User login
What Is Your Diagnosis? Confluent and Reticulate Papillomatosis (Gougerot-Carteaud Syndrome)
What's Eating You? Common Striped Bark Scorpion (Centruroides vittatus)
ICD narrows down obesity codes
There’s a code for that, as of Oct. 1.
Have you seen female genital cutting or mutilation in your practice?
There is a code for that.
Has your patient’s obesity made it difficult to obtain a diagnostic image?
You get the picture.
The new International Diagnostic Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) adds specific codes for these and other disorders.
Cancer codes clinch the case
Specific codes now describe findings that indicate a cancer diagnosis and support appropriate treatment.
Estrogen receptor status
V86.0 Estrogen receptor positive
V86.1 Estrogen receptor negative
The 2007 ICD-9-CM adds a new category: estrogen receptor status. This bit of diagnostic information is an important indicator of the type of treatment to which breast cancer will be responsive. For instance, an estrogen-receptor–positive (ER+) finding means estrogen is causing the tumor to grow. This information in conjunction with a primary diagnosis of malignant neoplasm of the breast (ICD-9-CM codes 174.0–174.9) instantly gives the payer a snapshot of the patient’s condition and supports hormone suppression treatment.
Elevated tumor markers
795.81 Elevated carcinoembryonic antigen [CEA]
795.82 Elevated cancer antigen 125 [CA 125]
795.89 Other abnormal tumor markers
Previously, an elevated CA-125 tumor marker was reported using the unspecified code 790.99 (other nonspecific findings in blood), but with the addition of a new code subcategory, 795.8x, to report elevated tumor-associated and specific antigens, this will no longer be a problem.
Abnormal cervical cytology
795.06 Papanicolaou smear of cervix with cytologic evidence of malignancy
The inclusion term “cytologic evidence of carcinoma” was deleted from code 795.04 (Papanicolaou smear of cervix and cervical HPV). A new code reports this finding, and this new code is now an “excludes” diagnosis under code 233.1 (carcinoma in situ of cervix uteri). Furthermore, code 233.1 has a new inclusion definition: cervical intraepithelial glandular neoplasia.
OB complications
649.xx Other conditions or status of the mother, complicating pregnancy, childbirth, or the puerperium
Preexisting conditions are covered in the new category.
Bariatric surgery and pregnancy
649.2X Bariatric surgery status complicating pregnancy, childbirth, or the puerperium
Until now, if you were monitoring a pregnant woman more closely because of her previous bariatric surgery, your only option was code 648.93 (other current conditions, classifiable elsewhere). The new code is for any intervention required during the pregnancy, if the mother has had obesity surgery such as gastric banding or gastric stapling.
A 5th digit must be appended: 0, unspecified episode of care; 1, delivered with or without mention of antepartum condition; 2, delivered with postpartum condition; 3, antepartum condition or complication; 4, postpartum complication.
Smoking, obesity, epilepsy, and more
649.0 [0–4] Tobacco use disorder
You must clearly indicate that the patient’s current smoking is complicating the management of her pregnancy.
649.1 [0–4] Obesity
A secondary code for type of obesity is required; for instance, 278.01 (morbid obesity).
649.3 [0–4] Coagulation defects
A second code from the 286 category (coagulation defects) must be added to identify the exact condition. If a coagulation defect causes antepartum hemorrhage, the correct code is 641.3x. A coagulation defect that appears only in the postpartum period is coded 666.3x.
649.4 [0–4] Epilepsy
A secondary code identifies the type of epilepsy (345.00–345.91). However, if the patient has eclampsia, use the code 642.6 (eclampsia with convulsions).
649.5 [0, 1, 3] Spotting
This code will be used predominately in early pregnancy when spotting is the chief complaint and there is no evidence of miscarriage. Note that the allowable 5th digits for this code exclude 2 and 4, because spotting is not considered a complication in the postpartum period. If the patient is bleeding heavily, other existing codes would be selected, such as 640.0x (threatened abortion) or 641.1x (hemorrhage from placenta previa).
649.6 [0–4] Uterine size-date discrepancy
This condition, which was formerly included under 646.8x (other specified complications of pregnancy), is used most often when an ultrasound is performed to date the pregnancy, especially when the last monthly period is unknown.
666.1x Other immediate postpartum hemorrhage
This code is revised, and now specifies uterine atony with hemorrhage. Uterine atony without hemorrhage is coded 669.8x.
More specific “other” codes
Several “other”-type codes for gynecologic conditions got more specific. For example, 2 new, more specific, 5-digit codes replace code 616.8 (other specified inflammatory diseases of cervix, vagina, and vulva).
616.81 Mucositis (ulcerative) of the cervix, vagina, and vulva
Requires an additional E code to identify the adverse affects of therapy that caused the mucositis, such as antineoplastic or immunosuppressive drugs or radiation therapy.
616.89 Other inflammatory disease of the cervix, vagina, and vulva
Identifies conditions such as a caruncle of the vagina or labium or ulcer of the vagina.
616.84 Cervical stump prolapse
Previously was reported with the code 618.39 (other specified genital prolapse).
629.29 Other types of female genital mutilation
This code includes female genital cutting or mutilation Type IV status, the collective term for other types of mutilation that can include such things as pricking the clitoris with needles, burning or scarring the genitals, and ripping or tearing the vagina.
Code 629.8 (other specified disorders of female genital organs) was deleted and replaced by these 2 new 5-digit codes:
629.81 Habitual aborter without current pregnancy
629.89 Other unspecified disorders of female genital organs
Index changes to ICD-9-CM are also important to note. This year the reference for vaginal intraepithelial neoplasia (VIN I and VIN II) was changed from code 624.8 (other specified noninflammatory disorders of vulva and perineum) to:
624.0 Dystrophy of vulva
New category: Pain control
338 Pain, not elsewhere classified
338.18 Other acute postoperative pain
338.28 Other chronic postoperative pain
338.3 Neoplasm-related pain (acute) (chronic)
Diagnostic coding just got easier if your practice includes insertion of an On-Q device for postoperative pain. A whole new category of codes groups pain into acute and chronic classifications and includes codes for both types of postoperative pain. These new codes would not be used to report generalized pain (780.96) or localized pain by site (eg, pelvic pain, 625.9), or pain disorders attributed to psychological factors. Listed above are some of the new codes in this category that may be of particular interest to ObGyns.
Imaging
Breast calcifications
793.81 Microcalcifications seen on a mammogram
793.89 Other abnormal findings on radiological examination of breast
ICD-9-CM now differentiates microcalcifications. The less-specific code is for findings documented as simply mammographic calcification or mammographic calculus.
Inconclusive imaging due to obesity
793.91 Image test inconclusive due to excess body fat
You must add a second code indicating the patient’s body mass index (BMI).
Other imaging abnormalities
793.99 Other nonspecific abnormal findings on radiological and other examination of body structure
This code could be reported for such things as an abnormal placental finding on ultrasound or an abnormal finding in the skin or subcutaneous tissue, where a more definitive diagnosis is not available.
Urinary symptoms
Additions to your diagnostic arsenal:
788.64 Urinary hesitancy
788.65 Straining on urination
Hyperglycemia
A new inclusion term is added
790.29 Other abnormal glucose
The existing code now includes a diagnosis of hyperglycemia not elsewhere specified.
V26.34 Testing of male for genetic disease carrier status
V26.35 Encounter for testing of male partner of habitual aborter
V26.39 Other genetic testing of male
Use these new codes to identify the male as the reason for doing the testing—something that has been lacking for years.
There’s a code for that, as of Oct. 1.
Have you seen female genital cutting or mutilation in your practice?
There is a code for that.
Has your patient’s obesity made it difficult to obtain a diagnostic image?
You get the picture.
The new International Diagnostic Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) adds specific codes for these and other disorders.
Cancer codes clinch the case
Specific codes now describe findings that indicate a cancer diagnosis and support appropriate treatment.
Estrogen receptor status
V86.0 Estrogen receptor positive
V86.1 Estrogen receptor negative
The 2007 ICD-9-CM adds a new category: estrogen receptor status. This bit of diagnostic information is an important indicator of the type of treatment to which breast cancer will be responsive. For instance, an estrogen-receptor–positive (ER+) finding means estrogen is causing the tumor to grow. This information in conjunction with a primary diagnosis of malignant neoplasm of the breast (ICD-9-CM codes 174.0–174.9) instantly gives the payer a snapshot of the patient’s condition and supports hormone suppression treatment.
Elevated tumor markers
795.81 Elevated carcinoembryonic antigen [CEA]
795.82 Elevated cancer antigen 125 [CA 125]
795.89 Other abnormal tumor markers
Previously, an elevated CA-125 tumor marker was reported using the unspecified code 790.99 (other nonspecific findings in blood), but with the addition of a new code subcategory, 795.8x, to report elevated tumor-associated and specific antigens, this will no longer be a problem.
Abnormal cervical cytology
795.06 Papanicolaou smear of cervix with cytologic evidence of malignancy
The inclusion term “cytologic evidence of carcinoma” was deleted from code 795.04 (Papanicolaou smear of cervix and cervical HPV). A new code reports this finding, and this new code is now an “excludes” diagnosis under code 233.1 (carcinoma in situ of cervix uteri). Furthermore, code 233.1 has a new inclusion definition: cervical intraepithelial glandular neoplasia.
OB complications
649.xx Other conditions or status of the mother, complicating pregnancy, childbirth, or the puerperium
Preexisting conditions are covered in the new category.
Bariatric surgery and pregnancy
649.2X Bariatric surgery status complicating pregnancy, childbirth, or the puerperium
Until now, if you were monitoring a pregnant woman more closely because of her previous bariatric surgery, your only option was code 648.93 (other current conditions, classifiable elsewhere). The new code is for any intervention required during the pregnancy, if the mother has had obesity surgery such as gastric banding or gastric stapling.
A 5th digit must be appended: 0, unspecified episode of care; 1, delivered with or without mention of antepartum condition; 2, delivered with postpartum condition; 3, antepartum condition or complication; 4, postpartum complication.
Smoking, obesity, epilepsy, and more
649.0 [0–4] Tobacco use disorder
You must clearly indicate that the patient’s current smoking is complicating the management of her pregnancy.
649.1 [0–4] Obesity
A secondary code for type of obesity is required; for instance, 278.01 (morbid obesity).
649.3 [0–4] Coagulation defects
A second code from the 286 category (coagulation defects) must be added to identify the exact condition. If a coagulation defect causes antepartum hemorrhage, the correct code is 641.3x. A coagulation defect that appears only in the postpartum period is coded 666.3x.
649.4 [0–4] Epilepsy
A secondary code identifies the type of epilepsy (345.00–345.91). However, if the patient has eclampsia, use the code 642.6 (eclampsia with convulsions).
649.5 [0, 1, 3] Spotting
This code will be used predominately in early pregnancy when spotting is the chief complaint and there is no evidence of miscarriage. Note that the allowable 5th digits for this code exclude 2 and 4, because spotting is not considered a complication in the postpartum period. If the patient is bleeding heavily, other existing codes would be selected, such as 640.0x (threatened abortion) or 641.1x (hemorrhage from placenta previa).
649.6 [0–4] Uterine size-date discrepancy
This condition, which was formerly included under 646.8x (other specified complications of pregnancy), is used most often when an ultrasound is performed to date the pregnancy, especially when the last monthly period is unknown.
666.1x Other immediate postpartum hemorrhage
This code is revised, and now specifies uterine atony with hemorrhage. Uterine atony without hemorrhage is coded 669.8x.
More specific “other” codes
Several “other”-type codes for gynecologic conditions got more specific. For example, 2 new, more specific, 5-digit codes replace code 616.8 (other specified inflammatory diseases of cervix, vagina, and vulva).
616.81 Mucositis (ulcerative) of the cervix, vagina, and vulva
Requires an additional E code to identify the adverse affects of therapy that caused the mucositis, such as antineoplastic or immunosuppressive drugs or radiation therapy.
616.89 Other inflammatory disease of the cervix, vagina, and vulva
Identifies conditions such as a caruncle of the vagina or labium or ulcer of the vagina.
616.84 Cervical stump prolapse
Previously was reported with the code 618.39 (other specified genital prolapse).
629.29 Other types of female genital mutilation
This code includes female genital cutting or mutilation Type IV status, the collective term for other types of mutilation that can include such things as pricking the clitoris with needles, burning or scarring the genitals, and ripping or tearing the vagina.
Code 629.8 (other specified disorders of female genital organs) was deleted and replaced by these 2 new 5-digit codes:
629.81 Habitual aborter without current pregnancy
629.89 Other unspecified disorders of female genital organs
Index changes to ICD-9-CM are also important to note. This year the reference for vaginal intraepithelial neoplasia (VIN I and VIN II) was changed from code 624.8 (other specified noninflammatory disorders of vulva and perineum) to:
624.0 Dystrophy of vulva
New category: Pain control
338 Pain, not elsewhere classified
338.18 Other acute postoperative pain
338.28 Other chronic postoperative pain
338.3 Neoplasm-related pain (acute) (chronic)
Diagnostic coding just got easier if your practice includes insertion of an On-Q device for postoperative pain. A whole new category of codes groups pain into acute and chronic classifications and includes codes for both types of postoperative pain. These new codes would not be used to report generalized pain (780.96) or localized pain by site (eg, pelvic pain, 625.9), or pain disorders attributed to psychological factors. Listed above are some of the new codes in this category that may be of particular interest to ObGyns.
Imaging
Breast calcifications
793.81 Microcalcifications seen on a mammogram
793.89 Other abnormal findings on radiological examination of breast
ICD-9-CM now differentiates microcalcifications. The less-specific code is for findings documented as simply mammographic calcification or mammographic calculus.
Inconclusive imaging due to obesity
793.91 Image test inconclusive due to excess body fat
You must add a second code indicating the patient’s body mass index (BMI).
Other imaging abnormalities
793.99 Other nonspecific abnormal findings on radiological and other examination of body structure
This code could be reported for such things as an abnormal placental finding on ultrasound or an abnormal finding in the skin or subcutaneous tissue, where a more definitive diagnosis is not available.
Urinary symptoms
Additions to your diagnostic arsenal:
788.64 Urinary hesitancy
788.65 Straining on urination
Hyperglycemia
A new inclusion term is added
790.29 Other abnormal glucose
The existing code now includes a diagnosis of hyperglycemia not elsewhere specified.
V26.34 Testing of male for genetic disease carrier status
V26.35 Encounter for testing of male partner of habitual aborter
V26.39 Other genetic testing of male
Use these new codes to identify the male as the reason for doing the testing—something that has been lacking for years.
There’s a code for that, as of Oct. 1.
Have you seen female genital cutting or mutilation in your practice?
There is a code for that.
Has your patient’s obesity made it difficult to obtain a diagnostic image?
You get the picture.
The new International Diagnostic Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) adds specific codes for these and other disorders.
Cancer codes clinch the case
Specific codes now describe findings that indicate a cancer diagnosis and support appropriate treatment.
Estrogen receptor status
V86.0 Estrogen receptor positive
V86.1 Estrogen receptor negative
The 2007 ICD-9-CM adds a new category: estrogen receptor status. This bit of diagnostic information is an important indicator of the type of treatment to which breast cancer will be responsive. For instance, an estrogen-receptor–positive (ER+) finding means estrogen is causing the tumor to grow. This information in conjunction with a primary diagnosis of malignant neoplasm of the breast (ICD-9-CM codes 174.0–174.9) instantly gives the payer a snapshot of the patient’s condition and supports hormone suppression treatment.
Elevated tumor markers
795.81 Elevated carcinoembryonic antigen [CEA]
795.82 Elevated cancer antigen 125 [CA 125]
795.89 Other abnormal tumor markers
Previously, an elevated CA-125 tumor marker was reported using the unspecified code 790.99 (other nonspecific findings in blood), but with the addition of a new code subcategory, 795.8x, to report elevated tumor-associated and specific antigens, this will no longer be a problem.
Abnormal cervical cytology
795.06 Papanicolaou smear of cervix with cytologic evidence of malignancy
The inclusion term “cytologic evidence of carcinoma” was deleted from code 795.04 (Papanicolaou smear of cervix and cervical HPV). A new code reports this finding, and this new code is now an “excludes” diagnosis under code 233.1 (carcinoma in situ of cervix uteri). Furthermore, code 233.1 has a new inclusion definition: cervical intraepithelial glandular neoplasia.
OB complications
649.xx Other conditions or status of the mother, complicating pregnancy, childbirth, or the puerperium
Preexisting conditions are covered in the new category.
Bariatric surgery and pregnancy
649.2X Bariatric surgery status complicating pregnancy, childbirth, or the puerperium
Until now, if you were monitoring a pregnant woman more closely because of her previous bariatric surgery, your only option was code 648.93 (other current conditions, classifiable elsewhere). The new code is for any intervention required during the pregnancy, if the mother has had obesity surgery such as gastric banding or gastric stapling.
A 5th digit must be appended: 0, unspecified episode of care; 1, delivered with or without mention of antepartum condition; 2, delivered with postpartum condition; 3, antepartum condition or complication; 4, postpartum complication.
Smoking, obesity, epilepsy, and more
649.0 [0–4] Tobacco use disorder
You must clearly indicate that the patient’s current smoking is complicating the management of her pregnancy.
649.1 [0–4] Obesity
A secondary code for type of obesity is required; for instance, 278.01 (morbid obesity).
649.3 [0–4] Coagulation defects
A second code from the 286 category (coagulation defects) must be added to identify the exact condition. If a coagulation defect causes antepartum hemorrhage, the correct code is 641.3x. A coagulation defect that appears only in the postpartum period is coded 666.3x.
649.4 [0–4] Epilepsy
A secondary code identifies the type of epilepsy (345.00–345.91). However, if the patient has eclampsia, use the code 642.6 (eclampsia with convulsions).
649.5 [0, 1, 3] Spotting
This code will be used predominately in early pregnancy when spotting is the chief complaint and there is no evidence of miscarriage. Note that the allowable 5th digits for this code exclude 2 and 4, because spotting is not considered a complication in the postpartum period. If the patient is bleeding heavily, other existing codes would be selected, such as 640.0x (threatened abortion) or 641.1x (hemorrhage from placenta previa).
649.6 [0–4] Uterine size-date discrepancy
This condition, which was formerly included under 646.8x (other specified complications of pregnancy), is used most often when an ultrasound is performed to date the pregnancy, especially when the last monthly period is unknown.
666.1x Other immediate postpartum hemorrhage
This code is revised, and now specifies uterine atony with hemorrhage. Uterine atony without hemorrhage is coded 669.8x.
More specific “other” codes
Several “other”-type codes for gynecologic conditions got more specific. For example, 2 new, more specific, 5-digit codes replace code 616.8 (other specified inflammatory diseases of cervix, vagina, and vulva).
616.81 Mucositis (ulcerative) of the cervix, vagina, and vulva
Requires an additional E code to identify the adverse affects of therapy that caused the mucositis, such as antineoplastic or immunosuppressive drugs or radiation therapy.
616.89 Other inflammatory disease of the cervix, vagina, and vulva
Identifies conditions such as a caruncle of the vagina or labium or ulcer of the vagina.
616.84 Cervical stump prolapse
Previously was reported with the code 618.39 (other specified genital prolapse).
629.29 Other types of female genital mutilation
This code includes female genital cutting or mutilation Type IV status, the collective term for other types of mutilation that can include such things as pricking the clitoris with needles, burning or scarring the genitals, and ripping or tearing the vagina.
Code 629.8 (other specified disorders of female genital organs) was deleted and replaced by these 2 new 5-digit codes:
629.81 Habitual aborter without current pregnancy
629.89 Other unspecified disorders of female genital organs
Index changes to ICD-9-CM are also important to note. This year the reference for vaginal intraepithelial neoplasia (VIN I and VIN II) was changed from code 624.8 (other specified noninflammatory disorders of vulva and perineum) to:
624.0 Dystrophy of vulva
New category: Pain control
338 Pain, not elsewhere classified
338.18 Other acute postoperative pain
338.28 Other chronic postoperative pain
338.3 Neoplasm-related pain (acute) (chronic)
Diagnostic coding just got easier if your practice includes insertion of an On-Q device for postoperative pain. A whole new category of codes groups pain into acute and chronic classifications and includes codes for both types of postoperative pain. These new codes would not be used to report generalized pain (780.96) or localized pain by site (eg, pelvic pain, 625.9), or pain disorders attributed to psychological factors. Listed above are some of the new codes in this category that may be of particular interest to ObGyns.
Imaging
Breast calcifications
793.81 Microcalcifications seen on a mammogram
793.89 Other abnormal findings on radiological examination of breast
ICD-9-CM now differentiates microcalcifications. The less-specific code is for findings documented as simply mammographic calcification or mammographic calculus.
Inconclusive imaging due to obesity
793.91 Image test inconclusive due to excess body fat
You must add a second code indicating the patient’s body mass index (BMI).
Other imaging abnormalities
793.99 Other nonspecific abnormal findings on radiological and other examination of body structure
This code could be reported for such things as an abnormal placental finding on ultrasound or an abnormal finding in the skin or subcutaneous tissue, where a more definitive diagnosis is not available.
Urinary symptoms
Additions to your diagnostic arsenal:
788.64 Urinary hesitancy
788.65 Straining on urination
Hyperglycemia
A new inclusion term is added
790.29 Other abnormal glucose
The existing code now includes a diagnosis of hyperglycemia not elsewhere specified.
V26.34 Testing of male for genetic disease carrier status
V26.35 Encounter for testing of male partner of habitual aborter
V26.39 Other genetic testing of male
Use these new codes to identify the male as the reason for doing the testing—something that has been lacking for years.
Prudent prescribing for patients with addictions
Did benzodiazepines prescribed to patient
with addiction cause delirium?
Maricopa County (AZ) Superior Court
A 40-year-old woman addicted to diazepam sought treatment from a psychiatric nurse who performed a psychological evaluation. The patient claimed that the nurse negligently prescribed benzodiazepines and other medications for anxiety, panic attacks, and depression.
The patient claimed that the prescriptions caused a drug-induced delirium, during which she put a nonlethal amount of the medication on her two minor daughters’ ice cream, then attempted suicide by overdosing with her prescriptions. The patient and her daughters survived.
The patient was charged with two counts of attempted murder and was incarcerated for 18 months while awaiting trail. She was acquitted of the charges but lost custody of her daughters.
The psychiatric nurse argued that the medication prescribed was appropriate and the patient was not in a drug-induced delirium when she tried to kill herself and her daughters. The defense alleged that other factors caused the patient to attempt suicide/homicide, including a pending divorce and financial problems.
- A defense verdict was returned
Woman claims she was prescribed narcotics
despite alprazolam addiction
Multnomah County (OR) Superior Court
The patient, age 57, began seeing a psychiatrist in March 1993 for anxiety and panic attacks. She had kicked a 10-year alprazolam addiction and had been drug-free for more than 6 months when she first visited the psychiatrist.
The patient claimed that over the next 11 years she developed an intimate friendship with the psychiatrist. The patient visited the psychiatrist’s office almost weekly—sometimes twice a week—and incurred almost $100,000 in fees. The patient says that the psychiatrist prescribed her narcotics, then sought the drugs from her for his personal use, and was negligent in his treatment.
- A $593,000 verdict was returned, which included $200,000 in punitive damages
- Try prescribing nonaddictive alternate medication first.
- Prescribe a limited amount for a short time when an abusable substance is clinically warranted.
- Document in the patient’s chart specific treatment needs that will be addressed by the medication, potential benefits and risks, the dosage, and date of the prescription.
- Use medication in combination with an ongoing discussion of the patient’s anxiety, history of addiction, and the clinician’s attempts to prevent future addictions.
- If prescription drug abuse develops, identify the problem and help the patient find appropriate treatment, such as detoxification inpatient chemical dependency treatment, or intensive outpatient dependency treatment.
Dr. Grant’s observations
Should benzodiazepines or other addictive substances be prescribed to a patient with a history of substance abuse? Little evidence guides clinicians,1,2 and limited research has examined whether former substance abusers are more likely than other patients to abuse benzodiazepines or if these medications increase the risk of substance abuse relapse.2
A psychiatrist can prescribe medication whenever a medical basis exists. In the first case a patient with anxiety and panic attacks was given benzodiazepines, an appropriate treatment for anxiety disorder.3 But what if the patient has a history of substance abuse? When is prescribing these medications negligent?
The fiduciary relationship between psychiatrist and patient states that the therapist is the patient’s ally and should always act in the patient’s best interest. With limited data, clinicians have no clear rule for a standard of care.
On one hand, benzodiazepine misuse is a problem and these medications must be prescribed cautiously. In 2004 roughly 300,000 Americans reported using prescription sedatives for nonmedical purposes.4 Many addiction specialists believe benzodiazepines are contraindicated for patients with current alcohol or drug abuse problems and for those in recovery. In this scenario, the clinician could choose an appropriate alternative to a benzodiazepine such as an antidepressant, buspirone, beta blocker, or anticonvulsant. Explain to the patient that these medications’ clinical effect is slower than that of benzodiazepines. Also consider psychotherapy to address anxiety.
On the other hand, benzodiazepines might be underused because of fear of addiction.5 Clinicians must consider whether their prescribing practices are designed to protect themselves or are in the patients’ best interests (Box 1). Of course, when treating a patient with a benzodiazepine addiction, the risk-benefit analysis shifts and abuse concerns may be more appropriate.
In the first case, the patient attempted suicide by overdosing on the prescribed medication. This fact might support the patient’s argument that she was not an appropriate candidate for benzodiazepines and the psychiatric nurse could be held liable—even though in this case she was not. One court found that a psychiatrist writing prescriptions for large amounts of controlled substances to someone addicted to drugs could be held liable for the patient’s suicide.6
In the second case, a psychiatrist prescribed narcotics to a patient with a history of addiction. The code of medical ethics is clear: A psychiatrist who regularly practices outside his or her area of professional competence should be considered as having acted in an unethical manner.7 So if you wish to prescribe narcotics, you must follow internal medicine’s ethical standards (Box 2).
Responsibility of care
Although the nurse in the first case could be liable for her actions, the psychiatrist who supervised the nurse might also be partially responsible. The law assumes that those who work under a physician’s supervision act as his or her agents. Nurses working for a physician are the physician’s agents, and the physician is responsible for a nurse’s acts. This legal principle is respondeat superior, or “let the master reply.”
Generally, the physician’s lack of knowledge about what the nurse prescribes is not a defense for a malpractice claim. In fact, the law requires that the physician know whether his or her agents meet the profession’s standard of care. In cases where a nurse prescribes an inappropriate medication, the psychiatrist can be charged with negligent supervision—that is, failing to provide to the nurse proper guidance and instruction.
Ethical conduct
Relationships with patients. The second case raises several egregious issues in patient care. Although intimate relationships with patients are prohibited, the fact that these cases still come before licensing boards and courts suggests that physicians are not getting the message. Although the report of this case is vague about what “intimate” means, several points are raised:
- Sexual relationships with current or former patients are not allowed.7 A patient is vulnerable, and the power differential makes it difficult for the patient to resist the therapist’s requests.
- Nonsexual, intimate relationships likely would be seen as a boundary violation, akin to a sexual relationship. In the case presented, the boundary violation is obvious even though the relationship may not have been sexual.
- Establish a patient-physician relationship.
- Perform and document a medical history and physical exam to justify the medication prescribed.
- Medication must be warranted and consistent with the physician’s diagnosis.
- Dosages and prolonged prescriptions need to be within the usual course of medical practice.
- Maintain accurate and complete treatment records.
Source: Snyder L, Leffler C. American College of Physicians ethics manual, 5th ed. Available at: http://www.acponline.org/ethics/ethicman5th.htm. Accessed August 30, 2006.
Medical ethics prohibit this behavior and state that psychiatrists should not:7
- use the unique position afforded by the psychotherapeutic situation to influence the patient in any way that is not directly relevant to treatment goals
- exploit information furnished by patients.
State medical boards have varying procedures in place to handle a physician’s substance abuse.
These programs’ goal is to assist recovery, eliminate risk to the public, and allow the physician to return to work. Clinicians should be aware of such programs in their jurisdictions.
