User login
Survival for older AML patients better with HSCT from unrelated donors
For adults aged 50 and older in first or second remission after induction therapy for acute myeloid leukemia, hematopoietic stem cell transplants (HSCT) from young matched unrelated donors was associated with better overall survival and lower risk for relapse than transplants from haploidentical donors, a retrospective study suggests,
Among 823 patients from the aged 50 to 75 with acute myeloid leukemia (AML) in a transplant registry, hazard ratios for both mortality and relapse were significantly higher for patients who received transplants from haploidentical siblings or offspring, compared with patients who received transplants from HLA-matched unrelated donors aged 40 or younger, reported Miguel-Angel Perales, MD, who is affiliated with Memorial Sloan Kettering Cancer Center in New York City, and colleagues.
“Our findings lend support to our hypothesis that a young [matched unrelated donor] should be the donor of choice when available. Furthermore, the data presented here suggest comparable times to transplantation in both treatment groups, confirming timely access to unrelated donors is no longer a barrier,” they wrote in Haematologica.Allogeneic transplants from matched unrelated donors have been performed for more than 30 years for treatment of patients with advanced myeloid and lymphoid malignancies. More recently, T-cell-replete bone marrow or peripheral blood transplants from haploidentical relatives, with post-transplant cyclophosphamide, tacrolimus, and mycophenolate mofetil to lower risk for graft-versus-host disease (GvHD) have become commonplace worldwide, and are established treatment options for patients with myeloid and lymphoid malignancies. There are conflicting studies suggesting that outcomes with haploidentical transplants are equivalent or superior to those seen with matched unrelated donors, the authors noted, but pointed to a 2018 study from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplant and the Center for International Blood and Marrow Transplant Research (CIBMTR). Those study results found that, among transplant recipients aged 55 through 76, graft failure, nonrelapse mortality, and overall mortality were higher when the donors were haploidentical offspring rather than HLA-matched siblings.
To see whether patients aged 50 and older with AML might benefit more with transplants from hapolidentical relatives or matched unrelated donors, the investigators used CIBMTR data to review outcomes for 823 adults with AML who received a transplant in first or second remission at one of 90 U.S. centers from 2008 through 2015.
Of this cohort, 192 patients received grafts from haploidentical donors (25% from siblings and 75% from offspring), and 631 received grafts from matched unrelated donors ranging from 18 to 40 years of age.
Although the two groups were generally similar in demographic and disease characteristics, patients in the matched unrelated donor group had significantly higher frequency of poor-risk cytogenetics (P = .03) and were significantly more likely to have received a myeloablative condition regimen than a reduced-intensity regimen (P less than .001).
In the haploidentical group, 76% of patients were in first complete remission, and the remaining 24% were in second complete remission. In the HLA-matched group the respective proportions were 83% and 17%.
The median follow-up was 42 months in the haploidentical group and 47 months in the HLA-matched group. Five-year overall survival rates were 32% and 42%, respectively.
In multivariable models controlling for donor and recipient age, sex, performance score, hematopoietic cell transplant comorbidity score, cytomegalovirus serostatus, disease status, cytogenetic risk, transplant conditioning regimen intensity and transplant period, the hazard ratio (HR) for the primary endpoint of overall mortality was 1.27 for haploidentical vs. HLA-matched grafts (P = .04). The HR for relapse risk with haploidentical transplants was 1.32 (P =.04). No significant differences in risk of nonrelapse mortality were found between the two study arms.
Bone marrow grafts from matched unrelated donors were associated with significantly higher risk for chronic GvHD than haploidentical grafts (HR, 3.12; P less than .001), but there was no difference in chronic graft-versus-host disease (GvHD) incidence between peripheral blood grafts from matched unrelated donors and haploidentical grafts.
“These data support the view that matched unrelated donor transplant with donors younger than 40 years is to be preferred,” the investigators wrote.
But in an interview, coauthor
“Even though there appears to be that clinical benefit for this older AML patient population, that benefit is not huge, and when you’re also accounting for the process of finding a donor and just getting someone into transplant, a lot of us weren’t sure if this was really going to be practice changing as the field does move into haploidentical transplants being more common,” he said.
He noted that the better outcomes among patients who received transplants from matched unrelated donors may be at least in part explained by the higher proportion of patients with unrelated donors who received myeloablative conditioning regimens. In this study, 65% of patients with haploidentical donors underwent reduced-intensity conditioning with total body irradiation, cyclophosphamide, and fludarabine.“If we do a comparison of equal conditioning regimens, are we really going to see the same outcomes in this setting? This might actually argue that, if you’re going to do a haploidentical transplant, you might start thinking about those newer, more ablative conditioning regimens,” he said.Dr. Tomlinson added that the data are reassuring, because of the modest size of the benefit, and because “many, many of our studies are showing that haploidentical transplants do almost as well as the matched ones. The big question mark will be what are the long-term outcomes? What happens after 3 years from those transplants? And that is going to take a lot more high quality, mature data.”In an editorial accompanying the study, Richard E. Champlin, MD, of the University of Texas MD Anderson Cancer Center in Houston, noted that the more frequent use of reduced-intensity conditioning used for most patients in the haploidentical group has been associated in other studies with higher relapse rates, compared with other, more intense reduced-intensity regimens.
While he agreed that the study by Dr. Perales and colleagues “should give pause for thought, however, for those considering jumping to haploidentical transplants as a preferred approach in general,” he also noted that the study’s conclusion might not apply to cases where time-to-transplant is critical, or when other conditioning and GvHD prophylaxis regimens are used.
“The ideal study would compare optimized versions of both haploidentical and unrelated donor transplants, and use “intention-to-treat” analysis, including all patients for whom a transplant is intended from the time of initial HLA typing,” he wrote.
The study was funded by grants from the National Institutes of Health and the Office of Naval Research. Dr. Tomlinson reported no relevant disclosures. Dr. Champlin did not report disclosures.
SOURCE: Perales M-A et al. Haematologica. 2020 Jan 31;105(2):407-13.
For adults aged 50 and older in first or second remission after induction therapy for acute myeloid leukemia, hematopoietic stem cell transplants (HSCT) from young matched unrelated donors was associated with better overall survival and lower risk for relapse than transplants from haploidentical donors, a retrospective study suggests,
Among 823 patients from the aged 50 to 75 with acute myeloid leukemia (AML) in a transplant registry, hazard ratios for both mortality and relapse were significantly higher for patients who received transplants from haploidentical siblings or offspring, compared with patients who received transplants from HLA-matched unrelated donors aged 40 or younger, reported Miguel-Angel Perales, MD, who is affiliated with Memorial Sloan Kettering Cancer Center in New York City, and colleagues.
“Our findings lend support to our hypothesis that a young [matched unrelated donor] should be the donor of choice when available. Furthermore, the data presented here suggest comparable times to transplantation in both treatment groups, confirming timely access to unrelated donors is no longer a barrier,” they wrote in Haematologica.Allogeneic transplants from matched unrelated donors have been performed for more than 30 years for treatment of patients with advanced myeloid and lymphoid malignancies. More recently, T-cell-replete bone marrow or peripheral blood transplants from haploidentical relatives, with post-transplant cyclophosphamide, tacrolimus, and mycophenolate mofetil to lower risk for graft-versus-host disease (GvHD) have become commonplace worldwide, and are established treatment options for patients with myeloid and lymphoid malignancies. There are conflicting studies suggesting that outcomes with haploidentical transplants are equivalent or superior to those seen with matched unrelated donors, the authors noted, but pointed to a 2018 study from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplant and the Center for International Blood and Marrow Transplant Research (CIBMTR). Those study results found that, among transplant recipients aged 55 through 76, graft failure, nonrelapse mortality, and overall mortality were higher when the donors were haploidentical offspring rather than HLA-matched siblings.
To see whether patients aged 50 and older with AML might benefit more with transplants from hapolidentical relatives or matched unrelated donors, the investigators used CIBMTR data to review outcomes for 823 adults with AML who received a transplant in first or second remission at one of 90 U.S. centers from 2008 through 2015.
Of this cohort, 192 patients received grafts from haploidentical donors (25% from siblings and 75% from offspring), and 631 received grafts from matched unrelated donors ranging from 18 to 40 years of age.
Although the two groups were generally similar in demographic and disease characteristics, patients in the matched unrelated donor group had significantly higher frequency of poor-risk cytogenetics (P = .03) and were significantly more likely to have received a myeloablative condition regimen than a reduced-intensity regimen (P less than .001).
In the haploidentical group, 76% of patients were in first complete remission, and the remaining 24% were in second complete remission. In the HLA-matched group the respective proportions were 83% and 17%.
The median follow-up was 42 months in the haploidentical group and 47 months in the HLA-matched group. Five-year overall survival rates were 32% and 42%, respectively.
In multivariable models controlling for donor and recipient age, sex, performance score, hematopoietic cell transplant comorbidity score, cytomegalovirus serostatus, disease status, cytogenetic risk, transplant conditioning regimen intensity and transplant period, the hazard ratio (HR) for the primary endpoint of overall mortality was 1.27 for haploidentical vs. HLA-matched grafts (P = .04). The HR for relapse risk with haploidentical transplants was 1.32 (P =.04). No significant differences in risk of nonrelapse mortality were found between the two study arms.
Bone marrow grafts from matched unrelated donors were associated with significantly higher risk for chronic GvHD than haploidentical grafts (HR, 3.12; P less than .001), but there was no difference in chronic graft-versus-host disease (GvHD) incidence between peripheral blood grafts from matched unrelated donors and haploidentical grafts.
“These data support the view that matched unrelated donor transplant with donors younger than 40 years is to be preferred,” the investigators wrote.
But in an interview, coauthor
“Even though there appears to be that clinical benefit for this older AML patient population, that benefit is not huge, and when you’re also accounting for the process of finding a donor and just getting someone into transplant, a lot of us weren’t sure if this was really going to be practice changing as the field does move into haploidentical transplants being more common,” he said.
He noted that the better outcomes among patients who received transplants from matched unrelated donors may be at least in part explained by the higher proportion of patients with unrelated donors who received myeloablative conditioning regimens. In this study, 65% of patients with haploidentical donors underwent reduced-intensity conditioning with total body irradiation, cyclophosphamide, and fludarabine.“If we do a comparison of equal conditioning regimens, are we really going to see the same outcomes in this setting? This might actually argue that, if you’re going to do a haploidentical transplant, you might start thinking about those newer, more ablative conditioning regimens,” he said.Dr. Tomlinson added that the data are reassuring, because of the modest size of the benefit, and because “many, many of our studies are showing that haploidentical transplants do almost as well as the matched ones. The big question mark will be what are the long-term outcomes? What happens after 3 years from those transplants? And that is going to take a lot more high quality, mature data.”In an editorial accompanying the study, Richard E. Champlin, MD, of the University of Texas MD Anderson Cancer Center in Houston, noted that the more frequent use of reduced-intensity conditioning used for most patients in the haploidentical group has been associated in other studies with higher relapse rates, compared with other, more intense reduced-intensity regimens.
While he agreed that the study by Dr. Perales and colleagues “should give pause for thought, however, for those considering jumping to haploidentical transplants as a preferred approach in general,” he also noted that the study’s conclusion might not apply to cases where time-to-transplant is critical, or when other conditioning and GvHD prophylaxis regimens are used.
“The ideal study would compare optimized versions of both haploidentical and unrelated donor transplants, and use “intention-to-treat” analysis, including all patients for whom a transplant is intended from the time of initial HLA typing,” he wrote.
The study was funded by grants from the National Institutes of Health and the Office of Naval Research. Dr. Tomlinson reported no relevant disclosures. Dr. Champlin did not report disclosures.
SOURCE: Perales M-A et al. Haematologica. 2020 Jan 31;105(2):407-13.
For adults aged 50 and older in first or second remission after induction therapy for acute myeloid leukemia, hematopoietic stem cell transplants (HSCT) from young matched unrelated donors was associated with better overall survival and lower risk for relapse than transplants from haploidentical donors, a retrospective study suggests,
Among 823 patients from the aged 50 to 75 with acute myeloid leukemia (AML) in a transplant registry, hazard ratios for both mortality and relapse were significantly higher for patients who received transplants from haploidentical siblings or offspring, compared with patients who received transplants from HLA-matched unrelated donors aged 40 or younger, reported Miguel-Angel Perales, MD, who is affiliated with Memorial Sloan Kettering Cancer Center in New York City, and colleagues.
“Our findings lend support to our hypothesis that a young [matched unrelated donor] should be the donor of choice when available. Furthermore, the data presented here suggest comparable times to transplantation in both treatment groups, confirming timely access to unrelated donors is no longer a barrier,” they wrote in Haematologica.Allogeneic transplants from matched unrelated donors have been performed for more than 30 years for treatment of patients with advanced myeloid and lymphoid malignancies. More recently, T-cell-replete bone marrow or peripheral blood transplants from haploidentical relatives, with post-transplant cyclophosphamide, tacrolimus, and mycophenolate mofetil to lower risk for graft-versus-host disease (GvHD) have become commonplace worldwide, and are established treatment options for patients with myeloid and lymphoid malignancies. There are conflicting studies suggesting that outcomes with haploidentical transplants are equivalent or superior to those seen with matched unrelated donors, the authors noted, but pointed to a 2018 study from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplant and the Center for International Blood and Marrow Transplant Research (CIBMTR). Those study results found that, among transplant recipients aged 55 through 76, graft failure, nonrelapse mortality, and overall mortality were higher when the donors were haploidentical offspring rather than HLA-matched siblings.
To see whether patients aged 50 and older with AML might benefit more with transplants from hapolidentical relatives or matched unrelated donors, the investigators used CIBMTR data to review outcomes for 823 adults with AML who received a transplant in first or second remission at one of 90 U.S. centers from 2008 through 2015.
Of this cohort, 192 patients received grafts from haploidentical donors (25% from siblings and 75% from offspring), and 631 received grafts from matched unrelated donors ranging from 18 to 40 years of age.
Although the two groups were generally similar in demographic and disease characteristics, patients in the matched unrelated donor group had significantly higher frequency of poor-risk cytogenetics (P = .03) and were significantly more likely to have received a myeloablative condition regimen than a reduced-intensity regimen (P less than .001).
In the haploidentical group, 76% of patients were in first complete remission, and the remaining 24% were in second complete remission. In the HLA-matched group the respective proportions were 83% and 17%.
The median follow-up was 42 months in the haploidentical group and 47 months in the HLA-matched group. Five-year overall survival rates were 32% and 42%, respectively.
In multivariable models controlling for donor and recipient age, sex, performance score, hematopoietic cell transplant comorbidity score, cytomegalovirus serostatus, disease status, cytogenetic risk, transplant conditioning regimen intensity and transplant period, the hazard ratio (HR) for the primary endpoint of overall mortality was 1.27 for haploidentical vs. HLA-matched grafts (P = .04). The HR for relapse risk with haploidentical transplants was 1.32 (P =.04). No significant differences in risk of nonrelapse mortality were found between the two study arms.
Bone marrow grafts from matched unrelated donors were associated with significantly higher risk for chronic GvHD than haploidentical grafts (HR, 3.12; P less than .001), but there was no difference in chronic graft-versus-host disease (GvHD) incidence between peripheral blood grafts from matched unrelated donors and haploidentical grafts.
“These data support the view that matched unrelated donor transplant with donors younger than 40 years is to be preferred,” the investigators wrote.
But in an interview, coauthor
“Even though there appears to be that clinical benefit for this older AML patient population, that benefit is not huge, and when you’re also accounting for the process of finding a donor and just getting someone into transplant, a lot of us weren’t sure if this was really going to be practice changing as the field does move into haploidentical transplants being more common,” he said.
He noted that the better outcomes among patients who received transplants from matched unrelated donors may be at least in part explained by the higher proportion of patients with unrelated donors who received myeloablative conditioning regimens. In this study, 65% of patients with haploidentical donors underwent reduced-intensity conditioning with total body irradiation, cyclophosphamide, and fludarabine.“If we do a comparison of equal conditioning regimens, are we really going to see the same outcomes in this setting? This might actually argue that, if you’re going to do a haploidentical transplant, you might start thinking about those newer, more ablative conditioning regimens,” he said.Dr. Tomlinson added that the data are reassuring, because of the modest size of the benefit, and because “many, many of our studies are showing that haploidentical transplants do almost as well as the matched ones. The big question mark will be what are the long-term outcomes? What happens after 3 years from those transplants? And that is going to take a lot more high quality, mature data.”In an editorial accompanying the study, Richard E. Champlin, MD, of the University of Texas MD Anderson Cancer Center in Houston, noted that the more frequent use of reduced-intensity conditioning used for most patients in the haploidentical group has been associated in other studies with higher relapse rates, compared with other, more intense reduced-intensity regimens.
While he agreed that the study by Dr. Perales and colleagues “should give pause for thought, however, for those considering jumping to haploidentical transplants as a preferred approach in general,” he also noted that the study’s conclusion might not apply to cases where time-to-transplant is critical, or when other conditioning and GvHD prophylaxis regimens are used.
“The ideal study would compare optimized versions of both haploidentical and unrelated donor transplants, and use “intention-to-treat” analysis, including all patients for whom a transplant is intended from the time of initial HLA typing,” he wrote.
The study was funded by grants from the National Institutes of Health and the Office of Naval Research. Dr. Tomlinson reported no relevant disclosures. Dr. Champlin did not report disclosures.
SOURCE: Perales M-A et al. Haematologica. 2020 Jan 31;105(2):407-13.
FROM HAEMATOLOGICA
Lidocaine-prilocaine cream tops lidocaine injections for vulvar biopsy pain
The median highest pain score in a randomized trial of 38 women undergoing vulvar biopsies was 25.7 mm lower, on a 100 mm visual analogue scale, when they received 5% lidocaine-prilocaine cream instead of a 1% lidocaine injection, according to a report from Duke University, in Durham, N.C.
“In the current study, we found that application of lidocaine-prilocaine cream, alone, for a minimum of 10 minutes before vulvar biopsy on a non–hair-bearing surface results in a significantly lower maximum pain score and a significantly better patient rating of the biopsy experience,” said investigators led by Logan K. Williams, MD, of the department of obstetrics and gynecology at Duke University, Durham, N.C.
Given the “clear advantage” of the cream, it “should be considered as an anesthetic method for vulvar biopsy in a non-hair-bearing area,” Dr. Williams and colleagues concluded (Obstet Gynecol. 2020 Feb;135{2]:311-8).
