question.
I like to say that a hospitalist is “a doctor who is an expert in taking care of people in the hospital.” Though not necessarily comprehensive, my definition usually does the job in casual conversation. In many ways I find this explanation easier than when I tried to describe myself as an “internist,” for which I never developed an easy definition. My favorite one-liner for internist was “pediatrician for adults,” but even that prompted blank stares or polite nods.
Early Definitions of Hospitalists
My definition certainly works in casual conversation. But the question gets to the heart of who we are, what we do, and what our field is about. Our ability to define these issues is critical to clarifying what hospitalists and hospital medicine are about.
It is interesting to look at early definitions of hospitalists. The first time the word hospitalist was published in 1996, hospitalists were defined as “specialists in inpatient medicine ... who will be responsible for managing the care of hospitalized patients in the same way that primary care physicians are responsible for managing the care of outpatients.”1
At the beginning there was a need to compare what hospitalists do, or will do, to something that was already known. The concept was so new that it needed an analogy to be explained. Even in 1999, a paper published in Annals of Internal Medicine defined hospitalists as “physicians who assume the care of hospitalized patients in place of the patients’ primary care provider.”2
Three years after the term was first coined, hospitalists were still being defined in relationship to other physicians. Another paper in Annals of Internal Medicine in 1999 defined a hospitalist as “a physician who spends at least 25% of his or her time serving as the physician-of-record for inpatients, during which time he or she accepts ‘hand-offs’ of hospitalized patients from primary care providers, returning patients to their primary care providers at the time of hospital discharge.”3 Of course that definition was quite a mouthful when explaining what you do to, say, your mother. But there were two important issues wrapped up in that definition.
The first was recognizing that some hospitalists were primarily engaged in research or leadership positions and did not provide a great deal of direct patient care, yet clearly defined themselves as hospitalists. The second was that we were still defined by our relationship to the primary care physician role. Our field was too new to be defined on its own and had to be explained in terms of the existing paradigm.
What became clear was that hospitalists should not be defined by the amount of inpatient care we provided but by our professional focus. For many hospitalists, the thought of caring for hospitalized patients only 25% of the time seemed ridiculous. To others involved in leadership or research who focused exclusively on hospital medicine yet did little patient care the definition seemed too restrictive.
In the end, any definition of hospitalists that depended on time could not encompass the wide range of roles and responsibilities that hospitalists held. Finally, a few months ago, hospitalist was included in the dictionary for the first time. The 2005 update of the Eleventh edition of Merriam-Webster’s Collegiate Dictionary defines a hospitalist as “a physician who specializes in treating hospitalized patients of other physicians in order to minimize the number of hospital visits by other physicians.” Although I am delighted to see hospitalist in the dictionary, this definition is too limited to be useful or accurate. It is certainly true that the presence of hospitalists means other physicians can come to the hospital less, but that is far from what hospitalists or hospital medicine are about.
SHM Definition of Hospitalists
Our society has an official definition of hospitalists: “Physicians whose primary professional focus is the general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to hospital medicine.”
I wish the dictionary had used this definition because it gets to the heart of what hospitalists are and defines us in a positive way, on our own terms, and not in relation to other physicians. This definition embraces the broad range of professional activities that hospitalists perform. Our definition even allows for hospitalists to engage in nonhospital-based activities such as outpatient care. The key to this definition is the emphasis of our professional focus being the care of hospitalized patients.
The Big Tent
What the SHM definition of hospitalists recognizes is the great diversity of physicians who serve as hospitalists and the wide variety of roles we all play in the service of caring for hospitalized patients. Both MDs and DOs serve as hospitalists, and they do so as internists, family physicians, and pediatricians. That all these physicians can come together in the same professional organization speaks to the importance of the unifying goal of caring for hospitalized patients that defines what each of us does.
Further, hospitalists can be involved exclusively in patient care, research, teaching, or leadership or in a combination of these roles. Once again the common principle is the focus on the care of hospitalized patients. In fact our society and field are better, more robust, more innovative, and more responsive to the needs of patients because we represent such a broad range of physicians in so many roles.
Our coming together in one organization creates a “big tent” for hospital medicine and allows for cross-fertilization of ideas. However, like any big tent, the strength of our diversity also creates challenges. For example, from an educational standpoint, we need to design programs and materials that meet the needs of all hospitalists. We have found that we share much, regardless of the setting in which we practice, the age of our patients, or the type of work we do. Patient safety, leadership, palliative care, and quality improvement are just a sample of the issues that pertain to all hospitalists.
Additionally, understanding these issues and addressing them takes people who are experts in patient care, teaching, research, and leadership—precisely the job descriptions found within the SHM. I am proud that SHM is one of the only professional societies to include internists, family physicians, and pediatricians from community practice, academia, and industry. Our big tent even extends beyond physicians to include nurse practitioners, physician assistants, pharmacists, nurses, and others who enrich our society and strengthen our field. In fact, our name—the Society of Hospital Medicine—was deliberately chosen to reflect the big tent. We specifically rejected a name that focused on the word hospitalist—not because we are not proud of it, but because we wanted all of those who work to improve the care of hospitalized patients to feel welcome in our society and to join in our mission.
Hospitalist Takes Hold
The phenomenon we now see is the emergence of “surgical” and “OB” hospitalists who care for hospitalized patients who otherwise do not have access to such physicians. Whether these physicians will assume the role of improving the system to provide better care to all inpatients or serve solely as technicians who work a shift and go home remains to be seen.
What is clear, however, is that in just 10 short years we have moved from having hospitalists defined in relationship to other physicians to having other physicians defined in relationship to hospitalists. This evolution is good for our field as we emerge from being the new kids on the block to being part of the existing paradigm.
Hope for the Future
The evolved definition of hospitalist reflects the maturing of our field and leaves me optimistic and hopeful for the future of hospitalists and hospital medicine. I hope that the dictionary will adopt our definition of hospitalist. I hope that one day hospitalist will be as well-known a word as pediatrician. I hope that as our field matures we never lose our enthusiasm and energy. And finally, I hope that our field stays unified and that the SHM continues to represent the broad range of physicians who work as hospitalists. Our field will be stronger and our achievements greater when we stand together, recognizing all that we share in common as hospitalists and respectful of the diversity that adds richness to our field. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
References
- Wachter RM, Goldman L. The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996;335:514-517.
- Lindenauer PK, Pantilat SZ, Katz PP, et al. Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians. Ann Intern Med. 1999;130(4Pt2):343-349.
- Wachter RM. An introduction to the hospitalist model. Ann Intern Med. 1999;130(4Pt2):338-342.
When I meet new people, I’m commonly asked, “So what do you do?” The first answer is easy: “I’m a doctor.” It’s the follow-up question that’s tricky: “What kind of doctor?”
“I’m a hospitalist,” I say.
“What’s that?”
I imagine that each of us faces similar questions almost daily from friends, family, patients, or strangers we meet. This tells me people are still learning who we are and what we are. I also imagine each of us has developed a standard way of answering that second question.
I like to say that a hospitalist is “a doctor who is an expert in taking care of people in the hospital.” Though not necessarily comprehensive, my definition usually does the job in casual conversation. In many ways I find this explanation easier than when I tried to describe myself as an “internist,” for which I never developed an easy definition. My favorite one-liner for internist was “pediatrician for adults,” but even that prompted blank stares or polite nods.
Early Definitions of Hospitalists
My definition certainly works in casual conversation. But the question gets to the heart of who we are, what we do, and what our field is about. Our ability to define these issues is critical to clarifying what hospitalists and hospital medicine are about.
It is interesting to look at early definitions of hospitalists. The first time the word hospitalist was published in 1996, hospitalists were defined as “specialists in inpatient medicine ... who will be responsible for managing the care of hospitalized patients in the same way that primary care physicians are responsible for managing the care of outpatients.”1
At the beginning there was a need to compare what hospitalists do, or will do, to something that was already known. The concept was so new that it needed an analogy to be explained. Even in 1999, a paper published in Annals of Internal Medicine defined hospitalists as “physicians who assume the care of hospitalized patients in place of the patients’ primary care provider.”2
Three years after the term was first coined, hospitalists were still being defined in relationship to other physicians. Another paper in Annals of Internal Medicine in 1999 defined a hospitalist as “a physician who spends at least 25% of his or her time serving as the physician-of-record for inpatients, during which time he or she accepts ‘hand-offs’ of hospitalized patients from primary care providers, returning patients to their primary care providers at the time of hospital discharge.”3 Of course that definition was quite a mouthful when explaining what you do to, say, your mother. But there were two important issues wrapped up in that definition.
The first was recognizing that some hospitalists were primarily engaged in research or leadership positions and did not provide a great deal of direct patient care, yet clearly defined themselves as hospitalists. The second was that we were still defined by our relationship to the primary care physician role. Our field was too new to be defined on its own and had to be explained in terms of the existing paradigm.
