User login
Novel coronavirus cases now at 11; entry ban and quarantine measures begin
, Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during a Centers for Disease Control and Prevention press briefing.
Four of the new cases are in California, and one in Massachusetts. Although four of the new cases have recent travel history to Wuhan, China, the epicenter of the 2019-nCoV outbreak, the fifth is a close household contact of one of the other California patients, said Dr. Messonnier. This last case is the second instance of person-to-person spread of 2019-nCoV in the United States.
“We expect to find additional cases of the novel coronavirus in the United States,” she said. “We expect to see more cases of person-to-person spread among close contacts. And we continue to expect this will happen given the explosive nature of this outbreak in China.”
As of the morning of Feb. 3, 167 persons under investigation, or PUIs, for possible 2019-nCoV have tested negative for the virus, and an additional 82 PUIs have testing pending – this latter figure includes some tests that are still in transit to the CDC, said Dr. Messonnier.
During the briefing, Dr. Messonnier emphasized both the aggressive nature of the U.S. public health response and the rationale for quick and assertive action. “The goal of our public health response is to protect and contain,” she said. “Strong measures now may blunt the impact of this virus on the United States.”
She cited the intensity of transmission in Hubei Province, the expansion of transmission to other provinces in China, the expansion of cases outside of China, and sporadic ongoing deaths from 2019-nCoV as drivers of the aggressive U.S. public health response.
A presidential proclamation is currently in place that bars U.S. entry to foreign nationals who have visited mainland China within the past 14 days; the ban does not apply to travelers from Hong Kong and Macao. Immediate family members of U.S. citizens and individuals who have U.S. permanent resident status are exempted from the entry ban and will be allowed entry into the United States.
However, explained Dr. Messonnier, those who have traveled to China recently and are permitted entry will be subject to screening. All passengers with such recent travel will be directed to one of 11 U.S. airports set up to perform additional screening.
As of Feb 3, the list of airports includes:
- San Francisco International Airport in California.
- Los Angeles International Airport in California.
- Hartsfield-Jackson Atlanta International Airport in Georgia.
- Daniel K. Inouye International Airport in Hawaii.
- O’Hare International Airport in Illinois.
- Detroit Metropolitan Airport in Michigan.
- Newark Liberty International Airport in New Jersey.
- John F. Kennedy International Airport in New York.
- Dallas/Fort Worth International Airport in Texas.
- Washington Dulles International Airport in Virginia.
- Seattle-Tacoma International Airport in Washington.
Travelers who have been to Hubei Province in the previous 14 days will have an additional health assessment at which they will be screened for fever, cough, or difficulty breathing. Any American citizens or exempt individuals who are symptomatic would then be transferred for further medical evaluation. Asymptomatic travelers in this category will be subject to a mandatory 14-day quarantine near their point of entry, rather than continuing on to their final destinations.
Dr. Messonnier emphasized that the mandatory 14-day quarantine is specifically for Americans or exempt individuals returning from Hubei Province, adding that the CDC is presently working with individual states to determine the exact venues for quarantine.
American citizens and exempt individuals returning from other parts of mainland China will be routed to one of the 11 airports and will also receive additional health screening. Symptomatic individuals in this travel category would be referred for further evaluation before being able to complete their itinerary.
Asymptomatic American citizens and exempt individuals who are returning from mainland China – but not Hubei Province – will be allowed to travel on to their final destinations, but will be asked to stay home as much as possible and to monitor their health during the 14 days after their return.
The U.S. Department of State is bringing back more Americans from Wuhan province this week, and these individuals will also be kept under federal quarantine for 14 days.
“There are likely to be confirmed infections among returning travelers,” said Dr. Messonnier. “It is important to note that this strategy is not meant to catch every single traveler returning from China with novel coronavirus; given the nature of this virus and how it’s spreading, that would be impossible, but working together we can catch the majority of them.
“The goal here is to slow the entry of this virus into the United States,” she said, adding that the nation’s health care and public health systems stand on high alert to detect the virus in community settings. In response to questioning from the press, Dr. Messonnier defended the stringent quarantine measures, noting that they are in line with those taken by some other nations, and with the aggressive action being taken by the Chinese government itself. “These actions are science based and aimed at protecting the health of all Americans,” she said.
The real-time reverse transcription polymerase chain reaction (rRT-PCR) assay that the CDC has developed detects 2019-nCoV in both respiratory and serum specimens. Dr. Messonnier reported that the CDC is today filing an emergency use authorization (EUA) application to the U.S. Food and Drug Administration to expedite access to the assay for public health laboratories across the country. “This will greatly enhance our capacity to test for this virus,” she said, noting that EUA approval may come as soon as the end of this week.
Although the CDC is poised to send an expert team to China, it’s still awaiting favorable results from the international negotiations currently underway. “This is a horrible situation in China,” said Dr. Messonnier. “Our presence on the ground in China would be a help to China. ... Science should trump everything else; that’s what we’re hoping – that the scientific expertise of the global community can be brought to bear on the incredibly complicated, difficult situation that our colleagues in China are dealing with.”
, Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during a Centers for Disease Control and Prevention press briefing.
Four of the new cases are in California, and one in Massachusetts. Although four of the new cases have recent travel history to Wuhan, China, the epicenter of the 2019-nCoV outbreak, the fifth is a close household contact of one of the other California patients, said Dr. Messonnier. This last case is the second instance of person-to-person spread of 2019-nCoV in the United States.
“We expect to find additional cases of the novel coronavirus in the United States,” she said. “We expect to see more cases of person-to-person spread among close contacts. And we continue to expect this will happen given the explosive nature of this outbreak in China.”
As of the morning of Feb. 3, 167 persons under investigation, or PUIs, for possible 2019-nCoV have tested negative for the virus, and an additional 82 PUIs have testing pending – this latter figure includes some tests that are still in transit to the CDC, said Dr. Messonnier.
During the briefing, Dr. Messonnier emphasized both the aggressive nature of the U.S. public health response and the rationale for quick and assertive action. “The goal of our public health response is to protect and contain,” she said. “Strong measures now may blunt the impact of this virus on the United States.”
She cited the intensity of transmission in Hubei Province, the expansion of transmission to other provinces in China, the expansion of cases outside of China, and sporadic ongoing deaths from 2019-nCoV as drivers of the aggressive U.S. public health response.
A presidential proclamation is currently in place that bars U.S. entry to foreign nationals who have visited mainland China within the past 14 days; the ban does not apply to travelers from Hong Kong and Macao. Immediate family members of U.S. citizens and individuals who have U.S. permanent resident status are exempted from the entry ban and will be allowed entry into the United States.
However, explained Dr. Messonnier, those who have traveled to China recently and are permitted entry will be subject to screening. All passengers with such recent travel will be directed to one of 11 U.S. airports set up to perform additional screening.
As of Feb 3, the list of airports includes:
- San Francisco International Airport in California.
- Los Angeles International Airport in California.
- Hartsfield-Jackson Atlanta International Airport in Georgia.
- Daniel K. Inouye International Airport in Hawaii.
- O’Hare International Airport in Illinois.
- Detroit Metropolitan Airport in Michigan.
- Newark Liberty International Airport in New Jersey.
- John F. Kennedy International Airport in New York.
- Dallas/Fort Worth International Airport in Texas.
- Washington Dulles International Airport in Virginia.
- Seattle-Tacoma International Airport in Washington.
Travelers who have been to Hubei Province in the previous 14 days will have an additional health assessment at which they will be screened for fever, cough, or difficulty breathing. Any American citizens or exempt individuals who are symptomatic would then be transferred for further medical evaluation. Asymptomatic travelers in this category will be subject to a mandatory 14-day quarantine near their point of entry, rather than continuing on to their final destinations.
Dr. Messonnier emphasized that the mandatory 14-day quarantine is specifically for Americans or exempt individuals returning from Hubei Province, adding that the CDC is presently working with individual states to determine the exact venues for quarantine.
American citizens and exempt individuals returning from other parts of mainland China will be routed to one of the 11 airports and will also receive additional health screening. Symptomatic individuals in this travel category would be referred for further evaluation before being able to complete their itinerary.
Asymptomatic American citizens and exempt individuals who are returning from mainland China – but not Hubei Province – will be allowed to travel on to their final destinations, but will be asked to stay home as much as possible and to monitor their health during the 14 days after their return.
The U.S. Department of State is bringing back more Americans from Wuhan province this week, and these individuals will also be kept under federal quarantine for 14 days.
“There are likely to be confirmed infections among returning travelers,” said Dr. Messonnier. “It is important to note that this strategy is not meant to catch every single traveler returning from China with novel coronavirus; given the nature of this virus and how it’s spreading, that would be impossible, but working together we can catch the majority of them.
“The goal here is to slow the entry of this virus into the United States,” she said, adding that the nation’s health care and public health systems stand on high alert to detect the virus in community settings. In response to questioning from the press, Dr. Messonnier defended the stringent quarantine measures, noting that they are in line with those taken by some other nations, and with the aggressive action being taken by the Chinese government itself. “These actions are science based and aimed at protecting the health of all Americans,” she said.
The real-time reverse transcription polymerase chain reaction (rRT-PCR) assay that the CDC has developed detects 2019-nCoV in both respiratory and serum specimens. Dr. Messonnier reported that the CDC is today filing an emergency use authorization (EUA) application to the U.S. Food and Drug Administration to expedite access to the assay for public health laboratories across the country. “This will greatly enhance our capacity to test for this virus,” she said, noting that EUA approval may come as soon as the end of this week.
Although the CDC is poised to send an expert team to China, it’s still awaiting favorable results from the international negotiations currently underway. “This is a horrible situation in China,” said Dr. Messonnier. “Our presence on the ground in China would be a help to China. ... Science should trump everything else; that’s what we’re hoping – that the scientific expertise of the global community can be brought to bear on the incredibly complicated, difficult situation that our colleagues in China are dealing with.”
, Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during a Centers for Disease Control and Prevention press briefing.
Four of the new cases are in California, and one in Massachusetts. Although four of the new cases have recent travel history to Wuhan, China, the epicenter of the 2019-nCoV outbreak, the fifth is a close household contact of one of the other California patients, said Dr. Messonnier. This last case is the second instance of person-to-person spread of 2019-nCoV in the United States.
“We expect to find additional cases of the novel coronavirus in the United States,” she said. “We expect to see more cases of person-to-person spread among close contacts. And we continue to expect this will happen given the explosive nature of this outbreak in China.”
As of the morning of Feb. 3, 167 persons under investigation, or PUIs, for possible 2019-nCoV have tested negative for the virus, and an additional 82 PUIs have testing pending – this latter figure includes some tests that are still in transit to the CDC, said Dr. Messonnier.
During the briefing, Dr. Messonnier emphasized both the aggressive nature of the U.S. public health response and the rationale for quick and assertive action. “The goal of our public health response is to protect and contain,” she said. “Strong measures now may blunt the impact of this virus on the United States.”
She cited the intensity of transmission in Hubei Province, the expansion of transmission to other provinces in China, the expansion of cases outside of China, and sporadic ongoing deaths from 2019-nCoV as drivers of the aggressive U.S. public health response.
A presidential proclamation is currently in place that bars U.S. entry to foreign nationals who have visited mainland China within the past 14 days; the ban does not apply to travelers from Hong Kong and Macao. Immediate family members of U.S. citizens and individuals who have U.S. permanent resident status are exempted from the entry ban and will be allowed entry into the United States.
However, explained Dr. Messonnier, those who have traveled to China recently and are permitted entry will be subject to screening. All passengers with such recent travel will be directed to one of 11 U.S. airports set up to perform additional screening.
As of Feb 3, the list of airports includes:
- San Francisco International Airport in California.
- Los Angeles International Airport in California.
- Hartsfield-Jackson Atlanta International Airport in Georgia.
- Daniel K. Inouye International Airport in Hawaii.
- O’Hare International Airport in Illinois.
- Detroit Metropolitan Airport in Michigan.
- Newark Liberty International Airport in New Jersey.
- John F. Kennedy International Airport in New York.
- Dallas/Fort Worth International Airport in Texas.
- Washington Dulles International Airport in Virginia.
- Seattle-Tacoma International Airport in Washington.
Travelers who have been to Hubei Province in the previous 14 days will have an additional health assessment at which they will be screened for fever, cough, or difficulty breathing. Any American citizens or exempt individuals who are symptomatic would then be transferred for further medical evaluation. Asymptomatic travelers in this category will be subject to a mandatory 14-day quarantine near their point of entry, rather than continuing on to their final destinations.
Dr. Messonnier emphasized that the mandatory 14-day quarantine is specifically for Americans or exempt individuals returning from Hubei Province, adding that the CDC is presently working with individual states to determine the exact venues for quarantine.
American citizens and exempt individuals returning from other parts of mainland China will be routed to one of the 11 airports and will also receive additional health screening. Symptomatic individuals in this travel category would be referred for further evaluation before being able to complete their itinerary.
Asymptomatic American citizens and exempt individuals who are returning from mainland China – but not Hubei Province – will be allowed to travel on to their final destinations, but will be asked to stay home as much as possible and to monitor their health during the 14 days after their return.
The U.S. Department of State is bringing back more Americans from Wuhan province this week, and these individuals will also be kept under federal quarantine for 14 days.