Drug brand names
- Alprazolam • Xanax
- Buspirone • BuSpar
- Diazepam • Valium
1. Brunette MF, Noordsy DL, Xie H, et al. Benzodiazepine use and abuse among patients with severe mental illness and co-occurring substance use disorders. Psychiatr Serv 2003;54:1395-401.
2. Posternak MA, Mueller TI. Assessing the risks and benefits of benzodiazepines for anxiety disorders in patients with a history of substance abuse or dependence. Am J Addict 2001;10:48-68.
3. Uhlenhuth EH, Balter MB, Ban TA, et al. International study of expert judgment on therapeutic use of benzodiazepines and other psychotherapeutic medications: IV. Therapeutic dose dependence and abuse liability of benzodiazepines in the long-term treatment of anxiety disorders. J Clin Psychopharmacol 1999;19(suppl 2):23S-29S.
4. U.S. Department of Health and Human Services. National Survey on Drug Use and Health. http://www.oas.samhsa.gov/nhsda.htm; accessed August 23, 2006.
5. American Psychiatric Association Practice guideline for the treatment of patients with panic disorder. Washington, DC: American Psychiatric Association; 1998.
6. Argus v Scheppegrell 472 So. 2d 573 (La. 1985).
7. American Psychiatric Association. Principles of medical ethics with annotations especially applicable to psychiatry, 2006 edition. Available at: http://www.psych.org/psych_pract/ethics/ppaethics.cfm. Accessed August 28, 2006.
8. Patten SB, Love EJ. Neuropsychiatric adverse drug reactions: passive reports to Health and Welfare Canada’s adverse reaction database (1965-present). Int J Psychiatry Med 1994;24:45-62.
9. Michel L, Lang JP. Benzodiazepines and forensic aspects. Encephale 2003;29:479-85.
10. Hughes PH, Brandenburg N, Baldwin DC, et al. Prevalence of substance abuse among US physicians. JAMA 1992;267:2333-9.
Did benzodiazepines prescribed to patient
with addiction cause delirium?
Maricopa County (AZ) Superior Court
A 40-year-old woman addicted to diazepam sought treatment from a psychiatric nurse who performed a psychological evaluation. The patient claimed that the nurse negligently prescribed benzodiazepines and other medications for anxiety, panic attacks, and depression.
The patient claimed that the prescriptions caused a drug-induced delirium, during which she put a nonlethal amount of the medication on her two minor daughters’ ice cream, then attempted suicide by overdosing with her prescriptions. The patient and her daughters survived.
The patient was charged with two counts of attempted murder and was incarcerated for 18 months while awaiting trail. She was acquitted of the charges but lost custody of her daughters.
The psychiatric nurse argued that the medication prescribed was appropriate and the patient was not in a drug-induced delirium when she tried to kill herself and her daughters. The defense alleged that other factors caused the patient to attempt suicide/homicide, including a pending divorce and financial problems.
- A defense verdict was returned
Woman claims she was prescribed narcotics
despite alprazolam addiction
Multnomah County (OR) Superior Court
The patient, age 57, began seeing a psychiatrist in March 1993 for anxiety and panic attacks. She had kicked a 10-year alprazolam addiction and had been drug-free for more than 6 months when she first visited the psychiatrist.
The patient claimed that over the next 11 years she developed an intimate friendship with the psychiatrist. The patient visited the psychiatrist’s office almost weekly—sometimes twice a week—and incurred almost $100,000 in fees. The patient says that the psychiatrist prescribed her narcotics, then sought the drugs from her for his personal use, and was negligent in his treatment.
- A $593,000 verdict was returned, which included $200,000 in punitive damages
- Try prescribing nonaddictive alternate medication first.
- Prescribe a limited amount for a short time when an abusable substance is clinically warranted.
- Document in the patient’s chart specific treatment needs that will be addressed by the medication, potential benefits and risks, the dosage, and date of the prescription.
- Use medication in combination with an ongoing discussion of the patient’s anxiety, history of addiction, and the clinician’s attempts to prevent future addictions.
- If prescription drug abuse develops, identify the problem and help the patient find appropriate treatment, such as detoxification inpatient chemical dependency treatment, or intensive outpatient dependency treatment.
Dr. Grant’s observations
Should benzodiazepines or other addictive substances be prescribed to a patient with a history of substance abuse? Little evidence guides clinicians,1,2 and limited research has examined whether former substance abusers are more likely than other patients to abuse benzodiazepines or if these medications increase the risk of substance abuse relapse.2
A psychiatrist can prescribe medication whenever a medical basis exists. In the first case a patient with anxiety and panic attacks was given benzodiazepines, an appropriate treatment for anxiety disorder.3 But what if the patient has a history of substance abuse? When is prescribing these medications negligent?
The fiduciary relationship between psychiatrist and patient states that the therapist is the patient’s ally and should always act in the patient’s best interest. With limited data, clinicians have no clear rule for a standard of care.
On one hand, benzodiazepine misuse is a problem and these medications must be prescribed cautiously. In 2004 roughly 300,000 Americans reported using prescription sedatives for nonmedical purposes.4 Many addiction specialists believe benzodiazepines are contraindicated for patients with current alcohol or drug abuse problems and for those in recovery. In this scenario, the clinician could choose an appropriate alternative to a benzodiazepine such as an antidepressant, buspirone, beta blocker, or anticonvulsant. Explain to the patient that these medications’ clinical effect is slower than that of benzodiazepines. Also consider psychotherapy to address anxiety.
On the other hand, benzodiazepines might be underused because of fear of addiction.5 Clinicians must consider whether their prescribing practices are designed to protect themselves or are in the patients’ best interests (Box 1). Of course, when treating a patient with a benzodiazepine addiction, the risk-benefit analysis shifts and abuse concerns may be more appropriate.
In the first case, the patient attempted suicide by overdosing on the prescribed medication. This fact might support the patient’s argument that she was not an appropriate candidate for benzodiazepines and the psychiatric nurse could be held liable—even though in this case she was not. One court found that a psychiatrist writing prescriptions for large amounts of controlled substances to someone addicted to drugs could be held liable for the patient’s suicide.6
In the second case, a psychiatrist prescribed narcotics to a patient with a history of addiction. The code of medical ethics is clear: A psychiatrist who regularly practices outside his or her area of professional competence should be considered as having acted in an unethical manner.7 So if you wish to prescribe narcotics, you must follow internal medicine’s ethical standards (Box 2).
Responsibility of care
Although the nurse in the first case could be liable for her actions, the psychiatrist who supervised the nurse might also be partially responsible. The law assumes that those who work under a physician’s supervision act as his or her agents. Nurses working for a physician are the physician’s agents, and the physician is responsible for a nurse’s acts. This legal principle is respondeat superior, or “let the master reply.”
Generally, the physician’s lack of knowledge about what the nurse prescribes is not a defense for a malpractice claim. In fact, the law requires that the physician know whether his or her agents meet the profession’s standard of care. In cases where a nurse prescribes an inappropriate medication, the psychiatrist can be charged with negligent supervision—that is, failing to provide to the nurse proper guidance and instruction.
Ethical conduct
Relationships with patients. The second case raises several egregious issues in patient care. Although intimate relationships with patients are prohibited, the fact that these cases still come before licensing boards and courts suggests that physicians are not getting the message. Although the report of this case is vague about what “intimate” means, several points are raised:
- Sexual relationships with current or former patients are not allowed.7 A patient is vulnerable, and the power differential makes it difficult for the patient to resist the therapist’s requests.
- Nonsexual, intimate relationships likely would be seen as a boundary violation, akin to a sexual relationship. In the case presented, the boundary violation is obvious even though the relationship may not have been sexual.
- Establish a patient-physician relationship.
- Perform and document a medical history and physical exam to justify the medication prescribed.
- Medication must be warranted and consistent with the physician’s diagnosis.
- Dosages and prolonged prescriptions need to be within the usual course of medical practice.
- Maintain accurate and complete treatment records.
Source: Snyder L, Leffler C. American College of Physicians ethics manual, 5th ed. Available at: http://www.acponline.org/ethics/ethicman5th.htm. Accessed August 30, 2006.
Medical ethics prohibit this behavior and state that psychiatrists should not:7
- use the unique position afforded by the psychotherapeutic situation to influence the patient in any way that is not directly relevant to treatment goals
- exploit information furnished by patients.
State medical boards have varying procedures in place to handle a physician’s substance abuse.
These programs’ goal is to assist recovery, eliminate risk to the public, and allow the physician to return to work. Clinicians should be aware of such programs in their jurisdictions.
Drug brand names
- Alprazolam • Xanax
- Buspirone • BuSpar
- Diazepam • Valium
Did benzodiazepines prescribed to patient
with addiction cause delirium?
Maricopa County (AZ) Superior Court
A 40-year-old woman addicted to diazepam sought treatment from a psychiatric nurse who performed a psychological evaluation. The patient claimed that the nurse negligently prescribed benzodiazepines and other medications for anxiety, panic attacks, and depression.
The patient claimed that the prescriptions caused a drug-induced delirium, during which she put a nonlethal amount of the medication on her two minor daughters’ ice cream, then attempted suicide by overdosing with her prescriptions. The patient and her daughters survived.
The patient was charged with two counts of attempted murder and was incarcerated for 18 months while awaiting trail. She was acquitted of the charges but lost custody of her daughters.
The psychiatric nurse argued that the medication prescribed was appropriate and the patient was not in a drug-induced delirium when she tried to kill herself and her daughters. The defense alleged that other factors caused the patient to attempt suicide/homicide, including a pending divorce and financial problems.
- A defense verdict was returned
Woman claims she was prescribed narcotics
despite alprazolam addiction
Multnomah County (OR) Superior Court
The patient, age 57, began seeing a psychiatrist in March 1993 for anxiety and panic attacks. She had kicked a 10-year alprazolam addiction and had been drug-free for more than 6 months when she first visited the psychiatrist.
The patient claimed that over the next 11 years she developed an intimate friendship with the psychiatrist. The patient visited the psychiatrist’s office almost weekly—sometimes twice a week—and incurred almost $100,000 in fees. The patient says that the psychiatrist prescribed her narcotics, then sought the drugs from her for his personal use, and was negligent in his treatment.
- A $593,000 verdict was returned, which included $200,000 in punitive damages
- Try prescribing nonaddictive alternate medication first.
- Prescribe a limited amount for a short time when an abusable substance is clinically warranted.
- Document in the patient’s chart specific treatment needs that will be addressed by the medication, potential benefits and risks, the dosage, and date of the prescription.
- Use medication in combination with an ongoing discussion of the patient’s anxiety, history of addiction, and the clinician’s attempts to prevent future addictions.
- If prescription drug abuse develops, identify the problem and help the patient find appropriate treatment, such as detoxification inpatient chemical dependency treatment, or intensive outpatient dependency treatment.
Dr. Grant’s observations
Should benzodiazepines or other addictive substances be prescribed to a patient with a history of substance abuse? Little evidence guides clinicians,1,2 and limited research has examined whether former substance abusers are more likely than other patients to abuse benzodiazepines or if these medications increase the risk of substance abuse relapse.2
A psychiatrist can prescribe medication whenever a medical basis exists. In the first case a patient with anxiety and panic attacks was given benzodiazepines, an appropriate treatment for anxiety disorder.3 But what if the patient has a history of substance abuse? When is prescribing these medications negligent?
The fiduciary relationship between psychiatrist and patient states that the therapist is the patient’s ally and should always act in the patient’s best interest. With limited data, clinicians have no clear rule for a standard of care.
On one hand, benzodiazepine misuse is a problem and these medications must be prescribed cautiously. In 2004 roughly 300,000 Americans reported using prescription sedatives for nonmedical purposes.4 Many addiction specialists believe benzodiazepines are contraindicated for patients with current alcohol or drug abuse problems and for those in recovery. In this scenario, the clinician could choose an appropriate alternative to a benzodiazepine such as an antidepressant, buspirone, beta blocker, or anticonvulsant. Explain to the patient that these medications’ clinical effect is slower than that of benzodiazepines. Also consider psychotherapy to address anxiety.
On the other hand, benzodiazepines might be underused because of fear of addiction.5 Clinicians must consider whether their prescribing practices are designed to protect themselves or are in the patients’ best interests (Box 1). Of course, when treating a patient with a benzodiazepine addiction, the risk-benefit analysis shifts and abuse concerns may be more appropriate.
In the first case, the patient attempted suicide by overdosing on the prescribed medication. This fact might support the patient’s argument that she was not an appropriate candidate for benzodiazepines and the psychiatric nurse could be held liable—even though in this case she was not. One court found that a psychiatrist writing prescriptions for large amounts of controlled substances to someone addicted to drugs could be held liable for the patient’s suicide.6
In the second case, a psychiatrist prescribed narcotics to a patient with a history of addiction. The code of medical ethics is clear: A psychiatrist who regularly practices outside his or her area of professional competence should be considered as having acted in an unethical manner.7 So if you wish to prescribe narcotics, you must follow internal medicine’s ethical standards (Box 2).
Responsibility of care
Although the nurse in the first case could be liable for her actions, the psychiatrist who supervised the nurse might also be partially responsible. The law assumes that those who work under a physician’s supervision act as his or her agents. Nurses working for a physician are the physician’s agents, and the physician is responsible for a nurse’s acts. This legal principle is respondeat superior, or “let the master reply.”
Generally, the physician’s lack of knowledge about what the nurse prescribes is not a defense for a malpractice claim. In fact, the law requires that the physician know whether his or her agents meet the profession’s standard of care. In cases where a nurse prescribes an inappropriate medication, the psychiatrist can be charged with negligent supervision—that is, failing to provide to the nurse proper guidance and instruction.
Ethical conduct
Relationships with patients. The second case raises several egregious issues in patient care. Although intimate relationships with patients are prohibited, the fact that these cases still come before licensing boards and courts suggests that physicians are not getting the message. Although the report of this case is vague about what “intimate” means, several points are raised:
- Sexual relationships with current or former patients are not allowed.7 A patient is vulnerable, and the power differential makes it difficult for the patient to resist the therapist’s requests.
- Nonsexual, intimate relationships likely would be seen as a boundary violation, akin to a sexual relationship. In the case presented, the boundary violation is obvious even though the relationship may not have been sexual.
- Establish a patient-physician relationship.
- Perform and document a medical history and physical exam to justify the medication prescribed.
- Medication must be warranted and consistent with the physician’s diagnosis.
- Dosages and prolonged prescriptions need to be within the usual course of medical practice.
- Maintain accurate and complete treatment records.
Source: Snyder L, Leffler C. American College of Physicians ethics manual, 5th ed. Available at: http://www.acponline.org/ethics/ethicman5th.htm. Accessed August 30, 2006.
Medical ethics prohibit this behavior and state that psychiatrists should not:7
- use the unique position afforded by the psychotherapeutic situation to influence the patient in any way that is not directly relevant to treatment goals
- exploit information furnished by patients.
State medical boards have varying procedures in place to handle a physician’s substance abuse.
These programs’ goal is to assist recovery, eliminate risk to the public, and allow the physician to return to work. Clinicians should be aware of such programs in their jurisdictions.
Drug brand names
- Alprazolam • Xanax
- Buspirone • BuSpar
- Diazepam • Valium
1. Brunette MF, Noordsy DL, Xie H, et al. Benzodiazepine use and abuse among patients with severe mental illness and co-occurring substance use disorders. Psychiatr Serv 2003;54:1395-401.
2. Posternak MA, Mueller TI. Assessing the risks and benefits of benzodiazepines for anxiety disorders in patients with a history of substance abuse or dependence. Am J Addict 2001;10:48-68.
3. Uhlenhuth EH, Balter MB, Ban TA, et al. International study of expert judgment on therapeutic use of benzodiazepines and other psychotherapeutic medications: IV. Therapeutic dose dependence and abuse liability of benzodiazepines in the long-term treatment of anxiety disorders. J Clin Psychopharmacol 1999;19(suppl 2):23S-29S.
4. U.S. Department of Health and Human Services. National Survey on Drug Use and Health. http://www.oas.samhsa.gov/nhsda.htm; accessed August 23, 2006.
5. American Psychiatric Association Practice guideline for the treatment of patients with panic disorder. Washington, DC: American Psychiatric Association; 1998.
6. Argus v Scheppegrell 472 So. 2d 573 (La. 1985).
7. American Psychiatric Association. Principles of medical ethics with annotations especially applicable to psychiatry, 2006 edition. Available at: http://www.psych.org/psych_pract/ethics/ppaethics.cfm. Accessed August 28, 2006.
8. Patten SB, Love EJ. Neuropsychiatric adverse drug reactions: passive reports to Health and Welfare Canada’s adverse reaction database (1965-present). Int J Psychiatry Med 1994;24:45-62.
9. Michel L, Lang JP. Benzodiazepines and forensic aspects. Encephale 2003;29:479-85.
10. Hughes PH, Brandenburg N, Baldwin DC, et al. Prevalence of substance abuse among US physicians. JAMA 1992;267:2333-9.
1. Brunette MF, Noordsy DL, Xie H, et al. Benzodiazepine use and abuse among patients with severe mental illness and co-occurring substance use disorders. Psychiatr Serv 2003;54:1395-401.
2. Posternak MA, Mueller TI. Assessing the risks and benefits of benzodiazepines for anxiety disorders in patients with a history of substance abuse or dependence. Am J Addict 2001;10:48-68.
3. Uhlenhuth EH, Balter MB, Ban TA, et al. International study of expert judgment on therapeutic use of benzodiazepines and other psychotherapeutic medications: IV. Therapeutic dose dependence and abuse liability of benzodiazepines in the long-term treatment of anxiety disorders. J Clin Psychopharmacol 1999;19(suppl 2):23S-29S.
4. U.S. Department of Health and Human Services. National Survey on Drug Use and Health. http://www.oas.samhsa.gov/nhsda.htm; accessed August 23, 2006.
5. American Psychiatric Association Practice guideline for the treatment of patients with panic disorder. Washington, DC: American Psychiatric Association; 1998.
6. Argus v Scheppegrell 472 So. 2d 573 (La. 1985).
7. American Psychiatric Association. Principles of medical ethics with annotations especially applicable to psychiatry, 2006 edition. Available at: http://www.psych.org/psych_pract/ethics/ppaethics.cfm. Accessed August 28, 2006.
8. Patten SB, Love EJ. Neuropsychiatric adverse drug reactions: passive reports to Health and Welfare Canada’s adverse reaction database (1965-present). Int J Psychiatry Med 1994;24:45-62.
9. Michel L, Lang JP. Benzodiazepines and forensic aspects. Encephale 2003;29:479-85.
10. Hughes PH, Brandenburg N, Baldwin DC, et al. Prevalence of substance abuse among US physicians. JAMA 1992;267:2333-9.
New warnings on stimulants for ADHD: Cause for alarm?
In August the FDA called for new warnings on stimulants used for attention-deficit/hyperactivity disorder (ADHD). Amphetamines now carry black box warnings that say, “Misuse of amphetamines may cause sudden death and serious cardiovascular adverse events.” Amphetamines and methylphenidates used for ADHD include expanded information about cardiovascular risks at usual dosages for patients with heart conditions.
To examine the clinical implications of these warnings, Current Psychiatry hosted a conversation between ADHD experts Anthony Rostain, MD, MA, and Lenard Adler, MD.
Dr. Rostain: Changes to warnings on ADHD medications have many psychiatrists looking for guidance on using stimulants. Can you give us some background and discuss the labeling changes?
Dr. Adler: Stimulants have been used for more than 40 years as ADHD treatments, and they’ve been shown to be highly effective. The FDA, which monitors issues of cardiovascular safety and stimulants in an ongoing way, examined specific isolated cases and changed some of the warnings as a result.
Dr. Rostain: What should practicing psychiatrists be concerned about if they’re thinking of prescribing stimulants for an ADHD patient?
Dr. Adler: The take-home point is that stimulants—because of the way they work—have been known to have minor effects of increasing blood pressure and pulse (Box 1).1-3 Clinicians have known about issues regarding stimulant use by patients with pre-existing cardiovascular conditions, but now the warnings are more formal for the methylphenidate and amphetamine products.
Dr. Rostain: An FDA committee recommended black box warnings on all stimulants used for ADHD, but the FDA decided instead to clarify warnings in prescription information for some medications. What was the FDA process?
Dr. Adler: The discussion was internal at the FDA, so I can’t say what their thinking was. The black box warning on amphetamines notes two issues. One is the potential for abuse and diversion, and the other warns of potential for sudden death and serious cardiovascular effects if the drug is misused. A warning has also been placed on all methylphenidate products regarding cardiovascular risk for patients with pre-existing cardiovascular conditions, but it is not a black box warning.
in healthy children and adults
Researchers at Massachusetts General Hospital have examined the effects of ADHD medications on blood pressure and heart rate in children and adults.
Children and adolescents. The first study1 was a 1-year extension of an open-label trial of once-daily, osmotic-release methylphenidate (MPH) in 432 children (age 6 to 13) with ADHD. Their blood pressure and heart rate were recorded at baseline and monthly.
At 12 months, MPH use at 18 to 54 mg/d was associated with minor but statistically significant mean increases in:
- systolic blood pressure (3.3 mm Hg [P<0.001])
- diastolic blood pressure (1.5 mm Hg [P<0.001])
- heart rate (3.9 bpm [P<0.0001]).
Adults. In a 24-month study,2 223 healthy adults with ADHD (age≥18) received mixed amphetamine salts extended-release (MAS XR) in an open-label extension of a 4-week, double-blind, placebo-controlled trial. MAS XR was started at 20 mg/d for 1 week, then increased up to 60 mg/d based on therapeutic effect, as measured by the ADHD Rating Scale IV.
Blood pressure and pulse were measured at baseline, weekly, then monthly, and 12-lead ECGs were obtained at baseline, weekly, then at 3- and 6-month intervals. Changes after 2 years were small and not statistically significant:
- systolic blood pressure (2.3±12.5 mm Hg)
- diastolic blood pressure (1.3±9.2 mm Hg)
- pulse (2.1±13.4 bpm).
A clinically insignificant increase was observed in the mean QTcB interval (7.2 msec; P<0.001), although no patient’s QTcB interval exceeded 480 msec. Seven patients dropped out because of cardiovascular side effects (5 with hypertension, and 2 with palpitation/tachycardia), which were not reported as being serious.
Stimulants and nonstimulants. In another study,3 the same researchers analyzed the cardiovascular effects of three stimulants (methylphenidate, amphetamine compounds, and pemoline) and two nonstimulants (bupropion and desipramine) used to treat ADHD in adults. Data on a total of 125 patients (mean age 39±9 years) from three previous placebo-controlled studies were re-examined for the medications’ effects on blood pressure and heart rate.
Minor but statistically significant changes in blood pressure and heart rate were found to be associated with both stimulant and nonstimulant medications:
- systolic blood pressure (bupropion, +5.9 mm Hg [P<0.05]; amphetamine, +5.4 mm Hg [P<0.05])
- diastolic blood pressure (desipramine, +7.1 mm Hg [P<0.05])
- heart rate (bupropion, +6.9 bpm [P<0.05]; amphetamine, +7.3 bpm [P<0.05]; methylphenidate, +4.5 bpm [P<0.05]).
In the last two studies, the authors concluded that although the cardiovascular effects of ADHD medications in healthy adults were minimal, clinicians should monitor vital signs at baseline and periodically during treatment.
Dr. Rostain: How were the warnings clarified?
Dr. Adler: The FDA has changed the language. Now physicians are warned that sudden death can occur at usual doses in patients with a pre-existing structural cardiac abnormality or other serious heart problem. So, stimulants generally should not be used in children or adolescents with known serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, or other serious cardiac problems that may place them at increased vulnerability to the sympathomimetic effects of a stimulant drug.
Dr. Rostain: What about adults?
Dr. Adler: The language is the same for adults. Adults have a greater likelihood than children of having a history of serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, coronary artery disease, or other cardiac problems. Adults with such abnormalities generally should not be treated with stimulant drugs.
Dr. Rostain: What’s the impact for clinicians?
Dr. Adler: Clinicians have known that stimulants should not be used in patients with significant pre-existing cardiovascular conditions. That generally includes structural abnormalities such as serious heart murmurs and abnormalities of the electro-conduction of the impulse through the heart. When patients present with a history of cardiac abnormalities, clinicians should speak to the pediatrician, primary care physician (PCP), or cardiologist, go over the risk factors, and decide whether these medications can be prescribed for the patient.
Dr. Rostain: Should psychiatrists perform screening tests before prescribing stimulants? When should they consult with a specialist?
Dr. Adler: There is no recommendation in the prescribing information. But clearly a clinician should determine whether a patient has structural cardiac abnormalities or serious heart problems. That means taking a history about heart murmur, syncope, or other serious heart problems. Also, you want to know if the patient is hypertensive. The burden is on the prescribing clinician.
Dr. Rostain: Suppose you have a patient with hypertension or a history of a heart condition, should that patient first be evaluated by a cardiologist? What about a screening ECG?
Dr. Adler: There are no specific recommendations. If clinicians have questions about prescribing the medication, they should consult with the patient’s PCP or cardiologist.
Dr. Rostain: Let’s say the patient has some heart issues, but the PCP or pediatrician gives the goahead to prescribe stimulants. What sort of monitoring do you recommend?
Dr. Adler: I can’t answer that directly. Clearly, you’re going to want to partner with the PCP to establish a plan of how to carefully monitor this patient. FDA guidelines recommend ongoing blood pressure monitoring, especially if the patient is hypertensive, but do not specify how often.
Dr. Rostain: What alternatives do psychiatrists have when treating ADHD in patients in whom stimulants may pose some risk?
Dr. Adler: The only approved nonstimulant ADHD medication is atomoxetine, the labeling of which carries language about possible effects on blood pressure. The FDA warning about structural cardiac abnormalities has not been extended to atomoxetine, but blood pressure needs to be monitored. Whether our medical colleagues feel comfortable using a nonstimulant in patients with structural cardiac abnormalities has not been determined.
Dr. Rostain: In the absence of guidelines in the new warnings on stimulants, are there any studies to help clinicians with treatment and monitoring?
Dr. Adler: There’s very little data. A group at Massachusetts General Hospital has been studying the effects of ADHD medication on adults with hypertension (Box 2).4 That’s a different issue than a structural cardiac abnormality, but at least we have some data. This group found that you can safely give stimulants to hypertensive patients by partnering with medical colleagues and monitoring the patient carefully. Antihypertensive dosages may need to be adjusted during psychostimulant treatment.
Dr. Rostain: How do you choose a medication if your patient has a structural heart abnormality?
Dr. Adler: Again, we don’t have a lot of data. The decision would depend on the cardiac abnormality and the consulting physician’s comfort level. Keep in mind that psychostimulants have a short duration of effect, so the effects of the medication can dissipate fairly quickly. Again, the decision to medicate a patient with pre-existing cardiac abnormalities must be done with medical guidance.
In a short-term, open-label trial by Wilens et al,4 13 adults with ADHD and hypertension received mixed amphetamine salts extended-release (MAS-XR), up to 60 mg/d, for 6 weeks (phase 1), then discontinued MAS-XR for 2 weeks (phase 2). All patients had normal blood pressure (<135/85 mm Hg) for at least 4 weeks before entering the study and received a comprehensive clinical assessment, including ECG. Blood pressure was measured manually at each clinic visit.
Single episodes of hypertension (>140/90 mm Hg) occurred at similar rates in each phase, but these episodes were not sustained at any two consecutive visits. Group mean systolic and diastolic blood pressures and pulse did not increase during stimulant treatment. No clinically significant ECG changes were observed, and no serious adverse events occurred.
The authors concluded that this preliminary trial suggests that adults with ADHD and controlled hypertension can be safely treated with stimulant medications.
Dr. Rostain: So are you saying clinicians should make decisions about prescribing stimulants for patients with ADHD on a case-by-case basis?
Dr. Adler: Exactly.
Dr. Rostain: What about children and adolescents who have unknown structural heart defects? A lot of parents are concerned about reports of sudden cardiac death in young athletes, such as when playing soccer or basketball. Is there any way for practitioners to protect children with ADHD from an unexpected event?