What became clear was that hospitalists should not be defined by the amount of inpatient care we provided but by our professional focus. For many hospitalists, the thought of caring for hospitalized patients only 25% of the time seemed ridiculous. To others involved in leadership or research who focused exclusively on hospital medicine yet did little patient care the definition seemed too restrictive.
In the end, any definition of hospitalists that depended on time could not encompass the wide range of roles and responsibilities that hospitalists held. Finally, a few months ago, hospitalist was included in the dictionary for the first time. The 2005 update of the Eleventh edition of Merriam-Webster’s Collegiate Dictionary defines a hospitalist as “a physician who specializes in treating hospitalized patients of other physicians in order to minimize the number of hospital visits by other physicians.” Although I am delighted to see hospitalist in the dictionary, this definition is too limited to be useful or accurate. It is certainly true that the presence of hospitalists means other physicians can come to the hospital less, but that is far from what hospitalists or hospital medicine are about.
SHM Definition of Hospitalists
Our society has an official definition of hospitalists: “Physicians whose primary professional focus is the general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to hospital medicine.”
I wish the dictionary had used this definition because it gets to the heart of what hospitalists are and defines us in a positive way, on our own terms, and not in relation to other physicians. This definition embraces the broad range of professional activities that hospitalists perform. Our definition even allows for hospitalists to engage in nonhospital-based activities such as outpatient care. The key to this definition is the emphasis of our professional focus being the care of hospitalized patients.
The Big Tent
What the SHM definition of hospitalists recognizes is the great diversity of physicians who serve as hospitalists and the wide variety of roles we all play in the service of caring for hospitalized patients. Both MDs and DOs serve as hospitalists, and they do so as internists, family physicians, and pediatricians. That all these physicians can come together in the same professional organization speaks to the importance of the unifying goal of caring for hospitalized patients that defines what each of us does.
Further, hospitalists can be involved exclusively in patient care, research, teaching, or leadership or in a combination of these roles. Once again the common principle is the focus on the care of hospitalized patients. In fact our society and field are better, more robust, more innovative, and more responsive to the needs of patients because we represent such a broad range of physicians in so many roles.
Our coming together in one organization creates a “big tent” for hospital medicine and allows for cross-fertilization of ideas. However, like any big tent, the strength of our diversity also creates challenges. For example, from an educational standpoint, we need to design programs and materials that meet the needs of all hospitalists. We have found that we share much, regardless of the setting in which we practice, the age of our patients, or the type of work we do. Patient safety, leadership, palliative care, and quality improvement are just a sample of the issues that pertain to all hospitalists.
Additionally, understanding these issues and addressing them takes people who are experts in patient care, teaching, research, and leadership—precisely the job descriptions found within the SHM. I am proud that SHM is one of the only professional societies to include internists, family physicians, and pediatricians from community practice, academia, and industry. Our big tent even extends beyond physicians to include nurse practitioners, physician assistants, pharmacists, nurses, and others who enrich our society and strengthen our field. In fact, our name—the Society of Hospital Medicine—was deliberately chosen to reflect the big tent. We specifically rejected a name that focused on the word hospitalist—not because we are not proud of it, but because we wanted all of those who work to improve the care of hospitalized patients to feel welcome in our society and to join in our mission.
Hospitalist Takes Hold
The phenomenon we now see is the emergence of “surgical” and “OB” hospitalists who care for hospitalized patients who otherwise do not have access to such physicians. Whether these physicians will assume the role of improving the system to provide better care to all inpatients or serve solely as technicians who work a shift and go home remains to be seen.
What is clear, however, is that in just 10 short years we have moved from having hospitalists defined in relationship to other physicians to having other physicians defined in relationship to hospitalists. This evolution is good for our field as we emerge from being the new kids on the block to being part of the existing paradigm.
Hope for the Future
The evolved definition of hospitalist reflects the maturing of our field and leaves me optimistic and hopeful for the future of hospitalists and hospital medicine. I hope that the dictionary will adopt our definition of hospitalist. I hope that one day hospitalist will be as well-known a word as pediatrician. I hope that as our field matures we never lose our enthusiasm and energy. And finally, I hope that our field stays unified and that the SHM continues to represent the broad range of physicians who work as hospitalists. Our field will be stronger and our achievements greater when we stand together, recognizing all that we share in common as hospitalists and respectful of the diversity that adds richness to our field. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
References
- Wachter RM, Goldman L. The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996;335:514-517.
- Lindenauer PK, Pantilat SZ, Katz PP, et al. Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians. Ann Intern Med. 1999;130(4Pt2):343-349.
- Wachter RM. An introduction to the hospitalist model. Ann Intern Med. 1999;130(4Pt2):338-342.
When I meet new people, I’m commonly asked, “So what do you do?” The first answer is easy: “I’m a doctor.” It’s the follow-up question that’s tricky: “What kind of doctor?”
“I’m a hospitalist,” I say.
“What’s that?”
I imagine that each of us faces similar questions almost daily from friends, family, patients, or strangers we meet. This tells me people are still learning who we are and what we are. I also imagine each of us has developed a standard way of answering that second question.
I like to say that a hospitalist is “a doctor who is an expert in taking care of people in the hospital.” Though not necessarily comprehensive, my definition usually does the job in casual conversation. In many ways I find this explanation easier than when I tried to describe myself as an “internist,” for which I never developed an easy definition. My favorite one-liner for internist was “pediatrician for adults,” but even that prompted blank stares or polite nods.
Early Definitions of Hospitalists
My definition certainly works in casual conversation. But the question gets to the heart of who we are, what we do, and what our field is about. Our ability to define these issues is critical to clarifying what hospitalists and hospital medicine are about.
It is interesting to look at early definitions of hospitalists. The first time the word hospitalist was published in 1996, hospitalists were defined as “specialists in inpatient medicine ... who will be responsible for managing the care of hospitalized patients in the same way that primary care physicians are responsible for managing the care of outpatients.”1
At the beginning there was a need to compare what hospitalists do, or will do, to something that was already known. The concept was so new that it needed an analogy to be explained. Even in 1999, a paper published in Annals of Internal Medicine defined hospitalists as “physicians who assume the care of hospitalized patients in place of the patients’ primary care provider.”2
Three years after the term was first coined, hospitalists were still being defined in relationship to other physicians. Another paper in Annals of Internal Medicine in 1999 defined a hospitalist as “a physician who spends at least 25% of his or her time serving as the physician-of-record for inpatients, during which time he or she accepts ‘hand-offs’ of hospitalized patients from primary care providers, returning patients to their primary care providers at the time of hospital discharge.”3 Of course that definition was quite a mouthful when explaining what you do to, say, your mother. But there were two important issues wrapped up in that definition.
The first was recognizing that some hospitalists were primarily engaged in research or leadership positions and did not provide a great deal of direct patient care, yet clearly defined themselves as hospitalists. The second was that we were still defined by our relationship to the primary care physician role. Our field was too new to be defined on its own and had to be explained in terms of the existing paradigm.
What became clear was that hospitalists should not be defined by the amount of inpatient care we provided but by our professional focus. For many hospitalists, the thought of caring for hospitalized patients only 25% of the time seemed ridiculous. To others involved in leadership or research who focused exclusively on hospital medicine yet did little patient care the definition seemed too restrictive.
In the end, any definition of hospitalists that depended on time could not encompass the wide range of roles and responsibilities that hospitalists held. Finally, a few months ago, hospitalist was included in the dictionary for the first time. The 2005 update of the Eleventh edition of Merriam-Webster’s Collegiate Dictionary defines a hospitalist as “a physician who specializes in treating hospitalized patients of other physicians in order to minimize the number of hospital visits by other physicians.” Although I am delighted to see hospitalist in the dictionary, this definition is too limited to be useful or accurate. It is certainly true that the presence of hospitalists means other physicians can come to the hospital less, but that is far from what hospitalists or hospital medicine are about.
SHM Definition of Hospitalists
Our society has an official definition of hospitalists: “Physicians whose primary professional focus is the general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to hospital medicine.”
I wish the dictionary had used this definition because it gets to the heart of what hospitalists are and defines us in a positive way, on our own terms, and not in relation to other physicians. This definition embraces the broad range of professional activities that hospitalists perform. Our definition even allows for hospitalists to engage in nonhospital-based activities such as outpatient care. The key to this definition is the emphasis of our professional focus being the care of hospitalized patients.
The Big Tent
What the SHM definition of hospitalists recognizes is the great diversity of physicians who serve as hospitalists and the wide variety of roles we all play in the service of caring for hospitalized patients. Both MDs and DOs serve as hospitalists, and they do so as internists, family physicians, and pediatricians. That all these physicians can come together in the same professional organization speaks to the importance of the unifying goal of caring for hospitalized patients that defines what each of us does.