Studies have pitted the cream against the injection before, but they did not compare patients’ maximal pain scores. The team wanted to do that because “comparing the highest score allows us to consider the possibility that the pain of anesthesia application” – injection versus cream – “may be greater than the pain of any other portion of the biopsy procedure.”
They randomized 19 women to the cream, approximately 5 g at the site of biopsy at least 10 minutes beforehand, and 18 others to the injection, 2 mL using a 27-gauge needle, at least 1 minute prior.
The median highest pain score in the lidocaine-prilocaine group was 20 mm, but 56.5 mm in the injection group. Patients randomized to lidocaine-prilocaine also had a significantly better (P = 0.02) experience than those receiving injected lidocaine, also assessed by visual analog scale (VAS). The median baseline pain level was 0 mm.
Anxiety was assessed after patients knew whether they were going to get the cream or the injection, but before the biopsy. The median score in the cream group was of 19 mm on another VAS, compared with 31.5 mm.
Participants were 60 years old on average, and almost all had prior vulvar biopsies. Two in the cream group and three in the injection group had punch biopsies; cervical biopsy forceps were used for the rest. More than half the women had benign findings, and most of the others had vulvar intraepithelial neoplasia, but there was one invasive cancer. At Duke, the cost of the injection was $0.99, compared with $7.36 for the cream.
Dr. Williams and colleagues cited a few limitations. One is that the patients and clinicians in the study were not blinded. Another is that most of the patients had undergone vulvar biopsy before, possibly predisposing them to bias.
“In the future, consideration could be taken to studying lidocaine-prilocaine cream applications to hair-bearing surfaces, which were excluded in this study.” Also, “there is a question of the histologic effect of lidocaine-prilocaine on tissues and whether this could affect pathologic diagnoses.
“We are conducting a separate ancillary study in conjunction with our dermatopathology colleagues to investigate this question,” the investigators said.
The work was funded by Duke and the National Institutes of Health. Dr. Williams had no disclosures.
aotto@mdedge.com
SOURCE: Williams LK et al. Obstet Gynecol. 2020 Feb;135(2):311-8.
The median highest pain score in a randomized trial of 38 women undergoing vulvar biopsies was 25.7 mm lower, on a 100 mm visual analogue scale, when they received 5% lidocaine-prilocaine cream instead of a 1% lidocaine injection, according to a report from Duke University, in Durham, N.C.
“In the current study, we found that application of lidocaine-prilocaine cream, alone, for a minimum of 10 minutes before vulvar biopsy on a non–hair-bearing surface results in a significantly lower maximum pain score and a significantly better patient rating of the biopsy experience,” said investigators led by Logan K. Williams, MD, of the department of obstetrics and gynecology at Duke University, Durham, N.C.
Given the “clear advantage” of the cream, it “should be considered as an anesthetic method for vulvar biopsy in a non-hair-bearing area,” Dr. Williams and colleagues concluded (Obstet Gynecol. 2020 Feb;135{2]:311-8).
Studies have pitted the cream against the injection before, but they did not compare patients’ maximal pain scores. The team wanted to do that because “comparing the highest score allows us to consider the possibility that the pain of anesthesia application” – injection versus cream – “may be greater than the pain of any other portion of the biopsy procedure.”
They randomized 19 women to the cream, approximately 5 g at the site of biopsy at least 10 minutes beforehand, and 18 others to the injection, 2 mL using a 27-gauge needle, at least 1 minute prior.
The median highest pain score in the lidocaine-prilocaine group was 20 mm, but 56.5 mm in the injection group. Patients randomized to lidocaine-prilocaine also had a significantly better (P = 0.02) experience than those receiving injected lidocaine, also assessed by visual analog scale (VAS). The median baseline pain level was 0 mm.
Anxiety was assessed after patients knew whether they were going to get the cream or the injection, but before the biopsy. The median score in the cream group was of 19 mm on another VAS, compared with 31.5 mm.
Participants were 60 years old on average, and almost all had prior vulvar biopsies. Two in the cream group and three in the injection group had punch biopsies; cervical biopsy forceps were used for the rest. More than half the women had benign findings, and most of the others had vulvar intraepithelial neoplasia, but there was one invasive cancer. At Duke, the cost of the injection was $0.99, compared with $7.36 for the cream.
Dr. Williams and colleagues cited a few limitations. One is that the patients and clinicians in the study were not blinded. Another is that most of the patients had undergone vulvar biopsy before, possibly predisposing them to bias.
“In the future, consideration could be taken to studying lidocaine-prilocaine cream applications to hair-bearing surfaces, which were excluded in this study.” Also, “there is a question of the histologic effect of lidocaine-prilocaine on tissues and whether this could affect pathologic diagnoses.
“We are conducting a separate ancillary study in conjunction with our dermatopathology colleagues to investigate this question,” the investigators said.
The work was funded by Duke and the National Institutes of Health. Dr. Williams had no disclosures.
aotto@mdedge.com
SOURCE: Williams LK et al. Obstet Gynecol. 2020 Feb;135(2):311-8.
The median highest pain score in a randomized trial of 38 women undergoing vulvar biopsies was 25.7 mm lower, on a 100 mm visual analogue scale, when they received 5% lidocaine-prilocaine cream instead of a 1% lidocaine injection, according to a report from Duke University, in Durham, N.C.
“In the current study, we found that application of lidocaine-prilocaine cream, alone, for a minimum of 10 minutes before vulvar biopsy on a non–hair-bearing surface results in a significantly lower maximum pain score and a significantly better patient rating of the biopsy experience,” said investigators led by Logan K. Williams, MD, of the department of obstetrics and gynecology at Duke University, Durham, N.C.
Given the “clear advantage” of the cream, it “should be considered as an anesthetic method for vulvar biopsy in a non-hair-bearing area,” Dr. Williams and colleagues concluded (Obstet Gynecol. 2020 Feb;135{2]:311-8).
Studies have pitted the cream against the injection before, but they did not compare patients’ maximal pain scores. The team wanted to do that because “comparing the highest score allows us to consider the possibility that the pain of anesthesia application” – injection versus cream – “may be greater than the pain of any other portion of the biopsy procedure.”
They randomized 19 women to the cream, approximately 5 g at the site of biopsy at least 10 minutes beforehand, and 18 others to the injection, 2 mL using a 27-gauge needle, at least 1 minute prior.
The median highest pain score in the lidocaine-prilocaine group was 20 mm, but 56.5 mm in the injection group. Patients randomized to lidocaine-prilocaine also had a significantly better (P = 0.02) experience than those receiving injected lidocaine, also assessed by visual analog scale (VAS). The median baseline pain level was 0 mm.
Anxiety was assessed after patients knew whether they were going to get the cream or the injection, but before the biopsy. The median score in the cream group was of 19 mm on another VAS, compared with 31.5 mm.
Participants were 60 years old on average, and almost all had prior vulvar biopsies. Two in the cream group and three in the injection group had punch biopsies; cervical biopsy forceps were used for the rest. More than half the women had benign findings, and most of the others had vulvar intraepithelial neoplasia, but there was one invasive cancer. At Duke, the cost of the injection was $0.99, compared with $7.36 for the cream.
Dr. Williams and colleagues cited a few limitations. One is that the patients and clinicians in the study were not blinded. Another is that most of the patients had undergone vulvar biopsy before, possibly predisposing them to bias.
“In the future, consideration could be taken to studying lidocaine-prilocaine cream applications to hair-bearing surfaces, which were excluded in this study.” Also, “there is a question of the histologic effect of lidocaine-prilocaine on tissues and whether this could affect pathologic diagnoses.
“We are conducting a separate ancillary study in conjunction with our dermatopathology colleagues to investigate this question,” the investigators said.
The work was funded by Duke and the National Institutes of Health. Dr. Williams had no disclosures.
aotto@mdedge.com
SOURCE: Williams LK et al. Obstet Gynecol. 2020 Feb;135(2):311-8.
FROM OBSTETRICS AND GYNECOLOGY
Data emerging to support personalized nutrition in oncology
SAN DIEGO – When Dawn Lemanne, MD, MPH, meets with cancer patients and their families, the question invariably comes up: “What should I eat?”

“The answer always is, ‘It depends,’” Dr. Lemanne, an oncologist who founded Oregon Integrative Oncology in Ashland, said at Natural Supplements: An Evidence-Based Update, presented by Scripps Center for Integrative Medicine. “The answers are not the same for each of these patients.”
According to Dr. Lemanne, targeted nutrition is evolving as a key component of cancer care. One of the goals of this approach is to decrease mTOR signaling. Normally, mTOR signaling promotes cell proliferation and metabolism; aberrant mTOR signaling can contribute to cancer initiation and progression.
“When mTOR speaks it says, ‘grow,’” said Dr. Lemanne, who is also an assistant professor of clinical medicine at the Andrew Weil Center for Integrative Medicine at the University of Arizona in Tucson. This message is meant to be heard by normal tissues, to stimulate normal tissue proliferation, such as in growing children or when a wound needs to be healed.
“However, cancer cells can hear and respond to mTOR’s message,” she said. “Normal cells may listen to mTOR’s ‘grow’ message or not, depending on the task they perform. Once we reach adulthood, we all likely have some precancerous or cancerous cells around, but they’re usually dormant. That’s why once you’re an adult, however, you don’t want too much mTOR signaling, because that might stimulate growth of things you definitely don’t want to grow.”
Having excessive levels of the growth hormone insulin-like growth factor-1 (IGF-1) also appears to play a role in cancer risk. Researchers studying members of a South American clan with Laron dwarfism – an inherited IGF-1 deficiency – found that besides being very short, affected members of this family rarely develop cancer (Cells. 2019;8[6]:596). “They also don’t get diabetes,” Dr. Lemanne said. “What we see in those with Laron dwarfism is that mTOR signaling is missing.”
She went on to note that studying type 2 diabetes gives physicians “a clue as to what dietary measures we might offer our patients in terms of decreasing their risk of dying from cancer or getting cancer.” The most common types of cancer are indeed more common in patients with type 2 diabetes. In addition, once someone with type 2 diabetes is diagnosed with cancer, their prognosis is poorer, compared with a cancer patient without diabetes.
“Metformin is often prescribed to patients with type 2 diabetes because it helps keep blood sugar low,” she said. “What’s fascinating is that diabetics on metformin develop cancer less frequently than diabetics not taking this drug. And also interesting, those diabetics who do develop cancer seem to do better if they’re on metformin before and after diagnosis.”
On the other hand, exogenous insulin therapy given to people with type 2 diabetes doubles the risk of cancer. Consistent with this is the two-decades-old finding that an elevated fasting insulin level also is associated with a poor breast cancer prognosis (J Clin Oncol. 2002 Jan 1;20[1]:42-51). “It’s really important to understand that, in a person destined to become a type 2 diabetic, the level of fasting insulin rises long before fasting glucose becomes abnormally high,” Dr. Lemanne explained. “A normal fasting glucose doesn’t let you off the hook in terms of checking your patient for insulin resistance.
“We will miss diagnosing many patients with dangerous insulin resistance and prediabetes if we don’t check the fasting glucose and the fasting insulin levels together. If the fasting insulin level is high, it’s important to limit carbohydrate intake enough to bring it down permanently, even when the fasting glucose is normal, or the patient is likely at increased risk for developing cancer.”
Two large, prospective randomized trials have examined breast cancer and diet: the Women’s Intervention Study (WINS) and the Women’s Health Eating and Living Study (WHEL). Patients in both trials had early stage breast cancer and were put on low-fat diets. In the end, there was a weak to negligible connection between breast cancer survival and dietary fat restriction. “That kind of shook up the oncology world,” Dr. Lemanne said, “because before these two studies, everyone ‘knew’ that dietary fat was related to breast cancer risk. These studies showed that wasn’t the case at all.”
According to Dr. Lemanne, unexpectedly, moderate carbohydrate restriction has been associated with lower risk of breast cancer recurrence in patients with postmenopausal hormone-receptor expressing breast cancer. Researchers at the University of California, San Diego, conducted a subanalysis of 265 postmenopausal patients with estrogen receptor positive breast cancer from the WHEL cohort (Cancer Epidemiol Biomarkers Prev. 2014 23[7]:1273-9). The recurrence risk was halved in those who cut their carbohydrate intake after diagnosis. The amount of decrease was modest, only 27 grams per day – the equivalent of one banana. “That is on par with a lot of our drugs, and maybe a little bit better,” she said. The effect was strongest if the breast tumor expressed IGF-1 receptor. Dr. Lemanne pointed out that decreasing dietary carbohydrate load was not the only treatment. These patients also had appropriate conventional cancer treatments, including surgery, radiation, and chemotherapy. “If we cut just some of the daily carb load in these patients, they might have a better cancer prognosis,” she said.
Overweight or obese patients with colon cancer also may benefit from moderate carbohydrate restriction. The CALGB 89803 study assessed 1,011 subjects with stage III colon cancer. It found that the subjects in the highest quintile of daily glycemic load and total carbohydrate intake had an increased risk of cancer recurrence and mortality (hazard ratio, 2.26; J Nat Cancer Inst. 2012;104[22]:1702-11). “This is pretty strong evidence that glycemic load and total carbohydrate intake play a role in colon cancer recurrence, but there’s a caveat here,” she said. “The effect was seen only in patients who were overweight or obese.” There was no association between carbohydrate intake and colon cancer recurrence in the absence of overweight or obesity.
Based on existing evidence, she said,
“That’s pretty modest; that’s 400 calories of carbohydrates per day,” Dr. Lemanne said. “I tell patients that they can have fruit, starchy vegetables, and even very small amounts of healthy whole grains, although I’m not a fan of grains due to the heavy carbohydrate load. All those things are OK. We’re not talking about jelly beans and white sugar.
“I also have them measure their fasting glucose each day, because different people have different blood glucose responses to the same food.” The goals she aims for with many of her patients are a fasting morning glucose between 79 and 83 mg/dL consistently, an HbA1c of 5.4 or less, and a BMI of 24.9 kg/m2 or less. “This set of goals, however, has to be individualized,” she said.
The ketogenic diet is another form of carb restriction, “but it’s much more drastic,” Dr. Lemanne said. “Most people require a carbohydrate load below 30 grams a day to enter a state of ketosis. But ketosis lowers the blood sugar and dampens the mTOR signaling.”
Evidence is emerging to support the use of a ketogenic diet as an adjunct to radiation therapy and as part of a complete course of treatment for glioblastoma multiforme and cancer cachexia. As an adjunct to radiation, a ketogenic diet decreases insulin and IGF-1 signaling. “This causes normal cells to enter dormancy, decreasing oxidative damage in normal cells,” Dr. Lemanne said. “There is also suppression of tumor angiogenesis, and thus poor DNA repair of radiation damage in tumor cells (Cancer Metastasis Rev. 2014;33[1]:217-29). Being in ketosis widens the therapeutic window. There are many animal studies which show that the ketogenic diet is helpful in cancer, mainly when combined with other anticancer treatments, such as radiation. Unfortunately, the evidence in humans is very anecdotal.”
One study found that if you feed mice with cancer ketogenic chow versus standard chow, they have a modestly improved survival (a mean of 43 days vs. 33 days; PLoS ONE. 2012;7[5]:e36197). However, when radiation was added to the keto diet, there was a dramatic improvement in survival (P less than 0.001). In fact, 75% survived to 250 days. “That’s pretty spectacular,” Dr. Lemanne said.
A ketogenic diet is standard therapy for several nonmalignant conditions, including glucose transporter 1 deficiency syndrome, pyruvate dehydrogenase deficiency syndrome, and refractory infantile epilepsy. The three major ketone bodies involved in human nutrition are acetoacetate, beta hydroxybutyrate, and acetone. Dr. Lemanne said beta hydroxybutyrate decreases inflammation and inhibits hexadecynoic acids (which induces apoptosis in cancer cells). Beta hydroxybutyrate also increases sirtuins, innate immunity, and seizure threshold; modulates circadian rhythm; and decreases insulin levels, she said.
In one case report from the scientific literature, a 38-year-old male with glioblastoma multiforme was placed on a hypocaloric ketogenic diet (Front Nutr. 2018 Mar 29;5:20). The patient had surgery, radiation, chemotherapy, and hyperbaric oxygen, and was given high doses of green tea extract in an attempt to antagonize glutamine metabolism. Two years after the beginning of his treatment, he was alive and had maintained a good level of tumor regression.
“We’ll see how he does,” said Dr. Lemanne, who was not involved in the report. “In my experience, I have a patient right now with a diagnosis of glioblastoma multiforme. She’s getting a keto diet in combo with intensive chemo, radiation, and surgery. She’s also had some hyperbaric oxygen and IV ozone therapy and is taking repurposed drugs. She has exceeded her expected survival, but she continues to have disease and symptoms. We are by no means out of the woods with this patient. But the keto diet has been quite feasible for her, because she has a lot of family and outside support.”
A ketogenic diet also may benefit patients with cancer cachexia, which is a loss of lean tissue. “Cancer cachexia is not completely understood,” Dr. Lemanne said. “What we know is that it is caused by inflammation created by the tumor itself, and this, in turn results in severe insulin resistance. Therefore, giving more calories as carbohydrate makes the cancer cachexia situation worse. Animal models of cancer cachexia have shown that the ketogenic diet normalizes metabolism and prevents lean tissue loss. Human studies are underway; we’ll see how they turn out.”
She closed her presentation by noting that in copious amounts of animal studies, fasting has been linked to improvements in chemotherapy efficacy and decreased side effects. In one study carried out at the University of Southern California in Los Angeles, volunteers fasted up to 140 hours before chemotherapy and an additional 156 hours afterward (Aging. 2009;1[12]:988-1007). The researchers found that the fasting was well-tolerated.
“The patients had some mild light-headedness, but there were no adverse effects on tumor volume or serum tumor markers,” Dr. Lemanne said. A more recent study of patients on cisplatin found that acaloric fasting led to decreased DNA damage in white blood cells, decreased IFG-1, and better white blood cell counts (BMC Cancer. 2016 Jun 10;16:360). “The benefits are immediate, and the optimal fasting time appears to be 48 hours,” Dr. Lemanne said.
One of her patients is a 64-year-old man on adjuvant cisplatin-based chemotherapy for cholangiocarcinoma. He fasts 24 hours before and 24 hours after each infusion, and has experienced no emesis or nausea. “His immune suppression and anemia are much milder than we expected, and he has not required any treatment for chemotherapy-related side effects,” Dr. Lemanne said. “That’s a big monetary value.”
