User login
Noninvasive carotid imaging can replace invasive imaging
-
CLINICAL QUESTION: Can noninvasive imaging replace invasive testing in patients with suspected carotid artery disease?
-
BOTTOM LINE: Noninvasive testing, especially contrast‐enhanced magnetic resonance angiography (CEMRA), compares very favorably with invasive angiography. Since noninvasive testing appears to be less accurate in patients with less severe stenosis, a reasonable strategy might begin with CEMRA. If CEMRA demonstrates a greater than 70% stenosis, the diagnosis is settled. If the stenosis appears to be less than 70%, invasive angiography might be considered. Of course, this diagnostic approach needs formal evaluation. (LOE = 1a‐).
-
REFERENCE: Wardlaw JM, Chappell FM, Best JJ, Wartolowska K, Berry E; NHS Research and Development Health Technology Assessment Carotid Stenosis Imaging Group. Non‐invasive imaging compared with intra‐arterial angiography in the diagnosis of symptomatic carotid stenosis: a meta‐analysis. Lancet 2006;367:1503‐1512.
-
STUDY DESIGN: Systematic review
-
FUNDING: Government
-
SETTING: Various (meta‐analysis)
-
SYNOPSIS: Two members of this research team searched MEDLINE and EMBASE and hand‐searched several journals to identify 41 prospective studies of at least 20 patients with suspected carotid artery disease who underwent 1 or more noninvasive test and invasive angiography. Any disagreements were settled by discussion with a third reviewer. Similarly, 2 reviewers extracted the data and discrepancies were arbitrated by a third reviewer. The identified studies included a total of 2541 patients. Overall, CEMRA generally performed best, although computed tomographic angiography, magnetic resonance angiography, and Doppler ultrasound also performed well. The authors found some variability in test performance, mainly due to differences in accuracy on the basis of the degree of stenosis. Nonetheless, depending on the degree of stenosis, CEMRA provided the most diagnostic information (positive likelihood ratio ranged from 13 to 26 and negative likelihood ratio from 0.04 to 0.24). Generally speaking, the noninvasive tests were not as accurate in patients with moderate stenosis (50%‐69%). Since this group also has a narrow surgical risk‐benefit margin, diagnostic certainty is critical. Finally, CEMRA results may be biased because of small study sizes and, as a new technology, the potential for reporting overly positive studies. Stay tuned.
-
CLINICAL QUESTION: Can noninvasive imaging replace invasive testing in patients with suspected carotid artery disease?
-
BOTTOM LINE: Noninvasive testing, especially contrast‐enhanced magnetic resonance angiography (CEMRA), compares very favorably with invasive angiography. Since noninvasive testing appears to be less accurate in patients with less severe stenosis, a reasonable strategy might begin with CEMRA. If CEMRA demonstrates a greater than 70% stenosis, the diagnosis is settled. If the stenosis appears to be less than 70%, invasive angiography might be considered. Of course, this diagnostic approach needs formal evaluation. (LOE = 1a‐).
-
REFERENCE: Wardlaw JM, Chappell FM, Best JJ, Wartolowska K, Berry E; NHS Research and Development Health Technology Assessment Carotid Stenosis Imaging Group. Non‐invasive imaging compared with intra‐arterial angiography in the diagnosis of symptomatic carotid stenosis: a meta‐analysis. Lancet 2006;367:1503‐1512.
-
STUDY DESIGN: Systematic review
-
FUNDING: Government
-
SETTING: Various (meta‐analysis)
-
SYNOPSIS: Two members of this research team searched MEDLINE and EMBASE and hand‐searched several journals to identify 41 prospective studies of at least 20 patients with suspected carotid artery disease who underwent 1 or more noninvasive test and invasive angiography. Any disagreements were settled by discussion with a third reviewer. Similarly, 2 reviewers extracted the data and discrepancies were arbitrated by a third reviewer. The identified studies included a total of 2541 patients. Overall, CEMRA generally performed best, although computed tomographic angiography, magnetic resonance angiography, and Doppler ultrasound also performed well. The authors found some variability in test performance, mainly due to differences in accuracy on the basis of the degree of stenosis. Nonetheless, depending on the degree of stenosis, CEMRA provided the most diagnostic information (positive likelihood ratio ranged from 13 to 26 and negative likelihood ratio from 0.04 to 0.24). Generally speaking, the noninvasive tests were not as accurate in patients with moderate stenosis (50%‐69%). Since this group also has a narrow surgical risk‐benefit margin, diagnostic certainty is critical. Finally, CEMRA results may be biased because of small study sizes and, as a new technology, the potential for reporting overly positive studies. Stay tuned.
-
CLINICAL QUESTION: Can noninvasive imaging replace invasive testing in patients with suspected carotid artery disease?
-
BOTTOM LINE: Noninvasive testing, especially contrast‐enhanced magnetic resonance angiography (CEMRA), compares very favorably with invasive angiography. Since noninvasive testing appears to be less accurate in patients with less severe stenosis, a reasonable strategy might begin with CEMRA. If CEMRA demonstrates a greater than 70% stenosis, the diagnosis is settled. If the stenosis appears to be less than 70%, invasive angiography might be considered. Of course, this diagnostic approach needs formal evaluation. (LOE = 1a‐).
-
REFERENCE: Wardlaw JM, Chappell FM, Best JJ, Wartolowska K, Berry E; NHS Research and Development Health Technology Assessment Carotid Stenosis Imaging Group. Non‐invasive imaging compared with intra‐arterial angiography in the diagnosis of symptomatic carotid stenosis: a meta‐analysis. Lancet 2006;367:1503‐1512.
-
STUDY DESIGN: Systematic review
-
FUNDING: Government
-
SETTING: Various (meta‐analysis)
-
SYNOPSIS: Two members of this research team searched MEDLINE and EMBASE and hand‐searched several journals to identify 41 prospective studies of at least 20 patients with suspected carotid artery disease who underwent 1 or more noninvasive test and invasive angiography. Any disagreements were settled by discussion with a third reviewer. Similarly, 2 reviewers extracted the data and discrepancies were arbitrated by a third reviewer. The identified studies included a total of 2541 patients. Overall, CEMRA generally performed best, although computed tomographic angiography, magnetic resonance angiography, and Doppler ultrasound also performed well. The authors found some variability in test performance, mainly due to differences in accuracy on the basis of the degree of stenosis. Nonetheless, depending on the degree of stenosis, CEMRA provided the most diagnostic information (positive likelihood ratio ranged from 13 to 26 and negative likelihood ratio from 0.04 to 0.24). Generally speaking, the noninvasive tests were not as accurate in patients with moderate stenosis (50%‐69%). Since this group also has a narrow surgical risk‐benefit margin, diagnostic certainty is critical. Finally, CEMRA results may be biased because of small study sizes and, as a new technology, the potential for reporting overly positive studies. Stay tuned.
Introducing Hospital Images Dx—A call for submissions
Of the many skills a hospitalist nurtures and develops, seeing and processing visual images is paramount. From the moment we enter the hospital each day, we look at patient faces, trying to fathom their levels of pain, of illness, and of response to therapy. We look at their rashes, facial droops, surgical wounds, and neck vein elevation. When we are done visually scrutinizing our patients, we inspect their rhythm strips or electrocardiograms and then move on to their X‐rays and advanced imaging.
Although we are, in a sense, slaves to the images before us, we also enjoy medicine for the challenge that these images providethere is always something novel to see. For the experienced clinician, a deep sense of satisfaction perfuses our limbic system with the quick recognition of the delta wave of Wolf‐Parkinson‐White on an EKG or the first vesicle of a zoster outbreak in a patient with initially unexplained cutaneous pain. What we recognize easily tends to come from having seen something beforefor better or worse, we depend on pattern recognition.
Unfortunately, we are all busier than we like and receive more journals than we have time to read. To make JHM even more germane and stimulating, we are initiating Hospital Images Dx. The main goal of Hospital Images Dx will be to show interesting images that a hospitalist might encounter, both the common and the obscure. Images, whether subtle or awe‐inspiring, should generally be able to speak the proverbial thousand words. To supplement those thousand words spoken by the submitted image, accompanying text will be limited to 250 words. The text should give a brief clinical summary of the patient's problem, relevant adjunct data, and 1 or 2 succinct teaching points related to the image. Our goal, simply stated, is for the reader to walk away after reading Hospital Images Dx with an image and a couple of key teaching points stored away for a rainy day.
We anticipate a substantial number of exciting submissions to Hospital Images Dx. Health care providers clearly get excited about the things they see as well as about the recordsthe imagesthat document both mundane and unusual encounters with a patient or a patient's data. We hope to tap into this enthusiasm and to teach a few things along the way. The editors look forward to receiving your Hospital Images Dx submission soon!
Of the many skills a hospitalist nurtures and develops, seeing and processing visual images is paramount. From the moment we enter the hospital each day, we look at patient faces, trying to fathom their levels of pain, of illness, and of response to therapy. We look at their rashes, facial droops, surgical wounds, and neck vein elevation. When we are done visually scrutinizing our patients, we inspect their rhythm strips or electrocardiograms and then move on to their X‐rays and advanced imaging.
Although we are, in a sense, slaves to the images before us, we also enjoy medicine for the challenge that these images providethere is always something novel to see. For the experienced clinician, a deep sense of satisfaction perfuses our limbic system with the quick recognition of the delta wave of Wolf‐Parkinson‐White on an EKG or the first vesicle of a zoster outbreak in a patient with initially unexplained cutaneous pain. What we recognize easily tends to come from having seen something beforefor better or worse, we depend on pattern recognition.
Unfortunately, we are all busier than we like and receive more journals than we have time to read. To make JHM even more germane and stimulating, we are initiating Hospital Images Dx. The main goal of Hospital Images Dx will be to show interesting images that a hospitalist might encounter, both the common and the obscure. Images, whether subtle or awe‐inspiring, should generally be able to speak the proverbial thousand words. To supplement those thousand words spoken by the submitted image, accompanying text will be limited to 250 words. The text should give a brief clinical summary of the patient's problem, relevant adjunct data, and 1 or 2 succinct teaching points related to the image. Our goal, simply stated, is for the reader to walk away after reading Hospital Images Dx with an image and a couple of key teaching points stored away for a rainy day.
We anticipate a substantial number of exciting submissions to Hospital Images Dx. Health care providers clearly get excited about the things they see as well as about the recordsthe imagesthat document both mundane and unusual encounters with a patient or a patient's data. We hope to tap into this enthusiasm and to teach a few things along the way. The editors look forward to receiving your Hospital Images Dx submission soon!
Of the many skills a hospitalist nurtures and develops, seeing and processing visual images is paramount. From the moment we enter the hospital each day, we look at patient faces, trying to fathom their levels of pain, of illness, and of response to therapy. We look at their rashes, facial droops, surgical wounds, and neck vein elevation. When we are done visually scrutinizing our patients, we inspect their rhythm strips or electrocardiograms and then move on to their X‐rays and advanced imaging.
Although we are, in a sense, slaves to the images before us, we also enjoy medicine for the challenge that these images providethere is always something novel to see. For the experienced clinician, a deep sense of satisfaction perfuses our limbic system with the quick recognition of the delta wave of Wolf‐Parkinson‐White on an EKG or the first vesicle of a zoster outbreak in a patient with initially unexplained cutaneous pain. What we recognize easily tends to come from having seen something beforefor better or worse, we depend on pattern recognition.
Unfortunately, we are all busier than we like and receive more journals than we have time to read. To make JHM even more germane and stimulating, we are initiating Hospital Images Dx. The main goal of Hospital Images Dx will be to show interesting images that a hospitalist might encounter, both the common and the obscure. Images, whether subtle or awe‐inspiring, should generally be able to speak the proverbial thousand words. To supplement those thousand words spoken by the submitted image, accompanying text will be limited to 250 words. The text should give a brief clinical summary of the patient's problem, relevant adjunct data, and 1 or 2 succinct teaching points related to the image. Our goal, simply stated, is for the reader to walk away after reading Hospital Images Dx with an image and a couple of key teaching points stored away for a rainy day.
We anticipate a substantial number of exciting submissions to Hospital Images Dx. Health care providers clearly get excited about the things they see as well as about the recordsthe imagesthat document both mundane and unusual encounters with a patient or a patient's data. We hope to tap into this enthusiasm and to teach a few things along the way. The editors look forward to receiving your Hospital Images Dx submission soon!
Improving Cost Effectiveness of Blood Cultures
Because as many as 90% of all blood cultures grow no organisms1 developing rules that predict which patients are at the lowest risk of having bacteremia could improve the utilization of this test and markedly reduce its cost. Of the approximate 10% of cultures that do grow organisms, only about half represent true bacteremia (ie, true positives), whereas the other half are considered contaminants (ie, false positives)2; the latter are known to increase both the cost and duration of care.3 Accordingly, reducing the number of contaminants could also reduce the cost of care. We assessed which of these two strategies would be the most cost effective. Although only 6% of the blood cultures obtained at our hospital represented contaminants, their associated cost was more than twice that associated with the 87% of cultures that were true negatives.
METHODS
We conducted a retrospective review of microbiological results and hospital records of patients for whom blood cultures were obtained in January 2002 at Denver Health Medical Center, a 400‐bed university‐affiliated public safety net hospital. The study was given exempt status by the Colorado Multiple Institutional Review Board. Patients were identified using a preexisting laboratory database.
We adopted the definitions used by Bates et al.3 for the inclusion and exclusion criteria and the definition of a blood culture episode so that we could apply the financial data presented by these authors to our results. Briefly, a blood culture set was defined as a single venipuncture, regardless of the number of bottles sent for culturing, and a blood culture episode was defined as the 48‐hour period beginning when a blood culture was drawn. All sets within the same 48‐hour period were considered part of the same episode. Cultures that grew bacteria were classified as either true positive, representing bacteremia, or false positive, representing contaminants. Determination of whether a patient had a true‐positive culture versus a contaminant was made in a weekly conference attended by the chief of the Infectious Disease Division, an Infectious Disease fellow, and at least one microbiologist, during which the species of organism cultured and the associated clinical data for each patient were considered. Organisms considered to indicate false positives included diphtheroids, Bacillus sp, Propionibacterium sp, coagulase‐negative staphylococci, and micrococci. All other organisms were considered true positives in the setting of appropriate clinical criteria as specified by the CDC guidelines.4 Hospital charges and lengths of stay were obtained from our institutional database.
The cost associated with a true‐negative blood culture was determined by summing the charges for phlebotomy and microbiological testing obtained from the January 2005 Denver Health hospital charge master and applying the cost‐to‐charge ratio reported on the Medicare Cost Report for inpatient services (not including the costs of physician salaries and benefits).
The cost of a false positive was determined two ways: (a) adjusting the data reported by Bates et al.3 for changes in the Consumer Price Index5 and (b) comparing the actual hospital charges of the patients in our sample who had false‐positive cultures with those who did not (adjusting both by the hospital's inpatient cost‐to‐charge ratio, again not including the cost of physician salaries and benefits).
The length of stay and cost of care for patients with true‐ and false‐positive blood cultures were compared by chi‐square analysis. P < .05 was considered statistically significant. The data were not normally distributed and, as such, are presented as medians and interquartile ranges.
RESULTS
Table 1 summarizes the interpretation of the 939 blood cultures drawn in January 2002. Only 6 culture sets (0.6%) could not be classified. The positive predictive value of a positive blood culture was only 53%.
| Blood cultures | Bacteremia | ||
|---|---|---|---|
| Number positive (%) | Number negative (%) | Total | |
| Number positive (%) | 62 (7) | 56 (6) | 118 (13) |
| Number negative (%) | 0 (0) | 815 (87) | 815 (87) |
| Total | 62 (7) | 871 (93) | 933 (100) |
Laboratory charges for patients with true‐negative and false‐positive blood cultures in January 2002 are shown in Table 2. Annualized, the associated charges were $1,781,292, and the costs were $748,143.
| Charge ($) | Tests (N) | Total ($) | |
|---|---|---|---|
| True‐negative cultures | |||
| Phlebotomy | $13.25 | ||
| Microbiology | $147.50 | ||
| Subtotal | $160.75 | 815 | $131,011 |
| False‐positive cultures | |||
| Phlebotomy | $13.25 | ||
| Microbiology | $147.50 | ||
| Identification | $60.75 | ||
| Sensitivity | $89.75 | ||
| Subtotal | $311.25 | 56 | $17,430 |
| $148,441 |
Bates et al.3 found that false‐positive blood cultures increased the length of hospital stay by 4.5 days and increased total charges by $4385 over those for patients with no contaminants. This adjusted to $6878 in 2005 according to the Consumer Price Index.5 After grouping our blood cultures into episodes as defined by Bates et al. (Table 3), we had 41 episodes of contaminated blood cultures that would annualize to charges of $3,383,976 and costs of $1,421,270 after applying the cost‐to‐charge ratio.
| Blood cultures | Bacteremia | ||
|---|---|---|---|
| Number positive (%) | Number negative (%) | Total | |
| |||
| Number positive (%) | 39 (9) | 41 (10) | 80 (19) |
| Number negative (%) | 0 (0) | 335 (81) | 335 (81) |
| Total | 39 (9) | 376 (91) | 415 (100) |
The median length of hospital stay and total charges for the patients with true‐negative and false‐positive blood cultures at Denver Health in January 2002 are summarized in Table 4. Using this approach, patients with false‐positive blood cultures at our institution added 1450‐2200 extra hospital days and accrued additional charges of $4,305,000 and costs of $1,808,100.
| Length of stay (days) | Interquartile range (days) | Total Charges ($) | Interquartile Range ($) | |
|---|---|---|---|---|
| ||||
| True negative | 5 | 2‐12 | $15,158 | $7,007‐$40,270 |
| False positive | 8a | 4‐13.5 | $23,908a | $14,083‐$52,031 |
| Difference | 3 | $8,750 | ||
DISCUSSION
The important finding of this study is that, despite there being nearly 15 times as many true‐negative blood cultures as false‐positive ones, the savings generated by reducing contaminants would be approximately twice that saved by reducing the true negatives (eg, a 50% reduction in the rate of contamination would reduce the total number of false‐positive episodes by 246 annually, saving $710,635‐$904,050, whereas reducing the true negatives by 50% would only save approximately $375,000.
There is no independent gold standard for evaluating the operating characteristics of a blood culture.6 Data from a series of repeated blood cultures represent the closest surrogate. Weinstein et al.7 drew at least 3 sets of cultures from 282 bacteremic patients and noted that bacteremia was documented in 91.5% of the first cultures, in 99.3% in 1 of the first 2 cultures, and in 99.6% in 1 of the first 3 cultures. Because 2 blood culture sets are drawn routinely, the difference between those 2 (if negative) and a third (if it represents a true positive) is 0.3% and would represent a false‐negative culture rate. Given that the true‐negative rate of blood cultures is 87%‐90%,1 the potential 0.3% false‐negative rate would not affect our analysis, and as such, we chose to ignore it. Accordingly, all sets of blood cultures with no growth were classified as true negatives.
Although we cannot show a cause‐and‐effect relationship between false‐positive cultures and the charges associated resulting from them, a recent study suggested that much of the excess length of stay of such patients is attributable to the false‐positive culture itself.8
Because health care costs have exceeded increases in general goods and services, adjusting the results of Bates et al.3 using the Consumer Price Index likely underestimated the projected cost of the false‐positive cultures. This limitation likely accounts for the observation that the difference in actual charges for our patients between those who did and those who did not have false‐positive blood cultures was greater than the cost of these false‐positive cultures as estimated by extrapolating from the data of Bates et al.3 Given the magnitude of the financial difference we observed, however, we suggest that this difference is not of sufficient size to alter our conclusion.
Physicians working at Denver Health are directly employed by the hospital, and the cost of physician salaries and benefits is included in the cost‐to‐charge ratio reported in our Medicare Cost Report. For purposes of this study, however, we elected to utilize a cost‐to‐charge ratio that was exclusive of physician salaries and benefits (ie, 0.42 rather than 0.66) because most hospitals in the United States do not employ their physicians. Accordingly, the costs we present underestimate the true cost to our institution by approximately 32% but are more representative of the costs of services provided by most hospitals in the United States.
Recent studies have shown that the rate of false‐positive cultures is higher when blood is drawn from indwelling catheters than when it is obtained by peripheral venipuncture.9, 10 The rates we cite from the literature2 and from our own institution (Table 1) are aggregate data that include samples drawn from both sites. Separating these would not alter our conclusion that a 50% reduction in false positives would save approximately twice as much as a 50% reduction in false negatives. These studies do, however, identify an important method for reducing false positives: sampling by venipuncture whenever possible, and only drawing through a catheter under very limited circumstances.
There are additional factors that favor a strategy of reducing contaminants over one that attempts to reduce the number of true‐negative cultures. First, reducing the total number of true‐negative blood cultures by 50% would require a very ambitious prediction rule that did not reduce the number of true positives to any meaningful extent. Prediction rules to reduce blood culture testing have been developed for patients with community‐acquired pneumonia, but the rules only reduced the number of cultures by 37% and, more importantly, left 11% of true bacteremias undetected.8 Reducing contaminants would have no effect on the detection of true positives, whereas any prediction rule would inevitably increase the risk of missing true bacteremia in at least a fraction of patients. Second, methods aimed at reducing contaminants can be implemented immediately, whereas deriving a prediction rule would take years to develop and test before it could be utilized. Third, implementing prediction rules may be difficult because many physicians prefer to rely on their clinical impressions.11
Reducing contaminants would require improving the technique by which blood cultures are obtained, with the objective of shifting a portion of false positives to true negatives. This might be accomplished in many ways: increasing the time spent on antiseptic scrubbing, improving the ways in which antiseptic devices are used, waiting for the antiseptic to air‐dry completely, choosing the antiseptic that is most effective in trials, drawing blood by venipuncture instead of through an indwelling catheter, limiting the number of venipuncture attempts before requiring a second site to be prepared, requiring all cultures be drawn by trained phlebotomists, and reducing phlebotomist turnover, among others. Denver Health has a 4‐page set of directions for phlebotomists to follow when obtaining blood cultures. Accordingly, there are numerous places the process could break down. Although having 2 phlebotomists involved (ie, one to perform the procedure and the other to observe and guide the first, assuring that all the appropriate steps are followed) might be considered an extraordinary step, our findings suggest the potential saving to the institution could far outweigh the additional personnel expense resulting from such an approach. Other potential solutions we have considered but not tested include providing a monthly salary bonus to the phlebotomist with the lowest contamination rate or giving bonuses to every phlebotomist who achieves a zero contamination rate.