Further, hospitalists can be involved exclusively in patient care, research, teaching, or leadership or in a combination of these roles. Once again the common principle is the focus on the care of hospitalized patients. In fact our society and field are better, more robust, more innovative, and more responsive to the needs of patients because we represent such a broad range of physicians in so many roles.
Our coming together in one organization creates a “big tent” for hospital medicine and allows for cross-fertilization of ideas. However, like any big tent, the strength of our diversity also creates challenges. For example, from an educational standpoint, we need to design programs and materials that meet the needs of all hospitalists. We have found that we share much, regardless of the setting in which we practice, the age of our patients, or the type of work we do. Patient safety, leadership, palliative care, and quality improvement are just a sample of the issues that pertain to all hospitalists.
Additionally, understanding these issues and addressing them takes people who are experts in patient care, teaching, research, and leadership—precisely the job descriptions found within the SHM. I am proud that SHM is one of the only professional societies to include internists, family physicians, and pediatricians from community practice, academia, and industry. Our big tent even extends beyond physicians to include nurse practitioners, physician assistants, pharmacists, nurses, and others who enrich our society and strengthen our field. In fact, our name—the Society of Hospital Medicine—was deliberately chosen to reflect the big tent. We specifically rejected a name that focused on the word hospitalist—not because we are not proud of it, but because we wanted all of those who work to improve the care of hospitalized patients to feel welcome in our society and to join in our mission.
Hospitalist Takes Hold
The phenomenon we now see is the emergence of “surgical” and “OB” hospitalists who care for hospitalized patients who otherwise do not have access to such physicians. Whether these physicians will assume the role of improving the system to provide better care to all inpatients or serve solely as technicians who work a shift and go home remains to be seen.
What is clear, however, is that in just 10 short years we have moved from having hospitalists defined in relationship to other physicians to having other physicians defined in relationship to hospitalists. This evolution is good for our field as we emerge from being the new kids on the block to being part of the existing paradigm.
Hope for the Future
The evolved definition of hospitalist reflects the maturing of our field and leaves me optimistic and hopeful for the future of hospitalists and hospital medicine. I hope that the dictionary will adopt our definition of hospitalist. I hope that one day hospitalist will be as well-known a word as pediatrician. I hope that as our field matures we never lose our enthusiasm and energy. And finally, I hope that our field stays unified and that the SHM continues to represent the broad range of physicians who work as hospitalists. Our field will be stronger and our achievements greater when we stand together, recognizing all that we share in common as hospitalists and respectful of the diversity that adds richness to our field. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
References
- Wachter RM, Goldman L. The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996;335:514-517.
- Lindenauer PK, Pantilat SZ, Katz PP, et al. Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians. Ann Intern Med. 1999;130(4Pt2):343-349.
- Wachter RM. An introduction to the hospitalist model. Ann Intern Med. 1999;130(4Pt2):338-342.
Risky Business
[H]ospitalists are in a very litigation-intensive and volatile environment. … [T]hey are practicing in a niche that has not been fully accepted by the medical community. There’s a lot of tension on various specialty groups as to the role of hospitalists, the value of hospitalists, whether for a variety of reasons they are creating impediments [to] the quality of care, possibly raising competitive concerns. And so the best trained, the best intentioned, and most capable hospitalist is choosing … a dangerous area of practice from a liability perspective.
—Barry Halpern, JD, Snell and Wilmer Law Offices, expert in medical malpractice law
As hospitalists move from patient to patient, consult to consult, and decision to decision, risk management—proactively identifying, assessing, and prioritizing risks with a goal of minimizing their negative consequences—may not stay uppermost in their minds. Yet for hospitalists, by virtue of their constant location and activity in hospitals, risks lurk at every corner, and the potential for being judged at fault is real and potentially costly.
What are the hospitalist’s risks of being sued for malpractice? How can hospitalists best protect themselves against malpractice claims? Does being liable for patient care ever cause hospitalists to handicap themselves, to hold back in some ways?
What Risks Do Hospitalists Face?
“I think the issue that hospitalists are facing from a medical-legal standpoint is there is not a lot of cumulative experience with case law, precedent, in the field of hospital medicine,” says Tom Baudendistel, MD, a hospitalist and associate program director at California Pacific Medical Center in San Francisco.
Besides errors of medical practice, hospitalists are at risk when they:
- Practice beyond the scope of their specialty;
- Fail to communicate or communicate poorly with patients, families, staff, and referring physicians; and
- Fail to exercise independent medical judgment.
Hospitalists work with sicker, more complicated patients in an environment where more things can go wrong. (See The Hospitalist, July/August 2002, “Hospitalists and the Malpractice Insurance Crisis.”) All things considered, hospital-based physicians are at greater risk of being sued than their colleagues who work in offices.
Case #1: The hospitalist failed to detect a vertebral artery dissection in a younger patient. Should they have been able to detect that? It’s a rather unusual stroke presentation. A neurologist would have picked it up—and certainly would have been held liable or negligent if they’d missed that diagnosis. During their training neurologists would have certainly seen this condition as a cause of stroke in someone below age 45. But internists, in general, don’t receive good neurologic training as part of their residencies, and in community hospitals there is no set neurology service.
Neurologists have now become more office-based and allow the hospitalists to do more. By doing more, they’re also exposed to more legal risk. Should the hospitalist be held negligent for missing an unusual stroke? It depends on what you think is a hospitalist’s scope of practice.
—Dr. Baudendistel
Scope of Practice
A hospitalist’s scope of practice is somewhat difficult to define, although the classification “hospitalist” is gaining clarity (including with insurance underwriters), and the hospitalist model is becoming more recognized as a subspecialty. (See “A Malpractice Primer,” The Hospitalist, Dec. 2005, p. 1.)
One challenge in defining the hospitalist’s scope of practice is that hospitalists do a variety of things and work in different departments of the hospital: Some spend more time in acute care, some are more in general care, and some of them are mostly in trauma care.
It is generally acknowledged that healthcare practitioners must employ the same degree of diligence and skill commonly possessed by other members of the healthcare profession who are engaged in the same kind of work in similar locales. Thus, hospitalists need to be acutely aware of how other hospitalists practice in similar settings with similar resources available.
Hospitalists in rural and suburban hospitals, which have fewer and less specialized staff readily available for consults, should expect to have a different scope of practice. In time further clarification of the roles, responsibilities, and clinical skills of hospitalists will be established so that the scope of practice is more clearly defined.
Dr. Baudendistel believes that residents tracking to specialize in hospital medicine could benefit from having more education in certain areas: neurology, perioperative medicine, and critical care.
SHM has recognized the need for better risk management strategies to protect hospitalists and will provide this information and continuing education in The Core Competencies in Hospital Medicine to be published the January/February 2006 issue of the Journal of Hospital Medicine.
Case #2: A male patient came into the ED at a rural hospital with an altered mental status. He had a history of falls and the CT scan in the ED showed a large subdural hematoma.
“We need to admit this patient to the hospital,” said the ED doc. “Call the hospitalist.”
“What does neurosurgery want to do?” asked the hospitalist.
The hospitalist tried to reach the neurosurgeon. And the ED doc wasn’t able to obtain neurosurgery consult because the neurosurgeon said that he wasn’t on call for that hospital. So the hospitalist was … left responsible without neurosurgery backup.
Ultimately, the patient worsened. The hospitalist called a different neurosurgeon at a different hospital who clearly wasn’t in charge of the patient. That doctor said, “Get the patient over to us, and we’ll take care of it.”
There was a 12-hour delay, and the patient finally got transferred to the other hospital, had surgery, and did OK. But he was definitely deteriorating.
The neurosurgeon who said he wasn’t on call for that hospital was wrong. He was lying or just didn’t know of his group’s call coverage. It was a clear violation. And it left the hospital in a situation that isn’t all that unfamiliar.
In this case, the hospitalist wasn’t at fault. There was clear chart documentation [provided as evidence] that said, “I called the neurosurgeon three times and they’re not calling back. Finally they called back the fourth time and said that they’re not coming in.” —Dr. Baudendistel
Communication
Communication is crucial in a clinician’s provision of quality care and also provides a safety net to help prevent liability. Communication with patients, families, staff, and other physicians—particularly their inpatients’ primary care physicians—provides the strongest armor against malpractice assaults. Timeliness and the urgency of the issue are key to patient care and are also are examined by those who review malpractice claims.
In recent years medical malpractice claims payouts have increased substantially for both jury verdicts and settlements. For monetary awards involving doctor-patient relations, which are largely predicated upon communication, the median payout is $230,000.1
Some hot-button areas that carry higher risk and call for meticulous communication between providers include:
- Inpatient postoperative care;
- Post-discharge communication (hand-offs);
- Diagnosis and treatment of a patient for whom there is an incomplete history; and
- Acceptance for treatment of patients whose medical conditions may either be unfamiliar to hospitalists or for which they have had limited or no training.