Dr. Adler: In general, stimulants are safe medications, but we don’t have guidelines to help us determine who will need an ECG and who will not. Children are less likely to have had an ECG in the past than an adult, so it’s important to do a history, obtain input from the pediatrician or PCP, and clearly review the risks and benefits of medication therapy with the patient’s family.
Dr. Rostain: What would you advise clinicians to tell parents of children with ADHD or adult patients who have concerns about the new labeling on stimulants?
Dr. Adler: It would be a shame if patients were not receiving treatment for ADHD because of unfounded medical concerns. When these medications are used appropriately, they have dramatic and positive affects on ADHD.
ADHD is common and highly impairing. Deciding not to treat it has serious consequences in terms of divorce, separation, underperformance in school and on the job, unemployment, smoking, substance use, and issues with motor vehicle accidents and driving.
The goal of treatment is for our patients to get better, and ADHD is highly treatable with medication. But we must be cognizant of the warnings and prescribe medications appropriately. The message is that we’ve got to work collaboratively with our partners in medicine and, in the absence of guidelines, use good common sense.
Related resources
- Wilens TE, Hammerness PG, Biederman J, et al. Blood pressure changes associated with medication treatment of adults with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2005;66:253-9.
Drug brand names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Methylphenidate • Concerta, Ritalin
- Mixed amphetamine salts • Adderall
- Pemoline • Cylert
Disclosures
Dr. Adler is a consultant to and receives grant/research support from Abbott Laboratories, Cephalon, Cortex Pharmaceuticals, Eli Lilly and Company, New River Pharmaceuticals, Novartis Pharmaceuticals Corp., Ortho-McNeil, Pfizer, and Shire. He also receives grant/research support from Bristol-Myers Squibb and Merck and Co., and is a speaker for Eli Lilly and Company.
Dr. Rostain is a consultant to Shire and a speaker for Eli Lilly and Company and Ortho-McNeil.
1. Wilens TE, Biederman J, Lerner M. Concerta Study Group. Effects of once-daily osmotic-release methylphenidate on blood pressure and heart rate in children with attention-deficit/hyperactivity disorder: results from a one-year follow-up study. J Clin Psychopharmacol 2004;24(1):36-41.
2. Biederman J, Spencer TJ, Wilens TE, et al. Long-term safety and effectiveness of mixed amphetamine salts extended release in adults with ADHD. CNS Spectr 2005;10(12 suppl 20):16-25.
3. Wilens TE, Hammerness PG, Biederman J, et al. Blood pressure changes associated with medication treatment of adults with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2005;66(2):253-9.
4. Wilens TE, Zusman RM, Hammerness PG, et al. An open-label study of the tolerability of mixed amphetamine salts in adults with attention-deficit/ hyperactivity disorder and treated primary essential hypertension. J Clin Psychiatry 2006;67(5):696-702.
Dr. Adler is associate professor of psychiatry and director of the adult ADHD program at New York University Medical Center. He recently published a book for patients, Scattered Minds: Hope and Help for Adults with ADHD.
Dr. Rostain is associate professor of psychiatry and pediatrics and director of education, department of psychiatry, University of Pennsylvania School of Medicine, Philadelphia.
In August the FDA called for new warnings on stimulants used for attention-deficit/hyperactivity disorder (ADHD). Amphetamines now carry black box warnings that say, “Misuse of amphetamines may cause sudden death and serious cardiovascular adverse events.” Amphetamines and methylphenidates used for ADHD include expanded information about cardiovascular risks at usual dosages for patients with heart conditions.
To examine the clinical implications of these warnings, Current Psychiatry hosted a conversation between ADHD experts Anthony Rostain, MD, MA, and Lenard Adler, MD.
Dr. Rostain: Changes to warnings on ADHD medications have many psychiatrists looking for guidance on using stimulants. Can you give us some background and discuss the labeling changes?
Dr. Adler: Stimulants have been used for more than 40 years as ADHD treatments, and they’ve been shown to be highly effective. The FDA, which monitors issues of cardiovascular safety and stimulants in an ongoing way, examined specific isolated cases and changed some of the warnings as a result.
Dr. Rostain: What should practicing psychiatrists be concerned about if they’re thinking of prescribing stimulants for an ADHD patient?
Dr. Adler: The take-home point is that stimulants—because of the way they work—have been known to have minor effects of increasing blood pressure and pulse (Box 1).1-3 Clinicians have known about issues regarding stimulant use by patients with pre-existing cardiovascular conditions, but now the warnings are more formal for the methylphenidate and amphetamine products.
Dr. Rostain: An FDA committee recommended black box warnings on all stimulants used for ADHD, but the FDA decided instead to clarify warnings in prescription information for some medications. What was the FDA process?
Dr. Adler: The discussion was internal at the FDA, so I can’t say what their thinking was. The black box warning on amphetamines notes two issues. One is the potential for abuse and diversion, and the other warns of potential for sudden death and serious cardiovascular effects if the drug is misused. A warning has also been placed on all methylphenidate products regarding cardiovascular risk for patients with pre-existing cardiovascular conditions, but it is not a black box warning.
in healthy children and adults
Researchers at Massachusetts General Hospital have examined the effects of ADHD medications on blood pressure and heart rate in children and adults.
Children and adolescents. The first study1 was a 1-year extension of an open-label trial of once-daily, osmotic-release methylphenidate (MPH) in 432 children (age 6 to 13) with ADHD. Their blood pressure and heart rate were recorded at baseline and monthly.
At 12 months, MPH use at 18 to 54 mg/d was associated with minor but statistically significant mean increases in:
- systolic blood pressure (3.3 mm Hg [P<0.001])
- diastolic blood pressure (1.5 mm Hg [P<0.001])
- heart rate (3.9 bpm [P<0.0001]).
Adults. In a 24-month study,2 223 healthy adults with ADHD (age≥18) received mixed amphetamine salts extended-release (MAS XR) in an open-label extension of a 4-week, double-blind, placebo-controlled trial. MAS XR was started at 20 mg/d for 1 week, then increased up to 60 mg/d based on therapeutic effect, as measured by the ADHD Rating Scale IV.
Blood pressure and pulse were measured at baseline, weekly, then monthly, and 12-lead ECGs were obtained at baseline, weekly, then at 3- and 6-month intervals. Changes after 2 years were small and not statistically significant:
- systolic blood pressure (2.3±12.5 mm Hg)
- diastolic blood pressure (1.3±9.2 mm Hg)
- pulse (2.1±13.4 bpm).
A clinically insignificant increase was observed in the mean QTcB interval (7.2 msec; P<0.001), although no patient’s QTcB interval exceeded 480 msec. Seven patients dropped out because of cardiovascular side effects (5 with hypertension, and 2 with palpitation/tachycardia), which were not reported as being serious.
Stimulants and nonstimulants. In another study,3 the same researchers analyzed the cardiovascular effects of three stimulants (methylphenidate, amphetamine compounds, and pemoline) and two nonstimulants (bupropion and desipramine) used to treat ADHD in adults. Data on a total of 125 patients (mean age 39±9 years) from three previous placebo-controlled studies were re-examined for the medications’ effects on blood pressure and heart rate.
Minor but statistically significant changes in blood pressure and heart rate were found to be associated with both stimulant and nonstimulant medications:
- systolic blood pressure (bupropion, +5.9 mm Hg [P<0.05]; amphetamine, +5.4 mm Hg [P<0.05])
- diastolic blood pressure (desipramine, +7.1 mm Hg [P<0.05])
- heart rate (bupropion, +6.9 bpm [P<0.05]; amphetamine, +7.3 bpm [P<0.05]; methylphenidate, +4.5 bpm [P<0.05]).
In the last two studies, the authors concluded that although the cardiovascular effects of ADHD medications in healthy adults were minimal, clinicians should monitor vital signs at baseline and periodically during treatment.
Dr. Rostain: How were the warnings clarified?
Dr. Adler: The FDA has changed the language. Now physicians are warned that sudden death can occur at usual doses in patients with a pre-existing structural cardiac abnormality or other serious heart problem. So, stimulants generally should not be used in children or adolescents with known serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, or other serious cardiac problems that may place them at increased vulnerability to the sympathomimetic effects of a stimulant drug.
Dr. Rostain: What about adults?
Dr. Adler: The language is the same for adults. Adults have a greater likelihood than children of having a history of serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, coronary artery disease, or other cardiac problems. Adults with such abnormalities generally should not be treated with stimulant drugs.
Dr. Rostain: What’s the impact for clinicians?
Dr. Adler: Clinicians have known that stimulants should not be used in patients with significant pre-existing cardiovascular conditions. That generally includes structural abnormalities such as serious heart murmurs and abnormalities of the electro-conduction of the impulse through the heart. When patients present with a history of cardiac abnormalities, clinicians should speak to the pediatrician, primary care physician (PCP), or cardiologist, go over the risk factors, and decide whether these medications can be prescribed for the patient.
Dr. Rostain: Should psychiatrists perform screening tests before prescribing stimulants? When should they consult with a specialist?
Dr. Adler: There is no recommendation in the prescribing information. But clearly a clinician should determine whether a patient has structural cardiac abnormalities or serious heart problems. That means taking a history about heart murmur, syncope, or other serious heart problems. Also, you want to know if the patient is hypertensive. The burden is on the prescribing clinician.
Dr. Rostain: Suppose you have a patient with hypertension or a history of a heart condition, should that patient first be evaluated by a cardiologist? What about a screening ECG?
Dr. Adler: There are no specific recommendations. If clinicians have questions about prescribing the medication, they should consult with the patient’s PCP or cardiologist.
Dr. Rostain: Let’s say the patient has some heart issues, but the PCP or pediatrician gives the goahead to prescribe stimulants. What sort of monitoring do you recommend?
Dr. Adler: I can’t answer that directly. Clearly, you’re going to want to partner with the PCP to establish a plan of how to carefully monitor this patient. FDA guidelines recommend ongoing blood pressure monitoring, especially if the patient is hypertensive, but do not specify how often.
Dr. Rostain: What alternatives do psychiatrists have when treating ADHD in patients in whom stimulants may pose some risk?
Dr. Adler: The only approved nonstimulant ADHD medication is atomoxetine, the labeling of which carries language about possible effects on blood pressure. The FDA warning about structural cardiac abnormalities has not been extended to atomoxetine, but blood pressure needs to be monitored. Whether our medical colleagues feel comfortable using a nonstimulant in patients with structural cardiac abnormalities has not been determined.
Dr. Rostain: In the absence of guidelines in the new warnings on stimulants, are there any studies to help clinicians with treatment and monitoring?
Dr. Adler: There’s very little data. A group at Massachusetts General Hospital has been studying the effects of ADHD medication on adults with hypertension (Box 2).4 That’s a different issue than a structural cardiac abnormality, but at least we have some data. This group found that you can safely give stimulants to hypertensive patients by partnering with medical colleagues and monitoring the patient carefully. Antihypertensive dosages may need to be adjusted during psychostimulant treatment.
Dr. Rostain: How do you choose a medication if your patient has a structural heart abnormality?
Dr. Adler: Again, we don’t have a lot of data. The decision would depend on the cardiac abnormality and the consulting physician’s comfort level. Keep in mind that psychostimulants have a short duration of effect, so the effects of the medication can dissipate fairly quickly. Again, the decision to medicate a patient with pre-existing cardiac abnormalities must be done with medical guidance.
In a short-term, open-label trial by Wilens et al,4 13 adults with ADHD and hypertension received mixed amphetamine salts extended-release (MAS-XR), up to 60 mg/d, for 6 weeks (phase 1), then discontinued MAS-XR for 2 weeks (phase 2). All patients had normal blood pressure (<135/85 mm Hg) for at least 4 weeks before entering the study and received a comprehensive clinical assessment, including ECG. Blood pressure was measured manually at each clinic visit.
Single episodes of hypertension (>140/90 mm Hg) occurred at similar rates in each phase, but these episodes were not sustained at any two consecutive visits. Group mean systolic and diastolic blood pressures and pulse did not increase during stimulant treatment. No clinically significant ECG changes were observed, and no serious adverse events occurred.
The authors concluded that this preliminary trial suggests that adults with ADHD and controlled hypertension can be safely treated with stimulant medications.
Dr. Rostain: So are you saying clinicians should make decisions about prescribing stimulants for patients with ADHD on a case-by-case basis?
Dr. Adler: Exactly.
Dr. Rostain: What about children and adolescents who have unknown structural heart defects? A lot of parents are concerned about reports of sudden cardiac death in young athletes, such as when playing soccer or basketball. Is there any way for practitioners to protect children with ADHD from an unexpected event?
Dr. Adler: In general, stimulants are safe medications, but we don’t have guidelines to help us determine who will need an ECG and who will not. Children are less likely to have had an ECG in the past than an adult, so it’s important to do a history, obtain input from the pediatrician or PCP, and clearly review the risks and benefits of medication therapy with the patient’s family.
Dr. Rostain: What would you advise clinicians to tell parents of children with ADHD or adult patients who have concerns about the new labeling on stimulants?
Dr. Adler: It would be a shame if patients were not receiving treatment for ADHD because of unfounded medical concerns. When these medications are used appropriately, they have dramatic and positive affects on ADHD.
ADHD is common and highly impairing. Deciding not to treat it has serious consequences in terms of divorce, separation, underperformance in school and on the job, unemployment, smoking, substance use, and issues with motor vehicle accidents and driving.
The goal of treatment is for our patients to get better, and ADHD is highly treatable with medication. But we must be cognizant of the warnings and prescribe medications appropriately. The message is that we’ve got to work collaboratively with our partners in medicine and, in the absence of guidelines, use good common sense.
Related resources
- Wilens TE, Hammerness PG, Biederman J, et al. Blood pressure changes associated with medication treatment of adults with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2005;66:253-9.
Drug brand names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Methylphenidate • Concerta, Ritalin
- Mixed amphetamine salts • Adderall
- Pemoline • Cylert
Disclosures
Dr. Adler is a consultant to and receives grant/research support from Abbott Laboratories, Cephalon, Cortex Pharmaceuticals, Eli Lilly and Company, New River Pharmaceuticals, Novartis Pharmaceuticals Corp., Ortho-McNeil, Pfizer, and Shire. He also receives grant/research support from Bristol-Myers Squibb and Merck and Co., and is a speaker for Eli Lilly and Company.
Dr. Rostain is a consultant to Shire and a speaker for Eli Lilly and Company and Ortho-McNeil.
In August the FDA called for new warnings on stimulants used for attention-deficit/hyperactivity disorder (ADHD). Amphetamines now carry black box warnings that say, “Misuse of amphetamines may cause sudden death and serious cardiovascular adverse events.” Amphetamines and methylphenidates used for ADHD include expanded information about cardiovascular risks at usual dosages for patients with heart conditions.
To examine the clinical implications of these warnings, Current Psychiatry hosted a conversation between ADHD experts Anthony Rostain, MD, MA, and Lenard Adler, MD.
Dr. Rostain: Changes to warnings on ADHD medications have many psychiatrists looking for guidance on using stimulants. Can you give us some background and discuss the labeling changes?
Dr. Adler: Stimulants have been used for more than 40 years as ADHD treatments, and they’ve been shown to be highly effective. The FDA, which monitors issues of cardiovascular safety and stimulants in an ongoing way, examined specific isolated cases and changed some of the warnings as a result.
Dr. Rostain: What should practicing psychiatrists be concerned about if they’re thinking of prescribing stimulants for an ADHD patient?
Dr. Adler: The take-home point is that stimulants—because of the way they work—have been known to have minor effects of increasing blood pressure and pulse (Box 1).1-3 Clinicians have known about issues regarding stimulant use by patients with pre-existing cardiovascular conditions, but now the warnings are more formal for the methylphenidate and amphetamine products.
Dr. Rostain: An FDA committee recommended black box warnings on all stimulants used for ADHD, but the FDA decided instead to clarify warnings in prescription information for some medications. What was the FDA process?
Dr. Adler: The discussion was internal at the FDA, so I can’t say what their thinking was. The black box warning on amphetamines notes two issues. One is the potential for abuse and diversion, and the other warns of potential for sudden death and serious cardiovascular effects if the drug is misused. A warning has also been placed on all methylphenidate products regarding cardiovascular risk for patients with pre-existing cardiovascular conditions, but it is not a black box warning.
in healthy children and adults
Researchers at Massachusetts General Hospital have examined the effects of ADHD medications on blood pressure and heart rate in children and adults.
Children and adolescents. The first study1 was a 1-year extension of an open-label trial of once-daily, osmotic-release methylphenidate (MPH) in 432 children (age 6 to 13) with ADHD. Their blood pressure and heart rate were recorded at baseline and monthly.
At 12 months, MPH use at 18 to 54 mg/d was associated with minor but statistically significant mean increases in:
- systolic blood pressure (3.3 mm Hg [P<0.001])
- diastolic blood pressure (1.5 mm Hg [P<0.001])
- heart rate (3.9 bpm [P<0.0001]).
Adults. In a 24-month study,2 223 healthy adults with ADHD (age≥18) received mixed amphetamine salts extended-release (MAS XR) in an open-label extension of a 4-week, double-blind, placebo-controlled trial. MAS XR was started at 20 mg/d for 1 week, then increased up to 60 mg/d based on therapeutic effect, as measured by the ADHD Rating Scale IV.
Blood pressure and pulse were measured at baseline, weekly, then monthly, and 12-lead ECGs were obtained at baseline, weekly, then at 3- and 6-month intervals. Changes after 2 years were small and not statistically significant:
- systolic blood pressure (2.3±12.5 mm Hg)
- diastolic blood pressure (1.3±9.2 mm Hg)
- pulse (2.1±13.4 bpm).
A clinically insignificant increase was observed in the mean QTcB interval (7.2 msec; P<0.001), although no patient’s QTcB interval exceeded 480 msec. Seven patients dropped out because of cardiovascular side effects (5 with hypertension, and 2 with palpitation/tachycardia), which were not reported as being serious.
Stimulants and nonstimulants. In another study,3 the same researchers analyzed the cardiovascular effects of three stimulants (methylphenidate, amphetamine compounds, and pemoline) and two nonstimulants (bupropion and desipramine) used to treat ADHD in adults. Data on a total of 125 patients (mean age 39±9 years) from three previous placebo-controlled studies were re-examined for the medications’ effects on blood pressure and heart rate.
Minor but statistically significant changes in blood pressure and heart rate were found to be associated with both stimulant and nonstimulant medications:
- systolic blood pressure (bupropion, +5.9 mm Hg [P<0.05]; amphetamine, +5.4 mm Hg [P<0.05])
- diastolic blood pressure (desipramine, +7.1 mm Hg [P<0.05])
- heart rate (bupropion, +6.9 bpm [P<0.05]; amphetamine, +7.3 bpm [P<0.05]; methylphenidate, +4.5 bpm [P<0.05]).
In the last two studies, the authors concluded that although the cardiovascular effects of ADHD medications in healthy adults were minimal, clinicians should monitor vital signs at baseline and periodically during treatment.
Dr. Rostain: How were the warnings clarified?
Dr. Adler: The FDA has changed the language. Now physicians are warned that sudden death can occur at usual doses in patients with a pre-existing structural cardiac abnormality or other serious heart problem. So, stimulants generally should not be used in children or adolescents with known serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, or other serious cardiac problems that may place them at increased vulnerability to the sympathomimetic effects of a stimulant drug.
Dr. Rostain: What about adults?
Dr. Adler: The language is the same for adults. Adults have a greater likelihood than children of having a history of serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, coronary artery disease, or other cardiac problems. Adults with such abnormalities generally should not be treated with stimulant drugs.
Dr. Rostain: What’s the impact for clinicians?
Dr. Adler: Clinicians have known that stimulants should not be used in patients with significant pre-existing cardiovascular conditions. That generally includes structural abnormalities such as serious heart murmurs and abnormalities of the electro-conduction of the impulse through the heart. When patients present with a history of cardiac abnormalities, clinicians should speak to the pediatrician, primary care physician (PCP), or cardiologist, go over the risk factors, and decide whether these medications can be prescribed for the patient.
Dr. Rostain: Should psychiatrists perform screening tests before prescribing stimulants? When should they consult with a specialist?
Dr. Adler: There is no recommendation in the prescribing information. But clearly a clinician should determine whether a patient has structural cardiac abnormalities or serious heart problems. That means taking a history about heart murmur, syncope, or other serious heart problems. Also, you want to know if the patient is hypertensive. The burden is on the prescribing clinician.
Dr. Rostain: Suppose you have a patient with hypertension or a history of a heart condition, should that patient first be evaluated by a cardiologist? What about a screening ECG?
Dr. Adler: There are no specific recommendations. If clinicians have questions about prescribing the medication, they should consult with the patient’s PCP or cardiologist.
Dr. Rostain: Let’s say the patient has some heart issues, but the PCP or pediatrician gives the goahead to prescribe stimulants. What sort of monitoring do you recommend?
Dr. Adler: I can’t answer that directly. Clearly, you’re going to want to partner with the PCP to establish a plan of how to carefully monitor this patient. FDA guidelines recommend ongoing blood pressure monitoring, especially if the patient is hypertensive, but do not specify how often.
Dr. Rostain: What alternatives do psychiatrists have when treating ADHD in patients in whom stimulants may pose some risk?
Dr. Adler: The only approved nonstimulant ADHD medication is atomoxetine, the labeling of which carries language about possible effects on blood pressure. The FDA warning about structural cardiac abnormalities has not been extended to atomoxetine, but blood pressure needs to be monitored. Whether our medical colleagues feel comfortable using a nonstimulant in patients with structural cardiac abnormalities has not been determined.
Dr. Rostain: In the absence of guidelines in the new warnings on stimulants, are there any studies to help clinicians with treatment and monitoring?
Dr. Adler: There’s very little data. A group at Massachusetts General Hospital has been studying the effects of ADHD medication on adults with hypertension (Box 2).4 That’s a different issue than a structural cardiac abnormality, but at least we have some data. This group found that you can safely give stimulants to hypertensive patients by partnering with medical colleagues and monitoring the patient carefully. Antihypertensive dosages may need to be adjusted during psychostimulant treatment.
Dr. Rostain: How do you choose a medication if your patient has a structural heart abnormality?
Dr. Adler: Again, we don’t have a lot of data. The decision would depend on the cardiac abnormality and the consulting physician’s comfort level. Keep in mind that psychostimulants have a short duration of effect, so the effects of the medication can dissipate fairly quickly. Again, the decision to medicate a patient with pre-existing cardiac abnormalities must be done with medical guidance.
In a short-term, open-label trial by Wilens et al,4 13 adults with ADHD and hypertension received mixed amphetamine salts extended-release (MAS-XR), up to 60 mg/d, for 6 weeks (phase 1), then discontinued MAS-XR for 2 weeks (phase 2). All patients had normal blood pressure (<135/85 mm Hg) for at least 4 weeks before entering the study and received a comprehensive clinical assessment, including ECG. Blood pressure was measured manually at each clinic visit.
Single episodes of hypertension (>140/90 mm Hg) occurred at similar rates in each phase, but these episodes were not sustained at any two consecutive visits. Group mean systolic and diastolic blood pressures and pulse did not increase during stimulant treatment. No clinically significant ECG changes were observed, and no serious adverse events occurred.
The authors concluded that this preliminary trial suggests that adults with ADHD and controlled hypertension can be safely treated with stimulant medications.
Dr. Rostain: So are you saying clinicians should make decisions about prescribing stimulants for patients with ADHD on a case-by-case basis?
Dr. Adler: Exactly.
Dr. Rostain: What about children and adolescents who have unknown structural heart defects? A lot of parents are concerned about reports of sudden cardiac death in young athletes, such as when playing soccer or basketball. Is there any way for practitioners to protect children with ADHD from an unexpected event?
Dr. Adler: In general, stimulants are safe medications, but we don’t have guidelines to help us determine who will need an ECG and who will not. Children are less likely to have had an ECG in the past than an adult, so it’s important to do a history, obtain input from the pediatrician or PCP, and clearly review the risks and benefits of medication therapy with the patient’s family.
Dr. Rostain: What would you advise clinicians to tell parents of children with ADHD or adult patients who have concerns about the new labeling on stimulants?
Dr. Adler: It would be a shame if patients were not receiving treatment for ADHD because of unfounded medical concerns. When these medications are used appropriately, they have dramatic and positive affects on ADHD.
ADHD is common and highly impairing. Deciding not to treat it has serious consequences in terms of divorce, separation, underperformance in school and on the job, unemployment, smoking, substance use, and issues with motor vehicle accidents and driving.
The goal of treatment is for our patients to get better, and ADHD is highly treatable with medication. But we must be cognizant of the warnings and prescribe medications appropriately. The message is that we’ve got to work collaboratively with our partners in medicine and, in the absence of guidelines, use good common sense.
Related resources
- Wilens TE, Hammerness PG, Biederman J, et al. Blood pressure changes associated with medication treatment of adults with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2005;66:253-9.
Drug brand names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Methylphenidate • Concerta, Ritalin
- Mixed amphetamine salts • Adderall
- Pemoline • Cylert
Disclosures
Dr. Adler is a consultant to and receives grant/research support from Abbott Laboratories, Cephalon, Cortex Pharmaceuticals, Eli Lilly and Company, New River Pharmaceuticals, Novartis Pharmaceuticals Corp., Ortho-McNeil, Pfizer, and Shire. He also receives grant/research support from Bristol-Myers Squibb and Merck and Co., and is a speaker for Eli Lilly and Company.
Dr. Rostain is a consultant to Shire and a speaker for Eli Lilly and Company and Ortho-McNeil.
1. Wilens TE, Biederman J, Lerner M. Concerta Study Group. Effects of once-daily osmotic-release methylphenidate on blood pressure and heart rate in children with attention-deficit/hyperactivity disorder: results from a one-year follow-up study. J Clin Psychopharmacol 2004;24(1):36-41.
2. Biederman J, Spencer TJ, Wilens TE, et al. Long-term safety and effectiveness of mixed amphetamine salts extended release in adults with ADHD. CNS Spectr 2005;10(12 suppl 20):16-25.
3. Wilens TE, Hammerness PG, Biederman J, et al. Blood pressure changes associated with medication treatment of adults with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2005;66(2):253-9.
4. Wilens TE, Zusman RM, Hammerness PG, et al. An open-label study of the tolerability of mixed amphetamine salts in adults with attention-deficit/ hyperactivity disorder and treated primary essential hypertension. J Clin Psychiatry 2006;67(5):696-702.
Dr. Adler is associate professor of psychiatry and director of the adult ADHD program at New York University Medical Center. He recently published a book for patients, Scattered Minds: Hope and Help for Adults with ADHD.
Dr. Rostain is associate professor of psychiatry and pediatrics and director of education, department of psychiatry, University of Pennsylvania School of Medicine, Philadelphia.
1. Wilens TE, Biederman J, Lerner M. Concerta Study Group. Effects of once-daily osmotic-release methylphenidate on blood pressure and heart rate in children with attention-deficit/hyperactivity disorder: results from a one-year follow-up study. J Clin Psychopharmacol 2004;24(1):36-41.
2. Biederman J, Spencer TJ, Wilens TE, et al. Long-term safety and effectiveness of mixed amphetamine salts extended release in adults with ADHD. CNS Spectr 2005;10(12 suppl 20):16-25.
3. Wilens TE, Hammerness PG, Biederman J, et al. Blood pressure changes associated with medication treatment of adults with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2005;66(2):253-9.
4. Wilens TE, Zusman RM, Hammerness PG, et al. An open-label study of the tolerability of mixed amphetamine salts in adults with attention-deficit/ hyperactivity disorder and treated primary essential hypertension. J Clin Psychiatry 2006;67(5):696-702.
Dr. Adler is associate professor of psychiatry and director of the adult ADHD program at New York University Medical Center. He recently published a book for patients, Scattered Minds: Hope and Help for Adults with ADHD.
Dr. Rostain is associate professor of psychiatry and pediatrics and director of education, department of psychiatry, University of Pennsylvania School of Medicine, Philadelphia.