In summary, we have concluded that the resource utilization associated with obtaining blood cultures can best be improved by reducing the small percentage of cultures that represent contaminants rather than by developing rules to reduce the much larger number of true negatives. The magnitude of the potential savings resulting from reducing contaminants is sufficiently large to warrant expending additional resources to accomplish this task.
- .Clinically relevant, cost‐effective clinical microbiology. Strategies to decrease unnecessary testing.Am J Clin Path.1997;107:154–167.
- ,,, et al.The clinical significance of positive blood cultures in the 1990s: A prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults.Clin Infect Dis.1997;24:584–602.
- ,,.Contaminant blood cultures and resource utilization: the true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,.Surveillance of nosocomial infection. In:Mayhall CG, ed.Hospital Epidemiology and Infection Control.3rd ed.Philadelphia:Lippincott Williams 106:246–253.
- ,,,.The clinical significance of positive blood cultures: a comprehensive analysis of 500 episodes of bacteremia and fungemia in adults. I. Laboratory and epidemiologic observations.Rev Infect Dis.1983;5:35–70.
- ,,,.Predicting bacteremia in patients with community acquired pneumonia.Am J Respir Crit Care Med.2004;169:342–347.
- ,,,,,.Clinical utility of blood cultures drawn from central venous or arterial catheters in critically ill surgical patients.Crit Care Med.2002;30:7–13.
- ,,.Comparison of contamination rates of catheter‐drawn and peripheral blood cultures.J Hosp Infect.2005;60:118–121.
- ,,,,.Physician response to a prediction rule for the triage of emergency department patients with chest pain.J Gen Intern Med.1994;9:241–247.
Because as many as 90% of all blood cultures grow no organisms1 developing rules that predict which patients are at the lowest risk of having bacteremia could improve the utilization of this test and markedly reduce its cost. Of the approximate 10% of cultures that do grow organisms, only about half represent true bacteremia (ie, true positives), whereas the other half are considered contaminants (ie, false positives)2; the latter are known to increase both the cost and duration of care.3 Accordingly, reducing the number of contaminants could also reduce the cost of care. We assessed which of these two strategies would be the most cost effective. Although only 6% of the blood cultures obtained at our hospital represented contaminants, their associated cost was more than twice that associated with the 87% of cultures that were true negatives.
METHODS
We conducted a retrospective review of microbiological results and hospital records of patients for whom blood cultures were obtained in January 2002 at Denver Health Medical Center, a 400‐bed university‐affiliated public safety net hospital. The study was given exempt status by the Colorado Multiple Institutional Review Board. Patients were identified using a preexisting laboratory database.
We adopted the definitions used by Bates et al.3 for the inclusion and exclusion criteria and the definition of a blood culture episode so that we could apply the financial data presented by these authors to our results. Briefly, a blood culture set was defined as a single venipuncture, regardless of the number of bottles sent for culturing, and a blood culture episode was defined as the 48‐hour period beginning when a blood culture was drawn. All sets within the same 48‐hour period were considered part of the same episode. Cultures that grew bacteria were classified as either true positive, representing bacteremia, or false positive, representing contaminants. Determination of whether a patient had a true‐positive culture versus a contaminant was made in a weekly conference attended by the chief of the Infectious Disease Division, an Infectious Disease fellow, and at least one microbiologist, during which the species of organism cultured and the associated clinical data for each patient were considered. Organisms considered to indicate false positives included diphtheroids, Bacillus sp, Propionibacterium sp, coagulase‐negative staphylococci, and micrococci. All other organisms were considered true positives in the setting of appropriate clinical criteria as specified by the CDC guidelines.4 Hospital charges and lengths of stay were obtained from our institutional database.
The cost associated with a true‐negative blood culture was determined by summing the charges for phlebotomy and microbiological testing obtained from the January 2005 Denver Health hospital charge master and applying the cost‐to‐charge ratio reported on the Medicare Cost Report for inpatient services (not including the costs of physician salaries and benefits).
The cost of a false positive was determined two ways: (a) adjusting the data reported by Bates et al.3 for changes in the Consumer Price Index5 and (b) comparing the actual hospital charges of the patients in our sample who had false‐positive cultures with those who did not (adjusting both by the hospital's inpatient cost‐to‐charge ratio, again not including the cost of physician salaries and benefits).
The length of stay and cost of care for patients with true‐ and false‐positive blood cultures were compared by chi‐square analysis. P < .05 was considered statistically significant. The data were not normally distributed and, as such, are presented as medians and interquartile ranges.
RESULTS
Table 1 summarizes the interpretation of the 939 blood cultures drawn in January 2002. Only 6 culture sets (0.6%) could not be classified. The positive predictive value of a positive blood culture was only 53%.
| Blood cultures | Bacteremia | ||
|---|---|---|---|
| Number positive (%) | Number negative (%) | Total | |
| Number positive (%) | 62 (7) | 56 (6) | 118 (13) |
| Number negative (%) | 0 (0) | 815 (87) | 815 (87) |
| Total | 62 (7) | 871 (93) | 933 (100) |
Laboratory charges for patients with true‐negative and false‐positive blood cultures in January 2002 are shown in Table 2. Annualized, the associated charges were $1,781,292, and the costs were $748,143.
| Charge ($) | Tests (N) | Total ($) | |
|---|---|---|---|
| True‐negative cultures | |||
| Phlebotomy | $13.25 | ||
| Microbiology | $147.50 | ||
| Subtotal | $160.75 | 815 | $131,011 |
| False‐positive cultures | |||
| Phlebotomy | $13.25 | ||
| Microbiology | $147.50 | ||
| Identification | $60.75 | ||
| Sensitivity | $89.75 | ||
| Subtotal | $311.25 | 56 | $17,430 |
| $148,441 |
Bates et al.3 found that false‐positive blood cultures increased the length of hospital stay by 4.5 days and increased total charges by $4385 over those for patients with no contaminants. This adjusted to $6878 in 2005 according to the Consumer Price Index.5 After grouping our blood cultures into episodes as defined by Bates et al. (Table 3), we had 41 episodes of contaminated blood cultures that would annualize to charges of $3,383,976 and costs of $1,421,270 after applying the cost‐to‐charge ratio.
| Blood cultures | Bacteremia | ||
|---|---|---|---|
| Number positive (%) | Number negative (%) | Total | |
| |||
| Number positive (%) | 39 (9) | 41 (10) | 80 (19) |
| Number negative (%) | 0 (0) | 335 (81) | 335 (81) |
| Total | 39 (9) | 376 (91) | 415 (100) |
The median length of hospital stay and total charges for the patients with true‐negative and false‐positive blood cultures at Denver Health in January 2002 are summarized in Table 4. Using this approach, patients with false‐positive blood cultures at our institution added 1450‐2200 extra hospital days and accrued additional charges of $4,305,000 and costs of $1,808,100.
| Length of stay (days) | Interquartile range (days) | Total Charges ($) | Interquartile Range ($) | |
|---|---|---|---|---|
| ||||
| True negative | 5 | 2‐12 | $15,158 | $7,007‐$40,270 |
| False positive | 8a | 4‐13.5 | $23,908a | $14,083‐$52,031 |
| Difference | 3 | $8,750 | ||
DISCUSSION
The important finding of this study is that, despite there being nearly 15 times as many true‐negative blood cultures as false‐positive ones, the savings generated by reducing contaminants would be approximately twice that saved by reducing the true negatives (eg, a 50% reduction in the rate of contamination would reduce the total number of false‐positive episodes by 246 annually, saving $710,635‐$904,050, whereas reducing the true negatives by 50% would only save approximately $375,000.
There is no independent gold standard for evaluating the operating characteristics of a blood culture.6 Data from a series of repeated blood cultures represent the closest surrogate. Weinstein et al.7 drew at least 3 sets of cultures from 282 bacteremic patients and noted that bacteremia was documented in 91.5% of the first cultures, in 99.3% in 1 of the first 2 cultures, and in 99.6% in 1 of the first 3 cultures. Because 2 blood culture sets are drawn routinely, the difference between those 2 (if negative) and a third (if it represents a true positive) is 0.3% and would represent a false‐negative culture rate. Given that the true‐negative rate of blood cultures is 87%‐90%,1 the potential 0.3% false‐negative rate would not affect our analysis, and as such, we chose to ignore it. Accordingly, all sets of blood cultures with no growth were classified as true negatives.
Although we cannot show a cause‐and‐effect relationship between false‐positive cultures and the charges associated resulting from them, a recent study suggested that much of the excess length of stay of such patients is attributable to the false‐positive culture itself.8
Because health care costs have exceeded increases in general goods and services, adjusting the results of Bates et al.3 using the Consumer Price Index likely underestimated the projected cost of the false‐positive cultures. This limitation likely accounts for the observation that the difference in actual charges for our patients between those who did and those who did not have false‐positive blood cultures was greater than the cost of these false‐positive cultures as estimated by extrapolating from the data of Bates et al.3 Given the magnitude of the financial difference we observed, however, we suggest that this difference is not of sufficient size to alter our conclusion.
Physicians working at Denver Health are directly employed by the hospital, and the cost of physician salaries and benefits is included in the cost‐to‐charge ratio reported in our Medicare Cost Report. For purposes of this study, however, we elected to utilize a cost‐to‐charge ratio that was exclusive of physician salaries and benefits (ie, 0.42 rather than 0.66) because most hospitals in the United States do not employ their physicians. Accordingly, the costs we present underestimate the true cost to our institution by approximately 32% but are more representative of the costs of services provided by most hospitals in the United States.
Recent studies have shown that the rate of false‐positive cultures is higher when blood is drawn from indwelling catheters than when it is obtained by peripheral venipuncture.9, 10 The rates we cite from the literature2 and from our own institution (Table 1) are aggregate data that include samples drawn from both sites. Separating these would not alter our conclusion that a 50% reduction in false positives would save approximately twice as much as a 50% reduction in false negatives. These studies do, however, identify an important method for reducing false positives: sampling by venipuncture whenever possible, and only drawing through a catheter under very limited circumstances.
There are additional factors that favor a strategy of reducing contaminants over one that attempts to reduce the number of true‐negative cultures. First, reducing the total number of true‐negative blood cultures by 50% would require a very ambitious prediction rule that did not reduce the number of true positives to any meaningful extent. Prediction rules to reduce blood culture testing have been developed for patients with community‐acquired pneumonia, but the rules only reduced the number of cultures by 37% and, more importantly, left 11% of true bacteremias undetected.8 Reducing contaminants would have no effect on the detection of true positives, whereas any prediction rule would inevitably increase the risk of missing true bacteremia in at least a fraction of patients. Second, methods aimed at reducing contaminants can be implemented immediately, whereas deriving a prediction rule would take years to develop and test before it could be utilized. Third, implementing prediction rules may be difficult because many physicians prefer to rely on their clinical impressions.11
Reducing contaminants would require improving the technique by which blood cultures are obtained, with the objective of shifting a portion of false positives to true negatives. This might be accomplished in many ways: increasing the time spent on antiseptic scrubbing, improving the ways in which antiseptic devices are used, waiting for the antiseptic to air‐dry completely, choosing the antiseptic that is most effective in trials, drawing blood by venipuncture instead of through an indwelling catheter, limiting the number of venipuncture attempts before requiring a second site to be prepared, requiring all cultures be drawn by trained phlebotomists, and reducing phlebotomist turnover, among others. Denver Health has a 4‐page set of directions for phlebotomists to follow when obtaining blood cultures. Accordingly, there are numerous places the process could break down. Although having 2 phlebotomists involved (ie, one to perform the procedure and the other to observe and guide the first, assuring that all the appropriate steps are followed) might be considered an extraordinary step, our findings suggest the potential saving to the institution could far outweigh the additional personnel expense resulting from such an approach. Other potential solutions we have considered but not tested include providing a monthly salary bonus to the phlebotomist with the lowest contamination rate or giving bonuses to every phlebotomist who achieves a zero contamination rate.
In summary, we have concluded that the resource utilization associated with obtaining blood cultures can best be improved by reducing the small percentage of cultures that represent contaminants rather than by developing rules to reduce the much larger number of true negatives. The magnitude of the potential savings resulting from reducing contaminants is sufficiently large to warrant expending additional resources to accomplish this task.
Because as many as 90% of all blood cultures grow no organisms1 developing rules that predict which patients are at the lowest risk of having bacteremia could improve the utilization of this test and markedly reduce its cost. Of the approximate 10% of cultures that do grow organisms, only about half represent true bacteremia (ie, true positives), whereas the other half are considered contaminants (ie, false positives)2; the latter are known to increase both the cost and duration of care.3 Accordingly, reducing the number of contaminants could also reduce the cost of care. We assessed which of these two strategies would be the most cost effective. Although only 6% of the blood cultures obtained at our hospital represented contaminants, their associated cost was more than twice that associated with the 87% of cultures that were true negatives.
METHODS
We conducted a retrospective review of microbiological results and hospital records of patients for whom blood cultures were obtained in January 2002 at Denver Health Medical Center, a 400‐bed university‐affiliated public safety net hospital. The study was given exempt status by the Colorado Multiple Institutional Review Board. Patients were identified using a preexisting laboratory database.
We adopted the definitions used by Bates et al.3 for the inclusion and exclusion criteria and the definition of a blood culture episode so that we could apply the financial data presented by these authors to our results. Briefly, a blood culture set was defined as a single venipuncture, regardless of the number of bottles sent for culturing, and a blood culture episode was defined as the 48‐hour period beginning when a blood culture was drawn. All sets within the same 48‐hour period were considered part of the same episode. Cultures that grew bacteria were classified as either true positive, representing bacteremia, or false positive, representing contaminants. Determination of whether a patient had a true‐positive culture versus a contaminant was made in a weekly conference attended by the chief of the Infectious Disease Division, an Infectious Disease fellow, and at least one microbiologist, during which the species of organism cultured and the associated clinical data for each patient were considered. Organisms considered to indicate false positives included diphtheroids, Bacillus sp, Propionibacterium sp, coagulase‐negative staphylococci, and micrococci. All other organisms were considered true positives in the setting of appropriate clinical criteria as specified by the CDC guidelines.4 Hospital charges and lengths of stay were obtained from our institutional database.
The cost associated with a true‐negative blood culture was determined by summing the charges for phlebotomy and microbiological testing obtained from the January 2005 Denver Health hospital charge master and applying the cost‐to‐charge ratio reported on the Medicare Cost Report for inpatient services (not including the costs of physician salaries and benefits).
The cost of a false positive was determined two ways: (a) adjusting the data reported by Bates et al.3 for changes in the Consumer Price Index5 and (b) comparing the actual hospital charges of the patients in our sample who had false‐positive cultures with those who did not (adjusting both by the hospital's inpatient cost‐to‐charge ratio, again not including the cost of physician salaries and benefits).
The length of stay and cost of care for patients with true‐ and false‐positive blood cultures were compared by chi‐square analysis. P < .05 was considered statistically significant. The data were not normally distributed and, as such, are presented as medians and interquartile ranges.
RESULTS
Table 1 summarizes the interpretation of the 939 blood cultures drawn in January 2002. Only 6 culture sets (0.6%) could not be classified. The positive predictive value of a positive blood culture was only 53%.
| Blood cultures | Bacteremia | ||
|---|---|---|---|
| Number positive (%) | Number negative (%) | Total | |
| Number positive (%) | 62 (7) | 56 (6) | 118 (13) |
| Number negative (%) | 0 (0) | 815 (87) | 815 (87) |
| Total | 62 (7) | 871 (93) | 933 (100) |
Laboratory charges for patients with true‐negative and false‐positive blood cultures in January 2002 are shown in Table 2. Annualized, the associated charges were $1,781,292, and the costs were $748,143.
| Charge ($) | Tests (N) | Total ($) | |
|---|---|---|---|
| True‐negative cultures | |||
| Phlebotomy | $13.25 | ||
| Microbiology | $147.50 | ||
| Subtotal | $160.75 | 815 | $131,011 |
| False‐positive cultures | |||
| Phlebotomy | $13.25 | ||
| Microbiology | $147.50 | ||
| Identification | $60.75 | ||
| Sensitivity | $89.75 | ||
| Subtotal | $311.25 | 56 | $17,430 |
| $148,441 |
Bates et al.3 found that false‐positive blood cultures increased the length of hospital stay by 4.5 days and increased total charges by $4385 over those for patients with no contaminants. This adjusted to $6878 in 2005 according to the Consumer Price Index.5 After grouping our blood cultures into episodes as defined by Bates et al. (Table 3), we had 41 episodes of contaminated blood cultures that would annualize to charges of $3,383,976 and costs of $1,421,270 after applying the cost‐to‐charge ratio.
| Blood cultures | Bacteremia | ||
|---|---|---|---|
| Number positive (%) | Number negative (%) | Total | |
| |||
| Number positive (%) | 39 (9) | 41 (10) | 80 (19) |
| Number negative (%) | 0 (0) | 335 (81) | 335 (81) |
| Total | 39 (9) | 376 (91) | 415 (100) |
The median length of hospital stay and total charges for the patients with true‐negative and false‐positive blood cultures at Denver Health in January 2002 are summarized in Table 4. Using this approach, patients with false‐positive blood cultures at our institution added 1450‐2200 extra hospital days and accrued additional charges of $4,305,000 and costs of $1,808,100.
| Length of stay (days) | Interquartile range (days) | Total Charges ($) | Interquartile Range ($) | |
|---|---|---|---|---|
| ||||
| True negative | 5 | 2‐12 | $15,158 | $7,007‐$40,270 |
| False positive | 8a | 4‐13.5 | $23,908a | $14,083‐$52,031 |
| Difference | 3 | $8,750 | ||
DISCUSSION
The important finding of this study is that, despite there being nearly 15 times as many true‐negative blood cultures as false‐positive ones, the savings generated by reducing contaminants would be approximately twice that saved by reducing the true negatives (eg, a 50% reduction in the rate of contamination would reduce the total number of false‐positive episodes by 246 annually, saving $710,635‐$904,050, whereas reducing the true negatives by 50% would only save approximately $375,000.
There is no independent gold standard for evaluating the operating characteristics of a blood culture.6 Data from a series of repeated blood cultures represent the closest surrogate. Weinstein et al.7 drew at least 3 sets of cultures from 282 bacteremic patients and noted that bacteremia was documented in 91.5% of the first cultures, in 99.3% in 1 of the first 2 cultures, and in 99.6% in 1 of the first 3 cultures. Because 2 blood culture sets are drawn routinely, the difference between those 2 (if negative) and a third (if it represents a true positive) is 0.3% and would represent a false‐negative culture rate. Given that the true‐negative rate of blood cultures is 87%‐90%,1 the potential 0.3% false‐negative rate would not affect our analysis, and as such, we chose to ignore it. Accordingly, all sets of blood cultures with no growth were classified as true negatives.
Although we cannot show a cause‐and‐effect relationship between false‐positive cultures and the charges associated resulting from them, a recent study suggested that much of the excess length of stay of such patients is attributable to the false‐positive culture itself.8
Because health care costs have exceeded increases in general goods and services, adjusting the results of Bates et al.3 using the Consumer Price Index likely underestimated the projected cost of the false‐positive cultures. This limitation likely accounts for the observation that the difference in actual charges for our patients between those who did and those who did not have false‐positive blood cultures was greater than the cost of these false‐positive cultures as estimated by extrapolating from the data of Bates et al.3 Given the magnitude of the financial difference we observed, however, we suggest that this difference is not of sufficient size to alter our conclusion.
Physicians working at Denver Health are directly employed by the hospital, and the cost of physician salaries and benefits is included in the cost‐to‐charge ratio reported in our Medicare Cost Report. For purposes of this study, however, we elected to utilize a cost‐to‐charge ratio that was exclusive of physician salaries and benefits (ie, 0.42 rather than 0.66) because most hospitals in the United States do not employ their physicians. Accordingly, the costs we present underestimate the true cost to our institution by approximately 32% but are more representative of the costs of services provided by most hospitals in the United States.
Recent studies have shown that the rate of false‐positive cultures is higher when blood is drawn from indwelling catheters than when it is obtained by peripheral venipuncture.9, 10 The rates we cite from the literature2 and from our own institution (Table 1) are aggregate data that include samples drawn from both sites. Separating these would not alter our conclusion that a 50% reduction in false positives would save approximately twice as much as a 50% reduction in false negatives. These studies do, however, identify an important method for reducing false positives: sampling by venipuncture whenever possible, and only drawing through a catheter under very limited circumstances.
There are additional factors that favor a strategy of reducing contaminants over one that attempts to reduce the number of true‐negative cultures. First, reducing the total number of true‐negative blood cultures by 50% would require a very ambitious prediction rule that did not reduce the number of true positives to any meaningful extent. Prediction rules to reduce blood culture testing have been developed for patients with community‐acquired pneumonia, but the rules only reduced the number of cultures by 37% and, more importantly, left 11% of true bacteremias undetected.8 Reducing contaminants would have no effect on the detection of true positives, whereas any prediction rule would inevitably increase the risk of missing true bacteremia in at least a fraction of patients. Second, methods aimed at reducing contaminants can be implemented immediately, whereas deriving a prediction rule would take years to develop and test before it could be utilized. Third, implementing prediction rules may be difficult because many physicians prefer to rely on their clinical impressions.11
Reducing contaminants would require improving the technique by which blood cultures are obtained, with the objective of shifting a portion of false positives to true negatives. This might be accomplished in many ways: increasing the time spent on antiseptic scrubbing, improving the ways in which antiseptic devices are used, waiting for the antiseptic to air‐dry completely, choosing the antiseptic that is most effective in trials, drawing blood by venipuncture instead of through an indwelling catheter, limiting the number of venipuncture attempts before requiring a second site to be prepared, requiring all cultures be drawn by trained phlebotomists, and reducing phlebotomist turnover, among others. Denver Health has a 4‐page set of directions for phlebotomists to follow when obtaining blood cultures. Accordingly, there are numerous places the process could break down. Although having 2 phlebotomists involved (ie, one to perform the procedure and the other to observe and guide the first, assuring that all the appropriate steps are followed) might be considered an extraordinary step, our findings suggest the potential saving to the institution could far outweigh the additional personnel expense resulting from such an approach. Other potential solutions we have considered but not tested include providing a monthly salary bonus to the phlebotomist with the lowest contamination rate or giving bonuses to every phlebotomist who achieves a zero contamination rate.
