User login
New guidelines for testosterone treatment in adult men with age-related low testosterone
Testosterone normally decreases with age in men beginning in their mid-30s, with a rate of decline averaging approximately 1.6% per year. Using a cutoff of a total testosterone less than 325 ng/dL, the incidence of low testosterone is approximately 20% after age 60 years, and 30% after age 70. While the change in labs values has been reasonably validated,

Additional potential symptoms of testosterone deficiency include changes in bone mineral density, decreased libido, depression, erectile dysfunction, loss of hair, and general weakness. Since the symptoms are nonspecific, it is often unclear if someone should be tested or treated for testosterone deficiency. To address this issue, the American College of Physicians commissioned a systematic review of the evidence on testosterone-replacement therapy for age-related testosterone deficiency.1
The evidence review of testosterone replacement in men with age-related low testosterone found the following.
- Low-certainty evidence of improvement in quality of life
- Moderate-certainty evidence of a small improvement in sexual function
- Low-certainty evidence of a small improvement in erectile function
- Low-certainty evidence showing little to no improvement in physical function
- Low-certainty evidence of a small increase to no difference in adverse cardiovascular events
- Moderate-certainty evidence of no increase in the risk for serious adverse events
The trials were not powered to assess mortality, but pool analysis showed fewer deaths among patients treated with testosterone than those who received placebo (odds ratio, 0.47; 95% confidence interval, 0.25-0.89). There were no differences in cognitive function, and the improvement in vitality and fatigue was “less than a small amount.” Evidence from an observational trial showed no increased risk for mortality, cardiovascular events, prostate cancer, or pulmonary embolus or deep vein thrombosis. Of note, most studies excluded men with recent cardiovascular disease.
This evidence review led to the following recommendations.2
Recommendation 1a
Clinicians should have a discussion regarding the potential risk and benefits of treatment with the patients who have documented age-related low testosterone (testosterone levels less than 10.4 nmol/L or 300 ng/dL) and are suffering from sexual dysfunction or have a desire to enhance their sexual function.
This recommendation was based on evidence showing small improvement in sexual function and erectile dysfunction.
Recommendation 1b
For patients who opt for treatment based on recommendation 1a, clinicians should reevaluate the benefit of treatment within 12 months. If a patient is not receiving any benefit in sexual function by 12 months, it is recommended that treatment be stopped at that time.
The ACP recommendation to stop treatment if a patient lacks improvement of sexual function within 12 months stems from low or insufficient evidence regarding potential harm of treatment. If the treatment is not helping the target symptom then the benefit no longer outweighs the potential harm.
Recommendation 1c
For patients who opt for treatment based on recommendation 1a, intramuscular replacement therapy rather than transdermal replacement therapy is recommended because of substantial differences in the cost.
It is important to note that both intramuscular and transdermal testosterone applications have been associated with improvements in sexual function, without any significant differences noted in benefit or harm for the patients. This recommendation is based on a per-person per-year average cost of the intramuscular formulation – $156.32, compared with the transdermal formulation – $2,135.32.
Recommendation 2
The ACP does not endorse the use of testosterone treatment for age-related low testosterone in patients desiring improvement in physical function, mood, energy, or cognitive function.
This clear recommendation is critical, as this might be the most common reason for prescriptions of testosterone – a misplaced belief that testosterone will help general quality of life. The evidence simply does not support this effect of testosterone replacement for age-related testosterone deficiency.
The bottom line
Testosterone levels in men decrease steadily with age, with a great deal of variability. Testosterone replacement therapy may be considered for men with age-related testosterone deficiency and sexual dysfunction. Testosterone replacement therapy is not recommended as a treatment for general fatigue, weakness or with an expectation that it will improve physical function, mood, energy, or cognitive function.
Dr. Hansen is a third-year resident in the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Hospital–Jefferson Health.
References
1. Diem SJ et al. Efficacy and safety of testosterone treatment in men: An evidence report for a clinical practice guideline by the American College of Physicians. Ann Intern Med. 2020 Jan 21. doi: 10.7326/M19-0830.
2. Qaseem A et al. Testosterone treatment in adult men with age-related low testosterone: A clinical guideline from the American College of Physicians. Ann Intern Med. 2020 Jan 21. doi: 10.7326/M19-0882.
Testosterone normally decreases with age in men beginning in their mid-30s, with a rate of decline averaging approximately 1.6% per year. Using a cutoff of a total testosterone less than 325 ng/dL, the incidence of low testosterone is approximately 20% after age 60 years, and 30% after age 70. While the change in labs values has been reasonably validated,
Additional potential symptoms of testosterone deficiency include changes in bone mineral density, decreased libido, depression, erectile dysfunction, loss of hair, and general weakness. Since the symptoms are nonspecific, it is often unclear if someone should be tested or treated for testosterone deficiency. To address this issue, the American College of Physicians commissioned a systematic review of the evidence on testosterone-replacement therapy for age-related testosterone deficiency.1
The evidence review of testosterone replacement in men with age-related low testosterone found the following.
- Low-certainty evidence of improvement in quality of life
- Moderate-certainty evidence of a small improvement in sexual function
- Low-certainty evidence of a small improvement in erectile function
- Low-certainty evidence showing little to no improvement in physical function
- Low-certainty evidence of a small increase to no difference in adverse cardiovascular events
- Moderate-certainty evidence of no increase in the risk for serious adverse events
The trials were not powered to assess mortality, but pool analysis showed fewer deaths among patients treated with testosterone than those who received placebo (odds ratio, 0.47; 95% confidence interval, 0.25-0.89). There were no differences in cognitive function, and the improvement in vitality and fatigue was “less than a small amount.” Evidence from an observational trial showed no increased risk for mortality, cardiovascular events, prostate cancer, or pulmonary embolus or deep vein thrombosis. Of note, most studies excluded men with recent cardiovascular disease.
This evidence review led to the following recommendations.2
Recommendation 1a
Clinicians should have a discussion regarding the potential risk and benefits of treatment with the patients who have documented age-related low testosterone (testosterone levels less than 10.4 nmol/L or 300 ng/dL) and are suffering from sexual dysfunction or have a desire to enhance their sexual function.
This recommendation was based on evidence showing small improvement in sexual function and erectile dysfunction.
Recommendation 1b
For patients who opt for treatment based on recommendation 1a, clinicians should reevaluate the benefit of treatment within 12 months. If a patient is not receiving any benefit in sexual function by 12 months, it is recommended that treatment be stopped at that time.
The ACP recommendation to stop treatment if a patient lacks improvement of sexual function within 12 months stems from low or insufficient evidence regarding potential harm of treatment. If the treatment is not helping the target symptom then the benefit no longer outweighs the potential harm.
Recommendation 1c
For patients who opt for treatment based on recommendation 1a, intramuscular replacement therapy rather than transdermal replacement therapy is recommended because of substantial differences in the cost.
It is important to note that both intramuscular and transdermal testosterone applications have been associated with improvements in sexual function, without any significant differences noted in benefit or harm for the patients. This recommendation is based on a per-person per-year average cost of the intramuscular formulation – $156.32, compared with the transdermal formulation – $2,135.32.
Recommendation 2
The ACP does not endorse the use of testosterone treatment for age-related low testosterone in patients desiring improvement in physical function, mood, energy, or cognitive function.
This clear recommendation is critical, as this might be the most common reason for prescriptions of testosterone – a misplaced belief that testosterone will help general quality of life. The evidence simply does not support this effect of testosterone replacement for age-related testosterone deficiency.
The bottom line
Testosterone levels in men decrease steadily with age, with a great deal of variability. Testosterone replacement therapy may be considered for men with age-related testosterone deficiency and sexual dysfunction. Testosterone replacement therapy is not recommended as a treatment for general fatigue, weakness or with an expectation that it will improve physical function, mood, energy, or cognitive function.
Dr. Hansen is a third-year resident in the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Hospital–Jefferson Health.
References
1. Diem SJ et al. Efficacy and safety of testosterone treatment in men: An evidence report for a clinical practice guideline by the American College of Physicians. Ann Intern Med. 2020 Jan 21. doi: 10.7326/M19-0830.
2. Qaseem A et al. Testosterone treatment in adult men with age-related low testosterone: A clinical guideline from the American College of Physicians. Ann Intern Med. 2020 Jan 21. doi: 10.7326/M19-0882.
Testosterone normally decreases with age in men beginning in their mid-30s, with a rate of decline averaging approximately 1.6% per year. Using a cutoff of a total testosterone less than 325 ng/dL, the incidence of low testosterone is approximately 20% after age 60 years, and 30% after age 70. While the change in labs values has been reasonably validated,
Additional potential symptoms of testosterone deficiency include changes in bone mineral density, decreased libido, depression, erectile dysfunction, loss of hair, and general weakness. Since the symptoms are nonspecific, it is often unclear if someone should be tested or treated for testosterone deficiency. To address this issue, the American College of Physicians commissioned a systematic review of the evidence on testosterone-replacement therapy for age-related testosterone deficiency.1
The evidence review of testosterone replacement in men with age-related low testosterone found the following.
- Low-certainty evidence of improvement in quality of life
- Moderate-certainty evidence of a small improvement in sexual function
- Low-certainty evidence of a small improvement in erectile function
- Low-certainty evidence showing little to no improvement in physical function
- Low-certainty evidence of a small increase to no difference in adverse cardiovascular events
- Moderate-certainty evidence of no increase in the risk for serious adverse events
The trials were not powered to assess mortality, but pool analysis showed fewer deaths among patients treated with testosterone than those who received placebo (odds ratio, 0.47; 95% confidence interval, 0.25-0.89). There were no differences in cognitive function, and the improvement in vitality and fatigue was “less than a small amount.” Evidence from an observational trial showed no increased risk for mortality, cardiovascular events, prostate cancer, or pulmonary embolus or deep vein thrombosis. Of note, most studies excluded men with recent cardiovascular disease.
This evidence review led to the following recommendations.2
Recommendation 1a
Clinicians should have a discussion regarding the potential risk and benefits of treatment with the patients who have documented age-related low testosterone (testosterone levels less than 10.4 nmol/L or 300 ng/dL) and are suffering from sexual dysfunction or have a desire to enhance their sexual function.
This recommendation was based on evidence showing small improvement in sexual function and erectile dysfunction.
Recommendation 1b
For patients who opt for treatment based on recommendation 1a, clinicians should reevaluate the benefit of treatment within 12 months. If a patient is not receiving any benefit in sexual function by 12 months, it is recommended that treatment be stopped at that time.
The ACP recommendation to stop treatment if a patient lacks improvement of sexual function within 12 months stems from low or insufficient evidence regarding potential harm of treatment. If the treatment is not helping the target symptom then the benefit no longer outweighs the potential harm.
Recommendation 1c
For patients who opt for treatment based on recommendation 1a, intramuscular replacement therapy rather than transdermal replacement therapy is recommended because of substantial differences in the cost.
It is important to note that both intramuscular and transdermal testosterone applications have been associated with improvements in sexual function, without any significant differences noted in benefit or harm for the patients. This recommendation is based on a per-person per-year average cost of the intramuscular formulation – $156.32, compared with the transdermal formulation – $2,135.32.
Recommendation 2
The ACP does not endorse the use of testosterone treatment for age-related low testosterone in patients desiring improvement in physical function, mood, energy, or cognitive function.
This clear recommendation is critical, as this might be the most common reason for prescriptions of testosterone – a misplaced belief that testosterone will help general quality of life. The evidence simply does not support this effect of testosterone replacement for age-related testosterone deficiency.
The bottom line
Testosterone levels in men decrease steadily with age, with a great deal of variability. Testosterone replacement therapy may be considered for men with age-related testosterone deficiency and sexual dysfunction. Testosterone replacement therapy is not recommended as a treatment for general fatigue, weakness or with an expectation that it will improve physical function, mood, energy, or cognitive function.
Dr. Hansen is a third-year resident in the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Hospital–Jefferson Health.
References
1. Diem SJ et al. Efficacy and safety of testosterone treatment in men: An evidence report for a clinical practice guideline by the American College of Physicians. Ann Intern Med. 2020 Jan 21. doi: 10.7326/M19-0830.
2. Qaseem A et al. Testosterone treatment in adult men with age-related low testosterone: A clinical guideline from the American College of Physicians. Ann Intern Med. 2020 Jan 21. doi: 10.7326/M19-0882.
Dermatomyositis without dermatitis correlates with autoantibodies
The prevalence of dermatomyositis without dermatitis among patients with biopsy-confirmed dermatomyositis was approximately 8% in a Japanese cohort study. “Dermatomyositis sine dermatitis does exist and is significantly associated with anti–nuclear matrix protein 2 [anti-NXP-2] autoantibodies,” the researchers reported in JAMA Neurology.
Few case reports of dermatomyositis sine dermatitis have been documented. To confirm the existence of the condition, study its prevalence, and characterize its serologic features, Michio Inoue, MD, PhD, of the National Center of Neurology and Psychiatry in Tokyo, and colleagues conducted a cohort study of patients seen at the center between January 2009 and August 2019.
Of more than 8,800 patients whose muscle biopsies were examined for diagnostic purposes, 199 were tested for dermatomyositis-specific autoantibodies. The investigators excluded patients who did not have myxovirus resistance protein A expression in myofibers on muscle biopsy. In all, 182 patients with dermatomyositis were enrolled in the study (51% women; median age at biopsy, 56 years). Fourteen patients without a skin rash at the time of muscle biopsy received a diagnosis of dermatomyositis sine dermatitis. Before the muscle biopsy, most patients without a rash had a diagnosis of polymyositis.
Association with anti-NXP-2 autoantibodies
Anti-NXP-2 autoantibodies were detected in 86% of the patients without a rash at the time of biopsy, compared with 28% of the patients with rashes. “No other clinical or pathological characteristics were associated with [dermatomyositis sine dermatitis] except increased probability of developing perifascicular atrophy (71% vs. 43%),” Dr. Inoue and colleagues said.
During a median follow-up of 34 months, patients with dermatomyositis sine dermatitis received oral prednisolone with or without additional immunotherapy, and two patients had subcutaneous edema. Calcification was not seen during follow-up. “One patient with ... anti-NXP-2 autoantibodies had severe interstitial lung disease and needed noninvasive positive-pressure ventilation support,” the researchers said.
Four of the 14 patients with dermatomyositis sine dermatitis “developed skin rashes after muscle biopsy,” the researchers noted. “Similarly, a patient with [dermatomyositis sine dermatitis] was reported to have developed a skin rash 2 years after muscle biopsy.”
Potential therapies for refractory dermatomyositis, such as Janus kinase inhibitors, may not be effective for other types of myositis, so identifying patients with dermatomyositis may be “more essential than ever,” the authors said.
Effects on organ systems vary
The study is the first to systematically examine dermatomyositis sine dermatitis, said David Fiorentino, MD, PhD, professor of dermatology and director of the multidisciplinary rheumatic skin disease clinic at the Stanford (Calif.) University.

On the one hand, the results are not surprising because dermatomyositis is a systemic autoimmune disease. “There are no rules about which organs it will or won’t affect in a given individual,” Dr. Fiorentino said in an interview.
At the same time, dermatomyositis’s historical association with rash persists even though there is “no biological reason why that would have to be the case.”
Some patients with dermatomyositis have skin-predominant disease without clinically significant muscle involvement. Lung-predominant disease also may exist, although it has not been carefully studied, he said.
The findings remind clinicians that they need to consider the diagnosis of dermatomyositis “even if they do not have the skin findings,” he said. Dr. Fiorentino cautioned against interpreting the results to mean that certain patients never have signs of cutaneous inflammation. In the study, about a one-third of patients without dermatitis at the time of biopsy developed a rash. In addition, clinicians often miss subtle disease under the fingernails or on the scalp, or mild rash on the elbows.
The cohort of patients who underwent muscle biopsy may not be representative of the spectrum of patients with dermatomyositis, and the findings need to be verified in other populations, Dr. Fiorentino said.
The study was supported by an intramural research grant of the National Center of Neurology and Psychiatry and a grant from the Japan Society for the Promotion of Science. Authors disclosed personal fees from pharmaceutical companies and government and corporate grants outside the submitted work. Dr. Fiorentino had no relevant disclosures.
SOURCE: Inoue M et al. JAMA Neurol. 2020 Apr 20. doi: 10.1001/jamaneurol.2020.0673.
The prevalence of dermatomyositis without dermatitis among patients with biopsy-confirmed dermatomyositis was approximately 8% in a Japanese cohort study. “Dermatomyositis sine dermatitis does exist and is significantly associated with anti–nuclear matrix protein 2 [anti-NXP-2] autoantibodies,” the researchers reported in JAMA Neurology.
Few case reports of dermatomyositis sine dermatitis have been documented. To confirm the existence of the condition, study its prevalence, and characterize its serologic features, Michio Inoue, MD, PhD, of the National Center of Neurology and Psychiatry in Tokyo, and colleagues conducted a cohort study of patients seen at the center between January 2009 and August 2019.
Of more than 8,800 patients whose muscle biopsies were examined for diagnostic purposes, 199 were tested for dermatomyositis-specific autoantibodies. The investigators excluded patients who did not have myxovirus resistance protein A expression in myofibers on muscle biopsy. In all, 182 patients with dermatomyositis were enrolled in the study (51% women; median age at biopsy, 56 years). Fourteen patients without a skin rash at the time of muscle biopsy received a diagnosis of dermatomyositis sine dermatitis. Before the muscle biopsy, most patients without a rash had a diagnosis of polymyositis.
Association with anti-NXP-2 autoantibodies
Anti-NXP-2 autoantibodies were detected in 86% of the patients without a rash at the time of biopsy, compared with 28% of the patients with rashes. “No other clinical or pathological characteristics were associated with [dermatomyositis sine dermatitis] except increased probability of developing perifascicular atrophy (71% vs. 43%),” Dr. Inoue and colleagues said.
During a median follow-up of 34 months, patients with dermatomyositis sine dermatitis received oral prednisolone with or without additional immunotherapy, and two patients had subcutaneous edema. Calcification was not seen during follow-up. “One patient with ... anti-NXP-2 autoantibodies had severe interstitial lung disease and needed noninvasive positive-pressure ventilation support,” the researchers said.
Four of the 14 patients with dermatomyositis sine dermatitis “developed skin rashes after muscle biopsy,” the researchers noted. “Similarly, a patient with [dermatomyositis sine dermatitis] was reported to have developed a skin rash 2 years after muscle biopsy.”
Potential therapies for refractory dermatomyositis, such as Janus kinase inhibitors, may not be effective for other types of myositis, so identifying patients with dermatomyositis may be “more essential than ever,” the authors said.
Effects on organ systems vary
The study is the first to systematically examine dermatomyositis sine dermatitis, said David Fiorentino, MD, PhD, professor of dermatology and director of the multidisciplinary rheumatic skin disease clinic at the Stanford (Calif.) University.
On the one hand, the results are not surprising because dermatomyositis is a systemic autoimmune disease. “There are no rules about which organs it will or won’t affect in a given individual,” Dr. Fiorentino said in an interview.
At the same time, dermatomyositis’s historical association with rash persists even though there is “no biological reason why that would have to be the case.”
Some patients with dermatomyositis have skin-predominant disease without clinically significant muscle involvement. Lung-predominant disease also may exist, although it has not been carefully studied, he said.
The findings remind clinicians that they need to consider the diagnosis of dermatomyositis “even if they do not have the skin findings,” he said. Dr. Fiorentino cautioned against interpreting the results to mean that certain patients never have signs of cutaneous inflammation. In the study, about a one-third of patients without dermatitis at the time of biopsy developed a rash. In addition, clinicians often miss subtle disease under the fingernails or on the scalp, or mild rash on the elbows.
The cohort of patients who underwent muscle biopsy may not be representative of the spectrum of patients with dermatomyositis, and the findings need to be verified in other populations, Dr. Fiorentino said.