Civil War Surgery

Thomas “Stonewall” Jackson and a small group of men rode at dusk along the still-steaming battlefield perimeter on May 2, 1863. During daylight the Confederates had won a stunning victory at Chancellorsville, Va. Despite marked manpower and hardware inferiority, the leadership of Generals Robert Lee and Stonewall Jackson sent Union General “Fighting” Joe Hooker literally running from the battlefield. Jackson’s evening patrol was to ensure stability and set his plan for the next day.
Encountering other Confederate soldiers on the path in the waning light, the Jackson patrol exchanged words with the men, but the North Carolina contingent of soldiers did not believe the approaching mounted men were Confederate, so they fired into their midst. General Jackson fell, having suffered two gunshot wounds. The large caliber (.58), soft-lead minie ball was heavy, and it expanded when it went through tissue, resulting in shattered bone and tearing of internal soft tissues. Minie ball injuries to an arm or a leg usually meant amputation, and torso or head wounds were most often fatal.
Friendly fire was the source of General Jackson’s mortal upper-arm wound. He was attended by the 27-year-old surgeon, Doctor Hunter McGuire, medical director of the left wing of the Army of Northern Virginia, under General Jackson’s command. Jackson had sustained a minor wound to his right hand and a severe, heavily bleeding wound to his left upper arm. Dr. McGuire amputated the left arm about two inches below the shoulder, administering chloroform anesthesia. Post-operatively, Dr. McGuire diagnosed his patient with pneumonia. Jackson remained ill and died a week later from, presumably, pneumonia. Interestingly, some historians wonder if he actually died of a pulmonary embolus because he had been in bed rest for a week and died of a respiratory event. Either way, he succumbed to complications of his initial injury.
Civil War-era surgery was a gruesome event; it is remarkable that so many of the soldiers actually survived the ordeal. Anesthesia was administered by placing a handkerchief over the nose and mouth and dropping chloroform on the cloth until the patient was unconscious. The surgeon then had about 10-15 minutes to accomplish the surgery with the patient asleep. The most common Civil War surgery was the amputation of an extremity and this was usually accomplished in about 10 minutes. First-person reports and photographic documentation confirm the mounds of discarded limbs outside Civil War field hospitals. It is interesting to note that the use of anesthesia without a protected airway—as in the case of Stonewall Jackson—was the likely etiology of his post-operative (aspiration) pneumonia.
Although the English surgeon Joseph Lister was on his way to setting the standard for antiseptic surgery, this concept did not make its way to the United States until after the 1860s. The Civil War ended in 1865. During the Civil War, surgical instruments were rinsed during and between cases in a tub of increasingly bloody cold water. The surgeon made his way from patient to patient in pus- and blood-splattered garments; it is little wonder that fever was a common and dreaded post-operative event. Surgical fever was often the result of pyemia, (literally pus in the blood), which presumably was the same diagnosis as sepsis. Other deadly complications included erysipelas, osteomyelitis, gangrene, tetanus, and pneumonia. Physicians had almost no way of treating penetrating torso injuries. Surgery was occasionally attempted, but usually fatal. Lacking any modality to localize the intra-abdominal or chest injury pre-operatively and realizing the need to complete the surgery in just minutes, torso surgery was usually not an option.
Those who survived their wounds—and their treatments—must have been a hardy lot. One wonders how many lives would have been saved with just a rudimentary understanding of aseptic technique. Today we face the same issues: amputation, post-operative pneumonia and pulmonary embolism, and wound infections. The problems of yesterday still remain the problems of today and tomorrow. TH
Thomas “Stonewall” Jackson and a small group of men rode at dusk along the still-steaming battlefield perimeter on May 2, 1863. During daylight the Confederates had won a stunning victory at Chancellorsville, Va. Despite marked manpower and hardware inferiority, the leadership of Generals Robert Lee and Stonewall Jackson sent Union General “Fighting” Joe Hooker literally running from the battlefield. Jackson’s evening patrol was to ensure stability and set his plan for the next day.
Encountering other Confederate soldiers on the path in the waning light, the Jackson patrol exchanged words with the men, but the North Carolina contingent of soldiers did not believe the approaching mounted men were Confederate, so they fired into their midst. General Jackson fell, having suffered two gunshot wounds. The large caliber (.58), soft-lead minie ball was heavy, and it expanded when it went through tissue, resulting in shattered bone and tearing of internal soft tissues. Minie ball injuries to an arm or a leg usually meant amputation, and torso or head wounds were most often fatal.
Friendly fire was the source of General Jackson’s mortal upper-arm wound. He was attended by the 27-year-old surgeon, Doctor Hunter McGuire, medical director of the left wing of the Army of Northern Virginia, under General Jackson’s command. Jackson had sustained a minor wound to his right hand and a severe, heavily bleeding wound to his left upper arm. Dr. McGuire amputated the left arm about two inches below the shoulder, administering chloroform anesthesia. Post-operatively, Dr. McGuire diagnosed his patient with pneumonia. Jackson remained ill and died a week later from, presumably, pneumonia. Interestingly, some historians wonder if he actually died of a pulmonary embolus because he had been in bed rest for a week and died of a respiratory event. Either way, he succumbed to complications of his initial injury.
Civil War-era surgery was a gruesome event; it is remarkable that so many of the soldiers actually survived the ordeal. Anesthesia was administered by placing a handkerchief over the nose and mouth and dropping chloroform on the cloth until the patient was unconscious. The surgeon then had about 10-15 minutes to accomplish the surgery with the patient asleep. The most common Civil War surgery was the amputation of an extremity and this was usually accomplished in about 10 minutes. First-person reports and photographic documentation confirm the mounds of discarded limbs outside Civil War field hospitals. It is interesting to note that the use of anesthesia without a protected airway—as in the case of Stonewall Jackson—was the likely etiology of his post-operative (aspiration) pneumonia.
Although the English surgeon Joseph Lister was on his way to setting the standard for antiseptic surgery, this concept did not make its way to the United States until after the 1860s. The Civil War ended in 1865. During the Civil War, surgical instruments were rinsed during and between cases in a tub of increasingly bloody cold water. The surgeon made his way from patient to patient in pus- and blood-splattered garments; it is little wonder that fever was a common and dreaded post-operative event. Surgical fever was often the result of pyemia, (literally pus in the blood), which presumably was the same diagnosis as sepsis. Other deadly complications included erysipelas, osteomyelitis, gangrene, tetanus, and pneumonia. Physicians had almost no way of treating penetrating torso injuries. Surgery was occasionally attempted, but usually fatal. Lacking any modality to localize the intra-abdominal or chest injury pre-operatively and realizing the need to complete the surgery in just minutes, torso surgery was usually not an option.
Those who survived their wounds—and their treatments—must have been a hardy lot. One wonders how many lives would have been saved with just a rudimentary understanding of aseptic technique. Today we face the same issues: amputation, post-operative pneumonia and pulmonary embolism, and wound infections. The problems of yesterday still remain the problems of today and tomorrow. TH
Thomas “Stonewall” Jackson and a small group of men rode at dusk along the still-steaming battlefield perimeter on May 2, 1863. During daylight the Confederates had won a stunning victory at Chancellorsville, Va. Despite marked manpower and hardware inferiority, the leadership of Generals Robert Lee and Stonewall Jackson sent Union General “Fighting” Joe Hooker literally running from the battlefield. Jackson’s evening patrol was to ensure stability and set his plan for the next day.
Encountering other Confederate soldiers on the path in the waning light, the Jackson patrol exchanged words with the men, but the North Carolina contingent of soldiers did not believe the approaching mounted men were Confederate, so they fired into their midst. General Jackson fell, having suffered two gunshot wounds. The large caliber (.58), soft-lead minie ball was heavy, and it expanded when it went through tissue, resulting in shattered bone and tearing of internal soft tissues. Minie ball injuries to an arm or a leg usually meant amputation, and torso or head wounds were most often fatal.
Friendly fire was the source of General Jackson’s mortal upper-arm wound. He was attended by the 27-year-old surgeon, Doctor Hunter McGuire, medical director of the left wing of the Army of Northern Virginia, under General Jackson’s command. Jackson had sustained a minor wound to his right hand and a severe, heavily bleeding wound to his left upper arm. Dr. McGuire amputated the left arm about two inches below the shoulder, administering chloroform anesthesia. Post-operatively, Dr. McGuire diagnosed his patient with pneumonia. Jackson remained ill and died a week later from, presumably, pneumonia. Interestingly, some historians wonder if he actually died of a pulmonary embolus because he had been in bed rest for a week and died of a respiratory event. Either way, he succumbed to complications of his initial injury.
Civil War-era surgery was a gruesome event; it is remarkable that so many of the soldiers actually survived the ordeal. Anesthesia was administered by placing a handkerchief over the nose and mouth and dropping chloroform on the cloth until the patient was unconscious. The surgeon then had about 10-15 minutes to accomplish the surgery with the patient asleep. The most common Civil War surgery was the amputation of an extremity and this was usually accomplished in about 10 minutes. First-person reports and photographic documentation confirm the mounds of discarded limbs outside Civil War field hospitals. It is interesting to note that the use of anesthesia without a protected airway—as in the case of Stonewall Jackson—was the likely etiology of his post-operative (aspiration) pneumonia.
Although the English surgeon Joseph Lister was on his way to setting the standard for antiseptic surgery, this concept did not make its way to the United States until after the 1860s. The Civil War ended in 1865. During the Civil War, surgical instruments were rinsed during and between cases in a tub of increasingly bloody cold water. The surgeon made his way from patient to patient in pus- and blood-splattered garments; it is little wonder that fever was a common and dreaded post-operative event. Surgical fever was often the result of pyemia, (literally pus in the blood), which presumably was the same diagnosis as sepsis. Other deadly complications included erysipelas, osteomyelitis, gangrene, tetanus, and pneumonia. Physicians had almost no way of treating penetrating torso injuries. Surgery was occasionally attempted, but usually fatal. Lacking any modality to localize the intra-abdominal or chest injury pre-operatively and realizing the need to complete the surgery in just minutes, torso surgery was usually not an option.
Those who survived their wounds—and their treatments—must have been a hardy lot. One wonders how many lives would have been saved with just a rudimentary understanding of aseptic technique. Today we face the same issues: amputation, post-operative pneumonia and pulmonary embolism, and wound infections. The problems of yesterday still remain the problems of today and tomorrow. TH
Old Doc Marsden

The Aspen were turning a golden brown, the cattle were fattened for market, and Doc Marsden was drunk again. His head lay on the two planks that served as a bar in what could only charitably be called a saloon. There were two places for a man to drink in Timberline, and this was Doc’s preferred watering hole.
Earlier that day Doc had been busy enough. There’d been a big brawl at the Triple H, and Billy Harkness had shot his younger brother, Lukas, after a lucky punch had broken Billy’s overlarge nose. It wasn’t a bad wound; Lukas had ducked, and the bullet had skimmed his back and lodged in his calf.
Doc had dressed the back wound with a poultice and fished the 0.45 slug from the gastrocnemius. He knew that much anatomy, but not much more. His hands had shaken ’till he had swigged a few swallows of what passed for bourbon. It was nervous work whittling on a Harkness. Luckily Lukas and Billy were a sight more intoxicated than Doc, and their big brother Boone Harkness was somewhere up the trail. The eldest Harkness brother had restless snake eyes. Boone never missed a thing, especially a target. He made Doc Marsden sweat. Doc gave Lukas a spoonful of laudanum, and his patient was soon snoring peacefully on the door they had used as an operating table. Doc took a small swig himself.
After he was sure that the Harkness boy was settled down and Doc’s helper Marty Johnson was there to watch over Lukas, Doc headed for the saloon and started drinking again. He pondered how he had ended up in Timberline. This hadn’t been his plan when he’d left Philadelphia all those years ago.
Back in Philadelphia his name had been Antonio Lombano. His parents had been immigrants, and he had been lucky to work for a butcher. He’d grown sick of slicing meat, and when the war came he enlisted. Anything to get away from the smell of blood and hanging beefs.
When he enlisted with the 37th infantry he’d expected to learn to shoot a gun and maybe even to die. He might have to kill a couple of Rebs, but at least he would leave Philadelphia. Instead, when they learned he had worked as a butcher, he was relegated to the cook’s tent. He was back to slicing meat. For two months the only flank he outmaneuvered was with his cutting blade.
He had been disemboweling a steer one day when a group of surgeons walked by, looking for an eyeball to dissect. They watched approvingly as he wielded his blade. Three days later he had been reassigned to the medical service as a surgeon’s assistant.
Antonio was assigned to work with Dr. Marsden, a fine surgeon from Boston. He watched with admiration as the surgeon amputated shattered arms and legs, sometimes twenty in a session. Antonio’s job was to help staunch the flow of blood with tourniquet or cautery, to brush the maggots from open wounds, and to count and burn the severed limbs. He was handling meat again.
During the months with Dr. Marsden, Antonio kept his eyes open and watched the doctor’s technique. When things got too busy, he would take up the knife as well. He became expert at sounding bullet wounds and was competent at below-the-knee amputations.
The war dragged on, and Antonio grew tired of endless surgery that seemed to be alleviated only by weeks of boredom. Dr. Marsden had been lying sick in his bunk for a week, febrile, jaundiced, and vomiting blood. Antonio suspected he’d picked up yellow jack in Texas. One day, he walked into the tent and found the surgeon dead. Without further thought, Antonio loaded the surgeon’s books and surgical kit into a bag, mounted a blue roan, and rode away from the war.
Fourteen years later, he sat with his head on a bar, vertiginous from the cheap liquor. He had become Old Doc Marsden, who liked a drink but sure was handy with a blade. He had pulled a thousand arrowheads, had sounded even more bullet wounds, and set countless fractures. He kept to the rough mining towns and frontier spaces where there was no shortage of injuries and no questions were asked. Timberline was just his speed. Recently, a second doctor had come to town. He did not mind the competition; in fact, he was glad to have someone to whom he could send the tougher cases.
Time passes.
It was a cool fall morning. There was a frost on the ground, and Doc Marsden was hung-over, sitting on his porch rolling his first morning cigarette. Boone Harkness had returned to town those many months ago with a wife, and she was pregnant. The new doctor in town had taken her case. Doc was glad; he wanted nothing to do with either Snake-Eye Harkness or his bride. He’d seen her only once, walking in town, and that was enough. She seemed a tiny china doll next to the tough man with the narrow hips and wide shoulders.
A rider approached his house. Some cowboy had probably been shot last night, or had stumbled down drunk and broken his leg. But it was Billy Harkness. He told Doc he was wanted on the Harkness ranch, pronto. The new doctor, Jenkins, was having trouble with Helena Harkness and wanted Doc’s help. That could only mean things were bad, real bad. Doc had foaled a few in his time, but he was no hand at tricky birthing. Doc Marsden said he’d be by shortly. Billy looked at him with pity. Snake-Eye had said now.
Doc ran into his home and took a quick drink from his whisky bottle, then grabbed his bag and his Colt. They rode out in the cool morning air, Billy leading the way. Doc Marsden thought about the gun in his holster. It would not be hard to put a slug in Billy’s back and make for the high country. He might get away. But then he’d spend the rest of his days looking over his shoulder. He might as well face his doom straight up. He was a fake and a drunk, but he was no coward. He had never shot a man, and he wouldn’t start now.
Halfway to the Harkness spread, Billy pulled up. He had another chore to run, he said; he’d be up at the big house later that day. This was Doc’s chance. He might not be willing to shoot Billy and run for it, but he was mounted, and the road was open to the north and west. He thought about the scene in the ranch house: thin-legged Helena trying to squeeze out that big Harkness baby, bleeding, crying, dying. If she died so would Doc, no question about that.
Doc turned north and headed up the road a mile, then stopped. He looked out over the prairie. He thought about the immigrant boy, the butcher shop, the war, the bullets and arrows. Philadelphia was a lifetime away. Antonio Lombano was long dead. He was Doc Marsden. He took a deep breath of mountain air, thought about the bottle in his saddlebag, and left it there. He turned the blue roan with the double snake brand south and headed toward the Harkness ranch. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
The Aspen were turning a golden brown, the cattle were fattened for market, and Doc Marsden was drunk again. His head lay on the two planks that served as a bar in what could only charitably be called a saloon. There were two places for a man to drink in Timberline, and this was Doc’s preferred watering hole.
Earlier that day Doc had been busy enough. There’d been a big brawl at the Triple H, and Billy Harkness had shot his younger brother, Lukas, after a lucky punch had broken Billy’s overlarge nose. It wasn’t a bad wound; Lukas had ducked, and the bullet had skimmed his back and lodged in his calf.
Doc had dressed the back wound with a poultice and fished the 0.45 slug from the gastrocnemius. He knew that much anatomy, but not much more. His hands had shaken ’till he had swigged a few swallows of what passed for bourbon. It was nervous work whittling on a Harkness. Luckily Lukas and Billy were a sight more intoxicated than Doc, and their big brother Boone Harkness was somewhere up the trail. The eldest Harkness brother had restless snake eyes. Boone never missed a thing, especially a target. He made Doc Marsden sweat. Doc gave Lukas a spoonful of laudanum, and his patient was soon snoring peacefully on the door they had used as an operating table. Doc took a small swig himself.
After he was sure that the Harkness boy was settled down and Doc’s helper Marty Johnson was there to watch over Lukas, Doc headed for the saloon and started drinking again. He pondered how he had ended up in Timberline. This hadn’t been his plan when he’d left Philadelphia all those years ago.
Back in Philadelphia his name had been Antonio Lombano. His parents had been immigrants, and he had been lucky to work for a butcher. He’d grown sick of slicing meat, and when the war came he enlisted. Anything to get away from the smell of blood and hanging beefs.
When he enlisted with the 37th infantry he’d expected to learn to shoot a gun and maybe even to die. He might have to kill a couple of Rebs, but at least he would leave Philadelphia. Instead, when they learned he had worked as a butcher, he was relegated to the cook’s tent. He was back to slicing meat. For two months the only flank he outmaneuvered was with his cutting blade.
He had been disemboweling a steer one day when a group of surgeons walked by, looking for an eyeball to dissect. They watched approvingly as he wielded his blade. Three days later he had been reassigned to the medical service as a surgeon’s assistant.
Antonio was assigned to work with Dr. Marsden, a fine surgeon from Boston. He watched with admiration as the surgeon amputated shattered arms and legs, sometimes twenty in a session. Antonio’s job was to help staunch the flow of blood with tourniquet or cautery, to brush the maggots from open wounds, and to count and burn the severed limbs. He was handling meat again.
During the months with Dr. Marsden, Antonio kept his eyes open and watched the doctor’s technique. When things got too busy, he would take up the knife as well. He became expert at sounding bullet wounds and was competent at below-the-knee amputations.
The war dragged on, and Antonio grew tired of endless surgery that seemed to be alleviated only by weeks of boredom. Dr. Marsden had been lying sick in his bunk for a week, febrile, jaundiced, and vomiting blood. Antonio suspected he’d picked up yellow jack in Texas. One day, he walked into the tent and found the surgeon dead. Without further thought, Antonio loaded the surgeon’s books and surgical kit into a bag, mounted a blue roan, and rode away from the war.
Fourteen years later, he sat with his head on a bar, vertiginous from the cheap liquor. He had become Old Doc Marsden, who liked a drink but sure was handy with a blade. He had pulled a thousand arrowheads, had sounded even more bullet wounds, and set countless fractures. He kept to the rough mining towns and frontier spaces where there was no shortage of injuries and no questions were asked. Timberline was just his speed. Recently, a second doctor had come to town. He did not mind the competition; in fact, he was glad to have someone to whom he could send the tougher cases.
Time passes.
It was a cool fall morning. There was a frost on the ground, and Doc Marsden was hung-over, sitting on his porch rolling his first morning cigarette. Boone Harkness had returned to town those many months ago with a wife, and she was pregnant. The new doctor in town had taken her case. Doc was glad; he wanted nothing to do with either Snake-Eye Harkness or his bride. He’d seen her only once, walking in town, and that was enough. She seemed a tiny china doll next to the tough man with the narrow hips and wide shoulders.
A rider approached his house. Some cowboy had probably been shot last night, or had stumbled down drunk and broken his leg. But it was Billy Harkness. He told Doc he was wanted on the Harkness ranch, pronto. The new doctor, Jenkins, was having trouble with Helena Harkness and wanted Doc’s help. That could only mean things were bad, real bad. Doc had foaled a few in his time, but he was no hand at tricky birthing. Doc Marsden said he’d be by shortly. Billy looked at him with pity. Snake-Eye had said now.
Doc ran into his home and took a quick drink from his whisky bottle, then grabbed his bag and his Colt. They rode out in the cool morning air, Billy leading the way. Doc Marsden thought about the gun in his holster. It would not be hard to put a slug in Billy’s back and make for the high country. He might get away. But then he’d spend the rest of his days looking over his shoulder. He might as well face his doom straight up. He was a fake and a drunk, but he was no coward. He had never shot a man, and he wouldn’t start now.
Halfway to the Harkness spread, Billy pulled up. He had another chore to run, he said; he’d be up at the big house later that day. This was Doc’s chance. He might not be willing to shoot Billy and run for it, but he was mounted, and the road was open to the north and west. He thought about the scene in the ranch house: thin-legged Helena trying to squeeze out that big Harkness baby, bleeding, crying, dying. If she died so would Doc, no question about that.
Doc turned north and headed up the road a mile, then stopped. He looked out over the prairie. He thought about the immigrant boy, the butcher shop, the war, the bullets and arrows. Philadelphia was a lifetime away. Antonio Lombano was long dead. He was Doc Marsden. He took a deep breath of mountain air, thought about the bottle in his saddlebag, and left it there. He turned the blue roan with the double snake brand south and headed toward the Harkness ranch. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
The Aspen were turning a golden brown, the cattle were fattened for market, and Doc Marsden was drunk again. His head lay on the two planks that served as a bar in what could only charitably be called a saloon. There were two places for a man to drink in Timberline, and this was Doc’s preferred watering hole.
Earlier that day Doc had been busy enough. There’d been a big brawl at the Triple H, and Billy Harkness had shot his younger brother, Lukas, after a lucky punch had broken Billy’s overlarge nose. It wasn’t a bad wound; Lukas had ducked, and the bullet had skimmed his back and lodged in his calf.
Doc had dressed the back wound with a poultice and fished the 0.45 slug from the gastrocnemius. He knew that much anatomy, but not much more. His hands had shaken ’till he had swigged a few swallows of what passed for bourbon. It was nervous work whittling on a Harkness. Luckily Lukas and Billy were a sight more intoxicated than Doc, and their big brother Boone Harkness was somewhere up the trail. The eldest Harkness brother had restless snake eyes. Boone never missed a thing, especially a target. He made Doc Marsden sweat. Doc gave Lukas a spoonful of laudanum, and his patient was soon snoring peacefully on the door they had used as an operating table. Doc took a small swig himself.
After he was sure that the Harkness boy was settled down and Doc’s helper Marty Johnson was there to watch over Lukas, Doc headed for the saloon and started drinking again. He pondered how he had ended up in Timberline. This hadn’t been his plan when he’d left Philadelphia all those years ago.
Back in Philadelphia his name had been Antonio Lombano. His parents had been immigrants, and he had been lucky to work for a butcher. He’d grown sick of slicing meat, and when the war came he enlisted. Anything to get away from the smell of blood and hanging beefs.
When he enlisted with the 37th infantry he’d expected to learn to shoot a gun and maybe even to die. He might have to kill a couple of Rebs, but at least he would leave Philadelphia. Instead, when they learned he had worked as a butcher, he was relegated to the cook’s tent. He was back to slicing meat. For two months the only flank he outmaneuvered was with his cutting blade.
He had been disemboweling a steer one day when a group of surgeons walked by, looking for an eyeball to dissect. They watched approvingly as he wielded his blade. Three days later he had been reassigned to the medical service as a surgeon’s assistant.
Antonio was assigned to work with Dr. Marsden, a fine surgeon from Boston. He watched with admiration as the surgeon amputated shattered arms and legs, sometimes twenty in a session. Antonio’s job was to help staunch the flow of blood with tourniquet or cautery, to brush the maggots from open wounds, and to count and burn the severed limbs. He was handling meat again.
During the months with Dr. Marsden, Antonio kept his eyes open and watched the doctor’s technique. When things got too busy, he would take up the knife as well. He became expert at sounding bullet wounds and was competent at below-the-knee amputations.
The war dragged on, and Antonio grew tired of endless surgery that seemed to be alleviated only by weeks of boredom. Dr. Marsden had been lying sick in his bunk for a week, febrile, jaundiced, and vomiting blood. Antonio suspected he’d picked up yellow jack in Texas. One day, he walked into the tent and found the surgeon dead. Without further thought, Antonio loaded the surgeon’s books and surgical kit into a bag, mounted a blue roan, and rode away from the war.
Fourteen years later, he sat with his head on a bar, vertiginous from the cheap liquor. He had become Old Doc Marsden, who liked a drink but sure was handy with a blade. He had pulled a thousand arrowheads, had sounded even more bullet wounds, and set countless fractures. He kept to the rough mining towns and frontier spaces where there was no shortage of injuries and no questions were asked. Timberline was just his speed. Recently, a second doctor had come to town. He did not mind the competition; in fact, he was glad to have someone to whom he could send the tougher cases.
Time passes.
It was a cool fall morning. There was a frost on the ground, and Doc Marsden was hung-over, sitting on his porch rolling his first morning cigarette. Boone Harkness had returned to town those many months ago with a wife, and she was pregnant. The new doctor in town had taken her case. Doc was glad; he wanted nothing to do with either Snake-Eye Harkness or his bride. He’d seen her only once, walking in town, and that was enough. She seemed a tiny china doll next to the tough man with the narrow hips and wide shoulders.
A rider approached his house. Some cowboy had probably been shot last night, or had stumbled down drunk and broken his leg. But it was Billy Harkness. He told Doc he was wanted on the Harkness ranch, pronto. The new doctor, Jenkins, was having trouble with Helena Harkness and wanted Doc’s help. That could only mean things were bad, real bad. Doc had foaled a few in his time, but he was no hand at tricky birthing. Doc Marsden said he’d be by shortly. Billy looked at him with pity. Snake-Eye had said now.
Doc ran into his home and took a quick drink from his whisky bottle, then grabbed his bag and his Colt. They rode out in the cool morning air, Billy leading the way. Doc Marsden thought about the gun in his holster. It would not be hard to put a slug in Billy’s back and make for the high country. He might get away. But then he’d spend the rest of his days looking over his shoulder. He might as well face his doom straight up. He was a fake and a drunk, but he was no coward. He had never shot a man, and he wouldn’t start now.
Halfway to the Harkness spread, Billy pulled up. He had another chore to run, he said; he’d be up at the big house later that day. This was Doc’s chance. He might not be willing to shoot Billy and run for it, but he was mounted, and the road was open to the north and west. He thought about the scene in the ranch house: thin-legged Helena trying to squeeze out that big Harkness baby, bleeding, crying, dying. If she died so would Doc, no question about that.
Doc turned north and headed up the road a mile, then stopped. He looked out over the prairie. He thought about the immigrant boy, the butcher shop, the war, the bullets and arrows. Philadelphia was a lifetime away. Antonio Lombano was long dead. He was Doc Marsden. He took a deep breath of mountain air, thought about the bottle in his saddlebag, and left it there. He turned the blue roan with the double snake brand south and headed toward the Harkness ranch. TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
Hip Fractures to Head Bleeds

In the mid-1970s I worked as a hospital orderly. I enjoyed getting an up-close view of the hospital culture and learning a little bit about sick people. And though I didn’t realize it at the time, I was watching the early maturation of a relatively new specialty in that hospital: emergency medicine.
One day I happened to be in the emergency room (I know they call it the emergency department now) when a panic stricken dad carried in his toddler who was having an impressive tonsillar hemorrhage as a complication of a tonsillectomy done a few days earlier. The ER staff took one look at this bloody child and told the dad to carry him way across the campus to the office tower where the ENT surgeon had his office practice. I was drafted to escort the dad, still carrying the child in his arms, and left father and child in the ENT’s office thinking everything would be fine.
