User login
Radioactive iodine can be first-line for hyperthyroidism, says UK
New UK guidelines for the treatment of hyperthyroidism, including Graves’ disease, place heavier emphasis on the use of radioactive iodine as the frontline treatment for patients unlikely to remain remission-free on the medications, as opposed to the alternative of antithyroid medications as a first choice.
senior author Kristien Boelaert, MD, PhD, who led the guideline committee, said in an interview.
“Recommending the use of radioactive iodine as first-line treatment for adults with Graves’ disease is a change to current practice and should reduce the variation between centers as to when radioactive iodine is considered appropriate,” the guidelines further state.
The new recommendations on hyperthyroidism are part of broader guidelines on thyroid disease by the UK National Institute for Health and Care Excellence (NICE), which concludes that radioactive iodine results in cure in as many as 90% of hyperthyroidism cases.
The recommendations were published in a guideline summary in BMJ by research fellow Melina Vasileiou of the National Guideline Centre, Royal College of Physicians, London, and colleagues.
Current guidelines in the United Kingdom and Europe typically call for radioactive iodine to be reserved for use as a definitive treatment only after relapse following antithyroid medication treatment. The latest European Thyroid Association guidelines were published in 2018.
Elsewhere guidelines vary, with many, including those by the American Thyroid Association (ATA) – the most recent published in 2016 – generally calling for treatment with either antithyroid medications, radioactive iodine, or total thyroidectomy, in the absence of any contraindications to each treatment option.
“The U.S. tends to use more radioactive iodine, while Europe, Latin America, and Japan lean more toward (perhaps longer) use of antithyroid medications,” Angela Leung, MD, associate clinical professor of medicine in the division of endocrinology, diabetes, and metabolism, department of medicine, University of California, Los Angeles, said in an interview.
“Preferences of deciding which treatment option, which may involve more than one option if antithyroid medications are used initially, depend on a variety of factors related to patient desire, comorbidities, and availability of the therapy,” she explained.
Concerns including worsening thyroid eye disease, cardiovascular disease, and development of secondary cancers have caused some hesitation in the use of frontline radioiodine therapy.
And one notably controversial article, published last year, suggested a link between radioactive iodine therapy and an increased risk of cancer mortality. However, as reported by Medscape Medical News, the article spurred debate, with the Society for Endocrinology and British Thyroid Association issuing a joint statement urging caution in interpretation of the findings.
Evidence supporting first-line radioactive iodine
Patients treated with radioactive iodine take a single tablet that contains iodine and a low dose of radiation, which is absorbed by the thyroid. After taking the treatment patients are advised to avoid prolonged close contact with children and pregnant women for a few days or weeks and to avoid getting pregnant or fathering a child for several months. The treatment is likely to lead to an underactive thyroid gland that will require ongoing treatment with thyroid hormone replacement.
In providing evidence in favor of the benefits of radioactive iodine over the risks, the new NICE guidelines cite five randomized controlled trials of people with hyperthyroid disease, which, though defined as “low quality” evidence, collectively indicate that long-term outcomes were improved with radioactive iodine treatment compared with antithyroid drugs – despite the former having a higher risk of thyroid eye disease (also known as Graves’ ophthalmopathy).
In addition, eight nonrandomized studies show no evidence of a clinically important increase in cancer diagnoses or deaths between people treated with radioactive iodine or surgery, or between people treated with radioactive iodine and healthy controls, the guideline committee notes.
“The strongest arguments (in favor of radioactive iodine as a first-line therapy) were the likelihood of inducing remission of Graves’ disease with radioactive iodine, the finding that radioiodine is a safe treatment (confirmed in the safety review undertaken by NICE), and the reduction in the need for patients to remain on antithyroid drugs, which may have significant side effects and treatment which usually requires repeated hospital visits or follow-up under a hospital service,” said Dr. Boelaert.
The new guideline does recommend that antithyroid medication is acceptable as the first-line treatment among patients considered likely to achieve remission.
Dr. Leung explains that the percentage of patients with Graves’ disease who can achieve remission with antithyroid drugs ranges from 30% to 50%. She noted some evidence does suggest the long-term use of the drugs may be acceptable.
“There are some data that ... report the relative safety of long-term use of antithyroid drugs (beyond 24 months) for both Graves’ disease and autonomous thyroid nodules,” Dr. Leung elaborated.
Pregnancy concerns and cost-effectiveness of radioactive iodine
Radioactive iodine therapy is meanwhile not suitable if malignancy is suspected, if the patient is pregnant or trying to become pregnant, or if the patient has active thyroid eye disease, the experts agree.
Dr. Leung noted that although “it is generally advised to not treat Graves’ disease with radioiodine if there is concurrent thyroid eye disease, steroids are a proven effective therapy to decrease this risk in select patients.”
And among pregnant patients, “antithyroid medications should be minimally used in the lowest possible doses,” Dr. Leung said, although she added that, despite their potential risks, the drugs “represent a viable option” for this patient population.
“Also, many would actually advocate for total thyroidectomy in women who are thinking of pregnancy in the near future,” she noted.
Another factor of relevance in the guideline recommendations – cost – also favors radioactive iodine, the committee noted.
“Economic evidence showed that radioactive iodine was the most cost-effective intervention,” the committee pointed out.
Trabs advised for determination of hyperthyroidism cause
The new U.K. guidelines further underscore the importance of establishing the underlying cause of hyperthyroidism to ensure appropriate treatment, and the preferred method for doing so is the measurement of thyroid-stimulating hormone receptor antibodies (TRAbs).
“It is important to identify the underlying cause of thyrotoxicosis through measurement of TRAbs, or radioisotope scanning, in order to distinguish hyperthyroidism from transient causes of thyrotoxicosis such as transient thyroiditis, which only requires supportive treatment,” explained Dr. Boelaert, consultant endocrinologist and director of the National Institute for Health Research Integrated Academic Training Program at the Institute of Applied Health Research, University of Birmingham (England).
“In addition, this will help distinguish Graves’ disease from toxic nodular hyperthyroidism, which is important as antithyroid drugs are not effective in inducing a cure in the latter,” she explained.
Meanwhile, the new guidelines further note that although use of diagnostic ultrasound is informative when palpation suggests thyroid nodules, it is of limited diagnostic value for Graves’ disease.
“The recommendation (suggests that) thyroid ultrasonography should only be offered if there is a palpable thyroid nodule,” Dr. Boelaert noted.
She concluded: “There has been uncertainty in the U.K. about the best treatment for hyperthyroidism despite radioactive iodine being the most common first-line treatment for this condition in the United States. We are very pleased to have been able to work with NICE to provide clear new guidance which we hope will improve outcomes for patients with this condition.”
The National Guideline Centre was commissioned and funded by NICE to develop the guideline. No authors received specific funding to write the summary. Dr. Boelaert has reported no relevant financial relationships. Disclosures for the other authors are listed in the article.
This article first appeared on Medscape.com.
New UK guidelines for the treatment of hyperthyroidism, including Graves’ disease, place heavier emphasis on the use of radioactive iodine as the frontline treatment for patients unlikely to remain remission-free on the medications, as opposed to the alternative of antithyroid medications as a first choice.
senior author Kristien Boelaert, MD, PhD, who led the guideline committee, said in an interview.
“Recommending the use of radioactive iodine as first-line treatment for adults with Graves’ disease is a change to current practice and should reduce the variation between centers as to when radioactive iodine is considered appropriate,” the guidelines further state.
The new recommendations on hyperthyroidism are part of broader guidelines on thyroid disease by the UK National Institute for Health and Care Excellence (NICE), which concludes that radioactive iodine results in cure in as many as 90% of hyperthyroidism cases.
The recommendations were published in a guideline summary in BMJ by research fellow Melina Vasileiou of the National Guideline Centre, Royal College of Physicians, London, and colleagues.
Current guidelines in the United Kingdom and Europe typically call for radioactive iodine to be reserved for use as a definitive treatment only after relapse following antithyroid medication treatment. The latest European Thyroid Association guidelines were published in 2018.
Elsewhere guidelines vary, with many, including those by the American Thyroid Association (ATA) – the most recent published in 2016 – generally calling for treatment with either antithyroid medications, radioactive iodine, or total thyroidectomy, in the absence of any contraindications to each treatment option.
“The U.S. tends to use more radioactive iodine, while Europe, Latin America, and Japan lean more toward (perhaps longer) use of antithyroid medications,” Angela Leung, MD, associate clinical professor of medicine in the division of endocrinology, diabetes, and metabolism, department of medicine, University of California, Los Angeles, said in an interview.
“Preferences of deciding which treatment option, which may involve more than one option if antithyroid medications are used initially, depend on a variety of factors related to patient desire, comorbidities, and availability of the therapy,” she explained.
Concerns including worsening thyroid eye disease, cardiovascular disease, and development of secondary cancers have caused some hesitation in the use of frontline radioiodine therapy.
And one notably controversial article, published last year, suggested a link between radioactive iodine therapy and an increased risk of cancer mortality. However, as reported by Medscape Medical News, the article spurred debate, with the Society for Endocrinology and British Thyroid Association issuing a joint statement urging caution in interpretation of the findings.
Evidence supporting first-line radioactive iodine
Patients treated with radioactive iodine take a single tablet that contains iodine and a low dose of radiation, which is absorbed by the thyroid. After taking the treatment patients are advised to avoid prolonged close contact with children and pregnant women for a few days or weeks and to avoid getting pregnant or fathering a child for several months. The treatment is likely to lead to an underactive thyroid gland that will require ongoing treatment with thyroid hormone replacement.
In providing evidence in favor of the benefits of radioactive iodine over the risks, the new NICE guidelines cite five randomized controlled trials of people with hyperthyroid disease, which, though defined as “low quality” evidence, collectively indicate that long-term outcomes were improved with radioactive iodine treatment compared with antithyroid drugs – despite the former having a higher risk of thyroid eye disease (also known as Graves’ ophthalmopathy).
In addition, eight nonrandomized studies show no evidence of a clinically important increase in cancer diagnoses or deaths between people treated with radioactive iodine or surgery, or between people treated with radioactive iodine and healthy controls, the guideline committee notes.
“The strongest arguments (in favor of radioactive iodine as a first-line therapy) were the likelihood of inducing remission of Graves’ disease with radioactive iodine, the finding that radioiodine is a safe treatment (confirmed in the safety review undertaken by NICE), and the reduction in the need for patients to remain on antithyroid drugs, which may have significant side effects and treatment which usually requires repeated hospital visits or follow-up under a hospital service,” said Dr. Boelaert.
The new guideline does recommend that antithyroid medication is acceptable as the first-line treatment among patients considered likely to achieve remission.
Dr. Leung explains that the percentage of patients with Graves’ disease who can achieve remission with antithyroid drugs ranges from 30% to 50%. She noted some evidence does suggest the long-term use of the drugs may be acceptable.
“There are some data that ... report the relative safety of long-term use of antithyroid drugs (beyond 24 months) for both Graves’ disease and autonomous thyroid nodules,” Dr. Leung elaborated.
Pregnancy concerns and cost-effectiveness of radioactive iodine
Radioactive iodine therapy is meanwhile not suitable if malignancy is suspected, if the patient is pregnant or trying to become pregnant, or if the patient has active thyroid eye disease, the experts agree.
Dr. Leung noted that although “it is generally advised to not treat Graves’ disease with radioiodine if there is concurrent thyroid eye disease, steroids are a proven effective therapy to decrease this risk in select patients.”
And among pregnant patients, “antithyroid medications should be minimally used in the lowest possible doses,” Dr. Leung said, although she added that, despite their potential risks, the drugs “represent a viable option” for this patient population.
“Also, many would actually advocate for total thyroidectomy in women who are thinking of pregnancy in the near future,” she noted.
Another factor of relevance in the guideline recommendations – cost – also favors radioactive iodine, the committee noted.
“Economic evidence showed that radioactive iodine was the most cost-effective intervention,” the committee pointed out.
Trabs advised for determination of hyperthyroidism cause
The new U.K. guidelines further underscore the importance of establishing the underlying cause of hyperthyroidism to ensure appropriate treatment, and the preferred method for doing so is the measurement of thyroid-stimulating hormone receptor antibodies (TRAbs).
“It is important to identify the underlying cause of thyrotoxicosis through measurement of TRAbs, or radioisotope scanning, in order to distinguish hyperthyroidism from transient causes of thyrotoxicosis such as transient thyroiditis, which only requires supportive treatment,” explained Dr. Boelaert, consultant endocrinologist and director of the National Institute for Health Research Integrated Academic Training Program at the Institute of Applied Health Research, University of Birmingham (England).
“In addition, this will help distinguish Graves’ disease from toxic nodular hyperthyroidism, which is important as antithyroid drugs are not effective in inducing a cure in the latter,” she explained.
Meanwhile, the new guidelines further note that although use of diagnostic ultrasound is informative when palpation suggests thyroid nodules, it is of limited diagnostic value for Graves’ disease.
“The recommendation (suggests that) thyroid ultrasonography should only be offered if there is a palpable thyroid nodule,” Dr. Boelaert noted.
She concluded: “There has been uncertainty in the U.K. about the best treatment for hyperthyroidism despite radioactive iodine being the most common first-line treatment for this condition in the United States. We are very pleased to have been able to work with NICE to provide clear new guidance which we hope will improve outcomes for patients with this condition.”
The National Guideline Centre was commissioned and funded by NICE to develop the guideline. No authors received specific funding to write the summary. Dr. Boelaert has reported no relevant financial relationships. Disclosures for the other authors are listed in the article.
This article first appeared on Medscape.com.
New UK guidelines for the treatment of hyperthyroidism, including Graves’ disease, place heavier emphasis on the use of radioactive iodine as the frontline treatment for patients unlikely to remain remission-free on the medications, as opposed to the alternative of antithyroid medications as a first choice.
senior author Kristien Boelaert, MD, PhD, who led the guideline committee, said in an interview.
“Recommending the use of radioactive iodine as first-line treatment for adults with Graves’ disease is a change to current practice and should reduce the variation between centers as to when radioactive iodine is considered appropriate,” the guidelines further state.
The new recommendations on hyperthyroidism are part of broader guidelines on thyroid disease by the UK National Institute for Health and Care Excellence (NICE), which concludes that radioactive iodine results in cure in as many as 90% of hyperthyroidism cases.
The recommendations were published in a guideline summary in BMJ by research fellow Melina Vasileiou of the National Guideline Centre, Royal College of Physicians, London, and colleagues.
Current guidelines in the United Kingdom and Europe typically call for radioactive iodine to be reserved for use as a definitive treatment only after relapse following antithyroid medication treatment. The latest European Thyroid Association guidelines were published in 2018.
Elsewhere guidelines vary, with many, including those by the American Thyroid Association (ATA) – the most recent published in 2016 – generally calling for treatment with either antithyroid medications, radioactive iodine, or total thyroidectomy, in the absence of any contraindications to each treatment option.
“The U.S. tends to use more radioactive iodine, while Europe, Latin America, and Japan lean more toward (perhaps longer) use of antithyroid medications,” Angela Leung, MD, associate clinical professor of medicine in the division of endocrinology, diabetes, and metabolism, department of medicine, University of California, Los Angeles, said in an interview.
“Preferences of deciding which treatment option, which may involve more than one option if antithyroid medications are used initially, depend on a variety of factors related to patient desire, comorbidities, and availability of the therapy,” she explained.
Concerns including worsening thyroid eye disease, cardiovascular disease, and development of secondary cancers have caused some hesitation in the use of frontline radioiodine therapy.
And one notably controversial article, published last year, suggested a link between radioactive iodine therapy and an increased risk of cancer mortality. However, as reported by Medscape Medical News, the article spurred debate, with the Society for Endocrinology and British Thyroid Association issuing a joint statement urging caution in interpretation of the findings.
Evidence supporting first-line radioactive iodine
Patients treated with radioactive iodine take a single tablet that contains iodine and a low dose of radiation, which is absorbed by the thyroid. After taking the treatment patients are advised to avoid prolonged close contact with children and pregnant women for a few days or weeks and to avoid getting pregnant or fathering a child for several months. The treatment is likely to lead to an underactive thyroid gland that will require ongoing treatment with thyroid hormone replacement.
In providing evidence in favor of the benefits of radioactive iodine over the risks, the new NICE guidelines cite five randomized controlled trials of people with hyperthyroid disease, which, though defined as “low quality” evidence, collectively indicate that long-term outcomes were improved with radioactive iodine treatment compared with antithyroid drugs – despite the former having a higher risk of thyroid eye disease (also known as Graves’ ophthalmopathy).
In addition, eight nonrandomized studies show no evidence of a clinically important increase in cancer diagnoses or deaths between people treated with radioactive iodine or surgery, or between people treated with radioactive iodine and healthy controls, the guideline committee notes.
“The strongest arguments (in favor of radioactive iodine as a first-line therapy) were the likelihood of inducing remission of Graves’ disease with radioactive iodine, the finding that radioiodine is a safe treatment (confirmed in the safety review undertaken by NICE), and the reduction in the need for patients to remain on antithyroid drugs, which may have significant side effects and treatment which usually requires repeated hospital visits or follow-up under a hospital service,” said Dr. Boelaert.
The new guideline does recommend that antithyroid medication is acceptable as the first-line treatment among patients considered likely to achieve remission.
Dr. Leung explains that the percentage of patients with Graves’ disease who can achieve remission with antithyroid drugs ranges from 30% to 50%. She noted some evidence does suggest the long-term use of the drugs may be acceptable.
“There are some data that ... report the relative safety of long-term use of antithyroid drugs (beyond 24 months) for both Graves’ disease and autonomous thyroid nodules,” Dr. Leung elaborated.
Pregnancy concerns and cost-effectiveness of radioactive iodine
Radioactive iodine therapy is meanwhile not suitable if malignancy is suspected, if the patient is pregnant or trying to become pregnant, or if the patient has active thyroid eye disease, the experts agree.
Dr. Leung noted that although “it is generally advised to not treat Graves’ disease with radioiodine if there is concurrent thyroid eye disease, steroids are a proven effective therapy to decrease this risk in select patients.”
And among pregnant patients, “antithyroid medications should be minimally used in the lowest possible doses,” Dr. Leung said, although she added that, despite their potential risks, the drugs “represent a viable option” for this patient population.
“Also, many would actually advocate for total thyroidectomy in women who are thinking of pregnancy in the near future,” she noted.
Another factor of relevance in the guideline recommendations – cost – also favors radioactive iodine, the committee noted.
“Economic evidence showed that radioactive iodine was the most cost-effective intervention,” the committee pointed out.
Trabs advised for determination of hyperthyroidism cause
The new U.K. guidelines further underscore the importance of establishing the underlying cause of hyperthyroidism to ensure appropriate treatment, and the preferred method for doing so is the measurement of thyroid-stimulating hormone receptor antibodies (TRAbs).
“It is important to identify the underlying cause of thyrotoxicosis through measurement of TRAbs, or radioisotope scanning, in order to distinguish hyperthyroidism from transient causes of thyrotoxicosis such as transient thyroiditis, which only requires supportive treatment,” explained Dr. Boelaert, consultant endocrinologist and director of the National Institute for Health Research Integrated Academic Training Program at the Institute of Applied Health Research, University of Birmingham (England).
“In addition, this will help distinguish Graves’ disease from toxic nodular hyperthyroidism, which is important as antithyroid drugs are not effective in inducing a cure in the latter,” she explained.