Fasting 13 hours overnight has been associated with fewer breast cancer-related problems in patients already diagnosed with the disease. Chronic caloric restriction, just cutting calories by 25%-40% daily, has been shown to delay all diseases of aging, including cancer, and is associated with increased longevity in many species. “Chronic caloric restriction is difficult, however, because it results in chronic hunger and weight loss,” she said. “Occasional fasting is superior to chronic caloric restriction because it maintains normal weight, preserves lean muscle mass, enhances tumor sensitivity to chemotherapy and radiotherapy, and diminishes the side effects of chemotherapy.”
Dr. Lemanne reported having no financial disclosures.
dbrunk@mdedge.com
SAN DIEGO – When Dawn Lemanne, MD, MPH, meets with cancer patients and their families, the question invariably comes up: “What should I eat?”
“The answer always is, ‘It depends,’” Dr. Lemanne, an oncologist who founded Oregon Integrative Oncology in Ashland, said at Natural Supplements: An Evidence-Based Update, presented by Scripps Center for Integrative Medicine. “The answers are not the same for each of these patients.”
According to Dr. Lemanne, targeted nutrition is evolving as a key component of cancer care. One of the goals of this approach is to decrease mTOR signaling. Normally, mTOR signaling promotes cell proliferation and metabolism; aberrant mTOR signaling can contribute to cancer initiation and progression.
“When mTOR speaks it says, ‘grow,’” said Dr. Lemanne, who is also an assistant professor of clinical medicine at the Andrew Weil Center for Integrative Medicine at the University of Arizona in Tucson. This message is meant to be heard by normal tissues, to stimulate normal tissue proliferation, such as in growing children or when a wound needs to be healed.
“However, cancer cells can hear and respond to mTOR’s message,” she said. “Normal cells may listen to mTOR’s ‘grow’ message or not, depending on the task they perform. Once we reach adulthood, we all likely have some precancerous or cancerous cells around, but they’re usually dormant. That’s why once you’re an adult, however, you don’t want too much mTOR signaling, because that might stimulate growth of things you definitely don’t want to grow.”
Having excessive levels of the growth hormone insulin-like growth factor-1 (IGF-1) also appears to play a role in cancer risk. Researchers studying members of a South American clan with Laron dwarfism – an inherited IGF-1 deficiency – found that besides being very short, affected members of this family rarely develop cancer (Cells. 2019;8[6]:596). “They also don’t get diabetes,” Dr. Lemanne said. “What we see in those with Laron dwarfism is that mTOR signaling is missing.”
She went on to note that studying type 2 diabetes gives physicians “a clue as to what dietary measures we might offer our patients in terms of decreasing their risk of dying from cancer or getting cancer.” The most common types of cancer are indeed more common in patients with type 2 diabetes. In addition, once someone with type 2 diabetes is diagnosed with cancer, their prognosis is poorer, compared with a cancer patient without diabetes.
“Metformin is often prescribed to patients with type 2 diabetes because it helps keep blood sugar low,” she said. “What’s fascinating is that diabetics on metformin develop cancer less frequently than diabetics not taking this drug. And also interesting, those diabetics who do develop cancer seem to do better if they’re on metformin before and after diagnosis.”
On the other hand, exogenous insulin therapy given to people with type 2 diabetes doubles the risk of cancer. Consistent with this is the two-decades-old finding that an elevated fasting insulin level also is associated with a poor breast cancer prognosis (J Clin Oncol. 2002 Jan 1;20[1]:42-51). “It’s really important to understand that, in a person destined to become a type 2 diabetic, the level of fasting insulin rises long before fasting glucose becomes abnormally high,” Dr. Lemanne explained. “A normal fasting glucose doesn’t let you off the hook in terms of checking your patient for insulin resistance.
“We will miss diagnosing many patients with dangerous insulin resistance and prediabetes if we don’t check the fasting glucose and the fasting insulin levels together. If the fasting insulin level is high, it’s important to limit carbohydrate intake enough to bring it down permanently, even when the fasting glucose is normal, or the patient is likely at increased risk for developing cancer.”
Two large, prospective randomized trials have examined breast cancer and diet: the Women’s Intervention Study (WINS) and the Women’s Health Eating and Living Study (WHEL). Patients in both trials had early stage breast cancer and were put on low-fat diets. In the end, there was a weak to negligible connection between breast cancer survival and dietary fat restriction. “That kind of shook up the oncology world,” Dr. Lemanne said, “because before these two studies, everyone ‘knew’ that dietary fat was related to breast cancer risk. These studies showed that wasn’t the case at all.”
According to Dr. Lemanne, unexpectedly, moderate carbohydrate restriction has been associated with lower risk of breast cancer recurrence in patients with postmenopausal hormone-receptor expressing breast cancer. Researchers at the University of California, San Diego, conducted a subanalysis of 265 postmenopausal patients with estrogen receptor positive breast cancer from the WHEL cohort (Cancer Epidemiol Biomarkers Prev. 2014 23[7]:1273-9). The recurrence risk was halved in those who cut their carbohydrate intake after diagnosis. The amount of decrease was modest, only 27 grams per day – the equivalent of one banana. “That is on par with a lot of our drugs, and maybe a little bit better,” she said. The effect was strongest if the breast tumor expressed IGF-1 receptor. Dr. Lemanne pointed out that decreasing dietary carbohydrate load was not the only treatment. These patients also had appropriate conventional cancer treatments, including surgery, radiation, and chemotherapy. “If we cut just some of the daily carb load in these patients, they might have a better cancer prognosis,” she said.
Overweight or obese patients with colon cancer also may benefit from moderate carbohydrate restriction. The CALGB 89803 study assessed 1,011 subjects with stage III colon cancer. It found that the subjects in the highest quintile of daily glycemic load and total carbohydrate intake had an increased risk of cancer recurrence and mortality (hazard ratio, 2.26; J Nat Cancer Inst. 2012;104[22]:1702-11). “This is pretty strong evidence that glycemic load and total carbohydrate intake play a role in colon cancer recurrence, but there’s a caveat here,” she said. “The effect was seen only in patients who were overweight or obese.” There was no association between carbohydrate intake and colon cancer recurrence in the absence of overweight or obesity.
Based on existing evidence, she said,
“That’s pretty modest; that’s 400 calories of carbohydrates per day,” Dr. Lemanne said. “I tell patients that they can have fruit, starchy vegetables, and even very small amounts of healthy whole grains, although I’m not a fan of grains due to the heavy carbohydrate load. All those things are OK. We’re not talking about jelly beans and white sugar.
“I also have them measure their fasting glucose each day, because different people have different blood glucose responses to the same food.” The goals she aims for with many of her patients are a fasting morning glucose between 79 and 83 mg/dL consistently, an HbA1c of 5.4 or less, and a BMI of 24.9 kg/m2 or less. “This set of goals, however, has to be individualized,” she said.
The ketogenic diet is another form of carb restriction, “but it’s much more drastic,” Dr. Lemanne said. “Most people require a carbohydrate load below 30 grams a day to enter a state of ketosis. But ketosis lowers the blood sugar and dampens the mTOR signaling.”
Evidence is emerging to support the use of a ketogenic diet as an adjunct to radiation therapy and as part of a complete course of treatment for glioblastoma multiforme and cancer cachexia. As an adjunct to radiation, a ketogenic diet decreases insulin and IGF-1 signaling. “This causes normal cells to enter dormancy, decreasing oxidative damage in normal cells,” Dr. Lemanne said. “There is also suppression of tumor angiogenesis, and thus poor DNA repair of radiation damage in tumor cells (Cancer Metastasis Rev. 2014;33[1]:217-29). Being in ketosis widens the therapeutic window. There are many animal studies which show that the ketogenic diet is helpful in cancer, mainly when combined with other anticancer treatments, such as radiation. Unfortunately, the evidence in humans is very anecdotal.”
One study found that if you feed mice with cancer ketogenic chow versus standard chow, they have a modestly improved survival (a mean of 43 days vs. 33 days; PLoS ONE. 2012;7[5]:e36197). However, when radiation was added to the keto diet, there was a dramatic improvement in survival (P less than 0.001). In fact, 75% survived to 250 days. “That’s pretty spectacular,” Dr. Lemanne said.
A ketogenic diet is standard therapy for several nonmalignant conditions, including glucose transporter 1 deficiency syndrome, pyruvate dehydrogenase deficiency syndrome, and refractory infantile epilepsy. The three major ketone bodies involved in human nutrition are acetoacetate, beta hydroxybutyrate, and acetone. Dr. Lemanne said beta hydroxybutyrate decreases inflammation and inhibits hexadecynoic acids (which induces apoptosis in cancer cells). Beta hydroxybutyrate also increases sirtuins, innate immunity, and seizure threshold; modulates circadian rhythm; and decreases insulin levels, she said.
In one case report from the scientific literature, a 38-year-old male with glioblastoma multiforme was placed on a hypocaloric ketogenic diet (Front Nutr. 2018 Mar 29;5:20). The patient had surgery, radiation, chemotherapy, and hyperbaric oxygen, and was given high doses of green tea extract in an attempt to antagonize glutamine metabolism. Two years after the beginning of his treatment, he was alive and had maintained a good level of tumor regression.
“We’ll see how he does,” said Dr. Lemanne, who was not involved in the report. “In my experience, I have a patient right now with a diagnosis of glioblastoma multiforme. She’s getting a keto diet in combo with intensive chemo, radiation, and surgery. She’s also had some hyperbaric oxygen and IV ozone therapy and is taking repurposed drugs. She has exceeded her expected survival, but she continues to have disease and symptoms. We are by no means out of the woods with this patient. But the keto diet has been quite feasible for her, because she has a lot of family and outside support.”
A ketogenic diet also may benefit patients with cancer cachexia, which is a loss of lean tissue. “Cancer cachexia is not completely understood,” Dr. Lemanne said. “What we know is that it is caused by inflammation created by the tumor itself, and this, in turn results in severe insulin resistance. Therefore, giving more calories as carbohydrate makes the cancer cachexia situation worse. Animal models of cancer cachexia have shown that the ketogenic diet normalizes metabolism and prevents lean tissue loss. Human studies are underway; we’ll see how they turn out.”
She closed her presentation by noting that in copious amounts of animal studies, fasting has been linked to improvements in chemotherapy efficacy and decreased side effects. In one study carried out at the University of Southern California in Los Angeles, volunteers fasted up to 140 hours before chemotherapy and an additional 156 hours afterward (Aging. 2009;1[12]:988-1007). The researchers found that the fasting was well-tolerated.
“The patients had some mild light-headedness, but there were no adverse effects on tumor volume or serum tumor markers,” Dr. Lemanne said. A more recent study of patients on cisplatin found that acaloric fasting led to decreased DNA damage in white blood cells, decreased IFG-1, and better white blood cell counts (BMC Cancer. 2016 Jun 10;16:360). “The benefits are immediate, and the optimal fasting time appears to be 48 hours,” Dr. Lemanne said.
One of her patients is a 64-year-old man on adjuvant cisplatin-based chemotherapy for cholangiocarcinoma. He fasts 24 hours before and 24 hours after each infusion, and has experienced no emesis or nausea. “His immune suppression and anemia are much milder than we expected, and he has not required any treatment for chemotherapy-related side effects,” Dr. Lemanne said. “That’s a big monetary value.”
Fasting 13 hours overnight has been associated with fewer breast cancer-related problems in patients already diagnosed with the disease. Chronic caloric restriction, just cutting calories by 25%-40% daily, has been shown to delay all diseases of aging, including cancer, and is associated with increased longevity in many species. “Chronic caloric restriction is difficult, however, because it results in chronic hunger and weight loss,” she said. “Occasional fasting is superior to chronic caloric restriction because it maintains normal weight, preserves lean muscle mass, enhances tumor sensitivity to chemotherapy and radiotherapy, and diminishes the side effects of chemotherapy.”
Dr. Lemanne reported having no financial disclosures.
dbrunk@mdedge.com
SAN DIEGO – When Dawn Lemanne, MD, MPH, meets with cancer patients and their families, the question invariably comes up: “What should I eat?”
“The answer always is, ‘It depends,’” Dr. Lemanne, an oncologist who founded Oregon Integrative Oncology in Ashland, said at Natural Supplements: An Evidence-Based Update, presented by Scripps Center for Integrative Medicine. “The answers are not the same for each of these patients.”
According to Dr. Lemanne, targeted nutrition is evolving as a key component of cancer care. One of the goals of this approach is to decrease mTOR signaling. Normally, mTOR signaling promotes cell proliferation and metabolism; aberrant mTOR signaling can contribute to cancer initiation and progression.
“When mTOR speaks it says, ‘grow,’” said Dr. Lemanne, who is also an assistant professor of clinical medicine at the Andrew Weil Center for Integrative Medicine at the University of Arizona in Tucson. This message is meant to be heard by normal tissues, to stimulate normal tissue proliferation, such as in growing children or when a wound needs to be healed.
“However, cancer cells can hear and respond to mTOR’s message,” she said. “Normal cells may listen to mTOR’s ‘grow’ message or not, depending on the task they perform. Once we reach adulthood, we all likely have some precancerous or cancerous cells around, but they’re usually dormant. That’s why once you’re an adult, however, you don’t want too much mTOR signaling, because that might stimulate growth of things you definitely don’t want to grow.”
Having excessive levels of the growth hormone insulin-like growth factor-1 (IGF-1) also appears to play a role in cancer risk. Researchers studying members of a South American clan with Laron dwarfism – an inherited IGF-1 deficiency – found that besides being very short, affected members of this family rarely develop cancer (Cells. 2019;8[6]:596). “They also don’t get diabetes,” Dr. Lemanne said. “What we see in those with Laron dwarfism is that mTOR signaling is missing.”
She went on to note that studying type 2 diabetes gives physicians “a clue as to what dietary measures we might offer our patients in terms of decreasing their risk of dying from cancer or getting cancer.” The most common types of cancer are indeed more common in patients with type 2 diabetes. In addition, once someone with type 2 diabetes is diagnosed with cancer, their prognosis is poorer, compared with a cancer patient without diabetes.
“Metformin is often prescribed to patients with type 2 diabetes because it helps keep blood sugar low,” she said. “What’s fascinating is that diabetics on metformin develop cancer less frequently than diabetics not taking this drug. And also interesting, those diabetics who do develop cancer seem to do better if they’re on metformin before and after diagnosis.”
On the other hand, exogenous insulin therapy given to people with type 2 diabetes doubles the risk of cancer. Consistent with this is the two-decades-old finding that an elevated fasting insulin level also is associated with a poor breast cancer prognosis (J Clin Oncol. 2002 Jan 1;20[1]:42-51). “It’s really important to understand that, in a person destined to become a type 2 diabetic, the level of fasting insulin rises long before fasting glucose becomes abnormally high,” Dr. Lemanne explained. “A normal fasting glucose doesn’t let you off the hook in terms of checking your patient for insulin resistance.
“We will miss diagnosing many patients with dangerous insulin resistance and prediabetes if we don’t check the fasting glucose and the fasting insulin levels together. If the fasting insulin level is high, it’s important to limit carbohydrate intake enough to bring it down permanently, even when the fasting glucose is normal, or the patient is likely at increased risk for developing cancer.”
Two large, prospective randomized trials have examined breast cancer and diet: the Women’s Intervention Study (WINS) and the Women’s Health Eating and Living Study (WHEL). Patients in both trials had early stage breast cancer and were put on low-fat diets. In the end, there was a weak to negligible connection between breast cancer survival and dietary fat restriction. “That kind of shook up the oncology world,” Dr. Lemanne said, “because before these two studies, everyone ‘knew’ that dietary fat was related to breast cancer risk. These studies showed that wasn’t the case at all.”
According to Dr. Lemanne, unexpectedly, moderate carbohydrate restriction has been associated with lower risk of breast cancer recurrence in patients with postmenopausal hormone-receptor expressing breast cancer. Researchers at the University of California, San Diego, conducted a subanalysis of 265 postmenopausal patients with estrogen receptor positive breast cancer from the WHEL cohort (Cancer Epidemiol Biomarkers Prev. 2014 23[7]:1273-9). The recurrence risk was halved in those who cut their carbohydrate intake after diagnosis. The amount of decrease was modest, only 27 grams per day – the equivalent of one banana. “That is on par with a lot of our drugs, and maybe a little bit better,” she said. The effect was strongest if the breast tumor expressed IGF-1 receptor. Dr. Lemanne pointed out that decreasing dietary carbohydrate load was not the only treatment. These patients also had appropriate conventional cancer treatments, including surgery, radiation, and chemotherapy. “If we cut just some of the daily carb load in these patients, they might have a better cancer prognosis,” she said.
Overweight or obese patients with colon cancer also may benefit from moderate carbohydrate restriction. The CALGB 89803 study assessed 1,011 subjects with stage III colon cancer. It found that the subjects in the highest quintile of daily glycemic load and total carbohydrate intake had an increased risk of cancer recurrence and mortality (hazard ratio, 2.26; J Nat Cancer Inst. 2012;104[22]:1702-11). “This is pretty strong evidence that glycemic load and total carbohydrate intake play a role in colon cancer recurrence, but there’s a caveat here,” she said. “The effect was seen only in patients who were overweight or obese.” There was no association between carbohydrate intake and colon cancer recurrence in the absence of overweight or obesity.
Based on existing evidence, she said,
“That’s pretty modest; that’s 400 calories of carbohydrates per day,” Dr. Lemanne said. “I tell patients that they can have fruit, starchy vegetables, and even very small amounts of healthy whole grains, although I’m not a fan of grains due to the heavy carbohydrate load. All those things are OK. We’re not talking about jelly beans and white sugar.
“I also have them measure their fasting glucose each day, because different people have different blood glucose responses to the same food.” The goals she aims for with many of her patients are a fasting morning glucose between 79 and 83 mg/dL consistently, an HbA1c of 5.4 or less, and a BMI of 24.9 kg/m2 or less. “This set of goals, however, has to be individualized,” she said.
The ketogenic diet is another form of carb restriction, “but it’s much more drastic,” Dr. Lemanne said. “Most people require a carbohydrate load below 30 grams a day to enter a state of ketosis. But ketosis lowers the blood sugar and dampens the mTOR signaling.”
Evidence is emerging to support the use of a ketogenic diet as an adjunct to radiation therapy and as part of a complete course of treatment for glioblastoma multiforme and cancer cachexia. As an adjunct to radiation, a ketogenic diet decreases insulin and IGF-1 signaling. “This causes normal cells to enter dormancy, decreasing oxidative damage in normal cells,” Dr. Lemanne said. “There is also suppression of tumor angiogenesis, and thus poor DNA repair of radiation damage in tumor cells (Cancer Metastasis Rev. 2014;33[1]:217-29). Being in ketosis widens the therapeutic window. There are many animal studies which show that the ketogenic diet is helpful in cancer, mainly when combined with other anticancer treatments, such as radiation. Unfortunately, the evidence in humans is very anecdotal.”