The study was supported by an intramural research grant of the National Center of Neurology and Psychiatry and a grant from the Japan Society for the Promotion of Science. Authors disclosed personal fees from pharmaceutical companies and government and corporate grants outside the submitted work. Dr. Fiorentino had no relevant disclosures.
SOURCE: Inoue M et al. JAMA Neurol. 2020 Apr 20. doi: 10.1001/jamaneurol.2020.0673.
The prevalence of dermatomyositis without dermatitis among patients with biopsy-confirmed dermatomyositis was approximately 8% in a Japanese cohort study. “Dermatomyositis sine dermatitis does exist and is significantly associated with anti–nuclear matrix protein 2 [anti-NXP-2] autoantibodies,” the researchers reported in JAMA Neurology.
Few case reports of dermatomyositis sine dermatitis have been documented. To confirm the existence of the condition, study its prevalence, and characterize its serologic features, Michio Inoue, MD, PhD, of the National Center of Neurology and Psychiatry in Tokyo, and colleagues conducted a cohort study of patients seen at the center between January 2009 and August 2019.
Of more than 8,800 patients whose muscle biopsies were examined for diagnostic purposes, 199 were tested for dermatomyositis-specific autoantibodies. The investigators excluded patients who did not have myxovirus resistance protein A expression in myofibers on muscle biopsy. In all, 182 patients with dermatomyositis were enrolled in the study (51% women; median age at biopsy, 56 years). Fourteen patients without a skin rash at the time of muscle biopsy received a diagnosis of dermatomyositis sine dermatitis. Before the muscle biopsy, most patients without a rash had a diagnosis of polymyositis.
Association with anti-NXP-2 autoantibodies
Anti-NXP-2 autoantibodies were detected in 86% of the patients without a rash at the time of biopsy, compared with 28% of the patients with rashes. “No other clinical or pathological characteristics were associated with [dermatomyositis sine dermatitis] except increased probability of developing perifascicular atrophy (71% vs. 43%),” Dr. Inoue and colleagues said.
During a median follow-up of 34 months, patients with dermatomyositis sine dermatitis received oral prednisolone with or without additional immunotherapy, and two patients had subcutaneous edema. Calcification was not seen during follow-up. “One patient with ... anti-NXP-2 autoantibodies had severe interstitial lung disease and needed noninvasive positive-pressure ventilation support,” the researchers said.
Four of the 14 patients with dermatomyositis sine dermatitis “developed skin rashes after muscle biopsy,” the researchers noted. “Similarly, a patient with [dermatomyositis sine dermatitis] was reported to have developed a skin rash 2 years after muscle biopsy.”
Potential therapies for refractory dermatomyositis, such as Janus kinase inhibitors, may not be effective for other types of myositis, so identifying patients with dermatomyositis may be “more essential than ever,” the authors said.
Effects on organ systems vary
The study is the first to systematically examine dermatomyositis sine dermatitis, said David Fiorentino, MD, PhD, professor of dermatology and director of the multidisciplinary rheumatic skin disease clinic at the Stanford (Calif.) University.
On the one hand, the results are not surprising because dermatomyositis is a systemic autoimmune disease. “There are no rules about which organs it will or won’t affect in a given individual,” Dr. Fiorentino said in an interview.
At the same time, dermatomyositis’s historical association with rash persists even though there is “no biological reason why that would have to be the case.”
Some patients with dermatomyositis have skin-predominant disease without clinically significant muscle involvement. Lung-predominant disease also may exist, although it has not been carefully studied, he said.
The findings remind clinicians that they need to consider the diagnosis of dermatomyositis “even if they do not have the skin findings,” he said. Dr. Fiorentino cautioned against interpreting the results to mean that certain patients never have signs of cutaneous inflammation. In the study, about a one-third of patients without dermatitis at the time of biopsy developed a rash. In addition, clinicians often miss subtle disease under the fingernails or on the scalp, or mild rash on the elbows.
The cohort of patients who underwent muscle biopsy may not be representative of the spectrum of patients with dermatomyositis, and the findings need to be verified in other populations, Dr. Fiorentino said.
The study was supported by an intramural research grant of the National Center of Neurology and Psychiatry and a grant from the Japan Society for the Promotion of Science. Authors disclosed personal fees from pharmaceutical companies and government and corporate grants outside the submitted work. Dr. Fiorentino had no relevant disclosures.
SOURCE: Inoue M et al. JAMA Neurol. 2020 Apr 20. doi: 10.1001/jamaneurol.2020.0673.
FROM JAMA NEUROLOGY
Brant Oliver, PhD, on patient-reported outcomes in MS

Brant Oliver, PhD, MS, MPH, APRN-BC, is a health care improvement and implementation scientist, educator, and board-certified family and psychiatric nurse practitioner (FNP-BC, PMHNP-BC). Dr. Oliver's work focuses on applied health care improvement science research, with a focus on "3C" (complex, costly, and chronic) conditions including MS, IBD, CF, RA, and others; coproduction; learning health systems; and shared decision making. He is Associate Professor at the Geisel School of Medicine at Dartmouth and also has been in clinical practice since 2003, working primarily as a certified MS specialist (MSCN) and a MS neurobehavioral nurse practitioner.
Which patient-reported outcomes (PROs) are commonly assessed in the care of patients with multiple sclerosis (MS)?
BRANT OLIVER, PhD: The current reality is that PROs are not being used routinely in MS clinical care in most settings. They are most commonly being used in research settings, either as part of clinical trials of new treatments, or in epidemiologic studies looking at the prevalence, incidence, and severity of certain symptoms or functional impairments in MS at the population level. A good example is the NARCOMS registry, which has been used to conduct high-quality epidemiologic studies of MS-related symptoms using self-report questionnaires.
We are starting to see some use of MS PROs in select clinical settings. Oftentimes these are measures of highly prevalent comorbid conditions that have an impact on quality of life, treatment adherence (depression severity and anxiety), and self-efficacy, which is a measure of perceived coping ability related to self-management of a chronic illness. Also, measures of patient experience are being employed in hospital-based clinics, such as the CG-CAHPS satisfaction measures.
The PROMIS (Patient-Reported Outcomes Measurement Information System) battery is a promising set of PRO measures that are being utilized across a number of conditions and that contain some MS-specific measures, such as the Fatigue MS measure. Fatigue is the most common and disabling symptom in MS, so having a good measure of fatigue is of critical importance. Having a sense of a patient’s experience with fatigue over time can also be very helpful from a clinical perspective. The PROMIS measure performs much better than its predecessor, the Modified Fatigue Impact Scale (MFIS). Another strength of the PROMIS measures is that they tend to do well correlating with other conditions. In certain research and improvement settings, PROMIS can help us understand the burden a particular disease or population places on total health system resources. For example, is fatigue burden in MS similar in severity to that in another 3C condition, such as inflammatory bowel disease?
There are other PRO measures that have not been used in MS but which I think we will see used in the future. One of these is called Collaborate, which falls into the category of patient-reported experience measures (PREMs). Collaborate measures the degree of shared decision-making that occurs in a clinical encounter, which becomes especially important as the complexity of disease-modifying treatment decisions increases as more disease-modifying therapies are introduced, each with their own profile of risks and benefits. I anticipate that the ability of clinics to facilitate effective shared decision-making will be of increasing interest to clinicians, patients, and also payers in the future.
What are some of the potential benefits of using PRO measures in terms of clinician/patient communication and clinical decision-making?
BRANT OLIVER, PhD: I think the most important benefit of measuring PROs is that it can make care more patient-centered. The big push for PROs in the first place was to incorporate more of the patient’s voice into their own care. Standard clinical measures, such as magnetic resonance imaging (MRI) or relapse rates, can be very precise and provide a good clinical picture of how the disease is behaving. But if we rely solely on that kind of information, we can lose sight of the person who is experiencing the disease.
PROs, be they just regular PROs (instruments that gather qualitative and/or quantitative patient-reported information) or PROMs (validated and standardized PRO measures) or PREMs (standardized and validated patient-reported experience measures), all aim to improve the ability to get a better story of the person who's experiencing the illness and how that condition affects them. We can also gain insight on what's most important to them regarding how their illness is managed, and what their experience of care is.
Sometimes the PRO picture and the clinical picture don't necessarily align. I'll tell a story about one a person, who's given me permission to share the story. She is an established professional, and her PRO measures concerning her quality of life, support from her workplace environment, and her ability to function in society are very high. She's very high functioning according to the PRO picture. However, her clinical measures suggest that she is significantly impaired. Her MRI burden is quite high, and her disability due to the MS, her EDSS (Expanded Disability Status Scale), is also quite high. So there are 2 very different stories provided by 2 different sets of data. The inclusion of PROs data, in connection with clinical data, can provide a more holistic view of this person, who is functioning well despite significant disease burden.
As a clinician working with patients with MS, this gives me much more to work with in trying to help people, not only treating the disease, but also trying to see where the person is most in need of help. A person could be very well controlled on MRI in terms of relapse rate, but have fatigue severity that is through the roof. If I weren't paying closer attention to that with a validated scale that measures fatigue severity over time, like the PROMIS Fatigue MS, I may not have a sense of how well treatment is helping that person's fatigue longitudinally, beyond what I can glean from the history and clinical examination.
PROs can also be helpful in terms of conditions that are harder to quantify. Depression is a significant cause of disability and a significant factor contributing to poor treatment adherence in MS. Also, the suicide rate in persons with MS is much higher than that in the general population. But there is no blood test for depression severity, and oftentimes a patient’s report on exam can be incomplete or misleading. Accompanying the mental status exam and the clinical evaluation with a validated depression severity measure (such as the PHQ9 [Patient Health Questionnaire-9], CES-D [Center for Epidemiologic Studies Depression Scale], or others) can help to determine whether treatments are having an initial effect, and this can also help with self-monitoring and treatment adherence.
That brings us to the second area where PROs show real promise in MS care: the learning health system (LHS) approach, which uses feed forward information to either predict the needs of people before they come to the office or optimize decision-making at the point of care (as discussed in our review article published in JCOM).1
PROs can play a significant role in the LHS approach in 2 ways. For example, if I have a good sense before a visit that the person has stable symptoms but is having a lot of trouble coping with MS, that may change how I allocate resources and focus the time at the visit to target the primary concern of the person before the visit even occurs. Over time I'd be able to monitor if those coping scores increase in response to the work we’re doing with the person.
The second part of this approach is a feedback mechanism. These measures can be aggregated at the population level and fed back to clinical MS centers to help clinicians who are trying to improve overall population health outcomes of people with MS to see how well they're doing on things like fatigue management, depression management, coping ability, and pain control, which can't be tested for with biologic methods. So in addition to looking at the MRI scan trends across the population and relapse rate annualized for the population over time, I'd also be able to see fatigue severity and depression severity at a clinic population level and assess the change in these severity levels over time, which I could then use to inform efforts to change how my system (clinic) provides MS care.
This capability of PROs could be of significant interest to payers, especially those who are looking to optimize the value of care that is being provided, given the high cost of MS care. MS treatments are very expensive, and MS care is multidisciplinary and requires a lot of resources. Payers, I think, will have an increasing interest in assessing the value of high-cost care. PROs could help to demonstrate that value, especially if they can help quantify that outcomes can be improved over time at the population level.
The third area where PROs are beneficial is population health research, especially in terms of the major improvement movements going on in the country, such as those advocated for by the Institute for Healthcare Improvement via the Triple Aim: improve population health outcomes, improve the experience of care, and minimize per capita cost. PROs can really help with the first 2 of those Triple Aim categories.
What are some of the factors that limit the use of PRO measures in MS research and clinical practice?
BRANT OLIVER, PhD: In our JCOM paper,1 we outlined major barriers or constraints or challenges to implementing PRO measures. One is time and technology in clinical care. It's busy. It's fast. A PRO measure requires patients to complete a questionnaire. And to do that, you need some time and space during the clinical visit, or before the visit, to collect this data. In the absence of appropriate technology, this is done using paper-based methods, which can be challenging. Technology can help. Examples include smart phone app-based collection systems, tablet PCs, or an online mechanism. But there are barriers to technology, too. Is the technology good enough? Is the interface with the people using it working well? Do you have an equal amount of access to and understanding of the technology from the people across your population? Is it only being used by a certain subset that is wealthier and more educated, or maybe who has English as a first language? Such constraints can be overcome, but they’re present in any situation where you are gathering PRO data.
Software constraints also extend to the electronic health record (EHR) capability of the clinics. If you can collect PRO data, does the EHR have the capability to present that data in a useful way during a 20- or 30-minute clinical visit? In other words, does it improve the quality of the visit, or does it generate just one more distraction during the visit? Some approaches, such as feed forward dashboards, provide easy visual displays that can quickly and easily add information at the point of care and can get around this limitation. However, a lot of MS care centers in private practice settings may not have the informatics capability of a large academic center.
Academic centers often have more EHR capability, but can also move much slower in implementation than more nimble private practice or community clinics. With many competing demands, it can sometimes take months to build one of these surveys into an EHR, for a task that takes just a day or so. But because other departments are in the queue for these changes, implementation often takes longer than we would intuitively think.
A second barrier is the burden on the individuals themselves. As much as we feel that PROs can make a difference, and the growing literature suggests that they really can, this is counterbalanced with the burden they may place on the patient. For example, a person may arrive at a clinic visit already with a lot on their mind, and then they get a questionnaire to complete in the waiting room before their visit (or perhaps they get asked to do it at home before the visit). The patient, rather than perceiving this as beneficial, may instead perceive it as an extra task or stressor. Explaining the purpose of the PRO measures, encouraging their use, and then actually using the results meaningfully during the visit can substantially improve their perceived value.
It’s important to limit the total amount of PROs used. In research, as well as in clinical settings, too many measures can lead to too little data. It's similar to an overly complex treatment plan: the chance that a person will adhere to all of it decreases with each level of complexity added. This can lead to decreased engagement by patients, and gradually they'll move away from participating in the PROs in general. Research and clinical efforts around PROs strive to get to a parsimonious set of critical measures, which will minimize the burden, but maximize the potential benefit.
A third challenge is interpretability. This gets into the psychometric properties of the PRO measures and setting appropriate clinical thresholds for what constitutes a “positive” or “actionable” result. What is a clinically significant level of fatigue severity on the PROMIS MS Fatigue? We know that the mean range of that instrument is somewhere between 50 and 60. Does that mean that scores above 60 suggest higher than average fatigue levels, or is it more complicated than that? In many cases, the instruments don't have extensive population level research for the populations in which they are used. Setting clinical thresholds can be difficult, and I suspect that this will be a major area of research in the coming years.
Another example is setting appropriate depression thresholds. We know that on the CES-D, for example, the positive threshold for active depression in a patient with MS may be different from that in a patient without MS, because fatigue is a contributing factor to the neurovegetative symptoms that are scored on the CES-D.
So even if we can incorporate PROs into general practice and minimize burden, we also have to pay attention to factors that limit their interpretability and employ them in a way whereby they provide clinically meaningful results that can help inform care. The good news is, for many PROs, even with these limitations, this can be done.
Following directly from this is error risk. Many PRO measures were designed for large-sample epidemiologic research, not for a smaller sample clinical practice, which can lead to a higher error risk, especially when following single individuals over time. Adjustments in how these scales are interpreted are required in many cases.
The limitations of many of the respondents completing questionnaires needs to be taken into account. Fatigue and cognitive impairment are very common in MS. Respondents may be selecting answers that are not entirely accurate if they're getting fatigued while doing the surveys, or if they have a comprehension deficit or a short-term memory deficit.
A final challenge is demonstrating, just like any treatment or assessment approach, that the benefit outweighs the burden. PRO measures that are fairly reliable, validated, and quick and easy to complete suddenly become quite valuable because their benefit far outweighs the potential constraints. I think as PROs and the ways of assessing them continue to develop, that will become a bigger issue. The question will be, okay, you can do this, but what is the value added by doing this? That added value could be demonstrated in terms of better clinical outcomes, reduced costs, reduced hospitalizations, better treatment adherence, and so on.
How do you see the use of patient-reported outcomes in MS care evolving over time?
BRANT OLIVER, PhD: I tend to be optimistic regarding PROs. I think they will become part of the new reality, especially in LHS-oriented models of care. As mentioned, LHSs use feed forward data to predict the needs of people or optimize shared decision-making. I think we're going to see more shared decision-making rather than less over time in complex chronic illnesses care.
In environments where there's an increasing focus on value for high-cost, such as complex chronic conditions like MS and inflammatory bowel disease, systems will have to justify the high cost of treatment. PROs will be a critical piece in making that value assessment, especially since that value assessment is coming from the voice of patients rather than only from clinicians or other stakeholders. Arguably, patients may be able to contribute the most to making the value proposition because it is their outcomes and their experiences that matter to payers. Because experience matters (and not just outcomes), I think we'll see more PREMs used over time, including in MS.
I also think over time we'll see studies working to optimize PROs in the clinical environment and for improvement and research. An early example of that is the MS Continuous Quality Improvement (MS-CQI) Collaborative. It is a prospective randomized multicenter study using patient-reported and clinical data in a LHS approach to study population health outcomes and the effect of quality improvement interventions on those outcomes. It's also optimizing how these PRO measures are actually used at the point of care. Studies like MS-CQI will help to better articulate how, when, and for what purpose PROs should best be used and also when they should be avoided.
I think over time the predictive analytics component of PROs will be emphasized. There is a big push in the MS field in developing biomarkers to help predict disease progression over time. From the predictive analytics or machine learning perspective, imagine a situation where PROs could be used to predict a person's trajectory over time: if they were more likely to be lost to follow-up, to be hospitalized, or to have a relapse in the next year or 2. Reliable PROs generating population health data at scale can inform the development of risk and outcome predictive models.
Dr. Oliver discloses that he has received research grant support (MS-CQI research study mentioned in interview). He is the principal investigator and developer of the MS-CQI study, which is grant funded by Biogen under a Sponsored Research Agreement.
1. Manohar N, Perkins T, Laurion R, Oliver B. Patient-reported outcomes in multiple sclerosis: an overview. J Clin Outcomes Manage. 2019;26:277-288.
Brant Oliver, PhD, MS, MPH, APRN-BC, is a health care improvement and implementation scientist, educator, and board-certified family and psychiatric nurse practitioner (FNP-BC, PMHNP-BC). Dr. Oliver's work focuses on applied health care improvement science research, with a focus on "3C" (complex, costly, and chronic) conditions including MS, IBD, CF, RA, and others; coproduction; learning health systems; and shared decision making. He is Associate Professor at the Geisel School of Medicine at Dartmouth and also has been in clinical practice since 2003, working primarily as a certified MS specialist (MSCN) and a MS neurobehavioral nurse practitioner.
Which patient-reported outcomes (PROs) are commonly assessed in the care of patients with multiple sclerosis (MS)?
BRANT OLIVER, PhD: The current reality is that PROs are not being used routinely in MS clinical care in most settings. They are most commonly being used in research settings, either as part of clinical trials of new treatments, or in epidemiologic studies looking at the prevalence, incidence, and severity of certain symptoms or functional impairments in MS at the population level. A good example is the NARCOMS registry, which has been used to conduct high-quality epidemiologic studies of MS-related symptoms using self-report questionnaires.
We are starting to see some use of MS PROs in select clinical settings. Oftentimes these are measures of highly prevalent comorbid conditions that have an impact on quality of life, treatment adherence (depression severity and anxiety), and self-efficacy, which is a measure of perceived coping ability related to self-management of a chronic illness. Also, measures of patient experience are being employed in hospital-based clinics, such as the CG-CAHPS satisfaction measures.
