User login
Fentanyl-related deaths show strong regional pattern
Fentanyl was involved in more overdose deaths than any other drug in 2017, and the death rate in New England was 15 times higher than in regions of the Midwest and West, according to the National Center for Health Statistics.
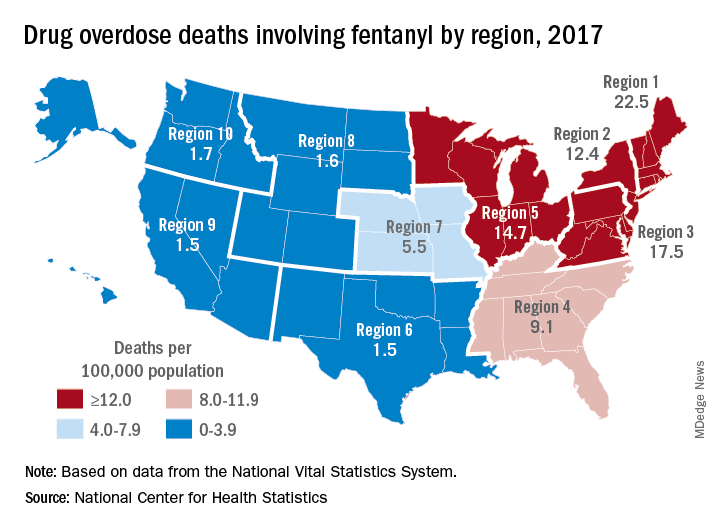
Nationally, fentanyl was involved in 39% of all drug overdose deaths and had an age-adjusted death rate of 8.7/100,000 standard population in 2017. In 2016, when fentanyl also was the most involved drug in the United States, the corresponding figures were 29% and 5.9/100,000, the agency said in a recent report.
Fentanyl was the most involved drug in overdose deaths for 6 of the country’s 10 public health regions in 2017, with a clear pattern of decreasing use from east to west. The highest death rate (22.5/100,000) occurred in Region 1 (New England) and the lowest rates (1.5/100,000) came in Region 6 (Arkansas, Louisiana, New Mexico, Oklahoma, and Texas) and Region 9 (Arizona, California, Hawaii, and Nevada), the researchers said.
A somewhat similar pattern was seen for heroin, which was second nationally on the list of drugs most frequently involved in overdose deaths (23%), except that New England was somewhat below three other regions in the East and upper Midwest. The highest heroin death rate (8.6/100,000) was seen in Region 2 (New Jersey and New York) and the lowest (2.2) occurred in Region 9, they said, based on data from the National Vital Statistics System’s mortality files.
The fentanyl pattern was even more closely repeated with cocaine, third in involvement nationally at 21% of overdose deaths in 2017. The high in overdose deaths (9.5/100,000) came in Region 1 again, and the low in Region 9 (1.3), along with Region 7 (Iowa, Kansas, Missouri, and Nebraska) and Region 10 (Alaska, Idaho, Oregon, and Washington), the report showed.
The regional pattern of overdose deaths for methamphetamine, which was fourth nationally in involvement (13.3%), basically reversed the other three drugs: highest in the West and lowest in the Northeast. Region 9 had the highest death rate (5.2/100,000) and Region 2 the lowest (0.4), with Region 1 just ahead at 0.6.
Fentanyl was involved in more overdose deaths than any other drug in 2017, and the death rate in New England was 15 times higher than in regions of the Midwest and West, according to the National Center for Health Statistics.
Nationally, fentanyl was involved in 39% of all drug overdose deaths and had an age-adjusted death rate of 8.7/100,000 standard population in 2017. In 2016, when fentanyl also was the most involved drug in the United States, the corresponding figures were 29% and 5.9/100,000, the agency said in a recent report.
Fentanyl was the most involved drug in overdose deaths for 6 of the country’s 10 public health regions in 2017, with a clear pattern of decreasing use from east to west. The highest death rate (22.5/100,000) occurred in Region 1 (New England) and the lowest rates (1.5/100,000) came in Region 6 (Arkansas, Louisiana, New Mexico, Oklahoma, and Texas) and Region 9 (Arizona, California, Hawaii, and Nevada), the researchers said.
A somewhat similar pattern was seen for heroin, which was second nationally on the list of drugs most frequently involved in overdose deaths (23%), except that New England was somewhat below three other regions in the East and upper Midwest. The highest heroin death rate (8.6/100,000) was seen in Region 2 (New Jersey and New York) and the lowest (2.2) occurred in Region 9, they said, based on data from the National Vital Statistics System’s mortality files.
The fentanyl pattern was even more closely repeated with cocaine, third in involvement nationally at 21% of overdose deaths in 2017. The high in overdose deaths (9.5/100,000) came in Region 1 again, and the low in Region 9 (1.3), along with Region 7 (Iowa, Kansas, Missouri, and Nebraska) and Region 10 (Alaska, Idaho, Oregon, and Washington), the report showed.
The regional pattern of overdose deaths for methamphetamine, which was fourth nationally in involvement (13.3%), basically reversed the other three drugs: highest in the West and lowest in the Northeast. Region 9 had the highest death rate (5.2/100,000) and Region 2 the lowest (0.4), with Region 1 just ahead at 0.6.
Fentanyl was involved in more overdose deaths than any other drug in 2017, and the death rate in New England was 15 times higher than in regions of the Midwest and West, according to the National Center for Health Statistics.
Nationally, fentanyl was involved in 39% of all drug overdose deaths and had an age-adjusted death rate of 8.7/100,000 standard population in 2017. In 2016, when fentanyl also was the most involved drug in the United States, the corresponding figures were 29% and 5.9/100,000, the agency said in a recent report.
Fentanyl was the most involved drug in overdose deaths for 6 of the country’s 10 public health regions in 2017, with a clear pattern of decreasing use from east to west. The highest death rate (22.5/100,000) occurred in Region 1 (New England) and the lowest rates (1.5/100,000) came in Region 6 (Arkansas, Louisiana, New Mexico, Oklahoma, and Texas) and Region 9 (Arizona, California, Hawaii, and Nevada), the researchers said.
A somewhat similar pattern was seen for heroin, which was second nationally on the list of drugs most frequently involved in overdose deaths (23%), except that New England was somewhat below three other regions in the East and upper Midwest. The highest heroin death rate (8.6/100,000) was seen in Region 2 (New Jersey and New York) and the lowest (2.2) occurred in Region 9, they said, based on data from the National Vital Statistics System’s mortality files.
The fentanyl pattern was even more closely repeated with cocaine, third in involvement nationally at 21% of overdose deaths in 2017. The high in overdose deaths (9.5/100,000) came in Region 1 again, and the low in Region 9 (1.3), along with Region 7 (Iowa, Kansas, Missouri, and Nebraska) and Region 10 (Alaska, Idaho, Oregon, and Washington), the report showed.
The regional pattern of overdose deaths for methamphetamine, which was fourth nationally in involvement (13.3%), basically reversed the other three drugs: highest in the West and lowest in the Northeast. Region 9 had the highest death rate (5.2/100,000) and Region 2 the lowest (0.4), with Region 1 just ahead at 0.6.
MS-related disability may be decreasing
STOCKHOLM – , according to an overview provided at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. Data consistently indicate that the time that elapses before a patient requires a cane for ambulation has increased, and survival has likewise improved. “Some of the improvement can be attributed confidently to treatment effect,” said Ilya Kister, MD, associate professor of neurology at NYU Langone Health in New York. “We hope to see an even greater change with newer therapies.”

At the same time, neurologists appear to be diagnosing more cases of MS than they previously did, said Dr. Kister, which suggests that neurologists probably are diagnosing milder cases. The overall societal burden of MS remains high.
The relative prevalence of mild disability has increased
About 25 years have elapsed since the first disease-modifying treatment (DMT) for MS became available, and treatment has become widespread during that time. Dr. Kister and colleagues sought to determine whether the current clinical population of patients with MS, who for the most part receive DMTs, has less disability than do untreated patients or patients from natural history studies do. They identified the MS Severity Score (MSSS) as a measure with which to compare populations. The MSSS assigns a patient a ranking according to his or her level of disability, using a reference population of patients with the same disease duration for comparison. “MSSS can be conceptualized as rate of disability accumulation,” said Dr. Kister. “Lower MSSS corresponds to relatively slower disability accumulation, and higher MSSS to higher disability accumulation.”
The MSSS was developed using the Expanded Disability Status Scale (EDSS) score as a measure of disability. Because many neurologists do not routinely obtain EDSS scores for their patients, Dr. Kister and colleagues used the Patient-Determined Disease Steps (PDDS) to measure disability. As its name implies, the PDDS is a patient-reported outcome measure that mainly measures ambulation. It correlates strongly with EDSS, said Dr. Kister. He and colleagues used the PDDS to develop a reference table of MS disability, which they called the Patient-Derived MSSS.
The investigators examined a large sample of patients at NYU MS Center and Barnabas MS Center in Livingston, N.J. They grouped patients into sextiles according to their Patient-Derived MSSS. Dr. Kister and colleagues found that, rather than arriving at sextiles that contained equal numbers of patients, as would be expected if disability were distributed as in the reference population, they had significantly more patients in the two lowest sextiles and significantly fewer patients in the two highest sextiles. “This [result] suggests that the disability curve has indeed shifted toward the more benign end of the spectrum in the contemporary clinic population,” said Dr. Kister.
Other researchers have observed a similar phenomenon. George et al. published the results of a large, international collaboration in Neurology Genetics in 2016. After examining more than 7,000 patients, the investigators noted a similar overrepresentation of patients with milder severity scores and underrepresentation of patients with higher severity scores. These results support the hypothesis of a shift toward milder disability, said Dr. Kister.
Trend toward milder disability
The investigators next examined whether the rate of accumulation of disability among patients with MS had changed from year to year since DMTs were introduced. They conducted a univariate analysis of MSSS for 6,238 patients who were enrolled in the N.Y. State MS Consortium during 1996-2007. They found that patients who were enrolled in more recent years had significantly lower MSSS than patients who were enrolled in earlier years, regardless of disease duration. When Dr. Kister and colleagues replicated their analysis using EDSS, they found significantly lower levels of disability for patients enrolled in more recent years, except for patients with disease duration of 26-30 years. A multivariate analysis showed that the median MSSS of enrollees into the N.Y. State MS Consortium decreased from 5.04 in 1996 to 3.78 in 2006.
In a subsequent study, Dr. Kister and colleagues examined the age at which patients in the MSBase registry reached various disability milestones (e.g., EDSS of 6, which indicates the need of a cane to walk outdoors), according to their year of enrollment in the registry. They found a significant increase in age at milestone achievement with each subsequent calendar year. For example, for every consecutive year of enrollment, the age at which patients attained an EDSS of 6 increased by 0.38 years. These analyses were confirmed for the subgroups of patients diagnosed according to the Poser and McDonald criteria. The increase in age “is probably not just related to the shift in diagnostic criteria,” said Dr. Kister. When the researchers calculated the net average gains in years over the 13-year follow-up period, they found that patients who entered at the end of the enrollment period were 4.9 years older when they reached an EDSS of 6, compared with patients with an EDSS of 6 who entered at the beginning of the enrollment period.
International data show similar trends
Research conducted around the world shows similar trends, said Dr. Kister. In 2009, Veugelers et al. published the results of a study that included 1,752 patients with MS in Nova Scotia. Before the 1998 introduction of a drug insurance program that provides DMTs, the time to an EDSS of 6 was 14.4 years. After the introduction of this program, the time to EDSS of 6 was 18.6 years.
More recently, Capra et al. examined 1,324 patients with MS who attended an MS center in Brescia, Italy, during 1980-2010. They found that the age at which 50% of patients reached an EDSS of 6 was approximately 55 years in 1990. By 2010, the age at achieving this milestone had increased to approximately 63 years.
In a prospective study, Cree et al. examined the evolution of disability in 448 actively treated patients with relapsing-remitting MS and 69 patients with progressive MS. Approximately 45% of patients had no disability worsening during a 10-year follow-up period. Furthermore, a comparatively low 11% of patients had reached an EDSS of 6 at 10 years. The average disease duration of the cohort at that time was 17 years, said Dr. Kister. The results indicated that about 50% of patients would be expected to reach an EDSS of 6 after a disease duration of approximately 38 years, “which is much longer than in the natural history studies,” he added.