One study found that if you feed mice with cancer ketogenic chow versus standard chow, they have a modestly improved survival (a mean of 43 days vs. 33 days; PLoS ONE. 2012;7[5]:e36197). However, when radiation was added to the keto diet, there was a dramatic improvement in survival (P less than 0.001). In fact, 75% survived to 250 days. “That’s pretty spectacular,” Dr. Lemanne said.
A ketogenic diet is standard therapy for several nonmalignant conditions, including glucose transporter 1 deficiency syndrome, pyruvate dehydrogenase deficiency syndrome, and refractory infantile epilepsy. The three major ketone bodies involved in human nutrition are acetoacetate, beta hydroxybutyrate, and acetone. Dr. Lemanne said beta hydroxybutyrate decreases inflammation and inhibits hexadecynoic acids (which induces apoptosis in cancer cells). Beta hydroxybutyrate also increases sirtuins, innate immunity, and seizure threshold; modulates circadian rhythm; and decreases insulin levels, she said.
In one case report from the scientific literature, a 38-year-old male with glioblastoma multiforme was placed on a hypocaloric ketogenic diet (Front Nutr. 2018 Mar 29;5:20). The patient had surgery, radiation, chemotherapy, and hyperbaric oxygen, and was given high doses of green tea extract in an attempt to antagonize glutamine metabolism. Two years after the beginning of his treatment, he was alive and had maintained a good level of tumor regression.
“We’ll see how he does,” said Dr. Lemanne, who was not involved in the report. “In my experience, I have a patient right now with a diagnosis of glioblastoma multiforme. She’s getting a keto diet in combo with intensive chemo, radiation, and surgery. She’s also had some hyperbaric oxygen and IV ozone therapy and is taking repurposed drugs. She has exceeded her expected survival, but she continues to have disease and symptoms. We are by no means out of the woods with this patient. But the keto diet has been quite feasible for her, because she has a lot of family and outside support.”
A ketogenic diet also may benefit patients with cancer cachexia, which is a loss of lean tissue. “Cancer cachexia is not completely understood,” Dr. Lemanne said. “What we know is that it is caused by inflammation created by the tumor itself, and this, in turn results in severe insulin resistance. Therefore, giving more calories as carbohydrate makes the cancer cachexia situation worse. Animal models of cancer cachexia have shown that the ketogenic diet normalizes metabolism and prevents lean tissue loss. Human studies are underway; we’ll see how they turn out.”
She closed her presentation by noting that in copious amounts of animal studies, fasting has been linked to improvements in chemotherapy efficacy and decreased side effects. In one study carried out at the University of Southern California in Los Angeles, volunteers fasted up to 140 hours before chemotherapy and an additional 156 hours afterward (Aging. 2009;1[12]:988-1007). The researchers found that the fasting was well-tolerated.
“The patients had some mild light-headedness, but there were no adverse effects on tumor volume or serum tumor markers,” Dr. Lemanne said. A more recent study of patients on cisplatin found that acaloric fasting led to decreased DNA damage in white blood cells, decreased IFG-1, and better white blood cell counts (BMC Cancer. 2016 Jun 10;16:360). “The benefits are immediate, and the optimal fasting time appears to be 48 hours,” Dr. Lemanne said.
One of her patients is a 64-year-old man on adjuvant cisplatin-based chemotherapy for cholangiocarcinoma. He fasts 24 hours before and 24 hours after each infusion, and has experienced no emesis or nausea. “His immune suppression and anemia are much milder than we expected, and he has not required any treatment for chemotherapy-related side effects,” Dr. Lemanne said. “That’s a big monetary value.”
Fasting 13 hours overnight has been associated with fewer breast cancer-related problems in patients already diagnosed with the disease. Chronic caloric restriction, just cutting calories by 25%-40% daily, has been shown to delay all diseases of aging, including cancer, and is associated with increased longevity in many species. “Chronic caloric restriction is difficult, however, because it results in chronic hunger and weight loss,” she said. “Occasional fasting is superior to chronic caloric restriction because it maintains normal weight, preserves lean muscle mass, enhances tumor sensitivity to chemotherapy and radiotherapy, and diminishes the side effects of chemotherapy.”
Dr. Lemanne reported having no financial disclosures.
dbrunk@mdedge.com
REPORTING FROM A NATURAL SUPPLEMENTS UPDATE
Blood pressure categories may signal maternal, perinatal risks
GRAPEVINE, TEX. – Blood pressure categories created by the American College of Cardiology (ACC) and American Heart Association (AHA) in 2017 identify patients with increased risk of preeclampsia, preterm birth, and perinatal death when applied to the first 20 weeks of pregnancy, according to a retrospective study presented at the meeting sponsored by the Society for Maternal-Fetal Medicine.

The absolute risk increases are small, and it is unknown whether treating these patients differently would be beneficial, said study author Martha Tesfalul, MD, maternal-fetal medicine clinical fellow at University of California, San Francisco. Nevertheless, , Dr. Tesfalul said.
Cutoffs with unclear implications
The ACC/AHA in November 2017 reclassified blood pressure in nonpregnant adults, but “implications of these categories in pregnancy are still unclear,” Dr. Tesfalul and colleagues said. Under the guidelines, normal blood pressure is systolic blood pressure less than 120 mm Hg and diastolic blood pressure less than 80 mm Hg. Elevated blood pressure is defined as systolic blood pressure between 120 and 129 mm Hg and diastolic blood pressure less than 80 mm Hg. Stage 1 hypertension is systolic blood pressure between 130 and 139 mm Hg or diastolic blood pressure between 80 and 89 mm Hg. And stage 2 hypertension is systolic blood pressure of at least 140 mm Hg or diastolic blood pressure of at least 90 mm Hg.
For the present analysis, the researchers retrospectively compared obstetric and perinatal outcomes for approximately 6,000 pregnancies at an academic center for which they had at least one blood pressure measurement prior to 20 weeks. The highest measurement was used to identify women with normal blood pressure, elevated blood pressure, or stage 1 hypertension according to the 2017 thresholds.
The researchers included singleton pregnancies with delivery between January 2014 and October 2017. They excluded patients with a prior diagnosis of chronic hypertension, autoimmune or chronic renal disease, or fetal anomalies. They examined rates of gestational hypertension, preeclampsia, preterm birth, neonatal intensive care admission, and perinatal death.
Adjusted relative risks
Dr. Tesfalul and colleagues identified about 3,500 pregnancies with normal blood pressure, more than 1,300 pregnancies with elevated blood pressure, and nearly 1,100 pregnancies with stage 1 hypertension.
After adjusting for relevant covariates – maternal age, nulliparity, race, body mass index, in vitro fertilization, tobacco use, pregestational diabetes, and aspirin use – elevated blood pressure and stage 1 hypertension were associated with a higher risk of preeclampsia and severe preeclampsia, relative to normal blood pressure. The proportion of patients with preeclampsia was 5.7% in the normal blood pressure group, 11.7% in the elevated blood pressure group (adjusted relative risk, 1.8), and 15% in the stage 1 hypertension group (adjusted RR, 2.1). The proportion with preeclampsia with severe features was 3.1% in the normal blood pressure group, 5.7% in the elevated blood pressure group (adjusted RR, 1.6), and 6.8% in the stage 1 hypertension group (adjusted RR, 1.8).
In addition, stage 1 hypertension, compared with normal blood pressure, was associated with increased odds of preterm birth at less than 37 weeks (7.9% vs. 5.1%; adjusted RR, 1.4) and perinatal death (0.7% vs. 0.4%; adjusted RR, 2.8).
“Patients with elevated blood pressure and stage 1 hypertension prior to 20 weeks are at increased risk of adverse outcomes,” the authors concluded. “Further research [is] needed to determine optimal care of patients with elevated blood pressure and stage 1 hypertension in pregnancy.”
Dr. Tesfalul receives support from the Foundation for SMFM.
SOURCE: Tesfalul M et al. Am J Obstet Gynecol. 2020 Jan;222(1):S92-3, Abstract 119.
GRAPEVINE, TEX. – Blood pressure categories created by the American College of Cardiology (ACC) and American Heart Association (AHA) in 2017 identify patients with increased risk of preeclampsia, preterm birth, and perinatal death when applied to the first 20 weeks of pregnancy, according to a retrospective study presented at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The absolute risk increases are small, and it is unknown whether treating these patients differently would be beneficial, said study author Martha Tesfalul, MD, maternal-fetal medicine clinical fellow at University of California, San Francisco. Nevertheless, , Dr. Tesfalul said.
Cutoffs with unclear implications
The ACC/AHA in November 2017 reclassified blood pressure in nonpregnant adults, but “implications of these categories in pregnancy are still unclear,” Dr. Tesfalul and colleagues said. Under the guidelines, normal blood pressure is systolic blood pressure less than 120 mm Hg and diastolic blood pressure less than 80 mm Hg. Elevated blood pressure is defined as systolic blood pressure between 120 and 129 mm Hg and diastolic blood pressure less than 80 mm Hg. Stage 1 hypertension is systolic blood pressure between 130 and 139 mm Hg or diastolic blood pressure between 80 and 89 mm Hg. And stage 2 hypertension is systolic blood pressure of at least 140 mm Hg or diastolic blood pressure of at least 90 mm Hg.
For the present analysis, the researchers retrospectively compared obstetric and perinatal outcomes for approximately 6,000 pregnancies at an academic center for which they had at least one blood pressure measurement prior to 20 weeks. The highest measurement was used to identify women with normal blood pressure, elevated blood pressure, or stage 1 hypertension according to the 2017 thresholds.
The researchers included singleton pregnancies with delivery between January 2014 and October 2017. They excluded patients with a prior diagnosis of chronic hypertension, autoimmune or chronic renal disease, or fetal anomalies. They examined rates of gestational hypertension, preeclampsia, preterm birth, neonatal intensive care admission, and perinatal death.
Adjusted relative risks
Dr. Tesfalul and colleagues identified about 3,500 pregnancies with normal blood pressure, more than 1,300 pregnancies with elevated blood pressure, and nearly 1,100 pregnancies with stage 1 hypertension.
After adjusting for relevant covariates – maternal age, nulliparity, race, body mass index, in vitro fertilization, tobacco use, pregestational diabetes, and aspirin use – elevated blood pressure and stage 1 hypertension were associated with a higher risk of preeclampsia and severe preeclampsia, relative to normal blood pressure. The proportion of patients with preeclampsia was 5.7% in the normal blood pressure group, 11.7% in the elevated blood pressure group (adjusted relative risk, 1.8), and 15% in the stage 1 hypertension group (adjusted RR, 2.1). The proportion with preeclampsia with severe features was 3.1% in the normal blood pressure group, 5.7% in the elevated blood pressure group (adjusted RR, 1.6), and 6.8% in the stage 1 hypertension group (adjusted RR, 1.8).
In addition, stage 1 hypertension, compared with normal blood pressure, was associated with increased odds of preterm birth at less than 37 weeks (7.9% vs. 5.1%; adjusted RR, 1.4) and perinatal death (0.7% vs. 0.4%; adjusted RR, 2.8).
“Patients with elevated blood pressure and stage 1 hypertension prior to 20 weeks are at increased risk of adverse outcomes,” the authors concluded. “Further research [is] needed to determine optimal care of patients with elevated blood pressure and stage 1 hypertension in pregnancy.”
Dr. Tesfalul receives support from the Foundation for SMFM.
SOURCE: Tesfalul M et al. Am J Obstet Gynecol. 2020 Jan;222(1):S92-3, Abstract 119.
GRAPEVINE, TEX. – Blood pressure categories created by the American College of Cardiology (ACC) and American Heart Association (AHA) in 2017 identify patients with increased risk of preeclampsia, preterm birth, and perinatal death when applied to the first 20 weeks of pregnancy, according to a retrospective study presented at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The absolute risk increases are small, and it is unknown whether treating these patients differently would be beneficial, said study author Martha Tesfalul, MD, maternal-fetal medicine clinical fellow at University of California, San Francisco. Nevertheless, , Dr. Tesfalul said.
Cutoffs with unclear implications
The ACC/AHA in November 2017 reclassified blood pressure in nonpregnant adults, but “implications of these categories in pregnancy are still unclear,” Dr. Tesfalul and colleagues said. Under the guidelines, normal blood pressure is systolic blood pressure less than 120 mm Hg and diastolic blood pressure less than 80 mm Hg. Elevated blood pressure is defined as systolic blood pressure between 120 and 129 mm Hg and diastolic blood pressure less than 80 mm Hg. Stage 1 hypertension is systolic blood pressure between 130 and 139 mm Hg or diastolic blood pressure between 80 and 89 mm Hg. And stage 2 hypertension is systolic blood pressure of at least 140 mm Hg or diastolic blood pressure of at least 90 mm Hg.
For the present analysis, the researchers retrospectively compared obstetric and perinatal outcomes for approximately 6,000 pregnancies at an academic center for which they had at least one blood pressure measurement prior to 20 weeks. The highest measurement was used to identify women with normal blood pressure, elevated blood pressure, or stage 1 hypertension according to the 2017 thresholds.
The researchers included singleton pregnancies with delivery between January 2014 and October 2017. They excluded patients with a prior diagnosis of chronic hypertension, autoimmune or chronic renal disease, or fetal anomalies. They examined rates of gestational hypertension, preeclampsia, preterm birth, neonatal intensive care admission, and perinatal death.
Adjusted relative risks
Dr. Tesfalul and colleagues identified about 3,500 pregnancies with normal blood pressure, more than 1,300 pregnancies with elevated blood pressure, and nearly 1,100 pregnancies with stage 1 hypertension.
After adjusting for relevant covariates – maternal age, nulliparity, race, body mass index, in vitro fertilization, tobacco use, pregestational diabetes, and aspirin use – elevated blood pressure and stage 1 hypertension were associated with a higher risk of preeclampsia and severe preeclampsia, relative to normal blood pressure. The proportion of patients with preeclampsia was 5.7% in the normal blood pressure group, 11.7% in the elevated blood pressure group (adjusted relative risk, 1.8), and 15% in the stage 1 hypertension group (adjusted RR, 2.1). The proportion with preeclampsia with severe features was 3.1% in the normal blood pressure group, 5.7% in the elevated blood pressure group (adjusted RR, 1.6), and 6.8% in the stage 1 hypertension group (adjusted RR, 1.8).
In addition, stage 1 hypertension, compared with normal blood pressure, was associated with increased odds of preterm birth at less than 37 weeks (7.9% vs. 5.1%; adjusted RR, 1.4) and perinatal death (0.7% vs. 0.4%; adjusted RR, 2.8).
“Patients with elevated blood pressure and stage 1 hypertension prior to 20 weeks are at increased risk of adverse outcomes,” the authors concluded. “Further research [is] needed to determine optimal care of patients with elevated blood pressure and stage 1 hypertension in pregnancy.”
Dr. Tesfalul receives support from the Foundation for SMFM.
SOURCE: Tesfalul M et al. Am J Obstet Gynecol. 2020 Jan;222(1):S92-3, Abstract 119.
REPORTING FROM THE PREGNANCY MEETING
Patients remain satisfied despite reduced use of opioids post partum
GRAPEVINE, TEX. – The amount of opioids prescribed post partum may decline over time without affecting levels of pain control satisfaction, according to research presented at the meeting sponsored by the Society for Maternal-Fetal Medicine.

Data from a large center indicate that trends in opioid use significantly declined from 2017 to 2019, but not at the expense of adequate pain control, said Nevert Badreldin, MD, assistant professor of obstetrics and gynecology at Northwestern University in Chicago. Patients consistently reported that they were satisfied with inpatient pain control, while opioid use per inpatient day decreased from about 30 morphine milligram equivalents (MME) to less than 20 MME during that time.
To assess trends in postpartum opioid prescribing, opioid use, and pain control satisfaction, Dr. Badreldin and colleagues evaluated data from a prospective observational study. Their analysis included data from women who used an opioid during postpartum hospitalization between May 2017 and July 2019. The researchers excluded women with NSAID or morphine allergies or recent opioid use, as well as those who received general anesthesia without concurrent neuraxial anesthesia, those who underwent peripartum hysterectomy, and women admitted to the ICU.
The investigators used nonparametric tests of trend to assess the difference over time in the proportion of patients who received an opioid prescription at discharge and in the total MME prescribed post partum.
Of 900 women with inpatient opioid use, 471 agreed to be followed after discharge. In that group, the amount of opioid use per inpatient day significantly declined. In addition, the percentage who received an opioid prescription at discharge significantly declined, as did the total MME prescribed at discharge.
“Both inpatient and outpatient satisfaction with pain control were unchanged,” the researchers reported. “In this population, both the frequency and amount of opioid use in the postpartum period declined from 2017 to 2019, without any change in satisfaction with pain control.”
The study was supported by the Society for Maternal-Fetal Medicine/AMAG 2017 Health Policy Award, and a coauthor received support from the National Institute of Child Health and Human Development.
Source: Badreldin N et al. Am J Obstet Gynecol. 2020 Jan;222(1):S93, Abstract 120.
GRAPEVINE, TEX. – The amount of opioids prescribed post partum may decline over time without affecting levels of pain control satisfaction, according to research presented at the meeting sponsored by the Society for Maternal-Fetal Medicine.
Data from a large center indicate that trends in opioid use significantly declined from 2017 to 2019, but not at the expense of adequate pain control, said Nevert Badreldin, MD, assistant professor of obstetrics and gynecology at Northwestern University in Chicago. Patients consistently reported that they were satisfied with inpatient pain control, while opioid use per inpatient day decreased from about 30 morphine milligram equivalents (MME) to less than 20 MME during that time.
To assess trends in postpartum opioid prescribing, opioid use, and pain control satisfaction, Dr. Badreldin and colleagues evaluated data from a prospective observational study. Their analysis included data from women who used an opioid during postpartum hospitalization between May 2017 and July 2019. The researchers excluded women with NSAID or morphine allergies or recent opioid use, as well as those who received general anesthesia without concurrent neuraxial anesthesia, those who underwent peripartum hysterectomy, and women admitted to the ICU.
The investigators used nonparametric tests of trend to assess the difference over time in the proportion of patients who received an opioid prescription at discharge and in the total MME prescribed post partum.