The PROMIS (Patient-Reported Outcomes Measurement Information System) battery is a promising set of PRO measures that are being utilized across a number of conditions and that contain some MS-specific measures, such as the Fatigue MS measure. Fatigue is the most common and disabling symptom in MS, so having a good measure of fatigue is of critical importance. Having a sense of a patient’s experience with fatigue over time can also be very helpful from a clinical perspective. The PROMIS measure performs much better than its predecessor, the Modified Fatigue Impact Scale (MFIS). Another strength of the PROMIS measures is that they tend to do well correlating with other conditions. In certain research and improvement settings, PROMIS can help us understand the burden a particular disease or population places on total health system resources. For example, is fatigue burden in MS similar in severity to that in another 3C condition, such as inflammatory bowel disease?
There are other PRO measures that have not been used in MS but which I think we will see used in the future. One of these is called Collaborate, which falls into the category of patient-reported experience measures (PREMs). Collaborate measures the degree of shared decision-making that occurs in a clinical encounter, which becomes especially important as the complexity of disease-modifying treatment decisions increases as more disease-modifying therapies are introduced, each with their own profile of risks and benefits. I anticipate that the ability of clinics to facilitate effective shared decision-making will be of increasing interest to clinicians, patients, and also payers in the future.
What are some of the potential benefits of using PRO measures in terms of clinician/patient communication and clinical decision-making?
BRANT OLIVER, PhD: I think the most important benefit of measuring PROs is that it can make care more patient-centered. The big push for PROs in the first place was to incorporate more of the patient’s voice into their own care. Standard clinical measures, such as magnetic resonance imaging (MRI) or relapse rates, can be very precise and provide a good clinical picture of how the disease is behaving. But if we rely solely on that kind of information, we can lose sight of the person who is experiencing the disease.
PROs, be they just regular PROs (instruments that gather qualitative and/or quantitative patient-reported information) or PROMs (validated and standardized PRO measures) or PREMs (standardized and validated patient-reported experience measures), all aim to improve the ability to get a better story of the person who's experiencing the illness and how that condition affects them. We can also gain insight on what's most important to them regarding how their illness is managed, and what their experience of care is.
Sometimes the PRO picture and the clinical picture don't necessarily align. I'll tell a story about one a person, who's given me permission to share the story. She is an established professional, and her PRO measures concerning her quality of life, support from her workplace environment, and her ability to function in society are very high. She's very high functioning according to the PRO picture. However, her clinical measures suggest that she is significantly impaired. Her MRI burden is quite high, and her disability due to the MS, her EDSS (Expanded Disability Status Scale), is also quite high. So there are 2 very different stories provided by 2 different sets of data. The inclusion of PROs data, in connection with clinical data, can provide a more holistic view of this person, who is functioning well despite significant disease burden.
As a clinician working with patients with MS, this gives me much more to work with in trying to help people, not only treating the disease, but also trying to see where the person is most in need of help. A person could be very well controlled on MRI in terms of relapse rate, but have fatigue severity that is through the roof. If I weren't paying closer attention to that with a validated scale that measures fatigue severity over time, like the PROMIS Fatigue MS, I may not have a sense of how well treatment is helping that person's fatigue longitudinally, beyond what I can glean from the history and clinical examination.
PROs can also be helpful in terms of conditions that are harder to quantify. Depression is a significant cause of disability and a significant factor contributing to poor treatment adherence in MS. Also, the suicide rate in persons with MS is much higher than that in the general population. But there is no blood test for depression severity, and oftentimes a patient’s report on exam can be incomplete or misleading. Accompanying the mental status exam and the clinical evaluation with a validated depression severity measure (such as the PHQ9 [Patient Health Questionnaire-9], CES-D [Center for Epidemiologic Studies Depression Scale], or others) can help to determine whether treatments are having an initial effect, and this can also help with self-monitoring and treatment adherence.
That brings us to the second area where PROs show real promise in MS care: the learning health system (LHS) approach, which uses feed forward information to either predict the needs of people before they come to the office or optimize decision-making at the point of care (as discussed in our review article published in JCOM).1
PROs can play a significant role in the LHS approach in 2 ways. For example, if I have a good sense before a visit that the person has stable symptoms but is having a lot of trouble coping with MS, that may change how I allocate resources and focus the time at the visit to target the primary concern of the person before the visit even occurs. Over time I'd be able to monitor if those coping scores increase in response to the work we’re doing with the person.
The second part of this approach is a feedback mechanism. These measures can be aggregated at the population level and fed back to clinical MS centers to help clinicians who are trying to improve overall population health outcomes of people with MS to see how well they're doing on things like fatigue management, depression management, coping ability, and pain control, which can't be tested for with biologic methods. So in addition to looking at the MRI scan trends across the population and relapse rate annualized for the population over time, I'd also be able to see fatigue severity and depression severity at a clinic population level and assess the change in these severity levels over time, which I could then use to inform efforts to change how my system (clinic) provides MS care.
This capability of PROs could be of significant interest to payers, especially those who are looking to optimize the value of care that is being provided, given the high cost of MS care. MS treatments are very expensive, and MS care is multidisciplinary and requires a lot of resources. Payers, I think, will have an increasing interest in assessing the value of high-cost care. PROs could help to demonstrate that value, especially if they can help quantify that outcomes can be improved over time at the population level.
The third area where PROs are beneficial is population health research, especially in terms of the major improvement movements going on in the country, such as those advocated for by the Institute for Healthcare Improvement via the Triple Aim: improve population health outcomes, improve the experience of care, and minimize per capita cost. PROs can really help with the first 2 of those Triple Aim categories.
What are some of the factors that limit the use of PRO measures in MS research and clinical practice?
BRANT OLIVER, PhD: In our JCOM paper,1 we outlined major barriers or constraints or challenges to implementing PRO measures. One is time and technology in clinical care. It's busy. It's fast. A PRO measure requires patients to complete a questionnaire. And to do that, you need some time and space during the clinical visit, or before the visit, to collect this data. In the absence of appropriate technology, this is done using paper-based methods, which can be challenging. Technology can help. Examples include smart phone app-based collection systems, tablet PCs, or an online mechanism. But there are barriers to technology, too. Is the technology good enough? Is the interface with the people using it working well? Do you have an equal amount of access to and understanding of the technology from the people across your population? Is it only being used by a certain subset that is wealthier and more educated, or maybe who has English as a first language? Such constraints can be overcome, but they’re present in any situation where you are gathering PRO data.
Software constraints also extend to the electronic health record (EHR) capability of the clinics. If you can collect PRO data, does the EHR have the capability to present that data in a useful way during a 20- or 30-minute clinical visit? In other words, does it improve the quality of the visit, or does it generate just one more distraction during the visit? Some approaches, such as feed forward dashboards, provide easy visual displays that can quickly and easily add information at the point of care and can get around this limitation. However, a lot of MS care centers in private practice settings may not have the informatics capability of a large academic center.
Academic centers often have more EHR capability, but can also move much slower in implementation than more nimble private practice or community clinics. With many competing demands, it can sometimes take months to build one of these surveys into an EHR, for a task that takes just a day or so. But because other departments are in the queue for these changes, implementation often takes longer than we would intuitively think.
A second barrier is the burden on the individuals themselves. As much as we feel that PROs can make a difference, and the growing literature suggests that they really can, this is counterbalanced with the burden they may place on the patient. For example, a person may arrive at a clinic visit already with a lot on their mind, and then they get a questionnaire to complete in the waiting room before their visit (or perhaps they get asked to do it at home before the visit). The patient, rather than perceiving this as beneficial, may instead perceive it as an extra task or stressor. Explaining the purpose of the PRO measures, encouraging their use, and then actually using the results meaningfully during the visit can substantially improve their perceived value.
It’s important to limit the total amount of PROs used. In research, as well as in clinical settings, too many measures can lead to too little data. It's similar to an overly complex treatment plan: the chance that a person will adhere to all of it decreases with each level of complexity added. This can lead to decreased engagement by patients, and gradually they'll move away from participating in the PROs in general. Research and clinical efforts around PROs strive to get to a parsimonious set of critical measures, which will minimize the burden, but maximize the potential benefit.
A third challenge is interpretability. This gets into the psychometric properties of the PRO measures and setting appropriate clinical thresholds for what constitutes a “positive” or “actionable” result. What is a clinically significant level of fatigue severity on the PROMIS MS Fatigue? We know that the mean range of that instrument is somewhere between 50 and 60. Does that mean that scores above 60 suggest higher than average fatigue levels, or is it more complicated than that? In many cases, the instruments don't have extensive population level research for the populations in which they are used. Setting clinical thresholds can be difficult, and I suspect that this will be a major area of research in the coming years.
Another example is setting appropriate depression thresholds. We know that on the CES-D, for example, the positive threshold for active depression in a patient with MS may be different from that in a patient without MS, because fatigue is a contributing factor to the neurovegetative symptoms that are scored on the CES-D.
So even if we can incorporate PROs into general practice and minimize burden, we also have to pay attention to factors that limit their interpretability and employ them in a way whereby they provide clinically meaningful results that can help inform care. The good news is, for many PROs, even with these limitations, this can be done.
Following directly from this is error risk. Many PRO measures were designed for large-sample epidemiologic research, not for a smaller sample clinical practice, which can lead to a higher error risk, especially when following single individuals over time. Adjustments in how these scales are interpreted are required in many cases.
The limitations of many of the respondents completing questionnaires needs to be taken into account. Fatigue and cognitive impairment are very common in MS. Respondents may be selecting answers that are not entirely accurate if they're getting fatigued while doing the surveys, or if they have a comprehension deficit or a short-term memory deficit.
A final challenge is demonstrating, just like any treatment or assessment approach, that the benefit outweighs the burden. PRO measures that are fairly reliable, validated, and quick and easy to complete suddenly become quite valuable because their benefit far outweighs the potential constraints. I think as PROs and the ways of assessing them continue to develop, that will become a bigger issue. The question will be, okay, you can do this, but what is the value added by doing this? That added value could be demonstrated in terms of better clinical outcomes, reduced costs, reduced hospitalizations, better treatment adherence, and so on.
How do you see the use of patient-reported outcomes in MS care evolving over time?
BRANT OLIVER, PhD: I tend to be optimistic regarding PROs. I think they will become part of the new reality, especially in LHS-oriented models of care. As mentioned, LHSs use feed forward data to predict the needs of people or optimize shared decision-making. I think we're going to see more shared decision-making rather than less over time in complex chronic illnesses care.
In environments where there's an increasing focus on value for high-cost, such as complex chronic conditions like MS and inflammatory bowel disease, systems will have to justify the high cost of treatment. PROs will be a critical piece in making that value assessment, especially since that value assessment is coming from the voice of patients rather than only from clinicians or other stakeholders. Arguably, patients may be able to contribute the most to making the value proposition because it is their outcomes and their experiences that matter to payers. Because experience matters (and not just outcomes), I think we'll see more PREMs used over time, including in MS.
I also think over time we'll see studies working to optimize PROs in the clinical environment and for improvement and research. An early example of that is the MS Continuous Quality Improvement (MS-CQI) Collaborative. It is a prospective randomized multicenter study using patient-reported and clinical data in a LHS approach to study population health outcomes and the effect of quality improvement interventions on those outcomes. It's also optimizing how these PRO measures are actually used at the point of care. Studies like MS-CQI will help to better articulate how, when, and for what purpose PROs should best be used and also when they should be avoided.
I think over time the predictive analytics component of PROs will be emphasized. There is a big push in the MS field in developing biomarkers to help predict disease progression over time. From the predictive analytics or machine learning perspective, imagine a situation where PROs could be used to predict a person's trajectory over time: if they were more likely to be lost to follow-up, to be hospitalized, or to have a relapse in the next year or 2. Reliable PROs generating population health data at scale can inform the development of risk and outcome predictive models.
Dr. Oliver discloses that he has received research grant support (MS-CQI research study mentioned in interview). He is the principal investigator and developer of the MS-CQI study, which is grant funded by Biogen under a Sponsored Research Agreement.
Brant Oliver, PhD, MS, MPH, APRN-BC, is a health care improvement and implementation scientist, educator, and board-certified family and psychiatric nurse practitioner (FNP-BC, PMHNP-BC). Dr. Oliver's work focuses on applied health care improvement science research, with a focus on "3C" (complex, costly, and chronic) conditions including MS, IBD, CF, RA, and others; coproduction; learning health systems; and shared decision making. He is Associate Professor at the Geisel School of Medicine at Dartmouth and also has been in clinical practice since 2003, working primarily as a certified MS specialist (MSCN) and a MS neurobehavioral nurse practitioner.
Which patient-reported outcomes (PROs) are commonly assessed in the care of patients with multiple sclerosis (MS)?
BRANT OLIVER, PhD: The current reality is that PROs are not being used routinely in MS clinical care in most settings. They are most commonly being used in research settings, either as part of clinical trials of new treatments, or in epidemiologic studies looking at the prevalence, incidence, and severity of certain symptoms or functional impairments in MS at the population level. A good example is the NARCOMS registry, which has been used to conduct high-quality epidemiologic studies of MS-related symptoms using self-report questionnaires.
We are starting to see some use of MS PROs in select clinical settings. Oftentimes these are measures of highly prevalent comorbid conditions that have an impact on quality of life, treatment adherence (depression severity and anxiety), and self-efficacy, which is a measure of perceived coping ability related to self-management of a chronic illness. Also, measures of patient experience are being employed in hospital-based clinics, such as the CG-CAHPS satisfaction measures.
The PROMIS (Patient-Reported Outcomes Measurement Information System) battery is a promising set of PRO measures that are being utilized across a number of conditions and that contain some MS-specific measures, such as the Fatigue MS measure. Fatigue is the most common and disabling symptom in MS, so having a good measure of fatigue is of critical importance. Having a sense of a patient’s experience with fatigue over time can also be very helpful from a clinical perspective. The PROMIS measure performs much better than its predecessor, the Modified Fatigue Impact Scale (MFIS). Another strength of the PROMIS measures is that they tend to do well correlating with other conditions. In certain research and improvement settings, PROMIS can help us understand the burden a particular disease or population places on total health system resources. For example, is fatigue burden in MS similar in severity to that in another 3C condition, such as inflammatory bowel disease?
There are other PRO measures that have not been used in MS but which I think we will see used in the future. One of these is called Collaborate, which falls into the category of patient-reported experience measures (PREMs). Collaborate measures the degree of shared decision-making that occurs in a clinical encounter, which becomes especially important as the complexity of disease-modifying treatment decisions increases as more disease-modifying therapies are introduced, each with their own profile of risks and benefits. I anticipate that the ability of clinics to facilitate effective shared decision-making will be of increasing interest to clinicians, patients, and also payers in the future.
What are some of the potential benefits of using PRO measures in terms of clinician/patient communication and clinical decision-making?
BRANT OLIVER, PhD: I think the most important benefit of measuring PROs is that it can make care more patient-centered. The big push for PROs in the first place was to incorporate more of the patient’s voice into their own care. Standard clinical measures, such as magnetic resonance imaging (MRI) or relapse rates, can be very precise and provide a good clinical picture of how the disease is behaving. But if we rely solely on that kind of information, we can lose sight of the person who is experiencing the disease.
PROs, be they just regular PROs (instruments that gather qualitative and/or quantitative patient-reported information) or PROMs (validated and standardized PRO measures) or PREMs (standardized and validated patient-reported experience measures), all aim to improve the ability to get a better story of the person who's experiencing the illness and how that condition affects them. We can also gain insight on what's most important to them regarding how their illness is managed, and what their experience of care is.
Sometimes the PRO picture and the clinical picture don't necessarily align. I'll tell a story about one a person, who's given me permission to share the story. She is an established professional, and her PRO measures concerning her quality of life, support from her workplace environment, and her ability to function in society are very high. She's very high functioning according to the PRO picture. However, her clinical measures suggest that she is significantly impaired. Her MRI burden is quite high, and her disability due to the MS, her EDSS (Expanded Disability Status Scale), is also quite high. So there are 2 very different stories provided by 2 different sets of data. The inclusion of PROs data, in connection with clinical data, can provide a more holistic view of this person, who is functioning well despite significant disease burden.
As a clinician working with patients with MS, this gives me much more to work with in trying to help people, not only treating the disease, but also trying to see where the person is most in need of help. A person could be very well controlled on MRI in terms of relapse rate, but have fatigue severity that is through the roof. If I weren't paying closer attention to that with a validated scale that measures fatigue severity over time, like the PROMIS Fatigue MS, I may not have a sense of how well treatment is helping that person's fatigue longitudinally, beyond what I can glean from the history and clinical examination.
PROs can also be helpful in terms of conditions that are harder to quantify. Depression is a significant cause of disability and a significant factor contributing to poor treatment adherence in MS. Also, the suicide rate in persons with MS is much higher than that in the general population. But there is no blood test for depression severity, and oftentimes a patient’s report on exam can be incomplete or misleading. Accompanying the mental status exam and the clinical evaluation with a validated depression severity measure (such as the PHQ9 [Patient Health Questionnaire-9], CES-D [Center for Epidemiologic Studies Depression Scale], or others) can help to determine whether treatments are having an initial effect, and this can also help with self-monitoring and treatment adherence.
That brings us to the second area where PROs show real promise in MS care: the learning health system (LHS) approach, which uses feed forward information to either predict the needs of people before they come to the office or optimize decision-making at the point of care (as discussed in our review article published in JCOM).1
PROs can play a significant role in the LHS approach in 2 ways. For example, if I have a good sense before a visit that the person has stable symptoms but is having a lot of trouble coping with MS, that may change how I allocate resources and focus the time at the visit to target the primary concern of the person before the visit even occurs. Over time I'd be able to monitor if those coping scores increase in response to the work we’re doing with the person.
The second part of this approach is a feedback mechanism. These measures can be aggregated at the population level and fed back to clinical MS centers to help clinicians who are trying to improve overall population health outcomes of people with MS to see how well they're doing on things like fatigue management, depression management, coping ability, and pain control, which can't be tested for with biologic methods. So in addition to looking at the MRI scan trends across the population and relapse rate annualized for the population over time, I'd also be able to see fatigue severity and depression severity at a clinic population level and assess the change in these severity levels over time, which I could then use to inform efforts to change how my system (clinic) provides MS care.
This capability of PROs could be of significant interest to payers, especially those who are looking to optimize the value of care that is being provided, given the high cost of MS care. MS treatments are very expensive, and MS care is multidisciplinary and requires a lot of resources. Payers, I think, will have an increasing interest in assessing the value of high-cost care. PROs could help to demonstrate that value, especially if they can help quantify that outcomes can be improved over time at the population level.
The third area where PROs are beneficial is population health research, especially in terms of the major improvement movements going on in the country, such as those advocated for by the Institute for Healthcare Improvement via the Triple Aim: improve population health outcomes, improve the experience of care, and minimize per capita cost. PROs can really help with the first 2 of those Triple Aim categories.
What are some of the factors that limit the use of PRO measures in MS research and clinical practice?
BRANT OLIVER, PhD: In our JCOM paper,1 we outlined major barriers or constraints or challenges to implementing PRO measures. One is time and technology in clinical care. It's busy. It's fast. A PRO measure requires patients to complete a questionnaire. And to do that, you need some time and space during the clinical visit, or before the visit, to collect this data. In the absence of appropriate technology, this is done using paper-based methods, which can be challenging. Technology can help. Examples include smart phone app-based collection systems, tablet PCs, or an online mechanism. But there are barriers to technology, too. Is the technology good enough? Is the interface with the people using it working well? Do you have an equal amount of access to and understanding of the technology from the people across your population? Is it only being used by a certain subset that is wealthier and more educated, or maybe who has English as a first language? Such constraints can be overcome, but they’re present in any situation where you are gathering PRO data.