In summary, we have concluded that the resource utilization associated with obtaining blood cultures can best be improved by reducing the small percentage of cultures that represent contaminants rather than by developing rules to reduce the much larger number of true negatives. The magnitude of the potential savings resulting from reducing contaminants is sufficiently large to warrant expending additional resources to accomplish this task.
- .Clinically relevant, cost‐effective clinical microbiology. Strategies to decrease unnecessary testing.Am J Clin Path.1997;107:154–167.
- ,,, et al.The clinical significance of positive blood cultures in the 1990s: A prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults.Clin Infect Dis.1997;24:584–602.
- ,,.Contaminant blood cultures and resource utilization: the true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,.Surveillance of nosocomial infection. In:Mayhall CG, ed.Hospital Epidemiology and Infection Control.3rd ed.Philadelphia:Lippincott Williams 106:246–253.
- ,,,.The clinical significance of positive blood cultures: a comprehensive analysis of 500 episodes of bacteremia and fungemia in adults. I. Laboratory and epidemiologic observations.Rev Infect Dis.1983;5:35–70.
- ,,,.Predicting bacteremia in patients with community acquired pneumonia.Am J Respir Crit Care Med.2004;169:342–347.
- ,,,,,.Clinical utility of blood cultures drawn from central venous or arterial catheters in critically ill surgical patients.Crit Care Med.2002;30:7–13.
- ,,.Comparison of contamination rates of catheter‐drawn and peripheral blood cultures.J Hosp Infect.2005;60:118–121.
- ,,,,.Physician response to a prediction rule for the triage of emergency department patients with chest pain.J Gen Intern Med.1994;9:241–247.
- .Clinically relevant, cost‐effective clinical microbiology. Strategies to decrease unnecessary testing.Am J Clin Path.1997;107:154–167.
- ,,, et al.The clinical significance of positive blood cultures in the 1990s: A prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults.Clin Infect Dis.1997;24:584–602.
- ,,.Contaminant blood cultures and resource utilization: the true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,.Surveillance of nosocomial infection. In:Mayhall CG, ed.Hospital Epidemiology and Infection Control.3rd ed.Philadelphia:Lippincott Williams 106:246–253.
- ,,,.The clinical significance of positive blood cultures: a comprehensive analysis of 500 episodes of bacteremia and fungemia in adults. I. Laboratory and epidemiologic observations.Rev Infect Dis.1983;5:35–70.
- ,,,.Predicting bacteremia in patients with community acquired pneumonia.Am J Respir Crit Care Med.2004;169:342–347.
- ,,,,,.Clinical utility of blood cultures drawn from central venous or arterial catheters in critically ill surgical patients.Crit Care Med.2002;30:7–13.
- ,,.Comparison of contamination rates of catheter‐drawn and peripheral blood cultures.J Hosp Infect.2005;60:118–121.
- ,,,,.Physician response to a prediction rule for the triage of emergency department patients with chest pain.J Gen Intern Med.1994;9:241–247.
Copyright © 2006 Society of Hospital Medicine
Editorial
In addition to marking my initial transition from student to physician, the commencement address by the medical informatics pioneer, Larry Weed, is my most enduring memory of medical school graduation. A provocative thinker in the field of decision support and structured medical records, Weed was credited by my teachers with developing the organized SOAP note. During his address he depressingly equated all the knowledge we had digested during the preceding mentally strenuous 4 years to shoveling a mountain of manure with a teaspoon. Although I agreed that some of the information I learned seemed to lack relevance (still don't know why I needed to learn the details of the Krebs cycle), as I began caring for patients as an intern, I found that much of it mattered. As I launched into residency training, I also discovered that lifelong learning would be a perpetual component of my medical career.
Despite becoming a passionate advocate of practicing evidence‐based medicine (EBM), I also recognized the impossibility of keeping up with the medical literature, given the relentless arrival of journals in the mail. Learning all the evidence is impossible, so we must develop information management skills and allow others to help us in identifying, reviewing, and summarizing salient and valid clinical information.1 One of my vital goals as editor of the Journal of Hospital Medicine is to ensure we provide our readers with useful clinical information that is concise, easily digested, and usable.
To that end we are introducing Patient‐Oriented Evidence that Matters, or POEMs. As described on the InfoPOEMs website (
-
They address a question that we face as clinicians.
-
They measure outcomes that we and our patients care about: symptoms, morbidity, quality of life, and mortality.
-
They have the potential to change the way we practice.
We are not the first journal to do this and join the company of the British Medical Journal and the Cleveland Clinic Journal of Medicine.2, 3 Staff physicians at InfoPOEMs screen more than 100 peer‐reviewed medical journals for relevant articles that practicing physicians can use at the point of care, the patient. A trained physician poet then summarizes selected articles in a standardized manner into a POEM. A POEM begins with a clinical question and then provides a bottom line answer from a recently published journal article. This is followed by a structured abstract that includes the study design and setting, followed by a synopsis of the article.
We will start with at least 2 POEMs per issue focused on clinical topics relevant to hospitalists. Soon, an experienced academic hospitalist and knowledgeable expert in EBM, Dr. Jennifer Kleinbart, will be writing POEMs for hospitalists. We look forward to your opinions about whether we should increase this content. Let me know.
- ,.Teaching evidence‐based medicine: should we be teaching information management instead?Acad Med.2005;80:685‐689.
- .A POEM a week for the BMJ.Br Med J.2002;325:983.
- POEMs: Keeping up with clinical research that can change your practice.Cleve Clin J Med.2004;71:222.
In addition to marking my initial transition from student to physician, the commencement address by the medical informatics pioneer, Larry Weed, is my most enduring memory of medical school graduation. A provocative thinker in the field of decision support and structured medical records, Weed was credited by my teachers with developing the organized SOAP note. During his address he depressingly equated all the knowledge we had digested during the preceding mentally strenuous 4 years to shoveling a mountain of manure with a teaspoon. Although I agreed that some of the information I learned seemed to lack relevance (still don't know why I needed to learn the details of the Krebs cycle), as I began caring for patients as an intern, I found that much of it mattered. As I launched into residency training, I also discovered that lifelong learning would be a perpetual component of my medical career.
Despite becoming a passionate advocate of practicing evidence‐based medicine (EBM), I also recognized the impossibility of keeping up with the medical literature, given the relentless arrival of journals in the mail. Learning all the evidence is impossible, so we must develop information management skills and allow others to help us in identifying, reviewing, and summarizing salient and valid clinical information.1 One of my vital goals as editor of the Journal of Hospital Medicine is to ensure we provide our readers with useful clinical information that is concise, easily digested, and usable.
To that end we are introducing Patient‐Oriented Evidence that Matters, or POEMs. As described on the InfoPOEMs website (
-
They address a question that we face as clinicians.
-
They measure outcomes that we and our patients care about: symptoms, morbidity, quality of life, and mortality.
-
They have the potential to change the way we practice.
We are not the first journal to do this and join the company of the British Medical Journal and the Cleveland Clinic Journal of Medicine.2, 3 Staff physicians at InfoPOEMs screen more than 100 peer‐reviewed medical journals for relevant articles that practicing physicians can use at the point of care, the patient. A trained physician poet then summarizes selected articles in a standardized manner into a POEM. A POEM begins with a clinical question and then provides a bottom line answer from a recently published journal article. This is followed by a structured abstract that includes the study design and setting, followed by a synopsis of the article.
We will start with at least 2 POEMs per issue focused on clinical topics relevant to hospitalists. Soon, an experienced academic hospitalist and knowledgeable expert in EBM, Dr. Jennifer Kleinbart, will be writing POEMs for hospitalists. We look forward to your opinions about whether we should increase this content. Let me know.
In addition to marking my initial transition from student to physician, the commencement address by the medical informatics pioneer, Larry Weed, is my most enduring memory of medical school graduation. A provocative thinker in the field of decision support and structured medical records, Weed was credited by my teachers with developing the organized SOAP note. During his address he depressingly equated all the knowledge we had digested during the preceding mentally strenuous 4 years to shoveling a mountain of manure with a teaspoon. Although I agreed that some of the information I learned seemed to lack relevance (still don't know why I needed to learn the details of the Krebs cycle), as I began caring for patients as an intern, I found that much of it mattered. As I launched into residency training, I also discovered that lifelong learning would be a perpetual component of my medical career.
Despite becoming a passionate advocate of practicing evidence‐based medicine (EBM), I also recognized the impossibility of keeping up with the medical literature, given the relentless arrival of journals in the mail. Learning all the evidence is impossible, so we must develop information management skills and allow others to help us in identifying, reviewing, and summarizing salient and valid clinical information.1 One of my vital goals as editor of the Journal of Hospital Medicine is to ensure we provide our readers with useful clinical information that is concise, easily digested, and usable.
To that end we are introducing Patient‐Oriented Evidence that Matters, or POEMs. As described on the InfoPOEMs website (
-
They address a question that we face as clinicians.
-
They measure outcomes that we and our patients care about: symptoms, morbidity, quality of life, and mortality.
-
They have the potential to change the way we practice.
We are not the first journal to do this and join the company of the British Medical Journal and the Cleveland Clinic Journal of Medicine.2, 3 Staff physicians at InfoPOEMs screen more than 100 peer‐reviewed medical journals for relevant articles that practicing physicians can use at the point of care, the patient. A trained physician poet then summarizes selected articles in a standardized manner into a POEM. A POEM begins with a clinical question and then provides a bottom line answer from a recently published journal article. This is followed by a structured abstract that includes the study design and setting, followed by a synopsis of the article.
We will start with at least 2 POEMs per issue focused on clinical topics relevant to hospitalists. Soon, an experienced academic hospitalist and knowledgeable expert in EBM, Dr. Jennifer Kleinbart, will be writing POEMs for hospitalists. We look forward to your opinions about whether we should increase this content. Let me know.
- ,.Teaching evidence‐based medicine: should we be teaching information management instead?Acad Med.2005;80:685‐689.
- .A POEM a week for the BMJ.Br Med J.2002;325:983.
- POEMs: Keeping up with clinical research that can change your practice.Cleve Clin J Med.2004;71:222.
- ,.Teaching evidence‐based medicine: should we be teaching information management instead?Acad Med.2005;80:685‐689.
- .A POEM a week for the BMJ.Br Med J.2002;325:983.
- POEMs: Keeping up with clinical research that can change your practice.Cleve Clin J Med.2004;71:222.
Morphine's Modest Origin
Pain is a powerful motivator. Any physician will tell you that pain is the catalyst for patients who have spent a lifetime avoiding the medical system to seek medical help. Not surprisingly, a mixture of societal and personal pain ultimately prompted the discovery of its most potent adversary.
A much different medical landscape existed in the early 1800s. It was an era in which natural remedies comprised a doctor’s primary arsenal against most common maladies—many of which have since been eradicated. Pain (an unfortunate consequence of most illness) was treated primarily with opium, a blessing for those treated with a good batch but worthless to those not so lucky. Imagine the frustration of those physicians responsible for healing the sick and ending suffering, but who were often unsuccessful at both.
Friedrich Sertürner (1783-1841) witnessed this frustration as a disgruntled German teenager forced into an apothecary apprenticeship. While doctors, exhausted after nights of unsuccessful attempts to relieve pain, blamed pharmacists for the unpredictable quality of opium, and pharmacists in turn scratched their heads and looked to their suppliers, the answer seemed apparent to young Sertürner. Though he lacked formal medical or research training, his rational thinking led him to believe that there must be an active ingredient in the opium which, if isolated, could be delivered in a safe, effective, and reliable dose.
In an effort to quell his boredom at the pharmacy, Sertürner spent his nights using old equipment to run experiments on opium, dissolving it in acid, neutralizing it with ammonia, and precipitating out various products. His first experiments yielded nothing more than inert compounds, but he was not easily dissuaded.
Months later, he isolated what he believed to be the active ingredient, the principium somniferum. His discovery contradicted current knowledge at that time because this compound was the first alkaloid ever derived from a plant source. He conducted many animal experiments with the new compound, demonstrating both its sedative properties and the dangerous consequences that often accompanied them. Sertürner initially named the drug Morpheus, after the Greek god of dreams; however, in keeping with the standardized naming of alkaloids, he finally settled on the name morphine. He eagerly submitted his research for publication, but his discovery was labeled unscientific and was not accepted by the medical community.
An insulted Sertürner set aside his research for years until one evening when a bout of personal pain prompted him to pick up where he had left off. In the midst of a terrible toothache, he took a small amount of his morphine, fell fast asleep, and awoke hours later to attest that this compound was in fact safe for human consumption. He went on to conduct dosing experiments with local children that would be frowned upon by even the most relaxed institutional review board today, but that at the time indicated he had achieved his goal of discovering a safe, effective, reliable dose of analgesic. His research was again disregarded. When university experiments in France began to confirm his results, however, he was ultimately credited with being the inventor of morphine.
The discovery of morphine not only spares many people today the pain of past eras, but its story also serves as an inspiration for further developments in medicine. Within the current medical landscape of specialties within specialties and with personalized genetic and drug therapy on the horizon, the idea of conducting research remains daunting. Still, the encompassing view and abundant experience of the generalist can be a great advantage to the advancement of medicine.
So, the next time you start a hydromorphone patient-controlled analgesia pump (PCA) or apply a fentanyl patch, think back a few hundred years, and imagine healing without the gift of Morpheus. TH
Larsen is a senior medical student at the Keck School of Medicine, University of Southern California, Los Angeles.
Resources
- Silverman MM. Magic in a Bottle. New York: The Macmillan Company; 1941.
- Hodgson B. In the Arms of Morpheus: The Tragic History of Laudanum, Morphine, and Patent Medicines. Richmond Hill, Ontario, Canada: Firefly Books; 2001.
Pain is a powerful motivator. Any physician will tell you that pain is the catalyst for patients who have spent a lifetime avoiding the medical system to seek medical help. Not surprisingly, a mixture of societal and personal pain ultimately prompted the discovery of its most potent adversary.
A much different medical landscape existed in the early 1800s. It was an era in which natural remedies comprised a doctor’s primary arsenal against most common maladies—many of which have since been eradicated. Pain (an unfortunate consequence of most illness) was treated primarily with opium, a blessing for those treated with a good batch but worthless to those not so lucky. Imagine the frustration of those physicians responsible for healing the sick and ending suffering, but who were often unsuccessful at both.
Friedrich Sertürner (1783-1841) witnessed this frustration as a disgruntled German teenager forced into an apothecary apprenticeship. While doctors, exhausted after nights of unsuccessful attempts to relieve pain, blamed pharmacists for the unpredictable quality of opium, and pharmacists in turn scratched their heads and looked to their suppliers, the answer seemed apparent to young Sertürner. Though he lacked formal medical or research training, his rational thinking led him to believe that there must be an active ingredient in the opium which, if isolated, could be delivered in a safe, effective, and reliable dose.
In an effort to quell his boredom at the pharmacy, Sertürner spent his nights using old equipment to run experiments on opium, dissolving it in acid, neutralizing it with ammonia, and precipitating out various products. His first experiments yielded nothing more than inert compounds, but he was not easily dissuaded.
Months later, he isolated what he believed to be the active ingredient, the principium somniferum. His discovery contradicted current knowledge at that time because this compound was the first alkaloid ever derived from a plant source. He conducted many animal experiments with the new compound, demonstrating both its sedative properties and the dangerous consequences that often accompanied them. Sertürner initially named the drug Morpheus, after the Greek god of dreams; however, in keeping with the standardized naming of alkaloids, he finally settled on the name morphine. He eagerly submitted his research for publication, but his discovery was labeled unscientific and was not accepted by the medical community.
An insulted Sertürner set aside his research for years until one evening when a bout of personal pain prompted him to pick up where he had left off. In the midst of a terrible toothache, he took a small amount of his morphine, fell fast asleep, and awoke hours later to attest that this compound was in fact safe for human consumption. He went on to conduct dosing experiments with local children that would be frowned upon by even the most relaxed institutional review board today, but that at the time indicated he had achieved his goal of discovering a safe, effective, reliable dose of analgesic. His research was again disregarded. When university experiments in France began to confirm his results, however, he was ultimately credited with being the inventor of morphine.
The discovery of morphine not only spares many people today the pain of past eras, but its story also serves as an inspiration for further developments in medicine. Within the current medical landscape of specialties within specialties and with personalized genetic and drug therapy on the horizon, the idea of conducting research remains daunting. Still, the encompassing view and abundant experience of the generalist can be a great advantage to the advancement of medicine.
So, the next time you start a hydromorphone patient-controlled analgesia pump (PCA) or apply a fentanyl patch, think back a few hundred years, and imagine healing without the gift of Morpheus. TH
Larsen is a senior medical student at the Keck School of Medicine, University of Southern California, Los Angeles.
Resources
- Silverman MM. Magic in a Bottle. New York: The Macmillan Company; 1941.
- Hodgson B. In the Arms of Morpheus: The Tragic History of Laudanum, Morphine, and Patent Medicines. Richmond Hill, Ontario, Canada: Firefly Books; 2001.
Pain is a powerful motivator. Any physician will tell you that pain is the catalyst for patients who have spent a lifetime avoiding the medical system to seek medical help. Not surprisingly, a mixture of societal and personal pain ultimately prompted the discovery of its most potent adversary.
A much different medical landscape existed in the early 1800s. It was an era in which natural remedies comprised a doctor’s primary arsenal against most common maladies—many of which have since been eradicated. Pain (an unfortunate consequence of most illness) was treated primarily with opium, a blessing for those treated with a good batch but worthless to those not so lucky. Imagine the frustration of those physicians responsible for healing the sick and ending suffering, but who were often unsuccessful at both.
Friedrich Sertürner (1783-1841) witnessed this frustration as a disgruntled German teenager forced into an apothecary apprenticeship. While doctors, exhausted after nights of unsuccessful attempts to relieve pain, blamed pharmacists for the unpredictable quality of opium, and pharmacists in turn scratched their heads and looked to their suppliers, the answer seemed apparent to young Sertürner. Though he lacked formal medical or research training, his rational thinking led him to believe that there must be an active ingredient in the opium which, if isolated, could be delivered in a safe, effective, and reliable dose.
In an effort to quell his boredom at the pharmacy, Sertürner spent his nights using old equipment to run experiments on opium, dissolving it in acid, neutralizing it with ammonia, and precipitating out various products. His first experiments yielded nothing more than inert compounds, but he was not easily dissuaded.
Months later, he isolated what he believed to be the active ingredient, the principium somniferum. His discovery contradicted current knowledge at that time because this compound was the first alkaloid ever derived from a plant source. He conducted many animal experiments with the new compound, demonstrating both its sedative properties and the dangerous consequences that often accompanied them. Sertürner initially named the drug Morpheus, after the Greek god of dreams; however, in keeping with the standardized naming of alkaloids, he finally settled on the name morphine. He eagerly submitted his research for publication, but his discovery was labeled unscientific and was not accepted by the medical community.
An insulted Sertürner set aside his research for years until one evening when a bout of personal pain prompted him to pick up where he had left off. In the midst of a terrible toothache, he took a small amount of his morphine, fell fast asleep, and awoke hours later to attest that this compound was in fact safe for human consumption. He went on to conduct dosing experiments with local children that would be frowned upon by even the most relaxed institutional review board today, but that at the time indicated he had achieved his goal of discovering a safe, effective, reliable dose of analgesic. His research was again disregarded. When university experiments in France began to confirm his results, however, he was ultimately credited with being the inventor of morphine.
The discovery of morphine not only spares many people today the pain of past eras, but its story also serves as an inspiration for further developments in medicine. Within the current medical landscape of specialties within specialties and with personalized genetic and drug therapy on the horizon, the idea of conducting research remains daunting. Still, the encompassing view and abundant experience of the generalist can be a great advantage to the advancement of medicine.
So, the next time you start a hydromorphone patient-controlled analgesia pump (PCA) or apply a fentanyl patch, think back a few hundred years, and imagine healing without the gift of Morpheus. TH
Larsen is a senior medical student at the Keck School of Medicine, University of Southern California, Los Angeles.
Resources
- Silverman MM. Magic in a Bottle. New York: The Macmillan Company; 1941.
- Hodgson B. In the Arms of Morpheus: The Tragic History of Laudanum, Morphine, and Patent Medicines. Richmond Hill, Ontario, Canada: Firefly Books; 2001.
Hot Potatoes

I always loved the game Hot Potato. A more stationary version of musical chairs, it involves the passing of the spud as the music plays or the clock ticks, then the last-minute handoff; the excitement of that game trained me for a life of brinkmanship.
The earliest version of the game involved passing a lit candle, with the loser holding the extinguished taper. I always enjoyed my cold war version, a wind-up fake bomb passed around the circle. Hot Potato was the name of a terrible Jim Kelly martial arts movie in 1976, and an even worse short-lived NBC game show in 1984. It is even a poorly rated video game. The newest “Hot Potato” is a computer routing system.
In the game Hot Potato, you never want to be the one with the spud when the music stops. Unfortunately, sometimes patients become that hot potato.