In 2019, Beiki et al. found that among patients with relapsing-remitting MS, the risk of reaching an EDSS of 6 decreased by 7% with each subsequent calendar year of diagnosis. The researchers did not observe a similar trend among patients with progressive MS. Their population-based, retrospective study included 7,331 patients in Sweden.
Two additional studies in Scandinavian populations add to the evidence of decreasing disability. In their examination of Swedish patients with MS who received a diagnosis of MS during 1968-2012, Burkill et al. found that the risk of death decreased over time. The hazard ratio of mortality for patients with MS, compared with a non-MS comparator group, decreased from 6.52 among those diagnosed during 1968-1980 to 2.08 for patients diagnosed during 2001-2012. The decrease in the risk of mortality was greater among patients with MS than in a matched comparator population. Similarly, in a nationwide, population-based study, Koch-Henriksen et al. found that all-cause excess mortality in Danish patients with MS decreased from 1950 through 1999.
The role of DMTs
The evidence suggests that DMTs are affecting the long-term progression of MS, said Dr. Kister. Palace et al. compared patients with MS in the UK who received treatment with interferon-beta with a modeled untreated cohort of patients in British Columbia. They found that treated patients reached an EDSS of 6 4 years later than did untreated patients.
Furthermore, an analysis by Brown et al. showed that the time to conversion to secondary progressive MS was longer among treated patients, compared with untreated patients. The risk of conversion was lower for patients treated with newer, more effective therapies (i.e., fingolimod, alemtuzumab, or natalizumab) than for those treated with glatiramer acetate or interferon beta.
Finally, Kingwell and colleagues examined the effect of treatment with interferon-beta on survival using an international cohort of approximately 6,000 patients with relapsing-remitting MS. They found that exposure to interferon-beta for more than 3 years was associated with a 32% reduction in the risk of mortality. They observed no similar risk reduction among patients exposed to interferon-beta for 6 months to 3 years.
Although these data are encouraging, other evidence indicates that the prevalence of MS in the United States has increased considerably in the past 40 years. Researchers estimate that 1 million Americans have MS, which “suggests that we are diagnosing many more mild cases,” said Dr. Kister. The burden of the disease remains high, he concluded.
Dr. Kister reported receiving consulting fees or research grants from Biogen, Roche, Genzyme and Genentech.
SOURCE: Kister I et al. ECTRIMS 2019. Abstract 281754.
STOCKHOLM – , according to an overview provided at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. Data consistently indicate that the time that elapses before a patient requires a cane for ambulation has increased, and survival has likewise improved. “Some of the improvement can be attributed confidently to treatment effect,” said Ilya Kister, MD, associate professor of neurology at NYU Langone Health in New York. “We hope to see an even greater change with newer therapies.”
At the same time, neurologists appear to be diagnosing more cases of MS than they previously did, said Dr. Kister, which suggests that neurologists probably are diagnosing milder cases. The overall societal burden of MS remains high.
The relative prevalence of mild disability has increased
About 25 years have elapsed since the first disease-modifying treatment (DMT) for MS became available, and treatment has become widespread during that time. Dr. Kister and colleagues sought to determine whether the current clinical population of patients with MS, who for the most part receive DMTs, has less disability than do untreated patients or patients from natural history studies do. They identified the MS Severity Score (MSSS) as a measure with which to compare populations. The MSSS assigns a patient a ranking according to his or her level of disability, using a reference population of patients with the same disease duration for comparison. “MSSS can be conceptualized as rate of disability accumulation,” said Dr. Kister. “Lower MSSS corresponds to relatively slower disability accumulation, and higher MSSS to higher disability accumulation.”
The MSSS was developed using the Expanded Disability Status Scale (EDSS) score as a measure of disability. Because many neurologists do not routinely obtain EDSS scores for their patients, Dr. Kister and colleagues used the Patient-Determined Disease Steps (PDDS) to measure disability. As its name implies, the PDDS is a patient-reported outcome measure that mainly measures ambulation. It correlates strongly with EDSS, said Dr. Kister. He and colleagues used the PDDS to develop a reference table of MS disability, which they called the Patient-Derived MSSS.
The investigators examined a large sample of patients at NYU MS Center and Barnabas MS Center in Livingston, N.J. They grouped patients into sextiles according to their Patient-Derived MSSS. Dr. Kister and colleagues found that, rather than arriving at sextiles that contained equal numbers of patients, as would be expected if disability were distributed as in the reference population, they had significantly more patients in the two lowest sextiles and significantly fewer patients in the two highest sextiles. “This [result] suggests that the disability curve has indeed shifted toward the more benign end of the spectrum in the contemporary clinic population,” said Dr. Kister.
Other researchers have observed a similar phenomenon. George et al. published the results of a large, international collaboration in Neurology Genetics in 2016. After examining more than 7,000 patients, the investigators noted a similar overrepresentation of patients with milder severity scores and underrepresentation of patients with higher severity scores. These results support the hypothesis of a shift toward milder disability, said Dr. Kister.
Trend toward milder disability
The investigators next examined whether the rate of accumulation of disability among patients with MS had changed from year to year since DMTs were introduced. They conducted a univariate analysis of MSSS for 6,238 patients who were enrolled in the N.Y. State MS Consortium during 1996-2007. They found that patients who were enrolled in more recent years had significantly lower MSSS than patients who were enrolled in earlier years, regardless of disease duration. When Dr. Kister and colleagues replicated their analysis using EDSS, they found significantly lower levels of disability for patients enrolled in more recent years, except for patients with disease duration of 26-30 years. A multivariate analysis showed that the median MSSS of enrollees into the N.Y. State MS Consortium decreased from 5.04 in 1996 to 3.78 in 2006.
In a subsequent study, Dr. Kister and colleagues examined the age at which patients in the MSBase registry reached various disability milestones (e.g., EDSS of 6, which indicates the need of a cane to walk outdoors), according to their year of enrollment in the registry. They found a significant increase in age at milestone achievement with each subsequent calendar year. For example, for every consecutive year of enrollment, the age at which patients attained an EDSS of 6 increased by 0.38 years. These analyses were confirmed for the subgroups of patients diagnosed according to the Poser and McDonald criteria. The increase in age “is probably not just related to the shift in diagnostic criteria,” said Dr. Kister. When the researchers calculated the net average gains in years over the 13-year follow-up period, they found that patients who entered at the end of the enrollment period were 4.9 years older when they reached an EDSS of 6, compared with patients with an EDSS of 6 who entered at the beginning of the enrollment period.
International data show similar trends
Research conducted around the world shows similar trends, said Dr. Kister. In 2009, Veugelers et al. published the results of a study that included 1,752 patients with MS in Nova Scotia. Before the 1998 introduction of a drug insurance program that provides DMTs, the time to an EDSS of 6 was 14.4 years. After the introduction of this program, the time to EDSS of 6 was 18.6 years.
More recently, Capra et al. examined 1,324 patients with MS who attended an MS center in Brescia, Italy, during 1980-2010. They found that the age at which 50% of patients reached an EDSS of 6 was approximately 55 years in 1990. By 2010, the age at achieving this milestone had increased to approximately 63 years.
In a prospective study, Cree et al. examined the evolution of disability in 448 actively treated patients with relapsing-remitting MS and 69 patients with progressive MS. Approximately 45% of patients had no disability worsening during a 10-year follow-up period. Furthermore, a comparatively low 11% of patients had reached an EDSS of 6 at 10 years. The average disease duration of the cohort at that time was 17 years, said Dr. Kister. The results indicated that about 50% of patients would be expected to reach an EDSS of 6 after a disease duration of approximately 38 years, “which is much longer than in the natural history studies,” he added.
In 2019, Beiki et al. found that among patients with relapsing-remitting MS, the risk of reaching an EDSS of 6 decreased by 7% with each subsequent calendar year of diagnosis. The researchers did not observe a similar trend among patients with progressive MS. Their population-based, retrospective study included 7,331 patients in Sweden.
Two additional studies in Scandinavian populations add to the evidence of decreasing disability. In their examination of Swedish patients with MS who received a diagnosis of MS during 1968-2012, Burkill et al. found that the risk of death decreased over time. The hazard ratio of mortality for patients with MS, compared with a non-MS comparator group, decreased from 6.52 among those diagnosed during 1968-1980 to 2.08 for patients diagnosed during 2001-2012. The decrease in the risk of mortality was greater among patients with MS than in a matched comparator population. Similarly, in a nationwide, population-based study, Koch-Henriksen et al. found that all-cause excess mortality in Danish patients with MS decreased from 1950 through 1999.
The role of DMTs
The evidence suggests that DMTs are affecting the long-term progression of MS, said Dr. Kister. Palace et al. compared patients with MS in the UK who received treatment with interferon-beta with a modeled untreated cohort of patients in British Columbia. They found that treated patients reached an EDSS of 6 4 years later than did untreated patients.
Furthermore, an analysis by Brown et al. showed that the time to conversion to secondary progressive MS was longer among treated patients, compared with untreated patients. The risk of conversion was lower for patients treated with newer, more effective therapies (i.e., fingolimod, alemtuzumab, or natalizumab) than for those treated with glatiramer acetate or interferon beta.
Finally, Kingwell and colleagues examined the effect of treatment with interferon-beta on survival using an international cohort of approximately 6,000 patients with relapsing-remitting MS. They found that exposure to interferon-beta for more than 3 years was associated with a 32% reduction in the risk of mortality. They observed no similar risk reduction among patients exposed to interferon-beta for 6 months to 3 years.
Although these data are encouraging, other evidence indicates that the prevalence of MS in the United States has increased considerably in the past 40 years. Researchers estimate that 1 million Americans have MS, which “suggests that we are diagnosing many more mild cases,” said Dr. Kister. The burden of the disease remains high, he concluded.
Dr. Kister reported receiving consulting fees or research grants from Biogen, Roche, Genzyme and Genentech.
SOURCE: Kister I et al. ECTRIMS 2019. Abstract 281754.
STOCKHOLM – , according to an overview provided at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. Data consistently indicate that the time that elapses before a patient requires a cane for ambulation has increased, and survival has likewise improved. “Some of the improvement can be attributed confidently to treatment effect,” said Ilya Kister, MD, associate professor of neurology at NYU Langone Health in New York. “We hope to see an even greater change with newer therapies.”
At the same time, neurologists appear to be diagnosing more cases of MS than they previously did, said Dr. Kister, which suggests that neurologists probably are diagnosing milder cases. The overall societal burden of MS remains high.
The relative prevalence of mild disability has increased
About 25 years have elapsed since the first disease-modifying treatment (DMT) for MS became available, and treatment has become widespread during that time. Dr. Kister and colleagues sought to determine whether the current clinical population of patients with MS, who for the most part receive DMTs, has less disability than do untreated patients or patients from natural history studies do. They identified the MS Severity Score (MSSS) as a measure with which to compare populations. The MSSS assigns a patient a ranking according to his or her level of disability, using a reference population of patients with the same disease duration for comparison. “MSSS can be conceptualized as rate of disability accumulation,” said Dr. Kister. “Lower MSSS corresponds to relatively slower disability accumulation, and higher MSSS to higher disability accumulation.”
The MSSS was developed using the Expanded Disability Status Scale (EDSS) score as a measure of disability. Because many neurologists do not routinely obtain EDSS scores for their patients, Dr. Kister and colleagues used the Patient-Determined Disease Steps (PDDS) to measure disability. As its name implies, the PDDS is a patient-reported outcome measure that mainly measures ambulation. It correlates strongly with EDSS, said Dr. Kister. He and colleagues used the PDDS to develop a reference table of MS disability, which they called the Patient-Derived MSSS.
The investigators examined a large sample of patients at NYU MS Center and Barnabas MS Center in Livingston, N.J. They grouped patients into sextiles according to their Patient-Derived MSSS. Dr. Kister and colleagues found that, rather than arriving at sextiles that contained equal numbers of patients, as would be expected if disability were distributed as in the reference population, they had significantly more patients in the two lowest sextiles and significantly fewer patients in the two highest sextiles. “This [result] suggests that the disability curve has indeed shifted toward the more benign end of the spectrum in the contemporary clinic population,” said Dr. Kister.