Software constraints also extend to the electronic health record (EHR) capability of the clinics. If you can collect PRO data, does the EHR have the capability to present that data in a useful way during a 20- or 30-minute clinical visit? In other words, does it improve the quality of the visit, or does it generate just one more distraction during the visit? Some approaches, such as feed forward dashboards, provide easy visual displays that can quickly and easily add information at the point of care and can get around this limitation. However, a lot of MS care centers in private practice settings may not have the informatics capability of a large academic center.
Academic centers often have more EHR capability, but can also move much slower in implementation than more nimble private practice or community clinics. With many competing demands, it can sometimes take months to build one of these surveys into an EHR, for a task that takes just a day or so. But because other departments are in the queue for these changes, implementation often takes longer than we would intuitively think.
A second barrier is the burden on the individuals themselves. As much as we feel that PROs can make a difference, and the growing literature suggests that they really can, this is counterbalanced with the burden they may place on the patient. For example, a person may arrive at a clinic visit already with a lot on their mind, and then they get a questionnaire to complete in the waiting room before their visit (or perhaps they get asked to do it at home before the visit). The patient, rather than perceiving this as beneficial, may instead perceive it as an extra task or stressor. Explaining the purpose of the PRO measures, encouraging their use, and then actually using the results meaningfully during the visit can substantially improve their perceived value.
It’s important to limit the total amount of PROs used. In research, as well as in clinical settings, too many measures can lead to too little data. It's similar to an overly complex treatment plan: the chance that a person will adhere to all of it decreases with each level of complexity added. This can lead to decreased engagement by patients, and gradually they'll move away from participating in the PROs in general. Research and clinical efforts around PROs strive to get to a parsimonious set of critical measures, which will minimize the burden, but maximize the potential benefit.
A third challenge is interpretability. This gets into the psychometric properties of the PRO measures and setting appropriate clinical thresholds for what constitutes a “positive” or “actionable” result. What is a clinically significant level of fatigue severity on the PROMIS MS Fatigue? We know that the mean range of that instrument is somewhere between 50 and 60. Does that mean that scores above 60 suggest higher than average fatigue levels, or is it more complicated than that? In many cases, the instruments don't have extensive population level research for the populations in which they are used. Setting clinical thresholds can be difficult, and I suspect that this will be a major area of research in the coming years.
Another example is setting appropriate depression thresholds. We know that on the CES-D, for example, the positive threshold for active depression in a patient with MS may be different from that in a patient without MS, because fatigue is a contributing factor to the neurovegetative symptoms that are scored on the CES-D.
So even if we can incorporate PROs into general practice and minimize burden, we also have to pay attention to factors that limit their interpretability and employ them in a way whereby they provide clinically meaningful results that can help inform care. The good news is, for many PROs, even with these limitations, this can be done.
Following directly from this is error risk. Many PRO measures were designed for large-sample epidemiologic research, not for a smaller sample clinical practice, which can lead to a higher error risk, especially when following single individuals over time. Adjustments in how these scales are interpreted are required in many cases.
The limitations of many of the respondents completing questionnaires needs to be taken into account. Fatigue and cognitive impairment are very common in MS. Respondents may be selecting answers that are not entirely accurate if they're getting fatigued while doing the surveys, or if they have a comprehension deficit or a short-term memory deficit.
A final challenge is demonstrating, just like any treatment or assessment approach, that the benefit outweighs the burden. PRO measures that are fairly reliable, validated, and quick and easy to complete suddenly become quite valuable because their benefit far outweighs the potential constraints. I think as PROs and the ways of assessing them continue to develop, that will become a bigger issue. The question will be, okay, you can do this, but what is the value added by doing this? That added value could be demonstrated in terms of better clinical outcomes, reduced costs, reduced hospitalizations, better treatment adherence, and so on.
How do you see the use of patient-reported outcomes in MS care evolving over time?
BRANT OLIVER, PhD: I tend to be optimistic regarding PROs. I think they will become part of the new reality, especially in LHS-oriented models of care. As mentioned, LHSs use feed forward data to predict the needs of people or optimize shared decision-making. I think we're going to see more shared decision-making rather than less over time in complex chronic illnesses care.
In environments where there's an increasing focus on value for high-cost, such as complex chronic conditions like MS and inflammatory bowel disease, systems will have to justify the high cost of treatment. PROs will be a critical piece in making that value assessment, especially since that value assessment is coming from the voice of patients rather than only from clinicians or other stakeholders. Arguably, patients may be able to contribute the most to making the value proposition because it is their outcomes and their experiences that matter to payers. Because experience matters (and not just outcomes), I think we'll see more PREMs used over time, including in MS.
I also think over time we'll see studies working to optimize PROs in the clinical environment and for improvement and research. An early example of that is the MS Continuous Quality Improvement (MS-CQI) Collaborative. It is a prospective randomized multicenter study using patient-reported and clinical data in a LHS approach to study population health outcomes and the effect of quality improvement interventions on those outcomes. It's also optimizing how these PRO measures are actually used at the point of care. Studies like MS-CQI will help to better articulate how, when, and for what purpose PROs should best be used and also when they should be avoided.
I think over time the predictive analytics component of PROs will be emphasized. There is a big push in the MS field in developing biomarkers to help predict disease progression over time. From the predictive analytics or machine learning perspective, imagine a situation where PROs could be used to predict a person's trajectory over time: if they were more likely to be lost to follow-up, to be hospitalized, or to have a relapse in the next year or 2. Reliable PROs generating population health data at scale can inform the development of risk and outcome predictive models.
Dr. Oliver discloses that he has received research grant support (MS-CQI research study mentioned in interview). He is the principal investigator and developer of the MS-CQI study, which is grant funded by Biogen under a Sponsored Research Agreement.
1. Manohar N, Perkins T, Laurion R, Oliver B. Patient-reported outcomes in multiple sclerosis: an overview. J Clin Outcomes Manage. 2019;26:277-288.
1. Manohar N, Perkins T, Laurion R, Oliver B. Patient-reported outcomes in multiple sclerosis: an overview. J Clin Outcomes Manage. 2019;26:277-288.
Six million childhood cancer deaths could be prevented over the next 30 years
Unless global investments are made to improve care worldwide, 11.1 million children will die from cancer over the next 30 years; 9.3 million of them (84%) will be in low- and lower-middle–income countries, according to a report in Lancet Oncology.
The report suggests that one in two new cases of childhood cancer are undiagnosed in low- and middle-income countries. If that trend continues, the number of children with cancer who are never diagnosed over the next 3 decades will exceed the number of those who are diagnosed.
Childhood cancer “is not complex, expensive, difficult to diagnose, or complicated to treat,” yet there’s a “worldwide inequity and a bleak picture for children with cancer” in low-income and middle-income countries, according to the report authors. The authors are 44 oncologists, pediatricians, and global health experts from around the world, led by Rifat Atun, MD, a professor of global health systems at Harvard University in Boston.
“For too long, there has been a widespread misconception that caring for children with cancer in low- and middle-income countries is expensive, unattainable, and inappropriate because of competing health priorities. Nothing could be further from the truth,” Dr. Atun said in a statement.
Dr. Atun and colleagues argued that the burden of childhood cancer “could be vastly reduced with new funding to scale up cost-effective interventions.” In fact, the authors estimated that scaling up interventions could prevent 6.2 million childhood cancer deaths between 2020 and 2050.
The reduction in deaths would translate to 318.4 million life-years gained, which would, in turn, translate to a global lifetime productivity gain of $2,580 billion, four times greater than the cumulative cost of $594 billion. This would mean a net return of $3 for every $1 spent.
Potential funders include governments, professional organizations, philanthropic groups, and industry, according to the authors. They also laid out the following six-pronged framework on how to proceed:
- Include childhood cancer in universal health coverage.
- Develop national cancer control plans for low-income and middle-income countries.
- End out-of-pocket costs for childhood cancer.
- Establish national and regional cancer networks to increase access to care.
- Expand population-based cancer registries to include children.
- Invest in research and innovations in low-income and middle-income countries.
“Success will be attained through political leadership, global solidarity, collective action, inclusive participation of all major stakeholders, and alignment of national and global efforts to expand access to effective and sustainable care for children with cancer,” the authors wrote.
No funding sources were reported. The authors didn’t have any disclosures.
SOURCE: Atun R et al. Lancet Oncol. 2020 Apr;21(4):e185-224.
Unless global investments are made to improve care worldwide, 11.1 million children will die from cancer over the next 30 years; 9.3 million of them (84%) will be in low- and lower-middle–income countries, according to a report in Lancet Oncology.
The report suggests that one in two new cases of childhood cancer are undiagnosed in low- and middle-income countries. If that trend continues, the number of children with cancer who are never diagnosed over the next 3 decades will exceed the number of those who are diagnosed.
Childhood cancer “is not complex, expensive, difficult to diagnose, or complicated to treat,” yet there’s a “worldwide inequity and a bleak picture for children with cancer” in low-income and middle-income countries, according to the report authors. The authors are 44 oncologists, pediatricians, and global health experts from around the world, led by Rifat Atun, MD, a professor of global health systems at Harvard University in Boston.
“For too long, there has been a widespread misconception that caring for children with cancer in low- and middle-income countries is expensive, unattainable, and inappropriate because of competing health priorities. Nothing could be further from the truth,” Dr. Atun said in a statement.
Dr. Atun and colleagues argued that the burden of childhood cancer “could be vastly reduced with new funding to scale up cost-effective interventions.” In fact, the authors estimated that scaling up interventions could prevent 6.2 million childhood cancer deaths between 2020 and 2050.
The reduction in deaths would translate to 318.4 million life-years gained, which would, in turn, translate to a global lifetime productivity gain of $2,580 billion, four times greater than the cumulative cost of $594 billion. This would mean a net return of $3 for every $1 spent.
Potential funders include governments, professional organizations, philanthropic groups, and industry, according to the authors. They also laid out the following six-pronged framework on how to proceed:
- Include childhood cancer in universal health coverage.
- Develop national cancer control plans for low-income and middle-income countries.
- End out-of-pocket costs for childhood cancer.
- Establish national and regional cancer networks to increase access to care.
- Expand population-based cancer registries to include children.
- Invest in research and innovations in low-income and middle-income countries.
“Success will be attained through political leadership, global solidarity, collective action, inclusive participation of all major stakeholders, and alignment of national and global efforts to expand access to effective and sustainable care for children with cancer,” the authors wrote.
No funding sources were reported. The authors didn’t have any disclosures.
SOURCE: Atun R et al. Lancet Oncol. 2020 Apr;21(4):e185-224.
Unless global investments are made to improve care worldwide, 11.1 million children will die from cancer over the next 30 years; 9.3 million of them (84%) will be in low- and lower-middle–income countries, according to a report in Lancet Oncology.
The report suggests that one in two new cases of childhood cancer are undiagnosed in low- and middle-income countries. If that trend continues, the number of children with cancer who are never diagnosed over the next 3 decades will exceed the number of those who are diagnosed.
Childhood cancer “is not complex, expensive, difficult to diagnose, or complicated to treat,” yet there’s a “worldwide inequity and a bleak picture for children with cancer” in low-income and middle-income countries, according to the report authors. The authors are 44 oncologists, pediatricians, and global health experts from around the world, led by Rifat Atun, MD, a professor of global health systems at Harvard University in Boston.
“For too long, there has been a widespread misconception that caring for children with cancer in low- and middle-income countries is expensive, unattainable, and inappropriate because of competing health priorities. Nothing could be further from the truth,” Dr. Atun said in a statement.
Dr. Atun and colleagues argued that the burden of childhood cancer “could be vastly reduced with new funding to scale up cost-effective interventions.” In fact, the authors estimated that scaling up interventions could prevent 6.2 million childhood cancer deaths between 2020 and 2050.
The reduction in deaths would translate to 318.4 million life-years gained, which would, in turn, translate to a global lifetime productivity gain of $2,580 billion, four times greater than the cumulative cost of $594 billion. This would mean a net return of $3 for every $1 spent.
Potential funders include governments, professional organizations, philanthropic groups, and industry, according to the authors. They also laid out the following six-pronged framework on how to proceed:
- Include childhood cancer in universal health coverage.
- Develop national cancer control plans for low-income and middle-income countries.
- End out-of-pocket costs for childhood cancer.
- Establish national and regional cancer networks to increase access to care.
- Expand population-based cancer registries to include children.
- Invest in research and innovations in low-income and middle-income countries.
“Success will be attained through political leadership, global solidarity, collective action, inclusive participation of all major stakeholders, and alignment of national and global efforts to expand access to effective and sustainable care for children with cancer,” the authors wrote.
No funding sources were reported. The authors didn’t have any disclosures.
SOURCE: Atun R et al. Lancet Oncol. 2020 Apr;21(4):e185-224.
FROM LANCET ONCOLOGY
Hydroxychloroquine ineffective for COVID-19, VA study suggests
Hydroxychloroquine (HCQ) with or without azithromycin (AZ) is not associated with a lower risk of requiring mechanical ventilation, according to a retrospective study of Veterans Affairs patients hospitalized with COVID-19.
The study, which was posted on a preprint server April 21 and has not been peer reviewed, also showed an increased risk of death associated with COVID-19 patients treated with HCQ alone.
“These findings highlight the importance of awaiting the results of ongoing prospective, randomized controlled studies before widespread adoption of these drugs,” write Joseph Magagnoli with Dorn Research Institute at the Columbia (S.C.) VA Health Care System and the department of clinical pharmacy & outcomes sciences, University of South Carolina, and colleagues.
A spokesperson with the University of Virginia, Charlottesville, where several of coauthors practice, said that the authors declined to comment for this article before peer review is completed.
The new data are not the first to suggest no benefit with HCQ among patients with COVID-19. A randomized trial showed no benefit and more side effects among 75 patients in China treated with HCQ, compared with 75 who received standard of care alone, according to a preprint posted online April 14.
No benefit in ventilation, death rates
The current analysis included data from all 368 male patients hospitalized with confirmed COVID-19 and treated at Veterans Health Administration medical centers in the United States through April 11.
Patients were categorized into three groups: those treated with HCQ in addition to standard of care (n = 97); those treated with HCQ and the antibiotic azithromycin plus standard of care (n = 113); and those who received standard supportive care only (n = 158).
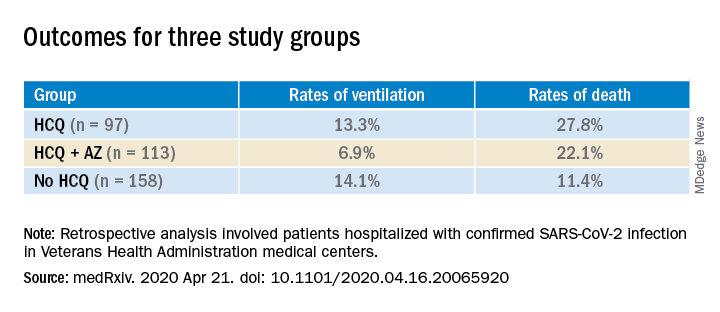
Compared with the no HCQ group, the risk of death from any cause was higher in the HCQ group (adjusted hazard ratio, 2.61; 95% confidence interval, 1.10-6.17; P = .03) but not in the HCQ+AZ group (aHR, 1.14; 95% CI, 0.56-2.32; P = .72).
The risk of ventilation was similar in the HCQ group (aHR, 1.43; 95% CI, 0.53-3.79; P = .48) and in the HCQ+AZ group (aHR, 0.43; 95% CI, 0.16-1.12; P = .09), compared with the no-HCQ group.
This study provides another counterbalance to claims of HCQ efficacy, David R. Wessner, PhD, professor of biology and chair of the department of health and human values at Davidson (N.C.) College, said in an interview.
Interest in HCQ spiked after an open-label, nonrandomized, single-center study of COVID-19 patients in France suggested that hydroxychloroquine helped clear the virus and had a potential enhanced effect when combined with azithromycin.
But the 36-patient trial has since been called into question.
Wait for convincing data
Dr. Wessner, whose research focuses on viral pathogenesis, says that, although the current data don’t definitively answer the question of whether HCQ is effective in treating COVID-19, taking a “let’s try it and see” approach is not reasonable.
“Until we have good, prospective randomized trials, it’s hard to know what to make of this. But this is more evidence that there’s not a good reason to use [HCQ],” Dr. Wessner said. He points out that the small randomized trial from China shows that HCQ comes with potential harms.
Anecdotal evidence is often cited by those who promote HCQ as a potential treatment, but “those are one-off examples,” Wessner continued. “That doesn’t really tell us anything.”
Some HCQ proponents have said that trials finding no benefit are flawed in that the drug is given too late. However, Dr. Wessner says, there’s no way to prove or disprove that claim without randomized controlled trials.
Conflicting messages
Despite lack of clear evidence of benefit for patients with COVID-19, HCQ is recommended off-label by the Chinese National guideline, and the U.S. Food and Drug Administration has issued an emergency-use authorization for the treatment of adult patients with COVID-19.
Conversely, the Infectious Diseases Society of America and a guideline panel convened by the National Institutes of Health each concluded recently that because of insufficient data, they could not recommend any specific treatments for patients with COVID-19.
The VA data for the current study came from the Veterans Affairs Informatics and Computing Infrastructure, which includes inpatient, outpatient and laboratory data and pharmacy claims.
The authors acknowledge some limitations, “including those inherent to all retrospective analyses such as nonrandomization of treatments.”
However, they note that they did adjust for potential confounders, including comorbidities, medications, and clinical and laboratory factors.
A coauthor, Jayakrishna Ambati, MD, is a cofounder of iVeena Holdings, iVeena Delivery Systems and Inflammasome Therapeutics, and has received consultancy fees from Allergan, Biogen, Boehringer Ingelheim, Immunovant, Janssen, Olix Pharmaceuticals, Retinal Solutions, and Saksin LifeSciences, all unrelated to this work. Dr. Ambati is named as an inventor on a patent application filed by the University of Virginia relating to COVID-19 but unrelated to this work. Another coauthor has received research grants from Boehringer Ingelheim, Gilead Sciences, Portola Pharmaceuticals, and United Therapeutics, all unrelated to this work. The other authors and Dr. Wessner have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Hydroxychloroquine (HCQ) with or without azithromycin (AZ) is not associated with a lower risk of requiring mechanical ventilation, according to a retrospective study of Veterans Affairs patients hospitalized with COVID-19.
The study, which was posted on a preprint server April 21 and has not been peer reviewed, also showed an increased risk of death associated with COVID-19 patients treated with HCQ alone.
“These findings highlight the importance of awaiting the results of ongoing prospective, randomized controlled studies before widespread adoption of these drugs,” write Joseph Magagnoli with Dorn Research Institute at the Columbia (S.C.) VA Health Care System and the department of clinical pharmacy & outcomes sciences, University of South Carolina, and colleagues.
A spokesperson with the University of Virginia, Charlottesville, where several of coauthors practice, said that the authors declined to comment for this article before peer review is completed.
The new data are not the first to suggest no benefit with HCQ among patients with COVID-19. A randomized trial showed no benefit and more side effects among 75 patients in China treated with HCQ, compared with 75 who received standard of care alone, according to a preprint posted online April 14.
No benefit in ventilation, death rates
The current analysis included data from all 368 male patients hospitalized with confirmed COVID-19 and treated at Veterans Health Administration medical centers in the United States through April 11.
Patients were categorized into three groups: those treated with HCQ in addition to standard of care (n = 97); those treated with HCQ and the antibiotic azithromycin plus standard of care (n = 113); and those who received standard supportive care only (n = 158).
Compared with the no HCQ group, the risk of death from any cause was higher in the HCQ group (adjusted hazard ratio, 2.61; 95% confidence interval, 1.10-6.17; P = .03) but not in the HCQ+AZ group (aHR, 1.14; 95% CI, 0.56-2.32; P = .72).
The risk of ventilation was similar in the HCQ group (aHR, 1.43; 95% CI, 0.53-3.79; P = .48) and in the HCQ+AZ group (aHR, 0.43; 95% CI, 0.16-1.12; P = .09), compared with the no-HCQ group.