Meanwhile, the new guidelines further note that although use of diagnostic ultrasound is informative when palpation suggests thyroid nodules, it is of limited diagnostic value for Graves’ disease.
“The recommendation (suggests that) thyroid ultrasonography should only be offered if there is a palpable thyroid nodule,” Dr. Boelaert noted.
She concluded: “There has been uncertainty in the U.K. about the best treatment for hyperthyroidism despite radioactive iodine being the most common first-line treatment for this condition in the United States. We are very pleased to have been able to work with NICE to provide clear new guidance which we hope will improve outcomes for patients with this condition.”
The National Guideline Centre was commissioned and funded by NICE to develop the guideline. No authors received specific funding to write the summary. Dr. Boelaert has reported no relevant financial relationships. Disclosures for the other authors are listed in the article.
This article first appeared on Medscape.com.
Consider allergic contact dermatitis in children with AD with disease flares, new rash
ORLANDO – Do you have ? Consider patch testing to assess whether they have allergic contact dermatitis.

“Of the patients who are sent to me by local pediatric dermatologists, 50% of them are positive” for allergens, said Jonathan H. Zippin, MD, PhD, director of the contact, occupational, and photodermatitis service at Cornell University, New York.
Speaking at the ODAC Dermatology, Aesthetic, and Surgical Conference, Dr. Zippin noted the prevalence of allergen sensitization is between 13% and 25% among children who are asymptomatic, while the prevalence of sensitization to at least one allergen among children with suspected allergic contact dermatitis (ACD) is between 25% and 96%. In 2014, a study from the National American Contact Dermatitis Group (NACDG) showed that of 883 children who were patch tested, 56.7% had at least one relevant positive patch test (RPPT) result.
“The take-home message here is that pediatric contact dermatitis is common, much more common than a lot of people realize,” Dr. Zippin said.
He described three common scenarios to keep in mind: a worsening rash, a new rash, and failure of a rash to improve after the patient avoids all of his or her positive allergens.
When a rash worsens, patch testing is likely to offer answers. In an analysis of 1,142 patients with suspected ACD aged 18 years or younger (mean age, 10.5 years; 64% female) in the Pediatric Contact Dermatitis Registry study database, 65% had at least one positive patch test, and 48% had at least 1 RPPT (Dermatitis 2016; 27[5] 293-302).
But not all patch testing is the same: The study also found that 24% of the RPPT cases would have been missed if assessed with the T.R.U.E. TEST compared with extended patch testing. If a T.R.U.E. TEST fails to explain generalized atopic dermatitis, the patient should be sent for more comprehensive testing where available, Dr. Zippin advised.
Pediatric patients also have unique allergens clinicians should consider. In the same study, children had a number of allergens similar to those of adults as reported in previous studies, such as nickel, cobalt, and neomycin. However, propylene glycol and cocamidopropyl betaine were allergens identified as unique to the pediatric population.
Another study looking at the same group of patients found that compared with children who did not have AD, children with AD had 7.4 times higher odds of having an RPPT to cocamidopropyl betaine, 7.6 times higher odds of having an RPPT to parthenolide, 5.3 times higher odds of having an RPPT to tixocortol pivalate, 4.2 times higher odds of having an RPPT to wool alcohols, and 4 times higher odds of having an RPPT to lanolin (JAMA Dermatology 2017;153[8]:765-70).
All of these are components of topical medicaments used to treat AD, “either components of emollients that we recommend, or components of steroids that we recommend,” Dr. Zippin pointed out.
One of these allergens could be the culprit when a child develops a new rash but there are no new apparent changes in products, exposures, and activities. Lanolin, also called wool grease, is used in many skin care products, for example. Dr. Zippin described the case of a 6-year-old girl with a history of AD, who presented with a new rash on her scalp and behind her ears, not explained by any obvious changes to products, exposures, or activities. Subsequent patch testing determined that the rash was caused by baby shampoo, which contained cocamidopropyl betaine, which is used in hypoallergenic products. The rash resolved after a different shampoo was used.
“Sometimes, we really have to be thinking when the rash is getting worse, is there something they’re being exposed to that might be an allergen?” Dr. Zippin said.
In patients who have avoided all their positive allergens but a rash has not improved, clinicians should consider systemic contact dermatitis (SCD). Patients can develop SCD through different types of exposures, including transepidermal, transmucosal, oral, intravenous, subcutaneous, intramuscular, inhalation, and implantation routes.
SCD also has a variety of presentations, including pompholyx/dyshidrosis/vesicular dermatitis, maculopapular eruption, chronic pruritus, exfoliative erythroderma/toxiderma, chronic urticaria, erythema multiforme and vasculitis, hyperkeratotic papules of the elbows, acute generalized exanthematous pustulosis, and pruritus ani, according to Dr. Zippin.
SCD should be considered when a patient has a positive patch test to an allergen that is known to cause SCD, and does not clear after avoiding cutaneous exposure to the allergen, Dr. Zippin advised.
Patients will most often develop SCD from plants and herbs, Dr. Zippin noted. Chrysanthemums and chamomile tea are common culprits for compositae allergy and can trigger SCD; other causes are Anacardiaceae, Balsam of Peru, and propolis. Metals (nickel, cobalt, gold, and chromium), medications (aminoglycosides, corticosteroids, and ethylenediamine), and other sources (formaldehyde, propylene glycol in frozen foods, gallates, and methylisothiazolinone) can cause SCD as well.
Methylisothiazolinone in particular is a very common sensitizer, Dr. Zippin said. “If you have a patient who is positive to this, it’s almost always the cause of their problem.”
Balsam of Peru is in a number of different foods, and patients who need to follow a diet free of Balsam of Peru should avoid a long list of foods including citrus; bakery goods; Danish pastry; candy; gum; spices such as cinnamon, cloves, vanilla, curry, allspice, anise, and ginger; spicy condiments such as ketchup, chili sauce, barbecue sauce; chili, pizza, and foods with red sauces; tomatoes; pickles; alcohol (wine, beer, gin, vermouth); tea (perfumed or flavored); tobacco; chocolate and ice cream; and soft drinks (cola or spiced soft drinks).
Patients starting a nickel-free diet should avoid soy, peanuts and other nuts, legumes, chocolate, cocoa, oats, fish, and whole wheat flours. Any elimination diet should last for 3 months but should at least be tried for 3-4 weeks, with gradual reintroduction of foods suspected as triggers once per week. Any type I allergies that are discovered or suspected can be referred to an allergist for allergen challenge and desensitization therapy.
For more information, Dr. Zippin recommended the American Contact Dermatitis Society website for more information.
Dr. Zippin reported that he is the founder and holds stock options at CEP Biotech; is on the medical advisory board and receives stock options from YouV Labs., is a paid consultant and performs industry-sponsored research for Pfizer, receives stock options from Regeneron, and is on the medical advisory board for Hoth Therapeutics Inc. He is on the board of directors for the American Contact Dermatitis Society.
ORLANDO – Do you have ? Consider patch testing to assess whether they have allergic contact dermatitis.
“Of the patients who are sent to me by local pediatric dermatologists, 50% of them are positive” for allergens, said Jonathan H. Zippin, MD, PhD, director of the contact, occupational, and photodermatitis service at Cornell University, New York.
Speaking at the ODAC Dermatology, Aesthetic, and Surgical Conference, Dr. Zippin noted the prevalence of allergen sensitization is between 13% and 25% among children who are asymptomatic, while the prevalence of sensitization to at least one allergen among children with suspected allergic contact dermatitis (ACD) is between 25% and 96%. In 2014, a study from the National American Contact Dermatitis Group (NACDG) showed that of 883 children who were patch tested, 56.7% had at least one relevant positive patch test (RPPT) result.
“The take-home message here is that pediatric contact dermatitis is common, much more common than a lot of people realize,” Dr. Zippin said.
He described three common scenarios to keep in mind: a worsening rash, a new rash, and failure of a rash to improve after the patient avoids all of his or her positive allergens.
When a rash worsens, patch testing is likely to offer answers. In an analysis of 1,142 patients with suspected ACD aged 18 years or younger (mean age, 10.5 years; 64% female) in the Pediatric Contact Dermatitis Registry study database, 65% had at least one positive patch test, and 48% had at least 1 RPPT (Dermatitis 2016; 27[5] 293-302).
But not all patch testing is the same: The study also found that 24% of the RPPT cases would have been missed if assessed with the T.R.U.E. TEST compared with extended patch testing. If a T.R.U.E. TEST fails to explain generalized atopic dermatitis, the patient should be sent for more comprehensive testing where available, Dr. Zippin advised.
Pediatric patients also have unique allergens clinicians should consider. In the same study, children had a number of allergens similar to those of adults as reported in previous studies, such as nickel, cobalt, and neomycin. However, propylene glycol and cocamidopropyl betaine were allergens identified as unique to the pediatric population.
Another study looking at the same group of patients found that compared with children who did not have AD, children with AD had 7.4 times higher odds of having an RPPT to cocamidopropyl betaine, 7.6 times higher odds of having an RPPT to parthenolide, 5.3 times higher odds of having an RPPT to tixocortol pivalate, 4.2 times higher odds of having an RPPT to wool alcohols, and 4 times higher odds of having an RPPT to lanolin (JAMA Dermatology 2017;153[8]:765-70).
All of these are components of topical medicaments used to treat AD, “either components of emollients that we recommend, or components of steroids that we recommend,” Dr. Zippin pointed out.
One of these allergens could be the culprit when a child develops a new rash but there are no new apparent changes in products, exposures, and activities. Lanolin, also called wool grease, is used in many skin care products, for example. Dr. Zippin described the case of a 6-year-old girl with a history of AD, who presented with a new rash on her scalp and behind her ears, not explained by any obvious changes to products, exposures, or activities. Subsequent patch testing determined that the rash was caused by baby shampoo, which contained cocamidopropyl betaine, which is used in hypoallergenic products. The rash resolved after a different shampoo was used.
“Sometimes, we really have to be thinking when the rash is getting worse, is there something they’re being exposed to that might be an allergen?” Dr. Zippin said.
In patients who have avoided all their positive allergens but a rash has not improved, clinicians should consider systemic contact dermatitis (SCD). Patients can develop SCD through different types of exposures, including transepidermal, transmucosal, oral, intravenous, subcutaneous, intramuscular, inhalation, and implantation routes.
SCD also has a variety of presentations, including pompholyx/dyshidrosis/vesicular dermatitis, maculopapular eruption, chronic pruritus, exfoliative erythroderma/toxiderma, chronic urticaria, erythema multiforme and vasculitis, hyperkeratotic papules of the elbows, acute generalized exanthematous pustulosis, and pruritus ani, according to Dr. Zippin.
SCD should be considered when a patient has a positive patch test to an allergen that is known to cause SCD, and does not clear after avoiding cutaneous exposure to the allergen, Dr. Zippin advised.
Patients will most often develop SCD from plants and herbs, Dr. Zippin noted. Chrysanthemums and chamomile tea are common culprits for compositae allergy and can trigger SCD; other causes are Anacardiaceae, Balsam of Peru, and propolis. Metals (nickel, cobalt, gold, and chromium), medications (aminoglycosides, corticosteroids, and ethylenediamine), and other sources (formaldehyde, propylene glycol in frozen foods, gallates, and methylisothiazolinone) can cause SCD as well.
Methylisothiazolinone in particular is a very common sensitizer, Dr. Zippin said. “If you have a patient who is positive to this, it’s almost always the cause of their problem.”
Balsam of Peru is in a number of different foods, and patients who need to follow a diet free of Balsam of Peru should avoid a long list of foods including citrus; bakery goods; Danish pastry; candy; gum; spices such as cinnamon, cloves, vanilla, curry, allspice, anise, and ginger; spicy condiments such as ketchup, chili sauce, barbecue sauce; chili, pizza, and foods with red sauces; tomatoes; pickles; alcohol (wine, beer, gin, vermouth); tea (perfumed or flavored); tobacco; chocolate and ice cream; and soft drinks (cola or spiced soft drinks).
Patients starting a nickel-free diet should avoid soy, peanuts and other nuts, legumes, chocolate, cocoa, oats, fish, and whole wheat flours. Any elimination diet should last for 3 months but should at least be tried for 3-4 weeks, with gradual reintroduction of foods suspected as triggers once per week. Any type I allergies that are discovered or suspected can be referred to an allergist for allergen challenge and desensitization therapy.
For more information, Dr. Zippin recommended the American Contact Dermatitis Society website for more information.
Dr. Zippin reported that he is the founder and holds stock options at CEP Biotech; is on the medical advisory board and receives stock options from YouV Labs., is a paid consultant and performs industry-sponsored research for Pfizer, receives stock options from Regeneron, and is on the medical advisory board for Hoth Therapeutics Inc. He is on the board of directors for the American Contact Dermatitis Society.
ORLANDO – Do you have ? Consider patch testing to assess whether they have allergic contact dermatitis.
“Of the patients who are sent to me by local pediatric dermatologists, 50% of them are positive” for allergens, said Jonathan H. Zippin, MD, PhD, director of the contact, occupational, and photodermatitis service at Cornell University, New York.
Speaking at the ODAC Dermatology, Aesthetic, and Surgical Conference, Dr. Zippin noted the prevalence of allergen sensitization is between 13% and 25% among children who are asymptomatic, while the prevalence of sensitization to at least one allergen among children with suspected allergic contact dermatitis (ACD) is between 25% and 96%. In 2014, a study from the National American Contact Dermatitis Group (NACDG) showed that of 883 children who were patch tested, 56.7% had at least one relevant positive patch test (RPPT) result.
“The take-home message here is that pediatric contact dermatitis is common, much more common than a lot of people realize,” Dr. Zippin said.
He described three common scenarios to keep in mind: a worsening rash, a new rash, and failure of a rash to improve after the patient avoids all of his or her positive allergens.
When a rash worsens, patch testing is likely to offer answers. In an analysis of 1,142 patients with suspected ACD aged 18 years or younger (mean age, 10.5 years; 64% female) in the Pediatric Contact Dermatitis Registry study database, 65% had at least one positive patch test, and 48% had at least 1 RPPT (Dermatitis 2016; 27[5] 293-302).
But not all patch testing is the same: The study also found that 24% of the RPPT cases would have been missed if assessed with the T.R.U.E. TEST compared with extended patch testing. If a T.R.U.E. TEST fails to explain generalized atopic dermatitis, the patient should be sent for more comprehensive testing where available, Dr. Zippin advised.
Pediatric patients also have unique allergens clinicians should consider. In the same study, children had a number of allergens similar to those of adults as reported in previous studies, such as nickel, cobalt, and neomycin. However, propylene glycol and cocamidopropyl betaine were allergens identified as unique to the pediatric population.
Another study looking at the same group of patients found that compared with children who did not have AD, children with AD had 7.4 times higher odds of having an RPPT to cocamidopropyl betaine, 7.6 times higher odds of having an RPPT to parthenolide, 5.3 times higher odds of having an RPPT to tixocortol pivalate, 4.2 times higher odds of having an RPPT to wool alcohols, and 4 times higher odds of having an RPPT to lanolin (JAMA Dermatology 2017;153[8]:765-70).
All of these are components of topical medicaments used to treat AD, “either components of emollients that we recommend, or components of steroids that we recommend,” Dr. Zippin pointed out.
One of these allergens could be the culprit when a child develops a new rash but there are no new apparent changes in products, exposures, and activities. Lanolin, also called wool grease, is used in many skin care products, for example. Dr. Zippin described the case of a 6-year-old girl with a history of AD, who presented with a new rash on her scalp and behind her ears, not explained by any obvious changes to products, exposures, or activities. Subsequent patch testing determined that the rash was caused by baby shampoo, which contained cocamidopropyl betaine, which is used in hypoallergenic products. The rash resolved after a different shampoo was used.
“Sometimes, we really have to be thinking when the rash is getting worse, is there something they’re being exposed to that might be an allergen?” Dr. Zippin said.
In patients who have avoided all their positive allergens but a rash has not improved, clinicians should consider systemic contact dermatitis (SCD). Patients can develop SCD through different types of exposures, including transepidermal, transmucosal, oral, intravenous, subcutaneous, intramuscular, inhalation, and implantation routes.
SCD also has a variety of presentations, including pompholyx/dyshidrosis/vesicular dermatitis, maculopapular eruption, chronic pruritus, exfoliative erythroderma/toxiderma, chronic urticaria, erythema multiforme and vasculitis, hyperkeratotic papules of the elbows, acute generalized exanthematous pustulosis, and pruritus ani, according to Dr. Zippin.
SCD should be considered when a patient has a positive patch test to an allergen that is known to cause SCD, and does not clear after avoiding cutaneous exposure to the allergen, Dr. Zippin advised.
Patients will most often develop SCD from plants and herbs, Dr. Zippin noted. Chrysanthemums and chamomile tea are common culprits for compositae allergy and can trigger SCD; other causes are Anacardiaceae, Balsam of Peru, and propolis. Metals (nickel, cobalt, gold, and chromium), medications (aminoglycosides, corticosteroids, and ethylenediamine), and other sources (formaldehyde, propylene glycol in frozen foods, gallates, and methylisothiazolinone) can cause SCD as well.
Methylisothiazolinone in particular is a very common sensitizer, Dr. Zippin said. “If you have a patient who is positive to this, it’s almost always the cause of their problem.”
Balsam of Peru is in a number of different foods, and patients who need to follow a diet free of Balsam of Peru should avoid a long list of foods including citrus; bakery goods; Danish pastry; candy; gum; spices such as cinnamon, cloves, vanilla, curry, allspice, anise, and ginger; spicy condiments such as ketchup, chili sauce, barbecue sauce; chili, pizza, and foods with red sauces; tomatoes; pickles; alcohol (wine, beer, gin, vermouth); tea (perfumed or flavored); tobacco; chocolate and ice cream; and soft drinks (cola or spiced soft drinks).
Patients starting a nickel-free diet should avoid soy, peanuts and other nuts, legumes, chocolate, cocoa, oats, fish, and whole wheat flours. Any elimination diet should last for 3 months but should at least be tried for 3-4 weeks, with gradual reintroduction of foods suspected as triggers once per week. Any type I allergies that are discovered or suspected can be referred to an allergist for allergen challenge and desensitization therapy.
For more information, Dr. Zippin recommended the American Contact Dermatitis Society website for more information.
Dr. Zippin reported that he is the founder and holds stock options at CEP Biotech; is on the medical advisory board and receives stock options from YouV Labs., is a paid consultant and performs industry-sponsored research for Pfizer, receives stock options from Regeneron, and is on the medical advisory board for Hoth Therapeutics Inc. He is on the board of directors for the American Contact Dermatitis Society.
EXPERT ANALYSIS FROM ODAC 2020
Equal Access Makes A Difference in Surviving Prostate Cancer
In the general US population, African American men are more than twice as likely as non-Hispanic white men to die of prostate cancer. Researchers from the University of California at San Diego, though, speculated that disparities in access to care and not racial differences might be driving the differing outcomes. They turned to the US Department of Veterans Affairs (VA) with its “equal-access medical system” to find out.
Using data from a longitudinal database of > 20 million veterans, the researchers followed 18,201 black and 41,834 white patients with prostate cancer who were diagnosed between 2000 and 2015 and received care through the VA. The results of the study were published in Cancer.