Communication with Patients
Communication—every aspect of it—is essential for the patient’s health, attitude, and satisfaction. Interestingly, legal data show that most patients who have bad outcomes don’t file suit.2 Although patients litigate for a variety of reasons, chief among them is when they perceive they have suffered because of administrative errors, rude practitioners or support staff, or the denial of tests and referrals they had requested and thought were reasonable.3 Data from a number of studies conducted within the past two decades show that although no particular communication skills can be directly associated with reducing malpractice claims, when patients perceive that their providers treat them genuinely and fairly, and update them honestly and regularly, they are less likely to sue.4-9
One-on-One with Barry Halpern, JD

My law firm practices throughout the western United States, and one of the areas that I see as a general pattern is when … continuity of care becomes an issue. The cases that are sometimes the most troublesome are those in which the hospitalist is involved.
There’s never a real clear demarcation of responsibility between, for instance, the surgery service and the hospitalist. Orders are written and then interpreted by the nursing staff in ways that, in retrospect, even the surgical service or the hospitalist are not pleased with. Yet the physicians aren’t talking to each other, and the documentation in the medical record is intermittent … .
Those kinds of situations, particularly where there is later alleged to have been, for instance, a medication error, become very difficult to defend. Because from the perspective of the lay jury that will be looking at the case, it’s easy for a plaintiff lawyer to depict a very disjointed and uncoordinated approach to care, when—in fact—the reality of practices is that they don’t always go perfectly and things aren’t always documented the instant that they are done.
And sometimes bad things happen despite everybody’s best efforts. But when you have a rough interface between the hospitalist and the other physicians with regard to responsibility for a patient, you are inviting a legal problem.
—Halpern is an attorney with Snell and Wilmer Law Offices, Phoenix
Case #3: A 72-year-old female who was pretty healthy (she had some high blood pressure) came in with abdominal pain. The ED doctor drew the laboratories, which suggested pancreatitis, and then investigated why she had pancreatitis. The ultrasound ordered by the ED doc showed gallstones. The physician then correctly inferred that she had gallstones causing her pancreatitis.
A hospitalist was called [and] admitted the patient. Surgery and GI consultants were called. The GI consultant first ordered an endoscopic retrograde cholangiopancreatography to clean the gallstones from the common bile duct. That went fine, and the next day the patient looked a little better. The GI service said, “Anticipated to go home in a couple days.” Surgery felt the same.
Then the consensus was to remove her gallbladder because eventually she would need to have it done. And that’s when things started to go badly.
On postoperative day two, the patient started having pain out of proportion to what should be expected. The internist (the hospitalist) raised that question in his note. The surgeon said, “No, that’s still postoperative pain,” and increased the pain medicine.
The hospitalist said, “I’m really concerned about this; I’ll talk to the surgeon.”
Again the surgeon said, “There’s nothing to worry about. I’ll at least order a HIDA scan.”
Initially the patient refused the scan, but the next day—postoperative day three—she was still having pain and was clearly worse. She had a high fever; her blood pressure dropped; and her white blood cell count climbed from 10,000 to 20,000, indicating infection/inflammation. Finally the hospitalist ordered a CT scan, which shows a perforation caused by the surgery.
The patient went to surgery for repair. As was predicted, she had a rocky hospital course and ultimately died a month later.
The surgeon was clearly in the wrong. … I was consulted and was asked, “What would you do with the hospitalist? What was their role in that case? Do you think he failed to meet the standard of care?”
—Dr. Baudendistel
Communication with Other Clinicians
“Communication between physicians is critical,” says Sally Whitaker, RN, BSN, risk manager with Rex Healthcare in Raleigh, N.C. “[Hospitalists] shouldn’t just rely on knowing they’ve put their notes on the discharge summary.”
At Rex Hospital (one of Rex Healthcare’s six facilities) where Whitaker works, when seminal events (those big bad things that happen) occur and result in severe trauma or death, the appropriate people meet to backtrack through the steps and scenarios that led to the breakdown.
“Fortunately we don’t have seminal events every day, but every day we do have things that go wrong,” she says. “ … And when we look at our Group Cause Analysis meetings, three-quarters of them [involve] communication issues.”
Exercise Independent Medical Judgment
Hospitalists should read their insurance and employer contracts carefully (especially those with a managed care organization) to ensure that the contract includes a statement allowing the physician to exercise independent medical judgment in the treatment of all patients. If that statement is not present, the hospitalist should request a revision in the contract to include such a statement.
In medical residency programs, a distinction is often made between being a consultant and being a co-manager, says Dr. Baudendistel, but “you have to assume there’s no legal difference between [the two].” Case #3 , he says, was a challenge to decide because the responsibilities of the surgeon and hospitalist in postoperative care were not clearly demarcated.
“I think the surgeon was probably saying, ‘I see this all the time and this is within the realm of what happens after one of these surgeries; let’s not be too worried yet,’” he says. “And I think the internist [hospitalist] ultimately pulled the trigger correctly and the [controversy later on pertained to] whether it should have been done a day or two earlier and whether that have mattered.”
This case illustrates that, although hospitalists are members of teams and partner with consultants and primary physicians, in the end they are managers of patient care and may (we hope rarely) have to break ranks to make aggressive care decisions.
“I think that the other thing that was in [the hospitalist’s] favor,” says Dr. Baudendistel of the case, “was that he was writing very thorough notes, [and] really was discussing everything with the family and everyone was on board. He was doing a very compassionate job … trying to manage this care.”
To Dr. Baudendistel, who is the chair of SHM’s ethics committee, this went a long way toward showing good faith.
Reducing Risks: Concern for the Medical Record
If the medical record is found deficient or illuminating in a negative way, it may serve the plaintiff attorney’s strategy well for establishing negligence or wrongdoing. The chart notes documented by nurses, attending staff, consultants, other residents, and therapists could either portray a smoothly managed case or a chronology of errors and omissions. The chart should never be cosigned and never merely assumed to be accurate.
When Things Go Wrong
Whitaker advises hospitalists to keep the lines of communication open. “Especially after something unexpected has happened,” she says. “So many times I think the human tendency is to just withdraw, or you feel terrible and you don’t know what to say, or you’re afraid you’re going to get emotional while you’re talking with the family.”
This is normal human response in these circumstances, but if you act on the impulse to withdraw and avoid the patient and family, or hold back, which may eventually lead to a filed claim from a family that feels abandoned.
“Until now the number of lawsuits has been really steady and the amount that we were paying in lawsuits was increasing,” says Whitaker. “However, we’re trying to work with the families earlier on so if we make a mistake and we realize that we made a mistake then we admit that. And we try to do what we can to make it right for that patient and their family.”
This often means reaching a fair and reasonable settlement, says Whitaker, “and [examining fair and reasonable means reviewing] the communication at the time the event occurred. Did we acknowledge that we made a mistake? Did we let them know we’d be willing to work with them? And did we let them know we [have since] made these changes … so they’ll … be reassured [that] hopefully it won’t happen again?”
Who’s in Charge?
Linda Greenwald, RN, MS, editor of risk management publications at ProMutual Insurance Group in Boston, wrote in the company’s newsletter, Perspectives on Clinical Risk Management, that in prior times, the question, “Who’s in charge?” was rhetorical.10 These days any number of generalists or specialists might claim that role. And therein lies the rub: Greenwald says that in many cases involving hospitalists the lines of responsibility are unclear and one or more systems may fail. If so, Greenwald writes, the result may be a malpractice claim alleging:
- Failure to diagnose when each of two physicians assumes the other has responsibility for follow-up;
- Negligence in treatment when one physician fails to monitor on an outpatient basis the medication first prescribed by another physician when the patient was an inpatient; and/or
- Negligent care when a patient misinterprets the information one physician asks him or her to relay to another physician.10
Halpern concurs that the modern mix of professionals working as a team on hospital care can be a major challenge.
“In olden days, when a primary care physician referred to a surgeon, and the surgeon performed surgery, and the surgeon took responsibility for postoperative care, and occasionally brought in a consultant, the lines were relatively clear,” says Halpern. “When a hospitalist is injected into the mix, unless the hospital has really clear procedures and unless everybody is comfortable with the system and everybody is talking to each other and agreeing on the lines of demarcation, you’re creating a soup that plaintiff lawyers would be happy to stir.”
The more murky the communication, the greater the liability. “And when you have murky lines of communication, murky lines of responsibility, and a medical catastrophe,” says Halpern, “human nature compounds the problem by frequently causing a finger-pointing contest, where each component of the patient care team circles its own wagons [and] points in a different direction. And that is the absolute worst thing that can happen when trying to deal with a patient injury claim.”