When I was a first-year medical student, I wanted my own patients. I shared the clinical experience with others grudgingly. Someone else would always ask the question I wanted to; they routinely heard the murmur first. Every patient was a new mystery to be solved, a reminder of how little I knew (and still don’t know). By my senior year of school, I still wanted my own patients, but I wanted the most exotic and difficult cases I could find, as a matter of principle.
By internship that glory had faded. I was harassed, sleep deprived, overworked, and underpaid, but otherwise I was OK. If I could avoid another admission, I was happy. New terminology entered my vocabulary. Expressions like “He’s a sieve” or “She’s a wall” described my coworkers in the emergency department (ED). Why would they admit that patient, were they crazy? Your chief resident was strong or weak based on turfing prowess. What could be sweeter than a bounce back to the other service?

As a resident, I perfected what Samuel Shem (a.k.a., Stephen Bergman, MD) described in the classic The House of God as the “buff and turf.” Transfer to surgery, no problem. Patient wants to leave AMA, just have him sign the paperwork. This negative attitude was pervasive. A team was judged by the strength of the resident, and measured by the relative size of the census. Of course, residents today would never feel this way, given work hour limits. That was in the old days.
As a newly minted private practice internist, I wanted all the patients I could see. I took every ED admit, opened all my slots. I was building my practice. I was on a productivity formula and wanted to surpass my targets. I was incentivized. It seemed odd to be working so hard to get patients when I had done the opposite just one year earlier. My colleagues looked on in amazement as I said yes to everything. The best advice I was ever given was to say no, but I did not heed it.
After a few years in practice, I was well stocked with patients. I still accepted all Medicare patients; at the time, I was the only one in private practice who would do so secondary to the lower pay rate. I didn’t mind because of my interest in geriatrics. I enjoyed these old folks, plus they brought in the best homegrown produce. My kids grew sick of okra.
When the HMOs came to town, with their IPAs and IPOs, along with other alphabetic acronyms too fierce to mention, I was once again incentivized to not see patients. It was fine for me to capture their PMPM (per member per month) fee, but I wasn’t encouraged to actually see them, and hospitalization involved a tremendous amount of paperwork and psychological conflict with my IPA handlers. “Do you really need that MRI?” was the question of the day.
I spent a brief and disastrous year in the world of practice management groups, where patients were subsidiary to stock value and practice acquisition. I emerged bent but not broken. Well, maybe slightly broken. Yes, money is the root of all evil.
Next, I began to work for a community-based university practice, on a straight salary. My financial incentives were eliminated, I saw as many as I comfortably could, and I forgot about the money. Life was good. I had a few medical students and an intern. We saw a large but comfortable volume of patients, mostly geriatric. I always tried to see the people who needed to be seen, but not so many that a visit was too brief.
The dark side reared its head again when I got a new boss who wanted the community university practice to go on productivity. Once again I was back to the bean counting rat race: see more patients and squeeze in an extra three this afternoon. “What do you mean you want a day off?”
But then I became a hospitalist and all was right with the world again. It was an excellent consultative practice with ample opportunities for teaching and research. Unfortunately, when the resident hours rules began, we found ourselves staffing services formerly run by teaching teams. We also found ourselves in rotation with the remaining teams.
This was the moment of truth. Would I return to my long abandoned roots? Would I begin once again to order the “surf and turf” platter? Happily, the answer has been “No.” The fullness of time has helped me to realize that patients are not hot potatoes. There are days when I find myself watching the admit board intently or wondering why one service or another is not taking their bounce backs. I have found, however, that the mental energy that is wasted in playing Hot Potato is needed to care for the patients who seek our help. Would I want my mother sitting in an ED while three services did their best to not have her on their lists? OK, in my mom’s case, I could understand. (Just joking, Arlene.)
So, the next time you get the call from the ED and find yourself wondering what that patient is doing on your service, think about the game of Hot Potato. Perhaps when the music stops, you are the right one to have the spud in hand. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
I always loved the game Hot Potato. A more stationary version of musical chairs, it involves the passing of the spud as the music plays or the clock ticks, then the last-minute handoff; the excitement of that game trained me for a life of brinkmanship.
The earliest version of the game involved passing a lit candle, with the loser holding the extinguished taper. I always enjoyed my cold war version, a wind-up fake bomb passed around the circle. Hot Potato was the name of a terrible Jim Kelly martial arts movie in 1976, and an even worse short-lived NBC game show in 1984. It is even a poorly rated video game. The newest “Hot Potato” is a computer routing system.
In the game Hot Potato, you never want to be the one with the spud when the music stops. Unfortunately, sometimes patients become that hot potato.
When I was a first-year medical student, I wanted my own patients. I shared the clinical experience with others grudgingly. Someone else would always ask the question I wanted to; they routinely heard the murmur first. Every patient was a new mystery to be solved, a reminder of how little I knew (and still don’t know). By my senior year of school, I still wanted my own patients, but I wanted the most exotic and difficult cases I could find, as a matter of principle.
By internship that glory had faded. I was harassed, sleep deprived, overworked, and underpaid, but otherwise I was OK. If I could avoid another admission, I was happy. New terminology entered my vocabulary. Expressions like “He’s a sieve” or “She’s a wall” described my coworkers in the emergency department (ED). Why would they admit that patient, were they crazy? Your chief resident was strong or weak based on turfing prowess. What could be sweeter than a bounce back to the other service?
As a resident, I perfected what Samuel Shem (a.k.a., Stephen Bergman, MD) described in the classic The House of God as the “buff and turf.” Transfer to surgery, no problem. Patient wants to leave AMA, just have him sign the paperwork. This negative attitude was pervasive. A team was judged by the strength of the resident, and measured by the relative size of the census. Of course, residents today would never feel this way, given work hour limits. That was in the old days.
As a newly minted private practice internist, I wanted all the patients I could see. I took every ED admit, opened all my slots. I was building my practice. I was on a productivity formula and wanted to surpass my targets. I was incentivized. It seemed odd to be working so hard to get patients when I had done the opposite just one year earlier. My colleagues looked on in amazement as I said yes to everything. The best advice I was ever given was to say no, but I did not heed it.
After a few years in practice, I was well stocked with patients. I still accepted all Medicare patients; at the time, I was the only one in private practice who would do so secondary to the lower pay rate. I didn’t mind because of my interest in geriatrics. I enjoyed these old folks, plus they brought in the best homegrown produce. My kids grew sick of okra.
When the HMOs came to town, with their IPAs and IPOs, along with other alphabetic acronyms too fierce to mention, I was once again incentivized to not see patients. It was fine for me to capture their PMPM (per member per month) fee, but I wasn’t encouraged to actually see them, and hospitalization involved a tremendous amount of paperwork and psychological conflict with my IPA handlers. “Do you really need that MRI?” was the question of the day.
I spent a brief and disastrous year in the world of practice management groups, where patients were subsidiary to stock value and practice acquisition. I emerged bent but not broken. Well, maybe slightly broken. Yes, money is the root of all evil.
Next, I began to work for a community-based university practice, on a straight salary. My financial incentives were eliminated, I saw as many as I comfortably could, and I forgot about the money. Life was good. I had a few medical students and an intern. We saw a large but comfortable volume of patients, mostly geriatric. I always tried to see the people who needed to be seen, but not so many that a visit was too brief.
The dark side reared its head again when I got a new boss who wanted the community university practice to go on productivity. Once again I was back to the bean counting rat race: see more patients and squeeze in an extra three this afternoon. “What do you mean you want a day off?”
But then I became a hospitalist and all was right with the world again. It was an excellent consultative practice with ample opportunities for teaching and research. Unfortunately, when the resident hours rules began, we found ourselves staffing services formerly run by teaching teams. We also found ourselves in rotation with the remaining teams.
This was the moment of truth. Would I return to my long abandoned roots? Would I begin once again to order the “surf and turf” platter? Happily, the answer has been “No.” The fullness of time has helped me to realize that patients are not hot potatoes. There are days when I find myself watching the admit board intently or wondering why one service or another is not taking their bounce backs. I have found, however, that the mental energy that is wasted in playing Hot Potato is needed to care for the patients who seek our help. Would I want my mother sitting in an ED while three services did their best to not have her on their lists? OK, in my mom’s case, I could understand. (Just joking, Arlene.)
So, the next time you get the call from the ED and find yourself wondering what that patient is doing on your service, think about the game of Hot Potato. Perhaps when the music stops, you are the right one to have the spud in hand. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
I always loved the game Hot Potato. A more stationary version of musical chairs, it involves the passing of the spud as the music plays or the clock ticks, then the last-minute handoff; the excitement of that game trained me for a life of brinkmanship.
The earliest version of the game involved passing a lit candle, with the loser holding the extinguished taper. I always enjoyed my cold war version, a wind-up fake bomb passed around the circle. Hot Potato was the name of a terrible Jim Kelly martial arts movie in 1976, and an even worse short-lived NBC game show in 1984. It is even a poorly rated video game. The newest “Hot Potato” is a computer routing system.
In the game Hot Potato, you never want to be the one with the spud when the music stops. Unfortunately, sometimes patients become that hot potato.
When I was a first-year medical student, I wanted my own patients. I shared the clinical experience with others grudgingly. Someone else would always ask the question I wanted to; they routinely heard the murmur first. Every patient was a new mystery to be solved, a reminder of how little I knew (and still don’t know). By my senior year of school, I still wanted my own patients, but I wanted the most exotic and difficult cases I could find, as a matter of principle.
By internship that glory had faded. I was harassed, sleep deprived, overworked, and underpaid, but otherwise I was OK. If I could avoid another admission, I was happy. New terminology entered my vocabulary. Expressions like “He’s a sieve” or “She’s a wall” described my coworkers in the emergency department (ED). Why would they admit that patient, were they crazy? Your chief resident was strong or weak based on turfing prowess. What could be sweeter than a bounce back to the other service?
As a resident, I perfected what Samuel Shem (a.k.a., Stephen Bergman, MD) described in the classic The House of God as the “buff and turf.” Transfer to surgery, no problem. Patient wants to leave AMA, just have him sign the paperwork. This negative attitude was pervasive. A team was judged by the strength of the resident, and measured by the relative size of the census. Of course, residents today would never feel this way, given work hour limits. That was in the old days.
As a newly minted private practice internist, I wanted all the patients I could see. I took every ED admit, opened all my slots. I was building my practice. I was on a productivity formula and wanted to surpass my targets. I was incentivized. It seemed odd to be working so hard to get patients when I had done the opposite just one year earlier. My colleagues looked on in amazement as I said yes to everything. The best advice I was ever given was to say no, but I did not heed it.
After a few years in practice, I was well stocked with patients. I still accepted all Medicare patients; at the time, I was the only one in private practice who would do so secondary to the lower pay rate. I didn’t mind because of my interest in geriatrics. I enjoyed these old folks, plus they brought in the best homegrown produce. My kids grew sick of okra.
When the HMOs came to town, with their IPAs and IPOs, along with other alphabetic acronyms too fierce to mention, I was once again incentivized to not see patients. It was fine for me to capture their PMPM (per member per month) fee, but I wasn’t encouraged to actually see them, and hospitalization involved a tremendous amount of paperwork and psychological conflict with my IPA handlers. “Do you really need that MRI?” was the question of the day.
I spent a brief and disastrous year in the world of practice management groups, where patients were subsidiary to stock value and practice acquisition. I emerged bent but not broken. Well, maybe slightly broken. Yes, money is the root of all evil.
Next, I began to work for a community-based university practice, on a straight salary. My financial incentives were eliminated, I saw as many as I comfortably could, and I forgot about the money. Life was good. I had a few medical students and an intern. We saw a large but comfortable volume of patients, mostly geriatric. I always tried to see the people who needed to be seen, but not so many that a visit was too brief.
The dark side reared its head again when I got a new boss who wanted the community university practice to go on productivity. Once again I was back to the bean counting rat race: see more patients and squeeze in an extra three this afternoon. “What do you mean you want a day off?”
But then I became a hospitalist and all was right with the world again. It was an excellent consultative practice with ample opportunities for teaching and research. Unfortunately, when the resident hours rules began, we found ourselves staffing services formerly run by teaching teams. We also found ourselves in rotation with the remaining teams.
This was the moment of truth. Would I return to my long abandoned roots? Would I begin once again to order the “surf and turf” platter? Happily, the answer has been “No.” The fullness of time has helped me to realize that patients are not hot potatoes. There are days when I find myself watching the admit board intently or wondering why one service or another is not taking their bounce backs. I have found, however, that the mental energy that is wasted in playing Hot Potato is needed to care for the patients who seek our help. Would I want my mother sitting in an ED while three services did their best to not have her on their lists? OK, in my mom’s case, I could understand. (Just joking, Arlene.)
So, the next time you get the call from the ED and find yourself wondering what that patient is doing on your service, think about the game of Hot Potato. Perhaps when the music stops, you are the right one to have the spud in hand. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
Keeping Patients in the Loop

A few years ago, I cared for an unfortunate homeless patient who seemed incapable of managing his own affairs and was probably illiterate. When he left the hospital, I gave him a copy of his discharge summary and stressed that he should carry it around and always show it to anyone taking care of him. A lot went on in the hospital, and I worried he wouldn’t follow through with the subsequent care I had arranged and would instead wind up in another emergency department (ED) the next time he had a problem.
A few weeks later I got a call from another ED in the area and learned that the patient hadn’t been able to provide any meaningful details of his health history or where he had received care previously. But he did pull a wrinkled copy of the discharge summary from his pocket to show the staff. In our phone conversation, the ED doctor remarked how helpful it had been to have this information that he probably would have never found otherwise. It saved the need to pursue workup for things that I had already investigated.
I tell this story because I think it would be great for hospitalists to ensure that all, or nearly all, of their patients receive a copy of their discharge summary as they leave the hospital—or soon thereafter. In fact, I suspect that if this became common for hospitalists, the idea might become de rigueur for all patients in the hospital.
I’ve been providing a copy for many of my patients for several years. I first started doing this for patients I cared for who lived out of my area (e.g., a different state) and I couldn’t rely on the hospital getting a copy of the summary to the patient’s primary care physician (PCP) at home. That experience convinced me it could be a good idea to give it to nearly all patients.
Giving each patient a copy of selected parts of the medical record and, when requested by patients, all of the medical record, is not a new idea. I think it is great that a number of clinics and other providers mail test results to patients, and neater still are the organizations that encourage patients to “visit our Web site to review your test results” and other such information. However routinely encouraging them to review all of the test results and other records generated during a hospital stay may be an idea that isn’t yet ready for prime time. Instead, I think it is useful to give the patient a copy of the discharge summary, which highlights relevant test results with accompanying explanation and analysis.
There are many reasons this can be a good idea. Of course, a discharge summary can’t replace or reduce the need for the doctor to discuss diagnoses, treatment, and follow-up plans with the patient. Still, it is a great summary of the diagnoses, medications, and discharge instructions that the patient can review later. Research shows that many patients forget most of what they have been told by the time they get home, and my hope is that the discharge summary will serve as a reminder.
Think about the other caregivers who will see the patient after discharge. They benefit from having a discharge summary to review. Sure I’ll send a copy of the summary to the patient’s primary care doctor and to the cardiologist who consulted during the hospital stay. But what about the visiting nurse who will start seeing the patient the day after discharge? The patient can show the summary to the nurse instead of trying to recall what he was told about his illness and showing the nurse his pill bottles. Also, the patient may end up seeing doctors that I didn’t know about who won’t be getting a copy of the summary from me (my hospital). He may see other doctors in the community that he didn’t think to tell me about and can take a copy of the summary to those visits. This is why I usually tell patients to carry the summary around with them and show it to all the providers they see.
What about the patients with low health literacy? I think they might be the ones to benefit the most from getting the summary. A patient with low literacy may often get assistance from other and can show the report to these caregivers (often friends or family members). Not every patient will show the report to someone who can read it, but I think a lot of them will. So I think it’s worthwhile to give the report to everyone, just in case. If a patient is demented or otherwise incompetent, I try to get the summary into the hands of a family member or other caregiver. (Of course this can raise HIPAA-related privacy issues, and consent may be needed in some cases.)
I think that most lay people can make sense of most of what is in a discharge summary. As for the more challenging technical language in nearly every summary, sophisticated people can turn to the Internet for help. I want patients to have written reminders when they need things like a follow-up chest X-ray or results of tests that were pending at discharge. The need for specific follow-up like this gets reported directly to the PCP (via the copy of the discharge summary sent directly to him/her), and I hope that patients who have read the summary will help remind the PCP of these things.
There are two principle costs or barriers to making this standard practice. The first is that doctors tend to resist it. They worry that patients won’t understand the information or—worse—will become needlessly worried and stressed, and that the doctor will have to spend significant time “talking the patient down” from a worry that would never have arisen if the patient hadn’t been nosing around in a record that is written in “medicalese.” Or maybe the patient will read an unflattering portrayal of his situation and become angry at the doctor. (“He called me a drug seeker!”) Yet my experience shows that these are infrequent problems.
I can recall only one such incident out of the thousands of patients who have left my care with a copy of their discharge summary. One reason is that it’s now a habit for me to dictate each report while keeping in mind the idea that the patient is likely to read it. So instead of referring to a patient as a likely drug seeker, I’m apt to say something like “the patient had difficult pain management problems.” And isn’t this better language anyway? I might be wrong about his drug seeking, and any future provider who sees my report will probably still understand that drug seeking is a possibility. There are rare cases in which I think it is best not to automatically give the patient a copy of the report. These could include a proven unflattering diagnosis that the patient disputes. But remember, the patient may eventually end up seeing any report you create, so it’s worth keeping this in mind with all of your medical record documentation.
The second reason for resisting this idea is the perceived difficulty or cost of implementing it. I’m fortunate that most of my patients can get a paper copy of the discharge summary I’ve prepared as they are leaving the hospital. Of course, this requires that I dictate the report at the time of the discharge visit, and it is transcribed immediately. If you can’t pull this off, then I suggest that you have a copy mailed (or e-mailed if feasible) within a day or two of discharge. If the summary isn’t available when the patient is ready to leave, I wouldn’t have him stay and needlessly tie up a hospital bed. When this happens to my patients, I have them go ahead and leave, and a copy is mailed to them.
So I hope you will consider making this a routine practice in your hospital. The costs are small, and the potential benefit to quality of care and patient satisfaction could be significant. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
A few years ago, I cared for an unfortunate homeless patient who seemed incapable of managing his own affairs and was probably illiterate. When he left the hospital, I gave him a copy of his discharge summary and stressed that he should carry it around and always show it to anyone taking care of him. A lot went on in the hospital, and I worried he wouldn’t follow through with the subsequent care I had arranged and would instead wind up in another emergency department (ED) the next time he had a problem.
A few weeks later I got a call from another ED in the area and learned that the patient hadn’t been able to provide any meaningful details of his health history or where he had received care previously. But he did pull a wrinkled copy of the discharge summary from his pocket to show the staff. In our phone conversation, the ED doctor remarked how helpful it had been to have this information that he probably would have never found otherwise. It saved the need to pursue workup for things that I had already investigated.
I tell this story because I think it would be great for hospitalists to ensure that all, or nearly all, of their patients receive a copy of their discharge summary as they leave the hospital—or soon thereafter. In fact, I suspect that if this became common for hospitalists, the idea might become de rigueur for all patients in the hospital.
I’ve been providing a copy for many of my patients for several years. I first started doing this for patients I cared for who lived out of my area (e.g., a different state) and I couldn’t rely on the hospital getting a copy of the summary to the patient’s primary care physician (PCP) at home. That experience convinced me it could be a good idea to give it to nearly all patients.
Giving each patient a copy of selected parts of the medical record and, when requested by patients, all of the medical record, is not a new idea. I think it is great that a number of clinics and other providers mail test results to patients, and neater still are the organizations that encourage patients to “visit our Web site to review your test results” and other such information. However routinely encouraging them to review all of the test results and other records generated during a hospital stay may be an idea that isn’t yet ready for prime time. Instead, I think it is useful to give the patient a copy of the discharge summary, which highlights relevant test results with accompanying explanation and analysis.
There are many reasons this can be a good idea. Of course, a discharge summary can’t replace or reduce the need for the doctor to discuss diagnoses, treatment, and follow-up plans with the patient. Still, it is a great summary of the diagnoses, medications, and discharge instructions that the patient can review later. Research shows that many patients forget most of what they have been told by the time they get home, and my hope is that the discharge summary will serve as a reminder.
Think about the other caregivers who will see the patient after discharge. They benefit from having a discharge summary to review. Sure I’ll send a copy of the summary to the patient’s primary care doctor and to the cardiologist who consulted during the hospital stay. But what about the visiting nurse who will start seeing the patient the day after discharge? The patient can show the summary to the nurse instead of trying to recall what he was told about his illness and showing the nurse his pill bottles. Also, the patient may end up seeing doctors that I didn’t know about who won’t be getting a copy of the summary from me (my hospital). He may see other doctors in the community that he didn’t think to tell me about and can take a copy of the summary to those visits. This is why I usually tell patients to carry the summary around with them and show it to all the providers they see.
What about the patients with low health literacy? I think they might be the ones to benefit the most from getting the summary. A patient with low literacy may often get assistance from other and can show the report to these caregivers (often friends or family members). Not every patient will show the report to someone who can read it, but I think a lot of them will. So I think it’s worthwhile to give the report to everyone, just in case. If a patient is demented or otherwise incompetent, I try to get the summary into the hands of a family member or other caregiver. (Of course this can raise HIPAA-related privacy issues, and consent may be needed in some cases.)
I think that most lay people can make sense of most of what is in a discharge summary. As for the more challenging technical language in nearly every summary, sophisticated people can turn to the Internet for help. I want patients to have written reminders when they need things like a follow-up chest X-ray or results of tests that were pending at discharge. The need for specific follow-up like this gets reported directly to the PCP (via the copy of the discharge summary sent directly to him/her), and I hope that patients who have read the summary will help remind the PCP of these things.