“There are likely to be confirmed infections among returning travelers,” said Dr. Messonnier. “It is important to note that this strategy is not meant to catch every single traveler returning from China with novel coronavirus; given the nature of this virus and how it’s spreading, that would be impossible, but working together we can catch the majority of them.
“The goal here is to slow the entry of this virus into the United States,” she said, adding that the nation’s health care and public health systems stand on high alert to detect the virus in community settings. In response to questioning from the press, Dr. Messonnier defended the stringent quarantine measures, noting that they are in line with those taken by some other nations, and with the aggressive action being taken by the Chinese government itself. “These actions are science based and aimed at protecting the health of all Americans,” she said.
The real-time reverse transcription polymerase chain reaction (rRT-PCR) assay that the CDC has developed detects 2019-nCoV in both respiratory and serum specimens. Dr. Messonnier reported that the CDC is today filing an emergency use authorization (EUA) application to the U.S. Food and Drug Administration to expedite access to the assay for public health laboratories across the country. “This will greatly enhance our capacity to test for this virus,” she said, noting that EUA approval may come as soon as the end of this week.
Although the CDC is poised to send an expert team to China, it’s still awaiting favorable results from the international negotiations currently underway. “This is a horrible situation in China,” said Dr. Messonnier. “Our presence on the ground in China would be a help to China. ... Science should trump everything else; that’s what we’re hoping – that the scientific expertise of the global community can be brought to bear on the incredibly complicated, difficult situation that our colleagues in China are dealing with.”
FROM A CDC PRESS BRIEFING
Who’ll get SAVR in 2020?
SNOWMASS, COLO. – The number of transcatheter aortic valve replacements (TAVRs) performed annually in the United States is forecast to rocket up from 75,000 in 2019 to 100,000 in 2020 in response to the procedure’s recent approval in low-surgical-risk patients with symptomatic aortic stenosis, Michael J. Mack, MD, said at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.

“In 2020, TAVR seems like a tsunami that’s totally overwhelming SAVR [surgical aortic valve replacement]. And the question is, after the wave hits shore, is there going to be anything left in the surgical arena?” asked Dr. Mack, who is medical director of cardiothoracic surgery and chairman of the Baylor Scott & White The Heart Hospital – Plano (Tex.) Research Center.
He answered his own question with a quote from Mark Twain: “Reports of my death are greatly exaggerated.”
The trend is clear: TAVR will take over the market for isolated aortic valve replacement in much the same way that endovascular abdominal aortic aneurysm repair (EVAR) has come to dominate open surgical repair by an 80:20 margin. And By one estimate, it could include some 270,000 individuals per year in North America and the European Union (Eur Heart J. 2018 Jul 21;39[28]:2635-42).
But there’s no need to shed a tear at the prospect of SAVR surgeons standing in unemployment lines. They will continue to have their hands full performing combined SAVR plus coronary artery bypass graft (CABG) procedures, SAVR plus mitral or tricuspid valve operations, and Bentall procedures, Dr. Mack predicted.
Who should get SAVR for aortic stenosis in 2020? For starters, he said, the sorts of patients who were excluded from the major TAVR-versus-SAVR randomized trials. The low-surgical-risk trials were restricted to patients who had symptomatic aortic stenosis involving a tricuspid valve, no left ventricular outflow tract calcium, no or minimal coronary artery disease (CAD), a relatively normal left ventricular ejection fraction, and an aortic valve anatomy suitable for TAVR. And, 92% of study participants were over age 65 years.
Dr. Mack called the evidence for the safety and effectiveness of TAVR “the most robust evidence base in the history of medical devices,” backed by nine U.S. trials and 8,000 randomized patients during the last dozen years. He has played a major role in developing that evidence base, having served most recently as cochair of the landmark PARTNER 3 trial, which demonstrated superiority for TAVR over SAVR in low-surgical-risk patients. But the evidence base doesn’t apply to patients not enrolled in the trials. So for the foreseeable future, patients younger than age 65 years should probably stick with SAVR, mainly because of the still-open question of tissue valve durability and TAVR’s high rate of associated conduction system impairment and need for new pacemaker implantation. Younger patients find permanent pacemakers particularly problematic, he noted.
Others who should stick with surgery include patients with bicuspid valves, especially when aortopathy is present, individuals with low-lying coronary arteries, patients with heavy calcium deposits at the left ventricular outflow tract, those with infective endocarditis or rheumatic valve disease, and patients with structural valve deterioration after a valve-in-valve TAVR.
“Once you get beyond the first valve-in-valve, the outcomes are not going to be good. Those patients should preferentially be considered for surgery. The results for valve-in-valve have been very disappointing, with a 33% all-cause mortality at 3 years in the PARTNER Aortic Valve-in-Valve Registry,” according to the surgeon.
In patients with aortic stenosis and CAD, the clinical decision making should be based on the coronary disease. In a patient with triple-vessel disease, diabetes, and/or a high Syntax score for whom the collaborative multidisciplinary heart team would recommend surgical revascularization if aortic stenosis wasn’t present, the most appropriate option is SAVR plus CABG. On the other hand, if the CAD is amenable to percutaneous coronary intervention (PCI) and the Syntax score is low, TAVR plus PCI is a safe and solid strategy, he continued.
In addition to the unresolved issue of tissue valve durability, another unanswered question pushing against universal adoption of TAVR involves the clinical implications of bioprosthetic valve leaflet thrombosis and the optimal antithrombotic therapy, both early and late. Leaflet thrombosis post-TAVR is common – as well as post-SAVR with bioprosthetic valves, albeit less so – but the lesions often come and go. Although there is a theoretical concern that they might be a precursor to leaflet destruction, at this point, their clinical significance remains unclear. In the recent GALILEO trial, TAVR patients randomized to low-dose rivaroxaban (Xarelto) plus aspirin showed fewer leaflet motion abnormalities and less leaflet thickening than did those on dual-antiplatelet therapy, but a significantly higher all-cause mortality (N Engl J Med 2020 Jan 9;382:120-9).
“I know that nowhere else in the body is thrombus a good thing, so thrombus in the valve can’t be a good thing. The only question is, how bad is it? And right now all we know is, some of our treatments for it are worse than the disease,” the surgeon commented.
Dr. Mack indicated that, at this time, clinical decision making in aortic stenosis should begin on the basis of patient age, which influences the key decision of whether to opt for a mechanical versus tissue replacement valve. For patients aged 50-70 years, shared decision making between the heart team and patient is appropriate. The evidence suggests SAVR with a mechanical valve is the better option, but many patients in this intermediate age group loathe the ideal of lifelong oral anticoagulation and favor a tissue valve.
For patients under age 50 years, the best evidence indicates that SAVR with a mechanical valve is clearly the best option; however, most young patients are instead opting for a tissue valve, even after being cautioned about the lingering uncertainty surrounding tissue valve durability, be it SAVR or TAVR. For patients over age 70 years, a tissue valve is the best choice based on the outcomes in PARTNER 3 and other low-surgical-risk trials. If the patient is younger than 65 years and wants a tissue valve, Dr. Mack thinks the best evidence-based option is SAVR. Above age 80 years, TAVR is the clear choice. Age 65-80 years is shared–decision making territory regarding TAVR versus SAVR.
Dr. Mack reported serving as a consultant to Gore and receiving research grants from Abbott Vascular, Edwards Lifesciences, and Medtronic.
SNOWMASS, COLO. – The number of transcatheter aortic valve replacements (TAVRs) performed annually in the United States is forecast to rocket up from 75,000 in 2019 to 100,000 in 2020 in response to the procedure’s recent approval in low-surgical-risk patients with symptomatic aortic stenosis, Michael J. Mack, MD, said at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
“In 2020, TAVR seems like a tsunami that’s totally overwhelming SAVR [surgical aortic valve replacement]. And the question is, after the wave hits shore, is there going to be anything left in the surgical arena?” asked Dr. Mack, who is medical director of cardiothoracic surgery and chairman of the Baylor Scott & White The Heart Hospital – Plano (Tex.) Research Center.
He answered his own question with a quote from Mark Twain: “Reports of my death are greatly exaggerated.”
The trend is clear: TAVR will take over the market for isolated aortic valve replacement in much the same way that endovascular abdominal aortic aneurysm repair (EVAR) has come to dominate open surgical repair by an 80:20 margin. And By one estimate, it could include some 270,000 individuals per year in North America and the European Union (Eur Heart J. 2018 Jul 21;39[28]:2635-42).
But there’s no need to shed a tear at the prospect of SAVR surgeons standing in unemployment lines. They will continue to have their hands full performing combined SAVR plus coronary artery bypass graft (CABG) procedures, SAVR plus mitral or tricuspid valve operations, and Bentall procedures, Dr. Mack predicted.
Who should get SAVR for aortic stenosis in 2020? For starters, he said, the sorts of patients who were excluded from the major TAVR-versus-SAVR randomized trials. The low-surgical-risk trials were restricted to patients who had symptomatic aortic stenosis involving a tricuspid valve, no left ventricular outflow tract calcium, no or minimal coronary artery disease (CAD), a relatively normal left ventricular ejection fraction, and an aortic valve anatomy suitable for TAVR. And, 92% of study participants were over age 65 years.
Dr. Mack called the evidence for the safety and effectiveness of TAVR “the most robust evidence base in the history of medical devices,” backed by nine U.S. trials and 8,000 randomized patients during the last dozen years. He has played a major role in developing that evidence base, having served most recently as cochair of the landmark PARTNER 3 trial, which demonstrated superiority for TAVR over SAVR in low-surgical-risk patients. But the evidence base doesn’t apply to patients not enrolled in the trials. So for the foreseeable future, patients younger than age 65 years should probably stick with SAVR, mainly because of the still-open question of tissue valve durability and TAVR’s high rate of associated conduction system impairment and need for new pacemaker implantation. Younger patients find permanent pacemakers particularly problematic, he noted.
Others who should stick with surgery include patients with bicuspid valves, especially when aortopathy is present, individuals with low-lying coronary arteries, patients with heavy calcium deposits at the left ventricular outflow tract, those with infective endocarditis or rheumatic valve disease, and patients with structural valve deterioration after a valve-in-valve TAVR.
“Once you get beyond the first valve-in-valve, the outcomes are not going to be good. Those patients should preferentially be considered for surgery. The results for valve-in-valve have been very disappointing, with a 33% all-cause mortality at 3 years in the PARTNER Aortic Valve-in-Valve Registry,” according to the surgeon.
In patients with aortic stenosis and CAD, the clinical decision making should be based on the coronary disease. In a patient with triple-vessel disease, diabetes, and/or a high Syntax score for whom the collaborative multidisciplinary heart team would recommend surgical revascularization if aortic stenosis wasn’t present, the most appropriate option is SAVR plus CABG. On the other hand, if the CAD is amenable to percutaneous coronary intervention (PCI) and the Syntax score is low, TAVR plus PCI is a safe and solid strategy, he continued.
In addition to the unresolved issue of tissue valve durability, another unanswered question pushing against universal adoption of TAVR involves the clinical implications of bioprosthetic valve leaflet thrombosis and the optimal antithrombotic therapy, both early and late. Leaflet thrombosis post-TAVR is common – as well as post-SAVR with bioprosthetic valves, albeit less so – but the lesions often come and go. Although there is a theoretical concern that they might be a precursor to leaflet destruction, at this point, their clinical significance remains unclear. In the recent GALILEO trial, TAVR patients randomized to low-dose rivaroxaban (Xarelto) plus aspirin showed fewer leaflet motion abnormalities and less leaflet thickening than did those on dual-antiplatelet therapy, but a significantly higher all-cause mortality (N Engl J Med 2020 Jan 9;382:120-9).
“I know that nowhere else in the body is thrombus a good thing, so thrombus in the valve can’t be a good thing. The only question is, how bad is it? And right now all we know is, some of our treatments for it are worse than the disease,” the surgeon commented.
Dr. Mack indicated that, at this time, clinical decision making in aortic stenosis should begin on the basis of patient age, which influences the key decision of whether to opt for a mechanical versus tissue replacement valve. For patients aged 50-70 years, shared decision making between the heart team and patient is appropriate. The evidence suggests SAVR with a mechanical valve is the better option, but many patients in this intermediate age group loathe the ideal of lifelong oral anticoagulation and favor a tissue valve.
For patients under age 50 years, the best evidence indicates that SAVR with a mechanical valve is clearly the best option; however, most young patients are instead opting for a tissue valve, even after being cautioned about the lingering uncertainty surrounding tissue valve durability, be it SAVR or TAVR. For patients over age 70 years, a tissue valve is the best choice based on the outcomes in PARTNER 3 and other low-surgical-risk trials. If the patient is younger than 65 years and wants a tissue valve, Dr. Mack thinks the best evidence-based option is SAVR. Above age 80 years, TAVR is the clear choice. Age 65-80 years is shared–decision making territory regarding TAVR versus SAVR.
Dr. Mack reported serving as a consultant to Gore and receiving research grants from Abbott Vascular, Edwards Lifesciences, and Medtronic.