Summary
The hospitalist’s primary risk for malpractice claims may be inadequate or absent patient follow-up resulting from a lack of communication. The best means of protection from claims is for hospitalists to incorporate a comprehensive risk management program into their practice.
Several strategies have proved successful to help prevent litigation. In general, hospitalists should make sure that their hospital has clearly delineated policies regarding responsibility for patients; clearly understand—and ensure that your coworkers, colleagues, and referring physicians understand—the hospital’s systems and protocols; exercise good communication skills; conform to the standard of care; know your own scope of care to the best of your ability; and exercise independent medical judgment, even when partnering with others. TH
Andrea Sattinger also writes the “Alliances” department for The Hospitalist.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003;348:2281-2284.
- Virshup BB, Oppenberg MPH, Coleman MM. Strategic risk management: reducing malpractice claims through more effective patient-doctor communication. Am J Med Quality. 1999;14:153-159.
- Gurwitz JH, Terry S, Field TS, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289:1107-1116.
- Shapiro RS, Simpson DE, Lawrence SL, et al.. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989;149:2190-2196.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;227:558-559.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370.
- Cohen JR. Apology and organizations: exploring an example from medical practice. Fordham Urban Law Journal. 2000;27:1447-1482.
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Greenwald L. Who's in charge? Perspectives on Clinical Risk Management. Boston, Mass: ProMutual Group Risk Management Services; Fall 2000.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
[H]ospitalists are in a very litigation-intensive and volatile environment. … [T]hey are practicing in a niche that has not been fully accepted by the medical community. There’s a lot of tension on various specialty groups as to the role of hospitalists, the value of hospitalists, whether for a variety of reasons they are creating impediments [to] the quality of care, possibly raising competitive concerns. And so the best trained, the best intentioned, and most capable hospitalist is choosing … a dangerous area of practice from a liability perspective.
—Barry Halpern, JD, Snell and Wilmer Law Offices, expert in medical malpractice law
As hospitalists move from patient to patient, consult to consult, and decision to decision, risk management—proactively identifying, assessing, and prioritizing risks with a goal of minimizing their negative consequences—may not stay uppermost in their minds. Yet for hospitalists, by virtue of their constant location and activity in hospitals, risks lurk at every corner, and the potential for being judged at fault is real and potentially costly.
What are the hospitalist’s risks of being sued for malpractice? How can hospitalists best protect themselves against malpractice claims? Does being liable for patient care ever cause hospitalists to handicap themselves, to hold back in some ways?
What Risks Do Hospitalists Face?
“I think the issue that hospitalists are facing from a medical-legal standpoint is there is not a lot of cumulative experience with case law, precedent, in the field of hospital medicine,” says Tom Baudendistel, MD, a hospitalist and associate program director at California Pacific Medical Center in San Francisco.
Besides errors of medical practice, hospitalists are at risk when they:
- Practice beyond the scope of their specialty;
- Fail to communicate or communicate poorly with patients, families, staff, and referring physicians; and
- Fail to exercise independent medical judgment.
Hospitalists work with sicker, more complicated patients in an environment where more things can go wrong. (See The Hospitalist, July/August 2002, “Hospitalists and the Malpractice Insurance Crisis.”) All things considered, hospital-based physicians are at greater risk of being sued than their colleagues who work in offices.
Case #1: The hospitalist failed to detect a vertebral artery dissection in a younger patient. Should they have been able to detect that? It’s a rather unusual stroke presentation. A neurologist would have picked it up—and certainly would have been held liable or negligent if they’d missed that diagnosis. During their training neurologists would have certainly seen this condition as a cause of stroke in someone below age 45. But internists, in general, don’t receive good neurologic training as part of their residencies, and in community hospitals there is no set neurology service.
Neurologists have now become more office-based and allow the hospitalists to do more. By doing more, they’re also exposed to more legal risk. Should the hospitalist be held negligent for missing an unusual stroke? It depends on what you think is a hospitalist’s scope of practice.
—Dr. Baudendistel
Scope of Practice
A hospitalist’s scope of practice is somewhat difficult to define, although the classification “hospitalist” is gaining clarity (including with insurance underwriters), and the hospitalist model is becoming more recognized as a subspecialty. (See “A Malpractice Primer,” The Hospitalist, Dec. 2005, p. 1.)
One challenge in defining the hospitalist’s scope of practice is that hospitalists do a variety of things and work in different departments of the hospital: Some spend more time in acute care, some are more in general care, and some of them are mostly in trauma care.
It is generally acknowledged that healthcare practitioners must employ the same degree of diligence and skill commonly possessed by other members of the healthcare profession who are engaged in the same kind of work in similar locales. Thus, hospitalists need to be acutely aware of how other hospitalists practice in similar settings with similar resources available.
Hospitalists in rural and suburban hospitals, which have fewer and less specialized staff readily available for consults, should expect to have a different scope of practice. In time further clarification of the roles, responsibilities, and clinical skills of hospitalists will be established so that the scope of practice is more clearly defined.
Dr. Baudendistel believes that residents tracking to specialize in hospital medicine could benefit from having more education in certain areas: neurology, perioperative medicine, and critical care.
SHM has recognized the need for better risk management strategies to protect hospitalists and will provide this information and continuing education in The Core Competencies in Hospital Medicine to be published the January/February 2006 issue of the Journal of Hospital Medicine.
Case #2: A male patient came into the ED at a rural hospital with an altered mental status. He had a history of falls and the CT scan in the ED showed a large subdural hematoma.
“We need to admit this patient to the hospital,” said the ED doc. “Call the hospitalist.”
“What does neurosurgery want to do?” asked the hospitalist.
The hospitalist tried to reach the neurosurgeon. And the ED doc wasn’t able to obtain neurosurgery consult because the neurosurgeon said that he wasn’t on call for that hospital. So the hospitalist was … left responsible without neurosurgery backup.
Ultimately, the patient worsened. The hospitalist called a different neurosurgeon at a different hospital who clearly wasn’t in charge of the patient. That doctor said, “Get the patient over to us, and we’ll take care of it.”
There was a 12-hour delay, and the patient finally got transferred to the other hospital, had surgery, and did OK. But he was definitely deteriorating.
The neurosurgeon who said he wasn’t on call for that hospital was wrong. He was lying or just didn’t know of his group’s call coverage. It was a clear violation. And it left the hospital in a situation that isn’t all that unfamiliar.
In this case, the hospitalist wasn’t at fault. There was clear chart documentation [provided as evidence] that said, “I called the neurosurgeon three times and they’re not calling back. Finally they called back the fourth time and said that they’re not coming in.” —Dr. Baudendistel
Communication
Communication is crucial in a clinician’s provision of quality care and also provides a safety net to help prevent liability. Communication with patients, families, staff, and other physicians—particularly their inpatients’ primary care physicians—provides the strongest armor against malpractice assaults. Timeliness and the urgency of the issue are key to patient care and are also are examined by those who review malpractice claims.
In recent years medical malpractice claims payouts have increased substantially for both jury verdicts and settlements. For monetary awards involving doctor-patient relations, which are largely predicated upon communication, the median payout is $230,000.1
Some hot-button areas that carry higher risk and call for meticulous communication between providers include:
- Inpatient postoperative care;
- Post-discharge communication (hand-offs);
- Diagnosis and treatment of a patient for whom there is an incomplete history; and
- Acceptance for treatment of patients whose medical conditions may either be unfamiliar to hospitalists or for which they have had limited or no training.
Communication with Patients
Communication—every aspect of it—is essential for the patient’s health, attitude, and satisfaction. Interestingly, legal data show that most patients who have bad outcomes don’t file suit.2 Although patients litigate for a variety of reasons, chief among them is when they perceive they have suffered because of administrative errors, rude practitioners or support staff, or the denial of tests and referrals they had requested and thought were reasonable.3 Data from a number of studies conducted within the past two decades show that although no particular communication skills can be directly associated with reducing malpractice claims, when patients perceive that their providers treat them genuinely and fairly, and update them honestly and regularly, they are less likely to sue.4-9
One-on-One with Barry Halpern, JD
My law firm practices throughout the western United States, and one of the areas that I see as a general pattern is when … continuity of care becomes an issue. The cases that are sometimes the most troublesome are those in which the hospitalist is involved.
There’s never a real clear demarcation of responsibility between, for instance, the surgery service and the hospitalist. Orders are written and then interpreted by the nursing staff in ways that, in retrospect, even the surgical service or the hospitalist are not pleased with. Yet the physicians aren’t talking to each other, and the documentation in the medical record is intermittent … .
Those kinds of situations, particularly where there is later alleged to have been, for instance, a medication error, become very difficult to defend. Because from the perspective of the lay jury that will be looking at the case, it’s easy for a plaintiff lawyer to depict a very disjointed and uncoordinated approach to care, when—in fact—the reality of practices is that they don’t always go perfectly and things aren’t always documented the instant that they are done.