Of 900 women with inpatient opioid use, 471 agreed to be followed after discharge. In that group, the amount of opioid use per inpatient day significantly declined. In addition, the percentage who received an opioid prescription at discharge significantly declined, as did the total MME prescribed at discharge.
“Both inpatient and outpatient satisfaction with pain control were unchanged,” the researchers reported. “In this population, both the frequency and amount of opioid use in the postpartum period declined from 2017 to 2019, without any change in satisfaction with pain control.”
The study was supported by the Society for Maternal-Fetal Medicine/AMAG 2017 Health Policy Award, and a coauthor received support from the National Institute of Child Health and Human Development.
Source: Badreldin N et al. Am J Obstet Gynecol. 2020 Jan;222(1):S93, Abstract 120.
GRAPEVINE, TEX. – The amount of opioids prescribed post partum may decline over time without affecting levels of pain control satisfaction, according to research presented at the meeting sponsored by the Society for Maternal-Fetal Medicine.
Data from a large center indicate that trends in opioid use significantly declined from 2017 to 2019, but not at the expense of adequate pain control, said Nevert Badreldin, MD, assistant professor of obstetrics and gynecology at Northwestern University in Chicago. Patients consistently reported that they were satisfied with inpatient pain control, while opioid use per inpatient day decreased from about 30 morphine milligram equivalents (MME) to less than 20 MME during that time.
To assess trends in postpartum opioid prescribing, opioid use, and pain control satisfaction, Dr. Badreldin and colleagues evaluated data from a prospective observational study. Their analysis included data from women who used an opioid during postpartum hospitalization between May 2017 and July 2019. The researchers excluded women with NSAID or morphine allergies or recent opioid use, as well as those who received general anesthesia without concurrent neuraxial anesthesia, those who underwent peripartum hysterectomy, and women admitted to the ICU.
The investigators used nonparametric tests of trend to assess the difference over time in the proportion of patients who received an opioid prescription at discharge and in the total MME prescribed post partum.
Of 900 women with inpatient opioid use, 471 agreed to be followed after discharge. In that group, the amount of opioid use per inpatient day significantly declined. In addition, the percentage who received an opioid prescription at discharge significantly declined, as did the total MME prescribed at discharge.
“Both inpatient and outpatient satisfaction with pain control were unchanged,” the researchers reported. “In this population, both the frequency and amount of opioid use in the postpartum period declined from 2017 to 2019, without any change in satisfaction with pain control.”
The study was supported by the Society for Maternal-Fetal Medicine/AMAG 2017 Health Policy Award, and a coauthor received support from the National Institute of Child Health and Human Development.
Source: Badreldin N et al. Am J Obstet Gynecol. 2020 Jan;222(1):S93, Abstract 120.
REPORTING FROM THE PREGNANCY MEETING
Myth busting: Sudden cardiac death in athletes
SNOWMASS, COLO. – Myths and misconceptions abound regarding the merits of universal incorporation of the resting 12-lead ECG into preparticipation cardiovascular screening of young athletes, Aaron L. Baggish, MD, declared at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.

Dr. Baggish, director of the Cardiovascular Performance Program at Massachusetts General Hospital and a cardiologist at Harvard Medical School, Boston, set out to pop the balloons of a handful of these widely floating myths. These are commonly held fictions: In an electronic poll at the outset of his talk, only one in five members of his large audience recognized all of the following boldface statements as false.
“Preparticipation cardiovascular screening (PPCVS) has been shown to reduce the incidence of sudden cardiac death (SCD) among young competitive athletes.”
FALSE. Not for PPCVS by history and physical examination alone, or with the addition of a screening 12-lead ECG. In Italy, where a cluster of high-profile sudden cardiac deaths led to passage of a 1982 national law mandating 12-lead ECG screening as part of the PPCVS, investigators presented studies purporting to demonstrate a subsequent reduction in the risk of SCD. But those studies were subsequently shown to be fraught with problems. And a high-quality study capable of convincingly demonstrating such a benefit would need to be prohibitively large and expensive. “Don’t hold your breath waiting for that to happen anytime soon,” advised Dr. Baggish, who is medical director for the Boston Marathon, as well as team cardiologist for Harvard University Athletics, the New England Patriots, the Boston Bruins, USRowing, and U.S. Soccer.
“Hypertrophic cardiomyopathy is the leading cause of sudden death among young competitive athletes.”
FALSE. A study of the National Collegiate Athletic Association (NCAA) comprehensive database, with 4.2 million athlete-years of follow-up, showed that the most common cause of SCD was autopsy-negative sudden unexplained death (SUD), accounting for 25% of cases. Hypertrophic cardiomyopathy was deemed the cause of 8% of the SCDs (Circulation. 2015 Jul 7;132[1]:10-9).
“The same thing has been shown in studies done in the United Kingdom and in Australia: . Over the next 10 years, I suspect that one of the most important areas that we’ll be looking into will be this SUD area, perhaps using molecular autopsy to make some headway there,” according to the cardiologist.
SCD is rare. In the NCAA study, the incidence was 1 in 53,703 athlete-years. In sobering contrast, accidents, suicide, and homicide accounted for 50% of all deaths in the collegiate athletes.
“When you think about what’s important in terms of educating young people to be safe, the history and physical exam and 12-lead ECG are nowhere near as important as talking with them about minimizing accident risk and staying away from guns,” Dr. Baggish commented.
“Contemporary ECG interpretation criteria designed specifically for use in young athletes have eliminated the problem of false-positive testing.”
FALSE. The story of adding ECG screening to the PPCVS is one of dramatically improved sensitivity over history and physical exam alone, but always at the cost of reduced specificity. In the Harvard Athlete Initiative Study, Dr. Baggish and coworkers reported that adding the 12-lead ECG resulted in a 17% false-positive rate (Ann Intern Med. 2010 Mar 2;152[5]:269-75). Similar findings were reported in independent studies at two other large universities.
“An ECG false-positive rate of 16%-20%? That’s big trouble. Remember, the conditions we’re looking for are uncommon, with a prevalence of maybe 1 in 500 at most. So if you’re flagging one-fifth or one-sixth of your athletes, the ECG is really not an appropriate tool for screening,” he commented.
Recognition of this limitation has led to development of refined, improved ECG criteria: most notably, the 2012 Seattle criteria, with an associated false-positive rate of 4%-8%, followed by the 2017 International Consensus Criteria (J Am Coll Cardiol. 2017 Feb 28;69[8]:1057-75), with a false-positive rate of 1%-2%. That’s a great improvement. Still, when Dr. Baggish, a marathoner himself, thinks about the roughly 32,000 Boston Marathon runners at the starting line each year, that false-positive rate would translate into 320-640 of those individuals being needlessly subjected to the not-insignificant time and expense of further testing, along with considerable anxiety for the runners and their families, and perhaps even inappropriate disqualification.
“Current ACC/AHA guidelines recommend against the use of the 12-lead ECG during the PPCVS.”
FALSE. Dr. Baggish was a coauthor of the current guidelines, which he described as “an open-door invitation to local decisions, with some important caveats” (Circulation. 2015 Dec 1;132[22]:e267-72).
The guidelines state that the minimum requirement and legal standard for PPCVS of young competitive athletes is a focused history and physical examination, such as the American College of Cardiology/American Heart Association 14-point screen, which consists of 10 elements addressing personal and family history and 4 focused on the physical examination, or the American Academy of Pediatrics Preparticipation Physical Evaluation. Further, while mandatory universal inclusion of the 12-lead ECG is not recommended – it’s rated Class III, meaning don’t do it – the guidelines state that screening programs are at liberty to choose the 12-lead ECG as an additional tool, “provided that close physician involvement and sufficient quality control can be achieved. If undertaken, such initiatives should recognize the known and anticipated limitations of the 12-lead ECG as a population screening test, including the expected frequency of false-positive and false-negative test results, as well as the cost required to support these initiatives over time.”
Dr. Baggish considers the ACC/AHA guidelines to be one of the two most important developments in the field of SCD during sports in recent years. The other is the NCAA-sponsored multidisciplinary Interassociation Consensus Statement on Cardiovascular Care of College Student-Athletes, which he also coauthored (J Am Coll Cardiol. 2016 Jun 28;67[25]:2981-95).
The report lays out the case for a much broader than traditional view of the PPCVS, with “goals that extend beyond detection of occult high-risk pathology.”
“The NCAA has done something very interesting,” Dr. Baggish explained. “It has said that, if we’re going to be screening, we should be thinking about screening with a much broader rationale. It’s not just about finding the needle-in-a-haystack hypertrophic cardiomyopathy or anomalous coronary arteries, it’s about engaging student-athletes at an early point in their collegiate career and trying to improve their health overall – and not just while they’re in college, but over their lifespan.”
He reported having no financial conflicts regarding his presentation.
SNOWMASS, COLO. – Myths and misconceptions abound regarding the merits of universal incorporation of the resting 12-lead ECG into preparticipation cardiovascular screening of young athletes, Aaron L. Baggish, MD, declared at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
Dr. Baggish, director of the Cardiovascular Performance Program at Massachusetts General Hospital and a cardiologist at Harvard Medical School, Boston, set out to pop the balloons of a handful of these widely floating myths. These are commonly held fictions: In an electronic poll at the outset of his talk, only one in five members of his large audience recognized all of the following boldface statements as false.
“Preparticipation cardiovascular screening (PPCVS) has been shown to reduce the incidence of sudden cardiac death (SCD) among young competitive athletes.”
FALSE. Not for PPCVS by history and physical examination alone, or with the addition of a screening 12-lead ECG. In Italy, where a cluster of high-profile sudden cardiac deaths led to passage of a 1982 national law mandating 12-lead ECG screening as part of the PPCVS, investigators presented studies purporting to demonstrate a subsequent reduction in the risk of SCD. But those studies were subsequently shown to be fraught with problems. And a high-quality study capable of convincingly demonstrating such a benefit would need to be prohibitively large and expensive. “Don’t hold your breath waiting for that to happen anytime soon,” advised Dr. Baggish, who is medical director for the Boston Marathon, as well as team cardiologist for Harvard University Athletics, the New England Patriots, the Boston Bruins, USRowing, and U.S. Soccer.
“Hypertrophic cardiomyopathy is the leading cause of sudden death among young competitive athletes.”
FALSE. A study of the National Collegiate Athletic Association (NCAA) comprehensive database, with 4.2 million athlete-years of follow-up, showed that the most common cause of SCD was autopsy-negative sudden unexplained death (SUD), accounting for 25% of cases. Hypertrophic cardiomyopathy was deemed the cause of 8% of the SCDs (Circulation. 2015 Jul 7;132[1]:10-9).
“The same thing has been shown in studies done in the United Kingdom and in Australia: . Over the next 10 years, I suspect that one of the most important areas that we’ll be looking into will be this SUD area, perhaps using molecular autopsy to make some headway there,” according to the cardiologist.
SCD is rare. In the NCAA study, the incidence was 1 in 53,703 athlete-years. In sobering contrast, accidents, suicide, and homicide accounted for 50% of all deaths in the collegiate athletes.
“When you think about what’s important in terms of educating young people to be safe, the history and physical exam and 12-lead ECG are nowhere near as important as talking with them about minimizing accident risk and staying away from guns,” Dr. Baggish commented.
“Contemporary ECG interpretation criteria designed specifically for use in young athletes have eliminated the problem of false-positive testing.”
FALSE. The story of adding ECG screening to the PPCVS is one of dramatically improved sensitivity over history and physical exam alone, but always at the cost of reduced specificity. In the Harvard Athlete Initiative Study, Dr. Baggish and coworkers reported that adding the 12-lead ECG resulted in a 17% false-positive rate (Ann Intern Med. 2010 Mar 2;152[5]:269-75). Similar findings were reported in independent studies at two other large universities.
“An ECG false-positive rate of 16%-20%? That’s big trouble. Remember, the conditions we’re looking for are uncommon, with a prevalence of maybe 1 in 500 at most. So if you’re flagging one-fifth or one-sixth of your athletes, the ECG is really not an appropriate tool for screening,” he commented.
Recognition of this limitation has led to development of refined, improved ECG criteria: most notably, the 2012 Seattle criteria, with an associated false-positive rate of 4%-8%, followed by the 2017 International Consensus Criteria (J Am Coll Cardiol. 2017 Feb 28;69[8]:1057-75), with a false-positive rate of 1%-2%. That’s a great improvement. Still, when Dr. Baggish, a marathoner himself, thinks about the roughly 32,000 Boston Marathon runners at the starting line each year, that false-positive rate would translate into 320-640 of those individuals being needlessly subjected to the not-insignificant time and expense of further testing, along with considerable anxiety for the runners and their families, and perhaps even inappropriate disqualification.
“Current ACC/AHA guidelines recommend against the use of the 12-lead ECG during the PPCVS.”
FALSE. Dr. Baggish was a coauthor of the current guidelines, which he described as “an open-door invitation to local decisions, with some important caveats” (Circulation. 2015 Dec 1;132[22]:e267-72).
The guidelines state that the minimum requirement and legal standard for PPCVS of young competitive athletes is a focused history and physical examination, such as the American College of Cardiology/American Heart Association 14-point screen, which consists of 10 elements addressing personal and family history and 4 focused on the physical examination, or the American Academy of Pediatrics Preparticipation Physical Evaluation. Further, while mandatory universal inclusion of the 12-lead ECG is not recommended – it’s rated Class III, meaning don’t do it – the guidelines state that screening programs are at liberty to choose the 12-lead ECG as an additional tool, “provided that close physician involvement and sufficient quality control can be achieved. If undertaken, such initiatives should recognize the known and anticipated limitations of the 12-lead ECG as a population screening test, including the expected frequency of false-positive and false-negative test results, as well as the cost required to support these initiatives over time.”
Dr. Baggish considers the ACC/AHA guidelines to be one of the two most important developments in the field of SCD during sports in recent years. The other is the NCAA-sponsored multidisciplinary Interassociation Consensus Statement on Cardiovascular Care of College Student-Athletes, which he also coauthored (J Am Coll Cardiol. 2016 Jun 28;67[25]:2981-95).
The report lays out the case for a much broader than traditional view of the PPCVS, with “goals that extend beyond detection of occult high-risk pathology.”
“The NCAA has done something very interesting,” Dr. Baggish explained. “It has said that, if we’re going to be screening, we should be thinking about screening with a much broader rationale. It’s not just about finding the needle-in-a-haystack hypertrophic cardiomyopathy or anomalous coronary arteries, it’s about engaging student-athletes at an early point in their collegiate career and trying to improve their health overall – and not just while they’re in college, but over their lifespan.”
He reported having no financial conflicts regarding his presentation.
SNOWMASS, COLO. – Myths and misconceptions abound regarding the merits of universal incorporation of the resting 12-lead ECG into preparticipation cardiovascular screening of young athletes, Aaron L. Baggish, MD, declared at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
Dr. Baggish, director of the Cardiovascular Performance Program at Massachusetts General Hospital and a cardiologist at Harvard Medical School, Boston, set out to pop the balloons of a handful of these widely floating myths. These are commonly held fictions: In an electronic poll at the outset of his talk, only one in five members of his large audience recognized all of the following boldface statements as false.
“Preparticipation cardiovascular screening (PPCVS) has been shown to reduce the incidence of sudden cardiac death (SCD) among young competitive athletes.”
FALSE. Not for PPCVS by history and physical examination alone, or with the addition of a screening 12-lead ECG. In Italy, where a cluster of high-profile sudden cardiac deaths led to passage of a 1982 national law mandating 12-lead ECG screening as part of the PPCVS, investigators presented studies purporting to demonstrate a subsequent reduction in the risk of SCD. But those studies were subsequently shown to be fraught with problems. And a high-quality study capable of convincingly demonstrating such a benefit would need to be prohibitively large and expensive. “Don’t hold your breath waiting for that to happen anytime soon,” advised Dr. Baggish, who is medical director for the Boston Marathon, as well as team cardiologist for Harvard University Athletics, the New England Patriots, the Boston Bruins, USRowing, and U.S. Soccer.
“Hypertrophic cardiomyopathy is the leading cause of sudden death among young competitive athletes.”
FALSE. A study of the National Collegiate Athletic Association (NCAA) comprehensive database, with 4.2 million athlete-years of follow-up, showed that the most common cause of SCD was autopsy-negative sudden unexplained death (SUD), accounting for 25% of cases. Hypertrophic cardiomyopathy was deemed the cause of 8% of the SCDs (Circulation. 2015 Jul 7;132[1]:10-9).
“The same thing has been shown in studies done in the United Kingdom and in Australia: . Over the next 10 years, I suspect that one of the most important areas that we’ll be looking into will be this SUD area, perhaps using molecular autopsy to make some headway there,” according to the cardiologist.
SCD is rare. In the NCAA study, the incidence was 1 in 53,703 athlete-years. In sobering contrast, accidents, suicide, and homicide accounted for 50% of all deaths in the collegiate athletes.
“When you think about what’s important in terms of educating young people to be safe, the history and physical exam and 12-lead ECG are nowhere near as important as talking with them about minimizing accident risk and staying away from guns,” Dr. Baggish commented.
“Contemporary ECG interpretation criteria designed specifically for use in young athletes have eliminated the problem of false-positive testing.”
FALSE. The story of adding ECG screening to the PPCVS is one of dramatically improved sensitivity over history and physical exam alone, but always at the cost of reduced specificity. In the Harvard Athlete Initiative Study, Dr. Baggish and coworkers reported that adding the 12-lead ECG resulted in a 17% false-positive rate (Ann Intern Med. 2010 Mar 2;152[5]:269-75). Similar findings were reported in independent studies at two other large universities.
“An ECG false-positive rate of 16%-20%? That’s big trouble. Remember, the conditions we’re looking for are uncommon, with a prevalence of maybe 1 in 500 at most. So if you’re flagging one-fifth or one-sixth of your athletes, the ECG is really not an appropriate tool for screening,” he commented.
Recognition of this limitation has led to development of refined, improved ECG criteria: most notably, the 2012 Seattle criteria, with an associated false-positive rate of 4%-8%, followed by the 2017 International Consensus Criteria (J Am Coll Cardiol. 2017 Feb 28;69[8]:1057-75), with a false-positive rate of 1%-2%. That’s a great improvement. Still, when Dr. Baggish, a marathoner himself, thinks about the roughly 32,000 Boston Marathon runners at the starting line each year, that false-positive rate would translate into 320-640 of those individuals being needlessly subjected to the not-insignificant time and expense of further testing, along with considerable anxiety for the runners and their families, and perhaps even inappropriate disqualification.