Other researchers have observed a similar phenomenon. George et al. published the results of a large, international collaboration in Neurology Genetics in 2016. After examining more than 7,000 patients, the investigators noted a similar overrepresentation of patients with milder severity scores and underrepresentation of patients with higher severity scores. These results support the hypothesis of a shift toward milder disability, said Dr. Kister.
Trend toward milder disability
The investigators next examined whether the rate of accumulation of disability among patients with MS had changed from year to year since DMTs were introduced. They conducted a univariate analysis of MSSS for 6,238 patients who were enrolled in the N.Y. State MS Consortium during 1996-2007. They found that patients who were enrolled in more recent years had significantly lower MSSS than patients who were enrolled in earlier years, regardless of disease duration. When Dr. Kister and colleagues replicated their analysis using EDSS, they found significantly lower levels of disability for patients enrolled in more recent years, except for patients with disease duration of 26-30 years. A multivariate analysis showed that the median MSSS of enrollees into the N.Y. State MS Consortium decreased from 5.04 in 1996 to 3.78 in 2006.
In a subsequent study, Dr. Kister and colleagues examined the age at which patients in the MSBase registry reached various disability milestones (e.g., EDSS of 6, which indicates the need of a cane to walk outdoors), according to their year of enrollment in the registry. They found a significant increase in age at milestone achievement with each subsequent calendar year. For example, for every consecutive year of enrollment, the age at which patients attained an EDSS of 6 increased by 0.38 years. These analyses were confirmed for the subgroups of patients diagnosed according to the Poser and McDonald criteria. The increase in age “is probably not just related to the shift in diagnostic criteria,” said Dr. Kister. When the researchers calculated the net average gains in years over the 13-year follow-up period, they found that patients who entered at the end of the enrollment period were 4.9 years older when they reached an EDSS of 6, compared with patients with an EDSS of 6 who entered at the beginning of the enrollment period.
International data show similar trends
Research conducted around the world shows similar trends, said Dr. Kister. In 2009, Veugelers et al. published the results of a study that included 1,752 patients with MS in Nova Scotia. Before the 1998 introduction of a drug insurance program that provides DMTs, the time to an EDSS of 6 was 14.4 years. After the introduction of this program, the time to EDSS of 6 was 18.6 years.
More recently, Capra et al. examined 1,324 patients with MS who attended an MS center in Brescia, Italy, during 1980-2010. They found that the age at which 50% of patients reached an EDSS of 6 was approximately 55 years in 1990. By 2010, the age at achieving this milestone had increased to approximately 63 years.
In a prospective study, Cree et al. examined the evolution of disability in 448 actively treated patients with relapsing-remitting MS and 69 patients with progressive MS. Approximately 45% of patients had no disability worsening during a 10-year follow-up period. Furthermore, a comparatively low 11% of patients had reached an EDSS of 6 at 10 years. The average disease duration of the cohort at that time was 17 years, said Dr. Kister. The results indicated that about 50% of patients would be expected to reach an EDSS of 6 after a disease duration of approximately 38 years, “which is much longer than in the natural history studies,” he added.
In 2019, Beiki et al. found that among patients with relapsing-remitting MS, the risk of reaching an EDSS of 6 decreased by 7% with each subsequent calendar year of diagnosis. The researchers did not observe a similar trend among patients with progressive MS. Their population-based, retrospective study included 7,331 patients in Sweden.
Two additional studies in Scandinavian populations add to the evidence of decreasing disability. In their examination of Swedish patients with MS who received a diagnosis of MS during 1968-2012, Burkill et al. found that the risk of death decreased over time. The hazard ratio of mortality for patients with MS, compared with a non-MS comparator group, decreased from 6.52 among those diagnosed during 1968-1980 to 2.08 for patients diagnosed during 2001-2012. The decrease in the risk of mortality was greater among patients with MS than in a matched comparator population. Similarly, in a nationwide, population-based study, Koch-Henriksen et al. found that all-cause excess mortality in Danish patients with MS decreased from 1950 through 1999.
The role of DMTs
The evidence suggests that DMTs are affecting the long-term progression of MS, said Dr. Kister. Palace et al. compared patients with MS in the UK who received treatment with interferon-beta with a modeled untreated cohort of patients in British Columbia. They found that treated patients reached an EDSS of 6 4 years later than did untreated patients.
Furthermore, an analysis by Brown et al. showed that the time to conversion to secondary progressive MS was longer among treated patients, compared with untreated patients. The risk of conversion was lower for patients treated with newer, more effective therapies (i.e., fingolimod, alemtuzumab, or natalizumab) than for those treated with glatiramer acetate or interferon beta.
Finally, Kingwell and colleagues examined the effect of treatment with interferon-beta on survival using an international cohort of approximately 6,000 patients with relapsing-remitting MS. They found that exposure to interferon-beta for more than 3 years was associated with a 32% reduction in the risk of mortality. They observed no similar risk reduction among patients exposed to interferon-beta for 6 months to 3 years.
Although these data are encouraging, other evidence indicates that the prevalence of MS in the United States has increased considerably in the past 40 years. Researchers estimate that 1 million Americans have MS, which “suggests that we are diagnosing many more mild cases,” said Dr. Kister. The burden of the disease remains high, he concluded.
Dr. Kister reported receiving consulting fees or research grants from Biogen, Roche, Genzyme and Genentech.
SOURCE: Kister I et al. ECTRIMS 2019. Abstract 281754.
EXPERT ANALYSIS FROM ECTRIMS 2019
Integrating lay navigation programs into cancer care is a challenge
The implementation of a lay navigation program as part of the delivery of cancer care presents a number of challenges, particularly because of the complexities of treating cancer, a new study has found.
Researchers looked at a lay navigator program, which uses nonclinical members to help provide information to cancer patients about their treatments, at the University of Alabama, and how the program was doing a year after its implementation.
“Integrating lay navigators into a complex clinical environment needs careful consideration at an organizational level, because this experience demonstrates that the integration process is not straightforward for clinical teams, patients, or navigators,” wrote Laura M. Holdsworth, PhD, Stanford (Calif.) University, and colleague. Their report is in the Journal of Oncology Practice.
A key difficulty discovered through the course of the research is that approximately two-thirds of concerns brought by patients to the lay navigators were clinical in nature, though only about a third (30%) required clinical follow-up and an additional 7% required social work follow-up.
“This seeming misalignment of nonclinical staff handling clinical issues is likely explained by the fact that clinical issues were often a request to repeat information previously delivered by a clinician,” the authors wrote. “The high proportion of clinical concerns brought to navigators is likely a consequence of navigators proactively contacting patients and thus being perceived as an accessible extension of the clinical team with whom to raise concern.”
Researchers found that clinical members did find navigators useful to the care team “specifically because they brought clinical issues to the attention of the clinical team that might otherwise have been missed.”
But on the other hand, some clinicians believed that “clinical concerns being raised with navigators were a source of concern and felt to be inappropriate, suggesting a lack of compatibility of a lay service layered onto complex clinical care,” Dr. Holdsworth and colleagues stated, adding that nurses “with a negative view of lay navigation seemed to lack knowledge and information about the navigator role, which created trust issues.”
Another potential issue is staff turnover within the navigator program and an ever-changing environment of patient education and support programs. Navigators can be very beneficial connecting patients to things such as support groups or helping to connect patients to insurers, but it requires a significant effort on the part of navigators to know, understand, and keep up to date with all the nonclinical opportunities that patients have, and high turnover can be an issue here.
Overall, though, the researchers note that the key finding “was that it was difficult to implement a lay navigation program outside of the clinical team for the purposes of cancer care coordination. The navigators were not integrated into the clinical teams and as such, the navigator role was treated with some suspicion by clinical team members; there was a sense of mistrust among some clinicians, and mismatched expectations around what navigators could or should be doing.”
SOURCE: Holdsworth L et al. J Oncol Pract, 2019 Nov. 6. doi: 10.1200/JOP.19.00339.
The implementation of a lay navigation program as part of the delivery of cancer care presents a number of challenges, particularly because of the complexities of treating cancer, a new study has found.
Researchers looked at a lay navigator program, which uses nonclinical members to help provide information to cancer patients about their treatments, at the University of Alabama, and how the program was doing a year after its implementation.
“Integrating lay navigators into a complex clinical environment needs careful consideration at an organizational level, because this experience demonstrates that the integration process is not straightforward for clinical teams, patients, or navigators,” wrote Laura M. Holdsworth, PhD, Stanford (Calif.) University, and colleague. Their report is in the Journal of Oncology Practice.
A key difficulty discovered through the course of the research is that approximately two-thirds of concerns brought by patients to the lay navigators were clinical in nature, though only about a third (30%) required clinical follow-up and an additional 7% required social work follow-up.
“This seeming misalignment of nonclinical staff handling clinical issues is likely explained by the fact that clinical issues were often a request to repeat information previously delivered by a clinician,” the authors wrote. “The high proportion of clinical concerns brought to navigators is likely a consequence of navigators proactively contacting patients and thus being perceived as an accessible extension of the clinical team with whom to raise concern.”
Researchers found that clinical members did find navigators useful to the care team “specifically because they brought clinical issues to the attention of the clinical team that might otherwise have been missed.”
But on the other hand, some clinicians believed that “clinical concerns being raised with navigators were a source of concern and felt to be inappropriate, suggesting a lack of compatibility of a lay service layered onto complex clinical care,” Dr. Holdsworth and colleagues stated, adding that nurses “with a negative view of lay navigation seemed to lack knowledge and information about the navigator role, which created trust issues.”
Another potential issue is staff turnover within the navigator program and an ever-changing environment of patient education and support programs. Navigators can be very beneficial connecting patients to things such as support groups or helping to connect patients to insurers, but it requires a significant effort on the part of navigators to know, understand, and keep up to date with all the nonclinical opportunities that patients have, and high turnover can be an issue here.
Overall, though, the researchers note that the key finding “was that it was difficult to implement a lay navigation program outside of the clinical team for the purposes of cancer care coordination. The navigators were not integrated into the clinical teams and as such, the navigator role was treated with some suspicion by clinical team members; there was a sense of mistrust among some clinicians, and mismatched expectations around what navigators could or should be doing.”
SOURCE: Holdsworth L et al. J Oncol Pract, 2019 Nov. 6. doi: 10.1200/JOP.19.00339.
The implementation of a lay navigation program as part of the delivery of cancer care presents a number of challenges, particularly because of the complexities of treating cancer, a new study has found.
Researchers looked at a lay navigator program, which uses nonclinical members to help provide information to cancer patients about their treatments, at the University of Alabama, and how the program was doing a year after its implementation.
“Integrating lay navigators into a complex clinical environment needs careful consideration at an organizational level, because this experience demonstrates that the integration process is not straightforward for clinical teams, patients, or navigators,” wrote Laura M. Holdsworth, PhD, Stanford (Calif.) University, and colleague. Their report is in the Journal of Oncology Practice.
A key difficulty discovered through the course of the research is that approximately two-thirds of concerns brought by patients to the lay navigators were clinical in nature, though only about a third (30%) required clinical follow-up and an additional 7% required social work follow-up.
“This seeming misalignment of nonclinical staff handling clinical issues is likely explained by the fact that clinical issues were often a request to repeat information previously delivered by a clinician,” the authors wrote. “The high proportion of clinical concerns brought to navigators is likely a consequence of navigators proactively contacting patients and thus being perceived as an accessible extension of the clinical team with whom to raise concern.”
Researchers found that clinical members did find navigators useful to the care team “specifically because they brought clinical issues to the attention of the clinical team that might otherwise have been missed.”
But on the other hand, some clinicians believed that “clinical concerns being raised with navigators were a source of concern and felt to be inappropriate, suggesting a lack of compatibility of a lay service layered onto complex clinical care,” Dr. Holdsworth and colleagues stated, adding that nurses “with a negative view of lay navigation seemed to lack knowledge and information about the navigator role, which created trust issues.”
Another potential issue is staff turnover within the navigator program and an ever-changing environment of patient education and support programs. Navigators can be very beneficial connecting patients to things such as support groups or helping to connect patients to insurers, but it requires a significant effort on the part of navigators to know, understand, and keep up to date with all the nonclinical opportunities that patients have, and high turnover can be an issue here.