This study provides another counterbalance to claims of HCQ efficacy, David R. Wessner, PhD, professor of biology and chair of the department of health and human values at Davidson (N.C.) College, said in an interview.
Interest in HCQ spiked after an open-label, nonrandomized, single-center study of COVID-19 patients in France suggested that hydroxychloroquine helped clear the virus and had a potential enhanced effect when combined with azithromycin.
But the 36-patient trial has since been called into question.
Wait for convincing data
Dr. Wessner, whose research focuses on viral pathogenesis, says that, although the current data don’t definitively answer the question of whether HCQ is effective in treating COVID-19, taking a “let’s try it and see” approach is not reasonable.
“Until we have good, prospective randomized trials, it’s hard to know what to make of this. But this is more evidence that there’s not a good reason to use [HCQ],” Dr. Wessner said. He points out that the small randomized trial from China shows that HCQ comes with potential harms.
Anecdotal evidence is often cited by those who promote HCQ as a potential treatment, but “those are one-off examples,” Wessner continued. “That doesn’t really tell us anything.”
Some HCQ proponents have said that trials finding no benefit are flawed in that the drug is given too late. However, Dr. Wessner says, there’s no way to prove or disprove that claim without randomized controlled trials.
Conflicting messages
Despite lack of clear evidence of benefit for patients with COVID-19, HCQ is recommended off-label by the Chinese National guideline, and the U.S. Food and Drug Administration has issued an emergency-use authorization for the treatment of adult patients with COVID-19.
Conversely, the Infectious Diseases Society of America and a guideline panel convened by the National Institutes of Health each concluded recently that because of insufficient data, they could not recommend any specific treatments for patients with COVID-19.
The VA data for the current study came from the Veterans Affairs Informatics and Computing Infrastructure, which includes inpatient, outpatient and laboratory data and pharmacy claims.
The authors acknowledge some limitations, “including those inherent to all retrospective analyses such as nonrandomization of treatments.”
However, they note that they did adjust for potential confounders, including comorbidities, medications, and clinical and laboratory factors.
A coauthor, Jayakrishna Ambati, MD, is a cofounder of iVeena Holdings, iVeena Delivery Systems and Inflammasome Therapeutics, and has received consultancy fees from Allergan, Biogen, Boehringer Ingelheim, Immunovant, Janssen, Olix Pharmaceuticals, Retinal Solutions, and Saksin LifeSciences, all unrelated to this work. Dr. Ambati is named as an inventor on a patent application filed by the University of Virginia relating to COVID-19 but unrelated to this work. Another coauthor has received research grants from Boehringer Ingelheim, Gilead Sciences, Portola Pharmaceuticals, and United Therapeutics, all unrelated to this work. The other authors and Dr. Wessner have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Hydroxychloroquine (HCQ) with or without azithromycin (AZ) is not associated with a lower risk of requiring mechanical ventilation, according to a retrospective study of Veterans Affairs patients hospitalized with COVID-19.
The study, which was posted on a preprint server April 21 and has not been peer reviewed, also showed an increased risk of death associated with COVID-19 patients treated with HCQ alone.
“These findings highlight the importance of awaiting the results of ongoing prospective, randomized controlled studies before widespread adoption of these drugs,” write Joseph Magagnoli with Dorn Research Institute at the Columbia (S.C.) VA Health Care System and the department of clinical pharmacy & outcomes sciences, University of South Carolina, and colleagues.
A spokesperson with the University of Virginia, Charlottesville, where several of coauthors practice, said that the authors declined to comment for this article before peer review is completed.
The new data are not the first to suggest no benefit with HCQ among patients with COVID-19. A randomized trial showed no benefit and more side effects among 75 patients in China treated with HCQ, compared with 75 who received standard of care alone, according to a preprint posted online April 14.
No benefit in ventilation, death rates
The current analysis included data from all 368 male patients hospitalized with confirmed COVID-19 and treated at Veterans Health Administration medical centers in the United States through April 11.
Patients were categorized into three groups: those treated with HCQ in addition to standard of care (n = 97); those treated with HCQ and the antibiotic azithromycin plus standard of care (n = 113); and those who received standard supportive care only (n = 158).
Compared with the no HCQ group, the risk of death from any cause was higher in the HCQ group (adjusted hazard ratio, 2.61; 95% confidence interval, 1.10-6.17; P = .03) but not in the HCQ+AZ group (aHR, 1.14; 95% CI, 0.56-2.32; P = .72).
The risk of ventilation was similar in the HCQ group (aHR, 1.43; 95% CI, 0.53-3.79; P = .48) and in the HCQ+AZ group (aHR, 0.43; 95% CI, 0.16-1.12; P = .09), compared with the no-HCQ group.
This study provides another counterbalance to claims of HCQ efficacy, David R. Wessner, PhD, professor of biology and chair of the department of health and human values at Davidson (N.C.) College, said in an interview.
Interest in HCQ spiked after an open-label, nonrandomized, single-center study of COVID-19 patients in France suggested that hydroxychloroquine helped clear the virus and had a potential enhanced effect when combined with azithromycin.
But the 36-patient trial has since been called into question.
Wait for convincing data
Dr. Wessner, whose research focuses on viral pathogenesis, says that, although the current data don’t definitively answer the question of whether HCQ is effective in treating COVID-19, taking a “let’s try it and see” approach is not reasonable.
“Until we have good, prospective randomized trials, it’s hard to know what to make of this. But this is more evidence that there’s not a good reason to use [HCQ],” Dr. Wessner said. He points out that the small randomized trial from China shows that HCQ comes with potential harms.
Anecdotal evidence is often cited by those who promote HCQ as a potential treatment, but “those are one-off examples,” Wessner continued. “That doesn’t really tell us anything.”
Some HCQ proponents have said that trials finding no benefit are flawed in that the drug is given too late. However, Dr. Wessner says, there’s no way to prove or disprove that claim without randomized controlled trials.
Conflicting messages
Despite lack of clear evidence of benefit for patients with COVID-19, HCQ is recommended off-label by the Chinese National guideline, and the U.S. Food and Drug Administration has issued an emergency-use authorization for the treatment of adult patients with COVID-19.
Conversely, the Infectious Diseases Society of America and a guideline panel convened by the National Institutes of Health each concluded recently that because of insufficient data, they could not recommend any specific treatments for patients with COVID-19.
The VA data for the current study came from the Veterans Affairs Informatics and Computing Infrastructure, which includes inpatient, outpatient and laboratory data and pharmacy claims.
The authors acknowledge some limitations, “including those inherent to all retrospective analyses such as nonrandomization of treatments.”
However, they note that they did adjust for potential confounders, including comorbidities, medications, and clinical and laboratory factors.
A coauthor, Jayakrishna Ambati, MD, is a cofounder of iVeena Holdings, iVeena Delivery Systems and Inflammasome Therapeutics, and has received consultancy fees from Allergan, Biogen, Boehringer Ingelheim, Immunovant, Janssen, Olix Pharmaceuticals, Retinal Solutions, and Saksin LifeSciences, all unrelated to this work. Dr. Ambati is named as an inventor on a patent application filed by the University of Virginia relating to COVID-19 but unrelated to this work. Another coauthor has received research grants from Boehringer Ingelheim, Gilead Sciences, Portola Pharmaceuticals, and United Therapeutics, all unrelated to this work. The other authors and Dr. Wessner have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Prioritizing ambulatory gynecology care during COVID-19: The latest guidance
What exactly constitutes appropriate ambulatory gynecology during this time of social distancing?
On March 30, 2020, the American College of Obstetricians and Gynecologists (ACOG) weighed in, releasing COVID-19 FAQs for Obstetrician-Gynecologists. These recommendations, which include information about obstetric and gynecologic surgery, are available to everyone, including the general public. They are intended to supplement guidance from the Centers for Disease Control and Prevention, as well as previously released ACOG guidance.
The recommendations include examples of patients needing in-person appointments, telehealth visits, or visits that should be deferred.
In-person appointments. Examples of patients for whom in-person appointments are appropriate include those with suspected ectopic pregnancy or profuse vaginal bleeding. With respect to contraceptive services, ACOG suggests that placement of IUDs and implants should continue whenever possible. If placement of the contraceptive device is deferred, use of self-administered hormonal contraceptives (including subcutaneous injections, oral, transdermal patch, and vaginal ring) should be encouraged as a bridge to later initiation of long-acting methods.
Telehealth visits. Video or telephone visits are advised for women desiring counseling and prescribing for contraception or menopausal symptoms.
Deferred. Deferral of office visits until after COVID-19 lockdowns is advised for average-risk women wishing routine well-woman visits. Other situations in which deferral should be considered include the following:
- For patients with abnormal cervical cancer screening results, ACOG suggests that colposcopy with cervical biopsies could be deferred for 6-12 months for patients with low-grade test results. In contrast, for patients with high-grade results, ACOG recommends that evaluation be performed within 3 months.
- For women who wish to discontinue their contraceptive, ACOG advises that removal of IUDs and implants be postponed when possible. These women should be counseled regarding extended use of these devices.
ACOG emphasizes that decisions regarding ambulatory gynecology should be individualized and take into consideration such issues as availability of local and regional resources, staffing, personal protective equipment, and the local prevalence of COVID-19.
As a gynecologist focused on ambulatory care, I believe that many clinicians will welcome this guidance from ACOG, which helps us provide optimal care during these challenging times.
Dr. Kaunitz is professor and associate chairman in the department of obstetrics and gynecology at the University of Florida, Jacksonville. He has disclosed receiving royalties from UpToDate, serving on the safety monitoring board for Femasys, and serving as a consultant for AMAG Pharmaceuticals, Merck & Co, Mithra, and Pfizer. His institution has received funding from pharmaceutical companies and nonprofits.
A version of this article originally appeared on Medscape.com.
What exactly constitutes appropriate ambulatory gynecology during this time of social distancing?
On March 30, 2020, the American College of Obstetricians and Gynecologists (ACOG) weighed in, releasing COVID-19 FAQs for Obstetrician-Gynecologists. These recommendations, which include information about obstetric and gynecologic surgery, are available to everyone, including the general public. They are intended to supplement guidance from the Centers for Disease Control and Prevention, as well as previously released ACOG guidance.
The recommendations include examples of patients needing in-person appointments, telehealth visits, or visits that should be deferred.
In-person appointments. Examples of patients for whom in-person appointments are appropriate include those with suspected ectopic pregnancy or profuse vaginal bleeding. With respect to contraceptive services, ACOG suggests that placement of IUDs and implants should continue whenever possible. If placement of the contraceptive device is deferred, use of self-administered hormonal contraceptives (including subcutaneous injections, oral, transdermal patch, and vaginal ring) should be encouraged as a bridge to later initiation of long-acting methods.
Telehealth visits. Video or telephone visits are advised for women desiring counseling and prescribing for contraception or menopausal symptoms.
Deferred. Deferral of office visits until after COVID-19 lockdowns is advised for average-risk women wishing routine well-woman visits. Other situations in which deferral should be considered include the following:
- For patients with abnormal cervical cancer screening results, ACOG suggests that colposcopy with cervical biopsies could be deferred for 6-12 months for patients with low-grade test results. In contrast, for patients with high-grade results, ACOG recommends that evaluation be performed within 3 months.
- For women who wish to discontinue their contraceptive, ACOG advises that removal of IUDs and implants be postponed when possible. These women should be counseled regarding extended use of these devices.
ACOG emphasizes that decisions regarding ambulatory gynecology should be individualized and take into consideration such issues as availability of local and regional resources, staffing, personal protective equipment, and the local prevalence of COVID-19.
As a gynecologist focused on ambulatory care, I believe that many clinicians will welcome this guidance from ACOG, which helps us provide optimal care during these challenging times.
Dr. Kaunitz is professor and associate chairman in the department of obstetrics and gynecology at the University of Florida, Jacksonville. He has disclosed receiving royalties from UpToDate, serving on the safety monitoring board for Femasys, and serving as a consultant for AMAG Pharmaceuticals, Merck & Co, Mithra, and Pfizer. His institution has received funding from pharmaceutical companies and nonprofits.
A version of this article originally appeared on Medscape.com.
What exactly constitutes appropriate ambulatory gynecology during this time of social distancing?
On March 30, 2020, the American College of Obstetricians and Gynecologists (ACOG) weighed in, releasing COVID-19 FAQs for Obstetrician-Gynecologists. These recommendations, which include information about obstetric and gynecologic surgery, are available to everyone, including the general public. They are intended to supplement guidance from the Centers for Disease Control and Prevention, as well as previously released ACOG guidance.
The recommendations include examples of patients needing in-person appointments, telehealth visits, or visits that should be deferred.
In-person appointments. Examples of patients for whom in-person appointments are appropriate include those with suspected ectopic pregnancy or profuse vaginal bleeding. With respect to contraceptive services, ACOG suggests that placement of IUDs and implants should continue whenever possible. If placement of the contraceptive device is deferred, use of self-administered hormonal contraceptives (including subcutaneous injections, oral, transdermal patch, and vaginal ring) should be encouraged as a bridge to later initiation of long-acting methods.
Telehealth visits. Video or telephone visits are advised for women desiring counseling and prescribing for contraception or menopausal symptoms.
Deferred. Deferral of office visits until after COVID-19 lockdowns is advised for average-risk women wishing routine well-woman visits. Other situations in which deferral should be considered include the following:
- For patients with abnormal cervical cancer screening results, ACOG suggests that colposcopy with cervical biopsies could be deferred for 6-12 months for patients with low-grade test results. In contrast, for patients with high-grade results, ACOG recommends that evaluation be performed within 3 months.
- For women who wish to discontinue their contraceptive, ACOG advises that removal of IUDs and implants be postponed when possible. These women should be counseled regarding extended use of these devices.
ACOG emphasizes that decisions regarding ambulatory gynecology should be individualized and take into consideration such issues as availability of local and regional resources, staffing, personal protective equipment, and the local prevalence of COVID-19.
As a gynecologist focused on ambulatory care, I believe that many clinicians will welcome this guidance from ACOG, which helps us provide optimal care during these challenging times.
Dr. Kaunitz is professor and associate chairman in the department of obstetrics and gynecology at the University of Florida, Jacksonville. He has disclosed receiving royalties from UpToDate, serving on the safety monitoring board for Femasys, and serving as a consultant for AMAG Pharmaceuticals, Merck & Co, Mithra, and Pfizer. His institution has received funding from pharmaceutical companies and nonprofits.
A version of this article originally appeared on Medscape.com.
Hip hemiarthroplasty outcomes found better with cement vs. no cement
In older patients undergoing hemiarthroplasty for repair of a hip fracture, cemented fixation reduces the risk of aseptic revisions, according to a large retrospective cohort analysis reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled due to COVID-19.
“These data suggest surgeons should consider cemented over uncemented femoral stem fixation in the absence of contraindications,” reported Kanu M. Okike, MD, an orthopedic surgeon with the Hawaii Permanente Medical Group, Kaiser Moanalua Medical Center, Honolulu.
The finding was drawn from a cohort analysis conducted in the United States. Several studies conducted in Europe and elsewhere, including randomized trials, have also favored cement.
“Cemented fixation is becoming a standard of care for elderly individuals outside of the U.S., but this study was conducted to evaluate the U.S. experience,” explained Dr. Okike in an interview.
Citing 2018 American Joint Replacement Registry data, Dr. Okike reported that more than half of hemiarthroplasties in the United States are still being fixed without cement.
The retrospective cohort analysis was undertaken with the Kaiser Permanente Hip Fracture Registry, selecting patients age 60 years or older who underwent hemiarthroplasty for hip fracture between 2009 and 2017. Of the 12,491 patients, 6,449 (51.6%) included cement fixation, and the remaining were uncemented.
After controlling for confounders, including age, sex, body mass index, and comorbidities, the incidence of aseptic revision 1 year after repair was 3.0% in the uncemented group and 1.3% in the cemented group. By hazard ratio (HR), the risk of aseptic revision, which was the primary endpoint, was increased by more than 75% (HR 1.77; 95% confidence interval, 1.43-2.19; P < .001).
Of the secondary outcomes evaluated, such as medical complications at 90 days or mortality at 1 year, none were significantly different between the two arms.
A post hoc analysis suggested that a higher risk of periprosthetic fracture explained the higher rates of aseptic revision in the uncemented group, according to Dr. Okike, whose data have now been published (JAMA. 2020;323:1077-84).
Surgeon preference was also evaluated in this study as an instrumental variable. When patients treated by a surgeon with a preference for cemented fixation were compared with those treated by a surgeon with a preference for cementless repair, the relative advantage of cement for the primary outcome was similar (HR, 1.74; P = .02).
These data are consistent with trials outside of the United States. For example, a randomized trial with 160 patients conducted in New Zealand associated cemented fixation with a lower risk of periprosthetic fracture (1 vs. 18) and superior Oxford hip scores (J Bone Joint Surg Am. 2012;94:577-83). Similarly, a randomized trial of 141 patients conducted in Sweden associated cemented fixation with lower rate of periprosthetic fracture (0 vs. 9) and improved outcomes on several instruments, including the Harris Hip Scale (Bone Joint J. 2015;97-B:1475-80).
Cemented fixation generally requires a slightly longer operating time, but it is not otherwise more difficult or more expensive, according to Dr. Okike. He believes these results encourage cemented fixation in older patients without contraindications. This is already specifically recommended in AAOS guidelines for the management of hip fractures in elderly patients.
An orthopedic surgeon who has published frequently on total hip arthroplasty, Emil van Haaren, MD, of Zuyderland Medical Center, Heerlen, the Netherlands, confirmed that cemented hemiarthroplasty is considered “the golden standard of care” at his institution. In one study for which he served as the senior author, survival was characterized as excellent in older patients receiving cemented hip arthroplasty that were followed for more than 10 years (J Arthroplasty. 2016;31:194-8).
“We routinely use cemented prosthesis in hip fracture management when an arthroplasty is indicated,” he reported, echoing the contention by Dr. Okike that this approach is dominant in many centers outside of the United States.
Dr. Okike reports no potential conflicts of interest.
SOURCE: Okiki KM et al. JAMA. 2020;323:1077-84.
In older patients undergoing hemiarthroplasty for repair of a hip fracture, cemented fixation reduces the risk of aseptic revisions, according to a large retrospective cohort analysis reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled due to COVID-19.
“These data suggest surgeons should consider cemented over uncemented femoral stem fixation in the absence of contraindications,” reported Kanu M. Okike, MD, an orthopedic surgeon with the Hawaii Permanente Medical Group, Kaiser Moanalua Medical Center, Honolulu.
The finding was drawn from a cohort analysis conducted in the United States. Several studies conducted in Europe and elsewhere, including randomized trials, have also favored cement.
“Cemented fixation is becoming a standard of care for elderly individuals outside of the U.S., but this study was conducted to evaluate the U.S. experience,” explained Dr. Okike in an interview.
Citing 2018 American Joint Replacement Registry data, Dr. Okike reported that more than half of hemiarthroplasties in the United States are still being fixed without cement.
The retrospective cohort analysis was undertaken with the Kaiser Permanente Hip Fracture Registry, selecting patients age 60 years or older who underwent hemiarthroplasty for hip fracture between 2009 and 2017. Of the 12,491 patients, 6,449 (51.6%) included cement fixation, and the remaining were uncemented.
After controlling for confounders, including age, sex, body mass index, and comorbidities, the incidence of aseptic revision 1 year after repair was 3.0% in the uncemented group and 1.3% in the cemented group. By hazard ratio (HR), the risk of aseptic revision, which was the primary endpoint, was increased by more than 75% (HR 1.77; 95% confidence interval, 1.43-2.19; P < .001).
Of the secondary outcomes evaluated, such as medical complications at 90 days or mortality at 1 year, none were significantly different between the two arms.