“Current ACC/AHA guidelines recommend against the use of the 12-lead ECG during the PPCVS.”
FALSE. Dr. Baggish was a coauthor of the current guidelines, which he described as “an open-door invitation to local decisions, with some important caveats” (Circulation. 2015 Dec 1;132[22]:e267-72).
The guidelines state that the minimum requirement and legal standard for PPCVS of young competitive athletes is a focused history and physical examination, such as the American College of Cardiology/American Heart Association 14-point screen, which consists of 10 elements addressing personal and family history and 4 focused on the physical examination, or the American Academy of Pediatrics Preparticipation Physical Evaluation. Further, while mandatory universal inclusion of the 12-lead ECG is not recommended – it’s rated Class III, meaning don’t do it – the guidelines state that screening programs are at liberty to choose the 12-lead ECG as an additional tool, “provided that close physician involvement and sufficient quality control can be achieved. If undertaken, such initiatives should recognize the known and anticipated limitations of the 12-lead ECG as a population screening test, including the expected frequency of false-positive and false-negative test results, as well as the cost required to support these initiatives over time.”
Dr. Baggish considers the ACC/AHA guidelines to be one of the two most important developments in the field of SCD during sports in recent years. The other is the NCAA-sponsored multidisciplinary Interassociation Consensus Statement on Cardiovascular Care of College Student-Athletes, which he also coauthored (J Am Coll Cardiol. 2016 Jun 28;67[25]:2981-95).
The report lays out the case for a much broader than traditional view of the PPCVS, with “goals that extend beyond detection of occult high-risk pathology.”
“The NCAA has done something very interesting,” Dr. Baggish explained. “It has said that, if we’re going to be screening, we should be thinking about screening with a much broader rationale. It’s not just about finding the needle-in-a-haystack hypertrophic cardiomyopathy or anomalous coronary arteries, it’s about engaging student-athletes at an early point in their collegiate career and trying to improve their health overall – and not just while they’re in college, but over their lifespan.”
He reported having no financial conflicts regarding his presentation.
REPORTING FROM ACC SNOWMASS 2020
CMS proposes second specialty tier for Medicare drugs
The Centers for Medicare & Medicaid Services’ latest maneuver to combat rising drug prices is the proposed addition of a second specialty drug tier for the Medicare Part D prescription drug benefit.
The proposal is part of a broader proposed update to Medicare Parts C and D for contract years 2021 and 2022.

In a fact sheet highlighting various elements of the overall proposal, CMS noted that Part D plan sponsors and pharmacy benefit managers have been requesting the option to add a second “preferred” specialty tier that would “encourage the use of more preferred, less expensive agents, reduce enrollee cost sharing, and reduce costs to CMS.”
Currently, all pharmaceuticals with a cost greater than $670 are placed in a single specialty tier.
During a Feb. 5 press briefing, CMS Administrator Seema Verma described this change as “giving plans more negotiating power so they can lower prices for beneficiaries even further.”
Ms. Verma used a hypothetical example of two rheumatoid arthritis drugs to illustrate how the change will work. Currently, if both are over the $670 threshold, they would both be on the specialty tier with the same cost sharing. “Creating a second preferred specialty tier would allow for a different copay and fosters a more competitive environment that places Part D plans in a better position to negotiate the price of similar drugs and pass those savings onto the patient through lower cost sharing,” she said.
CMS is proposing to allow plans to implement a preferred specialty tier for the 2021 plan year.
The agency is also seeking to drive more generic drug use as a means of lowering costs.
Ms. Verma noted that, typically, even after a generic drug is launched, health plan sponsors prefer to drive patients to the brand name product, if they can secure a greater rebate from the manufacturer.
In a separate Feb. 5 blog post, Ms. Verma noted that when a brand was included on a formulary, the generic was also on the formulary 91.8% of the time. For the times in which the generic was not, it was typically because the wholesale cost of the generic was only 5%-15% lower than the brand wholesale cost.
In an effort to encourage use of generics, CMS is seeking comment on the development of measures of generic and biosimilar use in Medicare Part D that could be incorporated in health plan star ratings.
Some of the measures proposed in the blog post include the generic substitution rate, the generic therapeutic alternative opportunity rate (which measures the number of brand fills divided by the sum of the brand and generic fills when both are available), and the biosimilar utilization rate.
gtwachtman@mdedge.com
The Centers for Medicare & Medicaid Services’ latest maneuver to combat rising drug prices is the proposed addition of a second specialty drug tier for the Medicare Part D prescription drug benefit.
The proposal is part of a broader proposed update to Medicare Parts C and D for contract years 2021 and 2022.
In a fact sheet highlighting various elements of the overall proposal, CMS noted that Part D plan sponsors and pharmacy benefit managers have been requesting the option to add a second “preferred” specialty tier that would “encourage the use of more preferred, less expensive agents, reduce enrollee cost sharing, and reduce costs to CMS.”
Currently, all pharmaceuticals with a cost greater than $670 are placed in a single specialty tier.
During a Feb. 5 press briefing, CMS Administrator Seema Verma described this change as “giving plans more negotiating power so they can lower prices for beneficiaries even further.”
Ms. Verma used a hypothetical example of two rheumatoid arthritis drugs to illustrate how the change will work. Currently, if both are over the $670 threshold, they would both be on the specialty tier with the same cost sharing. “Creating a second preferred specialty tier would allow for a different copay and fosters a more competitive environment that places Part D plans in a better position to negotiate the price of similar drugs and pass those savings onto the patient through lower cost sharing,” she said.
CMS is proposing to allow plans to implement a preferred specialty tier for the 2021 plan year.
The agency is also seeking to drive more generic drug use as a means of lowering costs.
Ms. Verma noted that, typically, even after a generic drug is launched, health plan sponsors prefer to drive patients to the brand name product, if they can secure a greater rebate from the manufacturer.
In a separate Feb. 5 blog post, Ms. Verma noted that when a brand was included on a formulary, the generic was also on the formulary 91.8% of the time. For the times in which the generic was not, it was typically because the wholesale cost of the generic was only 5%-15% lower than the brand wholesale cost.
In an effort to encourage use of generics, CMS is seeking comment on the development of measures of generic and biosimilar use in Medicare Part D that could be incorporated in health plan star ratings.
Some of the measures proposed in the blog post include the generic substitution rate, the generic therapeutic alternative opportunity rate (which measures the number of brand fills divided by the sum of the brand and generic fills when both are available), and the biosimilar utilization rate.
gtwachtman@mdedge.com
The Centers for Medicare & Medicaid Services’ latest maneuver to combat rising drug prices is the proposed addition of a second specialty drug tier for the Medicare Part D prescription drug benefit.
The proposal is part of a broader proposed update to Medicare Parts C and D for contract years 2021 and 2022.
In a fact sheet highlighting various elements of the overall proposal, CMS noted that Part D plan sponsors and pharmacy benefit managers have been requesting the option to add a second “preferred” specialty tier that would “encourage the use of more preferred, less expensive agents, reduce enrollee cost sharing, and reduce costs to CMS.”
Currently, all pharmaceuticals with a cost greater than $670 are placed in a single specialty tier.
During a Feb. 5 press briefing, CMS Administrator Seema Verma described this change as “giving plans more negotiating power so they can lower prices for beneficiaries even further.”
Ms. Verma used a hypothetical example of two rheumatoid arthritis drugs to illustrate how the change will work. Currently, if both are over the $670 threshold, they would both be on the specialty tier with the same cost sharing. “Creating a second preferred specialty tier would allow for a different copay and fosters a more competitive environment that places Part D plans in a better position to negotiate the price of similar drugs and pass those savings onto the patient through lower cost sharing,” she said.
CMS is proposing to allow plans to implement a preferred specialty tier for the 2021 plan year.
The agency is also seeking to drive more generic drug use as a means of lowering costs.
Ms. Verma noted that, typically, even after a generic drug is launched, health plan sponsors prefer to drive patients to the brand name product, if they can secure a greater rebate from the manufacturer.
In a separate Feb. 5 blog post, Ms. Verma noted that when a brand was included on a formulary, the generic was also on the formulary 91.8% of the time. For the times in which the generic was not, it was typically because the wholesale cost of the generic was only 5%-15% lower than the brand wholesale cost.
In an effort to encourage use of generics, CMS is seeking comment on the development of measures of generic and biosimilar use in Medicare Part D that could be incorporated in health plan star ratings.
Some of the measures proposed in the blog post include the generic substitution rate, the generic therapeutic alternative opportunity rate (which measures the number of brand fills divided by the sum of the brand and generic fills when both are available), and the biosimilar utilization rate.
gtwachtman@mdedge.com
Remdesivir under study as treatment for novel coronavirus
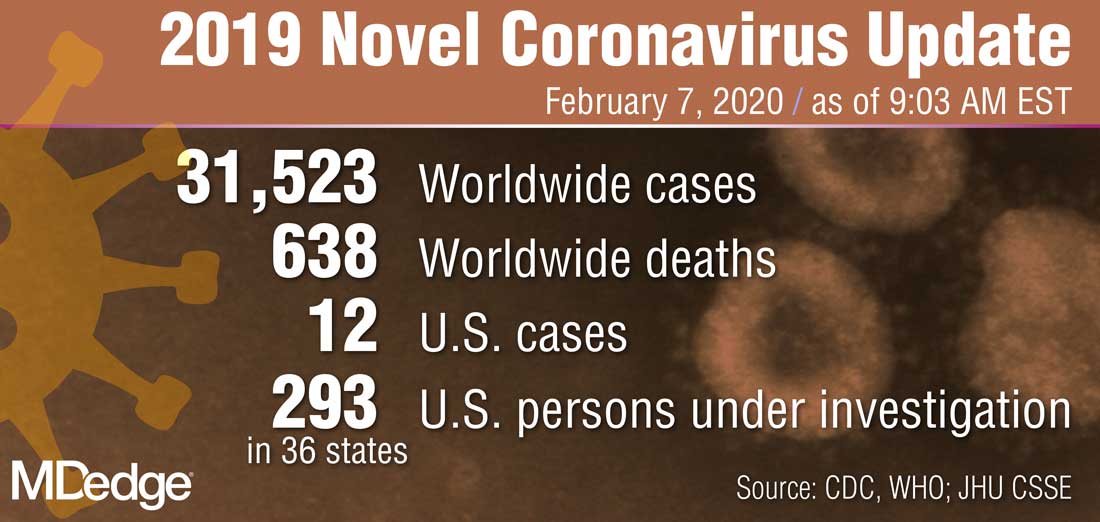
“What they’re looking at is the effect of this drug -- either the drug plus standard of care versus standard of care alone,” Anthony S. Fauci, MD, reported Feb. 7 during a press briefing held by members of President Trump’s Coronavirus Task Force. “I think pretty soon we are going to get a definitive answer, whether one of these among several drugs works.”
Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases, added that several organizations and individual investigators are developing vaccines for 2019-nCoV. In one such effort, the National Institutes of Health is working with Moderna Inc. to develop a vaccine built on a messenger RNA platform. “One of the first steps is to successfully get that [novel coronavirus] gene and insert it into the messenger RNA platform successfully and allow it to express proteins,” Dr. Fauci explained. “We’ve succeeded in that. The next [step] is to put it in a mouse animal model to induce immunogenicity, and to get the company to make [gold nanoparticle] products. All of those have been successfully implemented. There have been no glitches so far. If that continues, we will be in Phase 1 trials in people within the next two-and-a-half months.”
In another development on the same day, Robert R. Redfield, MD, director of the Centers for Disease Control and Prevention, announced that Heath & Human Services issued an interim final rule to amend foreign quarantine regulations in the wake of the public health threat posed by the 2019-nCoV. “This will enable CDC to collect certain contact information data regarding airline passengers and crew when they arrive from other countries. . .and may be exposed to communicable disease,” Dr. Redfield said. “This action is part of our multi-layered approach to the U.S. response and demonstrates our commitment to take all necessary actions to protect the American people.”
According to Alex Azar, secretary of Health and Human Services, and chair of President Trump’s Coronavirus Task Force, there are 12 confirmed cases of the novel coronavirus in the United States, including two cases of transmission to people who had not recently been in China. “Although the virus represents a potentially very serious public health threat, and we expect to continue seeing more cases here, the immediate risk to the American public is low at this time,” Mr. Azar said. “We are working as quickly as possible on the many unanswered questions about this virus. That includes exactly how it spreads, how deadly it is, whether it’s commonly transmitted by patients who are not yet displaying symptoms, and other issues.”
“What they’re looking at is the effect of this drug -- either the drug plus standard of care versus standard of care alone,” Anthony S. Fauci, MD, reported Feb. 7 during a press briefing held by members of President Trump’s Coronavirus Task Force. “I think pretty soon we are going to get a definitive answer, whether one of these among several drugs works.”
Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases, added that several organizations and individual investigators are developing vaccines for 2019-nCoV. In one such effort, the National Institutes of Health is working with Moderna Inc. to develop a vaccine built on a messenger RNA platform. “One of the first steps is to successfully get that [novel coronavirus] gene and insert it into the messenger RNA platform successfully and allow it to express proteins,” Dr. Fauci explained. “We’ve succeeded in that. The next [step] is to put it in a mouse animal model to induce immunogenicity, and to get the company to make [gold nanoparticle] products. All of those have been successfully implemented. There have been no glitches so far. If that continues, we will be in Phase 1 trials in people within the next two-and-a-half months.”
In another development on the same day, Robert R. Redfield, MD, director of the Centers for Disease Control and Prevention, announced that Heath & Human Services issued an interim final rule to amend foreign quarantine regulations in the wake of the public health threat posed by the 2019-nCoV. “This will enable CDC to collect certain contact information data regarding airline passengers and crew when they arrive from other countries. . .and may be exposed to communicable disease,” Dr. Redfield said. “This action is part of our multi-layered approach to the U.S. response and demonstrates our commitment to take all necessary actions to protect the American people.”
According to Alex Azar, secretary of Health and Human Services, and chair of President Trump’s Coronavirus Task Force, there are 12 confirmed cases of the novel coronavirus in the United States, including two cases of transmission to people who had not recently been in China. “Although the virus represents a potentially very serious public health threat, and we expect to continue seeing more cases here, the immediate risk to the American public is low at this time,” Mr. Azar said. “We are working as quickly as possible on the many unanswered questions about this virus. That includes exactly how it spreads, how deadly it is, whether it’s commonly transmitted by patients who are not yet displaying symptoms, and other issues.”
“What they’re looking at is the effect of this drug -- either the drug plus standard of care versus standard of care alone,” Anthony S. Fauci, MD, reported Feb. 7 during a press briefing held by members of President Trump’s Coronavirus Task Force. “I think pretty soon we are going to get a definitive answer, whether one of these among several drugs works.”
Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases, added that several organizations and individual investigators are developing vaccines for 2019-nCoV. In one such effort, the National Institutes of Health is working with Moderna Inc. to develop a vaccine built on a messenger RNA platform. “One of the first steps is to successfully get that [novel coronavirus] gene and insert it into the messenger RNA platform successfully and allow it to express proteins,” Dr. Fauci explained. “We’ve succeeded in that. The next [step] is to put it in a mouse animal model to induce immunogenicity, and to get the company to make [gold nanoparticle] products. All of those have been successfully implemented. There have been no glitches so far. If that continues, we will be in Phase 1 trials in people within the next two-and-a-half months.”
In another development on the same day, Robert R. Redfield, MD, director of the Centers for Disease Control and Prevention, announced that Heath & Human Services issued an interim final rule to amend foreign quarantine regulations in the wake of the public health threat posed by the 2019-nCoV. “This will enable CDC to collect certain contact information data regarding airline passengers and crew when they arrive from other countries. . .and may be exposed to communicable disease,” Dr. Redfield said. “This action is part of our multi-layered approach to the U.S. response and demonstrates our commitment to take all necessary actions to protect the American people.”
According to Alex Azar, secretary of Health and Human Services, and chair of President Trump’s Coronavirus Task Force, there are 12 confirmed cases of the novel coronavirus in the United States, including two cases of transmission to people who had not recently been in China. “Although the virus represents a potentially very serious public health threat, and we expect to continue seeing more cases here, the immediate risk to the American public is low at this time,” Mr. Azar said. “We are working as quickly as possible on the many unanswered questions about this virus. That includes exactly how it spreads, how deadly it is, whether it’s commonly transmitted by patients who are not yet displaying symptoms, and other issues.”
Progestin-only systemic hormone therapy for menopausal hot flashes
The field of menopause medicine is dominated by studies documenting the effectiveness of systemic estrogen or estrogen-progestin hormone therapy for the treatment of hot flashes caused by hypoestrogenism. The effectiveness of progestin-only systemic hormone therapy for the treatment of hot flashes is much less studied and seldom is utilized in clinical practice. A small number of studies have reported that progestins, including micronized progesterone, medroxyprogesterone acetate, and norethindrone acetate, are effective treatment for hot flashes. Progestin-only systemic hormone therapy might be especially helpful for postmenopausal women with moderate to severe hot flashes who have a contraindication to estrogen treatment.
Micronized progesterone
Micronized progesterone (Prometrium) 300 mg daily taken at bedtime has been reported to effectively treat hot flashes in postmenopausal women. In one study, 133 postmenopausal women with an average age of 55 years and approximately 3 years from their last menstrual period were randomly assigned to 12 weeks of treatment with placebo or micronized progesterone 300 mg daily taken at bedtime.1 Mean serum progesterone levels were 0.28 ng/mL (0.89 nM) and 27 ng/mL (86 nM) in the women taking placebo and micronized progesterone, respectively. Compared with placebo, micronized progesterone reduced daytime and nighttime hot flash frequency and severity. In addition, compared with placebo, micronized progesterone improved the quality of sleep.1
Most reviews conclude that micronized progesterone has minimal cardiovascular risk.2 Micronized progesterone therapy might be especially helpful for postmenopausal women with moderate to severe hot flashes who have a contraindication to estrogen treatment such as those at increased risk for cardiovascular disease or women with a thrombophilia. Many experts believe that systemic estrogen therapy is contraindicated in postmenopausal women with an American Heart Association risk score greater than 10% over 10 years.3 Additional contraindications to systemic estrogen include women with cardiac disease who have a thrombophilia, such as the Factor V Leiden mutation.4
For women who are at high risk for estrogen-induced cardiovascular events, micronized progesterone may be a better option than systemic estrogen for treating hot flashes. Alternatively, in these women at risk of cardiovascular disease a selective serotonin reuptake inhibitor, such as escitalopram, 10 mg to 20 mg daily, may be a good option for treating postmenopausal hot flashes.5
Medroxyprogesterone acetate
Medroxyprogesterone acetate, at a dosage of 20 mg daily, is an effective treatment for hot flashes. In a randomized clinical trial 27 postmenopausal women with hot flashes were randomly assigned to treatment with placebo or medroxyprogesterone acetate 20 mg daily for 4 weeks. Vasomotor flushes were decreased by 26% and 74% in the placebo and medroxyprogesterone groups, respectively.6
Depot medroxyprogesterone acetate injections at dosages from 150 mg to 400 mg also have been reported to effectively treat hot flashes.7,8 In a trial comparing the effectiveness of estrogen monotherapy (conjugated equine estrogen 0.6 mg daily) with progestin monotherapy (medroxyprogesterone acetate 10 mg daily), both treatments were equally effective in reducing hot flashes.9
Continue to: Micronized progesterone vs medroxyprogesterone acetate...