African American men at diagnosis were younger (median age, 63 vs 66 years), more likely to smoke, and had more general health problems than did white men. Black patients also had higher prostate-specific antigen levels (median, 6.7 ng/mL vs 6.2 ng/mL) but were less likely to have Gleason score 8 to 10 disease, a clinical T classification ≥ 3, or distant metastatic disease.
There was no difference between the groups in time from diagnosis to treatment. The 10-year prostate cancer-specific mortality rate was actually slightly lower for African American men: 4.4%, compared with 5.1% for white men.
Thus, the researchers concluded that because African American men who receive VA healthcare do not appear to present with more advanced disease, or experience worse outcomes than do white men—in contrast to national trends. Therefore, they determined that access to care may be an important determinant of racial equity.
“Prior outcomes for African Americans with prostate cancer don’t have to be a foregone conclusion,” the senior author, Brent Rose, MD, told The New York Times. “They are at least partly due to policy decisions we make about access to care.”
In the general US population, African American men are more than twice as likely as non-Hispanic white men to die of prostate cancer. Researchers from the University of California at San Diego, though, speculated that disparities in access to care and not racial differences might be driving the differing outcomes. They turned to the US Department of Veterans Affairs (VA) with its “equal-access medical system” to find out.
Using data from a longitudinal database of > 20 million veterans, the researchers followed 18,201 black and 41,834 white patients with prostate cancer who were diagnosed between 2000 and 2015 and received care through the VA. The results of the study were published in Cancer.
African American men at diagnosis were younger (median age, 63 vs 66 years), more likely to smoke, and had more general health problems than did white men. Black patients also had higher prostate-specific antigen levels (median, 6.7 ng/mL vs 6.2 ng/mL) but were less likely to have Gleason score 8 to 10 disease, a clinical T classification ≥ 3, or distant metastatic disease.
There was no difference between the groups in time from diagnosis to treatment. The 10-year prostate cancer-specific mortality rate was actually slightly lower for African American men: 4.4%, compared with 5.1% for white men.
Thus, the researchers concluded that because African American men who receive VA healthcare do not appear to present with more advanced disease, or experience worse outcomes than do white men—in contrast to national trends. Therefore, they determined that access to care may be an important determinant of racial equity.
“Prior outcomes for African Americans with prostate cancer don’t have to be a foregone conclusion,” the senior author, Brent Rose, MD, told The New York Times. “They are at least partly due to policy decisions we make about access to care.”
In the general US population, African American men are more than twice as likely as non-Hispanic white men to die of prostate cancer. Researchers from the University of California at San Diego, though, speculated that disparities in access to care and not racial differences might be driving the differing outcomes. They turned to the US Department of Veterans Affairs (VA) with its “equal-access medical system” to find out.
Using data from a longitudinal database of > 20 million veterans, the researchers followed 18,201 black and 41,834 white patients with prostate cancer who were diagnosed between 2000 and 2015 and received care through the VA. The results of the study were published in Cancer.
African American men at diagnosis were younger (median age, 63 vs 66 years), more likely to smoke, and had more general health problems than did white men. Black patients also had higher prostate-specific antigen levels (median, 6.7 ng/mL vs 6.2 ng/mL) but were less likely to have Gleason score 8 to 10 disease, a clinical T classification ≥ 3, or distant metastatic disease.
There was no difference between the groups in time from diagnosis to treatment. The 10-year prostate cancer-specific mortality rate was actually slightly lower for African American men: 4.4%, compared with 5.1% for white men.
Thus, the researchers concluded that because African American men who receive VA healthcare do not appear to present with more advanced disease, or experience worse outcomes than do white men—in contrast to national trends. Therefore, they determined that access to care may be an important determinant of racial equity.
“Prior outcomes for African Americans with prostate cancer don’t have to be a foregone conclusion,” the senior author, Brent Rose, MD, told The New York Times. “They are at least partly due to policy decisions we make about access to care.”
FDA not recommending recalls of diabetes drug metformin
The Food and Drug Administration says it has no plans to recall any metformin products, used for the treatment of type 2 diabetes, after tests it conducted did not show any evidence of contamination with N-nitrosodimethylamine (NDMA) at levels that would cause concern.

The FDA began testing samples of metformin for the carcinogen NDMA at the end of 2019. Contamination with this substance has led to recalls of hypertension and heartburn medications within the past 2 years.
That announcement came on the heels of a recall of three versions of metformin in Singapore and the European Medicines Agency’s request that manufacturers test for NDMA.
This week, the FDA posted laboratory results in which NDMA levels in some metformin products ranged from “not detectable to low.”
“To date, no sample of metformin that FDA has tested exceeds the acceptable daily intake for NDMA. FDA has not recommended metformin recalls in the U.S.,” the agency indicates.
More than 30 million people in the United States have diabetes; 90%-95% of cases are of type 2. Metformin is the fourth most prescribed drug in the United States.
“Patients should continue taking metformin to keep their diabetes under control,” the FDA emphasized. “It could be dangerous for patients with this serious condition to stop taking their metformin without first talking to their health care professionals.”
The agency plans to post the methods used in laboratory testing of metformin in the near future. The FDA is collaborating with international regulators to share testing results for metformin, along with testing results for other drugs.
The U.S. agency says it will continue to monitor NDMA in metformin, along with other drug products, and will provide timely updates of new developments, including product recalls.
For more information about NDMA, visit the FDA’s nitrosamines webpage.
The FDA also encourages health care professionals and patients to report adverse reactions or quality problems with any human drugs to the agency’s MedWatch Adverse Event Reporting program.
This article first appeared on Medscape.com.
The Food and Drug Administration says it has no plans to recall any metformin products, used for the treatment of type 2 diabetes, after tests it conducted did not show any evidence of contamination with N-nitrosodimethylamine (NDMA) at levels that would cause concern.
The FDA began testing samples of metformin for the carcinogen NDMA at the end of 2019. Contamination with this substance has led to recalls of hypertension and heartburn medications within the past 2 years.
That announcement came on the heels of a recall of three versions of metformin in Singapore and the European Medicines Agency’s request that manufacturers test for NDMA.
This week, the FDA posted laboratory results in which NDMA levels in some metformin products ranged from “not detectable to low.”
“To date, no sample of metformin that FDA has tested exceeds the acceptable daily intake for NDMA. FDA has not recommended metformin recalls in the U.S.,” the agency indicates.
More than 30 million people in the United States have diabetes; 90%-95% of cases are of type 2. Metformin is the fourth most prescribed drug in the United States.
“Patients should continue taking metformin to keep their diabetes under control,” the FDA emphasized. “It could be dangerous for patients with this serious condition to stop taking their metformin without first talking to their health care professionals.”
The agency plans to post the methods used in laboratory testing of metformin in the near future. The FDA is collaborating with international regulators to share testing results for metformin, along with testing results for other drugs.
The U.S. agency says it will continue to monitor NDMA in metformin, along with other drug products, and will provide timely updates of new developments, including product recalls.
For more information about NDMA, visit the FDA’s nitrosamines webpage.
The FDA also encourages health care professionals and patients to report adverse reactions or quality problems with any human drugs to the agency’s MedWatch Adverse Event Reporting program.
This article first appeared on Medscape.com.
The Food and Drug Administration says it has no plans to recall any metformin products, used for the treatment of type 2 diabetes, after tests it conducted did not show any evidence of contamination with N-nitrosodimethylamine (NDMA) at levels that would cause concern.
The FDA began testing samples of metformin for the carcinogen NDMA at the end of 2019. Contamination with this substance has led to recalls of hypertension and heartburn medications within the past 2 years.
That announcement came on the heels of a recall of three versions of metformin in Singapore and the European Medicines Agency’s request that manufacturers test for NDMA.
This week, the FDA posted laboratory results in which NDMA levels in some metformin products ranged from “not detectable to low.”
“To date, no sample of metformin that FDA has tested exceeds the acceptable daily intake for NDMA. FDA has not recommended metformin recalls in the U.S.,” the agency indicates.
More than 30 million people in the United States have diabetes; 90%-95% of cases are of type 2. Metformin is the fourth most prescribed drug in the United States.
“Patients should continue taking metformin to keep their diabetes under control,” the FDA emphasized. “It could be dangerous for patients with this serious condition to stop taking their metformin without first talking to their health care professionals.”
The agency plans to post the methods used in laboratory testing of metformin in the near future. The FDA is collaborating with international regulators to share testing results for metformin, along with testing results for other drugs.
The U.S. agency says it will continue to monitor NDMA in metformin, along with other drug products, and will provide timely updates of new developments, including product recalls.
For more information about NDMA, visit the FDA’s nitrosamines webpage.
The FDA also encourages health care professionals and patients to report adverse reactions or quality problems with any human drugs to the agency’s MedWatch Adverse Event Reporting program.
This article first appeared on Medscape.com.
Choice of infant sleep location is multifactorial
according to a recent nationally representative study.

Of 3,260 mothers surveyed, 59% of mothers said that they intended to room-share without bed-sharing, but only 45% practiced – and also had the intent to practice – room-sharing without bed-sharing. Of the 41% who said that they did not intend to bed-share, 24% actually did intend to practice at least some bed-sharing with their infants, who were all aged 2-6 months at the time of survey administration.
Mothers who were African American and those who were breastfeeding exclusively were most likely to report that they intended to bed-share, reported Ann Kellams, MD, of the department of pediatrics at the University of Virginia,Charlottesville, and coauthors. Mothers who were exclusively breastfeeding had a nearly threefold higher rate of intending to bed-share than mothers whose infants were fed formula.
How mothers perceived social norms about bed- and room-sharing practices also plays a role. Women who considered that social norms supported bed-sharing and discouraged room-sharing had almost 200 times the odds of intending to bed-share, compared with those who perceived that social norms supported room-sharing without bed-sharing.
Conversely, being advised by a doctor to follow the American Academy of Pediatrics–recommended practice of room-sharing without bed-sharing made it less likely that mothers would plan to share a bed with their infant (adjusted odds ratio, 0.56). Yet women who intended to room-share without bed-sharing but who actually did bed-share some of the time, their doctor’s advice to room-share only had no impact (aOR, 1.01).
The investigators noted that, “although other studies have investigated factors influencing maternal decisions, no studies to date have examined maternal intention regarding sleep location and what factors influence intention.”
The Study of Attitudes and Factors Effecting Infant Care drew from 32 U.S. hospitals, and asked mothers about feeding and care practices, including the infant’s usual sleep locations and all sleep locations over the 2 weeks preceding the survey. Additionally, the survey asked about future intent for sleeping practices, looking ahead to the next 2 weeks.
The survey design and the analysis performed in the study were based on the theory of planned behavior (TPB), “which hypothesizes that attitudes, subjective social norms, and perceptions about control over behavior impact one’s intention, which leads to actual behavior,” explained Dr. Kellams and coinvestigators. They reported that they had previously used TPB to analyze mothers’ intentions and actions regarding supine sleep position for infants, finding that a variety of behavioral and social facets accounted for by TPB affected maternal intention and decision making.
Additionally, the study’s design captured partial-night bed-sharing, where an infant may start the night in a separate bed but be brought to bed for feeding or comforting, then share a bed with the mother for the remainder of the night. “Unintended bed-sharing may explain our finding that there is frequent inconsistency between those whose near-future intention is to room-share without bed-sharing but whose actual practice includes bed-sharing,” the authors wrote.
“Attitudes, social norms, and doctor advice are associated with infant sleep location and may be potential targets for educational interventions,” concluded Dr. Kellams and coinvestigators.
Dr. Kellams and associates reported no relevant financial disclosures. The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health.
SOURCE: Kellams A et al. Pediatrics. 2020 Feb 7;145(3):e20191523.
according to a recent nationally representative study.
Of 3,260 mothers surveyed, 59% of mothers said that they intended to room-share without bed-sharing, but only 45% practiced – and also had the intent to practice – room-sharing without bed-sharing. Of the 41% who said that they did not intend to bed-share, 24% actually did intend to practice at least some bed-sharing with their infants, who were all aged 2-6 months at the time of survey administration.
Mothers who were African American and those who were breastfeeding exclusively were most likely to report that they intended to bed-share, reported Ann Kellams, MD, of the department of pediatrics at the University of Virginia,Charlottesville, and coauthors. Mothers who were exclusively breastfeeding had a nearly threefold higher rate of intending to bed-share than mothers whose infants were fed formula.
How mothers perceived social norms about bed- and room-sharing practices also plays a role. Women who considered that social norms supported bed-sharing and discouraged room-sharing had almost 200 times the odds of intending to bed-share, compared with those who perceived that social norms supported room-sharing without bed-sharing.
Conversely, being advised by a doctor to follow the American Academy of Pediatrics–recommended practice of room-sharing without bed-sharing made it less likely that mothers would plan to share a bed with their infant (adjusted odds ratio, 0.56). Yet women who intended to room-share without bed-sharing but who actually did bed-share some of the time, their doctor’s advice to room-share only had no impact (aOR, 1.01).
The investigators noted that, “although other studies have investigated factors influencing maternal decisions, no studies to date have examined maternal intention regarding sleep location and what factors influence intention.”
The Study of Attitudes and Factors Effecting Infant Care drew from 32 U.S. hospitals, and asked mothers about feeding and care practices, including the infant’s usual sleep locations and all sleep locations over the 2 weeks preceding the survey. Additionally, the survey asked about future intent for sleeping practices, looking ahead to the next 2 weeks.
The survey design and the analysis performed in the study were based on the theory of planned behavior (TPB), “which hypothesizes that attitudes, subjective social norms, and perceptions about control over behavior impact one’s intention, which leads to actual behavior,” explained Dr. Kellams and coinvestigators. They reported that they had previously used TPB to analyze mothers’ intentions and actions regarding supine sleep position for infants, finding that a variety of behavioral and social facets accounted for by TPB affected maternal intention and decision making.
Additionally, the study’s design captured partial-night bed-sharing, where an infant may start the night in a separate bed but be brought to bed for feeding or comforting, then share a bed with the mother for the remainder of the night. “Unintended bed-sharing may explain our finding that there is frequent inconsistency between those whose near-future intention is to room-share without bed-sharing but whose actual practice includes bed-sharing,” the authors wrote.
“Attitudes, social norms, and doctor advice are associated with infant sleep location and may be potential targets for educational interventions,” concluded Dr. Kellams and coinvestigators.
Dr. Kellams and associates reported no relevant financial disclosures. The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health.
SOURCE: Kellams A et al. Pediatrics. 2020 Feb 7;145(3):e20191523.
according to a recent nationally representative study.
Of 3,260 mothers surveyed, 59% of mothers said that they intended to room-share without bed-sharing, but only 45% practiced – and also had the intent to practice – room-sharing without bed-sharing. Of the 41% who said that they did not intend to bed-share, 24% actually did intend to practice at least some bed-sharing with their infants, who were all aged 2-6 months at the time of survey administration.
Mothers who were African American and those who were breastfeeding exclusively were most likely to report that they intended to bed-share, reported Ann Kellams, MD, of the department of pediatrics at the University of Virginia,Charlottesville, and coauthors. Mothers who were exclusively breastfeeding had a nearly threefold higher rate of intending to bed-share than mothers whose infants were fed formula.
How mothers perceived social norms about bed- and room-sharing practices also plays a role. Women who considered that social norms supported bed-sharing and discouraged room-sharing had almost 200 times the odds of intending to bed-share, compared with those who perceived that social norms supported room-sharing without bed-sharing.
Conversely, being advised by a doctor to follow the American Academy of Pediatrics–recommended practice of room-sharing without bed-sharing made it less likely that mothers would plan to share a bed with their infant (adjusted odds ratio, 0.56). Yet women who intended to room-share without bed-sharing but who actually did bed-share some of the time, their doctor’s advice to room-share only had no impact (aOR, 1.01).
The investigators noted that, “although other studies have investigated factors influencing maternal decisions, no studies to date have examined maternal intention regarding sleep location and what factors influence intention.”
The Study of Attitudes and Factors Effecting Infant Care drew from 32 U.S. hospitals, and asked mothers about feeding and care practices, including the infant’s usual sleep locations and all sleep locations over the 2 weeks preceding the survey. Additionally, the survey asked about future intent for sleeping practices, looking ahead to the next 2 weeks.
The survey design and the analysis performed in the study were based on the theory of planned behavior (TPB), “which hypothesizes that attitudes, subjective social norms, and perceptions about control over behavior impact one’s intention, which leads to actual behavior,” explained Dr. Kellams and coinvestigators. They reported that they had previously used TPB to analyze mothers’ intentions and actions regarding supine sleep position for infants, finding that a variety of behavioral and social facets accounted for by TPB affected maternal intention and decision making.
Additionally, the study’s design captured partial-night bed-sharing, where an infant may start the night in a separate bed but be brought to bed for feeding or comforting, then share a bed with the mother for the remainder of the night. “Unintended bed-sharing may explain our finding that there is frequent inconsistency between those whose near-future intention is to room-share without bed-sharing but whose actual practice includes bed-sharing,” the authors wrote.
“Attitudes, social norms, and doctor advice are associated with infant sleep location and may be potential targets for educational interventions,” concluded Dr. Kellams and coinvestigators.
Dr. Kellams and associates reported no relevant financial disclosures. The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health.
SOURCE: Kellams A et al. Pediatrics. 2020 Feb 7;145(3):e20191523.
FROM PEDIATRICS
Posttraumatic stress may persist up to 9 months after pregnancy loss
new research suggests.

The outcomes of a prospective cohort study involving 737 women who had experienced miscarriage or ectopic pregnancy and 171 controls with healthy pregnancies were presented in a report in the American Journal of Obstetrics & Gynecology.
One month after their pregnancy loss, 29% of these women met the criteria for posttraumatic stress, 24% reported moderate to severe anxiety, and 11% reported moderate to severe depression. In comparison, just 13% of women in the control group met the criteria for anxiety, and 2% met the criteria for depression, which meant women who had experienced early pregnancy loss had a greater than twofold odds of anxiety and nearly fourfold (odds ratio, 3.88) greater odds of depression, reported Jessica Farren, PhD, of the Queen Charlotte’s and Chelsea Hospital, London, and coauthors.
The most common posttraumatic symptom, experienced by 91% of respondents with posttraumatic stress at 1 month after the pregnancy, was reexperiencing symptoms, while 60% experienced avoidance and hyperarousal symptoms. At 3 months after the loss, 50% of those with posttraumatic stress reported an interruption of their general satisfaction with life.
While the incidence of posttraumatic stress, anxiety, and depression decreased over time in the women who had early pregnancy loss, by the third month 21% still met the criteria for posttraumatic stress, and by 9 months, 18% still were experiencing posttraumatic stress. Similarly, moderate to severe anxiety was still present in 23% of women at 3 months and 17% at 9 months, and moderate to severe depression was still experienced by 8% of women at 3 months and 6% of women at 9 months.
Dr. Farren and coauthors wrote that, given the incidence of miscarriage and ectopic pregnancy in the population, the high proportion of women still experiencing posttraumatic stress, anxiety, and depression at 9 months pointed to a significant public health issue. “It is recognized that PTSD in other contexts can have a significant impact on work, social interaction, health care utilization, and risks in future pregnancies,” they wrote. “Work is needed to evaluate strategies to effectively identify and treat affected women with these specific psychopathologies.”
The investigators also looked at the differences in outcomes in women who experienced miscarriage, compared with those who experienced ectopic pregnancy.