SNOWMASS, COLO. – The number of transcatheter aortic valve replacements (TAVRs) performed annually in the United States is forecast to rocket up from 75,000 in 2019 to 100,000 in 2020 in response to the procedure’s recent approval in low-surgical-risk patients with symptomatic aortic stenosis, Michael J. Mack, MD, said at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
“In 2020, TAVR seems like a tsunami that’s totally overwhelming SAVR [surgical aortic valve replacement]. And the question is, after the wave hits shore, is there going to be anything left in the surgical arena?” asked Dr. Mack, who is medical director of cardiothoracic surgery and chairman of the Baylor Scott & White The Heart Hospital – Plano (Tex.) Research Center.
He answered his own question with a quote from Mark Twain: “Reports of my death are greatly exaggerated.”
The trend is clear: TAVR will take over the market for isolated aortic valve replacement in much the same way that endovascular abdominal aortic aneurysm repair (EVAR) has come to dominate open surgical repair by an 80:20 margin. And By one estimate, it could include some 270,000 individuals per year in North America and the European Union (Eur Heart J. 2018 Jul 21;39[28]:2635-42).
But there’s no need to shed a tear at the prospect of SAVR surgeons standing in unemployment lines. They will continue to have their hands full performing combined SAVR plus coronary artery bypass graft (CABG) procedures, SAVR plus mitral or tricuspid valve operations, and Bentall procedures, Dr. Mack predicted.
Who should get SAVR for aortic stenosis in 2020? For starters, he said, the sorts of patients who were excluded from the major TAVR-versus-SAVR randomized trials. The low-surgical-risk trials were restricted to patients who had symptomatic aortic stenosis involving a tricuspid valve, no left ventricular outflow tract calcium, no or minimal coronary artery disease (CAD), a relatively normal left ventricular ejection fraction, and an aortic valve anatomy suitable for TAVR. And, 92% of study participants were over age 65 years.
Dr. Mack called the evidence for the safety and effectiveness of TAVR “the most robust evidence base in the history of medical devices,” backed by nine U.S. trials and 8,000 randomized patients during the last dozen years. He has played a major role in developing that evidence base, having served most recently as cochair of the landmark PARTNER 3 trial, which demonstrated superiority for TAVR over SAVR in low-surgical-risk patients. But the evidence base doesn’t apply to patients not enrolled in the trials. So for the foreseeable future, patients younger than age 65 years should probably stick with SAVR, mainly because of the still-open question of tissue valve durability and TAVR’s high rate of associated conduction system impairment and need for new pacemaker implantation. Younger patients find permanent pacemakers particularly problematic, he noted.
Others who should stick with surgery include patients with bicuspid valves, especially when aortopathy is present, individuals with low-lying coronary arteries, patients with heavy calcium deposits at the left ventricular outflow tract, those with infective endocarditis or rheumatic valve disease, and patients with structural valve deterioration after a valve-in-valve TAVR.
“Once you get beyond the first valve-in-valve, the outcomes are not going to be good. Those patients should preferentially be considered for surgery. The results for valve-in-valve have been very disappointing, with a 33% all-cause mortality at 3 years in the PARTNER Aortic Valve-in-Valve Registry,” according to the surgeon.
In patients with aortic stenosis and CAD, the clinical decision making should be based on the coronary disease. In a patient with triple-vessel disease, diabetes, and/or a high Syntax score for whom the collaborative multidisciplinary heart team would recommend surgical revascularization if aortic stenosis wasn’t present, the most appropriate option is SAVR plus CABG. On the other hand, if the CAD is amenable to percutaneous coronary intervention (PCI) and the Syntax score is low, TAVR plus PCI is a safe and solid strategy, he continued.
In addition to the unresolved issue of tissue valve durability, another unanswered question pushing against universal adoption of TAVR involves the clinical implications of bioprosthetic valve leaflet thrombosis and the optimal antithrombotic therapy, both early and late. Leaflet thrombosis post-TAVR is common – as well as post-SAVR with bioprosthetic valves, albeit less so – but the lesions often come and go. Although there is a theoretical concern that they might be a precursor to leaflet destruction, at this point, their clinical significance remains unclear. In the recent GALILEO trial, TAVR patients randomized to low-dose rivaroxaban (Xarelto) plus aspirin showed fewer leaflet motion abnormalities and less leaflet thickening than did those on dual-antiplatelet therapy, but a significantly higher all-cause mortality (N Engl J Med 2020 Jan 9;382:120-9).
“I know that nowhere else in the body is thrombus a good thing, so thrombus in the valve can’t be a good thing. The only question is, how bad is it? And right now all we know is, some of our treatments for it are worse than the disease,” the surgeon commented.
Dr. Mack indicated that, at this time, clinical decision making in aortic stenosis should begin on the basis of patient age, which influences the key decision of whether to opt for a mechanical versus tissue replacement valve. For patients aged 50-70 years, shared decision making between the heart team and patient is appropriate. The evidence suggests SAVR with a mechanical valve is the better option, but many patients in this intermediate age group loathe the ideal of lifelong oral anticoagulation and favor a tissue valve.
For patients under age 50 years, the best evidence indicates that SAVR with a mechanical valve is clearly the best option; however, most young patients are instead opting for a tissue valve, even after being cautioned about the lingering uncertainty surrounding tissue valve durability, be it SAVR or TAVR. For patients over age 70 years, a tissue valve is the best choice based on the outcomes in PARTNER 3 and other low-surgical-risk trials. If the patient is younger than 65 years and wants a tissue valve, Dr. Mack thinks the best evidence-based option is SAVR. Above age 80 years, TAVR is the clear choice. Age 65-80 years is shared–decision making territory regarding TAVR versus SAVR.
Dr. Mack reported serving as a consultant to Gore and receiving research grants from Abbott Vascular, Edwards Lifesciences, and Medtronic.
EXPERT ANALYSIS FROM ACC SNOWMASS 2020
Heart rhythm data from wearables confounds EP practice
NATIONAL HARBOR, MD. – or other warnings that flagged a possible cardiac arrhythmia.

While the clinical community has yet to reach an evidence-based consensus on how to deal with this information, or even asymptomatic arrhythmias identified by more standard means, the American public is voting with their wrists. People seem to like collecting and reviewing readouts on their heart rhythm and other vital data, and then they often take their numbers to a physician, especially when their device suggests a possible problem.
“The whole paradigm of ordering a test only if you intend to act on the result has been flipped. People now get what they want directly, and our job is to guide them” after the fact. “You need to teach people what’s actionable and what’s not,” Mintu P. Turakhia, MD, said at the annual International AF Symposium.
“We’re in a situation where the ability of a sensor to detect things is separate from access to the health care system. They are no longer coupled; they are disjointed. People can create their own ICU in their house just by shopping online, but what do we do with this information, whether it’s an irregular heart rhythm or their whole genome?” asked Dr. Turakhia, executive director of the Center for Digital Health at Stanford (Calif.) University and director of cardiac electrophysiology at the VA Palo Alto (Calif.) Health Care System.
“The main challenge is people without a diagnosis who get a notification. How much monitoring should you do until you can say it was a false positive? We don’t know what to do, so we monitor them. People are trying to figure this out.” Dr. Turakhia said. Some people who seek out electrophysiologists this way “may not even have a primary care physician,” he noted.
The potential implications of widespread monitoring for heartbeat irregularities in the general public began to surface in a study that Dr. Turakhia helped run that collected wearable data from nearly 420,000 Americans. Results from the Apple Heart Study showed that, during a median 117 days of monitoring with a smart watch, 2,161 people (0.5%) received a report of an irregular pulse, which led to further investigations that eventually diagnosed atrial fibrillation (AFib) in 153 people of the 450 who underwent follow-up assessment (N Engl J Med. 2019 Nov 14;381[20]:1909-17). These results “raise questions” about the large number of people who underwent follow-up testing who did not have arrhythmia, Dr. Turakhia noted.
“The dissemination of wearables has been quite dramatic, and electrophysiologists end up owning this,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director emeritus of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “I get a ton of calls from people whom I wish never bought a smart watch, and they say ‘I have atrial fibrillation. What do I do?’ ”
To document the growth of this trend, Dr. Turakhia cited results from a survey he collaborated on, run by Stanford and Rock Health, that found a 33% ownership rate among American adults of a wearable device capable of collecting health data, and a 42% rate of people who tracked their health data with a device, app, journal, or log. Both of these rates more than doubled what a similar survey found in 2015.
The cardiac electrophysiology community took a first step toward addressing one aspect of this evolving situation. In early 2020, the Heart Rhythm Society and the Consumer Technology Association jointly issued a guidance document targeted at consumers that walks them through the kinds of information their wearable devices might collect and how to approach this information. The main message: If you have questions or concerns about your data, consult a clinician. What remains in short supply is guidance to clinicians on what to do when they see these patients.
“Until recently, device-detected AFib was the sole purview of electrophysiologists using implanted rhythm-monitoring devices. Now mobile and other devices raise issues [of asymptomatic AFib] for a much broader population,” noted Daniel E. Singer, MD, professor of medicine and epidemiology at Harvard and Massachusetts General Hospital. “The world of device-detected AFib now includes watches.”
Researchers have tried for years to better understand the stroke risk faced by patients with asymptomatic or subclinical AFib that’s detected by an implanted device, as in the ASSERT study of nearly 2,600 patients followed for a median of 2.5 years that found an increased stroke risk when the duration of individual, subclinical AFib episodes surpassed 24 hours (Eur Heart J. 2017 May 1;38[17]:1339-44). More recently, a study of AFib duration collected by implanted cardiac devices in nearly 22,000 Americans showed a relationship between stroke risk and both the duration of AFib episodes and the underlying risk of a person for stroke as measured by their CHA2DS2-VAScscore (Circulation. 2019 Nov 12;140[20]:1639-46). Just under 30% of patients in the study were diagnosed with AFib at entry.
The implications of asymptomatic episodes of AFib have so far been largely studied in people with an implanted cardiac device, which may have limited applicability to wearable users. In addition, the field has not yet fully sorted out the relationships between the duration of individual AFib episodes and overall AFib burden, and a person’s stroke risk and the window of time when the potential stroke-preventing benefits of anticoagulation outweigh its bleeding risk.
The results of trials now in progress that are examining the safety and efficacy of medical interventions designed to avert strokes in patients with asymptomatic AFib “will bear on the use of anticoagulants in a large group of patients,” including people with AFib detected by a wearable, Dr. Singer predicted.
The Apple Heart Study was sponsored Apple. Dr. Turakhia has received funding from Apple, and he has received honoraria or research funding from several other companies. Dr. Ruskin has been a consultant or adviser to several companies, is a steering committee member for Pfizer, and holds equity or options in Portola, Element Science, NewPace, Gilead, and InfoBionic. Dr. Singer has been a consultant and adviser to Boehringer Ingelheim, Bristol-Myers Squibb, Johnson & Johnson, Merck, and Pfizer, and he has received research grants from Bristol-Myers Squibb.
NATIONAL HARBOR, MD. – or other warnings that flagged a possible cardiac arrhythmia.
While the clinical community has yet to reach an evidence-based consensus on how to deal with this information, or even asymptomatic arrhythmias identified by more standard means, the American public is voting with their wrists. People seem to like collecting and reviewing readouts on their heart rhythm and other vital data, and then they often take their numbers to a physician, especially when their device suggests a possible problem.
“The whole paradigm of ordering a test only if you intend to act on the result has been flipped. People now get what they want directly, and our job is to guide them” after the fact. “You need to teach people what’s actionable and what’s not,” Mintu P. Turakhia, MD, said at the annual International AF Symposium.
“We’re in a situation where the ability of a sensor to detect things is separate from access to the health care system. They are no longer coupled; they are disjointed. People can create their own ICU in their house just by shopping online, but what do we do with this information, whether it’s an irregular heart rhythm or their whole genome?” asked Dr. Turakhia, executive director of the Center for Digital Health at Stanford (Calif.) University and director of cardiac electrophysiology at the VA Palo Alto (Calif.) Health Care System.
“The main challenge is people without a diagnosis who get a notification. How much monitoring should you do until you can say it was a false positive? We don’t know what to do, so we monitor them. People are trying to figure this out.” Dr. Turakhia said. Some people who seek out electrophysiologists this way “may not even have a primary care physician,” he noted.
The potential implications of widespread monitoring for heartbeat irregularities in the general public began to surface in a study that Dr. Turakhia helped run that collected wearable data from nearly 420,000 Americans. Results from the Apple Heart Study showed that, during a median 117 days of monitoring with a smart watch, 2,161 people (0.5%) received a report of an irregular pulse, which led to further investigations that eventually diagnosed atrial fibrillation (AFib) in 153 people of the 450 who underwent follow-up assessment (N Engl J Med. 2019 Nov 14;381[20]:1909-17). These results “raise questions” about the large number of people who underwent follow-up testing who did not have arrhythmia, Dr. Turakhia noted.
“The dissemination of wearables has been quite dramatic, and electrophysiologists end up owning this,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director emeritus of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “I get a ton of calls from people whom I wish never bought a smart watch, and they say ‘I have atrial fibrillation. What do I do?’ ”
To document the growth of this trend, Dr. Turakhia cited results from a survey he collaborated on, run by Stanford and Rock Health, that found a 33% ownership rate among American adults of a wearable device capable of collecting health data, and a 42% rate of people who tracked their health data with a device, app, journal, or log. Both of these rates more than doubled what a similar survey found in 2015.