Overall, though, the researchers note that the key finding “was that it was difficult to implement a lay navigation program outside of the clinical team for the purposes of cancer care coordination. The navigators were not integrated into the clinical teams and as such, the navigator role was treated with some suspicion by clinical team members; there was a sense of mistrust among some clinicians, and mismatched expectations around what navigators could or should be doing.”
SOURCE: Holdsworth L et al. J Oncol Pract, 2019 Nov. 6. doi: 10.1200/JOP.19.00339.
FROM JOURNAL OF ONCOLOGY PRACTICE
Armored CAR T cells elicit responses in NHL patients
NATIONAL HARBOR, MD – An armored chimeric antigen receptor (CAR) T-cell therapy has demonstrated efficacy in vitro and in patients with relapsed or refractory non-Hodgkin lymphoma (NHL), according to findings presented at the annual meeting of the Society for Immunotherapy of Cancer.

ICTCAR014, a dominant negative PD-1 armored CAR T-cell therapy, proved more cytotoxic than traditional CAR T-cell therapy in vitro and produced responses in 12 of 13 NHL patients who received it.
Xiaobin Victor Lu, PhD, of Innovative Cellular Therapeutics, Shanghai, China, presented results with ICTCAR014 at the meeting.
Dr. Lu explained that ICTCAR014 consists of CD19-targeted CAR T cells genetically engineered to overexpress a PD-1 dominant negative protein with an altered intracellular signaling domain. The dominant negative protein can act as a “decoy receptor” to bind and block the PD-L1/2 inhibitory signal, thereby enhancing the efficacy of CAR T cells.
Innovative Cellular Therapeutics is developing ICTCAR014 because there is “some room to improve” with commercially available CAR T-cell products, Dr. Lu said. Specifically, tisagenlecleucel produced a 52% response rate in the JULIET trial (N Engl J Med. 2019;380:45-56), and axicabtagene ciloleucel produced an 82% response rate in the ZUMA-1 trial (N Engl J Med. 2017;377:2531-44).
There is also evidence to suggest that PD-1 blockade can modulate and “refuel” CAR T cells in relapsed/refractory NHL patients who fail or relapse after traditional anti-CD19 CAR T-cell therapy (Blood. 2017 Feb 23;129[8]:1039-41). This finding has prompted researchers to conduct trials of PD-1 inhibitors in combination with CAR T-cell therapies. But this combination approach may be expensive and cause more side effects than the armored CAR T-cell approach, Dr. Lu said.
In preclinical studies, Dr. Lu and colleagues found that ICTCAR014 was more effective than traditional anti-CD19 CAR T cells in killing Nalm6-PDL1 cells. In addition, the PD-1 dominant negative protein protected CAR T cells from exhaustion.
Dr. Lu also presented results in 13 NHL patients who have received ICTCAR014 in a phase 1 trial in China. Eleven patients had diffuse large B-cell lymphoma (DLBCL), and two had follicular lymphoma.
The objective response rate was 92.3% (12/13), which included five partial responses (38.5%) and seven complete responses (53.8%). Both follicular lymphoma patients and five DLBCL patients achieved a complete response. Five DLBCL patients achieved a partial response, and the remaining DLBCL patient did not respond.
Dr. Lu did not present safety data. However, he reported that there was no increased incidence of cytokine release syndrome or neurotoxicity in these patients, compared with patients receiving traditional CAR T-cell therapy.
Dr. Lu is employed by Innovative Cellular Therapeutics, which funded the research and is developing ICTCAR014.
SOURCE: Lu V et al. SITC 2019, Abstract O25.
NATIONAL HARBOR, MD – An armored chimeric antigen receptor (CAR) T-cell therapy has demonstrated efficacy in vitro and in patients with relapsed or refractory non-Hodgkin lymphoma (NHL), according to findings presented at the annual meeting of the Society for Immunotherapy of Cancer.
ICTCAR014, a dominant negative PD-1 armored CAR T-cell therapy, proved more cytotoxic than traditional CAR T-cell therapy in vitro and produced responses in 12 of 13 NHL patients who received it.
Xiaobin Victor Lu, PhD, of Innovative Cellular Therapeutics, Shanghai, China, presented results with ICTCAR014 at the meeting.
Dr. Lu explained that ICTCAR014 consists of CD19-targeted CAR T cells genetically engineered to overexpress a PD-1 dominant negative protein with an altered intracellular signaling domain. The dominant negative protein can act as a “decoy receptor” to bind and block the PD-L1/2 inhibitory signal, thereby enhancing the efficacy of CAR T cells.
Innovative Cellular Therapeutics is developing ICTCAR014 because there is “some room to improve” with commercially available CAR T-cell products, Dr. Lu said. Specifically, tisagenlecleucel produced a 52% response rate in the JULIET trial (N Engl J Med. 2019;380:45-56), and axicabtagene ciloleucel produced an 82% response rate in the ZUMA-1 trial (N Engl J Med. 2017;377:2531-44).
There is also evidence to suggest that PD-1 blockade can modulate and “refuel” CAR T cells in relapsed/refractory NHL patients who fail or relapse after traditional anti-CD19 CAR T-cell therapy (Blood. 2017 Feb 23;129[8]:1039-41). This finding has prompted researchers to conduct trials of PD-1 inhibitors in combination with CAR T-cell therapies. But this combination approach may be expensive and cause more side effects than the armored CAR T-cell approach, Dr. Lu said.
In preclinical studies, Dr. Lu and colleagues found that ICTCAR014 was more effective than traditional anti-CD19 CAR T cells in killing Nalm6-PDL1 cells. In addition, the PD-1 dominant negative protein protected CAR T cells from exhaustion.
Dr. Lu also presented results in 13 NHL patients who have received ICTCAR014 in a phase 1 trial in China. Eleven patients had diffuse large B-cell lymphoma (DLBCL), and two had follicular lymphoma.
The objective response rate was 92.3% (12/13), which included five partial responses (38.5%) and seven complete responses (53.8%). Both follicular lymphoma patients and five DLBCL patients achieved a complete response. Five DLBCL patients achieved a partial response, and the remaining DLBCL patient did not respond.
Dr. Lu did not present safety data. However, he reported that there was no increased incidence of cytokine release syndrome or neurotoxicity in these patients, compared with patients receiving traditional CAR T-cell therapy.
Dr. Lu is employed by Innovative Cellular Therapeutics, which funded the research and is developing ICTCAR014.
SOURCE: Lu V et al. SITC 2019, Abstract O25.
NATIONAL HARBOR, MD – An armored chimeric antigen receptor (CAR) T-cell therapy has demonstrated efficacy in vitro and in patients with relapsed or refractory non-Hodgkin lymphoma (NHL), according to findings presented at the annual meeting of the Society for Immunotherapy of Cancer.
ICTCAR014, a dominant negative PD-1 armored CAR T-cell therapy, proved more cytotoxic than traditional CAR T-cell therapy in vitro and produced responses in 12 of 13 NHL patients who received it.
Xiaobin Victor Lu, PhD, of Innovative Cellular Therapeutics, Shanghai, China, presented results with ICTCAR014 at the meeting.
Dr. Lu explained that ICTCAR014 consists of CD19-targeted CAR T cells genetically engineered to overexpress a PD-1 dominant negative protein with an altered intracellular signaling domain. The dominant negative protein can act as a “decoy receptor” to bind and block the PD-L1/2 inhibitory signal, thereby enhancing the efficacy of CAR T cells.
Innovative Cellular Therapeutics is developing ICTCAR014 because there is “some room to improve” with commercially available CAR T-cell products, Dr. Lu said. Specifically, tisagenlecleucel produced a 52% response rate in the JULIET trial (N Engl J Med. 2019;380:45-56), and axicabtagene ciloleucel produced an 82% response rate in the ZUMA-1 trial (N Engl J Med. 2017;377:2531-44).
There is also evidence to suggest that PD-1 blockade can modulate and “refuel” CAR T cells in relapsed/refractory NHL patients who fail or relapse after traditional anti-CD19 CAR T-cell therapy (Blood. 2017 Feb 23;129[8]:1039-41). This finding has prompted researchers to conduct trials of PD-1 inhibitors in combination with CAR T-cell therapies. But this combination approach may be expensive and cause more side effects than the armored CAR T-cell approach, Dr. Lu said.
In preclinical studies, Dr. Lu and colleagues found that ICTCAR014 was more effective than traditional anti-CD19 CAR T cells in killing Nalm6-PDL1 cells. In addition, the PD-1 dominant negative protein protected CAR T cells from exhaustion.
Dr. Lu also presented results in 13 NHL patients who have received ICTCAR014 in a phase 1 trial in China. Eleven patients had diffuse large B-cell lymphoma (DLBCL), and two had follicular lymphoma.
The objective response rate was 92.3% (12/13), which included five partial responses (38.5%) and seven complete responses (53.8%). Both follicular lymphoma patients and five DLBCL patients achieved a complete response. Five DLBCL patients achieved a partial response, and the remaining DLBCL patient did not respond.
Dr. Lu did not present safety data. However, he reported that there was no increased incidence of cytokine release syndrome or neurotoxicity in these patients, compared with patients receiving traditional CAR T-cell therapy.
Dr. Lu is employed by Innovative Cellular Therapeutics, which funded the research and is developing ICTCAR014.
SOURCE: Lu V et al. SITC 2019, Abstract O25.
REPORTING FROM SITC 2019

Combo shows promise for checkpoint inhibitor-refractory urothelial carcinoma
NATIONAL HARBOR, MD. – Sitravatinib may “restore or enhance” the activity of anti-PD-1 therapy in patients with checkpoint inhibitor–refractory urothelial carcinoma, an investigator reported at the annual meeting of the Society for Immunotherapy of Cancer.

Clinical activity was observed with combination sitravatinib and nivolumab in patients with urothelial carcinoma who had disease progression on or after an immune checkpoint inhibitor and were previously treated with platinum-based chemotherapy.
“Up until a few years ago, the only therapies we had [for urothelial carcinoma] were cytotoxic, platinum-based chemotherapies,” said Pavlos Msaouel, MD, PhD, of the University of Texas MD Anderson Cancer Center, Houston.
“Thankfully, since 2016, immune checkpoint therapy has become part of our toolbox. But even with single-agent, approved immune checkpoint therapies, anti-PD-1/anti-PD-L1, the response rates are still low, around 20%, and durable responses are only seen in a subset of patients. So we have to do better, if possible, potentially by combining immune checkpoint therapies with other immunotherapies such as sitravatinib.”
Dr. Msaouel explained that sitravatinib inhibits a spectrum of related receptor tyrosine kinases, including TAM family receptors (TYRO3, Axl, and Mer), split family receptors (VEGFR2/PDGFR and c-KIT), and c-Met. Researchers are investigating sitravatinib in combination with nivolumab in a phase 2 trial of patients with urothelial carcinoma (NCT03606174). Dr. Msaouel presented results from one cohort on this trial – 33 patients who had previously received platinum-based chemotherapy and a PD-1/PD-L1 inhibitor.
At baseline, the patients’ median age was 68 years (range, 47-83 years), and 70% were male. Patients had metastatic (n = 30) or locally advanced (n = 3) disease. They had received a median of two (range, one to four) prior systemic therapies.
For this study, patients received oral sitravatinib at 120 mg daily and intravenous nivolumab at 240 mg every 2 weeks or 480 mg every 4 weeks on continuous 28-day cycles. Tumor assessments were performed every 8 weeks.
Results
Of the 22 patients evaluable for efficacy, 1 patient achieved a complete response, 5 had a partial response, 15 had stable disease, and 1 progressed. Eight patients had tumor regression greater than 30%.
Treatment duration exceeded 26 weeks in six patients. Nine patients, including four responders, were still on study at the data cutoff in mid-October.
“This ongoing trial continues to show promising clinical activity, including tumor regression and prolonged duration on treatment,” Dr. Msaouel said.
He added that combination sitravatinib and nivolumab has “an acceptable side effect profile, with manageable adverse events.”
Common treatment-related adverse events, in all 33 patients, were fatigue (58%), diarrhea (48%), decreased appetite (33%), dysphonia (33%), nausea (33%), and alanine aminotransferase increase (21%).