Micronized progesterone vs medroxyprogesterone acetate
Experts in menopause medicine have suggested that in postmenopausal women micronized progesterone has a better pattern of benefits and fewer risks than medroxyprogesterone acetate.10,11 For example, in the E3N observational study of hormones and breast cancer risk, among 80,377 French postmenopausal women followed for a mean of 8 years, the combination of transdermal estradiol plus oral micronized progesterone was associated with no significantly increased risk of breast cancer (relative risk [RR], 1.08, 95% confidence interval [CI], 0.89–1.31) compared with never users of postmenopausal hormone therapy.12 By contrast, the combination of oral estrogen plus medroxyprogesterone acetate was associated with an increased risk of breast cancer (RR, 1.48; 95% CI, 1.02–2.16) compared with never users of postmenopausal hormone therapy. The E3N study indicates that micronized progesterone may have a more favorable breast health profile than medroxyprogesterone acetate.12

Norethindrone acetate
Norethindrone acetate monotherapy is not commonly prescribed for the treatment of menopausal hot flashes. However, a large clinical trial has demonstrated that norethindrone acetate effectively suppresses hot flashes in women with endometriosis treated with depot leuprolide acetate (LA). In one trial 201 women with endometriosis were randomly assigned to 12 months of treatment with13:
- LA plus placebo pills
- LA plus norethindrone acetate (NEA) 5 mg daily
- LA plus NEA 5 mg daily plus conjugated equine estrogen (CEE) 0.625 mg daily, or
- LA plus NEA 5 mg daily plus CEE 1.25 mg daily.
The median number of hot flashes in 24 hours was 6 in the LA plus placebo group and 0 in both the LA plus NEA 5 mg daily group and the LA plus NEA 5 mg plus CEE 1.25 mg daily group. This study demonstrates that NEA 5 mg daily is an effective treatment for hot flashes.
In the same study, LA plus placebo was associated with a significant decrease in lumbar spine bone mineral density. No significant decrease in bone mineral density was observed in the women who received LA plus NEA 5 mg daily. This finding indicates that NEA 5 mg reduces bone absorption caused by hypoestrogenism. In humans, norethindrone is a substrate for the aromatase enzyme system.14 Small quantities of ethinyl estradiol may be formed by aromatization of norethindrone in vivo,15,16 contributing to the effectiveness of NEA in suppressing hot flashes and preserving bone density.
Progestin: The estrogen alternative to hot flashes
For postmenopausal women with moderate to severe hot flashes, estrogen treatment reliably suppresses hot flashes and often improves sleep quality and mood. For postmenopausal women with a contraindication to estrogen treatment, progestin-only treatment with micronized progesterone or norethindrone acetate may be an effective option.
- Hitchcock CL, Prior JC. Oral micronized progesterone for vasomotor symptoms—a placebo-controlled randomized trial in healthy postmenopausal women. Menopause. 2012;19:886-893.
- Spark MJ, Willis J. Systematic review of progesterone use by midlife menopausal women. Maturitas 2012; 72: 192-202.
- Manson JE, Ames JM, Shapiro M, et al. Algorithm and mobile app for menopausal symptom management and hormonal/nonhormonal therapy decision making: a clinical decision-suport tool from The North American Menopause Society. Menopause. 2015;22:247-253.
- Herrington DM, Vittinghoff E, Howard TD, et al. Factor V Leiden, hormone replacement therapy, and risk of venous thromboembolic events in women with coronary disease. Arterioscler Thromb Vasc Biol. 2002;22:1012-1017.
- Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: a randomized controlled trial. Menopause. 2012;19:848-855.
- Schiff I, Tulchinsky D, Cramer D, et al. Oral medroxyprogesterone in the treatment of postmenopausal symptoms. JAMA. 1980;244:1443-1445.
- Bullock JL, Massey FM, Gambrell RD Jr. Use of medroxyprogesterone acetate to prevent menopausal symptoms. Obstet Gynecol. 1975;46:165-168.
- Loprinzi CL, Levitt R, Barton D, et al. Phase III comparison of depot medroxyprogesterone acetate to venlafaxine for managing hot flashes: North Central Cancer Treatment Group Trial N99C7. J Clin Oncol. 2006;24:1409-1414.
- Prior JC, Nielsen JD, Hitchcock CL, et al. Medroxyprogesterone and conjugated oestrogen are equivalent for hot flushes: 1-year randomized double-blind trial following premenopausal ovariectomy. Clin Sci (Lond). 2007;112:517-525.
- L’hermite M, Simoncini T, Fuller S, et al. Could transdermal estradiol + progesterone be a safer postmenopausal HRT? A review. Maturitas. 2008;60:185-201.
- Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? Menopause. 2014;21:769-783.
- Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat. 2008;107:103-111.
- Hornstein MD, Surrey ES, Weisberg GW, et al. Leuprolide acetate depot and hormonal add-back in endometriosis: a 12-month study. Lupron Add-Back Study Group. Obstet Gynecol. 1998;91:16-24.
- Barbieri RL, Canick JA, Ryan KJ. High-affinity steroid binding to rat testis 17 alpha-hydroxylase and human placental aromatase. J Steroid Biochem. 1981;14:387-393.
- Chu MC, Zhang X, Gentzschein E, et al. Formation of ethinyl estradiol in women during treatment with norethindrone acetate. J Clin Endocrinol Metab. 2007;92:2205-2207.
- Chwalisz K, Surrey E, Stanczyk FZ. The hormonal profile of norethindrone acetate: rationale for add-back therapy with gonadotropin-releasing hormone agonists in women with endometriosis. Reprod Sci. 2012;19:563-571.

Robert L. Barbieri, MD
Editor in Chief, OBG MANAGEMENT
Chair, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG MANAGEMENT
Chair, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG MANAGEMENT
Chair, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
The field of menopause medicine is dominated by studies documenting the effectiveness of systemic estrogen or estrogen-progestin hormone therapy for the treatment of hot flashes caused by hypoestrogenism. The effectiveness of progestin-only systemic hormone therapy for the treatment of hot flashes is much less studied and seldom is utilized in clinical practice. A small number of studies have reported that progestins, including micronized progesterone, medroxyprogesterone acetate, and norethindrone acetate, are effective treatment for hot flashes. Progestin-only systemic hormone therapy might be especially helpful for postmenopausal women with moderate to severe hot flashes who have a contraindication to estrogen treatment.
Micronized progesterone
Micronized progesterone (Prometrium) 300 mg daily taken at bedtime has been reported to effectively treat hot flashes in postmenopausal women. In one study, 133 postmenopausal women with an average age of 55 years and approximately 3 years from their last menstrual period were randomly assigned to 12 weeks of treatment with placebo or micronized progesterone 300 mg daily taken at bedtime.1 Mean serum progesterone levels were 0.28 ng/mL (0.89 nM) and 27 ng/mL (86 nM) in the women taking placebo and micronized progesterone, respectively. Compared with placebo, micronized progesterone reduced daytime and nighttime hot flash frequency and severity. In addition, compared with placebo, micronized progesterone improved the quality of sleep.1
Most reviews conclude that micronized progesterone has minimal cardiovascular risk.2 Micronized progesterone therapy might be especially helpful for postmenopausal women with moderate to severe hot flashes who have a contraindication to estrogen treatment such as those at increased risk for cardiovascular disease or women with a thrombophilia. Many experts believe that systemic estrogen therapy is contraindicated in postmenopausal women with an American Heart Association risk score greater than 10% over 10 years.3 Additional contraindications to systemic estrogen include women with cardiac disease who have a thrombophilia, such as the Factor V Leiden mutation.4
For women who are at high risk for estrogen-induced cardiovascular events, micronized progesterone may be a better option than systemic estrogen for treating hot flashes. Alternatively, in these women at risk of cardiovascular disease a selective serotonin reuptake inhibitor, such as escitalopram, 10 mg to 20 mg daily, may be a good option for treating postmenopausal hot flashes.5
Medroxyprogesterone acetate
Medroxyprogesterone acetate, at a dosage of 20 mg daily, is an effective treatment for hot flashes. In a randomized clinical trial 27 postmenopausal women with hot flashes were randomly assigned to treatment with placebo or medroxyprogesterone acetate 20 mg daily for 4 weeks. Vasomotor flushes were decreased by 26% and 74% in the placebo and medroxyprogesterone groups, respectively.6
Depot medroxyprogesterone acetate injections at dosages from 150 mg to 400 mg also have been reported to effectively treat hot flashes.7,8 In a trial comparing the effectiveness of estrogen monotherapy (conjugated equine estrogen 0.6 mg daily) with progestin monotherapy (medroxyprogesterone acetate 10 mg daily), both treatments were equally effective in reducing hot flashes.9
Continue to: Micronized progesterone vs medroxyprogesterone acetate...
Micronized progesterone vs medroxyprogesterone acetate
Experts in menopause medicine have suggested that in postmenopausal women micronized progesterone has a better pattern of benefits and fewer risks than medroxyprogesterone acetate.10,11 For example, in the E3N observational study of hormones and breast cancer risk, among 80,377 French postmenopausal women followed for a mean of 8 years, the combination of transdermal estradiol plus oral micronized progesterone was associated with no significantly increased risk of breast cancer (relative risk [RR], 1.08, 95% confidence interval [CI], 0.89–1.31) compared with never users of postmenopausal hormone therapy.12 By contrast, the combination of oral estrogen plus medroxyprogesterone acetate was associated with an increased risk of breast cancer (RR, 1.48; 95% CI, 1.02–2.16) compared with never users of postmenopausal hormone therapy. The E3N study indicates that micronized progesterone may have a more favorable breast health profile than medroxyprogesterone acetate.12
Norethindrone acetate
Norethindrone acetate monotherapy is not commonly prescribed for the treatment of menopausal hot flashes. However, a large clinical trial has demonstrated that norethindrone acetate effectively suppresses hot flashes in women with endometriosis treated with depot leuprolide acetate (LA). In one trial 201 women with endometriosis were randomly assigned to 12 months of treatment with13:
- LA plus placebo pills
- LA plus norethindrone acetate (NEA) 5 mg daily
- LA plus NEA 5 mg daily plus conjugated equine estrogen (CEE) 0.625 mg daily, or
- LA plus NEA 5 mg daily plus CEE 1.25 mg daily.
The median number of hot flashes in 24 hours was 6 in the LA plus placebo group and 0 in both the LA plus NEA 5 mg daily group and the LA plus NEA 5 mg plus CEE 1.25 mg daily group. This study demonstrates that NEA 5 mg daily is an effective treatment for hot flashes.
In the same study, LA plus placebo was associated with a significant decrease in lumbar spine bone mineral density. No significant decrease in bone mineral density was observed in the women who received LA plus NEA 5 mg daily. This finding indicates that NEA 5 mg reduces bone absorption caused by hypoestrogenism. In humans, norethindrone is a substrate for the aromatase enzyme system.14 Small quantities of ethinyl estradiol may be formed by aromatization of norethindrone in vivo,15,16 contributing to the effectiveness of NEA in suppressing hot flashes and preserving bone density.
Progestin: The estrogen alternative to hot flashes
For postmenopausal women with moderate to severe hot flashes, estrogen treatment reliably suppresses hot flashes and often improves sleep quality and mood. For postmenopausal women with a contraindication to estrogen treatment, progestin-only treatment with micronized progesterone or norethindrone acetate may be an effective option.
The field of menopause medicine is dominated by studies documenting the effectiveness of systemic estrogen or estrogen-progestin hormone therapy for the treatment of hot flashes caused by hypoestrogenism. The effectiveness of progestin-only systemic hormone therapy for the treatment of hot flashes is much less studied and seldom is utilized in clinical practice. A small number of studies have reported that progestins, including micronized progesterone, medroxyprogesterone acetate, and norethindrone acetate, are effective treatment for hot flashes. Progestin-only systemic hormone therapy might be especially helpful for postmenopausal women with moderate to severe hot flashes who have a contraindication to estrogen treatment.
Micronized progesterone
Micronized progesterone (Prometrium) 300 mg daily taken at bedtime has been reported to effectively treat hot flashes in postmenopausal women. In one study, 133 postmenopausal women with an average age of 55 years and approximately 3 years from their last menstrual period were randomly assigned to 12 weeks of treatment with placebo or micronized progesterone 300 mg daily taken at bedtime.1 Mean serum progesterone levels were 0.28 ng/mL (0.89 nM) and 27 ng/mL (86 nM) in the women taking placebo and micronized progesterone, respectively. Compared with placebo, micronized progesterone reduced daytime and nighttime hot flash frequency and severity. In addition, compared with placebo, micronized progesterone improved the quality of sleep.1
Most reviews conclude that micronized progesterone has minimal cardiovascular risk.2 Micronized progesterone therapy might be especially helpful for postmenopausal women with moderate to severe hot flashes who have a contraindication to estrogen treatment such as those at increased risk for cardiovascular disease or women with a thrombophilia. Many experts believe that systemic estrogen therapy is contraindicated in postmenopausal women with an American Heart Association risk score greater than 10% over 10 years.3 Additional contraindications to systemic estrogen include women with cardiac disease who have a thrombophilia, such as the Factor V Leiden mutation.4
For women who are at high risk for estrogen-induced cardiovascular events, micronized progesterone may be a better option than systemic estrogen for treating hot flashes. Alternatively, in these women at risk of cardiovascular disease a selective serotonin reuptake inhibitor, such as escitalopram, 10 mg to 20 mg daily, may be a good option for treating postmenopausal hot flashes.5
Medroxyprogesterone acetate
Medroxyprogesterone acetate, at a dosage of 20 mg daily, is an effective treatment for hot flashes. In a randomized clinical trial 27 postmenopausal women with hot flashes were randomly assigned to treatment with placebo or medroxyprogesterone acetate 20 mg daily for 4 weeks. Vasomotor flushes were decreased by 26% and 74% in the placebo and medroxyprogesterone groups, respectively.6
Depot medroxyprogesterone acetate injections at dosages from 150 mg to 400 mg also have been reported to effectively treat hot flashes.7,8 In a trial comparing the effectiveness of estrogen monotherapy (conjugated equine estrogen 0.6 mg daily) with progestin monotherapy (medroxyprogesterone acetate 10 mg daily), both treatments were equally effective in reducing hot flashes.9
Continue to: Micronized progesterone vs medroxyprogesterone acetate...
Micronized progesterone vs medroxyprogesterone acetate
Experts in menopause medicine have suggested that in postmenopausal women micronized progesterone has a better pattern of benefits and fewer risks than medroxyprogesterone acetate.10,11 For example, in the E3N observational study of hormones and breast cancer risk, among 80,377 French postmenopausal women followed for a mean of 8 years, the combination of transdermal estradiol plus oral micronized progesterone was associated with no significantly increased risk of breast cancer (relative risk [RR], 1.08, 95% confidence interval [CI], 0.89–1.31) compared with never users of postmenopausal hormone therapy.12 By contrast, the combination of oral estrogen plus medroxyprogesterone acetate was associated with an increased risk of breast cancer (RR, 1.48; 95% CI, 1.02–2.16) compared with never users of postmenopausal hormone therapy. The E3N study indicates that micronized progesterone may have a more favorable breast health profile than medroxyprogesterone acetate.12
Norethindrone acetate
Norethindrone acetate monotherapy is not commonly prescribed for the treatment of menopausal hot flashes. However, a large clinical trial has demonstrated that norethindrone acetate effectively suppresses hot flashes in women with endometriosis treated with depot leuprolide acetate (LA). In one trial 201 women with endometriosis were randomly assigned to 12 months of treatment with13:
- LA plus placebo pills
- LA plus norethindrone acetate (NEA) 5 mg daily
- LA plus NEA 5 mg daily plus conjugated equine estrogen (CEE) 0.625 mg daily, or
- LA plus NEA 5 mg daily plus CEE 1.25 mg daily.
The median number of hot flashes in 24 hours was 6 in the LA plus placebo group and 0 in both the LA plus NEA 5 mg daily group and the LA plus NEA 5 mg plus CEE 1.25 mg daily group. This study demonstrates that NEA 5 mg daily is an effective treatment for hot flashes.
In the same study, LA plus placebo was associated with a significant decrease in lumbar spine bone mineral density. No significant decrease in bone mineral density was observed in the women who received LA plus NEA 5 mg daily. This finding indicates that NEA 5 mg reduces bone absorption caused by hypoestrogenism. In humans, norethindrone is a substrate for the aromatase enzyme system.14 Small quantities of ethinyl estradiol may be formed by aromatization of norethindrone in vivo,15,16 contributing to the effectiveness of NEA in suppressing hot flashes and preserving bone density.
Progestin: The estrogen alternative to hot flashes
For postmenopausal women with moderate to severe hot flashes, estrogen treatment reliably suppresses hot flashes and often improves sleep quality and mood. For postmenopausal women with a contraindication to estrogen treatment, progestin-only treatment with micronized progesterone or norethindrone acetate may be an effective option.
- Hitchcock CL, Prior JC. Oral micronized progesterone for vasomotor symptoms—a placebo-controlled randomized trial in healthy postmenopausal women. Menopause. 2012;19:886-893.
- Spark MJ, Willis J. Systematic review of progesterone use by midlife menopausal women. Maturitas 2012; 72: 192-202.
- Manson JE, Ames JM, Shapiro M, et al. Algorithm and mobile app for menopausal symptom management and hormonal/nonhormonal therapy decision making: a clinical decision-suport tool from The North American Menopause Society. Menopause. 2015;22:247-253.