The cardiac electrophysiology community took a first step toward addressing one aspect of this evolving situation. In early 2020, the Heart Rhythm Society and the Consumer Technology Association jointly issued a guidance document targeted at consumers that walks them through the kinds of information their wearable devices might collect and how to approach this information. The main message: If you have questions or concerns about your data, consult a clinician. What remains in short supply is guidance to clinicians on what to do when they see these patients.
“Until recently, device-detected AFib was the sole purview of electrophysiologists using implanted rhythm-monitoring devices. Now mobile and other devices raise issues [of asymptomatic AFib] for a much broader population,” noted Daniel E. Singer, MD, professor of medicine and epidemiology at Harvard and Massachusetts General Hospital. “The world of device-detected AFib now includes watches.”
Researchers have tried for years to better understand the stroke risk faced by patients with asymptomatic or subclinical AFib that’s detected by an implanted device, as in the ASSERT study of nearly 2,600 patients followed for a median of 2.5 years that found an increased stroke risk when the duration of individual, subclinical AFib episodes surpassed 24 hours (Eur Heart J. 2017 May 1;38[17]:1339-44). More recently, a study of AFib duration collected by implanted cardiac devices in nearly 22,000 Americans showed a relationship between stroke risk and both the duration of AFib episodes and the underlying risk of a person for stroke as measured by their CHA2DS2-VAScscore (Circulation. 2019 Nov 12;140[20]:1639-46). Just under 30% of patients in the study were diagnosed with AFib at entry.
The implications of asymptomatic episodes of AFib have so far been largely studied in people with an implanted cardiac device, which may have limited applicability to wearable users. In addition, the field has not yet fully sorted out the relationships between the duration of individual AFib episodes and overall AFib burden, and a person’s stroke risk and the window of time when the potential stroke-preventing benefits of anticoagulation outweigh its bleeding risk.
The results of trials now in progress that are examining the safety and efficacy of medical interventions designed to avert strokes in patients with asymptomatic AFib “will bear on the use of anticoagulants in a large group of patients,” including people with AFib detected by a wearable, Dr. Singer predicted.
The Apple Heart Study was sponsored Apple. Dr. Turakhia has received funding from Apple, and he has received honoraria or research funding from several other companies. Dr. Ruskin has been a consultant or adviser to several companies, is a steering committee member for Pfizer, and holds equity or options in Portola, Element Science, NewPace, Gilead, and InfoBionic. Dr. Singer has been a consultant and adviser to Boehringer Ingelheim, Bristol-Myers Squibb, Johnson & Johnson, Merck, and Pfizer, and he has received research grants from Bristol-Myers Squibb.
NATIONAL HARBOR, MD. – or other warnings that flagged a possible cardiac arrhythmia.
While the clinical community has yet to reach an evidence-based consensus on how to deal with this information, or even asymptomatic arrhythmias identified by more standard means, the American public is voting with their wrists. People seem to like collecting and reviewing readouts on their heart rhythm and other vital data, and then they often take their numbers to a physician, especially when their device suggests a possible problem.
“The whole paradigm of ordering a test only if you intend to act on the result has been flipped. People now get what they want directly, and our job is to guide them” after the fact. “You need to teach people what’s actionable and what’s not,” Mintu P. Turakhia, MD, said at the annual International AF Symposium.
“We’re in a situation where the ability of a sensor to detect things is separate from access to the health care system. They are no longer coupled; they are disjointed. People can create their own ICU in their house just by shopping online, but what do we do with this information, whether it’s an irregular heart rhythm or their whole genome?” asked Dr. Turakhia, executive director of the Center for Digital Health at Stanford (Calif.) University and director of cardiac electrophysiology at the VA Palo Alto (Calif.) Health Care System.
“The main challenge is people without a diagnosis who get a notification. How much monitoring should you do until you can say it was a false positive? We don’t know what to do, so we monitor them. People are trying to figure this out.” Dr. Turakhia said. Some people who seek out electrophysiologists this way “may not even have a primary care physician,” he noted.
The potential implications of widespread monitoring for heartbeat irregularities in the general public began to surface in a study that Dr. Turakhia helped run that collected wearable data from nearly 420,000 Americans. Results from the Apple Heart Study showed that, during a median 117 days of monitoring with a smart watch, 2,161 people (0.5%) received a report of an irregular pulse, which led to further investigations that eventually diagnosed atrial fibrillation (AFib) in 153 people of the 450 who underwent follow-up assessment (N Engl J Med. 2019 Nov 14;381[20]:1909-17). These results “raise questions” about the large number of people who underwent follow-up testing who did not have arrhythmia, Dr. Turakhia noted.
“The dissemination of wearables has been quite dramatic, and electrophysiologists end up owning this,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director emeritus of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “I get a ton of calls from people whom I wish never bought a smart watch, and they say ‘I have atrial fibrillation. What do I do?’ ”
To document the growth of this trend, Dr. Turakhia cited results from a survey he collaborated on, run by Stanford and Rock Health, that found a 33% ownership rate among American adults of a wearable device capable of collecting health data, and a 42% rate of people who tracked their health data with a device, app, journal, or log. Both of these rates more than doubled what a similar survey found in 2015.
The cardiac electrophysiology community took a first step toward addressing one aspect of this evolving situation. In early 2020, the Heart Rhythm Society and the Consumer Technology Association jointly issued a guidance document targeted at consumers that walks them through the kinds of information their wearable devices might collect and how to approach this information. The main message: If you have questions or concerns about your data, consult a clinician. What remains in short supply is guidance to clinicians on what to do when they see these patients.
“Until recently, device-detected AFib was the sole purview of electrophysiologists using implanted rhythm-monitoring devices. Now mobile and other devices raise issues [of asymptomatic AFib] for a much broader population,” noted Daniel E. Singer, MD, professor of medicine and epidemiology at Harvard and Massachusetts General Hospital. “The world of device-detected AFib now includes watches.”
Researchers have tried for years to better understand the stroke risk faced by patients with asymptomatic or subclinical AFib that’s detected by an implanted device, as in the ASSERT study of nearly 2,600 patients followed for a median of 2.5 years that found an increased stroke risk when the duration of individual, subclinical AFib episodes surpassed 24 hours (Eur Heart J. 2017 May 1;38[17]:1339-44). More recently, a study of AFib duration collected by implanted cardiac devices in nearly 22,000 Americans showed a relationship between stroke risk and both the duration of AFib episodes and the underlying risk of a person for stroke as measured by their CHA2DS2-VAScscore (Circulation. 2019 Nov 12;140[20]:1639-46). Just under 30% of patients in the study were diagnosed with AFib at entry.
The implications of asymptomatic episodes of AFib have so far been largely studied in people with an implanted cardiac device, which may have limited applicability to wearable users. In addition, the field has not yet fully sorted out the relationships between the duration of individual AFib episodes and overall AFib burden, and a person’s stroke risk and the window of time when the potential stroke-preventing benefits of anticoagulation outweigh its bleeding risk.
The results of trials now in progress that are examining the safety and efficacy of medical interventions designed to avert strokes in patients with asymptomatic AFib “will bear on the use of anticoagulants in a large group of patients,” including people with AFib detected by a wearable, Dr. Singer predicted.
The Apple Heart Study was sponsored Apple. Dr. Turakhia has received funding from Apple, and he has received honoraria or research funding from several other companies. Dr. Ruskin has been a consultant or adviser to several companies, is a steering committee member for Pfizer, and holds equity or options in Portola, Element Science, NewPace, Gilead, and InfoBionic. Dr. Singer has been a consultant and adviser to Boehringer Ingelheim, Bristol-Myers Squibb, Johnson & Johnson, Merck, and Pfizer, and he has received research grants from Bristol-Myers Squibb.
REPORTING FROM THE AF SYMPOSIUM 2020
Endobronchial ultrasound with aspiration yields most lung lesions
, according to a multisite study of current and former smokers with suspected lung cancer.
Bronchoscopy has long played a role in the identification of lung lesions, but the yield varies according to many factors associated with the lesion and the type of bronchoscopy, and recent studies suggest that the yield may be lower than previously thought, wrote Gerard A. Silvestri, MD, of Medical University of South Carolina, Charleston, and colleagues.
In a study published in Chest, the researchers sought to assess the yield of bronchoscopy based on procedure and characteristics, as well as the physician-calculated pretest probability of cancer.
They conducted a secondary analysis of 687 patients from the AEGIS trial, a prospective 28-site study of current and former smokers who underwent bronchoscopy for suspected lung cancer. Patients under 21, those without a history of smoking, and those with a concurrent cancer or history of lung cancer were excluded. The average age of the participants was 63 years, and two-thirds were male. Of these, 474 had diagnostic bronchoscopies and 213 had nondiagnostic bronchoscopies.
The overall diagnostic yield was 69%. However, the diagnostic yield significantly higher (80%) with the use of EBUS-TBNA, compared with 55% for standard bronchoscopy with biopsy +/– fluoroscopy, 57% for electromagnetic navigation, and 74% for combination procedures.
Patients with diagnostic bronchoscopies were significantly more likely than were those who had nondiagnostic bronchoscopies to have lesions greater than 3 cm (67% vs. 45%), to have central locations (75% vs. 50%), and to have lymphadenopathy (57% vs. 55%).
In addition, yields were significantly higher (77%) for patients whose preprocedure physician-assessed probability of cancer was at least 60%, compared with yields in those whose preprocedure physician-assessed probability of cancer was less than 10% or 10%-60% (44% and 42%, respectively).
The study findings were limited by several factors including the high prevalence of cancer in the study population, a 1-year follow-up that may have missed slow-growing cancers, and lack of data on the presence or absence of a bronchus sign, the researchers noted. However, the results were strengthened by the large size, mixture of sites, and use of multiple technologies and presentations, they said.
The study is the largest to assess diagnostic yields and various bronchoscopy techniques and supports EBUS-TBNA as the most reliable, but patient selection and improved procedural training can help improve diagnostic yields, the researchers emphasized.
“While the overall yield of bronchoscopy is reasonable, EBUS-TBNA is the only technique that reliably provides a diagnosis in those suspected of having lung cancer, likely because the biopsy is targeting a central lymph node and there is direct visualization of the needle passing into the target,” they said. However,“better bronchoscopic technology is needed and there are devices in the development pipeline that promise improved diagnostic yield, though these products will require evaluation through prospective comparative effectiveness trials prior to widespread adoption,” they noted. Clinicians should be prepared to pursue alternatives to bronchoscopy if a diagnosis is unlikely, they concluded.
Dr. Silvestri disclosed research grant awards to his university from Olympus America, Auris robotics, Veracyte, and Veran Medical, as well as consulting fees from Olympus and Auris robotics.
SOURCE: Silvestri GA et al. CHEST. 2020 Jan 21. doi: 10.1016/j.chest.2019.12.024.
, according to a multisite study of current and former smokers with suspected lung cancer.
Bronchoscopy has long played a role in the identification of lung lesions, but the yield varies according to many factors associated with the lesion and the type of bronchoscopy, and recent studies suggest that the yield may be lower than previously thought, wrote Gerard A. Silvestri, MD, of Medical University of South Carolina, Charleston, and colleagues.
In a study published in Chest, the researchers sought to assess the yield of bronchoscopy based on procedure and characteristics, as well as the physician-calculated pretest probability of cancer.
They conducted a secondary analysis of 687 patients from the AEGIS trial, a prospective 28-site study of current and former smokers who underwent bronchoscopy for suspected lung cancer. Patients under 21, those without a history of smoking, and those with a concurrent cancer or history of lung cancer were excluded. The average age of the participants was 63 years, and two-thirds were male. Of these, 474 had diagnostic bronchoscopies and 213 had nondiagnostic bronchoscopies.
The overall diagnostic yield was 69%. However, the diagnostic yield significantly higher (80%) with the use of EBUS-TBNA, compared with 55% for standard bronchoscopy with biopsy +/– fluoroscopy, 57% for electromagnetic navigation, and 74% for combination procedures.
Patients with diagnostic bronchoscopies were significantly more likely than were those who had nondiagnostic bronchoscopies to have lesions greater than 3 cm (67% vs. 45%), to have central locations (75% vs. 50%), and to have lymphadenopathy (57% vs. 55%).
In addition, yields were significantly higher (77%) for patients whose preprocedure physician-assessed probability of cancer was at least 60%, compared with yields in those whose preprocedure physician-assessed probability of cancer was less than 10% or 10%-60% (44% and 42%, respectively).
The study findings were limited by several factors including the high prevalence of cancer in the study population, a 1-year follow-up that may have missed slow-growing cancers, and lack of data on the presence or absence of a bronchus sign, the researchers noted. However, the results were strengthened by the large size, mixture of sites, and use of multiple technologies and presentations, they said.
The study is the largest to assess diagnostic yields and various bronchoscopy techniques and supports EBUS-TBNA as the most reliable, but patient selection and improved procedural training can help improve diagnostic yields, the researchers emphasized.