Grade 3 treatment-related adverse events included fatigue (12%), hypertension (12%), diarrhea (9%), lipase increase (9%), decreased appetite (3%), and palmar-plantar erythrodysesthesia syndrome (3%). There were no grade 4 or 5 treatment-related events.
Mirati Therapeutics sponsored the trial. Dr. Msaouel disclosed relationships with Mirati, Bristol-Myers Squibb, Exelixis, Pfizer, and Takeda.
SOURCE: Msaouel P et al. SITC 2019. Abstract O23.
NATIONAL HARBOR, MD. – Sitravatinib may “restore or enhance” the activity of anti-PD-1 therapy in patients with checkpoint inhibitor–refractory urothelial carcinoma, an investigator reported at the annual meeting of the Society for Immunotherapy of Cancer.
Clinical activity was observed with combination sitravatinib and nivolumab in patients with urothelial carcinoma who had disease progression on or after an immune checkpoint inhibitor and were previously treated with platinum-based chemotherapy.
“Up until a few years ago, the only therapies we had [for urothelial carcinoma] were cytotoxic, platinum-based chemotherapies,” said Pavlos Msaouel, MD, PhD, of the University of Texas MD Anderson Cancer Center, Houston.
“Thankfully, since 2016, immune checkpoint therapy has become part of our toolbox. But even with single-agent, approved immune checkpoint therapies, anti-PD-1/anti-PD-L1, the response rates are still low, around 20%, and durable responses are only seen in a subset of patients. So we have to do better, if possible, potentially by combining immune checkpoint therapies with other immunotherapies such as sitravatinib.”
Dr. Msaouel explained that sitravatinib inhibits a spectrum of related receptor tyrosine kinases, including TAM family receptors (TYRO3, Axl, and Mer), split family receptors (VEGFR2/PDGFR and c-KIT), and c-Met. Researchers are investigating sitravatinib in combination with nivolumab in a phase 2 trial of patients with urothelial carcinoma (NCT03606174). Dr. Msaouel presented results from one cohort on this trial – 33 patients who had previously received platinum-based chemotherapy and a PD-1/PD-L1 inhibitor.
At baseline, the patients’ median age was 68 years (range, 47-83 years), and 70% were male. Patients had metastatic (n = 30) or locally advanced (n = 3) disease. They had received a median of two (range, one to four) prior systemic therapies.
For this study, patients received oral sitravatinib at 120 mg daily and intravenous nivolumab at 240 mg every 2 weeks or 480 mg every 4 weeks on continuous 28-day cycles. Tumor assessments were performed every 8 weeks.
Results
Of the 22 patients evaluable for efficacy, 1 patient achieved a complete response, 5 had a partial response, 15 had stable disease, and 1 progressed. Eight patients had tumor regression greater than 30%.
Treatment duration exceeded 26 weeks in six patients. Nine patients, including four responders, were still on study at the data cutoff in mid-October.
“This ongoing trial continues to show promising clinical activity, including tumor regression and prolonged duration on treatment,” Dr. Msaouel said.
He added that combination sitravatinib and nivolumab has “an acceptable side effect profile, with manageable adverse events.”
Common treatment-related adverse events, in all 33 patients, were fatigue (58%), diarrhea (48%), decreased appetite (33%), dysphonia (33%), nausea (33%), and alanine aminotransferase increase (21%).
Grade 3 treatment-related adverse events included fatigue (12%), hypertension (12%), diarrhea (9%), lipase increase (9%), decreased appetite (3%), and palmar-plantar erythrodysesthesia syndrome (3%). There were no grade 4 or 5 treatment-related events.
Mirati Therapeutics sponsored the trial. Dr. Msaouel disclosed relationships with Mirati, Bristol-Myers Squibb, Exelixis, Pfizer, and Takeda.
SOURCE: Msaouel P et al. SITC 2019. Abstract O23.
NATIONAL HARBOR, MD. – Sitravatinib may “restore or enhance” the activity of anti-PD-1 therapy in patients with checkpoint inhibitor–refractory urothelial carcinoma, an investigator reported at the annual meeting of the Society for Immunotherapy of Cancer.
Clinical activity was observed with combination sitravatinib and nivolumab in patients with urothelial carcinoma who had disease progression on or after an immune checkpoint inhibitor and were previously treated with platinum-based chemotherapy.
“Up until a few years ago, the only therapies we had [for urothelial carcinoma] were cytotoxic, platinum-based chemotherapies,” said Pavlos Msaouel, MD, PhD, of the University of Texas MD Anderson Cancer Center, Houston.
“Thankfully, since 2016, immune checkpoint therapy has become part of our toolbox. But even with single-agent, approved immune checkpoint therapies, anti-PD-1/anti-PD-L1, the response rates are still low, around 20%, and durable responses are only seen in a subset of patients. So we have to do better, if possible, potentially by combining immune checkpoint therapies with other immunotherapies such as sitravatinib.”
Dr. Msaouel explained that sitravatinib inhibits a spectrum of related receptor tyrosine kinases, including TAM family receptors (TYRO3, Axl, and Mer), split family receptors (VEGFR2/PDGFR and c-KIT), and c-Met. Researchers are investigating sitravatinib in combination with nivolumab in a phase 2 trial of patients with urothelial carcinoma (NCT03606174). Dr. Msaouel presented results from one cohort on this trial – 33 patients who had previously received platinum-based chemotherapy and a PD-1/PD-L1 inhibitor.
At baseline, the patients’ median age was 68 years (range, 47-83 years), and 70% were male. Patients had metastatic (n = 30) or locally advanced (n = 3) disease. They had received a median of two (range, one to four) prior systemic therapies.
For this study, patients received oral sitravatinib at 120 mg daily and intravenous nivolumab at 240 mg every 2 weeks or 480 mg every 4 weeks on continuous 28-day cycles. Tumor assessments were performed every 8 weeks.
Results
Of the 22 patients evaluable for efficacy, 1 patient achieved a complete response, 5 had a partial response, 15 had stable disease, and 1 progressed. Eight patients had tumor regression greater than 30%.
Treatment duration exceeded 26 weeks in six patients. Nine patients, including four responders, were still on study at the data cutoff in mid-October.
“This ongoing trial continues to show promising clinical activity, including tumor regression and prolonged duration on treatment,” Dr. Msaouel said.
He added that combination sitravatinib and nivolumab has “an acceptable side effect profile, with manageable adverse events.”
Common treatment-related adverse events, in all 33 patients, were fatigue (58%), diarrhea (48%), decreased appetite (33%), dysphonia (33%), nausea (33%), and alanine aminotransferase increase (21%).
Grade 3 treatment-related adverse events included fatigue (12%), hypertension (12%), diarrhea (9%), lipase increase (9%), decreased appetite (3%), and palmar-plantar erythrodysesthesia syndrome (3%). There were no grade 4 or 5 treatment-related events.
Mirati Therapeutics sponsored the trial. Dr. Msaouel disclosed relationships with Mirati, Bristol-Myers Squibb, Exelixis, Pfizer, and Takeda.
SOURCE: Msaouel P et al. SITC 2019. Abstract O23.
REPORTING FROM SITC 2019
Short-course DAA therapy may prevent hepatitis transmission in transplant patients
BOSTON – A short course of results of a recent study show.
The regimen, given right before transplantation and for 7 days afterward, reduced the cost of direct-acting antiviral (DAA) therapy and allowed patients to complete hepatitis C virus (HCV) therapy before hospital discharge, according to authors of the study, which was presented at the annual meeting of the American Association for the Study of Liver Diseases.
If confirmed in subsequent studies, this regimen could become the standard of care for donor-positive, recipient-negative transplantation, said lead study author Jordan J. Feld, MD, R. Phelan Chair in translational liver disease research at the University of Toronto and research director at the Toronto Centre for Liver Disease.
“Transplant recipients are understandably nervous about accepting organs from people with HCV infection,” said Dr. Feld in a press release. “This very short therapy allows them to leave hospital free of HCV, which is a huge benefit. Not only is it cheaper and likely safer, but the patients really prefer not having to worry about HCV with all of the other challenges after a transplant.”
Results of this study come at a time when the proportion of overdose death organ donors is on the rise, from just 1% in 2000 to 15% in 2016, according to Dr. Feld. Overdose deaths account for the largest percentage of HCV-infected donors, most of whom are young and often otherwise healthy, he added.
Recipients of HCV-infected organs can be cured after transplant as a number of studies have previously shown. However, preventing transmission would be better than cure, Dr. Feld said, in part because of issues with drug-drug interactions, potential for relapse, and issues with procuring the drugs after transplant.
Accordingly, Dr. Feld and colleagues sought to evaluate “preemptive” treatment with DAA therapy combined with ezetimibe, which they said has been shown to inhibit HCV entry blockers. The recipients, who were listed for heart, lung, kidney, or kidney-pancreas transplant, were given glecaprevir/pibrentasvir plus ezetimibe starting 6-12 hours prior to transplantation, and then daily for 7 days.
The median age was 36 years for the 16 donors reported, and 61 years for the 25 recipients. Most recipients (12 patients) had a lung transplant, while 8 had a heart transplant, 4 had a kidney transplant, and 1 had a kidney-pancreas transplant.
There were no virologic failures, according to the investigators, with sustained virologic response (SVR) after 6 weeks in 7 patients, and SVR after 12 weeks in the remaining 18. Three recipients did have detectable HCV RNA, though all cleared and had SVR at 6 weeks in one case, and SVR at 12 weeks in the other two, according to the investigators’ report.
Of 22 serious adverse events noted in the study, 1 was considered treatment related, according to the report, and there were 2 deaths among lung transplant patients, caused by sepsis in 1 case to sepsis and subarachnoid hemorrhage in another.
It’s not clear whether ezetimibe is needed in this short-duration regimen, but in any case, it is well tolerated and inexpensive, and so there is “minimal downside” to include it, Dr. Feld and coinvestigators wrote in their report.
Dr. Feld reported disclosures related to Abbvie, Abbott, Enanta Pharmaceuticals, Gilead, Janssen, Merck, and Roche.
SOURCE: Feld JJ et al. The Liver Meeting 2019, Abstract 38.
BOSTON – A short course of results of a recent study show.
The regimen, given right before transplantation and for 7 days afterward, reduced the cost of direct-acting antiviral (DAA) therapy and allowed patients to complete hepatitis C virus (HCV) therapy before hospital discharge, according to authors of the study, which was presented at the annual meeting of the American Association for the Study of Liver Diseases.
If confirmed in subsequent studies, this regimen could become the standard of care for donor-positive, recipient-negative transplantation, said lead study author Jordan J. Feld, MD, R. Phelan Chair in translational liver disease research at the University of Toronto and research director at the Toronto Centre for Liver Disease.
“Transplant recipients are understandably nervous about accepting organs from people with HCV infection,” said Dr. Feld in a press release. “This very short therapy allows them to leave hospital free of HCV, which is a huge benefit. Not only is it cheaper and likely safer, but the patients really prefer not having to worry about HCV with all of the other challenges after a transplant.”
Results of this study come at a time when the proportion of overdose death organ donors is on the rise, from just 1% in 2000 to 15% in 2016, according to Dr. Feld. Overdose deaths account for the largest percentage of HCV-infected donors, most of whom are young and often otherwise healthy, he added.
Recipients of HCV-infected organs can be cured after transplant as a number of studies have previously shown. However, preventing transmission would be better than cure, Dr. Feld said, in part because of issues with drug-drug interactions, potential for relapse, and issues with procuring the drugs after transplant.
Accordingly, Dr. Feld and colleagues sought to evaluate “preemptive” treatment with DAA therapy combined with ezetimibe, which they said has been shown to inhibit HCV entry blockers. The recipients, who were listed for heart, lung, kidney, or kidney-pancreas transplant, were given glecaprevir/pibrentasvir plus ezetimibe starting 6-12 hours prior to transplantation, and then daily for 7 days.
The median age was 36 years for the 16 donors reported, and 61 years for the 25 recipients. Most recipients (12 patients) had a lung transplant, while 8 had a heart transplant, 4 had a kidney transplant, and 1 had a kidney-pancreas transplant.
There were no virologic failures, according to the investigators, with sustained virologic response (SVR) after 6 weeks in 7 patients, and SVR after 12 weeks in the remaining 18. Three recipients did have detectable HCV RNA, though all cleared and had SVR at 6 weeks in one case, and SVR at 12 weeks in the other two, according to the investigators’ report.