I’ve thought about this incident periodically since then and come to two conclusions. The first is that I was totally unaware of how seriously ill this child was until talking later with some of the doctors and nurses at the hospital. Of course I’m now a lot better at recognizing which patients are really sick, but I’ve still had situations in which I failed to appreciate the seriousness of the patient’s condition until thinking about it after the fact. My second conclusion is that this child needed emergent intervention by the ER physician, and shouldn’t have been sent across the campus to an outpatient office.
I suspect the ER doctor thought that management of this acute surgical complication was beyond the scope of his training. So he decided that the risk of delaying intervention so the child could get to the ENT’s office was less than keeping him in the ER to get IV access and start volume replacement, and so on.
Though it would sound ridiculous now, you might imagine the ER doctor defending his decision by saying “I’m not trained in the acute management of surgical complications like that.” After all, like most ER doctors of the time, his training probably consisted of a one-year rotating internship or something similar. There were no (or very few) ER residencies at the time.
But if that doctor is still practicing in an ER somewhere, I’m pretty confident he has developed the expertise required to provide the initial management of patients like this one. Like all ER doctors, and the field of emergency medicine as a whole, he needed to adjust the scope of his practice to meet the needs of the institution and healthcare system where he worked. So even if it were reasonable for him to say initial intervention for acute tonsillar hemorrhage was out of the scope of his training and expertise in the 1970s, he can’t say it anymore. Like all ER doctors, he had to seek out ways to gain training and expertise in these kinds of problems in order to respond to the needs of the institution.
I tell this story because I think we as hospitalists—and the field of hospital medicine as a whole—sometimes find ourselves in situations similar to that of the 1970s ER doctor. We are sometimes asked to provide care that might not have been part of the usual scope of practice for someone with our training. I am trained as an internist, but am sometimes asked to admit patients with problems like hip fracture or hypertensive intracerebral hemorrhage when my first impulse is that an orthopedist or a neurosurgeon should admit that patient. Or I might be asked to admit a 17-year-old and wonder if it would be better for a pediatrician to take care of that patient.
On the one hand I want to say these aren’t really internal medicine problems, so I shouldn’t be the attending for these patients (but could serve as consultant). And while that might be a reasonable position to take today, I’m convinced that I can’t dig my heels in and insist that I never become the primary admitter for these patients. I think there is too big a need for a hospitalist to care for these kinds of patients at my hospital, and it’s unreasonable for me to take a hard line and insist I will never change.
While your list of diagnoses might be different than mine, I think there is a good chance that you’re often asked to care for patients that might be a little outside the traditional scope of the specialty you trained in. Do you think that the field of hospital medicine can—or should—avoid caring for these patients long term? I don’t. I think we need to gradually take on some of the new roles that our hospitals and physician colleagues request of us. Just like the ER doctors of the 1970s, I think we are in a period of significant evolution as our field “grows up.” And rather than resisting this change, I think we should thoughtfully decide where “the system” needs our services the most and work to develop the expertise to meet that need.
Some hospitalists are really uncomfortable with the idea of expanding the scope of their practice and raise a number of objections. They sometimes say “That’s fine if Nelson wants to care for patients with head bleeds, but there is no way I’m going to do it since it’s a sure path to a law suit.” Or “I’m happy to consult and manage the blood pressure, but there’s no way I’m willing to be attending.”
But don’t doctors in most specialties adjust their scope of practice regularly? Think about surgeons who have had to learn laparoscopic techniques after their residency training. And office-based internists who had little outpatient training during residency but have had to learn to be expert at it once they started practice. They are adapting the scope of their practice to the needs of the healthcare system, and they’ve found ways to gain competence and expertise in these areas.
I’m not suggesting we admit any type of patient someone might want us to. Nor am I confident that the two important areas for hospital medicine to become more involved in are hip fracture and hypertensive intracerebral hemorrhage (though they do seem to come up regularly). My point is that I don’t think we can dig our heels in and resist any change in our scope of practice. In our own local practices, and as a specialty, we need to decide the most valuable ways to adjust our practice scope and work diligently to become competent at them. We will still need an orthopedist to operate on the hip and a neurosurgeon to see patients with “head bleeds,” but maybe the system really needs, and could benefit from, hospitalists who have an increased role in caring for these patients. As our field evolves, training programs and CME courses will adapt to meet our need for more training in these areas that may feel new or unfamiliar to many of us.
Some days after the child with tonsillar hemorrhage presented, I learned that he had done OK and had gone home looking good. But the surgeon was furious that we had “dumped” this patient at his door without any warning and had sent the patient into his waiting room where other waiting patients were apparently horrified. The ER doctor could have responded that the surgeon should quit complaining and get used to this kind of thing because “it comes with the turf” of ENT practice. Or he could have told the ENT doctor he’d like for the two of them to work together to develop a way for the ER to play a much bigger role in the early emergent intervention.
I hope that when we find ourselves in a similar situation we try the latter response. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
In the mid-1970s I worked as a hospital orderly. I enjoyed getting an up-close view of the hospital culture and learning a little bit about sick people. And though I didn’t realize it at the time, I was watching the early maturation of a relatively new specialty in that hospital: emergency medicine.
One day I happened to be in the emergency room (I know they call it the emergency department now) when a panic stricken dad carried in his toddler who was having an impressive tonsillar hemorrhage as a complication of a tonsillectomy done a few days earlier. The ER staff took one look at this bloody child and told the dad to carry him way across the campus to the office tower where the ENT surgeon had his office practice. I was drafted to escort the dad, still carrying the child in his arms, and left father and child in the ENT’s office thinking everything would be fine.
I’ve thought about this incident periodically since then and come to two conclusions. The first is that I was totally unaware of how seriously ill this child was until talking later with some of the doctors and nurses at the hospital. Of course I’m now a lot better at recognizing which patients are really sick, but I’ve still had situations in which I failed to appreciate the seriousness of the patient’s condition until thinking about it after the fact. My second conclusion is that this child needed emergent intervention by the ER physician, and shouldn’t have been sent across the campus to an outpatient office.
I suspect the ER doctor thought that management of this acute surgical complication was beyond the scope of his training. So he decided that the risk of delaying intervention so the child could get to the ENT’s office was less than keeping him in the ER to get IV access and start volume replacement, and so on.
Though it would sound ridiculous now, you might imagine the ER doctor defending his decision by saying “I’m not trained in the acute management of surgical complications like that.” After all, like most ER doctors of the time, his training probably consisted of a one-year rotating internship or something similar. There were no (or very few) ER residencies at the time.
But if that doctor is still practicing in an ER somewhere, I’m pretty confident he has developed the expertise required to provide the initial management of patients like this one. Like all ER doctors, and the field of emergency medicine as a whole, he needed to adjust the scope of his practice to meet the needs of the institution and healthcare system where he worked. So even if it were reasonable for him to say initial intervention for acute tonsillar hemorrhage was out of the scope of his training and expertise in the 1970s, he can’t say it anymore. Like all ER doctors, he had to seek out ways to gain training and expertise in these kinds of problems in order to respond to the needs of the institution.
I tell this story because I think we as hospitalists—and the field of hospital medicine as a whole—sometimes find ourselves in situations similar to that of the 1970s ER doctor. We are sometimes asked to provide care that might not have been part of the usual scope of practice for someone with our training. I am trained as an internist, but am sometimes asked to admit patients with problems like hip fracture or hypertensive intracerebral hemorrhage when my first impulse is that an orthopedist or a neurosurgeon should admit that patient. Or I might be asked to admit a 17-year-old and wonder if it would be better for a pediatrician to take care of that patient.
On the one hand I want to say these aren’t really internal medicine problems, so I shouldn’t be the attending for these patients (but could serve as consultant). And while that might be a reasonable position to take today, I’m convinced that I can’t dig my heels in and insist that I never become the primary admitter for these patients. I think there is too big a need for a hospitalist to care for these kinds of patients at my hospital, and it’s unreasonable for me to take a hard line and insist I will never change.
While your list of diagnoses might be different than mine, I think there is a good chance that you’re often asked to care for patients that might be a little outside the traditional scope of the specialty you trained in. Do you think that the field of hospital medicine can—or should—avoid caring for these patients long term? I don’t. I think we need to gradually take on some of the new roles that our hospitals and physician colleagues request of us. Just like the ER doctors of the 1970s, I think we are in a period of significant evolution as our field “grows up.” And rather than resisting this change, I think we should thoughtfully decide where “the system” needs our services the most and work to develop the expertise to meet that need.
Some hospitalists are really uncomfortable with the idea of expanding the scope of their practice and raise a number of objections. They sometimes say “That’s fine if Nelson wants to care for patients with head bleeds, but there is no way I’m going to do it since it’s a sure path to a law suit.” Or “I’m happy to consult and manage the blood pressure, but there’s no way I’m willing to be attending.”
But don’t doctors in most specialties adjust their scope of practice regularly? Think about surgeons who have had to learn laparoscopic techniques after their residency training. And office-based internists who had little outpatient training during residency but have had to learn to be expert at it once they started practice. They are adapting the scope of their practice to the needs of the healthcare system, and they’ve found ways to gain competence and expertise in these areas.
I’m not suggesting we admit any type of patient someone might want us to. Nor am I confident that the two important areas for hospital medicine to become more involved in are hip fracture and hypertensive intracerebral hemorrhage (though they do seem to come up regularly). My point is that I don’t think we can dig our heels in and resist any change in our scope of practice. In our own local practices, and as a specialty, we need to decide the most valuable ways to adjust our practice scope and work diligently to become competent at them. We will still need an orthopedist to operate on the hip and a neurosurgeon to see patients with “head bleeds,” but maybe the system really needs, and could benefit from, hospitalists who have an increased role in caring for these patients. As our field evolves, training programs and CME courses will adapt to meet our need for more training in these areas that may feel new or unfamiliar to many of us.
Some days after the child with tonsillar hemorrhage presented, I learned that he had done OK and had gone home looking good. But the surgeon was furious that we had “dumped” this patient at his door without any warning and had sent the patient into his waiting room where other waiting patients were apparently horrified. The ER doctor could have responded that the surgeon should quit complaining and get used to this kind of thing because “it comes with the turf” of ENT practice. Or he could have told the ENT doctor he’d like for the two of them to work together to develop a way for the ER to play a much bigger role in the early emergent intervention.
I hope that when we find ourselves in a similar situation we try the latter response. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
In the mid-1970s I worked as a hospital orderly. I enjoyed getting an up-close view of the hospital culture and learning a little bit about sick people. And though I didn’t realize it at the time, I was watching the early maturation of a relatively new specialty in that hospital: emergency medicine.
One day I happened to be in the emergency room (I know they call it the emergency department now) when a panic stricken dad carried in his toddler who was having an impressive tonsillar hemorrhage as a complication of a tonsillectomy done a few days earlier. The ER staff took one look at this bloody child and told the dad to carry him way across the campus to the office tower where the ENT surgeon had his office practice. I was drafted to escort the dad, still carrying the child in his arms, and left father and child in the ENT’s office thinking everything would be fine.
I’ve thought about this incident periodically since then and come to two conclusions. The first is that I was totally unaware of how seriously ill this child was until talking later with some of the doctors and nurses at the hospital. Of course I’m now a lot better at recognizing which patients are really sick, but I’ve still had situations in which I failed to appreciate the seriousness of the patient’s condition until thinking about it after the fact. My second conclusion is that this child needed emergent intervention by the ER physician, and shouldn’t have been sent across the campus to an outpatient office.
I suspect the ER doctor thought that management of this acute surgical complication was beyond the scope of his training. So he decided that the risk of delaying intervention so the child could get to the ENT’s office was less than keeping him in the ER to get IV access and start volume replacement, and so on.
Though it would sound ridiculous now, you might imagine the ER doctor defending his decision by saying “I’m not trained in the acute management of surgical complications like that.” After all, like most ER doctors of the time, his training probably consisted of a one-year rotating internship or something similar. There were no (or very few) ER residencies at the time.
But if that doctor is still practicing in an ER somewhere, I’m pretty confident he has developed the expertise required to provide the initial management of patients like this one. Like all ER doctors, and the field of emergency medicine as a whole, he needed to adjust the scope of his practice to meet the needs of the institution and healthcare system where he worked. So even if it were reasonable for him to say initial intervention for acute tonsillar hemorrhage was out of the scope of his training and expertise in the 1970s, he can’t say it anymore. Like all ER doctors, he had to seek out ways to gain training and expertise in these kinds of problems in order to respond to the needs of the institution.
I tell this story because I think we as hospitalists—and the field of hospital medicine as a whole—sometimes find ourselves in situations similar to that of the 1970s ER doctor. We are sometimes asked to provide care that might not have been part of the usual scope of practice for someone with our training. I am trained as an internist, but am sometimes asked to admit patients with problems like hip fracture or hypertensive intracerebral hemorrhage when my first impulse is that an orthopedist or a neurosurgeon should admit that patient. Or I might be asked to admit a 17-year-old and wonder if it would be better for a pediatrician to take care of that patient.
On the one hand I want to say these aren’t really internal medicine problems, so I shouldn’t be the attending for these patients (but could serve as consultant). And while that might be a reasonable position to take today, I’m convinced that I can’t dig my heels in and insist that I never become the primary admitter for these patients. I think there is too big a need for a hospitalist to care for these kinds of patients at my hospital, and it’s unreasonable for me to take a hard line and insist I will never change.
While your list of diagnoses might be different than mine, I think there is a good chance that you’re often asked to care for patients that might be a little outside the traditional scope of the specialty you trained in. Do you think that the field of hospital medicine can—or should—avoid caring for these patients long term? I don’t. I think we need to gradually take on some of the new roles that our hospitals and physician colleagues request of us. Just like the ER doctors of the 1970s, I think we are in a period of significant evolution as our field “grows up.” And rather than resisting this change, I think we should thoughtfully decide where “the system” needs our services the most and work to develop the expertise to meet that need.
Some hospitalists are really uncomfortable with the idea of expanding the scope of their practice and raise a number of objections. They sometimes say “That’s fine if Nelson wants to care for patients with head bleeds, but there is no way I’m going to do it since it’s a sure path to a law suit.” Or “I’m happy to consult and manage the blood pressure, but there’s no way I’m willing to be attending.”
But don’t doctors in most specialties adjust their scope of practice regularly? Think about surgeons who have had to learn laparoscopic techniques after their residency training. And office-based internists who had little outpatient training during residency but have had to learn to be expert at it once they started practice. They are adapting the scope of their practice to the needs of the healthcare system, and they’ve found ways to gain competence and expertise in these areas.
I’m not suggesting we admit any type of patient someone might want us to. Nor am I confident that the two important areas for hospital medicine to become more involved in are hip fracture and hypertensive intracerebral hemorrhage (though they do seem to come up regularly). My point is that I don’t think we can dig our heels in and resist any change in our scope of practice. In our own local practices, and as a specialty, we need to decide the most valuable ways to adjust our practice scope and work diligently to become competent at them. We will still need an orthopedist to operate on the hip and a neurosurgeon to see patients with “head bleeds,” but maybe the system really needs, and could benefit from, hospitalists who have an increased role in caring for these patients. As our field evolves, training programs and CME courses will adapt to meet our need for more training in these areas that may feel new or unfamiliar to many of us.
Some days after the child with tonsillar hemorrhage presented, I learned that he had done OK and had gone home looking good. But the surgeon was furious that we had “dumped” this patient at his door without any warning and had sent the patient into his waiting room where other waiting patients were apparently horrified. The ER doctor could have responded that the surgeon should quit complaining and get used to this kind of thing because “it comes with the turf” of ENT practice. Or he could have told the ENT doctor he’d like for the two of them to work together to develop a way for the ER to play a much bigger role in the early emergent intervention.
I hope that when we find ourselves in a similar situation we try the latter response. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
PE in COPD, Board Certification, Neutropenic Cancer, and More
Gatifloxacin and Dysglycemia
Park-Wyllie LY, Juurlink DN, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med. 2006 Mar;354(13):1352-1361.
Fluoroquinolones are the most commonly prescribed antibiotics in the United States. Side effects associated with some fluoroquinolones (temafloxacin, grepafloxacin, sparfloxacin, and trovafloxacin) have prompted their restriction or withdrawal. Until now, dysglycemia had been associated with gatifloxacin only in small studies or case reports.
This study sought to examine, by a nested case control design, the association between gatifloxacin and dysglycemia that required hospital care. The researchers reviewed all prescription records from the Ontario (Canada) Drug Benefit database, which houses complete prescription drug sales for all patients older than age 65 (1.4 million residents). They linked this with a national Canadian database of those same patients’ emergency room visits and hospital admissions. Cases were patients who received hospital care for hypoglycemia (or hyperglycemia) within 30 days of filling an antibiotic prescription (macrolide, cephalosporin, or fluoroquinolone). Controls were patients who had not received hospital care after an antibiotic prescription in the same time period. They were matched by age, gender, whether or not they had been diagnosed as having diabetes, diabetic drug use, and time of antibiotic prescription. Patients were excluded if they turned 65 within the year, had been hospitalized within 90 days, had subsequent hospitalizations for dysglycemia, or had more than one antibiotic in 30 days. Logistic regression was used to determine the odds ratio for the association between dysglycemia and recent antibiotic use. In multivariable analysis, they adjusted for liver disease, renal disease, alcohol use, hospitalizations, physician visits, diabetic and P-450 medications, socioeconomic status, and number of prescription drugs. They were also stratified by diabetes status.
The cases treated for hypoglycemia were four times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 4.3, CI 2.9-6.3). The association was slightly less with levofloxacin (OR 1.5, CI 1.2-2.0), and there was no association of hypoglycemia with moxifloxacin, ciprofloxacin, or cephalosporins. The cases treated for hyperglycemia were 17 times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 16.7, CI 10.4-26.8). There was no association of hyperglycemia with the other fluoroquinolones or cephalosporins. The analyses were similar when stratified by diabetes status. In total, 1.1% of all gatifloxacin treatments were associated with dysglycemia requiring hospital care within 30 days. As to what to do with gatifloxacin, as stated precisely in an accompanying editorial, “For every approved indication for gatifloxacin, there are safer, equally effective, and less costly alternatives.”
Physician Board Certification and Acute MI Quality Measures.
Chen J, Rathore SS, Wang Y, et al. Physician board certification and the care and outcomes of elderly patients with acute myocardial infarction. J Gen Intern Med. 2006 Mar;21(3):238-244.
Board certification may have implications for practicing physicians because there is evidence that both hiring organizations and patients prefer board-certified physicians over non-board certified physicians. However, it is unknown if such certification translates into better quality of patient care.
In this study researchers sought to examine the relationship between physician board certification and quality of care in patients with acute myocardial infarction (AMI). Medical records were abstracted from the Cooperative Cardiovascular Project, a cohort of Medicare beneficiaries hospitalized with AMI. Board certification was obtained from the American Medical Association (AMA) Physician Masterfile, which is reportedly 94% accurate. Quality of care measures included ASA and beta-blocker use at the time of admission and discharge. Researchers also evaluated 30-day and one-year mortality.
They evaluated these quality measures on 101,251 patients and 36,668 physicians, of which 80% were board certified. In multivariable analyses adjusting for patient, hospital, and physician characteristics, board-certified internal medicine and cardiology physicians (but not family practitioners) were more likely to prescribe ASA and beta-blockers at admission and discharge than non-board certified physicians (adjusted relative risk ranged from 1.04 to 1.20). There was no difference in 30-day and one-year mortality among any specialty after multivariable adjustment.
These results, albeit modest, suggest that physician board certification may be associated with superior quality of care in elderly patients with AMI. The authors offer that board-certified physicians may be more aware or familiar with guidelines or may be more likely to agree with clinical guidelines. Although board-certified physicians have been shown to complete more hours of CME and spend more time reading journals, they caution that board certification should not be used as a surrogate marker of quality. Because 30% of U.S. practicing physicians are not currently board certified, these results certainly warrant further study.
PE in COPD
Tillie-Leblond I, Marquette CH, Perez T, et al. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Ann Intern Med. 2006 Mar 21;144(6):390-396.
This study sought to evaluate the prevalence and risk factors for pulmonary embolus (PE) in patients with unexplained exacerbations of COPD. All patients with an unexplained COPD exacerbation requiring hospitalization (not ICU) were evaluated for PE by spiral chest CT and lower limb venous ultrasound (USG). The COPD flare was “unexplained” if there were no signs or symptoms of respiratory tract infection, no pneumothorax, or a discrepancy between the clinical/radiologic features and the degree of hypoxemia. Patients were considered to have a PE if either of the two tests (CT or USG) were positive. Patients were not considered to have a PE if both tests were negative, and there was no evidence of PE at three-month follow-up.
Of 211 referred patients, 14 were not included due to inconclusive results or iodine intolerance. Of 197 enrolled patients, 25% had PE. There was no difference between the PE and non-PE groups with respect to referral location, clinical symptoms (dyspnea, pleuritic pain, hemoptysis, tachycardia, lower limb edema), need for long term oxygen therapy, admission P02 or PC02, recent trauma, recent surgery, obesity, or immobilization for more than seven days. Factors associated with PE on bivariate analysis included a decrease in PC02 >5mmHg from baseline, previous thromboembolism, and malignancy.
Researchers then calculated these patient’s Geneva score (a PE predictor score based on age, history, pulse, ABG, and chest X-ray findings. Those with a low probability Geneva score had a 9% incidence of PE, those with an intermediate score had a 47% incidence, and those with a high Geneva score had a 100% incidence.
In conclusion, in this study population of non-ICU patients with unexplained exacerbations of COPD, one in four had evidence of thromboembolic disease. Significant risk ratios between groups were found for patients with a prior history of thromboembolism, malignancy, or a decrease in their baseline PC02. These factors should be weighted heavily in determining which patients with unexplained COPD exacerbations should undergo workup to exclude a PE. The Geneva score also correlated well with PE incidence in this population.
Telithromycin in Asthma Exacerbations
Johnston SL, Blasi FB, Black PN, et al. The effect of telithromycin in acute exacerbations of asthma. New Engl J Med. 2006 Apr 13;354(15):1589-1600.
The use of antibiotics for uncomplicated asthma exacerbations is not currently considered standard of care. This randomized placebo controlled trial was designed to determine if telithromycin (a ketolide, structurally similar to macrolides, with efficacy against mycoplasma and chlamydia pneumonia) improves symptoms and peak flow rates in patients with asthma exacerbations. Researchers enrolled 278 patients age 18 to 55 with a history of asthma (less than six months) with an exacerbation (peak flow <80% and symptoms of wheeze and dyspnea). They excluded those requiring ICU care, smokers, known infection/recent antibiotic use, or regular use of oral steroids. Baseline demographics, pulmonary function, and acute medication use (steroids and beta agonists) were similar between the groups.
Intervention patients received telithromycin 800 mg a day for 10 days. The primary outcome was change in their asthma symptom score (rated on a seven-point scale) and change in their peak flows (recorded every morning for the study duration). Secondary outcomes were clinic pulmonary function tests (PFTs).
The intervention group had a mean decrease in their symptom score of 1.3 versus 1.0 in the placebo group (40% versus 27% reduction, p=.004). There was no difference between the groups in home peak flow measurements. There were statistically significant differences between the groups in clinic PFTs (FEV1, FVC, FEF 25%-75%), although the P values were not adjusted for multiple outcomes. The intervention group had a higher percentage of symptom-free days (16% versus 8%, P=.006). A total of 61% of the patients had serologic evidence of chlamydia or mycoplasma infection. Nausea (seven versus 0) and LFT elevations (two versus 0) were more frequent in the intervention group.
In conclusion, this is the first trial to report a benefit of antibiotic use in uncomplicated asthma exacerbations. This conclusion must be tempered by the underwhelming clinical improvement (1.3 versus 1.0 improvement in symptom scores), lack of peak flow improvement, recent reports of serious hepatotoxicity associated with telithromycin, and the possibility for antibiotic over-prescribing in unrefined patient populations.
Pneumonia Quality and Outcomes by Volume of Care
Lindenauer PK, Behal R, Murray CK, et al. Volume, quality of care, and outcome in pneumonia. Ann Intern Med. 2006 Feb 21;144(4):262-269.
It is widely known that, for many medical conditions and surgical procedures, outcomes are better when delivered by high-volume providers. It is not known if this holds true for patients with community-acquired pneumonia. To determine the association between physician/hospital volume and patient quality/outcomes, researchers utilized data from the Medicare National Pneumonia Quality Improvement Project. They included patients with an ICD9 diagnosis of pneumonia (850 patients were randomly selected from each state) at acute care hospitals with general or family medicine attendings. They excluded patients with no documentation of pneumonia, a normal chest X-ray, age <65, death on day one, comfort measures only, and departure against medical advice or transfer. Each physician and hospital volume were calculated from Medicare Part A claims for the same calendar year and analyzed by quartiles of volume.
Of the 9,741 physicians analyzed (13,480 patients), the median annual number of pneumonia patients was four, nine, 15, and 29 (in quartiles 1-4). Physician volume of care had little or no effect on performance rates of the timing of antibiotics, appropriate initial antibiotic, use of blood cultures, or in-hospital/30-day mortality rates. Low volume providers were significantly more likely to provide pneumococcal and influenza screening.
Of the 3,243 hospitals analyzed, the median annual pneumonia caseload was 57, 142, 262, and 465 (in quartiles 1-4). Hospital volume of care had little or no effect on performance rates of the appropriate initial antibiotic, use of blood cultures, pneumococcal/influenza screening, or in-hospital/30-day mortality rates (after severity of illness adjustment). Low volume centers were significantly more likely to give the first antibiotic within four hours.
In conclusion, volume of care by individual providers and hospital systems does not necessarily translate into better quality outcomes in pneumonia care. This may be partially explained by the challenges that larger medical centers face regarding delivering timely care (in overcrowded emergency rooms) and influencing behavior change (such as with standardized order sets).
By Debra Anoff, MD, assistant professor of medicine, Lucy Guerra, MD, assistant professor of medicine, Bjorn Holmstrom, MD, assistant professor of medicine, Asha Ramsakal, DO, assistant professor of medicine and chief, Richard Gross, MD, FACP, professor of medicine and chief, Division of Internal and Hospital Medicine H. Lee Moffitt Cancer Center and Research Institute, University of South Florida College of Medicine
Risk Factors for Mortality in Neutropenic Cancer Patients
Kuderer, NM, Dale DC, Crawford J, et al. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006 May 15;106(10):2258-2266.
Background: Neutropenic fever in a cancer patient is considered a medical emergency. Most episodes of febrile neutropenia result in hospital admission with prompt institution of broad spectrum antibiotics. The definition of neutropenia is usually regarded as an absolute neutrophil count (neutrophils plus bands) less than 500 cells/µL. The mortality rate of a cancer patient hospitalized with neutropenic fever ranges from 5 to 11%. There have been numerous small studies looking at risk factors associated with inpatient mortality. However, their small sample size and very select group of patients limit their generalizability to a standard hospitalist practice.
Methods: The authors used a longitudinal discharge database derived from 115 U.S. medical centers—both academic and community-based—in 39 states, looking retrospectively at all adult cancer patients hospitalized for febrile neutropenia between 1995 and 2000. The database included 55,276 hospitalizations and 41,779 patients and was analyzed for length of stay, cost per episode, mortality, and the clinical factors associated with mortality and prolonged hospitalization.
Results: The mortality rate for cancer patients with neutropenic fever averaged 9.5% per hospital. The average mortality rate was 14.3% for leukemia, 8.9% for lymphoma, and 8.0% for solid tumors. Lung cancer had the highest average mortality rate, 13.4%, followed by colorectal cancer at 8.8%, and breast cancer, which had the lowest mortality rate with 3.6%. Moreover, the highest mortality rate, 39.2%, was seen in those patients with a documented infection with invasive aspergillosis, while the rate of mortality for invasive candidiasis was 36.7%, followed by gram-negative bacteremia at 33.9%, pneumonia at 26.5%, and gram-positive bacteremia at 21.2%.
Patients without comorbidities, including common illnesses such as diabetes, congestive heart failure, and renal failure, had an average 2.6 % risk of dying. Those with one comorbidity had a 10.3% risk, and patients with more than one comorbidity had a mortality risk of 21.4%. Multivariate analysis revealed that the odds ratios for inpatient mortality were 3.94 for lung disease, 3.26 for cerebrovascular disease, 3.16 for renal disease, 2.89 for liver disease, 1.94 for pulmonary embolism, and 1.58 for heart disease.