“While the overall yield of bronchoscopy is reasonable, EBUS-TBNA is the only technique that reliably provides a diagnosis in those suspected of having lung cancer, likely because the biopsy is targeting a central lymph node and there is direct visualization of the needle passing into the target,” they said. However,“better bronchoscopic technology is needed and there are devices in the development pipeline that promise improved diagnostic yield, though these products will require evaluation through prospective comparative effectiveness trials prior to widespread adoption,” they noted. Clinicians should be prepared to pursue alternatives to bronchoscopy if a diagnosis is unlikely, they concluded.
Dr. Silvestri disclosed research grant awards to his university from Olympus America, Auris robotics, Veracyte, and Veran Medical, as well as consulting fees from Olympus and Auris robotics.
SOURCE: Silvestri GA et al. CHEST. 2020 Jan 21. doi: 10.1016/j.chest.2019.12.024.
, according to a multisite study of current and former smokers with suspected lung cancer.
Bronchoscopy has long played a role in the identification of lung lesions, but the yield varies according to many factors associated with the lesion and the type of bronchoscopy, and recent studies suggest that the yield may be lower than previously thought, wrote Gerard A. Silvestri, MD, of Medical University of South Carolina, Charleston, and colleagues.
In a study published in Chest, the researchers sought to assess the yield of bronchoscopy based on procedure and characteristics, as well as the physician-calculated pretest probability of cancer.
They conducted a secondary analysis of 687 patients from the AEGIS trial, a prospective 28-site study of current and former smokers who underwent bronchoscopy for suspected lung cancer. Patients under 21, those without a history of smoking, and those with a concurrent cancer or history of lung cancer were excluded. The average age of the participants was 63 years, and two-thirds were male. Of these, 474 had diagnostic bronchoscopies and 213 had nondiagnostic bronchoscopies.
The overall diagnostic yield was 69%. However, the diagnostic yield significantly higher (80%) with the use of EBUS-TBNA, compared with 55% for standard bronchoscopy with biopsy +/– fluoroscopy, 57% for electromagnetic navigation, and 74% for combination procedures.
Patients with diagnostic bronchoscopies were significantly more likely than were those who had nondiagnostic bronchoscopies to have lesions greater than 3 cm (67% vs. 45%), to have central locations (75% vs. 50%), and to have lymphadenopathy (57% vs. 55%).
In addition, yields were significantly higher (77%) for patients whose preprocedure physician-assessed probability of cancer was at least 60%, compared with yields in those whose preprocedure physician-assessed probability of cancer was less than 10% or 10%-60% (44% and 42%, respectively).
The study findings were limited by several factors including the high prevalence of cancer in the study population, a 1-year follow-up that may have missed slow-growing cancers, and lack of data on the presence or absence of a bronchus sign, the researchers noted. However, the results were strengthened by the large size, mixture of sites, and use of multiple technologies and presentations, they said.
The study is the largest to assess diagnostic yields and various bronchoscopy techniques and supports EBUS-TBNA as the most reliable, but patient selection and improved procedural training can help improve diagnostic yields, the researchers emphasized.
“While the overall yield of bronchoscopy is reasonable, EBUS-TBNA is the only technique that reliably provides a diagnosis in those suspected of having lung cancer, likely because the biopsy is targeting a central lymph node and there is direct visualization of the needle passing into the target,” they said. However,“better bronchoscopic technology is needed and there are devices in the development pipeline that promise improved diagnostic yield, though these products will require evaluation through prospective comparative effectiveness trials prior to widespread adoption,” they noted. Clinicians should be prepared to pursue alternatives to bronchoscopy if a diagnosis is unlikely, they concluded.
Dr. Silvestri disclosed research grant awards to his university from Olympus America, Auris robotics, Veracyte, and Veran Medical, as well as consulting fees from Olympus and Auris robotics.
SOURCE: Silvestri GA et al. CHEST. 2020 Jan 21. doi: 10.1016/j.chest.2019.12.024.
FROM CHEST
Physician groups push back on Medicaid block grant plan
It took less than a day for physician groups to start pushing back at the Centers for Medicare & Medicaid Services over its new Medicaid block grant plan, which was introduced on Jan. 30.
Dubbed “Healthy Adult Opportunity,” the agency is offering all states the chance to participate in a block grant program through the 1115 waiver process.
According to a fact sheet issued by the agency, the program will focus on “adults under age 65 who are not eligible for Medicaid on the basis of disability or their need for long term care services and supports, and who are not eligible under a state plan. Other very low-income parents, children, pregnant women, elderly adults, and people eligible on the basis of a disability will not be directly affected – except from the improvement that results from states reinvesting savings into strengthening their overall programs.”
States will be operating within a defined budget when participating in the program and expenditures exceeding that defined budget will not be eligible for additional federal funding. Budgets will be based on a state’s historic costs, as well as national and regional trends, and will be tied to inflation with the potential to have adjustments made for extraordinary events. States can set their baseline using the prior year’s total spending or a per-enrollee spending model.
A Jan. 30 letter to state Medicaid directors notes that states participating in the program “will be granted extensive flexibility to test alternative approaches to implementing their Medicaid programs, including the ability to make many ongoing program adjustments without the need for demonstration or state plan amendments that require prior approval.”
Among the activities states can engage in under this plan are adjusting cost-sharing requirements, adopting a closed formulary, and applying additional conditions of eligibility. Requests, if approved, will be approved for a 5-year initial period, with a renewal option of up to 10 years.
But physician groups are not seeing a benefit with this new block grant program.
“Moving to a block grant system will likely limit the ability of Medicaid patients to receive preventive and needed medical care from their family physicians, and it will only increase the health disparities that exist in these communities, worsen overall health outcomes, and ultimately increase costs,” Gary LeRoy, MD, president of the American Academy of Family Physicians, said in a statement.
The American Medical Association concurred.
“The AMA opposes caps on federal Medicaid funding, such as block grants, because they would increase the number of uninsured and undermine Medicaid’s role as an indispensable safety net,” Patrice Harris, MD, the AMA’s president, said in a statement. “The AMA supports flexibility in Medicaid and encourages CMS to work with states to develop and test new Medicaid models that best meet the needs and priorities of low-income patients. While encouraging flexibility, the AMA is mindful that expanding Medicaid has been a literal lifesaver for low-income patients. We need to find ways to build on this success. We look forward to reviewing the proposal in detail.”
Officials at the American College of Obstetricians and Gynecologists said the changes have the potential to harm women and children’s health, as well as negatively impact physician reimbursement and ultimately access to care.
“Limits on the federal contribution to the Medicaid program would negatively impact patients by forcing states to reduce the number of people who are eligible for Medicaid coverage, eliminate covered services, and increase beneficiary cost-sharing,” ACOG President Ted Anderson, MD, said in a statement. “ACOG is also concerned that this block grant opportunity could lower physician reimbursement for certain services, forcing providers out of the program and jeopardizing patients’ ability to access health care services. Given our nation’s stark rates of maternal mortality and severe maternal morbidity, we are alarmed by the Administration’s willingness to weaken physician payment in Medicaid.”
It took less than a day for physician groups to start pushing back at the Centers for Medicare & Medicaid Services over its new Medicaid block grant plan, which was introduced on Jan. 30.
Dubbed “Healthy Adult Opportunity,” the agency is offering all states the chance to participate in a block grant program through the 1115 waiver process.
According to a fact sheet issued by the agency, the program will focus on “adults under age 65 who are not eligible for Medicaid on the basis of disability or their need for long term care services and supports, and who are not eligible under a state plan. Other very low-income parents, children, pregnant women, elderly adults, and people eligible on the basis of a disability will not be directly affected – except from the improvement that results from states reinvesting savings into strengthening their overall programs.”
States will be operating within a defined budget when participating in the program and expenditures exceeding that defined budget will not be eligible for additional federal funding. Budgets will be based on a state’s historic costs, as well as national and regional trends, and will be tied to inflation with the potential to have adjustments made for extraordinary events. States can set their baseline using the prior year’s total spending or a per-enrollee spending model.
A Jan. 30 letter to state Medicaid directors notes that states participating in the program “will be granted extensive flexibility to test alternative approaches to implementing their Medicaid programs, including the ability to make many ongoing program adjustments without the need for demonstration or state plan amendments that require prior approval.”
Among the activities states can engage in under this plan are adjusting cost-sharing requirements, adopting a closed formulary, and applying additional conditions of eligibility. Requests, if approved, will be approved for a 5-year initial period, with a renewal option of up to 10 years.
But physician groups are not seeing a benefit with this new block grant program.
“Moving to a block grant system will likely limit the ability of Medicaid patients to receive preventive and needed medical care from their family physicians, and it will only increase the health disparities that exist in these communities, worsen overall health outcomes, and ultimately increase costs,” Gary LeRoy, MD, president of the American Academy of Family Physicians, said in a statement.
The American Medical Association concurred.
“The AMA opposes caps on federal Medicaid funding, such as block grants, because they would increase the number of uninsured and undermine Medicaid’s role as an indispensable safety net,” Patrice Harris, MD, the AMA’s president, said in a statement. “The AMA supports flexibility in Medicaid and encourages CMS to work with states to develop and test new Medicaid models that best meet the needs and priorities of low-income patients. While encouraging flexibility, the AMA is mindful that expanding Medicaid has been a literal lifesaver for low-income patients. We need to find ways to build on this success. We look forward to reviewing the proposal in detail.”
Officials at the American College of Obstetricians and Gynecologists said the changes have the potential to harm women and children’s health, as well as negatively impact physician reimbursement and ultimately access to care.
“Limits on the federal contribution to the Medicaid program would negatively impact patients by forcing states to reduce the number of people who are eligible for Medicaid coverage, eliminate covered services, and increase beneficiary cost-sharing,” ACOG President Ted Anderson, MD, said in a statement. “ACOG is also concerned that this block grant opportunity could lower physician reimbursement for certain services, forcing providers out of the program and jeopardizing patients’ ability to access health care services. Given our nation’s stark rates of maternal mortality and severe maternal morbidity, we are alarmed by the Administration’s willingness to weaken physician payment in Medicaid.”
It took less than a day for physician groups to start pushing back at the Centers for Medicare & Medicaid Services over its new Medicaid block grant plan, which was introduced on Jan. 30.
Dubbed “Healthy Adult Opportunity,” the agency is offering all states the chance to participate in a block grant program through the 1115 waiver process.
According to a fact sheet issued by the agency, the program will focus on “adults under age 65 who are not eligible for Medicaid on the basis of disability or their need for long term care services and supports, and who are not eligible under a state plan. Other very low-income parents, children, pregnant women, elderly adults, and people eligible on the basis of a disability will not be directly affected – except from the improvement that results from states reinvesting savings into strengthening their overall programs.”
States will be operating within a defined budget when participating in the program and expenditures exceeding that defined budget will not be eligible for additional federal funding. Budgets will be based on a state’s historic costs, as well as national and regional trends, and will be tied to inflation with the potential to have adjustments made for extraordinary events. States can set their baseline using the prior year’s total spending or a per-enrollee spending model.
A Jan. 30 letter to state Medicaid directors notes that states participating in the program “will be granted extensive flexibility to test alternative approaches to implementing their Medicaid programs, including the ability to make many ongoing program adjustments without the need for demonstration or state plan amendments that require prior approval.”
Among the activities states can engage in under this plan are adjusting cost-sharing requirements, adopting a closed formulary, and applying additional conditions of eligibility. Requests, if approved, will be approved for a 5-year initial period, with a renewal option of up to 10 years.
But physician groups are not seeing a benefit with this new block grant program.
“Moving to a block grant system will likely limit the ability of Medicaid patients to receive preventive and needed medical care from their family physicians, and it will only increase the health disparities that exist in these communities, worsen overall health outcomes, and ultimately increase costs,” Gary LeRoy, MD, president of the American Academy of Family Physicians, said in a statement.
The American Medical Association concurred.
“The AMA opposes caps on federal Medicaid funding, such as block grants, because they would increase the number of uninsured and undermine Medicaid’s role as an indispensable safety net,” Patrice Harris, MD, the AMA’s president, said in a statement. “The AMA supports flexibility in Medicaid and encourages CMS to work with states to develop and test new Medicaid models that best meet the needs and priorities of low-income patients. While encouraging flexibility, the AMA is mindful that expanding Medicaid has been a literal lifesaver for low-income patients. We need to find ways to build on this success. We look forward to reviewing the proposal in detail.”
Officials at the American College of Obstetricians and Gynecologists said the changes have the potential to harm women and children’s health, as well as negatively impact physician reimbursement and ultimately access to care.
“Limits on the federal contribution to the Medicaid program would negatively impact patients by forcing states to reduce the number of people who are eligible for Medicaid coverage, eliminate covered services, and increase beneficiary cost-sharing,” ACOG President Ted Anderson, MD, said in a statement. “ACOG is also concerned that this block grant opportunity could lower physician reimbursement for certain services, forcing providers out of the program and jeopardizing patients’ ability to access health care services. Given our nation’s stark rates of maternal mortality and severe maternal morbidity, we are alarmed by the Administration’s willingness to weaken physician payment in Medicaid.”
Colorectal cancer cases spike after start of routine screening
Incidence of colorectal cancer spiked among adults in the United States between the ages of 49 and 50 years, the age when many have routine screening colonoscopies, based on data from a cross-sectional study of 165,160 patients.