Of the 363 women who had a miscarriage, 30% met criteria for posttraumatic stress at 1 month, 20% at 3 months, and 17% at 9 months. Moderate to severe anxiety was reported by 25% women at 1 month, 22% at 3 months, and 17% at 9 months. Moderate to severe depression was reported by 12% at 1 month, 7% at 3 months, and 5% at 9 months.
Of the 74 women who had an ectopic pregnancy, 23% met criteria for posttraumatic stress at 1 month, 28% at 3 months, and 21% at 9 months. Moderate to severe anxiety was reported by 21% at 1 month, 30% at 3 months, and 23% at 9 months. Moderate to severe depression was reported by 7% at 1 month, 12% at 3 months, and 11% at 9 months.
The authors noted that the incidence of posttraumatic stress, anxiety, and depression decreased more strongly over time in women who had experienced miscarriage, compared with those who experienced ectopic pregnancy, although they commented that the confidence intervals were wide.
One coauthor was supported by an Imperial Health Charity grant and another by the National Institute for Health Research Biomedical Research Centre. No conflicts of interest were declared.
SOURCE: Farren J et al. Amer J Obstet Gynecol. 2019 Dec 13. doi: 10.1016/j.ajog.2019.10.102.
new research suggests.
The outcomes of a prospective cohort study involving 737 women who had experienced miscarriage or ectopic pregnancy and 171 controls with healthy pregnancies were presented in a report in the American Journal of Obstetrics & Gynecology.
One month after their pregnancy loss, 29% of these women met the criteria for posttraumatic stress, 24% reported moderate to severe anxiety, and 11% reported moderate to severe depression. In comparison, just 13% of women in the control group met the criteria for anxiety, and 2% met the criteria for depression, which meant women who had experienced early pregnancy loss had a greater than twofold odds of anxiety and nearly fourfold (odds ratio, 3.88) greater odds of depression, reported Jessica Farren, PhD, of the Queen Charlotte’s and Chelsea Hospital, London, and coauthors.
The most common posttraumatic symptom, experienced by 91% of respondents with posttraumatic stress at 1 month after the pregnancy, was reexperiencing symptoms, while 60% experienced avoidance and hyperarousal symptoms. At 3 months after the loss, 50% of those with posttraumatic stress reported an interruption of their general satisfaction with life.
While the incidence of posttraumatic stress, anxiety, and depression decreased over time in the women who had early pregnancy loss, by the third month 21% still met the criteria for posttraumatic stress, and by 9 months, 18% still were experiencing posttraumatic stress. Similarly, moderate to severe anxiety was still present in 23% of women at 3 months and 17% at 9 months, and moderate to severe depression was still experienced by 8% of women at 3 months and 6% of women at 9 months.
Dr. Farren and coauthors wrote that, given the incidence of miscarriage and ectopic pregnancy in the population, the high proportion of women still experiencing posttraumatic stress, anxiety, and depression at 9 months pointed to a significant public health issue. “It is recognized that PTSD in other contexts can have a significant impact on work, social interaction, health care utilization, and risks in future pregnancies,” they wrote. “Work is needed to evaluate strategies to effectively identify and treat affected women with these specific psychopathologies.”
The investigators also looked at the differences in outcomes in women who experienced miscarriage, compared with those who experienced ectopic pregnancy.
Of the 363 women who had a miscarriage, 30% met criteria for posttraumatic stress at 1 month, 20% at 3 months, and 17% at 9 months. Moderate to severe anxiety was reported by 25% women at 1 month, 22% at 3 months, and 17% at 9 months. Moderate to severe depression was reported by 12% at 1 month, 7% at 3 months, and 5% at 9 months.
Of the 74 women who had an ectopic pregnancy, 23% met criteria for posttraumatic stress at 1 month, 28% at 3 months, and 21% at 9 months. Moderate to severe anxiety was reported by 21% at 1 month, 30% at 3 months, and 23% at 9 months. Moderate to severe depression was reported by 7% at 1 month, 12% at 3 months, and 11% at 9 months.
The authors noted that the incidence of posttraumatic stress, anxiety, and depression decreased more strongly over time in women who had experienced miscarriage, compared with those who experienced ectopic pregnancy, although they commented that the confidence intervals were wide.
One coauthor was supported by an Imperial Health Charity grant and another by the National Institute for Health Research Biomedical Research Centre. No conflicts of interest were declared.
SOURCE: Farren J et al. Amer J Obstet Gynecol. 2019 Dec 13. doi: 10.1016/j.ajog.2019.10.102.
new research suggests.
The outcomes of a prospective cohort study involving 737 women who had experienced miscarriage or ectopic pregnancy and 171 controls with healthy pregnancies were presented in a report in the American Journal of Obstetrics & Gynecology.
One month after their pregnancy loss, 29% of these women met the criteria for posttraumatic stress, 24% reported moderate to severe anxiety, and 11% reported moderate to severe depression. In comparison, just 13% of women in the control group met the criteria for anxiety, and 2% met the criteria for depression, which meant women who had experienced early pregnancy loss had a greater than twofold odds of anxiety and nearly fourfold (odds ratio, 3.88) greater odds of depression, reported Jessica Farren, PhD, of the Queen Charlotte’s and Chelsea Hospital, London, and coauthors.
The most common posttraumatic symptom, experienced by 91% of respondents with posttraumatic stress at 1 month after the pregnancy, was reexperiencing symptoms, while 60% experienced avoidance and hyperarousal symptoms. At 3 months after the loss, 50% of those with posttraumatic stress reported an interruption of their general satisfaction with life.
While the incidence of posttraumatic stress, anxiety, and depression decreased over time in the women who had early pregnancy loss, by the third month 21% still met the criteria for posttraumatic stress, and by 9 months, 18% still were experiencing posttraumatic stress. Similarly, moderate to severe anxiety was still present in 23% of women at 3 months and 17% at 9 months, and moderate to severe depression was still experienced by 8% of women at 3 months and 6% of women at 9 months.
Dr. Farren and coauthors wrote that, given the incidence of miscarriage and ectopic pregnancy in the population, the high proportion of women still experiencing posttraumatic stress, anxiety, and depression at 9 months pointed to a significant public health issue. “It is recognized that PTSD in other contexts can have a significant impact on work, social interaction, health care utilization, and risks in future pregnancies,” they wrote. “Work is needed to evaluate strategies to effectively identify and treat affected women with these specific psychopathologies.”
The investigators also looked at the differences in outcomes in women who experienced miscarriage, compared with those who experienced ectopic pregnancy.
Of the 363 women who had a miscarriage, 30% met criteria for posttraumatic stress at 1 month, 20% at 3 months, and 17% at 9 months. Moderate to severe anxiety was reported by 25% women at 1 month, 22% at 3 months, and 17% at 9 months. Moderate to severe depression was reported by 12% at 1 month, 7% at 3 months, and 5% at 9 months.
Of the 74 women who had an ectopic pregnancy, 23% met criteria for posttraumatic stress at 1 month, 28% at 3 months, and 21% at 9 months. Moderate to severe anxiety was reported by 21% at 1 month, 30% at 3 months, and 23% at 9 months. Moderate to severe depression was reported by 7% at 1 month, 12% at 3 months, and 11% at 9 months.
The authors noted that the incidence of posttraumatic stress, anxiety, and depression decreased more strongly over time in women who had experienced miscarriage, compared with those who experienced ectopic pregnancy, although they commented that the confidence intervals were wide.
One coauthor was supported by an Imperial Health Charity grant and another by the National Institute for Health Research Biomedical Research Centre. No conflicts of interest were declared.
SOURCE: Farren J et al. Amer J Obstet Gynecol. 2019 Dec 13. doi: 10.1016/j.ajog.2019.10.102.
FROM THE AMERICAN JOURNAL OF OBSTETRICS & GYNECOLOGY
Mailed fecal testing may catch more cancer than endoscopic screening
On a population level, mailed fecal immunohistochemical tests (FITs) may catch more cases of advanced neoplasia than endoscopic methods, based on a Dutch screening study that invited more than 30,000 people to participate.
, reported lead author Esmée J. Grobbee, MD, of Erasmus University Medical Centre in Rotterdam, the Netherlands, and colleagues.
In addition to high participation, previous research has shown that successful FIT screening depends upon continued adherence to the screening program, the investigators wrote in Clinical Gastroenterology and Hepatology. They noted that, in the present study, just two rounds of FIT were needed to outperform endoscopic methods, and that these comparative findings are a first for the field.
“No literature is available on the comparison between endoscopic screening strategies and multiple rounds of FIT screening,” the investigators wrote. “It is of key importance for policy makers to know the impact of different screening programs over multiple rounds with long-term follow-up.”
To this end, the investigators invited 30,052 screening-naive people in the Netherlands to participate in the present study. Each invitation was for one of three groups: once-only colonoscopy, once-only flexible sigmoidoscopy, or four rounds of FIT. All individuals received an advanced notification by mail followed 2 weeks later by a more substantial information kit (and first FIT test when applicable). If these steps received no response, a reminder was sent 6 weeks later.
Participants in the FIT group received one test every 2 years. Patients who had a positive FIT (hemoglobin concentration of at least 10 mcg Hb/g feces) were scheduled for a colonoscopy. Similarly, colonoscopies were performed in patients who had concerning findings on flexible sigmoidoscopy (e.g., sessile serrated adenoma. This sequential system reduced the relative number of colonoscopies in these two groups; colonoscopy rates in the FIT group and flexible sigmoidoscopy group were 13% and 3%, respectively, compared with the 24% participation rate in the colonoscopy group.
At a population level, FIT screening had the highest advanced neoplasia detection rate, at 4.5%, compared with 2.3% and 2.2% for screening by sigmoidoscopy and colonoscopy, respectively.
“In the intention-to-screen analysis, FIT already detected significantly more advanced neoplasia and colorectal cancer (CRC) after only 2 rounds of FIT, and this difference increased over rounds,” the investigators noted.
Again in the intention-to-screen population, mailed FIT detected three times as many cases of CRC than either of the other two groups (0.6% vs. 0.2% for both). In contrast, colonoscopy and sigmoidoscopy had higher detection rates for nonadvanced adenomas, at 5.6% and 3.7%, respectively, compared with 3.2% for FIT, although the investigators noted that nonadvanced adenomas are “of uncertain clinical importance.” Sessile adenoma detection rates were similar across all three groups.
The as-screened analysis revealed higher detection rates of advanced neoplasia for colonoscopy (9.1%), compared with sigmoidoscopy (7.4%) and FIT (6.1%). In the same analysis, detection rates of colorectal cancer (CRC) were comparable across all three groups.
According to the investigators, the CRC-related findings require careful interpretation.
“Comparing CRC detection rates of FIT and endoscopic screening is complex … because CRCs detected in FIT screening could in theory have been prevented in a once-only colonoscopy by the removal of adenomas,” they wrote.
Still, the key takeaway of the study – that FIT screening was the most effective strategy – may have practical implications on a global scale, according to the investigators.
“Because many countries are considering implementing screening programs, the findings of this study aid in deciding on choice of screening strategies worldwide, which is based on expected participation rates and available colonoscopy resources,” they wrote.
The study was funded by the Netherlands Organization for Health Research and Development. The investigators disclosed no conflicts of interest.
SOURCE: Grobbee EJ et al. Clin Gastro Hepatol. 2019 Aug 13. doi: 10.1016/j.cgh.2019.08.015.
On a population level, mailed fecal immunohistochemical tests (FITs) may catch more cases of advanced neoplasia than endoscopic methods, based on a Dutch screening study that invited more than 30,000 people to participate.
, reported lead author Esmée J. Grobbee, MD, of Erasmus University Medical Centre in Rotterdam, the Netherlands, and colleagues.
In addition to high participation, previous research has shown that successful FIT screening depends upon continued adherence to the screening program, the investigators wrote in Clinical Gastroenterology and Hepatology. They noted that, in the present study, just two rounds of FIT were needed to outperform endoscopic methods, and that these comparative findings are a first for the field.
“No literature is available on the comparison between endoscopic screening strategies and multiple rounds of FIT screening,” the investigators wrote. “It is of key importance for policy makers to know the impact of different screening programs over multiple rounds with long-term follow-up.”
To this end, the investigators invited 30,052 screening-naive people in the Netherlands to participate in the present study. Each invitation was for one of three groups: once-only colonoscopy, once-only flexible sigmoidoscopy, or four rounds of FIT. All individuals received an advanced notification by mail followed 2 weeks later by a more substantial information kit (and first FIT test when applicable). If these steps received no response, a reminder was sent 6 weeks later.
Participants in the FIT group received one test every 2 years. Patients who had a positive FIT (hemoglobin concentration of at least 10 mcg Hb/g feces) were scheduled for a colonoscopy. Similarly, colonoscopies were performed in patients who had concerning findings on flexible sigmoidoscopy (e.g., sessile serrated adenoma. This sequential system reduced the relative number of colonoscopies in these two groups; colonoscopy rates in the FIT group and flexible sigmoidoscopy group were 13% and 3%, respectively, compared with the 24% participation rate in the colonoscopy group.
At a population level, FIT screening had the highest advanced neoplasia detection rate, at 4.5%, compared with 2.3% and 2.2% for screening by sigmoidoscopy and colonoscopy, respectively.
“In the intention-to-screen analysis, FIT already detected significantly more advanced neoplasia and colorectal cancer (CRC) after only 2 rounds of FIT, and this difference increased over rounds,” the investigators noted.
Again in the intention-to-screen population, mailed FIT detected three times as many cases of CRC than either of the other two groups (0.6% vs. 0.2% for both). In contrast, colonoscopy and sigmoidoscopy had higher detection rates for nonadvanced adenomas, at 5.6% and 3.7%, respectively, compared with 3.2% for FIT, although the investigators noted that nonadvanced adenomas are “of uncertain clinical importance.” Sessile adenoma detection rates were similar across all three groups.
The as-screened analysis revealed higher detection rates of advanced neoplasia for colonoscopy (9.1%), compared with sigmoidoscopy (7.4%) and FIT (6.1%). In the same analysis, detection rates of colorectal cancer (CRC) were comparable across all three groups.
According to the investigators, the CRC-related findings require careful interpretation.
“Comparing CRC detection rates of FIT and endoscopic screening is complex … because CRCs detected in FIT screening could in theory have been prevented in a once-only colonoscopy by the removal of adenomas,” they wrote.
Still, the key takeaway of the study – that FIT screening was the most effective strategy – may have practical implications on a global scale, according to the investigators.
“Because many countries are considering implementing screening programs, the findings of this study aid in deciding on choice of screening strategies worldwide, which is based on expected participation rates and available colonoscopy resources,” they wrote.
The study was funded by the Netherlands Organization for Health Research and Development. The investigators disclosed no conflicts of interest.
SOURCE: Grobbee EJ et al. Clin Gastro Hepatol. 2019 Aug 13. doi: 10.1016/j.cgh.2019.08.015.
On a population level, mailed fecal immunohistochemical tests (FITs) may catch more cases of advanced neoplasia than endoscopic methods, based on a Dutch screening study that invited more than 30,000 people to participate.
, reported lead author Esmée J. Grobbee, MD, of Erasmus University Medical Centre in Rotterdam, the Netherlands, and colleagues.
In addition to high participation, previous research has shown that successful FIT screening depends upon continued adherence to the screening program, the investigators wrote in Clinical Gastroenterology and Hepatology. They noted that, in the present study, just two rounds of FIT were needed to outperform endoscopic methods, and that these comparative findings are a first for the field.
“No literature is available on the comparison between endoscopic screening strategies and multiple rounds of FIT screening,” the investigators wrote. “It is of key importance for policy makers to know the impact of different screening programs over multiple rounds with long-term follow-up.”
To this end, the investigators invited 30,052 screening-naive people in the Netherlands to participate in the present study. Each invitation was for one of three groups: once-only colonoscopy, once-only flexible sigmoidoscopy, or four rounds of FIT. All individuals received an advanced notification by mail followed 2 weeks later by a more substantial information kit (and first FIT test when applicable). If these steps received no response, a reminder was sent 6 weeks later.
Participants in the FIT group received one test every 2 years. Patients who had a positive FIT (hemoglobin concentration of at least 10 mcg Hb/g feces) were scheduled for a colonoscopy. Similarly, colonoscopies were performed in patients who had concerning findings on flexible sigmoidoscopy (e.g., sessile serrated adenoma. This sequential system reduced the relative number of colonoscopies in these two groups; colonoscopy rates in the FIT group and flexible sigmoidoscopy group were 13% and 3%, respectively, compared with the 24% participation rate in the colonoscopy group.
At a population level, FIT screening had the highest advanced neoplasia detection rate, at 4.5%, compared with 2.3% and 2.2% for screening by sigmoidoscopy and colonoscopy, respectively.
“In the intention-to-screen analysis, FIT already detected significantly more advanced neoplasia and colorectal cancer (CRC) after only 2 rounds of FIT, and this difference increased over rounds,” the investigators noted.
Again in the intention-to-screen population, mailed FIT detected three times as many cases of CRC than either of the other two groups (0.6% vs. 0.2% for both). In contrast, colonoscopy and sigmoidoscopy had higher detection rates for nonadvanced adenomas, at 5.6% and 3.7%, respectively, compared with 3.2% for FIT, although the investigators noted that nonadvanced adenomas are “of uncertain clinical importance.” Sessile adenoma detection rates were similar across all three groups.
The as-screened analysis revealed higher detection rates of advanced neoplasia for colonoscopy (9.1%), compared with sigmoidoscopy (7.4%) and FIT (6.1%). In the same analysis, detection rates of colorectal cancer (CRC) were comparable across all three groups.
According to the investigators, the CRC-related findings require careful interpretation.
“Comparing CRC detection rates of FIT and endoscopic screening is complex … because CRCs detected in FIT screening could in theory have been prevented in a once-only colonoscopy by the removal of adenomas,” they wrote.
Still, the key takeaway of the study – that FIT screening was the most effective strategy – may have practical implications on a global scale, according to the investigators.
“Because many countries are considering implementing screening programs, the findings of this study aid in deciding on choice of screening strategies worldwide, which is based on expected participation rates and available colonoscopy resources,” they wrote.
The study was funded by the Netherlands Organization for Health Research and Development. The investigators disclosed no conflicts of interest.
SOURCE: Grobbee EJ et al. Clin Gastro Hepatol. 2019 Aug 13. doi: 10.1016/j.cgh.2019.08.015.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
GALAD score predicts NASH-HCC more than a year in advance
For patients with nonalcoholic steatohepatitis (NASH), the GALAD score may accurately predict hepatocellular carcinoma (HCC) as early as 560 days before diagnosis, according to investigators.
The GALAD score, which combines sex, age, alpha-fetoprotein-L3 (AFP-L3), alpha-fetoprotein, and des-gamma-carboxyprothrombin (DCP), could improve cancer surveillance among NASH patients whose obesity limits sensitivity of ultrasound, reported lead author Jan Best, MD, of the University Hospital Magdeburg in Germany, and colleagues.
“The limitations of ultrasound surveillance alone for early detection of HCC are particularly evident in patients with NASH,” the investigators wrote in Clinical Gastroenterology and Hepatology. “Serum-based biomarkers might be more effective, with or without ultrasound surveillance, for HCC surveillance in NASH patients, although data in this patient population are currently lacking. The current study assessed the performance of the GALAD score for early HCC detection in patients with NASH-related liver disease.”