A post hoc analysis suggested that a higher risk of periprosthetic fracture explained the higher rates of aseptic revision in the uncemented group, according to Dr. Okike, whose data have now been published (JAMA. 2020;323:1077-84).
Surgeon preference was also evaluated in this study as an instrumental variable. When patients treated by a surgeon with a preference for cemented fixation were compared with those treated by a surgeon with a preference for cementless repair, the relative advantage of cement for the primary outcome was similar (HR, 1.74; P = .02).
These data are consistent with trials outside of the United States. For example, a randomized trial with 160 patients conducted in New Zealand associated cemented fixation with a lower risk of periprosthetic fracture (1 vs. 18) and superior Oxford hip scores (J Bone Joint Surg Am. 2012;94:577-83). Similarly, a randomized trial of 141 patients conducted in Sweden associated cemented fixation with lower rate of periprosthetic fracture (0 vs. 9) and improved outcomes on several instruments, including the Harris Hip Scale (Bone Joint J. 2015;97-B:1475-80).
Cemented fixation generally requires a slightly longer operating time, but it is not otherwise more difficult or more expensive, according to Dr. Okike. He believes these results encourage cemented fixation in older patients without contraindications. This is already specifically recommended in AAOS guidelines for the management of hip fractures in elderly patients.
An orthopedic surgeon who has published frequently on total hip arthroplasty, Emil van Haaren, MD, of Zuyderland Medical Center, Heerlen, the Netherlands, confirmed that cemented hemiarthroplasty is considered “the golden standard of care” at his institution. In one study for which he served as the senior author, survival was characterized as excellent in older patients receiving cemented hip arthroplasty that were followed for more than 10 years (J Arthroplasty. 2016;31:194-8).
“We routinely use cemented prosthesis in hip fracture management when an arthroplasty is indicated,” he reported, echoing the contention by Dr. Okike that this approach is dominant in many centers outside of the United States.
Dr. Okike reports no potential conflicts of interest.
SOURCE: Okiki KM et al. JAMA. 2020;323:1077-84.
In older patients undergoing hemiarthroplasty for repair of a hip fracture, cemented fixation reduces the risk of aseptic revisions, according to a large retrospective cohort analysis reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled due to COVID-19.
“These data suggest surgeons should consider cemented over uncemented femoral stem fixation in the absence of contraindications,” reported Kanu M. Okike, MD, an orthopedic surgeon with the Hawaii Permanente Medical Group, Kaiser Moanalua Medical Center, Honolulu.
The finding was drawn from a cohort analysis conducted in the United States. Several studies conducted in Europe and elsewhere, including randomized trials, have also favored cement.
“Cemented fixation is becoming a standard of care for elderly individuals outside of the U.S., but this study was conducted to evaluate the U.S. experience,” explained Dr. Okike in an interview.
Citing 2018 American Joint Replacement Registry data, Dr. Okike reported that more than half of hemiarthroplasties in the United States are still being fixed without cement.
The retrospective cohort analysis was undertaken with the Kaiser Permanente Hip Fracture Registry, selecting patients age 60 years or older who underwent hemiarthroplasty for hip fracture between 2009 and 2017. Of the 12,491 patients, 6,449 (51.6%) included cement fixation, and the remaining were uncemented.
After controlling for confounders, including age, sex, body mass index, and comorbidities, the incidence of aseptic revision 1 year after repair was 3.0% in the uncemented group and 1.3% in the cemented group. By hazard ratio (HR), the risk of aseptic revision, which was the primary endpoint, was increased by more than 75% (HR 1.77; 95% confidence interval, 1.43-2.19; P < .001).
Of the secondary outcomes evaluated, such as medical complications at 90 days or mortality at 1 year, none were significantly different between the two arms.
A post hoc analysis suggested that a higher risk of periprosthetic fracture explained the higher rates of aseptic revision in the uncemented group, according to Dr. Okike, whose data have now been published (JAMA. 2020;323:1077-84).
Surgeon preference was also evaluated in this study as an instrumental variable. When patients treated by a surgeon with a preference for cemented fixation were compared with those treated by a surgeon with a preference for cementless repair, the relative advantage of cement for the primary outcome was similar (HR, 1.74; P = .02).
These data are consistent with trials outside of the United States. For example, a randomized trial with 160 patients conducted in New Zealand associated cemented fixation with a lower risk of periprosthetic fracture (1 vs. 18) and superior Oxford hip scores (J Bone Joint Surg Am. 2012;94:577-83). Similarly, a randomized trial of 141 patients conducted in Sweden associated cemented fixation with lower rate of periprosthetic fracture (0 vs. 9) and improved outcomes on several instruments, including the Harris Hip Scale (Bone Joint J. 2015;97-B:1475-80).
Cemented fixation generally requires a slightly longer operating time, but it is not otherwise more difficult or more expensive, according to Dr. Okike. He believes these results encourage cemented fixation in older patients without contraindications. This is already specifically recommended in AAOS guidelines for the management of hip fractures in elderly patients.
An orthopedic surgeon who has published frequently on total hip arthroplasty, Emil van Haaren, MD, of Zuyderland Medical Center, Heerlen, the Netherlands, confirmed that cemented hemiarthroplasty is considered “the golden standard of care” at his institution. In one study for which he served as the senior author, survival was characterized as excellent in older patients receiving cemented hip arthroplasty that were followed for more than 10 years (J Arthroplasty. 2016;31:194-8).
“We routinely use cemented prosthesis in hip fracture management when an arthroplasty is indicated,” he reported, echoing the contention by Dr. Okike that this approach is dominant in many centers outside of the United States.
Dr. Okike reports no potential conflicts of interest.
SOURCE: Okiki KM et al. JAMA. 2020;323:1077-84.
FROM AAOS 2020
Inactivated Bifidobacterium improves IBS symptoms
pointing the way to a therapeutic path that could avoid some risks of live probiotic use.
Of 443 patients taking part in a randomized, double-blind, placebo-controlled trial of a heat-inactivated nonviable Bifidobacterium probiotic, 221 received the probiotic while 222 received placebo capsules. The study’s primary endpoint was a composite of at least 30% improvement in abdominal pain and “adequate relief” of overall irritable bowel syndrome (IBS) symptoms in at least 4 of the 8 weeks of the study.
Within the B. bifidum group, 74 patients (34%) reached this endpoint, compared with 43 (19%) of those in the placebo group, for a risk ratio of 1.7 (P = .0007). Patients had no serious adverse events from the oral therapy, which they took in the form of two capsules daily for 8 weeks, and participants found both the inactivated Bifidobacterium treatment and placebo tolerable overall.
Bowel movements became more frequent in those who received B. bifidum capsules who had constipation-predominant IBS and less frequent in those with diarrhea-predominant IBS; the changes were statistically significant in both subgroups.
“Some probiotic strains can adhere well to epithelial cells and strengthen intestinal barrier function, providing an explanation for the efficacy of at least some probiotics in the treatment of IBS,” wrote Viola Andresen, MD, MSc, the study‘s lead author.
“Accordingly, enhancing the gut barrier is a useful treatment approach for patients with IBS,” added Dr. Andresen, of the department of internal medicine at the University of Hamburg (Germany) Teaching Hospital, and collaborators. The adherent properties of some strains of Bifidobacteria are mainly dependent on properties of the cell surface that are not changed by heat inactivation, which makes the bacteria nonviable – and removes the risk of infection.
Additional benefits of using nonviable bacteria for IBS therapy might include more stability and enhanced standardization, although previous studies have shown a reduction in efficacy when bacteria are made nonviable. Inactivated B. bifidum MIMBb75 was used in this study because it had previously been shown effective against IBS symptoms, noted Dr. Andresen and coauthors.
Adult patients were included if they met criteria for IBS according to Rome III and had abdominal pain rated at least 4 on an 11-point scale for at least 2 days of a 2-week run-in phase. Among the many criteria for exclusion from the study were history of inflammatory gastrointestinal disease, cancer, other serious stomach diseases, diabetes, many abdominal surgeries, and recent antipsychotic or steroid use.
During the study, participants recorded their abdominal pain over the last 24 hours daily; weekly averages were tallied for each patient. Patients were also asked to rate their relief of IBS symptoms, including abdominal pain, bowel habits, and other symptoms over the past week at weekly time points on a 7-point Likert scale, where scores of 3 or less indicated some measure of relief; IBS symptoms were considered to be adequately relieved with a score of 3 or less.
Secondary outcome measures for the study included changes in the Subjects’ Global Assessment of symptoms, and changes in individual symptoms. Number of bowel movements, stool form, sensation of incomplete evacuation, and medication use were also recorded daily.
Participants were aged a mean of 41 years, and about 70% were female. The mean body mass index was just under 25 kg/m2. About half of each study arm had diarrhea-predominant IBS. About a quarter had constipation-predominant IBS, and most of the rest were not subtyped.
Looking at the primary endpoint, the number needed to treat for benefit was 7.1 in favor of the inactivated bacterium, using an intention-to-treat analysis. Results were similar when a per-protocol analysis was applied. The investigators saw response to treatment climb through the duration of the study for both the probiotic and the placebo arms, with the gap in improvement between the groups widening over the 8-week study period.
“It might be assumed that the use of nonviable bacteria for the treatment of IBS could be a safe alternative, even in patients who are potentially susceptible to infection,” concluded Dr. Andresen and colleagues. A further advantage, noted the researchers, is greater product stability in fluctuating temperatures compared with viable bacteria, ensuring better standardization even in regions with warm or changing climates.
Perspective was offered in an accompanying commentary whose lead author was Nicholas Talley, MD, PhD, a gastroenterologist, adjunct professor, and pro vice-chancellor for global research at the University of Newcastle (Australia).
“By heat inactivating the bacteria the researchers did not administer a probiotic but a bacterial therapy,” wrote Dr. Talley and coauthors. In any event, they added, the exact mechanism by which probiotics benefit individuals with IBS is unknown.
“The concept that a probiotic might be efficacious in IBS even if nonviable organisms are administered is an important observation,” they wrote. Fewer benefits have been seen with oral probiotic therapy than with fecal microbial transfer, and oral therapy does not produce durable results unless administered on a chronic basis, Dr. Talley and coauthors added.
“The absence of fundamental knowledge in terms of how bacterial therapy alters mechanisms in IBS continues to hamper improvements in treatment, limiting any success to short-term symptom control rather than the true goal, reversal of disease,” they concluded.
The study was funded by Synformulas. Dr. Andresen reported financial relationships with several pharmaceutical companies. Dr. Talley reported financial relationships with several pharmaceutical and nutritional companies.
SOURCE: Andresen V et al. Lancet Gastroenterol Hepatol. 2020 Apr 8. doi: 10.1016/S2468-1253(20)30079-0
pointing the way to a therapeutic path that could avoid some risks of live probiotic use.
Of 443 patients taking part in a randomized, double-blind, placebo-controlled trial of a heat-inactivated nonviable Bifidobacterium probiotic, 221 received the probiotic while 222 received placebo capsules. The study’s primary endpoint was a composite of at least 30% improvement in abdominal pain and “adequate relief” of overall irritable bowel syndrome (IBS) symptoms in at least 4 of the 8 weeks of the study.
Within the B. bifidum group, 74 patients (34%) reached this endpoint, compared with 43 (19%) of those in the placebo group, for a risk ratio of 1.7 (P = .0007). Patients had no serious adverse events from the oral therapy, which they took in the form of two capsules daily for 8 weeks, and participants found both the inactivated Bifidobacterium treatment and placebo tolerable overall.
Bowel movements became more frequent in those who received B. bifidum capsules who had constipation-predominant IBS and less frequent in those with diarrhea-predominant IBS; the changes were statistically significant in both subgroups.
“Some probiotic strains can adhere well to epithelial cells and strengthen intestinal barrier function, providing an explanation for the efficacy of at least some probiotics in the treatment of IBS,” wrote Viola Andresen, MD, MSc, the study‘s lead author.
“Accordingly, enhancing the gut barrier is a useful treatment approach for patients with IBS,” added Dr. Andresen, of the department of internal medicine at the University of Hamburg (Germany) Teaching Hospital, and collaborators. The adherent properties of some strains of Bifidobacteria are mainly dependent on properties of the cell surface that are not changed by heat inactivation, which makes the bacteria nonviable – and removes the risk of infection.
Additional benefits of using nonviable bacteria for IBS therapy might include more stability and enhanced standardization, although previous studies have shown a reduction in efficacy when bacteria are made nonviable. Inactivated B. bifidum MIMBb75 was used in this study because it had previously been shown effective against IBS symptoms, noted Dr. Andresen and coauthors.
Adult patients were included if they met criteria for IBS according to Rome III and had abdominal pain rated at least 4 on an 11-point scale for at least 2 days of a 2-week run-in phase. Among the many criteria for exclusion from the study were history of inflammatory gastrointestinal disease, cancer, other serious stomach diseases, diabetes, many abdominal surgeries, and recent antipsychotic or steroid use.
During the study, participants recorded their abdominal pain over the last 24 hours daily; weekly averages were tallied for each patient. Patients were also asked to rate their relief of IBS symptoms, including abdominal pain, bowel habits, and other symptoms over the past week at weekly time points on a 7-point Likert scale, where scores of 3 or less indicated some measure of relief; IBS symptoms were considered to be adequately relieved with a score of 3 or less.
Secondary outcome measures for the study included changes in the Subjects’ Global Assessment of symptoms, and changes in individual symptoms. Number of bowel movements, stool form, sensation of incomplete evacuation, and medication use were also recorded daily.
Participants were aged a mean of 41 years, and about 70% were female. The mean body mass index was just under 25 kg/m2. About half of each study arm had diarrhea-predominant IBS. About a quarter had constipation-predominant IBS, and most of the rest were not subtyped.
Looking at the primary endpoint, the number needed to treat for benefit was 7.1 in favor of the inactivated bacterium, using an intention-to-treat analysis. Results were similar when a per-protocol analysis was applied. The investigators saw response to treatment climb through the duration of the study for both the probiotic and the placebo arms, with the gap in improvement between the groups widening over the 8-week study period.
“It might be assumed that the use of nonviable bacteria for the treatment of IBS could be a safe alternative, even in patients who are potentially susceptible to infection,” concluded Dr. Andresen and colleagues. A further advantage, noted the researchers, is greater product stability in fluctuating temperatures compared with viable bacteria, ensuring better standardization even in regions with warm or changing climates.
Perspective was offered in an accompanying commentary whose lead author was Nicholas Talley, MD, PhD, a gastroenterologist, adjunct professor, and pro vice-chancellor for global research at the University of Newcastle (Australia).
“By heat inactivating the bacteria the researchers did not administer a probiotic but a bacterial therapy,” wrote Dr. Talley and coauthors. In any event, they added, the exact mechanism by which probiotics benefit individuals with IBS is unknown.
“The concept that a probiotic might be efficacious in IBS even if nonviable organisms are administered is an important observation,” they wrote. Fewer benefits have been seen with oral probiotic therapy than with fecal microbial transfer, and oral therapy does not produce durable results unless administered on a chronic basis, Dr. Talley and coauthors added.
“The absence of fundamental knowledge in terms of how bacterial therapy alters mechanisms in IBS continues to hamper improvements in treatment, limiting any success to short-term symptom control rather than the true goal, reversal of disease,” they concluded.
The study was funded by Synformulas. Dr. Andresen reported financial relationships with several pharmaceutical companies. Dr. Talley reported financial relationships with several pharmaceutical and nutritional companies.
SOURCE: Andresen V et al. Lancet Gastroenterol Hepatol. 2020 Apr 8. doi: 10.1016/S2468-1253(20)30079-0
pointing the way to a therapeutic path that could avoid some risks of live probiotic use.
Of 443 patients taking part in a randomized, double-blind, placebo-controlled trial of a heat-inactivated nonviable Bifidobacterium probiotic, 221 received the probiotic while 222 received placebo capsules. The study’s primary endpoint was a composite of at least 30% improvement in abdominal pain and “adequate relief” of overall irritable bowel syndrome (IBS) symptoms in at least 4 of the 8 weeks of the study.
Within the B. bifidum group, 74 patients (34%) reached this endpoint, compared with 43 (19%) of those in the placebo group, for a risk ratio of 1.7 (P = .0007). Patients had no serious adverse events from the oral therapy, which they took in the form of two capsules daily for 8 weeks, and participants found both the inactivated Bifidobacterium treatment and placebo tolerable overall.
Bowel movements became more frequent in those who received B. bifidum capsules who had constipation-predominant IBS and less frequent in those with diarrhea-predominant IBS; the changes were statistically significant in both subgroups.
“Some probiotic strains can adhere well to epithelial cells and strengthen intestinal barrier function, providing an explanation for the efficacy of at least some probiotics in the treatment of IBS,” wrote Viola Andresen, MD, MSc, the study‘s lead author.
“Accordingly, enhancing the gut barrier is a useful treatment approach for patients with IBS,” added Dr. Andresen, of the department of internal medicine at the University of Hamburg (Germany) Teaching Hospital, and collaborators. The adherent properties of some strains of Bifidobacteria are mainly dependent on properties of the cell surface that are not changed by heat inactivation, which makes the bacteria nonviable – and removes the risk of infection.
Additional benefits of using nonviable bacteria for IBS therapy might include more stability and enhanced standardization, although previous studies have shown a reduction in efficacy when bacteria are made nonviable. Inactivated B. bifidum MIMBb75 was used in this study because it had previously been shown effective against IBS symptoms, noted Dr. Andresen and coauthors.
Adult patients were included if they met criteria for IBS according to Rome III and had abdominal pain rated at least 4 on an 11-point scale for at least 2 days of a 2-week run-in phase. Among the many criteria for exclusion from the study were history of inflammatory gastrointestinal disease, cancer, other serious stomach diseases, diabetes, many abdominal surgeries, and recent antipsychotic or steroid use.
During the study, participants recorded their abdominal pain over the last 24 hours daily; weekly averages were tallied for each patient. Patients were also asked to rate their relief of IBS symptoms, including abdominal pain, bowel habits, and other symptoms over the past week at weekly time points on a 7-point Likert scale, where scores of 3 or less indicated some measure of relief; IBS symptoms were considered to be adequately relieved with a score of 3 or less.
Secondary outcome measures for the study included changes in the Subjects’ Global Assessment of symptoms, and changes in individual symptoms. Number of bowel movements, stool form, sensation of incomplete evacuation, and medication use were also recorded daily.
Participants were aged a mean of 41 years, and about 70% were female. The mean body mass index was just under 25 kg/m2. About half of each study arm had diarrhea-predominant IBS. About a quarter had constipation-predominant IBS, and most of the rest were not subtyped.
Looking at the primary endpoint, the number needed to treat for benefit was 7.1 in favor of the inactivated bacterium, using an intention-to-treat analysis. Results were similar when a per-protocol analysis was applied. The investigators saw response to treatment climb through the duration of the study for both the probiotic and the placebo arms, with the gap in improvement between the groups widening over the 8-week study period.
“It might be assumed that the use of nonviable bacteria for the treatment of IBS could be a safe alternative, even in patients who are potentially susceptible to infection,” concluded Dr. Andresen and colleagues. A further advantage, noted the researchers, is greater product stability in fluctuating temperatures compared with viable bacteria, ensuring better standardization even in regions with warm or changing climates.
Perspective was offered in an accompanying commentary whose lead author was Nicholas Talley, MD, PhD, a gastroenterologist, adjunct professor, and pro vice-chancellor for global research at the University of Newcastle (Australia).
“By heat inactivating the bacteria the researchers did not administer a probiotic but a bacterial therapy,” wrote Dr. Talley and coauthors. In any event, they added, the exact mechanism by which probiotics benefit individuals with IBS is unknown.
“The concept that a probiotic might be efficacious in IBS even if nonviable organisms are administered is an important observation,” they wrote. Fewer benefits have been seen with oral probiotic therapy than with fecal microbial transfer, and oral therapy does not produce durable results unless administered on a chronic basis, Dr. Talley and coauthors added.