“We would expect to see some degree of CRC incidence increase from 49 to 50 years of age owing to screening uptake and diagnosis of preexisting CRCs that may have been clinically undetected,” wrote Wesal H. Abualkhair, MD, of Tulane University, New Orleans, and colleagues.
In a study published in JAMA Network Open, the researchers reviewed data from the Surveillance, Epidemiology, and End Results (SEER) registries from 2000 to 2015 on colorectal cancer incidence in 1-year intervals for adults aged 30-60 years, focusing on the year between ages 49 and 50.
Overall, the incidence of colorectal cancer increased by 46.1% from 49 to 50 years of age, and 93% of these cases were invasive.
The increase in cancer rates occurred across geographical regions, sex, and race, and likely reflects the impact of screening rather than advancing age, the researchers said.
They also found a significant increase in 5-year relative survival (6.9% absolute increase, 10% relative increase) for the transition between 49 and 50 years of age; no other age transitions showed a significant change.
The findings were limited by several factors, including the lack of specific outcomes data and inability to determine the number of years that the cancers existed before diagnosis, the researchers said. However, the results were strengthened by the large study population and detailed yearly assessment.
“Our analysis of the transition from 49 to 50 years provides new, registry-based data regarding risk among individuals younger than 50 years, which can add to preexisting modeling studies to help inform decision-making on the age at which to initiate screening,” the researchers said.
The study did not receive outside funding. Lead author Dr. Abualkhair had no financial conflicts to disclose.
SOURCE: Abualkhair WH et al. JAMA Network Open. 2020 Jan 31. doi: 10.1001/jamanetworkopen.2019.20407.
Incidence of colorectal cancer spiked among adults in the United States between the ages of 49 and 50 years, the age when many have routine screening colonoscopies, based on data from a cross-sectional study of 165,160 patients.
“We would expect to see some degree of CRC incidence increase from 49 to 50 years of age owing to screening uptake and diagnosis of preexisting CRCs that may have been clinically undetected,” wrote Wesal H. Abualkhair, MD, of Tulane University, New Orleans, and colleagues.
In a study published in JAMA Network Open, the researchers reviewed data from the Surveillance, Epidemiology, and End Results (SEER) registries from 2000 to 2015 on colorectal cancer incidence in 1-year intervals for adults aged 30-60 years, focusing on the year between ages 49 and 50.
Overall, the incidence of colorectal cancer increased by 46.1% from 49 to 50 years of age, and 93% of these cases were invasive.
The increase in cancer rates occurred across geographical regions, sex, and race, and likely reflects the impact of screening rather than advancing age, the researchers said.
They also found a significant increase in 5-year relative survival (6.9% absolute increase, 10% relative increase) for the transition between 49 and 50 years of age; no other age transitions showed a significant change.
The findings were limited by several factors, including the lack of specific outcomes data and inability to determine the number of years that the cancers existed before diagnosis, the researchers said. However, the results were strengthened by the large study population and detailed yearly assessment.
“Our analysis of the transition from 49 to 50 years provides new, registry-based data regarding risk among individuals younger than 50 years, which can add to preexisting modeling studies to help inform decision-making on the age at which to initiate screening,” the researchers said.
The study did not receive outside funding. Lead author Dr. Abualkhair had no financial conflicts to disclose.
SOURCE: Abualkhair WH et al. JAMA Network Open. 2020 Jan 31. doi: 10.1001/jamanetworkopen.2019.20407.
Incidence of colorectal cancer spiked among adults in the United States between the ages of 49 and 50 years, the age when many have routine screening colonoscopies, based on data from a cross-sectional study of 165,160 patients.
“We would expect to see some degree of CRC incidence increase from 49 to 50 years of age owing to screening uptake and diagnosis of preexisting CRCs that may have been clinically undetected,” wrote Wesal H. Abualkhair, MD, of Tulane University, New Orleans, and colleagues.
In a study published in JAMA Network Open, the researchers reviewed data from the Surveillance, Epidemiology, and End Results (SEER) registries from 2000 to 2015 on colorectal cancer incidence in 1-year intervals for adults aged 30-60 years, focusing on the year between ages 49 and 50.
Overall, the incidence of colorectal cancer increased by 46.1% from 49 to 50 years of age, and 93% of these cases were invasive.
The increase in cancer rates occurred across geographical regions, sex, and race, and likely reflects the impact of screening rather than advancing age, the researchers said.
They also found a significant increase in 5-year relative survival (6.9% absolute increase, 10% relative increase) for the transition between 49 and 50 years of age; no other age transitions showed a significant change.
The findings were limited by several factors, including the lack of specific outcomes data and inability to determine the number of years that the cancers existed before diagnosis, the researchers said. However, the results were strengthened by the large study population and detailed yearly assessment.
“Our analysis of the transition from 49 to 50 years provides new, registry-based data regarding risk among individuals younger than 50 years, which can add to preexisting modeling studies to help inform decision-making on the age at which to initiate screening,” the researchers said.
The study did not receive outside funding. Lead author Dr. Abualkhair had no financial conflicts to disclose.
SOURCE: Abualkhair WH et al. JAMA Network Open. 2020 Jan 31. doi: 10.1001/jamanetworkopen.2019.20407.
FROM JAMA NETWORK OPEN
Walk test may predict complications after lung cancer surgery
Risk of cardiopulmonary complications increased nearly eightfold in patients with moderate lung function decreases who failed to walk 400 m or more, according to the study, which included data on 416 patients with non–small cell lung cancer (NSCLC) who underwent lobectomy.
This is believed to be the first large study evaluating the utility of the 6-minute walk test (6MWT) to predict postoperative cardiopulmonary complications in this surgical setting, according to researchers led by Hyun Lee, MD, of Hanyang University in Seoul, South Korea.
“Our findings suggest that 6-minute walk distance would provide additional information in lung cancer patients with moderately decreased lung function who plan to undergo surgical resection,” said Dr. Lee and coauthors of the study report, which appears in CHEST.
More specifically, the option of curative resection should be considered in those lung cancer patients with moderately decreased lung function but a longer 6-minute walk distance, they added.
Exercise testing is currently recommended to further stratify risk of postoperative complications among patient with moderately decreased lung function, according to the researchers. The 6-minute walk test might be a good tool to evaluate feasibility for moderate risk patients, according to one recent review. However, studies so far have been limited by small numbers of patients, and larger studies have not specifically looked at predicted postoperative lung function status, they said.
Accordingly, the researchers evaluated data from patients expected to undergo curative lung cancer surgery who were enrolled in a prospective cohort study in Korea. They were classified as low or moderate risk based on pulmonary function tests, and further classified into short distance (less than 400 m) and long distance (400 m or more) groups based on their performance on the 6-minute walk test.
Postoperative cardiopulmonary complications were seen in 42.9% of the moderate-risk, short-distance group, versus 14.4% of patients in the moderate-risk, long-distance group. In the low-risk patients, those complications were seen in 9.5% and 8.3% of those in the long and short distance groups.
Odds for postoperative cardiopulmonary complications were significantly increased in the moderate-risk, short-distance group, compared with the low-risk, long-distance group (adjusted odds ratio, 7.84; 95% confidence interval, 2.24-27.46).
By contrast, odds for complications were not significantly increased in the moderate-risk, long-distance group, nor in the low-risk, short-distance groups, investigators said.
Dr. Lee and coauthors said they had no conflicts of interest to disclose.
SOURCE: Lee H et al. CHEST. 2020. doi: 10.1016/j.chest.2019.12.039.
Risk of cardiopulmonary complications increased nearly eightfold in patients with moderate lung function decreases who failed to walk 400 m or more, according to the study, which included data on 416 patients with non–small cell lung cancer (NSCLC) who underwent lobectomy.
This is believed to be the first large study evaluating the utility of the 6-minute walk test (6MWT) to predict postoperative cardiopulmonary complications in this surgical setting, according to researchers led by Hyun Lee, MD, of Hanyang University in Seoul, South Korea.
“Our findings suggest that 6-minute walk distance would provide additional information in lung cancer patients with moderately decreased lung function who plan to undergo surgical resection,” said Dr. Lee and coauthors of the study report, which appears in CHEST.
More specifically, the option of curative resection should be considered in those lung cancer patients with moderately decreased lung function but a longer 6-minute walk distance, they added.
Exercise testing is currently recommended to further stratify risk of postoperative complications among patient with moderately decreased lung function, according to the researchers. The 6-minute walk test might be a good tool to evaluate feasibility for moderate risk patients, according to one recent review. However, studies so far have been limited by small numbers of patients, and larger studies have not specifically looked at predicted postoperative lung function status, they said.
Accordingly, the researchers evaluated data from patients expected to undergo curative lung cancer surgery who were enrolled in a prospective cohort study in Korea. They were classified as low or moderate risk based on pulmonary function tests, and further classified into short distance (less than 400 m) and long distance (400 m or more) groups based on their performance on the 6-minute walk test.
Postoperative cardiopulmonary complications were seen in 42.9% of the moderate-risk, short-distance group, versus 14.4% of patients in the moderate-risk, long-distance group. In the low-risk patients, those complications were seen in 9.5% and 8.3% of those in the long and short distance groups.
Odds for postoperative cardiopulmonary complications were significantly increased in the moderate-risk, short-distance group, compared with the low-risk, long-distance group (adjusted odds ratio, 7.84; 95% confidence interval, 2.24-27.46).
By contrast, odds for complications were not significantly increased in the moderate-risk, long-distance group, nor in the low-risk, short-distance groups, investigators said.
Dr. Lee and coauthors said they had no conflicts of interest to disclose.
SOURCE: Lee H et al. CHEST. 2020. doi: 10.1016/j.chest.2019.12.039.
Risk of cardiopulmonary complications increased nearly eightfold in patients with moderate lung function decreases who failed to walk 400 m or more, according to the study, which included data on 416 patients with non–small cell lung cancer (NSCLC) who underwent lobectomy.
This is believed to be the first large study evaluating the utility of the 6-minute walk test (6MWT) to predict postoperative cardiopulmonary complications in this surgical setting, according to researchers led by Hyun Lee, MD, of Hanyang University in Seoul, South Korea.
“Our findings suggest that 6-minute walk distance would provide additional information in lung cancer patients with moderately decreased lung function who plan to undergo surgical resection,” said Dr. Lee and coauthors of the study report, which appears in CHEST.
More specifically, the option of curative resection should be considered in those lung cancer patients with moderately decreased lung function but a longer 6-minute walk distance, they added.
Exercise testing is currently recommended to further stratify risk of postoperative complications among patient with moderately decreased lung function, according to the researchers. The 6-minute walk test might be a good tool to evaluate feasibility for moderate risk patients, according to one recent review. However, studies so far have been limited by small numbers of patients, and larger studies have not specifically looked at predicted postoperative lung function status, they said.
Accordingly, the researchers evaluated data from patients expected to undergo curative lung cancer surgery who were enrolled in a prospective cohort study in Korea. They were classified as low or moderate risk based on pulmonary function tests, and further classified into short distance (less than 400 m) and long distance (400 m or more) groups based on their performance on the 6-minute walk test.
Postoperative cardiopulmonary complications were seen in 42.9% of the moderate-risk, short-distance group, versus 14.4% of patients in the moderate-risk, long-distance group. In the low-risk patients, those complications were seen in 9.5% and 8.3% of those in the long and short distance groups.
Odds for postoperative cardiopulmonary complications were significantly increased in the moderate-risk, short-distance group, compared with the low-risk, long-distance group (adjusted odds ratio, 7.84; 95% confidence interval, 2.24-27.46).
By contrast, odds for complications were not significantly increased in the moderate-risk, long-distance group, nor in the low-risk, short-distance groups, investigators said.
Dr. Lee and coauthors said they had no conflicts of interest to disclose.
SOURCE: Lee H et al. CHEST. 2020. doi: 10.1016/j.chest.2019.12.039.
FROM CHEST
Don’t forget about the flu: 2019-2010 season is not over
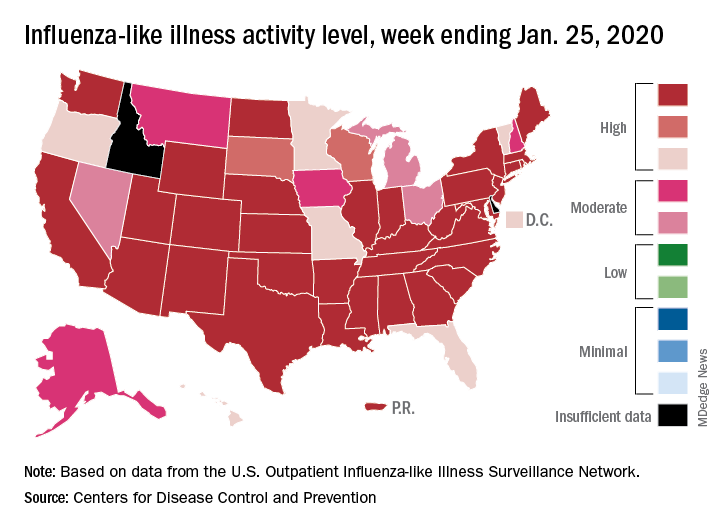
Nationally, an estimated 5.7% of all outpatients visiting health care providers had influenza-like illness (ILI) for the week ending Jan. 25, which was up from 5.1% the previous week but still lower than the current seasonal high of 7.1% recorded during the week of Dec. 22-28, the CDC’s influenza division reported.