And sometimes bad things happen despite everybody’s best efforts. But when you have a rough interface between the hospitalist and the other physicians with regard to responsibility for a patient, you are inviting a legal problem.
—Halpern is an attorney with Snell and Wilmer Law Offices, Phoenix
Case #3: A 72-year-old female who was pretty healthy (she had some high blood pressure) came in with abdominal pain. The ED doctor drew the laboratories, which suggested pancreatitis, and then investigated why she had pancreatitis. The ultrasound ordered by the ED doc showed gallstones. The physician then correctly inferred that she had gallstones causing her pancreatitis.
A hospitalist was called [and] admitted the patient. Surgery and GI consultants were called. The GI consultant first ordered an endoscopic retrograde cholangiopancreatography to clean the gallstones from the common bile duct. That went fine, and the next day the patient looked a little better. The GI service said, “Anticipated to go home in a couple days.” Surgery felt the same.
Then the consensus was to remove her gallbladder because eventually she would need to have it done. And that’s when things started to go badly.
On postoperative day two, the patient started having pain out of proportion to what should be expected. The internist (the hospitalist) raised that question in his note. The surgeon said, “No, that’s still postoperative pain,” and increased the pain medicine.
The hospitalist said, “I’m really concerned about this; I’ll talk to the surgeon.”
Again the surgeon said, “There’s nothing to worry about. I’ll at least order a HIDA scan.”
Initially the patient refused the scan, but the next day—postoperative day three—she was still having pain and was clearly worse. She had a high fever; her blood pressure dropped; and her white blood cell count climbed from 10,000 to 20,000, indicating infection/inflammation. Finally the hospitalist ordered a CT scan, which shows a perforation caused by the surgery.
The patient went to surgery for repair. As was predicted, she had a rocky hospital course and ultimately died a month later.
The surgeon was clearly in the wrong. … I was consulted and was asked, “What would you do with the hospitalist? What was their role in that case? Do you think he failed to meet the standard of care?”
—Dr. Baudendistel
Communication with Other Clinicians
“Communication between physicians is critical,” says Sally Whitaker, RN, BSN, risk manager with Rex Healthcare in Raleigh, N.C. “[Hospitalists] shouldn’t just rely on knowing they’ve put their notes on the discharge summary.”
At Rex Hospital (one of Rex Healthcare’s six facilities) where Whitaker works, when seminal events (those big bad things that happen) occur and result in severe trauma or death, the appropriate people meet to backtrack through the steps and scenarios that led to the breakdown.
“Fortunately we don’t have seminal events every day, but every day we do have things that go wrong,” she says. “ … And when we look at our Group Cause Analysis meetings, three-quarters of them [involve] communication issues.”
Exercise Independent Medical Judgment
Hospitalists should read their insurance and employer contracts carefully (especially those with a managed care organization) to ensure that the contract includes a statement allowing the physician to exercise independent medical judgment in the treatment of all patients. If that statement is not present, the hospitalist should request a revision in the contract to include such a statement.
In medical residency programs, a distinction is often made between being a consultant and being a co-manager, says Dr. Baudendistel, but “you have to assume there’s no legal difference between [the two].” Case #3 , he says, was a challenge to decide because the responsibilities of the surgeon and hospitalist in postoperative care were not clearly demarcated.
“I think the surgeon was probably saying, ‘I see this all the time and this is within the realm of what happens after one of these surgeries; let’s not be too worried yet,’” he says. “And I think the internist [hospitalist] ultimately pulled the trigger correctly and the [controversy later on pertained to] whether it should have been done a day or two earlier and whether that have mattered.”
This case illustrates that, although hospitalists are members of teams and partner with consultants and primary physicians, in the end they are managers of patient care and may (we hope rarely) have to break ranks to make aggressive care decisions.
“I think that the other thing that was in [the hospitalist’s] favor,” says Dr. Baudendistel of the case, “was that he was writing very thorough notes, [and] really was discussing everything with the family and everyone was on board. He was doing a very compassionate job … trying to manage this care.”
To Dr. Baudendistel, who is the chair of SHM’s ethics committee, this went a long way toward showing good faith.
Reducing Risks: Concern for the Medical Record
If the medical record is found deficient or illuminating in a negative way, it may serve the plaintiff attorney’s strategy well for establishing negligence or wrongdoing. The chart notes documented by nurses, attending staff, consultants, other residents, and therapists could either portray a smoothly managed case or a chronology of errors and omissions. The chart should never be cosigned and never merely assumed to be accurate.
When Things Go Wrong
Whitaker advises hospitalists to keep the lines of communication open. “Especially after something unexpected has happened,” she says. “So many times I think the human tendency is to just withdraw, or you feel terrible and you don’t know what to say, or you’re afraid you’re going to get emotional while you’re talking with the family.”
This is normal human response in these circumstances, but if you act on the impulse to withdraw and avoid the patient and family, or hold back, which may eventually lead to a filed claim from a family that feels abandoned.
“Until now the number of lawsuits has been really steady and the amount that we were paying in lawsuits was increasing,” says Whitaker. “However, we’re trying to work with the families earlier on so if we make a mistake and we realize that we made a mistake then we admit that. And we try to do what we can to make it right for that patient and their family.”
This often means reaching a fair and reasonable settlement, says Whitaker, “and [examining fair and reasonable means reviewing] the communication at the time the event occurred. Did we acknowledge that we made a mistake? Did we let them know we’d be willing to work with them? And did we let them know we [have since] made these changes … so they’ll … be reassured [that] hopefully it won’t happen again?”
Who’s in Charge?
Linda Greenwald, RN, MS, editor of risk management publications at ProMutual Insurance Group in Boston, wrote in the company’s newsletter, Perspectives on Clinical Risk Management, that in prior times, the question, “Who’s in charge?” was rhetorical.10 These days any number of generalists or specialists might claim that role. And therein lies the rub: Greenwald says that in many cases involving hospitalists the lines of responsibility are unclear and one or more systems may fail. If so, Greenwald writes, the result may be a malpractice claim alleging:
- Failure to diagnose when each of two physicians assumes the other has responsibility for follow-up;
- Negligence in treatment when one physician fails to monitor on an outpatient basis the medication first prescribed by another physician when the patient was an inpatient; and/or
- Negligent care when a patient misinterprets the information one physician asks him or her to relay to another physician.10
Halpern concurs that the modern mix of professionals working as a team on hospital care can be a major challenge.
“In olden days, when a primary care physician referred to a surgeon, and the surgeon performed surgery, and the surgeon took responsibility for postoperative care, and occasionally brought in a consultant, the lines were relatively clear,” says Halpern. “When a hospitalist is injected into the mix, unless the hospital has really clear procedures and unless everybody is comfortable with the system and everybody is talking to each other and agreeing on the lines of demarcation, you’re creating a soup that plaintiff lawyers would be happy to stir.”
The more murky the communication, the greater the liability. “And when you have murky lines of communication, murky lines of responsibility, and a medical catastrophe,” says Halpern, “human nature compounds the problem by frequently causing a finger-pointing contest, where each component of the patient care team circles its own wagons [and] points in a different direction. And that is the absolute worst thing that can happen when trying to deal with a patient injury claim.”
Summary
The hospitalist’s primary risk for malpractice claims may be inadequate or absent patient follow-up resulting from a lack of communication. The best means of protection from claims is for hospitalists to incorporate a comprehensive risk management program into their practice.
Several strategies have proved successful to help prevent litigation. In general, hospitalists should make sure that their hospital has clearly delineated policies regarding responsibility for patients; clearly understand—and ensure that your coworkers, colleagues, and referring physicians understand—the hospital’s systems and protocols; exercise good communication skills; conform to the standard of care; know your own scope of care to the best of your ability; and exercise independent medical judgment, even when partnering with others. TH
Andrea Sattinger also writes the “Alliances” department for The Hospitalist.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003;348:2281-2284.
- Virshup BB, Oppenberg MPH, Coleman MM. Strategic risk management: reducing malpractice claims through more effective patient-doctor communication. Am J Med Quality. 1999;14:153-159.
- Gurwitz JH, Terry S, Field TS, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289:1107-1116.
- Shapiro RS, Simpson DE, Lawrence SL, et al.. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989;149:2190-2196.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;227:558-559.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370.
- Cohen JR. Apology and organizations: exploring an example from medical practice. Fordham Urban Law Journal. 2000;27:1447-1482.