There are two principle costs or barriers to making this standard practice. The first is that doctors tend to resist it. They worry that patients won’t understand the information or—worse—will become needlessly worried and stressed, and that the doctor will have to spend significant time “talking the patient down” from a worry that would never have arisen if the patient hadn’t been nosing around in a record that is written in “medicalese.” Or maybe the patient will read an unflattering portrayal of his situation and become angry at the doctor. (“He called me a drug seeker!”) Yet my experience shows that these are infrequent problems.
I can recall only one such incident out of the thousands of patients who have left my care with a copy of their discharge summary. One reason is that it’s now a habit for me to dictate each report while keeping in mind the idea that the patient is likely to read it. So instead of referring to a patient as a likely drug seeker, I’m apt to say something like “the patient had difficult pain management problems.” And isn’t this better language anyway? I might be wrong about his drug seeking, and any future provider who sees my report will probably still understand that drug seeking is a possibility. There are rare cases in which I think it is best not to automatically give the patient a copy of the report. These could include a proven unflattering diagnosis that the patient disputes. But remember, the patient may eventually end up seeing any report you create, so it’s worth keeping this in mind with all of your medical record documentation.
The second reason for resisting this idea is the perceived difficulty or cost of implementing it. I’m fortunate that most of my patients can get a paper copy of the discharge summary I’ve prepared as they are leaving the hospital. Of course, this requires that I dictate the report at the time of the discharge visit, and it is transcribed immediately. If you can’t pull this off, then I suggest that you have a copy mailed (or e-mailed if feasible) within a day or two of discharge. If the summary isn’t available when the patient is ready to leave, I wouldn’t have him stay and needlessly tie up a hospital bed. When this happens to my patients, I have them go ahead and leave, and a copy is mailed to them.
So I hope you will consider making this a routine practice in your hospital. The costs are small, and the potential benefit to quality of care and patient satisfaction could be significant. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
A few years ago, I cared for an unfortunate homeless patient who seemed incapable of managing his own affairs and was probably illiterate. When he left the hospital, I gave him a copy of his discharge summary and stressed that he should carry it around and always show it to anyone taking care of him. A lot went on in the hospital, and I worried he wouldn’t follow through with the subsequent care I had arranged and would instead wind up in another emergency department (ED) the next time he had a problem.
A few weeks later I got a call from another ED in the area and learned that the patient hadn’t been able to provide any meaningful details of his health history or where he had received care previously. But he did pull a wrinkled copy of the discharge summary from his pocket to show the staff. In our phone conversation, the ED doctor remarked how helpful it had been to have this information that he probably would have never found otherwise. It saved the need to pursue workup for things that I had already investigated.
I tell this story because I think it would be great for hospitalists to ensure that all, or nearly all, of their patients receive a copy of their discharge summary as they leave the hospital—or soon thereafter. In fact, I suspect that if this became common for hospitalists, the idea might become de rigueur for all patients in the hospital.
I’ve been providing a copy for many of my patients for several years. I first started doing this for patients I cared for who lived out of my area (e.g., a different state) and I couldn’t rely on the hospital getting a copy of the summary to the patient’s primary care physician (PCP) at home. That experience convinced me it could be a good idea to give it to nearly all patients.
Giving each patient a copy of selected parts of the medical record and, when requested by patients, all of the medical record, is not a new idea. I think it is great that a number of clinics and other providers mail test results to patients, and neater still are the organizations that encourage patients to “visit our Web site to review your test results” and other such information. However routinely encouraging them to review all of the test results and other records generated during a hospital stay may be an idea that isn’t yet ready for prime time. Instead, I think it is useful to give the patient a copy of the discharge summary, which highlights relevant test results with accompanying explanation and analysis.
There are many reasons this can be a good idea. Of course, a discharge summary can’t replace or reduce the need for the doctor to discuss diagnoses, treatment, and follow-up plans with the patient. Still, it is a great summary of the diagnoses, medications, and discharge instructions that the patient can review later. Research shows that many patients forget most of what they have been told by the time they get home, and my hope is that the discharge summary will serve as a reminder.
Think about the other caregivers who will see the patient after discharge. They benefit from having a discharge summary to review. Sure I’ll send a copy of the summary to the patient’s primary care doctor and to the cardiologist who consulted during the hospital stay. But what about the visiting nurse who will start seeing the patient the day after discharge? The patient can show the summary to the nurse instead of trying to recall what he was told about his illness and showing the nurse his pill bottles. Also, the patient may end up seeing doctors that I didn’t know about who won’t be getting a copy of the summary from me (my hospital). He may see other doctors in the community that he didn’t think to tell me about and can take a copy of the summary to those visits. This is why I usually tell patients to carry the summary around with them and show it to all the providers they see.
What about the patients with low health literacy? I think they might be the ones to benefit the most from getting the summary. A patient with low literacy may often get assistance from other and can show the report to these caregivers (often friends or family members). Not every patient will show the report to someone who can read it, but I think a lot of them will. So I think it’s worthwhile to give the report to everyone, just in case. If a patient is demented or otherwise incompetent, I try to get the summary into the hands of a family member or other caregiver. (Of course this can raise HIPAA-related privacy issues, and consent may be needed in some cases.)
I think that most lay people can make sense of most of what is in a discharge summary. As for the more challenging technical language in nearly every summary, sophisticated people can turn to the Internet for help. I want patients to have written reminders when they need things like a follow-up chest X-ray or results of tests that were pending at discharge. The need for specific follow-up like this gets reported directly to the PCP (via the copy of the discharge summary sent directly to him/her), and I hope that patients who have read the summary will help remind the PCP of these things.
There are two principle costs or barriers to making this standard practice. The first is that doctors tend to resist it. They worry that patients won’t understand the information or—worse—will become needlessly worried and stressed, and that the doctor will have to spend significant time “talking the patient down” from a worry that would never have arisen if the patient hadn’t been nosing around in a record that is written in “medicalese.” Or maybe the patient will read an unflattering portrayal of his situation and become angry at the doctor. (“He called me a drug seeker!”) Yet my experience shows that these are infrequent problems.
I can recall only one such incident out of the thousands of patients who have left my care with a copy of their discharge summary. One reason is that it’s now a habit for me to dictate each report while keeping in mind the idea that the patient is likely to read it. So instead of referring to a patient as a likely drug seeker, I’m apt to say something like “the patient had difficult pain management problems.” And isn’t this better language anyway? I might be wrong about his drug seeking, and any future provider who sees my report will probably still understand that drug seeking is a possibility. There are rare cases in which I think it is best not to automatically give the patient a copy of the report. These could include a proven unflattering diagnosis that the patient disputes. But remember, the patient may eventually end up seeing any report you create, so it’s worth keeping this in mind with all of your medical record documentation.
The second reason for resisting this idea is the perceived difficulty or cost of implementing it. I’m fortunate that most of my patients can get a paper copy of the discharge summary I’ve prepared as they are leaving the hospital. Of course, this requires that I dictate the report at the time of the discharge visit, and it is transcribed immediately. If you can’t pull this off, then I suggest that you have a copy mailed (or e-mailed if feasible) within a day or two of discharge. If the summary isn’t available when the patient is ready to leave, I wouldn’t have him stay and needlessly tie up a hospital bed. When this happens to my patients, I have them go ahead and leave, and a copy is mailed to them.
So I hope you will consider making this a routine practice in your hospital. The costs are small, and the potential benefit to quality of care and patient satisfaction could be significant. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
A Work in Progress
Most hospitalist programs start when hospital administrators realize that having physicians dedicated exclusively to inpatient care is a great idea. Administrators then recruit a lead hospitalist—perhaps a stellar performer straight from residency, a community doctor closing his office, or a doctor located through a specialty staffing group.
Colorado Permanente Medical Group (CPMG), backed by a brand as powerful as Starbucks or Nordstrom, did things differently. So imbued with the Permanente culture are its physicians that its hospitalist group arose organically from physicians serving Denver’s Exempla St. Joseph Hospital and Boulder Community Hospital. (See “Kaiser Permanente Culture,” below.)
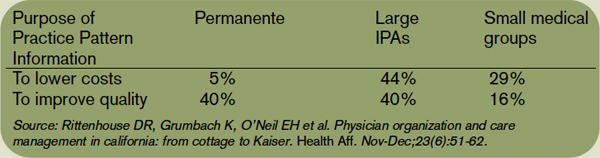
“Thirty years ago Permanente explored building their own versus finding a cost-effective hospital. They chose us, and their clinic doctors rounded on what grew to 70% of our department of medicine patients,” says Robert Gibbons, MD, St. Joseph’s residency program director. “Then they saw they needed to provide full-time inpatient coverage—the advent of the hospitalist program. Soon many CPMG clinic doctors disappeared, but the quality of medicine remained the same.”
Regional Department Chief Lauren Fraser, MD, oversees the now-mature hospitalist program, which keeps growing in size, complexity, and competence. “We’re always a work in progress, and that’s good,” she says.
According to Joe Heaton, MD, currently a Good Samaritan hospitalist and formerly CPMG regional department chief, CPMG’s primary care departments targeted three areas for better care early in 1995: streamlining patient scheduling, developing a centralized call center, and starting a hospitalist program.
The hospitalist program aimed for cost neutrality by limiting staffing at both hospitals to the same full-time equivalents (FTEs). To avoid forcing physicians into unwelcome assignments, the department offered its 70 internal medicine and 30 family practice doctors four tracks:
- Track A meant full-time hospital work;
- Track B offered a 50-50 hospital-clinic split;
- Track C provided for a 70% clinic, 30% hospital schedule; and
- Track D was full-time clinic work.
The family medicine department opted out of hospital duty, while the internists tracked themselves as follows: eight each for full-time hospital and half-time hospital duty, 34 for 30% hospital time, and 20 for full-time clinic. Fortunately, the tracks chosen matched the hospitals’ needs, and the program was off and running by July 1995.
“At the time, our group’s size created one of the largest hospitalist programs, allowing us to provide 24/7 coverage with at least two physicians on site,” says Dr. Heaton of the launch.
The hospitalist program had immediate measurable impact. Average length of stay dropped by 15%, and Track A and C physicians had similar utilization measures, suggesting that the model of care delivery was the key driver—rather than the amount of time physicians spent in the hospital. Dr. Gibbons was impressed with the hospitalist group’s results, noting that St. Joseph’s average reduced length of stay of 0.7 to one full day was consistent with national benchmarks. Because CPMG sees only Permanente patients, St. Joseph eventually contracted with two other hospitalist groups: the Exempla Faculty Inpatient Team, which covers half of its unassigned patients, and Midtown Inpatient Medicine, private internists who cover the other half of the unassigned patients, co-manage with orthopedic surgeons, and cover for internal medicine groups that no longer make hospital rounds.
CPMG hospitalists also covered Boulder Community Hospital in Denver’s rapidly expanding suburbs until 2005, when CPMG’s contract expired. All six hospitalists moved to nearby Exempla’s new Good Samaritan Hospital, where patient volume grew quickly from 25-30 patients a day to 80; 90% of the patients are Permanente members. Hospitalist staffing jumped to 13 FTEs (19 physicians). “We recruited very aggressively, including lots of locum tenens and moonlighters to cover the booming volume,” explains Brian Thom, MD, assistant regional department chief, Good Samaritan Hospital.
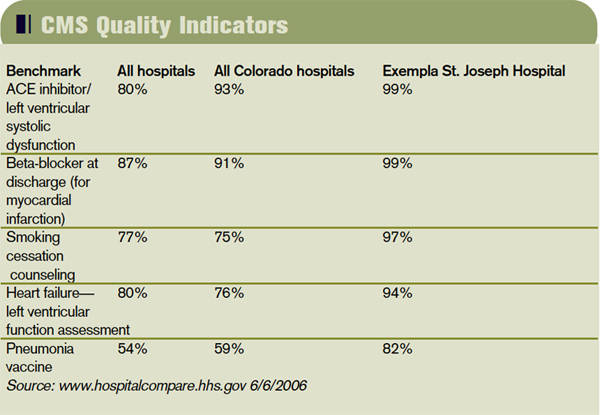
More Measures
In addition to length of stay, CPMG tracks the percentage of patients discharged in less than 24 hours, readmission rates, and disease-specific mortality by provider. All hospitalists get regular reports of department averages and statistical analyses of individual physicians. “This may be controversial, but we must look at outliers to see if [the problem is] case mix, such as many hospice patients, or something else,” says Dr. Heaton.
Striving for high levels of clinical expertise and consistency is a CPMG hallmark. Working for a medical behemoth in the Denver area, CPMG doctors—whether clinic-based or hospitalists—have a huge opportunity to integrate care and to co-manage many conditions with their colleagues. Hospitalists also staff the ICUs. In 2000, William Kinnard, MD, CPMG’s ICU co-director, commented that the group’s use of data-driven protocols allowed hospitalists to practice effectively in ICUs.
As for patient satisfaction, Dr. Heaton admits to “struggling for good measures,” noting that CPMG tackled it head-on in 1999 when Executive Medical Director Jack Cochran, MD, addressed the level of patient tenacity it took to navigate CPMG. Physician career satisfaction was sinking from long chaotic workdays that left both patients and doctors frustrated. By re-engineering scheduling and visit processes, Dr. Cochran made things run more smoothly. Other initiatives included an eight-hour physician-patient interaction course, video vignettes starring CPMG doctors illustrating communication techniques, and formal physician-to-physician coaching. Dr. Fraser still sends new hires to the course, recognizing that good communication satisfies both patients and physicians.
Scheduling: Every Program’s Mt. Everest
Because of the hospitalist program’s size and longevity, physicians have experimented extensively with scheduling. As do many groups, it started with seven 12-hour days on/seven days off blocks, which proved dissatisfying both personally and professionally.
“We experimented with scheduling to find what was sustainable for physicians and provided patient continuity,” says Dr. Fraser. “We’ve found that six eight-hour days in a row of rounding works best.”
Scheduling has evolved to the point that hospitalists provide the following to meet the hospitalist’s, the group’s, and the hospital’s needs: a dedicated triage physician 24/7 to handle calls from all sources of patient flow, two hospitalists on site at all times, eight-hour rounding days, and call physicians who admit and cross-cover after 4 p.m. Average daily census (ADC) is 10-12, plus one or two admissions. While that appears low, if CPMG hospitalists worked 12-hour shifts, their ADC would be 13-16, consistent with national norms.
“Dropping to eight-hour, as opposed to 12-hour, days keeps the job sustainable and helps doctors avoid burnout,” says Dr. Fraser. “However, we work more days per month, an average of 20-22.”
Overall, the scheduling strategy is working. “The majority of physicians who started over a decade ago remain, including many mid-life hospitalists in their 40s and 50s,” she adds. Physicians, rather than administrators, handle scheduling. Dr. Fraser has found that physicians can accept that third triage shift in a month (or an extra night shift when they’re short-handed) when another physician is filling the slots.
Other Features
All CPMG hospitalists can participate in St. Joseph’s residency program as “teaching attendings” for one month. From them, residents learn to co-manage care and participate in interdisciplinary rounds with nurses and social workers. Physicians note that residents make a hospitalist’s life smoother.
“At Good Sam, we do all our own procedures, unlike St. Joe’s, where they have residents. With our patient volumes, there’s little breathing room, especially when we have to cover non-Kaiser patients,” says Dr. Thom. Eventually, residents will rotate through Good Samaritan as well as St. Joseph.
One of the advantages of working in a brand-new hospital like Good Samaritan is establishing systems from scratch. That includes the new hospital’s electronic medical record (EMR), which is integrated with CPMG’s outpatient EMR. “We set up our own systems, complete with order sets and protocols,” explains Dr. Thom. “Considering that 90% of our patients are CPMG members, this gives us a high level of integration, clinically and electronically.”
Challenges Ahead
Despite CPMG’s size and stellar track record, challenges remain. Dr. Fraser identifies them as salaries that rank last within the group, making recruiting difficult; a hard time providing adequate back-up if a physician is unexpectedly absent; adjustments to fluctuations in patient census; time pressures of hospital committee work; and identification of an optimal scheduling model that fosters continuity of care yet provides a sustainable work life.
The group’s size has drawbacks, which Dr. Heaton identifies as the potential for a physician to not feel mission critical or to hide, and that communication and face-to-face meetings get complicated.
“Overall, the program can always use fine tuning, but we love who we work with and have the ultimate respect for our colleagues, which is the true benchmark of the quality of a medical career,” concludes Dr. Fraser. TH
Marlene Piturro regularly writes “Practice Profile.”
Most hospitalist programs start when hospital administrators realize that having physicians dedicated exclusively to inpatient care is a great idea. Administrators then recruit a lead hospitalist—perhaps a stellar performer straight from residency, a community doctor closing his office, or a doctor located through a specialty staffing group.
Colorado Permanente Medical Group (CPMG), backed by a brand as powerful as Starbucks or Nordstrom, did things differently. So imbued with the Permanente culture are its physicians that its hospitalist group arose organically from physicians serving Denver’s Exempla St. Joseph Hospital and Boulder Community Hospital. (See “Kaiser Permanente Culture,” below.)
“Thirty years ago Permanente explored building their own versus finding a cost-effective hospital. They chose us, and their clinic doctors rounded on what grew to 70% of our department of medicine patients,” says Robert Gibbons, MD, St. Joseph’s residency program director. “Then they saw they needed to provide full-time inpatient coverage—the advent of the hospitalist program. Soon many CPMG clinic doctors disappeared, but the quality of medicine remained the same.”
Regional Department Chief Lauren Fraser, MD, oversees the now-mature hospitalist program, which keeps growing in size, complexity, and competence. “We’re always a work in progress, and that’s good,” she says.
According to Joe Heaton, MD, currently a Good Samaritan hospitalist and formerly CPMG regional department chief, CPMG’s primary care departments targeted three areas for better care early in 1995: streamlining patient scheduling, developing a centralized call center, and starting a hospitalist program.
The hospitalist program aimed for cost neutrality by limiting staffing at both hospitals to the same full-time equivalents (FTEs). To avoid forcing physicians into unwelcome assignments, the department offered its 70 internal medicine and 30 family practice doctors four tracks:
- Track A meant full-time hospital work;
- Track B offered a 50-50 hospital-clinic split;
- Track C provided for a 70% clinic, 30% hospital schedule; and
- Track D was full-time clinic work.
The family medicine department opted out of hospital duty, while the internists tracked themselves as follows: eight each for full-time hospital and half-time hospital duty, 34 for 30% hospital time, and 20 for full-time clinic. Fortunately, the tracks chosen matched the hospitals’ needs, and the program was off and running by July 1995.
“At the time, our group’s size created one of the largest hospitalist programs, allowing us to provide 24/7 coverage with at least two physicians on site,” says Dr. Heaton of the launch.
The hospitalist program had immediate measurable impact. Average length of stay dropped by 15%, and Track A and C physicians had similar utilization measures, suggesting that the model of care delivery was the key driver—rather than the amount of time physicians spent in the hospital. Dr. Gibbons was impressed with the hospitalist group’s results, noting that St. Joseph’s average reduced length of stay of 0.7 to one full day was consistent with national benchmarks. Because CPMG sees only Permanente patients, St. Joseph eventually contracted with two other hospitalist groups: the Exempla Faculty Inpatient Team, which covers half of its unassigned patients, and Midtown Inpatient Medicine, private internists who cover the other half of the unassigned patients, co-manage with orthopedic surgeons, and cover for internal medicine groups that no longer make hospital rounds.
CPMG hospitalists also covered Boulder Community Hospital in Denver’s rapidly expanding suburbs until 2005, when CPMG’s contract expired. All six hospitalists moved to nearby Exempla’s new Good Samaritan Hospital, where patient volume grew quickly from 25-30 patients a day to 80; 90% of the patients are Permanente members. Hospitalist staffing jumped to 13 FTEs (19 physicians). “We recruited very aggressively, including lots of locum tenens and moonlighters to cover the booming volume,” explains Brian Thom, MD, assistant regional department chief, Good Samaritan Hospital.
More Measures
In addition to length of stay, CPMG tracks the percentage of patients discharged in less than 24 hours, readmission rates, and disease-specific mortality by provider. All hospitalists get regular reports of department averages and statistical analyses of individual physicians. “This may be controversial, but we must look at outliers to see if [the problem is] case mix, such as many hospice patients, or something else,” says Dr. Heaton.
Striving for high levels of clinical expertise and consistency is a CPMG hallmark. Working for a medical behemoth in the Denver area, CPMG doctors—whether clinic-based or hospitalists—have a huge opportunity to integrate care and to co-manage many conditions with their colleagues. Hospitalists also staff the ICUs. In 2000, William Kinnard, MD, CPMG’s ICU co-director, commented that the group’s use of data-driven protocols allowed hospitalists to practice effectively in ICUs.
As for patient satisfaction, Dr. Heaton admits to “struggling for good measures,” noting that CPMG tackled it head-on in 1999 when Executive Medical Director Jack Cochran, MD, addressed the level of patient tenacity it took to navigate CPMG. Physician career satisfaction was sinking from long chaotic workdays that left both patients and doctors frustrated. By re-engineering scheduling and visit processes, Dr. Cochran made things run more smoothly. Other initiatives included an eight-hour physician-patient interaction course, video vignettes starring CPMG doctors illustrating communication techniques, and formal physician-to-physician coaching. Dr. Fraser still sends new hires to the course, recognizing that good communication satisfies both patients and physicians.
Scheduling: Every Program’s Mt. Everest
Because of the hospitalist program’s size and longevity, physicians have experimented extensively with scheduling. As do many groups, it started with seven 12-hour days on/seven days off blocks, which proved dissatisfying both personally and professionally.
“We experimented with scheduling to find what was sustainable for physicians and provided patient continuity,” says Dr. Fraser. “We’ve found that six eight-hour days in a row of rounding works best.”
Scheduling has evolved to the point that hospitalists provide the following to meet the hospitalist’s, the group’s, and the hospital’s needs: a dedicated triage physician 24/7 to handle calls from all sources of patient flow, two hospitalists on site at all times, eight-hour rounding days, and call physicians who admit and cross-cover after 4 p.m. Average daily census (ADC) is 10-12, plus one or two admissions. While that appears low, if CPMG hospitalists worked 12-hour shifts, their ADC would be 13-16, consistent with national norms.