Of 22 serious adverse events noted in the study, 1 was considered treatment related, according to the report, and there were 2 deaths among lung transplant patients, caused by sepsis in 1 case to sepsis and subarachnoid hemorrhage in another.
It’s not clear whether ezetimibe is needed in this short-duration regimen, but in any case, it is well tolerated and inexpensive, and so there is “minimal downside” to include it, Dr. Feld and coinvestigators wrote in their report.
Dr. Feld reported disclosures related to Abbvie, Abbott, Enanta Pharmaceuticals, Gilead, Janssen, Merck, and Roche.
SOURCE: Feld JJ et al. The Liver Meeting 2019, Abstract 38.
BOSTON – A short course of results of a recent study show.
The regimen, given right before transplantation and for 7 days afterward, reduced the cost of direct-acting antiviral (DAA) therapy and allowed patients to complete hepatitis C virus (HCV) therapy before hospital discharge, according to authors of the study, which was presented at the annual meeting of the American Association for the Study of Liver Diseases.
If confirmed in subsequent studies, this regimen could become the standard of care for donor-positive, recipient-negative transplantation, said lead study author Jordan J. Feld, MD, R. Phelan Chair in translational liver disease research at the University of Toronto and research director at the Toronto Centre for Liver Disease.
“Transplant recipients are understandably nervous about accepting organs from people with HCV infection,” said Dr. Feld in a press release. “This very short therapy allows them to leave hospital free of HCV, which is a huge benefit. Not only is it cheaper and likely safer, but the patients really prefer not having to worry about HCV with all of the other challenges after a transplant.”
Results of this study come at a time when the proportion of overdose death organ donors is on the rise, from just 1% in 2000 to 15% in 2016, according to Dr. Feld. Overdose deaths account for the largest percentage of HCV-infected donors, most of whom are young and often otherwise healthy, he added.
Recipients of HCV-infected organs can be cured after transplant as a number of studies have previously shown. However, preventing transmission would be better than cure, Dr. Feld said, in part because of issues with drug-drug interactions, potential for relapse, and issues with procuring the drugs after transplant.
Accordingly, Dr. Feld and colleagues sought to evaluate “preemptive” treatment with DAA therapy combined with ezetimibe, which they said has been shown to inhibit HCV entry blockers. The recipients, who were listed for heart, lung, kidney, or kidney-pancreas transplant, were given glecaprevir/pibrentasvir plus ezetimibe starting 6-12 hours prior to transplantation, and then daily for 7 days.
The median age was 36 years for the 16 donors reported, and 61 years for the 25 recipients. Most recipients (12 patients) had a lung transplant, while 8 had a heart transplant, 4 had a kidney transplant, and 1 had a kidney-pancreas transplant.
There were no virologic failures, according to the investigators, with sustained virologic response (SVR) after 6 weeks in 7 patients, and SVR after 12 weeks in the remaining 18. Three recipients did have detectable HCV RNA, though all cleared and had SVR at 6 weeks in one case, and SVR at 12 weeks in the other two, according to the investigators’ report.
Of 22 serious adverse events noted in the study, 1 was considered treatment related, according to the report, and there were 2 deaths among lung transplant patients, caused by sepsis in 1 case to sepsis and subarachnoid hemorrhage in another.
It’s not clear whether ezetimibe is needed in this short-duration regimen, but in any case, it is well tolerated and inexpensive, and so there is “minimal downside” to include it, Dr. Feld and coinvestigators wrote in their report.
Dr. Feld reported disclosures related to Abbvie, Abbott, Enanta Pharmaceuticals, Gilead, Janssen, Merck, and Roche.
SOURCE: Feld JJ et al. The Liver Meeting 2019, Abstract 38.
REPORTING FROM THE LIVER MEETING 2019
Dextromethorphan/bupropion combo is remarkably fast-acting antidepressant
COPENHAGEN – A novel investigational oral combination of dextromethorphan and bupropion achieved a strikingly rapid and clinically meaningful reduction in depressive symptoms in patients with major depressive disorder in a phase 2, active comparator–controlled study, Cedric O’Gorman, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
– and the between-group difference continued to grow over the course of the 6-week, double-blind randomized trial. Thus, AXS-05 shows the potential to help meet the widely recognized need for faster-acting, higher-response antidepressant therapies than are currently available, observed Dr. O’Gorman, senior vice president for clinical development and medical affairs at Axsome Therapeutics in New York.
AXS-05 has multimodal mechanisms of action. As a result, it is not only in late-stage clinical development for major depressive disorder, but also for nicotine dependence and agitation in patients with Alzheimer’s disease.
Dextromethorphan is an NMDA (N-methyl-D-aspartate)–receptor antagonist, a serotonin and norepinephrine reuptake inhibitor, a sigma-1–receptor agonist, and a nicotinic-receptor antagonist. Bupropion, too, is a nicotinic-receptor antagonist. In addition, it’s a dopamine and norepinephrine reuptake inhibitor, and it boosts plasma levels of dextromethorphan by inhibiting its metabolism, the psychiatrist explained.
The phase 2, double-blind clinical trial included 80 patients with confirmed major depressive disorder who were experiencing an acute moderate to severe depressive episode. Slightly more than half of them had a history of three or more prior depressive episodes. Their mean baseline Montgomery-Åsberg Depression Rating Scale (MADRS) total score was 32, with a mean Clinical Global Impressions-Severity (CGI-S) score of 4.5 on a 1-7 scale. Participants were randomized to 45 mg dextromethorphan/105 mg bupropion or to 105 mg of bupropion-only, twice daily for 6 weeks.
The primary study endpoint was the average weekly change in MADRS score from baseline to week 6. The difference was highly significant: 13.7 points in the AXS-05 group, 8.8 with bupropion. At week 6, the AXS-05 group averaged a 17.2-point reduction from baseline in MADRS total score, compared with a 12.1-point decrease in controls. The between-group difference numerically favored AXS-05 at week 1, achieving statistically significant superiority from week 2 on. At week 6, 47% of the AXS-05 group had achieved clinical remission as defined by a MADRS score of 10 or less, as did 16% of the bupropion group.
At week 1 – again, the earliest assessment – 18% of AXS-05-treated patients were rated much or very much improved on the CGI, as were 3% of bupropion-treated controls. At week 6, 59% of the AXS-05 group and 27% of controls were rated very much improved.
Twelve percent of patients in both study arms discontinued treatment because of adverse events, none serious. The most common adverse events in the dextromethorphan/bupropion group were nausea, dizziness, dry mouth, reduced appetite, and anxiety. There were no instances of weight gain, sexual dysfunction, or psychomimetic effects.
Two phase 3, double-blind, 6-week RCTs of AXS-05 in depression are ongoing. STRIDE 1 includes 250 patients with treatment-resistant depression randomized to AXS-05 or bupropion. GEMINI is a study of 300 patients with major depressive disorder assigned to AXS-05 or placebo.
COPENHAGEN – A novel investigational oral combination of dextromethorphan and bupropion achieved a strikingly rapid and clinically meaningful reduction in depressive symptoms in patients with major depressive disorder in a phase 2, active comparator–controlled study, Cedric O’Gorman, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
– and the between-group difference continued to grow over the course of the 6-week, double-blind randomized trial. Thus, AXS-05 shows the potential to help meet the widely recognized need for faster-acting, higher-response antidepressant therapies than are currently available, observed Dr. O’Gorman, senior vice president for clinical development and medical affairs at Axsome Therapeutics in New York.
AXS-05 has multimodal mechanisms of action. As a result, it is not only in late-stage clinical development for major depressive disorder, but also for nicotine dependence and agitation in patients with Alzheimer’s disease.
Dextromethorphan is an NMDA (N-methyl-D-aspartate)–receptor antagonist, a serotonin and norepinephrine reuptake inhibitor, a sigma-1–receptor agonist, and a nicotinic-receptor antagonist. Bupropion, too, is a nicotinic-receptor antagonist. In addition, it’s a dopamine and norepinephrine reuptake inhibitor, and it boosts plasma levels of dextromethorphan by inhibiting its metabolism, the psychiatrist explained.
The phase 2, double-blind clinical trial included 80 patients with confirmed major depressive disorder who were experiencing an acute moderate to severe depressive episode. Slightly more than half of them had a history of three or more prior depressive episodes. Their mean baseline Montgomery-Åsberg Depression Rating Scale (MADRS) total score was 32, with a mean Clinical Global Impressions-Severity (CGI-S) score of 4.5 on a 1-7 scale. Participants were randomized to 45 mg dextromethorphan/105 mg bupropion or to 105 mg of bupropion-only, twice daily for 6 weeks.
The primary study endpoint was the average weekly change in MADRS score from baseline to week 6. The difference was highly significant: 13.7 points in the AXS-05 group, 8.8 with bupropion. At week 6, the AXS-05 group averaged a 17.2-point reduction from baseline in MADRS total score, compared with a 12.1-point decrease in controls. The between-group difference numerically favored AXS-05 at week 1, achieving statistically significant superiority from week 2 on. At week 6, 47% of the AXS-05 group had achieved clinical remission as defined by a MADRS score of 10 or less, as did 16% of the bupropion group.
At week 1 – again, the earliest assessment – 18% of AXS-05-treated patients were rated much or very much improved on the CGI, as were 3% of bupropion-treated controls. At week 6, 59% of the AXS-05 group and 27% of controls were rated very much improved.
Twelve percent of patients in both study arms discontinued treatment because of adverse events, none serious. The most common adverse events in the dextromethorphan/bupropion group were nausea, dizziness, dry mouth, reduced appetite, and anxiety. There were no instances of weight gain, sexual dysfunction, or psychomimetic effects.
Two phase 3, double-blind, 6-week RCTs of AXS-05 in depression are ongoing. STRIDE 1 includes 250 patients with treatment-resistant depression randomized to AXS-05 or bupropion. GEMINI is a study of 300 patients with major depressive disorder assigned to AXS-05 or placebo.
COPENHAGEN – A novel investigational oral combination of dextromethorphan and bupropion achieved a strikingly rapid and clinically meaningful reduction in depressive symptoms in patients with major depressive disorder in a phase 2, active comparator–controlled study, Cedric O’Gorman, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
– and the between-group difference continued to grow over the course of the 6-week, double-blind randomized trial. Thus, AXS-05 shows the potential to help meet the widely recognized need for faster-acting, higher-response antidepressant therapies than are currently available, observed Dr. O’Gorman, senior vice president for clinical development and medical affairs at Axsome Therapeutics in New York.
AXS-05 has multimodal mechanisms of action. As a result, it is not only in late-stage clinical development for major depressive disorder, but also for nicotine dependence and agitation in patients with Alzheimer’s disease.
Dextromethorphan is an NMDA (N-methyl-D-aspartate)–receptor antagonist, a serotonin and norepinephrine reuptake inhibitor, a sigma-1–receptor agonist, and a nicotinic-receptor antagonist. Bupropion, too, is a nicotinic-receptor antagonist. In addition, it’s a dopamine and norepinephrine reuptake inhibitor, and it boosts plasma levels of dextromethorphan by inhibiting its metabolism, the psychiatrist explained.
The phase 2, double-blind clinical trial included 80 patients with confirmed major depressive disorder who were experiencing an acute moderate to severe depressive episode. Slightly more than half of them had a history of three or more prior depressive episodes. Their mean baseline Montgomery-Åsberg Depression Rating Scale (MADRS) total score was 32, with a mean Clinical Global Impressions-Severity (CGI-S) score of 4.5 on a 1-7 scale. Participants were randomized to 45 mg dextromethorphan/105 mg bupropion or to 105 mg of bupropion-only, twice daily for 6 weeks.
The primary study endpoint was the average weekly change in MADRS score from baseline to week 6. The difference was highly significant: 13.7 points in the AXS-05 group, 8.8 with bupropion. At week 6, the AXS-05 group averaged a 17.2-point reduction from baseline in MADRS total score, compared with a 12.1-point decrease in controls. The between-group difference numerically favored AXS-05 at week 1, achieving statistically significant superiority from week 2 on. At week 6, 47% of the AXS-05 group had achieved clinical remission as defined by a MADRS score of 10 or less, as did 16% of the bupropion group.