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Greenwald L. Who's in charge? Perspectives on Clinical Risk Management. Boston, Mass: ProMutual Group Risk Management Services; Fall 2000.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
[H]ospitalists are in a very litigation-intensive and volatile environment. … [T]hey are practicing in a niche that has not been fully accepted by the medical community. There’s a lot of tension on various specialty groups as to the role of hospitalists, the value of hospitalists, whether for a variety of reasons they are creating impediments [to] the quality of care, possibly raising competitive concerns. And so the best trained, the best intentioned, and most capable hospitalist is choosing … a dangerous area of practice from a liability perspective.
—Barry Halpern, JD, Snell and Wilmer Law Offices, expert in medical malpractice law
As hospitalists move from patient to patient, consult to consult, and decision to decision, risk management—proactively identifying, assessing, and prioritizing risks with a goal of minimizing their negative consequences—may not stay uppermost in their minds. Yet for hospitalists, by virtue of their constant location and activity in hospitals, risks lurk at every corner, and the potential for being judged at fault is real and potentially costly.
What are the hospitalist’s risks of being sued for malpractice? How can hospitalists best protect themselves against malpractice claims? Does being liable for patient care ever cause hospitalists to handicap themselves, to hold back in some ways?
What Risks Do Hospitalists Face?
“I think the issue that hospitalists are facing from a medical-legal standpoint is there is not a lot of cumulative experience with case law, precedent, in the field of hospital medicine,” says Tom Baudendistel, MD, a hospitalist and associate program director at California Pacific Medical Center in San Francisco.
Besides errors of medical practice, hospitalists are at risk when they:
- Practice beyond the scope of their specialty;
- Fail to communicate or communicate poorly with patients, families, staff, and referring physicians; and
- Fail to exercise independent medical judgment.
Hospitalists work with sicker, more complicated patients in an environment where more things can go wrong. (See The Hospitalist, July/August 2002, “Hospitalists and the Malpractice Insurance Crisis.”) All things considered, hospital-based physicians are at greater risk of being sued than their colleagues who work in offices.
Case #1: The hospitalist failed to detect a vertebral artery dissection in a younger patient. Should they have been able to detect that? It’s a rather unusual stroke presentation. A neurologist would have picked it up—and certainly would have been held liable or negligent if they’d missed that diagnosis. During their training neurologists would have certainly seen this condition as a cause of stroke in someone below age 45. But internists, in general, don’t receive good neurologic training as part of their residencies, and in community hospitals there is no set neurology service.
Neurologists have now become more office-based and allow the hospitalists to do more. By doing more, they’re also exposed to more legal risk. Should the hospitalist be held negligent for missing an unusual stroke? It depends on what you think is a hospitalist’s scope of practice.
—Dr. Baudendistel
Scope of Practice
A hospitalist’s scope of practice is somewhat difficult to define, although the classification “hospitalist” is gaining clarity (including with insurance underwriters), and the hospitalist model is becoming more recognized as a subspecialty. (See “A Malpractice Primer,” The Hospitalist, Dec. 2005, p. 1.)
One challenge in defining the hospitalist’s scope of practice is that hospitalists do a variety of things and work in different departments of the hospital: Some spend more time in acute care, some are more in general care, and some of them are mostly in trauma care.
It is generally acknowledged that healthcare practitioners must employ the same degree of diligence and skill commonly possessed by other members of the healthcare profession who are engaged in the same kind of work in similar locales. Thus, hospitalists need to be acutely aware of how other hospitalists practice in similar settings with similar resources available.
Hospitalists in rural and suburban hospitals, which have fewer and less specialized staff readily available for consults, should expect to have a different scope of practice. In time further clarification of the roles, responsibilities, and clinical skills of hospitalists will be established so that the scope of practice is more clearly defined.
Dr. Baudendistel believes that residents tracking to specialize in hospital medicine could benefit from having more education in certain areas: neurology, perioperative medicine, and critical care.
SHM has recognized the need for better risk management strategies to protect hospitalists and will provide this information and continuing education in The Core Competencies in Hospital Medicine to be published the January/February 2006 issue of the Journal of Hospital Medicine.
Case #2: A male patient came into the ED at a rural hospital with an altered mental status. He had a history of falls and the CT scan in the ED showed a large subdural hematoma.
“We need to admit this patient to the hospital,” said the ED doc. “Call the hospitalist.”
“What does neurosurgery want to do?” asked the hospitalist.
The hospitalist tried to reach the neurosurgeon. And the ED doc wasn’t able to obtain neurosurgery consult because the neurosurgeon said that he wasn’t on call for that hospital. So the hospitalist was … left responsible without neurosurgery backup.
Ultimately, the patient worsened. The hospitalist called a different neurosurgeon at a different hospital who clearly wasn’t in charge of the patient. That doctor said, “Get the patient over to us, and we’ll take care of it.”
There was a 12-hour delay, and the patient finally got transferred to the other hospital, had surgery, and did OK. But he was definitely deteriorating.
The neurosurgeon who said he wasn’t on call for that hospital was wrong. He was lying or just didn’t know of his group’s call coverage. It was a clear violation. And it left the hospital in a situation that isn’t all that unfamiliar.
In this case, the hospitalist wasn’t at fault. There was clear chart documentation [provided as evidence] that said, “I called the neurosurgeon three times and they’re not calling back. Finally they called back the fourth time and said that they’re not coming in.” —Dr. Baudendistel
Communication
Communication is crucial in a clinician’s provision of quality care and also provides a safety net to help prevent liability. Communication with patients, families, staff, and other physicians—particularly their inpatients’ primary care physicians—provides the strongest armor against malpractice assaults. Timeliness and the urgency of the issue are key to patient care and are also are examined by those who review malpractice claims.
In recent years medical malpractice claims payouts have increased substantially for both jury verdicts and settlements. For monetary awards involving doctor-patient relations, which are largely predicated upon communication, the median payout is $230,000.1
Some hot-button areas that carry higher risk and call for meticulous communication between providers include:
- Inpatient postoperative care;
- Post-discharge communication (hand-offs);
- Diagnosis and treatment of a patient for whom there is an incomplete history; and
- Acceptance for treatment of patients whose medical conditions may either be unfamiliar to hospitalists or for which they have had limited or no training.
Communication with Patients
Communication—every aspect of it—is essential for the patient’s health, attitude, and satisfaction. Interestingly, legal data show that most patients who have bad outcomes don’t file suit.2 Although patients litigate for a variety of reasons, chief among them is when they perceive they have suffered because of administrative errors, rude practitioners or support staff, or the denial of tests and referrals they had requested and thought were reasonable.3 Data from a number of studies conducted within the past two decades show that although no particular communication skills can be directly associated with reducing malpractice claims, when patients perceive that their providers treat them genuinely and fairly, and update them honestly and regularly, they are less likely to sue.4-9
One-on-One with Barry Halpern, JD
My law firm practices throughout the western United States, and one of the areas that I see as a general pattern is when … continuity of care becomes an issue. The cases that are sometimes the most troublesome are those in which the hospitalist is involved.
There’s never a real clear demarcation of responsibility between, for instance, the surgery service and the hospitalist. Orders are written and then interpreted by the nursing staff in ways that, in retrospect, even the surgical service or the hospitalist are not pleased with. Yet the physicians aren’t talking to each other, and the documentation in the medical record is intermittent … .
Those kinds of situations, particularly where there is later alleged to have been, for instance, a medication error, become very difficult to defend. Because from the perspective of the lay jury that will be looking at the case, it’s easy for a plaintiff lawyer to depict a very disjointed and uncoordinated approach to care, when—in fact—the reality of practices is that they don’t always go perfectly and things aren’t always documented the instant that they are done.
And sometimes bad things happen despite everybody’s best efforts. But when you have a rough interface between the hospitalist and the other physicians with regard to responsibility for a patient, you are inviting a legal problem.
—Halpern is an attorney with Snell and Wilmer Law Offices, Phoenix
Case #3: A 72-year-old female who was pretty healthy (she had some high blood pressure) came in with abdominal pain. The ED doctor drew the laboratories, which suggested pancreatitis, and then investigated why she had pancreatitis. The ultrasound ordered by the ED doc showed gallstones. The physician then correctly inferred that she had gallstones causing her pancreatitis.
A hospitalist was called [and] admitted the patient. Surgery and GI consultants were called. The GI consultant first ordered an endoscopic retrograde cholangiopancreatography to clean the gallstones from the common bile duct. That went fine, and the next day the patient looked a little better. The GI service said, “Anticipated to go home in a couple days.” Surgery felt the same.
Then the consensus was to remove her gallbladder because eventually she would need to have it done. And that’s when things started to go badly.
On postoperative day two, the patient started having pain out of proportion to what should be expected. The internist (the hospitalist) raised that question in his note. The surgeon said, “No, that’s still postoperative pain,” and increased the pain medicine.
The hospitalist said, “I’m really concerned about this; I’ll talk to the surgeon.”
Again the surgeon said, “There’s nothing to worry about. I’ll at least order a HIDA scan.”