“Dropping to eight-hour, as opposed to 12-hour, days keeps the job sustainable and helps doctors avoid burnout,” says Dr. Fraser. “However, we work more days per month, an average of 20-22.”
Overall, the scheduling strategy is working. “The majority of physicians who started over a decade ago remain, including many mid-life hospitalists in their 40s and 50s,” she adds. Physicians, rather than administrators, handle scheduling. Dr. Fraser has found that physicians can accept that third triage shift in a month (or an extra night shift when they’re short-handed) when another physician is filling the slots.
Other Features
All CPMG hospitalists can participate in St. Joseph’s residency program as “teaching attendings” for one month. From them, residents learn to co-manage care and participate in interdisciplinary rounds with nurses and social workers. Physicians note that residents make a hospitalist’s life smoother.
“At Good Sam, we do all our own procedures, unlike St. Joe’s, where they have residents. With our patient volumes, there’s little breathing room, especially when we have to cover non-Kaiser patients,” says Dr. Thom. Eventually, residents will rotate through Good Samaritan as well as St. Joseph.
One of the advantages of working in a brand-new hospital like Good Samaritan is establishing systems from scratch. That includes the new hospital’s electronic medical record (EMR), which is integrated with CPMG’s outpatient EMR. “We set up our own systems, complete with order sets and protocols,” explains Dr. Thom. “Considering that 90% of our patients are CPMG members, this gives us a high level of integration, clinically and electronically.”
Challenges Ahead
Despite CPMG’s size and stellar track record, challenges remain. Dr. Fraser identifies them as salaries that rank last within the group, making recruiting difficult; a hard time providing adequate back-up if a physician is unexpectedly absent; adjustments to fluctuations in patient census; time pressures of hospital committee work; and identification of an optimal scheduling model that fosters continuity of care yet provides a sustainable work life.
The group’s size has drawbacks, which Dr. Heaton identifies as the potential for a physician to not feel mission critical or to hide, and that communication and face-to-face meetings get complicated.
“Overall, the program can always use fine tuning, but we love who we work with and have the ultimate respect for our colleagues, which is the true benchmark of the quality of a medical career,” concludes Dr. Fraser. TH
Marlene Piturro regularly writes “Practice Profile.”
Most hospitalist programs start when hospital administrators realize that having physicians dedicated exclusively to inpatient care is a great idea. Administrators then recruit a lead hospitalist—perhaps a stellar performer straight from residency, a community doctor closing his office, or a doctor located through a specialty staffing group.
Colorado Permanente Medical Group (CPMG), backed by a brand as powerful as Starbucks or Nordstrom, did things differently. So imbued with the Permanente culture are its physicians that its hospitalist group arose organically from physicians serving Denver’s Exempla St. Joseph Hospital and Boulder Community Hospital. (See “Kaiser Permanente Culture,” below.)
“Thirty years ago Permanente explored building their own versus finding a cost-effective hospital. They chose us, and their clinic doctors rounded on what grew to 70% of our department of medicine patients,” says Robert Gibbons, MD, St. Joseph’s residency program director. “Then they saw they needed to provide full-time inpatient coverage—the advent of the hospitalist program. Soon many CPMG clinic doctors disappeared, but the quality of medicine remained the same.”
Regional Department Chief Lauren Fraser, MD, oversees the now-mature hospitalist program, which keeps growing in size, complexity, and competence. “We’re always a work in progress, and that’s good,” she says.
According to Joe Heaton, MD, currently a Good Samaritan hospitalist and formerly CPMG regional department chief, CPMG’s primary care departments targeted three areas for better care early in 1995: streamlining patient scheduling, developing a centralized call center, and starting a hospitalist program.
The hospitalist program aimed for cost neutrality by limiting staffing at both hospitals to the same full-time equivalents (FTEs). To avoid forcing physicians into unwelcome assignments, the department offered its 70 internal medicine and 30 family practice doctors four tracks:
- Track A meant full-time hospital work;
- Track B offered a 50-50 hospital-clinic split;
- Track C provided for a 70% clinic, 30% hospital schedule; and
- Track D was full-time clinic work.
The family medicine department opted out of hospital duty, while the internists tracked themselves as follows: eight each for full-time hospital and half-time hospital duty, 34 for 30% hospital time, and 20 for full-time clinic. Fortunately, the tracks chosen matched the hospitals’ needs, and the program was off and running by July 1995.
“At the time, our group’s size created one of the largest hospitalist programs, allowing us to provide 24/7 coverage with at least two physicians on site,” says Dr. Heaton of the launch.
The hospitalist program had immediate measurable impact. Average length of stay dropped by 15%, and Track A and C physicians had similar utilization measures, suggesting that the model of care delivery was the key driver—rather than the amount of time physicians spent in the hospital. Dr. Gibbons was impressed with the hospitalist group’s results, noting that St. Joseph’s average reduced length of stay of 0.7 to one full day was consistent with national benchmarks. Because CPMG sees only Permanente patients, St. Joseph eventually contracted with two other hospitalist groups: the Exempla Faculty Inpatient Team, which covers half of its unassigned patients, and Midtown Inpatient Medicine, private internists who cover the other half of the unassigned patients, co-manage with orthopedic surgeons, and cover for internal medicine groups that no longer make hospital rounds.
CPMG hospitalists also covered Boulder Community Hospital in Denver’s rapidly expanding suburbs until 2005, when CPMG’s contract expired. All six hospitalists moved to nearby Exempla’s new Good Samaritan Hospital, where patient volume grew quickly from 25-30 patients a day to 80; 90% of the patients are Permanente members. Hospitalist staffing jumped to 13 FTEs (19 physicians). “We recruited very aggressively, including lots of locum tenens and moonlighters to cover the booming volume,” explains Brian Thom, MD, assistant regional department chief, Good Samaritan Hospital.
More Measures
In addition to length of stay, CPMG tracks the percentage of patients discharged in less than 24 hours, readmission rates, and disease-specific mortality by provider. All hospitalists get regular reports of department averages and statistical analyses of individual physicians. “This may be controversial, but we must look at outliers to see if [the problem is] case mix, such as many hospice patients, or something else,” says Dr. Heaton.
Striving for high levels of clinical expertise and consistency is a CPMG hallmark. Working for a medical behemoth in the Denver area, CPMG doctors—whether clinic-based or hospitalists—have a huge opportunity to integrate care and to co-manage many conditions with their colleagues. Hospitalists also staff the ICUs. In 2000, William Kinnard, MD, CPMG’s ICU co-director, commented that the group’s use of data-driven protocols allowed hospitalists to practice effectively in ICUs.
As for patient satisfaction, Dr. Heaton admits to “struggling for good measures,” noting that CPMG tackled it head-on in 1999 when Executive Medical Director Jack Cochran, MD, addressed the level of patient tenacity it took to navigate CPMG. Physician career satisfaction was sinking from long chaotic workdays that left both patients and doctors frustrated. By re-engineering scheduling and visit processes, Dr. Cochran made things run more smoothly. Other initiatives included an eight-hour physician-patient interaction course, video vignettes starring CPMG doctors illustrating communication techniques, and formal physician-to-physician coaching. Dr. Fraser still sends new hires to the course, recognizing that good communication satisfies both patients and physicians.
Scheduling: Every Program’s Mt. Everest
Because of the hospitalist program’s size and longevity, physicians have experimented extensively with scheduling. As do many groups, it started with seven 12-hour days on/seven days off blocks, which proved dissatisfying both personally and professionally.
“We experimented with scheduling to find what was sustainable for physicians and provided patient continuity,” says Dr. Fraser. “We’ve found that six eight-hour days in a row of rounding works best.”
Scheduling has evolved to the point that hospitalists provide the following to meet the hospitalist’s, the group’s, and the hospital’s needs: a dedicated triage physician 24/7 to handle calls from all sources of patient flow, two hospitalists on site at all times, eight-hour rounding days, and call physicians who admit and cross-cover after 4 p.m. Average daily census (ADC) is 10-12, plus one or two admissions. While that appears low, if CPMG hospitalists worked 12-hour shifts, their ADC would be 13-16, consistent with national norms.
“Dropping to eight-hour, as opposed to 12-hour, days keeps the job sustainable and helps doctors avoid burnout,” says Dr. Fraser. “However, we work more days per month, an average of 20-22.”
Overall, the scheduling strategy is working. “The majority of physicians who started over a decade ago remain, including many mid-life hospitalists in their 40s and 50s,” she adds. Physicians, rather than administrators, handle scheduling. Dr. Fraser has found that physicians can accept that third triage shift in a month (or an extra night shift when they’re short-handed) when another physician is filling the slots.
Other Features
All CPMG hospitalists can participate in St. Joseph’s residency program as “teaching attendings” for one month. From them, residents learn to co-manage care and participate in interdisciplinary rounds with nurses and social workers. Physicians note that residents make a hospitalist’s life smoother.
“At Good Sam, we do all our own procedures, unlike St. Joe’s, where they have residents. With our patient volumes, there’s little breathing room, especially when we have to cover non-Kaiser patients,” says Dr. Thom. Eventually, residents will rotate through Good Samaritan as well as St. Joseph.
One of the advantages of working in a brand-new hospital like Good Samaritan is establishing systems from scratch. That includes the new hospital’s electronic medical record (EMR), which is integrated with CPMG’s outpatient EMR. “We set up our own systems, complete with order sets and protocols,” explains Dr. Thom. “Considering that 90% of our patients are CPMG members, this gives us a high level of integration, clinically and electronically.”
Challenges Ahead
Despite CPMG’s size and stellar track record, challenges remain. Dr. Fraser identifies them as salaries that rank last within the group, making recruiting difficult; a hard time providing adequate back-up if a physician is unexpectedly absent; adjustments to fluctuations in patient census; time pressures of hospital committee work; and identification of an optimal scheduling model that fosters continuity of care yet provides a sustainable work life.
The group’s size has drawbacks, which Dr. Heaton identifies as the potential for a physician to not feel mission critical or to hide, and that communication and face-to-face meetings get complicated.
“Overall, the program can always use fine tuning, but we love who we work with and have the ultimate respect for our colleagues, which is the true benchmark of the quality of a medical career,” concludes Dr. Fraser. TH
Marlene Piturro regularly writes “Practice Profile.”
Sentinel Events
In July, a teenage mother-to-be entered a Madison, Wis., hospital to give birth. Within hours she was dead, though her baby survived.
An investigation by the Wisconsin State Department of Health revealed that the young woman had died after receiving an intravenous dose of an epidural anesthetic instead of the penicillin she was supposed to be given. Shortly after receiving the injection, the teenager had a seizure. She died less than two hours later.
In explaining what had happened, a nurse told investigators that the patient had been nervous about how she was to be anesthetized during the birth. To ease her concerns, the nurse brought out the epidural bag and told her how it worked. Unfortunately, it was one bag too many; the nurse later confused the epidural bag with the penicillin bag. The consequences were fatal.
The Human Toll
Such sentinel events are all too common. According to a just-released report, Preventing Medication Errors, prepared by the Institute of Medicine (IOM) at the behest of the Centers for Medicare and Medicaid Services, medication errors harm 1.5 million people yearly in the U.S. and kill thousands. The annual cost: at least $3.5 billion. But medication mistakes are just part of the picture.
Sentinel events—unexpected occurrences that result in death or serious physical or psychological injury, or the risk of their later occurrence—can happen anywhere along the healthcare continuum, in any setting. Statistics from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), however, show that 68% occur in general hospitals and another 11% in psychiatric hospitals. JCAHO tracked the sentinel events they reviewed from 1995 to March of 2006 and found that the most commonly reported sentinel events were patient suicide, wrong-site surgery, operative/postoperative complications, medication errors, and delay in treatment—in that order. Of the total number of cases reviewed, 73% resulted in the death of the patient and 10% in loss of function.
Hard-and-fast statistics on sentinel events are difficult to come by, however. Information from the JCAHO covers only the incidents reviewed by that organization, and experts agree that almost all types of sentinel events are under-reported. Researchers cite a number of reasons that many incidents go unreported; among them are lack of time, fear of punishment, and confusion about the severity of events that require notification. For example, do near misses count? (See “Near Misses,” The Hospitalist, May, p. 34.) Others see no benefit to themselves or their institutions from reporting.
Studies have attempted to define the true incidence of sentinel events, but a lack of consistent language and definitions makes it difficult to put the whole puzzle together, even when sentinel events do come to the surface.
Focus on Medication Errors
That said, we know that the incidence of sentinel events is much higher than it should be. As regularly reported by The Hospitalist, the problem most in the spotlight today—among researchers and the popular press—is medication errors. The IOM report says that, on average, a hospitalized patient is subject to at least one medication error per day, though error rates vary widely among hospitals. Fortunately, most errors cause no serious harm, but the costs for those that do are substantial. One study found that each preventable adverse drug event (ADE) costs a hospital approximately $8,750.
At least a quarter of medication-related injuries are preventable, according to the report. The irony is that many error-prevention methods are available today: “do not use” abbreviation lists; medication reconciliation (used to compare a patient’s medication orders with all other medications the patient is taking in order to avoid omissions, duplications, dosing errors, or drug interactions); and computerized physician order entry systems, to name a few.
With so much emphasis on patient safety and the increasing availability of sophisticated reporting and record-keeping technology, why haven’t incidence rates for ADEs and other sentinel events dropped dramatically? The answer is not that hospital personnel are lazy, incompetent, or indifferent to the safety of their patients. Experts agree that today’s doctors, nurses, pharmacists, and other medical staff are highly trained, dedicated professionals who want to practice the best medicine possible. The present system focuses on individual fault and does not foster disclosure that could lead to corrective procedures.
In fact, legal experts worry that JCAHO’s Sentinel Events Policy, which mandates self-reporting by hospitals accredited by the JCAHO, creates new problems. They suggest that self-reporting will have limited success in the absence of immunity from legal liability. One proposed solution calls for submitting self-regulatory reports to a neutral, nonsanctioning third-party entity. This approach has worked well for the airline industry.
New Patient-Care Focus
Abandoning a policy that concentrates on blame is at the heart of the improvements in patient safety proposed in the IOM report. Rather than pinpointing individual error, the new paradigm focuses on developing new systems of care that foster patient safety and help prevent sentinel events. In the absence of a finger-pointing environment, hospital personnel can freely examine what happened, discover the causes, and structure new procedures to prevent future occurrences – without fear of any retribution.
That’s the way they handle it at California Pacific Medical Center in San Francisco. In one case, when a nurse removed a dialysis catheter, the patient developed an air embolism and subsequently suffered a severe, permanently disabling stroke.
“When we investigated, we found that there was a written procedure in place to document a dialysis nurse’s credential,” says hospitalist Thomas E. Baudendistel, MD, FCAP, who is associate medical director of the hospital’s Internal Medicine Residency Program. “A, we weren’t aware of the credentialing procedure, and B, when we looked at it we weren’t sure it represented best practice. So we researched the literature and rewrote the policy. Now we schedule regular nursing education on pulling a dialysis catheter.”
In addition, the hospital set in place a follow-up plan to re-evaluate the procedure periodically. They also offer refresher training in catheter removal.
“We’ve used a similar approach in other situations,” says Dr. Baudendistel. “For example, our procedure with falls has changed. Now we use an event-based algorithm to determine whether a head CT scan is necessary.”
Hospitalists Can Lead
Hospital-based physicians are in an advantageous position to promote—as well as participate in—new initiatives for patient safety. Because they are involved in the day-to-day care of patients, hospitalists are firsthand observers when many errors occur. They have the experience and clinical judgment to give meaningful input to new incident-reporting protocols and to promote new policies through interdisciplinary teams that investigate and analyze adverse events.
Inevitably, electronic systems will replace paper-and-pen reporting and recordkeeping. Here hospitalists can take the lead, too. Unlike physicians who admit patients to multiple hospitals (each with a different information system), hospitalists practice in a single institution with only one system to learn. Hospitalists’ patient load may also help them to master new technology more quickly.
Surveys show that, while many hospitals have electronic ordering systems in place, relatively few physicians actually use them. In many cases, nurses or pharmacists place the electronic orders. Hospitalists who place their own orders can contribute to a reduction in medication errors by eliminating the pass-through of information that often causes misunderstandings.
Patient-Centric Healthcare: the New Paradigm
The traditional hospital system—and the healthcare system as a whole—are provider-oriented and provider-directed. Many patients, especially older ones, have a “doctor knows all” mindset, and they typically ask few questions—even when they don’t understand their treatment plans or exactly how they’re to take their medications when they go home. Case in point: A patient who was discharged from the hospital died at home shortly thereafter. The cause: His wife misunderstood the instructions for his pain medication and mistakenly applied six transdermal patches to his skin at one time instead of the single patch she should have applied. The multiple patches delivered a fatal overdose of the narcotic fentanyl.
Many experts believe that better informed—and empowered—patients are the key to reducing the number of sentinel events, including ADEs. The IOM report advocates a shift from a provider-centered to a patient-centered healthcare model. In this new paradigm, hospitalists would be much more expansive in their communications with patients. With regard to medications in particular, the report recommends that a physician:
- Review the patient’s medication list routinely and during care transitions.
- Review different treatment options.
- Review the names and purposes of all medications.
- Discuss when and how to take the medication.
- Discuss important and likely side effects and what to do about them.
- Discuss drug-drug, drug-food, and drug-disease interactions.
- Review the patient’s (or surrogate’s) role in appropriate medication use.
- Review the role of medications in the overall context of the patient’s health.
There are barriers to surmount before patients can become full partners in their healthcare. One of the most obvious is that patients need to be much better informed, and—when they are incapable of making appropriate decisions—they need surrogates to stand in for them. Patients need access to trustworthy and understandable information both online and in printed materials.
The IOM report recommends a government-sponsored national drug-information hotline; medication leaflets that provide standardized language in a manner that is appropriate for various age, literacy, and visual acuity levels; and development of personal health records.
PeaceHealth in Washington state took up the challenge of developing personal health records in 2001. PeaceHealth’s Project Manager, Mary Minniti, invited patients to design the system for self-management and communication among care team members. Today, the Shared Care Plan Personal Health Record is a reality, and Marc Pierson, MD, who is PeaceHealth’s regional vice president of Clinical Information and Special Projects, says “early evidence suggests that this type of tool promotes personal responsibility and positively affects patients’ confidence and active participation in their care.”
The tool is available on CD from www.peacehealth.org for those who would like to adopt it for their use.
Final Thought
The bad news is that sentinel events still take a staggering human and economic toll. The good news is that momentum is building for an important change in the way healthcare is delivered. Better communication, new technologies, and, perhaps most importantly, true provider-patient partnerships hold the promise of making hospital healthcare much safer. Hospitalists play a key role in this new scenario. TH
Joen Kinnan is a freelance medical writer based in Chicago.
In July, a teenage mother-to-be entered a Madison, Wis., hospital to give birth. Within hours she was dead, though her baby survived.
An investigation by the Wisconsin State Department of Health revealed that the young woman had died after receiving an intravenous dose of an epidural anesthetic instead of the penicillin she was supposed to be given. Shortly after receiving the injection, the teenager had a seizure. She died less than two hours later.
In explaining what had happened, a nurse told investigators that the patient had been nervous about how she was to be anesthetized during the birth. To ease her concerns, the nurse brought out the epidural bag and told her how it worked. Unfortunately, it was one bag too many; the nurse later confused the epidural bag with the penicillin bag. The consequences were fatal.
The Human Toll
Such sentinel events are all too common. According to a just-released report, Preventing Medication Errors, prepared by the Institute of Medicine (IOM) at the behest of the Centers for Medicare and Medicaid Services, medication errors harm 1.5 million people yearly in the U.S. and kill thousands. The annual cost: at least $3.5 billion. But medication mistakes are just part of the picture.
Sentinel events—unexpected occurrences that result in death or serious physical or psychological injury, or the risk of their later occurrence—can happen anywhere along the healthcare continuum, in any setting. Statistics from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), however, show that 68% occur in general hospitals and another 11% in psychiatric hospitals. JCAHO tracked the sentinel events they reviewed from 1995 to March of 2006 and found that the most commonly reported sentinel events were patient suicide, wrong-site surgery, operative/postoperative complications, medication errors, and delay in treatment—in that order. Of the total number of cases reviewed, 73% resulted in the death of the patient and 10% in loss of function.
Hard-and-fast statistics on sentinel events are difficult to come by, however. Information from the JCAHO covers only the incidents reviewed by that organization, and experts agree that almost all types of sentinel events are under-reported. Researchers cite a number of reasons that many incidents go unreported; among them are lack of time, fear of punishment, and confusion about the severity of events that require notification. For example, do near misses count? (See “Near Misses,” The Hospitalist, May, p. 34.) Others see no benefit to themselves or their institutions from reporting.
Studies have attempted to define the true incidence of sentinel events, but a lack of consistent language and definitions makes it difficult to put the whole puzzle together, even when sentinel events do come to the surface.
Focus on Medication Errors
That said, we know that the incidence of sentinel events is much higher than it should be. As regularly reported by The Hospitalist, the problem most in the spotlight today—among researchers and the popular press—is medication errors. The IOM report says that, on average, a hospitalized patient is subject to at least one medication error per day, though error rates vary widely among hospitals. Fortunately, most errors cause no serious harm, but the costs for those that do are substantial. One study found that each preventable adverse drug event (ADE) costs a hospital approximately $8,750.
At least a quarter of medication-related injuries are preventable, according to the report. The irony is that many error-prevention methods are available today: “do not use” abbreviation lists; medication reconciliation (used to compare a patient’s medication orders with all other medications the patient is taking in order to avoid omissions, duplications, dosing errors, or drug interactions); and computerized physician order entry systems, to name a few.