The study consisted of two parts: first, a retrospective case-control analysis, and second, a phase 3 prospective trial that implemented the GALAD score in a real-world population.
The retrospective component of the study involved 126 NASH patients with HCC (cases) and 231 NASH patients without HCC (controls), all of whom were treated at eight centers in Germany. The median GALAD score was significantly higher among NASH patients with HCC than in those without (2.93 vs. –3.96; P less than .001). At an optimal cutoff of –1.334, the GALAD score predicted HCC with a sensitivity of 91.2% and a specificity of 95.2%. Each component of the GALAD score aligned with previously published findings, as patients with HCC were predominantly older men with elevated serum AFP-L3, AFP, and DCP. But a closer look at the data showed that the GALAD score more accurately predicted HCC than any of its constituent serum measurements in isolation. For any stage of HCC, GALAD had an area under the curve (AUC) of 0.96, compared with significantly lower values for AFP (0.88), AFP-L3 (0.86), and DCP (0.87). Similarly, for early-stage HCC, GALAD score AUC was 0.92, compared with significantly lower values for AFP (0.77), AFP-L3 (0.74), and DCP (0.87).
The accuracy of the GALAD score – for detection of both any-stage and early-stage HCC — remained high regardless of cirrhosis status. Among patients with cirrhosis, the AUC for any-stage HCC was 0.93, and 0.85 for early-stage HCC. For patients without cirrhosis, GALAD was slightly more predictive, based on AUC’s of 0.98 and 0.94 for detection of any-stage and early-stage HCC, respectively. Again, these accuracy values significantly outmatched each serum measurement in isolation.
“These data on NASH-HCC patients demonstrate that GALAD can detect HCC independent of cirrhosis or stage of HCC,” the investigators wrote. “Indeed, even early noncirrhotic NASH-HCC seems clearly separable from NASH controls, as even small groups resulted in robust performance.”
The prospective component of the study involved screening 392 patients with NASH at a single treatment center in Japan. From this cohort, 28 patients developed HCC after a median of 10.1 years. Many patients in this group had significantly higher GALAD scores for 5 or more years before being diagnosed with HCC, and scores rose sharply in the months preceding diagnosis. Depending on selected cutoff value, the GALAD score predicted HCC from 200 to 560 days prior to diagnosis.
“While this specific result has to be confirmed in further prospective studies, it is a promising observation for potential use of GALAD as a screening tool in NASH patients,” the investigators wrote.
“In conclusion, our data confirm that the GALAD score is superior to individual serum markers for detection of HCC in NASH, independent of tumor stage or cirrhosis,” the investigators wrote. “The findings suggest that GALAD should be investigated as a potential tool for screening of NASH individuals to detect HCC at a resectable stage in a sufficiently large prospective study to identify a cutoff.”
The study was funded by Deutsche Forschungsgemeinschaft, the Wilhelm-Laupitz Foundation, and the Werner Jackstaedt Foundation. The investigators declared no conflicts of interest.
SOURCE: Best J et al. Clin Gastro Hepatol. 2019 Nov 8. doi: 10.1016/j.cgh.2019.11.012.
There has been increasing recognition that ultrasound-based HCC surveillance in patients with cirrhosis has suboptimal sensitivity and specificity for early HCC detection, particularly when applied to those with nonalcoholic steatohepatitis (NASH). These data highlight the critical need for novel biomarkers to improve early HCC detection and reduce mortality. The study by Dr. Best and colleagues evaluated a blood-based biomarker panel, GALAD, in patients with NASH and found that it was able to detect HCC at an early stage with a sensitivity of 68% and specificity of 95% - performance comparable, if not superior, to that of abdominal ultrasound. In an accompanying pilot prospective cohort study, the authors also found GALAD may detect HCC more than 1 year prior to diagnosis. Although earlier studies had similarly demonstrated high performance of GALAD for early HCC detection, this study specifically examined patients with NASH - a cohort that increasingly accounts for HCC cases in the Western world but has been underrepresented in prior studies. Therefore, it is reassuring to know that GALAD appears to have high sensitivity and specificity in this patient group. However, while the data by Best et al. are promising, validation of these results in larger cohort studies is needed before routine adoption in clinical practice. Fortunately, maturation of phase 3 biomarker cohorts, including the Early Detection Research Network Hepatocellular Early Detection Strategy (EDRN HEDS) and Texas HCC Consortium, will facilitate this evaluation in the near future and will hopefully translate promising biomarkers into clinical practice.
Amit G. Singal, MD, is an associate professor of medicine, medical director of the liver tumor program, and chief of hepatology at UT Southwestern Medical Center, Dallas. He has served as a consultant for Wako Diagnostics, Glycotest, Exact Sciences, Roche Diagnostics, and TARGET Pharmasolutions.
There has been increasing recognition that ultrasound-based HCC surveillance in patients with cirrhosis has suboptimal sensitivity and specificity for early HCC detection, particularly when applied to those with nonalcoholic steatohepatitis (NASH). These data highlight the critical need for novel biomarkers to improve early HCC detection and reduce mortality. The study by Dr. Best and colleagues evaluated a blood-based biomarker panel, GALAD, in patients with NASH and found that it was able to detect HCC at an early stage with a sensitivity of 68% and specificity of 95% - performance comparable, if not superior, to that of abdominal ultrasound. In an accompanying pilot prospective cohort study, the authors also found GALAD may detect HCC more than 1 year prior to diagnosis. Although earlier studies had similarly demonstrated high performance of GALAD for early HCC detection, this study specifically examined patients with NASH - a cohort that increasingly accounts for HCC cases in the Western world but has been underrepresented in prior studies. Therefore, it is reassuring to know that GALAD appears to have high sensitivity and specificity in this patient group. However, while the data by Best et al. are promising, validation of these results in larger cohort studies is needed before routine adoption in clinical practice. Fortunately, maturation of phase 3 biomarker cohorts, including the Early Detection Research Network Hepatocellular Early Detection Strategy (EDRN HEDS) and Texas HCC Consortium, will facilitate this evaluation in the near future and will hopefully translate promising biomarkers into clinical practice.
Amit G. Singal, MD, is an associate professor of medicine, medical director of the liver tumor program, and chief of hepatology at UT Southwestern Medical Center, Dallas. He has served as a consultant for Wako Diagnostics, Glycotest, Exact Sciences, Roche Diagnostics, and TARGET Pharmasolutions.
There has been increasing recognition that ultrasound-based HCC surveillance in patients with cirrhosis has suboptimal sensitivity and specificity for early HCC detection, particularly when applied to those with nonalcoholic steatohepatitis (NASH). These data highlight the critical need for novel biomarkers to improve early HCC detection and reduce mortality. The study by Dr. Best and colleagues evaluated a blood-based biomarker panel, GALAD, in patients with NASH and found that it was able to detect HCC at an early stage with a sensitivity of 68% and specificity of 95% - performance comparable, if not superior, to that of abdominal ultrasound. In an accompanying pilot prospective cohort study, the authors also found GALAD may detect HCC more than 1 year prior to diagnosis. Although earlier studies had similarly demonstrated high performance of GALAD for early HCC detection, this study specifically examined patients with NASH - a cohort that increasingly accounts for HCC cases in the Western world but has been underrepresented in prior studies. Therefore, it is reassuring to know that GALAD appears to have high sensitivity and specificity in this patient group. However, while the data by Best et al. are promising, validation of these results in larger cohort studies is needed before routine adoption in clinical practice. Fortunately, maturation of phase 3 biomarker cohorts, including the Early Detection Research Network Hepatocellular Early Detection Strategy (EDRN HEDS) and Texas HCC Consortium, will facilitate this evaluation in the near future and will hopefully translate promising biomarkers into clinical practice.
Amit G. Singal, MD, is an associate professor of medicine, medical director of the liver tumor program, and chief of hepatology at UT Southwestern Medical Center, Dallas. He has served as a consultant for Wako Diagnostics, Glycotest, Exact Sciences, Roche Diagnostics, and TARGET Pharmasolutions.
For patients with nonalcoholic steatohepatitis (NASH), the GALAD score may accurately predict hepatocellular carcinoma (HCC) as early as 560 days before diagnosis, according to investigators.
The GALAD score, which combines sex, age, alpha-fetoprotein-L3 (AFP-L3), alpha-fetoprotein, and des-gamma-carboxyprothrombin (DCP), could improve cancer surveillance among NASH patients whose obesity limits sensitivity of ultrasound, reported lead author Jan Best, MD, of the University Hospital Magdeburg in Germany, and colleagues.
“The limitations of ultrasound surveillance alone for early detection of HCC are particularly evident in patients with NASH,” the investigators wrote in Clinical Gastroenterology and Hepatology. “Serum-based biomarkers might be more effective, with or without ultrasound surveillance, for HCC surveillance in NASH patients, although data in this patient population are currently lacking. The current study assessed the performance of the GALAD score for early HCC detection in patients with NASH-related liver disease.”
The study consisted of two parts: first, a retrospective case-control analysis, and second, a phase 3 prospective trial that implemented the GALAD score in a real-world population.
The retrospective component of the study involved 126 NASH patients with HCC (cases) and 231 NASH patients without HCC (controls), all of whom were treated at eight centers in Germany. The median GALAD score was significantly higher among NASH patients with HCC than in those without (2.93 vs. –3.96; P less than .001). At an optimal cutoff of –1.334, the GALAD score predicted HCC with a sensitivity of 91.2% and a specificity of 95.2%. Each component of the GALAD score aligned with previously published findings, as patients with HCC were predominantly older men with elevated serum AFP-L3, AFP, and DCP. But a closer look at the data showed that the GALAD score more accurately predicted HCC than any of its constituent serum measurements in isolation. For any stage of HCC, GALAD had an area under the curve (AUC) of 0.96, compared with significantly lower values for AFP (0.88), AFP-L3 (0.86), and DCP (0.87). Similarly, for early-stage HCC, GALAD score AUC was 0.92, compared with significantly lower values for AFP (0.77), AFP-L3 (0.74), and DCP (0.87).
The accuracy of the GALAD score – for detection of both any-stage and early-stage HCC — remained high regardless of cirrhosis status. Among patients with cirrhosis, the AUC for any-stage HCC was 0.93, and 0.85 for early-stage HCC. For patients without cirrhosis, GALAD was slightly more predictive, based on AUC’s of 0.98 and 0.94 for detection of any-stage and early-stage HCC, respectively. Again, these accuracy values significantly outmatched each serum measurement in isolation.
“These data on NASH-HCC patients demonstrate that GALAD can detect HCC independent of cirrhosis or stage of HCC,” the investigators wrote. “Indeed, even early noncirrhotic NASH-HCC seems clearly separable from NASH controls, as even small groups resulted in robust performance.”
The prospective component of the study involved screening 392 patients with NASH at a single treatment center in Japan. From this cohort, 28 patients developed HCC after a median of 10.1 years. Many patients in this group had significantly higher GALAD scores for 5 or more years before being diagnosed with HCC, and scores rose sharply in the months preceding diagnosis. Depending on selected cutoff value, the GALAD score predicted HCC from 200 to 560 days prior to diagnosis.
“While this specific result has to be confirmed in further prospective studies, it is a promising observation for potential use of GALAD as a screening tool in NASH patients,” the investigators wrote.
“In conclusion, our data confirm that the GALAD score is superior to individual serum markers for detection of HCC in NASH, independent of tumor stage or cirrhosis,” the investigators wrote. “The findings suggest that GALAD should be investigated as a potential tool for screening of NASH individuals to detect HCC at a resectable stage in a sufficiently large prospective study to identify a cutoff.”
The study was funded by Deutsche Forschungsgemeinschaft, the Wilhelm-Laupitz Foundation, and the Werner Jackstaedt Foundation. The investigators declared no conflicts of interest.
SOURCE: Best J et al. Clin Gastro Hepatol. 2019 Nov 8. doi: 10.1016/j.cgh.2019.11.012.
For patients with nonalcoholic steatohepatitis (NASH), the GALAD score may accurately predict hepatocellular carcinoma (HCC) as early as 560 days before diagnosis, according to investigators.
The GALAD score, which combines sex, age, alpha-fetoprotein-L3 (AFP-L3), alpha-fetoprotein, and des-gamma-carboxyprothrombin (DCP), could improve cancer surveillance among NASH patients whose obesity limits sensitivity of ultrasound, reported lead author Jan Best, MD, of the University Hospital Magdeburg in Germany, and colleagues.
“The limitations of ultrasound surveillance alone for early detection of HCC are particularly evident in patients with NASH,” the investigators wrote in Clinical Gastroenterology and Hepatology. “Serum-based biomarkers might be more effective, with or without ultrasound surveillance, for HCC surveillance in NASH patients, although data in this patient population are currently lacking. The current study assessed the performance of the GALAD score for early HCC detection in patients with NASH-related liver disease.”
The study consisted of two parts: first, a retrospective case-control analysis, and second, a phase 3 prospective trial that implemented the GALAD score in a real-world population.
The retrospective component of the study involved 126 NASH patients with HCC (cases) and 231 NASH patients without HCC (controls), all of whom were treated at eight centers in Germany. The median GALAD score was significantly higher among NASH patients with HCC than in those without (2.93 vs. –3.96; P less than .001). At an optimal cutoff of –1.334, the GALAD score predicted HCC with a sensitivity of 91.2% and a specificity of 95.2%. Each component of the GALAD score aligned with previously published findings, as patients with HCC were predominantly older men with elevated serum AFP-L3, AFP, and DCP. But a closer look at the data showed that the GALAD score more accurately predicted HCC than any of its constituent serum measurements in isolation. For any stage of HCC, GALAD had an area under the curve (AUC) of 0.96, compared with significantly lower values for AFP (0.88), AFP-L3 (0.86), and DCP (0.87). Similarly, for early-stage HCC, GALAD score AUC was 0.92, compared with significantly lower values for AFP (0.77), AFP-L3 (0.74), and DCP (0.87).
The accuracy of the GALAD score – for detection of both any-stage and early-stage HCC — remained high regardless of cirrhosis status. Among patients with cirrhosis, the AUC for any-stage HCC was 0.93, and 0.85 for early-stage HCC. For patients without cirrhosis, GALAD was slightly more predictive, based on AUC’s of 0.98 and 0.94 for detection of any-stage and early-stage HCC, respectively. Again, these accuracy values significantly outmatched each serum measurement in isolation.
“These data on NASH-HCC patients demonstrate that GALAD can detect HCC independent of cirrhosis or stage of HCC,” the investigators wrote. “Indeed, even early noncirrhotic NASH-HCC seems clearly separable from NASH controls, as even small groups resulted in robust performance.”
The prospective component of the study involved screening 392 patients with NASH at a single treatment center in Japan. From this cohort, 28 patients developed HCC after a median of 10.1 years. Many patients in this group had significantly higher GALAD scores for 5 or more years before being diagnosed with HCC, and scores rose sharply in the months preceding diagnosis. Depending on selected cutoff value, the GALAD score predicted HCC from 200 to 560 days prior to diagnosis.
“While this specific result has to be confirmed in further prospective studies, it is a promising observation for potential use of GALAD as a screening tool in NASH patients,” the investigators wrote.
“In conclusion, our data confirm that the GALAD score is superior to individual serum markers for detection of HCC in NASH, independent of tumor stage or cirrhosis,” the investigators wrote. “The findings suggest that GALAD should be investigated as a potential tool for screening of NASH individuals to detect HCC at a resectable stage in a sufficiently large prospective study to identify a cutoff.”
The study was funded by Deutsche Forschungsgemeinschaft, the Wilhelm-Laupitz Foundation, and the Werner Jackstaedt Foundation. The investigators declared no conflicts of interest.
SOURCE: Best J et al. Clin Gastro Hepatol. 2019 Nov 8. doi: 10.1016/j.cgh.2019.11.012.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Fewer complications, better outcomes with outpatient UKA
according to a review from the University of Tennessee Campbell Clinic, Memphis.
“In carefully selected patients, the ASC [ambulatory surgery center] seems to be a safe alternative to the inpatient hospital setting,” concluded investigators led by led by Marcus Ford, MD, a Campbell Clinic orthopedic surgeon.
He and his colleagues have been doing outpatient unicompartmental knee arthroplasty (UKA) since 2009, and “based on the subjective success,” recently increased the number of total knee, hip, and shoulder arthroplasties performed in their ASC.
They wanted to make sure, however, that their impression of good outpatient UKA results was supported by the data, so they compared outcomes in 48 UKA patients treated at their ASC with 48 treated in the hospital. The operations were done by two surgeons using the same technique and same medial UKA implant.
“Naturally, surgeons select those patients who are deemed physically and mentally capable of succeeding with an accelerated discharge plan” for outpatient service, the investigators wrote. To address that potential selection bias, the team matched their subjects by age and comorbidities.
There was only one minor complication in the outpatient group, a superficial stitch abscess. No patient needed a second operation, and all went home the same day.
It was different on the inpatient side. The average length of stay was 2.9 days, and there were four major complications: a deep venous thrombosis, a pulmonary embolus, an acute postoperative infection, and a periprosthetic fracture. All four required hospital readmission, and two patients needed a second operation.
The report didn’t directly address the reasons for the differences, but Dr. Ford and colleagues did note that they “believe that the ASC allows the surgeon greater direct control of perioperative variables that can impact patient outcome.”
Patients were in their late 50s, on average, and there were more women than men in both groups. The mean American Society of Anesthesiologists physical status classification score was 1.94 and mean body mass index was 34.3 kg/m2 in the outpatient group, compared with a mean physical status classification score of 2.08 and mean body mass index of 32.9 kg/m2 in the inpatient group. The differences were not statistically significant.
No funding source was reported. The investigators did not report any disclosures.
SOURCE: Ford M et al. Orthop Clin North Am. 2020 Jan;51[1]:1-5. doi: 10.1016/j.ocl.2019.08.001
according to a review from the University of Tennessee Campbell Clinic, Memphis.
“In carefully selected patients, the ASC [ambulatory surgery center] seems to be a safe alternative to the inpatient hospital setting,” concluded investigators led by led by Marcus Ford, MD, a Campbell Clinic orthopedic surgeon.
He and his colleagues have been doing outpatient unicompartmental knee arthroplasty (UKA) since 2009, and “based on the subjective success,” recently increased the number of total knee, hip, and shoulder arthroplasties performed in their ASC.
They wanted to make sure, however, that their impression of good outpatient UKA results was supported by the data, so they compared outcomes in 48 UKA patients treated at their ASC with 48 treated in the hospital. The operations were done by two surgeons using the same technique and same medial UKA implant.
“Naturally, surgeons select those patients who are deemed physically and mentally capable of succeeding with an accelerated discharge plan” for outpatient service, the investigators wrote. To address that potential selection bias, the team matched their subjects by age and comorbidities.
There was only one minor complication in the outpatient group, a superficial stitch abscess. No patient needed a second operation, and all went home the same day.
It was different on the inpatient side. The average length of stay was 2.9 days, and there were four major complications: a deep venous thrombosis, a pulmonary embolus, an acute postoperative infection, and a periprosthetic fracture. All four required hospital readmission, and two patients needed a second operation.
The report didn’t directly address the reasons for the differences, but Dr. Ford and colleagues did note that they “believe that the ASC allows the surgeon greater direct control of perioperative variables that can impact patient outcome.”