At week 1 – again, the earliest assessment – 18% of AXS-05-treated patients were rated much or very much improved on the CGI, as were 3% of bupropion-treated controls. At week 6, 59% of the AXS-05 group and 27% of controls were rated very much improved.
Twelve percent of patients in both study arms discontinued treatment because of adverse events, none serious. The most common adverse events in the dextromethorphan/bupropion group were nausea, dizziness, dry mouth, reduced appetite, and anxiety. There were no instances of weight gain, sexual dysfunction, or psychomimetic effects.
Two phase 3, double-blind, 6-week RCTs of AXS-05 in depression are ongoing. STRIDE 1 includes 250 patients with treatment-resistant depression randomized to AXS-05 or bupropion. GEMINI is a study of 300 patients with major depressive disorder assigned to AXS-05 or placebo.
REPORTING FROM ECNP 2019
TLR9 agonist may overcome resistance to anti–PD-1 therapy in melanoma
NATIONAL HARBOR, MD. – A TLR9 agonist called CMP-001 can reverse resistance to anti–programmed death-1 (PD-1) therapy in patients with melanoma, a phase 1 trial suggests.
Combination CMP-001 and pembrolizumab produced durable responses in patients who had progressed on prior anti–PD-1 therapy, and the combination was considered well tolerated.
CMP-001 is a CpG-A TLR9 agonist packaged in a viruslike particle, John Kirkwood, MD, of University of Pittsburgh Medical Center, explained in a late-breaking abstract at the annual meeting of the Society for Immunotherapy of Cancer. CMP-001 activates tumor-associated plasmacytoid dendritic cells and induces systemic tumor-specific CD8+ T-cell responses.
Dr. Kirkwood and associates are investigating CMP-001, given alone or in combination with pembrolizumab, in a phase 1 trial (NCT02680184) of patients with metastatic or unresectable melanoma who are refractory to anti–PD-1 therapy.
Data were presented on 144 patients who received CMP-001 in combination with pembrolizumab. About 40% of patients (39.6%) had elevated lactate dehydrogenase at baseline, and 32.6% had BRAF mutations.
All patients had received prior anti–PD-1 therapy alone (75%) and/or in combination (50%). For most patients (93.1%), their last response to anti–PD-1 therapy was progression.
For this study, the patients received intratumoral CMP-001 injections at a range of doses (1 mg, 3 mg, 5 mg, 7.5 mg, and 10 mg). CMP-001 was given weekly for either 2 weeks or 7 weeks, then every 3 weeks until discontinuation. There were two different formulations of CMP-001 given – 0.01% polysorbate 20 (PS20; n = 83) and 0.00167% PS20 (n = 61).
Safety
“CMP-001 in combination with pembrolizumab is very well tolerated, with no apparent increase in autoimmune toxicities associated with anti–PD-1,” Dr. Kirkwood said.
The most common treatment-related adverse events were flulike symptoms, including chills (72%), pyrexia (56%), fatigue (51%), nausea (45%), vomiting (29%), and headache (28%). Another common event was injection-site pain (28%).
The most common grade 3 adverse events were hypotension (n = 9) and hypertension (n = 7). Grade 4 events included hypotension, aspartate aminotransferase increase, and alanine aminotransferase increase (n = 1 for all). There were no grade 5 events.
Six patients discontinued treatment because of adverse events.
Response
The overall response rate was 25% (21/83) among patients who received the 0.01% PS20 formulation of CMP-001 and 11.5% (7/61) among patients who received the 0.00167% PS20 formulation.
Responses were similar in injected and noninjected target lesions. The median duration of response has not been reached at a median follow-up of 16.9 months.
“Intratumoral CMP-001 reverses resistance to anti–PD-1 in patients who have progressed on prior anti–PD-1 therapy,” Dr. Kirkwood said, adding that these data support further clinical development of CMP-001.
The research is sponsored by Checkmate Pharmaceuticals. Dr. Kirkwood disclosed relationships with Amgen, BMS, Immunocore, Iovance, Novartis, Elsevier, Castle, Merck, and Checkmate.
SOURCE: Kirkwood J et al. SITC 2019, Abstract O85.
NATIONAL HARBOR, MD. – A TLR9 agonist called CMP-001 can reverse resistance to anti–programmed death-1 (PD-1) therapy in patients with melanoma, a phase 1 trial suggests.
Combination CMP-001 and pembrolizumab produced durable responses in patients who had progressed on prior anti–PD-1 therapy, and the combination was considered well tolerated.
CMP-001 is a CpG-A TLR9 agonist packaged in a viruslike particle, John Kirkwood, MD, of University of Pittsburgh Medical Center, explained in a late-breaking abstract at the annual meeting of the Society for Immunotherapy of Cancer. CMP-001 activates tumor-associated plasmacytoid dendritic cells and induces systemic tumor-specific CD8+ T-cell responses.
Dr. Kirkwood and associates are investigating CMP-001, given alone or in combination with pembrolizumab, in a phase 1 trial (NCT02680184) of patients with metastatic or unresectable melanoma who are refractory to anti–PD-1 therapy.
Data were presented on 144 patients who received CMP-001 in combination with pembrolizumab. About 40% of patients (39.6%) had elevated lactate dehydrogenase at baseline, and 32.6% had BRAF mutations.
All patients had received prior anti–PD-1 therapy alone (75%) and/or in combination (50%). For most patients (93.1%), their last response to anti–PD-1 therapy was progression.
For this study, the patients received intratumoral CMP-001 injections at a range of doses (1 mg, 3 mg, 5 mg, 7.5 mg, and 10 mg). CMP-001 was given weekly for either 2 weeks or 7 weeks, then every 3 weeks until discontinuation. There were two different formulations of CMP-001 given – 0.01% polysorbate 20 (PS20; n = 83) and 0.00167% PS20 (n = 61).
Safety
“CMP-001 in combination with pembrolizumab is very well tolerated, with no apparent increase in autoimmune toxicities associated with anti–PD-1,” Dr. Kirkwood said.
The most common treatment-related adverse events were flulike symptoms, including chills (72%), pyrexia (56%), fatigue (51%), nausea (45%), vomiting (29%), and headache (28%). Another common event was injection-site pain (28%).
The most common grade 3 adverse events were hypotension (n = 9) and hypertension (n = 7). Grade 4 events included hypotension, aspartate aminotransferase increase, and alanine aminotransferase increase (n = 1 for all). There were no grade 5 events.
Six patients discontinued treatment because of adverse events.
Response
The overall response rate was 25% (21/83) among patients who received the 0.01% PS20 formulation of CMP-001 and 11.5% (7/61) among patients who received the 0.00167% PS20 formulation.
Responses were similar in injected and noninjected target lesions. The median duration of response has not been reached at a median follow-up of 16.9 months.
“Intratumoral CMP-001 reverses resistance to anti–PD-1 in patients who have progressed on prior anti–PD-1 therapy,” Dr. Kirkwood said, adding that these data support further clinical development of CMP-001.
The research is sponsored by Checkmate Pharmaceuticals. Dr. Kirkwood disclosed relationships with Amgen, BMS, Immunocore, Iovance, Novartis, Elsevier, Castle, Merck, and Checkmate.
SOURCE: Kirkwood J et al. SITC 2019, Abstract O85.
NATIONAL HARBOR, MD. – A TLR9 agonist called CMP-001 can reverse resistance to anti–programmed death-1 (PD-1) therapy in patients with melanoma, a phase 1 trial suggests.
Combination CMP-001 and pembrolizumab produced durable responses in patients who had progressed on prior anti–PD-1 therapy, and the combination was considered well tolerated.
CMP-001 is a CpG-A TLR9 agonist packaged in a viruslike particle, John Kirkwood, MD, of University of Pittsburgh Medical Center, explained in a late-breaking abstract at the annual meeting of the Society for Immunotherapy of Cancer. CMP-001 activates tumor-associated plasmacytoid dendritic cells and induces systemic tumor-specific CD8+ T-cell responses.
Dr. Kirkwood and associates are investigating CMP-001, given alone or in combination with pembrolizumab, in a phase 1 trial (NCT02680184) of patients with metastatic or unresectable melanoma who are refractory to anti–PD-1 therapy.
Data were presented on 144 patients who received CMP-001 in combination with pembrolizumab. About 40% of patients (39.6%) had elevated lactate dehydrogenase at baseline, and 32.6% had BRAF mutations.
All patients had received prior anti–PD-1 therapy alone (75%) and/or in combination (50%). For most patients (93.1%), their last response to anti–PD-1 therapy was progression.
For this study, the patients received intratumoral CMP-001 injections at a range of doses (1 mg, 3 mg, 5 mg, 7.5 mg, and 10 mg). CMP-001 was given weekly for either 2 weeks or 7 weeks, then every 3 weeks until discontinuation. There were two different formulations of CMP-001 given – 0.01% polysorbate 20 (PS20; n = 83) and 0.00167% PS20 (n = 61).
Safety
“CMP-001 in combination with pembrolizumab is very well tolerated, with no apparent increase in autoimmune toxicities associated with anti–PD-1,” Dr. Kirkwood said.
The most common treatment-related adverse events were flulike symptoms, including chills (72%), pyrexia (56%), fatigue (51%), nausea (45%), vomiting (29%), and headache (28%). Another common event was injection-site pain (28%).
The most common grade 3 adverse events were hypotension (n = 9) and hypertension (n = 7). Grade 4 events included hypotension, aspartate aminotransferase increase, and alanine aminotransferase increase (n = 1 for all). There were no grade 5 events.
Six patients discontinued treatment because of adverse events.
Response
The overall response rate was 25% (21/83) among patients who received the 0.01% PS20 formulation of CMP-001 and 11.5% (7/61) among patients who received the 0.00167% PS20 formulation.
Responses were similar in injected and noninjected target lesions. The median duration of response has not been reached at a median follow-up of 16.9 months.
“Intratumoral CMP-001 reverses resistance to anti–PD-1 in patients who have progressed on prior anti–PD-1 therapy,” Dr. Kirkwood said, adding that these data support further clinical development of CMP-001.
The research is sponsored by Checkmate Pharmaceuticals. Dr. Kirkwood disclosed relationships with Amgen, BMS, Immunocore, Iovance, Novartis, Elsevier, Castle, Merck, and Checkmate.
SOURCE: Kirkwood J et al. SITC 2019, Abstract O85.
REPORTING FROM SITC 2019
Veterans at higher risk of sleep behavior disorders
Veterans may be at higher risk of idiopathic rapid eye movement sleep behavior disorders, particularly if they have traumatic brain injury (TBI) or posttraumatic stress disorder (PTSD) according to a paper published in Sleep.

In a prospective, cross-sectional study, researchers recruited 394 veterans – 94% of whom were male – who underwent in-lab video-polysomnography and questionnaires about REM sleep behavior disorder (RBD), as well as assessment of their trauma status and medical history.
Overall, 9% of subjects had RBD, a figure considerably higher than has been estimated in the general population (prevalence of 0.38%-1.0%). Seven percent had REM sleep without atonia, 31% had other parasomnias such as a history of dream enactment behavior, and 53% were classified as normal.
The majority of subjects determined to have RBD (n = 34) had either PTSD or comorbid TBI+PTSD (n = 19, 56%). The combined overall crude prevalence of RBD in subjects with either PTSD alone or TBI+PTSD was 16.8% (n = 19 out of 113).
The individuals with PTSD had a 2.81-fold greater odds of RBD and 3.13-fold greater odds of other parasomnias compared with those without PTSD.
Those with both traumatic brain injury and PTSD had 3.43-fold greater odds of RBD and 3.22-fold greater odds of other parasomnias compared with individuals without.
“Interestingly, the neuropathology underpinning PTSD shares common features with RBD, raising the question as to whether or not PTSD has a causal role in the development of RBD, or if a single pathophysiologic process generates two clinical entities,” wrote Jonathan E. Elliott, PhD, of the VA Portland Health Care System, and coauthors.
The researchers also looked for evidence of trauma-associated sleep disorder (TASD), a recently proposed phenomenological sleep disorder whose diagnostic criteria overlaps with REM sleep behavior disorder but includes subjects reporting having an inciting traumatic experience and a history of dreaming related to this experience as well as evidence of autonomic hyperarousal.