Another key indicator of influenza activity, the percentage of respiratory specimens testing positive, also remains high as it rose from 25.7% the week before to 27.7% for the week ending Jan. 25, the influenza division said. That is the highest rate of the 2019-2020 season so far, surpassing the 26.8% reached during Dec. 22-28.
Another new seasonal high involves the number of states, 33 plus Puerto Rico, at the highest level of ILI activity on the CDC’s 1-10 scale for the latest reporting week, topping the 32 jurisdictions from the last full week of December. Another eight states and the District of Columbia were in the “high” range with activity levels of 8 and 9, and no state with available data was lower than level 6, the CDC data show.
Going along with the recent 2-week increase in activity is a large increase in the number of ILI-related pediatric deaths, which rose from 39 on Jan. 11 to the current count of 68, the CDC said. At the same point last year, there had been 36 pediatric deaths.
Other indicators of ILI severity, however, “are not high at this point in the season,” the influenza division noted. “Overall, hospitalization rates remain similar to what has been seen at this time during recent seasons, but rates among children and young adults are higher at this time than in recent seasons.” Overall pneumonia and influenza mortality is also low, the CDC added.
Nationally, an estimated 5.7% of all outpatients visiting health care providers had influenza-like illness (ILI) for the week ending Jan. 25, which was up from 5.1% the previous week but still lower than the current seasonal high of 7.1% recorded during the week of Dec. 22-28, the CDC’s influenza division reported.
Another key indicator of influenza activity, the percentage of respiratory specimens testing positive, also remains high as it rose from 25.7% the week before to 27.7% for the week ending Jan. 25, the influenza division said. That is the highest rate of the 2019-2020 season so far, surpassing the 26.8% reached during Dec. 22-28.
Another new seasonal high involves the number of states, 33 plus Puerto Rico, at the highest level of ILI activity on the CDC’s 1-10 scale for the latest reporting week, topping the 32 jurisdictions from the last full week of December. Another eight states and the District of Columbia were in the “high” range with activity levels of 8 and 9, and no state with available data was lower than level 6, the CDC data show.
Going along with the recent 2-week increase in activity is a large increase in the number of ILI-related pediatric deaths, which rose from 39 on Jan. 11 to the current count of 68, the CDC said. At the same point last year, there had been 36 pediatric deaths.
Other indicators of ILI severity, however, “are not high at this point in the season,” the influenza division noted. “Overall, hospitalization rates remain similar to what has been seen at this time during recent seasons, but rates among children and young adults are higher at this time than in recent seasons.” Overall pneumonia and influenza mortality is also low, the CDC added.
Nationally, an estimated 5.7% of all outpatients visiting health care providers had influenza-like illness (ILI) for the week ending Jan. 25, which was up from 5.1% the previous week but still lower than the current seasonal high of 7.1% recorded during the week of Dec. 22-28, the CDC’s influenza division reported.
Another key indicator of influenza activity, the percentage of respiratory specimens testing positive, also remains high as it rose from 25.7% the week before to 27.7% for the week ending Jan. 25, the influenza division said. That is the highest rate of the 2019-2020 season so far, surpassing the 26.8% reached during Dec. 22-28.
Another new seasonal high involves the number of states, 33 plus Puerto Rico, at the highest level of ILI activity on the CDC’s 1-10 scale for the latest reporting week, topping the 32 jurisdictions from the last full week of December. Another eight states and the District of Columbia were in the “high” range with activity levels of 8 and 9, and no state with available data was lower than level 6, the CDC data show.
Going along with the recent 2-week increase in activity is a large increase in the number of ILI-related pediatric deaths, which rose from 39 on Jan. 11 to the current count of 68, the CDC said. At the same point last year, there had been 36 pediatric deaths.
Other indicators of ILI severity, however, “are not high at this point in the season,” the influenza division noted. “Overall, hospitalization rates remain similar to what has been seen at this time during recent seasons, but rates among children and young adults are higher at this time than in recent seasons.” Overall pneumonia and influenza mortality is also low, the CDC added.
High cost of wound dressings for epidermolysis bullosa highlighted
LONDON – More than £2.8 million (RDEB), according to a report at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA).

Results from the Prospective Epidermolysis Bullosa Longitudinal Evaluation Study (PEBLES), which is looking at the natural history of RDEB, showed that wound dressing and bandage costs were highest for study participants with the generalized severe (RDEB-GS) subtype, at just over £85,156 (about $112,450) per patient annually. Respective yearly costs for the generalized intermediate (RDEB-GI) and inversa (RDEB-INV) subtypes were £10,112 (about $13,350) and £1,699 (about $2,240) per patient.
Looking at the costs associated with EB is important, said one of the lead investigators for PEBLES, Jemima Mellerio, MD, FRCP, consultant dermatologist at St John’s Institute of Dermatology, at Guy’s & St. Thomas’ NHS Foundation Trust, London.
“If we are going to justify the kind of expenditure [associated with new treatments], we need to know that what we are treating is already a significant burden on our health care systems,” Dr. Mellerio said.
PEBLES is an ongoing London-based registry study that is enrolling patients with all subtypes of RDEB. Data are collected via a tablet device and include demographic data, information on clinical features, results of skin biopsies and genetic tests, and laboratory findings, as well as objective disease severity and subjective patient-orientated outcome scores.
So far, 60 patients – 49 adults and 11 children – have been enrolled in PEBLES since November 2014: 26 with RDEB-GS, 23 with RDEB-GI, 9 with RDEB-INV, and 2 with the pruriginosa RDEB subtype (RDEB-PR).
Most of the participants (71%) changed all their wound dressings at one time, patching up when required. Fourteen of 49 participants had paid people to help them change their dressings and when the total cost of combined wound dressings and paid care was taken into consideration, the mean annual cost per patient was around £2,500 (about $3,300) for RDEB-INV, £10,375 (about $13,700) per patient for RDEB-GS, and a staggering £98,000 (about $129,000) per patient for RDEB-GS. The total annual cost of dressings and associated care was an estimated £3,184,229 (about $4.2 million).
In addition to data on the cost of wound dressings, data on itch and pain and quality of life were presented at the EB World Congress and discussed by Dr. Mellerio.
A total of 42 participants older than 8 years of age had itch measured via the Leuven Itch Scale, she reported, noting that itch was a consistent symptom across all subtypes of RDEB. Itch is important as it not only causes problems with skin lesions and healing, but also significantly affects sleep and has a negative impact on patients’ mood, she emphasized.

Despite experiencing itch, more than half (58%) of participants were not using any kind of treatment for itch. This “likely reflects the lack of effectiveness of current medication for this debilitating symptom,” Dr. Mellerio and associates noted in one of their poster presentations of PEBLES data.
When treatment was used for itch, it consisted mainly of antihistamines (19% of patients), emollients (19%), or a combination of both (4%). However, treatment was generally “not very good,” with a satisfaction score of just 5 on a scale of 10, Dr. Mellerio pointed out. Participants “reported frustration with the lack of effective treatment for itch,” she said.
Itch was associated with disturbed sleep 1-3 nights per week in 20%-40% of participants, and every night in 20%-30%.
Pain was found to be a significant problem, with a median level of background pain scored as 4 on a 10-cm visual analog scale and a higher level (6) when associated with dressing changes.
Data on how RDEB affected quality of life were reported for 39 adults completing the 17-item Quality of Life in EB Questionnaire (QOLEB) and eight children who were able to complete the Pediatric Quality of Life Inventory (PedsQL) with the aid of their parents.
Dr. Mellerio reported that adults with RDEB-GS had an overall QOLEB score of 24 out of 50, an indication that their condition had a severe impact on their quality of life. The effect on quality of life was greater in terms of their physical functioning than emotional well-being, with respective scores of 19 out of 36, and 5 out of a possible 15. Less impact on quality of life was reported by participants with other RDEB subtypes.
PedsQL scores for the children indicated there might be a lesser effect of physical functioning on quality of life but a greater effect of emotional well-being on quality of life, but the numbers were small. “Interestingly, parents tended to rate their children’s impact on quality of life much higher than the children themselves,” Dr. Mellerio said.
The point of PEBLES is to start to understand the natural history of RDEB and to identify endpoints that might help in clinical trials of potential new treatments. Discussing the next steps for PEBLES, Dr. Mellerio said the aim was to recruit more pediatric patients and look at other data sets, such as bone health. The PEBLES team also hopes to extend recruitment to include other United Kingdom, and ultimately international, EB centers and, perhaps eventually to start to include other types of EB, such as EB simplex.
PEBLES is funded by DEBRA UK. Dr. Mellerio is a PEBLES investigator but had no conflicts of interest to disclose.
SOURCE: Mellerio JE et al. EB 2020. Pillay EI et al. Poster 77; Jeffs E et al. Poster 74; Jeffs et al. Poster 75. https://ebworldcongress.org/.
LONDON – More than £2.8 million (RDEB), according to a report at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA).
Results from the Prospective Epidermolysis Bullosa Longitudinal Evaluation Study (PEBLES), which is looking at the natural history of RDEB, showed that wound dressing and bandage costs were highest for study participants with the generalized severe (RDEB-GS) subtype, at just over £85,156 (about $112,450) per patient annually. Respective yearly costs for the generalized intermediate (RDEB-GI) and inversa (RDEB-INV) subtypes were £10,112 (about $13,350) and £1,699 (about $2,240) per patient.
Looking at the costs associated with EB is important, said one of the lead investigators for PEBLES, Jemima Mellerio, MD, FRCP, consultant dermatologist at St John’s Institute of Dermatology, at Guy’s & St. Thomas’ NHS Foundation Trust, London.
“If we are going to justify the kind of expenditure [associated with new treatments], we need to know that what we are treating is already a significant burden on our health care systems,” Dr. Mellerio said.
PEBLES is an ongoing London-based registry study that is enrolling patients with all subtypes of RDEB. Data are collected via a tablet device and include demographic data, information on clinical features, results of skin biopsies and genetic tests, and laboratory findings, as well as objective disease severity and subjective patient-orientated outcome scores.
So far, 60 patients – 49 adults and 11 children – have been enrolled in PEBLES since November 2014: 26 with RDEB-GS, 23 with RDEB-GI, 9 with RDEB-INV, and 2 with the pruriginosa RDEB subtype (RDEB-PR).
Most of the participants (71%) changed all their wound dressings at one time, patching up when required. Fourteen of 49 participants had paid people to help them change their dressings and when the total cost of combined wound dressings and paid care was taken into consideration, the mean annual cost per patient was around £2,500 (about $3,300) for RDEB-INV, £10,375 (about $13,700) per patient for RDEB-GS, and a staggering £98,000 (about $129,000) per patient for RDEB-GS. The total annual cost of dressings and associated care was an estimated £3,184,229 (about $4.2 million).
In addition to data on the cost of wound dressings, data on itch and pain and quality of life were presented at the EB World Congress and discussed by Dr. Mellerio.
A total of 42 participants older than 8 years of age had itch measured via the Leuven Itch Scale, she reported, noting that itch was a consistent symptom across all subtypes of RDEB. Itch is important as it not only causes problems with skin lesions and healing, but also significantly affects sleep and has a negative impact on patients’ mood, she emphasized.
Despite experiencing itch, more than half (58%) of participants were not using any kind of treatment for itch. This “likely reflects the lack of effectiveness of current medication for this debilitating symptom,” Dr. Mellerio and associates noted in one of their poster presentations of PEBLES data.
When treatment was used for itch, it consisted mainly of antihistamines (19% of patients), emollients (19%), or a combination of both (4%). However, treatment was generally “not very good,” with a satisfaction score of just 5 on a scale of 10, Dr. Mellerio pointed out. Participants “reported frustration with the lack of effective treatment for itch,” she said.
Itch was associated with disturbed sleep 1-3 nights per week in 20%-40% of participants, and every night in 20%-30%.
Pain was found to be a significant problem, with a median level of background pain scored as 4 on a 10-cm visual analog scale and a higher level (6) when associated with dressing changes.
Data on how RDEB affected quality of life were reported for 39 adults completing the 17-item Quality of Life in EB Questionnaire (QOLEB) and eight children who were able to complete the Pediatric Quality of Life Inventory (PedsQL) with the aid of their parents.
Dr. Mellerio reported that adults with RDEB-GS had an overall QOLEB score of 24 out of 50, an indication that their condition had a severe impact on their quality of life. The effect on quality of life was greater in terms of their physical functioning than emotional well-being, with respective scores of 19 out of 36, and 5 out of a possible 15. Less impact on quality of life was reported by participants with other RDEB subtypes.
PedsQL scores for the children indicated there might be a lesser effect of physical functioning on quality of life but a greater effect of emotional well-being on quality of life, but the numbers were small. “Interestingly, parents tended to rate their children’s impact on quality of life much higher than the children themselves,” Dr. Mellerio said.