Patients were in their late 50s, on average, and there were more women than men in both groups. The mean American Society of Anesthesiologists physical status classification score was 1.94 and mean body mass index was 34.3 kg/m2 in the outpatient group, compared with a mean physical status classification score of 2.08 and mean body mass index of 32.9 kg/m2 in the inpatient group. The differences were not statistically significant.
No funding source was reported. The investigators did not report any disclosures.
SOURCE: Ford M et al. Orthop Clin North Am. 2020 Jan;51[1]:1-5. doi: 10.1016/j.ocl.2019.08.001
according to a review from the University of Tennessee Campbell Clinic, Memphis.
“In carefully selected patients, the ASC [ambulatory surgery center] seems to be a safe alternative to the inpatient hospital setting,” concluded investigators led by led by Marcus Ford, MD, a Campbell Clinic orthopedic surgeon.
He and his colleagues have been doing outpatient unicompartmental knee arthroplasty (UKA) since 2009, and “based on the subjective success,” recently increased the number of total knee, hip, and shoulder arthroplasties performed in their ASC.
They wanted to make sure, however, that their impression of good outpatient UKA results was supported by the data, so they compared outcomes in 48 UKA patients treated at their ASC with 48 treated in the hospital. The operations were done by two surgeons using the same technique and same medial UKA implant.
“Naturally, surgeons select those patients who are deemed physically and mentally capable of succeeding with an accelerated discharge plan” for outpatient service, the investigators wrote. To address that potential selection bias, the team matched their subjects by age and comorbidities.
There was only one minor complication in the outpatient group, a superficial stitch abscess. No patient needed a second operation, and all went home the same day.
It was different on the inpatient side. The average length of stay was 2.9 days, and there were four major complications: a deep venous thrombosis, a pulmonary embolus, an acute postoperative infection, and a periprosthetic fracture. All four required hospital readmission, and two patients needed a second operation.
The report didn’t directly address the reasons for the differences, but Dr. Ford and colleagues did note that they “believe that the ASC allows the surgeon greater direct control of perioperative variables that can impact patient outcome.”
Patients were in their late 50s, on average, and there were more women than men in both groups. The mean American Society of Anesthesiologists physical status classification score was 1.94 and mean body mass index was 34.3 kg/m2 in the outpatient group, compared with a mean physical status classification score of 2.08 and mean body mass index of 32.9 kg/m2 in the inpatient group. The differences were not statistically significant.
No funding source was reported. The investigators did not report any disclosures.
SOURCE: Ford M et al. Orthop Clin North Am. 2020 Jan;51[1]:1-5. doi: 10.1016/j.ocl.2019.08.001
FROM ORTHOPEDIC CLINICS OF NORTH AMERICA
Effect of In-Office Samples on Dermatologists’ Prescribing Habits: A Retrospective Review
Over the years, there has been growing concern about the relationship between physicians and pharmaceutical companies. Many studies have demonstrated that pharmaceutical interactions and incentives can influence physicians’ prescribing habits.1-3 As a result, many academic centers have adopted policies that attempt to limit the pharmaceutical industry’s influence on faculty and in-training physicians. Although these policies can vary greatly, they generally limit access of pharmaceutical representatives to providers and restrict pharmaceutical samples.4,5 This policy shift has even been reported in private practice.6
At the heart of the matter is the question: What really influences physicians to write a prescription for a particular medication? Is it cost, efficacy, or representatives pushing a product? Prior studies illustrate that generic medications are equivalent to their brand-name counterparts. In fact, current regulations require no more than 5% to 7% difference in bioequivalence.7-9 Although most generic medications are bioequivalent, it may not be universal.10
Garrison and Levin11 distributed a survey to US-based prescribers in family practice, psychiatry, and internal medicine and found that prescribers deemed patient response and success as the highest priority when determining which drugs to prescribe. In contrast, drug representatives and free samples only slightly contributed.11 Considering the minimum duration for efficacy of a medication such as an antidepressant vs a topical steroid, this pattern may differ with samples in dermatologic settings. Interestingly, another survey concluded that samples were associated with “sticky” prescribing habits, noting that physicians would prescribe a brand-name medication after using a sample, despite increased cost to the patient.12 Further, it has been suggested that recipients of free samples may experience increased costs in the long run, which contrasts a stated goal of affordability to patients.12,13
Physician interaction with pharmaceutical companies begins as early as medical school,14 with physicians reporting interactions as often as 4 times each month.14-18 Interactions can include meetings with pharmaceutical representatives, sponsored meals, gifts, continuing medical education sponsorship, funding for travel, pharmaceutical representative speakers, research funding, and drug samples.3
A 2014 study reported that prescribing habits are influenced by the free drug samples provided by nongeneric pharmaceutical companies.19 Nationally, the number of brand-name and branded generic medications constitute 79% of prescriptions, yet together they only comprise 17% of medications prescribed at an academic medical clinic that does not provide samples. The number of medications with samples being prescribed by dermatologists increased by 15% over 9 years, which may correlate with the wider availability of medication samples, more specifically an increase in branded generic samples.19 This potential interaction is the reason why institutions question the current influence of pharmaceutical companies. Samples may appear convenient, allowing a patient to test the medication prior to committing; however, with brand-name samples being provided to the physician, he/she may become more inclined to prescribe the branded medication.12,15,19-22 Because brand-name medications are more expensive than generic medications, this practice can increase the cost of health care.13 One study found that over 1 year, the overuse of nongeneric medications led to a loss of potential savings throughout 49 states, equating to $229 million just through Medicaid; interestingly, it was noted that in some states, a maximum reimbursement is set by Medicaid, regardless of whether the generic or branded medication is dispensed. The authors also noted variability in the potential savings by state, which may be a function of the state-by-state maximum reimbursements for certain medications.23 Another study on oral combination medications estimated Medicare spending on branded drugs relative to the cost if generic combinations had been purchased instead. This study examined branded medications for which the active components were available as over-the-counter (OTC), generic, or same-class generic, and the authors estimated that $925 million could have been saved in 2016 by purchasing a generic substitute.24 The overuse of nongeneric medications when generic alternatives are available becomes an issue that not only financially impacts patients but all taxpayers. However, this pattern may differ if limited only to dermatologic medications, which was not the focus of the prior studies.
To limit conflicts of interest in interactions with the pharmaceutical, medical device, and biotechnology industries, the University of South Florida (USF) Morsani College of Medicine (COM)(Tampa, Florida) implemented its own set of regulations that eliminated in-office pharmaceutical samples, in addition to other restrictions. This study aimed to investigate if there was a change in the prescribing habits of academic dermatologists after their medical school implemented these new policies.
We hypothesized that the number of brand-name drugs prescribed by physicians in the Department of Dermatology & Cutaneous Surgery would change following USF Morsani COM pharmaceutical policy changes. We sought to determine how physician prescribing practices within the Department of Dermatology & Cutaneous Surgery changed following USF Morsani COM pharmaceutical policy changes.
Methods
Data Collection
A retrospective review of medical records was conducted to investigate the effect of the USF Morsani COM pharmaceutical policy changes on physician prescribing practices within the Department of Dermatology & Cutaneous Surgery. Medical records of patients seen for common dermatology diagnoses before (January 1, 2010, to May 30, 2010) and after (August 1, 2011, to December 31, 2011) the pharmaceutical policy changes were reviewed, and all medications prescribed were recorded. Data were collected from medical records within the USF Health electronic medical record system and included visits with each of the department’s 3 attending dermatologists. The diagnoses included in the study—acne vulgaris, atopic dermatitis, onychomycosis, psoriasis, and rosacea—were chosen because in-office samples were available. Prescribing data from the first 100 consecutive medical records were collected from each time period, and a medical record was included only if it contained at least 1 of the following diagnoses: acne vulgaris, atopic dermatitis, onychomycosis, psoriasis, or rosacea. The assessment and plan of each progress note were reviewed, and the exact medication name and associated diagnosis were recorded for each prescription. Subsequently, each medication was reviewed and placed in 1 of 3 categories: brand name, generic, and OTC. The total number of prescriptions for each diagnosis (per visit/note); the specific number of brand, generic, and OTC medications prescribed (per visit/note); and the percentage of brand, generic, and OTC medications prescribed (per visit/note and per diagnosis in total) were calculated. To ensure only intended medications were included, each medication recorded in the medical record note was cross-referenced with the prescribed medication in the electronic medical record. The primary objective of this study was to capture the prescribing physician’s intent as proxied by the pattern of prescription. Thus, changes made in prescriptions after the initial plan—whether insurance related or otherwise—were not relevant to this investigation.
The data were collected to compare the percentage of brand vs generic or OTC prescriptions per diagnosis to see if there was a difference in the prescribing habits before and after the pharmaceutical policy changes. Of note, several other pieces of data were collected from each medical record, including age, race, class of insurance (ie, Medicare, Medicaid, private health maintenance organization, private preferred provider organization), subtype diagnoses, and whether the prescription was new or a refill. The information gathered from the written record on the assessment and plan was verified using prescriptions ordered in the Allscripts electronic record, and any difference was noted. No identifying information that could be used to easily identify study participants was recorded.
Differences in prescribing habits across diagnoses before and after the policy changes were ascertained using a Fisher exact test and were further assessed using a mixed effects ordinal logistic regression model that accounted for within-provider clustering and baseline patient characteristics. An ordinal model was chosen to recognize differences in average cost among brand-name, generic, and OTC medications.
Results
In total, 200 medical records were collected. For the period analyzed before the policy change, 252 brand-name medications were prescribed compared to 231 prescribed for the period analyzed after the policy changes. There was insufficient evidence of an overall difference in brand-name medications prescribed before and after the policy changes (P=.145; Fisher exact test)(Table 1). There also was insufficient evidence of an overall difference in generic prescriptions, which totaled 153 before and 134 after the policy changes (P=.872; Fisher exact test)(Table 2). Over-the-counter prescriptions totaled 49 before and 69 after the policy changes. There was insufficient evidence of an overall difference before and after the policy changes for OTC medications (P=.192; Fisher exact test)(Table 3).
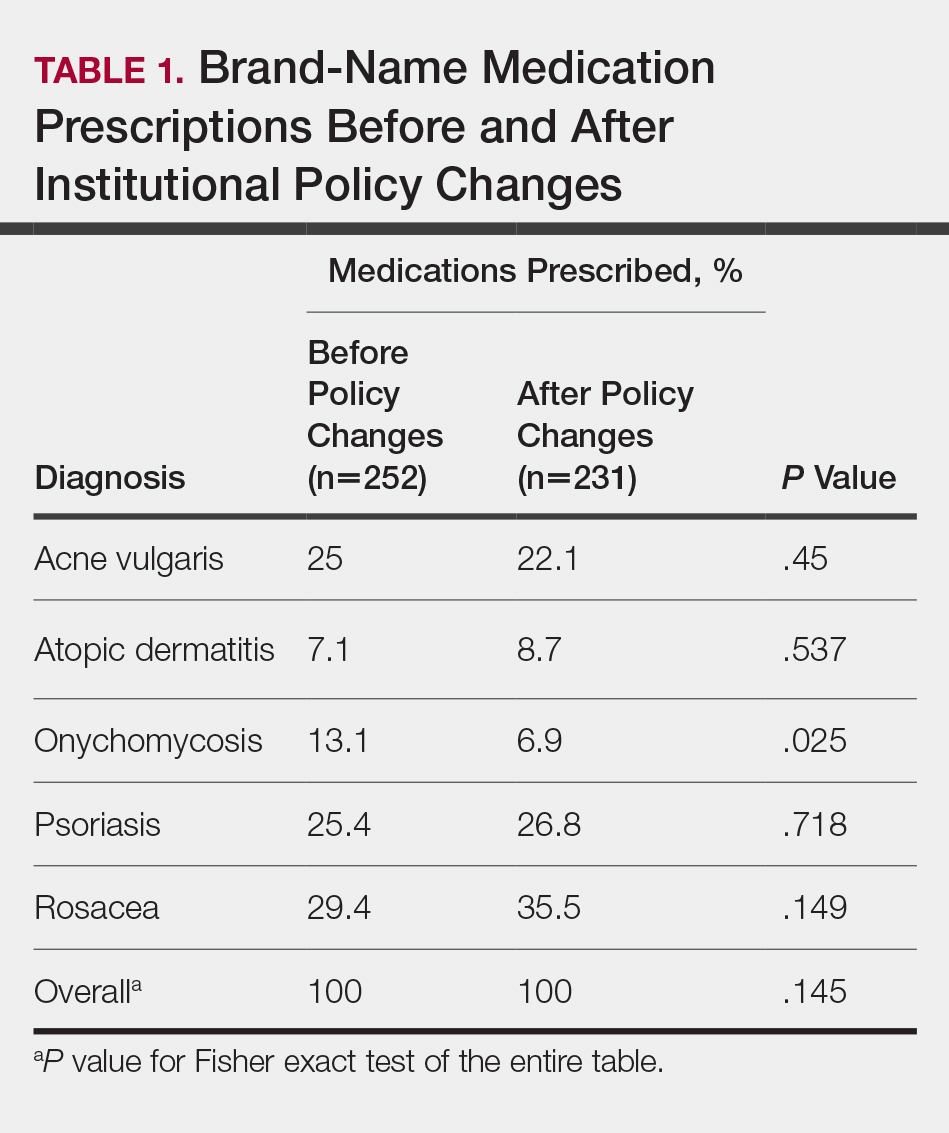

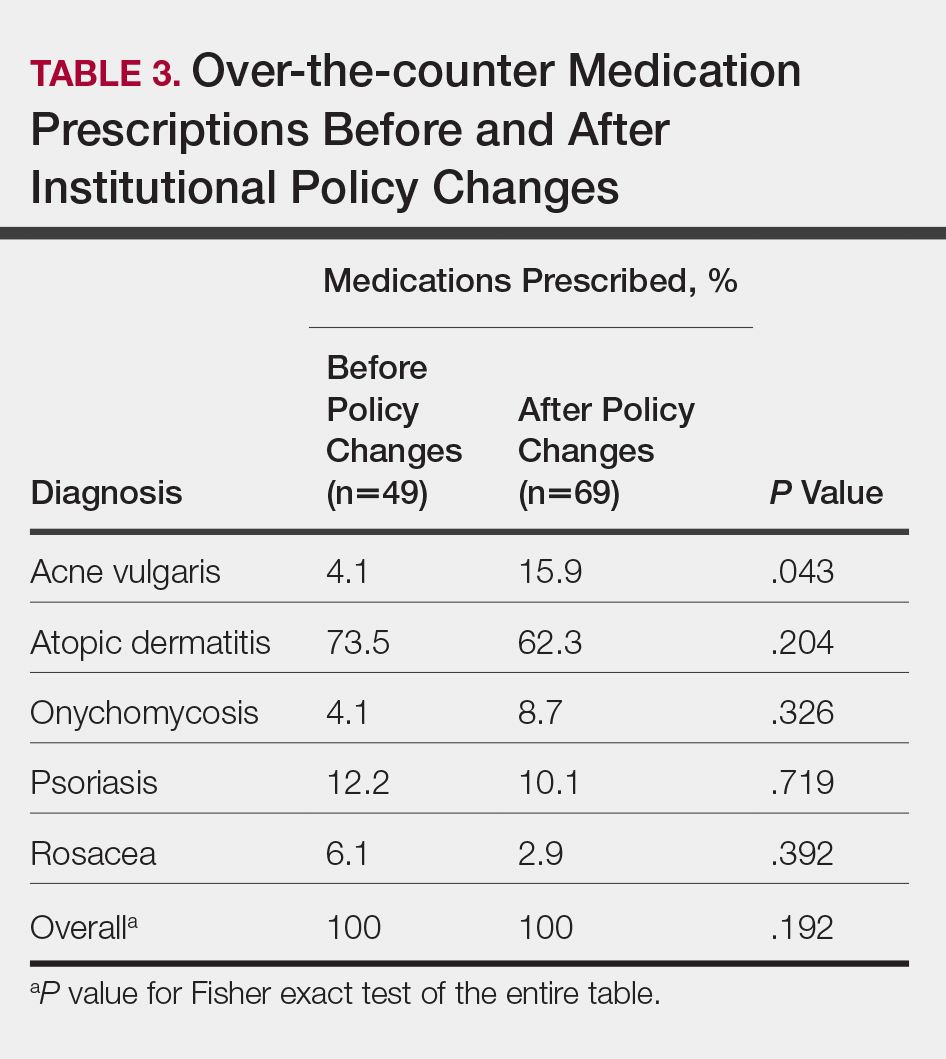
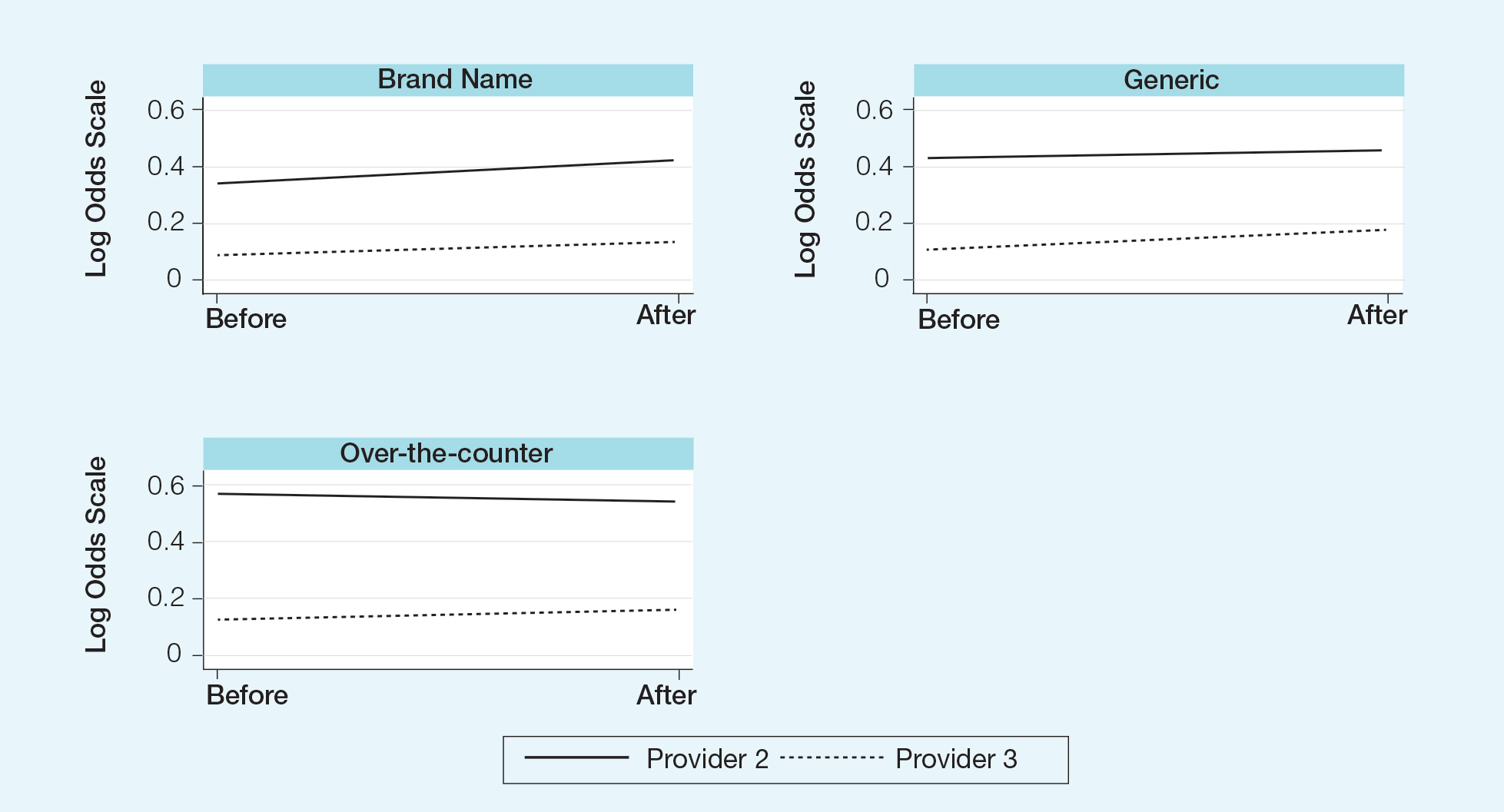
Comment
Although some medical institutions are diligently working to limit the potential influence pharmaceutical companies have on physician prescribing habits,4,5,25 the effect on physician prescribing habits is only now being established.15 Prior studies12,19,21 have found evidence that medication samples may lead to overuse of brand-name medications, but these findings do not hold true for the USF dermatologists included in this study, perhaps due to the difference in pharmaceutical company interactions or physicians maintaining prior prescription habits that were unrelated to the policy. Although this study focused on policy changes for in-office samples, prior studies either included other forms of interaction21 or did not include samples.22
Pharmaceutical samples allow patients to try a medication before committing to a long-term course of treatment with a particular medication, which has utility for physicians and patients. Although brand-name prescriptions may cost more, a trial period may assist the patient in deciding whether the medication is worth purchasing. Furthermore, physicians may feel more comfortable prescribing a medication once the individual patient has demonstrated a benefit from the sample, which may be particularly true in a specialty such as dermatology in which many branded topical medications contain a different vehicle than generic formulations, resulting in notable variations in active medication delivery and efficacy. Given the higher cost of branded topical medications, proving efficacy in patients through samples can provide a useful tool to the physician to determine the need for a branded formulation.