The study also showed that patients hospitalized for longer than 10 days (comprising 35% of all patients) accounted for the majority of overall deaths (65%), overall cost (78%), and overall days spent in the hospital (74%).
Conclusions: The study provided an estimate of inpatient mortality associated with neutropenic fever in cancer patients and highlighted those subgroups as being at heightened risk for death. Important limitations include the retrospective nature of the study, the use of administrative data sets as the primary data source, and a failure to analyze for the duration of neutropenia prior to treatment. The authors’ conclusion that the identified factors may be useful in determining which patients warrant “more aggressive supportive care measures” is plausible, but does not find enough support in the study to warrant general implementation.
Long-Term Value of Electrocardiogram Before Noncardiac Surgery
Jeger RV, Probst C, Arsenic R, et al. Long-term prognostic value of the preoperative 12-lead electrocardiogram before major noncardiac surgery in coronary artery disease. Am Heart J. 2006 Feb;151(2):508-513.
Background: The 12-lead electrocardiogram is commonly utilized as part of the cardiovascular preoperative risk stratification. Certain ECG abnormalities, such as left bundle branch block, Q waves, ST-T abnormalities, arrhythmias, and left ventricular hypertrophy (LVH), have been associated with elevated risk in the perioperative period.1,2 This article prospectively evaluated whether an exhaustive analysis of preoperative ECGs in this population would have long-term predictive validity.
Methods: The study utilized a “predefined” analysis applied retrospectively on data obtained for another study.3,4
The study analyzed 172 patients, all of whom had documented coronary artery disease (CAD) as defined by previous myocardial infarction (MI), prior revascularization, significant stenoses on prior catheterization, ischemia (by dobutamine stress echocardiogram or adenosine thallium imaging), or who were high risk for CAD. High risk required at least two of the following: age over 70, hypertension, diabetes mellitus, prior stroke, exercise intolerance, or a “pathological resting ECG.” These patients were to undergo noncardiac surgery. The primary endpoint was all-cause mortality after two years, and the secondary endpoint was major adverse cardiac events (MACE) after two years. The MACE were defined as nonfatal MI, coronary revascularization, re-hospitalization due to recurrent ischemia, and/or cardiac death.
The ECGs were obtained one day prior to surgery and analyzed using the Minnesota classification. Telephone interviews were done at six, 12, and 24 months to evaluate outcome, and the Swiss Mortality Registry was used to determine cause of death. Analyzed data were adjusted for current beta-blocker use and perioperative ischemia using a sensitivity analysis-like correction that is described briefly in the report.
Results: ST depression (odds ratio [OR] 4.5) and faster heart rate (OR 1.6) were independent predictors of all-cause mortality. Faster heart rate (OR 1.7) was also an independent predictor of MACE.
Commentary: The results of this relatively small study raise awareness of resting tachycardia and ST depression as possible markers for poor perioperative and two-year postoperative outcomes. The latter is already included in risk stratification guidelines5, and the former is of uncertain validity due to possible confounding variables such as anxiety or pain, beta blocker dosing differences, and lack of intra- and postoperative beta blocker usage data which may affect postoperative cardiac morbidity and mortality long after the drugs are stopped.
For hospitalists and other physicians performing cardiac risk stratification for noncardiac surgery patients, the current study does not warrant any change in current practice as recommended in the American College of Cardiology/American Heart Association Guidelines 2002.5 As to whether resting tachycardia should be considered as a predictive ECG criterion in this context, further valid and applicable evidence is needed.
References
- De Bacquer D, De Backer G, Kornitzer M, et al. Prognostic value of ECG findings for total, cardiovascular disease, and coronary heart disease death in men and women. Heart. 1998 Dec;80(6):570-577.
- Tervahauta M, Pekkanen J, Punsar S, et al. Resting electrocardiographic abnormalities as predictors of coronary events and total mortality among elderly men. Am J Med. 1996 Jun;100(6):641-645.
- Filipovic M, Jeger R, Probst C, et al. Heart rate variability and cardiac troponin I are incremental and independent predictors of one-year all-cause mortality after major noncardiac surgery in patients at risk of coronary artery disease. J Am Coll Cardiol. 2003 Nov 19;42(10):1767-76.
- Filipovic M, Jeger RV, Girard T, et al. Predictors of long-term mortality and cardiac events in patients with known or suspected coronary artery disease who survive major noncardiac surgery. Anaesthesia. 2005 Jan;60(1):5-11.
- Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery—executive summary. Circulation. 2002 Mar 12;105(10):1257-1267.
Statins and Cardiovascular Disease
Hackam DG, Mamdani M, Li P, et al. Statins and sepsis in patients with cardiovascular disease: a population-based cohort analysis. Lancet. 2006 Feb 4;367(9508):413-418.
Background: The benefits of statins in secondary prevention of MI and ischemic CVA, as well as in reduction of all-cause mortality and their primary prevention in diabetics, are well documented in the literature.1 The concept of statins reducing subsequent sepsis in humans with atherosclerotic cardiovascular disease (CVD) is relatively new. One hypothesis holds that such an effect may be due to several common pathophysiologic mechanisms of sepsis and CVD: endothelial instability, immune dysregulation, inflammation, and thrombogenesis. Statins have been shown to provide improved outcomes from sepsis in animal studies, and observational studies in humans have raised similar hypotheses. This study attempts to analyze whether statin use in humans is associated with similar benefits regarding prevention of sepsis.
Methods: This was a population-based cohort analysis of 141,487 patients in Ontario, Canada, during the period of time from 1997-2002, who were older than age 65 and had been hospitalized for acute coronary syndrome or ischemic stroke, or had revascularization and survived three months post discharge. Using four reputable linked administrative databases, the authors found that 46,662 (33%) patients were prescribed a statin within three months of the discharge date (the index date), and 94,825 (67%) were not. About 19% of enrolled patients died within nine months and were excluded from the analysis. Of the eligible patients, propensity-based matching was used to identify 69,168 patients, of whom half were prescribed a statin and half were not. The patients were then analyzed through provincial administrative databases for the end points of hospital admission with an International Classification of Disease (ICD) code of sepsis, severe sepsis, fatal sepsis, death, or the end of the study.
Results: A total of 551 out of 34,584 patients were admitted for sepsis from the statin group, and 667 out of 34,584 were admitted from the control group during a mean follow-up of 2.2 years. The rate of sepsis in the statin group was significantly lower than in the control group (71.2 versus 88.0 per 10,000 person-years; p=0.0003). Statin use was also associated with fewer episodes of sepsis in an extended duration of 3.8 years, and with a lower risk of severe and fatal sepsis where sepsis was the admission diagnosis. This protection was evident at both high and low doses. The hazard ratio for sepsis was .81. There was a 19% relative reduction in the risk of sepsis in patients older than 65 with atherosclerosis. The absolute risk reduction for the occurrence of sepsis per 10,000 person-years was 16.8%, or .168% per person-year, with a corresponding number needed to treat (NNT) of 595 patients to prevent one episode of sepsis per year.
Comments: Though sophisticated and diverse statistical methods were used to assess the robustness of the analysis, this study is retrospective. Unidentified confounders, clinical sepsis risk stratification (the presence of obstructive uropathy or impairments leading to aspiration or skin breakdown, for example) are not accounted for in the analysis. Nonetheless, the hypothesis is of high relevance to hospitalists; it has biologic plausibility, and the results are intriguing if not definitive.
From a practical perspective, it seems prudent to ensure ongoing statin use for all patients with appropriate traditional indications. Initiating statins for the sole purpose of reducing future risk of sepsis is not yet sufficiently supported by the available evidence, and the NNT of almost 600 patients per year in the current study does little to alter that recommendation. In reply to a subsequent letter to the editor, the authors pointed out that the high NNT in part reflects the low-risk profile of the cohort and would be lower in higher risk patients; for example, patients with chronic renal failure, previous infections, or corticosteroid use would have NNTs of 166, 250, and 250, respectively.2 A randomized, controlled prospective trial would be a welcome addition to the evidence on this important topic, as would studies of the use of statins solely as an acute intervention upon suspicion of sepsis.
References
- MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002 Jul 6;360(9326):7-22.
- Hackam DG, Redelmeier DA. Statins and sepsis—authors' reply. Lancet. 2006;367:1651.
Review: Impact of Health Information Technology
Advances in information technology have transformed the world of business and education and will undoubtedly change the delivery and implementation of medical services. What arguably sets the world of health information apart from other systems is, however, the extreme sensitivity of the data involved and the impact it has on human lives.
Methods and data sources: In the article, “Systemic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care,” the authors reviewed four data sources and extracted information on system design, effects on quality and cost benefit analysis. Four data sources were utilized including a MEDLINE analysis of articles indexed as health information technology (HIT) from 1995 to January 2004 utilizing:
- Cochrane Center Registry of Controlled Trials;
- Cochrane Database of Abstracts of Reviews of Effects;
- Periodical Abstracts Database; and
- Studies singled out by experts up to April of 2005
Of the four data sources, 24% of all studies came from the following academic centers: the Regenstrief Institute (Indianapolis), Brigham and Women’s Hospital (Boston), Department of Veterans Affairs, and the Latter Day Saints Hospital/Intermountain Health Care.
Inclusion criteria: The HIT evaluation and efficacy information derived was from these four academic institutions, each with its own EHR (electronic health record) system. Of 4,582 initial articles derived from a title review, 867 were deemed suitable given their title matter, but only 257 met inclusion criteria.
A modified framework from the Institute of Medicine’s six aims for care and a framework to analyze costs developed by the authors themselves was used for analysis.1
Reasons for rejection: Articles that did not have HIT as the subject, others that did not report outcomes data, and those that did not examine barriers for outcomes analysis were rejected.
Information examined: Extracted information on system capabilities including components of the system such as:
- User friendliness;
- Types of systems such as EHR that allowed for medical decision making support and e-prescribing; and
- Functional capabilities such as order entry and clinical documentation.
Common characteristics shared by the HIT systems evaluated by the four academic institutions: they were all multifunctional and included medical decision making support, all were internally developed by research experts and all had capabilities that had been improved upon and added incrementally over time.
The data supported five primary goals:
- Increasing delivery of healthcare according to established protocols and guidelines;
- Enhancing capacity to perform surveillance and monitoring of disease conditions and care delivery;
- Reducing medication error rates;
- Decreasing utilization of care; and
- Producing a mixed effect on time utilization.
Major findings: (see Figure 1, below).
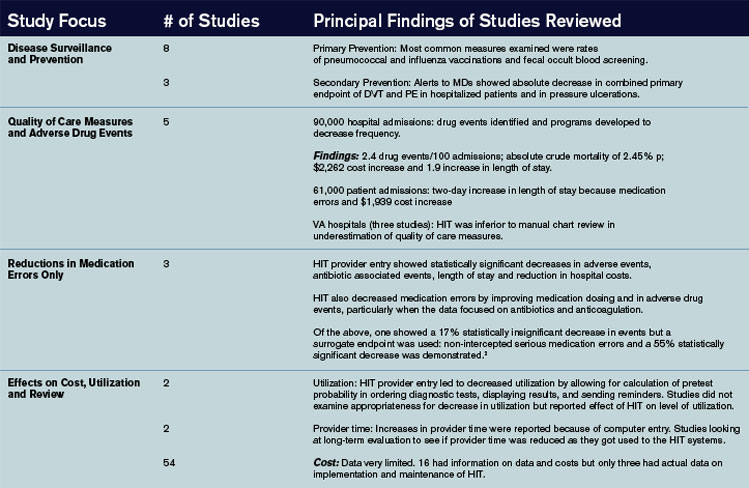
The authors of the article summarized 22 other studies in Appendix 22 from other institutions. The benefits noted were very similar to those found in the studies from the benchmark institutions; however, one major difference was the use of pre/post time-series designs that did not have a control or comparative group. Internally and commercially, HIT systems were evaluated in most of these studies with thirteen focusing on the former and nine on the later.
Summary and discussion: This study raises several questions worthy of further research and study:
- How are systems to interface with regard to the portability of health care information?
- Which are better: internally devised systems or commercially available systems?
- Who is going to be responsible for establishing standard guidelines for the implementation of HIT systems across the diverse healthcare systems in the United States? and
- How are the data to be used and analyzed by insurers and even public health entities?
HIT has shown many benefits with regard to quality of patient care issues and efficiency. Studies from these four benchmark institutions had one important limitation, however, and that is that the development of an internally developed HIT system took many years and is unlikely to be applicable to other institutions that have fewer resources and are struggling to implement the technology in a timely manner.
As the authors of the article acknowledge, it is not clear if HIT systems, though useful as tools, alter states of disease and health. More research looking at the direct impact of HIT information on morbidity and mortality is needed. As the authors state, this raises the question of a national HIT system, thereby making adoption of HIT a bipartisan initiative.
Providers need better evidence on information systems in order to make informed decisions about acquiring and implementing technology in community settings. The authors of this article made the first attempt to collate and appraise such evidence. Additional research is needed in academic, governmental, and community settings in both acute and nonacute facilities. As the authors point out, a uniform standard should be devised at the federal, state, and local level to report research on the implementation of HIT systems similar to the CONSORT and Quorum statement.
References
- Chaudry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742-752.
- Bates DW, Leape LL Cullen DJ. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998 Oct 21;280(15):1311-1316.
Gatifloxacin and Dysglycemia
Park-Wyllie LY, Juurlink DN, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med. 2006 Mar;354(13):1352-1361.
Fluoroquinolones are the most commonly prescribed antibiotics in the United States. Side effects associated with some fluoroquinolones (temafloxacin, grepafloxacin, sparfloxacin, and trovafloxacin) have prompted their restriction or withdrawal. Until now, dysglycemia had been associated with gatifloxacin only in small studies or case reports.
This study sought to examine, by a nested case control design, the association between gatifloxacin and dysglycemia that required hospital care. The researchers reviewed all prescription records from the Ontario (Canada) Drug Benefit database, which houses complete prescription drug sales for all patients older than age 65 (1.4 million residents). They linked this with a national Canadian database of those same patients’ emergency room visits and hospital admissions. Cases were patients who received hospital care for hypoglycemia (or hyperglycemia) within 30 days of filling an antibiotic prescription (macrolide, cephalosporin, or fluoroquinolone). Controls were patients who had not received hospital care after an antibiotic prescription in the same time period. They were matched by age, gender, whether or not they had been diagnosed as having diabetes, diabetic drug use, and time of antibiotic prescription. Patients were excluded if they turned 65 within the year, had been hospitalized within 90 days, had subsequent hospitalizations for dysglycemia, or had more than one antibiotic in 30 days. Logistic regression was used to determine the odds ratio for the association between dysglycemia and recent antibiotic use. In multivariable analysis, they adjusted for liver disease, renal disease, alcohol use, hospitalizations, physician visits, diabetic and P-450 medications, socioeconomic status, and number of prescription drugs. They were also stratified by diabetes status.
The cases treated for hypoglycemia were four times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 4.3, CI 2.9-6.3). The association was slightly less with levofloxacin (OR 1.5, CI 1.2-2.0), and there was no association of hypoglycemia with moxifloxacin, ciprofloxacin, or cephalosporins. The cases treated for hyperglycemia were 17 times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 16.7, CI 10.4-26.8). There was no association of hyperglycemia with the other fluoroquinolones or cephalosporins. The analyses were similar when stratified by diabetes status. In total, 1.1% of all gatifloxacin treatments were associated with dysglycemia requiring hospital care within 30 days. As to what to do with gatifloxacin, as stated precisely in an accompanying editorial, “For every approved indication for gatifloxacin, there are safer, equally effective, and less costly alternatives.”
Physician Board Certification and Acute MI Quality Measures.
Chen J, Rathore SS, Wang Y, et al. Physician board certification and the care and outcomes of elderly patients with acute myocardial infarction. J Gen Intern Med. 2006 Mar;21(3):238-244.
Board certification may have implications for practicing physicians because there is evidence that both hiring organizations and patients prefer board-certified physicians over non-board certified physicians. However, it is unknown if such certification translates into better quality of patient care.
In this study researchers sought to examine the relationship between physician board certification and quality of care in patients with acute myocardial infarction (AMI). Medical records were abstracted from the Cooperative Cardiovascular Project, a cohort of Medicare beneficiaries hospitalized with AMI. Board certification was obtained from the American Medical Association (AMA) Physician Masterfile, which is reportedly 94% accurate. Quality of care measures included ASA and beta-blocker use at the time of admission and discharge. Researchers also evaluated 30-day and one-year mortality.
They evaluated these quality measures on 101,251 patients and 36,668 physicians, of which 80% were board certified. In multivariable analyses adjusting for patient, hospital, and physician characteristics, board-certified internal medicine and cardiology physicians (but not family practitioners) were more likely to prescribe ASA and beta-blockers at admission and discharge than non-board certified physicians (adjusted relative risk ranged from 1.04 to 1.20). There was no difference in 30-day and one-year mortality among any specialty after multivariable adjustment.
These results, albeit modest, suggest that physician board certification may be associated with superior quality of care in elderly patients with AMI. The authors offer that board-certified physicians may be more aware or familiar with guidelines or may be more likely to agree with clinical guidelines. Although board-certified physicians have been shown to complete more hours of CME and spend more time reading journals, they caution that board certification should not be used as a surrogate marker of quality. Because 30% of U.S. practicing physicians are not currently board certified, these results certainly warrant further study.
PE in COPD
Tillie-Leblond I, Marquette CH, Perez T, et al. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Ann Intern Med. 2006 Mar 21;144(6):390-396.
This study sought to evaluate the prevalence and risk factors for pulmonary embolus (PE) in patients with unexplained exacerbations of COPD. All patients with an unexplained COPD exacerbation requiring hospitalization (not ICU) were evaluated for PE by spiral chest CT and lower limb venous ultrasound (USG). The COPD flare was “unexplained” if there were no signs or symptoms of respiratory tract infection, no pneumothorax, or a discrepancy between the clinical/radiologic features and the degree of hypoxemia. Patients were considered to have a PE if either of the two tests (CT or USG) were positive. Patients were not considered to have a PE if both tests were negative, and there was no evidence of PE at three-month follow-up.
Of 211 referred patients, 14 were not included due to inconclusive results or iodine intolerance. Of 197 enrolled patients, 25% had PE. There was no difference between the PE and non-PE groups with respect to referral location, clinical symptoms (dyspnea, pleuritic pain, hemoptysis, tachycardia, lower limb edema), need for long term oxygen therapy, admission P02 or PC02, recent trauma, recent surgery, obesity, or immobilization for more than seven days. Factors associated with PE on bivariate analysis included a decrease in PC02 >5mmHg from baseline, previous thromboembolism, and malignancy.
Researchers then calculated these patient’s Geneva score (a PE predictor score based on age, history, pulse, ABG, and chest X-ray findings. Those with a low probability Geneva score had a 9% incidence of PE, those with an intermediate score had a 47% incidence, and those with a high Geneva score had a 100% incidence.
In conclusion, in this study population of non-ICU patients with unexplained exacerbations of COPD, one in four had evidence of thromboembolic disease. Significant risk ratios between groups were found for patients with a prior history of thromboembolism, malignancy, or a decrease in their baseline PC02. These factors should be weighted heavily in determining which patients with unexplained COPD exacerbations should undergo workup to exclude a PE. The Geneva score also correlated well with PE incidence in this population.
Telithromycin in Asthma Exacerbations
Johnston SL, Blasi FB, Black PN, et al. The effect of telithromycin in acute exacerbations of asthma. New Engl J Med. 2006 Apr 13;354(15):1589-1600.
The use of antibiotics for uncomplicated asthma exacerbations is not currently considered standard of care. This randomized placebo controlled trial was designed to determine if telithromycin (a ketolide, structurally similar to macrolides, with efficacy against mycoplasma and chlamydia pneumonia) improves symptoms and peak flow rates in patients with asthma exacerbations. Researchers enrolled 278 patients age 18 to 55 with a history of asthma (less than six months) with an exacerbation (peak flow <80% and symptoms of wheeze and dyspnea). They excluded those requiring ICU care, smokers, known infection/recent antibiotic use, or regular use of oral steroids. Baseline demographics, pulmonary function, and acute medication use (steroids and beta agonists) were similar between the groups.
Intervention patients received telithromycin 800 mg a day for 10 days. The primary outcome was change in their asthma symptom score (rated on a seven-point scale) and change in their peak flows (recorded every morning for the study duration). Secondary outcomes were clinic pulmonary function tests (PFTs).
The intervention group had a mean decrease in their symptom score of 1.3 versus 1.0 in the placebo group (40% versus 27% reduction, p=.004). There was no difference between the groups in home peak flow measurements. There were statistically significant differences between the groups in clinic PFTs (FEV1, FVC, FEF 25%-75%), although the P values were not adjusted for multiple outcomes. The intervention group had a higher percentage of symptom-free days (16% versus 8%, P=.006). A total of 61% of the patients had serologic evidence of chlamydia or mycoplasma infection. Nausea (seven versus 0) and LFT elevations (two versus 0) were more frequent in the intervention group.
In conclusion, this is the first trial to report a benefit of antibiotic use in uncomplicated asthma exacerbations. This conclusion must be tempered by the underwhelming clinical improvement (1.3 versus 1.0 improvement in symptom scores), lack of peak flow improvement, recent reports of serious hepatotoxicity associated with telithromycin, and the possibility for antibiotic over-prescribing in unrefined patient populations.
Pneumonia Quality and Outcomes by Volume of Care
Lindenauer PK, Behal R, Murray CK, et al. Volume, quality of care, and outcome in pneumonia. Ann Intern Med. 2006 Feb 21;144(4):262-269.
It is widely known that, for many medical conditions and surgical procedures, outcomes are better when delivered by high-volume providers. It is not known if this holds true for patients with community-acquired pneumonia. To determine the association between physician/hospital volume and patient quality/outcomes, researchers utilized data from the Medicare National Pneumonia Quality Improvement Project. They included patients with an ICD9 diagnosis of pneumonia (850 patients were randomly selected from each state) at acute care hospitals with general or family medicine attendings. They excluded patients with no documentation of pneumonia, a normal chest X-ray, age <65, death on day one, comfort measures only, and departure against medical advice or transfer. Each physician and hospital volume were calculated from Medicare Part A claims for the same calendar year and analyzed by quartiles of volume.
Of the 9,741 physicians analyzed (13,480 patients), the median annual number of pneumonia patients was four, nine, 15, and 29 (in quartiles 1-4). Physician volume of care had little or no effect on performance rates of the timing of antibiotics, appropriate initial antibiotic, use of blood cultures, or in-hospital/30-day mortality rates. Low volume providers were significantly more likely to provide pneumococcal and influenza screening.
Of the 3,243 hospitals analyzed, the median annual pneumonia caseload was 57, 142, 262, and 465 (in quartiles 1-4). Hospital volume of care had little or no effect on performance rates of the appropriate initial antibiotic, use of blood cultures, pneumococcal/influenza screening, or in-hospital/30-day mortality rates (after severity of illness adjustment). Low volume centers were significantly more likely to give the first antibiotic within four hours.
In conclusion, volume of care by individual providers and hospital systems does not necessarily translate into better quality outcomes in pneumonia care. This may be partially explained by the challenges that larger medical centers face regarding delivering timely care (in overcrowded emergency rooms) and influencing behavior change (such as with standardized order sets).
By Debra Anoff, MD, assistant professor of medicine, Lucy Guerra, MD, assistant professor of medicine, Bjorn Holmstrom, MD, assistant professor of medicine, Asha Ramsakal, DO, assistant professor of medicine and chief, Richard Gross, MD, FACP, professor of medicine and chief, Division of Internal and Hospital Medicine H. Lee Moffitt Cancer Center and Research Institute, University of South Florida College of Medicine
Risk Factors for Mortality in Neutropenic Cancer Patients
Kuderer, NM, Dale DC, Crawford J, et al. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006 May 15;106(10):2258-2266.
Background: Neutropenic fever in a cancer patient is considered a medical emergency. Most episodes of febrile neutropenia result in hospital admission with prompt institution of broad spectrum antibiotics. The definition of neutropenia is usually regarded as an absolute neutrophil count (neutrophils plus bands) less than 500 cells/µL. The mortality rate of a cancer patient hospitalized with neutropenic fever ranges from 5 to 11%. There have been numerous small studies looking at risk factors associated with inpatient mortality. However, their small sample size and very select group of patients limit their generalizability to a standard hospitalist practice.
Methods: The authors used a longitudinal discharge database derived from 115 U.S. medical centers—both academic and community-based—in 39 states, looking retrospectively at all adult cancer patients hospitalized for febrile neutropenia between 1995 and 2000. The database included 55,276 hospitalizations and 41,779 patients and was analyzed for length of stay, cost per episode, mortality, and the clinical factors associated with mortality and prolonged hospitalization.
Results: The mortality rate for cancer patients with neutropenic fever averaged 9.5% per hospital. The average mortality rate was 14.3% for leukemia, 8.9% for lymphoma, and 8.0% for solid tumors. Lung cancer had the highest average mortality rate, 13.4%, followed by colorectal cancer at 8.8%, and breast cancer, which had the lowest mortality rate with 3.6%. Moreover, the highest mortality rate, 39.2%, was seen in those patients with a documented infection with invasive aspergillosis, while the rate of mortality for invasive candidiasis was 36.7%, followed by gram-negative bacteremia at 33.9%, pneumonia at 26.5%, and gram-positive bacteremia at 21.2%.
Patients without comorbidities, including common illnesses such as diabetes, congestive heart failure, and renal failure, had an average 2.6 % risk of dying. Those with one comorbidity had a 10.3% risk, and patients with more than one comorbidity had a mortality risk of 21.4%. Multivariate analysis revealed that the odds ratios for inpatient mortality were 3.94 for lung disease, 3.26 for cerebrovascular disease, 3.16 for renal disease, 2.89 for liver disease, 1.94 for pulmonary embolism, and 1.58 for heart disease.
The study also showed that patients hospitalized for longer than 10 days (comprising 35% of all patients) accounted for the majority of overall deaths (65%), overall cost (78%), and overall days spent in the hospital (74%).
Conclusions: The study provided an estimate of inpatient mortality associated with neutropenic fever in cancer patients and highlighted those subgroups as being at heightened risk for death. Important limitations include the retrospective nature of the study, the use of administrative data sets as the primary data source, and a failure to analyze for the duration of neutropenia prior to treatment. The authors’ conclusion that the identified factors may be useful in determining which patients warrant “more aggressive supportive care measures” is plausible, but does not find enough support in the study to warrant general implementation.
Long-Term Value of Electrocardiogram Before Noncardiac Surgery
Jeger RV, Probst C, Arsenic R, et al. Long-term prognostic value of the preoperative 12-lead electrocardiogram before major noncardiac surgery in coronary artery disease. Am Heart J. 2006 Feb;151(2):508-513.
Background: The 12-lead electrocardiogram is commonly utilized as part of the cardiovascular preoperative risk stratification. Certain ECG abnormalities, such as left bundle branch block, Q waves, ST-T abnormalities, arrhythmias, and left ventricular hypertrophy (LVH), have been associated with elevated risk in the perioperative period.1,2 This article prospectively evaluated whether an exhaustive analysis of preoperative ECGs in this population would have long-term predictive validity.
Methods: The study utilized a “predefined” analysis applied retrospectively on data obtained for another study.3,4
The study analyzed 172 patients, all of whom had documented coronary artery disease (CAD) as defined by previous myocardial infarction (MI), prior revascularization, significant stenoses on prior catheterization, ischemia (by dobutamine stress echocardiogram or adenosine thallium imaging), or who were high risk for CAD. High risk required at least two of the following: age over 70, hypertension, diabetes mellitus, prior stroke, exercise intolerance, or a “pathological resting ECG.” These patients were to undergo noncardiac surgery. The primary endpoint was all-cause mortality after two years, and the secondary endpoint was major adverse cardiac events (MACE) after two years. The MACE were defined as nonfatal MI, coronary revascularization, re-hospitalization due to recurrent ischemia, and/or cardiac death.