With so much emphasis on patient safety and the increasing availability of sophisticated reporting and record-keeping technology, why haven’t incidence rates for ADEs and other sentinel events dropped dramatically? The answer is not that hospital personnel are lazy, incompetent, or indifferent to the safety of their patients. Experts agree that today’s doctors, nurses, pharmacists, and other medical staff are highly trained, dedicated professionals who want to practice the best medicine possible. The present system focuses on individual fault and does not foster disclosure that could lead to corrective procedures.
In fact, legal experts worry that JCAHO’s Sentinel Events Policy, which mandates self-reporting by hospitals accredited by the JCAHO, creates new problems. They suggest that self-reporting will have limited success in the absence of immunity from legal liability. One proposed solution calls for submitting self-regulatory reports to a neutral, nonsanctioning third-party entity. This approach has worked well for the airline industry.
New Patient-Care Focus
Abandoning a policy that concentrates on blame is at the heart of the improvements in patient safety proposed in the IOM report. Rather than pinpointing individual error, the new paradigm focuses on developing new systems of care that foster patient safety and help prevent sentinel events. In the absence of a finger-pointing environment, hospital personnel can freely examine what happened, discover the causes, and structure new procedures to prevent future occurrences – without fear of any retribution.
That’s the way they handle it at California Pacific Medical Center in San Francisco. In one case, when a nurse removed a dialysis catheter, the patient developed an air embolism and subsequently suffered a severe, permanently disabling stroke.
“When we investigated, we found that there was a written procedure in place to document a dialysis nurse’s credential,” says hospitalist Thomas E. Baudendistel, MD, FCAP, who is associate medical director of the hospital’s Internal Medicine Residency Program. “A, we weren’t aware of the credentialing procedure, and B, when we looked at it we weren’t sure it represented best practice. So we researched the literature and rewrote the policy. Now we schedule regular nursing education on pulling a dialysis catheter.”
In addition, the hospital set in place a follow-up plan to re-evaluate the procedure periodically. They also offer refresher training in catheter removal.
“We’ve used a similar approach in other situations,” says Dr. Baudendistel. “For example, our procedure with falls has changed. Now we use an event-based algorithm to determine whether a head CT scan is necessary.”
Hospitalists Can Lead
Hospital-based physicians are in an advantageous position to promote—as well as participate in—new initiatives for patient safety. Because they are involved in the day-to-day care of patients, hospitalists are firsthand observers when many errors occur. They have the experience and clinical judgment to give meaningful input to new incident-reporting protocols and to promote new policies through interdisciplinary teams that investigate and analyze adverse events.
Inevitably, electronic systems will replace paper-and-pen reporting and recordkeeping. Here hospitalists can take the lead, too. Unlike physicians who admit patients to multiple hospitals (each with a different information system), hospitalists practice in a single institution with only one system to learn. Hospitalists’ patient load may also help them to master new technology more quickly.
Surveys show that, while many hospitals have electronic ordering systems in place, relatively few physicians actually use them. In many cases, nurses or pharmacists place the electronic orders. Hospitalists who place their own orders can contribute to a reduction in medication errors by eliminating the pass-through of information that often causes misunderstandings.
Patient-Centric Healthcare: the New Paradigm
The traditional hospital system—and the healthcare system as a whole—are provider-oriented and provider-directed. Many patients, especially older ones, have a “doctor knows all” mindset, and they typically ask few questions—even when they don’t understand their treatment plans or exactly how they’re to take their medications when they go home. Case in point: A patient who was discharged from the hospital died at home shortly thereafter. The cause: His wife misunderstood the instructions for his pain medication and mistakenly applied six transdermal patches to his skin at one time instead of the single patch she should have applied. The multiple patches delivered a fatal overdose of the narcotic fentanyl.
Many experts believe that better informed—and empowered—patients are the key to reducing the number of sentinel events, including ADEs. The IOM report advocates a shift from a provider-centered to a patient-centered healthcare model. In this new paradigm, hospitalists would be much more expansive in their communications with patients. With regard to medications in particular, the report recommends that a physician:
- Review the patient’s medication list routinely and during care transitions.
- Review different treatment options.
- Review the names and purposes of all medications.
- Discuss when and how to take the medication.
- Discuss important and likely side effects and what to do about them.
- Discuss drug-drug, drug-food, and drug-disease interactions.
- Review the patient’s (or surrogate’s) role in appropriate medication use.
- Review the role of medications in the overall context of the patient’s health.
There are barriers to surmount before patients can become full partners in their healthcare. One of the most obvious is that patients need to be much better informed, and—when they are incapable of making appropriate decisions—they need surrogates to stand in for them. Patients need access to trustworthy and understandable information both online and in printed materials.
The IOM report recommends a government-sponsored national drug-information hotline; medication leaflets that provide standardized language in a manner that is appropriate for various age, literacy, and visual acuity levels; and development of personal health records.
PeaceHealth in Washington state took up the challenge of developing personal health records in 2001. PeaceHealth’s Project Manager, Mary Minniti, invited patients to design the system for self-management and communication among care team members. Today, the Shared Care Plan Personal Health Record is a reality, and Marc Pierson, MD, who is PeaceHealth’s regional vice president of Clinical Information and Special Projects, says “early evidence suggests that this type of tool promotes personal responsibility and positively affects patients’ confidence and active participation in their care.”
The tool is available on CD from www.peacehealth.org for those who would like to adopt it for their use.
Final Thought
The bad news is that sentinel events still take a staggering human and economic toll. The good news is that momentum is building for an important change in the way healthcare is delivered. Better communication, new technologies, and, perhaps most importantly, true provider-patient partnerships hold the promise of making hospital healthcare much safer. Hospitalists play a key role in this new scenario. TH
Joen Kinnan is a freelance medical writer based in Chicago.
In July, a teenage mother-to-be entered a Madison, Wis., hospital to give birth. Within hours she was dead, though her baby survived.
An investigation by the Wisconsin State Department of Health revealed that the young woman had died after receiving an intravenous dose of an epidural anesthetic instead of the penicillin she was supposed to be given. Shortly after receiving the injection, the teenager had a seizure. She died less than two hours later.
In explaining what had happened, a nurse told investigators that the patient had been nervous about how she was to be anesthetized during the birth. To ease her concerns, the nurse brought out the epidural bag and told her how it worked. Unfortunately, it was one bag too many; the nurse later confused the epidural bag with the penicillin bag. The consequences were fatal.
The Human Toll
Such sentinel events are all too common. According to a just-released report, Preventing Medication Errors, prepared by the Institute of Medicine (IOM) at the behest of the Centers for Medicare and Medicaid Services, medication errors harm 1.5 million people yearly in the U.S. and kill thousands. The annual cost: at least $3.5 billion. But medication mistakes are just part of the picture.
Sentinel events—unexpected occurrences that result in death or serious physical or psychological injury, or the risk of their later occurrence—can happen anywhere along the healthcare continuum, in any setting. Statistics from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), however, show that 68% occur in general hospitals and another 11% in psychiatric hospitals. JCAHO tracked the sentinel events they reviewed from 1995 to March of 2006 and found that the most commonly reported sentinel events were patient suicide, wrong-site surgery, operative/postoperative complications, medication errors, and delay in treatment—in that order. Of the total number of cases reviewed, 73% resulted in the death of the patient and 10% in loss of function.
Hard-and-fast statistics on sentinel events are difficult to come by, however. Information from the JCAHO covers only the incidents reviewed by that organization, and experts agree that almost all types of sentinel events are under-reported. Researchers cite a number of reasons that many incidents go unreported; among them are lack of time, fear of punishment, and confusion about the severity of events that require notification. For example, do near misses count? (See “Near Misses,” The Hospitalist, May, p. 34.) Others see no benefit to themselves or their institutions from reporting.
Studies have attempted to define the true incidence of sentinel events, but a lack of consistent language and definitions makes it difficult to put the whole puzzle together, even when sentinel events do come to the surface.
Focus on Medication Errors
That said, we know that the incidence of sentinel events is much higher than it should be. As regularly reported by The Hospitalist, the problem most in the spotlight today—among researchers and the popular press—is medication errors. The IOM report says that, on average, a hospitalized patient is subject to at least one medication error per day, though error rates vary widely among hospitals. Fortunately, most errors cause no serious harm, but the costs for those that do are substantial. One study found that each preventable adverse drug event (ADE) costs a hospital approximately $8,750.
At least a quarter of medication-related injuries are preventable, according to the report. The irony is that many error-prevention methods are available today: “do not use” abbreviation lists; medication reconciliation (used to compare a patient’s medication orders with all other medications the patient is taking in order to avoid omissions, duplications, dosing errors, or drug interactions); and computerized physician order entry systems, to name a few.
With so much emphasis on patient safety and the increasing availability of sophisticated reporting and record-keeping technology, why haven’t incidence rates for ADEs and other sentinel events dropped dramatically? The answer is not that hospital personnel are lazy, incompetent, or indifferent to the safety of their patients. Experts agree that today’s doctors, nurses, pharmacists, and other medical staff are highly trained, dedicated professionals who want to practice the best medicine possible. The present system focuses on individual fault and does not foster disclosure that could lead to corrective procedures.
In fact, legal experts worry that JCAHO’s Sentinel Events Policy, which mandates self-reporting by hospitals accredited by the JCAHO, creates new problems. They suggest that self-reporting will have limited success in the absence of immunity from legal liability. One proposed solution calls for submitting self-regulatory reports to a neutral, nonsanctioning third-party entity. This approach has worked well for the airline industry.
New Patient-Care Focus
Abandoning a policy that concentrates on blame is at the heart of the improvements in patient safety proposed in the IOM report. Rather than pinpointing individual error, the new paradigm focuses on developing new systems of care that foster patient safety and help prevent sentinel events. In the absence of a finger-pointing environment, hospital personnel can freely examine what happened, discover the causes, and structure new procedures to prevent future occurrences – without fear of any retribution.
That’s the way they handle it at California Pacific Medical Center in San Francisco. In one case, when a nurse removed a dialysis catheter, the patient developed an air embolism and subsequently suffered a severe, permanently disabling stroke.
“When we investigated, we found that there was a written procedure in place to document a dialysis nurse’s credential,” says hospitalist Thomas E. Baudendistel, MD, FCAP, who is associate medical director of the hospital’s Internal Medicine Residency Program. “A, we weren’t aware of the credentialing procedure, and B, when we looked at it we weren’t sure it represented best practice. So we researched the literature and rewrote the policy. Now we schedule regular nursing education on pulling a dialysis catheter.”
In addition, the hospital set in place a follow-up plan to re-evaluate the procedure periodically. They also offer refresher training in catheter removal.
“We’ve used a similar approach in other situations,” says Dr. Baudendistel. “For example, our procedure with falls has changed. Now we use an event-based algorithm to determine whether a head CT scan is necessary.”
Hospitalists Can Lead
Hospital-based physicians are in an advantageous position to promote—as well as participate in—new initiatives for patient safety. Because they are involved in the day-to-day care of patients, hospitalists are firsthand observers when many errors occur. They have the experience and clinical judgment to give meaningful input to new incident-reporting protocols and to promote new policies through interdisciplinary teams that investigate and analyze adverse events.
Inevitably, electronic systems will replace paper-and-pen reporting and recordkeeping. Here hospitalists can take the lead, too. Unlike physicians who admit patients to multiple hospitals (each with a different information system), hospitalists practice in a single institution with only one system to learn. Hospitalists’ patient load may also help them to master new technology more quickly.
Surveys show that, while many hospitals have electronic ordering systems in place, relatively few physicians actually use them. In many cases, nurses or pharmacists place the electronic orders. Hospitalists who place their own orders can contribute to a reduction in medication errors by eliminating the pass-through of information that often causes misunderstandings.
Patient-Centric Healthcare: the New Paradigm
The traditional hospital system—and the healthcare system as a whole—are provider-oriented and provider-directed. Many patients, especially older ones, have a “doctor knows all” mindset, and they typically ask few questions—even when they don’t understand their treatment plans or exactly how they’re to take their medications when they go home. Case in point: A patient who was discharged from the hospital died at home shortly thereafter. The cause: His wife misunderstood the instructions for his pain medication and mistakenly applied six transdermal patches to his skin at one time instead of the single patch she should have applied. The multiple patches delivered a fatal overdose of the narcotic fentanyl.
Many experts believe that better informed—and empowered—patients are the key to reducing the number of sentinel events, including ADEs. The IOM report advocates a shift from a provider-centered to a patient-centered healthcare model. In this new paradigm, hospitalists would be much more expansive in their communications with patients. With regard to medications in particular, the report recommends that a physician:
- Review the patient’s medication list routinely and during care transitions.
- Review different treatment options.
- Review the names and purposes of all medications.
- Discuss when and how to take the medication.
- Discuss important and likely side effects and what to do about them.
- Discuss drug-drug, drug-food, and drug-disease interactions.
- Review the patient’s (or surrogate’s) role in appropriate medication use.
- Review the role of medications in the overall context of the patient’s health.
There are barriers to surmount before patients can become full partners in their healthcare. One of the most obvious is that patients need to be much better informed, and—when they are incapable of making appropriate decisions—they need surrogates to stand in for them. Patients need access to trustworthy and understandable information both online and in printed materials.
The IOM report recommends a government-sponsored national drug-information hotline; medication leaflets that provide standardized language in a manner that is appropriate for various age, literacy, and visual acuity levels; and development of personal health records.
PeaceHealth in Washington state took up the challenge of developing personal health records in 2001. PeaceHealth’s Project Manager, Mary Minniti, invited patients to design the system for self-management and communication among care team members. Today, the Shared Care Plan Personal Health Record is a reality, and Marc Pierson, MD, who is PeaceHealth’s regional vice president of Clinical Information and Special Projects, says “early evidence suggests that this type of tool promotes personal responsibility and positively affects patients’ confidence and active participation in their care.”
The tool is available on CD from www.peacehealth.org for those who would like to adopt it for their use.
Final Thought
The bad news is that sentinel events still take a staggering human and economic toll. The good news is that momentum is building for an important change in the way healthcare is delivered. Better communication, new technologies, and, perhaps most importantly, true provider-patient partnerships hold the promise of making hospital healthcare much safer. Hospitalists play a key role in this new scenario. TH
Joen Kinnan is a freelance medical writer based in Chicago.
Crucial Contact
If the secret to successful real estate investing is “location, location, location,” the key to maintaining good relationships with referring physicians is “communication, communication, communication.” While this may seem simplistic, the complexities of interpersonal communications can pose challenges even in the most straightforward of physician interchanges.
Recent studies and hospitalists consulted for this report maintain that hospitalists’ communications with referring physicians must be examined, practiced, and fine-tuned continually to ensure satisfaction for doctors—and their patients.
“It’s all about the communication,” says Bruce Becker, MD, chief medical officer at Medical Center Hospital in Odessa, Texas, and a family physician and professor of medicine for more than 20 years. “It’s sometimes not what you say, but how you say it.”
According to John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospital medicine groups with Nelson/Flores Associates and a columnist for The Hospitalist (“Practice Management”), it is key for hospitalists to examine and revise oral and written communication processes—especially at critical points during patient handoffs—rather than to assume that good communication will just happen naturally.
Gaining Acceptance
Some primary care physicians (PCPs) are more willing than others to refer patients to a hospitalist. Initially, new programs may have to work hard to gain acceptance with referring physicians. Some referring physicians may not be ready to give up hospital visits and may want to maintain collegiality and control. On the other hand, some family physicians are “ready to step away from hospital practice,” says Dr. Becker, citing diminishing reimbursements due to diagnosis-related groups (DRGs) and managed care.
John A. Bolinger, DO, FACP, medical director of the Hospitalist Program at Terre Haute (Ind.) Regional Hospital, believes that one way to promote a hospitalist program to PCPs is to emphasize hospitalists’ levels of training and efficiency.
“I try to make them aware of how [our hospitalist program] can be advantageous to them,” he explains. “Even if they have only one patient in the hospital, by the time they drive there, get the chart, make the rounds, make their notes, and do the required paperwork, it may take them an hour to see one patient. It makes good economic sense for them to stay in their offices, where they can see a minimum of four patients in the same amount of time for equal or better reimbursements.”
When primary care physicians voice resistance to using a hospitalist program, Dr. Bolinger says he tries to impress upon them the fact that hospitalists do not have outside practices, they will “never try to steal patients,” they stay within referral patterns, and they will make sure that PCPs get pertinent records as soon as possible. Dr. Bolinger believes referring physicians’ biggest concern when dealing with hospitalists is that they “don’t want to lose control.” The way to address those fears is to make sure referring physicians are always kept in the communications loop regarding their patients’ progress.
The policy for Dr. Bolinger’s hospitalist program is to make sure all dictated reports are transcribed and faxed immediately to the referring physician’s office. All scheduled follow-up appointments and medication changes are included in discharge summaries. “If need be,” says Dr. Bolinger, “we will even hand deliver information to physicians’ offices, which we have done multiple times.”
Become User-Friendly
The methods Dr. Bolinger describes often result in referring physicians’ satisfaction with hospitalist services, followed by increased referrals. Hospitalists can ensure continued referrals from their PCPs if they remember hospital medicine’s cardinal rules of availability and prompt, thorough reporting, says Dr. Nelson. It can help to view the interface with the hospitalist service from the PCP’s point of view.
For instance, how can physicians quickly reach the hospitalist service? “If you’re a referring doctor and you’ve got a patient in your office whom you think should be admitted today, who do you call? This can actually be a little tricky for most practices,” says Dr. Nelson. “Every practice should give some thought to making that contact as easy for the referring doctors as possible.”
Some important questions to ask: When trying to reach a hospitalist, is it best to call the group’s main number? Will a voicemail message be returned within an hour? Two hours? Is it better to call the hospital operator and have the hospitalist paged? Or do PCPs have access to hospitalists’ cell phone numbers?
Dr. Nelson suggests that hospitalist groups also give thought to standardizing admission and discharge reports, as well as other forms. Often, individual members of a hospitalist group use slightly different formats for reporting to referring physicians. He points out that this can be less user friendly for the reader, who may have a harder time scanning the document quickly to find a particular piece of important information. Other useful suggestions for making reports user friendly: Use similar headings on all reports; avoid dense text; list pending tests in a prominent place in the report document; and consider highlighting or underlining key words.
Preference for In-Person Contact
For a new hospitalist practice, telephone communication between the hospitalist and the primary physician is valuable, and the hospitalist should “pick up the phone liberally,” says Dr. Nelson.
Dr. Becker believes the best way for physicians to communicate is one on one—in person. “Too often,” he says, “we get used to communicating through a third party—usually a unit clerk, a nurse, or a resident. I believe that physician-to-physician communication is the ideal. If the attending physician and the consultant [hospitalist or subspecialist] speak in person, they can explain their thinking to each other, and “within one minute of precious time, figure out which way to go.”
In this way, without wasting time, the physician gives the consultant guidance as to the appropriate track to take and can also listen to the consultant’s suggestions.
“I feel that medicine has perhaps gotten a little bit away from that communication link,” continues Dr. Becker. “When we get further away from that direct communication—whether it is between doctors and consultants, nurses and doctors, or doctors and family members—you take that little bit of risk that there will be a missed step, either on the part of the communicator or on the receiving end as the listener.”
In a study exploring barriers to effective patient handoffs, Solet and colleagues focused on the communication between physicians as a vital link in patient care continuity. The authors concluded that, regardless of the method of managing patient handoffs (e.g., computer-assisted or paper-based), the best way to ensure effective handoffs of hospitalized patients was “precise, unambiguous, face-to-face communication.”1
In a 2001 study by Hruby, Pantilat, and colleagues at UCSF, the authors found that, for the most part, hospitalized patients with PCPs wanted contact with their primary physicians even while in the hospital. Approximately half of the surveyed patients also believed that the PCP, rather than an inpatient physician, should be the first to discuss with them serious diagnoses or disease management choices.2 Preferences such as those expressed in this study may play into referring physicians’ reluctance to make use of hospitalist services, says Dr. Bolinger. They may fear that patients will feel abandoned by the primary physician. Dr. Bolinger’s response to those sentiments: “Initially, some patients [in our hospital] were a little guarded and were not sure what to expect. But after a day or two of having us there, they are generally very, very pleased to have us on board. We are part of their medical team now.”
A Need for Marketing?
Dr. Becker has been actively developing a hospital medicine program at Medical Center Hospital for the past two years and joined SHM as part of that effort. Familiarizing himself with the tenets of hospital medicine, he discovered that, as a family doctor, “unknowingly, I was actually practicing hospital medicine for 20 years!”
As part of the hospital medicine program development process, he has solicited input from local physicians as well as patients. A simple survey to assess interest in a hospitalist program asked potential referring physicians, Would you use a hospitalist? Would you use a hospitalist after waiting a while to see how the process goes? Or, would you not consider using a hospitalist?
In two years, says Dr. Becker, response from the referring physician community has changed from “bah, humbug” to one of readiness for the program.
A mass mailing can serve to introduce a hospital medicine program in a community. Dr. Bolinger’s group used this method and, in his experience, local subspecialists—orthopedists, cardiologists, endocrinologists, pulmonologists—have proved the biggest source of referrals to their program. But PCPs are starting to use the hospitalist service for vacations and call-coverage issues and are beginning to value hospitalists’ services. “Physicians like coming to the hospital, but they’re starting to realize that the hospitalist program is a better system,” says Dr. Bolinger.
Dr. Nelson has been a hospitalist for 18 years. For most of that time he has had no shortage of referred patients. In fact, the bigger problem has been finding enough doctors to join the group and handle the existing referral volume. In that situation, it has not made sense to undertake marketing with the goal of increasing referrals. However, he advises, “It is always worth spending time and energy trying to maintain good relationships with physicians with whom you regularly share patients, and perhaps this could be called ‘marketing.’”
To maintain good relationships with referring physicians, his group conducts a survey on a yearly basis. A survey, he suggests, should be very short, consisting of only a few key questions, such as:
- Do we send reports promptly to your practice?
- Are your patients satisfied with the care they receive from us?
- Do you have any comments or feedback for our group?
Although his group gains information from these surveys, Dr. Nelson notes that the greater value of conducting such surveys may be in building public relations capital. By conducting a survey, hospitalists demonstrate that they care enough to ask for their referring physicians’ input.