The benefits described are subjective but should not be disregarded. Although Hurley et al19 found that the number of brand-name medications prescribed increases as more samples are given out, our study demonstrated that after eliminating medication samples, there was no significant difference in the percentage of brand-name medications prescribed compared to generic and OTC medications.
Physician education concerning the price of each brand-name medication prescribed in office may be one method of reducing the amount of such prescriptions. Physicians generally are uninformed of the cost of the medications being prescribed26 and may not recognize the financial burden one medication may have compared to its alternative. However, educating physicians will empower them to make the conscious decision to prefer or not prefer a brand-name medication. With some generic medications shown to have a difference in bioequivalence compared to their brand-name counterparts, a physician may find more success prescribing the brand-name medications, regardless of pharmaceutical company influence, which is an alternative solution to policy changes that eliminate samples entirely. Although this study found insufficient evidence that removing samples decreases brand-name medication prescriptions, it is imperative that solutions are established to reduce the country’s increasing burden of medical costs.
Possible shortfalls of this study include the short period of time between which prepolicy data and postpolicy data were collected. It is possible that providers did not have enough time to adjust their prescribing habits or that providers would not have changed a prescribing pattern or preference simply because of a policy change. Future studies could allow a time period greater than 2 years to compare prepolicy and postpolicy prescribing habits, or a future study might make comparisons of prescriber patterns at different institutions that have different policies. Another possible shortfall is that providers and patients were limited to those at the Department of Dermatology & Cutaneous Surgery at the USF Morsani COM. Although this study has found insufficient evidence of a difference in prescribing habits, it may be beneficial to conduct a larger study that encompasses multiple academic institutions with similar policy changes. Most importantly, this study only investigated the influence of in-office pharmaceutical samples on prescribing patterns. This study did not look at the many other ways in which providers may be influenced by pharmaceutical companies, which likely is a significant confounding variable in this study. Continued additional studies that specifically examine other methods through which providers may be influenced would be helpful in further examining the many ways in which physician prescription habits are influenced.
Conclusion
Changes in pharmaceutical policy in 2011 at USF Morsani COM specifically banned in-office samples. The totality of evidence in this study shows modest observational evidence of a change in the postpolicy odds relative to prepolicy odds, but the data also are compatible with no change between prescribing habits before and after the policy changes. Further study is needed to fully understand this relationship.
- Sondergaard J, Vach K, Kragstrup J, et al. Impact of pharmaceutical representative visits on GPs’ drug preferences. Fam Pract. 2009;26:204-209.
- Jelinek GA, Neate SL. The influence of the pharmaceutical industry in medicine. J Law Med. 2009;17:216-223.
- Wazana A. Physicians and the pharmaceutical industry: is a gift ever just a gift? JAMA. 2000;283:373-380.
- Coleman DL. Establishing policies for the relationship between industry and clinicians: lessons learned from two academic health centers. Acad Med. 2008;83:882-887.
- Coleman DL, Kazdin AE, Miller LA, et al. Guidelines for interactions between clinical faculty and the pharmaceutical industry: one medical school’s approach. Acad Med. 2006;81:154-160.
- Evans D, Hartung DM, Beasley D, et al. Breaking up is hard to do: lessons learned from a pharma-free practice transformation. J Am Board Fam Med. 2013;26:332-338.
- Davit BM, Nwakama PE, Buehler GJ, et al. Comparing generic and innovator drugs: a review of 12 years of bioequivalence data from the United States Food and Drug Administration. Ann Pharmacother. 2009;43:1583-1597.
- Kesselheim AS, Misono AS, Lee JL, et al. Clinical equivalence of generic and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008;300:2514-2526.
- McCormack J, Chmelicek JT. Generic versus brand name: the other drug war. Can Fam Physician. 2014;60:911.
- Borgheini G. The bioequivalence and therapeutic efficacy of generic versus brand-name psychoactive drugs. Clin Ther. 2003;25:1578-1592.
- Garrison GD, Levin GM. Factors affecting prescribing of the newer antidepressants. Ann Pharmacother. 2000;34:10-14.
- Rafique S, Sarwar W, Rashid A, et al. Influence of free drug samples on prescribing by physicians: a cross sectional survey. J Pak Med Assoc. 2017;67:465-467.
- Alexander GC, Zhang J, Basu A. Characteristics of patients receiving pharmaceutical samples and association between sample receipt and out-of-pocket prescription costs. Med Care. 2008;46:394-402.
- Hodges B. Interactions with the pharmaceutical industry: experiences and attitudes of psychiatry residents, interns and clerks. CMAJ. 1995;153:553-559.
- Brotzman GL, Mark DH. The effect on resident attitudes of regulatory policies regarding pharmaceutical representative activities. J Gen Intern Med. 1993;8:130-134.
- Keim SM, Sanders AB, Witzke DB, et al. Beliefs and practices of emergency medicine faculty and residents regarding professional interactions with the biomedical industry. Ann Emerg Med. 1993;22:1576-1581.
- Thomson AN, Craig BJ, Barham PM. Attitudes of general practitioners in New Zealand to pharmaceutical representatives. Br J Gen Pract. 1994;44:220-223.
- Ziegler MG, Lew P, Singer BC. The accuracy of drug information from pharmaceutical sales representatives. JAMA. 1995;273:1296-1298.
- Hurley MP, Stafford RS, Lane AT. Characterizing the relationship between free drug samples and prescription patterns for acne vulgaris and rosacea. JAMA Dermatol. 2014;150:487-493.
- Lexchin J. Interactions between physicians and the pharmaceutical industry: what does the literature say? CMAJ. 1993;149:1401-1407.
- Lieb K, Scheurich A. Contact between doctors and the pharmaceutical industry, their perceptions, and the effects on prescribing habits. PLoS One. 2014;9:e110130.
- Spurling GK, Mansfield PR, Montgomery BD, et al. Information from pharmaceutical companies and the quality, quantity, and cost of physicians’ prescribing: a systematic review. PLoS Med. 2010;7:e1000352.
- Fischer MA, Avorn J. Economic consequences of underuse of generic drugs: evidence from Medicaid and implications for prescription drug benefit plans. Health Serv Res. 2003;38:1051-1064.
- Sacks CA, Lee CC, Kesselheim AS, et al. Medicare spending on brand-name combination medications vs their generic constituents. JAMA. 2018;320:650-656.
- Brennan TA, Rothman DJ, Blank L, et al. Health industry practices that create conflicts of interest: a policy proposal for academic medical centers. JAMA. 2006;295:429-433.
- Allan GM, Lexchin J, Wiebe N. Physician awareness of drug cost: a systematic review. PLoS Med. 2007;4:e283.
Over the years, there has been growing concern about the relationship between physicians and pharmaceutical companies. Many studies have demonstrated that pharmaceutical interactions and incentives can influence physicians’ prescribing habits.1-3 As a result, many academic centers have adopted policies that attempt to limit the pharmaceutical industry’s influence on faculty and in-training physicians. Although these policies can vary greatly, they generally limit access of pharmaceutical representatives to providers and restrict pharmaceutical samples.4,5 This policy shift has even been reported in private practice.6
At the heart of the matter is the question: What really influences physicians to write a prescription for a particular medication? Is it cost, efficacy, or representatives pushing a product? Prior studies illustrate that generic medications are equivalent to their brand-name counterparts. In fact, current regulations require no more than 5% to 7% difference in bioequivalence.7-9 Although most generic medications are bioequivalent, it may not be universal.10
Garrison and Levin11 distributed a survey to US-based prescribers in family practice, psychiatry, and internal medicine and found that prescribers deemed patient response and success as the highest priority when determining which drugs to prescribe. In contrast, drug representatives and free samples only slightly contributed.11 Considering the minimum duration for efficacy of a medication such as an antidepressant vs a topical steroid, this pattern may differ with samples in dermatologic settings. Interestingly, another survey concluded that samples were associated with “sticky” prescribing habits, noting that physicians would prescribe a brand-name medication after using a sample, despite increased cost to the patient.12 Further, it has been suggested that recipients of free samples may experience increased costs in the long run, which contrasts a stated goal of affordability to patients.12,13
Physician interaction with pharmaceutical companies begins as early as medical school,14 with physicians reporting interactions as often as 4 times each month.14-18 Interactions can include meetings with pharmaceutical representatives, sponsored meals, gifts, continuing medical education sponsorship, funding for travel, pharmaceutical representative speakers, research funding, and drug samples.3
A 2014 study reported that prescribing habits are influenced by the free drug samples provided by nongeneric pharmaceutical companies.19 Nationally, the number of brand-name and branded generic medications constitute 79% of prescriptions, yet together they only comprise 17% of medications prescribed at an academic medical clinic that does not provide samples. The number of medications with samples being prescribed by dermatologists increased by 15% over 9 years, which may correlate with the wider availability of medication samples, more specifically an increase in branded generic samples.19 This potential interaction is the reason why institutions question the current influence of pharmaceutical companies. Samples may appear convenient, allowing a patient to test the medication prior to committing; however, with brand-name samples being provided to the physician, he/she may become more inclined to prescribe the branded medication.12,15,19-22 Because brand-name medications are more expensive than generic medications, this practice can increase the cost of health care.13 One study found that over 1 year, the overuse of nongeneric medications led to a loss of potential savings throughout 49 states, equating to $229 million just through Medicaid; interestingly, it was noted that in some states, a maximum reimbursement is set by Medicaid, regardless of whether the generic or branded medication is dispensed. The authors also noted variability in the potential savings by state, which may be a function of the state-by-state maximum reimbursements for certain medications.23 Another study on oral combination medications estimated Medicare spending on branded drugs relative to the cost if generic combinations had been purchased instead. This study examined branded medications for which the active components were available as over-the-counter (OTC), generic, or same-class generic, and the authors estimated that $925 million could have been saved in 2016 by purchasing a generic substitute.24 The overuse of nongeneric medications when generic alternatives are available becomes an issue that not only financially impacts patients but all taxpayers. However, this pattern may differ if limited only to dermatologic medications, which was not the focus of the prior studies.
To limit conflicts of interest in interactions with the pharmaceutical, medical device, and biotechnology industries, the University of South Florida (USF) Morsani College of Medicine (COM)(Tampa, Florida) implemented its own set of regulations that eliminated in-office pharmaceutical samples, in addition to other restrictions. This study aimed to investigate if there was a change in the prescribing habits of academic dermatologists after their medical school implemented these new policies.
We hypothesized that the number of brand-name drugs prescribed by physicians in the Department of Dermatology & Cutaneous Surgery would change following USF Morsani COM pharmaceutical policy changes. We sought to determine how physician prescribing practices within the Department of Dermatology & Cutaneous Surgery changed following USF Morsani COM pharmaceutical policy changes.
Methods
Data Collection
A retrospective review of medical records was conducted to investigate the effect of the USF Morsani COM pharmaceutical policy changes on physician prescribing practices within the Department of Dermatology & Cutaneous Surgery. Medical records of patients seen for common dermatology diagnoses before (January 1, 2010, to May 30, 2010) and after (August 1, 2011, to December 31, 2011) the pharmaceutical policy changes were reviewed, and all medications prescribed were recorded. Data were collected from medical records within the USF Health electronic medical record system and included visits with each of the department’s 3 attending dermatologists. The diagnoses included in the study—acne vulgaris, atopic dermatitis, onychomycosis, psoriasis, and rosacea—were chosen because in-office samples were available. Prescribing data from the first 100 consecutive medical records were collected from each time period, and a medical record was included only if it contained at least 1 of the following diagnoses: acne vulgaris, atopic dermatitis, onychomycosis, psoriasis, or rosacea. The assessment and plan of each progress note were reviewed, and the exact medication name and associated diagnosis were recorded for each prescription. Subsequently, each medication was reviewed and placed in 1 of 3 categories: brand name, generic, and OTC. The total number of prescriptions for each diagnosis (per visit/note); the specific number of brand, generic, and OTC medications prescribed (per visit/note); and the percentage of brand, generic, and OTC medications prescribed (per visit/note and per diagnosis in total) were calculated. To ensure only intended medications were included, each medication recorded in the medical record note was cross-referenced with the prescribed medication in the electronic medical record. The primary objective of this study was to capture the prescribing physician’s intent as proxied by the pattern of prescription. Thus, changes made in prescriptions after the initial plan—whether insurance related or otherwise—were not relevant to this investigation.
The data were collected to compare the percentage of brand vs generic or OTC prescriptions per diagnosis to see if there was a difference in the prescribing habits before and after the pharmaceutical policy changes. Of note, several other pieces of data were collected from each medical record, including age, race, class of insurance (ie, Medicare, Medicaid, private health maintenance organization, private preferred provider organization), subtype diagnoses, and whether the prescription was new or a refill. The information gathered from the written record on the assessment and plan was verified using prescriptions ordered in the Allscripts electronic record, and any difference was noted. No identifying information that could be used to easily identify study participants was recorded.
Differences in prescribing habits across diagnoses before and after the policy changes were ascertained using a Fisher exact test and were further assessed using a mixed effects ordinal logistic regression model that accounted for within-provider clustering and baseline patient characteristics. An ordinal model was chosen to recognize differences in average cost among brand-name, generic, and OTC medications.
Results
In total, 200 medical records were collected. For the period analyzed before the policy change, 252 brand-name medications were prescribed compared to 231 prescribed for the period analyzed after the policy changes. There was insufficient evidence of an overall difference in brand-name medications prescribed before and after the policy changes (P=.145; Fisher exact test)(Table 1). There also was insufficient evidence of an overall difference in generic prescriptions, which totaled 153 before and 134 after the policy changes (P=.872; Fisher exact test)(Table 2). Over-the-counter prescriptions totaled 49 before and 69 after the policy changes. There was insufficient evidence of an overall difference before and after the policy changes for OTC medications (P=.192; Fisher exact test)(Table 3).
Comment
Although some medical institutions are diligently working to limit the potential influence pharmaceutical companies have on physician prescribing habits,4,5,25 the effect on physician prescribing habits is only now being established.15 Prior studies12,19,21 have found evidence that medication samples may lead to overuse of brand-name medications, but these findings do not hold true for the USF dermatologists included in this study, perhaps due to the difference in pharmaceutical company interactions or physicians maintaining prior prescription habits that were unrelated to the policy. Although this study focused on policy changes for in-office samples, prior studies either included other forms of interaction21 or did not include samples.22
Pharmaceutical samples allow patients to try a medication before committing to a long-term course of treatment with a particular medication, which has utility for physicians and patients. Although brand-name prescriptions may cost more, a trial period may assist the patient in deciding whether the medication is worth purchasing. Furthermore, physicians may feel more comfortable prescribing a medication once the individual patient has demonstrated a benefit from the sample, which may be particularly true in a specialty such as dermatology in which many branded topical medications contain a different vehicle than generic formulations, resulting in notable variations in active medication delivery and efficacy. Given the higher cost of branded topical medications, proving efficacy in patients through samples can provide a useful tool to the physician to determine the need for a branded formulation.
The benefits described are subjective but should not be disregarded. Although Hurley et al19 found that the number of brand-name medications prescribed increases as more samples are given out, our study demonstrated that after eliminating medication samples, there was no significant difference in the percentage of brand-name medications prescribed compared to generic and OTC medications.
Physician education concerning the price of each brand-name medication prescribed in office may be one method of reducing the amount of such prescriptions. Physicians generally are uninformed of the cost of the medications being prescribed26 and may not recognize the financial burden one medication may have compared to its alternative. However, educating physicians will empower them to make the conscious decision to prefer or not prefer a brand-name medication. With some generic medications shown to have a difference in bioequivalence compared to their brand-name counterparts, a physician may find more success prescribing the brand-name medications, regardless of pharmaceutical company influence, which is an alternative solution to policy changes that eliminate samples entirely. Although this study found insufficient evidence that removing samples decreases brand-name medication prescriptions, it is imperative that solutions are established to reduce the country’s increasing burden of medical costs.
Possible shortfalls of this study include the short period of time between which prepolicy data and postpolicy data were collected. It is possible that providers did not have enough time to adjust their prescribing habits or that providers would not have changed a prescribing pattern or preference simply because of a policy change. Future studies could allow a time period greater than 2 years to compare prepolicy and postpolicy prescribing habits, or a future study might make comparisons of prescriber patterns at different institutions that have different policies. Another possible shortfall is that providers and patients were limited to those at the Department of Dermatology & Cutaneous Surgery at the USF Morsani COM. Although this study has found insufficient evidence of a difference in prescribing habits, it may be beneficial to conduct a larger study that encompasses multiple academic institutions with similar policy changes. Most importantly, this study only investigated the influence of in-office pharmaceutical samples on prescribing patterns. This study did not look at the many other ways in which providers may be influenced by pharmaceutical companies, which likely is a significant confounding variable in this study. Continued additional studies that specifically examine other methods through which providers may be influenced would be helpful in further examining the many ways in which physician prescription habits are influenced.
Conclusion
Changes in pharmaceutical policy in 2011 at USF Morsani COM specifically banned in-office samples. The totality of evidence in this study shows modest observational evidence of a change in the postpolicy odds relative to prepolicy odds, but the data also are compatible with no change between prescribing habits before and after the policy changes. Further study is needed to fully understand this relationship.