“The absence of fundamental knowledge in terms of how bacterial therapy alters mechanisms in IBS continues to hamper improvements in treatment, limiting any success to short-term symptom control rather than the true goal, reversal of disease,” they concluded.
The study was funded by Synformulas. Dr. Andresen reported financial relationships with several pharmaceutical companies. Dr. Talley reported financial relationships with several pharmaceutical and nutritional companies.
SOURCE: Andresen V et al. Lancet Gastroenterol Hepatol. 2020 Apr 8. doi: 10.1016/S2468-1253(20)30079-0
FROM THE LANCET GASTROENTEROLOGY AND HEPATOLOGY
Will coronavirus restrictions lead to more advanced cancers?
My pathology lab once faced a daily flood of colon polyps, pap smears, and prostate biopsies. Suddenly, our work has dried up. The coronavirus pandemic has cleared out operating rooms and clinics across the country. Endoscopy and radiology suites have gone dark.
Pathology is largely driven by mass screening programs, and the machinery of screening has grinded to a halt during the COVID-19 pandemic. The American Cancer Society currently recommends that “no one should go to a health care facility for routine cancer screening at this time.”
But malignancies are still growing and spreading even though a great deal of medical care is on hold. The most urgent cancer care is still taking place; the risks of delaying treatment for patients with advanced or symptomatic cancer are obvious—these tumors can cause severe pain and life-threatening complications.
But that leaves us with a more complex and uncomfortable question: Will the pause in screening ultimately leave patients with tiny, asymptomatic cancers or precursor lesions worse off? What will a delay mean for those with ductal carcinoma in situ or small breast cancers? What’s the long-term effect of all those dysplastic nevi and early melanoma left unexcised by dermatologists? Perhaps more troubling, what about the spreading kidney cancer that may have turned up as an incidental finding on a CT scan?
COVID-19: A natural experiment
For many years, we’ve been dealing with the other side of the screening question: overdiagnosing and treating cancers that would probably never harm the patient. Overdiagnosis has been on a decades-long rise due to organized screening like PSA testing and mammography, as well as through ad hoc detection from heavier use of medical imaging. All of these have been disrupted by the pandemic.
Because the correlation between medical interventions and cancer overdiagnosis is clear, we can safely assume that overdiagnosis will decline during the pandemic. But what will be the net effect? Early detection of cancer undoubtedly saves some lives, but how many and at what cost has been a seemingly intractable debate.
Until now.
The coronavirus outbreak will be a natural experiment like no other. Economists and epidemiologists love to study “natural experiments” – systemic shocks that shed light on a complex phenomenon.
The unexpected nationwide delay in screening will undoubtedly inform the debate on overdiagnosis. For one, we can learn whether less intensive screening leads to more advanced cancers. Because screening will probably return to normal at different times across the country, we can almost simulate a randomized trial. Will this transformative data be a silver lining to this awful time?
The pressure to ‘fight’
The pandemic has also raised a question about cancer screening that goes beyond data: Why has the loud epidemic of coronavirus so thoroughly trumped cancer’s silent one? To me, the necessary urgency of our coronavirus response stands in stark contrast to the overly aggressive public health messaging used for cancer screening.
The tools used to fight the coronavirus epidemic have been forceful. We’re all diligently washing our hands and staying inside. We’re making sacrifices in our jobs and personal lives to stop the virus’ spread.
Cancer screening has similarly been touted as dogma – an urgent public health intervention that only a fool would turn down. The American Cancer Society once ran an infamous advertisement suggesting that if you decline mammography, you “need more than your breasts examined.” Even today, well-intentioned organizations run cancer screening drives pushing people to pledge to “get screened now.” It is no surprise, then, that I have had patients and family members confide in me that they feel guilty about not pursuing all of their recommended screening tests. The thought of anyone feeling like they caused their own cancer appalls me.
This pressure extends into the clinic. In many practices, primary care doctors are evaluated based on how many patients “comply” with screening recommendations. There seems to be a relentless drive to reach 100% screening penetration. These oversimplified tactics run counter to the shared decision making and informed consent we profess to value in medicine.
The tricky thing about cancer screening is that because most people will never develop the cancer being screened for, we know that most people can also never be helped by it. This doesn’t make screening useless, just as washing your hands can help even if it doesn’t guarantee that you won’t catch coronavirus. We know that some individuals benefit, which we detect at the population level. Overdiagnosis arises in the same way, as a phenomenon detected within populations and not individuals. These aspects of screening are what has led to cancer being viewed as a “societal disease” requiring a uniform response – 100% screening compliance.
Metaphors of war
These assumptions fall apart now that we are facing a real societal disease, an infectious disease outbreak. Coronavirus has made us reflect on what actions individuals should take in order to protect others. But cancer is not a contagion. When we decide whether and how to screen, we make intimate decisions affecting primarily ourselves and our family – not society at large.
Countless articles have been written about the use of metaphor in cancer, perhaps most famously by essayist and breast cancer patient Susan Sontag. Sontag and others have been critical of the rampant use of war metaphors in the cancer community. Wars invoke sacrifice, duty, and suffering. The “battle” against coronavirus really puts the “war on cancer” in perspective. These pandemic weeks have terrified me. I have been willing to do anything to protect myself and others. They’ve also exhausted me. We can’t be at war forever.
When this current war ends, will the “war on cancer” resume unchanged? Screening will no doubt begin again, hopefully improved by data from the coronavirus natural experiment. But I wonder whether we will tolerate the same kinds of public health messages – and whether we should – having now experienced an infectious disease outbreak where our actions as individuals really do have an impact on the health of others.
After feeling helpless, besieged, and even guilt-ridden during the pandemic, I think many people would appreciate regaining a sense of control over other aspects of their health. Cancer screening can save lives, but it’s a choice we should make for ourselves based on an understanding of the trade-offs and our own preferences. When screening restarts, I hope its paternalistic dogma can be replaced by nuanced, empowering tactics more appropriate for peacetime.
Benjamin Mazer, MD, MBA, is an anatomic and clinical pathology resident at Yale with interests in diagnostic surgical pathology, laboratory management, and evidence-based medicine.
This article first appeared on Medscape.com.
My pathology lab once faced a daily flood of colon polyps, pap smears, and prostate biopsies. Suddenly, our work has dried up. The coronavirus pandemic has cleared out operating rooms and clinics across the country. Endoscopy and radiology suites have gone dark.
Pathology is largely driven by mass screening programs, and the machinery of screening has grinded to a halt during the COVID-19 pandemic. The American Cancer Society currently recommends that “no one should go to a health care facility for routine cancer screening at this time.”
But malignancies are still growing and spreading even though a great deal of medical care is on hold. The most urgent cancer care is still taking place; the risks of delaying treatment for patients with advanced or symptomatic cancer are obvious—these tumors can cause severe pain and life-threatening complications.
But that leaves us with a more complex and uncomfortable question: Will the pause in screening ultimately leave patients with tiny, asymptomatic cancers or precursor lesions worse off? What will a delay mean for those with ductal carcinoma in situ or small breast cancers? What’s the long-term effect of all those dysplastic nevi and early melanoma left unexcised by dermatologists? Perhaps more troubling, what about the spreading kidney cancer that may have turned up as an incidental finding on a CT scan?
COVID-19: A natural experiment
For many years, we’ve been dealing with the other side of the screening question: overdiagnosing and treating cancers that would probably never harm the patient. Overdiagnosis has been on a decades-long rise due to organized screening like PSA testing and mammography, as well as through ad hoc detection from heavier use of medical imaging. All of these have been disrupted by the pandemic.
Because the correlation between medical interventions and cancer overdiagnosis is clear, we can safely assume that overdiagnosis will decline during the pandemic. But what will be the net effect? Early detection of cancer undoubtedly saves some lives, but how many and at what cost has been a seemingly intractable debate.
Until now.
The coronavirus outbreak will be a natural experiment like no other. Economists and epidemiologists love to study “natural experiments” – systemic shocks that shed light on a complex phenomenon.
The unexpected nationwide delay in screening will undoubtedly inform the debate on overdiagnosis. For one, we can learn whether less intensive screening leads to more advanced cancers. Because screening will probably return to normal at different times across the country, we can almost simulate a randomized trial. Will this transformative data be a silver lining to this awful time?
The pressure to ‘fight’
The pandemic has also raised a question about cancer screening that goes beyond data: Why has the loud epidemic of coronavirus so thoroughly trumped cancer’s silent one? To me, the necessary urgency of our coronavirus response stands in stark contrast to the overly aggressive public health messaging used for cancer screening.
The tools used to fight the coronavirus epidemic have been forceful. We’re all diligently washing our hands and staying inside. We’re making sacrifices in our jobs and personal lives to stop the virus’ spread.
Cancer screening has similarly been touted as dogma – an urgent public health intervention that only a fool would turn down. The American Cancer Society once ran an infamous advertisement suggesting that if you decline mammography, you “need more than your breasts examined.” Even today, well-intentioned organizations run cancer screening drives pushing people to pledge to “get screened now.” It is no surprise, then, that I have had patients and family members confide in me that they feel guilty about not pursuing all of their recommended screening tests. The thought of anyone feeling like they caused their own cancer appalls me.
This pressure extends into the clinic. In many practices, primary care doctors are evaluated based on how many patients “comply” with screening recommendations. There seems to be a relentless drive to reach 100% screening penetration. These oversimplified tactics run counter to the shared decision making and informed consent we profess to value in medicine.
The tricky thing about cancer screening is that because most people will never develop the cancer being screened for, we know that most people can also never be helped by it. This doesn’t make screening useless, just as washing your hands can help even if it doesn’t guarantee that you won’t catch coronavirus. We know that some individuals benefit, which we detect at the population level. Overdiagnosis arises in the same way, as a phenomenon detected within populations and not individuals. These aspects of screening are what has led to cancer being viewed as a “societal disease” requiring a uniform response – 100% screening compliance.
Metaphors of war
These assumptions fall apart now that we are facing a real societal disease, an infectious disease outbreak. Coronavirus has made us reflect on what actions individuals should take in order to protect others. But cancer is not a contagion. When we decide whether and how to screen, we make intimate decisions affecting primarily ourselves and our family – not society at large.
Countless articles have been written about the use of metaphor in cancer, perhaps most famously by essayist and breast cancer patient Susan Sontag. Sontag and others have been critical of the rampant use of war metaphors in the cancer community. Wars invoke sacrifice, duty, and suffering. The “battle” against coronavirus really puts the “war on cancer” in perspective. These pandemic weeks have terrified me. I have been willing to do anything to protect myself and others. They’ve also exhausted me. We can’t be at war forever.
When this current war ends, will the “war on cancer” resume unchanged? Screening will no doubt begin again, hopefully improved by data from the coronavirus natural experiment. But I wonder whether we will tolerate the same kinds of public health messages – and whether we should – having now experienced an infectious disease outbreak where our actions as individuals really do have an impact on the health of others.
After feeling helpless, besieged, and even guilt-ridden during the pandemic, I think many people would appreciate regaining a sense of control over other aspects of their health. Cancer screening can save lives, but it’s a choice we should make for ourselves based on an understanding of the trade-offs and our own preferences. When screening restarts, I hope its paternalistic dogma can be replaced by nuanced, empowering tactics more appropriate for peacetime.
Benjamin Mazer, MD, MBA, is an anatomic and clinical pathology resident at Yale with interests in diagnostic surgical pathology, laboratory management, and evidence-based medicine.
This article first appeared on Medscape.com.
My pathology lab once faced a daily flood of colon polyps, pap smears, and prostate biopsies. Suddenly, our work has dried up. The coronavirus pandemic has cleared out operating rooms and clinics across the country. Endoscopy and radiology suites have gone dark.
Pathology is largely driven by mass screening programs, and the machinery of screening has grinded to a halt during the COVID-19 pandemic. The American Cancer Society currently recommends that “no one should go to a health care facility for routine cancer screening at this time.”
But malignancies are still growing and spreading even though a great deal of medical care is on hold. The most urgent cancer care is still taking place; the risks of delaying treatment for patients with advanced or symptomatic cancer are obvious—these tumors can cause severe pain and life-threatening complications.
But that leaves us with a more complex and uncomfortable question: Will the pause in screening ultimately leave patients with tiny, asymptomatic cancers or precursor lesions worse off? What will a delay mean for those with ductal carcinoma in situ or small breast cancers? What’s the long-term effect of all those dysplastic nevi and early melanoma left unexcised by dermatologists? Perhaps more troubling, what about the spreading kidney cancer that may have turned up as an incidental finding on a CT scan?
COVID-19: A natural experiment
For many years, we’ve been dealing with the other side of the screening question: overdiagnosing and treating cancers that would probably never harm the patient. Overdiagnosis has been on a decades-long rise due to organized screening like PSA testing and mammography, as well as through ad hoc detection from heavier use of medical imaging. All of these have been disrupted by the pandemic.
Because the correlation between medical interventions and cancer overdiagnosis is clear, we can safely assume that overdiagnosis will decline during the pandemic. But what will be the net effect? Early detection of cancer undoubtedly saves some lives, but how many and at what cost has been a seemingly intractable debate.
Until now.
The coronavirus outbreak will be a natural experiment like no other. Economists and epidemiologists love to study “natural experiments” – systemic shocks that shed light on a complex phenomenon.
The unexpected nationwide delay in screening will undoubtedly inform the debate on overdiagnosis. For one, we can learn whether less intensive screening leads to more advanced cancers. Because screening will probably return to normal at different times across the country, we can almost simulate a randomized trial. Will this transformative data be a silver lining to this awful time?
The pressure to ‘fight’
The pandemic has also raised a question about cancer screening that goes beyond data: Why has the loud epidemic of coronavirus so thoroughly trumped cancer’s silent one? To me, the necessary urgency of our coronavirus response stands in stark contrast to the overly aggressive public health messaging used for cancer screening.
The tools used to fight the coronavirus epidemic have been forceful. We’re all diligently washing our hands and staying inside. We’re making sacrifices in our jobs and personal lives to stop the virus’ spread.
Cancer screening has similarly been touted as dogma – an urgent public health intervention that only a fool would turn down. The American Cancer Society once ran an infamous advertisement suggesting that if you decline mammography, you “need more than your breasts examined.” Even today, well-intentioned organizations run cancer screening drives pushing people to pledge to “get screened now.” It is no surprise, then, that I have had patients and family members confide in me that they feel guilty about not pursuing all of their recommended screening tests. The thought of anyone feeling like they caused their own cancer appalls me.
This pressure extends into the clinic. In many practices, primary care doctors are evaluated based on how many patients “comply” with screening recommendations. There seems to be a relentless drive to reach 100% screening penetration. These oversimplified tactics run counter to the shared decision making and informed consent we profess to value in medicine.
The tricky thing about cancer screening is that because most people will never develop the cancer being screened for, we know that most people can also never be helped by it. This doesn’t make screening useless, just as washing your hands can help even if it doesn’t guarantee that you won’t catch coronavirus. We know that some individuals benefit, which we detect at the population level. Overdiagnosis arises in the same way, as a phenomenon detected within populations and not individuals. These aspects of screening are what has led to cancer being viewed as a “societal disease” requiring a uniform response – 100% screening compliance.
Metaphors of war
These assumptions fall apart now that we are facing a real societal disease, an infectious disease outbreak. Coronavirus has made us reflect on what actions individuals should take in order to protect others. But cancer is not a contagion. When we decide whether and how to screen, we make intimate decisions affecting primarily ourselves and our family – not society at large.
Countless articles have been written about the use of metaphor in cancer, perhaps most famously by essayist and breast cancer patient Susan Sontag. Sontag and others have been critical of the rampant use of war metaphors in the cancer community. Wars invoke sacrifice, duty, and suffering. The “battle” against coronavirus really puts the “war on cancer” in perspective. These pandemic weeks have terrified me. I have been willing to do anything to protect myself and others. They’ve also exhausted me. We can’t be at war forever.
When this current war ends, will the “war on cancer” resume unchanged? Screening will no doubt begin again, hopefully improved by data from the coronavirus natural experiment. But I wonder whether we will tolerate the same kinds of public health messages – and whether we should – having now experienced an infectious disease outbreak where our actions as individuals really do have an impact on the health of others.
After feeling helpless, besieged, and even guilt-ridden during the pandemic, I think many people would appreciate regaining a sense of control over other aspects of their health. Cancer screening can save lives, but it’s a choice we should make for ourselves based on an understanding of the trade-offs and our own preferences. When screening restarts, I hope its paternalistic dogma can be replaced by nuanced, empowering tactics more appropriate for peacetime.
Benjamin Mazer, MD, MBA, is an anatomic and clinical pathology resident at Yale with interests in diagnostic surgical pathology, laboratory management, and evidence-based medicine.
This article first appeared on Medscape.com.
European COVID-19 insights: Try helmet CPAP
Noninvasive ventilation with helmet continuous positive air pressure (CPAP) deserves to be embraced as an effective strategy in preventing self-induced lung injury, often a key factor in progression from the early milder expression of COVID-19 disease to classic severe acute respiratory distress syndrome, according to European physicians who have been through what they hope are the worst days of the pandemic in the Lombardy region of Northern Italy.

Helmet CPAP is a relatively inexpensive, convenient, well-tolerated intervention. It allows patients to remain conscious and responsive to commands such as “Time to roll over,” which in turn frees up nursing staff. The purpose of helmet CPAP is to curb the huge inspiratory drive that’s a defining feature of this disease and which, unchecked, can lead to self-induced lung injury (SILI), Luciano Gattinoni, MD, explained at a webinar hosted by the European Society of Anaesthesiology.
“Paranoid attention to inspiratory effort – checking it and correcting it – is something where we can make the difference between death and life. It’s extremely important,” said Dr. Gattinoni, guest professor of anesthesiology and intensive care at the University of Gottingen (Germany).
He and his fellow panelists were in accord regarding the merits of helmet CPAP as the premier method of noninvasive ventilatory assistance. They also addressed the importance of monitoring for hypercoagulation, as well as what they’ve come to see as the essential role of pronation in what they define as Type H disease, and the need to have detailed respiratory physiotherapy protocols in place.
“COVID-19 doesn’t like physiotherapy,” explained Paolo Pelosi, MD, professor of anesthesiology and intensive care medicine at the University of Genoa (Italy).
Dr. Gattinoni is credited for identification of two polar phenotypes of what he considers to be a single COVID-19 disease. Early on, many patients present with an atypical form of acute respiratory distress syndrome (ARDS), distinguished by an often-unexpected degree of hypoxia accompanied by high pulmonary compliance and surprisingly little shortness of breath. Dr. Gattinoni and colleagues call this Type L disease, which stands for low elastane, low ventilation to perfusion ratio, low lung weight on CT, and low lung recruitability, which means the patient has a high proportion of aerated lung tissue. Over time, because of either the natural history of the disease or SILI, this may shift to Type H disease, marked by high elastane, high right-to-left shunt, high lung weight, and high recruitability.
“If the pulmonary compliance is above 60 [mL/cm H2O], I’m pretty sure it’s Type L. If it’s 30 [mL/cm H2O] or less, I’m pretty sure it’s Type H. Don’t ask me about 45-55 [mL/cm H2O]; it’s a grey zone,” Dr. Gattinoni said.
Giuseppe Foti, MD, said helmet CPAP in patients with COVID-19 should be free flow, not attached to a ventilator, and the gas flow should be set high – at least 50 L/min – in order to prevent CO2 rebreathing. Although noninvasive ventilation is well accepted for patients with chronic obstructive pulmonary disease or acute cardiogenic pulmonary edema, it hasn’t been extensively studied in the setting of ARDS. A notable exception is a single-center randomized trial in which 83 patients with ARDS at the University of Chicago were assigned to noninvasive ventilation delivered by helmet or face mask (JAMA. 2016 Jun 14;315[22]:2435-41). The endotracheal intubation rate was just 18% in the helmet group, compared with 62% in the face mask group. The 90-day mortality rate was significantly lower in the helmet group as well, noted Dr. Foti, director of the department of anesthesia and intensive care at Monza University Hospital in Milan.