The researchers found 22 of the subjects with REM behavior disorder had a traumatic brain injury and/or PTSD, and 9 of these subjects reported evidence of altered dream mentation related to that prior traumatic experience. However, none showed evidence of autonomic nervous system hyperarousal that coincided with abnormal REM sleep activity.
The investigators noted that although the sample of 394 subjects with in-lab video-polysomnography is large, the study is underpowered to draw broader conclusions about prevalence of RBD among veterans. In addition, the study did not establish whether or not trauma exposure preceded, and contributed to, the development of parasomnias and this question should be pursued in further studies.
“Given the purported relationships between TBI, PTSD, RBD, and neurodegeneration, we sought to determine the crude prevalence and related associations of RBD following TBI and PTSD among veterans. Our data show that the prevalence of RBD and related parasomnias is significantly higher in veterans with PTSD and TBI+PTSD compared to veterans without a history of neuropsychiatric trauma,” the authors wrote.
No funding or conflicts of interest were declared.
SOURCE: Elliott JE et al. Sleep 2019 Oct 7. doi: 10.1093/sleep/zsz237.
Veterans may be at higher risk of idiopathic rapid eye movement sleep behavior disorders, particularly if they have traumatic brain injury (TBI) or posttraumatic stress disorder (PTSD) according to a paper published in Sleep.
In a prospective, cross-sectional study, researchers recruited 394 veterans – 94% of whom were male – who underwent in-lab video-polysomnography and questionnaires about REM sleep behavior disorder (RBD), as well as assessment of their trauma status and medical history.
Overall, 9% of subjects had RBD, a figure considerably higher than has been estimated in the general population (prevalence of 0.38%-1.0%). Seven percent had REM sleep without atonia, 31% had other parasomnias such as a history of dream enactment behavior, and 53% were classified as normal.
The majority of subjects determined to have RBD (n = 34) had either PTSD or comorbid TBI+PTSD (n = 19, 56%). The combined overall crude prevalence of RBD in subjects with either PTSD alone or TBI+PTSD was 16.8% (n = 19 out of 113).
The individuals with PTSD had a 2.81-fold greater odds of RBD and 3.13-fold greater odds of other parasomnias compared with those without PTSD.
Those with both traumatic brain injury and PTSD had 3.43-fold greater odds of RBD and 3.22-fold greater odds of other parasomnias compared with individuals without.
“Interestingly, the neuropathology underpinning PTSD shares common features with RBD, raising the question as to whether or not PTSD has a causal role in the development of RBD, or if a single pathophysiologic process generates two clinical entities,” wrote Jonathan E. Elliott, PhD, of the VA Portland Health Care System, and coauthors.
The researchers also looked for evidence of trauma-associated sleep disorder (TASD), a recently proposed phenomenological sleep disorder whose diagnostic criteria overlaps with REM sleep behavior disorder but includes subjects reporting having an inciting traumatic experience and a history of dreaming related to this experience as well as evidence of autonomic hyperarousal.
The researchers found 22 of the subjects with REM behavior disorder had a traumatic brain injury and/or PTSD, and 9 of these subjects reported evidence of altered dream mentation related to that prior traumatic experience. However, none showed evidence of autonomic nervous system hyperarousal that coincided with abnormal REM sleep activity.
The investigators noted that although the sample of 394 subjects with in-lab video-polysomnography is large, the study is underpowered to draw broader conclusions about prevalence of RBD among veterans. In addition, the study did not establish whether or not trauma exposure preceded, and contributed to, the development of parasomnias and this question should be pursued in further studies.
“Given the purported relationships between TBI, PTSD, RBD, and neurodegeneration, we sought to determine the crude prevalence and related associations of RBD following TBI and PTSD among veterans. Our data show that the prevalence of RBD and related parasomnias is significantly higher in veterans with PTSD and TBI+PTSD compared to veterans without a history of neuropsychiatric trauma,” the authors wrote.
No funding or conflicts of interest were declared.
SOURCE: Elliott JE et al. Sleep 2019 Oct 7. doi: 10.1093/sleep/zsz237.
Veterans may be at higher risk of idiopathic rapid eye movement sleep behavior disorders, particularly if they have traumatic brain injury (TBI) or posttraumatic stress disorder (PTSD) according to a paper published in Sleep.
In a prospective, cross-sectional study, researchers recruited 394 veterans – 94% of whom were male – who underwent in-lab video-polysomnography and questionnaires about REM sleep behavior disorder (RBD), as well as assessment of their trauma status and medical history.
Overall, 9% of subjects had RBD, a figure considerably higher than has been estimated in the general population (prevalence of 0.38%-1.0%). Seven percent had REM sleep without atonia, 31% had other parasomnias such as a history of dream enactment behavior, and 53% were classified as normal.
The majority of subjects determined to have RBD (n = 34) had either PTSD or comorbid TBI+PTSD (n = 19, 56%). The combined overall crude prevalence of RBD in subjects with either PTSD alone or TBI+PTSD was 16.8% (n = 19 out of 113).
The individuals with PTSD had a 2.81-fold greater odds of RBD and 3.13-fold greater odds of other parasomnias compared with those without PTSD.
Those with both traumatic brain injury and PTSD had 3.43-fold greater odds of RBD and 3.22-fold greater odds of other parasomnias compared with individuals without.
“Interestingly, the neuropathology underpinning PTSD shares common features with RBD, raising the question as to whether or not PTSD has a causal role in the development of RBD, or if a single pathophysiologic process generates two clinical entities,” wrote Jonathan E. Elliott, PhD, of the VA Portland Health Care System, and coauthors.
The researchers also looked for evidence of trauma-associated sleep disorder (TASD), a recently proposed phenomenological sleep disorder whose diagnostic criteria overlaps with REM sleep behavior disorder but includes subjects reporting having an inciting traumatic experience and a history of dreaming related to this experience as well as evidence of autonomic hyperarousal.
The researchers found 22 of the subjects with REM behavior disorder had a traumatic brain injury and/or PTSD, and 9 of these subjects reported evidence of altered dream mentation related to that prior traumatic experience. However, none showed evidence of autonomic nervous system hyperarousal that coincided with abnormal REM sleep activity.
The investigators noted that although the sample of 394 subjects with in-lab video-polysomnography is large, the study is underpowered to draw broader conclusions about prevalence of RBD among veterans. In addition, the study did not establish whether or not trauma exposure preceded, and contributed to, the development of parasomnias and this question should be pursued in further studies.
“Given the purported relationships between TBI, PTSD, RBD, and neurodegeneration, we sought to determine the crude prevalence and related associations of RBD following TBI and PTSD among veterans. Our data show that the prevalence of RBD and related parasomnias is significantly higher in veterans with PTSD and TBI+PTSD compared to veterans without a history of neuropsychiatric trauma,” the authors wrote.
No funding or conflicts of interest were declared.
SOURCE: Elliott JE et al. Sleep 2019 Oct 7. doi: 10.1093/sleep/zsz237.
FROM SLEEP
Resting-state cerebral blood flow tied to apathy in schizophrenia
Regional resting-state cerebral blood flow (rCBF) in the ventral and dorsal striatum is associated with apathy in patients with schizophrenia – but not with diminished expression, results of a small study suggest.
“This distinction is of high relevance when investigating striatal rCBF,” wrote Karoline Schneider, MD, and colleagues. “The paucity of reported associations beween striatal rCBF and negative symptoms could result from the fact that until now apathy and diminished expression have not been addressed separately.” The study was published in the Journal of Psychiatry & Neuroscience.
Dr. Schneider and colleagues used arterial spin labeling MRI to measure rCBF in 29 patients with schizophrenia from outpatient and inpatient units affiliated with the University of Zürich and in 20 controls without schizophrenia. Negative symptoms were assessed via the Brief Negative Symptom Scale and were divided into those of apathy or those of diminished expression.
, and between severity and higher rCBF in the left and right dorsal striatum (r = 0.48; P = .008). However, the correlations were nonsignificant for symptoms of diminished expression, reported Dr. Schneider, of the university’s department of psychiatry, psychotherapy, and psychosomatics.
“The association between increased striatal rCBF and the negative symptom dimension of apathy, but not diminished expression, provides further evidence for the assumption of different underlying neural bases,” Dr. Schneider and colleagues concluded. “These dimensions should be considered separately in future research on negative symptoms.”
Limitations of the study include its sample size. Another limitation is that all patients with schizophrenia in the study were taking second-generation antipsychotics, which in some research appears to influence striatal rCBF.
Grants from the Swiss National Science Foundation funded the study. Dr. Schneider reported no conflicts of interest. Two authors disclosed receiving grant support or honoraria from pharmaceutical companies but said those activities were unrelated to this study.
SOURCE: Schneider K et al. J Psychiatry Neurosci. 2019;44(2):102-10.
Regional resting-state cerebral blood flow (rCBF) in the ventral and dorsal striatum is associated with apathy in patients with schizophrenia – but not with diminished expression, results of a small study suggest.
“This distinction is of high relevance when investigating striatal rCBF,” wrote Karoline Schneider, MD, and colleagues. “The paucity of reported associations beween striatal rCBF and negative symptoms could result from the fact that until now apathy and diminished expression have not been addressed separately.” The study was published in the Journal of Psychiatry & Neuroscience.
Dr. Schneider and colleagues used arterial spin labeling MRI to measure rCBF in 29 patients with schizophrenia from outpatient and inpatient units affiliated with the University of Zürich and in 20 controls without schizophrenia. Negative symptoms were assessed via the Brief Negative Symptom Scale and were divided into those of apathy or those of diminished expression.
, and between severity and higher rCBF in the left and right dorsal striatum (r = 0.48; P = .008). However, the correlations were nonsignificant for symptoms of diminished expression, reported Dr. Schneider, of the university’s department of psychiatry, psychotherapy, and psychosomatics.
“The association between increased striatal rCBF and the negative symptom dimension of apathy, but not diminished expression, provides further evidence for the assumption of different underlying neural bases,” Dr. Schneider and colleagues concluded. “These dimensions should be considered separately in future research on negative symptoms.”
Limitations of the study include its sample size. Another limitation is that all patients with schizophrenia in the study were taking second-generation antipsychotics, which in some research appears to influence striatal rCBF.
Grants from the Swiss National Science Foundation funded the study. Dr. Schneider reported no conflicts of interest. Two authors disclosed receiving grant support or honoraria from pharmaceutical companies but said those activities were unrelated to this study.
SOURCE: Schneider K et al. J Psychiatry Neurosci. 2019;44(2):102-10.
Regional resting-state cerebral blood flow (rCBF) in the ventral and dorsal striatum is associated with apathy in patients with schizophrenia – but not with diminished expression, results of a small study suggest.
“This distinction is of high relevance when investigating striatal rCBF,” wrote Karoline Schneider, MD, and colleagues. “The paucity of reported associations beween striatal rCBF and negative symptoms could result from the fact that until now apathy and diminished expression have not been addressed separately.” The study was published in the Journal of Psychiatry & Neuroscience.
Dr. Schneider and colleagues used arterial spin labeling MRI to measure rCBF in 29 patients with schizophrenia from outpatient and inpatient units affiliated with the University of Zürich and in 20 controls without schizophrenia. Negative symptoms were assessed via the Brief Negative Symptom Scale and were divided into those of apathy or those of diminished expression.
, and between severity and higher rCBF in the left and right dorsal striatum (r = 0.48; P = .008). However, the correlations were nonsignificant for symptoms of diminished expression, reported Dr. Schneider, of the university’s department of psychiatry, psychotherapy, and psychosomatics.
“The association between increased striatal rCBF and the negative symptom dimension of apathy, but not diminished expression, provides further evidence for the assumption of different underlying neural bases,” Dr. Schneider and colleagues concluded. “These dimensions should be considered separately in future research on negative symptoms.”
Limitations of the study include its sample size. Another limitation is that all patients with schizophrenia in the study were taking second-generation antipsychotics, which in some research appears to influence striatal rCBF.
Grants from the Swiss National Science Foundation funded the study. Dr. Schneider reported no conflicts of interest. Two authors disclosed receiving grant support or honoraria from pharmaceutical companies but said those activities were unrelated to this study.
SOURCE: Schneider K et al. J Psychiatry Neurosci. 2019;44(2):102-10.
FROM THE JOURNAL OF PSYCHIATRY & NEUROSCIENCE