The point of PEBLES is to start to understand the natural history of RDEB and to identify endpoints that might help in clinical trials of potential new treatments. Discussing the next steps for PEBLES, Dr. Mellerio said the aim was to recruit more pediatric patients and look at other data sets, such as bone health. The PEBLES team also hopes to extend recruitment to include other United Kingdom, and ultimately international, EB centers and, perhaps eventually to start to include other types of EB, such as EB simplex.
PEBLES is funded by DEBRA UK. Dr. Mellerio is a PEBLES investigator but had no conflicts of interest to disclose.
SOURCE: Mellerio JE et al. EB 2020. Pillay EI et al. Poster 77; Jeffs E et al. Poster 74; Jeffs et al. Poster 75. https://ebworldcongress.org/.
LONDON – More than £2.8 million (RDEB), according to a report at the EB World Congress, organized by the Dystrophic Epidermolysis Bullosa Association (DEBRA).
Results from the Prospective Epidermolysis Bullosa Longitudinal Evaluation Study (PEBLES), which is looking at the natural history of RDEB, showed that wound dressing and bandage costs were highest for study participants with the generalized severe (RDEB-GS) subtype, at just over £85,156 (about $112,450) per patient annually. Respective yearly costs for the generalized intermediate (RDEB-GI) and inversa (RDEB-INV) subtypes were £10,112 (about $13,350) and £1,699 (about $2,240) per patient.
Looking at the costs associated with EB is important, said one of the lead investigators for PEBLES, Jemima Mellerio, MD, FRCP, consultant dermatologist at St John’s Institute of Dermatology, at Guy’s & St. Thomas’ NHS Foundation Trust, London.
“If we are going to justify the kind of expenditure [associated with new treatments], we need to know that what we are treating is already a significant burden on our health care systems,” Dr. Mellerio said.
PEBLES is an ongoing London-based registry study that is enrolling patients with all subtypes of RDEB. Data are collected via a tablet device and include demographic data, information on clinical features, results of skin biopsies and genetic tests, and laboratory findings, as well as objective disease severity and subjective patient-orientated outcome scores.
So far, 60 patients – 49 adults and 11 children – have been enrolled in PEBLES since November 2014: 26 with RDEB-GS, 23 with RDEB-GI, 9 with RDEB-INV, and 2 with the pruriginosa RDEB subtype (RDEB-PR).
Most of the participants (71%) changed all their wound dressings at one time, patching up when required. Fourteen of 49 participants had paid people to help them change their dressings and when the total cost of combined wound dressings and paid care was taken into consideration, the mean annual cost per patient was around £2,500 (about $3,300) for RDEB-INV, £10,375 (about $13,700) per patient for RDEB-GS, and a staggering £98,000 (about $129,000) per patient for RDEB-GS. The total annual cost of dressings and associated care was an estimated £3,184,229 (about $4.2 million).
In addition to data on the cost of wound dressings, data on itch and pain and quality of life were presented at the EB World Congress and discussed by Dr. Mellerio.
A total of 42 participants older than 8 years of age had itch measured via the Leuven Itch Scale, she reported, noting that itch was a consistent symptom across all subtypes of RDEB. Itch is important as it not only causes problems with skin lesions and healing, but also significantly affects sleep and has a negative impact on patients’ mood, she emphasized.
Despite experiencing itch, more than half (58%) of participants were not using any kind of treatment for itch. This “likely reflects the lack of effectiveness of current medication for this debilitating symptom,” Dr. Mellerio and associates noted in one of their poster presentations of PEBLES data.
When treatment was used for itch, it consisted mainly of antihistamines (19% of patients), emollients (19%), or a combination of both (4%). However, treatment was generally “not very good,” with a satisfaction score of just 5 on a scale of 10, Dr. Mellerio pointed out. Participants “reported frustration with the lack of effective treatment for itch,” she said.
Itch was associated with disturbed sleep 1-3 nights per week in 20%-40% of participants, and every night in 20%-30%.
Pain was found to be a significant problem, with a median level of background pain scored as 4 on a 10-cm visual analog scale and a higher level (6) when associated with dressing changes.
Data on how RDEB affected quality of life were reported for 39 adults completing the 17-item Quality of Life in EB Questionnaire (QOLEB) and eight children who were able to complete the Pediatric Quality of Life Inventory (PedsQL) with the aid of their parents.
Dr. Mellerio reported that adults with RDEB-GS had an overall QOLEB score of 24 out of 50, an indication that their condition had a severe impact on their quality of life. The effect on quality of life was greater in terms of their physical functioning than emotional well-being, with respective scores of 19 out of 36, and 5 out of a possible 15. Less impact on quality of life was reported by participants with other RDEB subtypes.
PedsQL scores for the children indicated there might be a lesser effect of physical functioning on quality of life but a greater effect of emotional well-being on quality of life, but the numbers were small. “Interestingly, parents tended to rate their children’s impact on quality of life much higher than the children themselves,” Dr. Mellerio said.
The point of PEBLES is to start to understand the natural history of RDEB and to identify endpoints that might help in clinical trials of potential new treatments. Discussing the next steps for PEBLES, Dr. Mellerio said the aim was to recruit more pediatric patients and look at other data sets, such as bone health. The PEBLES team also hopes to extend recruitment to include other United Kingdom, and ultimately international, EB centers and, perhaps eventually to start to include other types of EB, such as EB simplex.
PEBLES is funded by DEBRA UK. Dr. Mellerio is a PEBLES investigator but had no conflicts of interest to disclose.
SOURCE: Mellerio JE et al. EB 2020. Pillay EI et al. Poster 77; Jeffs E et al. Poster 74; Jeffs et al. Poster 75. https://ebworldcongress.org/.
REPORTING FROM EB 2020
Social media may negatively influence acne treatment
A small survey suggests many patients consult social media for advice on acne treatment and follow recommendations that don’t align with clinical guidelines.

Of the 130 patients surveyed, 45% consulted social media for advice on acne treatment, and 52% of those patients followed recommendations that don’t correspond to American Academy of Dermatology (AAD) guidelines. Most patients reported no improvement (40%) or minimal improvement (53%) in their acne after following advice from social media.
“These results suggest that dermatologists should inquire about social media acne treatment advice and directly address misinformation,” wrote Ahmed Yousaf, of West Virginia University, Morgantown, W.Va., and colleagues. Their report is in Pediatric Dermatology.
They conducted the survey of 130 patients treated for acne at West Virginia University. Most patients were female (60%), and a majority were adolescents (54%) or adults (44%). About half of the patients (51%) said their acne was moderate, 38% said it was severe, and 11% said it was mild.
Most patients said they consulted a medical professional for their first acne treatment (58%). However, 16% of patients said they first went to social media for advice, 26% said they consulted family or friends, and 10% took “other” steps as their first approach to acne treatment.
In all, 45% of patients consulted social media for acne treatment advice at some point. This includes 54% of women, 31% of men, 41% of adolescents, and 51% of adults. Social media consultation was more common among patients with severe acne (54%) than among those with mild (36%) or moderate (39%) acne.
The most common social media platforms used were YouTube and Instagram (58% each), followed by Pinterest (31%), Facebook (19%), Twitter (9%), Snapchat (7%), and Tumblr (3%). (Patients could select more than one social media platform.)
Roughly half (52%) of patients who consulted social media followed advice that does not align with AAD guidelines, 31% made changes that are recommended by the AAD, and 17% did not provide information on recommendations they followed.
The social media advice patients followed included using over-the-counter products (81%), making dietary changes (40%), using self-made products (19%), taking supplements (16%), and making changes in exercise routines (7%). (Patients could select more than one treatment approach.)
Among the patients who followed social media advice, 40% said they saw no change in their acne, and 53% reported minimal improvement.
“Only 7% of social media users reported significant improvement in their acne,” Mr. Yousaf and colleagues wrote. “This may be due to less accurate content found on social media compared to other health care sources.”
The authors acknowledged that the patients surveyed were recruited from a dermatology clinic. Therefore, these results “likely underestimate the percentage of patients who improve from social media acne treatment advice and do not consult a medical professional.”
Mr. Yousaf and colleagues did not disclose any conflicts of interest.
SOURCE: Yousaf A et al. Pediatr Dermatol. 2020 Jan 15. doi: 10.1111/pde.14091.
A small survey suggests many patients consult social media for advice on acne treatment and follow recommendations that don’t align with clinical guidelines.
Of the 130 patients surveyed, 45% consulted social media for advice on acne treatment, and 52% of those patients followed recommendations that don’t correspond to American Academy of Dermatology (AAD) guidelines. Most patients reported no improvement (40%) or minimal improvement (53%) in their acne after following advice from social media.
“These results suggest that dermatologists should inquire about social media acne treatment advice and directly address misinformation,” wrote Ahmed Yousaf, of West Virginia University, Morgantown, W.Va., and colleagues. Their report is in Pediatric Dermatology.
They conducted the survey of 130 patients treated for acne at West Virginia University. Most patients were female (60%), and a majority were adolescents (54%) or adults (44%). About half of the patients (51%) said their acne was moderate, 38% said it was severe, and 11% said it was mild.
Most patients said they consulted a medical professional for their first acne treatment (58%). However, 16% of patients said they first went to social media for advice, 26% said they consulted family or friends, and 10% took “other” steps as their first approach to acne treatment.
In all, 45% of patients consulted social media for acne treatment advice at some point. This includes 54% of women, 31% of men, 41% of adolescents, and 51% of adults. Social media consultation was more common among patients with severe acne (54%) than among those with mild (36%) or moderate (39%) acne.
The most common social media platforms used were YouTube and Instagram (58% each), followed by Pinterest (31%), Facebook (19%), Twitter (9%), Snapchat (7%), and Tumblr (3%). (Patients could select more than one social media platform.)
Roughly half (52%) of patients who consulted social media followed advice that does not align with AAD guidelines, 31% made changes that are recommended by the AAD, and 17% did not provide information on recommendations they followed.
The social media advice patients followed included using over-the-counter products (81%), making dietary changes (40%), using self-made products (19%), taking supplements (16%), and making changes in exercise routines (7%). (Patients could select more than one treatment approach.)
Among the patients who followed social media advice, 40% said they saw no change in their acne, and 53% reported minimal improvement.
“Only 7% of social media users reported significant improvement in their acne,” Mr. Yousaf and colleagues wrote. “This may be due to less accurate content found on social media compared to other health care sources.”
The authors acknowledged that the patients surveyed were recruited from a dermatology clinic. Therefore, these results “likely underestimate the percentage of patients who improve from social media acne treatment advice and do not consult a medical professional.”
Mr. Yousaf and colleagues did not disclose any conflicts of interest.
SOURCE: Yousaf A et al. Pediatr Dermatol. 2020 Jan 15. doi: 10.1111/pde.14091.
A small survey suggests many patients consult social media for advice on acne treatment and follow recommendations that don’t align with clinical guidelines.
Of the 130 patients surveyed, 45% consulted social media for advice on acne treatment, and 52% of those patients followed recommendations that don’t correspond to American Academy of Dermatology (AAD) guidelines. Most patients reported no improvement (40%) or minimal improvement (53%) in their acne after following advice from social media.
“These results suggest that dermatologists should inquire about social media acne treatment advice and directly address misinformation,” wrote Ahmed Yousaf, of West Virginia University, Morgantown, W.Va., and colleagues. Their report is in Pediatric Dermatology.
They conducted the survey of 130 patients treated for acne at West Virginia University. Most patients were female (60%), and a majority were adolescents (54%) or adults (44%). About half of the patients (51%) said their acne was moderate, 38% said it was severe, and 11% said it was mild.
Most patients said they consulted a medical professional for their first acne treatment (58%). However, 16% of patients said they first went to social media for advice, 26% said they consulted family or friends, and 10% took “other” steps as their first approach to acne treatment.
In all, 45% of patients consulted social media for acne treatment advice at some point. This includes 54% of women, 31% of men, 41% of adolescents, and 51% of adults. Social media consultation was more common among patients with severe acne (54%) than among those with mild (36%) or moderate (39%) acne.
The most common social media platforms used were YouTube and Instagram (58% each), followed by Pinterest (31%), Facebook (19%), Twitter (9%), Snapchat (7%), and Tumblr (3%). (Patients could select more than one social media platform.)
Roughly half (52%) of patients who consulted social media followed advice that does not align with AAD guidelines, 31% made changes that are recommended by the AAD, and 17% did not provide information on recommendations they followed.
The social media advice patients followed included using over-the-counter products (81%), making dietary changes (40%), using self-made products (19%), taking supplements (16%), and making changes in exercise routines (7%). (Patients could select more than one treatment approach.)
Among the patients who followed social media advice, 40% said they saw no change in their acne, and 53% reported minimal improvement.
“Only 7% of social media users reported significant improvement in their acne,” Mr. Yousaf and colleagues wrote. “This may be due to less accurate content found on social media compared to other health care sources.”
The authors acknowledged that the patients surveyed were recruited from a dermatology clinic. Therefore, these results “likely underestimate the percentage of patients who improve from social media acne treatment advice and do not consult a medical professional.”
Mr. Yousaf and colleagues did not disclose any conflicts of interest.
SOURCE: Yousaf A et al. Pediatr Dermatol. 2020 Jan 15. doi: 10.1111/pde.14091.
FROM PEDIATRIC DERMATOLOGY