Another good marketing tool is a patient education brochure, given to referring physicians, that explains hospitalists and hospitalist care. These brochures can help referring physicians prepare their patients for seeing a hospitalist in the inpatient setting, thus easing the initial reluctance patients sometimes experience when encountering a new physician.
Conclusion
On the cusp of launching his medical center’s hospital medicine program, Dr. Becker sees that good communication between referring physicians and hospitalists will ensure the program’s success. He advises physicians to remember their classes in communication as third-year medical students, when most participate in videotaped patient encounters. It’s always instructive, he says, to see how we come across to others in conversation.
Both verbal and nonverbal cues play a part in good communication. A 2003 study by Griffith and colleagues concluded that better nonverbal communication skills are associated with greater patient satisfaction, and that formal instruction in nonverbal communication can be a good addition to residency training.3
“I find that doctors talk to each other, in general, very easily,” says Dr. Becker. Sometimes [good communication] is just a matter of opening that door and essentially keeping the former attending, the PCP, apprised of what is going on.”
When hospitalists attend to thorough communication and promptly deliver complete discharge summaries, family physicians can report to their patients that they know what happened in the hospital and poll their patients about their experiences in the hospital. In this way, hospitalists and referring physicians can cement their relationship as team members for the patient. The success of any hospitalist program, Dr. Becker believes, lies in “making sure you fulfill the promise of what hospital medicine generates, and that is a continuity of care … , obtaining front-end communication so that patients get the best care throughout their [hospital] stay, and then follow up with discharge summaries to the primary physician’s office.” TH
Gretchen Henkel is a regular contributor to The Hospitalist.
References
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12): 1094-1099.
- Hruby M, Pantilat SZ, Lo B. How do patients view the role of the primary care physician in inpatient care? Am J Med. 2001;21;111(9B):21S-25S.
- Griffith CH III, Wilson JF, Langer S, et al. House staff nonverbal communication skills and standardized patient satisfaction. J Gen Intern Med. 2003 Mar;18(3):170-174.
If the secret to successful real estate investing is “location, location, location,” the key to maintaining good relationships with referring physicians is “communication, communication, communication.” While this may seem simplistic, the complexities of interpersonal communications can pose challenges even in the most straightforward of physician interchanges.
Recent studies and hospitalists consulted for this report maintain that hospitalists’ communications with referring physicians must be examined, practiced, and fine-tuned continually to ensure satisfaction for doctors—and their patients.
“It’s all about the communication,” says Bruce Becker, MD, chief medical officer at Medical Center Hospital in Odessa, Texas, and a family physician and professor of medicine for more than 20 years. “It’s sometimes not what you say, but how you say it.”
According to John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospital medicine groups with Nelson/Flores Associates and a columnist for The Hospitalist (“Practice Management”), it is key for hospitalists to examine and revise oral and written communication processes—especially at critical points during patient handoffs—rather than to assume that good communication will just happen naturally.
Gaining Acceptance
Some primary care physicians (PCPs) are more willing than others to refer patients to a hospitalist. Initially, new programs may have to work hard to gain acceptance with referring physicians. Some referring physicians may not be ready to give up hospital visits and may want to maintain collegiality and control. On the other hand, some family physicians are “ready to step away from hospital practice,” says Dr. Becker, citing diminishing reimbursements due to diagnosis-related groups (DRGs) and managed care.
John A. Bolinger, DO, FACP, medical director of the Hospitalist Program at Terre Haute (Ind.) Regional Hospital, believes that one way to promote a hospitalist program to PCPs is to emphasize hospitalists’ levels of training and efficiency.
“I try to make them aware of how [our hospitalist program] can be advantageous to them,” he explains. “Even if they have only one patient in the hospital, by the time they drive there, get the chart, make the rounds, make their notes, and do the required paperwork, it may take them an hour to see one patient. It makes good economic sense for them to stay in their offices, where they can see a minimum of four patients in the same amount of time for equal or better reimbursements.”
When primary care physicians voice resistance to using a hospitalist program, Dr. Bolinger says he tries to impress upon them the fact that hospitalists do not have outside practices, they will “never try to steal patients,” they stay within referral patterns, and they will make sure that PCPs get pertinent records as soon as possible. Dr. Bolinger believes referring physicians’ biggest concern when dealing with hospitalists is that they “don’t want to lose control.” The way to address those fears is to make sure referring physicians are always kept in the communications loop regarding their patients’ progress.
The policy for Dr. Bolinger’s hospitalist program is to make sure all dictated reports are transcribed and faxed immediately to the referring physician’s office. All scheduled follow-up appointments and medication changes are included in discharge summaries. “If need be,” says Dr. Bolinger, “we will even hand deliver information to physicians’ offices, which we have done multiple times.”
Become User-Friendly
The methods Dr. Bolinger describes often result in referring physicians’ satisfaction with hospitalist services, followed by increased referrals. Hospitalists can ensure continued referrals from their PCPs if they remember hospital medicine’s cardinal rules of availability and prompt, thorough reporting, says Dr. Nelson. It can help to view the interface with the hospitalist service from the PCP’s point of view.
For instance, how can physicians quickly reach the hospitalist service? “If you’re a referring doctor and you’ve got a patient in your office whom you think should be admitted today, who do you call? This can actually be a little tricky for most practices,” says Dr. Nelson. “Every practice should give some thought to making that contact as easy for the referring doctors as possible.”
Some important questions to ask: When trying to reach a hospitalist, is it best to call the group’s main number? Will a voicemail message be returned within an hour? Two hours? Is it better to call the hospital operator and have the hospitalist paged? Or do PCPs have access to hospitalists’ cell phone numbers?
Dr. Nelson suggests that hospitalist groups also give thought to standardizing admission and discharge reports, as well as other forms. Often, individual members of a hospitalist group use slightly different formats for reporting to referring physicians. He points out that this can be less user friendly for the reader, who may have a harder time scanning the document quickly to find a particular piece of important information. Other useful suggestions for making reports user friendly: Use similar headings on all reports; avoid dense text; list pending tests in a prominent place in the report document; and consider highlighting or underlining key words.
Preference for In-Person Contact
For a new hospitalist practice, telephone communication between the hospitalist and the primary physician is valuable, and the hospitalist should “pick up the phone liberally,” says Dr. Nelson.
Dr. Becker believes the best way for physicians to communicate is one on one—in person. “Too often,” he says, “we get used to communicating through a third party—usually a unit clerk, a nurse, or a resident. I believe that physician-to-physician communication is the ideal. If the attending physician and the consultant [hospitalist or subspecialist] speak in person, they can explain their thinking to each other, and “within one minute of precious time, figure out which way to go.”
In this way, without wasting time, the physician gives the consultant guidance as to the appropriate track to take and can also listen to the consultant’s suggestions.
“I feel that medicine has perhaps gotten a little bit away from that communication link,” continues Dr. Becker. “When we get further away from that direct communication—whether it is between doctors and consultants, nurses and doctors, or doctors and family members—you take that little bit of risk that there will be a missed step, either on the part of the communicator or on the receiving end as the listener.”
In a study exploring barriers to effective patient handoffs, Solet and colleagues focused on the communication between physicians as a vital link in patient care continuity. The authors concluded that, regardless of the method of managing patient handoffs (e.g., computer-assisted or paper-based), the best way to ensure effective handoffs of hospitalized patients was “precise, unambiguous, face-to-face communication.”1
In a 2001 study by Hruby, Pantilat, and colleagues at UCSF, the authors found that, for the most part, hospitalized patients with PCPs wanted contact with their primary physicians even while in the hospital. Approximately half of the surveyed patients also believed that the PCP, rather than an inpatient physician, should be the first to discuss with them serious diagnoses or disease management choices.2 Preferences such as those expressed in this study may play into referring physicians’ reluctance to make use of hospitalist services, says Dr. Bolinger. They may fear that patients will feel abandoned by the primary physician. Dr. Bolinger’s response to those sentiments: “Initially, some patients [in our hospital] were a little guarded and were not sure what to expect. But after a day or two of having us there, they are generally very, very pleased to have us on board. We are part of their medical team now.”
A Need for Marketing?
Dr. Becker has been actively developing a hospital medicine program at Medical Center Hospital for the past two years and joined SHM as part of that effort. Familiarizing himself with the tenets of hospital medicine, he discovered that, as a family doctor, “unknowingly, I was actually practicing hospital medicine for 20 years!”
As part of the hospital medicine program development process, he has solicited input from local physicians as well as patients. A simple survey to assess interest in a hospitalist program asked potential referring physicians, Would you use a hospitalist? Would you use a hospitalist after waiting a while to see how the process goes? Or, would you not consider using a hospitalist?
In two years, says Dr. Becker, response from the referring physician community has changed from “bah, humbug” to one of readiness for the program.
A mass mailing can serve to introduce a hospital medicine program in a community. Dr. Bolinger’s group used this method and, in his experience, local subspecialists—orthopedists, cardiologists, endocrinologists, pulmonologists—have proved the biggest source of referrals to their program. But PCPs are starting to use the hospitalist service for vacations and call-coverage issues and are beginning to value hospitalists’ services. “Physicians like coming to the hospital, but they’re starting to realize that the hospitalist program is a better system,” says Dr. Bolinger.
Dr. Nelson has been a hospitalist for 18 years. For most of that time he has had no shortage of referred patients. In fact, the bigger problem has been finding enough doctors to join the group and handle the existing referral volume. In that situation, it has not made sense to undertake marketing with the goal of increasing referrals. However, he advises, “It is always worth spending time and energy trying to maintain good relationships with physicians with whom you regularly share patients, and perhaps this could be called ‘marketing.’”
To maintain good relationships with referring physicians, his group conducts a survey on a yearly basis. A survey, he suggests, should be very short, consisting of only a few key questions, such as:
- Do we send reports promptly to your practice?
- Are your patients satisfied with the care they receive from us?
- Do you have any comments or feedback for our group?
Although his group gains information from these surveys, Dr. Nelson notes that the greater value of conducting such surveys may be in building public relations capital. By conducting a survey, hospitalists demonstrate that they care enough to ask for their referring physicians’ input.
Another good marketing tool is a patient education brochure, given to referring physicians, that explains hospitalists and hospitalist care. These brochures can help referring physicians prepare their patients for seeing a hospitalist in the inpatient setting, thus easing the initial reluctance patients sometimes experience when encountering a new physician.
Conclusion
On the cusp of launching his medical center’s hospital medicine program, Dr. Becker sees that good communication between referring physicians and hospitalists will ensure the program’s success. He advises physicians to remember their classes in communication as third-year medical students, when most participate in videotaped patient encounters. It’s always instructive, he says, to see how we come across to others in conversation.
Both verbal and nonverbal cues play a part in good communication. A 2003 study by Griffith and colleagues concluded that better nonverbal communication skills are associated with greater patient satisfaction, and that formal instruction in nonverbal communication can be a good addition to residency training.3
“I find that doctors talk to each other, in general, very easily,” says Dr. Becker. Sometimes [good communication] is just a matter of opening that door and essentially keeping the former attending, the PCP, apprised of what is going on.”
When hospitalists attend to thorough communication and promptly deliver complete discharge summaries, family physicians can report to their patients that they know what happened in the hospital and poll their patients about their experiences in the hospital. In this way, hospitalists and referring physicians can cement their relationship as team members for the patient. The success of any hospitalist program, Dr. Becker believes, lies in “making sure you fulfill the promise of what hospital medicine generates, and that is a continuity of care … , obtaining front-end communication so that patients get the best care throughout their [hospital] stay, and then follow up with discharge summaries to the primary physician’s office.” TH
Gretchen Henkel is a regular contributor to The Hospitalist.
References
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12): 1094-1099.
- Hruby M, Pantilat SZ, Lo B. How do patients view the role of the primary care physician in inpatient care? Am J Med. 2001;21;111(9B):21S-25S.
- Griffith CH III, Wilson JF, Langer S, et al. House staff nonverbal communication skills and standardized patient satisfaction. J Gen Intern Med. 2003 Mar;18(3):170-174.
If the secret to successful real estate investing is “location, location, location,” the key to maintaining good relationships with referring physicians is “communication, communication, communication.” While this may seem simplistic, the complexities of interpersonal communications can pose challenges even in the most straightforward of physician interchanges.
Recent studies and hospitalists consulted for this report maintain that hospitalists’ communications with referring physicians must be examined, practiced, and fine-tuned continually to ensure satisfaction for doctors—and their patients.
“It’s all about the communication,” says Bruce Becker, MD, chief medical officer at Medical Center Hospital in Odessa, Texas, and a family physician and professor of medicine for more than 20 years. “It’s sometimes not what you say, but how you say it.”
According to John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospital medicine groups with Nelson/Flores Associates and a columnist for The Hospitalist (“Practice Management”), it is key for hospitalists to examine and revise oral and written communication processes—especially at critical points during patient handoffs—rather than to assume that good communication will just happen naturally.
Gaining Acceptance
Some primary care physicians (PCPs) are more willing than others to refer patients to a hospitalist. Initially, new programs may have to work hard to gain acceptance with referring physicians. Some referring physicians may not be ready to give up hospital visits and may want to maintain collegiality and control. On the other hand, some family physicians are “ready to step away from hospital practice,” says Dr. Becker, citing diminishing reimbursements due to diagnosis-related groups (DRGs) and managed care.
John A. Bolinger, DO, FACP, medical director of the Hospitalist Program at Terre Haute (Ind.) Regional Hospital, believes that one way to promote a hospitalist program to PCPs is to emphasize hospitalists’ levels of training and efficiency.
“I try to make them aware of how [our hospitalist program] can be advantageous to them,” he explains. “Even if they have only one patient in the hospital, by the time they drive there, get the chart, make the rounds, make their notes, and do the required paperwork, it may take them an hour to see one patient. It makes good economic sense for them to stay in their offices, where they can see a minimum of four patients in the same amount of time for equal or better reimbursements.”
When primary care physicians voice resistance to using a hospitalist program, Dr. Bolinger says he tries to impress upon them the fact that hospitalists do not have outside practices, they will “never try to steal patients,” they stay within referral patterns, and they will make sure that PCPs get pertinent records as soon as possible. Dr. Bolinger believes referring physicians’ biggest concern when dealing with hospitalists is that they “don’t want to lose control.” The way to address those fears is to make sure referring physicians are always kept in the communications loop regarding their patients’ progress.
The policy for Dr. Bolinger’s hospitalist program is to make sure all dictated reports are transcribed and faxed immediately to the referring physician’s office. All scheduled follow-up appointments and medication changes are included in discharge summaries. “If need be,” says Dr. Bolinger, “we will even hand deliver information to physicians’ offices, which we have done multiple times.”
Become User-Friendly
The methods Dr. Bolinger describes often result in referring physicians’ satisfaction with hospitalist services, followed by increased referrals. Hospitalists can ensure continued referrals from their PCPs if they remember hospital medicine’s cardinal rules of availability and prompt, thorough reporting, says Dr. Nelson. It can help to view the interface with the hospitalist service from the PCP’s point of view.
For instance, how can physicians quickly reach the hospitalist service? “If you’re a referring doctor and you’ve got a patient in your office whom you think should be admitted today, who do you call? This can actually be a little tricky for most practices,” says Dr. Nelson. “Every practice should give some thought to making that contact as easy for the referring doctors as possible.”
Some important questions to ask: When trying to reach a hospitalist, is it best to call the group’s main number? Will a voicemail message be returned within an hour? Two hours? Is it better to call the hospital operator and have the hospitalist paged? Or do PCPs have access to hospitalists’ cell phone numbers?
Dr. Nelson suggests that hospitalist groups also give thought to standardizing admission and discharge reports, as well as other forms. Often, individual members of a hospitalist group use slightly different formats for reporting to referring physicians. He points out that this can be less user friendly for the reader, who may have a harder time scanning the document quickly to find a particular piece of important information. Other useful suggestions for making reports user friendly: Use similar headings on all reports; avoid dense text; list pending tests in a prominent place in the report document; and consider highlighting or underlining key words.
Preference for In-Person Contact
For a new hospitalist practice, telephone communication between the hospitalist and the primary physician is valuable, and the hospitalist should “pick up the phone liberally,” says Dr. Nelson.
Dr. Becker believes the best way for physicians to communicate is one on one—in person. “Too often,” he says, “we get used to communicating through a third party—usually a unit clerk, a nurse, or a resident. I believe that physician-to-physician communication is the ideal. If the attending physician and the consultant [hospitalist or subspecialist] speak in person, they can explain their thinking to each other, and “within one minute of precious time, figure out which way to go.”
In this way, without wasting time, the physician gives the consultant guidance as to the appropriate track to take and can also listen to the consultant’s suggestions.
“I feel that medicine has perhaps gotten a little bit away from that communication link,” continues Dr. Becker. “When we get further away from that direct communication—whether it is between doctors and consultants, nurses and doctors, or doctors and family members—you take that little bit of risk that there will be a missed step, either on the part of the communicator or on the receiving end as the listener.”
In a study exploring barriers to effective patient handoffs, Solet and colleagues focused on the communication between physicians as a vital link in patient care continuity. The authors concluded that, regardless of the method of managing patient handoffs (e.g., computer-assisted or paper-based), the best way to ensure effective handoffs of hospitalized patients was “precise, unambiguous, face-to-face communication.”1
In a 2001 study by Hruby, Pantilat, and colleagues at UCSF, the authors found that, for the most part, hospitalized patients with PCPs wanted contact with their primary physicians even while in the hospital. Approximately half of the surveyed patients also believed that the PCP, rather than an inpatient physician, should be the first to discuss with them serious diagnoses or disease management choices.2 Preferences such as those expressed in this study may play into referring physicians’ reluctance to make use of hospitalist services, says Dr. Bolinger. They may fear that patients will feel abandoned by the primary physician. Dr. Bolinger’s response to those sentiments: “Initially, some patients [in our hospital] were a little guarded and were not sure what to expect. But after a day or two of having us there, they are generally very, very pleased to have us on board. We are part of their medical team now.”
A Need for Marketing?
Dr. Becker has been actively developing a hospital medicine program at Medical Center Hospital for the past two years and joined SHM as part of that effort. Familiarizing himself with the tenets of hospital medicine, he discovered that, as a family doctor, “unknowingly, I was actually practicing hospital medicine for 20 years!”
As part of the hospital medicine program development process, he has solicited input from local physicians as well as patients. A simple survey to assess interest in a hospitalist program asked potential referring physicians, Would you use a hospitalist? Would you use a hospitalist after waiting a while to see how the process goes? Or, would you not consider using a hospitalist?
In two years, says Dr. Becker, response from the referring physician community has changed from “bah, humbug” to one of readiness for the program.
A mass mailing can serve to introduce a hospital medicine program in a community. Dr. Bolinger’s group used this method and, in his experience, local subspecialists—orthopedists, cardiologists, endocrinologists, pulmonologists—have proved the biggest source of referrals to their program. But PCPs are starting to use the hospitalist service for vacations and call-coverage issues and are beginning to value hospitalists’ services. “Physicians like coming to the hospital, but they’re starting to realize that the hospitalist program is a better system,” says Dr. Bolinger.
Dr. Nelson has been a hospitalist for 18 years. For most of that time he has had no shortage of referred patients. In fact, the bigger problem has been finding enough doctors to join the group and handle the existing referral volume. In that situation, it has not made sense to undertake marketing with the goal of increasing referrals. However, he advises, “It is always worth spending time and energy trying to maintain good relationships with physicians with whom you regularly share patients, and perhaps this could be called ‘marketing.’”
To maintain good relationships with referring physicians, his group conducts a survey on a yearly basis. A survey, he suggests, should be very short, consisting of only a few key questions, such as:
- Do we send reports promptly to your practice?
- Are your patients satisfied with the care they receive from us?
- Do you have any comments or feedback for our group?
Although his group gains information from these surveys, Dr. Nelson notes that the greater value of conducting such surveys may be in building public relations capital. By conducting a survey, hospitalists demonstrate that they care enough to ask for their referring physicians’ input.
Another good marketing tool is a patient education brochure, given to referring physicians, that explains hospitalists and hospitalist care. These brochures can help referring physicians prepare their patients for seeing a hospitalist in the inpatient setting, thus easing the initial reluctance patients sometimes experience when encountering a new physician.
Conclusion
On the cusp of launching his medical center’s hospital medicine program, Dr. Becker sees that good communication between referring physicians and hospitalists will ensure the program’s success. He advises physicians to remember their classes in communication as third-year medical students, when most participate in videotaped patient encounters. It’s always instructive, he says, to see how we come across to others in conversation.
Both verbal and nonverbal cues play a part in good communication. A 2003 study by Griffith and colleagues concluded that better nonverbal communication skills are associated with greater patient satisfaction, and that formal instruction in nonverbal communication can be a good addition to residency training.3
“I find that doctors talk to each other, in general, very easily,” says Dr. Becker. Sometimes [good communication] is just a matter of opening that door and essentially keeping the former attending, the PCP, apprised of what is going on.”
When hospitalists attend to thorough communication and promptly deliver complete discharge summaries, family physicians can report to their patients that they know what happened in the hospital and poll their patients about their experiences in the hospital. In this way, hospitalists and referring physicians can cement their relationship as team members for the patient. The success of any hospitalist program, Dr. Becker believes, lies in “making sure you fulfill the promise of what hospital medicine generates, and that is a continuity of care … , obtaining front-end communication so that patients get the best care throughout their [hospital] stay, and then follow up with discharge summaries to the primary physician’s office.” TH
Gretchen Henkel is a regular contributor to The Hospitalist.
References
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12): 1094-1099.
- Hruby M, Pantilat SZ, Lo B. How do patients view the role of the primary care physician in inpatient care? Am J Med. 2001;21;111(9B):21S-25S.
- Griffith CH III, Wilson JF, Langer S, et al. House staff nonverbal communication skills and standardized patient satisfaction. J Gen Intern Med. 2003 Mar;18(3):170-174.