Over the years, there has been growing concern about the relationship between physicians and pharmaceutical companies. Many studies have demonstrated that pharmaceutical interactions and incentives can influence physicians’ prescribing habits.1-3 As a result, many academic centers have adopted policies that attempt to limit the pharmaceutical industry’s influence on faculty and in-training physicians. Although these policies can vary greatly, they generally limit access of pharmaceutical representatives to providers and restrict pharmaceutical samples.4,5 This policy shift has even been reported in private practice.6
At the heart of the matter is the question: What really influences physicians to write a prescription for a particular medication? Is it cost, efficacy, or representatives pushing a product? Prior studies illustrate that generic medications are equivalent to their brand-name counterparts. In fact, current regulations require no more than 5% to 7% difference in bioequivalence.7-9 Although most generic medications are bioequivalent, it may not be universal.10
Garrison and Levin11 distributed a survey to US-based prescribers in family practice, psychiatry, and internal medicine and found that prescribers deemed patient response and success as the highest priority when determining which drugs to prescribe. In contrast, drug representatives and free samples only slightly contributed.11 Considering the minimum duration for efficacy of a medication such as an antidepressant vs a topical steroid, this pattern may differ with samples in dermatologic settings. Interestingly, another survey concluded that samples were associated with “sticky” prescribing habits, noting that physicians would prescribe a brand-name medication after using a sample, despite increased cost to the patient.12 Further, it has been suggested that recipients of free samples may experience increased costs in the long run, which contrasts a stated goal of affordability to patients.12,13
Physician interaction with pharmaceutical companies begins as early as medical school,14 with physicians reporting interactions as often as 4 times each month.14-18 Interactions can include meetings with pharmaceutical representatives, sponsored meals, gifts, continuing medical education sponsorship, funding for travel, pharmaceutical representative speakers, research funding, and drug samples.3
A 2014 study reported that prescribing habits are influenced by the free drug samples provided by nongeneric pharmaceutical companies.19 Nationally, the number of brand-name and branded generic medications constitute 79% of prescriptions, yet together they only comprise 17% of medications prescribed at an academic medical clinic that does not provide samples. The number of medications with samples being prescribed by dermatologists increased by 15% over 9 years, which may correlate with the wider availability of medication samples, more specifically an increase in branded generic samples.19 This potential interaction is the reason why institutions question the current influence of pharmaceutical companies. Samples may appear convenient, allowing a patient to test the medication prior to committing; however, with brand-name samples being provided to the physician, he/she may become more inclined to prescribe the branded medication.12,15,19-22 Because brand-name medications are more expensive than generic medications, this practice can increase the cost of health care.13 One study found that over 1 year, the overuse of nongeneric medications led to a loss of potential savings throughout 49 states, equating to $229 million just through Medicaid; interestingly, it was noted that in some states, a maximum reimbursement is set by Medicaid, regardless of whether the generic or branded medication is dispensed. The authors also noted variability in the potential savings by state, which may be a function of the state-by-state maximum reimbursements for certain medications.23 Another study on oral combination medications estimated Medicare spending on branded drugs relative to the cost if generic combinations had been purchased instead. This study examined branded medications for which the active components were available as over-the-counter (OTC), generic, or same-class generic, and the authors estimated that $925 million could have been saved in 2016 by purchasing a generic substitute.24 The overuse of nongeneric medications when generic alternatives are available becomes an issue that not only financially impacts patients but all taxpayers. However, this pattern may differ if limited only to dermatologic medications, which was not the focus of the prior studies.
To limit conflicts of interest in interactions with the pharmaceutical, medical device, and biotechnology industries, the University of South Florida (USF) Morsani College of Medicine (COM)(Tampa, Florida) implemented its own set of regulations that eliminated in-office pharmaceutical samples, in addition to other restrictions. This study aimed to investigate if there was a change in the prescribing habits of academic dermatologists after their medical school implemented these new policies.
We hypothesized that the number of brand-name drugs prescribed by physicians in the Department of Dermatology & Cutaneous Surgery would change following USF Morsani COM pharmaceutical policy changes. We sought to determine how physician prescribing practices within the Department of Dermatology & Cutaneous Surgery changed following USF Morsani COM pharmaceutical policy changes.
Methods
Data Collection
A retrospective review of medical records was conducted to investigate the effect of the USF Morsani COM pharmaceutical policy changes on physician prescribing practices within the Department of Dermatology & Cutaneous Surgery. Medical records of patients seen for common dermatology diagnoses before (January 1, 2010, to May 30, 2010) and after (August 1, 2011, to December 31, 2011) the pharmaceutical policy changes were reviewed, and all medications prescribed were recorded. Data were collected from medical records within the USF Health electronic medical record system and included visits with each of the department’s 3 attending dermatologists. The diagnoses included in the study—acne vulgaris, atopic dermatitis, onychomycosis, psoriasis, and rosacea—were chosen because in-office samples were available. Prescribing data from the first 100 consecutive medical records were collected from each time period, and a medical record was included only if it contained at least 1 of the following diagnoses: acne vulgaris, atopic dermatitis, onychomycosis, psoriasis, or rosacea. The assessment and plan of each progress note were reviewed, and the exact medication name and associated diagnosis were recorded for each prescription. Subsequently, each medication was reviewed and placed in 1 of 3 categories: brand name, generic, and OTC. The total number of prescriptions for each diagnosis (per visit/note); the specific number of brand, generic, and OTC medications prescribed (per visit/note); and the percentage of brand, generic, and OTC medications prescribed (per visit/note and per diagnosis in total) were calculated. To ensure only intended medications were included, each medication recorded in the medical record note was cross-referenced with the prescribed medication in the electronic medical record. The primary objective of this study was to capture the prescribing physician’s intent as proxied by the pattern of prescription. Thus, changes made in prescriptions after the initial plan—whether insurance related or otherwise—were not relevant to this investigation.
The data were collected to compare the percentage of brand vs generic or OTC prescriptions per diagnosis to see if there was a difference in the prescribing habits before and after the pharmaceutical policy changes. Of note, several other pieces of data were collected from each medical record, including age, race, class of insurance (ie, Medicare, Medicaid, private health maintenance organization, private preferred provider organization), subtype diagnoses, and whether the prescription was new or a refill. The information gathered from the written record on the assessment and plan was verified using prescriptions ordered in the Allscripts electronic record, and any difference was noted. No identifying information that could be used to easily identify study participants was recorded.
Differences in prescribing habits across diagnoses before and after the policy changes were ascertained using a Fisher exact test and were further assessed using a mixed effects ordinal logistic regression model that accounted for within-provider clustering and baseline patient characteristics. An ordinal model was chosen to recognize differences in average cost among brand-name, generic, and OTC medications.
Results
In total, 200 medical records were collected. For the period analyzed before the policy change, 252 brand-name medications were prescribed compared to 231 prescribed for the period analyzed after the policy changes. There was insufficient evidence of an overall difference in brand-name medications prescribed before and after the policy changes (P=.145; Fisher exact test)(Table 1). There also was insufficient evidence of an overall difference in generic prescriptions, which totaled 153 before and 134 after the policy changes (P=.872; Fisher exact test)(Table 2). Over-the-counter prescriptions totaled 49 before and 69 after the policy changes. There was insufficient evidence of an overall difference before and after the policy changes for OTC medications (P=.192; Fisher exact test)(Table 3).
Comment
Although some medical institutions are diligently working to limit the potential influence pharmaceutical companies have on physician prescribing habits,4,5,25 the effect on physician prescribing habits is only now being established.15 Prior studies12,19,21 have found evidence that medication samples may lead to overuse of brand-name medications, but these findings do not hold true for the USF dermatologists included in this study, perhaps due to the difference in pharmaceutical company interactions or physicians maintaining prior prescription habits that were unrelated to the policy. Although this study focused on policy changes for in-office samples, prior studies either included other forms of interaction21 or did not include samples.22
Pharmaceutical samples allow patients to try a medication before committing to a long-term course of treatment with a particular medication, which has utility for physicians and patients. Although brand-name prescriptions may cost more, a trial period may assist the patient in deciding whether the medication is worth purchasing. Furthermore, physicians may feel more comfortable prescribing a medication once the individual patient has demonstrated a benefit from the sample, which may be particularly true in a specialty such as dermatology in which many branded topical medications contain a different vehicle than generic formulations, resulting in notable variations in active medication delivery and efficacy. Given the higher cost of branded topical medications, proving efficacy in patients through samples can provide a useful tool to the physician to determine the need for a branded formulation.
The benefits described are subjective but should not be disregarded. Although Hurley et al19 found that the number of brand-name medications prescribed increases as more samples are given out, our study demonstrated that after eliminating medication samples, there was no significant difference in the percentage of brand-name medications prescribed compared to generic and OTC medications.
Physician education concerning the price of each brand-name medication prescribed in office may be one method of reducing the amount of such prescriptions. Physicians generally are uninformed of the cost of the medications being prescribed26 and may not recognize the financial burden one medication may have compared to its alternative. However, educating physicians will empower them to make the conscious decision to prefer or not prefer a brand-name medication. With some generic medications shown to have a difference in bioequivalence compared to their brand-name counterparts, a physician may find more success prescribing the brand-name medications, regardless of pharmaceutical company influence, which is an alternative solution to policy changes that eliminate samples entirely. Although this study found insufficient evidence that removing samples decreases brand-name medication prescriptions, it is imperative that solutions are established to reduce the country’s increasing burden of medical costs.
Possible shortfalls of this study include the short period of time between which prepolicy data and postpolicy data were collected. It is possible that providers did not have enough time to adjust their prescribing habits or that providers would not have changed a prescribing pattern or preference simply because of a policy change. Future studies could allow a time period greater than 2 years to compare prepolicy and postpolicy prescribing habits, or a future study might make comparisons of prescriber patterns at different institutions that have different policies. Another possible shortfall is that providers and patients were limited to those at the Department of Dermatology & Cutaneous Surgery at the USF Morsani COM. Although this study has found insufficient evidence of a difference in prescribing habits, it may be beneficial to conduct a larger study that encompasses multiple academic institutions with similar policy changes. Most importantly, this study only investigated the influence of in-office pharmaceutical samples on prescribing patterns. This study did not look at the many other ways in which providers may be influenced by pharmaceutical companies, which likely is a significant confounding variable in this study. Continued additional studies that specifically examine other methods through which providers may be influenced would be helpful in further examining the many ways in which physician prescription habits are influenced.
Conclusion
Changes in pharmaceutical policy in 2011 at USF Morsani COM specifically banned in-office samples. The totality of evidence in this study shows modest observational evidence of a change in the postpolicy odds relative to prepolicy odds, but the data also are compatible with no change between prescribing habits before and after the policy changes. Further study is needed to fully understand this relationship.
- Sondergaard J, Vach K, Kragstrup J, et al. Impact of pharmaceutical representative visits on GPs’ drug preferences. Fam Pract. 2009;26:204-209.
- Jelinek GA, Neate SL. The influence of the pharmaceutical industry in medicine. J Law Med. 2009;17:216-223.
- Wazana A. Physicians and the pharmaceutical industry: is a gift ever just a gift? JAMA. 2000;283:373-380.
- Coleman DL. Establishing policies for the relationship between industry and clinicians: lessons learned from two academic health centers. Acad Med. 2008;83:882-887.
- Coleman DL, Kazdin AE, Miller LA, et al. Guidelines for interactions between clinical faculty and the pharmaceutical industry: one medical school’s approach. Acad Med. 2006;81:154-160.
- Evans D, Hartung DM, Beasley D, et al. Breaking up is hard to do: lessons learned from a pharma-free practice transformation. J Am Board Fam Med. 2013;26:332-338.
- Davit BM, Nwakama PE, Buehler GJ, et al. Comparing generic and innovator drugs: a review of 12 years of bioequivalence data from the United States Food and Drug Administration. Ann Pharmacother. 2009;43:1583-1597.
- Kesselheim AS, Misono AS, Lee JL, et al. Clinical equivalence of generic and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008;300:2514-2526.
- McCormack J, Chmelicek JT. Generic versus brand name: the other drug war. Can Fam Physician. 2014;60:911.
- Borgheini G. The bioequivalence and therapeutic efficacy of generic versus brand-name psychoactive drugs. Clin Ther. 2003;25:1578-1592.
- Garrison GD, Levin GM. Factors affecting prescribing of the newer antidepressants. Ann Pharmacother. 2000;34:10-14.
- Rafique S, Sarwar W, Rashid A, et al. Influence of free drug samples on prescribing by physicians: a cross sectional survey. J Pak Med Assoc. 2017;67:465-467.
- Alexander GC, Zhang J, Basu A. Characteristics of patients receiving pharmaceutical samples and association between sample receipt and out-of-pocket prescription costs. Med Care. 2008;46:394-402.
- Hodges B. Interactions with the pharmaceutical industry: experiences and attitudes of psychiatry residents, interns and clerks. CMAJ. 1995;153:553-559.
- Brotzman GL, Mark DH. The effect on resident attitudes of regulatory policies regarding pharmaceutical representative activities. J Gen Intern Med. 1993;8:130-134.
- Keim SM, Sanders AB, Witzke DB, et al. Beliefs and practices of emergency medicine faculty and residents regarding professional interactions with the biomedical industry. Ann Emerg Med. 1993;22:1576-1581.
- Thomson AN, Craig BJ, Barham PM. Attitudes of general practitioners in New Zealand to pharmaceutical representatives. Br J Gen Pract. 1994;44:220-223.
- Ziegler MG, Lew P, Singer BC. The accuracy of drug information from pharmaceutical sales representatives. JAMA. 1995;273:1296-1298.
- Hurley MP, Stafford RS, Lane AT. Characterizing the relationship between free drug samples and prescription patterns for acne vulgaris and rosacea. JAMA Dermatol. 2014;150:487-493.
- Lexchin J. Interactions between physicians and the pharmaceutical industry: what does the literature say? CMAJ. 1993;149:1401-1407.
- Lieb K, Scheurich A. Contact between doctors and the pharmaceutical industry, their perceptions, and the effects on prescribing habits. PLoS One. 2014;9:e110130.
- Spurling GK, Mansfield PR, Montgomery BD, et al. Information from pharmaceutical companies and the quality, quantity, and cost of physicians’ prescribing: a systematic review. PLoS Med. 2010;7:e1000352.
- Fischer MA, Avorn J. Economic consequences of underuse of generic drugs: evidence from Medicaid and implications for prescription drug benefit plans. Health Serv Res. 2003;38:1051-1064.
- Sacks CA, Lee CC, Kesselheim AS, et al. Medicare spending on brand-name combination medications vs their generic constituents. JAMA. 2018;320:650-656.
- Brennan TA, Rothman DJ, Blank L, et al. Health industry practices that create conflicts of interest: a policy proposal for academic medical centers. JAMA. 2006;295:429-433.
- Allan GM, Lexchin J, Wiebe N. Physician awareness of drug cost: a systematic review. PLoS Med. 2007;4:e283.
- Sondergaard J, Vach K, Kragstrup J, et al. Impact of pharmaceutical representative visits on GPs’ drug preferences. Fam Pract. 2009;26:204-209.
- Jelinek GA, Neate SL. The influence of the pharmaceutical industry in medicine. J Law Med. 2009;17:216-223.
- Wazana A. Physicians and the pharmaceutical industry: is a gift ever just a gift? JAMA. 2000;283:373-380.
- Coleman DL. Establishing policies for the relationship between industry and clinicians: lessons learned from two academic health centers. Acad Med. 2008;83:882-887.
- Coleman DL, Kazdin AE, Miller LA, et al. Guidelines for interactions between clinical faculty and the pharmaceutical industry: one medical school’s approach. Acad Med. 2006;81:154-160.
- Evans D, Hartung DM, Beasley D, et al. Breaking up is hard to do: lessons learned from a pharma-free practice transformation. J Am Board Fam Med. 2013;26:332-338.
- Davit BM, Nwakama PE, Buehler GJ, et al. Comparing generic and innovator drugs: a review of 12 years of bioequivalence data from the United States Food and Drug Administration. Ann Pharmacother. 2009;43:1583-1597.
- Kesselheim AS, Misono AS, Lee JL, et al. Clinical equivalence of generic and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008;300:2514-2526.
- McCormack J, Chmelicek JT. Generic versus brand name: the other drug war. Can Fam Physician. 2014;60:911.
- Borgheini G. The bioequivalence and therapeutic efficacy of generic versus brand-name psychoactive drugs. Clin Ther. 2003;25:1578-1592.
- Garrison GD, Levin GM. Factors affecting prescribing of the newer antidepressants. Ann Pharmacother. 2000;34:10-14.
- Rafique S, Sarwar W, Rashid A, et al. Influence of free drug samples on prescribing by physicians: a cross sectional survey. J Pak Med Assoc. 2017;67:465-467.
- Alexander GC, Zhang J, Basu A. Characteristics of patients receiving pharmaceutical samples and association between sample receipt and out-of-pocket prescription costs. Med Care. 2008;46:394-402.
- Hodges B. Interactions with the pharmaceutical industry: experiences and attitudes of psychiatry residents, interns and clerks. CMAJ. 1995;153:553-559.
- Brotzman GL, Mark DH. The effect on resident attitudes of regulatory policies regarding pharmaceutical representative activities. J Gen Intern Med. 1993;8:130-134.
- Keim SM, Sanders AB, Witzke DB, et al. Beliefs and practices of emergency medicine faculty and residents regarding professional interactions with the biomedical industry. Ann Emerg Med. 1993;22:1576-1581.
- Thomson AN, Craig BJ, Barham PM. Attitudes of general practitioners in New Zealand to pharmaceutical representatives. Br J Gen Pract. 1994;44:220-223.
- Ziegler MG, Lew P, Singer BC. The accuracy of drug information from pharmaceutical sales representatives. JAMA. 1995;273:1296-1298.
- Hurley MP, Stafford RS, Lane AT. Characterizing the relationship between free drug samples and prescription patterns for acne vulgaris and rosacea. JAMA Dermatol. 2014;150:487-493.
- Lexchin J. Interactions between physicians and the pharmaceutical industry: what does the literature say? CMAJ. 1993;149:1401-1407.
- Lieb K, Scheurich A. Contact between doctors and the pharmaceutical industry, their perceptions, and the effects on prescribing habits. PLoS One. 2014;9:e110130.
- Spurling GK, Mansfield PR, Montgomery BD, et al. Information from pharmaceutical companies and the quality, quantity, and cost of physicians’ prescribing: a systematic review. PLoS Med. 2010;7:e1000352.
- Fischer MA, Avorn J. Economic consequences of underuse of generic drugs: evidence from Medicaid and implications for prescription drug benefit plans. Health Serv Res. 2003;38:1051-1064.
- Sacks CA, Lee CC, Kesselheim AS, et al. Medicare spending on brand-name combination medications vs their generic constituents. JAMA. 2018;320:650-656.
- Brennan TA, Rothman DJ, Blank L, et al. Health industry practices that create conflicts of interest: a policy proposal for academic medical centers. JAMA. 2006;295:429-433.
- Allan GM, Lexchin J, Wiebe N. Physician awareness of drug cost: a systematic review. PLoS Med. 2007;4:e283.
Practice Points
- There has been growing concern that pharmaceutical interactions and incentives can influence physicians’ prescribing habits.
- Many academic centers have adopted policies that attempt to limit the pharmaceutical industry’s influence on faculty and in-training physicians.
- This study aimed to investigate if there was a change in the prescribing habits of academic dermatologists after the medical school implemented new policies that banned in-office samples.