The ECGs were obtained one day prior to surgery and analyzed using the Minnesota classification. Telephone interviews were done at six, 12, and 24 months to evaluate outcome, and the Swiss Mortality Registry was used to determine cause of death. Analyzed data were adjusted for current beta-blocker use and perioperative ischemia using a sensitivity analysis-like correction that is described briefly in the report.
Results: ST depression (odds ratio [OR] 4.5) and faster heart rate (OR 1.6) were independent predictors of all-cause mortality. Faster heart rate (OR 1.7) was also an independent predictor of MACE.
Commentary: The results of this relatively small study raise awareness of resting tachycardia and ST depression as possible markers for poor perioperative and two-year postoperative outcomes. The latter is already included in risk stratification guidelines5, and the former is of uncertain validity due to possible confounding variables such as anxiety or pain, beta blocker dosing differences, and lack of intra- and postoperative beta blocker usage data which may affect postoperative cardiac morbidity and mortality long after the drugs are stopped.
For hospitalists and other physicians performing cardiac risk stratification for noncardiac surgery patients, the current study does not warrant any change in current practice as recommended in the American College of Cardiology/American Heart Association Guidelines 2002.5 As to whether resting tachycardia should be considered as a predictive ECG criterion in this context, further valid and applicable evidence is needed.
References
- De Bacquer D, De Backer G, Kornitzer M, et al. Prognostic value of ECG findings for total, cardiovascular disease, and coronary heart disease death in men and women. Heart. 1998 Dec;80(6):570-577.
- Tervahauta M, Pekkanen J, Punsar S, et al. Resting electrocardiographic abnormalities as predictors of coronary events and total mortality among elderly men. Am J Med. 1996 Jun;100(6):641-645.
- Filipovic M, Jeger R, Probst C, et al. Heart rate variability and cardiac troponin I are incremental and independent predictors of one-year all-cause mortality after major noncardiac surgery in patients at risk of coronary artery disease. J Am Coll Cardiol. 2003 Nov 19;42(10):1767-76.
- Filipovic M, Jeger RV, Girard T, et al. Predictors of long-term mortality and cardiac events in patients with known or suspected coronary artery disease who survive major noncardiac surgery. Anaesthesia. 2005 Jan;60(1):5-11.
- Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery—executive summary. Circulation. 2002 Mar 12;105(10):1257-1267.
Statins and Cardiovascular Disease
Hackam DG, Mamdani M, Li P, et al. Statins and sepsis in patients with cardiovascular disease: a population-based cohort analysis. Lancet. 2006 Feb 4;367(9508):413-418.
Background: The benefits of statins in secondary prevention of MI and ischemic CVA, as well as in reduction of all-cause mortality and their primary prevention in diabetics, are well documented in the literature.1 The concept of statins reducing subsequent sepsis in humans with atherosclerotic cardiovascular disease (CVD) is relatively new. One hypothesis holds that such an effect may be due to several common pathophysiologic mechanisms of sepsis and CVD: endothelial instability, immune dysregulation, inflammation, and thrombogenesis. Statins have been shown to provide improved outcomes from sepsis in animal studies, and observational studies in humans have raised similar hypotheses. This study attempts to analyze whether statin use in humans is associated with similar benefits regarding prevention of sepsis.
Methods: This was a population-based cohort analysis of 141,487 patients in Ontario, Canada, during the period of time from 1997-2002, who were older than age 65 and had been hospitalized for acute coronary syndrome or ischemic stroke, or had revascularization and survived three months post discharge. Using four reputable linked administrative databases, the authors found that 46,662 (33%) patients were prescribed a statin within three months of the discharge date (the index date), and 94,825 (67%) were not. About 19% of enrolled patients died within nine months and were excluded from the analysis. Of the eligible patients, propensity-based matching was used to identify 69,168 patients, of whom half were prescribed a statin and half were not. The patients were then analyzed through provincial administrative databases for the end points of hospital admission with an International Classification of Disease (ICD) code of sepsis, severe sepsis, fatal sepsis, death, or the end of the study.
Results: A total of 551 out of 34,584 patients were admitted for sepsis from the statin group, and 667 out of 34,584 were admitted from the control group during a mean follow-up of 2.2 years. The rate of sepsis in the statin group was significantly lower than in the control group (71.2 versus 88.0 per 10,000 person-years; p=0.0003). Statin use was also associated with fewer episodes of sepsis in an extended duration of 3.8 years, and with a lower risk of severe and fatal sepsis where sepsis was the admission diagnosis. This protection was evident at both high and low doses. The hazard ratio for sepsis was .81. There was a 19% relative reduction in the risk of sepsis in patients older than 65 with atherosclerosis. The absolute risk reduction for the occurrence of sepsis per 10,000 person-years was 16.8%, or .168% per person-year, with a corresponding number needed to treat (NNT) of 595 patients to prevent one episode of sepsis per year.
Comments: Though sophisticated and diverse statistical methods were used to assess the robustness of the analysis, this study is retrospective. Unidentified confounders, clinical sepsis risk stratification (the presence of obstructive uropathy or impairments leading to aspiration or skin breakdown, for example) are not accounted for in the analysis. Nonetheless, the hypothesis is of high relevance to hospitalists; it has biologic plausibility, and the results are intriguing if not definitive.
From a practical perspective, it seems prudent to ensure ongoing statin use for all patients with appropriate traditional indications. Initiating statins for the sole purpose of reducing future risk of sepsis is not yet sufficiently supported by the available evidence, and the NNT of almost 600 patients per year in the current study does little to alter that recommendation. In reply to a subsequent letter to the editor, the authors pointed out that the high NNT in part reflects the low-risk profile of the cohort and would be lower in higher risk patients; for example, patients with chronic renal failure, previous infections, or corticosteroid use would have NNTs of 166, 250, and 250, respectively.2 A randomized, controlled prospective trial would be a welcome addition to the evidence on this important topic, as would studies of the use of statins solely as an acute intervention upon suspicion of sepsis.
References
- MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002 Jul 6;360(9326):7-22.
- Hackam DG, Redelmeier DA. Statins and sepsis—authors' reply. Lancet. 2006;367:1651.
Review: Impact of Health Information Technology
Advances in information technology have transformed the world of business and education and will undoubtedly change the delivery and implementation of medical services. What arguably sets the world of health information apart from other systems is, however, the extreme sensitivity of the data involved and the impact it has on human lives.
Methods and data sources: In the article, “Systemic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care,” the authors reviewed four data sources and extracted information on system design, effects on quality and cost benefit analysis. Four data sources were utilized including a MEDLINE analysis of articles indexed as health information technology (HIT) from 1995 to January 2004 utilizing:
- Cochrane Center Registry of Controlled Trials;
- Cochrane Database of Abstracts of Reviews of Effects;
- Periodical Abstracts Database; and
- Studies singled out by experts up to April of 2005
Of the four data sources, 24% of all studies came from the following academic centers: the Regenstrief Institute (Indianapolis), Brigham and Women’s Hospital (Boston), Department of Veterans Affairs, and the Latter Day Saints Hospital/Intermountain Health Care.
Inclusion criteria: The HIT evaluation and efficacy information derived was from these four academic institutions, each with its own EHR (electronic health record) system. Of 4,582 initial articles derived from a title review, 867 were deemed suitable given their title matter, but only 257 met inclusion criteria.
A modified framework from the Institute of Medicine’s six aims for care and a framework to analyze costs developed by the authors themselves was used for analysis.1
Reasons for rejection: Articles that did not have HIT as the subject, others that did not report outcomes data, and those that did not examine barriers for outcomes analysis were rejected.
Information examined: Extracted information on system capabilities including components of the system such as:
- User friendliness;
- Types of systems such as EHR that allowed for medical decision making support and e-prescribing; and
- Functional capabilities such as order entry and clinical documentation.
Common characteristics shared by the HIT systems evaluated by the four academic institutions: they were all multifunctional and included medical decision making support, all were internally developed by research experts and all had capabilities that had been improved upon and added incrementally over time.
The data supported five primary goals:
- Increasing delivery of healthcare according to established protocols and guidelines;
- Enhancing capacity to perform surveillance and monitoring of disease conditions and care delivery;
- Reducing medication error rates;
- Decreasing utilization of care; and
- Producing a mixed effect on time utilization.
Major findings: (see Figure 1, below).
The authors of the article summarized 22 other studies in Appendix 22 from other institutions. The benefits noted were very similar to those found in the studies from the benchmark institutions; however, one major difference was the use of pre/post time-series designs that did not have a control or comparative group. Internally and commercially, HIT systems were evaluated in most of these studies with thirteen focusing on the former and nine on the later.
Summary and discussion: This study raises several questions worthy of further research and study:
- How are systems to interface with regard to the portability of health care information?
- Which are better: internally devised systems or commercially available systems?
- Who is going to be responsible for establishing standard guidelines for the implementation of HIT systems across the diverse healthcare systems in the United States? and
- How are the data to be used and analyzed by insurers and even public health entities?
HIT has shown many benefits with regard to quality of patient care issues and efficiency. Studies from these four benchmark institutions had one important limitation, however, and that is that the development of an internally developed HIT system took many years and is unlikely to be applicable to other institutions that have fewer resources and are struggling to implement the technology in a timely manner.
As the authors of the article acknowledge, it is not clear if HIT systems, though useful as tools, alter states of disease and health. More research looking at the direct impact of HIT information on morbidity and mortality is needed. As the authors state, this raises the question of a national HIT system, thereby making adoption of HIT a bipartisan initiative.
Providers need better evidence on information systems in order to make informed decisions about acquiring and implementing technology in community settings. The authors of this article made the first attempt to collate and appraise such evidence. Additional research is needed in academic, governmental, and community settings in both acute and nonacute facilities. As the authors point out, a uniform standard should be devised at the federal, state, and local level to report research on the implementation of HIT systems similar to the CONSORT and Quorum statement.
References
- Chaudry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742-752.
- Bates DW, Leape LL Cullen DJ. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998 Oct 21;280(15):1311-1316.
Gatifloxacin and Dysglycemia
Park-Wyllie LY, Juurlink DN, Kopp A, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med. 2006 Mar;354(13):1352-1361.
Fluoroquinolones are the most commonly prescribed antibiotics in the United States. Side effects associated with some fluoroquinolones (temafloxacin, grepafloxacin, sparfloxacin, and trovafloxacin) have prompted their restriction or withdrawal. Until now, dysglycemia had been associated with gatifloxacin only in small studies or case reports.
This study sought to examine, by a nested case control design, the association between gatifloxacin and dysglycemia that required hospital care. The researchers reviewed all prescription records from the Ontario (Canada) Drug Benefit database, which houses complete prescription drug sales for all patients older than age 65 (1.4 million residents). They linked this with a national Canadian database of those same patients’ emergency room visits and hospital admissions. Cases were patients who received hospital care for hypoglycemia (or hyperglycemia) within 30 days of filling an antibiotic prescription (macrolide, cephalosporin, or fluoroquinolone). Controls were patients who had not received hospital care after an antibiotic prescription in the same time period. They were matched by age, gender, whether or not they had been diagnosed as having diabetes, diabetic drug use, and time of antibiotic prescription. Patients were excluded if they turned 65 within the year, had been hospitalized within 90 days, had subsequent hospitalizations for dysglycemia, or had more than one antibiotic in 30 days. Logistic regression was used to determine the odds ratio for the association between dysglycemia and recent antibiotic use. In multivariable analysis, they adjusted for liver disease, renal disease, alcohol use, hospitalizations, physician visits, diabetic and P-450 medications, socioeconomic status, and number of prescription drugs. They were also stratified by diabetes status.
The cases treated for hypoglycemia were four times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 4.3, CI 2.9-6.3). The association was slightly less with levofloxacin (OR 1.5, CI 1.2-2.0), and there was no association of hypoglycemia with moxifloxacin, ciprofloxacin, or cephalosporins. The cases treated for hyperglycemia were 17 times more likely than controls to have been treated with gatifloxacin than with a macrolide (OR 16.7, CI 10.4-26.8). There was no association of hyperglycemia with the other fluoroquinolones or cephalosporins. The analyses were similar when stratified by diabetes status. In total, 1.1% of all gatifloxacin treatments were associated with dysglycemia requiring hospital care within 30 days. As to what to do with gatifloxacin, as stated precisely in an accompanying editorial, “For every approved indication for gatifloxacin, there are safer, equally effective, and less costly alternatives.”
Physician Board Certification and Acute MI Quality Measures.
Chen J, Rathore SS, Wang Y, et al. Physician board certification and the care and outcomes of elderly patients with acute myocardial infarction. J Gen Intern Med. 2006 Mar;21(3):238-244.
Board certification may have implications for practicing physicians because there is evidence that both hiring organizations and patients prefer board-certified physicians over non-board certified physicians. However, it is unknown if such certification translates into better quality of patient care.
In this study researchers sought to examine the relationship between physician board certification and quality of care in patients with acute myocardial infarction (AMI). Medical records were abstracted from the Cooperative Cardiovascular Project, a cohort of Medicare beneficiaries hospitalized with AMI. Board certification was obtained from the American Medical Association (AMA) Physician Masterfile, which is reportedly 94% accurate. Quality of care measures included ASA and beta-blocker use at the time of admission and discharge. Researchers also evaluated 30-day and one-year mortality.
They evaluated these quality measures on 101,251 patients and 36,668 physicians, of which 80% were board certified. In multivariable analyses adjusting for patient, hospital, and physician characteristics, board-certified internal medicine and cardiology physicians (but not family practitioners) were more likely to prescribe ASA and beta-blockers at admission and discharge than non-board certified physicians (adjusted relative risk ranged from 1.04 to 1.20). There was no difference in 30-day and one-year mortality among any specialty after multivariable adjustment.
These results, albeit modest, suggest that physician board certification may be associated with superior quality of care in elderly patients with AMI. The authors offer that board-certified physicians may be more aware or familiar with guidelines or may be more likely to agree with clinical guidelines. Although board-certified physicians have been shown to complete more hours of CME and spend more time reading journals, they caution that board certification should not be used as a surrogate marker of quality. Because 30% of U.S. practicing physicians are not currently board certified, these results certainly warrant further study.
PE in COPD
Tillie-Leblond I, Marquette CH, Perez T, et al. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Ann Intern Med. 2006 Mar 21;144(6):390-396.
This study sought to evaluate the prevalence and risk factors for pulmonary embolus (PE) in patients with unexplained exacerbations of COPD. All patients with an unexplained COPD exacerbation requiring hospitalization (not ICU) were evaluated for PE by spiral chest CT and lower limb venous ultrasound (USG). The COPD flare was “unexplained” if there were no signs or symptoms of respiratory tract infection, no pneumothorax, or a discrepancy between the clinical/radiologic features and the degree of hypoxemia. Patients were considered to have a PE if either of the two tests (CT or USG) were positive. Patients were not considered to have a PE if both tests were negative, and there was no evidence of PE at three-month follow-up.
Of 211 referred patients, 14 were not included due to inconclusive results or iodine intolerance. Of 197 enrolled patients, 25% had PE. There was no difference between the PE and non-PE groups with respect to referral location, clinical symptoms (dyspnea, pleuritic pain, hemoptysis, tachycardia, lower limb edema), need for long term oxygen therapy, admission P02 or PC02, recent trauma, recent surgery, obesity, or immobilization for more than seven days. Factors associated with PE on bivariate analysis included a decrease in PC02 >5mmHg from baseline, previous thromboembolism, and malignancy.
Researchers then calculated these patient’s Geneva score (a PE predictor score based on age, history, pulse, ABG, and chest X-ray findings. Those with a low probability Geneva score had a 9% incidence of PE, those with an intermediate score had a 47% incidence, and those with a high Geneva score had a 100% incidence.
In conclusion, in this study population of non-ICU patients with unexplained exacerbations of COPD, one in four had evidence of thromboembolic disease. Significant risk ratios between groups were found for patients with a prior history of thromboembolism, malignancy, or a decrease in their baseline PC02. These factors should be weighted heavily in determining which patients with unexplained COPD exacerbations should undergo workup to exclude a PE. The Geneva score also correlated well with PE incidence in this population.
Telithromycin in Asthma Exacerbations
Johnston SL, Blasi FB, Black PN, et al. The effect of telithromycin in acute exacerbations of asthma. New Engl J Med. 2006 Apr 13;354(15):1589-1600.
The use of antibiotics for uncomplicated asthma exacerbations is not currently considered standard of care. This randomized placebo controlled trial was designed to determine if telithromycin (a ketolide, structurally similar to macrolides, with efficacy against mycoplasma and chlamydia pneumonia) improves symptoms and peak flow rates in patients with asthma exacerbations. Researchers enrolled 278 patients age 18 to 55 with a history of asthma (less than six months) with an exacerbation (peak flow <80% and symptoms of wheeze and dyspnea). They excluded those requiring ICU care, smokers, known infection/recent antibiotic use, or regular use of oral steroids. Baseline demographics, pulmonary function, and acute medication use (steroids and beta agonists) were similar between the groups.
Intervention patients received telithromycin 800 mg a day for 10 days. The primary outcome was change in their asthma symptom score (rated on a seven-point scale) and change in their peak flows (recorded every morning for the study duration). Secondary outcomes were clinic pulmonary function tests (PFTs).
The intervention group had a mean decrease in their symptom score of 1.3 versus 1.0 in the placebo group (40% versus 27% reduction, p=.004). There was no difference between the groups in home peak flow measurements. There were statistically significant differences between the groups in clinic PFTs (FEV1, FVC, FEF 25%-75%), although the P values were not adjusted for multiple outcomes. The intervention group had a higher percentage of symptom-free days (16% versus 8%, P=.006). A total of 61% of the patients had serologic evidence of chlamydia or mycoplasma infection. Nausea (seven versus 0) and LFT elevations (two versus 0) were more frequent in the intervention group.
In conclusion, this is the first trial to report a benefit of antibiotic use in uncomplicated asthma exacerbations. This conclusion must be tempered by the underwhelming clinical improvement (1.3 versus 1.0 improvement in symptom scores), lack of peak flow improvement, recent reports of serious hepatotoxicity associated with telithromycin, and the possibility for antibiotic over-prescribing in unrefined patient populations.
Pneumonia Quality and Outcomes by Volume of Care
Lindenauer PK, Behal R, Murray CK, et al. Volume, quality of care, and outcome in pneumonia. Ann Intern Med. 2006 Feb 21;144(4):262-269.
It is widely known that, for many medical conditions and surgical procedures, outcomes are better when delivered by high-volume providers. It is not known if this holds true for patients with community-acquired pneumonia. To determine the association between physician/hospital volume and patient quality/outcomes, researchers utilized data from the Medicare National Pneumonia Quality Improvement Project. They included patients with an ICD9 diagnosis of pneumonia (850 patients were randomly selected from each state) at acute care hospitals with general or family medicine attendings. They excluded patients with no documentation of pneumonia, a normal chest X-ray, age <65, death on day one, comfort measures only, and departure against medical advice or transfer. Each physician and hospital volume were calculated from Medicare Part A claims for the same calendar year and analyzed by quartiles of volume.
Of the 9,741 physicians analyzed (13,480 patients), the median annual number of pneumonia patients was four, nine, 15, and 29 (in quartiles 1-4). Physician volume of care had little or no effect on performance rates of the timing of antibiotics, appropriate initial antibiotic, use of blood cultures, or in-hospital/30-day mortality rates. Low volume providers were significantly more likely to provide pneumococcal and influenza screening.
Of the 3,243 hospitals analyzed, the median annual pneumonia caseload was 57, 142, 262, and 465 (in quartiles 1-4). Hospital volume of care had little or no effect on performance rates of the appropriate initial antibiotic, use of blood cultures, pneumococcal/influenza screening, or in-hospital/30-day mortality rates (after severity of illness adjustment). Low volume centers were significantly more likely to give the first antibiotic within four hours.
In conclusion, volume of care by individual providers and hospital systems does not necessarily translate into better quality outcomes in pneumonia care. This may be partially explained by the challenges that larger medical centers face regarding delivering timely care (in overcrowded emergency rooms) and influencing behavior change (such as with standardized order sets).
By Debra Anoff, MD, assistant professor of medicine, Lucy Guerra, MD, assistant professor of medicine, Bjorn Holmstrom, MD, assistant professor of medicine, Asha Ramsakal, DO, assistant professor of medicine and chief, Richard Gross, MD, FACP, professor of medicine and chief, Division of Internal and Hospital Medicine H. Lee Moffitt Cancer Center and Research Institute, University of South Florida College of Medicine
Risk Factors for Mortality in Neutropenic Cancer Patients
Kuderer, NM, Dale DC, Crawford J, et al. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006 May 15;106(10):2258-2266.
Background: Neutropenic fever in a cancer patient is considered a medical emergency. Most episodes of febrile neutropenia result in hospital admission with prompt institution of broad spectrum antibiotics. The definition of neutropenia is usually regarded as an absolute neutrophil count (neutrophils plus bands) less than 500 cells/µL. The mortality rate of a cancer patient hospitalized with neutropenic fever ranges from 5 to 11%. There have been numerous small studies looking at risk factors associated with inpatient mortality. However, their small sample size and very select group of patients limit their generalizability to a standard hospitalist practice.
Methods: The authors used a longitudinal discharge database derived from 115 U.S. medical centers—both academic and community-based—in 39 states, looking retrospectively at all adult cancer patients hospitalized for febrile neutropenia between 1995 and 2000. The database included 55,276 hospitalizations and 41,779 patients and was analyzed for length of stay, cost per episode, mortality, and the clinical factors associated with mortality and prolonged hospitalization.
Results: The mortality rate for cancer patients with neutropenic fever averaged 9.5% per hospital. The average mortality rate was 14.3% for leukemia, 8.9% for lymphoma, and 8.0% for solid tumors. Lung cancer had the highest average mortality rate, 13.4%, followed by colorectal cancer at 8.8%, and breast cancer, which had the lowest mortality rate with 3.6%. Moreover, the highest mortality rate, 39.2%, was seen in those patients with a documented infection with invasive aspergillosis, while the rate of mortality for invasive candidiasis was 36.7%, followed by gram-negative bacteremia at 33.9%, pneumonia at 26.5%, and gram-positive bacteremia at 21.2%.
Patients without comorbidities, including common illnesses such as diabetes, congestive heart failure, and renal failure, had an average 2.6 % risk of dying. Those with one comorbidity had a 10.3% risk, and patients with more than one comorbidity had a mortality risk of 21.4%. Multivariate analysis revealed that the odds ratios for inpatient mortality were 3.94 for lung disease, 3.26 for cerebrovascular disease, 3.16 for renal disease, 2.89 for liver disease, 1.94 for pulmonary embolism, and 1.58 for heart disease.
The study also showed that patients hospitalized for longer than 10 days (comprising 35% of all patients) accounted for the majority of overall deaths (65%), overall cost (78%), and overall days spent in the hospital (74%).
Conclusions: The study provided an estimate of inpatient mortality associated with neutropenic fever in cancer patients and highlighted those subgroups as being at heightened risk for death. Important limitations include the retrospective nature of the study, the use of administrative data sets as the primary data source, and a failure to analyze for the duration of neutropenia prior to treatment. The authors’ conclusion that the identified factors may be useful in determining which patients warrant “more aggressive supportive care measures” is plausible, but does not find enough support in the study to warrant general implementation.
Long-Term Value of Electrocardiogram Before Noncardiac Surgery
Jeger RV, Probst C, Arsenic R, et al. Long-term prognostic value of the preoperative 12-lead electrocardiogram before major noncardiac surgery in coronary artery disease. Am Heart J. 2006 Feb;151(2):508-513.
Background: The 12-lead electrocardiogram is commonly utilized as part of the cardiovascular preoperative risk stratification. Certain ECG abnormalities, such as left bundle branch block, Q waves, ST-T abnormalities, arrhythmias, and left ventricular hypertrophy (LVH), have been associated with elevated risk in the perioperative period.1,2 This article prospectively evaluated whether an exhaustive analysis of preoperative ECGs in this population would have long-term predictive validity.
Methods: The study utilized a “predefined” analysis applied retrospectively on data obtained for another study.3,4
The study analyzed 172 patients, all of whom had documented coronary artery disease (CAD) as defined by previous myocardial infarction (MI), prior revascularization, significant stenoses on prior catheterization, ischemia (by dobutamine stress echocardiogram or adenosine thallium imaging), or who were high risk for CAD. High risk required at least two of the following: age over 70, hypertension, diabetes mellitus, prior stroke, exercise intolerance, or a “pathological resting ECG.” These patients were to undergo noncardiac surgery. The primary endpoint was all-cause mortality after two years, and the secondary endpoint was major adverse cardiac events (MACE) after two years. The MACE were defined as nonfatal MI, coronary revascularization, re-hospitalization due to recurrent ischemia, and/or cardiac death.
The ECGs were obtained one day prior to surgery and analyzed using the Minnesota classification. Telephone interviews were done at six, 12, and 24 months to evaluate outcome, and the Swiss Mortality Registry was used to determine cause of death. Analyzed data were adjusted for current beta-blocker use and perioperative ischemia using a sensitivity analysis-like correction that is described briefly in the report.
Results: ST depression (odds ratio [OR] 4.5) and faster heart rate (OR 1.6) were independent predictors of all-cause mortality. Faster heart rate (OR 1.7) was also an independent predictor of MACE.
Commentary: The results of this relatively small study raise awareness of resting tachycardia and ST depression as possible markers for poor perioperative and two-year postoperative outcomes. The latter is already included in risk stratification guidelines5, and the former is of uncertain validity due to possible confounding variables such as anxiety or pain, beta blocker dosing differences, and lack of intra- and postoperative beta blocker usage data which may affect postoperative cardiac morbidity and mortality long after the drugs are stopped.
For hospitalists and other physicians performing cardiac risk stratification for noncardiac surgery patients, the current study does not warrant any change in current practice as recommended in the American College of Cardiology/American Heart Association Guidelines 2002.5 As to whether resting tachycardia should be considered as a predictive ECG criterion in this context, further valid and applicable evidence is needed.
References
- De Bacquer D, De Backer G, Kornitzer M, et al. Prognostic value of ECG findings for total, cardiovascular disease, and coronary heart disease death in men and women. Heart. 1998 Dec;80(6):570-577.
- Tervahauta M, Pekkanen J, Punsar S, et al. Resting electrocardiographic abnormalities as predictors of coronary events and total mortality among elderly men. Am J Med. 1996 Jun;100(6):641-645.
- Filipovic M, Jeger R, Probst C, et al. Heart rate variability and cardiac troponin I are incremental and independent predictors of one-year all-cause mortality after major noncardiac surgery in patients at risk of coronary artery disease. J Am Coll Cardiol. 2003 Nov 19;42(10):1767-76.
- Filipovic M, Jeger RV, Girard T, et al. Predictors of long-term mortality and cardiac events in patients with known or suspected coronary artery disease who survive major noncardiac surgery. Anaesthesia. 2005 Jan;60(1):5-11.
- Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery—executive summary. Circulation. 2002 Mar 12;105(10):1257-1267.
Statins and Cardiovascular Disease
Hackam DG, Mamdani M, Li P, et al. Statins and sepsis in patients with cardiovascular disease: a population-based cohort analysis. Lancet. 2006 Feb 4;367(9508):413-418.
Background: The benefits of statins in secondary prevention of MI and ischemic CVA, as well as in reduction of all-cause mortality and their primary prevention in diabetics, are well documented in the literature.1 The concept of statins reducing subsequent sepsis in humans with atherosclerotic cardiovascular disease (CVD) is relatively new. One hypothesis holds that such an effect may be due to several common pathophysiologic mechanisms of sepsis and CVD: endothelial instability, immune dysregulation, inflammation, and thrombogenesis. Statins have been shown to provide improved outcomes from sepsis in animal studies, and observational studies in humans have raised similar hypotheses. This study attempts to analyze whether statin use in humans is associated with similar benefits regarding prevention of sepsis.