Christian Putensen, MD, said he views intubation for mechanical ventilation as wise in moderate or severe ARDS with an arterial oxygen partial pressure/fraction of inspired oxygen (PaO2/FiO2) ratio below 150. But in milder, Type L COVID-19 disease, he also likes helmet CPAP. It spares the patient from the traumatic compressive stress to the lung induced by mechanical ventilation, which may cause alveolar edema and SILI.
There is, however, a caveat: “Watch carefully and do not delay intubation if you see helmet CPAP is not working; that is, if the blood gas analysis doesn’t improve, the respiratory rate increases, tidal volume increases, and there is still increased respiratory drive,” advised Dr. Putensen, an anesthesiologist at the University of Bonn (Germany).
There is no agreed-upon practical quantitative measure of respiratory drive. A clinical evaluation of the patient’s depth of inspiration is the best guide, he added.
Dr. Gattinoni said that, when helmet CPAP can’t control respiratory drive in a patient with early-stage disease, he feels the only way to interrupt this destructive process is through early intubation and what he termed “gentle mechanical ventilation,” not with a positive end expiratory pressure of 20 cm H2O, but more like 4-5.
Watch for hypercoagulation
Thromboembolic complications are a common feature in COVID-19 disease.
“I’ve had occasion to see the autopsy results in more than 100 patients. It’s devastating to see the number of thromboses and microthromboses in the lungs, the liver, the kidney, and in the brain,” Dr. Gattinoni said.
“COVID-19 is a serial killer, no doubt,” Dr. Pelosi agreed. “He has no mercy for anyone. And he has two bullets: The first one is for the lung, the second is on the vascular side.”
Dr. Putensen is aggressive in utilizing prophylactic high-dose anticoagulation with heparin. He carefully monitors levels of fibrinogen, Factors V and VIII, and d-dimers. In the setting of COVID-19, he has found thromboelastography to be more reliable than partial thromboplastin time in guiding heparin titration.
Pronation
Panelists agreed that pronation is an especially valuable means of enhancing oxygenation in patients with Type H disease. Dr. Putensen tries for more than 16 hours per day. Dr. Foti is preparing a study of the impact of pronation in 50 awake, nonintubated patients, most of whom were on helmet CPAP. Seven of them couldn’t tolerate pronation for even an hour at a time; for the others, the median duration was 3.5 hours at a time.
“We saw a dramatic improvement, a nearly doubling in the PaO2/FiO2 ratio,” Dr. Foti said.
The helmet CPAP study was done outside of the ICU because, in March 2020, the Milan hospital was utterly overwhelmed by COVID-19. The university hospital ordinarily has 25 ICU beds. This was expanded to 100 ICU beds in an effort to meet the emergency, but that still wasn’t sufficient. Indeed, COVID-19 patients occupied 600 of the hospital’s 650 beds. Physicians were forced to do something formerly unthinkable: triage patients for intubation and mechanical ventilation based upon age, comorbidities, and survival prospects.
“We felt schizophrenic. I completely agree with Luciano’s idea to intubate early when we cannot control the respiratory drive that’s due to the disease. But we couldn’t do it because we had too many patients. So we had to triage,” Dr. Foti recalled, breaking off with a sob as other panelists wiped away their own tears during the webcast.
Respiratory physical therapy
Dr. Pelosi said he believes that optimal care of patients with COVID-19 disease requires a major commitment to physical therapy. He strongly recommends having thoughtfully designed separate written protocols in place for respiratory physiotherapy during mechanical ventilation, weaning, and postextubation. COVID-19 patients typically require 7-10 days of assisted ventilation before weaning, and weaning is a protracted process as well.
“I like to say COVID-19 always requires patience. You have to be very, very patient with this disease,” he emphasized. “These patients have a long and difficult weaning. If the patient isn’t improving during weaning, look at two issues: superinfection and thrombembolism, macro and micro.” The physical therapy measures routinely utilized at his hospital during mechanical ventilation include elevation of the bed head greater than 30 degrees, neuromuscular electrical stimulation, subglottic secretion suctioning, tracheal and oral aspiration, and cough assistance. Separate physical therapy menus are used during before and after extubation.
Dr. Gattinoni offered a final word: “We can do almost nothing with this disease. We try our best to keep the patient alive. What we can do is avoid excessive ventilation of the patient. Applying the typical treatment of ARDS in atypical [Type L] ARDS does not make sense and may be extremely harmful.”
Noninvasive ventilation with helmet continuous positive air pressure (CPAP) deserves to be embraced as an effective strategy in preventing self-induced lung injury, often a key factor in progression from the early milder expression of COVID-19 disease to classic severe acute respiratory distress syndrome, according to European physicians who have been through what they hope are the worst days of the pandemic in the Lombardy region of Northern Italy.
Helmet CPAP is a relatively inexpensive, convenient, well-tolerated intervention. It allows patients to remain conscious and responsive to commands such as “Time to roll over,” which in turn frees up nursing staff. The purpose of helmet CPAP is to curb the huge inspiratory drive that’s a defining feature of this disease and which, unchecked, can lead to self-induced lung injury (SILI), Luciano Gattinoni, MD, explained at a webinar hosted by the European Society of Anaesthesiology.
“Paranoid attention to inspiratory effort – checking it and correcting it – is something where we can make the difference between death and life. It’s extremely important,” said Dr. Gattinoni, guest professor of anesthesiology and intensive care at the University of Gottingen (Germany).
He and his fellow panelists were in accord regarding the merits of helmet CPAP as the premier method of noninvasive ventilatory assistance. They also addressed the importance of monitoring for hypercoagulation, as well as what they’ve come to see as the essential role of pronation in what they define as Type H disease, and the need to have detailed respiratory physiotherapy protocols in place.
“COVID-19 doesn’t like physiotherapy,” explained Paolo Pelosi, MD, professor of anesthesiology and intensive care medicine at the University of Genoa (Italy).
Dr. Gattinoni is credited for identification of two polar phenotypes of what he considers to be a single COVID-19 disease. Early on, many patients present with an atypical form of acute respiratory distress syndrome (ARDS), distinguished by an often-unexpected degree of hypoxia accompanied by high pulmonary compliance and surprisingly little shortness of breath. Dr. Gattinoni and colleagues call this Type L disease, which stands for low elastane, low ventilation to perfusion ratio, low lung weight on CT, and low lung recruitability, which means the patient has a high proportion of aerated lung tissue. Over time, because of either the natural history of the disease or SILI, this may shift to Type H disease, marked by high elastane, high right-to-left shunt, high lung weight, and high recruitability.
“If the pulmonary compliance is above 60 [mL/cm H2O], I’m pretty sure it’s Type L. If it’s 30 [mL/cm H2O] or less, I’m pretty sure it’s Type H. Don’t ask me about 45-55 [mL/cm H2O]; it’s a grey zone,” Dr. Gattinoni said.
Giuseppe Foti, MD, said helmet CPAP in patients with COVID-19 should be free flow, not attached to a ventilator, and the gas flow should be set high – at least 50 L/min – in order to prevent CO2 rebreathing. Although noninvasive ventilation is well accepted for patients with chronic obstructive pulmonary disease or acute cardiogenic pulmonary edema, it hasn’t been extensively studied in the setting of ARDS. A notable exception is a single-center randomized trial in which 83 patients with ARDS at the University of Chicago were assigned to noninvasive ventilation delivered by helmet or face mask (JAMA. 2016 Jun 14;315[22]:2435-41). The endotracheal intubation rate was just 18% in the helmet group, compared with 62% in the face mask group. The 90-day mortality rate was significantly lower in the helmet group as well, noted Dr. Foti, director of the department of anesthesia and intensive care at Monza University Hospital in Milan.
Christian Putensen, MD, said he views intubation for mechanical ventilation as wise in moderate or severe ARDS with an arterial oxygen partial pressure/fraction of inspired oxygen (PaO2/FiO2) ratio below 150. But in milder, Type L COVID-19 disease, he also likes helmet CPAP. It spares the patient from the traumatic compressive stress to the lung induced by mechanical ventilation, which may cause alveolar edema and SILI.
There is, however, a caveat: “Watch carefully and do not delay intubation if you see helmet CPAP is not working; that is, if the blood gas analysis doesn’t improve, the respiratory rate increases, tidal volume increases, and there is still increased respiratory drive,” advised Dr. Putensen, an anesthesiologist at the University of Bonn (Germany).
There is no agreed-upon practical quantitative measure of respiratory drive. A clinical evaluation of the patient’s depth of inspiration is the best guide, he added.
Dr. Gattinoni said that, when helmet CPAP can’t control respiratory drive in a patient with early-stage disease, he feels the only way to interrupt this destructive process is through early intubation and what he termed “gentle mechanical ventilation,” not with a positive end expiratory pressure of 20 cm H2O, but more like 4-5.
Watch for hypercoagulation
Thromboembolic complications are a common feature in COVID-19 disease.
“I’ve had occasion to see the autopsy results in more than 100 patients. It’s devastating to see the number of thromboses and microthromboses in the lungs, the liver, the kidney, and in the brain,” Dr. Gattinoni said.
“COVID-19 is a serial killer, no doubt,” Dr. Pelosi agreed. “He has no mercy for anyone. And he has two bullets: The first one is for the lung, the second is on the vascular side.”
Dr. Putensen is aggressive in utilizing prophylactic high-dose anticoagulation with heparin. He carefully monitors levels of fibrinogen, Factors V and VIII, and d-dimers. In the setting of COVID-19, he has found thromboelastography to be more reliable than partial thromboplastin time in guiding heparin titration.
Pronation
Panelists agreed that pronation is an especially valuable means of enhancing oxygenation in patients with Type H disease. Dr. Putensen tries for more than 16 hours per day. Dr. Foti is preparing a study of the impact of pronation in 50 awake, nonintubated patients, most of whom were on helmet CPAP. Seven of them couldn’t tolerate pronation for even an hour at a time; for the others, the median duration was 3.5 hours at a time.
“We saw a dramatic improvement, a nearly doubling in the PaO2/FiO2 ratio,” Dr. Foti said.
The helmet CPAP study was done outside of the ICU because, in March 2020, the Milan hospital was utterly overwhelmed by COVID-19. The university hospital ordinarily has 25 ICU beds. This was expanded to 100 ICU beds in an effort to meet the emergency, but that still wasn’t sufficient. Indeed, COVID-19 patients occupied 600 of the hospital’s 650 beds. Physicians were forced to do something formerly unthinkable: triage patients for intubation and mechanical ventilation based upon age, comorbidities, and survival prospects.
“We felt schizophrenic. I completely agree with Luciano’s idea to intubate early when we cannot control the respiratory drive that’s due to the disease. But we couldn’t do it because we had too many patients. So we had to triage,” Dr. Foti recalled, breaking off with a sob as other panelists wiped away their own tears during the webcast.
Respiratory physical therapy
Dr. Pelosi said he believes that optimal care of patients with COVID-19 disease requires a major commitment to physical therapy. He strongly recommends having thoughtfully designed separate written protocols in place for respiratory physiotherapy during mechanical ventilation, weaning, and postextubation. COVID-19 patients typically require 7-10 days of assisted ventilation before weaning, and weaning is a protracted process as well.
“I like to say COVID-19 always requires patience. You have to be very, very patient with this disease,” he emphasized. “These patients have a long and difficult weaning. If the patient isn’t improving during weaning, look at two issues: superinfection and thrombembolism, macro and micro.” The physical therapy measures routinely utilized at his hospital during mechanical ventilation include elevation of the bed head greater than 30 degrees, neuromuscular electrical stimulation, subglottic secretion suctioning, tracheal and oral aspiration, and cough assistance. Separate physical therapy menus are used during before and after extubation.
Dr. Gattinoni offered a final word: “We can do almost nothing with this disease. We try our best to keep the patient alive. What we can do is avoid excessive ventilation of the patient. Applying the typical treatment of ARDS in atypical [Type L] ARDS does not make sense and may be extremely harmful.”
Noninvasive ventilation with helmet continuous positive air pressure (CPAP) deserves to be embraced as an effective strategy in preventing self-induced lung injury, often a key factor in progression from the early milder expression of COVID-19 disease to classic severe acute respiratory distress syndrome, according to European physicians who have been through what they hope are the worst days of the pandemic in the Lombardy region of Northern Italy.
Helmet CPAP is a relatively inexpensive, convenient, well-tolerated intervention. It allows patients to remain conscious and responsive to commands such as “Time to roll over,” which in turn frees up nursing staff. The purpose of helmet CPAP is to curb the huge inspiratory drive that’s a defining feature of this disease and which, unchecked, can lead to self-induced lung injury (SILI), Luciano Gattinoni, MD, explained at a webinar hosted by the European Society of Anaesthesiology.
“Paranoid attention to inspiratory effort – checking it and correcting it – is something where we can make the difference between death and life. It’s extremely important,” said Dr. Gattinoni, guest professor of anesthesiology and intensive care at the University of Gottingen (Germany).
He and his fellow panelists were in accord regarding the merits of helmet CPAP as the premier method of noninvasive ventilatory assistance. They also addressed the importance of monitoring for hypercoagulation, as well as what they’ve come to see as the essential role of pronation in what they define as Type H disease, and the need to have detailed respiratory physiotherapy protocols in place.
“COVID-19 doesn’t like physiotherapy,” explained Paolo Pelosi, MD, professor of anesthesiology and intensive care medicine at the University of Genoa (Italy).
Dr. Gattinoni is credited for identification of two polar phenotypes of what he considers to be a single COVID-19 disease. Early on, many patients present with an atypical form of acute respiratory distress syndrome (ARDS), distinguished by an often-unexpected degree of hypoxia accompanied by high pulmonary compliance and surprisingly little shortness of breath. Dr. Gattinoni and colleagues call this Type L disease, which stands for low elastane, low ventilation to perfusion ratio, low lung weight on CT, and low lung recruitability, which means the patient has a high proportion of aerated lung tissue. Over time, because of either the natural history of the disease or SILI, this may shift to Type H disease, marked by high elastane, high right-to-left shunt, high lung weight, and high recruitability.
“If the pulmonary compliance is above 60 [mL/cm H2O], I’m pretty sure it’s Type L. If it’s 30 [mL/cm H2O] or less, I’m pretty sure it’s Type H. Don’t ask me about 45-55 [mL/cm H2O]; it’s a grey zone,” Dr. Gattinoni said.
Giuseppe Foti, MD, said helmet CPAP in patients with COVID-19 should be free flow, not attached to a ventilator, and the gas flow should be set high – at least 50 L/min – in order to prevent CO2 rebreathing. Although noninvasive ventilation is well accepted for patients with chronic obstructive pulmonary disease or acute cardiogenic pulmonary edema, it hasn’t been extensively studied in the setting of ARDS. A notable exception is a single-center randomized trial in which 83 patients with ARDS at the University of Chicago were assigned to noninvasive ventilation delivered by helmet or face mask (JAMA. 2016 Jun 14;315[22]:2435-41). The endotracheal intubation rate was just 18% in the helmet group, compared with 62% in the face mask group. The 90-day mortality rate was significantly lower in the helmet group as well, noted Dr. Foti, director of the department of anesthesia and intensive care at Monza University Hospital in Milan.
Christian Putensen, MD, said he views intubation for mechanical ventilation as wise in moderate or severe ARDS with an arterial oxygen partial pressure/fraction of inspired oxygen (PaO2/FiO2) ratio below 150. But in milder, Type L COVID-19 disease, he also likes helmet CPAP. It spares the patient from the traumatic compressive stress to the lung induced by mechanical ventilation, which may cause alveolar edema and SILI.
There is, however, a caveat: “Watch carefully and do not delay intubation if you see helmet CPAP is not working; that is, if the blood gas analysis doesn’t improve, the respiratory rate increases, tidal volume increases, and there is still increased respiratory drive,” advised Dr. Putensen, an anesthesiologist at the University of Bonn (Germany).
There is no agreed-upon practical quantitative measure of respiratory drive. A clinical evaluation of the patient’s depth of inspiration is the best guide, he added.
Dr. Gattinoni said that, when helmet CPAP can’t control respiratory drive in a patient with early-stage disease, he feels the only way to interrupt this destructive process is through early intubation and what he termed “gentle mechanical ventilation,” not with a positive end expiratory pressure of 20 cm H2O, but more like 4-5.
Watch for hypercoagulation
Thromboembolic complications are a common feature in COVID-19 disease.
“I’ve had occasion to see the autopsy results in more than 100 patients. It’s devastating to see the number of thromboses and microthromboses in the lungs, the liver, the kidney, and in the brain,” Dr. Gattinoni said.
“COVID-19 is a serial killer, no doubt,” Dr. Pelosi agreed. “He has no mercy for anyone. And he has two bullets: The first one is for the lung, the second is on the vascular side.”
Dr. Putensen is aggressive in utilizing prophylactic high-dose anticoagulation with heparin. He carefully monitors levels of fibrinogen, Factors V and VIII, and d-dimers. In the setting of COVID-19, he has found thromboelastography to be more reliable than partial thromboplastin time in guiding heparin titration.
Pronation
Panelists agreed that pronation is an especially valuable means of enhancing oxygenation in patients with Type H disease. Dr. Putensen tries for more than 16 hours per day. Dr. Foti is preparing a study of the impact of pronation in 50 awake, nonintubated patients, most of whom were on helmet CPAP. Seven of them couldn’t tolerate pronation for even an hour at a time; for the others, the median duration was 3.5 hours at a time.
“We saw a dramatic improvement, a nearly doubling in the PaO2/FiO2 ratio,” Dr. Foti said.
The helmet CPAP study was done outside of the ICU because, in March 2020, the Milan hospital was utterly overwhelmed by COVID-19. The university hospital ordinarily has 25 ICU beds. This was expanded to 100 ICU beds in an effort to meet the emergency, but that still wasn’t sufficient. Indeed, COVID-19 patients occupied 600 of the hospital’s 650 beds. Physicians were forced to do something formerly unthinkable: triage patients for intubation and mechanical ventilation based upon age, comorbidities, and survival prospects.
“We felt schizophrenic. I completely agree with Luciano’s idea to intubate early when we cannot control the respiratory drive that’s due to the disease. But we couldn’t do it because we had too many patients. So we had to triage,” Dr. Foti recalled, breaking off with a sob as other panelists wiped away their own tears during the webcast.
Respiratory physical therapy
Dr. Pelosi said he believes that optimal care of patients with COVID-19 disease requires a major commitment to physical therapy. He strongly recommends having thoughtfully designed separate written protocols in place for respiratory physiotherapy during mechanical ventilation, weaning, and postextubation. COVID-19 patients typically require 7-10 days of assisted ventilation before weaning, and weaning is a protracted process as well.
“I like to say COVID-19 always requires patience. You have to be very, very patient with this disease,” he emphasized. “These patients have a long and difficult weaning. If the patient isn’t improving during weaning, look at two issues: superinfection and thrombembolism, macro and micro.” The physical therapy measures routinely utilized at his hospital during mechanical ventilation include elevation of the bed head greater than 30 degrees, neuromuscular electrical stimulation, subglottic secretion suctioning, tracheal and oral aspiration, and cough assistance. Separate physical therapy menus are used during before and after extubation.
Dr. Gattinoni offered a final word: “We can do almost nothing with this disease. We try our best to keep the patient alive. What we can do is avoid excessive ventilation of the patient. Applying the typical treatment of ARDS in atypical [Type L] ARDS does not make sense and may be extremely harmful.”