Initially the patient refused the scan, but the next day—postoperative day three—she was still having pain and was clearly worse. She had a high fever; her blood pressure dropped; and her white blood cell count climbed from 10,000 to 20,000, indicating infection/inflammation. Finally the hospitalist ordered a CT scan, which shows a perforation caused by the surgery.
The patient went to surgery for repair. As was predicted, she had a rocky hospital course and ultimately died a month later.
The surgeon was clearly in the wrong. … I was consulted and was asked, “What would you do with the hospitalist? What was their role in that case? Do you think he failed to meet the standard of care?”
—Dr. Baudendistel
Communication with Other Clinicians
“Communication between physicians is critical,” says Sally Whitaker, RN, BSN, risk manager with Rex Healthcare in Raleigh, N.C. “[Hospitalists] shouldn’t just rely on knowing they’ve put their notes on the discharge summary.”
At Rex Hospital (one of Rex Healthcare’s six facilities) where Whitaker works, when seminal events (those big bad things that happen) occur and result in severe trauma or death, the appropriate people meet to backtrack through the steps and scenarios that led to the breakdown.
“Fortunately we don’t have seminal events every day, but every day we do have things that go wrong,” she says. “ … And when we look at our Group Cause Analysis meetings, three-quarters of them [involve] communication issues.”
Exercise Independent Medical Judgment
Hospitalists should read their insurance and employer contracts carefully (especially those with a managed care organization) to ensure that the contract includes a statement allowing the physician to exercise independent medical judgment in the treatment of all patients. If that statement is not present, the hospitalist should request a revision in the contract to include such a statement.
In medical residency programs, a distinction is often made between being a consultant and being a co-manager, says Dr. Baudendistel, but “you have to assume there’s no legal difference between [the two].” Case #3 , he says, was a challenge to decide because the responsibilities of the surgeon and hospitalist in postoperative care were not clearly demarcated.
“I think the surgeon was probably saying, ‘I see this all the time and this is within the realm of what happens after one of these surgeries; let’s not be too worried yet,’” he says. “And I think the internist [hospitalist] ultimately pulled the trigger correctly and the [controversy later on pertained to] whether it should have been done a day or two earlier and whether that have mattered.”
This case illustrates that, although hospitalists are members of teams and partner with consultants and primary physicians, in the end they are managers of patient care and may (we hope rarely) have to break ranks to make aggressive care decisions.
“I think that the other thing that was in [the hospitalist’s] favor,” says Dr. Baudendistel of the case, “was that he was writing very thorough notes, [and] really was discussing everything with the family and everyone was on board. He was doing a very compassionate job … trying to manage this care.”
To Dr. Baudendistel, who is the chair of SHM’s ethics committee, this went a long way toward showing good faith.
Reducing Risks: Concern for the Medical Record
If the medical record is found deficient or illuminating in a negative way, it may serve the plaintiff attorney’s strategy well for establishing negligence or wrongdoing. The chart notes documented by nurses, attending staff, consultants, other residents, and therapists could either portray a smoothly managed case or a chronology of errors and omissions. The chart should never be cosigned and never merely assumed to be accurate.
When Things Go Wrong
Whitaker advises hospitalists to keep the lines of communication open. “Especially after something unexpected has happened,” she says. “So many times I think the human tendency is to just withdraw, or you feel terrible and you don’t know what to say, or you’re afraid you’re going to get emotional while you’re talking with the family.”
This is normal human response in these circumstances, but if you act on the impulse to withdraw and avoid the patient and family, or hold back, which may eventually lead to a filed claim from a family that feels abandoned.
“Until now the number of lawsuits has been really steady and the amount that we were paying in lawsuits was increasing,” says Whitaker. “However, we’re trying to work with the families earlier on so if we make a mistake and we realize that we made a mistake then we admit that. And we try to do what we can to make it right for that patient and their family.”
This often means reaching a fair and reasonable settlement, says Whitaker, “and [examining fair and reasonable means reviewing] the communication at the time the event occurred. Did we acknowledge that we made a mistake? Did we let them know we’d be willing to work with them? And did we let them know we [have since] made these changes … so they’ll … be reassured [that] hopefully it won’t happen again?”
Who’s in Charge?
Linda Greenwald, RN, MS, editor of risk management publications at ProMutual Insurance Group in Boston, wrote in the company’s newsletter, Perspectives on Clinical Risk Management, that in prior times, the question, “Who’s in charge?” was rhetorical.10 These days any number of generalists or specialists might claim that role. And therein lies the rub: Greenwald says that in many cases involving hospitalists the lines of responsibility are unclear and one or more systems may fail. If so, Greenwald writes, the result may be a malpractice claim alleging:
- Failure to diagnose when each of two physicians assumes the other has responsibility for follow-up;
- Negligence in treatment when one physician fails to monitor on an outpatient basis the medication first prescribed by another physician when the patient was an inpatient; and/or
- Negligent care when a patient misinterprets the information one physician asks him or her to relay to another physician.10
Halpern concurs that the modern mix of professionals working as a team on hospital care can be a major challenge.
“In olden days, when a primary care physician referred to a surgeon, and the surgeon performed surgery, and the surgeon took responsibility for postoperative care, and occasionally brought in a consultant, the lines were relatively clear,” says Halpern. “When a hospitalist is injected into the mix, unless the hospital has really clear procedures and unless everybody is comfortable with the system and everybody is talking to each other and agreeing on the lines of demarcation, you’re creating a soup that plaintiff lawyers would be happy to stir.”
The more murky the communication, the greater the liability. “And when you have murky lines of communication, murky lines of responsibility, and a medical catastrophe,” says Halpern, “human nature compounds the problem by frequently causing a finger-pointing contest, where each component of the patient care team circles its own wagons [and] points in a different direction. And that is the absolute worst thing that can happen when trying to deal with a patient injury claim.”
Summary
The hospitalist’s primary risk for malpractice claims may be inadequate or absent patient follow-up resulting from a lack of communication. The best means of protection from claims is for hospitalists to incorporate a comprehensive risk management program into their practice.
Several strategies have proved successful to help prevent litigation. In general, hospitalists should make sure that their hospital has clearly delineated policies regarding responsibility for patients; clearly understand—and ensure that your coworkers, colleagues, and referring physicians understand—the hospital’s systems and protocols; exercise good communication skills; conform to the standard of care; know your own scope of care to the best of your ability; and exercise independent medical judgment, even when partnering with others. TH
Andrea Sattinger also writes the “Alliances” department for The Hospitalist.
References
- Mello MM, Studdert DM, Brennan TA. The new medical malpractice crisis. New Engl J Med. 2003;348:2281-2284.
- Virshup BB, Oppenberg MPH, Coleman MM. Strategic risk management: reducing malpractice claims through more effective patient-doctor communication. Am J Med Quality. 1999;14:153-159.
- Gurwitz JH, Terry S, Field TS, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289:1107-1116.
- Shapiro RS, Simpson DE, Lawrence SL, et al.. A survey of sued and nonsued physicians and suing patients. Arch Intern Med. 1989;149:2190-2196.
- Levinson W, Roter D, Mullooly JP, et al. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;227:558-559.
- Beckman HB, Markakis KM, Suchman AL, et al. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370.
- Cohen JR. Apology and organizations: exploring an example from medical practice. Fordham Urban Law Journal. 2000;27:1447-1482.
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1069.
- Entman SS, Glass CA, Hickson GB, et al. The relationship between malpractice claims history and subsequent obstetric care JAMA. 1994;272:1588-1591.
- Greenwald L. Who's in charge? Perspectives on Clinical Risk Management. Boston, Mass: ProMutual Group Risk Management Services; Fall 2000.
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9.
Evaluating and managing hypogammaglobulinemia
A Patch Test Study to Evaluate the Allergenicity of a Metallic Jewelry Alloy in Patients Allergic to Cobalt
Can a vaccine prevent Alzheimer’s disease?
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
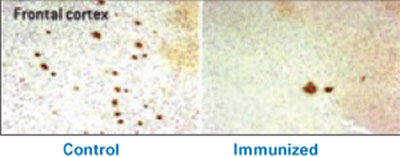
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
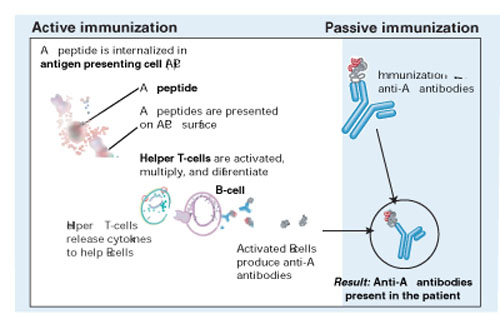
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-
What to tell patients about side effects
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Adult with ADHD? Try medication + psychotherapy
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.