Methods: This was a population-based cohort analysis of 141,487 patients in Ontario, Canada, during the period of time from 1997-2002, who were older than age 65 and had been hospitalized for acute coronary syndrome or ischemic stroke, or had revascularization and survived three months post discharge. Using four reputable linked administrative databases, the authors found that 46,662 (33%) patients were prescribed a statin within three months of the discharge date (the index date), and 94,825 (67%) were not. About 19% of enrolled patients died within nine months and were excluded from the analysis. Of the eligible patients, propensity-based matching was used to identify 69,168 patients, of whom half were prescribed a statin and half were not. The patients were then analyzed through provincial administrative databases for the end points of hospital admission with an International Classification of Disease (ICD) code of sepsis, severe sepsis, fatal sepsis, death, or the end of the study.
Results: A total of 551 out of 34,584 patients were admitted for sepsis from the statin group, and 667 out of 34,584 were admitted from the control group during a mean follow-up of 2.2 years. The rate of sepsis in the statin group was significantly lower than in the control group (71.2 versus 88.0 per 10,000 person-years; p=0.0003). Statin use was also associated with fewer episodes of sepsis in an extended duration of 3.8 years, and with a lower risk of severe and fatal sepsis where sepsis was the admission diagnosis. This protection was evident at both high and low doses. The hazard ratio for sepsis was .81. There was a 19% relative reduction in the risk of sepsis in patients older than 65 with atherosclerosis. The absolute risk reduction for the occurrence of sepsis per 10,000 person-years was 16.8%, or .168% per person-year, with a corresponding number needed to treat (NNT) of 595 patients to prevent one episode of sepsis per year.
Comments: Though sophisticated and diverse statistical methods were used to assess the robustness of the analysis, this study is retrospective. Unidentified confounders, clinical sepsis risk stratification (the presence of obstructive uropathy or impairments leading to aspiration or skin breakdown, for example) are not accounted for in the analysis. Nonetheless, the hypothesis is of high relevance to hospitalists; it has biologic plausibility, and the results are intriguing if not definitive.
From a practical perspective, it seems prudent to ensure ongoing statin use for all patients with appropriate traditional indications. Initiating statins for the sole purpose of reducing future risk of sepsis is not yet sufficiently supported by the available evidence, and the NNT of almost 600 patients per year in the current study does little to alter that recommendation. In reply to a subsequent letter to the editor, the authors pointed out that the high NNT in part reflects the low-risk profile of the cohort and would be lower in higher risk patients; for example, patients with chronic renal failure, previous infections, or corticosteroid use would have NNTs of 166, 250, and 250, respectively.2 A randomized, controlled prospective trial would be a welcome addition to the evidence on this important topic, as would studies of the use of statins solely as an acute intervention upon suspicion of sepsis.
References
- MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002 Jul 6;360(9326):7-22.
- Hackam DG, Redelmeier DA. Statins and sepsis—authors' reply. Lancet. 2006;367:1651.
Review: Impact of Health Information Technology
Advances in information technology have transformed the world of business and education and will undoubtedly change the delivery and implementation of medical services. What arguably sets the world of health information apart from other systems is, however, the extreme sensitivity of the data involved and the impact it has on human lives.
Methods and data sources: In the article, “Systemic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care,” the authors reviewed four data sources and extracted information on system design, effects on quality and cost benefit analysis. Four data sources were utilized including a MEDLINE analysis of articles indexed as health information technology (HIT) from 1995 to January 2004 utilizing:
- Cochrane Center Registry of Controlled Trials;
- Cochrane Database of Abstracts of Reviews of Effects;
- Periodical Abstracts Database; and
- Studies singled out by experts up to April of 2005
Of the four data sources, 24% of all studies came from the following academic centers: the Regenstrief Institute (Indianapolis), Brigham and Women’s Hospital (Boston), Department of Veterans Affairs, and the Latter Day Saints Hospital/Intermountain Health Care.
Inclusion criteria: The HIT evaluation and efficacy information derived was from these four academic institutions, each with its own EHR (electronic health record) system. Of 4,582 initial articles derived from a title review, 867 were deemed suitable given their title matter, but only 257 met inclusion criteria.
A modified framework from the Institute of Medicine’s six aims for care and a framework to analyze costs developed by the authors themselves was used for analysis.1
Reasons for rejection: Articles that did not have HIT as the subject, others that did not report outcomes data, and those that did not examine barriers for outcomes analysis were rejected.
Information examined: Extracted information on system capabilities including components of the system such as:
- User friendliness;
- Types of systems such as EHR that allowed for medical decision making support and e-prescribing; and
- Functional capabilities such as order entry and clinical documentation.
Common characteristics shared by the HIT systems evaluated by the four academic institutions: they were all multifunctional and included medical decision making support, all were internally developed by research experts and all had capabilities that had been improved upon and added incrementally over time.
The data supported five primary goals:
- Increasing delivery of healthcare according to established protocols and guidelines;
- Enhancing capacity to perform surveillance and monitoring of disease conditions and care delivery;
- Reducing medication error rates;
- Decreasing utilization of care; and
- Producing a mixed effect on time utilization.
Major findings: (see Figure 1, below).
The authors of the article summarized 22 other studies in Appendix 22 from other institutions. The benefits noted were very similar to those found in the studies from the benchmark institutions; however, one major difference was the use of pre/post time-series designs that did not have a control or comparative group. Internally and commercially, HIT systems were evaluated in most of these studies with thirteen focusing on the former and nine on the later.
Summary and discussion: This study raises several questions worthy of further research and study:
- How are systems to interface with regard to the portability of health care information?
- Which are better: internally devised systems or commercially available systems?
- Who is going to be responsible for establishing standard guidelines for the implementation of HIT systems across the diverse healthcare systems in the United States? and
- How are the data to be used and analyzed by insurers and even public health entities?
HIT has shown many benefits with regard to quality of patient care issues and efficiency. Studies from these four benchmark institutions had one important limitation, however, and that is that the development of an internally developed HIT system took many years and is unlikely to be applicable to other institutions that have fewer resources and are struggling to implement the technology in a timely manner.
As the authors of the article acknowledge, it is not clear if HIT systems, though useful as tools, alter states of disease and health. More research looking at the direct impact of HIT information on morbidity and mortality is needed. As the authors state, this raises the question of a national HIT system, thereby making adoption of HIT a bipartisan initiative.
Providers need better evidence on information systems in order to make informed decisions about acquiring and implementing technology in community settings. The authors of this article made the first attempt to collate and appraise such evidence. Additional research is needed in academic, governmental, and community settings in both acute and nonacute facilities. As the authors point out, a uniform standard should be devised at the federal, state, and local level to report research on the implementation of HIT systems similar to the CONSORT and Quorum statement.
References
- Chaudry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742-752.
- Bates DW, Leape LL Cullen DJ. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998 Oct 21;280(15):1311-1316.
Conference Report: AHRQ
The Agency for Healthcare Research and Quality (AHRQ) held its annual Patient Safety and Health IT (internet technology) Conference June 4-7, 2006, at the Renaissance Hotel in Washington, D.C. This annual meeting provides grantees, quality improvement and risk assessment managers, and all members of the healthcare team the opportunity to learn how AHRQ-funded patient safety and health IT research contributes to improved healthcare quality.
This was AHRQ’s sixth national conference with a focus on patient safety, and it was the second time the conference had a combined focus on patient safety and health IT. To highlight the importance of these two focus areas working together, the conference was entitled “Strengthening the Connections.” The significance of this relationship was further emphasized by holding the conference during the inaugural “National Health IT Week” and closing the sessions with a handoff (on National Health IT Day) to a health IT Summit held by the Healthcare Information and Management Systems Society (HIMSS).
This year’s conference opened with remarks from AHRQ Director Carolyn Clancy, MD, and opening keynote speaker David M. Sundwall, MD, director of the Utah Department of Health.
Dr. Clancy set the focus of the week by emphasizing that the pursuit of quality must be the shared ambition of patient safety and health IT. Quality healthcare is “the right treatment, for the right patient, at the right time” and the objectives of patient safety and health IT are best aligned when these goals are kept in sight by both focus areas. Dr. Clancy noted that AHRQ has helped pursue quality in patient safety and health IT by “fund[ing] some 240 Patient Safety and Health IT projects, and award[ing] more than $400 million in grants and contracts for both programs [since 2001].” Ultimately, “AHRQ’s efforts,” Dr. Clancy said, “are helping to light the path and measure the benefits for the average practice and community hospital. … [And they are] helping [to] show these providers [that] how to make a successful transition to health IT practice is a keystone in successfully adopting health IT.”
To share the work of this year’s presenting grantees, the sessions were categorized by topic into nine different, but concurrent, tracks. This allowed individuals with particular interests to easily identify which sessions would be most valuable to them. These tracks included:
- Track 1: Patient Safety and Health IT across Settings and Populations: These sessions covered the use of health IT in special populations, in outpatient clinics and physician offices, in emergency care, for the elderly, and in distance/telemedicine.
- Track 2: Implementation Issues in Patient Safety and Health IT: The track’s two sessions discussed how health IT will move into the 21st century, the relationship between clinical redesign and improved safety, process approaches to improving clinical performance, and the establishment and implementation of standards for e-prescribing.
- Track 3: Improving the Health of Communities through Regional Health Information Exchange (HIE): Track three featured ways to get started in HIE by gaining stakeholder support, ways to design and implement HIE at the front lines, and the development of sustainable business models for HIE, and offered updates on the shaping of the health IT vision at the Office of the National Coordinator.
- Track 4: Assessing Value and Evaluating Project Impact: Track four presentations covered the impact of certain health IT tools, a brainstorming session for rural health IT initiatives, an evaluation of medication administration technologies, an assessment of clinical decision support, new tools for assessing value, and an evaluation of regional health information exchange systems.
- Track 5: Achieving and Sustaining Improvements: This series of sessions highlighted the frequency of adverse medical-device events, socio-technical approaches to planning and assessing redesign with health IT, clinical decision support and reporting systems to improve population health and minimize harm in patient handoff settings, and ways to recognize and manage unintended consequences of health IT.
- Track 6: Using Reporting Systems for Safety and Quality Improvement: Track six presentations covered efforts to improve the accuracy and utility of reporting systems, ways to track changes over time through reporting systems, methods to track adverse drug events through reporting systems, and innovative applications of reporting systems.
- Track 7: Working Conditions Challenges in Patient Safety: Track seven described how health IT impacts provider working conditions and performance, how working conditions, and culture can impact performance of providers and patient outcomes, and how programs can be used to promote patient safety cultures.
- Track 8: Patient and Family Centered Health IT and Safety: The sessions in track eight presented strategies for improving medication management across transitions in care, as well as perceptions and approaches to patient-centered health IT.
- Track 9: Emerging Approaches to Drive Change in Healthcare: The ninth track discussed examples of how IT solutions intended to reduce error can sometimes induce new error, current uses of and research involving AHRQ’s patient safety indicators, appropriate and inappropriate use of technology in developing high reliability hospital systems, an introduction to and overview of using positive deviance as a quality improvement methodology, and the use of lean methodology in healthcare.
Of particular note is the involvement of five hospitalists in AHRQ-funded research. Jeff Greenwald, MD, Brian Jack, MD, Greg Maynard, MD, MS, Tosha Wetterneck, MD, and Mark Williams, MD, are each involved with quality improvement and patient safety research through AHRQ grants. (See The Hospitalist, June issue, p. 35.)
Doctors Jack and Greenwald are partners in researching the re-engineering of the hospital discharge process—a process that they note is not standardized and is often marked with poor quality as observed by the frequency of post-discharge adverse events and 30 day re-hospitalization rates—to improve patient safety. They have grants through AHRQ’s Partnerships in Implementing Patient Safety (PIPS) and Safe Practices Risk Assessment Challenge Grants (SPRACGS) research initiatives and presented their work as a part of track two.
Dr. Maynard is also funded through AHRQ’s PIPS research initiative as his research pursues the elimination of hospital-acquired venous thromboembolism (VTE). Noting that easy and cost effective prophylactic treatment exists, but is underutilized, Greg’s project involves the creation of a toolkit that allows institutions to acquire optimal prevention of hospital-acquired VTE, ultimately reducing morbidity, mortality, and the associated but unnecessary costs.
Dr. Wetterneck presented her work on medication administration technologies as a part of track four. Her research has focused on the development and evaluation of Smart IV pump technology that has been designed with human factors in mind.
Dr. Williams presented, along with John Bajha, PhD, his research on Hospital Patient Safe-D(ischarge). This initiative is funded by a PIPS grant and was presented as a part of track five. The project intends to first implement a “discharge bundle” that consists of medication reconciliation, patient-centered hospital discharge education, and a post-discharge continuity check by a clinician. Once the discharge bundle is established, its level of adoption and acceptance will be evaluated before the researchers develop an “implementation toolkit” for dissemination of the bundle. The bundle will be disseminated with the intended result of safer discharges.
The Patient Safety and Health IT Conference concluded on National Health IT Day and the start of the HIMSS Summit. Speakers included Dr. Clancy; Newt Gingrich, former speaker of the House and founder of the Center for Health Transformation; David Brailer, national coordinator for Health Information Technology; and Mark McClellan, MD, PhD, administrator of Centers for Medicare and Medicaid Services.
Additional panels throughout the day included leaders from outside of healthcare: David Hom, vice president, human resources strategic initiatives, Pitney Bowes; Bruce Bradley, director, health plan strategy and public policy, General Motors; and Dale Whitney, corporate health care manager, United Parcel Service; as well as a number of leaders from within the healthcare field who are actively involved with health IT implementation.
Ultimately, the day’s topics highlighted the importance of leveraging health IT in the pursuit of improved patient safety from the perspectives of policymakers, business leaders, and healthcare leaders and successfully served as a transition to the HIMSS Summit. TH
Resources
- For more information about the conference visit: http://healthit.ahrq.gov/PatientSafetyandHIT2006Conference.
- Webcasts and transcripts of the last day of the conference have been provided by the Kaiser Family Foundation: www.kaisernetwork.org/health_cast/hcast_index.cfm?display=detail&hc=1731
The Agency for Healthcare Research and Quality (AHRQ) held its annual Patient Safety and Health IT (internet technology) Conference June 4-7, 2006, at the Renaissance Hotel in Washington, D.C. This annual meeting provides grantees, quality improvement and risk assessment managers, and all members of the healthcare team the opportunity to learn how AHRQ-funded patient safety and health IT research contributes to improved healthcare quality.
This was AHRQ’s sixth national conference with a focus on patient safety, and it was the second time the conference had a combined focus on patient safety and health IT. To highlight the importance of these two focus areas working together, the conference was entitled “Strengthening the Connections.” The significance of this relationship was further emphasized by holding the conference during the inaugural “National Health IT Week” and closing the sessions with a handoff (on National Health IT Day) to a health IT Summit held by the Healthcare Information and Management Systems Society (HIMSS).
This year’s conference opened with remarks from AHRQ Director Carolyn Clancy, MD, and opening keynote speaker David M. Sundwall, MD, director of the Utah Department of Health.
Dr. Clancy set the focus of the week by emphasizing that the pursuit of quality must be the shared ambition of patient safety and health IT. Quality healthcare is “the right treatment, for the right patient, at the right time” and the objectives of patient safety and health IT are best aligned when these goals are kept in sight by both focus areas. Dr. Clancy noted that AHRQ has helped pursue quality in patient safety and health IT by “fund[ing] some 240 Patient Safety and Health IT projects, and award[ing] more than $400 million in grants and contracts for both programs [since 2001].” Ultimately, “AHRQ’s efforts,” Dr. Clancy said, “are helping to light the path and measure the benefits for the average practice and community hospital. … [And they are] helping [to] show these providers [that] how to make a successful transition to health IT practice is a keystone in successfully adopting health IT.”
To share the work of this year’s presenting grantees, the sessions were categorized by topic into nine different, but concurrent, tracks. This allowed individuals with particular interests to easily identify which sessions would be most valuable to them. These tracks included:
- Track 1: Patient Safety and Health IT across Settings and Populations: These sessions covered the use of health IT in special populations, in outpatient clinics and physician offices, in emergency care, for the elderly, and in distance/telemedicine.
- Track 2: Implementation Issues in Patient Safety and Health IT: The track’s two sessions discussed how health IT will move into the 21st century, the relationship between clinical redesign and improved safety, process approaches to improving clinical performance, and the establishment and implementation of standards for e-prescribing.
- Track 3: Improving the Health of Communities through Regional Health Information Exchange (HIE): Track three featured ways to get started in HIE by gaining stakeholder support, ways to design and implement HIE at the front lines, and the development of sustainable business models for HIE, and offered updates on the shaping of the health IT vision at the Office of the National Coordinator.
- Track 4: Assessing Value and Evaluating Project Impact: Track four presentations covered the impact of certain health IT tools, a brainstorming session for rural health IT initiatives, an evaluation of medication administration technologies, an assessment of clinical decision support, new tools for assessing value, and an evaluation of regional health information exchange systems.
- Track 5: Achieving and Sustaining Improvements: This series of sessions highlighted the frequency of adverse medical-device events, socio-technical approaches to planning and assessing redesign with health IT, clinical decision support and reporting systems to improve population health and minimize harm in patient handoff settings, and ways to recognize and manage unintended consequences of health IT.
- Track 6: Using Reporting Systems for Safety and Quality Improvement: Track six presentations covered efforts to improve the accuracy and utility of reporting systems, ways to track changes over time through reporting systems, methods to track adverse drug events through reporting systems, and innovative applications of reporting systems.
- Track 7: Working Conditions Challenges in Patient Safety: Track seven described how health IT impacts provider working conditions and performance, how working conditions, and culture can impact performance of providers and patient outcomes, and how programs can be used to promote patient safety cultures.
- Track 8: Patient and Family Centered Health IT and Safety: The sessions in track eight presented strategies for improving medication management across transitions in care, as well as perceptions and approaches to patient-centered health IT.
- Track 9: Emerging Approaches to Drive Change in Healthcare: The ninth track discussed examples of how IT solutions intended to reduce error can sometimes induce new error, current uses of and research involving AHRQ’s patient safety indicators, appropriate and inappropriate use of technology in developing high reliability hospital systems, an introduction to and overview of using positive deviance as a quality improvement methodology, and the use of lean methodology in healthcare.
Of particular note is the involvement of five hospitalists in AHRQ-funded research. Jeff Greenwald, MD, Brian Jack, MD, Greg Maynard, MD, MS, Tosha Wetterneck, MD, and Mark Williams, MD, are each involved with quality improvement and patient safety research through AHRQ grants. (See The Hospitalist, June issue, p. 35.)
Doctors Jack and Greenwald are partners in researching the re-engineering of the hospital discharge process—a process that they note is not standardized and is often marked with poor quality as observed by the frequency of post-discharge adverse events and 30 day re-hospitalization rates—to improve patient safety. They have grants through AHRQ’s Partnerships in Implementing Patient Safety (PIPS) and Safe Practices Risk Assessment Challenge Grants (SPRACGS) research initiatives and presented their work as a part of track two.
Dr. Maynard is also funded through AHRQ’s PIPS research initiative as his research pursues the elimination of hospital-acquired venous thromboembolism (VTE). Noting that easy and cost effective prophylactic treatment exists, but is underutilized, Greg’s project involves the creation of a toolkit that allows institutions to acquire optimal prevention of hospital-acquired VTE, ultimately reducing morbidity, mortality, and the associated but unnecessary costs.
Dr. Wetterneck presented her work on medication administration technologies as a part of track four. Her research has focused on the development and evaluation of Smart IV pump technology that has been designed with human factors in mind.
Dr. Williams presented, along with John Bajha, PhD, his research on Hospital Patient Safe-D(ischarge). This initiative is funded by a PIPS grant and was presented as a part of track five. The project intends to first implement a “discharge bundle” that consists of medication reconciliation, patient-centered hospital discharge education, and a post-discharge continuity check by a clinician. Once the discharge bundle is established, its level of adoption and acceptance will be evaluated before the researchers develop an “implementation toolkit” for dissemination of the bundle. The bundle will be disseminated with the intended result of safer discharges.
The Patient Safety and Health IT Conference concluded on National Health IT Day and the start of the HIMSS Summit. Speakers included Dr. Clancy; Newt Gingrich, former speaker of the House and founder of the Center for Health Transformation; David Brailer, national coordinator for Health Information Technology; and Mark McClellan, MD, PhD, administrator of Centers for Medicare and Medicaid Services.
Additional panels throughout the day included leaders from outside of healthcare: David Hom, vice president, human resources strategic initiatives, Pitney Bowes; Bruce Bradley, director, health plan strategy and public policy, General Motors; and Dale Whitney, corporate health care manager, United Parcel Service; as well as a number of leaders from within the healthcare field who are actively involved with health IT implementation.
Ultimately, the day’s topics highlighted the importance of leveraging health IT in the pursuit of improved patient safety from the perspectives of policymakers, business leaders, and healthcare leaders and successfully served as a transition to the HIMSS Summit. TH
Resources
- For more information about the conference visit: http://healthit.ahrq.gov/PatientSafetyandHIT2006Conference.
- Webcasts and transcripts of the last day of the conference have been provided by the Kaiser Family Foundation: www.kaisernetwork.org/health_cast/hcast_index.cfm?display=detail&hc=1731
The Agency for Healthcare Research and Quality (AHRQ) held its annual Patient Safety and Health IT (internet technology) Conference June 4-7, 2006, at the Renaissance Hotel in Washington, D.C. This annual meeting provides grantees, quality improvement and risk assessment managers, and all members of the healthcare team the opportunity to learn how AHRQ-funded patient safety and health IT research contributes to improved healthcare quality.
This was AHRQ’s sixth national conference with a focus on patient safety, and it was the second time the conference had a combined focus on patient safety and health IT. To highlight the importance of these two focus areas working together, the conference was entitled “Strengthening the Connections.” The significance of this relationship was further emphasized by holding the conference during the inaugural “National Health IT Week” and closing the sessions with a handoff (on National Health IT Day) to a health IT Summit held by the Healthcare Information and Management Systems Society (HIMSS).
This year’s conference opened with remarks from AHRQ Director Carolyn Clancy, MD, and opening keynote speaker David M. Sundwall, MD, director of the Utah Department of Health.
Dr. Clancy set the focus of the week by emphasizing that the pursuit of quality must be the shared ambition of patient safety and health IT. Quality healthcare is “the right treatment, for the right patient, at the right time” and the objectives of patient safety and health IT are best aligned when these goals are kept in sight by both focus areas. Dr. Clancy noted that AHRQ has helped pursue quality in patient safety and health IT by “fund[ing] some 240 Patient Safety and Health IT projects, and award[ing] more than $400 million in grants and contracts for both programs [since 2001].” Ultimately, “AHRQ’s efforts,” Dr. Clancy said, “are helping to light the path and measure the benefits for the average practice and community hospital. … [And they are] helping [to] show these providers [that] how to make a successful transition to health IT practice is a keystone in successfully adopting health IT.”
To share the work of this year’s presenting grantees, the sessions were categorized by topic into nine different, but concurrent, tracks. This allowed individuals with particular interests to easily identify which sessions would be most valuable to them. These tracks included:
- Track 1: Patient Safety and Health IT across Settings and Populations: These sessions covered the use of health IT in special populations, in outpatient clinics and physician offices, in emergency care, for the elderly, and in distance/telemedicine.
- Track 2: Implementation Issues in Patient Safety and Health IT: The track’s two sessions discussed how health IT will move into the 21st century, the relationship between clinical redesign and improved safety, process approaches to improving clinical performance, and the establishment and implementation of standards for e-prescribing.
- Track 3: Improving the Health of Communities through Regional Health Information Exchange (HIE): Track three featured ways to get started in HIE by gaining stakeholder support, ways to design and implement HIE at the front lines, and the development of sustainable business models for HIE, and offered updates on the shaping of the health IT vision at the Office of the National Coordinator.
- Track 4: Assessing Value and Evaluating Project Impact: Track four presentations covered the impact of certain health IT tools, a brainstorming session for rural health IT initiatives, an evaluation of medication administration technologies, an assessment of clinical decision support, new tools for assessing value, and an evaluation of regional health information exchange systems.
- Track 5: Achieving and Sustaining Improvements: This series of sessions highlighted the frequency of adverse medical-device events, socio-technical approaches to planning and assessing redesign with health IT, clinical decision support and reporting systems to improve population health and minimize harm in patient handoff settings, and ways to recognize and manage unintended consequences of health IT.
- Track 6: Using Reporting Systems for Safety and Quality Improvement: Track six presentations covered efforts to improve the accuracy and utility of reporting systems, ways to track changes over time through reporting systems, methods to track adverse drug events through reporting systems, and innovative applications of reporting systems.
- Track 7: Working Conditions Challenges in Patient Safety: Track seven described how health IT impacts provider working conditions and performance, how working conditions, and culture can impact performance of providers and patient outcomes, and how programs can be used to promote patient safety cultures.
- Track 8: Patient and Family Centered Health IT and Safety: The sessions in track eight presented strategies for improving medication management across transitions in care, as well as perceptions and approaches to patient-centered health IT.
- Track 9: Emerging Approaches to Drive Change in Healthcare: The ninth track discussed examples of how IT solutions intended to reduce error can sometimes induce new error, current uses of and research involving AHRQ’s patient safety indicators, appropriate and inappropriate use of technology in developing high reliability hospital systems, an introduction to and overview of using positive deviance as a quality improvement methodology, and the use of lean methodology in healthcare.
Of particular note is the involvement of five hospitalists in AHRQ-funded research. Jeff Greenwald, MD, Brian Jack, MD, Greg Maynard, MD, MS, Tosha Wetterneck, MD, and Mark Williams, MD, are each involved with quality improvement and patient safety research through AHRQ grants. (See The Hospitalist, June issue, p. 35.)
Doctors Jack and Greenwald are partners in researching the re-engineering of the hospital discharge process—a process that they note is not standardized and is often marked with poor quality as observed by the frequency of post-discharge adverse events and 30 day re-hospitalization rates—to improve patient safety. They have grants through AHRQ’s Partnerships in Implementing Patient Safety (PIPS) and Safe Practices Risk Assessment Challenge Grants (SPRACGS) research initiatives and presented their work as a part of track two.
Dr. Maynard is also funded through AHRQ’s PIPS research initiative as his research pursues the elimination of hospital-acquired venous thromboembolism (VTE). Noting that easy and cost effective prophylactic treatment exists, but is underutilized, Greg’s project involves the creation of a toolkit that allows institutions to acquire optimal prevention of hospital-acquired VTE, ultimately reducing morbidity, mortality, and the associated but unnecessary costs.
Dr. Wetterneck presented her work on medication administration technologies as a part of track four. Her research has focused on the development and evaluation of Smart IV pump technology that has been designed with human factors in mind.
Dr. Williams presented, along with John Bajha, PhD, his research on Hospital Patient Safe-D(ischarge). This initiative is funded by a PIPS grant and was presented as a part of track five. The project intends to first implement a “discharge bundle” that consists of medication reconciliation, patient-centered hospital discharge education, and a post-discharge continuity check by a clinician. Once the discharge bundle is established, its level of adoption and acceptance will be evaluated before the researchers develop an “implementation toolkit” for dissemination of the bundle. The bundle will be disseminated with the intended result of safer discharges.
The Patient Safety and Health IT Conference concluded on National Health IT Day and the start of the HIMSS Summit. Speakers included Dr. Clancy; Newt Gingrich, former speaker of the House and founder of the Center for Health Transformation; David Brailer, national coordinator for Health Information Technology; and Mark McClellan, MD, PhD, administrator of Centers for Medicare and Medicaid Services.
Additional panels throughout the day included leaders from outside of healthcare: David Hom, vice president, human resources strategic initiatives, Pitney Bowes; Bruce Bradley, director, health plan strategy and public policy, General Motors; and Dale Whitney, corporate health care manager, United Parcel Service; as well as a number of leaders from within the healthcare field who are actively involved with health IT implementation.
Ultimately, the day’s topics highlighted the importance of leveraging health IT in the pursuit of improved patient safety from the perspectives of policymakers, business leaders, and healthcare leaders and successfully served as a transition to the HIMSS Summit. TH
Resources
- For more information about the conference visit: http://healthit.ahrq.gov/PatientSafetyandHIT2006Conference.
- Webcasts and transcripts of the last day of the conference have been provided by the Kaiser Family Foundation: www.kaisernetwork.org/health_cast/hcast_index.cfm?display=detail&hc=1731