- Herrington DM, Vittinghoff E, Howard TD, et al. Factor V Leiden, hormone replacement therapy, and risk of venous thromboembolic events in women with coronary disease. Arterioscler Thromb Vasc Biol. 2002;22:1012-1017.
- Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: a randomized controlled trial. Menopause. 2012;19:848-855.
- Schiff I, Tulchinsky D, Cramer D, et al. Oral medroxyprogesterone in the treatment of postmenopausal symptoms. JAMA. 1980;244:1443-1445.
- Bullock JL, Massey FM, Gambrell RD Jr. Use of medroxyprogesterone acetate to prevent menopausal symptoms. Obstet Gynecol. 1975;46:165-168.
- Loprinzi CL, Levitt R, Barton D, et al. Phase III comparison of depot medroxyprogesterone acetate to venlafaxine for managing hot flashes: North Central Cancer Treatment Group Trial N99C7. J Clin Oncol. 2006;24:1409-1414.
- Prior JC, Nielsen JD, Hitchcock CL, et al. Medroxyprogesterone and conjugated oestrogen are equivalent for hot flushes: 1-year randomized double-blind trial following premenopausal ovariectomy. Clin Sci (Lond). 2007;112:517-525.
- L’hermite M, Simoncini T, Fuller S, et al. Could transdermal estradiol + progesterone be a safer postmenopausal HRT? A review. Maturitas. 2008;60:185-201.
- Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? Menopause. 2014;21:769-783.
- Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat. 2008;107:103-111.
- Hornstein MD, Surrey ES, Weisberg GW, et al. Leuprolide acetate depot and hormonal add-back in endometriosis: a 12-month study. Lupron Add-Back Study Group. Obstet Gynecol. 1998;91:16-24.
- Barbieri RL, Canick JA, Ryan KJ. High-affinity steroid binding to rat testis 17 alpha-hydroxylase and human placental aromatase. J Steroid Biochem. 1981;14:387-393.
- Chu MC, Zhang X, Gentzschein E, et al. Formation of ethinyl estradiol in women during treatment with norethindrone acetate. J Clin Endocrinol Metab. 2007;92:2205-2207.
- Chwalisz K, Surrey E, Stanczyk FZ. The hormonal profile of norethindrone acetate: rationale for add-back therapy with gonadotropin-releasing hormone agonists in women with endometriosis. Reprod Sci. 2012;19:563-571.
- Hitchcock CL, Prior JC. Oral micronized progesterone for vasomotor symptoms—a placebo-controlled randomized trial in healthy postmenopausal women. Menopause. 2012;19:886-893.
- Spark MJ, Willis J. Systematic review of progesterone use by midlife menopausal women. Maturitas 2012; 72: 192-202.
- Manson JE, Ames JM, Shapiro M, et al. Algorithm and mobile app for menopausal symptom management and hormonal/nonhormonal therapy decision making: a clinical decision-suport tool from The North American Menopause Society. Menopause. 2015;22:247-253.
- Herrington DM, Vittinghoff E, Howard TD, et al. Factor V Leiden, hormone replacement therapy, and risk of venous thromboembolic events in women with coronary disease. Arterioscler Thromb Vasc Biol. 2002;22:1012-1017.
- Ensrud KE, Joffe H, Guthrie KA, et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy perimenopausal and postmenopausal women with hot flashes: a randomized controlled trial. Menopause. 2012;19:848-855.
- Schiff I, Tulchinsky D, Cramer D, et al. Oral medroxyprogesterone in the treatment of postmenopausal symptoms. JAMA. 1980;244:1443-1445.
- Bullock JL, Massey FM, Gambrell RD Jr. Use of medroxyprogesterone acetate to prevent menopausal symptoms. Obstet Gynecol. 1975;46:165-168.
- Loprinzi CL, Levitt R, Barton D, et al. Phase III comparison of depot medroxyprogesterone acetate to venlafaxine for managing hot flashes: North Central Cancer Treatment Group Trial N99C7. J Clin Oncol. 2006;24:1409-1414.
- Prior JC, Nielsen JD, Hitchcock CL, et al. Medroxyprogesterone and conjugated oestrogen are equivalent for hot flushes: 1-year randomized double-blind trial following premenopausal ovariectomy. Clin Sci (Lond). 2007;112:517-525.
- L’hermite M, Simoncini T, Fuller S, et al. Could transdermal estradiol + progesterone be a safer postmenopausal HRT? A review. Maturitas. 2008;60:185-201.
- Simon JA. What if the Women’s Health Initiative had used transdermal estradiol and oral progesterone instead? Menopause. 2014;21:769-783.
- Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat. 2008;107:103-111.
- Hornstein MD, Surrey ES, Weisberg GW, et al. Leuprolide acetate depot and hormonal add-back in endometriosis: a 12-month study. Lupron Add-Back Study Group. Obstet Gynecol. 1998;91:16-24.
- Barbieri RL, Canick JA, Ryan KJ. High-affinity steroid binding to rat testis 17 alpha-hydroxylase and human placental aromatase. J Steroid Biochem. 1981;14:387-393.
- Chu MC, Zhang X, Gentzschein E, et al. Formation of ethinyl estradiol in women during treatment with norethindrone acetate. J Clin Endocrinol Metab. 2007;92:2205-2207.
- Chwalisz K, Surrey E, Stanczyk FZ. The hormonal profile of norethindrone acetate: rationale for add-back therapy with gonadotropin-releasing hormone agonists in women with endometriosis. Reprod Sci. 2012;19:563-571.

IBD quality initiative slashes ED utilization
AUSTIN, TEX. – A quality improvement initiative aimed at patients with inflammatory bowel disease (IBD) has reduced emergency department visits and hospitalizations by 20% or more and slashed opioid use by half, according to study results presented at the Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.

After 15 months, the quality improvement program saw emergency department visit rates decline from 18% to 14%, a 22% relative decrease, Gil Y. Melmed, MD, of Cedars-Sinai Medical Center, Los Angeles, said. Additionally, the study documented a similar decrease in the rate of hospitalization, declining from 14% to 11%, while opioid utilization rates declined from 8% to 4%. “We also found decreases in special-cause variation in other measures of interest, including CT scan utilization as well as corticosteroid use, which was reduced 29% during the course of the program,” he said.
The quality initiative was conducted through the Crohn’s & Colitis Foundation as an outgrowth of its IBD Qorus quality improvement program. The 15-month study involved 20,392 patient visits at 15 academic and 11 private/community practices from January 2018 to April 2019. “This specific project within Qorus is focused specifically around the concept of improving access during times of urgent care need,” Dr. Melmed told this news organization. The goal was to identify practice changes that can drive improvement.
The intervention consisted of 19 different strategies, called a “Change Package,” and participating sites could choose to test and implement one or more of them, Dr. Melmed said. Some examples included designating urgent care slots in the clinic schedule, installing a nurse hotline, a weekly “huddle” to review high-risk patients, and patient education on using urgent care.
One of the drivers of the program was to provide immediate care improvement to patients, Dr. Melmed said in the interview. “As opposed to investments into the cure of IBD that we need, but which can take years to develop, this research has immediate, practical applicability for patients today,” he said.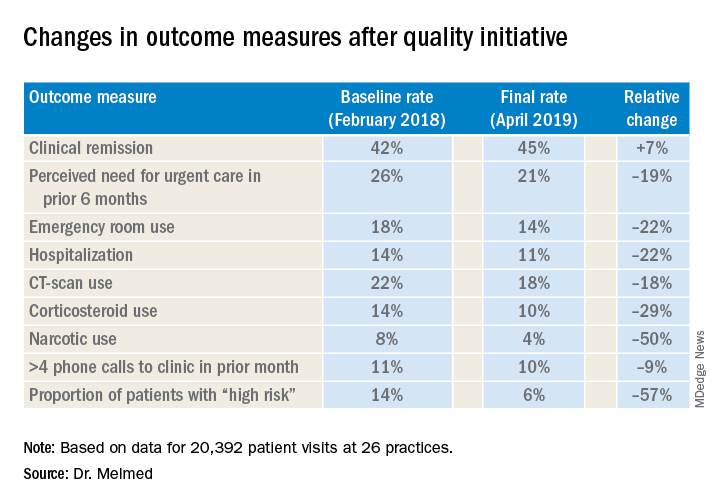
“The fact that we were able to demonstrate reduction in emergency room utilization and hospitalization, steroid use, and narcotic use has really energized the work that we were doing. We can now show that very-low-cost process changes at a site level lead to robust improvement in patient outcomes. These changes are potentially implementable in any practice setting,” Dr. Melmed said in the interview.
After Dr. Melmed’s presentation, Maria T. Abreu, MD, director of the Crohn’s and Colitis Center at the University of Miami, asked about the cost of the interventions. Dr. Melmed said the costs were nominal, such as paying for a new phone line for a patient hotline. “But overall the cost really involved in the program was the time that it took to review the high-risk list on a weekly basis with the team, and that is essentially a 15-minute huddle,” he said.
Later, Dr. Abreu said in an interview that the program was “a terrific example of how measuring outcomes and sharing ideas can make huge impacts in the lives of patients.” She added, “An enormous amount of money is spent on clinical trials of expensive biologics which have revolutionized treatment, yet the humanistic aspects of our care have just as great of an impact. In this study, each center focused on ways they could lower ER visits and hospitalizations. One size did not fit all, yet they could learn from each other. The very platform they used to conduct the study is a model for all of us.”
Corey A. Siegel, MD, of the Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and Dr. Melmed's coprincipal investigator on Qorus, said the quality initiative now includes 49 GI practices across the country with plans to grow to 60 by the end of the year. "We have created this 'collaboratory' for providers from actross the country to work togetherr to learn how to best deliver high-qulaity care for patients with IBD," he said.
Another feature of the quality initiative allowed participating sites to see how they compared with others anonymously, Dr. Melmed said. “Using the data, we called out high-performing sites to teach the rest of us what they were doing that enabled them to improve, so that all of us could learn from their successes,” he said.
The researchers are aiming to evaluate costs and identify the most successful interventions, with the plan to present the latter at Digestive Disease Week® 2020 and use them to develop a toolkit practices can use. “Ultimately,” said Dr. Melmed, “this is scalable.”
Dr. Melmed disclosed financial relationships with AbbVie, Boehringer-Ingelheim, Celgene, Jannsen, GSK, Medtronic, Pfizer, Samsung Bioepis, Takeda, and Techlab; IBD Qorus receives support from Abbvie, AMAG, Helmsley Charitable Trust, Janssen, Nephoroceuticals, Pfizer, Takeda, and UCB.
SOURCE: Melmed GT et al. Crohn’s & Colitis Congress 2020, Session 28.
AUSTIN, TEX. – A quality improvement initiative aimed at patients with inflammatory bowel disease (IBD) has reduced emergency department visits and hospitalizations by 20% or more and slashed opioid use by half, according to study results presented at the Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
After 15 months, the quality improvement program saw emergency department visit rates decline from 18% to 14%, a 22% relative decrease, Gil Y. Melmed, MD, of Cedars-Sinai Medical Center, Los Angeles, said. Additionally, the study documented a similar decrease in the rate of hospitalization, declining from 14% to 11%, while opioid utilization rates declined from 8% to 4%. “We also found decreases in special-cause variation in other measures of interest, including CT scan utilization as well as corticosteroid use, which was reduced 29% during the course of the program,” he said.
The quality initiative was conducted through the Crohn’s & Colitis Foundation as an outgrowth of its IBD Qorus quality improvement program. The 15-month study involved 20,392 patient visits at 15 academic and 11 private/community practices from January 2018 to April 2019. “This specific project within Qorus is focused specifically around the concept of improving access during times of urgent care need,” Dr. Melmed told this news organization. The goal was to identify practice changes that can drive improvement.
The intervention consisted of 19 different strategies, called a “Change Package,” and participating sites could choose to test and implement one or more of them, Dr. Melmed said. Some examples included designating urgent care slots in the clinic schedule, installing a nurse hotline, a weekly “huddle” to review high-risk patients, and patient education on using urgent care.
One of the drivers of the program was to provide immediate care improvement to patients, Dr. Melmed said in the interview. “As opposed to investments into the cure of IBD that we need, but which can take years to develop, this research has immediate, practical applicability for patients today,” he said.
“The fact that we were able to demonstrate reduction in emergency room utilization and hospitalization, steroid use, and narcotic use has really energized the work that we were doing. We can now show that very-low-cost process changes at a site level lead to robust improvement in patient outcomes. These changes are potentially implementable in any practice setting,” Dr. Melmed said in the interview.
After Dr. Melmed’s presentation, Maria T. Abreu, MD, director of the Crohn’s and Colitis Center at the University of Miami, asked about the cost of the interventions. Dr. Melmed said the costs were nominal, such as paying for a new phone line for a patient hotline. “But overall the cost really involved in the program was the time that it took to review the high-risk list on a weekly basis with the team, and that is essentially a 15-minute huddle,” he said.
Later, Dr. Abreu said in an interview that the program was “a terrific example of how measuring outcomes and sharing ideas can make huge impacts in the lives of patients.” She added, “An enormous amount of money is spent on clinical trials of expensive biologics which have revolutionized treatment, yet the humanistic aspects of our care have just as great of an impact. In this study, each center focused on ways they could lower ER visits and hospitalizations. One size did not fit all, yet they could learn from each other. The very platform they used to conduct the study is a model for all of us.”
Corey A. Siegel, MD, of the Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and Dr. Melmed's coprincipal investigator on Qorus, said the quality initiative now includes 49 GI practices across the country with plans to grow to 60 by the end of the year. "We have created this 'collaboratory' for providers from actross the country to work togetherr to learn how to best deliver high-qulaity care for patients with IBD," he said.
Another feature of the quality initiative allowed participating sites to see how they compared with others anonymously, Dr. Melmed said. “Using the data, we called out high-performing sites to teach the rest of us what they were doing that enabled them to improve, so that all of us could learn from their successes,” he said.
The researchers are aiming to evaluate costs and identify the most successful interventions, with the plan to present the latter at Digestive Disease Week® 2020 and use them to develop a toolkit practices can use. “Ultimately,” said Dr. Melmed, “this is scalable.”
Dr. Melmed disclosed financial relationships with AbbVie, Boehringer-Ingelheim, Celgene, Jannsen, GSK, Medtronic, Pfizer, Samsung Bioepis, Takeda, and Techlab; IBD Qorus receives support from Abbvie, AMAG, Helmsley Charitable Trust, Janssen, Nephoroceuticals, Pfizer, Takeda, and UCB.
SOURCE: Melmed GT et al. Crohn’s & Colitis Congress 2020, Session 28.
AUSTIN, TEX. – A quality improvement initiative aimed at patients with inflammatory bowel disease (IBD) has reduced emergency department visits and hospitalizations by 20% or more and slashed opioid use by half, according to study results presented at the Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
After 15 months, the quality improvement program saw emergency department visit rates decline from 18% to 14%, a 22% relative decrease, Gil Y. Melmed, MD, of Cedars-Sinai Medical Center, Los Angeles, said. Additionally, the study documented a similar decrease in the rate of hospitalization, declining from 14% to 11%, while opioid utilization rates declined from 8% to 4%. “We also found decreases in special-cause variation in other measures of interest, including CT scan utilization as well as corticosteroid use, which was reduced 29% during the course of the program,” he said.
The quality initiative was conducted through the Crohn’s & Colitis Foundation as an outgrowth of its IBD Qorus quality improvement program. The 15-month study involved 20,392 patient visits at 15 academic and 11 private/community practices from January 2018 to April 2019. “This specific project within Qorus is focused specifically around the concept of improving access during times of urgent care need,” Dr. Melmed told this news organization. The goal was to identify practice changes that can drive improvement.
The intervention consisted of 19 different strategies, called a “Change Package,” and participating sites could choose to test and implement one or more of them, Dr. Melmed said. Some examples included designating urgent care slots in the clinic schedule, installing a nurse hotline, a weekly “huddle” to review high-risk patients, and patient education on using urgent care.
One of the drivers of the program was to provide immediate care improvement to patients, Dr. Melmed said in the interview. “As opposed to investments into the cure of IBD that we need, but which can take years to develop, this research has immediate, practical applicability for patients today,” he said.
“The fact that we were able to demonstrate reduction in emergency room utilization and hospitalization, steroid use, and narcotic use has really energized the work that we were doing. We can now show that very-low-cost process changes at a site level lead to robust improvement in patient outcomes. These changes are potentially implementable in any practice setting,” Dr. Melmed said in the interview.
After Dr. Melmed’s presentation, Maria T. Abreu, MD, director of the Crohn’s and Colitis Center at the University of Miami, asked about the cost of the interventions. Dr. Melmed said the costs were nominal, such as paying for a new phone line for a patient hotline. “But overall the cost really involved in the program was the time that it took to review the high-risk list on a weekly basis with the team, and that is essentially a 15-minute huddle,” he said.
Later, Dr. Abreu said in an interview that the program was “a terrific example of how measuring outcomes and sharing ideas can make huge impacts in the lives of patients.” She added, “An enormous amount of money is spent on clinical trials of expensive biologics which have revolutionized treatment, yet the humanistic aspects of our care have just as great of an impact. In this study, each center focused on ways they could lower ER visits and hospitalizations. One size did not fit all, yet they could learn from each other. The very platform they used to conduct the study is a model for all of us.”
Corey A. Siegel, MD, of the Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and Dr. Melmed's coprincipal investigator on Qorus, said the quality initiative now includes 49 GI practices across the country with plans to grow to 60 by the end of the year. "We have created this 'collaboratory' for providers from actross the country to work togetherr to learn how to best deliver high-qulaity care for patients with IBD," he said.
Another feature of the quality initiative allowed participating sites to see how they compared with others anonymously, Dr. Melmed said. “Using the data, we called out high-performing sites to teach the rest of us what they were doing that enabled them to improve, so that all of us could learn from their successes,” he said.
The researchers are aiming to evaluate costs and identify the most successful interventions, with the plan to present the latter at Digestive Disease Week® 2020 and use them to develop a toolkit practices can use. “Ultimately,” said Dr. Melmed, “this is scalable.”
Dr. Melmed disclosed financial relationships with AbbVie, Boehringer-Ingelheim, Celgene, Jannsen, GSK, Medtronic, Pfizer, Samsung Bioepis, Takeda, and Techlab; IBD Qorus receives support from Abbvie, AMAG, Helmsley Charitable Trust, Janssen, Nephoroceuticals, Pfizer, Takeda, and UCB.
SOURCE: Melmed GT et al. Crohn’s & Colitis Congress 2020, Session 28.
REPORTING FROM CROHN’S & COLITIS CONGRESS